User login
Wide variability found in invasive mediastinal staging rates for lung cancer
COLORADO SPRINGS – Significant variability exists between hospitals in Washington state in their rates of invasive mediastinal staging for lung cancer, Farhood Farjah, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
“We found evidence of a fivefold variation in hospital-level rates of invasive mediastinal staging not explained by chance or case mix,” according to Dr. Farjah of the University of Washington, Seattle.

“This has led to substantial concerns about quality of thoracic surgical care in the community at large,” he noted.
The Washington study is the first to show hospital-by-hospital variation in rates of invasive mediastinal staging.
Invasive mediastinal staging for lung cancer is considered important because imaging is known to have a substantial false-negative rate, and staging results have a profound impact on treatment recommendations, which can range from surgery alone to additional chemoradiation therapy.
Yet the meaning of the hospital-level huge variability in practice observed in the Washington study remains unclear.
“Our understanding of the underutilization of invasive mediastinal staging is further complicated by the fact that patterns of invasive mediastinal staging are highly variable across hospitals staffed by at least one board-certified thoracic surgeon with a noncardiac practice,” Dr. Farjah explained. “This variability could be a marker of poor-quality care. However, because the guidelines are not supported by level 1 evidence, it’s equally plausible that this variability might represent uncertainty or even disagreement with the practice guidelines – and specifically about the appropriate indication for invasive staging.”
He presented a retrospective cohort study of 406 patients whose non–small cell lung cancer was resected during July 2011–December 2013 at one of five Washington hospitals, each with at least one board-certified thoracic surgeon with a noncardiac practice on staff. The four participating community hospitals and one academic medical center were involved in a National Cancer Institute–funded, physician-led quality improvement initiative.
Overall, 66% of the 406 patients underwent any form of invasive mediastinal staging: 85% by mediastinoscopy only; 12% by mediastinoscopy plus endobronchial ultrasound-guided nodal aspiration (EBUS); 3% by EBUS only; and the remaining handful by mediastinoscopy, EBUS, and esophageal ultrasound-guided nodal aspiration. The invasive staging was performed at the time of resection in 64% of cases. A median of three nodal stations were sampled.
After statistical adjustment for random variation and between-hospital differences in clinical stage, rates of invasive staging were all over the map. While an overall mean of 66% of the lung cancer patients underwent invasive mediastinal staging, the rates at the five hospitals were 94%, 84%, 31%, 80%, and 17%.
Dr. Farjah and his coinvestigators are now conducting provider interviews and focus groups in an effort to understand what drove the participating surgeons’ wide variability in performing invasive mediastinal staging.
Discussant Jane Yanagawa, MD, of the University of California, Los Angeles, commented, “I think this is a really interesting study because, historically, lower rates of mediastinoscopy are assumed to be a reflection of low-quality care – and you suggest that might not be the case, that it might be more complicated than that.”
Dr. Yanagawa sketched one fairly common scenario that might represent a surgeon’s reasonable avoidance of guideline-recommended invasive mediastinal staging: a patient who by all preoperative imaging appears to have stage IA lung cancer and wishes to avoid the morbidity, time, and cost of needle biopsy, instead choosing to go straight to the operating room for a diagnosis by wedge resection, followed by a completion lobectomy based upon the frozen section results. Could such a pathway account for the variability seen in the Washington study?
“I think it could have,” Dr. Farjah replied. “I would say that’s probably one driver of variability.”
As for the generalizability of the findings of a five-hospital study carried out in a single state, Dr. Farjah said he thinks the results are applicable to any academic or community hospital with at least one board-certified thoracic surgeon with a noncardiac practice.
He reported having no financial conflicts of interest regarding the study.
M. Patricia Rivera, MD, FCCP, comments: Staging of lung cancer is essential to select the best treatment strategy for a given patient. However, despite multiple guideline recommendations

M. Patricia Rivera, MD, FCCP, comments: Staging of lung cancer is essential to select the best treatment strategy for a given patient. However, despite multiple guideline recommendations
M. Patricia Rivera, MD, FCCP, comments: Staging of lung cancer is essential to select the best treatment strategy for a given patient. However, despite multiple guideline recommendations
COLORADO SPRINGS – Significant variability exists between hospitals in Washington state in their rates of invasive mediastinal staging for lung cancer, Farhood Farjah, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
“We found evidence of a fivefold variation in hospital-level rates of invasive mediastinal staging not explained by chance or case mix,” according to Dr. Farjah of the University of Washington, Seattle.
“This has led to substantial concerns about quality of thoracic surgical care in the community at large,” he noted.
The Washington study is the first to show hospital-by-hospital variation in rates of invasive mediastinal staging.
Invasive mediastinal staging for lung cancer is considered important because imaging is known to have a substantial false-negative rate, and staging results have a profound impact on treatment recommendations, which can range from surgery alone to additional chemoradiation therapy.
Yet the meaning of the hospital-level huge variability in practice observed in the Washington study remains unclear.
“Our understanding of the underutilization of invasive mediastinal staging is further complicated by the fact that patterns of invasive mediastinal staging are highly variable across hospitals staffed by at least one board-certified thoracic surgeon with a noncardiac practice,” Dr. Farjah explained. “This variability could be a marker of poor-quality care. However, because the guidelines are not supported by level 1 evidence, it’s equally plausible that this variability might represent uncertainty or even disagreement with the practice guidelines – and specifically about the appropriate indication for invasive staging.”
He presented a retrospective cohort study of 406 patients whose non–small cell lung cancer was resected during July 2011–December 2013 at one of five Washington hospitals, each with at least one board-certified thoracic surgeon with a noncardiac practice on staff. The four participating community hospitals and one academic medical center were involved in a National Cancer Institute–funded, physician-led quality improvement initiative.
Overall, 66% of the 406 patients underwent any form of invasive mediastinal staging: 85% by mediastinoscopy only; 12% by mediastinoscopy plus endobronchial ultrasound-guided nodal aspiration (EBUS); 3% by EBUS only; and the remaining handful by mediastinoscopy, EBUS, and esophageal ultrasound-guided nodal aspiration. The invasive staging was performed at the time of resection in 64% of cases. A median of three nodal stations were sampled.
After statistical adjustment for random variation and between-hospital differences in clinical stage, rates of invasive staging were all over the map. While an overall mean of 66% of the lung cancer patients underwent invasive mediastinal staging, the rates at the five hospitals were 94%, 84%, 31%, 80%, and 17%.
Dr. Farjah and his coinvestigators are now conducting provider interviews and focus groups in an effort to understand what drove the participating surgeons’ wide variability in performing invasive mediastinal staging.
Discussant Jane Yanagawa, MD, of the University of California, Los Angeles, commented, “I think this is a really interesting study because, historically, lower rates of mediastinoscopy are assumed to be a reflection of low-quality care – and you suggest that might not be the case, that it might be more complicated than that.”
Dr. Yanagawa sketched one fairly common scenario that might represent a surgeon’s reasonable avoidance of guideline-recommended invasive mediastinal staging: a patient who by all preoperative imaging appears to have stage IA lung cancer and wishes to avoid the morbidity, time, and cost of needle biopsy, instead choosing to go straight to the operating room for a diagnosis by wedge resection, followed by a completion lobectomy based upon the frozen section results. Could such a pathway account for the variability seen in the Washington study?
“I think it could have,” Dr. Farjah replied. “I would say that’s probably one driver of variability.”
As for the generalizability of the findings of a five-hospital study carried out in a single state, Dr. Farjah said he thinks the results are applicable to any academic or community hospital with at least one board-certified thoracic surgeon with a noncardiac practice.
He reported having no financial conflicts of interest regarding the study.
COLORADO SPRINGS – Significant variability exists between hospitals in Washington state in their rates of invasive mediastinal staging for lung cancer, Farhood Farjah, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
“We found evidence of a fivefold variation in hospital-level rates of invasive mediastinal staging not explained by chance or case mix,” according to Dr. Farjah of the University of Washington, Seattle.
“This has led to substantial concerns about quality of thoracic surgical care in the community at large,” he noted.
The Washington study is the first to show hospital-by-hospital variation in rates of invasive mediastinal staging.
Invasive mediastinal staging for lung cancer is considered important because imaging is known to have a substantial false-negative rate, and staging results have a profound impact on treatment recommendations, which can range from surgery alone to additional chemoradiation therapy.
Yet the meaning of the hospital-level huge variability in practice observed in the Washington study remains unclear.
“Our understanding of the underutilization of invasive mediastinal staging is further complicated by the fact that patterns of invasive mediastinal staging are highly variable across hospitals staffed by at least one board-certified thoracic surgeon with a noncardiac practice,” Dr. Farjah explained. “This variability could be a marker of poor-quality care. However, because the guidelines are not supported by level 1 evidence, it’s equally plausible that this variability might represent uncertainty or even disagreement with the practice guidelines – and specifically about the appropriate indication for invasive staging.”
He presented a retrospective cohort study of 406 patients whose non–small cell lung cancer was resected during July 2011–December 2013 at one of five Washington hospitals, each with at least one board-certified thoracic surgeon with a noncardiac practice on staff. The four participating community hospitals and one academic medical center were involved in a National Cancer Institute–funded, physician-led quality improvement initiative.
Overall, 66% of the 406 patients underwent any form of invasive mediastinal staging: 85% by mediastinoscopy only; 12% by mediastinoscopy plus endobronchial ultrasound-guided nodal aspiration (EBUS); 3% by EBUS only; and the remaining handful by mediastinoscopy, EBUS, and esophageal ultrasound-guided nodal aspiration. The invasive staging was performed at the time of resection in 64% of cases. A median of three nodal stations were sampled.
After statistical adjustment for random variation and between-hospital differences in clinical stage, rates of invasive staging were all over the map. While an overall mean of 66% of the lung cancer patients underwent invasive mediastinal staging, the rates at the five hospitals were 94%, 84%, 31%, 80%, and 17%.
Dr. Farjah and his coinvestigators are now conducting provider interviews and focus groups in an effort to understand what drove the participating surgeons’ wide variability in performing invasive mediastinal staging.
Discussant Jane Yanagawa, MD, of the University of California, Los Angeles, commented, “I think this is a really interesting study because, historically, lower rates of mediastinoscopy are assumed to be a reflection of low-quality care – and you suggest that might not be the case, that it might be more complicated than that.”
Dr. Yanagawa sketched one fairly common scenario that might represent a surgeon’s reasonable avoidance of guideline-recommended invasive mediastinal staging: a patient who by all preoperative imaging appears to have stage IA lung cancer and wishes to avoid the morbidity, time, and cost of needle biopsy, instead choosing to go straight to the operating room for a diagnosis by wedge resection, followed by a completion lobectomy based upon the frozen section results. Could such a pathway account for the variability seen in the Washington study?
“I think it could have,” Dr. Farjah replied. “I would say that’s probably one driver of variability.”
As for the generalizability of the findings of a five-hospital study carried out in a single state, Dr. Farjah said he thinks the results are applicable to any academic or community hospital with at least one board-certified thoracic surgeon with a noncardiac practice.
He reported having no financial conflicts of interest regarding the study.
AT THE WTSA ANNUAL MEETING
Key clinical point:
Major finding: Rates of invasive mediastinal staging after adjustment for clinical stage ranged from a low of 17% at one hospital to as high as 94% at another.
Data source: This retrospective cohort study included 406 patients.
Disclosures: Dr. Farjah reported having no financial conflicts of interest.
TAVR for failed surgical valves: the VIVA study
PARIS – Transcatheter aortic valve replacement using the self-expanding Evolut R device in high-surgical-risk patients with failing surgical aortic bioprostheses showed promising 30-day safety and effectiveness results in the ongoing VIVA study, Ran Kornowski, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“We had a lot of patients with small, failing valves in this study. Despite this, our valve gradients postprocedure were very, very low. This means to me that this platform is very well suited to deal with valve-in-valve procedures in general and with small bioprosthetic valves in particular,” observed Dr. Kornowski, chairman of the department of cardiology at Rabin Medical Center in Petah Tikva, Israel, and president of the Israel Heart Society.

The participants’ last surgical aortic valve replacement had been a mean of 9.3 years earlier. Seventy-one percent of subjects were New York Heart Association class III or IV. The mode of bioprosthetic failure was stenosis in 56% of cases, regurgitation in 23%, and both in the remainder. Ninety-three percent of their failing biosprothetic valves were stented devices. Forty-one percent of the devices were up to 21 mm and another 33% were more than 21 but less than 25 mm.
TAVR procedural access was by the iliofemoral route in 97% of cases. Local anesthesia was used in 42% of cases and conscious sedation in 35%. Fourteen percent of patients underwent preimplantation valvuloplasty; 21% postimplantation valvuloplasty. The procedural success rate was 98.5%.
The primary safety endpoint was 30-day cardiovascular mortality. The 2.0% rate was far lower than the prespecified cutoff which defined a positive outcome as less than a 10% rate in this high-surgical-risk population.
Other key 30-day outcomes:
• All-cause mortality occurred in 2.5% of patients.
• The 30-day stroke rate was 3%, with no disabling strokes.
• Major vascular complications occurred in 6.5% of the VIVA patients.
• Major bleeding occurred in 7%, minor bleeding in 7.9%. There were no cases of life-threatening bleeding.
• The incidence of Stage I acute kidney injury was rare, at 0.5%.
• Seven percent of patients received a permanent pacemaker.
• Eighty-seven percent of patients had no postprocedure paravalvular regurgitation (PVR), 11.4 had mild PVR, and 1.5% had moderate PVR.
• NYHA classification improved from baseline to 30 days in 81% of patients. At 30 days, 93% of participants were NYHA class I or II.
Turning to echocardiographic findings, the mean gradient improved from a mean baseline of 31.8 mm Hg to 12.6 mm Hg, while the effective orifice area rose from 1.0 to 1.5 cm2. The magnitude of both improvements was greater for patients with stenosis as their mode of valve failure.
“With the Evolut R, we aim for higher implantations – not more than about 4 mm below the ring – because going deeper could bring about higher gradients and functional deterioration later on,” the cardiologist explained.
The 1-year primary efficacy endpoint – lack of significant aortic stenosis as defined by a mean gradient less than 40 mm Hg – will be reported soon. The VIVA study is sponsored by Medtronic. Dr. Kornowski reported serving as a consultant to the company.
PARIS – Transcatheter aortic valve replacement using the self-expanding Evolut R device in high-surgical-risk patients with failing surgical aortic bioprostheses showed promising 30-day safety and effectiveness results in the ongoing VIVA study, Ran Kornowski, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“We had a lot of patients with small, failing valves in this study. Despite this, our valve gradients postprocedure were very, very low. This means to me that this platform is very well suited to deal with valve-in-valve procedures in general and with small bioprosthetic valves in particular,” observed Dr. Kornowski, chairman of the department of cardiology at Rabin Medical Center in Petah Tikva, Israel, and president of the Israel Heart Society.
The participants’ last surgical aortic valve replacement had been a mean of 9.3 years earlier. Seventy-one percent of subjects were New York Heart Association class III or IV. The mode of bioprosthetic failure was stenosis in 56% of cases, regurgitation in 23%, and both in the remainder. Ninety-three percent of their failing biosprothetic valves were stented devices. Forty-one percent of the devices were up to 21 mm and another 33% were more than 21 but less than 25 mm.
TAVR procedural access was by the iliofemoral route in 97% of cases. Local anesthesia was used in 42% of cases and conscious sedation in 35%. Fourteen percent of patients underwent preimplantation valvuloplasty; 21% postimplantation valvuloplasty. The procedural success rate was 98.5%.
The primary safety endpoint was 30-day cardiovascular mortality. The 2.0% rate was far lower than the prespecified cutoff which defined a positive outcome as less than a 10% rate in this high-surgical-risk population.
Other key 30-day outcomes:
• All-cause mortality occurred in 2.5% of patients.
• The 30-day stroke rate was 3%, with no disabling strokes.
• Major vascular complications occurred in 6.5% of the VIVA patients.
• Major bleeding occurred in 7%, minor bleeding in 7.9%. There were no cases of life-threatening bleeding.
• The incidence of Stage I acute kidney injury was rare, at 0.5%.
• Seven percent of patients received a permanent pacemaker.
• Eighty-seven percent of patients had no postprocedure paravalvular regurgitation (PVR), 11.4 had mild PVR, and 1.5% had moderate PVR.
• NYHA classification improved from baseline to 30 days in 81% of patients. At 30 days, 93% of participants were NYHA class I or II.
Turning to echocardiographic findings, the mean gradient improved from a mean baseline of 31.8 mm Hg to 12.6 mm Hg, while the effective orifice area rose from 1.0 to 1.5 cm2. The magnitude of both improvements was greater for patients with stenosis as their mode of valve failure.
“With the Evolut R, we aim for higher implantations – not more than about 4 mm below the ring – because going deeper could bring about higher gradients and functional deterioration later on,” the cardiologist explained.
The 1-year primary efficacy endpoint – lack of significant aortic stenosis as defined by a mean gradient less than 40 mm Hg – will be reported soon. The VIVA study is sponsored by Medtronic. Dr. Kornowski reported serving as a consultant to the company.
PARIS – Transcatheter aortic valve replacement using the self-expanding Evolut R device in high-surgical-risk patients with failing surgical aortic bioprostheses showed promising 30-day safety and effectiveness results in the ongoing VIVA study, Ran Kornowski, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“We had a lot of patients with small, failing valves in this study. Despite this, our valve gradients postprocedure were very, very low. This means to me that this platform is very well suited to deal with valve-in-valve procedures in general and with small bioprosthetic valves in particular,” observed Dr. Kornowski, chairman of the department of cardiology at Rabin Medical Center in Petah Tikva, Israel, and president of the Israel Heart Society.
The participants’ last surgical aortic valve replacement had been a mean of 9.3 years earlier. Seventy-one percent of subjects were New York Heart Association class III or IV. The mode of bioprosthetic failure was stenosis in 56% of cases, regurgitation in 23%, and both in the remainder. Ninety-three percent of their failing biosprothetic valves were stented devices. Forty-one percent of the devices were up to 21 mm and another 33% were more than 21 but less than 25 mm.
TAVR procedural access was by the iliofemoral route in 97% of cases. Local anesthesia was used in 42% of cases and conscious sedation in 35%. Fourteen percent of patients underwent preimplantation valvuloplasty; 21% postimplantation valvuloplasty. The procedural success rate was 98.5%.
The primary safety endpoint was 30-day cardiovascular mortality. The 2.0% rate was far lower than the prespecified cutoff which defined a positive outcome as less than a 10% rate in this high-surgical-risk population.
Other key 30-day outcomes:
• All-cause mortality occurred in 2.5% of patients.
• The 30-day stroke rate was 3%, with no disabling strokes.
• Major vascular complications occurred in 6.5% of the VIVA patients.
• Major bleeding occurred in 7%, minor bleeding in 7.9%. There were no cases of life-threatening bleeding.
• The incidence of Stage I acute kidney injury was rare, at 0.5%.
• Seven percent of patients received a permanent pacemaker.
• Eighty-seven percent of patients had no postprocedure paravalvular regurgitation (PVR), 11.4 had mild PVR, and 1.5% had moderate PVR.
• NYHA classification improved from baseline to 30 days in 81% of patients. At 30 days, 93% of participants were NYHA class I or II.
Turning to echocardiographic findings, the mean gradient improved from a mean baseline of 31.8 mm Hg to 12.6 mm Hg, while the effective orifice area rose from 1.0 to 1.5 cm2. The magnitude of both improvements was greater for patients with stenosis as their mode of valve failure.
“With the Evolut R, we aim for higher implantations – not more than about 4 mm below the ring – because going deeper could bring about higher gradients and functional deterioration later on,” the cardiologist explained.
The 1-year primary efficacy endpoint – lack of significant aortic stenosis as defined by a mean gradient less than 40 mm Hg – will be reported soon. The VIVA study is sponsored by Medtronic. Dr. Kornowski reported serving as a consultant to the company.
AT EuroPCR
Key clinical point:
Major finding: The 30-day cardiovascular mortality rate after transcatheter aortic valve replacement via a valve-in-valve procedure in patients with a failing surgically implanted bioprosthesis was 2%, compared with a projected rate of at least 10% with redo surgery.
Data source: VIVA, a prospective observational registry of 202 high-surgical-risk patients at 23 centers in four countries who underwent valve-in-valve transcatheter aortic valve replacement because of a failing surgically implanted aortic bioprosthesis.
Disclosures: VIVA is sponsored by Medtronic. The presenter reported serving as a consultant to the company.
Now boarding: How we can skip coach and bump our patients up to first class
Cruising above the earth at 37,000 feet on the way back from vacation, my mind starts wandering. The impending reality of returning to work is setting in, and I can’t help but reflect on how the experience of a weary traveler trying to get home is like that of a weary patient trying to navigate modern health care. As it turns out, there are more than a few similarities, and that is not necessarily a good thing.
The modern airline industry is often cited by experts as a model for safety, efficiency, and innovation, though just a few decades ago this wasn’t the case. Several factors (for example, catastrophic crashes; the events of September 11th, 2001; the economic downturn) forced airlines to make radical improvements in how they operated – many of which I am quite thankful for as I gaze down upon America’s heartland from my window seat. Still, there are many who would say that in spite of (and sometimes because of) these improvements, air travel is the worst it’s ever been; airport lines are longer than ever, costs have steadily increased, and customer service has become little more than a quaint idea from a bygone era.

Most people deride the frustrations of air travel yet accept them as normal. The same expectations have unfortunately been set in health care. Patients wait, though waiting only contributes to anxiety and leads them to question the quality of their care. They also expect their journey to have many layover stops, though these involve even more waiting and often unnecessary redundancy. We need to streamline the care delivery process, and this is where technology can help.
First of all, we need to address the waiting. In health care, we tend to call this “access,” an ever-present problem for patients and providers. Thankfully, some recent innovations have helped significantly. The first of these innovations is online scheduling, which allows patients to find openings and schedule visits without the need to pick up the phone. Much like the ability to book a dinner reservation online, this is becoming an expectation for health care consumers. Participating practices and health systems can also use it as a marketing advantage; it is a fantastic way to recruit new patients as they search for a new provider online (that is, seeing that a physician has immediate openings may make the decision easier).
There are several companies providing third-party online scheduling services, and many of these can interface directly with electronic health records. EHR vendors themselves also provide this functionality to existing patients through an online web portal or mobile app. Either way, if you haven’t considered it yet, you should. It’s a great way to fill last-minute schedule openings and increase your patient base, all while improving access and patient satisfaction.
Another way to improve access is through telemedicine. We’ve written about this in prior columns, but it has certainly become more prevalent and available since then. Now more insurers are reimbursing for telemedicine services, and consumers are starting to embrace it as well. Consider some advantages: it’s more convenient for patients and often less expensive for those without insurance – cash prices tend to be in the $50-$75 range. It can also be more convenient for providers, as the typical telemedicine visit lasts only about 10 minutes and can be easily fit in last-minute. Better still, telemedicine can be a way for providers to now be paid for services they might have previously provided for free by telephone. It is critical to choose patients and conditions appropriate for these “virtual visits.” Medication checks, lab follow-ups, or rash evaluations are just a few examples, but with a little bit of thought it is easy to find dozens of other opportunities to use telemedicine to improve access.
In addition to access, we need to look for ways to improve efficiency and decrease redundancy when sending patients for testing and consultations. Recently, I had the experience of visiting a specialist for a minor medical issue. In spite of the fact that the specialist was a member of the same health system as my PCP, I still spent the first 15 minutes of my visit filling out paperwork that requested information easily available from my health record. There must be a better way.
Patients are beginning to question why, in the world of ubiquitous social media and connectivity, our computerized medical records can’t communicate. This is especially true when they are seeing physicians who are part of the same health system (as in my case). Thankfully, vendors have gotten the message and have begun allowing providers to collaborate, not only with physicians using the same software, but also with those using other EHRs through Health Information Exchanges (HIEs). Unfortunately, this alone won’t be enough. We must continue to promote the notion of patient-owned medical records, as that will be the only way to ensure true patient-centered care. In a future column, we’ll explore this concept in greater detail, but for now we’ll confirm our belief that universal interoperability is reasonable and possible.
As we are getting ready to land, I reflect on the wonderful vacation I just had and the tasks ahead at home, most of which I enjoy. Patients aren’t always as lucky; they are accessing medical care because they have to, not because they want to. Their “destination” is all too often an unfortunate diagnosis, unexpected surgical procedure, or lifetime of chronic discomfort. It is therefore incumbent on us, their care providers, to use the tools at our disposal to offer them the most efficient, most comfortable, and most connected journey possible.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is also a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington Jefferson Health.
Cruising above the earth at 37,000 feet on the way back from vacation, my mind starts wandering. The impending reality of returning to work is setting in, and I can’t help but reflect on how the experience of a weary traveler trying to get home is like that of a weary patient trying to navigate modern health care. As it turns out, there are more than a few similarities, and that is not necessarily a good thing.
The modern airline industry is often cited by experts as a model for safety, efficiency, and innovation, though just a few decades ago this wasn’t the case. Several factors (for example, catastrophic crashes; the events of September 11th, 2001; the economic downturn) forced airlines to make radical improvements in how they operated – many of which I am quite thankful for as I gaze down upon America’s heartland from my window seat. Still, there are many who would say that in spite of (and sometimes because of) these improvements, air travel is the worst it’s ever been; airport lines are longer than ever, costs have steadily increased, and customer service has become little more than a quaint idea from a bygone era.
Most people deride the frustrations of air travel yet accept them as normal. The same expectations have unfortunately been set in health care. Patients wait, though waiting only contributes to anxiety and leads them to question the quality of their care. They also expect their journey to have many layover stops, though these involve even more waiting and often unnecessary redundancy. We need to streamline the care delivery process, and this is where technology can help.
First of all, we need to address the waiting. In health care, we tend to call this “access,” an ever-present problem for patients and providers. Thankfully, some recent innovations have helped significantly. The first of these innovations is online scheduling, which allows patients to find openings and schedule visits without the need to pick up the phone. Much like the ability to book a dinner reservation online, this is becoming an expectation for health care consumers. Participating practices and health systems can also use it as a marketing advantage; it is a fantastic way to recruit new patients as they search for a new provider online (that is, seeing that a physician has immediate openings may make the decision easier).
There are several companies providing third-party online scheduling services, and many of these can interface directly with electronic health records. EHR vendors themselves also provide this functionality to existing patients through an online web portal or mobile app. Either way, if you haven’t considered it yet, you should. It’s a great way to fill last-minute schedule openings and increase your patient base, all while improving access and patient satisfaction.
Another way to improve access is through telemedicine. We’ve written about this in prior columns, but it has certainly become more prevalent and available since then. Now more insurers are reimbursing for telemedicine services, and consumers are starting to embrace it as well. Consider some advantages: it’s more convenient for patients and often less expensive for those without insurance – cash prices tend to be in the $50-$75 range. It can also be more convenient for providers, as the typical telemedicine visit lasts only about 10 minutes and can be easily fit in last-minute. Better still, telemedicine can be a way for providers to now be paid for services they might have previously provided for free by telephone. It is critical to choose patients and conditions appropriate for these “virtual visits.” Medication checks, lab follow-ups, or rash evaluations are just a few examples, but with a little bit of thought it is easy to find dozens of other opportunities to use telemedicine to improve access.
In addition to access, we need to look for ways to improve efficiency and decrease redundancy when sending patients for testing and consultations. Recently, I had the experience of visiting a specialist for a minor medical issue. In spite of the fact that the specialist was a member of the same health system as my PCP, I still spent the first 15 minutes of my visit filling out paperwork that requested information easily available from my health record. There must be a better way.
Patients are beginning to question why, in the world of ubiquitous social media and connectivity, our computerized medical records can’t communicate. This is especially true when they are seeing physicians who are part of the same health system (as in my case). Thankfully, vendors have gotten the message and have begun allowing providers to collaborate, not only with physicians using the same software, but also with those using other EHRs through Health Information Exchanges (HIEs). Unfortunately, this alone won’t be enough. We must continue to promote the notion of patient-owned medical records, as that will be the only way to ensure true patient-centered care. In a future column, we’ll explore this concept in greater detail, but for now we’ll confirm our belief that universal interoperability is reasonable and possible.
As we are getting ready to land, I reflect on the wonderful vacation I just had and the tasks ahead at home, most of which I enjoy. Patients aren’t always as lucky; they are accessing medical care because they have to, not because they want to. Their “destination” is all too often an unfortunate diagnosis, unexpected surgical procedure, or lifetime of chronic discomfort. It is therefore incumbent on us, their care providers, to use the tools at our disposal to offer them the most efficient, most comfortable, and most connected journey possible.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is also a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington Jefferson Health.
Cruising above the earth at 37,000 feet on the way back from vacation, my mind starts wandering. The impending reality of returning to work is setting in, and I can’t help but reflect on how the experience of a weary traveler trying to get home is like that of a weary patient trying to navigate modern health care. As it turns out, there are more than a few similarities, and that is not necessarily a good thing.
The modern airline industry is often cited by experts as a model for safety, efficiency, and innovation, though just a few decades ago this wasn’t the case. Several factors (for example, catastrophic crashes; the events of September 11th, 2001; the economic downturn) forced airlines to make radical improvements in how they operated – many of which I am quite thankful for as I gaze down upon America’s heartland from my window seat. Still, there are many who would say that in spite of (and sometimes because of) these improvements, air travel is the worst it’s ever been; airport lines are longer than ever, costs have steadily increased, and customer service has become little more than a quaint idea from a bygone era.
Most people deride the frustrations of air travel yet accept them as normal. The same expectations have unfortunately been set in health care. Patients wait, though waiting only contributes to anxiety and leads them to question the quality of their care. They also expect their journey to have many layover stops, though these involve even more waiting and often unnecessary redundancy. We need to streamline the care delivery process, and this is where technology can help.
First of all, we need to address the waiting. In health care, we tend to call this “access,” an ever-present problem for patients and providers. Thankfully, some recent innovations have helped significantly. The first of these innovations is online scheduling, which allows patients to find openings and schedule visits without the need to pick up the phone. Much like the ability to book a dinner reservation online, this is becoming an expectation for health care consumers. Participating practices and health systems can also use it as a marketing advantage; it is a fantastic way to recruit new patients as they search for a new provider online (that is, seeing that a physician has immediate openings may make the decision easier).
There are several companies providing third-party online scheduling services, and many of these can interface directly with electronic health records. EHR vendors themselves also provide this functionality to existing patients through an online web portal or mobile app. Either way, if you haven’t considered it yet, you should. It’s a great way to fill last-minute schedule openings and increase your patient base, all while improving access and patient satisfaction.
Another way to improve access is through telemedicine. We’ve written about this in prior columns, but it has certainly become more prevalent and available since then. Now more insurers are reimbursing for telemedicine services, and consumers are starting to embrace it as well. Consider some advantages: it’s more convenient for patients and often less expensive for those without insurance – cash prices tend to be in the $50-$75 range. It can also be more convenient for providers, as the typical telemedicine visit lasts only about 10 minutes and can be easily fit in last-minute. Better still, telemedicine can be a way for providers to now be paid for services they might have previously provided for free by telephone. It is critical to choose patients and conditions appropriate for these “virtual visits.” Medication checks, lab follow-ups, or rash evaluations are just a few examples, but with a little bit of thought it is easy to find dozens of other opportunities to use telemedicine to improve access.
In addition to access, we need to look for ways to improve efficiency and decrease redundancy when sending patients for testing and consultations. Recently, I had the experience of visiting a specialist for a minor medical issue. In spite of the fact that the specialist was a member of the same health system as my PCP, I still spent the first 15 minutes of my visit filling out paperwork that requested information easily available from my health record. There must be a better way.
Patients are beginning to question why, in the world of ubiquitous social media and connectivity, our computerized medical records can’t communicate. This is especially true when they are seeing physicians who are part of the same health system (as in my case). Thankfully, vendors have gotten the message and have begun allowing providers to collaborate, not only with physicians using the same software, but also with those using other EHRs through Health Information Exchanges (HIEs). Unfortunately, this alone won’t be enough. We must continue to promote the notion of patient-owned medical records, as that will be the only way to ensure true patient-centered care. In a future column, we’ll explore this concept in greater detail, but for now we’ll confirm our belief that universal interoperability is reasonable and possible.
As we are getting ready to land, I reflect on the wonderful vacation I just had and the tasks ahead at home, most of which I enjoy. Patients aren’t always as lucky; they are accessing medical care because they have to, not because they want to. Their “destination” is all too often an unfortunate diagnosis, unexpected surgical procedure, or lifetime of chronic discomfort. It is therefore incumbent on us, their care providers, to use the tools at our disposal to offer them the most efficient, most comfortable, and most connected journey possible.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is also a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington Jefferson Health.
Solitary Nodule With White Hairs
The Diagnosis: Trichofolliculoma
Microscopic examination revealed a dilated cystic follicle that communicated with the skin surface (Figure). The follicle was lined with squamous epithelium and surrounded by numerous secondary follicles, many of which contained a hair shaft. A diagnosis of trichofolliculoma was made.
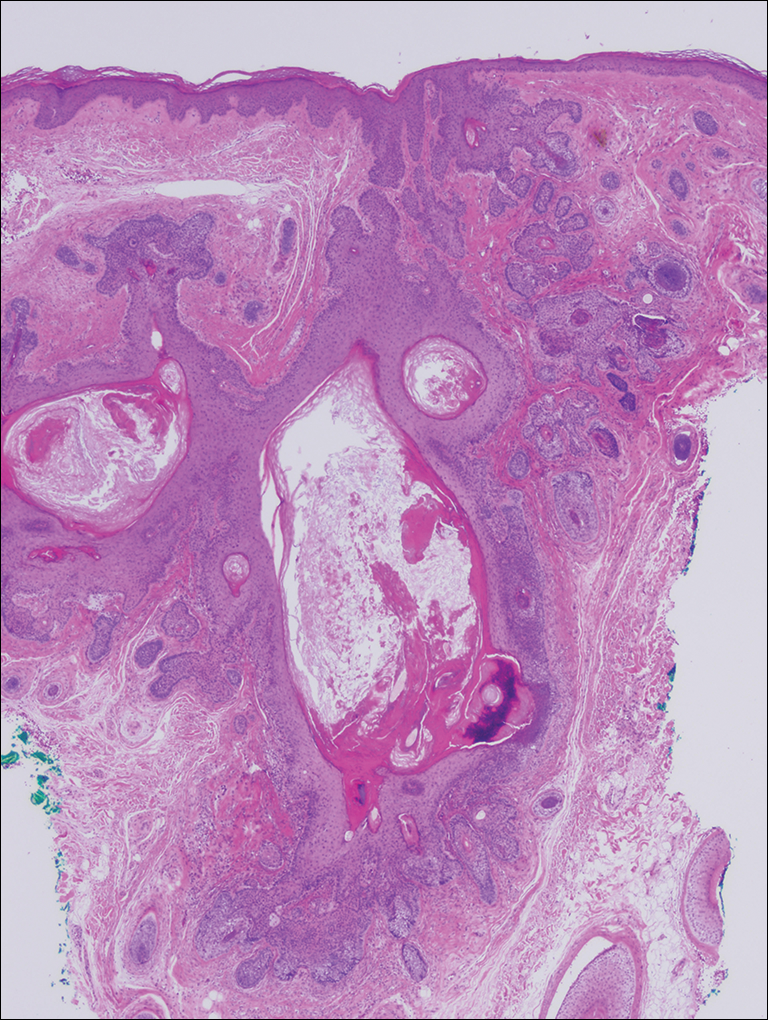
Clinically, the differential diagnosis of a flesh-colored papule on the scalp with prominent follicle includes dilated pore of Winer, epidermoid cyst, pilar sheath acanthoma, and trichoepithelioma.1,2 Multiple hair shafts present in a single follicle may be seen in pili multigemini, tufted folliculitis, trichostasis spinulosa, and trichofolliculoma. On histopathologic examination, a dilated central follicle surrounded with smaller secondary follicles was identified, consistent with trichofolliculoma.
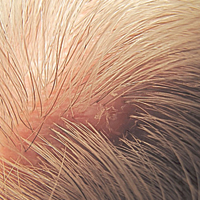
Trichofolliculoma is a rare follicular hamartoma typically occurring on the face, scalp, or trunk as a solitary papule or nodule due to the proliferation of abnormal hair follicle stem cells.3,4 It may present as a flesh-colored nodule with a central pore that may drain sebum or contain white vellus hairs. Trichofolliculoma is considered a benign entity, despite one case report of malignant transformation.5 Biopsy is diagnostic and no further treatment is needed. Recurrence rarely occurs at the primary site after surgical excision, which may be performed for cosmetic purposes or to alleviate functional impairment.
- Ghosh SK, Bandyopadhyay D, Barma KD. Perifollicular nodule on the face of a young man. Indian J Dermatol Venereol Leprol. 2011;77:531-533.
- Gokalp H, Gurer MA, Alan S. Trichofolliculoma: a rare variant of hair follicle hamartoma. Dermatol Online J. 2013;19:19264.
- Choi CM, Lew BL, Sim WY. Multiple trichofolliculomas on unusual sites: a case report and review of the literature. Int J Dermatol. 2013;52:87-89.
- Misago N, Kimura T, Toda S, et al. A revaluation of trichofolliculoma: the histopathological and immunohistochemical features. Am J Dermatopathol. 2010;32:35-43.
- Stem JB, Stout DA. Trichofolliculoma showing perineural invasion. trichofolliculocarcinoma? Arch Dermatol. 1979;115:1003-1004.
The Diagnosis: Trichofolliculoma
Microscopic examination revealed a dilated cystic follicle that communicated with the skin surface (Figure). The follicle was lined with squamous epithelium and surrounded by numerous secondary follicles, many of which contained a hair shaft. A diagnosis of trichofolliculoma was made.
Clinically, the differential diagnosis of a flesh-colored papule on the scalp with prominent follicle includes dilated pore of Winer, epidermoid cyst, pilar sheath acanthoma, and trichoepithelioma.1,2 Multiple hair shafts present in a single follicle may be seen in pili multigemini, tufted folliculitis, trichostasis spinulosa, and trichofolliculoma. On histopathologic examination, a dilated central follicle surrounded with smaller secondary follicles was identified, consistent with trichofolliculoma.
Trichofolliculoma is a rare follicular hamartoma typically occurring on the face, scalp, or trunk as a solitary papule or nodule due to the proliferation of abnormal hair follicle stem cells.3,4 It may present as a flesh-colored nodule with a central pore that may drain sebum or contain white vellus hairs. Trichofolliculoma is considered a benign entity, despite one case report of malignant transformation.5 Biopsy is diagnostic and no further treatment is needed. Recurrence rarely occurs at the primary site after surgical excision, which may be performed for cosmetic purposes or to alleviate functional impairment.
The Diagnosis: Trichofolliculoma
Microscopic examination revealed a dilated cystic follicle that communicated with the skin surface (Figure). The follicle was lined with squamous epithelium and surrounded by numerous secondary follicles, many of which contained a hair shaft. A diagnosis of trichofolliculoma was made.
Clinically, the differential diagnosis of a flesh-colored papule on the scalp with prominent follicle includes dilated pore of Winer, epidermoid cyst, pilar sheath acanthoma, and trichoepithelioma.1,2 Multiple hair shafts present in a single follicle may be seen in pili multigemini, tufted folliculitis, trichostasis spinulosa, and trichofolliculoma. On histopathologic examination, a dilated central follicle surrounded with smaller secondary follicles was identified, consistent with trichofolliculoma.
Trichofolliculoma is a rare follicular hamartoma typically occurring on the face, scalp, or trunk as a solitary papule or nodule due to the proliferation of abnormal hair follicle stem cells.3,4 It may present as a flesh-colored nodule with a central pore that may drain sebum or contain white vellus hairs. Trichofolliculoma is considered a benign entity, despite one case report of malignant transformation.5 Biopsy is diagnostic and no further treatment is needed. Recurrence rarely occurs at the primary site after surgical excision, which may be performed for cosmetic purposes or to alleviate functional impairment.
- Ghosh SK, Bandyopadhyay D, Barma KD. Perifollicular nodule on the face of a young man. Indian J Dermatol Venereol Leprol. 2011;77:531-533.
- Gokalp H, Gurer MA, Alan S. Trichofolliculoma: a rare variant of hair follicle hamartoma. Dermatol Online J. 2013;19:19264.
- Choi CM, Lew BL, Sim WY. Multiple trichofolliculomas on unusual sites: a case report and review of the literature. Int J Dermatol. 2013;52:87-89.
- Misago N, Kimura T, Toda S, et al. A revaluation of trichofolliculoma: the histopathological and immunohistochemical features. Am J Dermatopathol. 2010;32:35-43.
- Stem JB, Stout DA. Trichofolliculoma showing perineural invasion. trichofolliculocarcinoma? Arch Dermatol. 1979;115:1003-1004.
- Ghosh SK, Bandyopadhyay D, Barma KD. Perifollicular nodule on the face of a young man. Indian J Dermatol Venereol Leprol. 2011;77:531-533.
- Gokalp H, Gurer MA, Alan S. Trichofolliculoma: a rare variant of hair follicle hamartoma. Dermatol Online J. 2013;19:19264.
- Choi CM, Lew BL, Sim WY. Multiple trichofolliculomas on unusual sites: a case report and review of the literature. Int J Dermatol. 2013;52:87-89.
- Misago N, Kimura T, Toda S, et al. A revaluation of trichofolliculoma: the histopathological and immunohistochemical features. Am J Dermatopathol. 2010;32:35-43.
- Stem JB, Stout DA. Trichofolliculoma showing perineural invasion. trichofolliculocarcinoma? Arch Dermatol. 1979;115:1003-1004.

A 72-year-old man presented with a new asymptomatic 0.7-cm flesh-colored papule with a central tuft of white hairs on the posterior scalp. The remainder of the physical examination was unremarkable. Biopsy for histopathologic examination was performed to confirm diagnosis.
Campylobacteriosis incidence rises in U.S. from 2004 to 2012
Incidence of campylobacteriosis increased significantly in the United States from 2004 to 2012, according to Aimee Geissler, PhD, and her associates.
A total of 303,520 cases of campylobacteriosis were reported during the study period, with the average incidence rate growing from 10.5 cases per 100,000 persons during 2004-2006 to 12.7 cases per 100,000 persons during 2010-2012, an increase of 21%. The median number of Camplyobacter outbreaks doubled from 28 during 2004-2006 to 56 during 2010-2012; in total, 347 outbreaks were reported. Campylobacteriosis is the nation’s most common bacterial diarrheal illness.
The study findings “underscore the importance of standardizing national surveillance for campylobacteriosis, which is important in understanding the burden of infection, better describing geographic variations and differences among species, elucidating risk factors, and targeting prevention and control measures,” the investigators concluded.
Find the full study in Clinical Infectious Diseases (2017 Jul 20. doi: 10.1093/cid/cix624).
Incidence of campylobacteriosis increased significantly in the United States from 2004 to 2012, according to Aimee Geissler, PhD, and her associates.
A total of 303,520 cases of campylobacteriosis were reported during the study period, with the average incidence rate growing from 10.5 cases per 100,000 persons during 2004-2006 to 12.7 cases per 100,000 persons during 2010-2012, an increase of 21%. The median number of Camplyobacter outbreaks doubled from 28 during 2004-2006 to 56 during 2010-2012; in total, 347 outbreaks were reported. Campylobacteriosis is the nation’s most common bacterial diarrheal illness.
The study findings “underscore the importance of standardizing national surveillance for campylobacteriosis, which is important in understanding the burden of infection, better describing geographic variations and differences among species, elucidating risk factors, and targeting prevention and control measures,” the investigators concluded.
Find the full study in Clinical Infectious Diseases (2017 Jul 20. doi: 10.1093/cid/cix624).
Incidence of campylobacteriosis increased significantly in the United States from 2004 to 2012, according to Aimee Geissler, PhD, and her associates.
A total of 303,520 cases of campylobacteriosis were reported during the study period, with the average incidence rate growing from 10.5 cases per 100,000 persons during 2004-2006 to 12.7 cases per 100,000 persons during 2010-2012, an increase of 21%. The median number of Camplyobacter outbreaks doubled from 28 during 2004-2006 to 56 during 2010-2012; in total, 347 outbreaks were reported. Campylobacteriosis is the nation’s most common bacterial diarrheal illness.
The study findings “underscore the importance of standardizing national surveillance for campylobacteriosis, which is important in understanding the burden of infection, better describing geographic variations and differences among species, elucidating risk factors, and targeting prevention and control measures,” the investigators concluded.
Find the full study in Clinical Infectious Diseases (2017 Jul 20. doi: 10.1093/cid/cix624).
FROM CLINICAL INFECTIOUS DISEASES
Crisis in psychiatry: Top 5 problems, many solutions
Lack of access to psychiatric services has been a challenge for decades, resulting in significant delays to treatment with associated consequences in reduced quality of care, low patient satisfaction, poor patient outcomes, and higher costs.
The problem is exacerbated by a growing shortage of psychiatrists, an increased demand for psychiatric services, and inadequate payment rates. The result is a crisis that is resonating throughout the U.S. health care system.
As many know, a few months ago, the Medical Director Institute of the National Council for Behavioral Health, in partnership with the American Psychiatric Association, convened an expert panel to develop a report responding to this evolving quandary. The findings of our 60-page report, “The Psychiatric Shortage: Causes and Solutions,” suggest that psychiatry is uniquely positioned to address the issues that face our specialty.
The institute identified five areas of critical concern: workforce development, improved efficiency of service delivery, reducing burdensome regulations and confidentiality restrictions, broader implementation of innovative models, and adoption of novel reimbursement methods.
1. Workforce development
Psychiatrists come out of residency training without the skills they need to practice in today’s rapidly evolving health care environment. We need better preparation in measurement-based care, telepsychiatry, collaborative care, and other methods of efficient team collaboration with primary care.
Funding for graduate medical education and training programs must be expanded with an infusion of new funding – not only for psychiatrists – but also for psychiatric nurse practitioners and psychiatric physician assistants.
2. Improved efficiency of service delivery
Providers of psychiatric services in outpatient psychiatric programs face a cramped daily routine with increasingly briefer appointments scheduled back-to-back that limit in-depth clinical assessment, collaboration with other members of the treatment team, and consultation with primary care providers outside of the program. Such a schedule leads to lower-quality care.
Psychiatrists must have the same level of nurse and paraprofessional assistance and support provided to other medical specialties. In addition, regulations that prevent the broader use of telepsychiatry must be revised. All behavioral health providers should implement open access scheduling, a proven modality for reducing missed appointments.
3. Reducing burdensome regulations and confidentiality restrictions
Excessive documentation requirements, especially necessarily detailed, lengthy assessments and treatment must be revised and 42 CFR Part 2 must be made consistent with HIPAA requirements.
4. Broader implementation of innovative models
The shortage of psychiatrists will only worsen with the integration of primary care and behavioral health, and the shift to Accountable Care Organizations as part of health care reform (which, as of this writing, faces much uncertainty). Thanks to more efficient screening for mental health and substance use disorders now occurring in primary care, there will be growing demand for access to psychiatric services.
The collaborative care model for providing psychiatric services should be implemented throughout primary care. Behavioral health organizations must develop their own version of collaborative care that targets the limited psychiatric resource where it is most needed by using measurement-based care and collaborating more effectively with other team members.
5. Adoption of novel reimbursement methods
Inappropriately low rates limit access to care. Today, 40% of psychiatrists choose cash-only private practices, the second-highest among medical specialties after dermatologists, and 75% of provider organizations employing psychiatrists report that they lose money on their psychiatric services. At the same time, the shrinking number of inpatient psychiatric services has become a significant obstacle to improved access. Beds have been eliminated because of lower rates of reimbursement, compared with other medical-surgical procedures and difficulty in recruiting psychiatrists to staff inpatient units.
Psychiatric service rates must be reset to be consistent with the actual cost of providing care. Prospective payment models like Certified Community Behavioral Health Clinics should be expanded, and bundled payments for services like collaborative care and complex care should be covered by payers.
The Medical Director Institute recommends these solutions so that access to psychiatric services does not remain a barrier to the overall success of health care reform and service delivery improving the health of Americans. Multiple stakeholders – federal and state governments, payers, providers, provider trade associations, and advocates – must take action within their spheres of influence in the design, funding, regulation, and delivery of behavioral health care to improve access to psychiatric services. Such broad collaboration is imperative for our patients to get the care they need.
Dr. Parks is the medical director for the National Council for Behavioral Health. He practices psychiatry on an outpatient basis at Family Health Center, a federally funded community health center established to expand services to uninsured and underinsured patients in central Missouri. He also holds the position of Distinguished Research Professor of Science at the University of Missouri–St. Louis and is a clinical assistant professor of psychiatry at the University of Missouri–Columbia.
Lack of access to psychiatric services has been a challenge for decades, resulting in significant delays to treatment with associated consequences in reduced quality of care, low patient satisfaction, poor patient outcomes, and higher costs.
The problem is exacerbated by a growing shortage of psychiatrists, an increased demand for psychiatric services, and inadequate payment rates. The result is a crisis that is resonating throughout the U.S. health care system.
As many know, a few months ago, the Medical Director Institute of the National Council for Behavioral Health, in partnership with the American Psychiatric Association, convened an expert panel to develop a report responding to this evolving quandary. The findings of our 60-page report, “The Psychiatric Shortage: Causes and Solutions,” suggest that psychiatry is uniquely positioned to address the issues that face our specialty.
The institute identified five areas of critical concern: workforce development, improved efficiency of service delivery, reducing burdensome regulations and confidentiality restrictions, broader implementation of innovative models, and adoption of novel reimbursement methods.
1. Workforce development
Psychiatrists come out of residency training without the skills they need to practice in today’s rapidly evolving health care environment. We need better preparation in measurement-based care, telepsychiatry, collaborative care, and other methods of efficient team collaboration with primary care.
Funding for graduate medical education and training programs must be expanded with an infusion of new funding – not only for psychiatrists – but also for psychiatric nurse practitioners and psychiatric physician assistants.
2. Improved efficiency of service delivery
Providers of psychiatric services in outpatient psychiatric programs face a cramped daily routine with increasingly briefer appointments scheduled back-to-back that limit in-depth clinical assessment, collaboration with other members of the treatment team, and consultation with primary care providers outside of the program. Such a schedule leads to lower-quality care.
Psychiatrists must have the same level of nurse and paraprofessional assistance and support provided to other medical specialties. In addition, regulations that prevent the broader use of telepsychiatry must be revised. All behavioral health providers should implement open access scheduling, a proven modality for reducing missed appointments.
3. Reducing burdensome regulations and confidentiality restrictions
Excessive documentation requirements, especially necessarily detailed, lengthy assessments and treatment must be revised and 42 CFR Part 2 must be made consistent with HIPAA requirements.
4. Broader implementation of innovative models
The shortage of psychiatrists will only worsen with the integration of primary care and behavioral health, and the shift to Accountable Care Organizations as part of health care reform (which, as of this writing, faces much uncertainty). Thanks to more efficient screening for mental health and substance use disorders now occurring in primary care, there will be growing demand for access to psychiatric services.
The collaborative care model for providing psychiatric services should be implemented throughout primary care. Behavioral health organizations must develop their own version of collaborative care that targets the limited psychiatric resource where it is most needed by using measurement-based care and collaborating more effectively with other team members.
5. Adoption of novel reimbursement methods
Inappropriately low rates limit access to care. Today, 40% of psychiatrists choose cash-only private practices, the second-highest among medical specialties after dermatologists, and 75% of provider organizations employing psychiatrists report that they lose money on their psychiatric services. At the same time, the shrinking number of inpatient psychiatric services has become a significant obstacle to improved access. Beds have been eliminated because of lower rates of reimbursement, compared with other medical-surgical procedures and difficulty in recruiting psychiatrists to staff inpatient units.
Psychiatric service rates must be reset to be consistent with the actual cost of providing care. Prospective payment models like Certified Community Behavioral Health Clinics should be expanded, and bundled payments for services like collaborative care and complex care should be covered by payers.
The Medical Director Institute recommends these solutions so that access to psychiatric services does not remain a barrier to the overall success of health care reform and service delivery improving the health of Americans. Multiple stakeholders – federal and state governments, payers, providers, provider trade associations, and advocates – must take action within their spheres of influence in the design, funding, regulation, and delivery of behavioral health care to improve access to psychiatric services. Such broad collaboration is imperative for our patients to get the care they need.
Dr. Parks is the medical director for the National Council for Behavioral Health. He practices psychiatry on an outpatient basis at Family Health Center, a federally funded community health center established to expand services to uninsured and underinsured patients in central Missouri. He also holds the position of Distinguished Research Professor of Science at the University of Missouri–St. Louis and is a clinical assistant professor of psychiatry at the University of Missouri–Columbia.
Lack of access to psychiatric services has been a challenge for decades, resulting in significant delays to treatment with associated consequences in reduced quality of care, low patient satisfaction, poor patient outcomes, and higher costs.
The problem is exacerbated by a growing shortage of psychiatrists, an increased demand for psychiatric services, and inadequate payment rates. The result is a crisis that is resonating throughout the U.S. health care system.
As many know, a few months ago, the Medical Director Institute of the National Council for Behavioral Health, in partnership with the American Psychiatric Association, convened an expert panel to develop a report responding to this evolving quandary. The findings of our 60-page report, “The Psychiatric Shortage: Causes and Solutions,” suggest that psychiatry is uniquely positioned to address the issues that face our specialty.
The institute identified five areas of critical concern: workforce development, improved efficiency of service delivery, reducing burdensome regulations and confidentiality restrictions, broader implementation of innovative models, and adoption of novel reimbursement methods.
1. Workforce development
Psychiatrists come out of residency training without the skills they need to practice in today’s rapidly evolving health care environment. We need better preparation in measurement-based care, telepsychiatry, collaborative care, and other methods of efficient team collaboration with primary care.
Funding for graduate medical education and training programs must be expanded with an infusion of new funding – not only for psychiatrists – but also for psychiatric nurse practitioners and psychiatric physician assistants.
2. Improved efficiency of service delivery
Providers of psychiatric services in outpatient psychiatric programs face a cramped daily routine with increasingly briefer appointments scheduled back-to-back that limit in-depth clinical assessment, collaboration with other members of the treatment team, and consultation with primary care providers outside of the program. Such a schedule leads to lower-quality care.
Psychiatrists must have the same level of nurse and paraprofessional assistance and support provided to other medical specialties. In addition, regulations that prevent the broader use of telepsychiatry must be revised. All behavioral health providers should implement open access scheduling, a proven modality for reducing missed appointments.
3. Reducing burdensome regulations and confidentiality restrictions
Excessive documentation requirements, especially necessarily detailed, lengthy assessments and treatment must be revised and 42 CFR Part 2 must be made consistent with HIPAA requirements.
4. Broader implementation of innovative models
The shortage of psychiatrists will only worsen with the integration of primary care and behavioral health, and the shift to Accountable Care Organizations as part of health care reform (which, as of this writing, faces much uncertainty). Thanks to more efficient screening for mental health and substance use disorders now occurring in primary care, there will be growing demand for access to psychiatric services.
The collaborative care model for providing psychiatric services should be implemented throughout primary care. Behavioral health organizations must develop their own version of collaborative care that targets the limited psychiatric resource where it is most needed by using measurement-based care and collaborating more effectively with other team members.
5. Adoption of novel reimbursement methods
Inappropriately low rates limit access to care. Today, 40% of psychiatrists choose cash-only private practices, the second-highest among medical specialties after dermatologists, and 75% of provider organizations employing psychiatrists report that they lose money on their psychiatric services. At the same time, the shrinking number of inpatient psychiatric services has become a significant obstacle to improved access. Beds have been eliminated because of lower rates of reimbursement, compared with other medical-surgical procedures and difficulty in recruiting psychiatrists to staff inpatient units.
Psychiatric service rates must be reset to be consistent with the actual cost of providing care. Prospective payment models like Certified Community Behavioral Health Clinics should be expanded, and bundled payments for services like collaborative care and complex care should be covered by payers.
The Medical Director Institute recommends these solutions so that access to psychiatric services does not remain a barrier to the overall success of health care reform and service delivery improving the health of Americans. Multiple stakeholders – federal and state governments, payers, providers, provider trade associations, and advocates – must take action within their spheres of influence in the design, funding, regulation, and delivery of behavioral health care to improve access to psychiatric services. Such broad collaboration is imperative for our patients to get the care they need.
Dr. Parks is the medical director for the National Council for Behavioral Health. He practices psychiatry on an outpatient basis at Family Health Center, a federally funded community health center established to expand services to uninsured and underinsured patients in central Missouri. He also holds the position of Distinguished Research Professor of Science at the University of Missouri–St. Louis and is a clinical assistant professor of psychiatry at the University of Missouri–Columbia.
Bailout stenting for coronary bifurcations brings ‘unacceptable’ hazards
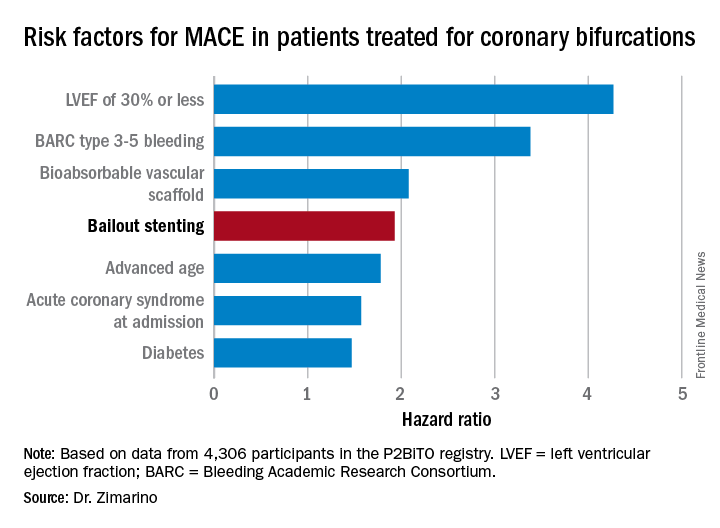
PARIS – Bailout stenting during percutaneous coronary intervention for coronary bifurcations doubled the risk of major adverse cardiovascular events in the world’s largest registry of patients with these often-challenging lesions treated using bioactive stents, Marco Zimarino, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
Indeed, resort to bailout stenting stood out as the major potentially modifiable risk factor for adverse outcomes among the 4,306 participants in the P2BiTO registry, an international collaboration supported by members of the EuroBifurcation Club. Most of the other independent risk factors identified in a multivariate regression analysis of the P2BiTO database were beyond operator control, including diabetes, advanced age, and presentation with an acute coronary syndrome, according to Dr. Zimarino of the University of Chieti (Italy).

Bailout stenting is largely avoidable through meticulous procedural planning, the interventional cardiologist added.
“Careful planning is always mandatory because bailout stenting is associated with an unacceptably higher risk of both in-hospital and 1-year adverse outcomes,” Dr. Zimarino emphasized. “It’s much better to leave a degraded side branch instead of using bailout stenting to get an excellent angiographic outcome that’s a predictor of a worse clinical outcome.”
Conventional wisdom holds that single stenting of either the main artery or a side branch in a patient with coronary bifurcation is safer than double stenting of both. However, that wasn’t really borne out in the P2BiTO registry provided the operator’s plan was for double stenting. The difference in 1-year major adverse cardiovascular events (MACE) between patients treated using a single- or double-stenting strategy wasn’t statistically significant, provided bailout stenting wasn’t utilized. If bailout stenting was employed, though, the risk of MACE was 2.2-fold greater than if the cardiologist stuck with the plan.
Ninety-eight percent of patients in the P2BiTO registry received drug-eluting stents. The other 2% got the Absorb bioabsorbable vascular scaffold. The percutaneous coronary intervention access site, treatment strategy, choice of stent, and duration of dual-antiplatelet therapy were left up to the operator’s discretion.
The risk of MACE was reduced by 39% in patients on dual-antiplatelet therapy for 6-12 months, compared with less than 6 months.
Discussant Graham Cassel, MD, director of the heart transplant unit at Milpark Hospital in Johannesburg, commented, “The message comes through very clearly that, if you plan your procedure well, the chance of bailout is far less – and if you do have to bail out, the results are uniformly bad. If you can avoid putting in two or three stents, that’s beneficial.”
Dr. Zimarino reported having no financial conflicts of interest regarding his presentation.

PARIS – Bailout stenting during percutaneous coronary intervention for coronary bifurcations doubled the risk of major adverse cardiovascular events in the world’s largest registry of patients with these often-challenging lesions treated using bioactive stents, Marco Zimarino, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
Indeed, resort to bailout stenting stood out as the major potentially modifiable risk factor for adverse outcomes among the 4,306 participants in the P2BiTO registry, an international collaboration supported by members of the EuroBifurcation Club. Most of the other independent risk factors identified in a multivariate regression analysis of the P2BiTO database were beyond operator control, including diabetes, advanced age, and presentation with an acute coronary syndrome, according to Dr. Zimarino of the University of Chieti (Italy).
Bailout stenting is largely avoidable through meticulous procedural planning, the interventional cardiologist added.
“Careful planning is always mandatory because bailout stenting is associated with an unacceptably higher risk of both in-hospital and 1-year adverse outcomes,” Dr. Zimarino emphasized. “It’s much better to leave a degraded side branch instead of using bailout stenting to get an excellent angiographic outcome that’s a predictor of a worse clinical outcome.”
Conventional wisdom holds that single stenting of either the main artery or a side branch in a patient with coronary bifurcation is safer than double stenting of both. However, that wasn’t really borne out in the P2BiTO registry provided the operator’s plan was for double stenting. The difference in 1-year major adverse cardiovascular events (MACE) between patients treated using a single- or double-stenting strategy wasn’t statistically significant, provided bailout stenting wasn’t utilized. If bailout stenting was employed, though, the risk of MACE was 2.2-fold greater than if the cardiologist stuck with the plan.
Ninety-eight percent of patients in the P2BiTO registry received drug-eluting stents. The other 2% got the Absorb bioabsorbable vascular scaffold. The percutaneous coronary intervention access site, treatment strategy, choice of stent, and duration of dual-antiplatelet therapy were left up to the operator’s discretion.
The risk of MACE was reduced by 39% in patients on dual-antiplatelet therapy for 6-12 months, compared with less than 6 months.
Discussant Graham Cassel, MD, director of the heart transplant unit at Milpark Hospital in Johannesburg, commented, “The message comes through very clearly that, if you plan your procedure well, the chance of bailout is far less – and if you do have to bail out, the results are uniformly bad. If you can avoid putting in two or three stents, that’s beneficial.”
Dr. Zimarino reported having no financial conflicts of interest regarding his presentation.
PARIS – Bailout stenting during percutaneous coronary intervention for coronary bifurcations doubled the risk of major adverse cardiovascular events in the world’s largest registry of patients with these often-challenging lesions treated using bioactive stents, Marco Zimarino, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
Indeed, resort to bailout stenting stood out as the major potentially modifiable risk factor for adverse outcomes among the 4,306 participants in the P2BiTO registry, an international collaboration supported by members of the EuroBifurcation Club. Most of the other independent risk factors identified in a multivariate regression analysis of the P2BiTO database were beyond operator control, including diabetes, advanced age, and presentation with an acute coronary syndrome, according to Dr. Zimarino of the University of Chieti (Italy).
Bailout stenting is largely avoidable through meticulous procedural planning, the interventional cardiologist added.
“Careful planning is always mandatory because bailout stenting is associated with an unacceptably higher risk of both in-hospital and 1-year adverse outcomes,” Dr. Zimarino emphasized. “It’s much better to leave a degraded side branch instead of using bailout stenting to get an excellent angiographic outcome that’s a predictor of a worse clinical outcome.”
Conventional wisdom holds that single stenting of either the main artery or a side branch in a patient with coronary bifurcation is safer than double stenting of both. However, that wasn’t really borne out in the P2BiTO registry provided the operator’s plan was for double stenting. The difference in 1-year major adverse cardiovascular events (MACE) between patients treated using a single- or double-stenting strategy wasn’t statistically significant, provided bailout stenting wasn’t utilized. If bailout stenting was employed, though, the risk of MACE was 2.2-fold greater than if the cardiologist stuck with the plan.
Ninety-eight percent of patients in the P2BiTO registry received drug-eluting stents. The other 2% got the Absorb bioabsorbable vascular scaffold. The percutaneous coronary intervention access site, treatment strategy, choice of stent, and duration of dual-antiplatelet therapy were left up to the operator’s discretion.
The risk of MACE was reduced by 39% in patients on dual-antiplatelet therapy for 6-12 months, compared with less than 6 months.
Discussant Graham Cassel, MD, director of the heart transplant unit at Milpark Hospital in Johannesburg, commented, “The message comes through very clearly that, if you plan your procedure well, the chance of bailout is far less – and if you do have to bail out, the results are uniformly bad. If you can avoid putting in two or three stents, that’s beneficial.”
Dr. Zimarino reported having no financial conflicts of interest regarding his presentation.
AT EUROPCR
Key clinical point:
Major finding: Bailout stenting during PCI for coronary bifurcations doubles the risk of major adverse cardiovascular events.
Data source: The P2BiTO registry includes 4,306 patients who received one or more drug-eluting stents or bioabsorbable vascular scaffolds for treatment of coronary bifurcations.
Disclosures: The study presenter reported having no financial conflicts of interest.
Revascularization of CTOs improves health status more than medical therapy
PARIS – The first randomized clinical trial to evaluate quality of life and clinical symptoms as the primary efficacy outcome in patients with coronary chronic total occlusion (CTO) showed a clear advantage for percutaneous revascularization over optimal medical therapy.
At 12 months’ follow-up in the 26-site, 396-patient EuroCTO trial, patients randomized to PCI with drug-eluting stents had significantly less angina and physical limitations coupled with greater improvement in quality of life than the optimal medical therapy (OMT) group on subscales of the Seattle Angina Questionnaire. On the angina frequency subscale, for example, the PCI group improved from a mean baseline score of 77.2 to 91.4 at 12 months, a significantly better result than the OMT group improvement from 80.6 to 87.5.
The PCI group also experienced greater mobility, better activity status, and less pain and discomfort as assessed by the EuroQOL five dimensions questionnaire (EQ-5D), Gerald S. Werner, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“PCI of a CTO should be considered as a primary option in symptomatic patients. It is a safe and effective treatment option in expert hands,” said Dr. Werner, director of cardiology and nonsurgical intensive care at the Darmstadt (Ger.) Clinic.
He emphasized the point about “expert hands,” drawing attention to the stellar 86.3% successful revascularization rate in the EuroCTO trial, even though these were often complex procedures. Indeed, in 36% of the CTO PCIs, a retrograde approach was used.
“CTO is a special field. Just like not everybody in every hospital will do a transcatheter aortic valve replacement, not everybody should do a CTO. It can be done safely and to the benefit of the patient, but it needs to be done by someone with expertise,” the cardiologist said.
Study participants were evenly split between those with single- and multivessel disease. Patients with additional nonocclusive disease had those lesions treated by PCI before the 2:1 randomization to CTO PCI or OMT.
The periprocedural complication rate was low at 2.9%, a figure that included a 1.5% incidence of pericardial tamponade as well as vascular repairs. There were no periprocedural MIs or deaths. The 1-year major adverse cardiac event rate was roughly 6% in both study arms.
The PCI group received 6-12 months of dual-antiplatelet therapy with clopidogrel and aspirin. So did roughly 40% of the OMT group because of prior PCI.
Both study arms had comparably high rates of guideline-directed medical therapy, including statins, beta-blockers, and ACE inhibitors. However, the PCI group made significantly less use of nitrates than the OMT group during follow-up, reflecting their greater reduction in angina frequency. The crossover rate from OMT to PCI because of ongoing angina was 7.3%.
The long-term safety and durability of the two treatment strategies will be assessed at 3 years of follow-up.
The EuroCTO trial was originally planned for 600 patients. The investigators eventually settled for less because of slow enrollment. Many interventionalists who are skilled in treating CTOs proved reluctant to randomize the patients.
Dr. Werner contrasted the positive EuroCTO findings regarding clinical symptoms and quality of life to the negative results of the Korean DECISION CTO trial presented at the 2017 meeting of the American College of Cardiology. DECISION CTO found that PCI plus OMT wasn’t superior to OMT alone in reducing MI and other major adverse cardiac events in patients with at least one CTO. In Dr. Werner’s view, the Korean investigators chose the wrong endpoint.
“The quality of life improvement we’ve shown after PCI in EuroCTO is a valid clinical goal in treating stable coronary artery disease. I don’t think we can aim at improving prognosis,” according to Dr. Werner.
The impetus for EuroCTO was a recognition that CTOs are common and seriously undertreated. CTOs account for 16%-18% of all coronary lesions in patients with stable coronary artery disease, yet U.S. national data indicate only 5% of PCIs are performed to treat CTOs.
The EuroCTO trial was sponsored by the Euro CTO Club and supported by research grants from Biosensors and Asahi.
PARIS – The first randomized clinical trial to evaluate quality of life and clinical symptoms as the primary efficacy outcome in patients with coronary chronic total occlusion (CTO) showed a clear advantage for percutaneous revascularization over optimal medical therapy.
At 12 months’ follow-up in the 26-site, 396-patient EuroCTO trial, patients randomized to PCI with drug-eluting stents had significantly less angina and physical limitations coupled with greater improvement in quality of life than the optimal medical therapy (OMT) group on subscales of the Seattle Angina Questionnaire. On the angina frequency subscale, for example, the PCI group improved from a mean baseline score of 77.2 to 91.4 at 12 months, a significantly better result than the OMT group improvement from 80.6 to 87.5.
The PCI group also experienced greater mobility, better activity status, and less pain and discomfort as assessed by the EuroQOL five dimensions questionnaire (EQ-5D), Gerald S. Werner, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“PCI of a CTO should be considered as a primary option in symptomatic patients. It is a safe and effective treatment option in expert hands,” said Dr. Werner, director of cardiology and nonsurgical intensive care at the Darmstadt (Ger.) Clinic.
He emphasized the point about “expert hands,” drawing attention to the stellar 86.3% successful revascularization rate in the EuroCTO trial, even though these were often complex procedures. Indeed, in 36% of the CTO PCIs, a retrograde approach was used.
“CTO is a special field. Just like not everybody in every hospital will do a transcatheter aortic valve replacement, not everybody should do a CTO. It can be done safely and to the benefit of the patient, but it needs to be done by someone with expertise,” the cardiologist said.
Study participants were evenly split between those with single- and multivessel disease. Patients with additional nonocclusive disease had those lesions treated by PCI before the 2:1 randomization to CTO PCI or OMT.
The periprocedural complication rate was low at 2.9%, a figure that included a 1.5% incidence of pericardial tamponade as well as vascular repairs. There were no periprocedural MIs or deaths. The 1-year major adverse cardiac event rate was roughly 6% in both study arms.
The PCI group received 6-12 months of dual-antiplatelet therapy with clopidogrel and aspirin. So did roughly 40% of the OMT group because of prior PCI.
Both study arms had comparably high rates of guideline-directed medical therapy, including statins, beta-blockers, and ACE inhibitors. However, the PCI group made significantly less use of nitrates than the OMT group during follow-up, reflecting their greater reduction in angina frequency. The crossover rate from OMT to PCI because of ongoing angina was 7.3%.
The long-term safety and durability of the two treatment strategies will be assessed at 3 years of follow-up.
The EuroCTO trial was originally planned for 600 patients. The investigators eventually settled for less because of slow enrollment. Many interventionalists who are skilled in treating CTOs proved reluctant to randomize the patients.
Dr. Werner contrasted the positive EuroCTO findings regarding clinical symptoms and quality of life to the negative results of the Korean DECISION CTO trial presented at the 2017 meeting of the American College of Cardiology. DECISION CTO found that PCI plus OMT wasn’t superior to OMT alone in reducing MI and other major adverse cardiac events in patients with at least one CTO. In Dr. Werner’s view, the Korean investigators chose the wrong endpoint.
“The quality of life improvement we’ve shown after PCI in EuroCTO is a valid clinical goal in treating stable coronary artery disease. I don’t think we can aim at improving prognosis,” according to Dr. Werner.
The impetus for EuroCTO was a recognition that CTOs are common and seriously undertreated. CTOs account for 16%-18% of all coronary lesions in patients with stable coronary artery disease, yet U.S. national data indicate only 5% of PCIs are performed to treat CTOs.
The EuroCTO trial was sponsored by the Euro CTO Club and supported by research grants from Biosensors and Asahi.
PARIS – The first randomized clinical trial to evaluate quality of life and clinical symptoms as the primary efficacy outcome in patients with coronary chronic total occlusion (CTO) showed a clear advantage for percutaneous revascularization over optimal medical therapy.
At 12 months’ follow-up in the 26-site, 396-patient EuroCTO trial, patients randomized to PCI with drug-eluting stents had significantly less angina and physical limitations coupled with greater improvement in quality of life than the optimal medical therapy (OMT) group on subscales of the Seattle Angina Questionnaire. On the angina frequency subscale, for example, the PCI group improved from a mean baseline score of 77.2 to 91.4 at 12 months, a significantly better result than the OMT group improvement from 80.6 to 87.5.
The PCI group also experienced greater mobility, better activity status, and less pain and discomfort as assessed by the EuroQOL five dimensions questionnaire (EQ-5D), Gerald S. Werner, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“PCI of a CTO should be considered as a primary option in symptomatic patients. It is a safe and effective treatment option in expert hands,” said Dr. Werner, director of cardiology and nonsurgical intensive care at the Darmstadt (Ger.) Clinic.
He emphasized the point about “expert hands,” drawing attention to the stellar 86.3% successful revascularization rate in the EuroCTO trial, even though these were often complex procedures. Indeed, in 36% of the CTO PCIs, a retrograde approach was used.
“CTO is a special field. Just like not everybody in every hospital will do a transcatheter aortic valve replacement, not everybody should do a CTO. It can be done safely and to the benefit of the patient, but it needs to be done by someone with expertise,” the cardiologist said.
Study participants were evenly split between those with single- and multivessel disease. Patients with additional nonocclusive disease had those lesions treated by PCI before the 2:1 randomization to CTO PCI or OMT.
The periprocedural complication rate was low at 2.9%, a figure that included a 1.5% incidence of pericardial tamponade as well as vascular repairs. There were no periprocedural MIs or deaths. The 1-year major adverse cardiac event rate was roughly 6% in both study arms.
The PCI group received 6-12 months of dual-antiplatelet therapy with clopidogrel and aspirin. So did roughly 40% of the OMT group because of prior PCI.
Both study arms had comparably high rates of guideline-directed medical therapy, including statins, beta-blockers, and ACE inhibitors. However, the PCI group made significantly less use of nitrates than the OMT group during follow-up, reflecting their greater reduction in angina frequency. The crossover rate from OMT to PCI because of ongoing angina was 7.3%.
The long-term safety and durability of the two treatment strategies will be assessed at 3 years of follow-up.
The EuroCTO trial was originally planned for 600 patients. The investigators eventually settled for less because of slow enrollment. Many interventionalists who are skilled in treating CTOs proved reluctant to randomize the patients.
Dr. Werner contrasted the positive EuroCTO findings regarding clinical symptoms and quality of life to the negative results of the Korean DECISION CTO trial presented at the 2017 meeting of the American College of Cardiology. DECISION CTO found that PCI plus OMT wasn’t superior to OMT alone in reducing MI and other major adverse cardiac events in patients with at least one CTO. In Dr. Werner’s view, the Korean investigators chose the wrong endpoint.
“The quality of life improvement we’ve shown after PCI in EuroCTO is a valid clinical goal in treating stable coronary artery disease. I don’t think we can aim at improving prognosis,” according to Dr. Werner.
The impetus for EuroCTO was a recognition that CTOs are common and seriously undertreated. CTOs account for 16%-18% of all coronary lesions in patients with stable coronary artery disease, yet U.S. national data indicate only 5% of PCIs are performed to treat CTOs.
The EuroCTO trial was sponsored by the Euro CTO Club and supported by research grants from Biosensors and Asahi.
AT EUROPCR
Key clinical point:
Major finding: Patients whose chronic total occlusions were treated by PCI rather than optimal medical therapy experienced significantly less angina and greater improvement in quality of life during 12 months of follow-up.
Data source: EuroCTO, a prospective, 26-site study in which 396 patients with coronary chronic total occlusions were randomized 2:1 to PCI or optimal medical therapy.
Disclosures: EuroCTO was sponsored by the Euro CTO Club and supported by research grants from Biosensors and Asahi.
Catching Up With Our CHEST Past Presidents
Where are they now? What have they been up to? CHEST’s Past Presidents each forged the way for the many successes of the American College of Chest Physicians, leading to enhanced patient care around the globe. Their outstanding leadership and vision are evidenced today in many of CHEST’s strategic initiatives. Let’s check in with Dr. Goldberg.
I arrived in Toronto in 1998 to start my term as President of the American College of Chest Physicians. (I had always loved Toronto, where I had spent months training in pediatric critical care at “Sick Kids” [Toronto’s Children’s Hospital] and collaborating with Audrey King on disability issues and public policy in Ontario.) CHEST 1998 in Toronto was equally exciting. What I remember - with humility – was that being CHEST President is not about “you.” It is about “The President,” who is honored and revered by all members for what CHEST truly represents … excellence in health-care education, communication, and information. Everyone came up to me to respect and honor the role … including awesome Past Presidents who lovingly shared their insights and experience and others (including many who became future presidents) to volunteer their assistance. I was in awe of these leaders and how they demonstrated selfless service.
And so I began my year of presidential service leadership. What I remember best is the respect all around the world for CHEST and what it does to unite people into actions that improve health globally. The President serves CHEST members to facilitate working together, which makes a difference. My presidential year culminated in the 65th anniversary conference in Chicago in 1999. All year, I had worked with my mentor (C. Everett Koop, MD, FCCP(Hon), to plan an opening ceremony that would be inspirational and unforgettable. For years, we had shared personal/private conversations. This time, we planned to communicate in public to inspire others and help them understand key issues we considered critical for the future of health care and global health.
Soon after my Presidential term, I took 2 years off for sabbatical to work more closely with Dr. Koop (2000-2002). Then, I retired to continue to focus on our work together and as personal caregiver for my wife, Evi Faure, MD, FCCP. Dr. Koop and I met many times and also held more public presentations, including the 2003 Surgeons’ General National Meeting on Overcoming Health Disparities at Howard University arranged with CHEST Past President Dr. Alvin Thomas.
All our joint efforts focused on the importance of Communication in Health Care. We shared the belief that communication of health information would create the “informed patient and family” who would then work together in partnership with health-care professional team members. We thought that this would be the best way to improve and reform health-care delivery. We sought to provide information (the “what”) in ways that it would be trusted, understandable, and easily usable (the “how) for patients and famili

My greatest learning was the importance of mentorship – both for the mentor and mentee. This fosters communication that enables learning and growth in our abilities to serve others by the profession we love.
http://www.chestnet.org/News/Blogs/CHEST-Thought-Leaders/2013/06/Dr-Koops-Legacy-Reflections-on-Mentorship
http://www.chestnet.org/News/Blogs/CHEST-Thought-Leaders/2013/08/The-Legacy-of-Dr-Koop-Reflections-on-Our-Fireside-Chat
Where are they now? What have they been up to? CHEST’s Past Presidents each forged the way for the many successes of the American College of Chest Physicians, leading to enhanced patient care around the globe. Their outstanding leadership and vision are evidenced today in many of CHEST’s strategic initiatives. Let’s check in with Dr. Goldberg.
I arrived in Toronto in 1998 to start my term as President of the American College of Chest Physicians. (I had always loved Toronto, where I had spent months training in pediatric critical care at “Sick Kids” [Toronto’s Children’s Hospital] and collaborating with Audrey King on disability issues and public policy in Ontario.) CHEST 1998 in Toronto was equally exciting. What I remember - with humility – was that being CHEST President is not about “you.” It is about “The President,” who is honored and revered by all members for what CHEST truly represents … excellence in health-care education, communication, and information. Everyone came up to me to respect and honor the role … including awesome Past Presidents who lovingly shared their insights and experience and others (including many who became future presidents) to volunteer their assistance. I was in awe of these leaders and how they demonstrated selfless service.
And so I began my year of presidential service leadership. What I remember best is the respect all around the world for CHEST and what it does to unite people into actions that improve health globally. The President serves CHEST members to facilitate working together, which makes a difference. My presidential year culminated in the 65th anniversary conference in Chicago in 1999. All year, I had worked with my mentor (C. Everett Koop, MD, FCCP(Hon), to plan an opening ceremony that would be inspirational and unforgettable. For years, we had shared personal/private conversations. This time, we planned to communicate in public to inspire others and help them understand key issues we considered critical for the future of health care and global health.
Soon after my Presidential term, I took 2 years off for sabbatical to work more closely with Dr. Koop (2000-2002). Then, I retired to continue to focus on our work together and as personal caregiver for my wife, Evi Faure, MD, FCCP. Dr. Koop and I met many times and also held more public presentations, including the 2003 Surgeons’ General National Meeting on Overcoming Health Disparities at Howard University arranged with CHEST Past President Dr. Alvin Thomas.
All our joint efforts focused on the importance of Communication in Health Care. We shared the belief that communication of health information would create the “informed patient and family” who would then work together in partnership with health-care professional team members. We thought that this would be the best way to improve and reform health-care delivery. We sought to provide information (the “what”) in ways that it would be trusted, understandable, and easily usable (the “how) for patients and famili
My greatest learning was the importance of mentorship – both for the mentor and mentee. This fosters communication that enables learning and growth in our abilities to serve others by the profession we love.
http://www.chestnet.org/News/Blogs/CHEST-Thought-Leaders/2013/06/Dr-Koops-Legacy-Reflections-on-Mentorship
http://www.chestnet.org/News/Blogs/CHEST-Thought-Leaders/2013/08/The-Legacy-of-Dr-Koop-Reflections-on-Our-Fireside-Chat
Where are they now? What have they been up to? CHEST’s Past Presidents each forged the way for the many successes of the American College of Chest Physicians, leading to enhanced patient care around the globe. Their outstanding leadership and vision are evidenced today in many of CHEST’s strategic initiatives. Let’s check in with Dr. Goldberg.
I arrived in Toronto in 1998 to start my term as President of the American College of Chest Physicians. (I had always loved Toronto, where I had spent months training in pediatric critical care at “Sick Kids” [Toronto’s Children’s Hospital] and collaborating with Audrey King on disability issues and public policy in Ontario.) CHEST 1998 in Toronto was equally exciting. What I remember - with humility – was that being CHEST President is not about “you.” It is about “The President,” who is honored and revered by all members for what CHEST truly represents … excellence in health-care education, communication, and information. Everyone came up to me to respect and honor the role … including awesome Past Presidents who lovingly shared their insights and experience and others (including many who became future presidents) to volunteer their assistance. I was in awe of these leaders and how they demonstrated selfless service.
And so I began my year of presidential service leadership. What I remember best is the respect all around the world for CHEST and what it does to unite people into actions that improve health globally. The President serves CHEST members to facilitate working together, which makes a difference. My presidential year culminated in the 65th anniversary conference in Chicago in 1999. All year, I had worked with my mentor (C. Everett Koop, MD, FCCP(Hon), to plan an opening ceremony that would be inspirational and unforgettable. For years, we had shared personal/private conversations. This time, we planned to communicate in public to inspire others and help them understand key issues we considered critical for the future of health care and global health.
Soon after my Presidential term, I took 2 years off for sabbatical to work more closely with Dr. Koop (2000-2002). Then, I retired to continue to focus on our work together and as personal caregiver for my wife, Evi Faure, MD, FCCP. Dr. Koop and I met many times and also held more public presentations, including the 2003 Surgeons’ General National Meeting on Overcoming Health Disparities at Howard University arranged with CHEST Past President Dr. Alvin Thomas.
All our joint efforts focused on the importance of Communication in Health Care. We shared the belief that communication of health information would create the “informed patient and family” who would then work together in partnership with health-care professional team members. We thought that this would be the best way to improve and reform health-care delivery. We sought to provide information (the “what”) in ways that it would be trusted, understandable, and easily usable (the “how) for patients and famili
My greatest learning was the importance of mentorship – both for the mentor and mentee. This fosters communication that enables learning and growth in our abilities to serve others by the profession we love.
http://www.chestnet.org/News/Blogs/CHEST-Thought-Leaders/2013/06/Dr-Koops-Legacy-Reflections-on-Mentorship
http://www.chestnet.org/News/Blogs/CHEST-Thought-Leaders/2013/08/The-Legacy-of-Dr-Koop-Reflections-on-Our-Fireside-Chat
Pediatric version of SOFA effective
An age-adjusted version of the Sequential Organ Failure Assessment score for sepsis has been found to be at least as good, if not better than, other pediatric organ dysfunction scores at predicting in-hospital mortality.
Writing in the Aug. 7 online edition of JAMA Pediatrics, researchers reported the outcome of a retrospective observational cohort study in 6,303 critically ill patients aged 21 years or younger, which was used to adapt and validate a pediatric version of the Sequential Organ Failure Assessment (SOFA) score.
“One of the major limitations of the SOFA score is that it was developed for adult patients and contains measures that vary significantly with age, which makes it unsuitable for children,” wrote Travis J. Matics, DO, and L. Nelson Sanchez-Pinto, MD, of the department of pediatrics at the University of Chicago.
Several pediatric organ dysfunction scores exist, but their range, scale, and coverage are different from those of the SOFA score, which makes them difficult to use concurrently (JAMA Pediatr. 2017 Aug 7. doi: 10.1001/jamapediatrics.2017.2352).
“Fundamentally, having different definitions of sepsis for patients above or below the pediatric-adult threshold has no known physiologic justification and should therefore be avoided,” the authors wrote.
In this study, they modified the age-dependent cardiovascular and renal variables of the adult SOFA score by using validated cut-offs from the updated Pediatric Logistic Organ Dysfunction (PELOD-2) scoring system. They also expanded the respiratory subscore to incorporate the SpO2:FiO2 ratio as an alternative surrogate of lung injury.
The neurologic subscore, based on the Glasgow Coma Scale, was changed to a pediatric version of the scale. The coagulation and hepatic criteria remained the same as the adult version of the score.
Validating the pediatric version of the SOFA score (pSOFA) score in 8,711 hospital encounters, researchers found that nonsurvivors had a significantly higher median maximum pSOFA score, compared with survivors (13 vs. 2, P less than .001). The area under the curve (AUC) for discriminating in-hospital mortality was 0.94 (95% confidence interval, 0.92-0.95) and remained stable across sex, age groups, and admission types.
The maximum pSOFA score was as good as the PELOD and PELOD-2 scales at discriminating in-hospital mortality and better than the Pediatric Multiple Organ Dysfunction Score. It also showed “excellent” discrimination of in-hospital mortality among the 48.4% of patients who had a confirmed or suspected infection in the pediatric intensive care unit (AUC, 0.92; 95% CI, 0.91-0.94), Dr. Matics and Dr. Sanchez-Pinto reported.
Researchers also looked at the clinical utility of pSOFA on the day of admission, compared with the Pediatric Risk of Mortality (PRISM) III score, and found the two were similar, while the pSOFA outperformed other organ dysfunction scores in this setting.
Overall, 14.1% of the pediatric intensive care population met the sepsis criteria according to the adapted definitions and pSOFA scores, and this group had a mortality of 12.1%. Four percent of the population met the criteria for septic shock, with a mortality of 32.3%.
The SOFA score incorporates respiratory, coagulation, renal, hepatic, cardiovascular, and neurologic variables. The authors, however, argued that it does not account for age-related variability, in particular in renal criteria and the detrimental effects of kidney dysfunction in younger patients.
“In addition, the respiratory subscore criteria – based on the ratio of PaO2 to the fraction of inspired oxygen (FiO2) – have not been modified in previous adaptations of the SOFA score even though the decreased use of arterial blood gases in children is a known limitation,” they wrote.
“Having a harmonized definition of sepsis across age groups while recognizing the importance of the age-based variation of its measures can have many benefits, including better design of clinical trials, improved accuracy of reported outcomes, and better translation of the research and clinical strategies in the management of sepsis,” Dr. Matics and Dr. Sanchez-Pinto said.
They acknowledged, however, that their findings were limited because they were generated using retrospective data and needed to be validated in a large multicenter sample of critically ill children. They also pointed out that they did not evaluate the performance of pSOFA as a longitudinal biomarker and suggested that such studies would improve understanding of pSOFA’s clinical utility.
No conflicts of interest were reported.

An age-adjusted version of the Sequential Organ Failure Assessment score for sepsis has been found to be at least as good, if not better than, other pediatric organ dysfunction scores at predicting in-hospital mortality.
Writing in the Aug. 7 online edition of JAMA Pediatrics, researchers reported the outcome of a retrospective observational cohort study in 6,303 critically ill patients aged 21 years or younger, which was used to adapt and validate a pediatric version of the Sequential Organ Failure Assessment (SOFA) score.
“One of the major limitations of the SOFA score is that it was developed for adult patients and contains measures that vary significantly with age, which makes it unsuitable for children,” wrote Travis J. Matics, DO, and L. Nelson Sanchez-Pinto, MD, of the department of pediatrics at the University of Chicago.
Several pediatric organ dysfunction scores exist, but their range, scale, and coverage are different from those of the SOFA score, which makes them difficult to use concurrently (JAMA Pediatr. 2017 Aug 7. doi: 10.1001/jamapediatrics.2017.2352).
“Fundamentally, having different definitions of sepsis for patients above or below the pediatric-adult threshold has no known physiologic justification and should therefore be avoided,” the authors wrote.
In this study, they modified the age-dependent cardiovascular and renal variables of the adult SOFA score by using validated cut-offs from the updated Pediatric Logistic Organ Dysfunction (PELOD-2) scoring system. They also expanded the respiratory subscore to incorporate the SpO2:FiO2 ratio as an alternative surrogate of lung injury.
The neurologic subscore, based on the Glasgow Coma Scale, was changed to a pediatric version of the scale. The coagulation and hepatic criteria remained the same as the adult version of the score.
Validating the pediatric version of the SOFA score (pSOFA) score in 8,711 hospital encounters, researchers found that nonsurvivors had a significantly higher median maximum pSOFA score, compared with survivors (13 vs. 2, P less than .001). The area under the curve (AUC) for discriminating in-hospital mortality was 0.94 (95% confidence interval, 0.92-0.95) and remained stable across sex, age groups, and admission types.
The maximum pSOFA score was as good as the PELOD and PELOD-2 scales at discriminating in-hospital mortality and better than the Pediatric Multiple Organ Dysfunction Score. It also showed “excellent” discrimination of in-hospital mortality among the 48.4% of patients who had a confirmed or suspected infection in the pediatric intensive care unit (AUC, 0.92; 95% CI, 0.91-0.94), Dr. Matics and Dr. Sanchez-Pinto reported.
Researchers also looked at the clinical utility of pSOFA on the day of admission, compared with the Pediatric Risk of Mortality (PRISM) III score, and found the two were similar, while the pSOFA outperformed other organ dysfunction scores in this setting.
Overall, 14.1% of the pediatric intensive care population met the sepsis criteria according to the adapted definitions and pSOFA scores, and this group had a mortality of 12.1%. Four percent of the population met the criteria for septic shock, with a mortality of 32.3%.
The SOFA score incorporates respiratory, coagulation, renal, hepatic, cardiovascular, and neurologic variables. The authors, however, argued that it does not account for age-related variability, in particular in renal criteria and the detrimental effects of kidney dysfunction in younger patients.
“In addition, the respiratory subscore criteria – based on the ratio of PaO2 to the fraction of inspired oxygen (FiO2) – have not been modified in previous adaptations of the SOFA score even though the decreased use of arterial blood gases in children is a known limitation,” they wrote.
“Having a harmonized definition of sepsis across age groups while recognizing the importance of the age-based variation of its measures can have many benefits, including better design of clinical trials, improved accuracy of reported outcomes, and better translation of the research and clinical strategies in the management of sepsis,” Dr. Matics and Dr. Sanchez-Pinto said.
They acknowledged, however, that their findings were limited because they were generated using retrospective data and needed to be validated in a large multicenter sample of critically ill children. They also pointed out that they did not evaluate the performance of pSOFA as a longitudinal biomarker and suggested that such studies would improve understanding of pSOFA’s clinical utility.
No conflicts of interest were reported.
An age-adjusted version of the Sequential Organ Failure Assessment score for sepsis has been found to be at least as good, if not better than, other pediatric organ dysfunction scores at predicting in-hospital mortality.
Writing in the Aug. 7 online edition of JAMA Pediatrics, researchers reported the outcome of a retrospective observational cohort study in 6,303 critically ill patients aged 21 years or younger, which was used to adapt and validate a pediatric version of the Sequential Organ Failure Assessment (SOFA) score.
“One of the major limitations of the SOFA score is that it was developed for adult patients and contains measures that vary significantly with age, which makes it unsuitable for children,” wrote Travis J. Matics, DO, and L. Nelson Sanchez-Pinto, MD, of the department of pediatrics at the University of Chicago.
Several pediatric organ dysfunction scores exist, but their range, scale, and coverage are different from those of the SOFA score, which makes them difficult to use concurrently (JAMA Pediatr. 2017 Aug 7. doi: 10.1001/jamapediatrics.2017.2352).
“Fundamentally, having different definitions of sepsis for patients above or below the pediatric-adult threshold has no known physiologic justification and should therefore be avoided,” the authors wrote.
In this study, they modified the age-dependent cardiovascular and renal variables of the adult SOFA score by using validated cut-offs from the updated Pediatric Logistic Organ Dysfunction (PELOD-2) scoring system. They also expanded the respiratory subscore to incorporate the SpO2:FiO2 ratio as an alternative surrogate of lung injury.
The neurologic subscore, based on the Glasgow Coma Scale, was changed to a pediatric version of the scale. The coagulation and hepatic criteria remained the same as the adult version of the score.
Validating the pediatric version of the SOFA score (pSOFA) score in 8,711 hospital encounters, researchers found that nonsurvivors had a significantly higher median maximum pSOFA score, compared with survivors (13 vs. 2, P less than .001). The area under the curve (AUC) for discriminating in-hospital mortality was 0.94 (95% confidence interval, 0.92-0.95) and remained stable across sex, age groups, and admission types.
The maximum pSOFA score was as good as the PELOD and PELOD-2 scales at discriminating in-hospital mortality and better than the Pediatric Multiple Organ Dysfunction Score. It also showed “excellent” discrimination of in-hospital mortality among the 48.4% of patients who had a confirmed or suspected infection in the pediatric intensive care unit (AUC, 0.92; 95% CI, 0.91-0.94), Dr. Matics and Dr. Sanchez-Pinto reported.
Researchers also looked at the clinical utility of pSOFA on the day of admission, compared with the Pediatric Risk of Mortality (PRISM) III score, and found the two were similar, while the pSOFA outperformed other organ dysfunction scores in this setting.
Overall, 14.1% of the pediatric intensive care population met the sepsis criteria according to the adapted definitions and pSOFA scores, and this group had a mortality of 12.1%. Four percent of the population met the criteria for septic shock, with a mortality of 32.3%.
The SOFA score incorporates respiratory, coagulation, renal, hepatic, cardiovascular, and neurologic variables. The authors, however, argued that it does not account for age-related variability, in particular in renal criteria and the detrimental effects of kidney dysfunction in younger patients.
“In addition, the respiratory subscore criteria – based on the ratio of PaO2 to the fraction of inspired oxygen (FiO2) – have not been modified in previous adaptations of the SOFA score even though the decreased use of arterial blood gases in children is a known limitation,” they wrote.
“Having a harmonized definition of sepsis across age groups while recognizing the importance of the age-based variation of its measures can have many benefits, including better design of clinical trials, improved accuracy of reported outcomes, and better translation of the research and clinical strategies in the management of sepsis,” Dr. Matics and Dr. Sanchez-Pinto said.
They acknowledged, however, that their findings were limited because they were generated using retrospective data and needed to be validated in a large multicenter sample of critically ill children. They also pointed out that they did not evaluate the performance of pSOFA as a longitudinal biomarker and suggested that such studies would improve understanding of pSOFA’s clinical utility.
No conflicts of interest were reported.
FROM JAMA PEDIATRICS
Key clinical point: A pediatric version of the Sequential Organ Failure Assessment score for sepsis can discriminate in-hospital mortality in critically ill children.
Major finding: An age-adjusted version of the SOFA score for sepsis has found to be at least as good, if not better than, other pediatric organ dysfunction scores at predicting in-hospital mortality.
Data source: A retrospective observational cohort study in 6,303 critically ill patients aged 21 years or younger.
Disclosures: No conflicts of interest were declared.