User login
Fungus makes mosquitoes more susceptible to malaria

Photo by James Gathany
Researchers say they have identified a fungus that compromises mosquitoes’ immune systems, making them more susceptible to infection with malaria parasites.
Malaria researchers have, in the past, identified microbes that prevent the Anopheles mosquito from being infected by malaria parasites, but this is the first time they have found a microorganism that appears to make the mosquito more likely to become infected with—and then spread—malaria.
The finding was published in Scientific Reports.
“This very common, naturally occurring fungus may have a significant impact on malaria transmission,” said study author George Dimopoulos, PhD, of the Johns Hopkins Bloomberg School of Public Health in Baltimore, Maryland.
“It doesn’t kill the mosquitoes. It doesn’t make them sick. It just makes them more likely to become infected and thereby to spread the disease. While this fungus is unlikely to be helpful as part of a malaria control strategy, our finding significantly advances our knowledge of the different factors that influence the transmission of malaria.”
For this study, Dr Dimopoulos and his colleagues isolated the Penicillium chrysogenum fungus from the gut of field-caught Anopheles mosquitoes. The team found this fungus made the mosquitoes more susceptible to being infected by Plasmodium parasites through a secreted heat-stable factor.
The researchers said the mechanism behind this increased susceptibility involves upregulation of the mosquitoes’ ornithine decarboxylase gene, which sequesters arginine for polyamine biosynthesis.
They noted that arginine plays an important role in the mosquitoes’ anti-Plasmodium defense as a substrate of nitric oxide production, so the availability of arginine has a direct impact on susceptibility to infection with Plasmodium parasites.
Dr Dimopoulos said Penicillium chrysogenum had not previously been studied in terms of mosquito biology, and he and his team had hoped the fungus would act like several other bacteria that researchers have identified, which prevent mosquitoes from becoming infected with malaria parasites.
Even though Penicillium chrysogenum actually appears to worsen infections, the team believes the fungus can still help researchers in their fight against malaria.
“We have questions we hope this finding will help us to answer, including, ‘Why do we have increased transmission of malaria in some areas and not others when the presence of mosquitoes is the same?’” Dr Dimopoulos said. “This gives us another piece of the complicated malaria puzzle.”
Because environmental microorganisms can vary greatly from region to region, Dr Dimopoulos and his colleagues believe their finding may help explain variations in the prevalence of malaria in different geographic areas. ![]()
Photo by James Gathany
Researchers say they have identified a fungus that compromises mosquitoes’ immune systems, making them more susceptible to infection with malaria parasites.
Malaria researchers have, in the past, identified microbes that prevent the Anopheles mosquito from being infected by malaria parasites, but this is the first time they have found a microorganism that appears to make the mosquito more likely to become infected with—and then spread—malaria.
The finding was published in Scientific Reports.
“This very common, naturally occurring fungus may have a significant impact on malaria transmission,” said study author George Dimopoulos, PhD, of the Johns Hopkins Bloomberg School of Public Health in Baltimore, Maryland.
“It doesn’t kill the mosquitoes. It doesn’t make them sick. It just makes them more likely to become infected and thereby to spread the disease. While this fungus is unlikely to be helpful as part of a malaria control strategy, our finding significantly advances our knowledge of the different factors that influence the transmission of malaria.”
For this study, Dr Dimopoulos and his colleagues isolated the Penicillium chrysogenum fungus from the gut of field-caught Anopheles mosquitoes. The team found this fungus made the mosquitoes more susceptible to being infected by Plasmodium parasites through a secreted heat-stable factor.
The researchers said the mechanism behind this increased susceptibility involves upregulation of the mosquitoes’ ornithine decarboxylase gene, which sequesters arginine for polyamine biosynthesis.
They noted that arginine plays an important role in the mosquitoes’ anti-Plasmodium defense as a substrate of nitric oxide production, so the availability of arginine has a direct impact on susceptibility to infection with Plasmodium parasites.
Dr Dimopoulos said Penicillium chrysogenum had not previously been studied in terms of mosquito biology, and he and his team had hoped the fungus would act like several other bacteria that researchers have identified, which prevent mosquitoes from becoming infected with malaria parasites.
Even though Penicillium chrysogenum actually appears to worsen infections, the team believes the fungus can still help researchers in their fight against malaria.
“We have questions we hope this finding will help us to answer, including, ‘Why do we have increased transmission of malaria in some areas and not others when the presence of mosquitoes is the same?’” Dr Dimopoulos said. “This gives us another piece of the complicated malaria puzzle.”
Because environmental microorganisms can vary greatly from region to region, Dr Dimopoulos and his colleagues believe their finding may help explain variations in the prevalence of malaria in different geographic areas. ![]()
Photo by James Gathany
Researchers say they have identified a fungus that compromises mosquitoes’ immune systems, making them more susceptible to infection with malaria parasites.
Malaria researchers have, in the past, identified microbes that prevent the Anopheles mosquito from being infected by malaria parasites, but this is the first time they have found a microorganism that appears to make the mosquito more likely to become infected with—and then spread—malaria.
The finding was published in Scientific Reports.
“This very common, naturally occurring fungus may have a significant impact on malaria transmission,” said study author George Dimopoulos, PhD, of the Johns Hopkins Bloomberg School of Public Health in Baltimore, Maryland.
“It doesn’t kill the mosquitoes. It doesn’t make them sick. It just makes them more likely to become infected and thereby to spread the disease. While this fungus is unlikely to be helpful as part of a malaria control strategy, our finding significantly advances our knowledge of the different factors that influence the transmission of malaria.”
For this study, Dr Dimopoulos and his colleagues isolated the Penicillium chrysogenum fungus from the gut of field-caught Anopheles mosquitoes. The team found this fungus made the mosquitoes more susceptible to being infected by Plasmodium parasites through a secreted heat-stable factor.
The researchers said the mechanism behind this increased susceptibility involves upregulation of the mosquitoes’ ornithine decarboxylase gene, which sequesters arginine for polyamine biosynthesis.
They noted that arginine plays an important role in the mosquitoes’ anti-Plasmodium defense as a substrate of nitric oxide production, so the availability of arginine has a direct impact on susceptibility to infection with Plasmodium parasites.
Dr Dimopoulos said Penicillium chrysogenum had not previously been studied in terms of mosquito biology, and he and his team had hoped the fungus would act like several other bacteria that researchers have identified, which prevent mosquitoes from becoming infected with malaria parasites.
Even though Penicillium chrysogenum actually appears to worsen infections, the team believes the fungus can still help researchers in their fight against malaria.
“We have questions we hope this finding will help us to answer, including, ‘Why do we have increased transmission of malaria in some areas and not others when the presence of mosquitoes is the same?’” Dr Dimopoulos said. “This gives us another piece of the complicated malaria puzzle.”
Because environmental microorganisms can vary greatly from region to region, Dr Dimopoulos and his colleagues believe their finding may help explain variations in the prevalence of malaria in different geographic areas. ![]()
Novel Method Reveals New Genetic Information on Depression
In a modern twist on clinical data gathering, crowd-sourcing has helped researchers identify “weak genetic signals” of depression. By combining data from the genetic information website 23andMe.com and previous genetic research, researchers identified for the first time 15 regions of the genome that may be associated with depression in people of European ancestry. Their findings should help “make clear that this is a brain disease,” said Roy Perlis, MD, MSc, a lead investigator and associate professor of psychiatry at Harvard Medical School, “which we hope will decrease the stigma still associated with these kinds of illnesses.”
Other studies have, of course, investigated genetic components of depression. But they may have been too small to uncover the subtle effects of the many genes influencing the risk of depression, these researchers say.
In their first analysis, using data from > 300,000 people of European ancestry who had purchased genetic profiles on 23andMe.com (and who consented to share their information with researchers), the researchers identified 2 genomic regions significantly associated with depression risk, including 1 previously associated with epilepsy and intellectual disability.
They then combined that information with data from genomewide association studies of 9,200 people with a history of depression and 9,500 controls, along with another group of 151,800 people with and without depression. That analysis revealed 15 genomic regions, including 17 specific sites, significantly associated with a diagnosis of depression. Several of the sites are located in or near genes known to be involved in brain development.
“The neurotransmitter-based models we are currently using to treat depression are more than 40 years old,” says Dr. Perlis. “We really need new treatment targets. We hope that finding these genes will point us toward novel treatment strategies. “[T]he traditional way of doing genetic studies is not the only way that works. Using existing large datasets or biobanks may be far more efficient.”
In a modern twist on clinical data gathering, crowd-sourcing has helped researchers identify “weak genetic signals” of depression. By combining data from the genetic information website 23andMe.com and previous genetic research, researchers identified for the first time 15 regions of the genome that may be associated with depression in people of European ancestry. Their findings should help “make clear that this is a brain disease,” said Roy Perlis, MD, MSc, a lead investigator and associate professor of psychiatry at Harvard Medical School, “which we hope will decrease the stigma still associated with these kinds of illnesses.”
Other studies have, of course, investigated genetic components of depression. But they may have been too small to uncover the subtle effects of the many genes influencing the risk of depression, these researchers say.
In their first analysis, using data from > 300,000 people of European ancestry who had purchased genetic profiles on 23andMe.com (and who consented to share their information with researchers), the researchers identified 2 genomic regions significantly associated with depression risk, including 1 previously associated with epilepsy and intellectual disability.
They then combined that information with data from genomewide association studies of 9,200 people with a history of depression and 9,500 controls, along with another group of 151,800 people with and without depression. That analysis revealed 15 genomic regions, including 17 specific sites, significantly associated with a diagnosis of depression. Several of the sites are located in or near genes known to be involved in brain development.
“The neurotransmitter-based models we are currently using to treat depression are more than 40 years old,” says Dr. Perlis. “We really need new treatment targets. We hope that finding these genes will point us toward novel treatment strategies. “[T]he traditional way of doing genetic studies is not the only way that works. Using existing large datasets or biobanks may be far more efficient.”
In a modern twist on clinical data gathering, crowd-sourcing has helped researchers identify “weak genetic signals” of depression. By combining data from the genetic information website 23andMe.com and previous genetic research, researchers identified for the first time 15 regions of the genome that may be associated with depression in people of European ancestry. Their findings should help “make clear that this is a brain disease,” said Roy Perlis, MD, MSc, a lead investigator and associate professor of psychiatry at Harvard Medical School, “which we hope will decrease the stigma still associated with these kinds of illnesses.”
Other studies have, of course, investigated genetic components of depression. But they may have been too small to uncover the subtle effects of the many genes influencing the risk of depression, these researchers say.
In their first analysis, using data from > 300,000 people of European ancestry who had purchased genetic profiles on 23andMe.com (and who consented to share their information with researchers), the researchers identified 2 genomic regions significantly associated with depression risk, including 1 previously associated with epilepsy and intellectual disability.
They then combined that information with data from genomewide association studies of 9,200 people with a history of depression and 9,500 controls, along with another group of 151,800 people with and without depression. That analysis revealed 15 genomic regions, including 17 specific sites, significantly associated with a diagnosis of depression. Several of the sites are located in or near genes known to be involved in brain development.
“The neurotransmitter-based models we are currently using to treat depression are more than 40 years old,” says Dr. Perlis. “We really need new treatment targets. We hope that finding these genes will point us toward novel treatment strategies. “[T]he traditional way of doing genetic studies is not the only way that works. Using existing large datasets or biobanks may be far more efficient.”
Resident SBML for Thoracentesis
There has been a nationwide shift away from general internists performing bedside thoracenteses and toward referring them to pulmonology and interventional radiology services.[1] Aligning with this trend, the American Board of Internal Medicine now only requires that internal medicine (IM)trained physicians understand the indications, complications, and management of bedside procedures.[2]
However, thoracentesis is still considered a core competency of practicing hospitalists, the fastest growing field within general IM.[3] Furthermore, evidence suggests that thoracenteses done by general internists have high patient satisfaction, reduce hospital length of stay, are more cost‐effective, and are as safe as those done by consultants.[4, 5, 6] It is thus important to understand the reasons for referrals to specialty services and to investigate potential interventions that increase performance of procedures by internists.
In this issue of the Journal of Hospital Medicine, Barsuk and colleagues present a prospective, single‐center study assessing the impact of simulation‐based mastery learning (SBML) on thoracentesis among a randomly selected group of IM residents.[7] They studied how their program influenced simulated skills, procedural self‐confidence, frequency of real‐world performance, and rate and reasons for referral to consultants. The authors compared the latter outcomes to traditionally trained residents and hospitalists, finding that SBML improved skills, self‐confidence, and the relative frequency of general internistperformed procedures. Low confidence and limited time were the primary reasons for referral.
To our knowledge, this is the first study to show that SBML can lead to a clinically and statistically significant change in thoracentesis referral patterns, which may have important implications for hospitalists. Given the inconsistent amount and quality of procedural training across IM residency programs, hospitalists may be increasingly ill prepared to perform thoracentesis and train future generations in its best practices.[2, 8, 9] This study demonstrates that SBML can provide trainees with essential hands‐on skills development and experience that is often missing from traditional training models.
Yet, although SBML seems to affect resident referral patterns, its potential impact on practicing hospitalists is less clear. Hospitalists provide the majority of care for general medicine inpatients around the country, and in this study had a dramatically lower rate of bedside procedure performance than even traditionally trained residents (0.7% vs 14.2$), which makes them vital to any strategy to increase bedside thoracentesis rates.[9] Yet the results by Barsuk et al. suggest that the effect size of SBML on hospitalists may be much smaller than on trainees. First, the primary driver of resident practice change appeared to be increased confidence, but baseline hospitalist confidence was significantly greater than that of traditionally trained residents. Second, it is unclear what, if any, effect SBML would have on the time needed to perform a thoracentesis, which was a major factor for hospitalists referring to consult services. Lastly, given the known decrement in procedural skills over time, the durability and associated costs of longitudinal SBML training are unknown.[10, 11, 12]
The fact that general internistperformed thoracenteses are as safe and more cost‐effective than those performed by consultants is a compelling argument to shift procedures back to the bedside. However, these cost analyses do not account for the opportunity cost for hospitalists, either in lost time spent caring for additional patients or in longer shift lengths. It is important to understand whether and how it can be feasible for general internists to perform more bedside thoracenteses so physician training and resource utilization can be optimized. Whereas confidence and time are likely limiting factors for all general internists, this study suggests that their relative importance may markedly differ between residents and hospitalists, and it is unclear how much the change in confidence resulting from SBML would affect the rates of thoracentesis by generalists beyond practice settings involving trainees. The feasibility, cost, and efficacy of SBML deserve more study in multiple clinical environments to understand its true impact. Ultimately, we suspect that only an intervention addressing procedural time demands will lead to meaningful, sustained increases in general internistperformed thoracenteses.
- , . The declining number and variety of procedures done by general internists: a resurvey of members of the American College of Physicians. Ann Intern Med. 2007;146(5):355–360.
- American Board of Internal Medicine. Internal medicine policies. Available at: http://www.abim.org/certification/policies/internal‐medicine‐subspecialty‐policies/internal‐medicine.aspx. Accessed July 18, 2016.
- Society of Hospital Medicine. SHM core competencies. Available at: http://www.hospitalmedicine.org/Web/Education/Core_Competencies/Web/Education/Core_Competencies.aspx. Accessed July 18, 2016.
- , , , . Patient satisfaction with a hospitalist procedure service: is bedside procedure teaching reassuring to patients? J Hosp Med. 2011;6(4):219–224.
- , , , , . Factors associated with inpatient thoracentesis procedure quality at university hospitals. Jt Comm J Qual Patient Saf. 2016;42(1):34–40.
- , , , , . Thoracentesis outcomes: a 12‐year experience. Thorax. 2015;70(2):127–132.
- , , , et al. The effect of simulation‐based mastery learning on thoracentesis referral patterns. J Hosp Med. 2016;11(11):792–795.
- . What we know about hospitalists. Innovative Thinking website. Available at: http://innovativesolutions.org/innovative‐thinking/what‐we‐know‐about‐hospitalists. Accessed July 18, 2016.
- , , , . Procedural skills training in internal medicine residencies. A survey of program directors. Ann intern Med. 1989;111(11):932–938.
- , , , et al. Beyond the comfort zone: residents assess their comfort performing inpatient medical procedures. Am J Med. 2006;119(1):71:e17–e24.
- . Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Acad Med. 2004;79(10 suppl):S70–S81
- , , , et al. Simulation training and its effect on long‐term resident performance in central venous catheterization. Simul Healthc. 2010;5(3):146–151.
There has been a nationwide shift away from general internists performing bedside thoracenteses and toward referring them to pulmonology and interventional radiology services.[1] Aligning with this trend, the American Board of Internal Medicine now only requires that internal medicine (IM)trained physicians understand the indications, complications, and management of bedside procedures.[2]
However, thoracentesis is still considered a core competency of practicing hospitalists, the fastest growing field within general IM.[3] Furthermore, evidence suggests that thoracenteses done by general internists have high patient satisfaction, reduce hospital length of stay, are more cost‐effective, and are as safe as those done by consultants.[4, 5, 6] It is thus important to understand the reasons for referrals to specialty services and to investigate potential interventions that increase performance of procedures by internists.
In this issue of the Journal of Hospital Medicine, Barsuk and colleagues present a prospective, single‐center study assessing the impact of simulation‐based mastery learning (SBML) on thoracentesis among a randomly selected group of IM residents.[7] They studied how their program influenced simulated skills, procedural self‐confidence, frequency of real‐world performance, and rate and reasons for referral to consultants. The authors compared the latter outcomes to traditionally trained residents and hospitalists, finding that SBML improved skills, self‐confidence, and the relative frequency of general internistperformed procedures. Low confidence and limited time were the primary reasons for referral.
To our knowledge, this is the first study to show that SBML can lead to a clinically and statistically significant change in thoracentesis referral patterns, which may have important implications for hospitalists. Given the inconsistent amount and quality of procedural training across IM residency programs, hospitalists may be increasingly ill prepared to perform thoracentesis and train future generations in its best practices.[2, 8, 9] This study demonstrates that SBML can provide trainees with essential hands‐on skills development and experience that is often missing from traditional training models.
Yet, although SBML seems to affect resident referral patterns, its potential impact on practicing hospitalists is less clear. Hospitalists provide the majority of care for general medicine inpatients around the country, and in this study had a dramatically lower rate of bedside procedure performance than even traditionally trained residents (0.7% vs 14.2$), which makes them vital to any strategy to increase bedside thoracentesis rates.[9] Yet the results by Barsuk et al. suggest that the effect size of SBML on hospitalists may be much smaller than on trainees. First, the primary driver of resident practice change appeared to be increased confidence, but baseline hospitalist confidence was significantly greater than that of traditionally trained residents. Second, it is unclear what, if any, effect SBML would have on the time needed to perform a thoracentesis, which was a major factor for hospitalists referring to consult services. Lastly, given the known decrement in procedural skills over time, the durability and associated costs of longitudinal SBML training are unknown.[10, 11, 12]
The fact that general internistperformed thoracenteses are as safe and more cost‐effective than those performed by consultants is a compelling argument to shift procedures back to the bedside. However, these cost analyses do not account for the opportunity cost for hospitalists, either in lost time spent caring for additional patients or in longer shift lengths. It is important to understand whether and how it can be feasible for general internists to perform more bedside thoracenteses so physician training and resource utilization can be optimized. Whereas confidence and time are likely limiting factors for all general internists, this study suggests that their relative importance may markedly differ between residents and hospitalists, and it is unclear how much the change in confidence resulting from SBML would affect the rates of thoracentesis by generalists beyond practice settings involving trainees. The feasibility, cost, and efficacy of SBML deserve more study in multiple clinical environments to understand its true impact. Ultimately, we suspect that only an intervention addressing procedural time demands will lead to meaningful, sustained increases in general internistperformed thoracenteses.
There has been a nationwide shift away from general internists performing bedside thoracenteses and toward referring them to pulmonology and interventional radiology services.[1] Aligning with this trend, the American Board of Internal Medicine now only requires that internal medicine (IM)trained physicians understand the indications, complications, and management of bedside procedures.[2]
However, thoracentesis is still considered a core competency of practicing hospitalists, the fastest growing field within general IM.[3] Furthermore, evidence suggests that thoracenteses done by general internists have high patient satisfaction, reduce hospital length of stay, are more cost‐effective, and are as safe as those done by consultants.[4, 5, 6] It is thus important to understand the reasons for referrals to specialty services and to investigate potential interventions that increase performance of procedures by internists.
In this issue of the Journal of Hospital Medicine, Barsuk and colleagues present a prospective, single‐center study assessing the impact of simulation‐based mastery learning (SBML) on thoracentesis among a randomly selected group of IM residents.[7] They studied how their program influenced simulated skills, procedural self‐confidence, frequency of real‐world performance, and rate and reasons for referral to consultants. The authors compared the latter outcomes to traditionally trained residents and hospitalists, finding that SBML improved skills, self‐confidence, and the relative frequency of general internistperformed procedures. Low confidence and limited time were the primary reasons for referral.
To our knowledge, this is the first study to show that SBML can lead to a clinically and statistically significant change in thoracentesis referral patterns, which may have important implications for hospitalists. Given the inconsistent amount and quality of procedural training across IM residency programs, hospitalists may be increasingly ill prepared to perform thoracentesis and train future generations in its best practices.[2, 8, 9] This study demonstrates that SBML can provide trainees with essential hands‐on skills development and experience that is often missing from traditional training models.
Yet, although SBML seems to affect resident referral patterns, its potential impact on practicing hospitalists is less clear. Hospitalists provide the majority of care for general medicine inpatients around the country, and in this study had a dramatically lower rate of bedside procedure performance than even traditionally trained residents (0.7% vs 14.2$), which makes them vital to any strategy to increase bedside thoracentesis rates.[9] Yet the results by Barsuk et al. suggest that the effect size of SBML on hospitalists may be much smaller than on trainees. First, the primary driver of resident practice change appeared to be increased confidence, but baseline hospitalist confidence was significantly greater than that of traditionally trained residents. Second, it is unclear what, if any, effect SBML would have on the time needed to perform a thoracentesis, which was a major factor for hospitalists referring to consult services. Lastly, given the known decrement in procedural skills over time, the durability and associated costs of longitudinal SBML training are unknown.[10, 11, 12]
The fact that general internistperformed thoracenteses are as safe and more cost‐effective than those performed by consultants is a compelling argument to shift procedures back to the bedside. However, these cost analyses do not account for the opportunity cost for hospitalists, either in lost time spent caring for additional patients or in longer shift lengths. It is important to understand whether and how it can be feasible for general internists to perform more bedside thoracenteses so physician training and resource utilization can be optimized. Whereas confidence and time are likely limiting factors for all general internists, this study suggests that their relative importance may markedly differ between residents and hospitalists, and it is unclear how much the change in confidence resulting from SBML would affect the rates of thoracentesis by generalists beyond practice settings involving trainees. The feasibility, cost, and efficacy of SBML deserve more study in multiple clinical environments to understand its true impact. Ultimately, we suspect that only an intervention addressing procedural time demands will lead to meaningful, sustained increases in general internistperformed thoracenteses.
- , . The declining number and variety of procedures done by general internists: a resurvey of members of the American College of Physicians. Ann Intern Med. 2007;146(5):355–360.
- American Board of Internal Medicine. Internal medicine policies. Available at: http://www.abim.org/certification/policies/internal‐medicine‐subspecialty‐policies/internal‐medicine.aspx. Accessed July 18, 2016.
- Society of Hospital Medicine. SHM core competencies. Available at: http://www.hospitalmedicine.org/Web/Education/Core_Competencies/Web/Education/Core_Competencies.aspx. Accessed July 18, 2016.
- , , , . Patient satisfaction with a hospitalist procedure service: is bedside procedure teaching reassuring to patients? J Hosp Med. 2011;6(4):219–224.
- , , , , . Factors associated with inpatient thoracentesis procedure quality at university hospitals. Jt Comm J Qual Patient Saf. 2016;42(1):34–40.
- , , , , . Thoracentesis outcomes: a 12‐year experience. Thorax. 2015;70(2):127–132.
- , , , et al. The effect of simulation‐based mastery learning on thoracentesis referral patterns. J Hosp Med. 2016;11(11):792–795.
- . What we know about hospitalists. Innovative Thinking website. Available at: http://innovativesolutions.org/innovative‐thinking/what‐we‐know‐about‐hospitalists. Accessed July 18, 2016.
- , , , . Procedural skills training in internal medicine residencies. A survey of program directors. Ann intern Med. 1989;111(11):932–938.
- , , , et al. Beyond the comfort zone: residents assess their comfort performing inpatient medical procedures. Am J Med. 2006;119(1):71:e17–e24.
- . Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Acad Med. 2004;79(10 suppl):S70–S81
- , , , et al. Simulation training and its effect on long‐term resident performance in central venous catheterization. Simul Healthc. 2010;5(3):146–151.
- , . The declining number and variety of procedures done by general internists: a resurvey of members of the American College of Physicians. Ann Intern Med. 2007;146(5):355–360.
- American Board of Internal Medicine. Internal medicine policies. Available at: http://www.abim.org/certification/policies/internal‐medicine‐subspecialty‐policies/internal‐medicine.aspx. Accessed July 18, 2016.
- Society of Hospital Medicine. SHM core competencies. Available at: http://www.hospitalmedicine.org/Web/Education/Core_Competencies/Web/Education/Core_Competencies.aspx. Accessed July 18, 2016.
- , , , . Patient satisfaction with a hospitalist procedure service: is bedside procedure teaching reassuring to patients? J Hosp Med. 2011;6(4):219–224.
- , , , , . Factors associated with inpatient thoracentesis procedure quality at university hospitals. Jt Comm J Qual Patient Saf. 2016;42(1):34–40.
- , , , , . Thoracentesis outcomes: a 12‐year experience. Thorax. 2015;70(2):127–132.
- , , , et al. The effect of simulation‐based mastery learning on thoracentesis referral patterns. J Hosp Med. 2016;11(11):792–795.
- . What we know about hospitalists. Innovative Thinking website. Available at: http://innovativesolutions.org/innovative‐thinking/what‐we‐know‐about‐hospitalists. Accessed July 18, 2016.
- , , , . Procedural skills training in internal medicine residencies. A survey of program directors. Ann intern Med. 1989;111(11):932–938.
- , , , et al. Beyond the comfort zone: residents assess their comfort performing inpatient medical procedures. Am J Med. 2006;119(1):71:e17–e24.
- . Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Acad Med. 2004;79(10 suppl):S70–S81
- , , , et al. Simulation training and its effect on long‐term resident performance in central venous catheterization. Simul Healthc. 2010;5(3):146–151.
GAO report calls out HHS for misdirecting ACA reinsurance funds
The Health and Human Services department is failing to properly administer a reinsurance program under the Affordable Care Act by unlawfully diverting funds intended for the U.S. Treasury, according to a nonpartisan watchdog report.
The Government Accountability Office (GAO) report, released Sept. 29, finds that HHS is breaking ACA regulations that require a portion of funds collected under its Transitional Reinsurance Program to go to the Treasury. Instead, the agency has redirected $5 billion so far to pay health insurers that enroll high-cost patients under the program.

“In light of the foregoing analysis, we conclude that HHS lacks authority to ignore the statute’s directive to deposit amounts from collections under the Transitional Reinsurance Program to the Treasury and instead make deposits in the Treasury only if its collections reach the amounts for reinsurance payments specified in section 1341,” Susan A. Poling, GAO general counsel, wrote in a legal opinion. “The agency is not authorized to prioritize collections in this manner.”
Republican lawmakers, including Sen. John Barrasso III (Wyo.), chair of the Senate Republican Policy Committee, praised the legal opinion, saying it shows the Obama administration is bending the rules when it comes to rolling out the ACA.
“This is a major victory for the American people who are suffering with higher premiums and fewer choices because of this failed law,” said Sen. Barrasso, who with several fellow Republican legislators requested the GAO investigation. “The administration should end this illegal scheme immediately, and focus on providing relief from the burdens of this law.”
At press time, neither the White House nor HHS had responded to request for comment on the report.
The Transitional Reinsurance Program is a 3-year initiative under the ACA that collects fees from employers and other private health insurance plans and directs the funds to health plans that face large claims for patients with high-cost medical conditions. The ACA specifies that between 2014 and 2016, HHS would collect $25 billion in fees, of which $5 billion would go into the Treasury.
But when HHS was unable to collect the full amount over the 3 years, it did not distribute funds into the Treasury, but instead used it pay the health plans. To justify that decision, HHS officials announced that the department would allocate all collections first for reinsurance payments until collections totaled the target amount set forth for reinsurance payments under the law, and that any remaining collections would go toward to administrative expenses and the Treasury, according to the GAO report.
But the GAO argues that HHS falling short of the projected collections does not alter the meaning of the statute.
“Specifically, where actual funding has fallen short of an agency’s original expectations, courts have directed the agency to distribute available funds to approximate the allocation plan Congress designed in anticipation of full funding,” Ms. Poling wrote. The HHS “assertion that the statute is silent with respect to allocation of collections overlooks the fact that section 1341 expressly directs HHS to collect amounts for the Treasury and prohibits the use of these amounts for any purpose other than deposit in the Treasury. HHS’s analysis focuses on words and phrases in the statute in isolation rather than in their appropriate context.”
While the GAO cannot force HHS to act with the opinion, lawmakers could use the report to craft legislation forcing HHS to repay the Treasury.

“This issue has been brewing for a while, and is another example of a series of attempts to challenge or limit payments being made to carriers under the ACA,” Katherine Hempstead, senior adviser to vice president at the Robert Wood Johnson Foundation, said in an interview. “It’s no mystery why making these payments is a pretty high priority for the [Centers for Medicare & Medicaid Services] right now, given the losses sustained by many market participants. My guess is that the can will probably be kicked down the road on this and a number of other issues for the next administration and Congress to resolve.”
The reinsurance program was one of three programs intended to protect against the negative impacts of adverse selection and risk selection, while working to stabilize premiums during the initial years of the health law’s implementation. The program aims to protect against premium increases in the individual market by offsetting expenses of high-cost patients.
On Twitter @legal_med
The Health and Human Services department is failing to properly administer a reinsurance program under the Affordable Care Act by unlawfully diverting funds intended for the U.S. Treasury, according to a nonpartisan watchdog report.
The Government Accountability Office (GAO) report, released Sept. 29, finds that HHS is breaking ACA regulations that require a portion of funds collected under its Transitional Reinsurance Program to go to the Treasury. Instead, the agency has redirected $5 billion so far to pay health insurers that enroll high-cost patients under the program.
“In light of the foregoing analysis, we conclude that HHS lacks authority to ignore the statute’s directive to deposit amounts from collections under the Transitional Reinsurance Program to the Treasury and instead make deposits in the Treasury only if its collections reach the amounts for reinsurance payments specified in section 1341,” Susan A. Poling, GAO general counsel, wrote in a legal opinion. “The agency is not authorized to prioritize collections in this manner.”
Republican lawmakers, including Sen. John Barrasso III (Wyo.), chair of the Senate Republican Policy Committee, praised the legal opinion, saying it shows the Obama administration is bending the rules when it comes to rolling out the ACA.
“This is a major victory for the American people who are suffering with higher premiums and fewer choices because of this failed law,” said Sen. Barrasso, who with several fellow Republican legislators requested the GAO investigation. “The administration should end this illegal scheme immediately, and focus on providing relief from the burdens of this law.”
At press time, neither the White House nor HHS had responded to request for comment on the report.
The Transitional Reinsurance Program is a 3-year initiative under the ACA that collects fees from employers and other private health insurance plans and directs the funds to health plans that face large claims for patients with high-cost medical conditions. The ACA specifies that between 2014 and 2016, HHS would collect $25 billion in fees, of which $5 billion would go into the Treasury.
But when HHS was unable to collect the full amount over the 3 years, it did not distribute funds into the Treasury, but instead used it pay the health plans. To justify that decision, HHS officials announced that the department would allocate all collections first for reinsurance payments until collections totaled the target amount set forth for reinsurance payments under the law, and that any remaining collections would go toward to administrative expenses and the Treasury, according to the GAO report.
But the GAO argues that HHS falling short of the projected collections does not alter the meaning of the statute.
“Specifically, where actual funding has fallen short of an agency’s original expectations, courts have directed the agency to distribute available funds to approximate the allocation plan Congress designed in anticipation of full funding,” Ms. Poling wrote. The HHS “assertion that the statute is silent with respect to allocation of collections overlooks the fact that section 1341 expressly directs HHS to collect amounts for the Treasury and prohibits the use of these amounts for any purpose other than deposit in the Treasury. HHS’s analysis focuses on words and phrases in the statute in isolation rather than in their appropriate context.”
While the GAO cannot force HHS to act with the opinion, lawmakers could use the report to craft legislation forcing HHS to repay the Treasury.
“This issue has been brewing for a while, and is another example of a series of attempts to challenge or limit payments being made to carriers under the ACA,” Katherine Hempstead, senior adviser to vice president at the Robert Wood Johnson Foundation, said in an interview. “It’s no mystery why making these payments is a pretty high priority for the [Centers for Medicare & Medicaid Services] right now, given the losses sustained by many market participants. My guess is that the can will probably be kicked down the road on this and a number of other issues for the next administration and Congress to resolve.”
The reinsurance program was one of three programs intended to protect against the negative impacts of adverse selection and risk selection, while working to stabilize premiums during the initial years of the health law’s implementation. The program aims to protect against premium increases in the individual market by offsetting expenses of high-cost patients.
On Twitter @legal_med
The Health and Human Services department is failing to properly administer a reinsurance program under the Affordable Care Act by unlawfully diverting funds intended for the U.S. Treasury, according to a nonpartisan watchdog report.
The Government Accountability Office (GAO) report, released Sept. 29, finds that HHS is breaking ACA regulations that require a portion of funds collected under its Transitional Reinsurance Program to go to the Treasury. Instead, the agency has redirected $5 billion so far to pay health insurers that enroll high-cost patients under the program.
“In light of the foregoing analysis, we conclude that HHS lacks authority to ignore the statute’s directive to deposit amounts from collections under the Transitional Reinsurance Program to the Treasury and instead make deposits in the Treasury only if its collections reach the amounts for reinsurance payments specified in section 1341,” Susan A. Poling, GAO general counsel, wrote in a legal opinion. “The agency is not authorized to prioritize collections in this manner.”
Republican lawmakers, including Sen. John Barrasso III (Wyo.), chair of the Senate Republican Policy Committee, praised the legal opinion, saying it shows the Obama administration is bending the rules when it comes to rolling out the ACA.
“This is a major victory for the American people who are suffering with higher premiums and fewer choices because of this failed law,” said Sen. Barrasso, who with several fellow Republican legislators requested the GAO investigation. “The administration should end this illegal scheme immediately, and focus on providing relief from the burdens of this law.”
At press time, neither the White House nor HHS had responded to request for comment on the report.
The Transitional Reinsurance Program is a 3-year initiative under the ACA that collects fees from employers and other private health insurance plans and directs the funds to health plans that face large claims for patients with high-cost medical conditions. The ACA specifies that between 2014 and 2016, HHS would collect $25 billion in fees, of which $5 billion would go into the Treasury.
But when HHS was unable to collect the full amount over the 3 years, it did not distribute funds into the Treasury, but instead used it pay the health plans. To justify that decision, HHS officials announced that the department would allocate all collections first for reinsurance payments until collections totaled the target amount set forth for reinsurance payments under the law, and that any remaining collections would go toward to administrative expenses and the Treasury, according to the GAO report.
But the GAO argues that HHS falling short of the projected collections does not alter the meaning of the statute.
“Specifically, where actual funding has fallen short of an agency’s original expectations, courts have directed the agency to distribute available funds to approximate the allocation plan Congress designed in anticipation of full funding,” Ms. Poling wrote. The HHS “assertion that the statute is silent with respect to allocation of collections overlooks the fact that section 1341 expressly directs HHS to collect amounts for the Treasury and prohibits the use of these amounts for any purpose other than deposit in the Treasury. HHS’s analysis focuses on words and phrases in the statute in isolation rather than in their appropriate context.”
While the GAO cannot force HHS to act with the opinion, lawmakers could use the report to craft legislation forcing HHS to repay the Treasury.
“This issue has been brewing for a while, and is another example of a series of attempts to challenge or limit payments being made to carriers under the ACA,” Katherine Hempstead, senior adviser to vice president at the Robert Wood Johnson Foundation, said in an interview. “It’s no mystery why making these payments is a pretty high priority for the [Centers for Medicare & Medicaid Services] right now, given the losses sustained by many market participants. My guess is that the can will probably be kicked down the road on this and a number of other issues for the next administration and Congress to resolve.”
The reinsurance program was one of three programs intended to protect against the negative impacts of adverse selection and risk selection, while working to stabilize premiums during the initial years of the health law’s implementation. The program aims to protect against premium increases in the individual market by offsetting expenses of high-cost patients.
On Twitter @legal_med

How Can Patient History Improve the Diagnosis of Chronic Migraine?
SAN DIEGO—Accurate diagnosis of chronic migraine may improve when patients use a “lumping” strategy versus a “splitting” strategy when sharing their headache history with providers, according to research presented at the 58th Annual Scientific Meeting of the American Headache Society.
Chronic migraine can be challenging to diagnose, especially for less experienced providers, said Priyanka Yadav, MBBS, a neurology resident at the University of Kentucky in Lexington. The International Classification of Headache Disorders, third edition, defines chronic migraine as headaches occurring on at least 15 days per month for three months, at least eight of which have features of migraine. Patients with chronic migraine can experience headaches similar to those of patients with tension-type headache. As a result, headache history is vital to achieving a correct diagnosis, Dr. Yadav added.
Although a provider may have sufficient information about the patient’s headache history, diagnosis may still be confusing if patients describe their headache history using a splitting strategy, in which patients distinguish multiple types of headache. For example, a patient may report that he or she had two types of headache that occurred over the previous three months. “This [history] can be confusing because inexperienced providers may not recognize that patients with chronic migraine experience headache days similar to [those of] tension headache,” said Dr. Yadav.

Dr. Yadav and colleagues hypothesized that a lumping strategy would help neurologists to reach a correct headache diagnosis, as opposed to the splitting strategy. In the lumping strategy, patients describe one type of headache. For example, a woman may report having a continuous, background, mild, pressure-like pain throughout her head, which can evolve into intense, throbbing pain associated with nausea and light and sound sensitivity, said Dr. Yadav.
For the study, researchers sent an unannounced electronic multiple choice quiz to 19 neurology residents at the University of Kentucky. The quiz assessed the residents’ ability to recognize the correct headache diagnoses of various case vignettes of episodic migraine, chronic tension-type headache, and chronic migraine. In addition, residents were asked to recognize the chronic migraine criteria. The main outcome measure was frequency of chronic migraine recognition as a function of history style, presented in either the lumping or splitting format.
The response rate to the quiz was 100%. Results indicated that correct recognition of chronic migraine was more likely when the headache history was presented in a lumping format, as opposed to a splitting format. “When presented with the splitting style, participants often thought that the patient had two headache diagnoses (eg, chronic tension-type headache and episodic migraine), instead of one unifying diagnosis (eg, chronic migraine),” said Jonathan H. Smith, MD, coauthor and Assistant Professor of Neurology at the University of Kentucky College of Medicine.
Participants were poor at recognizing that features of these primary headache disorders can coexist to contribute toward a uniform diagnosis of chronic migraine. “These results have strategic implications for how physicians should organize and teach the headache history,” said Dr. Yadav.
—Erica Robinson
Suggested Reading
Moriarty M, Mallick-Searle T. Diagnosis and treatment for chronic migraine. Nurse Pract. 2016;41(6):18-32.
Eross E, Dodick D, Eross M. The Sinus, Allergy and Migraine Study (SAMS). Headache. 2007;47(2):213-224.
SAN DIEGO—Accurate diagnosis of chronic migraine may improve when patients use a “lumping” strategy versus a “splitting” strategy when sharing their headache history with providers, according to research presented at the 58th Annual Scientific Meeting of the American Headache Society.
Chronic migraine can be challenging to diagnose, especially for less experienced providers, said Priyanka Yadav, MBBS, a neurology resident at the University of Kentucky in Lexington. The International Classification of Headache Disorders, third edition, defines chronic migraine as headaches occurring on at least 15 days per month for three months, at least eight of which have features of migraine. Patients with chronic migraine can experience headaches similar to those of patients with tension-type headache. As a result, headache history is vital to achieving a correct diagnosis, Dr. Yadav added.
Although a provider may have sufficient information about the patient’s headache history, diagnosis may still be confusing if patients describe their headache history using a splitting strategy, in which patients distinguish multiple types of headache. For example, a patient may report that he or she had two types of headache that occurred over the previous three months. “This [history] can be confusing because inexperienced providers may not recognize that patients with chronic migraine experience headache days similar to [those of] tension headache,” said Dr. Yadav.
Dr. Yadav and colleagues hypothesized that a lumping strategy would help neurologists to reach a correct headache diagnosis, as opposed to the splitting strategy. In the lumping strategy, patients describe one type of headache. For example, a woman may report having a continuous, background, mild, pressure-like pain throughout her head, which can evolve into intense, throbbing pain associated with nausea and light and sound sensitivity, said Dr. Yadav.
For the study, researchers sent an unannounced electronic multiple choice quiz to 19 neurology residents at the University of Kentucky. The quiz assessed the residents’ ability to recognize the correct headache diagnoses of various case vignettes of episodic migraine, chronic tension-type headache, and chronic migraine. In addition, residents were asked to recognize the chronic migraine criteria. The main outcome measure was frequency of chronic migraine recognition as a function of history style, presented in either the lumping or splitting format.
The response rate to the quiz was 100%. Results indicated that correct recognition of chronic migraine was more likely when the headache history was presented in a lumping format, as opposed to a splitting format. “When presented with the splitting style, participants often thought that the patient had two headache diagnoses (eg, chronic tension-type headache and episodic migraine), instead of one unifying diagnosis (eg, chronic migraine),” said Jonathan H. Smith, MD, coauthor and Assistant Professor of Neurology at the University of Kentucky College of Medicine.
Participants were poor at recognizing that features of these primary headache disorders can coexist to contribute toward a uniform diagnosis of chronic migraine. “These results have strategic implications for how physicians should organize and teach the headache history,” said Dr. Yadav.
—Erica Robinson
Suggested Reading
Moriarty M, Mallick-Searle T. Diagnosis and treatment for chronic migraine. Nurse Pract. 2016;41(6):18-32.
Eross E, Dodick D, Eross M. The Sinus, Allergy and Migraine Study (SAMS). Headache. 2007;47(2):213-224.
SAN DIEGO—Accurate diagnosis of chronic migraine may improve when patients use a “lumping” strategy versus a “splitting” strategy when sharing their headache history with providers, according to research presented at the 58th Annual Scientific Meeting of the American Headache Society.
Chronic migraine can be challenging to diagnose, especially for less experienced providers, said Priyanka Yadav, MBBS, a neurology resident at the University of Kentucky in Lexington. The International Classification of Headache Disorders, third edition, defines chronic migraine as headaches occurring on at least 15 days per month for three months, at least eight of which have features of migraine. Patients with chronic migraine can experience headaches similar to those of patients with tension-type headache. As a result, headache history is vital to achieving a correct diagnosis, Dr. Yadav added.
Although a provider may have sufficient information about the patient’s headache history, diagnosis may still be confusing if patients describe their headache history using a splitting strategy, in which patients distinguish multiple types of headache. For example, a patient may report that he or she had two types of headache that occurred over the previous three months. “This [history] can be confusing because inexperienced providers may not recognize that patients with chronic migraine experience headache days similar to [those of] tension headache,” said Dr. Yadav.
Dr. Yadav and colleagues hypothesized that a lumping strategy would help neurologists to reach a correct headache diagnosis, as opposed to the splitting strategy. In the lumping strategy, patients describe one type of headache. For example, a woman may report having a continuous, background, mild, pressure-like pain throughout her head, which can evolve into intense, throbbing pain associated with nausea and light and sound sensitivity, said Dr. Yadav.
For the study, researchers sent an unannounced electronic multiple choice quiz to 19 neurology residents at the University of Kentucky. The quiz assessed the residents’ ability to recognize the correct headache diagnoses of various case vignettes of episodic migraine, chronic tension-type headache, and chronic migraine. In addition, residents were asked to recognize the chronic migraine criteria. The main outcome measure was frequency of chronic migraine recognition as a function of history style, presented in either the lumping or splitting format.
The response rate to the quiz was 100%. Results indicated that correct recognition of chronic migraine was more likely when the headache history was presented in a lumping format, as opposed to a splitting format. “When presented with the splitting style, participants often thought that the patient had two headache diagnoses (eg, chronic tension-type headache and episodic migraine), instead of one unifying diagnosis (eg, chronic migraine),” said Jonathan H. Smith, MD, coauthor and Assistant Professor of Neurology at the University of Kentucky College of Medicine.
Participants were poor at recognizing that features of these primary headache disorders can coexist to contribute toward a uniform diagnosis of chronic migraine. “These results have strategic implications for how physicians should organize and teach the headache history,” said Dr. Yadav.
—Erica Robinson
Suggested Reading
Moriarty M, Mallick-Searle T. Diagnosis and treatment for chronic migraine. Nurse Pract. 2016;41(6):18-32.
Eross E, Dodick D, Eross M. The Sinus, Allergy and Migraine Study (SAMS). Headache. 2007;47(2):213-224.
USPSTF considers BP measurements in pregnancy to detect preeclampsia
All pregnant women should be screened with blood pressure measurements for preeclampsia throughout pregnancy, according to a new draft recommendation from the U.S. Preventive Services Task Force.
“Preeclampsia is a complex syndrome. It can quickly evolve into a severe disease that can result in serious, even fatal health outcomes for the mother and infant,” the USPSTF members wrote in their draft. “The ability to screen for preeclampsia using blood pressure measurements is important in order to identify and effectively treat a potentially unpredictable and fatal condition.”

The USPSTF noted that there is “adequate evidence” that supported the superior accuracy of blood pressure measurements over urinalysis as dipstick tests have “low diagnostic accuracy for proteinuria detection in pregnancy.”The USPSTF concluded “with moderate certainty” that screening for preeclampsia in all pregnant women with blood pressure measurements yields a substantial net benefit for mothers and newborns as there are “likely few harms” from screening with blood pressure measurements. The draft recommendation has a “B” grade, meaning that clinicians are encouraged to offer the service.
The American College of Obstetricians and Gynecologists applauded the USPSTF’s draft, noting that the recommendations align with their current guidance, which recommends that physicians use detailed medical histories to evaluate a patient’s risk for developing preeclampsia. Ob.gyns. already take a woman’s blood pressure at each routine visit, along with measuring weight, uterine size, and the presence of fetal heart activity, ACOG noted.
“Importantly, ACOG has found there are no accurate, predictive tests at this time to determine whether a woman will develop preeclampsia and therefore continues to recommend against other methods for predicting preeclampsia,” ACOG president Thomas Gellhaus, MD, said in a statement. “A detailed medical history and routine blood pressure measurements are the best tools available to alert ob.gyns. of a potential risk.”
In July, ACOG recommended an expanded list of risk factors for preeclampsia that include history of the condition, multifetal gestation, chronic hypertension, diabetes, renal disease, and autoimmune disease.
The USPSTF is accepting public comment on the draft recommendation until Oct. 24, 2016.
On Twitter @jessnicolecraig
All pregnant women should be screened with blood pressure measurements for preeclampsia throughout pregnancy, according to a new draft recommendation from the U.S. Preventive Services Task Force.
“Preeclampsia is a complex syndrome. It can quickly evolve into a severe disease that can result in serious, even fatal health outcomes for the mother and infant,” the USPSTF members wrote in their draft. “The ability to screen for preeclampsia using blood pressure measurements is important in order to identify and effectively treat a potentially unpredictable and fatal condition.”
The USPSTF noted that there is “adequate evidence” that supported the superior accuracy of blood pressure measurements over urinalysis as dipstick tests have “low diagnostic accuracy for proteinuria detection in pregnancy.”The USPSTF concluded “with moderate certainty” that screening for preeclampsia in all pregnant women with blood pressure measurements yields a substantial net benefit for mothers and newborns as there are “likely few harms” from screening with blood pressure measurements. The draft recommendation has a “B” grade, meaning that clinicians are encouraged to offer the service.
The American College of Obstetricians and Gynecologists applauded the USPSTF’s draft, noting that the recommendations align with their current guidance, which recommends that physicians use detailed medical histories to evaluate a patient’s risk for developing preeclampsia. Ob.gyns. already take a woman’s blood pressure at each routine visit, along with measuring weight, uterine size, and the presence of fetal heart activity, ACOG noted.
“Importantly, ACOG has found there are no accurate, predictive tests at this time to determine whether a woman will develop preeclampsia and therefore continues to recommend against other methods for predicting preeclampsia,” ACOG president Thomas Gellhaus, MD, said in a statement. “A detailed medical history and routine blood pressure measurements are the best tools available to alert ob.gyns. of a potential risk.”
In July, ACOG recommended an expanded list of risk factors for preeclampsia that include history of the condition, multifetal gestation, chronic hypertension, diabetes, renal disease, and autoimmune disease.
The USPSTF is accepting public comment on the draft recommendation until Oct. 24, 2016.
On Twitter @jessnicolecraig
All pregnant women should be screened with blood pressure measurements for preeclampsia throughout pregnancy, according to a new draft recommendation from the U.S. Preventive Services Task Force.
“Preeclampsia is a complex syndrome. It can quickly evolve into a severe disease that can result in serious, even fatal health outcomes for the mother and infant,” the USPSTF members wrote in their draft. “The ability to screen for preeclampsia using blood pressure measurements is important in order to identify and effectively treat a potentially unpredictable and fatal condition.”
The USPSTF noted that there is “adequate evidence” that supported the superior accuracy of blood pressure measurements over urinalysis as dipstick tests have “low diagnostic accuracy for proteinuria detection in pregnancy.”The USPSTF concluded “with moderate certainty” that screening for preeclampsia in all pregnant women with blood pressure measurements yields a substantial net benefit for mothers and newborns as there are “likely few harms” from screening with blood pressure measurements. The draft recommendation has a “B” grade, meaning that clinicians are encouraged to offer the service.
The American College of Obstetricians and Gynecologists applauded the USPSTF’s draft, noting that the recommendations align with their current guidance, which recommends that physicians use detailed medical histories to evaluate a patient’s risk for developing preeclampsia. Ob.gyns. already take a woman’s blood pressure at each routine visit, along with measuring weight, uterine size, and the presence of fetal heart activity, ACOG noted.
“Importantly, ACOG has found there are no accurate, predictive tests at this time to determine whether a woman will develop preeclampsia and therefore continues to recommend against other methods for predicting preeclampsia,” ACOG president Thomas Gellhaus, MD, said in a statement. “A detailed medical history and routine blood pressure measurements are the best tools available to alert ob.gyns. of a potential risk.”
In July, ACOG recommended an expanded list of risk factors for preeclampsia that include history of the condition, multifetal gestation, chronic hypertension, diabetes, renal disease, and autoimmune disease.
The USPSTF is accepting public comment on the draft recommendation until Oct. 24, 2016.
On Twitter @jessnicolecraig

QUIZ: Treating Infants Hospitalized With Viral Bronchiolitis
[WpProQuiz 14]
[WpProQuiz_toplist 14]
[WpProQuiz 14]
[WpProQuiz_toplist 14]
[WpProQuiz 14]
[WpProQuiz_toplist 14]
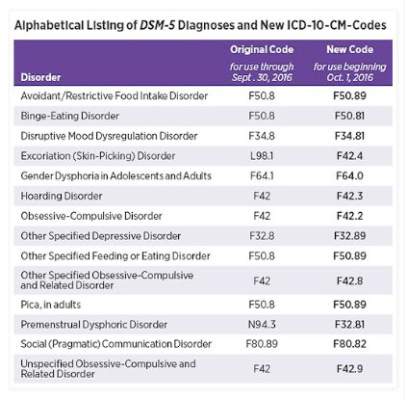
Changes in DSM-5 codes in ICD-10 go into effect Oct. 1
Earlier this month, the American Psychiatric Association released a supplement to the DSM-5 that updated codes for 14 diagnoses, including binge-eating disorder, disruptive mood dysregulation disorder, hoarding disorder, and premenstrual dysphoric disorder. On Oct. 1, those DSM-5 coding changes will be reflected within the International Classification of Diseases, Tenth Edition, Clinical Modification (ICD-10-CM).
Some of the changes are minor. For example, the code for binge-eating disorder is now F50.8 and will become F50.81 on Oct. 1. Disruptive mood dysregulation disorder will change from F34.8 to F34.81, and hoarding disorder will change from F42 to F42.3.
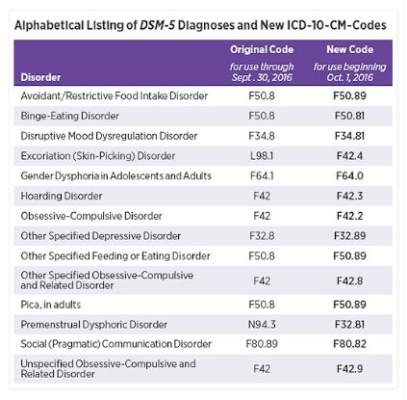
However, some of the changes are significant. The code for premenstrual dysphoric disorder, for example, will change from N94.3 to F32.81. The changes are aimed at improving diagnostic recording, communication among clinicians, and the collection of prevalence data.
To access the DSM-5 supplement, click here. A concise listing of the updated ICD-10-CM changes can be found here.
Earlier this month, the American Psychiatric Association released a supplement to the DSM-5 that updated codes for 14 diagnoses, including binge-eating disorder, disruptive mood dysregulation disorder, hoarding disorder, and premenstrual dysphoric disorder. On Oct. 1, those DSM-5 coding changes will be reflected within the International Classification of Diseases, Tenth Edition, Clinical Modification (ICD-10-CM).
Some of the changes are minor. For example, the code for binge-eating disorder is now F50.8 and will become F50.81 on Oct. 1. Disruptive mood dysregulation disorder will change from F34.8 to F34.81, and hoarding disorder will change from F42 to F42.3.
However, some of the changes are significant. The code for premenstrual dysphoric disorder, for example, will change from N94.3 to F32.81. The changes are aimed at improving diagnostic recording, communication among clinicians, and the collection of prevalence data.
To access the DSM-5 supplement, click here. A concise listing of the updated ICD-10-CM changes can be found here.
Earlier this month, the American Psychiatric Association released a supplement to the DSM-5 that updated codes for 14 diagnoses, including binge-eating disorder, disruptive mood dysregulation disorder, hoarding disorder, and premenstrual dysphoric disorder. On Oct. 1, those DSM-5 coding changes will be reflected within the International Classification of Diseases, Tenth Edition, Clinical Modification (ICD-10-CM).
Some of the changes are minor. For example, the code for binge-eating disorder is now F50.8 and will become F50.81 on Oct. 1. Disruptive mood dysregulation disorder will change from F34.8 to F34.81, and hoarding disorder will change from F42 to F42.3.
However, some of the changes are significant. The code for premenstrual dysphoric disorder, for example, will change from N94.3 to F32.81. The changes are aimed at improving diagnostic recording, communication among clinicians, and the collection of prevalence data.
To access the DSM-5 supplement, click here. A concise listing of the updated ICD-10-CM changes can be found here.
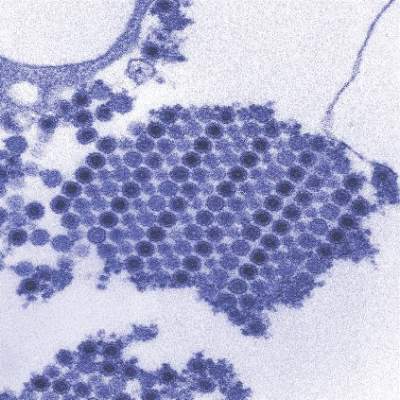
New chikungunya diagnostic assay proves quick, effective
A reverse transcription recombinase polymerase amplification (RT-RPA) assay was able to quickly and effectively identify chikungunya virus (CHIKV), according to a study published in PLOS Neglected Tropical Diseases.
Using chikungunya virus RNA samples, the RT-RPA assay detected down to 80 genome copies per reaction within 15 minutes, a time period four to six times faster than other molecular diagnostic techniques, such as reverse transcription-polymerase chain reaction (RT-PCR). In a sensitivity test involving all chikungunya serotypes and various alphaviruses, flaviviruses, and one phlebovirus, the RT-RPA assay identified all virus genotypes, with the only cross-reaction occurring with O’nyong’nyong virus.
In a test involving 58 plasma samples of suspected chikungunya fever from a trial in Thailand, two real-time RT-PCR tests identified 36 out of 58 samples (62%) as positive for chikungunya. The RT-RPA test successfully detected the virus in all 36 positive samples and did not detect the virus in any of the negative samples, giving a sensitivity and specificity of 100%.
“The CHIKV RPA assay presented here is a promising tool for CHIKV diagnostics at the point of need,” the investigators wrote. “Integration into a multimer or multiplex assay for simultaneous and differential detection of CHIKV, Dengue virus, and Zika virus, as well as an internal positive control would improve outbreak investigations, since the three viruses induce the same clinical picture upon infection and increasingly cocirculate in many parts of the world.”
Find the full study in PLOS Neglected Tropical Diseases (doi: 10.1371/journal.pntd.0004953).
A reverse transcription recombinase polymerase amplification (RT-RPA) assay was able to quickly and effectively identify chikungunya virus (CHIKV), according to a study published in PLOS Neglected Tropical Diseases.
Using chikungunya virus RNA samples, the RT-RPA assay detected down to 80 genome copies per reaction within 15 minutes, a time period four to six times faster than other molecular diagnostic techniques, such as reverse transcription-polymerase chain reaction (RT-PCR). In a sensitivity test involving all chikungunya serotypes and various alphaviruses, flaviviruses, and one phlebovirus, the RT-RPA assay identified all virus genotypes, with the only cross-reaction occurring with O’nyong’nyong virus.
In a test involving 58 plasma samples of suspected chikungunya fever from a trial in Thailand, two real-time RT-PCR tests identified 36 out of 58 samples (62%) as positive for chikungunya. The RT-RPA test successfully detected the virus in all 36 positive samples and did not detect the virus in any of the negative samples, giving a sensitivity and specificity of 100%.
“The CHIKV RPA assay presented here is a promising tool for CHIKV diagnostics at the point of need,” the investigators wrote. “Integration into a multimer or multiplex assay for simultaneous and differential detection of CHIKV, Dengue virus, and Zika virus, as well as an internal positive control would improve outbreak investigations, since the three viruses induce the same clinical picture upon infection and increasingly cocirculate in many parts of the world.”
Find the full study in PLOS Neglected Tropical Diseases (doi: 10.1371/journal.pntd.0004953).
A reverse transcription recombinase polymerase amplification (RT-RPA) assay was able to quickly and effectively identify chikungunya virus (CHIKV), according to a study published in PLOS Neglected Tropical Diseases.
Using chikungunya virus RNA samples, the RT-RPA assay detected down to 80 genome copies per reaction within 15 minutes, a time period four to six times faster than other molecular diagnostic techniques, such as reverse transcription-polymerase chain reaction (RT-PCR). In a sensitivity test involving all chikungunya serotypes and various alphaviruses, flaviviruses, and one phlebovirus, the RT-RPA assay identified all virus genotypes, with the only cross-reaction occurring with O’nyong’nyong virus.
In a test involving 58 plasma samples of suspected chikungunya fever from a trial in Thailand, two real-time RT-PCR tests identified 36 out of 58 samples (62%) as positive for chikungunya. The RT-RPA test successfully detected the virus in all 36 positive samples and did not detect the virus in any of the negative samples, giving a sensitivity and specificity of 100%.
“The CHIKV RPA assay presented here is a promising tool for CHIKV diagnostics at the point of need,” the investigators wrote. “Integration into a multimer or multiplex assay for simultaneous and differential detection of CHIKV, Dengue virus, and Zika virus, as well as an internal positive control would improve outbreak investigations, since the three viruses induce the same clinical picture upon infection and increasingly cocirculate in many parts of the world.”
Find the full study in PLOS Neglected Tropical Diseases (doi: 10.1371/journal.pntd.0004953).
FROM PLOS NEGLECTED TROPICAL DISEASES
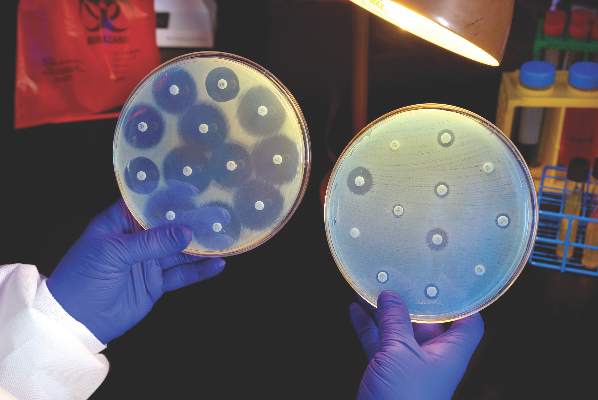
Ceftazidime-avibactam stands up to CRE, but resistance a problem
Intravenous ceftazidime-avibactam successfully treated 59% of carbapenem-resistant Enterobacteriaceae (CRE) infections, and 76% of patients remained alive at 30 days, according to a retrospective cohort study published in Clinical Infectious Diseases.
Those rates resemble previous reports of treatment with in vitro active agents, while the rate of acute kidney injury was about a third lower, said Ryan K. Shields, PharmD, of the University of Pittsburgh, and his associates. But 8% of CRE infections developed ceftazidime-avibactam resistance, which accounted for about a third of microbiological failures, the researchers said. “It is incumbent upon health care providers to share their clinical experiences with ceftazidime-avibactam and other new beta-lactamase inhibitors, so these agents can be used most effectively for the longest period of time,” they added.

Ceftazidime-avibactam (Avycaz) is a novel beta-lactam/beta-lactamase inhibitor combination approved by the Food and Drug Administration in 2015 for complicated intra-abdominal and urinary tract infections. It was hoped that the newly approved combination would prove safer and more effective than previously developed agents that showed in vitro activity against CRE, such as colistin, gentamicin, and tigecycline, the researchers noted.
They described CRE-infected patients treated with ceftazidime-avibactam (median, 14 days; range, 4-71 days) between April 2015 and February 2016. The average age of the patients was 64 years (range 26-78 years), and 57% were men. Infections included ventilator or health care–associated pneumonia, primary bacteremia, intra-abdominal infection, skin and soft tissue infections, pyelonephritis, mediastinitis, subdural empyema/ventriculitis, and purulent tracheobronchitis. All the CRE isolates were susceptible to ceftazidime-avibactam at baseline. In all, 70% of patients received ceftazidime-avibactam as monotherapy, while 30% received it in combination with intravenous or inhaled gentamicin, intravenous or intrathecal colistin, or tigecycline (Clin Infect Dis. 2016 Sep 13. doi: 10.1093/cid/ciw636).
A total of 28 (76%) patients were alive at 30 days and 62% were alive at 90 days, the investigators said. They calculated a 59% rate of clinical success, defined as absence of recurrence within 30 days of onset, resolution of signs and symptoms, and sterilization of site-specific cultures within 7 days of treatment. Combination therapy did not improve the chances of clinical success, they noted. Among the 15 clinical failures, 9 patients died, 4 developed recurrent CRE infections, and 2 did not clinically improve. Clinical success was less likely when patients needed continuous renal replacement therapy (17% vs. 68% for other patients; P = .03) or had higher Sequential Organ Failure Assessment (SOFA) scores (average, 5.2 in clinical successes vs. 8.8 in clinical failures; P = .047). In addition, 10% of patients developed acute kidney injury within 7 days of starting treatment, which was “considerably lower than the approximately 30% rate we previously reported with carbapenem-colistin or aminoglycoside-based combinations,” the investigators said.
The sample size was too small to definitively answer questions about whether combination regimens can overcome resistance, improve outcomes, or effectively treat specific types of CRE infection, the researchers noted. “Nevertheless, we can conclude that ceftazidime-avibactam offers an important advance in the treatment of CRE infections,” they wrote. “The development of resistance after as few as 10 days of therapy is troubling, and treatment failures and deaths in a significant minority of patients highlight the need for more agents with activity against CRE.”
The University of Pittsburgh Medical Center and the National Institutes of Health provided funding. One coauthor disclosed ties to Meiji, Shionogi, Tetraphase, Achaogen, Merck, and The Medicines Company. The other authors had no disclosures.
In the movie “Jaws,” after confidently setting out with an experienced shark hunter, upon catching his first glimpse of the predator, Chief Brody famously uttered, “We’re gonna need a bigger boat.” Similarly, we rejoiced at our triumph when ceftazidime-avibactam became available to treat our patients infected with [Klebsiella pneumoniae carbapenemase]-producing bacteria, and confidently set out to combat this killer. But like Chief Brody, we appear to have underestimated our foe; we too need a “bigger boat.”
We must not let the past repeat itself; hubris about the sudden availability of effective antibiotics has led to overconfidence and complacency among the medical and microbiological communities on several prior occasions in the last 80 years, with serious societal consequences. Shields and colleagues have provided us with a sobering reminder that there is no endpoint in our struggle against microbes. They will never stop adapting to what we conceive of to combat them, and in turn we must never stop conceiving of new ways to stay one step ahead.
Brad Spellberg, MD, is at Los Angeles County–USC Medical Center in Los Angeles. He disclosed ties to Cempra, The Medicines Company, MedImmune/AstraZeneca, PTC Therapeutics, Entasis, Tetraphase, Merck, Genentech, Dipexium, Motif, BioAIM, and Synthetic Biologics. He has received grants from AstraZeneca, Merck, Melinta, Steris, NIH, and Veterans Affairs Merit Review. These comments are from an editorial (Clin Infect Dis. 2016 Sept 13. doi: 10.1093/cid/ciw639).
In the movie “Jaws,” after confidently setting out with an experienced shark hunter, upon catching his first glimpse of the predator, Chief Brody famously uttered, “We’re gonna need a bigger boat.” Similarly, we rejoiced at our triumph when ceftazidime-avibactam became available to treat our patients infected with [Klebsiella pneumoniae carbapenemase]-producing bacteria, and confidently set out to combat this killer. But like Chief Brody, we appear to have underestimated our foe; we too need a “bigger boat.”
We must not let the past repeat itself; hubris about the sudden availability of effective antibiotics has led to overconfidence and complacency among the medical and microbiological communities on several prior occasions in the last 80 years, with serious societal consequences. Shields and colleagues have provided us with a sobering reminder that there is no endpoint in our struggle against microbes. They will never stop adapting to what we conceive of to combat them, and in turn we must never stop conceiving of new ways to stay one step ahead.
Brad Spellberg, MD, is at Los Angeles County–USC Medical Center in Los Angeles. He disclosed ties to Cempra, The Medicines Company, MedImmune/AstraZeneca, PTC Therapeutics, Entasis, Tetraphase, Merck, Genentech, Dipexium, Motif, BioAIM, and Synthetic Biologics. He has received grants from AstraZeneca, Merck, Melinta, Steris, NIH, and Veterans Affairs Merit Review. These comments are from an editorial (Clin Infect Dis. 2016 Sept 13. doi: 10.1093/cid/ciw639).
In the movie “Jaws,” after confidently setting out with an experienced shark hunter, upon catching his first glimpse of the predator, Chief Brody famously uttered, “We’re gonna need a bigger boat.” Similarly, we rejoiced at our triumph when ceftazidime-avibactam became available to treat our patients infected with [Klebsiella pneumoniae carbapenemase]-producing bacteria, and confidently set out to combat this killer. But like Chief Brody, we appear to have underestimated our foe; we too need a “bigger boat.”
We must not let the past repeat itself; hubris about the sudden availability of effective antibiotics has led to overconfidence and complacency among the medical and microbiological communities on several prior occasions in the last 80 years, with serious societal consequences. Shields and colleagues have provided us with a sobering reminder that there is no endpoint in our struggle against microbes. They will never stop adapting to what we conceive of to combat them, and in turn we must never stop conceiving of new ways to stay one step ahead.
Brad Spellberg, MD, is at Los Angeles County–USC Medical Center in Los Angeles. He disclosed ties to Cempra, The Medicines Company, MedImmune/AstraZeneca, PTC Therapeutics, Entasis, Tetraphase, Merck, Genentech, Dipexium, Motif, BioAIM, and Synthetic Biologics. He has received grants from AstraZeneca, Merck, Melinta, Steris, NIH, and Veterans Affairs Merit Review. These comments are from an editorial (Clin Infect Dis. 2016 Sept 13. doi: 10.1093/cid/ciw639).
Intravenous ceftazidime-avibactam successfully treated 59% of carbapenem-resistant Enterobacteriaceae (CRE) infections, and 76% of patients remained alive at 30 days, according to a retrospective cohort study published in Clinical Infectious Diseases.
Those rates resemble previous reports of treatment with in vitro active agents, while the rate of acute kidney injury was about a third lower, said Ryan K. Shields, PharmD, of the University of Pittsburgh, and his associates. But 8% of CRE infections developed ceftazidime-avibactam resistance, which accounted for about a third of microbiological failures, the researchers said. “It is incumbent upon health care providers to share their clinical experiences with ceftazidime-avibactam and other new beta-lactamase inhibitors, so these agents can be used most effectively for the longest period of time,” they added.
Ceftazidime-avibactam (Avycaz) is a novel beta-lactam/beta-lactamase inhibitor combination approved by the Food and Drug Administration in 2015 for complicated intra-abdominal and urinary tract infections. It was hoped that the newly approved combination would prove safer and more effective than previously developed agents that showed in vitro activity against CRE, such as colistin, gentamicin, and tigecycline, the researchers noted.
They described CRE-infected patients treated with ceftazidime-avibactam (median, 14 days; range, 4-71 days) between April 2015 and February 2016. The average age of the patients was 64 years (range 26-78 years), and 57% were men. Infections included ventilator or health care–associated pneumonia, primary bacteremia, intra-abdominal infection, skin and soft tissue infections, pyelonephritis, mediastinitis, subdural empyema/ventriculitis, and purulent tracheobronchitis. All the CRE isolates were susceptible to ceftazidime-avibactam at baseline. In all, 70% of patients received ceftazidime-avibactam as monotherapy, while 30% received it in combination with intravenous or inhaled gentamicin, intravenous or intrathecal colistin, or tigecycline (Clin Infect Dis. 2016 Sep 13. doi: 10.1093/cid/ciw636).
A total of 28 (76%) patients were alive at 30 days and 62% were alive at 90 days, the investigators said. They calculated a 59% rate of clinical success, defined as absence of recurrence within 30 days of onset, resolution of signs and symptoms, and sterilization of site-specific cultures within 7 days of treatment. Combination therapy did not improve the chances of clinical success, they noted. Among the 15 clinical failures, 9 patients died, 4 developed recurrent CRE infections, and 2 did not clinically improve. Clinical success was less likely when patients needed continuous renal replacement therapy (17% vs. 68% for other patients; P = .03) or had higher Sequential Organ Failure Assessment (SOFA) scores (average, 5.2 in clinical successes vs. 8.8 in clinical failures; P = .047). In addition, 10% of patients developed acute kidney injury within 7 days of starting treatment, which was “considerably lower than the approximately 30% rate we previously reported with carbapenem-colistin or aminoglycoside-based combinations,” the investigators said.
The sample size was too small to definitively answer questions about whether combination regimens can overcome resistance, improve outcomes, or effectively treat specific types of CRE infection, the researchers noted. “Nevertheless, we can conclude that ceftazidime-avibactam offers an important advance in the treatment of CRE infections,” they wrote. “The development of resistance after as few as 10 days of therapy is troubling, and treatment failures and deaths in a significant minority of patients highlight the need for more agents with activity against CRE.”
The University of Pittsburgh Medical Center and the National Institutes of Health provided funding. One coauthor disclosed ties to Meiji, Shionogi, Tetraphase, Achaogen, Merck, and The Medicines Company. The other authors had no disclosures.
Intravenous ceftazidime-avibactam successfully treated 59% of carbapenem-resistant Enterobacteriaceae (CRE) infections, and 76% of patients remained alive at 30 days, according to a retrospective cohort study published in Clinical Infectious Diseases.
Those rates resemble previous reports of treatment with in vitro active agents, while the rate of acute kidney injury was about a third lower, said Ryan K. Shields, PharmD, of the University of Pittsburgh, and his associates. But 8% of CRE infections developed ceftazidime-avibactam resistance, which accounted for about a third of microbiological failures, the researchers said. “It is incumbent upon health care providers to share their clinical experiences with ceftazidime-avibactam and other new beta-lactamase inhibitors, so these agents can be used most effectively for the longest period of time,” they added.
Ceftazidime-avibactam (Avycaz) is a novel beta-lactam/beta-lactamase inhibitor combination approved by the Food and Drug Administration in 2015 for complicated intra-abdominal and urinary tract infections. It was hoped that the newly approved combination would prove safer and more effective than previously developed agents that showed in vitro activity against CRE, such as colistin, gentamicin, and tigecycline, the researchers noted.
They described CRE-infected patients treated with ceftazidime-avibactam (median, 14 days; range, 4-71 days) between April 2015 and February 2016. The average age of the patients was 64 years (range 26-78 years), and 57% were men. Infections included ventilator or health care–associated pneumonia, primary bacteremia, intra-abdominal infection, skin and soft tissue infections, pyelonephritis, mediastinitis, subdural empyema/ventriculitis, and purulent tracheobronchitis. All the CRE isolates were susceptible to ceftazidime-avibactam at baseline. In all, 70% of patients received ceftazidime-avibactam as monotherapy, while 30% received it in combination with intravenous or inhaled gentamicin, intravenous or intrathecal colistin, or tigecycline (Clin Infect Dis. 2016 Sep 13. doi: 10.1093/cid/ciw636).
A total of 28 (76%) patients were alive at 30 days and 62% were alive at 90 days, the investigators said. They calculated a 59% rate of clinical success, defined as absence of recurrence within 30 days of onset, resolution of signs and symptoms, and sterilization of site-specific cultures within 7 days of treatment. Combination therapy did not improve the chances of clinical success, they noted. Among the 15 clinical failures, 9 patients died, 4 developed recurrent CRE infections, and 2 did not clinically improve. Clinical success was less likely when patients needed continuous renal replacement therapy (17% vs. 68% for other patients; P = .03) or had higher Sequential Organ Failure Assessment (SOFA) scores (average, 5.2 in clinical successes vs. 8.8 in clinical failures; P = .047). In addition, 10% of patients developed acute kidney injury within 7 days of starting treatment, which was “considerably lower than the approximately 30% rate we previously reported with carbapenem-colistin or aminoglycoside-based combinations,” the investigators said.
The sample size was too small to definitively answer questions about whether combination regimens can overcome resistance, improve outcomes, or effectively treat specific types of CRE infection, the researchers noted. “Nevertheless, we can conclude that ceftazidime-avibactam offers an important advance in the treatment of CRE infections,” they wrote. “The development of resistance after as few as 10 days of therapy is troubling, and treatment failures and deaths in a significant minority of patients highlight the need for more agents with activity against CRE.”
The University of Pittsburgh Medical Center and the National Institutes of Health provided funding. One coauthor disclosed ties to Meiji, Shionogi, Tetraphase, Achaogen, Merck, and The Medicines Company. The other authors had no disclosures.
FROM CLINICAL INFECTIOUS DISEASES
Key clinical point: Ceftazidime-avibactam effectively treated carbapenem-resistant Enterobacteriaceae (CRE) infections, but resistance emerged rapidly and in some cases led to microbiological failure.
Major finding: The rate of clinical success was 59%; 10% of patients developed acute kidney injury within 7 days of starting treatment; 8% developed resistance.
Data source: A single-center retrospective study of 37 patients with carbapenem-resistant Enterobacteriaceae infections treated with ceftazidime-avibactam.
Disclosures: The University of Pittsburgh Medical Center and the National Institutes of Health provided funding. A coauthor disclosed ties to Meiji, Shionogi, Tetraphase, Achaogen, Merck, and The Medicines Company. The other authors had no disclosures.