User login
Compound inhibits translation program to treat MM

A new compound has shown promise for treating multiple myeloma (MM) by inhibiting the oncogenic MYC-driven translation program supporting the disease, according to researchers.
The compound is CMLD01059, a derivative of natural products called rocaglates that are known to interfere with translation.
CMLD010509 induced apoptosis in MM cells in culture and exhibited anti-myeloma activity in 3 different mouse models.
In addition, the compound was well-tolerated by the mice and spared normal cells in culture.
Salomon Manier, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts, and his colleagues reported these results in Science Translational Medicine.
The researchers found that CMLD01059 treatment significantly reduced the levels of 54 proteins in MM cell lines, including 5 known drivers of tumor progression—MYC, MDM2, CCND1, MAF, and MCL-1.
Further investigation confirmed that CMLD010509 inhibits the translation of oncoproteins that support the proliferation and survival of MM cells.
The researchers also found that CMLD010509 triggered a “strong” and “rapid” apoptotic response in MM cells (NCI-H929 and MM1S).
So the team tested the anti-myeloma activity of CMLD010509 in mouse models.
In one model (mice injected with MM1S cells), CMLD010509 “caused a marked reduction in tumor burden,” according to the researchers.
The median survival was 47 days in CMLD010509-treated mice, compared to 35 days in control mice (P<0.001).
The researchers also noted that 4 weeks of CMLD010509 treatment was well-tolerated in the mice, who maintained their weight and normal complete blood counts.
In another MM model (mice injected with KMS-11 cells), the mice received CMLD010509 or vehicle control twice a week for 4 weeks and were sacrificed at the end of treatment.
Immunohistochemistry studies conducted on bone marrow samples revealed a decrease in CD138+ plasma cells, depletion of MYC, and inhibition of proliferation in the CMLD010509-treated mice.
For the last model, the researchers injected transplantable mouse MM cells into C57BL/6 mice. The team noted that these cells are driven by plasma cell-specific MYC overexpression (Vk*Myc cells).
The mice received CMLD010509 or vehicle control twice a week starting 1 week after cell inoculation.
The researchers said CMLD010509 was well-tolerated, and they observed a “robust” decrease of M-spike in the treated mice that was associated with a significant improvement in survival.
The median survival was 39 days in the control mice, but it had not been reached by 90 days in the treated mice (P=0.0019).
The researchers said these results support targeting translation with rocaglates to treat MM. ![]()
A new compound has shown promise for treating multiple myeloma (MM) by inhibiting the oncogenic MYC-driven translation program supporting the disease, according to researchers.
The compound is CMLD01059, a derivative of natural products called rocaglates that are known to interfere with translation.
CMLD010509 induced apoptosis in MM cells in culture and exhibited anti-myeloma activity in 3 different mouse models.
In addition, the compound was well-tolerated by the mice and spared normal cells in culture.
Salomon Manier, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts, and his colleagues reported these results in Science Translational Medicine.
The researchers found that CMLD01059 treatment significantly reduced the levels of 54 proteins in MM cell lines, including 5 known drivers of tumor progression—MYC, MDM2, CCND1, MAF, and MCL-1.
Further investigation confirmed that CMLD010509 inhibits the translation of oncoproteins that support the proliferation and survival of MM cells.
The researchers also found that CMLD010509 triggered a “strong” and “rapid” apoptotic response in MM cells (NCI-H929 and MM1S).
So the team tested the anti-myeloma activity of CMLD010509 in mouse models.
In one model (mice injected with MM1S cells), CMLD010509 “caused a marked reduction in tumor burden,” according to the researchers.
The median survival was 47 days in CMLD010509-treated mice, compared to 35 days in control mice (P<0.001).
The researchers also noted that 4 weeks of CMLD010509 treatment was well-tolerated in the mice, who maintained their weight and normal complete blood counts.
In another MM model (mice injected with KMS-11 cells), the mice received CMLD010509 or vehicle control twice a week for 4 weeks and were sacrificed at the end of treatment.
Immunohistochemistry studies conducted on bone marrow samples revealed a decrease in CD138+ plasma cells, depletion of MYC, and inhibition of proliferation in the CMLD010509-treated mice.
For the last model, the researchers injected transplantable mouse MM cells into C57BL/6 mice. The team noted that these cells are driven by plasma cell-specific MYC overexpression (Vk*Myc cells).
The mice received CMLD010509 or vehicle control twice a week starting 1 week after cell inoculation.
The researchers said CMLD010509 was well-tolerated, and they observed a “robust” decrease of M-spike in the treated mice that was associated with a significant improvement in survival.
The median survival was 39 days in the control mice, but it had not been reached by 90 days in the treated mice (P=0.0019).
The researchers said these results support targeting translation with rocaglates to treat MM. ![]()
A new compound has shown promise for treating multiple myeloma (MM) by inhibiting the oncogenic MYC-driven translation program supporting the disease, according to researchers.
The compound is CMLD01059, a derivative of natural products called rocaglates that are known to interfere with translation.
CMLD010509 induced apoptosis in MM cells in culture and exhibited anti-myeloma activity in 3 different mouse models.
In addition, the compound was well-tolerated by the mice and spared normal cells in culture.
Salomon Manier, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts, and his colleagues reported these results in Science Translational Medicine.
The researchers found that CMLD01059 treatment significantly reduced the levels of 54 proteins in MM cell lines, including 5 known drivers of tumor progression—MYC, MDM2, CCND1, MAF, and MCL-1.
Further investigation confirmed that CMLD010509 inhibits the translation of oncoproteins that support the proliferation and survival of MM cells.
The researchers also found that CMLD010509 triggered a “strong” and “rapid” apoptotic response in MM cells (NCI-H929 and MM1S).
So the team tested the anti-myeloma activity of CMLD010509 in mouse models.
In one model (mice injected with MM1S cells), CMLD010509 “caused a marked reduction in tumor burden,” according to the researchers.
The median survival was 47 days in CMLD010509-treated mice, compared to 35 days in control mice (P<0.001).
The researchers also noted that 4 weeks of CMLD010509 treatment was well-tolerated in the mice, who maintained their weight and normal complete blood counts.
In another MM model (mice injected with KMS-11 cells), the mice received CMLD010509 or vehicle control twice a week for 4 weeks and were sacrificed at the end of treatment.
Immunohistochemistry studies conducted on bone marrow samples revealed a decrease in CD138+ plasma cells, depletion of MYC, and inhibition of proliferation in the CMLD010509-treated mice.
For the last model, the researchers injected transplantable mouse MM cells into C57BL/6 mice. The team noted that these cells are driven by plasma cell-specific MYC overexpression (Vk*Myc cells).
The mice received CMLD010509 or vehicle control twice a week starting 1 week after cell inoculation.
The researchers said CMLD010509 was well-tolerated, and they observed a “robust” decrease of M-spike in the treated mice that was associated with a significant improvement in survival.
The median survival was 39 days in the control mice, but it had not been reached by 90 days in the treated mice (P=0.0019).
The researchers said these results support targeting translation with rocaglates to treat MM. ![]()
EMA recommends drug receive orphan designation for PNH

The European Medicines Agency (EMA) has recommended orphan drug designation for the complement C3 inhibitor APL-2 as a treatment for paroxysmal nocturnal hemoglobinuria (PNH).
APL-2 is a synthetic cyclic peptide conjugated to a polyethylene glycol polymer that binds specifically to C3 and C3b, blocking all 3 pathways of complement activation (classical, lectin, and alternative).
This comprehensive inhibition of complement-mediated pathology may have the potential to control symptoms and modify underlying disease in patients with PNH, according to Apellis Pharmaceuticals, Inc., the company developing APL-2.
APL-2 has been evaluated in a pair of phase 1 studies of healthy volunteers. Results from these studies were presented at the 2016 ASH Annual Meeting (abstract 1251).
Now, Apellis is evaluating APL-2 in PNH patients in a pair of phase 1b trials.
In PADDOCK (NCT02588833), researchers are assessing the safety, tolerability, pharmacokinetics, pharmacodynamics, and preliminary efficacy of multiple doses of APL-2 administered by daily subcutaneous injection in patients with PNH who have not received the standard of care in the past.
In PHAROAH (NCT02264639), researchers are assessing the safety, tolerability, pharmacokinetics, and pharmacodynamics of single and multiple doses of APL-2 administered by subcutaneous injection as an add-on to the standard of care in patients with PNH.
About orphan designation
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if the drug receives regulatory approval. The designation also provides incentives for companies seeking protocol assistance from the EMA during the product development phase and direct access to the centralized authorization procedure.
The EMA adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision. The European Commission typically makes a decision within 30 days. ![]()
The European Medicines Agency (EMA) has recommended orphan drug designation for the complement C3 inhibitor APL-2 as a treatment for paroxysmal nocturnal hemoglobinuria (PNH).
APL-2 is a synthetic cyclic peptide conjugated to a polyethylene glycol polymer that binds specifically to C3 and C3b, blocking all 3 pathways of complement activation (classical, lectin, and alternative).
This comprehensive inhibition of complement-mediated pathology may have the potential to control symptoms and modify underlying disease in patients with PNH, according to Apellis Pharmaceuticals, Inc., the company developing APL-2.
APL-2 has been evaluated in a pair of phase 1 studies of healthy volunteers. Results from these studies were presented at the 2016 ASH Annual Meeting (abstract 1251).
Now, Apellis is evaluating APL-2 in PNH patients in a pair of phase 1b trials.
In PADDOCK (NCT02588833), researchers are assessing the safety, tolerability, pharmacokinetics, pharmacodynamics, and preliminary efficacy of multiple doses of APL-2 administered by daily subcutaneous injection in patients with PNH who have not received the standard of care in the past.
In PHAROAH (NCT02264639), researchers are assessing the safety, tolerability, pharmacokinetics, and pharmacodynamics of single and multiple doses of APL-2 administered by subcutaneous injection as an add-on to the standard of care in patients with PNH.
About orphan designation
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if the drug receives regulatory approval. The designation also provides incentives for companies seeking protocol assistance from the EMA during the product development phase and direct access to the centralized authorization procedure.
The EMA adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision. The European Commission typically makes a decision within 30 days. ![]()
The European Medicines Agency (EMA) has recommended orphan drug designation for the complement C3 inhibitor APL-2 as a treatment for paroxysmal nocturnal hemoglobinuria (PNH).
APL-2 is a synthetic cyclic peptide conjugated to a polyethylene glycol polymer that binds specifically to C3 and C3b, blocking all 3 pathways of complement activation (classical, lectin, and alternative).
This comprehensive inhibition of complement-mediated pathology may have the potential to control symptoms and modify underlying disease in patients with PNH, according to Apellis Pharmaceuticals, Inc., the company developing APL-2.
APL-2 has been evaluated in a pair of phase 1 studies of healthy volunteers. Results from these studies were presented at the 2016 ASH Annual Meeting (abstract 1251).
Now, Apellis is evaluating APL-2 in PNH patients in a pair of phase 1b trials.
In PADDOCK (NCT02588833), researchers are assessing the safety, tolerability, pharmacokinetics, pharmacodynamics, and preliminary efficacy of multiple doses of APL-2 administered by daily subcutaneous injection in patients with PNH who have not received the standard of care in the past.
In PHAROAH (NCT02264639), researchers are assessing the safety, tolerability, pharmacokinetics, and pharmacodynamics of single and multiple doses of APL-2 administered by subcutaneous injection as an add-on to the standard of care in patients with PNH.
About orphan designation
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if the drug receives regulatory approval. The designation also provides incentives for companies seeking protocol assistance from the EMA during the product development phase and direct access to the centralized authorization procedure.
The EMA adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision. The European Commission typically makes a decision within 30 days. ![]()
Dry spots on lower legs

The FP made the presumptive diagnosis of nummular eczema, but recognized that a fungal infection and psoriasis were part of the differential diagnosis. He performed a potassium hydroxide (KOH) preparation, which was negative for hyphae and fungal elements. (See a video on how to perform a KOH preparation here: http://www.mdedge.com/jfponline/article/100603/dermatology/koh-preparation.) In order to explore whether this might be a case of guttate psoriasis, the FP asked about any preceding strep pharyngitis or other respiratory infections. The patient, however, had not had any preceding infections. The FP also checked her nails, scalp, and umbilicus for other signs of psoriasis, but found none. The FP was now confident in making a clinical diagnosis of nummular eczema (also known as nummular dermatitis).
Nummular eczema is a type of eczema characterized by circular or oval-shaped scaling plaques with well-defined borders. (“Nummus” is Latin for “coin.”) Nummular eczema produces multiple lesions that are most commonly found on the dorsa of the hands, arms, and legs.
Patients who have a history of atopic dermatitis are more likely to get nummular eczema even after they outgrow the atopic dermatitis. The 2 conditions involve problems with the barrier function of the skin, and emollients are helpful for the prevention and treatment of both.
In this case, the FP prescribed 0.1% triamcinolone ointment to be applied twice daily until the lesions resolved. At a one-month follow-up appointment, the patient indicated that her legs were now smooth and she was happy that she could shave them again. The FP told her that it would be a good idea to use emollients after bathing to keep the skin moist in order to prevent future episodes of nummular eczema.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Wah Y, Usatine R. Eczema. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP made the presumptive diagnosis of nummular eczema, but recognized that a fungal infection and psoriasis were part of the differential diagnosis. He performed a potassium hydroxide (KOH) preparation, which was negative for hyphae and fungal elements. (See a video on how to perform a KOH preparation here: http://www.mdedge.com/jfponline/article/100603/dermatology/koh-preparation.) In order to explore whether this might be a case of guttate psoriasis, the FP asked about any preceding strep pharyngitis or other respiratory infections. The patient, however, had not had any preceding infections. The FP also checked her nails, scalp, and umbilicus for other signs of psoriasis, but found none. The FP was now confident in making a clinical diagnosis of nummular eczema (also known as nummular dermatitis).
Nummular eczema is a type of eczema characterized by circular or oval-shaped scaling plaques with well-defined borders. (“Nummus” is Latin for “coin.”) Nummular eczema produces multiple lesions that are most commonly found on the dorsa of the hands, arms, and legs.
Patients who have a history of atopic dermatitis are more likely to get nummular eczema even after they outgrow the atopic dermatitis. The 2 conditions involve problems with the barrier function of the skin, and emollients are helpful for the prevention and treatment of both.
In this case, the FP prescribed 0.1% triamcinolone ointment to be applied twice daily until the lesions resolved. At a one-month follow-up appointment, the patient indicated that her legs were now smooth and she was happy that she could shave them again. The FP told her that it would be a good idea to use emollients after bathing to keep the skin moist in order to prevent future episodes of nummular eczema.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Wah Y, Usatine R. Eczema. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP made the presumptive diagnosis of nummular eczema, but recognized that a fungal infection and psoriasis were part of the differential diagnosis. He performed a potassium hydroxide (KOH) preparation, which was negative for hyphae and fungal elements. (See a video on how to perform a KOH preparation here: http://www.mdedge.com/jfponline/article/100603/dermatology/koh-preparation.) In order to explore whether this might be a case of guttate psoriasis, the FP asked about any preceding strep pharyngitis or other respiratory infections. The patient, however, had not had any preceding infections. The FP also checked her nails, scalp, and umbilicus for other signs of psoriasis, but found none. The FP was now confident in making a clinical diagnosis of nummular eczema (also known as nummular dermatitis).
Nummular eczema is a type of eczema characterized by circular or oval-shaped scaling plaques with well-defined borders. (“Nummus” is Latin for “coin.”) Nummular eczema produces multiple lesions that are most commonly found on the dorsa of the hands, arms, and legs.
Patients who have a history of atopic dermatitis are more likely to get nummular eczema even after they outgrow the atopic dermatitis. The 2 conditions involve problems with the barrier function of the skin, and emollients are helpful for the prevention and treatment of both.
In this case, the FP prescribed 0.1% triamcinolone ointment to be applied twice daily until the lesions resolved. At a one-month follow-up appointment, the patient indicated that her legs were now smooth and she was happy that she could shave them again. The FP told her that it would be a good idea to use emollients after bathing to keep the skin moist in order to prevent future episodes of nummular eczema.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Wah Y, Usatine R. Eczema. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

Boy’s Dark Side Comes Out
ANSWER
The correct answer is Becker nevus (BN; choice “c”).
Because the lesion was not congenital, a number of possibilities, including congenital melanocytic nevus (choice “a”), were ruled out. Another differential item that was eliminated was nevus spilus (choice “b”), a tan congenital nevus covered with darker, punctate macules that usually manifest on extremities. These have little, if any, malignant potential.
And while BN is not associated with malignancy, it is possible for it to co-exist with melanoma (choice “d”). Therefore, atypical BN cases may need to be followed or serially biopsied.
DISCUSSION
BN is unusual but not rare. Also referred to as Becker melanosis, the condition affects approximately 0.5% of the population. It primarily manifests in young men during early puberty, although women can develop BN.
Histologic signs of BN include epidermal thickening, elongation of rete ridges, and increased bundles of smooth muscle in the dermis.
Androgen causation is strongly indicated by the condition’s predominance in males and onset at puberty, as well as its associated hypertrichosis and increased density of androgen receptors in affected areas. Variations of the condition can involve the legs, arms, or face. It is possible for BN to manifest without additional hair growth. Hypoplasia of ipsilateral pectoral structures (or the ipsilateral breast in women) has also been reported.
Several types of lasers can be used to lighten the hyperpigmentation and remove hairs. This treatment modality yields variable results.
ANSWER
The correct answer is Becker nevus (BN; choice “c”).
Because the lesion was not congenital, a number of possibilities, including congenital melanocytic nevus (choice “a”), were ruled out. Another differential item that was eliminated was nevus spilus (choice “b”), a tan congenital nevus covered with darker, punctate macules that usually manifest on extremities. These have little, if any, malignant potential.
And while BN is not associated with malignancy, it is possible for it to co-exist with melanoma (choice “d”). Therefore, atypical BN cases may need to be followed or serially biopsied.
DISCUSSION
BN is unusual but not rare. Also referred to as Becker melanosis, the condition affects approximately 0.5% of the population. It primarily manifests in young men during early puberty, although women can develop BN.
Histologic signs of BN include epidermal thickening, elongation of rete ridges, and increased bundles of smooth muscle in the dermis.
Androgen causation is strongly indicated by the condition’s predominance in males and onset at puberty, as well as its associated hypertrichosis and increased density of androgen receptors in affected areas. Variations of the condition can involve the legs, arms, or face. It is possible for BN to manifest without additional hair growth. Hypoplasia of ipsilateral pectoral structures (or the ipsilateral breast in women) has also been reported.
Several types of lasers can be used to lighten the hyperpigmentation and remove hairs. This treatment modality yields variable results.
ANSWER
The correct answer is Becker nevus (BN; choice “c”).
Because the lesion was not congenital, a number of possibilities, including congenital melanocytic nevus (choice “a”), were ruled out. Another differential item that was eliminated was nevus spilus (choice “b”), a tan congenital nevus covered with darker, punctate macules that usually manifest on extremities. These have little, if any, malignant potential.
And while BN is not associated with malignancy, it is possible for it to co-exist with melanoma (choice “d”). Therefore, atypical BN cases may need to be followed or serially biopsied.
DISCUSSION
BN is unusual but not rare. Also referred to as Becker melanosis, the condition affects approximately 0.5% of the population. It primarily manifests in young men during early puberty, although women can develop BN.
Histologic signs of BN include epidermal thickening, elongation of rete ridges, and increased bundles of smooth muscle in the dermis.
Androgen causation is strongly indicated by the condition’s predominance in males and onset at puberty, as well as its associated hypertrichosis and increased density of androgen receptors in affected areas. Variations of the condition can involve the legs, arms, or face. It is possible for BN to manifest without additional hair growth. Hypoplasia of ipsilateral pectoral structures (or the ipsilateral breast in women) has also been reported.
Several types of lasers can be used to lighten the hyperpigmentation and remove hairs. This treatment modality yields variable results.

This 14-year-old boy’s family is alarmed by a darkening patch of skin on the right side of his chest and shoulder, which first appeared two years ago. Over the span of a few months, dark hairs grew on the hyperpigmented area.
The family’s primary care provider assured them that it was likely benign, but the lack of a specific diagnosis left them concerned. They requested referral to dermatology.
A large portion of the patient’s right anterior chest and shoulder is completely covered by uniformly hyperpigmented, hypertrichotic skin, which feels a bit thicker than the unaffected skin. The lesion’s borders are quite irregular and uneven; beyond them, no hairs can be seen. The problem is confined to the chest and shoulder; although the medial border extends to the sternal area, the lower edge stops short of the pectoral area.
The patient denies any symptoms and claims to be healthy in all other respects. There is no family history of similar problems.

Alpha blockers may facilitate the expulsion of larger ureteric stones
CLINICAL QUESTION: Are alpha blockers efficacious in patients with ureteric stones?
STUDY DESIGN: Systematic review & meta-analysis.
SETTING: Randomized controlled trials (RCTs); most conducted in Europe and Asia.
SYNOPSIS: Fifty-five unique RCTs (5,990 subjects) examining alpha blockers as the main treatment of ureteric stones versus placebo or control were included regardless of language and publication status.
Treatment with alpha blockers resulted in a 49% greater likelihood of stone passage (RR, 1.49; CI, 1.39-1.61) with a number needed to treat of four. A priori subgroup analysis revealed treatment was only beneficial in patients with larger stones (5mm or greater) independent of stone location or type of alpha blocker.
Secondary outcomes included reduced time to stone passage, fewer episodes of pain, decreased risk of surgical intervention, and lower risk of hospital admission with alpha blocker treatment without an increase in serious adverse events.
The meta-analysis was limited by the overall lack of methodological rigor of and clinical heterogeneity between the pooled studies.
BOTTOM LINE: Based on available evidence, it is reasonable to utilize an alpha blocker as medical expulsive therapy in patients with larger ureteric stones.
CITATIONS: Hollingsworth JM, Canales BK, Rogers MA, et al. Alpha blockers for treatment of ureteric stones: systematic review and meta-analysis. BMJ. 2016;355:i6112.
Dr. Ecker is the assistant director of education, Division of Hospital Medicine, University of Colorado School of Medicine, Aurora.
CLINICAL QUESTION: Are alpha blockers efficacious in patients with ureteric stones?
STUDY DESIGN: Systematic review & meta-analysis.
SETTING: Randomized controlled trials (RCTs); most conducted in Europe and Asia.
SYNOPSIS: Fifty-five unique RCTs (5,990 subjects) examining alpha blockers as the main treatment of ureteric stones versus placebo or control were included regardless of language and publication status.
Treatment with alpha blockers resulted in a 49% greater likelihood of stone passage (RR, 1.49; CI, 1.39-1.61) with a number needed to treat of four. A priori subgroup analysis revealed treatment was only beneficial in patients with larger stones (5mm or greater) independent of stone location or type of alpha blocker.
Secondary outcomes included reduced time to stone passage, fewer episodes of pain, decreased risk of surgical intervention, and lower risk of hospital admission with alpha blocker treatment without an increase in serious adverse events.
The meta-analysis was limited by the overall lack of methodological rigor of and clinical heterogeneity between the pooled studies.
BOTTOM LINE: Based on available evidence, it is reasonable to utilize an alpha blocker as medical expulsive therapy in patients with larger ureteric stones.
CITATIONS: Hollingsworth JM, Canales BK, Rogers MA, et al. Alpha blockers for treatment of ureteric stones: systematic review and meta-analysis. BMJ. 2016;355:i6112.
Dr. Ecker is the assistant director of education, Division of Hospital Medicine, University of Colorado School of Medicine, Aurora.
CLINICAL QUESTION: Are alpha blockers efficacious in patients with ureteric stones?
STUDY DESIGN: Systematic review & meta-analysis.
SETTING: Randomized controlled trials (RCTs); most conducted in Europe and Asia.
SYNOPSIS: Fifty-five unique RCTs (5,990 subjects) examining alpha blockers as the main treatment of ureteric stones versus placebo or control were included regardless of language and publication status.
Treatment with alpha blockers resulted in a 49% greater likelihood of stone passage (RR, 1.49; CI, 1.39-1.61) with a number needed to treat of four. A priori subgroup analysis revealed treatment was only beneficial in patients with larger stones (5mm or greater) independent of stone location or type of alpha blocker.
Secondary outcomes included reduced time to stone passage, fewer episodes of pain, decreased risk of surgical intervention, and lower risk of hospital admission with alpha blocker treatment without an increase in serious adverse events.
The meta-analysis was limited by the overall lack of methodological rigor of and clinical heterogeneity between the pooled studies.
BOTTOM LINE: Based on available evidence, it is reasonable to utilize an alpha blocker as medical expulsive therapy in patients with larger ureteric stones.
CITATIONS: Hollingsworth JM, Canales BK, Rogers MA, et al. Alpha blockers for treatment of ureteric stones: systematic review and meta-analysis. BMJ. 2016;355:i6112.
Dr. Ecker is the assistant director of education, Division of Hospital Medicine, University of Colorado School of Medicine, Aurora.
Interventions, especially those that are organization-directed, reduce burnout in physicians
CLINICAL QUESTION: How efficacious are interventions to reduce burnout in physicians?
BACKGROUND: Burnout is characterized by emotional exhaustion, depersonalization, and a diminished sense of personal accomplishment. It is driven by workplace stressors and affects nearly half of physicians practicing in the U.S.

SETTING: Randomized controlled trials and controlled before-after studies in primary, secondary, or intensive care settings; most conducted in North America and Europe.
SYNOPSIS: Twenty independent comparisons from 19 studies (1,550 physicians of any specialty including trainees) were included. All reported burnout outcomes after either physician- or organization-directed interventions designed to relieve stress and/or improve physician performance. Most physician-directed interventions utilized mindfulness-based stress reduction techniques or other educational interventions. Most organizational-directed interventions introduced reductions in workload or schedule changes.
Interventions were associated with small, significant reductions in burnout (standardized mean difference, –0.29; CI –0.42 to –0.16). A pre-specified subgroup analysis revealed organization-directed interventions had significantly improved effects, compared with physician-directed ones.
The generalizability of this meta-analysis is limited as the included studies significantly differed in their methodologies.
BOTTOM LINE: Burnout intervention programs for physicians are associated with small benefits, and the increased efficacy of organization-directed interventions suggest burnout is a problem of the health care system, rather than of individuals.
CITATIONS: Panagioti M, Panagopoulou E, Bower P, et al. Controlled interventions to reduce burnout in physicians: a systematic review and meta-analysis. JAMA Intern Med. 2017;177(2):195-205.
Dr. Ecker is the assistant director of education, Division of Hospital Medicine, University of Colorado School of Medicine, Aurora.
CLINICAL QUESTION: How efficacious are interventions to reduce burnout in physicians?
BACKGROUND: Burnout is characterized by emotional exhaustion, depersonalization, and a diminished sense of personal accomplishment. It is driven by workplace stressors and affects nearly half of physicians practicing in the U.S.
SETTING: Randomized controlled trials and controlled before-after studies in primary, secondary, or intensive care settings; most conducted in North America and Europe.
SYNOPSIS: Twenty independent comparisons from 19 studies (1,550 physicians of any specialty including trainees) were included. All reported burnout outcomes after either physician- or organization-directed interventions designed to relieve stress and/or improve physician performance. Most physician-directed interventions utilized mindfulness-based stress reduction techniques or other educational interventions. Most organizational-directed interventions introduced reductions in workload or schedule changes.
Interventions were associated with small, significant reductions in burnout (standardized mean difference, –0.29; CI –0.42 to –0.16). A pre-specified subgroup analysis revealed organization-directed interventions had significantly improved effects, compared with physician-directed ones.
The generalizability of this meta-analysis is limited as the included studies significantly differed in their methodologies.
BOTTOM LINE: Burnout intervention programs for physicians are associated with small benefits, and the increased efficacy of organization-directed interventions suggest burnout is a problem of the health care system, rather than of individuals.
CITATIONS: Panagioti M, Panagopoulou E, Bower P, et al. Controlled interventions to reduce burnout in physicians: a systematic review and meta-analysis. JAMA Intern Med. 2017;177(2):195-205.
Dr. Ecker is the assistant director of education, Division of Hospital Medicine, University of Colorado School of Medicine, Aurora.
CLINICAL QUESTION: How efficacious are interventions to reduce burnout in physicians?
BACKGROUND: Burnout is characterized by emotional exhaustion, depersonalization, and a diminished sense of personal accomplishment. It is driven by workplace stressors and affects nearly half of physicians practicing in the U.S.
SETTING: Randomized controlled trials and controlled before-after studies in primary, secondary, or intensive care settings; most conducted in North America and Europe.
SYNOPSIS: Twenty independent comparisons from 19 studies (1,550 physicians of any specialty including trainees) were included. All reported burnout outcomes after either physician- or organization-directed interventions designed to relieve stress and/or improve physician performance. Most physician-directed interventions utilized mindfulness-based stress reduction techniques or other educational interventions. Most organizational-directed interventions introduced reductions in workload or schedule changes.
Interventions were associated with small, significant reductions in burnout (standardized mean difference, –0.29; CI –0.42 to –0.16). A pre-specified subgroup analysis revealed organization-directed interventions had significantly improved effects, compared with physician-directed ones.
The generalizability of this meta-analysis is limited as the included studies significantly differed in their methodologies.
BOTTOM LINE: Burnout intervention programs for physicians are associated with small benefits, and the increased efficacy of organization-directed interventions suggest burnout is a problem of the health care system, rather than of individuals.
CITATIONS: Panagioti M, Panagopoulou E, Bower P, et al. Controlled interventions to reduce burnout in physicians: a systematic review and meta-analysis. JAMA Intern Med. 2017;177(2):195-205.
Dr. Ecker is the assistant director of education, Division of Hospital Medicine, University of Colorado School of Medicine, Aurora.
Deep infiltrating endometriosis lesions harbor cancer-driver mutations
Deep infiltrating endometriosis lesions were found to harbor several genetic mutations, including well-known cancer-driver mutations in the ARID1A, PIK3CA, KRAS, and PPP2R1A genes, investigators reported in the May 11 issue of the New England Journal of Medicine.
This finding was possible only through the use of a combination of next-generation sequencing tools, together with highly sensitive digital genomic assays. A finding of cancer-related mutations in noncancerous lesions – and, “in particular, in nonovarian deep infiltrating lesions that rarely (if ever) transform into cancer” – was very “surprising” and raises new questions about the pathobiology of endometriosis, said Michael S. Anglesio, PhD, of the University of British Columbia, Vancouver, and his associates.
All three subtypes of endometriosis exhibit “benign clinical behavior and normal-appearing histologic features,” and are considered to be nonmalignant inflammatory lesions, Dr. Anglesio and his associates said. However, they also “recapitulate some features of malignant neoplasms, including local invasion and resistance to apoptosis,” the investigators noted.
To further explore whether deep infiltrating endometriosis lesions harbor somatic mutations, they performed a series of genetic analyses on samples obtained from three independent cohorts of 27 affected patients in New York, Japan, and Vancouver. Whole-exome sequencing of lesions and adjacent normal tissue from 24 women revealed 80 different somatic mutations in 19 (79%) of the lesions.
The number of mutations per lesion varied widely, from 0 to 17, with a mean of 3.3 mutations per lesion. Five of these lesions harbored mutations in the cancer-driver genes ARID1A, PIK3CA, KRAS, or PPP2R1A.
In targeted-sequencing analyses of samples from three more patients, more activating mutations in the KRAS gene were found in two (66%). One woman had two different activating KRAS mutations, and the other had the same KRAS mutation in three separate lesions.
A further analysis of samples from an additional 12 patients showed KRAS mutations in 3 (25%) of them.
The data indicate that these mutations were very unlikely to have arisen by chance alone. In addition, “because cancer-driver mutations were present only in the epithelium but not the stroma of the same endometriosis lesion, we can assume that the observed mutations provide some key selective advantage to endometriotic epithelial cells,” Dr. Anglesio and his associates said (N Engl J Med. 2017 May 11. doi: 10.1056/NEJMoa1614814).
Their findings are consistent with those of recent studies of other organ systems, which reported cancer-driver mutations in benign lesions and in normal tissues from skin, neuronal, and ovarian samples, they added.
“Our findings challenge the current understanding of this invasive subtype of endometriosis and open the discussion on whether deep infiltrating endometriosis can be considered as a benign neoplasm,” the investigators wrote.
This study was sponsored by 27 nonindustry sources, including the Johns Hopkins University, the Virginia and D.K. Ludwig Fund for Cancer Research, the Ephraim and Wilma Shaw Roseman Foundation, the Endometriosis Foundation of America, and the National Institutes of Health. Dr. Anglesio reported having no relevant financial disclosures; some of his associates reported ties to several industry sources.
The variable patterns of somatic mutations discovered by Anglesio et al. are “intriguing” and raise many questions.
Do specific mutations in deep infiltrating endometriosis lesions contribute to the severity and progression of the disorder? Are such mutations to be found in other types of lesions? In endometrial precursor cells? Do specific mutations account for different presentations in different patients?
Exploring these questions will not be straightforward because of the difficulties in obtaining sufficient endometriotic tissue for genetic studies. Not only is it hard to get samples from peritoneal lesions, but the mutations occur in only one cell type – epithelium – which is even harder to isolate from mixed tissue samples.
Grant W. Montgomery, PhD, is at the Institute for Molecular Bioscience at the University of Queensland, Brisbane, Australia, and reported having no relevant financial disclosures. Linda C. Giudice, MD, PhD, is in the department of ob.gyn. and reproductive sciences at the University of California, San Francisco, and reported ties to AbbVie and Bayer. Dr. Montgomery and Dr. Giudice made these remarks in an editorial accompanying Dr. Anglesio’s report (N Engl J Med. 2017 May 11. doi: 10.1056/NEJMe1701700).
The variable patterns of somatic mutations discovered by Anglesio et al. are “intriguing” and raise many questions.
Do specific mutations in deep infiltrating endometriosis lesions contribute to the severity and progression of the disorder? Are such mutations to be found in other types of lesions? In endometrial precursor cells? Do specific mutations account for different presentations in different patients?
Exploring these questions will not be straightforward because of the difficulties in obtaining sufficient endometriotic tissue for genetic studies. Not only is it hard to get samples from peritoneal lesions, but the mutations occur in only one cell type – epithelium – which is even harder to isolate from mixed tissue samples.
Grant W. Montgomery, PhD, is at the Institute for Molecular Bioscience at the University of Queensland, Brisbane, Australia, and reported having no relevant financial disclosures. Linda C. Giudice, MD, PhD, is in the department of ob.gyn. and reproductive sciences at the University of California, San Francisco, and reported ties to AbbVie and Bayer. Dr. Montgomery and Dr. Giudice made these remarks in an editorial accompanying Dr. Anglesio’s report (N Engl J Med. 2017 May 11. doi: 10.1056/NEJMe1701700).
The variable patterns of somatic mutations discovered by Anglesio et al. are “intriguing” and raise many questions.
Do specific mutations in deep infiltrating endometriosis lesions contribute to the severity and progression of the disorder? Are such mutations to be found in other types of lesions? In endometrial precursor cells? Do specific mutations account for different presentations in different patients?
Exploring these questions will not be straightforward because of the difficulties in obtaining sufficient endometriotic tissue for genetic studies. Not only is it hard to get samples from peritoneal lesions, but the mutations occur in only one cell type – epithelium – which is even harder to isolate from mixed tissue samples.
Grant W. Montgomery, PhD, is at the Institute for Molecular Bioscience at the University of Queensland, Brisbane, Australia, and reported having no relevant financial disclosures. Linda C. Giudice, MD, PhD, is in the department of ob.gyn. and reproductive sciences at the University of California, San Francisco, and reported ties to AbbVie and Bayer. Dr. Montgomery and Dr. Giudice made these remarks in an editorial accompanying Dr. Anglesio’s report (N Engl J Med. 2017 May 11. doi: 10.1056/NEJMe1701700).
Deep infiltrating endometriosis lesions were found to harbor several genetic mutations, including well-known cancer-driver mutations in the ARID1A, PIK3CA, KRAS, and PPP2R1A genes, investigators reported in the May 11 issue of the New England Journal of Medicine.
This finding was possible only through the use of a combination of next-generation sequencing tools, together with highly sensitive digital genomic assays. A finding of cancer-related mutations in noncancerous lesions – and, “in particular, in nonovarian deep infiltrating lesions that rarely (if ever) transform into cancer” – was very “surprising” and raises new questions about the pathobiology of endometriosis, said Michael S. Anglesio, PhD, of the University of British Columbia, Vancouver, and his associates.
All three subtypes of endometriosis exhibit “benign clinical behavior and normal-appearing histologic features,” and are considered to be nonmalignant inflammatory lesions, Dr. Anglesio and his associates said. However, they also “recapitulate some features of malignant neoplasms, including local invasion and resistance to apoptosis,” the investigators noted.
To further explore whether deep infiltrating endometriosis lesions harbor somatic mutations, they performed a series of genetic analyses on samples obtained from three independent cohorts of 27 affected patients in New York, Japan, and Vancouver. Whole-exome sequencing of lesions and adjacent normal tissue from 24 women revealed 80 different somatic mutations in 19 (79%) of the lesions.
The number of mutations per lesion varied widely, from 0 to 17, with a mean of 3.3 mutations per lesion. Five of these lesions harbored mutations in the cancer-driver genes ARID1A, PIK3CA, KRAS, or PPP2R1A.
In targeted-sequencing analyses of samples from three more patients, more activating mutations in the KRAS gene were found in two (66%). One woman had two different activating KRAS mutations, and the other had the same KRAS mutation in three separate lesions.
A further analysis of samples from an additional 12 patients showed KRAS mutations in 3 (25%) of them.
The data indicate that these mutations were very unlikely to have arisen by chance alone. In addition, “because cancer-driver mutations were present only in the epithelium but not the stroma of the same endometriosis lesion, we can assume that the observed mutations provide some key selective advantage to endometriotic epithelial cells,” Dr. Anglesio and his associates said (N Engl J Med. 2017 May 11. doi: 10.1056/NEJMoa1614814).
Their findings are consistent with those of recent studies of other organ systems, which reported cancer-driver mutations in benign lesions and in normal tissues from skin, neuronal, and ovarian samples, they added.
“Our findings challenge the current understanding of this invasive subtype of endometriosis and open the discussion on whether deep infiltrating endometriosis can be considered as a benign neoplasm,” the investigators wrote.
This study was sponsored by 27 nonindustry sources, including the Johns Hopkins University, the Virginia and D.K. Ludwig Fund for Cancer Research, the Ephraim and Wilma Shaw Roseman Foundation, the Endometriosis Foundation of America, and the National Institutes of Health. Dr. Anglesio reported having no relevant financial disclosures; some of his associates reported ties to several industry sources.
Deep infiltrating endometriosis lesions were found to harbor several genetic mutations, including well-known cancer-driver mutations in the ARID1A, PIK3CA, KRAS, and PPP2R1A genes, investigators reported in the May 11 issue of the New England Journal of Medicine.
This finding was possible only through the use of a combination of next-generation sequencing tools, together with highly sensitive digital genomic assays. A finding of cancer-related mutations in noncancerous lesions – and, “in particular, in nonovarian deep infiltrating lesions that rarely (if ever) transform into cancer” – was very “surprising” and raises new questions about the pathobiology of endometriosis, said Michael S. Anglesio, PhD, of the University of British Columbia, Vancouver, and his associates.
All three subtypes of endometriosis exhibit “benign clinical behavior and normal-appearing histologic features,” and are considered to be nonmalignant inflammatory lesions, Dr. Anglesio and his associates said. However, they also “recapitulate some features of malignant neoplasms, including local invasion and resistance to apoptosis,” the investigators noted.
To further explore whether deep infiltrating endometriosis lesions harbor somatic mutations, they performed a series of genetic analyses on samples obtained from three independent cohorts of 27 affected patients in New York, Japan, and Vancouver. Whole-exome sequencing of lesions and adjacent normal tissue from 24 women revealed 80 different somatic mutations in 19 (79%) of the lesions.
The number of mutations per lesion varied widely, from 0 to 17, with a mean of 3.3 mutations per lesion. Five of these lesions harbored mutations in the cancer-driver genes ARID1A, PIK3CA, KRAS, or PPP2R1A.
In targeted-sequencing analyses of samples from three more patients, more activating mutations in the KRAS gene were found in two (66%). One woman had two different activating KRAS mutations, and the other had the same KRAS mutation in three separate lesions.
A further analysis of samples from an additional 12 patients showed KRAS mutations in 3 (25%) of them.
The data indicate that these mutations were very unlikely to have arisen by chance alone. In addition, “because cancer-driver mutations were present only in the epithelium but not the stroma of the same endometriosis lesion, we can assume that the observed mutations provide some key selective advantage to endometriotic epithelial cells,” Dr. Anglesio and his associates said (N Engl J Med. 2017 May 11. doi: 10.1056/NEJMoa1614814).
Their findings are consistent with those of recent studies of other organ systems, which reported cancer-driver mutations in benign lesions and in normal tissues from skin, neuronal, and ovarian samples, they added.
“Our findings challenge the current understanding of this invasive subtype of endometriosis and open the discussion on whether deep infiltrating endometriosis can be considered as a benign neoplasm,” the investigators wrote.
This study was sponsored by 27 nonindustry sources, including the Johns Hopkins University, the Virginia and D.K. Ludwig Fund for Cancer Research, the Ephraim and Wilma Shaw Roseman Foundation, the Endometriosis Foundation of America, and the National Institutes of Health. Dr. Anglesio reported having no relevant financial disclosures; some of his associates reported ties to several industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Deep infiltrating endometriosis lesions were found to harbor several genetic mutations, including well-known cancer-driver mutations in the ARID1A, PIK3CA, KRAS, and PPP2R1A genes.
Major finding: Endometriosis samples from 24 women revealed 80 different somatic mutations in 19 (79%) of the lesions; the number of mutations per lesion varied widely, from 0 to 17, with a mean of 3.3 mutations per lesion.
Data source: A series of genetic analyses of archived endometriosis samples from 27 women, and an additional analysis of KRAS mutations in samples from 12 more women.
Disclosures: This study was sponsored by 27 nonindustry sources, including Johns Hopkins University, the Virginia and D.K. Ludwig Fund for Cancer Research, the Ephraim and Wilma Shaw Roseman Foundation, the Endometriosis Foundation of America, and the National Institutes of Health. Dr. Anglesio reported having no relevant financial disclosures; some of his associates reported ties to several industry sources.
Safe, effective backup for U.S. MMR vaccine exists
Antibodies against measles, mumps, and rubella persisted for up to 2 years after vaccination of children 12-15 months with the MMR vaccine approved in the United States and a similar one approved in Europe, both of which are manufactured without human serum albumin, Andrea A. Berry, MD, at the University of Maryland, Baltimore, and her associates said.
In 752 children aged a mean 12 months who received either the United States MMR vaccine and the European one, seropositivity for measles, mumps, and rubella persisted for up to 2 years with both vaccines. Both vaccines also were well tolerated.
Because there is only one MMR vaccine licensed in the United States, interruption to this single supply line could present a public health risk, Dr. Berry and her associates said. As both the vaccines used in this study do not contain human serum albumin, the theoretical risk of microbial contamination is reduced, compared with previous formulations of MMR.
Read more at Human Vaccines Immunotherapeutics. (2017. doi: 10.1080/21645515.2017.1309486).
Antibodies against measles, mumps, and rubella persisted for up to 2 years after vaccination of children 12-15 months with the MMR vaccine approved in the United States and a similar one approved in Europe, both of which are manufactured without human serum albumin, Andrea A. Berry, MD, at the University of Maryland, Baltimore, and her associates said.
In 752 children aged a mean 12 months who received either the United States MMR vaccine and the European one, seropositivity for measles, mumps, and rubella persisted for up to 2 years with both vaccines. Both vaccines also were well tolerated.
Because there is only one MMR vaccine licensed in the United States, interruption to this single supply line could present a public health risk, Dr. Berry and her associates said. As both the vaccines used in this study do not contain human serum albumin, the theoretical risk of microbial contamination is reduced, compared with previous formulations of MMR.
Read more at Human Vaccines Immunotherapeutics. (2017. doi: 10.1080/21645515.2017.1309486).
Antibodies against measles, mumps, and rubella persisted for up to 2 years after vaccination of children 12-15 months with the MMR vaccine approved in the United States and a similar one approved in Europe, both of which are manufactured without human serum albumin, Andrea A. Berry, MD, at the University of Maryland, Baltimore, and her associates said.
In 752 children aged a mean 12 months who received either the United States MMR vaccine and the European one, seropositivity for measles, mumps, and rubella persisted for up to 2 years with both vaccines. Both vaccines also were well tolerated.
Because there is only one MMR vaccine licensed in the United States, interruption to this single supply line could present a public health risk, Dr. Berry and her associates said. As both the vaccines used in this study do not contain human serum albumin, the theoretical risk of microbial contamination is reduced, compared with previous formulations of MMR.
Read more at Human Vaccines Immunotherapeutics. (2017. doi: 10.1080/21645515.2017.1309486).
FROM HUMAN VACCINES & IMMUNOTHERAPEUTICS
Acquired Epidermodysplasia Verruciformis Occurring in a Renal Transplant Recipient
Acquired epidermodysplasia verruciformis (EDV) is a rare disorder occurring in patients with depressed cellular immunity, particularly individuals with human immunodeficiency virus (HIV). Rare cases of acquired EDV have been reported in stem cell or solid organ transplant recipients. Weakened cellular immunity predisposes the patient to human papillomavirus (HPV) infections, with 92% of renal transplant recipients developing warts within 5 years posttransplantation.1 Specific EDV-HPV subtypes have been isolated from lesions in several immunosuppressed individuals, with HPV-5 and HPV-8 being the most commonly isolated subtypes.2,3 Herein, we present the clinical findings of a renal transplant recipient who presented for evaluation of multiple skin lesions characteristic of EDV 5 years following transplantation and initiation of immunosuppressive therapy. Additionally, we review the current diagnostic findings, management, and treatment of acquired EDV.
A 44-year-old white woman presented for evaluation of several pruritic cutaneous lesions that had developed on the chest and neck of 1 month’s duration. The patient had been on the immunosuppressant medications cyclosporine and mycophenolate mofetil for more than 5 years following renal transplantation 7 years prior to the current presentation. She also was on low-dose prednisone for chronic systemic lupus erythematosus. Her family history was negative for any pertinent skin conditions.
On physical examination the patient exhibited several grouped 0.5-cm, shiny, pink lichenoid macules located on the upper mid chest, anterior neck, and left leg clinically resembling the lesions of pityriasis versicolor (Figure 1). A shave biopsy was taken from one of the newest lesions on the left leg. Histopathology revealed viral epidermal cytopathic changes, blue cytoplasm, and coarse hypergranulosis characteristic of EDV (Figure 2). A diagnosis of acquired EDV was made based on the clinical and histopathologic findings.
The patient’s skin lesions became more widespread despite several different treatment regimens, including cryosurgery; tazarotene cream 0.05% nightly; imiquimod cream 5% once weekly; and intermittent short courses of 5-fluorouracil cream 5%, which provided the best response. At her most recent clinic visit 8 years after initial presentation, she continued to have more widespread lesions on the trunk, arms, and legs, but no evidence of malignant transformation.
Comment
Epidermodysplasia verruciformis was first recognized as an inherited condition, most commonly inherited in an autosomal-dominant fashion; however, X-linked recessive cases have been reported.4,5 Patients with the inherited forms of this condition are prone to recurrent HPV infections secondary to a missense mutation in the epidermodysplasia verruciformis 1 and 2 genes, EVER1 and EVER2, on the EV1 locus located on chromosome 17q25.6 Because of this mutation, the patient’s cellular immunity becomes weakened. Cellular presentation of the EDV-HPV antigen to T lymphocytes becomes impaired, thereby inhibiting the body’s ability to successfully clear itself of the virus.5,6 The most commonly isolated EDV-HPV subtypes are HPV-5 and HPV-8, but HPV types 9, 12, 14, 15, 17, 19, 20, 21, 22, 23, 24, 25, and 50 also have been associated with EDV.1,3,7
Patients who have suppressed cellular immunity, such as transplant recipients on long-term immunosuppressant medications and individuals with HIV, graft-vs-host disease, systemic lupus erythematosus, and hematologic malignancies, are susceptible to EDV, as well as patients with atopic dermatitis being treated with topical calcineurin inhibitors.2,3,8-15 These patients acquire depressed cellular immunity and become increasingly susceptible to infections with the EDV-HPV subtypes. When clinical and histopathologic findings are consistent with EDV, a diagnosis of acquired EDV is given, which was further confirmed in a study conducted by Harwood et al.16 They found immunocompromised patients carry more EDV-HPV subtypes in skin lesions analyzed by polymerase chain reaction than immunocompetent individuals.16 Additionally, there is a positive correlation between the length of immunosuppression and the development of HPV lesions, with a majority of patients developing lesions within 5 years following initial immunosuppression.1,7,10,17
Epidermodysplasia verruciformis commonly presents with multiple hypopigmented to red macules that may coalesce into patches with a fine scale, clinically resembling the lesions of pityriasis versicolor.2,3,8-15 Epidermodysplasia verruciformis also may present as multiple flesh-colored, flat-topped, verrucous papules that clinically resemble the lesions of verruca plana on sun-exposed areas such as the face, arms, and legs.9 The characteristic histopathologic findings are enlarged keratinocytes with perinuclear halos and blue-gray cytoplasm as well as hypergranulosis.18 Immunocompromised hosts infected with EDV-HPV histologically tend to display more severe dysplasia than immunocompetent individuals.19 The differential diagnosis includes pityriasis versicolor, squamous cell carcinoma (SCC), and verruca plana. Tissue cultures and potassium hydroxide scrapings for microorganisms should be negative.
The specific EDV-HPV strains 5, 8, and 41 carry the highest oncogenic potential, with more than 60% of inherited EDV patients developing SCC by the fourth and fifth decades of life.16 Unlike inherited EDV, the clinical course of acquired EDV is less well known; however, UV light is thought to act synergistically with the EDV-HPV in oncogenic transformation of the lesions, as most of the SCCs develop on sun-exposed areas, and darker-skinned patients seem to have a decreased risk for malignant transformation of EDV lesions.4,9,20,21 Preventative measures such as strict sun protection and annual surveillance of lesions can help to prevent oncogenic progression of the lesions; however, several single- and multiple-agent regimens have been used in the treatment of EDV with variable results. Topical imiquimod, 5-fluorouracil, tretinoin, and tazarotene have been used with variable success. Acitretin alone and in combination with interferon alfa-2a also has been used.22,23 Highly active antiretroviral therapy in patients with HIV has effectively decreased the number of lesions in a subset of patients.24 We (anecdotal) and others25 also have had success using photodynamic therapy. Squamous cell carcinoma arising in patients with EDV can be managed by excision or by Mohs micrographic surgery.
Conclusion
We report a rare case of acquired EDV in a solid organ transplant recipient. Epidermodysplasia verruciformis can be acquired in immunosuppressed patients such as ours, and these patients should be followed closely due to the potential for malignant transformation. More studies regarding the anticipated clinical course of skin lesions in patients with acquired EDV are needed to better predict the time frame for malignant transformation.
- Dyall-Smith D, Trowell H, Dyall-Smith ML. Benign human papillomavirus infection in renal transplant recipients. Int J Dermatol. 1991;30:785-789.
- Lutzner MA, Orth G, Dutronquay V, et al. Detection of human papillomavirus type 5 DNA in skin cancers of an immunosuppressed renal allograft recipient. Lancet. 1983;2:422-424.
- Lutzner M, Croissant O, Ducasse MF, et al. A potentially oncogenic human papillomavirus (HPV-5) found in two renal allograft recipients. J Invest Dermatol. 1980;75:353-356.
- Androphy EJ, Dvoretzky I, Lowy DR. X-linked inheritance of epidermodysplasia verruciformis. genetic and virologic studies of a kindred. Arch Dermatol. 1985;121:864-868.
- Lutzner MA. Epidermodysplasia verruciformis. an autosomal recessive disease characterized by viral warts and skin cancer. a model for viral oncogenesis. Bull Cancer. 1978;65:169-182.
- Ramoz N, Rueda LA, Bouadjar B, et al. Mutations in two adjacent novel genes are associated with epidermodysplasia verruciformis. Nat Genet. 2002;32:579-581.
- Rüdlinger R, Smith IW, Bunney MH, et al. Human papillomavirus infections in a group of renal transplant recipients. Br J Dermatol. 1986;115:681-692.
- Kawai K, Egawa N, Kiyono T, et al. Epidermodysplasia-verruciformis-like eruption associated with gamma-papillomavirus infection in a patient with adult T-cell leukemia. Dermatology. 2009;219:274-278.
- Barr BB, Benton EC, McLaren K, et al. Human papilloma virus infection and skin cancer in renal allograft recipients. Lancet. 1989;1:124-129.
- Tanigaki T, Kanda R, Sato K. Epidermodysplasia verruciformis (L-L, 1922) in a patient with systemic lupus erythematosus. Arch Dermatol Res. 1986;278:247-248.
- Holmes C, Chong AH, Tabrizi SN, et al. Epidermodysplasia verruciformis-like syndrome in association with systemic lupus erythematosus. Australas J Dermatol. 2009;50:44-47.
- Gross G, Ellinger K, Roussaki A, et al. Epidermodysplasia verruciformis in a patient with Hodgkin’s disease: characterization of a new papillomavirus type and interferon treatment. J Invest Dermatol. 1988;91:43-48.
- Fernandez KH, Rady P, Tyring S, et al. Acquired epidermodysplasia verruciformis in a child with atopic dermatitis [published online September 3, 2012]. Pediatr Dermatol. 2014;31:400-402.
- Hultgren TL, Srinivasan SK, DiMaio DJ. Epidermodysplasia verruciformis occurring in a patient with human immunodeficiency virus: a case report. Cutis. 2007;79:307-311.
- Kunishige JH, Hymes SR, Madkan V, et al. Epidermodysplasia verruciformis in the setting of graft-versus-host disease. J Am Acad Dermatol. 2007;57(5 suppl):S78-S80.
- Harwood CA, Surentheran T, McGregor JM, et al. Human papillomavirus infection and non-melanoma skin cancer in immunosuppressed and immunocompetent individuals. J Med Virol. 2000;61:289-297.
- Moloney FJ, Keane S, O’Kelly P, et al. The impact of skin disease following renal transplantation on quality of life. Br J Dermatol. 2005;153:574-578.
- Tanigaki T, Endo H. A case of epidermodysplasia verruciformis (Lewandowsky-Lutz, 1922) with skin cancer: histopathology of malignant cutaneous changes. Dermatologica. 1984;169:97-101.
- Morrison C, Eliezri Y, Magro C, et al. The histologic spectrum of epidermodysplasia verruciformis in transplant and AIDS patients. J Cutan Pathol. 2002;29:480-489.
- Majewski S, Jabło´nska S. Epidermodysplasia verruciformis as a model of human papillomavirus-induced genetic cancer of the skin. Arch Dermatol. 1995;131:1312-1318.
- Jacyk WK, De Villiers EM. Epidermodysplasia verruciformis in Africans. Int J Dermatol. 1993;32:806-810.
- Gubinelli E, Posteraro P, Cocuroccia B, et al. Epidermodysplasia verruciformis with multiple mucosal carcinomas treated with pegylated interferon alfa and acitretin. J Dermatolog Treat. 2003;14:184-188.
- Anadolu R, Oskay T, Erdem C, et al. Treatment of epidermodysplasia verruciformis with a combination of acitretin and interferon alfa-2a. J Am Acad Dermatol. 2001;45:296-299.
- Haas N, Fuchs PG, Hermes B, et al. Remission of epidermodysplasia verruciformis-like skin eruption after highly active antiretroviral therapy in a human immunodeficiency virus-positive patient. Br J Dermatol. 2001;145:669-670.
- Karrer S, Szeimies RM, Abels C, et al. Epidermo-dysplasia verruciformis treated using topical 5-aminolaevulinic acid photodynamic therapy. Br J Dermatol. 1999;140:935-938.
Acquired epidermodysplasia verruciformis (EDV) is a rare disorder occurring in patients with depressed cellular immunity, particularly individuals with human immunodeficiency virus (HIV). Rare cases of acquired EDV have been reported in stem cell or solid organ transplant recipients. Weakened cellular immunity predisposes the patient to human papillomavirus (HPV) infections, with 92% of renal transplant recipients developing warts within 5 years posttransplantation.1 Specific EDV-HPV subtypes have been isolated from lesions in several immunosuppressed individuals, with HPV-5 and HPV-8 being the most commonly isolated subtypes.2,3 Herein, we present the clinical findings of a renal transplant recipient who presented for evaluation of multiple skin lesions characteristic of EDV 5 years following transplantation and initiation of immunosuppressive therapy. Additionally, we review the current diagnostic findings, management, and treatment of acquired EDV.
A 44-year-old white woman presented for evaluation of several pruritic cutaneous lesions that had developed on the chest and neck of 1 month’s duration. The patient had been on the immunosuppressant medications cyclosporine and mycophenolate mofetil for more than 5 years following renal transplantation 7 years prior to the current presentation. She also was on low-dose prednisone for chronic systemic lupus erythematosus. Her family history was negative for any pertinent skin conditions.
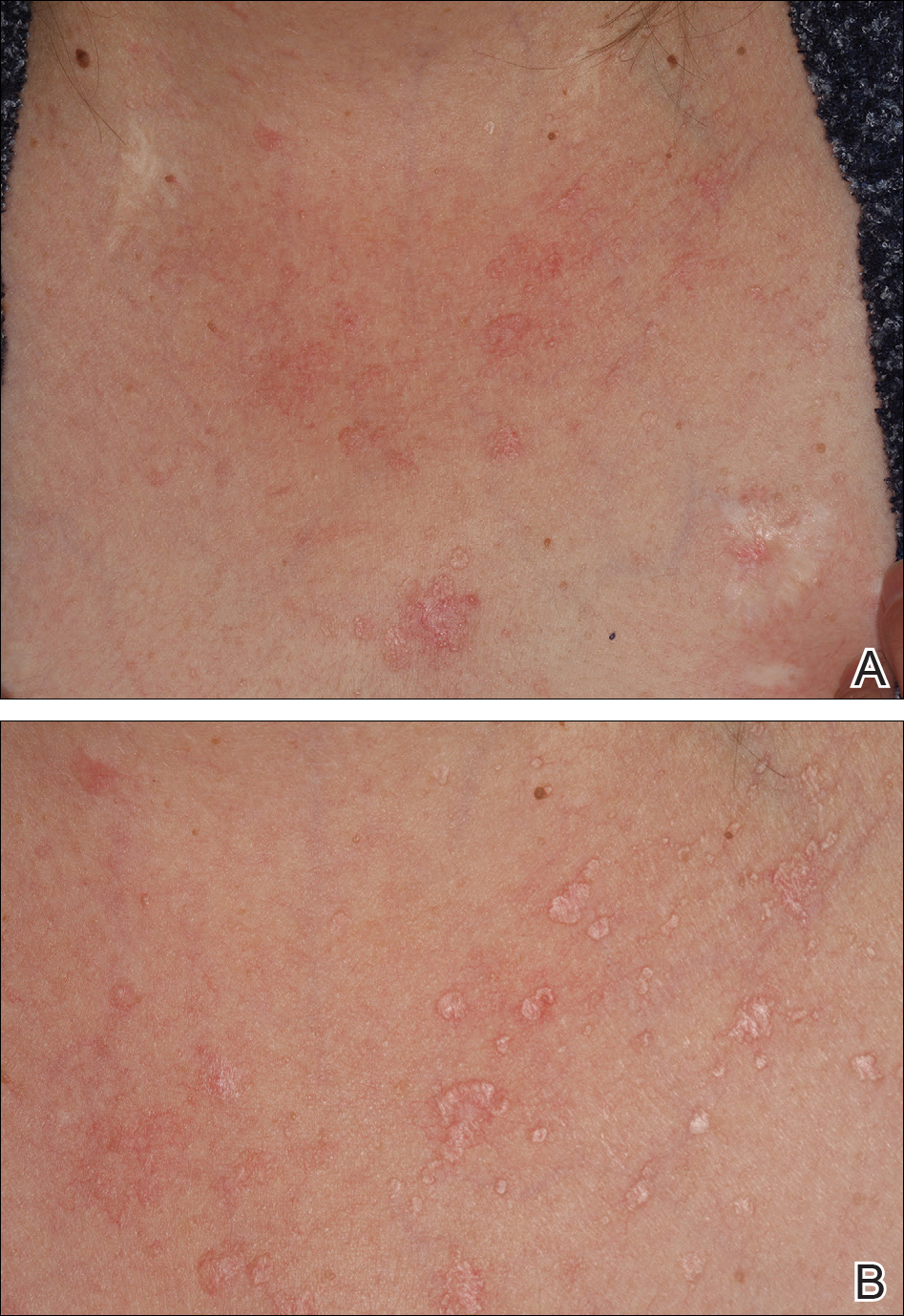
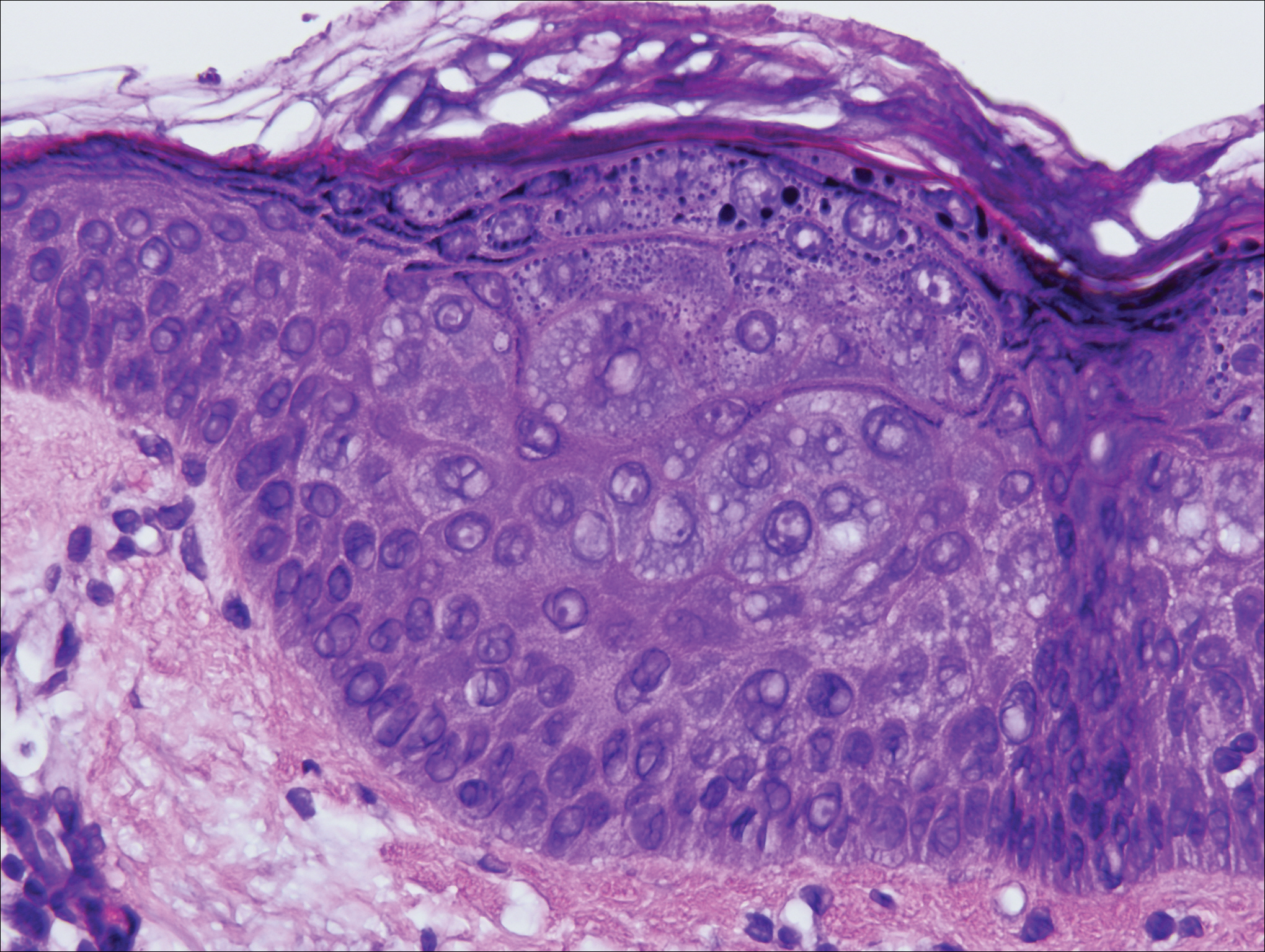
On physical examination the patient exhibited several grouped 0.5-cm, shiny, pink lichenoid macules located on the upper mid chest, anterior neck, and left leg clinically resembling the lesions of pityriasis versicolor (Figure 1). A shave biopsy was taken from one of the newest lesions on the left leg. Histopathology revealed viral epidermal cytopathic changes, blue cytoplasm, and coarse hypergranulosis characteristic of EDV (Figure 2). A diagnosis of acquired EDV was made based on the clinical and histopathologic findings.
The patient’s skin lesions became more widespread despite several different treatment regimens, including cryosurgery; tazarotene cream 0.05% nightly; imiquimod cream 5% once weekly; and intermittent short courses of 5-fluorouracil cream 5%, which provided the best response. At her most recent clinic visit 8 years after initial presentation, she continued to have more widespread lesions on the trunk, arms, and legs, but no evidence of malignant transformation.
Comment
Epidermodysplasia verruciformis was first recognized as an inherited condition, most commonly inherited in an autosomal-dominant fashion; however, X-linked recessive cases have been reported.4,5 Patients with the inherited forms of this condition are prone to recurrent HPV infections secondary to a missense mutation in the epidermodysplasia verruciformis 1 and 2 genes, EVER1 and EVER2, on the EV1 locus located on chromosome 17q25.6 Because of this mutation, the patient’s cellular immunity becomes weakened. Cellular presentation of the EDV-HPV antigen to T lymphocytes becomes impaired, thereby inhibiting the body’s ability to successfully clear itself of the virus.5,6 The most commonly isolated EDV-HPV subtypes are HPV-5 and HPV-8, but HPV types 9, 12, 14, 15, 17, 19, 20, 21, 22, 23, 24, 25, and 50 also have been associated with EDV.1,3,7
Patients who have suppressed cellular immunity, such as transplant recipients on long-term immunosuppressant medications and individuals with HIV, graft-vs-host disease, systemic lupus erythematosus, and hematologic malignancies, are susceptible to EDV, as well as patients with atopic dermatitis being treated with topical calcineurin inhibitors.2,3,8-15 These patients acquire depressed cellular immunity and become increasingly susceptible to infections with the EDV-HPV subtypes. When clinical and histopathologic findings are consistent with EDV, a diagnosis of acquired EDV is given, which was further confirmed in a study conducted by Harwood et al.16 They found immunocompromised patients carry more EDV-HPV subtypes in skin lesions analyzed by polymerase chain reaction than immunocompetent individuals.16 Additionally, there is a positive correlation between the length of immunosuppression and the development of HPV lesions, with a majority of patients developing lesions within 5 years following initial immunosuppression.1,7,10,17
Epidermodysplasia verruciformis commonly presents with multiple hypopigmented to red macules that may coalesce into patches with a fine scale, clinically resembling the lesions of pityriasis versicolor.2,3,8-15 Epidermodysplasia verruciformis also may present as multiple flesh-colored, flat-topped, verrucous papules that clinically resemble the lesions of verruca plana on sun-exposed areas such as the face, arms, and legs.9 The characteristic histopathologic findings are enlarged keratinocytes with perinuclear halos and blue-gray cytoplasm as well as hypergranulosis.18 Immunocompromised hosts infected with EDV-HPV histologically tend to display more severe dysplasia than immunocompetent individuals.19 The differential diagnosis includes pityriasis versicolor, squamous cell carcinoma (SCC), and verruca plana. Tissue cultures and potassium hydroxide scrapings for microorganisms should be negative.
The specific EDV-HPV strains 5, 8, and 41 carry the highest oncogenic potential, with more than 60% of inherited EDV patients developing SCC by the fourth and fifth decades of life.16 Unlike inherited EDV, the clinical course of acquired EDV is less well known; however, UV light is thought to act synergistically with the EDV-HPV in oncogenic transformation of the lesions, as most of the SCCs develop on sun-exposed areas, and darker-skinned patients seem to have a decreased risk for malignant transformation of EDV lesions.4,9,20,21 Preventative measures such as strict sun protection and annual surveillance of lesions can help to prevent oncogenic progression of the lesions; however, several single- and multiple-agent regimens have been used in the treatment of EDV with variable results. Topical imiquimod, 5-fluorouracil, tretinoin, and tazarotene have been used with variable success. Acitretin alone and in combination with interferon alfa-2a also has been used.22,23 Highly active antiretroviral therapy in patients with HIV has effectively decreased the number of lesions in a subset of patients.24 We (anecdotal) and others25 also have had success using photodynamic therapy. Squamous cell carcinoma arising in patients with EDV can be managed by excision or by Mohs micrographic surgery.
Conclusion
We report a rare case of acquired EDV in a solid organ transplant recipient. Epidermodysplasia verruciformis can be acquired in immunosuppressed patients such as ours, and these patients should be followed closely due to the potential for malignant transformation. More studies regarding the anticipated clinical course of skin lesions in patients with acquired EDV are needed to better predict the time frame for malignant transformation.
Acquired epidermodysplasia verruciformis (EDV) is a rare disorder occurring in patients with depressed cellular immunity, particularly individuals with human immunodeficiency virus (HIV). Rare cases of acquired EDV have been reported in stem cell or solid organ transplant recipients. Weakened cellular immunity predisposes the patient to human papillomavirus (HPV) infections, with 92% of renal transplant recipients developing warts within 5 years posttransplantation.1 Specific EDV-HPV subtypes have been isolated from lesions in several immunosuppressed individuals, with HPV-5 and HPV-8 being the most commonly isolated subtypes.2,3 Herein, we present the clinical findings of a renal transplant recipient who presented for evaluation of multiple skin lesions characteristic of EDV 5 years following transplantation and initiation of immunosuppressive therapy. Additionally, we review the current diagnostic findings, management, and treatment of acquired EDV.
A 44-year-old white woman presented for evaluation of several pruritic cutaneous lesions that had developed on the chest and neck of 1 month’s duration. The patient had been on the immunosuppressant medications cyclosporine and mycophenolate mofetil for more than 5 years following renal transplantation 7 years prior to the current presentation. She also was on low-dose prednisone for chronic systemic lupus erythematosus. Her family history was negative for any pertinent skin conditions.
On physical examination the patient exhibited several grouped 0.5-cm, shiny, pink lichenoid macules located on the upper mid chest, anterior neck, and left leg clinically resembling the lesions of pityriasis versicolor (Figure 1). A shave biopsy was taken from one of the newest lesions on the left leg. Histopathology revealed viral epidermal cytopathic changes, blue cytoplasm, and coarse hypergranulosis characteristic of EDV (Figure 2). A diagnosis of acquired EDV was made based on the clinical and histopathologic findings.
The patient’s skin lesions became more widespread despite several different treatment regimens, including cryosurgery; tazarotene cream 0.05% nightly; imiquimod cream 5% once weekly; and intermittent short courses of 5-fluorouracil cream 5%, which provided the best response. At her most recent clinic visit 8 years after initial presentation, she continued to have more widespread lesions on the trunk, arms, and legs, but no evidence of malignant transformation.
Comment
Epidermodysplasia verruciformis was first recognized as an inherited condition, most commonly inherited in an autosomal-dominant fashion; however, X-linked recessive cases have been reported.4,5 Patients with the inherited forms of this condition are prone to recurrent HPV infections secondary to a missense mutation in the epidermodysplasia verruciformis 1 and 2 genes, EVER1 and EVER2, on the EV1 locus located on chromosome 17q25.6 Because of this mutation, the patient’s cellular immunity becomes weakened. Cellular presentation of the EDV-HPV antigen to T lymphocytes becomes impaired, thereby inhibiting the body’s ability to successfully clear itself of the virus.5,6 The most commonly isolated EDV-HPV subtypes are HPV-5 and HPV-8, but HPV types 9, 12, 14, 15, 17, 19, 20, 21, 22, 23, 24, 25, and 50 also have been associated with EDV.1,3,7
Patients who have suppressed cellular immunity, such as transplant recipients on long-term immunosuppressant medications and individuals with HIV, graft-vs-host disease, systemic lupus erythematosus, and hematologic malignancies, are susceptible to EDV, as well as patients with atopic dermatitis being treated with topical calcineurin inhibitors.2,3,8-15 These patients acquire depressed cellular immunity and become increasingly susceptible to infections with the EDV-HPV subtypes. When clinical and histopathologic findings are consistent with EDV, a diagnosis of acquired EDV is given, which was further confirmed in a study conducted by Harwood et al.16 They found immunocompromised patients carry more EDV-HPV subtypes in skin lesions analyzed by polymerase chain reaction than immunocompetent individuals.16 Additionally, there is a positive correlation between the length of immunosuppression and the development of HPV lesions, with a majority of patients developing lesions within 5 years following initial immunosuppression.1,7,10,17
Epidermodysplasia verruciformis commonly presents with multiple hypopigmented to red macules that may coalesce into patches with a fine scale, clinically resembling the lesions of pityriasis versicolor.2,3,8-15 Epidermodysplasia verruciformis also may present as multiple flesh-colored, flat-topped, verrucous papules that clinically resemble the lesions of verruca plana on sun-exposed areas such as the face, arms, and legs.9 The characteristic histopathologic findings are enlarged keratinocytes with perinuclear halos and blue-gray cytoplasm as well as hypergranulosis.18 Immunocompromised hosts infected with EDV-HPV histologically tend to display more severe dysplasia than immunocompetent individuals.19 The differential diagnosis includes pityriasis versicolor, squamous cell carcinoma (SCC), and verruca plana. Tissue cultures and potassium hydroxide scrapings for microorganisms should be negative.
The specific EDV-HPV strains 5, 8, and 41 carry the highest oncogenic potential, with more than 60% of inherited EDV patients developing SCC by the fourth and fifth decades of life.16 Unlike inherited EDV, the clinical course of acquired EDV is less well known; however, UV light is thought to act synergistically with the EDV-HPV in oncogenic transformation of the lesions, as most of the SCCs develop on sun-exposed areas, and darker-skinned patients seem to have a decreased risk for malignant transformation of EDV lesions.4,9,20,21 Preventative measures such as strict sun protection and annual surveillance of lesions can help to prevent oncogenic progression of the lesions; however, several single- and multiple-agent regimens have been used in the treatment of EDV with variable results. Topical imiquimod, 5-fluorouracil, tretinoin, and tazarotene have been used with variable success. Acitretin alone and in combination with interferon alfa-2a also has been used.22,23 Highly active antiretroviral therapy in patients with HIV has effectively decreased the number of lesions in a subset of patients.24 We (anecdotal) and others25 also have had success using photodynamic therapy. Squamous cell carcinoma arising in patients with EDV can be managed by excision or by Mohs micrographic surgery.
Conclusion
We report a rare case of acquired EDV in a solid organ transplant recipient. Epidermodysplasia verruciformis can be acquired in immunosuppressed patients such as ours, and these patients should be followed closely due to the potential for malignant transformation. More studies regarding the anticipated clinical course of skin lesions in patients with acquired EDV are needed to better predict the time frame for malignant transformation.
- Dyall-Smith D, Trowell H, Dyall-Smith ML. Benign human papillomavirus infection in renal transplant recipients. Int J Dermatol. 1991;30:785-789.
- Lutzner MA, Orth G, Dutronquay V, et al. Detection of human papillomavirus type 5 DNA in skin cancers of an immunosuppressed renal allograft recipient. Lancet. 1983;2:422-424.
- Lutzner M, Croissant O, Ducasse MF, et al. A potentially oncogenic human papillomavirus (HPV-5) found in two renal allograft recipients. J Invest Dermatol. 1980;75:353-356.
- Androphy EJ, Dvoretzky I, Lowy DR. X-linked inheritance of epidermodysplasia verruciformis. genetic and virologic studies of a kindred. Arch Dermatol. 1985;121:864-868.
- Lutzner MA. Epidermodysplasia verruciformis. an autosomal recessive disease characterized by viral warts and skin cancer. a model for viral oncogenesis. Bull Cancer. 1978;65:169-182.
- Ramoz N, Rueda LA, Bouadjar B, et al. Mutations in two adjacent novel genes are associated with epidermodysplasia verruciformis. Nat Genet. 2002;32:579-581.
- Rüdlinger R, Smith IW, Bunney MH, et al. Human papillomavirus infections in a group of renal transplant recipients. Br J Dermatol. 1986;115:681-692.
- Kawai K, Egawa N, Kiyono T, et al. Epidermodysplasia-verruciformis-like eruption associated with gamma-papillomavirus infection in a patient with adult T-cell leukemia. Dermatology. 2009;219:274-278.
- Barr BB, Benton EC, McLaren K, et al. Human papilloma virus infection and skin cancer in renal allograft recipients. Lancet. 1989;1:124-129.
- Tanigaki T, Kanda R, Sato K. Epidermodysplasia verruciformis (L-L, 1922) in a patient with systemic lupus erythematosus. Arch Dermatol Res. 1986;278:247-248.
- Holmes C, Chong AH, Tabrizi SN, et al. Epidermodysplasia verruciformis-like syndrome in association with systemic lupus erythematosus. Australas J Dermatol. 2009;50:44-47.
- Gross G, Ellinger K, Roussaki A, et al. Epidermodysplasia verruciformis in a patient with Hodgkin’s disease: characterization of a new papillomavirus type and interferon treatment. J Invest Dermatol. 1988;91:43-48.
- Fernandez KH, Rady P, Tyring S, et al. Acquired epidermodysplasia verruciformis in a child with atopic dermatitis [published online September 3, 2012]. Pediatr Dermatol. 2014;31:400-402.
- Hultgren TL, Srinivasan SK, DiMaio DJ. Epidermodysplasia verruciformis occurring in a patient with human immunodeficiency virus: a case report. Cutis. 2007;79:307-311.
- Kunishige JH, Hymes SR, Madkan V, et al. Epidermodysplasia verruciformis in the setting of graft-versus-host disease. J Am Acad Dermatol. 2007;57(5 suppl):S78-S80.
- Harwood CA, Surentheran T, McGregor JM, et al. Human papillomavirus infection and non-melanoma skin cancer in immunosuppressed and immunocompetent individuals. J Med Virol. 2000;61:289-297.
- Moloney FJ, Keane S, O’Kelly P, et al. The impact of skin disease following renal transplantation on quality of life. Br J Dermatol. 2005;153:574-578.
- Tanigaki T, Endo H. A case of epidermodysplasia verruciformis (Lewandowsky-Lutz, 1922) with skin cancer: histopathology of malignant cutaneous changes. Dermatologica. 1984;169:97-101.
- Morrison C, Eliezri Y, Magro C, et al. The histologic spectrum of epidermodysplasia verruciformis in transplant and AIDS patients. J Cutan Pathol. 2002;29:480-489.
- Majewski S, Jabło´nska S. Epidermodysplasia verruciformis as a model of human papillomavirus-induced genetic cancer of the skin. Arch Dermatol. 1995;131:1312-1318.
- Jacyk WK, De Villiers EM. Epidermodysplasia verruciformis in Africans. Int J Dermatol. 1993;32:806-810.
- Gubinelli E, Posteraro P, Cocuroccia B, et al. Epidermodysplasia verruciformis with multiple mucosal carcinomas treated with pegylated interferon alfa and acitretin. J Dermatolog Treat. 2003;14:184-188.
- Anadolu R, Oskay T, Erdem C, et al. Treatment of epidermodysplasia verruciformis with a combination of acitretin and interferon alfa-2a. J Am Acad Dermatol. 2001;45:296-299.
- Haas N, Fuchs PG, Hermes B, et al. Remission of epidermodysplasia verruciformis-like skin eruption after highly active antiretroviral therapy in a human immunodeficiency virus-positive patient. Br J Dermatol. 2001;145:669-670.
- Karrer S, Szeimies RM, Abels C, et al. Epidermo-dysplasia verruciformis treated using topical 5-aminolaevulinic acid photodynamic therapy. Br J Dermatol. 1999;140:935-938.
- Dyall-Smith D, Trowell H, Dyall-Smith ML. Benign human papillomavirus infection in renal transplant recipients. Int J Dermatol. 1991;30:785-789.
- Lutzner MA, Orth G, Dutronquay V, et al. Detection of human papillomavirus type 5 DNA in skin cancers of an immunosuppressed renal allograft recipient. Lancet. 1983;2:422-424.
- Lutzner M, Croissant O, Ducasse MF, et al. A potentially oncogenic human papillomavirus (HPV-5) found in two renal allograft recipients. J Invest Dermatol. 1980;75:353-356.
- Androphy EJ, Dvoretzky I, Lowy DR. X-linked inheritance of epidermodysplasia verruciformis. genetic and virologic studies of a kindred. Arch Dermatol. 1985;121:864-868.
- Lutzner MA. Epidermodysplasia verruciformis. an autosomal recessive disease characterized by viral warts and skin cancer. a model for viral oncogenesis. Bull Cancer. 1978;65:169-182.
- Ramoz N, Rueda LA, Bouadjar B, et al. Mutations in two adjacent novel genes are associated with epidermodysplasia verruciformis. Nat Genet. 2002;32:579-581.
- Rüdlinger R, Smith IW, Bunney MH, et al. Human papillomavirus infections in a group of renal transplant recipients. Br J Dermatol. 1986;115:681-692.
- Kawai K, Egawa N, Kiyono T, et al. Epidermodysplasia-verruciformis-like eruption associated with gamma-papillomavirus infection in a patient with adult T-cell leukemia. Dermatology. 2009;219:274-278.
- Barr BB, Benton EC, McLaren K, et al. Human papilloma virus infection and skin cancer in renal allograft recipients. Lancet. 1989;1:124-129.
- Tanigaki T, Kanda R, Sato K. Epidermodysplasia verruciformis (L-L, 1922) in a patient with systemic lupus erythematosus. Arch Dermatol Res. 1986;278:247-248.
- Holmes C, Chong AH, Tabrizi SN, et al. Epidermodysplasia verruciformis-like syndrome in association with systemic lupus erythematosus. Australas J Dermatol. 2009;50:44-47.
- Gross G, Ellinger K, Roussaki A, et al. Epidermodysplasia verruciformis in a patient with Hodgkin’s disease: characterization of a new papillomavirus type and interferon treatment. J Invest Dermatol. 1988;91:43-48.
- Fernandez KH, Rady P, Tyring S, et al. Acquired epidermodysplasia verruciformis in a child with atopic dermatitis [published online September 3, 2012]. Pediatr Dermatol. 2014;31:400-402.
- Hultgren TL, Srinivasan SK, DiMaio DJ. Epidermodysplasia verruciformis occurring in a patient with human immunodeficiency virus: a case report. Cutis. 2007;79:307-311.
- Kunishige JH, Hymes SR, Madkan V, et al. Epidermodysplasia verruciformis in the setting of graft-versus-host disease. J Am Acad Dermatol. 2007;57(5 suppl):S78-S80.
- Harwood CA, Surentheran T, McGregor JM, et al. Human papillomavirus infection and non-melanoma skin cancer in immunosuppressed and immunocompetent individuals. J Med Virol. 2000;61:289-297.
- Moloney FJ, Keane S, O’Kelly P, et al. The impact of skin disease following renal transplantation on quality of life. Br J Dermatol. 2005;153:574-578.
- Tanigaki T, Endo H. A case of epidermodysplasia verruciformis (Lewandowsky-Lutz, 1922) with skin cancer: histopathology of malignant cutaneous changes. Dermatologica. 1984;169:97-101.
- Morrison C, Eliezri Y, Magro C, et al. The histologic spectrum of epidermodysplasia verruciformis in transplant and AIDS patients. J Cutan Pathol. 2002;29:480-489.
- Majewski S, Jabło´nska S. Epidermodysplasia verruciformis as a model of human papillomavirus-induced genetic cancer of the skin. Arch Dermatol. 1995;131:1312-1318.
- Jacyk WK, De Villiers EM. Epidermodysplasia verruciformis in Africans. Int J Dermatol. 1993;32:806-810.
- Gubinelli E, Posteraro P, Cocuroccia B, et al. Epidermodysplasia verruciformis with multiple mucosal carcinomas treated with pegylated interferon alfa and acitretin. J Dermatolog Treat. 2003;14:184-188.
- Anadolu R, Oskay T, Erdem C, et al. Treatment of epidermodysplasia verruciformis with a combination of acitretin and interferon alfa-2a. J Am Acad Dermatol. 2001;45:296-299.
- Haas N, Fuchs PG, Hermes B, et al. Remission of epidermodysplasia verruciformis-like skin eruption after highly active antiretroviral therapy in a human immunodeficiency virus-positive patient. Br J Dermatol. 2001;145:669-670.
- Karrer S, Szeimies RM, Abels C, et al. Epidermo-dysplasia verruciformis treated using topical 5-aminolaevulinic acid photodynamic therapy. Br J Dermatol. 1999;140:935-938.
Practice Points
- Acquired epidermodysplasia verruciformis (EDV) is a rare complication of iatrogenic immuno-suppression in the setting of solid organ transplantation.
- Patients with EDV should be counseled to avoid exposure to UV radiation to reduce the risk formalignant transformation.

Do you have to MIPS in 2017? CMS has a tool for that
Want to know if Medicare’s Merit-based Incentive Payment System (MIPS) is in your future?
The Centers for Medicare & Medicaid Services launched a Web tool on May 9. To see if you must participate in MIPS in 2017, just enter your national provider identifier. The agency is also in the process of mailing letters to update physicians on their status. The Web tool can be found at the CMS website.
Physicians who bill Medicare Part B more than $30,000 and see more than 100 Medicare patients must participate in MIPS this year. That threshold will be determined by means of claims submitted Sept. 1, 2015, through Aug. 31, 2016, and Sept. 1, 2016, through Aug. 31, 2017.
Those who don’t meet those criteria but want to participate may do so, but they won’t receive either a bonus or a penalty.
Under the MIPS “pick your pace” option, physicians who meet the threshold but are not ready to participate for either the 90-day period or the full year can report on one measure for 2017. Data on the lone measure need to be submitted to CMS no later than March 31, 2018.
Data need only be submitted for one patient, and, in 2017, all forms of submission – via registry, electronic health record, administrative claims, or attestation – are acceptable, though options may vary based on the performance option selected. Doing this minimum effort will result in no adjustment to Medicare payments in 2019.
Submitting no data at all for 2017, however, will mean a 4% Medicare pay cut in 2019.
To do the bare minimum to avoid any penalty, select a single data measurement from one of three categories: quality measures, improvement activity, or, in the case of Advancing Care Information, four or five base measures, depending on which certified EHR is being used.
There are 271 quality measures from which to choose, as well as 92 improvement activities. Improvement activities focus on care coordination, patient engagement, and patient safety.
For each measure, there is a downloadable spreadsheet that gives detailed information about the measure and how to meet it. The spreadsheet can also be used by physicians to track the data that are collected for submission.
Physicians who are new to Medicare in 2017 do not have to participate in MIPS in 2017.
Another way to be exempt from MIPS is to participate in the Advanced Alternative Payment Model track of the QPP. Doctors participating in APMs will have the opportunity to earn higher payment bonuses but will have to assume more risk and could see payment reductions if quality and value thresholds are not met.
Want to know if Medicare’s Merit-based Incentive Payment System (MIPS) is in your future?
The Centers for Medicare & Medicaid Services launched a Web tool on May 9. To see if you must participate in MIPS in 2017, just enter your national provider identifier. The agency is also in the process of mailing letters to update physicians on their status. The Web tool can be found at the CMS website.
Physicians who bill Medicare Part B more than $30,000 and see more than 100 Medicare patients must participate in MIPS this year. That threshold will be determined by means of claims submitted Sept. 1, 2015, through Aug. 31, 2016, and Sept. 1, 2016, through Aug. 31, 2017.
Those who don’t meet those criteria but want to participate may do so, but they won’t receive either a bonus or a penalty.
Under the MIPS “pick your pace” option, physicians who meet the threshold but are not ready to participate for either the 90-day period or the full year can report on one measure for 2017. Data on the lone measure need to be submitted to CMS no later than March 31, 2018.
Data need only be submitted for one patient, and, in 2017, all forms of submission – via registry, electronic health record, administrative claims, or attestation – are acceptable, though options may vary based on the performance option selected. Doing this minimum effort will result in no adjustment to Medicare payments in 2019.
Submitting no data at all for 2017, however, will mean a 4% Medicare pay cut in 2019.
To do the bare minimum to avoid any penalty, select a single data measurement from one of three categories: quality measures, improvement activity, or, in the case of Advancing Care Information, four or five base measures, depending on which certified EHR is being used.
There are 271 quality measures from which to choose, as well as 92 improvement activities. Improvement activities focus on care coordination, patient engagement, and patient safety.
For each measure, there is a downloadable spreadsheet that gives detailed information about the measure and how to meet it. The spreadsheet can also be used by physicians to track the data that are collected for submission.
Physicians who are new to Medicare in 2017 do not have to participate in MIPS in 2017.
Another way to be exempt from MIPS is to participate in the Advanced Alternative Payment Model track of the QPP. Doctors participating in APMs will have the opportunity to earn higher payment bonuses but will have to assume more risk and could see payment reductions if quality and value thresholds are not met.
Want to know if Medicare’s Merit-based Incentive Payment System (MIPS) is in your future?
The Centers for Medicare & Medicaid Services launched a Web tool on May 9. To see if you must participate in MIPS in 2017, just enter your national provider identifier. The agency is also in the process of mailing letters to update physicians on their status. The Web tool can be found at the CMS website.
Physicians who bill Medicare Part B more than $30,000 and see more than 100 Medicare patients must participate in MIPS this year. That threshold will be determined by means of claims submitted Sept. 1, 2015, through Aug. 31, 2016, and Sept. 1, 2016, through Aug. 31, 2017.
Those who don’t meet those criteria but want to participate may do so, but they won’t receive either a bonus or a penalty.
Under the MIPS “pick your pace” option, physicians who meet the threshold but are not ready to participate for either the 90-day period or the full year can report on one measure for 2017. Data on the lone measure need to be submitted to CMS no later than March 31, 2018.
Data need only be submitted for one patient, and, in 2017, all forms of submission – via registry, electronic health record, administrative claims, or attestation – are acceptable, though options may vary based on the performance option selected. Doing this minimum effort will result in no adjustment to Medicare payments in 2019.
Submitting no data at all for 2017, however, will mean a 4% Medicare pay cut in 2019.
To do the bare minimum to avoid any penalty, select a single data measurement from one of three categories: quality measures, improvement activity, or, in the case of Advancing Care Information, four or five base measures, depending on which certified EHR is being used.
There are 271 quality measures from which to choose, as well as 92 improvement activities. Improvement activities focus on care coordination, patient engagement, and patient safety.
For each measure, there is a downloadable spreadsheet that gives detailed information about the measure and how to meet it. The spreadsheet can also be used by physicians to track the data that are collected for submission.
Physicians who are new to Medicare in 2017 do not have to participate in MIPS in 2017.
Another way to be exempt from MIPS is to participate in the Advanced Alternative Payment Model track of the QPP. Doctors participating in APMs will have the opportunity to earn higher payment bonuses but will have to assume more risk and could see payment reductions if quality and value thresholds are not met.