User login
Multivessel PCI in STEMI gains traction
SNOWMASS, COLO. – The tide appears to have turned regarding the merits of percutaneous coronary intervention in non-infarct-related arteries in conjunction with primary PCI for ST-elevation MI in patients with multivessel disease, Douglas E. Drachman, MD, said at the Annual Cardiovascular Conference at Snowmass.
Previously, multivessel PCI in STEMI patients who are hemodynamically stable was believed harmful and was given a Class IIIb recommendation – meaning don’t do it – in the 2013 American College of Cardiology/American Heart Association STEMI guidelines. Just 2 years later, however, new evidence in the form of three randomized trials prompted a focused update of the joint guidelines in which the practice was upgraded to Class IIb status, meaning it could be considered and may be beneficial.

Roughly 50% of STEMI patients have significant lesions in non-infarct-related arteries (non-IRA). The question of how best to treat such patients is an important one because multivessel coronary disease in STEMI is associated with increased risks of both reinfarction and mortality, noted Dr. Drachman, an interventional cardiologist at Massachusetts General Hospital in Boston.
He offered several reasons why the findings of the three influential randomized trials differed from earlier negative retrospective observational studies: “I would argue there’s been significant improvement in our technique in doing PCI. We’re primarily doing transradial interventions now for our patients, so the risk associated with multiple accesses is reduced. Our ability to use more potent antithrombotic strategies is enhanced by our concern about bleeding risk. And the stent platforms that we use in our interventional strategies have improved to the point that we are tackling ever more challenging lesions with greater aplomb and less concern that we may cause harm. I think all these factors have enhanced the ability of the interventionalist to select and treat non-IRAs in a staged fashion and be less parsimonious at the point of care.”
The remaining questions are which non-IRA lesions should be treated, in whom, when relative to primary PCI, and what are the cost implications? These issues are being tackled in at least eight active randomized controlled trials. Depending upon the answers to come, multivessel PCI in STEMI patients could receive a further upgrade in the guidelines.
Since release of the 2015 focused guideline update, several large studies have provided further backing for multivessel PCI in STEMI patients with significant multivessel disease, although these weren’t randomized prospective studies and hence must be considered hypothesis-generating.
One of these major pieces of evidence was a meta-analysis of observational studies led by Eric R. Bates, MD, professor of internal medicine at the University of Michigan in Ann Arbor. He and his coinvestigators analyzed studies comparing culprit vessel-only primary PCI for STEMI patients with multivessel disease versus staged PCI in which primary PCI was done first, followed by PCI of a non-infarct-related vessel later during the same hospitalization or soon after. Staged PCI was the clear winner, with a 2.2-fold greater likelihood of freedom from mortality (J Am Coll Cardiol. 2016 Sep 6;68(10):1066-81).
When the investigators compared studies of staged PCI versus multivessel PCI in the same session as primary PCI, staged PCI was again the clear winner, with a 4-fold greater freedom from mortality.
Among the possible risks of performing PCI of a non-IRA in the same session as primary PCI are increased risks of thrombosis, contrast-induced nephropathy, stent undersizing due to vasospasm, and unintended jeopardy of distant viable myocardium due to microembolization or side branch occlusion, Dr. Drachman said.
“Maybe in certain circumstances it’s best to let the dust settle after the urgent vessel intervention. Wait a couple of days and then make your plan,” the cardiologist advised.
Another informative recent piece of evidence was provided by a Canadian retrospective observational study which compared revascularization strategies in 6,503 consecutive STEMI patients with multivessel disease. Staged multivessel PCI during the index hospitalization was performed in 658 patients, multivessel PCI during the primary PCI session in 1,325, and PCI limited to the infarct-related artery in 4,520. The study endpoints were 2-year all-cause mortality and repeat revascularization.
Staged multivessel PCI had the lowest mortality and repeat revascularization rates. The 2-year mortality rate associated with this strategy was 45% less than with multivessel intervention at the time of primary PCI and 35% lower than for culprit vessel-only PCI, which unsurprisingly had the highest repeat revascularization rate (JACC Cardiovasc Interv. 2017 Jan 9;10(1):11-23).
The first of the three randomized trials that led to a change in the guidelines was the UK PRAMI study (Preventive Angioplasty in Acute Myocardial Infarction). It showed at a mean 23-months followup that STEMI patients with multivessel disease had a 65% reduction in the relative risk of a composite endoint of cardiovascular death, MI, or refractory angina if they received non-IRA PCI at the same time as primary PCI compared with PCI limited to the IRA (N Engl J Med. 2013 Sep 19;369(12):1115-23).
Next came another UK trial: CvLPRIT (Complete vs. Culprit-Lesion Only Primary PCI) demonstrated a 65% reduction in the composite 12-month outcome of all-cause mortality, MI, heart failure, or ischemia-driven PCI with staged PCI during the index hospitalization compared with culprit vessel-only PCI (J Am Coll Cardiol. 2015 Mar 17;65(10):963-72).
Finally, DANAMI-3-PRIMULTI (the Third Danish Study of Optimal Acute Treatment of Patients with STEMI: Primary PCI in Multivessel Disease) showed a dramatic reduction in the risk of ischemia-driven PCI during a median 27 months of followup in patients who underwent staged multivessel PCI guided by the findings of fractional flow reserve measurement compared with primary PCI limited to the IRA (Lancet. 2015 Aug 15;386(9994):665-71). However, fractional flow reserve-guided multivessel PCI didn’t decrease the risk of death or nonfatal recurrent MI, leaving its role unsettled pending the results of ongoing clinical trials.
Dr. Drachman said it’s clear certain STEMI patients should not undergo non-IRA PCI. These include anyone in whom the procedure would be lengthy due to vessel tortuosity or chronic total occlusion, as well as patients with stable saphenous vein graft disease or heavily calcified lesions requiring atherectomy, since multivessel PCI in those settings would pose a high risk for additional left ventricular dysfunction.
“Be thoughtful about patients who have renal dysfunction,” he added.
Dr. Drachman reported having no financial conflicts of interest.
SNOWMASS, COLO. – The tide appears to have turned regarding the merits of percutaneous coronary intervention in non-infarct-related arteries in conjunction with primary PCI for ST-elevation MI in patients with multivessel disease, Douglas E. Drachman, MD, said at the Annual Cardiovascular Conference at Snowmass.
Previously, multivessel PCI in STEMI patients who are hemodynamically stable was believed harmful and was given a Class IIIb recommendation – meaning don’t do it – in the 2013 American College of Cardiology/American Heart Association STEMI guidelines. Just 2 years later, however, new evidence in the form of three randomized trials prompted a focused update of the joint guidelines in which the practice was upgraded to Class IIb status, meaning it could be considered and may be beneficial.
Roughly 50% of STEMI patients have significant lesions in non-infarct-related arteries (non-IRA). The question of how best to treat such patients is an important one because multivessel coronary disease in STEMI is associated with increased risks of both reinfarction and mortality, noted Dr. Drachman, an interventional cardiologist at Massachusetts General Hospital in Boston.
He offered several reasons why the findings of the three influential randomized trials differed from earlier negative retrospective observational studies: “I would argue there’s been significant improvement in our technique in doing PCI. We’re primarily doing transradial interventions now for our patients, so the risk associated with multiple accesses is reduced. Our ability to use more potent antithrombotic strategies is enhanced by our concern about bleeding risk. And the stent platforms that we use in our interventional strategies have improved to the point that we are tackling ever more challenging lesions with greater aplomb and less concern that we may cause harm. I think all these factors have enhanced the ability of the interventionalist to select and treat non-IRAs in a staged fashion and be less parsimonious at the point of care.”
The remaining questions are which non-IRA lesions should be treated, in whom, when relative to primary PCI, and what are the cost implications? These issues are being tackled in at least eight active randomized controlled trials. Depending upon the answers to come, multivessel PCI in STEMI patients could receive a further upgrade in the guidelines.
Since release of the 2015 focused guideline update, several large studies have provided further backing for multivessel PCI in STEMI patients with significant multivessel disease, although these weren’t randomized prospective studies and hence must be considered hypothesis-generating.
One of these major pieces of evidence was a meta-analysis of observational studies led by Eric R. Bates, MD, professor of internal medicine at the University of Michigan in Ann Arbor. He and his coinvestigators analyzed studies comparing culprit vessel-only primary PCI for STEMI patients with multivessel disease versus staged PCI in which primary PCI was done first, followed by PCI of a non-infarct-related vessel later during the same hospitalization or soon after. Staged PCI was the clear winner, with a 2.2-fold greater likelihood of freedom from mortality (J Am Coll Cardiol. 2016 Sep 6;68(10):1066-81).
When the investigators compared studies of staged PCI versus multivessel PCI in the same session as primary PCI, staged PCI was again the clear winner, with a 4-fold greater freedom from mortality.
Among the possible risks of performing PCI of a non-IRA in the same session as primary PCI are increased risks of thrombosis, contrast-induced nephropathy, stent undersizing due to vasospasm, and unintended jeopardy of distant viable myocardium due to microembolization or side branch occlusion, Dr. Drachman said.
“Maybe in certain circumstances it’s best to let the dust settle after the urgent vessel intervention. Wait a couple of days and then make your plan,” the cardiologist advised.
Another informative recent piece of evidence was provided by a Canadian retrospective observational study which compared revascularization strategies in 6,503 consecutive STEMI patients with multivessel disease. Staged multivessel PCI during the index hospitalization was performed in 658 patients, multivessel PCI during the primary PCI session in 1,325, and PCI limited to the infarct-related artery in 4,520. The study endpoints were 2-year all-cause mortality and repeat revascularization.
Staged multivessel PCI had the lowest mortality and repeat revascularization rates. The 2-year mortality rate associated with this strategy was 45% less than with multivessel intervention at the time of primary PCI and 35% lower than for culprit vessel-only PCI, which unsurprisingly had the highest repeat revascularization rate (JACC Cardiovasc Interv. 2017 Jan 9;10(1):11-23).
The first of the three randomized trials that led to a change in the guidelines was the UK PRAMI study (Preventive Angioplasty in Acute Myocardial Infarction). It showed at a mean 23-months followup that STEMI patients with multivessel disease had a 65% reduction in the relative risk of a composite endoint of cardiovascular death, MI, or refractory angina if they received non-IRA PCI at the same time as primary PCI compared with PCI limited to the IRA (N Engl J Med. 2013 Sep 19;369(12):1115-23).
Next came another UK trial: CvLPRIT (Complete vs. Culprit-Lesion Only Primary PCI) demonstrated a 65% reduction in the composite 12-month outcome of all-cause mortality, MI, heart failure, or ischemia-driven PCI with staged PCI during the index hospitalization compared with culprit vessel-only PCI (J Am Coll Cardiol. 2015 Mar 17;65(10):963-72).
Finally, DANAMI-3-PRIMULTI (the Third Danish Study of Optimal Acute Treatment of Patients with STEMI: Primary PCI in Multivessel Disease) showed a dramatic reduction in the risk of ischemia-driven PCI during a median 27 months of followup in patients who underwent staged multivessel PCI guided by the findings of fractional flow reserve measurement compared with primary PCI limited to the IRA (Lancet. 2015 Aug 15;386(9994):665-71). However, fractional flow reserve-guided multivessel PCI didn’t decrease the risk of death or nonfatal recurrent MI, leaving its role unsettled pending the results of ongoing clinical trials.
Dr. Drachman said it’s clear certain STEMI patients should not undergo non-IRA PCI. These include anyone in whom the procedure would be lengthy due to vessel tortuosity or chronic total occlusion, as well as patients with stable saphenous vein graft disease or heavily calcified lesions requiring atherectomy, since multivessel PCI in those settings would pose a high risk for additional left ventricular dysfunction.
“Be thoughtful about patients who have renal dysfunction,” he added.
Dr. Drachman reported having no financial conflicts of interest.
SNOWMASS, COLO. – The tide appears to have turned regarding the merits of percutaneous coronary intervention in non-infarct-related arteries in conjunction with primary PCI for ST-elevation MI in patients with multivessel disease, Douglas E. Drachman, MD, said at the Annual Cardiovascular Conference at Snowmass.
Previously, multivessel PCI in STEMI patients who are hemodynamically stable was believed harmful and was given a Class IIIb recommendation – meaning don’t do it – in the 2013 American College of Cardiology/American Heart Association STEMI guidelines. Just 2 years later, however, new evidence in the form of three randomized trials prompted a focused update of the joint guidelines in which the practice was upgraded to Class IIb status, meaning it could be considered and may be beneficial.
Roughly 50% of STEMI patients have significant lesions in non-infarct-related arteries (non-IRA). The question of how best to treat such patients is an important one because multivessel coronary disease in STEMI is associated with increased risks of both reinfarction and mortality, noted Dr. Drachman, an interventional cardiologist at Massachusetts General Hospital in Boston.
He offered several reasons why the findings of the three influential randomized trials differed from earlier negative retrospective observational studies: “I would argue there’s been significant improvement in our technique in doing PCI. We’re primarily doing transradial interventions now for our patients, so the risk associated with multiple accesses is reduced. Our ability to use more potent antithrombotic strategies is enhanced by our concern about bleeding risk. And the stent platforms that we use in our interventional strategies have improved to the point that we are tackling ever more challenging lesions with greater aplomb and less concern that we may cause harm. I think all these factors have enhanced the ability of the interventionalist to select and treat non-IRAs in a staged fashion and be less parsimonious at the point of care.”
The remaining questions are which non-IRA lesions should be treated, in whom, when relative to primary PCI, and what are the cost implications? These issues are being tackled in at least eight active randomized controlled trials. Depending upon the answers to come, multivessel PCI in STEMI patients could receive a further upgrade in the guidelines.
Since release of the 2015 focused guideline update, several large studies have provided further backing for multivessel PCI in STEMI patients with significant multivessel disease, although these weren’t randomized prospective studies and hence must be considered hypothesis-generating.
One of these major pieces of evidence was a meta-analysis of observational studies led by Eric R. Bates, MD, professor of internal medicine at the University of Michigan in Ann Arbor. He and his coinvestigators analyzed studies comparing culprit vessel-only primary PCI for STEMI patients with multivessel disease versus staged PCI in which primary PCI was done first, followed by PCI of a non-infarct-related vessel later during the same hospitalization or soon after. Staged PCI was the clear winner, with a 2.2-fold greater likelihood of freedom from mortality (J Am Coll Cardiol. 2016 Sep 6;68(10):1066-81).
When the investigators compared studies of staged PCI versus multivessel PCI in the same session as primary PCI, staged PCI was again the clear winner, with a 4-fold greater freedom from mortality.
Among the possible risks of performing PCI of a non-IRA in the same session as primary PCI are increased risks of thrombosis, contrast-induced nephropathy, stent undersizing due to vasospasm, and unintended jeopardy of distant viable myocardium due to microembolization or side branch occlusion, Dr. Drachman said.
“Maybe in certain circumstances it’s best to let the dust settle after the urgent vessel intervention. Wait a couple of days and then make your plan,” the cardiologist advised.
Another informative recent piece of evidence was provided by a Canadian retrospective observational study which compared revascularization strategies in 6,503 consecutive STEMI patients with multivessel disease. Staged multivessel PCI during the index hospitalization was performed in 658 patients, multivessel PCI during the primary PCI session in 1,325, and PCI limited to the infarct-related artery in 4,520. The study endpoints were 2-year all-cause mortality and repeat revascularization.
Staged multivessel PCI had the lowest mortality and repeat revascularization rates. The 2-year mortality rate associated with this strategy was 45% less than with multivessel intervention at the time of primary PCI and 35% lower than for culprit vessel-only PCI, which unsurprisingly had the highest repeat revascularization rate (JACC Cardiovasc Interv. 2017 Jan 9;10(1):11-23).
The first of the three randomized trials that led to a change in the guidelines was the UK PRAMI study (Preventive Angioplasty in Acute Myocardial Infarction). It showed at a mean 23-months followup that STEMI patients with multivessel disease had a 65% reduction in the relative risk of a composite endoint of cardiovascular death, MI, or refractory angina if they received non-IRA PCI at the same time as primary PCI compared with PCI limited to the IRA (N Engl J Med. 2013 Sep 19;369(12):1115-23).
Next came another UK trial: CvLPRIT (Complete vs. Culprit-Lesion Only Primary PCI) demonstrated a 65% reduction in the composite 12-month outcome of all-cause mortality, MI, heart failure, or ischemia-driven PCI with staged PCI during the index hospitalization compared with culprit vessel-only PCI (J Am Coll Cardiol. 2015 Mar 17;65(10):963-72).
Finally, DANAMI-3-PRIMULTI (the Third Danish Study of Optimal Acute Treatment of Patients with STEMI: Primary PCI in Multivessel Disease) showed a dramatic reduction in the risk of ischemia-driven PCI during a median 27 months of followup in patients who underwent staged multivessel PCI guided by the findings of fractional flow reserve measurement compared with primary PCI limited to the IRA (Lancet. 2015 Aug 15;386(9994):665-71). However, fractional flow reserve-guided multivessel PCI didn’t decrease the risk of death or nonfatal recurrent MI, leaving its role unsettled pending the results of ongoing clinical trials.
Dr. Drachman said it’s clear certain STEMI patients should not undergo non-IRA PCI. These include anyone in whom the procedure would be lengthy due to vessel tortuosity or chronic total occlusion, as well as patients with stable saphenous vein graft disease or heavily calcified lesions requiring atherectomy, since multivessel PCI in those settings would pose a high risk for additional left ventricular dysfunction.
“Be thoughtful about patients who have renal dysfunction,” he added.
Dr. Drachman reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
Flu activity up slightly, but still down from seasonal peak
After rising to a high point for the season in the last week of 2016, influenza activity dropped a bit in the first week of the new year but then rose again in the second week, according to the Centers for Disease Control and Prevention.
As measured by outpatient visits for influenza-like illness (ILI), activity slipped from 3.4% at the end of 2016 to 3.2% for the week ending Jan. 7 but then ticked up to 3.3% for the week ending Jan. 14, the CDC reported. The national baseline level of outpatient visits is 2.2% for ILI, which is defined as fever (temperature of 100° F or greater) and cough and/or sore throat.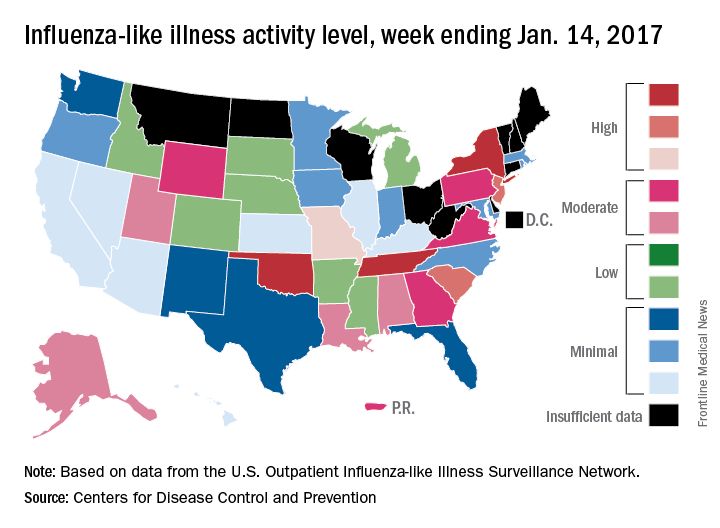
Two influenza-related pediatric deaths were reported for the week ending Jan. 14, although both occurred in earlier weeks: one during the week ending Dec. 10 and one during the week ending Jan. 7. So far for the 2016-2017 season, a total of five flu-related pediatric deaths have been reported, according to the CDC.
After rising to a high point for the season in the last week of 2016, influenza activity dropped a bit in the first week of the new year but then rose again in the second week, according to the Centers for Disease Control and Prevention.
As measured by outpatient visits for influenza-like illness (ILI), activity slipped from 3.4% at the end of 2016 to 3.2% for the week ending Jan. 7 but then ticked up to 3.3% for the week ending Jan. 14, the CDC reported. The national baseline level of outpatient visits is 2.2% for ILI, which is defined as fever (temperature of 100° F or greater) and cough and/or sore throat.
Two influenza-related pediatric deaths were reported for the week ending Jan. 14, although both occurred in earlier weeks: one during the week ending Dec. 10 and one during the week ending Jan. 7. So far for the 2016-2017 season, a total of five flu-related pediatric deaths have been reported, according to the CDC.
After rising to a high point for the season in the last week of 2016, influenza activity dropped a bit in the first week of the new year but then rose again in the second week, according to the Centers for Disease Control and Prevention.
As measured by outpatient visits for influenza-like illness (ILI), activity slipped from 3.4% at the end of 2016 to 3.2% for the week ending Jan. 7 but then ticked up to 3.3% for the week ending Jan. 14, the CDC reported. The national baseline level of outpatient visits is 2.2% for ILI, which is defined as fever (temperature of 100° F or greater) and cough and/or sore throat.
Two influenza-related pediatric deaths were reported for the week ending Jan. 14, although both occurred in earlier weeks: one during the week ending Dec. 10 and one during the week ending Jan. 7. So far for the 2016-2017 season, a total of five flu-related pediatric deaths have been reported, according to the CDC.
Resective epilepsy surgery found OK in septuagenarians
HOUSTON – With careful selection, patients in their 70s with refractory epilepsy may be offered resective epilepsy surgery, results from a small single-center study demonstrated.
The findings “were a surprise to us,” lead study author Ahmed Abdelkader, MD, said in an interview at the annual meeting of the American Epilepsy Society. “We expected that complications would be higher because this is a vulnerable age group with multiple comorbidities.”

Dr. Abdelkader and his associates searched the database of the Cleveland Clinic Epilepsy Center to identify patients aged 70 years and older who underwent respective epilepsy surgery between Jan. 1, 2000, and Sept. 30, 2015. They limited the analysis to seven patients who had at least one year of post-surgical follow-up. The mean age of the patients at surgery was 73 and the age of epilepsy onset ranged from 24-71 years, with a monthly frequency of 4.2 seizures. Their mean Charlson Combined Comorbidity Index score was 4, which translated into a 10-year mean survival probability of 53%. Four of the patients (57%) had a history of significant injuries due to seizures, while all but one had a positive MRI. Three of the patients had hippocampal sclerosis, “which is unique because most cases of hippocampal sclerosis are in younger age groups,” said Dr. Abdelkader, who is currently a research fellow at University Hospitals Case Medical Center, Cleveland.
All patients underwent anterior temporal lobectomy, four on the left side. None had a surgical complication. Six of the seven patients had a good surgical outcome, defined as a Class I or II on the Engel Epilepsy Surgery Outcome Scale, with four being completed free of seizures at one year of follow-up. One of the patients underwent two respective epilepsy surgeries: the first at age 72 and the second at age 75. He died of natural causes, 11 years after his first surgery, and was the only patient to pass away during the follow-up period.
In their abstract, the researchers called for future multi-center collaborative studies “to prospectively study factors influencing respective epilepsy surgery recommendation and its outcome in this rapidly growing population.”
Dr. Abdelkader reported having no financial disclosures.
HOUSTON – With careful selection, patients in their 70s with refractory epilepsy may be offered resective epilepsy surgery, results from a small single-center study demonstrated.
The findings “were a surprise to us,” lead study author Ahmed Abdelkader, MD, said in an interview at the annual meeting of the American Epilepsy Society. “We expected that complications would be higher because this is a vulnerable age group with multiple comorbidities.”
Dr. Abdelkader and his associates searched the database of the Cleveland Clinic Epilepsy Center to identify patients aged 70 years and older who underwent respective epilepsy surgery between Jan. 1, 2000, and Sept. 30, 2015. They limited the analysis to seven patients who had at least one year of post-surgical follow-up. The mean age of the patients at surgery was 73 and the age of epilepsy onset ranged from 24-71 years, with a monthly frequency of 4.2 seizures. Their mean Charlson Combined Comorbidity Index score was 4, which translated into a 10-year mean survival probability of 53%. Four of the patients (57%) had a history of significant injuries due to seizures, while all but one had a positive MRI. Three of the patients had hippocampal sclerosis, “which is unique because most cases of hippocampal sclerosis are in younger age groups,” said Dr. Abdelkader, who is currently a research fellow at University Hospitals Case Medical Center, Cleveland.
All patients underwent anterior temporal lobectomy, four on the left side. None had a surgical complication. Six of the seven patients had a good surgical outcome, defined as a Class I or II on the Engel Epilepsy Surgery Outcome Scale, with four being completed free of seizures at one year of follow-up. One of the patients underwent two respective epilepsy surgeries: the first at age 72 and the second at age 75. He died of natural causes, 11 years after his first surgery, and was the only patient to pass away during the follow-up period.
In their abstract, the researchers called for future multi-center collaborative studies “to prospectively study factors influencing respective epilepsy surgery recommendation and its outcome in this rapidly growing population.”
Dr. Abdelkader reported having no financial disclosures.
HOUSTON – With careful selection, patients in their 70s with refractory epilepsy may be offered resective epilepsy surgery, results from a small single-center study demonstrated.
The findings “were a surprise to us,” lead study author Ahmed Abdelkader, MD, said in an interview at the annual meeting of the American Epilepsy Society. “We expected that complications would be higher because this is a vulnerable age group with multiple comorbidities.”
Dr. Abdelkader and his associates searched the database of the Cleveland Clinic Epilepsy Center to identify patients aged 70 years and older who underwent respective epilepsy surgery between Jan. 1, 2000, and Sept. 30, 2015. They limited the analysis to seven patients who had at least one year of post-surgical follow-up. The mean age of the patients at surgery was 73 and the age of epilepsy onset ranged from 24-71 years, with a monthly frequency of 4.2 seizures. Their mean Charlson Combined Comorbidity Index score was 4, which translated into a 10-year mean survival probability of 53%. Four of the patients (57%) had a history of significant injuries due to seizures, while all but one had a positive MRI. Three of the patients had hippocampal sclerosis, “which is unique because most cases of hippocampal sclerosis are in younger age groups,” said Dr. Abdelkader, who is currently a research fellow at University Hospitals Case Medical Center, Cleveland.
All patients underwent anterior temporal lobectomy, four on the left side. None had a surgical complication. Six of the seven patients had a good surgical outcome, defined as a Class I or II on the Engel Epilepsy Surgery Outcome Scale, with four being completed free of seizures at one year of follow-up. One of the patients underwent two respective epilepsy surgeries: the first at age 72 and the second at age 75. He died of natural causes, 11 years after his first surgery, and was the only patient to pass away during the follow-up period.
In their abstract, the researchers called for future multi-center collaborative studies “to prospectively study factors influencing respective epilepsy surgery recommendation and its outcome in this rapidly growing population.”
Dr. Abdelkader reported having no financial disclosures.
AT AES 2016
Key clinical point:
Major finding: Six of the seven patients achieved good surgical outcome, with four being completed free of seizures at one year of follow-up.
Data source: A retrospective review of seven patients who underwent resective epilepsy surgery in their 70s.
Disclosures: Dr. Abdelkader reported having no financial disclosures.
Age and disease stage predict long-term survival in elderly lung cancer patients
AT THE STS ANNUAL MEETING
HOUSTON – Although certain medical factors predict long-term survival in patients over age 65 years with lung cancer, advanced age and disease stage are especially strong predictors, results from a large analysis of national data demonstrated.
The findings, which were presented by Mark Onaitis, MD, at the annual meeting of the Society of Thoracic Surgeons, come from a novel effort to pair Medicare data with files from the STS General Thoracic Surgery Database (GTSD).
For the current study, he and his associates linked GTSD data to Medicare data on 29,899 patients who underwent lung cancer resection from 2002 to 2013. They used Cox proportional hazards modeling to create a long-term survival model and used statistically significant univariate factors and known clinical predictors of outcome to perform variable selection.
Dr. Onaitis reported that the median age of patients was 73 years and that 52% were female. Of the 29,899 patients, 805 had a missing pathologic stage. Of the 29,094 patients not missing a pathologic stage, 69% were stage I, 18% stage II, 11% stage III, and 2% stage IV. Two-thirds of patients (66%) underwent lobectomy, followed by wedge resection (17%), segmentectomy (7%), bilobectomy (3%), pneumonectomy (3%), and sleeve lobectomy (1%). A thoracoscopic approach was performed in nearly half of resections (47%).
Cox analysis revealed the following strong negative predictors of long-term survival: having stage III or IV-V disease (hazard ratio, 1.23 and 1.37, respectively), being age 70-74 (HR, 1.19), 75-80 (HR, 1.40), or 80 and older (HR, 1.90).
After controlling for disease stage, the following procedures were associated with increased hazard of death, compared with lobectomy: wedge resection (HR, 1.22), segmentectomy (HR, 1.10), bilobectomy (HR, 1.30), and pneumonectomy (HR, 1.58). In addition, video-assisted thoracoscopic surgery was associated with improved long-term survival, compared with thoracotomy (HR, 0.86).
“Given the large number of patients and the excellent quality of the data, it was not surprising that age and stage and known medical conditions affect long-term survival,” Dr. Onaitis commented. “The deleterious effects of sublobar operations and open [as opposed to thoracoscopic or VATS] approach were more pronounced than expected.”
Other modifiable predictive factors include being a past or current smoker (HR, 1.35 and HR, 1.54, respectively) and having a body mass index below 18.5 kg/m2 (HR, 1.58).
Dr. Onaitis acknowledged certain limitations of the study, including its retrospective design. “Because the study involves linkage of STS data to Medicare data, the findings may not be applicable to patients less than 65 years of age,” he added. He reported having no financial disclosures.
AT THE STS ANNUAL MEETING
HOUSTON – Although certain medical factors predict long-term survival in patients over age 65 years with lung cancer, advanced age and disease stage are especially strong predictors, results from a large analysis of national data demonstrated.
The findings, which were presented by Mark Onaitis, MD, at the annual meeting of the Society of Thoracic Surgeons, come from a novel effort to pair Medicare data with files from the STS General Thoracic Surgery Database (GTSD).
For the current study, he and his associates linked GTSD data to Medicare data on 29,899 patients who underwent lung cancer resection from 2002 to 2013. They used Cox proportional hazards modeling to create a long-term survival model and used statistically significant univariate factors and known clinical predictors of outcome to perform variable selection.
Dr. Onaitis reported that the median age of patients was 73 years and that 52% were female. Of the 29,899 patients, 805 had a missing pathologic stage. Of the 29,094 patients not missing a pathologic stage, 69% were stage I, 18% stage II, 11% stage III, and 2% stage IV. Two-thirds of patients (66%) underwent lobectomy, followed by wedge resection (17%), segmentectomy (7%), bilobectomy (3%), pneumonectomy (3%), and sleeve lobectomy (1%). A thoracoscopic approach was performed in nearly half of resections (47%).
Cox analysis revealed the following strong negative predictors of long-term survival: having stage III or IV-V disease (hazard ratio, 1.23 and 1.37, respectively), being age 70-74 (HR, 1.19), 75-80 (HR, 1.40), or 80 and older (HR, 1.90).
After controlling for disease stage, the following procedures were associated with increased hazard of death, compared with lobectomy: wedge resection (HR, 1.22), segmentectomy (HR, 1.10), bilobectomy (HR, 1.30), and pneumonectomy (HR, 1.58). In addition, video-assisted thoracoscopic surgery was associated with improved long-term survival, compared with thoracotomy (HR, 0.86).
“Given the large number of patients and the excellent quality of the data, it was not surprising that age and stage and known medical conditions affect long-term survival,” Dr. Onaitis commented. “The deleterious effects of sublobar operations and open [as opposed to thoracoscopic or VATS] approach were more pronounced than expected.”
Other modifiable predictive factors include being a past or current smoker (HR, 1.35 and HR, 1.54, respectively) and having a body mass index below 18.5 kg/m2 (HR, 1.58).
Dr. Onaitis acknowledged certain limitations of the study, including its retrospective design. “Because the study involves linkage of STS data to Medicare data, the findings may not be applicable to patients less than 65 years of age,” he added. He reported having no financial disclosures.
AT THE STS ANNUAL MEETING
HOUSTON – Although certain medical factors predict long-term survival in patients over age 65 years with lung cancer, advanced age and disease stage are especially strong predictors, results from a large analysis of national data demonstrated.
The findings, which were presented by Mark Onaitis, MD, at the annual meeting of the Society of Thoracic Surgeons, come from a novel effort to pair Medicare data with files from the STS General Thoracic Surgery Database (GTSD).
For the current study, he and his associates linked GTSD data to Medicare data on 29,899 patients who underwent lung cancer resection from 2002 to 2013. They used Cox proportional hazards modeling to create a long-term survival model and used statistically significant univariate factors and known clinical predictors of outcome to perform variable selection.
Dr. Onaitis reported that the median age of patients was 73 years and that 52% were female. Of the 29,899 patients, 805 had a missing pathologic stage. Of the 29,094 patients not missing a pathologic stage, 69% were stage I, 18% stage II, 11% stage III, and 2% stage IV. Two-thirds of patients (66%) underwent lobectomy, followed by wedge resection (17%), segmentectomy (7%), bilobectomy (3%), pneumonectomy (3%), and sleeve lobectomy (1%). A thoracoscopic approach was performed in nearly half of resections (47%).
Cox analysis revealed the following strong negative predictors of long-term survival: having stage III or IV-V disease (hazard ratio, 1.23 and 1.37, respectively), being age 70-74 (HR, 1.19), 75-80 (HR, 1.40), or 80 and older (HR, 1.90).
After controlling for disease stage, the following procedures were associated with increased hazard of death, compared with lobectomy: wedge resection (HR, 1.22), segmentectomy (HR, 1.10), bilobectomy (HR, 1.30), and pneumonectomy (HR, 1.58). In addition, video-assisted thoracoscopic surgery was associated with improved long-term survival, compared with thoracotomy (HR, 0.86).
“Given the large number of patients and the excellent quality of the data, it was not surprising that age and stage and known medical conditions affect long-term survival,” Dr. Onaitis commented. “The deleterious effects of sublobar operations and open [as opposed to thoracoscopic or VATS] approach were more pronounced than expected.”
Other modifiable predictive factors include being a past or current smoker (HR, 1.35 and HR, 1.54, respectively) and having a body mass index below 18.5 kg/m2 (HR, 1.58).
Dr. Onaitis acknowledged certain limitations of the study, including its retrospective design. “Because the study involves linkage of STS data to Medicare data, the findings may not be applicable to patients less than 65 years of age,” he added. He reported having no financial disclosures.
Key clinical point:
Major finding: Strong negative predictors of long-term survival included having stage III or IV-V disease (HR, 1.23 and 1.37, respectively), being age 70-74 (HR, 1.19), 75-80 (HR, 1.40), or 80 and older (HR, 1.90).
Data source: A retrospective analysis of 29,899 patients over age 65 who underwent lung cancer resection from 2002 to 2013.
Disclosures: Dr. Onaitis reported having no financial disclosures.
Study IDs risk factors for ideal timing of stage 2 palliation following Norwood
HOUSTON – The optimal timing of stage 2 palliation after the Norwood operation depends on certain patient-specific risk factors, but in most cases should be done around 3-4 months of age, results from a multi-center study show.
While previous studies have investigated whether early stage-2 palliation (S2P) can be performed without increased post-S2P mortality, the effect of the timing of S2P on post-Norwood mortality remains unknown, Robert “Jake” Jaquiss, MD, said in an interview in advance of the annual meeting of the Society of Thoracic Surgeons.
“There has been a lot of dispute about how early is too early for S2P,” said Dr. Jaquiss, the study’s senior author, who is professor and division chief of pediatric cardiothoracic surgery at the University of Texas Southwestern Medical Center. “That is one of the few things that is in the control of the doctor. Most of the rest of the decisions are based entirely on the condition of the patient and the patient’s specific anatomy. So the timing of S2P is something that we can truly define most always. What we want to find out is, what is the ideal timing? How early is too early? Is there such a thing as too late?”
In an effort to determine the optimal timing of S2P that both minimizes pre-S2P attrition and maximizes long-term post-S2P survival, Dr. Jaquiss and his associates at 19 other institutions evaluated data from 534 neonates diagnosed with left ventricular outflow tract obstruction that precluded adequate systemic cardiac output through the aortic valve who initially underwent a Norwood operation from 2005 to 2016.

S2P was performed in 377 patients (71%) at a mean age of 5.4 months, while 115 (22%) died after Norwood, and the rest underwent biventricular repair or heart transplantation. After S2P, 38 (10%) died, 248 (66%) underwent Fontan, and the rest were alive awaiting Fontan or underwent heart transplantation.
Risk factors for death after Norwood included requiring pre-Norwood extracorporeal membrane oxygenation (P less than .0001), birth weight of less than 2.5 kg (P less than .0001), modified Blalock-Taussig shunt vs. a right ventricle to pulmonary artery conduit (P = .0003), larger baseline right pulmonary artery diameter (P = .0002), smaller baseline mitral valve diameter (P = .0002), smaller baseline tricuspid valve diameter (P = .0001), and nonwhite race (P = .03).
Risk factors for death after S2P included lower oxygen saturation at pre-S2P clinic visit (P = .02), having moderate or severe pre-S2P right ventricular dysfunction (P = .007), younger age at S2P (P = .03), and longer post-Norwood hospital length of stay (P = .03).
The risk-adjusted, 4-year, post-Norwood survival was 72%, with a confidence interval of 67%-75%. When plotted vs. the age at S2P, risk-adjusted, 4-year, post-Norwood survival for the 534 patients was maximized by S2P at 3-6 months of age. At the same time, risk-adjusted, 4-year survival in low-risk infants was compromised only by undergoing S2P earlier than 3 months of age. In high-risk infants, survival was severely compromised, especially when undergoing S2P earlier than 6 months of age.
“The results reinforced intuitions or expectations that most of the investigators already had,” Dr. Jaquiss said. “But we are in an era where evidence-based medicine is much preferable to intuition-based medicine. I’m very confident in the findings we have. I feel more confident in suggesting that we should be planning these surgeries around 3-4 months of age in usual-risk children and also more confident in suggesting that we need to consider transplantation earlier in children who are perceived to be at high risk. There is some hope [by clinicians in] some centers that you can convert a high-risk prognosis to a lower or intermediate risk prognosis by doing the S2P earlier or at some alternative time. Our data suggests that would not be helpful.”
Dr. Jaquiss and Dr. Meza reported having no financial disclosures.
HOUSTON – The optimal timing of stage 2 palliation after the Norwood operation depends on certain patient-specific risk factors, but in most cases should be done around 3-4 months of age, results from a multi-center study show.
While previous studies have investigated whether early stage-2 palliation (S2P) can be performed without increased post-S2P mortality, the effect of the timing of S2P on post-Norwood mortality remains unknown, Robert “Jake” Jaquiss, MD, said in an interview in advance of the annual meeting of the Society of Thoracic Surgeons.
“There has been a lot of dispute about how early is too early for S2P,” said Dr. Jaquiss, the study’s senior author, who is professor and division chief of pediatric cardiothoracic surgery at the University of Texas Southwestern Medical Center. “That is one of the few things that is in the control of the doctor. Most of the rest of the decisions are based entirely on the condition of the patient and the patient’s specific anatomy. So the timing of S2P is something that we can truly define most always. What we want to find out is, what is the ideal timing? How early is too early? Is there such a thing as too late?”
In an effort to determine the optimal timing of S2P that both minimizes pre-S2P attrition and maximizes long-term post-S2P survival, Dr. Jaquiss and his associates at 19 other institutions evaluated data from 534 neonates diagnosed with left ventricular outflow tract obstruction that precluded adequate systemic cardiac output through the aortic valve who initially underwent a Norwood operation from 2005 to 2016.
S2P was performed in 377 patients (71%) at a mean age of 5.4 months, while 115 (22%) died after Norwood, and the rest underwent biventricular repair or heart transplantation. After S2P, 38 (10%) died, 248 (66%) underwent Fontan, and the rest were alive awaiting Fontan or underwent heart transplantation.
Risk factors for death after Norwood included requiring pre-Norwood extracorporeal membrane oxygenation (P less than .0001), birth weight of less than 2.5 kg (P less than .0001), modified Blalock-Taussig shunt vs. a right ventricle to pulmonary artery conduit (P = .0003), larger baseline right pulmonary artery diameter (P = .0002), smaller baseline mitral valve diameter (P = .0002), smaller baseline tricuspid valve diameter (P = .0001), and nonwhite race (P = .03).
Risk factors for death after S2P included lower oxygen saturation at pre-S2P clinic visit (P = .02), having moderate or severe pre-S2P right ventricular dysfunction (P = .007), younger age at S2P (P = .03), and longer post-Norwood hospital length of stay (P = .03).
The risk-adjusted, 4-year, post-Norwood survival was 72%, with a confidence interval of 67%-75%. When plotted vs. the age at S2P, risk-adjusted, 4-year, post-Norwood survival for the 534 patients was maximized by S2P at 3-6 months of age. At the same time, risk-adjusted, 4-year survival in low-risk infants was compromised only by undergoing S2P earlier than 3 months of age. In high-risk infants, survival was severely compromised, especially when undergoing S2P earlier than 6 months of age.
“The results reinforced intuitions or expectations that most of the investigators already had,” Dr. Jaquiss said. “But we are in an era where evidence-based medicine is much preferable to intuition-based medicine. I’m very confident in the findings we have. I feel more confident in suggesting that we should be planning these surgeries around 3-4 months of age in usual-risk children and also more confident in suggesting that we need to consider transplantation earlier in children who are perceived to be at high risk. There is some hope [by clinicians in] some centers that you can convert a high-risk prognosis to a lower or intermediate risk prognosis by doing the S2P earlier or at some alternative time. Our data suggests that would not be helpful.”
Dr. Jaquiss and Dr. Meza reported having no financial disclosures.
HOUSTON – The optimal timing of stage 2 palliation after the Norwood operation depends on certain patient-specific risk factors, but in most cases should be done around 3-4 months of age, results from a multi-center study show.
While previous studies have investigated whether early stage-2 palliation (S2P) can be performed without increased post-S2P mortality, the effect of the timing of S2P on post-Norwood mortality remains unknown, Robert “Jake” Jaquiss, MD, said in an interview in advance of the annual meeting of the Society of Thoracic Surgeons.
“There has been a lot of dispute about how early is too early for S2P,” said Dr. Jaquiss, the study’s senior author, who is professor and division chief of pediatric cardiothoracic surgery at the University of Texas Southwestern Medical Center. “That is one of the few things that is in the control of the doctor. Most of the rest of the decisions are based entirely on the condition of the patient and the patient’s specific anatomy. So the timing of S2P is something that we can truly define most always. What we want to find out is, what is the ideal timing? How early is too early? Is there such a thing as too late?”
In an effort to determine the optimal timing of S2P that both minimizes pre-S2P attrition and maximizes long-term post-S2P survival, Dr. Jaquiss and his associates at 19 other institutions evaluated data from 534 neonates diagnosed with left ventricular outflow tract obstruction that precluded adequate systemic cardiac output through the aortic valve who initially underwent a Norwood operation from 2005 to 2016.
S2P was performed in 377 patients (71%) at a mean age of 5.4 months, while 115 (22%) died after Norwood, and the rest underwent biventricular repair or heart transplantation. After S2P, 38 (10%) died, 248 (66%) underwent Fontan, and the rest were alive awaiting Fontan or underwent heart transplantation.
Risk factors for death after Norwood included requiring pre-Norwood extracorporeal membrane oxygenation (P less than .0001), birth weight of less than 2.5 kg (P less than .0001), modified Blalock-Taussig shunt vs. a right ventricle to pulmonary artery conduit (P = .0003), larger baseline right pulmonary artery diameter (P = .0002), smaller baseline mitral valve diameter (P = .0002), smaller baseline tricuspid valve diameter (P = .0001), and nonwhite race (P = .03).
Risk factors for death after S2P included lower oxygen saturation at pre-S2P clinic visit (P = .02), having moderate or severe pre-S2P right ventricular dysfunction (P = .007), younger age at S2P (P = .03), and longer post-Norwood hospital length of stay (P = .03).
The risk-adjusted, 4-year, post-Norwood survival was 72%, with a confidence interval of 67%-75%. When plotted vs. the age at S2P, risk-adjusted, 4-year, post-Norwood survival for the 534 patients was maximized by S2P at 3-6 months of age. At the same time, risk-adjusted, 4-year survival in low-risk infants was compromised only by undergoing S2P earlier than 3 months of age. In high-risk infants, survival was severely compromised, especially when undergoing S2P earlier than 6 months of age.
“The results reinforced intuitions or expectations that most of the investigators already had,” Dr. Jaquiss said. “But we are in an era where evidence-based medicine is much preferable to intuition-based medicine. I’m very confident in the findings we have. I feel more confident in suggesting that we should be planning these surgeries around 3-4 months of age in usual-risk children and also more confident in suggesting that we need to consider transplantation earlier in children who are perceived to be at high risk. There is some hope [by clinicians in] some centers that you can convert a high-risk prognosis to a lower or intermediate risk prognosis by doing the S2P earlier or at some alternative time. Our data suggests that would not be helpful.”
Dr. Jaquiss and Dr. Meza reported having no financial disclosures.
Key clinical point:
Major finding: When plotted vs. the age at stage 2 palliation, risk-adjusted, 4-year, post-Norwood survival for the 534 patients was maximized by S2P at 3-6 months of age.
Data source: A multi-institutional analysis of 534 neonates diagnosed with left ventricular outflow tract obstruction that precluded adequate systemic cardiac output through the aortic valve who initially underwent a Norwood operation from 2005 to 2016.
Disclosures: Dr. Jaquiss and Dr. Meza reported having no financial disclosures.
New thinking on septal myectomy vs. alcohol ablation for obstructive cardiomyopathy
SNOWMASS, COLO. – The first-ever national study of the impact of hospital volume on outcomes of septal myectomy versus alcohol septal ablation for treatment of obstructive hypertrophic cardiomyopathy deserves to be practice-changing, Rick A. Nishimura, MD, said at the Annual Cardiovascular Conference at Snowmass.
Prior to release of these eye-opening data, conventional thinking held that referral for percutaneous septal ablation was the preferred option for elderly, sedentary patients with lots of comorbid conditions and a limited remaining lifespan, while surgical septal myectomy was the best fix for young, active, relatively healthy patients because of its impressive durability of benefit.
Similarly, 80% of alcohol ablations took place at centers doing less than 20 cases over 9 years. But the success of the percutaneous procedure was less dependent upon large institutional volumes. Only at the lowest-volume centers, where a total of fewer than 10 of the procedures were done over 9 years, was procedural mortality significantly higher – indeed, three- to fourfold higher – than at mid- or high-volume institutions or centers of excellence, all of which had similar mortality rates. The same was true for rates of postoperative complete heart block requiring a permanent pacemaker: significantly higher only at the lowest-volume institutions, according to the investigators from Weill Cornell Medical College in New York (JAMA Cardiol. 2016 Jun 1;1[3]:324-32).
“I think the bottom line is this: for the patient who is severely symptomatic with obstruction on optimal medical therapy, septal myectomy probably offers the best chance of excellent long-term symptomatic improvement, but the mortality depends on the center and the surgical expertise there, and complications do, too. This is something good to know that we never had data on before, that if you can’t get to a center with an experienced surgeon doing myectomies, it’s reasonable to go to a center doing ablations as long as there is some experience with the procedure there,” said Dr. Nishimura, professor of cardiovascular diseases and hypertension at the Mayo Clinic in Rochester, Minn.
Of the 11,248 patients treated for obstructive hypertrophic cardiomyopathy identified by the Cornell investigators using the Agency for Healthcare Research and Quality National Inpatient Sample database, 57% got myectomy and 43% underwent ablation. During the study years ablation increased in popularity by about 50%, rising from an annual rate of 1.6 to 2.5 procedures per million per year, while myectomy declined from 2.0 to 1.5 cases per million population per year. But that’s not what’s happened at the Mayo Clinic and other hypertrophic cardiomyopathy centers of excellence.
At the Mayo Clinic, for example, the volume of septal myectomies climbed from roughly 50 procedures per year in 2000 to close to 250 in 2015. Meanwhile the rate of alcohol septal ablation procedures remained steady at fewer than 20 per year.
“With shared decision making at Mayo, surgery has gone way up,” said Dr. Nishimura. “In an experienced surgeon’s hands, operative mortality is 0.8%, the gradient improves to 3%, and 94% of patients are postoperative New York Heart Association class I or II. This lasts for decades. We have 20-, 30-, and 40-year follow-up data now showing that over 90% of patients will have an excellent symptomatic benefit and be able to return to a normal lifestyle. The septum doesn’t come back. They’re good for life. So it’s a wonderful operation.”
In contrast, catheter-based septal ablation has a 4-year rate of survival free of death, NYHA class III or IV, or myectomy of 76%.
“One in four treated patients will not benefit,” the cardiologist emphasized.
The percutaneous procedure entails instilling alcohol into the septal perforator artery supplying the area of obstruction in order to cause a localized MI. Over a period of several weeks this causes the septum to shrink, thereby relieving the outflow tract obstruction.
When the procedure fails to bring about improvement, it’s often because the patient had a very long septal perforator artery and instilling the alcohol caused a large MI, making things worse. Or the patient didn’t have a septal perforator artery, or had one with so many branches that the cardiologist couldn’t identify the right one to treat to target the septum.
Dr. Nishimura reported having no financial conflicts.
SNOWMASS, COLO. – The first-ever national study of the impact of hospital volume on outcomes of septal myectomy versus alcohol septal ablation for treatment of obstructive hypertrophic cardiomyopathy deserves to be practice-changing, Rick A. Nishimura, MD, said at the Annual Cardiovascular Conference at Snowmass.
Prior to release of these eye-opening data, conventional thinking held that referral for percutaneous septal ablation was the preferred option for elderly, sedentary patients with lots of comorbid conditions and a limited remaining lifespan, while surgical septal myectomy was the best fix for young, active, relatively healthy patients because of its impressive durability of benefit.
Similarly, 80% of alcohol ablations took place at centers doing less than 20 cases over 9 years. But the success of the percutaneous procedure was less dependent upon large institutional volumes. Only at the lowest-volume centers, where a total of fewer than 10 of the procedures were done over 9 years, was procedural mortality significantly higher – indeed, three- to fourfold higher – than at mid- or high-volume institutions or centers of excellence, all of which had similar mortality rates. The same was true for rates of postoperative complete heart block requiring a permanent pacemaker: significantly higher only at the lowest-volume institutions, according to the investigators from Weill Cornell Medical College in New York (JAMA Cardiol. 2016 Jun 1;1[3]:324-32).
“I think the bottom line is this: for the patient who is severely symptomatic with obstruction on optimal medical therapy, septal myectomy probably offers the best chance of excellent long-term symptomatic improvement, but the mortality depends on the center and the surgical expertise there, and complications do, too. This is something good to know that we never had data on before, that if you can’t get to a center with an experienced surgeon doing myectomies, it’s reasonable to go to a center doing ablations as long as there is some experience with the procedure there,” said Dr. Nishimura, professor of cardiovascular diseases and hypertension at the Mayo Clinic in Rochester, Minn.
Of the 11,248 patients treated for obstructive hypertrophic cardiomyopathy identified by the Cornell investigators using the Agency for Healthcare Research and Quality National Inpatient Sample database, 57% got myectomy and 43% underwent ablation. During the study years ablation increased in popularity by about 50%, rising from an annual rate of 1.6 to 2.5 procedures per million per year, while myectomy declined from 2.0 to 1.5 cases per million population per year. But that’s not what’s happened at the Mayo Clinic and other hypertrophic cardiomyopathy centers of excellence.
At the Mayo Clinic, for example, the volume of septal myectomies climbed from roughly 50 procedures per year in 2000 to close to 250 in 2015. Meanwhile the rate of alcohol septal ablation procedures remained steady at fewer than 20 per year.
“With shared decision making at Mayo, surgery has gone way up,” said Dr. Nishimura. “In an experienced surgeon’s hands, operative mortality is 0.8%, the gradient improves to 3%, and 94% of patients are postoperative New York Heart Association class I or II. This lasts for decades. We have 20-, 30-, and 40-year follow-up data now showing that over 90% of patients will have an excellent symptomatic benefit and be able to return to a normal lifestyle. The septum doesn’t come back. They’re good for life. So it’s a wonderful operation.”
In contrast, catheter-based septal ablation has a 4-year rate of survival free of death, NYHA class III or IV, or myectomy of 76%.
“One in four treated patients will not benefit,” the cardiologist emphasized.
The percutaneous procedure entails instilling alcohol into the septal perforator artery supplying the area of obstruction in order to cause a localized MI. Over a period of several weeks this causes the septum to shrink, thereby relieving the outflow tract obstruction.
When the procedure fails to bring about improvement, it’s often because the patient had a very long septal perforator artery and instilling the alcohol caused a large MI, making things worse. Or the patient didn’t have a septal perforator artery, or had one with so many branches that the cardiologist couldn’t identify the right one to treat to target the septum.
Dr. Nishimura reported having no financial conflicts.
SNOWMASS, COLO. – The first-ever national study of the impact of hospital volume on outcomes of septal myectomy versus alcohol septal ablation for treatment of obstructive hypertrophic cardiomyopathy deserves to be practice-changing, Rick A. Nishimura, MD, said at the Annual Cardiovascular Conference at Snowmass.
Prior to release of these eye-opening data, conventional thinking held that referral for percutaneous septal ablation was the preferred option for elderly, sedentary patients with lots of comorbid conditions and a limited remaining lifespan, while surgical septal myectomy was the best fix for young, active, relatively healthy patients because of its impressive durability of benefit.
Similarly, 80% of alcohol ablations took place at centers doing less than 20 cases over 9 years. But the success of the percutaneous procedure was less dependent upon large institutional volumes. Only at the lowest-volume centers, where a total of fewer than 10 of the procedures were done over 9 years, was procedural mortality significantly higher – indeed, three- to fourfold higher – than at mid- or high-volume institutions or centers of excellence, all of which had similar mortality rates. The same was true for rates of postoperative complete heart block requiring a permanent pacemaker: significantly higher only at the lowest-volume institutions, according to the investigators from Weill Cornell Medical College in New York (JAMA Cardiol. 2016 Jun 1;1[3]:324-32).
“I think the bottom line is this: for the patient who is severely symptomatic with obstruction on optimal medical therapy, septal myectomy probably offers the best chance of excellent long-term symptomatic improvement, but the mortality depends on the center and the surgical expertise there, and complications do, too. This is something good to know that we never had data on before, that if you can’t get to a center with an experienced surgeon doing myectomies, it’s reasonable to go to a center doing ablations as long as there is some experience with the procedure there,” said Dr. Nishimura, professor of cardiovascular diseases and hypertension at the Mayo Clinic in Rochester, Minn.
Of the 11,248 patients treated for obstructive hypertrophic cardiomyopathy identified by the Cornell investigators using the Agency for Healthcare Research and Quality National Inpatient Sample database, 57% got myectomy and 43% underwent ablation. During the study years ablation increased in popularity by about 50%, rising from an annual rate of 1.6 to 2.5 procedures per million per year, while myectomy declined from 2.0 to 1.5 cases per million population per year. But that’s not what’s happened at the Mayo Clinic and other hypertrophic cardiomyopathy centers of excellence.
At the Mayo Clinic, for example, the volume of septal myectomies climbed from roughly 50 procedures per year in 2000 to close to 250 in 2015. Meanwhile the rate of alcohol septal ablation procedures remained steady at fewer than 20 per year.
“With shared decision making at Mayo, surgery has gone way up,” said Dr. Nishimura. “In an experienced surgeon’s hands, operative mortality is 0.8%, the gradient improves to 3%, and 94% of patients are postoperative New York Heart Association class I or II. This lasts for decades. We have 20-, 30-, and 40-year follow-up data now showing that over 90% of patients will have an excellent symptomatic benefit and be able to return to a normal lifestyle. The septum doesn’t come back. They’re good for life. So it’s a wonderful operation.”
In contrast, catheter-based septal ablation has a 4-year rate of survival free of death, NYHA class III or IV, or myectomy of 76%.
“One in four treated patients will not benefit,” the cardiologist emphasized.
The percutaneous procedure entails instilling alcohol into the septal perforator artery supplying the area of obstruction in order to cause a localized MI. Over a period of several weeks this causes the septum to shrink, thereby relieving the outflow tract obstruction.
When the procedure fails to bring about improvement, it’s often because the patient had a very long septal perforator artery and instilling the alcohol caused a large MI, making things worse. Or the patient didn’t have a septal perforator artery, or had one with so many branches that the cardiologist couldn’t identify the right one to treat to target the septum.
Dr. Nishimura reported having no financial conflicts.
Tertiary center repeat CT scans find additional trauma injuries
HOLLYWOOD, FLA. – Imaging obtained at nontertiary trauma centers probably doesn’t tell the whole story of a trauma patent’s injuries, according to a new retrospective study.
Repeat scans done at a Level 1 trauma center identified new injuries in 76% of patients who were transferred, Morgan Bonds, MD, reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma. About half of these previously unobserved injuries were considered clinically significant, said Dr. Bonds, a surgical resident at the University of Oklahoma, Oklahoma City.
Her study examined imaging and clinical assessment of 203 trauma patients who were initially worked up at a nontertiary trauma center (NTC), and then transferred to the Level 1 University of Oklahoma tertiary trauma Center (TTC). The facility’s primary radiologist reviewed all of the initial CT scans while blinded to the NTC interpretation. The initial scans and interpretations were then compared with those done at the TTC.

The team split imaging and interpretation disconnects into four categories:
• Type A errors: A missed injury on the NTC scan. “This represents the expertise and experience of our primary radiologist,” Dr. Bonds said.
• Type B errors: Missed injuries on scans where NTC radiologists saw other injuries that the TTC radiologist did not confirm. “This represents the experience of our radiologist and also the inexperience and overreaction of the NTC radiologists.
• Type C errors: New injuries seen on additional TTC imaging of the same body area. “This represents the quality of the image.”
• Type D errors: New injuries found upon any new imaging, whether of a previously scanned or newly scanned body area. “This represents quality of work-up – the decision of the trauma team to more fully investigate the patient’s injuries, as well as the quality of the CT tech performing the scan.”
During the study period, 203 patients presented at the TTC with prior scans conducted at an NTC.
The mean age of the patients was 43 years; most (67%) were men. The mean Injury Severity Score was 16; 97% had experienced blunt trauma. Shock was present in 3% and a traumatic brain injury in 8%. Repeat scans were most common for neck and cervical spine injuries (54%) and thoracic/lumbar spine injuries (53%) and least common for chest injuries (32%).
An inadequate NTC work-up as judged by the TTC attending was the most common reason for getting new images (76%). Poor image quality was the next most common reason (31%).
Among the 203 patients, 99 (49%) had a type A error. Of these injuries missed on the initial scan, 90% were considered to be clinically significant.
Type B errors occurred in 15% of patients.
Type C errors (new injuries in different body area) occurred in 54% of patients and, of these, 76% were considered clinically significant. Type D errors (new injuries seen in any imaging of any area) occurred in 73% of patients.
“This study confirms that images are often repeated or completed after having images done at nontertiary trauma centers,” Dr. Bonds said. “Relying on NTC image interpretation can lead to undertreating our patients. One potential solution to this issue could be image sharing between NTCs and TTCs. This might reduce both the rate of missed injuries and the need for repeat scans.”
Dr. Bonds had no financial disclosures.
On Twitter @Alz_Gal
HOLLYWOOD, FLA. – Imaging obtained at nontertiary trauma centers probably doesn’t tell the whole story of a trauma patent’s injuries, according to a new retrospective study.
Repeat scans done at a Level 1 trauma center identified new injuries in 76% of patients who were transferred, Morgan Bonds, MD, reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma. About half of these previously unobserved injuries were considered clinically significant, said Dr. Bonds, a surgical resident at the University of Oklahoma, Oklahoma City.
Her study examined imaging and clinical assessment of 203 trauma patients who were initially worked up at a nontertiary trauma center (NTC), and then transferred to the Level 1 University of Oklahoma tertiary trauma Center (TTC). The facility’s primary radiologist reviewed all of the initial CT scans while blinded to the NTC interpretation. The initial scans and interpretations were then compared with those done at the TTC.
The team split imaging and interpretation disconnects into four categories:
• Type A errors: A missed injury on the NTC scan. “This represents the expertise and experience of our primary radiologist,” Dr. Bonds said.
• Type B errors: Missed injuries on scans where NTC radiologists saw other injuries that the TTC radiologist did not confirm. “This represents the experience of our radiologist and also the inexperience and overreaction of the NTC radiologists.
• Type C errors: New injuries seen on additional TTC imaging of the same body area. “This represents the quality of the image.”
• Type D errors: New injuries found upon any new imaging, whether of a previously scanned or newly scanned body area. “This represents quality of work-up – the decision of the trauma team to more fully investigate the patient’s injuries, as well as the quality of the CT tech performing the scan.”
During the study period, 203 patients presented at the TTC with prior scans conducted at an NTC.
The mean age of the patients was 43 years; most (67%) were men. The mean Injury Severity Score was 16; 97% had experienced blunt trauma. Shock was present in 3% and a traumatic brain injury in 8%. Repeat scans were most common for neck and cervical spine injuries (54%) and thoracic/lumbar spine injuries (53%) and least common for chest injuries (32%).
An inadequate NTC work-up as judged by the TTC attending was the most common reason for getting new images (76%). Poor image quality was the next most common reason (31%).
Among the 203 patients, 99 (49%) had a type A error. Of these injuries missed on the initial scan, 90% were considered to be clinically significant.
Type B errors occurred in 15% of patients.
Type C errors (new injuries in different body area) occurred in 54% of patients and, of these, 76% were considered clinically significant. Type D errors (new injuries seen in any imaging of any area) occurred in 73% of patients.
“This study confirms that images are often repeated or completed after having images done at nontertiary trauma centers,” Dr. Bonds said. “Relying on NTC image interpretation can lead to undertreating our patients. One potential solution to this issue could be image sharing between NTCs and TTCs. This might reduce both the rate of missed injuries and the need for repeat scans.”
Dr. Bonds had no financial disclosures.
On Twitter @Alz_Gal
HOLLYWOOD, FLA. – Imaging obtained at nontertiary trauma centers probably doesn’t tell the whole story of a trauma patent’s injuries, according to a new retrospective study.
Repeat scans done at a Level 1 trauma center identified new injuries in 76% of patients who were transferred, Morgan Bonds, MD, reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma. About half of these previously unobserved injuries were considered clinically significant, said Dr. Bonds, a surgical resident at the University of Oklahoma, Oklahoma City.
Her study examined imaging and clinical assessment of 203 trauma patients who were initially worked up at a nontertiary trauma center (NTC), and then transferred to the Level 1 University of Oklahoma tertiary trauma Center (TTC). The facility’s primary radiologist reviewed all of the initial CT scans while blinded to the NTC interpretation. The initial scans and interpretations were then compared with those done at the TTC.
The team split imaging and interpretation disconnects into four categories:
• Type A errors: A missed injury on the NTC scan. “This represents the expertise and experience of our primary radiologist,” Dr. Bonds said.
• Type B errors: Missed injuries on scans where NTC radiologists saw other injuries that the TTC radiologist did not confirm. “This represents the experience of our radiologist and also the inexperience and overreaction of the NTC radiologists.
• Type C errors: New injuries seen on additional TTC imaging of the same body area. “This represents the quality of the image.”
• Type D errors: New injuries found upon any new imaging, whether of a previously scanned or newly scanned body area. “This represents quality of work-up – the decision of the trauma team to more fully investigate the patient’s injuries, as well as the quality of the CT tech performing the scan.”
During the study period, 203 patients presented at the TTC with prior scans conducted at an NTC.
The mean age of the patients was 43 years; most (67%) were men. The mean Injury Severity Score was 16; 97% had experienced blunt trauma. Shock was present in 3% and a traumatic brain injury in 8%. Repeat scans were most common for neck and cervical spine injuries (54%) and thoracic/lumbar spine injuries (53%) and least common for chest injuries (32%).
An inadequate NTC work-up as judged by the TTC attending was the most common reason for getting new images (76%). Poor image quality was the next most common reason (31%).
Among the 203 patients, 99 (49%) had a type A error. Of these injuries missed on the initial scan, 90% were considered to be clinically significant.
Type B errors occurred in 15% of patients.
Type C errors (new injuries in different body area) occurred in 54% of patients and, of these, 76% were considered clinically significant. Type D errors (new injuries seen in any imaging of any area) occurred in 73% of patients.
“This study confirms that images are often repeated or completed after having images done at nontertiary trauma centers,” Dr. Bonds said. “Relying on NTC image interpretation can lead to undertreating our patients. One potential solution to this issue could be image sharing between NTCs and TTCs. This might reduce both the rate of missed injuries and the need for repeat scans.”
Dr. Bonds had no financial disclosures.
On Twitter @Alz_Gal
Key clinical point:
Major finding: Overall, 76% of patients had missed injuries on their initial CT scans.
Data source: A study of 203 trauma patients.
Disclosures: Dr. Bonds had no financial disclosures.
Overcoming glucocorticoid resistance in lymphoma

Image by Ed Uthman
Targeting RUNX1 could combat glucocorticoid resistance in patients with lymphoma, according to research published in the Journal of Cellular Biochemistry.
Researchers found an over activity of RUNX1 in lymphoma cells interfered with sphingolipids and caused cells to become resistant to dexamethasone.
Dexamethasone works, in part, through the control of sphingolipid enzymes, which play a role in instructing cells to live or die.
Specifically, the researchers said they found that ectopic expression of RUNX1 in lymphoma cells consistently perturbs the sphingolipid rheostat and confers increased resistance to glucocorticoid-mediated apoptosis.
The team also described the mechanism of cross-talk between glucocorticoid and sphingolipid metabolism through the enzyme Sgpp1.
The researchers said dexamethasone induces expression of Sgpp1 in T-lymphoma cells and drives cell death, which is reduced by partial knockdown of Sgpp1 with short hairpin RNA or direct transcriptional repression of Sgpp1 by ectopic RUNX1.
These findings suggest that drugs targeting RUNX1 may be able to reverse glucocorticoid resistance in lymphoma patients.
“The possibility of making existing therapies more active and specific by combining [them] with drugs that inhibit RUNX is a new and exciting prospect,” said study author James Neil, of The University of Glasgow in Scotland.
“Our collaborators in the US have recently developed drugs that inhibit RUNX, and we plan to test these with existing therapies in blood cancers where MYC and RUNX are both implicated, including multiple myeloma and Burkitt lymphoma.”
An earlier study by Dr Neil and his colleagues suggested that RUNX1 was a potential therapeutic target in MYC-driven lymphomas. ![]()
Image by Ed Uthman
Targeting RUNX1 could combat glucocorticoid resistance in patients with lymphoma, according to research published in the Journal of Cellular Biochemistry.
Researchers found an over activity of RUNX1 in lymphoma cells interfered with sphingolipids and caused cells to become resistant to dexamethasone.
Dexamethasone works, in part, through the control of sphingolipid enzymes, which play a role in instructing cells to live or die.
Specifically, the researchers said they found that ectopic expression of RUNX1 in lymphoma cells consistently perturbs the sphingolipid rheostat and confers increased resistance to glucocorticoid-mediated apoptosis.
The team also described the mechanism of cross-talk between glucocorticoid and sphingolipid metabolism through the enzyme Sgpp1.
The researchers said dexamethasone induces expression of Sgpp1 in T-lymphoma cells and drives cell death, which is reduced by partial knockdown of Sgpp1 with short hairpin RNA or direct transcriptional repression of Sgpp1 by ectopic RUNX1.
These findings suggest that drugs targeting RUNX1 may be able to reverse glucocorticoid resistance in lymphoma patients.
“The possibility of making existing therapies more active and specific by combining [them] with drugs that inhibit RUNX is a new and exciting prospect,” said study author James Neil, of The University of Glasgow in Scotland.
“Our collaborators in the US have recently developed drugs that inhibit RUNX, and we plan to test these with existing therapies in blood cancers where MYC and RUNX are both implicated, including multiple myeloma and Burkitt lymphoma.”
An earlier study by Dr Neil and his colleagues suggested that RUNX1 was a potential therapeutic target in MYC-driven lymphomas. ![]()
Image by Ed Uthman
Targeting RUNX1 could combat glucocorticoid resistance in patients with lymphoma, according to research published in the Journal of Cellular Biochemistry.
Researchers found an over activity of RUNX1 in lymphoma cells interfered with sphingolipids and caused cells to become resistant to dexamethasone.
Dexamethasone works, in part, through the control of sphingolipid enzymes, which play a role in instructing cells to live or die.
Specifically, the researchers said they found that ectopic expression of RUNX1 in lymphoma cells consistently perturbs the sphingolipid rheostat and confers increased resistance to glucocorticoid-mediated apoptosis.
The team also described the mechanism of cross-talk between glucocorticoid and sphingolipid metabolism through the enzyme Sgpp1.
The researchers said dexamethasone induces expression of Sgpp1 in T-lymphoma cells and drives cell death, which is reduced by partial knockdown of Sgpp1 with short hairpin RNA or direct transcriptional repression of Sgpp1 by ectopic RUNX1.
These findings suggest that drugs targeting RUNX1 may be able to reverse glucocorticoid resistance in lymphoma patients.
“The possibility of making existing therapies more active and specific by combining [them] with drugs that inhibit RUNX is a new and exciting prospect,” said study author James Neil, of The University of Glasgow in Scotland.
“Our collaborators in the US have recently developed drugs that inhibit RUNX, and we plan to test these with existing therapies in blood cancers where MYC and RUNX are both implicated, including multiple myeloma and Burkitt lymphoma.”
An earlier study by Dr Neil and his colleagues suggested that RUNX1 was a potential therapeutic target in MYC-driven lymphomas. ![]()
Reducing the risk of device-related thrombosis

“superomniphobic” surface.
Photo from the Kota lab
at Colorado State University
Researchers say they have engineered “superhemophobic” titanium surfaces that could be used to create implantable medical devices that don’t pose a risk of thrombosis.
The team described this work in Advanced Healthcare Materials.
The undesirable interaction of blood with foreign materials is an ongoing problem in medical research, said study author Ketul Popat, PhD, of Colorado State University in Fort Collins, Colorado.
He and his colleagues noted that, when implanted medical devices come in contact with blood, platelet adhesion and activation occur, which may lead to thrombosis and device failure.
“If we can design materials where blood barely contacts the surface, there is virtually no chance of clotting, which is a coordinated set of events,” Dr Popat said. “Here, we’re targeting the prevention of the first set of events.”
Dr Popat and his colleagues started with sheets of titanium, which are commonly used in medical devices. The team then grew chemically altered surfaces that act as barriers between the titanium and blood.
They analyzed variations of titanium surfaces, including different textures and chemistries, and compared the extent of platelet adhesion and activation.
These experiments revealed that fluorinated nanotubes offered the best protection against clotting.
Having implantable medical devices that repel blood might seem counterintuitive, the researchers noted, as biomedical scientists often use materials with an affinity to blood to make them biologically compatible.
“What we are doing is the exact opposite,” said study author Arun Kota, PhD, of Colorado State University.
“We are taking a material that blood hates to come in contact with, in order to make it compatible with blood.”
In essence, the titanium surface is so repellent that blood is “tricked” into “believing” there’s virtually no foreign material there at all.
Growing a surface and testing it in the lab is only the beginning, the researchers said. They want to continue examining other clotting factors, and eventually, to test real medical devices. ![]()
“superomniphobic” surface.
Photo from the Kota lab
at Colorado State University
Researchers say they have engineered “superhemophobic” titanium surfaces that could be used to create implantable medical devices that don’t pose a risk of thrombosis.
The team described this work in Advanced Healthcare Materials.
The undesirable interaction of blood with foreign materials is an ongoing problem in medical research, said study author Ketul Popat, PhD, of Colorado State University in Fort Collins, Colorado.
He and his colleagues noted that, when implanted medical devices come in contact with blood, platelet adhesion and activation occur, which may lead to thrombosis and device failure.
“If we can design materials where blood barely contacts the surface, there is virtually no chance of clotting, which is a coordinated set of events,” Dr Popat said. “Here, we’re targeting the prevention of the first set of events.”
Dr Popat and his colleagues started with sheets of titanium, which are commonly used in medical devices. The team then grew chemically altered surfaces that act as barriers between the titanium and blood.
They analyzed variations of titanium surfaces, including different textures and chemistries, and compared the extent of platelet adhesion and activation.
These experiments revealed that fluorinated nanotubes offered the best protection against clotting.
Having implantable medical devices that repel blood might seem counterintuitive, the researchers noted, as biomedical scientists often use materials with an affinity to blood to make them biologically compatible.
“What we are doing is the exact opposite,” said study author Arun Kota, PhD, of Colorado State University.
“We are taking a material that blood hates to come in contact with, in order to make it compatible with blood.”
In essence, the titanium surface is so repellent that blood is “tricked” into “believing” there’s virtually no foreign material there at all.
Growing a surface and testing it in the lab is only the beginning, the researchers said. They want to continue examining other clotting factors, and eventually, to test real medical devices. ![]()
“superomniphobic” surface.
Photo from the Kota lab
at Colorado State University
Researchers say they have engineered “superhemophobic” titanium surfaces that could be used to create implantable medical devices that don’t pose a risk of thrombosis.
The team described this work in Advanced Healthcare Materials.
The undesirable interaction of blood with foreign materials is an ongoing problem in medical research, said study author Ketul Popat, PhD, of Colorado State University in Fort Collins, Colorado.
He and his colleagues noted that, when implanted medical devices come in contact with blood, platelet adhesion and activation occur, which may lead to thrombosis and device failure.
“If we can design materials where blood barely contacts the surface, there is virtually no chance of clotting, which is a coordinated set of events,” Dr Popat said. “Here, we’re targeting the prevention of the first set of events.”
Dr Popat and his colleagues started with sheets of titanium, which are commonly used in medical devices. The team then grew chemically altered surfaces that act as barriers between the titanium and blood.
They analyzed variations of titanium surfaces, including different textures and chemistries, and compared the extent of platelet adhesion and activation.
These experiments revealed that fluorinated nanotubes offered the best protection against clotting.
Having implantable medical devices that repel blood might seem counterintuitive, the researchers noted, as biomedical scientists often use materials with an affinity to blood to make them biologically compatible.
“What we are doing is the exact opposite,” said study author Arun Kota, PhD, of Colorado State University.
“We are taking a material that blood hates to come in contact with, in order to make it compatible with blood.”
In essence, the titanium surface is so repellent that blood is “tricked” into “believing” there’s virtually no foreign material there at all.
Growing a surface and testing it in the lab is only the beginning, the researchers said. They want to continue examining other clotting factors, and eventually, to test real medical devices. ![]()
Diabetes: Health Literacy Education Improves Veteran Outcomes
According to the National Academy of Medicine (NAM), health literacy is “the degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate health decisions.”1 Studies suggest that millions of patients have inadequate health literacy and cannot make fully informed decisions because of this lack of knowledge.2-4 A 2007 National Patient Safety Foundation report calculated that inadequate health literacy burdens the U.S. health care system with an additional $106 to $238 billion annually.5
In 2014, the American Diabetes Association reported that diabetes affects 29.1 million Americans (9.3%) and that by 2050 1 in 3 Americans will have diabetes.6 People with diabetes have health care costs 2.3 times higher than the cost for nondiabetic patients. The cost of taking care of patients with diabetes annually is about $245 billion.6 Without interventions that address health literacy and effective self-management to reduce the risks of complications and comorbidity, health care costs related to diabetes will continue to increase.
Literature Review
According to a U.S. Department of Education assessment on adult health literacy in 2003, 88% of adults in the U.S. have inadequate health literacy.2 About 90 million Americans lack health literacy skills, according to a 2004 NAM report.3 Heinrich, who conducted a review of U.S. studies on health literacy, concluded that about 25% of Americans have low health literacy.4
The Newest Vital Sign Tool
The Newest Vital Sign (NVS) tool is a free tool developed by Pfizer (New York, NY) for assessing health literacy. Participants are asked 6 questions about nutrition based on an ice cream nutrition label (Figure). The researcher records the participant’s responses, which accommodates participants who may have difficulty reading. The tool is scored from 0 to 6. A score of below 4 indicates the possibility of limited health literacy.7 This test can be completed in about 3 minutes, is widely accepted, and provides results comparable to more extensive literacy tests.8 A study conducted by Welch and colleagues suggested the NVS tool is both cost and time efficient.9 Ryan and colleagues found that 98% of patients in their study (n = 289) did not have objections to taking the NVS assessment.10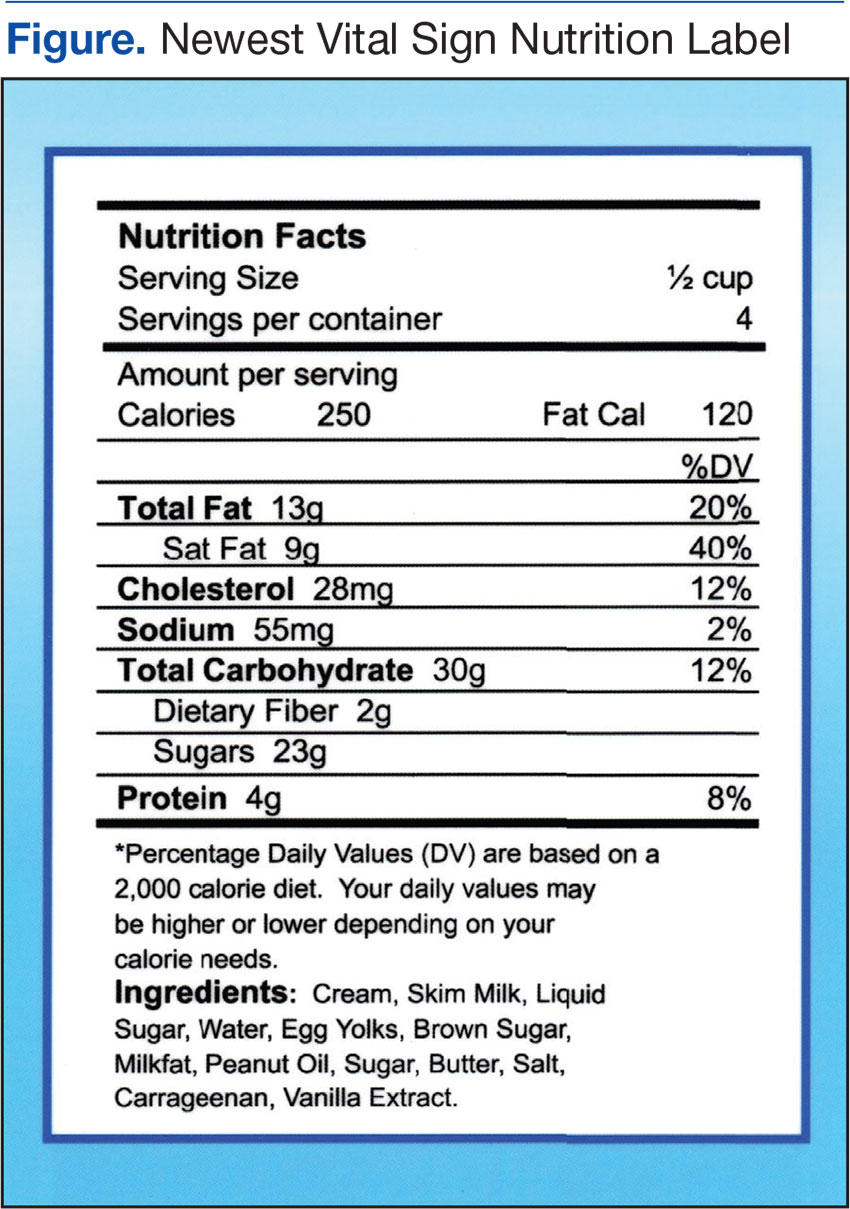
Escobedo and Weismuller’s study used the NVS health literacy tool to assess the health literacy of renal patients.3 In 2004, about 50,000 American patients with diabetes began treatment for kidney failure due to diabetes complications.6 Escobedo and Weismuller found that patients with diabetes with limited health literacy knowledge are more likely to be hospitalized, thus increasing health care costs.3 In addition, they discovered that these patients demonstrated poor adherence to prescribed treatment protocols. Welch, VanGeest, and Caskey conducted a case study on time, cost, and clinical utilization of the NVS health literacy tool and found that a patient’s lack of health literacy was linked to limited participation in personal medical decisions.7,9 Patient’s lack of knowledge was associated with delays in seeking treatment, poor self-management of the disease, and more hospital admissions.
Health Literacy and Diabetes
Studies specific to diabetes and inadequate health literacy support the premise that better health literacy leads to improved patient outcomes. Using the NVS tool, Heinrich conducted a study of the health literacy of 54 patients with diabetes in a primary care setting. The study showed that 65% had inadequate health literacy and that patients with diabetes with inadequate health literacy were more likely to have poor glycemic control compared with patients with diabetes and adequate health literacy levels.4 McCleary-Jones examined diet, foot care, and exercise of 50 African American participants with diabetes from a community health center, finding a positive relationship between health literacy and diabetes knowledge.11
Long and Gambling conducted a 2-year prospective, observational study that incorporated motivational interviewing and patient-centered care into a self-management program, examining the effectiveness of scheduled phone interventions to assist patients with diabetes in the management of their disease.12 The interventions used structured and consistent questions supported by a protocol and script that examined medication adherence and lifestyle choices. Long and Gambling concluded that “the findings demonstrate not only changes in the depth and detail of diabetes-related knowledge and confidence, but also enhanced competence in translating knowledge into every day self-care.”12 These researchers concluded that increased knowledge translated into better patient self-management of their disease. The Long and Gambling study included general self-management characteristics of monitoring HbA1c, diet, exercise, medication management, and general self-care. These researchers contend that diabetes self-management education must be a long-term endeavor to promote change.12
Mendoza and Rosenburg’s meta-analysis on self-management programs for diabetes and chronic conditions found a statistically significant 0.81% reduction in hemoglobin A1c (HbA1c). Characteristics of self-management programs that were linked to improved outcomes included nurse and provider education on medications, diet and/or exercise, and demonstrated use of motivational interviewing and biofeedback. Mendoza and Rosenburg suggested motivational interviewing focuses on the patient’s perspective and facilitates the process that the patient uses to assess their needs and to think about possible solutions.13 Mulimba and Bryo-Daniel found that motivational interviewing is a valuable tool for primary care nurses’ health promotion practice, and Thompson and colleagues found that it was effective in changing behavior.14,15
Nurse’s Role in Health Literacy
Nurses play a vital role in educating and securing adherence of patients in the management of their disease(s).13 In addition to educating patients, families, and friends of the family, nurses assist with helping them make informed decisions.16 The VHA uses the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) to teach health care staff about diabetes self-management education (DSME). Tisdel and colleagues found that DSME established through telemedicine or clinical mentoring improved patient outcomes.17 Mendoza and Rosenburgfound nurse-led DSME was linked to minimizing cardiovascular risk factors and improvements in HbA1c.13
Background
Staunton Community Based Outpatient Clinic (CBOC) in rural Virginia is a primary care clinic that serves veterans in the surrounding area. About one-fourth of the Staunton patients have diabetes. According to June 2014 data from the VHA Support Service Center, the physician at the Staunton CBOC was responsible for 946 patients (225 with diabetes) and the nurse practitioner was responsible for 707 (184 with diabetes). The VHA Support Service Center 2014 data indicated that veterans with poorly self-managed diabetes were at increased risk for poor outcomes, such as kidney failure, cardiovascular disease, and limb amputation. Veterans with diabetes use the emergency department more often and are admitted to the hospital more often than are veterans who do not have diabetes.18
Methods
The primary objective of this pilot study was to explore whether weekly structured nursing education sessions lasting 45 minutes and subsequent follow-up weekly conferences would improve their HbA1c for veterans identified as having ≥ 9 HbA1c and ≤ 3 health literacy score on the NVS 7 study assessment. Most recent HbA1c prior to beginning the study was used to identify potential participants. After completion of 12 weekly education interventions, an additional HbA1c was obtained.
The Salem VAMC and Eastern Mennonite University Institutional Review Board approved the study. Veterans’ questions were answered prior to signing consent forms. All data collected were kept confidential.
Veterans with ≥ 9 HbA1c were evaluated for possible participation. Forty-nine veterans met the criteria to participate in this pilot study. Exclusion criteria included diagnosis of any cognitive disorder, such as dementia, Alzheimer disease, or memory impairment. In addition, veterans unwilling or unable to commit to weekly follow-up sessions were excluded. The veterans eligible for participation were contacted by telephone, and 9 agreed to participate in the pilot study. Inclusion criteria included those aged ≥ 18 years and a diagnosis of diabetes with most recent HbA1c of ≥ 9 and a score of < 4 on the NVS health literacy assessment. After taking the NVS health literacy assessment, 6 of the 9 participants qualified to continue in the study.
Education interventions included assessing medication adherence, discussing diet, reviewing physical activity for the previous week (based on diet and activity logs), and reviewing home blood glucose monitoring. Weekly education sessions were either face-to-face or by telephone. This choice was given to accommodate veterans who may have had transportation issues. A total of 12 weekly appointments were scheduled for each participant, and education was directed at the specific needs and goals of each participant. Interventions for education were based on those found in previous studies.13,14,18,19
Data Collection and Analysis
All 6 participants were white male veterans who were diagnosed with diabetes for at least 3 years. Their ages ranged from 59 to 72. Three participants were service connected for diabetes and 3 were not. One participant dropped from the study after completing 4 appointments, stating he was just too busy to be available for a weekly appointment. Another participant completed 6 appointments and removed himself from the study due to time constraints. The 4 participants who completed the pilot study were followed for 12 weeks by a registered nurse (RN), and all had reductions in their HbA1c.
Participants were assessed at weekly appointments using a predetermined template for medication adherence, diet, activity, and blood glucose monitoring. Responses of the participants guided the education interventions to meet the individual veteran’s learning needs. For example, one veteran was given specific education on carbohydrate counting and another was educated on how to read food labels. Participants were also encouraged to express satisfaction, frustration, anger, or other emotions in managing their chronic illness. The premise for spending additional time with the veteran was to promote positive self-management behaviors as recommended by Radhakrishnan.19
Veterans who completed the study stated that the education interventions positively impacted their health status. One veteran was able to delay dialysis due to self-directed improvement in his lifestyle (exercising and watching his diet), which improved his HbA1c. This veteran attributed his health improvement to the individualized education sessions with the RN and knowing he had to be accountable to someone. Additionally, it was found there was a strong familial-social component to diabetes self-management. Several veterans were knowledgeable about diabetes self-management as evidenced by their responses to weekly questions. However, disease management for these veterans was strongly impacted by family and life events.
One veteran did not manage his disease for an entire week due to “being busy with a death in the family and planning for a wedding.” This veteran took his medication but did not check his blood glucose or monitor his diet. Another veteran spoke of eating ice cream and other concentrated sweets because his young grandson was with him for the week. A third veteran was able to manage his diet better when his wife packed snacks for him but when left to his own accord did not do well with his food selection. Even though these veterans understood how to effectively manage their diabetes, they may have chosen to inconsistently translate that knowledge into practice if they perceive those familial-social forces to be more important or more powerful.
Discussion
The findings from this small pilot study from a single clinic cannot be generalized. However, this pilot study adds to the literature of the positive impact of individualized, structured, tailored nursing interventions delivered with careful consideration of the participants’ personal goals and health care needs for diabetes self-management.
Participants monitored home blood glucose levels, diet, and activity and maintained adherence with prescribed diabetes medications. The HbA1c level for participants decreased by the end of the program. During the course of the pilot study a pharmacist managed the veterans’ medications. Participant 1 began a new medication regimen the first day of the study. Previously, the patient was self-regulating his medication. However, during the 12-week study, he had no medication adjustments. Participant 4 had several increases to his insulin dose (insulin aspart protamine and insulin aspart rdna origin) during the course of the study. Participants 5 and 6 had no medication adjustments during the study.
Even though participants had medication adjustments, which contributed to the HbA1c decrease, they became more aware of the medical need to control their blood sugar through the one-on-one education provided. Although there was variation in the depth and detail that participants maintained their food/activity log and home blood glucose monitoring, all participants agreed that they were more likely to be adherent with prescribed self-monitoring “knowing they were going to have to report self-monitoring information” to the RN.
Health care professionals may not realize the impact of familial-social events on blood glucose control. Veterans in this study found that having weekly sessions with the RN helped them through such events, even though they did not adhere strictly to their regimen. One suggestion is having veterans anticipate future familial-social events that may trigger nonadherence to their diabetes health plan and then discuss those events with the health care professional.
Future Research
This small exploratory pilot study has implications for future research. Increasing the study’s sample size and using a control group is recommended to compare veterans who have an educational intervention with those that do not and the impact it has on blood glucose control. The study was limited to 1 CBOC. Incorporating additional CBOCs could increase the sample size. Additionally, although this study was only 3 months in duration, a longer study could reveal significant patterns of change over time as well as the long-term benefit of a tailored educational intervention. In addition, adjusting the study inclusion criteria of > 9 HbA1c to include those with > 8 HbA1c also may increase the sample size.
Limited financial resources for the study could have negatively impacted the sample size. Incorporating recruitment or advertising strategy may increase the number of participants. Research also is needed on education interventions with a diverse group of male and female veterans that extends beyond 3 months. Exploring the value of including the veteran’s family in the education sessions is needed. Finally, this study examined only diabetes education. Researchers need to consider other diseases and the value of individualized education.
Limitations
Limitations included a small sample size and no control group. Due to the study’s small sample size, extrapolating data from it becomes difficult. However, this pilot study sets the groundwork for other researchers to expand the importance of education interventions and health literacy. Recruitment was challenging since an eligibility criterion was the NVS score, and patients were sometimes difficult to contact.7 The pilot study started with 6 white male participants but only 4 finished. During the course of the pilot study, 1 veteran had medication adjustments as part of routine care and 1 veteran had medication adjustments prior to the study, which could have altered the HbA1c results.
In hindsight, using the NVS to assess both prestudy with poststudy health literacy scores would have provided additional information about the education intervention. There is possible bias because the researcher was a VAMC employee, and the RN that implemented the interventions had previously worked with the patients.
Conclusion
Although this is a small descriptive pilot study, it adds to the body of research on the value of nurse-driven interventions to help veterans manage diabetes by enhancing their health literacy. It also raises questions and opportunities for further research into the power of familial-social influences on a veteran’s willingness to manage their diabetes. The majority of veterans who declined to participate in this study, even though they qualified, stated that they would “not follow any recommendations.” Further investigation is needed about why some veterans elect not to obtain help that could positively impact their health and possibly extend their life. Additionally, scientific quantitative and qualitative research is needed to evaluate the statistical significance between health care literacy and educational intervention on patient adherence among individuals diagnosed with diabetes.
1. Stiles E. Promoting health literacy in patients with diabetes. Nurs Stand. 2011;26(8):35-40.
2. Baum NH, Dowling RA. Health literacy: how do your patients rate? http://urologytimes.modernmedicine.com/urology-times/news/modernmedicine/modern-medicine-now/health-literacy-how-do-your-patients-rate. Published August 1, 2011. Accessed December 2, 2016.
3. Escobedo W, Weismuller P. Assessing health literacy in renal failure and kidney transplant patients. Prog Transplant. 2013;23(1):47-54.
4. Heinrich C. Health literacy: the sixth vital sign. J Am Acad Nurse Pract. 2012;24(4):218-223.
5. Roett MA, Wessel L. Help your patient “get” what you just said: health literacy guide. J Fam Pract. 2012;61(4):190-196.
6. American Diabetes Association. Statistics about diabetes. http://www.diabetes.org/diabetes-basics/statistics/?loc=feat1.Updated December 12, 2016. Accessed December 14, 2016.
7. Pfizer. The newest vital sign. http://www.pfizer.com/files/health/nvs_flipbook_english_final.pdf. Published February 2011. Accessed December 2, 2016.
8. Shah LC, West P, Bremmeyr K, Savoy-Moore RT. Health literacy instrument in family medicine: the “newest vital sign” ease of use and correlates. J Am Board Fam Med. 2010;23(2):195-203.
9. Welch VL, VanGeest JB, Caskey R. Time, costs, and clinical utilization of screening for health literacy: a case study using the Newest Vital Sign (NVS) instrument. J Am Board Fam Med. 2011;24(3):281-289.
10. Ryan JG, Leguen F, Weiss BD, et al. Will patients agree to have their literacy skills assessed in clinical practice? Health Educ Res. 2008;23(4):603-611.
11. McCleary-Jones V. Health literacy and its association with diabetes knowledge, self-efficacy and disease self-management among African Americans with diabetes mellitus. ABNF J. 2011;22(2):25-32.
12. Long AF, Gambling T. Enhancing health literacy and behavioral change within a tele-care education and support intervention for people with type 2 diabetes. Health Expect. 2012;15(3):267-282.
13. Mendoza M, Rosenberg T. Self-management of type 2 diabetes: A good idea-or not? J Fam Pract. 2013;62(5):244-248.
14. A Clifford Mulimba A, Byron-Daniel J. Motivational interviewing-based interventions and diabetes mellitus. Br J Nurs. 2014;23(1):8-14.
15. Thompson DR, Chair SY, Chan SW, Astin F, Davidson PM, Ski CF. Motivational interviewing: a useful approach to improving cardiovascular health? J Clin Nurs. 2011;20;(9-10):1236-1244.
16. Protheroe J, Rowlands G. Matching clinical information with levels of patient health literacy. Nurs Manag (Harrow). 2013;20(3):20-21.
17. Tisdel KA, Bedwell M, Tarkington PE, Mundy A, Fredrickson SK. Diabetes specialists share experience remotely with RN care managers. Fed Pract. 2013;30(suppl 7):15S-20S.
18. U.S. Department of Veterans Affairs, Veterans Health Administration Support Service Center. http://vssc.med.va.gov/AlphaIndex.asp?Ltr=D.
19. Radhakrishnan K. The efficacy of tailored interventions for self-management outcomes of type 2 diabetes, hypertension, or heart disease: a systemic review. J Adv Nurs. 2012;68(3):496-510.
According to the National Academy of Medicine (NAM), health literacy is “the degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate health decisions.”1 Studies suggest that millions of patients have inadequate health literacy and cannot make fully informed decisions because of this lack of knowledge.2-4 A 2007 National Patient Safety Foundation report calculated that inadequate health literacy burdens the U.S. health care system with an additional $106 to $238 billion annually.5
In 2014, the American Diabetes Association reported that diabetes affects 29.1 million Americans (9.3%) and that by 2050 1 in 3 Americans will have diabetes.6 People with diabetes have health care costs 2.3 times higher than the cost for nondiabetic patients. The cost of taking care of patients with diabetes annually is about $245 billion.6 Without interventions that address health literacy and effective self-management to reduce the risks of complications and comorbidity, health care costs related to diabetes will continue to increase.
Literature Review
According to a U.S. Department of Education assessment on adult health literacy in 2003, 88% of adults in the U.S. have inadequate health literacy.2 About 90 million Americans lack health literacy skills, according to a 2004 NAM report.3 Heinrich, who conducted a review of U.S. studies on health literacy, concluded that about 25% of Americans have low health literacy.4
The Newest Vital Sign Tool
The Newest Vital Sign (NVS) tool is a free tool developed by Pfizer (New York, NY) for assessing health literacy. Participants are asked 6 questions about nutrition based on an ice cream nutrition label (Figure). The researcher records the participant’s responses, which accommodates participants who may have difficulty reading. The tool is scored from 0 to 6. A score of below 4 indicates the possibility of limited health literacy.7 This test can be completed in about 3 minutes, is widely accepted, and provides results comparable to more extensive literacy tests.8 A study conducted by Welch and colleagues suggested the NVS tool is both cost and time efficient.9 Ryan and colleagues found that 98% of patients in their study (n = 289) did not have objections to taking the NVS assessment.10
Escobedo and Weismuller’s study used the NVS health literacy tool to assess the health literacy of renal patients.3 In 2004, about 50,000 American patients with diabetes began treatment for kidney failure due to diabetes complications.6 Escobedo and Weismuller found that patients with diabetes with limited health literacy knowledge are more likely to be hospitalized, thus increasing health care costs.3 In addition, they discovered that these patients demonstrated poor adherence to prescribed treatment protocols. Welch, VanGeest, and Caskey conducted a case study on time, cost, and clinical utilization of the NVS health literacy tool and found that a patient’s lack of health literacy was linked to limited participation in personal medical decisions.7,9 Patient’s lack of knowledge was associated with delays in seeking treatment, poor self-management of the disease, and more hospital admissions.
Health Literacy and Diabetes
Studies specific to diabetes and inadequate health literacy support the premise that better health literacy leads to improved patient outcomes. Using the NVS tool, Heinrich conducted a study of the health literacy of 54 patients with diabetes in a primary care setting. The study showed that 65% had inadequate health literacy and that patients with diabetes with inadequate health literacy were more likely to have poor glycemic control compared with patients with diabetes and adequate health literacy levels.4 McCleary-Jones examined diet, foot care, and exercise of 50 African American participants with diabetes from a community health center, finding a positive relationship between health literacy and diabetes knowledge.11
Long and Gambling conducted a 2-year prospective, observational study that incorporated motivational interviewing and patient-centered care into a self-management program, examining the effectiveness of scheduled phone interventions to assist patients with diabetes in the management of their disease.12 The interventions used structured and consistent questions supported by a protocol and script that examined medication adherence and lifestyle choices. Long and Gambling concluded that “the findings demonstrate not only changes in the depth and detail of diabetes-related knowledge and confidence, but also enhanced competence in translating knowledge into every day self-care.”12 These researchers concluded that increased knowledge translated into better patient self-management of their disease. The Long and Gambling study included general self-management characteristics of monitoring HbA1c, diet, exercise, medication management, and general self-care. These researchers contend that diabetes self-management education must be a long-term endeavor to promote change.12
Mendoza and Rosenburg’s meta-analysis on self-management programs for diabetes and chronic conditions found a statistically significant 0.81% reduction in hemoglobin A1c (HbA1c). Characteristics of self-management programs that were linked to improved outcomes included nurse and provider education on medications, diet and/or exercise, and demonstrated use of motivational interviewing and biofeedback. Mendoza and Rosenburg suggested motivational interviewing focuses on the patient’s perspective and facilitates the process that the patient uses to assess their needs and to think about possible solutions.13 Mulimba and Bryo-Daniel found that motivational interviewing is a valuable tool for primary care nurses’ health promotion practice, and Thompson and colleagues found that it was effective in changing behavior.14,15
Nurse’s Role in Health Literacy
Nurses play a vital role in educating and securing adherence of patients in the management of their disease(s).13 In addition to educating patients, families, and friends of the family, nurses assist with helping them make informed decisions.16 The VHA uses the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) to teach health care staff about diabetes self-management education (DSME). Tisdel and colleagues found that DSME established through telemedicine or clinical mentoring improved patient outcomes.17 Mendoza and Rosenburgfound nurse-led DSME was linked to minimizing cardiovascular risk factors and improvements in HbA1c.13
Background
Staunton Community Based Outpatient Clinic (CBOC) in rural Virginia is a primary care clinic that serves veterans in the surrounding area. About one-fourth of the Staunton patients have diabetes. According to June 2014 data from the VHA Support Service Center, the physician at the Staunton CBOC was responsible for 946 patients (225 with diabetes) and the nurse practitioner was responsible for 707 (184 with diabetes). The VHA Support Service Center 2014 data indicated that veterans with poorly self-managed diabetes were at increased risk for poor outcomes, such as kidney failure, cardiovascular disease, and limb amputation. Veterans with diabetes use the emergency department more often and are admitted to the hospital more often than are veterans who do not have diabetes.18
Methods
The primary objective of this pilot study was to explore whether weekly structured nursing education sessions lasting 45 minutes and subsequent follow-up weekly conferences would improve their HbA1c for veterans identified as having ≥ 9 HbA1c and ≤ 3 health literacy score on the NVS 7 study assessment. Most recent HbA1c prior to beginning the study was used to identify potential participants. After completion of 12 weekly education interventions, an additional HbA1c was obtained.
The Salem VAMC and Eastern Mennonite University Institutional Review Board approved the study. Veterans’ questions were answered prior to signing consent forms. All data collected were kept confidential.
Veterans with ≥ 9 HbA1c were evaluated for possible participation. Forty-nine veterans met the criteria to participate in this pilot study. Exclusion criteria included diagnosis of any cognitive disorder, such as dementia, Alzheimer disease, or memory impairment. In addition, veterans unwilling or unable to commit to weekly follow-up sessions were excluded. The veterans eligible for participation were contacted by telephone, and 9 agreed to participate in the pilot study. Inclusion criteria included those aged ≥ 18 years and a diagnosis of diabetes with most recent HbA1c of ≥ 9 and a score of < 4 on the NVS health literacy assessment. After taking the NVS health literacy assessment, 6 of the 9 participants qualified to continue in the study.
Education interventions included assessing medication adherence, discussing diet, reviewing physical activity for the previous week (based on diet and activity logs), and reviewing home blood glucose monitoring. Weekly education sessions were either face-to-face or by telephone. This choice was given to accommodate veterans who may have had transportation issues. A total of 12 weekly appointments were scheduled for each participant, and education was directed at the specific needs and goals of each participant. Interventions for education were based on those found in previous studies.13,14,18,19
Data Collection and Analysis
All 6 participants were white male veterans who were diagnosed with diabetes for at least 3 years. Their ages ranged from 59 to 72. Three participants were service connected for diabetes and 3 were not. One participant dropped from the study after completing 4 appointments, stating he was just too busy to be available for a weekly appointment. Another participant completed 6 appointments and removed himself from the study due to time constraints. The 4 participants who completed the pilot study were followed for 12 weeks by a registered nurse (RN), and all had reductions in their HbA1c.
Participants were assessed at weekly appointments using a predetermined template for medication adherence, diet, activity, and blood glucose monitoring. Responses of the participants guided the education interventions to meet the individual veteran’s learning needs. For example, one veteran was given specific education on carbohydrate counting and another was educated on how to read food labels. Participants were also encouraged to express satisfaction, frustration, anger, or other emotions in managing their chronic illness. The premise for spending additional time with the veteran was to promote positive self-management behaviors as recommended by Radhakrishnan.19
Veterans who completed the study stated that the education interventions positively impacted their health status. One veteran was able to delay dialysis due to self-directed improvement in his lifestyle (exercising and watching his diet), which improved his HbA1c. This veteran attributed his health improvement to the individualized education sessions with the RN and knowing he had to be accountable to someone. Additionally, it was found there was a strong familial-social component to diabetes self-management. Several veterans were knowledgeable about diabetes self-management as evidenced by their responses to weekly questions. However, disease management for these veterans was strongly impacted by family and life events.
One veteran did not manage his disease for an entire week due to “being busy with a death in the family and planning for a wedding.” This veteran took his medication but did not check his blood glucose or monitor his diet. Another veteran spoke of eating ice cream and other concentrated sweets because his young grandson was with him for the week. A third veteran was able to manage his diet better when his wife packed snacks for him but when left to his own accord did not do well with his food selection. Even though these veterans understood how to effectively manage their diabetes, they may have chosen to inconsistently translate that knowledge into practice if they perceive those familial-social forces to be more important or more powerful.
Discussion
The findings from this small pilot study from a single clinic cannot be generalized. However, this pilot study adds to the literature of the positive impact of individualized, structured, tailored nursing interventions delivered with careful consideration of the participants’ personal goals and health care needs for diabetes self-management.
Participants monitored home blood glucose levels, diet, and activity and maintained adherence with prescribed diabetes medications. The HbA1c level for participants decreased by the end of the program. During the course of the pilot study a pharmacist managed the veterans’ medications. Participant 1 began a new medication regimen the first day of the study. Previously, the patient was self-regulating his medication. However, during the 12-week study, he had no medication adjustments. Participant 4 had several increases to his insulin dose (insulin aspart protamine and insulin aspart rdna origin) during the course of the study. Participants 5 and 6 had no medication adjustments during the study.
Even though participants had medication adjustments, which contributed to the HbA1c decrease, they became more aware of the medical need to control their blood sugar through the one-on-one education provided. Although there was variation in the depth and detail that participants maintained their food/activity log and home blood glucose monitoring, all participants agreed that they were more likely to be adherent with prescribed self-monitoring “knowing they were going to have to report self-monitoring information” to the RN.
Health care professionals may not realize the impact of familial-social events on blood glucose control. Veterans in this study found that having weekly sessions with the RN helped them through such events, even though they did not adhere strictly to their regimen. One suggestion is having veterans anticipate future familial-social events that may trigger nonadherence to their diabetes health plan and then discuss those events with the health care professional.
Future Research
This small exploratory pilot study has implications for future research. Increasing the study’s sample size and using a control group is recommended to compare veterans who have an educational intervention with those that do not and the impact it has on blood glucose control. The study was limited to 1 CBOC. Incorporating additional CBOCs could increase the sample size. Additionally, although this study was only 3 months in duration, a longer study could reveal significant patterns of change over time as well as the long-term benefit of a tailored educational intervention. In addition, adjusting the study inclusion criteria of > 9 HbA1c to include those with > 8 HbA1c also may increase the sample size.
Limited financial resources for the study could have negatively impacted the sample size. Incorporating recruitment or advertising strategy may increase the number of participants. Research also is needed on education interventions with a diverse group of male and female veterans that extends beyond 3 months. Exploring the value of including the veteran’s family in the education sessions is needed. Finally, this study examined only diabetes education. Researchers need to consider other diseases and the value of individualized education.
Limitations
Limitations included a small sample size and no control group. Due to the study’s small sample size, extrapolating data from it becomes difficult. However, this pilot study sets the groundwork for other researchers to expand the importance of education interventions and health literacy. Recruitment was challenging since an eligibility criterion was the NVS score, and patients were sometimes difficult to contact.7 The pilot study started with 6 white male participants but only 4 finished. During the course of the pilot study, 1 veteran had medication adjustments as part of routine care and 1 veteran had medication adjustments prior to the study, which could have altered the HbA1c results.
In hindsight, using the NVS to assess both prestudy with poststudy health literacy scores would have provided additional information about the education intervention. There is possible bias because the researcher was a VAMC employee, and the RN that implemented the interventions had previously worked with the patients.
Conclusion
Although this is a small descriptive pilot study, it adds to the body of research on the value of nurse-driven interventions to help veterans manage diabetes by enhancing their health literacy. It also raises questions and opportunities for further research into the power of familial-social influences on a veteran’s willingness to manage their diabetes. The majority of veterans who declined to participate in this study, even though they qualified, stated that they would “not follow any recommendations.” Further investigation is needed about why some veterans elect not to obtain help that could positively impact their health and possibly extend their life. Additionally, scientific quantitative and qualitative research is needed to evaluate the statistical significance between health care literacy and educational intervention on patient adherence among individuals diagnosed with diabetes.
According to the National Academy of Medicine (NAM), health literacy is “the degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate health decisions.”1 Studies suggest that millions of patients have inadequate health literacy and cannot make fully informed decisions because of this lack of knowledge.2-4 A 2007 National Patient Safety Foundation report calculated that inadequate health literacy burdens the U.S. health care system with an additional $106 to $238 billion annually.5
In 2014, the American Diabetes Association reported that diabetes affects 29.1 million Americans (9.3%) and that by 2050 1 in 3 Americans will have diabetes.6 People with diabetes have health care costs 2.3 times higher than the cost for nondiabetic patients. The cost of taking care of patients with diabetes annually is about $245 billion.6 Without interventions that address health literacy and effective self-management to reduce the risks of complications and comorbidity, health care costs related to diabetes will continue to increase.
Literature Review
According to a U.S. Department of Education assessment on adult health literacy in 2003, 88% of adults in the U.S. have inadequate health literacy.2 About 90 million Americans lack health literacy skills, according to a 2004 NAM report.3 Heinrich, who conducted a review of U.S. studies on health literacy, concluded that about 25% of Americans have low health literacy.4
The Newest Vital Sign Tool
The Newest Vital Sign (NVS) tool is a free tool developed by Pfizer (New York, NY) for assessing health literacy. Participants are asked 6 questions about nutrition based on an ice cream nutrition label (Figure). The researcher records the participant’s responses, which accommodates participants who may have difficulty reading. The tool is scored from 0 to 6. A score of below 4 indicates the possibility of limited health literacy.7 This test can be completed in about 3 minutes, is widely accepted, and provides results comparable to more extensive literacy tests.8 A study conducted by Welch and colleagues suggested the NVS tool is both cost and time efficient.9 Ryan and colleagues found that 98% of patients in their study (n = 289) did not have objections to taking the NVS assessment.10
Escobedo and Weismuller’s study used the NVS health literacy tool to assess the health literacy of renal patients.3 In 2004, about 50,000 American patients with diabetes began treatment for kidney failure due to diabetes complications.6 Escobedo and Weismuller found that patients with diabetes with limited health literacy knowledge are more likely to be hospitalized, thus increasing health care costs.3 In addition, they discovered that these patients demonstrated poor adherence to prescribed treatment protocols. Welch, VanGeest, and Caskey conducted a case study on time, cost, and clinical utilization of the NVS health literacy tool and found that a patient’s lack of health literacy was linked to limited participation in personal medical decisions.7,9 Patient’s lack of knowledge was associated with delays in seeking treatment, poor self-management of the disease, and more hospital admissions.
Health Literacy and Diabetes
Studies specific to diabetes and inadequate health literacy support the premise that better health literacy leads to improved patient outcomes. Using the NVS tool, Heinrich conducted a study of the health literacy of 54 patients with diabetes in a primary care setting. The study showed that 65% had inadequate health literacy and that patients with diabetes with inadequate health literacy were more likely to have poor glycemic control compared with patients with diabetes and adequate health literacy levels.4 McCleary-Jones examined diet, foot care, and exercise of 50 African American participants with diabetes from a community health center, finding a positive relationship between health literacy and diabetes knowledge.11
Long and Gambling conducted a 2-year prospective, observational study that incorporated motivational interviewing and patient-centered care into a self-management program, examining the effectiveness of scheduled phone interventions to assist patients with diabetes in the management of their disease.12 The interventions used structured and consistent questions supported by a protocol and script that examined medication adherence and lifestyle choices. Long and Gambling concluded that “the findings demonstrate not only changes in the depth and detail of diabetes-related knowledge and confidence, but also enhanced competence in translating knowledge into every day self-care.”12 These researchers concluded that increased knowledge translated into better patient self-management of their disease. The Long and Gambling study included general self-management characteristics of monitoring HbA1c, diet, exercise, medication management, and general self-care. These researchers contend that diabetes self-management education must be a long-term endeavor to promote change.12
Mendoza and Rosenburg’s meta-analysis on self-management programs for diabetes and chronic conditions found a statistically significant 0.81% reduction in hemoglobin A1c (HbA1c). Characteristics of self-management programs that were linked to improved outcomes included nurse and provider education on medications, diet and/or exercise, and demonstrated use of motivational interviewing and biofeedback. Mendoza and Rosenburg suggested motivational interviewing focuses on the patient’s perspective and facilitates the process that the patient uses to assess their needs and to think about possible solutions.13 Mulimba and Bryo-Daniel found that motivational interviewing is a valuable tool for primary care nurses’ health promotion practice, and Thompson and colleagues found that it was effective in changing behavior.14,15
Nurse’s Role in Health Literacy
Nurses play a vital role in educating and securing adherence of patients in the management of their disease(s).13 In addition to educating patients, families, and friends of the family, nurses assist with helping them make informed decisions.16 The VHA uses the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) to teach health care staff about diabetes self-management education (DSME). Tisdel and colleagues found that DSME established through telemedicine or clinical mentoring improved patient outcomes.17 Mendoza and Rosenburgfound nurse-led DSME was linked to minimizing cardiovascular risk factors and improvements in HbA1c.13
Background
Staunton Community Based Outpatient Clinic (CBOC) in rural Virginia is a primary care clinic that serves veterans in the surrounding area. About one-fourth of the Staunton patients have diabetes. According to June 2014 data from the VHA Support Service Center, the physician at the Staunton CBOC was responsible for 946 patients (225 with diabetes) and the nurse practitioner was responsible for 707 (184 with diabetes). The VHA Support Service Center 2014 data indicated that veterans with poorly self-managed diabetes were at increased risk for poor outcomes, such as kidney failure, cardiovascular disease, and limb amputation. Veterans with diabetes use the emergency department more often and are admitted to the hospital more often than are veterans who do not have diabetes.18
Methods
The primary objective of this pilot study was to explore whether weekly structured nursing education sessions lasting 45 minutes and subsequent follow-up weekly conferences would improve their HbA1c for veterans identified as having ≥ 9 HbA1c and ≤ 3 health literacy score on the NVS 7 study assessment. Most recent HbA1c prior to beginning the study was used to identify potential participants. After completion of 12 weekly education interventions, an additional HbA1c was obtained.
The Salem VAMC and Eastern Mennonite University Institutional Review Board approved the study. Veterans’ questions were answered prior to signing consent forms. All data collected were kept confidential.
Veterans with ≥ 9 HbA1c were evaluated for possible participation. Forty-nine veterans met the criteria to participate in this pilot study. Exclusion criteria included diagnosis of any cognitive disorder, such as dementia, Alzheimer disease, or memory impairment. In addition, veterans unwilling or unable to commit to weekly follow-up sessions were excluded. The veterans eligible for participation were contacted by telephone, and 9 agreed to participate in the pilot study. Inclusion criteria included those aged ≥ 18 years and a diagnosis of diabetes with most recent HbA1c of ≥ 9 and a score of < 4 on the NVS health literacy assessment. After taking the NVS health literacy assessment, 6 of the 9 participants qualified to continue in the study.
Education interventions included assessing medication adherence, discussing diet, reviewing physical activity for the previous week (based on diet and activity logs), and reviewing home blood glucose monitoring. Weekly education sessions were either face-to-face or by telephone. This choice was given to accommodate veterans who may have had transportation issues. A total of 12 weekly appointments were scheduled for each participant, and education was directed at the specific needs and goals of each participant. Interventions for education were based on those found in previous studies.13,14,18,19
Data Collection and Analysis
All 6 participants were white male veterans who were diagnosed with diabetes for at least 3 years. Their ages ranged from 59 to 72. Three participants were service connected for diabetes and 3 were not. One participant dropped from the study after completing 4 appointments, stating he was just too busy to be available for a weekly appointment. Another participant completed 6 appointments and removed himself from the study due to time constraints. The 4 participants who completed the pilot study were followed for 12 weeks by a registered nurse (RN), and all had reductions in their HbA1c.
Participants were assessed at weekly appointments using a predetermined template for medication adherence, diet, activity, and blood glucose monitoring. Responses of the participants guided the education interventions to meet the individual veteran’s learning needs. For example, one veteran was given specific education on carbohydrate counting and another was educated on how to read food labels. Participants were also encouraged to express satisfaction, frustration, anger, or other emotions in managing their chronic illness. The premise for spending additional time with the veteran was to promote positive self-management behaviors as recommended by Radhakrishnan.19
Veterans who completed the study stated that the education interventions positively impacted their health status. One veteran was able to delay dialysis due to self-directed improvement in his lifestyle (exercising and watching his diet), which improved his HbA1c. This veteran attributed his health improvement to the individualized education sessions with the RN and knowing he had to be accountable to someone. Additionally, it was found there was a strong familial-social component to diabetes self-management. Several veterans were knowledgeable about diabetes self-management as evidenced by their responses to weekly questions. However, disease management for these veterans was strongly impacted by family and life events.
One veteran did not manage his disease for an entire week due to “being busy with a death in the family and planning for a wedding.” This veteran took his medication but did not check his blood glucose or monitor his diet. Another veteran spoke of eating ice cream and other concentrated sweets because his young grandson was with him for the week. A third veteran was able to manage his diet better when his wife packed snacks for him but when left to his own accord did not do well with his food selection. Even though these veterans understood how to effectively manage their diabetes, they may have chosen to inconsistently translate that knowledge into practice if they perceive those familial-social forces to be more important or more powerful.
Discussion
The findings from this small pilot study from a single clinic cannot be generalized. However, this pilot study adds to the literature of the positive impact of individualized, structured, tailored nursing interventions delivered with careful consideration of the participants’ personal goals and health care needs for diabetes self-management.
Participants monitored home blood glucose levels, diet, and activity and maintained adherence with prescribed diabetes medications. The HbA1c level for participants decreased by the end of the program. During the course of the pilot study a pharmacist managed the veterans’ medications. Participant 1 began a new medication regimen the first day of the study. Previously, the patient was self-regulating his medication. However, during the 12-week study, he had no medication adjustments. Participant 4 had several increases to his insulin dose (insulin aspart protamine and insulin aspart rdna origin) during the course of the study. Participants 5 and 6 had no medication adjustments during the study.
Even though participants had medication adjustments, which contributed to the HbA1c decrease, they became more aware of the medical need to control their blood sugar through the one-on-one education provided. Although there was variation in the depth and detail that participants maintained their food/activity log and home blood glucose monitoring, all participants agreed that they were more likely to be adherent with prescribed self-monitoring “knowing they were going to have to report self-monitoring information” to the RN.
Health care professionals may not realize the impact of familial-social events on blood glucose control. Veterans in this study found that having weekly sessions with the RN helped them through such events, even though they did not adhere strictly to their regimen. One suggestion is having veterans anticipate future familial-social events that may trigger nonadherence to their diabetes health plan and then discuss those events with the health care professional.
Future Research
This small exploratory pilot study has implications for future research. Increasing the study’s sample size and using a control group is recommended to compare veterans who have an educational intervention with those that do not and the impact it has on blood glucose control. The study was limited to 1 CBOC. Incorporating additional CBOCs could increase the sample size. Additionally, although this study was only 3 months in duration, a longer study could reveal significant patterns of change over time as well as the long-term benefit of a tailored educational intervention. In addition, adjusting the study inclusion criteria of > 9 HbA1c to include those with > 8 HbA1c also may increase the sample size.
Limited financial resources for the study could have negatively impacted the sample size. Incorporating recruitment or advertising strategy may increase the number of participants. Research also is needed on education interventions with a diverse group of male and female veterans that extends beyond 3 months. Exploring the value of including the veteran’s family in the education sessions is needed. Finally, this study examined only diabetes education. Researchers need to consider other diseases and the value of individualized education.
Limitations
Limitations included a small sample size and no control group. Due to the study’s small sample size, extrapolating data from it becomes difficult. However, this pilot study sets the groundwork for other researchers to expand the importance of education interventions and health literacy. Recruitment was challenging since an eligibility criterion was the NVS score, and patients were sometimes difficult to contact.7 The pilot study started with 6 white male participants but only 4 finished. During the course of the pilot study, 1 veteran had medication adjustments as part of routine care and 1 veteran had medication adjustments prior to the study, which could have altered the HbA1c results.
In hindsight, using the NVS to assess both prestudy with poststudy health literacy scores would have provided additional information about the education intervention. There is possible bias because the researcher was a VAMC employee, and the RN that implemented the interventions had previously worked with the patients.
Conclusion
Although this is a small descriptive pilot study, it adds to the body of research on the value of nurse-driven interventions to help veterans manage diabetes by enhancing their health literacy. It also raises questions and opportunities for further research into the power of familial-social influences on a veteran’s willingness to manage their diabetes. The majority of veterans who declined to participate in this study, even though they qualified, stated that they would “not follow any recommendations.” Further investigation is needed about why some veterans elect not to obtain help that could positively impact their health and possibly extend their life. Additionally, scientific quantitative and qualitative research is needed to evaluate the statistical significance between health care literacy and educational intervention on patient adherence among individuals diagnosed with diabetes.
1. Stiles E. Promoting health literacy in patients with diabetes. Nurs Stand. 2011;26(8):35-40.
2. Baum NH, Dowling RA. Health literacy: how do your patients rate? http://urologytimes.modernmedicine.com/urology-times/news/modernmedicine/modern-medicine-now/health-literacy-how-do-your-patients-rate. Published August 1, 2011. Accessed December 2, 2016.
3. Escobedo W, Weismuller P. Assessing health literacy in renal failure and kidney transplant patients. Prog Transplant. 2013;23(1):47-54.
4. Heinrich C. Health literacy: the sixth vital sign. J Am Acad Nurse Pract. 2012;24(4):218-223.
5. Roett MA, Wessel L. Help your patient “get” what you just said: health literacy guide. J Fam Pract. 2012;61(4):190-196.
6. American Diabetes Association. Statistics about diabetes. http://www.diabetes.org/diabetes-basics/statistics/?loc=feat1.Updated December 12, 2016. Accessed December 14, 2016.
7. Pfizer. The newest vital sign. http://www.pfizer.com/files/health/nvs_flipbook_english_final.pdf. Published February 2011. Accessed December 2, 2016.
8. Shah LC, West P, Bremmeyr K, Savoy-Moore RT. Health literacy instrument in family medicine: the “newest vital sign” ease of use and correlates. J Am Board Fam Med. 2010;23(2):195-203.
9. Welch VL, VanGeest JB, Caskey R. Time, costs, and clinical utilization of screening for health literacy: a case study using the Newest Vital Sign (NVS) instrument. J Am Board Fam Med. 2011;24(3):281-289.
10. Ryan JG, Leguen F, Weiss BD, et al. Will patients agree to have their literacy skills assessed in clinical practice? Health Educ Res. 2008;23(4):603-611.
11. McCleary-Jones V. Health literacy and its association with diabetes knowledge, self-efficacy and disease self-management among African Americans with diabetes mellitus. ABNF J. 2011;22(2):25-32.
12. Long AF, Gambling T. Enhancing health literacy and behavioral change within a tele-care education and support intervention for people with type 2 diabetes. Health Expect. 2012;15(3):267-282.
13. Mendoza M, Rosenberg T. Self-management of type 2 diabetes: A good idea-or not? J Fam Pract. 2013;62(5):244-248.
14. A Clifford Mulimba A, Byron-Daniel J. Motivational interviewing-based interventions and diabetes mellitus. Br J Nurs. 2014;23(1):8-14.
15. Thompson DR, Chair SY, Chan SW, Astin F, Davidson PM, Ski CF. Motivational interviewing: a useful approach to improving cardiovascular health? J Clin Nurs. 2011;20;(9-10):1236-1244.
16. Protheroe J, Rowlands G. Matching clinical information with levels of patient health literacy. Nurs Manag (Harrow). 2013;20(3):20-21.
17. Tisdel KA, Bedwell M, Tarkington PE, Mundy A, Fredrickson SK. Diabetes specialists share experience remotely with RN care managers. Fed Pract. 2013;30(suppl 7):15S-20S.
18. U.S. Department of Veterans Affairs, Veterans Health Administration Support Service Center. http://vssc.med.va.gov/AlphaIndex.asp?Ltr=D.
19. Radhakrishnan K. The efficacy of tailored interventions for self-management outcomes of type 2 diabetes, hypertension, or heart disease: a systemic review. J Adv Nurs. 2012;68(3):496-510.
1. Stiles E. Promoting health literacy in patients with diabetes. Nurs Stand. 2011;26(8):35-40.
2. Baum NH, Dowling RA. Health literacy: how do your patients rate? http://urologytimes.modernmedicine.com/urology-times/news/modernmedicine/modern-medicine-now/health-literacy-how-do-your-patients-rate. Published August 1, 2011. Accessed December 2, 2016.
3. Escobedo W, Weismuller P. Assessing health literacy in renal failure and kidney transplant patients. Prog Transplant. 2013;23(1):47-54.
4. Heinrich C. Health literacy: the sixth vital sign. J Am Acad Nurse Pract. 2012;24(4):218-223.
5. Roett MA, Wessel L. Help your patient “get” what you just said: health literacy guide. J Fam Pract. 2012;61(4):190-196.
6. American Diabetes Association. Statistics about diabetes. http://www.diabetes.org/diabetes-basics/statistics/?loc=feat1.Updated December 12, 2016. Accessed December 14, 2016.
7. Pfizer. The newest vital sign. http://www.pfizer.com/files/health/nvs_flipbook_english_final.pdf. Published February 2011. Accessed December 2, 2016.
8. Shah LC, West P, Bremmeyr K, Savoy-Moore RT. Health literacy instrument in family medicine: the “newest vital sign” ease of use and correlates. J Am Board Fam Med. 2010;23(2):195-203.
9. Welch VL, VanGeest JB, Caskey R. Time, costs, and clinical utilization of screening for health literacy: a case study using the Newest Vital Sign (NVS) instrument. J Am Board Fam Med. 2011;24(3):281-289.
10. Ryan JG, Leguen F, Weiss BD, et al. Will patients agree to have their literacy skills assessed in clinical practice? Health Educ Res. 2008;23(4):603-611.
11. McCleary-Jones V. Health literacy and its association with diabetes knowledge, self-efficacy and disease self-management among African Americans with diabetes mellitus. ABNF J. 2011;22(2):25-32.
12. Long AF, Gambling T. Enhancing health literacy and behavioral change within a tele-care education and support intervention for people with type 2 diabetes. Health Expect. 2012;15(3):267-282.
13. Mendoza M, Rosenberg T. Self-management of type 2 diabetes: A good idea-or not? J Fam Pract. 2013;62(5):244-248.
14. A Clifford Mulimba A, Byron-Daniel J. Motivational interviewing-based interventions and diabetes mellitus. Br J Nurs. 2014;23(1):8-14.
15. Thompson DR, Chair SY, Chan SW, Astin F, Davidson PM, Ski CF. Motivational interviewing: a useful approach to improving cardiovascular health? J Clin Nurs. 2011;20;(9-10):1236-1244.
16. Protheroe J, Rowlands G. Matching clinical information with levels of patient health literacy. Nurs Manag (Harrow). 2013;20(3):20-21.
17. Tisdel KA, Bedwell M, Tarkington PE, Mundy A, Fredrickson SK. Diabetes specialists share experience remotely with RN care managers. Fed Pract. 2013;30(suppl 7):15S-20S.
18. U.S. Department of Veterans Affairs, Veterans Health Administration Support Service Center. http://vssc.med.va.gov/AlphaIndex.asp?Ltr=D.
19. Radhakrishnan K. The efficacy of tailored interventions for self-management outcomes of type 2 diabetes, hypertension, or heart disease: a systemic review. J Adv Nurs. 2012;68(3):496-510.