User login
Dupilumab approval marks the first targeted treatment for AD
The approval of dupilumab, the first targeted biologic therapy approved in the United States for treatment of atopic dermatitis, provides a welcome, long-awaited alternative to currently available therapies for moderate to severe disease, according to two of the pivotal trial investigators.
In late March, the Food and Drug Administration approved dupilumab, a monoclonal antibody that inhibits signaling of both interleukin-4 and interleukin-13, for the treatment of moderate to severe AD in adults “whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.” It is administered subcutaneously, with an initial 600-mg dose, followed by 300 mg every other week, according to the prescribing information.
Dupilumab (Dupixent) was the second novel treatment approved for AD in less than 4 months – after years of no approvals of new therapies for this indication. In December, crisaborole ointment (Eucrisa) was approved for treatment of mild to moderate AD in patients aged 2 years and older. Crisaborole is a topical phosphodiesterase-4 inhibitor.
Dupilumab’s approval was based on three phase III studies of adults with moderate to severe AD: SOLO-1 and SOLO-2, which evaluated dupilumab as monotherapy, and the CHRONOS study, which compared dupilumab with topical corticosteroids to treatment with topical corticosteroids alone.
At 16 weeks in the SOLO trials, those treated with dupilumab had improvements in signs and symptoms of AD, including pruritus, anxiety and depression, and quality of life, compared with placebo. Almost 40% of those treated with dupilumab met the primary outcome – a score of clear or almost clear on the Investigator’s Global Assessment and a reduction of 2 points or more in that score from baseline – compared with 8%-10% of those on placebo (P less than .001). Injection-site reactions and conjunctivitis were more common among those treated with dupilumab (N Engl J Med. 2016;375:2335-48).

Emma Guttman-Yassky, MD, PhD, also an investigator in the SOLO 1 and SOLO 2 trials, said that prior to the approval, “we had nothing to treat our patients safely long term.”

“With dupilumab, because it’s specific, it provides the safety that we need,” while providing efficacy that is similar to or better than that of cyclosporine, with the caveat that dupilumab and cyclosporine have not been evaluated in a head-to-head study, Dr. Guttman-Yassky, professor and vice-chair of dermatology at the Icahn School of Medicine at Mount Sinai, New York, said in an interview.
About 5%-10% of those treated at her site had allergic conjunctivitis; most cases resolved with eye drops. So far, “it looks very safe but we need to have long-term data,” she added.
Dr. Simpson said that he was pleased to see the maintenance of therapeutic effects with no emergence of new side effects with the report of 52-week CHRONOS data in March at the American Academy of Dermatology annual meeting.
“We’re entering the era and the decade of atopic dermatitis,” he said. “Dermatologists should look out for many new topical and systemic therapies now that we’re uncovering and figuring out the pathophysiology of atopic dermatitis.”
Dupilumab, which costs $37,000 per year, is marketed by Regeneron and Sanofi. Studies in children and adolescents with AD are underway.
Dr. Guttman-Yassky has received funding from Regeneron for mechanistic studies and is working with most companies developing AD treatments. Dr. Simpson has received research grants from and serves as a consultant to Regeneron, as well as other pharmaceutical companies.
The approval of dupilumab, the first targeted biologic therapy approved in the United States for treatment of atopic dermatitis, provides a welcome, long-awaited alternative to currently available therapies for moderate to severe disease, according to two of the pivotal trial investigators.
In late March, the Food and Drug Administration approved dupilumab, a monoclonal antibody that inhibits signaling of both interleukin-4 and interleukin-13, for the treatment of moderate to severe AD in adults “whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.” It is administered subcutaneously, with an initial 600-mg dose, followed by 300 mg every other week, according to the prescribing information.
Dupilumab (Dupixent) was the second novel treatment approved for AD in less than 4 months – after years of no approvals of new therapies for this indication. In December, crisaborole ointment (Eucrisa) was approved for treatment of mild to moderate AD in patients aged 2 years and older. Crisaborole is a topical phosphodiesterase-4 inhibitor.
Dupilumab’s approval was based on three phase III studies of adults with moderate to severe AD: SOLO-1 and SOLO-2, which evaluated dupilumab as monotherapy, and the CHRONOS study, which compared dupilumab with topical corticosteroids to treatment with topical corticosteroids alone.
At 16 weeks in the SOLO trials, those treated with dupilumab had improvements in signs and symptoms of AD, including pruritus, anxiety and depression, and quality of life, compared with placebo. Almost 40% of those treated with dupilumab met the primary outcome – a score of clear or almost clear on the Investigator’s Global Assessment and a reduction of 2 points or more in that score from baseline – compared with 8%-10% of those on placebo (P less than .001). Injection-site reactions and conjunctivitis were more common among those treated with dupilumab (N Engl J Med. 2016;375:2335-48).
Emma Guttman-Yassky, MD, PhD, also an investigator in the SOLO 1 and SOLO 2 trials, said that prior to the approval, “we had nothing to treat our patients safely long term.”
“With dupilumab, because it’s specific, it provides the safety that we need,” while providing efficacy that is similar to or better than that of cyclosporine, with the caveat that dupilumab and cyclosporine have not been evaluated in a head-to-head study, Dr. Guttman-Yassky, professor and vice-chair of dermatology at the Icahn School of Medicine at Mount Sinai, New York, said in an interview.
About 5%-10% of those treated at her site had allergic conjunctivitis; most cases resolved with eye drops. So far, “it looks very safe but we need to have long-term data,” she added.
Dr. Simpson said that he was pleased to see the maintenance of therapeutic effects with no emergence of new side effects with the report of 52-week CHRONOS data in March at the American Academy of Dermatology annual meeting.
“We’re entering the era and the decade of atopic dermatitis,” he said. “Dermatologists should look out for many new topical and systemic therapies now that we’re uncovering and figuring out the pathophysiology of atopic dermatitis.”
Dupilumab, which costs $37,000 per year, is marketed by Regeneron and Sanofi. Studies in children and adolescents with AD are underway.
Dr. Guttman-Yassky has received funding from Regeneron for mechanistic studies and is working with most companies developing AD treatments. Dr. Simpson has received research grants from and serves as a consultant to Regeneron, as well as other pharmaceutical companies.
The approval of dupilumab, the first targeted biologic therapy approved in the United States for treatment of atopic dermatitis, provides a welcome, long-awaited alternative to currently available therapies for moderate to severe disease, according to two of the pivotal trial investigators.
In late March, the Food and Drug Administration approved dupilumab, a monoclonal antibody that inhibits signaling of both interleukin-4 and interleukin-13, for the treatment of moderate to severe AD in adults “whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.” It is administered subcutaneously, with an initial 600-mg dose, followed by 300 mg every other week, according to the prescribing information.
Dupilumab (Dupixent) was the second novel treatment approved for AD in less than 4 months – after years of no approvals of new therapies for this indication. In December, crisaborole ointment (Eucrisa) was approved for treatment of mild to moderate AD in patients aged 2 years and older. Crisaborole is a topical phosphodiesterase-4 inhibitor.
Dupilumab’s approval was based on three phase III studies of adults with moderate to severe AD: SOLO-1 and SOLO-2, which evaluated dupilumab as monotherapy, and the CHRONOS study, which compared dupilumab with topical corticosteroids to treatment with topical corticosteroids alone.
At 16 weeks in the SOLO trials, those treated with dupilumab had improvements in signs and symptoms of AD, including pruritus, anxiety and depression, and quality of life, compared with placebo. Almost 40% of those treated with dupilumab met the primary outcome – a score of clear or almost clear on the Investigator’s Global Assessment and a reduction of 2 points or more in that score from baseline – compared with 8%-10% of those on placebo (P less than .001). Injection-site reactions and conjunctivitis were more common among those treated with dupilumab (N Engl J Med. 2016;375:2335-48).
Emma Guttman-Yassky, MD, PhD, also an investigator in the SOLO 1 and SOLO 2 trials, said that prior to the approval, “we had nothing to treat our patients safely long term.”
“With dupilumab, because it’s specific, it provides the safety that we need,” while providing efficacy that is similar to or better than that of cyclosporine, with the caveat that dupilumab and cyclosporine have not been evaluated in a head-to-head study, Dr. Guttman-Yassky, professor and vice-chair of dermatology at the Icahn School of Medicine at Mount Sinai, New York, said in an interview.
About 5%-10% of those treated at her site had allergic conjunctivitis; most cases resolved with eye drops. So far, “it looks very safe but we need to have long-term data,” she added.
Dr. Simpson said that he was pleased to see the maintenance of therapeutic effects with no emergence of new side effects with the report of 52-week CHRONOS data in March at the American Academy of Dermatology annual meeting.
“We’re entering the era and the decade of atopic dermatitis,” he said. “Dermatologists should look out for many new topical and systemic therapies now that we’re uncovering and figuring out the pathophysiology of atopic dermatitis.”
Dupilumab, which costs $37,000 per year, is marketed by Regeneron and Sanofi. Studies in children and adolescents with AD are underway.
Dr. Guttman-Yassky has received funding from Regeneron for mechanistic studies and is working with most companies developing AD treatments. Dr. Simpson has received research grants from and serves as a consultant to Regeneron, as well as other pharmaceutical companies.
Avoid hysterectomy in POP repairs
SAN ANTONIO – The Systematic Review Group of the Society of Gynecologic Surgeons is suggesting uterine preservation, when not contraindicated, for most pelvic organ prolapse repairs to decrease mesh erosion, operating room time, and blood loss.
The advice is based on a review of 94 original studies, including 12 randomized controlled trials (RCTs) and 41 nonrandomized comparative studies, winnowed down to the strongest work from an original review of 7,324 abstracts through January 2017.
Short-term prolapse outcomes – 12-30 months in most of the studies – “are usually not clinically significant due to uterine preservation,” with the one exception of vaginal hysterectomy with native tissue reconstruction, which the group recommended over laparoscopic sacrohysteropexy, Kate Meriwether, MD, a gynecologic surgeon at the University of Louisville, Ky., said at the annual scientific meeting of the Society of Gynecologic Surgeons.
Hysterectomy for prolapse surgery is common: More than 74,000 hysterectomies are done in the United States each year with prolapse as the main indication. Even so, it’s not always necessary to take out the uterus, and perhaps more than a third of women would prefer to keep theirs, Dr. Meriwether said, speaking on behalf of the SGS Systematic Review Group.
The recommendations from the Systematic Review Group must be sent to the SGS board and the full membership before they can be approved as guidelines.*
The Review Group made a grade A recommendation for vaginal hysterectomy with native tissue reconstruction over laparoscopic sacrohysteropexy, meaning it was based on high-quality evidence. The rest of the advice came in the form of suggestions, based on moderate grade B evidence, often nonrandomized comparative studies and case reviews.
The Review Group suggested uterine preservation during laparoscopic native tissue prolapse repair to reduce operating room (OR) time and blood loss, and preserve vaginal length, based on four nonrandomized comparison studies using various approaches, with a total of 446 women and up to 3 years’ follow-up. There might be a higher risk of apical recurrence without hysterectomy, but without worsening of prolapse symptoms.
The Review Group also suggested uterine preservation in transvaginal mesh reconstruction for prolapse, based on four RCTs and nine comparison studies with 1,381 women and up to 30 months’ follow-up. The studies found a decreased risk of mesh erosion, reoperating for mesh erosion, blood loss, and postop bleeding, and improved posterior and apical Pelvic Organ Prolapse Quantification scores when women keep their uterus.
However, “the patient should be counseled that there may be increased de novo stress incontinence, overactive bladder,” postop constipation, and shorter vaginal length, Dr. Meriwether said.
Also, “we suggest preservation of the uterus in transvaginal apical native tissue repair of prolapse, as it does not worsen any outcomes and slightly reduces OR time and estimated blood loss,” based on 13 studies, including four RCTs, and a total of 1,449 women followed for up to 26 months, she said.
The Review Group also came out in favor of the Manchester procedure, when available, over vaginal hysterectomy with native tissue suspension, based on one RCT and five nonrandomized studies involving 1,126 women and up to 61 months’ follow-up. The Manchester procedure pushed back the time to prolapse reoperation 9 months in one study, and also decreased transfusions, OR time, and blood loss. It also better preserved perineal length.
The group suggested uterine preservation when considering mesh sacrocolpopexy versus mesh sacrohysteropexy, to reduce mesh erosion, OR time, blood loss, hospital stay, and surgery costs, although there might be a slight worsening of Pelvic Floor Distress Inventory and Pelvic Floor Impact scores. The advice was based on nine nonrandomized comparison studies involving 745 women followed for up to 39 months. There was no difference in prolapse resolution between the two techniques.
The one grade A recommendation, for vaginal hysterectomy with native tissue reconstruction over laparoscopic sacrohysteropexy, was based on two RCTs with 182 women followed for up to 12 months.
Hysterectomy in those studies significantly reduced the risk of repeat surgery for prolapse and urinary symptoms, shortened OR time, and improved quality of life scores. However, the benefits came at the cost of slightly shorter vaginal length, worse Pelvic Organ Prolapse Quantification point C scores, greater blood loss, and up to a day longer spent in the hospital.
Dr. Meriwether reported having no relevant financial disclosures.
*Correction, 6/8/2017: An earlier version of this story misstated the status of the Systematic Review Group's recommendations. The recommendations have not been approved as official SGS guidelines. Also, the meeting sponsor information was updated.
SAN ANTONIO – The Systematic Review Group of the Society of Gynecologic Surgeons is suggesting uterine preservation, when not contraindicated, for most pelvic organ prolapse repairs to decrease mesh erosion, operating room time, and blood loss.
The advice is based on a review of 94 original studies, including 12 randomized controlled trials (RCTs) and 41 nonrandomized comparative studies, winnowed down to the strongest work from an original review of 7,324 abstracts through January 2017.
Short-term prolapse outcomes – 12-30 months in most of the studies – “are usually not clinically significant due to uterine preservation,” with the one exception of vaginal hysterectomy with native tissue reconstruction, which the group recommended over laparoscopic sacrohysteropexy, Kate Meriwether, MD, a gynecologic surgeon at the University of Louisville, Ky., said at the annual scientific meeting of the Society of Gynecologic Surgeons.
Hysterectomy for prolapse surgery is common: More than 74,000 hysterectomies are done in the United States each year with prolapse as the main indication. Even so, it’s not always necessary to take out the uterus, and perhaps more than a third of women would prefer to keep theirs, Dr. Meriwether said, speaking on behalf of the SGS Systematic Review Group.
The recommendations from the Systematic Review Group must be sent to the SGS board and the full membership before they can be approved as guidelines.*
The Review Group made a grade A recommendation for vaginal hysterectomy with native tissue reconstruction over laparoscopic sacrohysteropexy, meaning it was based on high-quality evidence. The rest of the advice came in the form of suggestions, based on moderate grade B evidence, often nonrandomized comparative studies and case reviews.
The Review Group suggested uterine preservation during laparoscopic native tissue prolapse repair to reduce operating room (OR) time and blood loss, and preserve vaginal length, based on four nonrandomized comparison studies using various approaches, with a total of 446 women and up to 3 years’ follow-up. There might be a higher risk of apical recurrence without hysterectomy, but without worsening of prolapse symptoms.
The Review Group also suggested uterine preservation in transvaginal mesh reconstruction for prolapse, based on four RCTs and nine comparison studies with 1,381 women and up to 30 months’ follow-up. The studies found a decreased risk of mesh erosion, reoperating for mesh erosion, blood loss, and postop bleeding, and improved posterior and apical Pelvic Organ Prolapse Quantification scores when women keep their uterus.
However, “the patient should be counseled that there may be increased de novo stress incontinence, overactive bladder,” postop constipation, and shorter vaginal length, Dr. Meriwether said.
Also, “we suggest preservation of the uterus in transvaginal apical native tissue repair of prolapse, as it does not worsen any outcomes and slightly reduces OR time and estimated blood loss,” based on 13 studies, including four RCTs, and a total of 1,449 women followed for up to 26 months, she said.
The Review Group also came out in favor of the Manchester procedure, when available, over vaginal hysterectomy with native tissue suspension, based on one RCT and five nonrandomized studies involving 1,126 women and up to 61 months’ follow-up. The Manchester procedure pushed back the time to prolapse reoperation 9 months in one study, and also decreased transfusions, OR time, and blood loss. It also better preserved perineal length.
The group suggested uterine preservation when considering mesh sacrocolpopexy versus mesh sacrohysteropexy, to reduce mesh erosion, OR time, blood loss, hospital stay, and surgery costs, although there might be a slight worsening of Pelvic Floor Distress Inventory and Pelvic Floor Impact scores. The advice was based on nine nonrandomized comparison studies involving 745 women followed for up to 39 months. There was no difference in prolapse resolution between the two techniques.
The one grade A recommendation, for vaginal hysterectomy with native tissue reconstruction over laparoscopic sacrohysteropexy, was based on two RCTs with 182 women followed for up to 12 months.
Hysterectomy in those studies significantly reduced the risk of repeat surgery for prolapse and urinary symptoms, shortened OR time, and improved quality of life scores. However, the benefits came at the cost of slightly shorter vaginal length, worse Pelvic Organ Prolapse Quantification point C scores, greater blood loss, and up to a day longer spent in the hospital.
Dr. Meriwether reported having no relevant financial disclosures.
*Correction, 6/8/2017: An earlier version of this story misstated the status of the Systematic Review Group's recommendations. The recommendations have not been approved as official SGS guidelines. Also, the meeting sponsor information was updated.
SAN ANTONIO – The Systematic Review Group of the Society of Gynecologic Surgeons is suggesting uterine preservation, when not contraindicated, for most pelvic organ prolapse repairs to decrease mesh erosion, operating room time, and blood loss.
The advice is based on a review of 94 original studies, including 12 randomized controlled trials (RCTs) and 41 nonrandomized comparative studies, winnowed down to the strongest work from an original review of 7,324 abstracts through January 2017.
Short-term prolapse outcomes – 12-30 months in most of the studies – “are usually not clinically significant due to uterine preservation,” with the one exception of vaginal hysterectomy with native tissue reconstruction, which the group recommended over laparoscopic sacrohysteropexy, Kate Meriwether, MD, a gynecologic surgeon at the University of Louisville, Ky., said at the annual scientific meeting of the Society of Gynecologic Surgeons.
Hysterectomy for prolapse surgery is common: More than 74,000 hysterectomies are done in the United States each year with prolapse as the main indication. Even so, it’s not always necessary to take out the uterus, and perhaps more than a third of women would prefer to keep theirs, Dr. Meriwether said, speaking on behalf of the SGS Systematic Review Group.
The recommendations from the Systematic Review Group must be sent to the SGS board and the full membership before they can be approved as guidelines.*
The Review Group made a grade A recommendation for vaginal hysterectomy with native tissue reconstruction over laparoscopic sacrohysteropexy, meaning it was based on high-quality evidence. The rest of the advice came in the form of suggestions, based on moderate grade B evidence, often nonrandomized comparative studies and case reviews.
The Review Group suggested uterine preservation during laparoscopic native tissue prolapse repair to reduce operating room (OR) time and blood loss, and preserve vaginal length, based on four nonrandomized comparison studies using various approaches, with a total of 446 women and up to 3 years’ follow-up. There might be a higher risk of apical recurrence without hysterectomy, but without worsening of prolapse symptoms.
The Review Group also suggested uterine preservation in transvaginal mesh reconstruction for prolapse, based on four RCTs and nine comparison studies with 1,381 women and up to 30 months’ follow-up. The studies found a decreased risk of mesh erosion, reoperating for mesh erosion, blood loss, and postop bleeding, and improved posterior and apical Pelvic Organ Prolapse Quantification scores when women keep their uterus.
However, “the patient should be counseled that there may be increased de novo stress incontinence, overactive bladder,” postop constipation, and shorter vaginal length, Dr. Meriwether said.
Also, “we suggest preservation of the uterus in transvaginal apical native tissue repair of prolapse, as it does not worsen any outcomes and slightly reduces OR time and estimated blood loss,” based on 13 studies, including four RCTs, and a total of 1,449 women followed for up to 26 months, she said.
The Review Group also came out in favor of the Manchester procedure, when available, over vaginal hysterectomy with native tissue suspension, based on one RCT and five nonrandomized studies involving 1,126 women and up to 61 months’ follow-up. The Manchester procedure pushed back the time to prolapse reoperation 9 months in one study, and also decreased transfusions, OR time, and blood loss. It also better preserved perineal length.
The group suggested uterine preservation when considering mesh sacrocolpopexy versus mesh sacrohysteropexy, to reduce mesh erosion, OR time, blood loss, hospital stay, and surgery costs, although there might be a slight worsening of Pelvic Floor Distress Inventory and Pelvic Floor Impact scores. The advice was based on nine nonrandomized comparison studies involving 745 women followed for up to 39 months. There was no difference in prolapse resolution between the two techniques.
The one grade A recommendation, for vaginal hysterectomy with native tissue reconstruction over laparoscopic sacrohysteropexy, was based on two RCTs with 182 women followed for up to 12 months.
Hysterectomy in those studies significantly reduced the risk of repeat surgery for prolapse and urinary symptoms, shortened OR time, and improved quality of life scores. However, the benefits came at the cost of slightly shorter vaginal length, worse Pelvic Organ Prolapse Quantification point C scores, greater blood loss, and up to a day longer spent in the hospital.
Dr. Meriwether reported having no relevant financial disclosures.
*Correction, 6/8/2017: An earlier version of this story misstated the status of the Systematic Review Group's recommendations. The recommendations have not been approved as official SGS guidelines. Also, the meeting sponsor information was updated.
Ultrasound, cystoscopy combo tops CT for asymptomatic microscopic hematuria
Combining renal ultrasound and bladder cystoscopy is the most cost-effective approach for the initial evaluation of asymptomatic microscopic hematuria, even among patients at risk for genitourinary malignancy, according to a report published online April 17 in JAMA Internal Medicine.
“The superiority of this approach over the use of CT plus cystoscopy is driven primarily by higher costs of CT and the associated complications, albeit rare,” said Joshua A. Halpern, MD, of the department of urology, CornellUniversity, New York, and his associates. “Given the low prevalence of upper-tract malignant abnormalities in patients with asymptomatic microscopic hematuria, the small advantage in the sensitivity of CT imaging does not compensate for the significant additional costs.”
Every year, hundreds of thousands of patients undergo urinalysis for a variety of indications, and an estimated 40% are found to have microscopic hematuria in the absence of any urinary symptoms. This finding requires further evaluation because of one particular possible cause: a genitourinary malignancy. An estimated 11% of people with asymptomatic microscopic hematuria are found to have malignant abnormalities, the investigators said.
They assessed the cost-effectiveness of four common follow-up evaluations by creating a decision-analysis model to simulate the rates of cancer detection in adults with no history of cancer and with negative urine cultures that ruled out UTI as the cause of the hematuria.
The model was based on data from real-world experience in the medical literature and incorporated information on cancer incidence, diagnostic test accuracy, and complications.
The four approaches they examined were CT plus cystoscopy, which is considered the preferred method of diagnostic work-up by the American Urological Association; renal ultrasound plus cystoscopy, which many clinicians in the United States and other countries use instead; cystoscopy alone; and CT alone.
Compared with no follow-up evaluation, CT alone detected the fewest cancers (221 per 10,000 patients) at the highest cost ($9,300,000 per 10,000 patients). Cystoscopy alone detected 222 cancers per 10,000 at a cost of $10,287 per 10,000. Ultrasound plus cystoscopy detected 23 additional cancers per 10,000 patients at a relatively low cost of $53,810 per 10,000. Replacing ultrasound with CT detected just one additional cancer but cost an additional $6,480,484 per 10,000 patients.
The findings were similar in several sensitivity analyses, as well as in a subgroup analysis involving only higher-risk patients – men, smokers, and patients aged 50 years and older, the investigators noted (JAMA Intern Med. 2017 Apr 17. doi: 10.1001/jamaintenmed.2017.0739).
Dr. Halpern and his associates also applied their results to nationwide 2012 statistics for 485,222 patient visits to urologists to assess microscopic hematuria. If all urologists complied with AUA guidelines and used CT instead of ultrasound plus cystoscopy to assess these patients, they would have detected only 60 additional cancers, at an additional cost of $389,914,648.
Given these findings, renal ultrasound plus bladder cystoscopy should be considered the first-line assessment for these patients, Dr. Halpern and his associates said. Rewriting practice guidelines accordingly “will substantially reduce national expenditures associated with asymptomatic microscopic hematuria evaluation by up to $390 million.”
Moreover, recommending ultrasound rather than CT might have the unintended but beneficial consequence of improving compliance with further evaluation, because many primary care physicians are reluctant to refer these patients for radiocontrast CT studies, the researchers noted.
No sponsor was cited for this study. Dr. Halpern and his associates reported having no relevant financial disclosures.
The substantial differences between ultrasound and CT in cost per cancer detected, combined with the harm from CT-related contrast reactions and radiation exposure, strongly support renal ultrasound plus cystoscopy as the preferred first-line approach to assessing asymptomatic microscopic hematuria.
According to Halpern et al., this approach would cost approximately $54,000 per cancer detected. Replacing ultrasound with CT would detect just 1 additional cancer per 10,000 assessments, at an incremental cost of $6.5 million.
Leslee L. Subak, MD, and Deborah Grady, MD, are in the departments of obstetrics, gynecology, and reproductive sciences; urology; and epidemiology and biostatistics at the University of California, San Francisco. Dr. Subak reported receiving funding from Astellas to research urinary incontinence. Dr. Subak and Dr. Grady made these remarks in an invited commentary accompanying Dr. Halpern’s report (JAMA Intern Med. 2017 Apr 17. doi: 10.1001/jamainternmed.2017.0758).
The substantial differences between ultrasound and CT in cost per cancer detected, combined with the harm from CT-related contrast reactions and radiation exposure, strongly support renal ultrasound plus cystoscopy as the preferred first-line approach to assessing asymptomatic microscopic hematuria.
According to Halpern et al., this approach would cost approximately $54,000 per cancer detected. Replacing ultrasound with CT would detect just 1 additional cancer per 10,000 assessments, at an incremental cost of $6.5 million.
Leslee L. Subak, MD, and Deborah Grady, MD, are in the departments of obstetrics, gynecology, and reproductive sciences; urology; and epidemiology and biostatistics at the University of California, San Francisco. Dr. Subak reported receiving funding from Astellas to research urinary incontinence. Dr. Subak and Dr. Grady made these remarks in an invited commentary accompanying Dr. Halpern’s report (JAMA Intern Med. 2017 Apr 17. doi: 10.1001/jamainternmed.2017.0758).
The substantial differences between ultrasound and CT in cost per cancer detected, combined with the harm from CT-related contrast reactions and radiation exposure, strongly support renal ultrasound plus cystoscopy as the preferred first-line approach to assessing asymptomatic microscopic hematuria.
According to Halpern et al., this approach would cost approximately $54,000 per cancer detected. Replacing ultrasound with CT would detect just 1 additional cancer per 10,000 assessments, at an incremental cost of $6.5 million.
Leslee L. Subak, MD, and Deborah Grady, MD, are in the departments of obstetrics, gynecology, and reproductive sciences; urology; and epidemiology and biostatistics at the University of California, San Francisco. Dr. Subak reported receiving funding from Astellas to research urinary incontinence. Dr. Subak and Dr. Grady made these remarks in an invited commentary accompanying Dr. Halpern’s report (JAMA Intern Med. 2017 Apr 17. doi: 10.1001/jamainternmed.2017.0758).
Combining renal ultrasound and bladder cystoscopy is the most cost-effective approach for the initial evaluation of asymptomatic microscopic hematuria, even among patients at risk for genitourinary malignancy, according to a report published online April 17 in JAMA Internal Medicine.
“The superiority of this approach over the use of CT plus cystoscopy is driven primarily by higher costs of CT and the associated complications, albeit rare,” said Joshua A. Halpern, MD, of the department of urology, CornellUniversity, New York, and his associates. “Given the low prevalence of upper-tract malignant abnormalities in patients with asymptomatic microscopic hematuria, the small advantage in the sensitivity of CT imaging does not compensate for the significant additional costs.”
Every year, hundreds of thousands of patients undergo urinalysis for a variety of indications, and an estimated 40% are found to have microscopic hematuria in the absence of any urinary symptoms. This finding requires further evaluation because of one particular possible cause: a genitourinary malignancy. An estimated 11% of people with asymptomatic microscopic hematuria are found to have malignant abnormalities, the investigators said.
They assessed the cost-effectiveness of four common follow-up evaluations by creating a decision-analysis model to simulate the rates of cancer detection in adults with no history of cancer and with negative urine cultures that ruled out UTI as the cause of the hematuria.
The model was based on data from real-world experience in the medical literature and incorporated information on cancer incidence, diagnostic test accuracy, and complications.
The four approaches they examined were CT plus cystoscopy, which is considered the preferred method of diagnostic work-up by the American Urological Association; renal ultrasound plus cystoscopy, which many clinicians in the United States and other countries use instead; cystoscopy alone; and CT alone.
Compared with no follow-up evaluation, CT alone detected the fewest cancers (221 per 10,000 patients) at the highest cost ($9,300,000 per 10,000 patients). Cystoscopy alone detected 222 cancers per 10,000 at a cost of $10,287 per 10,000. Ultrasound plus cystoscopy detected 23 additional cancers per 10,000 patients at a relatively low cost of $53,810 per 10,000. Replacing ultrasound with CT detected just one additional cancer but cost an additional $6,480,484 per 10,000 patients.
The findings were similar in several sensitivity analyses, as well as in a subgroup analysis involving only higher-risk patients – men, smokers, and patients aged 50 years and older, the investigators noted (JAMA Intern Med. 2017 Apr 17. doi: 10.1001/jamaintenmed.2017.0739).
Dr. Halpern and his associates also applied their results to nationwide 2012 statistics for 485,222 patient visits to urologists to assess microscopic hematuria. If all urologists complied with AUA guidelines and used CT instead of ultrasound plus cystoscopy to assess these patients, they would have detected only 60 additional cancers, at an additional cost of $389,914,648.
Given these findings, renal ultrasound plus bladder cystoscopy should be considered the first-line assessment for these patients, Dr. Halpern and his associates said. Rewriting practice guidelines accordingly “will substantially reduce national expenditures associated with asymptomatic microscopic hematuria evaluation by up to $390 million.”
Moreover, recommending ultrasound rather than CT might have the unintended but beneficial consequence of improving compliance with further evaluation, because many primary care physicians are reluctant to refer these patients for radiocontrast CT studies, the researchers noted.
No sponsor was cited for this study. Dr. Halpern and his associates reported having no relevant financial disclosures.
Combining renal ultrasound and bladder cystoscopy is the most cost-effective approach for the initial evaluation of asymptomatic microscopic hematuria, even among patients at risk for genitourinary malignancy, according to a report published online April 17 in JAMA Internal Medicine.
“The superiority of this approach over the use of CT plus cystoscopy is driven primarily by higher costs of CT and the associated complications, albeit rare,” said Joshua A. Halpern, MD, of the department of urology, CornellUniversity, New York, and his associates. “Given the low prevalence of upper-tract malignant abnormalities in patients with asymptomatic microscopic hematuria, the small advantage in the sensitivity of CT imaging does not compensate for the significant additional costs.”
Every year, hundreds of thousands of patients undergo urinalysis for a variety of indications, and an estimated 40% are found to have microscopic hematuria in the absence of any urinary symptoms. This finding requires further evaluation because of one particular possible cause: a genitourinary malignancy. An estimated 11% of people with asymptomatic microscopic hematuria are found to have malignant abnormalities, the investigators said.
They assessed the cost-effectiveness of four common follow-up evaluations by creating a decision-analysis model to simulate the rates of cancer detection in adults with no history of cancer and with negative urine cultures that ruled out UTI as the cause of the hematuria.
The model was based on data from real-world experience in the medical literature and incorporated information on cancer incidence, diagnostic test accuracy, and complications.
The four approaches they examined were CT plus cystoscopy, which is considered the preferred method of diagnostic work-up by the American Urological Association; renal ultrasound plus cystoscopy, which many clinicians in the United States and other countries use instead; cystoscopy alone; and CT alone.
Compared with no follow-up evaluation, CT alone detected the fewest cancers (221 per 10,000 patients) at the highest cost ($9,300,000 per 10,000 patients). Cystoscopy alone detected 222 cancers per 10,000 at a cost of $10,287 per 10,000. Ultrasound plus cystoscopy detected 23 additional cancers per 10,000 patients at a relatively low cost of $53,810 per 10,000. Replacing ultrasound with CT detected just one additional cancer but cost an additional $6,480,484 per 10,000 patients.
The findings were similar in several sensitivity analyses, as well as in a subgroup analysis involving only higher-risk patients – men, smokers, and patients aged 50 years and older, the investigators noted (JAMA Intern Med. 2017 Apr 17. doi: 10.1001/jamaintenmed.2017.0739).
Dr. Halpern and his associates also applied their results to nationwide 2012 statistics for 485,222 patient visits to urologists to assess microscopic hematuria. If all urologists complied with AUA guidelines and used CT instead of ultrasound plus cystoscopy to assess these patients, they would have detected only 60 additional cancers, at an additional cost of $389,914,648.
Given these findings, renal ultrasound plus bladder cystoscopy should be considered the first-line assessment for these patients, Dr. Halpern and his associates said. Rewriting practice guidelines accordingly “will substantially reduce national expenditures associated with asymptomatic microscopic hematuria evaluation by up to $390 million.”
Moreover, recommending ultrasound rather than CT might have the unintended but beneficial consequence of improving compliance with further evaluation, because many primary care physicians are reluctant to refer these patients for radiocontrast CT studies, the researchers noted.
No sponsor was cited for this study. Dr. Halpern and his associates reported having no relevant financial disclosures.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Combining renal ultrasound and bladder cystoscopy is the most cost-effective approach for the initial evaluation of asymptomatic microscopic hematuria.
Major finding: If all urologists complied with AUA guidelines and used CT instead of ultrasound plus cystoscopy to assess the 485,222 patients who were seen for asymptomatic microscopic hematuria in 2012, they would have detected only 60 additional cancers, at an additional cost of $389,914,648.
Data source: Decision-analysis modeling of four common approaches to assessing asymptomatic microscopic hematuria.
Disclosures: No sponsor was cited for this study. Dr. Halpern and his associates reported having no relevant financial disclosures.
Lupus low disease activity definition gains momentum
MELBOURNE – A metric for low disease activity in lupus is nearly ready for prime-time in both clinical practice and clinical trials, according to speakers at a recent international conference on systemic lupus erythematosus.
The Lupus Low Disease Activity State definition, developed by the Asia Pacific Lupus Collaboration, represents a state which, if sustained, is associated with a low likelihood of adverse outcome, said Mandana Nikpour, MBBS, PhD, of St. Vincent’s Hospital and the University of Melbourne.

“On the other hand, patients that are overall doing relatively well have less active disease and tend to look a little more homogeneous and potentially are easier to define,” Dr. Nikpour said. “If we’re able to define this group of patients who are doing well, that definition could potentially serve as a therapeutic target.”
The consensus definition of a Lupus Low Disease Activity State (LLDAS), contains five items. The first is that the patient must have a SLEDAI-2K score of less than or equal to 4, with no activity in major organs. Secondly, patients must show no new features of lupus activity, compared with the previous assessment. The third LLDAS item is a Physician Global Assessment score of 1 or less on a scale of 0 to 3. The fourth item is a current prednisolone or equivalent dose of 7.5 mg/day or less, and the fifth is that patients are on well-tolerated standard doses of immunosuppressants and approved biologic agents.
While the definition has been retrospectively validated, Dr. Nikpour presented data from a prospective study that examined the agreement between LLDAS and the clinical judgment of 50 lupus experts on 50 cases.
These data showed overall agreement between experts and LLDAS rating of remission or low, moderate, or high disease activity in 78% of cases.
“Where there were disagreements, when we looked at the cases in more detail, it really boiled down to whether the expert felt that serologic activity [such as] low complement/raised anti-dsDNA was important, and some experts also accepted prednisone doses up to 10 mg per day in what they thought would be a low disease activity state,” Dr. Nikpour said.
In the same session, Chak-Sing Lau, MBChB, MD, chair of rheumatology and clinical immunology at the University of Hong Kong, presented data from another prospective, cross-sectional validation study of the LLDAS measure in 339 lupus patients who were followed for 30 months.
This study showed that 92.6% of patients had ever achieved LLDAS during the study period, and 62.1% of patient days were spent in LLDAS. Researchers also found that patients who spent a higher percentage of time in LLDAS had a significantly lower incidence of flare, even after adjustment for gender and age.
Commenting on the study, Dr. Nikpour said LLDAS could be a feasible target for lupus – or at least part of one – and a therapeutic endpoint or outcome measure in clinical trials.
“We now have a prospective validation of LLDAS in the Asia Pacific cohort, again looking at protection against future flares, damage accrual, and perhaps even mortality, and a state which confers better health-related quality of life,” she said in an interview.

The study involved 305 patients with active disease who were randomized to standard of care plus 300 mg or 1,000 mg anifrolumab every 4 weeks, or placebo, with follow-up at 28 and 52 weeks.
The analysis showed that LLDAS was strongly associated with the trial’s primary endpoint of SRI-4 response plus a sustained reduction of oral corticosteroid dose to below 10 mg/day, although LLDAS also proved itself more stringent than the SRI-4 response criteria.
Similarly, LLDAS attainment was strongly associated with BILAG (British Isles Lupus Assessment Group)–Based Composite Lupus Assessment response but again, was more stringent. However LLDAS was less stringent than the major clinical response definition used in the study, which was BILAG ‘C’ or less across all systems for a minimum of 6 months.
Patients who achieved a low disease activity state at week 52 also showed significantly greater improvements in patient global score, and in seven of the eight lupus quality of life domains, compared with patients who did not achieve LLDAS.
“The purpose of this analysis is not to evaluate the efficacy of anifrolumab but rather to evaluate the utility of this measure, and we believe that this has been attained,” Dr. Morand told the audience.
In an interview, Dr. Morand said the accumulating evidence for the validity of LLDAS both in clinical trials and clinical practice was approaching a tipping point, with numerous presentations at the conference addressing the question of LLDAS.
“Of course those findings have to be peer reviewed and published, and probably it needs to be tested in another clinical trial or two and still hold water, but I think it’s got momentum now.”
Dr. Nikpour declared research support, honoraria, and consultancies with several pharmaceutical companies. The MUSE trial was funded by MedImmune, and Dr. Morand declared research support, consultancies and travel funding from several pharmaceutical companies. Dr. Lau declared advisory board and consultancy roles with several pharmaceutical companies.
MELBOURNE – A metric for low disease activity in lupus is nearly ready for prime-time in both clinical practice and clinical trials, according to speakers at a recent international conference on systemic lupus erythematosus.
The Lupus Low Disease Activity State definition, developed by the Asia Pacific Lupus Collaboration, represents a state which, if sustained, is associated with a low likelihood of adverse outcome, said Mandana Nikpour, MBBS, PhD, of St. Vincent’s Hospital and the University of Melbourne.
“On the other hand, patients that are overall doing relatively well have less active disease and tend to look a little more homogeneous and potentially are easier to define,” Dr. Nikpour said. “If we’re able to define this group of patients who are doing well, that definition could potentially serve as a therapeutic target.”
The consensus definition of a Lupus Low Disease Activity State (LLDAS), contains five items. The first is that the patient must have a SLEDAI-2K score of less than or equal to 4, with no activity in major organs. Secondly, patients must show no new features of lupus activity, compared with the previous assessment. The third LLDAS item is a Physician Global Assessment score of 1 or less on a scale of 0 to 3. The fourth item is a current prednisolone or equivalent dose of 7.5 mg/day or less, and the fifth is that patients are on well-tolerated standard doses of immunosuppressants and approved biologic agents.
While the definition has been retrospectively validated, Dr. Nikpour presented data from a prospective study that examined the agreement between LLDAS and the clinical judgment of 50 lupus experts on 50 cases.
These data showed overall agreement between experts and LLDAS rating of remission or low, moderate, or high disease activity in 78% of cases.
“Where there were disagreements, when we looked at the cases in more detail, it really boiled down to whether the expert felt that serologic activity [such as] low complement/raised anti-dsDNA was important, and some experts also accepted prednisone doses up to 10 mg per day in what they thought would be a low disease activity state,” Dr. Nikpour said.
In the same session, Chak-Sing Lau, MBChB, MD, chair of rheumatology and clinical immunology at the University of Hong Kong, presented data from another prospective, cross-sectional validation study of the LLDAS measure in 339 lupus patients who were followed for 30 months.
This study showed that 92.6% of patients had ever achieved LLDAS during the study period, and 62.1% of patient days were spent in LLDAS. Researchers also found that patients who spent a higher percentage of time in LLDAS had a significantly lower incidence of flare, even after adjustment for gender and age.
Commenting on the study, Dr. Nikpour said LLDAS could be a feasible target for lupus – or at least part of one – and a therapeutic endpoint or outcome measure in clinical trials.
“We now have a prospective validation of LLDAS in the Asia Pacific cohort, again looking at protection against future flares, damage accrual, and perhaps even mortality, and a state which confers better health-related quality of life,” she said in an interview.
The study involved 305 patients with active disease who were randomized to standard of care plus 300 mg or 1,000 mg anifrolumab every 4 weeks, or placebo, with follow-up at 28 and 52 weeks.
The analysis showed that LLDAS was strongly associated with the trial’s primary endpoint of SRI-4 response plus a sustained reduction of oral corticosteroid dose to below 10 mg/day, although LLDAS also proved itself more stringent than the SRI-4 response criteria.
Similarly, LLDAS attainment was strongly associated with BILAG (British Isles Lupus Assessment Group)–Based Composite Lupus Assessment response but again, was more stringent. However LLDAS was less stringent than the major clinical response definition used in the study, which was BILAG ‘C’ or less across all systems for a minimum of 6 months.
Patients who achieved a low disease activity state at week 52 also showed significantly greater improvements in patient global score, and in seven of the eight lupus quality of life domains, compared with patients who did not achieve LLDAS.
“The purpose of this analysis is not to evaluate the efficacy of anifrolumab but rather to evaluate the utility of this measure, and we believe that this has been attained,” Dr. Morand told the audience.
In an interview, Dr. Morand said the accumulating evidence for the validity of LLDAS both in clinical trials and clinical practice was approaching a tipping point, with numerous presentations at the conference addressing the question of LLDAS.
“Of course those findings have to be peer reviewed and published, and probably it needs to be tested in another clinical trial or two and still hold water, but I think it’s got momentum now.”
Dr. Nikpour declared research support, honoraria, and consultancies with several pharmaceutical companies. The MUSE trial was funded by MedImmune, and Dr. Morand declared research support, consultancies and travel funding from several pharmaceutical companies. Dr. Lau declared advisory board and consultancy roles with several pharmaceutical companies.
MELBOURNE – A metric for low disease activity in lupus is nearly ready for prime-time in both clinical practice and clinical trials, according to speakers at a recent international conference on systemic lupus erythematosus.
The Lupus Low Disease Activity State definition, developed by the Asia Pacific Lupus Collaboration, represents a state which, if sustained, is associated with a low likelihood of adverse outcome, said Mandana Nikpour, MBBS, PhD, of St. Vincent’s Hospital and the University of Melbourne.
“On the other hand, patients that are overall doing relatively well have less active disease and tend to look a little more homogeneous and potentially are easier to define,” Dr. Nikpour said. “If we’re able to define this group of patients who are doing well, that definition could potentially serve as a therapeutic target.”
The consensus definition of a Lupus Low Disease Activity State (LLDAS), contains five items. The first is that the patient must have a SLEDAI-2K score of less than or equal to 4, with no activity in major organs. Secondly, patients must show no new features of lupus activity, compared with the previous assessment. The third LLDAS item is a Physician Global Assessment score of 1 or less on a scale of 0 to 3. The fourth item is a current prednisolone or equivalent dose of 7.5 mg/day or less, and the fifth is that patients are on well-tolerated standard doses of immunosuppressants and approved biologic agents.
While the definition has been retrospectively validated, Dr. Nikpour presented data from a prospective study that examined the agreement between LLDAS and the clinical judgment of 50 lupus experts on 50 cases.
These data showed overall agreement between experts and LLDAS rating of remission or low, moderate, or high disease activity in 78% of cases.
“Where there were disagreements, when we looked at the cases in more detail, it really boiled down to whether the expert felt that serologic activity [such as] low complement/raised anti-dsDNA was important, and some experts also accepted prednisone doses up to 10 mg per day in what they thought would be a low disease activity state,” Dr. Nikpour said.
In the same session, Chak-Sing Lau, MBChB, MD, chair of rheumatology and clinical immunology at the University of Hong Kong, presented data from another prospective, cross-sectional validation study of the LLDAS measure in 339 lupus patients who were followed for 30 months.
This study showed that 92.6% of patients had ever achieved LLDAS during the study period, and 62.1% of patient days were spent in LLDAS. Researchers also found that patients who spent a higher percentage of time in LLDAS had a significantly lower incidence of flare, even after adjustment for gender and age.
Commenting on the study, Dr. Nikpour said LLDAS could be a feasible target for lupus – or at least part of one – and a therapeutic endpoint or outcome measure in clinical trials.
“We now have a prospective validation of LLDAS in the Asia Pacific cohort, again looking at protection against future flares, damage accrual, and perhaps even mortality, and a state which confers better health-related quality of life,” she said in an interview.
The study involved 305 patients with active disease who were randomized to standard of care plus 300 mg or 1,000 mg anifrolumab every 4 weeks, or placebo, with follow-up at 28 and 52 weeks.
The analysis showed that LLDAS was strongly associated with the trial’s primary endpoint of SRI-4 response plus a sustained reduction of oral corticosteroid dose to below 10 mg/day, although LLDAS also proved itself more stringent than the SRI-4 response criteria.
Similarly, LLDAS attainment was strongly associated with BILAG (British Isles Lupus Assessment Group)–Based Composite Lupus Assessment response but again, was more stringent. However LLDAS was less stringent than the major clinical response definition used in the study, which was BILAG ‘C’ or less across all systems for a minimum of 6 months.
Patients who achieved a low disease activity state at week 52 also showed significantly greater improvements in patient global score, and in seven of the eight lupus quality of life domains, compared with patients who did not achieve LLDAS.
“The purpose of this analysis is not to evaluate the efficacy of anifrolumab but rather to evaluate the utility of this measure, and we believe that this has been attained,” Dr. Morand told the audience.
In an interview, Dr. Morand said the accumulating evidence for the validity of LLDAS both in clinical trials and clinical practice was approaching a tipping point, with numerous presentations at the conference addressing the question of LLDAS.
“Of course those findings have to be peer reviewed and published, and probably it needs to be tested in another clinical trial or two and still hold water, but I think it’s got momentum now.”
Dr. Nikpour declared research support, honoraria, and consultancies with several pharmaceutical companies. The MUSE trial was funded by MedImmune, and Dr. Morand declared research support, consultancies and travel funding from several pharmaceutical companies. Dr. Lau declared advisory board and consultancy roles with several pharmaceutical companies.
Key clinical point:
Major finding: The Lupus Low Disease Activity State definition shows significant agreement with clinical judgment and with other endpoints of treatment response, and is associated with a reduced risk of disease flare.
Data source: Three prospective validation studies, two cohort studies, and one clinical trial.
Disclosures: Dr. Nikpour declared research support, honoraria and consultancies with several pharmaceutical companies. The MUSE trial was funded by MedImmune, and Dr. Morand declared research support, consultancies, and travel funding from several pharmaceutical companies. Dr. Lau declared advisory board and consultancy roles with several pharmaceutical companies.
Neoadjuvant therapy timing may impact pancreatic cancer outcomes
SEATTLE – In patients with pancreatic cancer, an interval of 8 weeks between receiving neoadjuvant chemoradiation and surgical resection may improve resection margins, according to findings presented at the annual Society of Surgical Oncology Cancer Symposium.
The delay in resection did not negatively impact outcomes, and there was a modest improvement in overall survival among patients who had an 8-10 week interval between treatments.
“Attention should be focused on the treatment interval to time of resection in prospective studies,” said lead study author Raphael J. Louie, MD, of Dartmouth (N.H.) Hitchcock Norris Cotton Cancer Center.
Dr. Louie explained that for patients with pancreatic adenocarcinoma who receive neoadjuvant chemoradiation, it is unclear how long the optimal interval should be between therapy completion and surgical resection.
For this study, Dr. Louie and his colleagues sought to determine the optimal interval between neoadjuvant therapy and surgery to maximize response and oncologic outcomes.
“We hypothesized that there may be benefit to a delay,” he said.
The retrospective analysis included 637 patients who had been diagnosed with pancreatic adenocarcinoma at the Norris Cotton Cancer Center, and who had completed neoadjuvant chemoradiation and underwent R0 surgical resection between Jan. 1, 2004, and Dec. 31, 2015.
Of this group, 195 patients had metastatic disease, 28 underwent upfront surgical exploration, and 94 were lost to follow-up or had a poor performance status and were not included in the final analysis.
The cohort was grouped according to time from chemoradiation completion to surgery: 6-8 weeks, 8-10 weeks, and more than 10 weeks.
A total of 320 patients received neoadjuvant chemoradiation and 288 completed the full course. Of this group, 128 were evaluable by pathologic review.
Among patients with a 6- to 8-week interval, 61% had an R0 resection margin. This percentage rose to 72% for those who had an 8- to 10-week interval, and in similar fashion, 70% for those who had a 10- to 13-week interval (P = .6)
However, there was no statistical difference when the three groups were compared collectively.
Of 26 patients who were resected within 6-8 weeks of chemoradiation, 11% achieved a complete response (CR), 27% had a partial response (PR), and 61% had recurrence for an average disease-free survival of 20 months.
In the group (n = 58) of patients who were resected within 8-10 weeks, 7% had CR, 71% had PR, and 62% had recurrence, for an average disease-free survival of 17 months. Finally, the 44 patients who were resected within 10-13 weeks had similar outcomes; 5% had CR, 61% had PR, and 61% of patients had recurrence for an average disease-free survival of 14 months.
Dr. Louie noted that even though they observed improved PR in the 8- to 10-week group, there was no statistical significance in disease-free survival (P = .71) or overall survival (P = .19).
“Allowing more time from neoadjuvant therapy completion to surgical resection may improve the pathologic response,” said Dr. Louie. “Larger studies are needed to determine if the time interval to surgical resection has oncologic benefit for these patients.”
Dr. Louie has no disclosures.
SEATTLE – In patients with pancreatic cancer, an interval of 8 weeks between receiving neoadjuvant chemoradiation and surgical resection may improve resection margins, according to findings presented at the annual Society of Surgical Oncology Cancer Symposium.
The delay in resection did not negatively impact outcomes, and there was a modest improvement in overall survival among patients who had an 8-10 week interval between treatments.
“Attention should be focused on the treatment interval to time of resection in prospective studies,” said lead study author Raphael J. Louie, MD, of Dartmouth (N.H.) Hitchcock Norris Cotton Cancer Center.
Dr. Louie explained that for patients with pancreatic adenocarcinoma who receive neoadjuvant chemoradiation, it is unclear how long the optimal interval should be between therapy completion and surgical resection.
For this study, Dr. Louie and his colleagues sought to determine the optimal interval between neoadjuvant therapy and surgery to maximize response and oncologic outcomes.
“We hypothesized that there may be benefit to a delay,” he said.
The retrospective analysis included 637 patients who had been diagnosed with pancreatic adenocarcinoma at the Norris Cotton Cancer Center, and who had completed neoadjuvant chemoradiation and underwent R0 surgical resection between Jan. 1, 2004, and Dec. 31, 2015.
Of this group, 195 patients had metastatic disease, 28 underwent upfront surgical exploration, and 94 were lost to follow-up or had a poor performance status and were not included in the final analysis.
The cohort was grouped according to time from chemoradiation completion to surgery: 6-8 weeks, 8-10 weeks, and more than 10 weeks.
A total of 320 patients received neoadjuvant chemoradiation and 288 completed the full course. Of this group, 128 were evaluable by pathologic review.
Among patients with a 6- to 8-week interval, 61% had an R0 resection margin. This percentage rose to 72% for those who had an 8- to 10-week interval, and in similar fashion, 70% for those who had a 10- to 13-week interval (P = .6)
However, there was no statistical difference when the three groups were compared collectively.
Of 26 patients who were resected within 6-8 weeks of chemoradiation, 11% achieved a complete response (CR), 27% had a partial response (PR), and 61% had recurrence for an average disease-free survival of 20 months.
In the group (n = 58) of patients who were resected within 8-10 weeks, 7% had CR, 71% had PR, and 62% had recurrence, for an average disease-free survival of 17 months. Finally, the 44 patients who were resected within 10-13 weeks had similar outcomes; 5% had CR, 61% had PR, and 61% of patients had recurrence for an average disease-free survival of 14 months.
Dr. Louie noted that even though they observed improved PR in the 8- to 10-week group, there was no statistical significance in disease-free survival (P = .71) or overall survival (P = .19).
“Allowing more time from neoadjuvant therapy completion to surgical resection may improve the pathologic response,” said Dr. Louie. “Larger studies are needed to determine if the time interval to surgical resection has oncologic benefit for these patients.”
Dr. Louie has no disclosures.
SEATTLE – In patients with pancreatic cancer, an interval of 8 weeks between receiving neoadjuvant chemoradiation and surgical resection may improve resection margins, according to findings presented at the annual Society of Surgical Oncology Cancer Symposium.
The delay in resection did not negatively impact outcomes, and there was a modest improvement in overall survival among patients who had an 8-10 week interval between treatments.
“Attention should be focused on the treatment interval to time of resection in prospective studies,” said lead study author Raphael J. Louie, MD, of Dartmouth (N.H.) Hitchcock Norris Cotton Cancer Center.
Dr. Louie explained that for patients with pancreatic adenocarcinoma who receive neoadjuvant chemoradiation, it is unclear how long the optimal interval should be between therapy completion and surgical resection.
For this study, Dr. Louie and his colleagues sought to determine the optimal interval between neoadjuvant therapy and surgery to maximize response and oncologic outcomes.
“We hypothesized that there may be benefit to a delay,” he said.
The retrospective analysis included 637 patients who had been diagnosed with pancreatic adenocarcinoma at the Norris Cotton Cancer Center, and who had completed neoadjuvant chemoradiation and underwent R0 surgical resection between Jan. 1, 2004, and Dec. 31, 2015.
Of this group, 195 patients had metastatic disease, 28 underwent upfront surgical exploration, and 94 were lost to follow-up or had a poor performance status and were not included in the final analysis.
The cohort was grouped according to time from chemoradiation completion to surgery: 6-8 weeks, 8-10 weeks, and more than 10 weeks.
A total of 320 patients received neoadjuvant chemoradiation and 288 completed the full course. Of this group, 128 were evaluable by pathologic review.
Among patients with a 6- to 8-week interval, 61% had an R0 resection margin. This percentage rose to 72% for those who had an 8- to 10-week interval, and in similar fashion, 70% for those who had a 10- to 13-week interval (P = .6)
However, there was no statistical difference when the three groups were compared collectively.
Of 26 patients who were resected within 6-8 weeks of chemoradiation, 11% achieved a complete response (CR), 27% had a partial response (PR), and 61% had recurrence for an average disease-free survival of 20 months.
In the group (n = 58) of patients who were resected within 8-10 weeks, 7% had CR, 71% had PR, and 62% had recurrence, for an average disease-free survival of 17 months. Finally, the 44 patients who were resected within 10-13 weeks had similar outcomes; 5% had CR, 61% had PR, and 61% of patients had recurrence for an average disease-free survival of 14 months.
Dr. Louie noted that even though they observed improved PR in the 8- to 10-week group, there was no statistical significance in disease-free survival (P = .71) or overall survival (P = .19).
“Allowing more time from neoadjuvant therapy completion to surgical resection may improve the pathologic response,” said Dr. Louie. “Larger studies are needed to determine if the time interval to surgical resection has oncologic benefit for these patients.”
Dr. Louie has no disclosures.
AT SSO 2017
Key clinical point: A longer interval between neoadjuvant therapy and surgical resection could improve some outcomes in pancreatic cancer.
Major finding: Resection after 8 weeks may improve resection margins and may provide a modest improvement in survival for some patients.
Data source: Retrospective cohort study of 128 evaluable patients with biopsy-proven pancreatic adenocarcinoma who received neoadjuvant chemoradiation.
Disclosures: Dr. Louie has no disclosures.
Guideline endorses doublet therapy after pancreatic cancer surgery in chemo-naive patients
A recommendation on postop adjuvant chemotherapy has been updated in the Potentially Curable Pancreatic Cancer: American Society of Clinical Oncology Clinical Practice Guideline, according to an article published online on April 11 in the Journal of Clinical Oncology.
In the absence of medical or surgical contraindications, all patients who have resected pancreatic cancer and did not receive preoperative therapy should be offered 6 months of adjuvant chemotherapy, according to the new recommendation. “The doublet regimen of gemcitabine and capecitabine is preferred in the absence of concerns for toxicity or tolerance; alternatively, monotherapy with gemcitabine or fluorouracil plus folinic acid can be offered. Adjuvant treatment should be initiated within 8 weeks of surgical resection, assuming complete recovery,” Alok A. Khorana, MD, of the Cleveland Clinic, and members of the guideline committee wrote.
The recommendation was based on results of the ESPAC-4 study, a multicenter, international, open-label randomized controlled phase III trial (Lancet. 2017;389:1011-24). ESPAC-4 compared adjuvant combination chemotherapy of gemcitabine and capecitabine with gemcitabine monotherapy in 730 evaluable patients with resected pancreatic ductal adenocarcinoma.
Median overall survival was 28 months (95% confidence interval, 23.5-31.5 months) in the doublet arm and 25.5 months (95% CI, 22.7 to 27.9 months) for gemcitabine alone (hazard ratio, 0.82; 95% CI, 0.68-0.98; P = .032). Grade 3 and 4 adverse events were similar in both arms, although higher rates of hand-foot syndrome and diarrhea occurred in patients randomly assigned to the doublet arm.
The remaining recommendations from the original 2016 ASCO guideline are unchanged.
The revised guideline is available at this link.
[email protected]
On Twitter @maryjodales
A recommendation on postop adjuvant chemotherapy has been updated in the Potentially Curable Pancreatic Cancer: American Society of Clinical Oncology Clinical Practice Guideline, according to an article published online on April 11 in the Journal of Clinical Oncology.
In the absence of medical or surgical contraindications, all patients who have resected pancreatic cancer and did not receive preoperative therapy should be offered 6 months of adjuvant chemotherapy, according to the new recommendation. “The doublet regimen of gemcitabine and capecitabine is preferred in the absence of concerns for toxicity or tolerance; alternatively, monotherapy with gemcitabine or fluorouracil plus folinic acid can be offered. Adjuvant treatment should be initiated within 8 weeks of surgical resection, assuming complete recovery,” Alok A. Khorana, MD, of the Cleveland Clinic, and members of the guideline committee wrote.
The recommendation was based on results of the ESPAC-4 study, a multicenter, international, open-label randomized controlled phase III trial (Lancet. 2017;389:1011-24). ESPAC-4 compared adjuvant combination chemotherapy of gemcitabine and capecitabine with gemcitabine monotherapy in 730 evaluable patients with resected pancreatic ductal adenocarcinoma.
Median overall survival was 28 months (95% confidence interval, 23.5-31.5 months) in the doublet arm and 25.5 months (95% CI, 22.7 to 27.9 months) for gemcitabine alone (hazard ratio, 0.82; 95% CI, 0.68-0.98; P = .032). Grade 3 and 4 adverse events were similar in both arms, although higher rates of hand-foot syndrome and diarrhea occurred in patients randomly assigned to the doublet arm.
The remaining recommendations from the original 2016 ASCO guideline are unchanged.
The revised guideline is available at this link.
[email protected]
On Twitter @maryjodales
A recommendation on postop adjuvant chemotherapy has been updated in the Potentially Curable Pancreatic Cancer: American Society of Clinical Oncology Clinical Practice Guideline, according to an article published online on April 11 in the Journal of Clinical Oncology.
In the absence of medical or surgical contraindications, all patients who have resected pancreatic cancer and did not receive preoperative therapy should be offered 6 months of adjuvant chemotherapy, according to the new recommendation. “The doublet regimen of gemcitabine and capecitabine is preferred in the absence of concerns for toxicity or tolerance; alternatively, monotherapy with gemcitabine or fluorouracil plus folinic acid can be offered. Adjuvant treatment should be initiated within 8 weeks of surgical resection, assuming complete recovery,” Alok A. Khorana, MD, of the Cleveland Clinic, and members of the guideline committee wrote.
The recommendation was based on results of the ESPAC-4 study, a multicenter, international, open-label randomized controlled phase III trial (Lancet. 2017;389:1011-24). ESPAC-4 compared adjuvant combination chemotherapy of gemcitabine and capecitabine with gemcitabine monotherapy in 730 evaluable patients with resected pancreatic ductal adenocarcinoma.
Median overall survival was 28 months (95% confidence interval, 23.5-31.5 months) in the doublet arm and 25.5 months (95% CI, 22.7 to 27.9 months) for gemcitabine alone (hazard ratio, 0.82; 95% CI, 0.68-0.98; P = .032). Grade 3 and 4 adverse events were similar in both arms, although higher rates of hand-foot syndrome and diarrhea occurred in patients randomly assigned to the doublet arm.
The remaining recommendations from the original 2016 ASCO guideline are unchanged.
The revised guideline is available at this link.
[email protected]
On Twitter @maryjodales
FROM THE JOURNAL OF CLINICAL ONCOLOGY
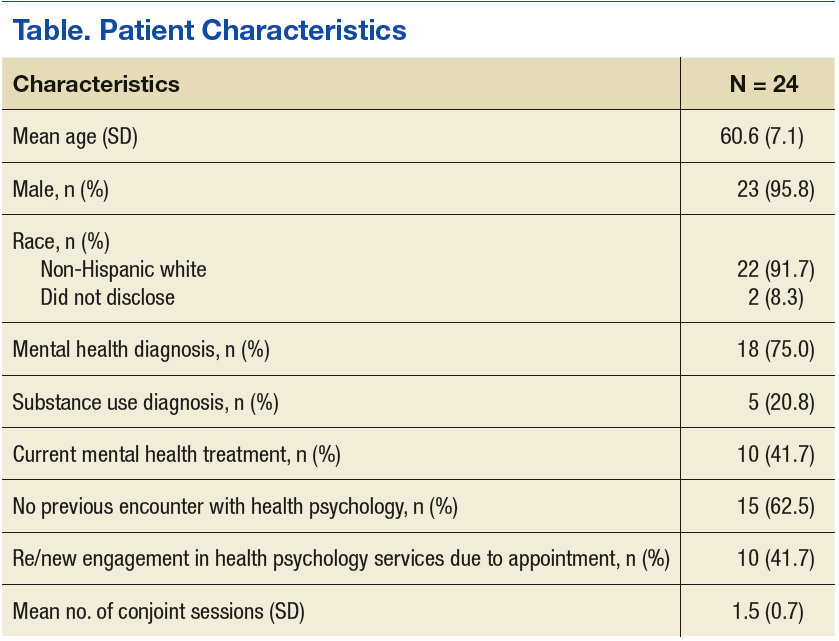
Conjoint Sessions With Clinical Pharmacy and Health Psychology for Chronic Pain
Providing comprehensive, integrated, behavioral intervention services to address the prevalent condition of chronic, noncancer pain is a growing concern. Although the biopsychosocial model (BPS) and stepped-care approaches have been understood and discussed for some time, clinician and patient understanding and investment in these approaches continue to face challenges. Moreover, even when resources (eg, staffing, referral options, space) are available, clinicians and patients must engage in meaningful communication to achieve this type of care.
Importantly, engagement means moving beyond diagnosis and assessment and offering interventions that provide psychoeducation related to the chronic pain cycle. These interventions address maladaptive cognitions and beliefs about movement and pain; promote paced, daily physical activity and engagement in life; and help increase coping skills to improve low mood or distress, all fundamental components of the BPS understanding of chronic pain.
Background
Chronic, noncancer pain is a prevalent presentation in primary care settings in the U.S. and even more so for veterans.1 Fifty percent of male veterans and 75% of female veterans report chronic pain as an important condition that impacts their health.2 An important aspect of this prevalence is the focus on opioid pain medication and medical procedures, both of which draw more narrowly on the biomedical model. Additional information on the longer term use of pain procedures and opioid medications is now available,and given some risks and limitations (eg, tolerance, decreasing efficacy, opioid-induced medical complications), the need to study and offer other options is gaining attention.3 Behavioral chronic pain management has a clear historic role that draws on the BPS modeland Gate Control Theory.3-6
More recently, the National Strategy of Chronic Pain collaborative and stepped-care models extended this literature, outlining collaboration and levels of care depending on the chronicity of the pain experience as well as co-occurring conditions and patient presentations.7,8 The Commission on Accreditation of Rehabilitation Facilities (CARF), the gold standard in interdisciplinary pain management programs, calls for further resources and coordination of these efforts, including a tertiary level of care representing the highest step in the stepped-care model.8
These interdisciplinary, integrative pain management programs, which include functional restoration and cognitive behavioral therapy (CBT) interventions, have been effective for the treatment of chronic pain.9-12However, the staffing, resources, clinical access, and coordination of this complex care may not be feasible in many health care settings. For example, a 2005 survey reported that there were only 200 multidisciplinary pain programs in the U.S., and only 84 of them were CARF accredited.13 By 2011 the number of CARF-accredited programs had decreased to 64 (the number of nonaccredited programs was not reported for 2011).13
Furthermore, engagement in behavioral pain management services is a challenge: Studies show that psychosocial interventions are underused, and a majority of studies may not report quantitatively or qualitatively on patient adherence or engagement in these services.14 These realities introduce the idea that coordinated appointments between 2 or 3 different disciplines available in primary care may be a feasible step toward implementing more comprehensive, optimal care models.
Behavioral pain management interventions that uphold the BPS also call on the idea of active self-management. Therefore, effective communication is fundamental at both the provider-patient and interprofessional levels to enhance engagement in health care, receptiveness to interventions, and to self-management of chronic pain.11,15 How clinicians conceptualize, hold assumptions about, and communicate with patients about chronic pain management has received more attention.15,16
Clinician Considerations for Pain Management
On theclinicians’ side, monitoring assumptions about patients and awareness of their beliefs as well as the care itself are foundational in patient interactions, impacting the success of patient engagement. Awareness of the language used in these interactions and how clinicians collaborate with other professionals become salient. Coupled with the reality of high attrition, this discussion lends itself in important ways to the motivational interviewing (MI) approach that aims to meet patients “where they are” by use of open-ended questions and reflective listening to guide the conversation in the direction of contemplating or actual behavior change.17 For example, “What do you think are the best ways to manage your pain?” and “It sounds like sometimes the medicine helps, but you also want more options to feel in control of your pain.”
Given the historic focus on the biomedical approach to chronic pain, including the use of opioid medications and medical procedures as well as traditional challenges to engagement in CBT, researchers have explored whether alternative methods may increase participation and improve outcomes for behavioral self-management.3 Drawing on a history of assessing readiness for change in pain management, Kerns and colleagues offered tailored cognitive strategies or behavioral skills training depending on patient preferences.18,19 These researchers also incorporated motivational enhancement strategies in the tailored interventions and compared engagement with standard CBT for chronic pain protocol. Although they did not find significant differences in engagement between the 2 groups, participation and treatment adherence were associated with posttreatment improvements in both groups.19 Taking a step back from enhancing intervention engagement, first assessing readiness to self-manage becomes another salient exploration and step in the process.
Another element of engagement in services is referral to other clinicians. Dorflinger and colleagues made this point in a conceptual paper that broadly outlined interdisciplinary, integrative, and more comprehensive models of care for chronic pain.15 We know from integrated models that referral-based care may decrease the likelihood of participation in health care services. That is, if a patient needs to make a separate appointment and meet with a new clinician, they are more likely to decline, cancel, or not show, particularly if they are not “ready” for change. Co-located or embedded care and conjoint sessions that include a warm handoff or another clinician who joins the first appointment may reduce stigma and other relevant barriers for introducing a patient to new ideas.20
Using a conjoint session that involves a clinical pharmacy pain specialist and a health psychologist is one way in which veterans can be exposed to more chronic pain-related BPS concepts and behavioral health services than they might be exposed to otherwise. The purpose of this project was to bring awareness to a practical and clinically relevant integrated approach to the dissemination of BPS information for chronic pain management.
In providing this information through effective communication at the patient-provider and interprofessional levels, the clinicians’ intention was to increase patient engagement and use of BPS strategies in the self-management of chronic pain. This project also aimed to enhance engagement and improve the quality of services before acquiring additional positions and funding for a specialized pain management team. These sessions were offered at the VA Ann Arbor Healthcare System (VAAAHS) in Michigan. Quantitative and qualitative information was examined from the conjoint and subsequent sessions that occurred in this setting.
Methods
With the above concepts in mind, VAAAHS offered veterans conjoint sessions involving a health psychologist and clinical pharmacy specialist during a 3-month period while this resource was available. The conjoint sessions were part of a preexisting pharmacist-run pain medication clinic embedded in primary care. The conjoint session was presented to patients as part of general clinic flow to reduce stigma of engagement in psychological services and allow for the dissemination of BPS information.
Participants
The electronic health records (EHR) of 24 veteran patients with chronic pain, who participated in a conjoint health psychology/pain pharmacy session, were reviewed for the current study. Most of the patients were male (95.8%) and non-Hispanic white (91.7%); the remaining participants did not disclose their ethnicity. The mean age was 60.6 years (SD 7.1; range 50-80). A total of 75% had a mental health diagnosis, and 41.7% were in mental health treatment at the time of the conjoint appointment. Among the sample, 20.8% had a current diagnosis of a substance use disorder (SUD), and no individuals were in treatment for a SUD at the time of the conjoint appointment. Patients received an average of 1.5 conjoint sessions (SD 0.7; range 1-3).
Procedure
The veterans for this project were chosen from a panel of patients followed by the pain medication clinical pharmacy specialist in the primary care pain medication clinic. The selected veterans were offered a joint session with their clinical pharmacy provider and the health psychology resident during their scheduled visit in the pain medication clinic. Each veteran was informed that the goal of the joint visit was to enhance self-directed nonpharmacologic chronic pain management skills as an additional set of tools in the tool kit for particularly difficult pain days. Veterans were assured that their usual care would not be compromised if they declined the session.
During the encounter(s), the health psychologist contributed to the veteran’s care by using MI and CBT for chronic pain skills. The health psychologist further assessed concerns and needs and guided the discussion as appropriate. With veteran readiness, these discussions explored the degree of knowledge and cognitive and behavioral coping skills the patient used. These conjoint sessions also documented the types of discussions and degree of engagement in the encounter(s) as well additional referrals, complementary services, and/or offered follow-up services for either additional conjoint sessions or further health psychology-related services.
A total of 24 EHRs from these conjoint and subsequent encounters were reviewed for evidence of the procedures by a psychology intern involved in chronic pain management services. Of these 24 records, 6 also were reviewed by a board-certified health psychologist for consensus building and agreement on coding (Sidebar, Record Coding).
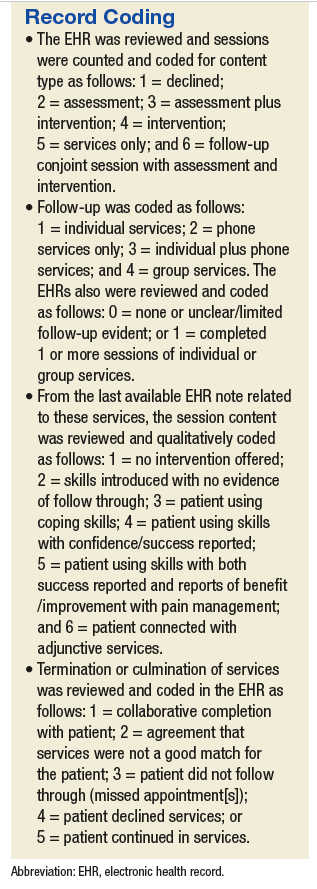
Using the coding system and SPSS Version 2.1 (IBM, Armonk NY), descriptive statistics were used to examine conjoint session content and new- or re-engagement in health psychology services following the conjoint sessions. For those patients who followed up with additional services, the content, type, and outcome of these services were explored. Next, linear regression was used to determine whether number of conjoint sessions was associated with a qualitative treatment outcome, and 2 logistic regressions were used to determine whether the number of sessions was associated with the likelihood of accepting services and follow-through with services after accepting them. An additional logistic regression examined whether having a mental health diagnosis (yes/no) was associated with whether the individual accepted additional health psychology services. Finally, independent sample t tests examined differences between those who accepted services vs those who declined follow-up services in substance use diagnosis, mental health diagnosis, and previous health psychology services engagement. Of note, given the small sample size, the Levene’s test for equality of variances was conducted and unequal variances were assumed.
Results
All 24 patients agreed to have the conjoint session with the clinical pharmacy specialist and health psychologist. Of the participants, 62.5% had no previous interaction with health psychology services. Among those who had previous encounters with health psychology services, 12.5% had participated in 1 or more group sessions, another 12.5% had participated in 1 or more individual sessions, and an additional 12.5% had been referred for health psychology services but had not followed through. A total of 10 participants represented a new- or re-engagement in health psychology services following the conjoint appointment. Two patients were referred for additional services as a result of their conjoint appointment (1 to specialty mental health and another to Primary Care-Mental Health Integration [PC-MHI]), and 1 of the participants followed through with the referral. Finally, with regard to the content of the initial session, 37.5% of the sessions contained some form of psychoeducation, 54.2% contained a functional assessment, and 41.7% contained an introduction of skills.
Half of the veterans participated in health psychology services beyond the initial conjoint session. Four of these veterans participated in additional conjoint sessions, and the remaining 8 engaged in health psychology services, which took the form of telephone sessions (3), in-person sessions (3), or a combination of both telephone and in-person sessions (2). Twelve veterans participated in an average of 3.4 (SD 3.7) follow-up sessions. In terms of the content of these follow-up sessions, across all formats and types, 3 included some introduction to coping skills, with no documented evidence of follow-through. For 2 of the veterans engaging in some type of follow-up, there was documented use of coping skills, and 2 used the coping skills with self-reported success and benefit. Finally, documentation revealed evidence that 3 of these veterans were not only using the coping skills with benefit, but also reported an improvement in pain management overall. One also was connected with a different service.
Regarding reasons for completion of services, 2 veterans were terminated due to completing treatment/meeting goals, 2 were terminated because they did not follow up after a session, 7 were terminated due to patient declining additional sessions, and 1 veteran was still receiving services at the time of the review. Linear regression indicated that the number of conjoint sessions was not associated with qualitative treatment outcome. Two logistic regressions indicated that number of conjoint sessions was not related to whether the veteran accepted follow-up services or whether the veteran followed through with services after accepting. Of note, logistic regression indicated that having a mental health diagnosiswas associated with a decreased likelihood of accepting health psychology services (P = .03). Regarding the independent samples t tests, veterans who did not accept follow-up services were more likely to have a mental health diagnosis (P = .03). The groups did not differ significantly with regard to substance use diagnosis or previous engagement in health psychology services.
Discussion
Results showed that all 24 veterans who were offered a conjoint session with a clinical pharmacy specialist and health psychologist engaged in at least 1 session. Half the veterans participated in further services as well. Both the initial conjoint and follow-up sessions offered a greater degree of communication related to the cognitive-behavioral and functional restoration components of behavioral pain management. Given that a majority of the sample had not participated in behavioral or mental health services previously, this may represent a greater penetration rate of exposure to mental health service for veterans than would have been available otherwise.
More specifically, qualitative results suggest that in these conjoint sessions, the veterans were exposed to behavioral psychotherapeutic approaches to chronic pain management (eg, health behavior change, motivational enhancement, health-related psychoeducation, and CBT for chronic pain) that again may not have been provided otherwise (ie, via referral and separately scheduled sessions). These findings are supported by theories consistent with the Transtheoretical Model, which indicates that individuals fall in varying degrees of readiness for behavioral change (ie, precontemplative, contemplative, planning, action, maintenance).21,22 Thus, behavioral intervention approaches must be adaptive and adjust format and communication, including the amount and type of psychoeducation offered. Moreover, the integrated theory of health behavior change in the context of chronic pain management calls for fostering awareness, knowledge, and beliefs through effective communication and education for a wide range of individuals who are at varying stages of change.23 In addition to the conjoint session and subsequent service(s) content that were reviewed and coded in this current project, future projects might draw on these theoretical models and code sessions for patients’ stages of change and assess whether a patient made progress across phases of change (eg, the patient shifted from contemplative to the planning stage of change).
Within this project’s conjoint sessions and consistent with MI principles, veterans were offered discussions related to the bidirectional and BPS aspects of their own chronic pain experience. That is, while discussing responses and adjustment to pain medication(s), veterans received reflections with MI and heard feedback related to their current coping strategies, methods to enhance coping, as well as potential psychosocial impacts of their chronic pain experience. With permission, veterans also were introduced to themes that comprised evidence-based CBT for chronic pain (CBT-CP) intervention. Understanding what change means in the context of chronic pain management is critical. That is, tipping the conversation toward consideration of alternative modalities (eg, relaxation, stress management, cognitions, and pain) in conjunction with or in place of the traditional modalities (eg, medication, pain procedures) is paramount.
Clinicians must listen for patient ambivalence related to procedures, interventions, medication changes, and/or the behavioral self-management of chronic pain. This type of active listening and exploration may be more likely when there is collaboration and effective team functioning among clinicians than when clinicians provide care independently. Future quality improvement (QI) or research projects could extend the EHR review and evaluate clinician-patient transcripts for fidelity to the CBT-CP and MI models. Such efforts could assess for associations between clinician MI consistent behaviors and change talk on the part of the patient. Furthermore, clinician communication and patient change talk from transcripts could be evaluated in relation to evidence from the EHR regarding patient use of coping skills and behavior change.
Consistent with behavioral health literature, having a mental health diagnosis was associated with declining additional behavioral health psychology services in this project. Research has shown that individuals with a mental health diagnosis tend to engage less in behavioral health self-management programs, such as chronic headache and weight management.24-26 This phenomenon lends support for the importance of health care professionals (HCPs) to increase access and exposure to mental and behavioral health services, such as the PC-MHI model.20 In fact, chronic pain management program development efforts within the VA system nationwide include collaboration with the PC-MHI services. One of the initial goals for PC-MHI services is to increase penetration rates into the general outpatient medical clinics and enhance engagement in mental health services.
Using conjoint sessions as was offered in the current project is one step in the development of more comprehensive interdisciplinary teams through interprofessional collaboration and the use of effective clinical communication. In turn, it will be important to directly explore the communication skills and attitudes of these HCPs with regard to interdisciplinary program development and collaboration as teams continue to integrate more broadly into the medical system and enhance chronic pain management services.11 Similarly, measuring the perceptions of clinical pharmacy specialists, physicians, health psychologists, or other clinical disciplines involved in chronic pain management could be another area to explore. More specific to MI, clinician confidence in the use of effective communication and MI skills represents still another area for future study.16
Limitations
Some limitations and suggested future directions found as part of this QI project have been outlined earlier. Other limitations include the used of a retrospective review of information available in patient medical charts. More developed measurement-based care or research could collect self-reports of patient satisfaction with care, functioning, knowledge, readiness for change, and mood in addition to what is noted and documented in clinical observations. Second, the sample was small and did not include any female and few younger veterans, even though these are important subpopulations when examining pain management services. When resources are available for a larger sample size, some exploratory analyses could be conducted for differences in engagement among subgroups. Third, this project may have further confounding variables as this was not an experimental or a controlled study, which could directly compare conjoint sessions with referral-based care and/or those not offered conjoint sessions.
Conclusion
The optimal method of behavioral pain management suggests the need for an interdisciplinary, coordinated team approach, in which the gold standard programs meet requirements set by CARF. However, on a practical level, optimal behavioral pain management may not be feasible at all health care facilities. Furthermore, in an effort to provide best practices to individuals with chronic pain, clinicians must be adaptive and skilled in using effective communication and specialized interventions, such as CBT and MI.
Approaching the more optimal behavioral self-management of chronic pain from a multimodal interdisciplinary perspective and further engaging veterans in this care is paramount. This project is merely one step in this effort that can shed light on the function and logistic outcomes of using a practical, integrated approach to chronic pain. It demonstrates that implementing best practices founded in sound theoretical models despite staffing and resource constraints is possible. Thus, continuing to explore the utility of alternate modalities may offer important applied and translational information to help disseminate and improve chronic pain management services.
Future research could focus on important subpopulations and enhance experimental design with pre- and postmeasures, controlling for possible confounding variables and if possible a controlled design.
Acknowledgments
This quality improvement project was unfunded, and approval was confirmed with the VA Ann Arbor Healthcare System Institutional Review Board and Research & Development committees. The authors also thank Associate Chief of Staff, Ambulatory Care, Clinton Greenstone, MD, and Chief of Primary Care Adam Tremblay, MD, for their leadership and support of these integrative services and quality improvement efforts. The authors especially recognize the veterans for whom they aim to provide the highest quality of services possible.
1. Brooks PM. The burden of musculoskeletal disease—a global perspective. Clin Rheumatol. 2006;25(6):778-781.
2. Haskell SG, Heapy A, Reid MC, Papas RK, Kerns RD. The prevalence and age-related characteristics of pain in a sample of women veterans receiving primary care. J Womens Health (Larchmt). 2006;15(7):862-869.
3. Roth RS, Geisser ME, Williams DA. Interventional pain medicine: retreat from the biopsychosocial model of pain. Transl Behav Med. 2012;2(1):106-116.
4. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129-136.
5. Borrell-Carrió F, Suchman AL, Epstein RM. The biopsychosocial model 25 years later: principles, practice, and scientific inquiry. Ann Fam Med. 2004;2(6):576-582.
6. Wall PD. The gate control theory of pain mechanisms: a re-examination and re-statement. Brain. 1978;101(1):1-18.
7. Dobscha SK, Corson K, Perrin NA, et al. Collaborative care for chronic pain in primary care: a cluster randomized trial. JAMA. 2009;301(12):1242-1252.
8. Von Korff, Moore JC. Stepped care for back pain: activating approaches for primary care. Ann Intern Med. 2001;134(9, pt 2):911-917.
9. Oslund S, Robinson RC, Clark TC, et al. Long-term effectiveness of a comprehensive pain management program: strengthening the case for interdisciplinary care. Proc (Bayl Univ Med Cent). 2009;22(3):211-214.
10. Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: a systematic review of interventions and outcomes. Rheumatology (Oxford). 2008;47(5):670-678.
11. Gatchel RJ, McGeary DD, McGeary CA, Lippe B. Interdisciplinary chronic pain management: past, present, and future. Am Psychol. 2014;69(2):119-130.
12. McCracken LM, Turk DC. Behavioral and cognitive-behavioral treatment for chronic pain: outcome, predictors of outcome, and treatment process. Spine (Phila Pa 1976). 2002;27(22): 2564-2573.
13. Jeffery MM, Butler M, Stark A, Kane RL. Multidisciplinary Pain Programs for Chronic Noncancer Pain. Comparative Effectiveness Technical Briefs, No 8. Rockville, MD: Agency for Healthcare Research and Quality; 2011.
14. Ehde DM, Dilworth TM, Turner JA. Cognitive-behavioral therapy for individuals with chronic pain: efficacy, innovations, and directions for research. Am Psychol. 2014;69(2):153-166.
15. Dorflinger L, Kerns RD, Auerbach SM. Providers’ roles in enhancing patients’ adherence to pain self management. Transl Behav Med. 2013;3(1):39-46.
16. Pellico LH, Gilliam WP, Lee AW, Kerns RD. Hearing new voices: registered nurses and health technicians experience caring for chronic pain patients in primary care clinics. Open Nurs J. 2014;8:25-33.
17. Rollnick S, Miller WR, Butler CC, eds. Motivational Interviewing in Health Care: Helping Patients Change Behavior. New York, NY: The Guilford Press; 2008.
18. Kerns RD, Habib S. A critical review of the pain readiness to change model. J Pain. 2004;5(7):357-367.19. Kerns RD, Burns JW, Shulman M, et al. Can we improve cognitive-behavior therapy for chronic back pain treatment engagement and adherence? A controlled trial of tailored versus standard therapy. Health Psychol. 2014;33(9):938-947.
20. Kearney LK, Post EP, Zeiss A, Goldstein MG, Dundon M. The role of mental and behavioral health in the application of the patient-centered medical home in the Department of Veterans Affairs. Transl Behav Med. 2011;1(4):624-628.
21. Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol. 1983;51(3):390-395.
22. Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol. 1992;47(9):1102-1114.
23. Ryan P. Integrated theory of health behavior change: background and intervention development. Clin Nurse Spec. 2009;23(3):161-172.
24. Evans DD , Blanchard EB. Prediction of early termination from the self-regulatory treatment of chronic headache. Biofeedback Self Regul. 1988;13(3):245-256.
25. Maguen S, Hoerster KD, Littman AJ, et al. Iraq and Afghanistan veterans with PTSD participate less in VA’s weight loss program than those without PTSD. J Affect Disord. 2016;193:289-294.
26. Bloor LE. Improving weight management services for female veterans: design and participation factors with a women only program, and comparisons with gender neutral services. Med Res Arch. 2015;2.
Providing comprehensive, integrated, behavioral intervention services to address the prevalent condition of chronic, noncancer pain is a growing concern. Although the biopsychosocial model (BPS) and stepped-care approaches have been understood and discussed for some time, clinician and patient understanding and investment in these approaches continue to face challenges. Moreover, even when resources (eg, staffing, referral options, space) are available, clinicians and patients must engage in meaningful communication to achieve this type of care.
Importantly, engagement means moving beyond diagnosis and assessment and offering interventions that provide psychoeducation related to the chronic pain cycle. These interventions address maladaptive cognitions and beliefs about movement and pain; promote paced, daily physical activity and engagement in life; and help increase coping skills to improve low mood or distress, all fundamental components of the BPS understanding of chronic pain.
Background
Chronic, noncancer pain is a prevalent presentation in primary care settings in the U.S. and even more so for veterans.1 Fifty percent of male veterans and 75% of female veterans report chronic pain as an important condition that impacts their health.2 An important aspect of this prevalence is the focus on opioid pain medication and medical procedures, both of which draw more narrowly on the biomedical model. Additional information on the longer term use of pain procedures and opioid medications is now available,and given some risks and limitations (eg, tolerance, decreasing efficacy, opioid-induced medical complications), the need to study and offer other options is gaining attention.3 Behavioral chronic pain management has a clear historic role that draws on the BPS modeland Gate Control Theory.3-6
More recently, the National Strategy of Chronic Pain collaborative and stepped-care models extended this literature, outlining collaboration and levels of care depending on the chronicity of the pain experience as well as co-occurring conditions and patient presentations.7,8 The Commission on Accreditation of Rehabilitation Facilities (CARF), the gold standard in interdisciplinary pain management programs, calls for further resources and coordination of these efforts, including a tertiary level of care representing the highest step in the stepped-care model.8
These interdisciplinary, integrative pain management programs, which include functional restoration and cognitive behavioral therapy (CBT) interventions, have been effective for the treatment of chronic pain.9-12However, the staffing, resources, clinical access, and coordination of this complex care may not be feasible in many health care settings. For example, a 2005 survey reported that there were only 200 multidisciplinary pain programs in the U.S., and only 84 of them were CARF accredited.13 By 2011 the number of CARF-accredited programs had decreased to 64 (the number of nonaccredited programs was not reported for 2011).13
Furthermore, engagement in behavioral pain management services is a challenge: Studies show that psychosocial interventions are underused, and a majority of studies may not report quantitatively or qualitatively on patient adherence or engagement in these services.14 These realities introduce the idea that coordinated appointments between 2 or 3 different disciplines available in primary care may be a feasible step toward implementing more comprehensive, optimal care models.
Behavioral pain management interventions that uphold the BPS also call on the idea of active self-management. Therefore, effective communication is fundamental at both the provider-patient and interprofessional levels to enhance engagement in health care, receptiveness to interventions, and to self-management of chronic pain.11,15 How clinicians conceptualize, hold assumptions about, and communicate with patients about chronic pain management has received more attention.15,16
Clinician Considerations for Pain Management
On theclinicians’ side, monitoring assumptions about patients and awareness of their beliefs as well as the care itself are foundational in patient interactions, impacting the success of patient engagement. Awareness of the language used in these interactions and how clinicians collaborate with other professionals become salient. Coupled with the reality of high attrition, this discussion lends itself in important ways to the motivational interviewing (MI) approach that aims to meet patients “where they are” by use of open-ended questions and reflective listening to guide the conversation in the direction of contemplating or actual behavior change.17 For example, “What do you think are the best ways to manage your pain?” and “It sounds like sometimes the medicine helps, but you also want more options to feel in control of your pain.”
Given the historic focus on the biomedical approach to chronic pain, including the use of opioid medications and medical procedures as well as traditional challenges to engagement in CBT, researchers have explored whether alternative methods may increase participation and improve outcomes for behavioral self-management.3 Drawing on a history of assessing readiness for change in pain management, Kerns and colleagues offered tailored cognitive strategies or behavioral skills training depending on patient preferences.18,19 These researchers also incorporated motivational enhancement strategies in the tailored interventions and compared engagement with standard CBT for chronic pain protocol. Although they did not find significant differences in engagement between the 2 groups, participation and treatment adherence were associated with posttreatment improvements in both groups.19 Taking a step back from enhancing intervention engagement, first assessing readiness to self-manage becomes another salient exploration and step in the process.
Another element of engagement in services is referral to other clinicians. Dorflinger and colleagues made this point in a conceptual paper that broadly outlined interdisciplinary, integrative, and more comprehensive models of care for chronic pain.15 We know from integrated models that referral-based care may decrease the likelihood of participation in health care services. That is, if a patient needs to make a separate appointment and meet with a new clinician, they are more likely to decline, cancel, or not show, particularly if they are not “ready” for change. Co-located or embedded care and conjoint sessions that include a warm handoff or another clinician who joins the first appointment may reduce stigma and other relevant barriers for introducing a patient to new ideas.20
Using a conjoint session that involves a clinical pharmacy pain specialist and a health psychologist is one way in which veterans can be exposed to more chronic pain-related BPS concepts and behavioral health services than they might be exposed to otherwise. The purpose of this project was to bring awareness to a practical and clinically relevant integrated approach to the dissemination of BPS information for chronic pain management.
In providing this information through effective communication at the patient-provider and interprofessional levels, the clinicians’ intention was to increase patient engagement and use of BPS strategies in the self-management of chronic pain. This project also aimed to enhance engagement and improve the quality of services before acquiring additional positions and funding for a specialized pain management team. These sessions were offered at the VA Ann Arbor Healthcare System (VAAAHS) in Michigan. Quantitative and qualitative information was examined from the conjoint and subsequent sessions that occurred in this setting.
Methods
With the above concepts in mind, VAAAHS offered veterans conjoint sessions involving a health psychologist and clinical pharmacy specialist during a 3-month period while this resource was available. The conjoint sessions were part of a preexisting pharmacist-run pain medication clinic embedded in primary care. The conjoint session was presented to patients as part of general clinic flow to reduce stigma of engagement in psychological services and allow for the dissemination of BPS information.
Participants
The electronic health records (EHR) of 24 veteran patients with chronic pain, who participated in a conjoint health psychology/pain pharmacy session, were reviewed for the current study. Most of the patients were male (95.8%) and non-Hispanic white (91.7%); the remaining participants did not disclose their ethnicity. The mean age was 60.6 years (SD 7.1; range 50-80). A total of 75% had a mental health diagnosis, and 41.7% were in mental health treatment at the time of the conjoint appointment. Among the sample, 20.8% had a current diagnosis of a substance use disorder (SUD), and no individuals were in treatment for a SUD at the time of the conjoint appointment. Patients received an average of 1.5 conjoint sessions (SD 0.7; range 1-3).
Procedure
The veterans for this project were chosen from a panel of patients followed by the pain medication clinical pharmacy specialist in the primary care pain medication clinic. The selected veterans were offered a joint session with their clinical pharmacy provider and the health psychology resident during their scheduled visit in the pain medication clinic. Each veteran was informed that the goal of the joint visit was to enhance self-directed nonpharmacologic chronic pain management skills as an additional set of tools in the tool kit for particularly difficult pain days. Veterans were assured that their usual care would not be compromised if they declined the session.
During the encounter(s), the health psychologist contributed to the veteran’s care by using MI and CBT for chronic pain skills. The health psychologist further assessed concerns and needs and guided the discussion as appropriate. With veteran readiness, these discussions explored the degree of knowledge and cognitive and behavioral coping skills the patient used. These conjoint sessions also documented the types of discussions and degree of engagement in the encounter(s) as well additional referrals, complementary services, and/or offered follow-up services for either additional conjoint sessions or further health psychology-related services.
A total of 24 EHRs from these conjoint and subsequent encounters were reviewed for evidence of the procedures by a psychology intern involved in chronic pain management services. Of these 24 records, 6 also were reviewed by a board-certified health psychologist for consensus building and agreement on coding (Sidebar, Record Coding).
Using the coding system and SPSS Version 2.1 (IBM, Armonk NY), descriptive statistics were used to examine conjoint session content and new- or re-engagement in health psychology services following the conjoint sessions. For those patients who followed up with additional services, the content, type, and outcome of these services were explored. Next, linear regression was used to determine whether number of conjoint sessions was associated with a qualitative treatment outcome, and 2 logistic regressions were used to determine whether the number of sessions was associated with the likelihood of accepting services and follow-through with services after accepting them. An additional logistic regression examined whether having a mental health diagnosis (yes/no) was associated with whether the individual accepted additional health psychology services. Finally, independent sample t tests examined differences between those who accepted services vs those who declined follow-up services in substance use diagnosis, mental health diagnosis, and previous health psychology services engagement. Of note, given the small sample size, the Levene’s test for equality of variances was conducted and unequal variances were assumed.
Results
All 24 patients agreed to have the conjoint session with the clinical pharmacy specialist and health psychologist. Of the participants, 62.5% had no previous interaction with health psychology services. Among those who had previous encounters with health psychology services, 12.5% had participated in 1 or more group sessions, another 12.5% had participated in 1 or more individual sessions, and an additional 12.5% had been referred for health psychology services but had not followed through. A total of 10 participants represented a new- or re-engagement in health psychology services following the conjoint appointment. Two patients were referred for additional services as a result of their conjoint appointment (1 to specialty mental health and another to Primary Care-Mental Health Integration [PC-MHI]), and 1 of the participants followed through with the referral. Finally, with regard to the content of the initial session, 37.5% of the sessions contained some form of psychoeducation, 54.2% contained a functional assessment, and 41.7% contained an introduction of skills.
Half of the veterans participated in health psychology services beyond the initial conjoint session. Four of these veterans participated in additional conjoint sessions, and the remaining 8 engaged in health psychology services, which took the form of telephone sessions (3), in-person sessions (3), or a combination of both telephone and in-person sessions (2). Twelve veterans participated in an average of 3.4 (SD 3.7) follow-up sessions. In terms of the content of these follow-up sessions, across all formats and types, 3 included some introduction to coping skills, with no documented evidence of follow-through. For 2 of the veterans engaging in some type of follow-up, there was documented use of coping skills, and 2 used the coping skills with self-reported success and benefit. Finally, documentation revealed evidence that 3 of these veterans were not only using the coping skills with benefit, but also reported an improvement in pain management overall. One also was connected with a different service.
Regarding reasons for completion of services, 2 veterans were terminated due to completing treatment/meeting goals, 2 were terminated because they did not follow up after a session, 7 were terminated due to patient declining additional sessions, and 1 veteran was still receiving services at the time of the review. Linear regression indicated that the number of conjoint sessions was not associated with qualitative treatment outcome. Two logistic regressions indicated that number of conjoint sessions was not related to whether the veteran accepted follow-up services or whether the veteran followed through with services after accepting. Of note, logistic regression indicated that having a mental health diagnosiswas associated with a decreased likelihood of accepting health psychology services (P = .03). Regarding the independent samples t tests, veterans who did not accept follow-up services were more likely to have a mental health diagnosis (P = .03). The groups did not differ significantly with regard to substance use diagnosis or previous engagement in health psychology services.
Discussion
Results showed that all 24 veterans who were offered a conjoint session with a clinical pharmacy specialist and health psychologist engaged in at least 1 session. Half the veterans participated in further services as well. Both the initial conjoint and follow-up sessions offered a greater degree of communication related to the cognitive-behavioral and functional restoration components of behavioral pain management. Given that a majority of the sample had not participated in behavioral or mental health services previously, this may represent a greater penetration rate of exposure to mental health service for veterans than would have been available otherwise.
More specifically, qualitative results suggest that in these conjoint sessions, the veterans were exposed to behavioral psychotherapeutic approaches to chronic pain management (eg, health behavior change, motivational enhancement, health-related psychoeducation, and CBT for chronic pain) that again may not have been provided otherwise (ie, via referral and separately scheduled sessions). These findings are supported by theories consistent with the Transtheoretical Model, which indicates that individuals fall in varying degrees of readiness for behavioral change (ie, precontemplative, contemplative, planning, action, maintenance).21,22 Thus, behavioral intervention approaches must be adaptive and adjust format and communication, including the amount and type of psychoeducation offered. Moreover, the integrated theory of health behavior change in the context of chronic pain management calls for fostering awareness, knowledge, and beliefs through effective communication and education for a wide range of individuals who are at varying stages of change.23 In addition to the conjoint session and subsequent service(s) content that were reviewed and coded in this current project, future projects might draw on these theoretical models and code sessions for patients’ stages of change and assess whether a patient made progress across phases of change (eg, the patient shifted from contemplative to the planning stage of change).
Within this project’s conjoint sessions and consistent with MI principles, veterans were offered discussions related to the bidirectional and BPS aspects of their own chronic pain experience. That is, while discussing responses and adjustment to pain medication(s), veterans received reflections with MI and heard feedback related to their current coping strategies, methods to enhance coping, as well as potential psychosocial impacts of their chronic pain experience. With permission, veterans also were introduced to themes that comprised evidence-based CBT for chronic pain (CBT-CP) intervention. Understanding what change means in the context of chronic pain management is critical. That is, tipping the conversation toward consideration of alternative modalities (eg, relaxation, stress management, cognitions, and pain) in conjunction with or in place of the traditional modalities (eg, medication, pain procedures) is paramount.
Clinicians must listen for patient ambivalence related to procedures, interventions, medication changes, and/or the behavioral self-management of chronic pain. This type of active listening and exploration may be more likely when there is collaboration and effective team functioning among clinicians than when clinicians provide care independently. Future quality improvement (QI) or research projects could extend the EHR review and evaluate clinician-patient transcripts for fidelity to the CBT-CP and MI models. Such efforts could assess for associations between clinician MI consistent behaviors and change talk on the part of the patient. Furthermore, clinician communication and patient change talk from transcripts could be evaluated in relation to evidence from the EHR regarding patient use of coping skills and behavior change.
Consistent with behavioral health literature, having a mental health diagnosis was associated with declining additional behavioral health psychology services in this project. Research has shown that individuals with a mental health diagnosis tend to engage less in behavioral health self-management programs, such as chronic headache and weight management.24-26 This phenomenon lends support for the importance of health care professionals (HCPs) to increase access and exposure to mental and behavioral health services, such as the PC-MHI model.20 In fact, chronic pain management program development efforts within the VA system nationwide include collaboration with the PC-MHI services. One of the initial goals for PC-MHI services is to increase penetration rates into the general outpatient medical clinics and enhance engagement in mental health services.
Using conjoint sessions as was offered in the current project is one step in the development of more comprehensive interdisciplinary teams through interprofessional collaboration and the use of effective clinical communication. In turn, it will be important to directly explore the communication skills and attitudes of these HCPs with regard to interdisciplinary program development and collaboration as teams continue to integrate more broadly into the medical system and enhance chronic pain management services.11 Similarly, measuring the perceptions of clinical pharmacy specialists, physicians, health psychologists, or other clinical disciplines involved in chronic pain management could be another area to explore. More specific to MI, clinician confidence in the use of effective communication and MI skills represents still another area for future study.16
Limitations
Some limitations and suggested future directions found as part of this QI project have been outlined earlier. Other limitations include the used of a retrospective review of information available in patient medical charts. More developed measurement-based care or research could collect self-reports of patient satisfaction with care, functioning, knowledge, readiness for change, and mood in addition to what is noted and documented in clinical observations. Second, the sample was small and did not include any female and few younger veterans, even though these are important subpopulations when examining pain management services. When resources are available for a larger sample size, some exploratory analyses could be conducted for differences in engagement among subgroups. Third, this project may have further confounding variables as this was not an experimental or a controlled study, which could directly compare conjoint sessions with referral-based care and/or those not offered conjoint sessions.
Conclusion
The optimal method of behavioral pain management suggests the need for an interdisciplinary, coordinated team approach, in which the gold standard programs meet requirements set by CARF. However, on a practical level, optimal behavioral pain management may not be feasible at all health care facilities. Furthermore, in an effort to provide best practices to individuals with chronic pain, clinicians must be adaptive and skilled in using effective communication and specialized interventions, such as CBT and MI.
Approaching the more optimal behavioral self-management of chronic pain from a multimodal interdisciplinary perspective and further engaging veterans in this care is paramount. This project is merely one step in this effort that can shed light on the function and logistic outcomes of using a practical, integrated approach to chronic pain. It demonstrates that implementing best practices founded in sound theoretical models despite staffing and resource constraints is possible. Thus, continuing to explore the utility of alternate modalities may offer important applied and translational information to help disseminate and improve chronic pain management services.
Future research could focus on important subpopulations and enhance experimental design with pre- and postmeasures, controlling for possible confounding variables and if possible a controlled design.
Acknowledgments
This quality improvement project was unfunded, and approval was confirmed with the VA Ann Arbor Healthcare System Institutional Review Board and Research & Development committees. The authors also thank Associate Chief of Staff, Ambulatory Care, Clinton Greenstone, MD, and Chief of Primary Care Adam Tremblay, MD, for their leadership and support of these integrative services and quality improvement efforts. The authors especially recognize the veterans for whom they aim to provide the highest quality of services possible.
Providing comprehensive, integrated, behavioral intervention services to address the prevalent condition of chronic, noncancer pain is a growing concern. Although the biopsychosocial model (BPS) and stepped-care approaches have been understood and discussed for some time, clinician and patient understanding and investment in these approaches continue to face challenges. Moreover, even when resources (eg, staffing, referral options, space) are available, clinicians and patients must engage in meaningful communication to achieve this type of care.
Importantly, engagement means moving beyond diagnosis and assessment and offering interventions that provide psychoeducation related to the chronic pain cycle. These interventions address maladaptive cognitions and beliefs about movement and pain; promote paced, daily physical activity and engagement in life; and help increase coping skills to improve low mood or distress, all fundamental components of the BPS understanding of chronic pain.
Background
Chronic, noncancer pain is a prevalent presentation in primary care settings in the U.S. and even more so for veterans.1 Fifty percent of male veterans and 75% of female veterans report chronic pain as an important condition that impacts their health.2 An important aspect of this prevalence is the focus on opioid pain medication and medical procedures, both of which draw more narrowly on the biomedical model. Additional information on the longer term use of pain procedures and opioid medications is now available,and given some risks and limitations (eg, tolerance, decreasing efficacy, opioid-induced medical complications), the need to study and offer other options is gaining attention.3 Behavioral chronic pain management has a clear historic role that draws on the BPS modeland Gate Control Theory.3-6
More recently, the National Strategy of Chronic Pain collaborative and stepped-care models extended this literature, outlining collaboration and levels of care depending on the chronicity of the pain experience as well as co-occurring conditions and patient presentations.7,8 The Commission on Accreditation of Rehabilitation Facilities (CARF), the gold standard in interdisciplinary pain management programs, calls for further resources and coordination of these efforts, including a tertiary level of care representing the highest step in the stepped-care model.8
These interdisciplinary, integrative pain management programs, which include functional restoration and cognitive behavioral therapy (CBT) interventions, have been effective for the treatment of chronic pain.9-12However, the staffing, resources, clinical access, and coordination of this complex care may not be feasible in many health care settings. For example, a 2005 survey reported that there were only 200 multidisciplinary pain programs in the U.S., and only 84 of them were CARF accredited.13 By 2011 the number of CARF-accredited programs had decreased to 64 (the number of nonaccredited programs was not reported for 2011).13
Furthermore, engagement in behavioral pain management services is a challenge: Studies show that psychosocial interventions are underused, and a majority of studies may not report quantitatively or qualitatively on patient adherence or engagement in these services.14 These realities introduce the idea that coordinated appointments between 2 or 3 different disciplines available in primary care may be a feasible step toward implementing more comprehensive, optimal care models.
Behavioral pain management interventions that uphold the BPS also call on the idea of active self-management. Therefore, effective communication is fundamental at both the provider-patient and interprofessional levels to enhance engagement in health care, receptiveness to interventions, and to self-management of chronic pain.11,15 How clinicians conceptualize, hold assumptions about, and communicate with patients about chronic pain management has received more attention.15,16
Clinician Considerations for Pain Management
On theclinicians’ side, monitoring assumptions about patients and awareness of their beliefs as well as the care itself are foundational in patient interactions, impacting the success of patient engagement. Awareness of the language used in these interactions and how clinicians collaborate with other professionals become salient. Coupled with the reality of high attrition, this discussion lends itself in important ways to the motivational interviewing (MI) approach that aims to meet patients “where they are” by use of open-ended questions and reflective listening to guide the conversation in the direction of contemplating or actual behavior change.17 For example, “What do you think are the best ways to manage your pain?” and “It sounds like sometimes the medicine helps, but you also want more options to feel in control of your pain.”
Given the historic focus on the biomedical approach to chronic pain, including the use of opioid medications and medical procedures as well as traditional challenges to engagement in CBT, researchers have explored whether alternative methods may increase participation and improve outcomes for behavioral self-management.3 Drawing on a history of assessing readiness for change in pain management, Kerns and colleagues offered tailored cognitive strategies or behavioral skills training depending on patient preferences.18,19 These researchers also incorporated motivational enhancement strategies in the tailored interventions and compared engagement with standard CBT for chronic pain protocol. Although they did not find significant differences in engagement between the 2 groups, participation and treatment adherence were associated with posttreatment improvements in both groups.19 Taking a step back from enhancing intervention engagement, first assessing readiness to self-manage becomes another salient exploration and step in the process.
Another element of engagement in services is referral to other clinicians. Dorflinger and colleagues made this point in a conceptual paper that broadly outlined interdisciplinary, integrative, and more comprehensive models of care for chronic pain.15 We know from integrated models that referral-based care may decrease the likelihood of participation in health care services. That is, if a patient needs to make a separate appointment and meet with a new clinician, they are more likely to decline, cancel, or not show, particularly if they are not “ready” for change. Co-located or embedded care and conjoint sessions that include a warm handoff or another clinician who joins the first appointment may reduce stigma and other relevant barriers for introducing a patient to new ideas.20
Using a conjoint session that involves a clinical pharmacy pain specialist and a health psychologist is one way in which veterans can be exposed to more chronic pain-related BPS concepts and behavioral health services than they might be exposed to otherwise. The purpose of this project was to bring awareness to a practical and clinically relevant integrated approach to the dissemination of BPS information for chronic pain management.
In providing this information through effective communication at the patient-provider and interprofessional levels, the clinicians’ intention was to increase patient engagement and use of BPS strategies in the self-management of chronic pain. This project also aimed to enhance engagement and improve the quality of services before acquiring additional positions and funding for a specialized pain management team. These sessions were offered at the VA Ann Arbor Healthcare System (VAAAHS) in Michigan. Quantitative and qualitative information was examined from the conjoint and subsequent sessions that occurred in this setting.
Methods
With the above concepts in mind, VAAAHS offered veterans conjoint sessions involving a health psychologist and clinical pharmacy specialist during a 3-month period while this resource was available. The conjoint sessions were part of a preexisting pharmacist-run pain medication clinic embedded in primary care. The conjoint session was presented to patients as part of general clinic flow to reduce stigma of engagement in psychological services and allow for the dissemination of BPS information.
Participants
The electronic health records (EHR) of 24 veteran patients with chronic pain, who participated in a conjoint health psychology/pain pharmacy session, were reviewed for the current study. Most of the patients were male (95.8%) and non-Hispanic white (91.7%); the remaining participants did not disclose their ethnicity. The mean age was 60.6 years (SD 7.1; range 50-80). A total of 75% had a mental health diagnosis, and 41.7% were in mental health treatment at the time of the conjoint appointment. Among the sample, 20.8% had a current diagnosis of a substance use disorder (SUD), and no individuals were in treatment for a SUD at the time of the conjoint appointment. Patients received an average of 1.5 conjoint sessions (SD 0.7; range 1-3).
Procedure
The veterans for this project were chosen from a panel of patients followed by the pain medication clinical pharmacy specialist in the primary care pain medication clinic. The selected veterans were offered a joint session with their clinical pharmacy provider and the health psychology resident during their scheduled visit in the pain medication clinic. Each veteran was informed that the goal of the joint visit was to enhance self-directed nonpharmacologic chronic pain management skills as an additional set of tools in the tool kit for particularly difficult pain days. Veterans were assured that their usual care would not be compromised if they declined the session.
During the encounter(s), the health psychologist contributed to the veteran’s care by using MI and CBT for chronic pain skills. The health psychologist further assessed concerns and needs and guided the discussion as appropriate. With veteran readiness, these discussions explored the degree of knowledge and cognitive and behavioral coping skills the patient used. These conjoint sessions also documented the types of discussions and degree of engagement in the encounter(s) as well additional referrals, complementary services, and/or offered follow-up services for either additional conjoint sessions or further health psychology-related services.
A total of 24 EHRs from these conjoint and subsequent encounters were reviewed for evidence of the procedures by a psychology intern involved in chronic pain management services. Of these 24 records, 6 also were reviewed by a board-certified health psychologist for consensus building and agreement on coding (Sidebar, Record Coding).
Using the coding system and SPSS Version 2.1 (IBM, Armonk NY), descriptive statistics were used to examine conjoint session content and new- or re-engagement in health psychology services following the conjoint sessions. For those patients who followed up with additional services, the content, type, and outcome of these services were explored. Next, linear regression was used to determine whether number of conjoint sessions was associated with a qualitative treatment outcome, and 2 logistic regressions were used to determine whether the number of sessions was associated with the likelihood of accepting services and follow-through with services after accepting them. An additional logistic regression examined whether having a mental health diagnosis (yes/no) was associated with whether the individual accepted additional health psychology services. Finally, independent sample t tests examined differences between those who accepted services vs those who declined follow-up services in substance use diagnosis, mental health diagnosis, and previous health psychology services engagement. Of note, given the small sample size, the Levene’s test for equality of variances was conducted and unequal variances were assumed.
Results
All 24 patients agreed to have the conjoint session with the clinical pharmacy specialist and health psychologist. Of the participants, 62.5% had no previous interaction with health psychology services. Among those who had previous encounters with health psychology services, 12.5% had participated in 1 or more group sessions, another 12.5% had participated in 1 or more individual sessions, and an additional 12.5% had been referred for health psychology services but had not followed through. A total of 10 participants represented a new- or re-engagement in health psychology services following the conjoint appointment. Two patients were referred for additional services as a result of their conjoint appointment (1 to specialty mental health and another to Primary Care-Mental Health Integration [PC-MHI]), and 1 of the participants followed through with the referral. Finally, with regard to the content of the initial session, 37.5% of the sessions contained some form of psychoeducation, 54.2% contained a functional assessment, and 41.7% contained an introduction of skills.
Half of the veterans participated in health psychology services beyond the initial conjoint session. Four of these veterans participated in additional conjoint sessions, and the remaining 8 engaged in health psychology services, which took the form of telephone sessions (3), in-person sessions (3), or a combination of both telephone and in-person sessions (2). Twelve veterans participated in an average of 3.4 (SD 3.7) follow-up sessions. In terms of the content of these follow-up sessions, across all formats and types, 3 included some introduction to coping skills, with no documented evidence of follow-through. For 2 of the veterans engaging in some type of follow-up, there was documented use of coping skills, and 2 used the coping skills with self-reported success and benefit. Finally, documentation revealed evidence that 3 of these veterans were not only using the coping skills with benefit, but also reported an improvement in pain management overall. One also was connected with a different service.
Regarding reasons for completion of services, 2 veterans were terminated due to completing treatment/meeting goals, 2 were terminated because they did not follow up after a session, 7 were terminated due to patient declining additional sessions, and 1 veteran was still receiving services at the time of the review. Linear regression indicated that the number of conjoint sessions was not associated with qualitative treatment outcome. Two logistic regressions indicated that number of conjoint sessions was not related to whether the veteran accepted follow-up services or whether the veteran followed through with services after accepting. Of note, logistic regression indicated that having a mental health diagnosiswas associated with a decreased likelihood of accepting health psychology services (P = .03). Regarding the independent samples t tests, veterans who did not accept follow-up services were more likely to have a mental health diagnosis (P = .03). The groups did not differ significantly with regard to substance use diagnosis or previous engagement in health psychology services.
Discussion
Results showed that all 24 veterans who were offered a conjoint session with a clinical pharmacy specialist and health psychologist engaged in at least 1 session. Half the veterans participated in further services as well. Both the initial conjoint and follow-up sessions offered a greater degree of communication related to the cognitive-behavioral and functional restoration components of behavioral pain management. Given that a majority of the sample had not participated in behavioral or mental health services previously, this may represent a greater penetration rate of exposure to mental health service for veterans than would have been available otherwise.
More specifically, qualitative results suggest that in these conjoint sessions, the veterans were exposed to behavioral psychotherapeutic approaches to chronic pain management (eg, health behavior change, motivational enhancement, health-related psychoeducation, and CBT for chronic pain) that again may not have been provided otherwise (ie, via referral and separately scheduled sessions). These findings are supported by theories consistent with the Transtheoretical Model, which indicates that individuals fall in varying degrees of readiness for behavioral change (ie, precontemplative, contemplative, planning, action, maintenance).21,22 Thus, behavioral intervention approaches must be adaptive and adjust format and communication, including the amount and type of psychoeducation offered. Moreover, the integrated theory of health behavior change in the context of chronic pain management calls for fostering awareness, knowledge, and beliefs through effective communication and education for a wide range of individuals who are at varying stages of change.23 In addition to the conjoint session and subsequent service(s) content that were reviewed and coded in this current project, future projects might draw on these theoretical models and code sessions for patients’ stages of change and assess whether a patient made progress across phases of change (eg, the patient shifted from contemplative to the planning stage of change).
Within this project’s conjoint sessions and consistent with MI principles, veterans were offered discussions related to the bidirectional and BPS aspects of their own chronic pain experience. That is, while discussing responses and adjustment to pain medication(s), veterans received reflections with MI and heard feedback related to their current coping strategies, methods to enhance coping, as well as potential psychosocial impacts of their chronic pain experience. With permission, veterans also were introduced to themes that comprised evidence-based CBT for chronic pain (CBT-CP) intervention. Understanding what change means in the context of chronic pain management is critical. That is, tipping the conversation toward consideration of alternative modalities (eg, relaxation, stress management, cognitions, and pain) in conjunction with or in place of the traditional modalities (eg, medication, pain procedures) is paramount.
Clinicians must listen for patient ambivalence related to procedures, interventions, medication changes, and/or the behavioral self-management of chronic pain. This type of active listening and exploration may be more likely when there is collaboration and effective team functioning among clinicians than when clinicians provide care independently. Future quality improvement (QI) or research projects could extend the EHR review and evaluate clinician-patient transcripts for fidelity to the CBT-CP and MI models. Such efforts could assess for associations between clinician MI consistent behaviors and change talk on the part of the patient. Furthermore, clinician communication and patient change talk from transcripts could be evaluated in relation to evidence from the EHR regarding patient use of coping skills and behavior change.
Consistent with behavioral health literature, having a mental health diagnosis was associated with declining additional behavioral health psychology services in this project. Research has shown that individuals with a mental health diagnosis tend to engage less in behavioral health self-management programs, such as chronic headache and weight management.24-26 This phenomenon lends support for the importance of health care professionals (HCPs) to increase access and exposure to mental and behavioral health services, such as the PC-MHI model.20 In fact, chronic pain management program development efforts within the VA system nationwide include collaboration with the PC-MHI services. One of the initial goals for PC-MHI services is to increase penetration rates into the general outpatient medical clinics and enhance engagement in mental health services.
Using conjoint sessions as was offered in the current project is one step in the development of more comprehensive interdisciplinary teams through interprofessional collaboration and the use of effective clinical communication. In turn, it will be important to directly explore the communication skills and attitudes of these HCPs with regard to interdisciplinary program development and collaboration as teams continue to integrate more broadly into the medical system and enhance chronic pain management services.11 Similarly, measuring the perceptions of clinical pharmacy specialists, physicians, health psychologists, or other clinical disciplines involved in chronic pain management could be another area to explore. More specific to MI, clinician confidence in the use of effective communication and MI skills represents still another area for future study.16
Limitations
Some limitations and suggested future directions found as part of this QI project have been outlined earlier. Other limitations include the used of a retrospective review of information available in patient medical charts. More developed measurement-based care or research could collect self-reports of patient satisfaction with care, functioning, knowledge, readiness for change, and mood in addition to what is noted and documented in clinical observations. Second, the sample was small and did not include any female and few younger veterans, even though these are important subpopulations when examining pain management services. When resources are available for a larger sample size, some exploratory analyses could be conducted for differences in engagement among subgroups. Third, this project may have further confounding variables as this was not an experimental or a controlled study, which could directly compare conjoint sessions with referral-based care and/or those not offered conjoint sessions.
Conclusion
The optimal method of behavioral pain management suggests the need for an interdisciplinary, coordinated team approach, in which the gold standard programs meet requirements set by CARF. However, on a practical level, optimal behavioral pain management may not be feasible at all health care facilities. Furthermore, in an effort to provide best practices to individuals with chronic pain, clinicians must be adaptive and skilled in using effective communication and specialized interventions, such as CBT and MI.
Approaching the more optimal behavioral self-management of chronic pain from a multimodal interdisciplinary perspective and further engaging veterans in this care is paramount. This project is merely one step in this effort that can shed light on the function and logistic outcomes of using a practical, integrated approach to chronic pain. It demonstrates that implementing best practices founded in sound theoretical models despite staffing and resource constraints is possible. Thus, continuing to explore the utility of alternate modalities may offer important applied and translational information to help disseminate and improve chronic pain management services.
Future research could focus on important subpopulations and enhance experimental design with pre- and postmeasures, controlling for possible confounding variables and if possible a controlled design.
Acknowledgments
This quality improvement project was unfunded, and approval was confirmed with the VA Ann Arbor Healthcare System Institutional Review Board and Research & Development committees. The authors also thank Associate Chief of Staff, Ambulatory Care, Clinton Greenstone, MD, and Chief of Primary Care Adam Tremblay, MD, for their leadership and support of these integrative services and quality improvement efforts. The authors especially recognize the veterans for whom they aim to provide the highest quality of services possible.
1. Brooks PM. The burden of musculoskeletal disease—a global perspective. Clin Rheumatol. 2006;25(6):778-781.
2. Haskell SG, Heapy A, Reid MC, Papas RK, Kerns RD. The prevalence and age-related characteristics of pain in a sample of women veterans receiving primary care. J Womens Health (Larchmt). 2006;15(7):862-869.
3. Roth RS, Geisser ME, Williams DA. Interventional pain medicine: retreat from the biopsychosocial model of pain. Transl Behav Med. 2012;2(1):106-116.
4. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129-136.
5. Borrell-Carrió F, Suchman AL, Epstein RM. The biopsychosocial model 25 years later: principles, practice, and scientific inquiry. Ann Fam Med. 2004;2(6):576-582.
6. Wall PD. The gate control theory of pain mechanisms: a re-examination and re-statement. Brain. 1978;101(1):1-18.
7. Dobscha SK, Corson K, Perrin NA, et al. Collaborative care for chronic pain in primary care: a cluster randomized trial. JAMA. 2009;301(12):1242-1252.
8. Von Korff, Moore JC. Stepped care for back pain: activating approaches for primary care. Ann Intern Med. 2001;134(9, pt 2):911-917.
9. Oslund S, Robinson RC, Clark TC, et al. Long-term effectiveness of a comprehensive pain management program: strengthening the case for interdisciplinary care. Proc (Bayl Univ Med Cent). 2009;22(3):211-214.
10. Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: a systematic review of interventions and outcomes. Rheumatology (Oxford). 2008;47(5):670-678.
11. Gatchel RJ, McGeary DD, McGeary CA, Lippe B. Interdisciplinary chronic pain management: past, present, and future. Am Psychol. 2014;69(2):119-130.
12. McCracken LM, Turk DC. Behavioral and cognitive-behavioral treatment for chronic pain: outcome, predictors of outcome, and treatment process. Spine (Phila Pa 1976). 2002;27(22): 2564-2573.
13. Jeffery MM, Butler M, Stark A, Kane RL. Multidisciplinary Pain Programs for Chronic Noncancer Pain. Comparative Effectiveness Technical Briefs, No 8. Rockville, MD: Agency for Healthcare Research and Quality; 2011.
14. Ehde DM, Dilworth TM, Turner JA. Cognitive-behavioral therapy for individuals with chronic pain: efficacy, innovations, and directions for research. Am Psychol. 2014;69(2):153-166.
15. Dorflinger L, Kerns RD, Auerbach SM. Providers’ roles in enhancing patients’ adherence to pain self management. Transl Behav Med. 2013;3(1):39-46.
16. Pellico LH, Gilliam WP, Lee AW, Kerns RD. Hearing new voices: registered nurses and health technicians experience caring for chronic pain patients in primary care clinics. Open Nurs J. 2014;8:25-33.
17. Rollnick S, Miller WR, Butler CC, eds. Motivational Interviewing in Health Care: Helping Patients Change Behavior. New York, NY: The Guilford Press; 2008.
18. Kerns RD, Habib S. A critical review of the pain readiness to change model. J Pain. 2004;5(7):357-367.19. Kerns RD, Burns JW, Shulman M, et al. Can we improve cognitive-behavior therapy for chronic back pain treatment engagement and adherence? A controlled trial of tailored versus standard therapy. Health Psychol. 2014;33(9):938-947.
20. Kearney LK, Post EP, Zeiss A, Goldstein MG, Dundon M. The role of mental and behavioral health in the application of the patient-centered medical home in the Department of Veterans Affairs. Transl Behav Med. 2011;1(4):624-628.
21. Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol. 1983;51(3):390-395.
22. Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol. 1992;47(9):1102-1114.
23. Ryan P. Integrated theory of health behavior change: background and intervention development. Clin Nurse Spec. 2009;23(3):161-172.
24. Evans DD , Blanchard EB. Prediction of early termination from the self-regulatory treatment of chronic headache. Biofeedback Self Regul. 1988;13(3):245-256.
25. Maguen S, Hoerster KD, Littman AJ, et al. Iraq and Afghanistan veterans with PTSD participate less in VA’s weight loss program than those without PTSD. J Affect Disord. 2016;193:289-294.
26. Bloor LE. Improving weight management services for female veterans: design and participation factors with a women only program, and comparisons with gender neutral services. Med Res Arch. 2015;2.
1. Brooks PM. The burden of musculoskeletal disease—a global perspective. Clin Rheumatol. 2006;25(6):778-781.
2. Haskell SG, Heapy A, Reid MC, Papas RK, Kerns RD. The prevalence and age-related characteristics of pain in a sample of women veterans receiving primary care. J Womens Health (Larchmt). 2006;15(7):862-869.
3. Roth RS, Geisser ME, Williams DA. Interventional pain medicine: retreat from the biopsychosocial model of pain. Transl Behav Med. 2012;2(1):106-116.
4. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129-136.
5. Borrell-Carrió F, Suchman AL, Epstein RM. The biopsychosocial model 25 years later: principles, practice, and scientific inquiry. Ann Fam Med. 2004;2(6):576-582.
6. Wall PD. The gate control theory of pain mechanisms: a re-examination and re-statement. Brain. 1978;101(1):1-18.
7. Dobscha SK, Corson K, Perrin NA, et al. Collaborative care for chronic pain in primary care: a cluster randomized trial. JAMA. 2009;301(12):1242-1252.
8. Von Korff, Moore JC. Stepped care for back pain: activating approaches for primary care. Ann Intern Med. 2001;134(9, pt 2):911-917.
9. Oslund S, Robinson RC, Clark TC, et al. Long-term effectiveness of a comprehensive pain management program: strengthening the case for interdisciplinary care. Proc (Bayl Univ Med Cent). 2009;22(3):211-214.
10. Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: a systematic review of interventions and outcomes. Rheumatology (Oxford). 2008;47(5):670-678.
11. Gatchel RJ, McGeary DD, McGeary CA, Lippe B. Interdisciplinary chronic pain management: past, present, and future. Am Psychol. 2014;69(2):119-130.
12. McCracken LM, Turk DC. Behavioral and cognitive-behavioral treatment for chronic pain: outcome, predictors of outcome, and treatment process. Spine (Phila Pa 1976). 2002;27(22): 2564-2573.
13. Jeffery MM, Butler M, Stark A, Kane RL. Multidisciplinary Pain Programs for Chronic Noncancer Pain. Comparative Effectiveness Technical Briefs, No 8. Rockville, MD: Agency for Healthcare Research and Quality; 2011.
14. Ehde DM, Dilworth TM, Turner JA. Cognitive-behavioral therapy for individuals with chronic pain: efficacy, innovations, and directions for research. Am Psychol. 2014;69(2):153-166.
15. Dorflinger L, Kerns RD, Auerbach SM. Providers’ roles in enhancing patients’ adherence to pain self management. Transl Behav Med. 2013;3(1):39-46.
16. Pellico LH, Gilliam WP, Lee AW, Kerns RD. Hearing new voices: registered nurses and health technicians experience caring for chronic pain patients in primary care clinics. Open Nurs J. 2014;8:25-33.
17. Rollnick S, Miller WR, Butler CC, eds. Motivational Interviewing in Health Care: Helping Patients Change Behavior. New York, NY: The Guilford Press; 2008.
18. Kerns RD, Habib S. A critical review of the pain readiness to change model. J Pain. 2004;5(7):357-367.19. Kerns RD, Burns JW, Shulman M, et al. Can we improve cognitive-behavior therapy for chronic back pain treatment engagement and adherence? A controlled trial of tailored versus standard therapy. Health Psychol. 2014;33(9):938-947.
20. Kearney LK, Post EP, Zeiss A, Goldstein MG, Dundon M. The role of mental and behavioral health in the application of the patient-centered medical home in the Department of Veterans Affairs. Transl Behav Med. 2011;1(4):624-628.
21. Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol. 1983;51(3):390-395.
22. Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol. 1992;47(9):1102-1114.
23. Ryan P. Integrated theory of health behavior change: background and intervention development. Clin Nurse Spec. 2009;23(3):161-172.
24. Evans DD , Blanchard EB. Prediction of early termination from the self-regulatory treatment of chronic headache. Biofeedback Self Regul. 1988;13(3):245-256.
25. Maguen S, Hoerster KD, Littman AJ, et al. Iraq and Afghanistan veterans with PTSD participate less in VA’s weight loss program than those without PTSD. J Affect Disord. 2016;193:289-294.
26. Bloor LE. Improving weight management services for female veterans: design and participation factors with a women only program, and comparisons with gender neutral services. Med Res Arch. 2015;2.
Early prophylaxis may preserve joint health in hemophilia patients

New research suggests that starting prophylactic factor VIII (FVIII) therapy early in life can preserve joint health in patients with hemophilia A.
In studying data on more than 6000 patients, researchers found the use of FVIII prophylaxis increased from 1999 to 2010.
And the rate of bleeding events, including joint bleeds, decreased over this time period.
The study also indicated that starting FVIII prophylaxis before age 4 decreases a patient’s risk of losing normal range of motion (ROM) in his joints.
Marilyn J. Manco-Johnson, MD, of the University of Colorado Denver in Aurora, Colorado, and her colleagues reported these findings in Blood.
The team studied information collected from 6196 males between 2 and 69 years of age with severe hemophilia A. Altogether, these patients had 26,614 visits to US hemophilia treatment centers between 1999 and 2010.
The data collected from the clinic visits were used to examine trends in FVIII prophylaxis use and changes in the patients’ health over the study period.
Prophylaxis and bleeds
Overall, prophylaxis use increased from 31% in 1999 to 59% in 2010. Three-quarters of patients younger than 20 years of age were on prophylaxis by 2010.
The rate of total bleeds fell 17% from 1999 to 2010 for patients receiving prophylaxis—from a mean of 4.91 bleeds every 6 months to a mean of 4.07 bleeds every 6 months. For patients not on prophylaxis, the rate of total bleeds fell 30%, from 14.2 to 9.87 bleeds.
For patients on prophylaxis, the rate of joint bleeding fell 22%, from a mean of 3.03 bleeds every 6 months in 1999 to a mean of 2.36 bleeds every 6 months in 2010. Among patients not on prophylaxis, the rate of joint bleeding fell 23%, from 9.42 to 7.25 bleeds.
The researchers noted that rates of joint bleeding and total bleeding events in patients not on prophylaxis were roughly twice the rates for patients who were using prophylaxis.
Joint ROM
The researchers also conducted longitudinal analyses to assess joint ROM on 3078 patients who had 14,130 visits to hemophilia treatment centers during the study period.
The team found a few factors that were significantly associated with a decrease in overall joint ROM at the patients’ initial visit. This included advancing age (P<0.001), non-white race (P<0.001), and obesity (P=0.003).
Obesity was associated with a significant increase in loss of joint ROM over time as well (P<0.001).
On the other hand, starting prophylaxis before age 4 was associated with a significant decrease in loss of joint ROM over time (P=0.03).
Questions and next steps
The researchers said it isn’t clear why prophylaxis is best able to protect joint ROM when treatment is started at a very young age. And it’s not clear why hemophilia patients who might benefit from prophylaxis aren’t using it.
The team said studies are needed to understand why some hemophilia patients don’t use prophylaxis and to develop strategies that are successful in changing this behavior.
In addition, more work is needed to understand the factors that may lead to joint bleeds and to develop treatment strategies for hemophilia patients who have a higher risk for joint disease. ![]()
New research suggests that starting prophylactic factor VIII (FVIII) therapy early in life can preserve joint health in patients with hemophilia A.
In studying data on more than 6000 patients, researchers found the use of FVIII prophylaxis increased from 1999 to 2010.
And the rate of bleeding events, including joint bleeds, decreased over this time period.
The study also indicated that starting FVIII prophylaxis before age 4 decreases a patient’s risk of losing normal range of motion (ROM) in his joints.
Marilyn J. Manco-Johnson, MD, of the University of Colorado Denver in Aurora, Colorado, and her colleagues reported these findings in Blood.
The team studied information collected from 6196 males between 2 and 69 years of age with severe hemophilia A. Altogether, these patients had 26,614 visits to US hemophilia treatment centers between 1999 and 2010.
The data collected from the clinic visits were used to examine trends in FVIII prophylaxis use and changes in the patients’ health over the study period.
Prophylaxis and bleeds
Overall, prophylaxis use increased from 31% in 1999 to 59% in 2010. Three-quarters of patients younger than 20 years of age were on prophylaxis by 2010.
The rate of total bleeds fell 17% from 1999 to 2010 for patients receiving prophylaxis—from a mean of 4.91 bleeds every 6 months to a mean of 4.07 bleeds every 6 months. For patients not on prophylaxis, the rate of total bleeds fell 30%, from 14.2 to 9.87 bleeds.
For patients on prophylaxis, the rate of joint bleeding fell 22%, from a mean of 3.03 bleeds every 6 months in 1999 to a mean of 2.36 bleeds every 6 months in 2010. Among patients not on prophylaxis, the rate of joint bleeding fell 23%, from 9.42 to 7.25 bleeds.
The researchers noted that rates of joint bleeding and total bleeding events in patients not on prophylaxis were roughly twice the rates for patients who were using prophylaxis.
Joint ROM
The researchers also conducted longitudinal analyses to assess joint ROM on 3078 patients who had 14,130 visits to hemophilia treatment centers during the study period.
The team found a few factors that were significantly associated with a decrease in overall joint ROM at the patients’ initial visit. This included advancing age (P<0.001), non-white race (P<0.001), and obesity (P=0.003).
Obesity was associated with a significant increase in loss of joint ROM over time as well (P<0.001).
On the other hand, starting prophylaxis before age 4 was associated with a significant decrease in loss of joint ROM over time (P=0.03).
Questions and next steps
The researchers said it isn’t clear why prophylaxis is best able to protect joint ROM when treatment is started at a very young age. And it’s not clear why hemophilia patients who might benefit from prophylaxis aren’t using it.
The team said studies are needed to understand why some hemophilia patients don’t use prophylaxis and to develop strategies that are successful in changing this behavior.
In addition, more work is needed to understand the factors that may lead to joint bleeds and to develop treatment strategies for hemophilia patients who have a higher risk for joint disease. ![]()
New research suggests that starting prophylactic factor VIII (FVIII) therapy early in life can preserve joint health in patients with hemophilia A.
In studying data on more than 6000 patients, researchers found the use of FVIII prophylaxis increased from 1999 to 2010.
And the rate of bleeding events, including joint bleeds, decreased over this time period.
The study also indicated that starting FVIII prophylaxis before age 4 decreases a patient’s risk of losing normal range of motion (ROM) in his joints.
Marilyn J. Manco-Johnson, MD, of the University of Colorado Denver in Aurora, Colorado, and her colleagues reported these findings in Blood.
The team studied information collected from 6196 males between 2 and 69 years of age with severe hemophilia A. Altogether, these patients had 26,614 visits to US hemophilia treatment centers between 1999 and 2010.
The data collected from the clinic visits were used to examine trends in FVIII prophylaxis use and changes in the patients’ health over the study period.
Prophylaxis and bleeds
Overall, prophylaxis use increased from 31% in 1999 to 59% in 2010. Three-quarters of patients younger than 20 years of age were on prophylaxis by 2010.
The rate of total bleeds fell 17% from 1999 to 2010 for patients receiving prophylaxis—from a mean of 4.91 bleeds every 6 months to a mean of 4.07 bleeds every 6 months. For patients not on prophylaxis, the rate of total bleeds fell 30%, from 14.2 to 9.87 bleeds.
For patients on prophylaxis, the rate of joint bleeding fell 22%, from a mean of 3.03 bleeds every 6 months in 1999 to a mean of 2.36 bleeds every 6 months in 2010. Among patients not on prophylaxis, the rate of joint bleeding fell 23%, from 9.42 to 7.25 bleeds.
The researchers noted that rates of joint bleeding and total bleeding events in patients not on prophylaxis were roughly twice the rates for patients who were using prophylaxis.
Joint ROM
The researchers also conducted longitudinal analyses to assess joint ROM on 3078 patients who had 14,130 visits to hemophilia treatment centers during the study period.
The team found a few factors that were significantly associated with a decrease in overall joint ROM at the patients’ initial visit. This included advancing age (P<0.001), non-white race (P<0.001), and obesity (P=0.003).
Obesity was associated with a significant increase in loss of joint ROM over time as well (P<0.001).
On the other hand, starting prophylaxis before age 4 was associated with a significant decrease in loss of joint ROM over time (P=0.03).
Questions and next steps
The researchers said it isn’t clear why prophylaxis is best able to protect joint ROM when treatment is started at a very young age. And it’s not clear why hemophilia patients who might benefit from prophylaxis aren’t using it.
The team said studies are needed to understand why some hemophilia patients don’t use prophylaxis and to develop strategies that are successful in changing this behavior.
In addition, more work is needed to understand the factors that may lead to joint bleeds and to develop treatment strategies for hemophilia patients who have a higher risk for joint disease. ![]()
Clinical Comestibles?
1. This 45-year-old woman’s skin has multiple small, soft, compressible papules, one of which is apt to bleed when scratched. She is concerned that these “cherry red” lesions are precancerous.

Diagnosis: Cherry angiomas, also known as de Morgan spots, are extremely common lesions; though usually asymptomatic, they may bleed with trauma. They occur most commonly as multiple asymptomatic lesions on the trunk and arms. These capillary hemangiomas are dome-shaped, small (0.1 to 0.5 cm in diameter), and bright red to violaceous; they can be flat, raised, or nodular.
Cherry angiomas form as a result of the development of multiple capillaries with narrow lumens and prominent endothelial cells arranged in a lobular pattern in the papillary dermis. Effective treatment options include curettage, laser ablation, and electrodesiccation.
For more information, see Kim, J-H, Park H-Y, Ahn SK. Cherry Angiomas on the Scalp. Case Rep Dermatol. 2009;1(1):82–86.
2. A 60-year-old African-American woman presents with painful swelling of two years’ duration. She delayed care due to lack of insurance. The patient is hypertensive, and her left breast and nipple are retracted, with darkened skin and a peau d’orange texture.

Diagnosis: Palpation of the firm, matted nodes in the left axilla elucidated the diagnosis of breast cancer with lymphedema. Lymphedema causes the skin of the breast to resemble that of an orange.
The patient was referred to the local university’s breast center. Although the prognosis was poor, it was important to make every effort to have the disease staged to determine the most appropriate therapy.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux, EJ. Breast cancer. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:551-556.
For more information, see “Swollen breast and arm.” The Journal of Family Practice. February 6, 2015.
3. This patient presents with her cheeks quite red and covered with hyperkeratotic, rough, pinpoint papules. No other blemishes or lesions are seen on her face, but there are hundreds of hyperkeratotic papules on her bilateral triceps, giving a “chicken skin” appearance.

Diagnosis: Keratosis pilaris (KP) is an extremely common and harmless problem that affects up to 70% of newborns, though it may not fully express until age 1 or 2. Caused by an overproduction of perifollicular keratin, KP is inherited in an autosomal dominant pattern and is often seen in conjunction with atopic dermatitis and related conditions (eg, eczema, xerosis, asthma, icthyosis). KP can manifest anywhere on the body except glabrous skin (palms and soles).
Variants of KP are also common; the one affecting this patient is keratosis pilaris rubra facei. This condition is often confused with acne, but treating it as such worsens irritation—especially in the wintertime, when humidity levels are low.
For more information, see “Acne: Maybe She's Born With It?” Clinician Reviews. 2016 July;26(7):W1.
4. A 5-year-old girl has a fever of 102.4°F and “strawberry tongue.” The posterior pharynx is erythematous with slight exudate visible. The anterior cervical lymph nodes are mildly tender and somewhat enlarged. No rashes are noted.

Diagnosis: The child’s strawberry tongue and scarlet fever were caused by strep pharyngitis. Strawberry tongue, identified by prominent papillae along with erythema (resembling a strawberry), is most commonly seen in children with scarlet fever or Kawasaki disease and usually develops within the first two to three days of illness. A white or yellowish coating typically precedes the distinctive red tongue with white papillae.
In this case, oral penicillin VK was prescribed, along with ibuprofen for the fever and sore throat. Improvement was noted within 24 hours, but the full 10-day course of pencillin was completed to prevent rheumatic fever.
For more information, see “Papillae on tongue.” Journal of Family Practice. January 24, 2014.
1. This 45-year-old woman’s skin has multiple small, soft, compressible papules, one of which is apt to bleed when scratched. She is concerned that these “cherry red” lesions are precancerous.
Diagnosis: Cherry angiomas, also known as de Morgan spots, are extremely common lesions; though usually asymptomatic, they may bleed with trauma. They occur most commonly as multiple asymptomatic lesions on the trunk and arms. These capillary hemangiomas are dome-shaped, small (0.1 to 0.5 cm in diameter), and bright red to violaceous; they can be flat, raised, or nodular.
Cherry angiomas form as a result of the development of multiple capillaries with narrow lumens and prominent endothelial cells arranged in a lobular pattern in the papillary dermis. Effective treatment options include curettage, laser ablation, and electrodesiccation.
For more information, see Kim, J-H, Park H-Y, Ahn SK. Cherry Angiomas on the Scalp. Case Rep Dermatol. 2009;1(1):82–86.
2. A 60-year-old African-American woman presents with painful swelling of two years’ duration. She delayed care due to lack of insurance. The patient is hypertensive, and her left breast and nipple are retracted, with darkened skin and a peau d’orange texture.
Diagnosis: Palpation of the firm, matted nodes in the left axilla elucidated the diagnosis of breast cancer with lymphedema. Lymphedema causes the skin of the breast to resemble that of an orange.
The patient was referred to the local university’s breast center. Although the prognosis was poor, it was important to make every effort to have the disease staged to determine the most appropriate therapy.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux, EJ. Breast cancer. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:551-556.
For more information, see “Swollen breast and arm.” The Journal of Family Practice. February 6, 2015.
3. This patient presents with her cheeks quite red and covered with hyperkeratotic, rough, pinpoint papules. No other blemishes or lesions are seen on her face, but there are hundreds of hyperkeratotic papules on her bilateral triceps, giving a “chicken skin” appearance.
Diagnosis: Keratosis pilaris (KP) is an extremely common and harmless problem that affects up to 70% of newborns, though it may not fully express until age 1 or 2. Caused by an overproduction of perifollicular keratin, KP is inherited in an autosomal dominant pattern and is often seen in conjunction with atopic dermatitis and related conditions (eg, eczema, xerosis, asthma, icthyosis). KP can manifest anywhere on the body except glabrous skin (palms and soles).
Variants of KP are also common; the one affecting this patient is keratosis pilaris rubra facei. This condition is often confused with acne, but treating it as such worsens irritation—especially in the wintertime, when humidity levels are low.
For more information, see “Acne: Maybe She's Born With It?” Clinician Reviews. 2016 July;26(7):W1.
4. A 5-year-old girl has a fever of 102.4°F and “strawberry tongue.” The posterior pharynx is erythematous with slight exudate visible. The anterior cervical lymph nodes are mildly tender and somewhat enlarged. No rashes are noted.
Diagnosis: The child’s strawberry tongue and scarlet fever were caused by strep pharyngitis. Strawberry tongue, identified by prominent papillae along with erythema (resembling a strawberry), is most commonly seen in children with scarlet fever or Kawasaki disease and usually develops within the first two to three days of illness. A white or yellowish coating typically precedes the distinctive red tongue with white papillae.
In this case, oral penicillin VK was prescribed, along with ibuprofen for the fever and sore throat. Improvement was noted within 24 hours, but the full 10-day course of pencillin was completed to prevent rheumatic fever.
For more information, see “Papillae on tongue.” Journal of Family Practice. January 24, 2014.
1. This 45-year-old woman’s skin has multiple small, soft, compressible papules, one of which is apt to bleed when scratched. She is concerned that these “cherry red” lesions are precancerous.
Diagnosis: Cherry angiomas, also known as de Morgan spots, are extremely common lesions; though usually asymptomatic, they may bleed with trauma. They occur most commonly as multiple asymptomatic lesions on the trunk and arms. These capillary hemangiomas are dome-shaped, small (0.1 to 0.5 cm in diameter), and bright red to violaceous; they can be flat, raised, or nodular.
Cherry angiomas form as a result of the development of multiple capillaries with narrow lumens and prominent endothelial cells arranged in a lobular pattern in the papillary dermis. Effective treatment options include curettage, laser ablation, and electrodesiccation.
For more information, see Kim, J-H, Park H-Y, Ahn SK. Cherry Angiomas on the Scalp. Case Rep Dermatol. 2009;1(1):82–86.
2. A 60-year-old African-American woman presents with painful swelling of two years’ duration. She delayed care due to lack of insurance. The patient is hypertensive, and her left breast and nipple are retracted, with darkened skin and a peau d’orange texture.
Diagnosis: Palpation of the firm, matted nodes in the left axilla elucidated the diagnosis of breast cancer with lymphedema. Lymphedema causes the skin of the breast to resemble that of an orange.
The patient was referred to the local university’s breast center. Although the prognosis was poor, it was important to make every effort to have the disease staged to determine the most appropriate therapy.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux, EJ. Breast cancer. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:551-556.
For more information, see “Swollen breast and arm.” The Journal of Family Practice. February 6, 2015.
3. This patient presents with her cheeks quite red and covered with hyperkeratotic, rough, pinpoint papules. No other blemishes or lesions are seen on her face, but there are hundreds of hyperkeratotic papules on her bilateral triceps, giving a “chicken skin” appearance.
Diagnosis: Keratosis pilaris (KP) is an extremely common and harmless problem that affects up to 70% of newborns, though it may not fully express until age 1 or 2. Caused by an overproduction of perifollicular keratin, KP is inherited in an autosomal dominant pattern and is often seen in conjunction with atopic dermatitis and related conditions (eg, eczema, xerosis, asthma, icthyosis). KP can manifest anywhere on the body except glabrous skin (palms and soles).
Variants of KP are also common; the one affecting this patient is keratosis pilaris rubra facei. This condition is often confused with acne, but treating it as such worsens irritation—especially in the wintertime, when humidity levels are low.
For more information, see “Acne: Maybe She's Born With It?” Clinician Reviews. 2016 July;26(7):W1.
4. A 5-year-old girl has a fever of 102.4°F and “strawberry tongue.” The posterior pharynx is erythematous with slight exudate visible. The anterior cervical lymph nodes are mildly tender and somewhat enlarged. No rashes are noted.
Diagnosis: The child’s strawberry tongue and scarlet fever were caused by strep pharyngitis. Strawberry tongue, identified by prominent papillae along with erythema (resembling a strawberry), is most commonly seen in children with scarlet fever or Kawasaki disease and usually develops within the first two to three days of illness. A white or yellowish coating typically precedes the distinctive red tongue with white papillae.
In this case, oral penicillin VK was prescribed, along with ibuprofen for the fever and sore throat. Improvement was noted within 24 hours, but the full 10-day course of pencillin was completed to prevent rheumatic fever.
For more information, see “Papillae on tongue.” Journal of Family Practice. January 24, 2014.
Best Practices: In the Management of Hemophilia

The treatment of patients with hemophilia has rapidly evolved from one-size-fits-all factor replacement strategies to highly individualized, patient-specific care.
Faculty:
Erik Berntorp, MD, PhD
Malmö Centre for Thrombosis and Haemostasis
Lund University
Malmö, Sweden
Faculty Disclosures:
This sponsored content was prepared by Dr. Berntorp and reviewed by Shire. Dr. Berntorp discloses that he is a consultant and on the advisory boards and speakers’ bureaus for Bayer, CSL Behring, Octapharma, Shire, and Sobi. The production of this section did not involve the news or editorial staff of Frontline Medical Communications.
S28001
2/17
Click here to read the supplement
The treatment of patients with hemophilia has rapidly evolved from one-size-fits-all factor replacement strategies to highly individualized, patient-specific care.
Faculty:
Erik Berntorp, MD, PhD
Malmö Centre for Thrombosis and Haemostasis
Lund University
Malmö, Sweden
Faculty Disclosures:
This sponsored content was prepared by Dr. Berntorp and reviewed by Shire. Dr. Berntorp discloses that he is a consultant and on the advisory boards and speakers’ bureaus for Bayer, CSL Behring, Octapharma, Shire, and Sobi. The production of this section did not involve the news or editorial staff of Frontline Medical Communications.
S28001
2/17
Click here to read the supplement
The treatment of patients with hemophilia has rapidly evolved from one-size-fits-all factor replacement strategies to highly individualized, patient-specific care.
Faculty:
Erik Berntorp, MD, PhD
Malmö Centre for Thrombosis and Haemostasis
Lund University
Malmö, Sweden
Faculty Disclosures:
This sponsored content was prepared by Dr. Berntorp and reviewed by Shire. Dr. Berntorp discloses that he is a consultant and on the advisory boards and speakers’ bureaus for Bayer, CSL Behring, Octapharma, Shire, and Sobi. The production of this section did not involve the news or editorial staff of Frontline Medical Communications.
S28001
2/17
Click here to read the supplement
