User login
Cognitive-behavioral therapy eases postconcussive symptoms in teens
Adolescents who underwent cognitive-behavioral therapy (CBT) as part of postconcussion care reported significantly lower levels of postconcussive symptoms and depressive symptoms in a randomized trial of 49 patients aged 11-17 years. The report was published online Sept. 12 in Pediatrics.
“Affective symptoms, including depression and anxiety, commonly co-occur with cognitive and somatic symptoms and may prolong recovery from postconcussive symptoms, wrote Carolyn A. McCarty, PhD, of Seattle Children’s Hospital, Washington, and her colleagues. “The complexities of managing persistent postconcussive symptoms in conjunction with comorbid psychological symptoms create a significant burden for injured children and adolescents, their families, and schools” (Pediatrics. 2016. doi: 10.1542/peds.2016-0459).

To determine the impact of CBT on persistent symptoms in adolescents with concussions, the researchers randomized 49 patients to usual care or a collaborative care plan that included usual care plus CBT.
After 6 months, approximately 13% of the teens in the CBT group reported high levels of postconcussive symptoms, compared with 42% of controls. In addition, 78% of CBT patients reported a depressive symptom reduction of more than 50%, compared with 46% of controls.
Concussions were diagnosed by sports medicine or rehabilitative medicine specialists. The patients assigned to CBT received usual care management, CBT, and possible psychopharmacological consultation. Control patients received usual concussion care, generally defined as an initial visit with a sports medicine physician and assessments at 1, 3, and 6 months. Usual care also could include MRI, sleep medication, and subthreshold exercise, depending on the patient. No serious adverse events were reported. The average age of the patients was 15 years, approximately 65% were girls, and 76% were white.
Overall, 83% of the CBT patients and 87% of their parents were “very satisfied” with their care, compared with 46% of patients and 29% of parents in the control group.
“Although patients in both groups showed symptom reduction in the first 3 months, only those who received collaborative care demonstrated sustained improvements through 6 months of follow-up,” Dr. McCarty and her colleagues wrote.
The results were limited by several factors including the small size of the study, the researchers said. However, the findings “prompt more investigation into the role of affective symptoms in perpetuating physical symptoms secondary to prolonged recovery from sports-related concussion,” and also suggest that collaborative care can help improve persistent postconcussive symptoms in teens.
Dr. McCarty and her colleagues had no relevant financial conflicts to disclose. The Seattle Sports Concussion Research Collaborative supported the study.
Increasing numbers of adolescents are presenting to physicians for management of concussions. This is mainly because of much greater awareness of the signs, symptoms, and potential adverse effects. While the majority of concussed teens recover in less than 2 weeks, 10%-15% will have prolonged symptoms (greater than 1 month), which has significant negative impact on their health, mood, social functioning, and academic performance. This is the first study to provide evidence-based guidance for treating these slow-to-recover teens.
I definitely believe there is value in adding CBT to postconcussive therapy for teens. I have seen CBT help a large number of my own patients who are suffering from prolonged postconcussion symptoms, so it is good to see the results of this well-done study support this approach. One caveat with CBT is that its success hinges on the patient’s being receptive to the idea of CBT and consistent with applying it in daily life, so it may not work for teens who are not motivated to learn and apply its techniques.
I am not surprised by these results of the study. A large proportion of the adolescents I treat for concussions are those referred from their pediatricians because they are suffering from prolonged symptoms. We have anecdotally noted that when a collaborative care model is applied, similar to what was provided for the intervention group in this study, including CBT, patients experience more rapid decrease in symptoms, improved mood, and smoother transition back to baseline functioning, especially in school. I suspect this is because CBT teaches them effective coping skills, and the bonus is that these skills are incredibly useful across one’s lifetime, not just for concussion recovery.
Adolescents who are slow to recover from a concussion commonly experience depressive symptoms. This study suggests CBT is a promising treatment for improving mood and facilitating recovery for these teens. However, a larger study is needed with more diverse subject population. This study included only 49 subjects, and the majority of them were white females. A larger study is needed to determine whether CBT is as feasible and effective for other populations of teens with prolonged concussion symptoms. Also, longer-term longitudinal studies are needed to better understand the etiology of persistent postconcussive symptoms and long-term effects 10-20 years down the road.
Cynthia LaBella, MD, is director of the concussion program at Ann & Robert H. Lurie Children’s Hospital of Chicago. Dr. LaBella said she had no relevant financial disclosures.
Increasing numbers of adolescents are presenting to physicians for management of concussions. This is mainly because of much greater awareness of the signs, symptoms, and potential adverse effects. While the majority of concussed teens recover in less than 2 weeks, 10%-15% will have prolonged symptoms (greater than 1 month), which has significant negative impact on their health, mood, social functioning, and academic performance. This is the first study to provide evidence-based guidance for treating these slow-to-recover teens.
I definitely believe there is value in adding CBT to postconcussive therapy for teens. I have seen CBT help a large number of my own patients who are suffering from prolonged postconcussion symptoms, so it is good to see the results of this well-done study support this approach. One caveat with CBT is that its success hinges on the patient’s being receptive to the idea of CBT and consistent with applying it in daily life, so it may not work for teens who are not motivated to learn and apply its techniques.
I am not surprised by these results of the study. A large proportion of the adolescents I treat for concussions are those referred from their pediatricians because they are suffering from prolonged symptoms. We have anecdotally noted that when a collaborative care model is applied, similar to what was provided for the intervention group in this study, including CBT, patients experience more rapid decrease in symptoms, improved mood, and smoother transition back to baseline functioning, especially in school. I suspect this is because CBT teaches them effective coping skills, and the bonus is that these skills are incredibly useful across one’s lifetime, not just for concussion recovery.
Adolescents who are slow to recover from a concussion commonly experience depressive symptoms. This study suggests CBT is a promising treatment for improving mood and facilitating recovery for these teens. However, a larger study is needed with more diverse subject population. This study included only 49 subjects, and the majority of them were white females. A larger study is needed to determine whether CBT is as feasible and effective for other populations of teens with prolonged concussion symptoms. Also, longer-term longitudinal studies are needed to better understand the etiology of persistent postconcussive symptoms and long-term effects 10-20 years down the road.
Cynthia LaBella, MD, is director of the concussion program at Ann & Robert H. Lurie Children’s Hospital of Chicago. Dr. LaBella said she had no relevant financial disclosures.
Increasing numbers of adolescents are presenting to physicians for management of concussions. This is mainly because of much greater awareness of the signs, symptoms, and potential adverse effects. While the majority of concussed teens recover in less than 2 weeks, 10%-15% will have prolonged symptoms (greater than 1 month), which has significant negative impact on their health, mood, social functioning, and academic performance. This is the first study to provide evidence-based guidance for treating these slow-to-recover teens.
I definitely believe there is value in adding CBT to postconcussive therapy for teens. I have seen CBT help a large number of my own patients who are suffering from prolonged postconcussion symptoms, so it is good to see the results of this well-done study support this approach. One caveat with CBT is that its success hinges on the patient’s being receptive to the idea of CBT and consistent with applying it in daily life, so it may not work for teens who are not motivated to learn and apply its techniques.
I am not surprised by these results of the study. A large proportion of the adolescents I treat for concussions are those referred from their pediatricians because they are suffering from prolonged symptoms. We have anecdotally noted that when a collaborative care model is applied, similar to what was provided for the intervention group in this study, including CBT, patients experience more rapid decrease in symptoms, improved mood, and smoother transition back to baseline functioning, especially in school. I suspect this is because CBT teaches them effective coping skills, and the bonus is that these skills are incredibly useful across one’s lifetime, not just for concussion recovery.
Adolescents who are slow to recover from a concussion commonly experience depressive symptoms. This study suggests CBT is a promising treatment for improving mood and facilitating recovery for these teens. However, a larger study is needed with more diverse subject population. This study included only 49 subjects, and the majority of them were white females. A larger study is needed to determine whether CBT is as feasible and effective for other populations of teens with prolonged concussion symptoms. Also, longer-term longitudinal studies are needed to better understand the etiology of persistent postconcussive symptoms and long-term effects 10-20 years down the road.
Cynthia LaBella, MD, is director of the concussion program at Ann & Robert H. Lurie Children’s Hospital of Chicago. Dr. LaBella said she had no relevant financial disclosures.
Adolescents who underwent cognitive-behavioral therapy (CBT) as part of postconcussion care reported significantly lower levels of postconcussive symptoms and depressive symptoms in a randomized trial of 49 patients aged 11-17 years. The report was published online Sept. 12 in Pediatrics.
“Affective symptoms, including depression and anxiety, commonly co-occur with cognitive and somatic symptoms and may prolong recovery from postconcussive symptoms, wrote Carolyn A. McCarty, PhD, of Seattle Children’s Hospital, Washington, and her colleagues. “The complexities of managing persistent postconcussive symptoms in conjunction with comorbid psychological symptoms create a significant burden for injured children and adolescents, their families, and schools” (Pediatrics. 2016. doi: 10.1542/peds.2016-0459).
To determine the impact of CBT on persistent symptoms in adolescents with concussions, the researchers randomized 49 patients to usual care or a collaborative care plan that included usual care plus CBT.
After 6 months, approximately 13% of the teens in the CBT group reported high levels of postconcussive symptoms, compared with 42% of controls. In addition, 78% of CBT patients reported a depressive symptom reduction of more than 50%, compared with 46% of controls.
Concussions were diagnosed by sports medicine or rehabilitative medicine specialists. The patients assigned to CBT received usual care management, CBT, and possible psychopharmacological consultation. Control patients received usual concussion care, generally defined as an initial visit with a sports medicine physician and assessments at 1, 3, and 6 months. Usual care also could include MRI, sleep medication, and subthreshold exercise, depending on the patient. No serious adverse events were reported. The average age of the patients was 15 years, approximately 65% were girls, and 76% were white.
Overall, 83% of the CBT patients and 87% of their parents were “very satisfied” with their care, compared with 46% of patients and 29% of parents in the control group.
“Although patients in both groups showed symptom reduction in the first 3 months, only those who received collaborative care demonstrated sustained improvements through 6 months of follow-up,” Dr. McCarty and her colleagues wrote.
The results were limited by several factors including the small size of the study, the researchers said. However, the findings “prompt more investigation into the role of affective symptoms in perpetuating physical symptoms secondary to prolonged recovery from sports-related concussion,” and also suggest that collaborative care can help improve persistent postconcussive symptoms in teens.
Dr. McCarty and her colleagues had no relevant financial conflicts to disclose. The Seattle Sports Concussion Research Collaborative supported the study.
Adolescents who underwent cognitive-behavioral therapy (CBT) as part of postconcussion care reported significantly lower levels of postconcussive symptoms and depressive symptoms in a randomized trial of 49 patients aged 11-17 years. The report was published online Sept. 12 in Pediatrics.
“Affective symptoms, including depression and anxiety, commonly co-occur with cognitive and somatic symptoms and may prolong recovery from postconcussive symptoms, wrote Carolyn A. McCarty, PhD, of Seattle Children’s Hospital, Washington, and her colleagues. “The complexities of managing persistent postconcussive symptoms in conjunction with comorbid psychological symptoms create a significant burden for injured children and adolescents, their families, and schools” (Pediatrics. 2016. doi: 10.1542/peds.2016-0459).
To determine the impact of CBT on persistent symptoms in adolescents with concussions, the researchers randomized 49 patients to usual care or a collaborative care plan that included usual care plus CBT.
After 6 months, approximately 13% of the teens in the CBT group reported high levels of postconcussive symptoms, compared with 42% of controls. In addition, 78% of CBT patients reported a depressive symptom reduction of more than 50%, compared with 46% of controls.
Concussions were diagnosed by sports medicine or rehabilitative medicine specialists. The patients assigned to CBT received usual care management, CBT, and possible psychopharmacological consultation. Control patients received usual concussion care, generally defined as an initial visit with a sports medicine physician and assessments at 1, 3, and 6 months. Usual care also could include MRI, sleep medication, and subthreshold exercise, depending on the patient. No serious adverse events were reported. The average age of the patients was 15 years, approximately 65% were girls, and 76% were white.
Overall, 83% of the CBT patients and 87% of their parents were “very satisfied” with their care, compared with 46% of patients and 29% of parents in the control group.
“Although patients in both groups showed symptom reduction in the first 3 months, only those who received collaborative care demonstrated sustained improvements through 6 months of follow-up,” Dr. McCarty and her colleagues wrote.
The results were limited by several factors including the small size of the study, the researchers said. However, the findings “prompt more investigation into the role of affective symptoms in perpetuating physical symptoms secondary to prolonged recovery from sports-related concussion,” and also suggest that collaborative care can help improve persistent postconcussive symptoms in teens.
Dr. McCarty and her colleagues had no relevant financial conflicts to disclose. The Seattle Sports Concussion Research Collaborative supported the study.
FROM PEDIATRICS
Key clinical point: Adolescents with persistent postconcussive symptoms and depressive symptoms improved significantly after the addition of CBT to usual care.
Major finding: After 6 months, 13% of teens who underwent CBT plus usual care reported high levels of postconcussive symptoms, compared with 42% of controls.
Data source: A randomized trial of 49 adolescents aged 11-17 years with persistent postconcussive symptoms at least 1 month after a sports-related concussion,
Disclosures: The researchers had no financial conflicts to disclose. The Seattle Sports Concussion Research Collaborative supported the study.

Think outside the ‘cardiac box’ to predict cardiac injury
WAIKOLOA, HI. – For gunshot wounds, the current “cardiac box” was the poorest predictor of cardiac injury, results from a single-center retrospective study demonstrated.
“We determined that, from a statistical standpoint, the cardiac box should be redefined to include the area of the thorax that extends from the clavicle to xiphoid and from the anterior midline to the posterior midline of the left thorax,” Bryan C. Morse, MD, said in an interview in advance of the annual meeting of the American Association for the Surgery of Trauma. “The classic cardiac box is inadequate to discriminate whether a gunshot wound will create a cardiac injury.”

Dr. Morse of Emory University and Grady Memorial Hospital, Atlanta, and his associates recently published their experience with penetrating cardiac injuries over the past 36 years and documented an increase in the number of cardiac injuries from gunshots over the past 10 years (J. Trauma Acute Care Surg. 2016 Jul 6. doi: 10.1097/TA.0000000000001165). They also noted that several of these injuries were caused by penetrating thoracic wounds outside the cardiac box.
The cardiac box is currently defined as the area of the chest overlying the heart, bounded by the midclavicular lines (laterally) and from the clavicles to the tip of the xiphoid. “Surgical teaching dictates that penetrating injuries (i.e. stab wounds and gunshot wounds) in the box have the highest likelihood of cardiac injury and thereby mandate further evaluation,” Dr. Morse said. “These studies, however, are based on small patient sample sizes in which the majority were stab wound victims and underwent minimal statistical scrutiny.”
In what he said is the largest study of its kind, Dr. Morse and his associates conducted a retrospective review of trauma registry data from Grady’s trauma center and autopsy reports to identify patients with penetrating thoracic gunshot wounds and cardiac injury from 2011 to 2013 and to evaluate the relationship between penetrating injuries and the likelihood of a cardiac injury. Using a circumferential grid system around the thorax, the researchers employed logistic regression analysis to compare differences in rates of cardiac injury from entrance/exit wounds in the cardiac box, versus outside the box. They repeated the process to identify potential regions that yield improved predictions for cardiac injury over the current definition of the cardiac box.
Over the 3-year study period, 263 patients sustained 735 penetrating thoracic wounds, of which 80% were gunshot wounds (GSWs). Most of the patients were males (89%) with a median of two injuries each. After stab wounds were excluded, 277 GSWs to the thorax were included for study and 95 (34%) injured the heart. Of the 233 GSWs entering the cardiac box, 30% caused cardiac injury while, of the 44 GSWs outside the cardiac box, 32% penetrated the heart, suggesting that the current cardiac box is a poor predictor of cardiac injury relative to the thoracic non–cardiac box regions (OR 1.1; P = .71).
The researchers observed that the regions from the anterior to the posterior midline of the left thorax provided the highest positive predictive value, with a sensitivity of 90% and a specificity of 31%, making this region the most statistically significant discriminator of cardiac injury (OR, 4.4; P less than .01). This finding was primarily based on the fact that gunshots to the left lateral chest (an area not currently included in the box) had a high rate of cardiac injury (41%; OR, 1.4).
“The current cardiac box is unable to discriminate between gunshot wounds that will cause a cardiac injury and those that will not,” Dr. Morse said. “Any gunshot wound to the chest can cause a cardiac injury. While clinically relevant box borders would include the left chest, the bottom line for surgeons is to think outside the current cardiac box.”
The improved cardiac box that he and his associates proposed includes the area from the clavicles to the xiphoid and from the anterior to the posterior midline over the left thorax. “While this may be intuitive, it is not what we as surgeons have been teaching,” he said. “Finally, gunshots to areas such as the right posterior and posterolateral chest were associated with rates of cardiac injury greater than 30% despite their distance from the heart. This led us to conclude that a gunshot anywhere to the chest should be considered to potentially cause a cardiac injury.”
Dr. Morse acknowledged certain limitations of the study, including the fact that the study excluded graze wounds and gunshots above the clavicles and below the xiphoid. “However, a small percentage of these did cause cardiac injuries, which emphasizes the point that gunshot wounds from any entrance can cause cardiac injury.”
Invited discussant Nicholas Namias, MD, professor and chief of the division of acute care surgery at Jackson Memorial Hospital, Miami, said that the study by Dr. Morse and his associates “confirms what Dr. [Grace] Rozycki showed 20 years ago: Forget the [cardiac] box; it’s dead. Just throw an ultrasound probe on.”
Dr. Morse reported having no relevant financial disclosures.
WAIKOLOA, HI. – For gunshot wounds, the current “cardiac box” was the poorest predictor of cardiac injury, results from a single-center retrospective study demonstrated.
“We determined that, from a statistical standpoint, the cardiac box should be redefined to include the area of the thorax that extends from the clavicle to xiphoid and from the anterior midline to the posterior midline of the left thorax,” Bryan C. Morse, MD, said in an interview in advance of the annual meeting of the American Association for the Surgery of Trauma. “The classic cardiac box is inadequate to discriminate whether a gunshot wound will create a cardiac injury.”
Dr. Morse of Emory University and Grady Memorial Hospital, Atlanta, and his associates recently published their experience with penetrating cardiac injuries over the past 36 years and documented an increase in the number of cardiac injuries from gunshots over the past 10 years (J. Trauma Acute Care Surg. 2016 Jul 6. doi: 10.1097/TA.0000000000001165). They also noted that several of these injuries were caused by penetrating thoracic wounds outside the cardiac box.
The cardiac box is currently defined as the area of the chest overlying the heart, bounded by the midclavicular lines (laterally) and from the clavicles to the tip of the xiphoid. “Surgical teaching dictates that penetrating injuries (i.e. stab wounds and gunshot wounds) in the box have the highest likelihood of cardiac injury and thereby mandate further evaluation,” Dr. Morse said. “These studies, however, are based on small patient sample sizes in which the majority were stab wound victims and underwent minimal statistical scrutiny.”
In what he said is the largest study of its kind, Dr. Morse and his associates conducted a retrospective review of trauma registry data from Grady’s trauma center and autopsy reports to identify patients with penetrating thoracic gunshot wounds and cardiac injury from 2011 to 2013 and to evaluate the relationship between penetrating injuries and the likelihood of a cardiac injury. Using a circumferential grid system around the thorax, the researchers employed logistic regression analysis to compare differences in rates of cardiac injury from entrance/exit wounds in the cardiac box, versus outside the box. They repeated the process to identify potential regions that yield improved predictions for cardiac injury over the current definition of the cardiac box.
Over the 3-year study period, 263 patients sustained 735 penetrating thoracic wounds, of which 80% were gunshot wounds (GSWs). Most of the patients were males (89%) with a median of two injuries each. After stab wounds were excluded, 277 GSWs to the thorax were included for study and 95 (34%) injured the heart. Of the 233 GSWs entering the cardiac box, 30% caused cardiac injury while, of the 44 GSWs outside the cardiac box, 32% penetrated the heart, suggesting that the current cardiac box is a poor predictor of cardiac injury relative to the thoracic non–cardiac box regions (OR 1.1; P = .71).
The researchers observed that the regions from the anterior to the posterior midline of the left thorax provided the highest positive predictive value, with a sensitivity of 90% and a specificity of 31%, making this region the most statistically significant discriminator of cardiac injury (OR, 4.4; P less than .01). This finding was primarily based on the fact that gunshots to the left lateral chest (an area not currently included in the box) had a high rate of cardiac injury (41%; OR, 1.4).
“The current cardiac box is unable to discriminate between gunshot wounds that will cause a cardiac injury and those that will not,” Dr. Morse said. “Any gunshot wound to the chest can cause a cardiac injury. While clinically relevant box borders would include the left chest, the bottom line for surgeons is to think outside the current cardiac box.”
The improved cardiac box that he and his associates proposed includes the area from the clavicles to the xiphoid and from the anterior to the posterior midline over the left thorax. “While this may be intuitive, it is not what we as surgeons have been teaching,” he said. “Finally, gunshots to areas such as the right posterior and posterolateral chest were associated with rates of cardiac injury greater than 30% despite their distance from the heart. This led us to conclude that a gunshot anywhere to the chest should be considered to potentially cause a cardiac injury.”
Dr. Morse acknowledged certain limitations of the study, including the fact that the study excluded graze wounds and gunshots above the clavicles and below the xiphoid. “However, a small percentage of these did cause cardiac injuries, which emphasizes the point that gunshot wounds from any entrance can cause cardiac injury.”
Invited discussant Nicholas Namias, MD, professor and chief of the division of acute care surgery at Jackson Memorial Hospital, Miami, said that the study by Dr. Morse and his associates “confirms what Dr. [Grace] Rozycki showed 20 years ago: Forget the [cardiac] box; it’s dead. Just throw an ultrasound probe on.”
Dr. Morse reported having no relevant financial disclosures.
WAIKOLOA, HI. – For gunshot wounds, the current “cardiac box” was the poorest predictor of cardiac injury, results from a single-center retrospective study demonstrated.
“We determined that, from a statistical standpoint, the cardiac box should be redefined to include the area of the thorax that extends from the clavicle to xiphoid and from the anterior midline to the posterior midline of the left thorax,” Bryan C. Morse, MD, said in an interview in advance of the annual meeting of the American Association for the Surgery of Trauma. “The classic cardiac box is inadequate to discriminate whether a gunshot wound will create a cardiac injury.”
Dr. Morse of Emory University and Grady Memorial Hospital, Atlanta, and his associates recently published their experience with penetrating cardiac injuries over the past 36 years and documented an increase in the number of cardiac injuries from gunshots over the past 10 years (J. Trauma Acute Care Surg. 2016 Jul 6. doi: 10.1097/TA.0000000000001165). They also noted that several of these injuries were caused by penetrating thoracic wounds outside the cardiac box.
The cardiac box is currently defined as the area of the chest overlying the heart, bounded by the midclavicular lines (laterally) and from the clavicles to the tip of the xiphoid. “Surgical teaching dictates that penetrating injuries (i.e. stab wounds and gunshot wounds) in the box have the highest likelihood of cardiac injury and thereby mandate further evaluation,” Dr. Morse said. “These studies, however, are based on small patient sample sizes in which the majority were stab wound victims and underwent minimal statistical scrutiny.”
In what he said is the largest study of its kind, Dr. Morse and his associates conducted a retrospective review of trauma registry data from Grady’s trauma center and autopsy reports to identify patients with penetrating thoracic gunshot wounds and cardiac injury from 2011 to 2013 and to evaluate the relationship between penetrating injuries and the likelihood of a cardiac injury. Using a circumferential grid system around the thorax, the researchers employed logistic regression analysis to compare differences in rates of cardiac injury from entrance/exit wounds in the cardiac box, versus outside the box. They repeated the process to identify potential regions that yield improved predictions for cardiac injury over the current definition of the cardiac box.
Over the 3-year study period, 263 patients sustained 735 penetrating thoracic wounds, of which 80% were gunshot wounds (GSWs). Most of the patients were males (89%) with a median of two injuries each. After stab wounds were excluded, 277 GSWs to the thorax were included for study and 95 (34%) injured the heart. Of the 233 GSWs entering the cardiac box, 30% caused cardiac injury while, of the 44 GSWs outside the cardiac box, 32% penetrated the heart, suggesting that the current cardiac box is a poor predictor of cardiac injury relative to the thoracic non–cardiac box regions (OR 1.1; P = .71).
The researchers observed that the regions from the anterior to the posterior midline of the left thorax provided the highest positive predictive value, with a sensitivity of 90% and a specificity of 31%, making this region the most statistically significant discriminator of cardiac injury (OR, 4.4; P less than .01). This finding was primarily based on the fact that gunshots to the left lateral chest (an area not currently included in the box) had a high rate of cardiac injury (41%; OR, 1.4).
“The current cardiac box is unable to discriminate between gunshot wounds that will cause a cardiac injury and those that will not,” Dr. Morse said. “Any gunshot wound to the chest can cause a cardiac injury. While clinically relevant box borders would include the left chest, the bottom line for surgeons is to think outside the current cardiac box.”
The improved cardiac box that he and his associates proposed includes the area from the clavicles to the xiphoid and from the anterior to the posterior midline over the left thorax. “While this may be intuitive, it is not what we as surgeons have been teaching,” he said. “Finally, gunshots to areas such as the right posterior and posterolateral chest were associated with rates of cardiac injury greater than 30% despite their distance from the heart. This led us to conclude that a gunshot anywhere to the chest should be considered to potentially cause a cardiac injury.”
Dr. Morse acknowledged certain limitations of the study, including the fact that the study excluded graze wounds and gunshots above the clavicles and below the xiphoid. “However, a small percentage of these did cause cardiac injuries, which emphasizes the point that gunshot wounds from any entrance can cause cardiac injury.”
Invited discussant Nicholas Namias, MD, professor and chief of the division of acute care surgery at Jackson Memorial Hospital, Miami, said that the study by Dr. Morse and his associates “confirms what Dr. [Grace] Rozycki showed 20 years ago: Forget the [cardiac] box; it’s dead. Just throw an ultrasound probe on.”
Dr. Morse reported having no relevant financial disclosures.
AT THE AAST ANNUAL MEETING
Key clinical point: The current cardiac box is inadequate to discriminate whether a gunshot wound will create a cardiac injury.
Major finding: Of the 233 gunshot wounds entering the cardiac box, 30% caused cardiac injury while, of the 44 GSWs outside the cardiac box, 32% penetrated the heart, suggesting that the current cardiac box is a poor predictor of cardiac injury relative to the thoracic non–cardiac box regions (OR 1.1; P = .71).
Data source: A retrospective review of 236 patients with penetrating thoracic gunshot wounds and cardiac injury from 2011 to 2013.
Disclosures: Dr. Morse reported having no relevant financial disclosures.

Can Neurologists Predict Long-Term Disability Trajectories in Primary Progressive MS?
LONDON—A dynamic model based on long-term observations and a statistical modeling approach can help neurologists predict the future disability trajectory of a new patient with primary progressive multiple sclerosis (MS), according to a study presented at the 32nd Congress of the European Committee for Treatment and Research in MS (ECTRIMS). The existence of heterogeneous classes of patients should be considered in the design of future clinical trials in primary progressive MS that have time-to-reach-disability milestones as their primary end points, said the researchers.
Several natural history studies of patients with primary progressive MS have been reported from international registries over the past decades. This population had a consistently heterogeneous rate of disability accumulation. Time to reach the milestone of an Expanded Disability Status Scale (EDSS) score of 6 ranged between seven and 14 years from disease onset.
Alessio Signori, PhD, postdoctoral researcher in biostatistics at the University of Genoa, Italy, and colleagues sought to identify subgroups of patients with primary progressive MS who had similar longitudinal EDSS trajectories over time. The investigators included in their analysis all patients with primary progressive MS in the MSBase international registry who had their first EDSS assessment within five years of disease onset. Longitudinal EDSS scores were modeled by a latent class mixed model (LCMM) using a nonlinear function of time from onset. LCMM is an advanced statistical approach that models heterogeneity between patients by classifying them into unobserved groups (ie, latent classes) that have similar characteristics.

A total of 853 participants with primary progressive MS (51.7% female) from 24 countries with a mean age at onset of 42.4, a median baseline EDSS of 4, and 2.4 years of disease duration were included. LCMM detected three distinct subgroups of patients with a mild (n = 143; 16.8%), a moderate (n = 378; 44.3%), and a severe (n = 332; 38.9%) disability trajectory, respectively. Time from disease onset to diagnosis was shortest for the severe group. Median time to an EDSS of 4 was 14, five, and 3.7 years for the three groups, respectively. The probability of reaching an EDSS of 6 at 10 years was 0%, 46.5%, and 83.1%, respectively. Increasing severity of the disability time course was related to a decreasing frequency of patients with at least one relapse during follow-up (ie, from 47.6% to 36.5%).
“Using this modeling approach, it is possible to predict the future disease course of a subject with primary progressive MS using early EDSS assessments,” said Dr. Signori. “By using only one year of EDSS monitoring, 73% of patients are correctly classified in their disability trajectory group (mild, moderate, or severe). After three years, this proportion is 87%, and after five years, it is 92%.”
LONDON—A dynamic model based on long-term observations and a statistical modeling approach can help neurologists predict the future disability trajectory of a new patient with primary progressive multiple sclerosis (MS), according to a study presented at the 32nd Congress of the European Committee for Treatment and Research in MS (ECTRIMS). The existence of heterogeneous classes of patients should be considered in the design of future clinical trials in primary progressive MS that have time-to-reach-disability milestones as their primary end points, said the researchers.
Several natural history studies of patients with primary progressive MS have been reported from international registries over the past decades. This population had a consistently heterogeneous rate of disability accumulation. Time to reach the milestone of an Expanded Disability Status Scale (EDSS) score of 6 ranged between seven and 14 years from disease onset.
Alessio Signori, PhD, postdoctoral researcher in biostatistics at the University of Genoa, Italy, and colleagues sought to identify subgroups of patients with primary progressive MS who had similar longitudinal EDSS trajectories over time. The investigators included in their analysis all patients with primary progressive MS in the MSBase international registry who had their first EDSS assessment within five years of disease onset. Longitudinal EDSS scores were modeled by a latent class mixed model (LCMM) using a nonlinear function of time from onset. LCMM is an advanced statistical approach that models heterogeneity between patients by classifying them into unobserved groups (ie, latent classes) that have similar characteristics.
A total of 853 participants with primary progressive MS (51.7% female) from 24 countries with a mean age at onset of 42.4, a median baseline EDSS of 4, and 2.4 years of disease duration were included. LCMM detected three distinct subgroups of patients with a mild (n = 143; 16.8%), a moderate (n = 378; 44.3%), and a severe (n = 332; 38.9%) disability trajectory, respectively. Time from disease onset to diagnosis was shortest for the severe group. Median time to an EDSS of 4 was 14, five, and 3.7 years for the three groups, respectively. The probability of reaching an EDSS of 6 at 10 years was 0%, 46.5%, and 83.1%, respectively. Increasing severity of the disability time course was related to a decreasing frequency of patients with at least one relapse during follow-up (ie, from 47.6% to 36.5%).
“Using this modeling approach, it is possible to predict the future disease course of a subject with primary progressive MS using early EDSS assessments,” said Dr. Signori. “By using only one year of EDSS monitoring, 73% of patients are correctly classified in their disability trajectory group (mild, moderate, or severe). After three years, this proportion is 87%, and after five years, it is 92%.”
LONDON—A dynamic model based on long-term observations and a statistical modeling approach can help neurologists predict the future disability trajectory of a new patient with primary progressive multiple sclerosis (MS), according to a study presented at the 32nd Congress of the European Committee for Treatment and Research in MS (ECTRIMS). The existence of heterogeneous classes of patients should be considered in the design of future clinical trials in primary progressive MS that have time-to-reach-disability milestones as their primary end points, said the researchers.
Several natural history studies of patients with primary progressive MS have been reported from international registries over the past decades. This population had a consistently heterogeneous rate of disability accumulation. Time to reach the milestone of an Expanded Disability Status Scale (EDSS) score of 6 ranged between seven and 14 years from disease onset.
Alessio Signori, PhD, postdoctoral researcher in biostatistics at the University of Genoa, Italy, and colleagues sought to identify subgroups of patients with primary progressive MS who had similar longitudinal EDSS trajectories over time. The investigators included in their analysis all patients with primary progressive MS in the MSBase international registry who had their first EDSS assessment within five years of disease onset. Longitudinal EDSS scores were modeled by a latent class mixed model (LCMM) using a nonlinear function of time from onset. LCMM is an advanced statistical approach that models heterogeneity between patients by classifying them into unobserved groups (ie, latent classes) that have similar characteristics.
A total of 853 participants with primary progressive MS (51.7% female) from 24 countries with a mean age at onset of 42.4, a median baseline EDSS of 4, and 2.4 years of disease duration were included. LCMM detected three distinct subgroups of patients with a mild (n = 143; 16.8%), a moderate (n = 378; 44.3%), and a severe (n = 332; 38.9%) disability trajectory, respectively. Time from disease onset to diagnosis was shortest for the severe group. Median time to an EDSS of 4 was 14, five, and 3.7 years for the three groups, respectively. The probability of reaching an EDSS of 6 at 10 years was 0%, 46.5%, and 83.1%, respectively. Increasing severity of the disability time course was related to a decreasing frequency of patients with at least one relapse during follow-up (ie, from 47.6% to 36.5%).
“Using this modeling approach, it is possible to predict the future disease course of a subject with primary progressive MS using early EDSS assessments,” said Dr. Signori. “By using only one year of EDSS monitoring, 73% of patients are correctly classified in their disability trajectory group (mild, moderate, or severe). After three years, this proportion is 87%, and after five years, it is 92%.”
The Ads Say ‘Get Your Flu Shot Today,’ But It May Be Wiser To Wait
The pharmacy chain pitches started in August: Come in and get your flu shot.
Convenience is touted. So are incentives: CVS offers a 20-percent-off shopping pass for everyone who gets a shot, while Walgreens donates toward international vaccination efforts.
The start of flu season is still weeks — if not months — away. Yet marketing of the vaccine has become an almost year-round effort, beginning when the shots become available in August and hyped as long as the supply lasts, often into April or May.
Not that long ago, most flu-shot campaigns started as the leaves began to turn in October. But the rise of retail medical clinics inside drug stores over the past decade — and state laws allowing pharmacists to give vaccinations — has stretched the flu-shot season.
The stores have figured out how “to deliver medical services in an on-demand way” which appeals to customers, particularly millennials, said Tom Charland, founder and CEO of Merchant Medicine, which tracks the walk-in clinic industry. “It’s a way to get people into the store to buy other things.”
But some experts say the marketing may be overtaking medical wisdom since it’s unclear how long the immunity imparted by the vaccine lasts, particularly in older people.
Federal health officials say it’s better to get the shot whenever you can. An early flu shot is better than no flu shot at all. But the science is mixed when it comes to how long a flu shot promoted and given during the waning days of summer will provide optimal protection, especially because flu season generally peaks in mid-winter or beyond. Experts are divided on how patients should respond to such offers.
“If you’re over 65, don’t get the flu vaccine in September. Or August. It’s a marketing scheme,” said Laura Haynes, an immunologist at the University of Connecticut Center on Aging.
That’s because a combination of factors makes it more difficult for the immune systems of people older than age 65 to respond to the vaccination in the first place. And its protective effects may wear off faster for this age group than it does for young people.
When is the best time to vaccinate? It’s a question even doctors have.
“Should I wait until October or November to vaccinate my elderly or medically frail patients?” That’s one of the queries on the website of the board that advises the Centers for Disease Control and Prevention on immunizations. The answer is that it is safe to make the shots available to all age groups when the vaccine becomes available, although it does include a caution.
The board says antibodies created by the vaccine decline in the months following vaccination “primarily affecting persons age 65 and older,” citing a study done during the 2011-2012 flu season. Still, while “delaying vaccination might permit greater immunity later in the season,” the CDC notes that “deferral could result in missed opportunities to vaccinate.”
How long will the immunity last?
“The data are very mixed,” said. John J. Treanor, a vaccine expert at the University of Rochester medical school. Some studies suggest vaccines lose some protectiveness during the course of a single flu season. Flu activity generally starts in the fall, but peaks in January or February and can run into the spring.
“So some might worry that if [they] got vaccinated very early and flu didn’t show up until very late, it might not work as well,” he said.
But other studies “show you still have protection from the shot you got last year if it’s a year when the strains didn’t change, Treanor said.
In any given flu season, vaccine effectiveness varies. One factor is how well the vaccines match the virus that is actually prevalent. Other factors influencing effectiveness include the age and general health of the recipient. In the overall population, the CDC says studies show vaccines can reduce the risk of flu by about 50 to 60 percent when the vaccines are well matched.
Health officials say it’s especially important to vaccinate children because they often spread the disease, are better able to develop antibodies from the vaccines and, if they don’t get sick, they won’t expose grandma and grandpa. While most people who get the flu recover, it is a serious disease responsible for many deaths each year, particularly among older adults and young children. Influenza’s intensity varies annually, with the CDC saying deaths associated with the flu have ranged from about 3,300 a year to 49,000 during the past 31 seasons.
To develop vaccines, manufacturers and scientists study what’s circulating in the Southern Hemisphere during its winter, which is our summer. Then — based on that evidence — forecast what flu strains might circulate here to make vaccines that are generally delivered in late July.
For the upcoming season, the vaccines will include three or four strains, including two A strains, an H1N1 and an H3N2, as well as one or two B strains, according to the CDC. It recommends that everyone older than 6 months get vaccinated, unless they have health conditions that would prevent it.
The vaccines can’t give a person the flu because the virus is killed before it’s included in the shot. This year, the nasal vaccine is not recommended for use, as studies showed it was not effective during several of the past flu seasons.
But when to go?
“The ideal time is between Halloween and Thanksgiving,” said Haynes at UConn. “If you can’t wait and the only chance is to get it in September, then go ahead and get it. It’s best to get it early rather than not at all.”
This Kaiser Health News story also ran on NPR.
The pharmacy chain pitches started in August: Come in and get your flu shot.
Convenience is touted. So are incentives: CVS offers a 20-percent-off shopping pass for everyone who gets a shot, while Walgreens donates toward international vaccination efforts.
The start of flu season is still weeks — if not months — away. Yet marketing of the vaccine has become an almost year-round effort, beginning when the shots become available in August and hyped as long as the supply lasts, often into April or May.
Not that long ago, most flu-shot campaigns started as the leaves began to turn in October. But the rise of retail medical clinics inside drug stores over the past decade — and state laws allowing pharmacists to give vaccinations — has stretched the flu-shot season.
The stores have figured out how “to deliver medical services in an on-demand way” which appeals to customers, particularly millennials, said Tom Charland, founder and CEO of Merchant Medicine, which tracks the walk-in clinic industry. “It’s a way to get people into the store to buy other things.”
But some experts say the marketing may be overtaking medical wisdom since it’s unclear how long the immunity imparted by the vaccine lasts, particularly in older people.
Federal health officials say it’s better to get the shot whenever you can. An early flu shot is better than no flu shot at all. But the science is mixed when it comes to how long a flu shot promoted and given during the waning days of summer will provide optimal protection, especially because flu season generally peaks in mid-winter or beyond. Experts are divided on how patients should respond to such offers.
“If you’re over 65, don’t get the flu vaccine in September. Or August. It’s a marketing scheme,” said Laura Haynes, an immunologist at the University of Connecticut Center on Aging.
That’s because a combination of factors makes it more difficult for the immune systems of people older than age 65 to respond to the vaccination in the first place. And its protective effects may wear off faster for this age group than it does for young people.
When is the best time to vaccinate? It’s a question even doctors have.
“Should I wait until October or November to vaccinate my elderly or medically frail patients?” That’s one of the queries on the website of the board that advises the Centers for Disease Control and Prevention on immunizations. The answer is that it is safe to make the shots available to all age groups when the vaccine becomes available, although it does include a caution.
The board says antibodies created by the vaccine decline in the months following vaccination “primarily affecting persons age 65 and older,” citing a study done during the 2011-2012 flu season. Still, while “delaying vaccination might permit greater immunity later in the season,” the CDC notes that “deferral could result in missed opportunities to vaccinate.”
How long will the immunity last?
“The data are very mixed,” said. John J. Treanor, a vaccine expert at the University of Rochester medical school. Some studies suggest vaccines lose some protectiveness during the course of a single flu season. Flu activity generally starts in the fall, but peaks in January or February and can run into the spring.
“So some might worry that if [they] got vaccinated very early and flu didn’t show up until very late, it might not work as well,” he said.
But other studies “show you still have protection from the shot you got last year if it’s a year when the strains didn’t change, Treanor said.
In any given flu season, vaccine effectiveness varies. One factor is how well the vaccines match the virus that is actually prevalent. Other factors influencing effectiveness include the age and general health of the recipient. In the overall population, the CDC says studies show vaccines can reduce the risk of flu by about 50 to 60 percent when the vaccines are well matched.
Health officials say it’s especially important to vaccinate children because they often spread the disease, are better able to develop antibodies from the vaccines and, if they don’t get sick, they won’t expose grandma and grandpa. While most people who get the flu recover, it is a serious disease responsible for many deaths each year, particularly among older adults and young children. Influenza’s intensity varies annually, with the CDC saying deaths associated with the flu have ranged from about 3,300 a year to 49,000 during the past 31 seasons.
To develop vaccines, manufacturers and scientists study what’s circulating in the Southern Hemisphere during its winter, which is our summer. Then — based on that evidence — forecast what flu strains might circulate here to make vaccines that are generally delivered in late July.
For the upcoming season, the vaccines will include three or four strains, including two A strains, an H1N1 and an H3N2, as well as one or two B strains, according to the CDC. It recommends that everyone older than 6 months get vaccinated, unless they have health conditions that would prevent it.
The vaccines can’t give a person the flu because the virus is killed before it’s included in the shot. This year, the nasal vaccine is not recommended for use, as studies showed it was not effective during several of the past flu seasons.
But when to go?
“The ideal time is between Halloween and Thanksgiving,” said Haynes at UConn. “If you can’t wait and the only chance is to get it in September, then go ahead and get it. It’s best to get it early rather than not at all.”
This Kaiser Health News story also ran on NPR.
The pharmacy chain pitches started in August: Come in and get your flu shot.
Convenience is touted. So are incentives: CVS offers a 20-percent-off shopping pass for everyone who gets a shot, while Walgreens donates toward international vaccination efforts.
The start of flu season is still weeks — if not months — away. Yet marketing of the vaccine has become an almost year-round effort, beginning when the shots become available in August and hyped as long as the supply lasts, often into April or May.
Not that long ago, most flu-shot campaigns started as the leaves began to turn in October. But the rise of retail medical clinics inside drug stores over the past decade — and state laws allowing pharmacists to give vaccinations — has stretched the flu-shot season.
The stores have figured out how “to deliver medical services in an on-demand way” which appeals to customers, particularly millennials, said Tom Charland, founder and CEO of Merchant Medicine, which tracks the walk-in clinic industry. “It’s a way to get people into the store to buy other things.”
But some experts say the marketing may be overtaking medical wisdom since it’s unclear how long the immunity imparted by the vaccine lasts, particularly in older people.
Federal health officials say it’s better to get the shot whenever you can. An early flu shot is better than no flu shot at all. But the science is mixed when it comes to how long a flu shot promoted and given during the waning days of summer will provide optimal protection, especially because flu season generally peaks in mid-winter or beyond. Experts are divided on how patients should respond to such offers.
“If you’re over 65, don’t get the flu vaccine in September. Or August. It’s a marketing scheme,” said Laura Haynes, an immunologist at the University of Connecticut Center on Aging.
That’s because a combination of factors makes it more difficult for the immune systems of people older than age 65 to respond to the vaccination in the first place. And its protective effects may wear off faster for this age group than it does for young people.
When is the best time to vaccinate? It’s a question even doctors have.
“Should I wait until October or November to vaccinate my elderly or medically frail patients?” That’s one of the queries on the website of the board that advises the Centers for Disease Control and Prevention on immunizations. The answer is that it is safe to make the shots available to all age groups when the vaccine becomes available, although it does include a caution.
The board says antibodies created by the vaccine decline in the months following vaccination “primarily affecting persons age 65 and older,” citing a study done during the 2011-2012 flu season. Still, while “delaying vaccination might permit greater immunity later in the season,” the CDC notes that “deferral could result in missed opportunities to vaccinate.”
How long will the immunity last?
“The data are very mixed,” said. John J. Treanor, a vaccine expert at the University of Rochester medical school. Some studies suggest vaccines lose some protectiveness during the course of a single flu season. Flu activity generally starts in the fall, but peaks in January or February and can run into the spring.
“So some might worry that if [they] got vaccinated very early and flu didn’t show up until very late, it might not work as well,” he said.
But other studies “show you still have protection from the shot you got last year if it’s a year when the strains didn’t change, Treanor said.
In any given flu season, vaccine effectiveness varies. One factor is how well the vaccines match the virus that is actually prevalent. Other factors influencing effectiveness include the age and general health of the recipient. In the overall population, the CDC says studies show vaccines can reduce the risk of flu by about 50 to 60 percent when the vaccines are well matched.
Health officials say it’s especially important to vaccinate children because they often spread the disease, are better able to develop antibodies from the vaccines and, if they don’t get sick, they won’t expose grandma and grandpa. While most people who get the flu recover, it is a serious disease responsible for many deaths each year, particularly among older adults and young children. Influenza’s intensity varies annually, with the CDC saying deaths associated with the flu have ranged from about 3,300 a year to 49,000 during the past 31 seasons.
To develop vaccines, manufacturers and scientists study what’s circulating in the Southern Hemisphere during its winter, which is our summer. Then — based on that evidence — forecast what flu strains might circulate here to make vaccines that are generally delivered in late July.
For the upcoming season, the vaccines will include three or four strains, including two A strains, an H1N1 and an H3N2, as well as one or two B strains, according to the CDC. It recommends that everyone older than 6 months get vaccinated, unless they have health conditions that would prevent it.
The vaccines can’t give a person the flu because the virus is killed before it’s included in the shot. This year, the nasal vaccine is not recommended for use, as studies showed it was not effective during several of the past flu seasons.
But when to go?
“The ideal time is between Halloween and Thanksgiving,” said Haynes at UConn. “If you can’t wait and the only chance is to get it in September, then go ahead and get it. It’s best to get it early rather than not at all.”
This Kaiser Health News story also ran on NPR.
Novel De Novo Heterozygous Frameshift Mutation of the ADAR1 Gene in Heavy Dyschromatosis Symmetrica Hereditaria
To the Editor:
Dyschromatosis symmetrica hereditaria (DSH)(Online Mendelian Inheritance in Man 127400), also called reticulate acropigmentation of Dohi, is a pigmentary genodermatosis characterized by a mixture of hyperpigmented and hypopigmented macules of various sizes on the dorsal aspects of the hands and feet. Linkage analysis has revealed that the DSH gene locus resides on chromosome 1q11-q21,1 and the adenosine deaminase RNA specific gene, ADAR1 (also called DSRAD), in this region has been identified as being responsible for the development of DSH.2 We report a sporadic case of severe DSH with the ADAR1 gene detected in a mutation analysis.
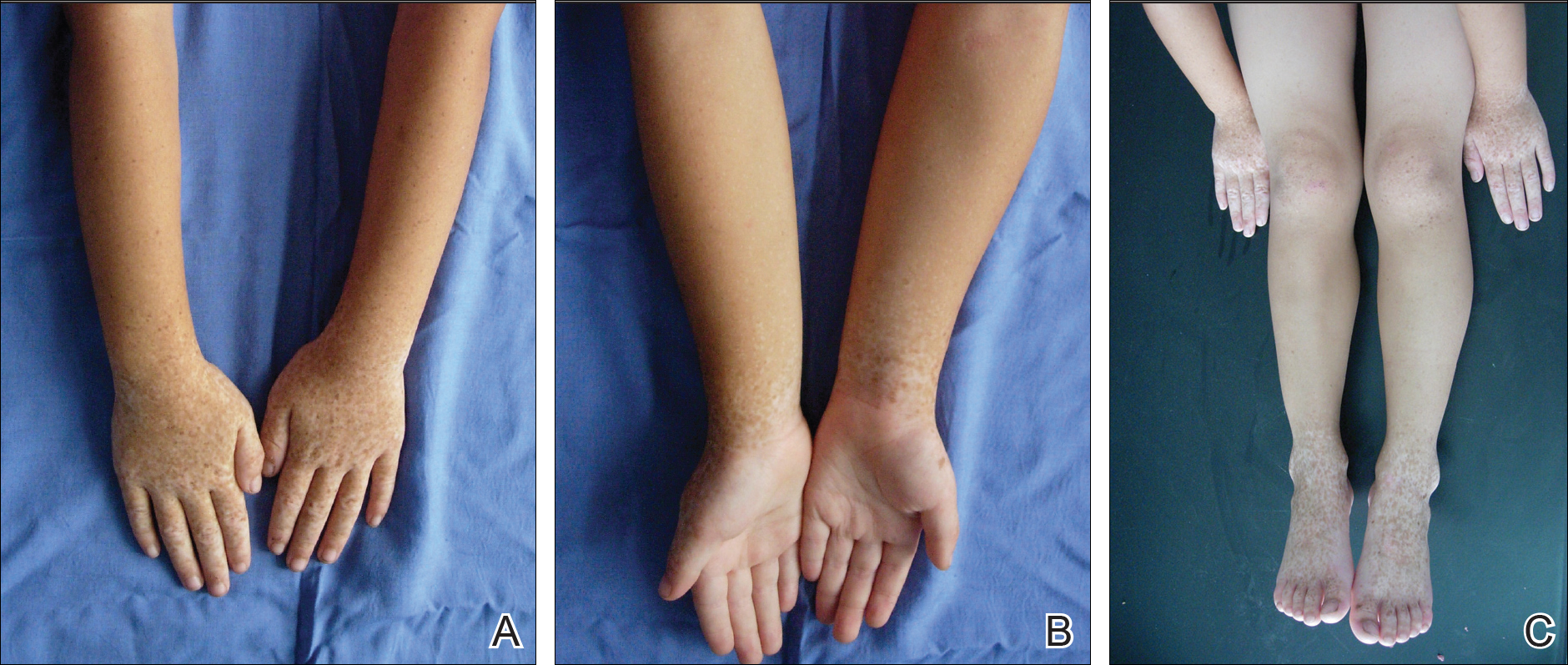
A 6-year-old girl presented with a mixture of hyperpigmented and hypopigmented macules on the dorsal aspects of the hands and feet and the curved side of the wrists, heels, and knees, as well as scattered frecklelike and depigmented spots on the face, ears, neck, arms, and upper back (Figure 1). Her parents noted that hyperpigmented and hypopigmented macules on the dorsal aspects of the hands developed at 5 months of age. Exacerbation after exposure to sunlight resulted in the eruption becoming remarkable in summer and fainter in winter. The skin lesions gradually became more progressive. Physical examination revealed that the patient generally was healthy.
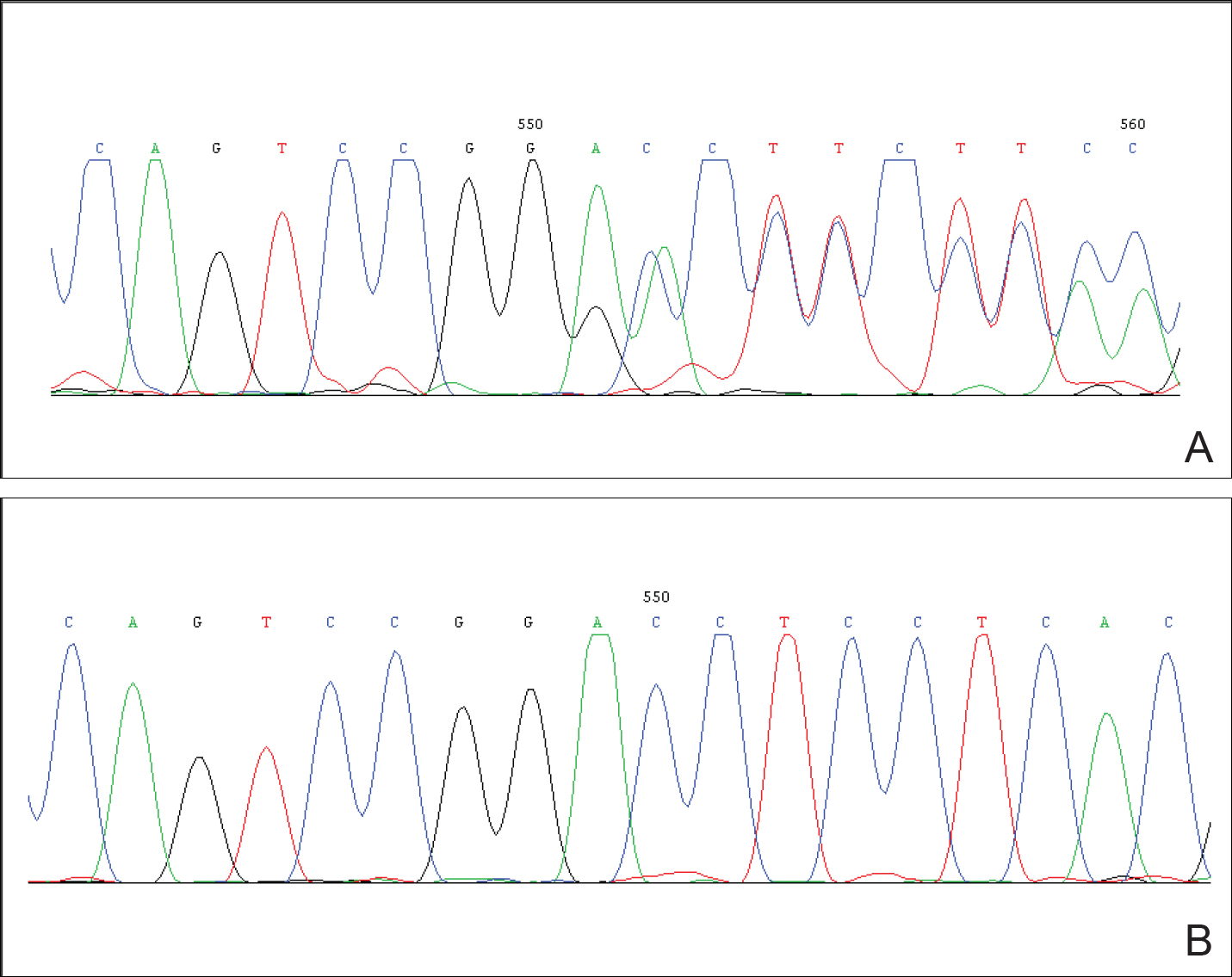
After obtaining informed consent, we performed a mutation analysis of the ADAR1 gene in our patient and her parents. We used a kit to extract genomic DNA from peripheral blood, which was then used to amplify the exons of the ADAR1 gene with intronic flanking sequences by polymerase chain reaction with the primer.3 After amplification, polymerase chain reaction products were purified. We sequenced the ADAR1 gene. Sequence comparisons and analysis found that the patient (proband) carried a heterozygous insertional mutation c.2253insG in exon 6 of the ADAR1 gene. This mutation was not detected in the proband’s healthy parents and 100 normal individuals (Figure 2).
Dyschromatosis symmetrica hereditaria is acquired by autosomal-dominant inheritance and is mainly reported in Asians, especially in Japan and China. Oyama et al4 reviewed 185 cases of DSH in Japan and found the onset of this disease usually was during infancy or childhood; 73% of patients developed the skin lesions before 6 years of age. Suzuki et al5 reported 10 unrelated Japanese patients and found the onset of disease ranged from 1 year of age to childhood. Zhang et al1,6 investigated 78 Chinese patients with DSH including 8 multigenerational families and 2 sporadic patients and found the age of disease onset ranged from 6 months to 15 years of age. The age of onset in our patient (5 months) was younger than these prior reports.
Patients with DSH have a characteristic appearance including a mixture of hyperpigmented and hypopigmented macules of various sizes on the dorsal aspects of the hands and feet. Few patients have similar lesions on the knees and elbows. Many patients have frecklelike macules on the face and arms.1-6 One patient has been described with scattered depigmented spots on the face and chest.1 Our patient had a characteristic appearance as well as some special manifestations including skin lesions on the curved side of the wrist, ears, neck, and upper back.
The human ADAR1 gene spans 30 kilobase and contains 15 exons. It encodes RNA-specific adenosine deaminase composed of 1226 amino acid residues. This enzyme is important for various functions such as site-specific RNA editing and nuclear translation. This enzyme has 2 Z-alpha domains, 3 double-stranded RNA–binding domains, and the putative deaminase domain corresponding to exon 2, exons 2 to 7, and exons 9 to 14 of ADAR1, respectively.6
Mutation analysis of the ADAR1 gene in this case showed heterozygous insertion mutation c.2253insG in exon 6 of the ADAR1 gene, which changed the reading frame, and 475 amino acid residues in C-terminus are replaced by 90 amino acid residues (TSSRAQVRLPSKSWGSLVPSRLRTQQEA RQAGSSRCGSPCLDWGEREGRTHGFHRG NPSDRGQSQKNYAPPLKVPRSTAKT DTPSHWQHLP). This mutation was not detected in the proband’s healthy parents and the 100 control individuals, which indicated that it was a de novo mutation and the pathogenic mutation of DSH rather than a common polymorphism.
In conclusion, we report a novel mutation of the ADAR1 gene with a heavy clinical phenotype in DSH. This study expands the spectrum of clinical manifestations and demonstrates the ADAR1 mutation in DSH.
Acknowledgments
We are most grateful to the patient and her family for taking part in our study.
- Zhang XJ, Gao M, Li M, et al. Identification of a locus for dyschromatosis symmetrica hereditaria at chromosome 1q11-1q21. J Invest Dermatol. 2003;120:776-780.
- Miyamura Y, Suzuki T, Kono M, et al. Mutations of the RNA-specific adenosine deaminase gene (DSRAD) are involved in dyschromatosis symmetrica hereditaria [published online August 11, 2003]. Am J Hum Genet. 2003;73:693-699.
- Li M, Li C, Hua H, et al. Identification of two novel mutations in Chinese patients with dyschromatosis symmetrica hereditaria [published online October 8, 2005]. Arch Dermatol Res. 2005;297:196-200.
- Oyama M, Shimizu H, Ohata Y, et al. Dyschromatosis symmetrica hereditaria (reticulate acropigmentation of Dohi): report of a Japanese family with the condition and a literature review of 185 cases. Br J Dermatol. 1999;140:491-496.
- Suzuki N, Suzuki T, Inagaki K, et al. Ten novel mutations of the ADAR1 gene in Japanese patients with dyschromatosis symmetrica hereditaria [published online August 17, 2006]. J Invest Dermatol. 2007;127:309-311.
- Zhang XJ, He PP, Li M, et al. Seven novel mutations of the ADAR gene in Chinese families and sporadic patients with dyschromatosis symmetrica hereditaria (DSH). Hum Mutat. 2004;23:629-630.
To the Editor:
Dyschromatosis symmetrica hereditaria (DSH)(Online Mendelian Inheritance in Man 127400), also called reticulate acropigmentation of Dohi, is a pigmentary genodermatosis characterized by a mixture of hyperpigmented and hypopigmented macules of various sizes on the dorsal aspects of the hands and feet. Linkage analysis has revealed that the DSH gene locus resides on chromosome 1q11-q21,1 and the adenosine deaminase RNA specific gene, ADAR1 (also called DSRAD), in this region has been identified as being responsible for the development of DSH.2 We report a sporadic case of severe DSH with the ADAR1 gene detected in a mutation analysis.
A 6-year-old girl presented with a mixture of hyperpigmented and hypopigmented macules on the dorsal aspects of the hands and feet and the curved side of the wrists, heels, and knees, as well as scattered frecklelike and depigmented spots on the face, ears, neck, arms, and upper back (Figure 1). Her parents noted that hyperpigmented and hypopigmented macules on the dorsal aspects of the hands developed at 5 months of age. Exacerbation after exposure to sunlight resulted in the eruption becoming remarkable in summer and fainter in winter. The skin lesions gradually became more progressive. Physical examination revealed that the patient generally was healthy.
After obtaining informed consent, we performed a mutation analysis of the ADAR1 gene in our patient and her parents. We used a kit to extract genomic DNA from peripheral blood, which was then used to amplify the exons of the ADAR1 gene with intronic flanking sequences by polymerase chain reaction with the primer.3 After amplification, polymerase chain reaction products were purified. We sequenced the ADAR1 gene. Sequence comparisons and analysis found that the patient (proband) carried a heterozygous insertional mutation c.2253insG in exon 6 of the ADAR1 gene. This mutation was not detected in the proband’s healthy parents and 100 normal individuals (Figure 2).
Dyschromatosis symmetrica hereditaria is acquired by autosomal-dominant inheritance and is mainly reported in Asians, especially in Japan and China. Oyama et al4 reviewed 185 cases of DSH in Japan and found the onset of this disease usually was during infancy or childhood; 73% of patients developed the skin lesions before 6 years of age. Suzuki et al5 reported 10 unrelated Japanese patients and found the onset of disease ranged from 1 year of age to childhood. Zhang et al1,6 investigated 78 Chinese patients with DSH including 8 multigenerational families and 2 sporadic patients and found the age of disease onset ranged from 6 months to 15 years of age. The age of onset in our patient (5 months) was younger than these prior reports.
Patients with DSH have a characteristic appearance including a mixture of hyperpigmented and hypopigmented macules of various sizes on the dorsal aspects of the hands and feet. Few patients have similar lesions on the knees and elbows. Many patients have frecklelike macules on the face and arms.1-6 One patient has been described with scattered depigmented spots on the face and chest.1 Our patient had a characteristic appearance as well as some special manifestations including skin lesions on the curved side of the wrist, ears, neck, and upper back.
The human ADAR1 gene spans 30 kilobase and contains 15 exons. It encodes RNA-specific adenosine deaminase composed of 1226 amino acid residues. This enzyme is important for various functions such as site-specific RNA editing and nuclear translation. This enzyme has 2 Z-alpha domains, 3 double-stranded RNA–binding domains, and the putative deaminase domain corresponding to exon 2, exons 2 to 7, and exons 9 to 14 of ADAR1, respectively.6
Mutation analysis of the ADAR1 gene in this case showed heterozygous insertion mutation c.2253insG in exon 6 of the ADAR1 gene, which changed the reading frame, and 475 amino acid residues in C-terminus are replaced by 90 amino acid residues (TSSRAQVRLPSKSWGSLVPSRLRTQQEA RQAGSSRCGSPCLDWGEREGRTHGFHRG NPSDRGQSQKNYAPPLKVPRSTAKT DTPSHWQHLP). This mutation was not detected in the proband’s healthy parents and the 100 control individuals, which indicated that it was a de novo mutation and the pathogenic mutation of DSH rather than a common polymorphism.
In conclusion, we report a novel mutation of the ADAR1 gene with a heavy clinical phenotype in DSH. This study expands the spectrum of clinical manifestations and demonstrates the ADAR1 mutation in DSH.
Acknowledgments
We are most grateful to the patient and her family for taking part in our study.
To the Editor:
Dyschromatosis symmetrica hereditaria (DSH)(Online Mendelian Inheritance in Man 127400), also called reticulate acropigmentation of Dohi, is a pigmentary genodermatosis characterized by a mixture of hyperpigmented and hypopigmented macules of various sizes on the dorsal aspects of the hands and feet. Linkage analysis has revealed that the DSH gene locus resides on chromosome 1q11-q21,1 and the adenosine deaminase RNA specific gene, ADAR1 (also called DSRAD), in this region has been identified as being responsible for the development of DSH.2 We report a sporadic case of severe DSH with the ADAR1 gene detected in a mutation analysis.
A 6-year-old girl presented with a mixture of hyperpigmented and hypopigmented macules on the dorsal aspects of the hands and feet and the curved side of the wrists, heels, and knees, as well as scattered frecklelike and depigmented spots on the face, ears, neck, arms, and upper back (Figure 1). Her parents noted that hyperpigmented and hypopigmented macules on the dorsal aspects of the hands developed at 5 months of age. Exacerbation after exposure to sunlight resulted in the eruption becoming remarkable in summer and fainter in winter. The skin lesions gradually became more progressive. Physical examination revealed that the patient generally was healthy.
After obtaining informed consent, we performed a mutation analysis of the ADAR1 gene in our patient and her parents. We used a kit to extract genomic DNA from peripheral blood, which was then used to amplify the exons of the ADAR1 gene with intronic flanking sequences by polymerase chain reaction with the primer.3 After amplification, polymerase chain reaction products were purified. We sequenced the ADAR1 gene. Sequence comparisons and analysis found that the patient (proband) carried a heterozygous insertional mutation c.2253insG in exon 6 of the ADAR1 gene. This mutation was not detected in the proband’s healthy parents and 100 normal individuals (Figure 2).
Dyschromatosis symmetrica hereditaria is acquired by autosomal-dominant inheritance and is mainly reported in Asians, especially in Japan and China. Oyama et al4 reviewed 185 cases of DSH in Japan and found the onset of this disease usually was during infancy or childhood; 73% of patients developed the skin lesions before 6 years of age. Suzuki et al5 reported 10 unrelated Japanese patients and found the onset of disease ranged from 1 year of age to childhood. Zhang et al1,6 investigated 78 Chinese patients with DSH including 8 multigenerational families and 2 sporadic patients and found the age of disease onset ranged from 6 months to 15 years of age. The age of onset in our patient (5 months) was younger than these prior reports.
Patients with DSH have a characteristic appearance including a mixture of hyperpigmented and hypopigmented macules of various sizes on the dorsal aspects of the hands and feet. Few patients have similar lesions on the knees and elbows. Many patients have frecklelike macules on the face and arms.1-6 One patient has been described with scattered depigmented spots on the face and chest.1 Our patient had a characteristic appearance as well as some special manifestations including skin lesions on the curved side of the wrist, ears, neck, and upper back.
The human ADAR1 gene spans 30 kilobase and contains 15 exons. It encodes RNA-specific adenosine deaminase composed of 1226 amino acid residues. This enzyme is important for various functions such as site-specific RNA editing and nuclear translation. This enzyme has 2 Z-alpha domains, 3 double-stranded RNA–binding domains, and the putative deaminase domain corresponding to exon 2, exons 2 to 7, and exons 9 to 14 of ADAR1, respectively.6
Mutation analysis of the ADAR1 gene in this case showed heterozygous insertion mutation c.2253insG in exon 6 of the ADAR1 gene, which changed the reading frame, and 475 amino acid residues in C-terminus are replaced by 90 amino acid residues (TSSRAQVRLPSKSWGSLVPSRLRTQQEA RQAGSSRCGSPCLDWGEREGRTHGFHRG NPSDRGQSQKNYAPPLKVPRSTAKT DTPSHWQHLP). This mutation was not detected in the proband’s healthy parents and the 100 control individuals, which indicated that it was a de novo mutation and the pathogenic mutation of DSH rather than a common polymorphism.
In conclusion, we report a novel mutation of the ADAR1 gene with a heavy clinical phenotype in DSH. This study expands the spectrum of clinical manifestations and demonstrates the ADAR1 mutation in DSH.
Acknowledgments
We are most grateful to the patient and her family for taking part in our study.
- Zhang XJ, Gao M, Li M, et al. Identification of a locus for dyschromatosis symmetrica hereditaria at chromosome 1q11-1q21. J Invest Dermatol. 2003;120:776-780.
- Miyamura Y, Suzuki T, Kono M, et al. Mutations of the RNA-specific adenosine deaminase gene (DSRAD) are involved in dyschromatosis symmetrica hereditaria [published online August 11, 2003]. Am J Hum Genet. 2003;73:693-699.
- Li M, Li C, Hua H, et al. Identification of two novel mutations in Chinese patients with dyschromatosis symmetrica hereditaria [published online October 8, 2005]. Arch Dermatol Res. 2005;297:196-200.
- Oyama M, Shimizu H, Ohata Y, et al. Dyschromatosis symmetrica hereditaria (reticulate acropigmentation of Dohi): report of a Japanese family with the condition and a literature review of 185 cases. Br J Dermatol. 1999;140:491-496.
- Suzuki N, Suzuki T, Inagaki K, et al. Ten novel mutations of the ADAR1 gene in Japanese patients with dyschromatosis symmetrica hereditaria [published online August 17, 2006]. J Invest Dermatol. 2007;127:309-311.
- Zhang XJ, He PP, Li M, et al. Seven novel mutations of the ADAR gene in Chinese families and sporadic patients with dyschromatosis symmetrica hereditaria (DSH). Hum Mutat. 2004;23:629-630.
- Zhang XJ, Gao M, Li M, et al. Identification of a locus for dyschromatosis symmetrica hereditaria at chromosome 1q11-1q21. J Invest Dermatol. 2003;120:776-780.
- Miyamura Y, Suzuki T, Kono M, et al. Mutations of the RNA-specific adenosine deaminase gene (DSRAD) are involved in dyschromatosis symmetrica hereditaria [published online August 11, 2003]. Am J Hum Genet. 2003;73:693-699.
- Li M, Li C, Hua H, et al. Identification of two novel mutations in Chinese patients with dyschromatosis symmetrica hereditaria [published online October 8, 2005]. Arch Dermatol Res. 2005;297:196-200.
- Oyama M, Shimizu H, Ohata Y, et al. Dyschromatosis symmetrica hereditaria (reticulate acropigmentation of Dohi): report of a Japanese family with the condition and a literature review of 185 cases. Br J Dermatol. 1999;140:491-496.
- Suzuki N, Suzuki T, Inagaki K, et al. Ten novel mutations of the ADAR1 gene in Japanese patients with dyschromatosis symmetrica hereditaria [published online August 17, 2006]. J Invest Dermatol. 2007;127:309-311.
- Zhang XJ, He PP, Li M, et al. Seven novel mutations of the ADAR gene in Chinese families and sporadic patients with dyschromatosis symmetrica hereditaria (DSH). Hum Mutat. 2004;23:629-630.
Practice Points
- The adenosine deaminase RNA specific gene, ADAR1, has been identified as being responsible for the development of dyschromatosis symmetrica hereditaria (DSH).
- The characteristic appearance of DSH is a mixture of hyperpigmented and hypopigmented macules of various sizes on the dorsal aspects of the hands and feet.

Should I throw out my expired medications?
A 55-year-old patient requests new prescriptions at a routine appointment. She will be traveling internationally next month and wants to replace her emergency medication kit, as the medications in it (ciprofloxacin, loperamide, and oxycodone) have all expired.
What do you do?
A) Replace the prescription for ciprofloxacin.
B) Replace all three medications.
C) Tell the patient that all the meds should still be fine.
This is a common concern brought up by patients. Many patients discard medications when they pass the expiration date on the package. Is this necessary? Is there a health risk to taking expired medications, and is it okay from a therapeutic standpoint to use medications past their expiration date?

The expiration date is not a date that the drug stops being effective or potentially becomes toxic. It is a date, required by law, that the manufacturer can guarantee greater than 90% original potency of the medication. There really isn’t incentive for pharmaceutical companies to extend the expiration dates, as it is profitable for patients to throw away expired medications and replace them with new prescriptions.
The U.S. military purchases a large stockpile of drugs and has the potential for having a great deal of expired medications. To help reduce this problem, the Food and Drug Administration administers the shelf-life extension program (SLEP) for the U.S. military as a testing and evaluation program designed to justify an extension of the shelf life of stockpiled drug products.1
Robbe Lyon, MD, and colleagues reported data from the SLEP.2 A total of 122 drugs were studied representing 3,005 lots, with 88% of these extended at least 1 year past the expiration date, with an average extension of more than 5 years. Several antibiotics were studied, including ciprofloxacin (mean extension, 55 months), amoxicillin (mean extension, 23 months), and doxycycline (mean extension, 50 months).
Lee Cantrell, PharmD, and coinvestigators looked at sealed drugs from a retail pharmacy that were 28-40 years past their expiration date.3 Amazingly, 12 of the 14 compounds tested were in concentrations that were at least 90% of the labeled amount. Among the drugs that were tested that maintained greater than 90% of the labeled amount were acetaminophen, codeine, hydrocodone, and barbiturates. Aspirin and amphetamine were the two drugs that did not have greater than 90% of the labeled amount. The aspirin amounts were very low, about 1% of the listed amount on the package.
The major myth surrounding expired medications is that taking an expired medication could be toxic.
There is one case report of toxicity from the use of expired tetracycline.4 This was a case series of three patients who developed reversible Fanconi syndrome linked to using an expired tetracycline preparation. That preparation of tetracycline is no longer available.
There are no other reports of toxicity due to use of expired medications.5,6 There appears to be no direct risk of toxicity to the patient by using medication past the expiration date.
The risk that isn’t answered is the risk of using medications that may not be effective if potency isn’t guaranteed beyond the expiration date. It appears that most drugs are effective for years past the expiration date.
This isn’t an issue for medications for treatment of chronic conditions, as patients take the medications every day, and the medications will be used up long before they expire. For medications that are used infrequently – analgesics, antihistamines, and medications for traveler’s diarrhea – they appear to be stable for years past expiration, and there is little risk to the patient if the medications are not fully effective.
I think aspirin should not be used past expiration, given the data showing that it breaks down more so than other medications. For the case at the start of this article, I think having the patient use the expired medications should be fine.
References
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
A 55-year-old patient requests new prescriptions at a routine appointment. She will be traveling internationally next month and wants to replace her emergency medication kit, as the medications in it (ciprofloxacin, loperamide, and oxycodone) have all expired.
What do you do?
A) Replace the prescription for ciprofloxacin.
B) Replace all three medications.
C) Tell the patient that all the meds should still be fine.
This is a common concern brought up by patients. Many patients discard medications when they pass the expiration date on the package. Is this necessary? Is there a health risk to taking expired medications, and is it okay from a therapeutic standpoint to use medications past their expiration date?
The expiration date is not a date that the drug stops being effective or potentially becomes toxic. It is a date, required by law, that the manufacturer can guarantee greater than 90% original potency of the medication. There really isn’t incentive for pharmaceutical companies to extend the expiration dates, as it is profitable for patients to throw away expired medications and replace them with new prescriptions.
The U.S. military purchases a large stockpile of drugs and has the potential for having a great deal of expired medications. To help reduce this problem, the Food and Drug Administration administers the shelf-life extension program (SLEP) for the U.S. military as a testing and evaluation program designed to justify an extension of the shelf life of stockpiled drug products.1
Robbe Lyon, MD, and colleagues reported data from the SLEP.2 A total of 122 drugs were studied representing 3,005 lots, with 88% of these extended at least 1 year past the expiration date, with an average extension of more than 5 years. Several antibiotics were studied, including ciprofloxacin (mean extension, 55 months), amoxicillin (mean extension, 23 months), and doxycycline (mean extension, 50 months).
Lee Cantrell, PharmD, and coinvestigators looked at sealed drugs from a retail pharmacy that were 28-40 years past their expiration date.3 Amazingly, 12 of the 14 compounds tested were in concentrations that were at least 90% of the labeled amount. Among the drugs that were tested that maintained greater than 90% of the labeled amount were acetaminophen, codeine, hydrocodone, and barbiturates. Aspirin and amphetamine were the two drugs that did not have greater than 90% of the labeled amount. The aspirin amounts were very low, about 1% of the listed amount on the package.
The major myth surrounding expired medications is that taking an expired medication could be toxic.
There is one case report of toxicity from the use of expired tetracycline.4 This was a case series of three patients who developed reversible Fanconi syndrome linked to using an expired tetracycline preparation. That preparation of tetracycline is no longer available.
There are no other reports of toxicity due to use of expired medications.5,6 There appears to be no direct risk of toxicity to the patient by using medication past the expiration date.
The risk that isn’t answered is the risk of using medications that may not be effective if potency isn’t guaranteed beyond the expiration date. It appears that most drugs are effective for years past the expiration date.
This isn’t an issue for medications for treatment of chronic conditions, as patients take the medications every day, and the medications will be used up long before they expire. For medications that are used infrequently – analgesics, antihistamines, and medications for traveler’s diarrhea – they appear to be stable for years past expiration, and there is little risk to the patient if the medications are not fully effective.
I think aspirin should not be used past expiration, given the data showing that it breaks down more so than other medications. For the case at the start of this article, I think having the patient use the expired medications should be fine.
References
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
A 55-year-old patient requests new prescriptions at a routine appointment. She will be traveling internationally next month and wants to replace her emergency medication kit, as the medications in it (ciprofloxacin, loperamide, and oxycodone) have all expired.
What do you do?
A) Replace the prescription for ciprofloxacin.
B) Replace all three medications.
C) Tell the patient that all the meds should still be fine.
This is a common concern brought up by patients. Many patients discard medications when they pass the expiration date on the package. Is this necessary? Is there a health risk to taking expired medications, and is it okay from a therapeutic standpoint to use medications past their expiration date?
The expiration date is not a date that the drug stops being effective or potentially becomes toxic. It is a date, required by law, that the manufacturer can guarantee greater than 90% original potency of the medication. There really isn’t incentive for pharmaceutical companies to extend the expiration dates, as it is profitable for patients to throw away expired medications and replace them with new prescriptions.
The U.S. military purchases a large stockpile of drugs and has the potential for having a great deal of expired medications. To help reduce this problem, the Food and Drug Administration administers the shelf-life extension program (SLEP) for the U.S. military as a testing and evaluation program designed to justify an extension of the shelf life of stockpiled drug products.1
Robbe Lyon, MD, and colleagues reported data from the SLEP.2 A total of 122 drugs were studied representing 3,005 lots, with 88% of these extended at least 1 year past the expiration date, with an average extension of more than 5 years. Several antibiotics were studied, including ciprofloxacin (mean extension, 55 months), amoxicillin (mean extension, 23 months), and doxycycline (mean extension, 50 months).
Lee Cantrell, PharmD, and coinvestigators looked at sealed drugs from a retail pharmacy that were 28-40 years past their expiration date.3 Amazingly, 12 of the 14 compounds tested were in concentrations that were at least 90% of the labeled amount. Among the drugs that were tested that maintained greater than 90% of the labeled amount were acetaminophen, codeine, hydrocodone, and barbiturates. Aspirin and amphetamine were the two drugs that did not have greater than 90% of the labeled amount. The aspirin amounts were very low, about 1% of the listed amount on the package.
The major myth surrounding expired medications is that taking an expired medication could be toxic.
There is one case report of toxicity from the use of expired tetracycline.4 This was a case series of three patients who developed reversible Fanconi syndrome linked to using an expired tetracycline preparation. That preparation of tetracycline is no longer available.
There are no other reports of toxicity due to use of expired medications.5,6 There appears to be no direct risk of toxicity to the patient by using medication past the expiration date.
The risk that isn’t answered is the risk of using medications that may not be effective if potency isn’t guaranteed beyond the expiration date. It appears that most drugs are effective for years past the expiration date.
This isn’t an issue for medications for treatment of chronic conditions, as patients take the medications every day, and the medications will be used up long before they expire. For medications that are used infrequently – analgesics, antihistamines, and medications for traveler’s diarrhea – they appear to be stable for years past expiration, and there is little risk to the patient if the medications are not fully effective.
I think aspirin should not be used past expiration, given the data showing that it breaks down more so than other medications. For the case at the start of this article, I think having the patient use the expired medications should be fine.
References
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].

Metastatic Crohn Disease Clinically Reminiscent of Erythema Nodosum on the Right Leg
Metastatic Crohn disease (MCD) is defined by the presence of cutaneous noncaseating granulomatous lesions that are noncontiguous with the gastrointestinal (GI) tract or fistulae.1 The clinical presentation of MCD is so variable that its diagnosis requires a high index of suspicion.1,2 In particular, the presence of erythematous tender nodules on the legs is easily mistaken for erythema nodosum (EN). Skin biopsy has an important role in confirming the diagnosis, as histopathological examination would reveal a noncaseating granuloma similar to those in the involved GI tract.2 Herein, we report a case of MCD on the right leg that was clinically reminiscent of unilateral EN.
Case Report
A 21-year-old woman presented to the dermatology department with 2 painful erythematous nodules on the lower right leg of 2 weeks’ duration. She also reported abdominal pain, diarrhea, and bloody stool. She had been diagnosed with Crohn disease (CD) 6 years prior that had been well controlled with systemic low-dose steroids (5–15 mg/d), metronidazole (750 mg/d), and intermittent mesalamine and antidiarrheal drugs. However, she had not taken her medication for several weeks on her own authority. Subsequently, the patient developed skin lesions, which were characterized by ill-defined erythematous nodules with tenderness on the right lower leg along with GI symptoms (Figure 1). Laboratory studies revealed anemia (hemoglobin, 9.9 g/dL [reference range, 12.0–16.0 g/dL]) and an elevated C-reactive protein level (4.3 mg/dL [reference range, 0–0.3 mg/dL]). Other routine laboratory findings were normal.

Histopathologically, a skin biopsy from the right ankle showed vague, ill-defined, noncaseating granulomas scattered in the deep dermis and lobules of the subcutis (Figure 2). The granulomas were composed of epithelioid cells and Langerhans-type giant cells. Lymphocytes and neutrophils also were present, but eosinophils were absent. Immunohistochemical staining revealed that the infiltrating cells were mostly CD4+ helper/inducer T cells intermixed with CD8+ suppressor/cytotoxic T cells. The CD4:CD8 ratio was approximately 2:1. Counts of CD20+ B cells were low. Epithelioid cells and giant cells were positive for CD68.
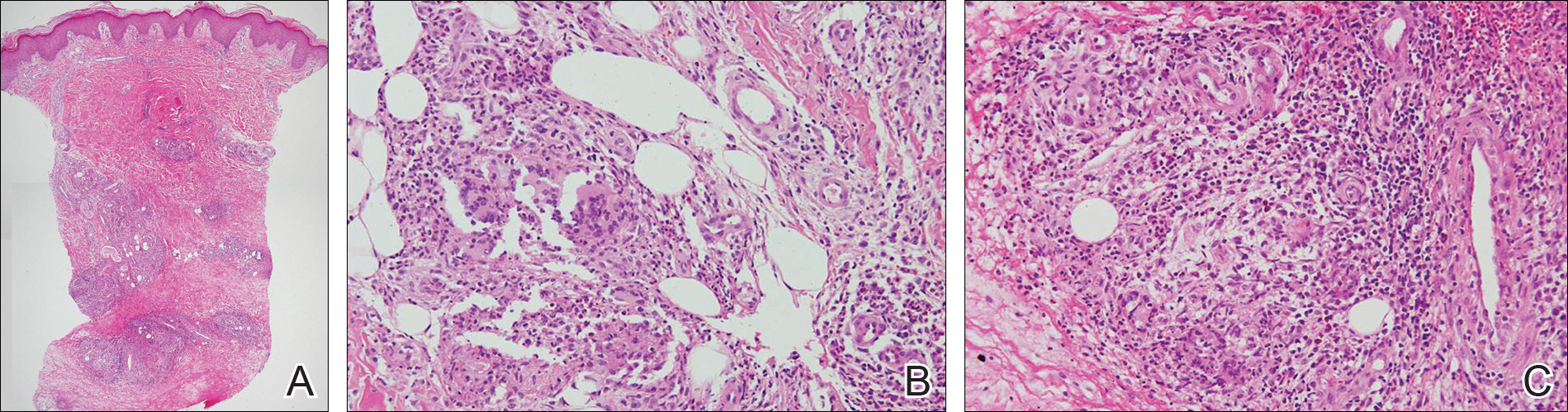
×20). The skin biopsy showed granulomas composed of epithelioid cells and multinucleated giant cells in the deep dermis and in the lobules of the subcutis (B)(H&E, original magnification ×200). Histopathologic features such as small vessel vasculitis characterized by a fibrin deposit in the small blood vessels and swelling of the endothelial cells as well as granulomatous perivasculitis with perivascular infiltration of the epithelioid cells were present (C)(H&E, original magnification ×200).
A colonoscopy was performed to evaluate the aggravation of CD. Multiple longitudinal ulcers were observed in the ileocecal valve area and from the transverse colon to the sigmoid colon (Figure 3A). Histopathologic findings from the colon showed mucosal ulceration and noncaseating granulomas with heavy infiltration of lymphocytes and plasma cells (Figure 3B). Staining for infectious microorganisms (eg, Ziehl-Neelsen, periodic acid–Schiff, Gram) was negative. A polymerase chain reaction performed on sections cut from the paraffin block of the skin biopsy was negative for Mycobacterium tuberculosis DNA.
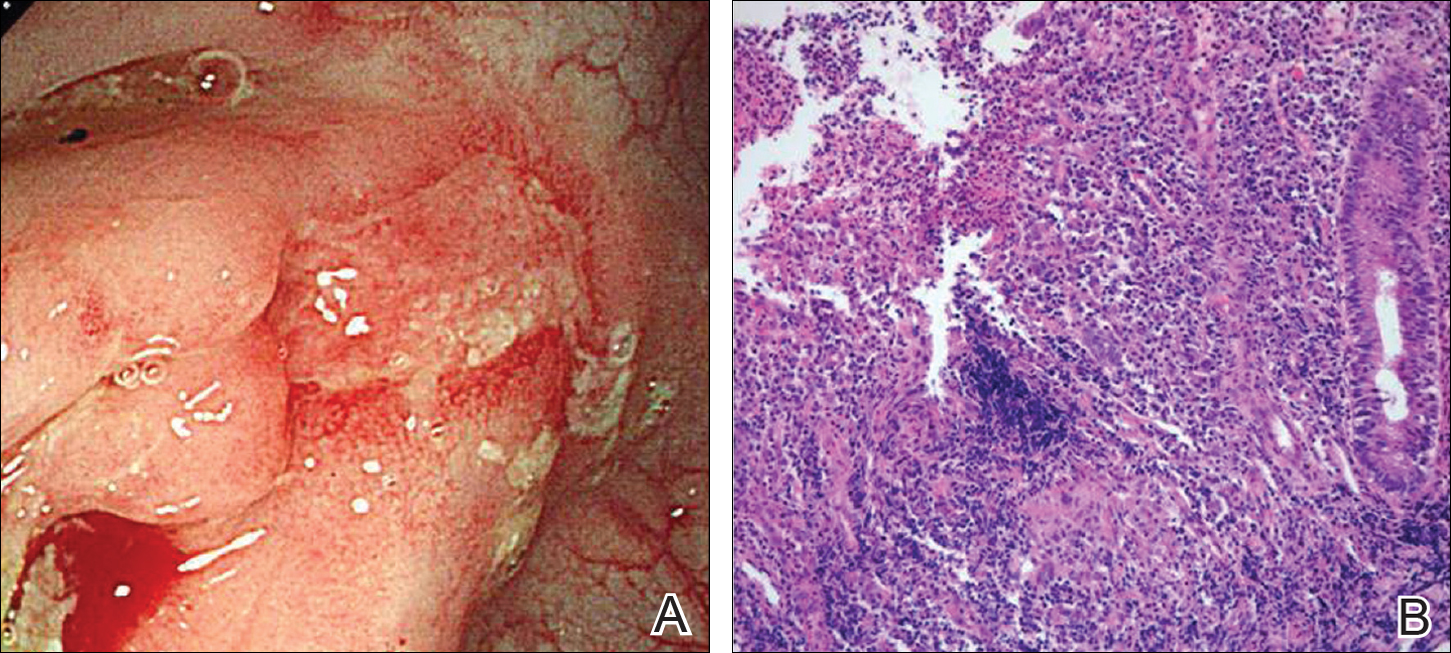
Based on the clinical and histopathologic findings, the patient was diagnosed with MCD that was clinically reminiscent of unilateral EN. Four weeks after the initiation of therapy with systemic corticosteroids (25 mg/d), oral metronidazole (750 mg/d), and mesalamine (1200 mg/d) for CD, the skin lesions were completely resolved and the patient’s GI symptoms improved simultaneously.
Comment
Crohn disease is a chronic inflammatory granulomatous disease of the GI tract that often is associated with reactive cutaneous lesions including EN, pyoderma gangrenosum, necrotizing vasculitis, and epidermolysis bullosa acquisita. Of these, EN is the most common to appear in CD patients and has been reported to occur in 1% to 15% of patients.3-5 In particular, skin lesions on the leg presenting as tender erythematous nodules and patches are often diagnosed as EN, which is relatively common. In our case, we initially suspected EN due to the rare presentation of MCD and lack of specific clinical features; however, the skin biopsy revealed noncaseating granulomas in the mid to deep dermis and subcutis consistent with MCD.
Metastatic Crohn disease is a rare disease entity and is characterized by the presence of noncaseating granulomas of the skin at sites separated from the GI tract by normal tissue.1 Although its pathogenesis is unclear, it has been suggested that immune complexes deposited in the skin could be responsible for the granulomatous reactions.4 A T lymphocyte–mediated type IV hypersensitivity reaction also could be responsible.6,7 Because antimicrobial therapy can be curative for infection-related MCD, special histologic stains and/or tissue cultures can help to exclude an infectious etiology.8
Clinical presentations of MCD vary greatly, with observations such as single or multiple erythematous swellings, papules, plaques, nodules, abscesses, and ulcers.1,2 The relationship between these clinical presentations and the intestinal activity of CD still is unknown; in some cases, however, the metastatic granulomatous lesions and the bowel disease show comparable severity.2,9,10 In a review of the literature, MCD was generally reported to present in the genital area in children. In adults, lesions most frequently present in the genital area, followed by ulcers on the arms and legs.1,2 These variations in clinical features and location resemble benign or infectious disease and can lead to delays in diagnosis.
Histopathologically, MCD lesions usually are ill-defined noncaseating granulomas with numerous multinucleated giant cells and lymphomononuclear cells located mostly in the dermis and occasionally extending into the subcutis. The cutaneous granulomata are similar to those present in the affected GI tract. Lymphocytes and plasma cells also are commonly present and eosinophils can be prominent.1,2,11 In some cases of MCD, granulomatous vasculitis of small- to medium-sized vessels can be found and is associated with dermal and subcutaneous granulomatous inflammation.8,11,12 Misago and Narisawa13 suggested that granulomatous vasculitis and panniculitis associated with CD is considered to be a rare subtype of MCD. Few cases of MCD presenting as granulomatous panniculitis have been described in the literature.14-16 Our patient presented with lesions that clinically resembled EN; however, the biopsy was more consistent with MCD. The Table summarizes the distinguishing clinical and histopathological features of MCD in our case and classic EN.
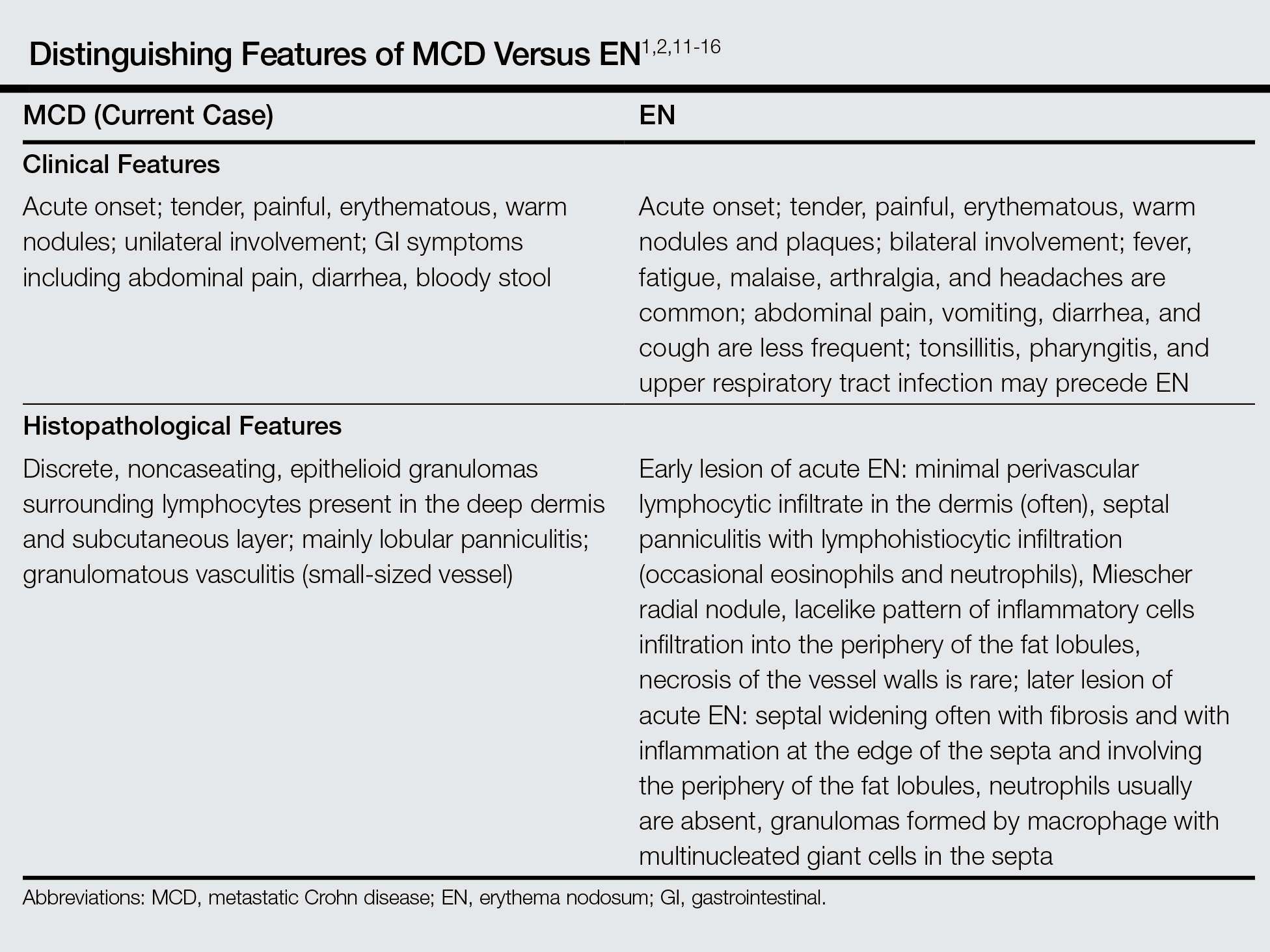
Although some authors believe that MCD is not related to CD activity, others assert that MCD lesions may parallel GI activity.1,2 Our patient was treated with systemic corticosteroids, oral metronidazole, and mesalamine to control the GI symptoms associated with CD. Four weeks after treatment, the GI symptoms and skin lesions improved simultaneously without any additional dermatologic treatment. We believe that MCD has the potential to serve as an early marker of the recurrence of CD and can help with the early diagnosis of CD aggravation, though an association between MCD and CD activity has not been confirmed.
Conclusion
We reported a case of MCD that was clinically reminiscent of unilateral EN and associated with GI disease activity. Physicians should be aware of the possibility of skin manifestations in CD, especially when erythematous nodular lesions are present on the leg.
- Calonje E, Brenn T, Lazar AJ, et al. Mckee’s Pathology of the Skin: With Clinical Correlations. 4th ed. Philadelphia, PA: Saunders Elsevier; 2012.
- Palamaras I, El-Jabbour J, Pietropaolo N, et al. Metastatic Crohn’s disease: a review. J Eur Acad Dermatol Venereol. 2008;22:1033-1043.
- Sonia F, Richard SB. Inflammatory bowel disease. In: Kasper DL, Braunwald E, Fauci AS, et al, eds. Harrison’s Principles of Internal Medicine. 16th ed. New York, NY: McGraw-Hill; 2005:1776-1789.
- Burgdorf W. Cutaneous manifestations of Crohn’s disease. J Am Acad Dermatol. 1981;5:689-695.
- Crowson AN, Nuovo GJ, Mihm MC Jr, et al. Cutaneous manifestations of Crohn’s disease, its spectrum, and its pathogenesis: intracellular consensus bacterial 16S rRNA is associated with the gastrointestinal but not the cutaneous manifestations of Crohn’s disease. Hum Pathol. 2003;34:1185-1192.
- Tatnall FM, Dodd HJ, Sarkany I. Crohn’s disease with metastatic cutaneous involvement and granulomatous cheilitis. J R Soc Med. 1987;80:49-51.
- Shum DT, Guenther L. Metastatic Crohn’s disease. case report and review of the literature. Arch Dermatol. 1990;126:645-648.
- Emanuel PO, Phelps RG. Metastatic Crohn’s disease: a histopathologic study of 12 cases. J Cutan Pathol. 2008;35:457-461.
- Chalvardjian A, Nethercott JR. Cutaneous granulomatous vasculitis associated with Crohn’s disease. Cutis. 1982;30:645-655.
- Lebwohl M, Fleischmajer R, Janowitz H, et al. Metastatic Crohn’s disease. J Am Acad Dermatol. 1984;10:33-38.
- Sabat M, Leulmo J, Saez A. Cutaneous granulomatous vasculitis in metastatic Crohn’s disease. J Eur Acad Dermatol Venereol. 2005;19:652-653.
- Burns AM, Walsh N, Green PJ. Granulomatous vasculitis in Crohn’s disease: a clinicopathologic correlate of two unusual cases. J Cutan Pathol. 2010;37:1077-1083.
- Misago N, Narisawa Y. Erythema induratum (nodular vasculitis) associated with Crohn’s disease: a rare type of metastatic Crohn’s disease. Am J Dermatopathol. 2012;34:325-329.
- Liebermann TR, Greene JF Jr. Transient subcutaneous granulomatosis of the upper extremities in Crohn’s disease. Am J Gastroenterol. 1979;72:89-91.
- Levine N, Bangert J. Cutaneous granulomatosis in Crohn’s disease. Arch Dermatol. 1982;118:1006-1009.
- Hackzell-Bradley M, Hedblad MA, Stephansson EA. Metastatic Crohn’s disease. report of 3 cases with special reference to histopathologic findings. Arch Dermatol. 1996;132:928-932.
Metastatic Crohn disease (MCD) is defined by the presence of cutaneous noncaseating granulomatous lesions that are noncontiguous with the gastrointestinal (GI) tract or fistulae.1 The clinical presentation of MCD is so variable that its diagnosis requires a high index of suspicion.1,2 In particular, the presence of erythematous tender nodules on the legs is easily mistaken for erythema nodosum (EN). Skin biopsy has an important role in confirming the diagnosis, as histopathological examination would reveal a noncaseating granuloma similar to those in the involved GI tract.2 Herein, we report a case of MCD on the right leg that was clinically reminiscent of unilateral EN.
Case Report
A 21-year-old woman presented to the dermatology department with 2 painful erythematous nodules on the lower right leg of 2 weeks’ duration. She also reported abdominal pain, diarrhea, and bloody stool. She had been diagnosed with Crohn disease (CD) 6 years prior that had been well controlled with systemic low-dose steroids (5–15 mg/d), metronidazole (750 mg/d), and intermittent mesalamine and antidiarrheal drugs. However, she had not taken her medication for several weeks on her own authority. Subsequently, the patient developed skin lesions, which were characterized by ill-defined erythematous nodules with tenderness on the right lower leg along with GI symptoms (Figure 1). Laboratory studies revealed anemia (hemoglobin, 9.9 g/dL [reference range, 12.0–16.0 g/dL]) and an elevated C-reactive protein level (4.3 mg/dL [reference range, 0–0.3 mg/dL]). Other routine laboratory findings were normal.
Histopathologically, a skin biopsy from the right ankle showed vague, ill-defined, noncaseating granulomas scattered in the deep dermis and lobules of the subcutis (Figure 2). The granulomas were composed of epithelioid cells and Langerhans-type giant cells. Lymphocytes and neutrophils also were present, but eosinophils were absent. Immunohistochemical staining revealed that the infiltrating cells were mostly CD4+ helper/inducer T cells intermixed with CD8+ suppressor/cytotoxic T cells. The CD4:CD8 ratio was approximately 2:1. Counts of CD20+ B cells were low. Epithelioid cells and giant cells were positive for CD68.
×20). The skin biopsy showed granulomas composed of epithelioid cells and multinucleated giant cells in the deep dermis and in the lobules of the subcutis (B)(H&E, original magnification ×200). Histopathologic features such as small vessel vasculitis characterized by a fibrin deposit in the small blood vessels and swelling of the endothelial cells as well as granulomatous perivasculitis with perivascular infiltration of the epithelioid cells were present (C)(H&E, original magnification ×200).
A colonoscopy was performed to evaluate the aggravation of CD. Multiple longitudinal ulcers were observed in the ileocecal valve area and from the transverse colon to the sigmoid colon (Figure 3A). Histopathologic findings from the colon showed mucosal ulceration and noncaseating granulomas with heavy infiltration of lymphocytes and plasma cells (Figure 3B). Staining for infectious microorganisms (eg, Ziehl-Neelsen, periodic acid–Schiff, Gram) was negative. A polymerase chain reaction performed on sections cut from the paraffin block of the skin biopsy was negative for Mycobacterium tuberculosis DNA.
Based on the clinical and histopathologic findings, the patient was diagnosed with MCD that was clinically reminiscent of unilateral EN. Four weeks after the initiation of therapy with systemic corticosteroids (25 mg/d), oral metronidazole (750 mg/d), and mesalamine (1200 mg/d) for CD, the skin lesions were completely resolved and the patient’s GI symptoms improved simultaneously.
Comment
Crohn disease is a chronic inflammatory granulomatous disease of the GI tract that often is associated with reactive cutaneous lesions including EN, pyoderma gangrenosum, necrotizing vasculitis, and epidermolysis bullosa acquisita. Of these, EN is the most common to appear in CD patients and has been reported to occur in 1% to 15% of patients.3-5 In particular, skin lesions on the leg presenting as tender erythematous nodules and patches are often diagnosed as EN, which is relatively common. In our case, we initially suspected EN due to the rare presentation of MCD and lack of specific clinical features; however, the skin biopsy revealed noncaseating granulomas in the mid to deep dermis and subcutis consistent with MCD.
Metastatic Crohn disease is a rare disease entity and is characterized by the presence of noncaseating granulomas of the skin at sites separated from the GI tract by normal tissue.1 Although its pathogenesis is unclear, it has been suggested that immune complexes deposited in the skin could be responsible for the granulomatous reactions.4 A T lymphocyte–mediated type IV hypersensitivity reaction also could be responsible.6,7 Because antimicrobial therapy can be curative for infection-related MCD, special histologic stains and/or tissue cultures can help to exclude an infectious etiology.8
Clinical presentations of MCD vary greatly, with observations such as single or multiple erythematous swellings, papules, plaques, nodules, abscesses, and ulcers.1,2 The relationship between these clinical presentations and the intestinal activity of CD still is unknown; in some cases, however, the metastatic granulomatous lesions and the bowel disease show comparable severity.2,9,10 In a review of the literature, MCD was generally reported to present in the genital area in children. In adults, lesions most frequently present in the genital area, followed by ulcers on the arms and legs.1,2 These variations in clinical features and location resemble benign or infectious disease and can lead to delays in diagnosis.
Histopathologically, MCD lesions usually are ill-defined noncaseating granulomas with numerous multinucleated giant cells and lymphomononuclear cells located mostly in the dermis and occasionally extending into the subcutis. The cutaneous granulomata are similar to those present in the affected GI tract. Lymphocytes and plasma cells also are commonly present and eosinophils can be prominent.1,2,11 In some cases of MCD, granulomatous vasculitis of small- to medium-sized vessels can be found and is associated with dermal and subcutaneous granulomatous inflammation.8,11,12 Misago and Narisawa13 suggested that granulomatous vasculitis and panniculitis associated with CD is considered to be a rare subtype of MCD. Few cases of MCD presenting as granulomatous panniculitis have been described in the literature.14-16 Our patient presented with lesions that clinically resembled EN; however, the biopsy was more consistent with MCD. The Table summarizes the distinguishing clinical and histopathological features of MCD in our case and classic EN.
Although some authors believe that MCD is not related to CD activity, others assert that MCD lesions may parallel GI activity.1,2 Our patient was treated with systemic corticosteroids, oral metronidazole, and mesalamine to control the GI symptoms associated with CD. Four weeks after treatment, the GI symptoms and skin lesions improved simultaneously without any additional dermatologic treatment. We believe that MCD has the potential to serve as an early marker of the recurrence of CD and can help with the early diagnosis of CD aggravation, though an association between MCD and CD activity has not been confirmed.
Conclusion
We reported a case of MCD that was clinically reminiscent of unilateral EN and associated with GI disease activity. Physicians should be aware of the possibility of skin manifestations in CD, especially when erythematous nodular lesions are present on the leg.
Metastatic Crohn disease (MCD) is defined by the presence of cutaneous noncaseating granulomatous lesions that are noncontiguous with the gastrointestinal (GI) tract or fistulae.1 The clinical presentation of MCD is so variable that its diagnosis requires a high index of suspicion.1,2 In particular, the presence of erythematous tender nodules on the legs is easily mistaken for erythema nodosum (EN). Skin biopsy has an important role in confirming the diagnosis, as histopathological examination would reveal a noncaseating granuloma similar to those in the involved GI tract.2 Herein, we report a case of MCD on the right leg that was clinically reminiscent of unilateral EN.
Case Report
A 21-year-old woman presented to the dermatology department with 2 painful erythematous nodules on the lower right leg of 2 weeks’ duration. She also reported abdominal pain, diarrhea, and bloody stool. She had been diagnosed with Crohn disease (CD) 6 years prior that had been well controlled with systemic low-dose steroids (5–15 mg/d), metronidazole (750 mg/d), and intermittent mesalamine and antidiarrheal drugs. However, she had not taken her medication for several weeks on her own authority. Subsequently, the patient developed skin lesions, which were characterized by ill-defined erythematous nodules with tenderness on the right lower leg along with GI symptoms (Figure 1). Laboratory studies revealed anemia (hemoglobin, 9.9 g/dL [reference range, 12.0–16.0 g/dL]) and an elevated C-reactive protein level (4.3 mg/dL [reference range, 0–0.3 mg/dL]). Other routine laboratory findings were normal.
Histopathologically, a skin biopsy from the right ankle showed vague, ill-defined, noncaseating granulomas scattered in the deep dermis and lobules of the subcutis (Figure 2). The granulomas were composed of epithelioid cells and Langerhans-type giant cells. Lymphocytes and neutrophils also were present, but eosinophils were absent. Immunohistochemical staining revealed that the infiltrating cells were mostly CD4+ helper/inducer T cells intermixed with CD8+ suppressor/cytotoxic T cells. The CD4:CD8 ratio was approximately 2:1. Counts of CD20+ B cells were low. Epithelioid cells and giant cells were positive for CD68.
×20). The skin biopsy showed granulomas composed of epithelioid cells and multinucleated giant cells in the deep dermis and in the lobules of the subcutis (B)(H&E, original magnification ×200). Histopathologic features such as small vessel vasculitis characterized by a fibrin deposit in the small blood vessels and swelling of the endothelial cells as well as granulomatous perivasculitis with perivascular infiltration of the epithelioid cells were present (C)(H&E, original magnification ×200).
A colonoscopy was performed to evaluate the aggravation of CD. Multiple longitudinal ulcers were observed in the ileocecal valve area and from the transverse colon to the sigmoid colon (Figure 3A). Histopathologic findings from the colon showed mucosal ulceration and noncaseating granulomas with heavy infiltration of lymphocytes and plasma cells (Figure 3B). Staining for infectious microorganisms (eg, Ziehl-Neelsen, periodic acid–Schiff, Gram) was negative. A polymerase chain reaction performed on sections cut from the paraffin block of the skin biopsy was negative for Mycobacterium tuberculosis DNA.
Based on the clinical and histopathologic findings, the patient was diagnosed with MCD that was clinically reminiscent of unilateral EN. Four weeks after the initiation of therapy with systemic corticosteroids (25 mg/d), oral metronidazole (750 mg/d), and mesalamine (1200 mg/d) for CD, the skin lesions were completely resolved and the patient’s GI symptoms improved simultaneously.
Comment
Crohn disease is a chronic inflammatory granulomatous disease of the GI tract that often is associated with reactive cutaneous lesions including EN, pyoderma gangrenosum, necrotizing vasculitis, and epidermolysis bullosa acquisita. Of these, EN is the most common to appear in CD patients and has been reported to occur in 1% to 15% of patients.3-5 In particular, skin lesions on the leg presenting as tender erythematous nodules and patches are often diagnosed as EN, which is relatively common. In our case, we initially suspected EN due to the rare presentation of MCD and lack of specific clinical features; however, the skin biopsy revealed noncaseating granulomas in the mid to deep dermis and subcutis consistent with MCD.
Metastatic Crohn disease is a rare disease entity and is characterized by the presence of noncaseating granulomas of the skin at sites separated from the GI tract by normal tissue.1 Although its pathogenesis is unclear, it has been suggested that immune complexes deposited in the skin could be responsible for the granulomatous reactions.4 A T lymphocyte–mediated type IV hypersensitivity reaction also could be responsible.6,7 Because antimicrobial therapy can be curative for infection-related MCD, special histologic stains and/or tissue cultures can help to exclude an infectious etiology.8
Clinical presentations of MCD vary greatly, with observations such as single or multiple erythematous swellings, papules, plaques, nodules, abscesses, and ulcers.1,2 The relationship between these clinical presentations and the intestinal activity of CD still is unknown; in some cases, however, the metastatic granulomatous lesions and the bowel disease show comparable severity.2,9,10 In a review of the literature, MCD was generally reported to present in the genital area in children. In adults, lesions most frequently present in the genital area, followed by ulcers on the arms and legs.1,2 These variations in clinical features and location resemble benign or infectious disease and can lead to delays in diagnosis.
Histopathologically, MCD lesions usually are ill-defined noncaseating granulomas with numerous multinucleated giant cells and lymphomononuclear cells located mostly in the dermis and occasionally extending into the subcutis. The cutaneous granulomata are similar to those present in the affected GI tract. Lymphocytes and plasma cells also are commonly present and eosinophils can be prominent.1,2,11 In some cases of MCD, granulomatous vasculitis of small- to medium-sized vessels can be found and is associated with dermal and subcutaneous granulomatous inflammation.8,11,12 Misago and Narisawa13 suggested that granulomatous vasculitis and panniculitis associated with CD is considered to be a rare subtype of MCD. Few cases of MCD presenting as granulomatous panniculitis have been described in the literature.14-16 Our patient presented with lesions that clinically resembled EN; however, the biopsy was more consistent with MCD. The Table summarizes the distinguishing clinical and histopathological features of MCD in our case and classic EN.
Although some authors believe that MCD is not related to CD activity, others assert that MCD lesions may parallel GI activity.1,2 Our patient was treated with systemic corticosteroids, oral metronidazole, and mesalamine to control the GI symptoms associated with CD. Four weeks after treatment, the GI symptoms and skin lesions improved simultaneously without any additional dermatologic treatment. We believe that MCD has the potential to serve as an early marker of the recurrence of CD and can help with the early diagnosis of CD aggravation, though an association between MCD and CD activity has not been confirmed.
Conclusion
We reported a case of MCD that was clinically reminiscent of unilateral EN and associated with GI disease activity. Physicians should be aware of the possibility of skin manifestations in CD, especially when erythematous nodular lesions are present on the leg.
- Calonje E, Brenn T, Lazar AJ, et al. Mckee’s Pathology of the Skin: With Clinical Correlations. 4th ed. Philadelphia, PA: Saunders Elsevier; 2012.
- Palamaras I, El-Jabbour J, Pietropaolo N, et al. Metastatic Crohn’s disease: a review. J Eur Acad Dermatol Venereol. 2008;22:1033-1043.
- Sonia F, Richard SB. Inflammatory bowel disease. In: Kasper DL, Braunwald E, Fauci AS, et al, eds. Harrison’s Principles of Internal Medicine. 16th ed. New York, NY: McGraw-Hill; 2005:1776-1789.
- Burgdorf W. Cutaneous manifestations of Crohn’s disease. J Am Acad Dermatol. 1981;5:689-695.
- Crowson AN, Nuovo GJ, Mihm MC Jr, et al. Cutaneous manifestations of Crohn’s disease, its spectrum, and its pathogenesis: intracellular consensus bacterial 16S rRNA is associated with the gastrointestinal but not the cutaneous manifestations of Crohn’s disease. Hum Pathol. 2003;34:1185-1192.
- Tatnall FM, Dodd HJ, Sarkany I. Crohn’s disease with metastatic cutaneous involvement and granulomatous cheilitis. J R Soc Med. 1987;80:49-51.
- Shum DT, Guenther L. Metastatic Crohn’s disease. case report and review of the literature. Arch Dermatol. 1990;126:645-648.
- Emanuel PO, Phelps RG. Metastatic Crohn’s disease: a histopathologic study of 12 cases. J Cutan Pathol. 2008;35:457-461.
- Chalvardjian A, Nethercott JR. Cutaneous granulomatous vasculitis associated with Crohn’s disease. Cutis. 1982;30:645-655.
- Lebwohl M, Fleischmajer R, Janowitz H, et al. Metastatic Crohn’s disease. J Am Acad Dermatol. 1984;10:33-38.
- Sabat M, Leulmo J, Saez A. Cutaneous granulomatous vasculitis in metastatic Crohn’s disease. J Eur Acad Dermatol Venereol. 2005;19:652-653.
- Burns AM, Walsh N, Green PJ. Granulomatous vasculitis in Crohn’s disease: a clinicopathologic correlate of two unusual cases. J Cutan Pathol. 2010;37:1077-1083.
- Misago N, Narisawa Y. Erythema induratum (nodular vasculitis) associated with Crohn’s disease: a rare type of metastatic Crohn’s disease. Am J Dermatopathol. 2012;34:325-329.
- Liebermann TR, Greene JF Jr. Transient subcutaneous granulomatosis of the upper extremities in Crohn’s disease. Am J Gastroenterol. 1979;72:89-91.
- Levine N, Bangert J. Cutaneous granulomatosis in Crohn’s disease. Arch Dermatol. 1982;118:1006-1009.
- Hackzell-Bradley M, Hedblad MA, Stephansson EA. Metastatic Crohn’s disease. report of 3 cases with special reference to histopathologic findings. Arch Dermatol. 1996;132:928-932.
- Calonje E, Brenn T, Lazar AJ, et al. Mckee’s Pathology of the Skin: With Clinical Correlations. 4th ed. Philadelphia, PA: Saunders Elsevier; 2012.
- Palamaras I, El-Jabbour J, Pietropaolo N, et al. Metastatic Crohn’s disease: a review. J Eur Acad Dermatol Venereol. 2008;22:1033-1043.
- Sonia F, Richard SB. Inflammatory bowel disease. In: Kasper DL, Braunwald E, Fauci AS, et al, eds. Harrison’s Principles of Internal Medicine. 16th ed. New York, NY: McGraw-Hill; 2005:1776-1789.
- Burgdorf W. Cutaneous manifestations of Crohn’s disease. J Am Acad Dermatol. 1981;5:689-695.
- Crowson AN, Nuovo GJ, Mihm MC Jr, et al. Cutaneous manifestations of Crohn’s disease, its spectrum, and its pathogenesis: intracellular consensus bacterial 16S rRNA is associated with the gastrointestinal but not the cutaneous manifestations of Crohn’s disease. Hum Pathol. 2003;34:1185-1192.
- Tatnall FM, Dodd HJ, Sarkany I. Crohn’s disease with metastatic cutaneous involvement and granulomatous cheilitis. J R Soc Med. 1987;80:49-51.
- Shum DT, Guenther L. Metastatic Crohn’s disease. case report and review of the literature. Arch Dermatol. 1990;126:645-648.
- Emanuel PO, Phelps RG. Metastatic Crohn’s disease: a histopathologic study of 12 cases. J Cutan Pathol. 2008;35:457-461.
- Chalvardjian A, Nethercott JR. Cutaneous granulomatous vasculitis associated with Crohn’s disease. Cutis. 1982;30:645-655.
- Lebwohl M, Fleischmajer R, Janowitz H, et al. Metastatic Crohn’s disease. J Am Acad Dermatol. 1984;10:33-38.
- Sabat M, Leulmo J, Saez A. Cutaneous granulomatous vasculitis in metastatic Crohn’s disease. J Eur Acad Dermatol Venereol. 2005;19:652-653.
- Burns AM, Walsh N, Green PJ. Granulomatous vasculitis in Crohn’s disease: a clinicopathologic correlate of two unusual cases. J Cutan Pathol. 2010;37:1077-1083.
- Misago N, Narisawa Y. Erythema induratum (nodular vasculitis) associated with Crohn’s disease: a rare type of metastatic Crohn’s disease. Am J Dermatopathol. 2012;34:325-329.
- Liebermann TR, Greene JF Jr. Transient subcutaneous granulomatosis of the upper extremities in Crohn’s disease. Am J Gastroenterol. 1979;72:89-91.
- Levine N, Bangert J. Cutaneous granulomatosis in Crohn’s disease. Arch Dermatol. 1982;118:1006-1009.
- Hackzell-Bradley M, Hedblad MA, Stephansson EA. Metastatic Crohn’s disease. report of 3 cases with special reference to histopathologic findings. Arch Dermatol. 1996;132:928-932.
Practice Points
- Metastatic Crohn disease (MCD) may be an initial sign indicating the aggravation of intestinal Crohn disease (CD).
- Metastatic Crohn disease on the legs could be clinically reminiscent of erythema nodosum (EN).
- Physicians should be aware of the possibility of MCD when encountering EN-like lesions on the legs in a CD patient.

Should we pursue board certification in Mohs micrographic surgery?
The medical director was direct and blunt: “You’ve got a problem with two very different levels of training in Mohs surgery. This is a big problem for your specialty.”
The remarks came at a medical director summit that I was attending to speak on the value of dermatology. I was explaining to medical directors how including small dermatology practices in their plans would realize cost savings when treating skin cancer in the office setting. An awkward silence followed the medical director’s remarks. Then I uttered a lame “we may have a board certification someday.”

My interview with the New York Times reporter before the meeting quickly became adversarial. “What about these guys who do Mohs after a 3-day course?” I explained that there is more involved than just the 3-day course, that there is a preceptorship and case reviews. Plus, some of “those guys” wrote some of the best Mohs textbooks. The reporter wasn’t buying it, and the rest of the interview went downhill.
And the training issues surrounding Mohs surgery are playing out in practice. One dermatologist wrote me complaining that an insurer will no longer let him bill for Mohs because “he can’t document his residency training in Mohs and did not do a fellowship.” Another wrote me saying he can no longer teach Mohs surgery at the VA or the medical school “because he didn’t do a formal Mohs fellowship.”
The issue of who is qualified to perform Mohs surgery is coming to a head. There are more than 2,500 dermatologists billing Medicare for Mohs, and insurers are groaning at the expense. They are looking for any possible reason to exclude dermatologists from billing for Mohs surgery.
A possible solution is a board certification in Mohs surgery. Osteopathic dermatologists have had this option for 20 years. Unfortunately, allopathic dermatologists cannot sit for the osteopathic exam. A new certification exam for allopathic dermatologists who have successfully completed a dermatology residency accredited by the Accreditation Council for Graduate Medical Education (ACGME) seems worthy of a discussion.
Downsides of certification include the likely $1,000 or more cost of a test, the costs of preparing for the test, and the risk of failing a test. A new certification would give the Maintenance of Certification (MOC) haters another reason to complain, since about 600 lifetime certified, board-exempt dermatologists would be dragged back into MOC to maintain a Mohs surgery subspecialty certification. Some of the current fellowship-trained Mohs surgeons will not like being grouped with the nonfellowship-trained surgeons, whom they consider their inferiors and who will now have the opportunity to be board certified.
The name of the fellowship, which is “micrographic surgery and dermatologic oncology,” also has some paranoid types fearing that they will lose the right to treat skin cancer if such a subspecialty is created. That shouldn’t be an issue, since all dermatologists are trained in residency to treat skin cancer. The formal fellowships already exist. There are already 1,600 fellowship-trained Mohs surgeons out there, and they have not cornered the market on skin cancer. The situation should not change since general dermatologists remain the gatekeepers – and entry point – for most skin cancer patients. Certification exams in dermatopathology and pediatric dermatology have not had a negative impact on general dermatologists, who still read their own slides and see kids for skin disease. In fact, having dermatopathology as a certified part of dermatology has been a huge benefit in our struggle to maintain the right to read our own slides.
Developing a certification exam would take at least 2 years if the American Board of Dermatology decided to do it. There would be no “grandfathering” automatic certification. Everyone would have to take the same exam – young, old, formally trained, or not.
Members of the American Board of Dermatology explained the qualifiers to sit for an exam (if there was an exam) at a summit I held in Cincinnati in 2015. They are interested in including all ABD dermatologists who currently practice Mohs surgery, fellowship trained or not. Suggested parameters included any ABD fellow whose practice is 20% Mohs and reconstructive surgery (by volume or income), or anyone who performs Mohs once a week. Fellowship-trained micrographic surgeons could be eligible, and this would be a self-attestation! There would be no case log reviews, no visits by inspectors, no secret questions or passwords. This pathway would remain open for 5 years as were the exams for dermatopathology and pediatric dermatology. After that point, only ACGME fellowship–trained Mohs surgeons would be eligible to take the exam.
Upsides to this approach include decreasing divisiveness in the specialty, creating a better brand, and elevating the specialty. A board certification will help in obtaining a Medicare specialty designation, which will help stop the delisting of Mohs surgeons from insurance networks based on their average charges compared with general dermatologists. This action would particularly help small practices.
The American Academy of Dermatology board of directors sent this issue to the education committee to inform and poll the membership. You should expect to hear more about the proposed process. As an AAD member, you will get to express your opinion so make sure you are well informed. The AAD membership opinion will be important in whether or not the American Board of Dermatology decides to pursue this. Remember, this is an American Board of Dermatology decision, not an AAD decision.
More reasons for a board certification include that the ACGME expects its fellowships to develop a board exam at some point (although not all have). The 1,000 ACGME fellowship–trained micrographic surgeons deserve a chance to be board certified, which is the medical profession’s way to demonstrate competence to the public.
Having all Mohs surgeons board certified would heal a huge rift in the house of dermatology, and give us a united, consistent face to present to other specialties, the Congress, and the media. Physicians are judged by their training and credentials. Love them or hate them, the ACGME is the gold standard. Perhaps the greatest beneficiaries would be those practicing Mohs who did not complete a formal fellowship. I think a board exam is overdue, and will be a boon to all of dermatology.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
The medical director was direct and blunt: “You’ve got a problem with two very different levels of training in Mohs surgery. This is a big problem for your specialty.”
The remarks came at a medical director summit that I was attending to speak on the value of dermatology. I was explaining to medical directors how including small dermatology practices in their plans would realize cost savings when treating skin cancer in the office setting. An awkward silence followed the medical director’s remarks. Then I uttered a lame “we may have a board certification someday.”
My interview with the New York Times reporter before the meeting quickly became adversarial. “What about these guys who do Mohs after a 3-day course?” I explained that there is more involved than just the 3-day course, that there is a preceptorship and case reviews. Plus, some of “those guys” wrote some of the best Mohs textbooks. The reporter wasn’t buying it, and the rest of the interview went downhill.
And the training issues surrounding Mohs surgery are playing out in practice. One dermatologist wrote me complaining that an insurer will no longer let him bill for Mohs because “he can’t document his residency training in Mohs and did not do a fellowship.” Another wrote me saying he can no longer teach Mohs surgery at the VA or the medical school “because he didn’t do a formal Mohs fellowship.”
The issue of who is qualified to perform Mohs surgery is coming to a head. There are more than 2,500 dermatologists billing Medicare for Mohs, and insurers are groaning at the expense. They are looking for any possible reason to exclude dermatologists from billing for Mohs surgery.
A possible solution is a board certification in Mohs surgery. Osteopathic dermatologists have had this option for 20 years. Unfortunately, allopathic dermatologists cannot sit for the osteopathic exam. A new certification exam for allopathic dermatologists who have successfully completed a dermatology residency accredited by the Accreditation Council for Graduate Medical Education (ACGME) seems worthy of a discussion.
Downsides of certification include the likely $1,000 or more cost of a test, the costs of preparing for the test, and the risk of failing a test. A new certification would give the Maintenance of Certification (MOC) haters another reason to complain, since about 600 lifetime certified, board-exempt dermatologists would be dragged back into MOC to maintain a Mohs surgery subspecialty certification. Some of the current fellowship-trained Mohs surgeons will not like being grouped with the nonfellowship-trained surgeons, whom they consider their inferiors and who will now have the opportunity to be board certified.
The name of the fellowship, which is “micrographic surgery and dermatologic oncology,” also has some paranoid types fearing that they will lose the right to treat skin cancer if such a subspecialty is created. That shouldn’t be an issue, since all dermatologists are trained in residency to treat skin cancer. The formal fellowships already exist. There are already 1,600 fellowship-trained Mohs surgeons out there, and they have not cornered the market on skin cancer. The situation should not change since general dermatologists remain the gatekeepers – and entry point – for most skin cancer patients. Certification exams in dermatopathology and pediatric dermatology have not had a negative impact on general dermatologists, who still read their own slides and see kids for skin disease. In fact, having dermatopathology as a certified part of dermatology has been a huge benefit in our struggle to maintain the right to read our own slides.
Developing a certification exam would take at least 2 years if the American Board of Dermatology decided to do it. There would be no “grandfathering” automatic certification. Everyone would have to take the same exam – young, old, formally trained, or not.
Members of the American Board of Dermatology explained the qualifiers to sit for an exam (if there was an exam) at a summit I held in Cincinnati in 2015. They are interested in including all ABD dermatologists who currently practice Mohs surgery, fellowship trained or not. Suggested parameters included any ABD fellow whose practice is 20% Mohs and reconstructive surgery (by volume or income), or anyone who performs Mohs once a week. Fellowship-trained micrographic surgeons could be eligible, and this would be a self-attestation! There would be no case log reviews, no visits by inspectors, no secret questions or passwords. This pathway would remain open for 5 years as were the exams for dermatopathology and pediatric dermatology. After that point, only ACGME fellowship–trained Mohs surgeons would be eligible to take the exam.
Upsides to this approach include decreasing divisiveness in the specialty, creating a better brand, and elevating the specialty. A board certification will help in obtaining a Medicare specialty designation, which will help stop the delisting of Mohs surgeons from insurance networks based on their average charges compared with general dermatologists. This action would particularly help small practices.
The American Academy of Dermatology board of directors sent this issue to the education committee to inform and poll the membership. You should expect to hear more about the proposed process. As an AAD member, you will get to express your opinion so make sure you are well informed. The AAD membership opinion will be important in whether or not the American Board of Dermatology decides to pursue this. Remember, this is an American Board of Dermatology decision, not an AAD decision.
More reasons for a board certification include that the ACGME expects its fellowships to develop a board exam at some point (although not all have). The 1,000 ACGME fellowship–trained micrographic surgeons deserve a chance to be board certified, which is the medical profession’s way to demonstrate competence to the public.
Having all Mohs surgeons board certified would heal a huge rift in the house of dermatology, and give us a united, consistent face to present to other specialties, the Congress, and the media. Physicians are judged by their training and credentials. Love them or hate them, the ACGME is the gold standard. Perhaps the greatest beneficiaries would be those practicing Mohs who did not complete a formal fellowship. I think a board exam is overdue, and will be a boon to all of dermatology.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
The medical director was direct and blunt: “You’ve got a problem with two very different levels of training in Mohs surgery. This is a big problem for your specialty.”
The remarks came at a medical director summit that I was attending to speak on the value of dermatology. I was explaining to medical directors how including small dermatology practices in their plans would realize cost savings when treating skin cancer in the office setting. An awkward silence followed the medical director’s remarks. Then I uttered a lame “we may have a board certification someday.”
My interview with the New York Times reporter before the meeting quickly became adversarial. “What about these guys who do Mohs after a 3-day course?” I explained that there is more involved than just the 3-day course, that there is a preceptorship and case reviews. Plus, some of “those guys” wrote some of the best Mohs textbooks. The reporter wasn’t buying it, and the rest of the interview went downhill.
And the training issues surrounding Mohs surgery are playing out in practice. One dermatologist wrote me complaining that an insurer will no longer let him bill for Mohs because “he can’t document his residency training in Mohs and did not do a fellowship.” Another wrote me saying he can no longer teach Mohs surgery at the VA or the medical school “because he didn’t do a formal Mohs fellowship.”
The issue of who is qualified to perform Mohs surgery is coming to a head. There are more than 2,500 dermatologists billing Medicare for Mohs, and insurers are groaning at the expense. They are looking for any possible reason to exclude dermatologists from billing for Mohs surgery.
A possible solution is a board certification in Mohs surgery. Osteopathic dermatologists have had this option for 20 years. Unfortunately, allopathic dermatologists cannot sit for the osteopathic exam. A new certification exam for allopathic dermatologists who have successfully completed a dermatology residency accredited by the Accreditation Council for Graduate Medical Education (ACGME) seems worthy of a discussion.
Downsides of certification include the likely $1,000 or more cost of a test, the costs of preparing for the test, and the risk of failing a test. A new certification would give the Maintenance of Certification (MOC) haters another reason to complain, since about 600 lifetime certified, board-exempt dermatologists would be dragged back into MOC to maintain a Mohs surgery subspecialty certification. Some of the current fellowship-trained Mohs surgeons will not like being grouped with the nonfellowship-trained surgeons, whom they consider their inferiors and who will now have the opportunity to be board certified.
The name of the fellowship, which is “micrographic surgery and dermatologic oncology,” also has some paranoid types fearing that they will lose the right to treat skin cancer if such a subspecialty is created. That shouldn’t be an issue, since all dermatologists are trained in residency to treat skin cancer. The formal fellowships already exist. There are already 1,600 fellowship-trained Mohs surgeons out there, and they have not cornered the market on skin cancer. The situation should not change since general dermatologists remain the gatekeepers – and entry point – for most skin cancer patients. Certification exams in dermatopathology and pediatric dermatology have not had a negative impact on general dermatologists, who still read their own slides and see kids for skin disease. In fact, having dermatopathology as a certified part of dermatology has been a huge benefit in our struggle to maintain the right to read our own slides.
Developing a certification exam would take at least 2 years if the American Board of Dermatology decided to do it. There would be no “grandfathering” automatic certification. Everyone would have to take the same exam – young, old, formally trained, or not.
Members of the American Board of Dermatology explained the qualifiers to sit for an exam (if there was an exam) at a summit I held in Cincinnati in 2015. They are interested in including all ABD dermatologists who currently practice Mohs surgery, fellowship trained or not. Suggested parameters included any ABD fellow whose practice is 20% Mohs and reconstructive surgery (by volume or income), or anyone who performs Mohs once a week. Fellowship-trained micrographic surgeons could be eligible, and this would be a self-attestation! There would be no case log reviews, no visits by inspectors, no secret questions or passwords. This pathway would remain open for 5 years as were the exams for dermatopathology and pediatric dermatology. After that point, only ACGME fellowship–trained Mohs surgeons would be eligible to take the exam.
Upsides to this approach include decreasing divisiveness in the specialty, creating a better brand, and elevating the specialty. A board certification will help in obtaining a Medicare specialty designation, which will help stop the delisting of Mohs surgeons from insurance networks based on their average charges compared with general dermatologists. This action would particularly help small practices.
The American Academy of Dermatology board of directors sent this issue to the education committee to inform and poll the membership. You should expect to hear more about the proposed process. As an AAD member, you will get to express your opinion so make sure you are well informed. The AAD membership opinion will be important in whether or not the American Board of Dermatology decides to pursue this. Remember, this is an American Board of Dermatology decision, not an AAD decision.
More reasons for a board certification include that the ACGME expects its fellowships to develop a board exam at some point (although not all have). The 1,000 ACGME fellowship–trained micrographic surgeons deserve a chance to be board certified, which is the medical profession’s way to demonstrate competence to the public.
Having all Mohs surgeons board certified would heal a huge rift in the house of dermatology, and give us a united, consistent face to present to other specialties, the Congress, and the media. Physicians are judged by their training and credentials. Love them or hate them, the ACGME is the gold standard. Perhaps the greatest beneficiaries would be those practicing Mohs who did not complete a formal fellowship. I think a board exam is overdue, and will be a boon to all of dermatology.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.

VIDEO: MOC + Me: Maintenance of Certification in Hospital Medicine
Dr. Marianne Green and Dr. Jeffrey Wiese, two members of the ABIM Council, talk about ABIM's Maintenance of Certification process, and the importance of professional assessment. Dr. Green works on Internal Medicine MOC, Dr. Wiese was part of the team that developed the Focused Practice in Hospital Medicine MOC.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Marianne Green and Dr. Jeffrey Wiese, two members of the ABIM Council, talk about ABIM's Maintenance of Certification process, and the importance of professional assessment. Dr. Green works on Internal Medicine MOC, Dr. Wiese was part of the team that developed the Focused Practice in Hospital Medicine MOC.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Marianne Green and Dr. Jeffrey Wiese, two members of the ABIM Council, talk about ABIM's Maintenance of Certification process, and the importance of professional assessment. Dr. Green works on Internal Medicine MOC, Dr. Wiese was part of the team that developed the Focused Practice in Hospital Medicine MOC.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Spending on Complementary Health Care
Americans spend billions of dollars out-of-pocket on complementary health care, according to an analysis of data from the 2012 National Health Interview Survey conducted by the National Center for Complementary and Integrative Health (NCCIH) and the CDC.
Of the more than $30 billion spent by consumers, nearly $15 billion went to visits to chiropractors, acupuncturists, massage therapists, and other complementary practitioners—almost 30% of what Americans spent on out-of-pocket services by conventional physicians. The mean annual out-of-pocket expenditure for practitioner visits was $433. This analysis also included the first-ever data on spending for children: almost $2 billion.
Related: Complementary Therapp-y
Americans also spent billions on natural product supplements for an annual mean of $368 or about one-fourth of what they spent on prescription drugs.
Income level made little difference in expenditure. People with family incomes of < $25,000 averaged $314 for visits to complementary practitioners, vs $518 for those with incomes of more than $100,000.
The fact that so many people spent money on complementary approaches is “an indication that users believe enough in the value of these approaches to pay for them,” said Richard Nahin, PhD, lead author of the analysis and lead epidemiologist for National Center for Complementary and Integrative Health, which conducted the analysis.
Related: Complementary and Alternative Medicine for Chronic Musculoskeletal Pain
It’s also the reason that it’s “extremely important for us to provide the public with evidence-based information to help inform decisions,” said Josephine Briggs, MD, director of NCCIH. “This underscores the importance of conducting rigorous research to know whether the products and practices being used are safe and effective.”
Americans spend billions of dollars out-of-pocket on complementary health care, according to an analysis of data from the 2012 National Health Interview Survey conducted by the National Center for Complementary and Integrative Health (NCCIH) and the CDC.
Of the more than $30 billion spent by consumers, nearly $15 billion went to visits to chiropractors, acupuncturists, massage therapists, and other complementary practitioners—almost 30% of what Americans spent on out-of-pocket services by conventional physicians. The mean annual out-of-pocket expenditure for practitioner visits was $433. This analysis also included the first-ever data on spending for children: almost $2 billion.
Related: Complementary Therapp-y
Americans also spent billions on natural product supplements for an annual mean of $368 or about one-fourth of what they spent on prescription drugs.
Income level made little difference in expenditure. People with family incomes of < $25,000 averaged $314 for visits to complementary practitioners, vs $518 for those with incomes of more than $100,000.
The fact that so many people spent money on complementary approaches is “an indication that users believe enough in the value of these approaches to pay for them,” said Richard Nahin, PhD, lead author of the analysis and lead epidemiologist for National Center for Complementary and Integrative Health, which conducted the analysis.
Related: Complementary and Alternative Medicine for Chronic Musculoskeletal Pain
It’s also the reason that it’s “extremely important for us to provide the public with evidence-based information to help inform decisions,” said Josephine Briggs, MD, director of NCCIH. “This underscores the importance of conducting rigorous research to know whether the products and practices being used are safe and effective.”
Americans spend billions of dollars out-of-pocket on complementary health care, according to an analysis of data from the 2012 National Health Interview Survey conducted by the National Center for Complementary and Integrative Health (NCCIH) and the CDC.
Of the more than $30 billion spent by consumers, nearly $15 billion went to visits to chiropractors, acupuncturists, massage therapists, and other complementary practitioners—almost 30% of what Americans spent on out-of-pocket services by conventional physicians. The mean annual out-of-pocket expenditure for practitioner visits was $433. This analysis also included the first-ever data on spending for children: almost $2 billion.
Related: Complementary Therapp-y
Americans also spent billions on natural product supplements for an annual mean of $368 or about one-fourth of what they spent on prescription drugs.
Income level made little difference in expenditure. People with family incomes of < $25,000 averaged $314 for visits to complementary practitioners, vs $518 for those with incomes of more than $100,000.
The fact that so many people spent money on complementary approaches is “an indication that users believe enough in the value of these approaches to pay for them,” said Richard Nahin, PhD, lead author of the analysis and lead epidemiologist for National Center for Complementary and Integrative Health, which conducted the analysis.
Related: Complementary and Alternative Medicine for Chronic Musculoskeletal Pain
It’s also the reason that it’s “extremely important for us to provide the public with evidence-based information to help inform decisions,” said Josephine Briggs, MD, director of NCCIH. “This underscores the importance of conducting rigorous research to know whether the products and practices being used are safe and effective.”