User login
In septic shock, vasopressin not better than norepinephrine
Vasopressin was no better than norepinephrine in preventing kidney failure when used as a first-line treatment for septic shock, according to a report published online Aug. 2 in JAMA.
In a multicenter, double-blind, randomized trial comparing the two approaches in 408 ICU patients with septic shock, the early use of vasopressin didn’t reduce the number of days free of kidney failure, compared with standard norepinephrine.

However, “the 95% confidence intervals of the difference between [study] groups has an upper limit of 5 days in favor of vasopressin, which could be clinically important,” said Anthony C. Gordon, MD, of Charing Cross Hospital and Imperial College London, and his associates. “Therefore, these results are still consistent with a potentially clinically important benefit for vasopressin; but a larger trial would be needed to confirm or refute this.”
Norepinephrine is the recommended first-line vasopressor for septic shock, but “there has been a growing interest in the use of vasopressin” ever since researchers described a relative deficiency of vasopressin in the disorder, Dr. Gordon and his associates noted.
“Preclinical and small clinical studies have suggested that vasopressin may be better able to maintain glomerular filtration rate and improve creatinine clearance, compared with norepinephrine,” the investigators said, and other studies have suggested that combining vasopressin with corticosteroids may prevent deterioration in organ function and reduce the duration of shock, thereby improving survival.
To examine those possibilities, they performed the VANISH (Vasopressin vs. Norepinephrine as Initial Therapy in Septic Shock) trial, assessing patients age 16 years and older at 18 general adult ICUs in the United Kingdom during a 2-year period. The study participants were randomly assigned to receive vasopressin plus hydrocortisone (100 patients), vasopressin plus matching placebo (104 patients), norepinephrine plus hydrocortisone (101 patients), or norepinephrine plus matching placebo (103 patients).
The primary outcome measure was the number of days alive and free of kidney failure during the 28 days following randomization. There was no significant difference among the four study groups in the number or the distribution of kidney-failure–free days, the investigators said (JAMA. 2016 Aug 2. doi: 10.1001/jama.2016.10485).
In addition, the percentage of survivors who never developed kidney failure was not significantly different between the two groups who received vasopressin (57.0%) and the two who received norepinephrine (59.2%). And the median number of days free of kidney failure in the subgroup of patients who died or developed kidney failure was not significantly different between those receiving vasopressin (9 days) and those receiving norepinephrine (13 days).
The quantities of IV fluids administered, the total fluid balance, serum lactate levels, and heart rate were all similar across the four study groups. There also was no significant difference in 28-day mortality between patients who received vasopressin (30.9%) and those who received norepinephrine (27.5%). Adverse event profiles also were comparable.
However, the rate of renal replacement therapy was 25.4% with vasopressin, significantly lower than the 35.3% rate in the norepinephrine group. The use of such therapy was not controlled in the trial and was initiated according to the treating physicians’ preference. “It is therefore not possible to know why renal replacement therapy was or was not started,” Dr. Gordon and his associates noted.
The use of renal replacement therapy wasn’t a primary outcome of the trial. Nevertheless, it is an important patient-centered outcome and may be a factor to consider when treating adults who have septic shock, the researchers added.
The study was supported by the U.K. National Institute for Health Research and the U.K. Intensive Care Foundation. Dr. Gordon reported ties to Ferring, HCA International, Orion, and Tenax Therapeutics; his associates reported having no relevant financial disclosures.
Vasopressin was no better than norepinephrine in preventing kidney failure when used as a first-line treatment for septic shock, according to a report published online Aug. 2 in JAMA.
In a multicenter, double-blind, randomized trial comparing the two approaches in 408 ICU patients with septic shock, the early use of vasopressin didn’t reduce the number of days free of kidney failure, compared with standard norepinephrine.
However, “the 95% confidence intervals of the difference between [study] groups has an upper limit of 5 days in favor of vasopressin, which could be clinically important,” said Anthony C. Gordon, MD, of Charing Cross Hospital and Imperial College London, and his associates. “Therefore, these results are still consistent with a potentially clinically important benefit for vasopressin; but a larger trial would be needed to confirm or refute this.”
Norepinephrine is the recommended first-line vasopressor for septic shock, but “there has been a growing interest in the use of vasopressin” ever since researchers described a relative deficiency of vasopressin in the disorder, Dr. Gordon and his associates noted.
“Preclinical and small clinical studies have suggested that vasopressin may be better able to maintain glomerular filtration rate and improve creatinine clearance, compared with norepinephrine,” the investigators said, and other studies have suggested that combining vasopressin with corticosteroids may prevent deterioration in organ function and reduce the duration of shock, thereby improving survival.
To examine those possibilities, they performed the VANISH (Vasopressin vs. Norepinephrine as Initial Therapy in Septic Shock) trial, assessing patients age 16 years and older at 18 general adult ICUs in the United Kingdom during a 2-year period. The study participants were randomly assigned to receive vasopressin plus hydrocortisone (100 patients), vasopressin plus matching placebo (104 patients), norepinephrine plus hydrocortisone (101 patients), or norepinephrine plus matching placebo (103 patients).
The primary outcome measure was the number of days alive and free of kidney failure during the 28 days following randomization. There was no significant difference among the four study groups in the number or the distribution of kidney-failure–free days, the investigators said (JAMA. 2016 Aug 2. doi: 10.1001/jama.2016.10485).
In addition, the percentage of survivors who never developed kidney failure was not significantly different between the two groups who received vasopressin (57.0%) and the two who received norepinephrine (59.2%). And the median number of days free of kidney failure in the subgroup of patients who died or developed kidney failure was not significantly different between those receiving vasopressin (9 days) and those receiving norepinephrine (13 days).
The quantities of IV fluids administered, the total fluid balance, serum lactate levels, and heart rate were all similar across the four study groups. There also was no significant difference in 28-day mortality between patients who received vasopressin (30.9%) and those who received norepinephrine (27.5%). Adverse event profiles also were comparable.
However, the rate of renal replacement therapy was 25.4% with vasopressin, significantly lower than the 35.3% rate in the norepinephrine group. The use of such therapy was not controlled in the trial and was initiated according to the treating physicians’ preference. “It is therefore not possible to know why renal replacement therapy was or was not started,” Dr. Gordon and his associates noted.
The use of renal replacement therapy wasn’t a primary outcome of the trial. Nevertheless, it is an important patient-centered outcome and may be a factor to consider when treating adults who have septic shock, the researchers added.
The study was supported by the U.K. National Institute for Health Research and the U.K. Intensive Care Foundation. Dr. Gordon reported ties to Ferring, HCA International, Orion, and Tenax Therapeutics; his associates reported having no relevant financial disclosures.
Vasopressin was no better than norepinephrine in preventing kidney failure when used as a first-line treatment for septic shock, according to a report published online Aug. 2 in JAMA.
In a multicenter, double-blind, randomized trial comparing the two approaches in 408 ICU patients with septic shock, the early use of vasopressin didn’t reduce the number of days free of kidney failure, compared with standard norepinephrine.
However, “the 95% confidence intervals of the difference between [study] groups has an upper limit of 5 days in favor of vasopressin, which could be clinically important,” said Anthony C. Gordon, MD, of Charing Cross Hospital and Imperial College London, and his associates. “Therefore, these results are still consistent with a potentially clinically important benefit for vasopressin; but a larger trial would be needed to confirm or refute this.”
Norepinephrine is the recommended first-line vasopressor for septic shock, but “there has been a growing interest in the use of vasopressin” ever since researchers described a relative deficiency of vasopressin in the disorder, Dr. Gordon and his associates noted.
“Preclinical and small clinical studies have suggested that vasopressin may be better able to maintain glomerular filtration rate and improve creatinine clearance, compared with norepinephrine,” the investigators said, and other studies have suggested that combining vasopressin with corticosteroids may prevent deterioration in organ function and reduce the duration of shock, thereby improving survival.
To examine those possibilities, they performed the VANISH (Vasopressin vs. Norepinephrine as Initial Therapy in Septic Shock) trial, assessing patients age 16 years and older at 18 general adult ICUs in the United Kingdom during a 2-year period. The study participants were randomly assigned to receive vasopressin plus hydrocortisone (100 patients), vasopressin plus matching placebo (104 patients), norepinephrine plus hydrocortisone (101 patients), or norepinephrine plus matching placebo (103 patients).
The primary outcome measure was the number of days alive and free of kidney failure during the 28 days following randomization. There was no significant difference among the four study groups in the number or the distribution of kidney-failure–free days, the investigators said (JAMA. 2016 Aug 2. doi: 10.1001/jama.2016.10485).
In addition, the percentage of survivors who never developed kidney failure was not significantly different between the two groups who received vasopressin (57.0%) and the two who received norepinephrine (59.2%). And the median number of days free of kidney failure in the subgroup of patients who died or developed kidney failure was not significantly different between those receiving vasopressin (9 days) and those receiving norepinephrine (13 days).
The quantities of IV fluids administered, the total fluid balance, serum lactate levels, and heart rate were all similar across the four study groups. There also was no significant difference in 28-day mortality between patients who received vasopressin (30.9%) and those who received norepinephrine (27.5%). Adverse event profiles also were comparable.
However, the rate of renal replacement therapy was 25.4% with vasopressin, significantly lower than the 35.3% rate in the norepinephrine group. The use of such therapy was not controlled in the trial and was initiated according to the treating physicians’ preference. “It is therefore not possible to know why renal replacement therapy was or was not started,” Dr. Gordon and his associates noted.
The use of renal replacement therapy wasn’t a primary outcome of the trial. Nevertheless, it is an important patient-centered outcome and may be a factor to consider when treating adults who have septic shock, the researchers added.
The study was supported by the U.K. National Institute for Health Research and the U.K. Intensive Care Foundation. Dr. Gordon reported ties to Ferring, HCA International, Orion, and Tenax Therapeutics; his associates reported having no relevant financial disclosures.
FROM JAMA
Key clinical point: Vasopressin didn’t perform better than norepinephrine in preventing kidney failure when used as a first-line treatment for septic shock.
Major finding: The primary outcome measure – the number of days alive and free of kidney failure during the first month of treatment – was not significantly different among the four study groups.
Data source: A multicenter, double-blind, randomized clinical trial involving 408 ICU patients treated in the United Kingdom during a 2-year period.
Disclosures: The study was supported by the U.K. National Institute for Health Research and the U.K. Intensive Care Foundation. Dr. Gordon reported ties to Ferring, HCA International, Orion, and Tenax Therapeutics; his associates reported having no relevant financial disclosures.
Psychiatric disorders often impair antiretroviral adherence in perinatally HIV-infected teens
DURBAN, SOUTH AFRICA – Adolescents who were perinatally infected with HIV have a high prevalence of selected psychiatric disorders that impede their adherence to antiretroviral therapy, Claude Ann Mellins, PhD, reported at the 21st International AIDS Conference.
Those psychiatric diagnoses were predictive of viremia over the ensuing 2-3 years in a new analysis from the ongoing Child and Adolescent Self-Awareness and Health (CASAH) study, according to Dr. Mellins, professor of medical psychology at Columbia University, New York, and codirector of CASAH.

The clinical implications of the CASAH findings are clear, she added. “Assessing and treating specific categories of psychiatric and substance abuse problems may enhance efforts to improve adherence and prevent poor health outcomes in these adolescents and young adults, who are especially vulnerable due to their very challenging circumstances,” Dr. Mellins said.
CASAH is a longitudinal study of perinatally HIV-infected and perinatally HIV-exposed but uninfected New York City youth. They were enrolled during 2003-2008, when they were 9-16 years old. They and their caregivers undergo detailed psychosocial interviews every 12-18 months. The goal is to identify risk factors as well as protective factors influencing their behavioral health outcomes, the clinical psychologist explained.
She reported on 179 perinatally infected adolescents who were at least 13 years old at the first of their three interviews conducted over a 2.7-year period. Of note, 53% of them met Diagnostic Interview Schedule for Children (DISC-IV) criteria for one or more psychiatric diagnoses at all three time points. The pattern of psychopathology was somewhat different from that previously described in adults with HIV, who have been studied much more extensively than perinatally infected teens.
“Much of the literature on adults has focused on depression and mood disorders as predictors of poor health outcomes. Our data suggest that among youth, disruptive behavioral disorders – things like [attention-deficit/hyperactivity disorder], conduct disorder, or oppositional defiant disorder – may be just as important, if not more so. Substance abuse was also a critical factor,” Dr. Mellins said.
In a cross-sectional multivariate logistic regression analysis, a behavior disorder diagnosed at the first interview was associated with a 2.57-fold increased likelihood of contemporaneous viremia as evidenced by a plasma HIV RNA viral load greater than 1,000 copies/mL, and with a threefold increased likelihood of self-reported missed doses of antiretroviral medications during the previous week.
Anxiety disorder was the most common psychiatric diagnosis at the initial interview, followed by disruptive behavior disorder and substance use disorder. A diagnosis of any psychiatric disorder at the time of the first interview was associated with a significantly increased risk of viremia across the next 2.7 years. Forty-seven percent of subjects had viremia at 2.7 years of follow-up, reflective of chronic suboptimal medication adherence.
She noted that the pattern of psychiatric disorders in perinatally infected patients shifts between adolescence and young adulthood.
“By the time perinatally infected adolescents become young adults, I will say that anxiety and mood disorders become much more prevalent. But the number of psychiatric problems actually goes down by young adulthood,” according to Dr. Mellins.
Indeed, in another CASAH analysis she presented at AIDS 2016, this one involving 136 perinatally infected young adults and 86 perinatally exposed but uninfected controls, the vast majority living in impoverished communities, there was no difference between the two groups in rates of psychiatric or substance use disorders, although the 27% prevalence of substance use disorders is higher than that found in the age-matched general population.
Eighty-four percent of the perinatally infected 18- to 28-year-olds had graduated from high school, 94% were in a stable housing situation, 59% were currently working or in school, 54% were paying rent, and 95% reported ever being in a romantic relationship. Rates were similar in the perinatally exposed but uninfected group with the exception that these individuals were less likely to be paying rent.
“In spite of substantive risks, there is a relatively large portion of both groups with positive behavioral health outcomes, achieving normative young adult transition milestones. We need to understand why. Identification of protective factors conferring resilience can inform evidence-based prevention efforts, which are critical given the staggering numbers of children and young adolescents worldwide affected by HIV who will be transitioning to adulthood,” she said.
Dr. Mellins said the CASAH findings constitute a persuasive argument in favor of integrating mental health as a component of HIV care.
“Young people don’t always go to mental health appointments that are separate from medical care, so integrating mental health as a component of HIV care might be one of the most effective ways to identify and treat mental health problems in infected youth while simultaneously improving medication adherence and health outcomes,” Dr. Mellins said.
The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – Adolescents who were perinatally infected with HIV have a high prevalence of selected psychiatric disorders that impede their adherence to antiretroviral therapy, Claude Ann Mellins, PhD, reported at the 21st International AIDS Conference.
Those psychiatric diagnoses were predictive of viremia over the ensuing 2-3 years in a new analysis from the ongoing Child and Adolescent Self-Awareness and Health (CASAH) study, according to Dr. Mellins, professor of medical psychology at Columbia University, New York, and codirector of CASAH.
The clinical implications of the CASAH findings are clear, she added. “Assessing and treating specific categories of psychiatric and substance abuse problems may enhance efforts to improve adherence and prevent poor health outcomes in these adolescents and young adults, who are especially vulnerable due to their very challenging circumstances,” Dr. Mellins said.
CASAH is a longitudinal study of perinatally HIV-infected and perinatally HIV-exposed but uninfected New York City youth. They were enrolled during 2003-2008, when they were 9-16 years old. They and their caregivers undergo detailed psychosocial interviews every 12-18 months. The goal is to identify risk factors as well as protective factors influencing their behavioral health outcomes, the clinical psychologist explained.
She reported on 179 perinatally infected adolescents who were at least 13 years old at the first of their three interviews conducted over a 2.7-year period. Of note, 53% of them met Diagnostic Interview Schedule for Children (DISC-IV) criteria for one or more psychiatric diagnoses at all three time points. The pattern of psychopathology was somewhat different from that previously described in adults with HIV, who have been studied much more extensively than perinatally infected teens.
“Much of the literature on adults has focused on depression and mood disorders as predictors of poor health outcomes. Our data suggest that among youth, disruptive behavioral disorders – things like [attention-deficit/hyperactivity disorder], conduct disorder, or oppositional defiant disorder – may be just as important, if not more so. Substance abuse was also a critical factor,” Dr. Mellins said.
In a cross-sectional multivariate logistic regression analysis, a behavior disorder diagnosed at the first interview was associated with a 2.57-fold increased likelihood of contemporaneous viremia as evidenced by a plasma HIV RNA viral load greater than 1,000 copies/mL, and with a threefold increased likelihood of self-reported missed doses of antiretroviral medications during the previous week.
Anxiety disorder was the most common psychiatric diagnosis at the initial interview, followed by disruptive behavior disorder and substance use disorder. A diagnosis of any psychiatric disorder at the time of the first interview was associated with a significantly increased risk of viremia across the next 2.7 years. Forty-seven percent of subjects had viremia at 2.7 years of follow-up, reflective of chronic suboptimal medication adherence.
She noted that the pattern of psychiatric disorders in perinatally infected patients shifts between adolescence and young adulthood.
“By the time perinatally infected adolescents become young adults, I will say that anxiety and mood disorders become much more prevalent. But the number of psychiatric problems actually goes down by young adulthood,” according to Dr. Mellins.
Indeed, in another CASAH analysis she presented at AIDS 2016, this one involving 136 perinatally infected young adults and 86 perinatally exposed but uninfected controls, the vast majority living in impoverished communities, there was no difference between the two groups in rates of psychiatric or substance use disorders, although the 27% prevalence of substance use disorders is higher than that found in the age-matched general population.
Eighty-four percent of the perinatally infected 18- to 28-year-olds had graduated from high school, 94% were in a stable housing situation, 59% were currently working or in school, 54% were paying rent, and 95% reported ever being in a romantic relationship. Rates were similar in the perinatally exposed but uninfected group with the exception that these individuals were less likely to be paying rent.
“In spite of substantive risks, there is a relatively large portion of both groups with positive behavioral health outcomes, achieving normative young adult transition milestones. We need to understand why. Identification of protective factors conferring resilience can inform evidence-based prevention efforts, which are critical given the staggering numbers of children and young adolescents worldwide affected by HIV who will be transitioning to adulthood,” she said.
Dr. Mellins said the CASAH findings constitute a persuasive argument in favor of integrating mental health as a component of HIV care.
“Young people don’t always go to mental health appointments that are separate from medical care, so integrating mental health as a component of HIV care might be one of the most effective ways to identify and treat mental health problems in infected youth while simultaneously improving medication adherence and health outcomes,” Dr. Mellins said.
The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – Adolescents who were perinatally infected with HIV have a high prevalence of selected psychiatric disorders that impede their adherence to antiretroviral therapy, Claude Ann Mellins, PhD, reported at the 21st International AIDS Conference.
Those psychiatric diagnoses were predictive of viremia over the ensuing 2-3 years in a new analysis from the ongoing Child and Adolescent Self-Awareness and Health (CASAH) study, according to Dr. Mellins, professor of medical psychology at Columbia University, New York, and codirector of CASAH.
The clinical implications of the CASAH findings are clear, she added. “Assessing and treating specific categories of psychiatric and substance abuse problems may enhance efforts to improve adherence and prevent poor health outcomes in these adolescents and young adults, who are especially vulnerable due to their very challenging circumstances,” Dr. Mellins said.
CASAH is a longitudinal study of perinatally HIV-infected and perinatally HIV-exposed but uninfected New York City youth. They were enrolled during 2003-2008, when they were 9-16 years old. They and their caregivers undergo detailed psychosocial interviews every 12-18 months. The goal is to identify risk factors as well as protective factors influencing their behavioral health outcomes, the clinical psychologist explained.
She reported on 179 perinatally infected adolescents who were at least 13 years old at the first of their three interviews conducted over a 2.7-year period. Of note, 53% of them met Diagnostic Interview Schedule for Children (DISC-IV) criteria for one or more psychiatric diagnoses at all three time points. The pattern of psychopathology was somewhat different from that previously described in adults with HIV, who have been studied much more extensively than perinatally infected teens.
“Much of the literature on adults has focused on depression and mood disorders as predictors of poor health outcomes. Our data suggest that among youth, disruptive behavioral disorders – things like [attention-deficit/hyperactivity disorder], conduct disorder, or oppositional defiant disorder – may be just as important, if not more so. Substance abuse was also a critical factor,” Dr. Mellins said.
In a cross-sectional multivariate logistic regression analysis, a behavior disorder diagnosed at the first interview was associated with a 2.57-fold increased likelihood of contemporaneous viremia as evidenced by a plasma HIV RNA viral load greater than 1,000 copies/mL, and with a threefold increased likelihood of self-reported missed doses of antiretroviral medications during the previous week.
Anxiety disorder was the most common psychiatric diagnosis at the initial interview, followed by disruptive behavior disorder and substance use disorder. A diagnosis of any psychiatric disorder at the time of the first interview was associated with a significantly increased risk of viremia across the next 2.7 years. Forty-seven percent of subjects had viremia at 2.7 years of follow-up, reflective of chronic suboptimal medication adherence.
She noted that the pattern of psychiatric disorders in perinatally infected patients shifts between adolescence and young adulthood.
“By the time perinatally infected adolescents become young adults, I will say that anxiety and mood disorders become much more prevalent. But the number of psychiatric problems actually goes down by young adulthood,” according to Dr. Mellins.
Indeed, in another CASAH analysis she presented at AIDS 2016, this one involving 136 perinatally infected young adults and 86 perinatally exposed but uninfected controls, the vast majority living in impoverished communities, there was no difference between the two groups in rates of psychiatric or substance use disorders, although the 27% prevalence of substance use disorders is higher than that found in the age-matched general population.
Eighty-four percent of the perinatally infected 18- to 28-year-olds had graduated from high school, 94% were in a stable housing situation, 59% were currently working or in school, 54% were paying rent, and 95% reported ever being in a romantic relationship. Rates were similar in the perinatally exposed but uninfected group with the exception that these individuals were less likely to be paying rent.
“In spite of substantive risks, there is a relatively large portion of both groups with positive behavioral health outcomes, achieving normative young adult transition milestones. We need to understand why. Identification of protective factors conferring resilience can inform evidence-based prevention efforts, which are critical given the staggering numbers of children and young adolescents worldwide affected by HIV who will be transitioning to adulthood,” she said.
Dr. Mellins said the CASAH findings constitute a persuasive argument in favor of integrating mental health as a component of HIV care.
“Young people don’t always go to mental health appointments that are separate from medical care, so integrating mental health as a component of HIV care might be one of the most effective ways to identify and treat mental health problems in infected youth while simultaneously improving medication adherence and health outcomes,” Dr. Mellins said.
The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.
AT AIDS 2016
Key clinical point: Look for and treat psychiatric disorders in perinatally HIV-infected adolescents as a means of optimizing their antiretroviral medication adherence.
Major finding: A majority of perinatally HIV-infected adolescents meet the criteria for at least one psychiatric diagnosis, and they are at significantly increased risk for poor medication adherence and viremia during the next 2-3 years.
Data source: The longitudinal CASAH study involving prospective follow-up of several hundred perinatally HIV-infected and perinatally exposed but uninfected subjects through adolescence and young adulthood.
Disclosures: The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.

A few 20-shot sessions might be enough for deoxycholic acid
NEWPORT BEACH, CALIF. – It’s unclear how well deoxycholic acid (Kybella) will work in the clinic because doctors and patients are generally opting for fewer injections and fewer treatment sessions than were evaluated in phase III studies, according to Lawrence Bass, MD.
The fat cytolytic was approved in 2015 for shrinking double chins, with up to six 50-injection sessions. In trials, patients tended to get more than 40 shots in their first two sessions and more than 30 in subsequent sessions. At that dosing, 40.5% of patients in one trial and 46% in another lost at least 10% of their submental volume on MRI, according to Food and Drug Administration review documents.

However, at the Summit in Aesthetic Medicine, Dr. Bass, a plastic surgeon in New York City, said that, in clinical practice, patients are typically being treated with 20 injections for two or three sessions – partly because of cost. “This product costs $300 for each 2 mL vial, which means in a typical 20-injection treatment, you use $600 of material,” he noted. An average treatment session in Manhattan costs patients about $1,500. In other parts of the country, sessions are probably around $1,200 each, he added.
Also, the necks of patients enrolled in trials “had to be pretty big, but the necks we are probably going to treat with this are the smaller and medium ones. The big ones are just going to do liposuction or something else,” he said. Given all the variables, “we don’t know how well the study experience is going to match clinical experience.”
Dr. Bass treated his first postapproval patient, a 52-year-old woman, with two 20-injection treatment sessions 2 months apart. “The fat definitely cleaned out” and her skin looked a bit tighter, but it’s tough to know if her skin truly tightened or simply draped flatter, he said.
FDA labeling notes that “the safe and effective use of Kybella for the treatment of subcutaneous fat outside the submental region has not been established and is not recommended,” but this advice is unlikely to keep doctors from trying it in off-label areas.
One issue is that “almost every other area is a whole lot bigger” than a double chin, Dr. Bass said. Treating a tummy with 50 injections six to eight times, for example, would cost patients $12,000-$15,000, which is “a whole lot more than lipo,” he added.
Also, administering more than 50 injections at a time for a larger area is not possible because of toxicity. Trying to get around that limit and cut costs by diluting deoxycholic acid or spacing the injections farther apart doesn’t seem to be an option, since phase II testing showed a loss of efficacy with that approach.
Dr. Bass tried deoxycholic acid on a woman with leftover tummy bulges following liposuction. After two 40-injection sessions, “there was still a little shape there, so I don’t think I’ll be doing that again,” he said at the meeting, which is held by Global Academy for Medical Education. Global Academy and this news organization are owned the same company.
Gynecomastia, meanwhile, would probably require too many shots, and the jowl, another potential target, is too close to the marginal mandibular branch of the facial nerve, “so you are not supposed to inject there,” Dr. Bass said. Diluted deoxycholic acid might be an option for bulging periorbital fat, “but I am going to let somebody who is braver than me try that for a while before I go there.”
Dr. Bass is an investigator and speaker for Cynosure, an investigator for Endo Pharmaceuticals and Neothetics, and an advisor to Merz. He participated in phase III testing of deoxycholic acid.
The indication approved for deoxycholic acid is “for improvement in the appearance of moderate to severe convexity or fullness associated with submental fat in adults.”
NEWPORT BEACH, CALIF. – It’s unclear how well deoxycholic acid (Kybella) will work in the clinic because doctors and patients are generally opting for fewer injections and fewer treatment sessions than were evaluated in phase III studies, according to Lawrence Bass, MD.
The fat cytolytic was approved in 2015 for shrinking double chins, with up to six 50-injection sessions. In trials, patients tended to get more than 40 shots in their first two sessions and more than 30 in subsequent sessions. At that dosing, 40.5% of patients in one trial and 46% in another lost at least 10% of their submental volume on MRI, according to Food and Drug Administration review documents.
However, at the Summit in Aesthetic Medicine, Dr. Bass, a plastic surgeon in New York City, said that, in clinical practice, patients are typically being treated with 20 injections for two or three sessions – partly because of cost. “This product costs $300 for each 2 mL vial, which means in a typical 20-injection treatment, you use $600 of material,” he noted. An average treatment session in Manhattan costs patients about $1,500. In other parts of the country, sessions are probably around $1,200 each, he added.
Also, the necks of patients enrolled in trials “had to be pretty big, but the necks we are probably going to treat with this are the smaller and medium ones. The big ones are just going to do liposuction or something else,” he said. Given all the variables, “we don’t know how well the study experience is going to match clinical experience.”
Dr. Bass treated his first postapproval patient, a 52-year-old woman, with two 20-injection treatment sessions 2 months apart. “The fat definitely cleaned out” and her skin looked a bit tighter, but it’s tough to know if her skin truly tightened or simply draped flatter, he said.
FDA labeling notes that “the safe and effective use of Kybella for the treatment of subcutaneous fat outside the submental region has not been established and is not recommended,” but this advice is unlikely to keep doctors from trying it in off-label areas.
One issue is that “almost every other area is a whole lot bigger” than a double chin, Dr. Bass said. Treating a tummy with 50 injections six to eight times, for example, would cost patients $12,000-$15,000, which is “a whole lot more than lipo,” he added.
Also, administering more than 50 injections at a time for a larger area is not possible because of toxicity. Trying to get around that limit and cut costs by diluting deoxycholic acid or spacing the injections farther apart doesn’t seem to be an option, since phase II testing showed a loss of efficacy with that approach.
Dr. Bass tried deoxycholic acid on a woman with leftover tummy bulges following liposuction. After two 40-injection sessions, “there was still a little shape there, so I don’t think I’ll be doing that again,” he said at the meeting, which is held by Global Academy for Medical Education. Global Academy and this news organization are owned the same company.
Gynecomastia, meanwhile, would probably require too many shots, and the jowl, another potential target, is too close to the marginal mandibular branch of the facial nerve, “so you are not supposed to inject there,” Dr. Bass said. Diluted deoxycholic acid might be an option for bulging periorbital fat, “but I am going to let somebody who is braver than me try that for a while before I go there.”
Dr. Bass is an investigator and speaker for Cynosure, an investigator for Endo Pharmaceuticals and Neothetics, and an advisor to Merz. He participated in phase III testing of deoxycholic acid.
The indication approved for deoxycholic acid is “for improvement in the appearance of moderate to severe convexity or fullness associated with submental fat in adults.”
NEWPORT BEACH, CALIF. – It’s unclear how well deoxycholic acid (Kybella) will work in the clinic because doctors and patients are generally opting for fewer injections and fewer treatment sessions than were evaluated in phase III studies, according to Lawrence Bass, MD.
The fat cytolytic was approved in 2015 for shrinking double chins, with up to six 50-injection sessions. In trials, patients tended to get more than 40 shots in their first two sessions and more than 30 in subsequent sessions. At that dosing, 40.5% of patients in one trial and 46% in another lost at least 10% of their submental volume on MRI, according to Food and Drug Administration review documents.
However, at the Summit in Aesthetic Medicine, Dr. Bass, a plastic surgeon in New York City, said that, in clinical practice, patients are typically being treated with 20 injections for two or three sessions – partly because of cost. “This product costs $300 for each 2 mL vial, which means in a typical 20-injection treatment, you use $600 of material,” he noted. An average treatment session in Manhattan costs patients about $1,500. In other parts of the country, sessions are probably around $1,200 each, he added.
Also, the necks of patients enrolled in trials “had to be pretty big, but the necks we are probably going to treat with this are the smaller and medium ones. The big ones are just going to do liposuction or something else,” he said. Given all the variables, “we don’t know how well the study experience is going to match clinical experience.”
Dr. Bass treated his first postapproval patient, a 52-year-old woman, with two 20-injection treatment sessions 2 months apart. “The fat definitely cleaned out” and her skin looked a bit tighter, but it’s tough to know if her skin truly tightened or simply draped flatter, he said.
FDA labeling notes that “the safe and effective use of Kybella for the treatment of subcutaneous fat outside the submental region has not been established and is not recommended,” but this advice is unlikely to keep doctors from trying it in off-label areas.
One issue is that “almost every other area is a whole lot bigger” than a double chin, Dr. Bass said. Treating a tummy with 50 injections six to eight times, for example, would cost patients $12,000-$15,000, which is “a whole lot more than lipo,” he added.
Also, administering more than 50 injections at a time for a larger area is not possible because of toxicity. Trying to get around that limit and cut costs by diluting deoxycholic acid or spacing the injections farther apart doesn’t seem to be an option, since phase II testing showed a loss of efficacy with that approach.
Dr. Bass tried deoxycholic acid on a woman with leftover tummy bulges following liposuction. After two 40-injection sessions, “there was still a little shape there, so I don’t think I’ll be doing that again,” he said at the meeting, which is held by Global Academy for Medical Education. Global Academy and this news organization are owned the same company.
Gynecomastia, meanwhile, would probably require too many shots, and the jowl, another potential target, is too close to the marginal mandibular branch of the facial nerve, “so you are not supposed to inject there,” Dr. Bass said. Diluted deoxycholic acid might be an option for bulging periorbital fat, “but I am going to let somebody who is braver than me try that for a while before I go there.”
Dr. Bass is an investigator and speaker for Cynosure, an investigator for Endo Pharmaceuticals and Neothetics, and an advisor to Merz. He participated in phase III testing of deoxycholic acid.
The indication approved for deoxycholic acid is “for improvement in the appearance of moderate to severe convexity or fullness associated with submental fat in adults.”
EXPERT ANALYSIS FROM THE SUMMIT IN AESTHETIC MEDICINE

Veteran Homelessness Drops 47% Since 2010
In the latest Department of Housing and Urban Development annual Point-in-Time (PIT) estimate of America’s homeless population, President Barak Obama revealed that since 2010 the rate of homelessness among veterans has dropped 47%. The January count found 13,000 homeless veterans, although the count fell well short of the President’s pledge to completely eliminate homelessness by 2016. “We will not stop until every veteran who fought for America has a home in America,” President Obama told the national Disabled American Veterans (DAV) convention on August 1. “This is something we’ve got to get done.”
“The dramatic decline in veteran homelessness is the result of the Obama administration’s investments in permanent supportive housing solutions, such as HUD-VASH [Housing and Urban Development-VA Supportive Housing] and Supportive Services for Veteran Families programs, extensive community partnerships, coordinated data and outreach, and other proven strategies that put Veterans first,” said VA Secretary Robert A. McDonald in a release. According to the VA, Virginia, Connecticut and 27 cities and towns across the country have “effectively ended” veteran homelessness.
In the DAV speech, President Obama also touted a number of VA health care programs, ranging from rural telehealth initiatives to increased funding for prosthetics and access to women’s health providers at all VA clinics. Pointing out that VA funding has increased during his administration, the President noted that “We’ve made VA benefits available to more than 2 million veterans who didn’t have them before.” The President also pointed out that veterans can apply for VA health care “…from any device, including your smartphone—simple, easy, in as little as 20 minutes.”
The White House also announced that the Million Veteran Program (MVP) had reached a new milestone with 500,000 veterans enrolled. About 62% of MVP enrollees reported a current or past diagnosis of high blood pressure and about one-third reported tinnitus. Also, nearly one-third, or 32%, of veterans present with a history or current diagnosis of cancer. “We believe MVP will accelerate our understanding of disease detection, progression, prevention and treatment by combining this rich clinical, environmental and genomic data,” said VA Under Secretary for Health David J. Shulkin, MD, in a statement. “VA has a deep history of innovation and research. The MVP will allow the nation’s top researchers to perform the most cutting-edge science to treat some of the nation’s most troubling diseases.”
“What this does is it gives us a better understanding of genetics, which will allow us to improve treatments for things like traumatic brain injury and posttraumatic stress, and diabetes, and cancer,” President Obama told the DAV audience. “And that won’t just help veterans. It will help all Americans. And it’s just one more example of how our veterans keep serving our country even after they come home.”
While Acknowledging the VA’s challenges to meet the needs of veterans, President Obama was insistent that VA care was essential for veterans. “Study after study shows that in many areas, like mental health, the quality of care at the VA is often better than in private care,” he told the DAV members. “So let’s listen to our veterans, who are telling us: Don’t destroy VA health care. Fix it and make it work, but don’t break our covenant with our veterans.”
In the latest Department of Housing and Urban Development annual Point-in-Time (PIT) estimate of America’s homeless population, President Barak Obama revealed that since 2010 the rate of homelessness among veterans has dropped 47%. The January count found 13,000 homeless veterans, although the count fell well short of the President’s pledge to completely eliminate homelessness by 2016. “We will not stop until every veteran who fought for America has a home in America,” President Obama told the national Disabled American Veterans (DAV) convention on August 1. “This is something we’ve got to get done.”
“The dramatic decline in veteran homelessness is the result of the Obama administration’s investments in permanent supportive housing solutions, such as HUD-VASH [Housing and Urban Development-VA Supportive Housing] and Supportive Services for Veteran Families programs, extensive community partnerships, coordinated data and outreach, and other proven strategies that put Veterans first,” said VA Secretary Robert A. McDonald in a release. According to the VA, Virginia, Connecticut and 27 cities and towns across the country have “effectively ended” veteran homelessness.
In the DAV speech, President Obama also touted a number of VA health care programs, ranging from rural telehealth initiatives to increased funding for prosthetics and access to women’s health providers at all VA clinics. Pointing out that VA funding has increased during his administration, the President noted that “We’ve made VA benefits available to more than 2 million veterans who didn’t have them before.” The President also pointed out that veterans can apply for VA health care “…from any device, including your smartphone—simple, easy, in as little as 20 minutes.”
The White House also announced that the Million Veteran Program (MVP) had reached a new milestone with 500,000 veterans enrolled. About 62% of MVP enrollees reported a current or past diagnosis of high blood pressure and about one-third reported tinnitus. Also, nearly one-third, or 32%, of veterans present with a history or current diagnosis of cancer. “We believe MVP will accelerate our understanding of disease detection, progression, prevention and treatment by combining this rich clinical, environmental and genomic data,” said VA Under Secretary for Health David J. Shulkin, MD, in a statement. “VA has a deep history of innovation and research. The MVP will allow the nation’s top researchers to perform the most cutting-edge science to treat some of the nation’s most troubling diseases.”
“What this does is it gives us a better understanding of genetics, which will allow us to improve treatments for things like traumatic brain injury and posttraumatic stress, and diabetes, and cancer,” President Obama told the DAV audience. “And that won’t just help veterans. It will help all Americans. And it’s just one more example of how our veterans keep serving our country even after they come home.”
While Acknowledging the VA’s challenges to meet the needs of veterans, President Obama was insistent that VA care was essential for veterans. “Study after study shows that in many areas, like mental health, the quality of care at the VA is often better than in private care,” he told the DAV members. “So let’s listen to our veterans, who are telling us: Don’t destroy VA health care. Fix it and make it work, but don’t break our covenant with our veterans.”
In the latest Department of Housing and Urban Development annual Point-in-Time (PIT) estimate of America’s homeless population, President Barak Obama revealed that since 2010 the rate of homelessness among veterans has dropped 47%. The January count found 13,000 homeless veterans, although the count fell well short of the President’s pledge to completely eliminate homelessness by 2016. “We will not stop until every veteran who fought for America has a home in America,” President Obama told the national Disabled American Veterans (DAV) convention on August 1. “This is something we’ve got to get done.”
“The dramatic decline in veteran homelessness is the result of the Obama administration’s investments in permanent supportive housing solutions, such as HUD-VASH [Housing and Urban Development-VA Supportive Housing] and Supportive Services for Veteran Families programs, extensive community partnerships, coordinated data and outreach, and other proven strategies that put Veterans first,” said VA Secretary Robert A. McDonald in a release. According to the VA, Virginia, Connecticut and 27 cities and towns across the country have “effectively ended” veteran homelessness.
In the DAV speech, President Obama also touted a number of VA health care programs, ranging from rural telehealth initiatives to increased funding for prosthetics and access to women’s health providers at all VA clinics. Pointing out that VA funding has increased during his administration, the President noted that “We’ve made VA benefits available to more than 2 million veterans who didn’t have them before.” The President also pointed out that veterans can apply for VA health care “…from any device, including your smartphone—simple, easy, in as little as 20 minutes.”
The White House also announced that the Million Veteran Program (MVP) had reached a new milestone with 500,000 veterans enrolled. About 62% of MVP enrollees reported a current or past diagnosis of high blood pressure and about one-third reported tinnitus. Also, nearly one-third, or 32%, of veterans present with a history or current diagnosis of cancer. “We believe MVP will accelerate our understanding of disease detection, progression, prevention and treatment by combining this rich clinical, environmental and genomic data,” said VA Under Secretary for Health David J. Shulkin, MD, in a statement. “VA has a deep history of innovation and research. The MVP will allow the nation’s top researchers to perform the most cutting-edge science to treat some of the nation’s most troubling diseases.”
“What this does is it gives us a better understanding of genetics, which will allow us to improve treatments for things like traumatic brain injury and posttraumatic stress, and diabetes, and cancer,” President Obama told the DAV audience. “And that won’t just help veterans. It will help all Americans. And it’s just one more example of how our veterans keep serving our country even after they come home.”
While Acknowledging the VA’s challenges to meet the needs of veterans, President Obama was insistent that VA care was essential for veterans. “Study after study shows that in many areas, like mental health, the quality of care at the VA is often better than in private care,” he told the DAV members. “So let’s listen to our veterans, who are telling us: Don’t destroy VA health care. Fix it and make it work, but don’t break our covenant with our veterans.”
Preorder 2016 State of Hospital Medicine Report
The State of Hospital Medicine (SoHM) report is the most comprehensive survey of hospital medicine in the country and provides current data on hospitalist compensation and productivity, plus covers practice demographics, staffing levels, staff growth, and compensation models.
Order now and be notified directly when the report is released in September 2016 at www.hospitalmedicine.org/survey.
The State of Hospital Medicine (SoHM) report is the most comprehensive survey of hospital medicine in the country and provides current data on hospitalist compensation and productivity, plus covers practice demographics, staffing levels, staff growth, and compensation models.
Order now and be notified directly when the report is released in September 2016 at www.hospitalmedicine.org/survey.
The State of Hospital Medicine (SoHM) report is the most comprehensive survey of hospital medicine in the country and provides current data on hospitalist compensation and productivity, plus covers practice demographics, staffing levels, staff growth, and compensation models.
Order now and be notified directly when the report is released in September 2016 at www.hospitalmedicine.org/survey.
PAs, NPs: Register for 2016 Adult Hospital Medicine Boot Camp

During the course, you will:
- Learn the most current evidence-based clinical practices for key topics in hospital medicine
- Augment your knowledge base to enhance your existing hospital medicine practice
- Expand your knowledge to transition into hospital medicine practice
- Network with like-minded practitioners
To learn more and register, visit www.aapa.org/bootcamp.
During the course, you will:
- Learn the most current evidence-based clinical practices for key topics in hospital medicine
- Augment your knowledge base to enhance your existing hospital medicine practice
- Expand your knowledge to transition into hospital medicine practice
- Network with like-minded practitioners
To learn more and register, visit www.aapa.org/bootcamp.
During the course, you will:
- Learn the most current evidence-based clinical practices for key topics in hospital medicine
- Augment your knowledge base to enhance your existing hospital medicine practice
- Expand your knowledge to transition into hospital medicine practice
- Network with like-minded practitioners
To learn more and register, visit www.aapa.org/bootcamp.

Gene therapy reduces need for FIX prophylaxis

Image courtesy of NIGMS
ORLANDO—The gene therapy AMT-060 can reduce the need for factor IX (FIX) prophylaxis in patients with severe hemophilia B, results of a phase 1/2 study suggest.
All of the patients treated in the low-dose cohort of this study have had sustained improvements in their disease phenotype and continue to maintain durable levels of FIX gene activity for up to 39 weeks post-treatment.
Four of the 5 patients were able to discontinue prophylactic FIX infusions.
In addition, AMT-060 was considered well-tolerated. There were 2 serious adverse events, but both were temporary. And none of the patients developed FIX inhibitors.
These data were presented at the World Federation of Hemophilia 2016 World Congress.* The research is sponsored by uniQure.
“I am very encouraged by the stability of increased FIX activity of AMT-060 and the significant reduction in required infusions of factor replacement,” said study investigator Wolfgang Miesbach, MD, of the University of Frankfurt in Germany.
“This effect is particularly important because it is seen in severe patients with established joint disease who experienced a high frequency of joint bleeds despite intense use of prophylactic FIX prior to study entry.”
Patients and treatment
AMT-060 consists of a codon-optimized wild-type FIX gene cassette, the LP1 liver promoter, and an AAV5 viral vector manufactured by uniQure using its proprietary insect cell-based technology platform.
In this phase 1/2 trial, Dr Miesbach and his colleagues are testing AMT-060 in 10 patients. All patients had severe or moderately severe hemophilia at baseline, including documented FIX levels less than 1% to 2% of normal, and required chronic infusions of prophylactic or on-demand FIX therapy at the time of enrollment.
Each patient received a 1-time, 30-minute, intravenous dose of AMT-060, without the use of corticosteroids. Five patients received AMT-060 at 5x1012 gc/kg, and 5 received AMT-060 at 2x1013 gc/kg.
Dr Miesbach presented results observed in the low-dose cohort. Patients in the high-dose cohort are still in the early stages of follow-up.
Most patients in the low-dose cohort were older than 50 years of age (range, 35-72). Four patients had severe hemophilia B, and 4 had advanced joint disease. All of the patients had frequent bleeding episodes, despite receiving once- or twice-weekly FIX prophylaxis.
Efficacy
For all 5 patients in the low-dose cohort, the mean annualized total FIX usage declined 75% after treatment with AMT-060.
“The majority of patients in this low-dose cohort of AMT-060 are showing FIX activity in the range of 5% of normal, and clinical experience has shown that patients in this range generally do not require prophylactic factor replacement and have a very low frequency of spontaneous joint bleeding episodes,” Dr Miesbach said.
Four patients discontinued prophylactic therapy. The 1 patient who remained on prophylactic therapy has sustained an improved disease phenotype and also required materially less FIX concentrate after treatment with AMT-060.
Through up to 9 months of follow-up, the mean steady-state FIX activity for the 4 patients who discontinued prophylactic FIX therapy was 5.4% of normal, with a range from 3.1% to 6.7% of normal. These patients had a mean reduction in annualized total FIX usage of 82%.
Safety and immunogenicity
Two patients experienced serious adverse events. One patient had self-limiting fever in the first 24 hours after receiving AMT-060.
The other patient had a transient elevation of alanine aminotransferase (ALT) that was responsive to tapering prednisolone (60 mg/day start dose) without loss of FIX activity. At baseline, this patient’s ALT was 26 IU/L. It hit a peak of 61 IU/L at week 10, but values returned to baseline levels within 2 weeks of treatment.
As expected, all of the patients developed anti-AAV5 antibodies after week 1. None of the patients developed inhibitory antibodies against FIX.
There was no evidence of sustained AAV5 capsid-specific T-cell activation, although 1 patient had transient T-cell activation slightly above the positive threshold at 1 time point. This patient did not have ALT elevation. ![]()
*Miesbach W et al, Updated results from a dose escalating study in adult patients with haemophilia B treated with AMT-060 (AAV5-hFIX) gene therapy, WFH 2016 World
Congress, July 2016.
Image courtesy of NIGMS
ORLANDO—The gene therapy AMT-060 can reduce the need for factor IX (FIX) prophylaxis in patients with severe hemophilia B, results of a phase 1/2 study suggest.
All of the patients treated in the low-dose cohort of this study have had sustained improvements in their disease phenotype and continue to maintain durable levels of FIX gene activity for up to 39 weeks post-treatment.
Four of the 5 patients were able to discontinue prophylactic FIX infusions.
In addition, AMT-060 was considered well-tolerated. There were 2 serious adverse events, but both were temporary. And none of the patients developed FIX inhibitors.
These data were presented at the World Federation of Hemophilia 2016 World Congress.* The research is sponsored by uniQure.
“I am very encouraged by the stability of increased FIX activity of AMT-060 and the significant reduction in required infusions of factor replacement,” said study investigator Wolfgang Miesbach, MD, of the University of Frankfurt in Germany.
“This effect is particularly important because it is seen in severe patients with established joint disease who experienced a high frequency of joint bleeds despite intense use of prophylactic FIX prior to study entry.”
Patients and treatment
AMT-060 consists of a codon-optimized wild-type FIX gene cassette, the LP1 liver promoter, and an AAV5 viral vector manufactured by uniQure using its proprietary insect cell-based technology platform.
In this phase 1/2 trial, Dr Miesbach and his colleagues are testing AMT-060 in 10 patients. All patients had severe or moderately severe hemophilia at baseline, including documented FIX levels less than 1% to 2% of normal, and required chronic infusions of prophylactic or on-demand FIX therapy at the time of enrollment.
Each patient received a 1-time, 30-minute, intravenous dose of AMT-060, without the use of corticosteroids. Five patients received AMT-060 at 5x1012 gc/kg, and 5 received AMT-060 at 2x1013 gc/kg.
Dr Miesbach presented results observed in the low-dose cohort. Patients in the high-dose cohort are still in the early stages of follow-up.
Most patients in the low-dose cohort were older than 50 years of age (range, 35-72). Four patients had severe hemophilia B, and 4 had advanced joint disease. All of the patients had frequent bleeding episodes, despite receiving once- or twice-weekly FIX prophylaxis.
Efficacy
For all 5 patients in the low-dose cohort, the mean annualized total FIX usage declined 75% after treatment with AMT-060.
“The majority of patients in this low-dose cohort of AMT-060 are showing FIX activity in the range of 5% of normal, and clinical experience has shown that patients in this range generally do not require prophylactic factor replacement and have a very low frequency of spontaneous joint bleeding episodes,” Dr Miesbach said.
Four patients discontinued prophylactic therapy. The 1 patient who remained on prophylactic therapy has sustained an improved disease phenotype and also required materially less FIX concentrate after treatment with AMT-060.
Through up to 9 months of follow-up, the mean steady-state FIX activity for the 4 patients who discontinued prophylactic FIX therapy was 5.4% of normal, with a range from 3.1% to 6.7% of normal. These patients had a mean reduction in annualized total FIX usage of 82%.
Safety and immunogenicity
Two patients experienced serious adverse events. One patient had self-limiting fever in the first 24 hours after receiving AMT-060.
The other patient had a transient elevation of alanine aminotransferase (ALT) that was responsive to tapering prednisolone (60 mg/day start dose) without loss of FIX activity. At baseline, this patient’s ALT was 26 IU/L. It hit a peak of 61 IU/L at week 10, but values returned to baseline levels within 2 weeks of treatment.
As expected, all of the patients developed anti-AAV5 antibodies after week 1. None of the patients developed inhibitory antibodies against FIX.
There was no evidence of sustained AAV5 capsid-specific T-cell activation, although 1 patient had transient T-cell activation slightly above the positive threshold at 1 time point. This patient did not have ALT elevation. ![]()
*Miesbach W et al, Updated results from a dose escalating study in adult patients with haemophilia B treated with AMT-060 (AAV5-hFIX) gene therapy, WFH 2016 World
Congress, July 2016.
Image courtesy of NIGMS
ORLANDO—The gene therapy AMT-060 can reduce the need for factor IX (FIX) prophylaxis in patients with severe hemophilia B, results of a phase 1/2 study suggest.
All of the patients treated in the low-dose cohort of this study have had sustained improvements in their disease phenotype and continue to maintain durable levels of FIX gene activity for up to 39 weeks post-treatment.
Four of the 5 patients were able to discontinue prophylactic FIX infusions.
In addition, AMT-060 was considered well-tolerated. There were 2 serious adverse events, but both were temporary. And none of the patients developed FIX inhibitors.
These data were presented at the World Federation of Hemophilia 2016 World Congress.* The research is sponsored by uniQure.
“I am very encouraged by the stability of increased FIX activity of AMT-060 and the significant reduction in required infusions of factor replacement,” said study investigator Wolfgang Miesbach, MD, of the University of Frankfurt in Germany.
“This effect is particularly important because it is seen in severe patients with established joint disease who experienced a high frequency of joint bleeds despite intense use of prophylactic FIX prior to study entry.”
Patients and treatment
AMT-060 consists of a codon-optimized wild-type FIX gene cassette, the LP1 liver promoter, and an AAV5 viral vector manufactured by uniQure using its proprietary insect cell-based technology platform.
In this phase 1/2 trial, Dr Miesbach and his colleagues are testing AMT-060 in 10 patients. All patients had severe or moderately severe hemophilia at baseline, including documented FIX levels less than 1% to 2% of normal, and required chronic infusions of prophylactic or on-demand FIX therapy at the time of enrollment.
Each patient received a 1-time, 30-minute, intravenous dose of AMT-060, without the use of corticosteroids. Five patients received AMT-060 at 5x1012 gc/kg, and 5 received AMT-060 at 2x1013 gc/kg.
Dr Miesbach presented results observed in the low-dose cohort. Patients in the high-dose cohort are still in the early stages of follow-up.
Most patients in the low-dose cohort were older than 50 years of age (range, 35-72). Four patients had severe hemophilia B, and 4 had advanced joint disease. All of the patients had frequent bleeding episodes, despite receiving once- or twice-weekly FIX prophylaxis.
Efficacy
For all 5 patients in the low-dose cohort, the mean annualized total FIX usage declined 75% after treatment with AMT-060.
“The majority of patients in this low-dose cohort of AMT-060 are showing FIX activity in the range of 5% of normal, and clinical experience has shown that patients in this range generally do not require prophylactic factor replacement and have a very low frequency of spontaneous joint bleeding episodes,” Dr Miesbach said.
Four patients discontinued prophylactic therapy. The 1 patient who remained on prophylactic therapy has sustained an improved disease phenotype and also required materially less FIX concentrate after treatment with AMT-060.
Through up to 9 months of follow-up, the mean steady-state FIX activity for the 4 patients who discontinued prophylactic FIX therapy was 5.4% of normal, with a range from 3.1% to 6.7% of normal. These patients had a mean reduction in annualized total FIX usage of 82%.
Safety and immunogenicity
Two patients experienced serious adverse events. One patient had self-limiting fever in the first 24 hours after receiving AMT-060.
The other patient had a transient elevation of alanine aminotransferase (ALT) that was responsive to tapering prednisolone (60 mg/day start dose) without loss of FIX activity. At baseline, this patient’s ALT was 26 IU/L. It hit a peak of 61 IU/L at week 10, but values returned to baseline levels within 2 weeks of treatment.
As expected, all of the patients developed anti-AAV5 antibodies after week 1. None of the patients developed inhibitory antibodies against FIX.
There was no evidence of sustained AAV5 capsid-specific T-cell activation, although 1 patient had transient T-cell activation slightly above the positive threshold at 1 time point. This patient did not have ALT elevation. ![]()
*Miesbach W et al, Updated results from a dose escalating study in adult patients with haemophilia B treated with AMT-060 (AAV5-hFIX) gene therapy, WFH 2016 World
Congress, July 2016.
Microneedle system could replace blood draws, team says
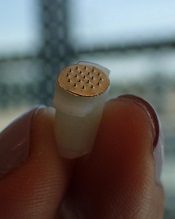
Photo courtesy of
Sahan Ranamukhaarachchi
A new microneedle drug monitoring system could one day replace invasive blood draws, according to researchers.
The system consists of a small, thin patch that is pressed against a patient’s arm during medical treatment and measures drugs in the bloodstream painlessly without drawing any blood.
The tiny projections on this patch resemble hollow cones and don’t pierce the skin like a standard hypodermic needle.
The researchers described this system in Scientific Reports.
“Many groups are researching microneedle technology for painless vaccines and drug delivery,” said study author Sahan Ranamukhaarachchi, a PhD student at the University of British Columbia (UBC) in Vancouver, British Columbia, Canada. “Using them to painlessly monitor drugs is a newer idea.”
The microneedle system Ranamukhaarachchi and his colleagues created was developed to monitor the antibiotic vancomycin. Patients taking vancomycin must be closely monitored because the drug can cause life-threatening side effects, so the patients undergo 3 to 4 blood draws per day.
The researchers discovered they could use fluid found just below the outer layer of skin, instead of blood, to monitor levels of vancomycin in the bloodstream.
The microneedle patch collects a tiny amount of the fluid, less than 1 nL, and a reaction occurs on the inside of the microneedles that can be detected using an optical sensor. This allows the user to quickly determine the concentration of vancomycin.
“This is probably one of the smallest probe volumes ever recorded for a medically relevant analysis,” said study author Urs Häfeli, PhD, of UBC.
This microneedle drug monitoring system was developed out of a research collaboration between Dr Häfeli and Boris Stoeber, PhD, also of UBC. The system is being commercialized by the UBC spin-off Microdermics Inc. ![]()
Photo courtesy of
Sahan Ranamukhaarachchi
A new microneedle drug monitoring system could one day replace invasive blood draws, according to researchers.
The system consists of a small, thin patch that is pressed against a patient’s arm during medical treatment and measures drugs in the bloodstream painlessly without drawing any blood.
The tiny projections on this patch resemble hollow cones and don’t pierce the skin like a standard hypodermic needle.
The researchers described this system in Scientific Reports.
“Many groups are researching microneedle technology for painless vaccines and drug delivery,” said study author Sahan Ranamukhaarachchi, a PhD student at the University of British Columbia (UBC) in Vancouver, British Columbia, Canada. “Using them to painlessly monitor drugs is a newer idea.”
The microneedle system Ranamukhaarachchi and his colleagues created was developed to monitor the antibiotic vancomycin. Patients taking vancomycin must be closely monitored because the drug can cause life-threatening side effects, so the patients undergo 3 to 4 blood draws per day.
The researchers discovered they could use fluid found just below the outer layer of skin, instead of blood, to monitor levels of vancomycin in the bloodstream.
The microneedle patch collects a tiny amount of the fluid, less than 1 nL, and a reaction occurs on the inside of the microneedles that can be detected using an optical sensor. This allows the user to quickly determine the concentration of vancomycin.
“This is probably one of the smallest probe volumes ever recorded for a medically relevant analysis,” said study author Urs Häfeli, PhD, of UBC.
This microneedle drug monitoring system was developed out of a research collaboration between Dr Häfeli and Boris Stoeber, PhD, also of UBC. The system is being commercialized by the UBC spin-off Microdermics Inc. ![]()
Photo courtesy of
Sahan Ranamukhaarachchi
A new microneedle drug monitoring system could one day replace invasive blood draws, according to researchers.
The system consists of a small, thin patch that is pressed against a patient’s arm during medical treatment and measures drugs in the bloodstream painlessly without drawing any blood.
The tiny projections on this patch resemble hollow cones and don’t pierce the skin like a standard hypodermic needle.
The researchers described this system in Scientific Reports.
“Many groups are researching microneedle technology for painless vaccines and drug delivery,” said study author Sahan Ranamukhaarachchi, a PhD student at the University of British Columbia (UBC) in Vancouver, British Columbia, Canada. “Using them to painlessly monitor drugs is a newer idea.”
The microneedle system Ranamukhaarachchi and his colleagues created was developed to monitor the antibiotic vancomycin. Patients taking vancomycin must be closely monitored because the drug can cause life-threatening side effects, so the patients undergo 3 to 4 blood draws per day.
The researchers discovered they could use fluid found just below the outer layer of skin, instead of blood, to monitor levels of vancomycin in the bloodstream.
The microneedle patch collects a tiny amount of the fluid, less than 1 nL, and a reaction occurs on the inside of the microneedles that can be detected using an optical sensor. This allows the user to quickly determine the concentration of vancomycin.
“This is probably one of the smallest probe volumes ever recorded for a medically relevant analysis,” said study author Urs Häfeli, PhD, of UBC.
This microneedle drug monitoring system was developed out of a research collaboration between Dr Häfeli and Boris Stoeber, PhD, also of UBC. The system is being commercialized by the UBC spin-off Microdermics Inc. ![]()
FDA approves reconstitution system for FVIII product

Photo courtesy of Baxalta
The US Food and Drug Administration (FDA) has approved the Baxject III reconstitution system for Adynovate, a pegylated recombinant factor VIII (FVIII) product.
The system is designed to mix a FVIII product with a diluent prior to infusion.
The Baxject III reconstitution system was previously FDA-approved for use with Advate, a recombinant FVIII product.
The latest FDA approval means the system will be available with Adynovate as well.
Adynovate and the diluent will come pre-packaged in the reconstitution system.
The Baxject III reconstitution system with Adynovate will be available to most customers in the fourth quarter of 2016, with a 2 mL diluent for the 250, 500, and 1000 IU potencies; and a 5 mL diluent for the 2000 IU potency.
Adynovate was approved by the FDA in 2015 for use in hemophilia A patients age 12 and older for on-demand treatment and control of bleeding and for prophylaxis to reduce the frequency of bleeding episodes. Full prescribing information is available here.
Advate was first approved by the FDA in 2003. The product is indicated for use in children and adults with hemophilia A for the control and prevention of bleeding episodes, perioperative management, and routine prophylaxis to prevent or reduce the frequency of bleeding episodes. Full prescribing information is available here.
The Baxject III reconstitution system, Adynovate, and Advate are all products of Baxalta, which is now a part of Shire. ![]()
Photo courtesy of Baxalta
The US Food and Drug Administration (FDA) has approved the Baxject III reconstitution system for Adynovate, a pegylated recombinant factor VIII (FVIII) product.
The system is designed to mix a FVIII product with a diluent prior to infusion.
The Baxject III reconstitution system was previously FDA-approved for use with Advate, a recombinant FVIII product.
The latest FDA approval means the system will be available with Adynovate as well.
Adynovate and the diluent will come pre-packaged in the reconstitution system.
The Baxject III reconstitution system with Adynovate will be available to most customers in the fourth quarter of 2016, with a 2 mL diluent for the 250, 500, and 1000 IU potencies; and a 5 mL diluent for the 2000 IU potency.
Adynovate was approved by the FDA in 2015 for use in hemophilia A patients age 12 and older for on-demand treatment and control of bleeding and for prophylaxis to reduce the frequency of bleeding episodes. Full prescribing information is available here.
Advate was first approved by the FDA in 2003. The product is indicated for use in children and adults with hemophilia A for the control and prevention of bleeding episodes, perioperative management, and routine prophylaxis to prevent or reduce the frequency of bleeding episodes. Full prescribing information is available here.
The Baxject III reconstitution system, Adynovate, and Advate are all products of Baxalta, which is now a part of Shire. ![]()
Photo courtesy of Baxalta
The US Food and Drug Administration (FDA) has approved the Baxject III reconstitution system for Adynovate, a pegylated recombinant factor VIII (FVIII) product.
The system is designed to mix a FVIII product with a diluent prior to infusion.
The Baxject III reconstitution system was previously FDA-approved for use with Advate, a recombinant FVIII product.
The latest FDA approval means the system will be available with Adynovate as well.
Adynovate and the diluent will come pre-packaged in the reconstitution system.
The Baxject III reconstitution system with Adynovate will be available to most customers in the fourth quarter of 2016, with a 2 mL diluent for the 250, 500, and 1000 IU potencies; and a 5 mL diluent for the 2000 IU potency.
Adynovate was approved by the FDA in 2015 for use in hemophilia A patients age 12 and older for on-demand treatment and control of bleeding and for prophylaxis to reduce the frequency of bleeding episodes. Full prescribing information is available here.
Advate was first approved by the FDA in 2003. The product is indicated for use in children and adults with hemophilia A for the control and prevention of bleeding episodes, perioperative management, and routine prophylaxis to prevent or reduce the frequency of bleeding episodes. Full prescribing information is available here.
The Baxject III reconstitution system, Adynovate, and Advate are all products of Baxalta, which is now a part of Shire. ![]()
HDAC inhibitor granted breakthrough designation

Image by Eric Smith
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for the histone deacetylase (HDAC) inhibitor pracinostat to be used in combination with azacitidine to treat newly diagnosed acute myeloid leukemia (AML) patients who are 75 and older or unfit for intensive chemotherapy.
The FDA’s breakthrough designation is intended to expedite the development and review of new therapies for serious or life-threatening conditions.
To earn the designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
The breakthrough therapy designation for pracinostat is supported by data from a phase 2 study of the HDAC inhibitor in combination with azacitidine in elderly patients with newly diagnosed AML who were not candidates for induction chemotherapy.
Detailed results from this trial were presented at the 20th Congress of the European Hematology Association last year. The research was sponsored by MEI Pharma, the company developing pracinostat.
The study included 50 AML patients who had a median age of 75 (range, 66-84).
The patients received pracinostat at 60 mg orally on days 1, 3, and 5 of each week for 21 days of each 28-day cycle. They received azacitidine subcutaneously or intravenously on days 1-7 or days 1-5 and 8-9 (per site preference) of each 28-day cycle.
According to updated data from MEI Pharma, the complete response rate was 42% (n=21), and the median overall survival was 19.1 months.
The company said these data compare favorably to a phase 3 study of azacitidine (AZA-AML-0011), which showed a median overall survival of 10.4 months with azacitidine alone and a complete response rate of 19.5% in a similar patient population.
The combination of pracinostat and azacitidine was thought to be well tolerated overall, with no unexpected toxicities. The most common grade 3-4 treatment-emergent adverse events included febrile neutropenia, thrombocytopenia, anemia, and fatigue. ![]()
Image by Eric Smith
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for the histone deacetylase (HDAC) inhibitor pracinostat to be used in combination with azacitidine to treat newly diagnosed acute myeloid leukemia (AML) patients who are 75 and older or unfit for intensive chemotherapy.
The FDA’s breakthrough designation is intended to expedite the development and review of new therapies for serious or life-threatening conditions.
To earn the designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
The breakthrough therapy designation for pracinostat is supported by data from a phase 2 study of the HDAC inhibitor in combination with azacitidine in elderly patients with newly diagnosed AML who were not candidates for induction chemotherapy.
Detailed results from this trial were presented at the 20th Congress of the European Hematology Association last year. The research was sponsored by MEI Pharma, the company developing pracinostat.
The study included 50 AML patients who had a median age of 75 (range, 66-84).
The patients received pracinostat at 60 mg orally on days 1, 3, and 5 of each week for 21 days of each 28-day cycle. They received azacitidine subcutaneously or intravenously on days 1-7 or days 1-5 and 8-9 (per site preference) of each 28-day cycle.
According to updated data from MEI Pharma, the complete response rate was 42% (n=21), and the median overall survival was 19.1 months.
The company said these data compare favorably to a phase 3 study of azacitidine (AZA-AML-0011), which showed a median overall survival of 10.4 months with azacitidine alone and a complete response rate of 19.5% in a similar patient population.
The combination of pracinostat and azacitidine was thought to be well tolerated overall, with no unexpected toxicities. The most common grade 3-4 treatment-emergent adverse events included febrile neutropenia, thrombocytopenia, anemia, and fatigue. ![]()
Image by Eric Smith
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for the histone deacetylase (HDAC) inhibitor pracinostat to be used in combination with azacitidine to treat newly diagnosed acute myeloid leukemia (AML) patients who are 75 and older or unfit for intensive chemotherapy.
The FDA’s breakthrough designation is intended to expedite the development and review of new therapies for serious or life-threatening conditions.
To earn the designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
The breakthrough therapy designation for pracinostat is supported by data from a phase 2 study of the HDAC inhibitor in combination with azacitidine in elderly patients with newly diagnosed AML who were not candidates for induction chemotherapy.
Detailed results from this trial were presented at the 20th Congress of the European Hematology Association last year. The research was sponsored by MEI Pharma, the company developing pracinostat.
The study included 50 AML patients who had a median age of 75 (range, 66-84).
The patients received pracinostat at 60 mg orally on days 1, 3, and 5 of each week for 21 days of each 28-day cycle. They received azacitidine subcutaneously or intravenously on days 1-7 or days 1-5 and 8-9 (per site preference) of each 28-day cycle.
According to updated data from MEI Pharma, the complete response rate was 42% (n=21), and the median overall survival was 19.1 months.
The company said these data compare favorably to a phase 3 study of azacitidine (AZA-AML-0011), which showed a median overall survival of 10.4 months with azacitidine alone and a complete response rate of 19.5% in a similar patient population.
The combination of pracinostat and azacitidine was thought to be well tolerated overall, with no unexpected toxicities. The most common grade 3-4 treatment-emergent adverse events included febrile neutropenia, thrombocytopenia, anemia, and fatigue. ![]()