User login
Pallor and weight loss
Ulcerative colitis is a chronic inflammatory condition that characteristically involves the large bowel. Disease activity usually follows a pattern of periods of active inflammation alternating with periods of remission. Approximately 15% of patients experience an aggressive course of ulcerative colitis. Acute severe ulcerative colitis (ASUC) is a life-threatening medical emergency, which may require hospitalization for prompt medical treatment and colectomy if medical treatment fails. Predictors of an aggressive disease course and colectomy include young age at the time of diagnosis, extensive disease, severe endoscopic disease activity, presence of extraintestinal manifestations, elevated inflammatory markers, and early need for corticosteroids.
The diagnosis of ASUC is based on the Mayo Clinic Score and the Truelove and Witts criteria which consists of the presence of six or more bloody stools per day and at least one of these signs of systemic toxicity:
• Pulse rate > 90 beats/min
• Temperature > 100.04 °F
• Hemoglobin < 10.5 g/dL
• Erythrocyte sedimentation rate (ESR) > 30 mm/h
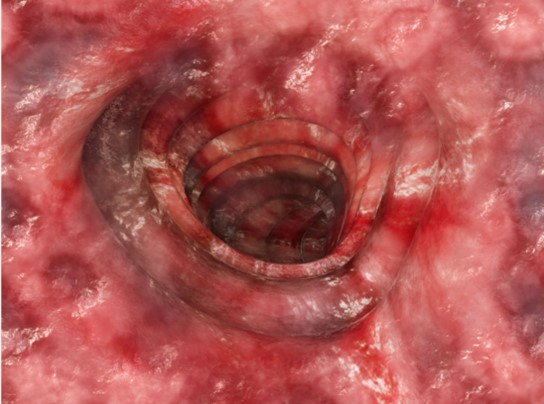
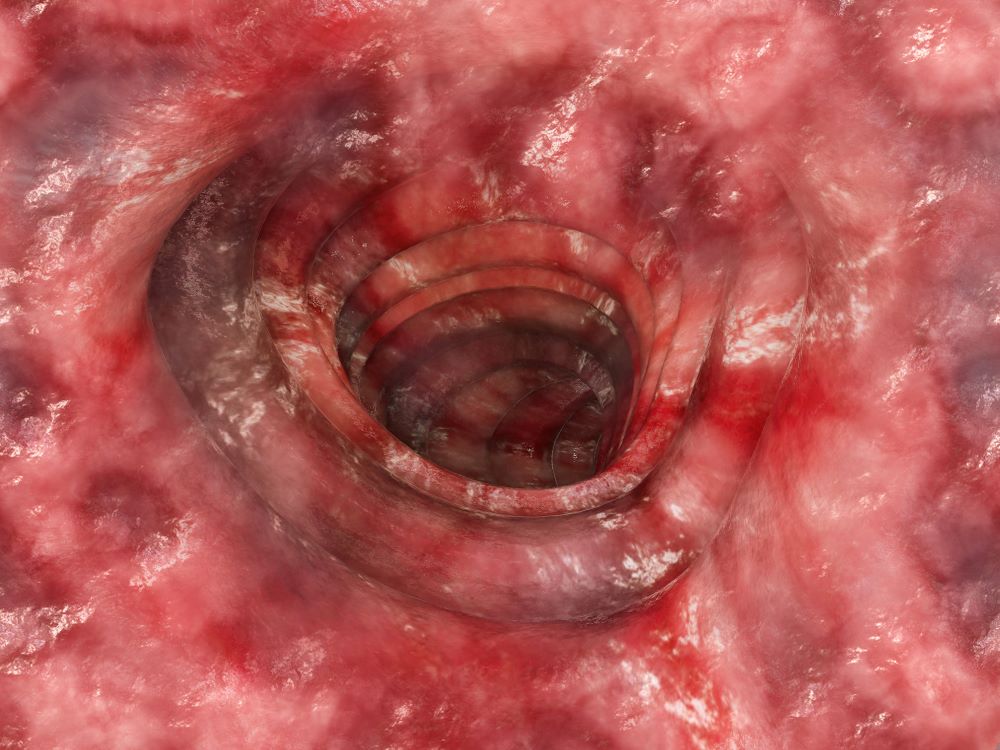
Further evaluation in patients with suspected ASUC aims to exclude alternative diagnoses and to determine the severity and extent of disease. Abdominal radiographs are obtained to rule out colonic dilatation and to evaluate for the possibility of microperforations. Stool studies should be obtained to evaluate for infections such as C difficile. To assess for the severity of mucosal disease a limited lower endoscopy is usually performed in hospitalized patients with ASUC. In addition, it allows for the opportunity to perform a biopsy to rule out cytomegalovirus as the cause of the disease flare. However, a colonoscopy should be avoided in these patients because of the increased risk for colonic dilation and perforation; a carefully performed flexible sigmoidoscopy with minimal insufflation by an experienced operator is sufficient for most patients. Endoscopic features of ASUC include erythema, absent vascular pattern, friability, erosions, and ulcerations.
The mainstay of management of hospitalized individuals with ASUC is intravenous corticosteroids. However, up to one third of patients may not show improvement in clinical or biochemical markers after treatment with steroids. In hospitalized patients with ASUC refractory to 3 to 5 days of intravenous corticosteroids infliximab or cyclosporin are suggested. Colectomy is a treatment option for patients unresponsive to medical therapy or for patients who develop life-threatening complications (colonic perforation, toxic megacolon, etc.)
Leyla Ghazi, MD, Physician, Dartmouth Health, GI Associates, Concord, New Hampshire.
Leyla Ghazi, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Ulcerative colitis is a chronic inflammatory condition that characteristically involves the large bowel. Disease activity usually follows a pattern of periods of active inflammation alternating with periods of remission. Approximately 15% of patients experience an aggressive course of ulcerative colitis. Acute severe ulcerative colitis (ASUC) is a life-threatening medical emergency, which may require hospitalization for prompt medical treatment and colectomy if medical treatment fails. Predictors of an aggressive disease course and colectomy include young age at the time of diagnosis, extensive disease, severe endoscopic disease activity, presence of extraintestinal manifestations, elevated inflammatory markers, and early need for corticosteroids.
The diagnosis of ASUC is based on the Mayo Clinic Score and the Truelove and Witts criteria which consists of the presence of six or more bloody stools per day and at least one of these signs of systemic toxicity:
• Pulse rate > 90 beats/min
• Temperature > 100.04 °F
• Hemoglobin < 10.5 g/dL
• Erythrocyte sedimentation rate (ESR) > 30 mm/h
Further evaluation in patients with suspected ASUC aims to exclude alternative diagnoses and to determine the severity and extent of disease. Abdominal radiographs are obtained to rule out colonic dilatation and to evaluate for the possibility of microperforations. Stool studies should be obtained to evaluate for infections such as C difficile. To assess for the severity of mucosal disease a limited lower endoscopy is usually performed in hospitalized patients with ASUC. In addition, it allows for the opportunity to perform a biopsy to rule out cytomegalovirus as the cause of the disease flare. However, a colonoscopy should be avoided in these patients because of the increased risk for colonic dilation and perforation; a carefully performed flexible sigmoidoscopy with minimal insufflation by an experienced operator is sufficient for most patients. Endoscopic features of ASUC include erythema, absent vascular pattern, friability, erosions, and ulcerations.
The mainstay of management of hospitalized individuals with ASUC is intravenous corticosteroids. However, up to one third of patients may not show improvement in clinical or biochemical markers after treatment with steroids. In hospitalized patients with ASUC refractory to 3 to 5 days of intravenous corticosteroids infliximab or cyclosporin are suggested. Colectomy is a treatment option for patients unresponsive to medical therapy or for patients who develop life-threatening complications (colonic perforation, toxic megacolon, etc.)
Leyla Ghazi, MD, Physician, Dartmouth Health, GI Associates, Concord, New Hampshire.
Leyla Ghazi, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Ulcerative colitis is a chronic inflammatory condition that characteristically involves the large bowel. Disease activity usually follows a pattern of periods of active inflammation alternating with periods of remission. Approximately 15% of patients experience an aggressive course of ulcerative colitis. Acute severe ulcerative colitis (ASUC) is a life-threatening medical emergency, which may require hospitalization for prompt medical treatment and colectomy if medical treatment fails. Predictors of an aggressive disease course and colectomy include young age at the time of diagnosis, extensive disease, severe endoscopic disease activity, presence of extraintestinal manifestations, elevated inflammatory markers, and early need for corticosteroids.
The diagnosis of ASUC is based on the Mayo Clinic Score and the Truelove and Witts criteria which consists of the presence of six or more bloody stools per day and at least one of these signs of systemic toxicity:
• Pulse rate > 90 beats/min
• Temperature > 100.04 °F
• Hemoglobin < 10.5 g/dL
• Erythrocyte sedimentation rate (ESR) > 30 mm/h
Further evaluation in patients with suspected ASUC aims to exclude alternative diagnoses and to determine the severity and extent of disease. Abdominal radiographs are obtained to rule out colonic dilatation and to evaluate for the possibility of microperforations. Stool studies should be obtained to evaluate for infections such as C difficile. To assess for the severity of mucosal disease a limited lower endoscopy is usually performed in hospitalized patients with ASUC. In addition, it allows for the opportunity to perform a biopsy to rule out cytomegalovirus as the cause of the disease flare. However, a colonoscopy should be avoided in these patients because of the increased risk for colonic dilation and perforation; a carefully performed flexible sigmoidoscopy with minimal insufflation by an experienced operator is sufficient for most patients. Endoscopic features of ASUC include erythema, absent vascular pattern, friability, erosions, and ulcerations.
The mainstay of management of hospitalized individuals with ASUC is intravenous corticosteroids. However, up to one third of patients may not show improvement in clinical or biochemical markers after treatment with steroids. In hospitalized patients with ASUC refractory to 3 to 5 days of intravenous corticosteroids infliximab or cyclosporin are suggested. Colectomy is a treatment option for patients unresponsive to medical therapy or for patients who develop life-threatening complications (colonic perforation, toxic megacolon, etc.)
Leyla Ghazi, MD, Physician, Dartmouth Health, GI Associates, Concord, New Hampshire.
Leyla Ghazi, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
A 36-year-old man presents reporting bouts of bloody diarrhea up to 10 times per day for the past 6 weeks. The diarrhea is associated with asymmetric polyarthralgia in the elbows and knees; a skin rash on the lower extremities; fatigue, weakness, and pallor; and a 12-lb weight loss. One month before, the patient had a colonoscopy that revealed left-sided ulcerative colitis (UC); results were confirmed with biopsy and the patient was started on mesalamine and prednisone.
Vital signs at the time of presentation include blood pressure 90/58, heart rate 112 beats/min, respiratory rate 21 breaths/min, and body temperature 101.9 °F. Examination shows generalized pallor with pale conjunctiva and dry mucosa. No heart murmurs are heard on auscultation. Palpation of the abdomen reveals no palpable masses or organomegaly. Mild pain is present on palpation of the left lower quadrant but without signs of peritoneal irritation. Bowel sounds are present. The lower extremities display erythematous nodular lesions and no edema. Peripheral pulses are present. Laboratory results showed an erythrocyte sedimentation rate of 60 mm, C-reactive protein of 20.2 mg/L, and hemoglobin of 9.8 g/dL. Abdominal radiographs were within normal limits. Stool cultures are pending. Flexible sigmoidoscopy was performed shortly after admission and showed the results above. Biopsies were taken to rule out infection.
Working with industry in private practice gastroenterology
In this video, Dr. Nadeem Baig of Allied Digestive Health in West Long Branck, N.J., discusses why he chose private practice gastroenterology and how his organization works with industry to support its mission of providing the best care for patients.
He has no financial conflicts relative to the topics in this video.

In this video, Dr. Nadeem Baig of Allied Digestive Health in West Long Branck, N.J., discusses why he chose private practice gastroenterology and how his organization works with industry to support its mission of providing the best care for patients.
He has no financial conflicts relative to the topics in this video.
In this video, Dr. Nadeem Baig of Allied Digestive Health in West Long Branck, N.J., discusses why he chose private practice gastroenterology and how his organization works with industry to support its mission of providing the best care for patients.
He has no financial conflicts relative to the topics in this video.

Roflumilast side effect benefits patients with psoriasis and overweight/obesity
BERLIN – .
Reporting secondary outcomes from the investigator-led trial at the annual congress of the European Academy of Dermatology and Venereology, Alexander Egeberg, MD, PhD, DMSc, noted that “clinically significant weight loss” was seen among patients who were treated with oral roflumilast, 500 mcg once daily, versus those receiving placebo.
Indeed, after 12 weeks of therapy, one in three patients treated with oral roflumilast experienced at least a 5% drop in their baseline body weight vs no patients who received placebo (35% vs. 0%; P < .05).
Additionally, a respective 17% versus 0% of patients lost 10% or more of their body weight, and 4% versus 0% lost 15% or more of their baseline body weight at 12 weeks.
After 24 weeks’ treatment, a substantial percentage of patients still had greater than or equal to 5%, greater than or equal to 10%, or greater than or equal to 15% weight loss, at 30%, 17%, and 13% for oral roflumilast, compared with 9%, 0%, and 0% for placebo, respectively.
“We saw that the higher baseline weight correlated with the proportion of weight loss, so that the more heavy patients at baseline also were the ones who experienced the greatest weight loss,” said Dr. Egeberg, who is professor of dermatology at the University of Copenhagen and a senior consultant at the department of dermatology at Bispebjerg Hospital, Copenhagen.
A beneficial side effect in psoriasis?
“You may have heard in psoriasis about topical roflumilast, but oral roflumilast is actually also shown to be effective in treating psoriasis,” said Egeberg.
Topical roflumilast is approved in the United States and Canada for treating plaque psoriasis.
Efficacy results from the PSORRO study were published earlier this year and showed a significantly greater improvement in Psoriasis Area and Severity Index (PASI) 75 with oral roflumilast vs. placebo at 12 weeks (35% vs. 0%), with a sustained effect seen at 24 weeks (44% vs. 40%).
Weight loss was among the most common side effects seen, leading Dr. Egeberg and fellow PSORRO investigators to wonder whether this may actually be a beneficial effect in patients with psoriasis.
“Oral roflumilast is actually a drug that has been on the market for quite a number of years,” Dr. Egeberg said.
Although only currently licensed for chronic obstructive pulmonary disease (COPD) in the United States, oral roflumilast, a phosphodiesterase (PDE) 4 inhibitor, is available as a generic, “which also means that it is extremely affordable,” suggested Dr. Edeberg.
Weight loss may be a problem in patients with COPD, he acknowledged; these patients tend to be underweight as a result of their poor state of health caused by the lung condition. Weight loss could be an advantage in patients with psoriasis who are overweight or living with obesity and have poor cardiometabolic parameters.
The psoriasis treatment with oral roflumilast study
The PSORRO study was a phase 2, multicenter, placebo-controlled, randomized trial performed between 2021 and 2022. A total of 46 adults with plaque psoriasis participated; half were initially treated with oral roflumilast and half with placebo.
Treatment was double-blind for the first 12 weeks, with all patients then receiving open-label treatment with roflumilast for 12 weeks.
The primary endpoint was the proportion of patients achieving at least 75% reduction from baseline PASI (PASI75). A host of secondary endpoints were studied, including weight and cardiometabolic parameters, which Dr. Egeberg reported at the EADV meeting.
Looking at the baseline characteristics of the oral roflumilast and placebo groups, the mean age was a respective 38 and 39 years, 65% and 83% were men, and the mean starting body weight was 102 kg and 105.1 kg.
After 12 weeks of treatment, body weight fell by a mean of 5.4 kg in the oral roflumilast group, with a further decrease of 1.4 kg by 24 weeks, bringing the total average weight loss to 6.8 kg. By comparison, weight loss among those in the placebo group was 0 kg at 12 weeks and around 2 kg at 24 weeks.
The majority of participants in both groups had high baseline BMIs; 70% of those who received oral roflumilast and 61% of those who received placebo had a BMI of 30 or higher.
“We wanted to investigate the impact of body weight, [so] we didn’t allow patients to be underweight when they were included,” Dr. Egeberg explained. Thus, for inclusion, patients had to have a BMI of 20 or higher.
An “extraordinary” finding was how some patients’ weight status based on their BMI changed throughout the study.
“We could see people that went from obese class 3, all the way to obese class 1. And we could see people going from being overweight to normal weight, which is really extraordinary for patients with psoriasis,” Dr. Egeberg said.
“But most importantly,” he added, “we didn’t have any patients who became underweight, suggesting that it actually is safe to use also in normal-weight patients.”
Reduced appetite behind benefit?
Trying to see why the weight loss occurred, Dr. Egeberg noted that it looked like it could be a result of a reduced appetite.
In common with other PDE-4 inhibitors, oral roflumilast treatment was associated with gastrointestinal symptoms – nausea, diarrhea, and abdominal pain – but all of these “decrease to placebo levels again, quite quickly,” he said.
“This really suggests that it’s not because of diarrhea, it’s not because of nausea and abdominal pain; it is because of a reduced appetite that patients actually lose weight when treated with roflumilast,” Dr. Egeberg said. It’s a potential bonus for the drug’s effects on the skin and could afford clinicians an opportunity to help motivate patients to eat well when they do eat, he observed.
Other cardiometabolic parameters assessed included blood pressure, glycated hemoglobin, total cholesterol and other key lipids, creatinine, alanine aminotransferase, and high-sensitivity C-reactive protein, but there were no noteworthy differences between the groups.
Roflumilast is an inexpensive drug because it is generic, Dr. Egeberg observed, but that also means that its use is likely to be off-label.
“It will be up to the treating physician to decide if this is an optimal therapy for their patients,” he suggested.
Cardiometabolic comorbidities important to target
Obesity is a cardiometabolic comorbidity that is important to consider when treating your patients with psoriasis, Paolo Gisondi, MD, of the University of Verona (Italy), said at a separate presentation at the EADV meeting.
While not directly commenting on the roflumilast study, he noted that moderate to severe psoriasis was “frequently associated” with metabolic disorders that put people at additional risk for cardiovascular and fatty liver diseases.
The PSORRO study was an investigator-initiated and investigator-led study and received no commercial funding. Research funding came from the Danish Psoriasis Foundation, Herlev and Gentofte Hospital, and several charitable and humanitarian organizations. Dr. Egeberg acknowledged acting as the principal investigator, speaker, and/or consultant to multiple pharma companies, all of which were unrelated to the study he presented. Dr. Gisondi’s comments were from a separate presentation, and he was not involved in the study.
A version of this article first appeared on Medscape.com.
BERLIN – .
Reporting secondary outcomes from the investigator-led trial at the annual congress of the European Academy of Dermatology and Venereology, Alexander Egeberg, MD, PhD, DMSc, noted that “clinically significant weight loss” was seen among patients who were treated with oral roflumilast, 500 mcg once daily, versus those receiving placebo.
Indeed, after 12 weeks of therapy, one in three patients treated with oral roflumilast experienced at least a 5% drop in their baseline body weight vs no patients who received placebo (35% vs. 0%; P < .05).
Additionally, a respective 17% versus 0% of patients lost 10% or more of their body weight, and 4% versus 0% lost 15% or more of their baseline body weight at 12 weeks.
After 24 weeks’ treatment, a substantial percentage of patients still had greater than or equal to 5%, greater than or equal to 10%, or greater than or equal to 15% weight loss, at 30%, 17%, and 13% for oral roflumilast, compared with 9%, 0%, and 0% for placebo, respectively.
“We saw that the higher baseline weight correlated with the proportion of weight loss, so that the more heavy patients at baseline also were the ones who experienced the greatest weight loss,” said Dr. Egeberg, who is professor of dermatology at the University of Copenhagen and a senior consultant at the department of dermatology at Bispebjerg Hospital, Copenhagen.
A beneficial side effect in psoriasis?
“You may have heard in psoriasis about topical roflumilast, but oral roflumilast is actually also shown to be effective in treating psoriasis,” said Egeberg.
Topical roflumilast is approved in the United States and Canada for treating plaque psoriasis.
Efficacy results from the PSORRO study were published earlier this year and showed a significantly greater improvement in Psoriasis Area and Severity Index (PASI) 75 with oral roflumilast vs. placebo at 12 weeks (35% vs. 0%), with a sustained effect seen at 24 weeks (44% vs. 40%).
Weight loss was among the most common side effects seen, leading Dr. Egeberg and fellow PSORRO investigators to wonder whether this may actually be a beneficial effect in patients with psoriasis.
“Oral roflumilast is actually a drug that has been on the market for quite a number of years,” Dr. Egeberg said.
Although only currently licensed for chronic obstructive pulmonary disease (COPD) in the United States, oral roflumilast, a phosphodiesterase (PDE) 4 inhibitor, is available as a generic, “which also means that it is extremely affordable,” suggested Dr. Edeberg.
Weight loss may be a problem in patients with COPD, he acknowledged; these patients tend to be underweight as a result of their poor state of health caused by the lung condition. Weight loss could be an advantage in patients with psoriasis who are overweight or living with obesity and have poor cardiometabolic parameters.
The psoriasis treatment with oral roflumilast study
The PSORRO study was a phase 2, multicenter, placebo-controlled, randomized trial performed between 2021 and 2022. A total of 46 adults with plaque psoriasis participated; half were initially treated with oral roflumilast and half with placebo.
Treatment was double-blind for the first 12 weeks, with all patients then receiving open-label treatment with roflumilast for 12 weeks.
The primary endpoint was the proportion of patients achieving at least 75% reduction from baseline PASI (PASI75). A host of secondary endpoints were studied, including weight and cardiometabolic parameters, which Dr. Egeberg reported at the EADV meeting.
Looking at the baseline characteristics of the oral roflumilast and placebo groups, the mean age was a respective 38 and 39 years, 65% and 83% were men, and the mean starting body weight was 102 kg and 105.1 kg.
After 12 weeks of treatment, body weight fell by a mean of 5.4 kg in the oral roflumilast group, with a further decrease of 1.4 kg by 24 weeks, bringing the total average weight loss to 6.8 kg. By comparison, weight loss among those in the placebo group was 0 kg at 12 weeks and around 2 kg at 24 weeks.
The majority of participants in both groups had high baseline BMIs; 70% of those who received oral roflumilast and 61% of those who received placebo had a BMI of 30 or higher.
“We wanted to investigate the impact of body weight, [so] we didn’t allow patients to be underweight when they were included,” Dr. Egeberg explained. Thus, for inclusion, patients had to have a BMI of 20 or higher.
An “extraordinary” finding was how some patients’ weight status based on their BMI changed throughout the study.
“We could see people that went from obese class 3, all the way to obese class 1. And we could see people going from being overweight to normal weight, which is really extraordinary for patients with psoriasis,” Dr. Egeberg said.
“But most importantly,” he added, “we didn’t have any patients who became underweight, suggesting that it actually is safe to use also in normal-weight patients.”
Reduced appetite behind benefit?
Trying to see why the weight loss occurred, Dr. Egeberg noted that it looked like it could be a result of a reduced appetite.
In common with other PDE-4 inhibitors, oral roflumilast treatment was associated with gastrointestinal symptoms – nausea, diarrhea, and abdominal pain – but all of these “decrease to placebo levels again, quite quickly,” he said.
“This really suggests that it’s not because of diarrhea, it’s not because of nausea and abdominal pain; it is because of a reduced appetite that patients actually lose weight when treated with roflumilast,” Dr. Egeberg said. It’s a potential bonus for the drug’s effects on the skin and could afford clinicians an opportunity to help motivate patients to eat well when they do eat, he observed.
Other cardiometabolic parameters assessed included blood pressure, glycated hemoglobin, total cholesterol and other key lipids, creatinine, alanine aminotransferase, and high-sensitivity C-reactive protein, but there were no noteworthy differences between the groups.
Roflumilast is an inexpensive drug because it is generic, Dr. Egeberg observed, but that also means that its use is likely to be off-label.
“It will be up to the treating physician to decide if this is an optimal therapy for their patients,” he suggested.
Cardiometabolic comorbidities important to target
Obesity is a cardiometabolic comorbidity that is important to consider when treating your patients with psoriasis, Paolo Gisondi, MD, of the University of Verona (Italy), said at a separate presentation at the EADV meeting.
While not directly commenting on the roflumilast study, he noted that moderate to severe psoriasis was “frequently associated” with metabolic disorders that put people at additional risk for cardiovascular and fatty liver diseases.
The PSORRO study was an investigator-initiated and investigator-led study and received no commercial funding. Research funding came from the Danish Psoriasis Foundation, Herlev and Gentofte Hospital, and several charitable and humanitarian organizations. Dr. Egeberg acknowledged acting as the principal investigator, speaker, and/or consultant to multiple pharma companies, all of which were unrelated to the study he presented. Dr. Gisondi’s comments were from a separate presentation, and he was not involved in the study.
A version of this article first appeared on Medscape.com.
BERLIN – .
Reporting secondary outcomes from the investigator-led trial at the annual congress of the European Academy of Dermatology and Venereology, Alexander Egeberg, MD, PhD, DMSc, noted that “clinically significant weight loss” was seen among patients who were treated with oral roflumilast, 500 mcg once daily, versus those receiving placebo.
Indeed, after 12 weeks of therapy, one in three patients treated with oral roflumilast experienced at least a 5% drop in their baseline body weight vs no patients who received placebo (35% vs. 0%; P < .05).
Additionally, a respective 17% versus 0% of patients lost 10% or more of their body weight, and 4% versus 0% lost 15% or more of their baseline body weight at 12 weeks.
After 24 weeks’ treatment, a substantial percentage of patients still had greater than or equal to 5%, greater than or equal to 10%, or greater than or equal to 15% weight loss, at 30%, 17%, and 13% for oral roflumilast, compared with 9%, 0%, and 0% for placebo, respectively.
“We saw that the higher baseline weight correlated with the proportion of weight loss, so that the more heavy patients at baseline also were the ones who experienced the greatest weight loss,” said Dr. Egeberg, who is professor of dermatology at the University of Copenhagen and a senior consultant at the department of dermatology at Bispebjerg Hospital, Copenhagen.
A beneficial side effect in psoriasis?
“You may have heard in psoriasis about topical roflumilast, but oral roflumilast is actually also shown to be effective in treating psoriasis,” said Egeberg.
Topical roflumilast is approved in the United States and Canada for treating plaque psoriasis.
Efficacy results from the PSORRO study were published earlier this year and showed a significantly greater improvement in Psoriasis Area and Severity Index (PASI) 75 with oral roflumilast vs. placebo at 12 weeks (35% vs. 0%), with a sustained effect seen at 24 weeks (44% vs. 40%).
Weight loss was among the most common side effects seen, leading Dr. Egeberg and fellow PSORRO investigators to wonder whether this may actually be a beneficial effect in patients with psoriasis.
“Oral roflumilast is actually a drug that has been on the market for quite a number of years,” Dr. Egeberg said.
Although only currently licensed for chronic obstructive pulmonary disease (COPD) in the United States, oral roflumilast, a phosphodiesterase (PDE) 4 inhibitor, is available as a generic, “which also means that it is extremely affordable,” suggested Dr. Edeberg.
Weight loss may be a problem in patients with COPD, he acknowledged; these patients tend to be underweight as a result of their poor state of health caused by the lung condition. Weight loss could be an advantage in patients with psoriasis who are overweight or living with obesity and have poor cardiometabolic parameters.
The psoriasis treatment with oral roflumilast study
The PSORRO study was a phase 2, multicenter, placebo-controlled, randomized trial performed between 2021 and 2022. A total of 46 adults with plaque psoriasis participated; half were initially treated with oral roflumilast and half with placebo.
Treatment was double-blind for the first 12 weeks, with all patients then receiving open-label treatment with roflumilast for 12 weeks.
The primary endpoint was the proportion of patients achieving at least 75% reduction from baseline PASI (PASI75). A host of secondary endpoints were studied, including weight and cardiometabolic parameters, which Dr. Egeberg reported at the EADV meeting.
Looking at the baseline characteristics of the oral roflumilast and placebo groups, the mean age was a respective 38 and 39 years, 65% and 83% were men, and the mean starting body weight was 102 kg and 105.1 kg.
After 12 weeks of treatment, body weight fell by a mean of 5.4 kg in the oral roflumilast group, with a further decrease of 1.4 kg by 24 weeks, bringing the total average weight loss to 6.8 kg. By comparison, weight loss among those in the placebo group was 0 kg at 12 weeks and around 2 kg at 24 weeks.
The majority of participants in both groups had high baseline BMIs; 70% of those who received oral roflumilast and 61% of those who received placebo had a BMI of 30 or higher.
“We wanted to investigate the impact of body weight, [so] we didn’t allow patients to be underweight when they were included,” Dr. Egeberg explained. Thus, for inclusion, patients had to have a BMI of 20 or higher.
An “extraordinary” finding was how some patients’ weight status based on their BMI changed throughout the study.
“We could see people that went from obese class 3, all the way to obese class 1. And we could see people going from being overweight to normal weight, which is really extraordinary for patients with psoriasis,” Dr. Egeberg said.
“But most importantly,” he added, “we didn’t have any patients who became underweight, suggesting that it actually is safe to use also in normal-weight patients.”
Reduced appetite behind benefit?
Trying to see why the weight loss occurred, Dr. Egeberg noted that it looked like it could be a result of a reduced appetite.
In common with other PDE-4 inhibitors, oral roflumilast treatment was associated with gastrointestinal symptoms – nausea, diarrhea, and abdominal pain – but all of these “decrease to placebo levels again, quite quickly,” he said.
“This really suggests that it’s not because of diarrhea, it’s not because of nausea and abdominal pain; it is because of a reduced appetite that patients actually lose weight when treated with roflumilast,” Dr. Egeberg said. It’s a potential bonus for the drug’s effects on the skin and could afford clinicians an opportunity to help motivate patients to eat well when they do eat, he observed.
Other cardiometabolic parameters assessed included blood pressure, glycated hemoglobin, total cholesterol and other key lipids, creatinine, alanine aminotransferase, and high-sensitivity C-reactive protein, but there were no noteworthy differences between the groups.
Roflumilast is an inexpensive drug because it is generic, Dr. Egeberg observed, but that also means that its use is likely to be off-label.
“It will be up to the treating physician to decide if this is an optimal therapy for their patients,” he suggested.
Cardiometabolic comorbidities important to target
Obesity is a cardiometabolic comorbidity that is important to consider when treating your patients with psoriasis, Paolo Gisondi, MD, of the University of Verona (Italy), said at a separate presentation at the EADV meeting.
While not directly commenting on the roflumilast study, he noted that moderate to severe psoriasis was “frequently associated” with metabolic disorders that put people at additional risk for cardiovascular and fatty liver diseases.
The PSORRO study was an investigator-initiated and investigator-led study and received no commercial funding. Research funding came from the Danish Psoriasis Foundation, Herlev and Gentofte Hospital, and several charitable and humanitarian organizations. Dr. Egeberg acknowledged acting as the principal investigator, speaker, and/or consultant to multiple pharma companies, all of which were unrelated to the study he presented. Dr. Gisondi’s comments were from a separate presentation, and he was not involved in the study.
A version of this article first appeared on Medscape.com.
AT THE EADV CONGRESS
MCL Guidelines
Autism spectrum disorders
According to the CDC, the prevalence of autism spectrum disorders (ASD) has gone from roughly 1 in 68 children in 2010 to 1 in 36 children in 2020.1 This is nearly a 50% increase over that 10-year period. Over the last several years, there has been evidence suggesting that increasing numbers of young people with ASD or other neurodivergent conditions identify as transgender or gender diverse.2 Experts agree more careful attention must be paid to these patients.

This includes things such as difficulty with communication, possible concrete thinking, and obsessive interests. While earlier research has shown a higher incidence of ASD in those referred to specialized gender medical clinics, it is important to realize that not all of these youth are seeking medical care. They may be brought to the attention of a primary care pediatrician (PCP) if the child has discussed their gender identity at home. It is important that PCPs approach these young people with an open mind and address any coexisting mental health conditions. PCPs must be careful not to dismiss any gender identity concerns as another of the patient’s “obsessions”; rather, they should ensure the patient receives the appropriate mental health care that they need to explore these concerns. One challenge for PCPs is that there is a dearth of mental health professionals who have experience in working with young people who have both gender dysphoria and a neurodivergent condition.
For those clinicians who provide gender-affirming medical care to these young people, it is imperative that they have a thorough understanding of the patient’s gender identity and medical goals before starting any treatment. This may require extensive collaboration with the patient’s mental health provider. The clinician providing medical care may also choose to proceed slower with the introduction of hormones and their subsequent dosing to allow the young person time to continue discussing their effects with their mental health provider. To help clinicians, Dr. John Strang and a multidisciplinary group of collaborators developed a set of guidelines for co-occurring ASD and gender dysphoria in adolescents.3 More recently, Dr. Strang and other collaborators have also developed a questionnaire that can be used by clinicians in the care of these patients.4 The goal of this questionnaire is to allow the young people to “communicate their experiences and needs in a report format attuned to common autistic thinking and communication styles.”
In summary, pediatricians and those who care for children and adolescents need to be aware of the increased association between those with ASD or other neurodivergent conditions and gender dysphoria. To ensure that these young people receive optimal care, it is important to connect them to experts (if possible) in coexisting ASD and gender dysphoria. If such experts are not readily available, the National LGBTQIA+ Health Education Center has developed a resource for providing an affirmative approach to care for these young people.5 While more research is needed to better understand young people with coexisting ASD (or other neurodivergent conditions), taking an individualized approach to their care can help ensure optimal outcomes.
Dr. Cooper is assistant professor of pediatrics at University of Texas Southwestern, Dallas, and an adolescent medicine specialist at Children’s Medical Center Dallas.
References
1. Data & Statistics on Autism Spectrum Disorder. https://www.cdc.gov/ncbddd/autism/data.html.
2. Glidden D et al. Gender dysphoria and autism spectrum disorder: A systematic review of the literature. Sex Med Rev. 2016;4(1):3-14. doi:10.1016/j.sxmr.2015.10.003.
3. Strang JF et al. Initial clinical guidelines for co-occurring autism spectrum disorder and gender dysphoria or incongruence in adolescents. J Clin Child Adolesc Psychol. 2018;47(1):105-15. doi:10.1080/15374416.2016.1228462.
4. Strang JF et. al. The Gender-Diversity and Autism Questionnaire: A Community-Developed Clinical, Research, and Self-Advocacy Tool for Autistic Transgender and Gender-Diverse Young Adults. Autism Adulthood. 2023 Jun 1;5(2):175-90. doi: 10.1089/aut.2023.0002.
5. National LGBT Health Education Center. Neurodiversity & gender-diverse youth: An affirming approach to care 2020. https://www.lgbtqiahealtheducation.org/publication/neurodiversity-gender-diverse-youth-an-affirming-approach-to-care-2020/download
According to the CDC, the prevalence of autism spectrum disorders (ASD) has gone from roughly 1 in 68 children in 2010 to 1 in 36 children in 2020.1 This is nearly a 50% increase over that 10-year period. Over the last several years, there has been evidence suggesting that increasing numbers of young people with ASD or other neurodivergent conditions identify as transgender or gender diverse.2 Experts agree more careful attention must be paid to these patients.
This includes things such as difficulty with communication, possible concrete thinking, and obsessive interests. While earlier research has shown a higher incidence of ASD in those referred to specialized gender medical clinics, it is important to realize that not all of these youth are seeking medical care. They may be brought to the attention of a primary care pediatrician (PCP) if the child has discussed their gender identity at home. It is important that PCPs approach these young people with an open mind and address any coexisting mental health conditions. PCPs must be careful not to dismiss any gender identity concerns as another of the patient’s “obsessions”; rather, they should ensure the patient receives the appropriate mental health care that they need to explore these concerns. One challenge for PCPs is that there is a dearth of mental health professionals who have experience in working with young people who have both gender dysphoria and a neurodivergent condition.
For those clinicians who provide gender-affirming medical care to these young people, it is imperative that they have a thorough understanding of the patient’s gender identity and medical goals before starting any treatment. This may require extensive collaboration with the patient’s mental health provider. The clinician providing medical care may also choose to proceed slower with the introduction of hormones and their subsequent dosing to allow the young person time to continue discussing their effects with their mental health provider. To help clinicians, Dr. John Strang and a multidisciplinary group of collaborators developed a set of guidelines for co-occurring ASD and gender dysphoria in adolescents.3 More recently, Dr. Strang and other collaborators have also developed a questionnaire that can be used by clinicians in the care of these patients.4 The goal of this questionnaire is to allow the young people to “communicate their experiences and needs in a report format attuned to common autistic thinking and communication styles.”
In summary, pediatricians and those who care for children and adolescents need to be aware of the increased association between those with ASD or other neurodivergent conditions and gender dysphoria. To ensure that these young people receive optimal care, it is important to connect them to experts (if possible) in coexisting ASD and gender dysphoria. If such experts are not readily available, the National LGBTQIA+ Health Education Center has developed a resource for providing an affirmative approach to care for these young people.5 While more research is needed to better understand young people with coexisting ASD (or other neurodivergent conditions), taking an individualized approach to their care can help ensure optimal outcomes.
Dr. Cooper is assistant professor of pediatrics at University of Texas Southwestern, Dallas, and an adolescent medicine specialist at Children’s Medical Center Dallas.
References
1. Data & Statistics on Autism Spectrum Disorder. https://www.cdc.gov/ncbddd/autism/data.html.
2. Glidden D et al. Gender dysphoria and autism spectrum disorder: A systematic review of the literature. Sex Med Rev. 2016;4(1):3-14. doi:10.1016/j.sxmr.2015.10.003.
3. Strang JF et al. Initial clinical guidelines for co-occurring autism spectrum disorder and gender dysphoria or incongruence in adolescents. J Clin Child Adolesc Psychol. 2018;47(1):105-15. doi:10.1080/15374416.2016.1228462.
4. Strang JF et. al. The Gender-Diversity and Autism Questionnaire: A Community-Developed Clinical, Research, and Self-Advocacy Tool for Autistic Transgender and Gender-Diverse Young Adults. Autism Adulthood. 2023 Jun 1;5(2):175-90. doi: 10.1089/aut.2023.0002.
5. National LGBT Health Education Center. Neurodiversity & gender-diverse youth: An affirming approach to care 2020. https://www.lgbtqiahealtheducation.org/publication/neurodiversity-gender-diverse-youth-an-affirming-approach-to-care-2020/download
According to the CDC, the prevalence of autism spectrum disorders (ASD) has gone from roughly 1 in 68 children in 2010 to 1 in 36 children in 2020.1 This is nearly a 50% increase over that 10-year period. Over the last several years, there has been evidence suggesting that increasing numbers of young people with ASD or other neurodivergent conditions identify as transgender or gender diverse.2 Experts agree more careful attention must be paid to these patients.
This includes things such as difficulty with communication, possible concrete thinking, and obsessive interests. While earlier research has shown a higher incidence of ASD in those referred to specialized gender medical clinics, it is important to realize that not all of these youth are seeking medical care. They may be brought to the attention of a primary care pediatrician (PCP) if the child has discussed their gender identity at home. It is important that PCPs approach these young people with an open mind and address any coexisting mental health conditions. PCPs must be careful not to dismiss any gender identity concerns as another of the patient’s “obsessions”; rather, they should ensure the patient receives the appropriate mental health care that they need to explore these concerns. One challenge for PCPs is that there is a dearth of mental health professionals who have experience in working with young people who have both gender dysphoria and a neurodivergent condition.
For those clinicians who provide gender-affirming medical care to these young people, it is imperative that they have a thorough understanding of the patient’s gender identity and medical goals before starting any treatment. This may require extensive collaboration with the patient’s mental health provider. The clinician providing medical care may also choose to proceed slower with the introduction of hormones and their subsequent dosing to allow the young person time to continue discussing their effects with their mental health provider. To help clinicians, Dr. John Strang and a multidisciplinary group of collaborators developed a set of guidelines for co-occurring ASD and gender dysphoria in adolescents.3 More recently, Dr. Strang and other collaborators have also developed a questionnaire that can be used by clinicians in the care of these patients.4 The goal of this questionnaire is to allow the young people to “communicate their experiences and needs in a report format attuned to common autistic thinking and communication styles.”
In summary, pediatricians and those who care for children and adolescents need to be aware of the increased association between those with ASD or other neurodivergent conditions and gender dysphoria. To ensure that these young people receive optimal care, it is important to connect them to experts (if possible) in coexisting ASD and gender dysphoria. If such experts are not readily available, the National LGBTQIA+ Health Education Center has developed a resource for providing an affirmative approach to care for these young people.5 While more research is needed to better understand young people with coexisting ASD (or other neurodivergent conditions), taking an individualized approach to their care can help ensure optimal outcomes.
Dr. Cooper is assistant professor of pediatrics at University of Texas Southwestern, Dallas, and an adolescent medicine specialist at Children’s Medical Center Dallas.
References
1. Data & Statistics on Autism Spectrum Disorder. https://www.cdc.gov/ncbddd/autism/data.html.
2. Glidden D et al. Gender dysphoria and autism spectrum disorder: A systematic review of the literature. Sex Med Rev. 2016;4(1):3-14. doi:10.1016/j.sxmr.2015.10.003.
3. Strang JF et al. Initial clinical guidelines for co-occurring autism spectrum disorder and gender dysphoria or incongruence in adolescents. J Clin Child Adolesc Psychol. 2018;47(1):105-15. doi:10.1080/15374416.2016.1228462.
4. Strang JF et. al. The Gender-Diversity and Autism Questionnaire: A Community-Developed Clinical, Research, and Self-Advocacy Tool for Autistic Transgender and Gender-Diverse Young Adults. Autism Adulthood. 2023 Jun 1;5(2):175-90. doi: 10.1089/aut.2023.0002.
5. National LGBT Health Education Center. Neurodiversity & gender-diverse youth: An affirming approach to care 2020. https://www.lgbtqiahealtheducation.org/publication/neurodiversity-gender-diverse-youth-an-affirming-approach-to-care-2020/download
New tool to guide transcatheter aortic valve replacement
TOPLINE:
, results of a new study suggest.
Researchers developed TJ-ICE–guided TAVR to facilitate implanting a heart valve at an optimal depth, guided by direct visualization of the membranous septum (MS) during the procedure.
METHODOLOGY:
- The single-center study included 163 patients with severe aortic stenosis (AS) from an ongoing registry, mean age 85 years, 71% women, and median Society of Thoracic Surgeons score of 6.3%, who underwent TAVR.
- The primary endpoint was the incidence at 30 days of PPMI; secondary endpoints included the feasibility of TJ-ICE–guided TAVR and safety, including complications related to TJ-ICE.
TAKEAWAY:
- Although all patients underwent valve placement in the proper anatomical location, moderate paravalvular leakage (PVL) occurred in four patients, and a second valve was required in two patients, resulting in a device success of 96.3%.
- New PPMI within 30 days was required in 11 patients (6.7%), all because of complete atrioventricular block; patients with baseline right bundle branch block (RBBB) had a higher incidence of new PPMI than did those without RBBB (23.8% vs. 4.2%; P < .001).
- Patients whose device was implanted inside the MS had a significantly lower incidence of new PPMI (overall 2.1% vs. 13.4%; P = .005); this finding was consistent in patients with baseline RBBB (6.7% vs. 66.7%; P = .004) or without RBBB (1.2% vs. 8.2%; P = .041).
- By 30 days, there was one death, which occurred as a result of bleeding in a patient with liver cirrhosis after a successful TAVR procedure; four patients experienced disabling strokes, and vascular complications developed in 16 patients.
IN PRACTICE:
The study demonstrated the “notable feasibility and safety” of TJ-ICE–guided TAVR, the authors write. They point to the “strong association of TAV position with new PPMI rate, which was clearly visualized by ICE during the procedure.”
In an accompanying editorial, Thomas Bartel, MD, PHD, Flexdoc Inc., Düsseldorf, Germany, noted that the study is the first to report a clinical benefit using a TJ-ICE approach, although barriers such as cost and lack of expertise could prevent interventional cardiologists from taking full advantage of ICE monitoring during TAVR, and further research is warranted.
Randomized and prospective trials comparing the accuracy, reproducibility, and outcomes of ICE guidance vs. guidance by transesophageal echocardiography, and pure fluoroscopy and angiography, “need to be performed before ICE imaging is adopted as the primary nonradiographic imaging modality for TAVR.”
SOURCE:
The study was carried out by Tsutomu Murakami, MD, department of cardiology, Tokai University, Isehara, Japan, and colleagues. It was published online in JACC: Asia.
LIMITATIONS:
The retrospective nonrandomized design has inherent limitations. The choice of intraprocedural imaging modality was decided based on heart team discussion, which may have introduced selection bias. Operators’ implantation skills could have influenced the results although most cases involved highly experienced board-certified operators. The limited number of subjects and the relatively low event rates preclude definitive conclusions.
DISCLOSURES:
Dr. Murakami has no relevant conflicts of interest; see paper for disclosures of other study authors. Dr. Bartel has no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
, results of a new study suggest.
Researchers developed TJ-ICE–guided TAVR to facilitate implanting a heart valve at an optimal depth, guided by direct visualization of the membranous septum (MS) during the procedure.
METHODOLOGY:
- The single-center study included 163 patients with severe aortic stenosis (AS) from an ongoing registry, mean age 85 years, 71% women, and median Society of Thoracic Surgeons score of 6.3%, who underwent TAVR.
- The primary endpoint was the incidence at 30 days of PPMI; secondary endpoints included the feasibility of TJ-ICE–guided TAVR and safety, including complications related to TJ-ICE.
TAKEAWAY:
- Although all patients underwent valve placement in the proper anatomical location, moderate paravalvular leakage (PVL) occurred in four patients, and a second valve was required in two patients, resulting in a device success of 96.3%.
- New PPMI within 30 days was required in 11 patients (6.7%), all because of complete atrioventricular block; patients with baseline right bundle branch block (RBBB) had a higher incidence of new PPMI than did those without RBBB (23.8% vs. 4.2%; P < .001).
- Patients whose device was implanted inside the MS had a significantly lower incidence of new PPMI (overall 2.1% vs. 13.4%; P = .005); this finding was consistent in patients with baseline RBBB (6.7% vs. 66.7%; P = .004) or without RBBB (1.2% vs. 8.2%; P = .041).
- By 30 days, there was one death, which occurred as a result of bleeding in a patient with liver cirrhosis after a successful TAVR procedure; four patients experienced disabling strokes, and vascular complications developed in 16 patients.
IN PRACTICE:
The study demonstrated the “notable feasibility and safety” of TJ-ICE–guided TAVR, the authors write. They point to the “strong association of TAV position with new PPMI rate, which was clearly visualized by ICE during the procedure.”
In an accompanying editorial, Thomas Bartel, MD, PHD, Flexdoc Inc., Düsseldorf, Germany, noted that the study is the first to report a clinical benefit using a TJ-ICE approach, although barriers such as cost and lack of expertise could prevent interventional cardiologists from taking full advantage of ICE monitoring during TAVR, and further research is warranted.
Randomized and prospective trials comparing the accuracy, reproducibility, and outcomes of ICE guidance vs. guidance by transesophageal echocardiography, and pure fluoroscopy and angiography, “need to be performed before ICE imaging is adopted as the primary nonradiographic imaging modality for TAVR.”
SOURCE:
The study was carried out by Tsutomu Murakami, MD, department of cardiology, Tokai University, Isehara, Japan, and colleagues. It was published online in JACC: Asia.
LIMITATIONS:
The retrospective nonrandomized design has inherent limitations. The choice of intraprocedural imaging modality was decided based on heart team discussion, which may have introduced selection bias. Operators’ implantation skills could have influenced the results although most cases involved highly experienced board-certified operators. The limited number of subjects and the relatively low event rates preclude definitive conclusions.
DISCLOSURES:
Dr. Murakami has no relevant conflicts of interest; see paper for disclosures of other study authors. Dr. Bartel has no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
, results of a new study suggest.
Researchers developed TJ-ICE–guided TAVR to facilitate implanting a heart valve at an optimal depth, guided by direct visualization of the membranous septum (MS) during the procedure.
METHODOLOGY:
- The single-center study included 163 patients with severe aortic stenosis (AS) from an ongoing registry, mean age 85 years, 71% women, and median Society of Thoracic Surgeons score of 6.3%, who underwent TAVR.
- The primary endpoint was the incidence at 30 days of PPMI; secondary endpoints included the feasibility of TJ-ICE–guided TAVR and safety, including complications related to TJ-ICE.
TAKEAWAY:
- Although all patients underwent valve placement in the proper anatomical location, moderate paravalvular leakage (PVL) occurred in four patients, and a second valve was required in two patients, resulting in a device success of 96.3%.
- New PPMI within 30 days was required in 11 patients (6.7%), all because of complete atrioventricular block; patients with baseline right bundle branch block (RBBB) had a higher incidence of new PPMI than did those without RBBB (23.8% vs. 4.2%; P < .001).
- Patients whose device was implanted inside the MS had a significantly lower incidence of new PPMI (overall 2.1% vs. 13.4%; P = .005); this finding was consistent in patients with baseline RBBB (6.7% vs. 66.7%; P = .004) or without RBBB (1.2% vs. 8.2%; P = .041).
- By 30 days, there was one death, which occurred as a result of bleeding in a patient with liver cirrhosis after a successful TAVR procedure; four patients experienced disabling strokes, and vascular complications developed in 16 patients.
IN PRACTICE:
The study demonstrated the “notable feasibility and safety” of TJ-ICE–guided TAVR, the authors write. They point to the “strong association of TAV position with new PPMI rate, which was clearly visualized by ICE during the procedure.”
In an accompanying editorial, Thomas Bartel, MD, PHD, Flexdoc Inc., Düsseldorf, Germany, noted that the study is the first to report a clinical benefit using a TJ-ICE approach, although barriers such as cost and lack of expertise could prevent interventional cardiologists from taking full advantage of ICE monitoring during TAVR, and further research is warranted.
Randomized and prospective trials comparing the accuracy, reproducibility, and outcomes of ICE guidance vs. guidance by transesophageal echocardiography, and pure fluoroscopy and angiography, “need to be performed before ICE imaging is adopted as the primary nonradiographic imaging modality for TAVR.”
SOURCE:
The study was carried out by Tsutomu Murakami, MD, department of cardiology, Tokai University, Isehara, Japan, and colleagues. It was published online in JACC: Asia.
LIMITATIONS:
The retrospective nonrandomized design has inherent limitations. The choice of intraprocedural imaging modality was decided based on heart team discussion, which may have introduced selection bias. Operators’ implantation skills could have influenced the results although most cases involved highly experienced board-certified operators. The limited number of subjects and the relatively low event rates preclude definitive conclusions.
DISCLOSURES:
Dr. Murakami has no relevant conflicts of interest; see paper for disclosures of other study authors. Dr. Bartel has no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Novel triple-threat approach to acne beats placebo
TOPLINE:
A topical fixed-dose combination of three approved acne treatments significantly improves moderate to severe acne with a strong safety profile.
METHODOLOGY:
- The two multicenter studies included 363 individuals aged 9 years and older with moderate to severe acne from 30 centers, including 15 in North America.
- Moderate to severe acne was defined as having 30-100 inflammatory lesions (papules, pustules, or nodules), 35-150 noninflammatory lesions (open or closed comedones), and at least two nodules.
- Participants were randomly assigned to receive treatment with a combination gel containing phosphate 1.2%, 0.15%, and 3.1% (known as IDP-126) or a vehicle gel for once-daily application for 12 weeks.
- Treatment success was defined as a reduction of at least two grades from baseline on the Evaluator’s Global Severity Score (EGSS) and lesion counts of clear (0) or almost clear (1) at weeks 2, 4, 8, and 12.
TAKEAWAY:
- Treatment success occurred in 49.6% of the IDP-126 group, vs 24.9% of the vehicle group in study 1, and in 50.5% of the IDP-126 group, vs 20.5% of the vehicle group in study 2. Overall treatment compliance was 93.7% and 91.3% for studies 1 and 2, respectively (P < .01 for both).
- Patients in the IDP-126 groups for both studies 1 and 2 had significantly greater absolute mean reductions in both inflammatory and noninflammatory lesions from baseline to week 12 compared to the vehicle patients (P ≤ .001 for all).
- Significantly more patients in the IDP-126 group achieved a grade reduction of 2 or more in EGSS compared with those who received the vehicle, with treatment differences of approximately 32% in both studies. Changes in lesion reductions between the treatment and the vehicle groups were significantly greater as early as week 4.
- The most common treatment-related adverse events among patients treated with IDP-126 were erythema, application-site pain, dryness, irritation, and exfoliation. Discontinuation of the study drug as a result of adverse events occurred in 2.5% and 3.3% of these patients in studies 1 and 2, respectively.
IN PRACTICE:
“With its simple treatment regimen containing 3 recommended acne treatments (benzoyl peroxide, a topical retinoid, and a topical antibiotic), IDP-126 is a potential new treatment option for acne,” the researchers concluded.
SOURCE:
The study was led by Linda Stein Gold, MD, of Henry Ford Hospital, Detroit. The study was published online in the Journal of the American Academy of Dermatology.
LIMITATIONS:
In both studies, treatment duration was short, and the studies may not reflect patients’ real-world experiences. The results may be affected by interobserver bias or variation in assessment of acne severity.
DISCLOSURES:
Gold has served as investigator/consultant or speaker for Ortho Dermatologics, LEO Pharma, Dermavant, Incyte, Novartis, AbbVie, Pfizer, Sun Pharma, UCB, Arcutis, and Lilly. Other study coauthors have relationships with multiple companies, including Ortho Dermatologics, which provided medical writing support for the study.
A version of this article first appeared on Medscape.com.
TOPLINE:
A topical fixed-dose combination of three approved acne treatments significantly improves moderate to severe acne with a strong safety profile.
METHODOLOGY:
- The two multicenter studies included 363 individuals aged 9 years and older with moderate to severe acne from 30 centers, including 15 in North America.
- Moderate to severe acne was defined as having 30-100 inflammatory lesions (papules, pustules, or nodules), 35-150 noninflammatory lesions (open or closed comedones), and at least two nodules.
- Participants were randomly assigned to receive treatment with a combination gel containing phosphate 1.2%, 0.15%, and 3.1% (known as IDP-126) or a vehicle gel for once-daily application for 12 weeks.
- Treatment success was defined as a reduction of at least two grades from baseline on the Evaluator’s Global Severity Score (EGSS) and lesion counts of clear (0) or almost clear (1) at weeks 2, 4, 8, and 12.
TAKEAWAY:
- Treatment success occurred in 49.6% of the IDP-126 group, vs 24.9% of the vehicle group in study 1, and in 50.5% of the IDP-126 group, vs 20.5% of the vehicle group in study 2. Overall treatment compliance was 93.7% and 91.3% for studies 1 and 2, respectively (P < .01 for both).
- Patients in the IDP-126 groups for both studies 1 and 2 had significantly greater absolute mean reductions in both inflammatory and noninflammatory lesions from baseline to week 12 compared to the vehicle patients (P ≤ .001 for all).
- Significantly more patients in the IDP-126 group achieved a grade reduction of 2 or more in EGSS compared with those who received the vehicle, with treatment differences of approximately 32% in both studies. Changes in lesion reductions between the treatment and the vehicle groups were significantly greater as early as week 4.
- The most common treatment-related adverse events among patients treated with IDP-126 were erythema, application-site pain, dryness, irritation, and exfoliation. Discontinuation of the study drug as a result of adverse events occurred in 2.5% and 3.3% of these patients in studies 1 and 2, respectively.
IN PRACTICE:
“With its simple treatment regimen containing 3 recommended acne treatments (benzoyl peroxide, a topical retinoid, and a topical antibiotic), IDP-126 is a potential new treatment option for acne,” the researchers concluded.
SOURCE:
The study was led by Linda Stein Gold, MD, of Henry Ford Hospital, Detroit. The study was published online in the Journal of the American Academy of Dermatology.
LIMITATIONS:
In both studies, treatment duration was short, and the studies may not reflect patients’ real-world experiences. The results may be affected by interobserver bias or variation in assessment of acne severity.
DISCLOSURES:
Gold has served as investigator/consultant or speaker for Ortho Dermatologics, LEO Pharma, Dermavant, Incyte, Novartis, AbbVie, Pfizer, Sun Pharma, UCB, Arcutis, and Lilly. Other study coauthors have relationships with multiple companies, including Ortho Dermatologics, which provided medical writing support for the study.
A version of this article first appeared on Medscape.com.
TOPLINE:
A topical fixed-dose combination of three approved acne treatments significantly improves moderate to severe acne with a strong safety profile.
METHODOLOGY:
- The two multicenter studies included 363 individuals aged 9 years and older with moderate to severe acne from 30 centers, including 15 in North America.
- Moderate to severe acne was defined as having 30-100 inflammatory lesions (papules, pustules, or nodules), 35-150 noninflammatory lesions (open or closed comedones), and at least two nodules.
- Participants were randomly assigned to receive treatment with a combination gel containing phosphate 1.2%, 0.15%, and 3.1% (known as IDP-126) or a vehicle gel for once-daily application for 12 weeks.
- Treatment success was defined as a reduction of at least two grades from baseline on the Evaluator’s Global Severity Score (EGSS) and lesion counts of clear (0) or almost clear (1) at weeks 2, 4, 8, and 12.
TAKEAWAY:
- Treatment success occurred in 49.6% of the IDP-126 group, vs 24.9% of the vehicle group in study 1, and in 50.5% of the IDP-126 group, vs 20.5% of the vehicle group in study 2. Overall treatment compliance was 93.7% and 91.3% for studies 1 and 2, respectively (P < .01 for both).
- Patients in the IDP-126 groups for both studies 1 and 2 had significantly greater absolute mean reductions in both inflammatory and noninflammatory lesions from baseline to week 12 compared to the vehicle patients (P ≤ .001 for all).
- Significantly more patients in the IDP-126 group achieved a grade reduction of 2 or more in EGSS compared with those who received the vehicle, with treatment differences of approximately 32% in both studies. Changes in lesion reductions between the treatment and the vehicle groups were significantly greater as early as week 4.
- The most common treatment-related adverse events among patients treated with IDP-126 were erythema, application-site pain, dryness, irritation, and exfoliation. Discontinuation of the study drug as a result of adverse events occurred in 2.5% and 3.3% of these patients in studies 1 and 2, respectively.
IN PRACTICE:
“With its simple treatment regimen containing 3 recommended acne treatments (benzoyl peroxide, a topical retinoid, and a topical antibiotic), IDP-126 is a potential new treatment option for acne,” the researchers concluded.
SOURCE:
The study was led by Linda Stein Gold, MD, of Henry Ford Hospital, Detroit. The study was published online in the Journal of the American Academy of Dermatology.
LIMITATIONS:
In both studies, treatment duration was short, and the studies may not reflect patients’ real-world experiences. The results may be affected by interobserver bias or variation in assessment of acne severity.
DISCLOSURES:
Gold has served as investigator/consultant or speaker for Ortho Dermatologics, LEO Pharma, Dermavant, Incyte, Novartis, AbbVie, Pfizer, Sun Pharma, UCB, Arcutis, and Lilly. Other study coauthors have relationships with multiple companies, including Ortho Dermatologics, which provided medical writing support for the study.
A version of this article first appeared on Medscape.com.
Antibiotics ‘like gold’ for some, driving inappropriate use
Personal beliefs and health care system barriers contribute to inappropriate antibiotic use by patients, report researchers presenting results at an annual scientific meeting on infectious diseases.
Nonprescription antibiotic use includes accessing medication left over from a prior prescribed course, obtained from social networks, and purchased over-the-counter in other countries or illegally in stores and markets in the United States.
Overuse and misuse of antibiotics contributes to a growing threat of antimicrobial resistance, and it is tough to say how common it is, Lindsey A. Laytner, PhD, MPH, with Baylor College of Medicine, Houston, pointed out in her presentation.
“This is an understudied area. We don’t routinely collect these data, so we don’t actually know what the true prevalence is. The factors that contribute to this unsafe practice in the U.S. are also underexplored,” Dr. Laytner said.
To investigate, the researchers conducted in-depth interviews with 86 adults (median age, 49 years; 62% women) to identify patients’ motivations to use antibiotics without a prescription. All of them answered “yes” when asked in a previous survey whether they would use antibiotics without contacting a doctor, nurse, dentist, or clinic.
Dr. Laytner said several prominent themes emerged.
Nearly all interviewees reported nonprescription antibiotic use for symptoms that mostly do not warrant antibiotics. These included symptoms of COVID-19, influenza, and the common cold, as well as for pain management, allergies, and even wounds.
Ineffectively treating symptoms
Many felt they “knew their body, knew what they had, and knew how to treat themselves” without a health care provider, Dr. Laytner said.
They also felt the over-the-counter medicines “don’t always work and that antibiotics are like gold or this cure-all and because they are difficult to get a prescription for, they should be kept on hand,” she explained.
A variety of health care system barriers also contribute to inappropriate antibiotic use, including long wait times to schedule appointments and to see the doctor while at their appointments; high costs for clinic visits and prescriptions; and transportation issues.
Many patients opted to use nonprescription antibiotics out of “convenience,” Laytner added.
She explains that the findings could help inform community-level education efforts on inappropriate use of antibiotics and help shape policies to promote antibiotic stewardship.
Access to care, education
Commenting on the study, Emily Sydnor Spivak, MD, associate professor of medicine at University of Utah, Salt Lake City, said she “wasn’t totally surprised by the results, but found it very interesting how there was a theme of autonomy, or ‘I know my body,’ that seemed to drive patients to get antibiotics for relief of symptoms.”
said Dr. Spivak, who is also medical director of antimicrobial stewardship programs at University of Utah Health and VA Salt Lake City Health Care System.
“Given the lack of access to health care as a reason some patients use nonprescription antibiotics, we need to think about access to the health care system and process changes and policy changes to allow better access. Without better access or interaction with the health care system, we can’t educate patients,” Dr. Spivak said.
The study had no commercial funding. Dr. Laytner and Dr. Spivak report no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
Personal beliefs and health care system barriers contribute to inappropriate antibiotic use by patients, report researchers presenting results at an annual scientific meeting on infectious diseases.
Nonprescription antibiotic use includes accessing medication left over from a prior prescribed course, obtained from social networks, and purchased over-the-counter in other countries or illegally in stores and markets in the United States.
Overuse and misuse of antibiotics contributes to a growing threat of antimicrobial resistance, and it is tough to say how common it is, Lindsey A. Laytner, PhD, MPH, with Baylor College of Medicine, Houston, pointed out in her presentation.
“This is an understudied area. We don’t routinely collect these data, so we don’t actually know what the true prevalence is. The factors that contribute to this unsafe practice in the U.S. are also underexplored,” Dr. Laytner said.
To investigate, the researchers conducted in-depth interviews with 86 adults (median age, 49 years; 62% women) to identify patients’ motivations to use antibiotics without a prescription. All of them answered “yes” when asked in a previous survey whether they would use antibiotics without contacting a doctor, nurse, dentist, or clinic.
Dr. Laytner said several prominent themes emerged.
Nearly all interviewees reported nonprescription antibiotic use for symptoms that mostly do not warrant antibiotics. These included symptoms of COVID-19, influenza, and the common cold, as well as for pain management, allergies, and even wounds.
Ineffectively treating symptoms
Many felt they “knew their body, knew what they had, and knew how to treat themselves” without a health care provider, Dr. Laytner said.
They also felt the over-the-counter medicines “don’t always work and that antibiotics are like gold or this cure-all and because they are difficult to get a prescription for, they should be kept on hand,” she explained.
A variety of health care system barriers also contribute to inappropriate antibiotic use, including long wait times to schedule appointments and to see the doctor while at their appointments; high costs for clinic visits and prescriptions; and transportation issues.
Many patients opted to use nonprescription antibiotics out of “convenience,” Laytner added.
She explains that the findings could help inform community-level education efforts on inappropriate use of antibiotics and help shape policies to promote antibiotic stewardship.
Access to care, education
Commenting on the study, Emily Sydnor Spivak, MD, associate professor of medicine at University of Utah, Salt Lake City, said she “wasn’t totally surprised by the results, but found it very interesting how there was a theme of autonomy, or ‘I know my body,’ that seemed to drive patients to get antibiotics for relief of symptoms.”
said Dr. Spivak, who is also medical director of antimicrobial stewardship programs at University of Utah Health and VA Salt Lake City Health Care System.
“Given the lack of access to health care as a reason some patients use nonprescription antibiotics, we need to think about access to the health care system and process changes and policy changes to allow better access. Without better access or interaction with the health care system, we can’t educate patients,” Dr. Spivak said.
The study had no commercial funding. Dr. Laytner and Dr. Spivak report no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
Personal beliefs and health care system barriers contribute to inappropriate antibiotic use by patients, report researchers presenting results at an annual scientific meeting on infectious diseases.
Nonprescription antibiotic use includes accessing medication left over from a prior prescribed course, obtained from social networks, and purchased over-the-counter in other countries or illegally in stores and markets in the United States.
Overuse and misuse of antibiotics contributes to a growing threat of antimicrobial resistance, and it is tough to say how common it is, Lindsey A. Laytner, PhD, MPH, with Baylor College of Medicine, Houston, pointed out in her presentation.
“This is an understudied area. We don’t routinely collect these data, so we don’t actually know what the true prevalence is. The factors that contribute to this unsafe practice in the U.S. are also underexplored,” Dr. Laytner said.
To investigate, the researchers conducted in-depth interviews with 86 adults (median age, 49 years; 62% women) to identify patients’ motivations to use antibiotics without a prescription. All of them answered “yes” when asked in a previous survey whether they would use antibiotics without contacting a doctor, nurse, dentist, or clinic.
Dr. Laytner said several prominent themes emerged.
Nearly all interviewees reported nonprescription antibiotic use for symptoms that mostly do not warrant antibiotics. These included symptoms of COVID-19, influenza, and the common cold, as well as for pain management, allergies, and even wounds.
Ineffectively treating symptoms
Many felt they “knew their body, knew what they had, and knew how to treat themselves” without a health care provider, Dr. Laytner said.
They also felt the over-the-counter medicines “don’t always work and that antibiotics are like gold or this cure-all and because they are difficult to get a prescription for, they should be kept on hand,” she explained.
A variety of health care system barriers also contribute to inappropriate antibiotic use, including long wait times to schedule appointments and to see the doctor while at their appointments; high costs for clinic visits and prescriptions; and transportation issues.
Many patients opted to use nonprescription antibiotics out of “convenience,” Laytner added.
She explains that the findings could help inform community-level education efforts on inappropriate use of antibiotics and help shape policies to promote antibiotic stewardship.
Access to care, education
Commenting on the study, Emily Sydnor Spivak, MD, associate professor of medicine at University of Utah, Salt Lake City, said she “wasn’t totally surprised by the results, but found it very interesting how there was a theme of autonomy, or ‘I know my body,’ that seemed to drive patients to get antibiotics for relief of symptoms.”
said Dr. Spivak, who is also medical director of antimicrobial stewardship programs at University of Utah Health and VA Salt Lake City Health Care System.
“Given the lack of access to health care as a reason some patients use nonprescription antibiotics, we need to think about access to the health care system and process changes and policy changes to allow better access. Without better access or interaction with the health care system, we can’t educate patients,” Dr. Spivak said.
The study had no commercial funding. Dr. Laytner and Dr. Spivak report no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
IDWEEK 2023
Trading one’s eggs for a service discount raises tough issues, says ethicist
This transcript has been edited for clarity.
I had a case come to me of a 32-year-old resident who works in a hospital near where I am and was very interested in freezing her eggs. She wasn’t married and was getting worried that maybe she wouldn’t have a partner soon. She was also getting worried that the potential ability of her eggs to be fertilized would begin to decline, which is a phenomenon that does occur with age. She thought, I’m 32; maybe I should freeze my eggs now, as it’s better than to try freezing them when I’m 35 or 37. The potency may be far less.
There are many programs out there now. There have been academic programs for a long time that have been doing egg freezing, and there are many children who have been born successfully. However, it’s also true that people freeze their eggs when they’re 40 years old, and the likelihood of their “working,” if you will, is far less. I wouldn’t say it’s impossible, but age matters. This medical resident knew that and she decided to look into egg freezing.
Well, it turned out that egg freezing is not something that her student insurance plan – or most insurance plans in general – covers. The opportunity to do this is probably going to cost her about $10,000. There are many new egg-freezing infertility programs that have stared up that aren’t part of hospitals. There are clinics that are run for profit. They sometimes encourage women to freeze their eggs.
The student resident quickly found out that there were companies near her who would do egg freezing but would cut a deal if she agreed to take drugs to super-ovulate, make a large number of eggs, and they would be procured if she agreed to give half of them to other women who needed eggs for their infertility treatment. She could keep half and she could get very discounted treatment of egg freezing.
That may be a deal that she’s going to accept. She doesn’t have a path forward. She’s worried about freezing her eggs right now. But there are many ethical considerations that really have to be thought through here.
First and foremost, she’s giving eggs to others. They’re going to use them to try to make children. They can’t make their own eggs, for some reason. She’s going to have some biologically related kids out there. It used to be that you could say to someone who donated sperm or eggs that this will be anonymous.
But in today’s day and age with 23andMe, Ancestry, and better genetic testing, there’s a pretty good likelihood that somebody is going to find out that the person they thought was their biological mom isn’t, and they have someone out there who was the person who, in this case, donated an egg.
Is she willing to risk having that connection, that contact, to have someone enter her life in the future? It’s a situation where she’s donating the eggs, but I’ll tell you that the clinic is going to make far more money using the donated eggs, probably getting $10,000 or $15,000 a cycle with people who are trying to have a child. They’ll make much more money than she’s going to get by donating.
She may get a $5,000 discount, if you will, but the clinic has a business interest. The more they get women involved in bartering their eggs, the more they’re going to profit. In a sense, she’s being coerced, perhaps – I’m going to put it glibly – to sell cheaply. She probably is getting undervalue, even though she needs a path to do this egg freezing.
The other big issue is that we don’t know that egg freezing is going to work for her until someone tries to use those eggs. She may have her own infertility problem not due to age but to other things. Approximately 8%-9% of couples do have infertility problems, sometimes related to gametes. She may never get a partner. Maybe she doesn’t want to use these eggs on her own as a single mom. All of these issues have to be talked through.
What really troubles me here is not so much that someone would choose to barter their eggs, but that they don’t get counseling. They don’t get independent advice about thinking this all through. It’s turning into a business. A business has a commodity – her eggs – that they want. She’s getting more and more desperate, willing to cut a deal to get where she needs to be, but perhaps is not really thinking through all of the ethical dimensions that bartering or trading one’s eggs in order to gain access to freezing entails.
We have to set up a system where there’s independent advice and independent counseling; otherwise, I think we’re closer to exploitation.
A version of this article first appeared on Medscape.com.
Dr. Caplan is director, division of medical ethics, New York University Langone Medical Center, New York. He has served as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use.
This transcript has been edited for clarity.
I had a case come to me of a 32-year-old resident who works in a hospital near where I am and was very interested in freezing her eggs. She wasn’t married and was getting worried that maybe she wouldn’t have a partner soon. She was also getting worried that the potential ability of her eggs to be fertilized would begin to decline, which is a phenomenon that does occur with age. She thought, I’m 32; maybe I should freeze my eggs now, as it’s better than to try freezing them when I’m 35 or 37. The potency may be far less.
There are many programs out there now. There have been academic programs for a long time that have been doing egg freezing, and there are many children who have been born successfully. However, it’s also true that people freeze their eggs when they’re 40 years old, and the likelihood of their “working,” if you will, is far less. I wouldn’t say it’s impossible, but age matters. This medical resident knew that and she decided to look into egg freezing.
Well, it turned out that egg freezing is not something that her student insurance plan – or most insurance plans in general – covers. The opportunity to do this is probably going to cost her about $10,000. There are many new egg-freezing infertility programs that have stared up that aren’t part of hospitals. There are clinics that are run for profit. They sometimes encourage women to freeze their eggs.
The student resident quickly found out that there were companies near her who would do egg freezing but would cut a deal if she agreed to take drugs to super-ovulate, make a large number of eggs, and they would be procured if she agreed to give half of them to other women who needed eggs for their infertility treatment. She could keep half and she could get very discounted treatment of egg freezing.
That may be a deal that she’s going to accept. She doesn’t have a path forward. She’s worried about freezing her eggs right now. But there are many ethical considerations that really have to be thought through here.
First and foremost, she’s giving eggs to others. They’re going to use them to try to make children. They can’t make their own eggs, for some reason. She’s going to have some biologically related kids out there. It used to be that you could say to someone who donated sperm or eggs that this will be anonymous.
But in today’s day and age with 23andMe, Ancestry, and better genetic testing, there’s a pretty good likelihood that somebody is going to find out that the person they thought was their biological mom isn’t, and they have someone out there who was the person who, in this case, donated an egg.
Is she willing to risk having that connection, that contact, to have someone enter her life in the future? It’s a situation where she’s donating the eggs, but I’ll tell you that the clinic is going to make far more money using the donated eggs, probably getting $10,000 or $15,000 a cycle with people who are trying to have a child. They’ll make much more money than she’s going to get by donating.
She may get a $5,000 discount, if you will, but the clinic has a business interest. The more they get women involved in bartering their eggs, the more they’re going to profit. In a sense, she’s being coerced, perhaps – I’m going to put it glibly – to sell cheaply. She probably is getting undervalue, even though she needs a path to do this egg freezing.
The other big issue is that we don’t know that egg freezing is going to work for her until someone tries to use those eggs. She may have her own infertility problem not due to age but to other things. Approximately 8%-9% of couples do have infertility problems, sometimes related to gametes. She may never get a partner. Maybe she doesn’t want to use these eggs on her own as a single mom. All of these issues have to be talked through.
What really troubles me here is not so much that someone would choose to barter their eggs, but that they don’t get counseling. They don’t get independent advice about thinking this all through. It’s turning into a business. A business has a commodity – her eggs – that they want. She’s getting more and more desperate, willing to cut a deal to get where she needs to be, but perhaps is not really thinking through all of the ethical dimensions that bartering or trading one’s eggs in order to gain access to freezing entails.
We have to set up a system where there’s independent advice and independent counseling; otherwise, I think we’re closer to exploitation.
A version of this article first appeared on Medscape.com.
Dr. Caplan is director, division of medical ethics, New York University Langone Medical Center, New York. He has served as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use.
This transcript has been edited for clarity.
I had a case come to me of a 32-year-old resident who works in a hospital near where I am and was very interested in freezing her eggs. She wasn’t married and was getting worried that maybe she wouldn’t have a partner soon. She was also getting worried that the potential ability of her eggs to be fertilized would begin to decline, which is a phenomenon that does occur with age. She thought, I’m 32; maybe I should freeze my eggs now, as it’s better than to try freezing them when I’m 35 or 37. The potency may be far less.
There are many programs out there now. There have been academic programs for a long time that have been doing egg freezing, and there are many children who have been born successfully. However, it’s also true that people freeze their eggs when they’re 40 years old, and the likelihood of their “working,” if you will, is far less. I wouldn’t say it’s impossible, but age matters. This medical resident knew that and she decided to look into egg freezing.
Well, it turned out that egg freezing is not something that her student insurance plan – or most insurance plans in general – covers. The opportunity to do this is probably going to cost her about $10,000. There are many new egg-freezing infertility programs that have stared up that aren’t part of hospitals. There are clinics that are run for profit. They sometimes encourage women to freeze their eggs.
The student resident quickly found out that there were companies near her who would do egg freezing but would cut a deal if she agreed to take drugs to super-ovulate, make a large number of eggs, and they would be procured if she agreed to give half of them to other women who needed eggs for their infertility treatment. She could keep half and she could get very discounted treatment of egg freezing.
That may be a deal that she’s going to accept. She doesn’t have a path forward. She’s worried about freezing her eggs right now. But there are many ethical considerations that really have to be thought through here.
First and foremost, she’s giving eggs to others. They’re going to use them to try to make children. They can’t make their own eggs, for some reason. She’s going to have some biologically related kids out there. It used to be that you could say to someone who donated sperm or eggs that this will be anonymous.
But in today’s day and age with 23andMe, Ancestry, and better genetic testing, there’s a pretty good likelihood that somebody is going to find out that the person they thought was their biological mom isn’t, and they have someone out there who was the person who, in this case, donated an egg.
Is she willing to risk having that connection, that contact, to have someone enter her life in the future? It’s a situation where she’s donating the eggs, but I’ll tell you that the clinic is going to make far more money using the donated eggs, probably getting $10,000 or $15,000 a cycle with people who are trying to have a child. They’ll make much more money than she’s going to get by donating.
She may get a $5,000 discount, if you will, but the clinic has a business interest. The more they get women involved in bartering their eggs, the more they’re going to profit. In a sense, she’s being coerced, perhaps – I’m going to put it glibly – to sell cheaply. She probably is getting undervalue, even though she needs a path to do this egg freezing.
The other big issue is that we don’t know that egg freezing is going to work for her until someone tries to use those eggs. She may have her own infertility problem not due to age but to other things. Approximately 8%-9% of couples do have infertility problems, sometimes related to gametes. She may never get a partner. Maybe she doesn’t want to use these eggs on her own as a single mom. All of these issues have to be talked through.
What really troubles me here is not so much that someone would choose to barter their eggs, but that they don’t get counseling. They don’t get independent advice about thinking this all through. It’s turning into a business. A business has a commodity – her eggs – that they want. She’s getting more and more desperate, willing to cut a deal to get where she needs to be, but perhaps is not really thinking through all of the ethical dimensions that bartering or trading one’s eggs in order to gain access to freezing entails.
We have to set up a system where there’s independent advice and independent counseling; otherwise, I think we’re closer to exploitation.
A version of this article first appeared on Medscape.com.
Dr. Caplan is director, division of medical ethics, New York University Langone Medical Center, New York. He has served as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use.