User login
LAA occlusion studied for stroke prevention in atrial fib with prior intracerebral hemorrhage
PARIS – Transcatheter left atrial appendage occlusion shows promise in providing a far better stroke prevention strategy than does standard medical management in patients with atrial fibrillation who have had a prior intracerebral hemorrhage, Dr. Jens E. Nielsen-Kudsk reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“This is a difficult group of patients because there is no consensus on how to treat patients with atrial fibrillation after an intracerebral hemorrhage. They are very often left without any antithrombotic therapy because physicians and the patients themselves fear to resume anticoagulant therapy. Left atrial appendage occlusion is a nice nonpharmacologic way to obtain stroke prevention,” said Dr. Nielsen-Kudsk of Aarhus (Denmark) University.

He presented a propensity-matched follow-up study of 147 pairs of such patients at seven Nordic heart centers. Half received the percutaneously delivered St. Jude Medical Amplatzer Amulet device, which is approved in Europe for stroke prevention in patients with atrial fibrillation (AF). These 147 device recipients were matched for stroke risk by CHA2DS2-VASc score and for bleeding risk by HASBLED score with 147 patients with AF and a prior intracerebral hemorrhage who received standard medical therapy, ranging from warfarin or a novel oral anticoagulant in nearly half of patients to no antithrombotic therapy in 44%. The Amplatzer recipients were most often placed on aspirin for 6 months afterward unless they had an indication for continued aspirin, such as known coronary artery disease.
During a mean of 166 days of follow-up, the primary study endpoint – a composite of ischemic stroke, major bleeding, or death – occurred in the standard medical therapy group at a rate of 278.9 events per 1,000 patient-years, compared with 47.9 per 1,000 patient-years in patients with left atrial appendage occlusion (LAAO). This translates to an 81% relative risk reduction.
Moreover, the risk of ischemic stroke in the LAAO group was reduced by 65%, major bleeding was reduced by 61%, the rate of intracerebral hemorrhage was reduced by 71%, and mortality was decreased by 92%, the cardiologist continued.
On the basis of these encouraging results, a randomized, prospective clinical trial of LAAO using the Amplatzer device versus standard medical therapy in patients with AF and a prior intracerebral hemorrhage will get underway in the Nordic countries within the next several months. It will be called STROKECLOSE, he added.
Asked if the Watchman, the only LAAO device approved in the United States, might be similarly amenable for stroke prevention in this high-stroke-and-bleeding-risk population, Dr. Nielsen-Kudsk said in theory, yes, but the device’s labeling calls for an initial 45 days of anticoagulation therapy. That’s a daunting prospect in patients who’ve already had an intracerebral bleed, he observed.

Dr. Nicolo Piazza, who chaired a press conference where the Nordic study was highlighted, said the Watchman labeling needn’t be a deal breaker.
“Although the Watchman recommendations suggest an anticoagulant for the first 45 days afterward, real-world practice is not necessarily that. Many of those patients are put on dual-antiplatelet therapy or a single antiplatelet agent for a period of 45 days, 3 months, 6 months – it’s very heterogeneous out there,” said Dr. Piazza of McGill University in Montreal.
He added that STROKEBLED will be a very important trial in terms of providing guidance for daily clinical practice. A propensity matched-pairs analysis can’t be considered the final word because of the possibility of unrecognized and unmatched variables that could affect outcomes.
Dr. Nielsen-Kudsk reported receiving research grants from and serving as a consultant to St. Jude Medical.
PARIS – Transcatheter left atrial appendage occlusion shows promise in providing a far better stroke prevention strategy than does standard medical management in patients with atrial fibrillation who have had a prior intracerebral hemorrhage, Dr. Jens E. Nielsen-Kudsk reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“This is a difficult group of patients because there is no consensus on how to treat patients with atrial fibrillation after an intracerebral hemorrhage. They are very often left without any antithrombotic therapy because physicians and the patients themselves fear to resume anticoagulant therapy. Left atrial appendage occlusion is a nice nonpharmacologic way to obtain stroke prevention,” said Dr. Nielsen-Kudsk of Aarhus (Denmark) University.
He presented a propensity-matched follow-up study of 147 pairs of such patients at seven Nordic heart centers. Half received the percutaneously delivered St. Jude Medical Amplatzer Amulet device, which is approved in Europe for stroke prevention in patients with atrial fibrillation (AF). These 147 device recipients were matched for stroke risk by CHA2DS2-VASc score and for bleeding risk by HASBLED score with 147 patients with AF and a prior intracerebral hemorrhage who received standard medical therapy, ranging from warfarin or a novel oral anticoagulant in nearly half of patients to no antithrombotic therapy in 44%. The Amplatzer recipients were most often placed on aspirin for 6 months afterward unless they had an indication for continued aspirin, such as known coronary artery disease.
During a mean of 166 days of follow-up, the primary study endpoint – a composite of ischemic stroke, major bleeding, or death – occurred in the standard medical therapy group at a rate of 278.9 events per 1,000 patient-years, compared with 47.9 per 1,000 patient-years in patients with left atrial appendage occlusion (LAAO). This translates to an 81% relative risk reduction.
Moreover, the risk of ischemic stroke in the LAAO group was reduced by 65%, major bleeding was reduced by 61%, the rate of intracerebral hemorrhage was reduced by 71%, and mortality was decreased by 92%, the cardiologist continued.
On the basis of these encouraging results, a randomized, prospective clinical trial of LAAO using the Amplatzer device versus standard medical therapy in patients with AF and a prior intracerebral hemorrhage will get underway in the Nordic countries within the next several months. It will be called STROKECLOSE, he added.
Asked if the Watchman, the only LAAO device approved in the United States, might be similarly amenable for stroke prevention in this high-stroke-and-bleeding-risk population, Dr. Nielsen-Kudsk said in theory, yes, but the device’s labeling calls for an initial 45 days of anticoagulation therapy. That’s a daunting prospect in patients who’ve already had an intracerebral bleed, he observed.
Dr. Nicolo Piazza, who chaired a press conference where the Nordic study was highlighted, said the Watchman labeling needn’t be a deal breaker.
“Although the Watchman recommendations suggest an anticoagulant for the first 45 days afterward, real-world practice is not necessarily that. Many of those patients are put on dual-antiplatelet therapy or a single antiplatelet agent for a period of 45 days, 3 months, 6 months – it’s very heterogeneous out there,” said Dr. Piazza of McGill University in Montreal.
He added that STROKEBLED will be a very important trial in terms of providing guidance for daily clinical practice. A propensity matched-pairs analysis can’t be considered the final word because of the possibility of unrecognized and unmatched variables that could affect outcomes.
Dr. Nielsen-Kudsk reported receiving research grants from and serving as a consultant to St. Jude Medical.
PARIS – Transcatheter left atrial appendage occlusion shows promise in providing a far better stroke prevention strategy than does standard medical management in patients with atrial fibrillation who have had a prior intracerebral hemorrhage, Dr. Jens E. Nielsen-Kudsk reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“This is a difficult group of patients because there is no consensus on how to treat patients with atrial fibrillation after an intracerebral hemorrhage. They are very often left without any antithrombotic therapy because physicians and the patients themselves fear to resume anticoagulant therapy. Left atrial appendage occlusion is a nice nonpharmacologic way to obtain stroke prevention,” said Dr. Nielsen-Kudsk of Aarhus (Denmark) University.
He presented a propensity-matched follow-up study of 147 pairs of such patients at seven Nordic heart centers. Half received the percutaneously delivered St. Jude Medical Amplatzer Amulet device, which is approved in Europe for stroke prevention in patients with atrial fibrillation (AF). These 147 device recipients were matched for stroke risk by CHA2DS2-VASc score and for bleeding risk by HASBLED score with 147 patients with AF and a prior intracerebral hemorrhage who received standard medical therapy, ranging from warfarin or a novel oral anticoagulant in nearly half of patients to no antithrombotic therapy in 44%. The Amplatzer recipients were most often placed on aspirin for 6 months afterward unless they had an indication for continued aspirin, such as known coronary artery disease.
During a mean of 166 days of follow-up, the primary study endpoint – a composite of ischemic stroke, major bleeding, or death – occurred in the standard medical therapy group at a rate of 278.9 events per 1,000 patient-years, compared with 47.9 per 1,000 patient-years in patients with left atrial appendage occlusion (LAAO). This translates to an 81% relative risk reduction.
Moreover, the risk of ischemic stroke in the LAAO group was reduced by 65%, major bleeding was reduced by 61%, the rate of intracerebral hemorrhage was reduced by 71%, and mortality was decreased by 92%, the cardiologist continued.
On the basis of these encouraging results, a randomized, prospective clinical trial of LAAO using the Amplatzer device versus standard medical therapy in patients with AF and a prior intracerebral hemorrhage will get underway in the Nordic countries within the next several months. It will be called STROKECLOSE, he added.
Asked if the Watchman, the only LAAO device approved in the United States, might be similarly amenable for stroke prevention in this high-stroke-and-bleeding-risk population, Dr. Nielsen-Kudsk said in theory, yes, but the device’s labeling calls for an initial 45 days of anticoagulation therapy. That’s a daunting prospect in patients who’ve already had an intracerebral bleed, he observed.
Dr. Nicolo Piazza, who chaired a press conference where the Nordic study was highlighted, said the Watchman labeling needn’t be a deal breaker.
“Although the Watchman recommendations suggest an anticoagulant for the first 45 days afterward, real-world practice is not necessarily that. Many of those patients are put on dual-antiplatelet therapy or a single antiplatelet agent for a period of 45 days, 3 months, 6 months – it’s very heterogeneous out there,” said Dr. Piazza of McGill University in Montreal.
He added that STROKEBLED will be a very important trial in terms of providing guidance for daily clinical practice. A propensity matched-pairs analysis can’t be considered the final word because of the possibility of unrecognized and unmatched variables that could affect outcomes.
Dr. Nielsen-Kudsk reported receiving research grants from and serving as a consultant to St. Jude Medical.
AT EUROPCR 2016
Key clinical point: Left atrial appendage occlusion appears to be better than medical management for stroke prevention in patients with AF and prior intracerebral hemorrhage.
Major finding: The risk of a combined endpoint of ischemic stroke, major bleeding, or death during follow-up was 81% lower in patients with atrial fibrillation and a prior intracerebral hemorrhage treated with a transcatheter left atrial appendage occlusion device than in controls on standard medical therapy.
Data source: This study included 147 patient pairs propensity-matched for stroke and bleeding risk.
Disclosures: The study presenter reported receiving research grants from and serving as a consultant to St. Jude Medical.

Does U.S. Healthcare Need More Diverse Leadership?
Throughout its history, the United States has been a nation of immigrants. From the early colonial settlements to the mid-20th century, most immigrants came from Western European countries. Since 1965, when the Immigration and Nationality Act abolished national-origin quotas, the diversity of immigrants has increased. “By the year 2043,” says Tomás León, president and CEO of the Institute for Diversity in Health Management in Chicago, “we will be a country where the majority of our population is comprised of racial and ethnic minorities.”

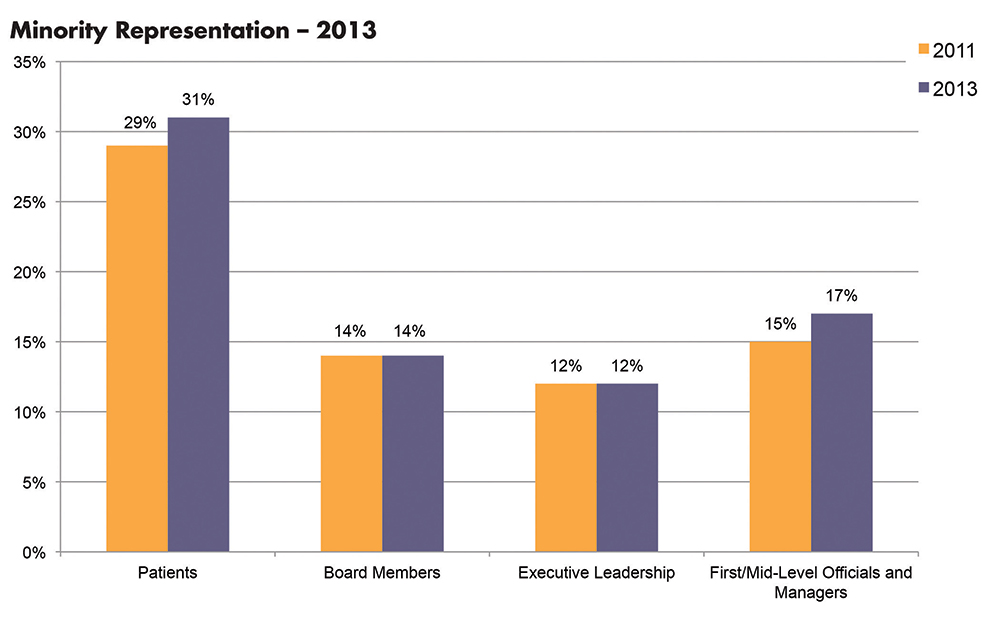
Those changing demographics, cited from the U.S. Census Bureau’s projections, already are evidenced in hospital patient populations. According to a benchmarking survey sponsored by the institute, which is an affiliate of the American Hospital Association, the percentage of minority patients seen in hospitals grew from 29% to 31% of patient census between 2011 and 2013.1 And yet, the survey found this increasing diversity is not currently reflected in leadership positions. During the same time period, underrepresented racial and ethnic minorities (UREM) on hospital boards of directors (14%) and in C-suite positions (14%) remained flat (see Figure 1).

Gender disparities in healthcare and academic leadership also have been slow to change. Periodic surveys conducted by the American College of Healthcare Executives indicate that women comprise only 11% of healthcare CEOs in the U.S.2 And despite the fact that women make up half of all medical students (and one-third of full-time faculty), the Association of American Medical Colleges (AAMC) finds that women still trail men when it comes to attaining full professorship and decanal positions at their academic institutions.3
The Hospitalist interviewed medical directors, researchers, diversity management professionals, and hospitalists to ascertain current solutions being pursued to narrow the gaps in leadership diversity.
Why Diversity in Leadership Matters

Eric E. Howell, MD, MHM, chief of the Division of Hospital Medicine at Johns Hopkins Bayview Medical Center in the Hopkins School of Medicine in Baltimore, believes there is a need to encourage the advancement to leadership positions for female and UREM physicians.
“In medicine, it’s really about service. If we are really here for our patients, we need representation of diversity in our faculty and leadership,” says Dr. Howell, a past SHM president and faculty member of SHM’s Leadership Academy since its inception in 2005. In addition, he says, “Diversity adds incredible strength to an organization and adds to the richness of the ideas and solutions to overcome challenging problems.”
With the implementation of the Affordable Care Act, formerly uninsured people are now accessing the healthcare system; many are bilingual and bicultural, notes George A. Zeppenfeldt-Cestero, president and CEO, Association of Hispanic Healthcare Executives.

“You want to make sure that providers, whether they are physicians, nurses, dentists, or health executives that drive policy issues, are also reflective of that population throughout the organization,” he says. “The real definition of diversity is making sure you have diversity in all layers of the workforce, including the C-suite.”
León points to the coming “seismic demographic shifts” and wonders if healthcare is ready to become more reflective of the communities it serves.
“Increasing diversity in healthcare leadership and governance is essential for the delivery and provision of culturally competent care,” León says. “Now, more than ever, it’s important that we collectively accelerate progress in this area.”
Advancing in Academic and Hospital Medicine
Might hospital medicine offer additional opportunities for women and minorities to advance into leadership positions? Hospitalist Flora Kisuule, MD, SFHM, assistant professor of medicine at Johns Hopkins School of Medicine and associate division director of the Collaborative Inpatient Medicine Service (CIMS) at Johns Hopkins Bayview Medical Center, believes this may be the case. She was with Dr. Howell’s group when he needed to fill the associate director position.
“My advancement speaks to hospital medicine and the fact that we are growing as a field,” she says. “Because of that, opportunities are presenting themselves.”
Dr. Kisuule’s ability to thrive in her position speaks to her professionalism but also to a number of other intentional factors: Dr. Howell’s continuing sponsorship to include her in leadership opportunities, an emergency call system for parents with sick children, and a women’s task force whose agenda calls for transparency in hiring and advancement.
Intentional Structure Change
Cardiologist Hannah A. Valantine, MD, recognizes the importance of addressing the lack of women and people from unrepresented groups in the Science, Technology, Engineering, and Mathematics (STEM) workforce. While at Stanford University School of Medicine, she developed and put into place a set of strategies to understand and mitigate the drivers of gender imbalance. Since then, Dr. Valantine was recruited to bring her expertise to the National Institutes of Health in Bethesda, Md., where she is the inaugural chief officer for scientific workforce diversity. In this role, she is committed “to promoting biomedical workforce diversity as an opportunity, not a problem.”
Dr. Valantine is pushing NIH to pursue a wide range of evidence-based programming to eliminate career-transition barriers that keep women and individuals from underrepresented groups from attaining spots in the top echelons of science and health leadership. She believes that applying scientific rigor to the issue of workforce diversity can lead to quantifiable, translatable, and repeatable methods for recruitment and retention of talent in the biomedical workforce (see “Building Blocks").
Before joining NIH, Dr. Valantine and her colleagues at Stanford surveyed gender composition and faculty satisfaction several years after initiating a multifaceted intervention to boost recruitment and development of women faculty.4 After making a visible commitment of resources to support faculty, with special attention to women, Stanford rose from below to above national benchmarks in the representation of women among faculty. Yet significant work remains to be done, Dr. Valantine says. Her work predicts that the estimated time to achieve 50% occupancy of full professorships by women nationally approaches 50 years—“far too long using current approaches.”
In a separate review article, Dr. Valantine and co-author Christy Sandborg, MD, described the Stanford University School of Medicine Academic Biomedical Career Customization (ABCC) model, which was adapted from Deloitte’s Mass Career Customization framework and allows for development of individual career plans that span a faculty member’s total career, not just a year or two at a time. Long-term planning can enable better alignment between the work culture and values of the workforce, which will improve the outlook for women faculty, Dr. Valantine says.
The issues of work-life balance may actually be generational, Dr. Valantine explains. Veteran hospitalist Janet Nagamine, MD, BSN, SFHM, of Santa Clara, Calif., agrees.
“Nowadays, men as well as women are looking for work-life balance,” she says.
In hospital medicine, Dr. Nagamine points out, the structural changes required to effect a work-life balance for hospital leaders are often difficult to achieve.
“As productivity surveys show, HM group leaders are putting in as many RVUs as the staff,” the former SHM board member says. “There is no dedicated time for administrative duties.”
Construct a Pipeline
Barriers to advancement often are particular to characteristics of diverse populations. For example, the AAMC’s report on the U.S. physician workforce documents that in African-American physicians 40 and younger, women outnumber their male counterparts. Therefore, in the association’s Diversity in Medical Education: Facts and Figures 2012 report, the executive summary points out the need to strengthen the medical education pipeline to increase the number of African-American males who enter the premed track.

Despite the fast-growing percentage of Latino and Hispanic populations in the United States, the shortage of Latino/Hispanic physicians increased from 1980 to 2010. Latinos/Hispanics are greatly underrepresented in the medical student, resident, and faculty populations, according to John Paul Sánchez, MD, MPH, assistant dean for diversity and inclusion in the Office for Diversity and Community Engagement at Rutgers, The State University of New Jersey. Likewise, Zeppenfeldt-Cestero believes that efforts must begin much earlier with Latino and other minority and underrepresented students.
“We have to make sure our students pursue the STEM disciplines and that they also later have the education and preparation to be competitive at the MBA or MPH levels,” he says.
Dr. Sánchez, an associate professor of emergency medicine and a diversity activist since his med school days, is the recipient of last year’s Association of Hispanic Healthcare Executives’ academic leader of the year award. Since September 2014, he has been involved with Building the Next Generation of Academic Physicians Inc., which collaborates with more than 40 medical schools across the country. The initiative offers conferences designed to develop diverse medical students’ and residents’ interest in pursuing academic medicine. Open to all medical students and residents, the conference curriculum is tailored for women, UREMs, and trainees who identify as lesbian, gay, bisexual, or transgender (LGBT), he says. Seven conferences were held in 2015, 10 are planned for this year, and seven for 2017.
Healthcare Leadership Gaps
Despite their omnipresence in healthcare, there is a dearth of women in chief executive and governance roles, as has been noted by both the American College of Healthcare Executives and the National Center for Healthcare Leadership. As with academic leadership positions, the leadership gap in the administrative sector does not seem to be due to a lack of women entering graduate programs in health administration. On the contrary, since the mid-1980s women have comprised 50% to 60% of graduate students.
“This is absolutely not a pipeline issue,” says Christy Harris Lemak, PhD, FACHE, professor and chair of the Department of Health Services Administration at the University of Alabama at Birmingham School of Health Professions and lead investigator of the National Center for Healthcare Leadership’s study of women in healthcare executive positions. Other factors come into play.
In the study, she and her co-authors queried female healthcare CEOs to ascertain the critical career inflection points that led to their success.6 Those who were strategic about their careers, sought out mentors, and voiced their intentions about pursuing leadership positions were more likely to be successful in those efforts. However, individual career efforts must be coupled with overall organizational commitment to fostering inclusion (see “Path to the Top: Strategic Advice for Women").
Hospitals and healthcare organizations must pursue the development of human capital (and the diversity of their leaders) in a systematic way. “We recommended [in the study] that organizations set expectations that leaders who mentor other potential leaders be rewarded in the same way as those who hit financial targets or readmission rate targets,” Dr. Lemak says.

Leadership matters, agrees Deborah J. Bowen, FACHE, CAE, president and CEO of Chicago-based American College of Healthcare Executives.
“I think we’re getting a little smarter. Organizational leaders and trustees have a better understanding that talent development is one of the most important jobs,” she says. “If you don’t have the right people in the right places making good decisions on behalf of the patients and the populations in the communities they’re serving, the rest falls apart.”
Nuances of Mentoring
Many conversations about encouraging diversity in healthcare leadership converge around the role of effective mentoring and sponsorship. A substantial body of research supports the impact of mentoring on retention, research productivity, career satisfaction, and career development for women. It’s important to ensure that the institutional culture is geared toward mentoring junior faculty, says Jessie Kimbrough Marshall, MD, MPH, assistant professor in the Division of General Medicine Hospitalist Program at the University of Michigan Health System in Ann Arbor (UMHS).
Several of our sources pointed out that leaders must learn how to be effective mentors. More attention is being given to enhancing leaders’ mentorship skills. One example is at the Institute for Diversity in Health Management, which conducts an intensive 12-month certificate in diversity management program for practitioners. León says the program fosters ongoing networking and support through the American Leadership Council on Diversity in Healthcare by building leadership competencies.
Dr. Valantine points out that mentoring is hardly a one-style-fits-all proposition but that it is a crucial element to creating and retaining diversity. She says it should be viewed “much more broadly than it is today, and it should focus beyond the trainer-trainee relationship.”

The process is a two-way street. Denege Ward, MD, hospitalist, assistant professor of internal medicine, and director of the medical short stay unit at UMHS, says minorities need to be ready to take a leap of faith.
“Underrepresented faculty and staff should take the risk of possible failure in challenging situations but learn from it and do better and not succumb to fear in face of challenges,” Dr. Ward says.
Although mentoring is one important component in building diversity in academic medicine, Dr. Sánchez asserts that role models, champions, and sponsors are equally important.
“In addition and separate from role models, there must be in place policies and procedures that promote a climate for diverse individuals to succeed,” he says. “What’s needed is an institutional vision and strategic plan that recognizes the importance of diversity. [It] has to become a core principle.”
Dr. Marshall echoes that refrain, noting the recruitment and retention of a diverse set of leaders will take time and intentionality. She is actively engaged in organizing annual meeting mentoring panels at the Society of General Internal Medicine.
“There are still quite a few barriers for women and minorities to advance into hospital leadership roles,” she says. “We still have a long way to go. However, I’m seeing more women and people of color get into these positions. The numbers are increasing, and that encourages me.” TH
Gretchen Henkel is a freelance writer in California.
References
- Institute for Diversity in Health Management. The state of health care diversity and disparities: a benchmarking study of U.S. hospitals. Available at: http://www.diversityconnection.org/diversityconnection/leadership-conferences/Benchmarking-Survey.jsp?fll=S11.
- Top issues confronting hospitals in 2015. American College of Healthcare Executives website. Available at: https://www.ache.org/pubs/research/ceoissues.cfm. Accessed March 5, 2016.
- Association of American Medical Colleges. Diversity in the physician workforce: facts & figures 2014. Available at: http://aamcdiversityfactsandfigures.org/.
- Valantine HA, Grewal D, Ku MC, et al. The gender gap in academic medicine: comparing results from a multifaceted intervention for Stanford faculty to peer and national cohorts. Acad Med. 2014;89(6):904-911.
- Valantine H, Sandborg CI. Changing the culture of academic medicine to eliminate the gender leadership gap: 50/50 by 2020. Acad Med. 2013;88(10):1411-1413.
- Sexton DW, Lemak CH, Wainio JA. Career inflection points of women who successfully achieved the hospital CEO position. J Healthc Manag. 2014;59(5):367-383.
Path to the Top: Strategic Advice for Women
One of the cornerstones of career advancement in healthcare is to stay connected by networking and attending meetings. For women and minorities, the path to leadership may not fit into the traditional linear model of the career ladder.
“For many leadership roles, you have to be visual and present; you have to attend meetings and functions,” says Denege Ward, MD, hospitalist, assistant professor of internal medicine, and director of the medical short stay unit at the University of Michigan Health System in Ann Arbor. “For women, this is difficult. We are still in charge of families and home.”
For some women, it may be more productive to employ the notion of the “leadership labyrinth.” Others refer to a “career lattice” or employ Deloitte’s Mass Career Customization framework.
“For women, the trajectory may include working part-time while their children are small or finding local training opportunities,” says Christy Harris Lemak, PhD, FACHE, professor and chair of the Department of Health Services Administration at the University of Alabama at Birmingham School of Health Professions and lead investigator of the National Center for Healthcare Leadership’s study of women in healthcare executive positions.
Hospitalist Flora Kisuule, MD, assistant professor of medicine at Johns Hopkins School of Medicine and associate division director of the Collaborative Inpatient Medicine Service (CIMS) at Johns Hopkins Bayview Medical Center in Baltimore, is a wife and mother of a 4-year-old. She agrees the leadership path for moms can take unexpected detours. She’s been able to complete some of her administrative tasks at home through the support of her medical director. If pursuing an MBA is too daunting, she encourages her hospitalist peers to take advantage of short courses and programs in leadership.
“As women, we like to do for others,” notes Elizabeth Gundersen, MD, FHM, assistant professor of clinical biomedical sciences at the Charles E. Schmidt College of Medicine at Florida Atlantic University in Boca Raton. While at the University of Massachusetts, she was one of eight physician quality officers and associate division chief of hospital medicine. To counter the impulse to say yes to everything, including roles that distract from ultimate career goals, one of the women leaders at UMass encouraged her mentees to “think of your ideal position—and then when a position is offered, assess that against your criteria.”

Jessie Kimbrough Marshall, MD, MPH, assistant professor in the Division of General Medicine Hospitalist Program at the University of Michigan Health System, seconds that opinion.
“Try to avoid professional commitments and activities that are not aligned to your career trajectory,” Dr. Marshall advises. “You can also identify someone who is in a position that is close to what you envision for yourself and reach out to that person.”
—Gretchen Henkel
Building Blocks: NIH’s Commitment to Enhance Diversity

The National Institutes of Health (NIH) has been committed to enhancing diversity for decades, according to cardiologist Hannah A. Valantine, MD.
“NIH has made considerable investments in programming,” says Dr. Valantine. However, despite these investments, “the change has not been as rapid or sustainable as we would like it to be.”
As a first step, in October 2014, NIH announced a new set of initiatives designed to enhance the ways in which participants are engaged and trained. Three components comprise the Enhancing Diversity in the NIH-Funded Workforce program. The Building Infrastructure Leading to Diversity (BUILD) program was awarded to 10 universities that met eligibility criteria for being under-resourced. The National Research Mentoring Network (NRMN) will recruit mentors and use methods (such as “train the trainer”) to bring a more deliberate and intentional approach to cultivating mentors. The third component, the Coordinating and Evaluation Center (CEC), focuses on evaluation and dissemination of identified best practices and competencies.
“We are moving away from the assumption that just because you are a leader in your research field that that means you are a good mentor,” Dr. Valantine says.
Throughout its history, the United States has been a nation of immigrants. From the early colonial settlements to the mid-20th century, most immigrants came from Western European countries. Since 1965, when the Immigration and Nationality Act abolished national-origin quotas, the diversity of immigrants has increased. “By the year 2043,” says Tomás León, president and CEO of the Institute for Diversity in Health Management in Chicago, “we will be a country where the majority of our population is comprised of racial and ethnic minorities.”
Those changing demographics, cited from the U.S. Census Bureau’s projections, already are evidenced in hospital patient populations. According to a benchmarking survey sponsored by the institute, which is an affiliate of the American Hospital Association, the percentage of minority patients seen in hospitals grew from 29% to 31% of patient census between 2011 and 2013.1 And yet, the survey found this increasing diversity is not currently reflected in leadership positions. During the same time period, underrepresented racial and ethnic minorities (UREM) on hospital boards of directors (14%) and in C-suite positions (14%) remained flat (see Figure 1).
Gender disparities in healthcare and academic leadership also have been slow to change. Periodic surveys conducted by the American College of Healthcare Executives indicate that women comprise only 11% of healthcare CEOs in the U.S.2 And despite the fact that women make up half of all medical students (and one-third of full-time faculty), the Association of American Medical Colleges (AAMC) finds that women still trail men when it comes to attaining full professorship and decanal positions at their academic institutions.3
The Hospitalist interviewed medical directors, researchers, diversity management professionals, and hospitalists to ascertain current solutions being pursued to narrow the gaps in leadership diversity.
Why Diversity in Leadership Matters
Eric E. Howell, MD, MHM, chief of the Division of Hospital Medicine at Johns Hopkins Bayview Medical Center in the Hopkins School of Medicine in Baltimore, believes there is a need to encourage the advancement to leadership positions for female and UREM physicians.
“In medicine, it’s really about service. If we are really here for our patients, we need representation of diversity in our faculty and leadership,” says Dr. Howell, a past SHM president and faculty member of SHM’s Leadership Academy since its inception in 2005. In addition, he says, “Diversity adds incredible strength to an organization and adds to the richness of the ideas and solutions to overcome challenging problems.”
With the implementation of the Affordable Care Act, formerly uninsured people are now accessing the healthcare system; many are bilingual and bicultural, notes George A. Zeppenfeldt-Cestero, president and CEO, Association of Hispanic Healthcare Executives.
“You want to make sure that providers, whether they are physicians, nurses, dentists, or health executives that drive policy issues, are also reflective of that population throughout the organization,” he says. “The real definition of diversity is making sure you have diversity in all layers of the workforce, including the C-suite.”
León points to the coming “seismic demographic shifts” and wonders if healthcare is ready to become more reflective of the communities it serves.
“Increasing diversity in healthcare leadership and governance is essential for the delivery and provision of culturally competent care,” León says. “Now, more than ever, it’s important that we collectively accelerate progress in this area.”
Advancing in Academic and Hospital Medicine
Might hospital medicine offer additional opportunities for women and minorities to advance into leadership positions? Hospitalist Flora Kisuule, MD, SFHM, assistant professor of medicine at Johns Hopkins School of Medicine and associate division director of the Collaborative Inpatient Medicine Service (CIMS) at Johns Hopkins Bayview Medical Center, believes this may be the case. She was with Dr. Howell’s group when he needed to fill the associate director position.
“My advancement speaks to hospital medicine and the fact that we are growing as a field,” she says. “Because of that, opportunities are presenting themselves.”
Dr. Kisuule’s ability to thrive in her position speaks to her professionalism but also to a number of other intentional factors: Dr. Howell’s continuing sponsorship to include her in leadership opportunities, an emergency call system for parents with sick children, and a women’s task force whose agenda calls for transparency in hiring and advancement.
Intentional Structure Change
Cardiologist Hannah A. Valantine, MD, recognizes the importance of addressing the lack of women and people from unrepresented groups in the Science, Technology, Engineering, and Mathematics (STEM) workforce. While at Stanford University School of Medicine, she developed and put into place a set of strategies to understand and mitigate the drivers of gender imbalance. Since then, Dr. Valantine was recruited to bring her expertise to the National Institutes of Health in Bethesda, Md., where she is the inaugural chief officer for scientific workforce diversity. In this role, she is committed “to promoting biomedical workforce diversity as an opportunity, not a problem.”
Dr. Valantine is pushing NIH to pursue a wide range of evidence-based programming to eliminate career-transition barriers that keep women and individuals from underrepresented groups from attaining spots in the top echelons of science and health leadership. She believes that applying scientific rigor to the issue of workforce diversity can lead to quantifiable, translatable, and repeatable methods for recruitment and retention of talent in the biomedical workforce (see “Building Blocks").
Before joining NIH, Dr. Valantine and her colleagues at Stanford surveyed gender composition and faculty satisfaction several years after initiating a multifaceted intervention to boost recruitment and development of women faculty.4 After making a visible commitment of resources to support faculty, with special attention to women, Stanford rose from below to above national benchmarks in the representation of women among faculty. Yet significant work remains to be done, Dr. Valantine says. Her work predicts that the estimated time to achieve 50% occupancy of full professorships by women nationally approaches 50 years—“far too long using current approaches.”
In a separate review article, Dr. Valantine and co-author Christy Sandborg, MD, described the Stanford University School of Medicine Academic Biomedical Career Customization (ABCC) model, which was adapted from Deloitte’s Mass Career Customization framework and allows for development of individual career plans that span a faculty member’s total career, not just a year or two at a time. Long-term planning can enable better alignment between the work culture and values of the workforce, which will improve the outlook for women faculty, Dr. Valantine says.
The issues of work-life balance may actually be generational, Dr. Valantine explains. Veteran hospitalist Janet Nagamine, MD, BSN, SFHM, of Santa Clara, Calif., agrees.
“Nowadays, men as well as women are looking for work-life balance,” she says.
In hospital medicine, Dr. Nagamine points out, the structural changes required to effect a work-life balance for hospital leaders are often difficult to achieve.
“As productivity surveys show, HM group leaders are putting in as many RVUs as the staff,” the former SHM board member says. “There is no dedicated time for administrative duties.”
Construct a Pipeline
Barriers to advancement often are particular to characteristics of diverse populations. For example, the AAMC’s report on the U.S. physician workforce documents that in African-American physicians 40 and younger, women outnumber their male counterparts. Therefore, in the association’s Diversity in Medical Education: Facts and Figures 2012 report, the executive summary points out the need to strengthen the medical education pipeline to increase the number of African-American males who enter the premed track.
Despite the fast-growing percentage of Latino and Hispanic populations in the United States, the shortage of Latino/Hispanic physicians increased from 1980 to 2010. Latinos/Hispanics are greatly underrepresented in the medical student, resident, and faculty populations, according to John Paul Sánchez, MD, MPH, assistant dean for diversity and inclusion in the Office for Diversity and Community Engagement at Rutgers, The State University of New Jersey. Likewise, Zeppenfeldt-Cestero believes that efforts must begin much earlier with Latino and other minority and underrepresented students.
“We have to make sure our students pursue the STEM disciplines and that they also later have the education and preparation to be competitive at the MBA or MPH levels,” he says.
Dr. Sánchez, an associate professor of emergency medicine and a diversity activist since his med school days, is the recipient of last year’s Association of Hispanic Healthcare Executives’ academic leader of the year award. Since September 2014, he has been involved with Building the Next Generation of Academic Physicians Inc., which collaborates with more than 40 medical schools across the country. The initiative offers conferences designed to develop diverse medical students’ and residents’ interest in pursuing academic medicine. Open to all medical students and residents, the conference curriculum is tailored for women, UREMs, and trainees who identify as lesbian, gay, bisexual, or transgender (LGBT), he says. Seven conferences were held in 2015, 10 are planned for this year, and seven for 2017.
Healthcare Leadership Gaps
Despite their omnipresence in healthcare, there is a dearth of women in chief executive and governance roles, as has been noted by both the American College of Healthcare Executives and the National Center for Healthcare Leadership. As with academic leadership positions, the leadership gap in the administrative sector does not seem to be due to a lack of women entering graduate programs in health administration. On the contrary, since the mid-1980s women have comprised 50% to 60% of graduate students.
“This is absolutely not a pipeline issue,” says Christy Harris Lemak, PhD, FACHE, professor and chair of the Department of Health Services Administration at the University of Alabama at Birmingham School of Health Professions and lead investigator of the National Center for Healthcare Leadership’s study of women in healthcare executive positions. Other factors come into play.
In the study, she and her co-authors queried female healthcare CEOs to ascertain the critical career inflection points that led to their success.6 Those who were strategic about their careers, sought out mentors, and voiced their intentions about pursuing leadership positions were more likely to be successful in those efforts. However, individual career efforts must be coupled with overall organizational commitment to fostering inclusion (see “Path to the Top: Strategic Advice for Women").
Hospitals and healthcare organizations must pursue the development of human capital (and the diversity of their leaders) in a systematic way. “We recommended [in the study] that organizations set expectations that leaders who mentor other potential leaders be rewarded in the same way as those who hit financial targets or readmission rate targets,” Dr. Lemak says.
Leadership matters, agrees Deborah J. Bowen, FACHE, CAE, president and CEO of Chicago-based American College of Healthcare Executives.
“I think we’re getting a little smarter. Organizational leaders and trustees have a better understanding that talent development is one of the most important jobs,” she says. “If you don’t have the right people in the right places making good decisions on behalf of the patients and the populations in the communities they’re serving, the rest falls apart.”
Nuances of Mentoring
Many conversations about encouraging diversity in healthcare leadership converge around the role of effective mentoring and sponsorship. A substantial body of research supports the impact of mentoring on retention, research productivity, career satisfaction, and career development for women. It’s important to ensure that the institutional culture is geared toward mentoring junior faculty, says Jessie Kimbrough Marshall, MD, MPH, assistant professor in the Division of General Medicine Hospitalist Program at the University of Michigan Health System in Ann Arbor (UMHS).
Several of our sources pointed out that leaders must learn how to be effective mentors. More attention is being given to enhancing leaders’ mentorship skills. One example is at the Institute for Diversity in Health Management, which conducts an intensive 12-month certificate in diversity management program for practitioners. León says the program fosters ongoing networking and support through the American Leadership Council on Diversity in Healthcare by building leadership competencies.
Dr. Valantine points out that mentoring is hardly a one-style-fits-all proposition but that it is a crucial element to creating and retaining diversity. She says it should be viewed “much more broadly than it is today, and it should focus beyond the trainer-trainee relationship.”
The process is a two-way street. Denege Ward, MD, hospitalist, assistant professor of internal medicine, and director of the medical short stay unit at UMHS, says minorities need to be ready to take a leap of faith.
“Underrepresented faculty and staff should take the risk of possible failure in challenging situations but learn from it and do better and not succumb to fear in face of challenges,” Dr. Ward says.
Although mentoring is one important component in building diversity in academic medicine, Dr. Sánchez asserts that role models, champions, and sponsors are equally important.
“In addition and separate from role models, there must be in place policies and procedures that promote a climate for diverse individuals to succeed,” he says. “What’s needed is an institutional vision and strategic plan that recognizes the importance of diversity. [It] has to become a core principle.”
Dr. Marshall echoes that refrain, noting the recruitment and retention of a diverse set of leaders will take time and intentionality. She is actively engaged in organizing annual meeting mentoring panels at the Society of General Internal Medicine.
“There are still quite a few barriers for women and minorities to advance into hospital leadership roles,” she says. “We still have a long way to go. However, I’m seeing more women and people of color get into these positions. The numbers are increasing, and that encourages me.” TH
Gretchen Henkel is a freelance writer in California.
References
- Institute for Diversity in Health Management. The state of health care diversity and disparities: a benchmarking study of U.S. hospitals. Available at: http://www.diversityconnection.org/diversityconnection/leadership-conferences/Benchmarking-Survey.jsp?fll=S11.
- Top issues confronting hospitals in 2015. American College of Healthcare Executives website. Available at: https://www.ache.org/pubs/research/ceoissues.cfm. Accessed March 5, 2016.
- Association of American Medical Colleges. Diversity in the physician workforce: facts & figures 2014. Available at: http://aamcdiversityfactsandfigures.org/.
- Valantine HA, Grewal D, Ku MC, et al. The gender gap in academic medicine: comparing results from a multifaceted intervention for Stanford faculty to peer and national cohorts. Acad Med. 2014;89(6):904-911.
- Valantine H, Sandborg CI. Changing the culture of academic medicine to eliminate the gender leadership gap: 50/50 by 2020. Acad Med. 2013;88(10):1411-1413.
- Sexton DW, Lemak CH, Wainio JA. Career inflection points of women who successfully achieved the hospital CEO position. J Healthc Manag. 2014;59(5):367-383.
Path to the Top: Strategic Advice for Women
One of the cornerstones of career advancement in healthcare is to stay connected by networking and attending meetings. For women and minorities, the path to leadership may not fit into the traditional linear model of the career ladder.
“For many leadership roles, you have to be visual and present; you have to attend meetings and functions,” says Denege Ward, MD, hospitalist, assistant professor of internal medicine, and director of the medical short stay unit at the University of Michigan Health System in Ann Arbor. “For women, this is difficult. We are still in charge of families and home.”
For some women, it may be more productive to employ the notion of the “leadership labyrinth.” Others refer to a “career lattice” or employ Deloitte’s Mass Career Customization framework.
“For women, the trajectory may include working part-time while their children are small or finding local training opportunities,” says Christy Harris Lemak, PhD, FACHE, professor and chair of the Department of Health Services Administration at the University of Alabama at Birmingham School of Health Professions and lead investigator of the National Center for Healthcare Leadership’s study of women in healthcare executive positions.
Hospitalist Flora Kisuule, MD, assistant professor of medicine at Johns Hopkins School of Medicine and associate division director of the Collaborative Inpatient Medicine Service (CIMS) at Johns Hopkins Bayview Medical Center in Baltimore, is a wife and mother of a 4-year-old. She agrees the leadership path for moms can take unexpected detours. She’s been able to complete some of her administrative tasks at home through the support of her medical director. If pursuing an MBA is too daunting, she encourages her hospitalist peers to take advantage of short courses and programs in leadership.
“As women, we like to do for others,” notes Elizabeth Gundersen, MD, FHM, assistant professor of clinical biomedical sciences at the Charles E. Schmidt College of Medicine at Florida Atlantic University in Boca Raton. While at the University of Massachusetts, she was one of eight physician quality officers and associate division chief of hospital medicine. To counter the impulse to say yes to everything, including roles that distract from ultimate career goals, one of the women leaders at UMass encouraged her mentees to “think of your ideal position—and then when a position is offered, assess that against your criteria.”
Jessie Kimbrough Marshall, MD, MPH, assistant professor in the Division of General Medicine Hospitalist Program at the University of Michigan Health System, seconds that opinion.
“Try to avoid professional commitments and activities that are not aligned to your career trajectory,” Dr. Marshall advises. “You can also identify someone who is in a position that is close to what you envision for yourself and reach out to that person.”
—Gretchen Henkel
Building Blocks: NIH’s Commitment to Enhance Diversity
The National Institutes of Health (NIH) has been committed to enhancing diversity for decades, according to cardiologist Hannah A. Valantine, MD.
“NIH has made considerable investments in programming,” says Dr. Valantine. However, despite these investments, “the change has not been as rapid or sustainable as we would like it to be.”
As a first step, in October 2014, NIH announced a new set of initiatives designed to enhance the ways in which participants are engaged and trained. Three components comprise the Enhancing Diversity in the NIH-Funded Workforce program. The Building Infrastructure Leading to Diversity (BUILD) program was awarded to 10 universities that met eligibility criteria for being under-resourced. The National Research Mentoring Network (NRMN) will recruit mentors and use methods (such as “train the trainer”) to bring a more deliberate and intentional approach to cultivating mentors. The third component, the Coordinating and Evaluation Center (CEC), focuses on evaluation and dissemination of identified best practices and competencies.
“We are moving away from the assumption that just because you are a leader in your research field that that means you are a good mentor,” Dr. Valantine says.
Throughout its history, the United States has been a nation of immigrants. From the early colonial settlements to the mid-20th century, most immigrants came from Western European countries. Since 1965, when the Immigration and Nationality Act abolished national-origin quotas, the diversity of immigrants has increased. “By the year 2043,” says Tomás León, president and CEO of the Institute for Diversity in Health Management in Chicago, “we will be a country where the majority of our population is comprised of racial and ethnic minorities.”
Those changing demographics, cited from the U.S. Census Bureau’s projections, already are evidenced in hospital patient populations. According to a benchmarking survey sponsored by the institute, which is an affiliate of the American Hospital Association, the percentage of minority patients seen in hospitals grew from 29% to 31% of patient census between 2011 and 2013.1 And yet, the survey found this increasing diversity is not currently reflected in leadership positions. During the same time period, underrepresented racial and ethnic minorities (UREM) on hospital boards of directors (14%) and in C-suite positions (14%) remained flat (see Figure 1).
Gender disparities in healthcare and academic leadership also have been slow to change. Periodic surveys conducted by the American College of Healthcare Executives indicate that women comprise only 11% of healthcare CEOs in the U.S.2 And despite the fact that women make up half of all medical students (and one-third of full-time faculty), the Association of American Medical Colleges (AAMC) finds that women still trail men when it comes to attaining full professorship and decanal positions at their academic institutions.3
The Hospitalist interviewed medical directors, researchers, diversity management professionals, and hospitalists to ascertain current solutions being pursued to narrow the gaps in leadership diversity.
Why Diversity in Leadership Matters
Eric E. Howell, MD, MHM, chief of the Division of Hospital Medicine at Johns Hopkins Bayview Medical Center in the Hopkins School of Medicine in Baltimore, believes there is a need to encourage the advancement to leadership positions for female and UREM physicians.
“In medicine, it’s really about service. If we are really here for our patients, we need representation of diversity in our faculty and leadership,” says Dr. Howell, a past SHM president and faculty member of SHM’s Leadership Academy since its inception in 2005. In addition, he says, “Diversity adds incredible strength to an organization and adds to the richness of the ideas and solutions to overcome challenging problems.”
With the implementation of the Affordable Care Act, formerly uninsured people are now accessing the healthcare system; many are bilingual and bicultural, notes George A. Zeppenfeldt-Cestero, president and CEO, Association of Hispanic Healthcare Executives.
“You want to make sure that providers, whether they are physicians, nurses, dentists, or health executives that drive policy issues, are also reflective of that population throughout the organization,” he says. “The real definition of diversity is making sure you have diversity in all layers of the workforce, including the C-suite.”
León points to the coming “seismic demographic shifts” and wonders if healthcare is ready to become more reflective of the communities it serves.
“Increasing diversity in healthcare leadership and governance is essential for the delivery and provision of culturally competent care,” León says. “Now, more than ever, it’s important that we collectively accelerate progress in this area.”
Advancing in Academic and Hospital Medicine
Might hospital medicine offer additional opportunities for women and minorities to advance into leadership positions? Hospitalist Flora Kisuule, MD, SFHM, assistant professor of medicine at Johns Hopkins School of Medicine and associate division director of the Collaborative Inpatient Medicine Service (CIMS) at Johns Hopkins Bayview Medical Center, believes this may be the case. She was with Dr. Howell’s group when he needed to fill the associate director position.
“My advancement speaks to hospital medicine and the fact that we are growing as a field,” she says. “Because of that, opportunities are presenting themselves.”
Dr. Kisuule’s ability to thrive in her position speaks to her professionalism but also to a number of other intentional factors: Dr. Howell’s continuing sponsorship to include her in leadership opportunities, an emergency call system for parents with sick children, and a women’s task force whose agenda calls for transparency in hiring and advancement.
Intentional Structure Change
Cardiologist Hannah A. Valantine, MD, recognizes the importance of addressing the lack of women and people from unrepresented groups in the Science, Technology, Engineering, and Mathematics (STEM) workforce. While at Stanford University School of Medicine, she developed and put into place a set of strategies to understand and mitigate the drivers of gender imbalance. Since then, Dr. Valantine was recruited to bring her expertise to the National Institutes of Health in Bethesda, Md., where she is the inaugural chief officer for scientific workforce diversity. In this role, she is committed “to promoting biomedical workforce diversity as an opportunity, not a problem.”
Dr. Valantine is pushing NIH to pursue a wide range of evidence-based programming to eliminate career-transition barriers that keep women and individuals from underrepresented groups from attaining spots in the top echelons of science and health leadership. She believes that applying scientific rigor to the issue of workforce diversity can lead to quantifiable, translatable, and repeatable methods for recruitment and retention of talent in the biomedical workforce (see “Building Blocks").
Before joining NIH, Dr. Valantine and her colleagues at Stanford surveyed gender composition and faculty satisfaction several years after initiating a multifaceted intervention to boost recruitment and development of women faculty.4 After making a visible commitment of resources to support faculty, with special attention to women, Stanford rose from below to above national benchmarks in the representation of women among faculty. Yet significant work remains to be done, Dr. Valantine says. Her work predicts that the estimated time to achieve 50% occupancy of full professorships by women nationally approaches 50 years—“far too long using current approaches.”
In a separate review article, Dr. Valantine and co-author Christy Sandborg, MD, described the Stanford University School of Medicine Academic Biomedical Career Customization (ABCC) model, which was adapted from Deloitte’s Mass Career Customization framework and allows for development of individual career plans that span a faculty member’s total career, not just a year or two at a time. Long-term planning can enable better alignment between the work culture and values of the workforce, which will improve the outlook for women faculty, Dr. Valantine says.
The issues of work-life balance may actually be generational, Dr. Valantine explains. Veteran hospitalist Janet Nagamine, MD, BSN, SFHM, of Santa Clara, Calif., agrees.
“Nowadays, men as well as women are looking for work-life balance,” she says.
In hospital medicine, Dr. Nagamine points out, the structural changes required to effect a work-life balance for hospital leaders are often difficult to achieve.
“As productivity surveys show, HM group leaders are putting in as many RVUs as the staff,” the former SHM board member says. “There is no dedicated time for administrative duties.”
Construct a Pipeline
Barriers to advancement often are particular to characteristics of diverse populations. For example, the AAMC’s report on the U.S. physician workforce documents that in African-American physicians 40 and younger, women outnumber their male counterparts. Therefore, in the association’s Diversity in Medical Education: Facts and Figures 2012 report, the executive summary points out the need to strengthen the medical education pipeline to increase the number of African-American males who enter the premed track.
Despite the fast-growing percentage of Latino and Hispanic populations in the United States, the shortage of Latino/Hispanic physicians increased from 1980 to 2010. Latinos/Hispanics are greatly underrepresented in the medical student, resident, and faculty populations, according to John Paul Sánchez, MD, MPH, assistant dean for diversity and inclusion in the Office for Diversity and Community Engagement at Rutgers, The State University of New Jersey. Likewise, Zeppenfeldt-Cestero believes that efforts must begin much earlier with Latino and other minority and underrepresented students.
“We have to make sure our students pursue the STEM disciplines and that they also later have the education and preparation to be competitive at the MBA or MPH levels,” he says.
Dr. Sánchez, an associate professor of emergency medicine and a diversity activist since his med school days, is the recipient of last year’s Association of Hispanic Healthcare Executives’ academic leader of the year award. Since September 2014, he has been involved with Building the Next Generation of Academic Physicians Inc., which collaborates with more than 40 medical schools across the country. The initiative offers conferences designed to develop diverse medical students’ and residents’ interest in pursuing academic medicine. Open to all medical students and residents, the conference curriculum is tailored for women, UREMs, and trainees who identify as lesbian, gay, bisexual, or transgender (LGBT), he says. Seven conferences were held in 2015, 10 are planned for this year, and seven for 2017.
Healthcare Leadership Gaps
Despite their omnipresence in healthcare, there is a dearth of women in chief executive and governance roles, as has been noted by both the American College of Healthcare Executives and the National Center for Healthcare Leadership. As with academic leadership positions, the leadership gap in the administrative sector does not seem to be due to a lack of women entering graduate programs in health administration. On the contrary, since the mid-1980s women have comprised 50% to 60% of graduate students.
“This is absolutely not a pipeline issue,” says Christy Harris Lemak, PhD, FACHE, professor and chair of the Department of Health Services Administration at the University of Alabama at Birmingham School of Health Professions and lead investigator of the National Center for Healthcare Leadership’s study of women in healthcare executive positions. Other factors come into play.
In the study, she and her co-authors queried female healthcare CEOs to ascertain the critical career inflection points that led to their success.6 Those who were strategic about their careers, sought out mentors, and voiced their intentions about pursuing leadership positions were more likely to be successful in those efforts. However, individual career efforts must be coupled with overall organizational commitment to fostering inclusion (see “Path to the Top: Strategic Advice for Women").
Hospitals and healthcare organizations must pursue the development of human capital (and the diversity of their leaders) in a systematic way. “We recommended [in the study] that organizations set expectations that leaders who mentor other potential leaders be rewarded in the same way as those who hit financial targets or readmission rate targets,” Dr. Lemak says.
Leadership matters, agrees Deborah J. Bowen, FACHE, CAE, president and CEO of Chicago-based American College of Healthcare Executives.
“I think we’re getting a little smarter. Organizational leaders and trustees have a better understanding that talent development is one of the most important jobs,” she says. “If you don’t have the right people in the right places making good decisions on behalf of the patients and the populations in the communities they’re serving, the rest falls apart.”
Nuances of Mentoring
Many conversations about encouraging diversity in healthcare leadership converge around the role of effective mentoring and sponsorship. A substantial body of research supports the impact of mentoring on retention, research productivity, career satisfaction, and career development for women. It’s important to ensure that the institutional culture is geared toward mentoring junior faculty, says Jessie Kimbrough Marshall, MD, MPH, assistant professor in the Division of General Medicine Hospitalist Program at the University of Michigan Health System in Ann Arbor (UMHS).
Several of our sources pointed out that leaders must learn how to be effective mentors. More attention is being given to enhancing leaders’ mentorship skills. One example is at the Institute for Diversity in Health Management, which conducts an intensive 12-month certificate in diversity management program for practitioners. León says the program fosters ongoing networking and support through the American Leadership Council on Diversity in Healthcare by building leadership competencies.
Dr. Valantine points out that mentoring is hardly a one-style-fits-all proposition but that it is a crucial element to creating and retaining diversity. She says it should be viewed “much more broadly than it is today, and it should focus beyond the trainer-trainee relationship.”
The process is a two-way street. Denege Ward, MD, hospitalist, assistant professor of internal medicine, and director of the medical short stay unit at UMHS, says minorities need to be ready to take a leap of faith.
“Underrepresented faculty and staff should take the risk of possible failure in challenging situations but learn from it and do better and not succumb to fear in face of challenges,” Dr. Ward says.
Although mentoring is one important component in building diversity in academic medicine, Dr. Sánchez asserts that role models, champions, and sponsors are equally important.
“In addition and separate from role models, there must be in place policies and procedures that promote a climate for diverse individuals to succeed,” he says. “What’s needed is an institutional vision and strategic plan that recognizes the importance of diversity. [It] has to become a core principle.”
Dr. Marshall echoes that refrain, noting the recruitment and retention of a diverse set of leaders will take time and intentionality. She is actively engaged in organizing annual meeting mentoring panels at the Society of General Internal Medicine.
“There are still quite a few barriers for women and minorities to advance into hospital leadership roles,” she says. “We still have a long way to go. However, I’m seeing more women and people of color get into these positions. The numbers are increasing, and that encourages me.” TH
Gretchen Henkel is a freelance writer in California.
References
- Institute for Diversity in Health Management. The state of health care diversity and disparities: a benchmarking study of U.S. hospitals. Available at: http://www.diversityconnection.org/diversityconnection/leadership-conferences/Benchmarking-Survey.jsp?fll=S11.
- Top issues confronting hospitals in 2015. American College of Healthcare Executives website. Available at: https://www.ache.org/pubs/research/ceoissues.cfm. Accessed March 5, 2016.
- Association of American Medical Colleges. Diversity in the physician workforce: facts & figures 2014. Available at: http://aamcdiversityfactsandfigures.org/.
- Valantine HA, Grewal D, Ku MC, et al. The gender gap in academic medicine: comparing results from a multifaceted intervention for Stanford faculty to peer and national cohorts. Acad Med. 2014;89(6):904-911.
- Valantine H, Sandborg CI. Changing the culture of academic medicine to eliminate the gender leadership gap: 50/50 by 2020. Acad Med. 2013;88(10):1411-1413.
- Sexton DW, Lemak CH, Wainio JA. Career inflection points of women who successfully achieved the hospital CEO position. J Healthc Manag. 2014;59(5):367-383.
Path to the Top: Strategic Advice for Women
One of the cornerstones of career advancement in healthcare is to stay connected by networking and attending meetings. For women and minorities, the path to leadership may not fit into the traditional linear model of the career ladder.
“For many leadership roles, you have to be visual and present; you have to attend meetings and functions,” says Denege Ward, MD, hospitalist, assistant professor of internal medicine, and director of the medical short stay unit at the University of Michigan Health System in Ann Arbor. “For women, this is difficult. We are still in charge of families and home.”
For some women, it may be more productive to employ the notion of the “leadership labyrinth.” Others refer to a “career lattice” or employ Deloitte’s Mass Career Customization framework.
“For women, the trajectory may include working part-time while their children are small or finding local training opportunities,” says Christy Harris Lemak, PhD, FACHE, professor and chair of the Department of Health Services Administration at the University of Alabama at Birmingham School of Health Professions and lead investigator of the National Center for Healthcare Leadership’s study of women in healthcare executive positions.
Hospitalist Flora Kisuule, MD, assistant professor of medicine at Johns Hopkins School of Medicine and associate division director of the Collaborative Inpatient Medicine Service (CIMS) at Johns Hopkins Bayview Medical Center in Baltimore, is a wife and mother of a 4-year-old. She agrees the leadership path for moms can take unexpected detours. She’s been able to complete some of her administrative tasks at home through the support of her medical director. If pursuing an MBA is too daunting, she encourages her hospitalist peers to take advantage of short courses and programs in leadership.
“As women, we like to do for others,” notes Elizabeth Gundersen, MD, FHM, assistant professor of clinical biomedical sciences at the Charles E. Schmidt College of Medicine at Florida Atlantic University in Boca Raton. While at the University of Massachusetts, she was one of eight physician quality officers and associate division chief of hospital medicine. To counter the impulse to say yes to everything, including roles that distract from ultimate career goals, one of the women leaders at UMass encouraged her mentees to “think of your ideal position—and then when a position is offered, assess that against your criteria.”
Jessie Kimbrough Marshall, MD, MPH, assistant professor in the Division of General Medicine Hospitalist Program at the University of Michigan Health System, seconds that opinion.
“Try to avoid professional commitments and activities that are not aligned to your career trajectory,” Dr. Marshall advises. “You can also identify someone who is in a position that is close to what you envision for yourself and reach out to that person.”
—Gretchen Henkel
Building Blocks: NIH’s Commitment to Enhance Diversity
The National Institutes of Health (NIH) has been committed to enhancing diversity for decades, according to cardiologist Hannah A. Valantine, MD.
“NIH has made considerable investments in programming,” says Dr. Valantine. However, despite these investments, “the change has not been as rapid or sustainable as we would like it to be.”
As a first step, in October 2014, NIH announced a new set of initiatives designed to enhance the ways in which participants are engaged and trained. Three components comprise the Enhancing Diversity in the NIH-Funded Workforce program. The Building Infrastructure Leading to Diversity (BUILD) program was awarded to 10 universities that met eligibility criteria for being under-resourced. The National Research Mentoring Network (NRMN) will recruit mentors and use methods (such as “train the trainer”) to bring a more deliberate and intentional approach to cultivating mentors. The third component, the Coordinating and Evaluation Center (CEC), focuses on evaluation and dissemination of identified best practices and competencies.
“We are moving away from the assumption that just because you are a leader in your research field that that means you are a good mentor,” Dr. Valantine says.
Venetoclax + LDAC has potential in older AML patients

site of ASCO Annual Meeting
© ASCO/Todd Buchanan
CHICAGO—Investigators are pursuing the combination of the selective BCL-2 inhibitor venetoclax plus low-dose cytarabine (LDAC) in older, treatment-naïve patients with acute myeloid leukemia (AML) who are unfit for intensive chemotherapy.
These patients have few treatment options, and to date, the combination is achieving significant reduction in bone marrow and peripheral blast counts.
The combination has also achieved some complete responses, including those with incomplete marrow recovery, for a complete response (CR) rate of 54%. By comparison, expected CR rates with LDAC are about 10%.
Tara L. Lin, MD, of the University of Kansas Medical Center in Kansas City, reported the results of the non-randomized, open-label phase 1/2 dose-escalation/expansion study as abstract 7007* at the 2016 ASCO Annual Meeting.
Dr Lin reported on the 18 patients enrolled in the phase 1 portion and on an additional 8 patients treated in the phase 2 portion.
Objectives of the study were safety, efficacy, and exploratory for biomarkers predictive of outcome.
Dr Lin noted that the entire study had almost reached full enrollment early in May, and an additional 50 patients had been treated on the phase 2 portion to date.
Eligibility criteria
Patients 65 years or older with untreated AML were eligible to enroll. They could not be eligible for standard induction therapy, and they had to have ECOG performance status of 0 – 2.
Patients were excluded if they had received cytarabine previously for a pre-existing myeloid disorder, acute promyelocytic leukemia, or active central nervous system involvement with AML.
Dosing schedule
In the phase 1 portion, patients received venetoclax orally once daily on days 2 – 28 of cycle 1 and days 1 – 28 of subsequent cycles, which were 28 days.
They received LDAC at 20 mg/m2 subcutaneously on days 1 – 10 of all cycles.
The venetoclax dose escalated from 50 mg to 600 mg in 6 days for dose level 1, and from 100 mg to 800 mg in 6 days for dose level 2.
Every patient was hospitalized prior to the initiation of therapy and aggressive tumor lysis prophylaxis begun at least 48 hours prior to venetoclax administration during cycle 1 and 24 hours prior to start of LDAC.
Once the patients had received prophylaxis and had a white blood cell count <25,000/μL, they were able to begin therapy starting with LDAC on day 1 and continuing through day 10.
No patient received venetoclax on day 1, Dr Lin emphasized.
Instead venetoclax began 24 hours after the LDAC, starting on day 2, and dose escalated each day until patients reached the maximum dose that was designed for their cohort level, which was then continued on days 6 – 28.
“A dose-limiting toxicity of thrombocytopenia was identified in the phase 1 portion,” Dr Lin said, “which led to the phase 2 dose recommendation of 600 mg daily of venetoclax.”
Demographics
Twenty-six patients were evaluable at the time of the presentation, 16 in the venetoclax 600-mg dose group and 10 in the 800-mg dose group.
The patients were a median of 75 years (range 66 – 87).
Sixty-five percent were males, 62% were ECOG status 1, and 19% (5 patients) had received prior hypomethylating treatment for pre-existing myelodysplastic syndromes.
Thirty-eight percent had bone marrow blast counts of 51% or greater.
Safety
Treatment-emergent adverse events (TEAEs), excluding cytopenias, occurring in 30% or more of patients included nausea (77%), fatigue (42%), febrile neutropenia (38%), diarrhea (35%), and vomiting (31%).
Grade 3/4 TEAEs, excluding cytopenias, occurring in 10% or more of patients included febrile neutropenia (38%), hypertension (12%), hyponatremia (12%), and hypophosphatemia (12%).
“In general,” Dr Lin said, “the drug was very well tolerated and patients were not discontinuing therapy because of side effects.”
Pharmacokinetics
At day 10, which coincided with the end day of the co-administration of the 2 drugs, and again, at day 18, when patients were receiving venetoclax alone, no differences were seen in either the Cmax per dose or AUC per dose between day 10 and day 18.
So the co-administration of LDAC did not markedly affect venetoclax exposures.
Efficacy
The overall response rate, consisting of CR plus CRi plus partial responses (PR), totaled 58% (15/26) of all patients.
Nine patients (35%) had resistant or progressive disease; 2 had incomplete data due to discontinuation.
Most patients (79%)—19 of 24—had a decrease in bone marrow blast count of over 50%, and 88% (15/17) had a decrease in peripheral blast count of over 50%.
Responses of patients who had received hypomethylating agents did not differ from those who had not.
The investigators also evaluated the impact of a prior myeloproliferative neoplasm (MPN) (n=4) on outcome and found that none of these patients had a response to therapy.
However, patients who did not have a previous MPN had a response rate of 68%.
Survival
At 12 months, overall survival (OS) in all patients was 57.6%. If MPN patients were not included in the analysis, the OS increased to 70.5%.
The 11 non-responders had a median OS of 4 months, while for the 15 responders (CR, Cri, PR) the median OS has not yet been reached.
“This data, in terms of taking into account the safety data, how well it appears to have been tolerated by the patients, and these overall response data,” Dr Lin said, “certainly suggest that venetoclax plus low-dose araC appears to have significant activity in this older patient population and . . . is worth further study for this patient group.”
Venetoclax has demonstrated single-agent activity in heavily pretreated patients with relapsed/refractory AML. It received accelerated approval from the US Food and Drug Administration (FDA) for the treatment of chronic lymphocytic leukemia (CLL), and has 3 breakthrough therapy designations from the FDA—one in combination with hypomethylating agents for treatment-naïve AML, one in relapsed or refractory CLL, and one in combination with rituximab for relapsed/refractory CLL.
The European Commission also granted venetoclax orphan designation for AML.
Venetoclax is being developed by AbbVie in collaboration with Genentech. AbbVie and Genentech provided financial support for the study and participated in the design, study conduct, analysis, and interpretation of data. ![]()
*Data in the abstract differ from the presentation.
site of ASCO Annual Meeting
© ASCO/Todd Buchanan
CHICAGO—Investigators are pursuing the combination of the selective BCL-2 inhibitor venetoclax plus low-dose cytarabine (LDAC) in older, treatment-naïve patients with acute myeloid leukemia (AML) who are unfit for intensive chemotherapy.
These patients have few treatment options, and to date, the combination is achieving significant reduction in bone marrow and peripheral blast counts.
The combination has also achieved some complete responses, including those with incomplete marrow recovery, for a complete response (CR) rate of 54%. By comparison, expected CR rates with LDAC are about 10%.
Tara L. Lin, MD, of the University of Kansas Medical Center in Kansas City, reported the results of the non-randomized, open-label phase 1/2 dose-escalation/expansion study as abstract 7007* at the 2016 ASCO Annual Meeting.
Dr Lin reported on the 18 patients enrolled in the phase 1 portion and on an additional 8 patients treated in the phase 2 portion.
Objectives of the study were safety, efficacy, and exploratory for biomarkers predictive of outcome.
Dr Lin noted that the entire study had almost reached full enrollment early in May, and an additional 50 patients had been treated on the phase 2 portion to date.
Eligibility criteria
Patients 65 years or older with untreated AML were eligible to enroll. They could not be eligible for standard induction therapy, and they had to have ECOG performance status of 0 – 2.
Patients were excluded if they had received cytarabine previously for a pre-existing myeloid disorder, acute promyelocytic leukemia, or active central nervous system involvement with AML.
Dosing schedule
In the phase 1 portion, patients received venetoclax orally once daily on days 2 – 28 of cycle 1 and days 1 – 28 of subsequent cycles, which were 28 days.
They received LDAC at 20 mg/m2 subcutaneously on days 1 – 10 of all cycles.
The venetoclax dose escalated from 50 mg to 600 mg in 6 days for dose level 1, and from 100 mg to 800 mg in 6 days for dose level 2.
Every patient was hospitalized prior to the initiation of therapy and aggressive tumor lysis prophylaxis begun at least 48 hours prior to venetoclax administration during cycle 1 and 24 hours prior to start of LDAC.
Once the patients had received prophylaxis and had a white blood cell count <25,000/μL, they were able to begin therapy starting with LDAC on day 1 and continuing through day 10.
No patient received venetoclax on day 1, Dr Lin emphasized.
Instead venetoclax began 24 hours after the LDAC, starting on day 2, and dose escalated each day until patients reached the maximum dose that was designed for their cohort level, which was then continued on days 6 – 28.
“A dose-limiting toxicity of thrombocytopenia was identified in the phase 1 portion,” Dr Lin said, “which led to the phase 2 dose recommendation of 600 mg daily of venetoclax.”
Demographics
Twenty-six patients were evaluable at the time of the presentation, 16 in the venetoclax 600-mg dose group and 10 in the 800-mg dose group.
The patients were a median of 75 years (range 66 – 87).
Sixty-five percent were males, 62% were ECOG status 1, and 19% (5 patients) had received prior hypomethylating treatment for pre-existing myelodysplastic syndromes.
Thirty-eight percent had bone marrow blast counts of 51% or greater.
Safety
Treatment-emergent adverse events (TEAEs), excluding cytopenias, occurring in 30% or more of patients included nausea (77%), fatigue (42%), febrile neutropenia (38%), diarrhea (35%), and vomiting (31%).
Grade 3/4 TEAEs, excluding cytopenias, occurring in 10% or more of patients included febrile neutropenia (38%), hypertension (12%), hyponatremia (12%), and hypophosphatemia (12%).
“In general,” Dr Lin said, “the drug was very well tolerated and patients were not discontinuing therapy because of side effects.”
Pharmacokinetics
At day 10, which coincided with the end day of the co-administration of the 2 drugs, and again, at day 18, when patients were receiving venetoclax alone, no differences were seen in either the Cmax per dose or AUC per dose between day 10 and day 18.
So the co-administration of LDAC did not markedly affect venetoclax exposures.
Efficacy
The overall response rate, consisting of CR plus CRi plus partial responses (PR), totaled 58% (15/26) of all patients.
Nine patients (35%) had resistant or progressive disease; 2 had incomplete data due to discontinuation.
Most patients (79%)—19 of 24—had a decrease in bone marrow blast count of over 50%, and 88% (15/17) had a decrease in peripheral blast count of over 50%.
Responses of patients who had received hypomethylating agents did not differ from those who had not.
The investigators also evaluated the impact of a prior myeloproliferative neoplasm (MPN) (n=4) on outcome and found that none of these patients had a response to therapy.
However, patients who did not have a previous MPN had a response rate of 68%.
Survival
At 12 months, overall survival (OS) in all patients was 57.6%. If MPN patients were not included in the analysis, the OS increased to 70.5%.
The 11 non-responders had a median OS of 4 months, while for the 15 responders (CR, Cri, PR) the median OS has not yet been reached.
“This data, in terms of taking into account the safety data, how well it appears to have been tolerated by the patients, and these overall response data,” Dr Lin said, “certainly suggest that venetoclax plus low-dose araC appears to have significant activity in this older patient population and . . . is worth further study for this patient group.”
Venetoclax has demonstrated single-agent activity in heavily pretreated patients with relapsed/refractory AML. It received accelerated approval from the US Food and Drug Administration (FDA) for the treatment of chronic lymphocytic leukemia (CLL), and has 3 breakthrough therapy designations from the FDA—one in combination with hypomethylating agents for treatment-naïve AML, one in relapsed or refractory CLL, and one in combination with rituximab for relapsed/refractory CLL.
The European Commission also granted venetoclax orphan designation for AML.
Venetoclax is being developed by AbbVie in collaboration with Genentech. AbbVie and Genentech provided financial support for the study and participated in the design, study conduct, analysis, and interpretation of data. ![]()
*Data in the abstract differ from the presentation.
site of ASCO Annual Meeting
© ASCO/Todd Buchanan
CHICAGO—Investigators are pursuing the combination of the selective BCL-2 inhibitor venetoclax plus low-dose cytarabine (LDAC) in older, treatment-naïve patients with acute myeloid leukemia (AML) who are unfit for intensive chemotherapy.
These patients have few treatment options, and to date, the combination is achieving significant reduction in bone marrow and peripheral blast counts.
The combination has also achieved some complete responses, including those with incomplete marrow recovery, for a complete response (CR) rate of 54%. By comparison, expected CR rates with LDAC are about 10%.
Tara L. Lin, MD, of the University of Kansas Medical Center in Kansas City, reported the results of the non-randomized, open-label phase 1/2 dose-escalation/expansion study as abstract 7007* at the 2016 ASCO Annual Meeting.
Dr Lin reported on the 18 patients enrolled in the phase 1 portion and on an additional 8 patients treated in the phase 2 portion.
Objectives of the study were safety, efficacy, and exploratory for biomarkers predictive of outcome.
Dr Lin noted that the entire study had almost reached full enrollment early in May, and an additional 50 patients had been treated on the phase 2 portion to date.
Eligibility criteria
Patients 65 years or older with untreated AML were eligible to enroll. They could not be eligible for standard induction therapy, and they had to have ECOG performance status of 0 – 2.
Patients were excluded if they had received cytarabine previously for a pre-existing myeloid disorder, acute promyelocytic leukemia, or active central nervous system involvement with AML.
Dosing schedule
In the phase 1 portion, patients received venetoclax orally once daily on days 2 – 28 of cycle 1 and days 1 – 28 of subsequent cycles, which were 28 days.
They received LDAC at 20 mg/m2 subcutaneously on days 1 – 10 of all cycles.
The venetoclax dose escalated from 50 mg to 600 mg in 6 days for dose level 1, and from 100 mg to 800 mg in 6 days for dose level 2.
Every patient was hospitalized prior to the initiation of therapy and aggressive tumor lysis prophylaxis begun at least 48 hours prior to venetoclax administration during cycle 1 and 24 hours prior to start of LDAC.
Once the patients had received prophylaxis and had a white blood cell count <25,000/μL, they were able to begin therapy starting with LDAC on day 1 and continuing through day 10.
No patient received venetoclax on day 1, Dr Lin emphasized.
Instead venetoclax began 24 hours after the LDAC, starting on day 2, and dose escalated each day until patients reached the maximum dose that was designed for their cohort level, which was then continued on days 6 – 28.
“A dose-limiting toxicity of thrombocytopenia was identified in the phase 1 portion,” Dr Lin said, “which led to the phase 2 dose recommendation of 600 mg daily of venetoclax.”
Demographics
Twenty-six patients were evaluable at the time of the presentation, 16 in the venetoclax 600-mg dose group and 10 in the 800-mg dose group.
The patients were a median of 75 years (range 66 – 87).
Sixty-five percent were males, 62% were ECOG status 1, and 19% (5 patients) had received prior hypomethylating treatment for pre-existing myelodysplastic syndromes.
Thirty-eight percent had bone marrow blast counts of 51% or greater.
Safety
Treatment-emergent adverse events (TEAEs), excluding cytopenias, occurring in 30% or more of patients included nausea (77%), fatigue (42%), febrile neutropenia (38%), diarrhea (35%), and vomiting (31%).
Grade 3/4 TEAEs, excluding cytopenias, occurring in 10% or more of patients included febrile neutropenia (38%), hypertension (12%), hyponatremia (12%), and hypophosphatemia (12%).
“In general,” Dr Lin said, “the drug was very well tolerated and patients were not discontinuing therapy because of side effects.”
Pharmacokinetics
At day 10, which coincided with the end day of the co-administration of the 2 drugs, and again, at day 18, when patients were receiving venetoclax alone, no differences were seen in either the Cmax per dose or AUC per dose between day 10 and day 18.
So the co-administration of LDAC did not markedly affect venetoclax exposures.
Efficacy
The overall response rate, consisting of CR plus CRi plus partial responses (PR), totaled 58% (15/26) of all patients.
Nine patients (35%) had resistant or progressive disease; 2 had incomplete data due to discontinuation.
Most patients (79%)—19 of 24—had a decrease in bone marrow blast count of over 50%, and 88% (15/17) had a decrease in peripheral blast count of over 50%.
Responses of patients who had received hypomethylating agents did not differ from those who had not.
The investigators also evaluated the impact of a prior myeloproliferative neoplasm (MPN) (n=4) on outcome and found that none of these patients had a response to therapy.
However, patients who did not have a previous MPN had a response rate of 68%.
Survival
At 12 months, overall survival (OS) in all patients was 57.6%. If MPN patients were not included in the analysis, the OS increased to 70.5%.
The 11 non-responders had a median OS of 4 months, while for the 15 responders (CR, Cri, PR) the median OS has not yet been reached.
“This data, in terms of taking into account the safety data, how well it appears to have been tolerated by the patients, and these overall response data,” Dr Lin said, “certainly suggest that venetoclax plus low-dose araC appears to have significant activity in this older patient population and . . . is worth further study for this patient group.”
Venetoclax has demonstrated single-agent activity in heavily pretreated patients with relapsed/refractory AML. It received accelerated approval from the US Food and Drug Administration (FDA) for the treatment of chronic lymphocytic leukemia (CLL), and has 3 breakthrough therapy designations from the FDA—one in combination with hypomethylating agents for treatment-naïve AML, one in relapsed or refractory CLL, and one in combination with rituximab for relapsed/refractory CLL.
The European Commission also granted venetoclax orphan designation for AML.
Venetoclax is being developed by AbbVie in collaboration with Genentech. AbbVie and Genentech provided financial support for the study and participated in the design, study conduct, analysis, and interpretation of data. ![]()
*Data in the abstract differ from the presentation.
Delaying therapy for HL/NHL likely safe for mom, baby

Photo credit: Vera Kratochvil
A single-center retrospective study of 39 pregnant women diagnosed with Hodgkin lymphoma (HL) or non-Hodgkin lymphoma (NHL) during pregnancy indicates that delaying treatment until the second trimester is “likely safe and results in acceptable” outcomes for both mother and child.
Investigators also found that deferring therapy until after delivery did not adversely affect maternal outcomes.
In order to clarify the sometimes conflicting reports regarding management of lymphoma during pregnancy, investigators at MD Anderson Cancer Center in Houston, Texas, undertook the study to determine whether administering standard chemotherapy during the second and third trimesters has acceptable maternal and fetal outcomes.
Michelle A. Fanale, MD, and colleagues published their findings in JAMA Oncology.
Patient characteristics
Investigators identified 31 women with HL and 8 with NHL who were diagnosed between 1991 and 2014 and had sufficient pregnancy and follow-up data.
The women were a median age of 28 years (range 19-38). The patients with NHL were significantly older, P=0.004.
Approximately 20% of patients had B symptoms. Most were stage II disease (72%), and 80% were ECOG performance status 0 or 1.
About two thirds of patients had hemoglobin levels less than 12 g/dL.
Most patients did not have extranodal nonbone-marrow disease (82%), although there was a significant difference between those with HL (90%) and NHL (50%), P=0.03.
One third of patients had bulky disease, and 88% were in their second or third trimesters at diagnosis.
Three women electively terminated their pregnancies at diagnosis. Of the 36 remaining patients, 24 (61%) began antenatal therapy and 12 (31%) postponed therapy until after delivery.
Four patients received radiation therapy above the diaphragm at a median dose of 40.4 Gy.
Obstetric outcomes
Antenatal therapy was not associated with increased incidence of preterm delivery. Of the 24 women who received treatment during pregnancy, 7 (29%) gave birth prematurely compared with 5 of the 12 women (42%) who postponed treatment until after delivery, P=0.73.
The investigators noted that the miscarriage rate was approximately 10%, which was higher than previous studies.
Four patients had miscarriages, 2 during the first trimester and 2 during the second. Both patients who had miscarriages in the first trimester had received lymphoma treatment during that time.
And one of the patients who had antenatal therapy during the second trimester and had a miscarriage was critically ill, which the investigators believed was a contributing factor.
The second woman who miscarried after therapy in the second trimester had conceived twins through in vitro fertilization and miscarried at 23 weeks after ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) therapy had been initiated at gestational week 15.
Investigators had fetal outcomes available for 31 of 32 patients who did not terminate or have a miscarriage. And these 31 infants had no anomalies at birth.
The investigators said that although the follow-up time is relatively short, they observed no malformations in the newborns.
Treatment responses and survival
The overall response rate (OR) was 91.7% and the complete response (CR) rate was 75.0% for the 24 patients who started treatment during pregnancy.
And for those 12 women who deferred therapy until delivery, both ORR and CR rates were 91.7%.
The 5-year progression-free survival (PFS) and OS were 74.7% and 82.4%, respectively, for all women. The median follow-up was 67.9 months (range 8.8 to 277.5).
For the 31 women with HL, the 5-year PFS and OS were 69.9% and 80%, respectively.
And for the 8 women with NHL, the 5-year PFS and OS were 85.7% and 83.3%, respectively.
Investigators found no difference in PFS or OS (P=0.84) based on undergoing antenatal lymphoma treatment among the 36 women who did not terminate their pregnancies at diagnosis.
The investigators conducted a univariate analysis and found that for the 36 women who did not electively terminate their pregnancies, the following were associated with increased risk of disease progression:
• Bulky disease—hazard ratio [HR] 3.6, P = 0.06
• Extranodal nonbone marrow involvement—HR 4.2, P = 0.04
• Poor ECOG performance status—HR 3.9, P = 0.005
Poor performance status was also associated with OS, HR 8.88, P = 0.004.
Multivariate analysis revealed significant associations in terms of OS and PFS for extranodal nonbone marrow involvement and performance status:
• Nonbone marrow involvement—OS HR, 73.5, P = 0.02; PFS HR 8.26, P = 0.01
• Performance status—OS HR, 26.7, P = 0.003; PFS HR, 4.89, P = 0.002
The investigators concluded that because they found no differences in PFS or OS according to whether patients received antenatal therapy, they believe that disease factors, rather than treatment-related factors, influence worse maternal outcomes.
They recommended delaying therapy until the second trimester if that can be accomplished without harm to the patient. ![]()
Photo credit: Vera Kratochvil
A single-center retrospective study of 39 pregnant women diagnosed with Hodgkin lymphoma (HL) or non-Hodgkin lymphoma (NHL) during pregnancy indicates that delaying treatment until the second trimester is “likely safe and results in acceptable” outcomes for both mother and child.
Investigators also found that deferring therapy until after delivery did not adversely affect maternal outcomes.
In order to clarify the sometimes conflicting reports regarding management of lymphoma during pregnancy, investigators at MD Anderson Cancer Center in Houston, Texas, undertook the study to determine whether administering standard chemotherapy during the second and third trimesters has acceptable maternal and fetal outcomes.
Michelle A. Fanale, MD, and colleagues published their findings in JAMA Oncology.
Patient characteristics
Investigators identified 31 women with HL and 8 with NHL who were diagnosed between 1991 and 2014 and had sufficient pregnancy and follow-up data.
The women were a median age of 28 years (range 19-38). The patients with NHL were significantly older, P=0.004.
Approximately 20% of patients had B symptoms. Most were stage II disease (72%), and 80% were ECOG performance status 0 or 1.
About two thirds of patients had hemoglobin levels less than 12 g/dL.
Most patients did not have extranodal nonbone-marrow disease (82%), although there was a significant difference between those with HL (90%) and NHL (50%), P=0.03.
One third of patients had bulky disease, and 88% were in their second or third trimesters at diagnosis.
Three women electively terminated their pregnancies at diagnosis. Of the 36 remaining patients, 24 (61%) began antenatal therapy and 12 (31%) postponed therapy until after delivery.
Four patients received radiation therapy above the diaphragm at a median dose of 40.4 Gy.
Obstetric outcomes
Antenatal therapy was not associated with increased incidence of preterm delivery. Of the 24 women who received treatment during pregnancy, 7 (29%) gave birth prematurely compared with 5 of the 12 women (42%) who postponed treatment until after delivery, P=0.73.
The investigators noted that the miscarriage rate was approximately 10%, which was higher than previous studies.
Four patients had miscarriages, 2 during the first trimester and 2 during the second. Both patients who had miscarriages in the first trimester had received lymphoma treatment during that time.
And one of the patients who had antenatal therapy during the second trimester and had a miscarriage was critically ill, which the investigators believed was a contributing factor.
The second woman who miscarried after therapy in the second trimester had conceived twins through in vitro fertilization and miscarried at 23 weeks after ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) therapy had been initiated at gestational week 15.
Investigators had fetal outcomes available for 31 of 32 patients who did not terminate or have a miscarriage. And these 31 infants had no anomalies at birth.
The investigators said that although the follow-up time is relatively short, they observed no malformations in the newborns.
Treatment responses and survival
The overall response rate (OR) was 91.7% and the complete response (CR) rate was 75.0% for the 24 patients who started treatment during pregnancy.
And for those 12 women who deferred therapy until delivery, both ORR and CR rates were 91.7%.
The 5-year progression-free survival (PFS) and OS were 74.7% and 82.4%, respectively, for all women. The median follow-up was 67.9 months (range 8.8 to 277.5).
For the 31 women with HL, the 5-year PFS and OS were 69.9% and 80%, respectively.
And for the 8 women with NHL, the 5-year PFS and OS were 85.7% and 83.3%, respectively.
Investigators found no difference in PFS or OS (P=0.84) based on undergoing antenatal lymphoma treatment among the 36 women who did not terminate their pregnancies at diagnosis.
The investigators conducted a univariate analysis and found that for the 36 women who did not electively terminate their pregnancies, the following were associated with increased risk of disease progression:
• Bulky disease—hazard ratio [HR] 3.6, P = 0.06
• Extranodal nonbone marrow involvement—HR 4.2, P = 0.04
• Poor ECOG performance status—HR 3.9, P = 0.005
Poor performance status was also associated with OS, HR 8.88, P = 0.004.
Multivariate analysis revealed significant associations in terms of OS and PFS for extranodal nonbone marrow involvement and performance status:
• Nonbone marrow involvement—OS HR, 73.5, P = 0.02; PFS HR 8.26, P = 0.01
• Performance status—OS HR, 26.7, P = 0.003; PFS HR, 4.89, P = 0.002
The investigators concluded that because they found no differences in PFS or OS according to whether patients received antenatal therapy, they believe that disease factors, rather than treatment-related factors, influence worse maternal outcomes.
They recommended delaying therapy until the second trimester if that can be accomplished without harm to the patient. ![]()
Photo credit: Vera Kratochvil
A single-center retrospective study of 39 pregnant women diagnosed with Hodgkin lymphoma (HL) or non-Hodgkin lymphoma (NHL) during pregnancy indicates that delaying treatment until the second trimester is “likely safe and results in acceptable” outcomes for both mother and child.
Investigators also found that deferring therapy until after delivery did not adversely affect maternal outcomes.
In order to clarify the sometimes conflicting reports regarding management of lymphoma during pregnancy, investigators at MD Anderson Cancer Center in Houston, Texas, undertook the study to determine whether administering standard chemotherapy during the second and third trimesters has acceptable maternal and fetal outcomes.
Michelle A. Fanale, MD, and colleagues published their findings in JAMA Oncology.
Patient characteristics
Investigators identified 31 women with HL and 8 with NHL who were diagnosed between 1991 and 2014 and had sufficient pregnancy and follow-up data.
The women were a median age of 28 years (range 19-38). The patients with NHL were significantly older, P=0.004.
Approximately 20% of patients had B symptoms. Most were stage II disease (72%), and 80% were ECOG performance status 0 or 1.
About two thirds of patients had hemoglobin levels less than 12 g/dL.
Most patients did not have extranodal nonbone-marrow disease (82%), although there was a significant difference between those with HL (90%) and NHL (50%), P=0.03.
One third of patients had bulky disease, and 88% were in their second or third trimesters at diagnosis.
Three women electively terminated their pregnancies at diagnosis. Of the 36 remaining patients, 24 (61%) began antenatal therapy and 12 (31%) postponed therapy until after delivery.
Four patients received radiation therapy above the diaphragm at a median dose of 40.4 Gy.
Obstetric outcomes
Antenatal therapy was not associated with increased incidence of preterm delivery. Of the 24 women who received treatment during pregnancy, 7 (29%) gave birth prematurely compared with 5 of the 12 women (42%) who postponed treatment until after delivery, P=0.73.
The investigators noted that the miscarriage rate was approximately 10%, which was higher than previous studies.
Four patients had miscarriages, 2 during the first trimester and 2 during the second. Both patients who had miscarriages in the first trimester had received lymphoma treatment during that time.
And one of the patients who had antenatal therapy during the second trimester and had a miscarriage was critically ill, which the investigators believed was a contributing factor.
The second woman who miscarried after therapy in the second trimester had conceived twins through in vitro fertilization and miscarried at 23 weeks after ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) therapy had been initiated at gestational week 15.
Investigators had fetal outcomes available for 31 of 32 patients who did not terminate or have a miscarriage. And these 31 infants had no anomalies at birth.
The investigators said that although the follow-up time is relatively short, they observed no malformations in the newborns.
Treatment responses and survival
The overall response rate (OR) was 91.7% and the complete response (CR) rate was 75.0% for the 24 patients who started treatment during pregnancy.
And for those 12 women who deferred therapy until delivery, both ORR and CR rates were 91.7%.
The 5-year progression-free survival (PFS) and OS were 74.7% and 82.4%, respectively, for all women. The median follow-up was 67.9 months (range 8.8 to 277.5).
For the 31 women with HL, the 5-year PFS and OS were 69.9% and 80%, respectively.
And for the 8 women with NHL, the 5-year PFS and OS were 85.7% and 83.3%, respectively.
Investigators found no difference in PFS or OS (P=0.84) based on undergoing antenatal lymphoma treatment among the 36 women who did not terminate their pregnancies at diagnosis.
The investigators conducted a univariate analysis and found that for the 36 women who did not electively terminate their pregnancies, the following were associated with increased risk of disease progression:
• Bulky disease—hazard ratio [HR] 3.6, P = 0.06
• Extranodal nonbone marrow involvement—HR 4.2, P = 0.04
• Poor ECOG performance status—HR 3.9, P = 0.005
Poor performance status was also associated with OS, HR 8.88, P = 0.004.
Multivariate analysis revealed significant associations in terms of OS and PFS for extranodal nonbone marrow involvement and performance status:
• Nonbone marrow involvement—OS HR, 73.5, P = 0.02; PFS HR 8.26, P = 0.01
• Performance status—OS HR, 26.7, P = 0.003; PFS HR, 4.89, P = 0.002
The investigators concluded that because they found no differences in PFS or OS according to whether patients received antenatal therapy, they believe that disease factors, rather than treatment-related factors, influence worse maternal outcomes.
They recommended delaying therapy until the second trimester if that can be accomplished without harm to the patient. ![]()
Tracking the Decline of AAA Repair in the United States
Has the advent of branched-fenestrated aortic endografts increased the number of abdominal aortic aneurysm (AAA) repairs due to patients who otherwise would not be offered open repair or infrarenal endovascular repair (EVAR)?
This is the question addressed by Dr. Bjoern D. Suckow, who will present the results of a study that he and his colleagues at the Dartmouth-Hitchcock Medical Center performed to evaluate trends in open AAA repair, EVAR, and branched-fenestrated EVAR (BEVAR) for AAA in Medicare beneficiaries from 2003 to 2013. They used a 100% sample of Medicare Part B claims to determine the number of each of these repair types and to compare them annually over the study period.
Between 2003 and 2013, the total number of AAA repairs significantly declined by 13% from 27,352 to 23,835, after a peak number of 29,924 repairs performed in 2005. The number of open AAA repairs significantly and steadily declined by 78%, from 15,385 in 2003 to 3,315 in 2013. In contrast, while the number of EVARs significantly increased from 11,967 in 2003 to 20,845 in 2008, that number has since declined a total of 13% to only 18,098 repairs in 2013, although this was not a significant difference.
Prior to 2011, there were no BEVAR cases among Medicare beneficiaries, according to Dr. Suckow. However, the number of BEVAR cases continuously and significantly rose more than 500% from 401 procedures in 2011 to 2,422 procedures in 2013. Over this same time period, the number of open repairs and the number of EVARs declined by 2,499 and 2,415 cases, respectively .
“The total number of AAA repairs in the Unites States has been declining annually since 2005,” said Dr. Suckow. “Our study shows that the continuous increase in BEVAR cases performed among Medicare patients over the last 3 years has not reversed the steady decline in overall numbers of AAA repairs, because of a concomitant decline in both open aneurysm repair and EVAR.”
Their results indicated that BEVAR was not likely responsible for the overall decline in open repair, as this trend was found to be present over a much longer time period, according to Dr. Suckow. Similarly, the rapid rise in BEVAR cases occurred when there was an almost equal decline in EVAR case numbers.
“These trends suggest a potential decline in the incidence of AAA in the U.S. Medicare population, with shifts in the type of repair based on available technology and perhaps patient preference,” said Dr. Suckow. “Future efforts are needed to determine the characteristics of patients treated with BEVAR as well as the long-term effectiveness of these new treatments,” he concluded.
Friday: Plenary Session 4
8:00 A.M. - 9:30 A.M.
Potomac Ballroom A/B
Has the advent of branched-fenestrated aortic endografts increased the number of abdominal aortic aneurysm (AAA) repairs due to patients who otherwise would not be offered open repair or infrarenal endovascular repair (EVAR)?
This is the question addressed by Dr. Bjoern D. Suckow, who will present the results of a study that he and his colleagues at the Dartmouth-Hitchcock Medical Center performed to evaluate trends in open AAA repair, EVAR, and branched-fenestrated EVAR (BEVAR) for AAA in Medicare beneficiaries from 2003 to 2013. They used a 100% sample of Medicare Part B claims to determine the number of each of these repair types and to compare them annually over the study period.
Between 2003 and 2013, the total number of AAA repairs significantly declined by 13% from 27,352 to 23,835, after a peak number of 29,924 repairs performed in 2005. The number of open AAA repairs significantly and steadily declined by 78%, from 15,385 in 2003 to 3,315 in 2013. In contrast, while the number of EVARs significantly increased from 11,967 in 2003 to 20,845 in 2008, that number has since declined a total of 13% to only 18,098 repairs in 2013, although this was not a significant difference.
Prior to 2011, there were no BEVAR cases among Medicare beneficiaries, according to Dr. Suckow. However, the number of BEVAR cases continuously and significantly rose more than 500% from 401 procedures in 2011 to 2,422 procedures in 2013. Over this same time period, the number of open repairs and the number of EVARs declined by 2,499 and 2,415 cases, respectively .
“The total number of AAA repairs in the Unites States has been declining annually since 2005,” said Dr. Suckow. “Our study shows that the continuous increase in BEVAR cases performed among Medicare patients over the last 3 years has not reversed the steady decline in overall numbers of AAA repairs, because of a concomitant decline in both open aneurysm repair and EVAR.”
Their results indicated that BEVAR was not likely responsible for the overall decline in open repair, as this trend was found to be present over a much longer time period, according to Dr. Suckow. Similarly, the rapid rise in BEVAR cases occurred when there was an almost equal decline in EVAR case numbers.
“These trends suggest a potential decline in the incidence of AAA in the U.S. Medicare population, with shifts in the type of repair based on available technology and perhaps patient preference,” said Dr. Suckow. “Future efforts are needed to determine the characteristics of patients treated with BEVAR as well as the long-term effectiveness of these new treatments,” he concluded.
Friday: Plenary Session 4
8:00 A.M. - 9:30 A.M.
Potomac Ballroom A/B
Has the advent of branched-fenestrated aortic endografts increased the number of abdominal aortic aneurysm (AAA) repairs due to patients who otherwise would not be offered open repair or infrarenal endovascular repair (EVAR)?
This is the question addressed by Dr. Bjoern D. Suckow, who will present the results of a study that he and his colleagues at the Dartmouth-Hitchcock Medical Center performed to evaluate trends in open AAA repair, EVAR, and branched-fenestrated EVAR (BEVAR) for AAA in Medicare beneficiaries from 2003 to 2013. They used a 100% sample of Medicare Part B claims to determine the number of each of these repair types and to compare them annually over the study period.
Between 2003 and 2013, the total number of AAA repairs significantly declined by 13% from 27,352 to 23,835, after a peak number of 29,924 repairs performed in 2005. The number of open AAA repairs significantly and steadily declined by 78%, from 15,385 in 2003 to 3,315 in 2013. In contrast, while the number of EVARs significantly increased from 11,967 in 2003 to 20,845 in 2008, that number has since declined a total of 13% to only 18,098 repairs in 2013, although this was not a significant difference.
Prior to 2011, there were no BEVAR cases among Medicare beneficiaries, according to Dr. Suckow. However, the number of BEVAR cases continuously and significantly rose more than 500% from 401 procedures in 2011 to 2,422 procedures in 2013. Over this same time period, the number of open repairs and the number of EVARs declined by 2,499 and 2,415 cases, respectively .
“The total number of AAA repairs in the Unites States has been declining annually since 2005,” said Dr. Suckow. “Our study shows that the continuous increase in BEVAR cases performed among Medicare patients over the last 3 years has not reversed the steady decline in overall numbers of AAA repairs, because of a concomitant decline in both open aneurysm repair and EVAR.”
Their results indicated that BEVAR was not likely responsible for the overall decline in open repair, as this trend was found to be present over a much longer time period, according to Dr. Suckow. Similarly, the rapid rise in BEVAR cases occurred when there was an almost equal decline in EVAR case numbers.
“These trends suggest a potential decline in the incidence of AAA in the U.S. Medicare population, with shifts in the type of repair based on available technology and perhaps patient preference,” said Dr. Suckow. “Future efforts are needed to determine the characteristics of patients treated with BEVAR as well as the long-term effectiveness of these new treatments,” he concluded.
Friday: Plenary Session 4
8:00 A.M. - 9:30 A.M.
Potomac Ballroom A/B

Learn Radiation Safety During Vascular Surgery
Practical tips for protecting your vascular surgery patients and yourselves from radiation exposure will be featured as part of this morning’s session “Radiation Safety for the Vascular Surgeon.”
“Since endovascular procedures became an essential part of the vascular field about 25 years ago, minimally invasive, radiation-guided procedures have become more sophisticated, more involved and more frequent while requiring better resolution,” said session co-moderator Dr. Peter Schneider of Kaiser Permanente Medical Group in Honolulu. “All of this means more radiation for the patient and for the physician. Going forward, as our field continues to develop, the likelihood is high that these requirements will continue and will intensify and that the radiation risk to patients and providers will increase.
“Radiation is a necessary tool in our ability to help our patients,” Dr. Schneider added. “Yet radiation has negative effects, such as radiation-induced cancers and cataracts. We need to do everything we can to minimize those negative effects.”
A good 60%-70% of vascular procedures involve endovascular techniques that utilize radiation, said session co-moderator Dr. Amy Reed of Rush University Medical Center in Chicago. “Even though your patient may be exposed multiple times in the future through CAT scans or cardiac catheterizations, you as the surgeon are going to be doing this for decades – so the long-term exposure to radiation is a concern. Usually it goes hand in hand that if you’re protecting the patient, you’re protecting yourself as well.”
There are a number of measures vascular surgeons can take to minimize radiation exposure, the moderators said. “These include simple things like the use of radiation filters during imaging, decreasing frame rates to the lowest level that gives the imaging required, being careful about maintaining distance from the image intensifier during fluoroscopy and use of radiation shielding,” Dr. Schneider said.
Additional steps can include collimating or focusing the view and changing table positions, Dr. Reed noted. Good radiation safety techniques are especially important for residency program directors, she added: “Trainees stand closer to the radiation, so it’s important to have good technique. Just like universal precautions measures such as wearing gloves and washing hands, trainees are going to learn radiation safety by emulating you.”
During the session, six expert clinicians knowledgeable about the effects of radiation will share their wisdom. Dr. Christopher Carsten of Greenville Health System in South Carolina will cover what is known about the clinically allowable limits of radiation to the provider and to the patient; Dr. Sunita Srivastava of the Cleveland Clinic will provide a basic understanding of the mechanism of the biological effects of radiation; Dr. Melissa Kirkwood of the University of Texas Southwestern Medical Center in Dallas will offer practical tips to the vascular surgeon for decreasing radiation; Dr. Audra Duncan of the University of Western Ontario will discuss the need for diagnostic tests or radiation-guided procedures in patients who are pregnant; Dr. Mark Farber of the University of North Carolina will discuss new technologies in radiation monitoring; and Dr. Lois Killewich of the University of Texas Medical Branch in Galveston will cover governmental regulations associated with the clinical use of radiation.
“We’re really trying to increase the awareness of radiation safety,” Dr. Reed said. “It’s not to go over all of the things radiation can cause – we know that – but what’s on the horizon that might be helpful for you, and what tips you can take back for protection if you’re not currently using them.”
Friday Breakfast Session B4
6:30 A.M. - 8:00 A.M.
Potomac Ballroom C
Practical tips for protecting your vascular surgery patients and yourselves from radiation exposure will be featured as part of this morning’s session “Radiation Safety for the Vascular Surgeon.”
“Since endovascular procedures became an essential part of the vascular field about 25 years ago, minimally invasive, radiation-guided procedures have become more sophisticated, more involved and more frequent while requiring better resolution,” said session co-moderator Dr. Peter Schneider of Kaiser Permanente Medical Group in Honolulu. “All of this means more radiation for the patient and for the physician. Going forward, as our field continues to develop, the likelihood is high that these requirements will continue and will intensify and that the radiation risk to patients and providers will increase.
“Radiation is a necessary tool in our ability to help our patients,” Dr. Schneider added. “Yet radiation has negative effects, such as radiation-induced cancers and cataracts. We need to do everything we can to minimize those negative effects.”
A good 60%-70% of vascular procedures involve endovascular techniques that utilize radiation, said session co-moderator Dr. Amy Reed of Rush University Medical Center in Chicago. “Even though your patient may be exposed multiple times in the future through CAT scans or cardiac catheterizations, you as the surgeon are going to be doing this for decades – so the long-term exposure to radiation is a concern. Usually it goes hand in hand that if you’re protecting the patient, you’re protecting yourself as well.”
There are a number of measures vascular surgeons can take to minimize radiation exposure, the moderators said. “These include simple things like the use of radiation filters during imaging, decreasing frame rates to the lowest level that gives the imaging required, being careful about maintaining distance from the image intensifier during fluoroscopy and use of radiation shielding,” Dr. Schneider said.
Additional steps can include collimating or focusing the view and changing table positions, Dr. Reed noted. Good radiation safety techniques are especially important for residency program directors, she added: “Trainees stand closer to the radiation, so it’s important to have good technique. Just like universal precautions measures such as wearing gloves and washing hands, trainees are going to learn radiation safety by emulating you.”
During the session, six expert clinicians knowledgeable about the effects of radiation will share their wisdom. Dr. Christopher Carsten of Greenville Health System in South Carolina will cover what is known about the clinically allowable limits of radiation to the provider and to the patient; Dr. Sunita Srivastava of the Cleveland Clinic will provide a basic understanding of the mechanism of the biological effects of radiation; Dr. Melissa Kirkwood of the University of Texas Southwestern Medical Center in Dallas will offer practical tips to the vascular surgeon for decreasing radiation; Dr. Audra Duncan of the University of Western Ontario will discuss the need for diagnostic tests or radiation-guided procedures in patients who are pregnant; Dr. Mark Farber of the University of North Carolina will discuss new technologies in radiation monitoring; and Dr. Lois Killewich of the University of Texas Medical Branch in Galveston will cover governmental regulations associated with the clinical use of radiation.
“We’re really trying to increase the awareness of radiation safety,” Dr. Reed said. “It’s not to go over all of the things radiation can cause – we know that – but what’s on the horizon that might be helpful for you, and what tips you can take back for protection if you’re not currently using them.”
Friday Breakfast Session B4
6:30 A.M. - 8:00 A.M.
Potomac Ballroom C
Practical tips for protecting your vascular surgery patients and yourselves from radiation exposure will be featured as part of this morning’s session “Radiation Safety for the Vascular Surgeon.”
“Since endovascular procedures became an essential part of the vascular field about 25 years ago, minimally invasive, radiation-guided procedures have become more sophisticated, more involved and more frequent while requiring better resolution,” said session co-moderator Dr. Peter Schneider of Kaiser Permanente Medical Group in Honolulu. “All of this means more radiation for the patient and for the physician. Going forward, as our field continues to develop, the likelihood is high that these requirements will continue and will intensify and that the radiation risk to patients and providers will increase.
“Radiation is a necessary tool in our ability to help our patients,” Dr. Schneider added. “Yet radiation has negative effects, such as radiation-induced cancers and cataracts. We need to do everything we can to minimize those negative effects.”
A good 60%-70% of vascular procedures involve endovascular techniques that utilize radiation, said session co-moderator Dr. Amy Reed of Rush University Medical Center in Chicago. “Even though your patient may be exposed multiple times in the future through CAT scans or cardiac catheterizations, you as the surgeon are going to be doing this for decades – so the long-term exposure to radiation is a concern. Usually it goes hand in hand that if you’re protecting the patient, you’re protecting yourself as well.”
There are a number of measures vascular surgeons can take to minimize radiation exposure, the moderators said. “These include simple things like the use of radiation filters during imaging, decreasing frame rates to the lowest level that gives the imaging required, being careful about maintaining distance from the image intensifier during fluoroscopy and use of radiation shielding,” Dr. Schneider said.
Additional steps can include collimating or focusing the view and changing table positions, Dr. Reed noted. Good radiation safety techniques are especially important for residency program directors, she added: “Trainees stand closer to the radiation, so it’s important to have good technique. Just like universal precautions measures such as wearing gloves and washing hands, trainees are going to learn radiation safety by emulating you.”
During the session, six expert clinicians knowledgeable about the effects of radiation will share their wisdom. Dr. Christopher Carsten of Greenville Health System in South Carolina will cover what is known about the clinically allowable limits of radiation to the provider and to the patient; Dr. Sunita Srivastava of the Cleveland Clinic will provide a basic understanding of the mechanism of the biological effects of radiation; Dr. Melissa Kirkwood of the University of Texas Southwestern Medical Center in Dallas will offer practical tips to the vascular surgeon for decreasing radiation; Dr. Audra Duncan of the University of Western Ontario will discuss the need for diagnostic tests or radiation-guided procedures in patients who are pregnant; Dr. Mark Farber of the University of North Carolina will discuss new technologies in radiation monitoring; and Dr. Lois Killewich of the University of Texas Medical Branch in Galveston will cover governmental regulations associated with the clinical use of radiation.
“We’re really trying to increase the awareness of radiation safety,” Dr. Reed said. “It’s not to go over all of the things radiation can cause – we know that – but what’s on the horizon that might be helpful for you, and what tips you can take back for protection if you’re not currently using them.”
Friday Breakfast Session B4
6:30 A.M. - 8:00 A.M.
Potomac Ballroom C

Enjoy a ‘Capitol’ Performance with the Capitol Steps
First, combine a Washington, D.C. venue and an upcoming and hotly debated presidential election. Add a date shortly before the GOP and Democratic national conventions.
What do you get? The perfect time and place for a political comedy show performed by the “Capitol Steps,” a group that’s been poking fun at politics, politicians and the headlines of the day since the Reagan administration.
The group will perform its particular brand of satirical humor – song parodies, standup comedy and more – at a special presentation for all VAM attendees from 8:30 to 9:30 p.m., Friday, in Potomac Ballroom A/B. The event is open at no charge to all registered attendees, guests and exhibitors.
No topic is safe, whether it’s the FBI’s fight earlier this year with Apple over a locked iPhone to Bill Clinton commenting on Hillary to Donald Trump and Sarah Palin. Perhaps the audience will hear Bernie Sanders sing a show tune or hear about “Deleter of the Facts.”
The group got its start in 1981. Senate staffers, planning entertainment for a Christmas party, created song parodies and skits from the headlines at the time and created the Capitol Steps in the process. The group has recorded more than 30 albums (the latest is “What to Expect When You’re Electing”) and has been featured on national television and radio.
“We are thrilled to offer the humor of the Capitol Steps to our members and guests,” said SVS President Dr. Bruce A. Perler, who was instrumental in bringing the “Steps” to VAM. “I am certain that, no matter what a particular member’s politics, in this most ‘unusual’ of presidential election campaigns, the Capitol Steps will provide plenty of laughs and remarkable satirical insights.”
First, combine a Washington, D.C. venue and an upcoming and hotly debated presidential election. Add a date shortly before the GOP and Democratic national conventions.
What do you get? The perfect time and place for a political comedy show performed by the “Capitol Steps,” a group that’s been poking fun at politics, politicians and the headlines of the day since the Reagan administration.
The group will perform its particular brand of satirical humor – song parodies, standup comedy and more – at a special presentation for all VAM attendees from 8:30 to 9:30 p.m., Friday, in Potomac Ballroom A/B. The event is open at no charge to all registered attendees, guests and exhibitors.
No topic is safe, whether it’s the FBI’s fight earlier this year with Apple over a locked iPhone to Bill Clinton commenting on Hillary to Donald Trump and Sarah Palin. Perhaps the audience will hear Bernie Sanders sing a show tune or hear about “Deleter of the Facts.”
The group got its start in 1981. Senate staffers, planning entertainment for a Christmas party, created song parodies and skits from the headlines at the time and created the Capitol Steps in the process. The group has recorded more than 30 albums (the latest is “What to Expect When You’re Electing”) and has been featured on national television and radio.
“We are thrilled to offer the humor of the Capitol Steps to our members and guests,” said SVS President Dr. Bruce A. Perler, who was instrumental in bringing the “Steps” to VAM. “I am certain that, no matter what a particular member’s politics, in this most ‘unusual’ of presidential election campaigns, the Capitol Steps will provide plenty of laughs and remarkable satirical insights.”
First, combine a Washington, D.C. venue and an upcoming and hotly debated presidential election. Add a date shortly before the GOP and Democratic national conventions.
What do you get? The perfect time and place for a political comedy show performed by the “Capitol Steps,” a group that’s been poking fun at politics, politicians and the headlines of the day since the Reagan administration.
The group will perform its particular brand of satirical humor – song parodies, standup comedy and more – at a special presentation for all VAM attendees from 8:30 to 9:30 p.m., Friday, in Potomac Ballroom A/B. The event is open at no charge to all registered attendees, guests and exhibitors.
No topic is safe, whether it’s the FBI’s fight earlier this year with Apple over a locked iPhone to Bill Clinton commenting on Hillary to Donald Trump and Sarah Palin. Perhaps the audience will hear Bernie Sanders sing a show tune or hear about “Deleter of the Facts.”
The group got its start in 1981. Senate staffers, planning entertainment for a Christmas party, created song parodies and skits from the headlines at the time and created the Capitol Steps in the process. The group has recorded more than 30 albums (the latest is “What to Expect When You’re Electing”) and has been featured on national television and radio.
“We are thrilled to offer the humor of the Capitol Steps to our members and guests,” said SVS President Dr. Bruce A. Perler, who was instrumental in bringing the “Steps” to VAM. “I am certain that, no matter what a particular member’s politics, in this most ‘unusual’ of presidential election campaigns, the Capitol Steps will provide plenty of laughs and remarkable satirical insights.”

Presidentially Speaking
Dr. Bruce Perler, Johns Hopkins Hospital, will give his SVS Presidential Address Friday after a short introduction by President-Elect Dr. Ronald Fairman.
Friday: 11 a.m. – 12:15 p.m. Potomac Ballroom A/B
Dr. Bruce Perler, Johns Hopkins Hospital, will give his SVS Presidential Address Friday after a short introduction by President-Elect Dr. Ronald Fairman.
Friday: 11 a.m. – 12:15 p.m. Potomac Ballroom A/B
Dr. Bruce Perler, Johns Hopkins Hospital, will give his SVS Presidential Address Friday after a short introduction by President-Elect Dr. Ronald Fairman.
Friday: 11 a.m. – 12:15 p.m. Potomac Ballroom A/B
Are You Going to the Fair? A Guide to What You Need to Know
There’s no Ferris Wheel or tilt-a-whirl at this fair – just useful information on 73 vascular training programs and the chance for aspiring vascular surgeons to find a good fit for their futures.
Programs are arranged on the floor by the types of offered paradigms: 0+5, 5+2 as well as those offering both training pathways. The configuration, introduced in 2015, makes it easier for attendees to locate the programs in which they are specifically interested.
This year residents/students will receive more data – such as if the program is academic- or community practice-based – to help them better locate the programs in which they are most interested in visiting in the time allotted. The change was made as the result of attendee feedback from earlier fairs.
The Residency Fair is the perfect way for residents and students to network and make connections. Program directors, faculty and current trainees from the 73 institutions will be on hand to talk with interested attendees.
More than 200 students and residents who have an active interest in vascular surgery are expected to participate.
A directory of all participating programs was distributed to students and residents earlier and also will be available at the fair. V
Friday: 5:00 P.M. - 6:30 P.M.
Exhibit Hall D
There’s no Ferris Wheel or tilt-a-whirl at this fair – just useful information on 73 vascular training programs and the chance for aspiring vascular surgeons to find a good fit for their futures.
Programs are arranged on the floor by the types of offered paradigms: 0+5, 5+2 as well as those offering both training pathways. The configuration, introduced in 2015, makes it easier for attendees to locate the programs in which they are specifically interested.
This year residents/students will receive more data – such as if the program is academic- or community practice-based – to help them better locate the programs in which they are most interested in visiting in the time allotted. The change was made as the result of attendee feedback from earlier fairs.
The Residency Fair is the perfect way for residents and students to network and make connections. Program directors, faculty and current trainees from the 73 institutions will be on hand to talk with interested attendees.
More than 200 students and residents who have an active interest in vascular surgery are expected to participate.
A directory of all participating programs was distributed to students and residents earlier and also will be available at the fair. V
Friday: 5:00 P.M. - 6:30 P.M.
Exhibit Hall D
There’s no Ferris Wheel or tilt-a-whirl at this fair – just useful information on 73 vascular training programs and the chance for aspiring vascular surgeons to find a good fit for their futures.
Programs are arranged on the floor by the types of offered paradigms: 0+5, 5+2 as well as those offering both training pathways. The configuration, introduced in 2015, makes it easier for attendees to locate the programs in which they are specifically interested.
This year residents/students will receive more data – such as if the program is academic- or community practice-based – to help them better locate the programs in which they are most interested in visiting in the time allotted. The change was made as the result of attendee feedback from earlier fairs.
The Residency Fair is the perfect way for residents and students to network and make connections. Program directors, faculty and current trainees from the 73 institutions will be on hand to talk with interested attendees.
More than 200 students and residents who have an active interest in vascular surgery are expected to participate.
A directory of all participating programs was distributed to students and residents earlier and also will be available at the fair. V
Friday: 5:00 P.M. - 6:30 P.M.
Exhibit Hall D

Study finds most antidepressants ineffective or harmful in children, adolescents
Most antidepressants prescribed to children and adolescents with acute major depression might not be nearly as effective as they are believed to be – and one might be harmful, according to a retrospective review published June 8 and including more than 5,000 participants.
“Our analysis found robust evidence to suggest a significantly increased risk for suicidality for young people given venlafaxine,” wrote Dr. Andrea Cipriani, Xinyu Zhou, Ph.D., and their colleagues. “Unfortunately, due to the absence of reliable data on suicidality for many antidepressants, it was not possible to comprehensively assess the risk of suicidality for all drugs.”
The review looked at 34 double-blind, randomized, controlled trials investigating at least one of 14 major drugs typically prescribed as antidepressants for pediatric patients. In addition to venlafaxine, the researchers looked at amitriptyline, citalopram, clomipramine, desipramine, duloxetine, escitalopram, fluoxetine, imipramine, mirtazapine, nefazodone, nortriptyline, paroxetine, and sertraline (Lancet. 2016 Jun 8. doi: 10.1016/S0140-6736[16]30385-3).
All trials were published before May 31, 2015, and were found in the PubMed, Cochrane Library, Web of Science, Embase, CINAHL, PsycINFO, and LiLACS databases, as well as regulatory agencies’ websites, and international registers for published and unpublished trials. Trials either compared one or more drugs against one another, or one or more drugs against a placebo.
Fluoxetine was the only drug found to be significantly more effective than placebo, and it also was found to be significantly more effective than nortriptyline. In addition, fluoxetine proved better tolerated than imipramine and duloxetine. “However, the clinical interpretation of these findings is limited not only by the uncertainty around these estimates, but also by the potential bias due to selective reporting and the small number of trials,” said Dr. Cipriani of the University of Oxford (England) and Dr. Zhou of the First Affiliated Hospital of Chongqing Medical University in China.
Regardless of which treatment clinicians choose, children and adolescents prescribed antidepressants should be monitored closely. Clinical guidelines for young people with major depression recommend psychotherapy, particularly cognitive-behavioral therapy or interpersonal therapy as first-line interventions, and “fluoxetine should be considered only for those patients with moderate to severe depression who do not have access to psychotherapy or have not responded to nonpharmacological interventions,” the researchers said.
The study was funded by the National Basic Research Program of China. The authors did not report any relevant financial disclosures.
The study by Dr. Andrea Cipriani, Xinyu Zhou, Ph.D., and their colleagues has “disturbing implications for clinical practice” in that it concludes that the risk-benefit profile of antidepressants in the acute treatment of major depression in children and adolescents “does not seem to offer a clear advantage” for these young patients, Dr. Jon Jureidini wrote in an accompanying editorial (Lancet. 2016 Jun 8. doi: 10.1016/S0140-6736[16]30385-2).
For clinicians, the implications are that every decision about whether and what to prescribe requires a calculation on the part of the clinician that is both complex and intuitive, he wrote.
“With research evidence as an important part of that calculation, we now know that we need to make a conscious correction for favorable misrepresentation of outcomes in published and unpublished study reports,” Dr. Jureidini wrote. “Only if the discounted benefit outweighs the boosted harm should the treatment be prescribed. For antidepressants in adolescents, this equation will rarely favor prescribing; in younger children, almost never.”
Dr. Jureidini is a research leader for the Robinson Research Institute at the University of Adelaide in North Adelaide, Australia.
The study by Dr. Andrea Cipriani, Xinyu Zhou, Ph.D., and their colleagues has “disturbing implications for clinical practice” in that it concludes that the risk-benefit profile of antidepressants in the acute treatment of major depression in children and adolescents “does not seem to offer a clear advantage” for these young patients, Dr. Jon Jureidini wrote in an accompanying editorial (Lancet. 2016 Jun 8. doi: 10.1016/S0140-6736[16]30385-2).
For clinicians, the implications are that every decision about whether and what to prescribe requires a calculation on the part of the clinician that is both complex and intuitive, he wrote.
“With research evidence as an important part of that calculation, we now know that we need to make a conscious correction for favorable misrepresentation of outcomes in published and unpublished study reports,” Dr. Jureidini wrote. “Only if the discounted benefit outweighs the boosted harm should the treatment be prescribed. For antidepressants in adolescents, this equation will rarely favor prescribing; in younger children, almost never.”
Dr. Jureidini is a research leader for the Robinson Research Institute at the University of Adelaide in North Adelaide, Australia.
The study by Dr. Andrea Cipriani, Xinyu Zhou, Ph.D., and their colleagues has “disturbing implications for clinical practice” in that it concludes that the risk-benefit profile of antidepressants in the acute treatment of major depression in children and adolescents “does not seem to offer a clear advantage” for these young patients, Dr. Jon Jureidini wrote in an accompanying editorial (Lancet. 2016 Jun 8. doi: 10.1016/S0140-6736[16]30385-2).
For clinicians, the implications are that every decision about whether and what to prescribe requires a calculation on the part of the clinician that is both complex and intuitive, he wrote.
“With research evidence as an important part of that calculation, we now know that we need to make a conscious correction for favorable misrepresentation of outcomes in published and unpublished study reports,” Dr. Jureidini wrote. “Only if the discounted benefit outweighs the boosted harm should the treatment be prescribed. For antidepressants in adolescents, this equation will rarely favor prescribing; in younger children, almost never.”
Dr. Jureidini is a research leader for the Robinson Research Institute at the University of Adelaide in North Adelaide, Australia.
Most antidepressants prescribed to children and adolescents with acute major depression might not be nearly as effective as they are believed to be – and one might be harmful, according to a retrospective review published June 8 and including more than 5,000 participants.
“Our analysis found robust evidence to suggest a significantly increased risk for suicidality for young people given venlafaxine,” wrote Dr. Andrea Cipriani, Xinyu Zhou, Ph.D., and their colleagues. “Unfortunately, due to the absence of reliable data on suicidality for many antidepressants, it was not possible to comprehensively assess the risk of suicidality for all drugs.”
The review looked at 34 double-blind, randomized, controlled trials investigating at least one of 14 major drugs typically prescribed as antidepressants for pediatric patients. In addition to venlafaxine, the researchers looked at amitriptyline, citalopram, clomipramine, desipramine, duloxetine, escitalopram, fluoxetine, imipramine, mirtazapine, nefazodone, nortriptyline, paroxetine, and sertraline (Lancet. 2016 Jun 8. doi: 10.1016/S0140-6736[16]30385-3).
All trials were published before May 31, 2015, and were found in the PubMed, Cochrane Library, Web of Science, Embase, CINAHL, PsycINFO, and LiLACS databases, as well as regulatory agencies’ websites, and international registers for published and unpublished trials. Trials either compared one or more drugs against one another, or one or more drugs against a placebo.
Fluoxetine was the only drug found to be significantly more effective than placebo, and it also was found to be significantly more effective than nortriptyline. In addition, fluoxetine proved better tolerated than imipramine and duloxetine. “However, the clinical interpretation of these findings is limited not only by the uncertainty around these estimates, but also by the potential bias due to selective reporting and the small number of trials,” said Dr. Cipriani of the University of Oxford (England) and Dr. Zhou of the First Affiliated Hospital of Chongqing Medical University in China.
Regardless of which treatment clinicians choose, children and adolescents prescribed antidepressants should be monitored closely. Clinical guidelines for young people with major depression recommend psychotherapy, particularly cognitive-behavioral therapy or interpersonal therapy as first-line interventions, and “fluoxetine should be considered only for those patients with moderate to severe depression who do not have access to psychotherapy or have not responded to nonpharmacological interventions,” the researchers said.
The study was funded by the National Basic Research Program of China. The authors did not report any relevant financial disclosures.
Most antidepressants prescribed to children and adolescents with acute major depression might not be nearly as effective as they are believed to be – and one might be harmful, according to a retrospective review published June 8 and including more than 5,000 participants.
“Our analysis found robust evidence to suggest a significantly increased risk for suicidality for young people given venlafaxine,” wrote Dr. Andrea Cipriani, Xinyu Zhou, Ph.D., and their colleagues. “Unfortunately, due to the absence of reliable data on suicidality for many antidepressants, it was not possible to comprehensively assess the risk of suicidality for all drugs.”
The review looked at 34 double-blind, randomized, controlled trials investigating at least one of 14 major drugs typically prescribed as antidepressants for pediatric patients. In addition to venlafaxine, the researchers looked at amitriptyline, citalopram, clomipramine, desipramine, duloxetine, escitalopram, fluoxetine, imipramine, mirtazapine, nefazodone, nortriptyline, paroxetine, and sertraline (Lancet. 2016 Jun 8. doi: 10.1016/S0140-6736[16]30385-3).
All trials were published before May 31, 2015, and were found in the PubMed, Cochrane Library, Web of Science, Embase, CINAHL, PsycINFO, and LiLACS databases, as well as regulatory agencies’ websites, and international registers for published and unpublished trials. Trials either compared one or more drugs against one another, or one or more drugs against a placebo.
Fluoxetine was the only drug found to be significantly more effective than placebo, and it also was found to be significantly more effective than nortriptyline. In addition, fluoxetine proved better tolerated than imipramine and duloxetine. “However, the clinical interpretation of these findings is limited not only by the uncertainty around these estimates, but also by the potential bias due to selective reporting and the small number of trials,” said Dr. Cipriani of the University of Oxford (England) and Dr. Zhou of the First Affiliated Hospital of Chongqing Medical University in China.
Regardless of which treatment clinicians choose, children and adolescents prescribed antidepressants should be monitored closely. Clinical guidelines for young people with major depression recommend psychotherapy, particularly cognitive-behavioral therapy or interpersonal therapy as first-line interventions, and “fluoxetine should be considered only for those patients with moderate to severe depression who do not have access to psychotherapy or have not responded to nonpharmacological interventions,” the researchers said.
The study was funded by the National Basic Research Program of China. The authors did not report any relevant financial disclosures.
FROM THE LANCET
Key clinical point: The majority of antidepressant drugs prescribed to children and adolescents are ineffective, with only fluoxetine showing significant improvement.
Major finding: Fluoxetine showed the most promising results among all 14 antidepressants studied.
Data source: Retrospective review of 34 studies with 5,260 participants investigating 14 distinct drugs used to treat depression in children and adolescents.
Disclosures: The study was funded by the National Basic Research Program of China. Authors did not report any relevant financial disclosures.