User login
Bevacizumab offers best value of anti-VEGF drugs to treat DME
Despite recent data showing that aflibercept is the most effective anti–vascular endothelial growth factor (anti-VEGF) treatment available for patients with diabetic macular edema, bevacizumab is still by far the best drug option available from a cost-effectiveness perspective, according to a post hoc analysis.
Dr. Joshua D. Stein of the University of Michigan, Ann Arbor, and his coauthors analyzed the anti-VEGF drugs prescribed to 624 diabetic macular edema (DME) patients – 209 taking aflibercept, 207 taking bevacizumab, and 208 taking ranibizumab – enrolled in the Diabetic Retinopathy Clinical Research Network Comparative Effectiveness Trial for incremental cost-effectiveness ratios (ICERs).
“On the basis of 2015 wholesale acquisition costs, aflibercept (2 mg) costs $1,850, ranibizumab (0.3mg) costs $1,170, and bevacizumab repackaged at compounding pharmacies into syringes for ophthalmologic use containing 1.25 mg of bevacizumab costs approximately $60 per dose,” Dr. Stein and his coauthors wrote (JAMA Ophthalmol. 2016 June 9. doi: 10.1001/jamaophthalmol.2016.1669). “Considering that these medicines may be given 9 to 11 times in the first year of treatment and, on average, 17 times during 5 years, total costs can be substantial.”
Data from the randomized clinical trial were used to calculate projected benefit, costs, and cost-effectiveness of aflibercept and ranibizumab compared with bevacizumab as baseline. In addition, the investigators also determined both ICERs and Quality Life-Adjusted Years (QALY) for each drug over periods of 1 and 10 years. Results indicated that for 1 year of treatment, the ICER of aflibercept was $1.11 million per QALY and for ranibizumab, $1.73 million per QALY. Over the course of 10 years, aflibercept would come out to $349,000 per QALY, while ranibizumab would be $603,000 per QALY. In an analysis of a subgroup with highly reduced eyesight due to DME, the 10-year ICER of aflibercept would be $287,000 per QALY and for ranibizumab, $817,000, according to Dr. Stein and his associates.
Over a 1-year period, bevacizumab would cost $4,100, compared to $26,100 for aflibercept and $18,600 for ranibizumab. Over a 10-year period, those costs would jump up to $102,500 for aflibercept and $79,400 for ranibizumab, while bevacizumab would cost $39,800. Overall, the costs of aflibercept and ranibizumab would have to decrease by 69% and 80%, respectively, for the costs to become competitive with bevacizumab.
“Aflibercept (2.0 mg) and ranibizumab (0.3 mg) are not cost-effective relative to bevacizumab for treatment of DME unless their prices decrease substantially [and] in contexts where bevacizumab is unavailable for DME treatment, aflibercept is not cost-effective relative to ranibizumab,” the authors concluded, adding that bevacizumab makes the most sense as a primary anti-VEGF treatment because it allows for the greatest overall value.
The National Eye Institute, the National Institute of Diabetes and Digestive and Kidney Diseases, and the U.S. Department of Health and Human Services funded the study. Dr. Stein did not report any relevant financial disclosures; however, other coauthors reported potentially relevant disclosures.
Despite recent data showing that aflibercept is the most effective anti–vascular endothelial growth factor (anti-VEGF) treatment available for patients with diabetic macular edema, bevacizumab is still by far the best drug option available from a cost-effectiveness perspective, according to a post hoc analysis.
Dr. Joshua D. Stein of the University of Michigan, Ann Arbor, and his coauthors analyzed the anti-VEGF drugs prescribed to 624 diabetic macular edema (DME) patients – 209 taking aflibercept, 207 taking bevacizumab, and 208 taking ranibizumab – enrolled in the Diabetic Retinopathy Clinical Research Network Comparative Effectiveness Trial for incremental cost-effectiveness ratios (ICERs).
“On the basis of 2015 wholesale acquisition costs, aflibercept (2 mg) costs $1,850, ranibizumab (0.3mg) costs $1,170, and bevacizumab repackaged at compounding pharmacies into syringes for ophthalmologic use containing 1.25 mg of bevacizumab costs approximately $60 per dose,” Dr. Stein and his coauthors wrote (JAMA Ophthalmol. 2016 June 9. doi: 10.1001/jamaophthalmol.2016.1669). “Considering that these medicines may be given 9 to 11 times in the first year of treatment and, on average, 17 times during 5 years, total costs can be substantial.”
Data from the randomized clinical trial were used to calculate projected benefit, costs, and cost-effectiveness of aflibercept and ranibizumab compared with bevacizumab as baseline. In addition, the investigators also determined both ICERs and Quality Life-Adjusted Years (QALY) for each drug over periods of 1 and 10 years. Results indicated that for 1 year of treatment, the ICER of aflibercept was $1.11 million per QALY and for ranibizumab, $1.73 million per QALY. Over the course of 10 years, aflibercept would come out to $349,000 per QALY, while ranibizumab would be $603,000 per QALY. In an analysis of a subgroup with highly reduced eyesight due to DME, the 10-year ICER of aflibercept would be $287,000 per QALY and for ranibizumab, $817,000, according to Dr. Stein and his associates.
Over a 1-year period, bevacizumab would cost $4,100, compared to $26,100 for aflibercept and $18,600 for ranibizumab. Over a 10-year period, those costs would jump up to $102,500 for aflibercept and $79,400 for ranibizumab, while bevacizumab would cost $39,800. Overall, the costs of aflibercept and ranibizumab would have to decrease by 69% and 80%, respectively, for the costs to become competitive with bevacizumab.
“Aflibercept (2.0 mg) and ranibizumab (0.3 mg) are not cost-effective relative to bevacizumab for treatment of DME unless their prices decrease substantially [and] in contexts where bevacizumab is unavailable for DME treatment, aflibercept is not cost-effective relative to ranibizumab,” the authors concluded, adding that bevacizumab makes the most sense as a primary anti-VEGF treatment because it allows for the greatest overall value.
The National Eye Institute, the National Institute of Diabetes and Digestive and Kidney Diseases, and the U.S. Department of Health and Human Services funded the study. Dr. Stein did not report any relevant financial disclosures; however, other coauthors reported potentially relevant disclosures.
Despite recent data showing that aflibercept is the most effective anti–vascular endothelial growth factor (anti-VEGF) treatment available for patients with diabetic macular edema, bevacizumab is still by far the best drug option available from a cost-effectiveness perspective, according to a post hoc analysis.
Dr. Joshua D. Stein of the University of Michigan, Ann Arbor, and his coauthors analyzed the anti-VEGF drugs prescribed to 624 diabetic macular edema (DME) patients – 209 taking aflibercept, 207 taking bevacizumab, and 208 taking ranibizumab – enrolled in the Diabetic Retinopathy Clinical Research Network Comparative Effectiveness Trial for incremental cost-effectiveness ratios (ICERs).
“On the basis of 2015 wholesale acquisition costs, aflibercept (2 mg) costs $1,850, ranibizumab (0.3mg) costs $1,170, and bevacizumab repackaged at compounding pharmacies into syringes for ophthalmologic use containing 1.25 mg of bevacizumab costs approximately $60 per dose,” Dr. Stein and his coauthors wrote (JAMA Ophthalmol. 2016 June 9. doi: 10.1001/jamaophthalmol.2016.1669). “Considering that these medicines may be given 9 to 11 times in the first year of treatment and, on average, 17 times during 5 years, total costs can be substantial.”
Data from the randomized clinical trial were used to calculate projected benefit, costs, and cost-effectiveness of aflibercept and ranibizumab compared with bevacizumab as baseline. In addition, the investigators also determined both ICERs and Quality Life-Adjusted Years (QALY) for each drug over periods of 1 and 10 years. Results indicated that for 1 year of treatment, the ICER of aflibercept was $1.11 million per QALY and for ranibizumab, $1.73 million per QALY. Over the course of 10 years, aflibercept would come out to $349,000 per QALY, while ranibizumab would be $603,000 per QALY. In an analysis of a subgroup with highly reduced eyesight due to DME, the 10-year ICER of aflibercept would be $287,000 per QALY and for ranibizumab, $817,000, according to Dr. Stein and his associates.
Over a 1-year period, bevacizumab would cost $4,100, compared to $26,100 for aflibercept and $18,600 for ranibizumab. Over a 10-year period, those costs would jump up to $102,500 for aflibercept and $79,400 for ranibizumab, while bevacizumab would cost $39,800. Overall, the costs of aflibercept and ranibizumab would have to decrease by 69% and 80%, respectively, for the costs to become competitive with bevacizumab.
“Aflibercept (2.0 mg) and ranibizumab (0.3 mg) are not cost-effective relative to bevacizumab for treatment of DME unless their prices decrease substantially [and] in contexts where bevacizumab is unavailable for DME treatment, aflibercept is not cost-effective relative to ranibizumab,” the authors concluded, adding that bevacizumab makes the most sense as a primary anti-VEGF treatment because it allows for the greatest overall value.
The National Eye Institute, the National Institute of Diabetes and Digestive and Kidney Diseases, and the U.S. Department of Health and Human Services funded the study. Dr. Stein did not report any relevant financial disclosures; however, other coauthors reported potentially relevant disclosures.
FROM JAMA OPHTHALMOLOGY
Key clinical point: Bevacizumab remains the best option, in terms of price and value, over aflibercept and ranibizumab for treatment of diabetic macular edema.
Major finding: Based on incremental cost-effectiveness ratios (ICERs) over 1- and 10-year periods, the costs of aflibercept and ranibizumab would have to decrease by 69% and 80%, respectively, to match the cost of bevacizumab over the same time periods.
Data source: Post hoc analysis of patients enrolled in the Diabetic Retinopathy Clinical Research Network Comparative Effectiveness Trial at 1-year follow-up.
Disclosures: The National Eye Institute, the National Institute of Diabetes and Digestive and Kidney Diseases, and the U.S. Department of Health and Human Services funded the study. Dr. Stein did not report any relevant financial disclosures.
Weighty issues: Exploring the connection between diabetes, depression
“You’re wearing an Unna boot – what happened?”
“Doc, my wife made too many tempting desserts while we were in Florida, and when we got back, I had an infected toe. My doctor gave me antibiotics, but the toe turned blue, so they had to amputate.”
I had been treating this man for depression for many years and did not know about his having diabetes, so I asked, “Are you diabetic?”
“No,” he answered. “My doctor says I’ve been prediabetic for 20 years, and he’s put me on a low dose of metformin. … My friends are on twice as much. I don’t even have to have one of those meters.

“I can just go to the senior center or stop by my doctor’s office once a week and have my sugar checked. My wife says she won’t tempt me with any more desserts; she’s buying fruit, which I’m not used to, and I’m not eating bread anymore.
“Hey, those pills you’re giving me for my depression are working great. I am eating and sleeping and doing things I love to do. The wife and I are getting over the kids’ divorces, and we are still able to help out with the grandchild, who has been so sick. When we got back home, I tried to get back with my poker buddies, but one of them is in cardiac rehab; he had a heart attack, and another one, his wife says he’s got Alzheimer’s – he did lose a lot last year and that wasn’t like him. … Yeah, I guess I’m OK. As soon as this toe heals, I’ll be 100%.”
This dialogue is a composite; the names have been changed to protect the innocent, but unfortunately, it is an oft-told tale. The relationship between diabetes and depression has been known for a long time.1Each one is a risk factor for the other, and together and separately, they are a risk factor for dementia.
For quite a while, it was thought that having a diabetes diagnosis and having to manage it in and of itself was depressing, and that therefore, people would become depressed. It was also thought that people who are depressed might try to soothe themselves with copious amounts of comfort food and alcohol, and would thereby develop diabetes. Certainly, many people’s routes to depression and diabetes are just that – psychological reactions to having the other disease. But research shows that there is a much deeper physiologic relationship between the two.
Since diabetes and depression or their sequelae are among the 14 leading causes of death in the United States, psychiatrists and other medical professionals need to collaborate in the treatment of these diseases in their patients. Medical homes are good, but most patients continue to receive treatment for all disorders separately and in isolation. If it were not for the medical professional asking directly, or discovering some medication after the patient has given permission for an electronic medication prescribing overview of all his medications, treatment for diabetes or depression might be unknown by the other medical professional. Our noncommunicative EHRs will not help here. The only thing that will help is open communication between the patient and all of his medical treaters.
Now that I am educated and alarmed about the diabetes-depression connection, I send a note to the primary care physician and follow up with a few articles from Science Daily such as “Depression, early death among seniors with diabetes: Strong link found by research,”2 or “Treating major depression in older adults with diabetes may lower risk of death”3, or the clincher, “Treatment for diabetes and depression improves both, researchers say.”4
For patients with type 2 diabetes, the form of the illness usually referred to in research on diabetes and depression, the body becomes insensitive to insulin, i.e., insulin resistance develops. We now know that insulin resistance occurs throughout the body, including the brain. Insulin receptors are present in all organs of the body, including the brain. We also know that the higher fasting glucose level seen in prediabetes is an indication of the development of insulin resistance. Insulin’s job is to get glucose into cells for ready availability of energy and into muscle for backup energy.
If glucose is too plentiful, as it is when sugary foods are overconsumed, insulin directs the rest of the glucose to be stored as fat in the liver, inside blood vessels, around organs, and subcutaneously. Ultimately, there is nowhere else to store the excess energy, and insulin resistance develops. The pancreas, which secretes insulin, keeps on pumping insulin and can poop out, requiring exogenous insulin to keep things moving.5Treatments can include insulin itself, medications that increase insulin sensitivity, diet, and exercise to deplete the energy stores, or bariatric surgery, which, by the way, is said to cure both diabetes and depression within 3 weeks after surgery (this effect is negated if patients regain their weight.)
What the research shows
Clinical research from the University of Pennsylvania6 and Massachusetts General Hospital7shows that having a third, nonphysician treater work with patients diagnosed with both disorders improves outcomes. Both of those protocols used cognitive-behavioral therapy (CBT) and motivational interviewing, group treatment, and telephone contact as modalities. One also used electronic monitoring of medication dosing and the record of the glucometer to follow patients’ progress.
In both studies, patients in the protocol groups did better than the treatment-as-usual groups in terms of relief of depression and control of diabetes. In the private primary care physician and psychiatrist office setting, a third party is not practical, but psychiatrists can add motivational interviewing and some aspects of CBT. Also, both psychiatrists and primary care physicians can use electronic medication monitoring and blood glucose monitoring. Recently, Apple released apps that the company said will make it easy for patients with those devices8, but the old glucometer and pharmacy follow-up for prescriptions also can be useful. Medication (bottle cap) monitors can be expensive and may not be practical for some patients.
A prospective study of 2,525 patients showed that those with depression and metabolic risk factors were more than six times more likely to develop diabetes than patients who had depression alone, metabolic risk factors alone, or neither. These results allow for gross sorting out of which people with depression are more likely to develop diabetes.9This can provide an opportunity to intervene before diabetes sets in – and would have saved the toe of the patient I described earlier.
At the cellular level, at least in mice, it appears that insulin resistance in the brain alters dopamine turnover and causes behavioral disorders that look like anxiety and depression.10Mice with a brain-specific knockout of the insulin receptor showed “mitochondrial dysfunction and oxidative distress in the dorsal striatum and the nucleus accumbens. Increased levels of MAO A and B leading to increased turnover of dopamine in the mesolimbic system were also observed.”
The depression in these mice was relieved with the use of imipramine and phenelzine, and the researchers also noted that previous research had shown a decrease in depressive-like behavior with the insulin sensitizer rosiglitazone, which reduces glucose in the brain when given to obese, diabetic mice. Certainly, further research is necessary, as is research in humans. But this demonstrates what might be happening to our patients who have metabolic syndrome or diabetes and depression, and may offer suggestions for appropriate treatments.
“If you see something, say something.”
In short, early effective intervention in the metabolic/prediabetes state is best. Taking weights and heights, calculating BMIs, and either measuring or observing waist circumference, can give us a hunch that metabolic syndrome exists. We do our patients a favor if we mention this – and enlist their curiosity and efforts in avoiding or mitigating the ravages of diabetes and worsening depression.
Dr. Harris, a diplomate of the American Board of Obesity Medicine, is in private practice and adult and geriatric psychiatry in Hartford, Conn. She also works as a psychiatric consultant to continuing care retirement organizations and professional groups. Dr. Harris, a former president of the Black Psychiatrists of America, is a Distinguished Fellow of the American Psychiatric Association. Besides psychotherapy, her major clinical interests include geriatrics, and the interface between general medicine and psychiatry.
References
1. U.S. Medicine, November 2009.
2. Science Daily, March 29, 2014.
3. Science Daily, Jan. 27, 2016.
4. Science Daily, Jan. 18, 2012.
5. “Diabetes Facts and Guidelines,” Yale Diabetes Center, 2011.
6. Ann Fam Med. 2012 Jan-Feb;10(1):15-22.
7. Diabetes Care. 2014;37(3):625-33.
8. Macworld, May 10, 2016.
9. Mol Psychiatry. 2016 Feb 23. doi: 10:1038/mp 2016.7.
10. Proc Natl Acad Sci USA. 2014 Mar 17;112(11):3463-8.
“You’re wearing an Unna boot – what happened?”
“Doc, my wife made too many tempting desserts while we were in Florida, and when we got back, I had an infected toe. My doctor gave me antibiotics, but the toe turned blue, so they had to amputate.”
I had been treating this man for depression for many years and did not know about his having diabetes, so I asked, “Are you diabetic?”
“No,” he answered. “My doctor says I’ve been prediabetic for 20 years, and he’s put me on a low dose of metformin. … My friends are on twice as much. I don’t even have to have one of those meters.
“I can just go to the senior center or stop by my doctor’s office once a week and have my sugar checked. My wife says she won’t tempt me with any more desserts; she’s buying fruit, which I’m not used to, and I’m not eating bread anymore.
“Hey, those pills you’re giving me for my depression are working great. I am eating and sleeping and doing things I love to do. The wife and I are getting over the kids’ divorces, and we are still able to help out with the grandchild, who has been so sick. When we got back home, I tried to get back with my poker buddies, but one of them is in cardiac rehab; he had a heart attack, and another one, his wife says he’s got Alzheimer’s – he did lose a lot last year and that wasn’t like him. … Yeah, I guess I’m OK. As soon as this toe heals, I’ll be 100%.”
This dialogue is a composite; the names have been changed to protect the innocent, but unfortunately, it is an oft-told tale. The relationship between diabetes and depression has been known for a long time.1Each one is a risk factor for the other, and together and separately, they are a risk factor for dementia.
For quite a while, it was thought that having a diabetes diagnosis and having to manage it in and of itself was depressing, and that therefore, people would become depressed. It was also thought that people who are depressed might try to soothe themselves with copious amounts of comfort food and alcohol, and would thereby develop diabetes. Certainly, many people’s routes to depression and diabetes are just that – psychological reactions to having the other disease. But research shows that there is a much deeper physiologic relationship between the two.
Since diabetes and depression or their sequelae are among the 14 leading causes of death in the United States, psychiatrists and other medical professionals need to collaborate in the treatment of these diseases in their patients. Medical homes are good, but most patients continue to receive treatment for all disorders separately and in isolation. If it were not for the medical professional asking directly, or discovering some medication after the patient has given permission for an electronic medication prescribing overview of all his medications, treatment for diabetes or depression might be unknown by the other medical professional. Our noncommunicative EHRs will not help here. The only thing that will help is open communication between the patient and all of his medical treaters.
Now that I am educated and alarmed about the diabetes-depression connection, I send a note to the primary care physician and follow up with a few articles from Science Daily such as “Depression, early death among seniors with diabetes: Strong link found by research,”2 or “Treating major depression in older adults with diabetes may lower risk of death”3, or the clincher, “Treatment for diabetes and depression improves both, researchers say.”4
For patients with type 2 diabetes, the form of the illness usually referred to in research on diabetes and depression, the body becomes insensitive to insulin, i.e., insulin resistance develops. We now know that insulin resistance occurs throughout the body, including the brain. Insulin receptors are present in all organs of the body, including the brain. We also know that the higher fasting glucose level seen in prediabetes is an indication of the development of insulin resistance. Insulin’s job is to get glucose into cells for ready availability of energy and into muscle for backup energy.
If glucose is too plentiful, as it is when sugary foods are overconsumed, insulin directs the rest of the glucose to be stored as fat in the liver, inside blood vessels, around organs, and subcutaneously. Ultimately, there is nowhere else to store the excess energy, and insulin resistance develops. The pancreas, which secretes insulin, keeps on pumping insulin and can poop out, requiring exogenous insulin to keep things moving.5Treatments can include insulin itself, medications that increase insulin sensitivity, diet, and exercise to deplete the energy stores, or bariatric surgery, which, by the way, is said to cure both diabetes and depression within 3 weeks after surgery (this effect is negated if patients regain their weight.)
What the research shows
Clinical research from the University of Pennsylvania6 and Massachusetts General Hospital7shows that having a third, nonphysician treater work with patients diagnosed with both disorders improves outcomes. Both of those protocols used cognitive-behavioral therapy (CBT) and motivational interviewing, group treatment, and telephone contact as modalities. One also used electronic monitoring of medication dosing and the record of the glucometer to follow patients’ progress.
In both studies, patients in the protocol groups did better than the treatment-as-usual groups in terms of relief of depression and control of diabetes. In the private primary care physician and psychiatrist office setting, a third party is not practical, but psychiatrists can add motivational interviewing and some aspects of CBT. Also, both psychiatrists and primary care physicians can use electronic medication monitoring and blood glucose monitoring. Recently, Apple released apps that the company said will make it easy for patients with those devices8, but the old glucometer and pharmacy follow-up for prescriptions also can be useful. Medication (bottle cap) monitors can be expensive and may not be practical for some patients.
A prospective study of 2,525 patients showed that those with depression and metabolic risk factors were more than six times more likely to develop diabetes than patients who had depression alone, metabolic risk factors alone, or neither. These results allow for gross sorting out of which people with depression are more likely to develop diabetes.9This can provide an opportunity to intervene before diabetes sets in – and would have saved the toe of the patient I described earlier.
At the cellular level, at least in mice, it appears that insulin resistance in the brain alters dopamine turnover and causes behavioral disorders that look like anxiety and depression.10Mice with a brain-specific knockout of the insulin receptor showed “mitochondrial dysfunction and oxidative distress in the dorsal striatum and the nucleus accumbens. Increased levels of MAO A and B leading to increased turnover of dopamine in the mesolimbic system were also observed.”
The depression in these mice was relieved with the use of imipramine and phenelzine, and the researchers also noted that previous research had shown a decrease in depressive-like behavior with the insulin sensitizer rosiglitazone, which reduces glucose in the brain when given to obese, diabetic mice. Certainly, further research is necessary, as is research in humans. But this demonstrates what might be happening to our patients who have metabolic syndrome or diabetes and depression, and may offer suggestions for appropriate treatments.
“If you see something, say something.”
In short, early effective intervention in the metabolic/prediabetes state is best. Taking weights and heights, calculating BMIs, and either measuring or observing waist circumference, can give us a hunch that metabolic syndrome exists. We do our patients a favor if we mention this – and enlist their curiosity and efforts in avoiding or mitigating the ravages of diabetes and worsening depression.
Dr. Harris, a diplomate of the American Board of Obesity Medicine, is in private practice and adult and geriatric psychiatry in Hartford, Conn. She also works as a psychiatric consultant to continuing care retirement organizations and professional groups. Dr. Harris, a former president of the Black Psychiatrists of America, is a Distinguished Fellow of the American Psychiatric Association. Besides psychotherapy, her major clinical interests include geriatrics, and the interface between general medicine and psychiatry.
References
1. U.S. Medicine, November 2009.
2. Science Daily, March 29, 2014.
3. Science Daily, Jan. 27, 2016.
4. Science Daily, Jan. 18, 2012.
5. “Diabetes Facts and Guidelines,” Yale Diabetes Center, 2011.
6. Ann Fam Med. 2012 Jan-Feb;10(1):15-22.
7. Diabetes Care. 2014;37(3):625-33.
8. Macworld, May 10, 2016.
9. Mol Psychiatry. 2016 Feb 23. doi: 10:1038/mp 2016.7.
10. Proc Natl Acad Sci USA. 2014 Mar 17;112(11):3463-8.
“You’re wearing an Unna boot – what happened?”
“Doc, my wife made too many tempting desserts while we were in Florida, and when we got back, I had an infected toe. My doctor gave me antibiotics, but the toe turned blue, so they had to amputate.”
I had been treating this man for depression for many years and did not know about his having diabetes, so I asked, “Are you diabetic?”
“No,” he answered. “My doctor says I’ve been prediabetic for 20 years, and he’s put me on a low dose of metformin. … My friends are on twice as much. I don’t even have to have one of those meters.
“I can just go to the senior center or stop by my doctor’s office once a week and have my sugar checked. My wife says she won’t tempt me with any more desserts; she’s buying fruit, which I’m not used to, and I’m not eating bread anymore.
“Hey, those pills you’re giving me for my depression are working great. I am eating and sleeping and doing things I love to do. The wife and I are getting over the kids’ divorces, and we are still able to help out with the grandchild, who has been so sick. When we got back home, I tried to get back with my poker buddies, but one of them is in cardiac rehab; he had a heart attack, and another one, his wife says he’s got Alzheimer’s – he did lose a lot last year and that wasn’t like him. … Yeah, I guess I’m OK. As soon as this toe heals, I’ll be 100%.”
This dialogue is a composite; the names have been changed to protect the innocent, but unfortunately, it is an oft-told tale. The relationship between diabetes and depression has been known for a long time.1Each one is a risk factor for the other, and together and separately, they are a risk factor for dementia.
For quite a while, it was thought that having a diabetes diagnosis and having to manage it in and of itself was depressing, and that therefore, people would become depressed. It was also thought that people who are depressed might try to soothe themselves with copious amounts of comfort food and alcohol, and would thereby develop diabetes. Certainly, many people’s routes to depression and diabetes are just that – psychological reactions to having the other disease. But research shows that there is a much deeper physiologic relationship between the two.
Since diabetes and depression or their sequelae are among the 14 leading causes of death in the United States, psychiatrists and other medical professionals need to collaborate in the treatment of these diseases in their patients. Medical homes are good, but most patients continue to receive treatment for all disorders separately and in isolation. If it were not for the medical professional asking directly, or discovering some medication after the patient has given permission for an electronic medication prescribing overview of all his medications, treatment for diabetes or depression might be unknown by the other medical professional. Our noncommunicative EHRs will not help here. The only thing that will help is open communication between the patient and all of his medical treaters.
Now that I am educated and alarmed about the diabetes-depression connection, I send a note to the primary care physician and follow up with a few articles from Science Daily such as “Depression, early death among seniors with diabetes: Strong link found by research,”2 or “Treating major depression in older adults with diabetes may lower risk of death”3, or the clincher, “Treatment for diabetes and depression improves both, researchers say.”4
For patients with type 2 diabetes, the form of the illness usually referred to in research on diabetes and depression, the body becomes insensitive to insulin, i.e., insulin resistance develops. We now know that insulin resistance occurs throughout the body, including the brain. Insulin receptors are present in all organs of the body, including the brain. We also know that the higher fasting glucose level seen in prediabetes is an indication of the development of insulin resistance. Insulin’s job is to get glucose into cells for ready availability of energy and into muscle for backup energy.
If glucose is too plentiful, as it is when sugary foods are overconsumed, insulin directs the rest of the glucose to be stored as fat in the liver, inside blood vessels, around organs, and subcutaneously. Ultimately, there is nowhere else to store the excess energy, and insulin resistance develops. The pancreas, which secretes insulin, keeps on pumping insulin and can poop out, requiring exogenous insulin to keep things moving.5Treatments can include insulin itself, medications that increase insulin sensitivity, diet, and exercise to deplete the energy stores, or bariatric surgery, which, by the way, is said to cure both diabetes and depression within 3 weeks after surgery (this effect is negated if patients regain their weight.)
What the research shows
Clinical research from the University of Pennsylvania6 and Massachusetts General Hospital7shows that having a third, nonphysician treater work with patients diagnosed with both disorders improves outcomes. Both of those protocols used cognitive-behavioral therapy (CBT) and motivational interviewing, group treatment, and telephone contact as modalities. One also used electronic monitoring of medication dosing and the record of the glucometer to follow patients’ progress.
In both studies, patients in the protocol groups did better than the treatment-as-usual groups in terms of relief of depression and control of diabetes. In the private primary care physician and psychiatrist office setting, a third party is not practical, but psychiatrists can add motivational interviewing and some aspects of CBT. Also, both psychiatrists and primary care physicians can use electronic medication monitoring and blood glucose monitoring. Recently, Apple released apps that the company said will make it easy for patients with those devices8, but the old glucometer and pharmacy follow-up for prescriptions also can be useful. Medication (bottle cap) monitors can be expensive and may not be practical for some patients.
A prospective study of 2,525 patients showed that those with depression and metabolic risk factors were more than six times more likely to develop diabetes than patients who had depression alone, metabolic risk factors alone, or neither. These results allow for gross sorting out of which people with depression are more likely to develop diabetes.9This can provide an opportunity to intervene before diabetes sets in – and would have saved the toe of the patient I described earlier.
At the cellular level, at least in mice, it appears that insulin resistance in the brain alters dopamine turnover and causes behavioral disorders that look like anxiety and depression.10Mice with a brain-specific knockout of the insulin receptor showed “mitochondrial dysfunction and oxidative distress in the dorsal striatum and the nucleus accumbens. Increased levels of MAO A and B leading to increased turnover of dopamine in the mesolimbic system were also observed.”
The depression in these mice was relieved with the use of imipramine and phenelzine, and the researchers also noted that previous research had shown a decrease in depressive-like behavior with the insulin sensitizer rosiglitazone, which reduces glucose in the brain when given to obese, diabetic mice. Certainly, further research is necessary, as is research in humans. But this demonstrates what might be happening to our patients who have metabolic syndrome or diabetes and depression, and may offer suggestions for appropriate treatments.
“If you see something, say something.”
In short, early effective intervention in the metabolic/prediabetes state is best. Taking weights and heights, calculating BMIs, and either measuring or observing waist circumference, can give us a hunch that metabolic syndrome exists. We do our patients a favor if we mention this – and enlist their curiosity and efforts in avoiding or mitigating the ravages of diabetes and worsening depression.
Dr. Harris, a diplomate of the American Board of Obesity Medicine, is in private practice and adult and geriatric psychiatry in Hartford, Conn. She also works as a psychiatric consultant to continuing care retirement organizations and professional groups. Dr. Harris, a former president of the Black Psychiatrists of America, is a Distinguished Fellow of the American Psychiatric Association. Besides psychotherapy, her major clinical interests include geriatrics, and the interface between general medicine and psychiatry.
References
1. U.S. Medicine, November 2009.
2. Science Daily, March 29, 2014.
3. Science Daily, Jan. 27, 2016.
4. Science Daily, Jan. 18, 2012.
5. “Diabetes Facts and Guidelines,” Yale Diabetes Center, 2011.
6. Ann Fam Med. 2012 Jan-Feb;10(1):15-22.
7. Diabetes Care. 2014;37(3):625-33.
8. Macworld, May 10, 2016.
9. Mol Psychiatry. 2016 Feb 23. doi: 10:1038/mp 2016.7.
10. Proc Natl Acad Sci USA. 2014 Mar 17;112(11):3463-8.

Over 20% of Americans skipped needed mental health care
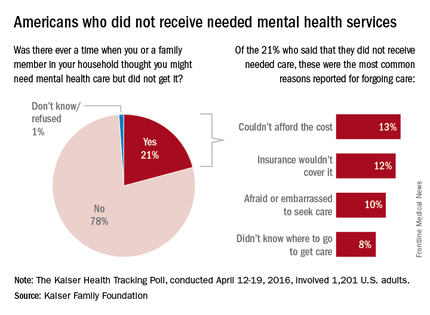
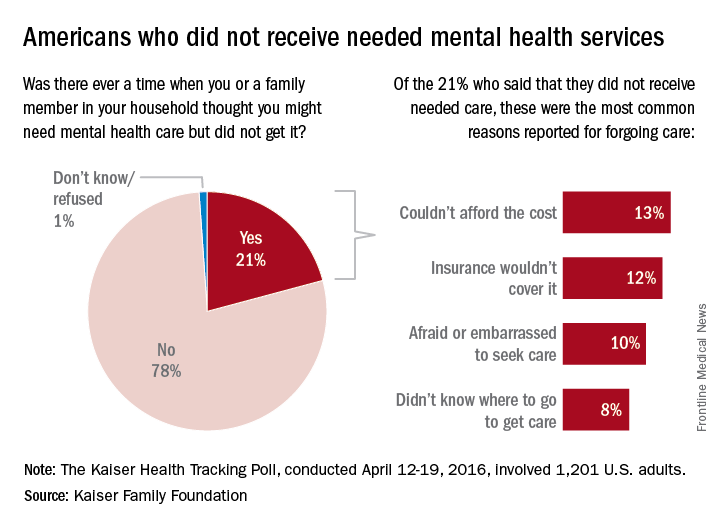
About one in five Americans report that there was a time when they or a family member in their household thought they needed mental health care but did not receive it for various reasons, according to a poll conducted by the Kaiser Family Foundation.
Among the 21% of Americans who did not get such care, the most common reason was “couldn’t afford the cost” (13%), which was closely followed by “insurance wouldn’t cover it” at 12%. “Afraid or embarrassed to seek care” was cited by 10% of those who had forgone mental health care, and 8% said that the reason was “didn’t know where to go to get care,” the Kaiser report said.
The Kaiser Health Tracking Poll was conducted April 12-19, 2016, among a nationally representative sample of 1,201 adults aged 18 years and older.
About one in five Americans report that there was a time when they or a family member in their household thought they needed mental health care but did not receive it for various reasons, according to a poll conducted by the Kaiser Family Foundation.
Among the 21% of Americans who did not get such care, the most common reason was “couldn’t afford the cost” (13%), which was closely followed by “insurance wouldn’t cover it” at 12%. “Afraid or embarrassed to seek care” was cited by 10% of those who had forgone mental health care, and 8% said that the reason was “didn’t know where to go to get care,” the Kaiser report said.
The Kaiser Health Tracking Poll was conducted April 12-19, 2016, among a nationally representative sample of 1,201 adults aged 18 years and older.
About one in five Americans report that there was a time when they or a family member in their household thought they needed mental health care but did not receive it for various reasons, according to a poll conducted by the Kaiser Family Foundation.
Among the 21% of Americans who did not get such care, the most common reason was “couldn’t afford the cost” (13%), which was closely followed by “insurance wouldn’t cover it” at 12%. “Afraid or embarrassed to seek care” was cited by 10% of those who had forgone mental health care, and 8% said that the reason was “didn’t know where to go to get care,” the Kaiser report said.
The Kaiser Health Tracking Poll was conducted April 12-19, 2016, among a nationally representative sample of 1,201 adults aged 18 years and older.
A new sort of consultant: Advising doctors, patients on California’s aid-in-dying law
BERKELEY, Calif. – Few people have the unusual set of professional experiences that Dr. Lonny Shavelson does. He worked as an emergency room physician in Berkeley for years – while also working as a journalist. He has written several books and takes hauntingly beautiful photographs.
Now, just as California’s aid-in-dying law takes effect June 9, Dr. Shavelson has added another specialty: A consultant to physicians and terminally ill patients who have questions about how it works.
“Can I just sit back and watch?” Dr. Shavelson asked from his cottage office. “This is really an amazing opportunity to be part of establishing policy and initiating something in medicine. This is a major change … [that] very, very few people know anything about and how to do it.”
Dr. Shavelson is the author of the 1995 book, “A Chosen Death,” which followed five terminally ill people over 2 years as they determined whether to amass drugs on their own and end their lives at a time of their choosing. He was present at the death of all of them.

He followed the issue closely for several years, but ultimately moved on to other projects – among them a book about addiction and a documentary about people who identify as neither male nor female.
Then last fall came the surprising passage of California’s End of Life Option Act, giving terminally ill adults with 6 months to live the right to request lethal medication to end their lives. The law takes effect June 9.
Dr. Shavelson decided he had to act, adding that he feels “quite guilty” about having been away from the issue while others pushed it forward.
His website, Bay Area End of Life Options, went up in April, and he’s outlined the law at “grand rounds” at several Bay Area hospitals this spring. His practice will be focused on consulting not only with physicians whose patients request aid-in-dying, but also with patients themselves. As he indicates on his site, he will offer care to patients who choose him as their “attending End-of-Life physician.”
Dr. Shavelson is adamant that this is “something that has to be done right.” To him, that means starting every patient encounter with a one-word question: “Why?”
“In fact, it’s the only initial approach that I think is acceptable. If somebody calls me and says, ‘I want to take the medication, my first question is, ‘Why? Let me talk to you about all the various alternatives and all the ways that we can think about this.’ ”
Dr. Shavelson worries that patients may seek aid-in-dying because they are in pain. So first, he would like all his patients to be enrolled in hospice care.
“This can only work when you’re sure that the patients have been given the best end-of-life care, which to me is most guaranteed by being a part of hospice or at least having a good palliative care physician. Then this is a rational decision. If you’re doing it otherwise, it’s because of lack of good care.”
California is the fifth state to legalize aid-in-dying, joining Oregon, Washington, Vermont, and Montana. The option is very rarely used. For example, in 2014 in Oregon, just 155 lethal prescriptions were written under the state’s law, and 105 people ultimately took the medicine and died.
Under the California law, two doctors must agree that a patient has 6 months or less to live. The patient must be mentally competent. At least one of the meetings between the patient and his or her doctor must be private, with no one else present, to ensure the patient is acting independently.
Patients must be able to swallow the medication themselves and must affirm in writing, within the 48 hours before taking the medication, that they will do so.
Dr. Shavelson says he has been surprised by the poor understanding of the law among some health care providers. One insisted the law was not taking effect this year; another asked how the law would benefit his patients with Alzheimer’s disease. (Patients with dementia don’t qualify under the law because they are not mentally competent.)
The law does not require that health care providers participate in ending terminally ill patients’ lives. Many physicians are “queasy” about the law, Dr. Shavelson said, and are unwilling to prescribe to patients who request the lethal medication – even when they think having such a law in place is the right thing to do.
“My response to that is as health care providers, you might have been uncomfortable the first time you drew blood. You might have been uncomfortable the first time you took out somebody’s gall bladder,” he said. “If it’s a medical procedure you believe in and you believe it’s the patient’s right, then it’s your obligation to learn how to do it – and do it correctly.”
Dr. Shavelson predicts that many physicians who are initially reluctant to provide this option to their patients may become more comfortable after the law goes into effect and they see how it works.
Dr. Burt Presberg, an East Bay psychiatrist who works with cancer patients and their families, attended a talk by Dr. Shavelson, and it led to some soul searching.
He wrestles with his own comfort level in handling patient requests. When he talks, he often pivots from his initial point to “on the other hand.”
Dr. Presberg says he is concerned that patients suffer from clinical depression at the end of life. Sometimes they feel they are a burden to family members who could “really push for the end of life to happen a little sooner than the patient themselves.”
His experience is that terminally ill patients with clinical depression can be successfully treated. He said he believes Dr. Shavelson will be aware of the need to treat depression,”but I do have concerns about other physicians.”
“On the other hand,” he added, “I think it’s really good that this is an option.”
Dr. Shavelson says he’s already received a handful of calls from patients, but mostly he’s spent his time before the law takes effect talking to other physicians. He needs a consulting physician and a pharmacist who will accept prescriptions for a lethal dose of medicine.
Then his mind returns to the patient. “It’s important … that we’re moving forward,” he said. “It’s crucial that we do that because this is part of the rights of patient care to have a certain level of autonomy in how they die.”
To him, this type of care “isn’t so tangibly different” from other kinds of questions doctors address.
“I’m just one of those docs who sees dying as a process, and [the] method of death is less important than making sure it’s a good death.”
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation. This story is part of a partnership that includes KQED, NPR, and Kaiser Health News.
BERKELEY, Calif. – Few people have the unusual set of professional experiences that Dr. Lonny Shavelson does. He worked as an emergency room physician in Berkeley for years – while also working as a journalist. He has written several books and takes hauntingly beautiful photographs.
Now, just as California’s aid-in-dying law takes effect June 9, Dr. Shavelson has added another specialty: A consultant to physicians and terminally ill patients who have questions about how it works.
“Can I just sit back and watch?” Dr. Shavelson asked from his cottage office. “This is really an amazing opportunity to be part of establishing policy and initiating something in medicine. This is a major change … [that] very, very few people know anything about and how to do it.”
Dr. Shavelson is the author of the 1995 book, “A Chosen Death,” which followed five terminally ill people over 2 years as they determined whether to amass drugs on their own and end their lives at a time of their choosing. He was present at the death of all of them.
He followed the issue closely for several years, but ultimately moved on to other projects – among them a book about addiction and a documentary about people who identify as neither male nor female.
Then last fall came the surprising passage of California’s End of Life Option Act, giving terminally ill adults with 6 months to live the right to request lethal medication to end their lives. The law takes effect June 9.
Dr. Shavelson decided he had to act, adding that he feels “quite guilty” about having been away from the issue while others pushed it forward.
His website, Bay Area End of Life Options, went up in April, and he’s outlined the law at “grand rounds” at several Bay Area hospitals this spring. His practice will be focused on consulting not only with physicians whose patients request aid-in-dying, but also with patients themselves. As he indicates on his site, he will offer care to patients who choose him as their “attending End-of-Life physician.”
Dr. Shavelson is adamant that this is “something that has to be done right.” To him, that means starting every patient encounter with a one-word question: “Why?”
“In fact, it’s the only initial approach that I think is acceptable. If somebody calls me and says, ‘I want to take the medication, my first question is, ‘Why? Let me talk to you about all the various alternatives and all the ways that we can think about this.’ ”
Dr. Shavelson worries that patients may seek aid-in-dying because they are in pain. So first, he would like all his patients to be enrolled in hospice care.
“This can only work when you’re sure that the patients have been given the best end-of-life care, which to me is most guaranteed by being a part of hospice or at least having a good palliative care physician. Then this is a rational decision. If you’re doing it otherwise, it’s because of lack of good care.”
California is the fifth state to legalize aid-in-dying, joining Oregon, Washington, Vermont, and Montana. The option is very rarely used. For example, in 2014 in Oregon, just 155 lethal prescriptions were written under the state’s law, and 105 people ultimately took the medicine and died.
Under the California law, two doctors must agree that a patient has 6 months or less to live. The patient must be mentally competent. At least one of the meetings between the patient and his or her doctor must be private, with no one else present, to ensure the patient is acting independently.
Patients must be able to swallow the medication themselves and must affirm in writing, within the 48 hours before taking the medication, that they will do so.
Dr. Shavelson says he has been surprised by the poor understanding of the law among some health care providers. One insisted the law was not taking effect this year; another asked how the law would benefit his patients with Alzheimer’s disease. (Patients with dementia don’t qualify under the law because they are not mentally competent.)
The law does not require that health care providers participate in ending terminally ill patients’ lives. Many physicians are “queasy” about the law, Dr. Shavelson said, and are unwilling to prescribe to patients who request the lethal medication – even when they think having such a law in place is the right thing to do.
“My response to that is as health care providers, you might have been uncomfortable the first time you drew blood. You might have been uncomfortable the first time you took out somebody’s gall bladder,” he said. “If it’s a medical procedure you believe in and you believe it’s the patient’s right, then it’s your obligation to learn how to do it – and do it correctly.”
Dr. Shavelson predicts that many physicians who are initially reluctant to provide this option to their patients may become more comfortable after the law goes into effect and they see how it works.
Dr. Burt Presberg, an East Bay psychiatrist who works with cancer patients and their families, attended a talk by Dr. Shavelson, and it led to some soul searching.
He wrestles with his own comfort level in handling patient requests. When he talks, he often pivots from his initial point to “on the other hand.”
Dr. Presberg says he is concerned that patients suffer from clinical depression at the end of life. Sometimes they feel they are a burden to family members who could “really push for the end of life to happen a little sooner than the patient themselves.”
His experience is that terminally ill patients with clinical depression can be successfully treated. He said he believes Dr. Shavelson will be aware of the need to treat depression,”but I do have concerns about other physicians.”
“On the other hand,” he added, “I think it’s really good that this is an option.”
Dr. Shavelson says he’s already received a handful of calls from patients, but mostly he’s spent his time before the law takes effect talking to other physicians. He needs a consulting physician and a pharmacist who will accept prescriptions for a lethal dose of medicine.
Then his mind returns to the patient. “It’s important … that we’re moving forward,” he said. “It’s crucial that we do that because this is part of the rights of patient care to have a certain level of autonomy in how they die.”
To him, this type of care “isn’t so tangibly different” from other kinds of questions doctors address.
“I’m just one of those docs who sees dying as a process, and [the] method of death is less important than making sure it’s a good death.”
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation. This story is part of a partnership that includes KQED, NPR, and Kaiser Health News.
BERKELEY, Calif. – Few people have the unusual set of professional experiences that Dr. Lonny Shavelson does. He worked as an emergency room physician in Berkeley for years – while also working as a journalist. He has written several books and takes hauntingly beautiful photographs.
Now, just as California’s aid-in-dying law takes effect June 9, Dr. Shavelson has added another specialty: A consultant to physicians and terminally ill patients who have questions about how it works.
“Can I just sit back and watch?” Dr. Shavelson asked from his cottage office. “This is really an amazing opportunity to be part of establishing policy and initiating something in medicine. This is a major change … [that] very, very few people know anything about and how to do it.”
Dr. Shavelson is the author of the 1995 book, “A Chosen Death,” which followed five terminally ill people over 2 years as they determined whether to amass drugs on their own and end their lives at a time of their choosing. He was present at the death of all of them.
He followed the issue closely for several years, but ultimately moved on to other projects – among them a book about addiction and a documentary about people who identify as neither male nor female.
Then last fall came the surprising passage of California’s End of Life Option Act, giving terminally ill adults with 6 months to live the right to request lethal medication to end their lives. The law takes effect June 9.
Dr. Shavelson decided he had to act, adding that he feels “quite guilty” about having been away from the issue while others pushed it forward.
His website, Bay Area End of Life Options, went up in April, and he’s outlined the law at “grand rounds” at several Bay Area hospitals this spring. His practice will be focused on consulting not only with physicians whose patients request aid-in-dying, but also with patients themselves. As he indicates on his site, he will offer care to patients who choose him as their “attending End-of-Life physician.”
Dr. Shavelson is adamant that this is “something that has to be done right.” To him, that means starting every patient encounter with a one-word question: “Why?”
“In fact, it’s the only initial approach that I think is acceptable. If somebody calls me and says, ‘I want to take the medication, my first question is, ‘Why? Let me talk to you about all the various alternatives and all the ways that we can think about this.’ ”
Dr. Shavelson worries that patients may seek aid-in-dying because they are in pain. So first, he would like all his patients to be enrolled in hospice care.
“This can only work when you’re sure that the patients have been given the best end-of-life care, which to me is most guaranteed by being a part of hospice or at least having a good palliative care physician. Then this is a rational decision. If you’re doing it otherwise, it’s because of lack of good care.”
California is the fifth state to legalize aid-in-dying, joining Oregon, Washington, Vermont, and Montana. The option is very rarely used. For example, in 2014 in Oregon, just 155 lethal prescriptions were written under the state’s law, and 105 people ultimately took the medicine and died.
Under the California law, two doctors must agree that a patient has 6 months or less to live. The patient must be mentally competent. At least one of the meetings between the patient and his or her doctor must be private, with no one else present, to ensure the patient is acting independently.
Patients must be able to swallow the medication themselves and must affirm in writing, within the 48 hours before taking the medication, that they will do so.
Dr. Shavelson says he has been surprised by the poor understanding of the law among some health care providers. One insisted the law was not taking effect this year; another asked how the law would benefit his patients with Alzheimer’s disease. (Patients with dementia don’t qualify under the law because they are not mentally competent.)
The law does not require that health care providers participate in ending terminally ill patients’ lives. Many physicians are “queasy” about the law, Dr. Shavelson said, and are unwilling to prescribe to patients who request the lethal medication – even when they think having such a law in place is the right thing to do.
“My response to that is as health care providers, you might have been uncomfortable the first time you drew blood. You might have been uncomfortable the first time you took out somebody’s gall bladder,” he said. “If it’s a medical procedure you believe in and you believe it’s the patient’s right, then it’s your obligation to learn how to do it – and do it correctly.”
Dr. Shavelson predicts that many physicians who are initially reluctant to provide this option to their patients may become more comfortable after the law goes into effect and they see how it works.
Dr. Burt Presberg, an East Bay psychiatrist who works with cancer patients and their families, attended a talk by Dr. Shavelson, and it led to some soul searching.
He wrestles with his own comfort level in handling patient requests. When he talks, he often pivots from his initial point to “on the other hand.”
Dr. Presberg says he is concerned that patients suffer from clinical depression at the end of life. Sometimes they feel they are a burden to family members who could “really push for the end of life to happen a little sooner than the patient themselves.”
His experience is that terminally ill patients with clinical depression can be successfully treated. He said he believes Dr. Shavelson will be aware of the need to treat depression,”but I do have concerns about other physicians.”
“On the other hand,” he added, “I think it’s really good that this is an option.”
Dr. Shavelson says he’s already received a handful of calls from patients, but mostly he’s spent his time before the law takes effect talking to other physicians. He needs a consulting physician and a pharmacist who will accept prescriptions for a lethal dose of medicine.
Then his mind returns to the patient. “It’s important … that we’re moving forward,” he said. “It’s crucial that we do that because this is part of the rights of patient care to have a certain level of autonomy in how they die.”
To him, this type of care “isn’t so tangibly different” from other kinds of questions doctors address.
“I’m just one of those docs who sees dying as a process, and [the] method of death is less important than making sure it’s a good death.”
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation. This story is part of a partnership that includes KQED, NPR, and Kaiser Health News.

Mental health disorders the leading cause of disease burden for females
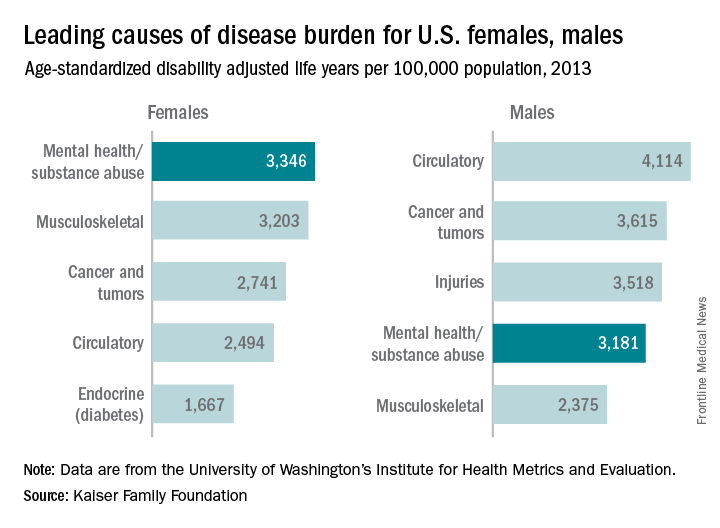
Mental health and substance abuse disorders are the leading cause of disease burden among U.S. females and the fourth-leading cause for males, according to the Kaiser Family Foundation.
Mental health/substance abuse conditions caused 3,346 age-standardized disability adjusted life years (DALYs) per 100,000 population for females in 2013, putting those conditions ahead of musculoskeletal conditions (3,203 DALYs per 100,000), cancer and tumors (2,741 DALYs), circulatory conditions (2,494 DALYs), and diabetes and other endocrine conditions (1,667 DALYs), Kaiser reported.
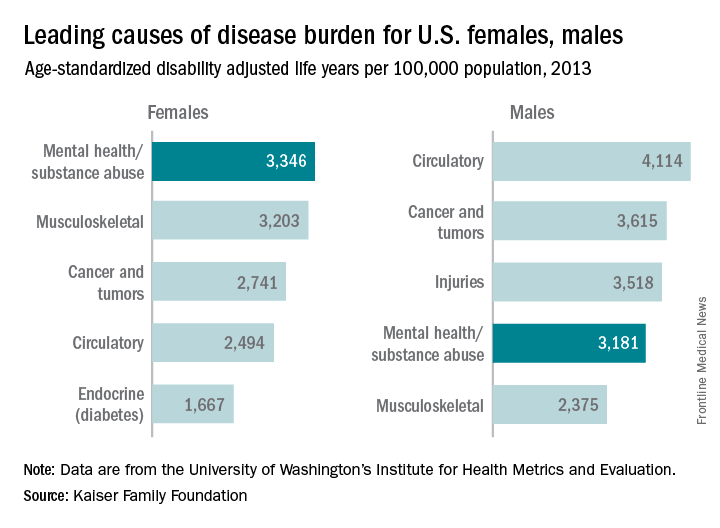
Among males, the disease burden resulting from mental health/substance abuse – 3,181 DALYs per 100,000 population – was less than that from circulatory conditions (4,114 DALYs per 100,000), cancer and tumors (3,615 DALYs), and injuries (3,518 DALYs). Musculoskeletal disorders were fifth at 2,375 DALYs, according to data from the Institute for Health Metrics and Evaluation’s Global Burden of Disease Study 2013.
The World Health Organization defines DALYs as “the sum of years of potential life lost due to premature mortality and the years of productive life lost due to disability.”
Mental health and substance abuse disorders are the leading cause of disease burden among U.S. females and the fourth-leading cause for males, according to the Kaiser Family Foundation.
Mental health/substance abuse conditions caused 3,346 age-standardized disability adjusted life years (DALYs) per 100,000 population for females in 2013, putting those conditions ahead of musculoskeletal conditions (3,203 DALYs per 100,000), cancer and tumors (2,741 DALYs), circulatory conditions (2,494 DALYs), and diabetes and other endocrine conditions (1,667 DALYs), Kaiser reported.
Among males, the disease burden resulting from mental health/substance abuse – 3,181 DALYs per 100,000 population – was less than that from circulatory conditions (4,114 DALYs per 100,000), cancer and tumors (3,615 DALYs), and injuries (3,518 DALYs). Musculoskeletal disorders were fifth at 2,375 DALYs, according to data from the Institute for Health Metrics and Evaluation’s Global Burden of Disease Study 2013.
The World Health Organization defines DALYs as “the sum of years of potential life lost due to premature mortality and the years of productive life lost due to disability.”
Mental health and substance abuse disorders are the leading cause of disease burden among U.S. females and the fourth-leading cause for males, according to the Kaiser Family Foundation.
Mental health/substance abuse conditions caused 3,346 age-standardized disability adjusted life years (DALYs) per 100,000 population for females in 2013, putting those conditions ahead of musculoskeletal conditions (3,203 DALYs per 100,000), cancer and tumors (2,741 DALYs), circulatory conditions (2,494 DALYs), and diabetes and other endocrine conditions (1,667 DALYs), Kaiser reported.
Among males, the disease burden resulting from mental health/substance abuse – 3,181 DALYs per 100,000 population – was less than that from circulatory conditions (4,114 DALYs per 100,000), cancer and tumors (3,615 DALYs), and injuries (3,518 DALYs). Musculoskeletal disorders were fifth at 2,375 DALYs, according to data from the Institute for Health Metrics and Evaluation’s Global Burden of Disease Study 2013.
The World Health Organization defines DALYs as “the sum of years of potential life lost due to premature mortality and the years of productive life lost due to disability.”
Bumps on arms

The FP diagnosed molluscum contagiosum because a few of the papules had central umbilication. While she noticed that many papules did not have central umbilication, she was aware that not all molluscum lesions would have this feature. Pearly papules are classic for molluscum, even when central umbilication is not visible.
Children with atopic dermatitis are more prone to molluscum infections and frequently get them in areas that have been, or presently are, involved with atopic dermatitis. In this case, the child had antecubital involvement with her atopic dermatitis (although her skin was relatively normal at the time). The altered barrier function found in atopic individuals makes them more prone to various viral and bacterial super infections, including molluscum, herpes, and bacterial impetigo.
In immunocompetent patients, lesions usually spontaneously resolve within 8 to 12 months. In a minority of cases, disease persists for a few years. Children do not have to be kept out of day care or school for this condition, even though it is somewhat contagious. Like warts, keeping kids out of school or day care is not useful to prevent the spread of disease and is not practical on a societal level.
The FP discussed cryotherapy with the mother and child, but the girl was not willing to allow it due to her fear of the pain. Other options included watch and wait, topical salicylic acid, tretinoin, and imiquimod—although none of these have been approved by the Food and Drug Administration. Cantharidin had also been used previously in this office, but it was not available because regulations have made it very difficult to obtain. Imiquimod is not suggested for children younger than 12; therefore, this costly medicine would not be covered by insurance.
The mother requested a prescription for tretinoin and stated that if the insurance would not cover it, she would go with over-the-counter salicylic acid. The FP wrote a prescription for 0.025% tretinoin cream to be applied daily and said to stop using it if irritation became too bothersome. Follow-up was to be done as needed, but was not completed.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux, EJ. Molluscum contagiosum. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:743-748.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP diagnosed molluscum contagiosum because a few of the papules had central umbilication. While she noticed that many papules did not have central umbilication, she was aware that not all molluscum lesions would have this feature. Pearly papules are classic for molluscum, even when central umbilication is not visible.
Children with atopic dermatitis are more prone to molluscum infections and frequently get them in areas that have been, or presently are, involved with atopic dermatitis. In this case, the child had antecubital involvement with her atopic dermatitis (although her skin was relatively normal at the time). The altered barrier function found in atopic individuals makes them more prone to various viral and bacterial super infections, including molluscum, herpes, and bacterial impetigo.
In immunocompetent patients, lesions usually spontaneously resolve within 8 to 12 months. In a minority of cases, disease persists for a few years. Children do not have to be kept out of day care or school for this condition, even though it is somewhat contagious. Like warts, keeping kids out of school or day care is not useful to prevent the spread of disease and is not practical on a societal level.
The FP discussed cryotherapy with the mother and child, but the girl was not willing to allow it due to her fear of the pain. Other options included watch and wait, topical salicylic acid, tretinoin, and imiquimod—although none of these have been approved by the Food and Drug Administration. Cantharidin had also been used previously in this office, but it was not available because regulations have made it very difficult to obtain. Imiquimod is not suggested for children younger than 12; therefore, this costly medicine would not be covered by insurance.
The mother requested a prescription for tretinoin and stated that if the insurance would not cover it, she would go with over-the-counter salicylic acid. The FP wrote a prescription for 0.025% tretinoin cream to be applied daily and said to stop using it if irritation became too bothersome. Follow-up was to be done as needed, but was not completed.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux, EJ. Molluscum contagiosum. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:743-748.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP diagnosed molluscum contagiosum because a few of the papules had central umbilication. While she noticed that many papules did not have central umbilication, she was aware that not all molluscum lesions would have this feature. Pearly papules are classic for molluscum, even when central umbilication is not visible.
Children with atopic dermatitis are more prone to molluscum infections and frequently get them in areas that have been, or presently are, involved with atopic dermatitis. In this case, the child had antecubital involvement with her atopic dermatitis (although her skin was relatively normal at the time). The altered barrier function found in atopic individuals makes them more prone to various viral and bacterial super infections, including molluscum, herpes, and bacterial impetigo.
In immunocompetent patients, lesions usually spontaneously resolve within 8 to 12 months. In a minority of cases, disease persists for a few years. Children do not have to be kept out of day care or school for this condition, even though it is somewhat contagious. Like warts, keeping kids out of school or day care is not useful to prevent the spread of disease and is not practical on a societal level.
The FP discussed cryotherapy with the mother and child, but the girl was not willing to allow it due to her fear of the pain. Other options included watch and wait, topical salicylic acid, tretinoin, and imiquimod—although none of these have been approved by the Food and Drug Administration. Cantharidin had also been used previously in this office, but it was not available because regulations have made it very difficult to obtain. Imiquimod is not suggested for children younger than 12; therefore, this costly medicine would not be covered by insurance.
The mother requested a prescription for tretinoin and stated that if the insurance would not cover it, she would go with over-the-counter salicylic acid. The FP wrote a prescription for 0.025% tretinoin cream to be applied daily and said to stop using it if irritation became too bothersome. Follow-up was to be done as needed, but was not completed.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux, EJ. Molluscum contagiosum. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:743-748.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

VIDEO: The ins and outs of JAK ihibitors for alopecia
NEWPORT BEACH, CALIF. – The promise of Janus kinase (JAK) inhibitors for alopecia seems to be holding up in the practice of Dr. Natasha Mesinkovska, a dermatologist at the University of California, Irvine.
There’s been much excitement about JAK inhibitors since Yale researchers reported in 2014 that tofacitinib (Xeljanz), a JAK inhibitor approved in the United States for rheumatoid arthritis, appeared to grow a full head of hair, plus body hair, in an essentially hairless 25-year-old man with plaque psoriasis. JAK inhibitors have been under investigation for alopecia ever since. Meanwhile, they are being used off label for hair loss around the country.
In her own practice, Dr. Mesinkovska estimates that about two-thirds of patients have some degree of hair regrowth, with particularly satisfying results in men. About 40 of her alopecia patients have opted for JAK inhibitors so far.
In an interview at the Summit in Aesthetic Medicine, Dr. Mesinkovska shared her insights and tips, as well as promising alopecia results for the psoriasis biologic ustekinumab (Stelara), an interleukin-12 and -23 antagonist. “This is a very exciting time for alopecia areata,” she said.
The Summit in Aesthetic Medicine is held by the Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NEWPORT BEACH, CALIF. – The promise of Janus kinase (JAK) inhibitors for alopecia seems to be holding up in the practice of Dr. Natasha Mesinkovska, a dermatologist at the University of California, Irvine.
There’s been much excitement about JAK inhibitors since Yale researchers reported in 2014 that tofacitinib (Xeljanz), a JAK inhibitor approved in the United States for rheumatoid arthritis, appeared to grow a full head of hair, plus body hair, in an essentially hairless 25-year-old man with plaque psoriasis. JAK inhibitors have been under investigation for alopecia ever since. Meanwhile, they are being used off label for hair loss around the country.
In her own practice, Dr. Mesinkovska estimates that about two-thirds of patients have some degree of hair regrowth, with particularly satisfying results in men. About 40 of her alopecia patients have opted for JAK inhibitors so far.
In an interview at the Summit in Aesthetic Medicine, Dr. Mesinkovska shared her insights and tips, as well as promising alopecia results for the psoriasis biologic ustekinumab (Stelara), an interleukin-12 and -23 antagonist. “This is a very exciting time for alopecia areata,” she said.
The Summit in Aesthetic Medicine is held by the Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NEWPORT BEACH, CALIF. – The promise of Janus kinase (JAK) inhibitors for alopecia seems to be holding up in the practice of Dr. Natasha Mesinkovska, a dermatologist at the University of California, Irvine.
There’s been much excitement about JAK inhibitors since Yale researchers reported in 2014 that tofacitinib (Xeljanz), a JAK inhibitor approved in the United States for rheumatoid arthritis, appeared to grow a full head of hair, plus body hair, in an essentially hairless 25-year-old man with plaque psoriasis. JAK inhibitors have been under investigation for alopecia ever since. Meanwhile, they are being used off label for hair loss around the country.
In her own practice, Dr. Mesinkovska estimates that about two-thirds of patients have some degree of hair regrowth, with particularly satisfying results in men. About 40 of her alopecia patients have opted for JAK inhibitors so far.
In an interview at the Summit in Aesthetic Medicine, Dr. Mesinkovska shared her insights and tips, as well as promising alopecia results for the psoriasis biologic ustekinumab (Stelara), an interleukin-12 and -23 antagonist. “This is a very exciting time for alopecia areata,” she said.
The Summit in Aesthetic Medicine is held by the Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM THE SUMMIT IN AESTHETIC MEDICINE

Adding calcipotriene to 5-FU dramatically reduced AKs
SCOTTSDALE, ARIZ. – A four-day topical combination regimen of 5-fluorouracil (5-FU) and calcipotriene removed almost 90% of facial actinic keratoses – significantly more than with 5-FU monotherapy, in a randomized, double-blind controlled study.
Calcipotriene (Dovonex) is a synthetic vitamin D3 derivative approved by the Food and Drug Association for treatment of scalp psoriasis. But calcipotriene is also an immunomodulator that induces thymic stromal lymphopoietin (TSLP), which suppresses the growth of early stage skin cancers, said Dr. Shawn Demehri, of Harvard Medical School, Boston.

To determine whether short-term TSLP induction could reduce AKs, he and his coinvestigators randomly assigned 131 men and women who were at least 50 years old and who had at least four AKs on the face, scalp, and/or upper arms to apply 5% 5-FU cream mixed with either 0.005% calcipotriene or Vaseline to affected areas twice daily for four days. The researchers counted and photographed the AKs at baseline and at subsequent follow-up visits.
The average age of the patients was 70 years, and 82% were men, said Dr. Demehri, who reported the results at the annual meeting of the Society for Investigative Dermatology. The combination of 5-FU and calcipotriene was associated with an 86% reduction in the number of facial AKs, compared with a 26% reduction among patients who used 5-FU monotherapy (P less than .0001).
The investigators observed equally dramatic differences in efficacy at other body sites. On the scalp, combination therapy reduced the number of AKs by 76%, while 5-FU alone reduced the number by only 6%. On the right upper arm, the dual regimen removed 70% of AKs compared with 10% for monotherapy, and on the left upper arm, combination treatment removed 80% of AKs, while 5-FU alone removed only 16% (all P values for these differences were less than .0001).
Notably, patients did not experience pain or crusting after using the combination cream, said Dr. Demehri, who is also a principal investigator in the department of dermatology and MGH Cancer Center, Massachusetts General Hospital, Boston. The combination of 5-FU and 0.005% calcipotriene “acts as a potent topical immunotherapeutic agent against actinic keratosis,” he concluded.
Dr. Demehri had no disclosures.
SCOTTSDALE, ARIZ. – A four-day topical combination regimen of 5-fluorouracil (5-FU) and calcipotriene removed almost 90% of facial actinic keratoses – significantly more than with 5-FU monotherapy, in a randomized, double-blind controlled study.
Calcipotriene (Dovonex) is a synthetic vitamin D3 derivative approved by the Food and Drug Association for treatment of scalp psoriasis. But calcipotriene is also an immunomodulator that induces thymic stromal lymphopoietin (TSLP), which suppresses the growth of early stage skin cancers, said Dr. Shawn Demehri, of Harvard Medical School, Boston.
To determine whether short-term TSLP induction could reduce AKs, he and his coinvestigators randomly assigned 131 men and women who were at least 50 years old and who had at least four AKs on the face, scalp, and/or upper arms to apply 5% 5-FU cream mixed with either 0.005% calcipotriene or Vaseline to affected areas twice daily for four days. The researchers counted and photographed the AKs at baseline and at subsequent follow-up visits.
The average age of the patients was 70 years, and 82% were men, said Dr. Demehri, who reported the results at the annual meeting of the Society for Investigative Dermatology. The combination of 5-FU and calcipotriene was associated with an 86% reduction in the number of facial AKs, compared with a 26% reduction among patients who used 5-FU monotherapy (P less than .0001).
The investigators observed equally dramatic differences in efficacy at other body sites. On the scalp, combination therapy reduced the number of AKs by 76%, while 5-FU alone reduced the number by only 6%. On the right upper arm, the dual regimen removed 70% of AKs compared with 10% for monotherapy, and on the left upper arm, combination treatment removed 80% of AKs, while 5-FU alone removed only 16% (all P values for these differences were less than .0001).
Notably, patients did not experience pain or crusting after using the combination cream, said Dr. Demehri, who is also a principal investigator in the department of dermatology and MGH Cancer Center, Massachusetts General Hospital, Boston. The combination of 5-FU and 0.005% calcipotriene “acts as a potent topical immunotherapeutic agent against actinic keratosis,” he concluded.
Dr. Demehri had no disclosures.
SCOTTSDALE, ARIZ. – A four-day topical combination regimen of 5-fluorouracil (5-FU) and calcipotriene removed almost 90% of facial actinic keratoses – significantly more than with 5-FU monotherapy, in a randomized, double-blind controlled study.
Calcipotriene (Dovonex) is a synthetic vitamin D3 derivative approved by the Food and Drug Association for treatment of scalp psoriasis. But calcipotriene is also an immunomodulator that induces thymic stromal lymphopoietin (TSLP), which suppresses the growth of early stage skin cancers, said Dr. Shawn Demehri, of Harvard Medical School, Boston.
To determine whether short-term TSLP induction could reduce AKs, he and his coinvestigators randomly assigned 131 men and women who were at least 50 years old and who had at least four AKs on the face, scalp, and/or upper arms to apply 5% 5-FU cream mixed with either 0.005% calcipotriene or Vaseline to affected areas twice daily for four days. The researchers counted and photographed the AKs at baseline and at subsequent follow-up visits.
The average age of the patients was 70 years, and 82% were men, said Dr. Demehri, who reported the results at the annual meeting of the Society for Investigative Dermatology. The combination of 5-FU and calcipotriene was associated with an 86% reduction in the number of facial AKs, compared with a 26% reduction among patients who used 5-FU monotherapy (P less than .0001).
The investigators observed equally dramatic differences in efficacy at other body sites. On the scalp, combination therapy reduced the number of AKs by 76%, while 5-FU alone reduced the number by only 6%. On the right upper arm, the dual regimen removed 70% of AKs compared with 10% for monotherapy, and on the left upper arm, combination treatment removed 80% of AKs, while 5-FU alone removed only 16% (all P values for these differences were less than .0001).
Notably, patients did not experience pain or crusting after using the combination cream, said Dr. Demehri, who is also a principal investigator in the department of dermatology and MGH Cancer Center, Massachusetts General Hospital, Boston. The combination of 5-FU and 0.005% calcipotriene “acts as a potent topical immunotherapeutic agent against actinic keratosis,” he concluded.
Dr. Demehri had no disclosures.
AT THE 2016 SID ANNUAL MEETING
Key clinical point: A combination of 5% 5-fluorouracil cream and 0.005% calcipotriene was significantly more effective at removing actinic keratoses at different anatomic sites as 5-FU monotherapy.
Major finding: At week 8, the combination group had an average 86% reduction in the number of facial AKs, compared with 26% with 5-FU monotherapy.
Data source: A randomized, double-blind, controlled study of 131 patients with at least four AKs on the face, scalp, and/or upper arms.
Disclosures: Dr. Demehri had no disclosures.

Nighttime extubations carry higher risks of reintubation, death
SAN FRANCISCO – Mechanically ventilated patients in the intensive care unit (ICU) have poorer outcomes if extubated during the night instead of during the day, finds a retrospective cohort study reported at an international conference of the American Thoracic Society.
Overall, 20.1% of the nearly 98,000 adult patients studied were extubated during nighttime hours, between 7:00 p.m. and 7:00 a.m., according to data presented in a session and a related press conference.

Compared with patients extubated during daytime hours, patients extubated during nighttime hours had higher rates of ICU and hospital death, with the absolute difference ranging from 1.0% to 5.1%. Additionally, among those mechanically ventilated for at least 12 hours, nighttime extubation was associated with an absolute 2% increase in the risk of reintubation.
“I think this is the first large-scale study that looks at a practice that, although not as common as we thought it was, is still done about a fifth of the time and even with decreasing rates, is not a rare practice on our units,” commented lead author Dr. Hayley B. Gershengorn of the department of medicine (critical care) and the Saul R. Korey department of neurology at the Albert Einstein College of Medicine, New York.
“As we have increasing staffing [overnight] and maybe an increasing push to move people through our ICUs, we need to probably take some care because although we can’t demonstrate a causal link, it is quite concerning, this consistent finding of increased mortality and reintubation in these folks,” she said.
There are several possible reasons for the observed heightened risks of death and reintubation with nighttime extubation that could not be fully explored in the study, Dr. Gershengorn said.
“We were not able to identify the indication for extubation or discontinuation of mechanical ventilation. So one of the concerns that we have is that it’s probably more common that folks unintentionally extubate themselves or someone unintentionally extubates them overnight, when staffing is less,” she explained. “The other part, which we tried to adjust for but we don’t have perfect data on, is what is the staffing overnight,” including factors such as the ratio of nurses to patients and how many units an intensivist is covering, not just whether he or she is present.
“In terms of the reintubation risk being higher in the [group with longer duration of mechanical ventilation], the question I have is whether or not there is less comfort with somebody looking less well when there is less staff around, and whether or not there may be a quicker trigger to reintubate them if they don’t look so great,” she said.
The majority of intubated patients are unlikely to improve enough physiologically to prompt nighttime extubation rather than waiting until daytime, according to Dr. Gershengorn. But there are at least two groups whom clinicians might want to extubate at night.
One group is those who underwent elective surgery during the day. “They are waiting to come out of anesthesia, and the plan is to discontinue mechanical ventilation at the time that that occurs,” she explained. Another group is those who are agitated on the ventilator, require more sedation than usual, and suddenly awake at night. “These patients are really hard to keep comfortable. I can [sedate them] again and try this problem all over again tomorrow morning, or I can just bite the bullet and pull the tube out,” she said.
The investigators analyzed data from the Project IMPACT critical care medicine database, in which data are prospectively collected for benchmarking purposes. In all, they studied 97,844 mechanically ventilated adults from 165 medical and surgical ICUs across the United States between 2000 and 2009.
Results showed that nighttime extubation was more common among elective surgical patients, those coming from the operating room or a postanesthesia care unit, and those mechanically ventilated for less than 12 hours.
In a finding that Dr. Gershengorn described as surprising, there was a temporal trend by which the adjusted proportion of extubations performed at night actually decreased in more recent years during the study period.
The investigators next looked at outcomes among 10,279 propensity-matched pairs of patients, one member of the pair having been extubated during the night and the other having been extubated during the day.
Among those mechanically ventilated for less than 12 hours, nighttime extubation was associated with higher ICU mortality (5.6% vs. 4.6%; P = .025) and hospital mortality (8.3% vs. 7.0%; P = .014). Findings were inconsistent for length of stay, with nighttime extubation associated with a shorter ICU stay but a longer hospital stay.
Among patients mechanically ventilated for 12 hours or longer, those extubated during the night had a higher rate of reintubation (14.6% vs. 12.4%; P less than .001), as well as higher ICU mortality (11.2% vs. 6.1%; P less than .001) and hospital mortality (16.0% vs. 11.1%; P less than .001). Lengths of stay did not differ by extubation time of day in this group.
In sensitivity analyses, findings were similar when the definition of nighttime extubation was altered to the hours of midnight to 5 a.m. and when analyses were restricted to nonpalliative patients, according to Dr. Gershengorn, who disclosed that she had no relevant conflicts of interest.
SAN FRANCISCO – Mechanically ventilated patients in the intensive care unit (ICU) have poorer outcomes if extubated during the night instead of during the day, finds a retrospective cohort study reported at an international conference of the American Thoracic Society.
Overall, 20.1% of the nearly 98,000 adult patients studied were extubated during nighttime hours, between 7:00 p.m. and 7:00 a.m., according to data presented in a session and a related press conference.
Compared with patients extubated during daytime hours, patients extubated during nighttime hours had higher rates of ICU and hospital death, with the absolute difference ranging from 1.0% to 5.1%. Additionally, among those mechanically ventilated for at least 12 hours, nighttime extubation was associated with an absolute 2% increase in the risk of reintubation.
“I think this is the first large-scale study that looks at a practice that, although not as common as we thought it was, is still done about a fifth of the time and even with decreasing rates, is not a rare practice on our units,” commented lead author Dr. Hayley B. Gershengorn of the department of medicine (critical care) and the Saul R. Korey department of neurology at the Albert Einstein College of Medicine, New York.
“As we have increasing staffing [overnight] and maybe an increasing push to move people through our ICUs, we need to probably take some care because although we can’t demonstrate a causal link, it is quite concerning, this consistent finding of increased mortality and reintubation in these folks,” she said.
There are several possible reasons for the observed heightened risks of death and reintubation with nighttime extubation that could not be fully explored in the study, Dr. Gershengorn said.
“We were not able to identify the indication for extubation or discontinuation of mechanical ventilation. So one of the concerns that we have is that it’s probably more common that folks unintentionally extubate themselves or someone unintentionally extubates them overnight, when staffing is less,” she explained. “The other part, which we tried to adjust for but we don’t have perfect data on, is what is the staffing overnight,” including factors such as the ratio of nurses to patients and how many units an intensivist is covering, not just whether he or she is present.
“In terms of the reintubation risk being higher in the [group with longer duration of mechanical ventilation], the question I have is whether or not there is less comfort with somebody looking less well when there is less staff around, and whether or not there may be a quicker trigger to reintubate them if they don’t look so great,” she said.
The majority of intubated patients are unlikely to improve enough physiologically to prompt nighttime extubation rather than waiting until daytime, according to Dr. Gershengorn. But there are at least two groups whom clinicians might want to extubate at night.
One group is those who underwent elective surgery during the day. “They are waiting to come out of anesthesia, and the plan is to discontinue mechanical ventilation at the time that that occurs,” she explained. Another group is those who are agitated on the ventilator, require more sedation than usual, and suddenly awake at night. “These patients are really hard to keep comfortable. I can [sedate them] again and try this problem all over again tomorrow morning, or I can just bite the bullet and pull the tube out,” she said.
The investigators analyzed data from the Project IMPACT critical care medicine database, in which data are prospectively collected for benchmarking purposes. In all, they studied 97,844 mechanically ventilated adults from 165 medical and surgical ICUs across the United States between 2000 and 2009.
Results showed that nighttime extubation was more common among elective surgical patients, those coming from the operating room or a postanesthesia care unit, and those mechanically ventilated for less than 12 hours.
In a finding that Dr. Gershengorn described as surprising, there was a temporal trend by which the adjusted proportion of extubations performed at night actually decreased in more recent years during the study period.
The investigators next looked at outcomes among 10,279 propensity-matched pairs of patients, one member of the pair having been extubated during the night and the other having been extubated during the day.
Among those mechanically ventilated for less than 12 hours, nighttime extubation was associated with higher ICU mortality (5.6% vs. 4.6%; P = .025) and hospital mortality (8.3% vs. 7.0%; P = .014). Findings were inconsistent for length of stay, with nighttime extubation associated with a shorter ICU stay but a longer hospital stay.
Among patients mechanically ventilated for 12 hours or longer, those extubated during the night had a higher rate of reintubation (14.6% vs. 12.4%; P less than .001), as well as higher ICU mortality (11.2% vs. 6.1%; P less than .001) and hospital mortality (16.0% vs. 11.1%; P less than .001). Lengths of stay did not differ by extubation time of day in this group.
In sensitivity analyses, findings were similar when the definition of nighttime extubation was altered to the hours of midnight to 5 a.m. and when analyses were restricted to nonpalliative patients, according to Dr. Gershengorn, who disclosed that she had no relevant conflicts of interest.
SAN FRANCISCO – Mechanically ventilated patients in the intensive care unit (ICU) have poorer outcomes if extubated during the night instead of during the day, finds a retrospective cohort study reported at an international conference of the American Thoracic Society.
Overall, 20.1% of the nearly 98,000 adult patients studied were extubated during nighttime hours, between 7:00 p.m. and 7:00 a.m., according to data presented in a session and a related press conference.
Compared with patients extubated during daytime hours, patients extubated during nighttime hours had higher rates of ICU and hospital death, with the absolute difference ranging from 1.0% to 5.1%. Additionally, among those mechanically ventilated for at least 12 hours, nighttime extubation was associated with an absolute 2% increase in the risk of reintubation.
“I think this is the first large-scale study that looks at a practice that, although not as common as we thought it was, is still done about a fifth of the time and even with decreasing rates, is not a rare practice on our units,” commented lead author Dr. Hayley B. Gershengorn of the department of medicine (critical care) and the Saul R. Korey department of neurology at the Albert Einstein College of Medicine, New York.
“As we have increasing staffing [overnight] and maybe an increasing push to move people through our ICUs, we need to probably take some care because although we can’t demonstrate a causal link, it is quite concerning, this consistent finding of increased mortality and reintubation in these folks,” she said.
There are several possible reasons for the observed heightened risks of death and reintubation with nighttime extubation that could not be fully explored in the study, Dr. Gershengorn said.
“We were not able to identify the indication for extubation or discontinuation of mechanical ventilation. So one of the concerns that we have is that it’s probably more common that folks unintentionally extubate themselves or someone unintentionally extubates them overnight, when staffing is less,” she explained. “The other part, which we tried to adjust for but we don’t have perfect data on, is what is the staffing overnight,” including factors such as the ratio of nurses to patients and how many units an intensivist is covering, not just whether he or she is present.
“In terms of the reintubation risk being higher in the [group with longer duration of mechanical ventilation], the question I have is whether or not there is less comfort with somebody looking less well when there is less staff around, and whether or not there may be a quicker trigger to reintubate them if they don’t look so great,” she said.
The majority of intubated patients are unlikely to improve enough physiologically to prompt nighttime extubation rather than waiting until daytime, according to Dr. Gershengorn. But there are at least two groups whom clinicians might want to extubate at night.
One group is those who underwent elective surgery during the day. “They are waiting to come out of anesthesia, and the plan is to discontinue mechanical ventilation at the time that that occurs,” she explained. Another group is those who are agitated on the ventilator, require more sedation than usual, and suddenly awake at night. “These patients are really hard to keep comfortable. I can [sedate them] again and try this problem all over again tomorrow morning, or I can just bite the bullet and pull the tube out,” she said.
The investigators analyzed data from the Project IMPACT critical care medicine database, in which data are prospectively collected for benchmarking purposes. In all, they studied 97,844 mechanically ventilated adults from 165 medical and surgical ICUs across the United States between 2000 and 2009.
Results showed that nighttime extubation was more common among elective surgical patients, those coming from the operating room or a postanesthesia care unit, and those mechanically ventilated for less than 12 hours.
In a finding that Dr. Gershengorn described as surprising, there was a temporal trend by which the adjusted proportion of extubations performed at night actually decreased in more recent years during the study period.
The investigators next looked at outcomes among 10,279 propensity-matched pairs of patients, one member of the pair having been extubated during the night and the other having been extubated during the day.
Among those mechanically ventilated for less than 12 hours, nighttime extubation was associated with higher ICU mortality (5.6% vs. 4.6%; P = .025) and hospital mortality (8.3% vs. 7.0%; P = .014). Findings were inconsistent for length of stay, with nighttime extubation associated with a shorter ICU stay but a longer hospital stay.
Among patients mechanically ventilated for 12 hours or longer, those extubated during the night had a higher rate of reintubation (14.6% vs. 12.4%; P less than .001), as well as higher ICU mortality (11.2% vs. 6.1%; P less than .001) and hospital mortality (16.0% vs. 11.1%; P less than .001). Lengths of stay did not differ by extubation time of day in this group.
In sensitivity analyses, findings were similar when the definition of nighttime extubation was altered to the hours of midnight to 5 a.m. and when analyses were restricted to nonpalliative patients, according to Dr. Gershengorn, who disclosed that she had no relevant conflicts of interest.
AT ATS 2016
Key clinical point: Mechanically ventilated ICU patients have poorer outcomes if they are extubated during the night instead of during the day.
Major finding: Compared with patients extubated during daytime hours, patients extubated during nighttime hours had higher rates of ICU and hospital death, with the absolute difference ranging from 1.0% to 5.1%.
Data source: A retrospective cohort study of 97,844 mechanically ventilated adult patients from 165 ICUs in the United States.
Disclosures: Dr. Gershengorn disclosed that she had no relevant conflicts of interest.

50 years of gynecologic surgery: A large dose of ingenuity, a small dose of controversy
Over the past 50 years, there has been explosive change in gynecologic surgery. Ob.Gyn. News has been at the forefront of capturing and chronicling this paradigm shift in the treatment of the female patient.
Our beginnings
From antiquity, physicians and surgeons have struggled with pelvic prolapse, uterine fibroids, ovarian cysts, urinary incontinence, vesicovaginal fistulas, pelvic pain, and abnormal uterine bleeding. At the time of the first edition of Ob.Gyn. News, it had been less than a century since Thomas Edison invented the light bulb; just over 50 years since Hans Christian Jacobaeus first created air pneumoperitoneum using a trocar, followed by the Nitze cystoscope; about 40 years since Richard Zollikofer created a carbon dioxide pneumoperitoneum; 25 years since F.H. Powers and A.C. Barnes had first described laparoscopic tubal sterilization by cautery; and about 20 years since Raoul Palmer, considered the father of modern laparoscopy, had first described the technique – left upper quadrant entry, testing insufflation, Trendelenburg positioning, and simple laparoscopic instrumentation.

In the 1950s, Hans Frangenheim would bring monopolar electrosurgery to laparoscopy and Harold Hopkins would introduce fiber optics. It was not until 1967 that Patrick Steptoe would publish the first textbook on laparoscopy in the English language.
Although usage as a diagnostic tool and a method of sterilization increased popularity of laparoscopy in the 1960s and early 1970s, there were few advances. In fact, a review of early editions of Ob.Gyn. News during that time period shows that the majority of articles involving laparoscopy dealt with sterilization; including the introduction of clips for tubal sterilization by Jaroslav Hulka in 1972. This did not deter the efforts of Jordan Phillips, who along with Jacques Rioux, Louis Keith, Richard Soderstrom – four early laparoscopists – incorporated a new society, the American Association of Gynecologic Laparoscopists (the AAGL) in 1971.
Simultaneously, in 1979, James Daniell in the United States, Maurice Bruhart in France, and Yona Tadir in Israel were promoting efforts to couple the carbon dioxide laser to the laparoscope to treat pelvic adhesions and endometriosis. Later on, fiber lasers, KTP, Nd:YAG, and Argon lasers would be utilized in our field. Still, only a few extirpative procedures were being performed via a laparoscope route. This included linear salpingostomy for the treatment of ectopic pregnancy, championed by Professor Bruhart and H. Manhes in Europe, and Alan DeCherney in the United States.
During the 1980s, laparoscopic surgery was at its innovative best. Through the pioneering efforts of Professor Kurt Semm and his protégée, Liselotte Mettler, the gynecologic laparoscopist was introduced to endoloops, simple suturing techniques, and mechanical morcellation techniques.
Procedures such as salpingo-oophorectomy, appendectomy, and myomectomy could now be performed via the laparoscope. Dr. Camran Nezhat coupled the carbon dioxide laser, the laparoscope, and the television monitor, coining the term laparoscopy. Most importantly, the laparoscopic surgeon was liberated; he or she could remain upright and perform surgery with both hands. Through the 1980s and 1990s, Dr. Nezhat, Dr. Harry Reich, and other innovators pushed the envelope in increasing the ability to extirpate endometriosis, excise severe pelvic adhesions, and perform discoid and segmental bowel resection.
The day the earth stood still
Every gynecologic laparoscopic surgeon should remember Jan. 26, 1988, as that was the date that Dr. Harry Reich performed the first total laparoscopic hysterectomy. Now, little more than 25 years later, in many parts of the country, a laparoscopic approach to hysterectomy is indeed the most common route. Over the years, with the evolution of instrumentation, including new energy systems (ultrasonic, advanced bipolar) and the introduction of barbed sutures, hysterectomy can now be performed via minilaparoscopy, single-site laparoscopy, robot-assisted, and robotic single site, all of which have been featured in the Ob.Gyn. News’ Master Class in Gynecologic Surgery.
But hysteroscopy came first
Abulkasim utilized a mirror to reflect light into the vaginal vault in 1,000 A.D. In 1806, Philipp Bozzini originated the idea of illuminating body cavities by an external light source. Through a system of mirrors and tubes, candlelight could be reflected into the body. In 1869, D.C. Pantaleoni used a cystoscope developed by Antoine Desormeaux – who has been called the father of endoscopy – to treat endometrial polyps with silver nitrate.
Through the 50 years of Ob.Gyn. News and over the past 12 years of the Master Class in Gynecologic Surgery, our community has been consistently updated as to advances in hysteroscopy, not only to enhance treatment efficacy, but safety as well. This has included such advances as the continuous flow hysteroscope, the Hamou contact hysteroscope, and fluid management systems to enhance visualization.
In 1978, Robert Neuwirth introduced loops to perform hysteroscopic myomectomy. The loop resectoscope was quickly followed by the rollerball to perform endometrial ablation. In the late 1990s, hysteroscopic bipolar cutting loops were introduced. This enabled use of ionic distension media saline, instead of nonionic media, thus decreasing risks related to hyponatremia.
In 2003, Mark Emanuel introduced hysteroscopic morcellation systems, which enabled more gynecologists to perform operative hysteroscopy safely. Resected tissue is removed immediately to allow superior visualization. The flexible hysteroscope coupled with vaginoscopy has enabled hysteroscopy to be done with minimal to no anesthesia in an in-office setting.
With advances in hysteroscopy over the past 35 years, hysteroscopic procedures such as polypectomy, myomectomy, lysis of adhesions, transection of endometriosis, evacuation of retained products of conception, and endometrial ablation/resection have become routine.
And now, the controversy
Since its inception, laparoscopic surgery has not been without controversy. In 1933, Karl Fervers described explosion and flashes of light from a combination of high frequency electric current and oxygen distension gas while performing laparoscopic adhesiolysis with the coagulation probe of the ureterocystoscope.
In the early 1970s, Professor Kurt Semm’s pioneering effort was not rewarded by his department, in Kiel, Germany, which instead recommended he schedule a brain scan and psychological testing.
Nearly 20 years later, in a 1992 edition of Current Science, Professor Semm, along with Alan DeCherney, stated that “over 80% of gynecological operations can now be performed by laparoscopy.” Shortly thereafter, however, Dr. Roy Pitkin, who at the time was president of the American College of Obstetricians and Gynecologists, wrote an editorial in the Journal of Obstetrics and Gynecology – “Operative Laparoscopy: Surgical Advance or Technical Gimmick?” (Obstet Gynecol. 1992 Mar;79[3]:441-2).
Fortunately, 18 years later, with the continued advances in laparoscopic surgery making it less expensive, safer, and more accessible, Dr. Pitkin did retract his statement (Obstet Gynecol. 2010 May;115[5]:890-1).
Currently, the gynecologic community is embroiled in controversies involving the use of the robot to assist in the performance of laparoscopic surgery, the incorporation of synthetic mesh to enhance urogynecologic procedures, the placement of Essure micro-inserts to occlude fallopian tubes, and the use of electronic power morcellation at time of laparoscopic or robot-assisted hysterectomy, myomectomy, or sacrocolpopexy.
After reading the 2013 article by Dr. Jason Wright, published in JAMA, comparing laparoscopic hysterectomy to robotic hysterectomy, no one can deny that the rise in a minimally invasive route to hysterectomy has coincided with the advent of the robot (JAMA. 2013 Feb 20;309[7]:689-98). On the other hand, many detractors, including Dr. James Breeden (past ACOG president 2012-2013), find the higher cost of robotic surgery very problematic. In fact, many of these detractors cite the paucity of data showing a significant advantage to use of robotics.
While certainly cost, more than ever, must be a major consideration, remember that during the 1990s, there were multiple articles in Ob.Gyn. News raising concerns about the cost of laparoscopic hysterectomy. Interestingly, studies over the past decade by Warren and Jonsdottir show a cost savings when hysterectomy is done laparoscopically as opposed to its being done by laparotomy. Thus, it certainly can be anticipated that with more physician experience, improved instrumentation, and robotic industry competition, the overall cost will become more comparable to a laparoscopic route.
In 1995, Ulf Ulmsten first described the use of tension-free tape (TVT) to treat stress urinary incontinence. In 1998, the Food and Drug Administration approved the use of the TVT sling in the United States. Since then, transobturator tension-free vaginal tape (TVT-O) and single incision mini-slings have been introduced. All of these techniques have been shown to be successful and have been well adapted into the armamentarium of physicians treating stress urinary incontinence.
With the success of synthetic mesh for the treatment of stress urinary incontinence, its use was extended to pelvic prolapse. In 2002, the first mesh device with indications for the treatment of pelvic organ prolapse was approved by the FDA. While the erosion rate utilizing synthetic mesh for stress urinary incontinence has been noted to be 2%, rates up to 8.3% have been noted in patients treated for pelvic prolapse.
In 2008, the FDA issued a warning regarding the use of mesh for prolapse and incontinence repair secondary to the sequelae of mesh erosion. Subsequently, in 2011, the concern was limited to vaginal mesh to correct pelvic organ prolapse. Finally, on Jan. 4, 2016, the FDA issued an order to reclassify surgical mesh to repair pelvic organ prolapse from class II, which includes moderate-risk devices, to class III, which includes high-risk devices. Moreover, the FDA issued a second order to manufacturers to submit a premarket approval application to support the safety and effectiveness of synthetic mesh for transvaginal repair of pelvic organ prolapse.

Essure micro-inserts for permanent birth control received initial approval from the FDA in November 2002. Despite the fact that Essure can be easily placed, is highly effective, and has seemingly low complication rates, concerns have been raised by the Facebook group “Essure Problems” and Erin Brockovich, the focus of the 2000 biographical film starring Julia Roberts.
After more than 5,000 women filed grievances with the FDA between November 2002 and May 2015, based on unintended pregnancies, miscarriages, stillbirths, severe pain, and bleeding, the FDA announced in 2016 that it would require a boxed warning label for Essure. The FDA also called upon Bayer, which makes and markets Essure, to conduct surveillance to assess “risks of the device in a real-world environment.” The agency stated it will use the results to “determine what, if any, further actions related to Essure are needed to protect public health.”
While Jan. 26, 1988, is a very special date in minimally invasive gynecologic surgery, April 17, 2014, is a day of infamy for the gynecologic laparoscopist. For on this day, the FDA announced a warning regarding electronic power morcellation. Many hospitals and hospital systems throughout the country issued bans on electronic power morcellation, leading to needless open laparotomy procedures and thus, introducing prolonged recovery times and increased risk.
At a time when the recent introduction of barbed suture had made both closure of the vaginal cuff at time of hysterectomy and repair of the hysterotomy at myomectomy easier and faster, the gynecologic laparoscopist was taking a step backward. The FDA based this decision and a subsequent boxed warning – issued in November 2014 – on a small number of studies showing potential upstaging of leiomyosarcoma post electronic power morcellation. Interestingly, many of the morcellation procedures cited did not use power morcellation. Furthermore, a more comprehensive meta-analysis by Elizabeth A. Pritts and colleagues, showed a far lower risk than suggested by the FDA (Gynecol Surg. 2015;12[3]:165-77).
Recently, an article by William Parker and colleagues recommended that the FDA reverse its position (Obstet Gynecol. 2016 Jan;127[1]:18-22). Many believe that ultimately, the solution will be morcellation in a containment bag, which I and my colleagues have been performing in virtually every power morcellation procedure since May 2014. During this current power morcellation controversy, the Master Class in Gynecologic Surgery has continued to update its readers with three different articles related to the subject.
And in conclusion
Without a doubt, the past 50 years of gynecologic surgery has been a time of unparalleled innovation with occasional controversy thrown in. Ob.Gyn. News and more recently, the Master Class in Gynecologic Surgery, has had a major leadership role in bringing this profound ingenuity to the gynecology community by introducing this explosion of surgical creativity to its readers.
And what will the next 50 years bring? I believe we will continue to see tremendous advancements in minimally invasive gynecologic surgery. There will be a definite impact of costs on the marketplace. Thus, many of the minor minimally invasive procedures currently performed in the hospital or surgery center will be brought into office settings. In addition, secondary to reimbursement, the more complex cases will be carried out by fewer gynecologic surgeons who have undergone more intense training in pelvic surgery and who can perform these cases more efficiently and with fewer complications. Our ability to perform surgery and what type of procedures we do will not only be based on randomized, controlled trials, but big data collection as well.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, and past president of the AAGL and the International Society for Gynecologic Endoscopy (ISGE). He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/Society of Reproductive Surgery fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller is a consultant and is on the speakers bureau for Ethicon.
Over the past 50 years, there has been explosive change in gynecologic surgery. Ob.Gyn. News has been at the forefront of capturing and chronicling this paradigm shift in the treatment of the female patient.
Our beginnings
From antiquity, physicians and surgeons have struggled with pelvic prolapse, uterine fibroids, ovarian cysts, urinary incontinence, vesicovaginal fistulas, pelvic pain, and abnormal uterine bleeding. At the time of the first edition of Ob.Gyn. News, it had been less than a century since Thomas Edison invented the light bulb; just over 50 years since Hans Christian Jacobaeus first created air pneumoperitoneum using a trocar, followed by the Nitze cystoscope; about 40 years since Richard Zollikofer created a carbon dioxide pneumoperitoneum; 25 years since F.H. Powers and A.C. Barnes had first described laparoscopic tubal sterilization by cautery; and about 20 years since Raoul Palmer, considered the father of modern laparoscopy, had first described the technique – left upper quadrant entry, testing insufflation, Trendelenburg positioning, and simple laparoscopic instrumentation.
In the 1950s, Hans Frangenheim would bring monopolar electrosurgery to laparoscopy and Harold Hopkins would introduce fiber optics. It was not until 1967 that Patrick Steptoe would publish the first textbook on laparoscopy in the English language.
Although usage as a diagnostic tool and a method of sterilization increased popularity of laparoscopy in the 1960s and early 1970s, there were few advances. In fact, a review of early editions of Ob.Gyn. News during that time period shows that the majority of articles involving laparoscopy dealt with sterilization; including the introduction of clips for tubal sterilization by Jaroslav Hulka in 1972. This did not deter the efforts of Jordan Phillips, who along with Jacques Rioux, Louis Keith, Richard Soderstrom – four early laparoscopists – incorporated a new society, the American Association of Gynecologic Laparoscopists (the AAGL) in 1971.
Simultaneously, in 1979, James Daniell in the United States, Maurice Bruhart in France, and Yona Tadir in Israel were promoting efforts to couple the carbon dioxide laser to the laparoscope to treat pelvic adhesions and endometriosis. Later on, fiber lasers, KTP, Nd:YAG, and Argon lasers would be utilized in our field. Still, only a few extirpative procedures were being performed via a laparoscope route. This included linear salpingostomy for the treatment of ectopic pregnancy, championed by Professor Bruhart and H. Manhes in Europe, and Alan DeCherney in the United States.
During the 1980s, laparoscopic surgery was at its innovative best. Through the pioneering efforts of Professor Kurt Semm and his protégée, Liselotte Mettler, the gynecologic laparoscopist was introduced to endoloops, simple suturing techniques, and mechanical morcellation techniques.
Procedures such as salpingo-oophorectomy, appendectomy, and myomectomy could now be performed via the laparoscope. Dr. Camran Nezhat coupled the carbon dioxide laser, the laparoscope, and the television monitor, coining the term laparoscopy. Most importantly, the laparoscopic surgeon was liberated; he or she could remain upright and perform surgery with both hands. Through the 1980s and 1990s, Dr. Nezhat, Dr. Harry Reich, and other innovators pushed the envelope in increasing the ability to extirpate endometriosis, excise severe pelvic adhesions, and perform discoid and segmental bowel resection.
The day the earth stood still
Every gynecologic laparoscopic surgeon should remember Jan. 26, 1988, as that was the date that Dr. Harry Reich performed the first total laparoscopic hysterectomy. Now, little more than 25 years later, in many parts of the country, a laparoscopic approach to hysterectomy is indeed the most common route. Over the years, with the evolution of instrumentation, including new energy systems (ultrasonic, advanced bipolar) and the introduction of barbed sutures, hysterectomy can now be performed via minilaparoscopy, single-site laparoscopy, robot-assisted, and robotic single site, all of which have been featured in the Ob.Gyn. News’ Master Class in Gynecologic Surgery.
But hysteroscopy came first
Abulkasim utilized a mirror to reflect light into the vaginal vault in 1,000 A.D. In 1806, Philipp Bozzini originated the idea of illuminating body cavities by an external light source. Through a system of mirrors and tubes, candlelight could be reflected into the body. In 1869, D.C. Pantaleoni used a cystoscope developed by Antoine Desormeaux – who has been called the father of endoscopy – to treat endometrial polyps with silver nitrate.
Through the 50 years of Ob.Gyn. News and over the past 12 years of the Master Class in Gynecologic Surgery, our community has been consistently updated as to advances in hysteroscopy, not only to enhance treatment efficacy, but safety as well. This has included such advances as the continuous flow hysteroscope, the Hamou contact hysteroscope, and fluid management systems to enhance visualization.
In 1978, Robert Neuwirth introduced loops to perform hysteroscopic myomectomy. The loop resectoscope was quickly followed by the rollerball to perform endometrial ablation. In the late 1990s, hysteroscopic bipolar cutting loops were introduced. This enabled use of ionic distension media saline, instead of nonionic media, thus decreasing risks related to hyponatremia.
In 2003, Mark Emanuel introduced hysteroscopic morcellation systems, which enabled more gynecologists to perform operative hysteroscopy safely. Resected tissue is removed immediately to allow superior visualization. The flexible hysteroscope coupled with vaginoscopy has enabled hysteroscopy to be done with minimal to no anesthesia in an in-office setting.
With advances in hysteroscopy over the past 35 years, hysteroscopic procedures such as polypectomy, myomectomy, lysis of adhesions, transection of endometriosis, evacuation of retained products of conception, and endometrial ablation/resection have become routine.
And now, the controversy
Since its inception, laparoscopic surgery has not been without controversy. In 1933, Karl Fervers described explosion and flashes of light from a combination of high frequency electric current and oxygen distension gas while performing laparoscopic adhesiolysis with the coagulation probe of the ureterocystoscope.
In the early 1970s, Professor Kurt Semm’s pioneering effort was not rewarded by his department, in Kiel, Germany, which instead recommended he schedule a brain scan and psychological testing.
Nearly 20 years later, in a 1992 edition of Current Science, Professor Semm, along with Alan DeCherney, stated that “over 80% of gynecological operations can now be performed by laparoscopy.” Shortly thereafter, however, Dr. Roy Pitkin, who at the time was president of the American College of Obstetricians and Gynecologists, wrote an editorial in the Journal of Obstetrics and Gynecology – “Operative Laparoscopy: Surgical Advance or Technical Gimmick?” (Obstet Gynecol. 1992 Mar;79[3]:441-2).
Fortunately, 18 years later, with the continued advances in laparoscopic surgery making it less expensive, safer, and more accessible, Dr. Pitkin did retract his statement (Obstet Gynecol. 2010 May;115[5]:890-1).
Currently, the gynecologic community is embroiled in controversies involving the use of the robot to assist in the performance of laparoscopic surgery, the incorporation of synthetic mesh to enhance urogynecologic procedures, the placement of Essure micro-inserts to occlude fallopian tubes, and the use of electronic power morcellation at time of laparoscopic or robot-assisted hysterectomy, myomectomy, or sacrocolpopexy.
After reading the 2013 article by Dr. Jason Wright, published in JAMA, comparing laparoscopic hysterectomy to robotic hysterectomy, no one can deny that the rise in a minimally invasive route to hysterectomy has coincided with the advent of the robot (JAMA. 2013 Feb 20;309[7]:689-98). On the other hand, many detractors, including Dr. James Breeden (past ACOG president 2012-2013), find the higher cost of robotic surgery very problematic. In fact, many of these detractors cite the paucity of data showing a significant advantage to use of robotics.
While certainly cost, more than ever, must be a major consideration, remember that during the 1990s, there were multiple articles in Ob.Gyn. News raising concerns about the cost of laparoscopic hysterectomy. Interestingly, studies over the past decade by Warren and Jonsdottir show a cost savings when hysterectomy is done laparoscopically as opposed to its being done by laparotomy. Thus, it certainly can be anticipated that with more physician experience, improved instrumentation, and robotic industry competition, the overall cost will become more comparable to a laparoscopic route.
In 1995, Ulf Ulmsten first described the use of tension-free tape (TVT) to treat stress urinary incontinence. In 1998, the Food and Drug Administration approved the use of the TVT sling in the United States. Since then, transobturator tension-free vaginal tape (TVT-O) and single incision mini-slings have been introduced. All of these techniques have been shown to be successful and have been well adapted into the armamentarium of physicians treating stress urinary incontinence.
With the success of synthetic mesh for the treatment of stress urinary incontinence, its use was extended to pelvic prolapse. In 2002, the first mesh device with indications for the treatment of pelvic organ prolapse was approved by the FDA. While the erosion rate utilizing synthetic mesh for stress urinary incontinence has been noted to be 2%, rates up to 8.3% have been noted in patients treated for pelvic prolapse.
In 2008, the FDA issued a warning regarding the use of mesh for prolapse and incontinence repair secondary to the sequelae of mesh erosion. Subsequently, in 2011, the concern was limited to vaginal mesh to correct pelvic organ prolapse. Finally, on Jan. 4, 2016, the FDA issued an order to reclassify surgical mesh to repair pelvic organ prolapse from class II, which includes moderate-risk devices, to class III, which includes high-risk devices. Moreover, the FDA issued a second order to manufacturers to submit a premarket approval application to support the safety and effectiveness of synthetic mesh for transvaginal repair of pelvic organ prolapse.
Essure micro-inserts for permanent birth control received initial approval from the FDA in November 2002. Despite the fact that Essure can be easily placed, is highly effective, and has seemingly low complication rates, concerns have been raised by the Facebook group “Essure Problems” and Erin Brockovich, the focus of the 2000 biographical film starring Julia Roberts.
After more than 5,000 women filed grievances with the FDA between November 2002 and May 2015, based on unintended pregnancies, miscarriages, stillbirths, severe pain, and bleeding, the FDA announced in 2016 that it would require a boxed warning label for Essure. The FDA also called upon Bayer, which makes and markets Essure, to conduct surveillance to assess “risks of the device in a real-world environment.” The agency stated it will use the results to “determine what, if any, further actions related to Essure are needed to protect public health.”
While Jan. 26, 1988, is a very special date in minimally invasive gynecologic surgery, April 17, 2014, is a day of infamy for the gynecologic laparoscopist. For on this day, the FDA announced a warning regarding electronic power morcellation. Many hospitals and hospital systems throughout the country issued bans on electronic power morcellation, leading to needless open laparotomy procedures and thus, introducing prolonged recovery times and increased risk.
At a time when the recent introduction of barbed suture had made both closure of the vaginal cuff at time of hysterectomy and repair of the hysterotomy at myomectomy easier and faster, the gynecologic laparoscopist was taking a step backward. The FDA based this decision and a subsequent boxed warning – issued in November 2014 – on a small number of studies showing potential upstaging of leiomyosarcoma post electronic power morcellation. Interestingly, many of the morcellation procedures cited did not use power morcellation. Furthermore, a more comprehensive meta-analysis by Elizabeth A. Pritts and colleagues, showed a far lower risk than suggested by the FDA (Gynecol Surg. 2015;12[3]:165-77).
Recently, an article by William Parker and colleagues recommended that the FDA reverse its position (Obstet Gynecol. 2016 Jan;127[1]:18-22). Many believe that ultimately, the solution will be morcellation in a containment bag, which I and my colleagues have been performing in virtually every power morcellation procedure since May 2014. During this current power morcellation controversy, the Master Class in Gynecologic Surgery has continued to update its readers with three different articles related to the subject.
And in conclusion
Without a doubt, the past 50 years of gynecologic surgery has been a time of unparalleled innovation with occasional controversy thrown in. Ob.Gyn. News and more recently, the Master Class in Gynecologic Surgery, has had a major leadership role in bringing this profound ingenuity to the gynecology community by introducing this explosion of surgical creativity to its readers.
And what will the next 50 years bring? I believe we will continue to see tremendous advancements in minimally invasive gynecologic surgery. There will be a definite impact of costs on the marketplace. Thus, many of the minor minimally invasive procedures currently performed in the hospital or surgery center will be brought into office settings. In addition, secondary to reimbursement, the more complex cases will be carried out by fewer gynecologic surgeons who have undergone more intense training in pelvic surgery and who can perform these cases more efficiently and with fewer complications. Our ability to perform surgery and what type of procedures we do will not only be based on randomized, controlled trials, but big data collection as well.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, and past president of the AAGL and the International Society for Gynecologic Endoscopy (ISGE). He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/Society of Reproductive Surgery fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller is a consultant and is on the speakers bureau for Ethicon.
Over the past 50 years, there has been explosive change in gynecologic surgery. Ob.Gyn. News has been at the forefront of capturing and chronicling this paradigm shift in the treatment of the female patient.
Our beginnings
From antiquity, physicians and surgeons have struggled with pelvic prolapse, uterine fibroids, ovarian cysts, urinary incontinence, vesicovaginal fistulas, pelvic pain, and abnormal uterine bleeding. At the time of the first edition of Ob.Gyn. News, it had been less than a century since Thomas Edison invented the light bulb; just over 50 years since Hans Christian Jacobaeus first created air pneumoperitoneum using a trocar, followed by the Nitze cystoscope; about 40 years since Richard Zollikofer created a carbon dioxide pneumoperitoneum; 25 years since F.H. Powers and A.C. Barnes had first described laparoscopic tubal sterilization by cautery; and about 20 years since Raoul Palmer, considered the father of modern laparoscopy, had first described the technique – left upper quadrant entry, testing insufflation, Trendelenburg positioning, and simple laparoscopic instrumentation.
In the 1950s, Hans Frangenheim would bring monopolar electrosurgery to laparoscopy and Harold Hopkins would introduce fiber optics. It was not until 1967 that Patrick Steptoe would publish the first textbook on laparoscopy in the English language.
Although usage as a diagnostic tool and a method of sterilization increased popularity of laparoscopy in the 1960s and early 1970s, there were few advances. In fact, a review of early editions of Ob.Gyn. News during that time period shows that the majority of articles involving laparoscopy dealt with sterilization; including the introduction of clips for tubal sterilization by Jaroslav Hulka in 1972. This did not deter the efforts of Jordan Phillips, who along with Jacques Rioux, Louis Keith, Richard Soderstrom – four early laparoscopists – incorporated a new society, the American Association of Gynecologic Laparoscopists (the AAGL) in 1971.
Simultaneously, in 1979, James Daniell in the United States, Maurice Bruhart in France, and Yona Tadir in Israel were promoting efforts to couple the carbon dioxide laser to the laparoscope to treat pelvic adhesions and endometriosis. Later on, fiber lasers, KTP, Nd:YAG, and Argon lasers would be utilized in our field. Still, only a few extirpative procedures were being performed via a laparoscope route. This included linear salpingostomy for the treatment of ectopic pregnancy, championed by Professor Bruhart and H. Manhes in Europe, and Alan DeCherney in the United States.
During the 1980s, laparoscopic surgery was at its innovative best. Through the pioneering efforts of Professor Kurt Semm and his protégée, Liselotte Mettler, the gynecologic laparoscopist was introduced to endoloops, simple suturing techniques, and mechanical morcellation techniques.
Procedures such as salpingo-oophorectomy, appendectomy, and myomectomy could now be performed via the laparoscope. Dr. Camran Nezhat coupled the carbon dioxide laser, the laparoscope, and the television monitor, coining the term laparoscopy. Most importantly, the laparoscopic surgeon was liberated; he or she could remain upright and perform surgery with both hands. Through the 1980s and 1990s, Dr. Nezhat, Dr. Harry Reich, and other innovators pushed the envelope in increasing the ability to extirpate endometriosis, excise severe pelvic adhesions, and perform discoid and segmental bowel resection.
The day the earth stood still
Every gynecologic laparoscopic surgeon should remember Jan. 26, 1988, as that was the date that Dr. Harry Reich performed the first total laparoscopic hysterectomy. Now, little more than 25 years later, in many parts of the country, a laparoscopic approach to hysterectomy is indeed the most common route. Over the years, with the evolution of instrumentation, including new energy systems (ultrasonic, advanced bipolar) and the introduction of barbed sutures, hysterectomy can now be performed via minilaparoscopy, single-site laparoscopy, robot-assisted, and robotic single site, all of which have been featured in the Ob.Gyn. News’ Master Class in Gynecologic Surgery.
But hysteroscopy came first
Abulkasim utilized a mirror to reflect light into the vaginal vault in 1,000 A.D. In 1806, Philipp Bozzini originated the idea of illuminating body cavities by an external light source. Through a system of mirrors and tubes, candlelight could be reflected into the body. In 1869, D.C. Pantaleoni used a cystoscope developed by Antoine Desormeaux – who has been called the father of endoscopy – to treat endometrial polyps with silver nitrate.
Through the 50 years of Ob.Gyn. News and over the past 12 years of the Master Class in Gynecologic Surgery, our community has been consistently updated as to advances in hysteroscopy, not only to enhance treatment efficacy, but safety as well. This has included such advances as the continuous flow hysteroscope, the Hamou contact hysteroscope, and fluid management systems to enhance visualization.
In 1978, Robert Neuwirth introduced loops to perform hysteroscopic myomectomy. The loop resectoscope was quickly followed by the rollerball to perform endometrial ablation. In the late 1990s, hysteroscopic bipolar cutting loops were introduced. This enabled use of ionic distension media saline, instead of nonionic media, thus decreasing risks related to hyponatremia.
In 2003, Mark Emanuel introduced hysteroscopic morcellation systems, which enabled more gynecologists to perform operative hysteroscopy safely. Resected tissue is removed immediately to allow superior visualization. The flexible hysteroscope coupled with vaginoscopy has enabled hysteroscopy to be done with minimal to no anesthesia in an in-office setting.
With advances in hysteroscopy over the past 35 years, hysteroscopic procedures such as polypectomy, myomectomy, lysis of adhesions, transection of endometriosis, evacuation of retained products of conception, and endometrial ablation/resection have become routine.
And now, the controversy
Since its inception, laparoscopic surgery has not been without controversy. In 1933, Karl Fervers described explosion and flashes of light from a combination of high frequency electric current and oxygen distension gas while performing laparoscopic adhesiolysis with the coagulation probe of the ureterocystoscope.
In the early 1970s, Professor Kurt Semm’s pioneering effort was not rewarded by his department, in Kiel, Germany, which instead recommended he schedule a brain scan and psychological testing.
Nearly 20 years later, in a 1992 edition of Current Science, Professor Semm, along with Alan DeCherney, stated that “over 80% of gynecological operations can now be performed by laparoscopy.” Shortly thereafter, however, Dr. Roy Pitkin, who at the time was president of the American College of Obstetricians and Gynecologists, wrote an editorial in the Journal of Obstetrics and Gynecology – “Operative Laparoscopy: Surgical Advance or Technical Gimmick?” (Obstet Gynecol. 1992 Mar;79[3]:441-2).
Fortunately, 18 years later, with the continued advances in laparoscopic surgery making it less expensive, safer, and more accessible, Dr. Pitkin did retract his statement (Obstet Gynecol. 2010 May;115[5]:890-1).
Currently, the gynecologic community is embroiled in controversies involving the use of the robot to assist in the performance of laparoscopic surgery, the incorporation of synthetic mesh to enhance urogynecologic procedures, the placement of Essure micro-inserts to occlude fallopian tubes, and the use of electronic power morcellation at time of laparoscopic or robot-assisted hysterectomy, myomectomy, or sacrocolpopexy.
After reading the 2013 article by Dr. Jason Wright, published in JAMA, comparing laparoscopic hysterectomy to robotic hysterectomy, no one can deny that the rise in a minimally invasive route to hysterectomy has coincided with the advent of the robot (JAMA. 2013 Feb 20;309[7]:689-98). On the other hand, many detractors, including Dr. James Breeden (past ACOG president 2012-2013), find the higher cost of robotic surgery very problematic. In fact, many of these detractors cite the paucity of data showing a significant advantage to use of robotics.
While certainly cost, more than ever, must be a major consideration, remember that during the 1990s, there were multiple articles in Ob.Gyn. News raising concerns about the cost of laparoscopic hysterectomy. Interestingly, studies over the past decade by Warren and Jonsdottir show a cost savings when hysterectomy is done laparoscopically as opposed to its being done by laparotomy. Thus, it certainly can be anticipated that with more physician experience, improved instrumentation, and robotic industry competition, the overall cost will become more comparable to a laparoscopic route.
In 1995, Ulf Ulmsten first described the use of tension-free tape (TVT) to treat stress urinary incontinence. In 1998, the Food and Drug Administration approved the use of the TVT sling in the United States. Since then, transobturator tension-free vaginal tape (TVT-O) and single incision mini-slings have been introduced. All of these techniques have been shown to be successful and have been well adapted into the armamentarium of physicians treating stress urinary incontinence.
With the success of synthetic mesh for the treatment of stress urinary incontinence, its use was extended to pelvic prolapse. In 2002, the first mesh device with indications for the treatment of pelvic organ prolapse was approved by the FDA. While the erosion rate utilizing synthetic mesh for stress urinary incontinence has been noted to be 2%, rates up to 8.3% have been noted in patients treated for pelvic prolapse.
In 2008, the FDA issued a warning regarding the use of mesh for prolapse and incontinence repair secondary to the sequelae of mesh erosion. Subsequently, in 2011, the concern was limited to vaginal mesh to correct pelvic organ prolapse. Finally, on Jan. 4, 2016, the FDA issued an order to reclassify surgical mesh to repair pelvic organ prolapse from class II, which includes moderate-risk devices, to class III, which includes high-risk devices. Moreover, the FDA issued a second order to manufacturers to submit a premarket approval application to support the safety and effectiveness of synthetic mesh for transvaginal repair of pelvic organ prolapse.
Essure micro-inserts for permanent birth control received initial approval from the FDA in November 2002. Despite the fact that Essure can be easily placed, is highly effective, and has seemingly low complication rates, concerns have been raised by the Facebook group “Essure Problems” and Erin Brockovich, the focus of the 2000 biographical film starring Julia Roberts.
After more than 5,000 women filed grievances with the FDA between November 2002 and May 2015, based on unintended pregnancies, miscarriages, stillbirths, severe pain, and bleeding, the FDA announced in 2016 that it would require a boxed warning label for Essure. The FDA also called upon Bayer, which makes and markets Essure, to conduct surveillance to assess “risks of the device in a real-world environment.” The agency stated it will use the results to “determine what, if any, further actions related to Essure are needed to protect public health.”
While Jan. 26, 1988, is a very special date in minimally invasive gynecologic surgery, April 17, 2014, is a day of infamy for the gynecologic laparoscopist. For on this day, the FDA announced a warning regarding electronic power morcellation. Many hospitals and hospital systems throughout the country issued bans on electronic power morcellation, leading to needless open laparotomy procedures and thus, introducing prolonged recovery times and increased risk.
At a time when the recent introduction of barbed suture had made both closure of the vaginal cuff at time of hysterectomy and repair of the hysterotomy at myomectomy easier and faster, the gynecologic laparoscopist was taking a step backward. The FDA based this decision and a subsequent boxed warning – issued in November 2014 – on a small number of studies showing potential upstaging of leiomyosarcoma post electronic power morcellation. Interestingly, many of the morcellation procedures cited did not use power morcellation. Furthermore, a more comprehensive meta-analysis by Elizabeth A. Pritts and colleagues, showed a far lower risk than suggested by the FDA (Gynecol Surg. 2015;12[3]:165-77).
Recently, an article by William Parker and colleagues recommended that the FDA reverse its position (Obstet Gynecol. 2016 Jan;127[1]:18-22). Many believe that ultimately, the solution will be morcellation in a containment bag, which I and my colleagues have been performing in virtually every power morcellation procedure since May 2014. During this current power morcellation controversy, the Master Class in Gynecologic Surgery has continued to update its readers with three different articles related to the subject.
And in conclusion
Without a doubt, the past 50 years of gynecologic surgery has been a time of unparalleled innovation with occasional controversy thrown in. Ob.Gyn. News and more recently, the Master Class in Gynecologic Surgery, has had a major leadership role in bringing this profound ingenuity to the gynecology community by introducing this explosion of surgical creativity to its readers.
And what will the next 50 years bring? I believe we will continue to see tremendous advancements in minimally invasive gynecologic surgery. There will be a definite impact of costs on the marketplace. Thus, many of the minor minimally invasive procedures currently performed in the hospital or surgery center will be brought into office settings. In addition, secondary to reimbursement, the more complex cases will be carried out by fewer gynecologic surgeons who have undergone more intense training in pelvic surgery and who can perform these cases more efficiently and with fewer complications. Our ability to perform surgery and what type of procedures we do will not only be based on randomized, controlled trials, but big data collection as well.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, and past president of the AAGL and the International Society for Gynecologic Endoscopy (ISGE). He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/Society of Reproductive Surgery fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller is a consultant and is on the speakers bureau for Ethicon.
