User login
Research Training Fellowship in Ataxia is Available
Do autologous blood and PRP injections effectively treat tennis elbow?
EVIDENCE-BASED ANSWER:
Yes, both approaches reduce pain, but the improvement with platelet-rich plasma (PRP) is not clinically meaningful. Autologous blood injections (ABIs) are more effective than corticosteroid injections for reducing pain and disability in patients with tennis elbow in both the short and long term (strength of recommendation [SOR]: B, consistent findings in 2 randomized controlled trials [RCTs]).
PRP injections reduce pain more than sham injections for chronic tennis elbow (SOR: B, high-quality RCT). However, the magnitude of the difference is small.
Autologous blood injections reduce pain
A 2013 RCT assessed the effectiveness of ABI (2 mL venous blood and 1 mL 2% lidocaine) compared with injection of 40 mg methylprednisolone and 1 mL 2% lidocaine in 50 patients with tennis elbow (mean age 38.2 years, mean duration of symptoms 4.5 weeks).1 The degree of pain and disability were evaluated at baseline, 2 weeks, and 6 weeks using a visual analog pain scale (VAS) and Nirschl functional staging, respectively, both measured on 10-point scales. Researchers found no statistical difference between the groups at baseline or 2 weeks. At 6 weeks, however, the ABI group showed significant improvements over the steroid group in pain (mean VAS=1.52 vs 2.28; P=.0396) and disability (mean Nirschl stage=1.40 vs 2.40; P=.0045).
A previous RCT, in 2012, compared ABI (2 mL of venous blood and 1 mL of 0.5% bupivacaine) in 30 patients (mean age 42.9 years, mean duration of symptoms 9.5 weeks) with a corticosteroid injection (80 mg of methylprednisolone and 1 mL of 0.5% bupivacaine) in another 30 patients (mean age 42.2 years, mean duration of symptoms 7.7 weeks). Outcomes were assessed at 12 weeks and 6 months on a 10-point VAS and 7-point Nirschl stage.2
The ABI group showed a significant decrease in pain and disability compared with the steroid group (mean VAS at 12 weeks=0.6 vs 1.5, P=.0127; mean VAS at 6 months=0.5 vs 1.8; P=.0058; mean Nirschl stage at 12 weeks=0.43 vs 1.0; P=.0184; mean Nirschl stage at 6 months=0.36 vs 1.2; P=.0064).
PRP: Some efficacy, little significance
A 2014 double-blinded RCT analyzed the efficacy of PRP injection vs control injection for treating tennis elbow of at least 3 months’ duration.3 A total of 112 patients (mean age 48.4 years) received a 2- to 3-mL injection of PRP at a site blocked with bupivacaine; 113 patients (mean age 47.4 years) received an injection of 2 to 3 mL 0.5% bupivacaine only. Success was defined as a ≥25% improvement in pain score on a 100-point VAS.
At 24 weeks, the PRP group demonstrated a success rate of 83.9% compared with 68.3% in the control group (number needed to treat=6; P=.037). However, the difference between the mean VAS improvement of 38 points in the PRP group and the mean decrease of 36 points in the control group carries little clinical significance.
1. Jindal N, Gaury Y, Banshiwal RC, et al. Comparison of short term results of single injection of autologous blood and steroid injection in tennis elbow: a prospective study. J Orthop Surg Res. 2013;8:10.
2. Dojode C. A randomised control trial to evaluate the efficacy of autologous blood injection versus local corticosteroid injection for treatment of lateral epicondylitis. Bone Joint Res. 2012;1:192-197.
3. Mishra A, Skrepnik NV, Edwards SG, et al. Efficacy of platelet-rich plasma for chronic tennis elbow: a double-blind, prospective, multicenter, randomized controlled trial of 230 patients. Am J Sports Med. 2014;42:463-471.
EVIDENCE-BASED ANSWER:
Yes, both approaches reduce pain, but the improvement with platelet-rich plasma (PRP) is not clinically meaningful. Autologous blood injections (ABIs) are more effective than corticosteroid injections for reducing pain and disability in patients with tennis elbow in both the short and long term (strength of recommendation [SOR]: B, consistent findings in 2 randomized controlled trials [RCTs]).
PRP injections reduce pain more than sham injections for chronic tennis elbow (SOR: B, high-quality RCT). However, the magnitude of the difference is small.
Autologous blood injections reduce pain
A 2013 RCT assessed the effectiveness of ABI (2 mL venous blood and 1 mL 2% lidocaine) compared with injection of 40 mg methylprednisolone and 1 mL 2% lidocaine in 50 patients with tennis elbow (mean age 38.2 years, mean duration of symptoms 4.5 weeks).1 The degree of pain and disability were evaluated at baseline, 2 weeks, and 6 weeks using a visual analog pain scale (VAS) and Nirschl functional staging, respectively, both measured on 10-point scales. Researchers found no statistical difference between the groups at baseline or 2 weeks. At 6 weeks, however, the ABI group showed significant improvements over the steroid group in pain (mean VAS=1.52 vs 2.28; P=.0396) and disability (mean Nirschl stage=1.40 vs 2.40; P=.0045).
A previous RCT, in 2012, compared ABI (2 mL of venous blood and 1 mL of 0.5% bupivacaine) in 30 patients (mean age 42.9 years, mean duration of symptoms 9.5 weeks) with a corticosteroid injection (80 mg of methylprednisolone and 1 mL of 0.5% bupivacaine) in another 30 patients (mean age 42.2 years, mean duration of symptoms 7.7 weeks). Outcomes were assessed at 12 weeks and 6 months on a 10-point VAS and 7-point Nirschl stage.2
The ABI group showed a significant decrease in pain and disability compared with the steroid group (mean VAS at 12 weeks=0.6 vs 1.5, P=.0127; mean VAS at 6 months=0.5 vs 1.8; P=.0058; mean Nirschl stage at 12 weeks=0.43 vs 1.0; P=.0184; mean Nirschl stage at 6 months=0.36 vs 1.2; P=.0064).
PRP: Some efficacy, little significance
A 2014 double-blinded RCT analyzed the efficacy of PRP injection vs control injection for treating tennis elbow of at least 3 months’ duration.3 A total of 112 patients (mean age 48.4 years) received a 2- to 3-mL injection of PRP at a site blocked with bupivacaine; 113 patients (mean age 47.4 years) received an injection of 2 to 3 mL 0.5% bupivacaine only. Success was defined as a ≥25% improvement in pain score on a 100-point VAS.
At 24 weeks, the PRP group demonstrated a success rate of 83.9% compared with 68.3% in the control group (number needed to treat=6; P=.037). However, the difference between the mean VAS improvement of 38 points in the PRP group and the mean decrease of 36 points in the control group carries little clinical significance.
EVIDENCE-BASED ANSWER:
Yes, both approaches reduce pain, but the improvement with platelet-rich plasma (PRP) is not clinically meaningful. Autologous blood injections (ABIs) are more effective than corticosteroid injections for reducing pain and disability in patients with tennis elbow in both the short and long term (strength of recommendation [SOR]: B, consistent findings in 2 randomized controlled trials [RCTs]).
PRP injections reduce pain more than sham injections for chronic tennis elbow (SOR: B, high-quality RCT). However, the magnitude of the difference is small.
Autologous blood injections reduce pain
A 2013 RCT assessed the effectiveness of ABI (2 mL venous blood and 1 mL 2% lidocaine) compared with injection of 40 mg methylprednisolone and 1 mL 2% lidocaine in 50 patients with tennis elbow (mean age 38.2 years, mean duration of symptoms 4.5 weeks).1 The degree of pain and disability were evaluated at baseline, 2 weeks, and 6 weeks using a visual analog pain scale (VAS) and Nirschl functional staging, respectively, both measured on 10-point scales. Researchers found no statistical difference between the groups at baseline or 2 weeks. At 6 weeks, however, the ABI group showed significant improvements over the steroid group in pain (mean VAS=1.52 vs 2.28; P=.0396) and disability (mean Nirschl stage=1.40 vs 2.40; P=.0045).
A previous RCT, in 2012, compared ABI (2 mL of venous blood and 1 mL of 0.5% bupivacaine) in 30 patients (mean age 42.9 years, mean duration of symptoms 9.5 weeks) with a corticosteroid injection (80 mg of methylprednisolone and 1 mL of 0.5% bupivacaine) in another 30 patients (mean age 42.2 years, mean duration of symptoms 7.7 weeks). Outcomes were assessed at 12 weeks and 6 months on a 10-point VAS and 7-point Nirschl stage.2
The ABI group showed a significant decrease in pain and disability compared with the steroid group (mean VAS at 12 weeks=0.6 vs 1.5, P=.0127; mean VAS at 6 months=0.5 vs 1.8; P=.0058; mean Nirschl stage at 12 weeks=0.43 vs 1.0; P=.0184; mean Nirschl stage at 6 months=0.36 vs 1.2; P=.0064).
PRP: Some efficacy, little significance
A 2014 double-blinded RCT analyzed the efficacy of PRP injection vs control injection for treating tennis elbow of at least 3 months’ duration.3 A total of 112 patients (mean age 48.4 years) received a 2- to 3-mL injection of PRP at a site blocked with bupivacaine; 113 patients (mean age 47.4 years) received an injection of 2 to 3 mL 0.5% bupivacaine only. Success was defined as a ≥25% improvement in pain score on a 100-point VAS.
At 24 weeks, the PRP group demonstrated a success rate of 83.9% compared with 68.3% in the control group (number needed to treat=6; P=.037). However, the difference between the mean VAS improvement of 38 points in the PRP group and the mean decrease of 36 points in the control group carries little clinical significance.
1. Jindal N, Gaury Y, Banshiwal RC, et al. Comparison of short term results of single injection of autologous blood and steroid injection in tennis elbow: a prospective study. J Orthop Surg Res. 2013;8:10.
2. Dojode C. A randomised control trial to evaluate the efficacy of autologous blood injection versus local corticosteroid injection for treatment of lateral epicondylitis. Bone Joint Res. 2012;1:192-197.
3. Mishra A, Skrepnik NV, Edwards SG, et al. Efficacy of platelet-rich plasma for chronic tennis elbow: a double-blind, prospective, multicenter, randomized controlled trial of 230 patients. Am J Sports Med. 2014;42:463-471.
1. Jindal N, Gaury Y, Banshiwal RC, et al. Comparison of short term results of single injection of autologous blood and steroid injection in tennis elbow: a prospective study. J Orthop Surg Res. 2013;8:10.
2. Dojode C. A randomised control trial to evaluate the efficacy of autologous blood injection versus local corticosteroid injection for treatment of lateral epicondylitis. Bone Joint Res. 2012;1:192-197.
3. Mishra A, Skrepnik NV, Edwards SG, et al. Efficacy of platelet-rich plasma for chronic tennis elbow: a double-blind, prospective, multicenter, randomized controlled trial of 230 patients. Am J Sports Med. 2014;42:463-471.
Evidence-based answers from the Family Physicians Inquiries Network

Which SSRIs most effectively treat depression in adolescents?
EVIDENCE-BASED ANSWER:
We don’t know which selective serotonin reuptake inhibitors (SSRIs) are the most effective and safe because no studies have compared these antidepressants with each other.
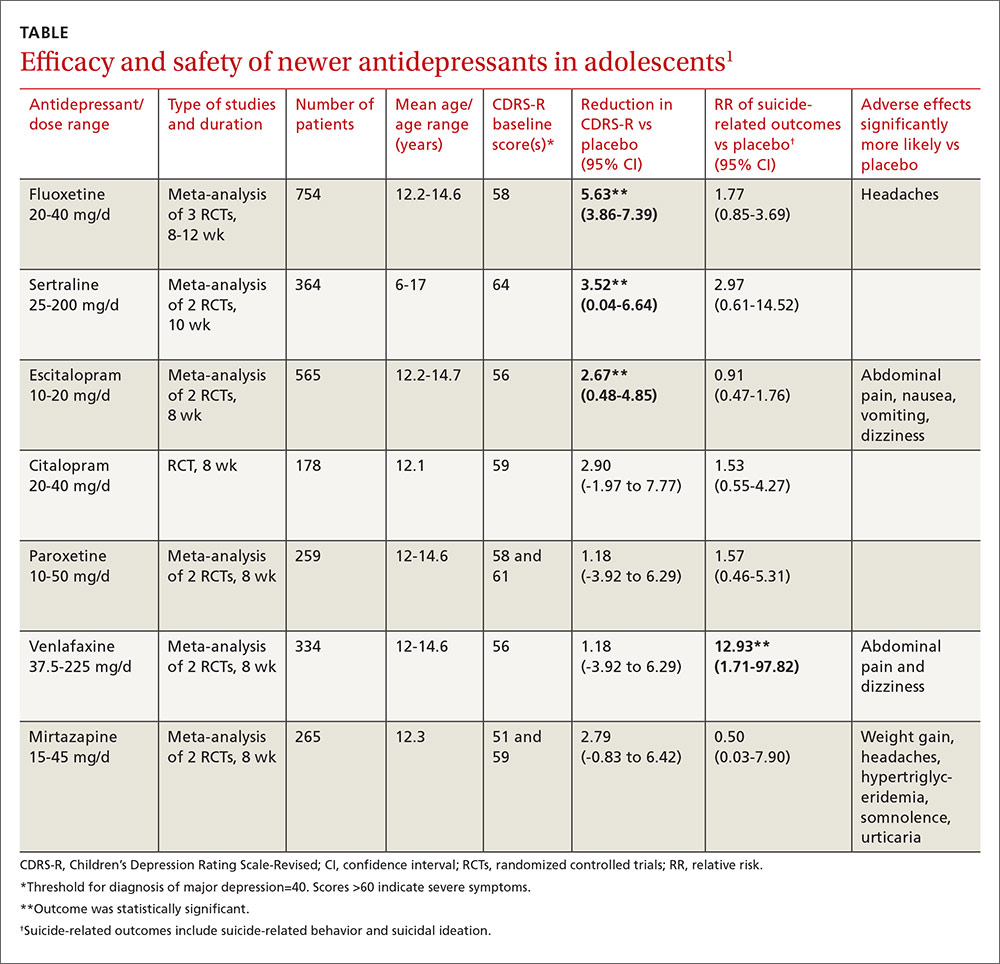
Three SSRI antidepressant medications—fluoxetine, sertraline, and escitalopram—produce modest improvements (about 5% to 10%) in standardized depression scores without a significant increase in the risk of suicide-related outcomes (suicidal behavior or ideation) in adolescent patients with major depression of moderate severity. As a group, however, the newer-generation antidepressants, including SSRIs, increase suicide-related outcomes by 50%. Citalopram, paroxetine, venlafaxine, and mirtazapine don’t improve depression scores (strength of recommendation [SOR]: A, meta-analyses of randomized controlled trials [RCTs]).
An updated national guideline recommends specific psychological therapy for adolescents with mild depression and combined psychotherapy and fluoxetine for moderate or severe depression, with sertraline or citalopram as second-line agents (SOR: A, RCTs).
EVIDENCE SUMMARY
A Cochrane systematic review (19 RCTs; 3335 patients, total) of newer-generation antidepressants for treating depression in adolescents found that, overall, they produced both a small decrease in symptom severity scores and an increased risk of suicide-related outcomes.1
Three SSRIs slightly lower one symptom severity score
Investigators performed a meta-analysis of all trials (14 RCTs; 2490 patients, total) that used the same standardized symptom severity score (the Children’s Depression Rating Scale—Revised [CDRS-R], range 17 to 113 points) to evaluate the following medications: fluoxetine, sertraline, escitalopram, citalopram, paroxetine, venlafaxine, and mirtazapine.1
All participants were outpatients who met criteria for a primary diagnosis of major depression, excluding comorbid conditions. The CDRS-R scores were evaluated by clinicians; the mean baseline score was 57 (40 is considered a threshold score for diagnosis, and above 60 indicates severe symptoms). Only 5 trials reported patients’ self-rated depression symptom severity (in patients taking fluoxetine and paroxetine) and none reported improvement. Treatment courses ranged from 8 to 12 weeks.
As a group, the newer antidepressants slightly reduced CDRS-R scores in adolescents (by 4.21 points, 95% confidence interval [CI], 0.41-5.95) but increased suicide-related outcomes (relative risk [RR]=1.47; 95% CI, 0.99-2.19). The individual antidepressants fluoxetine, sertraline, and escitalopram each produced statistically significant but clinically small reductions in CDRS-R scores of 5% to 10% without significantly increasing suicide-related outcomes (TABLE1). The other medications evaluated individually didn’t improve CDRS-R scores, and only venlafaxine increased suicide-related outcomes.
Other symptom severity scores show no improvement with SSRIs
Five additional RCTs not included in the meta-analysis that used standardized symptom severity scores other than the CDRS-R (Schedule for Affective Disorders and Schizophrenia for School-Aged Children [K-SADS], Montgomery-Asberg Depression Rating Scale [MADR], and Hamilton Depression Rating Scale [HAM-D]) found no improvement with fluoxetine (2 RCTs; 63 patients, total), citalopram (one RCT, 233 patients), or paroxetine (2 RCTs; 466 patients, total).
Certain drugs cause significantly more adverse events than placebo
Ten RCTs evaluated adverse events in adolescents treated with fluoxetine, escitalopram, citalopram, and paroxetine and reported a small increase over placebo when all medications were combined as a group (RR=1.11; 95% CI, 1.05-1.17). Investigators reported that the individual antidepressants fluoxetine, escitalopram, venlafaxine, and mirtazapine produced significantly more adverse events than placebo (P values not given). No studies compared antidepressant medications against each other for either efficacy or potential harms.
RECOMMENDATIONS
A newly revised expert guideline recommends treating mildly depressed adolescents with a specific psychological therapy—individual cognitive behavioral therapy, interpersonal therapy, family therapy, or psychodynamic psychotherapy—for at least 3 months.2
For adolescents with moderate to severe depression, the guideline advocates psychotherapy with the option of adding fluoxetine, although using antidepressants in adolescents who haven’t at least tried psychotherapy is outside of the drug’s indications.
The guideline also recommends careful monitoring for adverse effects and close review of mental state—weekly for the first 4 weeks of treatment, for example. If fluoxetine doesn’t help, sertraline and citalopram are recommended as alternatives.
1. Hetrick SE, McKenzie JE, Cox GR, et al. Newer generation antidepressants for depressive disorders in children and adolescents. Cochrane Database Syst Rev. 2012;11:CD004851.
2. Hopkins K, Crosland P, Elliott N, et al. Diagnosis and management of depression in children and young people: summary of updated NICE guidance. BMJ. 2015;350:h824.
EVIDENCE-BASED ANSWER:
We don’t know which selective serotonin reuptake inhibitors (SSRIs) are the most effective and safe because no studies have compared these antidepressants with each other.
Three SSRI antidepressant medications—fluoxetine, sertraline, and escitalopram—produce modest improvements (about 5% to 10%) in standardized depression scores without a significant increase in the risk of suicide-related outcomes (suicidal behavior or ideation) in adolescent patients with major depression of moderate severity. As a group, however, the newer-generation antidepressants, including SSRIs, increase suicide-related outcomes by 50%. Citalopram, paroxetine, venlafaxine, and mirtazapine don’t improve depression scores (strength of recommendation [SOR]: A, meta-analyses of randomized controlled trials [RCTs]).
An updated national guideline recommends specific psychological therapy for adolescents with mild depression and combined psychotherapy and fluoxetine for moderate or severe depression, with sertraline or citalopram as second-line agents (SOR: A, RCTs).
EVIDENCE SUMMARY
A Cochrane systematic review (19 RCTs; 3335 patients, total) of newer-generation antidepressants for treating depression in adolescents found that, overall, they produced both a small decrease in symptom severity scores and an increased risk of suicide-related outcomes.1
Three SSRIs slightly lower one symptom severity score
Investigators performed a meta-analysis of all trials (14 RCTs; 2490 patients, total) that used the same standardized symptom severity score (the Children’s Depression Rating Scale—Revised [CDRS-R], range 17 to 113 points) to evaluate the following medications: fluoxetine, sertraline, escitalopram, citalopram, paroxetine, venlafaxine, and mirtazapine.1
All participants were outpatients who met criteria for a primary diagnosis of major depression, excluding comorbid conditions. The CDRS-R scores were evaluated by clinicians; the mean baseline score was 57 (40 is considered a threshold score for diagnosis, and above 60 indicates severe symptoms). Only 5 trials reported patients’ self-rated depression symptom severity (in patients taking fluoxetine and paroxetine) and none reported improvement. Treatment courses ranged from 8 to 12 weeks.
As a group, the newer antidepressants slightly reduced CDRS-R scores in adolescents (by 4.21 points, 95% confidence interval [CI], 0.41-5.95) but increased suicide-related outcomes (relative risk [RR]=1.47; 95% CI, 0.99-2.19). The individual antidepressants fluoxetine, sertraline, and escitalopram each produced statistically significant but clinically small reductions in CDRS-R scores of 5% to 10% without significantly increasing suicide-related outcomes (TABLE1). The other medications evaluated individually didn’t improve CDRS-R scores, and only venlafaxine increased suicide-related outcomes.
Other symptom severity scores show no improvement with SSRIs
Five additional RCTs not included in the meta-analysis that used standardized symptom severity scores other than the CDRS-R (Schedule for Affective Disorders and Schizophrenia for School-Aged Children [K-SADS], Montgomery-Asberg Depression Rating Scale [MADR], and Hamilton Depression Rating Scale [HAM-D]) found no improvement with fluoxetine (2 RCTs; 63 patients, total), citalopram (one RCT, 233 patients), or paroxetine (2 RCTs; 466 patients, total).
Certain drugs cause significantly more adverse events than placebo
Ten RCTs evaluated adverse events in adolescents treated with fluoxetine, escitalopram, citalopram, and paroxetine and reported a small increase over placebo when all medications were combined as a group (RR=1.11; 95% CI, 1.05-1.17). Investigators reported that the individual antidepressants fluoxetine, escitalopram, venlafaxine, and mirtazapine produced significantly more adverse events than placebo (P values not given). No studies compared antidepressant medications against each other for either efficacy or potential harms.
RECOMMENDATIONS
A newly revised expert guideline recommends treating mildly depressed adolescents with a specific psychological therapy—individual cognitive behavioral therapy, interpersonal therapy, family therapy, or psychodynamic psychotherapy—for at least 3 months.2
For adolescents with moderate to severe depression, the guideline advocates psychotherapy with the option of adding fluoxetine, although using antidepressants in adolescents who haven’t at least tried psychotherapy is outside of the drug’s indications.
The guideline also recommends careful monitoring for adverse effects and close review of mental state—weekly for the first 4 weeks of treatment, for example. If fluoxetine doesn’t help, sertraline and citalopram are recommended as alternatives.
EVIDENCE-BASED ANSWER:
We don’t know which selective serotonin reuptake inhibitors (SSRIs) are the most effective and safe because no studies have compared these antidepressants with each other.
Three SSRI antidepressant medications—fluoxetine, sertraline, and escitalopram—produce modest improvements (about 5% to 10%) in standardized depression scores without a significant increase in the risk of suicide-related outcomes (suicidal behavior or ideation) in adolescent patients with major depression of moderate severity. As a group, however, the newer-generation antidepressants, including SSRIs, increase suicide-related outcomes by 50%. Citalopram, paroxetine, venlafaxine, and mirtazapine don’t improve depression scores (strength of recommendation [SOR]: A, meta-analyses of randomized controlled trials [RCTs]).
An updated national guideline recommends specific psychological therapy for adolescents with mild depression and combined psychotherapy and fluoxetine for moderate or severe depression, with sertraline or citalopram as second-line agents (SOR: A, RCTs).
EVIDENCE SUMMARY
A Cochrane systematic review (19 RCTs; 3335 patients, total) of newer-generation antidepressants for treating depression in adolescents found that, overall, they produced both a small decrease in symptom severity scores and an increased risk of suicide-related outcomes.1
Three SSRIs slightly lower one symptom severity score
Investigators performed a meta-analysis of all trials (14 RCTs; 2490 patients, total) that used the same standardized symptom severity score (the Children’s Depression Rating Scale—Revised [CDRS-R], range 17 to 113 points) to evaluate the following medications: fluoxetine, sertraline, escitalopram, citalopram, paroxetine, venlafaxine, and mirtazapine.1
All participants were outpatients who met criteria for a primary diagnosis of major depression, excluding comorbid conditions. The CDRS-R scores were evaluated by clinicians; the mean baseline score was 57 (40 is considered a threshold score for diagnosis, and above 60 indicates severe symptoms). Only 5 trials reported patients’ self-rated depression symptom severity (in patients taking fluoxetine and paroxetine) and none reported improvement. Treatment courses ranged from 8 to 12 weeks.
As a group, the newer antidepressants slightly reduced CDRS-R scores in adolescents (by 4.21 points, 95% confidence interval [CI], 0.41-5.95) but increased suicide-related outcomes (relative risk [RR]=1.47; 95% CI, 0.99-2.19). The individual antidepressants fluoxetine, sertraline, and escitalopram each produced statistically significant but clinically small reductions in CDRS-R scores of 5% to 10% without significantly increasing suicide-related outcomes (TABLE1). The other medications evaluated individually didn’t improve CDRS-R scores, and only venlafaxine increased suicide-related outcomes.
Other symptom severity scores show no improvement with SSRIs
Five additional RCTs not included in the meta-analysis that used standardized symptom severity scores other than the CDRS-R (Schedule for Affective Disorders and Schizophrenia for School-Aged Children [K-SADS], Montgomery-Asberg Depression Rating Scale [MADR], and Hamilton Depression Rating Scale [HAM-D]) found no improvement with fluoxetine (2 RCTs; 63 patients, total), citalopram (one RCT, 233 patients), or paroxetine (2 RCTs; 466 patients, total).
Certain drugs cause significantly more adverse events than placebo
Ten RCTs evaluated adverse events in adolescents treated with fluoxetine, escitalopram, citalopram, and paroxetine and reported a small increase over placebo when all medications were combined as a group (RR=1.11; 95% CI, 1.05-1.17). Investigators reported that the individual antidepressants fluoxetine, escitalopram, venlafaxine, and mirtazapine produced significantly more adverse events than placebo (P values not given). No studies compared antidepressant medications against each other for either efficacy or potential harms.
RECOMMENDATIONS
A newly revised expert guideline recommends treating mildly depressed adolescents with a specific psychological therapy—individual cognitive behavioral therapy, interpersonal therapy, family therapy, or psychodynamic psychotherapy—for at least 3 months.2
For adolescents with moderate to severe depression, the guideline advocates psychotherapy with the option of adding fluoxetine, although using antidepressants in adolescents who haven’t at least tried psychotherapy is outside of the drug’s indications.
The guideline also recommends careful monitoring for adverse effects and close review of mental state—weekly for the first 4 weeks of treatment, for example. If fluoxetine doesn’t help, sertraline and citalopram are recommended as alternatives.
1. Hetrick SE, McKenzie JE, Cox GR, et al. Newer generation antidepressants for depressive disorders in children and adolescents. Cochrane Database Syst Rev. 2012;11:CD004851.
2. Hopkins K, Crosland P, Elliott N, et al. Diagnosis and management of depression in children and young people: summary of updated NICE guidance. BMJ. 2015;350:h824.
1. Hetrick SE, McKenzie JE, Cox GR, et al. Newer generation antidepressants for depressive disorders in children and adolescents. Cochrane Database Syst Rev. 2012;11:CD004851.
2. Hopkins K, Crosland P, Elliott N, et al. Diagnosis and management of depression in children and young people: summary of updated NICE guidance. BMJ. 2015;350:h824.
Evidence-based answers from the Family Physicians Inquiries Network

A Melting Pot of Mail
VAPING DANGERS: CLEARING THE AIR
The liquid base of an e-cigarette contains either vegetable glycerin (VG) or propylene glycol, or more commonly, a proprietary combination of both. Each of these ingredients has varying effects on the body.
However, the first paragraph of Randy D. Danielsen’s editorial alluded to what I consider a bigger concern regarding the future medical complications of vaping. The description of a “… huge puff of cherry-scented smoke …” indicates that vapes are not puffed on the way cigarettes are.
Cigarette smoking is similar to drinking through a straw—the smoke is first captured in the mouth, then cooled and inhaled. In contrast, vaping involves inhaling smoke directly into the lungs. This action, along with the thick VG base, produces a high volume of smoke. Vape shops even sponsor contests to see who can produce the largest cloud of smoke.
Therefore, my concern regarding vaping is not limited to the toxicity of the ingredients; it extends to how the toxicants are delivered to the poor, unsuspecting alveoli.
Gary Dula, FNP-C
Houston, TX
Continue for Millenials: Not All Sitting at the Kids' Table >>
MILLENIALS: NOT ALL SITTING AT THE KIDS' TABLES
I received my master’s degree in 2015 and am nearing completion of a year-long FNP fellowship program. I was an Army nurse for four years and a float nurse at various hospitals for five. I am a “millennial”—and, according to the published letters about precepting, am hated by older nurses because of it. Considering I have practiced with many hard-working people my age who would lay down their lives for this country, I find this unprecedented.
I work hard, but the school I attended for my FNP did not prepare me well; it was difficult to get people to teach and precept me during school. This led me to apply for my current fellowship.
Throughout my nine-year nursing career, I have precepted many nurses, including those with associate degrees. I will continue to mentor and precept as an APRN. I take issue with the portrayal of millennials as lazy and unable to work hard. Why? Because we will not work for free, would like to collaboratively learn, and need help to develop our skills?
One day, you will grow old and need someone to take care of you. Why on earth would you berate the people who will be doing just that? Complaining about this generation is not going to change the fact that they are here and present in the workforce. We need more providers, and chastising the younger generation is not going to solve that problem.
Stephanie Butler-Cleland, FNP-BC
Colorado Springs, CO
Continue for The Pros of Precepting >>
THE PROS OF PRECEPTING
I am an urgent care NP in urban communities on the West Coast of Florida. I had taken a break from precepting as a result of negative experiences, but I recently resumed to precept my first NP student in years.
Prior to accepting the student I precepted, I received requests from two other students. One asked if I could change my schedule to be closer to where she lived. The other clearly didn’t want to commit to the drive or the hours I was available, and asked if I would work more weekends to accommodate her schedule. Needless to say, I refused both students.
Instead, I precepted a smart 28-year-old student from my alma mater, one of the Florida state universities. She was attentive, prepared, and eager. I was very, very impressed with her. She had been a nurse for four years and was a second-semester student. It was a pleasure to have her; I like being questioned and challenged. It was fun to see her enjoying my job, and it reminded me of why I love what I do.
Anne Conklin, MS, ARNP-C
Bradenton, FL
Continue for A Scheming Industry >>
A SCHEMING INDUSTRY
Intelligent health care policy has been frustrated by the enormous amount of money brought to bear on Congress by the insurance and pharmaceutical industries. Each dollar paid to an insurance company is used to construct buildings, hire workers, create a sales staff, and ultimately pay their shareholders a profit.
Since the insurance industry obtained an antitrust exemption in the 1940s, they are essentially immune from prosecution for price collusion. Until recently, it was difficult to know how much of the money paid was returned in the form of medical benefits. In order to keep profits rising, they must enroll more people. Promising coverage while impeding medical workups and care, making great profits, and needing more and more enrollees fits the definition of a Ponzi scheme.
Several years ago in California, the state insurance commission (under threat of decertification) got an industry representative to admit that the maximum percentage of dollars used for services was 70%. In other words, for each dollar spent, a patient would be lucky to get 70 cents worth of services.
All of us who practice know how the companies do this: We request a needed diagnostic test or treatment and are denied. I have interrupted my schedule on many days to call for a “peer to peer” review—only once was I denied. This is a roadblock that many busy practitioners will not challenge. Since insurance companies market how great their coverage is, patients often get angry at the provider.
The repeated argument is that the market forces will lower medical costs. This fallacy is easily debunked by noting the ever-escalating costs and comparing health care costs as a percent of gross domestic product (GDP) in our country versus others. France, for example, expends 12% of GDP on health and ranks first in health care outcomes by world standards. In the US, we are approaching 20% of GDP.
Since insurance adds nothing to care and increases costs dramatically (every provider has to have billers for the various insurance companies, since each has its own requirements), a single-payer system is the only system that will lower costs. Those who benefit from the current system declare that we can’t have “socialized medicine.” To which I would respond, fine; we’ll continue to pay 30% to 50% more so that insurance companies can have their profits at our expense.
Nelson Herilhy, PA-C, MHS
Concord, CA
VAPING DANGERS: CLEARING THE AIR
The liquid base of an e-cigarette contains either vegetable glycerin (VG) or propylene glycol, or more commonly, a proprietary combination of both. Each of these ingredients has varying effects on the body.
However, the first paragraph of Randy D. Danielsen’s editorial alluded to what I consider a bigger concern regarding the future medical complications of vaping. The description of a “… huge puff of cherry-scented smoke …” indicates that vapes are not puffed on the way cigarettes are.
Cigarette smoking is similar to drinking through a straw—the smoke is first captured in the mouth, then cooled and inhaled. In contrast, vaping involves inhaling smoke directly into the lungs. This action, along with the thick VG base, produces a high volume of smoke. Vape shops even sponsor contests to see who can produce the largest cloud of smoke.
Therefore, my concern regarding vaping is not limited to the toxicity of the ingredients; it extends to how the toxicants are delivered to the poor, unsuspecting alveoli.
Gary Dula, FNP-C
Houston, TX
Continue for Millenials: Not All Sitting at the Kids' Table >>
MILLENIALS: NOT ALL SITTING AT THE KIDS' TABLES
I received my master’s degree in 2015 and am nearing completion of a year-long FNP fellowship program. I was an Army nurse for four years and a float nurse at various hospitals for five. I am a “millennial”—and, according to the published letters about precepting, am hated by older nurses because of it. Considering I have practiced with many hard-working people my age who would lay down their lives for this country, I find this unprecedented.
I work hard, but the school I attended for my FNP did not prepare me well; it was difficult to get people to teach and precept me during school. This led me to apply for my current fellowship.
Throughout my nine-year nursing career, I have precepted many nurses, including those with associate degrees. I will continue to mentor and precept as an APRN. I take issue with the portrayal of millennials as lazy and unable to work hard. Why? Because we will not work for free, would like to collaboratively learn, and need help to develop our skills?
One day, you will grow old and need someone to take care of you. Why on earth would you berate the people who will be doing just that? Complaining about this generation is not going to change the fact that they are here and present in the workforce. We need more providers, and chastising the younger generation is not going to solve that problem.
Stephanie Butler-Cleland, FNP-BC
Colorado Springs, CO
Continue for The Pros of Precepting >>
THE PROS OF PRECEPTING
I am an urgent care NP in urban communities on the West Coast of Florida. I had taken a break from precepting as a result of negative experiences, but I recently resumed to precept my first NP student in years.
Prior to accepting the student I precepted, I received requests from two other students. One asked if I could change my schedule to be closer to where she lived. The other clearly didn’t want to commit to the drive or the hours I was available, and asked if I would work more weekends to accommodate her schedule. Needless to say, I refused both students.
Instead, I precepted a smart 28-year-old student from my alma mater, one of the Florida state universities. She was attentive, prepared, and eager. I was very, very impressed with her. She had been a nurse for four years and was a second-semester student. It was a pleasure to have her; I like being questioned and challenged. It was fun to see her enjoying my job, and it reminded me of why I love what I do.
Anne Conklin, MS, ARNP-C
Bradenton, FL
Continue for A Scheming Industry >>
A SCHEMING INDUSTRY
Intelligent health care policy has been frustrated by the enormous amount of money brought to bear on Congress by the insurance and pharmaceutical industries. Each dollar paid to an insurance company is used to construct buildings, hire workers, create a sales staff, and ultimately pay their shareholders a profit.
Since the insurance industry obtained an antitrust exemption in the 1940s, they are essentially immune from prosecution for price collusion. Until recently, it was difficult to know how much of the money paid was returned in the form of medical benefits. In order to keep profits rising, they must enroll more people. Promising coverage while impeding medical workups and care, making great profits, and needing more and more enrollees fits the definition of a Ponzi scheme.
Several years ago in California, the state insurance commission (under threat of decertification) got an industry representative to admit that the maximum percentage of dollars used for services was 70%. In other words, for each dollar spent, a patient would be lucky to get 70 cents worth of services.
All of us who practice know how the companies do this: We request a needed diagnostic test or treatment and are denied. I have interrupted my schedule on many days to call for a “peer to peer” review—only once was I denied. This is a roadblock that many busy practitioners will not challenge. Since insurance companies market how great their coverage is, patients often get angry at the provider.
The repeated argument is that the market forces will lower medical costs. This fallacy is easily debunked by noting the ever-escalating costs and comparing health care costs as a percent of gross domestic product (GDP) in our country versus others. France, for example, expends 12% of GDP on health and ranks first in health care outcomes by world standards. In the US, we are approaching 20% of GDP.
Since insurance adds nothing to care and increases costs dramatically (every provider has to have billers for the various insurance companies, since each has its own requirements), a single-payer system is the only system that will lower costs. Those who benefit from the current system declare that we can’t have “socialized medicine.” To which I would respond, fine; we’ll continue to pay 30% to 50% more so that insurance companies can have their profits at our expense.
Nelson Herilhy, PA-C, MHS
Concord, CA
VAPING DANGERS: CLEARING THE AIR
The liquid base of an e-cigarette contains either vegetable glycerin (VG) or propylene glycol, or more commonly, a proprietary combination of both. Each of these ingredients has varying effects on the body.
However, the first paragraph of Randy D. Danielsen’s editorial alluded to what I consider a bigger concern regarding the future medical complications of vaping. The description of a “… huge puff of cherry-scented smoke …” indicates that vapes are not puffed on the way cigarettes are.
Cigarette smoking is similar to drinking through a straw—the smoke is first captured in the mouth, then cooled and inhaled. In contrast, vaping involves inhaling smoke directly into the lungs. This action, along with the thick VG base, produces a high volume of smoke. Vape shops even sponsor contests to see who can produce the largest cloud of smoke.
Therefore, my concern regarding vaping is not limited to the toxicity of the ingredients; it extends to how the toxicants are delivered to the poor, unsuspecting alveoli.
Gary Dula, FNP-C
Houston, TX
Continue for Millenials: Not All Sitting at the Kids' Table >>
MILLENIALS: NOT ALL SITTING AT THE KIDS' TABLES
I received my master’s degree in 2015 and am nearing completion of a year-long FNP fellowship program. I was an Army nurse for four years and a float nurse at various hospitals for five. I am a “millennial”—and, according to the published letters about precepting, am hated by older nurses because of it. Considering I have practiced with many hard-working people my age who would lay down their lives for this country, I find this unprecedented.
I work hard, but the school I attended for my FNP did not prepare me well; it was difficult to get people to teach and precept me during school. This led me to apply for my current fellowship.
Throughout my nine-year nursing career, I have precepted many nurses, including those with associate degrees. I will continue to mentor and precept as an APRN. I take issue with the portrayal of millennials as lazy and unable to work hard. Why? Because we will not work for free, would like to collaboratively learn, and need help to develop our skills?
One day, you will grow old and need someone to take care of you. Why on earth would you berate the people who will be doing just that? Complaining about this generation is not going to change the fact that they are here and present in the workforce. We need more providers, and chastising the younger generation is not going to solve that problem.
Stephanie Butler-Cleland, FNP-BC
Colorado Springs, CO
Continue for The Pros of Precepting >>
THE PROS OF PRECEPTING
I am an urgent care NP in urban communities on the West Coast of Florida. I had taken a break from precepting as a result of negative experiences, but I recently resumed to precept my first NP student in years.
Prior to accepting the student I precepted, I received requests from two other students. One asked if I could change my schedule to be closer to where she lived. The other clearly didn’t want to commit to the drive or the hours I was available, and asked if I would work more weekends to accommodate her schedule. Needless to say, I refused both students.
Instead, I precepted a smart 28-year-old student from my alma mater, one of the Florida state universities. She was attentive, prepared, and eager. I was very, very impressed with her. She had been a nurse for four years and was a second-semester student. It was a pleasure to have her; I like being questioned and challenged. It was fun to see her enjoying my job, and it reminded me of why I love what I do.
Anne Conklin, MS, ARNP-C
Bradenton, FL
Continue for A Scheming Industry >>
A SCHEMING INDUSTRY
Intelligent health care policy has been frustrated by the enormous amount of money brought to bear on Congress by the insurance and pharmaceutical industries. Each dollar paid to an insurance company is used to construct buildings, hire workers, create a sales staff, and ultimately pay their shareholders a profit.
Since the insurance industry obtained an antitrust exemption in the 1940s, they are essentially immune from prosecution for price collusion. Until recently, it was difficult to know how much of the money paid was returned in the form of medical benefits. In order to keep profits rising, they must enroll more people. Promising coverage while impeding medical workups and care, making great profits, and needing more and more enrollees fits the definition of a Ponzi scheme.
Several years ago in California, the state insurance commission (under threat of decertification) got an industry representative to admit that the maximum percentage of dollars used for services was 70%. In other words, for each dollar spent, a patient would be lucky to get 70 cents worth of services.
All of us who practice know how the companies do this: We request a needed diagnostic test or treatment and are denied. I have interrupted my schedule on many days to call for a “peer to peer” review—only once was I denied. This is a roadblock that many busy practitioners will not challenge. Since insurance companies market how great their coverage is, patients often get angry at the provider.
The repeated argument is that the market forces will lower medical costs. This fallacy is easily debunked by noting the ever-escalating costs and comparing health care costs as a percent of gross domestic product (GDP) in our country versus others. France, for example, expends 12% of GDP on health and ranks first in health care outcomes by world standards. In the US, we are approaching 20% of GDP.
Since insurance adds nothing to care and increases costs dramatically (every provider has to have billers for the various insurance companies, since each has its own requirements), a single-payer system is the only system that will lower costs. Those who benefit from the current system declare that we can’t have “socialized medicine.” To which I would respond, fine; we’ll continue to pay 30% to 50% more so that insurance companies can have their profits at our expense.
Nelson Herilhy, PA-C, MHS
Concord, CA
“Unprecedented” VA Proposal? We Don’t Think So
On May 25, 2016, the Department of Veterans Affairs (VA) published a proposed rule change in the Federal Register under the simple heading “Advanced Practice Registered Nurses.” From such modest beginnings stemmed a potential game-changer for advanced practice clinicians in this country: In summary, the VA proposed to “amend its medical regulations to permit full practice authority of all VA advanced practice registered nurses (APRNs) when they are acting within the scope of their VA employment.”1
The impetus for the VA’s proposal is that 505,000 veterans wait 30 days to access care within the VA system—and 300,000 wait between 31 and 60 days for health services.2 Granting plenary practice to VA APRNs would enable them to respond to this backlog of patients, since veterans would have direct access to APRNs who practice within the VA system, regardless of their state of licensure.
More than 4,800 NPs work within the VA; they provide clinical assessments, order appropriate tests and medications, and develop patient-centered care plans.2,3 Research has documented that outcomes for patients whose care is managed by NPs are equal to or better than outcomes for similar patients who are managed by physicians.4 As Major General Vincent Boles of the US Army (retired) stated, “Veterans rely on VA health care to take care of them, and the VA’s nurse practitioners are qualified to provide our veterans with the care they need and deserve.”4
Allowing veterans access to high-quality care is a 21st century solution that is “zero risk, zero cost, zero delay,” according to Dr. Cindy Cooke, President of the American Association of Nurse Practitioners (AANP).4 And it is not just the AANP that supports this rule change. Ninety-one percent of US households that are home to a veteran, and 88% of Americans overall, express support for the VA proposal. In a Mellman Group survey of more than 1,000 adults, strong support was noted across party lines (91% of Republicans; 90% of Democrats)—a rarity in our current political climate.4
Support for full practice authority for NPs at the VA has come from more than 60 organizations, including the Military Officers’ Association of America, the Air Force Sergeants Association, AARP (with 3.7 million veteran households in its membership), and 80 bipartisan members of Congress.5 At the AANP annual conference in San Antonio, Dr. Cooke was joined by leaders from the local American Legion and retired military officers who announced their support for this “change in practice.”3
However, among the more than 162,000 comments received by the VA during the public comment period, there were dissenting opinions. On July 13, 2016, Dr. Robert Wergin, Chair of the Board of the American Academy of Family Physicians (AAFP), sent a letter to Dr. David Shulkin, the Undersecretary of Health in the VA, stating that there were “significant concerns” about the rule change. His main point was that granting full practice authority to NPs would “alter the consistent standards of care for veterans over nonveterans in the states; further fragment the health care system; and dismantle physician-led team-based health care models.” He also stated that “the AAFP strongly opposes the unprecedented proposal to dismiss state practice authority regarding the authority of NPs.”6
Unprecedented? I don’t think so. I practiced as a family NP in the Navy for more than 20 years. I had my own patient panel, cared for active duty members and their families, and evaluated outcomes the same way my physician colleagues did. We practiced collaboratively and respectfully. We discussed patient plan issues, provided peer review on one another’s charts, and accepted new patients into our panels. It was a true collaborative practice.
Military nurses only need to be licensed in one state. The guidelines for NP practice were not based on the rules of the state in which we were licensed but were established by our professional practice association—just as the guidelines for physician practice were not based on the rules extant in their licensing state. I practiced successfully in many states and overseas, although I was licensed in a state that did not recognize plenary practice at the time.
The VA is attempting to respond to veterans’ need for access to care by adopting a model similar to what the military employs. It’s not a matter of superseding state regulations; it’s a matter of recognizing the education and training of health care professionals who can improve patient outcomes.
The opportunity to respond to the proposed amendment has now closed. Through its grassroots Veterans Deserve Care campaign, the AANP and its partners and supporters—clinicians, veterans, families, and others—submitted nearly 60,000 comments.2 Now we wait for the VA to review the abundance of feedback and issue their final decision.
I am hopeful that the VA will acknowledge the overwhelming evidence that our veterans deserve access to care led by highly qualified professionals. The old system isn’t working. Einstein said that the definition of insanity was to do the same thing over and over and expect a different outcome; maintaining a faulty system fits that description. NPs have a well-tested, evidence-based, high-quality education that encourages their ability to lead health care teams, perform collaboratively, and improve outcomes for those who have served our country.
Caring for active duty military and veterans is in the DNA of nurses. Florence Nightingale spent much of her post-Crimea life using evidence-based proposals and political influence to improve the health care of the soldiers and veterans of the British Empire. In Notes on Nursing, she spurred nurses to political action: “Let whoever [sic] is in charge keep this simple question in her [sic] head (not how can I always do this right thing myself, but) how can I provide for this right thing to be always done?”7 This advice should be taken to heart by all health care professionals: We can honor our veterans by advocating for and providing the health care access they need.
To share your thoughts, please contact us at [email protected]
1. Advanced practice registered nurses [2016-12338]. Fed Regist. May 25, 2016. https://federalregister.gov/a/2016-12338.
2. American Association of Nurse Practitioners. AANP and Air Force Sergeants Association urge VA to swiftly enact proposed rule. July 25, 2016. www.aanp.org/legislation-regu lation/federal-legislation/va-proposed-rule/173-press-room/2016-press-releases/ 1987-aanp-and-air-force-sergeants-associa tion-urge-va-to-swiftly-enact-proposed-rule. Accessed August 9, 2016.
3. American Association of Nurse Practitioners. AANP and veterans groups call for streamlined access to veteran’s health care. June 23, 2016. www.aanp.org/press-room/press-releases/173-press-room/2016-press-releases/1959-aanp-veteran-groups-call-for-streamlined-access-to-veterans-health-care. Accessed August 9, 2016.
4. American Association of Nurse Practitioners. National survey finds overwhelming support for VA rule granting veterans direct access to nurse practitioner care. July 20, 2016. www.aanp.org/press-room/press-releases/173-press-room/2016-press-releases/1986-national-survey-finds-overwhelming-support-for-va-rule-granting-veterans-direct-access-to-nurse-practition er-care. Accessed August 9, 2016.
5. American Association of Nurse Anesthetists. Nursing coalition and veterans groups join forces in unprecedented response to VA proposed rule to increase veterans’ access to care. June 28, 2016. www.aana.com/newsandjournal/News/Pages/062816-Nursing-Coalition-and-Veterans-Groups-Join-Forces-in-Unprecedented-Response-to-VA-Proposed-Rule.aspx. Accessed August 9, 2016.
6. Wergin RL. Letter to David Shulkin. July 13, 2016. www.aafp.org/dam/AAFP/docu ments/advocacy/workforce/scope/LT-VHA-APRN-071316.pdf. Accessed August 9, 2016 .
7. Nightingale F. Notes on Nursing: What It Is and What It Is Not. New York, NY: D. Appleton and Company; 1860.
On May 25, 2016, the Department of Veterans Affairs (VA) published a proposed rule change in the Federal Register under the simple heading “Advanced Practice Registered Nurses.” From such modest beginnings stemmed a potential game-changer for advanced practice clinicians in this country: In summary, the VA proposed to “amend its medical regulations to permit full practice authority of all VA advanced practice registered nurses (APRNs) when they are acting within the scope of their VA employment.”1
The impetus for the VA’s proposal is that 505,000 veterans wait 30 days to access care within the VA system—and 300,000 wait between 31 and 60 days for health services.2 Granting plenary practice to VA APRNs would enable them to respond to this backlog of patients, since veterans would have direct access to APRNs who practice within the VA system, regardless of their state of licensure.
More than 4,800 NPs work within the VA; they provide clinical assessments, order appropriate tests and medications, and develop patient-centered care plans.2,3 Research has documented that outcomes for patients whose care is managed by NPs are equal to or better than outcomes for similar patients who are managed by physicians.4 As Major General Vincent Boles of the US Army (retired) stated, “Veterans rely on VA health care to take care of them, and the VA’s nurse practitioners are qualified to provide our veterans with the care they need and deserve.”4
Allowing veterans access to high-quality care is a 21st century solution that is “zero risk, zero cost, zero delay,” according to Dr. Cindy Cooke, President of the American Association of Nurse Practitioners (AANP).4 And it is not just the AANP that supports this rule change. Ninety-one percent of US households that are home to a veteran, and 88% of Americans overall, express support for the VA proposal. In a Mellman Group survey of more than 1,000 adults, strong support was noted across party lines (91% of Republicans; 90% of Democrats)—a rarity in our current political climate.4
Support for full practice authority for NPs at the VA has come from more than 60 organizations, including the Military Officers’ Association of America, the Air Force Sergeants Association, AARP (with 3.7 million veteran households in its membership), and 80 bipartisan members of Congress.5 At the AANP annual conference in San Antonio, Dr. Cooke was joined by leaders from the local American Legion and retired military officers who announced their support for this “change in practice.”3
However, among the more than 162,000 comments received by the VA during the public comment period, there were dissenting opinions. On July 13, 2016, Dr. Robert Wergin, Chair of the Board of the American Academy of Family Physicians (AAFP), sent a letter to Dr. David Shulkin, the Undersecretary of Health in the VA, stating that there were “significant concerns” about the rule change. His main point was that granting full practice authority to NPs would “alter the consistent standards of care for veterans over nonveterans in the states; further fragment the health care system; and dismantle physician-led team-based health care models.” He also stated that “the AAFP strongly opposes the unprecedented proposal to dismiss state practice authority regarding the authority of NPs.”6
Unprecedented? I don’t think so. I practiced as a family NP in the Navy for more than 20 years. I had my own patient panel, cared for active duty members and their families, and evaluated outcomes the same way my physician colleagues did. We practiced collaboratively and respectfully. We discussed patient plan issues, provided peer review on one another’s charts, and accepted new patients into our panels. It was a true collaborative practice.
Military nurses only need to be licensed in one state. The guidelines for NP practice were not based on the rules of the state in which we were licensed but were established by our professional practice association—just as the guidelines for physician practice were not based on the rules extant in their licensing state. I practiced successfully in many states and overseas, although I was licensed in a state that did not recognize plenary practice at the time.
The VA is attempting to respond to veterans’ need for access to care by adopting a model similar to what the military employs. It’s not a matter of superseding state regulations; it’s a matter of recognizing the education and training of health care professionals who can improve patient outcomes.
The opportunity to respond to the proposed amendment has now closed. Through its grassroots Veterans Deserve Care campaign, the AANP and its partners and supporters—clinicians, veterans, families, and others—submitted nearly 60,000 comments.2 Now we wait for the VA to review the abundance of feedback and issue their final decision.
I am hopeful that the VA will acknowledge the overwhelming evidence that our veterans deserve access to care led by highly qualified professionals. The old system isn’t working. Einstein said that the definition of insanity was to do the same thing over and over and expect a different outcome; maintaining a faulty system fits that description. NPs have a well-tested, evidence-based, high-quality education that encourages their ability to lead health care teams, perform collaboratively, and improve outcomes for those who have served our country.
Caring for active duty military and veterans is in the DNA of nurses. Florence Nightingale spent much of her post-Crimea life using evidence-based proposals and political influence to improve the health care of the soldiers and veterans of the British Empire. In Notes on Nursing, she spurred nurses to political action: “Let whoever [sic] is in charge keep this simple question in her [sic] head (not how can I always do this right thing myself, but) how can I provide for this right thing to be always done?”7 This advice should be taken to heart by all health care professionals: We can honor our veterans by advocating for and providing the health care access they need.
To share your thoughts, please contact us at [email protected]
On May 25, 2016, the Department of Veterans Affairs (VA) published a proposed rule change in the Federal Register under the simple heading “Advanced Practice Registered Nurses.” From such modest beginnings stemmed a potential game-changer for advanced practice clinicians in this country: In summary, the VA proposed to “amend its medical regulations to permit full practice authority of all VA advanced practice registered nurses (APRNs) when they are acting within the scope of their VA employment.”1
The impetus for the VA’s proposal is that 505,000 veterans wait 30 days to access care within the VA system—and 300,000 wait between 31 and 60 days for health services.2 Granting plenary practice to VA APRNs would enable them to respond to this backlog of patients, since veterans would have direct access to APRNs who practice within the VA system, regardless of their state of licensure.
More than 4,800 NPs work within the VA; they provide clinical assessments, order appropriate tests and medications, and develop patient-centered care plans.2,3 Research has documented that outcomes for patients whose care is managed by NPs are equal to or better than outcomes for similar patients who are managed by physicians.4 As Major General Vincent Boles of the US Army (retired) stated, “Veterans rely on VA health care to take care of them, and the VA’s nurse practitioners are qualified to provide our veterans with the care they need and deserve.”4
Allowing veterans access to high-quality care is a 21st century solution that is “zero risk, zero cost, zero delay,” according to Dr. Cindy Cooke, President of the American Association of Nurse Practitioners (AANP).4 And it is not just the AANP that supports this rule change. Ninety-one percent of US households that are home to a veteran, and 88% of Americans overall, express support for the VA proposal. In a Mellman Group survey of more than 1,000 adults, strong support was noted across party lines (91% of Republicans; 90% of Democrats)—a rarity in our current political climate.4
Support for full practice authority for NPs at the VA has come from more than 60 organizations, including the Military Officers’ Association of America, the Air Force Sergeants Association, AARP (with 3.7 million veteran households in its membership), and 80 bipartisan members of Congress.5 At the AANP annual conference in San Antonio, Dr. Cooke was joined by leaders from the local American Legion and retired military officers who announced their support for this “change in practice.”3
However, among the more than 162,000 comments received by the VA during the public comment period, there were dissenting opinions. On July 13, 2016, Dr. Robert Wergin, Chair of the Board of the American Academy of Family Physicians (AAFP), sent a letter to Dr. David Shulkin, the Undersecretary of Health in the VA, stating that there were “significant concerns” about the rule change. His main point was that granting full practice authority to NPs would “alter the consistent standards of care for veterans over nonveterans in the states; further fragment the health care system; and dismantle physician-led team-based health care models.” He also stated that “the AAFP strongly opposes the unprecedented proposal to dismiss state practice authority regarding the authority of NPs.”6
Unprecedented? I don’t think so. I practiced as a family NP in the Navy for more than 20 years. I had my own patient panel, cared for active duty members and their families, and evaluated outcomes the same way my physician colleagues did. We practiced collaboratively and respectfully. We discussed patient plan issues, provided peer review on one another’s charts, and accepted new patients into our panels. It was a true collaborative practice.
Military nurses only need to be licensed in one state. The guidelines for NP practice were not based on the rules of the state in which we were licensed but were established by our professional practice association—just as the guidelines for physician practice were not based on the rules extant in their licensing state. I practiced successfully in many states and overseas, although I was licensed in a state that did not recognize plenary practice at the time.
The VA is attempting to respond to veterans’ need for access to care by adopting a model similar to what the military employs. It’s not a matter of superseding state regulations; it’s a matter of recognizing the education and training of health care professionals who can improve patient outcomes.
The opportunity to respond to the proposed amendment has now closed. Through its grassroots Veterans Deserve Care campaign, the AANP and its partners and supporters—clinicians, veterans, families, and others—submitted nearly 60,000 comments.2 Now we wait for the VA to review the abundance of feedback and issue their final decision.
I am hopeful that the VA will acknowledge the overwhelming evidence that our veterans deserve access to care led by highly qualified professionals. The old system isn’t working. Einstein said that the definition of insanity was to do the same thing over and over and expect a different outcome; maintaining a faulty system fits that description. NPs have a well-tested, evidence-based, high-quality education that encourages their ability to lead health care teams, perform collaboratively, and improve outcomes for those who have served our country.
Caring for active duty military and veterans is in the DNA of nurses. Florence Nightingale spent much of her post-Crimea life using evidence-based proposals and political influence to improve the health care of the soldiers and veterans of the British Empire. In Notes on Nursing, she spurred nurses to political action: “Let whoever [sic] is in charge keep this simple question in her [sic] head (not how can I always do this right thing myself, but) how can I provide for this right thing to be always done?”7 This advice should be taken to heart by all health care professionals: We can honor our veterans by advocating for and providing the health care access they need.
To share your thoughts, please contact us at [email protected]
1. Advanced practice registered nurses [2016-12338]. Fed Regist. May 25, 2016. https://federalregister.gov/a/2016-12338.
2. American Association of Nurse Practitioners. AANP and Air Force Sergeants Association urge VA to swiftly enact proposed rule. July 25, 2016. www.aanp.org/legislation-regu lation/federal-legislation/va-proposed-rule/173-press-room/2016-press-releases/ 1987-aanp-and-air-force-sergeants-associa tion-urge-va-to-swiftly-enact-proposed-rule. Accessed August 9, 2016.
3. American Association of Nurse Practitioners. AANP and veterans groups call for streamlined access to veteran’s health care. June 23, 2016. www.aanp.org/press-room/press-releases/173-press-room/2016-press-releases/1959-aanp-veteran-groups-call-for-streamlined-access-to-veterans-health-care. Accessed August 9, 2016.
4. American Association of Nurse Practitioners. National survey finds overwhelming support for VA rule granting veterans direct access to nurse practitioner care. July 20, 2016. www.aanp.org/press-room/press-releases/173-press-room/2016-press-releases/1986-national-survey-finds-overwhelming-support-for-va-rule-granting-veterans-direct-access-to-nurse-practition er-care. Accessed August 9, 2016.
5. American Association of Nurse Anesthetists. Nursing coalition and veterans groups join forces in unprecedented response to VA proposed rule to increase veterans’ access to care. June 28, 2016. www.aana.com/newsandjournal/News/Pages/062816-Nursing-Coalition-and-Veterans-Groups-Join-Forces-in-Unprecedented-Response-to-VA-Proposed-Rule.aspx. Accessed August 9, 2016.
6. Wergin RL. Letter to David Shulkin. July 13, 2016. www.aafp.org/dam/AAFP/docu ments/advocacy/workforce/scope/LT-VHA-APRN-071316.pdf. Accessed August 9, 2016 .
7. Nightingale F. Notes on Nursing: What It Is and What It Is Not. New York, NY: D. Appleton and Company; 1860.
1. Advanced practice registered nurses [2016-12338]. Fed Regist. May 25, 2016. https://federalregister.gov/a/2016-12338.
2. American Association of Nurse Practitioners. AANP and Air Force Sergeants Association urge VA to swiftly enact proposed rule. July 25, 2016. www.aanp.org/legislation-regu lation/federal-legislation/va-proposed-rule/173-press-room/2016-press-releases/ 1987-aanp-and-air-force-sergeants-associa tion-urge-va-to-swiftly-enact-proposed-rule. Accessed August 9, 2016.
3. American Association of Nurse Practitioners. AANP and veterans groups call for streamlined access to veteran’s health care. June 23, 2016. www.aanp.org/press-room/press-releases/173-press-room/2016-press-releases/1959-aanp-veteran-groups-call-for-streamlined-access-to-veterans-health-care. Accessed August 9, 2016.
4. American Association of Nurse Practitioners. National survey finds overwhelming support for VA rule granting veterans direct access to nurse practitioner care. July 20, 2016. www.aanp.org/press-room/press-releases/173-press-room/2016-press-releases/1986-national-survey-finds-overwhelming-support-for-va-rule-granting-veterans-direct-access-to-nurse-practition er-care. Accessed August 9, 2016.
5. American Association of Nurse Anesthetists. Nursing coalition and veterans groups join forces in unprecedented response to VA proposed rule to increase veterans’ access to care. June 28, 2016. www.aana.com/newsandjournal/News/Pages/062816-Nursing-Coalition-and-Veterans-Groups-Join-Forces-in-Unprecedented-Response-to-VA-Proposed-Rule.aspx. Accessed August 9, 2016.
6. Wergin RL. Letter to David Shulkin. July 13, 2016. www.aafp.org/dam/AAFP/docu ments/advocacy/workforce/scope/LT-VHA-APRN-071316.pdf. Accessed August 9, 2016 .
7. Nightingale F. Notes on Nursing: What It Is and What It Is Not. New York, NY: D. Appleton and Company; 1860.
When Man’s Legs “Give Out,” His Buttocks Takes the Brunt
ANSWER
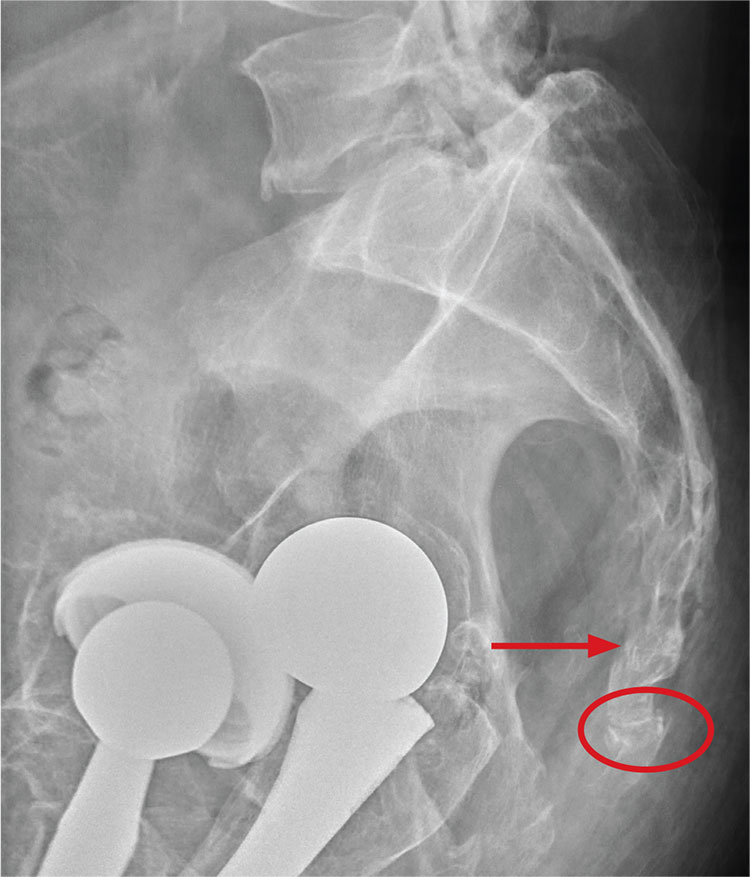
There are degenerative changes present. Bilateral hip prostheses are noted. Within the coccyx, there is bone remodeling and angulation that are likely chronic and related to remote trauma or injury (arrow). Below this, some cortical lucency (circled) is noted, most likely consistent with an acute fracture. The patient was prescribed a nonsteroidal medication and a mild narcotic pain medication.
ANSWER
There are degenerative changes present. Bilateral hip prostheses are noted. Within the coccyx, there is bone remodeling and angulation that are likely chronic and related to remote trauma or injury (arrow). Below this, some cortical lucency (circled) is noted, most likely consistent with an acute fracture. The patient was prescribed a nonsteroidal medication and a mild narcotic pain medication.
ANSWER
There are degenerative changes present. Bilateral hip prostheses are noted. Within the coccyx, there is bone remodeling and angulation that are likely chronic and related to remote trauma or injury (arrow). Below this, some cortical lucency (circled) is noted, most likely consistent with an acute fracture. The patient was prescribed a nonsteroidal medication and a mild narcotic pain medication.

A 75-year-old man presents to the urgent care center for evaluation of pain in his buttocks after a fall. He states he was walking when his “legs gave out” and he hit the ground. He landed squarely on his buttocks, causing immediate pain. He was eventually able to get up with some assistance. He denies current weakness or any bowel or bladder complaints.
His medical/surgical history is significant for coronary artery disease, hypertension, and bilateral hip replacements. Physical exam reveals an elderly male who is uncomfortable but in no obvious distress. His vital signs are stable. He has moderate point tenderness over his sacrum but is able to move all his extremities well, with normal strength.
Radiograph of his sacrum/coccyx is shown. What is your impression?
Maybe it is all in your head

Origin of pain: Brain vs body. Recent research provides strong evidence that in some cases of intractable chronic pain, the origin of the pain signal is in the brain—rather than the body. In this issue of JFP, Davis and Vanderah discuss this type of pain as “a third kind” that needs to be treated in a manner that completely differs from that for peripherally generated pain. They refer to the traditional kinds of pain as either nociceptive (resulting from tissue damage or insult), or neuropathic (due to dysfunctional stimulation of peripheral nerves). The neurophysiology of the third kind of pain, which I will call “centrally generated pain,” is not fully understood, but neuroimaging and other sophisticated methods are identifying areas of the brain that become activated by psychological trauma, leading to significant painful suffering in the absence of tissue damage, or that is far out of proportion to physical insult.
The bad news for primary care physicians is that this third kind of pain is difficult, if not impossible, to treat with our traditional armamentarium of pain medications and physical modalities. In fact, these patients are often at risk for addiction, as doses of ineffective narcotics are escalated.
The good news is that clinical researchers have begun to identify ways to effectively treat centrally generated pain. For example, Schubiner et al used a novel psychological approach that involved helping patients "learn that their pain is influenced primarily by central nervous system psychological processes, and to enhance awareness and expression of emotions related to psychological trauma or conflict."1 Thirty percent of the 72 participants in the preliminary, uncontrolled trial experienced a 70% reduction in pain. Dr. Schubiner’s research is ongoing and supported by funding from the National Institutes of Health.
Proper diagnosis is paramount. Of course, proper diagnosis is paramount because an individual may suffer from more than one of the 3 kinds of pain and require different approaches for each. Thorough evaluation at a multidisciplinary pain clinic is a good place to start. Once the diagnoses are sorted out, it will then be possible to treat each component of pain appropriately.
Dr. Schubiner’s methods and other new and developing treatment approaches to chronic pain will help us better relieve patients’ suffering, reduce narcotic overuse, and relieve our own anxiety about caring for these challenging patients.
1. Burger AJ, Lumley MA, Carty JN, et al. The effects of a novel psychological attribution and emotional awareness and expression therapy for chronic musculoskeletal pain: a preliminary, uncontrolled trial. J Psychosom Res. 2016;81:1-8.
Origin of pain: Brain vs body. Recent research provides strong evidence that in some cases of intractable chronic pain, the origin of the pain signal is in the brain—rather than the body. In this issue of JFP, Davis and Vanderah discuss this type of pain as “a third kind” that needs to be treated in a manner that completely differs from that for peripherally generated pain. They refer to the traditional kinds of pain as either nociceptive (resulting from tissue damage or insult), or neuropathic (due to dysfunctional stimulation of peripheral nerves). The neurophysiology of the third kind of pain, which I will call “centrally generated pain,” is not fully understood, but neuroimaging and other sophisticated methods are identifying areas of the brain that become activated by psychological trauma, leading to significant painful suffering in the absence of tissue damage, or that is far out of proportion to physical insult.
The bad news for primary care physicians is that this third kind of pain is difficult, if not impossible, to treat with our traditional armamentarium of pain medications and physical modalities. In fact, these patients are often at risk for addiction, as doses of ineffective narcotics are escalated.
The good news is that clinical researchers have begun to identify ways to effectively treat centrally generated pain. For example, Schubiner et al used a novel psychological approach that involved helping patients "learn that their pain is influenced primarily by central nervous system psychological processes, and to enhance awareness and expression of emotions related to psychological trauma or conflict."1 Thirty percent of the 72 participants in the preliminary, uncontrolled trial experienced a 70% reduction in pain. Dr. Schubiner’s research is ongoing and supported by funding from the National Institutes of Health.
Proper diagnosis is paramount. Of course, proper diagnosis is paramount because an individual may suffer from more than one of the 3 kinds of pain and require different approaches for each. Thorough evaluation at a multidisciplinary pain clinic is a good place to start. Once the diagnoses are sorted out, it will then be possible to treat each component of pain appropriately.
Dr. Schubiner’s methods and other new and developing treatment approaches to chronic pain will help us better relieve patients’ suffering, reduce narcotic overuse, and relieve our own anxiety about caring for these challenging patients.
1. Burger AJ, Lumley MA, Carty JN, et al. The effects of a novel psychological attribution and emotional awareness and expression therapy for chronic musculoskeletal pain: a preliminary, uncontrolled trial. J Psychosom Res. 2016;81:1-8.
Origin of pain: Brain vs body. Recent research provides strong evidence that in some cases of intractable chronic pain, the origin of the pain signal is in the brain—rather than the body. In this issue of JFP, Davis and Vanderah discuss this type of pain as “a third kind” that needs to be treated in a manner that completely differs from that for peripherally generated pain. They refer to the traditional kinds of pain as either nociceptive (resulting from tissue damage or insult), or neuropathic (due to dysfunctional stimulation of peripheral nerves). The neurophysiology of the third kind of pain, which I will call “centrally generated pain,” is not fully understood, but neuroimaging and other sophisticated methods are identifying areas of the brain that become activated by psychological trauma, leading to significant painful suffering in the absence of tissue damage, or that is far out of proportion to physical insult.
The bad news for primary care physicians is that this third kind of pain is difficult, if not impossible, to treat with our traditional armamentarium of pain medications and physical modalities. In fact, these patients are often at risk for addiction, as doses of ineffective narcotics are escalated.
The good news is that clinical researchers have begun to identify ways to effectively treat centrally generated pain. For example, Schubiner et al used a novel psychological approach that involved helping patients "learn that their pain is influenced primarily by central nervous system psychological processes, and to enhance awareness and expression of emotions related to psychological trauma or conflict."1 Thirty percent of the 72 participants in the preliminary, uncontrolled trial experienced a 70% reduction in pain. Dr. Schubiner’s research is ongoing and supported by funding from the National Institutes of Health.
Proper diagnosis is paramount. Of course, proper diagnosis is paramount because an individual may suffer from more than one of the 3 kinds of pain and require different approaches for each. Thorough evaluation at a multidisciplinary pain clinic is a good place to start. Once the diagnoses are sorted out, it will then be possible to treat each component of pain appropriately.
Dr. Schubiner’s methods and other new and developing treatment approaches to chronic pain will help us better relieve patients’ suffering, reduce narcotic overuse, and relieve our own anxiety about caring for these challenging patients.
1. Burger AJ, Lumley MA, Carty JN, et al. The effects of a novel psychological attribution and emotional awareness and expression therapy for chronic musculoskeletal pain: a preliminary, uncontrolled trial. J Psychosom Res. 2016;81:1-8.
Why did testing stop at EKG—especially given family history? ... More
Why did testing stop at EKG—especially given family history?
AFTER COMPLAINING OF CHEST PAIN, a 37-year-old man underwent an electrocardiogram (EKG) examination. The doctor concluded that the pain was not cardiac in nature. Two years later, the patient died of a sudden cardiac event associated with coronary atherosclerotic disease.
PLAINTIFF’S CLAIM The decedent suffered from high cholesterol and had a family history of cardiac issues, yet no additional testing was performed when the patient’s complaints continued.
THE DEFENSE No information on the defense is available.
VERDICT $3 million settlement.
COMMENT This is déjà vu for me. A colleague of mine had a nearly identical case a few years ago, but the patient died several days later. In the case described here, the high cholesterol and family history were red flags. A normal EKG does not rule out angina. I do wonder what happened, however, in the 2 years between the office visit and the patient’s sudden death. The chest pain at the office visit may well have been non-cardiac, but it appears the jury was not convinced.
2 FPs overlook boy’s proteinuria; delay in Dx costs him a kidney
AN 11-YEAR-OLD BOY underwent a laparoscopic appendectomy that included a urinalysis. Following the surgery, the surgeon notified the family physician (FP) that the patient’s urinalysis showed >300 mg/dL of protein. The result was unusual and required follow-up. The surgeon felt that the urinalysis result might be related to the proximity of the appendicitis to the boy’s ureter. The boy was evaluated on several other occasions by the FP, but no work-up was performed.
Three years later, the boy saw a different FP, who noted that the child had elevated blood pressure and blurry vision—among other symptoms. The boy’s renal function tests were documented as abnormal; however, the patient and his mother were never notified of this. Also, the patient was never referred to a nephrologist or neurologist and there was no intervention for a potential kidney abnormality.
Two years later, an associate of the FP ordered further blood tests that showed a clear abnormality with regard to the integrity of the child’s kidney function. The boy was evaluated at a hospital and diagnosed with end-stage renal disease. He received a kidney transplant 3 months later and requires lifetime medical care as a result of the transplant. The boy will likely require further transplants in 10-year increments.
PLAINTIFF’S CLAIM Both FPs deviated from the accepted standard of care when they failed to order further testing as a result of the abnormal laboratory tests. Earlier intervention may have prolonged the life of the boy’s kidney, thereby postponing the need for kidney replacements.
THE DEFENSE No information on the defense is available.
VERDICT $1.25 million Massachusetts settlement.
COMMENT 300 mg/dL is a significant amount of proteinuria and requires further testing. Why didn’t the FP follow up? Was a summary of the hospitalization sent to him/her? Certainly the diagnosis should have been made by the second FP, and the patient should’ve been referred to a nephrologist. A lawsuit would most likely have been averted had this happened. Delayed diagnosis accounts for a high proportion of malpractice suits against FPs.
Duodenal ulcer mistakenly attributed to Crohn’s disease
A 47-YEAR-OLD MAN with a history of Crohn’s disease began experiencing persistent abdominal pain. He hadn’t had symptoms of his Crohn’s disease in over 12 years. Nevertheless, doctors diagnosed his pain as an aggravation of the disease and gave him treatment based on this diagnosis. In fact, though, the man had an acute duodenal ulcer that had progressed and perforated. The patient underwent 12 surgeries (with complications) and almost 2 years of near-constant hospitalization as a result of the misdiagnosis. He now requires 24-hour care in all aspects of his life.
PLAINTIFF’S CLAIM The doctors were negligent in their failure to consider and diagnose a peptic ulcer when the plaintiff’s symptoms indicated issues other than Crohn’s disease.
THE DEFENSE No information on the defense is available.
VERDICT $28 million Maryland verdict.
COMMENT I suspect this was a tough diagnosis, given the patient’s prior history of Crohn’s disease. We are not told the nature of the abdominal pain. If the patient had classic epigastric pain, peptic ulcer disease should have been investigated. This case serves as a reminder that patients can have more than one disease of an organ system, and it reminds us of the need for a careful history and close follow-up if a complaint does not resolve.
Why did testing stop at EKG—especially given family history?
AFTER COMPLAINING OF CHEST PAIN, a 37-year-old man underwent an electrocardiogram (EKG) examination. The doctor concluded that the pain was not cardiac in nature. Two years later, the patient died of a sudden cardiac event associated with coronary atherosclerotic disease.
PLAINTIFF’S CLAIM The decedent suffered from high cholesterol and had a family history of cardiac issues, yet no additional testing was performed when the patient’s complaints continued.
THE DEFENSE No information on the defense is available.
VERDICT $3 million settlement.
COMMENT This is déjà vu for me. A colleague of mine had a nearly identical case a few years ago, but the patient died several days later. In the case described here, the high cholesterol and family history were red flags. A normal EKG does not rule out angina. I do wonder what happened, however, in the 2 years between the office visit and the patient’s sudden death. The chest pain at the office visit may well have been non-cardiac, but it appears the jury was not convinced.
2 FPs overlook boy’s proteinuria; delay in Dx costs him a kidney
AN 11-YEAR-OLD BOY underwent a laparoscopic appendectomy that included a urinalysis. Following the surgery, the surgeon notified the family physician (FP) that the patient’s urinalysis showed >300 mg/dL of protein. The result was unusual and required follow-up. The surgeon felt that the urinalysis result might be related to the proximity of the appendicitis to the boy’s ureter. The boy was evaluated on several other occasions by the FP, but no work-up was performed.
Three years later, the boy saw a different FP, who noted that the child had elevated blood pressure and blurry vision—among other symptoms. The boy’s renal function tests were documented as abnormal; however, the patient and his mother were never notified of this. Also, the patient was never referred to a nephrologist or neurologist and there was no intervention for a potential kidney abnormality.
Two years later, an associate of the FP ordered further blood tests that showed a clear abnormality with regard to the integrity of the child’s kidney function. The boy was evaluated at a hospital and diagnosed with end-stage renal disease. He received a kidney transplant 3 months later and requires lifetime medical care as a result of the transplant. The boy will likely require further transplants in 10-year increments.
PLAINTIFF’S CLAIM Both FPs deviated from the accepted standard of care when they failed to order further testing as a result of the abnormal laboratory tests. Earlier intervention may have prolonged the life of the boy’s kidney, thereby postponing the need for kidney replacements.
THE DEFENSE No information on the defense is available.
VERDICT $1.25 million Massachusetts settlement.
COMMENT 300 mg/dL is a significant amount of proteinuria and requires further testing. Why didn’t the FP follow up? Was a summary of the hospitalization sent to him/her? Certainly the diagnosis should have been made by the second FP, and the patient should’ve been referred to a nephrologist. A lawsuit would most likely have been averted had this happened. Delayed diagnosis accounts for a high proportion of malpractice suits against FPs.
Duodenal ulcer mistakenly attributed to Crohn’s disease
A 47-YEAR-OLD MAN with a history of Crohn’s disease began experiencing persistent abdominal pain. He hadn’t had symptoms of his Crohn’s disease in over 12 years. Nevertheless, doctors diagnosed his pain as an aggravation of the disease and gave him treatment based on this diagnosis. In fact, though, the man had an acute duodenal ulcer that had progressed and perforated. The patient underwent 12 surgeries (with complications) and almost 2 years of near-constant hospitalization as a result of the misdiagnosis. He now requires 24-hour care in all aspects of his life.
PLAINTIFF’S CLAIM The doctors were negligent in their failure to consider and diagnose a peptic ulcer when the plaintiff’s symptoms indicated issues other than Crohn’s disease.
THE DEFENSE No information on the defense is available.
VERDICT $28 million Maryland verdict.
COMMENT I suspect this was a tough diagnosis, given the patient’s prior history of Crohn’s disease. We are not told the nature of the abdominal pain. If the patient had classic epigastric pain, peptic ulcer disease should have been investigated. This case serves as a reminder that patients can have more than one disease of an organ system, and it reminds us of the need for a careful history and close follow-up if a complaint does not resolve.
Why did testing stop at EKG—especially given family history?
AFTER COMPLAINING OF CHEST PAIN, a 37-year-old man underwent an electrocardiogram (EKG) examination. The doctor concluded that the pain was not cardiac in nature. Two years later, the patient died of a sudden cardiac event associated with coronary atherosclerotic disease.
PLAINTIFF’S CLAIM The decedent suffered from high cholesterol and had a family history of cardiac issues, yet no additional testing was performed when the patient’s complaints continued.
THE DEFENSE No information on the defense is available.
VERDICT $3 million settlement.
COMMENT This is déjà vu for me. A colleague of mine had a nearly identical case a few years ago, but the patient died several days later. In the case described here, the high cholesterol and family history were red flags. A normal EKG does not rule out angina. I do wonder what happened, however, in the 2 years between the office visit and the patient’s sudden death. The chest pain at the office visit may well have been non-cardiac, but it appears the jury was not convinced.
2 FPs overlook boy’s proteinuria; delay in Dx costs him a kidney
AN 11-YEAR-OLD BOY underwent a laparoscopic appendectomy that included a urinalysis. Following the surgery, the surgeon notified the family physician (FP) that the patient’s urinalysis showed >300 mg/dL of protein. The result was unusual and required follow-up. The surgeon felt that the urinalysis result might be related to the proximity of the appendicitis to the boy’s ureter. The boy was evaluated on several other occasions by the FP, but no work-up was performed.
Three years later, the boy saw a different FP, who noted that the child had elevated blood pressure and blurry vision—among other symptoms. The boy’s renal function tests were documented as abnormal; however, the patient and his mother were never notified of this. Also, the patient was never referred to a nephrologist or neurologist and there was no intervention for a potential kidney abnormality.
Two years later, an associate of the FP ordered further blood tests that showed a clear abnormality with regard to the integrity of the child’s kidney function. The boy was evaluated at a hospital and diagnosed with end-stage renal disease. He received a kidney transplant 3 months later and requires lifetime medical care as a result of the transplant. The boy will likely require further transplants in 10-year increments.
PLAINTIFF’S CLAIM Both FPs deviated from the accepted standard of care when they failed to order further testing as a result of the abnormal laboratory tests. Earlier intervention may have prolonged the life of the boy’s kidney, thereby postponing the need for kidney replacements.
THE DEFENSE No information on the defense is available.
VERDICT $1.25 million Massachusetts settlement.
COMMENT 300 mg/dL is a significant amount of proteinuria and requires further testing. Why didn’t the FP follow up? Was a summary of the hospitalization sent to him/her? Certainly the diagnosis should have been made by the second FP, and the patient should’ve been referred to a nephrologist. A lawsuit would most likely have been averted had this happened. Delayed diagnosis accounts for a high proportion of malpractice suits against FPs.
Duodenal ulcer mistakenly attributed to Crohn’s disease
A 47-YEAR-OLD MAN with a history of Crohn’s disease began experiencing persistent abdominal pain. He hadn’t had symptoms of his Crohn’s disease in over 12 years. Nevertheless, doctors diagnosed his pain as an aggravation of the disease and gave him treatment based on this diagnosis. In fact, though, the man had an acute duodenal ulcer that had progressed and perforated. The patient underwent 12 surgeries (with complications) and almost 2 years of near-constant hospitalization as a result of the misdiagnosis. He now requires 24-hour care in all aspects of his life.
PLAINTIFF’S CLAIM The doctors were negligent in their failure to consider and diagnose a peptic ulcer when the plaintiff’s symptoms indicated issues other than Crohn’s disease.
THE DEFENSE No information on the defense is available.
VERDICT $28 million Maryland verdict.
COMMENT I suspect this was a tough diagnosis, given the patient’s prior history of Crohn’s disease. We are not told the nature of the abdominal pain. If the patient had classic epigastric pain, peptic ulcer disease should have been investigated. This case serves as a reminder that patients can have more than one disease of an organ system, and it reminds us of the need for a careful history and close follow-up if a complaint does not resolve.
Need-to-know information for the 2016-2017 flu season
The Advisory Committee on Immunization Practices (ACIP) took the unusual step at its June 2016 meeting of recommending against using a currently licensed vaccine, live attenuated influenza vaccine (LAIV), in the 2016-2017 influenza season.1 ACIP based its recommendation on surveillance data collected by the US Influenza Vaccine Effectiveness Network of the Centers for Disease Control and Prevention (CDC), which showed poor effectiveness by the LAIV vaccine among children and adolescents during the past 3 years.
The US Food and Drug Administration (FDA), however, has chosen not to take any action on this matter, saying on its Web site it “has determined that specific regulatory action is not warranted at this time. This determination is based on FDA’s review of manufacturing and clinical data supporting licensure … the totality of the evidence presented at the ACIP meeting, taking into account the inherent limitations of observational studies conducted to evaluate influenza vaccine effectiveness, as well as the well-known variability of influenza vaccine effectiveness across influenza seasons.”2
CDC data for the 2015-2016 flu season showed the effectiveness of LAIV to be just 3% among children 2 years through 17 years of age.3 The reason for this apparent lack of effectiveness is unknown. Other LAIV-effectiveness studies conducted in the 2015-2016 season—one each, in the United States, United Kingdom, and Finland—had results that differed from the CDC surveillance data, with effectiveness ranging from 46% to 58% against all strains combined.2 These results are comparable to vaccine effectiveness found in observational studies in children for both LAIV and inactivated influenza vaccines (IIV) in prior seasons.2
Vaccine manufacturers had projected that 171 to 176 million doses of flu vaccine, in all forms, would be available in the United States during the 2016-2017 season.3 LAIV accounts for about 8% of the total supply of influenza vaccine in the United States,3 and ACIP’s recommendation is not expected to create shortages of other options for the upcoming season. However, the LAIV accounts for one-third of flu vaccines administered to children, and clinicians who provide vaccinations to children have already ordered their vaccine supplies for the upcoming season. Also, it is not clear if children who have previously received the LAIV product will now accept other options for influenza vaccination—all of which involve an injection.
Whether the recommendation against LAIV will continue after this season is also unknown.
What happened during the 2015-2016 influenza season?
The 2015-2016 influenza season was relatively mild with the peak activity occurring in March, somewhat later than in previous years. The circulating influenza strains matched closely to those in the vaccine, making it more effective than the previous year’s vaccine. The predominant circulating strain was A (H1N1), accounting for 58% of illness; A (H3N2) caused 6% of cases and all B types together accounted for 34%.4 The hospitalization rate for all ages was 31.3/100,000 compared with 64.1 the year before.5 There were 85 pediatric deaths compared with 148 in 2014-2015.6
Vaccine effectiveness among all age groups and against all circulating strains was 47%.4 No major vaccine safety concerns were detected. Among those who received IIV3, there was a slight increase in the incidence of Guillain-Barré syndrome of 2.6 cases per one million vaccines.7
Other recommendations for 2016-2017
Once again, ACIP recommends influenza vaccine for all individuals 6 months and older.8 The CDC additionally specifies particular groups that should not skip vaccination given that they are at high risk of complications from influenza infection or because they could expose high-risk individuals to infection (TABLE 1).9
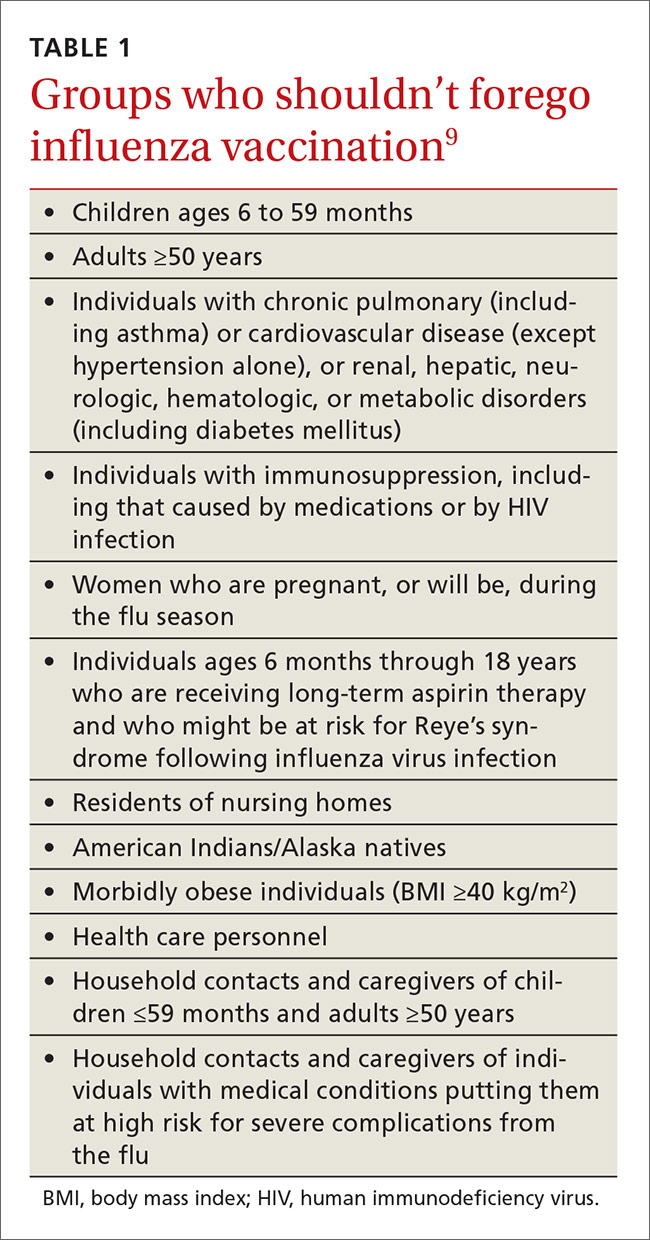
There will continue to be a selection of trivalent and quadrivalent influenza vaccine products in 2016-2017. Trivalent products will contain 3 viral strains: A/California/7/2009 (H1N1), A/Hong Kong/4801/2014 (H3N2) and B/Brisbane/60/2008.10 The quadrivalent products will contain those 3 antigens plus B/Phuket/3073/2013.10 The H3N2 strain is different from the one in last year’s vaccine. Each year, influenza experts analyze surveillance data to predict which circulating strains will predominate in North America, and these antigens constitute the vaccine formulation. The accuracy of this prediction in large part determines how effective the vaccine will be that season.
Two new vaccines have been approved for use in the United States. A quadrivalent cell culture inactivated vaccine (CCIV4), Flucelvax, was licensed in May 2016. It is prepared from virus propagated in canine kidney cells, not with an egg-based production process. It is approved for use in individuals 4 years of age and older.8 Fluad, an adjuvanted trivalent inactivated influenza vaccine, was licensed in late 2015 for individuals 65 years of age and older.8 This is the first adjuvanted influenza vaccine licensed in the United States and will compete with high-dose quadrivalent vaccine for use in older adults. ACIP does not express a preference for any vaccine in this age group.
Two other vaccines should also be available by this fall: Flublok, a quadrivalent recombinant influenza vaccine for individuals 18 years and older, and Flulaval, a quadrivalent inactivated influenza vaccine, for individuals 6 months of age and older. TABLE 211 lists approved influenza vaccines.
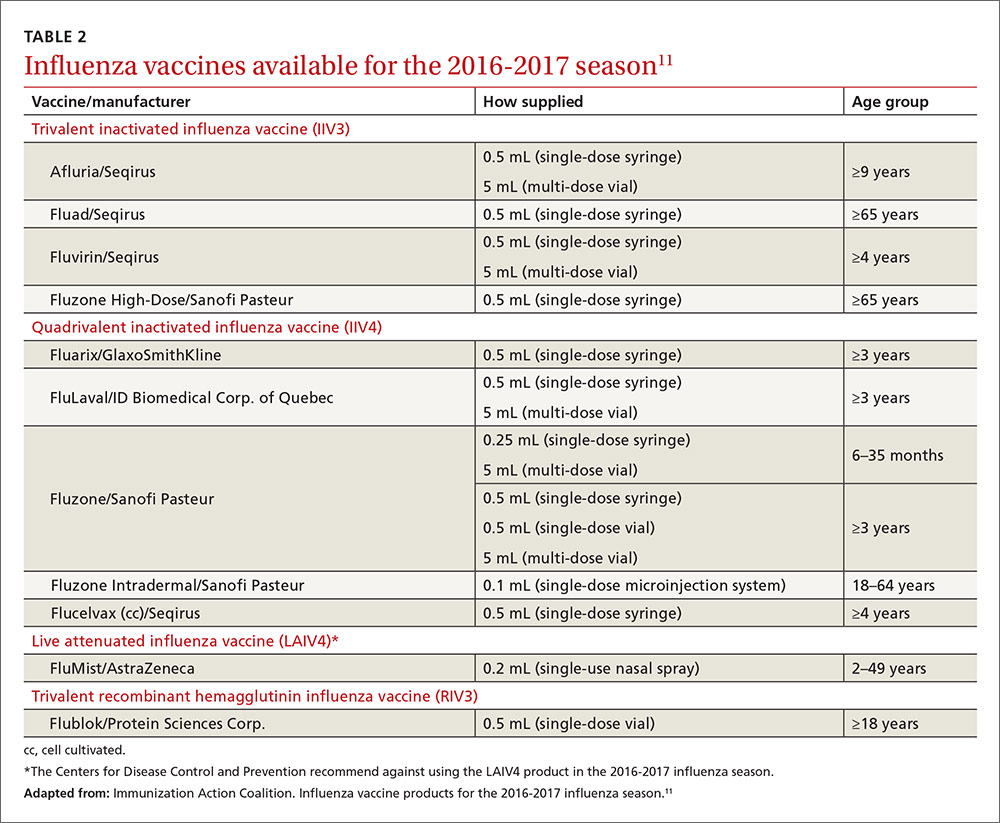
Issues specific to children
Deciding how many vaccine doses children need has been further simplified. Children younger than 9 years need 2 doses if they have received fewer than 2 doses of trivalent or quadrivalent influenza vaccine before July 1, 2016. The interval between the 2 doses should be at least 4 weeks. The 2 doses do not have to be the same product; importantly, do not delay a second dose just to obtain the same product used for the first dose. Also, one dose can be trivalent and the other one quadrivalent, although this offers less-than-optimal protection against the B-virus that is only in the quadrivalent product.
Children younger than 9 years require only one dose if they have received 2 or more total doses of trivalent or quadrivalent influenza vaccine before July 1, 2016. The 2 previous doses need not have been received during the same influenza season or consecutive influenza seasons.
In children ages 6 through 23 months there is a slight increased risk of febrile seizure if the influenza vaccine is co-administered with other vaccines, specifically pneumococcal conjugate vaccine (PCV 13) and diphtheria-tetanus-acellular-pertussis (DTaP). The 3 vaccines administered at the same time result in 30 febrile seizures per 100,000 children;12 the rate is lower when influenza vaccine is co-administered with only one of the others. ACIP believes that the risk of a febrile seizure, which does no long-term harm, does not warrant delaying vaccines that could be co-administered.13
Egg allergy requires no special precautions
Evidence continues to grow that influenza vaccine products do not contain enough egg protein to cause significant problems in those with a history of egg allergies. This year’s recommendations state that no special precautions are needed regarding the anatomic site of immunization or the length of observation after administering influenza vaccine in those with a history of allergies to eggs, no matter how severe. All vaccine-administration facilities should be able to respond to any hypersensitivity reaction, and the standard waiting time for observation after all vaccinations is 15 minutes.
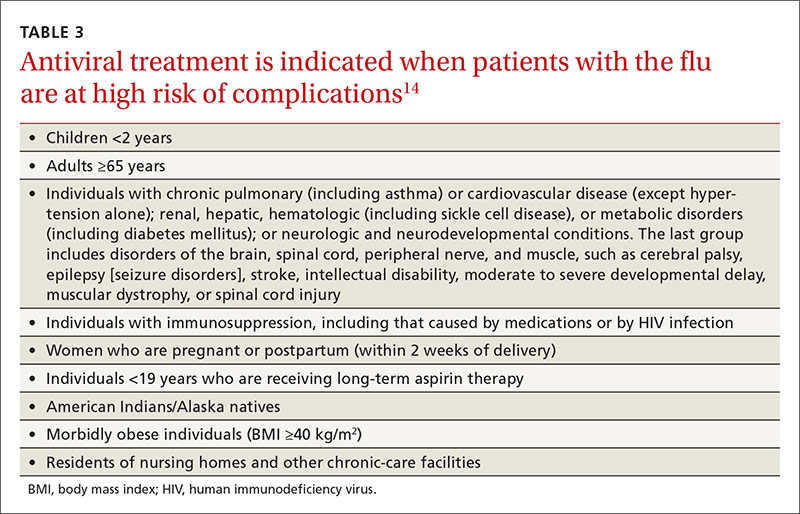
Antiviral medications for treatment or prevention
Most influenza strains circulating in 2016-2017 are expected to remain sensitive to oseltamivir and zanamivir, which can be used for treatment or disease prevention. A third neuraminidase inhibitor, peramivir, is available for intravenous use in adults 18 and older. Treatment is recommended for those who have confirmed or suspected influenza and are at high risk for complications (TABLE 3).14 Consideration of antiviral chemoprevention is recommended under certain circumstances (TABLE 4).15,16 The CDC influenza Web site lists recommended doses and duration for each antiviral for treatment and chemoprevention.15
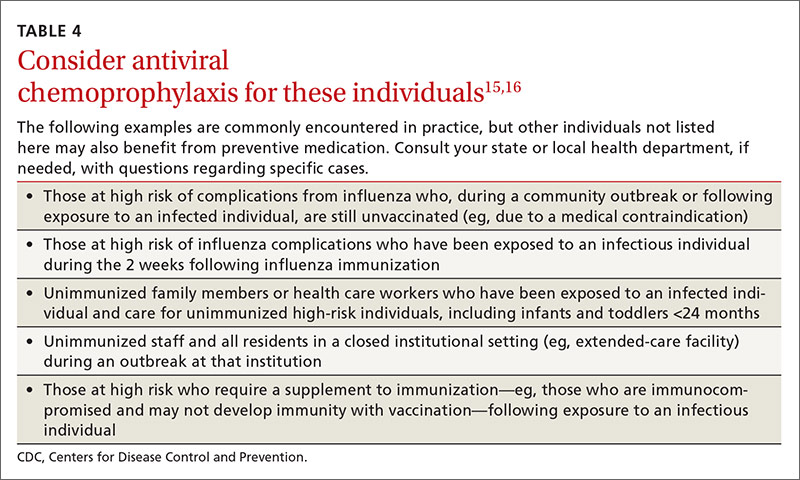
1. Grohskopf LA, Sokolow LZ, Broder KR, et al. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2016-17 influenza season. MMWR Recomm Rep. 2016;65:1-54.
2. U.S. Food and Drug Administration. FDA information regarding FluMist quadrivalent vaccine. Available at: http://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm508761.htm. Accessed July 13, 2016.
3. Centers for Disease Control and Prevention. ACIP votes down use of LAIV for 2016-2017 flu season. Available at: http://www.cdc.gov/media/releases/2016/s0622-laiv-flu.html. Accessed July 13, 2016.
4. Flannery B, Chung J. Influenza vaccine effectiveness, including LAIV vs IIV in children and adolescents, US Flu VE Network, 2015-2016. Presented at: meeting of the Advisory Committee on Immunization Practices; June 22, 2016; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2016-06/influenza-05-flannery.pdf. Accessed July 22, 2016.
5. Centers for Disease Control and Prevention. FluView. Laboratory-confirmed influenza hospitalizations. Available at: http://gis.cdc.gov/GRASP/Fluview/FluHospRates.html. Accessed July 25, 2016.
6. Centers for Disease Control and Prevention. FluView. Number of influenza-associated pediatric deaths by week of death. Available at: http://gis.cdc.gov/GRASP/Fluview/PedFluDeath.html. Accessed July 25, 2016.
7. Shimabukuro T. End-of-season update: 2015-2016 influenza vaccine safety monitoring. Presented at: meeting of the Advisory Committee on Immunization Practices; June 22, 2016; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2016-06/influenza-04-shimabukuro.pdf. Accessed July 22, 2016.
8. Grohskopf L. Proposed recommendations 2016-2017 influenza season. Presented at: meeting of the Advisory Committee on Immunization Practices; June 22, 2016; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2016-06/influenza-08-grohskopf.pdf. Accessed July 22, 2016.
9. Centers for Disease Control and Prevention. Influenza vaccination: a summary for clinicians. Available at: http://www.cdc.gov/flu/professionals/vaccination/vax-summary.htm. Accessed July 13, 2016.
10. Centers for Disease Control and Prevention. What you should know for the 2016-2017 influenza season. Available at: http://www.cdc.gov/flu/about/season/flu-season-2016-2017.htm. Accessed July 13, 2016.
11. Immunization Action Coalition. Influenza vaccine products for the 2016-2017 influenza season. Available at: http://www.immunize.org/catg.d/p4072.pdf. Accessed July 13, 2016.
12. Duffy J, Weintraub E, Hambidge SJ, et al. Febrile seizure risk after vaccination in children 6 to 23 months. Pediatrics. 2016;138.
13. Centers for Disease Control and Prevention. Childhood vaccines and febrile seizures. Available at: http://www.cdc.gov/vaccinesafety/concerns/febrile-seizures.html. Accessed August 11, 2016.
14. Centers for Disease Control and Prevention. Use of antivirals. Background and guidance on the use of influenza antiviral agents. Available at: http://www.cdc.gov/flu/professionals/antivirals/antiviral-use-influenza.htm. Accessed July 13, 2016.
15. Centers for Disease Control and Prevention. Influenza antiviral medications: summary for clinicians. Available at: http://www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm. Accessed July 13, 2016.
16. American Academy of Pediatrics. Recommendations for prevention and control of influenza in children, 2015-2016. Pediatrics. 2015;136:792-808.
The Advisory Committee on Immunization Practices (ACIP) took the unusual step at its June 2016 meeting of recommending against using a currently licensed vaccine, live attenuated influenza vaccine (LAIV), in the 2016-2017 influenza season.1 ACIP based its recommendation on surveillance data collected by the US Influenza Vaccine Effectiveness Network of the Centers for Disease Control and Prevention (CDC), which showed poor effectiveness by the LAIV vaccine among children and adolescents during the past 3 years.
The US Food and Drug Administration (FDA), however, has chosen not to take any action on this matter, saying on its Web site it “has determined that specific regulatory action is not warranted at this time. This determination is based on FDA’s review of manufacturing and clinical data supporting licensure … the totality of the evidence presented at the ACIP meeting, taking into account the inherent limitations of observational studies conducted to evaluate influenza vaccine effectiveness, as well as the well-known variability of influenza vaccine effectiveness across influenza seasons.”2
CDC data for the 2015-2016 flu season showed the effectiveness of LAIV to be just 3% among children 2 years through 17 years of age.3 The reason for this apparent lack of effectiveness is unknown. Other LAIV-effectiveness studies conducted in the 2015-2016 season—one each, in the United States, United Kingdom, and Finland—had results that differed from the CDC surveillance data, with effectiveness ranging from 46% to 58% against all strains combined.2 These results are comparable to vaccine effectiveness found in observational studies in children for both LAIV and inactivated influenza vaccines (IIV) in prior seasons.2
Vaccine manufacturers had projected that 171 to 176 million doses of flu vaccine, in all forms, would be available in the United States during the 2016-2017 season.3 LAIV accounts for about 8% of the total supply of influenza vaccine in the United States,3 and ACIP’s recommendation is not expected to create shortages of other options for the upcoming season. However, the LAIV accounts for one-third of flu vaccines administered to children, and clinicians who provide vaccinations to children have already ordered their vaccine supplies for the upcoming season. Also, it is not clear if children who have previously received the LAIV product will now accept other options for influenza vaccination—all of which involve an injection.
Whether the recommendation against LAIV will continue after this season is also unknown.
What happened during the 2015-2016 influenza season?
The 2015-2016 influenza season was relatively mild with the peak activity occurring in March, somewhat later than in previous years. The circulating influenza strains matched closely to those in the vaccine, making it more effective than the previous year’s vaccine. The predominant circulating strain was A (H1N1), accounting for 58% of illness; A (H3N2) caused 6% of cases and all B types together accounted for 34%.4 The hospitalization rate for all ages was 31.3/100,000 compared with 64.1 the year before.5 There were 85 pediatric deaths compared with 148 in 2014-2015.6
Vaccine effectiveness among all age groups and against all circulating strains was 47%.4 No major vaccine safety concerns were detected. Among those who received IIV3, there was a slight increase in the incidence of Guillain-Barré syndrome of 2.6 cases per one million vaccines.7
Other recommendations for 2016-2017
Once again, ACIP recommends influenza vaccine for all individuals 6 months and older.8 The CDC additionally specifies particular groups that should not skip vaccination given that they are at high risk of complications from influenza infection or because they could expose high-risk individuals to infection (TABLE 1).9
There will continue to be a selection of trivalent and quadrivalent influenza vaccine products in 2016-2017. Trivalent products will contain 3 viral strains: A/California/7/2009 (H1N1), A/Hong Kong/4801/2014 (H3N2) and B/Brisbane/60/2008.10 The quadrivalent products will contain those 3 antigens plus B/Phuket/3073/2013.10 The H3N2 strain is different from the one in last year’s vaccine. Each year, influenza experts analyze surveillance data to predict which circulating strains will predominate in North America, and these antigens constitute the vaccine formulation. The accuracy of this prediction in large part determines how effective the vaccine will be that season.
Two new vaccines have been approved for use in the United States. A quadrivalent cell culture inactivated vaccine (CCIV4), Flucelvax, was licensed in May 2016. It is prepared from virus propagated in canine kidney cells, not with an egg-based production process. It is approved for use in individuals 4 years of age and older.8 Fluad, an adjuvanted trivalent inactivated influenza vaccine, was licensed in late 2015 for individuals 65 years of age and older.8 This is the first adjuvanted influenza vaccine licensed in the United States and will compete with high-dose quadrivalent vaccine for use in older adults. ACIP does not express a preference for any vaccine in this age group.
Two other vaccines should also be available by this fall: Flublok, a quadrivalent recombinant influenza vaccine for individuals 18 years and older, and Flulaval, a quadrivalent inactivated influenza vaccine, for individuals 6 months of age and older. TABLE 211 lists approved influenza vaccines.
Issues specific to children
Deciding how many vaccine doses children need has been further simplified. Children younger than 9 years need 2 doses if they have received fewer than 2 doses of trivalent or quadrivalent influenza vaccine before July 1, 2016. The interval between the 2 doses should be at least 4 weeks. The 2 doses do not have to be the same product; importantly, do not delay a second dose just to obtain the same product used for the first dose. Also, one dose can be trivalent and the other one quadrivalent, although this offers less-than-optimal protection against the B-virus that is only in the quadrivalent product.
Children younger than 9 years require only one dose if they have received 2 or more total doses of trivalent or quadrivalent influenza vaccine before July 1, 2016. The 2 previous doses need not have been received during the same influenza season or consecutive influenza seasons.
In children ages 6 through 23 months there is a slight increased risk of febrile seizure if the influenza vaccine is co-administered with other vaccines, specifically pneumococcal conjugate vaccine (PCV 13) and diphtheria-tetanus-acellular-pertussis (DTaP). The 3 vaccines administered at the same time result in 30 febrile seizures per 100,000 children;12 the rate is lower when influenza vaccine is co-administered with only one of the others. ACIP believes that the risk of a febrile seizure, which does no long-term harm, does not warrant delaying vaccines that could be co-administered.13
Egg allergy requires no special precautions
Evidence continues to grow that influenza vaccine products do not contain enough egg protein to cause significant problems in those with a history of egg allergies. This year’s recommendations state that no special precautions are needed regarding the anatomic site of immunization or the length of observation after administering influenza vaccine in those with a history of allergies to eggs, no matter how severe. All vaccine-administration facilities should be able to respond to any hypersensitivity reaction, and the standard waiting time for observation after all vaccinations is 15 minutes.
Antiviral medications for treatment or prevention
Most influenza strains circulating in 2016-2017 are expected to remain sensitive to oseltamivir and zanamivir, which can be used for treatment or disease prevention. A third neuraminidase inhibitor, peramivir, is available for intravenous use in adults 18 and older. Treatment is recommended for those who have confirmed or suspected influenza and are at high risk for complications (TABLE 3).14 Consideration of antiviral chemoprevention is recommended under certain circumstances (TABLE 4).15,16 The CDC influenza Web site lists recommended doses and duration for each antiviral for treatment and chemoprevention.15
The Advisory Committee on Immunization Practices (ACIP) took the unusual step at its June 2016 meeting of recommending against using a currently licensed vaccine, live attenuated influenza vaccine (LAIV), in the 2016-2017 influenza season.1 ACIP based its recommendation on surveillance data collected by the US Influenza Vaccine Effectiveness Network of the Centers for Disease Control and Prevention (CDC), which showed poor effectiveness by the LAIV vaccine among children and adolescents during the past 3 years.
The US Food and Drug Administration (FDA), however, has chosen not to take any action on this matter, saying on its Web site it “has determined that specific regulatory action is not warranted at this time. This determination is based on FDA’s review of manufacturing and clinical data supporting licensure … the totality of the evidence presented at the ACIP meeting, taking into account the inherent limitations of observational studies conducted to evaluate influenza vaccine effectiveness, as well as the well-known variability of influenza vaccine effectiveness across influenza seasons.”2
CDC data for the 2015-2016 flu season showed the effectiveness of LAIV to be just 3% among children 2 years through 17 years of age.3 The reason for this apparent lack of effectiveness is unknown. Other LAIV-effectiveness studies conducted in the 2015-2016 season—one each, in the United States, United Kingdom, and Finland—had results that differed from the CDC surveillance data, with effectiveness ranging from 46% to 58% against all strains combined.2 These results are comparable to vaccine effectiveness found in observational studies in children for both LAIV and inactivated influenza vaccines (IIV) in prior seasons.2
Vaccine manufacturers had projected that 171 to 176 million doses of flu vaccine, in all forms, would be available in the United States during the 2016-2017 season.3 LAIV accounts for about 8% of the total supply of influenza vaccine in the United States,3 and ACIP’s recommendation is not expected to create shortages of other options for the upcoming season. However, the LAIV accounts for one-third of flu vaccines administered to children, and clinicians who provide vaccinations to children have already ordered their vaccine supplies for the upcoming season. Also, it is not clear if children who have previously received the LAIV product will now accept other options for influenza vaccination—all of which involve an injection.
Whether the recommendation against LAIV will continue after this season is also unknown.
What happened during the 2015-2016 influenza season?
The 2015-2016 influenza season was relatively mild with the peak activity occurring in March, somewhat later than in previous years. The circulating influenza strains matched closely to those in the vaccine, making it more effective than the previous year’s vaccine. The predominant circulating strain was A (H1N1), accounting for 58% of illness; A (H3N2) caused 6% of cases and all B types together accounted for 34%.4 The hospitalization rate for all ages was 31.3/100,000 compared with 64.1 the year before.5 There were 85 pediatric deaths compared with 148 in 2014-2015.6
Vaccine effectiveness among all age groups and against all circulating strains was 47%.4 No major vaccine safety concerns were detected. Among those who received IIV3, there was a slight increase in the incidence of Guillain-Barré syndrome of 2.6 cases per one million vaccines.7
Other recommendations for 2016-2017
Once again, ACIP recommends influenza vaccine for all individuals 6 months and older.8 The CDC additionally specifies particular groups that should not skip vaccination given that they are at high risk of complications from influenza infection or because they could expose high-risk individuals to infection (TABLE 1).9
There will continue to be a selection of trivalent and quadrivalent influenza vaccine products in 2016-2017. Trivalent products will contain 3 viral strains: A/California/7/2009 (H1N1), A/Hong Kong/4801/2014 (H3N2) and B/Brisbane/60/2008.10 The quadrivalent products will contain those 3 antigens plus B/Phuket/3073/2013.10 The H3N2 strain is different from the one in last year’s vaccine. Each year, influenza experts analyze surveillance data to predict which circulating strains will predominate in North America, and these antigens constitute the vaccine formulation. The accuracy of this prediction in large part determines how effective the vaccine will be that season.
Two new vaccines have been approved for use in the United States. A quadrivalent cell culture inactivated vaccine (CCIV4), Flucelvax, was licensed in May 2016. It is prepared from virus propagated in canine kidney cells, not with an egg-based production process. It is approved for use in individuals 4 years of age and older.8 Fluad, an adjuvanted trivalent inactivated influenza vaccine, was licensed in late 2015 for individuals 65 years of age and older.8 This is the first adjuvanted influenza vaccine licensed in the United States and will compete with high-dose quadrivalent vaccine for use in older adults. ACIP does not express a preference for any vaccine in this age group.
Two other vaccines should also be available by this fall: Flublok, a quadrivalent recombinant influenza vaccine for individuals 18 years and older, and Flulaval, a quadrivalent inactivated influenza vaccine, for individuals 6 months of age and older. TABLE 211 lists approved influenza vaccines.
Issues specific to children
Deciding how many vaccine doses children need has been further simplified. Children younger than 9 years need 2 doses if they have received fewer than 2 doses of trivalent or quadrivalent influenza vaccine before July 1, 2016. The interval between the 2 doses should be at least 4 weeks. The 2 doses do not have to be the same product; importantly, do not delay a second dose just to obtain the same product used for the first dose. Also, one dose can be trivalent and the other one quadrivalent, although this offers less-than-optimal protection against the B-virus that is only in the quadrivalent product.
Children younger than 9 years require only one dose if they have received 2 or more total doses of trivalent or quadrivalent influenza vaccine before July 1, 2016. The 2 previous doses need not have been received during the same influenza season or consecutive influenza seasons.
In children ages 6 through 23 months there is a slight increased risk of febrile seizure if the influenza vaccine is co-administered with other vaccines, specifically pneumococcal conjugate vaccine (PCV 13) and diphtheria-tetanus-acellular-pertussis (DTaP). The 3 vaccines administered at the same time result in 30 febrile seizures per 100,000 children;12 the rate is lower when influenza vaccine is co-administered with only one of the others. ACIP believes that the risk of a febrile seizure, which does no long-term harm, does not warrant delaying vaccines that could be co-administered.13
Egg allergy requires no special precautions
Evidence continues to grow that influenza vaccine products do not contain enough egg protein to cause significant problems in those with a history of egg allergies. This year’s recommendations state that no special precautions are needed regarding the anatomic site of immunization or the length of observation after administering influenza vaccine in those with a history of allergies to eggs, no matter how severe. All vaccine-administration facilities should be able to respond to any hypersensitivity reaction, and the standard waiting time for observation after all vaccinations is 15 minutes.
Antiviral medications for treatment or prevention
Most influenza strains circulating in 2016-2017 are expected to remain sensitive to oseltamivir and zanamivir, which can be used for treatment or disease prevention. A third neuraminidase inhibitor, peramivir, is available for intravenous use in adults 18 and older. Treatment is recommended for those who have confirmed or suspected influenza and are at high risk for complications (TABLE 3).14 Consideration of antiviral chemoprevention is recommended under certain circumstances (TABLE 4).15,16 The CDC influenza Web site lists recommended doses and duration for each antiviral for treatment and chemoprevention.15
1. Grohskopf LA, Sokolow LZ, Broder KR, et al. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2016-17 influenza season. MMWR Recomm Rep. 2016;65:1-54.
2. U.S. Food and Drug Administration. FDA information regarding FluMist quadrivalent vaccine. Available at: http://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm508761.htm. Accessed July 13, 2016.
3. Centers for Disease Control and Prevention. ACIP votes down use of LAIV for 2016-2017 flu season. Available at: http://www.cdc.gov/media/releases/2016/s0622-laiv-flu.html. Accessed July 13, 2016.
4. Flannery B, Chung J. Influenza vaccine effectiveness, including LAIV vs IIV in children and adolescents, US Flu VE Network, 2015-2016. Presented at: meeting of the Advisory Committee on Immunization Practices; June 22, 2016; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2016-06/influenza-05-flannery.pdf. Accessed July 22, 2016.
5. Centers for Disease Control and Prevention. FluView. Laboratory-confirmed influenza hospitalizations. Available at: http://gis.cdc.gov/GRASP/Fluview/FluHospRates.html. Accessed July 25, 2016.
6. Centers for Disease Control and Prevention. FluView. Number of influenza-associated pediatric deaths by week of death. Available at: http://gis.cdc.gov/GRASP/Fluview/PedFluDeath.html. Accessed July 25, 2016.
7. Shimabukuro T. End-of-season update: 2015-2016 influenza vaccine safety monitoring. Presented at: meeting of the Advisory Committee on Immunization Practices; June 22, 2016; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2016-06/influenza-04-shimabukuro.pdf. Accessed July 22, 2016.
8. Grohskopf L. Proposed recommendations 2016-2017 influenza season. Presented at: meeting of the Advisory Committee on Immunization Practices; June 22, 2016; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2016-06/influenza-08-grohskopf.pdf. Accessed July 22, 2016.
9. Centers for Disease Control and Prevention. Influenza vaccination: a summary for clinicians. Available at: http://www.cdc.gov/flu/professionals/vaccination/vax-summary.htm. Accessed July 13, 2016.
10. Centers for Disease Control and Prevention. What you should know for the 2016-2017 influenza season. Available at: http://www.cdc.gov/flu/about/season/flu-season-2016-2017.htm. Accessed July 13, 2016.
11. Immunization Action Coalition. Influenza vaccine products for the 2016-2017 influenza season. Available at: http://www.immunize.org/catg.d/p4072.pdf. Accessed July 13, 2016.
12. Duffy J, Weintraub E, Hambidge SJ, et al. Febrile seizure risk after vaccination in children 6 to 23 months. Pediatrics. 2016;138.
13. Centers for Disease Control and Prevention. Childhood vaccines and febrile seizures. Available at: http://www.cdc.gov/vaccinesafety/concerns/febrile-seizures.html. Accessed August 11, 2016.
14. Centers for Disease Control and Prevention. Use of antivirals. Background and guidance on the use of influenza antiviral agents. Available at: http://www.cdc.gov/flu/professionals/antivirals/antiviral-use-influenza.htm. Accessed July 13, 2016.
15. Centers for Disease Control and Prevention. Influenza antiviral medications: summary for clinicians. Available at: http://www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm. Accessed July 13, 2016.
16. American Academy of Pediatrics. Recommendations for prevention and control of influenza in children, 2015-2016. Pediatrics. 2015;136:792-808.
1. Grohskopf LA, Sokolow LZ, Broder KR, et al. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2016-17 influenza season. MMWR Recomm Rep. 2016;65:1-54.
2. U.S. Food and Drug Administration. FDA information regarding FluMist quadrivalent vaccine. Available at: http://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm508761.htm. Accessed July 13, 2016.
3. Centers for Disease Control and Prevention. ACIP votes down use of LAIV for 2016-2017 flu season. Available at: http://www.cdc.gov/media/releases/2016/s0622-laiv-flu.html. Accessed July 13, 2016.
4. Flannery B, Chung J. Influenza vaccine effectiveness, including LAIV vs IIV in children and adolescents, US Flu VE Network, 2015-2016. Presented at: meeting of the Advisory Committee on Immunization Practices; June 22, 2016; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2016-06/influenza-05-flannery.pdf. Accessed July 22, 2016.
5. Centers for Disease Control and Prevention. FluView. Laboratory-confirmed influenza hospitalizations. Available at: http://gis.cdc.gov/GRASP/Fluview/FluHospRates.html. Accessed July 25, 2016.
6. Centers for Disease Control and Prevention. FluView. Number of influenza-associated pediatric deaths by week of death. Available at: http://gis.cdc.gov/GRASP/Fluview/PedFluDeath.html. Accessed July 25, 2016.
7. Shimabukuro T. End-of-season update: 2015-2016 influenza vaccine safety monitoring. Presented at: meeting of the Advisory Committee on Immunization Practices; June 22, 2016; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2016-06/influenza-04-shimabukuro.pdf. Accessed July 22, 2016.
8. Grohskopf L. Proposed recommendations 2016-2017 influenza season. Presented at: meeting of the Advisory Committee on Immunization Practices; June 22, 2016; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2016-06/influenza-08-grohskopf.pdf. Accessed July 22, 2016.
9. Centers for Disease Control and Prevention. Influenza vaccination: a summary for clinicians. Available at: http://www.cdc.gov/flu/professionals/vaccination/vax-summary.htm. Accessed July 13, 2016.
10. Centers for Disease Control and Prevention. What you should know for the 2016-2017 influenza season. Available at: http://www.cdc.gov/flu/about/season/flu-season-2016-2017.htm. Accessed July 13, 2016.
11. Immunization Action Coalition. Influenza vaccine products for the 2016-2017 influenza season. Available at: http://www.immunize.org/catg.d/p4072.pdf. Accessed July 13, 2016.
12. Duffy J, Weintraub E, Hambidge SJ, et al. Febrile seizure risk after vaccination in children 6 to 23 months. Pediatrics. 2016;138.
13. Centers for Disease Control and Prevention. Childhood vaccines and febrile seizures. Available at: http://www.cdc.gov/vaccinesafety/concerns/febrile-seizures.html. Accessed August 11, 2016.
14. Centers for Disease Control and Prevention. Use of antivirals. Background and guidance on the use of influenza antiviral agents. Available at: http://www.cdc.gov/flu/professionals/antivirals/antiviral-use-influenza.htm. Accessed July 13, 2016.
15. Centers for Disease Control and Prevention. Influenza antiviral medications: summary for clinicians. Available at: http://www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm. Accessed July 13, 2016.
16. American Academy of Pediatrics. Recommendations for prevention and control of influenza in children, 2015-2016. Pediatrics. 2015;136:792-808.

Pruritus since childhood
A 48-year-old woman experiencing homelessness presented to our clinic with a 4-week history of an intensely pruritic rash on her upper back and bilateral upper extremities. She reported that she had experienced exacerbations and remissions of the rash in similar locations for the past several years and during childhood. Factors that exacerbated the rash included being outdoors and being exposed to heat. Her pruritus was intensified by scratching the skin and was significantly worse at night. Previous doctors had diagnosed her with psoriasis and prescribed a short trial of hydrocortisone cream and oral antihistamines, but they provided minimal relief.
The patient indicated that the itching interrupted her sleep and her skin’s appearance made it difficult to get a job. The physical exam revealed excoriated and erythematous papules and patches on her upper back, the extensor and flexor aspects of her bilateral forearms, and the dorsal surface of her bilateral wrists, hands, and fingers (FIGURE 1). Her skin was dry and scaly with pigmentary changes and skin thickening (FIGURE 2). She denied any other systemic symptoms. Her hair and nails were normal, she had no palpable lymph nodes, and she was afebrile. She reported suffering from seasonal allergies, but wasn’t aware of a family history of skin disorders.


WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Chronic atopic dermatitis
Although the patient was told she had psoriasis by previous doctors, we diagnosed her condition as atopic dermatitis based on its clinical appearance. There is no single test that can establish a diagnosis of atopic dermatitis. While serum total IgE levels are often elevated, testing is not currently recommended.
The United Kingdom working group on atopic dermatitis published diagnostic criteria based on clinical history and physical exam that include pruritic skin in addition to the presence of 3 or more of the following: skin crease involvement, chronically dry skin, symptom onset before 2 years of age, and visible evidence of dermatitis involving flexural surfaces.1 Our patient fulfilled all but one condition, as she wasn’t sure if her symptoms began before age 2.
Atopic dermatitis is a chronic and inflammatory cutaneous disease that affects approximately 10% to 12% of children and less than 1% of adults in the United States.2 Approximately 90% of cases present before the age of 5 and the literature demonstrates a slight female predominance.3,4
Disease severity is classified as mild, moderate, or severe.5 Mild disease is characterized by dry skin and minimal itching with little impairment of the patient’s physical and psychological wellbeing. Moderate disease includes frequent pruritus and erythema with or without secondary skin changes and a moderate impact on physical and mental health. In severe disease, extensive secondary skin changes exist and the patient’s daily activities, sleep, and mental health may be severely impaired.
Etiology is multifactorial. Causes of atopic dermatitis include abnormalities in the epidermal stratum corneum and tight junctions, a heightened type-2 helper T-cell response to environmental antigens, innate immunity defects, and altered microbial skin flora.6,7
Genetic influences appear to play a substantial role in disease development. Approximately 70% of patients have a positive family history of an atopic disease such as eczema, asthma, or allergic rhinitis.8 Genetic defects are believed to be related to defective proteins and lipids in the epidermis that lead to disruption of the epidermal barrier and subsequent cutaneous inflammation.6,7
Clinical presentation: Lesion distribution varies with age
Intense pruritus and dry scaly skin occur in both children and adults, although the distribution of lesions may vary with age. Children typically exhibit erythematous patches with papules and crusting on the face, scalp, extremities, or trunk. In adults, lesions are primarily located on the hands and feet, but may also present on the face, wrists, forearms, and flexural areas.3
Adults also frequently present with secondary skin changes such as thickened skin, pigmentation changes, lichenification, and excoriated papules due to chronic rubbing or scratching.3 Our patient presented with significant lichenification and hyperpigmentation of the skin that was most prominent on the wrists and forearms.
Additional clinical features consistent with atopic dermatitis include a personal history of allergic conditions and a disease course characterized by exacerbations and remissions. Exacerbations may be caused by heat exposure, dry climates, anxiety, rapid temperature variations, contact with certain chemical substances, or microbial infections.8
Differential Dx includes psoriasis and scabies
The differential diagnosis of chronic atopic dermatitis consists of allergic or irritant contact dermatitis, plaque psoriasis, seborrheic dermatitis, scabies, and drug eruptions. Early diagnosis of atopic dermatitis is imperative to prevent sleep disturbances, chronic secondary skin changes, scarring, and the development of skin infections.
Allergic or irritant contact dermatitis is a cutaneous inflammation occurring after contact with an allergen or irritant. The lesions include erythematous, scaling areas with marked borders that are commonly pruritic. Acute cases often present with vesicles and bullae, while lichenification with cracks and fissures are common among chronic cases. Patch testing may be performed if the diagnosis is suspected.
Plaque psoriasis is characterized by areas of dry, erythematous, and well-demarcated plaques with silver scales that are most commonly found on the knees, elbows, scalp, and lower back. Systemic manifestations can include joint pain and joint swelling. Nail pitting and onycholysis are also common. While our patient had skin thickening, it was from the lichenification that is common in atopic dermatitis.
Psoriasis and atopic dermatitis are often confused. Psoriasis has discrete plaques on extensor surfaces and is often associated with nail changes, while the thickening of the skin that comes with chronic itch and scratching of atopic dermatitis is often less well circumscribed and found on flexor surfaces. Family physicians are frequently the first to encounter patients with atopic dermatitis and psoriasis and must be able to distinguish these conditions, as their treatments differ.
Seborrheic dermatitis is a chronic, relapsing inflammatory condition characterized by pruritic, erythematous, greasy, scaly patches on sebum-rich skin such as the scalp, face, and upper trunk. Seborrheic dermatitis is a clinical diagnosis.
Scabies is a pruritic skin condition caused by Sarcoptes scabiei var hominis. Characteristic linear burrows often appear as serpiginous, gray, threadlike elevations in the webbed spaces of the fingers, scrotum, areolae, elbows, axillae, feet, and wrist flexors. Secondary lesions from scratching or inflammation include excoriations, erythema, and hyperpigmentation. The diagnosis is made clinically and confirmed by dermoscopy, when available. Alternatively, mites or eggs may be observed on skin scrapings using light microscopy.
Drug eruptions should be considered in individuals taking medications who develop acute, symmetric cutaneous eruptions that may be morbilliform, urticarial, papulosquamous, pustular, or bullous in nature.
Treatment depends on severity, area of involvement, and patient’s age
Components of atopic dermatitis treatment include skin hydration, negative stimuli avoidance, pharmacologic modalities, and patient education. Improved skin hydration can be achieved by applying thick emollients containing little to no water at least twice daily and after bathing.
Topical corticosteroids are added when emollient use alone fails. Potency selection is based upon the patient’s age, involved body region, and the severity of skin inflammation.8 In order to reduce cutaneous atrophy, only low-potency corticosteroids should be applied to the face, groin, and axillae. Patients with mild disease may apply desonide 0.05% or hydrocortisone 2.5% cream or ointment once or twice daily for 2 to 4 weeks.8 Patients without improvement or with moderate disease may need medium- to high-potency steroids such as fluocinolone 0.025% or triamcinolone 0.1%.
Patients with atopic dermatitis on the face, eyelids, neck, and skin folds or those who do not obtain relief from combined emollients and topical corticosteroids may benefit from topical calcineurin inhibitors such as pimecrolimus or tacrolimus.9 However, these agents should be utilized only for short periods of time and avoided in immunocompromised patients and those younger than 2 years of age.9
Patients with uncontrolled moderate to severe refractory disease may consider a trial of phototherapy or cyclosporine if phototherapy is ineffective or unavailable.10 A meta-analysis has shown that once remission is achieved, intermittent therapy with moderate- to high-potency corticosteroids or tacrolimus may be effective in reducing subsequent flares.11
In all cases, sedating antihistamines such as diphenhydramine or hydroxyzine can be utilized for pruritic relief, particularly at night. Additionally, signs suggestive of infection should prompt antibiotic treatment with agents that provide coverage for Staphylococcus and Streptococcus species. Lastly, patients must be adequately educated on stimuli avoidance (eg, hot water, wool) and counseled on the medical and psychological issues that often accompany atopic dermatitis.
Our patient was placed on triamcinolone 0.1% for 4 weeks and her condition improved.
CORRESPONDENCE
Andrea Richardson, MD, MPH, 7414 Carriage Bay, San Antonio, TX 78249; [email protected].
1. Williams HC, Burney PG, Pembroke AC, et al. The U.K. Working Party’s Diagnostic Criteria for Atopic Dermatitis. III. Independent hospital validation. Br J Dermatol. 1994;131:406-416.
2. Horii KA, Simon SD, Liu DY, et al. Atopic dermatitis in children in the United States, 1997-2004: visit trends, patient and provider characteristics, and prescribing patterns. Pediatrics. 2007;120:e527-e534.
3. Rudikoff D, Lebwohl M. Atopic dermatitis. Lancet. 1998;351:1715-1721.
4. Kang K, Polster AM, Nedorost ST, et al. Atopic dermatitis. In: Dermatology. Bolognia JL, Jorizzo JL, Rapini RP, et al, eds. Mosby, New York;2003:199.
5. Lewis-Jones S, Mugglestone MA; Guideline Development Group. Management of atopic eczema in children aged up to 12 years: summary of NICE guidance. BMJ. 2007;335:1263-1264.
6. Kuo IH, Yoshida T, De Benedetto A, et al. The cutaneous innate immune response in patients with atopic dermatitis. J Allergy Clin Immunol. 2013;131:266-278.
7. Boguniewicz M, Leung DY. Atopic dermatitis: a disease of altered skin barrier and immune dysregulation. Immunol Rev. 2011;242:233-246.
8. Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol. 2014;70:338-351.
9. Ashcroft DM, Dimmock P, Garside R, et al. Efficacy and tolerability of topical pimecrolimus and tacrolimus in the treatment of atopic dermatitis: meta-analysis of randomised controlled trials. BMJ. 2005;330:516.
10. Garritsen FM, Brouwer MW, Limpens J, et al. Photo(chemo)therapy in the management of atopic dermatitis: an updated systematic review with implications for practice and research. Br J Dermatol. 2014;170:501-513.
11. Schmitt J, von Kobyletzki L, Svensson A, et al. Efficacy and tolerability of proactive treatment with topical corticosteroids and calcineurin inhibitors for atopic eczema: systematic review and meta-analysis of randomized controlled trials. Br J Dermatol. 2011;164:415-428.
A 48-year-old woman experiencing homelessness presented to our clinic with a 4-week history of an intensely pruritic rash on her upper back and bilateral upper extremities. She reported that she had experienced exacerbations and remissions of the rash in similar locations for the past several years and during childhood. Factors that exacerbated the rash included being outdoors and being exposed to heat. Her pruritus was intensified by scratching the skin and was significantly worse at night. Previous doctors had diagnosed her with psoriasis and prescribed a short trial of hydrocortisone cream and oral antihistamines, but they provided minimal relief.
The patient indicated that the itching interrupted her sleep and her skin’s appearance made it difficult to get a job. The physical exam revealed excoriated and erythematous papules and patches on her upper back, the extensor and flexor aspects of her bilateral forearms, and the dorsal surface of her bilateral wrists, hands, and fingers (FIGURE 1). Her skin was dry and scaly with pigmentary changes and skin thickening (FIGURE 2). She denied any other systemic symptoms. Her hair and nails were normal, she had no palpable lymph nodes, and she was afebrile. She reported suffering from seasonal allergies, but wasn’t aware of a family history of skin disorders.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Chronic atopic dermatitis
Although the patient was told she had psoriasis by previous doctors, we diagnosed her condition as atopic dermatitis based on its clinical appearance. There is no single test that can establish a diagnosis of atopic dermatitis. While serum total IgE levels are often elevated, testing is not currently recommended.
The United Kingdom working group on atopic dermatitis published diagnostic criteria based on clinical history and physical exam that include pruritic skin in addition to the presence of 3 or more of the following: skin crease involvement, chronically dry skin, symptom onset before 2 years of age, and visible evidence of dermatitis involving flexural surfaces.1 Our patient fulfilled all but one condition, as she wasn’t sure if her symptoms began before age 2.
Atopic dermatitis is a chronic and inflammatory cutaneous disease that affects approximately 10% to 12% of children and less than 1% of adults in the United States.2 Approximately 90% of cases present before the age of 5 and the literature demonstrates a slight female predominance.3,4
Disease severity is classified as mild, moderate, or severe.5 Mild disease is characterized by dry skin and minimal itching with little impairment of the patient’s physical and psychological wellbeing. Moderate disease includes frequent pruritus and erythema with or without secondary skin changes and a moderate impact on physical and mental health. In severe disease, extensive secondary skin changes exist and the patient’s daily activities, sleep, and mental health may be severely impaired.
Etiology is multifactorial. Causes of atopic dermatitis include abnormalities in the epidermal stratum corneum and tight junctions, a heightened type-2 helper T-cell response to environmental antigens, innate immunity defects, and altered microbial skin flora.6,7
Genetic influences appear to play a substantial role in disease development. Approximately 70% of patients have a positive family history of an atopic disease such as eczema, asthma, or allergic rhinitis.8 Genetic defects are believed to be related to defective proteins and lipids in the epidermis that lead to disruption of the epidermal barrier and subsequent cutaneous inflammation.6,7
Clinical presentation: Lesion distribution varies with age
Intense pruritus and dry scaly skin occur in both children and adults, although the distribution of lesions may vary with age. Children typically exhibit erythematous patches with papules and crusting on the face, scalp, extremities, or trunk. In adults, lesions are primarily located on the hands and feet, but may also present on the face, wrists, forearms, and flexural areas.3
Adults also frequently present with secondary skin changes such as thickened skin, pigmentation changes, lichenification, and excoriated papules due to chronic rubbing or scratching.3 Our patient presented with significant lichenification and hyperpigmentation of the skin that was most prominent on the wrists and forearms.
Additional clinical features consistent with atopic dermatitis include a personal history of allergic conditions and a disease course characterized by exacerbations and remissions. Exacerbations may be caused by heat exposure, dry climates, anxiety, rapid temperature variations, contact with certain chemical substances, or microbial infections.8
Differential Dx includes psoriasis and scabies
The differential diagnosis of chronic atopic dermatitis consists of allergic or irritant contact dermatitis, plaque psoriasis, seborrheic dermatitis, scabies, and drug eruptions. Early diagnosis of atopic dermatitis is imperative to prevent sleep disturbances, chronic secondary skin changes, scarring, and the development of skin infections.
Allergic or irritant contact dermatitis is a cutaneous inflammation occurring after contact with an allergen or irritant. The lesions include erythematous, scaling areas with marked borders that are commonly pruritic. Acute cases often present with vesicles and bullae, while lichenification with cracks and fissures are common among chronic cases. Patch testing may be performed if the diagnosis is suspected.
Plaque psoriasis is characterized by areas of dry, erythematous, and well-demarcated plaques with silver scales that are most commonly found on the knees, elbows, scalp, and lower back. Systemic manifestations can include joint pain and joint swelling. Nail pitting and onycholysis are also common. While our patient had skin thickening, it was from the lichenification that is common in atopic dermatitis.
Psoriasis and atopic dermatitis are often confused. Psoriasis has discrete plaques on extensor surfaces and is often associated with nail changes, while the thickening of the skin that comes with chronic itch and scratching of atopic dermatitis is often less well circumscribed and found on flexor surfaces. Family physicians are frequently the first to encounter patients with atopic dermatitis and psoriasis and must be able to distinguish these conditions, as their treatments differ.
Seborrheic dermatitis is a chronic, relapsing inflammatory condition characterized by pruritic, erythematous, greasy, scaly patches on sebum-rich skin such as the scalp, face, and upper trunk. Seborrheic dermatitis is a clinical diagnosis.
Scabies is a pruritic skin condition caused by Sarcoptes scabiei var hominis. Characteristic linear burrows often appear as serpiginous, gray, threadlike elevations in the webbed spaces of the fingers, scrotum, areolae, elbows, axillae, feet, and wrist flexors. Secondary lesions from scratching or inflammation include excoriations, erythema, and hyperpigmentation. The diagnosis is made clinically and confirmed by dermoscopy, when available. Alternatively, mites or eggs may be observed on skin scrapings using light microscopy.
Drug eruptions should be considered in individuals taking medications who develop acute, symmetric cutaneous eruptions that may be morbilliform, urticarial, papulosquamous, pustular, or bullous in nature.
Treatment depends on severity, area of involvement, and patient’s age
Components of atopic dermatitis treatment include skin hydration, negative stimuli avoidance, pharmacologic modalities, and patient education. Improved skin hydration can be achieved by applying thick emollients containing little to no water at least twice daily and after bathing.
Topical corticosteroids are added when emollient use alone fails. Potency selection is based upon the patient’s age, involved body region, and the severity of skin inflammation.8 In order to reduce cutaneous atrophy, only low-potency corticosteroids should be applied to the face, groin, and axillae. Patients with mild disease may apply desonide 0.05% or hydrocortisone 2.5% cream or ointment once or twice daily for 2 to 4 weeks.8 Patients without improvement or with moderate disease may need medium- to high-potency steroids such as fluocinolone 0.025% or triamcinolone 0.1%.
Patients with atopic dermatitis on the face, eyelids, neck, and skin folds or those who do not obtain relief from combined emollients and topical corticosteroids may benefit from topical calcineurin inhibitors such as pimecrolimus or tacrolimus.9 However, these agents should be utilized only for short periods of time and avoided in immunocompromised patients and those younger than 2 years of age.9
Patients with uncontrolled moderate to severe refractory disease may consider a trial of phototherapy or cyclosporine if phototherapy is ineffective or unavailable.10 A meta-analysis has shown that once remission is achieved, intermittent therapy with moderate- to high-potency corticosteroids or tacrolimus may be effective in reducing subsequent flares.11
In all cases, sedating antihistamines such as diphenhydramine or hydroxyzine can be utilized for pruritic relief, particularly at night. Additionally, signs suggestive of infection should prompt antibiotic treatment with agents that provide coverage for Staphylococcus and Streptococcus species. Lastly, patients must be adequately educated on stimuli avoidance (eg, hot water, wool) and counseled on the medical and psychological issues that often accompany atopic dermatitis.
Our patient was placed on triamcinolone 0.1% for 4 weeks and her condition improved.
CORRESPONDENCE
Andrea Richardson, MD, MPH, 7414 Carriage Bay, San Antonio, TX 78249; [email protected].
A 48-year-old woman experiencing homelessness presented to our clinic with a 4-week history of an intensely pruritic rash on her upper back and bilateral upper extremities. She reported that she had experienced exacerbations and remissions of the rash in similar locations for the past several years and during childhood. Factors that exacerbated the rash included being outdoors and being exposed to heat. Her pruritus was intensified by scratching the skin and was significantly worse at night. Previous doctors had diagnosed her with psoriasis and prescribed a short trial of hydrocortisone cream and oral antihistamines, but they provided minimal relief.
The patient indicated that the itching interrupted her sleep and her skin’s appearance made it difficult to get a job. The physical exam revealed excoriated and erythematous papules and patches on her upper back, the extensor and flexor aspects of her bilateral forearms, and the dorsal surface of her bilateral wrists, hands, and fingers (FIGURE 1). Her skin was dry and scaly with pigmentary changes and skin thickening (FIGURE 2). She denied any other systemic symptoms. Her hair and nails were normal, she had no palpable lymph nodes, and she was afebrile. She reported suffering from seasonal allergies, but wasn’t aware of a family history of skin disorders.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Chronic atopic dermatitis
Although the patient was told she had psoriasis by previous doctors, we diagnosed her condition as atopic dermatitis based on its clinical appearance. There is no single test that can establish a diagnosis of atopic dermatitis. While serum total IgE levels are often elevated, testing is not currently recommended.
The United Kingdom working group on atopic dermatitis published diagnostic criteria based on clinical history and physical exam that include pruritic skin in addition to the presence of 3 or more of the following: skin crease involvement, chronically dry skin, symptom onset before 2 years of age, and visible evidence of dermatitis involving flexural surfaces.1 Our patient fulfilled all but one condition, as she wasn’t sure if her symptoms began before age 2.
Atopic dermatitis is a chronic and inflammatory cutaneous disease that affects approximately 10% to 12% of children and less than 1% of adults in the United States.2 Approximately 90% of cases present before the age of 5 and the literature demonstrates a slight female predominance.3,4
Disease severity is classified as mild, moderate, or severe.5 Mild disease is characterized by dry skin and minimal itching with little impairment of the patient’s physical and psychological wellbeing. Moderate disease includes frequent pruritus and erythema with or without secondary skin changes and a moderate impact on physical and mental health. In severe disease, extensive secondary skin changes exist and the patient’s daily activities, sleep, and mental health may be severely impaired.
Etiology is multifactorial. Causes of atopic dermatitis include abnormalities in the epidermal stratum corneum and tight junctions, a heightened type-2 helper T-cell response to environmental antigens, innate immunity defects, and altered microbial skin flora.6,7
Genetic influences appear to play a substantial role in disease development. Approximately 70% of patients have a positive family history of an atopic disease such as eczema, asthma, or allergic rhinitis.8 Genetic defects are believed to be related to defective proteins and lipids in the epidermis that lead to disruption of the epidermal barrier and subsequent cutaneous inflammation.6,7
Clinical presentation: Lesion distribution varies with age
Intense pruritus and dry scaly skin occur in both children and adults, although the distribution of lesions may vary with age. Children typically exhibit erythematous patches with papules and crusting on the face, scalp, extremities, or trunk. In adults, lesions are primarily located on the hands and feet, but may also present on the face, wrists, forearms, and flexural areas.3
Adults also frequently present with secondary skin changes such as thickened skin, pigmentation changes, lichenification, and excoriated papules due to chronic rubbing or scratching.3 Our patient presented with significant lichenification and hyperpigmentation of the skin that was most prominent on the wrists and forearms.
Additional clinical features consistent with atopic dermatitis include a personal history of allergic conditions and a disease course characterized by exacerbations and remissions. Exacerbations may be caused by heat exposure, dry climates, anxiety, rapid temperature variations, contact with certain chemical substances, or microbial infections.8
Differential Dx includes psoriasis and scabies
The differential diagnosis of chronic atopic dermatitis consists of allergic or irritant contact dermatitis, plaque psoriasis, seborrheic dermatitis, scabies, and drug eruptions. Early diagnosis of atopic dermatitis is imperative to prevent sleep disturbances, chronic secondary skin changes, scarring, and the development of skin infections.
Allergic or irritant contact dermatitis is a cutaneous inflammation occurring after contact with an allergen or irritant. The lesions include erythematous, scaling areas with marked borders that are commonly pruritic. Acute cases often present with vesicles and bullae, while lichenification with cracks and fissures are common among chronic cases. Patch testing may be performed if the diagnosis is suspected.
Plaque psoriasis is characterized by areas of dry, erythematous, and well-demarcated plaques with silver scales that are most commonly found on the knees, elbows, scalp, and lower back. Systemic manifestations can include joint pain and joint swelling. Nail pitting and onycholysis are also common. While our patient had skin thickening, it was from the lichenification that is common in atopic dermatitis.
Psoriasis and atopic dermatitis are often confused. Psoriasis has discrete plaques on extensor surfaces and is often associated with nail changes, while the thickening of the skin that comes with chronic itch and scratching of atopic dermatitis is often less well circumscribed and found on flexor surfaces. Family physicians are frequently the first to encounter patients with atopic dermatitis and psoriasis and must be able to distinguish these conditions, as their treatments differ.
Seborrheic dermatitis is a chronic, relapsing inflammatory condition characterized by pruritic, erythematous, greasy, scaly patches on sebum-rich skin such as the scalp, face, and upper trunk. Seborrheic dermatitis is a clinical diagnosis.
Scabies is a pruritic skin condition caused by Sarcoptes scabiei var hominis. Characteristic linear burrows often appear as serpiginous, gray, threadlike elevations in the webbed spaces of the fingers, scrotum, areolae, elbows, axillae, feet, and wrist flexors. Secondary lesions from scratching or inflammation include excoriations, erythema, and hyperpigmentation. The diagnosis is made clinically and confirmed by dermoscopy, when available. Alternatively, mites or eggs may be observed on skin scrapings using light microscopy.
Drug eruptions should be considered in individuals taking medications who develop acute, symmetric cutaneous eruptions that may be morbilliform, urticarial, papulosquamous, pustular, or bullous in nature.
Treatment depends on severity, area of involvement, and patient’s age
Components of atopic dermatitis treatment include skin hydration, negative stimuli avoidance, pharmacologic modalities, and patient education. Improved skin hydration can be achieved by applying thick emollients containing little to no water at least twice daily and after bathing.
Topical corticosteroids are added when emollient use alone fails. Potency selection is based upon the patient’s age, involved body region, and the severity of skin inflammation.8 In order to reduce cutaneous atrophy, only low-potency corticosteroids should be applied to the face, groin, and axillae. Patients with mild disease may apply desonide 0.05% or hydrocortisone 2.5% cream or ointment once or twice daily for 2 to 4 weeks.8 Patients without improvement or with moderate disease may need medium- to high-potency steroids such as fluocinolone 0.025% or triamcinolone 0.1%.
Patients with atopic dermatitis on the face, eyelids, neck, and skin folds or those who do not obtain relief from combined emollients and topical corticosteroids may benefit from topical calcineurin inhibitors such as pimecrolimus or tacrolimus.9 However, these agents should be utilized only for short periods of time and avoided in immunocompromised patients and those younger than 2 years of age.9
Patients with uncontrolled moderate to severe refractory disease may consider a trial of phototherapy or cyclosporine if phototherapy is ineffective or unavailable.10 A meta-analysis has shown that once remission is achieved, intermittent therapy with moderate- to high-potency corticosteroids or tacrolimus may be effective in reducing subsequent flares.11
In all cases, sedating antihistamines such as diphenhydramine or hydroxyzine can be utilized for pruritic relief, particularly at night. Additionally, signs suggestive of infection should prompt antibiotic treatment with agents that provide coverage for Staphylococcus and Streptococcus species. Lastly, patients must be adequately educated on stimuli avoidance (eg, hot water, wool) and counseled on the medical and psychological issues that often accompany atopic dermatitis.
Our patient was placed on triamcinolone 0.1% for 4 weeks and her condition improved.
CORRESPONDENCE
Andrea Richardson, MD, MPH, 7414 Carriage Bay, San Antonio, TX 78249; [email protected].
1. Williams HC, Burney PG, Pembroke AC, et al. The U.K. Working Party’s Diagnostic Criteria for Atopic Dermatitis. III. Independent hospital validation. Br J Dermatol. 1994;131:406-416.
2. Horii KA, Simon SD, Liu DY, et al. Atopic dermatitis in children in the United States, 1997-2004: visit trends, patient and provider characteristics, and prescribing patterns. Pediatrics. 2007;120:e527-e534.
3. Rudikoff D, Lebwohl M. Atopic dermatitis. Lancet. 1998;351:1715-1721.
4. Kang K, Polster AM, Nedorost ST, et al. Atopic dermatitis. In: Dermatology. Bolognia JL, Jorizzo JL, Rapini RP, et al, eds. Mosby, New York;2003:199.
5. Lewis-Jones S, Mugglestone MA; Guideline Development Group. Management of atopic eczema in children aged up to 12 years: summary of NICE guidance. BMJ. 2007;335:1263-1264.
6. Kuo IH, Yoshida T, De Benedetto A, et al. The cutaneous innate immune response in patients with atopic dermatitis. J Allergy Clin Immunol. 2013;131:266-278.
7. Boguniewicz M, Leung DY. Atopic dermatitis: a disease of altered skin barrier and immune dysregulation. Immunol Rev. 2011;242:233-246.
8. Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol. 2014;70:338-351.
9. Ashcroft DM, Dimmock P, Garside R, et al. Efficacy and tolerability of topical pimecrolimus and tacrolimus in the treatment of atopic dermatitis: meta-analysis of randomised controlled trials. BMJ. 2005;330:516.
10. Garritsen FM, Brouwer MW, Limpens J, et al. Photo(chemo)therapy in the management of atopic dermatitis: an updated systematic review with implications for practice and research. Br J Dermatol. 2014;170:501-513.
11. Schmitt J, von Kobyletzki L, Svensson A, et al. Efficacy and tolerability of proactive treatment with topical corticosteroids and calcineurin inhibitors for atopic eczema: systematic review and meta-analysis of randomized controlled trials. Br J Dermatol. 2011;164:415-428.
1. Williams HC, Burney PG, Pembroke AC, et al. The U.K. Working Party’s Diagnostic Criteria for Atopic Dermatitis. III. Independent hospital validation. Br J Dermatol. 1994;131:406-416.
2. Horii KA, Simon SD, Liu DY, et al. Atopic dermatitis in children in the United States, 1997-2004: visit trends, patient and provider characteristics, and prescribing patterns. Pediatrics. 2007;120:e527-e534.
3. Rudikoff D, Lebwohl M. Atopic dermatitis. Lancet. 1998;351:1715-1721.
4. Kang K, Polster AM, Nedorost ST, et al. Atopic dermatitis. In: Dermatology. Bolognia JL, Jorizzo JL, Rapini RP, et al, eds. Mosby, New York;2003:199.
5. Lewis-Jones S, Mugglestone MA; Guideline Development Group. Management of atopic eczema in children aged up to 12 years: summary of NICE guidance. BMJ. 2007;335:1263-1264.
6. Kuo IH, Yoshida T, De Benedetto A, et al. The cutaneous innate immune response in patients with atopic dermatitis. J Allergy Clin Immunol. 2013;131:266-278.
7. Boguniewicz M, Leung DY. Atopic dermatitis: a disease of altered skin barrier and immune dysregulation. Immunol Rev. 2011;242:233-246.
8. Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol. 2014;70:338-351.
9. Ashcroft DM, Dimmock P, Garside R, et al. Efficacy and tolerability of topical pimecrolimus and tacrolimus in the treatment of atopic dermatitis: meta-analysis of randomised controlled trials. BMJ. 2005;330:516.
10. Garritsen FM, Brouwer MW, Limpens J, et al. Photo(chemo)therapy in the management of atopic dermatitis: an updated systematic review with implications for practice and research. Br J Dermatol. 2014;170:501-513.
11. Schmitt J, von Kobyletzki L, Svensson A, et al. Efficacy and tolerability of proactive treatment with topical corticosteroids and calcineurin inhibitors for atopic eczema: systematic review and meta-analysis of randomized controlled trials. Br J Dermatol. 2011;164:415-428.
