User login
2018 Update on pelvic floor dysfunction
Using cystoscopy to evaluate ureteral efflux and bladder integrity following benign gynecologic surgery increases the detection rate of urinary tract injuries.1 Currently, it is standard of care to perform a cystoscopy following anti-incontinence procedures, but there is no consensus among ObGyns regarding the use of universal cystoscopy following benign gynecologic surgery.2 A number of studies, however, have suggested potential best practices for evaluating urinary tract injury during pelvic surgery for benign gynecologic conditions.
Pelvic surgeries for benign gynecologic conditions, including fibroids, menorrhagia, and pelvic organ prolapse (POP), are common. More than 500,000 hysterectomies are performed annually in the United States, and up to 11% of women will undergo at least one surgery for POP or urinary incontinence in their lifetime.3,4 During gynecologic surgery, the urinary tract is at risk, and the injury rate ranges from 0.02% to 2% for ureteral injury and from 1% to 5% for bladder injury.5,6
In a recent large randomized controlled trial, the rate of intraoperative ureteral obstruction following uterosacral ligament suspension (USLS) was 3.2%.7 Vaginal vault suspensions, as well as other vaginal cuff closure techniques, are common procedures associated with urinary tract injury.8 Additionally, ureteral injury during surgery for POP occurs in as many as 2% of anterior vaginal wall repairs.9
It is well documented that a delay in diagnosis of ureteral and/or bladder injuries is associated with increased morbidity, including the need for additional surgery to repair the injury; in addition, significant delay in identifying an injury may lead to subsequent sequela, such as renal injury and fistula formation.8
A large study in California found that 36.5% of hysterectomies performed for POP were performed by general gynecologists.10 General ObGyns performing these surgeries therefore must understand the risk of urinary tract injury during hysterectomy and reconstructive pelvic procedures so that they can appropriately identify, evaluate, and repair injuries in a timely fashion.
The best way to identify urinary tract injury at the time of gynecologic surgery is by cystoscopy, including a bladder survey and ureteral efflux evaluation. When should a cystoscopy be performed, and what is the best method for visualizing ureteral efflux? Can instituting universal cystoscopy for all gynecologic procedures make a difference in the rate of injury detection? In this Update, we summarize the data from 4 studies that help to answer these questions.
Continue to: About 30% of urinary tract injuries...
About 30% of urinary tract injuries identified prior to cystoscopy at hysterectomy (which detected 5 of 6 injuries)
Vakili B, Chesson RR, Kyle BL, et al. The incidence of urinary tract injury during hysterectomy: a prospective analysis based on universal cystoscopy. Am J Obstet Gynecol. 2005;192(5):1599–1604.
Vakili and colleagues conducted a multicenter prospective cohort study of women undergoing hysterectomy for benign indications; cystoscopy was performed in all cases. The 3 hospitals involved were all part of the Louisiana State University Health system. The investigators’ goal was to determine the rate of urinary tract injury in this patient population at the time of intraoperative cystoscopy.
Intraoperative cystoscopy beats visual evaluation
Four hundred and seventy-one women underwent hysterectomy and had intraoperative cystoscopy, including evaluation of ureteral patency with administration of intravenous (IV) indigo carmine. Patients underwent abdominal, vaginal, or laparoscopic hysterectomy, and 54 (11.4%) had concurrent POP or anti-incontinence procedures. The majority underwent an abdominal hysterectomy (59%), 31% had a vaginal hysterectomy, and 10% had a laparoscopic-assisted vaginal hysterectomy or total laparoscopic hysterectomy.
Rate of urinary tract injuries. The total urinary tract injury rate detected by cystoscopy was 4.8%. The ureteral injury rate was 1.7%, and the bladder injury rate was 3.6%. A combined ureteral and bladder injury occurred in 2 women.
Surgery for POP significantly increased the risk of ureteral injury (7.3% vs 1.2%; P = .025). All cases of ureteral injury during POP surgery occurred during USLS. There was a trend toward a higher rate of bladder injury in the group with concurrent anti-incontinence surgery (12.5% vs 3.1%; P = .049). Regarding the route of hysterectomy, the vaginal approach had the highest rate of ureteral injury; however, when prolapse cases were removed from the analysis, there were no differences between the abdominal, vaginal, and laparoscopic approaches for ureteral or bladder injuries.
Injury detection with cystoscopy. Importantly, the authors found that only 30% of injuries were identified prior to performing intraoperative cystoscopy. The majority of these were bladder injuries. In addition, despite visual confirmation of ureteral peristalsis during abdominal hysterectomy, when intraoperative cystoscopy was performed with evaluation for ureteral efflux, 5 of 6 ureteral injury cases were identified. The authors reported 1 postoperative vesicovaginal fistula and concluded that it was likely due to an unrecognized bladder injury. No other undetected injuries were identified.
Notably, no complications occurred as a result of cystoscopy.
Multiple surgical indications reflect real-world scenario
The study included physicians from 3 different hospitals and all routes of hysterectomy for multiple benign gynecologic indications as well as concomitant pelvic reconstructive procedures. While this enhances the generalizability of the study results, all study sites were located in Louisiana at hospitals with resident trainee involvement. Additionally, this study confirms previous retrospective studies that reported higher rates of injury with pelvic reconstructive procedures.
The study is limited by the inability to blind surgeons, which may have resulted in the surgeons altering their techniques and/or having a heightened awareness of the urinary tract. However, their rates of ureteral and bladder injuries were slightly higher than previously reported rates, suggesting that the procedures inherently carry risk. The study is further limited by the lack of a retrospective comparison group of hysterectomy without routine cystoscopy and a longer follow-up period that may have revealed additional missed delayed urologic injuries.
The rate of urinary tract injury, including both bladder and ureteral injuries, was more than 4% at the time of hysterectomy for benign conditions. Using intraoperative peristalsis or normal ureteral caliber could result in a false sense of security since these are not reliable signs of ureteral integrity. The majority of urinary tract injuries will not be identified without cystoscopic evaluation.
Continue to: Universal cystoscopy policy...
Universal cystoscopy policy proves protective, surgeon adherence is high
Chi AM, Curran DS, Morgan DM, Fenner DE, Swenson CW. Universal cystoscopy after benign hysterectomy: examining the effects of an institutional policy. Obstet Gynecol. 2016;127(2):369–375.
In a retrospective cohort study, Chi and colleagues evaluated urinary tract injuries at the time of hysterectomy before and after the institution of a universal cystoscopy policy. At the time of policy implementation at the University of Michigan, all faculty who performed hysterectomies attended a cystoscopy workshop. Attending physicians without prior cystoscopy training also were proctored in the operating room for 3 sessions and were required to demonstrate competency with bladder survey, visualizing ureteral efflux, and urethral assessment. Indigo carmine was used to visualize ureteral efflux.
Detection of urologic injury almost doubled with cystoscopy
A total of 2,822 hysterectomies were included in the study, with 973 in the pre–universal cystoscopy group and 1,849 in the post–universal cystoscopy group. The study period was 7 years, and data on complications were abstracted for 1 year after the completion of the study period.
The primary outcome had 3 components:
- the rate of urologic injury before and after the policy
- the cystoscopy detection rate of urologic injury
- the adherence rate to the policy.
The overall rate of bladder and ureteral injury was 2.1%; the rate of injury during pre–universal screening was 2.6%, and during post–universal screening was 1.8%. The intraoperative detection rate of injury nearly doubled, from 24% to 47%, when intraoperative cystoscopy was utilized. In addition, the percentage of delayed urologic complications decreased from 28% to 5.9% (P = .03) following implementation of the universal cystoscopy policy. With regard to surgeon adherence, cystoscopy was documented in 86.1% of the hysterectomy cases after the policy was implemented compared with 35.7% of cases before the policy.
The investigators performed a cost analysis and found that hospital costs were nearly twice as much if a delayed urologic injury was diagnosed.
Study had many strengths
This study evaluated aspects of implementing quality initiatives after proper training and proctoring of a procedure. The authors compared very large cohorts from a busy academic medical center in which surgeon adherence with routine cystoscopy was high. The majority of patient outcomes were tracked for an extended period following surgery, thereby minimizing the risk of missing delayed urologic injuries. Notably, however, there was shorter follow-up time for the post–universal cystoscopy group, which could result in underestimating the rate of delayed urologic injuries in this cohort.
Instituting a universal cystoscopy policy for hysterectomy was associated with a significant decrease in delayed postoperative urinary tract complications and an increase in the intraoperative detection rate of urologic injuries. Intraoperative detection and repair of a urinary tract injury is cost-effective compared with a delayed diagnosis.
Continue to: Cystoscopy reveals ureteral obstruction...
Cystoscopy reveals ureteral obstruction during various vaginal POP repair procedures
Gustilo-Ashby AM, Jelovsek JE, Barber MD, Yoo EH, Paraiso MF, Walters MD. The incidence of ureteral obstruction and the value of intraoperative cystoscopy during vaginal surgery for pelvic organ prolapse. Am J Obstet Gynecol. 2006;194(5):1478–1485.
To determine the rate of ureteral obstruction and ureteral injury during vaginal surgery for POP and the accuracy of using intraoperative cystoscopy to prevent upper urinary tract morbidity, Gustilo-Ashby and colleagues performed a retrospective review study of a large patient cohort.
Cystoscopy with indigo carmine is highly sensitive
The study included 700 patients who underwent vaginal surgery for anterior and/or apical POP. Patients had 1 or more of the following anterior and apical prolapse repair procedures: USLS (51%), distal McCall culdeplasty (26%), proximal McCall culdeplasty (29%), anterior colporrhaphy (82%), and colpocleisis (1.4%). Of note, distal McCall culdeplasty was defined as incorporation of the “vaginal epithelium into the uterosacral plication,” while proximal McCall culdeplasty involved plication of “the uterosacral ligaments in the midline proximal to the vaginal cuff.” All patients were given IV indigo carmine to aid in visualizing ureteral efflux.
The majority of patients had a hysterectomy (56%). When accounting for rare false-positive and negative cystoscopy results, the overall ureteral obstruction rate was 5.1% and the ureteral injury rate was 0.9%. The majority of obstructions occurred with USLS (5.9%), proximal McCall culdeplasty (4.4%), and colpocleisis (4.2%). Ureteral injuries occurred only in 6 cases: 3 USLS and 3 proximal McCall culdeplasty procedures.
Based on these findings, the authors calculated that cystoscopy at the time of vaginal surgery for anterior and/or apical prolapse has a sensitivity of 94.4% and a specificity of 99.5% for detecting ureteral obstruction. The positive predictive value of cystoscopy with the use of indigo carmine for detection of ureteral obstruction is 91.9% and the negative predictive value is 99.7%.
Impact of indigo carmine’s unavailability
This study’s strengths include its large sample size and the variety of surgical approaches used for repair of anterior vaginal wall and apical prolapse. Its retrospective design, however, is a limitation; this could result in underreporting of ureteral injuries if patients received care at another institution after surgery. Furthermore, it is unclear if cystoscopy would be as predictive of ureteral injury without the use of indigo carmine, which is no longer available at most institutions.
The utility of cystoscopy with IV indigo carmine as a screening test for ureteral obstruction is highlighted by the fact that most obstructions were relieved by intraoperative suture removal following positive cystoscopy. McCall culdeplasty procedures are commonly performed by general ObGyns at the time of vaginal hysterectomy. It is therefore important to note that rates of ureteral obstruction after proximal McCall culdeplasty were only slightly lower than those after USLS.
Continue to: Sodium fluorescein and 10% dextrose...
Sodium fluorescein and 10% dextrose provide clear visibility of ureteral jets in cystoscopy
Espaillat-Rijo L, Siff L, Alas AN, et al. Intraoperative cystoscopic evaluation of ureteral patency: a randomized controlled trial. Obstet Gynecol. 2016;128(6):1378–1383.
In a multicenter randomized controlled trial, Espaillat-Rijo and colleagues compared various methods for visualizing ureteral efflux in participants who underwent gynecologic or urogynecologic procedures in which cystoscopy was performed.
Study compared 4 media
The investigators enrolled 176 participants (174 completed the trial) and randomly assigned them to receive 1 of 4 modalities: 1) normal saline as a bladder distention medium (control), 2) 10% dextrose as a bladder distention medium, 3) 200 mg oral phenazopyridine given 30 minutes prior to cystoscopy, or 4) 50 mg IV sodium fluorescein at the start of cystoscopy. Indigo carmine was not included in this study because it has not been routinely available since 2014.
Surgeons were asked to categorize the ureteral jets as “clearly visible,” “somewhat visible,” or “not visible.”
The primary outcome was subjective visibility of the ureteral jet with each modality during cystoscopy. Secondary outcomes included surgeon satisfaction, adverse reactions to the modality used, postoperative urinary tract infection, postoperative urinary retention, and delayed diagnosis of ureteral injury.
Visibility assessment results. Overall, ureteral jets were “clearly visible” in 125 cases (71%) compared with “somewhat visible” in 45 (25.6%) and “not visible” in 4 (2.3%) cases. There was a statistically significant difference between the 4 groups. Use of sodium fluorescein and 10% dextrose resulted in significantly better visualization of ureteral jets (P < .001 and P = .004, respectively) compared with the control group. Visibility with phenazopyridine was not significantly different from that in the control group or in the 10% dextrose group (FIGURE).
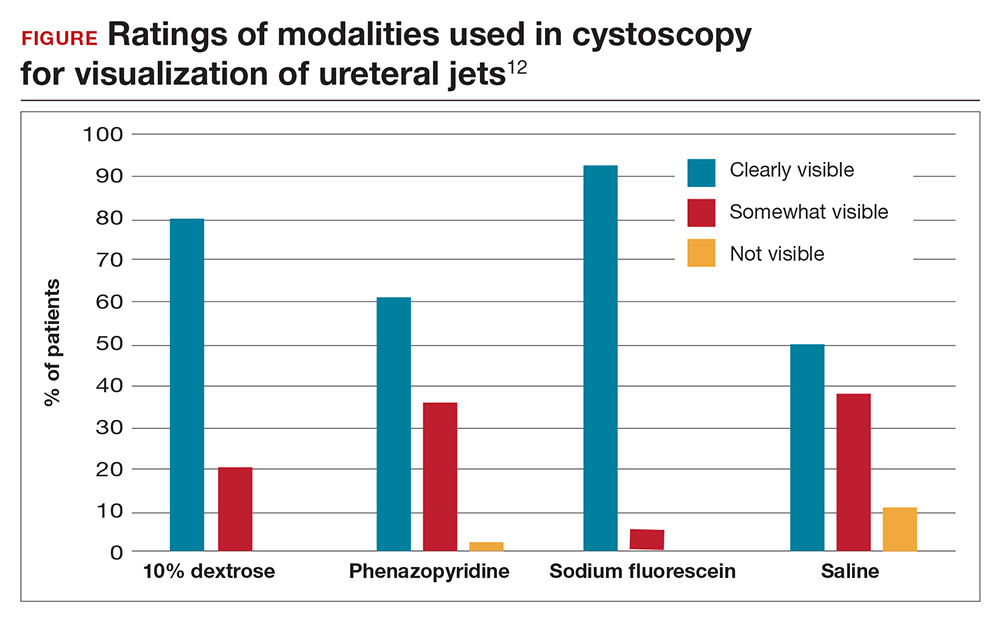
Surgeon satisfaction was highest with 10% dextrose and sodium fluorescein. In 6 cases, the surgeon was not satisfied with visualization of the ureteral jets and relied on fluorescein (5 times) or 10% dextrose (1 time) to ultimately see efflux. No significant adverse events occurred; the rate of urinary tract infection was 24.1% and did not differ between groups.
Results are widely generalizable
This was a well-designed randomized multicenter trial that included both benign gynecologic and urogynecologic procedures, thus strengthening the generalizability of the study. The study was timely since proven methods for visualization of ureteral patency became limited with the withdrawal of commercially available indigo carmine, the previous gold standard.
Intravenous sodium fluorescein and 10% dextrose as bladder distention media can both safely be used to visualize ureteral efflux and result in high surgeon satisfaction. Although 10% dextrose has been associated with higher rates of postoperative urinary tract infection,11 this was not found to be the case in this study. Preoperative administration of oral phenazopyridine was no different from the control modality with regard to visibility and surgeon satisfaction.
Continue to: The cost-effectiveness consideration
The cost-effectiveness consideration
The debate around universal cystoscopy following benign gynecologic surgery is ongoing.
The studies discussed in this Update demonstrate that cystoscopy following hysterectomy for benign indications:
- is superior to visualizing ureteral peristalsis
- increases detection of urinary tract injuries, and
- decreases delayed urologic injuries.
Although these articles emphasize the importance of detecting urologic injury, the picture would not be complete without mention of cost-effectiveness. Only one study, from 2001, has evaluated the cost-effectiveness of universal cystoscopy.1 Those authors concluded that universal cystoscopy is cost-effective only when the rate of urologic injury is 1.5% to 2%, but this conclusion, admittedly, was limited by the lack of data on medicolegal settlements, outpatient expenses, and nonmedical-related economic loss from decreased productivity. Given the extensive changes that have occurred in medical practice over the last 17 years and the emphasis on quality metrics and safety, an updated analysis would be needed to make definitive conclusions about cost-effectiveness.
While this Update cannot settle the ongoing debate of universal cystoscopy in gynecology, it is important to remember that the American College of Obstetricians and Gynecologists and the American Urogynecologic Society recommend cystoscopy following all surgeries for pelvic organ prolapse and stress urinary incontinence.2
References
- Visco AG, Taber KH, Weidner AD, Barber MD, Myers ER. Cost-effectiveness of universal cystoscopy to identify ureteral injury at hysterectomy. Obstet Gynecol. 2001;97(5 pt 1):685–692.
- ACOG Committee on Practice Bulletins–Gynecology and the American Urogynecologic Society. Urinary incontinence in women. Female Pelvic Med Reconstr Surg. 2015;21(6):304–314.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Ibeanu OA, Chesson RR, Echols KT, Nieves M, Busangu F, Nolan TE. Urinary tract injury during hysterectomy based on universal cystoscopy. Obstet Gynecol. 2009;113(1):6–10.
- ACOG Committee on Practice Bulletins–Gynecology and the American Urogynecologic Society. Urinary incontinence in women. Female Pelvic Med Reconstr Surg. 2015;21(6):304–314.
- Wilcox LS, Koonin LM, Pokras R, Strauss LT, Xia Z, Peterson HB. Hysterectomy in the United States, 1988–1990. Obstet Gynecol. 1994;83(4):549–555.
- Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol. 1997;89(4):501–506.
- Mäkinen J, Johansson J, Tomás C, et al. Morbidity of 10,110 hysterectomies by type of approach. Hum Reprod. 2001;16(7):1473–1478.
- Gilmour DT, Dwyer PL, Carey MP. Lower urinary tract injury during gynecologic surgery and its detection by intraoperative cystoscopy. Obstet Gynecol. 1999;94(5 pt 2):883–889.
- Barber MD, Brubaker L, Burgio KL, et al; Eunice Kennedy Schriver National Institute of Child Health and Human Development Pelvic Floor Disorders Network. Comparison of 2 transvaginal surgical approaches and perioperative behavioral therapy for apical vaginal prolapse: the OPTIMAL randomized trial. JAMA. 2014;311(10):1023–1034.
- Brandes S, Coburn M, Armenakas N, McAninch J. Diagnosis and management of ureteric injury: an evidence-based analysis. BJU Int. 2004;94(3):277–289.
- Kwon CH, Goldberg RP, Koduri S, Sand PK. The use of intraoperative cystoscopy in major vaginal and urogynecologic surgeries. Am J Obstet Gynecol. 2002;187(6):1466–1471.
- Adams-Piper ER, Guaderrama NM, Chen Q, Whitcomb EL. Impact of surgical training on the performance of proposed quality measures for hysterectomy for pelvic organ prolapse. Am J Obstet Gynecol. 2017;216(6):588.e1–588.e5.
- Siff LN, Unger CA, Jelovsek JE, Paraiso MF, Ridgeway BM Barber MD. Assessing ureteral patency using 10% dextrose cystoscopy fluid: evaluation of urinary tract infection rates. Am J Obstet Gynecol. 2016;215(1):74.e1–74.e6.
- Espaillat-Rijo L, Siff L, Alas AN, et al. Intraoperative cystoscopic evaluation of ureteral patency: a randomized controlled trial. Obstet Gynecol. 2016;128(6):1378–1383.
A. Rebecca Meekins, MD
Dr. Meekins is a Fellow in Female Pelvic Medicine and Reconstructive Surgery, Department of Obstetrics and Gynecology, Duke University School of Medicine, Durham, North Carolina.

Cindy L. Amundsen, MD
Dr. Amundsen is Roy T. Parker Professor in Obstetrics and Gynecology, Urogynecology and Reconstructive Pelvic Surgery; Associate Professor of Surgery, Division of Urology; Program Director of the Female Pelvic Medicine and Reconstructive Surgery Fellowship; Program Director of K12 Multidisciplinary Urologic Research Scholars Program; Program Director of BIRCWH, Duke University Medical Center.
The authors report no financial relationships relevant to this article.
A. Rebecca Meekins, MD
Dr. Meekins is a Fellow in Female Pelvic Medicine and Reconstructive Surgery, Department of Obstetrics and Gynecology, Duke University School of Medicine, Durham, North Carolina.
Cindy L. Amundsen, MD
Dr. Amundsen is Roy T. Parker Professor in Obstetrics and Gynecology, Urogynecology and Reconstructive Pelvic Surgery; Associate Professor of Surgery, Division of Urology; Program Director of the Female Pelvic Medicine and Reconstructive Surgery Fellowship; Program Director of K12 Multidisciplinary Urologic Research Scholars Program; Program Director of BIRCWH, Duke University Medical Center.
The authors report no financial relationships relevant to this article.
A. Rebecca Meekins, MD
Dr. Meekins is a Fellow in Female Pelvic Medicine and Reconstructive Surgery, Department of Obstetrics and Gynecology, Duke University School of Medicine, Durham, North Carolina.
Cindy L. Amundsen, MD
Dr. Amundsen is Roy T. Parker Professor in Obstetrics and Gynecology, Urogynecology and Reconstructive Pelvic Surgery; Associate Professor of Surgery, Division of Urology; Program Director of the Female Pelvic Medicine and Reconstructive Surgery Fellowship; Program Director of K12 Multidisciplinary Urologic Research Scholars Program; Program Director of BIRCWH, Duke University Medical Center.
The authors report no financial relationships relevant to this article.
Using cystoscopy to evaluate ureteral efflux and bladder integrity following benign gynecologic surgery increases the detection rate of urinary tract injuries.1 Currently, it is standard of care to perform a cystoscopy following anti-incontinence procedures, but there is no consensus among ObGyns regarding the use of universal cystoscopy following benign gynecologic surgery.2 A number of studies, however, have suggested potential best practices for evaluating urinary tract injury during pelvic surgery for benign gynecologic conditions.
Pelvic surgeries for benign gynecologic conditions, including fibroids, menorrhagia, and pelvic organ prolapse (POP), are common. More than 500,000 hysterectomies are performed annually in the United States, and up to 11% of women will undergo at least one surgery for POP or urinary incontinence in their lifetime.3,4 During gynecologic surgery, the urinary tract is at risk, and the injury rate ranges from 0.02% to 2% for ureteral injury and from 1% to 5% for bladder injury.5,6
In a recent large randomized controlled trial, the rate of intraoperative ureteral obstruction following uterosacral ligament suspension (USLS) was 3.2%.7 Vaginal vault suspensions, as well as other vaginal cuff closure techniques, are common procedures associated with urinary tract injury.8 Additionally, ureteral injury during surgery for POP occurs in as many as 2% of anterior vaginal wall repairs.9
It is well documented that a delay in diagnosis of ureteral and/or bladder injuries is associated with increased morbidity, including the need for additional surgery to repair the injury; in addition, significant delay in identifying an injury may lead to subsequent sequela, such as renal injury and fistula formation.8
A large study in California found that 36.5% of hysterectomies performed for POP were performed by general gynecologists.10 General ObGyns performing these surgeries therefore must understand the risk of urinary tract injury during hysterectomy and reconstructive pelvic procedures so that they can appropriately identify, evaluate, and repair injuries in a timely fashion.
The best way to identify urinary tract injury at the time of gynecologic surgery is by cystoscopy, including a bladder survey and ureteral efflux evaluation. When should a cystoscopy be performed, and what is the best method for visualizing ureteral efflux? Can instituting universal cystoscopy for all gynecologic procedures make a difference in the rate of injury detection? In this Update, we summarize the data from 4 studies that help to answer these questions.
Continue to: About 30% of urinary tract injuries...
About 30% of urinary tract injuries identified prior to cystoscopy at hysterectomy (which detected 5 of 6 injuries)
Vakili B, Chesson RR, Kyle BL, et al. The incidence of urinary tract injury during hysterectomy: a prospective analysis based on universal cystoscopy. Am J Obstet Gynecol. 2005;192(5):1599–1604.
Vakili and colleagues conducted a multicenter prospective cohort study of women undergoing hysterectomy for benign indications; cystoscopy was performed in all cases. The 3 hospitals involved were all part of the Louisiana State University Health system. The investigators’ goal was to determine the rate of urinary tract injury in this patient population at the time of intraoperative cystoscopy.
Intraoperative cystoscopy beats visual evaluation
Four hundred and seventy-one women underwent hysterectomy and had intraoperative cystoscopy, including evaluation of ureteral patency with administration of intravenous (IV) indigo carmine. Patients underwent abdominal, vaginal, or laparoscopic hysterectomy, and 54 (11.4%) had concurrent POP or anti-incontinence procedures. The majority underwent an abdominal hysterectomy (59%), 31% had a vaginal hysterectomy, and 10% had a laparoscopic-assisted vaginal hysterectomy or total laparoscopic hysterectomy.
Rate of urinary tract injuries. The total urinary tract injury rate detected by cystoscopy was 4.8%. The ureteral injury rate was 1.7%, and the bladder injury rate was 3.6%. A combined ureteral and bladder injury occurred in 2 women.
Surgery for POP significantly increased the risk of ureteral injury (7.3% vs 1.2%; P = .025). All cases of ureteral injury during POP surgery occurred during USLS. There was a trend toward a higher rate of bladder injury in the group with concurrent anti-incontinence surgery (12.5% vs 3.1%; P = .049). Regarding the route of hysterectomy, the vaginal approach had the highest rate of ureteral injury; however, when prolapse cases were removed from the analysis, there were no differences between the abdominal, vaginal, and laparoscopic approaches for ureteral or bladder injuries.
Injury detection with cystoscopy. Importantly, the authors found that only 30% of injuries were identified prior to performing intraoperative cystoscopy. The majority of these were bladder injuries. In addition, despite visual confirmation of ureteral peristalsis during abdominal hysterectomy, when intraoperative cystoscopy was performed with evaluation for ureteral efflux, 5 of 6 ureteral injury cases were identified. The authors reported 1 postoperative vesicovaginal fistula and concluded that it was likely due to an unrecognized bladder injury. No other undetected injuries were identified.
Notably, no complications occurred as a result of cystoscopy.
Multiple surgical indications reflect real-world scenario
The study included physicians from 3 different hospitals and all routes of hysterectomy for multiple benign gynecologic indications as well as concomitant pelvic reconstructive procedures. While this enhances the generalizability of the study results, all study sites were located in Louisiana at hospitals with resident trainee involvement. Additionally, this study confirms previous retrospective studies that reported higher rates of injury with pelvic reconstructive procedures.
The study is limited by the inability to blind surgeons, which may have resulted in the surgeons altering their techniques and/or having a heightened awareness of the urinary tract. However, their rates of ureteral and bladder injuries were slightly higher than previously reported rates, suggesting that the procedures inherently carry risk. The study is further limited by the lack of a retrospective comparison group of hysterectomy without routine cystoscopy and a longer follow-up period that may have revealed additional missed delayed urologic injuries.
The rate of urinary tract injury, including both bladder and ureteral injuries, was more than 4% at the time of hysterectomy for benign conditions. Using intraoperative peristalsis or normal ureteral caliber could result in a false sense of security since these are not reliable signs of ureteral integrity. The majority of urinary tract injuries will not be identified without cystoscopic evaluation.
Continue to: Universal cystoscopy policy...
Universal cystoscopy policy proves protective, surgeon adherence is high
Chi AM, Curran DS, Morgan DM, Fenner DE, Swenson CW. Universal cystoscopy after benign hysterectomy: examining the effects of an institutional policy. Obstet Gynecol. 2016;127(2):369–375.
In a retrospective cohort study, Chi and colleagues evaluated urinary tract injuries at the time of hysterectomy before and after the institution of a universal cystoscopy policy. At the time of policy implementation at the University of Michigan, all faculty who performed hysterectomies attended a cystoscopy workshop. Attending physicians without prior cystoscopy training also were proctored in the operating room for 3 sessions and were required to demonstrate competency with bladder survey, visualizing ureteral efflux, and urethral assessment. Indigo carmine was used to visualize ureteral efflux.
Detection of urologic injury almost doubled with cystoscopy
A total of 2,822 hysterectomies were included in the study, with 973 in the pre–universal cystoscopy group and 1,849 in the post–universal cystoscopy group. The study period was 7 years, and data on complications were abstracted for 1 year after the completion of the study period.
The primary outcome had 3 components:
- the rate of urologic injury before and after the policy
- the cystoscopy detection rate of urologic injury
- the adherence rate to the policy.
The overall rate of bladder and ureteral injury was 2.1%; the rate of injury during pre–universal screening was 2.6%, and during post–universal screening was 1.8%. The intraoperative detection rate of injury nearly doubled, from 24% to 47%, when intraoperative cystoscopy was utilized. In addition, the percentage of delayed urologic complications decreased from 28% to 5.9% (P = .03) following implementation of the universal cystoscopy policy. With regard to surgeon adherence, cystoscopy was documented in 86.1% of the hysterectomy cases after the policy was implemented compared with 35.7% of cases before the policy.
The investigators performed a cost analysis and found that hospital costs were nearly twice as much if a delayed urologic injury was diagnosed.
Study had many strengths
This study evaluated aspects of implementing quality initiatives after proper training and proctoring of a procedure. The authors compared very large cohorts from a busy academic medical center in which surgeon adherence with routine cystoscopy was high. The majority of patient outcomes were tracked for an extended period following surgery, thereby minimizing the risk of missing delayed urologic injuries. Notably, however, there was shorter follow-up time for the post–universal cystoscopy group, which could result in underestimating the rate of delayed urologic injuries in this cohort.
Instituting a universal cystoscopy policy for hysterectomy was associated with a significant decrease in delayed postoperative urinary tract complications and an increase in the intraoperative detection rate of urologic injuries. Intraoperative detection and repair of a urinary tract injury is cost-effective compared with a delayed diagnosis.
Continue to: Cystoscopy reveals ureteral obstruction...
Cystoscopy reveals ureteral obstruction during various vaginal POP repair procedures
Gustilo-Ashby AM, Jelovsek JE, Barber MD, Yoo EH, Paraiso MF, Walters MD. The incidence of ureteral obstruction and the value of intraoperative cystoscopy during vaginal surgery for pelvic organ prolapse. Am J Obstet Gynecol. 2006;194(5):1478–1485.
To determine the rate of ureteral obstruction and ureteral injury during vaginal surgery for POP and the accuracy of using intraoperative cystoscopy to prevent upper urinary tract morbidity, Gustilo-Ashby and colleagues performed a retrospective review study of a large patient cohort.
Cystoscopy with indigo carmine is highly sensitive
The study included 700 patients who underwent vaginal surgery for anterior and/or apical POP. Patients had 1 or more of the following anterior and apical prolapse repair procedures: USLS (51%), distal McCall culdeplasty (26%), proximal McCall culdeplasty (29%), anterior colporrhaphy (82%), and colpocleisis (1.4%). Of note, distal McCall culdeplasty was defined as incorporation of the “vaginal epithelium into the uterosacral plication,” while proximal McCall culdeplasty involved plication of “the uterosacral ligaments in the midline proximal to the vaginal cuff.” All patients were given IV indigo carmine to aid in visualizing ureteral efflux.
The majority of patients had a hysterectomy (56%). When accounting for rare false-positive and negative cystoscopy results, the overall ureteral obstruction rate was 5.1% and the ureteral injury rate was 0.9%. The majority of obstructions occurred with USLS (5.9%), proximal McCall culdeplasty (4.4%), and colpocleisis (4.2%). Ureteral injuries occurred only in 6 cases: 3 USLS and 3 proximal McCall culdeplasty procedures.
Based on these findings, the authors calculated that cystoscopy at the time of vaginal surgery for anterior and/or apical prolapse has a sensitivity of 94.4% and a specificity of 99.5% for detecting ureteral obstruction. The positive predictive value of cystoscopy with the use of indigo carmine for detection of ureteral obstruction is 91.9% and the negative predictive value is 99.7%.
Impact of indigo carmine’s unavailability
This study’s strengths include its large sample size and the variety of surgical approaches used for repair of anterior vaginal wall and apical prolapse. Its retrospective design, however, is a limitation; this could result in underreporting of ureteral injuries if patients received care at another institution after surgery. Furthermore, it is unclear if cystoscopy would be as predictive of ureteral injury without the use of indigo carmine, which is no longer available at most institutions.
The utility of cystoscopy with IV indigo carmine as a screening test for ureteral obstruction is highlighted by the fact that most obstructions were relieved by intraoperative suture removal following positive cystoscopy. McCall culdeplasty procedures are commonly performed by general ObGyns at the time of vaginal hysterectomy. It is therefore important to note that rates of ureteral obstruction after proximal McCall culdeplasty were only slightly lower than those after USLS.
Continue to: Sodium fluorescein and 10% dextrose...
Sodium fluorescein and 10% dextrose provide clear visibility of ureteral jets in cystoscopy
Espaillat-Rijo L, Siff L, Alas AN, et al. Intraoperative cystoscopic evaluation of ureteral patency: a randomized controlled trial. Obstet Gynecol. 2016;128(6):1378–1383.
In a multicenter randomized controlled trial, Espaillat-Rijo and colleagues compared various methods for visualizing ureteral efflux in participants who underwent gynecologic or urogynecologic procedures in which cystoscopy was performed.
Study compared 4 media
The investigators enrolled 176 participants (174 completed the trial) and randomly assigned them to receive 1 of 4 modalities: 1) normal saline as a bladder distention medium (control), 2) 10% dextrose as a bladder distention medium, 3) 200 mg oral phenazopyridine given 30 minutes prior to cystoscopy, or 4) 50 mg IV sodium fluorescein at the start of cystoscopy. Indigo carmine was not included in this study because it has not been routinely available since 2014.
Surgeons were asked to categorize the ureteral jets as “clearly visible,” “somewhat visible,” or “not visible.”
The primary outcome was subjective visibility of the ureteral jet with each modality during cystoscopy. Secondary outcomes included surgeon satisfaction, adverse reactions to the modality used, postoperative urinary tract infection, postoperative urinary retention, and delayed diagnosis of ureteral injury.
Visibility assessment results. Overall, ureteral jets were “clearly visible” in 125 cases (71%) compared with “somewhat visible” in 45 (25.6%) and “not visible” in 4 (2.3%) cases. There was a statistically significant difference between the 4 groups. Use of sodium fluorescein and 10% dextrose resulted in significantly better visualization of ureteral jets (P < .001 and P = .004, respectively) compared with the control group. Visibility with phenazopyridine was not significantly different from that in the control group or in the 10% dextrose group (FIGURE).
Surgeon satisfaction was highest with 10% dextrose and sodium fluorescein. In 6 cases, the surgeon was not satisfied with visualization of the ureteral jets and relied on fluorescein (5 times) or 10% dextrose (1 time) to ultimately see efflux. No significant adverse events occurred; the rate of urinary tract infection was 24.1% and did not differ between groups.
Results are widely generalizable
This was a well-designed randomized multicenter trial that included both benign gynecologic and urogynecologic procedures, thus strengthening the generalizability of the study. The study was timely since proven methods for visualization of ureteral patency became limited with the withdrawal of commercially available indigo carmine, the previous gold standard.
Intravenous sodium fluorescein and 10% dextrose as bladder distention media can both safely be used to visualize ureteral efflux and result in high surgeon satisfaction. Although 10% dextrose has been associated with higher rates of postoperative urinary tract infection,11 this was not found to be the case in this study. Preoperative administration of oral phenazopyridine was no different from the control modality with regard to visibility and surgeon satisfaction.
Continue to: The cost-effectiveness consideration
The cost-effectiveness consideration
The debate around universal cystoscopy following benign gynecologic surgery is ongoing.
The studies discussed in this Update demonstrate that cystoscopy following hysterectomy for benign indications:
- is superior to visualizing ureteral peristalsis
- increases detection of urinary tract injuries, and
- decreases delayed urologic injuries.
Although these articles emphasize the importance of detecting urologic injury, the picture would not be complete without mention of cost-effectiveness. Only one study, from 2001, has evaluated the cost-effectiveness of universal cystoscopy.1 Those authors concluded that universal cystoscopy is cost-effective only when the rate of urologic injury is 1.5% to 2%, but this conclusion, admittedly, was limited by the lack of data on medicolegal settlements, outpatient expenses, and nonmedical-related economic loss from decreased productivity. Given the extensive changes that have occurred in medical practice over the last 17 years and the emphasis on quality metrics and safety, an updated analysis would be needed to make definitive conclusions about cost-effectiveness.
While this Update cannot settle the ongoing debate of universal cystoscopy in gynecology, it is important to remember that the American College of Obstetricians and Gynecologists and the American Urogynecologic Society recommend cystoscopy following all surgeries for pelvic organ prolapse and stress urinary incontinence.2
References
- Visco AG, Taber KH, Weidner AD, Barber MD, Myers ER. Cost-effectiveness of universal cystoscopy to identify ureteral injury at hysterectomy. Obstet Gynecol. 2001;97(5 pt 1):685–692.
- ACOG Committee on Practice Bulletins–Gynecology and the American Urogynecologic Society. Urinary incontinence in women. Female Pelvic Med Reconstr Surg. 2015;21(6):304–314.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Using cystoscopy to evaluate ureteral efflux and bladder integrity following benign gynecologic surgery increases the detection rate of urinary tract injuries.1 Currently, it is standard of care to perform a cystoscopy following anti-incontinence procedures, but there is no consensus among ObGyns regarding the use of universal cystoscopy following benign gynecologic surgery.2 A number of studies, however, have suggested potential best practices for evaluating urinary tract injury during pelvic surgery for benign gynecologic conditions.
Pelvic surgeries for benign gynecologic conditions, including fibroids, menorrhagia, and pelvic organ prolapse (POP), are common. More than 500,000 hysterectomies are performed annually in the United States, and up to 11% of women will undergo at least one surgery for POP or urinary incontinence in their lifetime.3,4 During gynecologic surgery, the urinary tract is at risk, and the injury rate ranges from 0.02% to 2% for ureteral injury and from 1% to 5% for bladder injury.5,6
In a recent large randomized controlled trial, the rate of intraoperative ureteral obstruction following uterosacral ligament suspension (USLS) was 3.2%.7 Vaginal vault suspensions, as well as other vaginal cuff closure techniques, are common procedures associated with urinary tract injury.8 Additionally, ureteral injury during surgery for POP occurs in as many as 2% of anterior vaginal wall repairs.9
It is well documented that a delay in diagnosis of ureteral and/or bladder injuries is associated with increased morbidity, including the need for additional surgery to repair the injury; in addition, significant delay in identifying an injury may lead to subsequent sequela, such as renal injury and fistula formation.8
A large study in California found that 36.5% of hysterectomies performed for POP were performed by general gynecologists.10 General ObGyns performing these surgeries therefore must understand the risk of urinary tract injury during hysterectomy and reconstructive pelvic procedures so that they can appropriately identify, evaluate, and repair injuries in a timely fashion.
The best way to identify urinary tract injury at the time of gynecologic surgery is by cystoscopy, including a bladder survey and ureteral efflux evaluation. When should a cystoscopy be performed, and what is the best method for visualizing ureteral efflux? Can instituting universal cystoscopy for all gynecologic procedures make a difference in the rate of injury detection? In this Update, we summarize the data from 4 studies that help to answer these questions.
Continue to: About 30% of urinary tract injuries...
About 30% of urinary tract injuries identified prior to cystoscopy at hysterectomy (which detected 5 of 6 injuries)
Vakili B, Chesson RR, Kyle BL, et al. The incidence of urinary tract injury during hysterectomy: a prospective analysis based on universal cystoscopy. Am J Obstet Gynecol. 2005;192(5):1599–1604.
Vakili and colleagues conducted a multicenter prospective cohort study of women undergoing hysterectomy for benign indications; cystoscopy was performed in all cases. The 3 hospitals involved were all part of the Louisiana State University Health system. The investigators’ goal was to determine the rate of urinary tract injury in this patient population at the time of intraoperative cystoscopy.
Intraoperative cystoscopy beats visual evaluation
Four hundred and seventy-one women underwent hysterectomy and had intraoperative cystoscopy, including evaluation of ureteral patency with administration of intravenous (IV) indigo carmine. Patients underwent abdominal, vaginal, or laparoscopic hysterectomy, and 54 (11.4%) had concurrent POP or anti-incontinence procedures. The majority underwent an abdominal hysterectomy (59%), 31% had a vaginal hysterectomy, and 10% had a laparoscopic-assisted vaginal hysterectomy or total laparoscopic hysterectomy.
Rate of urinary tract injuries. The total urinary tract injury rate detected by cystoscopy was 4.8%. The ureteral injury rate was 1.7%, and the bladder injury rate was 3.6%. A combined ureteral and bladder injury occurred in 2 women.
Surgery for POP significantly increased the risk of ureteral injury (7.3% vs 1.2%; P = .025). All cases of ureteral injury during POP surgery occurred during USLS. There was a trend toward a higher rate of bladder injury in the group with concurrent anti-incontinence surgery (12.5% vs 3.1%; P = .049). Regarding the route of hysterectomy, the vaginal approach had the highest rate of ureteral injury; however, when prolapse cases were removed from the analysis, there were no differences between the abdominal, vaginal, and laparoscopic approaches for ureteral or bladder injuries.
Injury detection with cystoscopy. Importantly, the authors found that only 30% of injuries were identified prior to performing intraoperative cystoscopy. The majority of these were bladder injuries. In addition, despite visual confirmation of ureteral peristalsis during abdominal hysterectomy, when intraoperative cystoscopy was performed with evaluation for ureteral efflux, 5 of 6 ureteral injury cases were identified. The authors reported 1 postoperative vesicovaginal fistula and concluded that it was likely due to an unrecognized bladder injury. No other undetected injuries were identified.
Notably, no complications occurred as a result of cystoscopy.
Multiple surgical indications reflect real-world scenario
The study included physicians from 3 different hospitals and all routes of hysterectomy for multiple benign gynecologic indications as well as concomitant pelvic reconstructive procedures. While this enhances the generalizability of the study results, all study sites were located in Louisiana at hospitals with resident trainee involvement. Additionally, this study confirms previous retrospective studies that reported higher rates of injury with pelvic reconstructive procedures.
The study is limited by the inability to blind surgeons, which may have resulted in the surgeons altering their techniques and/or having a heightened awareness of the urinary tract. However, their rates of ureteral and bladder injuries were slightly higher than previously reported rates, suggesting that the procedures inherently carry risk. The study is further limited by the lack of a retrospective comparison group of hysterectomy without routine cystoscopy and a longer follow-up period that may have revealed additional missed delayed urologic injuries.
The rate of urinary tract injury, including both bladder and ureteral injuries, was more than 4% at the time of hysterectomy for benign conditions. Using intraoperative peristalsis or normal ureteral caliber could result in a false sense of security since these are not reliable signs of ureteral integrity. The majority of urinary tract injuries will not be identified without cystoscopic evaluation.
Continue to: Universal cystoscopy policy...
Universal cystoscopy policy proves protective, surgeon adherence is high
Chi AM, Curran DS, Morgan DM, Fenner DE, Swenson CW. Universal cystoscopy after benign hysterectomy: examining the effects of an institutional policy. Obstet Gynecol. 2016;127(2):369–375.
In a retrospective cohort study, Chi and colleagues evaluated urinary tract injuries at the time of hysterectomy before and after the institution of a universal cystoscopy policy. At the time of policy implementation at the University of Michigan, all faculty who performed hysterectomies attended a cystoscopy workshop. Attending physicians without prior cystoscopy training also were proctored in the operating room for 3 sessions and were required to demonstrate competency with bladder survey, visualizing ureteral efflux, and urethral assessment. Indigo carmine was used to visualize ureteral efflux.
Detection of urologic injury almost doubled with cystoscopy
A total of 2,822 hysterectomies were included in the study, with 973 in the pre–universal cystoscopy group and 1,849 in the post–universal cystoscopy group. The study period was 7 years, and data on complications were abstracted for 1 year after the completion of the study period.
The primary outcome had 3 components:
- the rate of urologic injury before and after the policy
- the cystoscopy detection rate of urologic injury
- the adherence rate to the policy.
The overall rate of bladder and ureteral injury was 2.1%; the rate of injury during pre–universal screening was 2.6%, and during post–universal screening was 1.8%. The intraoperative detection rate of injury nearly doubled, from 24% to 47%, when intraoperative cystoscopy was utilized. In addition, the percentage of delayed urologic complications decreased from 28% to 5.9% (P = .03) following implementation of the universal cystoscopy policy. With regard to surgeon adherence, cystoscopy was documented in 86.1% of the hysterectomy cases after the policy was implemented compared with 35.7% of cases before the policy.
The investigators performed a cost analysis and found that hospital costs were nearly twice as much if a delayed urologic injury was diagnosed.
Study had many strengths
This study evaluated aspects of implementing quality initiatives after proper training and proctoring of a procedure. The authors compared very large cohorts from a busy academic medical center in which surgeon adherence with routine cystoscopy was high. The majority of patient outcomes were tracked for an extended period following surgery, thereby minimizing the risk of missing delayed urologic injuries. Notably, however, there was shorter follow-up time for the post–universal cystoscopy group, which could result in underestimating the rate of delayed urologic injuries in this cohort.
Instituting a universal cystoscopy policy for hysterectomy was associated with a significant decrease in delayed postoperative urinary tract complications and an increase in the intraoperative detection rate of urologic injuries. Intraoperative detection and repair of a urinary tract injury is cost-effective compared with a delayed diagnosis.
Continue to: Cystoscopy reveals ureteral obstruction...
Cystoscopy reveals ureteral obstruction during various vaginal POP repair procedures
Gustilo-Ashby AM, Jelovsek JE, Barber MD, Yoo EH, Paraiso MF, Walters MD. The incidence of ureteral obstruction and the value of intraoperative cystoscopy during vaginal surgery for pelvic organ prolapse. Am J Obstet Gynecol. 2006;194(5):1478–1485.
To determine the rate of ureteral obstruction and ureteral injury during vaginal surgery for POP and the accuracy of using intraoperative cystoscopy to prevent upper urinary tract morbidity, Gustilo-Ashby and colleagues performed a retrospective review study of a large patient cohort.
Cystoscopy with indigo carmine is highly sensitive
The study included 700 patients who underwent vaginal surgery for anterior and/or apical POP. Patients had 1 or more of the following anterior and apical prolapse repair procedures: USLS (51%), distal McCall culdeplasty (26%), proximal McCall culdeplasty (29%), anterior colporrhaphy (82%), and colpocleisis (1.4%). Of note, distal McCall culdeplasty was defined as incorporation of the “vaginal epithelium into the uterosacral plication,” while proximal McCall culdeplasty involved plication of “the uterosacral ligaments in the midline proximal to the vaginal cuff.” All patients were given IV indigo carmine to aid in visualizing ureteral efflux.
The majority of patients had a hysterectomy (56%). When accounting for rare false-positive and negative cystoscopy results, the overall ureteral obstruction rate was 5.1% and the ureteral injury rate was 0.9%. The majority of obstructions occurred with USLS (5.9%), proximal McCall culdeplasty (4.4%), and colpocleisis (4.2%). Ureteral injuries occurred only in 6 cases: 3 USLS and 3 proximal McCall culdeplasty procedures.
Based on these findings, the authors calculated that cystoscopy at the time of vaginal surgery for anterior and/or apical prolapse has a sensitivity of 94.4% and a specificity of 99.5% for detecting ureteral obstruction. The positive predictive value of cystoscopy with the use of indigo carmine for detection of ureteral obstruction is 91.9% and the negative predictive value is 99.7%.
Impact of indigo carmine’s unavailability
This study’s strengths include its large sample size and the variety of surgical approaches used for repair of anterior vaginal wall and apical prolapse. Its retrospective design, however, is a limitation; this could result in underreporting of ureteral injuries if patients received care at another institution after surgery. Furthermore, it is unclear if cystoscopy would be as predictive of ureteral injury without the use of indigo carmine, which is no longer available at most institutions.
The utility of cystoscopy with IV indigo carmine as a screening test for ureteral obstruction is highlighted by the fact that most obstructions were relieved by intraoperative suture removal following positive cystoscopy. McCall culdeplasty procedures are commonly performed by general ObGyns at the time of vaginal hysterectomy. It is therefore important to note that rates of ureteral obstruction after proximal McCall culdeplasty were only slightly lower than those after USLS.
Continue to: Sodium fluorescein and 10% dextrose...
Sodium fluorescein and 10% dextrose provide clear visibility of ureteral jets in cystoscopy
Espaillat-Rijo L, Siff L, Alas AN, et al. Intraoperative cystoscopic evaluation of ureteral patency: a randomized controlled trial. Obstet Gynecol. 2016;128(6):1378–1383.
In a multicenter randomized controlled trial, Espaillat-Rijo and colleagues compared various methods for visualizing ureteral efflux in participants who underwent gynecologic or urogynecologic procedures in which cystoscopy was performed.
Study compared 4 media
The investigators enrolled 176 participants (174 completed the trial) and randomly assigned them to receive 1 of 4 modalities: 1) normal saline as a bladder distention medium (control), 2) 10% dextrose as a bladder distention medium, 3) 200 mg oral phenazopyridine given 30 minutes prior to cystoscopy, or 4) 50 mg IV sodium fluorescein at the start of cystoscopy. Indigo carmine was not included in this study because it has not been routinely available since 2014.
Surgeons were asked to categorize the ureteral jets as “clearly visible,” “somewhat visible,” or “not visible.”
The primary outcome was subjective visibility of the ureteral jet with each modality during cystoscopy. Secondary outcomes included surgeon satisfaction, adverse reactions to the modality used, postoperative urinary tract infection, postoperative urinary retention, and delayed diagnosis of ureteral injury.
Visibility assessment results. Overall, ureteral jets were “clearly visible” in 125 cases (71%) compared with “somewhat visible” in 45 (25.6%) and “not visible” in 4 (2.3%) cases. There was a statistically significant difference between the 4 groups. Use of sodium fluorescein and 10% dextrose resulted in significantly better visualization of ureteral jets (P < .001 and P = .004, respectively) compared with the control group. Visibility with phenazopyridine was not significantly different from that in the control group or in the 10% dextrose group (FIGURE).
Surgeon satisfaction was highest with 10% dextrose and sodium fluorescein. In 6 cases, the surgeon was not satisfied with visualization of the ureteral jets and relied on fluorescein (5 times) or 10% dextrose (1 time) to ultimately see efflux. No significant adverse events occurred; the rate of urinary tract infection was 24.1% and did not differ between groups.
Results are widely generalizable
This was a well-designed randomized multicenter trial that included both benign gynecologic and urogynecologic procedures, thus strengthening the generalizability of the study. The study was timely since proven methods for visualization of ureteral patency became limited with the withdrawal of commercially available indigo carmine, the previous gold standard.
Intravenous sodium fluorescein and 10% dextrose as bladder distention media can both safely be used to visualize ureteral efflux and result in high surgeon satisfaction. Although 10% dextrose has been associated with higher rates of postoperative urinary tract infection,11 this was not found to be the case in this study. Preoperative administration of oral phenazopyridine was no different from the control modality with regard to visibility and surgeon satisfaction.
Continue to: The cost-effectiveness consideration
The cost-effectiveness consideration
The debate around universal cystoscopy following benign gynecologic surgery is ongoing.
The studies discussed in this Update demonstrate that cystoscopy following hysterectomy for benign indications:
- is superior to visualizing ureteral peristalsis
- increases detection of urinary tract injuries, and
- decreases delayed urologic injuries.
Although these articles emphasize the importance of detecting urologic injury, the picture would not be complete without mention of cost-effectiveness. Only one study, from 2001, has evaluated the cost-effectiveness of universal cystoscopy.1 Those authors concluded that universal cystoscopy is cost-effective only when the rate of urologic injury is 1.5% to 2%, but this conclusion, admittedly, was limited by the lack of data on medicolegal settlements, outpatient expenses, and nonmedical-related economic loss from decreased productivity. Given the extensive changes that have occurred in medical practice over the last 17 years and the emphasis on quality metrics and safety, an updated analysis would be needed to make definitive conclusions about cost-effectiveness.
While this Update cannot settle the ongoing debate of universal cystoscopy in gynecology, it is important to remember that the American College of Obstetricians and Gynecologists and the American Urogynecologic Society recommend cystoscopy following all surgeries for pelvic organ prolapse and stress urinary incontinence.2
References
- Visco AG, Taber KH, Weidner AD, Barber MD, Myers ER. Cost-effectiveness of universal cystoscopy to identify ureteral injury at hysterectomy. Obstet Gynecol. 2001;97(5 pt 1):685–692.
- ACOG Committee on Practice Bulletins–Gynecology and the American Urogynecologic Society. Urinary incontinence in women. Female Pelvic Med Reconstr Surg. 2015;21(6):304–314.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Ibeanu OA, Chesson RR, Echols KT, Nieves M, Busangu F, Nolan TE. Urinary tract injury during hysterectomy based on universal cystoscopy. Obstet Gynecol. 2009;113(1):6–10.
- ACOG Committee on Practice Bulletins–Gynecology and the American Urogynecologic Society. Urinary incontinence in women. Female Pelvic Med Reconstr Surg. 2015;21(6):304–314.
- Wilcox LS, Koonin LM, Pokras R, Strauss LT, Xia Z, Peterson HB. Hysterectomy in the United States, 1988–1990. Obstet Gynecol. 1994;83(4):549–555.
- Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol. 1997;89(4):501–506.
- Mäkinen J, Johansson J, Tomás C, et al. Morbidity of 10,110 hysterectomies by type of approach. Hum Reprod. 2001;16(7):1473–1478.
- Gilmour DT, Dwyer PL, Carey MP. Lower urinary tract injury during gynecologic surgery and its detection by intraoperative cystoscopy. Obstet Gynecol. 1999;94(5 pt 2):883–889.
- Barber MD, Brubaker L, Burgio KL, et al; Eunice Kennedy Schriver National Institute of Child Health and Human Development Pelvic Floor Disorders Network. Comparison of 2 transvaginal surgical approaches and perioperative behavioral therapy for apical vaginal prolapse: the OPTIMAL randomized trial. JAMA. 2014;311(10):1023–1034.
- Brandes S, Coburn M, Armenakas N, McAninch J. Diagnosis and management of ureteric injury: an evidence-based analysis. BJU Int. 2004;94(3):277–289.
- Kwon CH, Goldberg RP, Koduri S, Sand PK. The use of intraoperative cystoscopy in major vaginal and urogynecologic surgeries. Am J Obstet Gynecol. 2002;187(6):1466–1471.
- Adams-Piper ER, Guaderrama NM, Chen Q, Whitcomb EL. Impact of surgical training on the performance of proposed quality measures for hysterectomy for pelvic organ prolapse. Am J Obstet Gynecol. 2017;216(6):588.e1–588.e5.
- Siff LN, Unger CA, Jelovsek JE, Paraiso MF, Ridgeway BM Barber MD. Assessing ureteral patency using 10% dextrose cystoscopy fluid: evaluation of urinary tract infection rates. Am J Obstet Gynecol. 2016;215(1):74.e1–74.e6.
- Espaillat-Rijo L, Siff L, Alas AN, et al. Intraoperative cystoscopic evaluation of ureteral patency: a randomized controlled trial. Obstet Gynecol. 2016;128(6):1378–1383.
- Ibeanu OA, Chesson RR, Echols KT, Nieves M, Busangu F, Nolan TE. Urinary tract injury during hysterectomy based on universal cystoscopy. Obstet Gynecol. 2009;113(1):6–10.
- ACOG Committee on Practice Bulletins–Gynecology and the American Urogynecologic Society. Urinary incontinence in women. Female Pelvic Med Reconstr Surg. 2015;21(6):304–314.
- Wilcox LS, Koonin LM, Pokras R, Strauss LT, Xia Z, Peterson HB. Hysterectomy in the United States, 1988–1990. Obstet Gynecol. 1994;83(4):549–555.
- Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol. 1997;89(4):501–506.
- Mäkinen J, Johansson J, Tomás C, et al. Morbidity of 10,110 hysterectomies by type of approach. Hum Reprod. 2001;16(7):1473–1478.
- Gilmour DT, Dwyer PL, Carey MP. Lower urinary tract injury during gynecologic surgery and its detection by intraoperative cystoscopy. Obstet Gynecol. 1999;94(5 pt 2):883–889.
- Barber MD, Brubaker L, Burgio KL, et al; Eunice Kennedy Schriver National Institute of Child Health and Human Development Pelvic Floor Disorders Network. Comparison of 2 transvaginal surgical approaches and perioperative behavioral therapy for apical vaginal prolapse: the OPTIMAL randomized trial. JAMA. 2014;311(10):1023–1034.
- Brandes S, Coburn M, Armenakas N, McAninch J. Diagnosis and management of ureteric injury: an evidence-based analysis. BJU Int. 2004;94(3):277–289.
- Kwon CH, Goldberg RP, Koduri S, Sand PK. The use of intraoperative cystoscopy in major vaginal and urogynecologic surgeries. Am J Obstet Gynecol. 2002;187(6):1466–1471.
- Adams-Piper ER, Guaderrama NM, Chen Q, Whitcomb EL. Impact of surgical training on the performance of proposed quality measures for hysterectomy for pelvic organ prolapse. Am J Obstet Gynecol. 2017;216(6):588.e1–588.e5.
- Siff LN, Unger CA, Jelovsek JE, Paraiso MF, Ridgeway BM Barber MD. Assessing ureteral patency using 10% dextrose cystoscopy fluid: evaluation of urinary tract infection rates. Am J Obstet Gynecol. 2016;215(1):74.e1–74.e6.
- Espaillat-Rijo L, Siff L, Alas AN, et al. Intraoperative cystoscopic evaluation of ureteral patency: a randomized controlled trial. Obstet Gynecol. 2016;128(6):1378–1383.
The Vampire Study, pathogenic puppies, and carbonated cannabis
What the duck?
Turns out it’s flu shot season for our feathered friends, too. After the bird flu pandemics that began in 2013, Chinese health officials worked hard to vaccinate their chickens and quell the spread of the disease. However, the ducks have outsmarted them: Two new genetic variations of the H7N9 and H7N2 flu subtypes have been found in unvaccinated ducks.
China consumes about 3 billion ducks per year, so officials are working rapidly to eliminate the virus. At press time, there was no word on whether the virus had affected any beloved rubber duckies, but we advise you to use caution when approaching bath time.
Toke-a-Cola
Cannabis is the world’s favorite illicit drug. And Coca-Cola makes the world’s favorite cola. Now there’s news of potential nuptials uniting these two global giants. BNN Bloomberg reports that Coke is talking tie-up with Canada’s Aurora Cannabis in a union that could give birth to cannabis-infused “wellness beverages.”

The fizzy federation would feature products containing cannabidiol, or CBD. Unlike its wilder psychoactive sibling tetrahydrocannabinol, or THC, the more sober-minded CBD is a nonpsychoactive cannabis compound credited with antidepressant, anxiolytic, and anti-inflammatory powers.
And what of Coca-Cola’s mortal cola enemy, Pepsi? Will the Choice of a New Generation let the Real Thing Bogart all the possible market opportunities? Sure, you could soon have a CBD Coke and a smile. But smiles are free. Frito-Lay’s parent, PepsiCo, could offer consumers a doubly profitable, Jeff Spicoli–approved pairing: carbonated cannabinoids and Cheetos.
I vant to suck MY blood
It’s not Halloween quite yet, but get into the spirit with the recently published and aptly named “Vampire Study.” Performed in Zürich, a team of researchers from the division of gastroenterology at Triemli Hospital convinced participants to ingest their own blood, all in the name of science.

Some lucky vamps drank their blood, while others ingested it via nasogastric tube. This isn’t “Saw 17,” though; there was a method to this madness. Researchers were investigating whether the ingestion of blood (as in gastrointestinal bleeding) can result in an increase in fecal calprotectin. Safe to say, though, the ingestion of blood is rarely a good sign – unless your name happens to be Nosferatu.
And they call it Campylobacter love
As any fan of Charles Schulz’s “Peanuts” comic strip can tell you, happiness is a warm puppy. Know what else warm puppies are? Carriers of Campylobacter jejuni.

Every year in the United States, Campylobacter causes an estimated 1.3 million diarrheal illnesses. A recent multistate investigation revealed that 118 people in 18 states across the nation – including 29 employees of an unnamed national pet store chain based in Ohio – got the puppy-borne bug between early 2016 and early 2018.
And the not-so-cuddly infections were resistant to all the antibiotics commonly used to quell Campylobacter. Why? Turns out, of the 149 puppies investigated by health officials, 55% of them got the drugs prophylactically – an approach that may have fueled the resistance. Stung by the canine controversy, the Daisy Hill Puppy Farm has assured Charlie Brown that it never slipped metronidazole into Snoopy’s water bowl.
What the duck?
Turns out it’s flu shot season for our feathered friends, too. After the bird flu pandemics that began in 2013, Chinese health officials worked hard to vaccinate their chickens and quell the spread of the disease. However, the ducks have outsmarted them: Two new genetic variations of the H7N9 and H7N2 flu subtypes have been found in unvaccinated ducks.
China consumes about 3 billion ducks per year, so officials are working rapidly to eliminate the virus. At press time, there was no word on whether the virus had affected any beloved rubber duckies, but we advise you to use caution when approaching bath time.
Toke-a-Cola
Cannabis is the world’s favorite illicit drug. And Coca-Cola makes the world’s favorite cola. Now there’s news of potential nuptials uniting these two global giants. BNN Bloomberg reports that Coke is talking tie-up with Canada’s Aurora Cannabis in a union that could give birth to cannabis-infused “wellness beverages.”
The fizzy federation would feature products containing cannabidiol, or CBD. Unlike its wilder psychoactive sibling tetrahydrocannabinol, or THC, the more sober-minded CBD is a nonpsychoactive cannabis compound credited with antidepressant, anxiolytic, and anti-inflammatory powers.
And what of Coca-Cola’s mortal cola enemy, Pepsi? Will the Choice of a New Generation let the Real Thing Bogart all the possible market opportunities? Sure, you could soon have a CBD Coke and a smile. But smiles are free. Frito-Lay’s parent, PepsiCo, could offer consumers a doubly profitable, Jeff Spicoli–approved pairing: carbonated cannabinoids and Cheetos.
I vant to suck MY blood
It’s not Halloween quite yet, but get into the spirit with the recently published and aptly named “Vampire Study.” Performed in Zürich, a team of researchers from the division of gastroenterology at Triemli Hospital convinced participants to ingest their own blood, all in the name of science.
Some lucky vamps drank their blood, while others ingested it via nasogastric tube. This isn’t “Saw 17,” though; there was a method to this madness. Researchers were investigating whether the ingestion of blood (as in gastrointestinal bleeding) can result in an increase in fecal calprotectin. Safe to say, though, the ingestion of blood is rarely a good sign – unless your name happens to be Nosferatu.
And they call it Campylobacter love
As any fan of Charles Schulz’s “Peanuts” comic strip can tell you, happiness is a warm puppy. Know what else warm puppies are? Carriers of Campylobacter jejuni.
Every year in the United States, Campylobacter causes an estimated 1.3 million diarrheal illnesses. A recent multistate investigation revealed that 118 people in 18 states across the nation – including 29 employees of an unnamed national pet store chain based in Ohio – got the puppy-borne bug between early 2016 and early 2018.
And the not-so-cuddly infections were resistant to all the antibiotics commonly used to quell Campylobacter. Why? Turns out, of the 149 puppies investigated by health officials, 55% of them got the drugs prophylactically – an approach that may have fueled the resistance. Stung by the canine controversy, the Daisy Hill Puppy Farm has assured Charlie Brown that it never slipped metronidazole into Snoopy’s water bowl.
What the duck?
Turns out it’s flu shot season for our feathered friends, too. After the bird flu pandemics that began in 2013, Chinese health officials worked hard to vaccinate their chickens and quell the spread of the disease. However, the ducks have outsmarted them: Two new genetic variations of the H7N9 and H7N2 flu subtypes have been found in unvaccinated ducks.
China consumes about 3 billion ducks per year, so officials are working rapidly to eliminate the virus. At press time, there was no word on whether the virus had affected any beloved rubber duckies, but we advise you to use caution when approaching bath time.
Toke-a-Cola
Cannabis is the world’s favorite illicit drug. And Coca-Cola makes the world’s favorite cola. Now there’s news of potential nuptials uniting these two global giants. BNN Bloomberg reports that Coke is talking tie-up with Canada’s Aurora Cannabis in a union that could give birth to cannabis-infused “wellness beverages.”
The fizzy federation would feature products containing cannabidiol, or CBD. Unlike its wilder psychoactive sibling tetrahydrocannabinol, or THC, the more sober-minded CBD is a nonpsychoactive cannabis compound credited with antidepressant, anxiolytic, and anti-inflammatory powers.
And what of Coca-Cola’s mortal cola enemy, Pepsi? Will the Choice of a New Generation let the Real Thing Bogart all the possible market opportunities? Sure, you could soon have a CBD Coke and a smile. But smiles are free. Frito-Lay’s parent, PepsiCo, could offer consumers a doubly profitable, Jeff Spicoli–approved pairing: carbonated cannabinoids and Cheetos.
I vant to suck MY blood
It’s not Halloween quite yet, but get into the spirit with the recently published and aptly named “Vampire Study.” Performed in Zürich, a team of researchers from the division of gastroenterology at Triemli Hospital convinced participants to ingest their own blood, all in the name of science.
Some lucky vamps drank their blood, while others ingested it via nasogastric tube. This isn’t “Saw 17,” though; there was a method to this madness. Researchers were investigating whether the ingestion of blood (as in gastrointestinal bleeding) can result in an increase in fecal calprotectin. Safe to say, though, the ingestion of blood is rarely a good sign – unless your name happens to be Nosferatu.
And they call it Campylobacter love
As any fan of Charles Schulz’s “Peanuts” comic strip can tell you, happiness is a warm puppy. Know what else warm puppies are? Carriers of Campylobacter jejuni.
Every year in the United States, Campylobacter causes an estimated 1.3 million diarrheal illnesses. A recent multistate investigation revealed that 118 people in 18 states across the nation – including 29 employees of an unnamed national pet store chain based in Ohio – got the puppy-borne bug between early 2016 and early 2018.
And the not-so-cuddly infections were resistant to all the antibiotics commonly used to quell Campylobacter. Why? Turns out, of the 149 puppies investigated by health officials, 55% of them got the drugs prophylactically – an approach that may have fueled the resistance. Stung by the canine controversy, the Daisy Hill Puppy Farm has assured Charlie Brown that it never slipped metronidazole into Snoopy’s water bowl.
FDA approves Seysara for treatment of moderate to severe acne
vulgaris for people aged 9 years and older, according to a press release from Paratek, the drug’s manufacturer.
FDA approval is based on results from two phase 3 clinical trials (NCT02320149 and NCT02322866), in which patients received either sarecycline at 1.5 mg/kg per day or placebo for 12 weeks. Patients who received sarecycline were significantly more likely to reach the primary endpoint of improved acne severity based on absolute change in facial lesion counts and percentage of participants with Investigator Global Assessment success.
Common adverse events reported in the sarecycline group were nausea (3.2%), nasopharyngitis (2.8%), and headache (2.8%). The discontinuation rate due to adverse events among sarecycline-treated patients in both studies combined was 1.4%.
Sarecycline is an oral, narrow spectrum tetracycline-derived antibiotic with anti-inflammatory properties, and is approved for once-daily use, according to Paratek. Seysara will be marketed in the United States by Almirall SA.
vulgaris for people aged 9 years and older, according to a press release from Paratek, the drug’s manufacturer.
FDA approval is based on results from two phase 3 clinical trials (NCT02320149 and NCT02322866), in which patients received either sarecycline at 1.5 mg/kg per day or placebo for 12 weeks. Patients who received sarecycline were significantly more likely to reach the primary endpoint of improved acne severity based on absolute change in facial lesion counts and percentage of participants with Investigator Global Assessment success.
Common adverse events reported in the sarecycline group were nausea (3.2%), nasopharyngitis (2.8%), and headache (2.8%). The discontinuation rate due to adverse events among sarecycline-treated patients in both studies combined was 1.4%.
Sarecycline is an oral, narrow spectrum tetracycline-derived antibiotic with anti-inflammatory properties, and is approved for once-daily use, according to Paratek. Seysara will be marketed in the United States by Almirall SA.
vulgaris for people aged 9 years and older, according to a press release from Paratek, the drug’s manufacturer.
FDA approval is based on results from two phase 3 clinical trials (NCT02320149 and NCT02322866), in which patients received either sarecycline at 1.5 mg/kg per day or placebo for 12 weeks. Patients who received sarecycline were significantly more likely to reach the primary endpoint of improved acne severity based on absolute change in facial lesion counts and percentage of participants with Investigator Global Assessment success.
Common adverse events reported in the sarecycline group were nausea (3.2%), nasopharyngitis (2.8%), and headache (2.8%). The discontinuation rate due to adverse events among sarecycline-treated patients in both studies combined was 1.4%.
Sarecycline is an oral, narrow spectrum tetracycline-derived antibiotic with anti-inflammatory properties, and is approved for once-daily use, according to Paratek. Seysara will be marketed in the United States by Almirall SA.
Checkpoint inhibitor linked to antiphospholipid syndrome in melanoma patient
A patient with melanoma experienced antiphospholipid syndrome following multiple infusions of the PD-1 inhibitor pembrolizumab, according to authors of a recent case report.
Presence of Raynaud phenomenon and high levels of antiphospholipid antibodies led to the diagnosis of antiphospholipid syndrome in the patient, who had stage IIIB unresectable melanoma.
This report provides additional evidence that this syndrome is an immune-related adverse event associated with checkpoint inhibitor therapy, said Alexandra Picard, MD, of Hôpital Archet, Nice, France, and coauthors.
“Due to the increased use of anti PD-1 therapies, clinicians should be aware of this new potential immune-mediated toxic effect that manifests as antiphospholipid syndrome,” the researchers wrote. The report is in JAMA Dermatology.
“Great caution” should be exercised when considering use of immune checkpoint inhibitors in patients with a history of antiphospholipid syndrome, the authors added.
The woman in this report was over 60 years of age and had first presented with superficial melanoma on her right calf, followed by recurrent lymph node metastases over the next few years, all of which were surgically treated.
Following a PET-CT scan showing a new metastatic lymph node, the woman started pembrolizumab 2 mg/kg every 3 weeks and had a partial response within 3 months, the investigators reported.
After the tenth infusion, however, the patient developed bilateral secondary Raynaud phenomenon that followed a typical discoloration sequence and resulted in a necrotic lesion at the tip of one finger.
The patient had no personal or family history of Raynaud phenomenon.
While beta2-glycoprotein 1 antibodies were not elevated, laboratory tests did show anticardiolipin antibodies and lupus anticoagulants at elevated levels, the investigators said, noting that repeat testing at 12 weeks confirmed positivity of antiphospholipid antibodies.
The Raynaud phenomenon disappeared and the necrotic lesion healed after pembrolizumab was stopped and prednisolone treatment was started, they added.
No recurrence of either was noted at the last follow-up.
Previous reports have described antiphospholipid syndrome in advanced melanoma patients treated with alfa-2b interferon alone or in combination with anti-interleukin 2, the authors said in their discussion of the case.
In addition, there has been another recent report of antiphospholipid syndrome associated with the CTLA4 inhibitor ipilimumab and the PD-1 inhibitor nivolumab, they said. In that case, testing for antiphospholipid antibodies revealed elevated beta2-glycoprotein 1 antibody levels.
“We hypothesize that [antiphospholipid syndrome] is a kind of autoimmunity induced by anti–PD-1 due to the expansive expression of the immune system against tumor cells,” the researchers wrote.
Although a case of cancer-associated antiphospholipid syndrome could not be ruled out in the present report, the rapid and complete resolution of symptoms after treatment discontinuation suggested that pembrolizumab, a “known immunostimulant,” was the cause, they said.
While antibodies against PD-1 have improved melanoma prognosis, they are associated with a wide range of immune-related adverse effects in the skin, gastrointestinal tract, liver, and endocrine system, Dr. Picard and coauthors noted.
They reported having no conflicts of interest.
SOURCE: Sanchez A, et al. JAMA Derm. 2018 Sep 19. doi: 10.1001/jamadermatol.2018.2770.
A patient with melanoma experienced antiphospholipid syndrome following multiple infusions of the PD-1 inhibitor pembrolizumab, according to authors of a recent case report.
Presence of Raynaud phenomenon and high levels of antiphospholipid antibodies led to the diagnosis of antiphospholipid syndrome in the patient, who had stage IIIB unresectable melanoma.
This report provides additional evidence that this syndrome is an immune-related adverse event associated with checkpoint inhibitor therapy, said Alexandra Picard, MD, of Hôpital Archet, Nice, France, and coauthors.
“Due to the increased use of anti PD-1 therapies, clinicians should be aware of this new potential immune-mediated toxic effect that manifests as antiphospholipid syndrome,” the researchers wrote. The report is in JAMA Dermatology.
“Great caution” should be exercised when considering use of immune checkpoint inhibitors in patients with a history of antiphospholipid syndrome, the authors added.
The woman in this report was over 60 years of age and had first presented with superficial melanoma on her right calf, followed by recurrent lymph node metastases over the next few years, all of which were surgically treated.
Following a PET-CT scan showing a new metastatic lymph node, the woman started pembrolizumab 2 mg/kg every 3 weeks and had a partial response within 3 months, the investigators reported.
After the tenth infusion, however, the patient developed bilateral secondary Raynaud phenomenon that followed a typical discoloration sequence and resulted in a necrotic lesion at the tip of one finger.
The patient had no personal or family history of Raynaud phenomenon.
While beta2-glycoprotein 1 antibodies were not elevated, laboratory tests did show anticardiolipin antibodies and lupus anticoagulants at elevated levels, the investigators said, noting that repeat testing at 12 weeks confirmed positivity of antiphospholipid antibodies.
The Raynaud phenomenon disappeared and the necrotic lesion healed after pembrolizumab was stopped and prednisolone treatment was started, they added.
No recurrence of either was noted at the last follow-up.
Previous reports have described antiphospholipid syndrome in advanced melanoma patients treated with alfa-2b interferon alone or in combination with anti-interleukin 2, the authors said in their discussion of the case.
In addition, there has been another recent report of antiphospholipid syndrome associated with the CTLA4 inhibitor ipilimumab and the PD-1 inhibitor nivolumab, they said. In that case, testing for antiphospholipid antibodies revealed elevated beta2-glycoprotein 1 antibody levels.
“We hypothesize that [antiphospholipid syndrome] is a kind of autoimmunity induced by anti–PD-1 due to the expansive expression of the immune system against tumor cells,” the researchers wrote.
Although a case of cancer-associated antiphospholipid syndrome could not be ruled out in the present report, the rapid and complete resolution of symptoms after treatment discontinuation suggested that pembrolizumab, a “known immunostimulant,” was the cause, they said.
While antibodies against PD-1 have improved melanoma prognosis, they are associated with a wide range of immune-related adverse effects in the skin, gastrointestinal tract, liver, and endocrine system, Dr. Picard and coauthors noted.
They reported having no conflicts of interest.
SOURCE: Sanchez A, et al. JAMA Derm. 2018 Sep 19. doi: 10.1001/jamadermatol.2018.2770.
A patient with melanoma experienced antiphospholipid syndrome following multiple infusions of the PD-1 inhibitor pembrolizumab, according to authors of a recent case report.
Presence of Raynaud phenomenon and high levels of antiphospholipid antibodies led to the diagnosis of antiphospholipid syndrome in the patient, who had stage IIIB unresectable melanoma.
This report provides additional evidence that this syndrome is an immune-related adverse event associated with checkpoint inhibitor therapy, said Alexandra Picard, MD, of Hôpital Archet, Nice, France, and coauthors.
“Due to the increased use of anti PD-1 therapies, clinicians should be aware of this new potential immune-mediated toxic effect that manifests as antiphospholipid syndrome,” the researchers wrote. The report is in JAMA Dermatology.
“Great caution” should be exercised when considering use of immune checkpoint inhibitors in patients with a history of antiphospholipid syndrome, the authors added.
The woman in this report was over 60 years of age and had first presented with superficial melanoma on her right calf, followed by recurrent lymph node metastases over the next few years, all of which were surgically treated.
Following a PET-CT scan showing a new metastatic lymph node, the woman started pembrolizumab 2 mg/kg every 3 weeks and had a partial response within 3 months, the investigators reported.
After the tenth infusion, however, the patient developed bilateral secondary Raynaud phenomenon that followed a typical discoloration sequence and resulted in a necrotic lesion at the tip of one finger.
The patient had no personal or family history of Raynaud phenomenon.
While beta2-glycoprotein 1 antibodies were not elevated, laboratory tests did show anticardiolipin antibodies and lupus anticoagulants at elevated levels, the investigators said, noting that repeat testing at 12 weeks confirmed positivity of antiphospholipid antibodies.
The Raynaud phenomenon disappeared and the necrotic lesion healed after pembrolizumab was stopped and prednisolone treatment was started, they added.
No recurrence of either was noted at the last follow-up.
Previous reports have described antiphospholipid syndrome in advanced melanoma patients treated with alfa-2b interferon alone or in combination with anti-interleukin 2, the authors said in their discussion of the case.
In addition, there has been another recent report of antiphospholipid syndrome associated with the CTLA4 inhibitor ipilimumab and the PD-1 inhibitor nivolumab, they said. In that case, testing for antiphospholipid antibodies revealed elevated beta2-glycoprotein 1 antibody levels.
“We hypothesize that [antiphospholipid syndrome] is a kind of autoimmunity induced by anti–PD-1 due to the expansive expression of the immune system against tumor cells,” the researchers wrote.
Although a case of cancer-associated antiphospholipid syndrome could not be ruled out in the present report, the rapid and complete resolution of symptoms after treatment discontinuation suggested that pembrolizumab, a “known immunostimulant,” was the cause, they said.
While antibodies against PD-1 have improved melanoma prognosis, they are associated with a wide range of immune-related adverse effects in the skin, gastrointestinal tract, liver, and endocrine system, Dr. Picard and coauthors noted.
They reported having no conflicts of interest.
SOURCE: Sanchez A, et al. JAMA Derm. 2018 Sep 19. doi: 10.1001/jamadermatol.2018.2770.
FROM JAMA DERMATOLOGY
Key clinical point: Antiphospholipid syndrome appears to be an immune-related adverse event associated with anti-PD-1 therapy.
Major finding: A melanoma patient receiving pembrolizumab was diagnosed with antiphospholipid syndrome that resolved following discontinuation of that treatment.
Study details: Case report of a woman in her 60s with stage IIIB unresectable melanoma who was treated with pembrolizumab 2 mg/kg every 3 weeks.
Disclosures: The authors reported no conflicts of interest.
Source: Sanchez A et al. JAMA Derm. 2018 Sep 19. doi: 10.1001/jamadermatol.2018.2770.
Previous psychiatric admissions predict suicide attempts
SAN DIEGO – Among patients presenting to the emergency department with suicidal ideation, the number of previous psychiatric admissions is the most important predictor of a subsequent suicide attempt, results from a 2-year-long study showed.

Momentary measures – significant current difficulties with sleep, energy, or appetite, and anhedonia – “are important considerations during suicide risk assessment, regardless of whether the patient meets the threshold for major depressive disorder, lead study author Anne C. Knorr said in an interview in advance of the annual meeting of the American College of Emergency Physicians.
“Many traditionally studied psychiatric risk factors do not significantly differ between individuals who think about suicide and those who act on their suicidal thoughts, an important distinction as only one-third of those who think about suicide carry out a suicide attempt. While there is support for some psychiatric factors – for example, anxiety, substance use disorders, sleep disturbance – being useful in differentiating these groups, the current study is unique in its use of a longitudinal design to identify influential risk factors that predict future suicide attempt among those with suicidal ideation,” she said.
Ms. Knorr, a research project manager at Geisinger Medical Center, Danville, Pa., and her colleagues collected electronic medical record data from 908 patients who had received a psychiatric evaluation at an index emergency department visit for suicidal ideation over a 2-year period. The mean age of patients was 39 years. The target sample was 30 patients who had returned to the ED following a suicide attempt within 6 months of their index ED visit.
The researchers analyzed 32 predictor variables from patient charts, including demographics, psychiatric history, and current psychiatric presentation. The evaluation was done with “a machine learning statistical approach which is more capable than traditional statistical approaches in handling a large number of predictor variables,” Ms. Knorr said.
The number of previous psychiatric admissions was the most important predictor of a subsequent suicide attempt. The next nine most important variables were sleep disturbance, history of family suicide, low energy, patient age, psychiatrist determination of severe suicide risk, psychiatrist determination of moderate suicide risk, appetite issues, presence of a support system, and loss of interest/pleasure.
These symptoms may not typically be weighed heavily in risk assessments, Ms. Knorr said. “Additionally, given that research suggests that the clinical determination of suicide risk is historically poor, it was interesting that psychiatrist determination of moderate or high risk was influential in predicting a return visit for suicide attempt. Finally, we were surprised that a past history of suicide attempt, often viewed as the strongest predictor of a future suicide attempt, did not emerge as one of the top 10 influential predictors.
“Limitations of this study include the use of a return visit to a Geisinger emergency department as the only measure of a future suicide attempt and the utilization of data from only one health system,” she noted.
The study was funded by the Geisinger Clinic Research Fund. One of the coauthors, Andrei Nemoianu, MD, reported receipt of a research grant from Takeda Pharmaceuticals for a separate study.
SOURCE: Knorr A et al. Ann Emerg Med. 2018 Oct;72;4:S23. doi. 10.1016/j.annemergmed.2018.08.055.
SAN DIEGO – Among patients presenting to the emergency department with suicidal ideation, the number of previous psychiatric admissions is the most important predictor of a subsequent suicide attempt, results from a 2-year-long study showed.
Momentary measures – significant current difficulties with sleep, energy, or appetite, and anhedonia – “are important considerations during suicide risk assessment, regardless of whether the patient meets the threshold for major depressive disorder, lead study author Anne C. Knorr said in an interview in advance of the annual meeting of the American College of Emergency Physicians.
“Many traditionally studied psychiatric risk factors do not significantly differ between individuals who think about suicide and those who act on their suicidal thoughts, an important distinction as only one-third of those who think about suicide carry out a suicide attempt. While there is support for some psychiatric factors – for example, anxiety, substance use disorders, sleep disturbance – being useful in differentiating these groups, the current study is unique in its use of a longitudinal design to identify influential risk factors that predict future suicide attempt among those with suicidal ideation,” she said.
Ms. Knorr, a research project manager at Geisinger Medical Center, Danville, Pa., and her colleagues collected electronic medical record data from 908 patients who had received a psychiatric evaluation at an index emergency department visit for suicidal ideation over a 2-year period. The mean age of patients was 39 years. The target sample was 30 patients who had returned to the ED following a suicide attempt within 6 months of their index ED visit.
The researchers analyzed 32 predictor variables from patient charts, including demographics, psychiatric history, and current psychiatric presentation. The evaluation was done with “a machine learning statistical approach which is more capable than traditional statistical approaches in handling a large number of predictor variables,” Ms. Knorr said.
The number of previous psychiatric admissions was the most important predictor of a subsequent suicide attempt. The next nine most important variables were sleep disturbance, history of family suicide, low energy, patient age, psychiatrist determination of severe suicide risk, psychiatrist determination of moderate suicide risk, appetite issues, presence of a support system, and loss of interest/pleasure.
These symptoms may not typically be weighed heavily in risk assessments, Ms. Knorr said. “Additionally, given that research suggests that the clinical determination of suicide risk is historically poor, it was interesting that psychiatrist determination of moderate or high risk was influential in predicting a return visit for suicide attempt. Finally, we were surprised that a past history of suicide attempt, often viewed as the strongest predictor of a future suicide attempt, did not emerge as one of the top 10 influential predictors.
“Limitations of this study include the use of a return visit to a Geisinger emergency department as the only measure of a future suicide attempt and the utilization of data from only one health system,” she noted.
The study was funded by the Geisinger Clinic Research Fund. One of the coauthors, Andrei Nemoianu, MD, reported receipt of a research grant from Takeda Pharmaceuticals for a separate study.
SOURCE: Knorr A et al. Ann Emerg Med. 2018 Oct;72;4:S23. doi. 10.1016/j.annemergmed.2018.08.055.
SAN DIEGO – Among patients presenting to the emergency department with suicidal ideation, the number of previous psychiatric admissions is the most important predictor of a subsequent suicide attempt, results from a 2-year-long study showed.
Momentary measures – significant current difficulties with sleep, energy, or appetite, and anhedonia – “are important considerations during suicide risk assessment, regardless of whether the patient meets the threshold for major depressive disorder, lead study author Anne C. Knorr said in an interview in advance of the annual meeting of the American College of Emergency Physicians.
“Many traditionally studied psychiatric risk factors do not significantly differ between individuals who think about suicide and those who act on their suicidal thoughts, an important distinction as only one-third of those who think about suicide carry out a suicide attempt. While there is support for some psychiatric factors – for example, anxiety, substance use disorders, sleep disturbance – being useful in differentiating these groups, the current study is unique in its use of a longitudinal design to identify influential risk factors that predict future suicide attempt among those with suicidal ideation,” she said.
Ms. Knorr, a research project manager at Geisinger Medical Center, Danville, Pa., and her colleagues collected electronic medical record data from 908 patients who had received a psychiatric evaluation at an index emergency department visit for suicidal ideation over a 2-year period. The mean age of patients was 39 years. The target sample was 30 patients who had returned to the ED following a suicide attempt within 6 months of their index ED visit.
The researchers analyzed 32 predictor variables from patient charts, including demographics, psychiatric history, and current psychiatric presentation. The evaluation was done with “a machine learning statistical approach which is more capable than traditional statistical approaches in handling a large number of predictor variables,” Ms. Knorr said.
The number of previous psychiatric admissions was the most important predictor of a subsequent suicide attempt. The next nine most important variables were sleep disturbance, history of family suicide, low energy, patient age, psychiatrist determination of severe suicide risk, psychiatrist determination of moderate suicide risk, appetite issues, presence of a support system, and loss of interest/pleasure.
These symptoms may not typically be weighed heavily in risk assessments, Ms. Knorr said. “Additionally, given that research suggests that the clinical determination of suicide risk is historically poor, it was interesting that psychiatrist determination of moderate or high risk was influential in predicting a return visit for suicide attempt. Finally, we were surprised that a past history of suicide attempt, often viewed as the strongest predictor of a future suicide attempt, did not emerge as one of the top 10 influential predictors.
“Limitations of this study include the use of a return visit to a Geisinger emergency department as the only measure of a future suicide attempt and the utilization of data from only one health system,” she noted.
The study was funded by the Geisinger Clinic Research Fund. One of the coauthors, Andrei Nemoianu, MD, reported receipt of a research grant from Takeda Pharmaceuticals for a separate study.
SOURCE: Knorr A et al. Ann Emerg Med. 2018 Oct;72;4:S23. doi. 10.1016/j.annemergmed.2018.08.055.
AT ACEP18
Key clinical point: A number of factors representing momentary experiences such as low energy emerged as predictors of suicide attempts among suicidal ideators following an ED visit.
Major finding: The number of past psychiatric admissions was the most influential predictor of a subsequent suicide attempt.
Study details: A study of 30 patients who had returned to the ED following a suicide attempt within 6 months of their index ED visit.
Disclosures: The Geisinger Clinic Research Fund supported the study. A coauthor, Andrei Nemoianu, MD, reported receipt of a research grant from Takeda Pharmaceuticals for a separate study.
Source: Knorr A et al. Ann Emerg Med. 2018 Oct;72;4:S23.
Hospital-level care coordination strategies and the patient experience
Clinical question: Does patient experience correlate with specific hospital care coordination and transition strategies, and if so, which strategies most strongly correlate with higher patient experience scores?
Background: Patient experience is an increasingly important measure in value-based payment programs. However, progress has been slow in improving patient experience, and little empirical data exist regarding which strategies are effective. Care transitions are critical times during a hospitalization, with many hospitals already implementing measures to improve the discharge process and prevent readmission of patients. It is not known whether those measures also influence patient experience scores, and if they do improve scores, which measures are most effective at doing so.
Study design: An analytic observational survey design.

Setting: Hospitals eligible for the Hospital Readmissions Reduction Program (HRRP) between June 2013 and December 2014.
Synopsis: A survey was developed and given to chief medical officers at 1,600 hospitals between June 2013 and December 2014; the survey assessed care coordination strategies employed by these institutions. 992 hospitals (62% response rate) were subsequently categorized as “low-strategy,” “mid-strategy,” or “high-strategy” hospitals. Patient satisfaction scores from the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey in 2014 were correlated to the number of strategies and the specific strategies each hospital employed. In general, the higher-strategy hospitals had significantly higher HCAHPS survey scores than did low-strategy hospitals (+2.23 points; P less than .001). Specifically, creating and sharing a discharge summary prior to discharge (+1.43 points; P less than .001), using a discharge planner (+1.71 points; P less than .001), and calling patients 48 hours post discharge (+1.64 points; P less than .001) all resulted in overall higher hospital ratings by patients.
One limitation of this study is that no causal inference can be made between the specific strategies associated with higher HCAHPS scores and care coordination strategies.
Bottom line: Hospital-led care transition strategies with direct patient interactions led to higher patient satisfaction scores.
Citation: Figueroa JF et al. Hospital-level care coordination strategies associated with better patient experience. BMJ Qual Saf. 2018 Apr 4. doi: 10.1136/bmjqs-2017-007597.
Dr. Tsien is a hospitalist in the division of hospital medicine in the department of medicine at Loyola University Chicago, Maywood, Ill.
Clinical question: Does patient experience correlate with specific hospital care coordination and transition strategies, and if so, which strategies most strongly correlate with higher patient experience scores?
Background: Patient experience is an increasingly important measure in value-based payment programs. However, progress has been slow in improving patient experience, and little empirical data exist regarding which strategies are effective. Care transitions are critical times during a hospitalization, with many hospitals already implementing measures to improve the discharge process and prevent readmission of patients. It is not known whether those measures also influence patient experience scores, and if they do improve scores, which measures are most effective at doing so.
Study design: An analytic observational survey design.
Setting: Hospitals eligible for the Hospital Readmissions Reduction Program (HRRP) between June 2013 and December 2014.
Synopsis: A survey was developed and given to chief medical officers at 1,600 hospitals between June 2013 and December 2014; the survey assessed care coordination strategies employed by these institutions. 992 hospitals (62% response rate) were subsequently categorized as “low-strategy,” “mid-strategy,” or “high-strategy” hospitals. Patient satisfaction scores from the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey in 2014 were correlated to the number of strategies and the specific strategies each hospital employed. In general, the higher-strategy hospitals had significantly higher HCAHPS survey scores than did low-strategy hospitals (+2.23 points; P less than .001). Specifically, creating and sharing a discharge summary prior to discharge (+1.43 points; P less than .001), using a discharge planner (+1.71 points; P less than .001), and calling patients 48 hours post discharge (+1.64 points; P less than .001) all resulted in overall higher hospital ratings by patients.
One limitation of this study is that no causal inference can be made between the specific strategies associated with higher HCAHPS scores and care coordination strategies.
Bottom line: Hospital-led care transition strategies with direct patient interactions led to higher patient satisfaction scores.
Citation: Figueroa JF et al. Hospital-level care coordination strategies associated with better patient experience. BMJ Qual Saf. 2018 Apr 4. doi: 10.1136/bmjqs-2017-007597.
Dr. Tsien is a hospitalist in the division of hospital medicine in the department of medicine at Loyola University Chicago, Maywood, Ill.
Clinical question: Does patient experience correlate with specific hospital care coordination and transition strategies, and if so, which strategies most strongly correlate with higher patient experience scores?
Background: Patient experience is an increasingly important measure in value-based payment programs. However, progress has been slow in improving patient experience, and little empirical data exist regarding which strategies are effective. Care transitions are critical times during a hospitalization, with many hospitals already implementing measures to improve the discharge process and prevent readmission of patients. It is not known whether those measures also influence patient experience scores, and if they do improve scores, which measures are most effective at doing so.
Study design: An analytic observational survey design.
Setting: Hospitals eligible for the Hospital Readmissions Reduction Program (HRRP) between June 2013 and December 2014.
Synopsis: A survey was developed and given to chief medical officers at 1,600 hospitals between June 2013 and December 2014; the survey assessed care coordination strategies employed by these institutions. 992 hospitals (62% response rate) were subsequently categorized as “low-strategy,” “mid-strategy,” or “high-strategy” hospitals. Patient satisfaction scores from the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey in 2014 were correlated to the number of strategies and the specific strategies each hospital employed. In general, the higher-strategy hospitals had significantly higher HCAHPS survey scores than did low-strategy hospitals (+2.23 points; P less than .001). Specifically, creating and sharing a discharge summary prior to discharge (+1.43 points; P less than .001), using a discharge planner (+1.71 points; P less than .001), and calling patients 48 hours post discharge (+1.64 points; P less than .001) all resulted in overall higher hospital ratings by patients.
One limitation of this study is that no causal inference can be made between the specific strategies associated with higher HCAHPS scores and care coordination strategies.
Bottom line: Hospital-led care transition strategies with direct patient interactions led to higher patient satisfaction scores.
Citation: Figueroa JF et al. Hospital-level care coordination strategies associated with better patient experience. BMJ Qual Saf. 2018 Apr 4. doi: 10.1136/bmjqs-2017-007597.
Dr. Tsien is a hospitalist in the division of hospital medicine in the department of medicine at Loyola University Chicago, Maywood, Ill.
Cervical cancer: Who should you screen?
Resource
US Preventive Services Task Force. Screening for cervical cancer: US Preventive Services Task Force recommendation statement. JAMA. 2018;320:674-686. https://jamanetwork.com/journals/jama/fullarticle/2697704. Accessed September 14, 2018.
Resource
US Preventive Services Task Force. Screening for cervical cancer: US Preventive Services Task Force recommendation statement. JAMA. 2018;320:674-686. https://jamanetwork.com/journals/jama/fullarticle/2697704. Accessed September 14, 2018.
Resource
US Preventive Services Task Force. Screening for cervical cancer: US Preventive Services Task Force recommendation statement. JAMA. 2018;320:674-686. https://jamanetwork.com/journals/jama/fullarticle/2697704. Accessed September 14, 2018.

ULTIMATE: IVUS-guided stent placement bests angiography
SAN DIEGO – Clinical outcomes were better when stent placement was guided by intravascular ultrasound rather than angiography, based on the results of a trial conducted in China. Unlike previous comparative studies, which focused on patients with more complex lesions, this trial included all patients undergoing drug-eluting stent (DES) placement.
In the ULTIMATE trial, 1,448 all-comer patients receiving DES were randomized to either intravascular ultrasound (IVUS)–guided or angiography-guided implantation, reported Junjie Zhang, PhD, of Nanjing Medical University in China, and colleagues. The study excluded patients who had a life expectancy shorter than 12 months, who were intolerant of dual antiplatelet therapy, and who had severe calcification needing rotational atherectomy.
At 30 days after stent placement, the incidence of target vessel failure was 0.8% in the IVUS group and 1.9% in the angiography group, a nonsignificant trend. However, outcomes were significantly different at 1 year, with target vessel failure occurring in 2.9% of IVUS patients and 5.4% of angiography patients (hazard ratio, 0.530; 95% confidence interval, 0.312-0.901; P = .019).
The work was simultaneously published in the Journal of the American College of Cardiology (2018 Sept. doi: 10.1016/j.jacc.2018.09.013) .
Despite good results in this and prior studies, uptake of the IVUS procedure is not high in the United States or Europe, according to members of a panel that reviewed the results at the Transcatheter Cardiovascular Therapeutics annual meeting.
“How can people continue to ignore the importance of imaging-guided stent optimization? Even with second-generation DES, the results are consistent across the studies. This is just another piece of irrefutable evidence,” said Gary S. Mintz, MD, chief medical officer at the Cardiovascular Research Foundation, and a discussant at the meeting, sponsored by the Cardiovascular Research Foundation.

That sentiment was generally echoed by the rest of the panel. John M. Hodson, MD, a professor of medicine at MetroHealth Medical Center in Cleveland, pointed out that the study included a variety of cases, and angiography was performed to a high standard in that arm of the study. “It shows that, even with a good angiographic approach, IVUS still wins. I’m amazed that there’s still some resistance to [IVUS] image guidance,” said Dr. Hodgson.
The ULTIMATE study also found that the procedural time was longer (60.88 minutes vs. 45.49 minutes; P less than .001), and the contrast volume was higher (178.29 mL vs. 161.96 mL; P less than .001) in the IVUS than in the angiography group.
A postprocedure IVUS assessment was performed to determine whether the stent was optimally deployed. The criteria for optimal deployment included minimal lumen area in the stented segment of at least 5 mm2, or 90% of the minimal lumen area at distal reference segment meeting that criteria; a less than 50% plaque burden at the 5 mm of vessel proximal or distal to the stent edge; and no edge dissection involving media greater than 3 mm in length.
In the IVUS group, 53% of patients had optimal placement. The rate of target vessel failure was 1.6% of patients with optimal placement and 4.4% of patients who failed to achieve all optimal criteria (HR, 0.349; 95% CI, 0.135-0.898; P = 0.029). Compared with angiography guidance, IVUS guidance was of similar benefit for patients with either American College of Cardiology/American Heart Association–defined B2/C lesions or A/B1 lesions in terms of the composite endpoint. The significant reduction of clinically driven target lesion revascularization or definite stent thrombosis (HR, 0.407; 95% CI: 0.188-0.880; P = 0.018) based on lesion-level analysis by IVUS guidance was not achieved when patient-level analysis was performed.
“I’m particularly impressed by the analysis of the optimal versus nonoptimal group. If you don’t use IVUS correctly, you don’t get a benefit. The ones [in the IVUS group] who did not get optimal stenting were very similar to the angiographic group,” said Dr. Mintz.
The study was funded by the National Science Foundation of China, Six Talent Peaks Project, Nanjing Health and Family Planning Commission, Nanjing Health Youth Talent Training Project, and the Nanjing Municipal Commission of Science & Technology. None of the study authors had relevant financial disclosures. Dr. Mintz reported received research support from Abbott Vascular and Boston Scientific. He has been a consultant for Boston Scientific, Volcano, and Infraredx. Dr. Hodgson reported received research support and consulted for Volcano.
SAN DIEGO – Clinical outcomes were better when stent placement was guided by intravascular ultrasound rather than angiography, based on the results of a trial conducted in China. Unlike previous comparative studies, which focused on patients with more complex lesions, this trial included all patients undergoing drug-eluting stent (DES) placement.
In the ULTIMATE trial, 1,448 all-comer patients receiving DES were randomized to either intravascular ultrasound (IVUS)–guided or angiography-guided implantation, reported Junjie Zhang, PhD, of Nanjing Medical University in China, and colleagues. The study excluded patients who had a life expectancy shorter than 12 months, who were intolerant of dual antiplatelet therapy, and who had severe calcification needing rotational atherectomy.
At 30 days after stent placement, the incidence of target vessel failure was 0.8% in the IVUS group and 1.9% in the angiography group, a nonsignificant trend. However, outcomes were significantly different at 1 year, with target vessel failure occurring in 2.9% of IVUS patients and 5.4% of angiography patients (hazard ratio, 0.530; 95% confidence interval, 0.312-0.901; P = .019).
The work was simultaneously published in the Journal of the American College of Cardiology (2018 Sept. doi: 10.1016/j.jacc.2018.09.013) .
Despite good results in this and prior studies, uptake of the IVUS procedure is not high in the United States or Europe, according to members of a panel that reviewed the results at the Transcatheter Cardiovascular Therapeutics annual meeting.
“How can people continue to ignore the importance of imaging-guided stent optimization? Even with second-generation DES, the results are consistent across the studies. This is just another piece of irrefutable evidence,” said Gary S. Mintz, MD, chief medical officer at the Cardiovascular Research Foundation, and a discussant at the meeting, sponsored by the Cardiovascular Research Foundation.
That sentiment was generally echoed by the rest of the panel. John M. Hodson, MD, a professor of medicine at MetroHealth Medical Center in Cleveland, pointed out that the study included a variety of cases, and angiography was performed to a high standard in that arm of the study. “It shows that, even with a good angiographic approach, IVUS still wins. I’m amazed that there’s still some resistance to [IVUS] image guidance,” said Dr. Hodgson.
The ULTIMATE study also found that the procedural time was longer (60.88 minutes vs. 45.49 minutes; P less than .001), and the contrast volume was higher (178.29 mL vs. 161.96 mL; P less than .001) in the IVUS than in the angiography group.
A postprocedure IVUS assessment was performed to determine whether the stent was optimally deployed. The criteria for optimal deployment included minimal lumen area in the stented segment of at least 5 mm2, or 90% of the minimal lumen area at distal reference segment meeting that criteria; a less than 50% plaque burden at the 5 mm of vessel proximal or distal to the stent edge; and no edge dissection involving media greater than 3 mm in length.
In the IVUS group, 53% of patients had optimal placement. The rate of target vessel failure was 1.6% of patients with optimal placement and 4.4% of patients who failed to achieve all optimal criteria (HR, 0.349; 95% CI, 0.135-0.898; P = 0.029). Compared with angiography guidance, IVUS guidance was of similar benefit for patients with either American College of Cardiology/American Heart Association–defined B2/C lesions or A/B1 lesions in terms of the composite endpoint. The significant reduction of clinically driven target lesion revascularization or definite stent thrombosis (HR, 0.407; 95% CI: 0.188-0.880; P = 0.018) based on lesion-level analysis by IVUS guidance was not achieved when patient-level analysis was performed.
“I’m particularly impressed by the analysis of the optimal versus nonoptimal group. If you don’t use IVUS correctly, you don’t get a benefit. The ones [in the IVUS group] who did not get optimal stenting were very similar to the angiographic group,” said Dr. Mintz.
The study was funded by the National Science Foundation of China, Six Talent Peaks Project, Nanjing Health and Family Planning Commission, Nanjing Health Youth Talent Training Project, and the Nanjing Municipal Commission of Science & Technology. None of the study authors had relevant financial disclosures. Dr. Mintz reported received research support from Abbott Vascular and Boston Scientific. He has been a consultant for Boston Scientific, Volcano, and Infraredx. Dr. Hodgson reported received research support and consulted for Volcano.
SAN DIEGO – Clinical outcomes were better when stent placement was guided by intravascular ultrasound rather than angiography, based on the results of a trial conducted in China. Unlike previous comparative studies, which focused on patients with more complex lesions, this trial included all patients undergoing drug-eluting stent (DES) placement.
In the ULTIMATE trial, 1,448 all-comer patients receiving DES were randomized to either intravascular ultrasound (IVUS)–guided or angiography-guided implantation, reported Junjie Zhang, PhD, of Nanjing Medical University in China, and colleagues. The study excluded patients who had a life expectancy shorter than 12 months, who were intolerant of dual antiplatelet therapy, and who had severe calcification needing rotational atherectomy.
At 30 days after stent placement, the incidence of target vessel failure was 0.8% in the IVUS group and 1.9% in the angiography group, a nonsignificant trend. However, outcomes were significantly different at 1 year, with target vessel failure occurring in 2.9% of IVUS patients and 5.4% of angiography patients (hazard ratio, 0.530; 95% confidence interval, 0.312-0.901; P = .019).
The work was simultaneously published in the Journal of the American College of Cardiology (2018 Sept. doi: 10.1016/j.jacc.2018.09.013) .
Despite good results in this and prior studies, uptake of the IVUS procedure is not high in the United States or Europe, according to members of a panel that reviewed the results at the Transcatheter Cardiovascular Therapeutics annual meeting.
“How can people continue to ignore the importance of imaging-guided stent optimization? Even with second-generation DES, the results are consistent across the studies. This is just another piece of irrefutable evidence,” said Gary S. Mintz, MD, chief medical officer at the Cardiovascular Research Foundation, and a discussant at the meeting, sponsored by the Cardiovascular Research Foundation.
That sentiment was generally echoed by the rest of the panel. John M. Hodson, MD, a professor of medicine at MetroHealth Medical Center in Cleveland, pointed out that the study included a variety of cases, and angiography was performed to a high standard in that arm of the study. “It shows that, even with a good angiographic approach, IVUS still wins. I’m amazed that there’s still some resistance to [IVUS] image guidance,” said Dr. Hodgson.
The ULTIMATE study also found that the procedural time was longer (60.88 minutes vs. 45.49 minutes; P less than .001), and the contrast volume was higher (178.29 mL vs. 161.96 mL; P less than .001) in the IVUS than in the angiography group.
A postprocedure IVUS assessment was performed to determine whether the stent was optimally deployed. The criteria for optimal deployment included minimal lumen area in the stented segment of at least 5 mm2, or 90% of the minimal lumen area at distal reference segment meeting that criteria; a less than 50% plaque burden at the 5 mm of vessel proximal or distal to the stent edge; and no edge dissection involving media greater than 3 mm in length.
In the IVUS group, 53% of patients had optimal placement. The rate of target vessel failure was 1.6% of patients with optimal placement and 4.4% of patients who failed to achieve all optimal criteria (HR, 0.349; 95% CI, 0.135-0.898; P = 0.029). Compared with angiography guidance, IVUS guidance was of similar benefit for patients with either American College of Cardiology/American Heart Association–defined B2/C lesions or A/B1 lesions in terms of the composite endpoint. The significant reduction of clinically driven target lesion revascularization or definite stent thrombosis (HR, 0.407; 95% CI: 0.188-0.880; P = 0.018) based on lesion-level analysis by IVUS guidance was not achieved when patient-level analysis was performed.
“I’m particularly impressed by the analysis of the optimal versus nonoptimal group. If you don’t use IVUS correctly, you don’t get a benefit. The ones [in the IVUS group] who did not get optimal stenting were very similar to the angiographic group,” said Dr. Mintz.
The study was funded by the National Science Foundation of China, Six Talent Peaks Project, Nanjing Health and Family Planning Commission, Nanjing Health Youth Talent Training Project, and the Nanjing Municipal Commission of Science & Technology. None of the study authors had relevant financial disclosures. Dr. Mintz reported received research support from Abbott Vascular and Boston Scientific. He has been a consultant for Boston Scientific, Volcano, and Infraredx. Dr. Hodgson reported received research support and consulted for Volcano.
REPORTING FROM TCT 2018
Key clinical point: Intravascular ultrasound–guided placement of drug-eluting stents resulted in a lower target vessel failure rate than did angiography guidance.
Major finding: The 1-year target vessel failure rate was 2.9% in the intravascular ultrasound–guided group and 5.4% in the angiography group.
Study details: A randomized, controlled trial of 1,448 all-comer patients.
Disclosures: The study was funded by the National Science Foundation of China, Six Talent Peaks Project, Nanjing Health and Family Planning Commission, Nanjing Health Youth Talent Training Project, and the Nanjing Municipal Commission of Science & Technology. None of the study authors had relevant financial disclosures. Dr. Mintz reported receiving research support from Abbott Vascular and Boston Scientific. He has been a consultant for Boston Scientific, Volcano, and Infraredx. Dr. Hodgson reported receiving research support and consulted for Volcano.
Refill disruptions for inhaled corticosteroids may mean more exacerbations
Interruptions of patients’ refills for combination inhaled corticosteroid medication caused by the Medicare Part D formulary switch may have resulted in increased exacerbations and hospitalizations, according to a study that will be presented at the CHEST 2018 annual meeting.
Katie Devane, PhD, and her colleagues examined pharmacy records of 44,832 patients aged 12 years and older who had received a combination inhaled corticosteroid (budesonide/formoterol) and a long-acting beta-agonist medication in 2016-2017. They were followed to track their refills, medication switches, and use of other medications such as oral corticosteroids, antibiotics, and rescue inhalers.
After the Medicare Part D formulary switch on Jan. 1, 2017, many of these patients experienced disruption of their refills. About half of the patients attempted to get a refill of their inhaled corticosteroid prescription but only 46% were approved. One-third of the patients studied did not replace their medication, 12% switched to monotherapy, and 17% had no inhaled medication, the study found.
The investigators concluded that the formulary block resulted in many patients going without optimal medication and potentially led to more exacerbations and ER visits.
View the study abstract here: https://journal.chestnet.org/article/S0012-3692(18)31877-4/fulltext
The study will be presented in the session Improving Care in COPD, Monday, Oct. 8, 2:15 p.m., Convention Center Room 207A.
Interruptions of patients’ refills for combination inhaled corticosteroid medication caused by the Medicare Part D formulary switch may have resulted in increased exacerbations and hospitalizations, according to a study that will be presented at the CHEST 2018 annual meeting.
Katie Devane, PhD, and her colleagues examined pharmacy records of 44,832 patients aged 12 years and older who had received a combination inhaled corticosteroid (budesonide/formoterol) and a long-acting beta-agonist medication in 2016-2017. They were followed to track their refills, medication switches, and use of other medications such as oral corticosteroids, antibiotics, and rescue inhalers.
After the Medicare Part D formulary switch on Jan. 1, 2017, many of these patients experienced disruption of their refills. About half of the patients attempted to get a refill of their inhaled corticosteroid prescription but only 46% were approved. One-third of the patients studied did not replace their medication, 12% switched to monotherapy, and 17% had no inhaled medication, the study found.
The investigators concluded that the formulary block resulted in many patients going without optimal medication and potentially led to more exacerbations and ER visits.
View the study abstract here: https://journal.chestnet.org/article/S0012-3692(18)31877-4/fulltext
The study will be presented in the session Improving Care in COPD, Monday, Oct. 8, 2:15 p.m., Convention Center Room 207A.
Interruptions of patients’ refills for combination inhaled corticosteroid medication caused by the Medicare Part D formulary switch may have resulted in increased exacerbations and hospitalizations, according to a study that will be presented at the CHEST 2018 annual meeting.
Katie Devane, PhD, and her colleagues examined pharmacy records of 44,832 patients aged 12 years and older who had received a combination inhaled corticosteroid (budesonide/formoterol) and a long-acting beta-agonist medication in 2016-2017. They were followed to track their refills, medication switches, and use of other medications such as oral corticosteroids, antibiotics, and rescue inhalers.
After the Medicare Part D formulary switch on Jan. 1, 2017, many of these patients experienced disruption of their refills. About half of the patients attempted to get a refill of their inhaled corticosteroid prescription but only 46% were approved. One-third of the patients studied did not replace their medication, 12% switched to monotherapy, and 17% had no inhaled medication, the study found.
The investigators concluded that the formulary block resulted in many patients going without optimal medication and potentially led to more exacerbations and ER visits.
View the study abstract here: https://journal.chestnet.org/article/S0012-3692(18)31877-4/fulltext
The study will be presented in the session Improving Care in COPD, Monday, Oct. 8, 2:15 p.m., Convention Center Room 207A.
Treatment adherence may trump environmental factors for children with asthma
Children with asthma who are provided with care and medication per National Asthma Education and Prevention Program guidelines can improve over time, despite the presence of environmental factors such as second-hand tobacco smoke and domestic pets, according to a study presented at the CHEST 2018 annual meeting.
A study conducted at the Nationwide Children’s Hospital in Columbus, Ohio, included 395 children aged 2-17 years with a diagnosis of uncontrolled asthma. These children were then treated using the NAEPP guidelines for acute care needs and symptom control. In this sample of patients, 25% were exposed to second-hand smoke, and 55% had a cat or dog in the home.
The investigators followed these patients and observed improvement of symptoms. But in a comparison of those with and without the potentially problematic environmental factors, improvement was independent of the presence of these factors. The findings suggest that NAEPP-recommended treatment of asthma is more important than are some environmental factors.
View the study abstract here: https://journal.chestnet.org/article/S0012-3692(18)31862-2/fulltext.
The findings will be presented in the session on Obstructive Lung Diseases, Wednesday, Oct. 10, at 1:00 p.m.
Children with asthma who are provided with care and medication per National Asthma Education and Prevention Program guidelines can improve over time, despite the presence of environmental factors such as second-hand tobacco smoke and domestic pets, according to a study presented at the CHEST 2018 annual meeting.
A study conducted at the Nationwide Children’s Hospital in Columbus, Ohio, included 395 children aged 2-17 years with a diagnosis of uncontrolled asthma. These children were then treated using the NAEPP guidelines for acute care needs and symptom control. In this sample of patients, 25% were exposed to second-hand smoke, and 55% had a cat or dog in the home.
The investigators followed these patients and observed improvement of symptoms. But in a comparison of those with and without the potentially problematic environmental factors, improvement was independent of the presence of these factors. The findings suggest that NAEPP-recommended treatment of asthma is more important than are some environmental factors.
View the study abstract here: https://journal.chestnet.org/article/S0012-3692(18)31862-2/fulltext.
The findings will be presented in the session on Obstructive Lung Diseases, Wednesday, Oct. 10, at 1:00 p.m.
Children with asthma who are provided with care and medication per National Asthma Education and Prevention Program guidelines can improve over time, despite the presence of environmental factors such as second-hand tobacco smoke and domestic pets, according to a study presented at the CHEST 2018 annual meeting.
A study conducted at the Nationwide Children’s Hospital in Columbus, Ohio, included 395 children aged 2-17 years with a diagnosis of uncontrolled asthma. These children were then treated using the NAEPP guidelines for acute care needs and symptom control. In this sample of patients, 25% were exposed to second-hand smoke, and 55% had a cat or dog in the home.
The investigators followed these patients and observed improvement of symptoms. But in a comparison of those with and without the potentially problematic environmental factors, improvement was independent of the presence of these factors. The findings suggest that NAEPP-recommended treatment of asthma is more important than are some environmental factors.
View the study abstract here: https://journal.chestnet.org/article/S0012-3692(18)31862-2/fulltext.
The findings will be presented in the session on Obstructive Lung Diseases, Wednesday, Oct. 10, at 1:00 p.m.