User login
Echocardiography can benefit use of stented bovine graft for MVR in infants
Mitral valve replacement in infants and young children is complicated because appropriately sized prostheses are difficult to come by and these patients need replacements later on as they continue to grow – thus the high rates of reintervention and death. Pediatric cardiac surgery specialists at Boston Children’s Hospital are among the few that have used stented jugular vein grafts in these patients, and they have reported on a refinement of their technique that uses echocardiography before and after graft placement to obtain valuable measurements for sizing and implanting a prosthesis and for identifying patients at risk of complications.
Lindsay R. Freud, MD, and her associates reported in the January 2017 issue of the Journal of Thoracic and Cardiovascular Surgery on pre- and postoperative echocardiograms of 24 patients who had mitral valve replacement (MVR) with the Melody stent-mounted, valved bovine jugular vein graft (Medtronic) (J Thorac Cardiovasc Surg. 2017;153:153-60). The device, which is approved for transcatheter pulmonary valve replacement, was adapted for implantation into the mitral position, an indication that is not yet Food and Drug Administration approved. “With the increasing use of the Melody valve in the mitral position in infants and young children, we sought to provide a framework for both pre- and early postoperative echocardiographic assessment,” Dr. Freud and her coauthors said.

“The potential dimensions often had normal z scores with fair correlation with intraoperative Melody dilation,” the investigators said. They also found that a ratio of the narrowest subaortic region in systole to the actual MV dimension (SubA:MV) less than 0.5 was associated with postoperative left ventricular outflow tract obstruction (LVOTO), which occurred in four patients. The median age of the study group was 8.5 months.
“Postoperatively, mitral gradients substantially improved, with low values relative to the effective orifice area of the Melody valve,” Dr. Freud and her associates said. None of the patients had significant regurgitation or perivalvar leak.
In early reports of the Melody valve in infants and small children, the surgeons determined the size of the replacement valve during the operation itself. Despite encouraging early results, reports of complications such as LVOTO soon followed. The Children’s Hospital Boston researchers undertook the study to determine if echocardiography before surgery would help to identify the correct valve size for expansion and predict which patients would be at risk for LVOTO.
“The preoperative SubA:MV ratio may help assess the risk for postoperative LVOTO, which is an important complication,” Dr. Freud and coauthors said. The presence of LVOTO preoperatively was also a risk factor, but only one of eight patients with an atrioventricular canal defect developed LVOTO. In patients with a SubA:MV ratio less than 0.5, preoperative LVOTO, or any other anatomic risk factor, surgeons should consider options to prevent LVOTO, Dr. Freud and her associates said. Those alternatives include more aggressive resection of stent material, atrial displacement of the valve, or less aggressive distal expansion of the valve.
Postoperative echocardiography enabled Dr. Freud and her coauthors to outline baseline values for the Melody valve in the mitral position by maximum intraoperative balloon diameter, ranging from 1 cm to 1.8 cm in 0.2-cm steps, and depending on five measurements at each step: peak and mean gradients, peak velocity, effective orifice area, and indexed effective orifice area.
“Validation of candidacy for Melody MVR and noninvasive assessment among larger series of patient will be necessary as greater experience with the Melody valve evolves,” Dr. Freud and her associates concluded.
Coauthor Sitaram Emani, MD, has filed a patent for an expandable valve through Boston Children’s Hospital. Dr. Freud and her other coauthors had no financial relationships to disclose.
The Melody valve is an “appealing solution” for MVR in infants and small children, Patrick Myers, MD, of Geneva University Hospitals said in his invited commentary (J Thorac Cardiovasc Surg. 2017;153:151-2) “This contribution brings further data to support Melody MVR,” he said of the report by Dr. Freud and her colleagues.
However, Dr. Myers noted that beyond the Boston Children’s Hospital experience, only two other reports of the Melody valve in the mitral position in children exist. “There are several outstanding technical issues that need to be investigated for the use of the Melody valve in the mitral position,” he said. Among those issues is the length of the stent itself – 28 mm, which can lead to LVOTO after placement “in a diminutive ventricle.” The fact that “only” four patients in the study group developed LVOTO after Melody MVR is “reassuring with regard to this theoretic limitation,” Dr. Myers said. “And the echocardiographic ratio of the narrowest subaortic region in systole to the actual mitral valve dimension could be of use in deciding when to be more aggressive in preventing LVOTO,” he said.
Dr. Myers also said that this report answered some questions about the durability of a venous valve under systemic pressures, but added, “Further echocardiographic and clinical follow-up data in this very challenging population are required,” he said.
Dr. Myers had no financial relationships to disclose.
The Melody valve is an “appealing solution” for MVR in infants and small children, Patrick Myers, MD, of Geneva University Hospitals said in his invited commentary (J Thorac Cardiovasc Surg. 2017;153:151-2) “This contribution brings further data to support Melody MVR,” he said of the report by Dr. Freud and her colleagues.
However, Dr. Myers noted that beyond the Boston Children’s Hospital experience, only two other reports of the Melody valve in the mitral position in children exist. “There are several outstanding technical issues that need to be investigated for the use of the Melody valve in the mitral position,” he said. Among those issues is the length of the stent itself – 28 mm, which can lead to LVOTO after placement “in a diminutive ventricle.” The fact that “only” four patients in the study group developed LVOTO after Melody MVR is “reassuring with regard to this theoretic limitation,” Dr. Myers said. “And the echocardiographic ratio of the narrowest subaortic region in systole to the actual mitral valve dimension could be of use in deciding when to be more aggressive in preventing LVOTO,” he said.
Dr. Myers also said that this report answered some questions about the durability of a venous valve under systemic pressures, but added, “Further echocardiographic and clinical follow-up data in this very challenging population are required,” he said.
Dr. Myers had no financial relationships to disclose.
The Melody valve is an “appealing solution” for MVR in infants and small children, Patrick Myers, MD, of Geneva University Hospitals said in his invited commentary (J Thorac Cardiovasc Surg. 2017;153:151-2) “This contribution brings further data to support Melody MVR,” he said of the report by Dr. Freud and her colleagues.
However, Dr. Myers noted that beyond the Boston Children’s Hospital experience, only two other reports of the Melody valve in the mitral position in children exist. “There are several outstanding technical issues that need to be investigated for the use of the Melody valve in the mitral position,” he said. Among those issues is the length of the stent itself – 28 mm, which can lead to LVOTO after placement “in a diminutive ventricle.” The fact that “only” four patients in the study group developed LVOTO after Melody MVR is “reassuring with regard to this theoretic limitation,” Dr. Myers said. “And the echocardiographic ratio of the narrowest subaortic region in systole to the actual mitral valve dimension could be of use in deciding when to be more aggressive in preventing LVOTO,” he said.
Dr. Myers also said that this report answered some questions about the durability of a venous valve under systemic pressures, but added, “Further echocardiographic and clinical follow-up data in this very challenging population are required,” he said.
Dr. Myers had no financial relationships to disclose.
Mitral valve replacement in infants and young children is complicated because appropriately sized prostheses are difficult to come by and these patients need replacements later on as they continue to grow – thus the high rates of reintervention and death. Pediatric cardiac surgery specialists at Boston Children’s Hospital are among the few that have used stented jugular vein grafts in these patients, and they have reported on a refinement of their technique that uses echocardiography before and after graft placement to obtain valuable measurements for sizing and implanting a prosthesis and for identifying patients at risk of complications.
Lindsay R. Freud, MD, and her associates reported in the January 2017 issue of the Journal of Thoracic and Cardiovascular Surgery on pre- and postoperative echocardiograms of 24 patients who had mitral valve replacement (MVR) with the Melody stent-mounted, valved bovine jugular vein graft (Medtronic) (J Thorac Cardiovasc Surg. 2017;153:153-60). The device, which is approved for transcatheter pulmonary valve replacement, was adapted for implantation into the mitral position, an indication that is not yet Food and Drug Administration approved. “With the increasing use of the Melody valve in the mitral position in infants and young children, we sought to provide a framework for both pre- and early postoperative echocardiographic assessment,” Dr. Freud and her coauthors said.
“The potential dimensions often had normal z scores with fair correlation with intraoperative Melody dilation,” the investigators said. They also found that a ratio of the narrowest subaortic region in systole to the actual MV dimension (SubA:MV) less than 0.5 was associated with postoperative left ventricular outflow tract obstruction (LVOTO), which occurred in four patients. The median age of the study group was 8.5 months.
“Postoperatively, mitral gradients substantially improved, with low values relative to the effective orifice area of the Melody valve,” Dr. Freud and her associates said. None of the patients had significant regurgitation or perivalvar leak.
In early reports of the Melody valve in infants and small children, the surgeons determined the size of the replacement valve during the operation itself. Despite encouraging early results, reports of complications such as LVOTO soon followed. The Children’s Hospital Boston researchers undertook the study to determine if echocardiography before surgery would help to identify the correct valve size for expansion and predict which patients would be at risk for LVOTO.
“The preoperative SubA:MV ratio may help assess the risk for postoperative LVOTO, which is an important complication,” Dr. Freud and coauthors said. The presence of LVOTO preoperatively was also a risk factor, but only one of eight patients with an atrioventricular canal defect developed LVOTO. In patients with a SubA:MV ratio less than 0.5, preoperative LVOTO, or any other anatomic risk factor, surgeons should consider options to prevent LVOTO, Dr. Freud and her associates said. Those alternatives include more aggressive resection of stent material, atrial displacement of the valve, or less aggressive distal expansion of the valve.
Postoperative echocardiography enabled Dr. Freud and her coauthors to outline baseline values for the Melody valve in the mitral position by maximum intraoperative balloon diameter, ranging from 1 cm to 1.8 cm in 0.2-cm steps, and depending on five measurements at each step: peak and mean gradients, peak velocity, effective orifice area, and indexed effective orifice area.
“Validation of candidacy for Melody MVR and noninvasive assessment among larger series of patient will be necessary as greater experience with the Melody valve evolves,” Dr. Freud and her associates concluded.
Coauthor Sitaram Emani, MD, has filed a patent for an expandable valve through Boston Children’s Hospital. Dr. Freud and her other coauthors had no financial relationships to disclose.
Mitral valve replacement in infants and young children is complicated because appropriately sized prostheses are difficult to come by and these patients need replacements later on as they continue to grow – thus the high rates of reintervention and death. Pediatric cardiac surgery specialists at Boston Children’s Hospital are among the few that have used stented jugular vein grafts in these patients, and they have reported on a refinement of their technique that uses echocardiography before and after graft placement to obtain valuable measurements for sizing and implanting a prosthesis and for identifying patients at risk of complications.
Lindsay R. Freud, MD, and her associates reported in the January 2017 issue of the Journal of Thoracic and Cardiovascular Surgery on pre- and postoperative echocardiograms of 24 patients who had mitral valve replacement (MVR) with the Melody stent-mounted, valved bovine jugular vein graft (Medtronic) (J Thorac Cardiovasc Surg. 2017;153:153-60). The device, which is approved for transcatheter pulmonary valve replacement, was adapted for implantation into the mitral position, an indication that is not yet Food and Drug Administration approved. “With the increasing use of the Melody valve in the mitral position in infants and young children, we sought to provide a framework for both pre- and early postoperative echocardiographic assessment,” Dr. Freud and her coauthors said.
“The potential dimensions often had normal z scores with fair correlation with intraoperative Melody dilation,” the investigators said. They also found that a ratio of the narrowest subaortic region in systole to the actual MV dimension (SubA:MV) less than 0.5 was associated with postoperative left ventricular outflow tract obstruction (LVOTO), which occurred in four patients. The median age of the study group was 8.5 months.
“Postoperatively, mitral gradients substantially improved, with low values relative to the effective orifice area of the Melody valve,” Dr. Freud and her associates said. None of the patients had significant regurgitation or perivalvar leak.
In early reports of the Melody valve in infants and small children, the surgeons determined the size of the replacement valve during the operation itself. Despite encouraging early results, reports of complications such as LVOTO soon followed. The Children’s Hospital Boston researchers undertook the study to determine if echocardiography before surgery would help to identify the correct valve size for expansion and predict which patients would be at risk for LVOTO.
“The preoperative SubA:MV ratio may help assess the risk for postoperative LVOTO, which is an important complication,” Dr. Freud and coauthors said. The presence of LVOTO preoperatively was also a risk factor, but only one of eight patients with an atrioventricular canal defect developed LVOTO. In patients with a SubA:MV ratio less than 0.5, preoperative LVOTO, or any other anatomic risk factor, surgeons should consider options to prevent LVOTO, Dr. Freud and her associates said. Those alternatives include more aggressive resection of stent material, atrial displacement of the valve, or less aggressive distal expansion of the valve.
Postoperative echocardiography enabled Dr. Freud and her coauthors to outline baseline values for the Melody valve in the mitral position by maximum intraoperative balloon diameter, ranging from 1 cm to 1.8 cm in 0.2-cm steps, and depending on five measurements at each step: peak and mean gradients, peak velocity, effective orifice area, and indexed effective orifice area.
“Validation of candidacy for Melody MVR and noninvasive assessment among larger series of patient will be necessary as greater experience with the Melody valve evolves,” Dr. Freud and her associates concluded.
Coauthor Sitaram Emani, MD, has filed a patent for an expandable valve through Boston Children’s Hospital. Dr. Freud and her other coauthors had no financial relationships to disclose.
FROM JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Preoperative echocardiography may help guide placement of modified stented jugular vein grafts in infants and small children with hypoplastic mitral and aortic valves.
Major finding: Echocardiography showed that a ratio of the narrowest subaortic region in systole to the actual mitral valve dimension of less than 0.5 was associated with postoperative left ventricular outflow tract obstruction.
Data source: Single-center, retrospective review of 24 patients who underwent mitral valve replacement with modified stented jugular vein grafts from March 2010 to March 2015.
Disclosures: Coauthor Sitaram Emani, MD, has filed a patent for an expandable valve through Boston Children’s Hospital. Dr. Freud and her other coauthors had no financial relationships to disclose.
AGA comment on ABIM announcement
For more than a year, AGA has pushed the American Board of Internal Medicine (ABIM) to eliminate high-stakes testing and reform the maintenance of certification (MOC) system into one that’s personalized and reflective of the realities of practice.
ABIM’s listening tour is over. In December 2016, they announced the addition of an option for a 2-year “knowledge check-in.” Although ABIM can point to nominal progress by making the assessment available outside its testing centers, they have not addressed cost, personalization, or the impact on patient care of such assessments.
Despite AGA’s diligent efforts to co-create a new MOC process – which included creating G-APP, constant communication, and participation in numerous summits – ABIM deemed AGA’s approach to be inconsistent with its own philosophy. Nonetheless, we are still in the midst of an evolution. AGA will continue to work with our sister GI and internal medicine societies to bring about change that supports meaningful lifelong learning through the least intrusive means possible.
In the meantime, if your professional situation requires you to maintain certification, please visit ABIM’s blog for more information. AGA tools such as the Digestive Diseases Self-Education Program® can help you prepare.
Visit http://www.gastro.org/career-center/maintenance-of-certification for the latest updates and information on MOC.
For more than a year, AGA has pushed the American Board of Internal Medicine (ABIM) to eliminate high-stakes testing and reform the maintenance of certification (MOC) system into one that’s personalized and reflective of the realities of practice.
ABIM’s listening tour is over. In December 2016, they announced the addition of an option for a 2-year “knowledge check-in.” Although ABIM can point to nominal progress by making the assessment available outside its testing centers, they have not addressed cost, personalization, or the impact on patient care of such assessments.
Despite AGA’s diligent efforts to co-create a new MOC process – which included creating G-APP, constant communication, and participation in numerous summits – ABIM deemed AGA’s approach to be inconsistent with its own philosophy. Nonetheless, we are still in the midst of an evolution. AGA will continue to work with our sister GI and internal medicine societies to bring about change that supports meaningful lifelong learning through the least intrusive means possible.
In the meantime, if your professional situation requires you to maintain certification, please visit ABIM’s blog for more information. AGA tools such as the Digestive Diseases Self-Education Program® can help you prepare.
Visit http://www.gastro.org/career-center/maintenance-of-certification for the latest updates and information on MOC.
For more than a year, AGA has pushed the American Board of Internal Medicine (ABIM) to eliminate high-stakes testing and reform the maintenance of certification (MOC) system into one that’s personalized and reflective of the realities of practice.
ABIM’s listening tour is over. In December 2016, they announced the addition of an option for a 2-year “knowledge check-in.” Although ABIM can point to nominal progress by making the assessment available outside its testing centers, they have not addressed cost, personalization, or the impact on patient care of such assessments.
Despite AGA’s diligent efforts to co-create a new MOC process – which included creating G-APP, constant communication, and participation in numerous summits – ABIM deemed AGA’s approach to be inconsistent with its own philosophy. Nonetheless, we are still in the midst of an evolution. AGA will continue to work with our sister GI and internal medicine societies to bring about change that supports meaningful lifelong learning through the least intrusive means possible.
In the meantime, if your professional situation requires you to maintain certification, please visit ABIM’s blog for more information. AGA tools such as the Digestive Diseases Self-Education Program® can help you prepare.
Visit http://www.gastro.org/career-center/maintenance-of-certification for the latest updates and information on MOC.
Access our MACRA resource collection
Prepare for 2017 with AGA’s Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) resources, which are available in the AGA Community resource library. This includes webinars, a tip sheet, and discussion threads.
The webinars and discussions in the community are available to members only, and contain information on the following topics:
- Intro to MACRA.
- 2016 PQRS Quality Reporting through the AGA Digestive Health Recognition Program (DHRP).
- Preparing for MIPS.
The materials were collected from a series of webinars and eQ&As in December, when topic experts presented a series of webinars on relevant MACRA protocols to help clinicians prepare for Medicare changes starting this year.
Each webinar preceded an Ask the Expert session in the AGA Community forum. Members brought their wide range of questions to the forum, including discussions about MACRA basics, as well as meticulous situation-based recording scenarios.
This members-only library can be accessed at community.gastro.org/MACRA. For more information, including a timeline, downloadable guides, and the latest MACRA news, visit gastro.org/MACRA.
Prepare for 2017 with AGA’s Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) resources, which are available in the AGA Community resource library. This includes webinars, a tip sheet, and discussion threads.
The webinars and discussions in the community are available to members only, and contain information on the following topics:
- Intro to MACRA.
- 2016 PQRS Quality Reporting through the AGA Digestive Health Recognition Program (DHRP).
- Preparing for MIPS.
The materials were collected from a series of webinars and eQ&As in December, when topic experts presented a series of webinars on relevant MACRA protocols to help clinicians prepare for Medicare changes starting this year.
Each webinar preceded an Ask the Expert session in the AGA Community forum. Members brought their wide range of questions to the forum, including discussions about MACRA basics, as well as meticulous situation-based recording scenarios.
This members-only library can be accessed at community.gastro.org/MACRA. For more information, including a timeline, downloadable guides, and the latest MACRA news, visit gastro.org/MACRA.
Prepare for 2017 with AGA’s Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) resources, which are available in the AGA Community resource library. This includes webinars, a tip sheet, and discussion threads.
The webinars and discussions in the community are available to members only, and contain information on the following topics:
- Intro to MACRA.
- 2016 PQRS Quality Reporting through the AGA Digestive Health Recognition Program (DHRP).
- Preparing for MIPS.
The materials were collected from a series of webinars and eQ&As in December, when topic experts presented a series of webinars on relevant MACRA protocols to help clinicians prepare for Medicare changes starting this year.
Each webinar preceded an Ask the Expert session in the AGA Community forum. Members brought their wide range of questions to the forum, including discussions about MACRA basics, as well as meticulous situation-based recording scenarios.
This members-only library can be accessed at community.gastro.org/MACRA. For more information, including a timeline, downloadable guides, and the latest MACRA news, visit gastro.org/MACRA.
Register for DDW® before the early-bird deadline
Registration for AGA members opened Jan. 11, and general registration opened on Jan. 18. Register by March 22 to save at least $80; registration is complimentary up until this date for member trainees, students, and postdoctoral fellows.
Why attend DDW?
DDW is the world’s leading educational forum for academicians, clinicians, researchers, students, and trainees working in gastroenterology, hepatology, GI endoscopy, gastrointestinal surgery, and related fields. Whether you work in patient care, research, education, or administration, the DDW program offers something for you.
For more information regarding why you should attend, what’s included in registration and more, visit www.ddw.org.
Registration for AGA members opened Jan. 11, and general registration opened on Jan. 18. Register by March 22 to save at least $80; registration is complimentary up until this date for member trainees, students, and postdoctoral fellows.
Why attend DDW?
DDW is the world’s leading educational forum for academicians, clinicians, researchers, students, and trainees working in gastroenterology, hepatology, GI endoscopy, gastrointestinal surgery, and related fields. Whether you work in patient care, research, education, or administration, the DDW program offers something for you.
For more information regarding why you should attend, what’s included in registration and more, visit www.ddw.org.
Registration for AGA members opened Jan. 11, and general registration opened on Jan. 18. Register by March 22 to save at least $80; registration is complimentary up until this date for member trainees, students, and postdoctoral fellows.
Why attend DDW?
DDW is the world’s leading educational forum for academicians, clinicians, researchers, students, and trainees working in gastroenterology, hepatology, GI endoscopy, gastrointestinal surgery, and related fields. Whether you work in patient care, research, education, or administration, the DDW program offers something for you.
For more information regarding why you should attend, what’s included in registration and more, visit www.ddw.org.
Annual AGA Tech Summit returns to Boston in 2017
AGA is excited to return to Boston for its eighth annual Tech Summit on April 12-14, 2017, at the InterContinental Hotel. We’ve assembled prominent individuals in the physician, medtech, and regulatory communities to lead attendees through a program that’s both informative and inspirational.
This is an ideal opportunity to explore critical elements impacting how GI technology evolves from concept to reality, including what it takes to obtain adoption, coverage, and reimbursement in a continually evolving health care environment.
We hope to see you this spring in Boston for a truly unique experience. Learn more and register at http://techsummit.gastro.org.
Have a novel idea or innovation? Apply for the AGA “Shark Tank”Calling all companies and entrepreneurs with an innovative technology or FDA-regulated product. If you are looking to get it financed, licensed, or distributed, you are encouraged to submit an application for an opportunity to present during the “Shark Tank” session at the 2017 AGA Tech Summit. A panel of business development leaders, investors, entrepreneurs, and other strategic partners will provide valuable feedback.
AGA is excited to return to Boston for its eighth annual Tech Summit on April 12-14, 2017, at the InterContinental Hotel. We’ve assembled prominent individuals in the physician, medtech, and regulatory communities to lead attendees through a program that’s both informative and inspirational.
This is an ideal opportunity to explore critical elements impacting how GI technology evolves from concept to reality, including what it takes to obtain adoption, coverage, and reimbursement in a continually evolving health care environment.
We hope to see you this spring in Boston for a truly unique experience. Learn more and register at http://techsummit.gastro.org.
Have a novel idea or innovation? Apply for the AGA “Shark Tank”Calling all companies and entrepreneurs with an innovative technology or FDA-regulated product. If you are looking to get it financed, licensed, or distributed, you are encouraged to submit an application for an opportunity to present during the “Shark Tank” session at the 2017 AGA Tech Summit. A panel of business development leaders, investors, entrepreneurs, and other strategic partners will provide valuable feedback.
AGA is excited to return to Boston for its eighth annual Tech Summit on April 12-14, 2017, at the InterContinental Hotel. We’ve assembled prominent individuals in the physician, medtech, and regulatory communities to lead attendees through a program that’s both informative and inspirational.
This is an ideal opportunity to explore critical elements impacting how GI technology evolves from concept to reality, including what it takes to obtain adoption, coverage, and reimbursement in a continually evolving health care environment.
We hope to see you this spring in Boston for a truly unique experience. Learn more and register at http://techsummit.gastro.org.
Have a novel idea or innovation? Apply for the AGA “Shark Tank”Calling all companies and entrepreneurs with an innovative technology or FDA-regulated product. If you are looking to get it financed, licensed, or distributed, you are encouraged to submit an application for an opportunity to present during the “Shark Tank” session at the 2017 AGA Tech Summit. A panel of business development leaders, investors, entrepreneurs, and other strategic partners will provide valuable feedback.
New histopathologic marker may aid dermatomyositis diagnosis
The detection of sarcoplasmic myxovirus resistance A expression in immunohistochemical analysis of muscle biopsy in patients suspected of having dermatomyositis may add greater sensitivity for the diagnosis when compared with conventional pathologic hallmarks of the disease, according to findings from a retrospective cohort study.
Myxovirus resistance A (MxA) is one of the type 1 interferon–inducible proteins whose overexpression is believed to play a role in the pathogenesis of dermatomyositis, and MxA expression has rarely been observed in other idiopathic inflammatory myopathies, said first author Akinori Uruha, MD, PhD, of the National Center of Neurology and Psychiatry, Tokyo, and his colleagues. They compared MxA expression in muscle biopsy samples from definite, probable, and possible dermatomyositis cases as well as other idiopathic inflammatory myopathies and other control conditions to assess its value against other muscle pathologic markers of dermatomyositis, such as the presence of perifascicular atrophy (PFA) and capillary membrane attack complex (MAC) deposition (Neurology. 2016 Dec 30. doi: 10.1212/WNL.0000000000003568).
The investigators studied muscle biopsy samples collected from 154 consecutive patients with idiopathic inflammatory myopathies seen from all over Japan, including 34 with dermatomyositis (10 juvenile cases), 8 with polymyositis (1 juvenile), 16 with anti–tRNA-synthetase antibody–associated myopathy (ASM); 46 with immune-mediated necrotizing myopathy (IMNM), and 50 with inclusion body myositis. The IMNM cases involved included 24 with anti–signal recognition particle (SRP) antibodies, 6 with anti–3-hydroxy-3-methylglutaryl-CoA reductase (HMGCR) antibodies, and 16 without anti-SRP, anti-HMGCR, or anti–tRNA-synthetase antibodies (3 juvenile patients). They used 51 patients with muscular dystrophy and 26 with neuropathies as controls.
Sarcoplasmic MxA expression proved to be more sensitive for a diagnosis of dermatomyositis than PFA and capillary MAC deposition (71% vs. 47% and 35%, respectively) but still had comparable specificity to those two markers (98% vs. 98% and 93%, respectively).
Of 18 cases with probable dermatomyositis, defined as typical skin rash but a lack of PFA, 8 (44%) showed sarcoplasmic MxA expression, and its sensitivity was 90% in juvenile cases overall and 63% in adult patients. Only 3 (17%) of the 18 showed capillary MAC deposition. Sarcoplasmic MxA expression occurred in all 12 patients with definite dermatomyositis, defined by the typical skin rash plus presence of PFA, whereas only 7 (58%) showed capillary MAC deposition. Among the four patients with possible dermatomyositis (PFA present but lacking typical skin rash), all showed sarcoplasmic MxA expression, compared with just two showing capillary MAC deposition.
In all other patients without definite, probable, or possible dermatomyositis, only two were positive for sarcoplasmic MxA expression (one with ASM and one with IMNM).
Dr. Uruha and his associates said that the results are “clearly demonstrating that sarcoplasmic MxA expression should be an excellent diagnostic marker of [dermatomyositis].”
The authors noted that the study was limited by the fact that they could not obtain full information about dermatomyositis-associated antibodies, and because other proteins of type 1 interferon signature are known to be upregulated in dermatomyositis, additional studies will need to determine which of the proteins is a better diagnostic marker.
The study was supported partly by an Intramural Research Grant of the National Center of Neurology and Psychiatry and grants from the Japanese Ministry of Education, Science, Sports and Culture and the Ministry of Health, Labor and Welfare of Japan. The investigators had no relevant disclosures.
The detection of sarcoplasmic myxovirus resistance A expression in immunohistochemical analysis of muscle biopsy in patients suspected of having dermatomyositis may add greater sensitivity for the diagnosis when compared with conventional pathologic hallmarks of the disease, according to findings from a retrospective cohort study.
Myxovirus resistance A (MxA) is one of the type 1 interferon–inducible proteins whose overexpression is believed to play a role in the pathogenesis of dermatomyositis, and MxA expression has rarely been observed in other idiopathic inflammatory myopathies, said first author Akinori Uruha, MD, PhD, of the National Center of Neurology and Psychiatry, Tokyo, and his colleagues. They compared MxA expression in muscle biopsy samples from definite, probable, and possible dermatomyositis cases as well as other idiopathic inflammatory myopathies and other control conditions to assess its value against other muscle pathologic markers of dermatomyositis, such as the presence of perifascicular atrophy (PFA) and capillary membrane attack complex (MAC) deposition (Neurology. 2016 Dec 30. doi: 10.1212/WNL.0000000000003568).
The investigators studied muscle biopsy samples collected from 154 consecutive patients with idiopathic inflammatory myopathies seen from all over Japan, including 34 with dermatomyositis (10 juvenile cases), 8 with polymyositis (1 juvenile), 16 with anti–tRNA-synthetase antibody–associated myopathy (ASM); 46 with immune-mediated necrotizing myopathy (IMNM), and 50 with inclusion body myositis. The IMNM cases involved included 24 with anti–signal recognition particle (SRP) antibodies, 6 with anti–3-hydroxy-3-methylglutaryl-CoA reductase (HMGCR) antibodies, and 16 without anti-SRP, anti-HMGCR, or anti–tRNA-synthetase antibodies (3 juvenile patients). They used 51 patients with muscular dystrophy and 26 with neuropathies as controls.
Sarcoplasmic MxA expression proved to be more sensitive for a diagnosis of dermatomyositis than PFA and capillary MAC deposition (71% vs. 47% and 35%, respectively) but still had comparable specificity to those two markers (98% vs. 98% and 93%, respectively).
Of 18 cases with probable dermatomyositis, defined as typical skin rash but a lack of PFA, 8 (44%) showed sarcoplasmic MxA expression, and its sensitivity was 90% in juvenile cases overall and 63% in adult patients. Only 3 (17%) of the 18 showed capillary MAC deposition. Sarcoplasmic MxA expression occurred in all 12 patients with definite dermatomyositis, defined by the typical skin rash plus presence of PFA, whereas only 7 (58%) showed capillary MAC deposition. Among the four patients with possible dermatomyositis (PFA present but lacking typical skin rash), all showed sarcoplasmic MxA expression, compared with just two showing capillary MAC deposition.
In all other patients without definite, probable, or possible dermatomyositis, only two were positive for sarcoplasmic MxA expression (one with ASM and one with IMNM).
Dr. Uruha and his associates said that the results are “clearly demonstrating that sarcoplasmic MxA expression should be an excellent diagnostic marker of [dermatomyositis].”
The authors noted that the study was limited by the fact that they could not obtain full information about dermatomyositis-associated antibodies, and because other proteins of type 1 interferon signature are known to be upregulated in dermatomyositis, additional studies will need to determine which of the proteins is a better diagnostic marker.
The study was supported partly by an Intramural Research Grant of the National Center of Neurology and Psychiatry and grants from the Japanese Ministry of Education, Science, Sports and Culture and the Ministry of Health, Labor and Welfare of Japan. The investigators had no relevant disclosures.
The detection of sarcoplasmic myxovirus resistance A expression in immunohistochemical analysis of muscle biopsy in patients suspected of having dermatomyositis may add greater sensitivity for the diagnosis when compared with conventional pathologic hallmarks of the disease, according to findings from a retrospective cohort study.
Myxovirus resistance A (MxA) is one of the type 1 interferon–inducible proteins whose overexpression is believed to play a role in the pathogenesis of dermatomyositis, and MxA expression has rarely been observed in other idiopathic inflammatory myopathies, said first author Akinori Uruha, MD, PhD, of the National Center of Neurology and Psychiatry, Tokyo, and his colleagues. They compared MxA expression in muscle biopsy samples from definite, probable, and possible dermatomyositis cases as well as other idiopathic inflammatory myopathies and other control conditions to assess its value against other muscle pathologic markers of dermatomyositis, such as the presence of perifascicular atrophy (PFA) and capillary membrane attack complex (MAC) deposition (Neurology. 2016 Dec 30. doi: 10.1212/WNL.0000000000003568).
The investigators studied muscle biopsy samples collected from 154 consecutive patients with idiopathic inflammatory myopathies seen from all over Japan, including 34 with dermatomyositis (10 juvenile cases), 8 with polymyositis (1 juvenile), 16 with anti–tRNA-synthetase antibody–associated myopathy (ASM); 46 with immune-mediated necrotizing myopathy (IMNM), and 50 with inclusion body myositis. The IMNM cases involved included 24 with anti–signal recognition particle (SRP) antibodies, 6 with anti–3-hydroxy-3-methylglutaryl-CoA reductase (HMGCR) antibodies, and 16 without anti-SRP, anti-HMGCR, or anti–tRNA-synthetase antibodies (3 juvenile patients). They used 51 patients with muscular dystrophy and 26 with neuropathies as controls.
Sarcoplasmic MxA expression proved to be more sensitive for a diagnosis of dermatomyositis than PFA and capillary MAC deposition (71% vs. 47% and 35%, respectively) but still had comparable specificity to those two markers (98% vs. 98% and 93%, respectively).
Of 18 cases with probable dermatomyositis, defined as typical skin rash but a lack of PFA, 8 (44%) showed sarcoplasmic MxA expression, and its sensitivity was 90% in juvenile cases overall and 63% in adult patients. Only 3 (17%) of the 18 showed capillary MAC deposition. Sarcoplasmic MxA expression occurred in all 12 patients with definite dermatomyositis, defined by the typical skin rash plus presence of PFA, whereas only 7 (58%) showed capillary MAC deposition. Among the four patients with possible dermatomyositis (PFA present but lacking typical skin rash), all showed sarcoplasmic MxA expression, compared with just two showing capillary MAC deposition.
In all other patients without definite, probable, or possible dermatomyositis, only two were positive for sarcoplasmic MxA expression (one with ASM and one with IMNM).
Dr. Uruha and his associates said that the results are “clearly demonstrating that sarcoplasmic MxA expression should be an excellent diagnostic marker of [dermatomyositis].”
The authors noted that the study was limited by the fact that they could not obtain full information about dermatomyositis-associated antibodies, and because other proteins of type 1 interferon signature are known to be upregulated in dermatomyositis, additional studies will need to determine which of the proteins is a better diagnostic marker.
The study was supported partly by an Intramural Research Grant of the National Center of Neurology and Psychiatry and grants from the Japanese Ministry of Education, Science, Sports and Culture and the Ministry of Health, Labor and Welfare of Japan. The investigators had no relevant disclosures.
FROM NEUROLOGY
Key clinical point:
Major finding: Sarcoplasmic MxA expression proved to be more sensitive for a diagnosis of dermatomyositis than PFA and capillary MAC deposition (71% vs. 47% and 35%, respectively) but still had comparable specificity to those two markers (98% vs. 98% and 93%, respectively).
Data source: A retrospective cohort study of 154 patients with idiopathic inflammatory myopathies, 51 with muscular dystrophy, and 26 with neuropathies.
Disclosures: The study was supported partly by an Intramural Research Grant of the National Center of Neurology and Psychiatry and grants from the Japanese Ministry of Education, Science, Sports and Culture and the Ministry of Health, Labor and Welfare of Japan. The investigators had no relevant disclosures.
Cosmetic Corner: Dermatologists Weigh in on Skin-Lightening Agents
To improve patient care and outcomes, leading dermatologists offered their recommendations on skin-lightening agents. Consideration must be given to:
- Even Better Clinical Dark Spot Corrector
Clinique Laboratories, LLC
Recommended by Gary Goldenberg, MD, New York, New York
- Lytera Skin Brightening Complex
SkinMedica, an Allergan compan
“It contains vitamin C, niacinamide, retinol, and licorice root extract to help lighten the skin and improve texture without hydroquinone.”—Anthony M. Rossi, MD, New York, New York
- Meladerm
Civant Skin Care
“This is an excellent hydroquinone-free cream for treating postinflammatory hyperpigmentation and melasma. It contains a combination of ingredients known to inhibit various steps along the melanogenesis pathway, such as retinyl palmitate, licorice extract, and arbutin, as well as lactic, kojic, and ascorbic acids.”—Cherise M. Levi, DO, New York, New York
Cutis invites readers to send us their recommendations. Cleansing devices, dry shampoos, athlete’s foot treatments, and face scrubs will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
[polldaddy:9711250]
To improve patient care and outcomes, leading dermatologists offered their recommendations on skin-lightening agents. Consideration must be given to:
- Even Better Clinical Dark Spot Corrector
Clinique Laboratories, LLC
Recommended by Gary Goldenberg, MD, New York, New York
- Lytera Skin Brightening Complex
SkinMedica, an Allergan compan
“It contains vitamin C, niacinamide, retinol, and licorice root extract to help lighten the skin and improve texture without hydroquinone.”—Anthony M. Rossi, MD, New York, New York
- Meladerm
Civant Skin Care
“This is an excellent hydroquinone-free cream for treating postinflammatory hyperpigmentation and melasma. It contains a combination of ingredients known to inhibit various steps along the melanogenesis pathway, such as retinyl palmitate, licorice extract, and arbutin, as well as lactic, kojic, and ascorbic acids.”—Cherise M. Levi, DO, New York, New York
Cutis invites readers to send us their recommendations. Cleansing devices, dry shampoos, athlete’s foot treatments, and face scrubs will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
[polldaddy:9711250]
To improve patient care and outcomes, leading dermatologists offered their recommendations on skin-lightening agents. Consideration must be given to:
- Even Better Clinical Dark Spot Corrector
Clinique Laboratories, LLC
Recommended by Gary Goldenberg, MD, New York, New York
- Lytera Skin Brightening Complex
SkinMedica, an Allergan compan
“It contains vitamin C, niacinamide, retinol, and licorice root extract to help lighten the skin and improve texture without hydroquinone.”—Anthony M. Rossi, MD, New York, New York
- Meladerm
Civant Skin Care
“This is an excellent hydroquinone-free cream for treating postinflammatory hyperpigmentation and melasma. It contains a combination of ingredients known to inhibit various steps along the melanogenesis pathway, such as retinyl palmitate, licorice extract, and arbutin, as well as lactic, kojic, and ascorbic acids.”—Cherise M. Levi, DO, New York, New York
Cutis invites readers to send us their recommendations. Cleansing devices, dry shampoos, athlete’s foot treatments, and face scrubs will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
[polldaddy:9711250]

Hybrid procedures may be better option for LVOTO in lower-weight neonates
Little outcomes data have been published comparing hybrid and Norwood stage 1 procedures for newborns with critical left ventricular outflow tract obstruction (LVOTO), but a prospective analysis of more than 500 operations over 9 years reported that while the Norwood has better survival rates overall, hybrid procedures may improve survival in low-birth-weight newborns.
“Although lower birth weight was identified as an important risk factor for death for the entire cohort, the detrimental impact of low birth weight was mitigated, to some degree, for patients who underwent a hybrid procedure,” said Travis Wilder, MD, of the Congenital Heart Surgeons’ Society (CHSS) Data Center, and his coauthors. They reported their findings in the January 2017 issue of the Journal of Thoracic and Cardiovascular Surgery (153:163-72).

Norwood operations involve major surgical reconstruction along with exposure to cardiopulmonary bypass (CPB), with either deep hypothermic circulatory arrest (DHCA) or regional cerebral perfusion, during aortic arch reconstruction. Previous reports have linked CPB to postoperative hemodynamic instability, complications, and death (Ann Thorac Surg. 2009 Jun;87:1885-92). “In addition, the early physiological stress imposed on neonates after Norwood operations raises concerns regarding adverse neurodevelopment,” Dr. Wilder and his coauthors wrote.
Dr. Wilder and his coauthors pointed out that the hybrid procedure has emerged to avoid CPB and DHCA or regional cerebral perfusion and the potential resulting physiologic instability. “In this light, hybrid palliation may be perceived as a lower-risk alternative to Norwood operations, especially for patients considered at high risk for mortality,” the researchers said. Despite that perception, the actual survival “remains incompletely defined,” they said.
The overall average 4-year unadjusted survival for the entire study population was 65%, but those who had the NW-RVPA procedure had significantly improved survival (73%) vs. both the NW-BT (61%) and the hybrid groups (60%).
Those who had the hybrid procedure were older at stage 1 (12 days vs. 8 and 6 days, respectively for NW-BT and NW-RVPA) and had lower birth weight (2.9 kg vs. 3.2 kg and 3.15 kg, respectively). Hybrid patients also had a higher prevalence of baseline right ventricle dysfunction, were more likely to have baseline tricuspid valve regurgitation, and had a lower prevalence of aortic and mitral valve atresia.
For all patients, birth weight of 2.0-2.5 kg had a strong association with poor survival, Dr. Wilder and his coauthors reported, but the drop-off in survival for low-birth-weight neonates was greater in the Norwood group than in the hybrid group. “This finding suggests that hybrid procedures may offer a modest survival advantage over NW-RVPA at birth weight less than or equal to 2.0 kg and over NW-BT at birth weight less than or equal to 3.0 kg,” the researchers said.
Dr. Wilder and his coauthors had no financial relationships to disclose.
While the study by Dr. Wilder and his coauthors may have drawn an accurate conclusion about low-birth-weight newborns possibly benefiting from a hybrid procedure for hypoplastic left heart syndrome, the number of patients in each strategy was small, Carlos M. Mery, MD, MPH, of Texas Children’s Hospital/Baylor College of Medicine, Houston, said in his invited commentary (J Thorac Cardiovasc Surg. 2017 Jan;153:173-4).
Dr. Mery noted other limitations of the study, namely the heterogeneity of procedures by participating center. “Of the 20 centers, only 11 performed any hybrid procedures, and 1 center accounted for 42% of all hybrid procedures performed,” he said. “Because centers may be associated with possibly unaccounted risk factors and different learning curves, the conclusions may not be easily generalizable.”
The conclusion that newborns of lower birth weight may benefit from the hybrid procedure helps to bring clarity for which patients may benefit from a specific procedure, Dr. Mery said. “We seem to be getting closer to the ultimate goal of being able to offer each individual patient the management strategy that will lead to the best possible outcome, not only for quantity but also for quality of life,” Dr. Mery said.
Dr. Mery had no financial relationships to disclose.
While the study by Dr. Wilder and his coauthors may have drawn an accurate conclusion about low-birth-weight newborns possibly benefiting from a hybrid procedure for hypoplastic left heart syndrome, the number of patients in each strategy was small, Carlos M. Mery, MD, MPH, of Texas Children’s Hospital/Baylor College of Medicine, Houston, said in his invited commentary (J Thorac Cardiovasc Surg. 2017 Jan;153:173-4).
Dr. Mery noted other limitations of the study, namely the heterogeneity of procedures by participating center. “Of the 20 centers, only 11 performed any hybrid procedures, and 1 center accounted for 42% of all hybrid procedures performed,” he said. “Because centers may be associated with possibly unaccounted risk factors and different learning curves, the conclusions may not be easily generalizable.”
The conclusion that newborns of lower birth weight may benefit from the hybrid procedure helps to bring clarity for which patients may benefit from a specific procedure, Dr. Mery said. “We seem to be getting closer to the ultimate goal of being able to offer each individual patient the management strategy that will lead to the best possible outcome, not only for quantity but also for quality of life,” Dr. Mery said.
Dr. Mery had no financial relationships to disclose.
While the study by Dr. Wilder and his coauthors may have drawn an accurate conclusion about low-birth-weight newborns possibly benefiting from a hybrid procedure for hypoplastic left heart syndrome, the number of patients in each strategy was small, Carlos M. Mery, MD, MPH, of Texas Children’s Hospital/Baylor College of Medicine, Houston, said in his invited commentary (J Thorac Cardiovasc Surg. 2017 Jan;153:173-4).
Dr. Mery noted other limitations of the study, namely the heterogeneity of procedures by participating center. “Of the 20 centers, only 11 performed any hybrid procedures, and 1 center accounted for 42% of all hybrid procedures performed,” he said. “Because centers may be associated with possibly unaccounted risk factors and different learning curves, the conclusions may not be easily generalizable.”
The conclusion that newborns of lower birth weight may benefit from the hybrid procedure helps to bring clarity for which patients may benefit from a specific procedure, Dr. Mery said. “We seem to be getting closer to the ultimate goal of being able to offer each individual patient the management strategy that will lead to the best possible outcome, not only for quantity but also for quality of life,” Dr. Mery said.
Dr. Mery had no financial relationships to disclose.
Little outcomes data have been published comparing hybrid and Norwood stage 1 procedures for newborns with critical left ventricular outflow tract obstruction (LVOTO), but a prospective analysis of more than 500 operations over 9 years reported that while the Norwood has better survival rates overall, hybrid procedures may improve survival in low-birth-weight newborns.
“Although lower birth weight was identified as an important risk factor for death for the entire cohort, the detrimental impact of low birth weight was mitigated, to some degree, for patients who underwent a hybrid procedure,” said Travis Wilder, MD, of the Congenital Heart Surgeons’ Society (CHSS) Data Center, and his coauthors. They reported their findings in the January 2017 issue of the Journal of Thoracic and Cardiovascular Surgery (153:163-72).
Norwood operations involve major surgical reconstruction along with exposure to cardiopulmonary bypass (CPB), with either deep hypothermic circulatory arrest (DHCA) or regional cerebral perfusion, during aortic arch reconstruction. Previous reports have linked CPB to postoperative hemodynamic instability, complications, and death (Ann Thorac Surg. 2009 Jun;87:1885-92). “In addition, the early physiological stress imposed on neonates after Norwood operations raises concerns regarding adverse neurodevelopment,” Dr. Wilder and his coauthors wrote.
Dr. Wilder and his coauthors pointed out that the hybrid procedure has emerged to avoid CPB and DHCA or regional cerebral perfusion and the potential resulting physiologic instability. “In this light, hybrid palliation may be perceived as a lower-risk alternative to Norwood operations, especially for patients considered at high risk for mortality,” the researchers said. Despite that perception, the actual survival “remains incompletely defined,” they said.
The overall average 4-year unadjusted survival for the entire study population was 65%, but those who had the NW-RVPA procedure had significantly improved survival (73%) vs. both the NW-BT (61%) and the hybrid groups (60%).
Those who had the hybrid procedure were older at stage 1 (12 days vs. 8 and 6 days, respectively for NW-BT and NW-RVPA) and had lower birth weight (2.9 kg vs. 3.2 kg and 3.15 kg, respectively). Hybrid patients also had a higher prevalence of baseline right ventricle dysfunction, were more likely to have baseline tricuspid valve regurgitation, and had a lower prevalence of aortic and mitral valve atresia.
For all patients, birth weight of 2.0-2.5 kg had a strong association with poor survival, Dr. Wilder and his coauthors reported, but the drop-off in survival for low-birth-weight neonates was greater in the Norwood group than in the hybrid group. “This finding suggests that hybrid procedures may offer a modest survival advantage over NW-RVPA at birth weight less than or equal to 2.0 kg and over NW-BT at birth weight less than or equal to 3.0 kg,” the researchers said.
Dr. Wilder and his coauthors had no financial relationships to disclose.
Little outcomes data have been published comparing hybrid and Norwood stage 1 procedures for newborns with critical left ventricular outflow tract obstruction (LVOTO), but a prospective analysis of more than 500 operations over 9 years reported that while the Norwood has better survival rates overall, hybrid procedures may improve survival in low-birth-weight newborns.
“Although lower birth weight was identified as an important risk factor for death for the entire cohort, the detrimental impact of low birth weight was mitigated, to some degree, for patients who underwent a hybrid procedure,” said Travis Wilder, MD, of the Congenital Heart Surgeons’ Society (CHSS) Data Center, and his coauthors. They reported their findings in the January 2017 issue of the Journal of Thoracic and Cardiovascular Surgery (153:163-72).
Norwood operations involve major surgical reconstruction along with exposure to cardiopulmonary bypass (CPB), with either deep hypothermic circulatory arrest (DHCA) or regional cerebral perfusion, during aortic arch reconstruction. Previous reports have linked CPB to postoperative hemodynamic instability, complications, and death (Ann Thorac Surg. 2009 Jun;87:1885-92). “In addition, the early physiological stress imposed on neonates after Norwood operations raises concerns regarding adverse neurodevelopment,” Dr. Wilder and his coauthors wrote.
Dr. Wilder and his coauthors pointed out that the hybrid procedure has emerged to avoid CPB and DHCA or regional cerebral perfusion and the potential resulting physiologic instability. “In this light, hybrid palliation may be perceived as a lower-risk alternative to Norwood operations, especially for patients considered at high risk for mortality,” the researchers said. Despite that perception, the actual survival “remains incompletely defined,” they said.
The overall average 4-year unadjusted survival for the entire study population was 65%, but those who had the NW-RVPA procedure had significantly improved survival (73%) vs. both the NW-BT (61%) and the hybrid groups (60%).
Those who had the hybrid procedure were older at stage 1 (12 days vs. 8 and 6 days, respectively for NW-BT and NW-RVPA) and had lower birth weight (2.9 kg vs. 3.2 kg and 3.15 kg, respectively). Hybrid patients also had a higher prevalence of baseline right ventricle dysfunction, were more likely to have baseline tricuspid valve regurgitation, and had a lower prevalence of aortic and mitral valve atresia.
For all patients, birth weight of 2.0-2.5 kg had a strong association with poor survival, Dr. Wilder and his coauthors reported, but the drop-off in survival for low-birth-weight neonates was greater in the Norwood group than in the hybrid group. “This finding suggests that hybrid procedures may offer a modest survival advantage over NW-RVPA at birth weight less than or equal to 2.0 kg and over NW-BT at birth weight less than or equal to 3.0 kg,” the researchers said.
Dr. Wilder and his coauthors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Norwood procedures have the best survival rates for neonates with critical left ventricular outflow tract obstruction, but hybrid procedures may improve survival for those with lower birth weight.
Major finding: Risk-adjusted 4-year survival was 76% for the Norwood operation with a right ventricle–to-pulmonary artery conduit, 61% for Norwood with a modified Blalock-Taussig shunt and 60% for the hybrid procedure.
Data source: Prospective observational cohort study of 564 neonates admitted to 21 Congenital Heart Surgeons’ Society institutions from 2005 to 2014.
Disclosures: Dr. Wilder and his coauthors had no financial relationships to disclose.
Zika virus slowdown continues
Zika activity is slowing as winter progresses, with less than a hundred new cases of pregnant women with laboratory evidence of infection reported over the 2 weeks ending Jan. 10, according to data from the Centers for Disease Control and Prevention.
The most recent CDC data show that, for the first time since early August, the majority of new cases of Zika infection among pregnant women were reported in the 50 states and the District of Columbia, compared with the U.S. territories. There were a total of 98 new cases, with 55 reported in the states and 43 in the U.S. territories.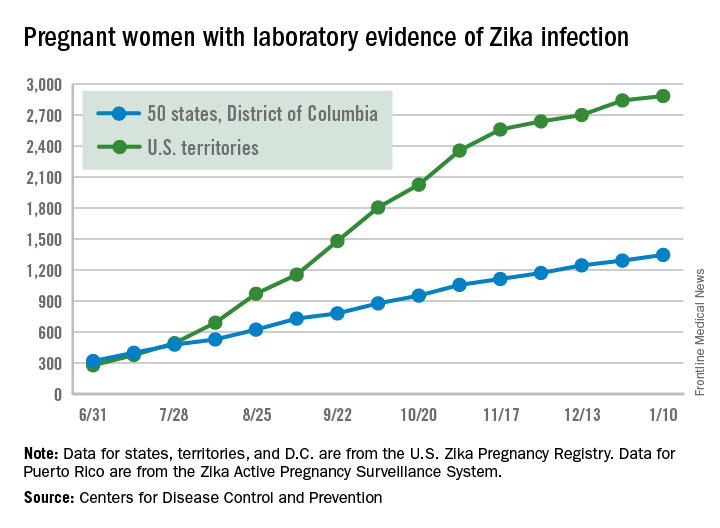
The total number of Zika-infected pregnant women in the United States is now 4,232 for 2016-2017. There have been 2,885 cases in the territories and 1,347 cases reported in the states/D.C. Among the cases in the states/D.C., 940 pregnancies have been completed, with Zika-related birth defects seen in 37 live-born infants and five pregnancy losses, the CDC said. The CDC is no longer reporting adverse pregnancy outcomes for the territories because Puerto Rico is not using the same inclusion criteria.
Zika cases among all Americans are still being reported weekly by the CDC, and the increase there has slowed as well: Total cases were up by 146 for the week ending Jan. 18, compared with 294 and 205 for each of the previous 2 weeks, according to CDC reports.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
Zika activity is slowing as winter progresses, with less than a hundred new cases of pregnant women with laboratory evidence of infection reported over the 2 weeks ending Jan. 10, according to data from the Centers for Disease Control and Prevention.
The most recent CDC data show that, for the first time since early August, the majority of new cases of Zika infection among pregnant women were reported in the 50 states and the District of Columbia, compared with the U.S. territories. There were a total of 98 new cases, with 55 reported in the states and 43 in the U.S. territories.
The total number of Zika-infected pregnant women in the United States is now 4,232 for 2016-2017. There have been 2,885 cases in the territories and 1,347 cases reported in the states/D.C. Among the cases in the states/D.C., 940 pregnancies have been completed, with Zika-related birth defects seen in 37 live-born infants and five pregnancy losses, the CDC said. The CDC is no longer reporting adverse pregnancy outcomes for the territories because Puerto Rico is not using the same inclusion criteria.
Zika cases among all Americans are still being reported weekly by the CDC, and the increase there has slowed as well: Total cases were up by 146 for the week ending Jan. 18, compared with 294 and 205 for each of the previous 2 weeks, according to CDC reports.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
Zika activity is slowing as winter progresses, with less than a hundred new cases of pregnant women with laboratory evidence of infection reported over the 2 weeks ending Jan. 10, according to data from the Centers for Disease Control and Prevention.
The most recent CDC data show that, for the first time since early August, the majority of new cases of Zika infection among pregnant women were reported in the 50 states and the District of Columbia, compared with the U.S. territories. There were a total of 98 new cases, with 55 reported in the states and 43 in the U.S. territories.
The total number of Zika-infected pregnant women in the United States is now 4,232 for 2016-2017. There have been 2,885 cases in the territories and 1,347 cases reported in the states/D.C. Among the cases in the states/D.C., 940 pregnancies have been completed, with Zika-related birth defects seen in 37 live-born infants and five pregnancy losses, the CDC said. The CDC is no longer reporting adverse pregnancy outcomes for the territories because Puerto Rico is not using the same inclusion criteria.
Zika cases among all Americans are still being reported weekly by the CDC, and the increase there has slowed as well: Total cases were up by 146 for the week ending Jan. 18, compared with 294 and 205 for each of the previous 2 weeks, according to CDC reports.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
Sleeve lobectomy appears better than pneumonectomy for NSCLC
Guidelines that recommend sleeve lobectomy as a means of avoiding pneumonectomy for lung cancer have been based on a limited retrospective series, but a large series drawn from a nationwide database in France has confirmed the preference for sleeve lobectomy because it leads to higher rates of survival, despite an increased risk of postoperative pulmonary complications.
“Whenever it is technically possible, surgeons must perform sleeve lobectomy to provide more long-term survival benefits to patients, even with the risk of more postoperative pulmonary complications,” said Pierre-Benoit Pagès, MD, PhD, and his coauthors in the January 2017 issue of the Journal of Thoracic and Cardiovascular Surgery (2017;153:184-95). Dr. Pagès is with the department of thoracic and cardiovascular surgery at the University Hospital Center Dijon (France) and Bocage Hospital.

Three-year overall survival was 71.9% for the sleeve lobectomy group vs. 60.8% for the pneumonectomy group. Three-year disease-free survival was 46.4% for the sleeve lobectomy group and 31.6% for the pneumonectomy group. In addition, compared with the sleeve lobectomy group, the pneumonectomy group had an increased risk of recurrence by matching (hazard ratio, 1.49; 95% CI, 1.1-2).
The researchers performed a propensity-matched analysis that favored sleeve lobectomy for early overall and disease-free survival, but the weighted analysis did not. Patients in the sleeve lobectomy group vs. the pneumonectomy group were younger (60.9 years vs. 61.9), had higher body mass index (25.6 vs. 25.1), had higher average forced expiratory volume (74.1% vs. 62.9%), and had lower American Society of Anesthesiologists scores (73.7% with scores of 1 and 2 vs. 70.8%). Sleeve lobectomy patients also were more likely to have right-sided surgery (69.6% vs. 41%) and squamous cell carcinoma (54.6% vs. 48.3%), and lower T and N stages (T1 and T2, 60.5% vs. 40.6%; N0, 40.9% vs. 26.2%).
Overall mortality after surgery was 5% in the sleeve lobectomy group vs. 5.9% in the pneumonectomy group, but propensity scoring showed far fewer postoperative pulmonary complications in the pneumonectomy group, with an odds ratio of 0.4, Dr. Pagès and his coauthors said. However, with other significant complications – arrhythmia, bronchopleural fistula, empyema, and hemorrhage – pneumonectomy had a propensity-matched odds ratio ranging from 1.6 to 7. “We found no significant difference regarding postoperative mortality in the sleeve lobectomy and pneumonectomy groups, whatever the statistical method used,” Dr. Pagès and his coauthors wrote.
The investigators had no financial relationships to disclose.
The study by Dr. Pagès and his colleagues is unique in the field of surgery for non–small cell lung cancer in that it drew on a nationwide database using data from 103 centers, Betty C. Tong, MD, MHS, of Duke University Medical Center, Durham, said in her invited commentary (J Thorac Cardiovasc Surg. 2017;153:196). “These results are likely as close to real life as possible,” she said.
She acknowledged that no prospective, randomized controlled trials have compared sleeve lobectomy to pneumonectomy, but she added, “it is unlikely that such a trial could be successfully executed.” The 5:1 ratio of patients having pneumonectomy vs. sleeve lobectomy in this study is similar to findings from the Society of Thoracic Surgeons General Thoracic Surgery database (J Thorac Cardiovasc Surg. 2008;132:247-54), Dr. Tong pointed out, “and likely reflects the fact that sleeve lobectomy can be technically more difficult to perform.”
The findings of the French Society of Thoracic and Cardiovascular Surgery group “should strongly encourage thoracic surgeons to perform pneumonectomy as sparingly as possible,” and consider sleeve lobectomy the standard for patients with central tumors, Dr. Tong said.
She had no financial relationships to disclose.
The study by Dr. Pagès and his colleagues is unique in the field of surgery for non–small cell lung cancer in that it drew on a nationwide database using data from 103 centers, Betty C. Tong, MD, MHS, of Duke University Medical Center, Durham, said in her invited commentary (J Thorac Cardiovasc Surg. 2017;153:196). “These results are likely as close to real life as possible,” she said.
She acknowledged that no prospective, randomized controlled trials have compared sleeve lobectomy to pneumonectomy, but she added, “it is unlikely that such a trial could be successfully executed.” The 5:1 ratio of patients having pneumonectomy vs. sleeve lobectomy in this study is similar to findings from the Society of Thoracic Surgeons General Thoracic Surgery database (J Thorac Cardiovasc Surg. 2008;132:247-54), Dr. Tong pointed out, “and likely reflects the fact that sleeve lobectomy can be technically more difficult to perform.”
The findings of the French Society of Thoracic and Cardiovascular Surgery group “should strongly encourage thoracic surgeons to perform pneumonectomy as sparingly as possible,” and consider sleeve lobectomy the standard for patients with central tumors, Dr. Tong said.
She had no financial relationships to disclose.
The study by Dr. Pagès and his colleagues is unique in the field of surgery for non–small cell lung cancer in that it drew on a nationwide database using data from 103 centers, Betty C. Tong, MD, MHS, of Duke University Medical Center, Durham, said in her invited commentary (J Thorac Cardiovasc Surg. 2017;153:196). “These results are likely as close to real life as possible,” she said.
She acknowledged that no prospective, randomized controlled trials have compared sleeve lobectomy to pneumonectomy, but she added, “it is unlikely that such a trial could be successfully executed.” The 5:1 ratio of patients having pneumonectomy vs. sleeve lobectomy in this study is similar to findings from the Society of Thoracic Surgeons General Thoracic Surgery database (J Thorac Cardiovasc Surg. 2008;132:247-54), Dr. Tong pointed out, “and likely reflects the fact that sleeve lobectomy can be technically more difficult to perform.”
The findings of the French Society of Thoracic and Cardiovascular Surgery group “should strongly encourage thoracic surgeons to perform pneumonectomy as sparingly as possible,” and consider sleeve lobectomy the standard for patients with central tumors, Dr. Tong said.
She had no financial relationships to disclose.
Guidelines that recommend sleeve lobectomy as a means of avoiding pneumonectomy for lung cancer have been based on a limited retrospective series, but a large series drawn from a nationwide database in France has confirmed the preference for sleeve lobectomy because it leads to higher rates of survival, despite an increased risk of postoperative pulmonary complications.
“Whenever it is technically possible, surgeons must perform sleeve lobectomy to provide more long-term survival benefits to patients, even with the risk of more postoperative pulmonary complications,” said Pierre-Benoit Pagès, MD, PhD, and his coauthors in the January 2017 issue of the Journal of Thoracic and Cardiovascular Surgery (2017;153:184-95). Dr. Pagès is with the department of thoracic and cardiovascular surgery at the University Hospital Center Dijon (France) and Bocage Hospital.
Three-year overall survival was 71.9% for the sleeve lobectomy group vs. 60.8% for the pneumonectomy group. Three-year disease-free survival was 46.4% for the sleeve lobectomy group and 31.6% for the pneumonectomy group. In addition, compared with the sleeve lobectomy group, the pneumonectomy group had an increased risk of recurrence by matching (hazard ratio, 1.49; 95% CI, 1.1-2).
The researchers performed a propensity-matched analysis that favored sleeve lobectomy for early overall and disease-free survival, but the weighted analysis did not. Patients in the sleeve lobectomy group vs. the pneumonectomy group were younger (60.9 years vs. 61.9), had higher body mass index (25.6 vs. 25.1), had higher average forced expiratory volume (74.1% vs. 62.9%), and had lower American Society of Anesthesiologists scores (73.7% with scores of 1 and 2 vs. 70.8%). Sleeve lobectomy patients also were more likely to have right-sided surgery (69.6% vs. 41%) and squamous cell carcinoma (54.6% vs. 48.3%), and lower T and N stages (T1 and T2, 60.5% vs. 40.6%; N0, 40.9% vs. 26.2%).
Overall mortality after surgery was 5% in the sleeve lobectomy group vs. 5.9% in the pneumonectomy group, but propensity scoring showed far fewer postoperative pulmonary complications in the pneumonectomy group, with an odds ratio of 0.4, Dr. Pagès and his coauthors said. However, with other significant complications – arrhythmia, bronchopleural fistula, empyema, and hemorrhage – pneumonectomy had a propensity-matched odds ratio ranging from 1.6 to 7. “We found no significant difference regarding postoperative mortality in the sleeve lobectomy and pneumonectomy groups, whatever the statistical method used,” Dr. Pagès and his coauthors wrote.
The investigators had no financial relationships to disclose.
Guidelines that recommend sleeve lobectomy as a means of avoiding pneumonectomy for lung cancer have been based on a limited retrospective series, but a large series drawn from a nationwide database in France has confirmed the preference for sleeve lobectomy because it leads to higher rates of survival, despite an increased risk of postoperative pulmonary complications.
“Whenever it is technically possible, surgeons must perform sleeve lobectomy to provide more long-term survival benefits to patients, even with the risk of more postoperative pulmonary complications,” said Pierre-Benoit Pagès, MD, PhD, and his coauthors in the January 2017 issue of the Journal of Thoracic and Cardiovascular Surgery (2017;153:184-95). Dr. Pagès is with the department of thoracic and cardiovascular surgery at the University Hospital Center Dijon (France) and Bocage Hospital.
Three-year overall survival was 71.9% for the sleeve lobectomy group vs. 60.8% for the pneumonectomy group. Three-year disease-free survival was 46.4% for the sleeve lobectomy group and 31.6% for the pneumonectomy group. In addition, compared with the sleeve lobectomy group, the pneumonectomy group had an increased risk of recurrence by matching (hazard ratio, 1.49; 95% CI, 1.1-2).
The researchers performed a propensity-matched analysis that favored sleeve lobectomy for early overall and disease-free survival, but the weighted analysis did not. Patients in the sleeve lobectomy group vs. the pneumonectomy group were younger (60.9 years vs. 61.9), had higher body mass index (25.6 vs. 25.1), had higher average forced expiratory volume (74.1% vs. 62.9%), and had lower American Society of Anesthesiologists scores (73.7% with scores of 1 and 2 vs. 70.8%). Sleeve lobectomy patients also were more likely to have right-sided surgery (69.6% vs. 41%) and squamous cell carcinoma (54.6% vs. 48.3%), and lower T and N stages (T1 and T2, 60.5% vs. 40.6%; N0, 40.9% vs. 26.2%).
Overall mortality after surgery was 5% in the sleeve lobectomy group vs. 5.9% in the pneumonectomy group, but propensity scoring showed far fewer postoperative pulmonary complications in the pneumonectomy group, with an odds ratio of 0.4, Dr. Pagès and his coauthors said. However, with other significant complications – arrhythmia, bronchopleural fistula, empyema, and hemorrhage – pneumonectomy had a propensity-matched odds ratio ranging from 1.6 to 7. “We found no significant difference regarding postoperative mortality in the sleeve lobectomy and pneumonectomy groups, whatever the statistical method used,” Dr. Pagès and his coauthors wrote.
The investigators had no financial relationships to disclose.
Key clinical point: Sleeve lobectomy for non–small cell lung cancer may lead to higher rates of overall and disease-free survival vs. pneumonectomy.
Major finding: Overall postoperative mortality was 5% in the sleeve lobectomy group vs. 5.9% in the pneumonectomy group.
Data source: An analysis of 941 sleeve lobectomy and 5,318 pneumonectomy procedures from 2005 to 2014 in the nationwide French database Epithor.
Disclosures: Dr. Pagès has received research grants from the Nuovo-Soldati Foundation for Cancer Research and the French Society of Thoracic and Cardiovascular Surgery, on whose behalf the study was performed. Dr. Pagès and his coauthors had no financial relationships to disclose.