User login
Highlights From the 2016 ECTRIMS Meeting

Modern breast surgery: What you should know
In a striking trend, the rate of contralateral prophylactic mastectomy (CPM) has risen by 30% over the last 10 years in the United States.1 Many women undergo CPM because of the fear and anxiety of cancer recurrence and their perceived risk of contralateral breast cancer; however, few women have a medical condition that necessitates removal of the contralateral breast. The medical indications for CPM include having a pathogenic genetic mutation (eg, BRCA1 and BRCA2), a strong family history of breast cancer, or prior mediastina chest radiation.
The actual risk of contralateral breast cancer is much lower than perceived. In women without a genetic mutation, the 10-year risk of contralateral breast cancer is only 3% to 5%.1 Also, CPM does not prevent the development of metastatic disease and offers no survival benefit over breast conservation or unilateral mastectomy.2 Furthermore, compared with unilateral therapeutic mastectomy, the “upgrade” to a CPM carries a 2.7-fold risk of a major surgical complication.3 It is therefore important that patients receive appropriate counseling regarding CPM, and that this counseling include cancer stage at diagnosis, family history and genetic risk, and cancer versus surgical risk (see “Counseling patients on contralateral prophylactic mastectomy” for key points to cover in patient discussions).
Counseling patients on contralateral prophylactic mastectomy
Commonly, patients diagnosed with breast cancer consider having their contralateral healthy breast removed as part of a bilateral mastectomy. They often experience severe anxiety about the cancer coming back and believe that removing both breasts will enable them to live longer. Keep the following key facts in mind when discussing treatment options with breast cancer patients.
Cancer stage at diagnosis. How long a patient lives from the time of her breast cancer diagnosis depends on the stage of the cancer at diagnosis, not the type of surgery performed. A woman with early stage I or stage II breast cancer has an 80% to 90% chance of being cancer free in 5 years.1 The chance of cancer recurring in the bones, liver, or lungs (metastatic breast cancer) will not be changed by removing the healthy breast. The risk of metastatic recurrence can be reduced, however, with chemotherapy and/or with hormone-blocker therapy.
Family history and genetic risk. Few women have a strong family history of breast and/or ovarian and other cancers, and this issue should be addressed with genetic counseling and testing prior to surgery. Those who carry a cancer-causing gene, such as BRCA1 or BRCA2, are at increased risk (40% to 60%) for a second or third breast cancer, especially if they are diagnosed at a young age (<50 years).2,3 In women who have a genetic mutation, removing both breasts and sometimes the ovaries can prevent development of another breast cancer. But this will not prevent spread of the cancer that is already present. Only chemotherapy and hormone blockers can prevent the spread of cancer.
Cancer risk versus surgical risk. For women with no family history of breast cancer, no genetic mutation, and no prior chest wall radiation, the risk of developing a new breast cancer in their other breast is only 3% to 5% every 10 years.3,4 This means that they have a 95% chance of not developing a new breast cancer in their healthy breast. Notably, removing the healthy breast can double the risk of postsurgical complications, including bleeding, infection, and loss of tissue and implant. The mastectomy site will be numb and the skin and nipple areola will not have any function other than cosmetic. Finally, wound complications from surgery could delay the start of important cancer treatment, such as chemotherapy or radiation.
The bottom line. Unless a woman has a strong family history of breast cancer, is diagnosed at a very young age, or has a genetic cancer-causing mutation, removing the contralateral healthy breast is not medically necessary and is not routinely recommended.
References
- Hennigs A, Riedel F, Gondos A, et al. Prognosis of breast cancer molecular subtypes in routine clinical care: a large prospective cohort study. BMC Cancer. 2016;16(1):734.
- Graeser MK, Engel C, Rhiem K, et al. Contralateral breast cancer risk in BRCA1 and BRCA2 mutation carriers. J Clin Oncol. 2009;27(35):5887–5992.
- Curtis RE, Ron E, Hankey BF, Hoover RN. New malignancies following breast cancer. In: Curtis RE, Freedman DM, Ron E, et al, eds. New Malignancies Among Cancer Survivors: SEER Cancer Registries, 1973-2000. Bethesda, MD: National Cancer Institute. NIH Publ. No. 05-5302. 2006:181–205. http://seer.cancer.gov/archive/publications/mpmono. Accessed September 18, 2016.
- Nichols HB, Berrington de Gonzalez A, Lacey JV Jr, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564–1569.
Women should be made aware that there are alternatives to mastectomy that have similar, or even better, outcomes with improved quality of life. Furthermore, a multi‑disciplinary, team-oriented approach with emphasis on minimally invasive biopsy and better cosmetic outcomes has enhanced quality of care. Knowledge of this team approach and of modern breast cancer treatments is essential for general ObGyns as this understanding improves the overall care and guidance—specifically regarding referral to expert, high-volume breast surgeons—provided to those women most in need.
Expanded treatment options for breast cancer
Advancements in breast surgery, better imaging, and targeted therapies are changing the paradigm of breast cancer treatment.
Image-guided biopsy is key in decision making
When an abnormality is found in the breast, surgical excision of an undiagnosed breast lesion is no longer considered an appropriate first step. Use of image-guided biopsy or minimally invasive core needle biopsy allows for accurate diagnosis of a breast lesion while avoiding a potentially breast deforming and expensive surgical operation. It is always better to go into the operating room (OR) with a diagnosis and do the right operation the first time.
A core needle biopsy, results of which demonstrate a benign lesion, helps avoid breast surgery in women who do not need it. If cancer is diagnosed on biopsy, the extent of disease can be better evaluated and decision making can be more informed, with a multidisciplinary approach used to consider the various options, including genetic counseling, plastic surgery consultation, or neoadjuvant therapy. Some lesions, such as those too close to the skin, chest wall, or an implant, may not be amenable to core needle biopsy and therefore require surgical excision for diagnosis.
Benefits of a multidisciplinary tumor conference
It is important for a multidisciplinary group of cancer specialists to review a patient’s case and discuss the ideal treatment plan prior to surgery. Some breast cancer subtypes (such as human epidermal growth factor receptor 2 [HER2]–overamplified breast cancer and many triple-negative breast cancers) are very sensitive to chemotherapy, and patients with these tumor types may benefit from receiving neoadjuvant chemotherapy prior to surgery. New types of chemotherapy may allow up to 60% of some breast cancers to diminish almost completely, with subsequent improved cosmetic results of breast surgery.4 It may also allow time for genetic counseling and testing prior to surgery. (See “How to code for a multidisciplinary tumor conference” for appropriate coding procedure.)
How to code for a multidisciplinary tumor conference
Melanie Witt, RN, MA
There are two coding choices for team conferences involving physician participation. If the patient and/or family is present, the CPT instruction is to bill a problem E/M service code (99201-99215) based on the time spent during this coordination of care/counseling. Documentation would include details about the conference decisions and implications for care, rather than history or examination.
If the patient is not present, report 99367 (Medical team conference with interdisciplinary team of health care professionals, patient and/or family not present, 30 minutes or more; participation by physician), but note that this code was developed under the assumption that the conference would be performed in a facility setting. Diagnostic coding would be breast cancer.
Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
This is an excerpt from a companion coding resource for breast cancer–related procedures by Ms. Witt. To read the companion article, “Coding for breast cancer–related procedures: A how-to guide,” in its entirety, click here.
Image-guided lumpectomy
Advances in breast imaging have led to increased identification of nonpalpable breast cancers. Surgical excision of nonpalpable breast lesions requires image guidance, which can be done using a variety of techniques.
Wire-guided localization (WGL) has been used in practice for the past 40 years. The procedure involves placement of a hooked wire under local anesthesia using either mammographic or ultrasound guidance. This procedure is mostly done in the radiology department on the same day as the surgery and requires that the radiologist coordinate with the OR schedule. Besides scheduling conflicts and delays in surgery, this procedure can be complicated by wires becoming dislodged, transected, or migrated, and limits the surgeon’s ability to cosmetically hide the scar in relation to position of the wire. It is uncomfortable for the patient, who must be transported from the radiology department to the OR with a wire extruding from her breast.
An alternative localization technique is placement of a radioactive source within the tumor, which can then be identified in the OR with a gamma probe.
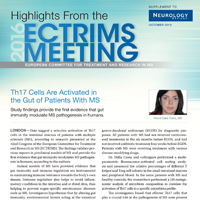
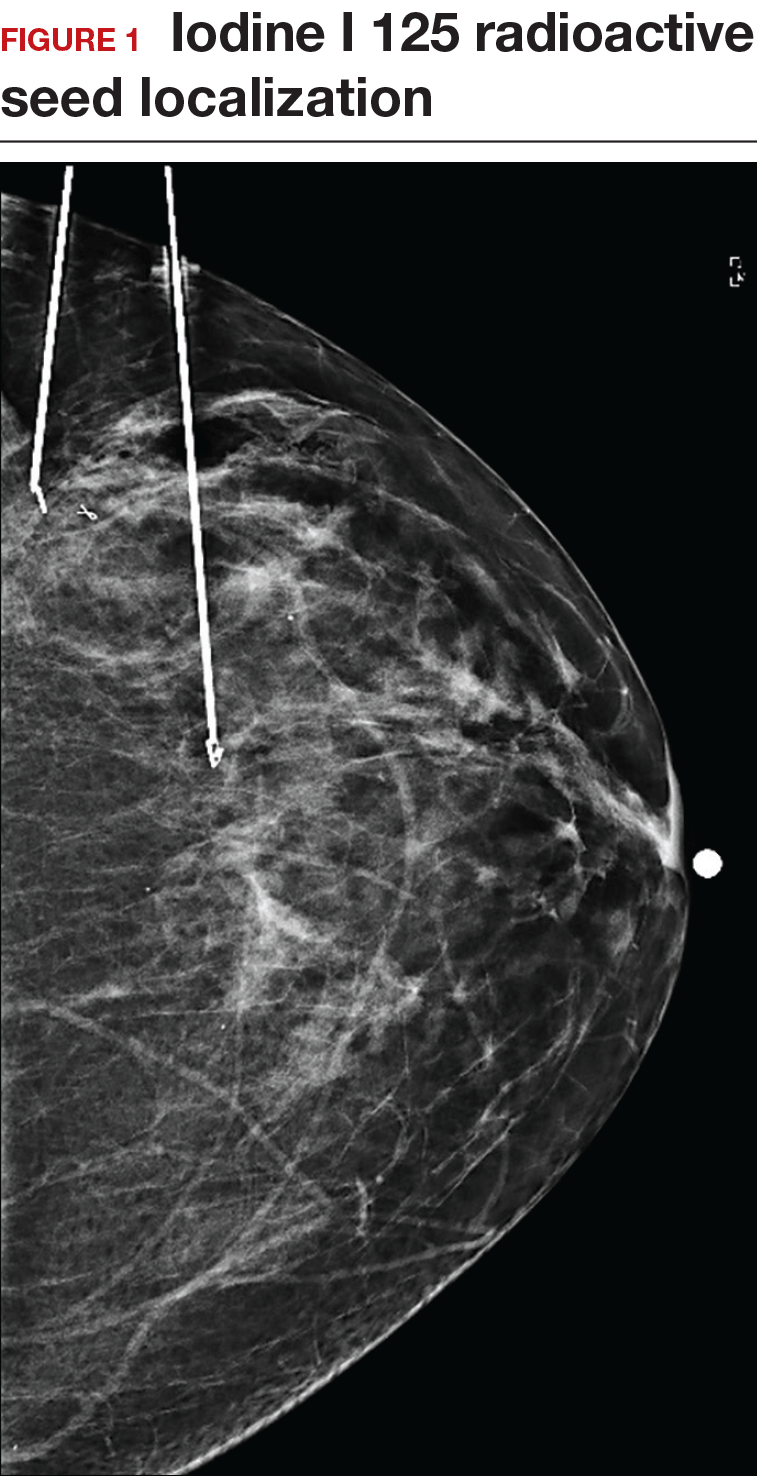
Iodine I 125 Radioactive seed localization (RSL) involves placing a 4-mm titanium radiolabeled seed into the breast lesion under mammographic or ultrasound guidance (FIGURES 1 and 2). The procedure can be performed a few days before surgery in the radiology department, and there is less chance for the seed to become displaced or dislodged. This technique provides scheduling flexibility for the radiologist and reduces OR delays. The surgeon uses the same gamma probe for sentinel node biopsy to find the lesion in the breast, using the setting specific for iodine I 125. Incisions can be tailored anywhere in the breast, and the seed is detected by a focal gamma signal. Once the lumpectomy is performed, the specimen is probed and radiographed to confirm removal of the seed and adequate margins.
Limitations of this procedure include potential loss of the seed during the operation and radiation safety issues regarding handling and disposal of the radioactive isotope. Once the seed has been placed in the patient’s body, it must be removed surgically, as the half-life of iodine I 125 is long (60 days).5 Care must therefore be taken to optimize medical clearance prior to seed placement and to avoid surgery cancellations.
Intraoperative ultrasound (IOUS) allows the surgeon to identify the lesion under general anesthesia in the OR, which is more comfortable for the patient. The surgical incision can be tailored cosmetically and the lumpectomy can be performed with real-time ultrasound visualization of the tumor during dissection. This technique eliminates the need for a separate preoperative seed or wire localization in radiology. However, it can be used only for lesions or clips that are visible by ultrasound. The excised specimen can be evaluated for confirmation of tumor removal and adequate margins via ultrasound and re-excision of close margins can be accomplished immediately if needed.
Results of a meta-analysis of WGL versus IOUS demonstrated a significant reduction of positive margins with the use of IOUS.6 Results of the COBALT trial, in which patients were assigned randomly to excision of palpable breast cancers with either IOUS or palpation, demonstrated a 14% reduction in positive margins in favor of IOUS.7 Surgeon-performed breast ultrasound requires advanced training and accreditation in breast ultrasound through a rigorous certification process offered by the American Society of Breast Surgeons (www.breastsurgeons.org).
Oncoplastic lumpectomy
This approach to lumpectomy combines adequate oncologist resection of the breast tumor with plastic surgery techniques to achieve superior cosmesis. This approach allows complete removal of the tumor with negative margins, yet maintains the normal shape and contour of the breast. Two techniques have been described: volume displacement and volume replacement.
With the volume displacement technique, the surgeon uses adjacent tissue advancement to fill the lumpectomy cavity with the patient’s own surrounding breast tissue (FIGURE 3). The volume replacement technique requires the transposition of autologous tissue from elsewhere in the body.

Oncoplastic lumpectomy allows more women with larger tumors to undergo breast conservation with better cosmetic results. It reduces the number of mastectomies performed without compromising local control and avoids the need for extensive plastic surgery reconstruction and implants. Special effort and attention must be paid to ensure adequate margins utilizing intraoperative specimen radiograph and pathology evaluation.
This procedure requires that the surgeon acquire specialized skills and knowledge of oncologic and plastic surgery techniques, and it is best performed with the collaboration of a multidisciplinary team. Compared with conventional lumpectomy or mastectomy, oncoplastic breast conservation has been shown to reduce re-excision rates, and it has similar rates of local and distant recurrence and similar disease-free survival and overall survival.8,9
Total skin- and nipple-sparing mastectomy
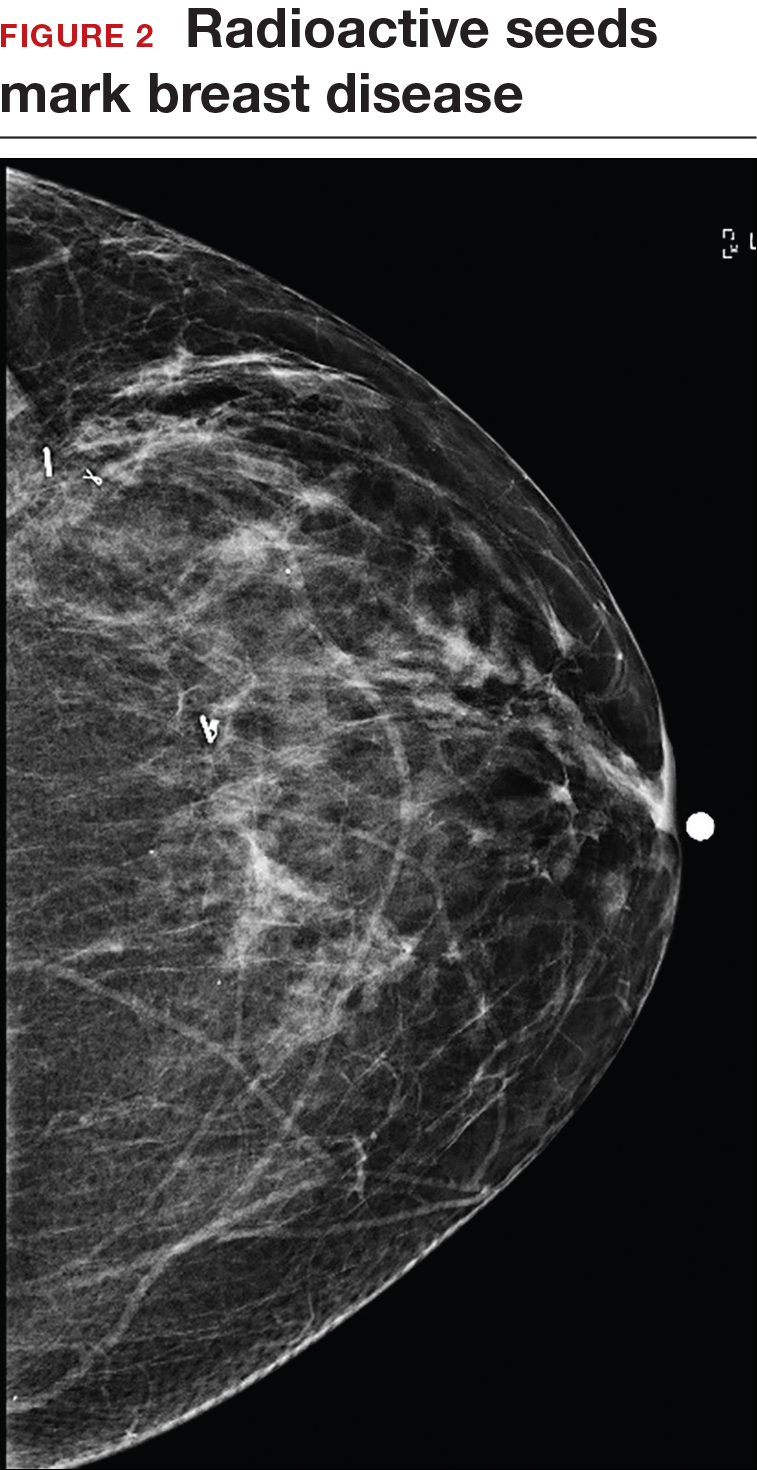
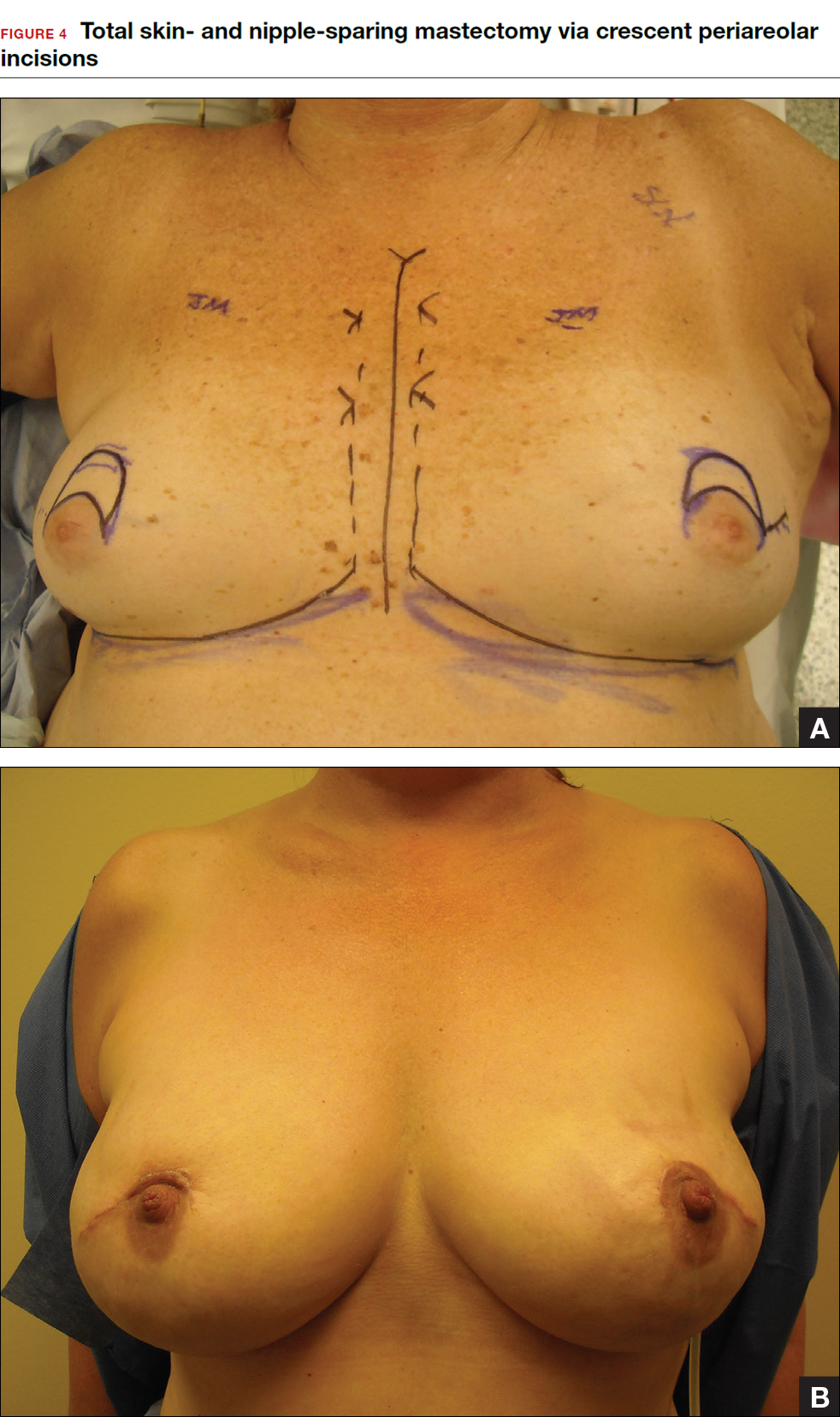
Some patients do not have the option of breast conservation. Women with multicentric breast cancer (more than 1 tumor in different quadrants of the breast) are better served with mastectomy. Surgical techniques for mastectomy have improved and provide women with various options. One option is skin- and nipple-sparing mastectomy, which preserves the skin envelope overlying the breast (including the skin of the nipple and areola) while removing the glandular elements of the breast and the majority of ductal tissue beneath the nipple-areola complex (FIGURE 4). This surgery can be performed via hidden scars at the inframammary crease or periareolar and is combined with immediate reconstruction, which provides an excellent cosmetic result.
Surgical considerations include removing glandular breast tissue within its anatomic boundaries while maintaining the blood supply to the skin and nipple-areola complex. Furthermore, there must be close dissection of ductal tissue beneath the nipple-areola complex and intraoperative frozen section of the nipple margin in cancer cases. Nipple-sparing mastectomy is oncologically safe in carefully selected patients who do not have cancer near or within the skin or nipple (eg, Paget disease).10 It is also safe as a prophylactic procedure for patients with genetic mutations, such as BRCA1 and BRCA2.11 The procedure is not ideal for smokers or patients with large, pendulous breasts. There is a 3% risk of breast cancer recurrence at the nipple or in the skin or muscle.10 Surgical complications include a 10% to 20% risk of skin or nipple necrosis.12
How do we manage the lymph nodes: Axillary dissection vs sentinel node biopsy?
Evaluation of the axillary nodes is currently part of breast cancer staging and can help the clinician determine the need for adjuvant chemotherapy. It also may assist in assessing the need for extending the radiation field beyond the breast to include the regional lymph nodes. Patients with early stage (stage I and II) breast cancer who do not have abnormal palpable lymph nodes or biopsy-proven metastasis to axillary nodes qualify for sentinel lymph node (SLN) biopsy.
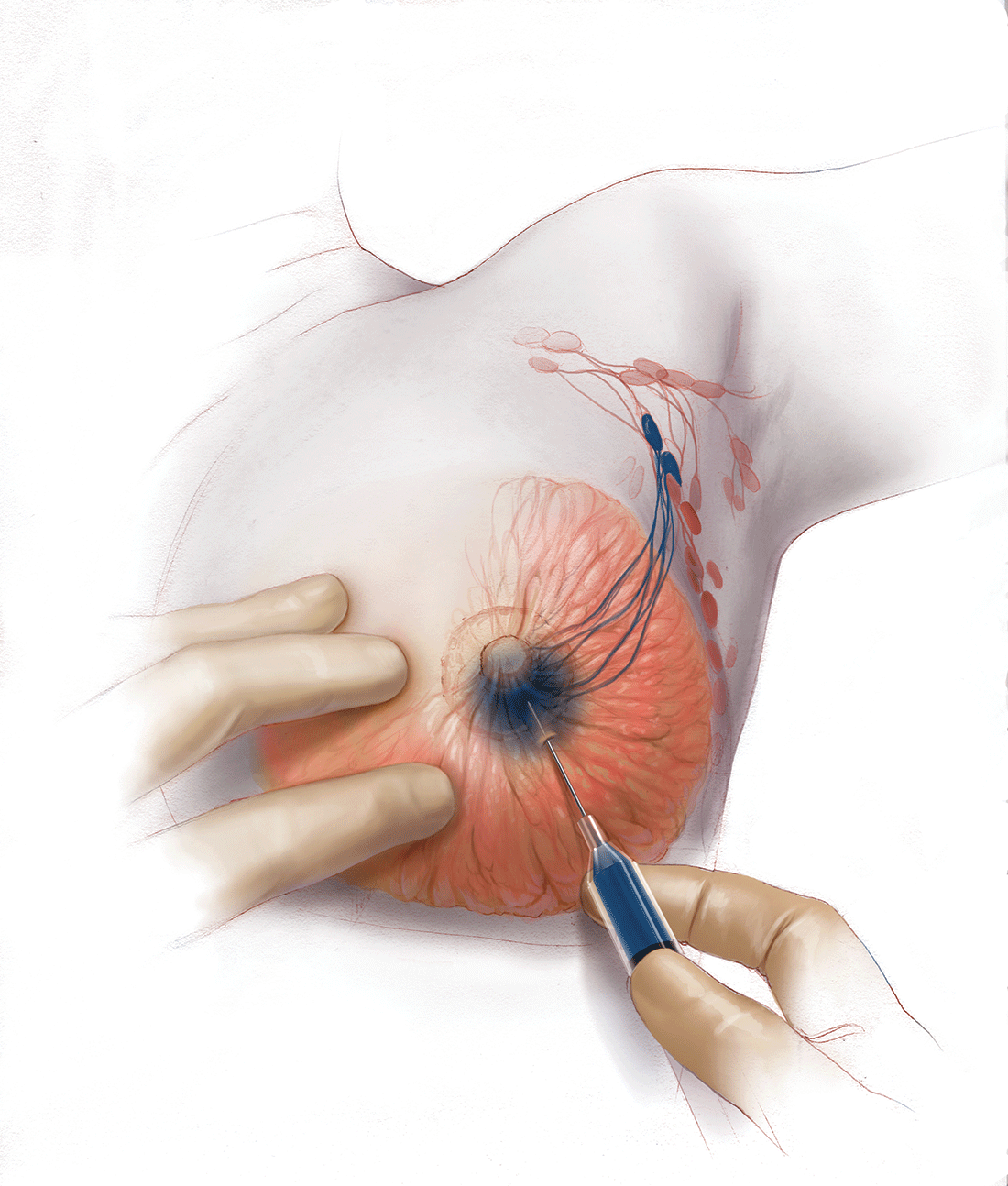
Sentinel node biopsy = less morbidity with no loss of accuracy. Compared with axillary lymph node dissection (ALND; removing all the level I and II nodes in the axilla), SLN biopsy has a 98% accuracy and is associated with less morbidity from lymphedema. The procedure involves injecting the breast with 2 tracers: a radioactive isotope, injected into the breast within 24 hours of the operation, and isosulfan blue dye, injected into the breast in the OR at the time of surgery (see illustration). Both tracers travel through the breast lymphatics and concentrate in the first few lymph nodes that drain the breast. The surgery is performed through a separate axillary incision, and the blue and radioactive lymph nodes are individually dissected and removed for pathologic evaluation. On average, 2 to 4 sentinel nodes are removed, including any suspicious palpable nodes. In experienced hands, this procedure has a false-negative rate of less than 5% to 10%.13
Axillary node dissection no longer standard of care. The indication for a completion ALND has changed based on the results of the randomized trial, ACOSOG Z0011.14 In this trial, patients with early stage breast cancer and 1 to 2 positive SLNs who were undergoing breast conservation therapy with radiation and adjuvant systemic therapy were randomly assigned to ALND or no ALND. (The trial did not include patients who were undergoing mastectomy, neoadjuvant chemotherapy, or who had more than 2 metastatic lymph nodes.) The investigators found no difference in overall or disease-free survival or local-regional recurrence between the 2 treatment groups over 9.2 years of follow up.14
Based on this practice-changing trial result, guidelines of the National Comprehensive Cancer Network no longer recommend completion ALND for patients who meet the ACOSOG Z0011 criteria. For patients who do not meet ACOSOG Z0011 criteria, we do intraoperative pathologic lymph node assessment with either frozen section or imprint cytology, and we perform immediate ALND when results are positive.
Indications for SLN biopsy include:
- invasive breast cancer with clinically negative axillary nodes
- ductal carcinoma in situ (DCIS) with microinvasion or extensive enough to require mastectomy
- clinically negative axillary nodes after neoadjuvant chemotherapy.
Contraindications for SLN biopsy include:
- bulky palpable lymphadenopathy
- pregnancy, as the safety of radioactive isotope and blue dye is not well studied; in isotope mapping the radiation dose is small and within safety limits for pregnant patients
- inflammatory breast cancer.
Complications of any axillary surgery may include risk of lymphedema (5% with SLN biopsy and 30% to 40% with ALND).15 Other complications include neuropathy of the affected arm with chronic pain and numbness of the skin.
Positive trends: Improved patient outcomes, specialized clinician training
Management of breast cancer has changed dramatically over the past several decades. More women are surviving breast cancer thanks to improvements in early detection, an individualized treatment approach with less aggressive surgery, and more effective targeted systemic therapies. A multidisciplinary, team-oriented approach with emphasis on minimally invasive biopsy and better cosmetic outcomes has enhanced quality of care.
Complexity in breast disease management has led to the development of formal fellowship training in breast surgical oncology. Studies have demonstrated that patients treated by high-volume breast surgeons are more satisfied with their care and have improved cancer outcomes.16,17 Women should be aware that they have different options for their breast cancer care, and surgeons with advanced specialization in this field may provide optimal results and better quality of care.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Nichols HB, Berrington de Gonzalez A, Lacey JV Jr, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564–1569.
- Wong SM, Freedman RA, Sagara Y, Aydogan F, Barry WT, Golshan M. Growing use of contralateral prophylactic mastectomy despite no improvement in long-term survival for invasive breast cancer [published online ahead of print March 8, 2016]. Ann Surg. doi:10.1097/SLA.0000000000001698.
- Miller ME, Czechura T, Martz B, et al. Operative risks associated with contralateral prophylactic mastectomy: a single institution experience. Ann Surg Oncol. 2013;20(13):4113–4120.
- Zhang X, Zhang XJ, Zhang TY, et al. Effect and safety of dual anti-human epidermal growth factor receptor 2 therapy compared to monotherapy in patients with human epidermal growth factor receptor 2-positive breast cancer: a systematic review. BMC Cancer. 2014;14:625.
- Ahmed M, Rubio IT, Klaase JM, Douek M. Surgical treatment of nonpalpable primary invasive and in situ breast cancer. Nat Rev Clin Oncol. 2015;12(11):645–663.
- Ahmed M, Douek M. Intra-operative ultrasound versus wire-guided localization in the surgical management of non-palpable breast cancers: systemic review and meta-analysis. Breast Cancer Res Treat. 2013;140(3):435–446.
- Krekel NM, Haloua MH, Lopes Cardozo AM, et al. Intraoperative ultrasound guidance for palpable breast cancer excision (COBALT trial): a multicentre, randomised controlled trial. Lancet Oncol. 2013;14(1):48–54.
- Chakravorty A, Shrestha AK, Sanmugalingam N, et al. How safe is oncoplastic breast conservation? Comparative analysis with standard breast conserving surgery. Eur J Surg Oncol. 2012;38(5):395–398.
- De Lorenzi F, Hubner G, Rotmensz N, et al. Oncological results of oncoplastic breast-conserving surgery: long term follow-up of a large series at a single institution: a matched-cohort analysis. Eur J Surg Oncol. 2016;42(1):71–77.
- De La Cruz L, Moody AM, Tappy EE, Blankenship AA, Hecht EM. Overall survival, disease-free survival, local recurrence, and nipple-areolar recurrence in the setting of nipple-sparing mastectomy: a meta-analysis and systematic review. Ann Surg Oncol. 2015;22(10):3241–3249.
- Yao K, Liederbach E, Tang R, et al. Nipple-sparing mastectomy in BRCA1/2 mutation carriers: an interim analysis and review of the literature. Ann Surg Oncol. 2015;22(2):370–376.
- Fortunato L, Loreti A, Andrich R, et al. When mastectomy is needed: is the nipple-sparing procedure a new standard with very few contraindications? J Surg Oncol. 2013;108(4):207–212.
- Veronesi U, Viale G, Paganelli G, et al. Sentinel lymph node biopsy in breast cancer: ten-year results of a randomized controlled study. Ann Surg. 2010;251(4):595–600.
- Giuliano AE, Hunt K, Ballman KV, et al. Ten-year survival results of ACOSOG Z0011: a randomized trial of axillary node dissection in women with clinical T1-2 N0 M0 breast cancer who have a positive sentinel node (Alliance). In: 2016 ASCO Annual Meeting; June 3-7, 2016. J Clin Oncol. 2016;34(15; May 20 suppl): Abstract 1007.
- DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013;14(6):500–515.
- Skinner KA, Helsper JT, Deapen D, Ye W, Sposto R. Breast cancer: do specialists make a difference? Ann Surg Oncol. 2003;10(6):606–615.
- Waljee JF, Hawley S, Alderman AK, Morrow M, Katz SJ. Patient satisfaction with treatment of breast cancer: does surgeon specialization matter? J Clin Oncol. 2007;25(24):3694–3698.

The author reports no financial relationships relevant to this article.
The author reports no financial relationships relevant to this article.
The author reports no financial relationships relevant to this article.
In a striking trend, the rate of contralateral prophylactic mastectomy (CPM) has risen by 30% over the last 10 years in the United States.1 Many women undergo CPM because of the fear and anxiety of cancer recurrence and their perceived risk of contralateral breast cancer; however, few women have a medical condition that necessitates removal of the contralateral breast. The medical indications for CPM include having a pathogenic genetic mutation (eg, BRCA1 and BRCA2), a strong family history of breast cancer, or prior mediastina chest radiation.
The actual risk of contralateral breast cancer is much lower than perceived. In women without a genetic mutation, the 10-year risk of contralateral breast cancer is only 3% to 5%.1 Also, CPM does not prevent the development of metastatic disease and offers no survival benefit over breast conservation or unilateral mastectomy.2 Furthermore, compared with unilateral therapeutic mastectomy, the “upgrade” to a CPM carries a 2.7-fold risk of a major surgical complication.3 It is therefore important that patients receive appropriate counseling regarding CPM, and that this counseling include cancer stage at diagnosis, family history and genetic risk, and cancer versus surgical risk (see “Counseling patients on contralateral prophylactic mastectomy” for key points to cover in patient discussions).
Counseling patients on contralateral prophylactic mastectomy
Commonly, patients diagnosed with breast cancer consider having their contralateral healthy breast removed as part of a bilateral mastectomy. They often experience severe anxiety about the cancer coming back and believe that removing both breasts will enable them to live longer. Keep the following key facts in mind when discussing treatment options with breast cancer patients.
Cancer stage at diagnosis. How long a patient lives from the time of her breast cancer diagnosis depends on the stage of the cancer at diagnosis, not the type of surgery performed. A woman with early stage I or stage II breast cancer has an 80% to 90% chance of being cancer free in 5 years.1 The chance of cancer recurring in the bones, liver, or lungs (metastatic breast cancer) will not be changed by removing the healthy breast. The risk of metastatic recurrence can be reduced, however, with chemotherapy and/or with hormone-blocker therapy.
Family history and genetic risk. Few women have a strong family history of breast and/or ovarian and other cancers, and this issue should be addressed with genetic counseling and testing prior to surgery. Those who carry a cancer-causing gene, such as BRCA1 or BRCA2, are at increased risk (40% to 60%) for a second or third breast cancer, especially if they are diagnosed at a young age (<50 years).2,3 In women who have a genetic mutation, removing both breasts and sometimes the ovaries can prevent development of another breast cancer. But this will not prevent spread of the cancer that is already present. Only chemotherapy and hormone blockers can prevent the spread of cancer.
Cancer risk versus surgical risk. For women with no family history of breast cancer, no genetic mutation, and no prior chest wall radiation, the risk of developing a new breast cancer in their other breast is only 3% to 5% every 10 years.3,4 This means that they have a 95% chance of not developing a new breast cancer in their healthy breast. Notably, removing the healthy breast can double the risk of postsurgical complications, including bleeding, infection, and loss of tissue and implant. The mastectomy site will be numb and the skin and nipple areola will not have any function other than cosmetic. Finally, wound complications from surgery could delay the start of important cancer treatment, such as chemotherapy or radiation.
The bottom line. Unless a woman has a strong family history of breast cancer, is diagnosed at a very young age, or has a genetic cancer-causing mutation, removing the contralateral healthy breast is not medically necessary and is not routinely recommended.
References
- Hennigs A, Riedel F, Gondos A, et al. Prognosis of breast cancer molecular subtypes in routine clinical care: a large prospective cohort study. BMC Cancer. 2016;16(1):734.
- Graeser MK, Engel C, Rhiem K, et al. Contralateral breast cancer risk in BRCA1 and BRCA2 mutation carriers. J Clin Oncol. 2009;27(35):5887–5992.
- Curtis RE, Ron E, Hankey BF, Hoover RN. New malignancies following breast cancer. In: Curtis RE, Freedman DM, Ron E, et al, eds. New Malignancies Among Cancer Survivors: SEER Cancer Registries, 1973-2000. Bethesda, MD: National Cancer Institute. NIH Publ. No. 05-5302. 2006:181–205. http://seer.cancer.gov/archive/publications/mpmono. Accessed September 18, 2016.
- Nichols HB, Berrington de Gonzalez A, Lacey JV Jr, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564–1569.
Women should be made aware that there are alternatives to mastectomy that have similar, or even better, outcomes with improved quality of life. Furthermore, a multi‑disciplinary, team-oriented approach with emphasis on minimally invasive biopsy and better cosmetic outcomes has enhanced quality of care. Knowledge of this team approach and of modern breast cancer treatments is essential for general ObGyns as this understanding improves the overall care and guidance—specifically regarding referral to expert, high-volume breast surgeons—provided to those women most in need.
Expanded treatment options for breast cancer
Advancements in breast surgery, better imaging, and targeted therapies are changing the paradigm of breast cancer treatment.
Image-guided biopsy is key in decision making
When an abnormality is found in the breast, surgical excision of an undiagnosed breast lesion is no longer considered an appropriate first step. Use of image-guided biopsy or minimally invasive core needle biopsy allows for accurate diagnosis of a breast lesion while avoiding a potentially breast deforming and expensive surgical operation. It is always better to go into the operating room (OR) with a diagnosis and do the right operation the first time.
A core needle biopsy, results of which demonstrate a benign lesion, helps avoid breast surgery in women who do not need it. If cancer is diagnosed on biopsy, the extent of disease can be better evaluated and decision making can be more informed, with a multidisciplinary approach used to consider the various options, including genetic counseling, plastic surgery consultation, or neoadjuvant therapy. Some lesions, such as those too close to the skin, chest wall, or an implant, may not be amenable to core needle biopsy and therefore require surgical excision for diagnosis.
Benefits of a multidisciplinary tumor conference
It is important for a multidisciplinary group of cancer specialists to review a patient’s case and discuss the ideal treatment plan prior to surgery. Some breast cancer subtypes (such as human epidermal growth factor receptor 2 [HER2]–overamplified breast cancer and many triple-negative breast cancers) are very sensitive to chemotherapy, and patients with these tumor types may benefit from receiving neoadjuvant chemotherapy prior to surgery. New types of chemotherapy may allow up to 60% of some breast cancers to diminish almost completely, with subsequent improved cosmetic results of breast surgery.4 It may also allow time for genetic counseling and testing prior to surgery. (See “How to code for a multidisciplinary tumor conference” for appropriate coding procedure.)
How to code for a multidisciplinary tumor conference
Melanie Witt, RN, MA
There are two coding choices for team conferences involving physician participation. If the patient and/or family is present, the CPT instruction is to bill a problem E/M service code (99201-99215) based on the time spent during this coordination of care/counseling. Documentation would include details about the conference decisions and implications for care, rather than history or examination.
If the patient is not present, report 99367 (Medical team conference with interdisciplinary team of health care professionals, patient and/or family not present, 30 minutes or more; participation by physician), but note that this code was developed under the assumption that the conference would be performed in a facility setting. Diagnostic coding would be breast cancer.
Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
This is an excerpt from a companion coding resource for breast cancer–related procedures by Ms. Witt. To read the companion article, “Coding for breast cancer–related procedures: A how-to guide,” in its entirety, click here.
Image-guided lumpectomy
Advances in breast imaging have led to increased identification of nonpalpable breast cancers. Surgical excision of nonpalpable breast lesions requires image guidance, which can be done using a variety of techniques.
Wire-guided localization (WGL) has been used in practice for the past 40 years. The procedure involves placement of a hooked wire under local anesthesia using either mammographic or ultrasound guidance. This procedure is mostly done in the radiology department on the same day as the surgery and requires that the radiologist coordinate with the OR schedule. Besides scheduling conflicts and delays in surgery, this procedure can be complicated by wires becoming dislodged, transected, or migrated, and limits the surgeon’s ability to cosmetically hide the scar in relation to position of the wire. It is uncomfortable for the patient, who must be transported from the radiology department to the OR with a wire extruding from her breast.
An alternative localization technique is placement of a radioactive source within the tumor, which can then be identified in the OR with a gamma probe.
Iodine I 125 Radioactive seed localization (RSL) involves placing a 4-mm titanium radiolabeled seed into the breast lesion under mammographic or ultrasound guidance (FIGURES 1 and 2). The procedure can be performed a few days before surgery in the radiology department, and there is less chance for the seed to become displaced or dislodged. This technique provides scheduling flexibility for the radiologist and reduces OR delays. The surgeon uses the same gamma probe for sentinel node biopsy to find the lesion in the breast, using the setting specific for iodine I 125. Incisions can be tailored anywhere in the breast, and the seed is detected by a focal gamma signal. Once the lumpectomy is performed, the specimen is probed and radiographed to confirm removal of the seed and adequate margins.
Limitations of this procedure include potential loss of the seed during the operation and radiation safety issues regarding handling and disposal of the radioactive isotope. Once the seed has been placed in the patient’s body, it must be removed surgically, as the half-life of iodine I 125 is long (60 days).5 Care must therefore be taken to optimize medical clearance prior to seed placement and to avoid surgery cancellations.
Intraoperative ultrasound (IOUS) allows the surgeon to identify the lesion under general anesthesia in the OR, which is more comfortable for the patient. The surgical incision can be tailored cosmetically and the lumpectomy can be performed with real-time ultrasound visualization of the tumor during dissection. This technique eliminates the need for a separate preoperative seed or wire localization in radiology. However, it can be used only for lesions or clips that are visible by ultrasound. The excised specimen can be evaluated for confirmation of tumor removal and adequate margins via ultrasound and re-excision of close margins can be accomplished immediately if needed.
Results of a meta-analysis of WGL versus IOUS demonstrated a significant reduction of positive margins with the use of IOUS.6 Results of the COBALT trial, in which patients were assigned randomly to excision of palpable breast cancers with either IOUS or palpation, demonstrated a 14% reduction in positive margins in favor of IOUS.7 Surgeon-performed breast ultrasound requires advanced training and accreditation in breast ultrasound through a rigorous certification process offered by the American Society of Breast Surgeons (www.breastsurgeons.org).
Oncoplastic lumpectomy
This approach to lumpectomy combines adequate oncologist resection of the breast tumor with plastic surgery techniques to achieve superior cosmesis. This approach allows complete removal of the tumor with negative margins, yet maintains the normal shape and contour of the breast. Two techniques have been described: volume displacement and volume replacement.
With the volume displacement technique, the surgeon uses adjacent tissue advancement to fill the lumpectomy cavity with the patient’s own surrounding breast tissue (FIGURE 3). The volume replacement technique requires the transposition of autologous tissue from elsewhere in the body.
Oncoplastic lumpectomy allows more women with larger tumors to undergo breast conservation with better cosmetic results. It reduces the number of mastectomies performed without compromising local control and avoids the need for extensive plastic surgery reconstruction and implants. Special effort and attention must be paid to ensure adequate margins utilizing intraoperative specimen radiograph and pathology evaluation.
This procedure requires that the surgeon acquire specialized skills and knowledge of oncologic and plastic surgery techniques, and it is best performed with the collaboration of a multidisciplinary team. Compared with conventional lumpectomy or mastectomy, oncoplastic breast conservation has been shown to reduce re-excision rates, and it has similar rates of local and distant recurrence and similar disease-free survival and overall survival.8,9
Total skin- and nipple-sparing mastectomy
Some patients do not have the option of breast conservation. Women with multicentric breast cancer (more than 1 tumor in different quadrants of the breast) are better served with mastectomy. Surgical techniques for mastectomy have improved and provide women with various options. One option is skin- and nipple-sparing mastectomy, which preserves the skin envelope overlying the breast (including the skin of the nipple and areola) while removing the glandular elements of the breast and the majority of ductal tissue beneath the nipple-areola complex (FIGURE 4). This surgery can be performed via hidden scars at the inframammary crease or periareolar and is combined with immediate reconstruction, which provides an excellent cosmetic result.
Surgical considerations include removing glandular breast tissue within its anatomic boundaries while maintaining the blood supply to the skin and nipple-areola complex. Furthermore, there must be close dissection of ductal tissue beneath the nipple-areola complex and intraoperative frozen section of the nipple margin in cancer cases. Nipple-sparing mastectomy is oncologically safe in carefully selected patients who do not have cancer near or within the skin or nipple (eg, Paget disease).10 It is also safe as a prophylactic procedure for patients with genetic mutations, such as BRCA1 and BRCA2.11 The procedure is not ideal for smokers or patients with large, pendulous breasts. There is a 3% risk of breast cancer recurrence at the nipple or in the skin or muscle.10 Surgical complications include a 10% to 20% risk of skin or nipple necrosis.12
How do we manage the lymph nodes: Axillary dissection vs sentinel node biopsy?
Evaluation of the axillary nodes is currently part of breast cancer staging and can help the clinician determine the need for adjuvant chemotherapy. It also may assist in assessing the need for extending the radiation field beyond the breast to include the regional lymph nodes. Patients with early stage (stage I and II) breast cancer who do not have abnormal palpable lymph nodes or biopsy-proven metastasis to axillary nodes qualify for sentinel lymph node (SLN) biopsy.
Sentinel node biopsy = less morbidity with no loss of accuracy. Compared with axillary lymph node dissection (ALND; removing all the level I and II nodes in the axilla), SLN biopsy has a 98% accuracy and is associated with less morbidity from lymphedema. The procedure involves injecting the breast with 2 tracers: a radioactive isotope, injected into the breast within 24 hours of the operation, and isosulfan blue dye, injected into the breast in the OR at the time of surgery (see illustration). Both tracers travel through the breast lymphatics and concentrate in the first few lymph nodes that drain the breast. The surgery is performed through a separate axillary incision, and the blue and radioactive lymph nodes are individually dissected and removed for pathologic evaluation. On average, 2 to 4 sentinel nodes are removed, including any suspicious palpable nodes. In experienced hands, this procedure has a false-negative rate of less than 5% to 10%.13
Axillary node dissection no longer standard of care. The indication for a completion ALND has changed based on the results of the randomized trial, ACOSOG Z0011.14 In this trial, patients with early stage breast cancer and 1 to 2 positive SLNs who were undergoing breast conservation therapy with radiation and adjuvant systemic therapy were randomly assigned to ALND or no ALND. (The trial did not include patients who were undergoing mastectomy, neoadjuvant chemotherapy, or who had more than 2 metastatic lymph nodes.) The investigators found no difference in overall or disease-free survival or local-regional recurrence between the 2 treatment groups over 9.2 years of follow up.14
Based on this practice-changing trial result, guidelines of the National Comprehensive Cancer Network no longer recommend completion ALND for patients who meet the ACOSOG Z0011 criteria. For patients who do not meet ACOSOG Z0011 criteria, we do intraoperative pathologic lymph node assessment with either frozen section or imprint cytology, and we perform immediate ALND when results are positive.
Indications for SLN biopsy include:
- invasive breast cancer with clinically negative axillary nodes
- ductal carcinoma in situ (DCIS) with microinvasion or extensive enough to require mastectomy
- clinically negative axillary nodes after neoadjuvant chemotherapy.
Contraindications for SLN biopsy include:
- bulky palpable lymphadenopathy
- pregnancy, as the safety of radioactive isotope and blue dye is not well studied; in isotope mapping the radiation dose is small and within safety limits for pregnant patients
- inflammatory breast cancer.
Complications of any axillary surgery may include risk of lymphedema (5% with SLN biopsy and 30% to 40% with ALND).15 Other complications include neuropathy of the affected arm with chronic pain and numbness of the skin.
Positive trends: Improved patient outcomes, specialized clinician training
Management of breast cancer has changed dramatically over the past several decades. More women are surviving breast cancer thanks to improvements in early detection, an individualized treatment approach with less aggressive surgery, and more effective targeted systemic therapies. A multidisciplinary, team-oriented approach with emphasis on minimally invasive biopsy and better cosmetic outcomes has enhanced quality of care.
Complexity in breast disease management has led to the development of formal fellowship training in breast surgical oncology. Studies have demonstrated that patients treated by high-volume breast surgeons are more satisfied with their care and have improved cancer outcomes.16,17 Women should be aware that they have different options for their breast cancer care, and surgeons with advanced specialization in this field may provide optimal results and better quality of care.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
In a striking trend, the rate of contralateral prophylactic mastectomy (CPM) has risen by 30% over the last 10 years in the United States.1 Many women undergo CPM because of the fear and anxiety of cancer recurrence and their perceived risk of contralateral breast cancer; however, few women have a medical condition that necessitates removal of the contralateral breast. The medical indications for CPM include having a pathogenic genetic mutation (eg, BRCA1 and BRCA2), a strong family history of breast cancer, or prior mediastina chest radiation.
The actual risk of contralateral breast cancer is much lower than perceived. In women without a genetic mutation, the 10-year risk of contralateral breast cancer is only 3% to 5%.1 Also, CPM does not prevent the development of metastatic disease and offers no survival benefit over breast conservation or unilateral mastectomy.2 Furthermore, compared with unilateral therapeutic mastectomy, the “upgrade” to a CPM carries a 2.7-fold risk of a major surgical complication.3 It is therefore important that patients receive appropriate counseling regarding CPM, and that this counseling include cancer stage at diagnosis, family history and genetic risk, and cancer versus surgical risk (see “Counseling patients on contralateral prophylactic mastectomy” for key points to cover in patient discussions).
Counseling patients on contralateral prophylactic mastectomy
Commonly, patients diagnosed with breast cancer consider having their contralateral healthy breast removed as part of a bilateral mastectomy. They often experience severe anxiety about the cancer coming back and believe that removing both breasts will enable them to live longer. Keep the following key facts in mind when discussing treatment options with breast cancer patients.
Cancer stage at diagnosis. How long a patient lives from the time of her breast cancer diagnosis depends on the stage of the cancer at diagnosis, not the type of surgery performed. A woman with early stage I or stage II breast cancer has an 80% to 90% chance of being cancer free in 5 years.1 The chance of cancer recurring in the bones, liver, or lungs (metastatic breast cancer) will not be changed by removing the healthy breast. The risk of metastatic recurrence can be reduced, however, with chemotherapy and/or with hormone-blocker therapy.
Family history and genetic risk. Few women have a strong family history of breast and/or ovarian and other cancers, and this issue should be addressed with genetic counseling and testing prior to surgery. Those who carry a cancer-causing gene, such as BRCA1 or BRCA2, are at increased risk (40% to 60%) for a second or third breast cancer, especially if they are diagnosed at a young age (<50 years).2,3 In women who have a genetic mutation, removing both breasts and sometimes the ovaries can prevent development of another breast cancer. But this will not prevent spread of the cancer that is already present. Only chemotherapy and hormone blockers can prevent the spread of cancer.
Cancer risk versus surgical risk. For women with no family history of breast cancer, no genetic mutation, and no prior chest wall radiation, the risk of developing a new breast cancer in their other breast is only 3% to 5% every 10 years.3,4 This means that they have a 95% chance of not developing a new breast cancer in their healthy breast. Notably, removing the healthy breast can double the risk of postsurgical complications, including bleeding, infection, and loss of tissue and implant. The mastectomy site will be numb and the skin and nipple areola will not have any function other than cosmetic. Finally, wound complications from surgery could delay the start of important cancer treatment, such as chemotherapy or radiation.
The bottom line. Unless a woman has a strong family history of breast cancer, is diagnosed at a very young age, or has a genetic cancer-causing mutation, removing the contralateral healthy breast is not medically necessary and is not routinely recommended.
References
- Hennigs A, Riedel F, Gondos A, et al. Prognosis of breast cancer molecular subtypes in routine clinical care: a large prospective cohort study. BMC Cancer. 2016;16(1):734.
- Graeser MK, Engel C, Rhiem K, et al. Contralateral breast cancer risk in BRCA1 and BRCA2 mutation carriers. J Clin Oncol. 2009;27(35):5887–5992.
- Curtis RE, Ron E, Hankey BF, Hoover RN. New malignancies following breast cancer. In: Curtis RE, Freedman DM, Ron E, et al, eds. New Malignancies Among Cancer Survivors: SEER Cancer Registries, 1973-2000. Bethesda, MD: National Cancer Institute. NIH Publ. No. 05-5302. 2006:181–205. http://seer.cancer.gov/archive/publications/mpmono. Accessed September 18, 2016.
- Nichols HB, Berrington de Gonzalez A, Lacey JV Jr, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564–1569.
Women should be made aware that there are alternatives to mastectomy that have similar, or even better, outcomes with improved quality of life. Furthermore, a multi‑disciplinary, team-oriented approach with emphasis on minimally invasive biopsy and better cosmetic outcomes has enhanced quality of care. Knowledge of this team approach and of modern breast cancer treatments is essential for general ObGyns as this understanding improves the overall care and guidance—specifically regarding referral to expert, high-volume breast surgeons—provided to those women most in need.
Expanded treatment options for breast cancer
Advancements in breast surgery, better imaging, and targeted therapies are changing the paradigm of breast cancer treatment.
Image-guided biopsy is key in decision making
When an abnormality is found in the breast, surgical excision of an undiagnosed breast lesion is no longer considered an appropriate first step. Use of image-guided biopsy or minimally invasive core needle biopsy allows for accurate diagnosis of a breast lesion while avoiding a potentially breast deforming and expensive surgical operation. It is always better to go into the operating room (OR) with a diagnosis and do the right operation the first time.
A core needle biopsy, results of which demonstrate a benign lesion, helps avoid breast surgery in women who do not need it. If cancer is diagnosed on biopsy, the extent of disease can be better evaluated and decision making can be more informed, with a multidisciplinary approach used to consider the various options, including genetic counseling, plastic surgery consultation, or neoadjuvant therapy. Some lesions, such as those too close to the skin, chest wall, or an implant, may not be amenable to core needle biopsy and therefore require surgical excision for diagnosis.
Benefits of a multidisciplinary tumor conference
It is important for a multidisciplinary group of cancer specialists to review a patient’s case and discuss the ideal treatment plan prior to surgery. Some breast cancer subtypes (such as human epidermal growth factor receptor 2 [HER2]–overamplified breast cancer and many triple-negative breast cancers) are very sensitive to chemotherapy, and patients with these tumor types may benefit from receiving neoadjuvant chemotherapy prior to surgery. New types of chemotherapy may allow up to 60% of some breast cancers to diminish almost completely, with subsequent improved cosmetic results of breast surgery.4 It may also allow time for genetic counseling and testing prior to surgery. (See “How to code for a multidisciplinary tumor conference” for appropriate coding procedure.)
How to code for a multidisciplinary tumor conference
Melanie Witt, RN, MA
There are two coding choices for team conferences involving physician participation. If the patient and/or family is present, the CPT instruction is to bill a problem E/M service code (99201-99215) based on the time spent during this coordination of care/counseling. Documentation would include details about the conference decisions and implications for care, rather than history or examination.
If the patient is not present, report 99367 (Medical team conference with interdisciplinary team of health care professionals, patient and/or family not present, 30 minutes or more; participation by physician), but note that this code was developed under the assumption that the conference would be performed in a facility setting. Diagnostic coding would be breast cancer.
Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
This is an excerpt from a companion coding resource for breast cancer–related procedures by Ms. Witt. To read the companion article, “Coding for breast cancer–related procedures: A how-to guide,” in its entirety, click here.
Image-guided lumpectomy
Advances in breast imaging have led to increased identification of nonpalpable breast cancers. Surgical excision of nonpalpable breast lesions requires image guidance, which can be done using a variety of techniques.
Wire-guided localization (WGL) has been used in practice for the past 40 years. The procedure involves placement of a hooked wire under local anesthesia using either mammographic or ultrasound guidance. This procedure is mostly done in the radiology department on the same day as the surgery and requires that the radiologist coordinate with the OR schedule. Besides scheduling conflicts and delays in surgery, this procedure can be complicated by wires becoming dislodged, transected, or migrated, and limits the surgeon’s ability to cosmetically hide the scar in relation to position of the wire. It is uncomfortable for the patient, who must be transported from the radiology department to the OR with a wire extruding from her breast.
An alternative localization technique is placement of a radioactive source within the tumor, which can then be identified in the OR with a gamma probe.
Iodine I 125 Radioactive seed localization (RSL) involves placing a 4-mm titanium radiolabeled seed into the breast lesion under mammographic or ultrasound guidance (FIGURES 1 and 2). The procedure can be performed a few days before surgery in the radiology department, and there is less chance for the seed to become displaced or dislodged. This technique provides scheduling flexibility for the radiologist and reduces OR delays. The surgeon uses the same gamma probe for sentinel node biopsy to find the lesion in the breast, using the setting specific for iodine I 125. Incisions can be tailored anywhere in the breast, and the seed is detected by a focal gamma signal. Once the lumpectomy is performed, the specimen is probed and radiographed to confirm removal of the seed and adequate margins.
Limitations of this procedure include potential loss of the seed during the operation and radiation safety issues regarding handling and disposal of the radioactive isotope. Once the seed has been placed in the patient’s body, it must be removed surgically, as the half-life of iodine I 125 is long (60 days).5 Care must therefore be taken to optimize medical clearance prior to seed placement and to avoid surgery cancellations.
Intraoperative ultrasound (IOUS) allows the surgeon to identify the lesion under general anesthesia in the OR, which is more comfortable for the patient. The surgical incision can be tailored cosmetically and the lumpectomy can be performed with real-time ultrasound visualization of the tumor during dissection. This technique eliminates the need for a separate preoperative seed or wire localization in radiology. However, it can be used only for lesions or clips that are visible by ultrasound. The excised specimen can be evaluated for confirmation of tumor removal and adequate margins via ultrasound and re-excision of close margins can be accomplished immediately if needed.
Results of a meta-analysis of WGL versus IOUS demonstrated a significant reduction of positive margins with the use of IOUS.6 Results of the COBALT trial, in which patients were assigned randomly to excision of palpable breast cancers with either IOUS or palpation, demonstrated a 14% reduction in positive margins in favor of IOUS.7 Surgeon-performed breast ultrasound requires advanced training and accreditation in breast ultrasound through a rigorous certification process offered by the American Society of Breast Surgeons (www.breastsurgeons.org).
Oncoplastic lumpectomy
This approach to lumpectomy combines adequate oncologist resection of the breast tumor with plastic surgery techniques to achieve superior cosmesis. This approach allows complete removal of the tumor with negative margins, yet maintains the normal shape and contour of the breast. Two techniques have been described: volume displacement and volume replacement.
With the volume displacement technique, the surgeon uses adjacent tissue advancement to fill the lumpectomy cavity with the patient’s own surrounding breast tissue (FIGURE 3). The volume replacement technique requires the transposition of autologous tissue from elsewhere in the body.
Oncoplastic lumpectomy allows more women with larger tumors to undergo breast conservation with better cosmetic results. It reduces the number of mastectomies performed without compromising local control and avoids the need for extensive plastic surgery reconstruction and implants. Special effort and attention must be paid to ensure adequate margins utilizing intraoperative specimen radiograph and pathology evaluation.
This procedure requires that the surgeon acquire specialized skills and knowledge of oncologic and plastic surgery techniques, and it is best performed with the collaboration of a multidisciplinary team. Compared with conventional lumpectomy or mastectomy, oncoplastic breast conservation has been shown to reduce re-excision rates, and it has similar rates of local and distant recurrence and similar disease-free survival and overall survival.8,9
Total skin- and nipple-sparing mastectomy
Some patients do not have the option of breast conservation. Women with multicentric breast cancer (more than 1 tumor in different quadrants of the breast) are better served with mastectomy. Surgical techniques for mastectomy have improved and provide women with various options. One option is skin- and nipple-sparing mastectomy, which preserves the skin envelope overlying the breast (including the skin of the nipple and areola) while removing the glandular elements of the breast and the majority of ductal tissue beneath the nipple-areola complex (FIGURE 4). This surgery can be performed via hidden scars at the inframammary crease or periareolar and is combined with immediate reconstruction, which provides an excellent cosmetic result.
Surgical considerations include removing glandular breast tissue within its anatomic boundaries while maintaining the blood supply to the skin and nipple-areola complex. Furthermore, there must be close dissection of ductal tissue beneath the nipple-areola complex and intraoperative frozen section of the nipple margin in cancer cases. Nipple-sparing mastectomy is oncologically safe in carefully selected patients who do not have cancer near or within the skin or nipple (eg, Paget disease).10 It is also safe as a prophylactic procedure for patients with genetic mutations, such as BRCA1 and BRCA2.11 The procedure is not ideal for smokers or patients with large, pendulous breasts. There is a 3% risk of breast cancer recurrence at the nipple or in the skin or muscle.10 Surgical complications include a 10% to 20% risk of skin or nipple necrosis.12
How do we manage the lymph nodes: Axillary dissection vs sentinel node biopsy?
Evaluation of the axillary nodes is currently part of breast cancer staging and can help the clinician determine the need for adjuvant chemotherapy. It also may assist in assessing the need for extending the radiation field beyond the breast to include the regional lymph nodes. Patients with early stage (stage I and II) breast cancer who do not have abnormal palpable lymph nodes or biopsy-proven metastasis to axillary nodes qualify for sentinel lymph node (SLN) biopsy.
Sentinel node biopsy = less morbidity with no loss of accuracy. Compared with axillary lymph node dissection (ALND; removing all the level I and II nodes in the axilla), SLN biopsy has a 98% accuracy and is associated with less morbidity from lymphedema. The procedure involves injecting the breast with 2 tracers: a radioactive isotope, injected into the breast within 24 hours of the operation, and isosulfan blue dye, injected into the breast in the OR at the time of surgery (see illustration). Both tracers travel through the breast lymphatics and concentrate in the first few lymph nodes that drain the breast. The surgery is performed through a separate axillary incision, and the blue and radioactive lymph nodes are individually dissected and removed for pathologic evaluation. On average, 2 to 4 sentinel nodes are removed, including any suspicious palpable nodes. In experienced hands, this procedure has a false-negative rate of less than 5% to 10%.13
Axillary node dissection no longer standard of care. The indication for a completion ALND has changed based on the results of the randomized trial, ACOSOG Z0011.14 In this trial, patients with early stage breast cancer and 1 to 2 positive SLNs who were undergoing breast conservation therapy with radiation and adjuvant systemic therapy were randomly assigned to ALND or no ALND. (The trial did not include patients who were undergoing mastectomy, neoadjuvant chemotherapy, or who had more than 2 metastatic lymph nodes.) The investigators found no difference in overall or disease-free survival or local-regional recurrence between the 2 treatment groups over 9.2 years of follow up.14
Based on this practice-changing trial result, guidelines of the National Comprehensive Cancer Network no longer recommend completion ALND for patients who meet the ACOSOG Z0011 criteria. For patients who do not meet ACOSOG Z0011 criteria, we do intraoperative pathologic lymph node assessment with either frozen section or imprint cytology, and we perform immediate ALND when results are positive.
Indications for SLN biopsy include:
- invasive breast cancer with clinically negative axillary nodes
- ductal carcinoma in situ (DCIS) with microinvasion or extensive enough to require mastectomy
- clinically negative axillary nodes after neoadjuvant chemotherapy.
Contraindications for SLN biopsy include:
- bulky palpable lymphadenopathy
- pregnancy, as the safety of radioactive isotope and blue dye is not well studied; in isotope mapping the radiation dose is small and within safety limits for pregnant patients
- inflammatory breast cancer.
Complications of any axillary surgery may include risk of lymphedema (5% with SLN biopsy and 30% to 40% with ALND).15 Other complications include neuropathy of the affected arm with chronic pain and numbness of the skin.
Positive trends: Improved patient outcomes, specialized clinician training
Management of breast cancer has changed dramatically over the past several decades. More women are surviving breast cancer thanks to improvements in early detection, an individualized treatment approach with less aggressive surgery, and more effective targeted systemic therapies. A multidisciplinary, team-oriented approach with emphasis on minimally invasive biopsy and better cosmetic outcomes has enhanced quality of care.
Complexity in breast disease management has led to the development of formal fellowship training in breast surgical oncology. Studies have demonstrated that patients treated by high-volume breast surgeons are more satisfied with their care and have improved cancer outcomes.16,17 Women should be aware that they have different options for their breast cancer care, and surgeons with advanced specialization in this field may provide optimal results and better quality of care.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Nichols HB, Berrington de Gonzalez A, Lacey JV Jr, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564–1569.
- Wong SM, Freedman RA, Sagara Y, Aydogan F, Barry WT, Golshan M. Growing use of contralateral prophylactic mastectomy despite no improvement in long-term survival for invasive breast cancer [published online ahead of print March 8, 2016]. Ann Surg. doi:10.1097/SLA.0000000000001698.
- Miller ME, Czechura T, Martz B, et al. Operative risks associated with contralateral prophylactic mastectomy: a single institution experience. Ann Surg Oncol. 2013;20(13):4113–4120.
- Zhang X, Zhang XJ, Zhang TY, et al. Effect and safety of dual anti-human epidermal growth factor receptor 2 therapy compared to monotherapy in patients with human epidermal growth factor receptor 2-positive breast cancer: a systematic review. BMC Cancer. 2014;14:625.
- Ahmed M, Rubio IT, Klaase JM, Douek M. Surgical treatment of nonpalpable primary invasive and in situ breast cancer. Nat Rev Clin Oncol. 2015;12(11):645–663.
- Ahmed M, Douek M. Intra-operative ultrasound versus wire-guided localization in the surgical management of non-palpable breast cancers: systemic review and meta-analysis. Breast Cancer Res Treat. 2013;140(3):435–446.
- Krekel NM, Haloua MH, Lopes Cardozo AM, et al. Intraoperative ultrasound guidance for palpable breast cancer excision (COBALT trial): a multicentre, randomised controlled trial. Lancet Oncol. 2013;14(1):48–54.
- Chakravorty A, Shrestha AK, Sanmugalingam N, et al. How safe is oncoplastic breast conservation? Comparative analysis with standard breast conserving surgery. Eur J Surg Oncol. 2012;38(5):395–398.
- De Lorenzi F, Hubner G, Rotmensz N, et al. Oncological results of oncoplastic breast-conserving surgery: long term follow-up of a large series at a single institution: a matched-cohort analysis. Eur J Surg Oncol. 2016;42(1):71–77.
- De La Cruz L, Moody AM, Tappy EE, Blankenship AA, Hecht EM. Overall survival, disease-free survival, local recurrence, and nipple-areolar recurrence in the setting of nipple-sparing mastectomy: a meta-analysis and systematic review. Ann Surg Oncol. 2015;22(10):3241–3249.
- Yao K, Liederbach E, Tang R, et al. Nipple-sparing mastectomy in BRCA1/2 mutation carriers: an interim analysis and review of the literature. Ann Surg Oncol. 2015;22(2):370–376.
- Fortunato L, Loreti A, Andrich R, et al. When mastectomy is needed: is the nipple-sparing procedure a new standard with very few contraindications? J Surg Oncol. 2013;108(4):207–212.
- Veronesi U, Viale G, Paganelli G, et al. Sentinel lymph node biopsy in breast cancer: ten-year results of a randomized controlled study. Ann Surg. 2010;251(4):595–600.
- Giuliano AE, Hunt K, Ballman KV, et al. Ten-year survival results of ACOSOG Z0011: a randomized trial of axillary node dissection in women with clinical T1-2 N0 M0 breast cancer who have a positive sentinel node (Alliance). In: 2016 ASCO Annual Meeting; June 3-7, 2016. J Clin Oncol. 2016;34(15; May 20 suppl): Abstract 1007.
- DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013;14(6):500–515.
- Skinner KA, Helsper JT, Deapen D, Ye W, Sposto R. Breast cancer: do specialists make a difference? Ann Surg Oncol. 2003;10(6):606–615.
- Waljee JF, Hawley S, Alderman AK, Morrow M, Katz SJ. Patient satisfaction with treatment of breast cancer: does surgeon specialization matter? J Clin Oncol. 2007;25(24):3694–3698.
- Nichols HB, Berrington de Gonzalez A, Lacey JV Jr, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564–1569.
- Wong SM, Freedman RA, Sagara Y, Aydogan F, Barry WT, Golshan M. Growing use of contralateral prophylactic mastectomy despite no improvement in long-term survival for invasive breast cancer [published online ahead of print March 8, 2016]. Ann Surg. doi:10.1097/SLA.0000000000001698.
- Miller ME, Czechura T, Martz B, et al. Operative risks associated with contralateral prophylactic mastectomy: a single institution experience. Ann Surg Oncol. 2013;20(13):4113–4120.
- Zhang X, Zhang XJ, Zhang TY, et al. Effect and safety of dual anti-human epidermal growth factor receptor 2 therapy compared to monotherapy in patients with human epidermal growth factor receptor 2-positive breast cancer: a systematic review. BMC Cancer. 2014;14:625.
- Ahmed M, Rubio IT, Klaase JM, Douek M. Surgical treatment of nonpalpable primary invasive and in situ breast cancer. Nat Rev Clin Oncol. 2015;12(11):645–663.
- Ahmed M, Douek M. Intra-operative ultrasound versus wire-guided localization in the surgical management of non-palpable breast cancers: systemic review and meta-analysis. Breast Cancer Res Treat. 2013;140(3):435–446.
- Krekel NM, Haloua MH, Lopes Cardozo AM, et al. Intraoperative ultrasound guidance for palpable breast cancer excision (COBALT trial): a multicentre, randomised controlled trial. Lancet Oncol. 2013;14(1):48–54.
- Chakravorty A, Shrestha AK, Sanmugalingam N, et al. How safe is oncoplastic breast conservation? Comparative analysis with standard breast conserving surgery. Eur J Surg Oncol. 2012;38(5):395–398.
- De Lorenzi F, Hubner G, Rotmensz N, et al. Oncological results of oncoplastic breast-conserving surgery: long term follow-up of a large series at a single institution: a matched-cohort analysis. Eur J Surg Oncol. 2016;42(1):71–77.
- De La Cruz L, Moody AM, Tappy EE, Blankenship AA, Hecht EM. Overall survival, disease-free survival, local recurrence, and nipple-areolar recurrence in the setting of nipple-sparing mastectomy: a meta-analysis and systematic review. Ann Surg Oncol. 2015;22(10):3241–3249.
- Yao K, Liederbach E, Tang R, et al. Nipple-sparing mastectomy in BRCA1/2 mutation carriers: an interim analysis and review of the literature. Ann Surg Oncol. 2015;22(2):370–376.
- Fortunato L, Loreti A, Andrich R, et al. When mastectomy is needed: is the nipple-sparing procedure a new standard with very few contraindications? J Surg Oncol. 2013;108(4):207–212.
- Veronesi U, Viale G, Paganelli G, et al. Sentinel lymph node biopsy in breast cancer: ten-year results of a randomized controlled study. Ann Surg. 2010;251(4):595–600.
- Giuliano AE, Hunt K, Ballman KV, et al. Ten-year survival results of ACOSOG Z0011: a randomized trial of axillary node dissection in women with clinical T1-2 N0 M0 breast cancer who have a positive sentinel node (Alliance). In: 2016 ASCO Annual Meeting; June 3-7, 2016. J Clin Oncol. 2016;34(15; May 20 suppl): Abstract 1007.
- DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013;14(6):500–515.
- Skinner KA, Helsper JT, Deapen D, Ye W, Sposto R. Breast cancer: do specialists make a difference? Ann Surg Oncol. 2003;10(6):606–615.
- Waljee JF, Hawley S, Alderman AK, Morrow M, Katz SJ. Patient satisfaction with treatment of breast cancer: does surgeon specialization matter? J Clin Oncol. 2007;25(24):3694–3698.
In this Article
- Counseling patients on CPM
- Oncoplastic lumpectomy approach
- How to manage the lymph nodes
Gait predicts cognitive decline in early Parkinson’s
PORTLAND, ORE. – Gait characteristics, rather than cognition, in early Parkinson’s disease predicted cognitive decline 3 years later in a small longitudinal study, suggesting that gait measures may provide a low cost clinical biomarker when combined with other predictors of cognitive decline in Parkinson’s disease.
Cognitive decline and dementia take a significant toll on patients’ personal, social, and economic affairs. Being able to identify at-risk individuals may allow for early behavioral and possibly pharmacological interventions. Gait has been shown to be a sensitive measure of cognitive decline in older adults, and the investigators here tested it as a predictor of cognitive decline in Parkinson’s disease (PD).
Led by Rosie Morris, PhD, of Newcastle University, Newcastle upon Tyne, England, researchers assessed gait characteristics and cognition in 119 patients within 4-6 months of a diagnosis of idiopathic PD and then 18 and 36 months later. The patients were recruited from the Incidence of Cognitive Impairment in Cohorts with Longitudinal Evaluation – Parkinson’s Disease (ICICLE-PD) study.
In this ICICLE-Gait substudy, participants walked for 2 minutes around a circuit that included a 7-meter instrumented walkway (GaitRite) that recorded 16 gait characteristics in the five independent domains of pace, variability, rhythm, asymmetry, and posture control. The investigators used the Montreal Cognitive Assessment (MoCA) battery of tests to assess global cognition, attention, fluctuating attention, executive function, working memory, visual memory, and visuospatial ability. They adjusted the results for covariates of age, education, gender, depression, and levodopa equivalent daily doses.

“We found that seven characteristics of gait were able to predict changes in measures of attention,” Dr. Morris said during a poster session at the World Parkinson Congress. The characteristics of gait were “mainly pace and variability and at diagnosis were sensitive to decline in tests of attention.”
With the multiple measures used in this study, a P value of less than or equal to .01 was considered statistically significant.
There were significant cognitive declines in the areas of attention, fluctuating attention, executive function, and visual memory. Fluctuating attention was predicted by measures of gait pace (step velocity, step length, and step swing: all P less than or equal to .007), gait variability (step stance and step length: both P less than or equal to .01), and postural control (P = .004). The pace measure of step length also predicted a decline in visual memory (P = .01).
Baseline MoCA predicted a decline in attention (P less than .001) but not in fluctuating attention or in visual memory.
The authors said that this study is the first “to demonstrate that discrete gait characteristics can predict measures of cognitive decline in early PD.” Asked why gait may predict cognitive decline, Dr. Morris postulated that certain characteristics of gait, such as speed and postural control, are related to cognition more so than other characteristics such as asymmetry.
These techniques may have clinical utility and not be merely of research interest. The parameters of gait may be measurable in the community using wearable sensors such as accelerometers “to measure discrete characteristics of gait ... So, ideally, it will be a possible future biomarker, and then we can measure them in the clinic and then identify risks from there,” she said, adding that she is planning research to explore the association of gait and cognition. Confounding factors yet to be examined are the effects of being on or off different medications and different medication cycles when patients are free-living in the community.
If researchers can validate that gait is a sensitive predictor of dementia, then the question becomes what to do about it. Dr. Morris suggested that physical therapy should incorporate more cognitive tasks.
Jori Fleisher, MD, a movement disorders neurologist at New York University Langone Medical Center, said that the study is “really interesting because right now there’s a huge search underway for biomarkers” to reliably predict progression of Parkinson’s disease or predict who is at risk for the disease.
“These investigators looked at whether something as seemingly simple as gait – so the way that someone walks, the way that their balance is, the pace of their walking – could predict decline in cognition. And that’s something of great interest to clinicians and to researchers: How do we figure out which of our patients are going to experience cognitive decline and in what different domains?” she said.
Although the researchers in this study used sophisticated and sensitive measures of several aspects of gait not generally available to clinicians, Dr. Fleisher predicted that it may be possible to extrapolate the findings to look for specific aspects of gait variability (possibly through the use of wearable devices) so the technique may become widely useful.
Once a patient is seen to be at high risk for cognitive decline, she said, exercise may be an appropriate intervention. “We know huge benefits of exercise, which have been shown in various aspects of cognitive decline ... [to] slow the decline in cognitive function.” Dr. Fleisher said the best exercise is any one that a patient will continue to do, whether it is walking, dancing, or any other exercise that the person will stick with.
The study was supported in the United Kingdom by the National Institute for Health Research, the National Health Service, and Parkinson’s UK. There was no commercial funding. Dr. Morris reported having no financial disclosures. Dr. Fleisher had no financial disclosures.
PORTLAND, ORE. – Gait characteristics, rather than cognition, in early Parkinson’s disease predicted cognitive decline 3 years later in a small longitudinal study, suggesting that gait measures may provide a low cost clinical biomarker when combined with other predictors of cognitive decline in Parkinson’s disease.
Cognitive decline and dementia take a significant toll on patients’ personal, social, and economic affairs. Being able to identify at-risk individuals may allow for early behavioral and possibly pharmacological interventions. Gait has been shown to be a sensitive measure of cognitive decline in older adults, and the investigators here tested it as a predictor of cognitive decline in Parkinson’s disease (PD).
Led by Rosie Morris, PhD, of Newcastle University, Newcastle upon Tyne, England, researchers assessed gait characteristics and cognition in 119 patients within 4-6 months of a diagnosis of idiopathic PD and then 18 and 36 months later. The patients were recruited from the Incidence of Cognitive Impairment in Cohorts with Longitudinal Evaluation – Parkinson’s Disease (ICICLE-PD) study.
In this ICICLE-Gait substudy, participants walked for 2 minutes around a circuit that included a 7-meter instrumented walkway (GaitRite) that recorded 16 gait characteristics in the five independent domains of pace, variability, rhythm, asymmetry, and posture control. The investigators used the Montreal Cognitive Assessment (MoCA) battery of tests to assess global cognition, attention, fluctuating attention, executive function, working memory, visual memory, and visuospatial ability. They adjusted the results for covariates of age, education, gender, depression, and levodopa equivalent daily doses.
“We found that seven characteristics of gait were able to predict changes in measures of attention,” Dr. Morris said during a poster session at the World Parkinson Congress. The characteristics of gait were “mainly pace and variability and at diagnosis were sensitive to decline in tests of attention.”
With the multiple measures used in this study, a P value of less than or equal to .01 was considered statistically significant.
There were significant cognitive declines in the areas of attention, fluctuating attention, executive function, and visual memory. Fluctuating attention was predicted by measures of gait pace (step velocity, step length, and step swing: all P less than or equal to .007), gait variability (step stance and step length: both P less than or equal to .01), and postural control (P = .004). The pace measure of step length also predicted a decline in visual memory (P = .01).
Baseline MoCA predicted a decline in attention (P less than .001) but not in fluctuating attention or in visual memory.
The authors said that this study is the first “to demonstrate that discrete gait characteristics can predict measures of cognitive decline in early PD.” Asked why gait may predict cognitive decline, Dr. Morris postulated that certain characteristics of gait, such as speed and postural control, are related to cognition more so than other characteristics such as asymmetry.
These techniques may have clinical utility and not be merely of research interest. The parameters of gait may be measurable in the community using wearable sensors such as accelerometers “to measure discrete characteristics of gait ... So, ideally, it will be a possible future biomarker, and then we can measure them in the clinic and then identify risks from there,” she said, adding that she is planning research to explore the association of gait and cognition. Confounding factors yet to be examined are the effects of being on or off different medications and different medication cycles when patients are free-living in the community.
If researchers can validate that gait is a sensitive predictor of dementia, then the question becomes what to do about it. Dr. Morris suggested that physical therapy should incorporate more cognitive tasks.
Jori Fleisher, MD, a movement disorders neurologist at New York University Langone Medical Center, said that the study is “really interesting because right now there’s a huge search underway for biomarkers” to reliably predict progression of Parkinson’s disease or predict who is at risk for the disease.
“These investigators looked at whether something as seemingly simple as gait – so the way that someone walks, the way that their balance is, the pace of their walking – could predict decline in cognition. And that’s something of great interest to clinicians and to researchers: How do we figure out which of our patients are going to experience cognitive decline and in what different domains?” she said.
Although the researchers in this study used sophisticated and sensitive measures of several aspects of gait not generally available to clinicians, Dr. Fleisher predicted that it may be possible to extrapolate the findings to look for specific aspects of gait variability (possibly through the use of wearable devices) so the technique may become widely useful.
Once a patient is seen to be at high risk for cognitive decline, she said, exercise may be an appropriate intervention. “We know huge benefits of exercise, which have been shown in various aspects of cognitive decline ... [to] slow the decline in cognitive function.” Dr. Fleisher said the best exercise is any one that a patient will continue to do, whether it is walking, dancing, or any other exercise that the person will stick with.
The study was supported in the United Kingdom by the National Institute for Health Research, the National Health Service, and Parkinson’s UK. There was no commercial funding. Dr. Morris reported having no financial disclosures. Dr. Fleisher had no financial disclosures.
PORTLAND, ORE. – Gait characteristics, rather than cognition, in early Parkinson’s disease predicted cognitive decline 3 years later in a small longitudinal study, suggesting that gait measures may provide a low cost clinical biomarker when combined with other predictors of cognitive decline in Parkinson’s disease.
Cognitive decline and dementia take a significant toll on patients’ personal, social, and economic affairs. Being able to identify at-risk individuals may allow for early behavioral and possibly pharmacological interventions. Gait has been shown to be a sensitive measure of cognitive decline in older adults, and the investigators here tested it as a predictor of cognitive decline in Parkinson’s disease (PD).
Led by Rosie Morris, PhD, of Newcastle University, Newcastle upon Tyne, England, researchers assessed gait characteristics and cognition in 119 patients within 4-6 months of a diagnosis of idiopathic PD and then 18 and 36 months later. The patients were recruited from the Incidence of Cognitive Impairment in Cohorts with Longitudinal Evaluation – Parkinson’s Disease (ICICLE-PD) study.
In this ICICLE-Gait substudy, participants walked for 2 minutes around a circuit that included a 7-meter instrumented walkway (GaitRite) that recorded 16 gait characteristics in the five independent domains of pace, variability, rhythm, asymmetry, and posture control. The investigators used the Montreal Cognitive Assessment (MoCA) battery of tests to assess global cognition, attention, fluctuating attention, executive function, working memory, visual memory, and visuospatial ability. They adjusted the results for covariates of age, education, gender, depression, and levodopa equivalent daily doses.
“We found that seven characteristics of gait were able to predict changes in measures of attention,” Dr. Morris said during a poster session at the World Parkinson Congress. The characteristics of gait were “mainly pace and variability and at diagnosis were sensitive to decline in tests of attention.”
With the multiple measures used in this study, a P value of less than or equal to .01 was considered statistically significant.
There were significant cognitive declines in the areas of attention, fluctuating attention, executive function, and visual memory. Fluctuating attention was predicted by measures of gait pace (step velocity, step length, and step swing: all P less than or equal to .007), gait variability (step stance and step length: both P less than or equal to .01), and postural control (P = .004). The pace measure of step length also predicted a decline in visual memory (P = .01).
Baseline MoCA predicted a decline in attention (P less than .001) but not in fluctuating attention or in visual memory.
The authors said that this study is the first “to demonstrate that discrete gait characteristics can predict measures of cognitive decline in early PD.” Asked why gait may predict cognitive decline, Dr. Morris postulated that certain characteristics of gait, such as speed and postural control, are related to cognition more so than other characteristics such as asymmetry.
These techniques may have clinical utility and not be merely of research interest. The parameters of gait may be measurable in the community using wearable sensors such as accelerometers “to measure discrete characteristics of gait ... So, ideally, it will be a possible future biomarker, and then we can measure them in the clinic and then identify risks from there,” she said, adding that she is planning research to explore the association of gait and cognition. Confounding factors yet to be examined are the effects of being on or off different medications and different medication cycles when patients are free-living in the community.
If researchers can validate that gait is a sensitive predictor of dementia, then the question becomes what to do about it. Dr. Morris suggested that physical therapy should incorporate more cognitive tasks.
Jori Fleisher, MD, a movement disorders neurologist at New York University Langone Medical Center, said that the study is “really interesting because right now there’s a huge search underway for biomarkers” to reliably predict progression of Parkinson’s disease or predict who is at risk for the disease.
“These investigators looked at whether something as seemingly simple as gait – so the way that someone walks, the way that their balance is, the pace of their walking – could predict decline in cognition. And that’s something of great interest to clinicians and to researchers: How do we figure out which of our patients are going to experience cognitive decline and in what different domains?” she said.
Although the researchers in this study used sophisticated and sensitive measures of several aspects of gait not generally available to clinicians, Dr. Fleisher predicted that it may be possible to extrapolate the findings to look for specific aspects of gait variability (possibly through the use of wearable devices) so the technique may become widely useful.
Once a patient is seen to be at high risk for cognitive decline, she said, exercise may be an appropriate intervention. “We know huge benefits of exercise, which have been shown in various aspects of cognitive decline ... [to] slow the decline in cognitive function.” Dr. Fleisher said the best exercise is any one that a patient will continue to do, whether it is walking, dancing, or any other exercise that the person will stick with.
The study was supported in the United Kingdom by the National Institute for Health Research, the National Health Service, and Parkinson’s UK. There was no commercial funding. Dr. Morris reported having no financial disclosures. Dr. Fleisher had no financial disclosures.
AT WPC 2016
Key clinical point: Gait characteristics, not cognition, predict cognitive decline in early Parkinson’s.
Major finding: Gait pace, variability, and postural control predict cognitive decline.
Data source: Observational study of 119 patients with early idiopathic Parkinson’s disease assessed at baseline and at 36 months.
Disclosures: The study was supported in the United Kingdom by the National Institute for Health Research, the National Health Service, and Parkinson’s UK. There was no commercial funding. Dr. Morris and Dr. Fleisher had no financial disclosures.

Mobility benefits of MS drug dalfampridine confirmed by patient-reported outcomes
LONDON – Patients with relapsing-remitting multiple sclerosis reported that their ability to walk was significantly improved following 6 months of treatment with extended-release dalfampridine – compared with patients on placebo – in a double-blind, randomized trial.
In the ENHANCE study, 43.2% of the 315 patients treated with extended-release dalfampridine (dalfampridine-ER; Ampyra) and 33.6% of the 318 who were given placebo achieved a clinically meaningful improvement of 8 or more points on the 12-item MS Walking Scale (MSWS-12) measured at week 24.

The odds ratio (OR) was 1.61, highlighting a significant difference between the two study arms (P = .006).
“This is one of the only studies to use a PRO [patient-reported outcome] as the primary outcome and to use an a priori threshold of clinical meaningfulness,” said Jeremy Hobart, MD, of Plymouth Hospitals NHS Trust (England), who reported the study’s findings at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis. This is an important, and challenging, development in MS trials, he added.
“We are all aware that walking impairments are one of the hallmarks of multiple sclerosis,” Dr. Hobart said, adding that it affects the “vast majority” of patients.
Dalfampridine-ER, which is known as prolonged-release fampridine in Europe, is the only therapy licensed to improve walking in MS, he observed. The pivotal studies that led to the drug’s approval, however, were of relatively short duration and the ENHANCE study was conducted to answer questions that have been raised about the durability of its effect on patients’ mobility.
Patients in ENHANCE received either dalfampridine-ER at a twice-daily dose of 10 mg or placebo for 24 weeks. The mean age of patients in each group was 49 and 48 years, respectively, and 59% and 57% of recruited patients in each arm were female. Patients were stratified according to their baseline Expanded Disability Status Scale (EDSS) score, with 78% and 77% in the dalfampridine-ER and placebo groups having a score of 6 or less.
Dr. Hobart noted that the mean change in MSWS-12 scores over time and an analysis of the cumulative proportion of responders at any particular threshold score on the MWSW-12 showed a clear benefit of dalfampridine-ER treatment over placebo.
The study investigators also assessed patients’ balance via the Timed Up and Go (TUG) test, with a benefit threshold set at obtaining at least a 15% or more improvement at 24 weeks. Significantly more dalfampridine-ER–treated than placebo-treated patients achieved this threshold (43.4% vs. 34.7%; OR, 1.46; P = .03).
There was a significant improvement between the two study arms on the 29-item physical scale of the Multiple Sclerosis Impact Scale (P less than .001).
However, there was no change seen in upper extremity function, with similar mean changes in the Berg Balance Scale score and the ABILHAND score at 24 weeks. The mean baseline scores for both of these measures were high, Dr. Hobart observed, which probably affected the findings. That said, patients with a baseline EDSS of 6 or higher had greater improvement in ABILHAND scores if they had received dalfampridine-ER, compared with placebo, but the difference was not statistically significant.
The safety profile was consistent with what has been seen in other trials, Dr. Hobart said, and there were no new safety concerns raised.
“The findings from ENHANCE expand and tend to ... confirm the favorable risk-benefit profile established in prior pivotal trials,” he said.
Biogen sponsored the study. Dr. Hobart disclosed receiving fees, honoraria, and research support from Biogen, Acorda, Genzyme, Global Blood Therapeutics, Merck Serono, Novartis, Tigercat, and Vanita.
LONDON – Patients with relapsing-remitting multiple sclerosis reported that their ability to walk was significantly improved following 6 months of treatment with extended-release dalfampridine – compared with patients on placebo – in a double-blind, randomized trial.
In the ENHANCE study, 43.2% of the 315 patients treated with extended-release dalfampridine (dalfampridine-ER; Ampyra) and 33.6% of the 318 who were given placebo achieved a clinically meaningful improvement of 8 or more points on the 12-item MS Walking Scale (MSWS-12) measured at week 24.
The odds ratio (OR) was 1.61, highlighting a significant difference between the two study arms (P = .006).
“This is one of the only studies to use a PRO [patient-reported outcome] as the primary outcome and to use an a priori threshold of clinical meaningfulness,” said Jeremy Hobart, MD, of Plymouth Hospitals NHS Trust (England), who reported the study’s findings at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis. This is an important, and challenging, development in MS trials, he added.
“We are all aware that walking impairments are one of the hallmarks of multiple sclerosis,” Dr. Hobart said, adding that it affects the “vast majority” of patients.
Dalfampridine-ER, which is known as prolonged-release fampridine in Europe, is the only therapy licensed to improve walking in MS, he observed. The pivotal studies that led to the drug’s approval, however, were of relatively short duration and the ENHANCE study was conducted to answer questions that have been raised about the durability of its effect on patients’ mobility.
Patients in ENHANCE received either dalfampridine-ER at a twice-daily dose of 10 mg or placebo for 24 weeks. The mean age of patients in each group was 49 and 48 years, respectively, and 59% and 57% of recruited patients in each arm were female. Patients were stratified according to their baseline Expanded Disability Status Scale (EDSS) score, with 78% and 77% in the dalfampridine-ER and placebo groups having a score of 6 or less.
Dr. Hobart noted that the mean change in MSWS-12 scores over time and an analysis of the cumulative proportion of responders at any particular threshold score on the MWSW-12 showed a clear benefit of dalfampridine-ER treatment over placebo.
The study investigators also assessed patients’ balance via the Timed Up and Go (TUG) test, with a benefit threshold set at obtaining at least a 15% or more improvement at 24 weeks. Significantly more dalfampridine-ER–treated than placebo-treated patients achieved this threshold (43.4% vs. 34.7%; OR, 1.46; P = .03).
There was a significant improvement between the two study arms on the 29-item physical scale of the Multiple Sclerosis Impact Scale (P less than .001).
However, there was no change seen in upper extremity function, with similar mean changes in the Berg Balance Scale score and the ABILHAND score at 24 weeks. The mean baseline scores for both of these measures were high, Dr. Hobart observed, which probably affected the findings. That said, patients with a baseline EDSS of 6 or higher had greater improvement in ABILHAND scores if they had received dalfampridine-ER, compared with placebo, but the difference was not statistically significant.
The safety profile was consistent with what has been seen in other trials, Dr. Hobart said, and there were no new safety concerns raised.
“The findings from ENHANCE expand and tend to ... confirm the favorable risk-benefit profile established in prior pivotal trials,” he said.
Biogen sponsored the study. Dr. Hobart disclosed receiving fees, honoraria, and research support from Biogen, Acorda, Genzyme, Global Blood Therapeutics, Merck Serono, Novartis, Tigercat, and Vanita.
LONDON – Patients with relapsing-remitting multiple sclerosis reported that their ability to walk was significantly improved following 6 months of treatment with extended-release dalfampridine – compared with patients on placebo – in a double-blind, randomized trial.
In the ENHANCE study, 43.2% of the 315 patients treated with extended-release dalfampridine (dalfampridine-ER; Ampyra) and 33.6% of the 318 who were given placebo achieved a clinically meaningful improvement of 8 or more points on the 12-item MS Walking Scale (MSWS-12) measured at week 24.
The odds ratio (OR) was 1.61, highlighting a significant difference between the two study arms (P = .006).
“This is one of the only studies to use a PRO [patient-reported outcome] as the primary outcome and to use an a priori threshold of clinical meaningfulness,” said Jeremy Hobart, MD, of Plymouth Hospitals NHS Trust (England), who reported the study’s findings at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis. This is an important, and challenging, development in MS trials, he added.
“We are all aware that walking impairments are one of the hallmarks of multiple sclerosis,” Dr. Hobart said, adding that it affects the “vast majority” of patients.
Dalfampridine-ER, which is known as prolonged-release fampridine in Europe, is the only therapy licensed to improve walking in MS, he observed. The pivotal studies that led to the drug’s approval, however, were of relatively short duration and the ENHANCE study was conducted to answer questions that have been raised about the durability of its effect on patients’ mobility.
Patients in ENHANCE received either dalfampridine-ER at a twice-daily dose of 10 mg or placebo for 24 weeks. The mean age of patients in each group was 49 and 48 years, respectively, and 59% and 57% of recruited patients in each arm were female. Patients were stratified according to their baseline Expanded Disability Status Scale (EDSS) score, with 78% and 77% in the dalfampridine-ER and placebo groups having a score of 6 or less.
Dr. Hobart noted that the mean change in MSWS-12 scores over time and an analysis of the cumulative proportion of responders at any particular threshold score on the MWSW-12 showed a clear benefit of dalfampridine-ER treatment over placebo.
The study investigators also assessed patients’ balance via the Timed Up and Go (TUG) test, with a benefit threshold set at obtaining at least a 15% or more improvement at 24 weeks. Significantly more dalfampridine-ER–treated than placebo-treated patients achieved this threshold (43.4% vs. 34.7%; OR, 1.46; P = .03).
There was a significant improvement between the two study arms on the 29-item physical scale of the Multiple Sclerosis Impact Scale (P less than .001).
However, there was no change seen in upper extremity function, with similar mean changes in the Berg Balance Scale score and the ABILHAND score at 24 weeks. The mean baseline scores for both of these measures were high, Dr. Hobart observed, which probably affected the findings. That said, patients with a baseline EDSS of 6 or higher had greater improvement in ABILHAND scores if they had received dalfampridine-ER, compared with placebo, but the difference was not statistically significant.
The safety profile was consistent with what has been seen in other trials, Dr. Hobart said, and there were no new safety concerns raised.
“The findings from ENHANCE expand and tend to ... confirm the favorable risk-benefit profile established in prior pivotal trials,” he said.
Biogen sponsored the study. Dr. Hobart disclosed receiving fees, honoraria, and research support from Biogen, Acorda, Genzyme, Global Blood Therapeutics, Merck Serono, Novartis, Tigercat, and Vanita.
AT ECTRIMS 2016
Key clinical point:The findings support the continued use of extended-release dalfampridine to improve multiple sclerosis patients’ mobility.
Major finding: Twelve-item Multiple Sclerosis Walking Scale scores at 24 weeks were significantly improved in more patients treated with dalfampridine, compared with those on placebo (43.2% vs. 33.6%; OR 1.61, P = .006).
Data source: Double-blind, randomized, placebo-controlled study of 636 patients with relapsing-remitting multiple sclerosis (RRMS) treated with extended-release dalfampridine or placebo for 24 weeks.
Disclosures: Biogen sponsored the study. Dr. Hobart disclosed receiving fees, honoraria, and research support from Biogen, Acorda, Genzyme, Global Blood Therapeutics, Merck Serono, Novartis, Tigercat, and Vanita.

Addressing Hospitalist Burnout with Mindfulness
As compared with the general population, hospitalists are especially prone to stress and burnout, according to an abstract published in the Journal of Hospital Medicine.
The study’s scoring showed that hospitalists started with higher levels of perceived stress than the general population of adults of similar ages. Among hospitalists who attended an average of two mindfulness sessions over five weeks, there was a statistically significant increase in mindfulness and a decrease in perceived stress.
The low number of participants, seven hospitalists, makes extrapolation difficult, but the results are suggestive.
“Even with those seven people, we did see there was a significant difference in their stress and an increase in their mindfulness, which I thought was kind of impressive just for going to only two or three sessions,” says study co-author Dennis Chang, MD, of the Icahn School of Medicine at Mount Sinai. “I think the biggest thing that I would like to see is if it actually improves how we take care of our patients, not just ourselves.”
Dr. Chang says one factor that inspired the study was a hospital survey.
“We do an annual survey of our hospitalists, and it seemed that we had, as a lot of hospital groups do, a burnout problem: People were feeling a little bit burnt out,” Dr. Chang says. “We read some articles on mindfulness, and we thought it might be interesting to see if it would help our hospital.”
Starting this Fall, Mount Sinai will offer a tailored mindfulness session for providers.
“We’re hoping we’ll see if these results really stand up,” Dr. Chang says.
He encourages hospitalists to learn more about mindfulness and to realize that small changes can have an impact.
“Even doing some breathing exercises for a couple of minutes a day can actually make a big difference,” he says. “It doesn’t take a lot of time. Maybe even going to one mindfulness session can give you some tools that you can use. It can make a huge difference in your stress levels and how you take care of patients.”
Reference
- Chablani S, Nguyen VT, Chang D. Mindfulness for hospitalists: a pilot study investigating the effect of a mindfulness initiative on mindfulness and perceived stress among hospitalists [abstract]. J Hosp Med. 2016;11(suppl 1). Accessed September 9, 2016.
As compared with the general population, hospitalists are especially prone to stress and burnout, according to an abstract published in the Journal of Hospital Medicine.
The study’s scoring showed that hospitalists started with higher levels of perceived stress than the general population of adults of similar ages. Among hospitalists who attended an average of two mindfulness sessions over five weeks, there was a statistically significant increase in mindfulness and a decrease in perceived stress.
The low number of participants, seven hospitalists, makes extrapolation difficult, but the results are suggestive.
“Even with those seven people, we did see there was a significant difference in their stress and an increase in their mindfulness, which I thought was kind of impressive just for going to only two or three sessions,” says study co-author Dennis Chang, MD, of the Icahn School of Medicine at Mount Sinai. “I think the biggest thing that I would like to see is if it actually improves how we take care of our patients, not just ourselves.”
Dr. Chang says one factor that inspired the study was a hospital survey.
“We do an annual survey of our hospitalists, and it seemed that we had, as a lot of hospital groups do, a burnout problem: People were feeling a little bit burnt out,” Dr. Chang says. “We read some articles on mindfulness, and we thought it might be interesting to see if it would help our hospital.”
Starting this Fall, Mount Sinai will offer a tailored mindfulness session for providers.
“We’re hoping we’ll see if these results really stand up,” Dr. Chang says.
He encourages hospitalists to learn more about mindfulness and to realize that small changes can have an impact.
“Even doing some breathing exercises for a couple of minutes a day can actually make a big difference,” he says. “It doesn’t take a lot of time. Maybe even going to one mindfulness session can give you some tools that you can use. It can make a huge difference in your stress levels and how you take care of patients.”
Reference
- Chablani S, Nguyen VT, Chang D. Mindfulness for hospitalists: a pilot study investigating the effect of a mindfulness initiative on mindfulness and perceived stress among hospitalists [abstract]. J Hosp Med. 2016;11(suppl 1). Accessed September 9, 2016.
As compared with the general population, hospitalists are especially prone to stress and burnout, according to an abstract published in the Journal of Hospital Medicine.
The study’s scoring showed that hospitalists started with higher levels of perceived stress than the general population of adults of similar ages. Among hospitalists who attended an average of two mindfulness sessions over five weeks, there was a statistically significant increase in mindfulness and a decrease in perceived stress.
The low number of participants, seven hospitalists, makes extrapolation difficult, but the results are suggestive.
“Even with those seven people, we did see there was a significant difference in their stress and an increase in their mindfulness, which I thought was kind of impressive just for going to only two or three sessions,” says study co-author Dennis Chang, MD, of the Icahn School of Medicine at Mount Sinai. “I think the biggest thing that I would like to see is if it actually improves how we take care of our patients, not just ourselves.”
Dr. Chang says one factor that inspired the study was a hospital survey.
“We do an annual survey of our hospitalists, and it seemed that we had, as a lot of hospital groups do, a burnout problem: People were feeling a little bit burnt out,” Dr. Chang says. “We read some articles on mindfulness, and we thought it might be interesting to see if it would help our hospital.”
Starting this Fall, Mount Sinai will offer a tailored mindfulness session for providers.
“We’re hoping we’ll see if these results really stand up,” Dr. Chang says.
He encourages hospitalists to learn more about mindfulness and to realize that small changes can have an impact.
“Even doing some breathing exercises for a couple of minutes a day can actually make a big difference,” he says. “It doesn’t take a lot of time. Maybe even going to one mindfulness session can give you some tools that you can use. It can make a huge difference in your stress levels and how you take care of patients.”
Reference
- Chablani S, Nguyen VT, Chang D. Mindfulness for hospitalists: a pilot study investigating the effect of a mindfulness initiative on mindfulness and perceived stress among hospitalists [abstract]. J Hosp Med. 2016;11(suppl 1). Accessed September 9, 2016.
Hepatitis C Virus Eradication Tied to Fewer Complications in Patients with Cirrhosis
NEW YORK (Reuters Health) - Sustained viral response (SVR) to hepatitis C virus (HCV) treatment is associated with a reduction in liver and non-liver complications in patients with compensated cirrhosis, researchers from France report.
"The achievement of HCV eradication strikingly decreases the risks of liver-related complications, a benefit that was up to now only suggested by retrospective studies," Dr. Pierre Nahon from Hôpital Jean Verdier in Bondy, France, told Reuters Health by email.
"These benefits extend beyond liver-related complications, in particular for cardiovascular disease and MACE (major adverse cardiovascular events) as well as bacterial infection," he said. "These positive effects are translated into survival benefits, whether considering liver-related or extra-hepatic mortality."
Dr. Nahon and colleagues from 35 clinical centers in France evaluated the impact of SVR in 1,671 patients, 1,323 of whom had HCV-related compensated cirrhosis.
After a median follow-up of 58.2 months, 59.5% of patients had a negative viral load, including 668 patients (51.7%) with SVR and 119 HCV-negative patients who were still undergoing antiviral treatment.
Male gender, absence of esophageal varices, and absence of diabetes were independent predictive factors for SVR, the researchers report in Gastroenterology, online the September 15.
SVR was associated with a significantly decreased risk of hepatocellular carcinoma (HCC; hazard ratio, 0.29) and mortality among patients who had HCC at baseline.
Patients who achieved SVR were also 74% less likely to develop liver decompensation during follow-up.
Extrahepatic events - including bacterial infections and cardiovascular events - were less than half as common among patients who achieved SVR than among others, but SVR had no apparent effect on the occurrence of extrahepatic malignancies.
SVR independently predicted a lower risk of hepatic and extrahepatic complications, a finding that was confirmed by a supporting propensity-matching analysis.
SVR was a protective factor for all-cause mortality (HR, 0.27; p<0.001), as well as a predictive factor for survival without liver-related or extrahepatic deaths.
"The present report, with the advantage of a longer follow-up and by studying virological clearance at endpoint as a time-dependent covariate after interferon- or direct-acting antivirals (DAA)-based regimen, now clearly shows that achieving SVR in HCV-infected cirrhotic patients leads to an improved prognosis," the researchers conclude.
"Overall, the present data are able to specifically highlight the independent influence of SVR on the incidence of liver complications, including HCC and mortality and interestingly a positive impact on the occurrence of extrahepatic manifestations," they add.
"However," the team notes, "the achievement of SVR in DAA-treated patients is too recent to draw any definite conclusion on this point, which will require a longer follow-up of the CirVir cohort to be adequately addressed."
"Although HCV eradication is achievable in almost all patients, physicians must be aware of the persisting risk of HCC occurrence in cirrhotic patients despite viral clearance, in particular in case of associated metabolic syndrome," Dr. Nahon cautioned. "These patients must be maintained in liver cancer surveillance programs."
The study did not have commercial funding. Several authors, including Dr. Nahon, reported financial ties to Gilead Sciences and other companies selling drugs for hepatitis C.
NEW YORK (Reuters Health) - Sustained viral response (SVR) to hepatitis C virus (HCV) treatment is associated with a reduction in liver and non-liver complications in patients with compensated cirrhosis, researchers from France report.
"The achievement of HCV eradication strikingly decreases the risks of liver-related complications, a benefit that was up to now only suggested by retrospective studies," Dr. Pierre Nahon from Hôpital Jean Verdier in Bondy, France, told Reuters Health by email.
"These benefits extend beyond liver-related complications, in particular for cardiovascular disease and MACE (major adverse cardiovascular events) as well as bacterial infection," he said. "These positive effects are translated into survival benefits, whether considering liver-related or extra-hepatic mortality."
Dr. Nahon and colleagues from 35 clinical centers in France evaluated the impact of SVR in 1,671 patients, 1,323 of whom had HCV-related compensated cirrhosis.
After a median follow-up of 58.2 months, 59.5% of patients had a negative viral load, including 668 patients (51.7%) with SVR and 119 HCV-negative patients who were still undergoing antiviral treatment.
Male gender, absence of esophageal varices, and absence of diabetes were independent predictive factors for SVR, the researchers report in Gastroenterology, online the September 15.
SVR was associated with a significantly decreased risk of hepatocellular carcinoma (HCC; hazard ratio, 0.29) and mortality among patients who had HCC at baseline.
Patients who achieved SVR were also 74% less likely to develop liver decompensation during follow-up.
Extrahepatic events - including bacterial infections and cardiovascular events - were less than half as common among patients who achieved SVR than among others, but SVR had no apparent effect on the occurrence of extrahepatic malignancies.
SVR independently predicted a lower risk of hepatic and extrahepatic complications, a finding that was confirmed by a supporting propensity-matching analysis.
SVR was a protective factor for all-cause mortality (HR, 0.27; p<0.001), as well as a predictive factor for survival without liver-related or extrahepatic deaths.
"The present report, with the advantage of a longer follow-up and by studying virological clearance at endpoint as a time-dependent covariate after interferon- or direct-acting antivirals (DAA)-based regimen, now clearly shows that achieving SVR in HCV-infected cirrhotic patients leads to an improved prognosis," the researchers conclude.
"Overall, the present data are able to specifically highlight the independent influence of SVR on the incidence of liver complications, including HCC and mortality and interestingly a positive impact on the occurrence of extrahepatic manifestations," they add.
"However," the team notes, "the achievement of SVR in DAA-treated patients is too recent to draw any definite conclusion on this point, which will require a longer follow-up of the CirVir cohort to be adequately addressed."
"Although HCV eradication is achievable in almost all patients, physicians must be aware of the persisting risk of HCC occurrence in cirrhotic patients despite viral clearance, in particular in case of associated metabolic syndrome," Dr. Nahon cautioned. "These patients must be maintained in liver cancer surveillance programs."
The study did not have commercial funding. Several authors, including Dr. Nahon, reported financial ties to Gilead Sciences and other companies selling drugs for hepatitis C.
NEW YORK (Reuters Health) - Sustained viral response (SVR) to hepatitis C virus (HCV) treatment is associated with a reduction in liver and non-liver complications in patients with compensated cirrhosis, researchers from France report.
"The achievement of HCV eradication strikingly decreases the risks of liver-related complications, a benefit that was up to now only suggested by retrospective studies," Dr. Pierre Nahon from Hôpital Jean Verdier in Bondy, France, told Reuters Health by email.
"These benefits extend beyond liver-related complications, in particular for cardiovascular disease and MACE (major adverse cardiovascular events) as well as bacterial infection," he said. "These positive effects are translated into survival benefits, whether considering liver-related or extra-hepatic mortality."
Dr. Nahon and colleagues from 35 clinical centers in France evaluated the impact of SVR in 1,671 patients, 1,323 of whom had HCV-related compensated cirrhosis.
After a median follow-up of 58.2 months, 59.5% of patients had a negative viral load, including 668 patients (51.7%) with SVR and 119 HCV-negative patients who were still undergoing antiviral treatment.
Male gender, absence of esophageal varices, and absence of diabetes were independent predictive factors for SVR, the researchers report in Gastroenterology, online the September 15.
SVR was associated with a significantly decreased risk of hepatocellular carcinoma (HCC; hazard ratio, 0.29) and mortality among patients who had HCC at baseline.
Patients who achieved SVR were also 74% less likely to develop liver decompensation during follow-up.
Extrahepatic events - including bacterial infections and cardiovascular events - were less than half as common among patients who achieved SVR than among others, but SVR had no apparent effect on the occurrence of extrahepatic malignancies.
SVR independently predicted a lower risk of hepatic and extrahepatic complications, a finding that was confirmed by a supporting propensity-matching analysis.
SVR was a protective factor for all-cause mortality (HR, 0.27; p<0.001), as well as a predictive factor for survival without liver-related or extrahepatic deaths.
"The present report, with the advantage of a longer follow-up and by studying virological clearance at endpoint as a time-dependent covariate after interferon- or direct-acting antivirals (DAA)-based regimen, now clearly shows that achieving SVR in HCV-infected cirrhotic patients leads to an improved prognosis," the researchers conclude.
"Overall, the present data are able to specifically highlight the independent influence of SVR on the incidence of liver complications, including HCC and mortality and interestingly a positive impact on the occurrence of extrahepatic manifestations," they add.
"However," the team notes, "the achievement of SVR in DAA-treated patients is too recent to draw any definite conclusion on this point, which will require a longer follow-up of the CirVir cohort to be adequately addressed."
"Although HCV eradication is achievable in almost all patients, physicians must be aware of the persisting risk of HCC occurrence in cirrhotic patients despite viral clearance, in particular in case of associated metabolic syndrome," Dr. Nahon cautioned. "These patients must be maintained in liver cancer surveillance programs."
The study did not have commercial funding. Several authors, including Dr. Nahon, reported financial ties to Gilead Sciences and other companies selling drugs for hepatitis C.
ASCO Expands Its Role in Cancer Care
The American Society of Clinical Oncology (ASCO) is redefining its role in cancer care. In a pair of presentations made at the Association of VA Hematology/Oncology (AVAHO) annual meeting, ASCO President Daniel F. Hayes, MD, FASCO, FACP, and Robin Zon, MD, FACP, FASCO, who chairs ASCO’s Pathways Task Force, each outlined key initiatives that promise to push the organization of more than 40,000 oncology care providers into new areas of research and care.
Rekated: Veteran Cancer Research Highlighted in ASCO Posters and Abstracts
Pathways
Responding to the burgeoning of clinical pathways for cancer care, ASCO stepped in to develop best practices and a better process for determining appropriate pathways. Concern over the lack of consensus on quality, efficiency, and transparency in developing pathways also spurred ASCO to action.
According to Dr. Zon, clinical pathways aims to improve efficient patient care based on evidence-based practices, optimize outcomes, and reduce variations and costs. “Pathways can promote high quality care,” Dr. Zon explained, “but they must be implemented responsibly. They are here to stay.”
The ASCO task force developed 9 recommendations for clinical pathways:
- A collaborative, national approach is necessary to remove administrative burdens.
- The process should be transparent and consistent, including its methodology.
- Pathways should address the full spectrum of cancer care from diagnosis to end of life.
- Pathways should promote the best evidence based care and be updated continuously.
- Patient variability and autonomy should be recognized.
- Pathways should increase efficiency and remove preauthorizations.
- Education, research, and access to clinical trials should be encouraged.
- A robust certification process is essential.
- Pathways developers should support research that examines how pathways impact patients.
Although the pathways currently have a more significant impact in private care settings, it is likely that truly evidence-based pathways can provide an important tool for oncology providers in the federal system.
TAPUR
The Targeted Agent and Profiling Utilization Registry (TAPUR) study is one of ASCO’s first forays into clinical trials and seeks to evaluate multiple the efficacy of precision medicine. Targeted therapies “should be more likely to help the patient,” asks Dr. Hayes, “but do they?” The trial is evaluating multiple molecularly guided therapies in a single master protocol with a common entry point for patients. TAPUR will include commercially available targeted drugs, but in different cancer types, ie, off label. The trial is supported by a number of pharmaceutical companies. For the trial, each tumor type-genomic variant-drug is a group with 19 patients per group. If 3 or fewer patients respond the group is stopped, but if at least 4 patients have a good overall response rate, 14 additional patients will be enrolled, with the prospect of growing further.
Related: ASCO's Chemotherapy Administration Safety Standards
Dr. Hayes also highlighted other key ASCO initiatives. The group is developing a value framework, which will provide an objective means for both patients and providers to assess the relative value for a specific patient of an intended therapy. Different patients may wish to differently weigh endpoints (overall survival [OS], progression-free survival, or response rate). The framework scores a drug based on its clinical benefits, toxicity, and cost among other factors. ASCO also is developing Cancer-LinQ, a data collection and storage system for oncology practices that consolidates data from electronic health records in a central database that can be
aggregated for research.
The American Society of Clinical Oncology (ASCO) is redefining its role in cancer care. In a pair of presentations made at the Association of VA Hematology/Oncology (AVAHO) annual meeting, ASCO President Daniel F. Hayes, MD, FASCO, FACP, and Robin Zon, MD, FACP, FASCO, who chairs ASCO’s Pathways Task Force, each outlined key initiatives that promise to push the organization of more than 40,000 oncology care providers into new areas of research and care.
Rekated: Veteran Cancer Research Highlighted in ASCO Posters and Abstracts
Pathways
Responding to the burgeoning of clinical pathways for cancer care, ASCO stepped in to develop best practices and a better process for determining appropriate pathways. Concern over the lack of consensus on quality, efficiency, and transparency in developing pathways also spurred ASCO to action.
According to Dr. Zon, clinical pathways aims to improve efficient patient care based on evidence-based practices, optimize outcomes, and reduce variations and costs. “Pathways can promote high quality care,” Dr. Zon explained, “but they must be implemented responsibly. They are here to stay.”
The ASCO task force developed 9 recommendations for clinical pathways:
- A collaborative, national approach is necessary to remove administrative burdens.
- The process should be transparent and consistent, including its methodology.
- Pathways should address the full spectrum of cancer care from diagnosis to end of life.
- Pathways should promote the best evidence based care and be updated continuously.
- Patient variability and autonomy should be recognized.
- Pathways should increase efficiency and remove preauthorizations.
- Education, research, and access to clinical trials should be encouraged.
- A robust certification process is essential.
- Pathways developers should support research that examines how pathways impact patients.
Although the pathways currently have a more significant impact in private care settings, it is likely that truly evidence-based pathways can provide an important tool for oncology providers in the federal system.
TAPUR
The Targeted Agent and Profiling Utilization Registry (TAPUR) study is one of ASCO’s first forays into clinical trials and seeks to evaluate multiple the efficacy of precision medicine. Targeted therapies “should be more likely to help the patient,” asks Dr. Hayes, “but do they?” The trial is evaluating multiple molecularly guided therapies in a single master protocol with a common entry point for patients. TAPUR will include commercially available targeted drugs, but in different cancer types, ie, off label. The trial is supported by a number of pharmaceutical companies. For the trial, each tumor type-genomic variant-drug is a group with 19 patients per group. If 3 or fewer patients respond the group is stopped, but if at least 4 patients have a good overall response rate, 14 additional patients will be enrolled, with the prospect of growing further.
Related: ASCO's Chemotherapy Administration Safety Standards
Dr. Hayes also highlighted other key ASCO initiatives. The group is developing a value framework, which will provide an objective means for both patients and providers to assess the relative value for a specific patient of an intended therapy. Different patients may wish to differently weigh endpoints (overall survival [OS], progression-free survival, or response rate). The framework scores a drug based on its clinical benefits, toxicity, and cost among other factors. ASCO also is developing Cancer-LinQ, a data collection and storage system for oncology practices that consolidates data from electronic health records in a central database that can be
aggregated for research.
The American Society of Clinical Oncology (ASCO) is redefining its role in cancer care. In a pair of presentations made at the Association of VA Hematology/Oncology (AVAHO) annual meeting, ASCO President Daniel F. Hayes, MD, FASCO, FACP, and Robin Zon, MD, FACP, FASCO, who chairs ASCO’s Pathways Task Force, each outlined key initiatives that promise to push the organization of more than 40,000 oncology care providers into new areas of research and care.
Rekated: Veteran Cancer Research Highlighted in ASCO Posters and Abstracts
Pathways
Responding to the burgeoning of clinical pathways for cancer care, ASCO stepped in to develop best practices and a better process for determining appropriate pathways. Concern over the lack of consensus on quality, efficiency, and transparency in developing pathways also spurred ASCO to action.
According to Dr. Zon, clinical pathways aims to improve efficient patient care based on evidence-based practices, optimize outcomes, and reduce variations and costs. “Pathways can promote high quality care,” Dr. Zon explained, “but they must be implemented responsibly. They are here to stay.”
The ASCO task force developed 9 recommendations for clinical pathways:
- A collaborative, national approach is necessary to remove administrative burdens.
- The process should be transparent and consistent, including its methodology.
- Pathways should address the full spectrum of cancer care from diagnosis to end of life.
- Pathways should promote the best evidence based care and be updated continuously.
- Patient variability and autonomy should be recognized.
- Pathways should increase efficiency and remove preauthorizations.
- Education, research, and access to clinical trials should be encouraged.
- A robust certification process is essential.
- Pathways developers should support research that examines how pathways impact patients.
Although the pathways currently have a more significant impact in private care settings, it is likely that truly evidence-based pathways can provide an important tool for oncology providers in the federal system.
TAPUR
The Targeted Agent and Profiling Utilization Registry (TAPUR) study is one of ASCO’s first forays into clinical trials and seeks to evaluate multiple the efficacy of precision medicine. Targeted therapies “should be more likely to help the patient,” asks Dr. Hayes, “but do they?” The trial is evaluating multiple molecularly guided therapies in a single master protocol with a common entry point for patients. TAPUR will include commercially available targeted drugs, but in different cancer types, ie, off label. The trial is supported by a number of pharmaceutical companies. For the trial, each tumor type-genomic variant-drug is a group with 19 patients per group. If 3 or fewer patients respond the group is stopped, but if at least 4 patients have a good overall response rate, 14 additional patients will be enrolled, with the prospect of growing further.
Related: ASCO's Chemotherapy Administration Safety Standards
Dr. Hayes also highlighted other key ASCO initiatives. The group is developing a value framework, which will provide an objective means for both patients and providers to assess the relative value for a specific patient of an intended therapy. Different patients may wish to differently weigh endpoints (overall survival [OS], progression-free survival, or response rate). The framework scores a drug based on its clinical benefits, toxicity, and cost among other factors. ASCO also is developing Cancer-LinQ, a data collection and storage system for oncology practices that consolidates data from electronic health records in a central database that can be
aggregated for research.
Don’t Miss the Celebration: AATS Centennial
Help us celebrate the AATS Centennial. Experience activities, events, historical artifacts and memorabilia commemorating the 100th anniversary of the American Association for Thoracic Surgery and the field of cardiothoracic surgery.
April 29 – May 3, 2017
Boston Hynes Convention Center
Boston, MA
A unique aspect of this year’s meeting is our collaboration with the American Society of Extracorporeal Technology (AmSECT). During the didactic portion of the program, the two organizations will be conducting joint panel sessions of interest to all members of the team.
AATS President & Annual Meeting Chair
Thoralf M. Sundt, III
AATS Annual Meeting Co-Chairs
Robert D. Jaquiss & Bryan F. Meyers
AmSECT President
Kenneth Shann
AmSECT International Conference Co-Chairs
Emily Saulitis & Larissa M.V. Teresi
Saturday Courses
Adult Cardiac Skills Chairs
Volkmar Falk, David Fitzgerald, Kenton Zehr
Congenital Skills Chairs
Ron Angona, David Bichell, Bohdan Maruszewski
General Thoracic Skills Chairs
Virginia Litle, Kazuhiro Yasufuku
Cardiothoracic Transplant and Mechanical Circulatory Support of Heart and Lung Failure Chairs
Matthew Bacchetta, Carmelo Milano, Rich Walczak
Surgical Ethics Forum Chairs
Bill DeBois, Martin McKneally, Robert Sade
Sunday Symposia
AATS/STS Adult Cardiac Surgery Symposium Chairs
David Fitzgerald, Hitoshi Ognio, Vinod Thourani
AATS/STS Congenital Heart Disease Symposium Chairs
Ron Angona, Michael Mitchell, Giovanni Stellin
AATS/STS General Thoracic Surgery Symposium Chairs
Seth Force, Moishe Liberman
Interprofessional Cardiothoracic Team Symposium Chairs
Steven Gottesfeld, Katherine Hoercher, Bruce Searles, Glenn Whitman
Saturday Course/Sunday Symposia Program
Share:
Help us celebrate the AATS Centennial. Experience activities, events, historical artifacts and memorabilia commemorating the 100th anniversary of the American Association for Thoracic Surgery and the field of cardiothoracic surgery.
April 29 – May 3, 2017
Boston Hynes Convention Center
Boston, MA
A unique aspect of this year’s meeting is our collaboration with the American Society of Extracorporeal Technology (AmSECT). During the didactic portion of the program, the two organizations will be conducting joint panel sessions of interest to all members of the team.
AATS President & Annual Meeting Chair
Thoralf M. Sundt, III
AATS Annual Meeting Co-Chairs
Robert D. Jaquiss & Bryan F. Meyers
AmSECT President
Kenneth Shann
AmSECT International Conference Co-Chairs
Emily Saulitis & Larissa M.V. Teresi
Saturday Courses
Adult Cardiac Skills Chairs
Volkmar Falk, David Fitzgerald, Kenton Zehr
Congenital Skills Chairs
Ron Angona, David Bichell, Bohdan Maruszewski
General Thoracic Skills Chairs
Virginia Litle, Kazuhiro Yasufuku
Cardiothoracic Transplant and Mechanical Circulatory Support of Heart and Lung Failure Chairs
Matthew Bacchetta, Carmelo Milano, Rich Walczak
Surgical Ethics Forum Chairs
Bill DeBois, Martin McKneally, Robert Sade
Sunday Symposia
AATS/STS Adult Cardiac Surgery Symposium Chairs
David Fitzgerald, Hitoshi Ognio, Vinod Thourani
AATS/STS Congenital Heart Disease Symposium Chairs
Ron Angona, Michael Mitchell, Giovanni Stellin
AATS/STS General Thoracic Surgery Symposium Chairs
Seth Force, Moishe Liberman
Interprofessional Cardiothoracic Team Symposium Chairs
Steven Gottesfeld, Katherine Hoercher, Bruce Searles, Glenn Whitman
Saturday Course/Sunday Symposia Program
Share:
Help us celebrate the AATS Centennial. Experience activities, events, historical artifacts and memorabilia commemorating the 100th anniversary of the American Association for Thoracic Surgery and the field of cardiothoracic surgery.
April 29 – May 3, 2017
Boston Hynes Convention Center
Boston, MA
A unique aspect of this year’s meeting is our collaboration with the American Society of Extracorporeal Technology (AmSECT). During the didactic portion of the program, the two organizations will be conducting joint panel sessions of interest to all members of the team.
AATS President & Annual Meeting Chair
Thoralf M. Sundt, III
AATS Annual Meeting Co-Chairs
Robert D. Jaquiss & Bryan F. Meyers
AmSECT President
Kenneth Shann
AmSECT International Conference Co-Chairs
Emily Saulitis & Larissa M.V. Teresi
Saturday Courses
Adult Cardiac Skills Chairs
Volkmar Falk, David Fitzgerald, Kenton Zehr
Congenital Skills Chairs
Ron Angona, David Bichell, Bohdan Maruszewski
General Thoracic Skills Chairs
Virginia Litle, Kazuhiro Yasufuku
Cardiothoracic Transplant and Mechanical Circulatory Support of Heart and Lung Failure Chairs
Matthew Bacchetta, Carmelo Milano, Rich Walczak
Surgical Ethics Forum Chairs
Bill DeBois, Martin McKneally, Robert Sade
Sunday Symposia
AATS/STS Adult Cardiac Surgery Symposium Chairs
David Fitzgerald, Hitoshi Ognio, Vinod Thourani
AATS/STS Congenital Heart Disease Symposium Chairs
Ron Angona, Michael Mitchell, Giovanni Stellin
AATS/STS General Thoracic Surgery Symposium Chairs
Seth Force, Moishe Liberman
Interprofessional Cardiothoracic Team Symposium Chairs
Steven Gottesfeld, Katherine Hoercher, Bruce Searles, Glenn Whitman
Saturday Course/Sunday Symposia Program
Share:
Improving the Quality of Life and Care for Cancer Survivors
As more and more patients with cancer become cancer survivors, the treatment landscape is changing. Increasingly, primary care providers bear much of the burden of care, but the lack of care coordination and clinical guidelines hamper efforts to care for the growing number of survivors. A number of speakers at the recent Association of VA Hematology/Oncology (AVAHO) sought to address these challenges and report on approaches to improving the quality of care for survivors.
Related: Putting the Focus on Quality of Life in Cancer Care
The VA Survivorship Interest Group (SIG) is trying to raise awareness and facilitate the delivery of high-quality survivorship care to veterans diagnosed with cancer, according to David A. Haggstrom, MD, MAS, of the Indianapolis VA Medical Center and Indiana University School of Medicine. Through monthly meetings, SIG is encouraging new research and promoting initiatives to develop survivorship related products and appropriate models of care delivery.
A Survivorship care plan that includes a treatment summary, and follow-up plan for a patient who has completed cancer treatment is one approach to improve care for cancer survivors. According to Haggstrom, the VA appears to be on track to meet the Commission on Care’s recommendation that ≥ 25% of eligible patients receive a survivorship care plan by the end of 2016, but more work needs to be done to get to the 2017 goal of ≥ 50%.
For example, the more than 2 million prostate cancer survivors have a number of complex problems that pose challenges to VA care providers, according to Ted A. Skolarus, MD, MPH, of the University of Michigan and VA Ann Arbor Healthcare System. Poor urinary control and sexual function can have a significant impact on quality of life for survivors. Furthermore, the lack of organized symptom assessment, clinical guidelines, and other support for patients and providers remains a challenge for providing high-quality care. Much of that burden is born by primary care providers, who are frequently uncomfortable addressing incontinence, impotence, and other psychosocial issues that are common among prostate cancer survivors.
Dr. Skolarus discussed an ongoing randomized self-management trial of veteran prostate cancer survivors, which tested self-management. Patients were assessed using an interactive voice response tool to administer a quality of life survey based on the Expanded Prostate Cancer Index Composite (EPIC), which measures urinary, sexual, bowel, and hormonal/vitality health. Patients are then provided with self-management tools that are specifically developed based on their EPIC responses. The trial is expected to close at the end of 2016.
Related: Cancer Survivorship Care
Sharon L. Bober, PhD, director of the Sexual Health Program at Dana-Farber Cancer Institute, delved in greater detail into the impact of sexual health on quality of life among cancer survivors. The majority of survivors are not prepared to deal with changes in sexual health, Dr. Bober reported, and “more than 50% have profound long lasting dysfunction.” Estimates of sexual dysfunction after cancer range from 40% to 100%, and while the issues for patients with breast or prostate cancer are more obvious, the sexual health problems are not limited to those types of cancer. Moreover, Dr. Bober argued, sexual health involves both physical and psychological aspects and proper treatment should address both.
As more and more patients with cancer become cancer survivors, the treatment landscape is changing. Increasingly, primary care providers bear much of the burden of care, but the lack of care coordination and clinical guidelines hamper efforts to care for the growing number of survivors. A number of speakers at the recent Association of VA Hematology/Oncology (AVAHO) sought to address these challenges and report on approaches to improving the quality of care for survivors.
Related: Putting the Focus on Quality of Life in Cancer Care
The VA Survivorship Interest Group (SIG) is trying to raise awareness and facilitate the delivery of high-quality survivorship care to veterans diagnosed with cancer, according to David A. Haggstrom, MD, MAS, of the Indianapolis VA Medical Center and Indiana University School of Medicine. Through monthly meetings, SIG is encouraging new research and promoting initiatives to develop survivorship related products and appropriate models of care delivery.
A Survivorship care plan that includes a treatment summary, and follow-up plan for a patient who has completed cancer treatment is one approach to improve care for cancer survivors. According to Haggstrom, the VA appears to be on track to meet the Commission on Care’s recommendation that ≥ 25% of eligible patients receive a survivorship care plan by the end of 2016, but more work needs to be done to get to the 2017 goal of ≥ 50%.
For example, the more than 2 million prostate cancer survivors have a number of complex problems that pose challenges to VA care providers, according to Ted A. Skolarus, MD, MPH, of the University of Michigan and VA Ann Arbor Healthcare System. Poor urinary control and sexual function can have a significant impact on quality of life for survivors. Furthermore, the lack of organized symptom assessment, clinical guidelines, and other support for patients and providers remains a challenge for providing high-quality care. Much of that burden is born by primary care providers, who are frequently uncomfortable addressing incontinence, impotence, and other psychosocial issues that are common among prostate cancer survivors.
Dr. Skolarus discussed an ongoing randomized self-management trial of veteran prostate cancer survivors, which tested self-management. Patients were assessed using an interactive voice response tool to administer a quality of life survey based on the Expanded Prostate Cancer Index Composite (EPIC), which measures urinary, sexual, bowel, and hormonal/vitality health. Patients are then provided with self-management tools that are specifically developed based on their EPIC responses. The trial is expected to close at the end of 2016.
Related: Cancer Survivorship Care
Sharon L. Bober, PhD, director of the Sexual Health Program at Dana-Farber Cancer Institute, delved in greater detail into the impact of sexual health on quality of life among cancer survivors. The majority of survivors are not prepared to deal with changes in sexual health, Dr. Bober reported, and “more than 50% have profound long lasting dysfunction.” Estimates of sexual dysfunction after cancer range from 40% to 100%, and while the issues for patients with breast or prostate cancer are more obvious, the sexual health problems are not limited to those types of cancer. Moreover, Dr. Bober argued, sexual health involves both physical and psychological aspects and proper treatment should address both.
As more and more patients with cancer become cancer survivors, the treatment landscape is changing. Increasingly, primary care providers bear much of the burden of care, but the lack of care coordination and clinical guidelines hamper efforts to care for the growing number of survivors. A number of speakers at the recent Association of VA Hematology/Oncology (AVAHO) sought to address these challenges and report on approaches to improving the quality of care for survivors.
Related: Putting the Focus on Quality of Life in Cancer Care
The VA Survivorship Interest Group (SIG) is trying to raise awareness and facilitate the delivery of high-quality survivorship care to veterans diagnosed with cancer, according to David A. Haggstrom, MD, MAS, of the Indianapolis VA Medical Center and Indiana University School of Medicine. Through monthly meetings, SIG is encouraging new research and promoting initiatives to develop survivorship related products and appropriate models of care delivery.
A Survivorship care plan that includes a treatment summary, and follow-up plan for a patient who has completed cancer treatment is one approach to improve care for cancer survivors. According to Haggstrom, the VA appears to be on track to meet the Commission on Care’s recommendation that ≥ 25% of eligible patients receive a survivorship care plan by the end of 2016, but more work needs to be done to get to the 2017 goal of ≥ 50%.
For example, the more than 2 million prostate cancer survivors have a number of complex problems that pose challenges to VA care providers, according to Ted A. Skolarus, MD, MPH, of the University of Michigan and VA Ann Arbor Healthcare System. Poor urinary control and sexual function can have a significant impact on quality of life for survivors. Furthermore, the lack of organized symptom assessment, clinical guidelines, and other support for patients and providers remains a challenge for providing high-quality care. Much of that burden is born by primary care providers, who are frequently uncomfortable addressing incontinence, impotence, and other psychosocial issues that are common among prostate cancer survivors.
Dr. Skolarus discussed an ongoing randomized self-management trial of veteran prostate cancer survivors, which tested self-management. Patients were assessed using an interactive voice response tool to administer a quality of life survey based on the Expanded Prostate Cancer Index Composite (EPIC), which measures urinary, sexual, bowel, and hormonal/vitality health. Patients are then provided with self-management tools that are specifically developed based on their EPIC responses. The trial is expected to close at the end of 2016.
Related: Cancer Survivorship Care
Sharon L. Bober, PhD, director of the Sexual Health Program at Dana-Farber Cancer Institute, delved in greater detail into the impact of sexual health on quality of life among cancer survivors. The majority of survivors are not prepared to deal with changes in sexual health, Dr. Bober reported, and “more than 50% have profound long lasting dysfunction.” Estimates of sexual dysfunction after cancer range from 40% to 100%, and while the issues for patients with breast or prostate cancer are more obvious, the sexual health problems are not limited to those types of cancer. Moreover, Dr. Bober argued, sexual health involves both physical and psychological aspects and proper treatment should address both.
Service can help lymphoma patients find clinical trials

The Lymphoma Association has launched Lymphoma TrialsLink, an online information service that can help lymphoma patients in the UK find clinical trials that might be right for them.
Lymphoma TrialsLink pulls information from different clinical trials databases and puts it in one place.
Lymphoma TrialsLink also provides information about different types of clinical trials and interviews with clinicians and patients who have participated in trials.
The service is available via the Lymphoma Association website: www.lymphomas.org.uk/TrialsLink.
At Lymphoma TrialsLink, patients can search by their type of lymphoma and geographical location to find easy-to-understand information about trials.
At present, treatment trials (phases 1/2 and 2/3), non-drug and non-treatment trials, and cross-tumoral trials that are currently recruiting participants in the UK are available on the Lymphoma TrialsLink website. Information on phase 1, phase 4, and invitation-only trials will be introduced in 2017.
Trial information, which is searchable by type of lymphoma and location, is sourced from a number of databases, including Cancer Research UK trials, UK clinical trials gateway, clinicaltrials.gov, and the NCRI Lymphoma Clinical Studies Group.
The data is verified by the coordinating trial center to ensure that closing dates and trial centers are up-to-date. The content on Lymphoma TrialsLink will be updated monthly.
“Clinical trials are essential for investigating drugs for the treatment of lymphatic cancer and improving survivorship rates,” said Jonathan Pearce, Lymphoma Association chief executive.
“Clinical trials aren’t right for everyone, but we want people to feel empowered to make an informed decision. Lymphoma TrialsLink will mean that lymphoma patients who aren’t currently aware of clinical trials will have the opportunity to find out more about relevant trials and make the best possible decisions about their healthcare.”
A recent Lymphoma Association survey of more than 3000 lymphoma patients* revealed that 78% were not given the option of participating in a clinical trial. Of those who were, the majority joined a trial.
“Lymphoma is the UK’s fifth most common cancer, yet it is neither well-known nor easily understood,” Pearce noted. “We are committed to supporting clinical research to help improve knowledge of lymphoma, to drive advances in treatments, and to deliver better outcomes for people affected by lymphoma.”
Lymphoma TrialsLink is funded by voluntary donations from Lymphoma Association supporters who responded to a fundraising appeal earlier this year. ![]()
*A quality health survey commissioned in 2016 by the Lymphoma Association. The full results of the survey are expected to be published soon.
The Lymphoma Association has launched Lymphoma TrialsLink, an online information service that can help lymphoma patients in the UK find clinical trials that might be right for them.
Lymphoma TrialsLink pulls information from different clinical trials databases and puts it in one place.
Lymphoma TrialsLink also provides information about different types of clinical trials and interviews with clinicians and patients who have participated in trials.
The service is available via the Lymphoma Association website: www.lymphomas.org.uk/TrialsLink.
At Lymphoma TrialsLink, patients can search by their type of lymphoma and geographical location to find easy-to-understand information about trials.
At present, treatment trials (phases 1/2 and 2/3), non-drug and non-treatment trials, and cross-tumoral trials that are currently recruiting participants in the UK are available on the Lymphoma TrialsLink website. Information on phase 1, phase 4, and invitation-only trials will be introduced in 2017.
Trial information, which is searchable by type of lymphoma and location, is sourced from a number of databases, including Cancer Research UK trials, UK clinical trials gateway, clinicaltrials.gov, and the NCRI Lymphoma Clinical Studies Group.
The data is verified by the coordinating trial center to ensure that closing dates and trial centers are up-to-date. The content on Lymphoma TrialsLink will be updated monthly.
“Clinical trials are essential for investigating drugs for the treatment of lymphatic cancer and improving survivorship rates,” said Jonathan Pearce, Lymphoma Association chief executive.
“Clinical trials aren’t right for everyone, but we want people to feel empowered to make an informed decision. Lymphoma TrialsLink will mean that lymphoma patients who aren’t currently aware of clinical trials will have the opportunity to find out more about relevant trials and make the best possible decisions about their healthcare.”
A recent Lymphoma Association survey of more than 3000 lymphoma patients* revealed that 78% were not given the option of participating in a clinical trial. Of those who were, the majority joined a trial.
“Lymphoma is the UK’s fifth most common cancer, yet it is neither well-known nor easily understood,” Pearce noted. “We are committed to supporting clinical research to help improve knowledge of lymphoma, to drive advances in treatments, and to deliver better outcomes for people affected by lymphoma.”
Lymphoma TrialsLink is funded by voluntary donations from Lymphoma Association supporters who responded to a fundraising appeal earlier this year. ![]()
*A quality health survey commissioned in 2016 by the Lymphoma Association. The full results of the survey are expected to be published soon.
The Lymphoma Association has launched Lymphoma TrialsLink, an online information service that can help lymphoma patients in the UK find clinical trials that might be right for them.
Lymphoma TrialsLink pulls information from different clinical trials databases and puts it in one place.
Lymphoma TrialsLink also provides information about different types of clinical trials and interviews with clinicians and patients who have participated in trials.
The service is available via the Lymphoma Association website: www.lymphomas.org.uk/TrialsLink.
At Lymphoma TrialsLink, patients can search by their type of lymphoma and geographical location to find easy-to-understand information about trials.
At present, treatment trials (phases 1/2 and 2/3), non-drug and non-treatment trials, and cross-tumoral trials that are currently recruiting participants in the UK are available on the Lymphoma TrialsLink website. Information on phase 1, phase 4, and invitation-only trials will be introduced in 2017.
Trial information, which is searchable by type of lymphoma and location, is sourced from a number of databases, including Cancer Research UK trials, UK clinical trials gateway, clinicaltrials.gov, and the NCRI Lymphoma Clinical Studies Group.
The data is verified by the coordinating trial center to ensure that closing dates and trial centers are up-to-date. The content on Lymphoma TrialsLink will be updated monthly.
“Clinical trials are essential for investigating drugs for the treatment of lymphatic cancer and improving survivorship rates,” said Jonathan Pearce, Lymphoma Association chief executive.
“Clinical trials aren’t right for everyone, but we want people to feel empowered to make an informed decision. Lymphoma TrialsLink will mean that lymphoma patients who aren’t currently aware of clinical trials will have the opportunity to find out more about relevant trials and make the best possible decisions about their healthcare.”
A recent Lymphoma Association survey of more than 3000 lymphoma patients* revealed that 78% were not given the option of participating in a clinical trial. Of those who were, the majority joined a trial.
“Lymphoma is the UK’s fifth most common cancer, yet it is neither well-known nor easily understood,” Pearce noted. “We are committed to supporting clinical research to help improve knowledge of lymphoma, to drive advances in treatments, and to deliver better outcomes for people affected by lymphoma.”
Lymphoma TrialsLink is funded by voluntary donations from Lymphoma Association supporters who responded to a fundraising appeal earlier this year. ![]()
*A quality health survey commissioned in 2016 by the Lymphoma Association. The full results of the survey are expected to be published soon.