User login
TRK inhibitor shows ‘striking’ activity, durability across diverse adult and pediatric cancers
CHICAGO – Larotrectinib, an oral inhibitor of tropomyosin receptor kinase (TRK), has durable efficacy across diverse adult and pediatric cancers that harbor a genetic aberration known as TRK fusion, finds an analysis of three trials reported at the annual meeting of the American Society of Clinical Oncology.
Fusion of a TRK gene with an unrelated gene leads to uncontrolled signaling in the TRK pathway, potentially causing tumor growth and addiction to this input, lead author David Hyman, MD, chief of early drug development at Memorial Sloan Kettering Cancer Center in New York explained in a press briefing.

Dr. Hyman and his colleagues analyzed data from 55 patients having 17 discrete types of advanced cancer harboring TRK fusions who were treated with larotrectinib in phase I and II trials. Results showed an overall response rate of 76%, and the large majority of responses were still ongoing at 12 months.
“I believe these data support larotrectinib as a potential new standard of care for these patients,” he said. “However, I want to emphasize that really recognizing this benefit in the community will require that we test patients more universally for the presence of TRK fusions or other tumor-agnostic biomarkers, such as microsatellite instability.”
On the basis of these promising data, the drug’s manufacturer, Loxo Oncology, plans to submit a New Drug Application to the Food and Drug Administration later this year or early next year. Larotrectinib has already been granted both orphan drug designation (for drugs used to treat rare conditions) and breakthrough therapy designation (for drugs used to treat serious conditions showing greater efficacy than available therapies).
A randomized trial pitting larotrectinib against other therapies is unlikely given the low prevalence of TRK fusions, the lack of treatment options for the fairly heavily pretreated trial patients, and the drug’s impressive performance, according to Dr. Hyman.
“The efficacy is so striking that it really exceeds almost any existing standard of care for solid tumors,” he elaborated. “There is hardly any chemotherapy or targeted therapy that has a response rate or durability that looks like larotrectinib in these patients.”
Expert perspective
The data for larotrectinib “really bring us into a new era where treatment is truly based on mutation, not location,” said Sumanta Kumar Pal, MD, a medical oncologist at City of Hope, in Duarte, Calif. “When I was in training, which was not too long ago, it really would have been a pipe dream to think that we could have treated cancers independent of their site of origin. … With the data presented by Dr. Hyman for larotrectinib, we may now be poised to treat many cancers in a manner that is agnostic of their site of origin and that is instead based on molecular criteria.

TRK testing
Several next-generation sequencing–based tests already available clinically can pick up TRK fusions, Dr. Hyman pointed out. “But it is important for the ordering physician to understand whether the tests they are ordering includes fusion detection and, if it’s an option, to select it. Otherwise, they will not find TRK fusions.
“The list price for these tests is in the kind of low thousands of dollars, which equates essentially to a PET scan for the cancer patient,” he noted. In cancers where sequential single-gene testing is already being done as standard of care, there is “minimal” incremental cost of instead using comprehensive testing that would detect TRK fusions.
Oncologists should be aware that obtaining test results can take weeks, Dr. Hyman stressed. “My personal opinion is that this [testing] should be more broadly adopted and should be adopted at a point in the patient’s treatment … [so that they] don’t become too sick, as we see in our own experience as well, and don’t have an opportunity to be treated even when the test results come back positive. So I would generally advocate early testing.”
Study details
For the study, which was funded by Loxo Oncology, the investigators analyzed data from three trials in which patients with advanced TRK fusion–positive solid cancers received larotrectinib (LOXO-101): a phase I trial among 8 adult patients, a phase I/II trial among 12 pediatric patients (SCOUT), and a phase II “basket” trial among 35 adult and adolescent patients (NAVIGATE).
“I want to emphasize that these patients were identified by local testing,” Dr. Hyman noted. “We did not perform central screening to find the TRK fusions, and in fact, 50 different laboratories identified the 55 patients. So this in a sense really represents the real-world identification of these patients.”
In an integrated analysis, the overall rate of confirmed response as assessed by investigators was 76%, with complete response in 12% of patients and partial response in 64%. Two patients had such deep tumor regression that they experienced downstaging enabling them to undergo potentially curative surgery. Efficacy was consistent regardless of tumor type, which TRK gene was affected, and the fusion partner gene.
Median time to response was 1.8 months. “This is actually just a reflection of when the first scan was obtained. But in the clinic, patients reported dramatic improvement of their symptoms within days of beginning therapy,” Dr. Hyman said.
With a median follow-up of 5.8 months, the median duration of response was not yet reached. Fully 79% of responses were still ongoing at 12 months. Median progression-free survival was likewise not reached; the 12-month rate was 63%.
The leading treatment-emergent adverse events were fatigue (38%), dizziness (27%), nausea (26%), and anemia (26%). “This is an extremely well tolerated therapy with only 13% of patients requiring any form of dose modification and not a single patient discontinuing due to adverse events,” he said.
It is unclear why some patients had apparent primary resistance to larotrectinib, but their TRK fusion test results may have been incorrect, Dr. Hyman speculated. Six patients developed acquired resistance to larotrectinib; five of them were found to have an identical resistance mutation, and two went on to receive and have a response to LOXO-195, a next-generation TRK inhibitor that appears to retain activity in the presence of this mutation (Cancer Discov. 2017 June 3. doi: 10.1158/2159-8290.CD-17-0507).
Dr. Hyman disclosed that he has a consulting or advisory role with Atara Biotherapeutics, Chugai Pharma, and CytomX Therapeutics, and that he receives research funding from AstraZeneca and Puma Biotechnology.
CHICAGO – Larotrectinib, an oral inhibitor of tropomyosin receptor kinase (TRK), has durable efficacy across diverse adult and pediatric cancers that harbor a genetic aberration known as TRK fusion, finds an analysis of three trials reported at the annual meeting of the American Society of Clinical Oncology.
Fusion of a TRK gene with an unrelated gene leads to uncontrolled signaling in the TRK pathway, potentially causing tumor growth and addiction to this input, lead author David Hyman, MD, chief of early drug development at Memorial Sloan Kettering Cancer Center in New York explained in a press briefing.
Dr. Hyman and his colleagues analyzed data from 55 patients having 17 discrete types of advanced cancer harboring TRK fusions who were treated with larotrectinib in phase I and II trials. Results showed an overall response rate of 76%, and the large majority of responses were still ongoing at 12 months.
“I believe these data support larotrectinib as a potential new standard of care for these patients,” he said. “However, I want to emphasize that really recognizing this benefit in the community will require that we test patients more universally for the presence of TRK fusions or other tumor-agnostic biomarkers, such as microsatellite instability.”
On the basis of these promising data, the drug’s manufacturer, Loxo Oncology, plans to submit a New Drug Application to the Food and Drug Administration later this year or early next year. Larotrectinib has already been granted both orphan drug designation (for drugs used to treat rare conditions) and breakthrough therapy designation (for drugs used to treat serious conditions showing greater efficacy than available therapies).
A randomized trial pitting larotrectinib against other therapies is unlikely given the low prevalence of TRK fusions, the lack of treatment options for the fairly heavily pretreated trial patients, and the drug’s impressive performance, according to Dr. Hyman.
“The efficacy is so striking that it really exceeds almost any existing standard of care for solid tumors,” he elaborated. “There is hardly any chemotherapy or targeted therapy that has a response rate or durability that looks like larotrectinib in these patients.”
Expert perspective
The data for larotrectinib “really bring us into a new era where treatment is truly based on mutation, not location,” said Sumanta Kumar Pal, MD, a medical oncologist at City of Hope, in Duarte, Calif. “When I was in training, which was not too long ago, it really would have been a pipe dream to think that we could have treated cancers independent of their site of origin. … With the data presented by Dr. Hyman for larotrectinib, we may now be poised to treat many cancers in a manner that is agnostic of their site of origin and that is instead based on molecular criteria.
TRK testing
Several next-generation sequencing–based tests already available clinically can pick up TRK fusions, Dr. Hyman pointed out. “But it is important for the ordering physician to understand whether the tests they are ordering includes fusion detection and, if it’s an option, to select it. Otherwise, they will not find TRK fusions.
“The list price for these tests is in the kind of low thousands of dollars, which equates essentially to a PET scan for the cancer patient,” he noted. In cancers where sequential single-gene testing is already being done as standard of care, there is “minimal” incremental cost of instead using comprehensive testing that would detect TRK fusions.
Oncologists should be aware that obtaining test results can take weeks, Dr. Hyman stressed. “My personal opinion is that this [testing] should be more broadly adopted and should be adopted at a point in the patient’s treatment … [so that they] don’t become too sick, as we see in our own experience as well, and don’t have an opportunity to be treated even when the test results come back positive. So I would generally advocate early testing.”
Study details
For the study, which was funded by Loxo Oncology, the investigators analyzed data from three trials in which patients with advanced TRK fusion–positive solid cancers received larotrectinib (LOXO-101): a phase I trial among 8 adult patients, a phase I/II trial among 12 pediatric patients (SCOUT), and a phase II “basket” trial among 35 adult and adolescent patients (NAVIGATE).
“I want to emphasize that these patients were identified by local testing,” Dr. Hyman noted. “We did not perform central screening to find the TRK fusions, and in fact, 50 different laboratories identified the 55 patients. So this in a sense really represents the real-world identification of these patients.”
In an integrated analysis, the overall rate of confirmed response as assessed by investigators was 76%, with complete response in 12% of patients and partial response in 64%. Two patients had such deep tumor regression that they experienced downstaging enabling them to undergo potentially curative surgery. Efficacy was consistent regardless of tumor type, which TRK gene was affected, and the fusion partner gene.
Median time to response was 1.8 months. “This is actually just a reflection of when the first scan was obtained. But in the clinic, patients reported dramatic improvement of their symptoms within days of beginning therapy,” Dr. Hyman said.
With a median follow-up of 5.8 months, the median duration of response was not yet reached. Fully 79% of responses were still ongoing at 12 months. Median progression-free survival was likewise not reached; the 12-month rate was 63%.
The leading treatment-emergent adverse events were fatigue (38%), dizziness (27%), nausea (26%), and anemia (26%). “This is an extremely well tolerated therapy with only 13% of patients requiring any form of dose modification and not a single patient discontinuing due to adverse events,” he said.
It is unclear why some patients had apparent primary resistance to larotrectinib, but their TRK fusion test results may have been incorrect, Dr. Hyman speculated. Six patients developed acquired resistance to larotrectinib; five of them were found to have an identical resistance mutation, and two went on to receive and have a response to LOXO-195, a next-generation TRK inhibitor that appears to retain activity in the presence of this mutation (Cancer Discov. 2017 June 3. doi: 10.1158/2159-8290.CD-17-0507).
Dr. Hyman disclosed that he has a consulting or advisory role with Atara Biotherapeutics, Chugai Pharma, and CytomX Therapeutics, and that he receives research funding from AstraZeneca and Puma Biotechnology.
CHICAGO – Larotrectinib, an oral inhibitor of tropomyosin receptor kinase (TRK), has durable efficacy across diverse adult and pediatric cancers that harbor a genetic aberration known as TRK fusion, finds an analysis of three trials reported at the annual meeting of the American Society of Clinical Oncology.
Fusion of a TRK gene with an unrelated gene leads to uncontrolled signaling in the TRK pathway, potentially causing tumor growth and addiction to this input, lead author David Hyman, MD, chief of early drug development at Memorial Sloan Kettering Cancer Center in New York explained in a press briefing.
Dr. Hyman and his colleagues analyzed data from 55 patients having 17 discrete types of advanced cancer harboring TRK fusions who were treated with larotrectinib in phase I and II trials. Results showed an overall response rate of 76%, and the large majority of responses were still ongoing at 12 months.
“I believe these data support larotrectinib as a potential new standard of care for these patients,” he said. “However, I want to emphasize that really recognizing this benefit in the community will require that we test patients more universally for the presence of TRK fusions or other tumor-agnostic biomarkers, such as microsatellite instability.”
On the basis of these promising data, the drug’s manufacturer, Loxo Oncology, plans to submit a New Drug Application to the Food and Drug Administration later this year or early next year. Larotrectinib has already been granted both orphan drug designation (for drugs used to treat rare conditions) and breakthrough therapy designation (for drugs used to treat serious conditions showing greater efficacy than available therapies).
A randomized trial pitting larotrectinib against other therapies is unlikely given the low prevalence of TRK fusions, the lack of treatment options for the fairly heavily pretreated trial patients, and the drug’s impressive performance, according to Dr. Hyman.
“The efficacy is so striking that it really exceeds almost any existing standard of care for solid tumors,” he elaborated. “There is hardly any chemotherapy or targeted therapy that has a response rate or durability that looks like larotrectinib in these patients.”
Expert perspective
The data for larotrectinib “really bring us into a new era where treatment is truly based on mutation, not location,” said Sumanta Kumar Pal, MD, a medical oncologist at City of Hope, in Duarte, Calif. “When I was in training, which was not too long ago, it really would have been a pipe dream to think that we could have treated cancers independent of their site of origin. … With the data presented by Dr. Hyman for larotrectinib, we may now be poised to treat many cancers in a manner that is agnostic of their site of origin and that is instead based on molecular criteria.
TRK testing
Several next-generation sequencing–based tests already available clinically can pick up TRK fusions, Dr. Hyman pointed out. “But it is important for the ordering physician to understand whether the tests they are ordering includes fusion detection and, if it’s an option, to select it. Otherwise, they will not find TRK fusions.
“The list price for these tests is in the kind of low thousands of dollars, which equates essentially to a PET scan for the cancer patient,” he noted. In cancers where sequential single-gene testing is already being done as standard of care, there is “minimal” incremental cost of instead using comprehensive testing that would detect TRK fusions.
Oncologists should be aware that obtaining test results can take weeks, Dr. Hyman stressed. “My personal opinion is that this [testing] should be more broadly adopted and should be adopted at a point in the patient’s treatment … [so that they] don’t become too sick, as we see in our own experience as well, and don’t have an opportunity to be treated even when the test results come back positive. So I would generally advocate early testing.”
Study details
For the study, which was funded by Loxo Oncology, the investigators analyzed data from three trials in which patients with advanced TRK fusion–positive solid cancers received larotrectinib (LOXO-101): a phase I trial among 8 adult patients, a phase I/II trial among 12 pediatric patients (SCOUT), and a phase II “basket” trial among 35 adult and adolescent patients (NAVIGATE).
“I want to emphasize that these patients were identified by local testing,” Dr. Hyman noted. “We did not perform central screening to find the TRK fusions, and in fact, 50 different laboratories identified the 55 patients. So this in a sense really represents the real-world identification of these patients.”
In an integrated analysis, the overall rate of confirmed response as assessed by investigators was 76%, with complete response in 12% of patients and partial response in 64%. Two patients had such deep tumor regression that they experienced downstaging enabling them to undergo potentially curative surgery. Efficacy was consistent regardless of tumor type, which TRK gene was affected, and the fusion partner gene.
Median time to response was 1.8 months. “This is actually just a reflection of when the first scan was obtained. But in the clinic, patients reported dramatic improvement of their symptoms within days of beginning therapy,” Dr. Hyman said.
With a median follow-up of 5.8 months, the median duration of response was not yet reached. Fully 79% of responses were still ongoing at 12 months. Median progression-free survival was likewise not reached; the 12-month rate was 63%.
The leading treatment-emergent adverse events were fatigue (38%), dizziness (27%), nausea (26%), and anemia (26%). “This is an extremely well tolerated therapy with only 13% of patients requiring any form of dose modification and not a single patient discontinuing due to adverse events,” he said.
It is unclear why some patients had apparent primary resistance to larotrectinib, but their TRK fusion test results may have been incorrect, Dr. Hyman speculated. Six patients developed acquired resistance to larotrectinib; five of them were found to have an identical resistance mutation, and two went on to receive and have a response to LOXO-195, a next-generation TRK inhibitor that appears to retain activity in the presence of this mutation (Cancer Discov. 2017 June 3. doi: 10.1158/2159-8290.CD-17-0507).
Dr. Hyman disclosed that he has a consulting or advisory role with Atara Biotherapeutics, Chugai Pharma, and CytomX Therapeutics, and that he receives research funding from AstraZeneca and Puma Biotechnology.
AT ASCO 2017
Key clinical point:
Major finding: The overall response rate was 76%, and 79% of responses were still ongoing at 12 months.
Data source: An integrated analysis of phase I and II trials among 55 children and adults having 17 discrete types of advanced cancer with TRK fusions.
Disclosures: Dr. Hyman disclosed that he has a consulting or advisory role with Atara Biotherapeutics, Chugai Pharma, and CytomX Therapeutics, and that he receives research funding from AstraZeneca and Puma Biotechnology. The study was funded by Loxo Oncology.

VIDEO: Survival improves when cancer patients self-report symptoms
CHICAGO – Patients with metastatic cancer who self-reported symptoms during routine cancer treatment experienced a number of benefits, including a statistically significant improvement in overall survival, according to findings from a randomized, controlled clinical trial.
The median overall survival among 441 patients receiving treatment for metastatic breast, lung, genitourinary, or gynecologic cancer who were randomized to the intervention arm was more than 5 months longer – a nearly 20% increase – than in 325 patients who received standard care (31.2 vs. 26 months), Ethan Basch, MD, reported at the annual meeting of the American Society of Clinical Oncology.

Additionally, 31% of patients in the intervention arm had better quality of life/physical functioning, compared with those in the control arm, and 7% fewer patients in the intervention arm visited an emergency room during the course of the study. The duration of potentially life-prolonging chemotherapy was increased by an average of 2 months in the intervention arm, he said.
The findings were simultaneously published online in a research letter in JAMA (2017 Jun 4. doi: 10.1001/jama.2017.7156).
Symptoms such as nausea, pain, and fatigue are common among patients with metastatic cancer, Dr. Basch said. “Unfortunately, they often go undetected by doctors and nurses until they become severe and physically debilitating,” he added, explaining that patients are often hesitant to call the office to report symptoms between visits.
Even at office visits, competing topics can interfere with communication about symptoms, he noted.
He and his colleagues hypothesized that self-reporting of patient symptoms between visits or prior to a visit while in the clinic waiting area would prompt earlier intervention and improve symptom control and outcomes.
Study subjects were patients at Memorial Sloan Kettering Cancer Center who had advanced solid genitourinary, gynecologic, breast, or lung tumors and who were receiving outpatient chemotherapy. Those assigned to the intervention group used tablet computers and an online web survey system to report on 12 symptoms commonly experienced during chemotherapy. The system triggers an alert to a nurse when a severe or worsening symptom is reported. Patients in the usual care group discussed symptoms during office visits and were encouraged to call the office between visits if they experienced concerning symptoms.
Patients remained on the study until discontinuation of all cancer treatment, hospice, or death.
One possible explanation for the findings is that this self-reporting approach prompts clinicians to manage symptoms before they cause serious downstream complications, Dr. Basch said.
The approach may also keep patients more physically functional, which is known from prior studies to have a strong association with better survival, and the approach may also improve management of chemotherapy side effects, enabling longer duration of beneficial cancer treatment, he said, explaining that, “in oncology, we often are limited in our ability to give life-prolonging treatment because people don’t tolerate it well.”
“This approach should be considered for inclusion in standard symptoms management as a component of high quality cancer care,” he concluded, noting that efforts are underway to test the next generation of systems to improve communication between patients and care teams and to figure out how best to integrate these tools into oncology practice.
The system used in the this study was designed for research, but a number of companies have tools currently available for patient-reported outcomes, and others are being developed, Dr. Basch said, noting that a National Cancer Institute questionnaire – the PRO-CTCAE – is publicly available and could be loaded into patients’ electronic health records for this purpose as well.
ASCO’s chief medical officer, Richard L. Schilsky, MD, said the findings demonstrate that “these frequent touches between the patient and their health care providers obviously can make a huge difference in their outcomes.”
Additionally, ASCO expert Harold J. Burstein, MD, of Dana-Farber Cancer Institute, Boston, said this “exciting and compelling study” validates the feeling among many clinicians that patient-focused, team-based care can improve outcomes in a meaningful way for patients. In a video interview, he further discusses the challenges with implementing a system like this and particularly with obtaining funding to support implementation.
“If this was a drug, if it was iPad-olizumab, it would be worth tens, if not hundreds of thousands, of dollars per year to have something that improved overall survival. We don’t have those same kinds of dollars to help implement these into our electronic health records or our systems. We need to find ways to support that and make it happen,” he said.
This study was supported by the National Institutes of Health and the Conquer Cancer Foundation of the American Society of Clinical Oncology. Dr. Basch and Dr. Burstein each reported having no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Patients with metastatic cancer who self-reported symptoms during routine cancer treatment experienced a number of benefits, including a statistically significant improvement in overall survival, according to findings from a randomized, controlled clinical trial.
The median overall survival among 441 patients receiving treatment for metastatic breast, lung, genitourinary, or gynecologic cancer who were randomized to the intervention arm was more than 5 months longer – a nearly 20% increase – than in 325 patients who received standard care (31.2 vs. 26 months), Ethan Basch, MD, reported at the annual meeting of the American Society of Clinical Oncology.
Additionally, 31% of patients in the intervention arm had better quality of life/physical functioning, compared with those in the control arm, and 7% fewer patients in the intervention arm visited an emergency room during the course of the study. The duration of potentially life-prolonging chemotherapy was increased by an average of 2 months in the intervention arm, he said.
The findings were simultaneously published online in a research letter in JAMA (2017 Jun 4. doi: 10.1001/jama.2017.7156).
Symptoms such as nausea, pain, and fatigue are common among patients with metastatic cancer, Dr. Basch said. “Unfortunately, they often go undetected by doctors and nurses until they become severe and physically debilitating,” he added, explaining that patients are often hesitant to call the office to report symptoms between visits.
Even at office visits, competing topics can interfere with communication about symptoms, he noted.
He and his colleagues hypothesized that self-reporting of patient symptoms between visits or prior to a visit while in the clinic waiting area would prompt earlier intervention and improve symptom control and outcomes.
Study subjects were patients at Memorial Sloan Kettering Cancer Center who had advanced solid genitourinary, gynecologic, breast, or lung tumors and who were receiving outpatient chemotherapy. Those assigned to the intervention group used tablet computers and an online web survey system to report on 12 symptoms commonly experienced during chemotherapy. The system triggers an alert to a nurse when a severe or worsening symptom is reported. Patients in the usual care group discussed symptoms during office visits and were encouraged to call the office between visits if they experienced concerning symptoms.
Patients remained on the study until discontinuation of all cancer treatment, hospice, or death.
One possible explanation for the findings is that this self-reporting approach prompts clinicians to manage symptoms before they cause serious downstream complications, Dr. Basch said.
The approach may also keep patients more physically functional, which is known from prior studies to have a strong association with better survival, and the approach may also improve management of chemotherapy side effects, enabling longer duration of beneficial cancer treatment, he said, explaining that, “in oncology, we often are limited in our ability to give life-prolonging treatment because people don’t tolerate it well.”
“This approach should be considered for inclusion in standard symptoms management as a component of high quality cancer care,” he concluded, noting that efforts are underway to test the next generation of systems to improve communication between patients and care teams and to figure out how best to integrate these tools into oncology practice.
The system used in the this study was designed for research, but a number of companies have tools currently available for patient-reported outcomes, and others are being developed, Dr. Basch said, noting that a National Cancer Institute questionnaire – the PRO-CTCAE – is publicly available and could be loaded into patients’ electronic health records for this purpose as well.
ASCO’s chief medical officer, Richard L. Schilsky, MD, said the findings demonstrate that “these frequent touches between the patient and their health care providers obviously can make a huge difference in their outcomes.”
Additionally, ASCO expert Harold J. Burstein, MD, of Dana-Farber Cancer Institute, Boston, said this “exciting and compelling study” validates the feeling among many clinicians that patient-focused, team-based care can improve outcomes in a meaningful way for patients. In a video interview, he further discusses the challenges with implementing a system like this and particularly with obtaining funding to support implementation.
“If this was a drug, if it was iPad-olizumab, it would be worth tens, if not hundreds of thousands, of dollars per year to have something that improved overall survival. We don’t have those same kinds of dollars to help implement these into our electronic health records or our systems. We need to find ways to support that and make it happen,” he said.
This study was supported by the National Institutes of Health and the Conquer Cancer Foundation of the American Society of Clinical Oncology. Dr. Basch and Dr. Burstein each reported having no disclosures.
CHICAGO – Patients with metastatic cancer who self-reported symptoms during routine cancer treatment experienced a number of benefits, including a statistically significant improvement in overall survival, according to findings from a randomized, controlled clinical trial.
The median overall survival among 441 patients receiving treatment for metastatic breast, lung, genitourinary, or gynecologic cancer who were randomized to the intervention arm was more than 5 months longer – a nearly 20% increase – than in 325 patients who received standard care (31.2 vs. 26 months), Ethan Basch, MD, reported at the annual meeting of the American Society of Clinical Oncology.
Additionally, 31% of patients in the intervention arm had better quality of life/physical functioning, compared with those in the control arm, and 7% fewer patients in the intervention arm visited an emergency room during the course of the study. The duration of potentially life-prolonging chemotherapy was increased by an average of 2 months in the intervention arm, he said.
The findings were simultaneously published online in a research letter in JAMA (2017 Jun 4. doi: 10.1001/jama.2017.7156).
Symptoms such as nausea, pain, and fatigue are common among patients with metastatic cancer, Dr. Basch said. “Unfortunately, they often go undetected by doctors and nurses until they become severe and physically debilitating,” he added, explaining that patients are often hesitant to call the office to report symptoms between visits.
Even at office visits, competing topics can interfere with communication about symptoms, he noted.
He and his colleagues hypothesized that self-reporting of patient symptoms between visits or prior to a visit while in the clinic waiting area would prompt earlier intervention and improve symptom control and outcomes.
Study subjects were patients at Memorial Sloan Kettering Cancer Center who had advanced solid genitourinary, gynecologic, breast, or lung tumors and who were receiving outpatient chemotherapy. Those assigned to the intervention group used tablet computers and an online web survey system to report on 12 symptoms commonly experienced during chemotherapy. The system triggers an alert to a nurse when a severe or worsening symptom is reported. Patients in the usual care group discussed symptoms during office visits and were encouraged to call the office between visits if they experienced concerning symptoms.
Patients remained on the study until discontinuation of all cancer treatment, hospice, or death.
One possible explanation for the findings is that this self-reporting approach prompts clinicians to manage symptoms before they cause serious downstream complications, Dr. Basch said.
The approach may also keep patients more physically functional, which is known from prior studies to have a strong association with better survival, and the approach may also improve management of chemotherapy side effects, enabling longer duration of beneficial cancer treatment, he said, explaining that, “in oncology, we often are limited in our ability to give life-prolonging treatment because people don’t tolerate it well.”
“This approach should be considered for inclusion in standard symptoms management as a component of high quality cancer care,” he concluded, noting that efforts are underway to test the next generation of systems to improve communication between patients and care teams and to figure out how best to integrate these tools into oncology practice.
The system used in the this study was designed for research, but a number of companies have tools currently available for patient-reported outcomes, and others are being developed, Dr. Basch said, noting that a National Cancer Institute questionnaire – the PRO-CTCAE – is publicly available and could be loaded into patients’ electronic health records for this purpose as well.
ASCO’s chief medical officer, Richard L. Schilsky, MD, said the findings demonstrate that “these frequent touches between the patient and their health care providers obviously can make a huge difference in their outcomes.”
Additionally, ASCO expert Harold J. Burstein, MD, of Dana-Farber Cancer Institute, Boston, said this “exciting and compelling study” validates the feeling among many clinicians that patient-focused, team-based care can improve outcomes in a meaningful way for patients. In a video interview, he further discusses the challenges with implementing a system like this and particularly with obtaining funding to support implementation.
“If this was a drug, if it was iPad-olizumab, it would be worth tens, if not hundreds of thousands, of dollars per year to have something that improved overall survival. We don’t have those same kinds of dollars to help implement these into our electronic health records or our systems. We need to find ways to support that and make it happen,” he said.
This study was supported by the National Institutes of Health and the Conquer Cancer Foundation of the American Society of Clinical Oncology. Dr. Basch and Dr. Burstein each reported having no disclosures.
AT THE 2017 ASCO ANNUAL MEETING
Key clinical point:
Major finding: Median overall survival was 31.2, vs. 26 months, with self-reporting of symptoms, vs. usual care.
Data source: A randomized controlled clinical trial of 766 patients.
Disclosures: This study was supported by the National Institutes of Health and the Conquer Cancer Foundation of the American Society of Clinical Oncology. Dr. Basch and Dr. Burstein each reported having no disclosures.

VIDEO: Routine genomic testing identifies actionable alterations in 52% of tumors
CHICAGO –
Molecular profiling, including genetic sequencing and copy number variation analysis, was performed in 1944 tumors from patients with advanced tumors enrolled in the profiLER study. Of the tumors screened, mutations deemed actionable were identified in 1,004 (52%), with 394 patients having two or more actionable targets, and the remainder having one identified targeted treatment. A molecular targeted treatment was recommended for 676 patients (35% of those tested).
“We showed that the patients who did receive the molecular targeted agents were doing better in terms of overall survival,” said Olivier Tredan, MD, PhD, the study’s lead investigator. Noting that these are trends as the trial was not randomized, he reported that the overall survival (OS) for those receiving targeted treatments was 53.7% at 3 years, compared with 46.1% for those who did not receive targeted treatment. The trend continued out to 5 years, with the OS for the targeted treatment group at 34.8%, compared with 28.1% OS for those who did not receive targeted treatment, he said at the annual meeting of the American Society of Clinical Oncology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Many patients either were too sick to receive the recommended treatment or died before they could be treated, Dr. Tredan said in a video interview.
Of the patients who did receive targeted treatment, over 60% received mTOR inhibitors. The next most common therapies were multitarget tyrosine kinase receptor (TKR)–inhibiting/antiangiogenic therapies, received by about one-third of patients. Fewer than one in five patients received any other therapies. Tumor types were colorectal, gynecological, breast, head and neck carcinomas, sarcomas, and brain tumors.
A new randomized clinical study, profiLER 2, is planned. The new study will pit a 315-gene commercial test against the 69-gene test used in profiLER 1, to see whether casting a wider net yields more targets for therapy.
Still, knowing that a treatment might help is useful only if the patient can actually receive the drug, said Dr. Tredan. “What we want is more molecular targeted agent initiation, so we need to have larger screening programs, but we need also to have access to novel targeted agents.”
Dr. Tredan reported financial relationships with Bayer, GlaxoSmithKline, and Novartis.
[email protected]
On Twitter @karioakes
CHICAGO –
Molecular profiling, including genetic sequencing and copy number variation analysis, was performed in 1944 tumors from patients with advanced tumors enrolled in the profiLER study. Of the tumors screened, mutations deemed actionable were identified in 1,004 (52%), with 394 patients having two or more actionable targets, and the remainder having one identified targeted treatment. A molecular targeted treatment was recommended for 676 patients (35% of those tested).
“We showed that the patients who did receive the molecular targeted agents were doing better in terms of overall survival,” said Olivier Tredan, MD, PhD, the study’s lead investigator. Noting that these are trends as the trial was not randomized, he reported that the overall survival (OS) for those receiving targeted treatments was 53.7% at 3 years, compared with 46.1% for those who did not receive targeted treatment. The trend continued out to 5 years, with the OS for the targeted treatment group at 34.8%, compared with 28.1% OS for those who did not receive targeted treatment, he said at the annual meeting of the American Society of Clinical Oncology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Many patients either were too sick to receive the recommended treatment or died before they could be treated, Dr. Tredan said in a video interview.
Of the patients who did receive targeted treatment, over 60% received mTOR inhibitors. The next most common therapies were multitarget tyrosine kinase receptor (TKR)–inhibiting/antiangiogenic therapies, received by about one-third of patients. Fewer than one in five patients received any other therapies. Tumor types were colorectal, gynecological, breast, head and neck carcinomas, sarcomas, and brain tumors.
A new randomized clinical study, profiLER 2, is planned. The new study will pit a 315-gene commercial test against the 69-gene test used in profiLER 1, to see whether casting a wider net yields more targets for therapy.
Still, knowing that a treatment might help is useful only if the patient can actually receive the drug, said Dr. Tredan. “What we want is more molecular targeted agent initiation, so we need to have larger screening programs, but we need also to have access to novel targeted agents.”
Dr. Tredan reported financial relationships with Bayer, GlaxoSmithKline, and Novartis.
[email protected]
On Twitter @karioakes
CHICAGO –
Molecular profiling, including genetic sequencing and copy number variation analysis, was performed in 1944 tumors from patients with advanced tumors enrolled in the profiLER study. Of the tumors screened, mutations deemed actionable were identified in 1,004 (52%), with 394 patients having two or more actionable targets, and the remainder having one identified targeted treatment. A molecular targeted treatment was recommended for 676 patients (35% of those tested).
“We showed that the patients who did receive the molecular targeted agents were doing better in terms of overall survival,” said Olivier Tredan, MD, PhD, the study’s lead investigator. Noting that these are trends as the trial was not randomized, he reported that the overall survival (OS) for those receiving targeted treatments was 53.7% at 3 years, compared with 46.1% for those who did not receive targeted treatment. The trend continued out to 5 years, with the OS for the targeted treatment group at 34.8%, compared with 28.1% OS for those who did not receive targeted treatment, he said at the annual meeting of the American Society of Clinical Oncology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Many patients either were too sick to receive the recommended treatment or died before they could be treated, Dr. Tredan said in a video interview.
Of the patients who did receive targeted treatment, over 60% received mTOR inhibitors. The next most common therapies were multitarget tyrosine kinase receptor (TKR)–inhibiting/antiangiogenic therapies, received by about one-third of patients. Fewer than one in five patients received any other therapies. Tumor types were colorectal, gynecological, breast, head and neck carcinomas, sarcomas, and brain tumors.
A new randomized clinical study, profiLER 2, is planned. The new study will pit a 315-gene commercial test against the 69-gene test used in profiLER 1, to see whether casting a wider net yields more targets for therapy.
Still, knowing that a treatment might help is useful only if the patient can actually receive the drug, said Dr. Tredan. “What we want is more molecular targeted agent initiation, so we need to have larger screening programs, but we need also to have access to novel targeted agents.”
Dr. Tredan reported financial relationships with Bayer, GlaxoSmithKline, and Novartis.
[email protected]
On Twitter @karioakes
AT ASCO 2017

Immune-agonist combo has activity against several tumor types
CHICAGO – A combination of the programmed death 1 (PD-1) inhibitor nivolumab (Opdivo) with an experimental immune-enhancing monoclonal antibody induced clinical responses in patients with several different solid tumor types, including some patients who had disease progression on a PD-1 inhibitor, investigators reported.
The investigational agent, euphoniously named BMS-986156 (986156), is a fully human immunoglobulin G1 agonist monoclonal antibody with high affinity binding for the glucocorticoid-induced tumor necrosis factor receptor–related gene (GITR).

BMS-986156156 “induces potent antitumor immunity by several mechanisms. First, it increases T-effector cell survival and function. Second, it promotes T-regulatory cell depletion and reduction through its conversion to other immune cells. As well, it reduces T-reg-mediated suppression of T-effector cells,” said Lillian L Siu, MD, from the Princess Margaret Hospital in Toronto.
In preclinical studies, the combination of an anti-GITR and an anti-PD-1 agent showed synergistic activity against murine tumor models.
Dr. Siu and colleagues conducted a phase I/IIa study of BMS-986156 with or without nivolumab in 66 patients with advanced solid tumors.
The 29 patients assigned to BMS-986156 monotherapy were started at 10 mg every 2 weeks, which was gradually titrated upward to find the maximum tolerated dose of 240 mg Q2 weeks.
The 37 patients assigned to the combination were started on a dose of 30-mg nivolumab and 240-mg BMS-986156. The nivolumab dose but not the BMS-986156 dose was then titrated upward to a maximum tolerated dose of 240 mg for each agent. This dose was based on pharmacodynamic and pharmacokinetic studies.
Tumor types included melanoma, cervical, colon, breast, renal, pancreatic, and ovarian cancers and cholangiocarcinoma.
Approximately one-third of patients in the monotherapy arm and nearly half of those in the combination arm had undergone three or more prior therapies for cancer. Seven patients in the monotherapy group and five in the combination group had previously received a PD-1 or PD-L1 inhibitor.
The median duration of treatment ranged from 7 to 15.5 weeks for 156 monotherapy and 8 to 18 weeks for the combination.
Safe and well tolerated
There were no dose-limiting toxicities or treatment-related deaths in either study arm, and patients tolerated both BMS-986156 monotherapy and the combination well. There were no grade 3 or 4 adverse events in the monotherapy arm.
“In the combination arm, the toxicity is very consistent with that observed with nivolumab monotherapy alone,” Dr. Siu said.
The only grade 4 event in this group was an increase in blood creatine phosphokinase. In this group, there were six grade 3 adverse events, including one each of colitis, dehydration, fatigue and increases in hepatic enzymes, lipase increase, and lung infection.
In pharmacokinetic studies, the action of the combinations was linear, with dose-related increases in exposure, and the combination had low immunogenicity, with no patients developing persistent antidrug antibodies.
The combination was also associated with increases in natural killer and CD8 cells in peripheral blood. Immunophenotyping of patients treated with the 240/240-mg dose of the combination showed increased proliferation and activation of CD8 effector cells, central memory cells, and CD4 cells.
Early promise
Dr. Siu reviewed interim efficacy results for the five patients treated with the combination who had responses.
For example, a 44-year-old woman with metastatic cervical cancer – a tumor type known to have high levels of GITR expression – had received more than three prior lines of therapy, including chemotherapy with a vascular endothelial growth factor inhibitor. She had a partial response with the combination, with an approximately 62% reduction in tumor burden. She had an ongoing response to the combination at the time of data cutoff in March 2017.

Two other patients had partial responses after progression on an anti-PD-1 agents, including one with nasopharyngeal cancer who had received three prior lines of therapy, including chemotherapy and a PD-1 inhibitor. This patient had an approximately 43% reduction in tumor burden, with a 17-week duration of response and ongoing response at data cutoff.
The other patient was a 59-year-old with malignant melanoma that had advanced on pembrolizumab (Keytruda). This patient too had received three prior lines of therapy, including a BRAF inhibitor, anti-PD-1, and BRAF/MEK inhibitor combination.
This patient had a response of 24-week duration at the time of data cutoff. It is ongoing, Dr. Liu said.
“This combination of immune agonists was safe with a low incidence of severe toxicity, and there was no maximum tolerated dose; however, the maximum administered dose may not be the most effective dose to move forward,” commented Siwen Hu-Lieskovan MD, PhD, from the Jonsson Comprehensive Cancer Center at the University of California, Los Angeles, the invited discussant.
She noted that activity of the combination has been seen in a wide range of tumor histologies but added that further biomarker studies will be critical for identifying patients who are likely to respond.
The study was funded by Bristol-Myers Squibb. Dr. Siu disclosed research funding from the company and others and consulting/advising several different companies. Dr. Hu-Lieskovan disclosed institutional research funding from BMS and other companies, as well as honoraria and consulting and serving in an advisory capacity for companies other than BMS. Several coauthors are employees of the company.
CHICAGO – A combination of the programmed death 1 (PD-1) inhibitor nivolumab (Opdivo) with an experimental immune-enhancing monoclonal antibody induced clinical responses in patients with several different solid tumor types, including some patients who had disease progression on a PD-1 inhibitor, investigators reported.
The investigational agent, euphoniously named BMS-986156 (986156), is a fully human immunoglobulin G1 agonist monoclonal antibody with high affinity binding for the glucocorticoid-induced tumor necrosis factor receptor–related gene (GITR).
BMS-986156156 “induces potent antitumor immunity by several mechanisms. First, it increases T-effector cell survival and function. Second, it promotes T-regulatory cell depletion and reduction through its conversion to other immune cells. As well, it reduces T-reg-mediated suppression of T-effector cells,” said Lillian L Siu, MD, from the Princess Margaret Hospital in Toronto.
In preclinical studies, the combination of an anti-GITR and an anti-PD-1 agent showed synergistic activity against murine tumor models.
Dr. Siu and colleagues conducted a phase I/IIa study of BMS-986156 with or without nivolumab in 66 patients with advanced solid tumors.
The 29 patients assigned to BMS-986156 monotherapy were started at 10 mg every 2 weeks, which was gradually titrated upward to find the maximum tolerated dose of 240 mg Q2 weeks.
The 37 patients assigned to the combination were started on a dose of 30-mg nivolumab and 240-mg BMS-986156. The nivolumab dose but not the BMS-986156 dose was then titrated upward to a maximum tolerated dose of 240 mg for each agent. This dose was based on pharmacodynamic and pharmacokinetic studies.
Tumor types included melanoma, cervical, colon, breast, renal, pancreatic, and ovarian cancers and cholangiocarcinoma.
Approximately one-third of patients in the monotherapy arm and nearly half of those in the combination arm had undergone three or more prior therapies for cancer. Seven patients in the monotherapy group and five in the combination group had previously received a PD-1 or PD-L1 inhibitor.
The median duration of treatment ranged from 7 to 15.5 weeks for 156 monotherapy and 8 to 18 weeks for the combination.
Safe and well tolerated
There were no dose-limiting toxicities or treatment-related deaths in either study arm, and patients tolerated both BMS-986156 monotherapy and the combination well. There were no grade 3 or 4 adverse events in the monotherapy arm.
“In the combination arm, the toxicity is very consistent with that observed with nivolumab monotherapy alone,” Dr. Siu said.
The only grade 4 event in this group was an increase in blood creatine phosphokinase. In this group, there were six grade 3 adverse events, including one each of colitis, dehydration, fatigue and increases in hepatic enzymes, lipase increase, and lung infection.
In pharmacokinetic studies, the action of the combinations was linear, with dose-related increases in exposure, and the combination had low immunogenicity, with no patients developing persistent antidrug antibodies.
The combination was also associated with increases in natural killer and CD8 cells in peripheral blood. Immunophenotyping of patients treated with the 240/240-mg dose of the combination showed increased proliferation and activation of CD8 effector cells, central memory cells, and CD4 cells.
Early promise
Dr. Siu reviewed interim efficacy results for the five patients treated with the combination who had responses.
For example, a 44-year-old woman with metastatic cervical cancer – a tumor type known to have high levels of GITR expression – had received more than three prior lines of therapy, including chemotherapy with a vascular endothelial growth factor inhibitor. She had a partial response with the combination, with an approximately 62% reduction in tumor burden. She had an ongoing response to the combination at the time of data cutoff in March 2017.
Two other patients had partial responses after progression on an anti-PD-1 agents, including one with nasopharyngeal cancer who had received three prior lines of therapy, including chemotherapy and a PD-1 inhibitor. This patient had an approximately 43% reduction in tumor burden, with a 17-week duration of response and ongoing response at data cutoff.
The other patient was a 59-year-old with malignant melanoma that had advanced on pembrolizumab (Keytruda). This patient too had received three prior lines of therapy, including a BRAF inhibitor, anti-PD-1, and BRAF/MEK inhibitor combination.
This patient had a response of 24-week duration at the time of data cutoff. It is ongoing, Dr. Liu said.
“This combination of immune agonists was safe with a low incidence of severe toxicity, and there was no maximum tolerated dose; however, the maximum administered dose may not be the most effective dose to move forward,” commented Siwen Hu-Lieskovan MD, PhD, from the Jonsson Comprehensive Cancer Center at the University of California, Los Angeles, the invited discussant.
She noted that activity of the combination has been seen in a wide range of tumor histologies but added that further biomarker studies will be critical for identifying patients who are likely to respond.
The study was funded by Bristol-Myers Squibb. Dr. Siu disclosed research funding from the company and others and consulting/advising several different companies. Dr. Hu-Lieskovan disclosed institutional research funding from BMS and other companies, as well as honoraria and consulting and serving in an advisory capacity for companies other than BMS. Several coauthors are employees of the company.
CHICAGO – A combination of the programmed death 1 (PD-1) inhibitor nivolumab (Opdivo) with an experimental immune-enhancing monoclonal antibody induced clinical responses in patients with several different solid tumor types, including some patients who had disease progression on a PD-1 inhibitor, investigators reported.
The investigational agent, euphoniously named BMS-986156 (986156), is a fully human immunoglobulin G1 agonist monoclonal antibody with high affinity binding for the glucocorticoid-induced tumor necrosis factor receptor–related gene (GITR).
BMS-986156156 “induces potent antitumor immunity by several mechanisms. First, it increases T-effector cell survival and function. Second, it promotes T-regulatory cell depletion and reduction through its conversion to other immune cells. As well, it reduces T-reg-mediated suppression of T-effector cells,” said Lillian L Siu, MD, from the Princess Margaret Hospital in Toronto.
In preclinical studies, the combination of an anti-GITR and an anti-PD-1 agent showed synergistic activity against murine tumor models.
Dr. Siu and colleagues conducted a phase I/IIa study of BMS-986156 with or without nivolumab in 66 patients with advanced solid tumors.
The 29 patients assigned to BMS-986156 monotherapy were started at 10 mg every 2 weeks, which was gradually titrated upward to find the maximum tolerated dose of 240 mg Q2 weeks.
The 37 patients assigned to the combination were started on a dose of 30-mg nivolumab and 240-mg BMS-986156. The nivolumab dose but not the BMS-986156 dose was then titrated upward to a maximum tolerated dose of 240 mg for each agent. This dose was based on pharmacodynamic and pharmacokinetic studies.
Tumor types included melanoma, cervical, colon, breast, renal, pancreatic, and ovarian cancers and cholangiocarcinoma.
Approximately one-third of patients in the monotherapy arm and nearly half of those in the combination arm had undergone three or more prior therapies for cancer. Seven patients in the monotherapy group and five in the combination group had previously received a PD-1 or PD-L1 inhibitor.
The median duration of treatment ranged from 7 to 15.5 weeks for 156 monotherapy and 8 to 18 weeks for the combination.
Safe and well tolerated
There were no dose-limiting toxicities or treatment-related deaths in either study arm, and patients tolerated both BMS-986156 monotherapy and the combination well. There were no grade 3 or 4 adverse events in the monotherapy arm.
“In the combination arm, the toxicity is very consistent with that observed with nivolumab monotherapy alone,” Dr. Siu said.
The only grade 4 event in this group was an increase in blood creatine phosphokinase. In this group, there were six grade 3 adverse events, including one each of colitis, dehydration, fatigue and increases in hepatic enzymes, lipase increase, and lung infection.
In pharmacokinetic studies, the action of the combinations was linear, with dose-related increases in exposure, and the combination had low immunogenicity, with no patients developing persistent antidrug antibodies.
The combination was also associated with increases in natural killer and CD8 cells in peripheral blood. Immunophenotyping of patients treated with the 240/240-mg dose of the combination showed increased proliferation and activation of CD8 effector cells, central memory cells, and CD4 cells.
Early promise
Dr. Siu reviewed interim efficacy results for the five patients treated with the combination who had responses.
For example, a 44-year-old woman with metastatic cervical cancer – a tumor type known to have high levels of GITR expression – had received more than three prior lines of therapy, including chemotherapy with a vascular endothelial growth factor inhibitor. She had a partial response with the combination, with an approximately 62% reduction in tumor burden. She had an ongoing response to the combination at the time of data cutoff in March 2017.
Two other patients had partial responses after progression on an anti-PD-1 agents, including one with nasopharyngeal cancer who had received three prior lines of therapy, including chemotherapy and a PD-1 inhibitor. This patient had an approximately 43% reduction in tumor burden, with a 17-week duration of response and ongoing response at data cutoff.
The other patient was a 59-year-old with malignant melanoma that had advanced on pembrolizumab (Keytruda). This patient too had received three prior lines of therapy, including a BRAF inhibitor, anti-PD-1, and BRAF/MEK inhibitor combination.
This patient had a response of 24-week duration at the time of data cutoff. It is ongoing, Dr. Liu said.
“This combination of immune agonists was safe with a low incidence of severe toxicity, and there was no maximum tolerated dose; however, the maximum administered dose may not be the most effective dose to move forward,” commented Siwen Hu-Lieskovan MD, PhD, from the Jonsson Comprehensive Cancer Center at the University of California, Los Angeles, the invited discussant.
She noted that activity of the combination has been seen in a wide range of tumor histologies but added that further biomarker studies will be critical for identifying patients who are likely to respond.
The study was funded by Bristol-Myers Squibb. Dr. Siu disclosed research funding from the company and others and consulting/advising several different companies. Dr. Hu-Lieskovan disclosed institutional research funding from BMS and other companies, as well as honoraria and consulting and serving in an advisory capacity for companies other than BMS. Several coauthors are employees of the company.
AT ASCO 2017
Key clinical point: A combination of a GITR-agonist and anti-PD-1 agent was safe and produced partial responses in patients with heavily pretreated advanced cancers.
Major finding: Two patients with cancers that had progression on a PD-1 inhibitor had durable partial responses.
Data source: A phase I/IIa dose-finding and safety study of BMS986156 alone or in combination with nivolumab (Opdivo).
Disclosures: The study was funded by Bristol-Myers Squibb. Dr. Siu disclosed research funding from the company and others and consulting/advising for several different companies. Dr. Hu-Lieskovan disclosed institutional research funding from BMS and other companies, as well as honoraria and consulting and serving in an advisory capacity for companies other than BMS. Several coauthors are employees of the company.
Cirrhosis linked to increased risk of stroke
reported online June 5 in JAMA Neurology.
Cirrhosis is known to be associated with “extrahepatic hemorrhagic and thrombotic processes, such as GI bleeding and venous thromboembolism. [But] the cerebrovascular complications of cirrhosis are comparatively less well understood.” Previous studies of the association with stroke have been small and have yielded conflicting results, with some finding a reduced incidence of stroke and others finding an increase among cirrhosis patients, said Neal S. Parikh, MD, of the Fell Family Brain and Mind Research Institute and Weill Cornell Medicine, both in New York, and his associates.
After the data were adjusted to account for stroke risk factors, relevant comorbidities, and demographic traits, the annual incidence of any type of stroke was significantly higher with cirrhosis than without cirrhosis (hazard ratio, 1.4). The association was stronger for intracranial hemorrhage (HR, 1.9) and subarachnoid hemorrhage (HR, 2.4) than for ischemic stroke (HR, 1.3).
The results of several secondary and sensitivity analyses were consistent with those of the primary analysis, regardless of whether the cirrhosis was alcohol-related or the stroke was fatal. The association was strongest among patients who had decompensated cirrhosis and was not evident at all among patients who had mild liver disease, Dr. Parikh and his associates said (JAMA Neurol. 2017 Jun 5 [doi: 10.1001/jamaneurol.2017.0923).
This study was not designed to explore the reasons for an association between cirrhosis and stroke, but the investigators noted many possible explanations. First, “cirrhosis is accompanied by a mixed coagulopathy, with potential implications for hemorrhagic and thrombotic processes.” It has been linked to many bleeding complications, including, most recently, cerebral microhemorrhages detectable on brain MRI. In addition, the underlying causes of cirrhosis, including alcohol abuse, hepatitis infection, and metabolic disease, may also contribute to stroke risk.
Alternatively, clinicians caring for patients with cirrhosis “may limit the aggressiveness of stroke prevention” – for example, by limiting antithrombotic medications or statins – because they are mindful of the patient’s increased risk of bleeding and hepatic toxicity, the investigators said.
reported online June 5 in JAMA Neurology.
Cirrhosis is known to be associated with “extrahepatic hemorrhagic and thrombotic processes, such as GI bleeding and venous thromboembolism. [But] the cerebrovascular complications of cirrhosis are comparatively less well understood.” Previous studies of the association with stroke have been small and have yielded conflicting results, with some finding a reduced incidence of stroke and others finding an increase among cirrhosis patients, said Neal S. Parikh, MD, of the Fell Family Brain and Mind Research Institute and Weill Cornell Medicine, both in New York, and his associates.
After the data were adjusted to account for stroke risk factors, relevant comorbidities, and demographic traits, the annual incidence of any type of stroke was significantly higher with cirrhosis than without cirrhosis (hazard ratio, 1.4). The association was stronger for intracranial hemorrhage (HR, 1.9) and subarachnoid hemorrhage (HR, 2.4) than for ischemic stroke (HR, 1.3).
The results of several secondary and sensitivity analyses were consistent with those of the primary analysis, regardless of whether the cirrhosis was alcohol-related or the stroke was fatal. The association was strongest among patients who had decompensated cirrhosis and was not evident at all among patients who had mild liver disease, Dr. Parikh and his associates said (JAMA Neurol. 2017 Jun 5 [doi: 10.1001/jamaneurol.2017.0923).
This study was not designed to explore the reasons for an association between cirrhosis and stroke, but the investigators noted many possible explanations. First, “cirrhosis is accompanied by a mixed coagulopathy, with potential implications for hemorrhagic and thrombotic processes.” It has been linked to many bleeding complications, including, most recently, cerebral microhemorrhages detectable on brain MRI. In addition, the underlying causes of cirrhosis, including alcohol abuse, hepatitis infection, and metabolic disease, may also contribute to stroke risk.
Alternatively, clinicians caring for patients with cirrhosis “may limit the aggressiveness of stroke prevention” – for example, by limiting antithrombotic medications or statins – because they are mindful of the patient’s increased risk of bleeding and hepatic toxicity, the investigators said.
reported online June 5 in JAMA Neurology.
Cirrhosis is known to be associated with “extrahepatic hemorrhagic and thrombotic processes, such as GI bleeding and venous thromboembolism. [But] the cerebrovascular complications of cirrhosis are comparatively less well understood.” Previous studies of the association with stroke have been small and have yielded conflicting results, with some finding a reduced incidence of stroke and others finding an increase among cirrhosis patients, said Neal S. Parikh, MD, of the Fell Family Brain and Mind Research Institute and Weill Cornell Medicine, both in New York, and his associates.
After the data were adjusted to account for stroke risk factors, relevant comorbidities, and demographic traits, the annual incidence of any type of stroke was significantly higher with cirrhosis than without cirrhosis (hazard ratio, 1.4). The association was stronger for intracranial hemorrhage (HR, 1.9) and subarachnoid hemorrhage (HR, 2.4) than for ischemic stroke (HR, 1.3).
The results of several secondary and sensitivity analyses were consistent with those of the primary analysis, regardless of whether the cirrhosis was alcohol-related or the stroke was fatal. The association was strongest among patients who had decompensated cirrhosis and was not evident at all among patients who had mild liver disease, Dr. Parikh and his associates said (JAMA Neurol. 2017 Jun 5 [doi: 10.1001/jamaneurol.2017.0923).
This study was not designed to explore the reasons for an association between cirrhosis and stroke, but the investigators noted many possible explanations. First, “cirrhosis is accompanied by a mixed coagulopathy, with potential implications for hemorrhagic and thrombotic processes.” It has been linked to many bleeding complications, including, most recently, cerebral microhemorrhages detectable on brain MRI. In addition, the underlying causes of cirrhosis, including alcohol abuse, hepatitis infection, and metabolic disease, may also contribute to stroke risk.
Alternatively, clinicians caring for patients with cirrhosis “may limit the aggressiveness of stroke prevention” – for example, by limiting antithrombotic medications or statins – because they are mindful of the patient’s increased risk of bleeding and hepatic toxicity, the investigators said.
FROM JAMA NEUROLOGY
Key clinical point: Cirrhosis was associated with an increased risk of stroke, especially hemorrhagic stroke, in a large nationally representative cohort study.
Major finding: The annual incidence of any type of stroke was significantly higher with cirrhosis than without cirrhosis (HR, 1.4), and this association was stronger for intracranial hemorrhage (HR, 1.9) and subarachnoid hemorrhage (HR, 2.4) than for ischemic stroke (HR, 1.3).
Data source: A retrospective cohort study involving a nationally representative sample of 1.6 million Medicare patients.
Disclosures: This study was supported by the National Institute of Neurological Disorders and Stroke and the Florence Gould Endowment for Discovery in Stroke. Dr. Parikh and his associates reported having no relevant financial disclosures.
VIDEO: Phase III results show promise for erenumab as migraine prevention drug
BOSTON – Two phase III trials of the investigational monoclonal antibody erenumab show promising results in reducing – but not eliminating – days affected by migraines and related disruptions in daily life with limited side effects, representing “an entirely new way forward” in migraine prevention, according to Peter Goadsby, MD.
In May, shortly after the results were released at the annual meeting of the American Academy of Neurology, Amgen filed regulatory documents for erenumab with the Food and Drug Administration.
Erenumab, also known as AMG 334, “is going to be the first mechanism-specific, migraine-targeted preventive treatment approach ever,” Dr. Goadsby, a University of California, San Francisco, neurologist, predicted at the annual meeting of the American Academy of Neurology. Erenumab is a fully human monoclonal antibody that is designed to block the calcitonin gene-related peptide (CGRP) receptor, which is linked to migraine.
Several drug makers are investigating CGRP-modulating treatments for migraine. Results suggest that the medications are “effective for episodic and migraine patients,” said Amaal Starling, MD, of the Mayo Clinic, Scottsdale, Ariz., who spoke about the drugs in a plenary session at the meeting. “They have rapid onset of efficacy, minimal side effects, and infrequent administration. All of these things may improve adherence.”
Dr. Goadsby is the lead author of the study reporting phase III results from the 24-week STRIVE trial, which tested two monthly subcutaneous doses of erenumab (70 mg and 140 mg) against placebo in a 1:1:1 ratio in 955 patients. The patients all had suffered from episodic migraine for at least a year.
“STRIVE has shown that the 70-mg and 140-mg doses are better than placebo at the regulatory endpoint and clinically relevant endpoints,” Dr. Goadsby said, “and there are improvements in function, everyday activities, and physical impairment. The overall frequency of adverse and serious events were comparable, even the same.”
The participants reported an average of 8.3 monthly migraine days (MMDs) at the beginning of the study. At the end, the number declined significantly by an average of 3.2 days (70-mg dose), 3.7 days (140-mg dose), and 1.8 days (placebo; P less than .001).
Half of those in the 140-mg group achieved at least a 50% reduction in MMDs, compared with 43% and 27% for the 70-mg and placebo groups, respectively (P less than .001).
The researchers also examined changes in scores regarding Physical Impairment (PI) and Impact on Everyday Activities (EA) as determined by the Migraine Physical Function Impact Diary. PI scores improved by 4.2, 4.8, and 2.4 points in the 70-mg, 140-mg, and placebo groups, respectively. EA scores improved by 5.5, 5.9, and 3.3 points, respectively (P less than .001).
The study authors reported that tolerability was similar for placebo and the drug. The most common adverse events were nasopharyngitis, upper respiratory tract infection, and sinusitis.
The researchers at the AAN meeting also released the results of a second study known as ARISE, led by David W. Dodick, MD, of the Mayo Clinic, Phoenix, Ariz. This double-blind, 12-week trial randomly assigned 577 adults with episodic migraine to a monthly subcutaneous dose of a placebo or 70 mg of erenumab.
The patients reported an average of 8.3 MMDs at the beginning of the trial. Those who took the medication reported an average 2.9 fewer MMDs while those who took the placebo reported 1.8 fewer MMDs (P less than .001) at 9-12 weeks.
Forty percent of those who took the drug saw a decrease of at least half in MMDs, compared with 30% of those who took placebo (odds ratio, 1.6; P = .010).
The PI levels declined by at least 5 points in 27% of placebo patients and 33% of erenumab patients (P = .13). EA levels declined by at least 5 points in 36% of placebo patients and 40% of erenumab patients (P = .26)
There were similar levels of adverse events in both drug and placebo groups, led by upper respiratory tract infection, injection site pain, and nasopharyngitis.
The Mayo Clinic’s Dr. Starling said anti-CGRP medications may dramatically improve the world of preventive migraine treatments, which are recommended for a third of migraine patients. Only about 3%-13% use them, she said.
In the future, it may be possible to be able to identify and target “super-responders” whose MMDs dip by 75% or more in some cases.
But there are questions, she said. The drugs’ specific mechanism for blocking migraine is not yet clear, and it’s also not clear if the CGRP antagonists could push patients at risk of TIA or cardiac angina to have a stroke instead.
Dr. Starling discussed some of the implications of the CGRP antagonists in development in a video interview.
Both studies were funded by Amgen. Dr. Goadsby reported numerous grants and personal fees from multiple drug makers, including Amgen. Dr. Starling reported support from Amgen, eNeura, and Eli Lilly. Dr. Dodick disclosed many relationships with pharmaceutical companies developing or marketing drugs for headache and migraine, including Amgen.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
BOSTON – Two phase III trials of the investigational monoclonal antibody erenumab show promising results in reducing – but not eliminating – days affected by migraines and related disruptions in daily life with limited side effects, representing “an entirely new way forward” in migraine prevention, according to Peter Goadsby, MD.
In May, shortly after the results were released at the annual meeting of the American Academy of Neurology, Amgen filed regulatory documents for erenumab with the Food and Drug Administration.
Erenumab, also known as AMG 334, “is going to be the first mechanism-specific, migraine-targeted preventive treatment approach ever,” Dr. Goadsby, a University of California, San Francisco, neurologist, predicted at the annual meeting of the American Academy of Neurology. Erenumab is a fully human monoclonal antibody that is designed to block the calcitonin gene-related peptide (CGRP) receptor, which is linked to migraine.
Several drug makers are investigating CGRP-modulating treatments for migraine. Results suggest that the medications are “effective for episodic and migraine patients,” said Amaal Starling, MD, of the Mayo Clinic, Scottsdale, Ariz., who spoke about the drugs in a plenary session at the meeting. “They have rapid onset of efficacy, minimal side effects, and infrequent administration. All of these things may improve adherence.”
Dr. Goadsby is the lead author of the study reporting phase III results from the 24-week STRIVE trial, which tested two monthly subcutaneous doses of erenumab (70 mg and 140 mg) against placebo in a 1:1:1 ratio in 955 patients. The patients all had suffered from episodic migraine for at least a year.
“STRIVE has shown that the 70-mg and 140-mg doses are better than placebo at the regulatory endpoint and clinically relevant endpoints,” Dr. Goadsby said, “and there are improvements in function, everyday activities, and physical impairment. The overall frequency of adverse and serious events were comparable, even the same.”
The participants reported an average of 8.3 monthly migraine days (MMDs) at the beginning of the study. At the end, the number declined significantly by an average of 3.2 days (70-mg dose), 3.7 days (140-mg dose), and 1.8 days (placebo; P less than .001).
Half of those in the 140-mg group achieved at least a 50% reduction in MMDs, compared with 43% and 27% for the 70-mg and placebo groups, respectively (P less than .001).
The researchers also examined changes in scores regarding Physical Impairment (PI) and Impact on Everyday Activities (EA) as determined by the Migraine Physical Function Impact Diary. PI scores improved by 4.2, 4.8, and 2.4 points in the 70-mg, 140-mg, and placebo groups, respectively. EA scores improved by 5.5, 5.9, and 3.3 points, respectively (P less than .001).
The study authors reported that tolerability was similar for placebo and the drug. The most common adverse events were nasopharyngitis, upper respiratory tract infection, and sinusitis.
The researchers at the AAN meeting also released the results of a second study known as ARISE, led by David W. Dodick, MD, of the Mayo Clinic, Phoenix, Ariz. This double-blind, 12-week trial randomly assigned 577 adults with episodic migraine to a monthly subcutaneous dose of a placebo or 70 mg of erenumab.
The patients reported an average of 8.3 MMDs at the beginning of the trial. Those who took the medication reported an average 2.9 fewer MMDs while those who took the placebo reported 1.8 fewer MMDs (P less than .001) at 9-12 weeks.
Forty percent of those who took the drug saw a decrease of at least half in MMDs, compared with 30% of those who took placebo (odds ratio, 1.6; P = .010).
The PI levels declined by at least 5 points in 27% of placebo patients and 33% of erenumab patients (P = .13). EA levels declined by at least 5 points in 36% of placebo patients and 40% of erenumab patients (P = .26)
There were similar levels of adverse events in both drug and placebo groups, led by upper respiratory tract infection, injection site pain, and nasopharyngitis.
The Mayo Clinic’s Dr. Starling said anti-CGRP medications may dramatically improve the world of preventive migraine treatments, which are recommended for a third of migraine patients. Only about 3%-13% use them, she said.
In the future, it may be possible to be able to identify and target “super-responders” whose MMDs dip by 75% or more in some cases.
But there are questions, she said. The drugs’ specific mechanism for blocking migraine is not yet clear, and it’s also not clear if the CGRP antagonists could push patients at risk of TIA or cardiac angina to have a stroke instead.
Dr. Starling discussed some of the implications of the CGRP antagonists in development in a video interview.
Both studies were funded by Amgen. Dr. Goadsby reported numerous grants and personal fees from multiple drug makers, including Amgen. Dr. Starling reported support from Amgen, eNeura, and Eli Lilly. Dr. Dodick disclosed many relationships with pharmaceutical companies developing or marketing drugs for headache and migraine, including Amgen.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
BOSTON – Two phase III trials of the investigational monoclonal antibody erenumab show promising results in reducing – but not eliminating – days affected by migraines and related disruptions in daily life with limited side effects, representing “an entirely new way forward” in migraine prevention, according to Peter Goadsby, MD.
In May, shortly after the results were released at the annual meeting of the American Academy of Neurology, Amgen filed regulatory documents for erenumab with the Food and Drug Administration.
Erenumab, also known as AMG 334, “is going to be the first mechanism-specific, migraine-targeted preventive treatment approach ever,” Dr. Goadsby, a University of California, San Francisco, neurologist, predicted at the annual meeting of the American Academy of Neurology. Erenumab is a fully human monoclonal antibody that is designed to block the calcitonin gene-related peptide (CGRP) receptor, which is linked to migraine.
Several drug makers are investigating CGRP-modulating treatments for migraine. Results suggest that the medications are “effective for episodic and migraine patients,” said Amaal Starling, MD, of the Mayo Clinic, Scottsdale, Ariz., who spoke about the drugs in a plenary session at the meeting. “They have rapid onset of efficacy, minimal side effects, and infrequent administration. All of these things may improve adherence.”
Dr. Goadsby is the lead author of the study reporting phase III results from the 24-week STRIVE trial, which tested two monthly subcutaneous doses of erenumab (70 mg and 140 mg) against placebo in a 1:1:1 ratio in 955 patients. The patients all had suffered from episodic migraine for at least a year.
“STRIVE has shown that the 70-mg and 140-mg doses are better than placebo at the regulatory endpoint and clinically relevant endpoints,” Dr. Goadsby said, “and there are improvements in function, everyday activities, and physical impairment. The overall frequency of adverse and serious events were comparable, even the same.”
The participants reported an average of 8.3 monthly migraine days (MMDs) at the beginning of the study. At the end, the number declined significantly by an average of 3.2 days (70-mg dose), 3.7 days (140-mg dose), and 1.8 days (placebo; P less than .001).
Half of those in the 140-mg group achieved at least a 50% reduction in MMDs, compared with 43% and 27% for the 70-mg and placebo groups, respectively (P less than .001).
The researchers also examined changes in scores regarding Physical Impairment (PI) and Impact on Everyday Activities (EA) as determined by the Migraine Physical Function Impact Diary. PI scores improved by 4.2, 4.8, and 2.4 points in the 70-mg, 140-mg, and placebo groups, respectively. EA scores improved by 5.5, 5.9, and 3.3 points, respectively (P less than .001).
The study authors reported that tolerability was similar for placebo and the drug. The most common adverse events were nasopharyngitis, upper respiratory tract infection, and sinusitis.
The researchers at the AAN meeting also released the results of a second study known as ARISE, led by David W. Dodick, MD, of the Mayo Clinic, Phoenix, Ariz. This double-blind, 12-week trial randomly assigned 577 adults with episodic migraine to a monthly subcutaneous dose of a placebo or 70 mg of erenumab.
The patients reported an average of 8.3 MMDs at the beginning of the trial. Those who took the medication reported an average 2.9 fewer MMDs while those who took the placebo reported 1.8 fewer MMDs (P less than .001) at 9-12 weeks.
Forty percent of those who took the drug saw a decrease of at least half in MMDs, compared with 30% of those who took placebo (odds ratio, 1.6; P = .010).
The PI levels declined by at least 5 points in 27% of placebo patients and 33% of erenumab patients (P = .13). EA levels declined by at least 5 points in 36% of placebo patients and 40% of erenumab patients (P = .26)
There were similar levels of adverse events in both drug and placebo groups, led by upper respiratory tract infection, injection site pain, and nasopharyngitis.
The Mayo Clinic’s Dr. Starling said anti-CGRP medications may dramatically improve the world of preventive migraine treatments, which are recommended for a third of migraine patients. Only about 3%-13% use them, she said.
In the future, it may be possible to be able to identify and target “super-responders” whose MMDs dip by 75% or more in some cases.
But there are questions, she said. The drugs’ specific mechanism for blocking migraine is not yet clear, and it’s also not clear if the CGRP antagonists could push patients at risk of TIA or cardiac angina to have a stroke instead.
Dr. Starling discussed some of the implications of the CGRP antagonists in development in a video interview.
Both studies were funded by Amgen. Dr. Goadsby reported numerous grants and personal fees from multiple drug makers, including Amgen. Dr. Starling reported support from Amgen, eNeura, and Eli Lilly. Dr. Dodick disclosed many relationships with pharmaceutical companies developing or marketing drugs for headache and migraine, including Amgen.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT AAN 2017

Female predisposition to anxiety disorders may have prenatal origin
SAN FRANCISCO – Why are anxiety disorders twice as prevalent in women as in men? As in Hawaiian hula dancing, the expressive hands may tell the tale.
The ratio of the length of the index finger to ring finger – known as the 2D:4D ratio – is a physical trait that remains stable across the lifetimes of males and females. It’s also a reliable indicator of prenatal exposure to androgens. In female college students, the higher the 2D:4D ratio, the greater their level of ruminative thinking, which is known to be both a risk factor and maintenance factor for anxiety, Ellie Shuo Jin reported at the annual conference of the Anxiety and Depression Association of America.
The findings shed new light on the relationship between testosterone and anxiety disorders, according to Ms. Jin, a doctoral student at the University of Texas, Austin. The hormone previously has been linked to reduced levels of anxiety, an observation consistent with the lower prevalence of anxiety disorders in men. However, it has been unclear whether prenatal exposure to testosterone, which encourages organizational effects, or the activational effects of postnatal exposure to the hormone is most protective against anxiety disorders.
Ms. Jin found that prenatal testosterone exposure as reflected in a low 2D:4D ratio was associated with a lower level of repetitive negative thinking as measured using the Perseverative Thinking Questionnaire but only in the female students.
She reported having no financial conflicts of interest regarding her study.
SAN FRANCISCO – Why are anxiety disorders twice as prevalent in women as in men? As in Hawaiian hula dancing, the expressive hands may tell the tale.
The ratio of the length of the index finger to ring finger – known as the 2D:4D ratio – is a physical trait that remains stable across the lifetimes of males and females. It’s also a reliable indicator of prenatal exposure to androgens. In female college students, the higher the 2D:4D ratio, the greater their level of ruminative thinking, which is known to be both a risk factor and maintenance factor for anxiety, Ellie Shuo Jin reported at the annual conference of the Anxiety and Depression Association of America.
The findings shed new light on the relationship between testosterone and anxiety disorders, according to Ms. Jin, a doctoral student at the University of Texas, Austin. The hormone previously has been linked to reduced levels of anxiety, an observation consistent with the lower prevalence of anxiety disorders in men. However, it has been unclear whether prenatal exposure to testosterone, which encourages organizational effects, or the activational effects of postnatal exposure to the hormone is most protective against anxiety disorders.
Ms. Jin found that prenatal testosterone exposure as reflected in a low 2D:4D ratio was associated with a lower level of repetitive negative thinking as measured using the Perseverative Thinking Questionnaire but only in the female students.
She reported having no financial conflicts of interest regarding her study.
SAN FRANCISCO – Why are anxiety disorders twice as prevalent in women as in men? As in Hawaiian hula dancing, the expressive hands may tell the tale.
The ratio of the length of the index finger to ring finger – known as the 2D:4D ratio – is a physical trait that remains stable across the lifetimes of males and females. It’s also a reliable indicator of prenatal exposure to androgens. In female college students, the higher the 2D:4D ratio, the greater their level of ruminative thinking, which is known to be both a risk factor and maintenance factor for anxiety, Ellie Shuo Jin reported at the annual conference of the Anxiety and Depression Association of America.
The findings shed new light on the relationship between testosterone and anxiety disorders, according to Ms. Jin, a doctoral student at the University of Texas, Austin. The hormone previously has been linked to reduced levels of anxiety, an observation consistent with the lower prevalence of anxiety disorders in men. However, it has been unclear whether prenatal exposure to testosterone, which encourages organizational effects, or the activational effects of postnatal exposure to the hormone is most protective against anxiety disorders.
Ms. Jin found that prenatal testosterone exposure as reflected in a low 2D:4D ratio was associated with a lower level of repetitive negative thinking as measured using the Perseverative Thinking Questionnaire but only in the female students.
She reported having no financial conflicts of interest regarding her study.
AT THE ANXIETY AND DEPRESSION CONFERENCE 2017
Key clinical point:
Major finding: The higher the ratio of the length of the index finger to the ring finger on the left hand, the greater the predisposition to repetitive negative thinking in women but not in men.
Data source: This cross-sectional study correlated the 2D:4D digit ratio to levels of repetitive negative thinking in 103 college students.
Disclosures: The presenter reported having no financial conflicts regarding her study.
What’s Eating You? Chiggers
Identifying Characteristics and Disease Transmission
Chiggers belong to the Trombiculidae family of mites and also are referred to as harvest mites, harvest bugs, harvest lice, mower’s mites, and redbugs.1 The term chigger specifically describes the larval stage of this mite’s life cycle, as it is the only stage responsible for chigger bites. The nymph and adult phases feed on vegetable matter. Trombiculid mites are most often found in forests, grassy areas, gardens, and moist areas of soil near bodies of water. Trombicula alfreddugesi is the most common species in the United States, and these mites mainly live in the southeastern and south central regions of the country. Conversely, Trombicula autumnalis is most predominant in Western Europe and East Asia.1
The life cycle of the mite includes the egg, larval, nymphal, and adult stages.2 Due to their need for air humidity greater than 80%, mites lay their eggs on low leaves, blades of grass, or on the ground. They spend most of their lives on vegetation no more than 30 cm above ground level.3 Eggs remain dormant for approximately 6 days until the hatching of the prelarvae, which have 6 legs and are nonfeeding. It takes another 6 days for the prelarvae to mature into larvae. Measuring 0.15 to 0.3 mm in length, mite larvae are a mere fraction of the size of adult mites, which generally are 1 to 2 mm in length, and are bright red or brown-red in color (Figure 1).

The biting larvae have many acceptable hosts including turtles, toads, birds, small mammals, and humans, which act as accidental hosts. Larvae remain on vegetation waiting for a suitable host to pass by so they may attach to its skin and remain there for several days. In the exploration for an ideal area to begin feeding (eg, thin epidermis,4 localized increased air humidity5), larvae can travel extensively on the skin; however, they often are stopped by tight-fitting sections of clothing (eg, waistbands), so bites are mostly found in clusters. To feed, mite larvae latch onto the skin using chelicerae, jawlike appendages found in the front of the mouth in arachnids.6 They then inject digestive enzymes that liquefy epidermal cells on direct contact, which results in the formation of a stylostome from which the mites may suck up lymph fluid and broken down tissue.7 Although the actual initial bite is painless, this feeding process leads to the localized inflammation and irritation noticed by infested patients.8
The classic clinical presentation includes severe pruritus and cutaneous swelling as well as erythema caused by the combination of several factors, such as enzyme-induced cellular mechanical damage, human immune response, and sometimes a superimposed bacterial infection. Papules and papulovesicles appear in groups, most commonly affecting the legs and waistline (Figure 2).9 Itching generally occurs within hours of larval latching and subsides within 72 hours. Cutaneous lesions typically take 1 to 2 weeks to heal. In some rare cases, patients may react with urticarial, bullous, or morbilliform eruptions, and the inflammation and pruritus can last for weeks.6 Summer penile syndrome has been noted in boys who display a local hypersensitivity to chigger bites.10 This syndrome represents a triad of penile swelling, dysuria, and pruritus, which lasts for a few days to a few weeks.

Disease Management
Because the lesions are self-healing, treatment is focused on symptomatic relief of itching by means of topical antipruritics (eg, camphor and menthol, pramoxine lotion) or oral antihistamines (eg, diphenhydramine, hydroxyzine). Potent topical corticosteroids may be used to alleviate inflammation and pruritus, especially when occluded under plastic wrap to increase absorption. In severe cases, an intralesional triamcinolone acetonide (2.5–5 mg/mL) injection may be required.9 The best practice, however, is to take preventative measures to avoid becoming a host for the mites. Patients should take special care when traveling in infested areas by completely covering their skin, tucking pant cuffs into their socks, and applying products containing DEET (N,N-diethyl-meta-toluamide or N,N-diethyl-3-methylbenzamide) to the skin and clothing. The odds of prevention are increased even further when clothing also is treated with permethrin.11
In parts of Asia and Australia, these mites may transmit Orientia tsutsugamushi, the organism responsible for scrub typhus, through their saliva during a bite.12 Scrub typhus is associated with an eschar, as well as fever, intense headache, and diffuse myalgia. It responds well to treatment with doxycycline 100 mg twice daily.13 Studies investigating genetic material found in trombiculid mites across the globe have detected Ehrlichia-specific DNA in Spain,14Borrelia-specific DNA in the Czech Republic,15,16 and Hantavirus-specific RNA in Texas.17 There is evidence that the mites play a role in maintenance of zoonotic reservoirs, while humans are infected via ingestion or inhalation of infectious rodent extreta.18
- McClain D, Dana AN, Goldenberg G. Mite infestations. Dermatol Ther. 2009;22:327-346.
- Lane RP, Crosskey RW. Medical Insects and Arachnids. London, England: Chapman & Hall; 1993.
- Gasser R, Wyniger R. Distribution and control of Trombiculidae with special reference to Trombicula autumnalis [article in German]. Acta Trop. 1955;12:308-326.
- Jones BM. The penetration of the host tissue by the harvest mite, Trombicula autumnalis Shaw. Parasitology. 1950;40:247-260.
- Farkas J. Concerning the predilected localisation of the manifestations of trombidiosis. predilected localisation and its relation to the ways of invasion [article in German]. Dermatol Monatsschr. 1979;165:858-861.
- Jones JG. Chiggers. Am Fam Physician. 1987;36:149-152.
- Shatrov AB. Stylostome formation in trombiculid mites (Acariformes: Trombiculidae). Exp Appl Acarol. 2009;49:261-280.
- Potts J. Eradication of ectoparasites in children. how to treat infestations of lice, scabies, and chiggers. Postgrad Med. 2001;110:57-59, 63-64.
- Elston DM. Arthropods and infestations. Infectious Diseases of the Skin. Boca Raton, FL; CRC Press; 2009:112-116.
- Smith GA, Sharma V, Knapp JF, et al. The summer penile syndrome: seasonal acute hypersensitivity reaction caused by chigger bites on the penis. Pediatr Emerg Care. 1998;14:116-118.
- Young GD, Evans S. Safety of DEET and permethrin in the prevention of arthropod attack. Military Med. 1998;163:324-330.
- Watt G, Parola P. Scrub typhus and tropical rickettsioses. Curr Opin Infect Dis. 2003;16:429-436.
- Panpanich R, Garner P. Antibiotics for treating scrub typhus. Cochrane Database Syst Rev. 2000;2:CD002150.
- Fernández-Soto P, Pérez-Sánchez R, Encinas-Grandes A. Molecular detection of Ehrlichia phagocytophila genogroup organisms in larvae of Neotrombicula autumnalis (Acari: Trombiculidae) captured in Spain. J Parasitol. 2001;87:1482-1483.
- Literak I, Stekolnikov AA, Sychra O, et al. Larvae of chigger mites Neotrombicula spp. (Acari: Trombiculidae) exhibited Borrelia but no Anaplasma infections: a field study including birds from the Czech Carpathians as hosts of chiggers. Exp Appl Acarol. 2008;44:307-314.
- Kampen H, Schöler A, Metzen M, et al. Neotrombicula autumnalis (Acari, Trombiculidae) as a vector for Borrelia burgdorferi sensu lato? Exp Appl Acarol. 2004;33:93-102.
- Houck MA, Qin H, Roberts HR. Hantavirus transmission: potential role of ectoparasites. Vector Borne Zoonotic Dis. 2001;1:75-79.
- Yu XJ, Tesh RB. The role of mites in the transmission and maintenance of Hantaan virus (Hantavirus: Bunyaviridae). J Infect Dis. 2014;210:1693-1699.
Identifying Characteristics and Disease Transmission
Chiggers belong to the Trombiculidae family of mites and also are referred to as harvest mites, harvest bugs, harvest lice, mower’s mites, and redbugs.1 The term chigger specifically describes the larval stage of this mite’s life cycle, as it is the only stage responsible for chigger bites. The nymph and adult phases feed on vegetable matter. Trombiculid mites are most often found in forests, grassy areas, gardens, and moist areas of soil near bodies of water. Trombicula alfreddugesi is the most common species in the United States, and these mites mainly live in the southeastern and south central regions of the country. Conversely, Trombicula autumnalis is most predominant in Western Europe and East Asia.1
The life cycle of the mite includes the egg, larval, nymphal, and adult stages.2 Due to their need for air humidity greater than 80%, mites lay their eggs on low leaves, blades of grass, or on the ground. They spend most of their lives on vegetation no more than 30 cm above ground level.3 Eggs remain dormant for approximately 6 days until the hatching of the prelarvae, which have 6 legs and are nonfeeding. It takes another 6 days for the prelarvae to mature into larvae. Measuring 0.15 to 0.3 mm in length, mite larvae are a mere fraction of the size of adult mites, which generally are 1 to 2 mm in length, and are bright red or brown-red in color (Figure 1).
The biting larvae have many acceptable hosts including turtles, toads, birds, small mammals, and humans, which act as accidental hosts. Larvae remain on vegetation waiting for a suitable host to pass by so they may attach to its skin and remain there for several days. In the exploration for an ideal area to begin feeding (eg, thin epidermis,4 localized increased air humidity5), larvae can travel extensively on the skin; however, they often are stopped by tight-fitting sections of clothing (eg, waistbands), so bites are mostly found in clusters. To feed, mite larvae latch onto the skin using chelicerae, jawlike appendages found in the front of the mouth in arachnids.6 They then inject digestive enzymes that liquefy epidermal cells on direct contact, which results in the formation of a stylostome from which the mites may suck up lymph fluid and broken down tissue.7 Although the actual initial bite is painless, this feeding process leads to the localized inflammation and irritation noticed by infested patients.8
The classic clinical presentation includes severe pruritus and cutaneous swelling as well as erythema caused by the combination of several factors, such as enzyme-induced cellular mechanical damage, human immune response, and sometimes a superimposed bacterial infection. Papules and papulovesicles appear in groups, most commonly affecting the legs and waistline (Figure 2).9 Itching generally occurs within hours of larval latching and subsides within 72 hours. Cutaneous lesions typically take 1 to 2 weeks to heal. In some rare cases, patients may react with urticarial, bullous, or morbilliform eruptions, and the inflammation and pruritus can last for weeks.6 Summer penile syndrome has been noted in boys who display a local hypersensitivity to chigger bites.10 This syndrome represents a triad of penile swelling, dysuria, and pruritus, which lasts for a few days to a few weeks.
Disease Management
Because the lesions are self-healing, treatment is focused on symptomatic relief of itching by means of topical antipruritics (eg, camphor and menthol, pramoxine lotion) or oral antihistamines (eg, diphenhydramine, hydroxyzine). Potent topical corticosteroids may be used to alleviate inflammation and pruritus, especially when occluded under plastic wrap to increase absorption. In severe cases, an intralesional triamcinolone acetonide (2.5–5 mg/mL) injection may be required.9 The best practice, however, is to take preventative measures to avoid becoming a host for the mites. Patients should take special care when traveling in infested areas by completely covering their skin, tucking pant cuffs into their socks, and applying products containing DEET (N,N-diethyl-meta-toluamide or N,N-diethyl-3-methylbenzamide) to the skin and clothing. The odds of prevention are increased even further when clothing also is treated with permethrin.11
In parts of Asia and Australia, these mites may transmit Orientia tsutsugamushi, the organism responsible for scrub typhus, through their saliva during a bite.12 Scrub typhus is associated with an eschar, as well as fever, intense headache, and diffuse myalgia. It responds well to treatment with doxycycline 100 mg twice daily.13 Studies investigating genetic material found in trombiculid mites across the globe have detected Ehrlichia-specific DNA in Spain,14Borrelia-specific DNA in the Czech Republic,15,16 and Hantavirus-specific RNA in Texas.17 There is evidence that the mites play a role in maintenance of zoonotic reservoirs, while humans are infected via ingestion or inhalation of infectious rodent extreta.18
Identifying Characteristics and Disease Transmission
Chiggers belong to the Trombiculidae family of mites and also are referred to as harvest mites, harvest bugs, harvest lice, mower’s mites, and redbugs.1 The term chigger specifically describes the larval stage of this mite’s life cycle, as it is the only stage responsible for chigger bites. The nymph and adult phases feed on vegetable matter. Trombiculid mites are most often found in forests, grassy areas, gardens, and moist areas of soil near bodies of water. Trombicula alfreddugesi is the most common species in the United States, and these mites mainly live in the southeastern and south central regions of the country. Conversely, Trombicula autumnalis is most predominant in Western Europe and East Asia.1
The life cycle of the mite includes the egg, larval, nymphal, and adult stages.2 Due to their need for air humidity greater than 80%, mites lay their eggs on low leaves, blades of grass, or on the ground. They spend most of their lives on vegetation no more than 30 cm above ground level.3 Eggs remain dormant for approximately 6 days until the hatching of the prelarvae, which have 6 legs and are nonfeeding. It takes another 6 days for the prelarvae to mature into larvae. Measuring 0.15 to 0.3 mm in length, mite larvae are a mere fraction of the size of adult mites, which generally are 1 to 2 mm in length, and are bright red or brown-red in color (Figure 1).
The biting larvae have many acceptable hosts including turtles, toads, birds, small mammals, and humans, which act as accidental hosts. Larvae remain on vegetation waiting for a suitable host to pass by so they may attach to its skin and remain there for several days. In the exploration for an ideal area to begin feeding (eg, thin epidermis,4 localized increased air humidity5), larvae can travel extensively on the skin; however, they often are stopped by tight-fitting sections of clothing (eg, waistbands), so bites are mostly found in clusters. To feed, mite larvae latch onto the skin using chelicerae, jawlike appendages found in the front of the mouth in arachnids.6 They then inject digestive enzymes that liquefy epidermal cells on direct contact, which results in the formation of a stylostome from which the mites may suck up lymph fluid and broken down tissue.7 Although the actual initial bite is painless, this feeding process leads to the localized inflammation and irritation noticed by infested patients.8
The classic clinical presentation includes severe pruritus and cutaneous swelling as well as erythema caused by the combination of several factors, such as enzyme-induced cellular mechanical damage, human immune response, and sometimes a superimposed bacterial infection. Papules and papulovesicles appear in groups, most commonly affecting the legs and waistline (Figure 2).9 Itching generally occurs within hours of larval latching and subsides within 72 hours. Cutaneous lesions typically take 1 to 2 weeks to heal. In some rare cases, patients may react with urticarial, bullous, or morbilliform eruptions, and the inflammation and pruritus can last for weeks.6 Summer penile syndrome has been noted in boys who display a local hypersensitivity to chigger bites.10 This syndrome represents a triad of penile swelling, dysuria, and pruritus, which lasts for a few days to a few weeks.
Disease Management
Because the lesions are self-healing, treatment is focused on symptomatic relief of itching by means of topical antipruritics (eg, camphor and menthol, pramoxine lotion) or oral antihistamines (eg, diphenhydramine, hydroxyzine). Potent topical corticosteroids may be used to alleviate inflammation and pruritus, especially when occluded under plastic wrap to increase absorption. In severe cases, an intralesional triamcinolone acetonide (2.5–5 mg/mL) injection may be required.9 The best practice, however, is to take preventative measures to avoid becoming a host for the mites. Patients should take special care when traveling in infested areas by completely covering their skin, tucking pant cuffs into their socks, and applying products containing DEET (N,N-diethyl-meta-toluamide or N,N-diethyl-3-methylbenzamide) to the skin and clothing. The odds of prevention are increased even further when clothing also is treated with permethrin.11
In parts of Asia and Australia, these mites may transmit Orientia tsutsugamushi, the organism responsible for scrub typhus, through their saliva during a bite.12 Scrub typhus is associated with an eschar, as well as fever, intense headache, and diffuse myalgia. It responds well to treatment with doxycycline 100 mg twice daily.13 Studies investigating genetic material found in trombiculid mites across the globe have detected Ehrlichia-specific DNA in Spain,14Borrelia-specific DNA in the Czech Republic,15,16 and Hantavirus-specific RNA in Texas.17 There is evidence that the mites play a role in maintenance of zoonotic reservoirs, while humans are infected via ingestion or inhalation of infectious rodent extreta.18
- McClain D, Dana AN, Goldenberg G. Mite infestations. Dermatol Ther. 2009;22:327-346.
- Lane RP, Crosskey RW. Medical Insects and Arachnids. London, England: Chapman & Hall; 1993.
- Gasser R, Wyniger R. Distribution and control of Trombiculidae with special reference to Trombicula autumnalis [article in German]. Acta Trop. 1955;12:308-326.
- Jones BM. The penetration of the host tissue by the harvest mite, Trombicula autumnalis Shaw. Parasitology. 1950;40:247-260.
- Farkas J. Concerning the predilected localisation of the manifestations of trombidiosis. predilected localisation and its relation to the ways of invasion [article in German]. Dermatol Monatsschr. 1979;165:858-861.
- Jones JG. Chiggers. Am Fam Physician. 1987;36:149-152.
- Shatrov AB. Stylostome formation in trombiculid mites (Acariformes: Trombiculidae). Exp Appl Acarol. 2009;49:261-280.
- Potts J. Eradication of ectoparasites in children. how to treat infestations of lice, scabies, and chiggers. Postgrad Med. 2001;110:57-59, 63-64.
- Elston DM. Arthropods and infestations. Infectious Diseases of the Skin. Boca Raton, FL; CRC Press; 2009:112-116.
- Smith GA, Sharma V, Knapp JF, et al. The summer penile syndrome: seasonal acute hypersensitivity reaction caused by chigger bites on the penis. Pediatr Emerg Care. 1998;14:116-118.
- Young GD, Evans S. Safety of DEET and permethrin in the prevention of arthropod attack. Military Med. 1998;163:324-330.
- Watt G, Parola P. Scrub typhus and tropical rickettsioses. Curr Opin Infect Dis. 2003;16:429-436.
- Panpanich R, Garner P. Antibiotics for treating scrub typhus. Cochrane Database Syst Rev. 2000;2:CD002150.
- Fernández-Soto P, Pérez-Sánchez R, Encinas-Grandes A. Molecular detection of Ehrlichia phagocytophila genogroup organisms in larvae of Neotrombicula autumnalis (Acari: Trombiculidae) captured in Spain. J Parasitol. 2001;87:1482-1483.
- Literak I, Stekolnikov AA, Sychra O, et al. Larvae of chigger mites Neotrombicula spp. (Acari: Trombiculidae) exhibited Borrelia but no Anaplasma infections: a field study including birds from the Czech Carpathians as hosts of chiggers. Exp Appl Acarol. 2008;44:307-314.
- Kampen H, Schöler A, Metzen M, et al. Neotrombicula autumnalis (Acari, Trombiculidae) as a vector for Borrelia burgdorferi sensu lato? Exp Appl Acarol. 2004;33:93-102.
- Houck MA, Qin H, Roberts HR. Hantavirus transmission: potential role of ectoparasites. Vector Borne Zoonotic Dis. 2001;1:75-79.
- Yu XJ, Tesh RB. The role of mites in the transmission and maintenance of Hantaan virus (Hantavirus: Bunyaviridae). J Infect Dis. 2014;210:1693-1699.
- McClain D, Dana AN, Goldenberg G. Mite infestations. Dermatol Ther. 2009;22:327-346.
- Lane RP, Crosskey RW. Medical Insects and Arachnids. London, England: Chapman & Hall; 1993.
- Gasser R, Wyniger R. Distribution and control of Trombiculidae with special reference to Trombicula autumnalis [article in German]. Acta Trop. 1955;12:308-326.
- Jones BM. The penetration of the host tissue by the harvest mite, Trombicula autumnalis Shaw. Parasitology. 1950;40:247-260.
- Farkas J. Concerning the predilected localisation of the manifestations of trombidiosis. predilected localisation and its relation to the ways of invasion [article in German]. Dermatol Monatsschr. 1979;165:858-861.
- Jones JG. Chiggers. Am Fam Physician. 1987;36:149-152.
- Shatrov AB. Stylostome formation in trombiculid mites (Acariformes: Trombiculidae). Exp Appl Acarol. 2009;49:261-280.
- Potts J. Eradication of ectoparasites in children. how to treat infestations of lice, scabies, and chiggers. Postgrad Med. 2001;110:57-59, 63-64.
- Elston DM. Arthropods and infestations. Infectious Diseases of the Skin. Boca Raton, FL; CRC Press; 2009:112-116.
- Smith GA, Sharma V, Knapp JF, et al. The summer penile syndrome: seasonal acute hypersensitivity reaction caused by chigger bites on the penis. Pediatr Emerg Care. 1998;14:116-118.
- Young GD, Evans S. Safety of DEET and permethrin in the prevention of arthropod attack. Military Med. 1998;163:324-330.
- Watt G, Parola P. Scrub typhus and tropical rickettsioses. Curr Opin Infect Dis. 2003;16:429-436.
- Panpanich R, Garner P. Antibiotics for treating scrub typhus. Cochrane Database Syst Rev. 2000;2:CD002150.
- Fernández-Soto P, Pérez-Sánchez R, Encinas-Grandes A. Molecular detection of Ehrlichia phagocytophila genogroup organisms in larvae of Neotrombicula autumnalis (Acari: Trombiculidae) captured in Spain. J Parasitol. 2001;87:1482-1483.
- Literak I, Stekolnikov AA, Sychra O, et al. Larvae of chigger mites Neotrombicula spp. (Acari: Trombiculidae) exhibited Borrelia but no Anaplasma infections: a field study including birds from the Czech Carpathians as hosts of chiggers. Exp Appl Acarol. 2008;44:307-314.
- Kampen H, Schöler A, Metzen M, et al. Neotrombicula autumnalis (Acari, Trombiculidae) as a vector for Borrelia burgdorferi sensu lato? Exp Appl Acarol. 2004;33:93-102.
- Houck MA, Qin H, Roberts HR. Hantavirus transmission: potential role of ectoparasites. Vector Borne Zoonotic Dis. 2001;1:75-79.
- Yu XJ, Tesh RB. The role of mites in the transmission and maintenance of Hantaan virus (Hantavirus: Bunyaviridae). J Infect Dis. 2014;210:1693-1699.
Practice Points
- The classic clinical presentation of chigger bites includes severe pruritus, cutaneous swelling, and erythematous papules and papulovesicles appearing in groups, most commonly affecting the legs and waistline.
- Because itching generally subsides within 72 hours of the chigger bite and cutaneous lesions typically heal within 1 to 2 weeks, treatment is focused on symptomatic relief.
- Symptomatic relief may be achieved by means of topical antipruritics or oral antihistamines as well as potent topical corticosteroids or an intralesional triamcinolone acetonide injection in severe cases.

NOTCH1 mutation predicts reduced ofatumumab efficacy in CLL
NEW YORK – NOTCH1 gene mutation appears to predict reduced efficacy of ofatumumab in patients with relapsed/refractory chronic lymphocytic leukemia, according to an analysis of patient DNA samples and data from the phase III COMPLEMENT 2 trial.
Recurrent mutations in NOTCH1, TP53, and SF3B1 are common in CLL and have been associated with adverse outcomes in previous studies; NOTCH1 mutation, in particular, was associated with poor outcome when rituximab was added to standard chemotherapy, indicating that the mutation is a predictive factor in the context of chemoimmunotherapy, Eugen Tausch, MD, of the University of Ulm, Germany, said at the annual International Workshop on Chronic Lymphocytic Leukemia.
The incidence and clinical impact of all three mutations were evaluated in relapsed/refractory CLL patients who were part of the COMPLEMENT 2 trial, which compared fludarabine and cyclophosphamide (FC) with FC+ofatumumab (FCO).
The mutation analysis of 325 available patient samples (out of 365) identified 221 mutations in 142 patients: 56 NOTCH1, 96 TP53, and 69 SF3B1 mutations, Dr. Tausch said.
The current study cohort was representative of the full COMPLEMENT 2 analysis set, he noted.
Additional TP53 mutations were found in 20 of 61 TP53 mutation patients, whereas only 4 of 64 SF3B1 mutation patients and 3 of 53 NOTCH1 mutation patients had additional mutations in SF3B1 and NOTCH1, respectively. TP53 mutation was associated with del(17p), and NOTCH1 mutation with +12q and elevated b2MG.
“We did not find associations with IGHV, gender, age, Binet stage, ECOG performance state, B symptoms, or WBC,” Dr. Tausch said.
In terms of outcomes as associated with the mutations, patients with TP53 mutation or SF3B1 mutation had a significantly worse overall response to treatment (overall response rate 67.8% vs. 84.4% for TP53 mutated vs. wild type, and 71.9% vs. 83.75% SF3B1 mutated vs. wild type, respectively). The findings were similar when looking at the treatment arms separately, he noted.
However, as in the full analysis set, progression-free survival among the subset of patients included in the current analysis was better in those who received FCO than in those who received FC (28.1 months vs. 18.1 months; hazard ratio, 0.67). TP53 mutation was an adverse prognostic factor overall in the current analysis (HR, 1.93), as well as in each treatment arm (HR for the FC arm, 2.14, and for the FCO arm, 1.81). TP53 mutation also was associated with decreased overall survival (HR, 2.11). Neither SF3B1 mutation nor NOTCH1 mutation were associated with differences in progression-free or overall survival, Dr. Tausch said.
CD20 expression on cell surface as measured using flow cytometry did not differ in wild-type vs. mutated patients, he said.
Multivariate analysis showed that independent prognostic factors for progression-free survival included FCO therapy (HR, 0.66), del(17p) (HR, 4.47), unmutated IGHV (HR, 2.17), and TP53 mutation (HR, 1.80), and independent prognostic factors for overall survival included del(17p) (HR, 5.02), unmutated IGHV (HR, 1.85), and TP53 mutation (HR, 1.68).
Adding ofatumumab to chemotherapy was beneficial, irrespective of TP53 mutation (HR, 0.52 for TP53 mutation, and HR, 0.68 for TP53 wild type), which confirms the prognostic value of TP53 mutation, he said.
With respect to NOTCH1, ofatumumab was beneficial in patients with NOTCH1 wild type but not in patients with NOTCH1 mutation (HR, 0.64 and 0.86, respectively).
This effect was not explained by CD20 expression levels, Dr. Tausch said.
The findings of this analysis suggest that NOTCH1 mutation is an independent predictive factor for reduced efficacy of ofatumumab, he said.
“Therefore, patients with a NOTCH1 mutation may be considered for chemotherapy without type1 CD20 antibodies or a treatment with novel compounds,” he concluded.
Dr. Tausch reported receiving research support from Novartis.
NEW YORK – NOTCH1 gene mutation appears to predict reduced efficacy of ofatumumab in patients with relapsed/refractory chronic lymphocytic leukemia, according to an analysis of patient DNA samples and data from the phase III COMPLEMENT 2 trial.
Recurrent mutations in NOTCH1, TP53, and SF3B1 are common in CLL and have been associated with adverse outcomes in previous studies; NOTCH1 mutation, in particular, was associated with poor outcome when rituximab was added to standard chemotherapy, indicating that the mutation is a predictive factor in the context of chemoimmunotherapy, Eugen Tausch, MD, of the University of Ulm, Germany, said at the annual International Workshop on Chronic Lymphocytic Leukemia.
The incidence and clinical impact of all three mutations were evaluated in relapsed/refractory CLL patients who were part of the COMPLEMENT 2 trial, which compared fludarabine and cyclophosphamide (FC) with FC+ofatumumab (FCO).
The mutation analysis of 325 available patient samples (out of 365) identified 221 mutations in 142 patients: 56 NOTCH1, 96 TP53, and 69 SF3B1 mutations, Dr. Tausch said.
The current study cohort was representative of the full COMPLEMENT 2 analysis set, he noted.
Additional TP53 mutations were found in 20 of 61 TP53 mutation patients, whereas only 4 of 64 SF3B1 mutation patients and 3 of 53 NOTCH1 mutation patients had additional mutations in SF3B1 and NOTCH1, respectively. TP53 mutation was associated with del(17p), and NOTCH1 mutation with +12q and elevated b2MG.
“We did not find associations with IGHV, gender, age, Binet stage, ECOG performance state, B symptoms, or WBC,” Dr. Tausch said.
In terms of outcomes as associated with the mutations, patients with TP53 mutation or SF3B1 mutation had a significantly worse overall response to treatment (overall response rate 67.8% vs. 84.4% for TP53 mutated vs. wild type, and 71.9% vs. 83.75% SF3B1 mutated vs. wild type, respectively). The findings were similar when looking at the treatment arms separately, he noted.
However, as in the full analysis set, progression-free survival among the subset of patients included in the current analysis was better in those who received FCO than in those who received FC (28.1 months vs. 18.1 months; hazard ratio, 0.67). TP53 mutation was an adverse prognostic factor overall in the current analysis (HR, 1.93), as well as in each treatment arm (HR for the FC arm, 2.14, and for the FCO arm, 1.81). TP53 mutation also was associated with decreased overall survival (HR, 2.11). Neither SF3B1 mutation nor NOTCH1 mutation were associated with differences in progression-free or overall survival, Dr. Tausch said.
CD20 expression on cell surface as measured using flow cytometry did not differ in wild-type vs. mutated patients, he said.
Multivariate analysis showed that independent prognostic factors for progression-free survival included FCO therapy (HR, 0.66), del(17p) (HR, 4.47), unmutated IGHV (HR, 2.17), and TP53 mutation (HR, 1.80), and independent prognostic factors for overall survival included del(17p) (HR, 5.02), unmutated IGHV (HR, 1.85), and TP53 mutation (HR, 1.68).
Adding ofatumumab to chemotherapy was beneficial, irrespective of TP53 mutation (HR, 0.52 for TP53 mutation, and HR, 0.68 for TP53 wild type), which confirms the prognostic value of TP53 mutation, he said.
With respect to NOTCH1, ofatumumab was beneficial in patients with NOTCH1 wild type but not in patients with NOTCH1 mutation (HR, 0.64 and 0.86, respectively).
This effect was not explained by CD20 expression levels, Dr. Tausch said.
The findings of this analysis suggest that NOTCH1 mutation is an independent predictive factor for reduced efficacy of ofatumumab, he said.
“Therefore, patients with a NOTCH1 mutation may be considered for chemotherapy without type1 CD20 antibodies or a treatment with novel compounds,” he concluded.
Dr. Tausch reported receiving research support from Novartis.
NEW YORK – NOTCH1 gene mutation appears to predict reduced efficacy of ofatumumab in patients with relapsed/refractory chronic lymphocytic leukemia, according to an analysis of patient DNA samples and data from the phase III COMPLEMENT 2 trial.
Recurrent mutations in NOTCH1, TP53, and SF3B1 are common in CLL and have been associated with adverse outcomes in previous studies; NOTCH1 mutation, in particular, was associated with poor outcome when rituximab was added to standard chemotherapy, indicating that the mutation is a predictive factor in the context of chemoimmunotherapy, Eugen Tausch, MD, of the University of Ulm, Germany, said at the annual International Workshop on Chronic Lymphocytic Leukemia.
The incidence and clinical impact of all three mutations were evaluated in relapsed/refractory CLL patients who were part of the COMPLEMENT 2 trial, which compared fludarabine and cyclophosphamide (FC) with FC+ofatumumab (FCO).
The mutation analysis of 325 available patient samples (out of 365) identified 221 mutations in 142 patients: 56 NOTCH1, 96 TP53, and 69 SF3B1 mutations, Dr. Tausch said.
The current study cohort was representative of the full COMPLEMENT 2 analysis set, he noted.
Additional TP53 mutations were found in 20 of 61 TP53 mutation patients, whereas only 4 of 64 SF3B1 mutation patients and 3 of 53 NOTCH1 mutation patients had additional mutations in SF3B1 and NOTCH1, respectively. TP53 mutation was associated with del(17p), and NOTCH1 mutation with +12q and elevated b2MG.
“We did not find associations with IGHV, gender, age, Binet stage, ECOG performance state, B symptoms, or WBC,” Dr. Tausch said.
In terms of outcomes as associated with the mutations, patients with TP53 mutation or SF3B1 mutation had a significantly worse overall response to treatment (overall response rate 67.8% vs. 84.4% for TP53 mutated vs. wild type, and 71.9% vs. 83.75% SF3B1 mutated vs. wild type, respectively). The findings were similar when looking at the treatment arms separately, he noted.
However, as in the full analysis set, progression-free survival among the subset of patients included in the current analysis was better in those who received FCO than in those who received FC (28.1 months vs. 18.1 months; hazard ratio, 0.67). TP53 mutation was an adverse prognostic factor overall in the current analysis (HR, 1.93), as well as in each treatment arm (HR for the FC arm, 2.14, and for the FCO arm, 1.81). TP53 mutation also was associated with decreased overall survival (HR, 2.11). Neither SF3B1 mutation nor NOTCH1 mutation were associated with differences in progression-free or overall survival, Dr. Tausch said.
CD20 expression on cell surface as measured using flow cytometry did not differ in wild-type vs. mutated patients, he said.
Multivariate analysis showed that independent prognostic factors for progression-free survival included FCO therapy (HR, 0.66), del(17p) (HR, 4.47), unmutated IGHV (HR, 2.17), and TP53 mutation (HR, 1.80), and independent prognostic factors for overall survival included del(17p) (HR, 5.02), unmutated IGHV (HR, 1.85), and TP53 mutation (HR, 1.68).
Adding ofatumumab to chemotherapy was beneficial, irrespective of TP53 mutation (HR, 0.52 for TP53 mutation, and HR, 0.68 for TP53 wild type), which confirms the prognostic value of TP53 mutation, he said.
With respect to NOTCH1, ofatumumab was beneficial in patients with NOTCH1 wild type but not in patients with NOTCH1 mutation (HR, 0.64 and 0.86, respectively).
This effect was not explained by CD20 expression levels, Dr. Tausch said.
The findings of this analysis suggest that NOTCH1 mutation is an independent predictive factor for reduced efficacy of ofatumumab, he said.
“Therefore, patients with a NOTCH1 mutation may be considered for chemotherapy without type1 CD20 antibodies or a treatment with novel compounds,” he concluded.
Dr. Tausch reported receiving research support from Novartis.
AT iwCLL MEETING
Key clinical point:
Major finding: Ofatumumab was beneficial in patients with NOTCH1 wild-type, but not in patients with NOTCH1 mutation (hazard ratios, 0.64 and 0.86, respectively).
Data source: A mutation analysis of 325 DNA samples from patients in the phase III COMPLEMENT 2 trial.
Disclosures: Dr. Tausch reported receiving research support from Novartis.
For Americans, less salt is still too much
Americans are buying less packaged food and beverages these days, and they’re getting less salt in the food that they do buy, but very few are getting the optimal sodium density in their purchases, according to a study involving more than 170,000 households.
First, salt content: In 2014, the households taking part in the Nielsen Homescan Consumer Panel were getting 361 mg of salt per 100 g of packaged food purchased, which is 12% less than the 411 mg per 100 g of food purchased in 2000. Overall sodium content, which includes beverages, dropped from 192 mg/100 g to 186 mg/100 g, said Jennifer M. Poti, PhD, of the University of North Carolina at Chapel Hill, and her associates.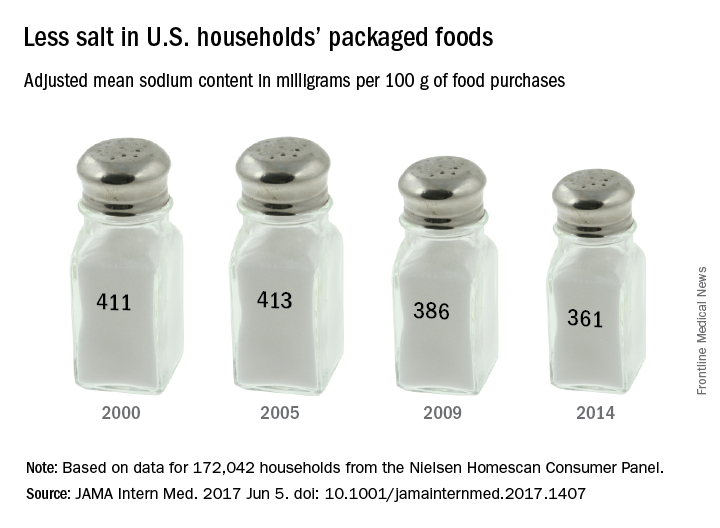
Total food and beverage purchases also were down from 1,328 g/day in 2000 to 1,134 in 2014, and the total sodium content of those purchases followed suit, dropping from 2,363 mg/day in 2000 to 1,967 mg/day in 2014. The decline in total purchases, however, was driven largely by beverages, which fell 21% from 2000 to 2014, while packaged food purchases fell by only 2%, the investigators reported (JAMA Intern Med. 2017 June 5. doi: 10.1001/jamainternmed.2017.1407).
Median sodium density was down significantly from 1,712 to 1,628 mg of sodium per 1,000 kcal, but by 2014, only 1.2% of the 172,042 households included in the study were purchasing the optimal level of 1,100 mg per 1,000 kcal, based on the DASH-Sodium trial and the Health Eating Index-2010, Dr. Poti and her associates said.
“Additional studies are needed to examine whether decreases in sodium from packaged foods were offset by increases in sodium from away-from-home sources,” they said, and since “there were no major shifts in the amount purchased for key food groups … sodium declines may relate mainly to reformulation.”
The study was funded by the Robert Wood Johnson Foundation, the National Institutes of Health, and the Carolina Population Center at the University of North Carolina. One of the investigators is supported by a National Health and Medical Research Council of Australia Early Career Fellowship. The investigators did not report any conflicts of interest.
Americans are buying less packaged food and beverages these days, and they’re getting less salt in the food that they do buy, but very few are getting the optimal sodium density in their purchases, according to a study involving more than 170,000 households.
First, salt content: In 2014, the households taking part in the Nielsen Homescan Consumer Panel were getting 361 mg of salt per 100 g of packaged food purchased, which is 12% less than the 411 mg per 100 g of food purchased in 2000. Overall sodium content, which includes beverages, dropped from 192 mg/100 g to 186 mg/100 g, said Jennifer M. Poti, PhD, of the University of North Carolina at Chapel Hill, and her associates.
Total food and beverage purchases also were down from 1,328 g/day in 2000 to 1,134 in 2014, and the total sodium content of those purchases followed suit, dropping from 2,363 mg/day in 2000 to 1,967 mg/day in 2014. The decline in total purchases, however, was driven largely by beverages, which fell 21% from 2000 to 2014, while packaged food purchases fell by only 2%, the investigators reported (JAMA Intern Med. 2017 June 5. doi: 10.1001/jamainternmed.2017.1407).
Median sodium density was down significantly from 1,712 to 1,628 mg of sodium per 1,000 kcal, but by 2014, only 1.2% of the 172,042 households included in the study were purchasing the optimal level of 1,100 mg per 1,000 kcal, based on the DASH-Sodium trial and the Health Eating Index-2010, Dr. Poti and her associates said.
“Additional studies are needed to examine whether decreases in sodium from packaged foods were offset by increases in sodium from away-from-home sources,” they said, and since “there were no major shifts in the amount purchased for key food groups … sodium declines may relate mainly to reformulation.”
The study was funded by the Robert Wood Johnson Foundation, the National Institutes of Health, and the Carolina Population Center at the University of North Carolina. One of the investigators is supported by a National Health and Medical Research Council of Australia Early Career Fellowship. The investigators did not report any conflicts of interest.
Americans are buying less packaged food and beverages these days, and they’re getting less salt in the food that they do buy, but very few are getting the optimal sodium density in their purchases, according to a study involving more than 170,000 households.
First, salt content: In 2014, the households taking part in the Nielsen Homescan Consumer Panel were getting 361 mg of salt per 100 g of packaged food purchased, which is 12% less than the 411 mg per 100 g of food purchased in 2000. Overall sodium content, which includes beverages, dropped from 192 mg/100 g to 186 mg/100 g, said Jennifer M. Poti, PhD, of the University of North Carolina at Chapel Hill, and her associates.
Total food and beverage purchases also were down from 1,328 g/day in 2000 to 1,134 in 2014, and the total sodium content of those purchases followed suit, dropping from 2,363 mg/day in 2000 to 1,967 mg/day in 2014. The decline in total purchases, however, was driven largely by beverages, which fell 21% from 2000 to 2014, while packaged food purchases fell by only 2%, the investigators reported (JAMA Intern Med. 2017 June 5. doi: 10.1001/jamainternmed.2017.1407).
Median sodium density was down significantly from 1,712 to 1,628 mg of sodium per 1,000 kcal, but by 2014, only 1.2% of the 172,042 households included in the study were purchasing the optimal level of 1,100 mg per 1,000 kcal, based on the DASH-Sodium trial and the Health Eating Index-2010, Dr. Poti and her associates said.
“Additional studies are needed to examine whether decreases in sodium from packaged foods were offset by increases in sodium from away-from-home sources,” they said, and since “there were no major shifts in the amount purchased for key food groups … sodium declines may relate mainly to reformulation.”
The study was funded by the Robert Wood Johnson Foundation, the National Institutes of Health, and the Carolina Population Center at the University of North Carolina. One of the investigators is supported by a National Health and Medical Research Council of Australia Early Career Fellowship. The investigators did not report any conflicts of interest.
FROM JAMA INTERNAL MEDICINE