User login
Physician Empathy Mitigates Patients’ Chronic Pain
Physicians who treat patients are potentially exposed to two opposing psychological processes: A positive feeling related to the experience of helping someone in need and, on the other hand, the adverse experience of seeing someone’s suffering and being frustrated about their inability to help. The ability to share the feelings of others is often referred to as empathy, while the ability to care for and show interest in others is the key aspect of compassion. Empathy makes it possible to share the positive and negative feelings of others in the same way: We can therefore feel happy when we indirectly share others’ joy and sad when we indirectly share others’ suffering.
Empathy in healthcare professionals is associated with patient satisfaction, diagnostic accuracy, adherence to treatment recommendations, clinical outcomes, clinical expertise, and physician retention. However, evidence indicates a tendency for empathy to decline during physicians’ training and specialization.
Estimating Empathy
Empathy studies are primarily based on observational data that include physician self-assessment or patient-perceived empathy. External evaluation of empathy by the recipient or observer is not the dominant approach, and a systematic review of the topic showed that, in 331 of the 470 studies examined (70.4%), individuals self-reported their level of empathy. The self-assessment system, particularly for doctors, is more likely to measure the doctor’s attitudes about empathy than empathy itself. The lack of correlation between physician and patient empathy assessments made it clear that patients cannot be disregarded when assessing physician empathy.
Consultation and Relational Empathy (CARE) is the primary assessment tool available to patients to measure physician empathy. It is a reliable and consistent system, particularly in primary care scenarios.
The CARE measure captures even small nuances of patient interactions with the physician and has been confirmed as a valuable tool in assessing the relational components of empathy.
Doctor-Patient Relationship
Communication with the physician is generally considered an important element of chronic pain care because it affects patient engagement and decision-making. A collaborative approach involving the patient and clinician in clinical decisions was associated with adherence to pain treatment and improved outcomes among patients with chronic lower back pain. The study conducted in a primary care setting of 1352 participants showed findings regarding physician empathy that did not necessarily involve a therapeutic alliance with the patient based on collaborative communication or expectation of a therapeutic effect of pharmacotherapy. Physician empathy remained the strongest factor associated with patient satisfaction, even after considering various potential confounders, including communication with the physician. In addition, ongoing empathy, especially when reported by patients with a long-term relationship with the physician, supported the hypothesis of a possible lasting effect on patient satisfaction.
Treating Chronic Pain
Empathy is an aspect of the doctor-patient relationship that may be particularly important in patients with chronic pain. A cohort study of 1470 patients with chronic low back pain analyzed whether and how it correlated with chronic pain outcomes. Patients reported their physician’s empathy at the time of enrollment using the CARE measure, which included 10 items on physician’s empathy characteristics during meetings. Physicians whose scores were 30 or higher (ie, rated as good, very good, or excellent in most items) were classified as very empathetic physicians (VEPs), while those whose scores were 29 or lower (ie, rated as poor or passable in most items) were classified as slightly empathetic physicians (SEPs).
Pain intensity was measured with a numerical rating scale (0-10) for the typical pain level within 7 days before each encounter. The long-term stability of CARE scores was assessed in patients who maintained the same physician for more than 24 months. The study showed the following results:
- The CARE score was inversely associated with pain intensity (P < .001).
- Pain intensity was lower in patients in the VEP group than those in the SEP group (6.3 vs 6.7; P < .001).
- The likelihood of having a more empathetic physician generally increased with the decrease in the cut point of the CARE score for greater or less empathy of the physician.
- The extent of the physician’s empathy effects exceeded that reported for nonpharmacological treatments, current opioid use, and lumbar spine surgery.
- The effects of the interaction of empathy with time tended to favor the VEP group with regard to pain but were not statistically significant.
Empathy is an essential aspect of the patient-physician relationship (particularly in delivering care), and these findings demonstrate its relevance in pain therapy. Empathy has high therapeutic value, compared with many pain treatments that are often recommended in clinical practice.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Physicians who treat patients are potentially exposed to two opposing psychological processes: A positive feeling related to the experience of helping someone in need and, on the other hand, the adverse experience of seeing someone’s suffering and being frustrated about their inability to help. The ability to share the feelings of others is often referred to as empathy, while the ability to care for and show interest in others is the key aspect of compassion. Empathy makes it possible to share the positive and negative feelings of others in the same way: We can therefore feel happy when we indirectly share others’ joy and sad when we indirectly share others’ suffering.
Empathy in healthcare professionals is associated with patient satisfaction, diagnostic accuracy, adherence to treatment recommendations, clinical outcomes, clinical expertise, and physician retention. However, evidence indicates a tendency for empathy to decline during physicians’ training and specialization.
Estimating Empathy
Empathy studies are primarily based on observational data that include physician self-assessment or patient-perceived empathy. External evaluation of empathy by the recipient or observer is not the dominant approach, and a systematic review of the topic showed that, in 331 of the 470 studies examined (70.4%), individuals self-reported their level of empathy. The self-assessment system, particularly for doctors, is more likely to measure the doctor’s attitudes about empathy than empathy itself. The lack of correlation between physician and patient empathy assessments made it clear that patients cannot be disregarded when assessing physician empathy.
Consultation and Relational Empathy (CARE) is the primary assessment tool available to patients to measure physician empathy. It is a reliable and consistent system, particularly in primary care scenarios.
The CARE measure captures even small nuances of patient interactions with the physician and has been confirmed as a valuable tool in assessing the relational components of empathy.
Doctor-Patient Relationship
Communication with the physician is generally considered an important element of chronic pain care because it affects patient engagement and decision-making. A collaborative approach involving the patient and clinician in clinical decisions was associated with adherence to pain treatment and improved outcomes among patients with chronic lower back pain. The study conducted in a primary care setting of 1352 participants showed findings regarding physician empathy that did not necessarily involve a therapeutic alliance with the patient based on collaborative communication or expectation of a therapeutic effect of pharmacotherapy. Physician empathy remained the strongest factor associated with patient satisfaction, even after considering various potential confounders, including communication with the physician. In addition, ongoing empathy, especially when reported by patients with a long-term relationship with the physician, supported the hypothesis of a possible lasting effect on patient satisfaction.
Treating Chronic Pain
Empathy is an aspect of the doctor-patient relationship that may be particularly important in patients with chronic pain. A cohort study of 1470 patients with chronic low back pain analyzed whether and how it correlated with chronic pain outcomes. Patients reported their physician’s empathy at the time of enrollment using the CARE measure, which included 10 items on physician’s empathy characteristics during meetings. Physicians whose scores were 30 or higher (ie, rated as good, very good, or excellent in most items) were classified as very empathetic physicians (VEPs), while those whose scores were 29 or lower (ie, rated as poor or passable in most items) were classified as slightly empathetic physicians (SEPs).
Pain intensity was measured with a numerical rating scale (0-10) for the typical pain level within 7 days before each encounter. The long-term stability of CARE scores was assessed in patients who maintained the same physician for more than 24 months. The study showed the following results:
- The CARE score was inversely associated with pain intensity (P < .001).
- Pain intensity was lower in patients in the VEP group than those in the SEP group (6.3 vs 6.7; P < .001).
- The likelihood of having a more empathetic physician generally increased with the decrease in the cut point of the CARE score for greater or less empathy of the physician.
- The extent of the physician’s empathy effects exceeded that reported for nonpharmacological treatments, current opioid use, and lumbar spine surgery.
- The effects of the interaction of empathy with time tended to favor the VEP group with regard to pain but were not statistically significant.
Empathy is an essential aspect of the patient-physician relationship (particularly in delivering care), and these findings demonstrate its relevance in pain therapy. Empathy has high therapeutic value, compared with many pain treatments that are often recommended in clinical practice.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Physicians who treat patients are potentially exposed to two opposing psychological processes: A positive feeling related to the experience of helping someone in need and, on the other hand, the adverse experience of seeing someone’s suffering and being frustrated about their inability to help. The ability to share the feelings of others is often referred to as empathy, while the ability to care for and show interest in others is the key aspect of compassion. Empathy makes it possible to share the positive and negative feelings of others in the same way: We can therefore feel happy when we indirectly share others’ joy and sad when we indirectly share others’ suffering.
Empathy in healthcare professionals is associated with patient satisfaction, diagnostic accuracy, adherence to treatment recommendations, clinical outcomes, clinical expertise, and physician retention. However, evidence indicates a tendency for empathy to decline during physicians’ training and specialization.
Estimating Empathy
Empathy studies are primarily based on observational data that include physician self-assessment or patient-perceived empathy. External evaluation of empathy by the recipient or observer is not the dominant approach, and a systematic review of the topic showed that, in 331 of the 470 studies examined (70.4%), individuals self-reported their level of empathy. The self-assessment system, particularly for doctors, is more likely to measure the doctor’s attitudes about empathy than empathy itself. The lack of correlation between physician and patient empathy assessments made it clear that patients cannot be disregarded when assessing physician empathy.
Consultation and Relational Empathy (CARE) is the primary assessment tool available to patients to measure physician empathy. It is a reliable and consistent system, particularly in primary care scenarios.
The CARE measure captures even small nuances of patient interactions with the physician and has been confirmed as a valuable tool in assessing the relational components of empathy.
Doctor-Patient Relationship
Communication with the physician is generally considered an important element of chronic pain care because it affects patient engagement and decision-making. A collaborative approach involving the patient and clinician in clinical decisions was associated with adherence to pain treatment and improved outcomes among patients with chronic lower back pain. The study conducted in a primary care setting of 1352 participants showed findings regarding physician empathy that did not necessarily involve a therapeutic alliance with the patient based on collaborative communication or expectation of a therapeutic effect of pharmacotherapy. Physician empathy remained the strongest factor associated with patient satisfaction, even after considering various potential confounders, including communication with the physician. In addition, ongoing empathy, especially when reported by patients with a long-term relationship with the physician, supported the hypothesis of a possible lasting effect on patient satisfaction.
Treating Chronic Pain
Empathy is an aspect of the doctor-patient relationship that may be particularly important in patients with chronic pain. A cohort study of 1470 patients with chronic low back pain analyzed whether and how it correlated with chronic pain outcomes. Patients reported their physician’s empathy at the time of enrollment using the CARE measure, which included 10 items on physician’s empathy characteristics during meetings. Physicians whose scores were 30 or higher (ie, rated as good, very good, or excellent in most items) were classified as very empathetic physicians (VEPs), while those whose scores were 29 or lower (ie, rated as poor or passable in most items) were classified as slightly empathetic physicians (SEPs).
Pain intensity was measured with a numerical rating scale (0-10) for the typical pain level within 7 days before each encounter. The long-term stability of CARE scores was assessed in patients who maintained the same physician for more than 24 months. The study showed the following results:
- The CARE score was inversely associated with pain intensity (P < .001).
- Pain intensity was lower in patients in the VEP group than those in the SEP group (6.3 vs 6.7; P < .001).
- The likelihood of having a more empathetic physician generally increased with the decrease in the cut point of the CARE score for greater or less empathy of the physician.
- The extent of the physician’s empathy effects exceeded that reported for nonpharmacological treatments, current opioid use, and lumbar spine surgery.
- The effects of the interaction of empathy with time tended to favor the VEP group with regard to pain but were not statistically significant.
Empathy is an essential aspect of the patient-physician relationship (particularly in delivering care), and these findings demonstrate its relevance in pain therapy. Empathy has high therapeutic value, compared with many pain treatments that are often recommended in clinical practice.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
GPs Urged to Embed Lifestyle Medicine into Primary Care
LIVERPOOL — “Healthy doctors make healthy patients”, stated a GP during a workshop at the Royal College of General Practitioners (RCGP) annual meeting. The session aimed to encourage GPs to embed lifestyle medicine into primary care through collaborative action.
Callum Leese from Aberfeldy Medical Practice in Scotland, who is also a lecturer at the University of Dundee for the Scottish Clinical Research Excellence Development Scheme (SCREDS), discussed the benefits of lifestyle medicine services in addressing lifestyle-related diseases, reducing their contribution towards the prevalence of chronic conditions, and helping prevent premature mortality.
Leese is leading a project to make Aberfeldy the healthiest town in Scotland by promoting physical activities, such as the 2-km, 5-km, and 7-km Santa Stride walking group in November, and a recent food festival to encourage healthy cooking and eating. “There’s loads of things that can be done to try and inspire change,” he said. “The research is fairly unequivocal in that healthy doctors make healthy patients,” Leese asserted. “The most important thing we can do is target our doctors and our nurses and make them advocates for what we want to see with our patients.”
Speaking to this news organization, he emphasized that, “if the doctors are moving, they’re much more likely to promote it, and if they’re eating well, they’re much more likely to be able to be evangelistic.”
Physical Activity Advice Shows High Return
About one-third of the population in the United Kingdom are physically inactive, which costs the economy £7.2 billion, with £1 billion attributed directly to the NHS, he informed the workshop.
As an honorary support fellow in physical activity and lifestyle medicine at the RCGP, Leese specializes in integrating physical activity into primary care settings. “We know it’s cost effective. If we compare it to smoking cessation advice, we know that we need to give advice to one person about 50 times for one person to stop smoking in primary care. But for physical activity, you need to give advice to 12 people for one person to increase their physical activity levels to meet the guidance,” he noted.
Leese stressed the importance of short but effective discussions between GPs and patients. He gave examples of online resources to recommend to patients, such as Moving Medicine, which aims to help healthcare professionals integrate physical activity into routine clinical conversations, or the RCGP toolkit (the Physical Activity Hub). “It really takes 1 minute of asking if the patient has ever considered being more active, and briefly explaining that being more active might have really significant outcomes for their condition,” he said.
In primary care, most patients who need to be more physically activity are directed toward 12-week exercise referral schemes, and sometimes we use social prescribing, for example, inviting patients to walk in groups, Leese explained. “However, despite the best intentions, about 78% of GPs aren’t doing it [advising on physical activity] regularly,” he noted. He cited four main challenges: lack of time, knowledge, resources, and financial support.
Geographical Variation in Social Prescribing
Social prescribing, which links patients with non–medical community support, also varies widely across the United Kingdom. “Social prescribing is a real example of that because it’s really well established in some places and not in others,” Leese remarked. He noted that inner-city and rural areas often have different needs. Contrary to some expectations, city dwellers are sometimes more active than those living in rural areas because despite having lots of green space for physical activity, “they tend to park the car outside the front door and park again right outside their place of work, whereas in London, for example, you can persuade people to get off a stop early on the Tube or a stop early in the bus.”
MAN v FAT 5-a-side Football
Leese also emphasized the importance of innovation in implementing lifestyle medicine, pointing out that nonmedical personnel, social prescribers, and health coaches can alleviate time pressures on GPs.
Citing an example of a physical activity-related intervention, he described a UK-wide organization developed for men in the 40s-50s age group, called MAN v FAT, which involves a novel weight-related way of playing five-a-side football. Players have a weigh-in before each game and teams are rewarded with points on the pitch for every pound lost as a team since their last match.
However, Leese acknowledged the need to tailor physical activity advice to different age groups. For example, “in an 80-year-old, physical activity might improve their balance and they’re less likely to fall and break something.”
Lifestyle Clinics
Leese cited the PCN Lifestyle Clinics, originating from the Leamington Primary Care Network (PCN), as an example of successful lifestyle medicine integration to help address the needs of people living with chronic conditions. “We don’t want to prescribe a model, but we can draw on a program run by the Leamington Spa PCN, that involves four group sessions of 6-10 people focused on lifestyle,” he said.
The weekly group-based sessions are run by a GP, a health and wellbeing coach, a dietitian, and a psychiatrist. Together, they cover four aspects of lifestyle and health comprising individual challenges, how community influences behavior and vice versa, food and nutrition, and physical activity for health and wellbeing.
“We try to debunk some of those myths around nutrition, compared with diet, and physical activity, compared with exercise. So, for example, the idea that exercise is usually considered to be using an elliptical cross-trainer whereas physical activity, which might be just dancing in your kitchen while you’re making dinner, is something that can be done more easily,” explained Leese.
Physical activities include running and swimming in collaboration with a leisure center. “It’s an amazing program,” he remarked.
Outcomes from 142 patients who attended the Lifestyle Clinic at a North Leamington GP practice over 14 months showed that 53% gained confidence in making lifestyle changes, 60% noticed a positive impact on their physical health, and 77% reported positive impacts on their mental health.
GP Embraces Lifestyle Medicine
Rachel Burnett, a GP from Park Medical Practice in Derby, a delegate who attended the session, commented on the central idea of incorporating lifestyle medicine into primary care practice. She told this news organization that, “I think it could prevent a lot of ill health and therefore a lot of health inequalities just by embedding lifestyle medicine into our work. To hear about the Leamington Spa project and how it›s been a success was really inspiring.”
Referring to her own practice, Burnett said: “My patients are familiar with the way I go on and on about lifestyle measures, but I believe the way forward is with group sessions because we need to give the same advice to a large number of patients, for example, with prediabetes. This could save time and resource, and I think patients who are more likely to make the changes will actually attend the sessions so we’re not wasting our breath.”
Neither Leese nor Burnett declared any relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
LIVERPOOL — “Healthy doctors make healthy patients”, stated a GP during a workshop at the Royal College of General Practitioners (RCGP) annual meeting. The session aimed to encourage GPs to embed lifestyle medicine into primary care through collaborative action.
Callum Leese from Aberfeldy Medical Practice in Scotland, who is also a lecturer at the University of Dundee for the Scottish Clinical Research Excellence Development Scheme (SCREDS), discussed the benefits of lifestyle medicine services in addressing lifestyle-related diseases, reducing their contribution towards the prevalence of chronic conditions, and helping prevent premature mortality.
Leese is leading a project to make Aberfeldy the healthiest town in Scotland by promoting physical activities, such as the 2-km, 5-km, and 7-km Santa Stride walking group in November, and a recent food festival to encourage healthy cooking and eating. “There’s loads of things that can be done to try and inspire change,” he said. “The research is fairly unequivocal in that healthy doctors make healthy patients,” Leese asserted. “The most important thing we can do is target our doctors and our nurses and make them advocates for what we want to see with our patients.”
Speaking to this news organization, he emphasized that, “if the doctors are moving, they’re much more likely to promote it, and if they’re eating well, they’re much more likely to be able to be evangelistic.”
Physical Activity Advice Shows High Return
About one-third of the population in the United Kingdom are physically inactive, which costs the economy £7.2 billion, with £1 billion attributed directly to the NHS, he informed the workshop.
As an honorary support fellow in physical activity and lifestyle medicine at the RCGP, Leese specializes in integrating physical activity into primary care settings. “We know it’s cost effective. If we compare it to smoking cessation advice, we know that we need to give advice to one person about 50 times for one person to stop smoking in primary care. But for physical activity, you need to give advice to 12 people for one person to increase their physical activity levels to meet the guidance,” he noted.
Leese stressed the importance of short but effective discussions between GPs and patients. He gave examples of online resources to recommend to patients, such as Moving Medicine, which aims to help healthcare professionals integrate physical activity into routine clinical conversations, or the RCGP toolkit (the Physical Activity Hub). “It really takes 1 minute of asking if the patient has ever considered being more active, and briefly explaining that being more active might have really significant outcomes for their condition,” he said.
In primary care, most patients who need to be more physically activity are directed toward 12-week exercise referral schemes, and sometimes we use social prescribing, for example, inviting patients to walk in groups, Leese explained. “However, despite the best intentions, about 78% of GPs aren’t doing it [advising on physical activity] regularly,” he noted. He cited four main challenges: lack of time, knowledge, resources, and financial support.
Geographical Variation in Social Prescribing
Social prescribing, which links patients with non–medical community support, also varies widely across the United Kingdom. “Social prescribing is a real example of that because it’s really well established in some places and not in others,” Leese remarked. He noted that inner-city and rural areas often have different needs. Contrary to some expectations, city dwellers are sometimes more active than those living in rural areas because despite having lots of green space for physical activity, “they tend to park the car outside the front door and park again right outside their place of work, whereas in London, for example, you can persuade people to get off a stop early on the Tube or a stop early in the bus.”
MAN v FAT 5-a-side Football
Leese also emphasized the importance of innovation in implementing lifestyle medicine, pointing out that nonmedical personnel, social prescribers, and health coaches can alleviate time pressures on GPs.
Citing an example of a physical activity-related intervention, he described a UK-wide organization developed for men in the 40s-50s age group, called MAN v FAT, which involves a novel weight-related way of playing five-a-side football. Players have a weigh-in before each game and teams are rewarded with points on the pitch for every pound lost as a team since their last match.
However, Leese acknowledged the need to tailor physical activity advice to different age groups. For example, “in an 80-year-old, physical activity might improve their balance and they’re less likely to fall and break something.”
Lifestyle Clinics
Leese cited the PCN Lifestyle Clinics, originating from the Leamington Primary Care Network (PCN), as an example of successful lifestyle medicine integration to help address the needs of people living with chronic conditions. “We don’t want to prescribe a model, but we can draw on a program run by the Leamington Spa PCN, that involves four group sessions of 6-10 people focused on lifestyle,” he said.
The weekly group-based sessions are run by a GP, a health and wellbeing coach, a dietitian, and a psychiatrist. Together, they cover four aspects of lifestyle and health comprising individual challenges, how community influences behavior and vice versa, food and nutrition, and physical activity for health and wellbeing.
“We try to debunk some of those myths around nutrition, compared with diet, and physical activity, compared with exercise. So, for example, the idea that exercise is usually considered to be using an elliptical cross-trainer whereas physical activity, which might be just dancing in your kitchen while you’re making dinner, is something that can be done more easily,” explained Leese.
Physical activities include running and swimming in collaboration with a leisure center. “It’s an amazing program,” he remarked.
Outcomes from 142 patients who attended the Lifestyle Clinic at a North Leamington GP practice over 14 months showed that 53% gained confidence in making lifestyle changes, 60% noticed a positive impact on their physical health, and 77% reported positive impacts on their mental health.
GP Embraces Lifestyle Medicine
Rachel Burnett, a GP from Park Medical Practice in Derby, a delegate who attended the session, commented on the central idea of incorporating lifestyle medicine into primary care practice. She told this news organization that, “I think it could prevent a lot of ill health and therefore a lot of health inequalities just by embedding lifestyle medicine into our work. To hear about the Leamington Spa project and how it›s been a success was really inspiring.”
Referring to her own practice, Burnett said: “My patients are familiar with the way I go on and on about lifestyle measures, but I believe the way forward is with group sessions because we need to give the same advice to a large number of patients, for example, with prediabetes. This could save time and resource, and I think patients who are more likely to make the changes will actually attend the sessions so we’re not wasting our breath.”
Neither Leese nor Burnett declared any relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
LIVERPOOL — “Healthy doctors make healthy patients”, stated a GP during a workshop at the Royal College of General Practitioners (RCGP) annual meeting. The session aimed to encourage GPs to embed lifestyle medicine into primary care through collaborative action.
Callum Leese from Aberfeldy Medical Practice in Scotland, who is also a lecturer at the University of Dundee for the Scottish Clinical Research Excellence Development Scheme (SCREDS), discussed the benefits of lifestyle medicine services in addressing lifestyle-related diseases, reducing their contribution towards the prevalence of chronic conditions, and helping prevent premature mortality.
Leese is leading a project to make Aberfeldy the healthiest town in Scotland by promoting physical activities, such as the 2-km, 5-km, and 7-km Santa Stride walking group in November, and a recent food festival to encourage healthy cooking and eating. “There’s loads of things that can be done to try and inspire change,” he said. “The research is fairly unequivocal in that healthy doctors make healthy patients,” Leese asserted. “The most important thing we can do is target our doctors and our nurses and make them advocates for what we want to see with our patients.”
Speaking to this news organization, he emphasized that, “if the doctors are moving, they’re much more likely to promote it, and if they’re eating well, they’re much more likely to be able to be evangelistic.”
Physical Activity Advice Shows High Return
About one-third of the population in the United Kingdom are physically inactive, which costs the economy £7.2 billion, with £1 billion attributed directly to the NHS, he informed the workshop.
As an honorary support fellow in physical activity and lifestyle medicine at the RCGP, Leese specializes in integrating physical activity into primary care settings. “We know it’s cost effective. If we compare it to smoking cessation advice, we know that we need to give advice to one person about 50 times for one person to stop smoking in primary care. But for physical activity, you need to give advice to 12 people for one person to increase their physical activity levels to meet the guidance,” he noted.
Leese stressed the importance of short but effective discussions between GPs and patients. He gave examples of online resources to recommend to patients, such as Moving Medicine, which aims to help healthcare professionals integrate physical activity into routine clinical conversations, or the RCGP toolkit (the Physical Activity Hub). “It really takes 1 minute of asking if the patient has ever considered being more active, and briefly explaining that being more active might have really significant outcomes for their condition,” he said.
In primary care, most patients who need to be more physically activity are directed toward 12-week exercise referral schemes, and sometimes we use social prescribing, for example, inviting patients to walk in groups, Leese explained. “However, despite the best intentions, about 78% of GPs aren’t doing it [advising on physical activity] regularly,” he noted. He cited four main challenges: lack of time, knowledge, resources, and financial support.
Geographical Variation in Social Prescribing
Social prescribing, which links patients with non–medical community support, also varies widely across the United Kingdom. “Social prescribing is a real example of that because it’s really well established in some places and not in others,” Leese remarked. He noted that inner-city and rural areas often have different needs. Contrary to some expectations, city dwellers are sometimes more active than those living in rural areas because despite having lots of green space for physical activity, “they tend to park the car outside the front door and park again right outside their place of work, whereas in London, for example, you can persuade people to get off a stop early on the Tube or a stop early in the bus.”
MAN v FAT 5-a-side Football
Leese also emphasized the importance of innovation in implementing lifestyle medicine, pointing out that nonmedical personnel, social prescribers, and health coaches can alleviate time pressures on GPs.
Citing an example of a physical activity-related intervention, he described a UK-wide organization developed for men in the 40s-50s age group, called MAN v FAT, which involves a novel weight-related way of playing five-a-side football. Players have a weigh-in before each game and teams are rewarded with points on the pitch for every pound lost as a team since their last match.
However, Leese acknowledged the need to tailor physical activity advice to different age groups. For example, “in an 80-year-old, physical activity might improve their balance and they’re less likely to fall and break something.”
Lifestyle Clinics
Leese cited the PCN Lifestyle Clinics, originating from the Leamington Primary Care Network (PCN), as an example of successful lifestyle medicine integration to help address the needs of people living with chronic conditions. “We don’t want to prescribe a model, but we can draw on a program run by the Leamington Spa PCN, that involves four group sessions of 6-10 people focused on lifestyle,” he said.
The weekly group-based sessions are run by a GP, a health and wellbeing coach, a dietitian, and a psychiatrist. Together, they cover four aspects of lifestyle and health comprising individual challenges, how community influences behavior and vice versa, food and nutrition, and physical activity for health and wellbeing.
“We try to debunk some of those myths around nutrition, compared with diet, and physical activity, compared with exercise. So, for example, the idea that exercise is usually considered to be using an elliptical cross-trainer whereas physical activity, which might be just dancing in your kitchen while you’re making dinner, is something that can be done more easily,” explained Leese.
Physical activities include running and swimming in collaboration with a leisure center. “It’s an amazing program,” he remarked.
Outcomes from 142 patients who attended the Lifestyle Clinic at a North Leamington GP practice over 14 months showed that 53% gained confidence in making lifestyle changes, 60% noticed a positive impact on their physical health, and 77% reported positive impacts on their mental health.
GP Embraces Lifestyle Medicine
Rachel Burnett, a GP from Park Medical Practice in Derby, a delegate who attended the session, commented on the central idea of incorporating lifestyle medicine into primary care practice. She told this news organization that, “I think it could prevent a lot of ill health and therefore a lot of health inequalities just by embedding lifestyle medicine into our work. To hear about the Leamington Spa project and how it›s been a success was really inspiring.”
Referring to her own practice, Burnett said: “My patients are familiar with the way I go on and on about lifestyle measures, but I believe the way forward is with group sessions because we need to give the same advice to a large number of patients, for example, with prediabetes. This could save time and resource, and I think patients who are more likely to make the changes will actually attend the sessions so we’re not wasting our breath.”
Neither Leese nor Burnett declared any relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Smartphone Data Flag Early Dementia Risk in Older Adults
a novel real-world study suggested.
During a smartphone-assisted scavenger hunt on a university campus, researchers observed that older adults with subjective cognitive decline (SCD) paused more frequently, likely to reorient themselves, than those without SCD. This behavior served as an identifier of individuals with SCD.
“Deficits in spatial navigation are one of the first signs of Alzheimer’s disease,” said study investigator Nadine Diersch, PhD, guest researcher with the German Center for Neurodegenerative Diseases (DZNE), Tübingen.
This study, said Diersch, provides “first evidence of how a digital footprint for early dementia-related cognitive decline might look like in real-world settings during a short (less than 30 minutes) and remotely performed wayfinding task.”
The study was published online in PLOS Digital Health.
Trouble With Orientation
A total of 72 men and women in their mid-20s to mid-60s participated in the study; 23 of the 48 older adults had SCD but still scored normally on neuropsychological assessments.
All study participants were instructed to independently find five buildings on the medical campus of the Otto-von-Guericke-University Magdeburg in Germany, guided by a smartphone app developed by the study team. Their patterns of movement were tracked by GPS.
All participants had similar knowledge of the campus, and all were experienced in using smartphones. They also practiced using the app beforehand.
In most cases, participants reached the five destinations in less than half an hour. The younger participants performed better than the older ones; on average, the younger adults walked shorter distances and generally did not use the help function on the app as often as the older ones.
In the older adults, the number of orientation stops was predictive of SCD status. The adults with SCD tended to hesitate more at intersections. A decline in executive functioning might explain this finding, Diersch said.
“Intact executive functioning is an important component of efficient navigation, for example, when switching between different navigation strategies or planning a route. However, since this was the first study on that subject, more research is needed to determine the precise contribution of different cognitive processes on digital wayfinding data,” said Diersch.
With more study, “we think that such a smartphone-assisted wayfinding task, performed in the immediate surroundings, could be used as a low-threshold screening tool — for example, to stratify subjects with regard to the need of extended cognitive and clinical diagnostics in specialized care,” she added.
‘A Game Changer’
Commenting on the research, Shaheen Lakhan, MD, PhD, neurologist and researcher based in Miami, Florida, who wasn’t involved in the research, said the findings have the potential to “revolutionize” dementia care.
“We’ve seen smartphones transform everything from banking to dating — now they’re set to reshape brain health monitoring. This ingenious digital scavenger hunt detects cognitive decline in real-world scenarios, bypassing costly, complex tests. It’s a game changer,” said Lakhan.
“Just as we track our steps and calories, we could soon track our cognitive health with a tap. This isn’t just innovation; it’s the future of dementia prevention and care unfolding on our smartphone screens. We’re not just talking about convenience. We’re talking about catching Alzheimer’s before it catches us,” he added.
The next phase, Lakhan noted, would be to develop smartphone apps as digital therapeutics, not just to detect cognitive decline but to treat or even prevent it.
“Imagine your phone not only flagging potential issues but also providing personalized brain training exercises to keep your mind sharp and resilient against dementia,” Lakhan said.
This work was funded by the Deutsche Forschungsgemeinschaft (German Research Foundation) within the Collaborative Research Center “Neural Resources of Cognition” and a DZNE Innovation-2-Application Award. Diersch is now a full-time employee of neotiv. Lakhan had no relevant disclosures.
A version of this article first appeared on Medscape.com.
a novel real-world study suggested.
During a smartphone-assisted scavenger hunt on a university campus, researchers observed that older adults with subjective cognitive decline (SCD) paused more frequently, likely to reorient themselves, than those without SCD. This behavior served as an identifier of individuals with SCD.
“Deficits in spatial navigation are one of the first signs of Alzheimer’s disease,” said study investigator Nadine Diersch, PhD, guest researcher with the German Center for Neurodegenerative Diseases (DZNE), Tübingen.
This study, said Diersch, provides “first evidence of how a digital footprint for early dementia-related cognitive decline might look like in real-world settings during a short (less than 30 minutes) and remotely performed wayfinding task.”
The study was published online in PLOS Digital Health.
Trouble With Orientation
A total of 72 men and women in their mid-20s to mid-60s participated in the study; 23 of the 48 older adults had SCD but still scored normally on neuropsychological assessments.
All study participants were instructed to independently find five buildings on the medical campus of the Otto-von-Guericke-University Magdeburg in Germany, guided by a smartphone app developed by the study team. Their patterns of movement were tracked by GPS.
All participants had similar knowledge of the campus, and all were experienced in using smartphones. They also practiced using the app beforehand.
In most cases, participants reached the five destinations in less than half an hour. The younger participants performed better than the older ones; on average, the younger adults walked shorter distances and generally did not use the help function on the app as often as the older ones.
In the older adults, the number of orientation stops was predictive of SCD status. The adults with SCD tended to hesitate more at intersections. A decline in executive functioning might explain this finding, Diersch said.
“Intact executive functioning is an important component of efficient navigation, for example, when switching between different navigation strategies or planning a route. However, since this was the first study on that subject, more research is needed to determine the precise contribution of different cognitive processes on digital wayfinding data,” said Diersch.
With more study, “we think that such a smartphone-assisted wayfinding task, performed in the immediate surroundings, could be used as a low-threshold screening tool — for example, to stratify subjects with regard to the need of extended cognitive and clinical diagnostics in specialized care,” she added.
‘A Game Changer’
Commenting on the research, Shaheen Lakhan, MD, PhD, neurologist and researcher based in Miami, Florida, who wasn’t involved in the research, said the findings have the potential to “revolutionize” dementia care.
“We’ve seen smartphones transform everything from banking to dating — now they’re set to reshape brain health monitoring. This ingenious digital scavenger hunt detects cognitive decline in real-world scenarios, bypassing costly, complex tests. It’s a game changer,” said Lakhan.
“Just as we track our steps and calories, we could soon track our cognitive health with a tap. This isn’t just innovation; it’s the future of dementia prevention and care unfolding on our smartphone screens. We’re not just talking about convenience. We’re talking about catching Alzheimer’s before it catches us,” he added.
The next phase, Lakhan noted, would be to develop smartphone apps as digital therapeutics, not just to detect cognitive decline but to treat or even prevent it.
“Imagine your phone not only flagging potential issues but also providing personalized brain training exercises to keep your mind sharp and resilient against dementia,” Lakhan said.
This work was funded by the Deutsche Forschungsgemeinschaft (German Research Foundation) within the Collaborative Research Center “Neural Resources of Cognition” and a DZNE Innovation-2-Application Award. Diersch is now a full-time employee of neotiv. Lakhan had no relevant disclosures.
A version of this article first appeared on Medscape.com.
a novel real-world study suggested.
During a smartphone-assisted scavenger hunt on a university campus, researchers observed that older adults with subjective cognitive decline (SCD) paused more frequently, likely to reorient themselves, than those without SCD. This behavior served as an identifier of individuals with SCD.
“Deficits in spatial navigation are one of the first signs of Alzheimer’s disease,” said study investigator Nadine Diersch, PhD, guest researcher with the German Center for Neurodegenerative Diseases (DZNE), Tübingen.
This study, said Diersch, provides “first evidence of how a digital footprint for early dementia-related cognitive decline might look like in real-world settings during a short (less than 30 minutes) and remotely performed wayfinding task.”
The study was published online in PLOS Digital Health.
Trouble With Orientation
A total of 72 men and women in their mid-20s to mid-60s participated in the study; 23 of the 48 older adults had SCD but still scored normally on neuropsychological assessments.
All study participants were instructed to independently find five buildings on the medical campus of the Otto-von-Guericke-University Magdeburg in Germany, guided by a smartphone app developed by the study team. Their patterns of movement were tracked by GPS.
All participants had similar knowledge of the campus, and all were experienced in using smartphones. They also practiced using the app beforehand.
In most cases, participants reached the five destinations in less than half an hour. The younger participants performed better than the older ones; on average, the younger adults walked shorter distances and generally did not use the help function on the app as often as the older ones.
In the older adults, the number of orientation stops was predictive of SCD status. The adults with SCD tended to hesitate more at intersections. A decline in executive functioning might explain this finding, Diersch said.
“Intact executive functioning is an important component of efficient navigation, for example, when switching between different navigation strategies or planning a route. However, since this was the first study on that subject, more research is needed to determine the precise contribution of different cognitive processes on digital wayfinding data,” said Diersch.
With more study, “we think that such a smartphone-assisted wayfinding task, performed in the immediate surroundings, could be used as a low-threshold screening tool — for example, to stratify subjects with regard to the need of extended cognitive and clinical diagnostics in specialized care,” she added.
‘A Game Changer’
Commenting on the research, Shaheen Lakhan, MD, PhD, neurologist and researcher based in Miami, Florida, who wasn’t involved in the research, said the findings have the potential to “revolutionize” dementia care.
“We’ve seen smartphones transform everything from banking to dating — now they’re set to reshape brain health monitoring. This ingenious digital scavenger hunt detects cognitive decline in real-world scenarios, bypassing costly, complex tests. It’s a game changer,” said Lakhan.
“Just as we track our steps and calories, we could soon track our cognitive health with a tap. This isn’t just innovation; it’s the future of dementia prevention and care unfolding on our smartphone screens. We’re not just talking about convenience. We’re talking about catching Alzheimer’s before it catches us,” he added.
The next phase, Lakhan noted, would be to develop smartphone apps as digital therapeutics, not just to detect cognitive decline but to treat or even prevent it.
“Imagine your phone not only flagging potential issues but also providing personalized brain training exercises to keep your mind sharp and resilient against dementia,” Lakhan said.
This work was funded by the Deutsche Forschungsgemeinschaft (German Research Foundation) within the Collaborative Research Center “Neural Resources of Cognition” and a DZNE Innovation-2-Application Award. Diersch is now a full-time employee of neotiv. Lakhan had no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM PLOS DIGITAL HEALTH
Do PFAs Cause Kidney Cancer? VA to Investigate
The US Department of Veterans Affairs (VA) will conduct a scientific assessment to find out in whether kidney cancer should be considered a presumptive service-connected condition for veterans exposed to per- and polyfluoroalkyl substances (PFAs). This assessment is the first step in the VA presumptive condition investigative process, which could allow exposed veterans who were exposed to PFAs during their service to access more VA services.
A class of more than 12,000 chemicals, PFAs have been used in the military since the early 1970s in many items, including military-grade firefighting foam. Studies have already suggested links between the so-called forever chemicals and cancer, particularly kidney cancer.
The US Department of Defense (DoD) is assessing contamination at hundreds of sites, while the National Defense Authorization Act in Fiscal Year 2020 mandated that DoD stop using those foams starting in October and remove all stocks from active and former installations and equipment. That may not happen until next year, though, because the DoD has requested a waiver through October 2025 and may extend it through 2026.
When a condition is considered presumptive, eligible veterans do not need to prove their service caused their disease to receive benefits. As part of the Biden Administration’s efforts to expand benefits and services for toxin-exposed veterans and their families, the VA expedited health care and benefits eligibility under the PACT Act by several years—including extending presumptions for head cancer, neck cancer, gastrointestinal cancer, reproductive cancer, lymphoma, pancreatic cancer, kidney cancer, melanoma, and hypertension for Vietnam era veterans. The VA has also extended presumptions for > 300 new conditions, most recently for male breast cancer, urethral cancer, and cancer of the paraurethral glands.
Whether a condition is an established presumptive condition or not, the VA will consider claims on a case-by-case basis and can grant disability compensation benefits if sufficient evidence of service connection is found. “[M]ake no mistake: Veterans should not wait for the outcome of this review to apply for the benefits and care they deserve,” VA Secretary Denis McDonough said in a release. “If you’re a veteran and believe your military service has negatively impacted your health, we encourage you to apply for VA care and benefits today.”
The public has 30 days to comment on the proposed scientific assessment between PFAs exposure and kidney cancer via the Federal Register. The VA is set to host a listening session on Nov. 19, 2024, to allow individuals to share research and input. Interested individuals may register to participate. The public may also comment via either forum on other conditions that would benefit from review for potential service-connection.
The US Department of Veterans Affairs (VA) will conduct a scientific assessment to find out in whether kidney cancer should be considered a presumptive service-connected condition for veterans exposed to per- and polyfluoroalkyl substances (PFAs). This assessment is the first step in the VA presumptive condition investigative process, which could allow exposed veterans who were exposed to PFAs during their service to access more VA services.
A class of more than 12,000 chemicals, PFAs have been used in the military since the early 1970s in many items, including military-grade firefighting foam. Studies have already suggested links between the so-called forever chemicals and cancer, particularly kidney cancer.
The US Department of Defense (DoD) is assessing contamination at hundreds of sites, while the National Defense Authorization Act in Fiscal Year 2020 mandated that DoD stop using those foams starting in October and remove all stocks from active and former installations and equipment. That may not happen until next year, though, because the DoD has requested a waiver through October 2025 and may extend it through 2026.
When a condition is considered presumptive, eligible veterans do not need to prove their service caused their disease to receive benefits. As part of the Biden Administration’s efforts to expand benefits and services for toxin-exposed veterans and their families, the VA expedited health care and benefits eligibility under the PACT Act by several years—including extending presumptions for head cancer, neck cancer, gastrointestinal cancer, reproductive cancer, lymphoma, pancreatic cancer, kidney cancer, melanoma, and hypertension for Vietnam era veterans. The VA has also extended presumptions for > 300 new conditions, most recently for male breast cancer, urethral cancer, and cancer of the paraurethral glands.
Whether a condition is an established presumptive condition or not, the VA will consider claims on a case-by-case basis and can grant disability compensation benefits if sufficient evidence of service connection is found. “[M]ake no mistake: Veterans should not wait for the outcome of this review to apply for the benefits and care they deserve,” VA Secretary Denis McDonough said in a release. “If you’re a veteran and believe your military service has negatively impacted your health, we encourage you to apply for VA care and benefits today.”
The public has 30 days to comment on the proposed scientific assessment between PFAs exposure and kidney cancer via the Federal Register. The VA is set to host a listening session on Nov. 19, 2024, to allow individuals to share research and input. Interested individuals may register to participate. The public may also comment via either forum on other conditions that would benefit from review for potential service-connection.
The US Department of Veterans Affairs (VA) will conduct a scientific assessment to find out in whether kidney cancer should be considered a presumptive service-connected condition for veterans exposed to per- and polyfluoroalkyl substances (PFAs). This assessment is the first step in the VA presumptive condition investigative process, which could allow exposed veterans who were exposed to PFAs during their service to access more VA services.
A class of more than 12,000 chemicals, PFAs have been used in the military since the early 1970s in many items, including military-grade firefighting foam. Studies have already suggested links between the so-called forever chemicals and cancer, particularly kidney cancer.
The US Department of Defense (DoD) is assessing contamination at hundreds of sites, while the National Defense Authorization Act in Fiscal Year 2020 mandated that DoD stop using those foams starting in October and remove all stocks from active and former installations and equipment. That may not happen until next year, though, because the DoD has requested a waiver through October 2025 and may extend it through 2026.
When a condition is considered presumptive, eligible veterans do not need to prove their service caused their disease to receive benefits. As part of the Biden Administration’s efforts to expand benefits and services for toxin-exposed veterans and their families, the VA expedited health care and benefits eligibility under the PACT Act by several years—including extending presumptions for head cancer, neck cancer, gastrointestinal cancer, reproductive cancer, lymphoma, pancreatic cancer, kidney cancer, melanoma, and hypertension for Vietnam era veterans. The VA has also extended presumptions for > 300 new conditions, most recently for male breast cancer, urethral cancer, and cancer of the paraurethral glands.
Whether a condition is an established presumptive condition or not, the VA will consider claims on a case-by-case basis and can grant disability compensation benefits if sufficient evidence of service connection is found. “[M]ake no mistake: Veterans should not wait for the outcome of this review to apply for the benefits and care they deserve,” VA Secretary Denis McDonough said in a release. “If you’re a veteran and believe your military service has negatively impacted your health, we encourage you to apply for VA care and benefits today.”
The public has 30 days to comment on the proposed scientific assessment between PFAs exposure and kidney cancer via the Federal Register. The VA is set to host a listening session on Nov. 19, 2024, to allow individuals to share research and input. Interested individuals may register to participate. The public may also comment via either forum on other conditions that would benefit from review for potential service-connection.
VA Tele-Emergency Care Program Expanded Nationwide
The US Department of Veterans Affairs (VA) has announced that tele-emergency care (tele-EC) is now available nationwide. According to the VA, the expansion has already helped > 61,000 callers with a 59.4% case resolution rate, meaning veterans’ needs were resolved without them having to travel to urgent care or an emergency department.
Tele-EC does not replace the need for in-person emergency evaluation, but offers quick, virtual triage assessments for veterans in rural areas or those with mobility and transportation challenges when in-person immediate care can be difficult to access. The program is a part of VA Health Connect, which connects the caller to a clinical triage nurse, who connects the veteran to tele-emergency care when clinically appropriate. Tele-EC practitioners evaluate the veteran over the phone or on video and recommend treatment or follow-up, including in-person care if needed. In life-threatening emergencies, the clinical triage nurse will call 911 and stay on the phone with the veteran until help arrives. The VA however, says the best step for a veteran experiencing a life-threatening emergency is to immediately contact 911 as opposed to seeking support via tele-EC.
The program can save time not only through on-the-spot evaluation, but by avoiding drive and wait times. “Sometimes, you’re not sure whether what you’re experiencing is a minor emergency or not — and tele-emergency care can help you resolve those questions,” VA Under Secretary for Health Shereef Elnahal, MD, says. “Veterans can get immediate, virtual triage with a VA medical provider who has direct access to their medical records. This avoids having to potentially drive to the nearest emergency department and wait to be evaluated, if appropriate.”
Veterans enrolled in VA health care can now access tele-EC nationwide by calling VA Health Connect and through the VA Health Chat app. Veterans can find their local VA Health Connect number by searching for their facility.
The US Department of Veterans Affairs (VA) has announced that tele-emergency care (tele-EC) is now available nationwide. According to the VA, the expansion has already helped > 61,000 callers with a 59.4% case resolution rate, meaning veterans’ needs were resolved without them having to travel to urgent care or an emergency department.
Tele-EC does not replace the need for in-person emergency evaluation, but offers quick, virtual triage assessments for veterans in rural areas or those with mobility and transportation challenges when in-person immediate care can be difficult to access. The program is a part of VA Health Connect, which connects the caller to a clinical triage nurse, who connects the veteran to tele-emergency care when clinically appropriate. Tele-EC practitioners evaluate the veteran over the phone or on video and recommend treatment or follow-up, including in-person care if needed. In life-threatening emergencies, the clinical triage nurse will call 911 and stay on the phone with the veteran until help arrives. The VA however, says the best step for a veteran experiencing a life-threatening emergency is to immediately contact 911 as opposed to seeking support via tele-EC.
The program can save time not only through on-the-spot evaluation, but by avoiding drive and wait times. “Sometimes, you’re not sure whether what you’re experiencing is a minor emergency or not — and tele-emergency care can help you resolve those questions,” VA Under Secretary for Health Shereef Elnahal, MD, says. “Veterans can get immediate, virtual triage with a VA medical provider who has direct access to their medical records. This avoids having to potentially drive to the nearest emergency department and wait to be evaluated, if appropriate.”
Veterans enrolled in VA health care can now access tele-EC nationwide by calling VA Health Connect and through the VA Health Chat app. Veterans can find their local VA Health Connect number by searching for their facility.
The US Department of Veterans Affairs (VA) has announced that tele-emergency care (tele-EC) is now available nationwide. According to the VA, the expansion has already helped > 61,000 callers with a 59.4% case resolution rate, meaning veterans’ needs were resolved without them having to travel to urgent care or an emergency department.
Tele-EC does not replace the need for in-person emergency evaluation, but offers quick, virtual triage assessments for veterans in rural areas or those with mobility and transportation challenges when in-person immediate care can be difficult to access. The program is a part of VA Health Connect, which connects the caller to a clinical triage nurse, who connects the veteran to tele-emergency care when clinically appropriate. Tele-EC practitioners evaluate the veteran over the phone or on video and recommend treatment or follow-up, including in-person care if needed. In life-threatening emergencies, the clinical triage nurse will call 911 and stay on the phone with the veteran until help arrives. The VA however, says the best step for a veteran experiencing a life-threatening emergency is to immediately contact 911 as opposed to seeking support via tele-EC.
The program can save time not only through on-the-spot evaluation, but by avoiding drive and wait times. “Sometimes, you’re not sure whether what you’re experiencing is a minor emergency or not — and tele-emergency care can help you resolve those questions,” VA Under Secretary for Health Shereef Elnahal, MD, says. “Veterans can get immediate, virtual triage with a VA medical provider who has direct access to their medical records. This avoids having to potentially drive to the nearest emergency department and wait to be evaluated, if appropriate.”
Veterans enrolled in VA health care can now access tele-EC nationwide by calling VA Health Connect and through the VA Health Chat app. Veterans can find their local VA Health Connect number by searching for their facility.
Persistent headaches and nightmares
The correct diagnosis is adolescent posttraumatic stress disorder (PTSD), as the patient's symptoms — recurrent nightmares, flashbacks, hypervigilance, and avoidance behaviors — are closely linked to her recent traumatic experience, fitting the clinical profile of PTSD. The MRI finding, although abnormal, does not correlate with a neurologic cause for her symptoms and may be incidental.
Temporal lobe epilepsy can cause behavioral changes but does not explain the specific PTSD symptoms like flashbacks and nightmares.
Chronic migraine could explain the headaches but not the full spectrum of PTSD symptoms.
Major depressive disorder could account for some of the emotional and social symptoms but lacks the characteristic re-experiencing and avoidance behaviors typical of PTSD.
Adolescent PTSD is a significant public health concern, causing significant distress to a small portion of the youth population. By late adolescence, approximately two thirds of youths have been exposed to trauma, and 8% of these individuals meet the criteria for PTSD by age 18. The incidence is exceptionally high in cases of sexual abuse and assault, with rates reaching up to 40%. PTSD in adolescents is associated with severe psychological distress, reduced academic performance, and a high rate of comorbidities, including anxiety and depression. There are specific populations (including children who are evacuated from home, asylum seekers, etc.) that show higher rates of PTSD.
PTSD can lead to chronic impairments, comorbid psychiatric disorders, and an increased risk for suicide, with cases documented in toddlers as young as 1 year old. Thus, it is important to consider the individual's background and social history, as older children with PTSD may present with symptoms from early childhood trauma, often distant from the time of clinical evaluation.
Intrusion symptoms are a hallmark of PTSD, characterized by persistent and uncontrollable thoughts, dreams, and emotional reactions related to the traumatic event. These symptoms distinguish PTSD from other anxiety and mood disorders. Children with PTSD often experience involuntary, distressing thoughts and memories triggered by trauma cues, such as sights, sounds, or smells associated with the traumatic event. In younger children, these intrusive thoughts may manifest through repetitive play that re-enacts aspects of the trauma.
Nightmares are also common, although in children the content may not always directly relate to the traumatic event. Chronic nightmares contribute to sleep disturbances, exacerbating PTSD symptoms. Trauma reminders, which can be both internal (thoughts, memories) and external (places, sensory experiences), can provoke severe distress and physiologic reactions.
Avoidance symptoms often develop as a coping mechanism in response to distressing re-experiencing symptoms. Children may avoid thoughts, feelings, and memories of the traumatic event or people, places, and activities associated with the trauma. In young children, avoidance may manifest as restricted play or reduced exploration of their environment.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) outlines specific criteria for diagnosing PTSD in individuals over 6 years old, which includes exposure to actual or threatened death, serious injury, or sexual violence, and the presence of symptoms such as intrusion, avoidance, negative mood alterations, and heightened arousal. The DSM-5-TR provides tailored diagnostic criteria for developmental differences in symptom expression for children under 6.
Managing PTSD in children requires a patient-specific approach, with an emphasis on obtaining consent from both the patient and guardian. The American Academy of Child and Adolescent Psychiatry (AACAP) recommends psychotherapy as the first-line treatment for pediatric PTSD. However, patients with severe symptoms or comorbidities may initially be unable to engage in meaningful therapy and may require medication to stabilize symptoms before starting psychotherapy.
Trauma-focused psychotherapy, including cognitive-behavioral therapy (CBT), exposure-based therapy, and eye movement desensitization and reprocessing (EMDR) therapy, is the preferred treatment for PTSD. Clinical studies have shown that patients receiving trauma-focused psychotherapy experience more remarkable symptom improvement than those who do not receive treatment and, in children, psychotherapy generally yields better outcomes than pharmacotherapy.
While selective serotonin reuptake inhibitors like sertraline and paroxetine are FDA-approved for PTSD treatment in adults, their efficacy in children often produces outcomes similar to those of placebo. Medications are typically reserved for severe symptoms and are used as an off-label treatment in pediatric cases. Pharmacologic management may be necessary when the severity of symptoms prevents the use of trauma-focused psychotherapy or requires immediate stabilization.
Heidi Moawad, MD, Clinical Assistant Professor, Department of Medical Education, Case Western Reserve University School of Medicine, Cleveland, Ohio.
Heidi Moawad, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The correct diagnosis is adolescent posttraumatic stress disorder (PTSD), as the patient's symptoms — recurrent nightmares, flashbacks, hypervigilance, and avoidance behaviors — are closely linked to her recent traumatic experience, fitting the clinical profile of PTSD. The MRI finding, although abnormal, does not correlate with a neurologic cause for her symptoms and may be incidental.
Temporal lobe epilepsy can cause behavioral changes but does not explain the specific PTSD symptoms like flashbacks and nightmares.
Chronic migraine could explain the headaches but not the full spectrum of PTSD symptoms.
Major depressive disorder could account for some of the emotional and social symptoms but lacks the characteristic re-experiencing and avoidance behaviors typical of PTSD.
Adolescent PTSD is a significant public health concern, causing significant distress to a small portion of the youth population. By late adolescence, approximately two thirds of youths have been exposed to trauma, and 8% of these individuals meet the criteria for PTSD by age 18. The incidence is exceptionally high in cases of sexual abuse and assault, with rates reaching up to 40%. PTSD in adolescents is associated with severe psychological distress, reduced academic performance, and a high rate of comorbidities, including anxiety and depression. There are specific populations (including children who are evacuated from home, asylum seekers, etc.) that show higher rates of PTSD.
PTSD can lead to chronic impairments, comorbid psychiatric disorders, and an increased risk for suicide, with cases documented in toddlers as young as 1 year old. Thus, it is important to consider the individual's background and social history, as older children with PTSD may present with symptoms from early childhood trauma, often distant from the time of clinical evaluation.
Intrusion symptoms are a hallmark of PTSD, characterized by persistent and uncontrollable thoughts, dreams, and emotional reactions related to the traumatic event. These symptoms distinguish PTSD from other anxiety and mood disorders. Children with PTSD often experience involuntary, distressing thoughts and memories triggered by trauma cues, such as sights, sounds, or smells associated with the traumatic event. In younger children, these intrusive thoughts may manifest through repetitive play that re-enacts aspects of the trauma.
Nightmares are also common, although in children the content may not always directly relate to the traumatic event. Chronic nightmares contribute to sleep disturbances, exacerbating PTSD symptoms. Trauma reminders, which can be both internal (thoughts, memories) and external (places, sensory experiences), can provoke severe distress and physiologic reactions.
Avoidance symptoms often develop as a coping mechanism in response to distressing re-experiencing symptoms. Children may avoid thoughts, feelings, and memories of the traumatic event or people, places, and activities associated with the trauma. In young children, avoidance may manifest as restricted play or reduced exploration of their environment.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) outlines specific criteria for diagnosing PTSD in individuals over 6 years old, which includes exposure to actual or threatened death, serious injury, or sexual violence, and the presence of symptoms such as intrusion, avoidance, negative mood alterations, and heightened arousal. The DSM-5-TR provides tailored diagnostic criteria for developmental differences in symptom expression for children under 6.
Managing PTSD in children requires a patient-specific approach, with an emphasis on obtaining consent from both the patient and guardian. The American Academy of Child and Adolescent Psychiatry (AACAP) recommends psychotherapy as the first-line treatment for pediatric PTSD. However, patients with severe symptoms or comorbidities may initially be unable to engage in meaningful therapy and may require medication to stabilize symptoms before starting psychotherapy.
Trauma-focused psychotherapy, including cognitive-behavioral therapy (CBT), exposure-based therapy, and eye movement desensitization and reprocessing (EMDR) therapy, is the preferred treatment for PTSD. Clinical studies have shown that patients receiving trauma-focused psychotherapy experience more remarkable symptom improvement than those who do not receive treatment and, in children, psychotherapy generally yields better outcomes than pharmacotherapy.
While selective serotonin reuptake inhibitors like sertraline and paroxetine are FDA-approved for PTSD treatment in adults, their efficacy in children often produces outcomes similar to those of placebo. Medications are typically reserved for severe symptoms and are used as an off-label treatment in pediatric cases. Pharmacologic management may be necessary when the severity of symptoms prevents the use of trauma-focused psychotherapy or requires immediate stabilization.
Heidi Moawad, MD, Clinical Assistant Professor, Department of Medical Education, Case Western Reserve University School of Medicine, Cleveland, Ohio.
Heidi Moawad, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The correct diagnosis is adolescent posttraumatic stress disorder (PTSD), as the patient's symptoms — recurrent nightmares, flashbacks, hypervigilance, and avoidance behaviors — are closely linked to her recent traumatic experience, fitting the clinical profile of PTSD. The MRI finding, although abnormal, does not correlate with a neurologic cause for her symptoms and may be incidental.
Temporal lobe epilepsy can cause behavioral changes but does not explain the specific PTSD symptoms like flashbacks and nightmares.
Chronic migraine could explain the headaches but not the full spectrum of PTSD symptoms.
Major depressive disorder could account for some of the emotional and social symptoms but lacks the characteristic re-experiencing and avoidance behaviors typical of PTSD.
Adolescent PTSD is a significant public health concern, causing significant distress to a small portion of the youth population. By late adolescence, approximately two thirds of youths have been exposed to trauma, and 8% of these individuals meet the criteria for PTSD by age 18. The incidence is exceptionally high in cases of sexual abuse and assault, with rates reaching up to 40%. PTSD in adolescents is associated with severe psychological distress, reduced academic performance, and a high rate of comorbidities, including anxiety and depression. There are specific populations (including children who are evacuated from home, asylum seekers, etc.) that show higher rates of PTSD.
PTSD can lead to chronic impairments, comorbid psychiatric disorders, and an increased risk for suicide, with cases documented in toddlers as young as 1 year old. Thus, it is important to consider the individual's background and social history, as older children with PTSD may present with symptoms from early childhood trauma, often distant from the time of clinical evaluation.
Intrusion symptoms are a hallmark of PTSD, characterized by persistent and uncontrollable thoughts, dreams, and emotional reactions related to the traumatic event. These symptoms distinguish PTSD from other anxiety and mood disorders. Children with PTSD often experience involuntary, distressing thoughts and memories triggered by trauma cues, such as sights, sounds, or smells associated with the traumatic event. In younger children, these intrusive thoughts may manifest through repetitive play that re-enacts aspects of the trauma.
Nightmares are also common, although in children the content may not always directly relate to the traumatic event. Chronic nightmares contribute to sleep disturbances, exacerbating PTSD symptoms. Trauma reminders, which can be both internal (thoughts, memories) and external (places, sensory experiences), can provoke severe distress and physiologic reactions.
Avoidance symptoms often develop as a coping mechanism in response to distressing re-experiencing symptoms. Children may avoid thoughts, feelings, and memories of the traumatic event or people, places, and activities associated with the trauma. In young children, avoidance may manifest as restricted play or reduced exploration of their environment.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) outlines specific criteria for diagnosing PTSD in individuals over 6 years old, which includes exposure to actual or threatened death, serious injury, or sexual violence, and the presence of symptoms such as intrusion, avoidance, negative mood alterations, and heightened arousal. The DSM-5-TR provides tailored diagnostic criteria for developmental differences in symptom expression for children under 6.
Managing PTSD in children requires a patient-specific approach, with an emphasis on obtaining consent from both the patient and guardian. The American Academy of Child and Adolescent Psychiatry (AACAP) recommends psychotherapy as the first-line treatment for pediatric PTSD. However, patients with severe symptoms or comorbidities may initially be unable to engage in meaningful therapy and may require medication to stabilize symptoms before starting psychotherapy.
Trauma-focused psychotherapy, including cognitive-behavioral therapy (CBT), exposure-based therapy, and eye movement desensitization and reprocessing (EMDR) therapy, is the preferred treatment for PTSD. Clinical studies have shown that patients receiving trauma-focused psychotherapy experience more remarkable symptom improvement than those who do not receive treatment and, in children, psychotherapy generally yields better outcomes than pharmacotherapy.
While selective serotonin reuptake inhibitors like sertraline and paroxetine are FDA-approved for PTSD treatment in adults, their efficacy in children often produces outcomes similar to those of placebo. Medications are typically reserved for severe symptoms and are used as an off-label treatment in pediatric cases. Pharmacologic management may be necessary when the severity of symptoms prevents the use of trauma-focused psychotherapy or requires immediate stabilization.
Heidi Moawad, MD, Clinical Assistant Professor, Department of Medical Education, Case Western Reserve University School of Medicine, Cleveland, Ohio.
Heidi Moawad, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
A 15-year-old girl presented to the emergency department with complaints of persistent headaches, nightmares, and difficulty concentrating in school over the past 3 months. The patient had recently experienced a traumatic event, a severe car accident in which a close friend was critically injured. Since the incident, the patient has been exhibiting increased irritability, avoidance of activities that she previously enjoyed, and a noticeable withdrawal from social interactions. Additionally, she reported recurrent flashbacks to the accident, often triggered by sounds resembling car engines. On physical examination, the patient appeared anxious and exhibited hypervigilance. An MRI of the brain was performed to rule out any organic causes of her symptoms, revealing an area of increased signal intensity in the left cerebellar hemisphere (as highlighted in the image).
Suicide Screening and Safety Plans Moved Needle on Attempts and Deaths Moving the Needle
In the winter of 2023, Cynthia Smith, MD, an internal medicine physician in Philadelphia and the chief membership and engagement officer for the American College of Physicians, treated a high-achieving, middle-aged man who said he felt completely alone and isolated.
Smith used depression and suicide screeners and found the man was actively thinking of harming himself. She and the man created a safety plan. Then, she connected her patient to a clinical social worker within her health system who helped him enter an intensive outpatient treatment program for depression.
“I am not sure if screening this patient for depression saved his life, but I do think he left the office feeling less alone and more supported than when he arrived. Screening him helped us achieve that outcome,” said Smith. “Our patient needed to know that we cared about him.”
Smith’s experience is part of a broader movement to screen patients for depression and suicide with the goal of getting people into treatment.
Prior research has shown more than 40% people who die by suicide visit a primary care clinician in the month before death, and more than 75% see a primary care physician in the year before a suicide death.
New research published in Annals of Internal Medicine showed these screening processes reduced suicide attempts and deaths by suicide by 25% in one health system.
Clinicians using screening questions to engage patients in safety planning “can know that this work is valuable, and that it will save lives,” said Julie Angerhofer, PhD, MPH, a collaborative scientist at Kaiser Permanente Washington Health Research Institute in Seattle, and a coauthor of the study. “For those who are considering investing in doing this work, it is good news because it is going to have an effect. We did not know that until we did this trial.”
Suicide is the 11th leading cause of death in the United States, accounting for 49,000 fatalities in 2022, according to the Centers for Disease Control and Prevention.
The new study findings “are significant when it comes to working with people who are at risk for suicide in primary care practice and shows that it is both feasible and effective,” said Julie Goldstein Grumet, PhD, vice president for suicide prevention strategy and director of the Zero Suicide Institute at the nonprofit Education Development Center.
Grumet said the use of standardized screening tools, like those used in the study protocol, is key.
When patients screened positive for depression with the Patient Health Questionnaire 2 (PHQ-2), they were asked to complete the additional questions of the PHQ-9. If patients reported frequent suicidal thoughts, they received a brief, self-administered version of the Columbia-Suicide Severity Rating Scale. The analysis included 333,593 patients who had 1.56 million visits for any reason to their primary care clinician.
Patients who reported some level of intent or planning for a suicide attempt in the prior month were connected to a clinical social worker for same day safety planning.
The study showed that the rate of documented fatal or nonfatal suicide attempts within 90 days of a primary care visit was 25% lower in the suicide care than in the usual care period and 24% lower in the 60 days after a visit, both statistically significant findings.
These tools help clinicians “to determine the type of care needed and to provide the right level of intervention,” Grumet said.
Both Smith and the study utilized social workers to help with safety planning. But because many clinicians do not work in integrated health systems with access to these professionals, other workflows can also support the screening and safety planning process, Angerhofer said. For instance, nurses can be trained to conduct a safety plan.
“Some systems also use centralized groups of providers trained in safety planning to support primary care teams virtually,” she said. Clinicians can also refer to free trainings on safety planning available online — including the one on the Zero Suicide website.
Smith said one of the biggest barriers to suicide care is the lack of resources needed to follow-up on a positive screen.
The study findings are “a call to action, but it can’t be the straw breaking the backs of primary care doctors; it has to be supported,” Smith said.
A safety plan includes:
- Helping patients recognize warning signs of an impending suicidal crisis
- Using social contacts as a means of distraction from suicidal thoughts
- Contacting family members or friends who may help resolve the crisis
- Contacting mental health professionals or agencies
- Making the patient’s home environment safer by reducing the potential use and availability of lethal means
The study was supported by a grant from the National Institute of Mental Health. Various study authors reported receiving consulting fees, honoraria, and grants from the University of Washington, Advocate Aurora Health, the Donaghue Medical Research Foundation’s Greater Value Portfolio program, and the Patient-Centered Outcomes Research Institute, among others.
A version of this article first appeared on Medscape.com.
In the winter of 2023, Cynthia Smith, MD, an internal medicine physician in Philadelphia and the chief membership and engagement officer for the American College of Physicians, treated a high-achieving, middle-aged man who said he felt completely alone and isolated.
Smith used depression and suicide screeners and found the man was actively thinking of harming himself. She and the man created a safety plan. Then, she connected her patient to a clinical social worker within her health system who helped him enter an intensive outpatient treatment program for depression.
“I am not sure if screening this patient for depression saved his life, but I do think he left the office feeling less alone and more supported than when he arrived. Screening him helped us achieve that outcome,” said Smith. “Our patient needed to know that we cared about him.”
Smith’s experience is part of a broader movement to screen patients for depression and suicide with the goal of getting people into treatment.
Prior research has shown more than 40% people who die by suicide visit a primary care clinician in the month before death, and more than 75% see a primary care physician in the year before a suicide death.
New research published in Annals of Internal Medicine showed these screening processes reduced suicide attempts and deaths by suicide by 25% in one health system.
Clinicians using screening questions to engage patients in safety planning “can know that this work is valuable, and that it will save lives,” said Julie Angerhofer, PhD, MPH, a collaborative scientist at Kaiser Permanente Washington Health Research Institute in Seattle, and a coauthor of the study. “For those who are considering investing in doing this work, it is good news because it is going to have an effect. We did not know that until we did this trial.”
Suicide is the 11th leading cause of death in the United States, accounting for 49,000 fatalities in 2022, according to the Centers for Disease Control and Prevention.
The new study findings “are significant when it comes to working with people who are at risk for suicide in primary care practice and shows that it is both feasible and effective,” said Julie Goldstein Grumet, PhD, vice president for suicide prevention strategy and director of the Zero Suicide Institute at the nonprofit Education Development Center.
Grumet said the use of standardized screening tools, like those used in the study protocol, is key.
When patients screened positive for depression with the Patient Health Questionnaire 2 (PHQ-2), they were asked to complete the additional questions of the PHQ-9. If patients reported frequent suicidal thoughts, they received a brief, self-administered version of the Columbia-Suicide Severity Rating Scale. The analysis included 333,593 patients who had 1.56 million visits for any reason to their primary care clinician.
Patients who reported some level of intent or planning for a suicide attempt in the prior month were connected to a clinical social worker for same day safety planning.
The study showed that the rate of documented fatal or nonfatal suicide attempts within 90 days of a primary care visit was 25% lower in the suicide care than in the usual care period and 24% lower in the 60 days after a visit, both statistically significant findings.
These tools help clinicians “to determine the type of care needed and to provide the right level of intervention,” Grumet said.
Both Smith and the study utilized social workers to help with safety planning. But because many clinicians do not work in integrated health systems with access to these professionals, other workflows can also support the screening and safety planning process, Angerhofer said. For instance, nurses can be trained to conduct a safety plan.
“Some systems also use centralized groups of providers trained in safety planning to support primary care teams virtually,” she said. Clinicians can also refer to free trainings on safety planning available online — including the one on the Zero Suicide website.
Smith said one of the biggest barriers to suicide care is the lack of resources needed to follow-up on a positive screen.
The study findings are “a call to action, but it can’t be the straw breaking the backs of primary care doctors; it has to be supported,” Smith said.
A safety plan includes:
- Helping patients recognize warning signs of an impending suicidal crisis
- Using social contacts as a means of distraction from suicidal thoughts
- Contacting family members or friends who may help resolve the crisis
- Contacting mental health professionals or agencies
- Making the patient’s home environment safer by reducing the potential use and availability of lethal means
The study was supported by a grant from the National Institute of Mental Health. Various study authors reported receiving consulting fees, honoraria, and grants from the University of Washington, Advocate Aurora Health, the Donaghue Medical Research Foundation’s Greater Value Portfolio program, and the Patient-Centered Outcomes Research Institute, among others.
A version of this article first appeared on Medscape.com.
In the winter of 2023, Cynthia Smith, MD, an internal medicine physician in Philadelphia and the chief membership and engagement officer for the American College of Physicians, treated a high-achieving, middle-aged man who said he felt completely alone and isolated.
Smith used depression and suicide screeners and found the man was actively thinking of harming himself. She and the man created a safety plan. Then, she connected her patient to a clinical social worker within her health system who helped him enter an intensive outpatient treatment program for depression.
“I am not sure if screening this patient for depression saved his life, but I do think he left the office feeling less alone and more supported than when he arrived. Screening him helped us achieve that outcome,” said Smith. “Our patient needed to know that we cared about him.”
Smith’s experience is part of a broader movement to screen patients for depression and suicide with the goal of getting people into treatment.
Prior research has shown more than 40% people who die by suicide visit a primary care clinician in the month before death, and more than 75% see a primary care physician in the year before a suicide death.
New research published in Annals of Internal Medicine showed these screening processes reduced suicide attempts and deaths by suicide by 25% in one health system.
Clinicians using screening questions to engage patients in safety planning “can know that this work is valuable, and that it will save lives,” said Julie Angerhofer, PhD, MPH, a collaborative scientist at Kaiser Permanente Washington Health Research Institute in Seattle, and a coauthor of the study. “For those who are considering investing in doing this work, it is good news because it is going to have an effect. We did not know that until we did this trial.”
Suicide is the 11th leading cause of death in the United States, accounting for 49,000 fatalities in 2022, according to the Centers for Disease Control and Prevention.
The new study findings “are significant when it comes to working with people who are at risk for suicide in primary care practice and shows that it is both feasible and effective,” said Julie Goldstein Grumet, PhD, vice president for suicide prevention strategy and director of the Zero Suicide Institute at the nonprofit Education Development Center.
Grumet said the use of standardized screening tools, like those used in the study protocol, is key.
When patients screened positive for depression with the Patient Health Questionnaire 2 (PHQ-2), they were asked to complete the additional questions of the PHQ-9. If patients reported frequent suicidal thoughts, they received a brief, self-administered version of the Columbia-Suicide Severity Rating Scale. The analysis included 333,593 patients who had 1.56 million visits for any reason to their primary care clinician.
Patients who reported some level of intent or planning for a suicide attempt in the prior month were connected to a clinical social worker for same day safety planning.
The study showed that the rate of documented fatal or nonfatal suicide attempts within 90 days of a primary care visit was 25% lower in the suicide care than in the usual care period and 24% lower in the 60 days after a visit, both statistically significant findings.
These tools help clinicians “to determine the type of care needed and to provide the right level of intervention,” Grumet said.
Both Smith and the study utilized social workers to help with safety planning. But because many clinicians do not work in integrated health systems with access to these professionals, other workflows can also support the screening and safety planning process, Angerhofer said. For instance, nurses can be trained to conduct a safety plan.
“Some systems also use centralized groups of providers trained in safety planning to support primary care teams virtually,” she said. Clinicians can also refer to free trainings on safety planning available online — including the one on the Zero Suicide website.
Smith said one of the biggest barriers to suicide care is the lack of resources needed to follow-up on a positive screen.
The study findings are “a call to action, but it can’t be the straw breaking the backs of primary care doctors; it has to be supported,” Smith said.
A safety plan includes:
- Helping patients recognize warning signs of an impending suicidal crisis
- Using social contacts as a means of distraction from suicidal thoughts
- Contacting family members or friends who may help resolve the crisis
- Contacting mental health professionals or agencies
- Making the patient’s home environment safer by reducing the potential use and availability of lethal means
The study was supported by a grant from the National Institute of Mental Health. Various study authors reported receiving consulting fees, honoraria, and grants from the University of Washington, Advocate Aurora Health, the Donaghue Medical Research Foundation’s Greater Value Portfolio program, and the Patient-Centered Outcomes Research Institute, among others.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE
Caffeine Brings Benefits and Risks
Coffee and tea are among the plants that are highest in caffeine. Their use as beverages makes caffeine the most consumed psychoactive agent in the world. Coffee is commonly used to increase alertness and work productivity. Synthetic caffeine is added to soft drinks, energy drinks, and products intended to reduce fatigue or promote weight loss.
The caffeine content varies with the type of drink: It is high in coffee, energy drinks, and caffeine tablets; intermediate in tea; and low in soft drinks. Coffee is the predominant source of the caffeine ingested by adults. The evidence for caffeine’s effects on people is ambiguous, and some risks and benefits deserve special attention because of the impact they may have on our health.
Characteristics of Caffeine
The half-life of caffeine varies according to age. In adults, it is 2.5-4.5 hours; in newborns, 80 hours; in children older than 6 months, it remains stable over time with respect to weight. Smoking accelerates caffeine metabolism by reducing the half-life by 50%. Oral contraceptives, however, double caffeine’s half-life. Caffeine metabolism is reduced during pregnancy (it is greater in the first trimester), with a half-life of more than 15 hours. Caffeine clearance can be slowed by several classes of drugs (eg, quinolones, cardiovascular drugs, bronchodilators, and antidepressants) that increase its half-life because they are metabolized by the same liver enzymes.
Caffeine passes the blood-brain barrier and, having an adenosine-like structure, inhibits adenosine’s effects by binding to adenosine receptors. In the brain, caffeine reduces fatigue, increases alertness, reduces reaction times, may reduce the risk for depression, and increases the effectiveness of nonsteroidal anti-inflammatory drugs in treating headaches and other types of pain.
Caffeine and Chronic Diseases
The evidence available on the relationship between caffeine and health has several methodological limitations. Observations of the acute effects of caffeine may not reflect long-term effects because tolerance to caffeine’s effects may develop over time. Smoking and unhealthy lifestyles are confounding factors in epidemiological studies of caffeine intake. In addition, the estimate of the amount and frequency of caffeine intake is often inaccurate because it is mainly based on self-assessment systems. Finally, prospective studies of caffeine consumption are mainly based on coffee and tea consumption, but it is unclear how much the observed outcomes can be translated to intake of other beverages such as energy drinks.
Considering the very high prevalence of arterial hypertension worldwide (31.1% of adults), many questions have been raised about the influence of coffee consumption on blood pressure (BP) and the risk for arterial hypertension. Administration of 200-300 mg caffeine is shown to induce a mean increase of 8.1 mm Hg systolic BP and 5.7 mm Hg diastolic BP. The increase is observed in the first hour after caffeine intake and lasts no longer than 3 hours.
Yet, the moderate and usual consumption of coffee does not increase, but may even reduce, the risk of developing high BP. In contrast, occasional coffee consumption can have hypertensive effects, and moderate and usual consumption in patients with high BP does not appear to increase the risk for uncontrolled BP and can reduce the risk for death from any cause. The inverse association between coffee consumption and hypertension risk was confirmed in a review and meta-analysis of cross-sectional and cohort studies.
With respect to lipid metabolism, cholesterol levels may increase after caffeine consumption because of cafestol. Concentrations of cafestol are high in unfiltered coffee, intermediate in espresso and moka pot coffee, and negligible in instant or filtered coffee. Studies on the impact of coffee on lipid levels have led to inconsistent results, however. Data have shown that people who drink more coffee have higher triglycerides, total cholesterol, and low-density lipoprotein cholesterol (LDL-C) levels. Other data have shown that caffeine promotes LDL receptor expression and clearance of LDL cholesterol.
Experimental and cohort studies have not shown an association between coffee consumption and atrial fibrillation (AF). In fact, evidence suggests that coffee consumption tends to reduce the risk for AF in a dose-response relationship. Similarly, coffee consumption is not associated with increased risk for cardiovascular events in the general population or among patients with a history of hypertension, diabetes, or cardiovascular disease.
The Coffee and Real-Time Atrial and Ventricular Ectopy study evaluated the acute effects of coffee consumption on cardiac ectopy using wearable sensors with continuous recording. It did not demonstrate any increase in daily premature atrial contractions with coffee consumption, compared with abstaining from caffeine.
In patients with type 2 diabetes, a study performed in Japan showed that coffee consumption was associated with reduced all-cause mortality. The results suggested a dose-response relationship, and drinking coffee and green tea appeared to reduce mortality risk further. The results were not generalizable, however, because of the study population’s ethnic homogeneity.
Dose and Toxicity
Caffeine at high doses (> 400 mg daily) and in susceptible patients can induce anxiety, but the effects of caffeine on sleep and anxiety can differ from patient to patient. This variation reflects differences in caffeine metabolism rate and adenosine receptor gene variants.
High caffeine intake can stimulate diuresis, but without causing damaging effects on hydration when taking moderate doses of caffeine (≤ 400 mg daily) for long periods. Stopping caffeine suddenly, in a regular consumer, can lead to withdrawal symptoms such as headache, asthenia, decreased attention, depressed mood, and flu-like symptoms.
The toxic effects of caffeine occur with intake > 1.2 g. A dose of 10-14 g is considered fatal. Caffeine overdose is rare when considering traditional methods of intake (coffee and tea) because 70-100 cups of coffee should be sufficient for caffeine poisoning. Severe events can occur following the use of caffeine tablets or as energy drinks for the following reasons:
- The episodic consumption of caffeine does not allow for tolerance to develop.
- Young people are more vulnerable to the effects of caffeine.
- Caffeine has a synergistic effect in combination with other components in energy drinks.
- Taking caffeine in combination with alcohol or intense exertion causes serious, even fatal, outcomes.
Products Containing Caffeine
Evidence supports the relationship between high consumption (approximately 1 L) of energy drinks with a caffeine content of 320 mg and short-term cardiovascular adverse events, such as increased BP, QT-segment prolongation corrected for heart rate, and palpitations. These tests prompt the recommendation to avoid consuming these beverages in high quantities and in association with alcohol.
Weight loss products generally contain caffeine coupled with herbal extracts that are expected to improve fat metabolism, lipolysis, and oxidation. These products, because of their easy availability, presumed benefits, and high caffeine concentration, may be more susceptible to misuse because they can be taken in larger portions than recommended. The combination of multiple ingredients, concentrated amounts of caffeine, and excessive consumption increases the likelihood of adverse effects.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Coffee and tea are among the plants that are highest in caffeine. Their use as beverages makes caffeine the most consumed psychoactive agent in the world. Coffee is commonly used to increase alertness and work productivity. Synthetic caffeine is added to soft drinks, energy drinks, and products intended to reduce fatigue or promote weight loss.
The caffeine content varies with the type of drink: It is high in coffee, energy drinks, and caffeine tablets; intermediate in tea; and low in soft drinks. Coffee is the predominant source of the caffeine ingested by adults. The evidence for caffeine’s effects on people is ambiguous, and some risks and benefits deserve special attention because of the impact they may have on our health.
Characteristics of Caffeine
The half-life of caffeine varies according to age. In adults, it is 2.5-4.5 hours; in newborns, 80 hours; in children older than 6 months, it remains stable over time with respect to weight. Smoking accelerates caffeine metabolism by reducing the half-life by 50%. Oral contraceptives, however, double caffeine’s half-life. Caffeine metabolism is reduced during pregnancy (it is greater in the first trimester), with a half-life of more than 15 hours. Caffeine clearance can be slowed by several classes of drugs (eg, quinolones, cardiovascular drugs, bronchodilators, and antidepressants) that increase its half-life because they are metabolized by the same liver enzymes.
Caffeine passes the blood-brain barrier and, having an adenosine-like structure, inhibits adenosine’s effects by binding to adenosine receptors. In the brain, caffeine reduces fatigue, increases alertness, reduces reaction times, may reduce the risk for depression, and increases the effectiveness of nonsteroidal anti-inflammatory drugs in treating headaches and other types of pain.
Caffeine and Chronic Diseases
The evidence available on the relationship between caffeine and health has several methodological limitations. Observations of the acute effects of caffeine may not reflect long-term effects because tolerance to caffeine’s effects may develop over time. Smoking and unhealthy lifestyles are confounding factors in epidemiological studies of caffeine intake. In addition, the estimate of the amount and frequency of caffeine intake is often inaccurate because it is mainly based on self-assessment systems. Finally, prospective studies of caffeine consumption are mainly based on coffee and tea consumption, but it is unclear how much the observed outcomes can be translated to intake of other beverages such as energy drinks.
Considering the very high prevalence of arterial hypertension worldwide (31.1% of adults), many questions have been raised about the influence of coffee consumption on blood pressure (BP) and the risk for arterial hypertension. Administration of 200-300 mg caffeine is shown to induce a mean increase of 8.1 mm Hg systolic BP and 5.7 mm Hg diastolic BP. The increase is observed in the first hour after caffeine intake and lasts no longer than 3 hours.
Yet, the moderate and usual consumption of coffee does not increase, but may even reduce, the risk of developing high BP. In contrast, occasional coffee consumption can have hypertensive effects, and moderate and usual consumption in patients with high BP does not appear to increase the risk for uncontrolled BP and can reduce the risk for death from any cause. The inverse association between coffee consumption and hypertension risk was confirmed in a review and meta-analysis of cross-sectional and cohort studies.
With respect to lipid metabolism, cholesterol levels may increase after caffeine consumption because of cafestol. Concentrations of cafestol are high in unfiltered coffee, intermediate in espresso and moka pot coffee, and negligible in instant or filtered coffee. Studies on the impact of coffee on lipid levels have led to inconsistent results, however. Data have shown that people who drink more coffee have higher triglycerides, total cholesterol, and low-density lipoprotein cholesterol (LDL-C) levels. Other data have shown that caffeine promotes LDL receptor expression and clearance of LDL cholesterol.
Experimental and cohort studies have not shown an association between coffee consumption and atrial fibrillation (AF). In fact, evidence suggests that coffee consumption tends to reduce the risk for AF in a dose-response relationship. Similarly, coffee consumption is not associated with increased risk for cardiovascular events in the general population or among patients with a history of hypertension, diabetes, or cardiovascular disease.
The Coffee and Real-Time Atrial and Ventricular Ectopy study evaluated the acute effects of coffee consumption on cardiac ectopy using wearable sensors with continuous recording. It did not demonstrate any increase in daily premature atrial contractions with coffee consumption, compared with abstaining from caffeine.
In patients with type 2 diabetes, a study performed in Japan showed that coffee consumption was associated with reduced all-cause mortality. The results suggested a dose-response relationship, and drinking coffee and green tea appeared to reduce mortality risk further. The results were not generalizable, however, because of the study population’s ethnic homogeneity.
Dose and Toxicity
Caffeine at high doses (> 400 mg daily) and in susceptible patients can induce anxiety, but the effects of caffeine on sleep and anxiety can differ from patient to patient. This variation reflects differences in caffeine metabolism rate and adenosine receptor gene variants.
High caffeine intake can stimulate diuresis, but without causing damaging effects on hydration when taking moderate doses of caffeine (≤ 400 mg daily) for long periods. Stopping caffeine suddenly, in a regular consumer, can lead to withdrawal symptoms such as headache, asthenia, decreased attention, depressed mood, and flu-like symptoms.
The toxic effects of caffeine occur with intake > 1.2 g. A dose of 10-14 g is considered fatal. Caffeine overdose is rare when considering traditional methods of intake (coffee and tea) because 70-100 cups of coffee should be sufficient for caffeine poisoning. Severe events can occur following the use of caffeine tablets or as energy drinks for the following reasons:
- The episodic consumption of caffeine does not allow for tolerance to develop.
- Young people are more vulnerable to the effects of caffeine.
- Caffeine has a synergistic effect in combination with other components in energy drinks.
- Taking caffeine in combination with alcohol or intense exertion causes serious, even fatal, outcomes.
Products Containing Caffeine
Evidence supports the relationship between high consumption (approximately 1 L) of energy drinks with a caffeine content of 320 mg and short-term cardiovascular adverse events, such as increased BP, QT-segment prolongation corrected for heart rate, and palpitations. These tests prompt the recommendation to avoid consuming these beverages in high quantities and in association with alcohol.
Weight loss products generally contain caffeine coupled with herbal extracts that are expected to improve fat metabolism, lipolysis, and oxidation. These products, because of their easy availability, presumed benefits, and high caffeine concentration, may be more susceptible to misuse because they can be taken in larger portions than recommended. The combination of multiple ingredients, concentrated amounts of caffeine, and excessive consumption increases the likelihood of adverse effects.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Coffee and tea are among the plants that are highest in caffeine. Their use as beverages makes caffeine the most consumed psychoactive agent in the world. Coffee is commonly used to increase alertness and work productivity. Synthetic caffeine is added to soft drinks, energy drinks, and products intended to reduce fatigue or promote weight loss.
The caffeine content varies with the type of drink: It is high in coffee, energy drinks, and caffeine tablets; intermediate in tea; and low in soft drinks. Coffee is the predominant source of the caffeine ingested by adults. The evidence for caffeine’s effects on people is ambiguous, and some risks and benefits deserve special attention because of the impact they may have on our health.
Characteristics of Caffeine
The half-life of caffeine varies according to age. In adults, it is 2.5-4.5 hours; in newborns, 80 hours; in children older than 6 months, it remains stable over time with respect to weight. Smoking accelerates caffeine metabolism by reducing the half-life by 50%. Oral contraceptives, however, double caffeine’s half-life. Caffeine metabolism is reduced during pregnancy (it is greater in the first trimester), with a half-life of more than 15 hours. Caffeine clearance can be slowed by several classes of drugs (eg, quinolones, cardiovascular drugs, bronchodilators, and antidepressants) that increase its half-life because they are metabolized by the same liver enzymes.
Caffeine passes the blood-brain barrier and, having an adenosine-like structure, inhibits adenosine’s effects by binding to adenosine receptors. In the brain, caffeine reduces fatigue, increases alertness, reduces reaction times, may reduce the risk for depression, and increases the effectiveness of nonsteroidal anti-inflammatory drugs in treating headaches and other types of pain.
Caffeine and Chronic Diseases
The evidence available on the relationship between caffeine and health has several methodological limitations. Observations of the acute effects of caffeine may not reflect long-term effects because tolerance to caffeine’s effects may develop over time. Smoking and unhealthy lifestyles are confounding factors in epidemiological studies of caffeine intake. In addition, the estimate of the amount and frequency of caffeine intake is often inaccurate because it is mainly based on self-assessment systems. Finally, prospective studies of caffeine consumption are mainly based on coffee and tea consumption, but it is unclear how much the observed outcomes can be translated to intake of other beverages such as energy drinks.
Considering the very high prevalence of arterial hypertension worldwide (31.1% of adults), many questions have been raised about the influence of coffee consumption on blood pressure (BP) and the risk for arterial hypertension. Administration of 200-300 mg caffeine is shown to induce a mean increase of 8.1 mm Hg systolic BP and 5.7 mm Hg diastolic BP. The increase is observed in the first hour after caffeine intake and lasts no longer than 3 hours.
Yet, the moderate and usual consumption of coffee does not increase, but may even reduce, the risk of developing high BP. In contrast, occasional coffee consumption can have hypertensive effects, and moderate and usual consumption in patients with high BP does not appear to increase the risk for uncontrolled BP and can reduce the risk for death from any cause. The inverse association between coffee consumption and hypertension risk was confirmed in a review and meta-analysis of cross-sectional and cohort studies.
With respect to lipid metabolism, cholesterol levels may increase after caffeine consumption because of cafestol. Concentrations of cafestol are high in unfiltered coffee, intermediate in espresso and moka pot coffee, and negligible in instant or filtered coffee. Studies on the impact of coffee on lipid levels have led to inconsistent results, however. Data have shown that people who drink more coffee have higher triglycerides, total cholesterol, and low-density lipoprotein cholesterol (LDL-C) levels. Other data have shown that caffeine promotes LDL receptor expression and clearance of LDL cholesterol.
Experimental and cohort studies have not shown an association between coffee consumption and atrial fibrillation (AF). In fact, evidence suggests that coffee consumption tends to reduce the risk for AF in a dose-response relationship. Similarly, coffee consumption is not associated with increased risk for cardiovascular events in the general population or among patients with a history of hypertension, diabetes, or cardiovascular disease.
The Coffee and Real-Time Atrial and Ventricular Ectopy study evaluated the acute effects of coffee consumption on cardiac ectopy using wearable sensors with continuous recording. It did not demonstrate any increase in daily premature atrial contractions with coffee consumption, compared with abstaining from caffeine.
In patients with type 2 diabetes, a study performed in Japan showed that coffee consumption was associated with reduced all-cause mortality. The results suggested a dose-response relationship, and drinking coffee and green tea appeared to reduce mortality risk further. The results were not generalizable, however, because of the study population’s ethnic homogeneity.
Dose and Toxicity
Caffeine at high doses (> 400 mg daily) and in susceptible patients can induce anxiety, but the effects of caffeine on sleep and anxiety can differ from patient to patient. This variation reflects differences in caffeine metabolism rate and adenosine receptor gene variants.
High caffeine intake can stimulate diuresis, but without causing damaging effects on hydration when taking moderate doses of caffeine (≤ 400 mg daily) for long periods. Stopping caffeine suddenly, in a regular consumer, can lead to withdrawal symptoms such as headache, asthenia, decreased attention, depressed mood, and flu-like symptoms.
The toxic effects of caffeine occur with intake > 1.2 g. A dose of 10-14 g is considered fatal. Caffeine overdose is rare when considering traditional methods of intake (coffee and tea) because 70-100 cups of coffee should be sufficient for caffeine poisoning. Severe events can occur following the use of caffeine tablets or as energy drinks for the following reasons:
- The episodic consumption of caffeine does not allow for tolerance to develop.
- Young people are more vulnerable to the effects of caffeine.
- Caffeine has a synergistic effect in combination with other components in energy drinks.
- Taking caffeine in combination with alcohol or intense exertion causes serious, even fatal, outcomes.
Products Containing Caffeine
Evidence supports the relationship between high consumption (approximately 1 L) of energy drinks with a caffeine content of 320 mg and short-term cardiovascular adverse events, such as increased BP, QT-segment prolongation corrected for heart rate, and palpitations. These tests prompt the recommendation to avoid consuming these beverages in high quantities and in association with alcohol.
Weight loss products generally contain caffeine coupled with herbal extracts that are expected to improve fat metabolism, lipolysis, and oxidation. These products, because of their easy availability, presumed benefits, and high caffeine concentration, may be more susceptible to misuse because they can be taken in larger portions than recommended. The combination of multiple ingredients, concentrated amounts of caffeine, and excessive consumption increases the likelihood of adverse effects.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Utilization, Cost, and Prescription Trends of Antipsychotics Prescribed by Dermatologists for Medicare Patients
To the Editor:
Patients with primary psychiatric disorders with dermatologic manifestations often seek treatment from dermatologists instead of psychiatrists.1 For example, patients with delusions of parasitosis may lack insight into the underlying etiology of their disease and instead fixate on establishing an organic cause for their symptoms. As a result, it is an increasingly common practice for dermatologists to diagnose and treat psychiatric conditions.1 The goal of this study was to evaluate trends for the top 5 antipsychotics most frequently prescribed by dermatologists in the Medicare Part D database.
In this retrospective analysis, we consulted the Medicare Provider Utilization and Payment Data for January 2013 through December 2020, which is provided to the public by the Centers for Medicare & Medicaid Services.2 Only prescribing data from dermatologists were included in this study by using the built-in filter on the website to select “dermatology” as the prescriber type. All other provider types were excluded. We chose the top 5 most prescribed antipsychotics based on the number of supply days reported. Supply days—defined by Medicare as the number of days’ worth of medication that is prescribed—were used as a metric for utilization; therefore, each drug’s total supply days prescribed by dermatologists were calculated using this combined filter of drug name and total supply days using the database.
To analyze utilization over time, the annual average growth rate (AAGR) was calculated by determining the growth rate in total supply days annually from 2013 to 2020 and then averaging those rates to determine the overall AAGR. For greater clinical relevance, we calculated the average growth in supply days for the entire study period by determining the difference in the number of supply days for each year and then averaging these values. This was done to consider overall trends across dermatology rather than individual dermatologist prescribing patterns.
Based on our analysis, the antipsychotics most frequently prescribed by dermatologists for Medicare patients from January 2013 to December 2020 were pimozide, quetiapine, risperidone, olanzapine, and aripiprazole. The AAGR for each drug was 2.35%, 4.89%, 5.59%, 9.48%, and 20.72%, respectively, which is consistent with increased utilization over the study period for all 5 drugs (Table 1). The change in cost per supply day for the same period was 1.3%, –66.1%, –60.2%, –81.7%, and –84.3%, respectively. The net difference in cost per supply day over this entire period was $0.02, –$2.79, –$1.06, –$5.37, and –$21.22, respectively (Table 2).
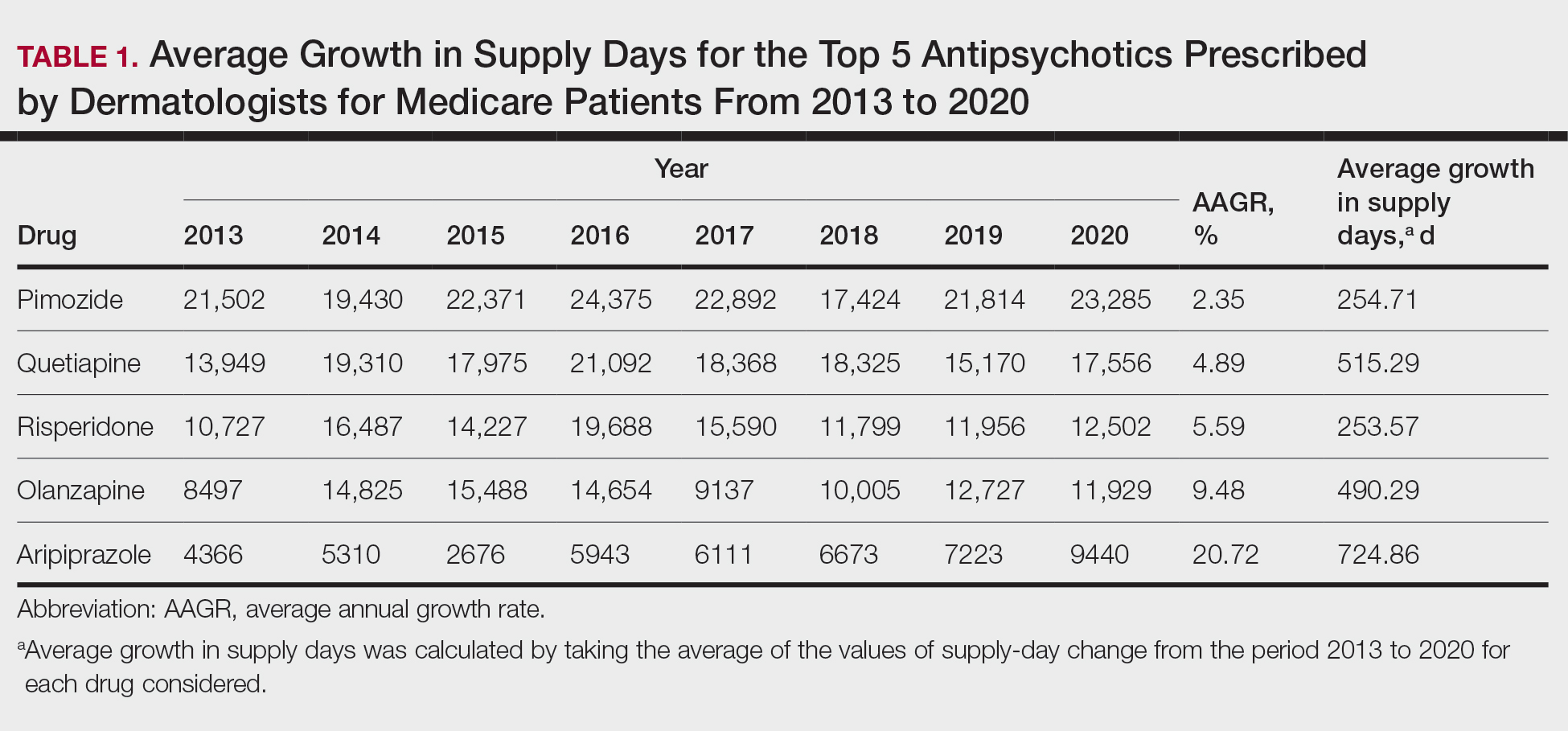
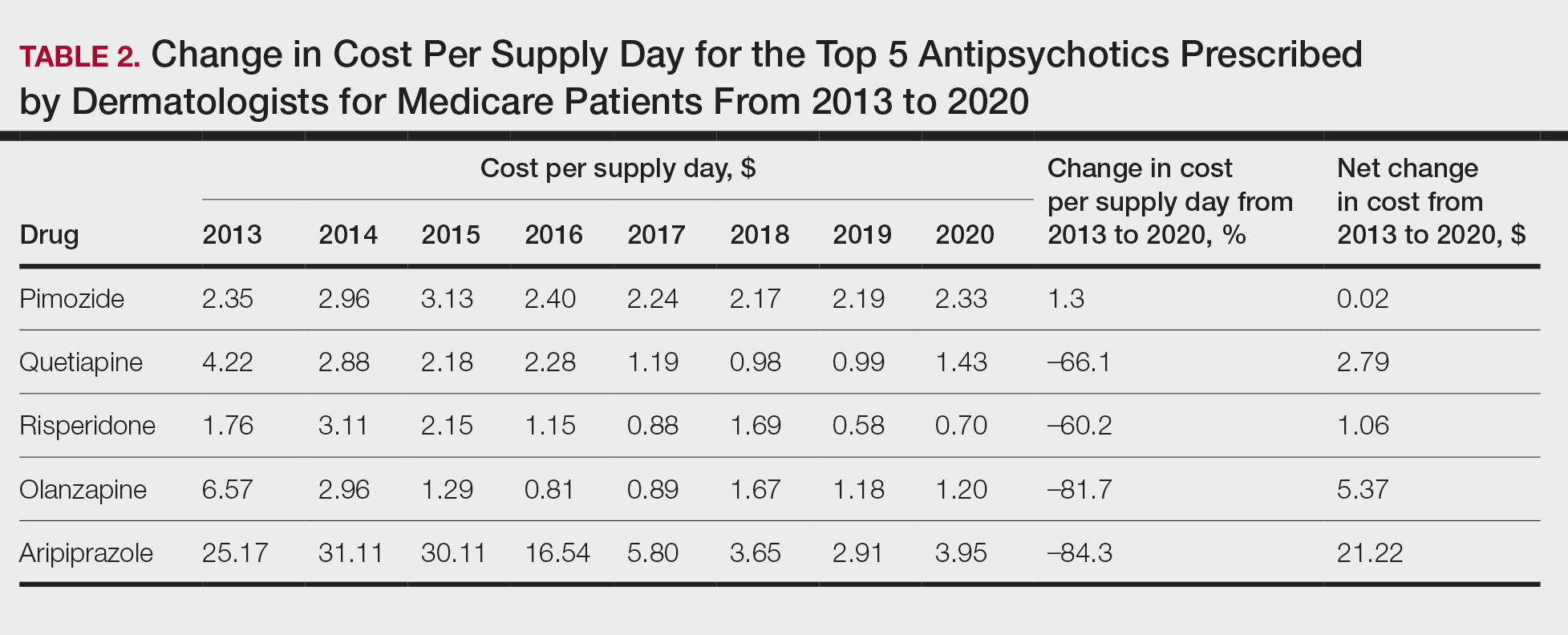
There were several limitations to our study. Our analysis was limited to the Medicare population. Uninsured patients and those with Medicare Advantage or private health insurance plans were not included. In the Medicare database, only prescribers who prescribed a medication 10 times or more were recorded; therefore, some prescribers were not captured.
Although there was an increase in the dermatologic use of all 5 drugs in this study, perhaps the most marked growth was exhibited by aripiprazole, which had an AAGR of 20.72% (Table 1). Affordability may have been a factor, as the most marked reduction in price per supply day was noted for aripiprazole during the study period. Pimozide, which traditionally has been the first-line therapy for delusions of parasitosis, is the only first-generation antipsychotic drug among the 5 most frequently prescribed antipsychotics.3 Interestingly, pimozide had the lowest AAGR compared with the 4 second-generation antipsychotics. This finding also is corroborated by the average growth in supply days. While pimozide is a first-generation antipsychotic and had the lowest AAGR, pimozide still was the most prescribed antipsychotic in this study. Considering the average growth in Medicare beneficiaries during the study period was 2.70% per year,2 the AAGR of the 4 other drugs excluding pimozide shows that this growth was larger than what can be attributed to an increase in population size.
The most common conditions for which dermatologists prescribe antipsychotics are primary delusional infestation disorders as well as a range of self-inflicted dermatologic manifestations of dermatitis artefacta.4 Particularly, dermatologist-prescribed antipsychotics are first-line for these conditions in which perception of a persistent disease state is present.4 Importantly, dermatologists must differentiate between other dermatology-related psychiatric conditions such as trichotillomania and body dysmorphic disorder, which tend to respond better to selective serotonin reuptake inhibitors.4 Our data suggest that dermatologists are increasing their utilization of second-generation antipsychotics at a higher rate than first-generation antipsychotics, likely due to the lower risk of extrapyramidal symptoms. Patients are more willing to initiate a trial of psychiatric medication when it is prescribed by a dermatologist vs a psychiatrist due to lack of perceived stigma, which can lead to greater treatment compliance rates.5 As mentioned previously, as part of the differential, dermatologists also can effectively prescribe medications such as selective serotonin reuptake inhibitors for symptoms including anxiety, trichotillomania, body dysmorphic disorder, or secondary psychiatric disorders as a result of the burden of skin disease.5
In many cases, a dermatologist may be the first and only specialist to evaluate patients with conditions that overlap within the jurisdiction of dermatology and psychiatry. It is imperative that dermatologists feel comfortable treating this vulnerable patient population. As demonstrated by Medicare prescription data, the increasing utilization of antipsychotics in our specialty demands that dermatologists possess an adequate working knowledge of psychopharmacology, which may be accomplished during residency training through several directives, including focused didactic sessions, elective rotations in psychiatry, increased exposure to psychocutaneous lectures at national conferences, and finally through the establishment of joint dermatology-psychiatry clinics with interdepartmental collaboration.
- Weber MB, Recuero JK, Almeida CS. Use of psychiatric drugs in dermatology. An Bras Dermatol. 2020;95:133-143. doi:10.1016/j.abd.2019.12.002
- Centers for Medicare & Medicaid Services. Medicare provider utilization and payment data: part D prescriber. Updated September 10, 2024. Accessed October 7, 2024. https://www.cms.gov/data -research/statistics-trends-and-reports/medicare-provider-utilization-payment-data/part-d-prescriber
- Bolognia J, Schaffe JV, Lorenzo C. Dermatology. In: Duncan KO, Koo JYM, eds. Psychocutaneous Diseases. Elsevier; 2017:128-136.
- Gupta MA, Vujcic B, Pur DR, et al. Use of antipsychotic drugs in dermatology. Clin Dermatol. 2018;36:765-773. doi:10.1016/j.clindermatol.2018.08.006
- Jafferany M, Stamu-O’Brien C, Mkhoyan R, et al. Psychotropic drugs in dermatology: a dermatologist’s approach and choice of medications. Dermatol Ther. 2020;33:E13385. doi:10.1111/dth.13385
To the Editor:
Patients with primary psychiatric disorders with dermatologic manifestations often seek treatment from dermatologists instead of psychiatrists.1 For example, patients with delusions of parasitosis may lack insight into the underlying etiology of their disease and instead fixate on establishing an organic cause for their symptoms. As a result, it is an increasingly common practice for dermatologists to diagnose and treat psychiatric conditions.1 The goal of this study was to evaluate trends for the top 5 antipsychotics most frequently prescribed by dermatologists in the Medicare Part D database.
In this retrospective analysis, we consulted the Medicare Provider Utilization and Payment Data for January 2013 through December 2020, which is provided to the public by the Centers for Medicare & Medicaid Services.2 Only prescribing data from dermatologists were included in this study by using the built-in filter on the website to select “dermatology” as the prescriber type. All other provider types were excluded. We chose the top 5 most prescribed antipsychotics based on the number of supply days reported. Supply days—defined by Medicare as the number of days’ worth of medication that is prescribed—were used as a metric for utilization; therefore, each drug’s total supply days prescribed by dermatologists were calculated using this combined filter of drug name and total supply days using the database.
To analyze utilization over time, the annual average growth rate (AAGR) was calculated by determining the growth rate in total supply days annually from 2013 to 2020 and then averaging those rates to determine the overall AAGR. For greater clinical relevance, we calculated the average growth in supply days for the entire study period by determining the difference in the number of supply days for each year and then averaging these values. This was done to consider overall trends across dermatology rather than individual dermatologist prescribing patterns.
Based on our analysis, the antipsychotics most frequently prescribed by dermatologists for Medicare patients from January 2013 to December 2020 were pimozide, quetiapine, risperidone, olanzapine, and aripiprazole. The AAGR for each drug was 2.35%, 4.89%, 5.59%, 9.48%, and 20.72%, respectively, which is consistent with increased utilization over the study period for all 5 drugs (Table 1). The change in cost per supply day for the same period was 1.3%, –66.1%, –60.2%, –81.7%, and –84.3%, respectively. The net difference in cost per supply day over this entire period was $0.02, –$2.79, –$1.06, –$5.37, and –$21.22, respectively (Table 2).
There were several limitations to our study. Our analysis was limited to the Medicare population. Uninsured patients and those with Medicare Advantage or private health insurance plans were not included. In the Medicare database, only prescribers who prescribed a medication 10 times or more were recorded; therefore, some prescribers were not captured.
Although there was an increase in the dermatologic use of all 5 drugs in this study, perhaps the most marked growth was exhibited by aripiprazole, which had an AAGR of 20.72% (Table 1). Affordability may have been a factor, as the most marked reduction in price per supply day was noted for aripiprazole during the study period. Pimozide, which traditionally has been the first-line therapy for delusions of parasitosis, is the only first-generation antipsychotic drug among the 5 most frequently prescribed antipsychotics.3 Interestingly, pimozide had the lowest AAGR compared with the 4 second-generation antipsychotics. This finding also is corroborated by the average growth in supply days. While pimozide is a first-generation antipsychotic and had the lowest AAGR, pimozide still was the most prescribed antipsychotic in this study. Considering the average growth in Medicare beneficiaries during the study period was 2.70% per year,2 the AAGR of the 4 other drugs excluding pimozide shows that this growth was larger than what can be attributed to an increase in population size.
The most common conditions for which dermatologists prescribe antipsychotics are primary delusional infestation disorders as well as a range of self-inflicted dermatologic manifestations of dermatitis artefacta.4 Particularly, dermatologist-prescribed antipsychotics are first-line for these conditions in which perception of a persistent disease state is present.4 Importantly, dermatologists must differentiate between other dermatology-related psychiatric conditions such as trichotillomania and body dysmorphic disorder, which tend to respond better to selective serotonin reuptake inhibitors.4 Our data suggest that dermatologists are increasing their utilization of second-generation antipsychotics at a higher rate than first-generation antipsychotics, likely due to the lower risk of extrapyramidal symptoms. Patients are more willing to initiate a trial of psychiatric medication when it is prescribed by a dermatologist vs a psychiatrist due to lack of perceived stigma, which can lead to greater treatment compliance rates.5 As mentioned previously, as part of the differential, dermatologists also can effectively prescribe medications such as selective serotonin reuptake inhibitors for symptoms including anxiety, trichotillomania, body dysmorphic disorder, or secondary psychiatric disorders as a result of the burden of skin disease.5
In many cases, a dermatologist may be the first and only specialist to evaluate patients with conditions that overlap within the jurisdiction of dermatology and psychiatry. It is imperative that dermatologists feel comfortable treating this vulnerable patient population. As demonstrated by Medicare prescription data, the increasing utilization of antipsychotics in our specialty demands that dermatologists possess an adequate working knowledge of psychopharmacology, which may be accomplished during residency training through several directives, including focused didactic sessions, elective rotations in psychiatry, increased exposure to psychocutaneous lectures at national conferences, and finally through the establishment of joint dermatology-psychiatry clinics with interdepartmental collaboration.
To the Editor:
Patients with primary psychiatric disorders with dermatologic manifestations often seek treatment from dermatologists instead of psychiatrists.1 For example, patients with delusions of parasitosis may lack insight into the underlying etiology of their disease and instead fixate on establishing an organic cause for their symptoms. As a result, it is an increasingly common practice for dermatologists to diagnose and treat psychiatric conditions.1 The goal of this study was to evaluate trends for the top 5 antipsychotics most frequently prescribed by dermatologists in the Medicare Part D database.
In this retrospective analysis, we consulted the Medicare Provider Utilization and Payment Data for January 2013 through December 2020, which is provided to the public by the Centers for Medicare & Medicaid Services.2 Only prescribing data from dermatologists were included in this study by using the built-in filter on the website to select “dermatology” as the prescriber type. All other provider types were excluded. We chose the top 5 most prescribed antipsychotics based on the number of supply days reported. Supply days—defined by Medicare as the number of days’ worth of medication that is prescribed—were used as a metric for utilization; therefore, each drug’s total supply days prescribed by dermatologists were calculated using this combined filter of drug name and total supply days using the database.
To analyze utilization over time, the annual average growth rate (AAGR) was calculated by determining the growth rate in total supply days annually from 2013 to 2020 and then averaging those rates to determine the overall AAGR. For greater clinical relevance, we calculated the average growth in supply days for the entire study period by determining the difference in the number of supply days for each year and then averaging these values. This was done to consider overall trends across dermatology rather than individual dermatologist prescribing patterns.
Based on our analysis, the antipsychotics most frequently prescribed by dermatologists for Medicare patients from January 2013 to December 2020 were pimozide, quetiapine, risperidone, olanzapine, and aripiprazole. The AAGR for each drug was 2.35%, 4.89%, 5.59%, 9.48%, and 20.72%, respectively, which is consistent with increased utilization over the study period for all 5 drugs (Table 1). The change in cost per supply day for the same period was 1.3%, –66.1%, –60.2%, –81.7%, and –84.3%, respectively. The net difference in cost per supply day over this entire period was $0.02, –$2.79, –$1.06, –$5.37, and –$21.22, respectively (Table 2).
There were several limitations to our study. Our analysis was limited to the Medicare population. Uninsured patients and those with Medicare Advantage or private health insurance plans were not included. In the Medicare database, only prescribers who prescribed a medication 10 times or more were recorded; therefore, some prescribers were not captured.
Although there was an increase in the dermatologic use of all 5 drugs in this study, perhaps the most marked growth was exhibited by aripiprazole, which had an AAGR of 20.72% (Table 1). Affordability may have been a factor, as the most marked reduction in price per supply day was noted for aripiprazole during the study period. Pimozide, which traditionally has been the first-line therapy for delusions of parasitosis, is the only first-generation antipsychotic drug among the 5 most frequently prescribed antipsychotics.3 Interestingly, pimozide had the lowest AAGR compared with the 4 second-generation antipsychotics. This finding also is corroborated by the average growth in supply days. While pimozide is a first-generation antipsychotic and had the lowest AAGR, pimozide still was the most prescribed antipsychotic in this study. Considering the average growth in Medicare beneficiaries during the study period was 2.70% per year,2 the AAGR of the 4 other drugs excluding pimozide shows that this growth was larger than what can be attributed to an increase in population size.
The most common conditions for which dermatologists prescribe antipsychotics are primary delusional infestation disorders as well as a range of self-inflicted dermatologic manifestations of dermatitis artefacta.4 Particularly, dermatologist-prescribed antipsychotics are first-line for these conditions in which perception of a persistent disease state is present.4 Importantly, dermatologists must differentiate between other dermatology-related psychiatric conditions such as trichotillomania and body dysmorphic disorder, which tend to respond better to selective serotonin reuptake inhibitors.4 Our data suggest that dermatologists are increasing their utilization of second-generation antipsychotics at a higher rate than first-generation antipsychotics, likely due to the lower risk of extrapyramidal symptoms. Patients are more willing to initiate a trial of psychiatric medication when it is prescribed by a dermatologist vs a psychiatrist due to lack of perceived stigma, which can lead to greater treatment compliance rates.5 As mentioned previously, as part of the differential, dermatologists also can effectively prescribe medications such as selective serotonin reuptake inhibitors for symptoms including anxiety, trichotillomania, body dysmorphic disorder, or secondary psychiatric disorders as a result of the burden of skin disease.5
In many cases, a dermatologist may be the first and only specialist to evaluate patients with conditions that overlap within the jurisdiction of dermatology and psychiatry. It is imperative that dermatologists feel comfortable treating this vulnerable patient population. As demonstrated by Medicare prescription data, the increasing utilization of antipsychotics in our specialty demands that dermatologists possess an adequate working knowledge of psychopharmacology, which may be accomplished during residency training through several directives, including focused didactic sessions, elective rotations in psychiatry, increased exposure to psychocutaneous lectures at national conferences, and finally through the establishment of joint dermatology-psychiatry clinics with interdepartmental collaboration.
- Weber MB, Recuero JK, Almeida CS. Use of psychiatric drugs in dermatology. An Bras Dermatol. 2020;95:133-143. doi:10.1016/j.abd.2019.12.002
- Centers for Medicare & Medicaid Services. Medicare provider utilization and payment data: part D prescriber. Updated September 10, 2024. Accessed October 7, 2024. https://www.cms.gov/data -research/statistics-trends-and-reports/medicare-provider-utilization-payment-data/part-d-prescriber
- Bolognia J, Schaffe JV, Lorenzo C. Dermatology. In: Duncan KO, Koo JYM, eds. Psychocutaneous Diseases. Elsevier; 2017:128-136.
- Gupta MA, Vujcic B, Pur DR, et al. Use of antipsychotic drugs in dermatology. Clin Dermatol. 2018;36:765-773. doi:10.1016/j.clindermatol.2018.08.006
- Jafferany M, Stamu-O’Brien C, Mkhoyan R, et al. Psychotropic drugs in dermatology: a dermatologist’s approach and choice of medications. Dermatol Ther. 2020;33:E13385. doi:10.1111/dth.13385
- Weber MB, Recuero JK, Almeida CS. Use of psychiatric drugs in dermatology. An Bras Dermatol. 2020;95:133-143. doi:10.1016/j.abd.2019.12.002
- Centers for Medicare & Medicaid Services. Medicare provider utilization and payment data: part D prescriber. Updated September 10, 2024. Accessed October 7, 2024. https://www.cms.gov/data -research/statistics-trends-and-reports/medicare-provider-utilization-payment-data/part-d-prescriber
- Bolognia J, Schaffe JV, Lorenzo C. Dermatology. In: Duncan KO, Koo JYM, eds. Psychocutaneous Diseases. Elsevier; 2017:128-136.
- Gupta MA, Vujcic B, Pur DR, et al. Use of antipsychotic drugs in dermatology. Clin Dermatol. 2018;36:765-773. doi:10.1016/j.clindermatol.2018.08.006
- Jafferany M, Stamu-O’Brien C, Mkhoyan R, et al. Psychotropic drugs in dermatology: a dermatologist’s approach and choice of medications. Dermatol Ther. 2020;33:E13385. doi:10.1111/dth.13385
Practice Points
- Dermatologists are frontline medical providers who can be useful in screening for primary psychiatric disorders in patients with dermatologic manifestations.
- Second-generation antipsychotics are effective for treating many psychiatric disorders.
New Scanner Creates Highly Detailed, 3D Images of Blood Vessels in Seconds
A new scanner can provide three-dimensional (3D) photoacoustic images of millimeter-scale veins and arteries in seconds.
The scanner, developed by researchers at University College London (UCL) in England, could help clinicians better visualize and track microvascular changes for a wide range of diseases, including cancer, rheumatoid arthritis (RA), and peripheral vascular disease (PVD).
The case studies “illustrate potential areas of application that warrant future, more comprehensive clinical studies,” the authors wrote. “Moreover, they demonstrate the feasibility of using the scanner on a real-world patient cohort where imaging is more challenging due to frailty, comorbidity, or pain that may limit their ability to tolerate prolonged scan times.”
The work was published online in Nature Biomedical Engineering.
Improving Photoacoustic Imaging
PAT works using the photoacoustic effect, a phenomenon where sound waves are generated when light is absorbed by a material. When pulsed light from a laser is directed at tissue, some of that light is absorbed and causes an increase in heat in the targeted area. This localized heat also increases pressure, which generates ultrasound waves that can be detected by specialized sensors.
While previous PAT scanners translated these sound waves to electric signals directly to generate imaging, UCL engineers developed a sensor in the early 2000s that can detect these ultrasound waves using light. The result was much clearer, 3D images.
“That was great, but the problem was it was very slow, and it would take 5 minutes to get an image,” explained Paul Beard, PhD, professor of biomedical photoacoustics at UCL and senior author of the study. “That’s fine if you’re imaging a dead mouse or an anesthetized mouse, but not so useful for human imaging,” he continued, where motion would blur the image.
In this new paper, Beard and colleagues outlined how they cut scanning times to an order of seconds (or fraction of a second) rather than minutes. While previous iterations could detect only acoustic waves from one point at a time, this new scanner can detect waves from multiple points simultaneously. The scanner can visualize veins and arteries up to 15 mm deep in human tissue and can also provide dynamic, 3D images of “time-varying tissue perfusion and other hemodynamic events,” the authors wrote.
With these types of scanners, there is always a trade-off between imaging quality and imaging speed, explained Srivalleesha Mallidi, PhD, an assistant professor of biomedical engineering at Tufts University in Medford, Massachusetts. She was not involved with the work.
“With the resolution that [the authors] are providing and the depth at which they are seeing the signals, it is one of the fastest systems,” she said.
Clinical Utility
Beard and colleagues also tested the scanner to visualize blood vessels in participants with RA, suspected PVD, and skin inflammation. The scanning images “illustrated how vascular abnormalities such as increased vessel tortuosity, which has previously been linked to PVD, and the neovascularization associated with inflammation can be visualized and quantified,” the authors wrote.
The next step, Beard noted, is testing whether these characteristics can be used as a marker for the progression of disease.
Nehal Mehta, MD, a cardiologist and professor of medicine at the George Washington University, Washington, DC, agreed that more longitudinal research is needed to understand how the abnormalities captured in these images can inform detection and diagnosis of various diseases.
“You don’t know whether these images look bad because of reverse causation — the disease is doing this — or true causation — that this is actually detecting the root cause of the disease,” he explained. “Until we have a bank of normal and abnormal scans, we don’t know what any of these things mean.”
Though still some time away from entering the clinic, Mehta likened the technology to the introduction of optical coherence tomography in the 1980s. Before being adapted for clinical use, researchers first needed to visualize differences between normal coronary vasculature and myocardial infarction.
“I think this is an amazingly strong first proof of concept,” Mehta said. “This technology is showing a true promise in the field imaging.”
The work was funded by grants from Cancer Research UK, the Engineering & Physical Sciences Research Council, Wellcome Trust, the European Research Council, and the National Institute for Health and Care Research University College London Hospitals Biomedical Research Centre. Beard and two coauthors are shareholders of DeepColor Imaging to which the intellectual property associated with the new scanner has been licensed, but the company was not involved in any of this research. Mallidi and Mehta had no relevant disclosures.
A version of this article first appeared on Medscape.com.
A new scanner can provide three-dimensional (3D) photoacoustic images of millimeter-scale veins and arteries in seconds.
The scanner, developed by researchers at University College London (UCL) in England, could help clinicians better visualize and track microvascular changes for a wide range of diseases, including cancer, rheumatoid arthritis (RA), and peripheral vascular disease (PVD).
The case studies “illustrate potential areas of application that warrant future, more comprehensive clinical studies,” the authors wrote. “Moreover, they demonstrate the feasibility of using the scanner on a real-world patient cohort where imaging is more challenging due to frailty, comorbidity, or pain that may limit their ability to tolerate prolonged scan times.”
The work was published online in Nature Biomedical Engineering.
Improving Photoacoustic Imaging
PAT works using the photoacoustic effect, a phenomenon where sound waves are generated when light is absorbed by a material. When pulsed light from a laser is directed at tissue, some of that light is absorbed and causes an increase in heat in the targeted area. This localized heat also increases pressure, which generates ultrasound waves that can be detected by specialized sensors.
While previous PAT scanners translated these sound waves to electric signals directly to generate imaging, UCL engineers developed a sensor in the early 2000s that can detect these ultrasound waves using light. The result was much clearer, 3D images.
“That was great, but the problem was it was very slow, and it would take 5 minutes to get an image,” explained Paul Beard, PhD, professor of biomedical photoacoustics at UCL and senior author of the study. “That’s fine if you’re imaging a dead mouse or an anesthetized mouse, but not so useful for human imaging,” he continued, where motion would blur the image.
In this new paper, Beard and colleagues outlined how they cut scanning times to an order of seconds (or fraction of a second) rather than minutes. While previous iterations could detect only acoustic waves from one point at a time, this new scanner can detect waves from multiple points simultaneously. The scanner can visualize veins and arteries up to 15 mm deep in human tissue and can also provide dynamic, 3D images of “time-varying tissue perfusion and other hemodynamic events,” the authors wrote.
With these types of scanners, there is always a trade-off between imaging quality and imaging speed, explained Srivalleesha Mallidi, PhD, an assistant professor of biomedical engineering at Tufts University in Medford, Massachusetts. She was not involved with the work.
“With the resolution that [the authors] are providing and the depth at which they are seeing the signals, it is one of the fastest systems,” she said.
Clinical Utility
Beard and colleagues also tested the scanner to visualize blood vessels in participants with RA, suspected PVD, and skin inflammation. The scanning images “illustrated how vascular abnormalities such as increased vessel tortuosity, which has previously been linked to PVD, and the neovascularization associated with inflammation can be visualized and quantified,” the authors wrote.
The next step, Beard noted, is testing whether these characteristics can be used as a marker for the progression of disease.
Nehal Mehta, MD, a cardiologist and professor of medicine at the George Washington University, Washington, DC, agreed that more longitudinal research is needed to understand how the abnormalities captured in these images can inform detection and diagnosis of various diseases.
“You don’t know whether these images look bad because of reverse causation — the disease is doing this — or true causation — that this is actually detecting the root cause of the disease,” he explained. “Until we have a bank of normal and abnormal scans, we don’t know what any of these things mean.”
Though still some time away from entering the clinic, Mehta likened the technology to the introduction of optical coherence tomography in the 1980s. Before being adapted for clinical use, researchers first needed to visualize differences between normal coronary vasculature and myocardial infarction.
“I think this is an amazingly strong first proof of concept,” Mehta said. “This technology is showing a true promise in the field imaging.”
The work was funded by grants from Cancer Research UK, the Engineering & Physical Sciences Research Council, Wellcome Trust, the European Research Council, and the National Institute for Health and Care Research University College London Hospitals Biomedical Research Centre. Beard and two coauthors are shareholders of DeepColor Imaging to which the intellectual property associated with the new scanner has been licensed, but the company was not involved in any of this research. Mallidi and Mehta had no relevant disclosures.
A version of this article first appeared on Medscape.com.
A new scanner can provide three-dimensional (3D) photoacoustic images of millimeter-scale veins and arteries in seconds.
The scanner, developed by researchers at University College London (UCL) in England, could help clinicians better visualize and track microvascular changes for a wide range of diseases, including cancer, rheumatoid arthritis (RA), and peripheral vascular disease (PVD).
The case studies “illustrate potential areas of application that warrant future, more comprehensive clinical studies,” the authors wrote. “Moreover, they demonstrate the feasibility of using the scanner on a real-world patient cohort where imaging is more challenging due to frailty, comorbidity, or pain that may limit their ability to tolerate prolonged scan times.”
The work was published online in Nature Biomedical Engineering.
Improving Photoacoustic Imaging
PAT works using the photoacoustic effect, a phenomenon where sound waves are generated when light is absorbed by a material. When pulsed light from a laser is directed at tissue, some of that light is absorbed and causes an increase in heat in the targeted area. This localized heat also increases pressure, which generates ultrasound waves that can be detected by specialized sensors.
While previous PAT scanners translated these sound waves to electric signals directly to generate imaging, UCL engineers developed a sensor in the early 2000s that can detect these ultrasound waves using light. The result was much clearer, 3D images.
“That was great, but the problem was it was very slow, and it would take 5 minutes to get an image,” explained Paul Beard, PhD, professor of biomedical photoacoustics at UCL and senior author of the study. “That’s fine if you’re imaging a dead mouse or an anesthetized mouse, but not so useful for human imaging,” he continued, where motion would blur the image.
In this new paper, Beard and colleagues outlined how they cut scanning times to an order of seconds (or fraction of a second) rather than minutes. While previous iterations could detect only acoustic waves from one point at a time, this new scanner can detect waves from multiple points simultaneously. The scanner can visualize veins and arteries up to 15 mm deep in human tissue and can also provide dynamic, 3D images of “time-varying tissue perfusion and other hemodynamic events,” the authors wrote.
With these types of scanners, there is always a trade-off between imaging quality and imaging speed, explained Srivalleesha Mallidi, PhD, an assistant professor of biomedical engineering at Tufts University in Medford, Massachusetts. She was not involved with the work.
“With the resolution that [the authors] are providing and the depth at which they are seeing the signals, it is one of the fastest systems,” she said.
Clinical Utility
Beard and colleagues also tested the scanner to visualize blood vessels in participants with RA, suspected PVD, and skin inflammation. The scanning images “illustrated how vascular abnormalities such as increased vessel tortuosity, which has previously been linked to PVD, and the neovascularization associated with inflammation can be visualized and quantified,” the authors wrote.
The next step, Beard noted, is testing whether these characteristics can be used as a marker for the progression of disease.
Nehal Mehta, MD, a cardiologist and professor of medicine at the George Washington University, Washington, DC, agreed that more longitudinal research is needed to understand how the abnormalities captured in these images can inform detection and diagnosis of various diseases.
“You don’t know whether these images look bad because of reverse causation — the disease is doing this — or true causation — that this is actually detecting the root cause of the disease,” he explained. “Until we have a bank of normal and abnormal scans, we don’t know what any of these things mean.”
Though still some time away from entering the clinic, Mehta likened the technology to the introduction of optical coherence tomography in the 1980s. Before being adapted for clinical use, researchers first needed to visualize differences between normal coronary vasculature and myocardial infarction.
“I think this is an amazingly strong first proof of concept,” Mehta said. “This technology is showing a true promise in the field imaging.”
The work was funded by grants from Cancer Research UK, the Engineering & Physical Sciences Research Council, Wellcome Trust, the European Research Council, and the National Institute for Health and Care Research University College London Hospitals Biomedical Research Centre. Beard and two coauthors are shareholders of DeepColor Imaging to which the intellectual property associated with the new scanner has been licensed, but the company was not involved in any of this research. Mallidi and Mehta had no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM NATURE BIOMEDICAL ENGINEERING