User login
Miscellany
Many interesting things happen in a medical office, most of which don’t merit a full column. Here are some from my own past few months:
Endocrine Knee? I was hard put to explain the calluses on both my patient’s knees. As I tried to formulate a question, he rescued me by saying, “I’m an endocrinologist. I spend a lot of my time on my knees, trimming the toenails of elderly diabetics.”

Who knew? At least bending the knee to insurers and regulators doesn’t require keratolytics ...
You can get anything online. My patient was about to graduate with a degree in psychoanalysis. “I have to set up my office,” she said, “drapes, analyst couch, and so forth.”
“Where do you buy an analyst couch?” I asked.
“Analyticcouch.com,” she explained. “Available in a variety of colors.”
What a country!
No I’m not, Officer! Many patients consider removing facial red spots that make them self-conscious, but Harriet’s reason was unique. “I got pulled over by a cop for an illegal change of lanes,” she said. “When he saw the red spot under my eye, he assumed I was a drunk. ‘Get over there, punk,’ he said.”
The other bathroom is upstairs. Stan listed his occupation as “muralist.” Picturing him sneaking up to blank walls on street corners in the middle of the night with a can of Benjamin Moore to ply his trade, I asked where he draws his murals.
“Most of my work is residential,” he said. “For instance, last year I did a bathroom in Framingham. The motif they wanted was ancient Egypt. I had to do a lot of research on the 18th dynasty, to get the details exactly right.”
That made sense. You wouldn’t want a dangling hieroglyphic participle in your downstairs lavatory. I asked him how it worked out.
“The client was delighted,” he said, “only there was one problem. Whenever guests came over for a dinner party, there was always a long line, because whoever was in the bathroom wouldn’t come out.”
There are always alternatives. By now I am used to hearing patients extol the virtues of exotic treatments: Vicks VapoRub for toenail tinea, tea tree oil for most anything. Apple cider vinegar for everything else.
Then the other day Marcy surprised me with this:
“I stopped the minocycline,” she said, “Instead I started using celery, which I ground up and boiled and then froze and then applied to the face.”
A little bit of a production, perhaps – grinding, boiling, freezing. As long as it works ...
You need a different kind of doctor. “I see I won’t be able to shower for 3 days,” said the new patient.
My jaw dropped, but no words came out.
“It’s that sign you put up,” he said, “right on the exam room door.”
As I don’t usually read my own signs, I turned to look. The sign read:
“If you have no-showed without notice three times, we reserve the right to reschedule you at our convenience.”
“It says, ‘No-Showed,” I said. Not ‘No Showers.”
I resisted the urge to refer him to an optometrist.
This reminded me of another episode some time ago, when a patient listed his Chief Complaint as, “I want Lasik Surgery.”
“Forgive me,” I said, “but why would you ask a dermatologist for Lasik surgery?”
“Doesn’t the sign on your door say, “Boston Ophthalmology?” he asked.
“Upstairs,” I said. “Seventh floor.”
Negotiating with Father Time. We suspected porphyria, and ordered a 24-hour urine collection. “I’m a busy executive,” said the patient. “I haven’t got time to collect it for that long.”
“But it has to be a whole day ...”
“Fifteen hours,” he said. “I’ll give you 15 hours.”
“But we need ...”
“Eighteen hours. OK?”
“Well, not really. You see, the test has to be a whole day ...”
“All right, 21 hours. That’s my best offer.”
Maybe if I could get him to spend the day in that Egyptian bathroom ...
Dr. Rockoff practices dermatology in Brookline, Mass, and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book, “Act Like a Doctor, Think Like a Patient,” is now available on amazon.com and barnesandnoble.com. This is his second book. Write to him at [email protected].
Many interesting things happen in a medical office, most of which don’t merit a full column. Here are some from my own past few months:
Endocrine Knee? I was hard put to explain the calluses on both my patient’s knees. As I tried to formulate a question, he rescued me by saying, “I’m an endocrinologist. I spend a lot of my time on my knees, trimming the toenails of elderly diabetics.”
Who knew? At least bending the knee to insurers and regulators doesn’t require keratolytics ...
You can get anything online. My patient was about to graduate with a degree in psychoanalysis. “I have to set up my office,” she said, “drapes, analyst couch, and so forth.”
“Where do you buy an analyst couch?” I asked.
“Analyticcouch.com,” she explained. “Available in a variety of colors.”
What a country!
No I’m not, Officer! Many patients consider removing facial red spots that make them self-conscious, but Harriet’s reason was unique. “I got pulled over by a cop for an illegal change of lanes,” she said. “When he saw the red spot under my eye, he assumed I was a drunk. ‘Get over there, punk,’ he said.”
The other bathroom is upstairs. Stan listed his occupation as “muralist.” Picturing him sneaking up to blank walls on street corners in the middle of the night with a can of Benjamin Moore to ply his trade, I asked where he draws his murals.
“Most of my work is residential,” he said. “For instance, last year I did a bathroom in Framingham. The motif they wanted was ancient Egypt. I had to do a lot of research on the 18th dynasty, to get the details exactly right.”
That made sense. You wouldn’t want a dangling hieroglyphic participle in your downstairs lavatory. I asked him how it worked out.
“The client was delighted,” he said, “only there was one problem. Whenever guests came over for a dinner party, there was always a long line, because whoever was in the bathroom wouldn’t come out.”
There are always alternatives. By now I am used to hearing patients extol the virtues of exotic treatments: Vicks VapoRub for toenail tinea, tea tree oil for most anything. Apple cider vinegar for everything else.
Then the other day Marcy surprised me with this:
“I stopped the minocycline,” she said, “Instead I started using celery, which I ground up and boiled and then froze and then applied to the face.”
A little bit of a production, perhaps – grinding, boiling, freezing. As long as it works ...
You need a different kind of doctor. “I see I won’t be able to shower for 3 days,” said the new patient.
My jaw dropped, but no words came out.
“It’s that sign you put up,” he said, “right on the exam room door.”
As I don’t usually read my own signs, I turned to look. The sign read:
“If you have no-showed without notice three times, we reserve the right to reschedule you at our convenience.”
“It says, ‘No-Showed,” I said. Not ‘No Showers.”
I resisted the urge to refer him to an optometrist.
This reminded me of another episode some time ago, when a patient listed his Chief Complaint as, “I want Lasik Surgery.”
“Forgive me,” I said, “but why would you ask a dermatologist for Lasik surgery?”
“Doesn’t the sign on your door say, “Boston Ophthalmology?” he asked.
“Upstairs,” I said. “Seventh floor.”
Negotiating with Father Time. We suspected porphyria, and ordered a 24-hour urine collection. “I’m a busy executive,” said the patient. “I haven’t got time to collect it for that long.”
“But it has to be a whole day ...”
“Fifteen hours,” he said. “I’ll give you 15 hours.”
“But we need ...”
“Eighteen hours. OK?”
“Well, not really. You see, the test has to be a whole day ...”
“All right, 21 hours. That’s my best offer.”
Maybe if I could get him to spend the day in that Egyptian bathroom ...
Dr. Rockoff practices dermatology in Brookline, Mass, and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book, “Act Like a Doctor, Think Like a Patient,” is now available on amazon.com and barnesandnoble.com. This is his second book. Write to him at [email protected].
Many interesting things happen in a medical office, most of which don’t merit a full column. Here are some from my own past few months:
Endocrine Knee? I was hard put to explain the calluses on both my patient’s knees. As I tried to formulate a question, he rescued me by saying, “I’m an endocrinologist. I spend a lot of my time on my knees, trimming the toenails of elderly diabetics.”
Who knew? At least bending the knee to insurers and regulators doesn’t require keratolytics ...
You can get anything online. My patient was about to graduate with a degree in psychoanalysis. “I have to set up my office,” she said, “drapes, analyst couch, and so forth.”
“Where do you buy an analyst couch?” I asked.
“Analyticcouch.com,” she explained. “Available in a variety of colors.”
What a country!
No I’m not, Officer! Many patients consider removing facial red spots that make them self-conscious, but Harriet’s reason was unique. “I got pulled over by a cop for an illegal change of lanes,” she said. “When he saw the red spot under my eye, he assumed I was a drunk. ‘Get over there, punk,’ he said.”
The other bathroom is upstairs. Stan listed his occupation as “muralist.” Picturing him sneaking up to blank walls on street corners in the middle of the night with a can of Benjamin Moore to ply his trade, I asked where he draws his murals.
“Most of my work is residential,” he said. “For instance, last year I did a bathroom in Framingham. The motif they wanted was ancient Egypt. I had to do a lot of research on the 18th dynasty, to get the details exactly right.”
That made sense. You wouldn’t want a dangling hieroglyphic participle in your downstairs lavatory. I asked him how it worked out.
“The client was delighted,” he said, “only there was one problem. Whenever guests came over for a dinner party, there was always a long line, because whoever was in the bathroom wouldn’t come out.”
There are always alternatives. By now I am used to hearing patients extol the virtues of exotic treatments: Vicks VapoRub for toenail tinea, tea tree oil for most anything. Apple cider vinegar for everything else.
Then the other day Marcy surprised me with this:
“I stopped the minocycline,” she said, “Instead I started using celery, which I ground up and boiled and then froze and then applied to the face.”
A little bit of a production, perhaps – grinding, boiling, freezing. As long as it works ...
You need a different kind of doctor. “I see I won’t be able to shower for 3 days,” said the new patient.
My jaw dropped, but no words came out.
“It’s that sign you put up,” he said, “right on the exam room door.”
As I don’t usually read my own signs, I turned to look. The sign read:
“If you have no-showed without notice three times, we reserve the right to reschedule you at our convenience.”
“It says, ‘No-Showed,” I said. Not ‘No Showers.”
I resisted the urge to refer him to an optometrist.
This reminded me of another episode some time ago, when a patient listed his Chief Complaint as, “I want Lasik Surgery.”
“Forgive me,” I said, “but why would you ask a dermatologist for Lasik surgery?”
“Doesn’t the sign on your door say, “Boston Ophthalmology?” he asked.
“Upstairs,” I said. “Seventh floor.”
Negotiating with Father Time. We suspected porphyria, and ordered a 24-hour urine collection. “I’m a busy executive,” said the patient. “I haven’t got time to collect it for that long.”
“But it has to be a whole day ...”
“Fifteen hours,” he said. “I’ll give you 15 hours.”
“But we need ...”
“Eighteen hours. OK?”
“Well, not really. You see, the test has to be a whole day ...”
“All right, 21 hours. That’s my best offer.”
Maybe if I could get him to spend the day in that Egyptian bathroom ...
Dr. Rockoff practices dermatology in Brookline, Mass, and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book, “Act Like a Doctor, Think Like a Patient,” is now available on amazon.com and barnesandnoble.com. This is his second book. Write to him at [email protected].

FDA to streamline development of antimicrobials, susceptibility test devices
The Food and Drug Administration has released a draft guidance document intended to help drug sponsors and device manufacturers coordinate the development of new antimicrobial drugs and antimicrobial susceptibility test devices (ASTs).
The FDA said it wants the guidance document, entitled “Coordinated Development of Antimicrobial Drugs and Antimicrobial Susceptibility Test Devices,” to help harmonize “development of these products such that the AST device could be cleared either at the time of new drug approval or shortly thereafter.” The agency acknowledged in the guidance document that development of antimicrobial drugs and ASTs – which test for in vitro susceptibility of bacterial pathogens isolated from clinical specimens to antimicrobials – has traditionally occurred independently, with AST device development “often initiated following drug approval.” A coordinated approach to developing new antimicrobial drugs with AST devices ideally would minimize the time between the approval of a new antimicrobial drug and clearance of an AST device.
The FDA highlighted three key goals of the guidance document:
• Describe interactions between antimicrobial drug sponsors and AST device manufacturers to help improve coordinated development of a new antimicrobial drug and an AST device to streamline the clearance process.
• Explain the considerations for submitting separate applications to the Center for Drug Evaluation and Research and the Center for Devices and Radiological Health when seeking to facilitate clearance of an AST device as close in time as possible to antimicrobial drug approval.
• Emphasize that the review of the new antimicrobial drug product and AST device(s) will remain independent, and that coordinated development does not influence the review timelines for either product.
The FDA will accept comments and suggestions on the draft guidance document within 60 days of publication in the Federal Register.
On Twitter @richpizzi
The Food and Drug Administration has released a draft guidance document intended to help drug sponsors and device manufacturers coordinate the development of new antimicrobial drugs and antimicrobial susceptibility test devices (ASTs).
The FDA said it wants the guidance document, entitled “Coordinated Development of Antimicrobial Drugs and Antimicrobial Susceptibility Test Devices,” to help harmonize “development of these products such that the AST device could be cleared either at the time of new drug approval or shortly thereafter.” The agency acknowledged in the guidance document that development of antimicrobial drugs and ASTs – which test for in vitro susceptibility of bacterial pathogens isolated from clinical specimens to antimicrobials – has traditionally occurred independently, with AST device development “often initiated following drug approval.” A coordinated approach to developing new antimicrobial drugs with AST devices ideally would minimize the time between the approval of a new antimicrobial drug and clearance of an AST device.
The FDA highlighted three key goals of the guidance document:
• Describe interactions between antimicrobial drug sponsors and AST device manufacturers to help improve coordinated development of a new antimicrobial drug and an AST device to streamline the clearance process.
• Explain the considerations for submitting separate applications to the Center for Drug Evaluation and Research and the Center for Devices and Radiological Health when seeking to facilitate clearance of an AST device as close in time as possible to antimicrobial drug approval.
• Emphasize that the review of the new antimicrobial drug product and AST device(s) will remain independent, and that coordinated development does not influence the review timelines for either product.
The FDA will accept comments and suggestions on the draft guidance document within 60 days of publication in the Federal Register.
On Twitter @richpizzi
The Food and Drug Administration has released a draft guidance document intended to help drug sponsors and device manufacturers coordinate the development of new antimicrobial drugs and antimicrobial susceptibility test devices (ASTs).
The FDA said it wants the guidance document, entitled “Coordinated Development of Antimicrobial Drugs and Antimicrobial Susceptibility Test Devices,” to help harmonize “development of these products such that the AST device could be cleared either at the time of new drug approval or shortly thereafter.” The agency acknowledged in the guidance document that development of antimicrobial drugs and ASTs – which test for in vitro susceptibility of bacterial pathogens isolated from clinical specimens to antimicrobials – has traditionally occurred independently, with AST device development “often initiated following drug approval.” A coordinated approach to developing new antimicrobial drugs with AST devices ideally would minimize the time between the approval of a new antimicrobial drug and clearance of an AST device.
The FDA highlighted three key goals of the guidance document:
• Describe interactions between antimicrobial drug sponsors and AST device manufacturers to help improve coordinated development of a new antimicrobial drug and an AST device to streamline the clearance process.
• Explain the considerations for submitting separate applications to the Center for Drug Evaluation and Research and the Center for Devices and Radiological Health when seeking to facilitate clearance of an AST device as close in time as possible to antimicrobial drug approval.
• Emphasize that the review of the new antimicrobial drug product and AST device(s) will remain independent, and that coordinated development does not influence the review timelines for either product.
The FDA will accept comments and suggestions on the draft guidance document within 60 days of publication in the Federal Register.
On Twitter @richpizzi
Do as I say, not as I do! A futile plea
I am constantly amazed when parents come in complaining about their child’s nail biting or irritable attitude “no matter how many times I tell her” as they do these same things in front of me!
We have not evolved that far from our nonverbal ancestors to expect that words will speak louder than actions. Looking closely, you can see even very young infants gazing closely at their parents, then mirroring their facial expressions a few minutes later (because of slower processing). Mirroring is probably the correct word for this as the mirror neuron system of the brain has as its primary and crucial function allowing humans to copy what they see in others.

Children look to model, especially those who are slightly older and more adept than they are. Older siblings bask in this adoration at times and squeal in frustration at other times that their younger sister is “mocking” them by copying their speech and actions. When children are picking up serious negative behaviors from siblings or peers, particularly in adolescence, we need to coach parents to take action.
But watching parents is the most powerful or “salient” stimulus for learning. Some theorize that the long period of childhood evolved to allow children to learn the incredible amount of information necessary to live independently in our complex culture. This learning begins very early and requires close contact and careful observation of the minute details of how the parent survives every day.
Eating is a great primitive example of why children must model their parents. How do animals know which plants are poisonous? By watching others eat and spit, choke, or vomit. Entire families have nonpreferred foods passed on by modeling refusal as well as lack of exposure on the table. Conversely, picky eaters need to observe others, preferably admired peers and parents, eating those vegetables. (Tasting is also necessary, but that’s a topic for another day!) It is worth asking about family meals, without the distraction of a TV, as they are key moments to model nutritious eating for their lifetime.
In “underdeveloped” countries, infants are naturally carried everywhere and observing constantly. In our “developed” country, many infants spend hours each day at day care, modeling their caregivers or watching media examples of people interacting, which may not be the models parents would consciously choose. Parents often ask us about childcare, anxious about the extremely rare threat of abduction, when we should instead be advising them about what models they want for their children during this critical learning period.
Emotion cueing is a crucial component of modeling and an untaught constant of typical parent-child interaction. Crawling infants placed on a clear surface over a “visual cliff” that appeared to be a sudden precipice look to the parent’s affect to decide how to act. The mother was instructed to show fear or joy when her baby reached the apparent danger and looked up for a warning. When fear was shown, the infants backed off and cried. When joy was shown, the baby crawled gaily across the “cliff.” For parents who do not come by signaling confidence naturally but want to model this for their children, I advise they “fake it until you make it!”
Parents are instructing their progeny in how to feel and act in every situation, whether they know it or not. Confident parents model bravery; kind parents model compassion; flexible parents model resilience; patient parents model tolerance; anxious parents model caution; angry parents model aggression. Ignoring parents (think: on their cellphone, distracted, depressed, inebriated, or high) leave their children to feel confused and insecure. An adaptive child of an ignoring parent may demand information by crying, clinging, fighting with siblings, or hitting the parent. They are desperate for the parental attention to teach them and keep them safe. A more passive child may become increasingly inhibited in their exploration of the world. We need to consider possible modeling failures when such child reaction patterns are the complaint, and remember that the adverse model may not be in the room, requiring us to ask, “What other adult models does he see?”
Studies have shown that infants learn resilience when experiencing “mistakes” in parent-infant interaction; learning how to tolerate and repair an interaction that is not perfect. This is really good news for parents who feel that they must be perfect models for their children! For parents of anxious or obsessive children, I sometimes prescribe making mistakes and saying “Oh well,” as well as rewarding the child when they can say “Oh well” themselves. No child is too old to benefit from observing a parent apologize sincerely for a mistake.
Language is modeled, right down to accent. But when parents complain about their child cussing, raising their voice in anger, having an “attitude,” or “talking back,” it is worth asking (parent and child) “Where do you think they/you have heard talk like that?” It may be childcare providers, peers, TV, video games or online media (all of which may warrant a change), but it also may reflect interactions at home.
Children make stronger memories when emotions are high as these may signal danger, making recall more salient to survival. This salience helps explain the lasting detriments to learning and health of growing up with psychological abuse, marital discord, partner violence, mental illness, or criminal behavior (among the Adverse Childhood Experiences). Such experiences cause stress and a sense of the world as a dangerous place, but also become models for the child’s own later relationships as adults. While unavoidable, they can be buffered by parents’ explaining them and providing alternative positive modeling.
Watching the parent conduct their craft, a key component of apprenticeship and family businesses in the past, has been replaced by YouTube and avatars for learning physical skills. But “modeling the process” of pride in craftsmanship, persistence in a task, and recovering and starting over when things go awry are omitted from training videos. These are good reasons to assure that parents do chores, crafts, cooking, or camping with their children as some things will surely go wrong, giving parents the chance to model resilience and problem solving!
Although teens may protest conversations and activities, they are watching their parents for how to be a spouse, a neighbor, a friend, a leader, a citizen. Parents, who may be cutting their teens loose, need to continue to expect/require participation in family meals and outings. Those are opportunities to model adult-level interactions with each other and with the community as well as to talk about their activities at work, in volunteering, in charity, and in religious practice. The moral development of the adolescent is shaped by what they see to the degree that when parents state one moral code but violate it themselves (for example, cheating on taxes, running red lights), the teen is less likely to follow the principles long term that the parents have verbalized.
Parents often relate to us as though we were their own parents. While this “projection” can interfere with disclosure on touchy subjects, it is also an opportunity for us to model ways of relating and reacting from sympathizing with the 4-year-old screaming about vaccines to asking an 8-year-old why he thinks his parents are getting a divorce.
Parenting (and being a pediatrician) is an opportunity to enjoy reliving your youth or to get a “do over” of parts you would like to have different for your child. Playfulness and silliness model joy for the child that can last a lifetime.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at [email protected].
I am constantly amazed when parents come in complaining about their child’s nail biting or irritable attitude “no matter how many times I tell her” as they do these same things in front of me!
We have not evolved that far from our nonverbal ancestors to expect that words will speak louder than actions. Looking closely, you can see even very young infants gazing closely at their parents, then mirroring their facial expressions a few minutes later (because of slower processing). Mirroring is probably the correct word for this as the mirror neuron system of the brain has as its primary and crucial function allowing humans to copy what they see in others.
Children look to model, especially those who are slightly older and more adept than they are. Older siblings bask in this adoration at times and squeal in frustration at other times that their younger sister is “mocking” them by copying their speech and actions. When children are picking up serious negative behaviors from siblings or peers, particularly in adolescence, we need to coach parents to take action.
But watching parents is the most powerful or “salient” stimulus for learning. Some theorize that the long period of childhood evolved to allow children to learn the incredible amount of information necessary to live independently in our complex culture. This learning begins very early and requires close contact and careful observation of the minute details of how the parent survives every day.
Eating is a great primitive example of why children must model their parents. How do animals know which plants are poisonous? By watching others eat and spit, choke, or vomit. Entire families have nonpreferred foods passed on by modeling refusal as well as lack of exposure on the table. Conversely, picky eaters need to observe others, preferably admired peers and parents, eating those vegetables. (Tasting is also necessary, but that’s a topic for another day!) It is worth asking about family meals, without the distraction of a TV, as they are key moments to model nutritious eating for their lifetime.
In “underdeveloped” countries, infants are naturally carried everywhere and observing constantly. In our “developed” country, many infants spend hours each day at day care, modeling their caregivers or watching media examples of people interacting, which may not be the models parents would consciously choose. Parents often ask us about childcare, anxious about the extremely rare threat of abduction, when we should instead be advising them about what models they want for their children during this critical learning period.
Emotion cueing is a crucial component of modeling and an untaught constant of typical parent-child interaction. Crawling infants placed on a clear surface over a “visual cliff” that appeared to be a sudden precipice look to the parent’s affect to decide how to act. The mother was instructed to show fear or joy when her baby reached the apparent danger and looked up for a warning. When fear was shown, the infants backed off and cried. When joy was shown, the baby crawled gaily across the “cliff.” For parents who do not come by signaling confidence naturally but want to model this for their children, I advise they “fake it until you make it!”
Parents are instructing their progeny in how to feel and act in every situation, whether they know it or not. Confident parents model bravery; kind parents model compassion; flexible parents model resilience; patient parents model tolerance; anxious parents model caution; angry parents model aggression. Ignoring parents (think: on their cellphone, distracted, depressed, inebriated, or high) leave their children to feel confused and insecure. An adaptive child of an ignoring parent may demand information by crying, clinging, fighting with siblings, or hitting the parent. They are desperate for the parental attention to teach them and keep them safe. A more passive child may become increasingly inhibited in their exploration of the world. We need to consider possible modeling failures when such child reaction patterns are the complaint, and remember that the adverse model may not be in the room, requiring us to ask, “What other adult models does he see?”
Studies have shown that infants learn resilience when experiencing “mistakes” in parent-infant interaction; learning how to tolerate and repair an interaction that is not perfect. This is really good news for parents who feel that they must be perfect models for their children! For parents of anxious or obsessive children, I sometimes prescribe making mistakes and saying “Oh well,” as well as rewarding the child when they can say “Oh well” themselves. No child is too old to benefit from observing a parent apologize sincerely for a mistake.
Language is modeled, right down to accent. But when parents complain about their child cussing, raising their voice in anger, having an “attitude,” or “talking back,” it is worth asking (parent and child) “Where do you think they/you have heard talk like that?” It may be childcare providers, peers, TV, video games or online media (all of which may warrant a change), but it also may reflect interactions at home.
Children make stronger memories when emotions are high as these may signal danger, making recall more salient to survival. This salience helps explain the lasting detriments to learning and health of growing up with psychological abuse, marital discord, partner violence, mental illness, or criminal behavior (among the Adverse Childhood Experiences). Such experiences cause stress and a sense of the world as a dangerous place, but also become models for the child’s own later relationships as adults. While unavoidable, they can be buffered by parents’ explaining them and providing alternative positive modeling.
Watching the parent conduct their craft, a key component of apprenticeship and family businesses in the past, has been replaced by YouTube and avatars for learning physical skills. But “modeling the process” of pride in craftsmanship, persistence in a task, and recovering and starting over when things go awry are omitted from training videos. These are good reasons to assure that parents do chores, crafts, cooking, or camping with their children as some things will surely go wrong, giving parents the chance to model resilience and problem solving!
Although teens may protest conversations and activities, they are watching their parents for how to be a spouse, a neighbor, a friend, a leader, a citizen. Parents, who may be cutting their teens loose, need to continue to expect/require participation in family meals and outings. Those are opportunities to model adult-level interactions with each other and with the community as well as to talk about their activities at work, in volunteering, in charity, and in religious practice. The moral development of the adolescent is shaped by what they see to the degree that when parents state one moral code but violate it themselves (for example, cheating on taxes, running red lights), the teen is less likely to follow the principles long term that the parents have verbalized.
Parents often relate to us as though we were their own parents. While this “projection” can interfere with disclosure on touchy subjects, it is also an opportunity for us to model ways of relating and reacting from sympathizing with the 4-year-old screaming about vaccines to asking an 8-year-old why he thinks his parents are getting a divorce.
Parenting (and being a pediatrician) is an opportunity to enjoy reliving your youth or to get a “do over” of parts you would like to have different for your child. Playfulness and silliness model joy for the child that can last a lifetime.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at [email protected].
I am constantly amazed when parents come in complaining about their child’s nail biting or irritable attitude “no matter how many times I tell her” as they do these same things in front of me!
We have not evolved that far from our nonverbal ancestors to expect that words will speak louder than actions. Looking closely, you can see even very young infants gazing closely at their parents, then mirroring their facial expressions a few minutes later (because of slower processing). Mirroring is probably the correct word for this as the mirror neuron system of the brain has as its primary and crucial function allowing humans to copy what they see in others.
Children look to model, especially those who are slightly older and more adept than they are. Older siblings bask in this adoration at times and squeal in frustration at other times that their younger sister is “mocking” them by copying their speech and actions. When children are picking up serious negative behaviors from siblings or peers, particularly in adolescence, we need to coach parents to take action.
But watching parents is the most powerful or “salient” stimulus for learning. Some theorize that the long period of childhood evolved to allow children to learn the incredible amount of information necessary to live independently in our complex culture. This learning begins very early and requires close contact and careful observation of the minute details of how the parent survives every day.
Eating is a great primitive example of why children must model their parents. How do animals know which plants are poisonous? By watching others eat and spit, choke, or vomit. Entire families have nonpreferred foods passed on by modeling refusal as well as lack of exposure on the table. Conversely, picky eaters need to observe others, preferably admired peers and parents, eating those vegetables. (Tasting is also necessary, but that’s a topic for another day!) It is worth asking about family meals, without the distraction of a TV, as they are key moments to model nutritious eating for their lifetime.
In “underdeveloped” countries, infants are naturally carried everywhere and observing constantly. In our “developed” country, many infants spend hours each day at day care, modeling their caregivers or watching media examples of people interacting, which may not be the models parents would consciously choose. Parents often ask us about childcare, anxious about the extremely rare threat of abduction, when we should instead be advising them about what models they want for their children during this critical learning period.
Emotion cueing is a crucial component of modeling and an untaught constant of typical parent-child interaction. Crawling infants placed on a clear surface over a “visual cliff” that appeared to be a sudden precipice look to the parent’s affect to decide how to act. The mother was instructed to show fear or joy when her baby reached the apparent danger and looked up for a warning. When fear was shown, the infants backed off and cried. When joy was shown, the baby crawled gaily across the “cliff.” For parents who do not come by signaling confidence naturally but want to model this for their children, I advise they “fake it until you make it!”
Parents are instructing their progeny in how to feel and act in every situation, whether they know it or not. Confident parents model bravery; kind parents model compassion; flexible parents model resilience; patient parents model tolerance; anxious parents model caution; angry parents model aggression. Ignoring parents (think: on their cellphone, distracted, depressed, inebriated, or high) leave their children to feel confused and insecure. An adaptive child of an ignoring parent may demand information by crying, clinging, fighting with siblings, or hitting the parent. They are desperate for the parental attention to teach them and keep them safe. A more passive child may become increasingly inhibited in their exploration of the world. We need to consider possible modeling failures when such child reaction patterns are the complaint, and remember that the adverse model may not be in the room, requiring us to ask, “What other adult models does he see?”
Studies have shown that infants learn resilience when experiencing “mistakes” in parent-infant interaction; learning how to tolerate and repair an interaction that is not perfect. This is really good news for parents who feel that they must be perfect models for their children! For parents of anxious or obsessive children, I sometimes prescribe making mistakes and saying “Oh well,” as well as rewarding the child when they can say “Oh well” themselves. No child is too old to benefit from observing a parent apologize sincerely for a mistake.
Language is modeled, right down to accent. But when parents complain about their child cussing, raising their voice in anger, having an “attitude,” or “talking back,” it is worth asking (parent and child) “Where do you think they/you have heard talk like that?” It may be childcare providers, peers, TV, video games or online media (all of which may warrant a change), but it also may reflect interactions at home.
Children make stronger memories when emotions are high as these may signal danger, making recall more salient to survival. This salience helps explain the lasting detriments to learning and health of growing up with psychological abuse, marital discord, partner violence, mental illness, or criminal behavior (among the Adverse Childhood Experiences). Such experiences cause stress and a sense of the world as a dangerous place, but also become models for the child’s own later relationships as adults. While unavoidable, they can be buffered by parents’ explaining them and providing alternative positive modeling.
Watching the parent conduct their craft, a key component of apprenticeship and family businesses in the past, has been replaced by YouTube and avatars for learning physical skills. But “modeling the process” of pride in craftsmanship, persistence in a task, and recovering and starting over when things go awry are omitted from training videos. These are good reasons to assure that parents do chores, crafts, cooking, or camping with their children as some things will surely go wrong, giving parents the chance to model resilience and problem solving!
Although teens may protest conversations and activities, they are watching their parents for how to be a spouse, a neighbor, a friend, a leader, a citizen. Parents, who may be cutting their teens loose, need to continue to expect/require participation in family meals and outings. Those are opportunities to model adult-level interactions with each other and with the community as well as to talk about their activities at work, in volunteering, in charity, and in religious practice. The moral development of the adolescent is shaped by what they see to the degree that when parents state one moral code but violate it themselves (for example, cheating on taxes, running red lights), the teen is less likely to follow the principles long term that the parents have verbalized.
Parents often relate to us as though we were their own parents. While this “projection” can interfere with disclosure on touchy subjects, it is also an opportunity for us to model ways of relating and reacting from sympathizing with the 4-year-old screaming about vaccines to asking an 8-year-old why he thinks his parents are getting a divorce.
Parenting (and being a pediatrician) is an opportunity to enjoy reliving your youth or to get a “do over” of parts you would like to have different for your child. Playfulness and silliness model joy for the child that can last a lifetime.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at [email protected].

Hospital managers identify barriers to antimicrobial stewardship
Antimicrobial stewardship programs are being introduced in hospitals internationally amidst the problem of escalating antimicrobial resistance. But sustained behavioral change in the area of antibiotic prescribing has been difficult to achieve.
While we have an understanding of doctors’ roles in antibiotic optimization within hospital contexts, the role of hospital management in successes or failures of antimicrobial stewardship programs (and optimization of antibiotics more broadly) has not been explored. Our new study published in the Journal of Hospital Infection examines this very question – the role of the manager as an enabler, or indeed a barrier, to antibiotic optimization.

Researchers in the study performed semistructured interviews with 23 hospital managers at three hospitals in two different states in Australia to specifically examine their opinions on antibiotic resistance, antibiotic governance, and their roles as senior management. The results illustrate how hospital managers prioritize financial pressures and immediate clinical demands over longer-term issues such as antibiotic prescribing and resistance. Here is an example of those pressures, described by one manager:
“I think the problem is [antimicrobial stewardship] in a competitive market. Are the waiting lists more newsworthy than antibiotic prescribing? Absolutely. You get more adverse events happening because of the waiting lists. … So, of course it’s not going to be the [antibiotic] prescribing that comes up to the top of that.” –Departmental Director
The study results also showed how managers find it challenging to comprehend, or act on the basis of, antibiotic-prescribing audits and had little faith in the value of data on antibiotic use and appropriateness. Other clinical areas with more clearly defined targets (and consequences for failing to meet targets) were prioritized over antibiotic prescribing in medical management decision making. Managers also found it difficult to influence the behavior of doctors and thought that it was a clinical responsibility to improve practice. In the words of one:
“I am a believer in delegated accountability and people on the shop floor knowing what they’re doing and being held accountable for it.” – Divisional Director

Managers perceived that there was limited accountability among doctors for antibiotic use and limited education and feedback to doctors:
“Those figures [on suboptimal prescribing] you give me, I haven’t heard them before. So, that in itself is a problem, and I would suggest you’d probably find a large number of medical staff haven’t been exposed to that.”
– Divisional Director
This study was performed in three hospitals with active antimicrobial stewardship programs. In Australia, as is becoming the pattern in countries within the Organisation for Economic Co-operation and Development (OECD), there is a legislative requirement for hospitals to have an effective antimicrobial stewardship program. And yet, meaningful sustained change in antibiotic prescribing is elusive, as evidenced by national antibiotic-prescribing data. The study results raise the important question of who is perceived as responsible for antibiotic-prescribing improvement and the actual and potential role of hospital managers in enacting change. It seems likely that both “top-down” influence (by managers and executive) and “bottom-up” influence (clinician-driven processes) will be required for effective and sustained practice change.
It is also clear from the results of this study that hospital managers do not perceive clear or immediate consequences for failing to improve antibiotic prescribing, and the perceived “distant” threat of antimicrobial resistance is not prioritized among other competing pressures. In addition, the widespread nature of antibiotic use makes it difficult to audit and even more difficult to communicate the extent of the problem.
These data would suggest that to move forward we need to look at an incentive structure for antibiotic-prescribing improvements or consequences in the short term for failing to optimize antibiotic use, and clearly defined goals for antibiotic optimization in hospitals.
Jennifer Broom, MBChB, PhD, is an infectious diseases physician at the Sunshine Coast Hospital and Health Service and an associate professor of medicine at the University of Queensland, Brisbane, Australia. Alex Broom, PhD, is professor of sociology in the School of Social Sciences at the University of New South Wales, Sydney.
Antimicrobial stewardship programs are being introduced in hospitals internationally amidst the problem of escalating antimicrobial resistance. But sustained behavioral change in the area of antibiotic prescribing has been difficult to achieve.
While we have an understanding of doctors’ roles in antibiotic optimization within hospital contexts, the role of hospital management in successes or failures of antimicrobial stewardship programs (and optimization of antibiotics more broadly) has not been explored. Our new study published in the Journal of Hospital Infection examines this very question – the role of the manager as an enabler, or indeed a barrier, to antibiotic optimization.
Researchers in the study performed semistructured interviews with 23 hospital managers at three hospitals in two different states in Australia to specifically examine their opinions on antibiotic resistance, antibiotic governance, and their roles as senior management. The results illustrate how hospital managers prioritize financial pressures and immediate clinical demands over longer-term issues such as antibiotic prescribing and resistance. Here is an example of those pressures, described by one manager:
“I think the problem is [antimicrobial stewardship] in a competitive market. Are the waiting lists more newsworthy than antibiotic prescribing? Absolutely. You get more adverse events happening because of the waiting lists. … So, of course it’s not going to be the [antibiotic] prescribing that comes up to the top of that.” –Departmental Director
The study results also showed how managers find it challenging to comprehend, or act on the basis of, antibiotic-prescribing audits and had little faith in the value of data on antibiotic use and appropriateness. Other clinical areas with more clearly defined targets (and consequences for failing to meet targets) were prioritized over antibiotic prescribing in medical management decision making. Managers also found it difficult to influence the behavior of doctors and thought that it was a clinical responsibility to improve practice. In the words of one:
“I am a believer in delegated accountability and people on the shop floor knowing what they’re doing and being held accountable for it.” – Divisional Director
Managers perceived that there was limited accountability among doctors for antibiotic use and limited education and feedback to doctors:
“Those figures [on suboptimal prescribing] you give me, I haven’t heard them before. So, that in itself is a problem, and I would suggest you’d probably find a large number of medical staff haven’t been exposed to that.”
– Divisional Director
This study was performed in three hospitals with active antimicrobial stewardship programs. In Australia, as is becoming the pattern in countries within the Organisation for Economic Co-operation and Development (OECD), there is a legislative requirement for hospitals to have an effective antimicrobial stewardship program. And yet, meaningful sustained change in antibiotic prescribing is elusive, as evidenced by national antibiotic-prescribing data. The study results raise the important question of who is perceived as responsible for antibiotic-prescribing improvement and the actual and potential role of hospital managers in enacting change. It seems likely that both “top-down” influence (by managers and executive) and “bottom-up” influence (clinician-driven processes) will be required for effective and sustained practice change.
It is also clear from the results of this study that hospital managers do not perceive clear or immediate consequences for failing to improve antibiotic prescribing, and the perceived “distant” threat of antimicrobial resistance is not prioritized among other competing pressures. In addition, the widespread nature of antibiotic use makes it difficult to audit and even more difficult to communicate the extent of the problem.
These data would suggest that to move forward we need to look at an incentive structure for antibiotic-prescribing improvements or consequences in the short term for failing to optimize antibiotic use, and clearly defined goals for antibiotic optimization in hospitals.
Jennifer Broom, MBChB, PhD, is an infectious diseases physician at the Sunshine Coast Hospital and Health Service and an associate professor of medicine at the University of Queensland, Brisbane, Australia. Alex Broom, PhD, is professor of sociology in the School of Social Sciences at the University of New South Wales, Sydney.
Antimicrobial stewardship programs are being introduced in hospitals internationally amidst the problem of escalating antimicrobial resistance. But sustained behavioral change in the area of antibiotic prescribing has been difficult to achieve.
While we have an understanding of doctors’ roles in antibiotic optimization within hospital contexts, the role of hospital management in successes or failures of antimicrobial stewardship programs (and optimization of antibiotics more broadly) has not been explored. Our new study published in the Journal of Hospital Infection examines this very question – the role of the manager as an enabler, or indeed a barrier, to antibiotic optimization.
Researchers in the study performed semistructured interviews with 23 hospital managers at three hospitals in two different states in Australia to specifically examine their opinions on antibiotic resistance, antibiotic governance, and their roles as senior management. The results illustrate how hospital managers prioritize financial pressures and immediate clinical demands over longer-term issues such as antibiotic prescribing and resistance. Here is an example of those pressures, described by one manager:
“I think the problem is [antimicrobial stewardship] in a competitive market. Are the waiting lists more newsworthy than antibiotic prescribing? Absolutely. You get more adverse events happening because of the waiting lists. … So, of course it’s not going to be the [antibiotic] prescribing that comes up to the top of that.” –Departmental Director
The study results also showed how managers find it challenging to comprehend, or act on the basis of, antibiotic-prescribing audits and had little faith in the value of data on antibiotic use and appropriateness. Other clinical areas with more clearly defined targets (and consequences for failing to meet targets) were prioritized over antibiotic prescribing in medical management decision making. Managers also found it difficult to influence the behavior of doctors and thought that it was a clinical responsibility to improve practice. In the words of one:
“I am a believer in delegated accountability and people on the shop floor knowing what they’re doing and being held accountable for it.” – Divisional Director
Managers perceived that there was limited accountability among doctors for antibiotic use and limited education and feedback to doctors:
“Those figures [on suboptimal prescribing] you give me, I haven’t heard them before. So, that in itself is a problem, and I would suggest you’d probably find a large number of medical staff haven’t been exposed to that.”
– Divisional Director
This study was performed in three hospitals with active antimicrobial stewardship programs. In Australia, as is becoming the pattern in countries within the Organisation for Economic Co-operation and Development (OECD), there is a legislative requirement for hospitals to have an effective antimicrobial stewardship program. And yet, meaningful sustained change in antibiotic prescribing is elusive, as evidenced by national antibiotic-prescribing data. The study results raise the important question of who is perceived as responsible for antibiotic-prescribing improvement and the actual and potential role of hospital managers in enacting change. It seems likely that both “top-down” influence (by managers and executive) and “bottom-up” influence (clinician-driven processes) will be required for effective and sustained practice change.
It is also clear from the results of this study that hospital managers do not perceive clear or immediate consequences for failing to improve antibiotic prescribing, and the perceived “distant” threat of antimicrobial resistance is not prioritized among other competing pressures. In addition, the widespread nature of antibiotic use makes it difficult to audit and even more difficult to communicate the extent of the problem.
These data would suggest that to move forward we need to look at an incentive structure for antibiotic-prescribing improvements or consequences in the short term for failing to optimize antibiotic use, and clearly defined goals for antibiotic optimization in hospitals.
Jennifer Broom, MBChB, PhD, is an infectious diseases physician at the Sunshine Coast Hospital and Health Service and an associate professor of medicine at the University of Queensland, Brisbane, Australia. Alex Broom, PhD, is professor of sociology in the School of Social Sciences at the University of New South Wales, Sydney.

CABG best for diabetes patients with CKD – or is it?
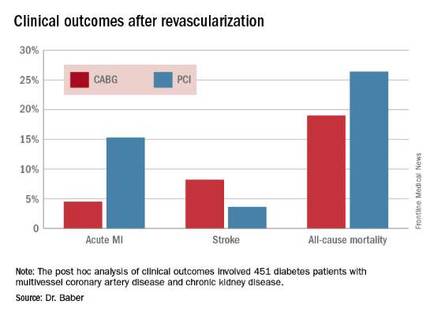
ROME – The use of coronary artery bypass graft surgery for revascularization in patients with multivessel CAD and comorbid diabetes plus chronic kidney disease was associated with a significantly lower risk of major cardiovascular and cerebrovascular events than was PCI with first-generation drug-eluting stents in a new secondary analysis from the landmark FREEDOM trial.
“The reason for this presentation is that even though chronic kidney disease is common in patients with diabetes, until now there has not been a large study of the efficacy and safety of coronary revascularization with drug-eluting stents versus CABG in this population in a randomized trial cohort,” explained Usman Baber, MD, who reported the results at the annual congress of the European Society of Cardiology.

FREEDOM (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease) randomized 1,900 diabetic patients with multivessel CAD to PCI or CABG. As previously reported, CABG proved superior to PCI, with a significantly lower rate of the composite primary endpoint composed of all-cause mortality, MI, or stroke (N Engl J Med. 2012 Dec 20;367[25]:2375-84).
Dr. Baber presented a post hoc analysis of the 451 FREEDOM participants with baseline comorbid chronic kidney disease (CKD). Their mean SYNTAX score was 27, and their mean baseline estimated glomerular filtration rate was 44 mL/min per 1.73 m2, indicative of mild to moderate CKD.
“Only 28 patients in the FREEDOM trial had an estimated GFR below 30, therefore we can’t make any inferences about revascularization in that setting, which I think is a completely different population,” he noted.
The 5-year rate of major adverse cardiovascular and cerebrovascular events in patients with CKD was 26% in the CABG group, an absolute 9.4% less than the 35.6% rate in subjects randomized to PCI.
Roughly one-quarter of FREEDOM participants had CKD. They fared significantly worse than did those without CKD. The 5-year incidence of major adverse cardiovascular and cerebrovascular events was 30.8% in patients with CKD and 20.1% in patients without renal impairment. In a multivariate analysis adjusted for age, gender, hypertension, peripheral vascular disease, and other potential confounders, the risk of all-cause mortality was twofold higher in the CKD group. Their risk of cardiac death was increased 1.8-fold, and they were at 1.9-fold increased risk for stroke. Interestingly, however, the acute MI risk did not differ between patients with or without CKD, Dr. Baber observed.
Drilling deeper into the data, the cardiologist reported that CABG was associated with significantly lower rates of MI and a nonsignificant trend for fewer deaths, but with a significantly higher stroke rate than PCI.
One audience member rose to complain that this information won’t be helpful in counseling his diabetic patients with CKD and multivessel CAD because the choices look so grim: a higher risk of MI with percutaneous therapy, and a greater risk of stroke with surgery.
Dr. Baber replied by pointing out that the 10.8% absolute reduction in the risk of MI with CABG compared with PCI was more than twice as large as the absolute 4.6% increase in stroke risk with surgery.

“Most people would say that a heart attack is an inconvenience, and a stroke is a life-changing experience for them and their family,” said session cochair Kim A. Williams, MD, professor of medicine and chairman of cardiology at Rush University Medical Center in Chicago.
At that, Dr. Baber backtracked a bit, observing that since this was a post hoc analysis, the FREEDOM findings in patients with CKD must be viewed as hypothesis-generating rather than definitive. And, of course, contemporary second-generation drug-eluting stents have a better risk/benefit profile than do those used in FREEDOM.
“The number needed to treat/number needed to harm ratio for CABG and PCI probably ends up being roughly equal. The pertinence of an analysis like this is if you look at real-world registry-based data, you find a therapeutic nihilism that’s highly prevalent in CKD patients, where many patients who might benefit are not provided with revascularization therapy. It’s clear that we as clinicians – either because we don’t know there is a benefit or we are too concerned about potential harm – deprive patients of a treatment that might be beneficial. This analysis makes clinicians who might be concerned feel somewhat comforted that there is not unacceptable harm and that there is benefit,” Dr. Baber said.
Follow-up of FREEDOM participants continues and will be the subject of future reports, he added.
The FREEDOM trial was sponsored by the National Heart, Lung and Blood Institute. Dr. Baber reported having no financial conflicts of interest.
ROME – The use of coronary artery bypass graft surgery for revascularization in patients with multivessel CAD and comorbid diabetes plus chronic kidney disease was associated with a significantly lower risk of major cardiovascular and cerebrovascular events than was PCI with first-generation drug-eluting stents in a new secondary analysis from the landmark FREEDOM trial.
“The reason for this presentation is that even though chronic kidney disease is common in patients with diabetes, until now there has not been a large study of the efficacy and safety of coronary revascularization with drug-eluting stents versus CABG in this population in a randomized trial cohort,” explained Usman Baber, MD, who reported the results at the annual congress of the European Society of Cardiology.
FREEDOM (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease) randomized 1,900 diabetic patients with multivessel CAD to PCI or CABG. As previously reported, CABG proved superior to PCI, with a significantly lower rate of the composite primary endpoint composed of all-cause mortality, MI, or stroke (N Engl J Med. 2012 Dec 20;367[25]:2375-84).
Dr. Baber presented a post hoc analysis of the 451 FREEDOM participants with baseline comorbid chronic kidney disease (CKD). Their mean SYNTAX score was 27, and their mean baseline estimated glomerular filtration rate was 44 mL/min per 1.73 m2, indicative of mild to moderate CKD.
“Only 28 patients in the FREEDOM trial had an estimated GFR below 30, therefore we can’t make any inferences about revascularization in that setting, which I think is a completely different population,” he noted.
The 5-year rate of major adverse cardiovascular and cerebrovascular events in patients with CKD was 26% in the CABG group, an absolute 9.4% less than the 35.6% rate in subjects randomized to PCI.
Roughly one-quarter of FREEDOM participants had CKD. They fared significantly worse than did those without CKD. The 5-year incidence of major adverse cardiovascular and cerebrovascular events was 30.8% in patients with CKD and 20.1% in patients without renal impairment. In a multivariate analysis adjusted for age, gender, hypertension, peripheral vascular disease, and other potential confounders, the risk of all-cause mortality was twofold higher in the CKD group. Their risk of cardiac death was increased 1.8-fold, and they were at 1.9-fold increased risk for stroke. Interestingly, however, the acute MI risk did not differ between patients with or without CKD, Dr. Baber observed.
Drilling deeper into the data, the cardiologist reported that CABG was associated with significantly lower rates of MI and a nonsignificant trend for fewer deaths, but with a significantly higher stroke rate than PCI.
One audience member rose to complain that this information won’t be helpful in counseling his diabetic patients with CKD and multivessel CAD because the choices look so grim: a higher risk of MI with percutaneous therapy, and a greater risk of stroke with surgery.
Dr. Baber replied by pointing out that the 10.8% absolute reduction in the risk of MI with CABG compared with PCI was more than twice as large as the absolute 4.6% increase in stroke risk with surgery.
“Most people would say that a heart attack is an inconvenience, and a stroke is a life-changing experience for them and their family,” said session cochair Kim A. Williams, MD, professor of medicine and chairman of cardiology at Rush University Medical Center in Chicago.
At that, Dr. Baber backtracked a bit, observing that since this was a post hoc analysis, the FREEDOM findings in patients with CKD must be viewed as hypothesis-generating rather than definitive. And, of course, contemporary second-generation drug-eluting stents have a better risk/benefit profile than do those used in FREEDOM.
“The number needed to treat/number needed to harm ratio for CABG and PCI probably ends up being roughly equal. The pertinence of an analysis like this is if you look at real-world registry-based data, you find a therapeutic nihilism that’s highly prevalent in CKD patients, where many patients who might benefit are not provided with revascularization therapy. It’s clear that we as clinicians – either because we don’t know there is a benefit or we are too concerned about potential harm – deprive patients of a treatment that might be beneficial. This analysis makes clinicians who might be concerned feel somewhat comforted that there is not unacceptable harm and that there is benefit,” Dr. Baber said.
Follow-up of FREEDOM participants continues and will be the subject of future reports, he added.
The FREEDOM trial was sponsored by the National Heart, Lung and Blood Institute. Dr. Baber reported having no financial conflicts of interest.
ROME – The use of coronary artery bypass graft surgery for revascularization in patients with multivessel CAD and comorbid diabetes plus chronic kidney disease was associated with a significantly lower risk of major cardiovascular and cerebrovascular events than was PCI with first-generation drug-eluting stents in a new secondary analysis from the landmark FREEDOM trial.
“The reason for this presentation is that even though chronic kidney disease is common in patients with diabetes, until now there has not been a large study of the efficacy and safety of coronary revascularization with drug-eluting stents versus CABG in this population in a randomized trial cohort,” explained Usman Baber, MD, who reported the results at the annual congress of the European Society of Cardiology.
FREEDOM (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease) randomized 1,900 diabetic patients with multivessel CAD to PCI or CABG. As previously reported, CABG proved superior to PCI, with a significantly lower rate of the composite primary endpoint composed of all-cause mortality, MI, or stroke (N Engl J Med. 2012 Dec 20;367[25]:2375-84).
Dr. Baber presented a post hoc analysis of the 451 FREEDOM participants with baseline comorbid chronic kidney disease (CKD). Their mean SYNTAX score was 27, and their mean baseline estimated glomerular filtration rate was 44 mL/min per 1.73 m2, indicative of mild to moderate CKD.
“Only 28 patients in the FREEDOM trial had an estimated GFR below 30, therefore we can’t make any inferences about revascularization in that setting, which I think is a completely different population,” he noted.
The 5-year rate of major adverse cardiovascular and cerebrovascular events in patients with CKD was 26% in the CABG group, an absolute 9.4% less than the 35.6% rate in subjects randomized to PCI.
Roughly one-quarter of FREEDOM participants had CKD. They fared significantly worse than did those without CKD. The 5-year incidence of major adverse cardiovascular and cerebrovascular events was 30.8% in patients with CKD and 20.1% in patients without renal impairment. In a multivariate analysis adjusted for age, gender, hypertension, peripheral vascular disease, and other potential confounders, the risk of all-cause mortality was twofold higher in the CKD group. Their risk of cardiac death was increased 1.8-fold, and they were at 1.9-fold increased risk for stroke. Interestingly, however, the acute MI risk did not differ between patients with or without CKD, Dr. Baber observed.
Drilling deeper into the data, the cardiologist reported that CABG was associated with significantly lower rates of MI and a nonsignificant trend for fewer deaths, but with a significantly higher stroke rate than PCI.
One audience member rose to complain that this information won’t be helpful in counseling his diabetic patients with CKD and multivessel CAD because the choices look so grim: a higher risk of MI with percutaneous therapy, and a greater risk of stroke with surgery.
Dr. Baber replied by pointing out that the 10.8% absolute reduction in the risk of MI with CABG compared with PCI was more than twice as large as the absolute 4.6% increase in stroke risk with surgery.
“Most people would say that a heart attack is an inconvenience, and a stroke is a life-changing experience for them and their family,” said session cochair Kim A. Williams, MD, professor of medicine and chairman of cardiology at Rush University Medical Center in Chicago.
At that, Dr. Baber backtracked a bit, observing that since this was a post hoc analysis, the FREEDOM findings in patients with CKD must be viewed as hypothesis-generating rather than definitive. And, of course, contemporary second-generation drug-eluting stents have a better risk/benefit profile than do those used in FREEDOM.
“The number needed to treat/number needed to harm ratio for CABG and PCI probably ends up being roughly equal. The pertinence of an analysis like this is if you look at real-world registry-based data, you find a therapeutic nihilism that’s highly prevalent in CKD patients, where many patients who might benefit are not provided with revascularization therapy. It’s clear that we as clinicians – either because we don’t know there is a benefit or we are too concerned about potential harm – deprive patients of a treatment that might be beneficial. This analysis makes clinicians who might be concerned feel somewhat comforted that there is not unacceptable harm and that there is benefit,” Dr. Baber said.
Follow-up of FREEDOM participants continues and will be the subject of future reports, he added.
The FREEDOM trial was sponsored by the National Heart, Lung and Blood Institute. Dr. Baber reported having no financial conflicts of interest.
AT THE ESC CONGRESS 2016
Key clinical point: Coronary artery bypass graft surgery resulted in fewer myocardial infarctions but more strokes than did percutaneous coronary intervention at 5 years of follow-up in diabetic patients with multivessel coronary artery disease and chronic kidney disease.
Major finding: The cumulative MI rates in patients randomized to CABG versus PCI were 4.5% and 15.3%, respectively, while the stroke rates were 8.2% versus 3.6%.
Data source: A post hoc analysis of clinical outcomes in 451 diabetic patients with multivessel CAD and chronic kidney disease who were randomized to CABG or PCI in the prospective multicenter FREEDOM trial.
Disclosures: The FREEDOM trial was sponsored by the National Heart, Lung, and Blood Institute. The presenter reported having no financial conflicts of interest.

Parkinson’s cell transplant trials require better standardization
PORTLAND, ORE. – Implantation of dopamine-producing cells to replace those lost in the substantia nigra has been seen as the cure for Parkinson’s disease, with many attempts in patients over the years. Along the way, a few successes have occurred, but in general, cell-based therapies have produced mixed results.
“When it works well, it works very well with fetal dopamine cells, but it does not always work well,” said Roger Barker, MBBS, PhD, of the department of clinical neurosciences at the University of Cambridge (England). In his lecture to a large, capacity crowd at the World Parkinson Congress, he reviewed the field going back more than three decades and drew “lessons learned” from the results of animal experiments and human trials.

He said dopamine-producing cell therapy will never cure the disease, although it works well early in the disease “but creates problems later,” with off-target and nonphysiologic effects in other parts of the brain, such as overstimulation. One exception was the use of fetal dopamine cells in an animal model, showing that cells could survive long-term, connect and integrate into the brain, release dopamine, and restore behaviors to normal if cells from the same species were used at the right developmental stage of the animal and implanted where dopamine normally works, that is, in the striatum.
Other problems reported from human trials using embryonic dopamine neurons or fetal nigral transplants have been graft-induced dyskinesias, but without clinical benefit, as well as Lewy bodies in grafted neurons, suggesting host-to-graft disease propagation. However, in another report, a patient had a clinical benefit and showed extensive graft-derived dopaminergic innervation 24 years after transplantation, at which time the patient died.
Lessons learned over time
Dr. Barker explained that the variable results that have been achieved in various trials using different protocols and nonstandardized approaches over the years make it “extremely difficult to make any conclusions.” These variations included performing tests on different kinds of patients and using different doses of cells, delivery approaches, immunosuppression, primary endpoints of the trials, and levels of follow-up.
The age of the patient, disease stage, and graft technique emerged as key issues in data gathered from the trials, he said. The best chance of success occurred in younger patients with less advanced disease, when grafting occurred across the whole striatum evenly, and when contamination with 5-hydroxytryptamine (serotonin) neurons was avoided.
Going forward, trials in Parkinson’s disease are planned or underway using embryonic/fetal stem cells or adult stem cells. Such cells provide logistical advantages in that their differentiation can be controlled more easily and they are a defined product. Nigral dopaminergic cells can be produced from human embryonic stem cells that behave like human fetal ventral midbrain dopamine cells in vitro and in vivo in rats and show similar efficacy and potency.
The Center for iPS Cell Research and Application in Kyoto, Japan, will conduct a trial using induced pluripotent stem (iPS) cells beginning next year, the New York State Stem Cell Science Consortia (NYSTEM) will use human embryonic stem cells beginning in 2018, and around the same time the European Union’s NeuroStemCellRepair network will also use human embryonic stem cells. In addition, the European TRANSEURO trial, coordinated by Dr. Barker, is planning a single-arm, multicenter, dose-escalation trial for 2018/2019 using intracerebral neurotransplantation of dopaminergic neurons derived from human embryonic stem cells. Participating patients will be younger than 65 years with less than 10 years disease duration, no significant levodopa-induced dyskinesia, and no cognitive or psychiatric problems.
From these trials, scientists hope to eventually produce a human embryonic stem cell–derived dopaminergic cell product made under GMP (good manufacturing practice) conditions that can be tested for safety and efficacy and put into clinical trials, with an ultimate goal of production and commercialization.
Finally, Dr. Barker alerted physicians to published guidance from the International Society for Stem Cell Research that can help them critically evaluate any cell-based clinical trial that they may be asked to run. And for patients, large numbers of whom attended the conference, he advised avoiding any “trial” that would charge them to participate because legitimate research trials do not charge for experimental therapies.
Asked to comment on the field, Peter LeWitt, MD, director of the Parkinson’s Disease and Movement Disorders Program at Henry Ford Hospital, West Bloomfield, Mich., and professor of neurology at Wayne State University, Detroit, said, “The jury is out and is coming back on stem cells and its alternative, such as fetal tissue. It’s pointing to the bright future of restoring the brain and not just using drugs to mask symptoms.”
He said the critical review of evidence from past trials “sounds like it’s heading towards a more focused view of how to enhance the successes that have occurred already – the 24-year outcomes [of] the patients who have met all biological plausibility improvements at this point. ... The science has moved along to improve their techniques of judging success and failure and sorting out partial benefits.”
Dr. Barker reported that he sits on an advisory board of Teva-Lundbeck and has advised and received honoraria from Solvay, GSK, Eli Lilly, and Pfizer, receives royalties from Springer, Wiley, and Cambridge University Press, and receives grant support from various institutes and foundations, Dr. LeWitt reported no relevant conflicts of interest.
PORTLAND, ORE. – Implantation of dopamine-producing cells to replace those lost in the substantia nigra has been seen as the cure for Parkinson’s disease, with many attempts in patients over the years. Along the way, a few successes have occurred, but in general, cell-based therapies have produced mixed results.
“When it works well, it works very well with fetal dopamine cells, but it does not always work well,” said Roger Barker, MBBS, PhD, of the department of clinical neurosciences at the University of Cambridge (England). In his lecture to a large, capacity crowd at the World Parkinson Congress, he reviewed the field going back more than three decades and drew “lessons learned” from the results of animal experiments and human trials.
He said dopamine-producing cell therapy will never cure the disease, although it works well early in the disease “but creates problems later,” with off-target and nonphysiologic effects in other parts of the brain, such as overstimulation. One exception was the use of fetal dopamine cells in an animal model, showing that cells could survive long-term, connect and integrate into the brain, release dopamine, and restore behaviors to normal if cells from the same species were used at the right developmental stage of the animal and implanted where dopamine normally works, that is, in the striatum.
Other problems reported from human trials using embryonic dopamine neurons or fetal nigral transplants have been graft-induced dyskinesias, but without clinical benefit, as well as Lewy bodies in grafted neurons, suggesting host-to-graft disease propagation. However, in another report, a patient had a clinical benefit and showed extensive graft-derived dopaminergic innervation 24 years after transplantation, at which time the patient died.
Lessons learned over time
Dr. Barker explained that the variable results that have been achieved in various trials using different protocols and nonstandardized approaches over the years make it “extremely difficult to make any conclusions.” These variations included performing tests on different kinds of patients and using different doses of cells, delivery approaches, immunosuppression, primary endpoints of the trials, and levels of follow-up.
The age of the patient, disease stage, and graft technique emerged as key issues in data gathered from the trials, he said. The best chance of success occurred in younger patients with less advanced disease, when grafting occurred across the whole striatum evenly, and when contamination with 5-hydroxytryptamine (serotonin) neurons was avoided.
Going forward, trials in Parkinson’s disease are planned or underway using embryonic/fetal stem cells or adult stem cells. Such cells provide logistical advantages in that their differentiation can be controlled more easily and they are a defined product. Nigral dopaminergic cells can be produced from human embryonic stem cells that behave like human fetal ventral midbrain dopamine cells in vitro and in vivo in rats and show similar efficacy and potency.
The Center for iPS Cell Research and Application in Kyoto, Japan, will conduct a trial using induced pluripotent stem (iPS) cells beginning next year, the New York State Stem Cell Science Consortia (NYSTEM) will use human embryonic stem cells beginning in 2018, and around the same time the European Union’s NeuroStemCellRepair network will also use human embryonic stem cells. In addition, the European TRANSEURO trial, coordinated by Dr. Barker, is planning a single-arm, multicenter, dose-escalation trial for 2018/2019 using intracerebral neurotransplantation of dopaminergic neurons derived from human embryonic stem cells. Participating patients will be younger than 65 years with less than 10 years disease duration, no significant levodopa-induced dyskinesia, and no cognitive or psychiatric problems.
From these trials, scientists hope to eventually produce a human embryonic stem cell–derived dopaminergic cell product made under GMP (good manufacturing practice) conditions that can be tested for safety and efficacy and put into clinical trials, with an ultimate goal of production and commercialization.
Finally, Dr. Barker alerted physicians to published guidance from the International Society for Stem Cell Research that can help them critically evaluate any cell-based clinical trial that they may be asked to run. And for patients, large numbers of whom attended the conference, he advised avoiding any “trial” that would charge them to participate because legitimate research trials do not charge for experimental therapies.
Asked to comment on the field, Peter LeWitt, MD, director of the Parkinson’s Disease and Movement Disorders Program at Henry Ford Hospital, West Bloomfield, Mich., and professor of neurology at Wayne State University, Detroit, said, “The jury is out and is coming back on stem cells and its alternative, such as fetal tissue. It’s pointing to the bright future of restoring the brain and not just using drugs to mask symptoms.”
He said the critical review of evidence from past trials “sounds like it’s heading towards a more focused view of how to enhance the successes that have occurred already – the 24-year outcomes [of] the patients who have met all biological plausibility improvements at this point. ... The science has moved along to improve their techniques of judging success and failure and sorting out partial benefits.”
Dr. Barker reported that he sits on an advisory board of Teva-Lundbeck and has advised and received honoraria from Solvay, GSK, Eli Lilly, and Pfizer, receives royalties from Springer, Wiley, and Cambridge University Press, and receives grant support from various institutes and foundations, Dr. LeWitt reported no relevant conflicts of interest.
PORTLAND, ORE. – Implantation of dopamine-producing cells to replace those lost in the substantia nigra has been seen as the cure for Parkinson’s disease, with many attempts in patients over the years. Along the way, a few successes have occurred, but in general, cell-based therapies have produced mixed results.
“When it works well, it works very well with fetal dopamine cells, but it does not always work well,” said Roger Barker, MBBS, PhD, of the department of clinical neurosciences at the University of Cambridge (England). In his lecture to a large, capacity crowd at the World Parkinson Congress, he reviewed the field going back more than three decades and drew “lessons learned” from the results of animal experiments and human trials.
He said dopamine-producing cell therapy will never cure the disease, although it works well early in the disease “but creates problems later,” with off-target and nonphysiologic effects in other parts of the brain, such as overstimulation. One exception was the use of fetal dopamine cells in an animal model, showing that cells could survive long-term, connect and integrate into the brain, release dopamine, and restore behaviors to normal if cells from the same species were used at the right developmental stage of the animal and implanted where dopamine normally works, that is, in the striatum.
Other problems reported from human trials using embryonic dopamine neurons or fetal nigral transplants have been graft-induced dyskinesias, but without clinical benefit, as well as Lewy bodies in grafted neurons, suggesting host-to-graft disease propagation. However, in another report, a patient had a clinical benefit and showed extensive graft-derived dopaminergic innervation 24 years after transplantation, at which time the patient died.
Lessons learned over time
Dr. Barker explained that the variable results that have been achieved in various trials using different protocols and nonstandardized approaches over the years make it “extremely difficult to make any conclusions.” These variations included performing tests on different kinds of patients and using different doses of cells, delivery approaches, immunosuppression, primary endpoints of the trials, and levels of follow-up.
The age of the patient, disease stage, and graft technique emerged as key issues in data gathered from the trials, he said. The best chance of success occurred in younger patients with less advanced disease, when grafting occurred across the whole striatum evenly, and when contamination with 5-hydroxytryptamine (serotonin) neurons was avoided.
Going forward, trials in Parkinson’s disease are planned or underway using embryonic/fetal stem cells or adult stem cells. Such cells provide logistical advantages in that their differentiation can be controlled more easily and they are a defined product. Nigral dopaminergic cells can be produced from human embryonic stem cells that behave like human fetal ventral midbrain dopamine cells in vitro and in vivo in rats and show similar efficacy and potency.
The Center for iPS Cell Research and Application in Kyoto, Japan, will conduct a trial using induced pluripotent stem (iPS) cells beginning next year, the New York State Stem Cell Science Consortia (NYSTEM) will use human embryonic stem cells beginning in 2018, and around the same time the European Union’s NeuroStemCellRepair network will also use human embryonic stem cells. In addition, the European TRANSEURO trial, coordinated by Dr. Barker, is planning a single-arm, multicenter, dose-escalation trial for 2018/2019 using intracerebral neurotransplantation of dopaminergic neurons derived from human embryonic stem cells. Participating patients will be younger than 65 years with less than 10 years disease duration, no significant levodopa-induced dyskinesia, and no cognitive or psychiatric problems.
From these trials, scientists hope to eventually produce a human embryonic stem cell–derived dopaminergic cell product made under GMP (good manufacturing practice) conditions that can be tested for safety and efficacy and put into clinical trials, with an ultimate goal of production and commercialization.
Finally, Dr. Barker alerted physicians to published guidance from the International Society for Stem Cell Research that can help them critically evaluate any cell-based clinical trial that they may be asked to run. And for patients, large numbers of whom attended the conference, he advised avoiding any “trial” that would charge them to participate because legitimate research trials do not charge for experimental therapies.
Asked to comment on the field, Peter LeWitt, MD, director of the Parkinson’s Disease and Movement Disorders Program at Henry Ford Hospital, West Bloomfield, Mich., and professor of neurology at Wayne State University, Detroit, said, “The jury is out and is coming back on stem cells and its alternative, such as fetal tissue. It’s pointing to the bright future of restoring the brain and not just using drugs to mask symptoms.”
He said the critical review of evidence from past trials “sounds like it’s heading towards a more focused view of how to enhance the successes that have occurred already – the 24-year outcomes [of] the patients who have met all biological plausibility improvements at this point. ... The science has moved along to improve their techniques of judging success and failure and sorting out partial benefits.”
Dr. Barker reported that he sits on an advisory board of Teva-Lundbeck and has advised and received honoraria from Solvay, GSK, Eli Lilly, and Pfizer, receives royalties from Springer, Wiley, and Cambridge University Press, and receives grant support from various institutes and foundations, Dr. LeWitt reported no relevant conflicts of interest.
EXPERT ANALYSIS FROM WPC 2016

Americas are declared measles free by PAHO
The Americas are measles free.
The region is the first in the world to have eradicated the disease, according to Pan-American Health Organization officials who spoke during a media briefing.
“Bye-bye measles,” said PAHO director Carissa F. Etienne, MD, during the briefing.

In 1994, countries across the Americas collectively declared their determination to rid the region of endemic measles transmission by 2000, agreeing to implement PAHO-recommended surveillance and immunization strategies, including the introduction and expanded use of the triple viral vaccine (MMR) against measles, mumps, and rubella.
In 2007, an expert international committee began verifying absence of the disease regionally. Although the disease was largely thought to have been wiped out in the Americas by 2002, officials postponed making an announcement until elimination of both measles and rubella could be declared jointly. An outbreak of measles in 2013 thwarted this plan, with the last confirmed case of reported endemic measles in the Americas not occurring until July 2015 in Brazil. In all, five vaccine-preventable diseases have been eliminated in the region, according to PAHO: smallpox in 1971, polio in 1994, and rubella and congenital rubella syndrome in 2015.
“The tasks of verification was not without its challenges, and countries overcame a number of geopolitical difficulties, including [maintaining] high vaccination coverage for very mobile populations, limited – and often no – access to deprived areas, and the presence of conflict situations,” Merceline Dahl-Regis, MD, the Bahamas’ chief medical officer and chair of PAHO’s elimination verification committee, said during the media briefing. She credited the expansion of national immunization programs, the “stellar work” conducted by various national commissions, and excellent communication between the nations’ respective governments, local and federal, as critical to the success of the effort. Also credited by other officials is PAHO’s revolving vaccine fund, which provides five-dose vials of MMR for about 1 dollar each.
Globally, since use of the MMR vaccine began, there has been a 95% drop in cases over a 35-year period, from 4.5 million cases in 1980 to approximately 244,700 in 2015. At the time the initiative to eradicate the disease was announced, measles was among the top five most common killers of children under the age of 5 years worldwide. The vaccine-preventable disease took the lives of 114,900 children globally in 2014, according to the World Health Organization. Worldwide, about 85% of children are vaccinated against measles by their first birthday, up from 73% in 2000.
Keeping vaccination rates high and immediately reporting any imported cases of the disease are essential to maintaining this milestone, according to PAHO officials.
“Importation of measles from other parts of the world into the Americas will continue, and we must be ready to detect and respond quickly, but today, let us celebrate,” Capt. Mary Agocs, MD, a Red Cross senior adviser to the elimination initiative, said during the briefing.
On Twitter @whitneymcknight
The Americas are measles free.
The region is the first in the world to have eradicated the disease, according to Pan-American Health Organization officials who spoke during a media briefing.
“Bye-bye measles,” said PAHO director Carissa F. Etienne, MD, during the briefing.
In 1994, countries across the Americas collectively declared their determination to rid the region of endemic measles transmission by 2000, agreeing to implement PAHO-recommended surveillance and immunization strategies, including the introduction and expanded use of the triple viral vaccine (MMR) against measles, mumps, and rubella.
In 2007, an expert international committee began verifying absence of the disease regionally. Although the disease was largely thought to have been wiped out in the Americas by 2002, officials postponed making an announcement until elimination of both measles and rubella could be declared jointly. An outbreak of measles in 2013 thwarted this plan, with the last confirmed case of reported endemic measles in the Americas not occurring until July 2015 in Brazil. In all, five vaccine-preventable diseases have been eliminated in the region, according to PAHO: smallpox in 1971, polio in 1994, and rubella and congenital rubella syndrome in 2015.
“The tasks of verification was not without its challenges, and countries overcame a number of geopolitical difficulties, including [maintaining] high vaccination coverage for very mobile populations, limited – and often no – access to deprived areas, and the presence of conflict situations,” Merceline Dahl-Regis, MD, the Bahamas’ chief medical officer and chair of PAHO’s elimination verification committee, said during the media briefing. She credited the expansion of national immunization programs, the “stellar work” conducted by various national commissions, and excellent communication between the nations’ respective governments, local and federal, as critical to the success of the effort. Also credited by other officials is PAHO’s revolving vaccine fund, which provides five-dose vials of MMR for about 1 dollar each.
Globally, since use of the MMR vaccine began, there has been a 95% drop in cases over a 35-year period, from 4.5 million cases in 1980 to approximately 244,700 in 2015. At the time the initiative to eradicate the disease was announced, measles was among the top five most common killers of children under the age of 5 years worldwide. The vaccine-preventable disease took the lives of 114,900 children globally in 2014, according to the World Health Organization. Worldwide, about 85% of children are vaccinated against measles by their first birthday, up from 73% in 2000.
Keeping vaccination rates high and immediately reporting any imported cases of the disease are essential to maintaining this milestone, according to PAHO officials.
“Importation of measles from other parts of the world into the Americas will continue, and we must be ready to detect and respond quickly, but today, let us celebrate,” Capt. Mary Agocs, MD, a Red Cross senior adviser to the elimination initiative, said during the briefing.
On Twitter @whitneymcknight
The Americas are measles free.
The region is the first in the world to have eradicated the disease, according to Pan-American Health Organization officials who spoke during a media briefing.
“Bye-bye measles,” said PAHO director Carissa F. Etienne, MD, during the briefing.
In 1994, countries across the Americas collectively declared their determination to rid the region of endemic measles transmission by 2000, agreeing to implement PAHO-recommended surveillance and immunization strategies, including the introduction and expanded use of the triple viral vaccine (MMR) against measles, mumps, and rubella.
In 2007, an expert international committee began verifying absence of the disease regionally. Although the disease was largely thought to have been wiped out in the Americas by 2002, officials postponed making an announcement until elimination of both measles and rubella could be declared jointly. An outbreak of measles in 2013 thwarted this plan, with the last confirmed case of reported endemic measles in the Americas not occurring until July 2015 in Brazil. In all, five vaccine-preventable diseases have been eliminated in the region, according to PAHO: smallpox in 1971, polio in 1994, and rubella and congenital rubella syndrome in 2015.
“The tasks of verification was not without its challenges, and countries overcame a number of geopolitical difficulties, including [maintaining] high vaccination coverage for very mobile populations, limited – and often no – access to deprived areas, and the presence of conflict situations,” Merceline Dahl-Regis, MD, the Bahamas’ chief medical officer and chair of PAHO’s elimination verification committee, said during the media briefing. She credited the expansion of national immunization programs, the “stellar work” conducted by various national commissions, and excellent communication between the nations’ respective governments, local and federal, as critical to the success of the effort. Also credited by other officials is PAHO’s revolving vaccine fund, which provides five-dose vials of MMR for about 1 dollar each.
Globally, since use of the MMR vaccine began, there has been a 95% drop in cases over a 35-year period, from 4.5 million cases in 1980 to approximately 244,700 in 2015. At the time the initiative to eradicate the disease was announced, measles was among the top five most common killers of children under the age of 5 years worldwide. The vaccine-preventable disease took the lives of 114,900 children globally in 2014, according to the World Health Organization. Worldwide, about 85% of children are vaccinated against measles by their first birthday, up from 73% in 2000.
Keeping vaccination rates high and immediately reporting any imported cases of the disease are essential to maintaining this milestone, according to PAHO officials.
“Importation of measles from other parts of the world into the Americas will continue, and we must be ready to detect and respond quickly, but today, let us celebrate,” Capt. Mary Agocs, MD, a Red Cross senior adviser to the elimination initiative, said during the briefing.
On Twitter @whitneymcknight
FROM A PAHO MEDIA BRIEFING

Aspirin not prescribed appropriately to cut cardiovascular risk in diabetes
MUNICH – Many patients with diabetes who could benefit from low-dose aspirin therapy may not be getting it – and many who are getting aspirin should not be, according to data presented at the annual meeting of the European Association for the Study of Diabetes.
A large, randomized trial concluded that 21% of diabetes patients who qualified for aspirin therapy for cardiovascular risk reduction were not getting it, and that it was contraindicated in almost 60% of those who were taking it, Lauren Crain, PhD, reported at the meeting.

Balancing the risks and benefits of aspirin therapy is not an easy challenge, said Dr. Crain, a health behavior researcher at HealthPartners Institute, Minneapolis. The clinical information necessary for the assessment is “rather lengthy, and not always readily available in primary care settings,” she said, and it’s clear from this study that clinicians could use some help in this area. Unfortunately, the electronic algorithm tested, which was meant to improve appropriate aspirin prescribing, didn’t improve the situation very much.
“At the final visit in the diabetes group [after the algorithm was employed], the total proportion of patients using aspirin was higher than at the first visit,” Dr. Crain noted. “However, that was the case regardless of whether patients were over- or underusing aspirin at the first visit.”
The aspirin findings were part of a large, randomized trial testing the algorithm as a way to reduce cardiovascular risk factors. The study was conducted in 19 primary care practices.
The decision-making algorithm, Cardiovascular Wizard, uses electronic health records to identify and advise patients with uncontrolled cardiovascular risk factors. Priorities and clinical recommendations are displayed for the provider and patient in the hope of facilitating shared decision making, Dr. Crain said.
One of the Wizard’s algorithms concerns aspirin prescribing. It is programmed with data from the United States Preventive Services Task Force, and recommends aspirin if cardiovascular risk scores are high and if consistent with providing a benefit greater than the risk of gastrointestinal bleeding. Aspirin is not recommended if the benefit is determined to be low or if major contraindications are present, including anticoagulant use or history of intracerebral hemorrhage.
The tool also alerts providers to the presence of other potential risks including aspirin allergy or intolerance, history of GI bleeds or risk conditions, and the concomitant use of nonsteroidal anti-inflammatory drugs.
The study comprised 11,000 adults, 4,000 of whom had diabetes. The remainder had high-risk, reversible cardiovascular risk factors (hypertension, dyslipidemia, or tobacco use). Each group was randomized to either cardiovascular risk assessment by usual care or with the Cardiovascular Wizard program.
The aspirin substudy looked at aspirin use at the baseline visit and the patient’s final, 1-year follow-up visit. At both visits, aspirin use was documented, and the clinician used the Wizard to assess whether or not it was indicated.
At the baseline visit, 71% of the diabetes group was using aspirin. However, according to the Wizard tool, more than one-third of them should not have been taking it – and among these, 57% were doing so. Among the remaining two-thirds of patients, all of whom should have been using aspirin, 21% were not taking it, Dr. Crain said.
Among the patients with reversible high-risk factors, 27% were using aspirin. However, according to the Wizard tool, the drug was contraindicated in 34% of those patients. “Most importantly, however, among those for whom aspirin was indicated, only 25% were using it – so, we’re talking about a 75% underusage,” Dr. Crain said.
By the 1-year follow-up visit, the situation was not much changed, despite the tool’s recommendations. Among those with diabetes, 56% in the usual care group and 60% in Wizard group were still overusing aspirin. Underuse was occurring in 21% of the usual care group and 17% of the Wizard group.
Patients with reversible high-risk factors fared a little better at 1 year, especially those who, at baseline, should have been taking aspirin but were not. Among these, 10% in the usual care group and 13% in the Wizard group had started taking aspirin.
The results were a bit of a disappointment, Dr. Crain said, but they don’t invalidate the investigators’ faith in an algorithmic advising system.
“We do think that electronic health record tools like this can help providers follow guidelines and improve the quality of their aspirin recommendations and prescribing, and hopefully reduce cardiovascular events and aspirin-related hazards,” she said. “Unfortunately, that didn’t happen here in the diabetes patients,” and the results in the second group were not stellar.
She added that the Wizard development team will be tweaking the tool to clarify some of the choices available as it guides patients and providers through the algorithm, in hopes of improving its efficacy.
Dr. Crain made no financial disclosures.
On Twitter @alz_gal
MUNICH – Many patients with diabetes who could benefit from low-dose aspirin therapy may not be getting it – and many who are getting aspirin should not be, according to data presented at the annual meeting of the European Association for the Study of Diabetes.
A large, randomized trial concluded that 21% of diabetes patients who qualified for aspirin therapy for cardiovascular risk reduction were not getting it, and that it was contraindicated in almost 60% of those who were taking it, Lauren Crain, PhD, reported at the meeting.
Balancing the risks and benefits of aspirin therapy is not an easy challenge, said Dr. Crain, a health behavior researcher at HealthPartners Institute, Minneapolis. The clinical information necessary for the assessment is “rather lengthy, and not always readily available in primary care settings,” she said, and it’s clear from this study that clinicians could use some help in this area. Unfortunately, the electronic algorithm tested, which was meant to improve appropriate aspirin prescribing, didn’t improve the situation very much.
“At the final visit in the diabetes group [after the algorithm was employed], the total proportion of patients using aspirin was higher than at the first visit,” Dr. Crain noted. “However, that was the case regardless of whether patients were over- or underusing aspirin at the first visit.”
The aspirin findings were part of a large, randomized trial testing the algorithm as a way to reduce cardiovascular risk factors. The study was conducted in 19 primary care practices.
The decision-making algorithm, Cardiovascular Wizard, uses electronic health records to identify and advise patients with uncontrolled cardiovascular risk factors. Priorities and clinical recommendations are displayed for the provider and patient in the hope of facilitating shared decision making, Dr. Crain said.
One of the Wizard’s algorithms concerns aspirin prescribing. It is programmed with data from the United States Preventive Services Task Force, and recommends aspirin if cardiovascular risk scores are high and if consistent with providing a benefit greater than the risk of gastrointestinal bleeding. Aspirin is not recommended if the benefit is determined to be low or if major contraindications are present, including anticoagulant use or history of intracerebral hemorrhage.
The tool also alerts providers to the presence of other potential risks including aspirin allergy or intolerance, history of GI bleeds or risk conditions, and the concomitant use of nonsteroidal anti-inflammatory drugs.
The study comprised 11,000 adults, 4,000 of whom had diabetes. The remainder had high-risk, reversible cardiovascular risk factors (hypertension, dyslipidemia, or tobacco use). Each group was randomized to either cardiovascular risk assessment by usual care or with the Cardiovascular Wizard program.
The aspirin substudy looked at aspirin use at the baseline visit and the patient’s final, 1-year follow-up visit. At both visits, aspirin use was documented, and the clinician used the Wizard to assess whether or not it was indicated.
At the baseline visit, 71% of the diabetes group was using aspirin. However, according to the Wizard tool, more than one-third of them should not have been taking it – and among these, 57% were doing so. Among the remaining two-thirds of patients, all of whom should have been using aspirin, 21% were not taking it, Dr. Crain said.
Among the patients with reversible high-risk factors, 27% were using aspirin. However, according to the Wizard tool, the drug was contraindicated in 34% of those patients. “Most importantly, however, among those for whom aspirin was indicated, only 25% were using it – so, we’re talking about a 75% underusage,” Dr. Crain said.
By the 1-year follow-up visit, the situation was not much changed, despite the tool’s recommendations. Among those with diabetes, 56% in the usual care group and 60% in Wizard group were still overusing aspirin. Underuse was occurring in 21% of the usual care group and 17% of the Wizard group.
Patients with reversible high-risk factors fared a little better at 1 year, especially those who, at baseline, should have been taking aspirin but were not. Among these, 10% in the usual care group and 13% in the Wizard group had started taking aspirin.
The results were a bit of a disappointment, Dr. Crain said, but they don’t invalidate the investigators’ faith in an algorithmic advising system.
“We do think that electronic health record tools like this can help providers follow guidelines and improve the quality of their aspirin recommendations and prescribing, and hopefully reduce cardiovascular events and aspirin-related hazards,” she said. “Unfortunately, that didn’t happen here in the diabetes patients,” and the results in the second group were not stellar.
She added that the Wizard development team will be tweaking the tool to clarify some of the choices available as it guides patients and providers through the algorithm, in hopes of improving its efficacy.
Dr. Crain made no financial disclosures.
On Twitter @alz_gal
MUNICH – Many patients with diabetes who could benefit from low-dose aspirin therapy may not be getting it – and many who are getting aspirin should not be, according to data presented at the annual meeting of the European Association for the Study of Diabetes.
A large, randomized trial concluded that 21% of diabetes patients who qualified for aspirin therapy for cardiovascular risk reduction were not getting it, and that it was contraindicated in almost 60% of those who were taking it, Lauren Crain, PhD, reported at the meeting.
Balancing the risks and benefits of aspirin therapy is not an easy challenge, said Dr. Crain, a health behavior researcher at HealthPartners Institute, Minneapolis. The clinical information necessary for the assessment is “rather lengthy, and not always readily available in primary care settings,” she said, and it’s clear from this study that clinicians could use some help in this area. Unfortunately, the electronic algorithm tested, which was meant to improve appropriate aspirin prescribing, didn’t improve the situation very much.
“At the final visit in the diabetes group [after the algorithm was employed], the total proportion of patients using aspirin was higher than at the first visit,” Dr. Crain noted. “However, that was the case regardless of whether patients were over- or underusing aspirin at the first visit.”
The aspirin findings were part of a large, randomized trial testing the algorithm as a way to reduce cardiovascular risk factors. The study was conducted in 19 primary care practices.
The decision-making algorithm, Cardiovascular Wizard, uses electronic health records to identify and advise patients with uncontrolled cardiovascular risk factors. Priorities and clinical recommendations are displayed for the provider and patient in the hope of facilitating shared decision making, Dr. Crain said.
One of the Wizard’s algorithms concerns aspirin prescribing. It is programmed with data from the United States Preventive Services Task Force, and recommends aspirin if cardiovascular risk scores are high and if consistent with providing a benefit greater than the risk of gastrointestinal bleeding. Aspirin is not recommended if the benefit is determined to be low or if major contraindications are present, including anticoagulant use or history of intracerebral hemorrhage.
The tool also alerts providers to the presence of other potential risks including aspirin allergy or intolerance, history of GI bleeds or risk conditions, and the concomitant use of nonsteroidal anti-inflammatory drugs.
The study comprised 11,000 adults, 4,000 of whom had diabetes. The remainder had high-risk, reversible cardiovascular risk factors (hypertension, dyslipidemia, or tobacco use). Each group was randomized to either cardiovascular risk assessment by usual care or with the Cardiovascular Wizard program.
The aspirin substudy looked at aspirin use at the baseline visit and the patient’s final, 1-year follow-up visit. At both visits, aspirin use was documented, and the clinician used the Wizard to assess whether or not it was indicated.
At the baseline visit, 71% of the diabetes group was using aspirin. However, according to the Wizard tool, more than one-third of them should not have been taking it – and among these, 57% were doing so. Among the remaining two-thirds of patients, all of whom should have been using aspirin, 21% were not taking it, Dr. Crain said.
Among the patients with reversible high-risk factors, 27% were using aspirin. However, according to the Wizard tool, the drug was contraindicated in 34% of those patients. “Most importantly, however, among those for whom aspirin was indicated, only 25% were using it – so, we’re talking about a 75% underusage,” Dr. Crain said.
By the 1-year follow-up visit, the situation was not much changed, despite the tool’s recommendations. Among those with diabetes, 56% in the usual care group and 60% in Wizard group were still overusing aspirin. Underuse was occurring in 21% of the usual care group and 17% of the Wizard group.
Patients with reversible high-risk factors fared a little better at 1 year, especially those who, at baseline, should have been taking aspirin but were not. Among these, 10% in the usual care group and 13% in the Wizard group had started taking aspirin.
The results were a bit of a disappointment, Dr. Crain said, but they don’t invalidate the investigators’ faith in an algorithmic advising system.
“We do think that electronic health record tools like this can help providers follow guidelines and improve the quality of their aspirin recommendations and prescribing, and hopefully reduce cardiovascular events and aspirin-related hazards,” she said. “Unfortunately, that didn’t happen here in the diabetes patients,” and the results in the second group were not stellar.
She added that the Wizard development team will be tweaking the tool to clarify some of the choices available as it guides patients and providers through the algorithm, in hopes of improving its efficacy.
Dr. Crain made no financial disclosures.
On Twitter @alz_gal
AT EASD 2016
Key clinical point: Many diabetes patients who should be taking aspirin for cardiovascular risk reduction are not doing so, and many who should not be taking it are.
Major finding: Aspirin was underused in 21% of diabetes patients and overused in 57% of patients.
Data source: A randomized study of 11,000 patients.
Disclosures: Dr. Lauren Crain had no financial disclosures.

Nearly half of patients readmitted after liver transplant
Nearly half of patients were readmitted to the hospital within 90 days of liver transplantation, according to a single-center retrospective study.
“As readmission portends decreased survival, an emphasis should be placed on identifying and optimizing those at increased risk. If readmission does occur, however, it presents an opportunity to intervene, as virtually no patients died during initial readmission,” Madhukar S. Patel, MD, and his associates at Massachusetts General Hospital, Boston, wrote online in HPB.
Long wait times for liver transplantation in this part of the country lead to “high patient acuity,” the researchers noted. To better understand the correlates and consequences of posttransplant readmissions, they reviewed the records for 325 adults who underwent liver transplantation at their hospital between 2005 and 2015. Patients averaged 56 years old and had awaited transplant for a mean of 1 year (standard deviation, 506 days). Their average MELD (Model for End-Stage Liver Disease) scores were 30.3 at transplant (SD, 5.8), and 16.9 (SD, 9.4) on postoperative day 5. Their average hospital length of stay was 12 days, the investigators reported (HPB. 2016 Sep 15. doi: 10.1016/j.hpb.2016.08.003). A total of 149 patients (46%) were readmitted within 90 days of discharge, most often for infections (28% of readmissions), followed by medication issues (19%) and biliary complications (11%). The strongest predictor of posttransplant readmission was hepatitis C virus (HCV) infection, which more than doubled the odds of readmission, compared with alcoholic liver disease (odds ratio, 2.37; 95% confidence interval, 1.44-3.91; P = .001). Transplantees with HCV might benefit from closer outpatient follow-up to detect worsening liver function, diagnostic algorithms to help prevent unnecessary readmissions, and associated nosocomial infections, and pre- and posttransplant direct-acting antiviral therapy, “although the impact [of direct-acting antiviral] therapy on readmissions] is unknown at this time,” the investigators said.
The multivariable analysis also linked readmissions to longer hospital stays (OR, 1.03; P = .04), while age and male sex were protective factors, the investigators said. “Although speculative, it is possible that these factors may be protective due to differences in social support structures upon discharge,” they wrote, noting that women are more likely than men to outlive their partners and thus to live alone in later life.
Readmission within 90 days was associated with a significantly lower rate of survival at 5 years (75% vs. 88% for patients who were not readmitted; P = .008). But only one patient died during the initial readmission, “suggesting that when readmission does occur, it may be an opportunity to intervene,” the researchers said. Strategies include earlier extubation and removal of indwelling catheters, decreasing levels of immunosuppression, lowering treatment thresholds, and shifting patients with laboratory abnormalities to the outpatient setting, they noted. “At our center a process has been initiated in which the inpatient transplant attending surgeon directly passes off discharged patients to the outpatient team,” the investigators wrote. “Additionally, for patients discharged to an acute rehabilitation facility, a specific transplant physician point of contact is provided to the team at the rehab center in case any questions or issues arise [after] discharge. Although these strategies are a reasonable starting point, follow-up studies remain necessary in order to evaluate the impact of these interventions in this patient cohort.”
The researchers reported no funding sources and had no relevant financial disclosures.
Nearly half of patients were readmitted to the hospital within 90 days of liver transplantation, according to a single-center retrospective study.
“As readmission portends decreased survival, an emphasis should be placed on identifying and optimizing those at increased risk. If readmission does occur, however, it presents an opportunity to intervene, as virtually no patients died during initial readmission,” Madhukar S. Patel, MD, and his associates at Massachusetts General Hospital, Boston, wrote online in HPB.
Long wait times for liver transplantation in this part of the country lead to “high patient acuity,” the researchers noted. To better understand the correlates and consequences of posttransplant readmissions, they reviewed the records for 325 adults who underwent liver transplantation at their hospital between 2005 and 2015. Patients averaged 56 years old and had awaited transplant for a mean of 1 year (standard deviation, 506 days). Their average MELD (Model for End-Stage Liver Disease) scores were 30.3 at transplant (SD, 5.8), and 16.9 (SD, 9.4) on postoperative day 5. Their average hospital length of stay was 12 days, the investigators reported (HPB. 2016 Sep 15. doi: 10.1016/j.hpb.2016.08.003). A total of 149 patients (46%) were readmitted within 90 days of discharge, most often for infections (28% of readmissions), followed by medication issues (19%) and biliary complications (11%). The strongest predictor of posttransplant readmission was hepatitis C virus (HCV) infection, which more than doubled the odds of readmission, compared with alcoholic liver disease (odds ratio, 2.37; 95% confidence interval, 1.44-3.91; P = .001). Transplantees with HCV might benefit from closer outpatient follow-up to detect worsening liver function, diagnostic algorithms to help prevent unnecessary readmissions, and associated nosocomial infections, and pre- and posttransplant direct-acting antiviral therapy, “although the impact [of direct-acting antiviral] therapy on readmissions] is unknown at this time,” the investigators said.
The multivariable analysis also linked readmissions to longer hospital stays (OR, 1.03; P = .04), while age and male sex were protective factors, the investigators said. “Although speculative, it is possible that these factors may be protective due to differences in social support structures upon discharge,” they wrote, noting that women are more likely than men to outlive their partners and thus to live alone in later life.
Readmission within 90 days was associated with a significantly lower rate of survival at 5 years (75% vs. 88% for patients who were not readmitted; P = .008). But only one patient died during the initial readmission, “suggesting that when readmission does occur, it may be an opportunity to intervene,” the researchers said. Strategies include earlier extubation and removal of indwelling catheters, decreasing levels of immunosuppression, lowering treatment thresholds, and shifting patients with laboratory abnormalities to the outpatient setting, they noted. “At our center a process has been initiated in which the inpatient transplant attending surgeon directly passes off discharged patients to the outpatient team,” the investigators wrote. “Additionally, for patients discharged to an acute rehabilitation facility, a specific transplant physician point of contact is provided to the team at the rehab center in case any questions or issues arise [after] discharge. Although these strategies are a reasonable starting point, follow-up studies remain necessary in order to evaluate the impact of these interventions in this patient cohort.”
The researchers reported no funding sources and had no relevant financial disclosures.
Nearly half of patients were readmitted to the hospital within 90 days of liver transplantation, according to a single-center retrospective study.
“As readmission portends decreased survival, an emphasis should be placed on identifying and optimizing those at increased risk. If readmission does occur, however, it presents an opportunity to intervene, as virtually no patients died during initial readmission,” Madhukar S. Patel, MD, and his associates at Massachusetts General Hospital, Boston, wrote online in HPB.
Long wait times for liver transplantation in this part of the country lead to “high patient acuity,” the researchers noted. To better understand the correlates and consequences of posttransplant readmissions, they reviewed the records for 325 adults who underwent liver transplantation at their hospital between 2005 and 2015. Patients averaged 56 years old and had awaited transplant for a mean of 1 year (standard deviation, 506 days). Their average MELD (Model for End-Stage Liver Disease) scores were 30.3 at transplant (SD, 5.8), and 16.9 (SD, 9.4) on postoperative day 5. Their average hospital length of stay was 12 days, the investigators reported (HPB. 2016 Sep 15. doi: 10.1016/j.hpb.2016.08.003). A total of 149 patients (46%) were readmitted within 90 days of discharge, most often for infections (28% of readmissions), followed by medication issues (19%) and biliary complications (11%). The strongest predictor of posttransplant readmission was hepatitis C virus (HCV) infection, which more than doubled the odds of readmission, compared with alcoholic liver disease (odds ratio, 2.37; 95% confidence interval, 1.44-3.91; P = .001). Transplantees with HCV might benefit from closer outpatient follow-up to detect worsening liver function, diagnostic algorithms to help prevent unnecessary readmissions, and associated nosocomial infections, and pre- and posttransplant direct-acting antiviral therapy, “although the impact [of direct-acting antiviral] therapy on readmissions] is unknown at this time,” the investigators said.
The multivariable analysis also linked readmissions to longer hospital stays (OR, 1.03; P = .04), while age and male sex were protective factors, the investigators said. “Although speculative, it is possible that these factors may be protective due to differences in social support structures upon discharge,” they wrote, noting that women are more likely than men to outlive their partners and thus to live alone in later life.
Readmission within 90 days was associated with a significantly lower rate of survival at 5 years (75% vs. 88% for patients who were not readmitted; P = .008). But only one patient died during the initial readmission, “suggesting that when readmission does occur, it may be an opportunity to intervene,” the researchers said. Strategies include earlier extubation and removal of indwelling catheters, decreasing levels of immunosuppression, lowering treatment thresholds, and shifting patients with laboratory abnormalities to the outpatient setting, they noted. “At our center a process has been initiated in which the inpatient transplant attending surgeon directly passes off discharged patients to the outpatient team,” the investigators wrote. “Additionally, for patients discharged to an acute rehabilitation facility, a specific transplant physician point of contact is provided to the team at the rehab center in case any questions or issues arise [after] discharge. Although these strategies are a reasonable starting point, follow-up studies remain necessary in order to evaluate the impact of these interventions in this patient cohort.”
The researchers reported no funding sources and had no relevant financial disclosures.
FROM HPB
Key clinical point: Nearly half of liver recipients at Massachusetts General Hospital were readmitted within 90 days.
Major finding: A total of 46% of patients were readmitted, with hepatitis C virus infection being the strongest predictor of readmission (odds ratio, 2.37, compared with alcoholic liver disease).
Data source: A single-center retrospective study of 325 liver transplant patients between 2005 and 2015.
Disclosures: The researchers reported no funding sources and had no relevant financial disclosures.
AATS Submission Opportunities
Current and future CT surgery division chiefs/department chairs are invited to apply for the AATS Leadership Academy Program.
Friday, April 28, 2017
AATS Centennial
Boston, MA
This intensive, didactic and interactive program brings together up to 20 international surgeons who have demonstrated significant promise as potential future division chiefs or have recent assumed that role. The program provides participants with administrative, interpersonal, mentoring and negotiating skills, as well as the opportunity to network with well-known thoracic surgeon leaders and potential mentors.
Deadline: November 30, 2016
Qualifications/More Information
Don’t miss the opportunity to submit to one of these AATS scholarship programs.
Deadline: January 20, 2017
AATS Member for a Day
North American medical students, and general and up to third year integrated CT Surgery
(I-6) surgery residents can accompany an AATS Member during portions of the AATS Centennial as an AATS Member for a Day.
The meeting takes place April 29-May 3, 2017 in Boston, MA.
Those selected will receive free hotel accommodations for three to four night in an AATS Centennial hotel. They will also be given a $250 meal and $500 travel stipend at the end of the meeting.
Eligibility/More information
Summer Internship Opportunity for First/Second Year Medical Students
First and second year medical students can spend the summer being exposed to cardiothoracic surgery thanks to the AATS Summer Intern Scholarship. For eight weeks (June – September), students will work in the CT department of an AATS member.
Those chosen receive $2,500 for living expenses. They also will be able to attend the AATS Centennial gratis.
The meeting takes place April 29 – May 3, 2017 in Boston, MA.
More information
AATS Resident Poster Competition
International cardiothoracic surgery residents and/or congenital heart surgery fellows: Take advantage of this opportunity to represent your institution and present a scientific poster of your clinical/investigative research at the AATS Centennial.
The meeting will take place April 29 - May 3, 2017 in Boston, MA.
Awardee institutions get a $500 stipend to offset meal/travel costs. Each winner receives free registration to the AATS Centennial and access to the Skills Course (April 30) and Postgraduate Course (May 1).
More information
Non-MD CT Surgical Team Scientific Poster Competition
Non-MD cardiothoracic team professionals can submit a scientific poster for the Perioperative/Team-Based Care Poster Competition.
Winning posters will be displayed at the AATS Centennial, April 29 – May 3, 2017 in Boston, MA.
The competition winner will receive a $1,000 stipend to offset travel and accommodation costs.
More information
Share:
Current and future CT surgery division chiefs/department chairs are invited to apply for the AATS Leadership Academy Program.
Friday, April 28, 2017
AATS Centennial
Boston, MA
This intensive, didactic and interactive program brings together up to 20 international surgeons who have demonstrated significant promise as potential future division chiefs or have recent assumed that role. The program provides participants with administrative, interpersonal, mentoring and negotiating skills, as well as the opportunity to network with well-known thoracic surgeon leaders and potential mentors.
Deadline: November 30, 2016
Qualifications/More Information
Don’t miss the opportunity to submit to one of these AATS scholarship programs.
Deadline: January 20, 2017
AATS Member for a Day
North American medical students, and general and up to third year integrated CT Surgery
(I-6) surgery residents can accompany an AATS Member during portions of the AATS Centennial as an AATS Member for a Day.
The meeting takes place April 29-May 3, 2017 in Boston, MA.
Those selected will receive free hotel accommodations for three to four night in an AATS Centennial hotel. They will also be given a $250 meal and $500 travel stipend at the end of the meeting.
Eligibility/More information
Summer Internship Opportunity for First/Second Year Medical Students
First and second year medical students can spend the summer being exposed to cardiothoracic surgery thanks to the AATS Summer Intern Scholarship. For eight weeks (June – September), students will work in the CT department of an AATS member.
Those chosen receive $2,500 for living expenses. They also will be able to attend the AATS Centennial gratis.
The meeting takes place April 29 – May 3, 2017 in Boston, MA.
More information
AATS Resident Poster Competition
International cardiothoracic surgery residents and/or congenital heart surgery fellows: Take advantage of this opportunity to represent your institution and present a scientific poster of your clinical/investigative research at the AATS Centennial.
The meeting will take place April 29 - May 3, 2017 in Boston, MA.
Awardee institutions get a $500 stipend to offset meal/travel costs. Each winner receives free registration to the AATS Centennial and access to the Skills Course (April 30) and Postgraduate Course (May 1).
More information
Non-MD CT Surgical Team Scientific Poster Competition
Non-MD cardiothoracic team professionals can submit a scientific poster for the Perioperative/Team-Based Care Poster Competition.
Winning posters will be displayed at the AATS Centennial, April 29 – May 3, 2017 in Boston, MA.
The competition winner will receive a $1,000 stipend to offset travel and accommodation costs.
More information
Share:
Current and future CT surgery division chiefs/department chairs are invited to apply for the AATS Leadership Academy Program.
Friday, April 28, 2017
AATS Centennial
Boston, MA
This intensive, didactic and interactive program brings together up to 20 international surgeons who have demonstrated significant promise as potential future division chiefs or have recent assumed that role. The program provides participants with administrative, interpersonal, mentoring and negotiating skills, as well as the opportunity to network with well-known thoracic surgeon leaders and potential mentors.
Deadline: November 30, 2016
Qualifications/More Information
Don’t miss the opportunity to submit to one of these AATS scholarship programs.
Deadline: January 20, 2017
AATS Member for a Day
North American medical students, and general and up to third year integrated CT Surgery
(I-6) surgery residents can accompany an AATS Member during portions of the AATS Centennial as an AATS Member for a Day.
The meeting takes place April 29-May 3, 2017 in Boston, MA.
Those selected will receive free hotel accommodations for three to four night in an AATS Centennial hotel. They will also be given a $250 meal and $500 travel stipend at the end of the meeting.
Eligibility/More information
Summer Internship Opportunity for First/Second Year Medical Students
First and second year medical students can spend the summer being exposed to cardiothoracic surgery thanks to the AATS Summer Intern Scholarship. For eight weeks (June – September), students will work in the CT department of an AATS member.
Those chosen receive $2,500 for living expenses. They also will be able to attend the AATS Centennial gratis.
The meeting takes place April 29 – May 3, 2017 in Boston, MA.
More information
AATS Resident Poster Competition
International cardiothoracic surgery residents and/or congenital heart surgery fellows: Take advantage of this opportunity to represent your institution and present a scientific poster of your clinical/investigative research at the AATS Centennial.
The meeting will take place April 29 - May 3, 2017 in Boston, MA.
Awardee institutions get a $500 stipend to offset meal/travel costs. Each winner receives free registration to the AATS Centennial and access to the Skills Course (April 30) and Postgraduate Course (May 1).
More information
Non-MD CT Surgical Team Scientific Poster Competition
Non-MD cardiothoracic team professionals can submit a scientific poster for the Perioperative/Team-Based Care Poster Competition.
Winning posters will be displayed at the AATS Centennial, April 29 – May 3, 2017 in Boston, MA.
The competition winner will receive a $1,000 stipend to offset travel and accommodation costs.
More information
Share:
