User login
Balancing speed, safety in device approvals
WASHINGTON – Regulators from two continents are slowly inching toward more common ground when it comes to device approvals, a move that should strike a better balance between the time to approval and safety of the products.
It is no surprise that for devices to be approved in the United States, a much more rigorous evidence standard exists than it does in Europe, but the Food and Drug Administration is looking for ways to make changes to allow for quicker approval times without compromising safety.
Meanwhile, across the Atlantic, European regulators are looking for increased evidence requirements that will not stifle innovation.

However, health information technology may help relieve some inefficiencies going forward.
“If we combine quality registries, claims data, the evolving improving electronic health records, and the data warehouses that all of our health systems have, we can conduct prospective, observational, and clinical trials at a dramatically lower cost, answering many more questions per unit of time,” Dr. Califf added.
Other areas that will help improve the efficiency of the U.S. approval process is the work on developing a framework to bring feasibility studies back to America.
“I want to really accelerate that because we are hearing from a lot of people that they want to access the technology early; it’s the right thing to do, and we are hearing from industry that they’d like to work in the United States,” he said.
However, that is going to require one group that is generally more risk adverse to be willing to participate more in the process.
“The main limiting factors at this point in time are the health systems that we are all working in,” Dr. Califf noted. “They are very risk adverse. So while it is nice to argue and advertise that your interventional cardiologists are the best in town on your billboard, protecting those interventional cardiologists to do the high-risk, early studies that are really needed to develop devices is a different matter.”
He called on doctors to go back to their health systems to help better develop those early feasibility pathways to help bring some of that innovation back the United States.
Finally, Dr. Califf addressed the idea of developing evidence that can function not only for device approval, but for payment as well, especially as reimbursement systems are becoming more value driven.
“We are going to move to a system where reimbursement will increasingly move away from fee for service and increasingly gravitate to payment for value,” Dr. Califf said. “In order for this to work, we’ve got to develop the kinds of clinical trials [that include] the calculation of value, so the winners can be promoted on a wider scale and the procedures and technologies that don’t provide incremental value are left behind.”
He continued: “We need your help in figuring out the common source of information so that the FDA can make its decision – which is different from CMS’s decision – but where there’s a continuum of knowledge that allows for products to be approved if they are worthwhile, and then to be paid for and allowed to be marketed.”
Meanwhile, developers are facing a different situation in Europe, where more regulation and more stringent evidence standards could be coming down the pike.
Dr. Fraser noted research that has shown that devices first approved in Europe, compared with their U.S. counterparts, are associated with an increased incidence of recalls or safety alerts.
That being said, he noted that there are several proposed regulations that would increase the evidence requirements related to regulatory approval that manufacturers could face in the coming year, a challenge as it will require some level of harmonization across countries and regulatory systems within each country.
“In Europe, we are on the dawn of a new era regarding medical device assessment, but it is going to pose a very large challenge for our colleagues in the regulatory agencies because of their personnel, funding, and the integration between all these bodies and national systems. There are also tremendous challenges for us as physicians to ensure that we seek the evidence, we assess and contribute to it, and particularly now, that we also routinely take part in new systems for postmarket surveillance,” he said.
WASHINGTON – Regulators from two continents are slowly inching toward more common ground when it comes to device approvals, a move that should strike a better balance between the time to approval and safety of the products.
It is no surprise that for devices to be approved in the United States, a much more rigorous evidence standard exists than it does in Europe, but the Food and Drug Administration is looking for ways to make changes to allow for quicker approval times without compromising safety.
Meanwhile, across the Atlantic, European regulators are looking for increased evidence requirements that will not stifle innovation.
However, health information technology may help relieve some inefficiencies going forward.
“If we combine quality registries, claims data, the evolving improving electronic health records, and the data warehouses that all of our health systems have, we can conduct prospective, observational, and clinical trials at a dramatically lower cost, answering many more questions per unit of time,” Dr. Califf added.
Other areas that will help improve the efficiency of the U.S. approval process is the work on developing a framework to bring feasibility studies back to America.
“I want to really accelerate that because we are hearing from a lot of people that they want to access the technology early; it’s the right thing to do, and we are hearing from industry that they’d like to work in the United States,” he said.
However, that is going to require one group that is generally more risk adverse to be willing to participate more in the process.
“The main limiting factors at this point in time are the health systems that we are all working in,” Dr. Califf noted. “They are very risk adverse. So while it is nice to argue and advertise that your interventional cardiologists are the best in town on your billboard, protecting those interventional cardiologists to do the high-risk, early studies that are really needed to develop devices is a different matter.”
He called on doctors to go back to their health systems to help better develop those early feasibility pathways to help bring some of that innovation back the United States.
Finally, Dr. Califf addressed the idea of developing evidence that can function not only for device approval, but for payment as well, especially as reimbursement systems are becoming more value driven.
“We are going to move to a system where reimbursement will increasingly move away from fee for service and increasingly gravitate to payment for value,” Dr. Califf said. “In order for this to work, we’ve got to develop the kinds of clinical trials [that include] the calculation of value, so the winners can be promoted on a wider scale and the procedures and technologies that don’t provide incremental value are left behind.”
He continued: “We need your help in figuring out the common source of information so that the FDA can make its decision – which is different from CMS’s decision – but where there’s a continuum of knowledge that allows for products to be approved if they are worthwhile, and then to be paid for and allowed to be marketed.”
Meanwhile, developers are facing a different situation in Europe, where more regulation and more stringent evidence standards could be coming down the pike.
Dr. Fraser noted research that has shown that devices first approved in Europe, compared with their U.S. counterparts, are associated with an increased incidence of recalls or safety alerts.
That being said, he noted that there are several proposed regulations that would increase the evidence requirements related to regulatory approval that manufacturers could face in the coming year, a challenge as it will require some level of harmonization across countries and regulatory systems within each country.
“In Europe, we are on the dawn of a new era regarding medical device assessment, but it is going to pose a very large challenge for our colleagues in the regulatory agencies because of their personnel, funding, and the integration between all these bodies and national systems. There are also tremendous challenges for us as physicians to ensure that we seek the evidence, we assess and contribute to it, and particularly now, that we also routinely take part in new systems for postmarket surveillance,” he said.
WASHINGTON – Regulators from two continents are slowly inching toward more common ground when it comes to device approvals, a move that should strike a better balance between the time to approval and safety of the products.
It is no surprise that for devices to be approved in the United States, a much more rigorous evidence standard exists than it does in Europe, but the Food and Drug Administration is looking for ways to make changes to allow for quicker approval times without compromising safety.
Meanwhile, across the Atlantic, European regulators are looking for increased evidence requirements that will not stifle innovation.
However, health information technology may help relieve some inefficiencies going forward.
“If we combine quality registries, claims data, the evolving improving electronic health records, and the data warehouses that all of our health systems have, we can conduct prospective, observational, and clinical trials at a dramatically lower cost, answering many more questions per unit of time,” Dr. Califf added.
Other areas that will help improve the efficiency of the U.S. approval process is the work on developing a framework to bring feasibility studies back to America.
“I want to really accelerate that because we are hearing from a lot of people that they want to access the technology early; it’s the right thing to do, and we are hearing from industry that they’d like to work in the United States,” he said.
However, that is going to require one group that is generally more risk adverse to be willing to participate more in the process.
“The main limiting factors at this point in time are the health systems that we are all working in,” Dr. Califf noted. “They are very risk adverse. So while it is nice to argue and advertise that your interventional cardiologists are the best in town on your billboard, protecting those interventional cardiologists to do the high-risk, early studies that are really needed to develop devices is a different matter.”
He called on doctors to go back to their health systems to help better develop those early feasibility pathways to help bring some of that innovation back the United States.
Finally, Dr. Califf addressed the idea of developing evidence that can function not only for device approval, but for payment as well, especially as reimbursement systems are becoming more value driven.
“We are going to move to a system where reimbursement will increasingly move away from fee for service and increasingly gravitate to payment for value,” Dr. Califf said. “In order for this to work, we’ve got to develop the kinds of clinical trials [that include] the calculation of value, so the winners can be promoted on a wider scale and the procedures and technologies that don’t provide incremental value are left behind.”
He continued: “We need your help in figuring out the common source of information so that the FDA can make its decision – which is different from CMS’s decision – but where there’s a continuum of knowledge that allows for products to be approved if they are worthwhile, and then to be paid for and allowed to be marketed.”
Meanwhile, developers are facing a different situation in Europe, where more regulation and more stringent evidence standards could be coming down the pike.
Dr. Fraser noted research that has shown that devices first approved in Europe, compared with their U.S. counterparts, are associated with an increased incidence of recalls or safety alerts.
That being said, he noted that there are several proposed regulations that would increase the evidence requirements related to regulatory approval that manufacturers could face in the coming year, a challenge as it will require some level of harmonization across countries and regulatory systems within each country.
“In Europe, we are on the dawn of a new era regarding medical device assessment, but it is going to pose a very large challenge for our colleagues in the regulatory agencies because of their personnel, funding, and the integration between all these bodies and national systems. There are also tremendous challenges for us as physicians to ensure that we seek the evidence, we assess and contribute to it, and particularly now, that we also routinely take part in new systems for postmarket surveillance,” he said.
AT TCT 2016
Welcome to the 2016 VEITHsymposium
Welcome to the 43rd annual Vascular & Endovascular, Issues, Techniques and Horizons Symposium (VEITHsymposium). This year’s program promises to be one of the best, most comprehensive, and most thought-provoking of any of our meetings. This year we celebrate our 43rd anniversary and have introduced several improvements.
Nearly 600 international clinician/educators have gathered to provide attendees with the latest topics and advances that are important to the global vascular community. These data span the breadth of vascular diseases, diagnostic procedures, medical treatments, interventional procedures and open surgical advances for treating vascular disease. As is the hallmark of the VEITHsymposium, the 5-day program will run from dawn to dusk daily and will be fully captured in our online library.

Top vascular experts from around the world will provide updates on the latest clinical trials and offer insight into the real-life application of the most recent data to close the gap between the current state of knowledge and actual clinical practice.
Controversial issues will be approached from multiple perspectives to ensure a balanced, unbiased exposure of topics and to provide audience members with the information they need to make informed choices in their own practices.
This year our meeting continues its increased emphasis on venous disease. Three full days of the meeting are developments in venous disease of all sorts and active endovascular treatments in this rapidly expanding area of opportunity.
Some of the program’s other hot topics will be the continuing controversies surrounding parallel grafts (chimneys, and snorkel and sandwich grafts); multilayer open stents versus fenestrated and branched endografts; new developments in carotid stenting; new developments in the treatment of aortic dissections; a day devoted to the management of arteriovenous malformations (AVMs); new developments in the endovascular treatment of lower-extremity ischemia, particularly below the knee; the latest developments in EVAR and TEVAR including experiences with a plethora of new endovascular grafts and devices that have appeared on the scene in the last year; and improvements in the medical treatment of vascular disease and vascular patients undergoing surgery and other interventions. Important issues to vascular specialists and outpatient vascular treatment will also be highlighted.
This year’s program will include a special session all-day Tuesday, focused in the morning on management options for pulmonary embolism led by Dr. Michael R. Jaff. The afternoon part of the day will focus on new developments in the management of acute and chronic large vein occlusion, and will be led by Dr. Kenneth Ouriel.
This year there will also be sessions devoted to crucial issues for vascular specialists including changing relationships with government and the FDA and how to survive under new reimbursement rules and regulations including Obamacare. Our physician/educators will also offer a glimpse into some new techniques and technologies that have been available overseas, but are just gaining approval in the United States, such as drug-eluting balloons and stents.
Attendees will notice some other exciting changes or additions to this year’s program. We have included a new Job Fair Program on Friday in the Americas Hall 1 on the 3rd floor. In addition, there will be more breaks in the schedule to encourage exploration of state-of-the-art technology, products, and services available in the Exhibit areas and Pavilions. The Exhibit Halls are crowded with displays and booths of particular interest to vascular surgeons and vascular specialists. The Pavilions and Exhibits also offer attendees the chance to meet faculty and to network with other attendees and industry partners. This is one place to learn more about exciting new technologies and developments in our field.
Other new additions to our meeting this year will be an exciting Abbott Pavilion in the Americas Hall as well as an expanded Innovations and Investment Summit which facilitates interaction between innovators, industry and investors. This non-CME Session will be held from 8 AM to 3 PM on Thursday, November 17th in the Gramercy Suites on the 2nd floor, and will be led by Kenneth Ouriel, Jean Bismuth and Chris Cheng.
Also new this year will be an expanded VEITHsymposium mobile app, provided courtesy of Cook Medical. Download the app for your iPhone, iPad or Android phone or tablet! Search the App Store (iPhone/iPad) or Google Play Store (Android) for “VEITHsymposium 2016” and install the app. You will be able to access the complete program, create your personal program, add your notes, view the location of sessions and exhibitors on the floor plan, and much more. After you have installed the app and opened it for the first time, you can continue to use it offline. To receive the latest updates and announcements, you will need to be connected to the internet.
In addition, there will be expanded Associate Faculty programs which will give younger and less well-known vascular specialists the opportunity to present their work at the podium with leading experts as session moderators.
Again this year, an Online Library will be available for a minimal fee of $75 for clinical meeting attendees and will include access to talks, slides, videos, and panels from the meeting. This Library will enable all attendees to see and hear key presentations they may miss because of the concurrent sessions or other reasons. This library will be available 10-14 days after the meeting. Attendees should note in their program talks they wish to hear but could not, and then revisit the missed talks on the Online Library which is indexed exactly to the program. The talks are also indexed in the Library by presenter, topic, or session. This Library is a great resource for study, research or review for any purpose.
On behalf of all the meeting Co-Chairmen and our entire staff, we greatly appreciate you coming to our meeting. We hope it is our best meeting ever and that you find it educational, most useful and exciting so that you return next year.
Welcome to the 43rd annual Vascular & Endovascular, Issues, Techniques and Horizons Symposium (VEITHsymposium). This year’s program promises to be one of the best, most comprehensive, and most thought-provoking of any of our meetings. This year we celebrate our 43rd anniversary and have introduced several improvements.
Nearly 600 international clinician/educators have gathered to provide attendees with the latest topics and advances that are important to the global vascular community. These data span the breadth of vascular diseases, diagnostic procedures, medical treatments, interventional procedures and open surgical advances for treating vascular disease. As is the hallmark of the VEITHsymposium, the 5-day program will run from dawn to dusk daily and will be fully captured in our online library.
Top vascular experts from around the world will provide updates on the latest clinical trials and offer insight into the real-life application of the most recent data to close the gap between the current state of knowledge and actual clinical practice.
Controversial issues will be approached from multiple perspectives to ensure a balanced, unbiased exposure of topics and to provide audience members with the information they need to make informed choices in their own practices.
This year our meeting continues its increased emphasis on venous disease. Three full days of the meeting are developments in venous disease of all sorts and active endovascular treatments in this rapidly expanding area of opportunity.
Some of the program’s other hot topics will be the continuing controversies surrounding parallel grafts (chimneys, and snorkel and sandwich grafts); multilayer open stents versus fenestrated and branched endografts; new developments in carotid stenting; new developments in the treatment of aortic dissections; a day devoted to the management of arteriovenous malformations (AVMs); new developments in the endovascular treatment of lower-extremity ischemia, particularly below the knee; the latest developments in EVAR and TEVAR including experiences with a plethora of new endovascular grafts and devices that have appeared on the scene in the last year; and improvements in the medical treatment of vascular disease and vascular patients undergoing surgery and other interventions. Important issues to vascular specialists and outpatient vascular treatment will also be highlighted.
This year’s program will include a special session all-day Tuesday, focused in the morning on management options for pulmonary embolism led by Dr. Michael R. Jaff. The afternoon part of the day will focus on new developments in the management of acute and chronic large vein occlusion, and will be led by Dr. Kenneth Ouriel.
This year there will also be sessions devoted to crucial issues for vascular specialists including changing relationships with government and the FDA and how to survive under new reimbursement rules and regulations including Obamacare. Our physician/educators will also offer a glimpse into some new techniques and technologies that have been available overseas, but are just gaining approval in the United States, such as drug-eluting balloons and stents.
Attendees will notice some other exciting changes or additions to this year’s program. We have included a new Job Fair Program on Friday in the Americas Hall 1 on the 3rd floor. In addition, there will be more breaks in the schedule to encourage exploration of state-of-the-art technology, products, and services available in the Exhibit areas and Pavilions. The Exhibit Halls are crowded with displays and booths of particular interest to vascular surgeons and vascular specialists. The Pavilions and Exhibits also offer attendees the chance to meet faculty and to network with other attendees and industry partners. This is one place to learn more about exciting new technologies and developments in our field.
Other new additions to our meeting this year will be an exciting Abbott Pavilion in the Americas Hall as well as an expanded Innovations and Investment Summit which facilitates interaction between innovators, industry and investors. This non-CME Session will be held from 8 AM to 3 PM on Thursday, November 17th in the Gramercy Suites on the 2nd floor, and will be led by Kenneth Ouriel, Jean Bismuth and Chris Cheng.
Also new this year will be an expanded VEITHsymposium mobile app, provided courtesy of Cook Medical. Download the app for your iPhone, iPad or Android phone or tablet! Search the App Store (iPhone/iPad) or Google Play Store (Android) for “VEITHsymposium 2016” and install the app. You will be able to access the complete program, create your personal program, add your notes, view the location of sessions and exhibitors on the floor plan, and much more. After you have installed the app and opened it for the first time, you can continue to use it offline. To receive the latest updates and announcements, you will need to be connected to the internet.
In addition, there will be expanded Associate Faculty programs which will give younger and less well-known vascular specialists the opportunity to present their work at the podium with leading experts as session moderators.
Again this year, an Online Library will be available for a minimal fee of $75 for clinical meeting attendees and will include access to talks, slides, videos, and panels from the meeting. This Library will enable all attendees to see and hear key presentations they may miss because of the concurrent sessions or other reasons. This library will be available 10-14 days after the meeting. Attendees should note in their program talks they wish to hear but could not, and then revisit the missed talks on the Online Library which is indexed exactly to the program. The talks are also indexed in the Library by presenter, topic, or session. This Library is a great resource for study, research or review for any purpose.
On behalf of all the meeting Co-Chairmen and our entire staff, we greatly appreciate you coming to our meeting. We hope it is our best meeting ever and that you find it educational, most useful and exciting so that you return next year.
Welcome to the 43rd annual Vascular & Endovascular, Issues, Techniques and Horizons Symposium (VEITHsymposium). This year’s program promises to be one of the best, most comprehensive, and most thought-provoking of any of our meetings. This year we celebrate our 43rd anniversary and have introduced several improvements.
Nearly 600 international clinician/educators have gathered to provide attendees with the latest topics and advances that are important to the global vascular community. These data span the breadth of vascular diseases, diagnostic procedures, medical treatments, interventional procedures and open surgical advances for treating vascular disease. As is the hallmark of the VEITHsymposium, the 5-day program will run from dawn to dusk daily and will be fully captured in our online library.
Top vascular experts from around the world will provide updates on the latest clinical trials and offer insight into the real-life application of the most recent data to close the gap between the current state of knowledge and actual clinical practice.
Controversial issues will be approached from multiple perspectives to ensure a balanced, unbiased exposure of topics and to provide audience members with the information they need to make informed choices in their own practices.
This year our meeting continues its increased emphasis on venous disease. Three full days of the meeting are developments in venous disease of all sorts and active endovascular treatments in this rapidly expanding area of opportunity.
Some of the program’s other hot topics will be the continuing controversies surrounding parallel grafts (chimneys, and snorkel and sandwich grafts); multilayer open stents versus fenestrated and branched endografts; new developments in carotid stenting; new developments in the treatment of aortic dissections; a day devoted to the management of arteriovenous malformations (AVMs); new developments in the endovascular treatment of lower-extremity ischemia, particularly below the knee; the latest developments in EVAR and TEVAR including experiences with a plethora of new endovascular grafts and devices that have appeared on the scene in the last year; and improvements in the medical treatment of vascular disease and vascular patients undergoing surgery and other interventions. Important issues to vascular specialists and outpatient vascular treatment will also be highlighted.
This year’s program will include a special session all-day Tuesday, focused in the morning on management options for pulmonary embolism led by Dr. Michael R. Jaff. The afternoon part of the day will focus on new developments in the management of acute and chronic large vein occlusion, and will be led by Dr. Kenneth Ouriel.
This year there will also be sessions devoted to crucial issues for vascular specialists including changing relationships with government and the FDA and how to survive under new reimbursement rules and regulations including Obamacare. Our physician/educators will also offer a glimpse into some new techniques and technologies that have been available overseas, but are just gaining approval in the United States, such as drug-eluting balloons and stents.
Attendees will notice some other exciting changes or additions to this year’s program. We have included a new Job Fair Program on Friday in the Americas Hall 1 on the 3rd floor. In addition, there will be more breaks in the schedule to encourage exploration of state-of-the-art technology, products, and services available in the Exhibit areas and Pavilions. The Exhibit Halls are crowded with displays and booths of particular interest to vascular surgeons and vascular specialists. The Pavilions and Exhibits also offer attendees the chance to meet faculty and to network with other attendees and industry partners. This is one place to learn more about exciting new technologies and developments in our field.
Other new additions to our meeting this year will be an exciting Abbott Pavilion in the Americas Hall as well as an expanded Innovations and Investment Summit which facilitates interaction between innovators, industry and investors. This non-CME Session will be held from 8 AM to 3 PM on Thursday, November 17th in the Gramercy Suites on the 2nd floor, and will be led by Kenneth Ouriel, Jean Bismuth and Chris Cheng.
Also new this year will be an expanded VEITHsymposium mobile app, provided courtesy of Cook Medical. Download the app for your iPhone, iPad or Android phone or tablet! Search the App Store (iPhone/iPad) or Google Play Store (Android) for “VEITHsymposium 2016” and install the app. You will be able to access the complete program, create your personal program, add your notes, view the location of sessions and exhibitors on the floor plan, and much more. After you have installed the app and opened it for the first time, you can continue to use it offline. To receive the latest updates and announcements, you will need to be connected to the internet.
In addition, there will be expanded Associate Faculty programs which will give younger and less well-known vascular specialists the opportunity to present their work at the podium with leading experts as session moderators.
Again this year, an Online Library will be available for a minimal fee of $75 for clinical meeting attendees and will include access to talks, slides, videos, and panels from the meeting. This Library will enable all attendees to see and hear key presentations they may miss because of the concurrent sessions or other reasons. This library will be available 10-14 days after the meeting. Attendees should note in their program talks they wish to hear but could not, and then revisit the missed talks on the Online Library which is indexed exactly to the program. The talks are also indexed in the Library by presenter, topic, or session. This Library is a great resource for study, research or review for any purpose.
On behalf of all the meeting Co-Chairmen and our entire staff, we greatly appreciate you coming to our meeting. We hope it is our best meeting ever and that you find it educational, most useful and exciting so that you return next year.
Give guidance, not just Viagra, to men with diabetes and related impotence
Diabetic men with erectile dysfunction might consider a prescription for a drug like Viagra to be a permanent cure for a temporary issue: Take a pill, problem solved. But the truth, a leading urologist says, is entirely different.
“If a diabetic patient has erectile dysfunction, it’s not enough to provide Viagra [sildenafil] or Cialis [tadalafil] and then send him on his merry way,” J. Francois Eid, MD, a New York City urologist, said at the annual meeting of the American Association of Diabetes Educators. “It’s important to let individuals know the drug has not cured the erectile dysfunction. If patients don’t take care of the diabetes, the erectile dysfunction progresses.”
In an interview, Dr. Eid shared several messages for medical professionals who treat men with diabetes and related erectile dysfunction:
• Diabetes has “devastating” effects on the penis, and may even cause it to shrink.
• Long-term uncontrolled diabetes can make ED permanent.
• While ED drugs often fail in men with diabetes, several other options exist; and penis implants may provide significant relief.
How big is the problem? An estimated 50%-75% of men with diabetes experience from some degree of ED, which is thought to be three times more common in diabetic men than other men, according to Dr. Eid.
“Diabetes has a devastating effect on the muscle tissue inside the penis,” he said. “All the tiny little arteries that feed blood to the muscle get occluded. Little by little, the muscle inside the penis shrinks.” Indeed, some diabetics with ED complain that their penises have shrunk, he said.
Diabetic damage doesn’t stop with these small vessels, he said. “You really have two parallel situations: You need blood flow that feeds the muscle of the penis, and you need an artery dedicated to bringing blood rapidly when a man becomes aroused and wants to be sexually active,” he said. “That artery is also affected by diabetes. They’ll say ‘I can get a partial erection, but I can’t maintain it.’ ”
What comes after an ED diagnosis in diabetic patients? Often, Dr. Eid will instantly refer these men to a cardiologist. “If a patient has diabetes and is newly diagnosed, a significant portion of these men are going to develop coronary artery disease in the next 2-3 years,” he said. “One of the things we do is recommend is that they see a cardiologist and perhaps have a stress test or some sort of evaluation.”
Dr. Eid also urges these patients to treat their diabetes in order to avoid developing ED for life. “They need to manage their diabetes and make sure they control it so the ED will not progress and will stabilize, as a result,” he said. “If the diabetes is controlled after the patient is first diagnosed, then the erections will come back. But if the patient has diabetes for many years, and suddenly decides it’s time to control it, they cannot prevent the damage that’s already been done.”
As for treatments, patients with diabetes and related ED should begin with medications like sildenafil and tadalafil, he recommended. But research findings suggest that the drugs will fail in half of men with type 2 diabetes, he said.
Other options include penile self-injections, vacuum devices, and penile implants.
The injections “can work well and are painless, but men detest having to inject themselves before sexual activity,” Dr. Eid said. And he said men rarely have success using vacuum devices, which are available over the counter.
By contrast, penis implants can successfully treat erectile dysfunction in many cases, Dr. Eid said. Men trigger erections by squeezing a pump that is implanted into the scrotum. Fluid then flows from an implanted reservoir into a cylinder implanted in the penis.
Men are often pleased by penis implants because they can have sex spontaneously without having to plan for it ahead of time, as required by medications. “They’re completely transformed,” Dr. Eid said. “They feel that they’re cured.”
Dr. Eid receives or has received research support/grants from American Medical Systems, Coloplast, Lilly ICOS, Bayer, Vivus, Pharmacia-Upjohn, and Pfizer. He is or was a consultant and on the speakers bureau for Coloplast, American Medical Systems, Lilly ICOS, Bayer and Pfizer.
Diabetic men with erectile dysfunction might consider a prescription for a drug like Viagra to be a permanent cure for a temporary issue: Take a pill, problem solved. But the truth, a leading urologist says, is entirely different.
“If a diabetic patient has erectile dysfunction, it’s not enough to provide Viagra [sildenafil] or Cialis [tadalafil] and then send him on his merry way,” J. Francois Eid, MD, a New York City urologist, said at the annual meeting of the American Association of Diabetes Educators. “It’s important to let individuals know the drug has not cured the erectile dysfunction. If patients don’t take care of the diabetes, the erectile dysfunction progresses.”
In an interview, Dr. Eid shared several messages for medical professionals who treat men with diabetes and related erectile dysfunction:
• Diabetes has “devastating” effects on the penis, and may even cause it to shrink.
• Long-term uncontrolled diabetes can make ED permanent.
• While ED drugs often fail in men with diabetes, several other options exist; and penis implants may provide significant relief.
How big is the problem? An estimated 50%-75% of men with diabetes experience from some degree of ED, which is thought to be three times more common in diabetic men than other men, according to Dr. Eid.
“Diabetes has a devastating effect on the muscle tissue inside the penis,” he said. “All the tiny little arteries that feed blood to the muscle get occluded. Little by little, the muscle inside the penis shrinks.” Indeed, some diabetics with ED complain that their penises have shrunk, he said.
Diabetic damage doesn’t stop with these small vessels, he said. “You really have two parallel situations: You need blood flow that feeds the muscle of the penis, and you need an artery dedicated to bringing blood rapidly when a man becomes aroused and wants to be sexually active,” he said. “That artery is also affected by diabetes. They’ll say ‘I can get a partial erection, but I can’t maintain it.’ ”
What comes after an ED diagnosis in diabetic patients? Often, Dr. Eid will instantly refer these men to a cardiologist. “If a patient has diabetes and is newly diagnosed, a significant portion of these men are going to develop coronary artery disease in the next 2-3 years,” he said. “One of the things we do is recommend is that they see a cardiologist and perhaps have a stress test or some sort of evaluation.”
Dr. Eid also urges these patients to treat their diabetes in order to avoid developing ED for life. “They need to manage their diabetes and make sure they control it so the ED will not progress and will stabilize, as a result,” he said. “If the diabetes is controlled after the patient is first diagnosed, then the erections will come back. But if the patient has diabetes for many years, and suddenly decides it’s time to control it, they cannot prevent the damage that’s already been done.”
As for treatments, patients with diabetes and related ED should begin with medications like sildenafil and tadalafil, he recommended. But research findings suggest that the drugs will fail in half of men with type 2 diabetes, he said.
Other options include penile self-injections, vacuum devices, and penile implants.
The injections “can work well and are painless, but men detest having to inject themselves before sexual activity,” Dr. Eid said. And he said men rarely have success using vacuum devices, which are available over the counter.
By contrast, penis implants can successfully treat erectile dysfunction in many cases, Dr. Eid said. Men trigger erections by squeezing a pump that is implanted into the scrotum. Fluid then flows from an implanted reservoir into a cylinder implanted in the penis.
Men are often pleased by penis implants because they can have sex spontaneously without having to plan for it ahead of time, as required by medications. “They’re completely transformed,” Dr. Eid said. “They feel that they’re cured.”
Dr. Eid receives or has received research support/grants from American Medical Systems, Coloplast, Lilly ICOS, Bayer, Vivus, Pharmacia-Upjohn, and Pfizer. He is or was a consultant and on the speakers bureau for Coloplast, American Medical Systems, Lilly ICOS, Bayer and Pfizer.
Diabetic men with erectile dysfunction might consider a prescription for a drug like Viagra to be a permanent cure for a temporary issue: Take a pill, problem solved. But the truth, a leading urologist says, is entirely different.
“If a diabetic patient has erectile dysfunction, it’s not enough to provide Viagra [sildenafil] or Cialis [tadalafil] and then send him on his merry way,” J. Francois Eid, MD, a New York City urologist, said at the annual meeting of the American Association of Diabetes Educators. “It’s important to let individuals know the drug has not cured the erectile dysfunction. If patients don’t take care of the diabetes, the erectile dysfunction progresses.”
In an interview, Dr. Eid shared several messages for medical professionals who treat men with diabetes and related erectile dysfunction:
• Diabetes has “devastating” effects on the penis, and may even cause it to shrink.
• Long-term uncontrolled diabetes can make ED permanent.
• While ED drugs often fail in men with diabetes, several other options exist; and penis implants may provide significant relief.
How big is the problem? An estimated 50%-75% of men with diabetes experience from some degree of ED, which is thought to be three times more common in diabetic men than other men, according to Dr. Eid.
“Diabetes has a devastating effect on the muscle tissue inside the penis,” he said. “All the tiny little arteries that feed blood to the muscle get occluded. Little by little, the muscle inside the penis shrinks.” Indeed, some diabetics with ED complain that their penises have shrunk, he said.
Diabetic damage doesn’t stop with these small vessels, he said. “You really have two parallel situations: You need blood flow that feeds the muscle of the penis, and you need an artery dedicated to bringing blood rapidly when a man becomes aroused and wants to be sexually active,” he said. “That artery is also affected by diabetes. They’ll say ‘I can get a partial erection, but I can’t maintain it.’ ”
What comes after an ED diagnosis in diabetic patients? Often, Dr. Eid will instantly refer these men to a cardiologist. “If a patient has diabetes and is newly diagnosed, a significant portion of these men are going to develop coronary artery disease in the next 2-3 years,” he said. “One of the things we do is recommend is that they see a cardiologist and perhaps have a stress test or some sort of evaluation.”
Dr. Eid also urges these patients to treat their diabetes in order to avoid developing ED for life. “They need to manage their diabetes and make sure they control it so the ED will not progress and will stabilize, as a result,” he said. “If the diabetes is controlled after the patient is first diagnosed, then the erections will come back. But if the patient has diabetes for many years, and suddenly decides it’s time to control it, they cannot prevent the damage that’s already been done.”
As for treatments, patients with diabetes and related ED should begin with medications like sildenafil and tadalafil, he recommended. But research findings suggest that the drugs will fail in half of men with type 2 diabetes, he said.
Other options include penile self-injections, vacuum devices, and penile implants.
The injections “can work well and are painless, but men detest having to inject themselves before sexual activity,” Dr. Eid said. And he said men rarely have success using vacuum devices, which are available over the counter.
By contrast, penis implants can successfully treat erectile dysfunction in many cases, Dr. Eid said. Men trigger erections by squeezing a pump that is implanted into the scrotum. Fluid then flows from an implanted reservoir into a cylinder implanted in the penis.
Men are often pleased by penis implants because they can have sex spontaneously without having to plan for it ahead of time, as required by medications. “They’re completely transformed,” Dr. Eid said. “They feel that they’re cured.”
Dr. Eid receives or has received research support/grants from American Medical Systems, Coloplast, Lilly ICOS, Bayer, Vivus, Pharmacia-Upjohn, and Pfizer. He is or was a consultant and on the speakers bureau for Coloplast, American Medical Systems, Lilly ICOS, Bayer and Pfizer.
EXPERT ANALYSIS FROM AADE 16
An enlightened approach to weight loss using liraglutide
NEW ORLEANS – Early weight loss on liraglutide – specifically, dropping at least 4% of body weight at 16 weeks – is a strong and clinically useful identifier of patients with a high likelihood of significant weight loss 13 months into treatment, with an accompanying improvement in cardiometabolic risk factors, according to Ken Fujioka, MD.
Conversely, patients who aren’t early responders to subcutaneous liraglutide at 3 mg/day are unlikely to achieve at least 5% weight loss after a full year on the drug, the regulatory benchmark for clinically meaningful weight loss, added Dr. Fujioka, an internist and director of the center for weight management at the Scripps Clinic in La Jolla, Calif.
“Using this early response criterion at week 16 to predict long-term weight loss is to me a very valuable tool. Obesity is an odd disease because it has so many different causes. Finding the right drug is tough, and how long to keep trying with a particular medication is something we haven’t known. So I think the biggest change in obesity medicine is the creation of stopping rules that allow you to say, ‘OK, maybe this isn’t going to work. There’s some other reason you’re gaining weight, so let’s move on to something else,’” Dr. Fujioka said at the meeting presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
“When you stop the medication, you improve the risk-benefit ratio by removing all risk. That’s a win-win to me, and I applaud the FDA for getting on the pharmaceutical companies to make sure they put stopping rules in their medication labels,” he added.
He presented a post hoc pooled analysis of two previously published large, double-blind phase III clinical trials of subcutaneous liraglutide at 3 mg/day (Saxenda) or placebo in combination with a diet and exercise intervention for weight loss: the 3,731-patient SCALE Obesity and Prediabetes trial and the 846-patient SCALE Diabetes trial. In both trials liraglutide was started at a dose of 0.6 mg and titrated to 3.0 mg by week 4. The lifestyle intervention entailed a 500-kcal/day deficit diet and a minimum of 150 minutes of physical activity per week.
The purpose of the pooled analysis was to identify the best early predictor of response status at 56 weeks by examining the impact of 3%, 4%, and 5% weight loss after 8, 12, and 16 weeks of treatment as cut points. This post hoc analysis was prespecified at the request of the Food and Drug Administration before the trials were completed.
The bottom line: The best predictor of long-term outcome on liraglutide, a glucagonlike peptide–1 analog, proved to be a weight loss of 4% or greater at 16 weeks. It had an 81% positive predictive value and a 76% negative predictive value for at least a 5% weight loss at 56 weeks. It correctly predicted weight outcomes at 56 weeks in 80.1% of patients, the highest success rate of all the combinations studied. This finding was the impetus for the current product labeling, which contains the stopping rule. Dr. Fujioka shared study data not included in the labeling; namely, the marked contrast in how early responders and early nonresponders fared at 56 weeks.
The mean weight loss at 56 weeks in nondiabetic early responders to liraglutide was 10.8%, compared with only 3% in early nondiabetic nonresponders. Diabetic early responders averaged an 8.5% weight loss at 56 weeks, while early nonresponders had a mean 3.1% weight loss.
In the SCALE Obesity and Prediabetes trial, 50% of early responders to liraglutide ended up with a greater than 10% weight loss at 56 weeks, and 21% had more than 15% weight loss, compared with rates of 6% and 2%, respectively, in early nonresponders.
In the SCALE Diabetes study, 38% of early responders had greater than 10% weight loss long term, a rate nearly fourfold higher than in early nonresponders. Moreover, 10% of early responder diabetic patients had greater than 15% weight loss, versus a mere 2% of early nonresponders, the internist continued.
The ratio of early responders to early nonresponders in the nondiabetic population was 77%:23%. In diabetic patients, it was 63%:37%.
Turning to cardiometabolic endpoints, Dr. Fujioka noted that early responders in the SCALE Obesity and Prediabetes trial went on to show a mean reduction in systolic blood pressure of 5.1 mm Hg at 56 weeks, compared with a 2–mm Hg decrease in early nonresponders. Early responders also averaged a 10.5-cm shrinkage in waist circumference from a baseline of 115 cm, which was more than twice that observed at 56 weeks in early nonresponders. HDL-cholesterol level rose by 3.9% in early responders but remained unchanged over time in early nonresponders.
Diabetic patients who were early responders to liraglutide 3.0 mg/day had a mean 44.2-mg/dL reduction in fasting plasma glucose at 56 weeks from a baseline of 158 mg/dL, compared with a 30.1-mg/dL decrease in early nonresponders.
“The drop in fasting blood glucose is very quick – within a matter of weeks – so if you already have diabetic patients on drugs that are going to bring their blood sugar down, you may have to back titrate those other drugs really quickly. You don’t want to make your patients hypoglycemic,” the physician said.
Mean hemoglobin A1c values in early responder diabetic patients fell by 1.6% from a baseline of 7.9%, a full 0.5% greater reduction than in early nonresponders.
By far the most frequent adverse events in the two SCALE trials were gastrointestinal, with nausea leading the way. Rates were modestly higher in the early responders.
This analysis and the clinical trials on which it was based were sponsored by Novo Nordisk, which markets liraglutide under the brand names Saxenda and Voctoza. The presenter reported receiving research grants from and serving as a consultant to Novo Nordisk and other pharmaceutical companies.
NEW ORLEANS – Early weight loss on liraglutide – specifically, dropping at least 4% of body weight at 16 weeks – is a strong and clinically useful identifier of patients with a high likelihood of significant weight loss 13 months into treatment, with an accompanying improvement in cardiometabolic risk factors, according to Ken Fujioka, MD.
Conversely, patients who aren’t early responders to subcutaneous liraglutide at 3 mg/day are unlikely to achieve at least 5% weight loss after a full year on the drug, the regulatory benchmark for clinically meaningful weight loss, added Dr. Fujioka, an internist and director of the center for weight management at the Scripps Clinic in La Jolla, Calif.
“Using this early response criterion at week 16 to predict long-term weight loss is to me a very valuable tool. Obesity is an odd disease because it has so many different causes. Finding the right drug is tough, and how long to keep trying with a particular medication is something we haven’t known. So I think the biggest change in obesity medicine is the creation of stopping rules that allow you to say, ‘OK, maybe this isn’t going to work. There’s some other reason you’re gaining weight, so let’s move on to something else,’” Dr. Fujioka said at the meeting presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
“When you stop the medication, you improve the risk-benefit ratio by removing all risk. That’s a win-win to me, and I applaud the FDA for getting on the pharmaceutical companies to make sure they put stopping rules in their medication labels,” he added.
He presented a post hoc pooled analysis of two previously published large, double-blind phase III clinical trials of subcutaneous liraglutide at 3 mg/day (Saxenda) or placebo in combination with a diet and exercise intervention for weight loss: the 3,731-patient SCALE Obesity and Prediabetes trial and the 846-patient SCALE Diabetes trial. In both trials liraglutide was started at a dose of 0.6 mg and titrated to 3.0 mg by week 4. The lifestyle intervention entailed a 500-kcal/day deficit diet and a minimum of 150 minutes of physical activity per week.
The purpose of the pooled analysis was to identify the best early predictor of response status at 56 weeks by examining the impact of 3%, 4%, and 5% weight loss after 8, 12, and 16 weeks of treatment as cut points. This post hoc analysis was prespecified at the request of the Food and Drug Administration before the trials were completed.
The bottom line: The best predictor of long-term outcome on liraglutide, a glucagonlike peptide–1 analog, proved to be a weight loss of 4% or greater at 16 weeks. It had an 81% positive predictive value and a 76% negative predictive value for at least a 5% weight loss at 56 weeks. It correctly predicted weight outcomes at 56 weeks in 80.1% of patients, the highest success rate of all the combinations studied. This finding was the impetus for the current product labeling, which contains the stopping rule. Dr. Fujioka shared study data not included in the labeling; namely, the marked contrast in how early responders and early nonresponders fared at 56 weeks.
The mean weight loss at 56 weeks in nondiabetic early responders to liraglutide was 10.8%, compared with only 3% in early nondiabetic nonresponders. Diabetic early responders averaged an 8.5% weight loss at 56 weeks, while early nonresponders had a mean 3.1% weight loss.
In the SCALE Obesity and Prediabetes trial, 50% of early responders to liraglutide ended up with a greater than 10% weight loss at 56 weeks, and 21% had more than 15% weight loss, compared with rates of 6% and 2%, respectively, in early nonresponders.
In the SCALE Diabetes study, 38% of early responders had greater than 10% weight loss long term, a rate nearly fourfold higher than in early nonresponders. Moreover, 10% of early responder diabetic patients had greater than 15% weight loss, versus a mere 2% of early nonresponders, the internist continued.
The ratio of early responders to early nonresponders in the nondiabetic population was 77%:23%. In diabetic patients, it was 63%:37%.
Turning to cardiometabolic endpoints, Dr. Fujioka noted that early responders in the SCALE Obesity and Prediabetes trial went on to show a mean reduction in systolic blood pressure of 5.1 mm Hg at 56 weeks, compared with a 2–mm Hg decrease in early nonresponders. Early responders also averaged a 10.5-cm shrinkage in waist circumference from a baseline of 115 cm, which was more than twice that observed at 56 weeks in early nonresponders. HDL-cholesterol level rose by 3.9% in early responders but remained unchanged over time in early nonresponders.
Diabetic patients who were early responders to liraglutide 3.0 mg/day had a mean 44.2-mg/dL reduction in fasting plasma glucose at 56 weeks from a baseline of 158 mg/dL, compared with a 30.1-mg/dL decrease in early nonresponders.
“The drop in fasting blood glucose is very quick – within a matter of weeks – so if you already have diabetic patients on drugs that are going to bring their blood sugar down, you may have to back titrate those other drugs really quickly. You don’t want to make your patients hypoglycemic,” the physician said.
Mean hemoglobin A1c values in early responder diabetic patients fell by 1.6% from a baseline of 7.9%, a full 0.5% greater reduction than in early nonresponders.
By far the most frequent adverse events in the two SCALE trials were gastrointestinal, with nausea leading the way. Rates were modestly higher in the early responders.
This analysis and the clinical trials on which it was based were sponsored by Novo Nordisk, which markets liraglutide under the brand names Saxenda and Voctoza. The presenter reported receiving research grants from and serving as a consultant to Novo Nordisk and other pharmaceutical companies.
NEW ORLEANS – Early weight loss on liraglutide – specifically, dropping at least 4% of body weight at 16 weeks – is a strong and clinically useful identifier of patients with a high likelihood of significant weight loss 13 months into treatment, with an accompanying improvement in cardiometabolic risk factors, according to Ken Fujioka, MD.
Conversely, patients who aren’t early responders to subcutaneous liraglutide at 3 mg/day are unlikely to achieve at least 5% weight loss after a full year on the drug, the regulatory benchmark for clinically meaningful weight loss, added Dr. Fujioka, an internist and director of the center for weight management at the Scripps Clinic in La Jolla, Calif.
“Using this early response criterion at week 16 to predict long-term weight loss is to me a very valuable tool. Obesity is an odd disease because it has so many different causes. Finding the right drug is tough, and how long to keep trying with a particular medication is something we haven’t known. So I think the biggest change in obesity medicine is the creation of stopping rules that allow you to say, ‘OK, maybe this isn’t going to work. There’s some other reason you’re gaining weight, so let’s move on to something else,’” Dr. Fujioka said at the meeting presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
“When you stop the medication, you improve the risk-benefit ratio by removing all risk. That’s a win-win to me, and I applaud the FDA for getting on the pharmaceutical companies to make sure they put stopping rules in their medication labels,” he added.
He presented a post hoc pooled analysis of two previously published large, double-blind phase III clinical trials of subcutaneous liraglutide at 3 mg/day (Saxenda) or placebo in combination with a diet and exercise intervention for weight loss: the 3,731-patient SCALE Obesity and Prediabetes trial and the 846-patient SCALE Diabetes trial. In both trials liraglutide was started at a dose of 0.6 mg and titrated to 3.0 mg by week 4. The lifestyle intervention entailed a 500-kcal/day deficit diet and a minimum of 150 minutes of physical activity per week.
The purpose of the pooled analysis was to identify the best early predictor of response status at 56 weeks by examining the impact of 3%, 4%, and 5% weight loss after 8, 12, and 16 weeks of treatment as cut points. This post hoc analysis was prespecified at the request of the Food and Drug Administration before the trials were completed.
The bottom line: The best predictor of long-term outcome on liraglutide, a glucagonlike peptide–1 analog, proved to be a weight loss of 4% or greater at 16 weeks. It had an 81% positive predictive value and a 76% negative predictive value for at least a 5% weight loss at 56 weeks. It correctly predicted weight outcomes at 56 weeks in 80.1% of patients, the highest success rate of all the combinations studied. This finding was the impetus for the current product labeling, which contains the stopping rule. Dr. Fujioka shared study data not included in the labeling; namely, the marked contrast in how early responders and early nonresponders fared at 56 weeks.
The mean weight loss at 56 weeks in nondiabetic early responders to liraglutide was 10.8%, compared with only 3% in early nondiabetic nonresponders. Diabetic early responders averaged an 8.5% weight loss at 56 weeks, while early nonresponders had a mean 3.1% weight loss.
In the SCALE Obesity and Prediabetes trial, 50% of early responders to liraglutide ended up with a greater than 10% weight loss at 56 weeks, and 21% had more than 15% weight loss, compared with rates of 6% and 2%, respectively, in early nonresponders.
In the SCALE Diabetes study, 38% of early responders had greater than 10% weight loss long term, a rate nearly fourfold higher than in early nonresponders. Moreover, 10% of early responder diabetic patients had greater than 15% weight loss, versus a mere 2% of early nonresponders, the internist continued.
The ratio of early responders to early nonresponders in the nondiabetic population was 77%:23%. In diabetic patients, it was 63%:37%.
Turning to cardiometabolic endpoints, Dr. Fujioka noted that early responders in the SCALE Obesity and Prediabetes trial went on to show a mean reduction in systolic blood pressure of 5.1 mm Hg at 56 weeks, compared with a 2–mm Hg decrease in early nonresponders. Early responders also averaged a 10.5-cm shrinkage in waist circumference from a baseline of 115 cm, which was more than twice that observed at 56 weeks in early nonresponders. HDL-cholesterol level rose by 3.9% in early responders but remained unchanged over time in early nonresponders.
Diabetic patients who were early responders to liraglutide 3.0 mg/day had a mean 44.2-mg/dL reduction in fasting plasma glucose at 56 weeks from a baseline of 158 mg/dL, compared with a 30.1-mg/dL decrease in early nonresponders.
“The drop in fasting blood glucose is very quick – within a matter of weeks – so if you already have diabetic patients on drugs that are going to bring their blood sugar down, you may have to back titrate those other drugs really quickly. You don’t want to make your patients hypoglycemic,” the physician said.
Mean hemoglobin A1c values in early responder diabetic patients fell by 1.6% from a baseline of 7.9%, a full 0.5% greater reduction than in early nonresponders.
By far the most frequent adverse events in the two SCALE trials were gastrointestinal, with nausea leading the way. Rates were modestly higher in the early responders.
This analysis and the clinical trials on which it was based were sponsored by Novo Nordisk, which markets liraglutide under the brand names Saxenda and Voctoza. The presenter reported receiving research grants from and serving as a consultant to Novo Nordisk and other pharmaceutical companies.
AT OBESITY WEEK 2016
Key clinical point:
Major finding: A 4% or greater weight loss at week 16 on liraglutide 3 mg/day had an 81.4% positive predictive value and a 76% negative predictive value for achievement of at least 5% weight loss at week 56 on the drug.
Data source: This was a prespecified post hoc analysis of two phase III randomized, double-blind clinical trials of liraglutide 3 mg/day for weight loss in more than 4,500 subjects.
Disclosures: This analysis and the clinical trials on which it is based were sponsored by Novo Nordisk, which markets liraglutide under the brand names Saxenda and Voctoza. The presenter reported receiving research grants from and serving as a consultant to Novo Nordisk and other pharmaceutical companies.
Body-size awareness linked with BMI decrease in obese children, teens
SAN FRANCISCO – Body-size awareness was associated with a decrease in BMI among Latino children and teens, said Grace Lim, MD, a pediatrician in King City, Calif.
Awareness of body size, as a proxy for motivation to change behavior, was based on choices of sex-specific body silhouettes in comparison to actual body mass index (BMI) z-scores. Dr. Lim and her coauthor, Dr. Nazrat Mirza, conducted a study at Children’s National Medical Center in Washington of 80 overweight or obese Latino youths aged 7-15 years who were taking part in a 12-week, community-based weight management program: 68% of study participants demonstrated awareness of overweight or obese body sizes. They were more likely to be older (P less than .001) and with higher maternal age (P = .02). Body-size awareness in the child was positively associated with a decrease in BMI during the intervention period (P less than .001).
Dr. Lim said that she had no relevant financial disclosures.
SAN FRANCISCO – Body-size awareness was associated with a decrease in BMI among Latino children and teens, said Grace Lim, MD, a pediatrician in King City, Calif.
Awareness of body size, as a proxy for motivation to change behavior, was based on choices of sex-specific body silhouettes in comparison to actual body mass index (BMI) z-scores. Dr. Lim and her coauthor, Dr. Nazrat Mirza, conducted a study at Children’s National Medical Center in Washington of 80 overweight or obese Latino youths aged 7-15 years who were taking part in a 12-week, community-based weight management program: 68% of study participants demonstrated awareness of overweight or obese body sizes. They were more likely to be older (P less than .001) and with higher maternal age (P = .02). Body-size awareness in the child was positively associated with a decrease in BMI during the intervention period (P less than .001).
Dr. Lim said that she had no relevant financial disclosures.
SAN FRANCISCO – Body-size awareness was associated with a decrease in BMI among Latino children and teens, said Grace Lim, MD, a pediatrician in King City, Calif.
Awareness of body size, as a proxy for motivation to change behavior, was based on choices of sex-specific body silhouettes in comparison to actual body mass index (BMI) z-scores. Dr. Lim and her coauthor, Dr. Nazrat Mirza, conducted a study at Children’s National Medical Center in Washington of 80 overweight or obese Latino youths aged 7-15 years who were taking part in a 12-week, community-based weight management program: 68% of study participants demonstrated awareness of overweight or obese body sizes. They were more likely to be older (P less than .001) and with higher maternal age (P = .02). Body-size awareness in the child was positively associated with a decrease in BMI during the intervention period (P less than .001).
Dr. Lim said that she had no relevant financial disclosures.
AT AAP 16
Key clinical point:
Major finding: 68% of 80 the children demonstrated awareness of overweight or obese body sizes and were more likely to drop their BMI.
Data source: A study of 80 overweight or obese Latino youths aged 7-15 years taking part in a 12-week, community-based weight management program.
Disclosures: Dr. Lim said she that had no relevant financial disclosures.
He/O2 does not reduce NIV failure in severe COPD exacerbations
Inhaling He/O2 did not result in a lower NIV failure rate than inhaling Air/O2 in COPD patients requiring noninvasive ventilation, in a randomized, controlled study.
In the study, known as the E.C.H.O.ICU trial, patients either received He/02 (a 78%/22% mixture blended with 100% O2) or a conventional Air/O2 mixture for up to 72 hours, during both noninvasive ventilation (NIV) and spontaneous breathing.
Previous research had demonstrated that during hypercapnic COPD exacerbations, the He/O2 mixture reduces airway resistance, partial pressure of carbon dioxide in arterial blood (PaCO2), intrinsic positive end-expiratory pressure, and work of breathing during both spontaneous breathing and NIV, compared with Air/O2, said Philippe Jolliet, MD, and his colleagues.
The two treatment groups in the E.C.H.O.ICU trial had similar NIV failure rates – defined as endotracheal intubation or death without intubation. The rates were 14.7% for the patients who received He/O2 and 14.5% for the patients who received Air/O2. The NIV failures for 31 the patients in the He/O2 group resulted in intubation; the remaining two patients who were classified as having NIV failure died. All 32 of the patients in the Air/O2 group who had NIV failures were intubated.
The length of ICU stay was also comparable between the two groups. In the subgroups of patients with severe acidosis (having a pH of less than 7.30) from both the He/O2 and Air/O2 groups, the NIV failure rates were again nearly identical (AJRCCM. 2016 Oct 13; doi: 10.1164/rccm.201601-0083OC).
The average times to NIV failure were 93 hours in the He/O2 group (N = 33) and 52 hours in the Air/O2 group (N = 32, P = .12). The He/O2 group achieved a significantly quicker improvement in respiratory acidosis, encephalopathy score, and respiratory rate.
Patients intubated following an NIV failure who had received He/O2 had a shorter ventilation duration and a shorter ICU stay than did the intubated patients who had received Air/O2 (7.4 days, vs. 13.6 days, P = .02, and 15.8 vs. 26.7 days, P = .01).
No significant differences appeared in the safety profile of the two groups, nor were significant differences seen in ICU, hospital, or 6-month mortality rates; or in 6-month hospital readmission rates.
“[The] study was stopped prematurely after a futility analysis due the low event rate identified by [an independent adjudication committee],” said Dr. Jolliet of the intensive care and burn unit at Le Centre Hospitalier Universitaire Vaudois (CHUV), in Lausanne, Switzerland, and his fellow researchers.
The study included 445 patients from ICUs or intermediate care units in six countries. The inclusion criteria were presenting with current COPD exacerbation with hypercapnic acute respiratory failure, a PaCO2 of at least 45 mm Hg, an arterial pH of less than or equal to 7.35, and at least one of the following: respiration rate of at least 25 breaths per minute, a PaO2 less than or equal to 50 mm Hg, and an arterial oxygen saturation of less than or equal to 90%.
Half of the patients in each group were already receiving NIV prior to enrollment in the study. Males constituted two thirds of all enrolled patients.
HeO2 administration was limited to 72 hours for each patient and about a third of NIV failures occurred after the end of the HeO2 administration, the researchers said.
“The main reason for the absence of observed benefit on outcome in the He/O2 probably lies in the very low NIV failure rate now observed in both groups. One possible mechanism explaining the low intubation rate could be that some patients had received uncontrolled oxygen therapy prior to ICU admission, thereby worsening initial hypercapnia and acidosis, a problem that can easily be corrected by adequate titration,” the researchers said. “The 14.5% failure rate in the Air/O2 group was much lower than the 25% rate used in designing the study,” which was based on previous research.
The trial’s sponsor, Air Liquide Healthcare, provided input into the design and conduct of the study; oversaw the collection, management, and statistical analysis of data; and contributed to the manuscript’s preparation and review.
Inhaling He/O2 did not result in a lower NIV failure rate than inhaling Air/O2 in COPD patients requiring noninvasive ventilation, in a randomized, controlled study.
In the study, known as the E.C.H.O.ICU trial, patients either received He/02 (a 78%/22% mixture blended with 100% O2) or a conventional Air/O2 mixture for up to 72 hours, during both noninvasive ventilation (NIV) and spontaneous breathing.
Previous research had demonstrated that during hypercapnic COPD exacerbations, the He/O2 mixture reduces airway resistance, partial pressure of carbon dioxide in arterial blood (PaCO2), intrinsic positive end-expiratory pressure, and work of breathing during both spontaneous breathing and NIV, compared with Air/O2, said Philippe Jolliet, MD, and his colleagues.
The two treatment groups in the E.C.H.O.ICU trial had similar NIV failure rates – defined as endotracheal intubation or death without intubation. The rates were 14.7% for the patients who received He/O2 and 14.5% for the patients who received Air/O2. The NIV failures for 31 the patients in the He/O2 group resulted in intubation; the remaining two patients who were classified as having NIV failure died. All 32 of the patients in the Air/O2 group who had NIV failures were intubated.
The length of ICU stay was also comparable between the two groups. In the subgroups of patients with severe acidosis (having a pH of less than 7.30) from both the He/O2 and Air/O2 groups, the NIV failure rates were again nearly identical (AJRCCM. 2016 Oct 13; doi: 10.1164/rccm.201601-0083OC).
The average times to NIV failure were 93 hours in the He/O2 group (N = 33) and 52 hours in the Air/O2 group (N = 32, P = .12). The He/O2 group achieved a significantly quicker improvement in respiratory acidosis, encephalopathy score, and respiratory rate.
Patients intubated following an NIV failure who had received He/O2 had a shorter ventilation duration and a shorter ICU stay than did the intubated patients who had received Air/O2 (7.4 days, vs. 13.6 days, P = .02, and 15.8 vs. 26.7 days, P = .01).
No significant differences appeared in the safety profile of the two groups, nor were significant differences seen in ICU, hospital, or 6-month mortality rates; or in 6-month hospital readmission rates.
“[The] study was stopped prematurely after a futility analysis due the low event rate identified by [an independent adjudication committee],” said Dr. Jolliet of the intensive care and burn unit at Le Centre Hospitalier Universitaire Vaudois (CHUV), in Lausanne, Switzerland, and his fellow researchers.
The study included 445 patients from ICUs or intermediate care units in six countries. The inclusion criteria were presenting with current COPD exacerbation with hypercapnic acute respiratory failure, a PaCO2 of at least 45 mm Hg, an arterial pH of less than or equal to 7.35, and at least one of the following: respiration rate of at least 25 breaths per minute, a PaO2 less than or equal to 50 mm Hg, and an arterial oxygen saturation of less than or equal to 90%.
Half of the patients in each group were already receiving NIV prior to enrollment in the study. Males constituted two thirds of all enrolled patients.
HeO2 administration was limited to 72 hours for each patient and about a third of NIV failures occurred after the end of the HeO2 administration, the researchers said.
“The main reason for the absence of observed benefit on outcome in the He/O2 probably lies in the very low NIV failure rate now observed in both groups. One possible mechanism explaining the low intubation rate could be that some patients had received uncontrolled oxygen therapy prior to ICU admission, thereby worsening initial hypercapnia and acidosis, a problem that can easily be corrected by adequate titration,” the researchers said. “The 14.5% failure rate in the Air/O2 group was much lower than the 25% rate used in designing the study,” which was based on previous research.
The trial’s sponsor, Air Liquide Healthcare, provided input into the design and conduct of the study; oversaw the collection, management, and statistical analysis of data; and contributed to the manuscript’s preparation and review.
Inhaling He/O2 did not result in a lower NIV failure rate than inhaling Air/O2 in COPD patients requiring noninvasive ventilation, in a randomized, controlled study.
In the study, known as the E.C.H.O.ICU trial, patients either received He/02 (a 78%/22% mixture blended with 100% O2) or a conventional Air/O2 mixture for up to 72 hours, during both noninvasive ventilation (NIV) and spontaneous breathing.
Previous research had demonstrated that during hypercapnic COPD exacerbations, the He/O2 mixture reduces airway resistance, partial pressure of carbon dioxide in arterial blood (PaCO2), intrinsic positive end-expiratory pressure, and work of breathing during both spontaneous breathing and NIV, compared with Air/O2, said Philippe Jolliet, MD, and his colleagues.
The two treatment groups in the E.C.H.O.ICU trial had similar NIV failure rates – defined as endotracheal intubation or death without intubation. The rates were 14.7% for the patients who received He/O2 and 14.5% for the patients who received Air/O2. The NIV failures for 31 the patients in the He/O2 group resulted in intubation; the remaining two patients who were classified as having NIV failure died. All 32 of the patients in the Air/O2 group who had NIV failures were intubated.
The length of ICU stay was also comparable between the two groups. In the subgroups of patients with severe acidosis (having a pH of less than 7.30) from both the He/O2 and Air/O2 groups, the NIV failure rates were again nearly identical (AJRCCM. 2016 Oct 13; doi: 10.1164/rccm.201601-0083OC).
The average times to NIV failure were 93 hours in the He/O2 group (N = 33) and 52 hours in the Air/O2 group (N = 32, P = .12). The He/O2 group achieved a significantly quicker improvement in respiratory acidosis, encephalopathy score, and respiratory rate.
Patients intubated following an NIV failure who had received He/O2 had a shorter ventilation duration and a shorter ICU stay than did the intubated patients who had received Air/O2 (7.4 days, vs. 13.6 days, P = .02, and 15.8 vs. 26.7 days, P = .01).
No significant differences appeared in the safety profile of the two groups, nor were significant differences seen in ICU, hospital, or 6-month mortality rates; or in 6-month hospital readmission rates.
“[The] study was stopped prematurely after a futility analysis due the low event rate identified by [an independent adjudication committee],” said Dr. Jolliet of the intensive care and burn unit at Le Centre Hospitalier Universitaire Vaudois (CHUV), in Lausanne, Switzerland, and his fellow researchers.
The study included 445 patients from ICUs or intermediate care units in six countries. The inclusion criteria were presenting with current COPD exacerbation with hypercapnic acute respiratory failure, a PaCO2 of at least 45 mm Hg, an arterial pH of less than or equal to 7.35, and at least one of the following: respiration rate of at least 25 breaths per minute, a PaO2 less than or equal to 50 mm Hg, and an arterial oxygen saturation of less than or equal to 90%.
Half of the patients in each group were already receiving NIV prior to enrollment in the study. Males constituted two thirds of all enrolled patients.
HeO2 administration was limited to 72 hours for each patient and about a third of NIV failures occurred after the end of the HeO2 administration, the researchers said.
“The main reason for the absence of observed benefit on outcome in the He/O2 probably lies in the very low NIV failure rate now observed in both groups. One possible mechanism explaining the low intubation rate could be that some patients had received uncontrolled oxygen therapy prior to ICU admission, thereby worsening initial hypercapnia and acidosis, a problem that can easily be corrected by adequate titration,” the researchers said. “The 14.5% failure rate in the Air/O2 group was much lower than the 25% rate used in designing the study,” which was based on previous research.
The trial’s sponsor, Air Liquide Healthcare, provided input into the design and conduct of the study; oversaw the collection, management, and statistical analysis of data; and contributed to the manuscript’s preparation and review.
FROM AJRCCM
Key clinical point: .
Major finding: The trial was stopped prematurely due to a low event rate. The NIV failure rates for patients who received Air/O2 and He/O2 were 14.5% (N = 32) and 14.7% ( N = 33, P = .97), respectively.
Data source: A prospective, open-label, randomized, controlled trial of 445 patients.
Disclosures: Air Liquide Healthcare sponsored and contributed to the study.
Comorbidities common in COPD patients
LOS ANGELES – Comorbidities are common in patients with chronic obstructive pulmonary disease, especially cardiovascular disease, diabetes, anemia, and osteoporosis, results from a single-center analysis showed.
“These affect the course and outcome of COPD, so identification and treatment of these comorbidities is very important,” Hamdy Mohammadien, MD, said in an interview in advance of the annual meeting of the American College of Chest Physicians.
In an effort to estimate the presence of comorbidities in patients with COPD and to assess the relationship of comorbid diseases with age, sex, C-reactive protein, and COPD severity, Dr. Mohammadien and his associates at Sohag (Egypt) University, retrospectively evaluated 400 COPD patients who were at least 40 years of age. Those who presented with bronchial asthma or other lung diseases were excluded from the analysis. The mean age of patients was 62 years, 69% were male, and 36% were current smokers. Their mean FEV1/FVC ratio (forced expiratory volume in 1 second/forced vital capacity) was 48%, and 57% had two or more exacerbations in the previous year.
Dr. Mohammadien reported that all patients had at least one comorbidity. The most common comorbidities were cardiovascular diseases (85%), diabetes (35%), dyslipidemia (23%), osteopenia (11%), anemia (10%), muscle wasting (9%), pneumonia (7%), osteoporosis (6%), GERD (2%), and lung cancer (2%). He also noted that the association between cardiovascular events, dyslipidemia, diabetes, osteoporosis, muscle wasting, and anemia was highly significant in COPD patients aged 60 years and older, in men, and in patients with stage III and IV COPD. In addition, a significant relationship was observed between a positive CRP level and each comorbidity, with the exception of gastroesophageal reflux disease and lung cancer. The three comorbidities with the greatest significance were ischemic heart disease (P = .0001), dyslipidemia (P = .0001), and pneumonia (P = .0003). Finally, frequent exacerbators were significantly more likely to have two or more comorbidities (odds ratio 2; P = .04) and to have more hospitalizations in the past year (P less than .01).
“Comorbidities are common in patients with COPD, and have a significant impact on health status and prognosis, thus justifying the need for a comprehensive and integrating therapeutic approach,” Dr. Mohammadien said at the meeting. “In the management of COPD all these conditions need to be carefully evaluated and treated.”
He acknowledged certain limitations of the study, including its relatively small sample size and the fact that bone density was measured by sonar and not by dual-energy x-ray absorptiometry. Dr. Mohammadien reported having no financial disclosures.
LOS ANGELES – Comorbidities are common in patients with chronic obstructive pulmonary disease, especially cardiovascular disease, diabetes, anemia, and osteoporosis, results from a single-center analysis showed.
“These affect the course and outcome of COPD, so identification and treatment of these comorbidities is very important,” Hamdy Mohammadien, MD, said in an interview in advance of the annual meeting of the American College of Chest Physicians.
In an effort to estimate the presence of comorbidities in patients with COPD and to assess the relationship of comorbid diseases with age, sex, C-reactive protein, and COPD severity, Dr. Mohammadien and his associates at Sohag (Egypt) University, retrospectively evaluated 400 COPD patients who were at least 40 years of age. Those who presented with bronchial asthma or other lung diseases were excluded from the analysis. The mean age of patients was 62 years, 69% were male, and 36% were current smokers. Their mean FEV1/FVC ratio (forced expiratory volume in 1 second/forced vital capacity) was 48%, and 57% had two or more exacerbations in the previous year.
Dr. Mohammadien reported that all patients had at least one comorbidity. The most common comorbidities were cardiovascular diseases (85%), diabetes (35%), dyslipidemia (23%), osteopenia (11%), anemia (10%), muscle wasting (9%), pneumonia (7%), osteoporosis (6%), GERD (2%), and lung cancer (2%). He also noted that the association between cardiovascular events, dyslipidemia, diabetes, osteoporosis, muscle wasting, and anemia was highly significant in COPD patients aged 60 years and older, in men, and in patients with stage III and IV COPD. In addition, a significant relationship was observed between a positive CRP level and each comorbidity, with the exception of gastroesophageal reflux disease and lung cancer. The three comorbidities with the greatest significance were ischemic heart disease (P = .0001), dyslipidemia (P = .0001), and pneumonia (P = .0003). Finally, frequent exacerbators were significantly more likely to have two or more comorbidities (odds ratio 2; P = .04) and to have more hospitalizations in the past year (P less than .01).
“Comorbidities are common in patients with COPD, and have a significant impact on health status and prognosis, thus justifying the need for a comprehensive and integrating therapeutic approach,” Dr. Mohammadien said at the meeting. “In the management of COPD all these conditions need to be carefully evaluated and treated.”
He acknowledged certain limitations of the study, including its relatively small sample size and the fact that bone density was measured by sonar and not by dual-energy x-ray absorptiometry. Dr. Mohammadien reported having no financial disclosures.
LOS ANGELES – Comorbidities are common in patients with chronic obstructive pulmonary disease, especially cardiovascular disease, diabetes, anemia, and osteoporosis, results from a single-center analysis showed.
“These affect the course and outcome of COPD, so identification and treatment of these comorbidities is very important,” Hamdy Mohammadien, MD, said in an interview in advance of the annual meeting of the American College of Chest Physicians.
In an effort to estimate the presence of comorbidities in patients with COPD and to assess the relationship of comorbid diseases with age, sex, C-reactive protein, and COPD severity, Dr. Mohammadien and his associates at Sohag (Egypt) University, retrospectively evaluated 400 COPD patients who were at least 40 years of age. Those who presented with bronchial asthma or other lung diseases were excluded from the analysis. The mean age of patients was 62 years, 69% were male, and 36% were current smokers. Their mean FEV1/FVC ratio (forced expiratory volume in 1 second/forced vital capacity) was 48%, and 57% had two or more exacerbations in the previous year.
Dr. Mohammadien reported that all patients had at least one comorbidity. The most common comorbidities were cardiovascular diseases (85%), diabetes (35%), dyslipidemia (23%), osteopenia (11%), anemia (10%), muscle wasting (9%), pneumonia (7%), osteoporosis (6%), GERD (2%), and lung cancer (2%). He also noted that the association between cardiovascular events, dyslipidemia, diabetes, osteoporosis, muscle wasting, and anemia was highly significant in COPD patients aged 60 years and older, in men, and in patients with stage III and IV COPD. In addition, a significant relationship was observed between a positive CRP level and each comorbidity, with the exception of gastroesophageal reflux disease and lung cancer. The three comorbidities with the greatest significance were ischemic heart disease (P = .0001), dyslipidemia (P = .0001), and pneumonia (P = .0003). Finally, frequent exacerbators were significantly more likely to have two or more comorbidities (odds ratio 2; P = .04) and to have more hospitalizations in the past year (P less than .01).
“Comorbidities are common in patients with COPD, and have a significant impact on health status and prognosis, thus justifying the need for a comprehensive and integrating therapeutic approach,” Dr. Mohammadien said at the meeting. “In the management of COPD all these conditions need to be carefully evaluated and treated.”
He acknowledged certain limitations of the study, including its relatively small sample size and the fact that bone density was measured by sonar and not by dual-energy x-ray absorptiometry. Dr. Mohammadien reported having no financial disclosures.
AT CHEST 2016
Key clinical point:
Major finding: The three most common comorbidities in COPD patients were cardiovascular diseases (85%), diabetes (35%), and dyslipidemia (23%).
Data source: A retrospective study of 400 patients with COPD.
Disclosures: Dr. Mohammadien reported having no financial disclosures.
Employer-provided insurance stable after ACA implementation
Concerns that Affordable Care Act (ACA) provisions implemented in 2014 would lead large numbers of employers to drop health insurance coverage appear to have been unfounded, according to a study published in the journal Health Affairs.
More than 95% of employers did not change their insurance coverage policy between 2013 and 2014: 46.4% offered coverage in 2013 and continued it in 2014 and 49.1% did not offer coverage either year. Of the 21,900 private-sector employers included in the analysis, 3.5% provided coverage in 2013 but not in 2014 and 1.1% did not offer it in 2013 but did in 2014, reported Jean Abraham, PhD, of the University of Minnesota, Minneapolis, and her associates (Health Aff. 2016 Oct 26;35[11]. doi: 10.1377/hlthaff.2016.0631).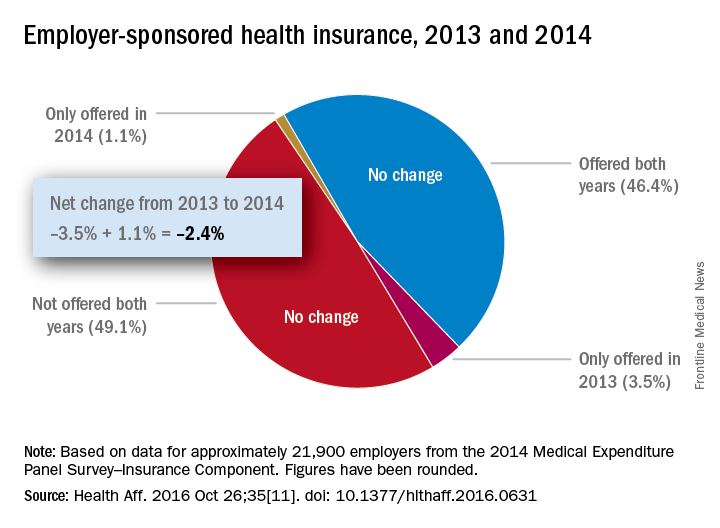
The analysis of data from the 2014 Medical Expenditure Panel Survey–Insurance Component, however, did show associations between coverage changes and several workforce and employer characteristics. “Small firms were more likely to drop coverage compared to large ones, as were those with more low-wage workers compared to those with fewer such workers, newer establishments compared to older ones, and those in the service sector compared to those in blue- and white-collar industries,” Dr. Abraham and her associates wrote.
The Robert Wood Johnson Foundation’s State Health Access Reform Evaluation program supported the study. No other financial disclosures were provided.
Concerns that Affordable Care Act (ACA) provisions implemented in 2014 would lead large numbers of employers to drop health insurance coverage appear to have been unfounded, according to a study published in the journal Health Affairs.
More than 95% of employers did not change their insurance coverage policy between 2013 and 2014: 46.4% offered coverage in 2013 and continued it in 2014 and 49.1% did not offer coverage either year. Of the 21,900 private-sector employers included in the analysis, 3.5% provided coverage in 2013 but not in 2014 and 1.1% did not offer it in 2013 but did in 2014, reported Jean Abraham, PhD, of the University of Minnesota, Minneapolis, and her associates (Health Aff. 2016 Oct 26;35[11]. doi: 10.1377/hlthaff.2016.0631).
The analysis of data from the 2014 Medical Expenditure Panel Survey–Insurance Component, however, did show associations between coverage changes and several workforce and employer characteristics. “Small firms were more likely to drop coverage compared to large ones, as were those with more low-wage workers compared to those with fewer such workers, newer establishments compared to older ones, and those in the service sector compared to those in blue- and white-collar industries,” Dr. Abraham and her associates wrote.
The Robert Wood Johnson Foundation’s State Health Access Reform Evaluation program supported the study. No other financial disclosures were provided.
Concerns that Affordable Care Act (ACA) provisions implemented in 2014 would lead large numbers of employers to drop health insurance coverage appear to have been unfounded, according to a study published in the journal Health Affairs.
More than 95% of employers did not change their insurance coverage policy between 2013 and 2014: 46.4% offered coverage in 2013 and continued it in 2014 and 49.1% did not offer coverage either year. Of the 21,900 private-sector employers included in the analysis, 3.5% provided coverage in 2013 but not in 2014 and 1.1% did not offer it in 2013 but did in 2014, reported Jean Abraham, PhD, of the University of Minnesota, Minneapolis, and her associates (Health Aff. 2016 Oct 26;35[11]. doi: 10.1377/hlthaff.2016.0631).
The analysis of data from the 2014 Medical Expenditure Panel Survey–Insurance Component, however, did show associations between coverage changes and several workforce and employer characteristics. “Small firms were more likely to drop coverage compared to large ones, as were those with more low-wage workers compared to those with fewer such workers, newer establishments compared to older ones, and those in the service sector compared to those in blue- and white-collar industries,” Dr. Abraham and her associates wrote.
The Robert Wood Johnson Foundation’s State Health Access Reform Evaluation program supported the study. No other financial disclosures were provided.
Number of Medicare part D drug plans continues to decline
There will be 16% fewer Medicare part D prescription drug plans available in 2017, compared with 2016, according to an analysis by the Kaiser Family Foundation.
In 2017, there will be 746 stand-alone prescription drug plans available to Medicare beneficiaries in the 50 states and the District of Columbia, which is 140 (16%) less than were available in 2016 and 1,129 (60%) less than the peak in 2007, Kaiser reported.
Of the nearly 41 million people enrolled in Medicare part D plans in 2016, about 12 million receive the low-income subsidy. The Congressional Budget Office estimates that spending on part D benefits will be $94 billion in 2017, which is 15.6% of overall Medicare costs. Medicare actuaries have projected that the cost per enrollee will increase by 5.8% annually from 2015 to 2025, Kaiser reported.
There will be 16% fewer Medicare part D prescription drug plans available in 2017, compared with 2016, according to an analysis by the Kaiser Family Foundation.
In 2017, there will be 746 stand-alone prescription drug plans available to Medicare beneficiaries in the 50 states and the District of Columbia, which is 140 (16%) less than were available in 2016 and 1,129 (60%) less than the peak in 2007, Kaiser reported.
Of the nearly 41 million people enrolled in Medicare part D plans in 2016, about 12 million receive the low-income subsidy. The Congressional Budget Office estimates that spending on part D benefits will be $94 billion in 2017, which is 15.6% of overall Medicare costs. Medicare actuaries have projected that the cost per enrollee will increase by 5.8% annually from 2015 to 2025, Kaiser reported.
There will be 16% fewer Medicare part D prescription drug plans available in 2017, compared with 2016, according to an analysis by the Kaiser Family Foundation.
In 2017, there will be 746 stand-alone prescription drug plans available to Medicare beneficiaries in the 50 states and the District of Columbia, which is 140 (16%) less than were available in 2016 and 1,129 (60%) less than the peak in 2007, Kaiser reported.
Of the nearly 41 million people enrolled in Medicare part D plans in 2016, about 12 million receive the low-income subsidy. The Congressional Budget Office estimates that spending on part D benefits will be $94 billion in 2017, which is 15.6% of overall Medicare costs. Medicare actuaries have projected that the cost per enrollee will increase by 5.8% annually from 2015 to 2025, Kaiser reported.
Woman with rash in groin

The family physician (FP) suspected that the patient had tinea cruris, but hadn’t ever seen it spread so far from the inguinal area. The rash had central clearing, which is typical of tinea corporis, but is not seen as often with tinea cruris. The FP performed a potassium hydroxide (KOH) preparation, which was positive for branching septate hyphae. (See video on how to perform a KOH preparation here.)
The FP discussed the treatment options, which consisted of topical antifungal medicine vs oral antifungal medicine. The patient was willing to try the topical terbinafine and return for a follow-up appointment in a month. The FP told the patient that he would give her oral terbinafine if the topical terbinafine didn’t work. One month later, the skin had cleared and the patient was happy with the results.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Smith M. Tinea cruris. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:795-798.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The family physician (FP) suspected that the patient had tinea cruris, but hadn’t ever seen it spread so far from the inguinal area. The rash had central clearing, which is typical of tinea corporis, but is not seen as often with tinea cruris. The FP performed a potassium hydroxide (KOH) preparation, which was positive for branching septate hyphae. (See video on how to perform a KOH preparation here.)
The FP discussed the treatment options, which consisted of topical antifungal medicine vs oral antifungal medicine. The patient was willing to try the topical terbinafine and return for a follow-up appointment in a month. The FP told the patient that he would give her oral terbinafine if the topical terbinafine didn’t work. One month later, the skin had cleared and the patient was happy with the results.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Smith M. Tinea cruris. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:795-798.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The family physician (FP) suspected that the patient had tinea cruris, but hadn’t ever seen it spread so far from the inguinal area. The rash had central clearing, which is typical of tinea corporis, but is not seen as often with tinea cruris. The FP performed a potassium hydroxide (KOH) preparation, which was positive for branching septate hyphae. (See video on how to perform a KOH preparation here.)
The FP discussed the treatment options, which consisted of topical antifungal medicine vs oral antifungal medicine. The patient was willing to try the topical terbinafine and return for a follow-up appointment in a month. The FP told the patient that he would give her oral terbinafine if the topical terbinafine didn’t work. One month later, the skin had cleared and the patient was happy with the results.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Smith M. Tinea cruris. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:795-798.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
