User login
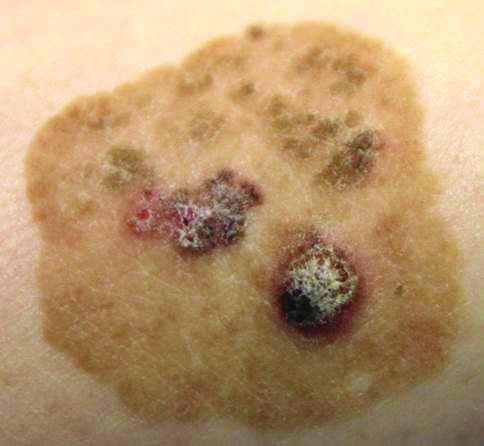
Brown Papules and a Plaque on the Calf
The Diagnosis: Irritated Seborrheic Keratosis
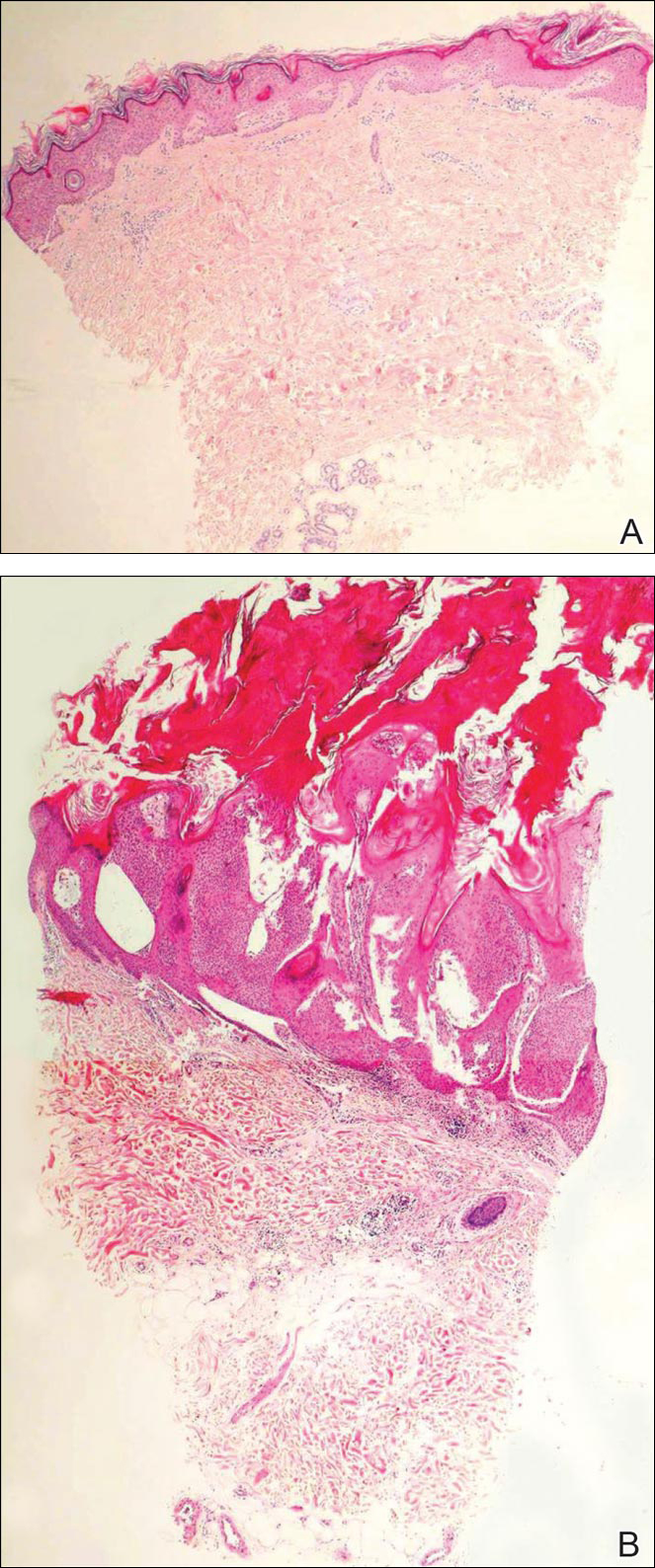
Biopsies of one of the protruding papules and the underlying plaque were performed. The specimen from the papule showed hyperkeratosis, acanthosis, papillomatosis, and a flattened dermoepidermal junction with demarcated horizontal margin, which demonstrated apparent upward growth of the epidermis. Moderate lymphocytic infiltration in the upper dermis also was observed (Figure, A). The histologic findings of the plaque showed acanthosis, several pseudohorn cysts, hyperpigmentation of the basal layer, and a horizontal demarcation of the dermoepidermal junction (Figure, B).
Seborrheic keratosis is the most common benign epidermal tumor of the skin with variable appearance.1 It usually begins with well-circumscribed, dull, flat, tan or brown patches that then grow into waxy verrucous papules.1 There are many clinicopathologic variants of SK such as common SK, stucco keratosis, and dermatosis papulosa nigra in clinical variation, as well as acanthotic, hyperkeratotic, clonal, reticulated, irritated, and melanoacanthoma subtypes based on histological variation.2,3
Seborrheic keratosis is a tumor of keratinocytic origin. Although genetics, sun exposure,4 and human papillomavirus infection5 are thought to be causative factors, the precise etiology of SK is unknown.1
The histology of SK shows monotonous basaloid tumor cells without atypia. It generally is comprised of focal acanthosis and papillomatosis with a sharp flat base. Intraepithelial horn pseudocysts are notable features of SK and increased melanin often is seen.2,6
Irritated SK is a histologic variant of SK that has been mechanically or chemically irritated or is involved in immunologic responses. Histologically, the dermis underlying an SK lesion filled with a dense lymphocytic infiltration is characteristic.1,2
For symptomatic or cosmetically undesirable lesions, complete removal of the lesion is the preferred treatment. Cryotherapy, electrodesiccation followed by curettage, curettage followed by desiccation, laser ablation, and surgical excision are effective treatments.1
- Valencia DT, Nicholas RS, Ken KL, et al. Benign epithelial tumors, hamartomas, and hyperplasias. In: Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill Professional; 2012:1319-1336.
- Kirkharn N. Tumors and cysts of the epidermis. In: Elder DE, Elenitsas R, Johnson BL Jr, eds. Lever’s Histopathology of the Skin. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:791-850.
- Rajesh G, Thappa DM, Jaisankar TJ, et al. Spectrum of seborrheic keratoses in South Indians: a clinical and dermoscopic study. Indian J Dermatol Venereol Leprol. 2011;77:483-488.
- Yeatman JM, Kilkenny M, Marks R. The prevalence of seborrhoeic keratoses in an Australian population: does exposure to sunlight play a part in their frequency? Br J Dermatol. 1997;137:411-414.
- Li YH, Chen G, Dong XP, et al. Detection of epidermodysplasia verruciformis-associated human papillomavirus DNA in nongenital seborrhoeic keratosis. Br J Dermatol. 2004;151:1060-1065.
- Brinster NK, Liu V, Diwan AH, et al. Dermatopathology. Philadelphia, PA: Saunders/Elsevier; 2011.
The Diagnosis: Irritated Seborrheic Keratosis
Biopsies of one of the protruding papules and the underlying plaque were performed. The specimen from the papule showed hyperkeratosis, acanthosis, papillomatosis, and a flattened dermoepidermal junction with demarcated horizontal margin, which demonstrated apparent upward growth of the epidermis. Moderate lymphocytic infiltration in the upper dermis also was observed (Figure, A). The histologic findings of the plaque showed acanthosis, several pseudohorn cysts, hyperpigmentation of the basal layer, and a horizontal demarcation of the dermoepidermal junction (Figure, B).
Seborrheic keratosis is the most common benign epidermal tumor of the skin with variable appearance.1 It usually begins with well-circumscribed, dull, flat, tan or brown patches that then grow into waxy verrucous papules.1 There are many clinicopathologic variants of SK such as common SK, stucco keratosis, and dermatosis papulosa nigra in clinical variation, as well as acanthotic, hyperkeratotic, clonal, reticulated, irritated, and melanoacanthoma subtypes based on histological variation.2,3
Seborrheic keratosis is a tumor of keratinocytic origin. Although genetics, sun exposure,4 and human papillomavirus infection5 are thought to be causative factors, the precise etiology of SK is unknown.1
The histology of SK shows monotonous basaloid tumor cells without atypia. It generally is comprised of focal acanthosis and papillomatosis with a sharp flat base. Intraepithelial horn pseudocysts are notable features of SK and increased melanin often is seen.2,6
Irritated SK is a histologic variant of SK that has been mechanically or chemically irritated or is involved in immunologic responses. Histologically, the dermis underlying an SK lesion filled with a dense lymphocytic infiltration is characteristic.1,2
For symptomatic or cosmetically undesirable lesions, complete removal of the lesion is the preferred treatment. Cryotherapy, electrodesiccation followed by curettage, curettage followed by desiccation, laser ablation, and surgical excision are effective treatments.1
The Diagnosis: Irritated Seborrheic Keratosis
Biopsies of one of the protruding papules and the underlying plaque were performed. The specimen from the papule showed hyperkeratosis, acanthosis, papillomatosis, and a flattened dermoepidermal junction with demarcated horizontal margin, which demonstrated apparent upward growth of the epidermis. Moderate lymphocytic infiltration in the upper dermis also was observed (Figure, A). The histologic findings of the plaque showed acanthosis, several pseudohorn cysts, hyperpigmentation of the basal layer, and a horizontal demarcation of the dermoepidermal junction (Figure, B).
Seborrheic keratosis is the most common benign epidermal tumor of the skin with variable appearance.1 It usually begins with well-circumscribed, dull, flat, tan or brown patches that then grow into waxy verrucous papules.1 There are many clinicopathologic variants of SK such as common SK, stucco keratosis, and dermatosis papulosa nigra in clinical variation, as well as acanthotic, hyperkeratotic, clonal, reticulated, irritated, and melanoacanthoma subtypes based on histological variation.2,3
Seborrheic keratosis is a tumor of keratinocytic origin. Although genetics, sun exposure,4 and human papillomavirus infection5 are thought to be causative factors, the precise etiology of SK is unknown.1
The histology of SK shows monotonous basaloid tumor cells without atypia. It generally is comprised of focal acanthosis and papillomatosis with a sharp flat base. Intraepithelial horn pseudocysts are notable features of SK and increased melanin often is seen.2,6
Irritated SK is a histologic variant of SK that has been mechanically or chemically irritated or is involved in immunologic responses. Histologically, the dermis underlying an SK lesion filled with a dense lymphocytic infiltration is characteristic.1,2
For symptomatic or cosmetically undesirable lesions, complete removal of the lesion is the preferred treatment. Cryotherapy, electrodesiccation followed by curettage, curettage followed by desiccation, laser ablation, and surgical excision are effective treatments.1
- Valencia DT, Nicholas RS, Ken KL, et al. Benign epithelial tumors, hamartomas, and hyperplasias. In: Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill Professional; 2012:1319-1336.
- Kirkharn N. Tumors and cysts of the epidermis. In: Elder DE, Elenitsas R, Johnson BL Jr, eds. Lever’s Histopathology of the Skin. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:791-850.
- Rajesh G, Thappa DM, Jaisankar TJ, et al. Spectrum of seborrheic keratoses in South Indians: a clinical and dermoscopic study. Indian J Dermatol Venereol Leprol. 2011;77:483-488.
- Yeatman JM, Kilkenny M, Marks R. The prevalence of seborrhoeic keratoses in an Australian population: does exposure to sunlight play a part in their frequency? Br J Dermatol. 1997;137:411-414.
- Li YH, Chen G, Dong XP, et al. Detection of epidermodysplasia verruciformis-associated human papillomavirus DNA in nongenital seborrhoeic keratosis. Br J Dermatol. 2004;151:1060-1065.
- Brinster NK, Liu V, Diwan AH, et al. Dermatopathology. Philadelphia, PA: Saunders/Elsevier; 2011.
- Valencia DT, Nicholas RS, Ken KL, et al. Benign epithelial tumors, hamartomas, and hyperplasias. In: Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill Professional; 2012:1319-1336.
- Kirkharn N. Tumors and cysts of the epidermis. In: Elder DE, Elenitsas R, Johnson BL Jr, eds. Lever’s Histopathology of the Skin. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:791-850.
- Rajesh G, Thappa DM, Jaisankar TJ, et al. Spectrum of seborrheic keratoses in South Indians: a clinical and dermoscopic study. Indian J Dermatol Venereol Leprol. 2011;77:483-488.
- Yeatman JM, Kilkenny M, Marks R. The prevalence of seborrhoeic keratoses in an Australian population: does exposure to sunlight play a part in their frequency? Br J Dermatol. 1997;137:411-414.
- Li YH, Chen G, Dong XP, et al. Detection of epidermodysplasia verruciformis-associated human papillomavirus DNA in nongenital seborrhoeic keratosis. Br J Dermatol. 2004;151:1060-1065.
- Brinster NK, Liu V, Diwan AH, et al. Dermatopathology. Philadelphia, PA: Saunders/Elsevier; 2011.

Phentermine-topiramate tops competition for long-term weight loss
SAN DIEGO – Phentermine-topiramate was the most effective long-term weight loss drug, based on findings from a network meta-analysis from the University of California, San Diego.
The investigators pooled data from 28 studies of phentermine-topiramate (Qsymia) and four other drugs: orlistat (Xenical, Alli), lorcaserin (Belviq), naltrexone-bupropion (Contrave), and liraglutide (Victoza, Saxenda). The most commonly prescribed weight loss drug in the United States – generic phentermine – was not included because it’s not indicated for long-term use.

“It’s good to have a problem of plenty,” said Dr. Siddharth Singh, but it also makes it hard to figure out which drug to prescribe, especially given the lack of head-to-head studies. He said he hopes the results will help. However, the 30%-45% attrition rate across the studies means that the results have to be interpreted cautiously, said Dr. Singh, who is in the division of gastroenterology in the department of internal medicine, UCSD.
Most of the studies were company-funded phase III trials of weight loss drugs vs. placebo; the trials all were at least 1 year long and included more than 29,000 overweight or obese adults. The analysis was limited to patients on the maximum recommended dose of each drug.
All the drugs were more effective than placebo, but phentermine-topiramate was the most effective, with about 75% of patients losing at least 5% of their weight at 1 year and more than half losing at least 10%, with an average weight loss above placebo of 9 kg. Phentermine-topiramate patients were 10 times more likely than patients on placebo to hit the 5% mark at 1 year; liraglutide patients were 5.5 times more likely to do so; naltrexone-bupropion patients were 4 times more likely; lorcaserin patients, 3.1 times more likely; and orlistat patients, 2.7 times more likely to hit the 5% mark. The spread was similar for weight loss of 10% or more at 1 year vs. placebo.
Phentermine-topiramate’s tolerability profile was acceptable, with 10% of patients quitting the drug by 1 year because of adverse events. The best tolerated was lorcaserin, with a discontinuation rate of 6%, and the least tolerated was liraglutide, with a 13% discontinuation rate. Patients were more likely to quit active drug than placebo in all the studies.
Of course, there are other considerations, especially comorbidities; liraglutide might be the best choice in diabetics, for instance, and patients with psychiatric issues might want to avoid naltrexone-bupropion and lorcaserin, Dr. Singh said.
Subjects were a median of 46 years old, and 74% were women. The median body mass index was 36 kg/m2. All the patients had lifestyle and nutrition counseling along with their study medications.
The investigators next plan to compare the drugs’ safety and efficacy in real world settings.
There was no industry funding for the work, and Dr. Singh had no relevant financial disclosures.

|
Dr. John Morton |
The findings do not correlate with the way weight loss drugs are prescribed. The drug that’s being prescribed the most – outside of generic phentermine – is Contrave (naltrexone-bupropion), but the one that seemed to have the most effect was Qsymia (phentermine-topiramate), which is not being prescribed as often. Qsymia is probably underprescribed, perhaps as a result of its high price tag. Cost is a big factor for these drugs.
Dr. John Morton is chief of bariatric and minimally invasive surgery at Stanford (Calif.) University. He moderated Dr. Singh’s presentation, and had no disclosures.
|
|
Dr. John Morton |
The findings do not correlate with the way weight loss drugs are prescribed. The drug that’s being prescribed the most – outside of generic phentermine – is Contrave (naltrexone-bupropion), but the one that seemed to have the most effect was Qsymia (phentermine-topiramate), which is not being prescribed as often. Qsymia is probably underprescribed, perhaps as a result of its high price tag. Cost is a big factor for these drugs.
Dr. John Morton is chief of bariatric and minimally invasive surgery at Stanford (Calif.) University. He moderated Dr. Singh’s presentation, and had no disclosures.
|
|
Dr. John Morton |
The findings do not correlate with the way weight loss drugs are prescribed. The drug that’s being prescribed the most – outside of generic phentermine – is Contrave (naltrexone-bupropion), but the one that seemed to have the most effect was Qsymia (phentermine-topiramate), which is not being prescribed as often. Qsymia is probably underprescribed, perhaps as a result of its high price tag. Cost is a big factor for these drugs.
Dr. John Morton is chief of bariatric and minimally invasive surgery at Stanford (Calif.) University. He moderated Dr. Singh’s presentation, and had no disclosures.
SAN DIEGO – Phentermine-topiramate was the most effective long-term weight loss drug, based on findings from a network meta-analysis from the University of California, San Diego.
The investigators pooled data from 28 studies of phentermine-topiramate (Qsymia) and four other drugs: orlistat (Xenical, Alli), lorcaserin (Belviq), naltrexone-bupropion (Contrave), and liraglutide (Victoza, Saxenda). The most commonly prescribed weight loss drug in the United States – generic phentermine – was not included because it’s not indicated for long-term use.
“It’s good to have a problem of plenty,” said Dr. Siddharth Singh, but it also makes it hard to figure out which drug to prescribe, especially given the lack of head-to-head studies. He said he hopes the results will help. However, the 30%-45% attrition rate across the studies means that the results have to be interpreted cautiously, said Dr. Singh, who is in the division of gastroenterology in the department of internal medicine, UCSD.
Most of the studies were company-funded phase III trials of weight loss drugs vs. placebo; the trials all were at least 1 year long and included more than 29,000 overweight or obese adults. The analysis was limited to patients on the maximum recommended dose of each drug.
All the drugs were more effective than placebo, but phentermine-topiramate was the most effective, with about 75% of patients losing at least 5% of their weight at 1 year and more than half losing at least 10%, with an average weight loss above placebo of 9 kg. Phentermine-topiramate patients were 10 times more likely than patients on placebo to hit the 5% mark at 1 year; liraglutide patients were 5.5 times more likely to do so; naltrexone-bupropion patients were 4 times more likely; lorcaserin patients, 3.1 times more likely; and orlistat patients, 2.7 times more likely to hit the 5% mark. The spread was similar for weight loss of 10% or more at 1 year vs. placebo.
Phentermine-topiramate’s tolerability profile was acceptable, with 10% of patients quitting the drug by 1 year because of adverse events. The best tolerated was lorcaserin, with a discontinuation rate of 6%, and the least tolerated was liraglutide, with a 13% discontinuation rate. Patients were more likely to quit active drug than placebo in all the studies.
Of course, there are other considerations, especially comorbidities; liraglutide might be the best choice in diabetics, for instance, and patients with psychiatric issues might want to avoid naltrexone-bupropion and lorcaserin, Dr. Singh said.
Subjects were a median of 46 years old, and 74% were women. The median body mass index was 36 kg/m2. All the patients had lifestyle and nutrition counseling along with their study medications.
The investigators next plan to compare the drugs’ safety and efficacy in real world settings.
There was no industry funding for the work, and Dr. Singh had no relevant financial disclosures.
SAN DIEGO – Phentermine-topiramate was the most effective long-term weight loss drug, based on findings from a network meta-analysis from the University of California, San Diego.
The investigators pooled data from 28 studies of phentermine-topiramate (Qsymia) and four other drugs: orlistat (Xenical, Alli), lorcaserin (Belviq), naltrexone-bupropion (Contrave), and liraglutide (Victoza, Saxenda). The most commonly prescribed weight loss drug in the United States – generic phentermine – was not included because it’s not indicated for long-term use.
“It’s good to have a problem of plenty,” said Dr. Siddharth Singh, but it also makes it hard to figure out which drug to prescribe, especially given the lack of head-to-head studies. He said he hopes the results will help. However, the 30%-45% attrition rate across the studies means that the results have to be interpreted cautiously, said Dr. Singh, who is in the division of gastroenterology in the department of internal medicine, UCSD.
Most of the studies were company-funded phase III trials of weight loss drugs vs. placebo; the trials all were at least 1 year long and included more than 29,000 overweight or obese adults. The analysis was limited to patients on the maximum recommended dose of each drug.
All the drugs were more effective than placebo, but phentermine-topiramate was the most effective, with about 75% of patients losing at least 5% of their weight at 1 year and more than half losing at least 10%, with an average weight loss above placebo of 9 kg. Phentermine-topiramate patients were 10 times more likely than patients on placebo to hit the 5% mark at 1 year; liraglutide patients were 5.5 times more likely to do so; naltrexone-bupropion patients were 4 times more likely; lorcaserin patients, 3.1 times more likely; and orlistat patients, 2.7 times more likely to hit the 5% mark. The spread was similar for weight loss of 10% or more at 1 year vs. placebo.
Phentermine-topiramate’s tolerability profile was acceptable, with 10% of patients quitting the drug by 1 year because of adverse events. The best tolerated was lorcaserin, with a discontinuation rate of 6%, and the least tolerated was liraglutide, with a 13% discontinuation rate. Patients were more likely to quit active drug than placebo in all the studies.
Of course, there are other considerations, especially comorbidities; liraglutide might be the best choice in diabetics, for instance, and patients with psychiatric issues might want to avoid naltrexone-bupropion and lorcaserin, Dr. Singh said.
Subjects were a median of 46 years old, and 74% were women. The median body mass index was 36 kg/m2. All the patients had lifestyle and nutrition counseling along with their study medications.
The investigators next plan to compare the drugs’ safety and efficacy in real world settings.
There was no industry funding for the work, and Dr. Singh had no relevant financial disclosures.
AT DDW® 2016
Key clinical point: Phentermine-topiramate was the most effective long-term weight loss drug in a network meta-analysis from the University of California, San Diego.
Major finding: All the drugs were better than placebo, but phentermine-topiramate was the most effective, with 75% of patients losing at least 5% of their weight at 1 year and more than half losing at least 10%.
Data source: Twenty-eight clinical trials involving more than 29,000 overweight or obese adults
Disclosures: There was no industry funding, and the presenter didn’t have any relevant financial disclosures.

VIDEO: RA patients on subcutaneous methotrexate avoid biologics
LONDON – Subcutaneous methotrexate monotherapy may be more effective at helping recently diagnosed patients with rheumatoid arthritis avoid biologic therapy, compared with similar patients on oral methotrexate, based on an analysis of data collected from 483 Canadian patients in routine care and enrolled in a national registry.
“This is a signal for improved efficacy with subcutaneous methotrexate, compared with oral methotrexate,” said Dr. Stephanie Gottheil, who reported these results at the European Congress of Rheumatology.
“In general, as long as patients with rheumatoid arthritis are under good control without a biologic drug, that is preferable” to initiating biologic treatment, said Dr. Gottheil, a researcher at Western University in London, Ont. Delaying the start of biologic treatment saves money, avoids the increased risk of infection that comes with biologic treatment, and defers a patient’s immune response to a biologic drug that can eventually compromise the biologic’s efficacy, she said in an interview.
“These data did not come from a randomized trial and so are by no means conclusive, but this is a signal that supports other data that subcutaneous methotrexate potentially puts patients into remission faster, and we know that earlier remission predicts more sustained remission,” she said.
“The biggest barrier to subcutaneous administration of methotrexate is patient preference to not inject themselves, but results from some studies have also shown that subcutaneous methotrexate is better tolerated,” compared with oral dosing, she added.
The study used data collected in the Canadian Early Arthritis Cohort (CATCH), which enrolls patients at several centers throughout Canada diagnosed with rheumatoid arthritis for less than 12 months. Dr. Gottheil and her associates particularly focused on 1,189 early RA patients with moderate to severe disease activity enrolled in CATCH during 2007-2012 who received methotrexate and had never previously received a biologic drug. The study’s primary endpoint was time to first treatment with a biologic during 3 years of follow-up after entry into the registry.
The patients’ average age at enrollment was 56 years, more than two-thirds were women, and their average methotrexate dosage was 20 mg/week. The cohort included 483 patients on methotrexate monotherapy – with virtually equal numbers on oral methotrexate and subcutaneous methotrexate – and 706 on a regimen that combined methotrexate with one or more additional (nonbiologic) drugs at baseline. The patients in each of the methotrexate monotherapy subgroups, those on oral or subcutaneous therapy, were very similar in their demographic and clinical profiles.
The analysis showed no statistically significant difference in time to first biologic use between the patients on a combination regimen and those on oral methotrexate monotherapy.
But when the researchers compared the time to first biologic among those on subcutaneous methotrexate monotherapy with those on oral methotrexate monotherapy, the subcutaneous patients showed a statistically significant, 47% reduced rate of starting any biologic drug during follow-up in an analysis that controlled for age, sex, education, comorbidities, disease duration, baseline disease activity, baseline corticosteroid use, joint erosions at baseline, and score on the health-assessment questionnaire at baseline, Dr. Gottheil reported.
The analysis also revealed three other variables that significantly linked with a slower progression to biologic treatment: older age, no use of corticosteroid treatment at baseline, and lower disease activity at baseline.
The CATCH registry research program is sponsored by AbbVie, Amgen, Bristol-Myers Squibb, Hoffmann-La Roche, Janssen, Pfizer, and UCB. Dr. Gottheil had no relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
LONDON – Subcutaneous methotrexate monotherapy may be more effective at helping recently diagnosed patients with rheumatoid arthritis avoid biologic therapy, compared with similar patients on oral methotrexate, based on an analysis of data collected from 483 Canadian patients in routine care and enrolled in a national registry.
“This is a signal for improved efficacy with subcutaneous methotrexate, compared with oral methotrexate,” said Dr. Stephanie Gottheil, who reported these results at the European Congress of Rheumatology.
“In general, as long as patients with rheumatoid arthritis are under good control without a biologic drug, that is preferable” to initiating biologic treatment, said Dr. Gottheil, a researcher at Western University in London, Ont. Delaying the start of biologic treatment saves money, avoids the increased risk of infection that comes with biologic treatment, and defers a patient’s immune response to a biologic drug that can eventually compromise the biologic’s efficacy, she said in an interview.
“These data did not come from a randomized trial and so are by no means conclusive, but this is a signal that supports other data that subcutaneous methotrexate potentially puts patients into remission faster, and we know that earlier remission predicts more sustained remission,” she said.
“The biggest barrier to subcutaneous administration of methotrexate is patient preference to not inject themselves, but results from some studies have also shown that subcutaneous methotrexate is better tolerated,” compared with oral dosing, she added.
The study used data collected in the Canadian Early Arthritis Cohort (CATCH), which enrolls patients at several centers throughout Canada diagnosed with rheumatoid arthritis for less than 12 months. Dr. Gottheil and her associates particularly focused on 1,189 early RA patients with moderate to severe disease activity enrolled in CATCH during 2007-2012 who received methotrexate and had never previously received a biologic drug. The study’s primary endpoint was time to first treatment with a biologic during 3 years of follow-up after entry into the registry.
The patients’ average age at enrollment was 56 years, more than two-thirds were women, and their average methotrexate dosage was 20 mg/week. The cohort included 483 patients on methotrexate monotherapy – with virtually equal numbers on oral methotrexate and subcutaneous methotrexate – and 706 on a regimen that combined methotrexate with one or more additional (nonbiologic) drugs at baseline. The patients in each of the methotrexate monotherapy subgroups, those on oral or subcutaneous therapy, were very similar in their demographic and clinical profiles.
The analysis showed no statistically significant difference in time to first biologic use between the patients on a combination regimen and those on oral methotrexate monotherapy.
But when the researchers compared the time to first biologic among those on subcutaneous methotrexate monotherapy with those on oral methotrexate monotherapy, the subcutaneous patients showed a statistically significant, 47% reduced rate of starting any biologic drug during follow-up in an analysis that controlled for age, sex, education, comorbidities, disease duration, baseline disease activity, baseline corticosteroid use, joint erosions at baseline, and score on the health-assessment questionnaire at baseline, Dr. Gottheil reported.
The analysis also revealed three other variables that significantly linked with a slower progression to biologic treatment: older age, no use of corticosteroid treatment at baseline, and lower disease activity at baseline.
The CATCH registry research program is sponsored by AbbVie, Amgen, Bristol-Myers Squibb, Hoffmann-La Roche, Janssen, Pfizer, and UCB. Dr. Gottheil had no relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
LONDON – Subcutaneous methotrexate monotherapy may be more effective at helping recently diagnosed patients with rheumatoid arthritis avoid biologic therapy, compared with similar patients on oral methotrexate, based on an analysis of data collected from 483 Canadian patients in routine care and enrolled in a national registry.
“This is a signal for improved efficacy with subcutaneous methotrexate, compared with oral methotrexate,” said Dr. Stephanie Gottheil, who reported these results at the European Congress of Rheumatology.
“In general, as long as patients with rheumatoid arthritis are under good control without a biologic drug, that is preferable” to initiating biologic treatment, said Dr. Gottheil, a researcher at Western University in London, Ont. Delaying the start of biologic treatment saves money, avoids the increased risk of infection that comes with biologic treatment, and defers a patient’s immune response to a biologic drug that can eventually compromise the biologic’s efficacy, she said in an interview.
“These data did not come from a randomized trial and so are by no means conclusive, but this is a signal that supports other data that subcutaneous methotrexate potentially puts patients into remission faster, and we know that earlier remission predicts more sustained remission,” she said.
“The biggest barrier to subcutaneous administration of methotrexate is patient preference to not inject themselves, but results from some studies have also shown that subcutaneous methotrexate is better tolerated,” compared with oral dosing, she added.
The study used data collected in the Canadian Early Arthritis Cohort (CATCH), which enrolls patients at several centers throughout Canada diagnosed with rheumatoid arthritis for less than 12 months. Dr. Gottheil and her associates particularly focused on 1,189 early RA patients with moderate to severe disease activity enrolled in CATCH during 2007-2012 who received methotrexate and had never previously received a biologic drug. The study’s primary endpoint was time to first treatment with a biologic during 3 years of follow-up after entry into the registry.
The patients’ average age at enrollment was 56 years, more than two-thirds were women, and their average methotrexate dosage was 20 mg/week. The cohort included 483 patients on methotrexate monotherapy – with virtually equal numbers on oral methotrexate and subcutaneous methotrexate – and 706 on a regimen that combined methotrexate with one or more additional (nonbiologic) drugs at baseline. The patients in each of the methotrexate monotherapy subgroups, those on oral or subcutaneous therapy, were very similar in their demographic and clinical profiles.
The analysis showed no statistically significant difference in time to first biologic use between the patients on a combination regimen and those on oral methotrexate monotherapy.
But when the researchers compared the time to first biologic among those on subcutaneous methotrexate monotherapy with those on oral methotrexate monotherapy, the subcutaneous patients showed a statistically significant, 47% reduced rate of starting any biologic drug during follow-up in an analysis that controlled for age, sex, education, comorbidities, disease duration, baseline disease activity, baseline corticosteroid use, joint erosions at baseline, and score on the health-assessment questionnaire at baseline, Dr. Gottheil reported.
The analysis also revealed three other variables that significantly linked with a slower progression to biologic treatment: older age, no use of corticosteroid treatment at baseline, and lower disease activity at baseline.
The CATCH registry research program is sponsored by AbbVie, Amgen, Bristol-Myers Squibb, Hoffmann-La Roche, Janssen, Pfizer, and UCB. Dr. Gottheil had no relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
AT THE EULAR 2016 CONGRESS
Key clinical point: Among patients with recently diagnosed, moderate to severe rheumatoid arthritis, subcutaneous methotrexate monotherapy postponed the need for biologic therapy longer than did oral methotrexate monotherapy.
Major finding: Progression to biologic therapy was 47% less common among RA patients on subcutaneous methotrexate monotherapy, compared with oral methotrexate.
Data source: Three-year follow-up of 483 Canadian patients with recently diagnosed rheumatoid arthritis enrolled in CATCH, a national, real-world registry.
Disclosures: The CATCH registry research program is sponsored by AbbVie, Amgen, Bristol-Myers Squibb, Hoffmann-La Roche, Janssen, Pfizer, and UCB. Dr. Gottheil had no relevant disclosures.

Updated Behçet’s disease recommendations expand biologic treatment
LONDON – A EULAR task force issued the first update to recommendations for managing Behçet’s disease since 2008, with revised recommendations that reflect expanded use of biologic agents, and increased evidence to guide management of gastrointestinal involvement, use of anticoagulants in patients with venous involvement, and use of surgical and interventional treatments, Dr. Gülen Hatemi said while presenting the update at the European Congress of Rheumatology.
The task force, which included more than 20 members, identified 304 articles to apply to the update, and produced five overarching principal and 18 specific recommendations divided among six categories of clinical manifestations of Behçet’s disease, said Dr. Hatemi, convenor of the task force and a rheumatologist at Istanbul University.

For mucocutaneous involvement, the update included five items that all received a “strong” recommendation from the task force: For an oral or genital ulcer, use a topical agent, such as a local steroid. Try colchicine first to prevent recurrent mucocutaneous lesions, especially when the dominant lesion is erythema nodosum or a genital ulcer. Treat papulopustular or acnelike lesions with topical or systemic agents, as when treating acne vulgaris. Coordinate treatment of leg ulcers, which can be caused by venous stasis or obliterative vasculitis, with a dermatologist and vascular surgeon. And azathioprine, thalidomide, interferon-alpha, a tumor necrosis factor (TNF)–alpha antagonist, or apremilast (Otezla) may be necessary for selected patients.
The task force issued two strong recommendations for managing eye involvement along with one conditional recommendation. The first strong recommendation was that managing uveitis requires close collaboration with an ophthalmologist, with the goal of inducing and maintaining remission. Patients with an inflammatory eye disease affecting the posterior segment should receive treatment with azathioprine, cyclosporine, interferon-alpha, or a monoclonal TNF-alpha antagonist. Treatment with a systemic corticosteroid should occur only when combined with azathioprine or another systemic immunosuppressant.
The second strong recommendation was that patients who present with an initial or recurrent acute episode of sight-threatening uveitis should receive treatment with a high-dose glucocorticoid, infliximab, or interferon-alpha. Intravitreal injection with a glucocorticoid as an adjunct to systemic therapy is an option for patients with a unilateral exacerbation. The conditional recommendation was for patients with isolated anterior uveitis. When these patients have markers of a poor prognosis – such as young age, male sex, or early disease onset – systemic treatment with an immunosuppressant is a possible option.
The panel issued three strong recommendations along with one conditional recommendation for managing vascular involvement. One of the strong recommendations called for treating acute deep vein thrombosis with a glucocorticoid as well as an immunosuppresant such as azathioprine, cyclophosphamide, or cyclosporine. A conditional recommendation said patients with refractory venous thrombosis could be considered for treatment with a monoclonal TNF-alpha antagonist, along with an anticoagulant if the patient’s risk for bleeding was generally low and a coexistent pulmonary artery aneurysm was ruled out.
Management of arterial aneurysms received the other two strong recommendations. The panel recommended high-dose glucocorticoid plus cyclophosphamide for a pulmonary artery aneurysm, followed by a monoclonal TNF-alpha antagonist for refractory cases. Patients with these aneurysms who are at high risk for major bleeding should undergo embolization in preference to open surgery. When patients have aortic or peripheral artery aneurysms, treatment should start with cyclophosphamide and a corticosteroid before an aneurysm repair is attempted. But surgery or stenting of the aneurysm should not be delayed when patients are symptomatic.
Gastrointestinal involvement received one strong and two conditional recommendations. The panel strongly recommended confirming gastrointestinal involvement using endoscopy, imaging, or both, while also ruling out treatment with a nonsteroidal anti-inflammatory drug, inflammatory bowel disease, or an infection such as tuberculosis as the cause of gastrointestinal symptoms. One of the conditional recommendations called for an urgent surgical consult when patients have perforation, major bleeding, or obstruction. The second conditional recommendation called for considering glucocorticoid treatment to treat an acute exacerbation of gastrointestinal involvement. Additional treatment options to pair with a glucocorticoid include a disease-modifying drug such as 5-aminosalicylic acid or azathioprine. For patients with severe or refractory gastrointestinal symptoms or both, a monoclonal TNF-alpha antagonist or thalidomide is another potential option.
The panel issued two strong recommendations for managing nervous system involvement. The top treatment option for parenchymal involvement is a high-dose glucocorticoid followed by slow tapering while also treating with an immunosuppressant such as azathioprine. Treatment with cyclosporine should be avoided, the panel said. Treatment with a monoclonal TNF-alpha antagonist is an option to consider as first-line treatment for patients with severe nervous system involvement or for those with refractory disease. The second strong recommendation was to treat a cerebral venous thrombus with a high-dose glucocorticoid followed by tapering, with short-term anticoagulant treatment as an option. Patients also need screening for the presence of vascular disease at an extracranial location.
The panel’s final recommendation was a strong endorsement of colchicine as first-line treatment for arthritis in Behçet’s patients, although patients with acute monoarticular disease can be managed with an intra-articular injection of a glucocorticoid. For patients with recurrent or chronic arthritis, treatment options include azathioprine, interferon-alpha, or a TNF-alpha antagonist.
Dr. Hatemi has received research support from, received honoraria from, or has been a speaker for AbbVie, Celgene, Merck Sharp & Dohme, and Pfizer.
On Twitter @mitchelzoler
LONDON – A EULAR task force issued the first update to recommendations for managing Behçet’s disease since 2008, with revised recommendations that reflect expanded use of biologic agents, and increased evidence to guide management of gastrointestinal involvement, use of anticoagulants in patients with venous involvement, and use of surgical and interventional treatments, Dr. Gülen Hatemi said while presenting the update at the European Congress of Rheumatology.
The task force, which included more than 20 members, identified 304 articles to apply to the update, and produced five overarching principal and 18 specific recommendations divided among six categories of clinical manifestations of Behçet’s disease, said Dr. Hatemi, convenor of the task force and a rheumatologist at Istanbul University.
For mucocutaneous involvement, the update included five items that all received a “strong” recommendation from the task force: For an oral or genital ulcer, use a topical agent, such as a local steroid. Try colchicine first to prevent recurrent mucocutaneous lesions, especially when the dominant lesion is erythema nodosum or a genital ulcer. Treat papulopustular or acnelike lesions with topical or systemic agents, as when treating acne vulgaris. Coordinate treatment of leg ulcers, which can be caused by venous stasis or obliterative vasculitis, with a dermatologist and vascular surgeon. And azathioprine, thalidomide, interferon-alpha, a tumor necrosis factor (TNF)–alpha antagonist, or apremilast (Otezla) may be necessary for selected patients.
The task force issued two strong recommendations for managing eye involvement along with one conditional recommendation. The first strong recommendation was that managing uveitis requires close collaboration with an ophthalmologist, with the goal of inducing and maintaining remission. Patients with an inflammatory eye disease affecting the posterior segment should receive treatment with azathioprine, cyclosporine, interferon-alpha, or a monoclonal TNF-alpha antagonist. Treatment with a systemic corticosteroid should occur only when combined with azathioprine or another systemic immunosuppressant.
The second strong recommendation was that patients who present with an initial or recurrent acute episode of sight-threatening uveitis should receive treatment with a high-dose glucocorticoid, infliximab, or interferon-alpha. Intravitreal injection with a glucocorticoid as an adjunct to systemic therapy is an option for patients with a unilateral exacerbation. The conditional recommendation was for patients with isolated anterior uveitis. When these patients have markers of a poor prognosis – such as young age, male sex, or early disease onset – systemic treatment with an immunosuppressant is a possible option.
The panel issued three strong recommendations along with one conditional recommendation for managing vascular involvement. One of the strong recommendations called for treating acute deep vein thrombosis with a glucocorticoid as well as an immunosuppresant such as azathioprine, cyclophosphamide, or cyclosporine. A conditional recommendation said patients with refractory venous thrombosis could be considered for treatment with a monoclonal TNF-alpha antagonist, along with an anticoagulant if the patient’s risk for bleeding was generally low and a coexistent pulmonary artery aneurysm was ruled out.
Management of arterial aneurysms received the other two strong recommendations. The panel recommended high-dose glucocorticoid plus cyclophosphamide for a pulmonary artery aneurysm, followed by a monoclonal TNF-alpha antagonist for refractory cases. Patients with these aneurysms who are at high risk for major bleeding should undergo embolization in preference to open surgery. When patients have aortic or peripheral artery aneurysms, treatment should start with cyclophosphamide and a corticosteroid before an aneurysm repair is attempted. But surgery or stenting of the aneurysm should not be delayed when patients are symptomatic.
Gastrointestinal involvement received one strong and two conditional recommendations. The panel strongly recommended confirming gastrointestinal involvement using endoscopy, imaging, or both, while also ruling out treatment with a nonsteroidal anti-inflammatory drug, inflammatory bowel disease, or an infection such as tuberculosis as the cause of gastrointestinal symptoms. One of the conditional recommendations called for an urgent surgical consult when patients have perforation, major bleeding, or obstruction. The second conditional recommendation called for considering glucocorticoid treatment to treat an acute exacerbation of gastrointestinal involvement. Additional treatment options to pair with a glucocorticoid include a disease-modifying drug such as 5-aminosalicylic acid or azathioprine. For patients with severe or refractory gastrointestinal symptoms or both, a monoclonal TNF-alpha antagonist or thalidomide is another potential option.
The panel issued two strong recommendations for managing nervous system involvement. The top treatment option for parenchymal involvement is a high-dose glucocorticoid followed by slow tapering while also treating with an immunosuppressant such as azathioprine. Treatment with cyclosporine should be avoided, the panel said. Treatment with a monoclonal TNF-alpha antagonist is an option to consider as first-line treatment for patients with severe nervous system involvement or for those with refractory disease. The second strong recommendation was to treat a cerebral venous thrombus with a high-dose glucocorticoid followed by tapering, with short-term anticoagulant treatment as an option. Patients also need screening for the presence of vascular disease at an extracranial location.
The panel’s final recommendation was a strong endorsement of colchicine as first-line treatment for arthritis in Behçet’s patients, although patients with acute monoarticular disease can be managed with an intra-articular injection of a glucocorticoid. For patients with recurrent or chronic arthritis, treatment options include azathioprine, interferon-alpha, or a TNF-alpha antagonist.
Dr. Hatemi has received research support from, received honoraria from, or has been a speaker for AbbVie, Celgene, Merck Sharp & Dohme, and Pfizer.
On Twitter @mitchelzoler
LONDON – A EULAR task force issued the first update to recommendations for managing Behçet’s disease since 2008, with revised recommendations that reflect expanded use of biologic agents, and increased evidence to guide management of gastrointestinal involvement, use of anticoagulants in patients with venous involvement, and use of surgical and interventional treatments, Dr. Gülen Hatemi said while presenting the update at the European Congress of Rheumatology.
The task force, which included more than 20 members, identified 304 articles to apply to the update, and produced five overarching principal and 18 specific recommendations divided among six categories of clinical manifestations of Behçet’s disease, said Dr. Hatemi, convenor of the task force and a rheumatologist at Istanbul University.
For mucocutaneous involvement, the update included five items that all received a “strong” recommendation from the task force: For an oral or genital ulcer, use a topical agent, such as a local steroid. Try colchicine first to prevent recurrent mucocutaneous lesions, especially when the dominant lesion is erythema nodosum or a genital ulcer. Treat papulopustular or acnelike lesions with topical or systemic agents, as when treating acne vulgaris. Coordinate treatment of leg ulcers, which can be caused by venous stasis or obliterative vasculitis, with a dermatologist and vascular surgeon. And azathioprine, thalidomide, interferon-alpha, a tumor necrosis factor (TNF)–alpha antagonist, or apremilast (Otezla) may be necessary for selected patients.
The task force issued two strong recommendations for managing eye involvement along with one conditional recommendation. The first strong recommendation was that managing uveitis requires close collaboration with an ophthalmologist, with the goal of inducing and maintaining remission. Patients with an inflammatory eye disease affecting the posterior segment should receive treatment with azathioprine, cyclosporine, interferon-alpha, or a monoclonal TNF-alpha antagonist. Treatment with a systemic corticosteroid should occur only when combined with azathioprine or another systemic immunosuppressant.
The second strong recommendation was that patients who present with an initial or recurrent acute episode of sight-threatening uveitis should receive treatment with a high-dose glucocorticoid, infliximab, or interferon-alpha. Intravitreal injection with a glucocorticoid as an adjunct to systemic therapy is an option for patients with a unilateral exacerbation. The conditional recommendation was for patients with isolated anterior uveitis. When these patients have markers of a poor prognosis – such as young age, male sex, or early disease onset – systemic treatment with an immunosuppressant is a possible option.
The panel issued three strong recommendations along with one conditional recommendation for managing vascular involvement. One of the strong recommendations called for treating acute deep vein thrombosis with a glucocorticoid as well as an immunosuppresant such as azathioprine, cyclophosphamide, or cyclosporine. A conditional recommendation said patients with refractory venous thrombosis could be considered for treatment with a monoclonal TNF-alpha antagonist, along with an anticoagulant if the patient’s risk for bleeding was generally low and a coexistent pulmonary artery aneurysm was ruled out.
Management of arterial aneurysms received the other two strong recommendations. The panel recommended high-dose glucocorticoid plus cyclophosphamide for a pulmonary artery aneurysm, followed by a monoclonal TNF-alpha antagonist for refractory cases. Patients with these aneurysms who are at high risk for major bleeding should undergo embolization in preference to open surgery. When patients have aortic or peripheral artery aneurysms, treatment should start with cyclophosphamide and a corticosteroid before an aneurysm repair is attempted. But surgery or stenting of the aneurysm should not be delayed when patients are symptomatic.
Gastrointestinal involvement received one strong and two conditional recommendations. The panel strongly recommended confirming gastrointestinal involvement using endoscopy, imaging, or both, while also ruling out treatment with a nonsteroidal anti-inflammatory drug, inflammatory bowel disease, or an infection such as tuberculosis as the cause of gastrointestinal symptoms. One of the conditional recommendations called for an urgent surgical consult when patients have perforation, major bleeding, or obstruction. The second conditional recommendation called for considering glucocorticoid treatment to treat an acute exacerbation of gastrointestinal involvement. Additional treatment options to pair with a glucocorticoid include a disease-modifying drug such as 5-aminosalicylic acid or azathioprine. For patients with severe or refractory gastrointestinal symptoms or both, a monoclonal TNF-alpha antagonist or thalidomide is another potential option.
The panel issued two strong recommendations for managing nervous system involvement. The top treatment option for parenchymal involvement is a high-dose glucocorticoid followed by slow tapering while also treating with an immunosuppressant such as azathioprine. Treatment with cyclosporine should be avoided, the panel said. Treatment with a monoclonal TNF-alpha antagonist is an option to consider as first-line treatment for patients with severe nervous system involvement or for those with refractory disease. The second strong recommendation was to treat a cerebral venous thrombus with a high-dose glucocorticoid followed by tapering, with short-term anticoagulant treatment as an option. Patients also need screening for the presence of vascular disease at an extracranial location.
The panel’s final recommendation was a strong endorsement of colchicine as first-line treatment for arthritis in Behçet’s patients, although patients with acute monoarticular disease can be managed with an intra-articular injection of a glucocorticoid. For patients with recurrent or chronic arthritis, treatment options include azathioprine, interferon-alpha, or a TNF-alpha antagonist.
Dr. Hatemi has received research support from, received honoraria from, or has been a speaker for AbbVie, Celgene, Merck Sharp & Dohme, and Pfizer.
On Twitter @mitchelzoler
AT THE EULAR 2016 CONGRESS
One meal increases odds of doctors prescribing drugs
Doctors who accepted a single, industry-sponsored meal worth less than $20 were significantly more likely to prescribe the featured drug to Medicare patients, based on data from a cross-sectional study of 279,669 physicians. The findings were published online June 20 in JAMA Internal Medicine (JAMA Intern. Med. 2016 Jun. doi: 10.1001/jamainternmed.2016.2765).
In a multivariate analysis, physicians who received a single meal related to the promoted drug were 1.8 times more likely to prescribe rosuvastatin than other statins, 1.7 times more likely to prescribe nebivolol than other beta-blockers, 1.5 times more likely to prescribe olmesartan than other ACE inhibitors or ARBs, and more than twice as likely to prescribe desvenlafaxine than other SSRIs and serotonin norepinephrine reuptake inhibitors (odds ratio, 2.18).

These differences remained significant after controlling for factors including prescribing volume, physician specialty, practice setting, and demographics. Prescribing rates increased with additional meals and more expensive meals.
Previous studies have identified associations between increased prescribing and industry payments to physicians, wrote Colette DeJong, a research fellow at the University of California, San Francisco, Center for Healthcare Value, and her colleagues. However, “It is not known whether much smaller payments, such as sponsored meals, are associated with increased prescribing of the promoted brand-name drug over therapeutic alternatives,” they noted.
The researchers reviewed data from the federal Open Payments program from Aug. 1 through Dec. 31, 2013, as well as Medicare Part D prescribing data for 2013.
The results were limited by the cross-sectional nature of the study and the limitations of data from the Open Payments program, and the data reflect an association, not a cause-and-effect relationship, the researchers noted. However, “Our results are consistent with recent analyses that linked federal or state-level physician payment records with Medicare Part D prescribing data,” and with smaller studies, they said. “Future research could compare industry-sponsored meals and other methods for disseminating drug information, such as academic detailing and independent drug bulletins, with respect to the cost and quality of prescribing,” they added. The researchers had no financial conflicts to disclose.
Read the full study here: http://archinte.jamanetwork.com/article.aspx?doi=10.1001/jamainternmed.2016.2765.
“Is it necessary to prove a causal relationship between industry payments to physicians and the prescribing of brand-name medications?” asked Dr. Robert Steinbrook in an editor’s note accompanying the study. “Other than research support, product development, and bona fide consulting related to specific research programs and projects, it is already evident that there are few reasons for physicians to have financial associations with industry,” he wrote. “Although the association between industry payments to physicians and higher rates of prescribing of brand-name medications is not in dispute, none of these studies have established a cause-and-effect relationship,” he noted. One possible reason for the association: “Physicians may choose to attend industry events where information is provided about drugs that they already prefer,” he said. However, if drug companies and device manufacturers spent less money on physician activities and more on independent safety, effectiveness, and affordability studies, “our patients and the health care system would be better off,” he said (JAMA Intern. Med. 2016, published online June 20).
Dr. Steinbrook is editor at large for JAMA Internal Medicine. He had no relevant financial conflicts to disclose.
“Is it necessary to prove a causal relationship between industry payments to physicians and the prescribing of brand-name medications?” asked Dr. Robert Steinbrook in an editor’s note accompanying the study. “Other than research support, product development, and bona fide consulting related to specific research programs and projects, it is already evident that there are few reasons for physicians to have financial associations with industry,” he wrote. “Although the association between industry payments to physicians and higher rates of prescribing of brand-name medications is not in dispute, none of these studies have established a cause-and-effect relationship,” he noted. One possible reason for the association: “Physicians may choose to attend industry events where information is provided about drugs that they already prefer,” he said. However, if drug companies and device manufacturers spent less money on physician activities and more on independent safety, effectiveness, and affordability studies, “our patients and the health care system would be better off,” he said (JAMA Intern. Med. 2016, published online June 20).
Dr. Steinbrook is editor at large for JAMA Internal Medicine. He had no relevant financial conflicts to disclose.
“Is it necessary to prove a causal relationship between industry payments to physicians and the prescribing of brand-name medications?” asked Dr. Robert Steinbrook in an editor’s note accompanying the study. “Other than research support, product development, and bona fide consulting related to specific research programs and projects, it is already evident that there are few reasons for physicians to have financial associations with industry,” he wrote. “Although the association between industry payments to physicians and higher rates of prescribing of brand-name medications is not in dispute, none of these studies have established a cause-and-effect relationship,” he noted. One possible reason for the association: “Physicians may choose to attend industry events where information is provided about drugs that they already prefer,” he said. However, if drug companies and device manufacturers spent less money on physician activities and more on independent safety, effectiveness, and affordability studies, “our patients and the health care system would be better off,” he said (JAMA Intern. Med. 2016, published online June 20).
Dr. Steinbrook is editor at large for JAMA Internal Medicine. He had no relevant financial conflicts to disclose.
Doctors who accepted a single, industry-sponsored meal worth less than $20 were significantly more likely to prescribe the featured drug to Medicare patients, based on data from a cross-sectional study of 279,669 physicians. The findings were published online June 20 in JAMA Internal Medicine (JAMA Intern. Med. 2016 Jun. doi: 10.1001/jamainternmed.2016.2765).
In a multivariate analysis, physicians who received a single meal related to the promoted drug were 1.8 times more likely to prescribe rosuvastatin than other statins, 1.7 times more likely to prescribe nebivolol than other beta-blockers, 1.5 times more likely to prescribe olmesartan than other ACE inhibitors or ARBs, and more than twice as likely to prescribe desvenlafaxine than other SSRIs and serotonin norepinephrine reuptake inhibitors (odds ratio, 2.18).
These differences remained significant after controlling for factors including prescribing volume, physician specialty, practice setting, and demographics. Prescribing rates increased with additional meals and more expensive meals.
Previous studies have identified associations between increased prescribing and industry payments to physicians, wrote Colette DeJong, a research fellow at the University of California, San Francisco, Center for Healthcare Value, and her colleagues. However, “It is not known whether much smaller payments, such as sponsored meals, are associated with increased prescribing of the promoted brand-name drug over therapeutic alternatives,” they noted.
The researchers reviewed data from the federal Open Payments program from Aug. 1 through Dec. 31, 2013, as well as Medicare Part D prescribing data for 2013.
The results were limited by the cross-sectional nature of the study and the limitations of data from the Open Payments program, and the data reflect an association, not a cause-and-effect relationship, the researchers noted. However, “Our results are consistent with recent analyses that linked federal or state-level physician payment records with Medicare Part D prescribing data,” and with smaller studies, they said. “Future research could compare industry-sponsored meals and other methods for disseminating drug information, such as academic detailing and independent drug bulletins, with respect to the cost and quality of prescribing,” they added. The researchers had no financial conflicts to disclose.
Read the full study here: http://archinte.jamanetwork.com/article.aspx?doi=10.1001/jamainternmed.2016.2765.
Doctors who accepted a single, industry-sponsored meal worth less than $20 were significantly more likely to prescribe the featured drug to Medicare patients, based on data from a cross-sectional study of 279,669 physicians. The findings were published online June 20 in JAMA Internal Medicine (JAMA Intern. Med. 2016 Jun. doi: 10.1001/jamainternmed.2016.2765).
In a multivariate analysis, physicians who received a single meal related to the promoted drug were 1.8 times more likely to prescribe rosuvastatin than other statins, 1.7 times more likely to prescribe nebivolol than other beta-blockers, 1.5 times more likely to prescribe olmesartan than other ACE inhibitors or ARBs, and more than twice as likely to prescribe desvenlafaxine than other SSRIs and serotonin norepinephrine reuptake inhibitors (odds ratio, 2.18).
These differences remained significant after controlling for factors including prescribing volume, physician specialty, practice setting, and demographics. Prescribing rates increased with additional meals and more expensive meals.
Previous studies have identified associations between increased prescribing and industry payments to physicians, wrote Colette DeJong, a research fellow at the University of California, San Francisco, Center for Healthcare Value, and her colleagues. However, “It is not known whether much smaller payments, such as sponsored meals, are associated with increased prescribing of the promoted brand-name drug over therapeutic alternatives,” they noted.
The researchers reviewed data from the federal Open Payments program from Aug. 1 through Dec. 31, 2013, as well as Medicare Part D prescribing data for 2013.
The results were limited by the cross-sectional nature of the study and the limitations of data from the Open Payments program, and the data reflect an association, not a cause-and-effect relationship, the researchers noted. However, “Our results are consistent with recent analyses that linked federal or state-level physician payment records with Medicare Part D prescribing data,” and with smaller studies, they said. “Future research could compare industry-sponsored meals and other methods for disseminating drug information, such as academic detailing and independent drug bulletins, with respect to the cost and quality of prescribing,” they added. The researchers had no financial conflicts to disclose.
Read the full study here: http://archinte.jamanetwork.com/article.aspx?doi=10.1001/jamainternmed.2016.2765.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Industry-sponsored meals were associated with higher prescribing rates of the featured drug to Medicare patients.
Major finding: Doctors were significantly more likely to prescribe rosuvastatin, nebivolol, and olmesartan, and more than twice as likely to prescribe desvenlafaxine (OR, 2.18) over those drugs’ competitors if they received a $20 or less complimentary meal from the company promoting the drug of interest.
Data source: A cross-sectional study of 279,669 physicians.
Disclosures: The researchers had no financial conflicts to disclose.

Sweet spot found for LDL-C reduction to minimize risk
Researchers have identified a “sweet spot” target for reducing low-density lipoprotein cholesterol levels with statin therapy that is associated with the lowest risk of adverse cardiac outcomes.
A study published online June 20 in JAMA Internal Medicine analyzed data from an Israeli health care organization between 2009-2013 and identified 31,619 patients with ischemic heart disease, aged 30-84 years, who were being treated with statins and were at least 80% adherent to the medication regime.

The analysis showed individuals who achieved a “moderate” LDL-C level – between 70.1-100.0 mg/dL – after 1 year of statin treatment had an 11% lower incidence of major adverse cardiac events, compared with those with a “high” LDL-C level – between 100.1-130.0 mg/dL (95% confidence interval, 0.84-0.94; P less than .001).
However researchers observed no significant difference in the risk of adverse cardiac events between the moderate group and those who achieved a “low” LDL-C equal to or less than 70.0mg/dL (hazard ratio, 1.02; 95% CI, 0.97-1.07; P = .54).
In a further analysis that included 54,884 individuals who were at least 50% adherent to their statin therapy, there was a slightly increased risk of major cardiac events in patients who achieved a low LDL-C, compared with those in the moderate LDL-C group, and a significant 13% reduction in risk in the moderate LDL-C group, compared with the high LDL-C group.
“Whereas this may reflect clinical risk of low levels of LDL-C, these results further support the main findings of this study that achieving a level below 70 mg/dL is not beneficial for all patients,” wrote Dr. Morton Leibowitz, from the Clalit Research Institute, Tel Aviv, and his coauthors.
Adjustment for age did not significantly alter the interaction between LDL-C levels and the risk of adverse cardiac events (JAMA Intern Med. 2016 Jun 20. doi: 10.1001/jamainternmed.2016.2751).
“The question of the association between achieved LDL-C levels and major adverse cardiac events for secondary prevention has become highly relevant, particularly in the real-world context of patients excluded from [randomized, controlled trials],” the authors wrote, suggesting that their data only partially support recent claims that lower LDL-C is better for cardiac outcomes.
“Our findings of significantly lower risk of MACEs associated with achieved LDL-C level of less than 100.0 mg/dL but not with achieved LDL-C of less than 70.0 mg/dL suggest a target for long-term statin treatment.”
The study was funded by the Clalit Research Institute. No conflicts of interest were reported.
Researchers have identified a “sweet spot” target for reducing low-density lipoprotein cholesterol levels with statin therapy that is associated with the lowest risk of adverse cardiac outcomes.
A study published online June 20 in JAMA Internal Medicine analyzed data from an Israeli health care organization between 2009-2013 and identified 31,619 patients with ischemic heart disease, aged 30-84 years, who were being treated with statins and were at least 80% adherent to the medication regime.
The analysis showed individuals who achieved a “moderate” LDL-C level – between 70.1-100.0 mg/dL – after 1 year of statin treatment had an 11% lower incidence of major adverse cardiac events, compared with those with a “high” LDL-C level – between 100.1-130.0 mg/dL (95% confidence interval, 0.84-0.94; P less than .001).
However researchers observed no significant difference in the risk of adverse cardiac events between the moderate group and those who achieved a “low” LDL-C equal to or less than 70.0mg/dL (hazard ratio, 1.02; 95% CI, 0.97-1.07; P = .54).
In a further analysis that included 54,884 individuals who were at least 50% adherent to their statin therapy, there was a slightly increased risk of major cardiac events in patients who achieved a low LDL-C, compared with those in the moderate LDL-C group, and a significant 13% reduction in risk in the moderate LDL-C group, compared with the high LDL-C group.
“Whereas this may reflect clinical risk of low levels of LDL-C, these results further support the main findings of this study that achieving a level below 70 mg/dL is not beneficial for all patients,” wrote Dr. Morton Leibowitz, from the Clalit Research Institute, Tel Aviv, and his coauthors.
Adjustment for age did not significantly alter the interaction between LDL-C levels and the risk of adverse cardiac events (JAMA Intern Med. 2016 Jun 20. doi: 10.1001/jamainternmed.2016.2751).
“The question of the association between achieved LDL-C levels and major adverse cardiac events for secondary prevention has become highly relevant, particularly in the real-world context of patients excluded from [randomized, controlled trials],” the authors wrote, suggesting that their data only partially support recent claims that lower LDL-C is better for cardiac outcomes.
“Our findings of significantly lower risk of MACEs associated with achieved LDL-C level of less than 100.0 mg/dL but not with achieved LDL-C of less than 70.0 mg/dL suggest a target for long-term statin treatment.”
The study was funded by the Clalit Research Institute. No conflicts of interest were reported.
Researchers have identified a “sweet spot” target for reducing low-density lipoprotein cholesterol levels with statin therapy that is associated with the lowest risk of adverse cardiac outcomes.
A study published online June 20 in JAMA Internal Medicine analyzed data from an Israeli health care organization between 2009-2013 and identified 31,619 patients with ischemic heart disease, aged 30-84 years, who were being treated with statins and were at least 80% adherent to the medication regime.
The analysis showed individuals who achieved a “moderate” LDL-C level – between 70.1-100.0 mg/dL – after 1 year of statin treatment had an 11% lower incidence of major adverse cardiac events, compared with those with a “high” LDL-C level – between 100.1-130.0 mg/dL (95% confidence interval, 0.84-0.94; P less than .001).
However researchers observed no significant difference in the risk of adverse cardiac events between the moderate group and those who achieved a “low” LDL-C equal to or less than 70.0mg/dL (hazard ratio, 1.02; 95% CI, 0.97-1.07; P = .54).
In a further analysis that included 54,884 individuals who were at least 50% adherent to their statin therapy, there was a slightly increased risk of major cardiac events in patients who achieved a low LDL-C, compared with those in the moderate LDL-C group, and a significant 13% reduction in risk in the moderate LDL-C group, compared with the high LDL-C group.
“Whereas this may reflect clinical risk of low levels of LDL-C, these results further support the main findings of this study that achieving a level below 70 mg/dL is not beneficial for all patients,” wrote Dr. Morton Leibowitz, from the Clalit Research Institute, Tel Aviv, and his coauthors.
Adjustment for age did not significantly alter the interaction between LDL-C levels and the risk of adverse cardiac events (JAMA Intern Med. 2016 Jun 20. doi: 10.1001/jamainternmed.2016.2751).
“The question of the association between achieved LDL-C levels and major adverse cardiac events for secondary prevention has become highly relevant, particularly in the real-world context of patients excluded from [randomized, controlled trials],” the authors wrote, suggesting that their data only partially support recent claims that lower LDL-C is better for cardiac outcomes.
“Our findings of significantly lower risk of MACEs associated with achieved LDL-C level of less than 100.0 mg/dL but not with achieved LDL-C of less than 70.0 mg/dL suggest a target for long-term statin treatment.”
The study was funded by the Clalit Research Institute. No conflicts of interest were reported.
FROM JAMA INTERNAL MEDICINE
Key clinical point: A moderate target for LDL-C reduction achieves the greatest reduction in the risk of adverse events, compared with low or high targets.
Major finding: Achieving an LDL-C of 70.1-100.0 mg/dL is associated with an 11% lower incidence of major adverse cardiac events, compared with an LDL-C between 100.1-130.0 mg/dL.
Data source: A population-based cohort study tracked 31,619 patients with ischemic heart disease who were being treated with statins and were at least 80% adherent to the medication regime.
Disclosures: The study was funded by the Clalit Research Institute. No conflicts of interest were reported.

The June issue of Vascular Specialist is now online
Check out the June issue of Vascular Specialist now online in our enhanced digital edition and standard PDF. This month includes stories on vascular trainee case loads, the difficulties surgeons have at estimating blood loss, and an editorial by Dr. Russell Samson asking “Why be a vascular surgeon?”

Our Point/Counterpoint features a debate on the importance of the angiosome concept in revascularization for limb salvage between Dr. Richard Neville and Dr. Bauer Sumpio, and our Medicolegal Issues column examines the liability issues raised by the new move to value-based care.
Check out the June issue of Vascular Specialist now online in our enhanced digital edition and standard PDF. This month includes stories on vascular trainee case loads, the difficulties surgeons have at estimating blood loss, and an editorial by Dr. Russell Samson asking “Why be a vascular surgeon?”
Our Point/Counterpoint features a debate on the importance of the angiosome concept in revascularization for limb salvage between Dr. Richard Neville and Dr. Bauer Sumpio, and our Medicolegal Issues column examines the liability issues raised by the new move to value-based care.
Check out the June issue of Vascular Specialist now online in our enhanced digital edition and standard PDF. This month includes stories on vascular trainee case loads, the difficulties surgeons have at estimating blood loss, and an editorial by Dr. Russell Samson asking “Why be a vascular surgeon?”
Our Point/Counterpoint features a debate on the importance of the angiosome concept in revascularization for limb salvage between Dr. Richard Neville and Dr. Bauer Sumpio, and our Medicolegal Issues column examines the liability issues raised by the new move to value-based care.

Red Alert: Can Topical Skin Care Products Promote Melanoma Metastasis?

Le Gal et al (Sci Transl Med. 2015;7:308re8) discovered that antioxidant administration in mice not only increased lymph node metastases but also increased the migration and invasive properties of human melanoma cells. However, the antioxidant N-acetylcysteine (NAC) had no impact on the number and size of the primary tumors (in mice), and neither NAC nor Trolox (6-hydroxy-2,5,7,8-tetramethylchroman-2-carboxylic acid), a structurally unrelated antioxidant and soluble vitamin E analogue, affected the proliferation of human melanoma cells. Hence, the progression of malignant melanoma (MM), a cancer that is sensitive to changes in reduction-oxidation status, may be influenced by exposure to antioxidants and vitamin E.
What’s the issue?
Healthy individuals and oncology patients commonly use supplements containing antioxidants to prevent cancer and fight malignancy, respectively. However, animal studies and human clinical trials have shown that antioxidants increase cancer risk and accelerate the progression of primary lung tumors. Le Gal et al’s study regarding progression of melanoma metastases following exposure to antioxidants extends the observations demonstrated for lung neoplasms. N-acetylcysteine was added to the drinking water of mice, whereas NAC and Trolox were added to a panel of human MM cell lines. N-acetylcysteine increased lymph node metastases in the endogenous mouse model of MM, and both NAC and Trolox markedly increased the migrations and invasive properties of human MM cells.
Cancers may be caused or exacerbated by free radicals. It has been assumed that antioxidants may protect against malignancy by destroying free radicals. Although prior studies have concluded that antioxidants prevent healthy cells from transforming into cancer after exposure to free radicals, Le Gal et al’s research suggests that antioxidants may not only protect but also enhance tumor progression once a cancer has developed.
If one extends the results of animal and tissue culture studies to humans, exposure to antioxidants may potentially influence the course of metastatic disease in patients who have already developed melanoma. In addition to systemic exposure after receiving oral antioxidants, melanoma patients also can be topically exposed to antioxidants. For example, nonprescription skin care products such as cutaneous rejuvenation treatments, emollients, and sunscreens can contain β-carotene, vitamin E, and other antioxidants. It remains to be determined whether topical exposure to antioxidants can cause the same observations that have occurred following systemic absorption in mice or tissue culture studies in human cell lines. Should we caution our melanoma patients with regards to what they apply to their skin?
Le Gal et al (Sci Transl Med. 2015;7:308re8) discovered that antioxidant administration in mice not only increased lymph node metastases but also increased the migration and invasive properties of human melanoma cells. However, the antioxidant N-acetylcysteine (NAC) had no impact on the number and size of the primary tumors (in mice), and neither NAC nor Trolox (6-hydroxy-2,5,7,8-tetramethylchroman-2-carboxylic acid), a structurally unrelated antioxidant and soluble vitamin E analogue, affected the proliferation of human melanoma cells. Hence, the progression of malignant melanoma (MM), a cancer that is sensitive to changes in reduction-oxidation status, may be influenced by exposure to antioxidants and vitamin E.
What’s the issue?
Healthy individuals and oncology patients commonly use supplements containing antioxidants to prevent cancer and fight malignancy, respectively. However, animal studies and human clinical trials have shown that antioxidants increase cancer risk and accelerate the progression of primary lung tumors. Le Gal et al’s study regarding progression of melanoma metastases following exposure to antioxidants extends the observations demonstrated for lung neoplasms. N-acetylcysteine was added to the drinking water of mice, whereas NAC and Trolox were added to a panel of human MM cell lines. N-acetylcysteine increased lymph node metastases in the endogenous mouse model of MM, and both NAC and Trolox markedly increased the migrations and invasive properties of human MM cells.
Cancers may be caused or exacerbated by free radicals. It has been assumed that antioxidants may protect against malignancy by destroying free radicals. Although prior studies have concluded that antioxidants prevent healthy cells from transforming into cancer after exposure to free radicals, Le Gal et al’s research suggests that antioxidants may not only protect but also enhance tumor progression once a cancer has developed.
If one extends the results of animal and tissue culture studies to humans, exposure to antioxidants may potentially influence the course of metastatic disease in patients who have already developed melanoma. In addition to systemic exposure after receiving oral antioxidants, melanoma patients also can be topically exposed to antioxidants. For example, nonprescription skin care products such as cutaneous rejuvenation treatments, emollients, and sunscreens can contain β-carotene, vitamin E, and other antioxidants. It remains to be determined whether topical exposure to antioxidants can cause the same observations that have occurred following systemic absorption in mice or tissue culture studies in human cell lines. Should we caution our melanoma patients with regards to what they apply to their skin?
Le Gal et al (Sci Transl Med. 2015;7:308re8) discovered that antioxidant administration in mice not only increased lymph node metastases but also increased the migration and invasive properties of human melanoma cells. However, the antioxidant N-acetylcysteine (NAC) had no impact on the number and size of the primary tumors (in mice), and neither NAC nor Trolox (6-hydroxy-2,5,7,8-tetramethylchroman-2-carboxylic acid), a structurally unrelated antioxidant and soluble vitamin E analogue, affected the proliferation of human melanoma cells. Hence, the progression of malignant melanoma (MM), a cancer that is sensitive to changes in reduction-oxidation status, may be influenced by exposure to antioxidants and vitamin E.
What’s the issue?
Healthy individuals and oncology patients commonly use supplements containing antioxidants to prevent cancer and fight malignancy, respectively. However, animal studies and human clinical trials have shown that antioxidants increase cancer risk and accelerate the progression of primary lung tumors. Le Gal et al’s study regarding progression of melanoma metastases following exposure to antioxidants extends the observations demonstrated for lung neoplasms. N-acetylcysteine was added to the drinking water of mice, whereas NAC and Trolox were added to a panel of human MM cell lines. N-acetylcysteine increased lymph node metastases in the endogenous mouse model of MM, and both NAC and Trolox markedly increased the migrations and invasive properties of human MM cells.
Cancers may be caused or exacerbated by free radicals. It has been assumed that antioxidants may protect against malignancy by destroying free radicals. Although prior studies have concluded that antioxidants prevent healthy cells from transforming into cancer after exposure to free radicals, Le Gal et al’s research suggests that antioxidants may not only protect but also enhance tumor progression once a cancer has developed.
If one extends the results of animal and tissue culture studies to humans, exposure to antioxidants may potentially influence the course of metastatic disease in patients who have already developed melanoma. In addition to systemic exposure after receiving oral antioxidants, melanoma patients also can be topically exposed to antioxidants. For example, nonprescription skin care products such as cutaneous rejuvenation treatments, emollients, and sunscreens can contain β-carotene, vitamin E, and other antioxidants. It remains to be determined whether topical exposure to antioxidants can cause the same observations that have occurred following systemic absorption in mice or tissue culture studies in human cell lines. Should we caution our melanoma patients with regards to what they apply to their skin?

Member Decisions Coming July 1
We understand membership applicants are anxious for a decision!
Check your mailbox. All those who submitted applications to be members of SVS will receive a letter about the membership decision around July 1.
We understand membership applicants are anxious for a decision!
Check your mailbox. All those who submitted applications to be members of SVS will receive a letter about the membership decision around July 1.
We understand membership applicants are anxious for a decision!
Check your mailbox. All those who submitted applications to be members of SVS will receive a letter about the membership decision around July 1.

New SVS Officers Elected at Annual Meeting
At the Vascular Annual Meeting last week, members voted on new officers and approved selection of new members of the Board of Directors.
Officers elected are:
• Vice president, Dr. Michel Makaroun
• Secretary, Dr. Ali AbuRahma
• Treasurer, Dr. Kim Hodgson
New members of the Board of Directors are:
Dr. Frank Pomposelli, Clinical Practice Council chair
Dr. Michael Golden, Eastern Vascular Society
Dr. Thomas Forbes, Canadian Society for Vascular Surgery
Dr. Donald Jacobs, Midwestern Vascular Surgical Society
Dr. William Marston, Southern Association for Vascular Surgery
Dr. Thomas Bower, Society for Clinical Vascular Surgery
Dr. Darrin Clouse, Vascular and Endovascular Surgery Society
Dr. William Jordan, Association of Program Directors in Vascular Surgery.
At the Vascular Annual Meeting last week, members voted on new officers and approved selection of new members of the Board of Directors.
Officers elected are:
• Vice president, Dr. Michel Makaroun
• Secretary, Dr. Ali AbuRahma
• Treasurer, Dr. Kim Hodgson
New members of the Board of Directors are:
Dr. Frank Pomposelli, Clinical Practice Council chair
Dr. Michael Golden, Eastern Vascular Society
Dr. Thomas Forbes, Canadian Society for Vascular Surgery
Dr. Donald Jacobs, Midwestern Vascular Surgical Society
Dr. William Marston, Southern Association for Vascular Surgery
Dr. Thomas Bower, Society for Clinical Vascular Surgery
Dr. Darrin Clouse, Vascular and Endovascular Surgery Society
Dr. William Jordan, Association of Program Directors in Vascular Surgery.
At the Vascular Annual Meeting last week, members voted on new officers and approved selection of new members of the Board of Directors.
Officers elected are:
• Vice president, Dr. Michel Makaroun
• Secretary, Dr. Ali AbuRahma
• Treasurer, Dr. Kim Hodgson
New members of the Board of Directors are:
Dr. Frank Pomposelli, Clinical Practice Council chair
Dr. Michael Golden, Eastern Vascular Society
Dr. Thomas Forbes, Canadian Society for Vascular Surgery
Dr. Donald Jacobs, Midwestern Vascular Surgical Society
Dr. William Marston, Southern Association for Vascular Surgery
Dr. Thomas Bower, Society for Clinical Vascular Surgery
Dr. Darrin Clouse, Vascular and Endovascular Surgery Society
Dr. William Jordan, Association of Program Directors in Vascular Surgery.
