User login
Daily fish oil dose boosts healing after heart attack
A daily dose of omega-3 fatty acids from fish oil significantly improved heart function in adults after heart attacks, based on data from a randomized trial of 358 heart attack survivors. The findings were published online Aug. 1 in Circulation.
Patients who received 4 grams of omega-3 fatty acids from fish oil (O-3FA) for 6 months had significant reductions in left ventricular end-systolic volume index (–5.8%) and noninfarct myocardial fibrosis (–5.6%), compared with placebo patients, Bobak Heydari, MD, MPH, of Brigham and Women’s Hospital, Boston, and colleagues.
The effects remained significant after adjusting for factors including guideline-based standard post-heart attack medical therapies, they noted.
Treatment with omega-3 fatty acids (O-3FA) “also was associated with a significant reduction of both biomarkers of inflammation (myeloperoxidase, lipoprotein-associated phospholipase A2) and myocardial fibrosis (ST2),” the researchers wrote. “We therefore speculate that O-3FA treatment provides the aforementioned improvement in LV remodeling and noninfarct myocardial fibrosis through suppression of inflammation at both systemic and myocardial levels during the convalescent healing phase after acute MI,” they noted.
The results build on data from a previous study showing an association between daily doses of O-3FA and improved survival rates in heart attack patients, but the specific impact on heart structure and tissue has not been well studied, the researchers noted (Circulation. 2016;134:378-91 doi: 10.1161/circulationaha.115.019949).
The OMEGA-REMODEL trial (Omega-3 Acid Ethyl Esters on Left Ventricular Remodeling After Acute Myocardial Infarction) was designed to assess the impact of omega-3 fatty acids on heart healing after a heart attack. The average age of the patients was about 60 years. Demographic characteristics and cardiovascular disease histories were not significantly different between the groups.
Compliance for both treatment and placebo groups was 96% based on pill counts. Nausea was the most common side effect, reported by 5.9% of treatment patients and 5.4% of placebo patients. No serious adverse events associated with treatment were reported.
The findings were limited by several factors, including the possible use of over-the-counter fish oil supplementation by patients, the researchers noted. “However, dose-response relationship between O-3FA therapy and our main study endpoints strongly supported our intention-to-treat analysis,” they said.
The study was funded by the National Heart, Lung, and Blood Institute. The researchers had no financial conflicts to disclose.
A daily dose of omega-3 fatty acids from fish oil significantly improved heart function in adults after heart attacks, based on data from a randomized trial of 358 heart attack survivors. The findings were published online Aug. 1 in Circulation.
Patients who received 4 grams of omega-3 fatty acids from fish oil (O-3FA) for 6 months had significant reductions in left ventricular end-systolic volume index (–5.8%) and noninfarct myocardial fibrosis (–5.6%), compared with placebo patients, Bobak Heydari, MD, MPH, of Brigham and Women’s Hospital, Boston, and colleagues.
The effects remained significant after adjusting for factors including guideline-based standard post-heart attack medical therapies, they noted.
Treatment with omega-3 fatty acids (O-3FA) “also was associated with a significant reduction of both biomarkers of inflammation (myeloperoxidase, lipoprotein-associated phospholipase A2) and myocardial fibrosis (ST2),” the researchers wrote. “We therefore speculate that O-3FA treatment provides the aforementioned improvement in LV remodeling and noninfarct myocardial fibrosis through suppression of inflammation at both systemic and myocardial levels during the convalescent healing phase after acute MI,” they noted.
The results build on data from a previous study showing an association between daily doses of O-3FA and improved survival rates in heart attack patients, but the specific impact on heart structure and tissue has not been well studied, the researchers noted (Circulation. 2016;134:378-91 doi: 10.1161/circulationaha.115.019949).
The OMEGA-REMODEL trial (Omega-3 Acid Ethyl Esters on Left Ventricular Remodeling After Acute Myocardial Infarction) was designed to assess the impact of omega-3 fatty acids on heart healing after a heart attack. The average age of the patients was about 60 years. Demographic characteristics and cardiovascular disease histories were not significantly different between the groups.
Compliance for both treatment and placebo groups was 96% based on pill counts. Nausea was the most common side effect, reported by 5.9% of treatment patients and 5.4% of placebo patients. No serious adverse events associated with treatment were reported.
The findings were limited by several factors, including the possible use of over-the-counter fish oil supplementation by patients, the researchers noted. “However, dose-response relationship between O-3FA therapy and our main study endpoints strongly supported our intention-to-treat analysis,” they said.
The study was funded by the National Heart, Lung, and Blood Institute. The researchers had no financial conflicts to disclose.
A daily dose of omega-3 fatty acids from fish oil significantly improved heart function in adults after heart attacks, based on data from a randomized trial of 358 heart attack survivors. The findings were published online Aug. 1 in Circulation.
Patients who received 4 grams of omega-3 fatty acids from fish oil (O-3FA) for 6 months had significant reductions in left ventricular end-systolic volume index (–5.8%) and noninfarct myocardial fibrosis (–5.6%), compared with placebo patients, Bobak Heydari, MD, MPH, of Brigham and Women’s Hospital, Boston, and colleagues.
The effects remained significant after adjusting for factors including guideline-based standard post-heart attack medical therapies, they noted.
Treatment with omega-3 fatty acids (O-3FA) “also was associated with a significant reduction of both biomarkers of inflammation (myeloperoxidase, lipoprotein-associated phospholipase A2) and myocardial fibrosis (ST2),” the researchers wrote. “We therefore speculate that O-3FA treatment provides the aforementioned improvement in LV remodeling and noninfarct myocardial fibrosis through suppression of inflammation at both systemic and myocardial levels during the convalescent healing phase after acute MI,” they noted.
The results build on data from a previous study showing an association between daily doses of O-3FA and improved survival rates in heart attack patients, but the specific impact on heart structure and tissue has not been well studied, the researchers noted (Circulation. 2016;134:378-91 doi: 10.1161/circulationaha.115.019949).
The OMEGA-REMODEL trial (Omega-3 Acid Ethyl Esters on Left Ventricular Remodeling After Acute Myocardial Infarction) was designed to assess the impact of omega-3 fatty acids on heart healing after a heart attack. The average age of the patients was about 60 years. Demographic characteristics and cardiovascular disease histories were not significantly different between the groups.
Compliance for both treatment and placebo groups was 96% based on pill counts. Nausea was the most common side effect, reported by 5.9% of treatment patients and 5.4% of placebo patients. No serious adverse events associated with treatment were reported.
The findings were limited by several factors, including the possible use of over-the-counter fish oil supplementation by patients, the researchers noted. “However, dose-response relationship between O-3FA therapy and our main study endpoints strongly supported our intention-to-treat analysis,” they said.
The study was funded by the National Heart, Lung, and Blood Institute. The researchers had no financial conflicts to disclose.
FROM CIRCULATION
Key clinical point: A daily dose of omega-3 fatty acids for 6 months after a heart attack improved heart function and reduced scarring.
Major finding: Heart attack patients who received 4 grams of omega-3 fatty acids from fish oil daily had significant reductions in both left ventricular end-systolic volume index (-5.8%) and noninfarct myocardial fibrosis (-5.6%), compared with placebo patients after 6 months.
Data source: A randomized trial of 360 heart attack survivors.
Disclosures: The study was funded by the National Heart, Lung, and Blood Institute. The researchers had no financial conflicts to disclose.
Young age, tumor subtype linked in breast cancer survival
Younger age at diagnosis of breast cancer predicts poor survival only with certain molecular subtypes of tumor, according to a report published online Aug. 1 in the Journal of Clinical Oncology.
An age of 40 years or younger “has long been considered a poor prognostic factor, because young women, on average, have an increased risk of disease recurrence and decreased survival. In recent years, however, with improved understanding of tumor biology, this assertion has been challenged with increased recognition of the prognostic and predictive role of tumor subtype and awareness that young women are more likely to develop more aggressive phenotypes,” said Ann H. Partridge, MD, of the Dana-Farber Cancer Institute, and Brigham and Women’s Hospital, both in Boston, and her associates.
To examine the relationships among patient age, tumor subtypes, and outcomes, they analyzed data for 17,575 women treated at eight U.S. cancer centers in 2000-2007 and enrolled in a National Comprehensive Cancer Network registry. The study participants (mean age, 35 years) all had newly diagnosed unilateral stage I, II, or III breast cancer and were followed for a median of 6.4 years. Their data were stratified by age at diagnosis: 40 years or younger, 41-50 years, 51-60 years, 61-70 years, or over 70 years.
In the initial analysis, younger women were 90% more likely to die of breast cancer than older women. This probability decreased to 50% when the data were adjusted to control for treatment, stage at diagnosis, and tumor grade, then decreased further to 30% when the data were further adjusted to control for tumor molecular subtype and method of detection, the investigators said (J Clin Oncol. 2016 Aug 1; doi:10.1200/JCO.2015.65.8013).
However, when the data were analyzed according to tumor subtype, women who had luminal A breast cancer (7,738 participants) were more than twice as likely to die of their disease if they were aged 40 or younger at diagnosis than if they were older (hazard ratio, 2.1). The age-related increase in risk was slightly lower for luminal B breast cancer (HR, 1.4), and appeared to be largely confined to those with HER2-negative luminal B tumors.
There also was a borderline increased risk of death in younger women who had triple-negative breast cancer (HR, 1.4), compared with older women who had that tumor subtype. In contrast, younger age did not correlate with increased breast cancer mortality among women with HER2-positive disease.
These findings “support the growing evidence that the relationship between age at diagnosis and breast-cancer-specific survival varies by tumor subtype, which has implications for both treatment decisions and future research directions. ....In women with luminal disease, younger age does have a substantial prognostic role, which may reflect inadequate therapy, including lower treatment efficacy and less therapeutic adherence and persistence, as well as residual differences in tumor biology,” Dr. Partridge and her associates said.
No specific source of funding was identified for this study. Dr. Partridge reported serving as a consultant for Pfizer; her associates reported ties to Pfizer, Tokai, Bristol-Myers Squibb, Carevive Systems, Oncothyreon, Amgen, and BeyondSpring Pharmaceuticals.
Younger age at diagnosis of breast cancer predicts poor survival only with certain molecular subtypes of tumor, according to a report published online Aug. 1 in the Journal of Clinical Oncology.
An age of 40 years or younger “has long been considered a poor prognostic factor, because young women, on average, have an increased risk of disease recurrence and decreased survival. In recent years, however, with improved understanding of tumor biology, this assertion has been challenged with increased recognition of the prognostic and predictive role of tumor subtype and awareness that young women are more likely to develop more aggressive phenotypes,” said Ann H. Partridge, MD, of the Dana-Farber Cancer Institute, and Brigham and Women’s Hospital, both in Boston, and her associates.
To examine the relationships among patient age, tumor subtypes, and outcomes, they analyzed data for 17,575 women treated at eight U.S. cancer centers in 2000-2007 and enrolled in a National Comprehensive Cancer Network registry. The study participants (mean age, 35 years) all had newly diagnosed unilateral stage I, II, or III breast cancer and were followed for a median of 6.4 years. Their data were stratified by age at diagnosis: 40 years or younger, 41-50 years, 51-60 years, 61-70 years, or over 70 years.
In the initial analysis, younger women were 90% more likely to die of breast cancer than older women. This probability decreased to 50% when the data were adjusted to control for treatment, stage at diagnosis, and tumor grade, then decreased further to 30% when the data were further adjusted to control for tumor molecular subtype and method of detection, the investigators said (J Clin Oncol. 2016 Aug 1; doi:10.1200/JCO.2015.65.8013).
However, when the data were analyzed according to tumor subtype, women who had luminal A breast cancer (7,738 participants) were more than twice as likely to die of their disease if they were aged 40 or younger at diagnosis than if they were older (hazard ratio, 2.1). The age-related increase in risk was slightly lower for luminal B breast cancer (HR, 1.4), and appeared to be largely confined to those with HER2-negative luminal B tumors.
There also was a borderline increased risk of death in younger women who had triple-negative breast cancer (HR, 1.4), compared with older women who had that tumor subtype. In contrast, younger age did not correlate with increased breast cancer mortality among women with HER2-positive disease.
These findings “support the growing evidence that the relationship between age at diagnosis and breast-cancer-specific survival varies by tumor subtype, which has implications for both treatment decisions and future research directions. ....In women with luminal disease, younger age does have a substantial prognostic role, which may reflect inadequate therapy, including lower treatment efficacy and less therapeutic adherence and persistence, as well as residual differences in tumor biology,” Dr. Partridge and her associates said.
No specific source of funding was identified for this study. Dr. Partridge reported serving as a consultant for Pfizer; her associates reported ties to Pfizer, Tokai, Bristol-Myers Squibb, Carevive Systems, Oncothyreon, Amgen, and BeyondSpring Pharmaceuticals.
Younger age at diagnosis of breast cancer predicts poor survival only with certain molecular subtypes of tumor, according to a report published online Aug. 1 in the Journal of Clinical Oncology.
An age of 40 years or younger “has long been considered a poor prognostic factor, because young women, on average, have an increased risk of disease recurrence and decreased survival. In recent years, however, with improved understanding of tumor biology, this assertion has been challenged with increased recognition of the prognostic and predictive role of tumor subtype and awareness that young women are more likely to develop more aggressive phenotypes,” said Ann H. Partridge, MD, of the Dana-Farber Cancer Institute, and Brigham and Women’s Hospital, both in Boston, and her associates.
To examine the relationships among patient age, tumor subtypes, and outcomes, they analyzed data for 17,575 women treated at eight U.S. cancer centers in 2000-2007 and enrolled in a National Comprehensive Cancer Network registry. The study participants (mean age, 35 years) all had newly diagnosed unilateral stage I, II, or III breast cancer and were followed for a median of 6.4 years. Their data were stratified by age at diagnosis: 40 years or younger, 41-50 years, 51-60 years, 61-70 years, or over 70 years.
In the initial analysis, younger women were 90% more likely to die of breast cancer than older women. This probability decreased to 50% when the data were adjusted to control for treatment, stage at diagnosis, and tumor grade, then decreased further to 30% when the data were further adjusted to control for tumor molecular subtype and method of detection, the investigators said (J Clin Oncol. 2016 Aug 1; doi:10.1200/JCO.2015.65.8013).
However, when the data were analyzed according to tumor subtype, women who had luminal A breast cancer (7,738 participants) were more than twice as likely to die of their disease if they were aged 40 or younger at diagnosis than if they were older (hazard ratio, 2.1). The age-related increase in risk was slightly lower for luminal B breast cancer (HR, 1.4), and appeared to be largely confined to those with HER2-negative luminal B tumors.
There also was a borderline increased risk of death in younger women who had triple-negative breast cancer (HR, 1.4), compared with older women who had that tumor subtype. In contrast, younger age did not correlate with increased breast cancer mortality among women with HER2-positive disease.
These findings “support the growing evidence that the relationship between age at diagnosis and breast-cancer-specific survival varies by tumor subtype, which has implications for both treatment decisions and future research directions. ....In women with luminal disease, younger age does have a substantial prognostic role, which may reflect inadequate therapy, including lower treatment efficacy and less therapeutic adherence and persistence, as well as residual differences in tumor biology,” Dr. Partridge and her associates said.
No specific source of funding was identified for this study. Dr. Partridge reported serving as a consultant for Pfizer; her associates reported ties to Pfizer, Tokai, Bristol-Myers Squibb, Carevive Systems, Oncothyreon, Amgen, and BeyondSpring Pharmaceuticals.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Younger age at diagnosis of breast cancer predicts poor survival only with certain molecular subtypes of tumor.
Major finding: Women who had luminal A breast cancer (7,738 participants) were more than twice as likely to die of their disease if they were aged 40 or younger at diagnosis than if they were older (HR, 2.1).
Data source: A longitudinal cohort study assessing the role of age, tumor subtype, and survival among 17,575 breast cancer patients treated in 2000-2007 and followed for 6 years.
Disclosures: No specific source of funding was identified for this study. Dr. Partridge reported serving as a consultant for Pfizer; her associates reported ties to Pfizer, Tokai, Bristol-Myers Squibb, Carevive Systems, Oncothyreon, Amgen, and BeyondSpring Pharmaceuticals.
Biomarker-driven targeted therapy feasible for NSCLC
Biomarker-driven targeted therapy was found feasible for heavily pretreated, metastatic non–small-cell lung cancer in a phase II trial reported online Aug. 1 in the Journal of Clinical Oncology.
The open-label multicenter umbrella study under the Biomarker-Integrated Approaches of Targeted Therapy for Lung Cancer Elimination (BATTLE) trial, called the BATTLE-2, involved 200 patients with advanced NSCLC refractory to platinum-based chemotherapy and multiple other treatments. All patients underwent tumor tissue biopsies for biomarker and gene expression analyses.
The results of those assessments were then used to perform “adaptive randomization” in which the patients were assigned to one of four treatment arms deemed most likely to control their particular malignancy, said Vassiliki Papadimitrakopoulou, MD, professor of medicine in the department of thoracic/head and neck medical oncology at the University of Texas MD Anderson Cancer Center, Houston, and her associates.
One group of 22 patients received 150 mg erlotinib once daily; the second group (42 patients) received 150 mg erlotinib daily plus 135 mg of the AKT inhibitor MK-2206 once weekly; the third group (75 patients) received 100 mg per week of MK-2206 plus 100 mg of the MEK inhibitor AZD6244 once daily; and the fourth group (61 patients) received 400 mg of sorafenib twice daily. A total of 186 patients were evaluable at 8 weeks, and the overall rate of disease control was 48% at that time. After a median follow-up of 20 months, the median progression-free survival was 2.0 months, median overall survival was 6.5 months, and the 1-year survival was 28%.
The primary endpoint of the study – disease control rate at 8 weeks – was not significantly different among the four treatment groups. It was 32% in group 1, 50% in group 2, 53% in group 3, and 46% in group 4. There were no complete responses and only 6 partial responses: 3 patients in group 3 and 3 patients in group 4. However, the study demonstrated “the utility of real-time biopsies for broad profiling of tumors that serve as a discovery vehicle for better target selection,” the investigators said (J Clin Oncol. 2016 Aug 1. doi:10.1200/JCO.2015.66.0084).
“We are currently pursuing alternative strategies in targeting KRAS mut+ tumors by incorporating knowledge derived from BATTLE 2,” they added.
This study was supported by Merck, Bayer Healthcare Pharmaceuticals, and the National Cancer Institute. Dr. Papadimitrakopoulou and her associates reported ties to numerous industry sources.
“Notwithstanding the low bar of the relatively unconventional endpoint of 8-week [disease control rate], BATTLE-2 should be recognized as a valuable contribution to the field, despite it failing to demonstrate encouraging efficacy in any of the treatment arms or patient subsets,” Howard (Jack) West, MD, wrote in an accompanying editorial (J Clin Oncol. 2016 Aug 1. doi: 10.1200/JCO.2016.68.8226).
But the main result of this study was that all treatment arms produced a disappointing 8-week disease control rate averaging 48%, with no treatment proving to be more promising than the others, with no complete responses and only rare partial responses, and with a progression-free survival of only 2 months in every group, he wrote. However, molecular targeting sometimes benefits small subgroups of patients, such as when advanced squamous NSCLC responds to afatinib. In this study, a subgroup of 52 patients whose tumors showed KRAS mut+ mutations had a significantly longer progression-free survival if they did not receive erlotinib.
Dr. West is affiliated with the Swedish Cancer Institute, Seattle. He reported ties to numerous industry sources.
“Notwithstanding the low bar of the relatively unconventional endpoint of 8-week [disease control rate], BATTLE-2 should be recognized as a valuable contribution to the field, despite it failing to demonstrate encouraging efficacy in any of the treatment arms or patient subsets,” Howard (Jack) West, MD, wrote in an accompanying editorial (J Clin Oncol. 2016 Aug 1. doi: 10.1200/JCO.2016.68.8226).
But the main result of this study was that all treatment arms produced a disappointing 8-week disease control rate averaging 48%, with no treatment proving to be more promising than the others, with no complete responses and only rare partial responses, and with a progression-free survival of only 2 months in every group, he wrote. However, molecular targeting sometimes benefits small subgroups of patients, such as when advanced squamous NSCLC responds to afatinib. In this study, a subgroup of 52 patients whose tumors showed KRAS mut+ mutations had a significantly longer progression-free survival if they did not receive erlotinib.
Dr. West is affiliated with the Swedish Cancer Institute, Seattle. He reported ties to numerous industry sources.
“Notwithstanding the low bar of the relatively unconventional endpoint of 8-week [disease control rate], BATTLE-2 should be recognized as a valuable contribution to the field, despite it failing to demonstrate encouraging efficacy in any of the treatment arms or patient subsets,” Howard (Jack) West, MD, wrote in an accompanying editorial (J Clin Oncol. 2016 Aug 1. doi: 10.1200/JCO.2016.68.8226).
But the main result of this study was that all treatment arms produced a disappointing 8-week disease control rate averaging 48%, with no treatment proving to be more promising than the others, with no complete responses and only rare partial responses, and with a progression-free survival of only 2 months in every group, he wrote. However, molecular targeting sometimes benefits small subgroups of patients, such as when advanced squamous NSCLC responds to afatinib. In this study, a subgroup of 52 patients whose tumors showed KRAS mut+ mutations had a significantly longer progression-free survival if they did not receive erlotinib.
Dr. West is affiliated with the Swedish Cancer Institute, Seattle. He reported ties to numerous industry sources.
Biomarker-driven targeted therapy was found feasible for heavily pretreated, metastatic non–small-cell lung cancer in a phase II trial reported online Aug. 1 in the Journal of Clinical Oncology.
The open-label multicenter umbrella study under the Biomarker-Integrated Approaches of Targeted Therapy for Lung Cancer Elimination (BATTLE) trial, called the BATTLE-2, involved 200 patients with advanced NSCLC refractory to platinum-based chemotherapy and multiple other treatments. All patients underwent tumor tissue biopsies for biomarker and gene expression analyses.
The results of those assessments were then used to perform “adaptive randomization” in which the patients were assigned to one of four treatment arms deemed most likely to control their particular malignancy, said Vassiliki Papadimitrakopoulou, MD, professor of medicine in the department of thoracic/head and neck medical oncology at the University of Texas MD Anderson Cancer Center, Houston, and her associates.
One group of 22 patients received 150 mg erlotinib once daily; the second group (42 patients) received 150 mg erlotinib daily plus 135 mg of the AKT inhibitor MK-2206 once weekly; the third group (75 patients) received 100 mg per week of MK-2206 plus 100 mg of the MEK inhibitor AZD6244 once daily; and the fourth group (61 patients) received 400 mg of sorafenib twice daily. A total of 186 patients were evaluable at 8 weeks, and the overall rate of disease control was 48% at that time. After a median follow-up of 20 months, the median progression-free survival was 2.0 months, median overall survival was 6.5 months, and the 1-year survival was 28%.
The primary endpoint of the study – disease control rate at 8 weeks – was not significantly different among the four treatment groups. It was 32% in group 1, 50% in group 2, 53% in group 3, and 46% in group 4. There were no complete responses and only 6 partial responses: 3 patients in group 3 and 3 patients in group 4. However, the study demonstrated “the utility of real-time biopsies for broad profiling of tumors that serve as a discovery vehicle for better target selection,” the investigators said (J Clin Oncol. 2016 Aug 1. doi:10.1200/JCO.2015.66.0084).
“We are currently pursuing alternative strategies in targeting KRAS mut+ tumors by incorporating knowledge derived from BATTLE 2,” they added.
This study was supported by Merck, Bayer Healthcare Pharmaceuticals, and the National Cancer Institute. Dr. Papadimitrakopoulou and her associates reported ties to numerous industry sources.
Biomarker-driven targeted therapy was found feasible for heavily pretreated, metastatic non–small-cell lung cancer in a phase II trial reported online Aug. 1 in the Journal of Clinical Oncology.
The open-label multicenter umbrella study under the Biomarker-Integrated Approaches of Targeted Therapy for Lung Cancer Elimination (BATTLE) trial, called the BATTLE-2, involved 200 patients with advanced NSCLC refractory to platinum-based chemotherapy and multiple other treatments. All patients underwent tumor tissue biopsies for biomarker and gene expression analyses.
The results of those assessments were then used to perform “adaptive randomization” in which the patients were assigned to one of four treatment arms deemed most likely to control their particular malignancy, said Vassiliki Papadimitrakopoulou, MD, professor of medicine in the department of thoracic/head and neck medical oncology at the University of Texas MD Anderson Cancer Center, Houston, and her associates.
One group of 22 patients received 150 mg erlotinib once daily; the second group (42 patients) received 150 mg erlotinib daily plus 135 mg of the AKT inhibitor MK-2206 once weekly; the third group (75 patients) received 100 mg per week of MK-2206 plus 100 mg of the MEK inhibitor AZD6244 once daily; and the fourth group (61 patients) received 400 mg of sorafenib twice daily. A total of 186 patients were evaluable at 8 weeks, and the overall rate of disease control was 48% at that time. After a median follow-up of 20 months, the median progression-free survival was 2.0 months, median overall survival was 6.5 months, and the 1-year survival was 28%.
The primary endpoint of the study – disease control rate at 8 weeks – was not significantly different among the four treatment groups. It was 32% in group 1, 50% in group 2, 53% in group 3, and 46% in group 4. There were no complete responses and only 6 partial responses: 3 patients in group 3 and 3 patients in group 4. However, the study demonstrated “the utility of real-time biopsies for broad profiling of tumors that serve as a discovery vehicle for better target selection,” the investigators said (J Clin Oncol. 2016 Aug 1. doi:10.1200/JCO.2015.66.0084).
“We are currently pursuing alternative strategies in targeting KRAS mut+ tumors by incorporating knowledge derived from BATTLE 2,” they added.
This study was supported by Merck, Bayer Healthcare Pharmaceuticals, and the National Cancer Institute. Dr. Papadimitrakopoulou and her associates reported ties to numerous industry sources.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Biomarker-driven targeted therapy was found feasible for heavily pretreated, metastatic NSCLC.
Major finding: The primary endpoint – disease control rate at 8 weeks – was 32% in group 1, 50% in group 2, 53% in group 3, and 46% in group 4.
Data source: A randomized open-label phase II study involving 200 patients with heavily pretreated, metastatic NSCLC.
Disclosures: This study was supported by Merck, Bayer Healthcare Pharmaceuticals, and the National Cancer Institute. Dr. Papadimitrakopoulou and her associates reported ties to numerous industry sources.
Statins in Chronic Kidney Disease: When and When Not to Use Them
2016 Obstetric code changes that could affect your reimbursement (very soon)
By now the upheaval of changing to the new International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10) diagnostic coding system has settled. The code freeze that was initiated in 2012 has ended, and the new and revised codes that will go into effect on October 1, 2016, are being revealed. Good documentation will lead to more accurate diagnostic coding, which in turn assists decision makers in their quest to report the health of our population and to make good decisions for resource allocation. You are in the unique position to assist in this process, so keep up the good work.
In this article, I focus on ICD-10 diagnostic coding for obstetric services. I will cover diagnostic coding for gynecologic services in the September issue of OBG Management.
Code revisions for uterine scar and more changes to note
With the upcoming edition of ICD-10, the code Z3A, Weeks’ gestation, will be changed from mandatory reporting to reporting if known. This means that if the patient is no longer pregnant, a Z3A code no longer needs to be reported, and if at the time of service the provider does not know the weeks’ gestation, Z3A would not be required. However, this information should be readily available during the antepartum period and should still be considered important to record and report. And it would still be reported for hospitalization for delivery.
If the code O09.81, Supervision of pregnancy resulting from assisted reproductive technology, is reported, the code Z33.3, Gestational carrier status, may be reported in addition for informational purposes.
When the code O34.29, Maternal care due to uterine scar from other previous surgery, is reported, the tabular index clarifies that this refers to a uterine scar from a transmural uterine incision other than that used for cesarean delivery. This would include incision into the uterine wall to remove fibroids.
The O42 code category, relating to Premature rupture of membranes, should now be interpreted to mean rupture of membranes at or after 37 completed weeks of gestation, rather than after 37 completed weeks.
The code category O99.6, Diseases of the digestive system complicating pregnancy, childbirth, and the puerperium, has been clarified: it does not include hemorrhoids in pregnancy. Therefore, a code from O22.4_ (a final digit of 0 [unspecified], 1, 2, or 3 is required for the trimester) also can be reported if hemorrhoids are present.
A note now clarifies that O99.82, Streptococcus B carrier state complicating pregnancy, childbirth, and the puerperium, cannot be reported with Z22.330, Carrier of streptococcus group B (GBS) in a nonpregnant woman.
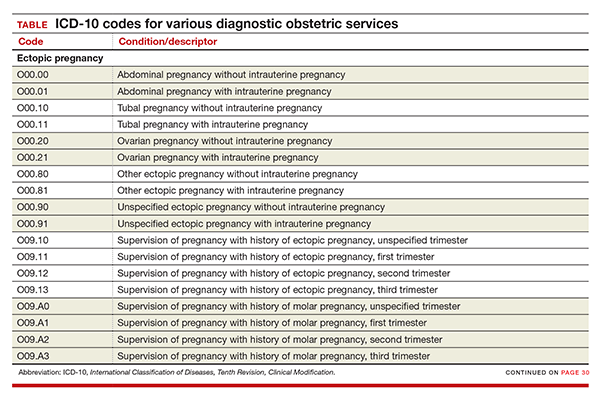
New codes for specifying types of ectopic pregnancy
ICD-10 did not initially recognize ectopic pregnancy with and without intrauterine pregnancy, as was the case in ICD-9, but starting in October it will do so. In addition, a history of ectopic or molar pregnancy during a current pregnancy is now reported separately. Each of these codes will require a final digit to indicate the trimester (TABLE).
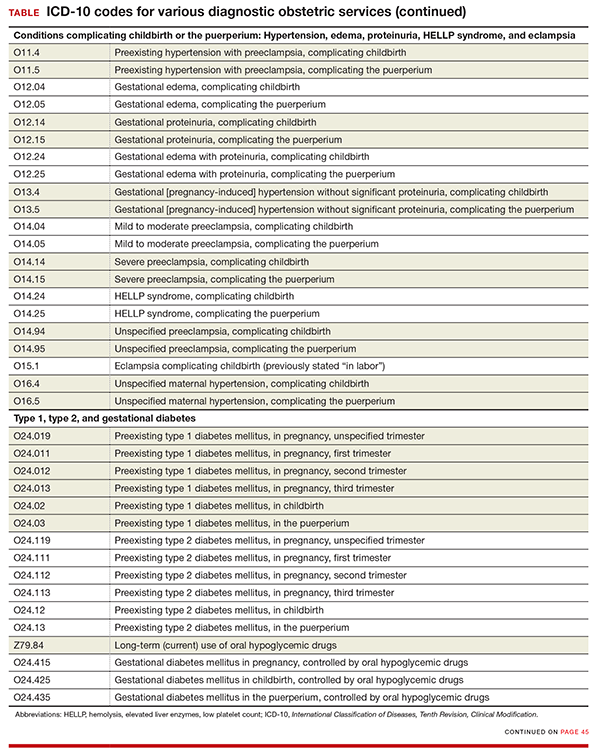
Codes added for complicating conditions of childbirth and the puerperium
Missing from the ICD-10 lineup last year were codes for conditions related to hypertension, edema, proteinuria, HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome, and eclampsia that were complicating the pregnancy at the time of delivery or after delivery (TABLE).
Note that the “childbirth” code is reported only when a patient delivers at the current episode of care. Once a patient delivers and is discharged, the “puerperium” code should be selected.
Revised descriptions, new reporting instruction for diabetes
The code descriptions for preexisting type 1 and type 2 diabetes were revised, but this change does not impact reporting the codes. However, for type 2 diabetes, the instruction for reporting an additional code has changed. Now, in addition to reporting the code for current use of insulin (Z79.4), when appropriate, report the new added code for use of hypoglycemic agents (Z79.84), such as glyburide or metformin.
For gestational diabetes, new codes have been added for the use of hypoglycemic agents; therefore, no additional code is reported (TABLE).
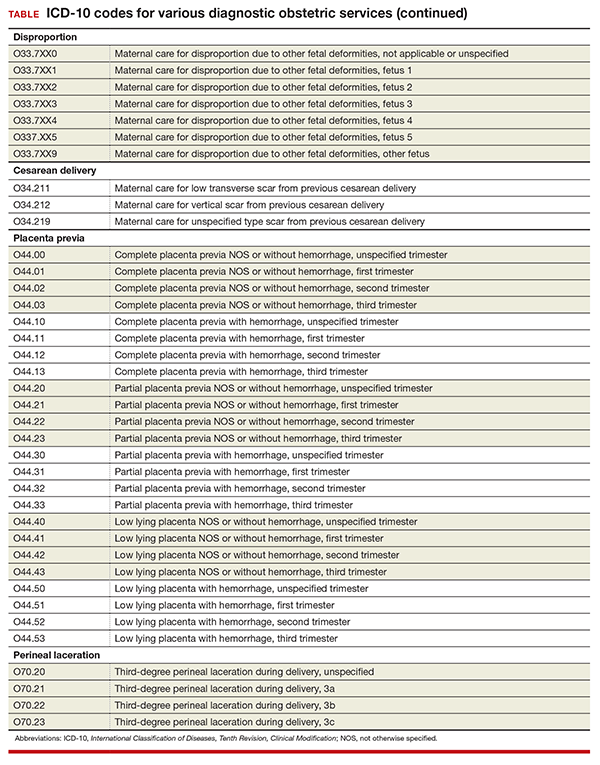
Disproportion code includes numeric specifier for fetus
The disproportion code category was expanded to include a final digit for the fetus with the deformity (TABLE). The final digit of the code number denotes which fetus; for example, “0” means a singleton pregnancy, “1” means fetus 1 (number range from 1 to 5), and “9” denotes any fetus after the fifth.
Cesarean delivery scar codes expanded
The code for maternal care for a scar from a previous cesarean delivery has been expanded to 3 different codes (TABLE). Clinicians should make every effort to document and report the location of the previous cesarean as low transverse or vertical. From a coding standpoint, a vertical scar can also be referred to as a classical scar.
Changes to placenta previa codes
The code category for placenta previa has been expanded to capture the degree of previa as complete, partial, or low lying and with or without hemorrhage (TABLE). Going forward, it will be important to carefully document the circumstances so that the most specific code can be reported and tracked. Trimester specification is required as the final digit.
New subclassifications for perineal laceration
The code category for perineal laceration has been expanded with new codes to capture subclassifications for a third-degree laceration that can involve the external and internal anal sphincter (TABLE). Through its collaborative hub, the Women’s Health Registry Alliance (reVITALize) initiative, the American Congress of Obstetricians and Gynecologists (ACOG) worked on the current classification of third- and fourth-degree perineal lacerations, which has been adopted by the Royal College of Obstetricians and Gynaecologists.1
Under this subclassification, a 3a laceration would involve a tear of less than 50% of the external anal sphincter (EAS); 3b would involve a tear of more than 50% of the EAS; and 3c would mean that both the external and internal anal sphincter are torn. ACOG and its collaborative group encourage clinicians to use these subclassifications in documentation to allow for more robust data collection and complete repair information. From a payment standpoint, such information may go a long way to substantiating the severity of a tear, which may require more physician work.
Z code additions
Finally, the ever-popular diagnostic code for Rho(D) immunization is back, and 2 codes have been added for a gestational carrier and 1 for a family history of sudden infant death syndrome. The codes are:
- Z29.13 Encounter for prophylactic Rho(D) immune globulin
- Z31.7 Encounter for procreative management and counseling for gestational carrier
- Z33.3 Pregnant state, gestational carrier
- Z84.82 Family history of sudden infant death syndrome.
- Centers for Disease Control and Prevention. ICD-10 Coordination and Maintenance Committee meeting: diagnosis agenda. September 23-24, 2014;38, 39. http://www.cdc.gov/nchs/data/icd/topic_packet_09_23_2012.pdf. Accessed July 5, 2016.

Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
By now the upheaval of changing to the new International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10) diagnostic coding system has settled. The code freeze that was initiated in 2012 has ended, and the new and revised codes that will go into effect on October 1, 2016, are being revealed. Good documentation will lead to more accurate diagnostic coding, which in turn assists decision makers in their quest to report the health of our population and to make good decisions for resource allocation. You are in the unique position to assist in this process, so keep up the good work.
In this article, I focus on ICD-10 diagnostic coding for obstetric services. I will cover diagnostic coding for gynecologic services in the September issue of OBG Management.
Code revisions for uterine scar and more changes to note
With the upcoming edition of ICD-10, the code Z3A, Weeks’ gestation, will be changed from mandatory reporting to reporting if known. This means that if the patient is no longer pregnant, a Z3A code no longer needs to be reported, and if at the time of service the provider does not know the weeks’ gestation, Z3A would not be required. However, this information should be readily available during the antepartum period and should still be considered important to record and report. And it would still be reported for hospitalization for delivery.
If the code O09.81, Supervision of pregnancy resulting from assisted reproductive technology, is reported, the code Z33.3, Gestational carrier status, may be reported in addition for informational purposes.
When the code O34.29, Maternal care due to uterine scar from other previous surgery, is reported, the tabular index clarifies that this refers to a uterine scar from a transmural uterine incision other than that used for cesarean delivery. This would include incision into the uterine wall to remove fibroids.
The O42 code category, relating to Premature rupture of membranes, should now be interpreted to mean rupture of membranes at or after 37 completed weeks of gestation, rather than after 37 completed weeks.
The code category O99.6, Diseases of the digestive system complicating pregnancy, childbirth, and the puerperium, has been clarified: it does not include hemorrhoids in pregnancy. Therefore, a code from O22.4_ (a final digit of 0 [unspecified], 1, 2, or 3 is required for the trimester) also can be reported if hemorrhoids are present.
A note now clarifies that O99.82, Streptococcus B carrier state complicating pregnancy, childbirth, and the puerperium, cannot be reported with Z22.330, Carrier of streptococcus group B (GBS) in a nonpregnant woman.
New codes for specifying types of ectopic pregnancy
ICD-10 did not initially recognize ectopic pregnancy with and without intrauterine pregnancy, as was the case in ICD-9, but starting in October it will do so. In addition, a history of ectopic or molar pregnancy during a current pregnancy is now reported separately. Each of these codes will require a final digit to indicate the trimester (TABLE).
Codes added for complicating conditions of childbirth and the puerperium
Missing from the ICD-10 lineup last year were codes for conditions related to hypertension, edema, proteinuria, HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome, and eclampsia that were complicating the pregnancy at the time of delivery or after delivery (TABLE).
Note that the “childbirth” code is reported only when a patient delivers at the current episode of care. Once a patient delivers and is discharged, the “puerperium” code should be selected.
Revised descriptions, new reporting instruction for diabetes
The code descriptions for preexisting type 1 and type 2 diabetes were revised, but this change does not impact reporting the codes. However, for type 2 diabetes, the instruction for reporting an additional code has changed. Now, in addition to reporting the code for current use of insulin (Z79.4), when appropriate, report the new added code for use of hypoglycemic agents (Z79.84), such as glyburide or metformin.
For gestational diabetes, new codes have been added for the use of hypoglycemic agents; therefore, no additional code is reported (TABLE).
Disproportion code includes numeric specifier for fetus
The disproportion code category was expanded to include a final digit for the fetus with the deformity (TABLE). The final digit of the code number denotes which fetus; for example, “0” means a singleton pregnancy, “1” means fetus 1 (number range from 1 to 5), and “9” denotes any fetus after the fifth.
Cesarean delivery scar codes expanded
The code for maternal care for a scar from a previous cesarean delivery has been expanded to 3 different codes (TABLE). Clinicians should make every effort to document and report the location of the previous cesarean as low transverse or vertical. From a coding standpoint, a vertical scar can also be referred to as a classical scar.
Changes to placenta previa codes
The code category for placenta previa has been expanded to capture the degree of previa as complete, partial, or low lying and with or without hemorrhage (TABLE). Going forward, it will be important to carefully document the circumstances so that the most specific code can be reported and tracked. Trimester specification is required as the final digit.
New subclassifications for perineal laceration
The code category for perineal laceration has been expanded with new codes to capture subclassifications for a third-degree laceration that can involve the external and internal anal sphincter (TABLE). Through its collaborative hub, the Women’s Health Registry Alliance (reVITALize) initiative, the American Congress of Obstetricians and Gynecologists (ACOG) worked on the current classification of third- and fourth-degree perineal lacerations, which has been adopted by the Royal College of Obstetricians and Gynaecologists.1
Under this subclassification, a 3a laceration would involve a tear of less than 50% of the external anal sphincter (EAS); 3b would involve a tear of more than 50% of the EAS; and 3c would mean that both the external and internal anal sphincter are torn. ACOG and its collaborative group encourage clinicians to use these subclassifications in documentation to allow for more robust data collection and complete repair information. From a payment standpoint, such information may go a long way to substantiating the severity of a tear, which may require more physician work.
Z code additions
Finally, the ever-popular diagnostic code for Rho(D) immunization is back, and 2 codes have been added for a gestational carrier and 1 for a family history of sudden infant death syndrome. The codes are:
- Z29.13 Encounter for prophylactic Rho(D) immune globulin
- Z31.7 Encounter for procreative management and counseling for gestational carrier
- Z33.3 Pregnant state, gestational carrier
- Z84.82 Family history of sudden infant death syndrome.
By now the upheaval of changing to the new International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10) diagnostic coding system has settled. The code freeze that was initiated in 2012 has ended, and the new and revised codes that will go into effect on October 1, 2016, are being revealed. Good documentation will lead to more accurate diagnostic coding, which in turn assists decision makers in their quest to report the health of our population and to make good decisions for resource allocation. You are in the unique position to assist in this process, so keep up the good work.
In this article, I focus on ICD-10 diagnostic coding for obstetric services. I will cover diagnostic coding for gynecologic services in the September issue of OBG Management.
Code revisions for uterine scar and more changes to note
With the upcoming edition of ICD-10, the code Z3A, Weeks’ gestation, will be changed from mandatory reporting to reporting if known. This means that if the patient is no longer pregnant, a Z3A code no longer needs to be reported, and if at the time of service the provider does not know the weeks’ gestation, Z3A would not be required. However, this information should be readily available during the antepartum period and should still be considered important to record and report. And it would still be reported for hospitalization for delivery.
If the code O09.81, Supervision of pregnancy resulting from assisted reproductive technology, is reported, the code Z33.3, Gestational carrier status, may be reported in addition for informational purposes.
When the code O34.29, Maternal care due to uterine scar from other previous surgery, is reported, the tabular index clarifies that this refers to a uterine scar from a transmural uterine incision other than that used for cesarean delivery. This would include incision into the uterine wall to remove fibroids.
The O42 code category, relating to Premature rupture of membranes, should now be interpreted to mean rupture of membranes at or after 37 completed weeks of gestation, rather than after 37 completed weeks.
The code category O99.6, Diseases of the digestive system complicating pregnancy, childbirth, and the puerperium, has been clarified: it does not include hemorrhoids in pregnancy. Therefore, a code from O22.4_ (a final digit of 0 [unspecified], 1, 2, or 3 is required for the trimester) also can be reported if hemorrhoids are present.
A note now clarifies that O99.82, Streptococcus B carrier state complicating pregnancy, childbirth, and the puerperium, cannot be reported with Z22.330, Carrier of streptococcus group B (GBS) in a nonpregnant woman.
New codes for specifying types of ectopic pregnancy
ICD-10 did not initially recognize ectopic pregnancy with and without intrauterine pregnancy, as was the case in ICD-9, but starting in October it will do so. In addition, a history of ectopic or molar pregnancy during a current pregnancy is now reported separately. Each of these codes will require a final digit to indicate the trimester (TABLE).
Codes added for complicating conditions of childbirth and the puerperium
Missing from the ICD-10 lineup last year were codes for conditions related to hypertension, edema, proteinuria, HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome, and eclampsia that were complicating the pregnancy at the time of delivery or after delivery (TABLE).
Note that the “childbirth” code is reported only when a patient delivers at the current episode of care. Once a patient delivers and is discharged, the “puerperium” code should be selected.
Revised descriptions, new reporting instruction for diabetes
The code descriptions for preexisting type 1 and type 2 diabetes were revised, but this change does not impact reporting the codes. However, for type 2 diabetes, the instruction for reporting an additional code has changed. Now, in addition to reporting the code for current use of insulin (Z79.4), when appropriate, report the new added code for use of hypoglycemic agents (Z79.84), such as glyburide or metformin.
For gestational diabetes, new codes have been added for the use of hypoglycemic agents; therefore, no additional code is reported (TABLE).
Disproportion code includes numeric specifier for fetus
The disproportion code category was expanded to include a final digit for the fetus with the deformity (TABLE). The final digit of the code number denotes which fetus; for example, “0” means a singleton pregnancy, “1” means fetus 1 (number range from 1 to 5), and “9” denotes any fetus after the fifth.
Cesarean delivery scar codes expanded
The code for maternal care for a scar from a previous cesarean delivery has been expanded to 3 different codes (TABLE). Clinicians should make every effort to document and report the location of the previous cesarean as low transverse or vertical. From a coding standpoint, a vertical scar can also be referred to as a classical scar.
Changes to placenta previa codes
The code category for placenta previa has been expanded to capture the degree of previa as complete, partial, or low lying and with or without hemorrhage (TABLE). Going forward, it will be important to carefully document the circumstances so that the most specific code can be reported and tracked. Trimester specification is required as the final digit.
New subclassifications for perineal laceration
The code category for perineal laceration has been expanded with new codes to capture subclassifications for a third-degree laceration that can involve the external and internal anal sphincter (TABLE). Through its collaborative hub, the Women’s Health Registry Alliance (reVITALize) initiative, the American Congress of Obstetricians and Gynecologists (ACOG) worked on the current classification of third- and fourth-degree perineal lacerations, which has been adopted by the Royal College of Obstetricians and Gynaecologists.1
Under this subclassification, a 3a laceration would involve a tear of less than 50% of the external anal sphincter (EAS); 3b would involve a tear of more than 50% of the EAS; and 3c would mean that both the external and internal anal sphincter are torn. ACOG and its collaborative group encourage clinicians to use these subclassifications in documentation to allow for more robust data collection and complete repair information. From a payment standpoint, such information may go a long way to substantiating the severity of a tear, which may require more physician work.
Z code additions
Finally, the ever-popular diagnostic code for Rho(D) immunization is back, and 2 codes have been added for a gestational carrier and 1 for a family history of sudden infant death syndrome. The codes are:
- Z29.13 Encounter for prophylactic Rho(D) immune globulin
- Z31.7 Encounter for procreative management and counseling for gestational carrier
- Z33.3 Pregnant state, gestational carrier
- Z84.82 Family history of sudden infant death syndrome.
- Centers for Disease Control and Prevention. ICD-10 Coordination and Maintenance Committee meeting: diagnosis agenda. September 23-24, 2014;38, 39. http://www.cdc.gov/nchs/data/icd/topic_packet_09_23_2012.pdf. Accessed July 5, 2016.
- Centers for Disease Control and Prevention. ICD-10 Coordination and Maintenance Committee meeting: diagnosis agenda. September 23-24, 2014;38, 39. http://www.cdc.gov/nchs/data/icd/topic_packet_09_23_2012.pdf. Accessed July 5, 2016.
In this Article
- New and expanded codes
- Z code additions
- Table of codes
PHM16: Visual Clues Can Help Establish a Diagnosis
PHM16’s Visual Diagnosis: Signs and Why They Matter session led by Dr. Kenneth Roberts and guest presenters was a review of case presentations in which visual clues were vital to establishing a diagnosis. Though much of the content was presented with pictures, the emphasis was placed on the importance of correct diagnosis to avoid both misdiagnoses/over-diagnoses and the potential harm that may result from inappropriate treatment. This may also translate into poor utilization of resources and significant financial burden that can result from the unnecessary hospitalization of a patient.
Many of the presented cases (such as the Gianotti-Crosti toddler over-diagnosed as eczema herpeticum, a child with pseudochromhidrosis misdiagnosed as a cyanotic disease, the case of phytophotodermatitis mistaken as child abuse, and a teen treated for 2 years for JIA before diagnosis of hypertrophic osteoarthropathy was made) highlighted examples in which there was extensive workup, hospitalization, subspecialty evaluation, and even incorrect treatment of patients.
In other instances, such as Henoch-Schonlein purpura, Waardenburg syndrome, or McCune-Albright syndrome, the correct diagnosis is necessary to help guide management and future treatment, including subspecialty evaluation.
Many diseases with visual presentations also have a benign course and require no treatment, and acknowledging this is important in providing reassurance to a family that may be very anxious over the physical appearance of their child.
This session underscores the need for experience and exposure to various signs, not only with rare medical conditions, but also in common illnesses such as Kawasaki and scarlet fever that may present similarly.
Key Takeaway:
Providers should have a high index of suspicion and use visual clues to make the correct diagnosis in order to guide treatment, avoid harm in children, and ensure appropriate utilization of resources.
Chandani DeZure, MD, FAAP, is a pediatric Hospitalist at Children’s National Health System, Instruction of Pediatrics at George Washington University’s School of Medicine and Health Sciences in Washington, D.C.

PHM16’s Visual Diagnosis: Signs and Why They Matter session led by Dr. Kenneth Roberts and guest presenters was a review of case presentations in which visual clues were vital to establishing a diagnosis. Though much of the content was presented with pictures, the emphasis was placed on the importance of correct diagnosis to avoid both misdiagnoses/over-diagnoses and the potential harm that may result from inappropriate treatment. This may also translate into poor utilization of resources and significant financial burden that can result from the unnecessary hospitalization of a patient.
Many of the presented cases (such as the Gianotti-Crosti toddler over-diagnosed as eczema herpeticum, a child with pseudochromhidrosis misdiagnosed as a cyanotic disease, the case of phytophotodermatitis mistaken as child abuse, and a teen treated for 2 years for JIA before diagnosis of hypertrophic osteoarthropathy was made) highlighted examples in which there was extensive workup, hospitalization, subspecialty evaluation, and even incorrect treatment of patients.
In other instances, such as Henoch-Schonlein purpura, Waardenburg syndrome, or McCune-Albright syndrome, the correct diagnosis is necessary to help guide management and future treatment, including subspecialty evaluation.
Many diseases with visual presentations also have a benign course and require no treatment, and acknowledging this is important in providing reassurance to a family that may be very anxious over the physical appearance of their child.
This session underscores the need for experience and exposure to various signs, not only with rare medical conditions, but also in common illnesses such as Kawasaki and scarlet fever that may present similarly.
Key Takeaway:
Providers should have a high index of suspicion and use visual clues to make the correct diagnosis in order to guide treatment, avoid harm in children, and ensure appropriate utilization of resources.
Chandani DeZure, MD, FAAP, is a pediatric Hospitalist at Children’s National Health System, Instruction of Pediatrics at George Washington University’s School of Medicine and Health Sciences in Washington, D.C.
PHM16’s Visual Diagnosis: Signs and Why They Matter session led by Dr. Kenneth Roberts and guest presenters was a review of case presentations in which visual clues were vital to establishing a diagnosis. Though much of the content was presented with pictures, the emphasis was placed on the importance of correct diagnosis to avoid both misdiagnoses/over-diagnoses and the potential harm that may result from inappropriate treatment. This may also translate into poor utilization of resources and significant financial burden that can result from the unnecessary hospitalization of a patient.
Many of the presented cases (such as the Gianotti-Crosti toddler over-diagnosed as eczema herpeticum, a child with pseudochromhidrosis misdiagnosed as a cyanotic disease, the case of phytophotodermatitis mistaken as child abuse, and a teen treated for 2 years for JIA before diagnosis of hypertrophic osteoarthropathy was made) highlighted examples in which there was extensive workup, hospitalization, subspecialty evaluation, and even incorrect treatment of patients.
In other instances, such as Henoch-Schonlein purpura, Waardenburg syndrome, or McCune-Albright syndrome, the correct diagnosis is necessary to help guide management and future treatment, including subspecialty evaluation.
Many diseases with visual presentations also have a benign course and require no treatment, and acknowledging this is important in providing reassurance to a family that may be very anxious over the physical appearance of their child.
This session underscores the need for experience and exposure to various signs, not only with rare medical conditions, but also in common illnesses such as Kawasaki and scarlet fever that may present similarly.
Key Takeaway:
Providers should have a high index of suspicion and use visual clues to make the correct diagnosis in order to guide treatment, avoid harm in children, and ensure appropriate utilization of resources.
Chandani DeZure, MD, FAAP, is a pediatric Hospitalist at Children’s National Health System, Instruction of Pediatrics at George Washington University’s School of Medicine and Health Sciences in Washington, D.C.

NSQIP Study: Symptomatic AAAs have a twofold increased periop mortality risk over asymptomatic
A recent small study suggested that, in the age of endovascular aortic aneurysm repair (EVAR), the mortality rates between symptomatic and asymptomatic abdominal aortic aneurysm (AAA) repair have become similar, according to Peter A. Soden, MD, of Beth Deaconess Medical Center, Boston, and his colleagues. However, in their large database study, Dr. Soden and his colleagues found that outcomes for the repair of abdominal aortic aneurysms were increasingly worse from asymptomatic to symptomatic to ruptured AAA.
The researchers assessed all patients undergoing endovascular and open AAA repair in the 2011-2013 American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) data set, according to a report published in the August issue of the Journal of Vascular Surgery.
Symptomatic AAA was defined as lack of evidence of rupture but with the presence of abdominal or back pain or symptoms from local compression by the aneurysm causing early satiety, hydronephrosis, or deep vein thrombosis. Ruptured aneurysms were divided into two categories: hypotensive (defined as systolic blood pressure less than 90 mmm Hg or drop of greater than 40 mm HG from baseline) and nonhypotensive (J Vasc Surg. 2016;64:297-305).
There were numerous demographic and comorbidity differences between asymptomatic and symptomatic patients and between symptomatic and ruptured patients, with a general trend of increasing of commodities and factors influencing operative risk.
The final study included 5,502 patients undergoing repair of infrarenal (85%; 92% EVAR) or juxtarenal (15%;20% EVAR) aneurysms. These differences in the use of EVAR were statistically significant.
This population comprised 4,495 asymptomatic patients (82% EVAR), 455 symptomatic patients (69% EVAR), and 552 ruptured patients (52% EVAR).
The overall 30-day mortality rate was significantly higher in symptomatic over asymptomatic patients (5.1% vs. 1.9%; P less than .001).Similarly, for EVAR, the overall 30-day mortality rate was significantly higher in symptomatic over asymptomatic patients (3.8% vs. 1.4%; P less than .001). For open repair, there was no significant difference in mortality (7.7% vs. 4.3%) between symptomatic and asymptomatic patients, respectively.
Multivariate analysis showed that symptomatic patients had twice the operative mortality as asymptomatic patients (odds ratio, 2.1). A symptomatic aneurysm was also predictive of a major adverse event (OR, 1.5). Ruptured aneurysms had a significant nearly sevenfold increase in mortality risk vs. symptomatic aneurysms (OR, 6.5) and a fivefold increase of risk of a major adverse event (OR 5.1), with all ORs within their 95% confidence interval levels).
“In this large contemporary study of symptomatic AAA patients, in which the majority were treated with EVAR, we found that symptomatic patients have twice the perioperative mortality compared with asymptomatic patients. Despite this, we also find a reduction in perioperative mortality for symptomatic aneurysms compared with prior reports in which the majority were treated with open repair, and we believe this supports an EVAR-first approach for symptomatic aneurysms with suitable anatomy,” the researchers concluded.
The authors reported that they had no relevant disclosures.
A recent small study suggested that, in the age of endovascular aortic aneurysm repair (EVAR), the mortality rates between symptomatic and asymptomatic abdominal aortic aneurysm (AAA) repair have become similar, according to Peter A. Soden, MD, of Beth Deaconess Medical Center, Boston, and his colleagues. However, in their large database study, Dr. Soden and his colleagues found that outcomes for the repair of abdominal aortic aneurysms were increasingly worse from asymptomatic to symptomatic to ruptured AAA.
The researchers assessed all patients undergoing endovascular and open AAA repair in the 2011-2013 American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) data set, according to a report published in the August issue of the Journal of Vascular Surgery.
Symptomatic AAA was defined as lack of evidence of rupture but with the presence of abdominal or back pain or symptoms from local compression by the aneurysm causing early satiety, hydronephrosis, or deep vein thrombosis. Ruptured aneurysms were divided into two categories: hypotensive (defined as systolic blood pressure less than 90 mmm Hg or drop of greater than 40 mm HG from baseline) and nonhypotensive (J Vasc Surg. 2016;64:297-305).
There were numerous demographic and comorbidity differences between asymptomatic and symptomatic patients and between symptomatic and ruptured patients, with a general trend of increasing of commodities and factors influencing operative risk.
The final study included 5,502 patients undergoing repair of infrarenal (85%; 92% EVAR) or juxtarenal (15%;20% EVAR) aneurysms. These differences in the use of EVAR were statistically significant.
This population comprised 4,495 asymptomatic patients (82% EVAR), 455 symptomatic patients (69% EVAR), and 552 ruptured patients (52% EVAR).
The overall 30-day mortality rate was significantly higher in symptomatic over asymptomatic patients (5.1% vs. 1.9%; P less than .001).Similarly, for EVAR, the overall 30-day mortality rate was significantly higher in symptomatic over asymptomatic patients (3.8% vs. 1.4%; P less than .001). For open repair, there was no significant difference in mortality (7.7% vs. 4.3%) between symptomatic and asymptomatic patients, respectively.
Multivariate analysis showed that symptomatic patients had twice the operative mortality as asymptomatic patients (odds ratio, 2.1). A symptomatic aneurysm was also predictive of a major adverse event (OR, 1.5). Ruptured aneurysms had a significant nearly sevenfold increase in mortality risk vs. symptomatic aneurysms (OR, 6.5) and a fivefold increase of risk of a major adverse event (OR 5.1), with all ORs within their 95% confidence interval levels).
“In this large contemporary study of symptomatic AAA patients, in which the majority were treated with EVAR, we found that symptomatic patients have twice the perioperative mortality compared with asymptomatic patients. Despite this, we also find a reduction in perioperative mortality for symptomatic aneurysms compared with prior reports in which the majority were treated with open repair, and we believe this supports an EVAR-first approach for symptomatic aneurysms with suitable anatomy,” the researchers concluded.
The authors reported that they had no relevant disclosures.
A recent small study suggested that, in the age of endovascular aortic aneurysm repair (EVAR), the mortality rates between symptomatic and asymptomatic abdominal aortic aneurysm (AAA) repair have become similar, according to Peter A. Soden, MD, of Beth Deaconess Medical Center, Boston, and his colleagues. However, in their large database study, Dr. Soden and his colleagues found that outcomes for the repair of abdominal aortic aneurysms were increasingly worse from asymptomatic to symptomatic to ruptured AAA.
The researchers assessed all patients undergoing endovascular and open AAA repair in the 2011-2013 American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) data set, according to a report published in the August issue of the Journal of Vascular Surgery.
Symptomatic AAA was defined as lack of evidence of rupture but with the presence of abdominal or back pain or symptoms from local compression by the aneurysm causing early satiety, hydronephrosis, or deep vein thrombosis. Ruptured aneurysms were divided into two categories: hypotensive (defined as systolic blood pressure less than 90 mmm Hg or drop of greater than 40 mm HG from baseline) and nonhypotensive (J Vasc Surg. 2016;64:297-305).
There were numerous demographic and comorbidity differences between asymptomatic and symptomatic patients and between symptomatic and ruptured patients, with a general trend of increasing of commodities and factors influencing operative risk.
The final study included 5,502 patients undergoing repair of infrarenal (85%; 92% EVAR) or juxtarenal (15%;20% EVAR) aneurysms. These differences in the use of EVAR were statistically significant.
This population comprised 4,495 asymptomatic patients (82% EVAR), 455 symptomatic patients (69% EVAR), and 552 ruptured patients (52% EVAR).
The overall 30-day mortality rate was significantly higher in symptomatic over asymptomatic patients (5.1% vs. 1.9%; P less than .001).Similarly, for EVAR, the overall 30-day mortality rate was significantly higher in symptomatic over asymptomatic patients (3.8% vs. 1.4%; P less than .001). For open repair, there was no significant difference in mortality (7.7% vs. 4.3%) between symptomatic and asymptomatic patients, respectively.
Multivariate analysis showed that symptomatic patients had twice the operative mortality as asymptomatic patients (odds ratio, 2.1). A symptomatic aneurysm was also predictive of a major adverse event (OR, 1.5). Ruptured aneurysms had a significant nearly sevenfold increase in mortality risk vs. symptomatic aneurysms (OR, 6.5) and a fivefold increase of risk of a major adverse event (OR 5.1), with all ORs within their 95% confidence interval levels).
“In this large contemporary study of symptomatic AAA patients, in which the majority were treated with EVAR, we found that symptomatic patients have twice the perioperative mortality compared with asymptomatic patients. Despite this, we also find a reduction in perioperative mortality for symptomatic aneurysms compared with prior reports in which the majority were treated with open repair, and we believe this supports an EVAR-first approach for symptomatic aneurysms with suitable anatomy,” the researchers concluded.
The authors reported that they had no relevant disclosures.
FROM THE JOURNAL OF VASCULAR SURGERY
Key clinical point: Outcomes for repair of abdominal aortic aneurysm repair were increasingly worse from asymptomatic to symptomatic to ruptured AAA.
Major finding: Patients with symptomatic AAA had a twofold increased risk of perioperative mortality, compared with patients with asymptomatic AAA undergoing repair.
Data source: The study assessed all patients undergoing AAA repair in the 2011-2013 American College of Surgeons NSQIP data set.
Disclosures: The authors reported that they had no relevant disclosures.

PHM16: The New AAP Clinical Practice Guideline on Evaluating, Managing Febrile Infants
One of PHM16’s most highly-attended sessions was an update on the anticipated AAP guidelines for febrile infants between ages 7-90 days given by Dr. Kenneth Roberts. The goal is to give evidence-based guidelines, not rules, from the most recent literature available. It also stresses the need to separate individual components of serious bacterial infections (UTI, bacteremia, and meningitis) as the incidence and clinical course can vary greatly in this population.
The inclusion criteria for infants for this upcoming algorithm require an infant to be full-term (37-43 weeks gestation), aged 7-90 days, well-appearing, and presenting with a temperature of 38 degrees Celsius.
Exclusion criteria include perinatal/prenatal/neonatal: maternal fever, infection, or antimicrobial treatment, the presence of any evident infection, being technology-dependent, and the presence of congenital anomalies.
The updated guideline will aim to stratify management by age 7-28 days, 29-60 days, and 61 to 90 days to provide the most appropriate and directed treatment.
It will also include a role for inflammatory markers, and allow for a “kinder, gentler” approach to the management of febrile infants aged 7-90 days including withholding certain treatments and procedures if infants are at low risk of infection. An active, not passive, need for observation may be appropriate for certain infants as well. These guidelines should be tailored for individual patients to provide the best care possible while minimizing risk in this population.
Key Takeaway:
An updated AAP Practice guideline algorithm for the management of well-appearing febrile infants 7-28 days, 29-60 days, and 60-90 days will be coming in the near future that will help standardize care in this population, but should not be used as a substitute for clinical judgment.
Chandani DeZure, MD, FAAP, is a pediatric hospitalist at Children’s National Health System, Instruction of Pediatrics at George Washington University’s School of Medicine and Health Sciences in Washington, D.C.
One of PHM16’s most highly-attended sessions was an update on the anticipated AAP guidelines for febrile infants between ages 7-90 days given by Dr. Kenneth Roberts. The goal is to give evidence-based guidelines, not rules, from the most recent literature available. It also stresses the need to separate individual components of serious bacterial infections (UTI, bacteremia, and meningitis) as the incidence and clinical course can vary greatly in this population.
The inclusion criteria for infants for this upcoming algorithm require an infant to be full-term (37-43 weeks gestation), aged 7-90 days, well-appearing, and presenting with a temperature of 38 degrees Celsius.
Exclusion criteria include perinatal/prenatal/neonatal: maternal fever, infection, or antimicrobial treatment, the presence of any evident infection, being technology-dependent, and the presence of congenital anomalies.
The updated guideline will aim to stratify management by age 7-28 days, 29-60 days, and 61 to 90 days to provide the most appropriate and directed treatment.
It will also include a role for inflammatory markers, and allow for a “kinder, gentler” approach to the management of febrile infants aged 7-90 days including withholding certain treatments and procedures if infants are at low risk of infection. An active, not passive, need for observation may be appropriate for certain infants as well. These guidelines should be tailored for individual patients to provide the best care possible while minimizing risk in this population.
Key Takeaway:
An updated AAP Practice guideline algorithm for the management of well-appearing febrile infants 7-28 days, 29-60 days, and 60-90 days will be coming in the near future that will help standardize care in this population, but should not be used as a substitute for clinical judgment.
Chandani DeZure, MD, FAAP, is a pediatric hospitalist at Children’s National Health System, Instruction of Pediatrics at George Washington University’s School of Medicine and Health Sciences in Washington, D.C.
One of PHM16’s most highly-attended sessions was an update on the anticipated AAP guidelines for febrile infants between ages 7-90 days given by Dr. Kenneth Roberts. The goal is to give evidence-based guidelines, not rules, from the most recent literature available. It also stresses the need to separate individual components of serious bacterial infections (UTI, bacteremia, and meningitis) as the incidence and clinical course can vary greatly in this population.
The inclusion criteria for infants for this upcoming algorithm require an infant to be full-term (37-43 weeks gestation), aged 7-90 days, well-appearing, and presenting with a temperature of 38 degrees Celsius.
Exclusion criteria include perinatal/prenatal/neonatal: maternal fever, infection, or antimicrobial treatment, the presence of any evident infection, being technology-dependent, and the presence of congenital anomalies.
The updated guideline will aim to stratify management by age 7-28 days, 29-60 days, and 61 to 90 days to provide the most appropriate and directed treatment.
It will also include a role for inflammatory markers, and allow for a “kinder, gentler” approach to the management of febrile infants aged 7-90 days including withholding certain treatments and procedures if infants are at low risk of infection. An active, not passive, need for observation may be appropriate for certain infants as well. These guidelines should be tailored for individual patients to provide the best care possible while minimizing risk in this population.
Key Takeaway:
An updated AAP Practice guideline algorithm for the management of well-appearing febrile infants 7-28 days, 29-60 days, and 60-90 days will be coming in the near future that will help standardize care in this population, but should not be used as a substitute for clinical judgment.
Chandani DeZure, MD, FAAP, is a pediatric hospitalist at Children’s National Health System, Instruction of Pediatrics at George Washington University’s School of Medicine and Health Sciences in Washington, D.C.
Post-AMI Death Risk Model Has High Predictive Accuracy
An updated risk model based on data from patients presenting after acute myocardial infarction to a broad spectrum of U.S. hospitals appears to predict with a high degree of accuracy which patients are at the greatest risk for in-hospital mortality, investigators say.
Created from data on more than 240,000 patients presenting to one of 655 U.S. hospitals in 2012 and 2013 following ST-segment elevation myocardial infarction (STEMI) or non–ST-segment elevation MI (NSTEMI), the model identified the following independent risk factors for in-hospital mortality: age, heart rate, systolic blood pressure, presentation to the hospital after cardiac arrest, presentation in cardiogenic shock, presentation in heart failure, presentation with STEMI, creatinine clearance, and troponin ratio, reported Robert L. McNamara, MD, of Yale University, New Haven, Conn.

The investigators are participants in the ACTION (Acute Coronary Treatment and Intervention Outcomes Network) Registry–GWTG (Get With the Guidelines).
“The new ACTION Registry–GWTG in-hospital mortality risk model and risk score represent robust, parsimonious, and contemporary risk adjustment methodology for use in routine clinical care and hospital quality assessment. The addition of risk adjustment for patients presenting after cardiac arrest is critically important and enables a fairer assessment across hospitals with varied case mix,” they wrote (J Am Coll Cardiol. 2016 Aug 1;68[6]:626-35).
The revised risk model has the potential to facilitate hospital quality assessments and help investigators to identify specific factors that could help clinicians even further lower death rates, the investigators write.
Further mortality reductions?
Although improvements in care of patients with acute MI over the last several decades have driven the in-hospital death rate from 29% in 1969 down to less than 7% today, there are still more than 100,000 AMI-related in-hospital deaths in the United States annually, with wide variations across hospitals, Dr. McNamara and colleagues noted.
A previous risk model published by ACTION Registry–GWTG members included data on patients treated at 306 U.S. hospitals and provided a simple, validated in-hospital mortality and risk score.
Since that model was published, however, the dataset was expanded to include patients presenting after cardiac arrest at the time of AMI presentation.
“Being able to adjust for cardiac arrest is critical because it is a well-documented predictor of mortality. Moreover, continued improvement in AMI care mandates periodic updates to the risk models so that hospitals can assess their quality as contemporary care continues to evolve,” the authors wrote.
To see whether they could develop a new and improved model and risk score, they analyzed data on 243,440 patients treated at one of 655 hospitals in the voluntary network. Data on 145,952 patients (60% of the total), 57,039 of whom presented with STEMI, and 88,913 of whom presented with NSTEMI, were used to for the derivation sample.
Data on the remaining 97,488 (38,060 with STEMI and 59,428 with NSTEMI) were used to create the validation sample.
The authors found that for the total cohort, the in-hospital mortality rate was 4.6%. In multivariate models controlled for demographic and clinical factors, independent risk factors significantly associated with in-hospital mortality (validation cohort) were:
• Presentation after cardiac arrest (odds ratio, 5.15).
• Presentation in cardiogenic shock (OR, 4.22).
• Presentation in heart failure (OR, 1.83).
• STEMI on electrocardiography (OR, 1.81).
• Age, per 5 years (OR, 1.24).
• Systolic BP, per 10 mm Hg decrease (OR, 1.19).
• Creatinine clearance per 5/mL/min/1.73 m2 decrease (OR, 1.11).
• Heart rate per 10 beats/min (OR, 1.09).
• Troponin ratio, per 5 units (OR, 1.05).
The 95% confidence intervals for all of the above factors were significant.
The C-statistic, a standard measure of the predictive accuracy of a logistic regression model, was 0.88, indicating that the final ACTION Registry–GWTG in-hospital mortality model had a high level of discrimination in both the derivation and validation populations, the authors state.
The ACTION Registry–GWTG is a Program of the American College of Cardiology and the American Heart Association, with funding from Schering-Plough and the Bristol-Myers Squibb/Sanofi Pharmaceutical Partnership. Dr. McNamara serves on a clinical trials endpoint adjudication committee for Pfizer. Other coauthors reported multiple financial relationships with pharmaceutical and medical device companies.
Data analyses for the risk models developed by the ACTION Registry generally showed good accuracy and precision. The calibration information showed that patients with a cardiac arrest experienced much greater risk for mortality than did the other major groups (STEMI, NSTEMI, or no cardiac arrest). Until now, clinicians and researchers have generally used either the TIMI [Thrombolysis in Myocardial Infarction] or GRACE [Global Registry of Acute Coronary Events] score to guide therapeutic decisions. With the advent of the ACTION score, which appears to be most helpful for patients with moderate to severe disease, and the HEART [history, ECG, age, risk factor, troponin] score, which targets care for patients with minimal to mild disease, there are other options. Recently, the DAPT (Dual Antiplatelet Therapy) investigators published a prediction algorithm that provides yet another prognostic score to assess risk of ischemic events and risk of bleeding in patients who have undergone percutaneous coronary intervention. The key variables in the DAPT score are age, cigarette smoking, diabetes, MI at presentation, previous percutaneous coronary intervention or previous MI, use of a paclitaxel-eluting stent, stent diameter of less than 3 mm, heart failure or reduced ejection fraction, and use of a vein graft stent.
A comprehensive cross validation and comparison across at least some of the algorithms – TIMI, GRACE, HEART, DAPT, and ACTION – would help at this point. Interventions and decision points have evolved over the past 15 years, and evaluation of relatively contemporary data would be especially helpful. For example, the HEART score is likely to be used in situations in which the negative predictive capabilities are most important. The ACTION score is likely to be most useful in severely ill patients and to provide guidance for newer interventions. If detailed information concerning stents is available, then the DAPT score should prove helpful.
It is likely that one score does not fit all. Each algorithm provides a useful summary of risk to help guide decision making for patients with ischemic symptoms, depending on the severity of the signs and symptoms at presentation and the duration of the follow-up interval. Consensus building would help to move this field forward for hospital-based management of patients evaluated for cardiac ischemia.
Peter W.F. Wilson, MD, of the Atlanta VAMC and Emory Clinical Cardiovascular Research
Institute, Atlanta; and Ralph B. D’Agostino Sr., PhD, of the department of mathematics and statistics, Boston University, made these comments in an accompanying editorial (J Am Coll Cardiol. 2016 Aug 1;68[6]:636-8). They reported no relevant disclosures.
Data analyses for the risk models developed by the ACTION Registry generally showed good accuracy and precision. The calibration information showed that patients with a cardiac arrest experienced much greater risk for mortality than did the other major groups (STEMI, NSTEMI, or no cardiac arrest). Until now, clinicians and researchers have generally used either the TIMI [Thrombolysis in Myocardial Infarction] or GRACE [Global Registry of Acute Coronary Events] score to guide therapeutic decisions. With the advent of the ACTION score, which appears to be most helpful for patients with moderate to severe disease, and the HEART [history, ECG, age, risk factor, troponin] score, which targets care for patients with minimal to mild disease, there are other options. Recently, the DAPT (Dual Antiplatelet Therapy) investigators published a prediction algorithm that provides yet another prognostic score to assess risk of ischemic events and risk of bleeding in patients who have undergone percutaneous coronary intervention. The key variables in the DAPT score are age, cigarette smoking, diabetes, MI at presentation, previous percutaneous coronary intervention or previous MI, use of a paclitaxel-eluting stent, stent diameter of less than 3 mm, heart failure or reduced ejection fraction, and use of a vein graft stent.
A comprehensive cross validation and comparison across at least some of the algorithms – TIMI, GRACE, HEART, DAPT, and ACTION – would help at this point. Interventions and decision points have evolved over the past 15 years, and evaluation of relatively contemporary data would be especially helpful. For example, the HEART score is likely to be used in situations in which the negative predictive capabilities are most important. The ACTION score is likely to be most useful in severely ill patients and to provide guidance for newer interventions. If detailed information concerning stents is available, then the DAPT score should prove helpful.
It is likely that one score does not fit all. Each algorithm provides a useful summary of risk to help guide decision making for patients with ischemic symptoms, depending on the severity of the signs and symptoms at presentation and the duration of the follow-up interval. Consensus building would help to move this field forward for hospital-based management of patients evaluated for cardiac ischemia.
Peter W.F. Wilson, MD, of the Atlanta VAMC and Emory Clinical Cardiovascular Research
Institute, Atlanta; and Ralph B. D’Agostino Sr., PhD, of the department of mathematics and statistics, Boston University, made these comments in an accompanying editorial (J Am Coll Cardiol. 2016 Aug 1;68[6]:636-8). They reported no relevant disclosures.
Data analyses for the risk models developed by the ACTION Registry generally showed good accuracy and precision. The calibration information showed that patients with a cardiac arrest experienced much greater risk for mortality than did the other major groups (STEMI, NSTEMI, or no cardiac arrest). Until now, clinicians and researchers have generally used either the TIMI [Thrombolysis in Myocardial Infarction] or GRACE [Global Registry of Acute Coronary Events] score to guide therapeutic decisions. With the advent of the ACTION score, which appears to be most helpful for patients with moderate to severe disease, and the HEART [history, ECG, age, risk factor, troponin] score, which targets care for patients with minimal to mild disease, there are other options. Recently, the DAPT (Dual Antiplatelet Therapy) investigators published a prediction algorithm that provides yet another prognostic score to assess risk of ischemic events and risk of bleeding in patients who have undergone percutaneous coronary intervention. The key variables in the DAPT score are age, cigarette smoking, diabetes, MI at presentation, previous percutaneous coronary intervention or previous MI, use of a paclitaxel-eluting stent, stent diameter of less than 3 mm, heart failure or reduced ejection fraction, and use of a vein graft stent.
A comprehensive cross validation and comparison across at least some of the algorithms – TIMI, GRACE, HEART, DAPT, and ACTION – would help at this point. Interventions and decision points have evolved over the past 15 years, and evaluation of relatively contemporary data would be especially helpful. For example, the HEART score is likely to be used in situations in which the negative predictive capabilities are most important. The ACTION score is likely to be most useful in severely ill patients and to provide guidance for newer interventions. If detailed information concerning stents is available, then the DAPT score should prove helpful.
It is likely that one score does not fit all. Each algorithm provides a useful summary of risk to help guide decision making for patients with ischemic symptoms, depending on the severity of the signs and symptoms at presentation and the duration of the follow-up interval. Consensus building would help to move this field forward for hospital-based management of patients evaluated for cardiac ischemia.
Peter W.F. Wilson, MD, of the Atlanta VAMC and Emory Clinical Cardiovascular Research
Institute, Atlanta; and Ralph B. D’Agostino Sr., PhD, of the department of mathematics and statistics, Boston University, made these comments in an accompanying editorial (J Am Coll Cardiol. 2016 Aug 1;68[6]:636-8). They reported no relevant disclosures.
An updated risk model based on data from patients presenting after acute myocardial infarction to a broad spectrum of U.S. hospitals appears to predict with a high degree of accuracy which patients are at the greatest risk for in-hospital mortality, investigators say.
Created from data on more than 240,000 patients presenting to one of 655 U.S. hospitals in 2012 and 2013 following ST-segment elevation myocardial infarction (STEMI) or non–ST-segment elevation MI (NSTEMI), the model identified the following independent risk factors for in-hospital mortality: age, heart rate, systolic blood pressure, presentation to the hospital after cardiac arrest, presentation in cardiogenic shock, presentation in heart failure, presentation with STEMI, creatinine clearance, and troponin ratio, reported Robert L. McNamara, MD, of Yale University, New Haven, Conn.
The investigators are participants in the ACTION (Acute Coronary Treatment and Intervention Outcomes Network) Registry–GWTG (Get With the Guidelines).
“The new ACTION Registry–GWTG in-hospital mortality risk model and risk score represent robust, parsimonious, and contemporary risk adjustment methodology for use in routine clinical care and hospital quality assessment. The addition of risk adjustment for patients presenting after cardiac arrest is critically important and enables a fairer assessment across hospitals with varied case mix,” they wrote (J Am Coll Cardiol. 2016 Aug 1;68[6]:626-35).
The revised risk model has the potential to facilitate hospital quality assessments and help investigators to identify specific factors that could help clinicians even further lower death rates, the investigators write.
Further mortality reductions?
Although improvements in care of patients with acute MI over the last several decades have driven the in-hospital death rate from 29% in 1969 down to less than 7% today, there are still more than 100,000 AMI-related in-hospital deaths in the United States annually, with wide variations across hospitals, Dr. McNamara and colleagues noted.
A previous risk model published by ACTION Registry–GWTG members included data on patients treated at 306 U.S. hospitals and provided a simple, validated in-hospital mortality and risk score.
Since that model was published, however, the dataset was expanded to include patients presenting after cardiac arrest at the time of AMI presentation.
“Being able to adjust for cardiac arrest is critical because it is a well-documented predictor of mortality. Moreover, continued improvement in AMI care mandates periodic updates to the risk models so that hospitals can assess their quality as contemporary care continues to evolve,” the authors wrote.
To see whether they could develop a new and improved model and risk score, they analyzed data on 243,440 patients treated at one of 655 hospitals in the voluntary network. Data on 145,952 patients (60% of the total), 57,039 of whom presented with STEMI, and 88,913 of whom presented with NSTEMI, were used to for the derivation sample.
Data on the remaining 97,488 (38,060 with STEMI and 59,428 with NSTEMI) were used to create the validation sample.
The authors found that for the total cohort, the in-hospital mortality rate was 4.6%. In multivariate models controlled for demographic and clinical factors, independent risk factors significantly associated with in-hospital mortality (validation cohort) were:
• Presentation after cardiac arrest (odds ratio, 5.15).
• Presentation in cardiogenic shock (OR, 4.22).
• Presentation in heart failure (OR, 1.83).
• STEMI on electrocardiography (OR, 1.81).
• Age, per 5 years (OR, 1.24).
• Systolic BP, per 10 mm Hg decrease (OR, 1.19).
• Creatinine clearance per 5/mL/min/1.73 m2 decrease (OR, 1.11).
• Heart rate per 10 beats/min (OR, 1.09).
• Troponin ratio, per 5 units (OR, 1.05).
The 95% confidence intervals for all of the above factors were significant.
The C-statistic, a standard measure of the predictive accuracy of a logistic regression model, was 0.88, indicating that the final ACTION Registry–GWTG in-hospital mortality model had a high level of discrimination in both the derivation and validation populations, the authors state.
The ACTION Registry–GWTG is a Program of the American College of Cardiology and the American Heart Association, with funding from Schering-Plough and the Bristol-Myers Squibb/Sanofi Pharmaceutical Partnership. Dr. McNamara serves on a clinical trials endpoint adjudication committee for Pfizer. Other coauthors reported multiple financial relationships with pharmaceutical and medical device companies.
An updated risk model based on data from patients presenting after acute myocardial infarction to a broad spectrum of U.S. hospitals appears to predict with a high degree of accuracy which patients are at the greatest risk for in-hospital mortality, investigators say.
Created from data on more than 240,000 patients presenting to one of 655 U.S. hospitals in 2012 and 2013 following ST-segment elevation myocardial infarction (STEMI) or non–ST-segment elevation MI (NSTEMI), the model identified the following independent risk factors for in-hospital mortality: age, heart rate, systolic blood pressure, presentation to the hospital after cardiac arrest, presentation in cardiogenic shock, presentation in heart failure, presentation with STEMI, creatinine clearance, and troponin ratio, reported Robert L. McNamara, MD, of Yale University, New Haven, Conn.
The investigators are participants in the ACTION (Acute Coronary Treatment and Intervention Outcomes Network) Registry–GWTG (Get With the Guidelines).
“The new ACTION Registry–GWTG in-hospital mortality risk model and risk score represent robust, parsimonious, and contemporary risk adjustment methodology for use in routine clinical care and hospital quality assessment. The addition of risk adjustment for patients presenting after cardiac arrest is critically important and enables a fairer assessment across hospitals with varied case mix,” they wrote (J Am Coll Cardiol. 2016 Aug 1;68[6]:626-35).
The revised risk model has the potential to facilitate hospital quality assessments and help investigators to identify specific factors that could help clinicians even further lower death rates, the investigators write.
Further mortality reductions?
Although improvements in care of patients with acute MI over the last several decades have driven the in-hospital death rate from 29% in 1969 down to less than 7% today, there are still more than 100,000 AMI-related in-hospital deaths in the United States annually, with wide variations across hospitals, Dr. McNamara and colleagues noted.
A previous risk model published by ACTION Registry–GWTG members included data on patients treated at 306 U.S. hospitals and provided a simple, validated in-hospital mortality and risk score.
Since that model was published, however, the dataset was expanded to include patients presenting after cardiac arrest at the time of AMI presentation.
“Being able to adjust for cardiac arrest is critical because it is a well-documented predictor of mortality. Moreover, continued improvement in AMI care mandates periodic updates to the risk models so that hospitals can assess their quality as contemporary care continues to evolve,” the authors wrote.
To see whether they could develop a new and improved model and risk score, they analyzed data on 243,440 patients treated at one of 655 hospitals in the voluntary network. Data on 145,952 patients (60% of the total), 57,039 of whom presented with STEMI, and 88,913 of whom presented with NSTEMI, were used to for the derivation sample.
Data on the remaining 97,488 (38,060 with STEMI and 59,428 with NSTEMI) were used to create the validation sample.
The authors found that for the total cohort, the in-hospital mortality rate was 4.6%. In multivariate models controlled for demographic and clinical factors, independent risk factors significantly associated with in-hospital mortality (validation cohort) were:
• Presentation after cardiac arrest (odds ratio, 5.15).
• Presentation in cardiogenic shock (OR, 4.22).
• Presentation in heart failure (OR, 1.83).
• STEMI on electrocardiography (OR, 1.81).
• Age, per 5 years (OR, 1.24).
• Systolic BP, per 10 mm Hg decrease (OR, 1.19).
• Creatinine clearance per 5/mL/min/1.73 m2 decrease (OR, 1.11).
• Heart rate per 10 beats/min (OR, 1.09).
• Troponin ratio, per 5 units (OR, 1.05).
The 95% confidence intervals for all of the above factors were significant.
The C-statistic, a standard measure of the predictive accuracy of a logistic regression model, was 0.88, indicating that the final ACTION Registry–GWTG in-hospital mortality model had a high level of discrimination in both the derivation and validation populations, the authors state.
The ACTION Registry–GWTG is a Program of the American College of Cardiology and the American Heart Association, with funding from Schering-Plough and the Bristol-Myers Squibb/Sanofi Pharmaceutical Partnership. Dr. McNamara serves on a clinical trials endpoint adjudication committee for Pfizer. Other coauthors reported multiple financial relationships with pharmaceutical and medical device companies.
FROM JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY

Post-AMI death risk model has high predictive accuracy
An updated risk model based on data from patients presenting after acute myocardial infarction to a broad spectrum of U.S. hospitals appears to predict with a high degree of accuracy which patients are at the greatest risk for in-hospital mortality, investigators say.
Created from data on more than 240,000 patients presenting to one of 655 U.S. hospitals in 2012 and 2013 following ST-segment elevation myocardial infarction (STEMI) or non–ST-segment elevation MI (NSTEMI), the model identified the following independent risk factors for in-hospital mortality: age, heart rate, systolic blood pressure, presentation to the hospital after cardiac arrest, presentation in cardiogenic shock, presentation in heart failure, presentation with STEMI, creatinine clearance, and troponin ratio, reported Robert L. McNamara, MD, of Yale University, New Haven, Conn.

The investigators are participants in the ACTION (Acute Coronary Treatment and Intervention Outcomes Network) Registry–GWTG (Get With the Guidelines).
“The new ACTION Registry–GWTG in-hospital mortality risk model and risk score represent robust, parsimonious, and contemporary risk adjustment methodology for use in routine clinical care and hospital quality assessment. The addition of risk adjustment for patients presenting after cardiac arrest is critically important and enables a fairer assessment across hospitals with varied case mix,” they wrote (J Am Coll Cardiol. 2016 Aug 1;68[6]:626-35).
The revised risk model has the potential to facilitate hospital quality assessments and help investigators to identify specific factors that could help clinicians even further lower death rates, the investigators write.
Further mortality reductions?
Although improvements in care of patients with acute MI over the last several decades have driven the in-hospital death rate from 29% in 1969 down to less than 7% today, there are still more than 100,000 AMI-related in-hospital deaths in the United States annually, with wide variations across hospitals, Dr. McNamara and colleagues noted.
A previous risk model published by ACTION Registry–GWTG members included data on patients treated at 306 U.S. hospitals and provided a simple, validated in-hospital mortality and risk score.
Since that model was published, however, the dataset was expanded to include patients presenting after cardiac arrest at the time of AMI presentation.
“Being able to adjust for cardiac arrest is critical because it is a well-documented predictor of mortality. Moreover, continued improvement in AMI care mandates periodic updates to the risk models so that hospitals can assess their quality as contemporary care continues to evolve,” the authors wrote.
To see whether they could develop a new and improved model and risk score, they analyzed data on 243,440 patients treated at one of 655 hospitals in the voluntary network. Data on 145,952 patients (60% of the total), 57,039 of whom presented with STEMI, and 88,913 of whom presented with NSTEMI, were used to for the derivation sample.
Data on the remaining 97,488 (38,060 with STEMI and 59,428 with NSTEMI) were used to create the validation sample.
The authors found that for the total cohort, the in-hospital mortality rate was 4.6%. In multivariate models controlled for demographic and clinical factors, independent risk factors significantly associated with in-hospital mortality (validation cohort) were:
• Presentation after cardiac arrest (odds ratio, 5.15).
• Presentation in cardiogenic shock (OR, 4.22).
• Presentation in heart failure (OR, 1.83).
• STEMI on electrocardiography (OR, 1.81).
• Age, per 5 years (OR, 1.24).
• Systolic BP, per 10 mm Hg decrease (OR, 1.19).
• Creatinine clearance per 5/mL/min/1.73 m2 decrease (OR, 1.11).
• Heart rate per 10 beats/min (OR, 1.09).
• Troponin ratio, per 5 units (OR, 1.05).
The 95% confidence intervals for all of the above factors were significant.
The C-statistic, a standard measure of the predictive accuracy of a logistic regression model, was 0.88, indicating that the final ACTION Registry–GWTG in-hospital mortality model had a high level of discrimination in both the derivation and validation populations, the authors state.
The ACTION Registry–GWTG is a Program of the American College of Cardiology and the American Heart Association, with funding from Schering-Plough and the Bristol-Myers Squibb/Sanofi Pharmaceutical Partnership. Dr. McNamara serves on a clinical trials endpoint adjudication committee for Pfizer. Other coauthors reported multiple financial relationships with pharmaceutical and medical device companies.
Data analyses for the risk models developed by the ACTION Registry generally showed good accuracy and precision. The calibration information showed that patients with a cardiac arrest experienced much greater risk for mortality than did the other major groups (STEMI, NSTEMI, or no cardiac arrest). Until now, clinicians and researchers have generally used either the TIMI [Thrombolysis in Myocardial Infarction] or GRACE [Global Registry of Acute Coronary Events] score to guide therapeutic decisions. With the advent of the ACTION score, which appears to be most helpful for patients with moderate to severe disease, and the HEART [history, ECG, age, risk factor, troponin] score, which targets care for patients with minimal to mild disease, there are other options. Recently, the DAPT (Dual Antiplatelet Therapy) investigators published a prediction algorithm that provides yet another prognostic score to assess risk of ischemic events and risk of bleeding in patients who have undergone percutaneous coronary intervention. The key variables in the DAPT score are age, cigarette smoking, diabetes, MI at presentation, previous percutaneous coronary intervention or previous MI, use of a paclitaxel-eluting stent, stent diameter of less than 3 mm, heart failure or reduced ejection fraction, and use of a vein graft stent.
A comprehensive cross validation and comparison across at least some of the algorithms – TIMI, GRACE, HEART, DAPT, and ACTION – would help at this point. Interventions and decision points have evolved over the past 15 years, and evaluation of relatively contemporary data would be especially helpful. For example, the HEART score is likely to be used in situations in which the negative predictive capabilities are most important. The ACTION score is likely to be most useful in severely ill patients and to provide guidance for newer interventions. If detailed information concerning stents is available, then the DAPT score should prove helpful.
It is likely that one score does not fit all. Each algorithm provides a useful summary of risk to help guide decision making for patients with ischemic symptoms, depending on the severity of the signs and symptoms at presentation and the duration of the follow-up interval. Consensus building would help to move this field forward for hospital-based management of patients evaluated for cardiac ischemia.
Peter W.F. Wilson, MD, of the Atlanta VAMC and Emory Clinical Cardiovascular Research
Institute, Atlanta; and Ralph B. D’Agostino Sr., PhD, of the department of mathematics and statistics, Boston University, made these comments in an accompanying editorial (J Am Coll Cardiol. 2016 Aug 1;68[6]:636-8). They reported no relevant disclosures.
Data analyses for the risk models developed by the ACTION Registry generally showed good accuracy and precision. The calibration information showed that patients with a cardiac arrest experienced much greater risk for mortality than did the other major groups (STEMI, NSTEMI, or no cardiac arrest). Until now, clinicians and researchers have generally used either the TIMI [Thrombolysis in Myocardial Infarction] or GRACE [Global Registry of Acute Coronary Events] score to guide therapeutic decisions. With the advent of the ACTION score, which appears to be most helpful for patients with moderate to severe disease, and the HEART [history, ECG, age, risk factor, troponin] score, which targets care for patients with minimal to mild disease, there are other options. Recently, the DAPT (Dual Antiplatelet Therapy) investigators published a prediction algorithm that provides yet another prognostic score to assess risk of ischemic events and risk of bleeding in patients who have undergone percutaneous coronary intervention. The key variables in the DAPT score are age, cigarette smoking, diabetes, MI at presentation, previous percutaneous coronary intervention or previous MI, use of a paclitaxel-eluting stent, stent diameter of less than 3 mm, heart failure or reduced ejection fraction, and use of a vein graft stent.
A comprehensive cross validation and comparison across at least some of the algorithms – TIMI, GRACE, HEART, DAPT, and ACTION – would help at this point. Interventions and decision points have evolved over the past 15 years, and evaluation of relatively contemporary data would be especially helpful. For example, the HEART score is likely to be used in situations in which the negative predictive capabilities are most important. The ACTION score is likely to be most useful in severely ill patients and to provide guidance for newer interventions. If detailed information concerning stents is available, then the DAPT score should prove helpful.
It is likely that one score does not fit all. Each algorithm provides a useful summary of risk to help guide decision making for patients with ischemic symptoms, depending on the severity of the signs and symptoms at presentation and the duration of the follow-up interval. Consensus building would help to move this field forward for hospital-based management of patients evaluated for cardiac ischemia.
Peter W.F. Wilson, MD, of the Atlanta VAMC and Emory Clinical Cardiovascular Research
Institute, Atlanta; and Ralph B. D’Agostino Sr., PhD, of the department of mathematics and statistics, Boston University, made these comments in an accompanying editorial (J Am Coll Cardiol. 2016 Aug 1;68[6]:636-8). They reported no relevant disclosures.
Data analyses for the risk models developed by the ACTION Registry generally showed good accuracy and precision. The calibration information showed that patients with a cardiac arrest experienced much greater risk for mortality than did the other major groups (STEMI, NSTEMI, or no cardiac arrest). Until now, clinicians and researchers have generally used either the TIMI [Thrombolysis in Myocardial Infarction] or GRACE [Global Registry of Acute Coronary Events] score to guide therapeutic decisions. With the advent of the ACTION score, which appears to be most helpful for patients with moderate to severe disease, and the HEART [history, ECG, age, risk factor, troponin] score, which targets care for patients with minimal to mild disease, there are other options. Recently, the DAPT (Dual Antiplatelet Therapy) investigators published a prediction algorithm that provides yet another prognostic score to assess risk of ischemic events and risk of bleeding in patients who have undergone percutaneous coronary intervention. The key variables in the DAPT score are age, cigarette smoking, diabetes, MI at presentation, previous percutaneous coronary intervention or previous MI, use of a paclitaxel-eluting stent, stent diameter of less than 3 mm, heart failure or reduced ejection fraction, and use of a vein graft stent.
A comprehensive cross validation and comparison across at least some of the algorithms – TIMI, GRACE, HEART, DAPT, and ACTION – would help at this point. Interventions and decision points have evolved over the past 15 years, and evaluation of relatively contemporary data would be especially helpful. For example, the HEART score is likely to be used in situations in which the negative predictive capabilities are most important. The ACTION score is likely to be most useful in severely ill patients and to provide guidance for newer interventions. If detailed information concerning stents is available, then the DAPT score should prove helpful.
It is likely that one score does not fit all. Each algorithm provides a useful summary of risk to help guide decision making for patients with ischemic symptoms, depending on the severity of the signs and symptoms at presentation and the duration of the follow-up interval. Consensus building would help to move this field forward for hospital-based management of patients evaluated for cardiac ischemia.
Peter W.F. Wilson, MD, of the Atlanta VAMC and Emory Clinical Cardiovascular Research
Institute, Atlanta; and Ralph B. D’Agostino Sr., PhD, of the department of mathematics and statistics, Boston University, made these comments in an accompanying editorial (J Am Coll Cardiol. 2016 Aug 1;68[6]:636-8). They reported no relevant disclosures.
An updated risk model based on data from patients presenting after acute myocardial infarction to a broad spectrum of U.S. hospitals appears to predict with a high degree of accuracy which patients are at the greatest risk for in-hospital mortality, investigators say.
Created from data on more than 240,000 patients presenting to one of 655 U.S. hospitals in 2012 and 2013 following ST-segment elevation myocardial infarction (STEMI) or non–ST-segment elevation MI (NSTEMI), the model identified the following independent risk factors for in-hospital mortality: age, heart rate, systolic blood pressure, presentation to the hospital after cardiac arrest, presentation in cardiogenic shock, presentation in heart failure, presentation with STEMI, creatinine clearance, and troponin ratio, reported Robert L. McNamara, MD, of Yale University, New Haven, Conn.
The investigators are participants in the ACTION (Acute Coronary Treatment and Intervention Outcomes Network) Registry–GWTG (Get With the Guidelines).
“The new ACTION Registry–GWTG in-hospital mortality risk model and risk score represent robust, parsimonious, and contemporary risk adjustment methodology for use in routine clinical care and hospital quality assessment. The addition of risk adjustment for patients presenting after cardiac arrest is critically important and enables a fairer assessment across hospitals with varied case mix,” they wrote (J Am Coll Cardiol. 2016 Aug 1;68[6]:626-35).
The revised risk model has the potential to facilitate hospital quality assessments and help investigators to identify specific factors that could help clinicians even further lower death rates, the investigators write.
Further mortality reductions?
Although improvements in care of patients with acute MI over the last several decades have driven the in-hospital death rate from 29% in 1969 down to less than 7% today, there are still more than 100,000 AMI-related in-hospital deaths in the United States annually, with wide variations across hospitals, Dr. McNamara and colleagues noted.
A previous risk model published by ACTION Registry–GWTG members included data on patients treated at 306 U.S. hospitals and provided a simple, validated in-hospital mortality and risk score.
Since that model was published, however, the dataset was expanded to include patients presenting after cardiac arrest at the time of AMI presentation.
“Being able to adjust for cardiac arrest is critical because it is a well-documented predictor of mortality. Moreover, continued improvement in AMI care mandates periodic updates to the risk models so that hospitals can assess their quality as contemporary care continues to evolve,” the authors wrote.
To see whether they could develop a new and improved model and risk score, they analyzed data on 243,440 patients treated at one of 655 hospitals in the voluntary network. Data on 145,952 patients (60% of the total), 57,039 of whom presented with STEMI, and 88,913 of whom presented with NSTEMI, were used to for the derivation sample.
Data on the remaining 97,488 (38,060 with STEMI and 59,428 with NSTEMI) were used to create the validation sample.
The authors found that for the total cohort, the in-hospital mortality rate was 4.6%. In multivariate models controlled for demographic and clinical factors, independent risk factors significantly associated with in-hospital mortality (validation cohort) were:
• Presentation after cardiac arrest (odds ratio, 5.15).
• Presentation in cardiogenic shock (OR, 4.22).
• Presentation in heart failure (OR, 1.83).
• STEMI on electrocardiography (OR, 1.81).
• Age, per 5 years (OR, 1.24).
• Systolic BP, per 10 mm Hg decrease (OR, 1.19).
• Creatinine clearance per 5/mL/min/1.73 m2 decrease (OR, 1.11).
• Heart rate per 10 beats/min (OR, 1.09).
• Troponin ratio, per 5 units (OR, 1.05).
The 95% confidence intervals for all of the above factors were significant.
The C-statistic, a standard measure of the predictive accuracy of a logistic regression model, was 0.88, indicating that the final ACTION Registry–GWTG in-hospital mortality model had a high level of discrimination in both the derivation and validation populations, the authors state.
The ACTION Registry–GWTG is a Program of the American College of Cardiology and the American Heart Association, with funding from Schering-Plough and the Bristol-Myers Squibb/Sanofi Pharmaceutical Partnership. Dr. McNamara serves on a clinical trials endpoint adjudication committee for Pfizer. Other coauthors reported multiple financial relationships with pharmaceutical and medical device companies.
An updated risk model based on data from patients presenting after acute myocardial infarction to a broad spectrum of U.S. hospitals appears to predict with a high degree of accuracy which patients are at the greatest risk for in-hospital mortality, investigators say.
Created from data on more than 240,000 patients presenting to one of 655 U.S. hospitals in 2012 and 2013 following ST-segment elevation myocardial infarction (STEMI) or non–ST-segment elevation MI (NSTEMI), the model identified the following independent risk factors for in-hospital mortality: age, heart rate, systolic blood pressure, presentation to the hospital after cardiac arrest, presentation in cardiogenic shock, presentation in heart failure, presentation with STEMI, creatinine clearance, and troponin ratio, reported Robert L. McNamara, MD, of Yale University, New Haven, Conn.
The investigators are participants in the ACTION (Acute Coronary Treatment and Intervention Outcomes Network) Registry–GWTG (Get With the Guidelines).
“The new ACTION Registry–GWTG in-hospital mortality risk model and risk score represent robust, parsimonious, and contemporary risk adjustment methodology for use in routine clinical care and hospital quality assessment. The addition of risk adjustment for patients presenting after cardiac arrest is critically important and enables a fairer assessment across hospitals with varied case mix,” they wrote (J Am Coll Cardiol. 2016 Aug 1;68[6]:626-35).
The revised risk model has the potential to facilitate hospital quality assessments and help investigators to identify specific factors that could help clinicians even further lower death rates, the investigators write.
Further mortality reductions?
Although improvements in care of patients with acute MI over the last several decades have driven the in-hospital death rate from 29% in 1969 down to less than 7% today, there are still more than 100,000 AMI-related in-hospital deaths in the United States annually, with wide variations across hospitals, Dr. McNamara and colleagues noted.
A previous risk model published by ACTION Registry–GWTG members included data on patients treated at 306 U.S. hospitals and provided a simple, validated in-hospital mortality and risk score.
Since that model was published, however, the dataset was expanded to include patients presenting after cardiac arrest at the time of AMI presentation.
“Being able to adjust for cardiac arrest is critical because it is a well-documented predictor of mortality. Moreover, continued improvement in AMI care mandates periodic updates to the risk models so that hospitals can assess their quality as contemporary care continues to evolve,” the authors wrote.
To see whether they could develop a new and improved model and risk score, they analyzed data on 243,440 patients treated at one of 655 hospitals in the voluntary network. Data on 145,952 patients (60% of the total), 57,039 of whom presented with STEMI, and 88,913 of whom presented with NSTEMI, were used to for the derivation sample.
Data on the remaining 97,488 (38,060 with STEMI and 59,428 with NSTEMI) were used to create the validation sample.
The authors found that for the total cohort, the in-hospital mortality rate was 4.6%. In multivariate models controlled for demographic and clinical factors, independent risk factors significantly associated with in-hospital mortality (validation cohort) were:
• Presentation after cardiac arrest (odds ratio, 5.15).
• Presentation in cardiogenic shock (OR, 4.22).
• Presentation in heart failure (OR, 1.83).
• STEMI on electrocardiography (OR, 1.81).
• Age, per 5 years (OR, 1.24).
• Systolic BP, per 10 mm Hg decrease (OR, 1.19).
• Creatinine clearance per 5/mL/min/1.73 m2 decrease (OR, 1.11).
• Heart rate per 10 beats/min (OR, 1.09).
• Troponin ratio, per 5 units (OR, 1.05).
The 95% confidence intervals for all of the above factors were significant.
The C-statistic, a standard measure of the predictive accuracy of a logistic regression model, was 0.88, indicating that the final ACTION Registry–GWTG in-hospital mortality model had a high level of discrimination in both the derivation and validation populations, the authors state.
The ACTION Registry–GWTG is a Program of the American College of Cardiology and the American Heart Association, with funding from Schering-Plough and the Bristol-Myers Squibb/Sanofi Pharmaceutical Partnership. Dr. McNamara serves on a clinical trials endpoint adjudication committee for Pfizer. Other coauthors reported multiple financial relationships with pharmaceutical and medical device companies.
FROM JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Key clinical point: An updated cardiac mortality risk model may help to further reduce in-hospital deaths following acute myocardial infarction.
Major finding: The C-statistic for the model, a measure of predictive accuracy, was 0.88.
Data source: Updated risk model and in-hospital mortality score based on data from 243,440 patients following an AMI in 655 U.S. hospitals.
Disclosures: The ACTION Registry-GWTG is a Program of the American College of Cardiology and the American Heart Association, with funding from Schering-Plough and the Bristol-Myers Squibb/Sanofi Pharmaceutical Partnership. Dr. McNamara serves on a clinical trials endpoint adjudication committee for Pfizer. Other coauthors reported multiple financial relationships with pharmaceutical and medical device companies.
