User login
CHEST Clinical Trials Registry
Are you a clinical trials investigator with unused capacity? Would you like to refer patients to participate in groundbreaking clinical trials?
The CHEST Clinical Trials Registry is a free service that connects physicians to information about clinical trials in respiratory disease conducted by participating pharmaceutical companies.
Ongoing groundbreaking research could have a measurable impact on patient care, but a lack of clinical trial participants is significantly slowing research and threatening the development of new treatments. Recruiting and retaining trial participants are the greatest challenges to developing the next generation of treatment options.
Participation in clinical trials provides an opportunity to advance and accelerate medical research and contribute to an improved health outlook for future generations. Use our registry to get immediate information on how you can be involved in a clinical trial.
Access this site to learn more: www.chestnet.org/Guidelines-and-Resources/Clinical-Trials/Clinical-Trials-Registry.
Are you a clinical trials investigator with unused capacity? Would you like to refer patients to participate in groundbreaking clinical trials?
The CHEST Clinical Trials Registry is a free service that connects physicians to information about clinical trials in respiratory disease conducted by participating pharmaceutical companies.
Ongoing groundbreaking research could have a measurable impact on patient care, but a lack of clinical trial participants is significantly slowing research and threatening the development of new treatments. Recruiting and retaining trial participants are the greatest challenges to developing the next generation of treatment options.
Participation in clinical trials provides an opportunity to advance and accelerate medical research and contribute to an improved health outlook for future generations. Use our registry to get immediate information on how you can be involved in a clinical trial.
Access this site to learn more: www.chestnet.org/Guidelines-and-Resources/Clinical-Trials/Clinical-Trials-Registry.
Are you a clinical trials investigator with unused capacity? Would you like to refer patients to participate in groundbreaking clinical trials?
The CHEST Clinical Trials Registry is a free service that connects physicians to information about clinical trials in respiratory disease conducted by participating pharmaceutical companies.
Ongoing groundbreaking research could have a measurable impact on patient care, but a lack of clinical trial participants is significantly slowing research and threatening the development of new treatments. Recruiting and retaining trial participants are the greatest challenges to developing the next generation of treatment options.
Participation in clinical trials provides an opportunity to advance and accelerate medical research and contribute to an improved health outlook for future generations. Use our registry to get immediate information on how you can be involved in a clinical trial.
Access this site to learn more: www.chestnet.org/Guidelines-and-Resources/Clinical-Trials/Clinical-Trials-Registry.
Rheumatoid arthritis increases heart failure risk
ROME – Rheumatoid arthritis is associated with a significantly increased risk of hospitalization for heart failure, according to a nationwide Danish study, Usman Khalid, MD, reported at the annual congress of the European Society of Cardiology.
As a chronic systemic inflammatory disease, rheumatoid arthritis (RA) has been associated with increased risk of a variety of comorbid conditions, including cardiovascular disease. But RA’s relationship specifically with heart failure hasn’t previously been looked at in the comprehensive way that’s possible in Denmark, where linked national registries enable researchers to follow health issues in the entire population from birth to death, noted Dr. Khalid of the University of Copenhagen.

In an analysis adjusted for age, sex, and calendar year, individuals with RA were 83% more likely to be hospitalized for heart failure than were the non-RA Danish population. In a fully adjusted analysis that controlled for those potential confounders as well as comorbid conditions, smoking, alcohol intake, socioeconomic status, and prescription medications, patients with RA remained at a statistically significant and clinically meaningful 38% increased risk of heart failure hospitalization.
Further studies are planned to determine the underlying mechanisms of this association, Dr. Khalid added.
He reported having no financial conflicts of interest regarding this study, which was supported by an unrestricted grant from Leo Pharma.
ROME – Rheumatoid arthritis is associated with a significantly increased risk of hospitalization for heart failure, according to a nationwide Danish study, Usman Khalid, MD, reported at the annual congress of the European Society of Cardiology.
As a chronic systemic inflammatory disease, rheumatoid arthritis (RA) has been associated with increased risk of a variety of comorbid conditions, including cardiovascular disease. But RA’s relationship specifically with heart failure hasn’t previously been looked at in the comprehensive way that’s possible in Denmark, where linked national registries enable researchers to follow health issues in the entire population from birth to death, noted Dr. Khalid of the University of Copenhagen.
In an analysis adjusted for age, sex, and calendar year, individuals with RA were 83% more likely to be hospitalized for heart failure than were the non-RA Danish population. In a fully adjusted analysis that controlled for those potential confounders as well as comorbid conditions, smoking, alcohol intake, socioeconomic status, and prescription medications, patients with RA remained at a statistically significant and clinically meaningful 38% increased risk of heart failure hospitalization.
Further studies are planned to determine the underlying mechanisms of this association, Dr. Khalid added.
He reported having no financial conflicts of interest regarding this study, which was supported by an unrestricted grant from Leo Pharma.
ROME – Rheumatoid arthritis is associated with a significantly increased risk of hospitalization for heart failure, according to a nationwide Danish study, Usman Khalid, MD, reported at the annual congress of the European Society of Cardiology.
As a chronic systemic inflammatory disease, rheumatoid arthritis (RA) has been associated with increased risk of a variety of comorbid conditions, including cardiovascular disease. But RA’s relationship specifically with heart failure hasn’t previously been looked at in the comprehensive way that’s possible in Denmark, where linked national registries enable researchers to follow health issues in the entire population from birth to death, noted Dr. Khalid of the University of Copenhagen.
In an analysis adjusted for age, sex, and calendar year, individuals with RA were 83% more likely to be hospitalized for heart failure than were the non-RA Danish population. In a fully adjusted analysis that controlled for those potential confounders as well as comorbid conditions, smoking, alcohol intake, socioeconomic status, and prescription medications, patients with RA remained at a statistically significant and clinically meaningful 38% increased risk of heart failure hospitalization.
Further studies are planned to determine the underlying mechanisms of this association, Dr. Khalid added.
He reported having no financial conflicts of interest regarding this study, which was supported by an unrestricted grant from Leo Pharma.
AT THE ESC CONGRESS 2016
Key clinical point:
Major finding: The incidence rate for heart failure hospitalization was 7.37 per 1,000 person-years in Danish adults with rheumatoid arthritis, compared with 2.45 per 1,000 in the general population.
Data source: This study utilized Danish comprehensive national registries to determine the rate at which 13,800 Danes with rheumatoid arthritis and no baseline history of heart failure were hospitalized for heart failure during 15 years of follow-up.
Disclosures: The study was supported by an unrestricted grant from Leo Pharma. The presenter reported having no financial conflicts of interest.
Lessons learned from using CDK 4/6 inhibitors to treat metastatic breast cancer
45 new cancer drugs – a significant jump from the average 26 approvals annually from 2006 to 2014. This major shift in the number of approvals is due to many factors, including the intensified efforts by scientists and clinicians to develop new drugs, especially novel immunotherapies, and changes in the FDA’s drug approval process under the leadership of Dr Richard Pazdur.
Click on the PDF icon at the top of this introduction to read the full article.
45 new cancer drugs – a significant jump from the average 26 approvals annually from 2006 to 2014. This major shift in the number of approvals is due to many factors, including the intensified efforts by scientists and clinicians to develop new drugs, especially novel immunotherapies, and changes in the FDA’s drug approval process under the leadership of Dr Richard Pazdur.
Click on the PDF icon at the top of this introduction to read the full article.
45 new cancer drugs – a significant jump from the average 26 approvals annually from 2006 to 2014. This major shift in the number of approvals is due to many factors, including the intensified efforts by scientists and clinicians to develop new drugs, especially novel immunotherapies, and changes in the FDA’s drug approval process under the leadership of Dr Richard Pazdur.
Click on the PDF icon at the top of this introduction to read the full article.

Can carotid interventions affect cognitive function?
COLUMBUS, OHIO – The primary goal of carotid artery revascularization is to prevent stroke, heart attack or death, but carotid artery stenting and carotid endarterectomy may also cause changes in cognitive skills, according Raghu Motaganahalli, MD, of the Indiana University, Indianapolis.
“What about cognitive dysfunction as a result of carotid artery stenting (CAS) or carotid endarterectomy (CEA)?” Dr. Motaganahalli asked at the annual meeting of the Midwestern Vascular Surgical Society. “I think this is real, that there’s some truth to the matter. The question is how much and what domains of cognitive functions are affected?”

“Cerebrovascular hemodynamics status plays a role in cognitive function, but we need a better understanding of cerebrovascular hemodynamic failure and either improvement or decline of cognitive function after CAS or CEA,” he said.
A review of published trials shows that 10%-20% of patients who have either CAS or CEA have some degree of cognitive dysfunction as early as a day after the procedure. “It’s not a small number, compared to stoke, risk of myocardial infarction and death,” he said.
Some series have reported up to 40% of patients showed some cognitive dysfunction, and post–carotid endarterectomy cognitive dysfunction has been associated with early death, Dr. Motaganahalli said.
Cognitive dysfunction manifests in various forms, ranging from level of consciousness and memory to mood and ability to make calculations. Although the Mini-Mental State Examination Global Cognitive Assessment tool provides a method for evaluating cognitive function, “There is no uniformly accepted neurocognition test,” Dr. Motaganahalli said. That explains the wide variability of findings among published studies.
Vascular surgeons take a somewhat casual approach to their patients’ cognitive abilities after carotid revascularization, Dr. Motaganahalli said. “We don’t evaluate their memory and their cognitive functions on post-op day one; we just look to see whether they have neurologic dysfunction up front and that they’re capable of going home after that.”
But predicting in advance which patients are predisposed to cognitive decline after the procedures is difficult, he said. He cited a systematic review of 32 studies published between 1990-2007 that showed variable results (Stroke. 2008;39:3116-27): 11 studies during 1990-2005 suggested cognition actually improved after CEA; 9 studies during 1994-2006 suggested the opposite; 4 trials during 1992-2005 suggested no change in cognition after CEA; 5 studies during 2003-2007 showed improvement in cognition after CAS; and 3 trials comparing CAS and CEA and cognition found no differences in how the two procedures affect cognition.
Dr. Motaganahalli also cited a systematic review of 37 studies, 18 of which examined CEA, 12 CAS and seven compared CEA and CAS, found that either cognitive improvement or impairment for CEA and CAS separately were 10–15% of patients (Cerebrovasc Dis Extra. 2014;4:132-48).
“We have 69 papers that looked at cognitive function alone, but unfortunately, we don’t know whether cognitive function really improved based on this data set,” he said. “None of them are making the argument so clearly that there is cognitive improvement after revascularization.”
The variability in study findings can be due to differences in methodologies, the types of psychometric tests used, statistical analyses and the timing of cognitive assessments, Dr. Motaganahalli said.
Cognitive impairment after stroke caused by carotid disease is better understood than is cognitive impairment in the absence of a major stroke, Dr. Motaganahalli said.
“The mechanisms of how carotid disease can cause the cognitive impairment are threefold: It could be microembolism and hypoperfusion, which together can cause white matter disease and thereby some cognitive dysfunction in the long term,” he said (Neuroimaging Clin N Am. 2007 Aug;17:313-24).
Functional neurons may be a biomarker of cognitive outcome, he said. Hypoperfusion of functional neurons may lead to hypofunctional neurons, which can increase cerebral blood flow and cerebral metabolic rate for oxygen (CMRO2), and thus improve cognition. However, when additional variables are introduced to the hypofunctional neurons – such as microembolism, white matter disease, and prolonged hypoperfusion – that can lead to neuronal infarction that, while increasing cerebral blood flow, causes no change in CMRO2 and, thus, no cognitive improvement. The interval between hypofunctional neurons and neuronal infarction “is the time to do the revascularization, as long as you can demonstrate that there may be some truth to matter that it influences cognition,” Dr. Motaganahalli said.
While vascular surgeons may not be able to predict who will have cognitive decline after carotid interventions, “There are some pointers for possibly picking those patients who may benefit,” Dr. Motaganahalli said.
That choice of patients revolves around recognizing that chronic ischemia induces and increases the severity of cognitive dysfunction. Therefore, incorporating the pathophysiology of chronic ischemia into the algorithm for carotid artery disease may provide an opportunity to extend the goals of carotid artery revascularization to include preventing or reversing cognitive decline, he said.
Dr. Motaganahalli disclosed he is a consultant to Silk Road Medical.
COLUMBUS, OHIO – The primary goal of carotid artery revascularization is to prevent stroke, heart attack or death, but carotid artery stenting and carotid endarterectomy may also cause changes in cognitive skills, according Raghu Motaganahalli, MD, of the Indiana University, Indianapolis.
“What about cognitive dysfunction as a result of carotid artery stenting (CAS) or carotid endarterectomy (CEA)?” Dr. Motaganahalli asked at the annual meeting of the Midwestern Vascular Surgical Society. “I think this is real, that there’s some truth to the matter. The question is how much and what domains of cognitive functions are affected?”
“Cerebrovascular hemodynamics status plays a role in cognitive function, but we need a better understanding of cerebrovascular hemodynamic failure and either improvement or decline of cognitive function after CAS or CEA,” he said.
A review of published trials shows that 10%-20% of patients who have either CAS or CEA have some degree of cognitive dysfunction as early as a day after the procedure. “It’s not a small number, compared to stoke, risk of myocardial infarction and death,” he said.
Some series have reported up to 40% of patients showed some cognitive dysfunction, and post–carotid endarterectomy cognitive dysfunction has been associated with early death, Dr. Motaganahalli said.
Cognitive dysfunction manifests in various forms, ranging from level of consciousness and memory to mood and ability to make calculations. Although the Mini-Mental State Examination Global Cognitive Assessment tool provides a method for evaluating cognitive function, “There is no uniformly accepted neurocognition test,” Dr. Motaganahalli said. That explains the wide variability of findings among published studies.
Vascular surgeons take a somewhat casual approach to their patients’ cognitive abilities after carotid revascularization, Dr. Motaganahalli said. “We don’t evaluate their memory and their cognitive functions on post-op day one; we just look to see whether they have neurologic dysfunction up front and that they’re capable of going home after that.”
But predicting in advance which patients are predisposed to cognitive decline after the procedures is difficult, he said. He cited a systematic review of 32 studies published between 1990-2007 that showed variable results (Stroke. 2008;39:3116-27): 11 studies during 1990-2005 suggested cognition actually improved after CEA; 9 studies during 1994-2006 suggested the opposite; 4 trials during 1992-2005 suggested no change in cognition after CEA; 5 studies during 2003-2007 showed improvement in cognition after CAS; and 3 trials comparing CAS and CEA and cognition found no differences in how the two procedures affect cognition.
Dr. Motaganahalli also cited a systematic review of 37 studies, 18 of which examined CEA, 12 CAS and seven compared CEA and CAS, found that either cognitive improvement or impairment for CEA and CAS separately were 10–15% of patients (Cerebrovasc Dis Extra. 2014;4:132-48).
“We have 69 papers that looked at cognitive function alone, but unfortunately, we don’t know whether cognitive function really improved based on this data set,” he said. “None of them are making the argument so clearly that there is cognitive improvement after revascularization.”
The variability in study findings can be due to differences in methodologies, the types of psychometric tests used, statistical analyses and the timing of cognitive assessments, Dr. Motaganahalli said.
Cognitive impairment after stroke caused by carotid disease is better understood than is cognitive impairment in the absence of a major stroke, Dr. Motaganahalli said.
“The mechanisms of how carotid disease can cause the cognitive impairment are threefold: It could be microembolism and hypoperfusion, which together can cause white matter disease and thereby some cognitive dysfunction in the long term,” he said (Neuroimaging Clin N Am. 2007 Aug;17:313-24).
Functional neurons may be a biomarker of cognitive outcome, he said. Hypoperfusion of functional neurons may lead to hypofunctional neurons, which can increase cerebral blood flow and cerebral metabolic rate for oxygen (CMRO2), and thus improve cognition. However, when additional variables are introduced to the hypofunctional neurons – such as microembolism, white matter disease, and prolonged hypoperfusion – that can lead to neuronal infarction that, while increasing cerebral blood flow, causes no change in CMRO2 and, thus, no cognitive improvement. The interval between hypofunctional neurons and neuronal infarction “is the time to do the revascularization, as long as you can demonstrate that there may be some truth to matter that it influences cognition,” Dr. Motaganahalli said.
While vascular surgeons may not be able to predict who will have cognitive decline after carotid interventions, “There are some pointers for possibly picking those patients who may benefit,” Dr. Motaganahalli said.
That choice of patients revolves around recognizing that chronic ischemia induces and increases the severity of cognitive dysfunction. Therefore, incorporating the pathophysiology of chronic ischemia into the algorithm for carotid artery disease may provide an opportunity to extend the goals of carotid artery revascularization to include preventing or reversing cognitive decline, he said.
Dr. Motaganahalli disclosed he is a consultant to Silk Road Medical.
COLUMBUS, OHIO – The primary goal of carotid artery revascularization is to prevent stroke, heart attack or death, but carotid artery stenting and carotid endarterectomy may also cause changes in cognitive skills, according Raghu Motaganahalli, MD, of the Indiana University, Indianapolis.
“What about cognitive dysfunction as a result of carotid artery stenting (CAS) or carotid endarterectomy (CEA)?” Dr. Motaganahalli asked at the annual meeting of the Midwestern Vascular Surgical Society. “I think this is real, that there’s some truth to the matter. The question is how much and what domains of cognitive functions are affected?”
“Cerebrovascular hemodynamics status plays a role in cognitive function, but we need a better understanding of cerebrovascular hemodynamic failure and either improvement or decline of cognitive function after CAS or CEA,” he said.
A review of published trials shows that 10%-20% of patients who have either CAS or CEA have some degree of cognitive dysfunction as early as a day after the procedure. “It’s not a small number, compared to stoke, risk of myocardial infarction and death,” he said.
Some series have reported up to 40% of patients showed some cognitive dysfunction, and post–carotid endarterectomy cognitive dysfunction has been associated with early death, Dr. Motaganahalli said.
Cognitive dysfunction manifests in various forms, ranging from level of consciousness and memory to mood and ability to make calculations. Although the Mini-Mental State Examination Global Cognitive Assessment tool provides a method for evaluating cognitive function, “There is no uniformly accepted neurocognition test,” Dr. Motaganahalli said. That explains the wide variability of findings among published studies.
Vascular surgeons take a somewhat casual approach to their patients’ cognitive abilities after carotid revascularization, Dr. Motaganahalli said. “We don’t evaluate their memory and their cognitive functions on post-op day one; we just look to see whether they have neurologic dysfunction up front and that they’re capable of going home after that.”
But predicting in advance which patients are predisposed to cognitive decline after the procedures is difficult, he said. He cited a systematic review of 32 studies published between 1990-2007 that showed variable results (Stroke. 2008;39:3116-27): 11 studies during 1990-2005 suggested cognition actually improved after CEA; 9 studies during 1994-2006 suggested the opposite; 4 trials during 1992-2005 suggested no change in cognition after CEA; 5 studies during 2003-2007 showed improvement in cognition after CAS; and 3 trials comparing CAS and CEA and cognition found no differences in how the two procedures affect cognition.
Dr. Motaganahalli also cited a systematic review of 37 studies, 18 of which examined CEA, 12 CAS and seven compared CEA and CAS, found that either cognitive improvement or impairment for CEA and CAS separately were 10–15% of patients (Cerebrovasc Dis Extra. 2014;4:132-48).
“We have 69 papers that looked at cognitive function alone, but unfortunately, we don’t know whether cognitive function really improved based on this data set,” he said. “None of them are making the argument so clearly that there is cognitive improvement after revascularization.”
The variability in study findings can be due to differences in methodologies, the types of psychometric tests used, statistical analyses and the timing of cognitive assessments, Dr. Motaganahalli said.
Cognitive impairment after stroke caused by carotid disease is better understood than is cognitive impairment in the absence of a major stroke, Dr. Motaganahalli said.
“The mechanisms of how carotid disease can cause the cognitive impairment are threefold: It could be microembolism and hypoperfusion, which together can cause white matter disease and thereby some cognitive dysfunction in the long term,” he said (Neuroimaging Clin N Am. 2007 Aug;17:313-24).
Functional neurons may be a biomarker of cognitive outcome, he said. Hypoperfusion of functional neurons may lead to hypofunctional neurons, which can increase cerebral blood flow and cerebral metabolic rate for oxygen (CMRO2), and thus improve cognition. However, when additional variables are introduced to the hypofunctional neurons – such as microembolism, white matter disease, and prolonged hypoperfusion – that can lead to neuronal infarction that, while increasing cerebral blood flow, causes no change in CMRO2 and, thus, no cognitive improvement. The interval between hypofunctional neurons and neuronal infarction “is the time to do the revascularization, as long as you can demonstrate that there may be some truth to matter that it influences cognition,” Dr. Motaganahalli said.
While vascular surgeons may not be able to predict who will have cognitive decline after carotid interventions, “There are some pointers for possibly picking those patients who may benefit,” Dr. Motaganahalli said.
That choice of patients revolves around recognizing that chronic ischemia induces and increases the severity of cognitive dysfunction. Therefore, incorporating the pathophysiology of chronic ischemia into the algorithm for carotid artery disease may provide an opportunity to extend the goals of carotid artery revascularization to include preventing or reversing cognitive decline, he said.
Dr. Motaganahalli disclosed he is a consultant to Silk Road Medical.
AT THE ANNUAL MEETING OF THE MIDWESTERN VASCULAR SURGERY SOCIETY
Key clinical point: Incorporating the pathophysiology of chronic ischemia into the algorithm for carotid artery disease could expand the goals of revascularization to encompass cognitive decline.
Major finding: Cerebrovascular hemodynamic status plays a role in cognitive function after carotid artery interventions, but the mechanisms of either improvement or decline need better understanding.
Data source: Systematic review of 32 papers on neurocognition after carotid interventions published between 1990-2007 and analysis of 37 studies of CAS or CEA or both published since 2007.
Disclosures: Dr. Motaganahalli disclosed he is a consultant to Silk Road Medical Inc.
Open Surgical Repair Session to Highlight CLI
Attendees at Tuesday afternoon’s “Topics Related to Open Surgery and Aortic Coarctations” session will learn when open surgery is the best choice despite remarkable advances in endovascular treatment.
“There are still open procedures that every vascular surgeon needs to know how to do well,” said moderator Dr. Fred Weaver of the University of Southern California, Los Angeles.
Coral reef lesions, aortoesophageal fistulas, extensive aortobifemoral occlusions, and celiac axis compression syndromes are often just too complex and extensive for endovascular approaches, and endovascular procedures are less likely to work when patients have underlying problems such as Marfan syndrome and Takayasu arteritis. In addition, open fixes for renal artery disease better preserve kidney function, Dr. Weaver noted. They also make sense for young patients needing a durable, one-time fix. “We don’t have much long-term follow-up experience with endovascular procedures, but we have almost a half-century of experience with open vascular procedures. We know how durable they can be,” he said.
Issues surrounding open procedures and more will be addressed in the session. “Open surgical solutions are oftentimes deferred or not even offered for fear of bad outcomes,” but “they can be successful, and you have to have them in your playbook,” said co-moderator Dr. James Black of Johns Hopkins University.
Three presentations will tackle critical limb ischemia (CLI), a “hot topic that is still very controversial,” Dr. Weaver noted.
Dr. Julien Sfeir of Lebanese University, Beirut, will discuss open salvage after failed endovascular CLI intervention. Dr. R. Clement Darling of Albany Medical College in New York, and also a moderator, will discuss the role of open procedures in the endovascular era, and Dr. Carlo Setacci of the University of Siena, Italy, will address combining open and endovascular techniques for especially difficult cases.
BEST-CLI, an ongoing randomized controlled trial comparing endovascular therapy with open surgical bypass in CLI, will likely be discussed, which is “one of the reasons someone might want to come to this session. Nobody really knows what’s the best option in a lot of situations,” Dr. Weaver said.
Dr. Black will also address when open repair is best – and how to do it – when there’s a distal aortic failure after thoracic endovascular aortic repair (TEVAR). “Stents may palliate dissection in the chest, but dissection beyond the stent into the abdomen remains untreated, and there can life-threatening growth of the aortic diameter. Because the dissection anatomy can be so variable, open surgery is the most expeditious fix, especially in a patient with acute symptoms” he said.
One presentation will buck the theme: a new endovascular approach for aortic coarctation. With the recent approval of the NuMED Cheatham Platinum Stent System, “we now have a viable device solution to handle what otherwise would be a major surgery. It’s a very large diameter, balloon-expandable stent graft with significant radial force made to order for this problem. We’ve totally reversed the treatment paradigm, from 10 days in the hospital and 2 months recovery to 1 night in the hospital and you are driving in 2 days,” Dr. Black said.
Yet “whether it works over the long term is an area of considerable uncertainty. This is an area which is in flux,” Dr. Weaver noted. Dr. Elchanan Bruckheimer will speak about the COAST 1 and 2 trials that preceded the Food and Drug Administration approval of the Cheatham Platinum Stent System.
Session 16:
Topics Related to Open Surgery and Aortic Coarctations
Tuesday, 4:32 p.m. – 5:58 p.m.
Grand Ballroom West, 3rd Floor
Attendees at Tuesday afternoon’s “Topics Related to Open Surgery and Aortic Coarctations” session will learn when open surgery is the best choice despite remarkable advances in endovascular treatment.
“There are still open procedures that every vascular surgeon needs to know how to do well,” said moderator Dr. Fred Weaver of the University of Southern California, Los Angeles.
Coral reef lesions, aortoesophageal fistulas, extensive aortobifemoral occlusions, and celiac axis compression syndromes are often just too complex and extensive for endovascular approaches, and endovascular procedures are less likely to work when patients have underlying problems such as Marfan syndrome and Takayasu arteritis. In addition, open fixes for renal artery disease better preserve kidney function, Dr. Weaver noted. They also make sense for young patients needing a durable, one-time fix. “We don’t have much long-term follow-up experience with endovascular procedures, but we have almost a half-century of experience with open vascular procedures. We know how durable they can be,” he said.
Issues surrounding open procedures and more will be addressed in the session. “Open surgical solutions are oftentimes deferred or not even offered for fear of bad outcomes,” but “they can be successful, and you have to have them in your playbook,” said co-moderator Dr. James Black of Johns Hopkins University.
Three presentations will tackle critical limb ischemia (CLI), a “hot topic that is still very controversial,” Dr. Weaver noted.
Dr. Julien Sfeir of Lebanese University, Beirut, will discuss open salvage after failed endovascular CLI intervention. Dr. R. Clement Darling of Albany Medical College in New York, and also a moderator, will discuss the role of open procedures in the endovascular era, and Dr. Carlo Setacci of the University of Siena, Italy, will address combining open and endovascular techniques for especially difficult cases.
BEST-CLI, an ongoing randomized controlled trial comparing endovascular therapy with open surgical bypass in CLI, will likely be discussed, which is “one of the reasons someone might want to come to this session. Nobody really knows what’s the best option in a lot of situations,” Dr. Weaver said.
Dr. Black will also address when open repair is best – and how to do it – when there’s a distal aortic failure after thoracic endovascular aortic repair (TEVAR). “Stents may palliate dissection in the chest, but dissection beyond the stent into the abdomen remains untreated, and there can life-threatening growth of the aortic diameter. Because the dissection anatomy can be so variable, open surgery is the most expeditious fix, especially in a patient with acute symptoms” he said.
One presentation will buck the theme: a new endovascular approach for aortic coarctation. With the recent approval of the NuMED Cheatham Platinum Stent System, “we now have a viable device solution to handle what otherwise would be a major surgery. It’s a very large diameter, balloon-expandable stent graft with significant radial force made to order for this problem. We’ve totally reversed the treatment paradigm, from 10 days in the hospital and 2 months recovery to 1 night in the hospital and you are driving in 2 days,” Dr. Black said.
Yet “whether it works over the long term is an area of considerable uncertainty. This is an area which is in flux,” Dr. Weaver noted. Dr. Elchanan Bruckheimer will speak about the COAST 1 and 2 trials that preceded the Food and Drug Administration approval of the Cheatham Platinum Stent System.
Session 16:
Topics Related to Open Surgery and Aortic Coarctations
Tuesday, 4:32 p.m. – 5:58 p.m.
Grand Ballroom West, 3rd Floor
Attendees at Tuesday afternoon’s “Topics Related to Open Surgery and Aortic Coarctations” session will learn when open surgery is the best choice despite remarkable advances in endovascular treatment.
“There are still open procedures that every vascular surgeon needs to know how to do well,” said moderator Dr. Fred Weaver of the University of Southern California, Los Angeles.
Coral reef lesions, aortoesophageal fistulas, extensive aortobifemoral occlusions, and celiac axis compression syndromes are often just too complex and extensive for endovascular approaches, and endovascular procedures are less likely to work when patients have underlying problems such as Marfan syndrome and Takayasu arteritis. In addition, open fixes for renal artery disease better preserve kidney function, Dr. Weaver noted. They also make sense for young patients needing a durable, one-time fix. “We don’t have much long-term follow-up experience with endovascular procedures, but we have almost a half-century of experience with open vascular procedures. We know how durable they can be,” he said.
Issues surrounding open procedures and more will be addressed in the session. “Open surgical solutions are oftentimes deferred or not even offered for fear of bad outcomes,” but “they can be successful, and you have to have them in your playbook,” said co-moderator Dr. James Black of Johns Hopkins University.
Three presentations will tackle critical limb ischemia (CLI), a “hot topic that is still very controversial,” Dr. Weaver noted.
Dr. Julien Sfeir of Lebanese University, Beirut, will discuss open salvage after failed endovascular CLI intervention. Dr. R. Clement Darling of Albany Medical College in New York, and also a moderator, will discuss the role of open procedures in the endovascular era, and Dr. Carlo Setacci of the University of Siena, Italy, will address combining open and endovascular techniques for especially difficult cases.
BEST-CLI, an ongoing randomized controlled trial comparing endovascular therapy with open surgical bypass in CLI, will likely be discussed, which is “one of the reasons someone might want to come to this session. Nobody really knows what’s the best option in a lot of situations,” Dr. Weaver said.
Dr. Black will also address when open repair is best – and how to do it – when there’s a distal aortic failure after thoracic endovascular aortic repair (TEVAR). “Stents may palliate dissection in the chest, but dissection beyond the stent into the abdomen remains untreated, and there can life-threatening growth of the aortic diameter. Because the dissection anatomy can be so variable, open surgery is the most expeditious fix, especially in a patient with acute symptoms” he said.
One presentation will buck the theme: a new endovascular approach for aortic coarctation. With the recent approval of the NuMED Cheatham Platinum Stent System, “we now have a viable device solution to handle what otherwise would be a major surgery. It’s a very large diameter, balloon-expandable stent graft with significant radial force made to order for this problem. We’ve totally reversed the treatment paradigm, from 10 days in the hospital and 2 months recovery to 1 night in the hospital and you are driving in 2 days,” Dr. Black said.
Yet “whether it works over the long term is an area of considerable uncertainty. This is an area which is in flux,” Dr. Weaver noted. Dr. Elchanan Bruckheimer will speak about the COAST 1 and 2 trials that preceded the Food and Drug Administration approval of the Cheatham Platinum Stent System.
Session 16:
Topics Related to Open Surgery and Aortic Coarctations
Tuesday, 4:32 p.m. – 5:58 p.m.
Grand Ballroom West, 3rd Floor
Identifying the ‘No Option for Treatment’ Patient in Critical Limb Ischemia
Over the last decade, advanced techniques for extreme limb salvage have become available, but are not necessarily preferable for every patient. The focus of the Wednesday afternoon session, “More About CLI: The ‘No Option for Treatment’ Limb and Extreme Limb Salvage Techniques and Results,” is identifying patients for whom limb salvage is a feasible option and those for whom it is not.
“This is an important session, addressing those patients in whom it may be futile to continue pressing for the high-end, complex reconstructions we can perform,” said co-moderator Dr. Richard F. Neville, of the Heart and Vascular Institute in Fairfax, Va.
“There are patients in whom we should just say, ‘Let’s not do four angioplasties, a bypass, and multiple plastic surgeries. The best thing is to give them amputation and rehab them,” said Dr. Neville. The global crisis of type 2 diabetes, the costs and morbidities associated with leg amputation, and mortality rates post amputation have gained the attention of policy makers who have begun pressuring health systems to find less costly alternatives.
“The government has realized what many physicians have known for a while: In the long run, it costs the health care system a lot more to amputate than to save a leg,” said Dr. Neville.
The co-moderator of the session, Dr. Sean P. Lyden of the Cleveland Clinic College of Medicine at Case Western University, argued that new therapies are in high demand. “We still have a lot of patients where our current options of open surgery or endovascular therapy fail [but] too many patients get amputations yearly in the United States. Finding new options for these patients is critical.”
The typical VEITHsymposium attendee is well aware that limbs can be salvaged, but there is a lack of awareness of the range of possibilities for critical limb ischemia across most other specialties. “We vascular surgeons know it’s possible, but we have to get the word out to the primary care doctors, the endocrinologists, and others to let them know that this can be done,” said Dr. Neville.
The criteria for which patients make the best candidates for extreme limb salvage are still evolving. “It’s harder than you think,” said Dr. Neville. “There are many different opinions about what should even go into the decision-making process. Even thought leaders from vascular surgery, podiatry, and plastic surgery are struggling to decide on what factors are most implicated. It’s not that the specialties are in disagreement, but we can’t quite come to a consensus yet.”
Data surrounding critical limb ischemia outcomes will be discussed at the session, and the panel will debate what are the best criteria for determining extreme limb salvation algorithms.
“If we could come up with guidelines or a scoring system, that would allow us to have a helpful tool when discussing treatment options with the patient’s family who typically want us to do everything, even when we know it’s not the best thing to do,” said Dr. Neville.
Session 27:
More About CLI: The ‘No Option for Treatment’ Limb and Extreme Limb Salvage Techniques nd Results
Wednesday, 1:00 p.m. – 2:06 p.m.
Grand Ballroom East, 3rd Floor
Over the last decade, advanced techniques for extreme limb salvage have become available, but are not necessarily preferable for every patient. The focus of the Wednesday afternoon session, “More About CLI: The ‘No Option for Treatment’ Limb and Extreme Limb Salvage Techniques and Results,” is identifying patients for whom limb salvage is a feasible option and those for whom it is not.
“This is an important session, addressing those patients in whom it may be futile to continue pressing for the high-end, complex reconstructions we can perform,” said co-moderator Dr. Richard F. Neville, of the Heart and Vascular Institute in Fairfax, Va.
“There are patients in whom we should just say, ‘Let’s not do four angioplasties, a bypass, and multiple plastic surgeries. The best thing is to give them amputation and rehab them,” said Dr. Neville. The global crisis of type 2 diabetes, the costs and morbidities associated with leg amputation, and mortality rates post amputation have gained the attention of policy makers who have begun pressuring health systems to find less costly alternatives.
“The government has realized what many physicians have known for a while: In the long run, it costs the health care system a lot more to amputate than to save a leg,” said Dr. Neville.
The co-moderator of the session, Dr. Sean P. Lyden of the Cleveland Clinic College of Medicine at Case Western University, argued that new therapies are in high demand. “We still have a lot of patients where our current options of open surgery or endovascular therapy fail [but] too many patients get amputations yearly in the United States. Finding new options for these patients is critical.”
The typical VEITHsymposium attendee is well aware that limbs can be salvaged, but there is a lack of awareness of the range of possibilities for critical limb ischemia across most other specialties. “We vascular surgeons know it’s possible, but we have to get the word out to the primary care doctors, the endocrinologists, and others to let them know that this can be done,” said Dr. Neville.
The criteria for which patients make the best candidates for extreme limb salvage are still evolving. “It’s harder than you think,” said Dr. Neville. “There are many different opinions about what should even go into the decision-making process. Even thought leaders from vascular surgery, podiatry, and plastic surgery are struggling to decide on what factors are most implicated. It’s not that the specialties are in disagreement, but we can’t quite come to a consensus yet.”
Data surrounding critical limb ischemia outcomes will be discussed at the session, and the panel will debate what are the best criteria for determining extreme limb salvation algorithms.
“If we could come up with guidelines or a scoring system, that would allow us to have a helpful tool when discussing treatment options with the patient’s family who typically want us to do everything, even when we know it’s not the best thing to do,” said Dr. Neville.
Session 27:
More About CLI: The ‘No Option for Treatment’ Limb and Extreme Limb Salvage Techniques nd Results
Wednesday, 1:00 p.m. – 2:06 p.m.
Grand Ballroom East, 3rd Floor
Over the last decade, advanced techniques for extreme limb salvage have become available, but are not necessarily preferable for every patient. The focus of the Wednesday afternoon session, “More About CLI: The ‘No Option for Treatment’ Limb and Extreme Limb Salvage Techniques and Results,” is identifying patients for whom limb salvage is a feasible option and those for whom it is not.
“This is an important session, addressing those patients in whom it may be futile to continue pressing for the high-end, complex reconstructions we can perform,” said co-moderator Dr. Richard F. Neville, of the Heart and Vascular Institute in Fairfax, Va.
“There are patients in whom we should just say, ‘Let’s not do four angioplasties, a bypass, and multiple plastic surgeries. The best thing is to give them amputation and rehab them,” said Dr. Neville. The global crisis of type 2 diabetes, the costs and morbidities associated with leg amputation, and mortality rates post amputation have gained the attention of policy makers who have begun pressuring health systems to find less costly alternatives.
“The government has realized what many physicians have known for a while: In the long run, it costs the health care system a lot more to amputate than to save a leg,” said Dr. Neville.
The co-moderator of the session, Dr. Sean P. Lyden of the Cleveland Clinic College of Medicine at Case Western University, argued that new therapies are in high demand. “We still have a lot of patients where our current options of open surgery or endovascular therapy fail [but] too many patients get amputations yearly in the United States. Finding new options for these patients is critical.”
The typical VEITHsymposium attendee is well aware that limbs can be salvaged, but there is a lack of awareness of the range of possibilities for critical limb ischemia across most other specialties. “We vascular surgeons know it’s possible, but we have to get the word out to the primary care doctors, the endocrinologists, and others to let them know that this can be done,” said Dr. Neville.
The criteria for which patients make the best candidates for extreme limb salvage are still evolving. “It’s harder than you think,” said Dr. Neville. “There are many different opinions about what should even go into the decision-making process. Even thought leaders from vascular surgery, podiatry, and plastic surgery are struggling to decide on what factors are most implicated. It’s not that the specialties are in disagreement, but we can’t quite come to a consensus yet.”
Data surrounding critical limb ischemia outcomes will be discussed at the session, and the panel will debate what are the best criteria for determining extreme limb salvation algorithms.
“If we could come up with guidelines or a scoring system, that would allow us to have a helpful tool when discussing treatment options with the patient’s family who typically want us to do everything, even when we know it’s not the best thing to do,” said Dr. Neville.
Session 27:
More About CLI: The ‘No Option for Treatment’ Limb and Extreme Limb Salvage Techniques nd Results
Wednesday, 1:00 p.m. – 2:06 p.m.
Grand Ballroom East, 3rd Floor
Ulipristal acetate meets primary endpoint in pivotal uterine fibroids trial
SALT LAKE CITY – The selective progesterone receptor modulator ulipristal acetate significantly reduced bleeding associated with fibroids in VENUS-I, a pivotal phase III trial of 147 premenopausal women.
A total of 58% of patients who took 10 mg ulipristal acetate per day had no bleeding except spotting during the last 35 days of treatment, compared with 2% of the placebo group (P less than .0001), James Simon, MD, said at the annual meeting of the American Society for Reproductive Medicine. Forty-seven percent of patients who took 5 mg ulipristal acetate per day also met the primary endpoint (P less than .0001, compared with placebo), he said.
The most common treatment-related adverse effect was hypertension, which affected 8% of women in the 10-mg group and 4% of women in the 5-mg group, he added during the late-breaking oral presentation.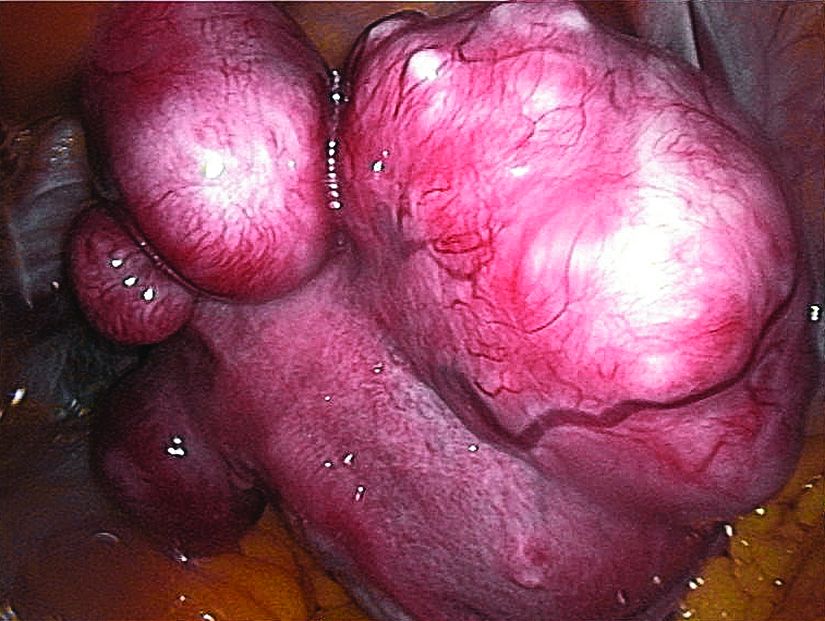
Ulipristal acetate is currently approved in the United States as an emergency contraceptive, but is marketed for treating symptomatic fibroids in Canada and Europe. The drug reduced bleeding in about 90% of patients in the European trials (N Engl J Med. 2012;366:409-20; Fertil Steril. 2014 Jun;101[6]:1565-73).
The VENUS-I trial included premenopausal women aged 18-50 years who had experienced 22-35 days of bleeding during at least four of their last six menstrual cycles, with at least 80 mL menstrual blood loss, and at least one fibroid confirmed by transvaginal ultrasound.
“The women in our study were more severely affected, in terms of the amount of bleeding and in terms of fibroid size and uterine size, than what was reported in the European trials,” Dr. Simon said.
The average age of the patients was 41 years, and 69% were African-American, reflecting the disproportionate burden of severely symptomatic fibroids in this group, he said.
Patients were randomly assigned to oral treatment with either placebo or 10 mg or 5 mg ulipristal acetate for 12 weeks, followed by a 12-week drug-free observation period. The primary endpoint was amenorrhea, not including spotting, during the last 35 consecutive days of treatment.
The 10-mg group was 49 times more likely to reach this endpoint than was the placebo arm (P less than .0001), even after the researchers controlled for multiple potential confounders, Dr. Simon reported. The hazard ratio for the 5-mg group was also highly statistically significant at 35.5 (P less than .0001).
“Almost all patients who achieved amenorrhea in the ulipristal acetate groups did so by day 11,” Dr. Simon said.
Rates of amenorrhea from day 11 through the end of treatment were 58% in the 10-mg group, 43% in the 5-mg group, and 0% in the placebo group (P less than .0001 for differences among groups). Patients who received ulipristal acetate also reported significantly greater improvements on the Uterine Fibroid Symptom and Quality of Life (UFS-QOL) questionnaire than did the placebo group.
No patients stopped treatment because of adverse effects. Of the six patients who developed hypertension while on ulipristal acetate, five had a history of high blood pressure, and the increases were generally “slight,” Dr. Simon said. The other common treatment-emergent adverse effects included increased creatinine phosphokinase, hot flashes, acne, and nausea.
Blinded pathologists interpreted endometrial biopsies at baseline, the end of treatment, and at the end of the drug-free observation period. These revealed no cases of atypical endometrial hyperplasia or malignancy, and no baseline increases in rates of progesterone receptor modulator–associated endometrial changes, Dr. Simon said. One patient developed endometrial hyperplasia without atypia at the end of treatment, which resolved by the end of the 12-week drug-free observation period.
VENUS-I is one of two pivotal trials of ulipristal acetate for the treatment of uterine fibroids in the United States. Results from the second trial, VENUS-II, are expected in 2017.
The VENUS-I trial was supported by Allergan and Gedeon Richter. Dr. Simon reported ties to numerous other pharmaceutical companies, but not to Allergan or Gedeon Richter.
SALT LAKE CITY – The selective progesterone receptor modulator ulipristal acetate significantly reduced bleeding associated with fibroids in VENUS-I, a pivotal phase III trial of 147 premenopausal women.
A total of 58% of patients who took 10 mg ulipristal acetate per day had no bleeding except spotting during the last 35 days of treatment, compared with 2% of the placebo group (P less than .0001), James Simon, MD, said at the annual meeting of the American Society for Reproductive Medicine. Forty-seven percent of patients who took 5 mg ulipristal acetate per day also met the primary endpoint (P less than .0001, compared with placebo), he said.
The most common treatment-related adverse effect was hypertension, which affected 8% of women in the 10-mg group and 4% of women in the 5-mg group, he added during the late-breaking oral presentation.
Ulipristal acetate is currently approved in the United States as an emergency contraceptive, but is marketed for treating symptomatic fibroids in Canada and Europe. The drug reduced bleeding in about 90% of patients in the European trials (N Engl J Med. 2012;366:409-20; Fertil Steril. 2014 Jun;101[6]:1565-73).
The VENUS-I trial included premenopausal women aged 18-50 years who had experienced 22-35 days of bleeding during at least four of their last six menstrual cycles, with at least 80 mL menstrual blood loss, and at least one fibroid confirmed by transvaginal ultrasound.
“The women in our study were more severely affected, in terms of the amount of bleeding and in terms of fibroid size and uterine size, than what was reported in the European trials,” Dr. Simon said.
The average age of the patients was 41 years, and 69% were African-American, reflecting the disproportionate burden of severely symptomatic fibroids in this group, he said.
Patients were randomly assigned to oral treatment with either placebo or 10 mg or 5 mg ulipristal acetate for 12 weeks, followed by a 12-week drug-free observation period. The primary endpoint was amenorrhea, not including spotting, during the last 35 consecutive days of treatment.
The 10-mg group was 49 times more likely to reach this endpoint than was the placebo arm (P less than .0001), even after the researchers controlled for multiple potential confounders, Dr. Simon reported. The hazard ratio for the 5-mg group was also highly statistically significant at 35.5 (P less than .0001).
“Almost all patients who achieved amenorrhea in the ulipristal acetate groups did so by day 11,” Dr. Simon said.
Rates of amenorrhea from day 11 through the end of treatment were 58% in the 10-mg group, 43% in the 5-mg group, and 0% in the placebo group (P less than .0001 for differences among groups). Patients who received ulipristal acetate also reported significantly greater improvements on the Uterine Fibroid Symptom and Quality of Life (UFS-QOL) questionnaire than did the placebo group.
No patients stopped treatment because of adverse effects. Of the six patients who developed hypertension while on ulipristal acetate, five had a history of high blood pressure, and the increases were generally “slight,” Dr. Simon said. The other common treatment-emergent adverse effects included increased creatinine phosphokinase, hot flashes, acne, and nausea.
Blinded pathologists interpreted endometrial biopsies at baseline, the end of treatment, and at the end of the drug-free observation period. These revealed no cases of atypical endometrial hyperplasia or malignancy, and no baseline increases in rates of progesterone receptor modulator–associated endometrial changes, Dr. Simon said. One patient developed endometrial hyperplasia without atypia at the end of treatment, which resolved by the end of the 12-week drug-free observation period.
VENUS-I is one of two pivotal trials of ulipristal acetate for the treatment of uterine fibroids in the United States. Results from the second trial, VENUS-II, are expected in 2017.
The VENUS-I trial was supported by Allergan and Gedeon Richter. Dr. Simon reported ties to numerous other pharmaceutical companies, but not to Allergan or Gedeon Richter.
SALT LAKE CITY – The selective progesterone receptor modulator ulipristal acetate significantly reduced bleeding associated with fibroids in VENUS-I, a pivotal phase III trial of 147 premenopausal women.
A total of 58% of patients who took 10 mg ulipristal acetate per day had no bleeding except spotting during the last 35 days of treatment, compared with 2% of the placebo group (P less than .0001), James Simon, MD, said at the annual meeting of the American Society for Reproductive Medicine. Forty-seven percent of patients who took 5 mg ulipristal acetate per day also met the primary endpoint (P less than .0001, compared with placebo), he said.
The most common treatment-related adverse effect was hypertension, which affected 8% of women in the 10-mg group and 4% of women in the 5-mg group, he added during the late-breaking oral presentation.
Ulipristal acetate is currently approved in the United States as an emergency contraceptive, but is marketed for treating symptomatic fibroids in Canada and Europe. The drug reduced bleeding in about 90% of patients in the European trials (N Engl J Med. 2012;366:409-20; Fertil Steril. 2014 Jun;101[6]:1565-73).
The VENUS-I trial included premenopausal women aged 18-50 years who had experienced 22-35 days of bleeding during at least four of their last six menstrual cycles, with at least 80 mL menstrual blood loss, and at least one fibroid confirmed by transvaginal ultrasound.
“The women in our study were more severely affected, in terms of the amount of bleeding and in terms of fibroid size and uterine size, than what was reported in the European trials,” Dr. Simon said.
The average age of the patients was 41 years, and 69% were African-American, reflecting the disproportionate burden of severely symptomatic fibroids in this group, he said.
Patients were randomly assigned to oral treatment with either placebo or 10 mg or 5 mg ulipristal acetate for 12 weeks, followed by a 12-week drug-free observation period. The primary endpoint was amenorrhea, not including spotting, during the last 35 consecutive days of treatment.
The 10-mg group was 49 times more likely to reach this endpoint than was the placebo arm (P less than .0001), even after the researchers controlled for multiple potential confounders, Dr. Simon reported. The hazard ratio for the 5-mg group was also highly statistically significant at 35.5 (P less than .0001).
“Almost all patients who achieved amenorrhea in the ulipristal acetate groups did so by day 11,” Dr. Simon said.
Rates of amenorrhea from day 11 through the end of treatment were 58% in the 10-mg group, 43% in the 5-mg group, and 0% in the placebo group (P less than .0001 for differences among groups). Patients who received ulipristal acetate also reported significantly greater improvements on the Uterine Fibroid Symptom and Quality of Life (UFS-QOL) questionnaire than did the placebo group.
No patients stopped treatment because of adverse effects. Of the six patients who developed hypertension while on ulipristal acetate, five had a history of high blood pressure, and the increases were generally “slight,” Dr. Simon said. The other common treatment-emergent adverse effects included increased creatinine phosphokinase, hot flashes, acne, and nausea.
Blinded pathologists interpreted endometrial biopsies at baseline, the end of treatment, and at the end of the drug-free observation period. These revealed no cases of atypical endometrial hyperplasia or malignancy, and no baseline increases in rates of progesterone receptor modulator–associated endometrial changes, Dr. Simon said. One patient developed endometrial hyperplasia without atypia at the end of treatment, which resolved by the end of the 12-week drug-free observation period.
VENUS-I is one of two pivotal trials of ulipristal acetate for the treatment of uterine fibroids in the United States. Results from the second trial, VENUS-II, are expected in 2017.
The VENUS-I trial was supported by Allergan and Gedeon Richter. Dr. Simon reported ties to numerous other pharmaceutical companies, but not to Allergan or Gedeon Richter.
AT 2016 ASRM
Key clinical point:
Major finding: Rates of amenorrhea during the last 35 consecutive days of treatment were 58% in the 10-mg group, compared with 2% in the placebo group (P less than .0001).
Data source: A randomized, double-blind trial of 147 premenopausal women with uterine fibroids and an average of 80 mL menstrual blood loss.
Disclosures: VENUS-I was supported by Allergan and Gedeon Richter. Dr. Simon reported ties to numerous other pharmaceutical companies, but not to Allergan or Gedeon Richter.
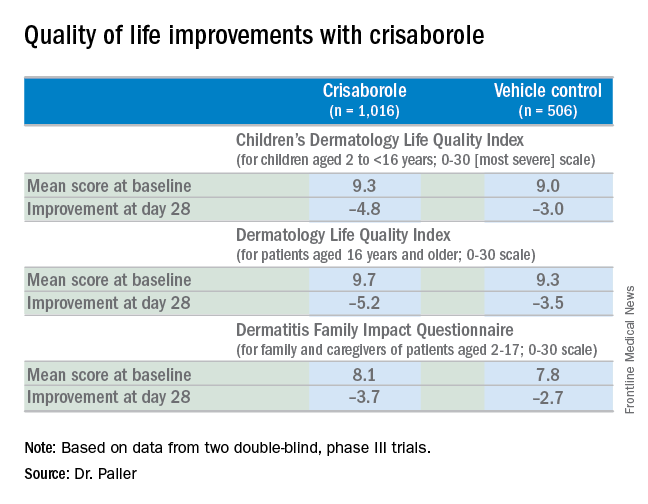
Topical crisaborole boosts quality of life in atopic dermatitis
VIENNA – Topical crisaborole 2% ointment administered twice a day was consistently associated with clinically meaningful quality of life improvement scores on multiple measures in the two pivotal phase III, randomized, controlled trials of atopic dermatitis (AD) patients aged 2 years old through adulthood, Amy S. Paller, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
AD in children and adolescents is infamous for the adverse quality of life impact it imposes upon the patients’ parents, family, and caregivers. So the significant improvement seen with crisaborole, compared with its vehicle on the Dermatitis Family Impact (DFI) Questionnaire was particularly gratifying. The DFI questionnaire assesses quality of life in key domains, including family, parent, and caregiver sleep, emotional distress, relationships, family leisure, and ability to do housework or go shopping.

“If approved, crisaborole ... could improve the quality of life for patients with mild to moderate atopic dermatitis and, very importantly, for their families as well,” declared Dr. Paller, professor of dermatology and chair of the department of dermatology and professor of pediatrics at Northwestern University, Chicago.
Crisaborole’s developer, Anacor Pharmaceuticals, has filed an application for approval for treating mild to moderate AD in patients aged 2 years and older, now under review at the Food and Drug Administration.
In a separate presentation at the EADV congress, Lawrence F. Eichenfield, MD, presented the results of a long-term, open-label crisaborole safety study of 48-52 weeks duration. The long-term study involved 517 participants in the two pivotal phase III trials. There were no serious adverse events and no long-term cutaneous adverse events such as the skin atrophy or telangiectasias that can occur with topical steroids. The safety profile was favorable for long-term treatment of patients 2 years of age or older with mild to moderate AD.

Crisaborole 2% topical ointment is a novel, boron-based, nonsteroidal inhibitor of phosphodiesterase 4 (PDE-4). AD is marked by overactivity of PDE-4, which results in decreased levels of cyclic AMP and resultant increased release of inflammatory cytokines.
Dr. Paller noted that, in the previously reported efficacy results of the two pivotal, double-blind, 28-day, phase III trials, crisaborole treatment reduced global disease severity and provided early and sustained improvement in itch severity. She presented the prespecified quality of life results for the two identically designed, parallel pivotal trials, which totaled 1,016 patients on crisaborole and 506 on its vehicle. At baseline, 39% of subjects had mild AD, and 61% had moderate AD. The mean body surface area affected was 18%. Participants’ mean age was 12.3 years, and 14% were aged 8 years old or older.
The structure of the long-term safety study suggests how crisaborole might be used in clinical practice. During the year-long, open-label study, patients were evaluated every 28 days. If their skin was deemed clear or almost clear on the basis of an Investigator’s Static Global Assessment (ISGA) score of 0 or 1, they were taken off crisaborole and could use only emollients for the next 28 days, at which time they would be reevaluated. At that point, if they had an ISGA of 2 or more, they went back on crisaborole twice a day for 28 days until their next evaluation.
Dr. Eichenfield reported that 10.2% of participants in the long-term safety study reported treatment-related adverse events, which were mild to moderate. The most frequently reported of these were mild to moderate flares of AD during a 28-day off-treatment period in 1.3% of patients, application site pain in 2.3%, and application site infection in 1.2%.
Dr. Paller and Dr. Eichenfield reported serving as consultants to Anacor Pharmaceuticals.
The FDA review of crisaborole is expected to be completed by early January 2017, according to Anacor.
VIENNA – Topical crisaborole 2% ointment administered twice a day was consistently associated with clinically meaningful quality of life improvement scores on multiple measures in the two pivotal phase III, randomized, controlled trials of atopic dermatitis (AD) patients aged 2 years old through adulthood, Amy S. Paller, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
AD in children and adolescents is infamous for the adverse quality of life impact it imposes upon the patients’ parents, family, and caregivers. So the significant improvement seen with crisaborole, compared with its vehicle on the Dermatitis Family Impact (DFI) Questionnaire was particularly gratifying. The DFI questionnaire assesses quality of life in key domains, including family, parent, and caregiver sleep, emotional distress, relationships, family leisure, and ability to do housework or go shopping.
“If approved, crisaborole ... could improve the quality of life for patients with mild to moderate atopic dermatitis and, very importantly, for their families as well,” declared Dr. Paller, professor of dermatology and chair of the department of dermatology and professor of pediatrics at Northwestern University, Chicago.
Crisaborole’s developer, Anacor Pharmaceuticals, has filed an application for approval for treating mild to moderate AD in patients aged 2 years and older, now under review at the Food and Drug Administration.
In a separate presentation at the EADV congress, Lawrence F. Eichenfield, MD, presented the results of a long-term, open-label crisaborole safety study of 48-52 weeks duration. The long-term study involved 517 participants in the two pivotal phase III trials. There were no serious adverse events and no long-term cutaneous adverse events such as the skin atrophy or telangiectasias that can occur with topical steroids. The safety profile was favorable for long-term treatment of patients 2 years of age or older with mild to moderate AD.
Crisaborole 2% topical ointment is a novel, boron-based, nonsteroidal inhibitor of phosphodiesterase 4 (PDE-4). AD is marked by overactivity of PDE-4, which results in decreased levels of cyclic AMP and resultant increased release of inflammatory cytokines.
Dr. Paller noted that, in the previously reported efficacy results of the two pivotal, double-blind, 28-day, phase III trials, crisaborole treatment reduced global disease severity and provided early and sustained improvement in itch severity. She presented the prespecified quality of life results for the two identically designed, parallel pivotal trials, which totaled 1,016 patients on crisaborole and 506 on its vehicle. At baseline, 39% of subjects had mild AD, and 61% had moderate AD. The mean body surface area affected was 18%. Participants’ mean age was 12.3 years, and 14% were aged 8 years old or older.
The structure of the long-term safety study suggests how crisaborole might be used in clinical practice. During the year-long, open-label study, patients were evaluated every 28 days. If their skin was deemed clear or almost clear on the basis of an Investigator’s Static Global Assessment (ISGA) score of 0 or 1, they were taken off crisaborole and could use only emollients for the next 28 days, at which time they would be reevaluated. At that point, if they had an ISGA of 2 or more, they went back on crisaborole twice a day for 28 days until their next evaluation.
Dr. Eichenfield reported that 10.2% of participants in the long-term safety study reported treatment-related adverse events, which were mild to moderate. The most frequently reported of these were mild to moderate flares of AD during a 28-day off-treatment period in 1.3% of patients, application site pain in 2.3%, and application site infection in 1.2%.
Dr. Paller and Dr. Eichenfield reported serving as consultants to Anacor Pharmaceuticals.
The FDA review of crisaborole is expected to be completed by early January 2017, according to Anacor.
VIENNA – Topical crisaborole 2% ointment administered twice a day was consistently associated with clinically meaningful quality of life improvement scores on multiple measures in the two pivotal phase III, randomized, controlled trials of atopic dermatitis (AD) patients aged 2 years old through adulthood, Amy S. Paller, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
AD in children and adolescents is infamous for the adverse quality of life impact it imposes upon the patients’ parents, family, and caregivers. So the significant improvement seen with crisaborole, compared with its vehicle on the Dermatitis Family Impact (DFI) Questionnaire was particularly gratifying. The DFI questionnaire assesses quality of life in key domains, including family, parent, and caregiver sleep, emotional distress, relationships, family leisure, and ability to do housework or go shopping.
“If approved, crisaborole ... could improve the quality of life for patients with mild to moderate atopic dermatitis and, very importantly, for their families as well,” declared Dr. Paller, professor of dermatology and chair of the department of dermatology and professor of pediatrics at Northwestern University, Chicago.
Crisaborole’s developer, Anacor Pharmaceuticals, has filed an application for approval for treating mild to moderate AD in patients aged 2 years and older, now under review at the Food and Drug Administration.
In a separate presentation at the EADV congress, Lawrence F. Eichenfield, MD, presented the results of a long-term, open-label crisaborole safety study of 48-52 weeks duration. The long-term study involved 517 participants in the two pivotal phase III trials. There were no serious adverse events and no long-term cutaneous adverse events such as the skin atrophy or telangiectasias that can occur with topical steroids. The safety profile was favorable for long-term treatment of patients 2 years of age or older with mild to moderate AD.
Crisaborole 2% topical ointment is a novel, boron-based, nonsteroidal inhibitor of phosphodiesterase 4 (PDE-4). AD is marked by overactivity of PDE-4, which results in decreased levels of cyclic AMP and resultant increased release of inflammatory cytokines.
Dr. Paller noted that, in the previously reported efficacy results of the two pivotal, double-blind, 28-day, phase III trials, crisaborole treatment reduced global disease severity and provided early and sustained improvement in itch severity. She presented the prespecified quality of life results for the two identically designed, parallel pivotal trials, which totaled 1,016 patients on crisaborole and 506 on its vehicle. At baseline, 39% of subjects had mild AD, and 61% had moderate AD. The mean body surface area affected was 18%. Participants’ mean age was 12.3 years, and 14% were aged 8 years old or older.
The structure of the long-term safety study suggests how crisaborole might be used in clinical practice. During the year-long, open-label study, patients were evaluated every 28 days. If their skin was deemed clear or almost clear on the basis of an Investigator’s Static Global Assessment (ISGA) score of 0 or 1, they were taken off crisaborole and could use only emollients for the next 28 days, at which time they would be reevaluated. At that point, if they had an ISGA of 2 or more, they went back on crisaborole twice a day for 28 days until their next evaluation.
Dr. Eichenfield reported that 10.2% of participants in the long-term safety study reported treatment-related adverse events, which were mild to moderate. The most frequently reported of these were mild to moderate flares of AD during a 28-day off-treatment period in 1.3% of patients, application site pain in 2.3%, and application site infection in 1.2%.
Dr. Paller and Dr. Eichenfield reported serving as consultants to Anacor Pharmaceuticals.
The FDA review of crisaborole is expected to be completed by early January 2017, according to Anacor.
EXPERT ANALYSIS FROM THE EADV CONGRESS
Take a Bite of the Big Apple at the VEITHsymposium
New York City is a global destination renowned for its unparalleled variety of things to do and see to match all tastes and interests. In your time between and after the VEITHsymposium sessions, you can enjoy a Broadway show, take in some of the city’s famous museums, go on a shopping spree, or dine at some of the best restaurants in the world. Whether with family or on your own, there is something for everyone.
For a quick look at current entertainment and dining options, pick up a copy of TimeOut New York or visit www.timeout.com/newyork, where you’ll find current listings for what is playing at theaters off and on Broadway as well as live music, special events, shopping, fine dining, and more.
For a more comprehensive listing of Broadway and off-Broadway shows, visit www.Broadway.com.
For the sports fan, you can find a complete online calendar listing of sporting events that are going during the VEITHsymposium (www.nycgo.com/things-to-do/events-in-nyc/sports-calendar). Pick up the New York Knicks basketball team playing the Detroit Pistons on Nov. 16 at Madison Square Garden. College basketball will also be featured at the Garden with the Champions Classic on Nov. 15.
If you’re a classical music enthusiast, you should make time to attend a performance at Lincoln Center (www.lincolncenter.org), which plays host to the New York Philharmonic and the Metropolitan Opera. During the VEITHsymposium, the operas “Aida,” “La Boheme,” and “Manon Lescaut” are all being performed.
And for the forever young crowd, Billy Joel is in concert at Madison Square Garden on Nov. 19.
No matter where your music tastes lie, for the most up-to-date accounting of musical performances in the city, pick up a copy of the free weekly newspaper, the Village Voice, or visit it online (www.villagevoice.com).
For your exercise pleasure and a literal change of pace, there are a number of interesting walking tours available, including ones that amble through the historic lower East Side, the Metropolitan Opera, and Broadway theaters (www.walksofnewyork.com).
The New York food scene is both vast and varied, so to choose your dining from fine to fun, you can visit the venerable New York Times website (www.nytimes.com/reviews/dining) to plan your eating experience by rating, price, neighborhood, and choice of cuisine.
You will find several notable museums and landmarks within a few blocks of the VEITHsymposium. The Museum of Modern Art is the closest to the New York Hilton Midtown, at 11 West 53rd St., between Fifth and Sixth Avenues. MoMA houses more than 150,000 paintings, sculptures, drawings, prints, photographs, architectural models and drawings, and design objects. The Metropolitan Museum of Art is a bit farther away (1000 Fifth Ave. at 82nd St.). The holdings include 2 million works spanning 5,000 years of art history from around the world from Egyptian mummies to Rembrandts and Picassos.
The American Museum of Natural History is on the Upper West Side of Central Park (at 79th St.) and has something for museum goers of all ages: dinosaurs, fossils, stuffed specimens, minerals, gems, and human cultural artifacts.
The memorial at the site of the World Trade Center towers stands witness to a national tragedy and to the spirit of the people of New York. The names of nearly 3,000 men, women, and children killed in the attacks of Sept. 11, 2001, and Feb. 26, 1993, are inscribed on the parapets surrounding the two memorial pools (www.911memorial.org/visit).
In addition the famous Central Park, don’t overlook the less-noted Bryant Park (between 40th and 42nd Streets and Fifth and Sixth Avenues), which offers an opportunity to do some holiday shopping at the annual Holiday Shops fair. This outdoor, European-style market features everything from handcrafted items to gourmet treats.
If you’re a first-time visitor, the Empire State Building, the Statue of Liberty, and Ellis Island remain the must-see symbols of New York. Be prepared for long lines to get to the top of the Empire State Building (www.esbnyc.com). Dress warmly for the ferry ride from Battery Park (www.statuecruises.com) to the Statue of Liberty.
Above all, while you’re at the VEITHsymposium, be sure that you and your guests enjoy some of the many pleasures that New York has to offer. It’s your kind of town.
New York City is a global destination renowned for its unparalleled variety of things to do and see to match all tastes and interests. In your time between and after the VEITHsymposium sessions, you can enjoy a Broadway show, take in some of the city’s famous museums, go on a shopping spree, or dine at some of the best restaurants in the world. Whether with family or on your own, there is something for everyone.
For a quick look at current entertainment and dining options, pick up a copy of TimeOut New York or visit www.timeout.com/newyork, where you’ll find current listings for what is playing at theaters off and on Broadway as well as live music, special events, shopping, fine dining, and more.
For a more comprehensive listing of Broadway and off-Broadway shows, visit www.Broadway.com.
For the sports fan, you can find a complete online calendar listing of sporting events that are going during the VEITHsymposium (www.nycgo.com/things-to-do/events-in-nyc/sports-calendar). Pick up the New York Knicks basketball team playing the Detroit Pistons on Nov. 16 at Madison Square Garden. College basketball will also be featured at the Garden with the Champions Classic on Nov. 15.
If you’re a classical music enthusiast, you should make time to attend a performance at Lincoln Center (www.lincolncenter.org), which plays host to the New York Philharmonic and the Metropolitan Opera. During the VEITHsymposium, the operas “Aida,” “La Boheme,” and “Manon Lescaut” are all being performed.
And for the forever young crowd, Billy Joel is in concert at Madison Square Garden on Nov. 19.
No matter where your music tastes lie, for the most up-to-date accounting of musical performances in the city, pick up a copy of the free weekly newspaper, the Village Voice, or visit it online (www.villagevoice.com).
For your exercise pleasure and a literal change of pace, there are a number of interesting walking tours available, including ones that amble through the historic lower East Side, the Metropolitan Opera, and Broadway theaters (www.walksofnewyork.com).
The New York food scene is both vast and varied, so to choose your dining from fine to fun, you can visit the venerable New York Times website (www.nytimes.com/reviews/dining) to plan your eating experience by rating, price, neighborhood, and choice of cuisine.
You will find several notable museums and landmarks within a few blocks of the VEITHsymposium. The Museum of Modern Art is the closest to the New York Hilton Midtown, at 11 West 53rd St., between Fifth and Sixth Avenues. MoMA houses more than 150,000 paintings, sculptures, drawings, prints, photographs, architectural models and drawings, and design objects. The Metropolitan Museum of Art is a bit farther away (1000 Fifth Ave. at 82nd St.). The holdings include 2 million works spanning 5,000 years of art history from around the world from Egyptian mummies to Rembrandts and Picassos.
The American Museum of Natural History is on the Upper West Side of Central Park (at 79th St.) and has something for museum goers of all ages: dinosaurs, fossils, stuffed specimens, minerals, gems, and human cultural artifacts.
The memorial at the site of the World Trade Center towers stands witness to a national tragedy and to the spirit of the people of New York. The names of nearly 3,000 men, women, and children killed in the attacks of Sept. 11, 2001, and Feb. 26, 1993, are inscribed on the parapets surrounding the two memorial pools (www.911memorial.org/visit).
In addition the famous Central Park, don’t overlook the less-noted Bryant Park (between 40th and 42nd Streets and Fifth and Sixth Avenues), which offers an opportunity to do some holiday shopping at the annual Holiday Shops fair. This outdoor, European-style market features everything from handcrafted items to gourmet treats.
If you’re a first-time visitor, the Empire State Building, the Statue of Liberty, and Ellis Island remain the must-see symbols of New York. Be prepared for long lines to get to the top of the Empire State Building (www.esbnyc.com). Dress warmly for the ferry ride from Battery Park (www.statuecruises.com) to the Statue of Liberty.
Above all, while you’re at the VEITHsymposium, be sure that you and your guests enjoy some of the many pleasures that New York has to offer. It’s your kind of town.
New York City is a global destination renowned for its unparalleled variety of things to do and see to match all tastes and interests. In your time between and after the VEITHsymposium sessions, you can enjoy a Broadway show, take in some of the city’s famous museums, go on a shopping spree, or dine at some of the best restaurants in the world. Whether with family or on your own, there is something for everyone.
For a quick look at current entertainment and dining options, pick up a copy of TimeOut New York or visit www.timeout.com/newyork, where you’ll find current listings for what is playing at theaters off and on Broadway as well as live music, special events, shopping, fine dining, and more.
For a more comprehensive listing of Broadway and off-Broadway shows, visit www.Broadway.com.
For the sports fan, you can find a complete online calendar listing of sporting events that are going during the VEITHsymposium (www.nycgo.com/things-to-do/events-in-nyc/sports-calendar). Pick up the New York Knicks basketball team playing the Detroit Pistons on Nov. 16 at Madison Square Garden. College basketball will also be featured at the Garden with the Champions Classic on Nov. 15.
If you’re a classical music enthusiast, you should make time to attend a performance at Lincoln Center (www.lincolncenter.org), which plays host to the New York Philharmonic and the Metropolitan Opera. During the VEITHsymposium, the operas “Aida,” “La Boheme,” and “Manon Lescaut” are all being performed.
And for the forever young crowd, Billy Joel is in concert at Madison Square Garden on Nov. 19.
No matter where your music tastes lie, for the most up-to-date accounting of musical performances in the city, pick up a copy of the free weekly newspaper, the Village Voice, or visit it online (www.villagevoice.com).
For your exercise pleasure and a literal change of pace, there are a number of interesting walking tours available, including ones that amble through the historic lower East Side, the Metropolitan Opera, and Broadway theaters (www.walksofnewyork.com).
The New York food scene is both vast and varied, so to choose your dining from fine to fun, you can visit the venerable New York Times website (www.nytimes.com/reviews/dining) to plan your eating experience by rating, price, neighborhood, and choice of cuisine.
You will find several notable museums and landmarks within a few blocks of the VEITHsymposium. The Museum of Modern Art is the closest to the New York Hilton Midtown, at 11 West 53rd St., between Fifth and Sixth Avenues. MoMA houses more than 150,000 paintings, sculptures, drawings, prints, photographs, architectural models and drawings, and design objects. The Metropolitan Museum of Art is a bit farther away (1000 Fifth Ave. at 82nd St.). The holdings include 2 million works spanning 5,000 years of art history from around the world from Egyptian mummies to Rembrandts and Picassos.
The American Museum of Natural History is on the Upper West Side of Central Park (at 79th St.) and has something for museum goers of all ages: dinosaurs, fossils, stuffed specimens, minerals, gems, and human cultural artifacts.
The memorial at the site of the World Trade Center towers stands witness to a national tragedy and to the spirit of the people of New York. The names of nearly 3,000 men, women, and children killed in the attacks of Sept. 11, 2001, and Feb. 26, 1993, are inscribed on the parapets surrounding the two memorial pools (www.911memorial.org/visit).
In addition the famous Central Park, don’t overlook the less-noted Bryant Park (between 40th and 42nd Streets and Fifth and Sixth Avenues), which offers an opportunity to do some holiday shopping at the annual Holiday Shops fair. This outdoor, European-style market features everything from handcrafted items to gourmet treats.
If you’re a first-time visitor, the Empire State Building, the Statue of Liberty, and Ellis Island remain the must-see symbols of New York. Be prepared for long lines to get to the top of the Empire State Building (www.esbnyc.com). Dress warmly for the ferry ride from Battery Park (www.statuecruises.com) to the Statue of Liberty.
Above all, while you’re at the VEITHsymposium, be sure that you and your guests enjoy some of the many pleasures that New York has to offer. It’s your kind of town.
Prognostic scores helpful in subset of COPD patients
LOS ANGELES – The Sequential Organ Failure Assessment (SOFA) score and the Glasgow Coma Scale (GCS) are simple, accurate tools for risk stratification of hospitalized patients with acute exacerbation of COPD, results from a single-center study showed.
“Acute exacerbations of chronic obstructive pulmonary disease often require hospitalization, may necessitate mechanical ventilation, and can be fatal,” Mohamed Metwally, MD, FCCP, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “There are currently no validated disease-specific scores that measure the severity of acute exacerbation. Prognostic tools are needed to assess acute exacerbations of chronic obstructive pulmonary disease.”

For the 2-year study, Dr. Metwally and his associates prospectively evaluated 250 critically ill ICU AECOPD patients, mean age 65 years, at Assiut University Hospital between December 2012 and December 2014. The primary outcome was in-hospital mortality while the secondary endpoint was need for intubation and mechanical ventilation. The researchers excluded patients who died less than 24 hours after admission, those with underlying COPD who were admitted with another primary diagnosis such as an accident or a stroke, or for elective hospitalizations such as elective surgery or diagnostic procedures.
Dr. Metwally and his associates collected sociodemographic data, vital signs, and other clinical variables, and collected scores from five tools used to measure mortality prediction: the Acute Physiology and Chronic Health Evaluation (APACHE II), the SOFA score, the Early Warning Score (EWS), the GCS, and the Charlson Comorbidity Index (CCI). To assess performance of the scores, they used area under the receiver operating characteristic curve (AUC) analysis and the Hosmer-Lemeshow goodness-of-fit test for logistic regression.
Of the 250 patients, 43 (17%) died during their hospital stay and 54% required mechanical ventilation. All recorded scores were significantly higher in nonsurvivors, compared with survivors, and the risk of clinical deterioration increased with increasing scores. The discriminatory power of each score varied as measured by AUC analysis. The AUC of APACHE II, SOFA, EWS, GCS, and CCI were 0.79, 0.81, 0.76, 0.69, and 0.68, respectively “and all these models had good calibration in mortality prediction,” Dr. Metwally said. The SOFA score was the best in predicting mortality (its predicted mortality was 16%, compared with the actual mortality of 17%), while the APACHE II score overestimated mortality by at least twofold (46% vs. 17%). In addition, the EWS outperformed the GCS in predicting mortality. “This may be due to EWS containing all vital signs plus level of consciousness,” he said in an interview.
The GCS was found to be the most useful in predicting need for mechanical ventilation, with an AUC of 0.81. The AUCs of APACHE II, SOFA, EWS, and CCI were 0.79, 0.80, 0.73, and 0.61, respectively. All of the scores had good calibration in mortality prediction, Dr. Metwally said, with the exception of SOFA.
As for the APACHE II, Dr. Metwally said that instrument “can be used as a tool to predict both mortality and intubation in a specific group of patients, but with low discriminatory power.” He acknowledged certain limitations of the study, including the fact that it was limited to patients with AECOPD. “Future studies should include any critically ill respiratory patients,” he said.
He reported having no financial disclosures.
LOS ANGELES – The Sequential Organ Failure Assessment (SOFA) score and the Glasgow Coma Scale (GCS) are simple, accurate tools for risk stratification of hospitalized patients with acute exacerbation of COPD, results from a single-center study showed.
“Acute exacerbations of chronic obstructive pulmonary disease often require hospitalization, may necessitate mechanical ventilation, and can be fatal,” Mohamed Metwally, MD, FCCP, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “There are currently no validated disease-specific scores that measure the severity of acute exacerbation. Prognostic tools are needed to assess acute exacerbations of chronic obstructive pulmonary disease.”
For the 2-year study, Dr. Metwally and his associates prospectively evaluated 250 critically ill ICU AECOPD patients, mean age 65 years, at Assiut University Hospital between December 2012 and December 2014. The primary outcome was in-hospital mortality while the secondary endpoint was need for intubation and mechanical ventilation. The researchers excluded patients who died less than 24 hours after admission, those with underlying COPD who were admitted with another primary diagnosis such as an accident or a stroke, or for elective hospitalizations such as elective surgery or diagnostic procedures.
Dr. Metwally and his associates collected sociodemographic data, vital signs, and other clinical variables, and collected scores from five tools used to measure mortality prediction: the Acute Physiology and Chronic Health Evaluation (APACHE II), the SOFA score, the Early Warning Score (EWS), the GCS, and the Charlson Comorbidity Index (CCI). To assess performance of the scores, they used area under the receiver operating characteristic curve (AUC) analysis and the Hosmer-Lemeshow goodness-of-fit test for logistic regression.
Of the 250 patients, 43 (17%) died during their hospital stay and 54% required mechanical ventilation. All recorded scores were significantly higher in nonsurvivors, compared with survivors, and the risk of clinical deterioration increased with increasing scores. The discriminatory power of each score varied as measured by AUC analysis. The AUC of APACHE II, SOFA, EWS, GCS, and CCI were 0.79, 0.81, 0.76, 0.69, and 0.68, respectively “and all these models had good calibration in mortality prediction,” Dr. Metwally said. The SOFA score was the best in predicting mortality (its predicted mortality was 16%, compared with the actual mortality of 17%), while the APACHE II score overestimated mortality by at least twofold (46% vs. 17%). In addition, the EWS outperformed the GCS in predicting mortality. “This may be due to EWS containing all vital signs plus level of consciousness,” he said in an interview.
The GCS was found to be the most useful in predicting need for mechanical ventilation, with an AUC of 0.81. The AUCs of APACHE II, SOFA, EWS, and CCI were 0.79, 0.80, 0.73, and 0.61, respectively. All of the scores had good calibration in mortality prediction, Dr. Metwally said, with the exception of SOFA.
As for the APACHE II, Dr. Metwally said that instrument “can be used as a tool to predict both mortality and intubation in a specific group of patients, but with low discriminatory power.” He acknowledged certain limitations of the study, including the fact that it was limited to patients with AECOPD. “Future studies should include any critically ill respiratory patients,” he said.
He reported having no financial disclosures.
LOS ANGELES – The Sequential Organ Failure Assessment (SOFA) score and the Glasgow Coma Scale (GCS) are simple, accurate tools for risk stratification of hospitalized patients with acute exacerbation of COPD, results from a single-center study showed.
“Acute exacerbations of chronic obstructive pulmonary disease often require hospitalization, may necessitate mechanical ventilation, and can be fatal,” Mohamed Metwally, MD, FCCP, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “There are currently no validated disease-specific scores that measure the severity of acute exacerbation. Prognostic tools are needed to assess acute exacerbations of chronic obstructive pulmonary disease.”
For the 2-year study, Dr. Metwally and his associates prospectively evaluated 250 critically ill ICU AECOPD patients, mean age 65 years, at Assiut University Hospital between December 2012 and December 2014. The primary outcome was in-hospital mortality while the secondary endpoint was need for intubation and mechanical ventilation. The researchers excluded patients who died less than 24 hours after admission, those with underlying COPD who were admitted with another primary diagnosis such as an accident or a stroke, or for elective hospitalizations such as elective surgery or diagnostic procedures.
Dr. Metwally and his associates collected sociodemographic data, vital signs, and other clinical variables, and collected scores from five tools used to measure mortality prediction: the Acute Physiology and Chronic Health Evaluation (APACHE II), the SOFA score, the Early Warning Score (EWS), the GCS, and the Charlson Comorbidity Index (CCI). To assess performance of the scores, they used area under the receiver operating characteristic curve (AUC) analysis and the Hosmer-Lemeshow goodness-of-fit test for logistic regression.
Of the 250 patients, 43 (17%) died during their hospital stay and 54% required mechanical ventilation. All recorded scores were significantly higher in nonsurvivors, compared with survivors, and the risk of clinical deterioration increased with increasing scores. The discriminatory power of each score varied as measured by AUC analysis. The AUC of APACHE II, SOFA, EWS, GCS, and CCI were 0.79, 0.81, 0.76, 0.69, and 0.68, respectively “and all these models had good calibration in mortality prediction,” Dr. Metwally said. The SOFA score was the best in predicting mortality (its predicted mortality was 16%, compared with the actual mortality of 17%), while the APACHE II score overestimated mortality by at least twofold (46% vs. 17%). In addition, the EWS outperformed the GCS in predicting mortality. “This may be due to EWS containing all vital signs plus level of consciousness,” he said in an interview.
The GCS was found to be the most useful in predicting need for mechanical ventilation, with an AUC of 0.81. The AUCs of APACHE II, SOFA, EWS, and CCI were 0.79, 0.80, 0.73, and 0.61, respectively. All of the scores had good calibration in mortality prediction, Dr. Metwally said, with the exception of SOFA.
As for the APACHE II, Dr. Metwally said that instrument “can be used as a tool to predict both mortality and intubation in a specific group of patients, but with low discriminatory power.” He acknowledged certain limitations of the study, including the fact that it was limited to patients with AECOPD. “Future studies should include any critically ill respiratory patients,” he said.
He reported having no financial disclosures.
AT CHEST 2016
Key clinical point:
Major finding: The Sequential Organ Failure Assessment score was the best in predicting mortality of patients with acute exacerbation of COPD (its predicted mortality was 16%, compared with the actual mortality of 17%).
Data source: A prospective evaluation of 250 critically ill ICU patients hospitalized with acute exacerbation of COPD.
Disclosures: Dr. Metwally reported having no financial disclosures.