User login
Researchers develop genetics-based prognostic tool for MDS

Researchers have developed a new risk model for primary myelodysplastic syndromes (MDS) that integrates genetic and clinical information.
The research team considered the current standard for prognostication—the revised International Prognostic Scoring System (IPSS-R)—to be too complex, limited to newly diagnosed cases, and missing information on mutations and age.
So they devised a “simpler and more contemporary” prognostic system, the Mayo Alliance Prognostic Model for MDS.
The team, from the Mayo Clinic in Rochester, Minnesota, and the National Taiwan University Hospital (NTUH), described the new model in Mayo Clinic Proceedings.
Lead author Ayalew Tefferi, MD, of the Mayo Clinic, said the new model “is not an enhancement of the international prognostic scoring system tool, it's a complete makeover."
The team analyzed mutation information from 357 patients with primary MDS or leukemic transformation treated at the Mayo Clinic from the end of December 1994 through mid-December 2017.
The patients were a median age of 74 and 70% were males.
They compared the Mayo patients to 328 NTUH patients, who were a median age of 66 and 65% were males.
Multivariate analysis of the Mayo cohort identified the following as predictors of inferior overall survival:
- Monosomal karyotype (hazard ratio [HR], 5.2; 95% CI, 3.1-8.6)
- Non-monosomal karyotype abnormalities other than single/double del(5q) (HR, 1.8; 95% CI, 1.3-2.6)
- RUNX1 (HR, 2.0; 95% CI, 1.2-3.1)
- ASXL1 (HR, 1.7; 95% CI, 1.2-2.3) mutations
- Absence of SF3B1 mutations (HR, 1.6; 95% CI, 1.1-2.4)
- Age greater than 70 years (HR, 2.2; 95% CI, 1.6-3.1)
- Hemoglobin level less than 8 g/dL in women or less than 9 g/dL in men (HR, 2.3; 95% CI, 1.7-3.1)
- Platelet count less than 75 x 109/L (HR, 1.5; 95% CI, 1.1-2.1)
- 10% or more bone marrow blasts (HR, 1.7; 95% CI, 1.1-2.8)
They then provided values to reflect the prognostic contribution of each of the above predictors and devised the new 4-tiered Mayo prognostic model.
Median 5-year overall survival rates in the 4 categories in the Mayo model were 73% (low risk), 34% (intermediate-1), 7% (intermediate-2), and 0% (high risk; 9-month median survival).
The team then validated the Mayo alliance model by using the NTUH cohort and compared it to the IPSS-R.
The investigators were able to confirm superior predictive accuracy of their model and a substantial discordance between the the Mayo model and the IPSS-R in terms of the pattern of risk distribution.
Examples of discordance included:
- More than 25% of patients belonging to the high-risk category according to the Mayo alliance model were classified as IPSS-R low or intermediate risk
- Almost 50% of patients with intermediate-2 risk category according to the Mayo alliance model were classified as IPSS-R very low or low risk
- Almost 50% of patients with IPSS-R very low risk were classified as intermediate-2 or intermediate-1 risk according to the Mayo alliance model
The authors wrote that this “suggests a fundamental and not incremental advantage for the new Mayo alliance model.”
Researchers have developed a new risk model for primary myelodysplastic syndromes (MDS) that integrates genetic and clinical information.
The research team considered the current standard for prognostication—the revised International Prognostic Scoring System (IPSS-R)—to be too complex, limited to newly diagnosed cases, and missing information on mutations and age.
So they devised a “simpler and more contemporary” prognostic system, the Mayo Alliance Prognostic Model for MDS.
The team, from the Mayo Clinic in Rochester, Minnesota, and the National Taiwan University Hospital (NTUH), described the new model in Mayo Clinic Proceedings.
Lead author Ayalew Tefferi, MD, of the Mayo Clinic, said the new model “is not an enhancement of the international prognostic scoring system tool, it's a complete makeover."
The team analyzed mutation information from 357 patients with primary MDS or leukemic transformation treated at the Mayo Clinic from the end of December 1994 through mid-December 2017.
The patients were a median age of 74 and 70% were males.
They compared the Mayo patients to 328 NTUH patients, who were a median age of 66 and 65% were males.
Multivariate analysis of the Mayo cohort identified the following as predictors of inferior overall survival:
- Monosomal karyotype (hazard ratio [HR], 5.2; 95% CI, 3.1-8.6)
- Non-monosomal karyotype abnormalities other than single/double del(5q) (HR, 1.8; 95% CI, 1.3-2.6)
- RUNX1 (HR, 2.0; 95% CI, 1.2-3.1)
- ASXL1 (HR, 1.7; 95% CI, 1.2-2.3) mutations
- Absence of SF3B1 mutations (HR, 1.6; 95% CI, 1.1-2.4)
- Age greater than 70 years (HR, 2.2; 95% CI, 1.6-3.1)
- Hemoglobin level less than 8 g/dL in women or less than 9 g/dL in men (HR, 2.3; 95% CI, 1.7-3.1)
- Platelet count less than 75 x 109/L (HR, 1.5; 95% CI, 1.1-2.1)
- 10% or more bone marrow blasts (HR, 1.7; 95% CI, 1.1-2.8)
They then provided values to reflect the prognostic contribution of each of the above predictors and devised the new 4-tiered Mayo prognostic model.
Median 5-year overall survival rates in the 4 categories in the Mayo model were 73% (low risk), 34% (intermediate-1), 7% (intermediate-2), and 0% (high risk; 9-month median survival).
The team then validated the Mayo alliance model by using the NTUH cohort and compared it to the IPSS-R.
The investigators were able to confirm superior predictive accuracy of their model and a substantial discordance between the the Mayo model and the IPSS-R in terms of the pattern of risk distribution.
Examples of discordance included:
- More than 25% of patients belonging to the high-risk category according to the Mayo alliance model were classified as IPSS-R low or intermediate risk
- Almost 50% of patients with intermediate-2 risk category according to the Mayo alliance model were classified as IPSS-R very low or low risk
- Almost 50% of patients with IPSS-R very low risk were classified as intermediate-2 or intermediate-1 risk according to the Mayo alliance model
The authors wrote that this “suggests a fundamental and not incremental advantage for the new Mayo alliance model.”
Researchers have developed a new risk model for primary myelodysplastic syndromes (MDS) that integrates genetic and clinical information.
The research team considered the current standard for prognostication—the revised International Prognostic Scoring System (IPSS-R)—to be too complex, limited to newly diagnosed cases, and missing information on mutations and age.
So they devised a “simpler and more contemporary” prognostic system, the Mayo Alliance Prognostic Model for MDS.
The team, from the Mayo Clinic in Rochester, Minnesota, and the National Taiwan University Hospital (NTUH), described the new model in Mayo Clinic Proceedings.
Lead author Ayalew Tefferi, MD, of the Mayo Clinic, said the new model “is not an enhancement of the international prognostic scoring system tool, it's a complete makeover."
The team analyzed mutation information from 357 patients with primary MDS or leukemic transformation treated at the Mayo Clinic from the end of December 1994 through mid-December 2017.
The patients were a median age of 74 and 70% were males.
They compared the Mayo patients to 328 NTUH patients, who were a median age of 66 and 65% were males.
Multivariate analysis of the Mayo cohort identified the following as predictors of inferior overall survival:
- Monosomal karyotype (hazard ratio [HR], 5.2; 95% CI, 3.1-8.6)
- Non-monosomal karyotype abnormalities other than single/double del(5q) (HR, 1.8; 95% CI, 1.3-2.6)
- RUNX1 (HR, 2.0; 95% CI, 1.2-3.1)
- ASXL1 (HR, 1.7; 95% CI, 1.2-2.3) mutations
- Absence of SF3B1 mutations (HR, 1.6; 95% CI, 1.1-2.4)
- Age greater than 70 years (HR, 2.2; 95% CI, 1.6-3.1)
- Hemoglobin level less than 8 g/dL in women or less than 9 g/dL in men (HR, 2.3; 95% CI, 1.7-3.1)
- Platelet count less than 75 x 109/L (HR, 1.5; 95% CI, 1.1-2.1)
- 10% or more bone marrow blasts (HR, 1.7; 95% CI, 1.1-2.8)
They then provided values to reflect the prognostic contribution of each of the above predictors and devised the new 4-tiered Mayo prognostic model.
Median 5-year overall survival rates in the 4 categories in the Mayo model were 73% (low risk), 34% (intermediate-1), 7% (intermediate-2), and 0% (high risk; 9-month median survival).
The team then validated the Mayo alliance model by using the NTUH cohort and compared it to the IPSS-R.
The investigators were able to confirm superior predictive accuracy of their model and a substantial discordance between the the Mayo model and the IPSS-R in terms of the pattern of risk distribution.
Examples of discordance included:
- More than 25% of patients belonging to the high-risk category according to the Mayo alliance model were classified as IPSS-R low or intermediate risk
- Almost 50% of patients with intermediate-2 risk category according to the Mayo alliance model were classified as IPSS-R very low or low risk
- Almost 50% of patients with IPSS-R very low risk were classified as intermediate-2 or intermediate-1 risk according to the Mayo alliance model
The authors wrote that this “suggests a fundamental and not incremental advantage for the new Mayo alliance model.”
Carfilzomib receives approval for once-weekly dosing

The U.S. Food and Drug Administration (FDA) has approved carfilzomib (Kyprolis) for a once-weekly dosing option in combination with dexamethasone for patients with relapsed or refractory multiple myeloma (MM).
Carfilzomib administered once-weekly at 70 mg/m2 with dexamethasone achieved a superior progression-free survival (PFS) and overall response rates (ORR) compared to twice-weekly carfilzomib at doses of 27 mg/m2.
Carfilzomib is not, however, approved for the twice-weekly 27 mg/m2 dose with dexamethasone alone, but with dexamethasone and lenalidomide.
The FDA based its approval on data from the phase 3 ARROW trial.
The FDA reviewed and approved the supplemental New Drug Application under its Oncology Center of Excellence Real-Time Oncology Review and Assessment Aid pilot program. The program is exploring a more efficient review process to ensure that safe and effective treatments are available to patients as soon as possible.
The FDA approved the carfilzomib application in just over a month.
ARROW
The ARROW study, reported at the 2018 ASCO annual meeting and published in The Lancet, evaluated 478 patients with relapsed or refractory MM who had received at least two but no more than three prior therapies. Prior therapies could include bortezomib and an immunomodulatory drug.
Patients randomized to the investigational arm receive a 30-minute infusion of once-weekly carfilzomib (20 mg/m2 on day 1 of cycle 1; 70 mg/m2 on days 8 and 15 of cycle 1; and 70 mg/m2 on days 1, 8 and 15 of subsequent cycles) with 40 mg of dexamethasone.
Patients randomized to the comparator arm received a 10-minute infusion of twice-weekly carfilzomib (20 mg/m2 on days 1 and 2 of cycle 1; 27 mg/m2 on days 8, 9, 15 and 16 of cycle 1; and 27 mg/m2 on days 1, 2, 8, 9, 15 and 16 of subsequent cycles) with 40 mg of dexamethasone.
Patients in the once-weekly arm achieved a statistically significant 3.7-month improvement in PFS compared to the twice-weekly regimen. Median PFS was 11.2 months for the once-weekly patients and 7.6 months for the twice-weekly group (P=0.0014).
Patients in the once-weekly group had a 62.9% ORR compared to 40.8% for those treated twice weekly (P<0.0001).
More patients (7.1%) in the once-weekly group had complete responses or better than those in the twice-weekly arm (1.7%).
The safety profile of the two arms were comparable, with no new safety risks identified in the once-weekly arm.
Treatment-emergent adverse events occurring in 20% or more patients in either arm included anemia, diarrhea, fatigue, hypertension, insomnia, and pyrexia.
First approved in 2012, carfilzomib has indications for the following in the U.S.:
- Treatment of patients with relapsed or refractory multiple myeloma who have received one to three lines of therapy in combination with dexamethasone or with lenalidomide plus dexamethasone.
- As a single agent for the treatment of patients with relapsed or refractory multiple myeloma who have received one or more lines of therapy.
Amgen manufactures carfilzomib for Onyx Pharmaceuticals, Inc.
Prescribing information for carfilzomib is available online.
The U.S. Food and Drug Administration (FDA) has approved carfilzomib (Kyprolis) for a once-weekly dosing option in combination with dexamethasone for patients with relapsed or refractory multiple myeloma (MM).
Carfilzomib administered once-weekly at 70 mg/m2 with dexamethasone achieved a superior progression-free survival (PFS) and overall response rates (ORR) compared to twice-weekly carfilzomib at doses of 27 mg/m2.
Carfilzomib is not, however, approved for the twice-weekly 27 mg/m2 dose with dexamethasone alone, but with dexamethasone and lenalidomide.
The FDA based its approval on data from the phase 3 ARROW trial.
The FDA reviewed and approved the supplemental New Drug Application under its Oncology Center of Excellence Real-Time Oncology Review and Assessment Aid pilot program. The program is exploring a more efficient review process to ensure that safe and effective treatments are available to patients as soon as possible.
The FDA approved the carfilzomib application in just over a month.
ARROW
The ARROW study, reported at the 2018 ASCO annual meeting and published in The Lancet, evaluated 478 patients with relapsed or refractory MM who had received at least two but no more than three prior therapies. Prior therapies could include bortezomib and an immunomodulatory drug.
Patients randomized to the investigational arm receive a 30-minute infusion of once-weekly carfilzomib (20 mg/m2 on day 1 of cycle 1; 70 mg/m2 on days 8 and 15 of cycle 1; and 70 mg/m2 on days 1, 8 and 15 of subsequent cycles) with 40 mg of dexamethasone.
Patients randomized to the comparator arm received a 10-minute infusion of twice-weekly carfilzomib (20 mg/m2 on days 1 and 2 of cycle 1; 27 mg/m2 on days 8, 9, 15 and 16 of cycle 1; and 27 mg/m2 on days 1, 2, 8, 9, 15 and 16 of subsequent cycles) with 40 mg of dexamethasone.
Patients in the once-weekly arm achieved a statistically significant 3.7-month improvement in PFS compared to the twice-weekly regimen. Median PFS was 11.2 months for the once-weekly patients and 7.6 months for the twice-weekly group (P=0.0014).
Patients in the once-weekly group had a 62.9% ORR compared to 40.8% for those treated twice weekly (P<0.0001).
More patients (7.1%) in the once-weekly group had complete responses or better than those in the twice-weekly arm (1.7%).
The safety profile of the two arms were comparable, with no new safety risks identified in the once-weekly arm.
Treatment-emergent adverse events occurring in 20% or more patients in either arm included anemia, diarrhea, fatigue, hypertension, insomnia, and pyrexia.
First approved in 2012, carfilzomib has indications for the following in the U.S.:
- Treatment of patients with relapsed or refractory multiple myeloma who have received one to three lines of therapy in combination with dexamethasone or with lenalidomide plus dexamethasone.
- As a single agent for the treatment of patients with relapsed or refractory multiple myeloma who have received one or more lines of therapy.
Amgen manufactures carfilzomib for Onyx Pharmaceuticals, Inc.
Prescribing information for carfilzomib is available online.
The U.S. Food and Drug Administration (FDA) has approved carfilzomib (Kyprolis) for a once-weekly dosing option in combination with dexamethasone for patients with relapsed or refractory multiple myeloma (MM).
Carfilzomib administered once-weekly at 70 mg/m2 with dexamethasone achieved a superior progression-free survival (PFS) and overall response rates (ORR) compared to twice-weekly carfilzomib at doses of 27 mg/m2.
Carfilzomib is not, however, approved for the twice-weekly 27 mg/m2 dose with dexamethasone alone, but with dexamethasone and lenalidomide.
The FDA based its approval on data from the phase 3 ARROW trial.
The FDA reviewed and approved the supplemental New Drug Application under its Oncology Center of Excellence Real-Time Oncology Review and Assessment Aid pilot program. The program is exploring a more efficient review process to ensure that safe and effective treatments are available to patients as soon as possible.
The FDA approved the carfilzomib application in just over a month.
ARROW
The ARROW study, reported at the 2018 ASCO annual meeting and published in The Lancet, evaluated 478 patients with relapsed or refractory MM who had received at least two but no more than three prior therapies. Prior therapies could include bortezomib and an immunomodulatory drug.
Patients randomized to the investigational arm receive a 30-minute infusion of once-weekly carfilzomib (20 mg/m2 on day 1 of cycle 1; 70 mg/m2 on days 8 and 15 of cycle 1; and 70 mg/m2 on days 1, 8 and 15 of subsequent cycles) with 40 mg of dexamethasone.
Patients randomized to the comparator arm received a 10-minute infusion of twice-weekly carfilzomib (20 mg/m2 on days 1 and 2 of cycle 1; 27 mg/m2 on days 8, 9, 15 and 16 of cycle 1; and 27 mg/m2 on days 1, 2, 8, 9, 15 and 16 of subsequent cycles) with 40 mg of dexamethasone.
Patients in the once-weekly arm achieved a statistically significant 3.7-month improvement in PFS compared to the twice-weekly regimen. Median PFS was 11.2 months for the once-weekly patients and 7.6 months for the twice-weekly group (P=0.0014).
Patients in the once-weekly group had a 62.9% ORR compared to 40.8% for those treated twice weekly (P<0.0001).
More patients (7.1%) in the once-weekly group had complete responses or better than those in the twice-weekly arm (1.7%).
The safety profile of the two arms were comparable, with no new safety risks identified in the once-weekly arm.
Treatment-emergent adverse events occurring in 20% or more patients in either arm included anemia, diarrhea, fatigue, hypertension, insomnia, and pyrexia.
First approved in 2012, carfilzomib has indications for the following in the U.S.:
- Treatment of patients with relapsed or refractory multiple myeloma who have received one to three lines of therapy in combination with dexamethasone or with lenalidomide plus dexamethasone.
- As a single agent for the treatment of patients with relapsed or refractory multiple myeloma who have received one or more lines of therapy.
Amgen manufactures carfilzomib for Onyx Pharmaceuticals, Inc.
Prescribing information for carfilzomib is available online.
The Rancher, the Roof, and the Rogue Heart
ANSWER
The correct interpretation of this ECG includes atrial fibrillation with variable atrioventricular (AV) block and a left-axis deviation.
Atrial fibrillation is evidenced by the absence of P waves, a consistent PR interval, and an irregularly irregular rhythm. The ventricular rate in atrial fibrillation is due to variable conduction through the AV node, and the 1.6-second pause prior to the last beat on this ECG is due to variable block in the conduction system below the AV node. Pauses such as these may result in clinical symptoms; when seen, the clinician should exercise caution in determining which method (six-second rule, 300/150/100 method) to use to measure the overall heart rate. Note that a pause of undetermined time also exists prior to the first QRS complex seen on the rhythm strip.
Finally, a left-axis deviation is evidenced by an R-wave axis between –30 and –120°.
ANSWER
The correct interpretation of this ECG includes atrial fibrillation with variable atrioventricular (AV) block and a left-axis deviation.
Atrial fibrillation is evidenced by the absence of P waves, a consistent PR interval, and an irregularly irregular rhythm. The ventricular rate in atrial fibrillation is due to variable conduction through the AV node, and the 1.6-second pause prior to the last beat on this ECG is due to variable block in the conduction system below the AV node. Pauses such as these may result in clinical symptoms; when seen, the clinician should exercise caution in determining which method (six-second rule, 300/150/100 method) to use to measure the overall heart rate. Note that a pause of undetermined time also exists prior to the first QRS complex seen on the rhythm strip.
Finally, a left-axis deviation is evidenced by an R-wave axis between –30 and –120°.
ANSWER
The correct interpretation of this ECG includes atrial fibrillation with variable atrioventricular (AV) block and a left-axis deviation.
Atrial fibrillation is evidenced by the absence of P waves, a consistent PR interval, and an irregularly irregular rhythm. The ventricular rate in atrial fibrillation is due to variable conduction through the AV node, and the 1.6-second pause prior to the last beat on this ECG is due to variable block in the conduction system below the AV node. Pauses such as these may result in clinical symptoms; when seen, the clinician should exercise caution in determining which method (six-second rule, 300/150/100 method) to use to measure the overall heart rate. Note that a pause of undetermined time also exists prior to the first QRS complex seen on the rhythm strip.
Finally, a left-axis deviation is evidenced by an R-wave axis between –30 and –120°.

Three days ago, a 74-year-old man fell from his roof, sustaining three fractured ribs and a right-sided hemothorax. He was admitted for treatment: a chest tube to drain the hemothorax and a decortication procedure the following day. His pain has been well controlled postoperatively, and he has been ambulating with his chest tube drainage system on water seal.
This morning, the telemetry technician notices pauses on the patient’s rhythm strips and pages you for interpretation and management. Puzzled as to why this patient was placed on telemetry, you order a 12-lead ECG and review the patient’s electronic medical record (EMR).
Medical history is remarkable for chronic atrial fibrillation, hypertension, hypothyroidism, and a remote history of two transient ischemic attacks (TIAs). His CHA2DS2-VASc score is calculated to be 4, given his age and medical history. When you talk to the patient, he reports no episodes of syncope, near syncope, chest pain, or shortness of breath. He explains that he’s very active and was repairing his roof in preparation for winter when he reached too far and the ladder tipped over.
The patient’s medications include warfarin, hydrochlorothiazide, metoprolol, and propylthiouracil. He has no known drug allergies and denies recreational or homeopathic medication use.
The patient has been a rancher his entire life and doesn’t see himself retiring. He has lived alone on a 200-acre ranch since his wife died of non-Hodgkin lymphoma 12 years ago. He has two adult sons, both in good health, who visit during holidays. The patient was adopted and does not know his family history. He smoked as a young adult but says he hasn’t done so “since cigarettes reached $1.00 per pack.” He has an occasional drink when friends visit but otherwise doesn’t consume alcohol.
The review of systems is remarkable only for a resolving paronychia on his left middle finger.
According to the EMR, his vital signs as of this morning include a blood pressure of 138/94 mm Hg; heart rate, 66 beats/min; respiratory rate, 14 breaths/min; and O2 saturation, 98% on 2L of oxygen via nasal prongs. His height is 6’2” and his weight, 184 lb.
Physical exam reveals an otherwise healthy yet weathered man in no distress. He has multiple old and new areas of ecchymosis on his upper and lower extremities and his right chest. A chest tube is evident exiting the right anterior chest wall. Breath sounds are distant with rhonchi on the right chest and clear and full on the left. The cardiac exam reveals no evidence of jugular venous distention. Heart rhythm is irregularly irregular at a rate of 60 beats/min. There are no murmurs, bruits, or extra heart sounds. The abdomen is soft and scaphoid with no palpable masses. His lower extremities show no evidence of pitting edema, and pulses are strong and full bilaterally. He is alert, oriented, and conversive and does not demonstrate any focal signs.
The ECG you ordered shows an unmeasurable PR interval; QRS duration, 102 ms; QT/QTc interval, 392/397 ms; P axis, unmeasured; R axis, –61°; and T axis, 76°. What is your interpretation?

Physical assaults in the emergency department on the rise, survey finds

Those are key findings from an email-based survey administered to ACEP members in August of 2018.
“The results are quite troubling,” Vidor E. Friedman, MD, FACEP, president of ACEP, said during a press briefing at the group’s annual meeting. “Emergency physicians are reporting that violence in emergency departments is increasing and that it’s harming not only physicians and nurses, but also patients and the care that’s being provided to them.”
Dr. Friedman, who practices emergency medicine in Maitland, Fla., recalled one afternoon shift when police brought in a drunk man they had cited for vagrancy after finding him in a ditch by the roadside. It was the man’s first day out of jail in 10 years. “He was a pretty intimidating looking guy,” Dr. Friedman said. “He threatened me and he threatened the staff, so we appropriately restrained him, which only increased his agitation. The fourth time he said he was going to kill me, he told me he was going to put an ice pick in my heart. When his buddies came to pick him up, I had the police escort him to the city limits, and I didn’t sleep at home for a week. This is the kind of thing that health care workers are exposed to on a fairly regular basis.”
The ACEP survey found that emergency physicians across all demographics experience various forms of violence and are increasingly concerned about violence in the ED. “We know that there is gross underreporting of [violence in the ED],” said Terry Kowalenko, MD, FACEP, chair of emergency medicine at Oakland University William Beaumont School of Medicine, Rochester, Mich., and coauthor of a new study that assessed violence against emergency physicians in that state. “Some studies have shown it to be under 50%. The other thing is, it’s very difficult to predict who the perpetrator will be, or who the victim will be. We did find that the time you spend with the patient certainly increases your chances of violence perpetrated against you. Clearly, there are consequences to the victim, the perpetrator, the institution, and potentially, other patients.”

According to Dr. Kowalenko’s own research, 72% of emergency medicine physicians in Michigan reported experiencing violence in the past year. In 2018, an increasing proportion of that state’s emergency physicians reported feeling “constantly fearful” of becoming a victim of violence (8.1% vs. 1.2% in 2005), with 22% reporting feeling frequently fearful (up from 9.4% in 2005).
For the ACEP-sponsored survey, on Aug. 21, 2018, Alexandria, Va.–based Marketing General sent an email to 31,389 ACEP members, inviting them to answer 22 questions in an effort to understand emergency physicians’ views on the level, type, frequency, and impact of violence experienced in the ED. By the time polling closed 6 days later, 3,539 surveys were completed, for a response rate of about 11%. Clinicians in California led the way with 8% of total responses, followed by those in Texas (7%), New York (7%), Florida (5%), Pennsylvania (5%), and Ohio (5%). Nearly two-thirds of respondents (71%) were male, and 25% work for emergency departments with annual patient volumes between 50,001 and 75,000, while another 39% work for departments with even higher volumes.
Nearly half of respondents (47%) reported being physically assaulted while at work in the ED, while 71% have witnessed an assault. Only 10% have experienced neither. The majority of assaults were committed by patients (97%), but 28% involved a patient’s family member or friend. The most common form of assault was a hit or a slap (44%), while other frequent forms of violence included being spit on (30%), punched (28%), or kicked (27%).
Among those who have been physically assaulted, 48% reported that at least half of all assaults were committed by people believed to be seeking drugs or who were under the influence of drugs or alcohol, while 41% said that more than half of assaults were committed by psychiatric patients.
“Our emergency departments are kind of a microcosm of all the challenges that we face today in society: gang violence, gun violence, domestic violence, and psychiatric illnesses [for which] we have a shortage of beds,” said Leigh Vinocur, MD, FACEP, former chair of ACEP’s Emergency Department Violence Committee. “Then there is the opioid crisis.” She added that being in an emergency department can be “an emotionally volatile experience for people from all walks of life. People come in hurt. They’re at their worst; they’re frightened, they’re vulnerable and stressed.”
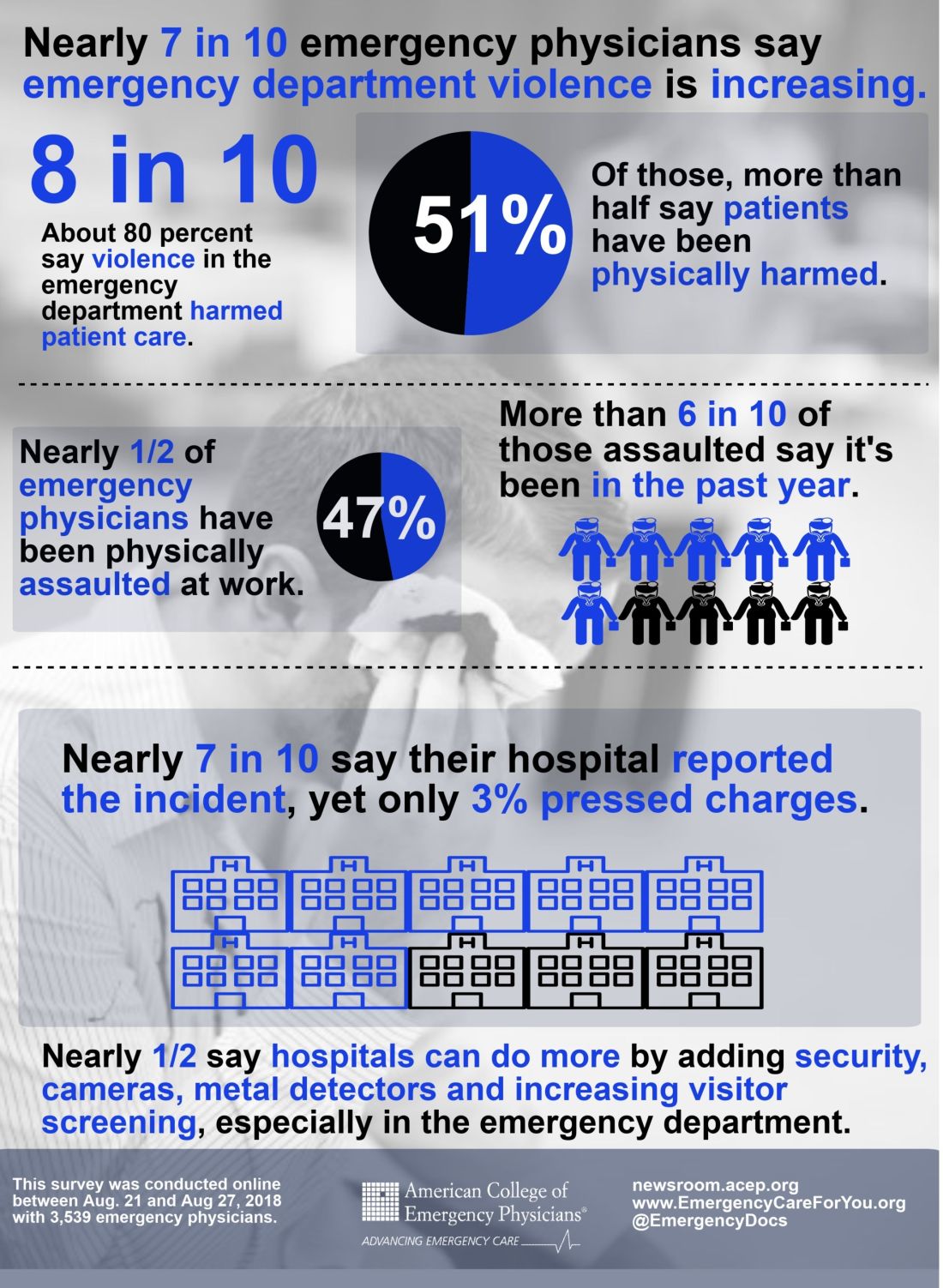
More than three-quarters of ACEP survey respondents (77%) believe that violence in the ED has harmed patient care, primarily by loss of productivity (81%), emotional trauma (81%), increased wait times (80%), and less focus from emergency staff or physicians (76%). In addition, 49% ranked “increase security” as the most important step hospitals can take to increase ED safety, while the top three contributing factors to violence in the ED were no adequate punitive consequence or response toward the attacker (34%), behavioral health patients (32%), and absence of adequate protective mechanisms for physicians/staff (15%).
When asked how the hospital administration or hospital security responded to the assault, 28% said that the hospital or nursing staff put a behavioral flag in the patient’s medical chart, while 21% said that hospital security arrested the patient for the assault or enlisted law enforcement to arrest the patient.
Finally, nearly half of respondents indicated that hospitals could do more by adding security cameras, metal detectors, and increasing visitor screening. “Obviously this is site-specific,” Dr. Friedman said. “We’re not saying that every emergency department in America needs to have a metal detector out front, but this needs to be something that institutions take seriously, to protect both patients and the providers that work there.”
[email protected]
Those are key findings from an email-based survey administered to ACEP members in August of 2018.
“The results are quite troubling,” Vidor E. Friedman, MD, FACEP, president of ACEP, said during a press briefing at the group’s annual meeting. “Emergency physicians are reporting that violence in emergency departments is increasing and that it’s harming not only physicians and nurses, but also patients and the care that’s being provided to them.”
Dr. Friedman, who practices emergency medicine in Maitland, Fla., recalled one afternoon shift when police brought in a drunk man they had cited for vagrancy after finding him in a ditch by the roadside. It was the man’s first day out of jail in 10 years. “He was a pretty intimidating looking guy,” Dr. Friedman said. “He threatened me and he threatened the staff, so we appropriately restrained him, which only increased his agitation. The fourth time he said he was going to kill me, he told me he was going to put an ice pick in my heart. When his buddies came to pick him up, I had the police escort him to the city limits, and I didn’t sleep at home for a week. This is the kind of thing that health care workers are exposed to on a fairly regular basis.”
The ACEP survey found that emergency physicians across all demographics experience various forms of violence and are increasingly concerned about violence in the ED. “We know that there is gross underreporting of [violence in the ED],” said Terry Kowalenko, MD, FACEP, chair of emergency medicine at Oakland University William Beaumont School of Medicine, Rochester, Mich., and coauthor of a new study that assessed violence against emergency physicians in that state. “Some studies have shown it to be under 50%. The other thing is, it’s very difficult to predict who the perpetrator will be, or who the victim will be. We did find that the time you spend with the patient certainly increases your chances of violence perpetrated against you. Clearly, there are consequences to the victim, the perpetrator, the institution, and potentially, other patients.”
According to Dr. Kowalenko’s own research, 72% of emergency medicine physicians in Michigan reported experiencing violence in the past year. In 2018, an increasing proportion of that state’s emergency physicians reported feeling “constantly fearful” of becoming a victim of violence (8.1% vs. 1.2% in 2005), with 22% reporting feeling frequently fearful (up from 9.4% in 2005).
For the ACEP-sponsored survey, on Aug. 21, 2018, Alexandria, Va.–based Marketing General sent an email to 31,389 ACEP members, inviting them to answer 22 questions in an effort to understand emergency physicians’ views on the level, type, frequency, and impact of violence experienced in the ED. By the time polling closed 6 days later, 3,539 surveys were completed, for a response rate of about 11%. Clinicians in California led the way with 8% of total responses, followed by those in Texas (7%), New York (7%), Florida (5%), Pennsylvania (5%), and Ohio (5%). Nearly two-thirds of respondents (71%) were male, and 25% work for emergency departments with annual patient volumes between 50,001 and 75,000, while another 39% work for departments with even higher volumes.
Nearly half of respondents (47%) reported being physically assaulted while at work in the ED, while 71% have witnessed an assault. Only 10% have experienced neither. The majority of assaults were committed by patients (97%), but 28% involved a patient’s family member or friend. The most common form of assault was a hit or a slap (44%), while other frequent forms of violence included being spit on (30%), punched (28%), or kicked (27%).
Among those who have been physically assaulted, 48% reported that at least half of all assaults were committed by people believed to be seeking drugs or who were under the influence of drugs or alcohol, while 41% said that more than half of assaults were committed by psychiatric patients.
“Our emergency departments are kind of a microcosm of all the challenges that we face today in society: gang violence, gun violence, domestic violence, and psychiatric illnesses [for which] we have a shortage of beds,” said Leigh Vinocur, MD, FACEP, former chair of ACEP’s Emergency Department Violence Committee. “Then there is the opioid crisis.” She added that being in an emergency department can be “an emotionally volatile experience for people from all walks of life. People come in hurt. They’re at their worst; they’re frightened, they’re vulnerable and stressed.”
More than three-quarters of ACEP survey respondents (77%) believe that violence in the ED has harmed patient care, primarily by loss of productivity (81%), emotional trauma (81%), increased wait times (80%), and less focus from emergency staff or physicians (76%). In addition, 49% ranked “increase security” as the most important step hospitals can take to increase ED safety, while the top three contributing factors to violence in the ED were no adequate punitive consequence or response toward the attacker (34%), behavioral health patients (32%), and absence of adequate protective mechanisms for physicians/staff (15%).
When asked how the hospital administration or hospital security responded to the assault, 28% said that the hospital or nursing staff put a behavioral flag in the patient’s medical chart, while 21% said that hospital security arrested the patient for the assault or enlisted law enforcement to arrest the patient.
Finally, nearly half of respondents indicated that hospitals could do more by adding security cameras, metal detectors, and increasing visitor screening. “Obviously this is site-specific,” Dr. Friedman said. “We’re not saying that every emergency department in America needs to have a metal detector out front, but this needs to be something that institutions take seriously, to protect both patients and the providers that work there.”
[email protected]
Those are key findings from an email-based survey administered to ACEP members in August of 2018.
“The results are quite troubling,” Vidor E. Friedman, MD, FACEP, president of ACEP, said during a press briefing at the group’s annual meeting. “Emergency physicians are reporting that violence in emergency departments is increasing and that it’s harming not only physicians and nurses, but also patients and the care that’s being provided to them.”
Dr. Friedman, who practices emergency medicine in Maitland, Fla., recalled one afternoon shift when police brought in a drunk man they had cited for vagrancy after finding him in a ditch by the roadside. It was the man’s first day out of jail in 10 years. “He was a pretty intimidating looking guy,” Dr. Friedman said. “He threatened me and he threatened the staff, so we appropriately restrained him, which only increased his agitation. The fourth time he said he was going to kill me, he told me he was going to put an ice pick in my heart. When his buddies came to pick him up, I had the police escort him to the city limits, and I didn’t sleep at home for a week. This is the kind of thing that health care workers are exposed to on a fairly regular basis.”
The ACEP survey found that emergency physicians across all demographics experience various forms of violence and are increasingly concerned about violence in the ED. “We know that there is gross underreporting of [violence in the ED],” said Terry Kowalenko, MD, FACEP, chair of emergency medicine at Oakland University William Beaumont School of Medicine, Rochester, Mich., and coauthor of a new study that assessed violence against emergency physicians in that state. “Some studies have shown it to be under 50%. The other thing is, it’s very difficult to predict who the perpetrator will be, or who the victim will be. We did find that the time you spend with the patient certainly increases your chances of violence perpetrated against you. Clearly, there are consequences to the victim, the perpetrator, the institution, and potentially, other patients.”
According to Dr. Kowalenko’s own research, 72% of emergency medicine physicians in Michigan reported experiencing violence in the past year. In 2018, an increasing proportion of that state’s emergency physicians reported feeling “constantly fearful” of becoming a victim of violence (8.1% vs. 1.2% in 2005), with 22% reporting feeling frequently fearful (up from 9.4% in 2005).
For the ACEP-sponsored survey, on Aug. 21, 2018, Alexandria, Va.–based Marketing General sent an email to 31,389 ACEP members, inviting them to answer 22 questions in an effort to understand emergency physicians’ views on the level, type, frequency, and impact of violence experienced in the ED. By the time polling closed 6 days later, 3,539 surveys were completed, for a response rate of about 11%. Clinicians in California led the way with 8% of total responses, followed by those in Texas (7%), New York (7%), Florida (5%), Pennsylvania (5%), and Ohio (5%). Nearly two-thirds of respondents (71%) were male, and 25% work for emergency departments with annual patient volumes between 50,001 and 75,000, while another 39% work for departments with even higher volumes.
Nearly half of respondents (47%) reported being physically assaulted while at work in the ED, while 71% have witnessed an assault. Only 10% have experienced neither. The majority of assaults were committed by patients (97%), but 28% involved a patient’s family member or friend. The most common form of assault was a hit or a slap (44%), while other frequent forms of violence included being spit on (30%), punched (28%), or kicked (27%).
Among those who have been physically assaulted, 48% reported that at least half of all assaults were committed by people believed to be seeking drugs or who were under the influence of drugs or alcohol, while 41% said that more than half of assaults were committed by psychiatric patients.
“Our emergency departments are kind of a microcosm of all the challenges that we face today in society: gang violence, gun violence, domestic violence, and psychiatric illnesses [for which] we have a shortage of beds,” said Leigh Vinocur, MD, FACEP, former chair of ACEP’s Emergency Department Violence Committee. “Then there is the opioid crisis.” She added that being in an emergency department can be “an emotionally volatile experience for people from all walks of life. People come in hurt. They’re at their worst; they’re frightened, they’re vulnerable and stressed.”
More than three-quarters of ACEP survey respondents (77%) believe that violence in the ED has harmed patient care, primarily by loss of productivity (81%), emotional trauma (81%), increased wait times (80%), and less focus from emergency staff or physicians (76%). In addition, 49% ranked “increase security” as the most important step hospitals can take to increase ED safety, while the top three contributing factors to violence in the ED were no adequate punitive consequence or response toward the attacker (34%), behavioral health patients (32%), and absence of adequate protective mechanisms for physicians/staff (15%).
When asked how the hospital administration or hospital security responded to the assault, 28% said that the hospital or nursing staff put a behavioral flag in the patient’s medical chart, while 21% said that hospital security arrested the patient for the assault or enlisted law enforcement to arrest the patient.
Finally, nearly half of respondents indicated that hospitals could do more by adding security cameras, metal detectors, and increasing visitor screening. “Obviously this is site-specific,” Dr. Friedman said. “We’re not saying that every emergency department in America needs to have a metal detector out front, but this needs to be something that institutions take seriously, to protect both patients and the providers that work there.”
[email protected]
AT ACEP18
Anti-TNF agents preferred for severe psoriasis in pregnancy
CHICAGO – according to Kenneth B. Gordon, MD, professor and chair of dermatology at Medical College of Wisconsin in Milwaukee.
“We always had this concept that psoriasis gets better during pregnancy, that you might have 20% or 30% of patients who might have a little bit of a flare or maintain, but most keep on getting better,” Dr. Gordon told attendees at the American Academy of Dermatology summer meeting.
But the majority doesn’t mean everyone. He shared the case of one pregnant woman who came to him with severe psoriasis, covering the whole of her inner thigh, to underscore that severe cases do happen in pregnancy.
“These are real situations, and when you talk about maternal health, this woman is uncomfortable, she can’t sleep, and she’s having huge stressors that are not only going to impact her and her pregnancy but also that impact her child,” Dr. Gordon said.
Dr. Gordon clarified that he is not referring to patients with limited psoriasis or those who respond to topicals or phototherapy. But because methotrexate or acitretin are “hands-off during pregnancy,” he said, the only systemic therapy available for serious cases besides biologics is cyclosporine, which has its own risks. “We know that [cyclosporine] is associated with preterm labor and preterm birth and significant low birth weight, so even in the best scenario, when we have someone with persistent severe psoriasis in pregnancy, our best agent has a lot of downsides.”
Too few data exist on anti–interleukin (IL)-17 or anti-IL-23 therapies to draw conclusions about their use, he said, and but gastroenterology and rheumatology have a fair amount of evidence on anti–tumor necrosis factor (TNF) therapies during pregnancy because it’s usually too risky to stop treating conditions such as Crohn’s with these drugs. Still, Dr. Gordon cautioned, much of the data on biologics in pregnancy are conflicting.
The question of what medications to use, and in whom, centers on balancing risks to the fetus from the medication versus risks from the condition.
“There are impacts on the fetus of having severe psoriasis, and it varies with severity of disease,” Dr. Gordon said. For example, data suggest an increased likelihood of low birth weight in children born to mothers with severe psoriasis, and that risk may extend to preterm birth as well, although “we don’t know exactly the magnitude of that effect.”
Meanwhile, the consensus from the literature throughout dermatology, rheumatology, and gastroenterology is that anti-TNF agents do not cause birth defects or affect risk of preterm birth or low birth weight.
“The bigger question is what’s the impact on the immune system of the child,” Dr. Gordon said. Data from a small Scandinavian study suggested no increased risk of allergies, infections, or similar immunologic outcomes, but evidence remains limited.
Research has shown that infants’ exposure to anti-TNF medications persists for 3-6 months after delivery, and the American Academy of Pediatrics recommends delaying immunization in children exposed to anti-TNF agents in pregnancy. But actual evidence on immunization outcomes shows no reduced immunogenicity in such children.
“Clearly there is persistence of drug in the child, but in fact you have normal responses to immunization,” Dr. Gordon said. “The pediatricians’ argument is not based on data of what actually happens in immunization; it’s based on the fact that the drug is there.”
So what’s the bottom line?
The National Psoriasis Foundation recommends moisturizers and topical corticosteroids as first-line therapy in pregnant women with psoriasis, followed by phototherapy for second-line treatment.
But some patients will need systemic therapy during pregnancy, although it’s “best not to introduce more medications than needed in pregnancy,” Dr. Gordon said. For women with a significant flare-up or very persistent volatile disease, NPF first recommends cyclosporine, but Dr. Gordon disagrees and would go with anti-TNF agents before cyclosporine.
Data show that certolizumab is not actively transported across the placenta therefore reducing fetal exposure, so Dr. Gordon would specifically use certolizumab first, all other things being equal.
“But if the patient has been on another anti-TNF that’s been working, I don’t really have an issue with staying with it,” he added.
Existing evidence so far shows no impact in terms of genetic abnormalities, birth weight, premature birth, or even infant immunizations from anti-TNF agents. But beyond those, “there is simply not enough information on pregnancy with other forms of biologic therapy to draw conclusions.” Dr. Gordon said.
Dr. Gordon disclosed that he has received grant support and/or honoraria from Abbvie, Amgen, Almirall, and Boehringer Ingelheim.
CHICAGO – according to Kenneth B. Gordon, MD, professor and chair of dermatology at Medical College of Wisconsin in Milwaukee.
“We always had this concept that psoriasis gets better during pregnancy, that you might have 20% or 30% of patients who might have a little bit of a flare or maintain, but most keep on getting better,” Dr. Gordon told attendees at the American Academy of Dermatology summer meeting.
But the majority doesn’t mean everyone. He shared the case of one pregnant woman who came to him with severe psoriasis, covering the whole of her inner thigh, to underscore that severe cases do happen in pregnancy.
“These are real situations, and when you talk about maternal health, this woman is uncomfortable, she can’t sleep, and she’s having huge stressors that are not only going to impact her and her pregnancy but also that impact her child,” Dr. Gordon said.
Dr. Gordon clarified that he is not referring to patients with limited psoriasis or those who respond to topicals or phototherapy. But because methotrexate or acitretin are “hands-off during pregnancy,” he said, the only systemic therapy available for serious cases besides biologics is cyclosporine, which has its own risks. “We know that [cyclosporine] is associated with preterm labor and preterm birth and significant low birth weight, so even in the best scenario, when we have someone with persistent severe psoriasis in pregnancy, our best agent has a lot of downsides.”
Too few data exist on anti–interleukin (IL)-17 or anti-IL-23 therapies to draw conclusions about their use, he said, and but gastroenterology and rheumatology have a fair amount of evidence on anti–tumor necrosis factor (TNF) therapies during pregnancy because it’s usually too risky to stop treating conditions such as Crohn’s with these drugs. Still, Dr. Gordon cautioned, much of the data on biologics in pregnancy are conflicting.
The question of what medications to use, and in whom, centers on balancing risks to the fetus from the medication versus risks from the condition.
“There are impacts on the fetus of having severe psoriasis, and it varies with severity of disease,” Dr. Gordon said. For example, data suggest an increased likelihood of low birth weight in children born to mothers with severe psoriasis, and that risk may extend to preterm birth as well, although “we don’t know exactly the magnitude of that effect.”
Meanwhile, the consensus from the literature throughout dermatology, rheumatology, and gastroenterology is that anti-TNF agents do not cause birth defects or affect risk of preterm birth or low birth weight.
“The bigger question is what’s the impact on the immune system of the child,” Dr. Gordon said. Data from a small Scandinavian study suggested no increased risk of allergies, infections, or similar immunologic outcomes, but evidence remains limited.
Research has shown that infants’ exposure to anti-TNF medications persists for 3-6 months after delivery, and the American Academy of Pediatrics recommends delaying immunization in children exposed to anti-TNF agents in pregnancy. But actual evidence on immunization outcomes shows no reduced immunogenicity in such children.
“Clearly there is persistence of drug in the child, but in fact you have normal responses to immunization,” Dr. Gordon said. “The pediatricians’ argument is not based on data of what actually happens in immunization; it’s based on the fact that the drug is there.”
So what’s the bottom line?
The National Psoriasis Foundation recommends moisturizers and topical corticosteroids as first-line therapy in pregnant women with psoriasis, followed by phototherapy for second-line treatment.
But some patients will need systemic therapy during pregnancy, although it’s “best not to introduce more medications than needed in pregnancy,” Dr. Gordon said. For women with a significant flare-up or very persistent volatile disease, NPF first recommends cyclosporine, but Dr. Gordon disagrees and would go with anti-TNF agents before cyclosporine.
Data show that certolizumab is not actively transported across the placenta therefore reducing fetal exposure, so Dr. Gordon would specifically use certolizumab first, all other things being equal.
“But if the patient has been on another anti-TNF that’s been working, I don’t really have an issue with staying with it,” he added.
Existing evidence so far shows no impact in terms of genetic abnormalities, birth weight, premature birth, or even infant immunizations from anti-TNF agents. But beyond those, “there is simply not enough information on pregnancy with other forms of biologic therapy to draw conclusions.” Dr. Gordon said.
Dr. Gordon disclosed that he has received grant support and/or honoraria from Abbvie, Amgen, Almirall, and Boehringer Ingelheim.
CHICAGO – according to Kenneth B. Gordon, MD, professor and chair of dermatology at Medical College of Wisconsin in Milwaukee.
“We always had this concept that psoriasis gets better during pregnancy, that you might have 20% or 30% of patients who might have a little bit of a flare or maintain, but most keep on getting better,” Dr. Gordon told attendees at the American Academy of Dermatology summer meeting.
But the majority doesn’t mean everyone. He shared the case of one pregnant woman who came to him with severe psoriasis, covering the whole of her inner thigh, to underscore that severe cases do happen in pregnancy.
“These are real situations, and when you talk about maternal health, this woman is uncomfortable, she can’t sleep, and she’s having huge stressors that are not only going to impact her and her pregnancy but also that impact her child,” Dr. Gordon said.
Dr. Gordon clarified that he is not referring to patients with limited psoriasis or those who respond to topicals or phototherapy. But because methotrexate or acitretin are “hands-off during pregnancy,” he said, the only systemic therapy available for serious cases besides biologics is cyclosporine, which has its own risks. “We know that [cyclosporine] is associated with preterm labor and preterm birth and significant low birth weight, so even in the best scenario, when we have someone with persistent severe psoriasis in pregnancy, our best agent has a lot of downsides.”
Too few data exist on anti–interleukin (IL)-17 or anti-IL-23 therapies to draw conclusions about their use, he said, and but gastroenterology and rheumatology have a fair amount of evidence on anti–tumor necrosis factor (TNF) therapies during pregnancy because it’s usually too risky to stop treating conditions such as Crohn’s with these drugs. Still, Dr. Gordon cautioned, much of the data on biologics in pregnancy are conflicting.
The question of what medications to use, and in whom, centers on balancing risks to the fetus from the medication versus risks from the condition.
“There are impacts on the fetus of having severe psoriasis, and it varies with severity of disease,” Dr. Gordon said. For example, data suggest an increased likelihood of low birth weight in children born to mothers with severe psoriasis, and that risk may extend to preterm birth as well, although “we don’t know exactly the magnitude of that effect.”
Meanwhile, the consensus from the literature throughout dermatology, rheumatology, and gastroenterology is that anti-TNF agents do not cause birth defects or affect risk of preterm birth or low birth weight.
“The bigger question is what’s the impact on the immune system of the child,” Dr. Gordon said. Data from a small Scandinavian study suggested no increased risk of allergies, infections, or similar immunologic outcomes, but evidence remains limited.
Research has shown that infants’ exposure to anti-TNF medications persists for 3-6 months after delivery, and the American Academy of Pediatrics recommends delaying immunization in children exposed to anti-TNF agents in pregnancy. But actual evidence on immunization outcomes shows no reduced immunogenicity in such children.
“Clearly there is persistence of drug in the child, but in fact you have normal responses to immunization,” Dr. Gordon said. “The pediatricians’ argument is not based on data of what actually happens in immunization; it’s based on the fact that the drug is there.”
So what’s the bottom line?
The National Psoriasis Foundation recommends moisturizers and topical corticosteroids as first-line therapy in pregnant women with psoriasis, followed by phototherapy for second-line treatment.
But some patients will need systemic therapy during pregnancy, although it’s “best not to introduce more medications than needed in pregnancy,” Dr. Gordon said. For women with a significant flare-up or very persistent volatile disease, NPF first recommends cyclosporine, but Dr. Gordon disagrees and would go with anti-TNF agents before cyclosporine.
Data show that certolizumab is not actively transported across the placenta therefore reducing fetal exposure, so Dr. Gordon would specifically use certolizumab first, all other things being equal.
“But if the patient has been on another anti-TNF that’s been working, I don’t really have an issue with staying with it,” he added.
Existing evidence so far shows no impact in terms of genetic abnormalities, birth weight, premature birth, or even infant immunizations from anti-TNF agents. But beyond those, “there is simply not enough information on pregnancy with other forms of biologic therapy to draw conclusions.” Dr. Gordon said.
Dr. Gordon disclosed that he has received grant support and/or honoraria from Abbvie, Amgen, Almirall, and Boehringer Ingelheim.
EXPERT ANALYSIS FROM SUMMER AAD 2018
Now is the time to be heard: October is Advocacy Month!
The American College of Obstetricians and Gynecologists (ACOG) and specifically the Junior Fellow College Advisory Council (JFCAC) are rolling out steps to help you make your voice heard. Starting October 1, head to acog.org/advocacy to check out the ACOG Physician Advocacy video to get inspired. (Or watch it here!) Whether you are a seasoned advocate or just getting started, ACOG and women across the country are counting on you!
Week 1 (October 1–7): Why I advocate
The focus of this week is on delving into topics that interest you, learning why advocacy is critically important, and developing your own message to advocate for women’s health.
- View advocacy videos here to understand what advocacy is and why it is so important.
- See ACOG’s 2018 list of legislative priorities here to find topics that inspire you.
Week 2 (October 8–14): Use your voice
Explore the multitude of platforms available today for amplifying your message. Learn to use social media smartly, get advice for how to write op-eds for local outlets, add your name to support current legislative efforts, and find out who your representatives are to schedule sit-down meetings.
- For tips on communicating with elected officials, click here.
- Connect with ACOG and your district on social media, and remember to use social media responsibly to advocate effectively. See this link for more information!
- Don’t forget to include #JFadvoMonth in your posts while highlighting your advocacy work on social media!
Continued to: Week 3 (October 15–19): Empower your patients
Week 3 (October 15–21): Empower your patients
As a physician, advocating for your patient extends into the clinic itself. Access toolkits, patient websites, handouts, and resources available through ACOG.
- Familiarize yourself with the Patient Page for videos, infographics, and FAQs that are useful resources for your patients.
- Toolkits for providers are available here—use these to enhance your practice and empower your patients!
Week 4 (October 22–28): Take it forward
Advocacy happens year-round. Be sure you are actively involved in ACOG’s efforts. Participate in calls to action and remember on November 6 to GET OUT THE VOTE!
- Participate in the annual Congressional Leadership Conference (March 10–12, 2019) in Washington, DC. Descend on Washington with hundreds of fellow ObGyns to advocate to Congress on important issues. For more information, click here.
- Donate to the Ob-GynPAC, ACOG’s political action committee dedicated to electing officials who support our specialty.
- Run for office! ACOG has resources to support you. Be on the lookout for opportunities to attend candidate workshops sponsored by the Ob-GynPAC!
Get active now!
We are at a critical moment for women’s health and the future of our specialty. Key issues nationally include advocating to Congress to move forward with bills in the Senate (S 1112) and House (HR 1318) to support efforts to reduce maternal mortality. (See this article for background information on these bills.)
To find your elected officials and take action now, click here and tell Congress to help prevent maternal mortality, defend patient protections, and improve access and quality of maternity care.
You can be an advocate for your patients and your profession. Your voice matters. Now is the time to be heard.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
The American College of Obstetricians and Gynecologists (ACOG) and specifically the Junior Fellow College Advisory Council (JFCAC) are rolling out steps to help you make your voice heard. Starting October 1, head to acog.org/advocacy to check out the ACOG Physician Advocacy video to get inspired. (Or watch it here!) Whether you are a seasoned advocate or just getting started, ACOG and women across the country are counting on you!
Week 1 (October 1–7): Why I advocate
The focus of this week is on delving into topics that interest you, learning why advocacy is critically important, and developing your own message to advocate for women’s health.
- View advocacy videos here to understand what advocacy is and why it is so important.
- See ACOG’s 2018 list of legislative priorities here to find topics that inspire you.
Week 2 (October 8–14): Use your voice
Explore the multitude of platforms available today for amplifying your message. Learn to use social media smartly, get advice for how to write op-eds for local outlets, add your name to support current legislative efforts, and find out who your representatives are to schedule sit-down meetings.
- For tips on communicating with elected officials, click here.
- Connect with ACOG and your district on social media, and remember to use social media responsibly to advocate effectively. See this link for more information!
- Don’t forget to include #JFadvoMonth in your posts while highlighting your advocacy work on social media!
Continued to: Week 3 (October 15–19): Empower your patients
Week 3 (October 15–21): Empower your patients
As a physician, advocating for your patient extends into the clinic itself. Access toolkits, patient websites, handouts, and resources available through ACOG.
- Familiarize yourself with the Patient Page for videos, infographics, and FAQs that are useful resources for your patients.
- Toolkits for providers are available here—use these to enhance your practice and empower your patients!
Week 4 (October 22–28): Take it forward
Advocacy happens year-round. Be sure you are actively involved in ACOG’s efforts. Participate in calls to action and remember on November 6 to GET OUT THE VOTE!
- Participate in the annual Congressional Leadership Conference (March 10–12, 2019) in Washington, DC. Descend on Washington with hundreds of fellow ObGyns to advocate to Congress on important issues. For more information, click here.
- Donate to the Ob-GynPAC, ACOG’s political action committee dedicated to electing officials who support our specialty.
- Run for office! ACOG has resources to support you. Be on the lookout for opportunities to attend candidate workshops sponsored by the Ob-GynPAC!
Get active now!
We are at a critical moment for women’s health and the future of our specialty. Key issues nationally include advocating to Congress to move forward with bills in the Senate (S 1112) and House (HR 1318) to support efforts to reduce maternal mortality. (See this article for background information on these bills.)
To find your elected officials and take action now, click here and tell Congress to help prevent maternal mortality, defend patient protections, and improve access and quality of maternity care.
You can be an advocate for your patients and your profession. Your voice matters. Now is the time to be heard.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
The American College of Obstetricians and Gynecologists (ACOG) and specifically the Junior Fellow College Advisory Council (JFCAC) are rolling out steps to help you make your voice heard. Starting October 1, head to acog.org/advocacy to check out the ACOG Physician Advocacy video to get inspired. (Or watch it here!) Whether you are a seasoned advocate or just getting started, ACOG and women across the country are counting on you!
Week 1 (October 1–7): Why I advocate
The focus of this week is on delving into topics that interest you, learning why advocacy is critically important, and developing your own message to advocate for women’s health.
- View advocacy videos here to understand what advocacy is and why it is so important.
- See ACOG’s 2018 list of legislative priorities here to find topics that inspire you.
Week 2 (October 8–14): Use your voice
Explore the multitude of platforms available today for amplifying your message. Learn to use social media smartly, get advice for how to write op-eds for local outlets, add your name to support current legislative efforts, and find out who your representatives are to schedule sit-down meetings.
- For tips on communicating with elected officials, click here.
- Connect with ACOG and your district on social media, and remember to use social media responsibly to advocate effectively. See this link for more information!
- Don’t forget to include #JFadvoMonth in your posts while highlighting your advocacy work on social media!
Continued to: Week 3 (October 15–19): Empower your patients
Week 3 (October 15–21): Empower your patients
As a physician, advocating for your patient extends into the clinic itself. Access toolkits, patient websites, handouts, and resources available through ACOG.
- Familiarize yourself with the Patient Page for videos, infographics, and FAQs that are useful resources for your patients.
- Toolkits for providers are available here—use these to enhance your practice and empower your patients!
Week 4 (October 22–28): Take it forward
Advocacy happens year-round. Be sure you are actively involved in ACOG’s efforts. Participate in calls to action and remember on November 6 to GET OUT THE VOTE!
- Participate in the annual Congressional Leadership Conference (March 10–12, 2019) in Washington, DC. Descend on Washington with hundreds of fellow ObGyns to advocate to Congress on important issues. For more information, click here.
- Donate to the Ob-GynPAC, ACOG’s political action committee dedicated to electing officials who support our specialty.
- Run for office! ACOG has resources to support you. Be on the lookout for opportunities to attend candidate workshops sponsored by the Ob-GynPAC!
Get active now!
We are at a critical moment for women’s health and the future of our specialty. Key issues nationally include advocating to Congress to move forward with bills in the Senate (S 1112) and House (HR 1318) to support efforts to reduce maternal mortality. (See this article for background information on these bills.)
To find your elected officials and take action now, click here and tell Congress to help prevent maternal mortality, defend patient protections, and improve access and quality of maternity care.
You can be an advocate for your patients and your profession. Your voice matters. Now is the time to be heard.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.

Vaginal and bilateral thigh removal of a transobturator sling

Additional videos from SGS are available here, including these recent offerings:
- Morcellation at the time of vaginal hysterectomy
- Surgical management of non-tubal ectopic pregnancies
- Size can matter: Laparoscopic hysterectomy for the very large uterus
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Additional videos from SGS are available here, including these recent offerings:
- Morcellation at the time of vaginal hysterectomy
- Surgical management of non-tubal ectopic pregnancies
- Size can matter: Laparoscopic hysterectomy for the very large uterus
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Additional videos from SGS are available here, including these recent offerings:
- Morcellation at the time of vaginal hysterectomy
- Surgical management of non-tubal ectopic pregnancies
- Size can matter: Laparoscopic hysterectomy for the very large uterus
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
This video is brought to you by![]()

Better therapy, not earlier diagnosis, explains improved RCC survival
Credit improvements in therapy rather than diagnosis at an earlier stage for improved survival of renal cell carcinoma in recent years, investigators say.
A review of records on nearly 263,000 patients diagnosed with renal cell carcinoma (RCC ) from 2004 through 2015 showed that better 5-year overall survival (OS) in later years was likely attributable to better treatments rather than an uptick in detection of cancers at an earlier stage, a trend known as “stage migration,” reported Hiten D. Patel, MD, of the Brady Urological Institute at Johns Hopkins Medicine in Baltimore, and his colleagues.
“While survival has improved over time when considering all RCC patients, the primary benefit was observed in advanced RCC (stage III–IV), with 5-year survival increasing from 9.8% in 2004 to 13.2% in 2010 for patients with distant metastatic disease. The results indicate that stage migration no longer contributes to improvements in survival for RCC, and additional gains reflect improvements in advanced treatment options,” they wrote in European Urology Oncology.
Dr. Patel and colleagues noted that the incidence of RCC has been on the rise worldwide for nearly 3 decades because of both environmental risk factors and improvements in medical imaging that have resulted in an increase in incidental cancers.
“Data from the National Cancer Database (NCDB) indicated an increase in the proportion of patients presenting with cT1 RCC from 40% before 1993 to 60% through 2004. However, it is unknown if clinical stage migration has continued into recent years, which has implications for patient outcomes,” they wrote.
To try to answer this question, they sifted through data on 262,597 patients diagnosed with RCC from 2004 through 2015 at more than 1,500 facilities covered by the U.S. National Cancer Database.
They found that, up to 2007, there were statistically significant trends toward more frequent diagnosis of clinical stage I disease (70% of cases) and less frequent diagnoses of stage III (8%) and stage IV (11%; P less than .001 for all comparisons). From 2008 through 2015, however, the respective rates stabilized.
They also noticed a trend throughout the study period for decreased size of localized tumors at diagnosis, with a mean decrease of 0.22 cm for stage I lesions, and 1.24 cm for stage II tumors.
When they looked at 5-year overall survival by Kaplan-Meier analysis, they saw that it improved from 67.9% in 2004 to 72.3% in 2010. As noted before, most of the benefit was attributable to gains in survival among patients with stage III or IV disease.
In multivariable Cox proportional hazard models, diagnosis in recent years was a statistically significant predictor of improved survival, even after adjustment for stage distribution. In addition, receipt of systemic therapy was associated with improved survival, with a hazard ratio of 0.811 (P less than .001).
The authors acknowledged that a limitation of the findings is the reliance on the NCDB, which includes data on most cancer diagnoses in the United States, but is not a population-based sample.
No study funding source was reported. Dr. Patel and coauthors reported having no conflicts of interest to disclose.
SOURCE: Patel HD et al. Eur Urol Oncol. 2018 Sep 25. doi: 10.1016/j.euo.2018.08.023.
Credit improvements in therapy rather than diagnosis at an earlier stage for improved survival of renal cell carcinoma in recent years, investigators say.
A review of records on nearly 263,000 patients diagnosed with renal cell carcinoma (RCC ) from 2004 through 2015 showed that better 5-year overall survival (OS) in later years was likely attributable to better treatments rather than an uptick in detection of cancers at an earlier stage, a trend known as “stage migration,” reported Hiten D. Patel, MD, of the Brady Urological Institute at Johns Hopkins Medicine in Baltimore, and his colleagues.
“While survival has improved over time when considering all RCC patients, the primary benefit was observed in advanced RCC (stage III–IV), with 5-year survival increasing from 9.8% in 2004 to 13.2% in 2010 for patients with distant metastatic disease. The results indicate that stage migration no longer contributes to improvements in survival for RCC, and additional gains reflect improvements in advanced treatment options,” they wrote in European Urology Oncology.
Dr. Patel and colleagues noted that the incidence of RCC has been on the rise worldwide for nearly 3 decades because of both environmental risk factors and improvements in medical imaging that have resulted in an increase in incidental cancers.
“Data from the National Cancer Database (NCDB) indicated an increase in the proportion of patients presenting with cT1 RCC from 40% before 1993 to 60% through 2004. However, it is unknown if clinical stage migration has continued into recent years, which has implications for patient outcomes,” they wrote.
To try to answer this question, they sifted through data on 262,597 patients diagnosed with RCC from 2004 through 2015 at more than 1,500 facilities covered by the U.S. National Cancer Database.
They found that, up to 2007, there were statistically significant trends toward more frequent diagnosis of clinical stage I disease (70% of cases) and less frequent diagnoses of stage III (8%) and stage IV (11%; P less than .001 for all comparisons). From 2008 through 2015, however, the respective rates stabilized.
They also noticed a trend throughout the study period for decreased size of localized tumors at diagnosis, with a mean decrease of 0.22 cm for stage I lesions, and 1.24 cm for stage II tumors.
When they looked at 5-year overall survival by Kaplan-Meier analysis, they saw that it improved from 67.9% in 2004 to 72.3% in 2010. As noted before, most of the benefit was attributable to gains in survival among patients with stage III or IV disease.
In multivariable Cox proportional hazard models, diagnosis in recent years was a statistically significant predictor of improved survival, even after adjustment for stage distribution. In addition, receipt of systemic therapy was associated with improved survival, with a hazard ratio of 0.811 (P less than .001).
The authors acknowledged that a limitation of the findings is the reliance on the NCDB, which includes data on most cancer diagnoses in the United States, but is not a population-based sample.
No study funding source was reported. Dr. Patel and coauthors reported having no conflicts of interest to disclose.
SOURCE: Patel HD et al. Eur Urol Oncol. 2018 Sep 25. doi: 10.1016/j.euo.2018.08.023.
Credit improvements in therapy rather than diagnosis at an earlier stage for improved survival of renal cell carcinoma in recent years, investigators say.
A review of records on nearly 263,000 patients diagnosed with renal cell carcinoma (RCC ) from 2004 through 2015 showed that better 5-year overall survival (OS) in later years was likely attributable to better treatments rather than an uptick in detection of cancers at an earlier stage, a trend known as “stage migration,” reported Hiten D. Patel, MD, of the Brady Urological Institute at Johns Hopkins Medicine in Baltimore, and his colleagues.
“While survival has improved over time when considering all RCC patients, the primary benefit was observed in advanced RCC (stage III–IV), with 5-year survival increasing from 9.8% in 2004 to 13.2% in 2010 for patients with distant metastatic disease. The results indicate that stage migration no longer contributes to improvements in survival for RCC, and additional gains reflect improvements in advanced treatment options,” they wrote in European Urology Oncology.
Dr. Patel and colleagues noted that the incidence of RCC has been on the rise worldwide for nearly 3 decades because of both environmental risk factors and improvements in medical imaging that have resulted in an increase in incidental cancers.
“Data from the National Cancer Database (NCDB) indicated an increase in the proportion of patients presenting with cT1 RCC from 40% before 1993 to 60% through 2004. However, it is unknown if clinical stage migration has continued into recent years, which has implications for patient outcomes,” they wrote.
To try to answer this question, they sifted through data on 262,597 patients diagnosed with RCC from 2004 through 2015 at more than 1,500 facilities covered by the U.S. National Cancer Database.
They found that, up to 2007, there were statistically significant trends toward more frequent diagnosis of clinical stage I disease (70% of cases) and less frequent diagnoses of stage III (8%) and stage IV (11%; P less than .001 for all comparisons). From 2008 through 2015, however, the respective rates stabilized.
They also noticed a trend throughout the study period for decreased size of localized tumors at diagnosis, with a mean decrease of 0.22 cm for stage I lesions, and 1.24 cm for stage II tumors.
When they looked at 5-year overall survival by Kaplan-Meier analysis, they saw that it improved from 67.9% in 2004 to 72.3% in 2010. As noted before, most of the benefit was attributable to gains in survival among patients with stage III or IV disease.
In multivariable Cox proportional hazard models, diagnosis in recent years was a statistically significant predictor of improved survival, even after adjustment for stage distribution. In addition, receipt of systemic therapy was associated with improved survival, with a hazard ratio of 0.811 (P less than .001).
The authors acknowledged that a limitation of the findings is the reliance on the NCDB, which includes data on most cancer diagnoses in the United States, but is not a population-based sample.
No study funding source was reported. Dr. Patel and coauthors reported having no conflicts of interest to disclose.
SOURCE: Patel HD et al. Eur Urol Oncol. 2018 Sep 25. doi: 10.1016/j.euo.2018.08.023.
FROM EUROPEAN UROLOGY ONCOLOGY
Key clinical point: Improved renal cell carcinoma survival appears to be attributable to improvements in therapy rather than increased diagnosis of early-stage disease.
Major finding: 5-year survival increased from 9.8% in 2004 to 13.2% in 2010 for patients with distant metastatic disease.
Study details: Retrospective analysis of data from the National Cancer Database on 262,597 patients diagnosed with RCC from 2004 through 2015.
Disclosures: No study funding source was reported. Dr. Patel and coauthors reported having no conflicts of interest to disclose.
Source: Patel HD et al. Eur Urol Oncol. 2018 Sep 25. doi: 10.1016/j.euo.2018.08.023.
Could group CBT help survivors of Florence?
Rising waters forced hundreds of people, mainly in the Carolinas, to call for emergency rescues, and some people were forced to abandon their cars because of flooding. One man reportedly died by electrocution while trying to hook up a generator. Another man died after going out to check the status of hunting dogs, according to media reports. And in one of the most heart-wrenching tragedies, a mother and her infant were killed when a tree fell on their home.

Watching the TV reports and listening to the news of Hurricane Florence’s devastating impact on so many millions of people has been shocking. The death toll from this catastrophic weather event as of this writing stands at 39. Besides the current and future physical problems and illnesses left in Florence’s wake, the extent of property damage and loss must be overwhelming for the survivors.
I worry about the extent of the emotional toll left behind by Florence, just as Hurricane Maria did last year in Puerto Rico. The storm and its subsequent damage to the individual psyche – including the loss of identity and the fracturing of social structures and networks – almost certainly will lead to posttraumatic stress disorder, depression, and utter despair for many survivors.
While monitoring Florence’s impact, I thought about Hurricane Sandy, which upended me personally when it hit New York in 2012. As I’ve written previously, Sandy’s impact left me without power, running water, or toilet facilities. Almost 3 days of this uncertainty shook me from my comfort zone and truly affected my emotions. Before day 3, I left my home and drove (yes, I could still use my car; the roads were clear and my garage was not flooded) to my older son’s home – where I had a great support system and was able to continue to live a relatively normal life while watching the storm’s developments on TV. To this day, many areas of New York, New Jersey, and Connecticut that were hit by Sandy have not fully recovered.
Back to the human tragedy still unfolding for the survivors of Florence: I believe – and the data suggest – that early intervention and treatment of PTSD leads to better outcomes and should be addressed sooner than later. There is no specific medicinal “magic bullet” for PTSD, although some medications may help as well as treat a depressive component of the disorder and other medications may assist in improving sleep and disruptive sleep patterns. It’s been shown, time and again, that cognitive-behavioral therapy, various types of prolonged exposure therapy, and eye movement desensitization therapies work best. The most updated federal guidelines from the Department of Veterans Affairs and the Department of Defense, coauthored by Lori L. Davis, MD, of the University of Alabama at Birmingham, reinforce those treatments.
I also believe that, in situations in which masses of people are affected or potentially affected by PTSD, another first line of care that should be added is supportive, educational, interactive group therapy. In other words, it is possible that a cognitive-behavioral group therapy (CBGT) approach would reach many more people, make psychiatric intervention acceptable, and help the survivors of Florence. A recent study by researchers at the University of Massachusetts Boston that examined the role of “decentering” as part of CBGT for patients with specific anxiety disorders, for example, social anxiety disorder, might provide some hints. Decentering involves learning to observe thoughts and feelings as objective events in the mind rather than identifying with them personally. Aaron T. Beck, MD, and others hypothesized decentering as a mechanism of change in CBT.
In the UMass study, researchers recruited 81 people with a principal diagnosis of social anxiety disorder based on the Anxiety Disorders Interview Scheduled for DSM-IV. Other inclusion criteria for the study included stability on medications for 3 months or 1 month on benzodiazepines (Behav Ther. 2018 Sep;49[5]:809-12). Sixty-three of participants had 12 sessions of CBGT. The researchers found that people who received the CBGT experienced an increase in decentering. An increase in decentering, in turn, predicted improvement on most outcome measures.
Just as primary care physicians and surgeons know how to address serious physical health issues related natural and man-made disasters, psychiatrists must quickly know how to address the mental health aspects of care. Group therapy has the greatest potential to help more people and perhaps treat – and even prevent not only PTSD but many anxiety disorders as well.
Dr. London, a psychiatrist who practices in New York, developed and ran a short-term psychotherapy program for 20 years at NYU Langone Medical Center and has been writing columns for 35 years. His new book about helping people feel better fast is expected to be published in fall 2018. He has no disclosures.
Rising waters forced hundreds of people, mainly in the Carolinas, to call for emergency rescues, and some people were forced to abandon their cars because of flooding. One man reportedly died by electrocution while trying to hook up a generator. Another man died after going out to check the status of hunting dogs, according to media reports. And in one of the most heart-wrenching tragedies, a mother and her infant were killed when a tree fell on their home.
Watching the TV reports and listening to the news of Hurricane Florence’s devastating impact on so many millions of people has been shocking. The death toll from this catastrophic weather event as of this writing stands at 39. Besides the current and future physical problems and illnesses left in Florence’s wake, the extent of property damage and loss must be overwhelming for the survivors.
I worry about the extent of the emotional toll left behind by Florence, just as Hurricane Maria did last year in Puerto Rico. The storm and its subsequent damage to the individual psyche – including the loss of identity and the fracturing of social structures and networks – almost certainly will lead to posttraumatic stress disorder, depression, and utter despair for many survivors.
While monitoring Florence’s impact, I thought about Hurricane Sandy, which upended me personally when it hit New York in 2012. As I’ve written previously, Sandy’s impact left me without power, running water, or toilet facilities. Almost 3 days of this uncertainty shook me from my comfort zone and truly affected my emotions. Before day 3, I left my home and drove (yes, I could still use my car; the roads were clear and my garage was not flooded) to my older son’s home – where I had a great support system and was able to continue to live a relatively normal life while watching the storm’s developments on TV. To this day, many areas of New York, New Jersey, and Connecticut that were hit by Sandy have not fully recovered.
Back to the human tragedy still unfolding for the survivors of Florence: I believe – and the data suggest – that early intervention and treatment of PTSD leads to better outcomes and should be addressed sooner than later. There is no specific medicinal “magic bullet” for PTSD, although some medications may help as well as treat a depressive component of the disorder and other medications may assist in improving sleep and disruptive sleep patterns. It’s been shown, time and again, that cognitive-behavioral therapy, various types of prolonged exposure therapy, and eye movement desensitization therapies work best. The most updated federal guidelines from the Department of Veterans Affairs and the Department of Defense, coauthored by Lori L. Davis, MD, of the University of Alabama at Birmingham, reinforce those treatments.
I also believe that, in situations in which masses of people are affected or potentially affected by PTSD, another first line of care that should be added is supportive, educational, interactive group therapy. In other words, it is possible that a cognitive-behavioral group therapy (CBGT) approach would reach many more people, make psychiatric intervention acceptable, and help the survivors of Florence. A recent study by researchers at the University of Massachusetts Boston that examined the role of “decentering” as part of CBGT for patients with specific anxiety disorders, for example, social anxiety disorder, might provide some hints. Decentering involves learning to observe thoughts and feelings as objective events in the mind rather than identifying with them personally. Aaron T. Beck, MD, and others hypothesized decentering as a mechanism of change in CBT.
In the UMass study, researchers recruited 81 people with a principal diagnosis of social anxiety disorder based on the Anxiety Disorders Interview Scheduled for DSM-IV. Other inclusion criteria for the study included stability on medications for 3 months or 1 month on benzodiazepines (Behav Ther. 2018 Sep;49[5]:809-12). Sixty-three of participants had 12 sessions of CBGT. The researchers found that people who received the CBGT experienced an increase in decentering. An increase in decentering, in turn, predicted improvement on most outcome measures.
Just as primary care physicians and surgeons know how to address serious physical health issues related natural and man-made disasters, psychiatrists must quickly know how to address the mental health aspects of care. Group therapy has the greatest potential to help more people and perhaps treat – and even prevent not only PTSD but many anxiety disorders as well.
Dr. London, a psychiatrist who practices in New York, developed and ran a short-term psychotherapy program for 20 years at NYU Langone Medical Center and has been writing columns for 35 years. His new book about helping people feel better fast is expected to be published in fall 2018. He has no disclosures.
Rising waters forced hundreds of people, mainly in the Carolinas, to call for emergency rescues, and some people were forced to abandon their cars because of flooding. One man reportedly died by electrocution while trying to hook up a generator. Another man died after going out to check the status of hunting dogs, according to media reports. And in one of the most heart-wrenching tragedies, a mother and her infant were killed when a tree fell on their home.
Watching the TV reports and listening to the news of Hurricane Florence’s devastating impact on so many millions of people has been shocking. The death toll from this catastrophic weather event as of this writing stands at 39. Besides the current and future physical problems and illnesses left in Florence’s wake, the extent of property damage and loss must be overwhelming for the survivors.
I worry about the extent of the emotional toll left behind by Florence, just as Hurricane Maria did last year in Puerto Rico. The storm and its subsequent damage to the individual psyche – including the loss of identity and the fracturing of social structures and networks – almost certainly will lead to posttraumatic stress disorder, depression, and utter despair for many survivors.
While monitoring Florence’s impact, I thought about Hurricane Sandy, which upended me personally when it hit New York in 2012. As I’ve written previously, Sandy’s impact left me without power, running water, or toilet facilities. Almost 3 days of this uncertainty shook me from my comfort zone and truly affected my emotions. Before day 3, I left my home and drove (yes, I could still use my car; the roads were clear and my garage was not flooded) to my older son’s home – where I had a great support system and was able to continue to live a relatively normal life while watching the storm’s developments on TV. To this day, many areas of New York, New Jersey, and Connecticut that were hit by Sandy have not fully recovered.
Back to the human tragedy still unfolding for the survivors of Florence: I believe – and the data suggest – that early intervention and treatment of PTSD leads to better outcomes and should be addressed sooner than later. There is no specific medicinal “magic bullet” for PTSD, although some medications may help as well as treat a depressive component of the disorder and other medications may assist in improving sleep and disruptive sleep patterns. It’s been shown, time and again, that cognitive-behavioral therapy, various types of prolonged exposure therapy, and eye movement desensitization therapies work best. The most updated federal guidelines from the Department of Veterans Affairs and the Department of Defense, coauthored by Lori L. Davis, MD, of the University of Alabama at Birmingham, reinforce those treatments.
I also believe that, in situations in which masses of people are affected or potentially affected by PTSD, another first line of care that should be added is supportive, educational, interactive group therapy. In other words, it is possible that a cognitive-behavioral group therapy (CBGT) approach would reach many more people, make psychiatric intervention acceptable, and help the survivors of Florence. A recent study by researchers at the University of Massachusetts Boston that examined the role of “decentering” as part of CBGT for patients with specific anxiety disorders, for example, social anxiety disorder, might provide some hints. Decentering involves learning to observe thoughts and feelings as objective events in the mind rather than identifying with them personally. Aaron T. Beck, MD, and others hypothesized decentering as a mechanism of change in CBT.
In the UMass study, researchers recruited 81 people with a principal diagnosis of social anxiety disorder based on the Anxiety Disorders Interview Scheduled for DSM-IV. Other inclusion criteria for the study included stability on medications for 3 months or 1 month on benzodiazepines (Behav Ther. 2018 Sep;49[5]:809-12). Sixty-three of participants had 12 sessions of CBGT. The researchers found that people who received the CBGT experienced an increase in decentering. An increase in decentering, in turn, predicted improvement on most outcome measures.
Just as primary care physicians and surgeons know how to address serious physical health issues related natural and man-made disasters, psychiatrists must quickly know how to address the mental health aspects of care. Group therapy has the greatest potential to help more people and perhaps treat – and even prevent not only PTSD but many anxiety disorders as well.
Dr. London, a psychiatrist who practices in New York, developed and ran a short-term psychotherapy program for 20 years at NYU Langone Medical Center and has been writing columns for 35 years. His new book about helping people feel better fast is expected to be published in fall 2018. He has no disclosures.
Web-based lifestyle program aids in weight loss for NAFLD patients
A web-based intervention for management of nonalcoholic fatty liver disease – which researchers said may help reach busy or remote patients not able to attend in-person sessions – had a similar number of patients reach a target weight-loss goal of at least 10% of body weight, compared with a group-based intervention.
“The use of web education in the management of noncommunicable diseases has long been suggested, considering the huge number of cases at risk and patients’ needs,” wrote Arianna Mazzotti, MD, of the department of medical and surgical sciences, Alma Mater University, Bologna, Italy, and her colleagues. Their report was published in the Journal of Hepatology.
“The majority of cases are in an age range where job constraints make it difficult to implement a systematic face-to-face or group approach, whereas the eHealth procedures may keep the contact between patients and therapists without disrupting normal daily living.”
Dr. Mazzotti and her colleagues studied 716 patients with nonalcoholic fatty liver disease (NAFLD) at the university between January 2010 and December 2015 who attended either a web-based NAFLD intervention (278 patients) or an in-person, group-based lifestyle modification program (438 patients). Patients in the web-based intervention tended to be younger males with a higher education level, similar mean body mass index (33 kg/m2), and significantly lower blood pressure and rates of type 2 diabetes mellitus. The primary outcome included weight loss of at least 10%; secondary outcomes included changes in weight, changes in lifestyle, surrogate markers of steatosis and fibrosis, and alanine aminotransferase (ALT) within normal limits, researchers said.
The group-based program consisted of five 2-hour weekly sessions counseling patients on diet and physical activity, whereas the web-based intervention reproduced these sessions in addition to questionnaires, “highly interactive” slides, examples, and games as well as a mechanism to ask questions. Regardless of intervention, patients attended a 6-month in-person follow-up where they received treatment and reinforcement for comorbidities such as type 2 diabetes mellitus.
In the web-based intervention, 76% of patients attended the 6-month follow-up, 58% attended the 12-month follow-up, and 43% attended the 24-month follow-up, compared with 87%, 80%, and 69% of patients in the group-based intervention, respectively. Patients in the web-based intervention had a significantly decreased intake of calories after 6 months (273 kcal/day vs. 193 kcal/day; P = .006) compared with the group-based intervention. Physical activity significantly increased at 6 months for both groups, but there were no significant differences between groups.
Body weight decreased for the web-based intervention by 3.4% at 6 months, 4.9% at 12 months, and 5.5% at 24 months, compared with 3.1% at 6 months, 4.0% at 12 months, and 4.2% at 24 months in the group-based intervention. There was a nearly two-point reduction in body mass index for both groups, with 20% of web-based intervention patients and 15% of group-based intervention patients achieving the 10% weight-loss target; and, when the researchers performed a logistic regression analysis, the web-based intervention group was not associated with less short- and long-term 10% weight reduction after attrition rates and confounders were adjusted for.
At 24-month follow-up, the researchers found a decrease in ALT levels by an average of 22 ± 32 mU/mL, with the web-based intervention group having normalized ALT levels in 18% of cases at 6 months, 32% at 12 months, and 35% at 24 months, compared with 16% of cases at 6 months, 22% of cases at 12 months, and 29% of cases at 24 months in the group-based intervention. Compared with the group-based intervention, there was a higher reduction in fatty liver index scores at 12-month follow-up (71.3 vs. 78.0; P less than .001) and 24-month follow-up (68.9 vs. 76.3; P = .002) for the web-based intervention group. The researchers noted NAFLD fibrosis score and Fib-4 scores were reduced in both groups.
“The [web-based intervention] program might be extended to other units and/or general practitioners, increasing its impact in the community in prevention and treatment of progressive NAFLD,” Dr. Mazzotti and her colleagues wrote. “It might also be superimposed to drug treatment in the most severe cases, with possible additive effects.”
This study was supported by a grant from the European Community Seventh Framework Program. The authors report no relevant conflicts of interest.
*This story was updated on 10/4/2018.
SOURCE: Mazzotti A et al. J Hepatol. 2018 Oct 2. doi: 10.1016/j.jhep.2018.07.013.
A web-based intervention for management of nonalcoholic fatty liver disease – which researchers said may help reach busy or remote patients not able to attend in-person sessions – had a similar number of patients reach a target weight-loss goal of at least 10% of body weight, compared with a group-based intervention.
“The use of web education in the management of noncommunicable diseases has long been suggested, considering the huge number of cases at risk and patients’ needs,” wrote Arianna Mazzotti, MD, of the department of medical and surgical sciences, Alma Mater University, Bologna, Italy, and her colleagues. Their report was published in the Journal of Hepatology.
“The majority of cases are in an age range where job constraints make it difficult to implement a systematic face-to-face or group approach, whereas the eHealth procedures may keep the contact between patients and therapists without disrupting normal daily living.”
Dr. Mazzotti and her colleagues studied 716 patients with nonalcoholic fatty liver disease (NAFLD) at the university between January 2010 and December 2015 who attended either a web-based NAFLD intervention (278 patients) or an in-person, group-based lifestyle modification program (438 patients). Patients in the web-based intervention tended to be younger males with a higher education level, similar mean body mass index (33 kg/m2), and significantly lower blood pressure and rates of type 2 diabetes mellitus. The primary outcome included weight loss of at least 10%; secondary outcomes included changes in weight, changes in lifestyle, surrogate markers of steatosis and fibrosis, and alanine aminotransferase (ALT) within normal limits, researchers said.
The group-based program consisted of five 2-hour weekly sessions counseling patients on diet and physical activity, whereas the web-based intervention reproduced these sessions in addition to questionnaires, “highly interactive” slides, examples, and games as well as a mechanism to ask questions. Regardless of intervention, patients attended a 6-month in-person follow-up where they received treatment and reinforcement for comorbidities such as type 2 diabetes mellitus.
In the web-based intervention, 76% of patients attended the 6-month follow-up, 58% attended the 12-month follow-up, and 43% attended the 24-month follow-up, compared with 87%, 80%, and 69% of patients in the group-based intervention, respectively. Patients in the web-based intervention had a significantly decreased intake of calories after 6 months (273 kcal/day vs. 193 kcal/day; P = .006) compared with the group-based intervention. Physical activity significantly increased at 6 months for both groups, but there were no significant differences between groups.
Body weight decreased for the web-based intervention by 3.4% at 6 months, 4.9% at 12 months, and 5.5% at 24 months, compared with 3.1% at 6 months, 4.0% at 12 months, and 4.2% at 24 months in the group-based intervention. There was a nearly two-point reduction in body mass index for both groups, with 20% of web-based intervention patients and 15% of group-based intervention patients achieving the 10% weight-loss target; and, when the researchers performed a logistic regression analysis, the web-based intervention group was not associated with less short- and long-term 10% weight reduction after attrition rates and confounders were adjusted for.
At 24-month follow-up, the researchers found a decrease in ALT levels by an average of 22 ± 32 mU/mL, with the web-based intervention group having normalized ALT levels in 18% of cases at 6 months, 32% at 12 months, and 35% at 24 months, compared with 16% of cases at 6 months, 22% of cases at 12 months, and 29% of cases at 24 months in the group-based intervention. Compared with the group-based intervention, there was a higher reduction in fatty liver index scores at 12-month follow-up (71.3 vs. 78.0; P less than .001) and 24-month follow-up (68.9 vs. 76.3; P = .002) for the web-based intervention group. The researchers noted NAFLD fibrosis score and Fib-4 scores were reduced in both groups.
“The [web-based intervention] program might be extended to other units and/or general practitioners, increasing its impact in the community in prevention and treatment of progressive NAFLD,” Dr. Mazzotti and her colleagues wrote. “It might also be superimposed to drug treatment in the most severe cases, with possible additive effects.”
This study was supported by a grant from the European Community Seventh Framework Program. The authors report no relevant conflicts of interest.
*This story was updated on 10/4/2018.
SOURCE: Mazzotti A et al. J Hepatol. 2018 Oct 2. doi: 10.1016/j.jhep.2018.07.013.
A web-based intervention for management of nonalcoholic fatty liver disease – which researchers said may help reach busy or remote patients not able to attend in-person sessions – had a similar number of patients reach a target weight-loss goal of at least 10% of body weight, compared with a group-based intervention.
“The use of web education in the management of noncommunicable diseases has long been suggested, considering the huge number of cases at risk and patients’ needs,” wrote Arianna Mazzotti, MD, of the department of medical and surgical sciences, Alma Mater University, Bologna, Italy, and her colleagues. Their report was published in the Journal of Hepatology.
“The majority of cases are in an age range where job constraints make it difficult to implement a systematic face-to-face or group approach, whereas the eHealth procedures may keep the contact between patients and therapists without disrupting normal daily living.”
Dr. Mazzotti and her colleagues studied 716 patients with nonalcoholic fatty liver disease (NAFLD) at the university between January 2010 and December 2015 who attended either a web-based NAFLD intervention (278 patients) or an in-person, group-based lifestyle modification program (438 patients). Patients in the web-based intervention tended to be younger males with a higher education level, similar mean body mass index (33 kg/m2), and significantly lower blood pressure and rates of type 2 diabetes mellitus. The primary outcome included weight loss of at least 10%; secondary outcomes included changes in weight, changes in lifestyle, surrogate markers of steatosis and fibrosis, and alanine aminotransferase (ALT) within normal limits, researchers said.
The group-based program consisted of five 2-hour weekly sessions counseling patients on diet and physical activity, whereas the web-based intervention reproduced these sessions in addition to questionnaires, “highly interactive” slides, examples, and games as well as a mechanism to ask questions. Regardless of intervention, patients attended a 6-month in-person follow-up where they received treatment and reinforcement for comorbidities such as type 2 diabetes mellitus.
In the web-based intervention, 76% of patients attended the 6-month follow-up, 58% attended the 12-month follow-up, and 43% attended the 24-month follow-up, compared with 87%, 80%, and 69% of patients in the group-based intervention, respectively. Patients in the web-based intervention had a significantly decreased intake of calories after 6 months (273 kcal/day vs. 193 kcal/day; P = .006) compared with the group-based intervention. Physical activity significantly increased at 6 months for both groups, but there were no significant differences between groups.
Body weight decreased for the web-based intervention by 3.4% at 6 months, 4.9% at 12 months, and 5.5% at 24 months, compared with 3.1% at 6 months, 4.0% at 12 months, and 4.2% at 24 months in the group-based intervention. There was a nearly two-point reduction in body mass index for both groups, with 20% of web-based intervention patients and 15% of group-based intervention patients achieving the 10% weight-loss target; and, when the researchers performed a logistic regression analysis, the web-based intervention group was not associated with less short- and long-term 10% weight reduction after attrition rates and confounders were adjusted for.
At 24-month follow-up, the researchers found a decrease in ALT levels by an average of 22 ± 32 mU/mL, with the web-based intervention group having normalized ALT levels in 18% of cases at 6 months, 32% at 12 months, and 35% at 24 months, compared with 16% of cases at 6 months, 22% of cases at 12 months, and 29% of cases at 24 months in the group-based intervention. Compared with the group-based intervention, there was a higher reduction in fatty liver index scores at 12-month follow-up (71.3 vs. 78.0; P less than .001) and 24-month follow-up (68.9 vs. 76.3; P = .002) for the web-based intervention group. The researchers noted NAFLD fibrosis score and Fib-4 scores were reduced in both groups.
“The [web-based intervention] program might be extended to other units and/or general practitioners, increasing its impact in the community in prevention and treatment of progressive NAFLD,” Dr. Mazzotti and her colleagues wrote. “It might also be superimposed to drug treatment in the most severe cases, with possible additive effects.”
This study was supported by a grant from the European Community Seventh Framework Program. The authors report no relevant conflicts of interest.
*This story was updated on 10/4/2018.
SOURCE: Mazzotti A et al. J Hepatol. 2018 Oct 2. doi: 10.1016/j.jhep.2018.07.013.
FROM THE JOURNAL OF HEPATOLOGY
Key clinical point: A web-based lifestyle modification intervention was similarly effective as a group intervention in reducing weight for patients with nonalcoholic fatty liver disease.
Major finding: In the web-based intervention, body weight decreased by 3.4% at 6 months, 4.9% at 12 months, and 5.5% at 24 months, compared with 3.1% at 6 months, 4.0% at 12 months, and 4.2% at 24 months in the group-based intervention. A similar number of patients in both groups achieved the 10% weight-loss target.
Study details: An observational study of 716 patients participating in web-based or group nonalcoholic fatty liver disease interventions at the University of Bologna between January 2010 and December 2015.
Disclosures: The European Community Seventh Framework Program supported the study. The authors report no conflicts of interest.
Source: Mazzotti A et al. J Hepatol. 2018 Oct 2. doi: 10.1016/j.jhep.2018.07.013.