User login
MRSA patients report signs of stigma tied to illness
About half of individuals infected with methicillin-resistant Staphylococcus aureus report feeling stigmatized in interactions with hospital staff, data from a survey of 61 adult patients show.
“Hospital care for people who carry MRSA calls for a dedicated and patient-centered approach in both the way the care is delivered ... as well as the way the care is organized at the institutional level,” wrote Babette Rump, MD, of the Regional Health Service Utrecht region, Zeist, the Netherlands, and her coauthors (J Hosp Infect. 2016. doi: 10.1016/j.jhin.2016.09.010). “Prevention of unnecessary intrusive measures, while as the same time applying appropriate precautionary measures, is key to successful and respectful MRSA management.”
Dr. Rump and her associates set out to identify and quantify stigma tied to MRSA and “explore its association with mental health within a country with a MRSA ‘search and destroy’ policy.” In the Netherlands and Scandinavian countries, this policy includes isolating MRSA carriers, wearing personal protective equipment, and disinfecting the room after patients are discharged (Antimicrob Resist Infect Control. 2014 Jan 15;3[1]3). The U.S. Centers for Disease Control and Prevention, in its 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings, recommends similar methods, including application of infection control precautions during patient care and environmental measures, such as cleaning and disinfection of the patient care environment and dedicated single-patient use of noncritical equipment.
In the current study, 60-item questionnaires were provided to all adult patients at two hospitals and two regional health services who had acquired MRSA between Oct. 1, 2013, and April 1, 2014. Stigma was assessed using the 40-item Berger HIV Stigma Scale, reported Dr. Rump.
Overall, 56% of survey respondents reported stigma, including 14% who reported clear stigma and 42% who reported suggestive stigma. The remaining 44% reported no stigma. A total of 80% of the patients received MRSA eradication treatment, which was strongly associated with higher stigma, the researchers noted.
Written comments provided by 40 patients (68%) along with the questionnaires “offer valuable insights to set the focus for improvement,” the researchers said.
The most frequent comments involved patients’ perceived organizational problems with the hospital (8 patients), lack of staff knowledge (4 patients), as well as little attention paid to patient perspectives (4 patients) and unnecessarily intrusive treatments (3 patients). Also of note, 5 patients blamed and 2 “shamed” the hospital as their source of MRSA.
The results were limited by several factors, including the small study size, the researchers wrote. However, the findings suggest that “a substantial proportion of people that carry MRSA experience signs of stigma and that anticipation on MRSA-associated stigma is warranted,” they said.
The researchers had no financial conflicts to disclose.
About half of individuals infected with methicillin-resistant Staphylococcus aureus report feeling stigmatized in interactions with hospital staff, data from a survey of 61 adult patients show.
“Hospital care for people who carry MRSA calls for a dedicated and patient-centered approach in both the way the care is delivered ... as well as the way the care is organized at the institutional level,” wrote Babette Rump, MD, of the Regional Health Service Utrecht region, Zeist, the Netherlands, and her coauthors (J Hosp Infect. 2016. doi: 10.1016/j.jhin.2016.09.010). “Prevention of unnecessary intrusive measures, while as the same time applying appropriate precautionary measures, is key to successful and respectful MRSA management.”
Dr. Rump and her associates set out to identify and quantify stigma tied to MRSA and “explore its association with mental health within a country with a MRSA ‘search and destroy’ policy.” In the Netherlands and Scandinavian countries, this policy includes isolating MRSA carriers, wearing personal protective equipment, and disinfecting the room after patients are discharged (Antimicrob Resist Infect Control. 2014 Jan 15;3[1]3). The U.S. Centers for Disease Control and Prevention, in its 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings, recommends similar methods, including application of infection control precautions during patient care and environmental measures, such as cleaning and disinfection of the patient care environment and dedicated single-patient use of noncritical equipment.
In the current study, 60-item questionnaires were provided to all adult patients at two hospitals and two regional health services who had acquired MRSA between Oct. 1, 2013, and April 1, 2014. Stigma was assessed using the 40-item Berger HIV Stigma Scale, reported Dr. Rump.
Overall, 56% of survey respondents reported stigma, including 14% who reported clear stigma and 42% who reported suggestive stigma. The remaining 44% reported no stigma. A total of 80% of the patients received MRSA eradication treatment, which was strongly associated with higher stigma, the researchers noted.
Written comments provided by 40 patients (68%) along with the questionnaires “offer valuable insights to set the focus for improvement,” the researchers said.
The most frequent comments involved patients’ perceived organizational problems with the hospital (8 patients), lack of staff knowledge (4 patients), as well as little attention paid to patient perspectives (4 patients) and unnecessarily intrusive treatments (3 patients). Also of note, 5 patients blamed and 2 “shamed” the hospital as their source of MRSA.
The results were limited by several factors, including the small study size, the researchers wrote. However, the findings suggest that “a substantial proportion of people that carry MRSA experience signs of stigma and that anticipation on MRSA-associated stigma is warranted,” they said.
The researchers had no financial conflicts to disclose.
About half of individuals infected with methicillin-resistant Staphylococcus aureus report feeling stigmatized in interactions with hospital staff, data from a survey of 61 adult patients show.
“Hospital care for people who carry MRSA calls for a dedicated and patient-centered approach in both the way the care is delivered ... as well as the way the care is organized at the institutional level,” wrote Babette Rump, MD, of the Regional Health Service Utrecht region, Zeist, the Netherlands, and her coauthors (J Hosp Infect. 2016. doi: 10.1016/j.jhin.2016.09.010). “Prevention of unnecessary intrusive measures, while as the same time applying appropriate precautionary measures, is key to successful and respectful MRSA management.”
Dr. Rump and her associates set out to identify and quantify stigma tied to MRSA and “explore its association with mental health within a country with a MRSA ‘search and destroy’ policy.” In the Netherlands and Scandinavian countries, this policy includes isolating MRSA carriers, wearing personal protective equipment, and disinfecting the room after patients are discharged (Antimicrob Resist Infect Control. 2014 Jan 15;3[1]3). The U.S. Centers for Disease Control and Prevention, in its 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings, recommends similar methods, including application of infection control precautions during patient care and environmental measures, such as cleaning and disinfection of the patient care environment and dedicated single-patient use of noncritical equipment.
In the current study, 60-item questionnaires were provided to all adult patients at two hospitals and two regional health services who had acquired MRSA between Oct. 1, 2013, and April 1, 2014. Stigma was assessed using the 40-item Berger HIV Stigma Scale, reported Dr. Rump.
Overall, 56% of survey respondents reported stigma, including 14% who reported clear stigma and 42% who reported suggestive stigma. The remaining 44% reported no stigma. A total of 80% of the patients received MRSA eradication treatment, which was strongly associated with higher stigma, the researchers noted.
Written comments provided by 40 patients (68%) along with the questionnaires “offer valuable insights to set the focus for improvement,” the researchers said.
The most frequent comments involved patients’ perceived organizational problems with the hospital (8 patients), lack of staff knowledge (4 patients), as well as little attention paid to patient perspectives (4 patients) and unnecessarily intrusive treatments (3 patients). Also of note, 5 patients blamed and 2 “shamed” the hospital as their source of MRSA.
The results were limited by several factors, including the small study size, the researchers wrote. However, the findings suggest that “a substantial proportion of people that carry MRSA experience signs of stigma and that anticipation on MRSA-associated stigma is warranted,” they said.
The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF HOSPITAL INFECTION
Key clinical point: Adults with methicillin-resistant Staphylococcus aureus (MRSA) are susceptible to stigma.
Major finding: Approximately half (56%) of adults being treated for MRSA reported stigma associated with their illness.
Data source: A cross-sectional study including 61 adults with MRSA.
Disclosures: The researchers had no financial conflicts to disclose.
A Modified Levering Technique for Removing a Broken Solid Intramedullary Tibial Nail: A Technical Tip
In both elective and revision surgery, removal of retained hardware can be unpredictable. Broken hardware, whether identified before or during surgery, presents a significant challenge. Cases often require enlisting a large variety of equipment and techniques that often result in larger dissection and potential for wider soft-tissue or bony destruction. Broken intramedullary devices, located entirely within the cortices of bone, pose unique challenges.1,2 Various techniques have been used to remove broken cannulated nails.1-9 There is, however, a paucity of techniques for removing broken solid nails from within the tibia.1,2 Moreover, many of these techniques require significant metaphyseal and cortical bone destruction that may compromise the integrity of the long bone.1,3,9 In this article, we describe a modified technique for removal of a broken solid nail, with minimal cortical bone destruction, in the setting of a tibial nonunion.
Technique
A 23-year-old man presented with a symptomatic valgus nonunion of the tibia, which had been treated with a solid intramedullary 9-mm nail (Orthofix). The patient was taken to the operative theater for nonunion takedown and exchanged reamed intramedullary nailing. The proximal fragment of the anterograde intramedullary nail was removed in standard fashion using the Winquist Universal Extraction Set (Shukla Medical). When threading the extractor into the proximal aspect of the nail, we found it helpful to leave one of the cross-locks in place to prevent nail rotation.10 Inspection of the removed nail revealed a fracture of the device at the more proximal of 2 distal cross-locks (Figures 1A, 1B, 2). 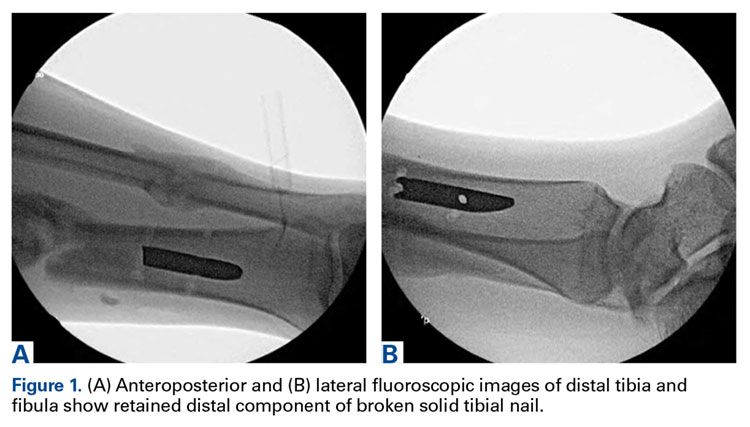

To remove the distal fragment of the nail, we used a 5.0-mm smooth Steinmann pin. After cross-lock removal, the pin was placed unicortically through the distal medial cortex at the tip of the retained implant. The distal nail fragment was pushed proximally using the pin as a lever with the interposed cortical bone serving as a fulcrum (Figures 3A, 3B). 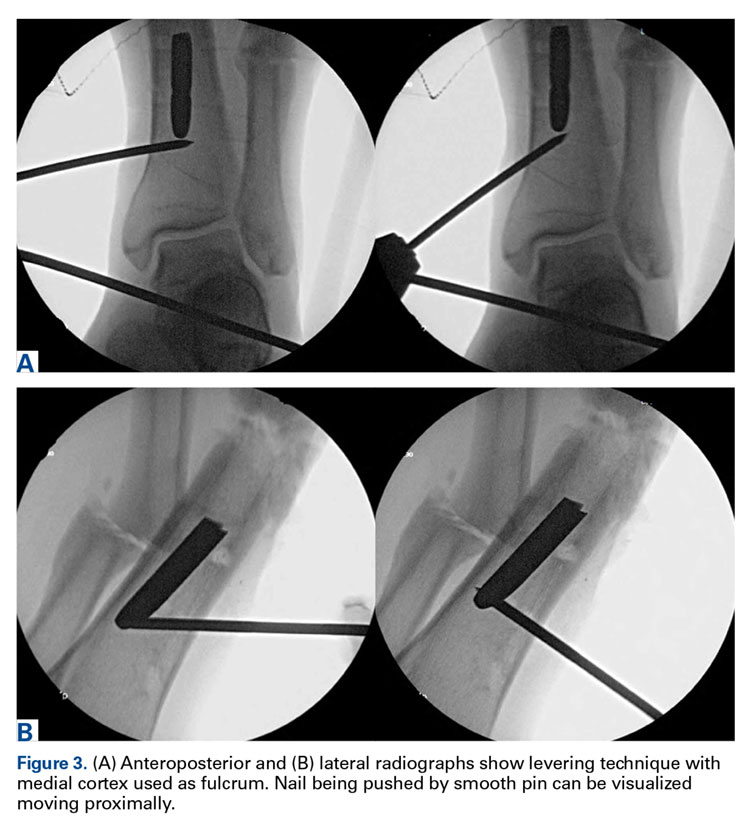
Discussion
Removal of broken solid intramedullary tibial nails presents orthopedic surgeons with a unique challenge. We have described a technique that modifies and incorporates previously described techniques while exploiting available surgical windows to facilitate hardware removal. This technique obviates the need for further bony and soft-tissue dissection, potentially mitigating surgical morbidity.
Other techniques for removing broken solid intramedullary devices have been reported. Krettek and colleagues7 described a technique in which the short distal fragment of a broken solid femoral intramedullary nail was removed with use of retrograde levering through a cortical window just proximal to the articular surface. The same window was then used for anterograde nail removal with a small Hohmann retractor serving as a guide. This technique is limited by the need for a large bony window, which potentially creates a stress riser within the distal segment. In addition, a short, distal nail fragment is required in order to facilitate manipulation through the metaphyseal bone. This technique is more readily used within the distal femur, given the large metaphyseal volume, in contrast with the distal tibial metaphysis. Giannoudis and colleagues1 described a method (for both tibia and femur) in which the intramedullary canal was proximally reamed to permit retrograde removal of an anterograde nail. The authors described reaming the canal to 4 mm larger than the nail to create access for a cleaning trephine and then a ratcheting extractor. This technique can be easily applied to the tibia or femur but requires special equipment that may not be readily available. Other retrograde techniques for the femur8 are not as suitable for the tibia, as they would cause significant chondral damage to the tibiotalar joint.
In developing our technique, which includes modifications of other methods, we used cortical windows, levering, and anterograde reaming to permit removal of a broken solid fragment through a nonunion site and with minimal additional destruction of bone. Although an existing cortical window was used, the newly created cortical window was significantly smaller than windows used in other techniques, and it avoids the articular surface. This technique can be performed with common, readily accessible equipment, which may be helpful in situations in which broken nails are encountered unexpectedly. In summary, this simple, safe, and effective technique uses standard equipment to preserve bone, decrease operative time, and alleviate surgeon frustration in complicated hardware removal surgeries.
Am J Orthop. 2016;45(6):E352-E354. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Giannoudis PV, Matthews SJ, Smith RM. Removal of the retained fragment of broken solid nails by the intra-medullary route. Injury. 2001;32(5):407-410.
2. Hak DJ, McElvany M. Removal of broken hardware. J Am Acad Orthop Surg. 2008;16(2):113-120.
3. Abdelgawad AA, Kanlic E. Removal of a broken cannulated intramedullary nail: review of the literature and a case report of a new technique. Case Rep Orthop. 2013;2013:461703.
4. Dawson GR Jr, Stader RO. Extractor for removing broken stuck intramedullary nail. Am J Orthop Surg. 1968;10(6):150-151.
5. Gosling T, Allami M, Koenemann B, Hankemeier S, Krettek C. Minimally invasive exchange tibial nailing for a broken solid nail: case report and description of a new technique. J Orthop Trauma. 2005;19(10):744-747.
6. Hellemondt FJ, Haeff MJ. Removal of a broken solid intramedullary interlocking nail. A technical note. Acta Orthop Scand. 1996;67(5):512.
7. Krettek C, Schandelmaier P, Tscherne H. Removal of a broken solid femoral nail: a simple push-out technique. A case report. J Bone Joint Surg Am. 1997;79(2):247-251.
8. Milia MJ, Vincent AB, Bosse MJ. Retrograde removal of an incarcerated solid titanium femoral nail after subtrochanteric fracture. J Orthop Trauma. 2003;17(7):521-524.
9. Whalley H, Thomas G, Hull P, Porter K. Surgeon versus metalwork—tips to remove a retained intramedullary nail fragment. Injury. 2009;40(7):783-789.
10. Smith G, Khan A, Marsh A. A novel way to remove a broken intramedullary nail. Ann R Coll Surg Engl. 2012;94(8):605.
In both elective and revision surgery, removal of retained hardware can be unpredictable. Broken hardware, whether identified before or during surgery, presents a significant challenge. Cases often require enlisting a large variety of equipment and techniques that often result in larger dissection and potential for wider soft-tissue or bony destruction. Broken intramedullary devices, located entirely within the cortices of bone, pose unique challenges.1,2 Various techniques have been used to remove broken cannulated nails.1-9 There is, however, a paucity of techniques for removing broken solid nails from within the tibia.1,2 Moreover, many of these techniques require significant metaphyseal and cortical bone destruction that may compromise the integrity of the long bone.1,3,9 In this article, we describe a modified technique for removal of a broken solid nail, with minimal cortical bone destruction, in the setting of a tibial nonunion.
Technique
A 23-year-old man presented with a symptomatic valgus nonunion of the tibia, which had been treated with a solid intramedullary 9-mm nail (Orthofix). The patient was taken to the operative theater for nonunion takedown and exchanged reamed intramedullary nailing. The proximal fragment of the anterograde intramedullary nail was removed in standard fashion using the Winquist Universal Extraction Set (Shukla Medical). When threading the extractor into the proximal aspect of the nail, we found it helpful to leave one of the cross-locks in place to prevent nail rotation.10 Inspection of the removed nail revealed a fracture of the device at the more proximal of 2 distal cross-locks (Figures 1A, 1B, 2).
To remove the distal fragment of the nail, we used a 5.0-mm smooth Steinmann pin. After cross-lock removal, the pin was placed unicortically through the distal medial cortex at the tip of the retained implant. The distal nail fragment was pushed proximally using the pin as a lever with the interposed cortical bone serving as a fulcrum (Figures 3A, 3B).
Discussion
Removal of broken solid intramedullary tibial nails presents orthopedic surgeons with a unique challenge. We have described a technique that modifies and incorporates previously described techniques while exploiting available surgical windows to facilitate hardware removal. This technique obviates the need for further bony and soft-tissue dissection, potentially mitigating surgical morbidity.
Other techniques for removing broken solid intramedullary devices have been reported. Krettek and colleagues7 described a technique in which the short distal fragment of a broken solid femoral intramedullary nail was removed with use of retrograde levering through a cortical window just proximal to the articular surface. The same window was then used for anterograde nail removal with a small Hohmann retractor serving as a guide. This technique is limited by the need for a large bony window, which potentially creates a stress riser within the distal segment. In addition, a short, distal nail fragment is required in order to facilitate manipulation through the metaphyseal bone. This technique is more readily used within the distal femur, given the large metaphyseal volume, in contrast with the distal tibial metaphysis. Giannoudis and colleagues1 described a method (for both tibia and femur) in which the intramedullary canal was proximally reamed to permit retrograde removal of an anterograde nail. The authors described reaming the canal to 4 mm larger than the nail to create access for a cleaning trephine and then a ratcheting extractor. This technique can be easily applied to the tibia or femur but requires special equipment that may not be readily available. Other retrograde techniques for the femur8 are not as suitable for the tibia, as they would cause significant chondral damage to the tibiotalar joint.
In developing our technique, which includes modifications of other methods, we used cortical windows, levering, and anterograde reaming to permit removal of a broken solid fragment through a nonunion site and with minimal additional destruction of bone. Although an existing cortical window was used, the newly created cortical window was significantly smaller than windows used in other techniques, and it avoids the articular surface. This technique can be performed with common, readily accessible equipment, which may be helpful in situations in which broken nails are encountered unexpectedly. In summary, this simple, safe, and effective technique uses standard equipment to preserve bone, decrease operative time, and alleviate surgeon frustration in complicated hardware removal surgeries.
Am J Orthop. 2016;45(6):E352-E354. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
In both elective and revision surgery, removal of retained hardware can be unpredictable. Broken hardware, whether identified before or during surgery, presents a significant challenge. Cases often require enlisting a large variety of equipment and techniques that often result in larger dissection and potential for wider soft-tissue or bony destruction. Broken intramedullary devices, located entirely within the cortices of bone, pose unique challenges.1,2 Various techniques have been used to remove broken cannulated nails.1-9 There is, however, a paucity of techniques for removing broken solid nails from within the tibia.1,2 Moreover, many of these techniques require significant metaphyseal and cortical bone destruction that may compromise the integrity of the long bone.1,3,9 In this article, we describe a modified technique for removal of a broken solid nail, with minimal cortical bone destruction, in the setting of a tibial nonunion.
Technique
A 23-year-old man presented with a symptomatic valgus nonunion of the tibia, which had been treated with a solid intramedullary 9-mm nail (Orthofix). The patient was taken to the operative theater for nonunion takedown and exchanged reamed intramedullary nailing. The proximal fragment of the anterograde intramedullary nail was removed in standard fashion using the Winquist Universal Extraction Set (Shukla Medical). When threading the extractor into the proximal aspect of the nail, we found it helpful to leave one of the cross-locks in place to prevent nail rotation.10 Inspection of the removed nail revealed a fracture of the device at the more proximal of 2 distal cross-locks (Figures 1A, 1B, 2).
To remove the distal fragment of the nail, we used a 5.0-mm smooth Steinmann pin. After cross-lock removal, the pin was placed unicortically through the distal medial cortex at the tip of the retained implant. The distal nail fragment was pushed proximally using the pin as a lever with the interposed cortical bone serving as a fulcrum (Figures 3A, 3B).
Discussion
Removal of broken solid intramedullary tibial nails presents orthopedic surgeons with a unique challenge. We have described a technique that modifies and incorporates previously described techniques while exploiting available surgical windows to facilitate hardware removal. This technique obviates the need for further bony and soft-tissue dissection, potentially mitigating surgical morbidity.
Other techniques for removing broken solid intramedullary devices have been reported. Krettek and colleagues7 described a technique in which the short distal fragment of a broken solid femoral intramedullary nail was removed with use of retrograde levering through a cortical window just proximal to the articular surface. The same window was then used for anterograde nail removal with a small Hohmann retractor serving as a guide. This technique is limited by the need for a large bony window, which potentially creates a stress riser within the distal segment. In addition, a short, distal nail fragment is required in order to facilitate manipulation through the metaphyseal bone. This technique is more readily used within the distal femur, given the large metaphyseal volume, in contrast with the distal tibial metaphysis. Giannoudis and colleagues1 described a method (for both tibia and femur) in which the intramedullary canal was proximally reamed to permit retrograde removal of an anterograde nail. The authors described reaming the canal to 4 mm larger than the nail to create access for a cleaning trephine and then a ratcheting extractor. This technique can be easily applied to the tibia or femur but requires special equipment that may not be readily available. Other retrograde techniques for the femur8 are not as suitable for the tibia, as they would cause significant chondral damage to the tibiotalar joint.
In developing our technique, which includes modifications of other methods, we used cortical windows, levering, and anterograde reaming to permit removal of a broken solid fragment through a nonunion site and with minimal additional destruction of bone. Although an existing cortical window was used, the newly created cortical window was significantly smaller than windows used in other techniques, and it avoids the articular surface. This technique can be performed with common, readily accessible equipment, which may be helpful in situations in which broken nails are encountered unexpectedly. In summary, this simple, safe, and effective technique uses standard equipment to preserve bone, decrease operative time, and alleviate surgeon frustration in complicated hardware removal surgeries.
Am J Orthop. 2016;45(6):E352-E354. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Giannoudis PV, Matthews SJ, Smith RM. Removal of the retained fragment of broken solid nails by the intra-medullary route. Injury. 2001;32(5):407-410.
2. Hak DJ, McElvany M. Removal of broken hardware. J Am Acad Orthop Surg. 2008;16(2):113-120.
3. Abdelgawad AA, Kanlic E. Removal of a broken cannulated intramedullary nail: review of the literature and a case report of a new technique. Case Rep Orthop. 2013;2013:461703.
4. Dawson GR Jr, Stader RO. Extractor for removing broken stuck intramedullary nail. Am J Orthop Surg. 1968;10(6):150-151.
5. Gosling T, Allami M, Koenemann B, Hankemeier S, Krettek C. Minimally invasive exchange tibial nailing for a broken solid nail: case report and description of a new technique. J Orthop Trauma. 2005;19(10):744-747.
6. Hellemondt FJ, Haeff MJ. Removal of a broken solid intramedullary interlocking nail. A technical note. Acta Orthop Scand. 1996;67(5):512.
7. Krettek C, Schandelmaier P, Tscherne H. Removal of a broken solid femoral nail: a simple push-out technique. A case report. J Bone Joint Surg Am. 1997;79(2):247-251.
8. Milia MJ, Vincent AB, Bosse MJ. Retrograde removal of an incarcerated solid titanium femoral nail after subtrochanteric fracture. J Orthop Trauma. 2003;17(7):521-524.
9. Whalley H, Thomas G, Hull P, Porter K. Surgeon versus metalwork—tips to remove a retained intramedullary nail fragment. Injury. 2009;40(7):783-789.
10. Smith G, Khan A, Marsh A. A novel way to remove a broken intramedullary nail. Ann R Coll Surg Engl. 2012;94(8):605.
1. Giannoudis PV, Matthews SJ, Smith RM. Removal of the retained fragment of broken solid nails by the intra-medullary route. Injury. 2001;32(5):407-410.
2. Hak DJ, McElvany M. Removal of broken hardware. J Am Acad Orthop Surg. 2008;16(2):113-120.
3. Abdelgawad AA, Kanlic E. Removal of a broken cannulated intramedullary nail: review of the literature and a case report of a new technique. Case Rep Orthop. 2013;2013:461703.
4. Dawson GR Jr, Stader RO. Extractor for removing broken stuck intramedullary nail. Am J Orthop Surg. 1968;10(6):150-151.
5. Gosling T, Allami M, Koenemann B, Hankemeier S, Krettek C. Minimally invasive exchange tibial nailing for a broken solid nail: case report and description of a new technique. J Orthop Trauma. 2005;19(10):744-747.
6. Hellemondt FJ, Haeff MJ. Removal of a broken solid intramedullary interlocking nail. A technical note. Acta Orthop Scand. 1996;67(5):512.
7. Krettek C, Schandelmaier P, Tscherne H. Removal of a broken solid femoral nail: a simple push-out technique. A case report. J Bone Joint Surg Am. 1997;79(2):247-251.
8. Milia MJ, Vincent AB, Bosse MJ. Retrograde removal of an incarcerated solid titanium femoral nail after subtrochanteric fracture. J Orthop Trauma. 2003;17(7):521-524.
9. Whalley H, Thomas G, Hull P, Porter K. Surgeon versus metalwork—tips to remove a retained intramedullary nail fragment. Injury. 2009;40(7):783-789.
10. Smith G, Khan A, Marsh A. A novel way to remove a broken intramedullary nail. Ann R Coll Surg Engl. 2012;94(8):605.
Does Accelerated Physical Therapy After Elective Primary Hip and Knee Arthroplasty Facilitate Early Discharge?
Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are among the most effective surgical procedures in modern medicine. Use of primary THA in the United States is projected to increase by 174% by 2030, to 532,000 cases annually, and the estimate for TKA is even greater.1 Hospital length of stay (LOS) accounts for a significant portion of the overall cost of these procedures. Reducing LOS to limit costs without compromising patient safety, satisfaction, and outcomes remains the goal at all joint arthroplasty centers. Rapid-recovery or fast-track clinical pathways limiting opioid use and emphasizing patient education and early (day-of-surgery) mobilization have been shown to reduce LOS without compromising patient outcomes.2-5 Factors correlated with LOS after THA include surgical approach, use of multimodal analgesia, obesity, age, and social situations or living conditions.4,6-10
Our institution recently implemented a protocol in which certified physical therapists provide accelerated (day-of-surgery) physical therapy (PT) for all total joint arthroplasty patients. For the study reported here, we hypothesized that, compared with PT started on postoperative day 1 (POD-1), PT started day of surgery (Day 0) would result in shorter LOS for unilateral primary THA and TKA patients. In addition, we wanted to evaluate any predischarge differences in function, as measured by gait distance, between the groups.
Methods
After obtaining Institutional Review Board approval, we retrospectively evaluated use of the new postoperative protocol (Day 0 PT) for primary THA and TKA patients. We reviewed all cases of primary unilateral THA or TKA performed by a single surgeon over the 12-month period immediately following initiation of the protocol. There were 116 THA cases and 126 TKA cases. Charts were reviewed for patient demographics, intraoperative data, in-hospital course, and PT session notes. Patients who had a PT session at any point on day of surgery were designated the Day 0 group, and patients who had PT starting the next day (POD-1) were designated the Non-Day 0 group. Although the medical records showed that Day 0 PT had been ordered in all cases, not all patients received PT on the day of their surgery; the most common reason was that they returned from postanesthesia care after the physical therapists’ work shift had ended. Another reason was patient noncompliance or unwillingness stemming from the prolonged effects of general anesthesia, diminished mental orientation, excess fatigue, or inadequate pain control. PT sessions after THA and TKA remained consistent over the study period, with twice daily sessions directed at patient mobility, range of motion, and gentle strengthening exercise. PT was performed only with patient consent.
Surgery
A combination of general and spinal anesthesia was used in almost all THA and TKA cases. In <5% of cases, either the patient refused spinal anesthesia, or it was unsuccessful. In addition, tranexamic acid was administered to limit blood loss in all THA and TKA cases. Of the 116 THAs performed over the study period, 3 were excluded (see below). Of the 113 patients included in the study, 88 (77.9%) used a minimally invasive posterolateral approach, 18 (15.9%) a direct anterior approach, and 7 (6.2%) an anterolateral approach. All THAs were performed with conventional instruments and uncemented components. All TKAs were performed with a standard medial parapatellar approach, conventional instruments, and a tourniquet; in each case, the patella was resurfaced, and cemented fixation was used. Drains were not used in any THA or TKA cases. A local anesthetic cocktail (100 mL of 0.25% ropivacaine, 15 mL of 0.5% ropivacaine, and 1 mL of 1:1000 epinephrine) was injected for postoperative analgesia in all THA and TKA cases.
There were 3 important intraoperative findings in the THA Day 0 group: 2 cases of incidental gluteus medius tendon tears requiring repair and 1 case of nondisplaced calcar fracture treated with a cerclage cable. The THA Non-Day 0 group and both TKA groups had no major intraoperative findings.
Physical Therapy
Day-of-surgery PT was ordered for all patients. Patients did not receive formal PT before surgery. The PT protocol consisted of subjective assessment of patient condition, expectations, and goals; lower limb strengthening exercises; and maximum gait training with use of an assistive device as tolerated. Standard hip movement restrictions were ordered for posterolateral approach patients to protect the soft-tissue repair. Continuous passive motion (CPM) was not used during this study period.
Discharge Criteria
Patients were cleared for discharge by a multidisciplinary team using several criteria: no medical condition that would require readmission, intact surgical incision without discharge or concerning erythema, adequate analgesia (oral medications), intact neurovascular examination, and PT goals achieved (independence with bed mobility, transfers, standing balance, and minimum gait distance of 150 feet). Patients who could not be discharged home because of family or occupation issues or because of problems with gait or transfer were referred to skilled nursing or home healthcare. Follow-up for wound assessment and for examination of radiographs and functional range of motion was planned for 2 to 3 weeks after surgery (all patients followed up). Two patients, 1 in the THA Non-Day 0 group and 1 in the TKA Day 0 group, had a mechanical fall 1 day before discharge, but there were no complication-related discharge delays. In addition, there were no readmissions during the first 4 weeks after surgery.
Excluded Patients
Of the 116 THA cases, 113 (63 Day 0, 50 Non-Day 0) were analyzed. To establish homogeneity between groups and remove potential confounding factors, we excluded 4 THA patients (all Non-Day 0) from analysis because of medical complications prolonging LOS. In 1 of these cases, the patient developed respiratory insufficiency and myocardial infarction on POD-3, and critical care support was required (LOS, 16 days). In another case, anticoagulation treatment led to the development of a hip hematoma on POD-9 and to treatment (evacuation) in the operating room (LOS, 14 days). The other 2 cases involved exacerbation of dysphagia from preexisting myasthenia gravis (LOS, 5 days) and Ogilvie syndrome, managed conservatively (LOS, 9 days).
Of the 126 TKA cases, 123 (97 Day 0, 26 Non-Day 0) were analyzed. Three TKA patients were excluded because of prolonged hospitalization for medical reasons: One developed a deep vein thrombosis, 1 acquired Clostridium difficile colitis (history of lung transplantation, multiple immunosuppressive drugs), and 1 developed respiratory insufficiency from asthma exacerbation.
Statistical Analysis
Power analysis (G*Power) was used to determine an appropriate sample size for comparison.11 Given a previously published mean LOS after THA of 4 days, the hypothesized mean LOS reducing that by at least 0.5 day to 3.5 days, a significance level set at 5%, a power of test set at 0.95, and an allocation ratio of 1, a minimum of 23 subjects would be needed in each group to attain a statistically significant difference using the nonparametric Mann-Whitney test. The Shapiro-Wilk test was used to assess data normality. Regarding statistical significance, the Mann-Whitney U test was used for non-normally distributed data, the 2-sided Fisher exact test and χ2 test for qualitative data and contingency, and the 2-tailed, unpaired, independent-samples Student t test for normally distributed data. Data were analyzed with SPSS Statistics for Windows Version 20 (IBM).
Results
TKA and THA patients had similar demographic profiles, types of anesthesia, operating room and surgery times, surgical approaches, and total number of PT sessions before discharge. Estimated blood loss, however, was significantly (P < .05) higher for Non-Day 0 patients than for Non-Day 0 patients (Table 1). 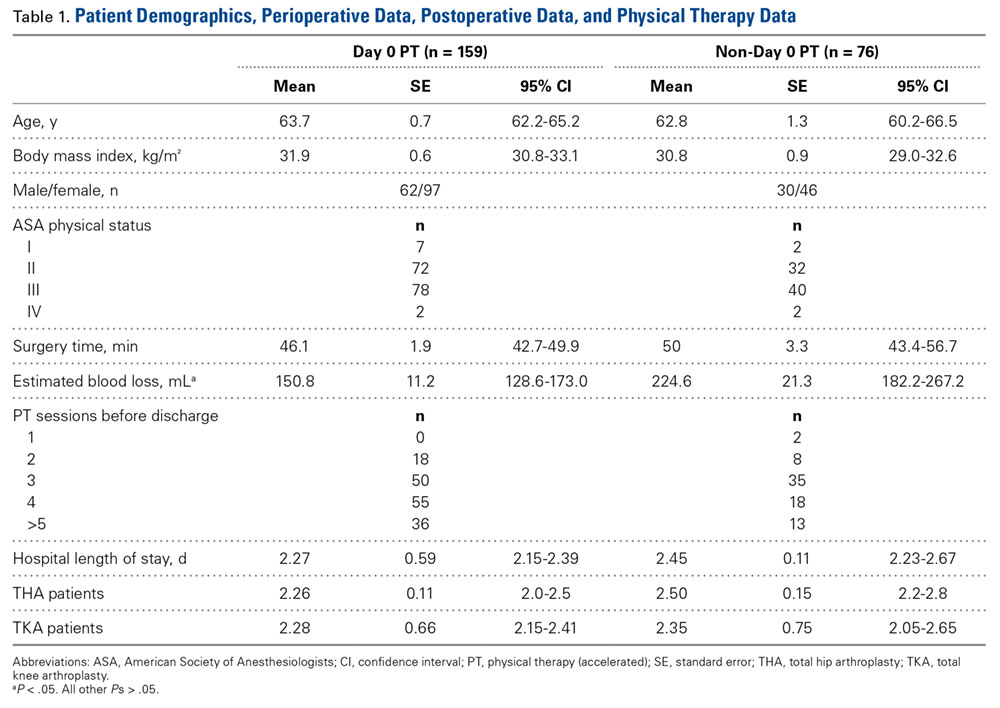
Mean (SD) distance ambulated during first PT session was 2-fold farther (P = .014) for Non-Day 0 patients, 84.1 (10.4) feet, than for Day 0 patients, 42.1 (6.4) feet. On POD-1, mean (SD) gait was significantly (P = .019) longer for Day 0 patients, 162.4 (12.9) feet, than for Non-Day 0 patients, 118 (11.7) feet (Figure 2). 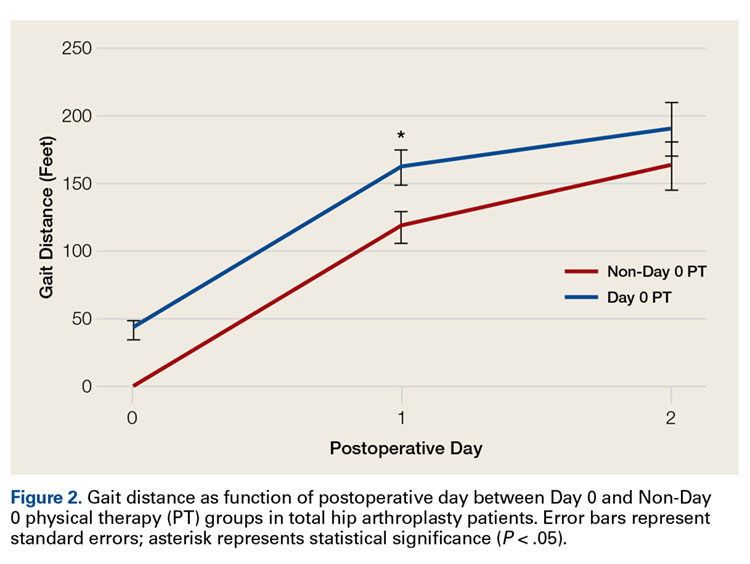
In TKA patients, although mean (SD) distance ambulated tended to be farther for the Day 0 group than for the Non-Day 0 group—114 (12.3) feet on POD-1 and 176 (15.2) feet on POD-2 for Day 0 vs 94 (22.2) feet on POD-1 and 148 (22.1) feet on POD-2 for Non-Day 0—the differences were not statistically significant. In addition, knee arc of motion during first PT session was statistically significantly (P = .3) higher for Day 0 patients, 69.1° (18.7°), than for Non-Day 0 patients, 61.7° (18.8°).
Statistical analysis revealed no difference in LOS based on surgical approach to the hip: 2.4 days for posterolateral (2.2 days for Day 0 and 2.6 days for Non-Day 0; P = .06); 2.1 days for direct anterior (2.1 days for Day 0 and 2.0 days for Non-Day 0; P = .7); and 2.7 days for anterolateral (3.0 days for Day 0 and 2.6 days for Non-Day 0; P = .6).
Discussion
Protocols for PT after THA and TKA remain unstandardized and largely dependent on institutions and surgeons. Factors permitting successful implementation of accelerated rehabilitation include patient motivation, adequate analgesia, and adequate support by physical therapists.12 A potential risk associated with accelerated PT after THA is dislocation, which did not occur in any patient in our Day 0 group. Other risks are increased pain and swelling leading to increased risk of falling and bleeding, which were not observed in our cohort. Although Day 0 PT was ordered in all cases in this study, only 55% of THA patients and 79% of TKA patients received PT the same day as their surgery. The delay can be addressed by making physical therapists’ work shifts more flexible for cases that finish later in the day and by providing preoperative education on the importance of day-of-surgery PT. Dr. Incavo and office staff routinely discuss discharge planning with all patients before surgery, but there was no stimulus protocol or communication to discuss or emphasize LOS with patients before surgery, and there was no questionnaire or survey given to assess patient expectations about PT and discharge.
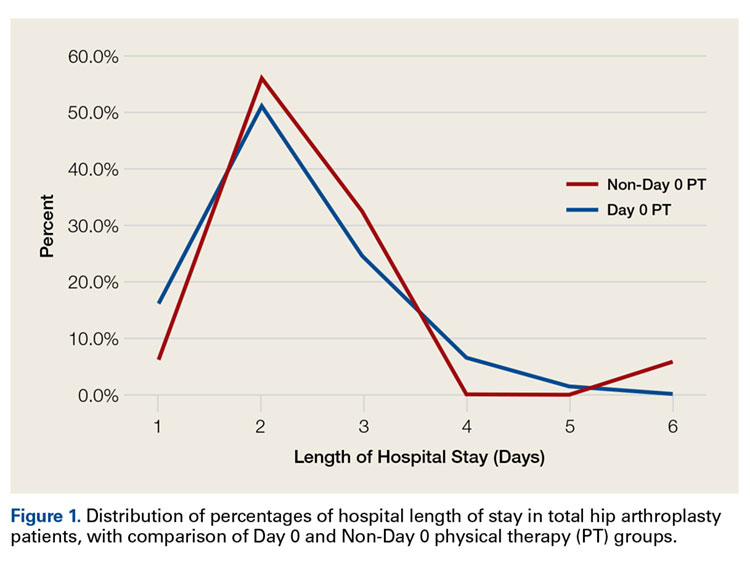
Our finding of no statistically significant reduction in mean LOS after implementation of accelerated PT for THA or TKA differs from findings in multiple other reports.4,5,13-17 Baseline or control group mean LOS tended to be higher in previous studies3,5,18-23 (3.4-11.4 days) than in our control group (2.5 days) (Table 2). 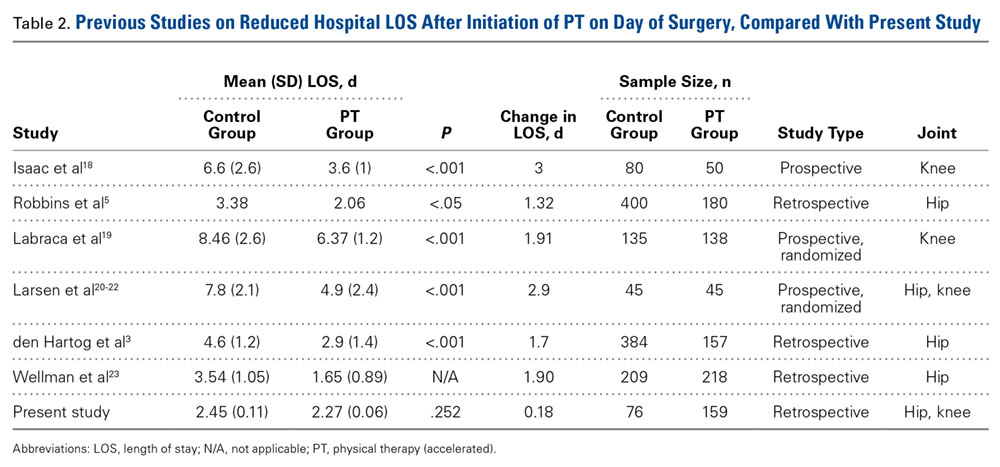
Conclusion
These results provide useful information for providers who are managing primary THA and TKA cases and seeking continual improvement in postoperative patient care and better resource allocation. Hospitals, particularly those operating in bundled-care environments, are increasingly coming under scrutiny to control costs. Our study results showed that the costs associated with Day 0 PT are justified for THA but not for TKA.
Am J Orthop. 2016;45(6):E337-E342. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780-785.
2. Barbieri A, Vanhaecht K, Van Herck P, et al. Effects of clinical pathways in the joint replacement: a meta-analysis. BMC Med. 2009;7:32.
3. den Hartog YM, Mathijssen NM, Vehmeijer SB. Reduced length of hospital stay after the introduction of a rapid recovery protocol for primary THA procedures. Acta Orthop. 2013;84(5):444-447.
4. Husted H, Holm G, Jacobsen S. Predictors of length of stay and patient satisfaction after hip and knee replacement surgery: fast-track experience in 712 patients. Acta Orthop. 2008;79(2):168-173.
5. Robbins CE, Casey D, Bono JV, Murphy SB, Talmo CT, Ward DM. A multidisciplinary total hip arthroplasty protocol with accelerated postoperative rehabilitation: does the patient benefit? Am J Orthop. 2014;43(4):178-181.
6. den Hartog YM, Mathijssen NM, Hannink G, Vehmeijer SB. Which patient characteristics influence length of hospital stay after primary total hip arthroplasty in a ‘fast-track’ setting? Bone Joint J. 2015;97(1):19-23.
7. Forrest G, Fuchs M, Gutierrez A, Girardy J. Factors affecting length of stay and need for rehabilitation after hip and knee arthroplasty. J Arthroplasty. 1998;13(2):186-190.
8. Foote J, Panchoo K, Blair P, Bannister G. Length of stay following primary total hip replacement. Ann R Coll Surg Engl. 2009;91(6):500-504.
9. Sharma V, Morgan PM, Cheng EY. Factors influencing early rehabilitation after THA: a systematic review. Clin Orthop Relat Res. 2009;467(6):1400-1411.
10. Dorr LD, Maheshwari AV, Long WT, Wan Z, Sirianni LE. Early pain relief and function after posterior minimally invasive and conventional total hip arthroplasty. A prospective, randomized, blinded study. J Bone Joint Surg Am. 2007;89(6):1153-1160.
11. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175-191.
12. Ranawat AS, Ranawat CS. Pain management and accelerated rehabilitation for total hip and total knee arthroplasty. J Arthroplasty. 2007;22(7 suppl 3):12-15.
13. Husted H, Otte KS, Kristensen BB, Orsnes T, Kehlet H. Readmissions after fast-track hip and knee arthroplasty. Arch Orthop Trauma Surg. 2010;130(9):1185-1191.
14. Husted H, Lunn TH, Troelsen A, Gaarn-Larsen L, Kristensen BB, Kehlet H. Why still in hospital after fast-track hip and knee arthroplasty? Acta Orthop. 2011;82(6):679-684.
15. Husted H, Jensen CM, Solgaard S, Kehlet H. Reduced length of stay following hip and knee arthroplasty in Denmark 2000-2009: from research to implementation. Arch Orthop Trauma Surg. 2012;132(1):101-104.
16. Berger RA, Sanders SA, Thill ES, Sporer SM, Della Valle C. Newer anesthesia and rehabilitation protocols enable outpatient hip replacement in selected patients. Clin Orthop Relat Res. 2009;467(6):1424-1430.
17. Peck CN, Foster A, McLauchlan GJ. Reducing incision length or intensifying rehabilitation: what makes the difference to length of stay in total hip replacement in a UK setting? Int Orthop. 2006;30(5):395-398.
18. Isaac D, Falode T, Liu P, I’Anson H, Dillow K, Gill P. Accelerated rehabilitation after total knee replacement. Knee. 2005;12(5):346-350.
19. Labraca NS, Castro-Sánchez AM, Matarán-Peñarrocha GA, Arroyo-Morales M, Sánchez-Joya Mdel M, Moreno-Lorenzo C. Benefits of starting rehabilitation within 24 hours of primary total knee arthroplasty: randomized clinical trial. Clin Rehabil. 2011;25(6):557-566.
20. Larsen K, Hansen TB, Søballe K. Hip arthroplasty patients benefit from accelerated perioperative care and rehabilitation: a quasi-experimental study of 98 patients. Acta Orthop. 2008;79(5):624-630.
21. Larsen K, Hansen TB, Thomsen PB, Christiansen T, Søballe K. Cost-effectiveness of accelerated perioperative care and rehabilitation after total hip and knee arthroplasty. J Bone Joint Surg Am. 2009;91(4):761-772.
22. Larsen K, Sørensen OG, Hansen TB, Thomsen PB, Søballe K. Accelerated perioperative care and rehabilitation intervention for hip and knee replacement is effective: a randomized clinical trial involving 87 patients with 3 months of follow-up. Acta Orthop. 2008;79(2):149-159.
23. Wellman SS, Murphy AC, Gulcynski D. Murphy SB. Implementation of an accelerated mobilization protocol following primary total hip arthroplasty: impact on length of stay and disposition. Curr Rev Musculoskelet Med. 2011;4(3):84-90.
Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are among the most effective surgical procedures in modern medicine. Use of primary THA in the United States is projected to increase by 174% by 2030, to 532,000 cases annually, and the estimate for TKA is even greater.1 Hospital length of stay (LOS) accounts for a significant portion of the overall cost of these procedures. Reducing LOS to limit costs without compromising patient safety, satisfaction, and outcomes remains the goal at all joint arthroplasty centers. Rapid-recovery or fast-track clinical pathways limiting opioid use and emphasizing patient education and early (day-of-surgery) mobilization have been shown to reduce LOS without compromising patient outcomes.2-5 Factors correlated with LOS after THA include surgical approach, use of multimodal analgesia, obesity, age, and social situations or living conditions.4,6-10
Our institution recently implemented a protocol in which certified physical therapists provide accelerated (day-of-surgery) physical therapy (PT) for all total joint arthroplasty patients. For the study reported here, we hypothesized that, compared with PT started on postoperative day 1 (POD-1), PT started day of surgery (Day 0) would result in shorter LOS for unilateral primary THA and TKA patients. In addition, we wanted to evaluate any predischarge differences in function, as measured by gait distance, between the groups.
Methods
After obtaining Institutional Review Board approval, we retrospectively evaluated use of the new postoperative protocol (Day 0 PT) for primary THA and TKA patients. We reviewed all cases of primary unilateral THA or TKA performed by a single surgeon over the 12-month period immediately following initiation of the protocol. There were 116 THA cases and 126 TKA cases. Charts were reviewed for patient demographics, intraoperative data, in-hospital course, and PT session notes. Patients who had a PT session at any point on day of surgery were designated the Day 0 group, and patients who had PT starting the next day (POD-1) were designated the Non-Day 0 group. Although the medical records showed that Day 0 PT had been ordered in all cases, not all patients received PT on the day of their surgery; the most common reason was that they returned from postanesthesia care after the physical therapists’ work shift had ended. Another reason was patient noncompliance or unwillingness stemming from the prolonged effects of general anesthesia, diminished mental orientation, excess fatigue, or inadequate pain control. PT sessions after THA and TKA remained consistent over the study period, with twice daily sessions directed at patient mobility, range of motion, and gentle strengthening exercise. PT was performed only with patient consent.
Surgery
A combination of general and spinal anesthesia was used in almost all THA and TKA cases. In <5% of cases, either the patient refused spinal anesthesia, or it was unsuccessful. In addition, tranexamic acid was administered to limit blood loss in all THA and TKA cases. Of the 116 THAs performed over the study period, 3 were excluded (see below). Of the 113 patients included in the study, 88 (77.9%) used a minimally invasive posterolateral approach, 18 (15.9%) a direct anterior approach, and 7 (6.2%) an anterolateral approach. All THAs were performed with conventional instruments and uncemented components. All TKAs were performed with a standard medial parapatellar approach, conventional instruments, and a tourniquet; in each case, the patella was resurfaced, and cemented fixation was used. Drains were not used in any THA or TKA cases. A local anesthetic cocktail (100 mL of 0.25% ropivacaine, 15 mL of 0.5% ropivacaine, and 1 mL of 1:1000 epinephrine) was injected for postoperative analgesia in all THA and TKA cases.
There were 3 important intraoperative findings in the THA Day 0 group: 2 cases of incidental gluteus medius tendon tears requiring repair and 1 case of nondisplaced calcar fracture treated with a cerclage cable. The THA Non-Day 0 group and both TKA groups had no major intraoperative findings.
Physical Therapy
Day-of-surgery PT was ordered for all patients. Patients did not receive formal PT before surgery. The PT protocol consisted of subjective assessment of patient condition, expectations, and goals; lower limb strengthening exercises; and maximum gait training with use of an assistive device as tolerated. Standard hip movement restrictions were ordered for posterolateral approach patients to protect the soft-tissue repair. Continuous passive motion (CPM) was not used during this study period.
Discharge Criteria
Patients were cleared for discharge by a multidisciplinary team using several criteria: no medical condition that would require readmission, intact surgical incision without discharge or concerning erythema, adequate analgesia (oral medications), intact neurovascular examination, and PT goals achieved (independence with bed mobility, transfers, standing balance, and minimum gait distance of 150 feet). Patients who could not be discharged home because of family or occupation issues or because of problems with gait or transfer were referred to skilled nursing or home healthcare. Follow-up for wound assessment and for examination of radiographs and functional range of motion was planned for 2 to 3 weeks after surgery (all patients followed up). Two patients, 1 in the THA Non-Day 0 group and 1 in the TKA Day 0 group, had a mechanical fall 1 day before discharge, but there were no complication-related discharge delays. In addition, there were no readmissions during the first 4 weeks after surgery.
Excluded Patients
Of the 116 THA cases, 113 (63 Day 0, 50 Non-Day 0) were analyzed. To establish homogeneity between groups and remove potential confounding factors, we excluded 4 THA patients (all Non-Day 0) from analysis because of medical complications prolonging LOS. In 1 of these cases, the patient developed respiratory insufficiency and myocardial infarction on POD-3, and critical care support was required (LOS, 16 days). In another case, anticoagulation treatment led to the development of a hip hematoma on POD-9 and to treatment (evacuation) in the operating room (LOS, 14 days). The other 2 cases involved exacerbation of dysphagia from preexisting myasthenia gravis (LOS, 5 days) and Ogilvie syndrome, managed conservatively (LOS, 9 days).
Of the 126 TKA cases, 123 (97 Day 0, 26 Non-Day 0) were analyzed. Three TKA patients were excluded because of prolonged hospitalization for medical reasons: One developed a deep vein thrombosis, 1 acquired Clostridium difficile colitis (history of lung transplantation, multiple immunosuppressive drugs), and 1 developed respiratory insufficiency from asthma exacerbation.
Statistical Analysis
Power analysis (G*Power) was used to determine an appropriate sample size for comparison.11 Given a previously published mean LOS after THA of 4 days, the hypothesized mean LOS reducing that by at least 0.5 day to 3.5 days, a significance level set at 5%, a power of test set at 0.95, and an allocation ratio of 1, a minimum of 23 subjects would be needed in each group to attain a statistically significant difference using the nonparametric Mann-Whitney test. The Shapiro-Wilk test was used to assess data normality. Regarding statistical significance, the Mann-Whitney U test was used for non-normally distributed data, the 2-sided Fisher exact test and χ2 test for qualitative data and contingency, and the 2-tailed, unpaired, independent-samples Student t test for normally distributed data. Data were analyzed with SPSS Statistics for Windows Version 20 (IBM).
Results
TKA and THA patients had similar demographic profiles, types of anesthesia, operating room and surgery times, surgical approaches, and total number of PT sessions before discharge. Estimated blood loss, however, was significantly (P < .05) higher for Non-Day 0 patients than for Non-Day 0 patients (Table 1).
Mean (SD) distance ambulated during first PT session was 2-fold farther (P = .014) for Non-Day 0 patients, 84.1 (10.4) feet, than for Day 0 patients, 42.1 (6.4) feet. On POD-1, mean (SD) gait was significantly (P = .019) longer for Day 0 patients, 162.4 (12.9) feet, than for Non-Day 0 patients, 118 (11.7) feet (Figure 2).
In TKA patients, although mean (SD) distance ambulated tended to be farther for the Day 0 group than for the Non-Day 0 group—114 (12.3) feet on POD-1 and 176 (15.2) feet on POD-2 for Day 0 vs 94 (22.2) feet on POD-1 and 148 (22.1) feet on POD-2 for Non-Day 0—the differences were not statistically significant. In addition, knee arc of motion during first PT session was statistically significantly (P = .3) higher for Day 0 patients, 69.1° (18.7°), than for Non-Day 0 patients, 61.7° (18.8°).
Statistical analysis revealed no difference in LOS based on surgical approach to the hip: 2.4 days for posterolateral (2.2 days for Day 0 and 2.6 days for Non-Day 0; P = .06); 2.1 days for direct anterior (2.1 days for Day 0 and 2.0 days for Non-Day 0; P = .7); and 2.7 days for anterolateral (3.0 days for Day 0 and 2.6 days for Non-Day 0; P = .6).
Discussion
Protocols for PT after THA and TKA remain unstandardized and largely dependent on institutions and surgeons. Factors permitting successful implementation of accelerated rehabilitation include patient motivation, adequate analgesia, and adequate support by physical therapists.12 A potential risk associated with accelerated PT after THA is dislocation, which did not occur in any patient in our Day 0 group. Other risks are increased pain and swelling leading to increased risk of falling and bleeding, which were not observed in our cohort. Although Day 0 PT was ordered in all cases in this study, only 55% of THA patients and 79% of TKA patients received PT the same day as their surgery. The delay can be addressed by making physical therapists’ work shifts more flexible for cases that finish later in the day and by providing preoperative education on the importance of day-of-surgery PT. Dr. Incavo and office staff routinely discuss discharge planning with all patients before surgery, but there was no stimulus protocol or communication to discuss or emphasize LOS with patients before surgery, and there was no questionnaire or survey given to assess patient expectations about PT and discharge.
Our finding of no statistically significant reduction in mean LOS after implementation of accelerated PT for THA or TKA differs from findings in multiple other reports.4,5,13-17 Baseline or control group mean LOS tended to be higher in previous studies3,5,18-23 (3.4-11.4 days) than in our control group (2.5 days) (Table 2).
Conclusion
These results provide useful information for providers who are managing primary THA and TKA cases and seeking continual improvement in postoperative patient care and better resource allocation. Hospitals, particularly those operating in bundled-care environments, are increasingly coming under scrutiny to control costs. Our study results showed that the costs associated with Day 0 PT are justified for THA but not for TKA.
Am J Orthop. 2016;45(6):E337-E342. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are among the most effective surgical procedures in modern medicine. Use of primary THA in the United States is projected to increase by 174% by 2030, to 532,000 cases annually, and the estimate for TKA is even greater.1 Hospital length of stay (LOS) accounts for a significant portion of the overall cost of these procedures. Reducing LOS to limit costs without compromising patient safety, satisfaction, and outcomes remains the goal at all joint arthroplasty centers. Rapid-recovery or fast-track clinical pathways limiting opioid use and emphasizing patient education and early (day-of-surgery) mobilization have been shown to reduce LOS without compromising patient outcomes.2-5 Factors correlated with LOS after THA include surgical approach, use of multimodal analgesia, obesity, age, and social situations or living conditions.4,6-10
Our institution recently implemented a protocol in which certified physical therapists provide accelerated (day-of-surgery) physical therapy (PT) for all total joint arthroplasty patients. For the study reported here, we hypothesized that, compared with PT started on postoperative day 1 (POD-1), PT started day of surgery (Day 0) would result in shorter LOS for unilateral primary THA and TKA patients. In addition, we wanted to evaluate any predischarge differences in function, as measured by gait distance, between the groups.
Methods
After obtaining Institutional Review Board approval, we retrospectively evaluated use of the new postoperative protocol (Day 0 PT) for primary THA and TKA patients. We reviewed all cases of primary unilateral THA or TKA performed by a single surgeon over the 12-month period immediately following initiation of the protocol. There were 116 THA cases and 126 TKA cases. Charts were reviewed for patient demographics, intraoperative data, in-hospital course, and PT session notes. Patients who had a PT session at any point on day of surgery were designated the Day 0 group, and patients who had PT starting the next day (POD-1) were designated the Non-Day 0 group. Although the medical records showed that Day 0 PT had been ordered in all cases, not all patients received PT on the day of their surgery; the most common reason was that they returned from postanesthesia care after the physical therapists’ work shift had ended. Another reason was patient noncompliance or unwillingness stemming from the prolonged effects of general anesthesia, diminished mental orientation, excess fatigue, or inadequate pain control. PT sessions after THA and TKA remained consistent over the study period, with twice daily sessions directed at patient mobility, range of motion, and gentle strengthening exercise. PT was performed only with patient consent.
Surgery
A combination of general and spinal anesthesia was used in almost all THA and TKA cases. In <5% of cases, either the patient refused spinal anesthesia, or it was unsuccessful. In addition, tranexamic acid was administered to limit blood loss in all THA and TKA cases. Of the 116 THAs performed over the study period, 3 were excluded (see below). Of the 113 patients included in the study, 88 (77.9%) used a minimally invasive posterolateral approach, 18 (15.9%) a direct anterior approach, and 7 (6.2%) an anterolateral approach. All THAs were performed with conventional instruments and uncemented components. All TKAs were performed with a standard medial parapatellar approach, conventional instruments, and a tourniquet; in each case, the patella was resurfaced, and cemented fixation was used. Drains were not used in any THA or TKA cases. A local anesthetic cocktail (100 mL of 0.25% ropivacaine, 15 mL of 0.5% ropivacaine, and 1 mL of 1:1000 epinephrine) was injected for postoperative analgesia in all THA and TKA cases.
There were 3 important intraoperative findings in the THA Day 0 group: 2 cases of incidental gluteus medius tendon tears requiring repair and 1 case of nondisplaced calcar fracture treated with a cerclage cable. The THA Non-Day 0 group and both TKA groups had no major intraoperative findings.
Physical Therapy
Day-of-surgery PT was ordered for all patients. Patients did not receive formal PT before surgery. The PT protocol consisted of subjective assessment of patient condition, expectations, and goals; lower limb strengthening exercises; and maximum gait training with use of an assistive device as tolerated. Standard hip movement restrictions were ordered for posterolateral approach patients to protect the soft-tissue repair. Continuous passive motion (CPM) was not used during this study period.
Discharge Criteria
Patients were cleared for discharge by a multidisciplinary team using several criteria: no medical condition that would require readmission, intact surgical incision without discharge or concerning erythema, adequate analgesia (oral medications), intact neurovascular examination, and PT goals achieved (independence with bed mobility, transfers, standing balance, and minimum gait distance of 150 feet). Patients who could not be discharged home because of family or occupation issues or because of problems with gait or transfer were referred to skilled nursing or home healthcare. Follow-up for wound assessment and for examination of radiographs and functional range of motion was planned for 2 to 3 weeks after surgery (all patients followed up). Two patients, 1 in the THA Non-Day 0 group and 1 in the TKA Day 0 group, had a mechanical fall 1 day before discharge, but there were no complication-related discharge delays. In addition, there were no readmissions during the first 4 weeks after surgery.
Excluded Patients
Of the 116 THA cases, 113 (63 Day 0, 50 Non-Day 0) were analyzed. To establish homogeneity between groups and remove potential confounding factors, we excluded 4 THA patients (all Non-Day 0) from analysis because of medical complications prolonging LOS. In 1 of these cases, the patient developed respiratory insufficiency and myocardial infarction on POD-3, and critical care support was required (LOS, 16 days). In another case, anticoagulation treatment led to the development of a hip hematoma on POD-9 and to treatment (evacuation) in the operating room (LOS, 14 days). The other 2 cases involved exacerbation of dysphagia from preexisting myasthenia gravis (LOS, 5 days) and Ogilvie syndrome, managed conservatively (LOS, 9 days).
Of the 126 TKA cases, 123 (97 Day 0, 26 Non-Day 0) were analyzed. Three TKA patients were excluded because of prolonged hospitalization for medical reasons: One developed a deep vein thrombosis, 1 acquired Clostridium difficile colitis (history of lung transplantation, multiple immunosuppressive drugs), and 1 developed respiratory insufficiency from asthma exacerbation.
Statistical Analysis
Power analysis (G*Power) was used to determine an appropriate sample size for comparison.11 Given a previously published mean LOS after THA of 4 days, the hypothesized mean LOS reducing that by at least 0.5 day to 3.5 days, a significance level set at 5%, a power of test set at 0.95, and an allocation ratio of 1, a minimum of 23 subjects would be needed in each group to attain a statistically significant difference using the nonparametric Mann-Whitney test. The Shapiro-Wilk test was used to assess data normality. Regarding statistical significance, the Mann-Whitney U test was used for non-normally distributed data, the 2-sided Fisher exact test and χ2 test for qualitative data and contingency, and the 2-tailed, unpaired, independent-samples Student t test for normally distributed data. Data were analyzed with SPSS Statistics for Windows Version 20 (IBM).
Results
TKA and THA patients had similar demographic profiles, types of anesthesia, operating room and surgery times, surgical approaches, and total number of PT sessions before discharge. Estimated blood loss, however, was significantly (P < .05) higher for Non-Day 0 patients than for Non-Day 0 patients (Table 1).
Mean (SD) distance ambulated during first PT session was 2-fold farther (P = .014) for Non-Day 0 patients, 84.1 (10.4) feet, than for Day 0 patients, 42.1 (6.4) feet. On POD-1, mean (SD) gait was significantly (P = .019) longer for Day 0 patients, 162.4 (12.9) feet, than for Non-Day 0 patients, 118 (11.7) feet (Figure 2).
In TKA patients, although mean (SD) distance ambulated tended to be farther for the Day 0 group than for the Non-Day 0 group—114 (12.3) feet on POD-1 and 176 (15.2) feet on POD-2 for Day 0 vs 94 (22.2) feet on POD-1 and 148 (22.1) feet on POD-2 for Non-Day 0—the differences were not statistically significant. In addition, knee arc of motion during first PT session was statistically significantly (P = .3) higher for Day 0 patients, 69.1° (18.7°), than for Non-Day 0 patients, 61.7° (18.8°).
Statistical analysis revealed no difference in LOS based on surgical approach to the hip: 2.4 days for posterolateral (2.2 days for Day 0 and 2.6 days for Non-Day 0; P = .06); 2.1 days for direct anterior (2.1 days for Day 0 and 2.0 days for Non-Day 0; P = .7); and 2.7 days for anterolateral (3.0 days for Day 0 and 2.6 days for Non-Day 0; P = .6).
Discussion
Protocols for PT after THA and TKA remain unstandardized and largely dependent on institutions and surgeons. Factors permitting successful implementation of accelerated rehabilitation include patient motivation, adequate analgesia, and adequate support by physical therapists.12 A potential risk associated with accelerated PT after THA is dislocation, which did not occur in any patient in our Day 0 group. Other risks are increased pain and swelling leading to increased risk of falling and bleeding, which were not observed in our cohort. Although Day 0 PT was ordered in all cases in this study, only 55% of THA patients and 79% of TKA patients received PT the same day as their surgery. The delay can be addressed by making physical therapists’ work shifts more flexible for cases that finish later in the day and by providing preoperative education on the importance of day-of-surgery PT. Dr. Incavo and office staff routinely discuss discharge planning with all patients before surgery, but there was no stimulus protocol or communication to discuss or emphasize LOS with patients before surgery, and there was no questionnaire or survey given to assess patient expectations about PT and discharge.
Our finding of no statistically significant reduction in mean LOS after implementation of accelerated PT for THA or TKA differs from findings in multiple other reports.4,5,13-17 Baseline or control group mean LOS tended to be higher in previous studies3,5,18-23 (3.4-11.4 days) than in our control group (2.5 days) (Table 2).
Conclusion
These results provide useful information for providers who are managing primary THA and TKA cases and seeking continual improvement in postoperative patient care and better resource allocation. Hospitals, particularly those operating in bundled-care environments, are increasingly coming under scrutiny to control costs. Our study results showed that the costs associated with Day 0 PT are justified for THA but not for TKA.
Am J Orthop. 2016;45(6):E337-E342. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780-785.
2. Barbieri A, Vanhaecht K, Van Herck P, et al. Effects of clinical pathways in the joint replacement: a meta-analysis. BMC Med. 2009;7:32.
3. den Hartog YM, Mathijssen NM, Vehmeijer SB. Reduced length of hospital stay after the introduction of a rapid recovery protocol for primary THA procedures. Acta Orthop. 2013;84(5):444-447.
4. Husted H, Holm G, Jacobsen S. Predictors of length of stay and patient satisfaction after hip and knee replacement surgery: fast-track experience in 712 patients. Acta Orthop. 2008;79(2):168-173.
5. Robbins CE, Casey D, Bono JV, Murphy SB, Talmo CT, Ward DM. A multidisciplinary total hip arthroplasty protocol with accelerated postoperative rehabilitation: does the patient benefit? Am J Orthop. 2014;43(4):178-181.
6. den Hartog YM, Mathijssen NM, Hannink G, Vehmeijer SB. Which patient characteristics influence length of hospital stay after primary total hip arthroplasty in a ‘fast-track’ setting? Bone Joint J. 2015;97(1):19-23.
7. Forrest G, Fuchs M, Gutierrez A, Girardy J. Factors affecting length of stay and need for rehabilitation after hip and knee arthroplasty. J Arthroplasty. 1998;13(2):186-190.
8. Foote J, Panchoo K, Blair P, Bannister G. Length of stay following primary total hip replacement. Ann R Coll Surg Engl. 2009;91(6):500-504.
9. Sharma V, Morgan PM, Cheng EY. Factors influencing early rehabilitation after THA: a systematic review. Clin Orthop Relat Res. 2009;467(6):1400-1411.
10. Dorr LD, Maheshwari AV, Long WT, Wan Z, Sirianni LE. Early pain relief and function after posterior minimally invasive and conventional total hip arthroplasty. A prospective, randomized, blinded study. J Bone Joint Surg Am. 2007;89(6):1153-1160.
11. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175-191.
12. Ranawat AS, Ranawat CS. Pain management and accelerated rehabilitation for total hip and total knee arthroplasty. J Arthroplasty. 2007;22(7 suppl 3):12-15.
13. Husted H, Otte KS, Kristensen BB, Orsnes T, Kehlet H. Readmissions after fast-track hip and knee arthroplasty. Arch Orthop Trauma Surg. 2010;130(9):1185-1191.
14. Husted H, Lunn TH, Troelsen A, Gaarn-Larsen L, Kristensen BB, Kehlet H. Why still in hospital after fast-track hip and knee arthroplasty? Acta Orthop. 2011;82(6):679-684.
15. Husted H, Jensen CM, Solgaard S, Kehlet H. Reduced length of stay following hip and knee arthroplasty in Denmark 2000-2009: from research to implementation. Arch Orthop Trauma Surg. 2012;132(1):101-104.
16. Berger RA, Sanders SA, Thill ES, Sporer SM, Della Valle C. Newer anesthesia and rehabilitation protocols enable outpatient hip replacement in selected patients. Clin Orthop Relat Res. 2009;467(6):1424-1430.
17. Peck CN, Foster A, McLauchlan GJ. Reducing incision length or intensifying rehabilitation: what makes the difference to length of stay in total hip replacement in a UK setting? Int Orthop. 2006;30(5):395-398.
18. Isaac D, Falode T, Liu P, I’Anson H, Dillow K, Gill P. Accelerated rehabilitation after total knee replacement. Knee. 2005;12(5):346-350.
19. Labraca NS, Castro-Sánchez AM, Matarán-Peñarrocha GA, Arroyo-Morales M, Sánchez-Joya Mdel M, Moreno-Lorenzo C. Benefits of starting rehabilitation within 24 hours of primary total knee arthroplasty: randomized clinical trial. Clin Rehabil. 2011;25(6):557-566.
20. Larsen K, Hansen TB, Søballe K. Hip arthroplasty patients benefit from accelerated perioperative care and rehabilitation: a quasi-experimental study of 98 patients. Acta Orthop. 2008;79(5):624-630.
21. Larsen K, Hansen TB, Thomsen PB, Christiansen T, Søballe K. Cost-effectiveness of accelerated perioperative care and rehabilitation after total hip and knee arthroplasty. J Bone Joint Surg Am. 2009;91(4):761-772.
22. Larsen K, Sørensen OG, Hansen TB, Thomsen PB, Søballe K. Accelerated perioperative care and rehabilitation intervention for hip and knee replacement is effective: a randomized clinical trial involving 87 patients with 3 months of follow-up. Acta Orthop. 2008;79(2):149-159.
23. Wellman SS, Murphy AC, Gulcynski D. Murphy SB. Implementation of an accelerated mobilization protocol following primary total hip arthroplasty: impact on length of stay and disposition. Curr Rev Musculoskelet Med. 2011;4(3):84-90.
1. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780-785.
2. Barbieri A, Vanhaecht K, Van Herck P, et al. Effects of clinical pathways in the joint replacement: a meta-analysis. BMC Med. 2009;7:32.
3. den Hartog YM, Mathijssen NM, Vehmeijer SB. Reduced length of hospital stay after the introduction of a rapid recovery protocol for primary THA procedures. Acta Orthop. 2013;84(5):444-447.
4. Husted H, Holm G, Jacobsen S. Predictors of length of stay and patient satisfaction after hip and knee replacement surgery: fast-track experience in 712 patients. Acta Orthop. 2008;79(2):168-173.
5. Robbins CE, Casey D, Bono JV, Murphy SB, Talmo CT, Ward DM. A multidisciplinary total hip arthroplasty protocol with accelerated postoperative rehabilitation: does the patient benefit? Am J Orthop. 2014;43(4):178-181.
6. den Hartog YM, Mathijssen NM, Hannink G, Vehmeijer SB. Which patient characteristics influence length of hospital stay after primary total hip arthroplasty in a ‘fast-track’ setting? Bone Joint J. 2015;97(1):19-23.
7. Forrest G, Fuchs M, Gutierrez A, Girardy J. Factors affecting length of stay and need for rehabilitation after hip and knee arthroplasty. J Arthroplasty. 1998;13(2):186-190.
8. Foote J, Panchoo K, Blair P, Bannister G. Length of stay following primary total hip replacement. Ann R Coll Surg Engl. 2009;91(6):500-504.
9. Sharma V, Morgan PM, Cheng EY. Factors influencing early rehabilitation after THA: a systematic review. Clin Orthop Relat Res. 2009;467(6):1400-1411.
10. Dorr LD, Maheshwari AV, Long WT, Wan Z, Sirianni LE. Early pain relief and function after posterior minimally invasive and conventional total hip arthroplasty. A prospective, randomized, blinded study. J Bone Joint Surg Am. 2007;89(6):1153-1160.
11. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175-191.
12. Ranawat AS, Ranawat CS. Pain management and accelerated rehabilitation for total hip and total knee arthroplasty. J Arthroplasty. 2007;22(7 suppl 3):12-15.
13. Husted H, Otte KS, Kristensen BB, Orsnes T, Kehlet H. Readmissions after fast-track hip and knee arthroplasty. Arch Orthop Trauma Surg. 2010;130(9):1185-1191.
14. Husted H, Lunn TH, Troelsen A, Gaarn-Larsen L, Kristensen BB, Kehlet H. Why still in hospital after fast-track hip and knee arthroplasty? Acta Orthop. 2011;82(6):679-684.
15. Husted H, Jensen CM, Solgaard S, Kehlet H. Reduced length of stay following hip and knee arthroplasty in Denmark 2000-2009: from research to implementation. Arch Orthop Trauma Surg. 2012;132(1):101-104.
16. Berger RA, Sanders SA, Thill ES, Sporer SM, Della Valle C. Newer anesthesia and rehabilitation protocols enable outpatient hip replacement in selected patients. Clin Orthop Relat Res. 2009;467(6):1424-1430.
17. Peck CN, Foster A, McLauchlan GJ. Reducing incision length or intensifying rehabilitation: what makes the difference to length of stay in total hip replacement in a UK setting? Int Orthop. 2006;30(5):395-398.
18. Isaac D, Falode T, Liu P, I’Anson H, Dillow K, Gill P. Accelerated rehabilitation after total knee replacement. Knee. 2005;12(5):346-350.
19. Labraca NS, Castro-Sánchez AM, Matarán-Peñarrocha GA, Arroyo-Morales M, Sánchez-Joya Mdel M, Moreno-Lorenzo C. Benefits of starting rehabilitation within 24 hours of primary total knee arthroplasty: randomized clinical trial. Clin Rehabil. 2011;25(6):557-566.
20. Larsen K, Hansen TB, Søballe K. Hip arthroplasty patients benefit from accelerated perioperative care and rehabilitation: a quasi-experimental study of 98 patients. Acta Orthop. 2008;79(5):624-630.
21. Larsen K, Hansen TB, Thomsen PB, Christiansen T, Søballe K. Cost-effectiveness of accelerated perioperative care and rehabilitation after total hip and knee arthroplasty. J Bone Joint Surg Am. 2009;91(4):761-772.
22. Larsen K, Sørensen OG, Hansen TB, Thomsen PB, Søballe K. Accelerated perioperative care and rehabilitation intervention for hip and knee replacement is effective: a randomized clinical trial involving 87 patients with 3 months of follow-up. Acta Orthop. 2008;79(2):149-159.
23. Wellman SS, Murphy AC, Gulcynski D. Murphy SB. Implementation of an accelerated mobilization protocol following primary total hip arthroplasty: impact on length of stay and disposition. Curr Rev Musculoskelet Med. 2011;4(3):84-90.

Glenohumeral Joint Sepsis Caused by Streptococcus mitis: A Case Report
Septic arthritis predominantly involves the weight-bearing joints of the hip and knee, which account for nearly 60% of cases.1 In contrast, the shoulder joint is involved in 10% to 15% of cases, though this number may be higher among intravenous (IV) drug users.2 The most common causative organisms are the Staphylococcus species, followed closely by β-hemolytic streptococci, with these 2 groups accounting for more than 90% of all cases.3 The Streptococcus viridans group belongs to normal oral flora residing predominantly on the surface of teeth. Although well known for its ability to colonize heart valves and frequently cause bacterial endocarditis, this group has rarely been associated with septic arthritis. Furthermore, Streptococcus mitis, a subgroup of S viridans, has been implicated even less commonly.
In this article, we report a case of glenohumeral joint septic arthritis caused by S mitis. To our knowledge, such a case has not been previously reported in the English literature. Given the low virulence of this orally based bacterium, treating physicians must maintain clinical suspicion for the organism in the setting of persistent joint effusion and pain in association with periodontal disease or trauma. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A right-hand-dominant 54-year-old man presented to Dr. Gruson with complaints of persistent right shoulder pain associated with worsening range of motion (ROM). Three weeks earlier, the patient reported being assaulted and noted progressive swelling about the right shoulder. He denied fevers, chills, or prior shoulder problems. Although his past medical history was remarkable for hepatitis C and diabetes, he was not taking any diabetic medications at that time. A review of systems was remarkable for poor dental hygiene, and the patient was missing several teeth, which he said had been knocked out during the assault. Physical examination revealed diffuse tenderness about the right shoulder and severe pain with all passive movement. The shoulder was pseudoparalyzed. There were no subcutaneous collections, wounds, or ecchymosis about the shoulder. Mild calor was noted on the right shoulder relative to the left. Radiographs of the right shoulder showed no acute osseous abnormalities.
Magnetic resonance imaging (MRI), which was urgently obtained to assess the integrity of the rotator cuff and the location of the effusion, showed a large subacromial and glenohumeral joint effusion as well as diffuse muscular edema (Figures 1A-1C). 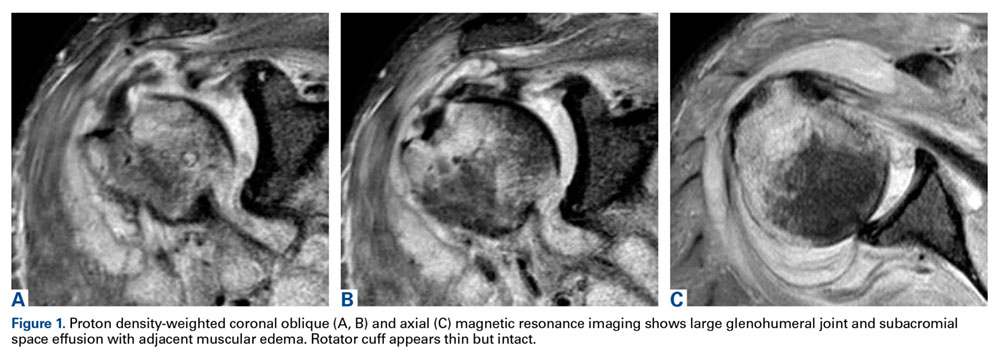
In light of the elevated infection findings of the laboratory tests and the positive culture, urgent arthroscopic irrigation and débridement of the right shoulder were indicated. Given the organism identified, transesophageal echocardiography was performed; there were no valvular vegetations. Creation of the posterior glenohumeral portal resulted in egress of turbid fluid, which was sent for culture. The subacromial space and the glenohumeral joint were thoroughly lavaged and the copious hemorrhagic synovitis débrided (Figures 2A, 2B). 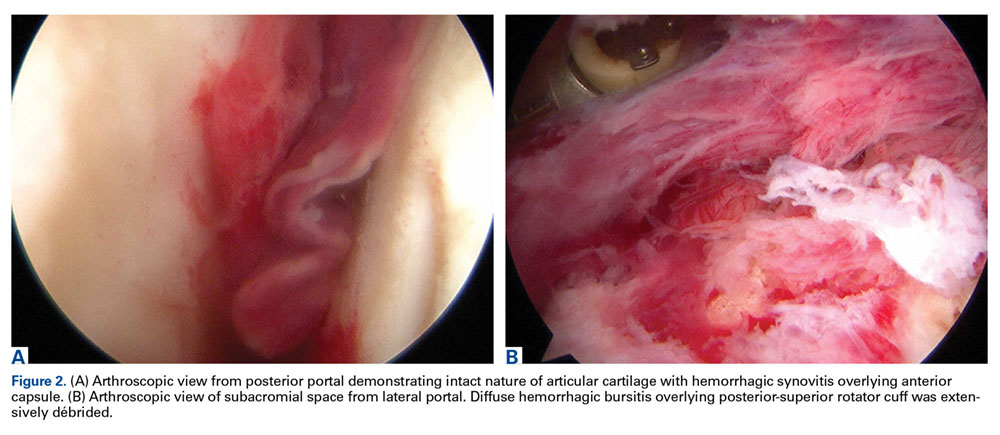
The 8-week course of antibiotics normalized the patient’s ESR to 13 mm/h. Follow-up MRI showed improvement in the soft-tissue edema. Clinically, the patient reported minimal shoulder pain. He was undergoing physical therapy to regain strength and ROM.
Discussion
Staphylococcus aureus is the leading causative organism of septic arthritis, accounting for more than 60% of all cases.4 Conversely, the Streptococcus viridans group is rarely implicated in septic arthritis, accounting for <1% of cases.4S viridans is part of the commensal oral flora and has low virulence. This heterogeneous group is subdivided into S mitis, S salivarius, S anginosus, S mutans, and S bovis. The S mitis group is further subdivided into S sanguinis (formerly known as S sanguis) and S mitis. Infection by an organism of the S viridans group usually occurs on a previously injured focus, and the organism is a causative agent of bacterial endocarditis.5 Reported cases of septic arthritis caused by S viridans have predominantly involved the knee joint—with severe osteoarthritis, poor dental hygiene, and prior IV drug use identified as risk factors.5-7The shoulder joint is seldom involved in septic arthritis; estimated incidence is under 8%.8 Although overall incidence may rise in an increasingly elderly patient population, incidence of shoulder infection remains low.2,9
The main routes for developing septic arthritis include direct inoculation secondary to penetrating trauma or hematologic spread.10 Coatsworth and colleagues11 reported on iatrogenic S mitis septic arthritis of a shoulder arthroplasty during ultrasonography-guided aspiration by a technician who was not wearing a mask. Our institutional policy is to perform joint aspiration under strictly sterile conditions, which were adhered to in the present case. We surmise our patient developed transient bacteremia from the loss of several teeth, particularly given his poor dentition. Yombi and colleagues5 documented 2 cases of septic arthritis caused by Streptococcus gordonii, a relative of S sanguinis. One involved a previously replaced knee, and the other a native knee joint. Other cases of S viridans group septic arthritis have involved the knee,6,7,12,13 the sternoclavicular joint,14-16 and the acromioclavicular joint.17S sanguinis6,7,12,15,16 and S gordonii5 have been implicated in most cases, and an unspeciated S viridans in others.13,14,17 Concomitant periodontal disease has been reported in most cases as well,6,7,12,15 including our patient’s case. In the English-language literature, we found no other reports of S mitis as the causative agent of acute septic glenohumeral joint arthritis from hematogenous spread.
There should be no delay in diagnosing septic arthritis, and infected material should be removed from the joint. In animal models, complete joint destruction occurred only 5 weeks after inoculation with Staphylococcus aureus.10 Garofalo and colleagues18 reported a trend toward improved functional outcomes after earlier operative treatment. The choice of open surgical drainage vs repeat needle aspiration seems to be of little consequence, as both have good long-term outcomes, but open surgical drainage seems to result in better long-term functional ROM.2,9 However, results of a recent study suggested surgical treatment is not always superior to medical treatment for septic arthritis in native joints.19 In some cases involving S viridans species, treatment consisted of a combination of IV antibiotics and onetime or repeat aspiration;6,12-15 treatment in the remaining cases was surgical débridement.5,7,16,17 Given that S viridans is associated with bacterial endocarditis, echocardiography is essential if this organism is to be identified. Medical management and antibiotic treatment should be initiated after consultation with medical and infectious disease specialists.19We have reported a case of septic shoulder caused by S mitis, a low-virulence organism seldom associated with joint infection. The patient’s infection likely resulted from hematogenous spread from the oral cavity (dentition was poor). Urgent aspiration of the joint and baseline infection laboratory tests are recommended. MRI of the shoulder may show an effusion. Urgent arthroscopic irrigation and débridement can yield good clinical outcomes.
Am J Orthop. 2016;45(6):E343-E346. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Mathews CJ, Kingsley G, Field M, et al. Management of septic arthritis: a systematic review. Ann Rheum Dis. 2007;66(4):440-445.
2. Leslie BM, Harris JM 3rd, Driscoll D. Septic arthritis of the shoulder in adults. J Bone Joint Surg Am. 1989;71(10):1516-1522.
3. Gupta MN, Sturrock RD, Field M. A prospective 2-year study of 75 patients with adult-onset septic arthritis. Rheumatology. 2001;40(1):24-30.
4. Dubost JJ, Soubrier M, De Champs C, Ristori JM, Bussiere JL, Sauvezie B. No changes in the distribution of organisms responsible for septic arthritis over a 20 year period. Ann Rheum Dis. 2002;61(3):267-269.
5. Yombi J, Belkhir L, Jonckheere S, et al. Streptococcus gordonii septic arthritis: two cases and review of literature. BMC Infect Dis. 2012;12:215.
6. Papaioannides D, Boniatsi L, Korantzopoulos P, Sinapidis D, Giotis C. Acute septic arthritis due to Streptococcus sanguis. Med Princ Pract. 2006;15(1):77-79.
7. Edson RS, Osmon DR, Berry DJ. Septic arthritis due to Streptococcus sanguis. Mayo Clin Proc. 2002;77(7):709-710.
8. Weston VC, Jones AC, Bradbury N, Fawthrop F, Doherty M. Clinical features and outcome of septic arthritis in a single UK health district 1982-1991. Ann Rheum Dis. 1999;58(4):214-219.
9. Lossos IS, Yossepowitch O, Kandel L, Yardeni D, Arber N. Septic arthritis of the glenohumeral joint. A report of 11 cases and review of the literature. Medicine. 1998;77(3):177-187.
10. Esterhai JL Jr, Gelb I. Adult septic arthritis. Orthop Clin North Am. 1991;22(3):503-514.
11. Coatsworth NR, Huntington PG, Giuffre B, Kotsiou G. The doctor and the mask: iatrogenic septic arthritis caused by Streptoccocus mitis. Med J Aust. 2013;198(5):285-286.
12. Patrick MR, Lewis D. Short of a length: Streptococcus sanguis knee infection from dental source. Br J Rheumatol. 1992;31(8):569.
13. Barbadillo C, Trujillo A, Cuende E, Mazzucchelli R, Mulero J, Andreu JL. Septic arthritis due to Streptococcus viridans. Clin Exp Rheumatol. 1990;8(5):520-521.
14. Mata P, Molins A, de Oya M. Sternal arthritis caused by Streptococcus viridans in a heroin addict [in Spanish]. Med Clin. 1984;83(16):689.
15. Mandac I, Prkacin I, Sabljar Matovinovic M, Sustercic D. Septic arthritis due to Streptococcus sanguis. Coll Antropol. 2010;34(2):661-664.
16. Nitsche JF, Vaughan JH, Williams G, Curd JG. Septic sternoclavicular arthritis with Pasteurella multocida and Streptococcus sanguis. Arthritis Rheum. 1982;25(4):467-469.
17. Blankstein A, Amsallem JL, Rubenstein E, Horoszowski H, Farin I. Septic arthritis of the acromioclavicular joint. Arch Orthop Trauma Surg. 1985;103(6):417-418.
18. Garofalo R, Flanagin B, Cesari E, Vinci E, Conti M, Castagna A. Destructive septic arthritis of shoulder in adults. Musculoskelet Surg. 2014;98(supp 1):S35-S39.
19. Ravindran V, Logan I, Bourke BE. Medical vs surgical treatment for the native joint in septic arthritis: a 6-year, single UK academic centre experience. Rheumatology. 2009;48(10):1320-1322.
Septic arthritis predominantly involves the weight-bearing joints of the hip and knee, which account for nearly 60% of cases.1 In contrast, the shoulder joint is involved in 10% to 15% of cases, though this number may be higher among intravenous (IV) drug users.2 The most common causative organisms are the Staphylococcus species, followed closely by β-hemolytic streptococci, with these 2 groups accounting for more than 90% of all cases.3 The Streptococcus viridans group belongs to normal oral flora residing predominantly on the surface of teeth. Although well known for its ability to colonize heart valves and frequently cause bacterial endocarditis, this group has rarely been associated with septic arthritis. Furthermore, Streptococcus mitis, a subgroup of S viridans, has been implicated even less commonly.
In this article, we report a case of glenohumeral joint septic arthritis caused by S mitis. To our knowledge, such a case has not been previously reported in the English literature. Given the low virulence of this orally based bacterium, treating physicians must maintain clinical suspicion for the organism in the setting of persistent joint effusion and pain in association with periodontal disease or trauma. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A right-hand-dominant 54-year-old man presented to Dr. Gruson with complaints of persistent right shoulder pain associated with worsening range of motion (ROM). Three weeks earlier, the patient reported being assaulted and noted progressive swelling about the right shoulder. He denied fevers, chills, or prior shoulder problems. Although his past medical history was remarkable for hepatitis C and diabetes, he was not taking any diabetic medications at that time. A review of systems was remarkable for poor dental hygiene, and the patient was missing several teeth, which he said had been knocked out during the assault. Physical examination revealed diffuse tenderness about the right shoulder and severe pain with all passive movement. The shoulder was pseudoparalyzed. There were no subcutaneous collections, wounds, or ecchymosis about the shoulder. Mild calor was noted on the right shoulder relative to the left. Radiographs of the right shoulder showed no acute osseous abnormalities.
Magnetic resonance imaging (MRI), which was urgently obtained to assess the integrity of the rotator cuff and the location of the effusion, showed a large subacromial and glenohumeral joint effusion as well as diffuse muscular edema (Figures 1A-1C).
In light of the elevated infection findings of the laboratory tests and the positive culture, urgent arthroscopic irrigation and débridement of the right shoulder were indicated. Given the organism identified, transesophageal echocardiography was performed; there were no valvular vegetations. Creation of the posterior glenohumeral portal resulted in egress of turbid fluid, which was sent for culture. The subacromial space and the glenohumeral joint were thoroughly lavaged and the copious hemorrhagic synovitis débrided (Figures 2A, 2B).
The 8-week course of antibiotics normalized the patient’s ESR to 13 mm/h. Follow-up MRI showed improvement in the soft-tissue edema. Clinically, the patient reported minimal shoulder pain. He was undergoing physical therapy to regain strength and ROM.
Discussion
Staphylococcus aureus is the leading causative organism of septic arthritis, accounting for more than 60% of all cases.4 Conversely, the Streptococcus viridans group is rarely implicated in septic arthritis, accounting for <1% of cases.4S viridans is part of the commensal oral flora and has low virulence. This heterogeneous group is subdivided into S mitis, S salivarius, S anginosus, S mutans, and S bovis. The S mitis group is further subdivided into S sanguinis (formerly known as S sanguis) and S mitis. Infection by an organism of the S viridans group usually occurs on a previously injured focus, and the organism is a causative agent of bacterial endocarditis.5 Reported cases of septic arthritis caused by S viridans have predominantly involved the knee joint—with severe osteoarthritis, poor dental hygiene, and prior IV drug use identified as risk factors.5-7The shoulder joint is seldom involved in septic arthritis; estimated incidence is under 8%.8 Although overall incidence may rise in an increasingly elderly patient population, incidence of shoulder infection remains low.2,9
The main routes for developing septic arthritis include direct inoculation secondary to penetrating trauma or hematologic spread.10 Coatsworth and colleagues11 reported on iatrogenic S mitis septic arthritis of a shoulder arthroplasty during ultrasonography-guided aspiration by a technician who was not wearing a mask. Our institutional policy is to perform joint aspiration under strictly sterile conditions, which were adhered to in the present case. We surmise our patient developed transient bacteremia from the loss of several teeth, particularly given his poor dentition. Yombi and colleagues5 documented 2 cases of septic arthritis caused by Streptococcus gordonii, a relative of S sanguinis. One involved a previously replaced knee, and the other a native knee joint. Other cases of S viridans group septic arthritis have involved the knee,6,7,12,13 the sternoclavicular joint,14-16 and the acromioclavicular joint.17S sanguinis6,7,12,15,16 and S gordonii5 have been implicated in most cases, and an unspeciated S viridans in others.13,14,17 Concomitant periodontal disease has been reported in most cases as well,6,7,12,15 including our patient’s case. In the English-language literature, we found no other reports of S mitis as the causative agent of acute septic glenohumeral joint arthritis from hematogenous spread.
There should be no delay in diagnosing septic arthritis, and infected material should be removed from the joint. In animal models, complete joint destruction occurred only 5 weeks after inoculation with Staphylococcus aureus.10 Garofalo and colleagues18 reported a trend toward improved functional outcomes after earlier operative treatment. The choice of open surgical drainage vs repeat needle aspiration seems to be of little consequence, as both have good long-term outcomes, but open surgical drainage seems to result in better long-term functional ROM.2,9 However, results of a recent study suggested surgical treatment is not always superior to medical treatment for septic arthritis in native joints.19 In some cases involving S viridans species, treatment consisted of a combination of IV antibiotics and onetime or repeat aspiration;6,12-15 treatment in the remaining cases was surgical débridement.5,7,16,17 Given that S viridans is associated with bacterial endocarditis, echocardiography is essential if this organism is to be identified. Medical management and antibiotic treatment should be initiated after consultation with medical and infectious disease specialists.19We have reported a case of septic shoulder caused by S mitis, a low-virulence organism seldom associated with joint infection. The patient’s infection likely resulted from hematogenous spread from the oral cavity (dentition was poor). Urgent aspiration of the joint and baseline infection laboratory tests are recommended. MRI of the shoulder may show an effusion. Urgent arthroscopic irrigation and débridement can yield good clinical outcomes.
Am J Orthop. 2016;45(6):E343-E346. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
Septic arthritis predominantly involves the weight-bearing joints of the hip and knee, which account for nearly 60% of cases.1 In contrast, the shoulder joint is involved in 10% to 15% of cases, though this number may be higher among intravenous (IV) drug users.2 The most common causative organisms are the Staphylococcus species, followed closely by β-hemolytic streptococci, with these 2 groups accounting for more than 90% of all cases.3 The Streptococcus viridans group belongs to normal oral flora residing predominantly on the surface of teeth. Although well known for its ability to colonize heart valves and frequently cause bacterial endocarditis, this group has rarely been associated with septic arthritis. Furthermore, Streptococcus mitis, a subgroup of S viridans, has been implicated even less commonly.
In this article, we report a case of glenohumeral joint septic arthritis caused by S mitis. To our knowledge, such a case has not been previously reported in the English literature. Given the low virulence of this orally based bacterium, treating physicians must maintain clinical suspicion for the organism in the setting of persistent joint effusion and pain in association with periodontal disease or trauma. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A right-hand-dominant 54-year-old man presented to Dr. Gruson with complaints of persistent right shoulder pain associated with worsening range of motion (ROM). Three weeks earlier, the patient reported being assaulted and noted progressive swelling about the right shoulder. He denied fevers, chills, or prior shoulder problems. Although his past medical history was remarkable for hepatitis C and diabetes, he was not taking any diabetic medications at that time. A review of systems was remarkable for poor dental hygiene, and the patient was missing several teeth, which he said had been knocked out during the assault. Physical examination revealed diffuse tenderness about the right shoulder and severe pain with all passive movement. The shoulder was pseudoparalyzed. There were no subcutaneous collections, wounds, or ecchymosis about the shoulder. Mild calor was noted on the right shoulder relative to the left. Radiographs of the right shoulder showed no acute osseous abnormalities.
Magnetic resonance imaging (MRI), which was urgently obtained to assess the integrity of the rotator cuff and the location of the effusion, showed a large subacromial and glenohumeral joint effusion as well as diffuse muscular edema (Figures 1A-1C).
In light of the elevated infection findings of the laboratory tests and the positive culture, urgent arthroscopic irrigation and débridement of the right shoulder were indicated. Given the organism identified, transesophageal echocardiography was performed; there were no valvular vegetations. Creation of the posterior glenohumeral portal resulted in egress of turbid fluid, which was sent for culture. The subacromial space and the glenohumeral joint were thoroughly lavaged and the copious hemorrhagic synovitis débrided (Figures 2A, 2B).
The 8-week course of antibiotics normalized the patient’s ESR to 13 mm/h. Follow-up MRI showed improvement in the soft-tissue edema. Clinically, the patient reported minimal shoulder pain. He was undergoing physical therapy to regain strength and ROM.
Discussion
Staphylococcus aureus is the leading causative organism of septic arthritis, accounting for more than 60% of all cases.4 Conversely, the Streptococcus viridans group is rarely implicated in septic arthritis, accounting for <1% of cases.4S viridans is part of the commensal oral flora and has low virulence. This heterogeneous group is subdivided into S mitis, S salivarius, S anginosus, S mutans, and S bovis. The S mitis group is further subdivided into S sanguinis (formerly known as S sanguis) and S mitis. Infection by an organism of the S viridans group usually occurs on a previously injured focus, and the organism is a causative agent of bacterial endocarditis.5 Reported cases of septic arthritis caused by S viridans have predominantly involved the knee joint—with severe osteoarthritis, poor dental hygiene, and prior IV drug use identified as risk factors.5-7The shoulder joint is seldom involved in septic arthritis; estimated incidence is under 8%.8 Although overall incidence may rise in an increasingly elderly patient population, incidence of shoulder infection remains low.2,9
The main routes for developing septic arthritis include direct inoculation secondary to penetrating trauma or hematologic spread.10 Coatsworth and colleagues11 reported on iatrogenic S mitis septic arthritis of a shoulder arthroplasty during ultrasonography-guided aspiration by a technician who was not wearing a mask. Our institutional policy is to perform joint aspiration under strictly sterile conditions, which were adhered to in the present case. We surmise our patient developed transient bacteremia from the loss of several teeth, particularly given his poor dentition. Yombi and colleagues5 documented 2 cases of septic arthritis caused by Streptococcus gordonii, a relative of S sanguinis. One involved a previously replaced knee, and the other a native knee joint. Other cases of S viridans group septic arthritis have involved the knee,6,7,12,13 the sternoclavicular joint,14-16 and the acromioclavicular joint.17S sanguinis6,7,12,15,16 and S gordonii5 have been implicated in most cases, and an unspeciated S viridans in others.13,14,17 Concomitant periodontal disease has been reported in most cases as well,6,7,12,15 including our patient’s case. In the English-language literature, we found no other reports of S mitis as the causative agent of acute septic glenohumeral joint arthritis from hematogenous spread.
There should be no delay in diagnosing septic arthritis, and infected material should be removed from the joint. In animal models, complete joint destruction occurred only 5 weeks after inoculation with Staphylococcus aureus.10 Garofalo and colleagues18 reported a trend toward improved functional outcomes after earlier operative treatment. The choice of open surgical drainage vs repeat needle aspiration seems to be of little consequence, as both have good long-term outcomes, but open surgical drainage seems to result in better long-term functional ROM.2,9 However, results of a recent study suggested surgical treatment is not always superior to medical treatment for septic arthritis in native joints.19 In some cases involving S viridans species, treatment consisted of a combination of IV antibiotics and onetime or repeat aspiration;6,12-15 treatment in the remaining cases was surgical débridement.5,7,16,17 Given that S viridans is associated with bacterial endocarditis, echocardiography is essential if this organism is to be identified. Medical management and antibiotic treatment should be initiated after consultation with medical and infectious disease specialists.19We have reported a case of septic shoulder caused by S mitis, a low-virulence organism seldom associated with joint infection. The patient’s infection likely resulted from hematogenous spread from the oral cavity (dentition was poor). Urgent aspiration of the joint and baseline infection laboratory tests are recommended. MRI of the shoulder may show an effusion. Urgent arthroscopic irrigation and débridement can yield good clinical outcomes.
Am J Orthop. 2016;45(6):E343-E346. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Mathews CJ, Kingsley G, Field M, et al. Management of septic arthritis: a systematic review. Ann Rheum Dis. 2007;66(4):440-445.
2. Leslie BM, Harris JM 3rd, Driscoll D. Septic arthritis of the shoulder in adults. J Bone Joint Surg Am. 1989;71(10):1516-1522.
3. Gupta MN, Sturrock RD, Field M. A prospective 2-year study of 75 patients with adult-onset septic arthritis. Rheumatology. 2001;40(1):24-30.
4. Dubost JJ, Soubrier M, De Champs C, Ristori JM, Bussiere JL, Sauvezie B. No changes in the distribution of organisms responsible for septic arthritis over a 20 year period. Ann Rheum Dis. 2002;61(3):267-269.
5. Yombi J, Belkhir L, Jonckheere S, et al. Streptococcus gordonii septic arthritis: two cases and review of literature. BMC Infect Dis. 2012;12:215.
6. Papaioannides D, Boniatsi L, Korantzopoulos P, Sinapidis D, Giotis C. Acute septic arthritis due to Streptococcus sanguis. Med Princ Pract. 2006;15(1):77-79.
7. Edson RS, Osmon DR, Berry DJ. Septic arthritis due to Streptococcus sanguis. Mayo Clin Proc. 2002;77(7):709-710.
8. Weston VC, Jones AC, Bradbury N, Fawthrop F, Doherty M. Clinical features and outcome of septic arthritis in a single UK health district 1982-1991. Ann Rheum Dis. 1999;58(4):214-219.
9. Lossos IS, Yossepowitch O, Kandel L, Yardeni D, Arber N. Septic arthritis of the glenohumeral joint. A report of 11 cases and review of the literature. Medicine. 1998;77(3):177-187.
10. Esterhai JL Jr, Gelb I. Adult septic arthritis. Orthop Clin North Am. 1991;22(3):503-514.
11. Coatsworth NR, Huntington PG, Giuffre B, Kotsiou G. The doctor and the mask: iatrogenic septic arthritis caused by Streptoccocus mitis. Med J Aust. 2013;198(5):285-286.
12. Patrick MR, Lewis D. Short of a length: Streptococcus sanguis knee infection from dental source. Br J Rheumatol. 1992;31(8):569.
13. Barbadillo C, Trujillo A, Cuende E, Mazzucchelli R, Mulero J, Andreu JL. Septic arthritis due to Streptococcus viridans. Clin Exp Rheumatol. 1990;8(5):520-521.
14. Mata P, Molins A, de Oya M. Sternal arthritis caused by Streptococcus viridans in a heroin addict [in Spanish]. Med Clin. 1984;83(16):689.
15. Mandac I, Prkacin I, Sabljar Matovinovic M, Sustercic D. Septic arthritis due to Streptococcus sanguis. Coll Antropol. 2010;34(2):661-664.
16. Nitsche JF, Vaughan JH, Williams G, Curd JG. Septic sternoclavicular arthritis with Pasteurella multocida and Streptococcus sanguis. Arthritis Rheum. 1982;25(4):467-469.
17. Blankstein A, Amsallem JL, Rubenstein E, Horoszowski H, Farin I. Septic arthritis of the acromioclavicular joint. Arch Orthop Trauma Surg. 1985;103(6):417-418.
18. Garofalo R, Flanagin B, Cesari E, Vinci E, Conti M, Castagna A. Destructive septic arthritis of shoulder in adults. Musculoskelet Surg. 2014;98(supp 1):S35-S39.
19. Ravindran V, Logan I, Bourke BE. Medical vs surgical treatment for the native joint in septic arthritis: a 6-year, single UK academic centre experience. Rheumatology. 2009;48(10):1320-1322.
1. Mathews CJ, Kingsley G, Field M, et al. Management of septic arthritis: a systematic review. Ann Rheum Dis. 2007;66(4):440-445.
2. Leslie BM, Harris JM 3rd, Driscoll D. Septic arthritis of the shoulder in adults. J Bone Joint Surg Am. 1989;71(10):1516-1522.
3. Gupta MN, Sturrock RD, Field M. A prospective 2-year study of 75 patients with adult-onset septic arthritis. Rheumatology. 2001;40(1):24-30.
4. Dubost JJ, Soubrier M, De Champs C, Ristori JM, Bussiere JL, Sauvezie B. No changes in the distribution of organisms responsible for septic arthritis over a 20 year period. Ann Rheum Dis. 2002;61(3):267-269.
5. Yombi J, Belkhir L, Jonckheere S, et al. Streptococcus gordonii septic arthritis: two cases and review of literature. BMC Infect Dis. 2012;12:215.
6. Papaioannides D, Boniatsi L, Korantzopoulos P, Sinapidis D, Giotis C. Acute septic arthritis due to Streptococcus sanguis. Med Princ Pract. 2006;15(1):77-79.
7. Edson RS, Osmon DR, Berry DJ. Septic arthritis due to Streptococcus sanguis. Mayo Clin Proc. 2002;77(7):709-710.
8. Weston VC, Jones AC, Bradbury N, Fawthrop F, Doherty M. Clinical features and outcome of septic arthritis in a single UK health district 1982-1991. Ann Rheum Dis. 1999;58(4):214-219.
9. Lossos IS, Yossepowitch O, Kandel L, Yardeni D, Arber N. Septic arthritis of the glenohumeral joint. A report of 11 cases and review of the literature. Medicine. 1998;77(3):177-187.
10. Esterhai JL Jr, Gelb I. Adult septic arthritis. Orthop Clin North Am. 1991;22(3):503-514.
11. Coatsworth NR, Huntington PG, Giuffre B, Kotsiou G. The doctor and the mask: iatrogenic septic arthritis caused by Streptoccocus mitis. Med J Aust. 2013;198(5):285-286.
12. Patrick MR, Lewis D. Short of a length: Streptococcus sanguis knee infection from dental source. Br J Rheumatol. 1992;31(8):569.
13. Barbadillo C, Trujillo A, Cuende E, Mazzucchelli R, Mulero J, Andreu JL. Septic arthritis due to Streptococcus viridans. Clin Exp Rheumatol. 1990;8(5):520-521.
14. Mata P, Molins A, de Oya M. Sternal arthritis caused by Streptococcus viridans in a heroin addict [in Spanish]. Med Clin. 1984;83(16):689.
15. Mandac I, Prkacin I, Sabljar Matovinovic M, Sustercic D. Septic arthritis due to Streptococcus sanguis. Coll Antropol. 2010;34(2):661-664.
16. Nitsche JF, Vaughan JH, Williams G, Curd JG. Septic sternoclavicular arthritis with Pasteurella multocida and Streptococcus sanguis. Arthritis Rheum. 1982;25(4):467-469.
17. Blankstein A, Amsallem JL, Rubenstein E, Horoszowski H, Farin I. Septic arthritis of the acromioclavicular joint. Arch Orthop Trauma Surg. 1985;103(6):417-418.
18. Garofalo R, Flanagin B, Cesari E, Vinci E, Conti M, Castagna A. Destructive septic arthritis of shoulder in adults. Musculoskelet Surg. 2014;98(supp 1):S35-S39.
19. Ravindran V, Logan I, Bourke BE. Medical vs surgical treatment for the native joint in septic arthritis: a 6-year, single UK academic centre experience. Rheumatology. 2009;48(10):1320-1322.

Experts offer tips on anxiety, depression, and psychosis in Parkinson’s
SAN FRANCISCO – Depression and psychosis were strongly correlated in Parkinson’s disease, while the presence of clinical anxiety upped the odds of psychosis by a statistically significant 8%, in a cross-sectional study presented at the 2016 congress of the International Psychogeriatric Association.
Felicia C. Goldstein, PhD, professor of neurology at Emory University, Atlanta, compared 48 patients with Parkinson’s disease and psychosis with 96 nonpsychotic controls who also had Parkinson’s disease. The groups were similar in terms of age, age of disease onset, educational level, Montreal Cognitive Assessment score (MoCA), and Unified Parkinson’s Disease Rating Scale (UPDRS) score, although patients with psychosis had about a 1.5-year longer mean duration of Parkinson’s disease than did controls (8.8 years vs. 7.3 years; P = .06).

Patients with psychosis were significantly more likely than controls to meet DSM-5 and Beck Depression Inventory II criteria for depression, with odds ratios of 8.0 (95% confidence interval, 2.5-25.6; P = .001) and 1.1 (1.02-1.1; P = .01), respectively. Patients with psychosis also were significantly more likely to have a positive result on the Beck Anxiety Inventory (OR, 1.1; 95% CI, 1.01-1.15; P = .01), and met DSM-5 criteria for anxiety more often than did controls (OR, 3.0; 95% CI, 0.9-9.5), although the latter correlation did not reach statistical significance (P = .07).
“The association between psychosis and anxiety has not been previously reported,” Dr. Goldstein noted. The findings underscore the link between psychosis and mood disorders in Parkinson’s disease and the need to treat these comorbidities, she said.
Neuropsychiatric symptoms in Parkinson’s disease also merit close monitoring and treatment, because they correlate with greater disability, faster progression of motor symptoms, and increased mortality, Adriana P. Hermida, MD, said in a separate oral presentation at the congress. In particular, depression is “the elephant in the room when it comes to Parkinson’s disease,” she said. “It is there, it is underrecognized, and it is undertreated.” Suicidal ideation is common, and patients should be treated even if they do not meet all criteria for a depressive disorder, added Dr. Hermida of the department of psychiatry and behavioral sciences at Emory.

For depression in Parkinson’s disease, Dr. Hermida said she typically starts with a selective serotonin reuptake inhibitor, most often escitalopram or sertraline. If the patient has a partial response, she adds another antidepressant, but if there is no response, she switches antidepressants. Second-line options for add-ons and switches include mirtazapine, which improves sleep and appetite and may improve tremor; venlafaxine extended release, which can raise blood pressure and may benefit hypotensive patients; and bupropion extended release, which is best for patients who need more activation, do not have substantial concerns with anxiety, and have REM sleep behavior disorder, she said. She said she also will consider dopamine agonists such as pramipexole, but they can increase the risk of psychosis, impulse control disorders, and dopamine dysregulation syndrome. She also noted that electroconvulsive therapy can rapidly improve both depression and motor symptoms, and should not be reserved for last-resort cases. Parkinson’s medications should be held the day of ECT, and cognition should be monitored afterward, she said.
Approximately 30% of Parkinson’s patients meet DSM-5 criteria for an anxiety disorder, and more than half have significant symptoms of anxiety, Dr. Hermida continued. Anxiety, like other signs and symptoms of Parkinson’s disease, can fluctuate throughout the day and tends to occur most frequently during “off” periods. No randomized controlled trials have examined anxiolytics in Parkinson’s disease patients, but studies of mindfulness-based cognitive therapy have yielded good results, she noted. Benzodiazepines “should be used sparingly, if at all,” as they increase the risk of confusion, gait abnormalities, and falls.
Psychosis should be treated if symptoms are ego-dystonic, she said. She said she uses first-line clozapine, which is more effective for delusions than quetiapine and has fewer adverse motor effects. She said she has not yet used pimavanserin (Nuplazid), a selective 5-HT2A inverse agonist that in April 2016 became the first drug approved by the Food and Drug Administration for treating hallucinations and delusions in Parkinson’s disease. The pivotal trial lasted 6 weeks and included 199 patients; those who received pimavanserin had a median 5.8-point drop on the Scale to Access Psychosis in Parkinson’s Disease (SAPS-PD), compared with 2.7 for placebo (P = .001), Dr. Hermida noted. Patients did not experience sedation or motor impairment, which are common adverse effects of other antipsychotics in this population.
Dr. Goldstein and Dr. Hermida reported no funding sources or conflicts of interest.
SAN FRANCISCO – Depression and psychosis were strongly correlated in Parkinson’s disease, while the presence of clinical anxiety upped the odds of psychosis by a statistically significant 8%, in a cross-sectional study presented at the 2016 congress of the International Psychogeriatric Association.
Felicia C. Goldstein, PhD, professor of neurology at Emory University, Atlanta, compared 48 patients with Parkinson’s disease and psychosis with 96 nonpsychotic controls who also had Parkinson’s disease. The groups were similar in terms of age, age of disease onset, educational level, Montreal Cognitive Assessment score (MoCA), and Unified Parkinson’s Disease Rating Scale (UPDRS) score, although patients with psychosis had about a 1.5-year longer mean duration of Parkinson’s disease than did controls (8.8 years vs. 7.3 years; P = .06).
Patients with psychosis were significantly more likely than controls to meet DSM-5 and Beck Depression Inventory II criteria for depression, with odds ratios of 8.0 (95% confidence interval, 2.5-25.6; P = .001) and 1.1 (1.02-1.1; P = .01), respectively. Patients with psychosis also were significantly more likely to have a positive result on the Beck Anxiety Inventory (OR, 1.1; 95% CI, 1.01-1.15; P = .01), and met DSM-5 criteria for anxiety more often than did controls (OR, 3.0; 95% CI, 0.9-9.5), although the latter correlation did not reach statistical significance (P = .07).
“The association between psychosis and anxiety has not been previously reported,” Dr. Goldstein noted. The findings underscore the link between psychosis and mood disorders in Parkinson’s disease and the need to treat these comorbidities, she said.
Neuropsychiatric symptoms in Parkinson’s disease also merit close monitoring and treatment, because they correlate with greater disability, faster progression of motor symptoms, and increased mortality, Adriana P. Hermida, MD, said in a separate oral presentation at the congress. In particular, depression is “the elephant in the room when it comes to Parkinson’s disease,” she said. “It is there, it is underrecognized, and it is undertreated.” Suicidal ideation is common, and patients should be treated even if they do not meet all criteria for a depressive disorder, added Dr. Hermida of the department of psychiatry and behavioral sciences at Emory.
For depression in Parkinson’s disease, Dr. Hermida said she typically starts with a selective serotonin reuptake inhibitor, most often escitalopram or sertraline. If the patient has a partial response, she adds another antidepressant, but if there is no response, she switches antidepressants. Second-line options for add-ons and switches include mirtazapine, which improves sleep and appetite and may improve tremor; venlafaxine extended release, which can raise blood pressure and may benefit hypotensive patients; and bupropion extended release, which is best for patients who need more activation, do not have substantial concerns with anxiety, and have REM sleep behavior disorder, she said. She said she also will consider dopamine agonists such as pramipexole, but they can increase the risk of psychosis, impulse control disorders, and dopamine dysregulation syndrome. She also noted that electroconvulsive therapy can rapidly improve both depression and motor symptoms, and should not be reserved for last-resort cases. Parkinson’s medications should be held the day of ECT, and cognition should be monitored afterward, she said.
Approximately 30% of Parkinson’s patients meet DSM-5 criteria for an anxiety disorder, and more than half have significant symptoms of anxiety, Dr. Hermida continued. Anxiety, like other signs and symptoms of Parkinson’s disease, can fluctuate throughout the day and tends to occur most frequently during “off” periods. No randomized controlled trials have examined anxiolytics in Parkinson’s disease patients, but studies of mindfulness-based cognitive therapy have yielded good results, she noted. Benzodiazepines “should be used sparingly, if at all,” as they increase the risk of confusion, gait abnormalities, and falls.
Psychosis should be treated if symptoms are ego-dystonic, she said. She said she uses first-line clozapine, which is more effective for delusions than quetiapine and has fewer adverse motor effects. She said she has not yet used pimavanserin (Nuplazid), a selective 5-HT2A inverse agonist that in April 2016 became the first drug approved by the Food and Drug Administration for treating hallucinations and delusions in Parkinson’s disease. The pivotal trial lasted 6 weeks and included 199 patients; those who received pimavanserin had a median 5.8-point drop on the Scale to Access Psychosis in Parkinson’s Disease (SAPS-PD), compared with 2.7 for placebo (P = .001), Dr. Hermida noted. Patients did not experience sedation or motor impairment, which are common adverse effects of other antipsychotics in this population.
Dr. Goldstein and Dr. Hermida reported no funding sources or conflicts of interest.
SAN FRANCISCO – Depression and psychosis were strongly correlated in Parkinson’s disease, while the presence of clinical anxiety upped the odds of psychosis by a statistically significant 8%, in a cross-sectional study presented at the 2016 congress of the International Psychogeriatric Association.
Felicia C. Goldstein, PhD, professor of neurology at Emory University, Atlanta, compared 48 patients with Parkinson’s disease and psychosis with 96 nonpsychotic controls who also had Parkinson’s disease. The groups were similar in terms of age, age of disease onset, educational level, Montreal Cognitive Assessment score (MoCA), and Unified Parkinson’s Disease Rating Scale (UPDRS) score, although patients with psychosis had about a 1.5-year longer mean duration of Parkinson’s disease than did controls (8.8 years vs. 7.3 years; P = .06).
Patients with psychosis were significantly more likely than controls to meet DSM-5 and Beck Depression Inventory II criteria for depression, with odds ratios of 8.0 (95% confidence interval, 2.5-25.6; P = .001) and 1.1 (1.02-1.1; P = .01), respectively. Patients with psychosis also were significantly more likely to have a positive result on the Beck Anxiety Inventory (OR, 1.1; 95% CI, 1.01-1.15; P = .01), and met DSM-5 criteria for anxiety more often than did controls (OR, 3.0; 95% CI, 0.9-9.5), although the latter correlation did not reach statistical significance (P = .07).
“The association between psychosis and anxiety has not been previously reported,” Dr. Goldstein noted. The findings underscore the link between psychosis and mood disorders in Parkinson’s disease and the need to treat these comorbidities, she said.
Neuropsychiatric symptoms in Parkinson’s disease also merit close monitoring and treatment, because they correlate with greater disability, faster progression of motor symptoms, and increased mortality, Adriana P. Hermida, MD, said in a separate oral presentation at the congress. In particular, depression is “the elephant in the room when it comes to Parkinson’s disease,” she said. “It is there, it is underrecognized, and it is undertreated.” Suicidal ideation is common, and patients should be treated even if they do not meet all criteria for a depressive disorder, added Dr. Hermida of the department of psychiatry and behavioral sciences at Emory.
For depression in Parkinson’s disease, Dr. Hermida said she typically starts with a selective serotonin reuptake inhibitor, most often escitalopram or sertraline. If the patient has a partial response, she adds another antidepressant, but if there is no response, she switches antidepressants. Second-line options for add-ons and switches include mirtazapine, which improves sleep and appetite and may improve tremor; venlafaxine extended release, which can raise blood pressure and may benefit hypotensive patients; and bupropion extended release, which is best for patients who need more activation, do not have substantial concerns with anxiety, and have REM sleep behavior disorder, she said. She said she also will consider dopamine agonists such as pramipexole, but they can increase the risk of psychosis, impulse control disorders, and dopamine dysregulation syndrome. She also noted that electroconvulsive therapy can rapidly improve both depression and motor symptoms, and should not be reserved for last-resort cases. Parkinson’s medications should be held the day of ECT, and cognition should be monitored afterward, she said.
Approximately 30% of Parkinson’s patients meet DSM-5 criteria for an anxiety disorder, and more than half have significant symptoms of anxiety, Dr. Hermida continued. Anxiety, like other signs and symptoms of Parkinson’s disease, can fluctuate throughout the day and tends to occur most frequently during “off” periods. No randomized controlled trials have examined anxiolytics in Parkinson’s disease patients, but studies of mindfulness-based cognitive therapy have yielded good results, she noted. Benzodiazepines “should be used sparingly, if at all,” as they increase the risk of confusion, gait abnormalities, and falls.
Psychosis should be treated if symptoms are ego-dystonic, she said. She said she uses first-line clozapine, which is more effective for delusions than quetiapine and has fewer adverse motor effects. She said she has not yet used pimavanserin (Nuplazid), a selective 5-HT2A inverse agonist that in April 2016 became the first drug approved by the Food and Drug Administration for treating hallucinations and delusions in Parkinson’s disease. The pivotal trial lasted 6 weeks and included 199 patients; those who received pimavanserin had a median 5.8-point drop on the Scale to Access Psychosis in Parkinson’s Disease (SAPS-PD), compared with 2.7 for placebo (P = .001), Dr. Hermida noted. Patients did not experience sedation or motor impairment, which are common adverse effects of other antipsychotics in this population.
Dr. Goldstein and Dr. Hermida reported no funding sources or conflicts of interest.
AT IPA 2016
Key clinical point: A cross-sectional study uncovered a statistically significant link between anxiety and psychosis in Parkinson’s disease.
Major finding: Patients with psychosis also were significantly more likely to have a positive result on the Beck Anxiety Inventory (odds ratio, 1.1; 95% confidence interval, 1.01-1.15; P = .01).
Data source: A cross-sectional study of 48 patients with Parkinson’s disease and psychosis and 96 nonpsychotic controls who also had Parkinson’s disease.
Disclosures: Dr. Goldstein and Dr. Hermida disclosed no funding sources or conflicts of interest.
2016 GYN coding changes to note for your maximized reimbursement
In the August 2016 issue of OBG
Urogynecology diagnostic codes
Urogynecologists will find a large number of changes to codes they can select on October 1, 2016. While some codes improve reporting for conditions or symptoms related to urinary issues, many more concern postoperative complications following surgery for devices and grafts applied to the genitourinary system.
The American Urological Association requested new codes to align with a 2009 joint report on the terminology for female pelvic floor dysfunction.1 These codes, along with others, are listed in TABLE 1.
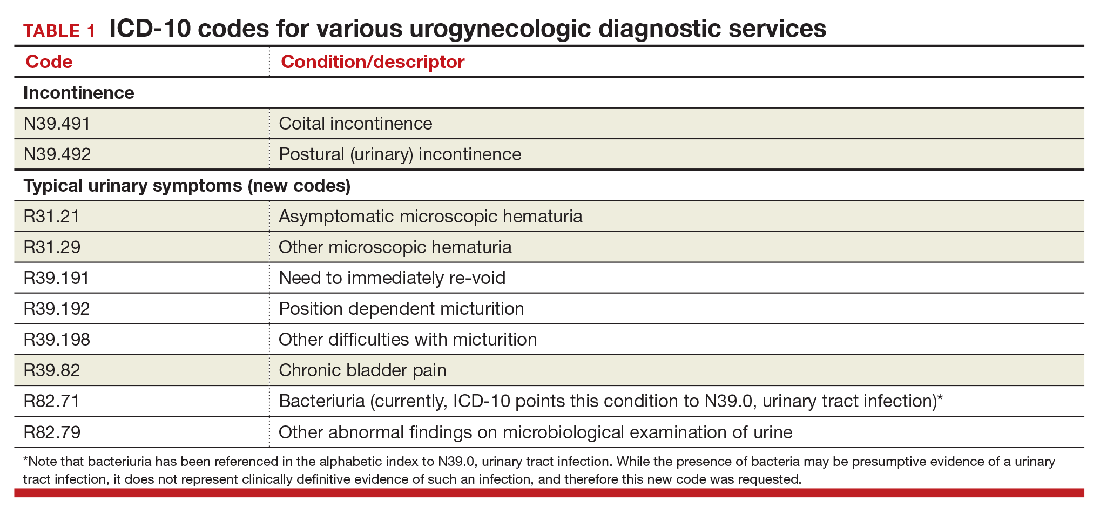
Urinary procedure complication codes
Not every urogynecologist will have an issue after surgery for incontinence, but if they do, there are tons of new and revised codes to address every possible complication the patient may have (TABLE 2). Each of these codes is reported based on whether the complication is being actively treated (initial encounter: final character is A), is being followed up after treatment (subsequent encounter: final character is D), or is caused by another condition (sequela: final character is S).
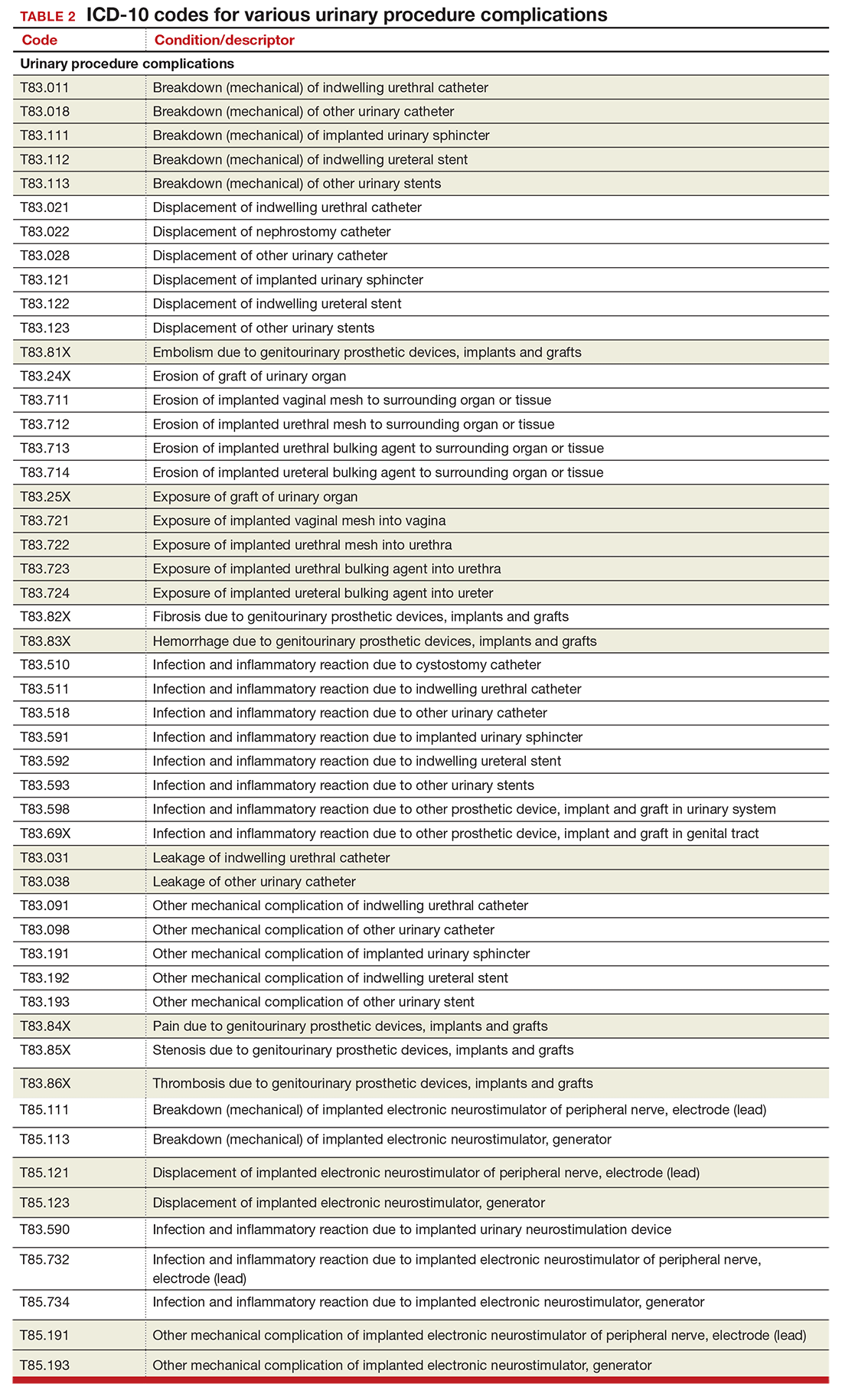
Gynecology-related diagnostic codes
Laterality
If there are 2 organs in the genitourinary system, the chances are good that there is now a right and a left designation code in ICD-10. Documentation should be clear, of course, and if the condition exists on both the right and the left side (even if only one side is being treated actively), list both codes, as there is no bilateral designation in the codes (TABLE 3). And while there is a code for “unspecified side,” providers normally do know which side, so use of this code should be avoided, if possible.
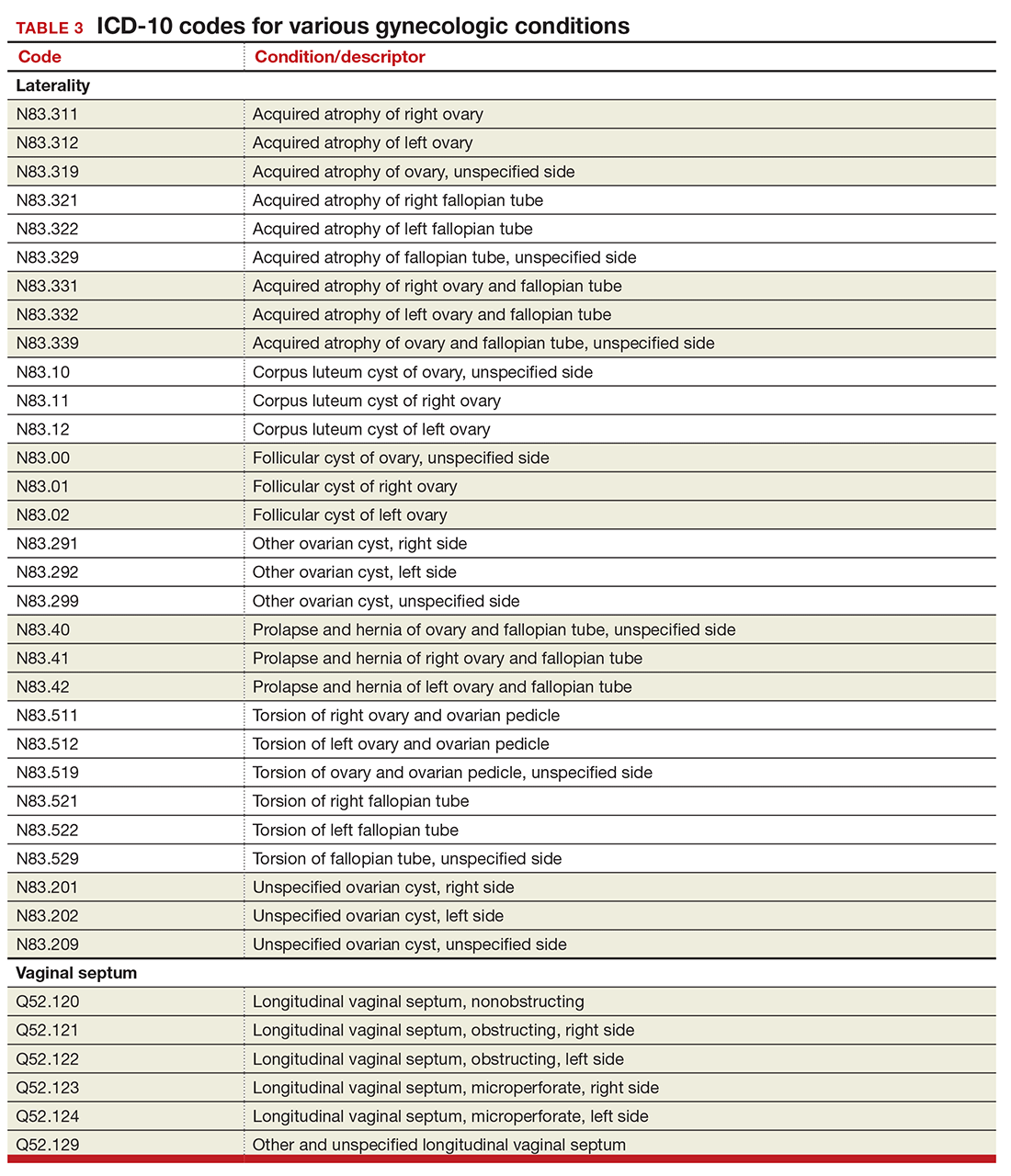
Vaginal septum
The right and left designations extend to the congenital codes for vaginal septum, but they go one step further. The American Congress of Obstetricians and Gynecologists (ACOG) requested that the codes for longitudinal vaginal septum be expanded to differentiate a nonobstructing vaginal septum from an obstructing vaginal septum, in addition to adding laterality to these codes (TABLE 3).2
Mastitis
There are now 2 new codes for inflammation of the breast; one describes mastitis without abscess, while the other code includes an abscess of the breast and nipple (TABLE 4). Once again, documentation will lead to the most specific code to describe the findings.

Childhood and prepubertal concerns
The single code for hypertrophy of the vulva has been expanded to include asymmetric labium majus enlargement. This code was requested by ACOG because this is a known clinical diagnosis and the currently available vulvar codes are inadequate for capturing this condition. The vulvar enlargement appears to be in response to hormonal surges during prepuberty and early puberty. Adult hypertrophy, either congenital or acquired from childbirth or as a late result of an old injury, would be reported by the “other specified” code (TABLE 5).
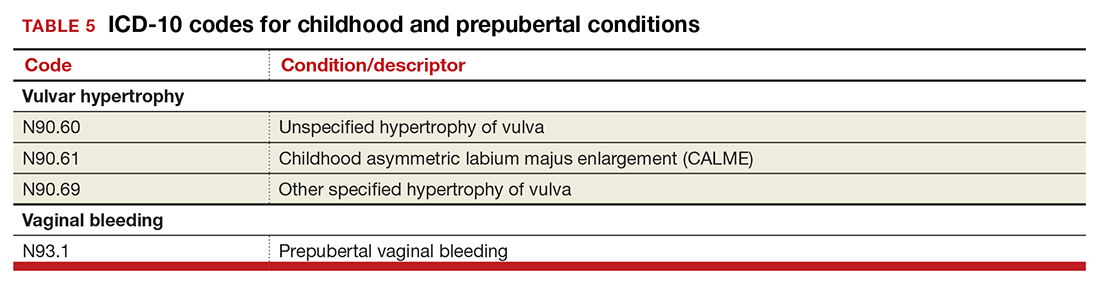
The causes of prepubertal bleeding vary and include the presence of a foreign object, tumors, or fluctuations in hormones, but prepubertal bleeding differs from the bleeding associated with normal menstruation. For that reason, ACOG requested a code that better captures the nature of the condition before a thorough work-up has pinpointed the cause (TABLE 5). Once the cause of the bleeding is known, a more specific diagnosis would then be reported (eg, D28.1, Benign neoplasm of vagina, or T19.2XXA, Foreign body in vulva and vagina, initial encounter).
Dypareunia
Additional documentation for dyspareunia will now be required to ensure that the most specific code is reported. In this case, the clinician should identify whether the pain is superficial or deep to better report on female pelvic floor dysfunction and to support the different treatments based on the location of the pain (TABLE 6). Deep dyspareunia would be felt in the mid or upper vagina.

Postoperative hemorrhage and hematoma
The codes for postprocedural hemorrhage and hematomas have received a face-lift: the single codes for these 2 complications will be split so that each can be reported separately (TABLE 7). Note that the new codes require that the condition be found following the initial surgery, and the code selected depends on whether the surgery involved the genitourinary system or another system.
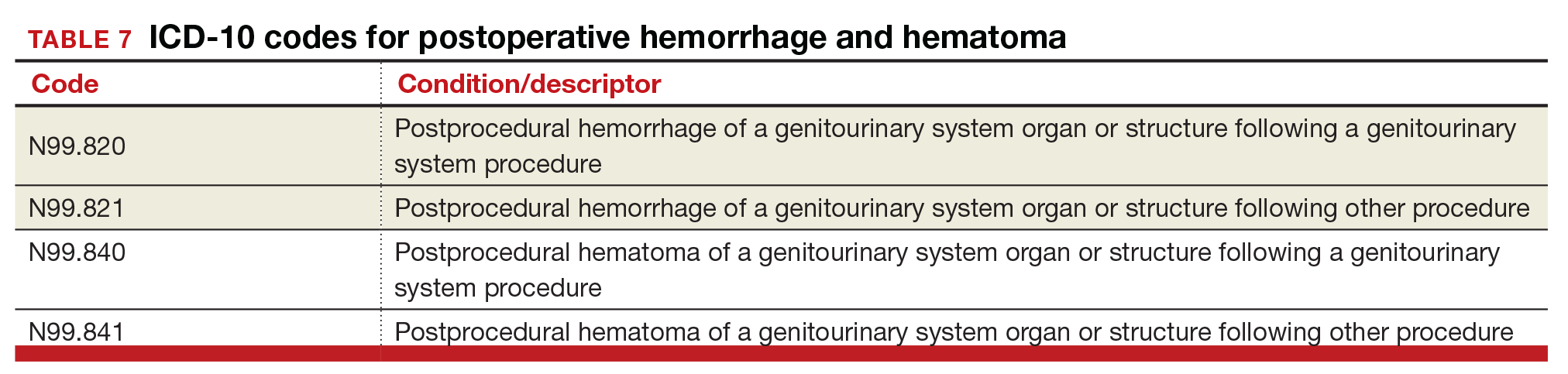
Hormone malignancy status
The new Z19 codes will augment information known about a patient’s neoplasm (TABLE 8). The ICD-10 rule states that the type and location of the neoplasm are always coded first, followed by one of the new Z19 codes, if known.

Viral hepatitis carrier
The more specific code for type of viral hepatitis the patient is a carrier of has been bundled into a single code for viral hepatitis (TABLE 9). Carrier status in ICD-10 is defined as a person who harbors the specific organisms of a disease, does not currently have any symptoms, but is capable of transmitting the infection.
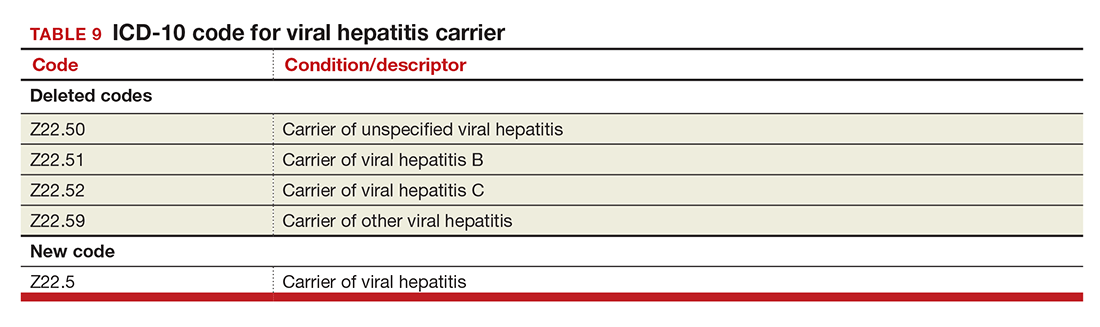
Contraception
The good news is that the ICD-9 code for contraceptive subdermal implants has been added to ICD-10 coding. In addition, the codes for contraceptive methods have been expanded to also include vaginal rings and transdermal patches (TABLE 10).
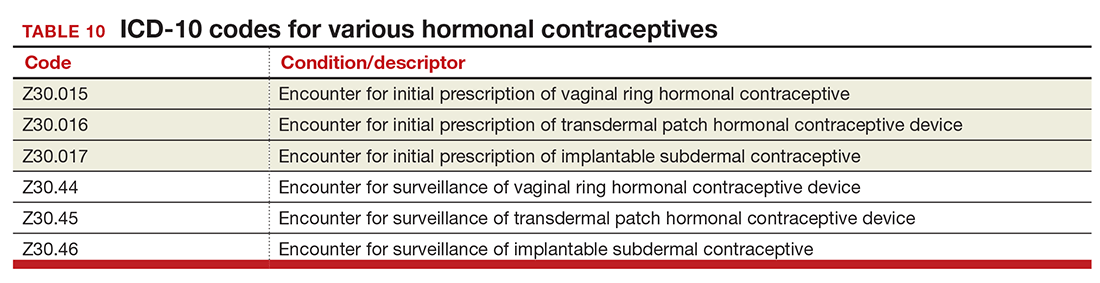
Miscellaneous code changes
Counseling a patient prior to pregnancy just got easier with the addition of a code for gestational carriers. Also, the old ICD-9 code that let a payer know that a procedure was converted from a laparoscopic to an open abdominal procedure is back (TABLE 11).

Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Centers for Disease Control and Prevention. ICD-10 Coordination and Maintenance Committee Meeting: diagnosis agenda. September 23–24, 2014;28–29. https://www.cdc.gov/nchs/data/icd/topic_packet_09_23_2012.pdf. Accessed August 30, 2016.
- Centers for Disease Control and Prevention. ICD-10 Coordination and Maintenance Committee Meeting: diagnosis agenda. March 18–19, 2015. http://www.cdc.gov/nchs/data/icd/Tentative_Agenda_March%202015_Final.pdf. Accessed August 30, 2016.

Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
In the August 2016 issue of OBG
Urogynecology diagnostic codes
Urogynecologists will find a large number of changes to codes they can select on October 1, 2016. While some codes improve reporting for conditions or symptoms related to urinary issues, many more concern postoperative complications following surgery for devices and grafts applied to the genitourinary system.
The American Urological Association requested new codes to align with a 2009 joint report on the terminology for female pelvic floor dysfunction.1 These codes, along with others, are listed in TABLE 1.
Urinary procedure complication codes
Not every urogynecologist will have an issue after surgery for incontinence, but if they do, there are tons of new and revised codes to address every possible complication the patient may have (TABLE 2). Each of these codes is reported based on whether the complication is being actively treated (initial encounter: final character is A), is being followed up after treatment (subsequent encounter: final character is D), or is caused by another condition (sequela: final character is S).
Gynecology-related diagnostic codes
Laterality
If there are 2 organs in the genitourinary system, the chances are good that there is now a right and a left designation code in ICD-10. Documentation should be clear, of course, and if the condition exists on both the right and the left side (even if only one side is being treated actively), list both codes, as there is no bilateral designation in the codes (TABLE 3). And while there is a code for “unspecified side,” providers normally do know which side, so use of this code should be avoided, if possible.
Vaginal septum
The right and left designations extend to the congenital codes for vaginal septum, but they go one step further. The American Congress of Obstetricians and Gynecologists (ACOG) requested that the codes for longitudinal vaginal septum be expanded to differentiate a nonobstructing vaginal septum from an obstructing vaginal septum, in addition to adding laterality to these codes (TABLE 3).2
Mastitis
There are now 2 new codes for inflammation of the breast; one describes mastitis without abscess, while the other code includes an abscess of the breast and nipple (TABLE 4). Once again, documentation will lead to the most specific code to describe the findings.
Childhood and prepubertal concerns
The single code for hypertrophy of the vulva has been expanded to include asymmetric labium majus enlargement. This code was requested by ACOG because this is a known clinical diagnosis and the currently available vulvar codes are inadequate for capturing this condition. The vulvar enlargement appears to be in response to hormonal surges during prepuberty and early puberty. Adult hypertrophy, either congenital or acquired from childbirth or as a late result of an old injury, would be reported by the “other specified” code (TABLE 5).
The causes of prepubertal bleeding vary and include the presence of a foreign object, tumors, or fluctuations in hormones, but prepubertal bleeding differs from the bleeding associated with normal menstruation. For that reason, ACOG requested a code that better captures the nature of the condition before a thorough work-up has pinpointed the cause (TABLE 5). Once the cause of the bleeding is known, a more specific diagnosis would then be reported (eg, D28.1, Benign neoplasm of vagina, or T19.2XXA, Foreign body in vulva and vagina, initial encounter).
Dypareunia
Additional documentation for dyspareunia will now be required to ensure that the most specific code is reported. In this case, the clinician should identify whether the pain is superficial or deep to better report on female pelvic floor dysfunction and to support the different treatments based on the location of the pain (TABLE 6). Deep dyspareunia would be felt in the mid or upper vagina.
Postoperative hemorrhage and hematoma
The codes for postprocedural hemorrhage and hematomas have received a face-lift: the single codes for these 2 complications will be split so that each can be reported separately (TABLE 7). Note that the new codes require that the condition be found following the initial surgery, and the code selected depends on whether the surgery involved the genitourinary system or another system.
Hormone malignancy status
The new Z19 codes will augment information known about a patient’s neoplasm (TABLE 8). The ICD-10 rule states that the type and location of the neoplasm are always coded first, followed by one of the new Z19 codes, if known.
Viral hepatitis carrier
The more specific code for type of viral hepatitis the patient is a carrier of has been bundled into a single code for viral hepatitis (TABLE 9). Carrier status in ICD-10 is defined as a person who harbors the specific organisms of a disease, does not currently have any symptoms, but is capable of transmitting the infection.
Contraception
The good news is that the ICD-9 code for contraceptive subdermal implants has been added to ICD-10 coding. In addition, the codes for contraceptive methods have been expanded to also include vaginal rings and transdermal patches (TABLE 10).
Miscellaneous code changes
Counseling a patient prior to pregnancy just got easier with the addition of a code for gestational carriers. Also, the old ICD-9 code that let a payer know that a procedure was converted from a laparoscopic to an open abdominal procedure is back (TABLE 11).
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
In the August 2016 issue of OBG
Urogynecology diagnostic codes
Urogynecologists will find a large number of changes to codes they can select on October 1, 2016. While some codes improve reporting for conditions or symptoms related to urinary issues, many more concern postoperative complications following surgery for devices and grafts applied to the genitourinary system.
The American Urological Association requested new codes to align with a 2009 joint report on the terminology for female pelvic floor dysfunction.1 These codes, along with others, are listed in TABLE 1.
Urinary procedure complication codes
Not every urogynecologist will have an issue after surgery for incontinence, but if they do, there are tons of new and revised codes to address every possible complication the patient may have (TABLE 2). Each of these codes is reported based on whether the complication is being actively treated (initial encounter: final character is A), is being followed up after treatment (subsequent encounter: final character is D), or is caused by another condition (sequela: final character is S).
Gynecology-related diagnostic codes
Laterality
If there are 2 organs in the genitourinary system, the chances are good that there is now a right and a left designation code in ICD-10. Documentation should be clear, of course, and if the condition exists on both the right and the left side (even if only one side is being treated actively), list both codes, as there is no bilateral designation in the codes (TABLE 3). And while there is a code for “unspecified side,” providers normally do know which side, so use of this code should be avoided, if possible.
Vaginal septum
The right and left designations extend to the congenital codes for vaginal septum, but they go one step further. The American Congress of Obstetricians and Gynecologists (ACOG) requested that the codes for longitudinal vaginal septum be expanded to differentiate a nonobstructing vaginal septum from an obstructing vaginal septum, in addition to adding laterality to these codes (TABLE 3).2
Mastitis
There are now 2 new codes for inflammation of the breast; one describes mastitis without abscess, while the other code includes an abscess of the breast and nipple (TABLE 4). Once again, documentation will lead to the most specific code to describe the findings.
Childhood and prepubertal concerns
The single code for hypertrophy of the vulva has been expanded to include asymmetric labium majus enlargement. This code was requested by ACOG because this is a known clinical diagnosis and the currently available vulvar codes are inadequate for capturing this condition. The vulvar enlargement appears to be in response to hormonal surges during prepuberty and early puberty. Adult hypertrophy, either congenital or acquired from childbirth or as a late result of an old injury, would be reported by the “other specified” code (TABLE 5).
The causes of prepubertal bleeding vary and include the presence of a foreign object, tumors, or fluctuations in hormones, but prepubertal bleeding differs from the bleeding associated with normal menstruation. For that reason, ACOG requested a code that better captures the nature of the condition before a thorough work-up has pinpointed the cause (TABLE 5). Once the cause of the bleeding is known, a more specific diagnosis would then be reported (eg, D28.1, Benign neoplasm of vagina, or T19.2XXA, Foreign body in vulva and vagina, initial encounter).
Dypareunia
Additional documentation for dyspareunia will now be required to ensure that the most specific code is reported. In this case, the clinician should identify whether the pain is superficial or deep to better report on female pelvic floor dysfunction and to support the different treatments based on the location of the pain (TABLE 6). Deep dyspareunia would be felt in the mid or upper vagina.
Postoperative hemorrhage and hematoma
The codes for postprocedural hemorrhage and hematomas have received a face-lift: the single codes for these 2 complications will be split so that each can be reported separately (TABLE 7). Note that the new codes require that the condition be found following the initial surgery, and the code selected depends on whether the surgery involved the genitourinary system or another system.
Hormone malignancy status
The new Z19 codes will augment information known about a patient’s neoplasm (TABLE 8). The ICD-10 rule states that the type and location of the neoplasm are always coded first, followed by one of the new Z19 codes, if known.
Viral hepatitis carrier
The more specific code for type of viral hepatitis the patient is a carrier of has been bundled into a single code for viral hepatitis (TABLE 9). Carrier status in ICD-10 is defined as a person who harbors the specific organisms of a disease, does not currently have any symptoms, but is capable of transmitting the infection.
Contraception
The good news is that the ICD-9 code for contraceptive subdermal implants has been added to ICD-10 coding. In addition, the codes for contraceptive methods have been expanded to also include vaginal rings and transdermal patches (TABLE 10).
Miscellaneous code changes
Counseling a patient prior to pregnancy just got easier with the addition of a code for gestational carriers. Also, the old ICD-9 code that let a payer know that a procedure was converted from a laparoscopic to an open abdominal procedure is back (TABLE 11).
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Centers for Disease Control and Prevention. ICD-10 Coordination and Maintenance Committee Meeting: diagnosis agenda. September 23–24, 2014;28–29. https://www.cdc.gov/nchs/data/icd/topic_packet_09_23_2012.pdf. Accessed August 30, 2016.
- Centers for Disease Control and Prevention. ICD-10 Coordination and Maintenance Committee Meeting: diagnosis agenda. March 18–19, 2015. http://www.cdc.gov/nchs/data/icd/Tentative_Agenda_March%202015_Final.pdf. Accessed August 30, 2016.
- Centers for Disease Control and Prevention. ICD-10 Coordination and Maintenance Committee Meeting: diagnosis agenda. September 23–24, 2014;28–29. https://www.cdc.gov/nchs/data/icd/topic_packet_09_23_2012.pdf. Accessed August 30, 2016.
- Centers for Disease Control and Prevention. ICD-10 Coordination and Maintenance Committee Meeting: diagnosis agenda. March 18–19, 2015. http://www.cdc.gov/nchs/data/icd/Tentative_Agenda_March%202015_Final.pdf. Accessed August 30, 2016.
In this Article
- Urogynecology dx codes
- Gynecology dx codes
- Codes for hormonal contraceptives
Medicare’s revaluation of gastrointestinal endoscopic procedures: Implications for academic and community-based practices
No sentient gastroenterologist has missed the fact that, over the past 3 years, Medicare revalued our endoscopy codes. The impact of those reimbursement changes has been felt both by community gastroenterologists and by those practicing in academic centers. Impacts are different, however, because funds flow, opportunities for ancillary income and compensation formulas all are different for private versus academic physicians. In this month’s Road Ahead column, I have invited leaders from both camps (private practice and academic GI) to describe how reduced procedural reimbursement is affecting their practices. I was impressed and surprised at the level of detail and analysis provided by Dr. Dorn and Dr. Vesy. There are few other sources of financial data that are embedded in real-world experience. We all are concerned about our futures, and this article should spur us into serious discussions about practice strategies going forward. As I wrote in a recent article in Gastroenterology (2016;150:295-9), this is “No Time for WIMPs.”
Gastroenterology practices generate the bulk of their revenue from endoscopic procedures. Over the past decade, the professional fees Medicare pays for these procedures have generally declined. Meanwhile, associated hospital outpatient facility fees have increased while ambulatory surgery center (ASC) fees remain below 2007 levels. This article surveys these changes and examines their significant impact on academic and private gastroenterology practices.
Professional fees for endoscopic procedures
Since 1992 physician professional fees have been linked to the Medicare Physician Fee Schedule, which assigns each service a certain number of relative value units (RVUs). First, the work RVU (wRVU) is based on the estimated physician time, mental effort, technical skill, and psychological stress required to provide a service. Second, a practice expense RVU (PE RVU) reflects the direct and indirect costs of providing the service. For procedures performed in office-based settings the PE RVU includes rent, nonclinician staff, equipment, and supplies, on average amounting to 44% of the total RVU. For procedures performed in hospital outpatient departments (HOPDs) and ASCs, the PE RVU is much lower, because most costs are incurred by the facility (which receives a separate facility fee), rather than the physician practice. Third, a small proportion of the overall RVU is linked to malpractice insurance costs (MP RVU). The RVU components are geographically adjusted, combined, and then multiplied by a conversion factor (CF, which in 2016 is $35.80) to determine actual Medicare payment (Payment = [wRVU + PE RVU + MP RVU] × CF).1
To address potential distortions in this physician fee schedule, The Affordable Care Act directed the Secretary of Health and Human Services to establish a formal process to review potentially misvalued procedure codes. During 2012 and 2014, multiple gastroenterological and surgical societies surveyed practicing physicians on the physician work, time, and intensity required to perform more than 120 services in question, including esophagoscopy, esophagogastroduodenoscopy, endoscopic retrograde cholangiopancreatography, flexible sigmoidoscopy and ileoscopy, pouchoscopy, and colonoscopy. At the same time, these societies assembled an expert panel of practicing physicians to determine the practice expenses associated with these procedures. The societies analyzed the results and presented recommendations to the American Medical Association/Specialty Society Relative Value Scale Update Committee, which, in turn, presented their recommendations to the Centers for Medicare and Medicaid Services.2 In 2014, CMS accepted approximately three-quarters of the Relative Value Scale Update Committee’s recommendations, ultimately decreasing wRVUs, increasing PE RVUs for procedures performed in office-based settings, and leaving MP RVUs unchanged for most upper endoscopy and endoscopic retrograde cholangiopancreatography procedures. These changes translated into significant 2015 payment reductions for esophagoscopy and esophagogastroduodenoscopy (4%-42%), endoscopic ultrasound (10%-35%), and endoscopic retrograde cholangiopancreatography (0%-37%) performed within facilities, with less effect for those performed in office-based settings. At that time, “in light of the substantial nature of [the colonoscopy] code revision and its relationship to the policies on moderate sedation,” CMS delayed revaluation of the lower gastrointestinal (GI) endoscopy codes.3 This reprieve is now over: The 2016 Medicare Physician Fee Schedule Final Rule includes up to 17% cuts (12% on average) to the wRVU associated with these lower GI procedures (Table 1). For office-based procedures (but not facility-based procedures) these wRVU cuts are buffered (and sometimes offset) by general increases in PE RVUs.
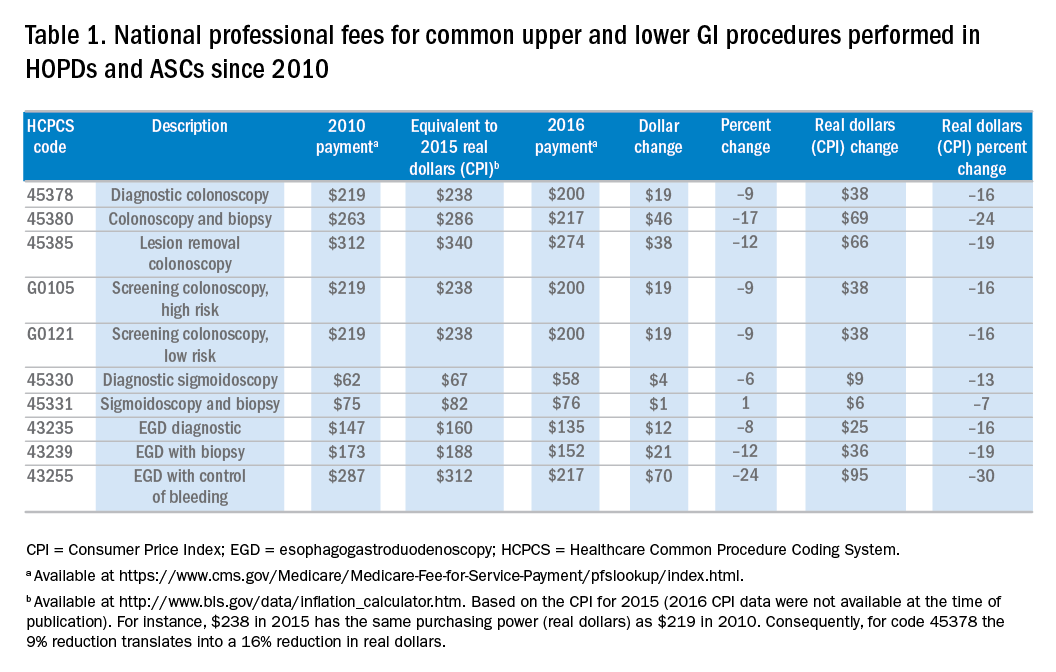
Facility fees for endoscopic procedures
Compared with the small percentage of endoscopic procedures that are performed in office-based settings, those performed in HOPDs and ASCs entail a lower professional fee plus a separate facility fee. Since 2000 CMS has paid for services provided in HOPDs using the outpatient prospective payment system (OPPS). Clinical services are first classified into ambulatory payment classifications (APC) on the basis of clinical and cost similarity. Next, services within an APC are assigned a single relative payment rate, which is linked to the resources required to perform the service. The APC payment rate is geographically adjusted and then multiplied by a CF to determine an actual dollar amount.4
Since 2008, CMS has used a nearly identical mechanism to pay for facility services provided in ASCs. Services are classified using the same APCs and same relative weights as the OPPS. The difference is that the ASC CF is less than the OPPS CF (the 2016 ASC CF is 58% of the OPPS CF), translating into lower dollar payments for ASC services.5 Of note, in 2008 ASC rates were cut significantly when CMS adopted this methodology for determining ASC facility fees (previously, ASC rates were approximately 85% of HOPD rates).
CMS reviews the APCs and their relative weights annually, and may adjust how specific services are classified and how APCs are weighed. Since 2006, HOPD rates for the 10 common procedures listed in Table 1 have increased by 26%-93% real (i.e., Consumer Price Index–adjusted) dollars. Meanwhile, given the steep 2008 ASC fee cuts the 2016 ASC fees are still significantly lower than they were 1 decade ago, especially when accounting for inflation. In fact, ASC fees for the most common procedures have decreased by 20% in real dollars (Supplementary Tables 1 and 2 at http://dx.doi.org/10.1016/j.cgh.2016.03.032).
Putting these changes in context
It is important to consider these changes within a broader context. First, the full economic impact of these changes on an individual gastroenterology practice depends on where it performs its services and whether it collects associated facility fees, and fees for anesthesia and pathology services. Second, the Medicare population is growing by more than 10,000 people each day.6 Third, beyond Medicare, most commercial insurers peg their reimbursement rates to a percentage of the Medicare Fee Schedule. Although the details of specific contracts vary, gastroenterologists should expect to see commercial rates move in a similar direction within the next 1–2 years. Fourth, in the 2016 Fee Schedule CMS described its future intention to remove the value of moderate sedation from all GI procedures valued with moderate sedation inherent to the procedure. The more that moderate sedation is ultimately valued, the less that endoscopic procedures will be valued. Consequently, gastroenterologists who rely on anesthesiology professionals to sedate their patients will receive less revenue per procedure. Finally, the 2015 Medicare Access and Children’s Health Insurance Program Reauthorization Act (MACRA) links a higher proportion of these dwindling fee-for-service payments to performance. Starting in 2018, physicians who elect to remain on a fee-for-service tract will receive a composite Merit-Based Incentive Payment System (MIPS) score that will translate into either performance bonuses or penalties (as much as 4% in 2019 and going up to 9% in 2022). Alternatively, providers who “sufficiently” participate in “two-sided” (i.e., risk-bearing) alternative payment models (e.g., bundled payments and accountable care organizations) instead of fee-for-service payments will receive 5% across-the-board bonuses. In sum, it is possible that fee-for-service payments may eventually become so unattractive that many gastroenterologists decide (or hope) to move to alternative payment models that combine both professional and facility fees, such as the CMS now-mandatory Comprehensive Care for Joint Replacement (CJR) program.7
Impact on academic practices
For most academic gastroenterology practices, clinical revenue far exceeds all other sources of funding, including research grants, teaching support, philanthropy, and partnerships with industry. Although a select few academic GI divisions have managed to build their own ASCs to share facility fees, for most academic practices, clinical revenue comes solely from the professional fees for endoscopic procedures and, less so, from office and hospital-based consultations and management of established patients.8 Thus, steep cuts to professional fees for endoscopic procedures, the leading source of overall revenue, will severely strain most academic gastroenterology practices.
In one of our practices (SDD), the 10 common procedures listed in Table 1 accounted for 27% of total direct clinical revenue over the past year. Roughly one-fourth of our patients are Medicare beneficiaries. Assuming no change in volume, the 2016 fee schedule cuts will amount to a 0.9% drop in direct clinical revenue. If all other payers follow with identical cuts, then direct clinical revenue will drop by 3.7%. Although our practice is fortunate to have other well-developed clinical and nonclinical revenue streams, these cuts are not insignificant.
How can academic practices continue to provide accessible clinical care in the face of these fee cuts? It can help to first consider how revenue is distributed for a Medicare beneficiary who undergoes a diagnostic colonoscopy with biopsy to evaluate unexplained diarrhea in an academic medical center’s hospital-based facility. The academic gastroenterologist receives $212 (CPT 45380). From this $212, the academic gastroenterology practice must pay assessments to various entities (sometimes including the school of medicine, department of medicine, and faculty practice plan) that may amount to more than 30% of total revenue. The roughly $150 that remains is used to pay faculty member salaries (the median salary for an academic gastroenterologist is $300,009) and benefits (estimated at $74,000/year); MP insurance (estimated at $2,275/year, higher in certain parts of the United States); and overhead for support staff, supplies, and other expenses (estimated at $50,550/year). Thus, a purely clinical academic gastroenterologist who is paid at the Medical Group Management Association (MGMA) median must generate $610,179 in preassessment revenue. If this hypothetical academic gastroenterologist solely treated Medicare beneficiaries, at $35.82 per RVU he or she would need to generate a staggering 17,035 RVUs per year, an amount that far exceeds the MGMA median (6,445) and 90th percentile (10,991) for academic gastroenterologists. Of course, real-world academic gastroenterologists also treat commercially insured patients and many spend time on nonclinical activities (although clinical income typically supports time devoted to research and teaching, not vice versa). Still, this example highlights a clear fact: Academic gastroenterology practices take a major financial loss delivering services to Medicare beneficiaries. Meanwhile, the HOPD charges more than $2,200 for the procedure. Although it receives $752 facility fee from Medicare (Disproportionate Share Hospitals and NCI Cancer Centers receive more), with a cost-to-charge ratio of roughly 0.2, revenue still clearly exceeds expenses. Finally, the anesthesia professional (if any) receives roughly $198 (CPT 00810) and the pathologist $74 (CPT 88305).
Although some may argue that academic gastroenterologists should simply accept a pay cut, lower salaries may drive many away from academia. To hire enough new (or even maintain enough existing) faculty members to maintain and grow volume, academic gastroenterology practices must find ways to supplement declining professional fees. One option is for academic practices to open their own ASCs, either alone or jointly with their health care system. But this assumes, often erroneously, that the health care system is willing to share facility fees. A second option is to develop incentive programs that transfer revenue from the health care system to the physicians. Importantly, these must be at fair market value and for nonemployed physicians cannot be linked to volume.10 Examples include medical directorships and non–volume-based performance bonuses. A third option is to consider alternative payment models, such as bundled payments that include a single lump sum payment for both professional and facility fees. The practice and health system then negotiates how the bundle is shared. Bundles should motivate hospitals and academic practices to work together to improve care and reduce overall expenses. Along these lines, CMS recently announced the CJR program under which hospitals and physicians in 75 locations will be required to participate. Although AGA recently published a bundled payment framework for screening and surveillance colonoscopy,11 bundles for other endoscopic procedures remain to be defined. But, a clearly defined, attractively priced, and skillfully negotiated bundle could be a means for redistributing revenue in ways that are more favorable to academic practices. No matter the approach, it is critical for academic gastroenterology practices and their health care systems to align their goals and integrate their services. But this is easier said than done.
Impact on private gastroenterology practices
The impact of these professional and facility fee changes on private practice depends on the practice’s payer mix, and whether it owns an ASC and directly provides anesthesia and pathology services. Consider Texas Digestive Disease Consultants (TDDC), an 80-gastroenterologist practice that provides GI care and endoscopic procedures throughout north and central Texas. TDDC revenue comes solely from professional fees generated by gastroenterologists and the pathologists that the practice employs. TDDC operating expenses include employee salaries and benefits, rent, and taxes. Based on an expected work-year of 2,080 hours, each TDDC gastroenterologist must generate $219 per hour to cover practice expenses. Physicians receive income only after practice revenue exceeds $219 per hour.
In the 2016 Medicare Physician Fee Schedule, colonoscopy code 45387 is assigned 3.36 RVUs, based on 67 minutes in total time. Based on this information, 2016 CMS payment for a screening colonoscopy ($200) will result in a loss of $45 in practice revenue over expenses. Across the TDDC practices in 2015, CMS patients represented 29% of all colonoscopies performed, but only 11% of revenue from those procedures. In aggregate, assuming no change in volume, the 2016 fee schedule cuts will translate into $5,472 less physician income for each gastroenterologist. If all other payers follow with identical cuts then each gastroenterologist would forfeit $50,896 of income.
For pathology services, code 88305 reimburses a global service per specimen. The average number of specimens per outpatient GI procedure at TDDC is 1.5. Based on CMS’ per specimen payment of $73 (down from $107 in 2012), average pathology reimbursement per a CMS endoscopic procedure is $110.
What about facility fees? Many TDDC physicians separately own and operate ASCs and anesthesia practices. Because the physician owners of these facilities funded, developed, and operate these facilities on their own, any revenue over expenses from these facilities flow directly to the ASC, rather than to TDDC. Since 2008, when ASC payments were severely reduced, ASC revenue over expenses for a Medicare colonoscopy has ranged from $0 to $70. For anesthesia services, the ASC receives approximately $159 per screening colonoscopy, which is not enough to actually cover the costs of providing anesthesia services. In sum, when TDDC gastroenterologists perform colonoscopies on Medicare patients at an HOPD the physician loses money. When the same procedure is performed at an ASC the physician barely break even.
How can private practice gastroenterologists respond to these fee cuts? First, some gastroenterologists may be forced to accept lower salaries. Second, practices can offset fee cuts by improving efficiency and reducing overall cost of care, assuming they are not already maximally efficient. Third, some private practices can increase Medicare professional payments by reclassifying as nonparticipating with Medicare. Nonparticipating status allows practices to charge the patient up to approximately 109.25% of the Medicare approved rate, with the patient submitting the claim directly to Medicare (“balance billing”). The downside is that patients shoulder the additional cost and may potentially decide to seek care elsewhere. Fourth, private practices should explore alternative payment models, such as bundled payment as described previously, either on their own or by partnering with local health systems to share risk. Finally, some practices may sell equity to and become employees of local health systems.
Conclusions
Changes to Medicare professional and facility fee payments for endoscopic procedures significantly affect academic and private gastroenterology practices. Dwindling professional fees – alongside increasing HOPD facility fees – make academic gastroenterology practices increasingly reliant on support from their parent health care systems. Like academic practices, private gastroenterology practices experience financial losses when treating Medicare beneficiaries. Academic and private gastroenterology practices should consider several potential responses. Although beyond the scope of this article, all practices must continuously strive to improve the quality and reduce the costs of the endoscopic procedures they perform.
Acknowledgments
The authors thank Leslie Narramore, MPA, for her insights and help with reimbursement data. They also thank Bryan Rhodes for providing financial data and Shivan Mehta, MD, MBA, for his feedback on the Relative Value Scale Update Committee process.
References
1. MEDPAC. Payment basics: physician and other health professional payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
2. Mehta, S.J., Brill, J.V. What is the RUC and how does it impact gastroenterology?. Clin Gastroenterol Hepatol. 2014;12:1208-11.
3. American College of Gastroenterology, American Gastroenterological Association, American Society for Gastrointestinal Endoscopy. Key Provisions in the CY 2015 Medicare Physician Fee Schedule Final Rule, 2015. Available at: http://gi.org/wp-content/uploads/2014/11/Tri-Soc_CY15_MPFS_Final_Rule_Summary.pdf.
4. MEDPAC. Payment basics: Outpatient hospital services payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
5. MEDPAC. Payment basics: Ambulatory surgery center services payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
6. Diamond, D. 10,000 people are now enrolling in Medicare – every day. Forbes; 2015 (Available at: http://www.forbes.com/sites/dandiamond/2015/07/13/aging-in-america-10000-people-enroll-in-medicare-every-day/#5177f1f35e07. Accessed January 3, 2016)
7. Mechanic, R.E. Mandatory Medicare bundled payment: Is it ready for prime time?. N Engl J Med. 2015;373:1291-3.
8. Rustgi, A.K., Allen, J.I. The house of gastrointestinal medicine: How academic medical centers can build a sustainable economic clinical model. Clin Gastroenterol Hepatol. 2013;11:1370-3.
9. Academic Practice Compensation and Production Report. Medical Group Management Association, Englewood, Colo.; 2015.
10. Becker S., Townshend G., Carnell H., et al. Physician compensation: 10 core legal and regulatory concepts. Becker’s Hospital Review Available at: http://www.beckershospitalreview.com/legal-regulatory-issues/physician-compensation-10-core-legal-and-regulatory-concepts.html. Accessed Jan. 20, 2016.
11. Brill, J.V., Jain, R., Margolis, P.S., et al. A bundled payment framework for colonoscopy performed for colorectal cancer screening or surveillance. Gastroenterology. 2014;146:849-53, e9.
Dr. Dorn is vice chief, division of gastroenterology and hepatology, associate professor of medicine, health policy & management, University of North Carolina at Chapel Hill; he has received honoraria for consulting and presentations on health reform from AbbVie and Olympus. Dr. Vesy is a gastroenterologist affiliated with Baylor University Medical Center, Dallas.
No sentient gastroenterologist has missed the fact that, over the past 3 years, Medicare revalued our endoscopy codes. The impact of those reimbursement changes has been felt both by community gastroenterologists and by those practicing in academic centers. Impacts are different, however, because funds flow, opportunities for ancillary income and compensation formulas all are different for private versus academic physicians. In this month’s Road Ahead column, I have invited leaders from both camps (private practice and academic GI) to describe how reduced procedural reimbursement is affecting their practices. I was impressed and surprised at the level of detail and analysis provided by Dr. Dorn and Dr. Vesy. There are few other sources of financial data that are embedded in real-world experience. We all are concerned about our futures, and this article should spur us into serious discussions about practice strategies going forward. As I wrote in a recent article in Gastroenterology (2016;150:295-9), this is “No Time for WIMPs.”
Gastroenterology practices generate the bulk of their revenue from endoscopic procedures. Over the past decade, the professional fees Medicare pays for these procedures have generally declined. Meanwhile, associated hospital outpatient facility fees have increased while ambulatory surgery center (ASC) fees remain below 2007 levels. This article surveys these changes and examines their significant impact on academic and private gastroenterology practices.
Professional fees for endoscopic procedures
Since 1992 physician professional fees have been linked to the Medicare Physician Fee Schedule, which assigns each service a certain number of relative value units (RVUs). First, the work RVU (wRVU) is based on the estimated physician time, mental effort, technical skill, and psychological stress required to provide a service. Second, a practice expense RVU (PE RVU) reflects the direct and indirect costs of providing the service. For procedures performed in office-based settings the PE RVU includes rent, nonclinician staff, equipment, and supplies, on average amounting to 44% of the total RVU. For procedures performed in hospital outpatient departments (HOPDs) and ASCs, the PE RVU is much lower, because most costs are incurred by the facility (which receives a separate facility fee), rather than the physician practice. Third, a small proportion of the overall RVU is linked to malpractice insurance costs (MP RVU). The RVU components are geographically adjusted, combined, and then multiplied by a conversion factor (CF, which in 2016 is $35.80) to determine actual Medicare payment (Payment = [wRVU + PE RVU + MP RVU] × CF).1
To address potential distortions in this physician fee schedule, The Affordable Care Act directed the Secretary of Health and Human Services to establish a formal process to review potentially misvalued procedure codes. During 2012 and 2014, multiple gastroenterological and surgical societies surveyed practicing physicians on the physician work, time, and intensity required to perform more than 120 services in question, including esophagoscopy, esophagogastroduodenoscopy, endoscopic retrograde cholangiopancreatography, flexible sigmoidoscopy and ileoscopy, pouchoscopy, and colonoscopy. At the same time, these societies assembled an expert panel of practicing physicians to determine the practice expenses associated with these procedures. The societies analyzed the results and presented recommendations to the American Medical Association/Specialty Society Relative Value Scale Update Committee, which, in turn, presented their recommendations to the Centers for Medicare and Medicaid Services.2 In 2014, CMS accepted approximately three-quarters of the Relative Value Scale Update Committee’s recommendations, ultimately decreasing wRVUs, increasing PE RVUs for procedures performed in office-based settings, and leaving MP RVUs unchanged for most upper endoscopy and endoscopic retrograde cholangiopancreatography procedures. These changes translated into significant 2015 payment reductions for esophagoscopy and esophagogastroduodenoscopy (4%-42%), endoscopic ultrasound (10%-35%), and endoscopic retrograde cholangiopancreatography (0%-37%) performed within facilities, with less effect for those performed in office-based settings. At that time, “in light of the substantial nature of [the colonoscopy] code revision and its relationship to the policies on moderate sedation,” CMS delayed revaluation of the lower gastrointestinal (GI) endoscopy codes.3 This reprieve is now over: The 2016 Medicare Physician Fee Schedule Final Rule includes up to 17% cuts (12% on average) to the wRVU associated with these lower GI procedures (Table 1). For office-based procedures (but not facility-based procedures) these wRVU cuts are buffered (and sometimes offset) by general increases in PE RVUs.
Facility fees for endoscopic procedures
Compared with the small percentage of endoscopic procedures that are performed in office-based settings, those performed in HOPDs and ASCs entail a lower professional fee plus a separate facility fee. Since 2000 CMS has paid for services provided in HOPDs using the outpatient prospective payment system (OPPS). Clinical services are first classified into ambulatory payment classifications (APC) on the basis of clinical and cost similarity. Next, services within an APC are assigned a single relative payment rate, which is linked to the resources required to perform the service. The APC payment rate is geographically adjusted and then multiplied by a CF to determine an actual dollar amount.4
Since 2008, CMS has used a nearly identical mechanism to pay for facility services provided in ASCs. Services are classified using the same APCs and same relative weights as the OPPS. The difference is that the ASC CF is less than the OPPS CF (the 2016 ASC CF is 58% of the OPPS CF), translating into lower dollar payments for ASC services.5 Of note, in 2008 ASC rates were cut significantly when CMS adopted this methodology for determining ASC facility fees (previously, ASC rates were approximately 85% of HOPD rates).
CMS reviews the APCs and their relative weights annually, and may adjust how specific services are classified and how APCs are weighed. Since 2006, HOPD rates for the 10 common procedures listed in Table 1 have increased by 26%-93% real (i.e., Consumer Price Index–adjusted) dollars. Meanwhile, given the steep 2008 ASC fee cuts the 2016 ASC fees are still significantly lower than they were 1 decade ago, especially when accounting for inflation. In fact, ASC fees for the most common procedures have decreased by 20% in real dollars (Supplementary Tables 1 and 2 at http://dx.doi.org/10.1016/j.cgh.2016.03.032).
Putting these changes in context
It is important to consider these changes within a broader context. First, the full economic impact of these changes on an individual gastroenterology practice depends on where it performs its services and whether it collects associated facility fees, and fees for anesthesia and pathology services. Second, the Medicare population is growing by more than 10,000 people each day.6 Third, beyond Medicare, most commercial insurers peg their reimbursement rates to a percentage of the Medicare Fee Schedule. Although the details of specific contracts vary, gastroenterologists should expect to see commercial rates move in a similar direction within the next 1–2 years. Fourth, in the 2016 Fee Schedule CMS described its future intention to remove the value of moderate sedation from all GI procedures valued with moderate sedation inherent to the procedure. The more that moderate sedation is ultimately valued, the less that endoscopic procedures will be valued. Consequently, gastroenterologists who rely on anesthesiology professionals to sedate their patients will receive less revenue per procedure. Finally, the 2015 Medicare Access and Children’s Health Insurance Program Reauthorization Act (MACRA) links a higher proportion of these dwindling fee-for-service payments to performance. Starting in 2018, physicians who elect to remain on a fee-for-service tract will receive a composite Merit-Based Incentive Payment System (MIPS) score that will translate into either performance bonuses or penalties (as much as 4% in 2019 and going up to 9% in 2022). Alternatively, providers who “sufficiently” participate in “two-sided” (i.e., risk-bearing) alternative payment models (e.g., bundled payments and accountable care organizations) instead of fee-for-service payments will receive 5% across-the-board bonuses. In sum, it is possible that fee-for-service payments may eventually become so unattractive that many gastroenterologists decide (or hope) to move to alternative payment models that combine both professional and facility fees, such as the CMS now-mandatory Comprehensive Care for Joint Replacement (CJR) program.7
Impact on academic practices
For most academic gastroenterology practices, clinical revenue far exceeds all other sources of funding, including research grants, teaching support, philanthropy, and partnerships with industry. Although a select few academic GI divisions have managed to build their own ASCs to share facility fees, for most academic practices, clinical revenue comes solely from the professional fees for endoscopic procedures and, less so, from office and hospital-based consultations and management of established patients.8 Thus, steep cuts to professional fees for endoscopic procedures, the leading source of overall revenue, will severely strain most academic gastroenterology practices.
In one of our practices (SDD), the 10 common procedures listed in Table 1 accounted for 27% of total direct clinical revenue over the past year. Roughly one-fourth of our patients are Medicare beneficiaries. Assuming no change in volume, the 2016 fee schedule cuts will amount to a 0.9% drop in direct clinical revenue. If all other payers follow with identical cuts, then direct clinical revenue will drop by 3.7%. Although our practice is fortunate to have other well-developed clinical and nonclinical revenue streams, these cuts are not insignificant.
How can academic practices continue to provide accessible clinical care in the face of these fee cuts? It can help to first consider how revenue is distributed for a Medicare beneficiary who undergoes a diagnostic colonoscopy with biopsy to evaluate unexplained diarrhea in an academic medical center’s hospital-based facility. The academic gastroenterologist receives $212 (CPT 45380). From this $212, the academic gastroenterology practice must pay assessments to various entities (sometimes including the school of medicine, department of medicine, and faculty practice plan) that may amount to more than 30% of total revenue. The roughly $150 that remains is used to pay faculty member salaries (the median salary for an academic gastroenterologist is $300,009) and benefits (estimated at $74,000/year); MP insurance (estimated at $2,275/year, higher in certain parts of the United States); and overhead for support staff, supplies, and other expenses (estimated at $50,550/year). Thus, a purely clinical academic gastroenterologist who is paid at the Medical Group Management Association (MGMA) median must generate $610,179 in preassessment revenue. If this hypothetical academic gastroenterologist solely treated Medicare beneficiaries, at $35.82 per RVU he or she would need to generate a staggering 17,035 RVUs per year, an amount that far exceeds the MGMA median (6,445) and 90th percentile (10,991) for academic gastroenterologists. Of course, real-world academic gastroenterologists also treat commercially insured patients and many spend time on nonclinical activities (although clinical income typically supports time devoted to research and teaching, not vice versa). Still, this example highlights a clear fact: Academic gastroenterology practices take a major financial loss delivering services to Medicare beneficiaries. Meanwhile, the HOPD charges more than $2,200 for the procedure. Although it receives $752 facility fee from Medicare (Disproportionate Share Hospitals and NCI Cancer Centers receive more), with a cost-to-charge ratio of roughly 0.2, revenue still clearly exceeds expenses. Finally, the anesthesia professional (if any) receives roughly $198 (CPT 00810) and the pathologist $74 (CPT 88305).
Although some may argue that academic gastroenterologists should simply accept a pay cut, lower salaries may drive many away from academia. To hire enough new (or even maintain enough existing) faculty members to maintain and grow volume, academic gastroenterology practices must find ways to supplement declining professional fees. One option is for academic practices to open their own ASCs, either alone or jointly with their health care system. But this assumes, often erroneously, that the health care system is willing to share facility fees. A second option is to develop incentive programs that transfer revenue from the health care system to the physicians. Importantly, these must be at fair market value and for nonemployed physicians cannot be linked to volume.10 Examples include medical directorships and non–volume-based performance bonuses. A third option is to consider alternative payment models, such as bundled payments that include a single lump sum payment for both professional and facility fees. The practice and health system then negotiates how the bundle is shared. Bundles should motivate hospitals and academic practices to work together to improve care and reduce overall expenses. Along these lines, CMS recently announced the CJR program under which hospitals and physicians in 75 locations will be required to participate. Although AGA recently published a bundled payment framework for screening and surveillance colonoscopy,11 bundles for other endoscopic procedures remain to be defined. But, a clearly defined, attractively priced, and skillfully negotiated bundle could be a means for redistributing revenue in ways that are more favorable to academic practices. No matter the approach, it is critical for academic gastroenterology practices and their health care systems to align their goals and integrate their services. But this is easier said than done.
Impact on private gastroenterology practices
The impact of these professional and facility fee changes on private practice depends on the practice’s payer mix, and whether it owns an ASC and directly provides anesthesia and pathology services. Consider Texas Digestive Disease Consultants (TDDC), an 80-gastroenterologist practice that provides GI care and endoscopic procedures throughout north and central Texas. TDDC revenue comes solely from professional fees generated by gastroenterologists and the pathologists that the practice employs. TDDC operating expenses include employee salaries and benefits, rent, and taxes. Based on an expected work-year of 2,080 hours, each TDDC gastroenterologist must generate $219 per hour to cover practice expenses. Physicians receive income only after practice revenue exceeds $219 per hour.
In the 2016 Medicare Physician Fee Schedule, colonoscopy code 45387 is assigned 3.36 RVUs, based on 67 minutes in total time. Based on this information, 2016 CMS payment for a screening colonoscopy ($200) will result in a loss of $45 in practice revenue over expenses. Across the TDDC practices in 2015, CMS patients represented 29% of all colonoscopies performed, but only 11% of revenue from those procedures. In aggregate, assuming no change in volume, the 2016 fee schedule cuts will translate into $5,472 less physician income for each gastroenterologist. If all other payers follow with identical cuts then each gastroenterologist would forfeit $50,896 of income.
For pathology services, code 88305 reimburses a global service per specimen. The average number of specimens per outpatient GI procedure at TDDC is 1.5. Based on CMS’ per specimen payment of $73 (down from $107 in 2012), average pathology reimbursement per a CMS endoscopic procedure is $110.
What about facility fees? Many TDDC physicians separately own and operate ASCs and anesthesia practices. Because the physician owners of these facilities funded, developed, and operate these facilities on their own, any revenue over expenses from these facilities flow directly to the ASC, rather than to TDDC. Since 2008, when ASC payments were severely reduced, ASC revenue over expenses for a Medicare colonoscopy has ranged from $0 to $70. For anesthesia services, the ASC receives approximately $159 per screening colonoscopy, which is not enough to actually cover the costs of providing anesthesia services. In sum, when TDDC gastroenterologists perform colonoscopies on Medicare patients at an HOPD the physician loses money. When the same procedure is performed at an ASC the physician barely break even.
How can private practice gastroenterologists respond to these fee cuts? First, some gastroenterologists may be forced to accept lower salaries. Second, practices can offset fee cuts by improving efficiency and reducing overall cost of care, assuming they are not already maximally efficient. Third, some private practices can increase Medicare professional payments by reclassifying as nonparticipating with Medicare. Nonparticipating status allows practices to charge the patient up to approximately 109.25% of the Medicare approved rate, with the patient submitting the claim directly to Medicare (“balance billing”). The downside is that patients shoulder the additional cost and may potentially decide to seek care elsewhere. Fourth, private practices should explore alternative payment models, such as bundled payment as described previously, either on their own or by partnering with local health systems to share risk. Finally, some practices may sell equity to and become employees of local health systems.
Conclusions
Changes to Medicare professional and facility fee payments for endoscopic procedures significantly affect academic and private gastroenterology practices. Dwindling professional fees – alongside increasing HOPD facility fees – make academic gastroenterology practices increasingly reliant on support from their parent health care systems. Like academic practices, private gastroenterology practices experience financial losses when treating Medicare beneficiaries. Academic and private gastroenterology practices should consider several potential responses. Although beyond the scope of this article, all practices must continuously strive to improve the quality and reduce the costs of the endoscopic procedures they perform.
Acknowledgments
The authors thank Leslie Narramore, MPA, for her insights and help with reimbursement data. They also thank Bryan Rhodes for providing financial data and Shivan Mehta, MD, MBA, for his feedback on the Relative Value Scale Update Committee process.
References
1. MEDPAC. Payment basics: physician and other health professional payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
2. Mehta, S.J., Brill, J.V. What is the RUC and how does it impact gastroenterology?. Clin Gastroenterol Hepatol. 2014;12:1208-11.
3. American College of Gastroenterology, American Gastroenterological Association, American Society for Gastrointestinal Endoscopy. Key Provisions in the CY 2015 Medicare Physician Fee Schedule Final Rule, 2015. Available at: http://gi.org/wp-content/uploads/2014/11/Tri-Soc_CY15_MPFS_Final_Rule_Summary.pdf.
4. MEDPAC. Payment basics: Outpatient hospital services payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
5. MEDPAC. Payment basics: Ambulatory surgery center services payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
6. Diamond, D. 10,000 people are now enrolling in Medicare – every day. Forbes; 2015 (Available at: http://www.forbes.com/sites/dandiamond/2015/07/13/aging-in-america-10000-people-enroll-in-medicare-every-day/#5177f1f35e07. Accessed January 3, 2016)
7. Mechanic, R.E. Mandatory Medicare bundled payment: Is it ready for prime time?. N Engl J Med. 2015;373:1291-3.
8. Rustgi, A.K., Allen, J.I. The house of gastrointestinal medicine: How academic medical centers can build a sustainable economic clinical model. Clin Gastroenterol Hepatol. 2013;11:1370-3.
9. Academic Practice Compensation and Production Report. Medical Group Management Association, Englewood, Colo.; 2015.
10. Becker S., Townshend G., Carnell H., et al. Physician compensation: 10 core legal and regulatory concepts. Becker’s Hospital Review Available at: http://www.beckershospitalreview.com/legal-regulatory-issues/physician-compensation-10-core-legal-and-regulatory-concepts.html. Accessed Jan. 20, 2016.
11. Brill, J.V., Jain, R., Margolis, P.S., et al. A bundled payment framework for colonoscopy performed for colorectal cancer screening or surveillance. Gastroenterology. 2014;146:849-53, e9.
Dr. Dorn is vice chief, division of gastroenterology and hepatology, associate professor of medicine, health policy & management, University of North Carolina at Chapel Hill; he has received honoraria for consulting and presentations on health reform from AbbVie and Olympus. Dr. Vesy is a gastroenterologist affiliated with Baylor University Medical Center, Dallas.
No sentient gastroenterologist has missed the fact that, over the past 3 years, Medicare revalued our endoscopy codes. The impact of those reimbursement changes has been felt both by community gastroenterologists and by those practicing in academic centers. Impacts are different, however, because funds flow, opportunities for ancillary income and compensation formulas all are different for private versus academic physicians. In this month’s Road Ahead column, I have invited leaders from both camps (private practice and academic GI) to describe how reduced procedural reimbursement is affecting their practices. I was impressed and surprised at the level of detail and analysis provided by Dr. Dorn and Dr. Vesy. There are few other sources of financial data that are embedded in real-world experience. We all are concerned about our futures, and this article should spur us into serious discussions about practice strategies going forward. As I wrote in a recent article in Gastroenterology (2016;150:295-9), this is “No Time for WIMPs.”
Gastroenterology practices generate the bulk of their revenue from endoscopic procedures. Over the past decade, the professional fees Medicare pays for these procedures have generally declined. Meanwhile, associated hospital outpatient facility fees have increased while ambulatory surgery center (ASC) fees remain below 2007 levels. This article surveys these changes and examines their significant impact on academic and private gastroenterology practices.
Professional fees for endoscopic procedures
Since 1992 physician professional fees have been linked to the Medicare Physician Fee Schedule, which assigns each service a certain number of relative value units (RVUs). First, the work RVU (wRVU) is based on the estimated physician time, mental effort, technical skill, and psychological stress required to provide a service. Second, a practice expense RVU (PE RVU) reflects the direct and indirect costs of providing the service. For procedures performed in office-based settings the PE RVU includes rent, nonclinician staff, equipment, and supplies, on average amounting to 44% of the total RVU. For procedures performed in hospital outpatient departments (HOPDs) and ASCs, the PE RVU is much lower, because most costs are incurred by the facility (which receives a separate facility fee), rather than the physician practice. Third, a small proportion of the overall RVU is linked to malpractice insurance costs (MP RVU). The RVU components are geographically adjusted, combined, and then multiplied by a conversion factor (CF, which in 2016 is $35.80) to determine actual Medicare payment (Payment = [wRVU + PE RVU + MP RVU] × CF).1
To address potential distortions in this physician fee schedule, The Affordable Care Act directed the Secretary of Health and Human Services to establish a formal process to review potentially misvalued procedure codes. During 2012 and 2014, multiple gastroenterological and surgical societies surveyed practicing physicians on the physician work, time, and intensity required to perform more than 120 services in question, including esophagoscopy, esophagogastroduodenoscopy, endoscopic retrograde cholangiopancreatography, flexible sigmoidoscopy and ileoscopy, pouchoscopy, and colonoscopy. At the same time, these societies assembled an expert panel of practicing physicians to determine the practice expenses associated with these procedures. The societies analyzed the results and presented recommendations to the American Medical Association/Specialty Society Relative Value Scale Update Committee, which, in turn, presented their recommendations to the Centers for Medicare and Medicaid Services.2 In 2014, CMS accepted approximately three-quarters of the Relative Value Scale Update Committee’s recommendations, ultimately decreasing wRVUs, increasing PE RVUs for procedures performed in office-based settings, and leaving MP RVUs unchanged for most upper endoscopy and endoscopic retrograde cholangiopancreatography procedures. These changes translated into significant 2015 payment reductions for esophagoscopy and esophagogastroduodenoscopy (4%-42%), endoscopic ultrasound (10%-35%), and endoscopic retrograde cholangiopancreatography (0%-37%) performed within facilities, with less effect for those performed in office-based settings. At that time, “in light of the substantial nature of [the colonoscopy] code revision and its relationship to the policies on moderate sedation,” CMS delayed revaluation of the lower gastrointestinal (GI) endoscopy codes.3 This reprieve is now over: The 2016 Medicare Physician Fee Schedule Final Rule includes up to 17% cuts (12% on average) to the wRVU associated with these lower GI procedures (Table 1). For office-based procedures (but not facility-based procedures) these wRVU cuts are buffered (and sometimes offset) by general increases in PE RVUs.
Facility fees for endoscopic procedures
Compared with the small percentage of endoscopic procedures that are performed in office-based settings, those performed in HOPDs and ASCs entail a lower professional fee plus a separate facility fee. Since 2000 CMS has paid for services provided in HOPDs using the outpatient prospective payment system (OPPS). Clinical services are first classified into ambulatory payment classifications (APC) on the basis of clinical and cost similarity. Next, services within an APC are assigned a single relative payment rate, which is linked to the resources required to perform the service. The APC payment rate is geographically adjusted and then multiplied by a CF to determine an actual dollar amount.4
Since 2008, CMS has used a nearly identical mechanism to pay for facility services provided in ASCs. Services are classified using the same APCs and same relative weights as the OPPS. The difference is that the ASC CF is less than the OPPS CF (the 2016 ASC CF is 58% of the OPPS CF), translating into lower dollar payments for ASC services.5 Of note, in 2008 ASC rates were cut significantly when CMS adopted this methodology for determining ASC facility fees (previously, ASC rates were approximately 85% of HOPD rates).
CMS reviews the APCs and their relative weights annually, and may adjust how specific services are classified and how APCs are weighed. Since 2006, HOPD rates for the 10 common procedures listed in Table 1 have increased by 26%-93% real (i.e., Consumer Price Index–adjusted) dollars. Meanwhile, given the steep 2008 ASC fee cuts the 2016 ASC fees are still significantly lower than they were 1 decade ago, especially when accounting for inflation. In fact, ASC fees for the most common procedures have decreased by 20% in real dollars (Supplementary Tables 1 and 2 at http://dx.doi.org/10.1016/j.cgh.2016.03.032).
Putting these changes in context
It is important to consider these changes within a broader context. First, the full economic impact of these changes on an individual gastroenterology practice depends on where it performs its services and whether it collects associated facility fees, and fees for anesthesia and pathology services. Second, the Medicare population is growing by more than 10,000 people each day.6 Third, beyond Medicare, most commercial insurers peg their reimbursement rates to a percentage of the Medicare Fee Schedule. Although the details of specific contracts vary, gastroenterologists should expect to see commercial rates move in a similar direction within the next 1–2 years. Fourth, in the 2016 Fee Schedule CMS described its future intention to remove the value of moderate sedation from all GI procedures valued with moderate sedation inherent to the procedure. The more that moderate sedation is ultimately valued, the less that endoscopic procedures will be valued. Consequently, gastroenterologists who rely on anesthesiology professionals to sedate their patients will receive less revenue per procedure. Finally, the 2015 Medicare Access and Children’s Health Insurance Program Reauthorization Act (MACRA) links a higher proportion of these dwindling fee-for-service payments to performance. Starting in 2018, physicians who elect to remain on a fee-for-service tract will receive a composite Merit-Based Incentive Payment System (MIPS) score that will translate into either performance bonuses or penalties (as much as 4% in 2019 and going up to 9% in 2022). Alternatively, providers who “sufficiently” participate in “two-sided” (i.e., risk-bearing) alternative payment models (e.g., bundled payments and accountable care organizations) instead of fee-for-service payments will receive 5% across-the-board bonuses. In sum, it is possible that fee-for-service payments may eventually become so unattractive that many gastroenterologists decide (or hope) to move to alternative payment models that combine both professional and facility fees, such as the CMS now-mandatory Comprehensive Care for Joint Replacement (CJR) program.7
Impact on academic practices
For most academic gastroenterology practices, clinical revenue far exceeds all other sources of funding, including research grants, teaching support, philanthropy, and partnerships with industry. Although a select few academic GI divisions have managed to build their own ASCs to share facility fees, for most academic practices, clinical revenue comes solely from the professional fees for endoscopic procedures and, less so, from office and hospital-based consultations and management of established patients.8 Thus, steep cuts to professional fees for endoscopic procedures, the leading source of overall revenue, will severely strain most academic gastroenterology practices.
In one of our practices (SDD), the 10 common procedures listed in Table 1 accounted for 27% of total direct clinical revenue over the past year. Roughly one-fourth of our patients are Medicare beneficiaries. Assuming no change in volume, the 2016 fee schedule cuts will amount to a 0.9% drop in direct clinical revenue. If all other payers follow with identical cuts, then direct clinical revenue will drop by 3.7%. Although our practice is fortunate to have other well-developed clinical and nonclinical revenue streams, these cuts are not insignificant.
How can academic practices continue to provide accessible clinical care in the face of these fee cuts? It can help to first consider how revenue is distributed for a Medicare beneficiary who undergoes a diagnostic colonoscopy with biopsy to evaluate unexplained diarrhea in an academic medical center’s hospital-based facility. The academic gastroenterologist receives $212 (CPT 45380). From this $212, the academic gastroenterology practice must pay assessments to various entities (sometimes including the school of medicine, department of medicine, and faculty practice plan) that may amount to more than 30% of total revenue. The roughly $150 that remains is used to pay faculty member salaries (the median salary for an academic gastroenterologist is $300,009) and benefits (estimated at $74,000/year); MP insurance (estimated at $2,275/year, higher in certain parts of the United States); and overhead for support staff, supplies, and other expenses (estimated at $50,550/year). Thus, a purely clinical academic gastroenterologist who is paid at the Medical Group Management Association (MGMA) median must generate $610,179 in preassessment revenue. If this hypothetical academic gastroenterologist solely treated Medicare beneficiaries, at $35.82 per RVU he or she would need to generate a staggering 17,035 RVUs per year, an amount that far exceeds the MGMA median (6,445) and 90th percentile (10,991) for academic gastroenterologists. Of course, real-world academic gastroenterologists also treat commercially insured patients and many spend time on nonclinical activities (although clinical income typically supports time devoted to research and teaching, not vice versa). Still, this example highlights a clear fact: Academic gastroenterology practices take a major financial loss delivering services to Medicare beneficiaries. Meanwhile, the HOPD charges more than $2,200 for the procedure. Although it receives $752 facility fee from Medicare (Disproportionate Share Hospitals and NCI Cancer Centers receive more), with a cost-to-charge ratio of roughly 0.2, revenue still clearly exceeds expenses. Finally, the anesthesia professional (if any) receives roughly $198 (CPT 00810) and the pathologist $74 (CPT 88305).
Although some may argue that academic gastroenterologists should simply accept a pay cut, lower salaries may drive many away from academia. To hire enough new (or even maintain enough existing) faculty members to maintain and grow volume, academic gastroenterology practices must find ways to supplement declining professional fees. One option is for academic practices to open their own ASCs, either alone or jointly with their health care system. But this assumes, often erroneously, that the health care system is willing to share facility fees. A second option is to develop incentive programs that transfer revenue from the health care system to the physicians. Importantly, these must be at fair market value and for nonemployed physicians cannot be linked to volume.10 Examples include medical directorships and non–volume-based performance bonuses. A third option is to consider alternative payment models, such as bundled payments that include a single lump sum payment for both professional and facility fees. The practice and health system then negotiates how the bundle is shared. Bundles should motivate hospitals and academic practices to work together to improve care and reduce overall expenses. Along these lines, CMS recently announced the CJR program under which hospitals and physicians in 75 locations will be required to participate. Although AGA recently published a bundled payment framework for screening and surveillance colonoscopy,11 bundles for other endoscopic procedures remain to be defined. But, a clearly defined, attractively priced, and skillfully negotiated bundle could be a means for redistributing revenue in ways that are more favorable to academic practices. No matter the approach, it is critical for academic gastroenterology practices and their health care systems to align their goals and integrate their services. But this is easier said than done.
Impact on private gastroenterology practices
The impact of these professional and facility fee changes on private practice depends on the practice’s payer mix, and whether it owns an ASC and directly provides anesthesia and pathology services. Consider Texas Digestive Disease Consultants (TDDC), an 80-gastroenterologist practice that provides GI care and endoscopic procedures throughout north and central Texas. TDDC revenue comes solely from professional fees generated by gastroenterologists and the pathologists that the practice employs. TDDC operating expenses include employee salaries and benefits, rent, and taxes. Based on an expected work-year of 2,080 hours, each TDDC gastroenterologist must generate $219 per hour to cover practice expenses. Physicians receive income only after practice revenue exceeds $219 per hour.
In the 2016 Medicare Physician Fee Schedule, colonoscopy code 45387 is assigned 3.36 RVUs, based on 67 minutes in total time. Based on this information, 2016 CMS payment for a screening colonoscopy ($200) will result in a loss of $45 in practice revenue over expenses. Across the TDDC practices in 2015, CMS patients represented 29% of all colonoscopies performed, but only 11% of revenue from those procedures. In aggregate, assuming no change in volume, the 2016 fee schedule cuts will translate into $5,472 less physician income for each gastroenterologist. If all other payers follow with identical cuts then each gastroenterologist would forfeit $50,896 of income.
For pathology services, code 88305 reimburses a global service per specimen. The average number of specimens per outpatient GI procedure at TDDC is 1.5. Based on CMS’ per specimen payment of $73 (down from $107 in 2012), average pathology reimbursement per a CMS endoscopic procedure is $110.
What about facility fees? Many TDDC physicians separately own and operate ASCs and anesthesia practices. Because the physician owners of these facilities funded, developed, and operate these facilities on their own, any revenue over expenses from these facilities flow directly to the ASC, rather than to TDDC. Since 2008, when ASC payments were severely reduced, ASC revenue over expenses for a Medicare colonoscopy has ranged from $0 to $70. For anesthesia services, the ASC receives approximately $159 per screening colonoscopy, which is not enough to actually cover the costs of providing anesthesia services. In sum, when TDDC gastroenterologists perform colonoscopies on Medicare patients at an HOPD the physician loses money. When the same procedure is performed at an ASC the physician barely break even.
How can private practice gastroenterologists respond to these fee cuts? First, some gastroenterologists may be forced to accept lower salaries. Second, practices can offset fee cuts by improving efficiency and reducing overall cost of care, assuming they are not already maximally efficient. Third, some private practices can increase Medicare professional payments by reclassifying as nonparticipating with Medicare. Nonparticipating status allows practices to charge the patient up to approximately 109.25% of the Medicare approved rate, with the patient submitting the claim directly to Medicare (“balance billing”). The downside is that patients shoulder the additional cost and may potentially decide to seek care elsewhere. Fourth, private practices should explore alternative payment models, such as bundled payment as described previously, either on their own or by partnering with local health systems to share risk. Finally, some practices may sell equity to and become employees of local health systems.
Conclusions
Changes to Medicare professional and facility fee payments for endoscopic procedures significantly affect academic and private gastroenterology practices. Dwindling professional fees – alongside increasing HOPD facility fees – make academic gastroenterology practices increasingly reliant on support from their parent health care systems. Like academic practices, private gastroenterology practices experience financial losses when treating Medicare beneficiaries. Academic and private gastroenterology practices should consider several potential responses. Although beyond the scope of this article, all practices must continuously strive to improve the quality and reduce the costs of the endoscopic procedures they perform.
Acknowledgments
The authors thank Leslie Narramore, MPA, for her insights and help with reimbursement data. They also thank Bryan Rhodes for providing financial data and Shivan Mehta, MD, MBA, for his feedback on the Relative Value Scale Update Committee process.
References
1. MEDPAC. Payment basics: physician and other health professional payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
2. Mehta, S.J., Brill, J.V. What is the RUC and how does it impact gastroenterology?. Clin Gastroenterol Hepatol. 2014;12:1208-11.
3. American College of Gastroenterology, American Gastroenterological Association, American Society for Gastrointestinal Endoscopy. Key Provisions in the CY 2015 Medicare Physician Fee Schedule Final Rule, 2015. Available at: http://gi.org/wp-content/uploads/2014/11/Tri-Soc_CY15_MPFS_Final_Rule_Summary.pdf.
4. MEDPAC. Payment basics: Outpatient hospital services payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
5. MEDPAC. Payment basics: Ambulatory surgery center services payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
6. Diamond, D. 10,000 people are now enrolling in Medicare – every day. Forbes; 2015 (Available at: http://www.forbes.com/sites/dandiamond/2015/07/13/aging-in-america-10000-people-enroll-in-medicare-every-day/#5177f1f35e07. Accessed January 3, 2016)
7. Mechanic, R.E. Mandatory Medicare bundled payment: Is it ready for prime time?. N Engl J Med. 2015;373:1291-3.
8. Rustgi, A.K., Allen, J.I. The house of gastrointestinal medicine: How academic medical centers can build a sustainable economic clinical model. Clin Gastroenterol Hepatol. 2013;11:1370-3.
9. Academic Practice Compensation and Production Report. Medical Group Management Association, Englewood, Colo.; 2015.
10. Becker S., Townshend G., Carnell H., et al. Physician compensation: 10 core legal and regulatory concepts. Becker’s Hospital Review Available at: http://www.beckershospitalreview.com/legal-regulatory-issues/physician-compensation-10-core-legal-and-regulatory-concepts.html. Accessed Jan. 20, 2016.
11. Brill, J.V., Jain, R., Margolis, P.S., et al. A bundled payment framework for colonoscopy performed for colorectal cancer screening or surveillance. Gastroenterology. 2014;146:849-53, e9.
Dr. Dorn is vice chief, division of gastroenterology and hepatology, associate professor of medicine, health policy & management, University of North Carolina at Chapel Hill; he has received honoraria for consulting and presentations on health reform from AbbVie and Olympus. Dr. Vesy is a gastroenterologist affiliated with Baylor University Medical Center, Dallas.

Merck Manual available as free app
The Merck Manual professional app is now available for free for use on either Android or Apple devices.
“In today’s mobile world, health care professionals expect critical health information at their fingertips, with or without an Internet connection,” said Robert S. Porter, MD, Merck Manuals’ editor-in-chief.

The app contains more than 1,000 photos and illustrations, and offline content can be stored on the device. A Wi-Fi connection is not needed to access the manual. When a cell phone is connected to the Internet, the app allows access to features such as videos of procedures, quizzes, medical news, editorials, and drug reference information.
The Merck Manual professional app is now available for free for use on either Android or Apple devices.
“In today’s mobile world, health care professionals expect critical health information at their fingertips, with or without an Internet connection,” said Robert S. Porter, MD, Merck Manuals’ editor-in-chief.
The app contains more than 1,000 photos and illustrations, and offline content can be stored on the device. A Wi-Fi connection is not needed to access the manual. When a cell phone is connected to the Internet, the app allows access to features such as videos of procedures, quizzes, medical news, editorials, and drug reference information.
The Merck Manual professional app is now available for free for use on either Android or Apple devices.
“In today’s mobile world, health care professionals expect critical health information at their fingertips, with or without an Internet connection,” said Robert S. Porter, MD, Merck Manuals’ editor-in-chief.
The app contains more than 1,000 photos and illustrations, and offline content can be stored on the device. A Wi-Fi connection is not needed to access the manual. When a cell phone is connected to the Internet, the app allows access to features such as videos of procedures, quizzes, medical news, editorials, and drug reference information.
Preparing for the GI boards
The latest installment of AGA’s Digestive Diseases Self Education Program® (DDSEP®) 8 not only helps prepare you for the in-depth gastroenterology and hepatology material on the GI board exam, but also for the test-taking process itself, thanks to a helpful piece by Suzanne Rose, MD, MSEd, and Norma Saks, EdD.
Dr. Rose, professor of medicine and senior associate dean for education at the University of Connecticut School of Medicine, and Dr. Saks, professor of the department of psychiatry, assistant dean for educational programs and director of the Cognitive Skills Program at the Robert Wood Johnson Medical School, compiled their experience and knowledge into a helpful and comprehensive list of test-taking tips for practitioners taking the GI board exams.
The article, “How to Prepare for the Gastroenterology Boards,” delves into each stage of test preparation, including studying, practice testing, and taking the test itself. Below are just a few summaries of the many tips they provide. You can access the full article by purchasing DDSEP® 8. To learn more about AGA’s DDSEP® offerings, visit http://buyddsep8.gastro.org.
Before the exam
Get to know the rules and familiarize yourself with the American Board of Internal Medicine’s (ABIM) certification process. Make sure you allow enough time to prepare for the exam when you’re signing up, and also get familiar with the location, scheduling, and potential penalties of the exam.
Preparing for the exam
While studying, Dr. Rose and Dr. Saks recommend first identifying your strengths and weaknesses so that you can take the time to prepare where you need it. Also, make a study schedule and take practice tests so that you can better identify topics you should spend more time studying for. For instance, even though you might think something’s a test strength, practicing could help show you that you’re overthinking topics you’re most comfortable with. Also, consider working with a partner or larger group to help increase learning retention and keep you on track with your study schedule.
Taking the exam
In addition to obvious things like double-checking ABIM’s website before the test day and getting a good night’s sleep, the authors provide some helpful time management suggestions. Some topics they address include guessing, pacing yourself during the exam and how to best address those difficult questions. One big tip they offer: don’t leave questions blank, as those will automatically be counted as incorrect answers.
The latest installment of AGA’s Digestive Diseases Self Education Program® (DDSEP®) 8 not only helps prepare you for the in-depth gastroenterology and hepatology material on the GI board exam, but also for the test-taking process itself, thanks to a helpful piece by Suzanne Rose, MD, MSEd, and Norma Saks, EdD.
Dr. Rose, professor of medicine and senior associate dean for education at the University of Connecticut School of Medicine, and Dr. Saks, professor of the department of psychiatry, assistant dean for educational programs and director of the Cognitive Skills Program at the Robert Wood Johnson Medical School, compiled their experience and knowledge into a helpful and comprehensive list of test-taking tips for practitioners taking the GI board exams.
The article, “How to Prepare for the Gastroenterology Boards,” delves into each stage of test preparation, including studying, practice testing, and taking the test itself. Below are just a few summaries of the many tips they provide. You can access the full article by purchasing DDSEP® 8. To learn more about AGA’s DDSEP® offerings, visit http://buyddsep8.gastro.org.
Before the exam
Get to know the rules and familiarize yourself with the American Board of Internal Medicine’s (ABIM) certification process. Make sure you allow enough time to prepare for the exam when you’re signing up, and also get familiar with the location, scheduling, and potential penalties of the exam.
Preparing for the exam
While studying, Dr. Rose and Dr. Saks recommend first identifying your strengths and weaknesses so that you can take the time to prepare where you need it. Also, make a study schedule and take practice tests so that you can better identify topics you should spend more time studying for. For instance, even though you might think something’s a test strength, practicing could help show you that you’re overthinking topics you’re most comfortable with. Also, consider working with a partner or larger group to help increase learning retention and keep you on track with your study schedule.
Taking the exam
In addition to obvious things like double-checking ABIM’s website before the test day and getting a good night’s sleep, the authors provide some helpful time management suggestions. Some topics they address include guessing, pacing yourself during the exam and how to best address those difficult questions. One big tip they offer: don’t leave questions blank, as those will automatically be counted as incorrect answers.
The latest installment of AGA’s Digestive Diseases Self Education Program® (DDSEP®) 8 not only helps prepare you for the in-depth gastroenterology and hepatology material on the GI board exam, but also for the test-taking process itself, thanks to a helpful piece by Suzanne Rose, MD, MSEd, and Norma Saks, EdD.
Dr. Rose, professor of medicine and senior associate dean for education at the University of Connecticut School of Medicine, and Dr. Saks, professor of the department of psychiatry, assistant dean for educational programs and director of the Cognitive Skills Program at the Robert Wood Johnson Medical School, compiled their experience and knowledge into a helpful and comprehensive list of test-taking tips for practitioners taking the GI board exams.
The article, “How to Prepare for the Gastroenterology Boards,” delves into each stage of test preparation, including studying, practice testing, and taking the test itself. Below are just a few summaries of the many tips they provide. You can access the full article by purchasing DDSEP® 8. To learn more about AGA’s DDSEP® offerings, visit http://buyddsep8.gastro.org.
Before the exam
Get to know the rules and familiarize yourself with the American Board of Internal Medicine’s (ABIM) certification process. Make sure you allow enough time to prepare for the exam when you’re signing up, and also get familiar with the location, scheduling, and potential penalties of the exam.
Preparing for the exam
While studying, Dr. Rose and Dr. Saks recommend first identifying your strengths and weaknesses so that you can take the time to prepare where you need it. Also, make a study schedule and take practice tests so that you can better identify topics you should spend more time studying for. For instance, even though you might think something’s a test strength, practicing could help show you that you’re overthinking topics you’re most comfortable with. Also, consider working with a partner or larger group to help increase learning retention and keep you on track with your study schedule.
Taking the exam
In addition to obvious things like double-checking ABIM’s website before the test day and getting a good night’s sleep, the authors provide some helpful time management suggestions. Some topics they address include guessing, pacing yourself during the exam and how to best address those difficult questions. One big tip they offer: don’t leave questions blank, as those will automatically be counted as incorrect answers.
PAD Toolkit Available
For SVS members, every month is PAD month. But with September PAD Awareness Month, it's a good time to remind members that SVS offers a digital toolkit to share with colleagues, patients and referring physicians.
If you have ever wished you had a YouTube playlist of video information on PAD that patients can watch, we’ve got it. We also provide links to printable brochures, articles, practice guidelines and more.
Visit the SVS PAD Resources page here.
For SVS members, every month is PAD month. But with September PAD Awareness Month, it's a good time to remind members that SVS offers a digital toolkit to share with colleagues, patients and referring physicians.
If you have ever wished you had a YouTube playlist of video information on PAD that patients can watch, we’ve got it. We also provide links to printable brochures, articles, practice guidelines and more.
Visit the SVS PAD Resources page here.
For SVS members, every month is PAD month. But with September PAD Awareness Month, it's a good time to remind members that SVS offers a digital toolkit to share with colleagues, patients and referring physicians.
If you have ever wished you had a YouTube playlist of video information on PAD that patients can watch, we’ve got it. We also provide links to printable brochures, articles, practice guidelines and more.
Visit the SVS PAD Resources page here.
