User login
Early escitalopram for post-ACS depression improves MACE, 8 years on
Even years after their cardiac events, acute coronary syndrome patients whose depression was treated with 6 months of an antidepressant had fewer cardiovascular events, according to a randomized, controlled trial.
Compared with patients who were given placebo for depression after experiencing acute coronary syndrome (ACS), patients who received escitalopram experienced a lower incidence of a composite outcome of major adverse cardiovascular events (MACE), in this extension study of a 6-month trial reported previously (J Clin Psychiatry. 2015 Jan;76[1]:62-8).
After a median of 8.1 years, MACE, the study’s primary outcome, was experienced by 40.9% of patients taking escitalopram, compared with 53.6% of those taking placebo (hazard ratio 0.69, 95% confidence interval 0.49-0.96, P = .03). The investigators also tracked the individual MACE components (all-cause mortality, myocardial infarction, and percutaneous coronary intervention), finding that MI was also significantly less common in the escitalopram group compared with those who took placebo (8.7% vs. 15.2%, HR 0.54, 95% CI, 0.27-0.96, P = .04).
The other MACE components were seen less frequently in the escitalopram group, but the differences from those taking placebo were not statistically significant. The study did not show a mortality benefit for those who took escitalopram, noted first author Jae-Min Kim, MD, of the department of psychiatry at Chonnam University Medical School, Gwangju, South Korea, and his coauthors.
The randomized, double-blind, placebo-controlled trial comprised 300 patients who recently had ACS and also met DSM-IV criteria for major or minor depression.
Over a 5-year period at a single site, patients were randomized to receive escitalopram at an initial dose of 10 mg daily (149 patients), or placebo (151), for 24 weeks after their ACS event. Escitalopram doses could be adjusted according to clinician judgment from 5 to 20 mg daily.
Patients who consented to participate were enrolled and screened for depression within 2 weeks of their ACS event, and any who scored higher than 10 on the Beck Depression Inventory at the initial screen or at follow-up appointments up to 12 weeks post enrollment went on for further screening.
Demographic data were collected with an eye toward identifying factors that could affect cardiac outcomes, said Dr. Kim and his colleagues. So in addition to age, sex, and educational level, the investigators tracked participants’ living situations and marital and employment status.
Patients were a mean of 60 years old, and about 60% were male. The median Beck Depression Inventory score was 16-17.
The study differed from others, said the investigators, because it followed patients for a longer period of time. In previous studies, “[E]ffects on cardiac outcomes have not generally been found within the treatment period,” they wrote.
Though the study’s generalizability might be limited by the fact that it was conducted at a single site and all participants were Asian, the single-site design and South Korea’s comprehensive patient data registries also allowed for complete data collection over a very long follow-up period, noted Dr. Kim and his colleagues.
Adherence was high, at 93% for those taking escitalopram and 95% for those taking placebo. Other work published from the study has shown that those taking 24 weeks of escitalopram had less depression than did those taking placebo, they added.
One coauthor reported receiving financial support from Janssen and Roche. The study was supported by the National Research Foundation of Korea.
SOURCE: Kim J-M et al. JAMA. 2018;320(4):350-8.
Even years after their cardiac events, acute coronary syndrome patients whose depression was treated with 6 months of an antidepressant had fewer cardiovascular events, according to a randomized, controlled trial.
Compared with patients who were given placebo for depression after experiencing acute coronary syndrome (ACS), patients who received escitalopram experienced a lower incidence of a composite outcome of major adverse cardiovascular events (MACE), in this extension study of a 6-month trial reported previously (J Clin Psychiatry. 2015 Jan;76[1]:62-8).
After a median of 8.1 years, MACE, the study’s primary outcome, was experienced by 40.9% of patients taking escitalopram, compared with 53.6% of those taking placebo (hazard ratio 0.69, 95% confidence interval 0.49-0.96, P = .03). The investigators also tracked the individual MACE components (all-cause mortality, myocardial infarction, and percutaneous coronary intervention), finding that MI was also significantly less common in the escitalopram group compared with those who took placebo (8.7% vs. 15.2%, HR 0.54, 95% CI, 0.27-0.96, P = .04).
The other MACE components were seen less frequently in the escitalopram group, but the differences from those taking placebo were not statistically significant. The study did not show a mortality benefit for those who took escitalopram, noted first author Jae-Min Kim, MD, of the department of psychiatry at Chonnam University Medical School, Gwangju, South Korea, and his coauthors.
The randomized, double-blind, placebo-controlled trial comprised 300 patients who recently had ACS and also met DSM-IV criteria for major or minor depression.
Over a 5-year period at a single site, patients were randomized to receive escitalopram at an initial dose of 10 mg daily (149 patients), or placebo (151), for 24 weeks after their ACS event. Escitalopram doses could be adjusted according to clinician judgment from 5 to 20 mg daily.
Patients who consented to participate were enrolled and screened for depression within 2 weeks of their ACS event, and any who scored higher than 10 on the Beck Depression Inventory at the initial screen or at follow-up appointments up to 12 weeks post enrollment went on for further screening.
Demographic data were collected with an eye toward identifying factors that could affect cardiac outcomes, said Dr. Kim and his colleagues. So in addition to age, sex, and educational level, the investigators tracked participants’ living situations and marital and employment status.
Patients were a mean of 60 years old, and about 60% were male. The median Beck Depression Inventory score was 16-17.
The study differed from others, said the investigators, because it followed patients for a longer period of time. In previous studies, “[E]ffects on cardiac outcomes have not generally been found within the treatment period,” they wrote.
Though the study’s generalizability might be limited by the fact that it was conducted at a single site and all participants were Asian, the single-site design and South Korea’s comprehensive patient data registries also allowed for complete data collection over a very long follow-up period, noted Dr. Kim and his colleagues.
Adherence was high, at 93% for those taking escitalopram and 95% for those taking placebo. Other work published from the study has shown that those taking 24 weeks of escitalopram had less depression than did those taking placebo, they added.
One coauthor reported receiving financial support from Janssen and Roche. The study was supported by the National Research Foundation of Korea.
SOURCE: Kim J-M et al. JAMA. 2018;320(4):350-8.
Even years after their cardiac events, acute coronary syndrome patients whose depression was treated with 6 months of an antidepressant had fewer cardiovascular events, according to a randomized, controlled trial.
Compared with patients who were given placebo for depression after experiencing acute coronary syndrome (ACS), patients who received escitalopram experienced a lower incidence of a composite outcome of major adverse cardiovascular events (MACE), in this extension study of a 6-month trial reported previously (J Clin Psychiatry. 2015 Jan;76[1]:62-8).
After a median of 8.1 years, MACE, the study’s primary outcome, was experienced by 40.9% of patients taking escitalopram, compared with 53.6% of those taking placebo (hazard ratio 0.69, 95% confidence interval 0.49-0.96, P = .03). The investigators also tracked the individual MACE components (all-cause mortality, myocardial infarction, and percutaneous coronary intervention), finding that MI was also significantly less common in the escitalopram group compared with those who took placebo (8.7% vs. 15.2%, HR 0.54, 95% CI, 0.27-0.96, P = .04).
The other MACE components were seen less frequently in the escitalopram group, but the differences from those taking placebo were not statistically significant. The study did not show a mortality benefit for those who took escitalopram, noted first author Jae-Min Kim, MD, of the department of psychiatry at Chonnam University Medical School, Gwangju, South Korea, and his coauthors.
The randomized, double-blind, placebo-controlled trial comprised 300 patients who recently had ACS and also met DSM-IV criteria for major or minor depression.
Over a 5-year period at a single site, patients were randomized to receive escitalopram at an initial dose of 10 mg daily (149 patients), or placebo (151), for 24 weeks after their ACS event. Escitalopram doses could be adjusted according to clinician judgment from 5 to 20 mg daily.
Patients who consented to participate were enrolled and screened for depression within 2 weeks of their ACS event, and any who scored higher than 10 on the Beck Depression Inventory at the initial screen or at follow-up appointments up to 12 weeks post enrollment went on for further screening.
Demographic data were collected with an eye toward identifying factors that could affect cardiac outcomes, said Dr. Kim and his colleagues. So in addition to age, sex, and educational level, the investigators tracked participants’ living situations and marital and employment status.
Patients were a mean of 60 years old, and about 60% were male. The median Beck Depression Inventory score was 16-17.
The study differed from others, said the investigators, because it followed patients for a longer period of time. In previous studies, “[E]ffects on cardiac outcomes have not generally been found within the treatment period,” they wrote.
Though the study’s generalizability might be limited by the fact that it was conducted at a single site and all participants were Asian, the single-site design and South Korea’s comprehensive patient data registries also allowed for complete data collection over a very long follow-up period, noted Dr. Kim and his colleagues.
Adherence was high, at 93% for those taking escitalopram and 95% for those taking placebo. Other work published from the study has shown that those taking 24 weeks of escitalopram had less depression than did those taking placebo, they added.
One coauthor reported receiving financial support from Janssen and Roche. The study was supported by the National Research Foundation of Korea.
SOURCE: Kim J-M et al. JAMA. 2018;320(4):350-8.
FROM JAMA
Key clinical point: .
Major finding: The hazard ratio was 0.69 for MACE in the escitalopram group compared with placebo (P = .03).
Study details: Randomized, double-blind, placebo-controlled trial of 300 patients with ACS given escitalopram or placebo.
Disclosures: The National Research Council of Korea sponsored the study. One author reported funding from Janssen and Roche.
Source: Kim J-M et al. JAMA. 2018;320(4):350-8.
How to bring behavioral care into your office
There is consensus within both the medical and public health communities that an integrated model of health care, in which behavioral health is integrated into primary care settings, is the optimal way to improve the health of a population (not just treat disease) while managing costs and improving the patient’s experience of care. Such a model is especially compelling for pediatric care.
There are 74 million children under 18 years in the United States and the prevalence of psychiatric disorders in youth is 20%, or 15 million; after vaccinations and following development, managing psychiatric symptoms is the most common issue in pediatric primary care.
While some psychiatric illnesses can be well managed by primary care clinicians alone, some illnesses require specialized therapy or more complex pharmacologic treatment. Untreated or inadequately treated childhood mental illness can lead to a longer and worse course of illness, academic difficulties, emergence of associated illnesses (such as substance use disorders), and legal problems. For those children with chronic medical conditions, emotional disorders cause distress, and affect adherence and family functioning. We will discuss some practical strategies to begin to bring behavioral health care into the pediatric primary care setting.
Start by implementing behavioral health screening into annual and sick visits. Broad instruments, such as the Pediatric Symptom Checklist (PSC, 35 items) or the Child Behavior Check List (CBCL, 113 items) can be filled out by caregivers in the waiting room or online before a visit, and can suggest specific disorders or simply the need for a full psychiatric assessment. Electronic medical records may have publicly available questionnaires such as PSC built into their software, facilitating use of a tablet or home computer, and may ease scoring and downloading of results. Depending on the structure of your practice, you could have one clinician in charge of managing screening. You may become comfortable diagnosing certain disorders, such as ADHD, a major depressive episode, or an anxiety disorder, and you may begin medication treatment when appropriate. You can use instruments developed for specific disease entities (such as ADHD, obsessive compulsive disorder [OCD], anxiety, or depression) to monitor your patient’s treatment response, and they may be done virtually to minimize unnecessary visits.
Treatment algorithms for most psychiatric illnesses are available through the American Academy of Pediatrics and the American Academy of Child and Adolescent Psychiatry, and can guide you through the early stages of treatment. Psychotherapy is the first-line treatment for mild to moderate anxiety and mood disorders, and it is critical to the treatment of more severe disorders. Difficulty in finding a therapist who is skilled in a specific treatment, is a good fit, and accepts insurance can be a significant barrier to care. Establishing a coordinated relationship with a team of therapists can facilitate referrals. Some states have programs in which primary care physicians can have telephone consultations with mental health clinicians or to access referral services for therapy, such as the Massachusetts Child Psychiatry Access Project.
If you have a busy enough practice, consider bringing a social worker or psychologist to work with you. Such a clinician could perform diagnostic assessments, ongoing therapy, parent guidance, family work, or care coordination. Consider how to make it cost-effective for this clinician and your group, whether by inviting that person to sublet one of your offices, or having that person directly employed by you and benefiting from your office staff and patient flow. Many states now reimburse for screening and these funds could contribute to the expense of a social worker. This approach would bring you from coordination to true colocation, which greatly improves the likelihood of compliance with therapy, enhances coordination of a patient’s care, creates opportunities for ongoing education between disciplines, and diminishes stigma of acknowledging a mental illness. Anxiety disorders are the most common illnesses of youth, with mood disorders emerging in adolescence, and substance use disorders in later adolescence. Consider this in seeking a clinician with a specific interest or skill set (such as cognitive behavioral therapy for anxiety or mood problems, dialectical behavior therapy for chronic suicidality, or motivational interviewing for substance abuse).

Beyond diagnosing and treating psychiatric illness in your patients, a primary care pediatric setting with integrated behavioral health would improve the health of our young patients by investing in prevention and parental support. Universal prevention efforts are a hallmark of good pediatric care, from vaccines to educating parents and children about injury prevention (bike helmets, smoke detectors, and car seats) and risky behaviors (smoking). Educate your patients and their parents about best practices to promote good mental health, from good sleep hygiene to regular exercise and healthy stress management techniques. You could use posters and pamphlets, videos and smartphone apps, or screening instruments and discussion.
If you invest in a colocated mental health clinician, you can expand your prevention efforts beyond the universal. Screen for a family history of anxiety, mood, and substance use disorders, and screen for adverse childhood experiences scores. Chronic stress and a family history of specific psychiatric illnesses significantly increase the risk of specific illnesses in your patients. There are evidence-based interventions that can be used to prevent the emergence of many disorders in young people at specific risk. For example, parents who have struggled with anxiety can learn specific strategies for managing their children’s anxiety, significantly lowering the risk of anxiety disorders in their children. These skills can be taught individually or in groups, depending on the prevalence in your practice. Those insurers who reimburse for therapy have a reimbursement schedule for work with parents as well.

There may be funds available to support your investment in integrated care. Under the Affordable Care Act, Medicaid enhanced funding for Health Homes for enrolled children. There have been federal grants for primary care offices to engage in different levels of integration and measure outcomes (Project LAUNCH – Linking Actions for Unmet Needs in Children’s Health). There may be funding at the state level or from private foundations dedicated to public health research and initiatives. Even if you do not invest in procuring outside funding, you should consider how to measure patient outcomes once you are making any efforts at integrating behavioral health care into your practice. Outcome measures include questionnaire scores, treatment adherence, number of school absences, number of office or ED visits, or global measurements, such as the Child Global Assessment Scale (CGAS). Such data can inform you about how to adjust your approach, and could contribute to the larger effort to understand what strategies are most effective and feasible. Addressing the behavioral health needs of your patients could meaningfully contribute to the efforts to make the vision of integrated care – that which truly promotes health in our young people – a reality.

Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. Email them at [email protected].
There is consensus within both the medical and public health communities that an integrated model of health care, in which behavioral health is integrated into primary care settings, is the optimal way to improve the health of a population (not just treat disease) while managing costs and improving the patient’s experience of care. Such a model is especially compelling for pediatric care.
There are 74 million children under 18 years in the United States and the prevalence of psychiatric disorders in youth is 20%, or 15 million; after vaccinations and following development, managing psychiatric symptoms is the most common issue in pediatric primary care.
While some psychiatric illnesses can be well managed by primary care clinicians alone, some illnesses require specialized therapy or more complex pharmacologic treatment. Untreated or inadequately treated childhood mental illness can lead to a longer and worse course of illness, academic difficulties, emergence of associated illnesses (such as substance use disorders), and legal problems. For those children with chronic medical conditions, emotional disorders cause distress, and affect adherence and family functioning. We will discuss some practical strategies to begin to bring behavioral health care into the pediatric primary care setting.
Start by implementing behavioral health screening into annual and sick visits. Broad instruments, such as the Pediatric Symptom Checklist (PSC, 35 items) or the Child Behavior Check List (CBCL, 113 items) can be filled out by caregivers in the waiting room or online before a visit, and can suggest specific disorders or simply the need for a full psychiatric assessment. Electronic medical records may have publicly available questionnaires such as PSC built into their software, facilitating use of a tablet or home computer, and may ease scoring and downloading of results. Depending on the structure of your practice, you could have one clinician in charge of managing screening. You may become comfortable diagnosing certain disorders, such as ADHD, a major depressive episode, or an anxiety disorder, and you may begin medication treatment when appropriate. You can use instruments developed for specific disease entities (such as ADHD, obsessive compulsive disorder [OCD], anxiety, or depression) to monitor your patient’s treatment response, and they may be done virtually to minimize unnecessary visits.
Treatment algorithms for most psychiatric illnesses are available through the American Academy of Pediatrics and the American Academy of Child and Adolescent Psychiatry, and can guide you through the early stages of treatment. Psychotherapy is the first-line treatment for mild to moderate anxiety and mood disorders, and it is critical to the treatment of more severe disorders. Difficulty in finding a therapist who is skilled in a specific treatment, is a good fit, and accepts insurance can be a significant barrier to care. Establishing a coordinated relationship with a team of therapists can facilitate referrals. Some states have programs in which primary care physicians can have telephone consultations with mental health clinicians or to access referral services for therapy, such as the Massachusetts Child Psychiatry Access Project.
If you have a busy enough practice, consider bringing a social worker or psychologist to work with you. Such a clinician could perform diagnostic assessments, ongoing therapy, parent guidance, family work, or care coordination. Consider how to make it cost-effective for this clinician and your group, whether by inviting that person to sublet one of your offices, or having that person directly employed by you and benefiting from your office staff and patient flow. Many states now reimburse for screening and these funds could contribute to the expense of a social worker. This approach would bring you from coordination to true colocation, which greatly improves the likelihood of compliance with therapy, enhances coordination of a patient’s care, creates opportunities for ongoing education between disciplines, and diminishes stigma of acknowledging a mental illness. Anxiety disorders are the most common illnesses of youth, with mood disorders emerging in adolescence, and substance use disorders in later adolescence. Consider this in seeking a clinician with a specific interest or skill set (such as cognitive behavioral therapy for anxiety or mood problems, dialectical behavior therapy for chronic suicidality, or motivational interviewing for substance abuse).
Beyond diagnosing and treating psychiatric illness in your patients, a primary care pediatric setting with integrated behavioral health would improve the health of our young patients by investing in prevention and parental support. Universal prevention efforts are a hallmark of good pediatric care, from vaccines to educating parents and children about injury prevention (bike helmets, smoke detectors, and car seats) and risky behaviors (smoking). Educate your patients and their parents about best practices to promote good mental health, from good sleep hygiene to regular exercise and healthy stress management techniques. You could use posters and pamphlets, videos and smartphone apps, or screening instruments and discussion.
If you invest in a colocated mental health clinician, you can expand your prevention efforts beyond the universal. Screen for a family history of anxiety, mood, and substance use disorders, and screen for adverse childhood experiences scores. Chronic stress and a family history of specific psychiatric illnesses significantly increase the risk of specific illnesses in your patients. There are evidence-based interventions that can be used to prevent the emergence of many disorders in young people at specific risk. For example, parents who have struggled with anxiety can learn specific strategies for managing their children’s anxiety, significantly lowering the risk of anxiety disorders in their children. These skills can be taught individually or in groups, depending on the prevalence in your practice. Those insurers who reimburse for therapy have a reimbursement schedule for work with parents as well.
There may be funds available to support your investment in integrated care. Under the Affordable Care Act, Medicaid enhanced funding for Health Homes for enrolled children. There have been federal grants for primary care offices to engage in different levels of integration and measure outcomes (Project LAUNCH – Linking Actions for Unmet Needs in Children’s Health). There may be funding at the state level or from private foundations dedicated to public health research and initiatives. Even if you do not invest in procuring outside funding, you should consider how to measure patient outcomes once you are making any efforts at integrating behavioral health care into your practice. Outcome measures include questionnaire scores, treatment adherence, number of school absences, number of office or ED visits, or global measurements, such as the Child Global Assessment Scale (CGAS). Such data can inform you about how to adjust your approach, and could contribute to the larger effort to understand what strategies are most effective and feasible. Addressing the behavioral health needs of your patients could meaningfully contribute to the efforts to make the vision of integrated care – that which truly promotes health in our young people – a reality.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. Email them at [email protected].
There is consensus within both the medical and public health communities that an integrated model of health care, in which behavioral health is integrated into primary care settings, is the optimal way to improve the health of a population (not just treat disease) while managing costs and improving the patient’s experience of care. Such a model is especially compelling for pediatric care.
There are 74 million children under 18 years in the United States and the prevalence of psychiatric disorders in youth is 20%, or 15 million; after vaccinations and following development, managing psychiatric symptoms is the most common issue in pediatric primary care.
While some psychiatric illnesses can be well managed by primary care clinicians alone, some illnesses require specialized therapy or more complex pharmacologic treatment. Untreated or inadequately treated childhood mental illness can lead to a longer and worse course of illness, academic difficulties, emergence of associated illnesses (such as substance use disorders), and legal problems. For those children with chronic medical conditions, emotional disorders cause distress, and affect adherence and family functioning. We will discuss some practical strategies to begin to bring behavioral health care into the pediatric primary care setting.
Start by implementing behavioral health screening into annual and sick visits. Broad instruments, such as the Pediatric Symptom Checklist (PSC, 35 items) or the Child Behavior Check List (CBCL, 113 items) can be filled out by caregivers in the waiting room or online before a visit, and can suggest specific disorders or simply the need for a full psychiatric assessment. Electronic medical records may have publicly available questionnaires such as PSC built into their software, facilitating use of a tablet or home computer, and may ease scoring and downloading of results. Depending on the structure of your practice, you could have one clinician in charge of managing screening. You may become comfortable diagnosing certain disorders, such as ADHD, a major depressive episode, or an anxiety disorder, and you may begin medication treatment when appropriate. You can use instruments developed for specific disease entities (such as ADHD, obsessive compulsive disorder [OCD], anxiety, or depression) to monitor your patient’s treatment response, and they may be done virtually to minimize unnecessary visits.
Treatment algorithms for most psychiatric illnesses are available through the American Academy of Pediatrics and the American Academy of Child and Adolescent Psychiatry, and can guide you through the early stages of treatment. Psychotherapy is the first-line treatment for mild to moderate anxiety and mood disorders, and it is critical to the treatment of more severe disorders. Difficulty in finding a therapist who is skilled in a specific treatment, is a good fit, and accepts insurance can be a significant barrier to care. Establishing a coordinated relationship with a team of therapists can facilitate referrals. Some states have programs in which primary care physicians can have telephone consultations with mental health clinicians or to access referral services for therapy, such as the Massachusetts Child Psychiatry Access Project.
If you have a busy enough practice, consider bringing a social worker or psychologist to work with you. Such a clinician could perform diagnostic assessments, ongoing therapy, parent guidance, family work, or care coordination. Consider how to make it cost-effective for this clinician and your group, whether by inviting that person to sublet one of your offices, or having that person directly employed by you and benefiting from your office staff and patient flow. Many states now reimburse for screening and these funds could contribute to the expense of a social worker. This approach would bring you from coordination to true colocation, which greatly improves the likelihood of compliance with therapy, enhances coordination of a patient’s care, creates opportunities for ongoing education between disciplines, and diminishes stigma of acknowledging a mental illness. Anxiety disorders are the most common illnesses of youth, with mood disorders emerging in adolescence, and substance use disorders in later adolescence. Consider this in seeking a clinician with a specific interest or skill set (such as cognitive behavioral therapy for anxiety or mood problems, dialectical behavior therapy for chronic suicidality, or motivational interviewing for substance abuse).
Beyond diagnosing and treating psychiatric illness in your patients, a primary care pediatric setting with integrated behavioral health would improve the health of our young patients by investing in prevention and parental support. Universal prevention efforts are a hallmark of good pediatric care, from vaccines to educating parents and children about injury prevention (bike helmets, smoke detectors, and car seats) and risky behaviors (smoking). Educate your patients and their parents about best practices to promote good mental health, from good sleep hygiene to regular exercise and healthy stress management techniques. You could use posters and pamphlets, videos and smartphone apps, or screening instruments and discussion.
If you invest in a colocated mental health clinician, you can expand your prevention efforts beyond the universal. Screen for a family history of anxiety, mood, and substance use disorders, and screen for adverse childhood experiences scores. Chronic stress and a family history of specific psychiatric illnesses significantly increase the risk of specific illnesses in your patients. There are evidence-based interventions that can be used to prevent the emergence of many disorders in young people at specific risk. For example, parents who have struggled with anxiety can learn specific strategies for managing their children’s anxiety, significantly lowering the risk of anxiety disorders in their children. These skills can be taught individually or in groups, depending on the prevalence in your practice. Those insurers who reimburse for therapy have a reimbursement schedule for work with parents as well.
There may be funds available to support your investment in integrated care. Under the Affordable Care Act, Medicaid enhanced funding for Health Homes for enrolled children. There have been federal grants for primary care offices to engage in different levels of integration and measure outcomes (Project LAUNCH – Linking Actions for Unmet Needs in Children’s Health). There may be funding at the state level or from private foundations dedicated to public health research and initiatives. Even if you do not invest in procuring outside funding, you should consider how to measure patient outcomes once you are making any efforts at integrating behavioral health care into your practice. Outcome measures include questionnaire scores, treatment adherence, number of school absences, number of office or ED visits, or global measurements, such as the Child Global Assessment Scale (CGAS). Such data can inform you about how to adjust your approach, and could contribute to the larger effort to understand what strategies are most effective and feasible. Addressing the behavioral health needs of your patients could meaningfully contribute to the efforts to make the vision of integrated care – that which truly promotes health in our young people – a reality.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. Email them at [email protected].
Real-World Evidence for Safety and Effectiveness of Repeated Courses of Hyaluronic Acid Injections on the Time to Knee Replacement Surgery
ABSTRACT
Osteoarthritis (OA) of the knee is a top cause of disability among the elderly. Total knee replacement (TKR) has been available as an effective and definite surgical method to treat severe OA of the knee. However, TKR is a significant procedure with potential risk for serious complications and high costs. Alternative lower risk therapies that can delay or obviate TKR are valuable to those who are poor candidates for surgery or wish to avoid TKR as long as possible. Given the chondroprotective effects of hyaluronic acid (HA) injections, they are a safe and effective treatment to improve pain, function, and longevity of the knee. Thus, HA features the potential to delay or obviate TKR.
We aim to study the safety and effectiveness of repeated courses of HA on the time to TKR over a 3-year period using data from a large US health plan administrative claims database.
Retrospective analyses were conducted by identifying knee OA patients during the selection period (2007-2010). The follow-up period was 36 months, post-index date of initial HA injection. Procedural outcomes and adverse events of interest were tabulated and analyzed. A Cox proportional hazards model was used to model the risk of TKR.
A total of 50,389 patients who received HA for treatment of knee OA and met the study inclusion criteria were analyzed. Successive courses of HA showed a good safety profile and led to high proportions of patients without TKR 3 years after treatment initiation. Multivariate statistical modeling showed that multiple courses of HA injections significantly decreased the rates of TKR (95.0% without TKR for ≥5 courses vs 71.6% without TKR for 1 course; hazard ratio, 0.138; P < .0001).
Repeated courses of treatment with HA are safe and are associated with the delay of TKR for up to 3 years. Additional research is needed to evaluate the effect of repeated HA courses on delaying TKR beyond a 3-year time horizon.
Continue to: Osteoarthritis (OA) of the knee...
Osteoarthritis (OA) of the knee has emerged as one of the main causes of disability in the United States. Although no currently known cure of OA can reverse the progression of the disease, total knee replacement (TKR) is an effective and definitive treatment. However, TKR is an invasive procedure with potential risk for serious complications, and it has imposed high costs on the US healthcare system, with expenses accounting for hospital expenditures of TKR estimated at $28.5 billion in 2009.1Alternative low-risk therapies that can delay or obviate TKR are valuable to a number of patients, especially the poor candidates for surgery or those who wish to avoid TKR.
Intra-articular (IA) hyaluronic acid (HA) injections have been available as a safe and effective treatment option to alleviate pain and to improve joint functions.2 Results of randomized double-blind controlled clinical trials have demonstrated the pain-relieving effect of IA HA injections.3-5 Furthermore, a recent network meta-analysis comparing various pharmacologic interventions for knee OA has confirmed the efficacy of IA HA injections, which outperformed other interventions when compared with oral placebos.6,7 IA therapies are more effective than oral therapies for knee OA pain, with IA HA injections demonstrating the most pain reduction, potentially due to the benefit associated with needle injection and aspiration. Recent experimental studies have also suggested that IA HA may provide cartilage protection, reduce inflammation, and boost the viscosity of synovial fluid;8 IA HA may also exert therapeutic effects by inhibiting bone formation in OA patients.9,10 HA possesses the potential to delay or obviate TKR. Previous research with a case series review of patients in an orthopedic specialty practice reported that the use of IA HA injections in patients with grade IV OA delayed TKR substantially.11 One study analyzed retrospective medical claims data from a single private insurer and discovered potential evidence for the modest benefit of IA HA injections in delaying TKR.12
More detailed research work on a large sample of patients with knee OA and the requirement of TKR as a condition for inclusion using US administrative claims data has demonstrated the TKR-delaying effects of IA HA injections in comparison with a control group without claims for IA HA injections.13,14 This study also uses real-world US administrative data but utilizes a different approach by starting with a sample of patients with knee OA and evidence of IA HA injections and then assessing the effect of repeated courses of HA treatment on the delay of TKR, without TKR as a mandatory condition for inclusion. All patients with knee OA within the time window were included, regardless of the need for TKR compared with previous studies which only considered patients who ultimately received TKR. Safety information and effectiveness information were examined to achieve a balanced risk-benefit assessment. We also analyzed how multiple courses of HA treatment and other potentially relevant covariates at baseline affected the risk of receiving TKR in a multivariate survival model. We aimed to achieve a realistic assessment of the clinical utility of HA injections in delaying TKR in a real-world setting using both safety and effectiveness data.
METHODS
DATA SOURCE
A retrospective cohort observational study using IMS Health’s PharMetrics Plus Health Plan Claims Database was conducted by identifying knee OA patients with claims indicating initiation of HA injection at an index date during the selection period (July 1, 2007 to June 30, 2010). All common HA agents in the US market during this period (Euflexxa, Hyalgan, Orthovisc, Supartz, and Synvisc) were selected via the corresponding J-codes and pooled for investigation of HA class effects. The follow-up period was 36 months, post-index date of the initial HA injection. Outcomes were measured, and adverse events were identified during this period. The time window for identification of adverse events was within 2 weeks from any injection during the course of therapy (evidence of an emergency room visit and/or physician office visit with requisite code). The data during the 12-month pre-index baseline period from the claims database was used to obtain information about baseline patient characteristics, such as age, gender, type of coverage, physician specialty, Charlson Comorbidity Index (CCI), major comorbidities, and major medications of interest commonly used among patients with knee OA.
STUDY SAMPLE SELECTION
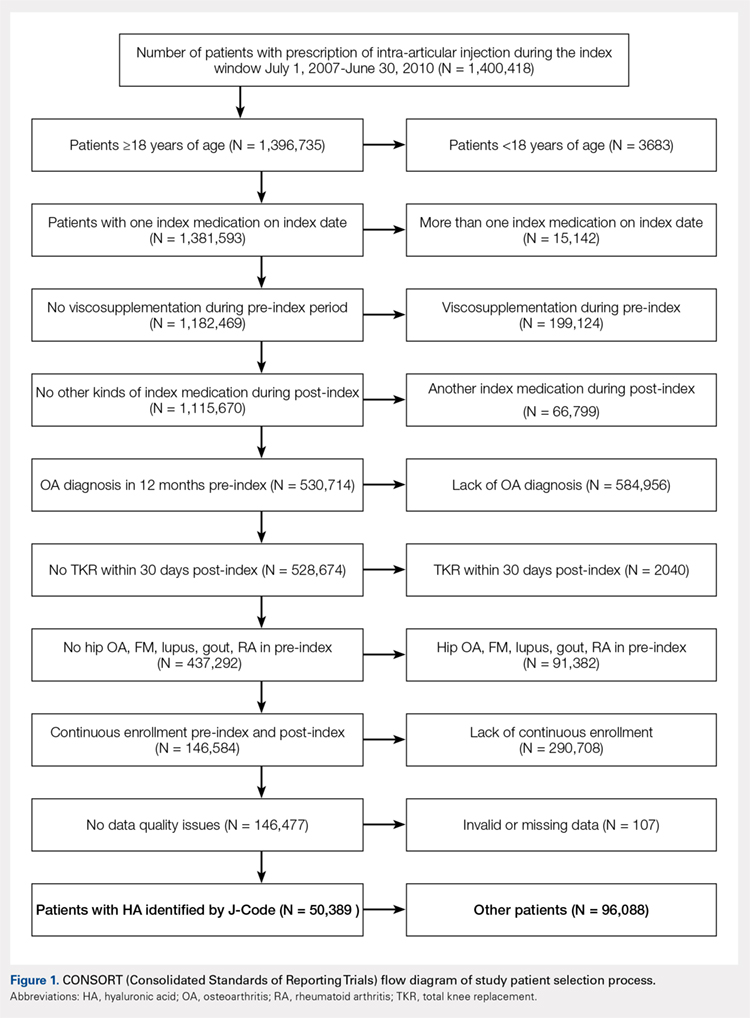
The eligible patients required an outpatient claim indicating the initiation of HA injection. The date of the first claim for the patient within the selection window was defined as their index date. Patients had to be ≥18 years of age in the year of their index date. They had to present at least 1 clinical knee OA diagnosis at any point in the 12-month pre-index period (including the index date), and only patients who were continuously enrolled from 12 months pre-index to 36 months post-index date were evaluated. Among these patients (approximately 1.4 million), the following were excluded to minimize complications in data analysis and interpretation: patients with evidence of any HA use in the pre-index period; patients with evidence of a different kind of HA index medication in the post-index period; patients with evidence of TKR within 30 days of the index event during the post-index period; patients with evidence of 2 different kinds of HA index medications on the index date; and patients with evidence of diagnosis of hip OA, fibromyalgia, rheumatoid arthritis, lupus, or gout during the pre-index period.
Five patient cohorts were defined according to the number of courses of IA HA injections over the entire post-index period.
Continue to: Statistical analysis...
STATISTICAL ANALYSIS
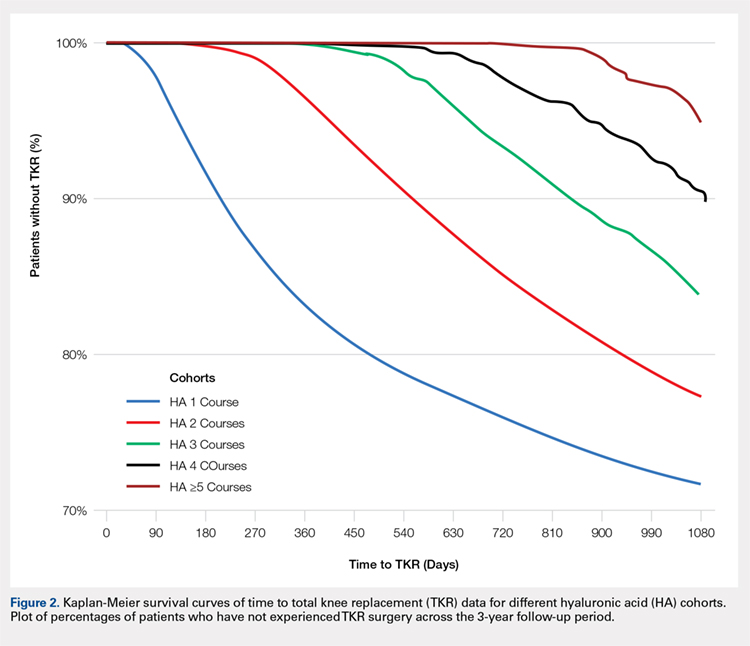
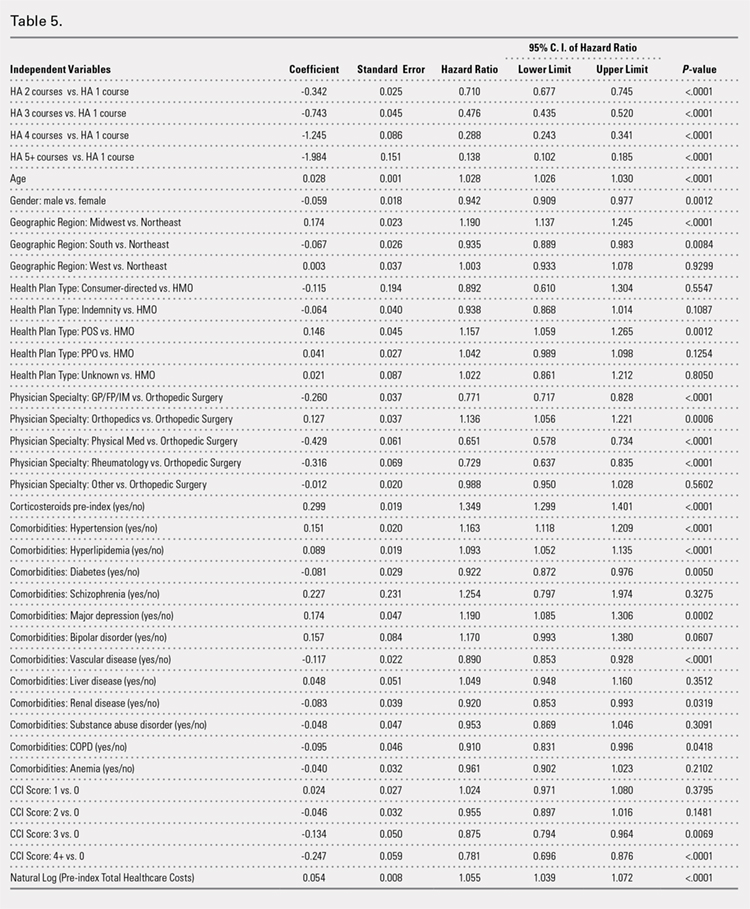
All statistical analyses were performed using SAS version 9.2 (SAS Institute Inc.). Descriptive statistics such as means, standard deviations, medians, and 25% and 75% percentiles (Q1 and Q3, respectively) were provided for the continuous variables. Numbers and percentages were provided for the categorical variables. For statistical testing, Student’s t-tests were applied for the continuous variables and chi-square tests for the categorical variables. All the statistical tests were two-tailed. The sample sizes in this database study are remarkably large, such that differences that are not clinically important could still be statistically significant at the conventional alpha level of 0.05. Thus, we applied a more stringent requirement of the alpha level of 0.0001 to identify highly statistically significant results. The number and percentage of patients within each cohort with at least 1 instance of an adverse event of interest (those adverse events commonly expected for patients who receive IA injections for knee OA) were assessed. Times to TKR during the 36-month post-index period were analyzed and compared among different cohorts. Any patients who had not undergone TKR by the end of the post-index period were considered censored at 36 months. The Kaplan-Meier method was employed to model survival curves with time to TKR data, and log-rank tests were used to compare survival curves among different cohorts. A Cox proportional hazards model (PHM) was used to model the risk of TKR with a pre-specified set of covariates adjusted for baseline attributes, such as age, gender, comorbidities, and pre-index healthcare costs. Hazard ratios with 95% confidence intervals were used to examine the measures of event risk.
RESULTS
PATIENT CHARACTERISTICS
Applying study selection criteria to the claims database yielded 50,389 patients (Figure 1), providing an ample sample size for the statistical analysis. Only patients with evidence of knee OA and use of HA injections (the index medication of interest) were selected, regardless of whether they received TKR during the post-index period. The requirement for a knee OA diagnosis during the 12-month pre-index period resulted in the significant attrition of patients, with 584,956 patients being excluded. Among the 50,389 patients who received HA for treatment of knee OA, 36,260 (72.0%) received a single course of treatment, 8709 (17.3%) received 2 courses, 3179 (6.3%) received 3 courses, 1354 (2.7%) received 4 courses, and 887 (1.8%) received ≥5 courses of treatment.
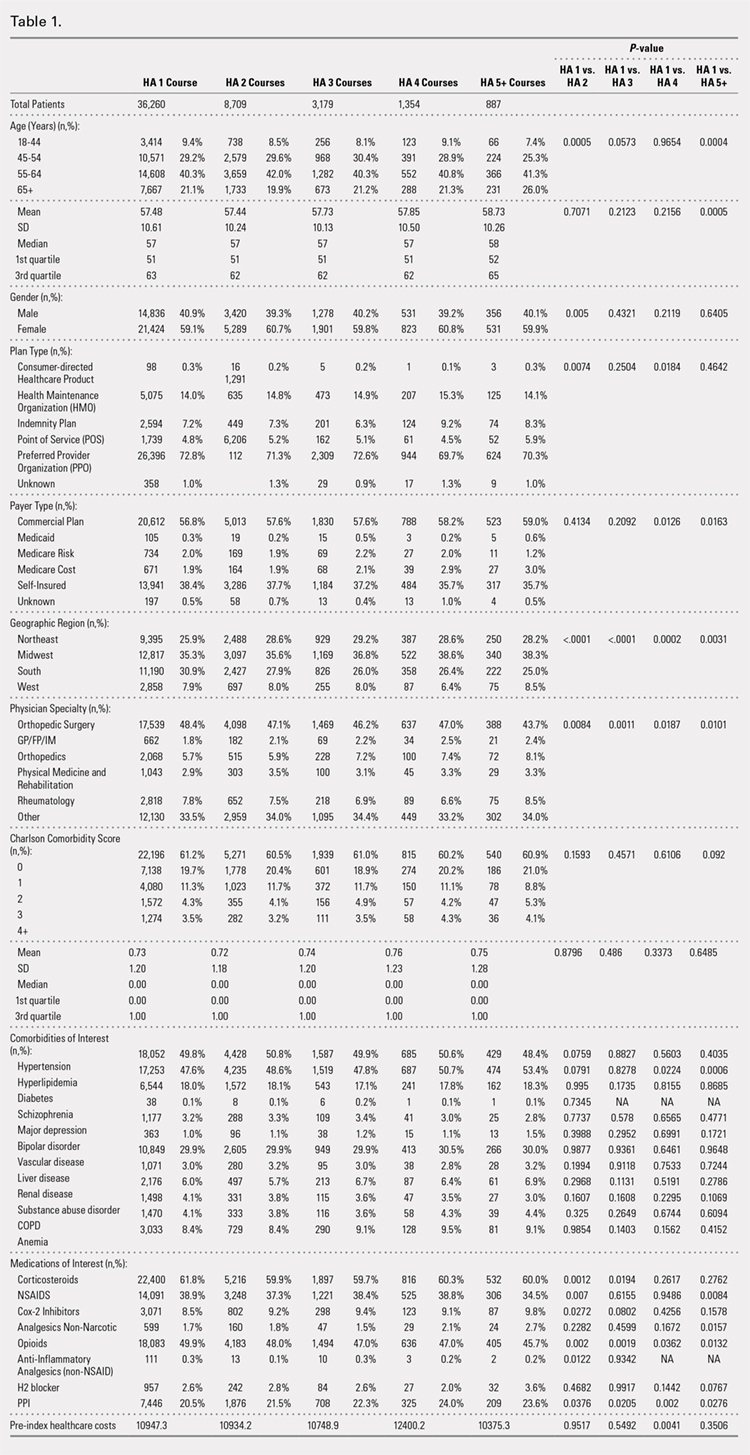
Comparison of baseline characteristics among the 5 IA HA cohorts showed the fairly similar baseline characteristics of all cohorts (Table 1). Geographic region, physician specialty, and opioid use showed differences among the cohorts. Cohorts with ≥5 HA courses presented lower proportions of patients from Southern US states, patients seeing orthopedic surgeons, and patients using opioids than cohorts with fewer HA courses.
PROCEDURES OF INTEREST
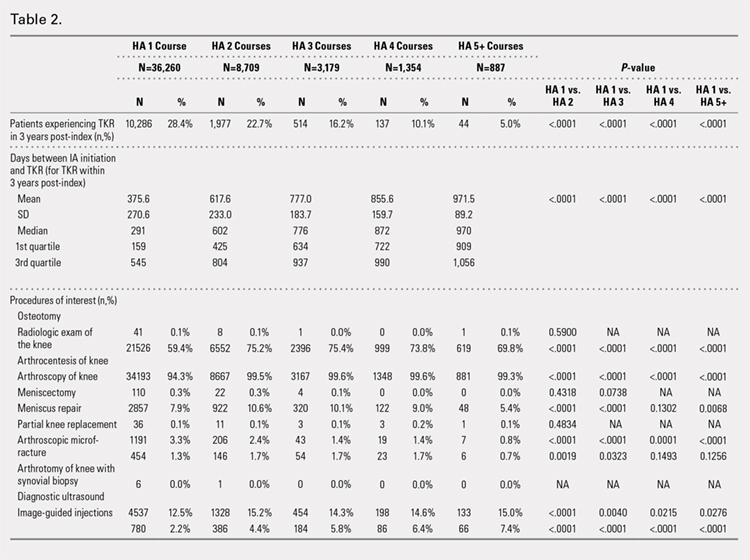
An analysis of the procedures patients received after HA treatment initiation showed that higher numbers of HA treatment courses resulted in lower proportions of patients receiving TKR within 3 years after HA treatment initiation (Table 2). With an increasing number of HA treatment courses, the proportion of patients with TKR within 3 years post-index consistently decreased from 28.4% (for 1 HA course) to 5.0% (for ≥5 HA courses), with all differences being highly statistically significant (P < .0001). Similarly, partial knee replacement exhibited a similar trend, with the proportion of patients decreasing from 3.3% (for 1 HA course) to 0.8% (for ≥5 HA courses; P < .0001). Among the patients with TKR within 3 years post-index, increasing numbers of treatment courses correlated with increasing time to TKR, with a mean of 375.6 days (for 1 HA course) rising to a mean of 971.5 days (for ≥5 HA courses; P < .0001). On the other hand, patients with multiple courses of HA treatment were more likely to undergo radiologic examinations of the knee, arthrocenteses, and image-guided injections than patients with only a single course of HA treatment (P < .0001).
ADVERSE EVENTS
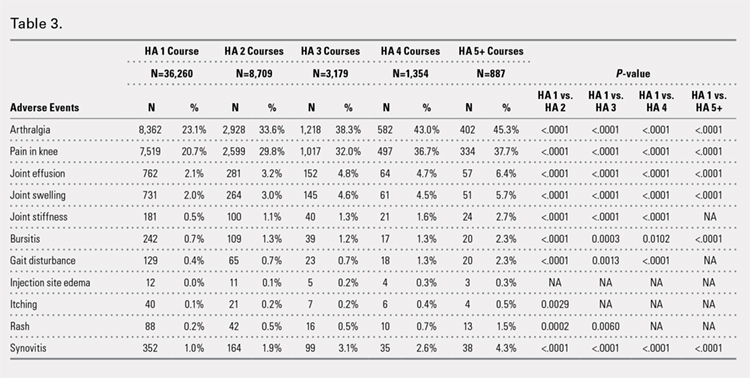
Arthralgia and joint pain in the knee were the most commonly recorded adverse events (Table 3). More courses of HA treatment were associated with higher rates of adverse events. Overall, the reported adverse events profile of repeated courses of HA treatment consisted of mostly common and mild adverse events and displayed no safety concern for patients with knee OA that was followed-up for 3 years. The causality of these adverse events directly related to HA injections vs a specific disease state cannot be determined from an administrative claims data set.
TIME TO TKR
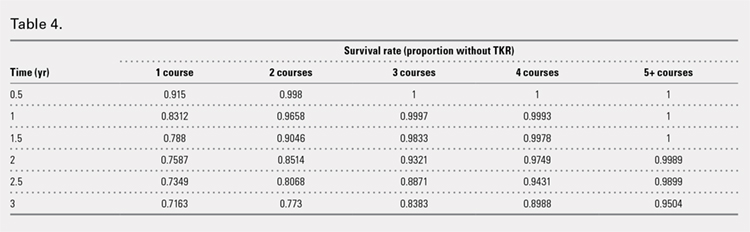
Successive courses of HA led to high proportions of patients without TKR 3 years after HA treatment initiation. This result is evident in the Kaplan-Meier survival curves of time to TKR for different HA cohorts (Figure 2), with log-rank tests of multiple courses vs a single course of HA (P < .0001) showing highly statistically significance. Tabulation of proportions of patients without TKR by various time points showed that increasing numbers of HA treatment courses correlated with higher proportions of patients without TKR at almost all time points (Table 4); within 3 years post-index, 71.6% of patients in the 1 HA course cohort exhibited no TKR, whereas 95.0% of patients in ≥5 HA courses cohort presented no TKR. We also performed a multivariate Cox PHM (Table 5) to account for baseline characteristics of different HA cohorts with covariates when estimating the risks of receiving TKR. The results of the Cox PHM showed that multiple courses of HA treatment significantly decreased the risk of TKR (hazard ratio, 0.138 for ≥5 HA courses vs 1 HA course; P < .0001). Inspection of other highly significant covariates showed that being older, living in the Midwest region of the US (vs the Northeast), receiving pre-index corticosteroids, having an orthopedic surgeon as a treating physician (vs a general practitioner, a rheumatologist, or a physical medicine and rehabilitation specialist), experiencing hypertension or hyperlipidemia, and higher pre-index total healthcare costs were associated with an increased risk of TKR (all P < .0001). Vascular disease and high CCI scores were associated with a decreased risk of TKR (P < .0001).
Continue to: Discussion...
DISCUSSION
This study demonstrated that multiple courses of HA treatment can delay the need for surgery for up to 3 years, with risk for both TKR and partial knee replacement decreasing in a dose-dependent manner. The potentially confounding effect of differences in baseline characteristics that could influence patients’ propensity to receive TKR in a database study was controlled by performing a multivariate analysis with covariate adjustment. The TKR-delaying effect of HA injection was more prominent in cohorts with a high number of HA treatment courses: 19 out of 20 patients in the cohort of ≥5 HA courses were free of TKR at the end of the 3-year post-index period. Such a high proportion of patients avoiding TKR with repeated courses of HA suggests that some patients may be able to successfully delay TKR well beyond the 3-year time span. This finding is counter-evidence to the frequently made assumption15 that all patients with knee OA will eventually progress to a state of disability, making TKR inevitable. The patients with end-stage radiographic knee OA can also benefit from IA HA injections for an extended period of time;16 the latest evidence indicates that nonoperative management can improve symptoms irrespective of radiographic disease severity, implying that TKR needs not to be the only therapeutic option for patients with end-stage radiographic knee OA.17 This finding suggests that HA treatment should be considered an important clinical treatment option for patients with knee OA.
Although the incidence rates of certain adverse events, such as arthralgia/joint pain, are sizable, these temporary adverse events commonly occur among patients who receive IA injections for knee OA; most of these events may simply include symptoms of the remaining underlying knee OA. These results are consistent with those of previous literature reporting the safety of repeated treatment with IA HA injections in a prospective clinical trial18 and demonstrating that repeated courses of HA treatment pose no greater safety risk than a single course of HA treatment.
Multivariate modeling outcomes of factors influencing risk of receiving TKR are broadly consistent with the generally accepted notions that different levels of disease severity and patients’ willingness to consider TKR at baseline influence the likelihood and timing of receiving TKR.19,20 Age and obesity are common risk factors for progression of OA. Orthopedic surgeons are more likely to recommend surgery than non-surgeons. The pre-index use of corticosteroids and high pre-index healthcare costs could be associated with more severe symptoms at baseline. Patients with vascular disease or severe comorbidities, as evidenced by high CCI scores, make poor candidates for major elective surgeries such as TKR. These results are intuitive and validate the clinical insights of this study. Moreover, inclusion of these covariates in the analysis model allows for indirect adjustment of the most important prognostic factors for TKR at baseline, permitting proper statistical comparison of the results for different cohort groups.
Recently, the efficacy of HA injections for OA patients has become the subject of debate when the American Academy of Orthopaedic Surgeons (AAOS) revised its clinical practice guideline, recommending against the use of HA.21 The AAOS’ findings differ from those of other clinical societies, such as the American College of Rheumatology22 and the European League Against Rheumatism,23 which provide no strong recommendation against the use of HA injections. The announcement of the new guideline by AAOS caused concern among clinicians and payers who had valued IA HA injections as a means to control knee OA pain before patients progress to TKR;24 on the other hand, the demand for nonoperative treatment of knee OA remains high. Utilization rates of TKR have increased dramatically, and surgeries are now performed on younger patients with increasing burden on the healthcare system,25,26 in spite of the fact that as high as a third of TKR surgeries may have been performed in inappropriate patients.27 Part of the confusion surrounding clinical utility of HA stems from the fact that up until recently, relatively little research looked into the practical benefits of HA in actual clinical practice. Analyses of databases such as registries are now gaining attention to overcome that problem. Examination of large administrative databases maintained by commercial payers offers the benefit of probing realistically the safety and efficacy of treatments in actual clinical environments in a very large number of patients with heterogeneous backgrounds. Recently, the Agency for Healthcare Research and Quality’s Technology Assessment Program in the US called for such studies to determine whether HA injections can delay progression to TKR.28 The results of this study and several others11,13,14,16 suggest that use of HA to treat OA of the knee is associated with the delay of TKR, supporting the utility of HA in clinical practice and the healthcare system. Potential clinical benefits of delaying TKR may include the reduced risk of aseptic loosening if younger patients can wait for TKR or more time to allow the modification of risk factors in patients who will ultimately undergo TKR.
LIMITATIONS
Follow-up period was limited to 3 years post-index date because longer follow-up data were not available at the time of the study design. If an incorrect adverse event or OA diagnosis was listed in the medical record, or if the medical record was incomplete, then patients might have been misclassified, resulting in selection bias. The claims dataset includes no uninsured and Medicare patients, as the population in the database consisted primarily of commercially-insured patients in the US. Therefore, the results are most generalizable to other commercially-insured patients in the US. Generalizability to other populations may not be assured if they differ in their accessibility to physician services or prescriptions from the patients in this study. Other treatments such as the nonsteroidal anti-inflammatory drugs used by patients were not included within the pre-specified statistical model because their potential effects were assumed to be short-lived and much less than those of corticosteroid. Including these treatments would overload the statistical model with too many covariates, leading to potential computational instability. The database used provides no information on systemic factors, including plan limits on medication use, that could affect care. Given the large and diverse nature of the healthcare plans in the database. However, these factors should not have materially affected our study results. The claims database also lacks direct indicators of OA disease severity, such as Kellgren-Lawrence scores or patient-reported outcomes, including pain and function questionnaire scores. Our multivariate analysis indirectly makes up for this deficiency by considering other baseline characteristics or clinical indicators that may be correlated with information unavailable in a claims database. Patients who opt to undergo repeated courses of HA treatment may be more inclined to avoid surgery or may naturally experience OA disease progression more slowly, making them potentially different from patients who select to undergo surgery earlier without repeated courses of HA treatment. This condition may introduce a bias that causes difficulty in proving the causality between repeated HA use and delay of TKR.
CONCLUSION
Analysis of the knee OA patient data from a real-world database showed that repeated courses of treatment with HA are safe and are associated with the delay of TKR for up to 3 years. Additional research is needed to evaluate the effects of repeated HA courses on delaying TKR beyond a 3-year period.
- Murphy L, Helmick CG. The impact of osteoarthritis in the United States: a population-health perspective. Am J Nurs. 2012;112(3 Suppl 1):S13-S19.
- Arnold W, Fullerton DS, Holder S, May CS. Viscosupplementation: managed care issues for osteoarthritis of the knee. J Manag Care Pharm. 2007;13(4 Suppl):S3-S19.
- Strand V, Conaghan PG, Lohmander LS, et al. An integrated analysis of five double-blind, randomized controlled trials evaluating the safety and efficacy of a hyaluronan product for intra-articular injection in osteoarthritis of the knee. Osteoarthritis Cartilage. 2006;14(9):859-866.
- Strand V, Baraf HS, Lavin PT, Lim S, Hosokawa H. A multicenter, randomized controlled trial comparing a single intra-articular injection of Gel-200, a new cross-linked formulation of hyaluronic acid, to phosphate buffered saline for treatment of osteoarthritis of the knee. Osteoarthritis Cartilage. 2012;20(5):350-356.
- Strand V, McIntyre LF, Beach WR, Miller LE, Block JE. Safety and efficacy of US-approved viscosupplements for knee osteoarthritis: a systematic review and meta-analysis of randomized, saline-controlled trials. J Pain Res. 2015;8:217-228.
- Bannuru RR, Schmid CH, Kent DM, Vaysbrott EE, Wong JB, McAlindon TE. Comparative effectiveness of pharmacologic interventions for knee osteoarthritis: a systematic review and network meta-analysis. Ann Intern Med. 2015;162(1):46-54.
- Mandl LA, Losina E. Relative efficacy of knee osteoarthritis treatments: are all placebos created equal? Ann Intern Med. 2015;162(1):71-72.
- Kusayama Y, Akamatsu Y, Kumagai K, Kobayashi H, Aratake M, Saito T. Changes in synovial fluid biomarkers and clinical efficacy of intra-articular injections of hyaluronic acid for patients with knee osteoarthritis. J Exp Orthop. 2014;1(1):16. doi:10.1186/s40634-014-0016-7.
- Kaneko K, Higuchi C, Kunugiza Y, et al. Hyaluronan inhibits BMP-induced osteoblast differentiation. FEBS Lett. 2015;589(4):447-454. doi:10.1016/j.febslet.2014.
- Altman RD, Manjoo A, Fierlinger A, Niazi F, Nicholls M. The mechanism of action for hyaluronic acid treatment in the osteoarthritic knee: a systematic review. BMC Musculoskelet Disord. 2015;16:321. doi:10.1186/s12891-015-0775-z.
- Waddell DD, Bricker DC. Total knee replacement delayed with hylan G-F 20 use in patients with grade IV osteoarthritis. J Manag Care Pharm. 2007;13(2):113-121.
- Khan T, Nanchanatt G, Farber K, Jan S. Analysis of the effectiveness of hyaluronic acid in prevention of total knee replacement in osteoarthritis patients. J Manag Care Pharm. 2014;20:S49.
- Abbott T, Altman RD, Dimeff R, et al. Do hyaluronic acid injections delay total knee replacement surgery? Arthritis Rheum. 2013;65(Suppl 10):2139.
- Altman R, Lim S, Steen R, Dasa V. Intra-articular hyaluronic acid delays total knee replacement in patients with knee osteoarthritis: evidence from a large U.S. health claims database. Osteoarthritis Cartilage. 2015;23(Suppl 2):A403-A404.
- Mather RC 3rd, Hug KT, Orlando LA, et al. Economic evaluation of access to musculoskeletal care: the case of waiting for total knee arthroplasty. BMC Musculoskelet Disord. 2014;15:22. doi:10.1186/1471-2474-15-22.
- Waddell DD, Joseph B. Delayed total knee replacement with Hylan G-F 20. J Knee Surg. 2016;29(2):159-168. doi:10.1055/s-0034-1395281.
- Atukorala I, Makovey J, Williams M, Ochoa Albiztegui E, Eyles JP, Hunter DJ. If you have end-stage radiographic knee osteoarthritis can you respond to non-surgical management? Osteoarthritis Cartilage. 2015;23(Suppl 2):A329.
- Strand V, Baraf HS, Lavin PT, Lim S, Hosokawa H. Effectiveness and safety of a multicenter extension and retreatment trial of Gel-200 in patients with knee osteoarthritis. Cartilage. 2012;3(4):297-304. doi:10.1177/1947603512451024.
- Riddle DL, Kong X, Jiranek WA. Two-year incidence and predictors of future knee arthroplasty in persons with symptomatic knee osteoarthritis: preliminary analysis of longitudinal data from the osteoarthritis initiative. Knee. 2009;16(6):494-500.
- Hawker GA, Guan J, Croxford R, et al. A prospective population-based study of the predictors of undergoing total joint arthroplasty. Arthritis Rheum. 2006;54(10):3212-3220.
- Jevsevar DS. Treatment of osteoarthritis of the knee: evidence-based guideline, 2nd edition. J Am Acad Orthop Surg. 2013;21(9):571-576. doi:10.5435/JAAOS-21-09-571.
- Hochberg MC, Altman RD, April KT, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken). 2012;64(4):465-474.
- Jordan KM, Arden NK, Doherty M, et al. EULAR Recommendations 2003: an evidence based approach to the management of knee osteoarthritis: report of a task force of the standing committee for international clinical studies including therapeutic trials (ESCISIT). Ann Rheum Dis. 2003;62(12):1145-1155.
- Bannuru RR, Vaysbrot EE, McIntyre LF. Did the American Academy of Orthopaedic Surgeons osteoarthritis guidelines miss the mark? Arthroscopy. 2014;30(1):86-89. doi:10.1016/j.arthro.2013.10.007.
- Losina E, Thornhill TS, Rome BN, Wright J, Katz JN. The dramatic increase in total knee replacement utilization rates in the United States cannot be fully explained by growth in population size and the obesity epidemic. J Bone Joint Surg Am. 2012;94(3):201-207. doi:10.2106/JBJS.J.01958.
- Weinstein AM, Rome BN, Reichmann WM, et al. Estimating the burden of total knee replacement in the United States. J Bone Joint Surg Am. 2013;95(5):385-392. doi:10.2106/JBJS.L.00206.
- Riddle DL, Jiranek WA, Hayes CW. Use of a validated algorithm to judge the appropriateness of total knee arthroplasty in the United States: a multicenter longitudinal cohort study. Arthritis Rheumatol. 2014;66(8):2134-2143. doi:10.1002/art.38685.
- NewBerry SJ, Fitzgerald JD, Maglione MA, et al. Agency for Healthcare Research and Quality Web site. Systematic Review for Effectiveness of Hyaluronic Acid in the Treatment of Severe Degenerative Joint Disease (DJD) of the Knee: Technology Assessment Report. http://www.ahrq.gov/research/findings/ta/call-for-public-review.html. Published July 23, 2015. Accessed December 22, 2014.
ABSTRACT
Osteoarthritis (OA) of the knee is a top cause of disability among the elderly. Total knee replacement (TKR) has been available as an effective and definite surgical method to treat severe OA of the knee. However, TKR is a significant procedure with potential risk for serious complications and high costs. Alternative lower risk therapies that can delay or obviate TKR are valuable to those who are poor candidates for surgery or wish to avoid TKR as long as possible. Given the chondroprotective effects of hyaluronic acid (HA) injections, they are a safe and effective treatment to improve pain, function, and longevity of the knee. Thus, HA features the potential to delay or obviate TKR.
We aim to study the safety and effectiveness of repeated courses of HA on the time to TKR over a 3-year period using data from a large US health plan administrative claims database.
Retrospective analyses were conducted by identifying knee OA patients during the selection period (2007-2010). The follow-up period was 36 months, post-index date of initial HA injection. Procedural outcomes and adverse events of interest were tabulated and analyzed. A Cox proportional hazards model was used to model the risk of TKR.
A total of 50,389 patients who received HA for treatment of knee OA and met the study inclusion criteria were analyzed. Successive courses of HA showed a good safety profile and led to high proportions of patients without TKR 3 years after treatment initiation. Multivariate statistical modeling showed that multiple courses of HA injections significantly decreased the rates of TKR (95.0% without TKR for ≥5 courses vs 71.6% without TKR for 1 course; hazard ratio, 0.138; P < .0001).
Repeated courses of treatment with HA are safe and are associated with the delay of TKR for up to 3 years. Additional research is needed to evaluate the effect of repeated HA courses on delaying TKR beyond a 3-year time horizon.
Continue to: Osteoarthritis (OA) of the knee...
Osteoarthritis (OA) of the knee has emerged as one of the main causes of disability in the United States. Although no currently known cure of OA can reverse the progression of the disease, total knee replacement (TKR) is an effective and definitive treatment. However, TKR is an invasive procedure with potential risk for serious complications, and it has imposed high costs on the US healthcare system, with expenses accounting for hospital expenditures of TKR estimated at $28.5 billion in 2009.1Alternative low-risk therapies that can delay or obviate TKR are valuable to a number of patients, especially the poor candidates for surgery or those who wish to avoid TKR.
Intra-articular (IA) hyaluronic acid (HA) injections have been available as a safe and effective treatment option to alleviate pain and to improve joint functions.2 Results of randomized double-blind controlled clinical trials have demonstrated the pain-relieving effect of IA HA injections.3-5 Furthermore, a recent network meta-analysis comparing various pharmacologic interventions for knee OA has confirmed the efficacy of IA HA injections, which outperformed other interventions when compared with oral placebos.6,7 IA therapies are more effective than oral therapies for knee OA pain, with IA HA injections demonstrating the most pain reduction, potentially due to the benefit associated with needle injection and aspiration. Recent experimental studies have also suggested that IA HA may provide cartilage protection, reduce inflammation, and boost the viscosity of synovial fluid;8 IA HA may also exert therapeutic effects by inhibiting bone formation in OA patients.9,10 HA possesses the potential to delay or obviate TKR. Previous research with a case series review of patients in an orthopedic specialty practice reported that the use of IA HA injections in patients with grade IV OA delayed TKR substantially.11 One study analyzed retrospective medical claims data from a single private insurer and discovered potential evidence for the modest benefit of IA HA injections in delaying TKR.12
More detailed research work on a large sample of patients with knee OA and the requirement of TKR as a condition for inclusion using US administrative claims data has demonstrated the TKR-delaying effects of IA HA injections in comparison with a control group without claims for IA HA injections.13,14 This study also uses real-world US administrative data but utilizes a different approach by starting with a sample of patients with knee OA and evidence of IA HA injections and then assessing the effect of repeated courses of HA treatment on the delay of TKR, without TKR as a mandatory condition for inclusion. All patients with knee OA within the time window were included, regardless of the need for TKR compared with previous studies which only considered patients who ultimately received TKR. Safety information and effectiveness information were examined to achieve a balanced risk-benefit assessment. We also analyzed how multiple courses of HA treatment and other potentially relevant covariates at baseline affected the risk of receiving TKR in a multivariate survival model. We aimed to achieve a realistic assessment of the clinical utility of HA injections in delaying TKR in a real-world setting using both safety and effectiveness data.
METHODS
DATA SOURCE
A retrospective cohort observational study using IMS Health’s PharMetrics Plus Health Plan Claims Database was conducted by identifying knee OA patients with claims indicating initiation of HA injection at an index date during the selection period (July 1, 2007 to June 30, 2010). All common HA agents in the US market during this period (Euflexxa, Hyalgan, Orthovisc, Supartz, and Synvisc) were selected via the corresponding J-codes and pooled for investigation of HA class effects. The follow-up period was 36 months, post-index date of the initial HA injection. Outcomes were measured, and adverse events were identified during this period. The time window for identification of adverse events was within 2 weeks from any injection during the course of therapy (evidence of an emergency room visit and/or physician office visit with requisite code). The data during the 12-month pre-index baseline period from the claims database was used to obtain information about baseline patient characteristics, such as age, gender, type of coverage, physician specialty, Charlson Comorbidity Index (CCI), major comorbidities, and major medications of interest commonly used among patients with knee OA.
STUDY SAMPLE SELECTION
The eligible patients required an outpatient claim indicating the initiation of HA injection. The date of the first claim for the patient within the selection window was defined as their index date. Patients had to be ≥18 years of age in the year of their index date. They had to present at least 1 clinical knee OA diagnosis at any point in the 12-month pre-index period (including the index date), and only patients who were continuously enrolled from 12 months pre-index to 36 months post-index date were evaluated. Among these patients (approximately 1.4 million), the following were excluded to minimize complications in data analysis and interpretation: patients with evidence of any HA use in the pre-index period; patients with evidence of a different kind of HA index medication in the post-index period; patients with evidence of TKR within 30 days of the index event during the post-index period; patients with evidence of 2 different kinds of HA index medications on the index date; and patients with evidence of diagnosis of hip OA, fibromyalgia, rheumatoid arthritis, lupus, or gout during the pre-index period.
Five patient cohorts were defined according to the number of courses of IA HA injections over the entire post-index period.
Continue to: Statistical analysis...
STATISTICAL ANALYSIS
All statistical analyses were performed using SAS version 9.2 (SAS Institute Inc.). Descriptive statistics such as means, standard deviations, medians, and 25% and 75% percentiles (Q1 and Q3, respectively) were provided for the continuous variables. Numbers and percentages were provided for the categorical variables. For statistical testing, Student’s t-tests were applied for the continuous variables and chi-square tests for the categorical variables. All the statistical tests were two-tailed. The sample sizes in this database study are remarkably large, such that differences that are not clinically important could still be statistically significant at the conventional alpha level of 0.05. Thus, we applied a more stringent requirement of the alpha level of 0.0001 to identify highly statistically significant results. The number and percentage of patients within each cohort with at least 1 instance of an adverse event of interest (those adverse events commonly expected for patients who receive IA injections for knee OA) were assessed. Times to TKR during the 36-month post-index period were analyzed and compared among different cohorts. Any patients who had not undergone TKR by the end of the post-index period were considered censored at 36 months. The Kaplan-Meier method was employed to model survival curves with time to TKR data, and log-rank tests were used to compare survival curves among different cohorts. A Cox proportional hazards model (PHM) was used to model the risk of TKR with a pre-specified set of covariates adjusted for baseline attributes, such as age, gender, comorbidities, and pre-index healthcare costs. Hazard ratios with 95% confidence intervals were used to examine the measures of event risk.
RESULTS
PATIENT CHARACTERISTICS
Applying study selection criteria to the claims database yielded 50,389 patients (Figure 1), providing an ample sample size for the statistical analysis. Only patients with evidence of knee OA and use of HA injections (the index medication of interest) were selected, regardless of whether they received TKR during the post-index period. The requirement for a knee OA diagnosis during the 12-month pre-index period resulted in the significant attrition of patients, with 584,956 patients being excluded. Among the 50,389 patients who received HA for treatment of knee OA, 36,260 (72.0%) received a single course of treatment, 8709 (17.3%) received 2 courses, 3179 (6.3%) received 3 courses, 1354 (2.7%) received 4 courses, and 887 (1.8%) received ≥5 courses of treatment.
Comparison of baseline characteristics among the 5 IA HA cohorts showed the fairly similar baseline characteristics of all cohorts (Table 1). Geographic region, physician specialty, and opioid use showed differences among the cohorts. Cohorts with ≥5 HA courses presented lower proportions of patients from Southern US states, patients seeing orthopedic surgeons, and patients using opioids than cohorts with fewer HA courses.
PROCEDURES OF INTEREST
An analysis of the procedures patients received after HA treatment initiation showed that higher numbers of HA treatment courses resulted in lower proportions of patients receiving TKR within 3 years after HA treatment initiation (Table 2). With an increasing number of HA treatment courses, the proportion of patients with TKR within 3 years post-index consistently decreased from 28.4% (for 1 HA course) to 5.0% (for ≥5 HA courses), with all differences being highly statistically significant (P < .0001). Similarly, partial knee replacement exhibited a similar trend, with the proportion of patients decreasing from 3.3% (for 1 HA course) to 0.8% (for ≥5 HA courses; P < .0001). Among the patients with TKR within 3 years post-index, increasing numbers of treatment courses correlated with increasing time to TKR, with a mean of 375.6 days (for 1 HA course) rising to a mean of 971.5 days (for ≥5 HA courses; P < .0001). On the other hand, patients with multiple courses of HA treatment were more likely to undergo radiologic examinations of the knee, arthrocenteses, and image-guided injections than patients with only a single course of HA treatment (P < .0001).
ADVERSE EVENTS
Arthralgia and joint pain in the knee were the most commonly recorded adverse events (Table 3). More courses of HA treatment were associated with higher rates of adverse events. Overall, the reported adverse events profile of repeated courses of HA treatment consisted of mostly common and mild adverse events and displayed no safety concern for patients with knee OA that was followed-up for 3 years. The causality of these adverse events directly related to HA injections vs a specific disease state cannot be determined from an administrative claims data set.
TIME TO TKR
Successive courses of HA led to high proportions of patients without TKR 3 years after HA treatment initiation. This result is evident in the Kaplan-Meier survival curves of time to TKR for different HA cohorts (Figure 2), with log-rank tests of multiple courses vs a single course of HA (P < .0001) showing highly statistically significance. Tabulation of proportions of patients without TKR by various time points showed that increasing numbers of HA treatment courses correlated with higher proportions of patients without TKR at almost all time points (Table 4); within 3 years post-index, 71.6% of patients in the 1 HA course cohort exhibited no TKR, whereas 95.0% of patients in ≥5 HA courses cohort presented no TKR. We also performed a multivariate Cox PHM (Table 5) to account for baseline characteristics of different HA cohorts with covariates when estimating the risks of receiving TKR. The results of the Cox PHM showed that multiple courses of HA treatment significantly decreased the risk of TKR (hazard ratio, 0.138 for ≥5 HA courses vs 1 HA course; P < .0001). Inspection of other highly significant covariates showed that being older, living in the Midwest region of the US (vs the Northeast), receiving pre-index corticosteroids, having an orthopedic surgeon as a treating physician (vs a general practitioner, a rheumatologist, or a physical medicine and rehabilitation specialist), experiencing hypertension or hyperlipidemia, and higher pre-index total healthcare costs were associated with an increased risk of TKR (all P < .0001). Vascular disease and high CCI scores were associated with a decreased risk of TKR (P < .0001).
Continue to: Discussion...
DISCUSSION
This study demonstrated that multiple courses of HA treatment can delay the need for surgery for up to 3 years, with risk for both TKR and partial knee replacement decreasing in a dose-dependent manner. The potentially confounding effect of differences in baseline characteristics that could influence patients’ propensity to receive TKR in a database study was controlled by performing a multivariate analysis with covariate adjustment. The TKR-delaying effect of HA injection was more prominent in cohorts with a high number of HA treatment courses: 19 out of 20 patients in the cohort of ≥5 HA courses were free of TKR at the end of the 3-year post-index period. Such a high proportion of patients avoiding TKR with repeated courses of HA suggests that some patients may be able to successfully delay TKR well beyond the 3-year time span. This finding is counter-evidence to the frequently made assumption15 that all patients with knee OA will eventually progress to a state of disability, making TKR inevitable. The patients with end-stage radiographic knee OA can also benefit from IA HA injections for an extended period of time;16 the latest evidence indicates that nonoperative management can improve symptoms irrespective of radiographic disease severity, implying that TKR needs not to be the only therapeutic option for patients with end-stage radiographic knee OA.17 This finding suggests that HA treatment should be considered an important clinical treatment option for patients with knee OA.
Although the incidence rates of certain adverse events, such as arthralgia/joint pain, are sizable, these temporary adverse events commonly occur among patients who receive IA injections for knee OA; most of these events may simply include symptoms of the remaining underlying knee OA. These results are consistent with those of previous literature reporting the safety of repeated treatment with IA HA injections in a prospective clinical trial18 and demonstrating that repeated courses of HA treatment pose no greater safety risk than a single course of HA treatment.
Multivariate modeling outcomes of factors influencing risk of receiving TKR are broadly consistent with the generally accepted notions that different levels of disease severity and patients’ willingness to consider TKR at baseline influence the likelihood and timing of receiving TKR.19,20 Age and obesity are common risk factors for progression of OA. Orthopedic surgeons are more likely to recommend surgery than non-surgeons. The pre-index use of corticosteroids and high pre-index healthcare costs could be associated with more severe symptoms at baseline. Patients with vascular disease or severe comorbidities, as evidenced by high CCI scores, make poor candidates for major elective surgeries such as TKR. These results are intuitive and validate the clinical insights of this study. Moreover, inclusion of these covariates in the analysis model allows for indirect adjustment of the most important prognostic factors for TKR at baseline, permitting proper statistical comparison of the results for different cohort groups.
Recently, the efficacy of HA injections for OA patients has become the subject of debate when the American Academy of Orthopaedic Surgeons (AAOS) revised its clinical practice guideline, recommending against the use of HA.21 The AAOS’ findings differ from those of other clinical societies, such as the American College of Rheumatology22 and the European League Against Rheumatism,23 which provide no strong recommendation against the use of HA injections. The announcement of the new guideline by AAOS caused concern among clinicians and payers who had valued IA HA injections as a means to control knee OA pain before patients progress to TKR;24 on the other hand, the demand for nonoperative treatment of knee OA remains high. Utilization rates of TKR have increased dramatically, and surgeries are now performed on younger patients with increasing burden on the healthcare system,25,26 in spite of the fact that as high as a third of TKR surgeries may have been performed in inappropriate patients.27 Part of the confusion surrounding clinical utility of HA stems from the fact that up until recently, relatively little research looked into the practical benefits of HA in actual clinical practice. Analyses of databases such as registries are now gaining attention to overcome that problem. Examination of large administrative databases maintained by commercial payers offers the benefit of probing realistically the safety and efficacy of treatments in actual clinical environments in a very large number of patients with heterogeneous backgrounds. Recently, the Agency for Healthcare Research and Quality’s Technology Assessment Program in the US called for such studies to determine whether HA injections can delay progression to TKR.28 The results of this study and several others11,13,14,16 suggest that use of HA to treat OA of the knee is associated with the delay of TKR, supporting the utility of HA in clinical practice and the healthcare system. Potential clinical benefits of delaying TKR may include the reduced risk of aseptic loosening if younger patients can wait for TKR or more time to allow the modification of risk factors in patients who will ultimately undergo TKR.
LIMITATIONS
Follow-up period was limited to 3 years post-index date because longer follow-up data were not available at the time of the study design. If an incorrect adverse event or OA diagnosis was listed in the medical record, or if the medical record was incomplete, then patients might have been misclassified, resulting in selection bias. The claims dataset includes no uninsured and Medicare patients, as the population in the database consisted primarily of commercially-insured patients in the US. Therefore, the results are most generalizable to other commercially-insured patients in the US. Generalizability to other populations may not be assured if they differ in their accessibility to physician services or prescriptions from the patients in this study. Other treatments such as the nonsteroidal anti-inflammatory drugs used by patients were not included within the pre-specified statistical model because their potential effects were assumed to be short-lived and much less than those of corticosteroid. Including these treatments would overload the statistical model with too many covariates, leading to potential computational instability. The database used provides no information on systemic factors, including plan limits on medication use, that could affect care. Given the large and diverse nature of the healthcare plans in the database. However, these factors should not have materially affected our study results. The claims database also lacks direct indicators of OA disease severity, such as Kellgren-Lawrence scores or patient-reported outcomes, including pain and function questionnaire scores. Our multivariate analysis indirectly makes up for this deficiency by considering other baseline characteristics or clinical indicators that may be correlated with information unavailable in a claims database. Patients who opt to undergo repeated courses of HA treatment may be more inclined to avoid surgery or may naturally experience OA disease progression more slowly, making them potentially different from patients who select to undergo surgery earlier without repeated courses of HA treatment. This condition may introduce a bias that causes difficulty in proving the causality between repeated HA use and delay of TKR.
CONCLUSION
Analysis of the knee OA patient data from a real-world database showed that repeated courses of treatment with HA are safe and are associated with the delay of TKR for up to 3 years. Additional research is needed to evaluate the effects of repeated HA courses on delaying TKR beyond a 3-year period.
ABSTRACT
Osteoarthritis (OA) of the knee is a top cause of disability among the elderly. Total knee replacement (TKR) has been available as an effective and definite surgical method to treat severe OA of the knee. However, TKR is a significant procedure with potential risk for serious complications and high costs. Alternative lower risk therapies that can delay or obviate TKR are valuable to those who are poor candidates for surgery or wish to avoid TKR as long as possible. Given the chondroprotective effects of hyaluronic acid (HA) injections, they are a safe and effective treatment to improve pain, function, and longevity of the knee. Thus, HA features the potential to delay or obviate TKR.
We aim to study the safety and effectiveness of repeated courses of HA on the time to TKR over a 3-year period using data from a large US health plan administrative claims database.
Retrospective analyses were conducted by identifying knee OA patients during the selection period (2007-2010). The follow-up period was 36 months, post-index date of initial HA injection. Procedural outcomes and adverse events of interest were tabulated and analyzed. A Cox proportional hazards model was used to model the risk of TKR.
A total of 50,389 patients who received HA for treatment of knee OA and met the study inclusion criteria were analyzed. Successive courses of HA showed a good safety profile and led to high proportions of patients without TKR 3 years after treatment initiation. Multivariate statistical modeling showed that multiple courses of HA injections significantly decreased the rates of TKR (95.0% without TKR for ≥5 courses vs 71.6% without TKR for 1 course; hazard ratio, 0.138; P < .0001).
Repeated courses of treatment with HA are safe and are associated with the delay of TKR for up to 3 years. Additional research is needed to evaluate the effect of repeated HA courses on delaying TKR beyond a 3-year time horizon.
Continue to: Osteoarthritis (OA) of the knee...
Osteoarthritis (OA) of the knee has emerged as one of the main causes of disability in the United States. Although no currently known cure of OA can reverse the progression of the disease, total knee replacement (TKR) is an effective and definitive treatment. However, TKR is an invasive procedure with potential risk for serious complications, and it has imposed high costs on the US healthcare system, with expenses accounting for hospital expenditures of TKR estimated at $28.5 billion in 2009.1Alternative low-risk therapies that can delay or obviate TKR are valuable to a number of patients, especially the poor candidates for surgery or those who wish to avoid TKR.
Intra-articular (IA) hyaluronic acid (HA) injections have been available as a safe and effective treatment option to alleviate pain and to improve joint functions.2 Results of randomized double-blind controlled clinical trials have demonstrated the pain-relieving effect of IA HA injections.3-5 Furthermore, a recent network meta-analysis comparing various pharmacologic interventions for knee OA has confirmed the efficacy of IA HA injections, which outperformed other interventions when compared with oral placebos.6,7 IA therapies are more effective than oral therapies for knee OA pain, with IA HA injections demonstrating the most pain reduction, potentially due to the benefit associated with needle injection and aspiration. Recent experimental studies have also suggested that IA HA may provide cartilage protection, reduce inflammation, and boost the viscosity of synovial fluid;8 IA HA may also exert therapeutic effects by inhibiting bone formation in OA patients.9,10 HA possesses the potential to delay or obviate TKR. Previous research with a case series review of patients in an orthopedic specialty practice reported that the use of IA HA injections in patients with grade IV OA delayed TKR substantially.11 One study analyzed retrospective medical claims data from a single private insurer and discovered potential evidence for the modest benefit of IA HA injections in delaying TKR.12
More detailed research work on a large sample of patients with knee OA and the requirement of TKR as a condition for inclusion using US administrative claims data has demonstrated the TKR-delaying effects of IA HA injections in comparison with a control group without claims for IA HA injections.13,14 This study also uses real-world US administrative data but utilizes a different approach by starting with a sample of patients with knee OA and evidence of IA HA injections and then assessing the effect of repeated courses of HA treatment on the delay of TKR, without TKR as a mandatory condition for inclusion. All patients with knee OA within the time window were included, regardless of the need for TKR compared with previous studies which only considered patients who ultimately received TKR. Safety information and effectiveness information were examined to achieve a balanced risk-benefit assessment. We also analyzed how multiple courses of HA treatment and other potentially relevant covariates at baseline affected the risk of receiving TKR in a multivariate survival model. We aimed to achieve a realistic assessment of the clinical utility of HA injections in delaying TKR in a real-world setting using both safety and effectiveness data.
METHODS
DATA SOURCE
A retrospective cohort observational study using IMS Health’s PharMetrics Plus Health Plan Claims Database was conducted by identifying knee OA patients with claims indicating initiation of HA injection at an index date during the selection period (July 1, 2007 to June 30, 2010). All common HA agents in the US market during this period (Euflexxa, Hyalgan, Orthovisc, Supartz, and Synvisc) were selected via the corresponding J-codes and pooled for investigation of HA class effects. The follow-up period was 36 months, post-index date of the initial HA injection. Outcomes were measured, and adverse events were identified during this period. The time window for identification of adverse events was within 2 weeks from any injection during the course of therapy (evidence of an emergency room visit and/or physician office visit with requisite code). The data during the 12-month pre-index baseline period from the claims database was used to obtain information about baseline patient characteristics, such as age, gender, type of coverage, physician specialty, Charlson Comorbidity Index (CCI), major comorbidities, and major medications of interest commonly used among patients with knee OA.
STUDY SAMPLE SELECTION
The eligible patients required an outpatient claim indicating the initiation of HA injection. The date of the first claim for the patient within the selection window was defined as their index date. Patients had to be ≥18 years of age in the year of their index date. They had to present at least 1 clinical knee OA diagnosis at any point in the 12-month pre-index period (including the index date), and only patients who were continuously enrolled from 12 months pre-index to 36 months post-index date were evaluated. Among these patients (approximately 1.4 million), the following were excluded to minimize complications in data analysis and interpretation: patients with evidence of any HA use in the pre-index period; patients with evidence of a different kind of HA index medication in the post-index period; patients with evidence of TKR within 30 days of the index event during the post-index period; patients with evidence of 2 different kinds of HA index medications on the index date; and patients with evidence of diagnosis of hip OA, fibromyalgia, rheumatoid arthritis, lupus, or gout during the pre-index period.
Five patient cohorts were defined according to the number of courses of IA HA injections over the entire post-index period.
Continue to: Statistical analysis...
STATISTICAL ANALYSIS
All statistical analyses were performed using SAS version 9.2 (SAS Institute Inc.). Descriptive statistics such as means, standard deviations, medians, and 25% and 75% percentiles (Q1 and Q3, respectively) were provided for the continuous variables. Numbers and percentages were provided for the categorical variables. For statistical testing, Student’s t-tests were applied for the continuous variables and chi-square tests for the categorical variables. All the statistical tests were two-tailed. The sample sizes in this database study are remarkably large, such that differences that are not clinically important could still be statistically significant at the conventional alpha level of 0.05. Thus, we applied a more stringent requirement of the alpha level of 0.0001 to identify highly statistically significant results. The number and percentage of patients within each cohort with at least 1 instance of an adverse event of interest (those adverse events commonly expected for patients who receive IA injections for knee OA) were assessed. Times to TKR during the 36-month post-index period were analyzed and compared among different cohorts. Any patients who had not undergone TKR by the end of the post-index period were considered censored at 36 months. The Kaplan-Meier method was employed to model survival curves with time to TKR data, and log-rank tests were used to compare survival curves among different cohorts. A Cox proportional hazards model (PHM) was used to model the risk of TKR with a pre-specified set of covariates adjusted for baseline attributes, such as age, gender, comorbidities, and pre-index healthcare costs. Hazard ratios with 95% confidence intervals were used to examine the measures of event risk.
RESULTS
PATIENT CHARACTERISTICS
Applying study selection criteria to the claims database yielded 50,389 patients (Figure 1), providing an ample sample size for the statistical analysis. Only patients with evidence of knee OA and use of HA injections (the index medication of interest) were selected, regardless of whether they received TKR during the post-index period. The requirement for a knee OA diagnosis during the 12-month pre-index period resulted in the significant attrition of patients, with 584,956 patients being excluded. Among the 50,389 patients who received HA for treatment of knee OA, 36,260 (72.0%) received a single course of treatment, 8709 (17.3%) received 2 courses, 3179 (6.3%) received 3 courses, 1354 (2.7%) received 4 courses, and 887 (1.8%) received ≥5 courses of treatment.
Comparison of baseline characteristics among the 5 IA HA cohorts showed the fairly similar baseline characteristics of all cohorts (Table 1). Geographic region, physician specialty, and opioid use showed differences among the cohorts. Cohorts with ≥5 HA courses presented lower proportions of patients from Southern US states, patients seeing orthopedic surgeons, and patients using opioids than cohorts with fewer HA courses.
PROCEDURES OF INTEREST
An analysis of the procedures patients received after HA treatment initiation showed that higher numbers of HA treatment courses resulted in lower proportions of patients receiving TKR within 3 years after HA treatment initiation (Table 2). With an increasing number of HA treatment courses, the proportion of patients with TKR within 3 years post-index consistently decreased from 28.4% (for 1 HA course) to 5.0% (for ≥5 HA courses), with all differences being highly statistically significant (P < .0001). Similarly, partial knee replacement exhibited a similar trend, with the proportion of patients decreasing from 3.3% (for 1 HA course) to 0.8% (for ≥5 HA courses; P < .0001). Among the patients with TKR within 3 years post-index, increasing numbers of treatment courses correlated with increasing time to TKR, with a mean of 375.6 days (for 1 HA course) rising to a mean of 971.5 days (for ≥5 HA courses; P < .0001). On the other hand, patients with multiple courses of HA treatment were more likely to undergo radiologic examinations of the knee, arthrocenteses, and image-guided injections than patients with only a single course of HA treatment (P < .0001).
ADVERSE EVENTS
Arthralgia and joint pain in the knee were the most commonly recorded adverse events (Table 3). More courses of HA treatment were associated with higher rates of adverse events. Overall, the reported adverse events profile of repeated courses of HA treatment consisted of mostly common and mild adverse events and displayed no safety concern for patients with knee OA that was followed-up for 3 years. The causality of these adverse events directly related to HA injections vs a specific disease state cannot be determined from an administrative claims data set.
TIME TO TKR
Successive courses of HA led to high proportions of patients without TKR 3 years after HA treatment initiation. This result is evident in the Kaplan-Meier survival curves of time to TKR for different HA cohorts (Figure 2), with log-rank tests of multiple courses vs a single course of HA (P < .0001) showing highly statistically significance. Tabulation of proportions of patients without TKR by various time points showed that increasing numbers of HA treatment courses correlated with higher proportions of patients without TKR at almost all time points (Table 4); within 3 years post-index, 71.6% of patients in the 1 HA course cohort exhibited no TKR, whereas 95.0% of patients in ≥5 HA courses cohort presented no TKR. We also performed a multivariate Cox PHM (Table 5) to account for baseline characteristics of different HA cohorts with covariates when estimating the risks of receiving TKR. The results of the Cox PHM showed that multiple courses of HA treatment significantly decreased the risk of TKR (hazard ratio, 0.138 for ≥5 HA courses vs 1 HA course; P < .0001). Inspection of other highly significant covariates showed that being older, living in the Midwest region of the US (vs the Northeast), receiving pre-index corticosteroids, having an orthopedic surgeon as a treating physician (vs a general practitioner, a rheumatologist, or a physical medicine and rehabilitation specialist), experiencing hypertension or hyperlipidemia, and higher pre-index total healthcare costs were associated with an increased risk of TKR (all P < .0001). Vascular disease and high CCI scores were associated with a decreased risk of TKR (P < .0001).
Continue to: Discussion...
DISCUSSION
This study demonstrated that multiple courses of HA treatment can delay the need for surgery for up to 3 years, with risk for both TKR and partial knee replacement decreasing in a dose-dependent manner. The potentially confounding effect of differences in baseline characteristics that could influence patients’ propensity to receive TKR in a database study was controlled by performing a multivariate analysis with covariate adjustment. The TKR-delaying effect of HA injection was more prominent in cohorts with a high number of HA treatment courses: 19 out of 20 patients in the cohort of ≥5 HA courses were free of TKR at the end of the 3-year post-index period. Such a high proportion of patients avoiding TKR with repeated courses of HA suggests that some patients may be able to successfully delay TKR well beyond the 3-year time span. This finding is counter-evidence to the frequently made assumption15 that all patients with knee OA will eventually progress to a state of disability, making TKR inevitable. The patients with end-stage radiographic knee OA can also benefit from IA HA injections for an extended period of time;16 the latest evidence indicates that nonoperative management can improve symptoms irrespective of radiographic disease severity, implying that TKR needs not to be the only therapeutic option for patients with end-stage radiographic knee OA.17 This finding suggests that HA treatment should be considered an important clinical treatment option for patients with knee OA.
Although the incidence rates of certain adverse events, such as arthralgia/joint pain, are sizable, these temporary adverse events commonly occur among patients who receive IA injections for knee OA; most of these events may simply include symptoms of the remaining underlying knee OA. These results are consistent with those of previous literature reporting the safety of repeated treatment with IA HA injections in a prospective clinical trial18 and demonstrating that repeated courses of HA treatment pose no greater safety risk than a single course of HA treatment.
Multivariate modeling outcomes of factors influencing risk of receiving TKR are broadly consistent with the generally accepted notions that different levels of disease severity and patients’ willingness to consider TKR at baseline influence the likelihood and timing of receiving TKR.19,20 Age and obesity are common risk factors for progression of OA. Orthopedic surgeons are more likely to recommend surgery than non-surgeons. The pre-index use of corticosteroids and high pre-index healthcare costs could be associated with more severe symptoms at baseline. Patients with vascular disease or severe comorbidities, as evidenced by high CCI scores, make poor candidates for major elective surgeries such as TKR. These results are intuitive and validate the clinical insights of this study. Moreover, inclusion of these covariates in the analysis model allows for indirect adjustment of the most important prognostic factors for TKR at baseline, permitting proper statistical comparison of the results for different cohort groups.
Recently, the efficacy of HA injections for OA patients has become the subject of debate when the American Academy of Orthopaedic Surgeons (AAOS) revised its clinical practice guideline, recommending against the use of HA.21 The AAOS’ findings differ from those of other clinical societies, such as the American College of Rheumatology22 and the European League Against Rheumatism,23 which provide no strong recommendation against the use of HA injections. The announcement of the new guideline by AAOS caused concern among clinicians and payers who had valued IA HA injections as a means to control knee OA pain before patients progress to TKR;24 on the other hand, the demand for nonoperative treatment of knee OA remains high. Utilization rates of TKR have increased dramatically, and surgeries are now performed on younger patients with increasing burden on the healthcare system,25,26 in spite of the fact that as high as a third of TKR surgeries may have been performed in inappropriate patients.27 Part of the confusion surrounding clinical utility of HA stems from the fact that up until recently, relatively little research looked into the practical benefits of HA in actual clinical practice. Analyses of databases such as registries are now gaining attention to overcome that problem. Examination of large administrative databases maintained by commercial payers offers the benefit of probing realistically the safety and efficacy of treatments in actual clinical environments in a very large number of patients with heterogeneous backgrounds. Recently, the Agency for Healthcare Research and Quality’s Technology Assessment Program in the US called for such studies to determine whether HA injections can delay progression to TKR.28 The results of this study and several others11,13,14,16 suggest that use of HA to treat OA of the knee is associated with the delay of TKR, supporting the utility of HA in clinical practice and the healthcare system. Potential clinical benefits of delaying TKR may include the reduced risk of aseptic loosening if younger patients can wait for TKR or more time to allow the modification of risk factors in patients who will ultimately undergo TKR.
LIMITATIONS
Follow-up period was limited to 3 years post-index date because longer follow-up data were not available at the time of the study design. If an incorrect adverse event or OA diagnosis was listed in the medical record, or if the medical record was incomplete, then patients might have been misclassified, resulting in selection bias. The claims dataset includes no uninsured and Medicare patients, as the population in the database consisted primarily of commercially-insured patients in the US. Therefore, the results are most generalizable to other commercially-insured patients in the US. Generalizability to other populations may not be assured if they differ in their accessibility to physician services or prescriptions from the patients in this study. Other treatments such as the nonsteroidal anti-inflammatory drugs used by patients were not included within the pre-specified statistical model because their potential effects were assumed to be short-lived and much less than those of corticosteroid. Including these treatments would overload the statistical model with too many covariates, leading to potential computational instability. The database used provides no information on systemic factors, including plan limits on medication use, that could affect care. Given the large and diverse nature of the healthcare plans in the database. However, these factors should not have materially affected our study results. The claims database also lacks direct indicators of OA disease severity, such as Kellgren-Lawrence scores or patient-reported outcomes, including pain and function questionnaire scores. Our multivariate analysis indirectly makes up for this deficiency by considering other baseline characteristics or clinical indicators that may be correlated with information unavailable in a claims database. Patients who opt to undergo repeated courses of HA treatment may be more inclined to avoid surgery or may naturally experience OA disease progression more slowly, making them potentially different from patients who select to undergo surgery earlier without repeated courses of HA treatment. This condition may introduce a bias that causes difficulty in proving the causality between repeated HA use and delay of TKR.
CONCLUSION
Analysis of the knee OA patient data from a real-world database showed that repeated courses of treatment with HA are safe and are associated with the delay of TKR for up to 3 years. Additional research is needed to evaluate the effects of repeated HA courses on delaying TKR beyond a 3-year period.
- Murphy L, Helmick CG. The impact of osteoarthritis in the United States: a population-health perspective. Am J Nurs. 2012;112(3 Suppl 1):S13-S19.
- Arnold W, Fullerton DS, Holder S, May CS. Viscosupplementation: managed care issues for osteoarthritis of the knee. J Manag Care Pharm. 2007;13(4 Suppl):S3-S19.
- Strand V, Conaghan PG, Lohmander LS, et al. An integrated analysis of five double-blind, randomized controlled trials evaluating the safety and efficacy of a hyaluronan product for intra-articular injection in osteoarthritis of the knee. Osteoarthritis Cartilage. 2006;14(9):859-866.
- Strand V, Baraf HS, Lavin PT, Lim S, Hosokawa H. A multicenter, randomized controlled trial comparing a single intra-articular injection of Gel-200, a new cross-linked formulation of hyaluronic acid, to phosphate buffered saline for treatment of osteoarthritis of the knee. Osteoarthritis Cartilage. 2012;20(5):350-356.
- Strand V, McIntyre LF, Beach WR, Miller LE, Block JE. Safety and efficacy of US-approved viscosupplements for knee osteoarthritis: a systematic review and meta-analysis of randomized, saline-controlled trials. J Pain Res. 2015;8:217-228.
- Bannuru RR, Schmid CH, Kent DM, Vaysbrott EE, Wong JB, McAlindon TE. Comparative effectiveness of pharmacologic interventions for knee osteoarthritis: a systematic review and network meta-analysis. Ann Intern Med. 2015;162(1):46-54.
- Mandl LA, Losina E. Relative efficacy of knee osteoarthritis treatments: are all placebos created equal? Ann Intern Med. 2015;162(1):71-72.
- Kusayama Y, Akamatsu Y, Kumagai K, Kobayashi H, Aratake M, Saito T. Changes in synovial fluid biomarkers and clinical efficacy of intra-articular injections of hyaluronic acid for patients with knee osteoarthritis. J Exp Orthop. 2014;1(1):16. doi:10.1186/s40634-014-0016-7.
- Kaneko K, Higuchi C, Kunugiza Y, et al. Hyaluronan inhibits BMP-induced osteoblast differentiation. FEBS Lett. 2015;589(4):447-454. doi:10.1016/j.febslet.2014.
- Altman RD, Manjoo A, Fierlinger A, Niazi F, Nicholls M. The mechanism of action for hyaluronic acid treatment in the osteoarthritic knee: a systematic review. BMC Musculoskelet Disord. 2015;16:321. doi:10.1186/s12891-015-0775-z.
- Waddell DD, Bricker DC. Total knee replacement delayed with hylan G-F 20 use in patients with grade IV osteoarthritis. J Manag Care Pharm. 2007;13(2):113-121.
- Khan T, Nanchanatt G, Farber K, Jan S. Analysis of the effectiveness of hyaluronic acid in prevention of total knee replacement in osteoarthritis patients. J Manag Care Pharm. 2014;20:S49.
- Abbott T, Altman RD, Dimeff R, et al. Do hyaluronic acid injections delay total knee replacement surgery? Arthritis Rheum. 2013;65(Suppl 10):2139.
- Altman R, Lim S, Steen R, Dasa V. Intra-articular hyaluronic acid delays total knee replacement in patients with knee osteoarthritis: evidence from a large U.S. health claims database. Osteoarthritis Cartilage. 2015;23(Suppl 2):A403-A404.
- Mather RC 3rd, Hug KT, Orlando LA, et al. Economic evaluation of access to musculoskeletal care: the case of waiting for total knee arthroplasty. BMC Musculoskelet Disord. 2014;15:22. doi:10.1186/1471-2474-15-22.
- Waddell DD, Joseph B. Delayed total knee replacement with Hylan G-F 20. J Knee Surg. 2016;29(2):159-168. doi:10.1055/s-0034-1395281.
- Atukorala I, Makovey J, Williams M, Ochoa Albiztegui E, Eyles JP, Hunter DJ. If you have end-stage radiographic knee osteoarthritis can you respond to non-surgical management? Osteoarthritis Cartilage. 2015;23(Suppl 2):A329.
- Strand V, Baraf HS, Lavin PT, Lim S, Hosokawa H. Effectiveness and safety of a multicenter extension and retreatment trial of Gel-200 in patients with knee osteoarthritis. Cartilage. 2012;3(4):297-304. doi:10.1177/1947603512451024.
- Riddle DL, Kong X, Jiranek WA. Two-year incidence and predictors of future knee arthroplasty in persons with symptomatic knee osteoarthritis: preliminary analysis of longitudinal data from the osteoarthritis initiative. Knee. 2009;16(6):494-500.
- Hawker GA, Guan J, Croxford R, et al. A prospective population-based study of the predictors of undergoing total joint arthroplasty. Arthritis Rheum. 2006;54(10):3212-3220.
- Jevsevar DS. Treatment of osteoarthritis of the knee: evidence-based guideline, 2nd edition. J Am Acad Orthop Surg. 2013;21(9):571-576. doi:10.5435/JAAOS-21-09-571.
- Hochberg MC, Altman RD, April KT, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken). 2012;64(4):465-474.
- Jordan KM, Arden NK, Doherty M, et al. EULAR Recommendations 2003: an evidence based approach to the management of knee osteoarthritis: report of a task force of the standing committee for international clinical studies including therapeutic trials (ESCISIT). Ann Rheum Dis. 2003;62(12):1145-1155.
- Bannuru RR, Vaysbrot EE, McIntyre LF. Did the American Academy of Orthopaedic Surgeons osteoarthritis guidelines miss the mark? Arthroscopy. 2014;30(1):86-89. doi:10.1016/j.arthro.2013.10.007.
- Losina E, Thornhill TS, Rome BN, Wright J, Katz JN. The dramatic increase in total knee replacement utilization rates in the United States cannot be fully explained by growth in population size and the obesity epidemic. J Bone Joint Surg Am. 2012;94(3):201-207. doi:10.2106/JBJS.J.01958.
- Weinstein AM, Rome BN, Reichmann WM, et al. Estimating the burden of total knee replacement in the United States. J Bone Joint Surg Am. 2013;95(5):385-392. doi:10.2106/JBJS.L.00206.
- Riddle DL, Jiranek WA, Hayes CW. Use of a validated algorithm to judge the appropriateness of total knee arthroplasty in the United States: a multicenter longitudinal cohort study. Arthritis Rheumatol. 2014;66(8):2134-2143. doi:10.1002/art.38685.
- NewBerry SJ, Fitzgerald JD, Maglione MA, et al. Agency for Healthcare Research and Quality Web site. Systematic Review for Effectiveness of Hyaluronic Acid in the Treatment of Severe Degenerative Joint Disease (DJD) of the Knee: Technology Assessment Report. http://www.ahrq.gov/research/findings/ta/call-for-public-review.html. Published July 23, 2015. Accessed December 22, 2014.
- Murphy L, Helmick CG. The impact of osteoarthritis in the United States: a population-health perspective. Am J Nurs. 2012;112(3 Suppl 1):S13-S19.
- Arnold W, Fullerton DS, Holder S, May CS. Viscosupplementation: managed care issues for osteoarthritis of the knee. J Manag Care Pharm. 2007;13(4 Suppl):S3-S19.
- Strand V, Conaghan PG, Lohmander LS, et al. An integrated analysis of five double-blind, randomized controlled trials evaluating the safety and efficacy of a hyaluronan product for intra-articular injection in osteoarthritis of the knee. Osteoarthritis Cartilage. 2006;14(9):859-866.
- Strand V, Baraf HS, Lavin PT, Lim S, Hosokawa H. A multicenter, randomized controlled trial comparing a single intra-articular injection of Gel-200, a new cross-linked formulation of hyaluronic acid, to phosphate buffered saline for treatment of osteoarthritis of the knee. Osteoarthritis Cartilage. 2012;20(5):350-356.
- Strand V, McIntyre LF, Beach WR, Miller LE, Block JE. Safety and efficacy of US-approved viscosupplements for knee osteoarthritis: a systematic review and meta-analysis of randomized, saline-controlled trials. J Pain Res. 2015;8:217-228.
- Bannuru RR, Schmid CH, Kent DM, Vaysbrott EE, Wong JB, McAlindon TE. Comparative effectiveness of pharmacologic interventions for knee osteoarthritis: a systematic review and network meta-analysis. Ann Intern Med. 2015;162(1):46-54.
- Mandl LA, Losina E. Relative efficacy of knee osteoarthritis treatments: are all placebos created equal? Ann Intern Med. 2015;162(1):71-72.
- Kusayama Y, Akamatsu Y, Kumagai K, Kobayashi H, Aratake M, Saito T. Changes in synovial fluid biomarkers and clinical efficacy of intra-articular injections of hyaluronic acid for patients with knee osteoarthritis. J Exp Orthop. 2014;1(1):16. doi:10.1186/s40634-014-0016-7.
- Kaneko K, Higuchi C, Kunugiza Y, et al. Hyaluronan inhibits BMP-induced osteoblast differentiation. FEBS Lett. 2015;589(4):447-454. doi:10.1016/j.febslet.2014.
- Altman RD, Manjoo A, Fierlinger A, Niazi F, Nicholls M. The mechanism of action for hyaluronic acid treatment in the osteoarthritic knee: a systematic review. BMC Musculoskelet Disord. 2015;16:321. doi:10.1186/s12891-015-0775-z.
- Waddell DD, Bricker DC. Total knee replacement delayed with hylan G-F 20 use in patients with grade IV osteoarthritis. J Manag Care Pharm. 2007;13(2):113-121.
- Khan T, Nanchanatt G, Farber K, Jan S. Analysis of the effectiveness of hyaluronic acid in prevention of total knee replacement in osteoarthritis patients. J Manag Care Pharm. 2014;20:S49.
- Abbott T, Altman RD, Dimeff R, et al. Do hyaluronic acid injections delay total knee replacement surgery? Arthritis Rheum. 2013;65(Suppl 10):2139.
- Altman R, Lim S, Steen R, Dasa V. Intra-articular hyaluronic acid delays total knee replacement in patients with knee osteoarthritis: evidence from a large U.S. health claims database. Osteoarthritis Cartilage. 2015;23(Suppl 2):A403-A404.
- Mather RC 3rd, Hug KT, Orlando LA, et al. Economic evaluation of access to musculoskeletal care: the case of waiting for total knee arthroplasty. BMC Musculoskelet Disord. 2014;15:22. doi:10.1186/1471-2474-15-22.
- Waddell DD, Joseph B. Delayed total knee replacement with Hylan G-F 20. J Knee Surg. 2016;29(2):159-168. doi:10.1055/s-0034-1395281.
- Atukorala I, Makovey J, Williams M, Ochoa Albiztegui E, Eyles JP, Hunter DJ. If you have end-stage radiographic knee osteoarthritis can you respond to non-surgical management? Osteoarthritis Cartilage. 2015;23(Suppl 2):A329.
- Strand V, Baraf HS, Lavin PT, Lim S, Hosokawa H. Effectiveness and safety of a multicenter extension and retreatment trial of Gel-200 in patients with knee osteoarthritis. Cartilage. 2012;3(4):297-304. doi:10.1177/1947603512451024.
- Riddle DL, Kong X, Jiranek WA. Two-year incidence and predictors of future knee arthroplasty in persons with symptomatic knee osteoarthritis: preliminary analysis of longitudinal data from the osteoarthritis initiative. Knee. 2009;16(6):494-500.
- Hawker GA, Guan J, Croxford R, et al. A prospective population-based study of the predictors of undergoing total joint arthroplasty. Arthritis Rheum. 2006;54(10):3212-3220.
- Jevsevar DS. Treatment of osteoarthritis of the knee: evidence-based guideline, 2nd edition. J Am Acad Orthop Surg. 2013;21(9):571-576. doi:10.5435/JAAOS-21-09-571.
- Hochberg MC, Altman RD, April KT, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken). 2012;64(4):465-474.
- Jordan KM, Arden NK, Doherty M, et al. EULAR Recommendations 2003: an evidence based approach to the management of knee osteoarthritis: report of a task force of the standing committee for international clinical studies including therapeutic trials (ESCISIT). Ann Rheum Dis. 2003;62(12):1145-1155.
- Bannuru RR, Vaysbrot EE, McIntyre LF. Did the American Academy of Orthopaedic Surgeons osteoarthritis guidelines miss the mark? Arthroscopy. 2014;30(1):86-89. doi:10.1016/j.arthro.2013.10.007.
- Losina E, Thornhill TS, Rome BN, Wright J, Katz JN. The dramatic increase in total knee replacement utilization rates in the United States cannot be fully explained by growth in population size and the obesity epidemic. J Bone Joint Surg Am. 2012;94(3):201-207. doi:10.2106/JBJS.J.01958.
- Weinstein AM, Rome BN, Reichmann WM, et al. Estimating the burden of total knee replacement in the United States. J Bone Joint Surg Am. 2013;95(5):385-392. doi:10.2106/JBJS.L.00206.
- Riddle DL, Jiranek WA, Hayes CW. Use of a validated algorithm to judge the appropriateness of total knee arthroplasty in the United States: a multicenter longitudinal cohort study. Arthritis Rheumatol. 2014;66(8):2134-2143. doi:10.1002/art.38685.
- NewBerry SJ, Fitzgerald JD, Maglione MA, et al. Agency for Healthcare Research and Quality Web site. Systematic Review for Effectiveness of Hyaluronic Acid in the Treatment of Severe Degenerative Joint Disease (DJD) of the Knee: Technology Assessment Report. http://www.ahrq.gov/research/findings/ta/call-for-public-review.html. Published July 23, 2015. Accessed December 22, 2014.
TAKE-HOME POINTS
- Repeated courses of treatment with HA are safe and are associated with the delay of TKR for up to 3 years.
- HA treatment should be considered an important clinical treatment option for patients with knee OA.
- Repeated courses of treatment with HA are safe.
- Repeated courses of HA treatment pose no greater safety risk than a single course of HA treatment.
- Additional research is needed to evaluate the effects of repeated HA courses on delaying TKR beyond a 3-year period.
How to prescribe effectively for opioid use disorder
NEW ORLEANS – Physicians committed to fighting the national opioid epidemic really need to take the 8-hour training course on addiction treatment required to obtain a Drug Enforcement Administration ‘X’ number, because it will enable them to prescribe buprenorphine, a drug with unique advantages for many affected patients, Ellie Grossman, MD, asserted at the annual meeting of the American College of Physicians.

Buprenorphine (Subutex) is one of the three medications approved for treatment of opioid use disorder (OUD), along with methadone and naltrexone (Revia). And for certain patients, it’s clearly the best choice, according to Dr. Grossman, a general internist at Harvard Medical School, Boston, and the primary care lead for behavioral health integration at the Cambridge (Mass.) Health Alliance.
The DEA X number certification process, which entails obtaining a waiver through SAMHSA – the Substance Abuse and Mental Health Services Administration – is bureaucratic. It’s unpopular with many physicians. But it’s well worth 8 hours of an internist’s time to get the waiver and gain the ability to prescribe buprenorphine.
“The requirement is admittedly clunky, and many people have strong feelings about whether this is a regulation that should exist,” according to Dr. Grossman. “I myself didn’t need to have special training to prescribe methadone, a full opioid agonist that my patients could easily die from. But I did have to undergo an 8-hour training to prescribe buprenorphine, and it’s much harder to die from that drug.”
She addressed which of the three medications for OUD is the best fit in a given patient, the appropriate treatment duration, and the role of adjunctive counseling, which – spoiler alert – has been cast into question by the results of a major government-funded randomized trial.
Dr. Grossman’s overriding message: “You are saving lives by getting people on medication.”
Indeed, studies have shown that patients with OUD who receive no treatment have a sixfold increase in the standardized mortality ratio, compared with the general population. Contrast that with the less than 2-fold increased risk with medication-assisted treatment and roughly a 2.5-fold increased risk when medication is given short term to cover withdrawal and then tapered and discontinued.
Other documented benefits of long-term medication-assisted treatment of patients with OUD as described in a 2014 Cochrane review include reductions in injection drug use, crime days, HIV-related risk behaviors and seroconversion, and improved health and social functioning.
Of note, those well-documented benefits apply only to methadone, a full opioid agonist, and buprenorphine, a partial agonist, because those two drugs have been around long enough to generate long-term outcome data. Naltrexone, which has a completely different mechanism of action – it’s a full opioid antagonist – has not as of yet.
Individualizing medical therapy for OUD
Physicians can’t write a prescription for methadone. The drug must be administered at a certified opioid treatment program, or OTP, otherwise known as a methadone clinic. Those clinics are highly regulated at both the federal and state levels, with lots of minutia involved. Patient counseling and drug screening are required.
In contrast, a physician with a DEA X number can write a prescription for buprenorphine and have a patient fill it at a pharmacy. There is inherently less structure surrounding buprenorphine therapy than that of methadone, Dr. Grossman noted. There are no hard and fast rules about how often a physician has to see the patient or do drug screens or counseling. Buprenorphine is available as once-daily oral sublingual therapy and, more recently, in long-acting injectable and implantable formulations, although Dr. Grossman believes the jury is still out about how these nonoral agents are best utilized.
“I’m often asked, ‘Which is better, methadone or buprenorphine?’ Really, the answer is they’re both pretty darn good,” according to Dr. Grossman.
The Cochrane review concluded that, in the studies that have used real-world dosing – that is, higher doses than in the initial studies – high-dose buprenorphine and high-dose methadone have similar rates of retention in treatment.
“What I tell patients is that a lot hinges on the structure of the treatment delivery system,” Dr. Grossman said. “If it’s methadone, they’re going to the OTP every day. Some people need more structure; they need a set of eyes on them every day. Or if they are at high risk for medication diversion – for example, someone else in their household might want to steal their medications – going to a methadone program gets around that. Also, when somebody has been on methadone in the past and did well on it and wants to go on it again, I’m likely to say, ‘That sounds like a good fit.’”
Buprenorphine is a good option for patients who don’t require close, structured supervision. It has fewer drug interactions than does methadone and is less prone to cause QTc prolongation. Also, it’s a more realistic option for patients who live so far from an OTP that daily attendance is impractical. And ob.gyns increasingly favor buprenorphine, because the problem of neonatal abstinence syndrome is less severe than when mothers are on methadone.
As for extended-release naltrexone (Vivitrol), the pivotal double-blind Russian trial that won FDA approval for treatment of OUD showed a dramatic improvement in opioid-free weeks (Lancet. 2011 Apr 30;377[9776]:1506-13).
More recently, the 24-week, multicenter, open-label X:BOT trial randomized 570 U.S. patients with OUD to once-monthly extended-release naltrexone or daily sublingual buprenorphine-naloxone (Suboxone). The dropout rate was higher in the extended-release naltrexone arm because patients had to be opioid free for 2 weeks before starting on the opioid antagonist. As a practical matter, that can be difficult to achieve unless a patient has just been released from jail or prison. But the per-protocol relapse rates were similar (Lancet. 2018 Jan 27;391[10118]:309-18).
“Many people interpret this study as saying, with the right patient who can get into an opioid-free state or, if you inherit an opioid-free state, the choice between extended-release naltrexone and buprenorphine-naloxone may be a bit of a wash in terms of clinical effectiveness, as best we can detect,” Dr. Grossman explained. “That said, they’re very different experiences: One is a shot in your butt once a month, the other is something you put in your mouth once a day. Patients typically have a strong point of view regarding what they’re up for.”
Extended-release naltrexone doesn’t require a DEA waiver or attendance at an OTP. But it costs roughly $800 per injection, although many insurers do cover it after additional paperwork is completed. While Dr. Grossman does use extended-release naltrexone in her own practice, it comes with some baggage. The drug comes in a powder, which is mixed with a diluent in the office, creating a thick, frothy substance that’s slow to inject. It has to be kept refrigerated, then warmed up in time for the patient visit.
“If you live somewhere where there’s no OTP and you don’t have a DEA X number, and you have a patient with OUD who’s interested in extended-release naltrexone, it’s not crazy to think about,” she noted.
Duration of medical therapy
Study after study demonstrates that, when treatment stops, the risk of relapse goes up.
“We as health care providers are used to the mentality of chronic diseases, like diabetes, where you’re probably on medicine for the rest of your life,” Dr. Grossman said. “OUD is another chronic disease where you might have a patient on medication for the rest of their life, although you may not want to drum that into their head right up front. It’s kind of scary. I don’t usually talk that way with my diabetic patients when I give them their diagnosis. So, I don’t push it.
“But the reality is, to give them the best chance of health, they should be on medication for a good long time,” she added. “And that’s true for all of the OUD medications.”
The role of counseling
The best evidence of the utility of adjunctive counseling in the treatment of OUD comes from the landmark Prescription Opioid Addiction Treatment Study (POATS), a 653-patient multicenter trial conducted by the National Drug Abuse Treatment Network and funded by the National Institute on Drug Abuse. Participants were randomized to standard medical management including medication and a meeting with a physician every 1-2 weeks, or to standard therapy plus individual counseling with a trained substance use counselor.
To the surprise of many, given that SAMHSA guidance strongly recommends counseling and other forms of behavioral therapy, there was no difference in outcomes between the two groups (Drug Alcohol Depend. 2015 May 1;150:112-9).
Subsequent parsing of the POATS data showed that the subgroup of people who were using heroin rather than prescription pills and who actually attended at least 60% of their counseling sessions did better than if they were randomized to no counseling.
“There’s still room for quibbling about the study, but many people would say, ‘You know, it’s not a slam dunk that everybody needs counseling,’ ” the internist commented.
“So, how do we pick the right treatment for our patients with OUD? It’s what feels right for them,” Dr. Grossman cautioned. “This gets back to what we do every day in managing chronic diseases: We nudge, we encourage, we use our motivational interviewing skills to help people figure out how they can change their lives and get healthier. There’s a long list of things going on in our patients’ lives that are going to help guide that decision.
“The message here: Medication is better than no medication, but it’s not a slam dunk which medication or how,” she concluded.
NEW ORLEANS – Physicians committed to fighting the national opioid epidemic really need to take the 8-hour training course on addiction treatment required to obtain a Drug Enforcement Administration ‘X’ number, because it will enable them to prescribe buprenorphine, a drug with unique advantages for many affected patients, Ellie Grossman, MD, asserted at the annual meeting of the American College of Physicians.
Buprenorphine (Subutex) is one of the three medications approved for treatment of opioid use disorder (OUD), along with methadone and naltrexone (Revia). And for certain patients, it’s clearly the best choice, according to Dr. Grossman, a general internist at Harvard Medical School, Boston, and the primary care lead for behavioral health integration at the Cambridge (Mass.) Health Alliance.
The DEA X number certification process, which entails obtaining a waiver through SAMHSA – the Substance Abuse and Mental Health Services Administration – is bureaucratic. It’s unpopular with many physicians. But it’s well worth 8 hours of an internist’s time to get the waiver and gain the ability to prescribe buprenorphine.
“The requirement is admittedly clunky, and many people have strong feelings about whether this is a regulation that should exist,” according to Dr. Grossman. “I myself didn’t need to have special training to prescribe methadone, a full opioid agonist that my patients could easily die from. But I did have to undergo an 8-hour training to prescribe buprenorphine, and it’s much harder to die from that drug.”
She addressed which of the three medications for OUD is the best fit in a given patient, the appropriate treatment duration, and the role of adjunctive counseling, which – spoiler alert – has been cast into question by the results of a major government-funded randomized trial.
Dr. Grossman’s overriding message: “You are saving lives by getting people on medication.”
Indeed, studies have shown that patients with OUD who receive no treatment have a sixfold increase in the standardized mortality ratio, compared with the general population. Contrast that with the less than 2-fold increased risk with medication-assisted treatment and roughly a 2.5-fold increased risk when medication is given short term to cover withdrawal and then tapered and discontinued.
Other documented benefits of long-term medication-assisted treatment of patients with OUD as described in a 2014 Cochrane review include reductions in injection drug use, crime days, HIV-related risk behaviors and seroconversion, and improved health and social functioning.
Of note, those well-documented benefits apply only to methadone, a full opioid agonist, and buprenorphine, a partial agonist, because those two drugs have been around long enough to generate long-term outcome data. Naltrexone, which has a completely different mechanism of action – it’s a full opioid antagonist – has not as of yet.
Individualizing medical therapy for OUD
Physicians can’t write a prescription for methadone. The drug must be administered at a certified opioid treatment program, or OTP, otherwise known as a methadone clinic. Those clinics are highly regulated at both the federal and state levels, with lots of minutia involved. Patient counseling and drug screening are required.
In contrast, a physician with a DEA X number can write a prescription for buprenorphine and have a patient fill it at a pharmacy. There is inherently less structure surrounding buprenorphine therapy than that of methadone, Dr. Grossman noted. There are no hard and fast rules about how often a physician has to see the patient or do drug screens or counseling. Buprenorphine is available as once-daily oral sublingual therapy and, more recently, in long-acting injectable and implantable formulations, although Dr. Grossman believes the jury is still out about how these nonoral agents are best utilized.
“I’m often asked, ‘Which is better, methadone or buprenorphine?’ Really, the answer is they’re both pretty darn good,” according to Dr. Grossman.
The Cochrane review concluded that, in the studies that have used real-world dosing – that is, higher doses than in the initial studies – high-dose buprenorphine and high-dose methadone have similar rates of retention in treatment.
“What I tell patients is that a lot hinges on the structure of the treatment delivery system,” Dr. Grossman said. “If it’s methadone, they’re going to the OTP every day. Some people need more structure; they need a set of eyes on them every day. Or if they are at high risk for medication diversion – for example, someone else in their household might want to steal their medications – going to a methadone program gets around that. Also, when somebody has been on methadone in the past and did well on it and wants to go on it again, I’m likely to say, ‘That sounds like a good fit.’”
Buprenorphine is a good option for patients who don’t require close, structured supervision. It has fewer drug interactions than does methadone and is less prone to cause QTc prolongation. Also, it’s a more realistic option for patients who live so far from an OTP that daily attendance is impractical. And ob.gyns increasingly favor buprenorphine, because the problem of neonatal abstinence syndrome is less severe than when mothers are on methadone.
As for extended-release naltrexone (Vivitrol), the pivotal double-blind Russian trial that won FDA approval for treatment of OUD showed a dramatic improvement in opioid-free weeks (Lancet. 2011 Apr 30;377[9776]:1506-13).
More recently, the 24-week, multicenter, open-label X:BOT trial randomized 570 U.S. patients with OUD to once-monthly extended-release naltrexone or daily sublingual buprenorphine-naloxone (Suboxone). The dropout rate was higher in the extended-release naltrexone arm because patients had to be opioid free for 2 weeks before starting on the opioid antagonist. As a practical matter, that can be difficult to achieve unless a patient has just been released from jail or prison. But the per-protocol relapse rates were similar (Lancet. 2018 Jan 27;391[10118]:309-18).
“Many people interpret this study as saying, with the right patient who can get into an opioid-free state or, if you inherit an opioid-free state, the choice between extended-release naltrexone and buprenorphine-naloxone may be a bit of a wash in terms of clinical effectiveness, as best we can detect,” Dr. Grossman explained. “That said, they’re very different experiences: One is a shot in your butt once a month, the other is something you put in your mouth once a day. Patients typically have a strong point of view regarding what they’re up for.”
Extended-release naltrexone doesn’t require a DEA waiver or attendance at an OTP. But it costs roughly $800 per injection, although many insurers do cover it after additional paperwork is completed. While Dr. Grossman does use extended-release naltrexone in her own practice, it comes with some baggage. The drug comes in a powder, which is mixed with a diluent in the office, creating a thick, frothy substance that’s slow to inject. It has to be kept refrigerated, then warmed up in time for the patient visit.
“If you live somewhere where there’s no OTP and you don’t have a DEA X number, and you have a patient with OUD who’s interested in extended-release naltrexone, it’s not crazy to think about,” she noted.
Duration of medical therapy
Study after study demonstrates that, when treatment stops, the risk of relapse goes up.
“We as health care providers are used to the mentality of chronic diseases, like diabetes, where you’re probably on medicine for the rest of your life,” Dr. Grossman said. “OUD is another chronic disease where you might have a patient on medication for the rest of their life, although you may not want to drum that into their head right up front. It’s kind of scary. I don’t usually talk that way with my diabetic patients when I give them their diagnosis. So, I don’t push it.
“But the reality is, to give them the best chance of health, they should be on medication for a good long time,” she added. “And that’s true for all of the OUD medications.”
The role of counseling
The best evidence of the utility of adjunctive counseling in the treatment of OUD comes from the landmark Prescription Opioid Addiction Treatment Study (POATS), a 653-patient multicenter trial conducted by the National Drug Abuse Treatment Network and funded by the National Institute on Drug Abuse. Participants were randomized to standard medical management including medication and a meeting with a physician every 1-2 weeks, or to standard therapy plus individual counseling with a trained substance use counselor.
To the surprise of many, given that SAMHSA guidance strongly recommends counseling and other forms of behavioral therapy, there was no difference in outcomes between the two groups (Drug Alcohol Depend. 2015 May 1;150:112-9).
Subsequent parsing of the POATS data showed that the subgroup of people who were using heroin rather than prescription pills and who actually attended at least 60% of their counseling sessions did better than if they were randomized to no counseling.
“There’s still room for quibbling about the study, but many people would say, ‘You know, it’s not a slam dunk that everybody needs counseling,’ ” the internist commented.
“So, how do we pick the right treatment for our patients with OUD? It’s what feels right for them,” Dr. Grossman cautioned. “This gets back to what we do every day in managing chronic diseases: We nudge, we encourage, we use our motivational interviewing skills to help people figure out how they can change their lives and get healthier. There’s a long list of things going on in our patients’ lives that are going to help guide that decision.
“The message here: Medication is better than no medication, but it’s not a slam dunk which medication or how,” she concluded.
NEW ORLEANS – Physicians committed to fighting the national opioid epidemic really need to take the 8-hour training course on addiction treatment required to obtain a Drug Enforcement Administration ‘X’ number, because it will enable them to prescribe buprenorphine, a drug with unique advantages for many affected patients, Ellie Grossman, MD, asserted at the annual meeting of the American College of Physicians.
Buprenorphine (Subutex) is one of the three medications approved for treatment of opioid use disorder (OUD), along with methadone and naltrexone (Revia). And for certain patients, it’s clearly the best choice, according to Dr. Grossman, a general internist at Harvard Medical School, Boston, and the primary care lead for behavioral health integration at the Cambridge (Mass.) Health Alliance.
The DEA X number certification process, which entails obtaining a waiver through SAMHSA – the Substance Abuse and Mental Health Services Administration – is bureaucratic. It’s unpopular with many physicians. But it’s well worth 8 hours of an internist’s time to get the waiver and gain the ability to prescribe buprenorphine.
“The requirement is admittedly clunky, and many people have strong feelings about whether this is a regulation that should exist,” according to Dr. Grossman. “I myself didn’t need to have special training to prescribe methadone, a full opioid agonist that my patients could easily die from. But I did have to undergo an 8-hour training to prescribe buprenorphine, and it’s much harder to die from that drug.”
She addressed which of the three medications for OUD is the best fit in a given patient, the appropriate treatment duration, and the role of adjunctive counseling, which – spoiler alert – has been cast into question by the results of a major government-funded randomized trial.
Dr. Grossman’s overriding message: “You are saving lives by getting people on medication.”
Indeed, studies have shown that patients with OUD who receive no treatment have a sixfold increase in the standardized mortality ratio, compared with the general population. Contrast that with the less than 2-fold increased risk with medication-assisted treatment and roughly a 2.5-fold increased risk when medication is given short term to cover withdrawal and then tapered and discontinued.
Other documented benefits of long-term medication-assisted treatment of patients with OUD as described in a 2014 Cochrane review include reductions in injection drug use, crime days, HIV-related risk behaviors and seroconversion, and improved health and social functioning.
Of note, those well-documented benefits apply only to methadone, a full opioid agonist, and buprenorphine, a partial agonist, because those two drugs have been around long enough to generate long-term outcome data. Naltrexone, which has a completely different mechanism of action – it’s a full opioid antagonist – has not as of yet.
Individualizing medical therapy for OUD
Physicians can’t write a prescription for methadone. The drug must be administered at a certified opioid treatment program, or OTP, otherwise known as a methadone clinic. Those clinics are highly regulated at both the federal and state levels, with lots of minutia involved. Patient counseling and drug screening are required.
In contrast, a physician with a DEA X number can write a prescription for buprenorphine and have a patient fill it at a pharmacy. There is inherently less structure surrounding buprenorphine therapy than that of methadone, Dr. Grossman noted. There are no hard and fast rules about how often a physician has to see the patient or do drug screens or counseling. Buprenorphine is available as once-daily oral sublingual therapy and, more recently, in long-acting injectable and implantable formulations, although Dr. Grossman believes the jury is still out about how these nonoral agents are best utilized.
“I’m often asked, ‘Which is better, methadone or buprenorphine?’ Really, the answer is they’re both pretty darn good,” according to Dr. Grossman.
The Cochrane review concluded that, in the studies that have used real-world dosing – that is, higher doses than in the initial studies – high-dose buprenorphine and high-dose methadone have similar rates of retention in treatment.
“What I tell patients is that a lot hinges on the structure of the treatment delivery system,” Dr. Grossman said. “If it’s methadone, they’re going to the OTP every day. Some people need more structure; they need a set of eyes on them every day. Or if they are at high risk for medication diversion – for example, someone else in their household might want to steal their medications – going to a methadone program gets around that. Also, when somebody has been on methadone in the past and did well on it and wants to go on it again, I’m likely to say, ‘That sounds like a good fit.’”
Buprenorphine is a good option for patients who don’t require close, structured supervision. It has fewer drug interactions than does methadone and is less prone to cause QTc prolongation. Also, it’s a more realistic option for patients who live so far from an OTP that daily attendance is impractical. And ob.gyns increasingly favor buprenorphine, because the problem of neonatal abstinence syndrome is less severe than when mothers are on methadone.
As for extended-release naltrexone (Vivitrol), the pivotal double-blind Russian trial that won FDA approval for treatment of OUD showed a dramatic improvement in opioid-free weeks (Lancet. 2011 Apr 30;377[9776]:1506-13).
More recently, the 24-week, multicenter, open-label X:BOT trial randomized 570 U.S. patients with OUD to once-monthly extended-release naltrexone or daily sublingual buprenorphine-naloxone (Suboxone). The dropout rate was higher in the extended-release naltrexone arm because patients had to be opioid free for 2 weeks before starting on the opioid antagonist. As a practical matter, that can be difficult to achieve unless a patient has just been released from jail or prison. But the per-protocol relapse rates were similar (Lancet. 2018 Jan 27;391[10118]:309-18).
“Many people interpret this study as saying, with the right patient who can get into an opioid-free state or, if you inherit an opioid-free state, the choice between extended-release naltrexone and buprenorphine-naloxone may be a bit of a wash in terms of clinical effectiveness, as best we can detect,” Dr. Grossman explained. “That said, they’re very different experiences: One is a shot in your butt once a month, the other is something you put in your mouth once a day. Patients typically have a strong point of view regarding what they’re up for.”
Extended-release naltrexone doesn’t require a DEA waiver or attendance at an OTP. But it costs roughly $800 per injection, although many insurers do cover it after additional paperwork is completed. While Dr. Grossman does use extended-release naltrexone in her own practice, it comes with some baggage. The drug comes in a powder, which is mixed with a diluent in the office, creating a thick, frothy substance that’s slow to inject. It has to be kept refrigerated, then warmed up in time for the patient visit.
“If you live somewhere where there’s no OTP and you don’t have a DEA X number, and you have a patient with OUD who’s interested in extended-release naltrexone, it’s not crazy to think about,” she noted.
Duration of medical therapy
Study after study demonstrates that, when treatment stops, the risk of relapse goes up.
“We as health care providers are used to the mentality of chronic diseases, like diabetes, where you’re probably on medicine for the rest of your life,” Dr. Grossman said. “OUD is another chronic disease where you might have a patient on medication for the rest of their life, although you may not want to drum that into their head right up front. It’s kind of scary. I don’t usually talk that way with my diabetic patients when I give them their diagnosis. So, I don’t push it.
“But the reality is, to give them the best chance of health, they should be on medication for a good long time,” she added. “And that’s true for all of the OUD medications.”
The role of counseling
The best evidence of the utility of adjunctive counseling in the treatment of OUD comes from the landmark Prescription Opioid Addiction Treatment Study (POATS), a 653-patient multicenter trial conducted by the National Drug Abuse Treatment Network and funded by the National Institute on Drug Abuse. Participants were randomized to standard medical management including medication and a meeting with a physician every 1-2 weeks, or to standard therapy plus individual counseling with a trained substance use counselor.
To the surprise of many, given that SAMHSA guidance strongly recommends counseling and other forms of behavioral therapy, there was no difference in outcomes between the two groups (Drug Alcohol Depend. 2015 May 1;150:112-9).
Subsequent parsing of the POATS data showed that the subgroup of people who were using heroin rather than prescription pills and who actually attended at least 60% of their counseling sessions did better than if they were randomized to no counseling.
“There’s still room for quibbling about the study, but many people would say, ‘You know, it’s not a slam dunk that everybody needs counseling,’ ” the internist commented.
“So, how do we pick the right treatment for our patients with OUD? It’s what feels right for them,” Dr. Grossman cautioned. “This gets back to what we do every day in managing chronic diseases: We nudge, we encourage, we use our motivational interviewing skills to help people figure out how they can change their lives and get healthier. There’s a long list of things going on in our patients’ lives that are going to help guide that decision.
“The message here: Medication is better than no medication, but it’s not a slam dunk which medication or how,” she concluded.
REPORTING FROM ACP INTERNAL MEDICINE
FDA approves Orilissa for endometriosis pain
The Food and Drug Administration has approved elagolix (Orilissa) for oral treatment of moderate to severe pain associated with endometriosis, announced AbbVie and Neurocrine Biosciences; this approval makes it the first such treatment in more than a decade. It is expected to be available in the United States in early August.

Elagolix is a gonadotropin-releasing hormone (GnRH) antagonist and the first and only one developed specifically for managing this kind of pain.
The approval is based on two 6-month, randomized, double-blind, placebo-controlled phase 3 trials that compared a total of 952 adult women treated with either elagolix with 734 treated with placebo. All of the women experienced moderate to severe endometriosis pain; their ages ranged from 18 to 49 years.
Of the women in the treatment group, 475 were treated with a 150-mg daily dose, and 477 were treated with a 200-mg twice-daily dose. Both treatment groups showed significantly greater mean reductions in pain – both daily menstrual and nonmenstrual pelvic pain – at 6 months. Furthermore, women in the 200-mg twice-daily group also showed statistically significant greater reductions in pain with sex at 3 months, compared with placebo. Altogether, these represent the three most common kinds of endometriosis pain.
The most concerning adverse event associated with elagolix is dose-dependent decreases in bone mineral density; this effect limits treatment to either 150 mg daily for up to 24 months or 200 mg twice daily for up to 6 months. Bone mineral density loss might not be completely reversible, even with treatment cessation. Common adverse events (occurring in at least 5%) included hot flush/night sweats, headache, and nausea. Elagolix is not recommended for women who are or may be pregnant, have osteoporosis, have severe liver disease, or take strong OATP1B1 inhibitors.
Full prescribing information, as well as further details on the approval, can be found on the AbbVie website.
The Food and Drug Administration has approved elagolix (Orilissa) for oral treatment of moderate to severe pain associated with endometriosis, announced AbbVie and Neurocrine Biosciences; this approval makes it the first such treatment in more than a decade. It is expected to be available in the United States in early August.
Elagolix is a gonadotropin-releasing hormone (GnRH) antagonist and the first and only one developed specifically for managing this kind of pain.
The approval is based on two 6-month, randomized, double-blind, placebo-controlled phase 3 trials that compared a total of 952 adult women treated with either elagolix with 734 treated with placebo. All of the women experienced moderate to severe endometriosis pain; their ages ranged from 18 to 49 years.
Of the women in the treatment group, 475 were treated with a 150-mg daily dose, and 477 were treated with a 200-mg twice-daily dose. Both treatment groups showed significantly greater mean reductions in pain – both daily menstrual and nonmenstrual pelvic pain – at 6 months. Furthermore, women in the 200-mg twice-daily group also showed statistically significant greater reductions in pain with sex at 3 months, compared with placebo. Altogether, these represent the three most common kinds of endometriosis pain.
The most concerning adverse event associated with elagolix is dose-dependent decreases in bone mineral density; this effect limits treatment to either 150 mg daily for up to 24 months or 200 mg twice daily for up to 6 months. Bone mineral density loss might not be completely reversible, even with treatment cessation. Common adverse events (occurring in at least 5%) included hot flush/night sweats, headache, and nausea. Elagolix is not recommended for women who are or may be pregnant, have osteoporosis, have severe liver disease, or take strong OATP1B1 inhibitors.
Full prescribing information, as well as further details on the approval, can be found on the AbbVie website.
The Food and Drug Administration has approved elagolix (Orilissa) for oral treatment of moderate to severe pain associated with endometriosis, announced AbbVie and Neurocrine Biosciences; this approval makes it the first such treatment in more than a decade. It is expected to be available in the United States in early August.
Elagolix is a gonadotropin-releasing hormone (GnRH) antagonist and the first and only one developed specifically for managing this kind of pain.
The approval is based on two 6-month, randomized, double-blind, placebo-controlled phase 3 trials that compared a total of 952 adult women treated with either elagolix with 734 treated with placebo. All of the women experienced moderate to severe endometriosis pain; their ages ranged from 18 to 49 years.
Of the women in the treatment group, 475 were treated with a 150-mg daily dose, and 477 were treated with a 200-mg twice-daily dose. Both treatment groups showed significantly greater mean reductions in pain – both daily menstrual and nonmenstrual pelvic pain – at 6 months. Furthermore, women in the 200-mg twice-daily group also showed statistically significant greater reductions in pain with sex at 3 months, compared with placebo. Altogether, these represent the three most common kinds of endometriosis pain.
The most concerning adverse event associated with elagolix is dose-dependent decreases in bone mineral density; this effect limits treatment to either 150 mg daily for up to 24 months or 200 mg twice daily for up to 6 months. Bone mineral density loss might not be completely reversible, even with treatment cessation. Common adverse events (occurring in at least 5%) included hot flush/night sweats, headache, and nausea. Elagolix is not recommended for women who are or may be pregnant, have osteoporosis, have severe liver disease, or take strong OATP1B1 inhibitors.
Full prescribing information, as well as further details on the approval, can be found on the AbbVie website.
Fathers and mothers report similar rates of depression at well-child visit
Prevalence of depression in fathers was similar to that of mothers screened at well-child visits, according to a research letter published in JAMA Pediatrics.
An analysis of data obtained from the Child Health Improvement through Computer Automation (CHICA) pediatric health surveillance system found that 4.4% of fathers who attended the well-child visit and completed a prescreening form scored positive for depression, comparable with the rate in mothers (5%). Overall, fathers composed 11.7% of parents who screened positive for depression, reported Erika R. Cheng, PhD, of Indiana University, Indianapolis, and her colleagues.
Dr. Cheng and her colleagues estimated prevalence of paternal depression using CHICA data from parents of children aged 15 months and younger from five community health centers in Indianapolis between August 1, 2016, and December 31, 2017. CHICA is a 20-question prescreen of pediatric health conditions based on the patient’s existing data.
Maternal postpartum depression was assessed using a modified version of the Edinburgh Postnatal Depression Scale, administered every 90 days during the child’s first 15 months of life, Dr. Cheng and her colleagues wrote.
Fathers were present at 30.8% of well-child visits (2,946 of 9,572) and completed the prescreening at 806 visits (8.4% of total visits). A total of 36 (4.4%) fathers screened positive for depression, compared with 273 (5%) mothers. However, since CHICA assesses depression for only one parent, some cases of paternal depression may have been missed, the investigators added.
“Pediatric clinics are thus promising settings in which to address depression in both parents as part of a family-centered approach to care,” Dr. Cheng and her coauthors concluded. “Addressing these gaps could improve detection and treatment rates of postnatal depression in both mothers and fathers.”
Two of the authors coinvented the CHICA system, and one is a co-owner of Digital Health Solutions, which licensed the system. No other disclosures were reported.
SOURCE: Cheng ER et al. JAMA Pediatr. 2018 Jul 23. doi:10.1001/jamapediatrics.2018.1505.
Prevalence of depression in fathers was similar to that of mothers screened at well-child visits, according to a research letter published in JAMA Pediatrics.
An analysis of data obtained from the Child Health Improvement through Computer Automation (CHICA) pediatric health surveillance system found that 4.4% of fathers who attended the well-child visit and completed a prescreening form scored positive for depression, comparable with the rate in mothers (5%). Overall, fathers composed 11.7% of parents who screened positive for depression, reported Erika R. Cheng, PhD, of Indiana University, Indianapolis, and her colleagues.
Dr. Cheng and her colleagues estimated prevalence of paternal depression using CHICA data from parents of children aged 15 months and younger from five community health centers in Indianapolis between August 1, 2016, and December 31, 2017. CHICA is a 20-question prescreen of pediatric health conditions based on the patient’s existing data.
Maternal postpartum depression was assessed using a modified version of the Edinburgh Postnatal Depression Scale, administered every 90 days during the child’s first 15 months of life, Dr. Cheng and her colleagues wrote.
Fathers were present at 30.8% of well-child visits (2,946 of 9,572) and completed the prescreening at 806 visits (8.4% of total visits). A total of 36 (4.4%) fathers screened positive for depression, compared with 273 (5%) mothers. However, since CHICA assesses depression for only one parent, some cases of paternal depression may have been missed, the investigators added.
“Pediatric clinics are thus promising settings in which to address depression in both parents as part of a family-centered approach to care,” Dr. Cheng and her coauthors concluded. “Addressing these gaps could improve detection and treatment rates of postnatal depression in both mothers and fathers.”
Two of the authors coinvented the CHICA system, and one is a co-owner of Digital Health Solutions, which licensed the system. No other disclosures were reported.
SOURCE: Cheng ER et al. JAMA Pediatr. 2018 Jul 23. doi:10.1001/jamapediatrics.2018.1505.
Prevalence of depression in fathers was similar to that of mothers screened at well-child visits, according to a research letter published in JAMA Pediatrics.
An analysis of data obtained from the Child Health Improvement through Computer Automation (CHICA) pediatric health surveillance system found that 4.4% of fathers who attended the well-child visit and completed a prescreening form scored positive for depression, comparable with the rate in mothers (5%). Overall, fathers composed 11.7% of parents who screened positive for depression, reported Erika R. Cheng, PhD, of Indiana University, Indianapolis, and her colleagues.
Dr. Cheng and her colleagues estimated prevalence of paternal depression using CHICA data from parents of children aged 15 months and younger from five community health centers in Indianapolis between August 1, 2016, and December 31, 2017. CHICA is a 20-question prescreen of pediatric health conditions based on the patient’s existing data.
Maternal postpartum depression was assessed using a modified version of the Edinburgh Postnatal Depression Scale, administered every 90 days during the child’s first 15 months of life, Dr. Cheng and her colleagues wrote.
Fathers were present at 30.8% of well-child visits (2,946 of 9,572) and completed the prescreening at 806 visits (8.4% of total visits). A total of 36 (4.4%) fathers screened positive for depression, compared with 273 (5%) mothers. However, since CHICA assesses depression for only one parent, some cases of paternal depression may have been missed, the investigators added.
“Pediatric clinics are thus promising settings in which to address depression in both parents as part of a family-centered approach to care,” Dr. Cheng and her coauthors concluded. “Addressing these gaps could improve detection and treatment rates of postnatal depression in both mothers and fathers.”
Two of the authors coinvented the CHICA system, and one is a co-owner of Digital Health Solutions, which licensed the system. No other disclosures were reported.
SOURCE: Cheng ER et al. JAMA Pediatr. 2018 Jul 23. doi:10.1001/jamapediatrics.2018.1505.
FROM JAMA PEDIATRICS
Key clinical point: Depression prevalence during pediatric well-child care visits was similar in fathers and mothers.
Major finding: Fathers screened positive for depression at a rate of 4.4%, compared with 5% of mothers.
Study details: An analysis of parent responses from 9,572 clinic visits between August 2016 and December 2017.
Disclosures: Two of the authors coinvented the CHICA system, and one is a co-owner of Digital Health Solutions, which licensed the system. No other disclosures were reported.
Source: Cheng ER et al. JAMA Pediatr. 2018 Jul 23. doi:10.1001/jamapediatrics.2018.1505.
Mandated 1-hour sepsis care protocol lowers mortality in children
A bundle of blood cultures, broad-spectrum antibiotics, and intravenous fluid replacement reduces risk of in-hospital mortality among children with sepsis if all three forms of management are initiated within an hour, according to a cohort study published in JAMA.

Although published guidelines already recommend prompt initiation of these three elements of care, a mandate created in New York in 2013 called for these interventions to be initiated in children within 1 hour of sepsis recognition. The newly published cohort study shows a mortality benefit when this is done.
In the study, which evaluated the impact of the bundle as well as each of the components in 1,179 pediatric patients with sepsis treated at 54 hospitals, the risk-adjusted odds ratio of in-hospital mortality was 0.59 (P = .02) among patients receiving the mandated protocol, compared with those who did not.
When provided within 1 hour, none of the individual components of the bundles were associated with a significant reduction of risk-adjusted, in-hospital mortality by themselves. However, there were trends for benefit with blood cultures (OR, 0.73; P = .1) and broad-spectrum antibiotics (OR, 0.78; P = .18). There was no trend for administration of intravenous fluids (OR, 0.88; P = .56), for which the mandate specified 20 mL/kg.
Although 46.5% of patients received intravenous fluids, 62.8% received broad-spectrum antibiotics, and blood cultures were obtained in 67.7% of the children within 1 hour, only 24.9% were managed with the entire sepsis bundle. Across hospitals, the proportion of children completing the bundle ranged from 7.3% to 46.1%.
Bundle completion was more common in hospitals already treating a relatively high volume of pediatric patients and in those with pediatric specialty services, but the study authors noted that this was not a linear relationship. Rather, they called this association “hypothesis generating” and speculated that other factors might also be important.
The children in this cohort ranged in age from under 1 month to 17 years. Slightly more than half were aged 6 years or older and nearly one-third were older than 12 years. Nearly 45% had no comorbidities. Slightly more than one-third had a malignancy or were immunosuppressed.
None of the study authors reported any relevant financial relationships with industry.
SOURCE: Evans IVR et al. JAMA. 2018 Jul 24. doi:10.1001/jama.2018.9071.
The data published by Evans et al support a protocol approach to sepsis management in children as well as prompt delivery of the components outlined in the New York state mandate, according to an accompanying editorial written by Robert J. Vinci, MD, of Boston Medical Center, and Elliot Melendez, MD, of Johns Hopkins All Children’s Hospital, St. Petersburg, Fla. However, it cannot be determined from this study whether it is prompt delivery of these three mandated components or a more rigorous approach to pediatric sepsis management that deserves the most credit for the mortality benefit.
“Organizations that undertake quality improvement initiatives may have systems of care that promote the bundle completion, which then leads to improved outcomes,” they wrote. As a result, bundle completion may be a marker of expertise in managing critically ill children. They agreed that the data support the tested protocol, but they questioned whether this is sufficient.
“Organizations should be cautious about merely adopting a bundle of care without ensuring they have a universal culture of safety and quality that is adopted and supported from front-line clinical caregivers to organizational leaders and administrators,” they stated.
Dr. Vinci and Dr. Melendez had no disclosures to report.
SOURCE: JAMA. 2018;320(4):345-346. doi:10.1001/jama.2018.9183.
The data published by Evans et al support a protocol approach to sepsis management in children as well as prompt delivery of the components outlined in the New York state mandate, according to an accompanying editorial written by Robert J. Vinci, MD, of Boston Medical Center, and Elliot Melendez, MD, of Johns Hopkins All Children’s Hospital, St. Petersburg, Fla. However, it cannot be determined from this study whether it is prompt delivery of these three mandated components or a more rigorous approach to pediatric sepsis management that deserves the most credit for the mortality benefit.
“Organizations that undertake quality improvement initiatives may have systems of care that promote the bundle completion, which then leads to improved outcomes,” they wrote. As a result, bundle completion may be a marker of expertise in managing critically ill children. They agreed that the data support the tested protocol, but they questioned whether this is sufficient.
“Organizations should be cautious about merely adopting a bundle of care without ensuring they have a universal culture of safety and quality that is adopted and supported from front-line clinical caregivers to organizational leaders and administrators,” they stated.
Dr. Vinci and Dr. Melendez had no disclosures to report.
SOURCE: JAMA. 2018;320(4):345-346. doi:10.1001/jama.2018.9183.
The data published by Evans et al support a protocol approach to sepsis management in children as well as prompt delivery of the components outlined in the New York state mandate, according to an accompanying editorial written by Robert J. Vinci, MD, of Boston Medical Center, and Elliot Melendez, MD, of Johns Hopkins All Children’s Hospital, St. Petersburg, Fla. However, it cannot be determined from this study whether it is prompt delivery of these three mandated components or a more rigorous approach to pediatric sepsis management that deserves the most credit for the mortality benefit.
“Organizations that undertake quality improvement initiatives may have systems of care that promote the bundle completion, which then leads to improved outcomes,” they wrote. As a result, bundle completion may be a marker of expertise in managing critically ill children. They agreed that the data support the tested protocol, but they questioned whether this is sufficient.
“Organizations should be cautious about merely adopting a bundle of care without ensuring they have a universal culture of safety and quality that is adopted and supported from front-line clinical caregivers to organizational leaders and administrators,” they stated.
Dr. Vinci and Dr. Melendez had no disclosures to report.
SOURCE: JAMA. 2018;320(4):345-346. doi:10.1001/jama.2018.9183.
A bundle of blood cultures, broad-spectrum antibiotics, and intravenous fluid replacement reduces risk of in-hospital mortality among children with sepsis if all three forms of management are initiated within an hour, according to a cohort study published in JAMA.
Although published guidelines already recommend prompt initiation of these three elements of care, a mandate created in New York in 2013 called for these interventions to be initiated in children within 1 hour of sepsis recognition. The newly published cohort study shows a mortality benefit when this is done.
In the study, which evaluated the impact of the bundle as well as each of the components in 1,179 pediatric patients with sepsis treated at 54 hospitals, the risk-adjusted odds ratio of in-hospital mortality was 0.59 (P = .02) among patients receiving the mandated protocol, compared with those who did not.
When provided within 1 hour, none of the individual components of the bundles were associated with a significant reduction of risk-adjusted, in-hospital mortality by themselves. However, there were trends for benefit with blood cultures (OR, 0.73; P = .1) and broad-spectrum antibiotics (OR, 0.78; P = .18). There was no trend for administration of intravenous fluids (OR, 0.88; P = .56), for which the mandate specified 20 mL/kg.
Although 46.5% of patients received intravenous fluids, 62.8% received broad-spectrum antibiotics, and blood cultures were obtained in 67.7% of the children within 1 hour, only 24.9% were managed with the entire sepsis bundle. Across hospitals, the proportion of children completing the bundle ranged from 7.3% to 46.1%.
Bundle completion was more common in hospitals already treating a relatively high volume of pediatric patients and in those with pediatric specialty services, but the study authors noted that this was not a linear relationship. Rather, they called this association “hypothesis generating” and speculated that other factors might also be important.
The children in this cohort ranged in age from under 1 month to 17 years. Slightly more than half were aged 6 years or older and nearly one-third were older than 12 years. Nearly 45% had no comorbidities. Slightly more than one-third had a malignancy or were immunosuppressed.
None of the study authors reported any relevant financial relationships with industry.
SOURCE: Evans IVR et al. JAMA. 2018 Jul 24. doi:10.1001/jama.2018.9071.
A bundle of blood cultures, broad-spectrum antibiotics, and intravenous fluid replacement reduces risk of in-hospital mortality among children with sepsis if all three forms of management are initiated within an hour, according to a cohort study published in JAMA.
Although published guidelines already recommend prompt initiation of these three elements of care, a mandate created in New York in 2013 called for these interventions to be initiated in children within 1 hour of sepsis recognition. The newly published cohort study shows a mortality benefit when this is done.
In the study, which evaluated the impact of the bundle as well as each of the components in 1,179 pediatric patients with sepsis treated at 54 hospitals, the risk-adjusted odds ratio of in-hospital mortality was 0.59 (P = .02) among patients receiving the mandated protocol, compared with those who did not.
When provided within 1 hour, none of the individual components of the bundles were associated with a significant reduction of risk-adjusted, in-hospital mortality by themselves. However, there were trends for benefit with blood cultures (OR, 0.73; P = .1) and broad-spectrum antibiotics (OR, 0.78; P = .18). There was no trend for administration of intravenous fluids (OR, 0.88; P = .56), for which the mandate specified 20 mL/kg.
Although 46.5% of patients received intravenous fluids, 62.8% received broad-spectrum antibiotics, and blood cultures were obtained in 67.7% of the children within 1 hour, only 24.9% were managed with the entire sepsis bundle. Across hospitals, the proportion of children completing the bundle ranged from 7.3% to 46.1%.
Bundle completion was more common in hospitals already treating a relatively high volume of pediatric patients and in those with pediatric specialty services, but the study authors noted that this was not a linear relationship. Rather, they called this association “hypothesis generating” and speculated that other factors might also be important.
The children in this cohort ranged in age from under 1 month to 17 years. Slightly more than half were aged 6 years or older and nearly one-third were older than 12 years. Nearly 45% had no comorbidities. Slightly more than one-third had a malignancy or were immunosuppressed.
None of the study authors reported any relevant financial relationships with industry.
SOURCE: Evans IVR et al. JAMA. 2018 Jul 24. doi:10.1001/jama.2018.9071.
FROM JAMA
Key clinical point: Delivery of all three parts of the bundled pediatric sepsis management protocol was required for a mortality benefit.
Major finding: With timely delivery of the complete bundle, the odds ratio for in-hospital mortality was reduced 41% (OR, 0.59; P = .02).
Study details: A cohort study including 1,179 pediatric patients with sepsis at 54 New York hospitals.
Disclosures: None of the study authors reported any relevant financial relationships with industry.
Source: Evans IVR et al. JAMA. 2018 Jul 24. doi:10.1001/jama.2018.9071.
HIV guidelines: Update recommends immediate treatment, three-drug therapy
For adult patients with HIV, earlier treatment results in faster and more likely virologic suppression along with greater linkage to care, according to the 2018 Recommendations of the International Antiviral Society-USA (IAS-USA).
The updated treatment and prevention guidelines also have outlined drug selection, including three-drug therapy (usually as a single-tablet combination) and two-drug switch therapy, as well as discouragement of cash incentives for treatment. The guidelines, written by Michael S. Saag, MD, of the University of Alabama at Birmingham and his coauthors, were published in JAMA.

Since the previous IAS-USA guidelines were published in 2016 (JAMA. 2016;316(2):191-210), multiple studies have investigated the importance of timely antiretroviral therapy (ART). In one study, patients with HIV began ART within 24 hours of diagnosis. These patients achieved virologic suppression (fewer than 200 HIV RNA copies/mL) quicker than patients treated according to previous guidelines (medians, 1.8 months vs. 4.3 months; P = .0001). Another study found that patients who began ART immediately were more likely to achieve viral suppression at 12 months (50% vs. 34%; P = .007) and become linked to care at 3 months (68% vs. 43%). As such, the updated guidelines recommended that ART should be started as soon as possible (even without supporting laboratory results). Exceptions were maintained for patients not ready to start therapy and those at risk for immune reconstitution syndrome.
With regard to initial treatment selection, three-drug therapy is recommended, incorporating an integrase single-strand transfer inhibitor (InSTI) with 2 nucleoside reverse transcriptase inhibitors.
Single-tablet formulations are effective, well tolerated, and promote medication adherence. Dolutegravir is not recommended in women who are pregnant or may become pregnant because it may increase the risk of neural tube defects. It is unclear whether other InSTIs pose similar risks. Although two-drug regimens are not recommended for initial therapy, they may be considered as switch therapy to reduce cost and complications.
The 2018 guidelines have discouraged cash incentives for ART adherence because such programs have proven ineffective. Conversely, noncash incentives are likely to be beneficial. Further recommendations to improve outcomes were wide ranging and included identification of patients subject to food scarcity or psychiatric disorders. For the latter, chronic depression has been associated with worse outcomes – including a two-fold mortality risk – and so appropriate treatment is recommended.
The researchers concluded with a brief review of future directions for HIV treatment and prevention. Long-acting injectable and oral antiretrovirals are under investigation, along with implantable and nanoparticle therapies.
“Clinicians who care for patients with HIV have a major role in advocating for programs and their patients at the local, national, and international levels,” the authors wrote. “Advocacy should go beyond access to ART and include access to mental health and substance abuse services, as well as efforts to end policies such as HIV criminalization that impede the ability to provide evidence-based care and prevention services.”
The authors reported support from Gilead, ViiV, Merck, and other sources. The current guidelines were funded by IAS-USA.
SOURCE: Saag MS et al. JAMA. 2018;320[4]:379-96.
New antiretroviral regimens, coupled with an improved understanding of HIV biology, have “led to improved treatment strategies and a significant decrease in mortality, transforming AIDS into a chronic, manageable disease in many countries of the world,” James Riddell IV, MD, wrote in an editorial in JAMA.
Recent research highlights the importance of early treatment with antiretroviral therapy. Patients treated as soon as possible are more likely to achieve viral suppression sooner and are more likely to be linked to care. Viral suppression not only improves patient quality of life but also prevents viral transmission.
Dr. Riddell praised the role of guidelines in raising quality of care for a broad range of patients but cautioned that “guidelines serve only as a starting point, as evidenced by the fact that implementation has proved to be much more challenging.”
Even as diagnostic and treatment abilities have advanced, a 2014 study showed that “only 49% of the approximately 1.1 million people living with HIV in the United States were virologically suppressed. Therefore, it is clear that new strategies are needed to reach HIV-infected individuals who are not receiving effective treatment.” To tackle the HIV epidemic, Dr. Riddell called for “a multipronged approach …that includes new HIV prevention strategies (HIV preexposure prophylaxis, education regarding condom use), expanded HIV testing, rapid and immediate linkage to care when possible, viral suppression for persons who are HIV infected, and strategies to enhance adherence to therapy and retention in care.”
James Riddell IV, MD, is with the division of infectious diseases in the department of internal medicine at the University of Michigan Medical Center. These comments are adapted from an editorial (JAMA 2018;320[4]:347-9).
New antiretroviral regimens, coupled with an improved understanding of HIV biology, have “led to improved treatment strategies and a significant decrease in mortality, transforming AIDS into a chronic, manageable disease in many countries of the world,” James Riddell IV, MD, wrote in an editorial in JAMA.
Recent research highlights the importance of early treatment with antiretroviral therapy. Patients treated as soon as possible are more likely to achieve viral suppression sooner and are more likely to be linked to care. Viral suppression not only improves patient quality of life but also prevents viral transmission.
Dr. Riddell praised the role of guidelines in raising quality of care for a broad range of patients but cautioned that “guidelines serve only as a starting point, as evidenced by the fact that implementation has proved to be much more challenging.”
Even as diagnostic and treatment abilities have advanced, a 2014 study showed that “only 49% of the approximately 1.1 million people living with HIV in the United States were virologically suppressed. Therefore, it is clear that new strategies are needed to reach HIV-infected individuals who are not receiving effective treatment.” To tackle the HIV epidemic, Dr. Riddell called for “a multipronged approach …that includes new HIV prevention strategies (HIV preexposure prophylaxis, education regarding condom use), expanded HIV testing, rapid and immediate linkage to care when possible, viral suppression for persons who are HIV infected, and strategies to enhance adherence to therapy and retention in care.”
James Riddell IV, MD, is with the division of infectious diseases in the department of internal medicine at the University of Michigan Medical Center. These comments are adapted from an editorial (JAMA 2018;320[4]:347-9).
New antiretroviral regimens, coupled with an improved understanding of HIV biology, have “led to improved treatment strategies and a significant decrease in mortality, transforming AIDS into a chronic, manageable disease in many countries of the world,” James Riddell IV, MD, wrote in an editorial in JAMA.
Recent research highlights the importance of early treatment with antiretroviral therapy. Patients treated as soon as possible are more likely to achieve viral suppression sooner and are more likely to be linked to care. Viral suppression not only improves patient quality of life but also prevents viral transmission.
Dr. Riddell praised the role of guidelines in raising quality of care for a broad range of patients but cautioned that “guidelines serve only as a starting point, as evidenced by the fact that implementation has proved to be much more challenging.”
Even as diagnostic and treatment abilities have advanced, a 2014 study showed that “only 49% of the approximately 1.1 million people living with HIV in the United States were virologically suppressed. Therefore, it is clear that new strategies are needed to reach HIV-infected individuals who are not receiving effective treatment.” To tackle the HIV epidemic, Dr. Riddell called for “a multipronged approach …that includes new HIV prevention strategies (HIV preexposure prophylaxis, education regarding condom use), expanded HIV testing, rapid and immediate linkage to care when possible, viral suppression for persons who are HIV infected, and strategies to enhance adherence to therapy and retention in care.”
James Riddell IV, MD, is with the division of infectious diseases in the department of internal medicine at the University of Michigan Medical Center. These comments are adapted from an editorial (JAMA 2018;320[4]:347-9).
For adult patients with HIV, earlier treatment results in faster and more likely virologic suppression along with greater linkage to care, according to the 2018 Recommendations of the International Antiviral Society-USA (IAS-USA).
The updated treatment and prevention guidelines also have outlined drug selection, including three-drug therapy (usually as a single-tablet combination) and two-drug switch therapy, as well as discouragement of cash incentives for treatment. The guidelines, written by Michael S. Saag, MD, of the University of Alabama at Birmingham and his coauthors, were published in JAMA.
Since the previous IAS-USA guidelines were published in 2016 (JAMA. 2016;316(2):191-210), multiple studies have investigated the importance of timely antiretroviral therapy (ART). In one study, patients with HIV began ART within 24 hours of diagnosis. These patients achieved virologic suppression (fewer than 200 HIV RNA copies/mL) quicker than patients treated according to previous guidelines (medians, 1.8 months vs. 4.3 months; P = .0001). Another study found that patients who began ART immediately were more likely to achieve viral suppression at 12 months (50% vs. 34%; P = .007) and become linked to care at 3 months (68% vs. 43%). As such, the updated guidelines recommended that ART should be started as soon as possible (even without supporting laboratory results). Exceptions were maintained for patients not ready to start therapy and those at risk for immune reconstitution syndrome.
With regard to initial treatment selection, three-drug therapy is recommended, incorporating an integrase single-strand transfer inhibitor (InSTI) with 2 nucleoside reverse transcriptase inhibitors.
Single-tablet formulations are effective, well tolerated, and promote medication adherence. Dolutegravir is not recommended in women who are pregnant or may become pregnant because it may increase the risk of neural tube defects. It is unclear whether other InSTIs pose similar risks. Although two-drug regimens are not recommended for initial therapy, they may be considered as switch therapy to reduce cost and complications.
The 2018 guidelines have discouraged cash incentives for ART adherence because such programs have proven ineffective. Conversely, noncash incentives are likely to be beneficial. Further recommendations to improve outcomes were wide ranging and included identification of patients subject to food scarcity or psychiatric disorders. For the latter, chronic depression has been associated with worse outcomes – including a two-fold mortality risk – and so appropriate treatment is recommended.
The researchers concluded with a brief review of future directions for HIV treatment and prevention. Long-acting injectable and oral antiretrovirals are under investigation, along with implantable and nanoparticle therapies.
“Clinicians who care for patients with HIV have a major role in advocating for programs and their patients at the local, national, and international levels,” the authors wrote. “Advocacy should go beyond access to ART and include access to mental health and substance abuse services, as well as efforts to end policies such as HIV criminalization that impede the ability to provide evidence-based care and prevention services.”
The authors reported support from Gilead, ViiV, Merck, and other sources. The current guidelines were funded by IAS-USA.
SOURCE: Saag MS et al. JAMA. 2018;320[4]:379-96.
For adult patients with HIV, earlier treatment results in faster and more likely virologic suppression along with greater linkage to care, according to the 2018 Recommendations of the International Antiviral Society-USA (IAS-USA).
The updated treatment and prevention guidelines also have outlined drug selection, including three-drug therapy (usually as a single-tablet combination) and two-drug switch therapy, as well as discouragement of cash incentives for treatment. The guidelines, written by Michael S. Saag, MD, of the University of Alabama at Birmingham and his coauthors, were published in JAMA.
Since the previous IAS-USA guidelines were published in 2016 (JAMA. 2016;316(2):191-210), multiple studies have investigated the importance of timely antiretroviral therapy (ART). In one study, patients with HIV began ART within 24 hours of diagnosis. These patients achieved virologic suppression (fewer than 200 HIV RNA copies/mL) quicker than patients treated according to previous guidelines (medians, 1.8 months vs. 4.3 months; P = .0001). Another study found that patients who began ART immediately were more likely to achieve viral suppression at 12 months (50% vs. 34%; P = .007) and become linked to care at 3 months (68% vs. 43%). As such, the updated guidelines recommended that ART should be started as soon as possible (even without supporting laboratory results). Exceptions were maintained for patients not ready to start therapy and those at risk for immune reconstitution syndrome.
With regard to initial treatment selection, three-drug therapy is recommended, incorporating an integrase single-strand transfer inhibitor (InSTI) with 2 nucleoside reverse transcriptase inhibitors.
Single-tablet formulations are effective, well tolerated, and promote medication adherence. Dolutegravir is not recommended in women who are pregnant or may become pregnant because it may increase the risk of neural tube defects. It is unclear whether other InSTIs pose similar risks. Although two-drug regimens are not recommended for initial therapy, they may be considered as switch therapy to reduce cost and complications.
The 2018 guidelines have discouraged cash incentives for ART adherence because such programs have proven ineffective. Conversely, noncash incentives are likely to be beneficial. Further recommendations to improve outcomes were wide ranging and included identification of patients subject to food scarcity or psychiatric disorders. For the latter, chronic depression has been associated with worse outcomes – including a two-fold mortality risk – and so appropriate treatment is recommended.
The researchers concluded with a brief review of future directions for HIV treatment and prevention. Long-acting injectable and oral antiretrovirals are under investigation, along with implantable and nanoparticle therapies.
“Clinicians who care for patients with HIV have a major role in advocating for programs and their patients at the local, national, and international levels,” the authors wrote. “Advocacy should go beyond access to ART and include access to mental health and substance abuse services, as well as efforts to end policies such as HIV criminalization that impede the ability to provide evidence-based care and prevention services.”
The authors reported support from Gilead, ViiV, Merck, and other sources. The current guidelines were funded by IAS-USA.
SOURCE: Saag MS et al. JAMA. 2018;320[4]:379-96.
FROM JAMA
Key clinical point: For patients with HIV, earlier treatment results in faster virologic suppression.
Major finding: Patients with HIV who started antiretroviral therapy within 24 hours of HIV diagnosis achieved virologic suppression ( 200 HIV RNA copies/mL) in a median time of 1.8 months, compared with 4.3 months for those treated in accordance with previous recommendations (P = .0001).
Study details: 2018 HIV treatment and prevention guidelines by the International Antiviral Society-USA Panel; based on numerous studies.
Disclosures: The authors reported funding from Gilead, ViiV, Merck, and others. The guidelines were sponsored by the International Antiviral Society-USA (IAS-USA).
Source: Saag et al. JAMA. 2018:320(4);379-96.
New studies expand on Aimovig for migraine
SAN FRANCISCO – Now that erenumab has won approval as the first-in-class calcitonin gene-related peptide inhibitor for prevention of episodic and chronic migraine, a flurry of new studies shedding light on how the drug might best be used in clinical practice emerged as a highlight of the annual meeting of the American Headache Society.
Erenumab (Aimovig) is a fully human monoclonal antibody targeting the calcitonin gene-related peptide (CGRP) receptor. It was approved by the Food and Drug Administration at 140 and 70 mg monthly by subcutaneous injection on the strength of the required 12-week, double-blind, placebo-controlled clinical trial data. Among the fresh data presented at the headache meeting was reassuring evidence of the monoclonal antibody’s continued high degree of safety and tolerability for episodic migraine after more than 3 years of therapy, as well as a suggestion that the biologic’s efficacy for chronic migraine was not only sustained but actually increased over the course of a 1-year study.
Also, erenumab appears to be a novel treatment option for patients who have previously failed adequate trials of two to four standard preventive therapies. In addition, it has now demonstrated efficacy in reducing overuse of acute migraine drugs such as triptans, ergots, and opioids.
Here are the highlights:
One-year safety and efficacy for chronic migraine
Stewart J. Tepper, MD, presented results of a 1-year, open-label extension study that began after participants completed a pivotal 12-week, placebo-controlled, double-blind, randomized trial whose findings have been published (Lancet Neurol. 2017 Jun;16[6]:425-34). At the end of the 12-week, double-blind period, the mean number of monthly migraine days (MMD) in the erenumab group had dropped by 6.6 days from 18.1 at baseline. Subsequently, after 52 weeks of open-label erenumab at 140 mg monthly, that figure had further improved to 10.5 fewer MMDs than at baseline.

“That’s encouraging for our patients in that we will be able to tell them that if you’re a responder, you’re likely to show some continued improvement over time,” observed Dr. Tepper, professor of neurology and director of the headache clinic at Dartmouth University in Hanover, N.H.
During 527 patient-years of open-label therapy, at least a 50% reduction in MMDs was achieved by 67% of patients in the 140-mg group and 53% in the 70-mg group.
“I think it’s also important to look at the rate of 75% or greater reduction in MMDs, which is the responder rate most closely linked to a drop in disability. That rate at 52 weeks was 42% at 140 mg and 27% at 70 mg,” the neurologist continued.
At week 52, 12.7% of patients on erenumab at 140 mg monthly had no migraines at all during the previous month.
The mean number of acute migraine-specific medication days per month decreased by about 4 days in the erenumab group during the 12-week, double-blind trial and continued to fall during the open-label extension study, with a mean reduction from baseline of 6.7 days at week 52.
“That’s clearly sustained efficacy, and it looks like some accumulating efficacy,” Dr. Tepper said.
Safety and tolerability continued to be excellent, as in the parent 12-week study.
“One of the very interesting findings we saw which differentiates erenumab from, say, onabotulinumtoxinA, is that if you looked at the patients who were on placebo during the 12 weeks of the double-blind study and then looked at the first month they went on erenumab, they caught up immediately to the patients who’d been receiving the monoclonal antibody from the beginning. That’s unlike onabotulinumtoxinA in the regulatory trials, where the patients who initially received placebo never quite caught up to those who received active therapy from the beginning,” he said.
Dr. Tepper emphasized that a clear-eyed view of an open-label study needs to recognize that only responders would have stayed in the erenumab study for a full 52 weeks, so the results paint an overly rosy picture of overall efficacy. Even so, he found the results impressive. Of 609 patients who enrolled in the study, 74% completed it.
“It’s a very encouraging 1-year study for erenumab,” he concluded.
Safety and tolerability for episodic migraine at 3-plus years
Among 383 episodic migraine patients who enrolled in an ongoing 5-year, open-label extension study of erenumab after completing a 12-week, placebo-controlled, double-blind clinical trial, there have been no new safety signals at a mean 3.2 years of follow-up. The incidence rates and types of adverse events remain indistinguishable from placebo as noted in the parent 12-week double-blind trial, with the exception of an increased rate of mild injection site reactions, reported Daniel D. Mikol, MD, PhD, executive medical director for global neuroscience development at Amgen in Thousand Oaks, Calif.

Erenumab proves effective in patients who have failed multiple preventive therapies
Jan Klatt, MD, presented the results of the 12-week, double-blind portion of the phase 3b LIBERTY study, the first clinical trial specifically designed to assess the effects of CGRP-directed therapy in patients who have previously failed to respond to and/or tolerate two to four currently available preventive medications at adequate doses for at least 2-3 months.

The rationale for the trial was straightforward: “There is a particularly high unmet need in patients who have failed currently available preventive therapies, and who are usually considered difficult to treat,” explained Dr. Klatt of Novartis in Basel, Switzerland.
LIBERTY included 246 such patients with episodic migraine who were randomized to 12 weeks of erenumab at 140 mg monthly or placebo. The primary endpoint – the proportion of patients with at least a 50% reduction in MMDs during weeks 9-12 from the baseline of 9.3 – occurred in 30.3% of the erenumab group, significantly better than the 13.7% rate with placebo, with an adjusted odds ratio of 2.73 for success with erenumab. An open-label extension study is ongoing.
A clear separation was already evident at week 4 of the randomized trial, a prespecified secondary endpoint. A 50% or greater reduction in MMDs was seen at that point in 23.5% of the erenumab group versus 4.8% in placebo-treated controls, for a response odds ratio of 6.16. A 75% or greater reduction in MMDs during weeks 9-12 occurred in 11.8% of the erenumab group and 4% of controls. A 100% response rate – that is, no migraines during weeks 9-12 – occurred in 5.9% of the active treatment arm and none of the controls. Outcomes on two novel patient-reported outcomes – the Migraine Physical Function Impact Diary–physical impairment and –everyday activities subscales – were also significantly better in the active treatment arm.
Treatment outcomes with erenumab were similar regardless of which drug classes patients had previously failed on, the three most common of which were beta-blockers, topiramate, and amitriptyline, which is approved for migraine prevention in Europe, where the LIBERTY trial was conducted.
One audience member observed that the 13.7% primary endpoint placebo response rate was far lower than typically seen in double-blind migraine trials.
“This is something we see quite consistently,” Dr. Klatt replied. “Once you proceed to this kind of more difficult-to-treat population, your placebo response rates drop to really low levels. It’s probably due to the fact that those patients have low expectations for any new therapy.”
Erenumab quells acute migraine medication overuse
Dr. Tepper presented a separate analysis of the 52-week, open-label extension study of erenumab, this time comparing outcomes in 252 chronic migraine patients who met criteria for acute medication overuse (AMO) at baseline and 357 who did not. Overuse was defined via International Headache Society criteria: The use of triptans, ergots, or combination analgesics on 10 or more days per month, or simple analgesics on at least 15 days monthly. Combination analgesics feature a simple analgesic plus opiates or butalbital.
“The bottom line here is that the drug worked about the same and in a very encouraging way in the AMO and nonoveruse patients,” he said. “This is obviously something that’s very, very important to us because we’d like to take our patients who are overusing acute migraine medications and use the monoclonal antibody as a way of getting them off overuse and into episodic migraine.”
After 52 weeks of open-label erenumab, 61% of the non-AMO group and 56% of those with baseline AMO had at least a 50% reduction from baseline in MMDs. The use of acute migraine-specific medications fell by 3.7 days in the non-AMO group and by 6.7 days in those with AMO at baseline.
Safety in patients with stable angina
Although no signal of any cardiovascular issues arose in four randomized, double-blind clinical trials or in the long-term extension studies, it was appropriate to take a more focused look at erenumab’s effects in a high-risk population with stable angina and proven ischemic coronary artery disease. That’s because CGRP is a neuropeptide that not only affects migraine, it also acts as a cytoprotective mediator released by cardiac nerve fibers during myocardial ischemia. Thus, erenumab posed a theoretic cardiovascular risk, explained Christophe Depre, MD, PhD, of Amgen.
He presented a 12-week, randomized, double-blind study in which 89 patients with stable angina were assigned to a single IV infusion of 140 mg of erenumab or placebo followed by an exercise treadmill test. Reassuringly, the CGRP inhibitor had no adverse effect on exercise time, time to onset of at least 1 mm of ST segment depression. Nor did it affect heart rate or blood pressure during or after exercise.
Dr. Tepper reported serving as a consultant to numerous pharmaceutical and medical device companies, including Amgen and Novartis, which sponsored the erenumab studies. Dr. Depre and Dr. Mikol are Amgen employees, while Dr. Klatt is employed by Novartis.
SAN FRANCISCO – Now that erenumab has won approval as the first-in-class calcitonin gene-related peptide inhibitor for prevention of episodic and chronic migraine, a flurry of new studies shedding light on how the drug might best be used in clinical practice emerged as a highlight of the annual meeting of the American Headache Society.
Erenumab (Aimovig) is a fully human monoclonal antibody targeting the calcitonin gene-related peptide (CGRP) receptor. It was approved by the Food and Drug Administration at 140 and 70 mg monthly by subcutaneous injection on the strength of the required 12-week, double-blind, placebo-controlled clinical trial data. Among the fresh data presented at the headache meeting was reassuring evidence of the monoclonal antibody’s continued high degree of safety and tolerability for episodic migraine after more than 3 years of therapy, as well as a suggestion that the biologic’s efficacy for chronic migraine was not only sustained but actually increased over the course of a 1-year study.
Also, erenumab appears to be a novel treatment option for patients who have previously failed adequate trials of two to four standard preventive therapies. In addition, it has now demonstrated efficacy in reducing overuse of acute migraine drugs such as triptans, ergots, and opioids.
Here are the highlights:
One-year safety and efficacy for chronic migraine
Stewart J. Tepper, MD, presented results of a 1-year, open-label extension study that began after participants completed a pivotal 12-week, placebo-controlled, double-blind, randomized trial whose findings have been published (Lancet Neurol. 2017 Jun;16[6]:425-34). At the end of the 12-week, double-blind period, the mean number of monthly migraine days (MMD) in the erenumab group had dropped by 6.6 days from 18.1 at baseline. Subsequently, after 52 weeks of open-label erenumab at 140 mg monthly, that figure had further improved to 10.5 fewer MMDs than at baseline.
“That’s encouraging for our patients in that we will be able to tell them that if you’re a responder, you’re likely to show some continued improvement over time,” observed Dr. Tepper, professor of neurology and director of the headache clinic at Dartmouth University in Hanover, N.H.
During 527 patient-years of open-label therapy, at least a 50% reduction in MMDs was achieved by 67% of patients in the 140-mg group and 53% in the 70-mg group.
“I think it’s also important to look at the rate of 75% or greater reduction in MMDs, which is the responder rate most closely linked to a drop in disability. That rate at 52 weeks was 42% at 140 mg and 27% at 70 mg,” the neurologist continued.
At week 52, 12.7% of patients on erenumab at 140 mg monthly had no migraines at all during the previous month.
The mean number of acute migraine-specific medication days per month decreased by about 4 days in the erenumab group during the 12-week, double-blind trial and continued to fall during the open-label extension study, with a mean reduction from baseline of 6.7 days at week 52.
“That’s clearly sustained efficacy, and it looks like some accumulating efficacy,” Dr. Tepper said.
Safety and tolerability continued to be excellent, as in the parent 12-week study.
“One of the very interesting findings we saw which differentiates erenumab from, say, onabotulinumtoxinA, is that if you looked at the patients who were on placebo during the 12 weeks of the double-blind study and then looked at the first month they went on erenumab, they caught up immediately to the patients who’d been receiving the monoclonal antibody from the beginning. That’s unlike onabotulinumtoxinA in the regulatory trials, where the patients who initially received placebo never quite caught up to those who received active therapy from the beginning,” he said.
Dr. Tepper emphasized that a clear-eyed view of an open-label study needs to recognize that only responders would have stayed in the erenumab study for a full 52 weeks, so the results paint an overly rosy picture of overall efficacy. Even so, he found the results impressive. Of 609 patients who enrolled in the study, 74% completed it.
“It’s a very encouraging 1-year study for erenumab,” he concluded.
Safety and tolerability for episodic migraine at 3-plus years
Among 383 episodic migraine patients who enrolled in an ongoing 5-year, open-label extension study of erenumab after completing a 12-week, placebo-controlled, double-blind clinical trial, there have been no new safety signals at a mean 3.2 years of follow-up. The incidence rates and types of adverse events remain indistinguishable from placebo as noted in the parent 12-week double-blind trial, with the exception of an increased rate of mild injection site reactions, reported Daniel D. Mikol, MD, PhD, executive medical director for global neuroscience development at Amgen in Thousand Oaks, Calif.
Erenumab proves effective in patients who have failed multiple preventive therapies
Jan Klatt, MD, presented the results of the 12-week, double-blind portion of the phase 3b LIBERTY study, the first clinical trial specifically designed to assess the effects of CGRP-directed therapy in patients who have previously failed to respond to and/or tolerate two to four currently available preventive medications at adequate doses for at least 2-3 months.
The rationale for the trial was straightforward: “There is a particularly high unmet need in patients who have failed currently available preventive therapies, and who are usually considered difficult to treat,” explained Dr. Klatt of Novartis in Basel, Switzerland.
LIBERTY included 246 such patients with episodic migraine who were randomized to 12 weeks of erenumab at 140 mg monthly or placebo. The primary endpoint – the proportion of patients with at least a 50% reduction in MMDs during weeks 9-12 from the baseline of 9.3 – occurred in 30.3% of the erenumab group, significantly better than the 13.7% rate with placebo, with an adjusted odds ratio of 2.73 for success with erenumab. An open-label extension study is ongoing.
A clear separation was already evident at week 4 of the randomized trial, a prespecified secondary endpoint. A 50% or greater reduction in MMDs was seen at that point in 23.5% of the erenumab group versus 4.8% in placebo-treated controls, for a response odds ratio of 6.16. A 75% or greater reduction in MMDs during weeks 9-12 occurred in 11.8% of the erenumab group and 4% of controls. A 100% response rate – that is, no migraines during weeks 9-12 – occurred in 5.9% of the active treatment arm and none of the controls. Outcomes on two novel patient-reported outcomes – the Migraine Physical Function Impact Diary–physical impairment and –everyday activities subscales – were also significantly better in the active treatment arm.
Treatment outcomes with erenumab were similar regardless of which drug classes patients had previously failed on, the three most common of which were beta-blockers, topiramate, and amitriptyline, which is approved for migraine prevention in Europe, where the LIBERTY trial was conducted.
One audience member observed that the 13.7% primary endpoint placebo response rate was far lower than typically seen in double-blind migraine trials.
“This is something we see quite consistently,” Dr. Klatt replied. “Once you proceed to this kind of more difficult-to-treat population, your placebo response rates drop to really low levels. It’s probably due to the fact that those patients have low expectations for any new therapy.”
Erenumab quells acute migraine medication overuse
Dr. Tepper presented a separate analysis of the 52-week, open-label extension study of erenumab, this time comparing outcomes in 252 chronic migraine patients who met criteria for acute medication overuse (AMO) at baseline and 357 who did not. Overuse was defined via International Headache Society criteria: The use of triptans, ergots, or combination analgesics on 10 or more days per month, or simple analgesics on at least 15 days monthly. Combination analgesics feature a simple analgesic plus opiates or butalbital.
“The bottom line here is that the drug worked about the same and in a very encouraging way in the AMO and nonoveruse patients,” he said. “This is obviously something that’s very, very important to us because we’d like to take our patients who are overusing acute migraine medications and use the monoclonal antibody as a way of getting them off overuse and into episodic migraine.”
After 52 weeks of open-label erenumab, 61% of the non-AMO group and 56% of those with baseline AMO had at least a 50% reduction from baseline in MMDs. The use of acute migraine-specific medications fell by 3.7 days in the non-AMO group and by 6.7 days in those with AMO at baseline.
Safety in patients with stable angina
Although no signal of any cardiovascular issues arose in four randomized, double-blind clinical trials or in the long-term extension studies, it was appropriate to take a more focused look at erenumab’s effects in a high-risk population with stable angina and proven ischemic coronary artery disease. That’s because CGRP is a neuropeptide that not only affects migraine, it also acts as a cytoprotective mediator released by cardiac nerve fibers during myocardial ischemia. Thus, erenumab posed a theoretic cardiovascular risk, explained Christophe Depre, MD, PhD, of Amgen.
He presented a 12-week, randomized, double-blind study in which 89 patients with stable angina were assigned to a single IV infusion of 140 mg of erenumab or placebo followed by an exercise treadmill test. Reassuringly, the CGRP inhibitor had no adverse effect on exercise time, time to onset of at least 1 mm of ST segment depression. Nor did it affect heart rate or blood pressure during or after exercise.
Dr. Tepper reported serving as a consultant to numerous pharmaceutical and medical device companies, including Amgen and Novartis, which sponsored the erenumab studies. Dr. Depre and Dr. Mikol are Amgen employees, while Dr. Klatt is employed by Novartis.
SAN FRANCISCO – Now that erenumab has won approval as the first-in-class calcitonin gene-related peptide inhibitor for prevention of episodic and chronic migraine, a flurry of new studies shedding light on how the drug might best be used in clinical practice emerged as a highlight of the annual meeting of the American Headache Society.
Erenumab (Aimovig) is a fully human monoclonal antibody targeting the calcitonin gene-related peptide (CGRP) receptor. It was approved by the Food and Drug Administration at 140 and 70 mg monthly by subcutaneous injection on the strength of the required 12-week, double-blind, placebo-controlled clinical trial data. Among the fresh data presented at the headache meeting was reassuring evidence of the monoclonal antibody’s continued high degree of safety and tolerability for episodic migraine after more than 3 years of therapy, as well as a suggestion that the biologic’s efficacy for chronic migraine was not only sustained but actually increased over the course of a 1-year study.
Also, erenumab appears to be a novel treatment option for patients who have previously failed adequate trials of two to four standard preventive therapies. In addition, it has now demonstrated efficacy in reducing overuse of acute migraine drugs such as triptans, ergots, and opioids.
Here are the highlights:
One-year safety and efficacy for chronic migraine
Stewart J. Tepper, MD, presented results of a 1-year, open-label extension study that began after participants completed a pivotal 12-week, placebo-controlled, double-blind, randomized trial whose findings have been published (Lancet Neurol. 2017 Jun;16[6]:425-34). At the end of the 12-week, double-blind period, the mean number of monthly migraine days (MMD) in the erenumab group had dropped by 6.6 days from 18.1 at baseline. Subsequently, after 52 weeks of open-label erenumab at 140 mg monthly, that figure had further improved to 10.5 fewer MMDs than at baseline.
“That’s encouraging for our patients in that we will be able to tell them that if you’re a responder, you’re likely to show some continued improvement over time,” observed Dr. Tepper, professor of neurology and director of the headache clinic at Dartmouth University in Hanover, N.H.
During 527 patient-years of open-label therapy, at least a 50% reduction in MMDs was achieved by 67% of patients in the 140-mg group and 53% in the 70-mg group.
“I think it’s also important to look at the rate of 75% or greater reduction in MMDs, which is the responder rate most closely linked to a drop in disability. That rate at 52 weeks was 42% at 140 mg and 27% at 70 mg,” the neurologist continued.
At week 52, 12.7% of patients on erenumab at 140 mg monthly had no migraines at all during the previous month.
The mean number of acute migraine-specific medication days per month decreased by about 4 days in the erenumab group during the 12-week, double-blind trial and continued to fall during the open-label extension study, with a mean reduction from baseline of 6.7 days at week 52.
“That’s clearly sustained efficacy, and it looks like some accumulating efficacy,” Dr. Tepper said.
Safety and tolerability continued to be excellent, as in the parent 12-week study.
“One of the very interesting findings we saw which differentiates erenumab from, say, onabotulinumtoxinA, is that if you looked at the patients who were on placebo during the 12 weeks of the double-blind study and then looked at the first month they went on erenumab, they caught up immediately to the patients who’d been receiving the monoclonal antibody from the beginning. That’s unlike onabotulinumtoxinA in the regulatory trials, where the patients who initially received placebo never quite caught up to those who received active therapy from the beginning,” he said.
Dr. Tepper emphasized that a clear-eyed view of an open-label study needs to recognize that only responders would have stayed in the erenumab study for a full 52 weeks, so the results paint an overly rosy picture of overall efficacy. Even so, he found the results impressive. Of 609 patients who enrolled in the study, 74% completed it.
“It’s a very encouraging 1-year study for erenumab,” he concluded.
Safety and tolerability for episodic migraine at 3-plus years
Among 383 episodic migraine patients who enrolled in an ongoing 5-year, open-label extension study of erenumab after completing a 12-week, placebo-controlled, double-blind clinical trial, there have been no new safety signals at a mean 3.2 years of follow-up. The incidence rates and types of adverse events remain indistinguishable from placebo as noted in the parent 12-week double-blind trial, with the exception of an increased rate of mild injection site reactions, reported Daniel D. Mikol, MD, PhD, executive medical director for global neuroscience development at Amgen in Thousand Oaks, Calif.
Erenumab proves effective in patients who have failed multiple preventive therapies
Jan Klatt, MD, presented the results of the 12-week, double-blind portion of the phase 3b LIBERTY study, the first clinical trial specifically designed to assess the effects of CGRP-directed therapy in patients who have previously failed to respond to and/or tolerate two to four currently available preventive medications at adequate doses for at least 2-3 months.
The rationale for the trial was straightforward: “There is a particularly high unmet need in patients who have failed currently available preventive therapies, and who are usually considered difficult to treat,” explained Dr. Klatt of Novartis in Basel, Switzerland.
LIBERTY included 246 such patients with episodic migraine who were randomized to 12 weeks of erenumab at 140 mg monthly or placebo. The primary endpoint – the proportion of patients with at least a 50% reduction in MMDs during weeks 9-12 from the baseline of 9.3 – occurred in 30.3% of the erenumab group, significantly better than the 13.7% rate with placebo, with an adjusted odds ratio of 2.73 for success with erenumab. An open-label extension study is ongoing.
A clear separation was already evident at week 4 of the randomized trial, a prespecified secondary endpoint. A 50% or greater reduction in MMDs was seen at that point in 23.5% of the erenumab group versus 4.8% in placebo-treated controls, for a response odds ratio of 6.16. A 75% or greater reduction in MMDs during weeks 9-12 occurred in 11.8% of the erenumab group and 4% of controls. A 100% response rate – that is, no migraines during weeks 9-12 – occurred in 5.9% of the active treatment arm and none of the controls. Outcomes on two novel patient-reported outcomes – the Migraine Physical Function Impact Diary–physical impairment and –everyday activities subscales – were also significantly better in the active treatment arm.
Treatment outcomes with erenumab were similar regardless of which drug classes patients had previously failed on, the three most common of which were beta-blockers, topiramate, and amitriptyline, which is approved for migraine prevention in Europe, where the LIBERTY trial was conducted.
One audience member observed that the 13.7% primary endpoint placebo response rate was far lower than typically seen in double-blind migraine trials.
“This is something we see quite consistently,” Dr. Klatt replied. “Once you proceed to this kind of more difficult-to-treat population, your placebo response rates drop to really low levels. It’s probably due to the fact that those patients have low expectations for any new therapy.”
Erenumab quells acute migraine medication overuse
Dr. Tepper presented a separate analysis of the 52-week, open-label extension study of erenumab, this time comparing outcomes in 252 chronic migraine patients who met criteria for acute medication overuse (AMO) at baseline and 357 who did not. Overuse was defined via International Headache Society criteria: The use of triptans, ergots, or combination analgesics on 10 or more days per month, or simple analgesics on at least 15 days monthly. Combination analgesics feature a simple analgesic plus opiates or butalbital.
“The bottom line here is that the drug worked about the same and in a very encouraging way in the AMO and nonoveruse patients,” he said. “This is obviously something that’s very, very important to us because we’d like to take our patients who are overusing acute migraine medications and use the monoclonal antibody as a way of getting them off overuse and into episodic migraine.”
After 52 weeks of open-label erenumab, 61% of the non-AMO group and 56% of those with baseline AMO had at least a 50% reduction from baseline in MMDs. The use of acute migraine-specific medications fell by 3.7 days in the non-AMO group and by 6.7 days in those with AMO at baseline.
Safety in patients with stable angina
Although no signal of any cardiovascular issues arose in four randomized, double-blind clinical trials or in the long-term extension studies, it was appropriate to take a more focused look at erenumab’s effects in a high-risk population with stable angina and proven ischemic coronary artery disease. That’s because CGRP is a neuropeptide that not only affects migraine, it also acts as a cytoprotective mediator released by cardiac nerve fibers during myocardial ischemia. Thus, erenumab posed a theoretic cardiovascular risk, explained Christophe Depre, MD, PhD, of Amgen.
He presented a 12-week, randomized, double-blind study in which 89 patients with stable angina were assigned to a single IV infusion of 140 mg of erenumab or placebo followed by an exercise treadmill test. Reassuringly, the CGRP inhibitor had no adverse effect on exercise time, time to onset of at least 1 mm of ST segment depression. Nor did it affect heart rate or blood pressure during or after exercise.
Dr. Tepper reported serving as a consultant to numerous pharmaceutical and medical device companies, including Amgen and Novartis, which sponsored the erenumab studies. Dr. Depre and Dr. Mikol are Amgen employees, while Dr. Klatt is employed by Novartis.
REPORTING FROM THE AHS ANNUAL MEETING
European experts envy U.S. pediatric flu vaccination approach
MALMO, SWEDEN – When American physicians think about health care in Europe, what typically comes to mind are government-funded, single-payer national health services with cradle-to-grave coverage of essential services, a strong public health bent, and perhaps some queuing.

“It’s complicated. There is no common strategic approach,” Hanna Nohynek, MD, PhD, observed at a session on childhood immunization against flu held during the annual meeting of the European Society for Paediatric Infectious Diseases.
“In real life, influenza coverage among [European] children is either not known or quite low. Impact assessments in children are done in only a few countries,” said Dr. Nohynek, chief physician in the infectious diseases control and vaccinations unit of the National Institute for Health and Welfare in Helsinki, Finland.
“The only country doing as well coverage-wise as the U.S. is the U.K., with rates of 50%-65%. In Finland it’s less than 40%,” according to Dr. Nohynek.
“We have 28 countries today in the E.U. [European Union], and we have 28 different recommendations in Europe. So where do we go from here? It’s really not easy,” observed session cochair Alberticus Osterhaus, DVM, PhD, emeritus professor of virology at Erasmus University in Rotterdam, the Netherlands.
For all the oft-cited shortcomings of health care in the United States, That’s why Jon S. Abramson, MD, a former chair of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP), was invited to explain how the U.S. strategy was accomplished.
The U.S. approach
The current U.S. policy, implemented in 2010, is to recommend an annual flu shot for all persons older than 6 months of age.
Influenza vaccination has been part of the U.S. public health program since 1960. Children aged 6-23 months, as well as their household contacts and women who will be pregnant during flu season, were added in 2004. In 2006, the flu vaccine recommendation was expanded to include children aged 6-59 months as a result of persuasive data showing that the rate of flu-associated hospitalizations and deaths in children up to 4 years old was second only to the rate in the elderly population.
The rationale for expanding the recommendation to include all school-age children and adolescents stemmed from evidence that the highest average flu-related illness rate in the United States was in that age group, which confirmed that schools are a powerful vector for the spread of influenza. Vaccinating this age-group also was seen as having an indirect benefit for their household contacts.
The current policy of recommending vaccination of everyone over age 6 months was adopted because it checked off a lot of boxes: “It’s a single recommendation, easy to apply; it eliminates the need to look for indications and risk factors; it increases vaccination coverage rates; annual vaccination is safe and effective; and flu-related morbidity and mortality occur in all age groups,” Dr. Abramson continued.
The rate of influenza vaccine coverage in pregnant women has improved over time from less than 15% to about 50%. To place that in perspective, however, the rate in Argentina is 95%, the pediatrician noted.
“We’re doing better in children than we are in adults in terms of seasonal coverage rates,” he added. “In 2015, it was 59%, versus 42% in adults.”
Dr. Abramson said there remains some skepticism in the United States regarding the effectiveness of flu vaccines in preventing flu-related illness. That’s because of the difficulty in communicating that vaccine effectiveness varies from year to year, sometimes substantially, depending upon two factors: the transmission characteristics of the circulating strains and how well the vaccines match up against those strains.
“I think we have to learn to live with that. I don’t think we’ll see a universal flu vaccine that we can give once every 10 years,” he said.
“The bottom line is, even if a vaccine is only 50% efficacious overall, we’re still impacting huge numbers,” the pediatrician added.
Dr. Abramson cited a CDC estimate that, for the 2012-2013 season, where the vaccine was 49% efficacious, the result of vaccination was 6.6 million fewer cases of influenza-associated illnesses nationally, 3.2 million fewer flu-associated medical visits, and 79,000 hospitalizations avoided.
“I think we have a fairly good program in the United States. We’re doing well in children. We certainly could be doing better. Not having FluMist for the past 2 seasons probably hurt us some,” according to Dr. Abramson.
The FluMist experience
The FluMist episode is viewed by many European pediatric infectious disease experts as a debacle. Europeans eager to develop a pan-European strategy for seasonal immunization against influenza in children and adolescents viewed the U.S. FluMist episode with dismay. For the 2016-2017 and 2017-2018 flu seasons, the ACIP recommended against FluMist, a previously approved intranasally administered quadrivalent live attenuated virus vaccine, on the basis of a single study showing subpar effectiveness against influenza A H1NI. Then at its October 2017 meeting, ACIP reversed itself and reinstated FluMist for the 2018-2019 season after viewing data from Finland and several other countries demonstrating that, in countries where it hadn’t been taken off the market, the vaccine had performed as well as injectable inactivated influenza vaccines in the 2016-2017 flu season.
“I think from the European side, it’s been a bit of a sorry spectacle,” commented Dr. Osterhaus, referring to the ACIP’s waffling. After all, authorities in Canada and European countries where FluMist was available had looked at the same data that caused ACIP to derecommend the vaccine but hadn’t found it convincing.
“We’re very happy to see ACIP has reinstated the vaccine,” Dr. Nohynek said.
Dr. Abramson declined to defend the ACIP decision to drop FluMist.
“From my standpoint, knowing that influenza B kills more children than A does, if I had been on the ACIP committee – and I’m not anymore – that would not have been my vote,” he said. “Whatever you want to say about the live attenuated influenza vaccine, about how good it is against some A strains or not, it’s better than other vaccines against influenza B. And the death rate is higher from B than A in children, although that is not true in adults.”
Plus, FluMist was an important option for people avoiding immunization because they dislike shots.
“The vast majority of deaths due to flu in children in 2010-2016 have been in kids who didn’t get vaccinated,” he noted.
Dr. Nohynek said the Finnish real-world experience recorded in comprehensive national registries for the 2017-2018 flu season – a bad year for vaccine/virus mismatch in Europe – confirmed Dr. Abramson’s comments about the superiority of quadrivalent live attenuated influenza vaccine against influenza B. Among 54,611 Finnish children aged 24-35 months, the laboratory-confirmed vaccine effectiveness of trivalent inactivated virus vaccine, with 9% coverage, was 4.5% for influenza A and 12.2% for influenza B. In contrast, the vaccine effectiveness for the intranasal quadrivalent live attenuated influenza vaccine was 32% for A and a whopping 80% for B.
“It’s quite amazing, at least to me, to see figures like this in real world data,” she commented.
Session cochair Adam Finn, MD, PhD, said he has found it instructive to take a closer look at the U.K. data for the past several flu seasons.
“We’ve seen greater control of the epidemic in Scotland and Northern Ireland, where coverage in primary school kids was higher, in the 60%-70% area, and lower in England and Wales, where it was more like 50%. So we’re beginning to think that’s the kind of level of annual coverage in children we might need to suppress an epidemic. I think that’s a really important message that people should understand: We’re not looking for 95% coverage,” observed Dr. Finn, aprofessor of pediatrics at the University of Bristol (England).
Vaccine effectiveness will improve
Dr. Osterhaus predicted better times are coming in terms of vaccine effectiveness. Vaccine production times will become shorter as recombinant technologies replace the traditional lengthy chicken egg-based vaccine production; as a result, there will be less drift-associated mismatch. Improved surveillance, including the ability to follow strain mobility patterns and population-based antibody landscapes, are another important advance.
“We’ve always been looking at one side of the coin: the virus. Once or twice a year eminent gray people sitting together in Geneva at WHO decide which strains should be selected for the next vaccine. But if you know what antibodies are present in the population, this can be quite important information as well,” he said.
Dr. Nohynek reported receiving research funding from GlaxoSmithKline and Pfizer. The other speakers reported having no relevant financial conflicts of interest.
MALMO, SWEDEN – When American physicians think about health care in Europe, what typically comes to mind are government-funded, single-payer national health services with cradle-to-grave coverage of essential services, a strong public health bent, and perhaps some queuing.
“It’s complicated. There is no common strategic approach,” Hanna Nohynek, MD, PhD, observed at a session on childhood immunization against flu held during the annual meeting of the European Society for Paediatric Infectious Diseases.
“In real life, influenza coverage among [European] children is either not known or quite low. Impact assessments in children are done in only a few countries,” said Dr. Nohynek, chief physician in the infectious diseases control and vaccinations unit of the National Institute for Health and Welfare in Helsinki, Finland.
“The only country doing as well coverage-wise as the U.S. is the U.K., with rates of 50%-65%. In Finland it’s less than 40%,” according to Dr. Nohynek.
“We have 28 countries today in the E.U. [European Union], and we have 28 different recommendations in Europe. So where do we go from here? It’s really not easy,” observed session cochair Alberticus Osterhaus, DVM, PhD, emeritus professor of virology at Erasmus University in Rotterdam, the Netherlands.
For all the oft-cited shortcomings of health care in the United States, That’s why Jon S. Abramson, MD, a former chair of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP), was invited to explain how the U.S. strategy was accomplished.
The U.S. approach
The current U.S. policy, implemented in 2010, is to recommend an annual flu shot for all persons older than 6 months of age.
Influenza vaccination has been part of the U.S. public health program since 1960. Children aged 6-23 months, as well as their household contacts and women who will be pregnant during flu season, were added in 2004. In 2006, the flu vaccine recommendation was expanded to include children aged 6-59 months as a result of persuasive data showing that the rate of flu-associated hospitalizations and deaths in children up to 4 years old was second only to the rate in the elderly population.
The rationale for expanding the recommendation to include all school-age children and adolescents stemmed from evidence that the highest average flu-related illness rate in the United States was in that age group, which confirmed that schools are a powerful vector for the spread of influenza. Vaccinating this age-group also was seen as having an indirect benefit for their household contacts.
The current policy of recommending vaccination of everyone over age 6 months was adopted because it checked off a lot of boxes: “It’s a single recommendation, easy to apply; it eliminates the need to look for indications and risk factors; it increases vaccination coverage rates; annual vaccination is safe and effective; and flu-related morbidity and mortality occur in all age groups,” Dr. Abramson continued.
The rate of influenza vaccine coverage in pregnant women has improved over time from less than 15% to about 50%. To place that in perspective, however, the rate in Argentina is 95%, the pediatrician noted.
“We’re doing better in children than we are in adults in terms of seasonal coverage rates,” he added. “In 2015, it was 59%, versus 42% in adults.”
Dr. Abramson said there remains some skepticism in the United States regarding the effectiveness of flu vaccines in preventing flu-related illness. That’s because of the difficulty in communicating that vaccine effectiveness varies from year to year, sometimes substantially, depending upon two factors: the transmission characteristics of the circulating strains and how well the vaccines match up against those strains.
“I think we have to learn to live with that. I don’t think we’ll see a universal flu vaccine that we can give once every 10 years,” he said.
“The bottom line is, even if a vaccine is only 50% efficacious overall, we’re still impacting huge numbers,” the pediatrician added.
Dr. Abramson cited a CDC estimate that, for the 2012-2013 season, where the vaccine was 49% efficacious, the result of vaccination was 6.6 million fewer cases of influenza-associated illnesses nationally, 3.2 million fewer flu-associated medical visits, and 79,000 hospitalizations avoided.
“I think we have a fairly good program in the United States. We’re doing well in children. We certainly could be doing better. Not having FluMist for the past 2 seasons probably hurt us some,” according to Dr. Abramson.
The FluMist experience
The FluMist episode is viewed by many European pediatric infectious disease experts as a debacle. Europeans eager to develop a pan-European strategy for seasonal immunization against influenza in children and adolescents viewed the U.S. FluMist episode with dismay. For the 2016-2017 and 2017-2018 flu seasons, the ACIP recommended against FluMist, a previously approved intranasally administered quadrivalent live attenuated virus vaccine, on the basis of a single study showing subpar effectiveness against influenza A H1NI. Then at its October 2017 meeting, ACIP reversed itself and reinstated FluMist for the 2018-2019 season after viewing data from Finland and several other countries demonstrating that, in countries where it hadn’t been taken off the market, the vaccine had performed as well as injectable inactivated influenza vaccines in the 2016-2017 flu season.
“I think from the European side, it’s been a bit of a sorry spectacle,” commented Dr. Osterhaus, referring to the ACIP’s waffling. After all, authorities in Canada and European countries where FluMist was available had looked at the same data that caused ACIP to derecommend the vaccine but hadn’t found it convincing.
“We’re very happy to see ACIP has reinstated the vaccine,” Dr. Nohynek said.
Dr. Abramson declined to defend the ACIP decision to drop FluMist.
“From my standpoint, knowing that influenza B kills more children than A does, if I had been on the ACIP committee – and I’m not anymore – that would not have been my vote,” he said. “Whatever you want to say about the live attenuated influenza vaccine, about how good it is against some A strains or not, it’s better than other vaccines against influenza B. And the death rate is higher from B than A in children, although that is not true in adults.”
Plus, FluMist was an important option for people avoiding immunization because they dislike shots.
“The vast majority of deaths due to flu in children in 2010-2016 have been in kids who didn’t get vaccinated,” he noted.
Dr. Nohynek said the Finnish real-world experience recorded in comprehensive national registries for the 2017-2018 flu season – a bad year for vaccine/virus mismatch in Europe – confirmed Dr. Abramson’s comments about the superiority of quadrivalent live attenuated influenza vaccine against influenza B. Among 54,611 Finnish children aged 24-35 months, the laboratory-confirmed vaccine effectiveness of trivalent inactivated virus vaccine, with 9% coverage, was 4.5% for influenza A and 12.2% for influenza B. In contrast, the vaccine effectiveness for the intranasal quadrivalent live attenuated influenza vaccine was 32% for A and a whopping 80% for B.
“It’s quite amazing, at least to me, to see figures like this in real world data,” she commented.
Session cochair Adam Finn, MD, PhD, said he has found it instructive to take a closer look at the U.K. data for the past several flu seasons.
“We’ve seen greater control of the epidemic in Scotland and Northern Ireland, where coverage in primary school kids was higher, in the 60%-70% area, and lower in England and Wales, where it was more like 50%. So we’re beginning to think that’s the kind of level of annual coverage in children we might need to suppress an epidemic. I think that’s a really important message that people should understand: We’re not looking for 95% coverage,” observed Dr. Finn, aprofessor of pediatrics at the University of Bristol (England).
Vaccine effectiveness will improve
Dr. Osterhaus predicted better times are coming in terms of vaccine effectiveness. Vaccine production times will become shorter as recombinant technologies replace the traditional lengthy chicken egg-based vaccine production; as a result, there will be less drift-associated mismatch. Improved surveillance, including the ability to follow strain mobility patterns and population-based antibody landscapes, are another important advance.
“We’ve always been looking at one side of the coin: the virus. Once or twice a year eminent gray people sitting together in Geneva at WHO decide which strains should be selected for the next vaccine. But if you know what antibodies are present in the population, this can be quite important information as well,” he said.
Dr. Nohynek reported receiving research funding from GlaxoSmithKline and Pfizer. The other speakers reported having no relevant financial conflicts of interest.
MALMO, SWEDEN – When American physicians think about health care in Europe, what typically comes to mind are government-funded, single-payer national health services with cradle-to-grave coverage of essential services, a strong public health bent, and perhaps some queuing.
“It’s complicated. There is no common strategic approach,” Hanna Nohynek, MD, PhD, observed at a session on childhood immunization against flu held during the annual meeting of the European Society for Paediatric Infectious Diseases.
“In real life, influenza coverage among [European] children is either not known or quite low. Impact assessments in children are done in only a few countries,” said Dr. Nohynek, chief physician in the infectious diseases control and vaccinations unit of the National Institute for Health and Welfare in Helsinki, Finland.
“The only country doing as well coverage-wise as the U.S. is the U.K., with rates of 50%-65%. In Finland it’s less than 40%,” according to Dr. Nohynek.
“We have 28 countries today in the E.U. [European Union], and we have 28 different recommendations in Europe. So where do we go from here? It’s really not easy,” observed session cochair Alberticus Osterhaus, DVM, PhD, emeritus professor of virology at Erasmus University in Rotterdam, the Netherlands.
For all the oft-cited shortcomings of health care in the United States, That’s why Jon S. Abramson, MD, a former chair of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP), was invited to explain how the U.S. strategy was accomplished.
The U.S. approach
The current U.S. policy, implemented in 2010, is to recommend an annual flu shot for all persons older than 6 months of age.
Influenza vaccination has been part of the U.S. public health program since 1960. Children aged 6-23 months, as well as their household contacts and women who will be pregnant during flu season, were added in 2004. In 2006, the flu vaccine recommendation was expanded to include children aged 6-59 months as a result of persuasive data showing that the rate of flu-associated hospitalizations and deaths in children up to 4 years old was second only to the rate in the elderly population.
The rationale for expanding the recommendation to include all school-age children and adolescents stemmed from evidence that the highest average flu-related illness rate in the United States was in that age group, which confirmed that schools are a powerful vector for the spread of influenza. Vaccinating this age-group also was seen as having an indirect benefit for their household contacts.
The current policy of recommending vaccination of everyone over age 6 months was adopted because it checked off a lot of boxes: “It’s a single recommendation, easy to apply; it eliminates the need to look for indications and risk factors; it increases vaccination coverage rates; annual vaccination is safe and effective; and flu-related morbidity and mortality occur in all age groups,” Dr. Abramson continued.
The rate of influenza vaccine coverage in pregnant women has improved over time from less than 15% to about 50%. To place that in perspective, however, the rate in Argentina is 95%, the pediatrician noted.
“We’re doing better in children than we are in adults in terms of seasonal coverage rates,” he added. “In 2015, it was 59%, versus 42% in adults.”
Dr. Abramson said there remains some skepticism in the United States regarding the effectiveness of flu vaccines in preventing flu-related illness. That’s because of the difficulty in communicating that vaccine effectiveness varies from year to year, sometimes substantially, depending upon two factors: the transmission characteristics of the circulating strains and how well the vaccines match up against those strains.
“I think we have to learn to live with that. I don’t think we’ll see a universal flu vaccine that we can give once every 10 years,” he said.
“The bottom line is, even if a vaccine is only 50% efficacious overall, we’re still impacting huge numbers,” the pediatrician added.
Dr. Abramson cited a CDC estimate that, for the 2012-2013 season, where the vaccine was 49% efficacious, the result of vaccination was 6.6 million fewer cases of influenza-associated illnesses nationally, 3.2 million fewer flu-associated medical visits, and 79,000 hospitalizations avoided.
“I think we have a fairly good program in the United States. We’re doing well in children. We certainly could be doing better. Not having FluMist for the past 2 seasons probably hurt us some,” according to Dr. Abramson.
The FluMist experience
The FluMist episode is viewed by many European pediatric infectious disease experts as a debacle. Europeans eager to develop a pan-European strategy for seasonal immunization against influenza in children and adolescents viewed the U.S. FluMist episode with dismay. For the 2016-2017 and 2017-2018 flu seasons, the ACIP recommended against FluMist, a previously approved intranasally administered quadrivalent live attenuated virus vaccine, on the basis of a single study showing subpar effectiveness against influenza A H1NI. Then at its October 2017 meeting, ACIP reversed itself and reinstated FluMist for the 2018-2019 season after viewing data from Finland and several other countries demonstrating that, in countries where it hadn’t been taken off the market, the vaccine had performed as well as injectable inactivated influenza vaccines in the 2016-2017 flu season.
“I think from the European side, it’s been a bit of a sorry spectacle,” commented Dr. Osterhaus, referring to the ACIP’s waffling. After all, authorities in Canada and European countries where FluMist was available had looked at the same data that caused ACIP to derecommend the vaccine but hadn’t found it convincing.
“We’re very happy to see ACIP has reinstated the vaccine,” Dr. Nohynek said.
Dr. Abramson declined to defend the ACIP decision to drop FluMist.
“From my standpoint, knowing that influenza B kills more children than A does, if I had been on the ACIP committee – and I’m not anymore – that would not have been my vote,” he said. “Whatever you want to say about the live attenuated influenza vaccine, about how good it is against some A strains or not, it’s better than other vaccines against influenza B. And the death rate is higher from B than A in children, although that is not true in adults.”
Plus, FluMist was an important option for people avoiding immunization because they dislike shots.
“The vast majority of deaths due to flu in children in 2010-2016 have been in kids who didn’t get vaccinated,” he noted.
Dr. Nohynek said the Finnish real-world experience recorded in comprehensive national registries for the 2017-2018 flu season – a bad year for vaccine/virus mismatch in Europe – confirmed Dr. Abramson’s comments about the superiority of quadrivalent live attenuated influenza vaccine against influenza B. Among 54,611 Finnish children aged 24-35 months, the laboratory-confirmed vaccine effectiveness of trivalent inactivated virus vaccine, with 9% coverage, was 4.5% for influenza A and 12.2% for influenza B. In contrast, the vaccine effectiveness for the intranasal quadrivalent live attenuated influenza vaccine was 32% for A and a whopping 80% for B.
“It’s quite amazing, at least to me, to see figures like this in real world data,” she commented.
Session cochair Adam Finn, MD, PhD, said he has found it instructive to take a closer look at the U.K. data for the past several flu seasons.
“We’ve seen greater control of the epidemic in Scotland and Northern Ireland, where coverage in primary school kids was higher, in the 60%-70% area, and lower in England and Wales, where it was more like 50%. So we’re beginning to think that’s the kind of level of annual coverage in children we might need to suppress an epidemic. I think that’s a really important message that people should understand: We’re not looking for 95% coverage,” observed Dr. Finn, aprofessor of pediatrics at the University of Bristol (England).
Vaccine effectiveness will improve
Dr. Osterhaus predicted better times are coming in terms of vaccine effectiveness. Vaccine production times will become shorter as recombinant technologies replace the traditional lengthy chicken egg-based vaccine production; as a result, there will be less drift-associated mismatch. Improved surveillance, including the ability to follow strain mobility patterns and population-based antibody landscapes, are another important advance.
“We’ve always been looking at one side of the coin: the virus. Once or twice a year eminent gray people sitting together in Geneva at WHO decide which strains should be selected for the next vaccine. But if you know what antibodies are present in the population, this can be quite important information as well,” he said.
Dr. Nohynek reported receiving research funding from GlaxoSmithKline and Pfizer. The other speakers reported having no relevant financial conflicts of interest.
EXPERT ANALYSIS FROM ESPID 2018