User login
Diabetes Programs Aren’t Reaching Their Targets
The CDC’s lifestyle change program (LCP), part of the National Diabetes Prevention Program, teaches people with prediabetes practical, real-life changes. Those changes can be enough to reduce the risk of type 2 diabetes by as much as 58%—or even 71% for people aged > 60 years. But are enough people getting the opportunity to participate?
CDC researchers assessed the availability of in-person LCP classes by diabetes incidence and socioeconomic status at the county level. They mapped 1,558 LCP class locations. They found classes in 711 (23%) US counties as of March 2017 (there may be more now, the researchers say).
But the classes were not necessarily located where they could do the most good, the researchers found. Only 17% of the counties with the highest diabetes incidence and 10% of counties with the most socioeconomic disadvantage had a publicly available class location. By contrast, 26.8% of counties in the lowest tertile of incidence had class locations.
The researchers say policy makers, program planners, and others engaged in expanding the availability of the classes can use the information to prioritize locations, especially for underrepresented populations.
The CDC’s lifestyle change program (LCP), part of the National Diabetes Prevention Program, teaches people with prediabetes practical, real-life changes. Those changes can be enough to reduce the risk of type 2 diabetes by as much as 58%—or even 71% for people aged > 60 years. But are enough people getting the opportunity to participate?
CDC researchers assessed the availability of in-person LCP classes by diabetes incidence and socioeconomic status at the county level. They mapped 1,558 LCP class locations. They found classes in 711 (23%) US counties as of March 2017 (there may be more now, the researchers say).
But the classes were not necessarily located where they could do the most good, the researchers found. Only 17% of the counties with the highest diabetes incidence and 10% of counties with the most socioeconomic disadvantage had a publicly available class location. By contrast, 26.8% of counties in the lowest tertile of incidence had class locations.
The researchers say policy makers, program planners, and others engaged in expanding the availability of the classes can use the information to prioritize locations, especially for underrepresented populations.
The CDC’s lifestyle change program (LCP), part of the National Diabetes Prevention Program, teaches people with prediabetes practical, real-life changes. Those changes can be enough to reduce the risk of type 2 diabetes by as much as 58%—or even 71% for people aged > 60 years. But are enough people getting the opportunity to participate?
CDC researchers assessed the availability of in-person LCP classes by diabetes incidence and socioeconomic status at the county level. They mapped 1,558 LCP class locations. They found classes in 711 (23%) US counties as of March 2017 (there may be more now, the researchers say).
But the classes were not necessarily located where they could do the most good, the researchers found. Only 17% of the counties with the highest diabetes incidence and 10% of counties with the most socioeconomic disadvantage had a publicly available class location. By contrast, 26.8% of counties in the lowest tertile of incidence had class locations.
The researchers say policy makers, program planners, and others engaged in expanding the availability of the classes can use the information to prioritize locations, especially for underrepresented populations.
MDM2 inhibitors could treat resistant AML

Preclinical research has revealed a potential treatment for chemotherapy-resistant acute myeloid leukemia (AML).
Researchers characterized a mechanism of chemotherapy resistance in AML and found that MDM2 is a key player in this dysregulated signaling pathway.
They tested MDM2 inhibitors and found these drugs could sensitize resistant AML to chemotherapy in vitro and in vivo.
In fact, mice with refractory AML responded to standard induction therapy when combined with an MDM2 inhibitor, showing no signs of disease and prolonged survival.
These results were published in Cancer Discovery.
“We were blown away when we saw the results,” said study author William Stanford, PhD, of Ottawa Hospital Research Institute in Ontario, Canada.
“If these findings hold up in clinical trials, we could have a new treatment for people who would almost certainly die of their disease today.”
Mechanism of resistance
Dr. Stanford’s research began with the protein MTF2. He and his colleagues previously found that MTF2 plays a role in erythropoiesis, and the team wanted to determine if MTF2 also plays a role in AML.
Using AML samples from patients treated at The Ottawa Hospital, the researchers found the mean survival was three times longer in patients with normal MTF2 activity than in patients with low MTF2 activity.
“Initially, we thought that MTF2 could be an important biomarker to identify patients who might benefit from experimental therapies,” Dr. Stanford said. “But then we started thinking that if we could understand what MTF2 was doing, maybe we could use this information to develop a new treatment.”
Dr. Stanford and his colleagues discovered that MTF2 represses MDM2, a protein that helps cells resist chemotherapy.
The team found that MTF2-deficient cells overexpress MDM2, which inhibits p53, and this leads to defects in cell-cycle regulation and apoptosis that enable resistance to chemotherapy.
Testing MDM2 inhibitors
Since MDM2 inhibitors are already being tested in clinical trials for other cancers, Dr. Stanford and his colleagues tested these inhibitors in vitro and in mouse models of chemotherapy-resistant AML.
The in vitro experiments included two MDM2 inhibitors—Nutlin3A and MI-773—combined with daunorubicin or cytarabine.
The researchers found that refractory, MTF2-deficient AML cells underwent apoptosis when treated with either daunorubicin or cytarabine in combination with Nutlin3A or MI-773. The effect was comparable to that observed in AML cells with normal MTF2.
The team found that Nutlin3A was more efficient at sensitizing refractory, MTF2-deficient AML cells to daunorubicin, so they used Nutlin3A in the in vivo experiments.
For these experiments, the researchers tested Nutlin3A in mice injected with either chemotherapy-responsive AML cells (with normal MTF2) or refractory, MTF2-deficient AML cells.
Once the mice had “a substantial leukemic burden” (≥ 20% CD45+CD33+ leukemic blasts in their peripheral blood), they were randomized to receive vehicle control, Nutlin3A, standard induction therapy, or induction plus Nutlin3A.
The mice engrafted with chemotherapy-responsive AML cells did not respond to vehicle control or Nutlin3A alone. However, they did respond to standard induction and induction plus Nutlin3A, surviving until the end of the experiment at 16 weeks.
Among the mice engrafted with refractory, MTF2-deficient AML cells, only those animals treated with induction plus Nutlin3A survived until the end of the experiment.
The researchers also noted a “dramatic loss” in the blast-containing CD45+CD33+ and CD34+CD38− populations in mice treated with induction plus Nutlin3A.
To assess residual disease, the researchers performed secondary transplants with cells from mice that had engrafted with refractory, MTF2-deficient AML cells but responded to induction plus Nutlin3A.
The recipient mice had no evidence of AML at 16 weeks after transplant when the experiment ended.
Dr. Stanford and his colleagues are now trying to obtain pharmaceutical-grade MDM2 inhibitors to conduct trials in AML patients at The Ottawa Hospital.
The researchers are also screening libraries of approved drugs to see if any of these can block MDM2, and they are working with a biotech company to develop a test to identify chemotherapy-resistant AML patients who would respond to MDM2 inhibitors.
The current research was supported by grants from the Canadian Cancer Society Research Institute, Canadian Institutes of Health Research, Cancer Research Society, National Institutes of Health, and a Tier 1 Canada Research Chair in Integrative Stem Cell Biology. One study author reported a relationship with Epicypher, Inc. No other conflicts of interest were reported.
Preclinical research has revealed a potential treatment for chemotherapy-resistant acute myeloid leukemia (AML).
Researchers characterized a mechanism of chemotherapy resistance in AML and found that MDM2 is a key player in this dysregulated signaling pathway.
They tested MDM2 inhibitors and found these drugs could sensitize resistant AML to chemotherapy in vitro and in vivo.
In fact, mice with refractory AML responded to standard induction therapy when combined with an MDM2 inhibitor, showing no signs of disease and prolonged survival.
These results were published in Cancer Discovery.
“We were blown away when we saw the results,” said study author William Stanford, PhD, of Ottawa Hospital Research Institute in Ontario, Canada.
“If these findings hold up in clinical trials, we could have a new treatment for people who would almost certainly die of their disease today.”
Mechanism of resistance
Dr. Stanford’s research began with the protein MTF2. He and his colleagues previously found that MTF2 plays a role in erythropoiesis, and the team wanted to determine if MTF2 also plays a role in AML.
Using AML samples from patients treated at The Ottawa Hospital, the researchers found the mean survival was three times longer in patients with normal MTF2 activity than in patients with low MTF2 activity.
“Initially, we thought that MTF2 could be an important biomarker to identify patients who might benefit from experimental therapies,” Dr. Stanford said. “But then we started thinking that if we could understand what MTF2 was doing, maybe we could use this information to develop a new treatment.”
Dr. Stanford and his colleagues discovered that MTF2 represses MDM2, a protein that helps cells resist chemotherapy.
The team found that MTF2-deficient cells overexpress MDM2, which inhibits p53, and this leads to defects in cell-cycle regulation and apoptosis that enable resistance to chemotherapy.
Testing MDM2 inhibitors
Since MDM2 inhibitors are already being tested in clinical trials for other cancers, Dr. Stanford and his colleagues tested these inhibitors in vitro and in mouse models of chemotherapy-resistant AML.
The in vitro experiments included two MDM2 inhibitors—Nutlin3A and MI-773—combined with daunorubicin or cytarabine.
The researchers found that refractory, MTF2-deficient AML cells underwent apoptosis when treated with either daunorubicin or cytarabine in combination with Nutlin3A or MI-773. The effect was comparable to that observed in AML cells with normal MTF2.
The team found that Nutlin3A was more efficient at sensitizing refractory, MTF2-deficient AML cells to daunorubicin, so they used Nutlin3A in the in vivo experiments.
For these experiments, the researchers tested Nutlin3A in mice injected with either chemotherapy-responsive AML cells (with normal MTF2) or refractory, MTF2-deficient AML cells.
Once the mice had “a substantial leukemic burden” (≥ 20% CD45+CD33+ leukemic blasts in their peripheral blood), they were randomized to receive vehicle control, Nutlin3A, standard induction therapy, or induction plus Nutlin3A.
The mice engrafted with chemotherapy-responsive AML cells did not respond to vehicle control or Nutlin3A alone. However, they did respond to standard induction and induction plus Nutlin3A, surviving until the end of the experiment at 16 weeks.
Among the mice engrafted with refractory, MTF2-deficient AML cells, only those animals treated with induction plus Nutlin3A survived until the end of the experiment.
The researchers also noted a “dramatic loss” in the blast-containing CD45+CD33+ and CD34+CD38− populations in mice treated with induction plus Nutlin3A.
To assess residual disease, the researchers performed secondary transplants with cells from mice that had engrafted with refractory, MTF2-deficient AML cells but responded to induction plus Nutlin3A.
The recipient mice had no evidence of AML at 16 weeks after transplant when the experiment ended.
Dr. Stanford and his colleagues are now trying to obtain pharmaceutical-grade MDM2 inhibitors to conduct trials in AML patients at The Ottawa Hospital.
The researchers are also screening libraries of approved drugs to see if any of these can block MDM2, and they are working with a biotech company to develop a test to identify chemotherapy-resistant AML patients who would respond to MDM2 inhibitors.
The current research was supported by grants from the Canadian Cancer Society Research Institute, Canadian Institutes of Health Research, Cancer Research Society, National Institutes of Health, and a Tier 1 Canada Research Chair in Integrative Stem Cell Biology. One study author reported a relationship with Epicypher, Inc. No other conflicts of interest were reported.
Preclinical research has revealed a potential treatment for chemotherapy-resistant acute myeloid leukemia (AML).
Researchers characterized a mechanism of chemotherapy resistance in AML and found that MDM2 is a key player in this dysregulated signaling pathway.
They tested MDM2 inhibitors and found these drugs could sensitize resistant AML to chemotherapy in vitro and in vivo.
In fact, mice with refractory AML responded to standard induction therapy when combined with an MDM2 inhibitor, showing no signs of disease and prolonged survival.
These results were published in Cancer Discovery.
“We were blown away when we saw the results,” said study author William Stanford, PhD, of Ottawa Hospital Research Institute in Ontario, Canada.
“If these findings hold up in clinical trials, we could have a new treatment for people who would almost certainly die of their disease today.”
Mechanism of resistance
Dr. Stanford’s research began with the protein MTF2. He and his colleagues previously found that MTF2 plays a role in erythropoiesis, and the team wanted to determine if MTF2 also plays a role in AML.
Using AML samples from patients treated at The Ottawa Hospital, the researchers found the mean survival was three times longer in patients with normal MTF2 activity than in patients with low MTF2 activity.
“Initially, we thought that MTF2 could be an important biomarker to identify patients who might benefit from experimental therapies,” Dr. Stanford said. “But then we started thinking that if we could understand what MTF2 was doing, maybe we could use this information to develop a new treatment.”
Dr. Stanford and his colleagues discovered that MTF2 represses MDM2, a protein that helps cells resist chemotherapy.
The team found that MTF2-deficient cells overexpress MDM2, which inhibits p53, and this leads to defects in cell-cycle regulation and apoptosis that enable resistance to chemotherapy.
Testing MDM2 inhibitors
Since MDM2 inhibitors are already being tested in clinical trials for other cancers, Dr. Stanford and his colleagues tested these inhibitors in vitro and in mouse models of chemotherapy-resistant AML.
The in vitro experiments included two MDM2 inhibitors—Nutlin3A and MI-773—combined with daunorubicin or cytarabine.
The researchers found that refractory, MTF2-deficient AML cells underwent apoptosis when treated with either daunorubicin or cytarabine in combination with Nutlin3A or MI-773. The effect was comparable to that observed in AML cells with normal MTF2.
The team found that Nutlin3A was more efficient at sensitizing refractory, MTF2-deficient AML cells to daunorubicin, so they used Nutlin3A in the in vivo experiments.
For these experiments, the researchers tested Nutlin3A in mice injected with either chemotherapy-responsive AML cells (with normal MTF2) or refractory, MTF2-deficient AML cells.
Once the mice had “a substantial leukemic burden” (≥ 20% CD45+CD33+ leukemic blasts in their peripheral blood), they were randomized to receive vehicle control, Nutlin3A, standard induction therapy, or induction plus Nutlin3A.
The mice engrafted with chemotherapy-responsive AML cells did not respond to vehicle control or Nutlin3A alone. However, they did respond to standard induction and induction plus Nutlin3A, surviving until the end of the experiment at 16 weeks.
Among the mice engrafted with refractory, MTF2-deficient AML cells, only those animals treated with induction plus Nutlin3A survived until the end of the experiment.
The researchers also noted a “dramatic loss” in the blast-containing CD45+CD33+ and CD34+CD38− populations in mice treated with induction plus Nutlin3A.
To assess residual disease, the researchers performed secondary transplants with cells from mice that had engrafted with refractory, MTF2-deficient AML cells but responded to induction plus Nutlin3A.
The recipient mice had no evidence of AML at 16 weeks after transplant when the experiment ended.
Dr. Stanford and his colleagues are now trying to obtain pharmaceutical-grade MDM2 inhibitors to conduct trials in AML patients at The Ottawa Hospital.
The researchers are also screening libraries of approved drugs to see if any of these can block MDM2, and they are working with a biotech company to develop a test to identify chemotherapy-resistant AML patients who would respond to MDM2 inhibitors.
The current research was supported by grants from the Canadian Cancer Society Research Institute, Canadian Institutes of Health Research, Cancer Research Society, National Institutes of Health, and a Tier 1 Canada Research Chair in Integrative Stem Cell Biology. One study author reported a relationship with Epicypher, Inc. No other conflicts of interest were reported.
SNPs linked to bleeding in African Americans on warfarin

Researchers say they have identified single-nucleotide polymorphisms (SNPs) that are associated with increased bleeding risk in African-American patients on warfarin.
A retrospective study revealed four SNPs associated with increased bleeding risk in African Americans with an international normalized ratio (INR) of less than 4.
One of these SNPs was seen in more than a third of bleeding cases and less than 5% of controls.
These preliminary findings could have implications for patients of African descent, but independent validation of the study results are needed, according to Minoli A. Perera, PharmD, PhD, of Northwestern University in Chicago, and her coauthors.
The researchers reported their findings in JAMA.
The report covered findings in a discovery cohort of African-American patients from a genome-wide study conducted at the University of Chicago and a replication cohort of patients who self-identified as African American and had routinely received care at University of Chicago hospitals.
The discovery cohort included 31 patients with major bleeding that occurred at an INR less than 4 and 184 controls with no documented history of bleeding related to warfarin.
In that cohort, Dr. Perera and her colleagues found four SNPs in linkage disequilibrium on chromosome 6 associated with warfarin-related bleeding:
- rs115112393
- rs16871327
- rs78132896
- rs114504854.
In particular, rs78132896 was found in 35.5% of cases (11/31) and 4.9% of controls (9/184), with an odds ratio of 8.31 (95% confidence interval [CI], 3.2-21.5).
The replication cohort, including 40 cases and 148 warfarin-treated controls, was genotyped specifically for rs78132896. The SNP was similarly found in 35.0% of cases (14/40) and 4.8% of controls (7/148), with an odds ratio of 8.24 (95% CI, 3.1-25.3).
“Genome-wide significance of this cohort was achieved when the cohorts were combined via meta-analysis,” the researchers wrote. They reported an odds ratio of 8.27 for that analysis (95% CI, 4.18-16.38).
Further analysis showed that, compared with wild-type alleles, the rs16871327 and rs78132896 risk alleles increased EPHA7 gene transcription.
Expression of the EPHA7 gene on vascular endothelial cells and peripheral lymphocytes is increased during inflammation, according to Dr. Perera and her coauthors. Increased EPHA7 expression might lead to bleeding in patients who are taking warfarin.
“This haplotype might also have potential implications for bleeding risk with direct oral anticoagulants,” the researchers wrote.
Dr. Perera and her coauthors reported no conflicts of interest related to their work on this study, which was funded by grants from the National Heart, Lung, and Blood Institute; the National Institute of General Medicine; the National Institutes of Health; and the American Heart Association Midwest Affiliate; as well as a research award from the University of Illinois at Chicago College of Pharmacy.
Researchers say they have identified single-nucleotide polymorphisms (SNPs) that are associated with increased bleeding risk in African-American patients on warfarin.
A retrospective study revealed four SNPs associated with increased bleeding risk in African Americans with an international normalized ratio (INR) of less than 4.
One of these SNPs was seen in more than a third of bleeding cases and less than 5% of controls.
These preliminary findings could have implications for patients of African descent, but independent validation of the study results are needed, according to Minoli A. Perera, PharmD, PhD, of Northwestern University in Chicago, and her coauthors.
The researchers reported their findings in JAMA.
The report covered findings in a discovery cohort of African-American patients from a genome-wide study conducted at the University of Chicago and a replication cohort of patients who self-identified as African American and had routinely received care at University of Chicago hospitals.
The discovery cohort included 31 patients with major bleeding that occurred at an INR less than 4 and 184 controls with no documented history of bleeding related to warfarin.
In that cohort, Dr. Perera and her colleagues found four SNPs in linkage disequilibrium on chromosome 6 associated with warfarin-related bleeding:
- rs115112393
- rs16871327
- rs78132896
- rs114504854.
In particular, rs78132896 was found in 35.5% of cases (11/31) and 4.9% of controls (9/184), with an odds ratio of 8.31 (95% confidence interval [CI], 3.2-21.5).
The replication cohort, including 40 cases and 148 warfarin-treated controls, was genotyped specifically for rs78132896. The SNP was similarly found in 35.0% of cases (14/40) and 4.8% of controls (7/148), with an odds ratio of 8.24 (95% CI, 3.1-25.3).
“Genome-wide significance of this cohort was achieved when the cohorts were combined via meta-analysis,” the researchers wrote. They reported an odds ratio of 8.27 for that analysis (95% CI, 4.18-16.38).
Further analysis showed that, compared with wild-type alleles, the rs16871327 and rs78132896 risk alleles increased EPHA7 gene transcription.
Expression of the EPHA7 gene on vascular endothelial cells and peripheral lymphocytes is increased during inflammation, according to Dr. Perera and her coauthors. Increased EPHA7 expression might lead to bleeding in patients who are taking warfarin.
“This haplotype might also have potential implications for bleeding risk with direct oral anticoagulants,” the researchers wrote.
Dr. Perera and her coauthors reported no conflicts of interest related to their work on this study, which was funded by grants from the National Heart, Lung, and Blood Institute; the National Institute of General Medicine; the National Institutes of Health; and the American Heart Association Midwest Affiliate; as well as a research award from the University of Illinois at Chicago College of Pharmacy.
Researchers say they have identified single-nucleotide polymorphisms (SNPs) that are associated with increased bleeding risk in African-American patients on warfarin.
A retrospective study revealed four SNPs associated with increased bleeding risk in African Americans with an international normalized ratio (INR) of less than 4.
One of these SNPs was seen in more than a third of bleeding cases and less than 5% of controls.
These preliminary findings could have implications for patients of African descent, but independent validation of the study results are needed, according to Minoli A. Perera, PharmD, PhD, of Northwestern University in Chicago, and her coauthors.
The researchers reported their findings in JAMA.
The report covered findings in a discovery cohort of African-American patients from a genome-wide study conducted at the University of Chicago and a replication cohort of patients who self-identified as African American and had routinely received care at University of Chicago hospitals.
The discovery cohort included 31 patients with major bleeding that occurred at an INR less than 4 and 184 controls with no documented history of bleeding related to warfarin.
In that cohort, Dr. Perera and her colleagues found four SNPs in linkage disequilibrium on chromosome 6 associated with warfarin-related bleeding:
- rs115112393
- rs16871327
- rs78132896
- rs114504854.
In particular, rs78132896 was found in 35.5% of cases (11/31) and 4.9% of controls (9/184), with an odds ratio of 8.31 (95% confidence interval [CI], 3.2-21.5).
The replication cohort, including 40 cases and 148 warfarin-treated controls, was genotyped specifically for rs78132896. The SNP was similarly found in 35.0% of cases (14/40) and 4.8% of controls (7/148), with an odds ratio of 8.24 (95% CI, 3.1-25.3).
“Genome-wide significance of this cohort was achieved when the cohorts were combined via meta-analysis,” the researchers wrote. They reported an odds ratio of 8.27 for that analysis (95% CI, 4.18-16.38).
Further analysis showed that, compared with wild-type alleles, the rs16871327 and rs78132896 risk alleles increased EPHA7 gene transcription.
Expression of the EPHA7 gene on vascular endothelial cells and peripheral lymphocytes is increased during inflammation, according to Dr. Perera and her coauthors. Increased EPHA7 expression might lead to bleeding in patients who are taking warfarin.
“This haplotype might also have potential implications for bleeding risk with direct oral anticoagulants,” the researchers wrote.
Dr. Perera and her coauthors reported no conflicts of interest related to their work on this study, which was funded by grants from the National Heart, Lung, and Blood Institute; the National Institute of General Medicine; the National Institutes of Health; and the American Heart Association Midwest Affiliate; as well as a research award from the University of Illinois at Chicago College of Pharmacy.
Engineered MSCs could treat GVHD
LAUSANNE, SWITZERLAND—A mesenchymal stem cell (MSC) product could treat acute graft-versus-host disease (GVHD), according to preclinical research.
The product, apceth-201, improved symptoms of GVHD and prolonged survival in two mouse models.
Researchers described results with apceth-201 in a poster presentation at the Annual Congress of the European Society of Gene and Cell Therapy.
Most of the researchers involved in this study work for apceth Biopharma, the company developing apceth-201.
Apceth-201 consists of allogeneic human MSCs that have been genetically modified to express alpha-1 antitrypsin, a protease inhibitor exerting anti-inflammatory and tissue-protective functions.
In vitro assays showed that apceth-201 suppresses T-cell proliferation, polarizes macrophages to an anti-inflammatory M2 type, converts dendritic cells to a tolerogenic phenotype, and increases induction of regulatory T cells.
Apeceth-201 also demonstrated activity in vivo.
In a humanized GVHD model, treatment with apceth-201 improved bone marrow cellularity and reduced levels of inflammatory markers.
Additionally, mice treated with apceth-201 had double the median survival of mice treated with native MSCs.
Researchers also tested the effects of apceth-201 against GVHD in a model of haploidentical hematopoietic stem cell transplant.
All control mice succumbed to GVHD within 22 days, but more than half of mice treated with apceth-201 survived until the end of the experiment, which was 100 days.
All of the survivors had complete resolution of GVHD symptoms.
The researchers also said apceth-201 was safe. It did not impair T-cell-dependent antibody responses, and host resistance was similar in treated mice and controls.
“We are very excited with these results that clearly show the transformative therapeutic potential of apceth-201 in an immune-mediated disease with high unmet medical need and few treatment options,” said Christine Guenther, CEO of apceth Biopharma.
“Based on these promising and impressive data, we are currently preparing to initiate a phase 1/2 clinical study assessing the safety and efficacy of apceth-201 in adult steroid-refractory GVHD patients.”
LAUSANNE, SWITZERLAND—A mesenchymal stem cell (MSC) product could treat acute graft-versus-host disease (GVHD), according to preclinical research.
The product, apceth-201, improved symptoms of GVHD and prolonged survival in two mouse models.
Researchers described results with apceth-201 in a poster presentation at the Annual Congress of the European Society of Gene and Cell Therapy.
Most of the researchers involved in this study work for apceth Biopharma, the company developing apceth-201.
Apceth-201 consists of allogeneic human MSCs that have been genetically modified to express alpha-1 antitrypsin, a protease inhibitor exerting anti-inflammatory and tissue-protective functions.
In vitro assays showed that apceth-201 suppresses T-cell proliferation, polarizes macrophages to an anti-inflammatory M2 type, converts dendritic cells to a tolerogenic phenotype, and increases induction of regulatory T cells.
Apeceth-201 also demonstrated activity in vivo.
In a humanized GVHD model, treatment with apceth-201 improved bone marrow cellularity and reduced levels of inflammatory markers.
Additionally, mice treated with apceth-201 had double the median survival of mice treated with native MSCs.
Researchers also tested the effects of apceth-201 against GVHD in a model of haploidentical hematopoietic stem cell transplant.
All control mice succumbed to GVHD within 22 days, but more than half of mice treated with apceth-201 survived until the end of the experiment, which was 100 days.
All of the survivors had complete resolution of GVHD symptoms.
The researchers also said apceth-201 was safe. It did not impair T-cell-dependent antibody responses, and host resistance was similar in treated mice and controls.
“We are very excited with these results that clearly show the transformative therapeutic potential of apceth-201 in an immune-mediated disease with high unmet medical need and few treatment options,” said Christine Guenther, CEO of apceth Biopharma.
“Based on these promising and impressive data, we are currently preparing to initiate a phase 1/2 clinical study assessing the safety and efficacy of apceth-201 in adult steroid-refractory GVHD patients.”
LAUSANNE, SWITZERLAND—A mesenchymal stem cell (MSC) product could treat acute graft-versus-host disease (GVHD), according to preclinical research.
The product, apceth-201, improved symptoms of GVHD and prolonged survival in two mouse models.
Researchers described results with apceth-201 in a poster presentation at the Annual Congress of the European Society of Gene and Cell Therapy.
Most of the researchers involved in this study work for apceth Biopharma, the company developing apceth-201.
Apceth-201 consists of allogeneic human MSCs that have been genetically modified to express alpha-1 antitrypsin, a protease inhibitor exerting anti-inflammatory and tissue-protective functions.
In vitro assays showed that apceth-201 suppresses T-cell proliferation, polarizes macrophages to an anti-inflammatory M2 type, converts dendritic cells to a tolerogenic phenotype, and increases induction of regulatory T cells.
Apeceth-201 also demonstrated activity in vivo.
In a humanized GVHD model, treatment with apceth-201 improved bone marrow cellularity and reduced levels of inflammatory markers.
Additionally, mice treated with apceth-201 had double the median survival of mice treated with native MSCs.
Researchers also tested the effects of apceth-201 against GVHD in a model of haploidentical hematopoietic stem cell transplant.
All control mice succumbed to GVHD within 22 days, but more than half of mice treated with apceth-201 survived until the end of the experiment, which was 100 days.
All of the survivors had complete resolution of GVHD symptoms.
The researchers also said apceth-201 was safe. It did not impair T-cell-dependent antibody responses, and host resistance was similar in treated mice and controls.
“We are very excited with these results that clearly show the transformative therapeutic potential of apceth-201 in an immune-mediated disease with high unmet medical need and few treatment options,” said Christine Guenther, CEO of apceth Biopharma.
“Based on these promising and impressive data, we are currently preparing to initiate a phase 1/2 clinical study assessing the safety and efficacy of apceth-201 in adult steroid-refractory GVHD patients.”
New Registry Offers Insight Into Opsoclonus-Myoclonus Syndrome
WASHINGTON – a rare disease affecting only 1 in 5,000,000 individuals, mostly aged 1-5 years, based on data from a new patient registry.
In partnership with the National Organization of Rare Disorders (NORD) the nonprofit OMSLife Foundation has created a patient registry to better understand the disease experience in patients, wrote Mike Michaelis, chairman of OMSLife, and his colleagues. Early data from 275 enrolled patients were presented in a poster at the NORD Rare Summit, held by the National Organization for Rare Disorders.
The registry patients were mainly born in the United States (86%) and white (74%); approximately half were female. Of 150 patients who indicated symptoms at onset, 87% reported ataxia. Additional symptoms at onset were myoclonus (61%), opsoclonus (59%), tremors (46%), sleep disturbances (45%), temper tantrums (38%), vomiting (27%), fever (13%), headache (9%) and other symptoms (13%).
The researchers reviewed associations of symptoms at onset to determine the frequency of other symptoms for each individual symptom. Ataxia was present with 89% or higher instances of the other reported symptoms. Of note, some symptoms occurred more frequently than expected, such as temper tantrums and tremors in approximately 70% of patients with sleep disturbances. Myoclonus and opsoclonus, as well as fever and vomiting, also were significantly associated with the presence of other symptoms.
Two-thirds of the registry patients (69%) were diagnosed within 3 months of symptom onset, and 83% of these were diagnosed by a neurologist. Based on the Mitchell-Pike OMS severity scale, 59% of the patients met criteria for severe disease, 34% were classified as moderate, and 7% were mild. The registry is ongoing, but the current data provide insight on the clinical picture and common symptoms of OMS, the researchers said.
OMS Life was established in 2012 to support patients, caregivers, and researchers in raising awareness of opsoclonus-myoclonus syndrome as well as funds for research.
The study was supported by the OMSLife Foundation, NORD, and Trio Health Analytics. The researchers are employed by these organizations.
WASHINGTON – a rare disease affecting only 1 in 5,000,000 individuals, mostly aged 1-5 years, based on data from a new patient registry.
In partnership with the National Organization of Rare Disorders (NORD) the nonprofit OMSLife Foundation has created a patient registry to better understand the disease experience in patients, wrote Mike Michaelis, chairman of OMSLife, and his colleagues. Early data from 275 enrolled patients were presented in a poster at the NORD Rare Summit, held by the National Organization for Rare Disorders.
The registry patients were mainly born in the United States (86%) and white (74%); approximately half were female. Of 150 patients who indicated symptoms at onset, 87% reported ataxia. Additional symptoms at onset were myoclonus (61%), opsoclonus (59%), tremors (46%), sleep disturbances (45%), temper tantrums (38%), vomiting (27%), fever (13%), headache (9%) and other symptoms (13%).
The researchers reviewed associations of symptoms at onset to determine the frequency of other symptoms for each individual symptom. Ataxia was present with 89% or higher instances of the other reported symptoms. Of note, some symptoms occurred more frequently than expected, such as temper tantrums and tremors in approximately 70% of patients with sleep disturbances. Myoclonus and opsoclonus, as well as fever and vomiting, also were significantly associated with the presence of other symptoms.
Two-thirds of the registry patients (69%) were diagnosed within 3 months of symptom onset, and 83% of these were diagnosed by a neurologist. Based on the Mitchell-Pike OMS severity scale, 59% of the patients met criteria for severe disease, 34% were classified as moderate, and 7% were mild. The registry is ongoing, but the current data provide insight on the clinical picture and common symptoms of OMS, the researchers said.
OMS Life was established in 2012 to support patients, caregivers, and researchers in raising awareness of opsoclonus-myoclonus syndrome as well as funds for research.
The study was supported by the OMSLife Foundation, NORD, and Trio Health Analytics. The researchers are employed by these organizations.
WASHINGTON – a rare disease affecting only 1 in 5,000,000 individuals, mostly aged 1-5 years, based on data from a new patient registry.
In partnership with the National Organization of Rare Disorders (NORD) the nonprofit OMSLife Foundation has created a patient registry to better understand the disease experience in patients, wrote Mike Michaelis, chairman of OMSLife, and his colleagues. Early data from 275 enrolled patients were presented in a poster at the NORD Rare Summit, held by the National Organization for Rare Disorders.
The registry patients were mainly born in the United States (86%) and white (74%); approximately half were female. Of 150 patients who indicated symptoms at onset, 87% reported ataxia. Additional symptoms at onset were myoclonus (61%), opsoclonus (59%), tremors (46%), sleep disturbances (45%), temper tantrums (38%), vomiting (27%), fever (13%), headache (9%) and other symptoms (13%).
The researchers reviewed associations of symptoms at onset to determine the frequency of other symptoms for each individual symptom. Ataxia was present with 89% or higher instances of the other reported symptoms. Of note, some symptoms occurred more frequently than expected, such as temper tantrums and tremors in approximately 70% of patients with sleep disturbances. Myoclonus and opsoclonus, as well as fever and vomiting, also were significantly associated with the presence of other symptoms.
Two-thirds of the registry patients (69%) were diagnosed within 3 months of symptom onset, and 83% of these were diagnosed by a neurologist. Based on the Mitchell-Pike OMS severity scale, 59% of the patients met criteria for severe disease, 34% were classified as moderate, and 7% were mild. The registry is ongoing, but the current data provide insight on the clinical picture and common symptoms of OMS, the researchers said.
OMS Life was established in 2012 to support patients, caregivers, and researchers in raising awareness of opsoclonus-myoclonus syndrome as well as funds for research.
The study was supported by the OMSLife Foundation, NORD, and Trio Health Analytics. The researchers are employed by these organizations.
REPORTING FROM NORD SUMMIT 2018
Key clinical point: Most patients with OMS experienced multiple symptoms at disease onset; ataxia was the most common.
Major finding: Approximately 87% of patients with OMS reported ataxia at disease onset and 59% experienced severe disease.
Study details: The data come from a registry including 275 OMS patients.
Disclosures: The study was supported by the OMSLife Foundation, NORD, and Trio Health Analytics. The researchers are employed by these organizations.
Physician Commentary: Neurology Community Responds to Diclofenac Cardiovascular Risks
In July 2018, The BMJ published a study examining the cardiovascular risks of diclofenac initiation compared with initiation of other traditional non-steroidal anti-inflammatory drugs, initiation of paracetamol, and no initiation. The results showed a 50% increase in adverse events among diclofenac initiators compared with non-initiators (as well as a 20% increase over paracetamol/ibuprofen initiators, and 30% increase over naproxen initiators). (Read the full study here). Here, I asked several of my colleagues to weigh in on the results of this study and its implications for our practices, and then I share my own thoughts on these findings:

Stewart J. Tepper, MD, FAHS
Professor of Neurology
Geisel School of Medicine at Dartmouth
There have been previous studies and meta-analyses demonstrating the cardiovascular risks of diclofenac. This very large cohort study highlights the magnitude of effects for both those patients at high risk and at low risk for cardiovascular disease. Diclofenac has many advantages for migraine treatment, such as a rapid onset of action in its liquid form, but it has higher risks for major cardiac events than most currently available nonsteroidal anti-inflammatory drugs (NSAIDs). As providers, we must be judicious in diclofenac use and informative with our patients.

Marcelo Bigal, MD, PhD
Chief Medical Officer, Purdue Pharma
It is well established that NSAIDs are associated with increased risk of poor cardiovascular outcomes. This study offers powerful evidence that the risk after frequent diclofenac use is disproportionally increased relative to other commonly used NSAIDs, such as ibuprofen or naproxen. It is relevant to discuss the implications of the findings for the treatment of migraine.
The acute treatment of migraine associated with attack-related disability should favor triptans as first line therapy, not NSAIDs. Because triptans are vasoconstrictive medications, unmet needs exist in patients at cardiovascular risk. Anti-CGRP acute migraine therapies, as well as “ditans” (5HT-1f antagonist) are under regulatory review and may address the needs of these patients. In the context of acute migraine therapy, diclofenac and NSAIDs are typically used instead of triptans, or with triptans when additional efficacy is needed. We certainly find that the use of diclofenac in these situations should be judicious, and reserved to those who clearly need it, have infrequent migraine attacks, and are otherwise healthy.
Diclofenac is also often used in the emergency department in many countries as a rescue therapy. In a series of clinical trials where we tested most commonly used drugs in this setting in Brazil, we found that efficacies were 83.6% for intravenous dipyrone, 66.7% for intramuscular diclofenac and 81.8% for intravenous chlorpromazine. We continue to believe that diclofenac is an important, non-sedative and non-opioid option for the management of headaches in the emergency department, assuming that at discharge, patients would receive proper guidance on the management of migraine without relying on frequent use of NSAIDs.
Jack Schim, MD
Co-Director, The Headache Center of Southern California
This article supports findings of prior epidemiologic studies correlating exposure to NSAIDs with increased cerebrovascular and cardiovascular risk. Prior studies have shown a dose-related response in risk associated with NSAID therapy, supporting a causal association. However, while relative risk is significantly higher in individuals with NSAID exposure, the absolute risk remains very low. The greater risk from NSAIDs continues to be to the kidneys, and to the stomach.
As with all therapies, we need to weigh the advantages and disadvantages of NSAID therapy with our headache patients. All medications carry their own risks. For acute treatment of migraines, our primary tool, triptans, are contraindicated in a significant subset of individuals, including patients with ischemic coronary artery as well as those with history of stroke or transient ischemic attack (TIA). The alternatives, NSAIDs, dopamine blocking agents, have utility and risks.
Diclofenac powder to be dissolved in water is an effective abortive for migraine for many individuals. In general, our patients have intermittent exposure, preferably not more than 2 days per week. For the appropriate individual, NSAIDS, including diclofenac, remain an important tool in the acute care armamentarium.

Rob Cowan, MD, FAAN, FAHS
Higgins Professor of Neurology and Neurosciences
Chief, Division of Headache Medicine, Dept. of Neurology and Neurosciences
Director, Stanford University School of Medicine
These kinds of large, population-based studies must be interpreted with caution. While they may emulate the protocol of prospective studies, they lack proper inclusion/exclusion criteria, particularly with respect to indication. It may be reasonable to assume that the population of diclofenac users is "sicker" than the general population and the population that is using cheaper, more accessible NSAIDs or paracetamol. Without knowing the access and economic issues in Denmark, it is difficult to weigh these variables in the study. Thus, while it is certainly an important issue to explore (the relative risks and benefits of a given medication within a class), the absence of a well-designed, prospective study precludes any definitive conclusion regarding relative safety and risk profile for Diclofenac.
+++
These are great comments by my colleagues. My impression after seeing the data and reading my colleague’s comments, is that diclofenac may be riskier than other NSAIDs in this study; but when used properly in generally healthy migraineurs, it is probably more effective than dangerous when evaluating the risk/benefit ratio. When diclofenac is used as an oral solution (Cambia), 2 days per week or less, in a patient without serious gastrointestinal, renal, cardiac or hypertensive issues, it appears to pose little risk to the patient. When given to the wrong patient, or when taken too frequently, is could be dangerous. What I really like about this preparation is that it causes fewer adverse events compared to triptans and works very quickly. It can be used when triptans have been used enough that week or if they tend to cause significant adverse events when taken. We can use diclofenac for our headache patients, but we should remain vigilant to give it cautiously and only to patients who have no contraindication to its use.
Please write to us at Neurology Reviews Migraine Resource Center ([email protected]) with your opinions.
Alan M. Rapoport, M.D.
Editor-in-Chief
Migraine Resource Center
Clinical Professor of Neurology
The David Geffen School of Medicine at UCLA
Los Angeles, California
In July 2018, The BMJ published a study examining the cardiovascular risks of diclofenac initiation compared with initiation of other traditional non-steroidal anti-inflammatory drugs, initiation of paracetamol, and no initiation. The results showed a 50% increase in adverse events among diclofenac initiators compared with non-initiators (as well as a 20% increase over paracetamol/ibuprofen initiators, and 30% increase over naproxen initiators). (Read the full study here). Here, I asked several of my colleagues to weigh in on the results of this study and its implications for our practices, and then I share my own thoughts on these findings:
Stewart J. Tepper, MD, FAHS
Professor of Neurology
Geisel School of Medicine at Dartmouth
There have been previous studies and meta-analyses demonstrating the cardiovascular risks of diclofenac. This very large cohort study highlights the magnitude of effects for both those patients at high risk and at low risk for cardiovascular disease. Diclofenac has many advantages for migraine treatment, such as a rapid onset of action in its liquid form, but it has higher risks for major cardiac events than most currently available nonsteroidal anti-inflammatory drugs (NSAIDs). As providers, we must be judicious in diclofenac use and informative with our patients.
Marcelo Bigal, MD, PhD
Chief Medical Officer, Purdue Pharma
It is well established that NSAIDs are associated with increased risk of poor cardiovascular outcomes. This study offers powerful evidence that the risk after frequent diclofenac use is disproportionally increased relative to other commonly used NSAIDs, such as ibuprofen or naproxen. It is relevant to discuss the implications of the findings for the treatment of migraine.
The acute treatment of migraine associated with attack-related disability should favor triptans as first line therapy, not NSAIDs. Because triptans are vasoconstrictive medications, unmet needs exist in patients at cardiovascular risk. Anti-CGRP acute migraine therapies, as well as “ditans” (5HT-1f antagonist) are under regulatory review and may address the needs of these patients. In the context of acute migraine therapy, diclofenac and NSAIDs are typically used instead of triptans, or with triptans when additional efficacy is needed. We certainly find that the use of diclofenac in these situations should be judicious, and reserved to those who clearly need it, have infrequent migraine attacks, and are otherwise healthy.
Diclofenac is also often used in the emergency department in many countries as a rescue therapy. In a series of clinical trials where we tested most commonly used drugs in this setting in Brazil, we found that efficacies were 83.6% for intravenous dipyrone, 66.7% for intramuscular diclofenac and 81.8% for intravenous chlorpromazine. We continue to believe that diclofenac is an important, non-sedative and non-opioid option for the management of headaches in the emergency department, assuming that at discharge, patients would receive proper guidance on the management of migraine without relying on frequent use of NSAIDs.
Jack Schim, MD
Co-Director, The Headache Center of Southern California
This article supports findings of prior epidemiologic studies correlating exposure to NSAIDs with increased cerebrovascular and cardiovascular risk. Prior studies have shown a dose-related response in risk associated with NSAID therapy, supporting a causal association. However, while relative risk is significantly higher in individuals with NSAID exposure, the absolute risk remains very low. The greater risk from NSAIDs continues to be to the kidneys, and to the stomach.
As with all therapies, we need to weigh the advantages and disadvantages of NSAID therapy with our headache patients. All medications carry their own risks. For acute treatment of migraines, our primary tool, triptans, are contraindicated in a significant subset of individuals, including patients with ischemic coronary artery as well as those with history of stroke or transient ischemic attack (TIA). The alternatives, NSAIDs, dopamine blocking agents, have utility and risks.
Diclofenac powder to be dissolved in water is an effective abortive for migraine for many individuals. In general, our patients have intermittent exposure, preferably not more than 2 days per week. For the appropriate individual, NSAIDS, including diclofenac, remain an important tool in the acute care armamentarium.
Rob Cowan, MD, FAAN, FAHS
Higgins Professor of Neurology and Neurosciences
Chief, Division of Headache Medicine, Dept. of Neurology and Neurosciences
Director, Stanford University School of Medicine
These kinds of large, population-based studies must be interpreted with caution. While they may emulate the protocol of prospective studies, they lack proper inclusion/exclusion criteria, particularly with respect to indication. It may be reasonable to assume that the population of diclofenac users is "sicker" than the general population and the population that is using cheaper, more accessible NSAIDs or paracetamol. Without knowing the access and economic issues in Denmark, it is difficult to weigh these variables in the study. Thus, while it is certainly an important issue to explore (the relative risks and benefits of a given medication within a class), the absence of a well-designed, prospective study precludes any definitive conclusion regarding relative safety and risk profile for Diclofenac.
+++
These are great comments by my colleagues. My impression after seeing the data and reading my colleague’s comments, is that diclofenac may be riskier than other NSAIDs in this study; but when used properly in generally healthy migraineurs, it is probably more effective than dangerous when evaluating the risk/benefit ratio. When diclofenac is used as an oral solution (Cambia), 2 days per week or less, in a patient without serious gastrointestinal, renal, cardiac or hypertensive issues, it appears to pose little risk to the patient. When given to the wrong patient, or when taken too frequently, is could be dangerous. What I really like about this preparation is that it causes fewer adverse events compared to triptans and works very quickly. It can be used when triptans have been used enough that week or if they tend to cause significant adverse events when taken. We can use diclofenac for our headache patients, but we should remain vigilant to give it cautiously and only to patients who have no contraindication to its use.
Please write to us at Neurology Reviews Migraine Resource Center ([email protected]) with your opinions.
Alan M. Rapoport, M.D.
Editor-in-Chief
Migraine Resource Center
Clinical Professor of Neurology
The David Geffen School of Medicine at UCLA
Los Angeles, California
In July 2018, The BMJ published a study examining the cardiovascular risks of diclofenac initiation compared with initiation of other traditional non-steroidal anti-inflammatory drugs, initiation of paracetamol, and no initiation. The results showed a 50% increase in adverse events among diclofenac initiators compared with non-initiators (as well as a 20% increase over paracetamol/ibuprofen initiators, and 30% increase over naproxen initiators). (Read the full study here). Here, I asked several of my colleagues to weigh in on the results of this study and its implications for our practices, and then I share my own thoughts on these findings:
Stewart J. Tepper, MD, FAHS
Professor of Neurology
Geisel School of Medicine at Dartmouth
There have been previous studies and meta-analyses demonstrating the cardiovascular risks of diclofenac. This very large cohort study highlights the magnitude of effects for both those patients at high risk and at low risk for cardiovascular disease. Diclofenac has many advantages for migraine treatment, such as a rapid onset of action in its liquid form, but it has higher risks for major cardiac events than most currently available nonsteroidal anti-inflammatory drugs (NSAIDs). As providers, we must be judicious in diclofenac use and informative with our patients.
Marcelo Bigal, MD, PhD
Chief Medical Officer, Purdue Pharma
It is well established that NSAIDs are associated with increased risk of poor cardiovascular outcomes. This study offers powerful evidence that the risk after frequent diclofenac use is disproportionally increased relative to other commonly used NSAIDs, such as ibuprofen or naproxen. It is relevant to discuss the implications of the findings for the treatment of migraine.
The acute treatment of migraine associated with attack-related disability should favor triptans as first line therapy, not NSAIDs. Because triptans are vasoconstrictive medications, unmet needs exist in patients at cardiovascular risk. Anti-CGRP acute migraine therapies, as well as “ditans” (5HT-1f antagonist) are under regulatory review and may address the needs of these patients. In the context of acute migraine therapy, diclofenac and NSAIDs are typically used instead of triptans, or with triptans when additional efficacy is needed. We certainly find that the use of diclofenac in these situations should be judicious, and reserved to those who clearly need it, have infrequent migraine attacks, and are otherwise healthy.
Diclofenac is also often used in the emergency department in many countries as a rescue therapy. In a series of clinical trials where we tested most commonly used drugs in this setting in Brazil, we found that efficacies were 83.6% for intravenous dipyrone, 66.7% for intramuscular diclofenac and 81.8% for intravenous chlorpromazine. We continue to believe that diclofenac is an important, non-sedative and non-opioid option for the management of headaches in the emergency department, assuming that at discharge, patients would receive proper guidance on the management of migraine without relying on frequent use of NSAIDs.
Jack Schim, MD
Co-Director, The Headache Center of Southern California
This article supports findings of prior epidemiologic studies correlating exposure to NSAIDs with increased cerebrovascular and cardiovascular risk. Prior studies have shown a dose-related response in risk associated with NSAID therapy, supporting a causal association. However, while relative risk is significantly higher in individuals with NSAID exposure, the absolute risk remains very low. The greater risk from NSAIDs continues to be to the kidneys, and to the stomach.
As with all therapies, we need to weigh the advantages and disadvantages of NSAID therapy with our headache patients. All medications carry their own risks. For acute treatment of migraines, our primary tool, triptans, are contraindicated in a significant subset of individuals, including patients with ischemic coronary artery as well as those with history of stroke or transient ischemic attack (TIA). The alternatives, NSAIDs, dopamine blocking agents, have utility and risks.
Diclofenac powder to be dissolved in water is an effective abortive for migraine for many individuals. In general, our patients have intermittent exposure, preferably not more than 2 days per week. For the appropriate individual, NSAIDS, including diclofenac, remain an important tool in the acute care armamentarium.
Rob Cowan, MD, FAAN, FAHS
Higgins Professor of Neurology and Neurosciences
Chief, Division of Headache Medicine, Dept. of Neurology and Neurosciences
Director, Stanford University School of Medicine
These kinds of large, population-based studies must be interpreted with caution. While they may emulate the protocol of prospective studies, they lack proper inclusion/exclusion criteria, particularly with respect to indication. It may be reasonable to assume that the population of diclofenac users is "sicker" than the general population and the population that is using cheaper, more accessible NSAIDs or paracetamol. Without knowing the access and economic issues in Denmark, it is difficult to weigh these variables in the study. Thus, while it is certainly an important issue to explore (the relative risks and benefits of a given medication within a class), the absence of a well-designed, prospective study precludes any definitive conclusion regarding relative safety and risk profile for Diclofenac.
+++
These are great comments by my colleagues. My impression after seeing the data and reading my colleague’s comments, is that diclofenac may be riskier than other NSAIDs in this study; but when used properly in generally healthy migraineurs, it is probably more effective than dangerous when evaluating the risk/benefit ratio. When diclofenac is used as an oral solution (Cambia), 2 days per week or less, in a patient without serious gastrointestinal, renal, cardiac or hypertensive issues, it appears to pose little risk to the patient. When given to the wrong patient, or when taken too frequently, is could be dangerous. What I really like about this preparation is that it causes fewer adverse events compared to triptans and works very quickly. It can be used when triptans have been used enough that week or if they tend to cause significant adverse events when taken. We can use diclofenac for our headache patients, but we should remain vigilant to give it cautiously and only to patients who have no contraindication to its use.
Please write to us at Neurology Reviews Migraine Resource Center ([email protected]) with your opinions.
Alan M. Rapoport, M.D.
Editor-in-Chief
Migraine Resource Center
Clinical Professor of Neurology
The David Geffen School of Medicine at UCLA
Los Angeles, California
Breast cancer in men comparable with women, gonadal therapy debated
MUNICH – Men with metastatic breast cancer (MBC) have a similar prognosis, compared with women, but gonadal suppression remains a topic of debate, according to recent trials and conference proceedings.
Male breast cancer is a rare, little-studied disease that was highlighted at the annual meeting of the European Society for Medical Oncology.
“This is a truly magnificent effort made by these authors,” said invited discussant Carolien Schroeder, MD, PhD, of the University Medical Center Groningen in the Netherlands, noting the challenges inherent to studies of niche cancer populations.
Previous studies have shown that men with MBC are usually hormone receptor positive (HR+) and older than women with MBC. Male patients also tend to present with more severe disease.
“[Male breast cancer patients] usually present with higher stages of disease; larger tumors, more nodal involvement, and more metastatic disease,” Dr. Schroeder said. “And 4%-16% may have genetic predisposition, usually due to a BRCA2 mutation.”
One retrospective study used data from the Epidemiological Strategy and Medical Economics Metastatic Breast Cancer (ESME MBC) platform to further knowledge of male patient characteristics, treatment types, and disease outcomes. ESME is a national database that stores patient information from 18 cancer centers in France.
“We have reported on one of the biggest series of men with metastatic disease, with comprehensive data on their management and outcome with different types of treatment,” said principal investigator Jean-Sébastien Frénel, MD, of the Institut de Cancérologie de l’Ouest in Nantes, France, in an interview.
The ESME study evaluated 16,701 patients with MBC: 16,552 women (99.11%) and 149 men (0.89%). Patients received at least one treatment between January 2008 and December 2014.
On average, male patients were older than females (mean: 68.1 years vs. 60.6 years), which lines up with existing data; in contrast, 78.4% of men were HR+, which is slightly lower than the widely described figure of 90%. Almost half of the HR+/human epidermal growth factor 2– (HER2–) male patients were given a frontline hormonal therapy (43%); of those, 44% received tamoxifen, 40% received an aromatase inhibitor (with or without a gonadotropin-releasing hormone analog [GnRH]), and 16% received other therapies. Outcomes were relatively similar between men and women: median progression-free survival (PFS) was 9.8 months for men, compared with 13.0 months for women. About one-quarter of HR+/HER2– men (27.6%) received frontline chemotherapy, resulting in a PFS of 6.9 months compared with 6.3 months for matched women. Overall survival was also slightly longer for men than matched women (41.8 months vs 34.9 months). In general, these statistics show that men and women received similar treatments and had similar outcomes.
“Most of the patients receiving hormonal therapy were treated with tamoxifen and the remainder received aromatase inhibitors,” Dr. Frénel said. “But few patients received aromatase inhibitors plus [GnRH] analogs despite some guidelines recommending that they should be given in combination.”
GnRH for men remains a topic of debate. Although aromatase inhibitors should be given with GnRH to avoid a negative feedback loop, gonadal suppression causes erectile dysfunction, thereby decreasing well-being. This dilemma is made worse by a lack of data on hormonal therapy for men with breast cancer.
To address this shortcoming, a prospective, randomized trial compared three different hormonal regimens for men. Male-GBG54 involved 55 men with breast cancer. For 6 months, patients received 1 of 3 treatment regimens: tamoxifen (20 mg/day), tamoxifen + GnRH (subcutaneous every 3 months), or exemestane (25 mg daily) + GnRH. Median estradiol levels were measured at 3 months and 6 months, and wellbeing was measured using questionnaires.
As expected, the results showed increased estradiol levels in the tamoxifen group and decreased levels in the GnRH group. Men were generally dissatisfied with GnRH therapy because of the erectile dysfunction it caused.
“Tamoxifen monotherapy should be kept as standard hormonal therapy for men with breast cancer. The side effects are moderate, hardly impairing sexual behavior. The combination with GnRH influenced patients’ well-being and erectile function profoundly,” lead author Mattea Reinisch, MD, of Klinikum Essen-Mitte (Germany), said in an interview.
Dr. Schroeder agreed that tamoxifen should remain the standard treatment but suggested that the benefits of gonadal suppression may outweigh the downsides. “We need efficacy data for gonadal suppression,” she said. “After all, we are advising our premenopausal breast cancer patients to undergo the gonadal suppression therapy on a daily basis because of the oncological superiority, despite the toxicity they are also experiencing.”
Dr. Schroeder again called for efficacy data and described shortcomings of Male-GBG54: “[Dr. Reinisch and her colleagues] have chosen a biological surrogate endpoint, but what we’d really like, of course, [are] the efficacy data. The quality of life data are not breast-cancer specific, and these are only data for 6 months, whereas, particularly in the metastatic setting, the compliance issue after 6 months is also relevant.”
Reflecting on the data from ESME and Male-GBG54, Dr. Schroeder said, “I think this field is maturing, and intervention trials have proven themselves to be possible in this niche population.”
Looking to the future, Dr. Schroeder suggested that male breast cancer can be studied either in separate trials from women (focusing on sex-specific targets), or in shared studies, as many disease characteristics are the same regardless of sex. She also said that worse disease in men is likely due to delayed presentation rather than biological differences between men and women.
“This leaves room for improvement,” Dr. Schroeder said. “We still need to work on the awareness of this disease.”
Discussant Dr. Schroeder disclosed financial relationships with Novartis, Roche, Genentech, and others. Male-GBG54 was funded by Claudia von Schilling Foundation.
SOURCES: Sirieix J et al. ESMO 2018, Abstract 294PD; Reinisch et al. ESMO 2018, Abstract 273PD.
MUNICH – Men with metastatic breast cancer (MBC) have a similar prognosis, compared with women, but gonadal suppression remains a topic of debate, according to recent trials and conference proceedings.
Male breast cancer is a rare, little-studied disease that was highlighted at the annual meeting of the European Society for Medical Oncology.
“This is a truly magnificent effort made by these authors,” said invited discussant Carolien Schroeder, MD, PhD, of the University Medical Center Groningen in the Netherlands, noting the challenges inherent to studies of niche cancer populations.
Previous studies have shown that men with MBC are usually hormone receptor positive (HR+) and older than women with MBC. Male patients also tend to present with more severe disease.
“[Male breast cancer patients] usually present with higher stages of disease; larger tumors, more nodal involvement, and more metastatic disease,” Dr. Schroeder said. “And 4%-16% may have genetic predisposition, usually due to a BRCA2 mutation.”
One retrospective study used data from the Epidemiological Strategy and Medical Economics Metastatic Breast Cancer (ESME MBC) platform to further knowledge of male patient characteristics, treatment types, and disease outcomes. ESME is a national database that stores patient information from 18 cancer centers in France.
“We have reported on one of the biggest series of men with metastatic disease, with comprehensive data on their management and outcome with different types of treatment,” said principal investigator Jean-Sébastien Frénel, MD, of the Institut de Cancérologie de l’Ouest in Nantes, France, in an interview.
The ESME study evaluated 16,701 patients with MBC: 16,552 women (99.11%) and 149 men (0.89%). Patients received at least one treatment between January 2008 and December 2014.
On average, male patients were older than females (mean: 68.1 years vs. 60.6 years), which lines up with existing data; in contrast, 78.4% of men were HR+, which is slightly lower than the widely described figure of 90%. Almost half of the HR+/human epidermal growth factor 2– (HER2–) male patients were given a frontline hormonal therapy (43%); of those, 44% received tamoxifen, 40% received an aromatase inhibitor (with or without a gonadotropin-releasing hormone analog [GnRH]), and 16% received other therapies. Outcomes were relatively similar between men and women: median progression-free survival (PFS) was 9.8 months for men, compared with 13.0 months for women. About one-quarter of HR+/HER2– men (27.6%) received frontline chemotherapy, resulting in a PFS of 6.9 months compared with 6.3 months for matched women. Overall survival was also slightly longer for men than matched women (41.8 months vs 34.9 months). In general, these statistics show that men and women received similar treatments and had similar outcomes.
“Most of the patients receiving hormonal therapy were treated with tamoxifen and the remainder received aromatase inhibitors,” Dr. Frénel said. “But few patients received aromatase inhibitors plus [GnRH] analogs despite some guidelines recommending that they should be given in combination.”
GnRH for men remains a topic of debate. Although aromatase inhibitors should be given with GnRH to avoid a negative feedback loop, gonadal suppression causes erectile dysfunction, thereby decreasing well-being. This dilemma is made worse by a lack of data on hormonal therapy for men with breast cancer.
To address this shortcoming, a prospective, randomized trial compared three different hormonal regimens for men. Male-GBG54 involved 55 men with breast cancer. For 6 months, patients received 1 of 3 treatment regimens: tamoxifen (20 mg/day), tamoxifen + GnRH (subcutaneous every 3 months), or exemestane (25 mg daily) + GnRH. Median estradiol levels were measured at 3 months and 6 months, and wellbeing was measured using questionnaires.
As expected, the results showed increased estradiol levels in the tamoxifen group and decreased levels in the GnRH group. Men were generally dissatisfied with GnRH therapy because of the erectile dysfunction it caused.
“Tamoxifen monotherapy should be kept as standard hormonal therapy for men with breast cancer. The side effects are moderate, hardly impairing sexual behavior. The combination with GnRH influenced patients’ well-being and erectile function profoundly,” lead author Mattea Reinisch, MD, of Klinikum Essen-Mitte (Germany), said in an interview.
Dr. Schroeder agreed that tamoxifen should remain the standard treatment but suggested that the benefits of gonadal suppression may outweigh the downsides. “We need efficacy data for gonadal suppression,” she said. “After all, we are advising our premenopausal breast cancer patients to undergo the gonadal suppression therapy on a daily basis because of the oncological superiority, despite the toxicity they are also experiencing.”
Dr. Schroeder again called for efficacy data and described shortcomings of Male-GBG54: “[Dr. Reinisch and her colleagues] have chosen a biological surrogate endpoint, but what we’d really like, of course, [are] the efficacy data. The quality of life data are not breast-cancer specific, and these are only data for 6 months, whereas, particularly in the metastatic setting, the compliance issue after 6 months is also relevant.”
Reflecting on the data from ESME and Male-GBG54, Dr. Schroeder said, “I think this field is maturing, and intervention trials have proven themselves to be possible in this niche population.”
Looking to the future, Dr. Schroeder suggested that male breast cancer can be studied either in separate trials from women (focusing on sex-specific targets), or in shared studies, as many disease characteristics are the same regardless of sex. She also said that worse disease in men is likely due to delayed presentation rather than biological differences between men and women.
“This leaves room for improvement,” Dr. Schroeder said. “We still need to work on the awareness of this disease.”
Discussant Dr. Schroeder disclosed financial relationships with Novartis, Roche, Genentech, and others. Male-GBG54 was funded by Claudia von Schilling Foundation.
SOURCES: Sirieix J et al. ESMO 2018, Abstract 294PD; Reinisch et al. ESMO 2018, Abstract 273PD.
MUNICH – Men with metastatic breast cancer (MBC) have a similar prognosis, compared with women, but gonadal suppression remains a topic of debate, according to recent trials and conference proceedings.
Male breast cancer is a rare, little-studied disease that was highlighted at the annual meeting of the European Society for Medical Oncology.
“This is a truly magnificent effort made by these authors,” said invited discussant Carolien Schroeder, MD, PhD, of the University Medical Center Groningen in the Netherlands, noting the challenges inherent to studies of niche cancer populations.
Previous studies have shown that men with MBC are usually hormone receptor positive (HR+) and older than women with MBC. Male patients also tend to present with more severe disease.
“[Male breast cancer patients] usually present with higher stages of disease; larger tumors, more nodal involvement, and more metastatic disease,” Dr. Schroeder said. “And 4%-16% may have genetic predisposition, usually due to a BRCA2 mutation.”
One retrospective study used data from the Epidemiological Strategy and Medical Economics Metastatic Breast Cancer (ESME MBC) platform to further knowledge of male patient characteristics, treatment types, and disease outcomes. ESME is a national database that stores patient information from 18 cancer centers in France.
“We have reported on one of the biggest series of men with metastatic disease, with comprehensive data on their management and outcome with different types of treatment,” said principal investigator Jean-Sébastien Frénel, MD, of the Institut de Cancérologie de l’Ouest in Nantes, France, in an interview.
The ESME study evaluated 16,701 patients with MBC: 16,552 women (99.11%) and 149 men (0.89%). Patients received at least one treatment between January 2008 and December 2014.
On average, male patients were older than females (mean: 68.1 years vs. 60.6 years), which lines up with existing data; in contrast, 78.4% of men were HR+, which is slightly lower than the widely described figure of 90%. Almost half of the HR+/human epidermal growth factor 2– (HER2–) male patients were given a frontline hormonal therapy (43%); of those, 44% received tamoxifen, 40% received an aromatase inhibitor (with or without a gonadotropin-releasing hormone analog [GnRH]), and 16% received other therapies. Outcomes were relatively similar between men and women: median progression-free survival (PFS) was 9.8 months for men, compared with 13.0 months for women. About one-quarter of HR+/HER2– men (27.6%) received frontline chemotherapy, resulting in a PFS of 6.9 months compared with 6.3 months for matched women. Overall survival was also slightly longer for men than matched women (41.8 months vs 34.9 months). In general, these statistics show that men and women received similar treatments and had similar outcomes.
“Most of the patients receiving hormonal therapy were treated with tamoxifen and the remainder received aromatase inhibitors,” Dr. Frénel said. “But few patients received aromatase inhibitors plus [GnRH] analogs despite some guidelines recommending that they should be given in combination.”
GnRH for men remains a topic of debate. Although aromatase inhibitors should be given with GnRH to avoid a negative feedback loop, gonadal suppression causes erectile dysfunction, thereby decreasing well-being. This dilemma is made worse by a lack of data on hormonal therapy for men with breast cancer.
To address this shortcoming, a prospective, randomized trial compared three different hormonal regimens for men. Male-GBG54 involved 55 men with breast cancer. For 6 months, patients received 1 of 3 treatment regimens: tamoxifen (20 mg/day), tamoxifen + GnRH (subcutaneous every 3 months), or exemestane (25 mg daily) + GnRH. Median estradiol levels were measured at 3 months and 6 months, and wellbeing was measured using questionnaires.
As expected, the results showed increased estradiol levels in the tamoxifen group and decreased levels in the GnRH group. Men were generally dissatisfied with GnRH therapy because of the erectile dysfunction it caused.
“Tamoxifen monotherapy should be kept as standard hormonal therapy for men with breast cancer. The side effects are moderate, hardly impairing sexual behavior. The combination with GnRH influenced patients’ well-being and erectile function profoundly,” lead author Mattea Reinisch, MD, of Klinikum Essen-Mitte (Germany), said in an interview.
Dr. Schroeder agreed that tamoxifen should remain the standard treatment but suggested that the benefits of gonadal suppression may outweigh the downsides. “We need efficacy data for gonadal suppression,” she said. “After all, we are advising our premenopausal breast cancer patients to undergo the gonadal suppression therapy on a daily basis because of the oncological superiority, despite the toxicity they are also experiencing.”
Dr. Schroeder again called for efficacy data and described shortcomings of Male-GBG54: “[Dr. Reinisch and her colleagues] have chosen a biological surrogate endpoint, but what we’d really like, of course, [are] the efficacy data. The quality of life data are not breast-cancer specific, and these are only data for 6 months, whereas, particularly in the metastatic setting, the compliance issue after 6 months is also relevant.”
Reflecting on the data from ESME and Male-GBG54, Dr. Schroeder said, “I think this field is maturing, and intervention trials have proven themselves to be possible in this niche population.”
Looking to the future, Dr. Schroeder suggested that male breast cancer can be studied either in separate trials from women (focusing on sex-specific targets), or in shared studies, as many disease characteristics are the same regardless of sex. She also said that worse disease in men is likely due to delayed presentation rather than biological differences between men and women.
“This leaves room for improvement,” Dr. Schroeder said. “We still need to work on the awareness of this disease.”
Discussant Dr. Schroeder disclosed financial relationships with Novartis, Roche, Genentech, and others. Male-GBG54 was funded by Claudia von Schilling Foundation.
SOURCES: Sirieix J et al. ESMO 2018, Abstract 294PD; Reinisch et al. ESMO 2018, Abstract 273PD.
REPORTING FROM ESMO 2018
Key clinical point: Men with metastatic breast cancer (MBC) have a similar prognosis, compared with women, but gonadal suppression remains a topic of debate.
Major finding: Median PFS was 9.8 months in men, compared with 13.0 months in matched women.
Study details: The ESME study was a large-scale retrospective analysis of 16,701 patients, 149 of whom were men with MBC. Male-GBG54 was a prospective, randomized trial involving 46 MBC patients who received three different endocrine therapies.
Disclosures: Discussant Dr. Schroeder disclosed financial relationships with Novartis, Roche, Genentech, and others. Male-GBG54 was funded by Claudia von Schilling Foundation.
Source: Sirieix et al. ESMO 2018, Abstract 294PD; Reinisch et al. ESMO 2018, Abstract 273PD.
Private practice gastroenterology models: Weighing the options
Editor’s note: It is my pleasure to introduce this new quarterly column in The New Gastroenterologist that will be dedicated to addressing important topics for early-career GIs who are either considering a career or starting a career as an independent GI physician in practice. This column is a collaboration between the AGA’s The New Gastroenterologist and the Digestive Health Physicians Association (DHPA), a national advocacy organization of more than 1,800 gastroenterologists in 79 member practices, which is focused exclusively on policies that promote and protect the high-quality, cost-efficient care provided to patients in the independent GI-practice setting.
Bryson W. Katona, MD, PhD
Editor in Chief, The New Gastroenterologist
Educating and training for your life’s work has likely occupied much of the past 10 years including medical school, residency, and fellowship. When it comes to deciding the next steps, the options can seem daunting.
As a long-standing private practice gastroenterologist, I think it is important for early-career GIs to understand the different private practice options and the new challenges and opportunities that private practitioners are experiencing.
According to recent data, there are approximately 12,500 clinical gastroenterologists divided among private gastroenterology practice models, hospital-based employees, and large multispecialty groups. There are nearly 6,000 private practice gastroenterologists.

There has been ongoing dialogue among all health care system stakeholders and the public regarding health care delivery, access, and financing. For the past several years, private practice advocacy groups, including DHPA, have been urging the elimination of the Medicare “site of service” differential between hospital and nonhospital settings, which typically results in substantially higher costs for hospital-based services.
In the 2015 Balanced Budget Act, Congress mandated that patient services provided in off-campus locations acquired by hospitals after Nov.1, 2015, be paid at the nonhospital rate. The 2019 Medicare Outpatient Prospective Payment System/Ambulatory Surgical Center proposed rule takes additional steps in achieving site neutrality and will likely have the effect of tamping down hospitals’ incentives to acquire independent physician practices.
This is a positive step forward in preserving the cost-efficient, high-quality care provided in the independent GI medical setting. And, with the growing health needs of an aging population and an aging GI physician workforce (nearly half of gastroenterologists are older than 55 years old), there is sure to be an ongoing high demand for providers in our specialty.
Selecting the career path that best fits your goals, ambitions, and lifestyle can be challenging. But, our professional training has taught us that the best method for arriving at the correct course of action is to first understand the questions and then seek the answers – let’s get to it.
Private practice models: What are the options?
A lot has changed since I completed my fellowship training in 1978. But the most dramatic changes have happened in the past decade, including the trend of smaller practices consolidating into larger groups.
Traditionally, physicians and patients have favored individual and very-small-group practices. Patients view small-group practices as highly personalized. They come to appreciate knowing all the physicians and staff in a practice. These long-standing “family type” relationships among patients and providers that often develop in this clinical care setting engenders in both the patient and provider a high level of satisfaction with the type and experience of care provided.
New physicians who are part of a small group practice often have the opportunity to take an earlier and more active role within the leadership of the practice. Small groups typically look to new physicians to function as “innovators” who can introduce into the practice those cutting-edge treatments and procedures learned during fellowship.
In the past decade, however, the trend toward the disappearance of solo and very-small-group practices has accelerated. Today, very small groups face several challenges. Providing all the “necessities” that are now part of today’s medical practice can be daunting. Small-sized practices are less likely to integrate ancillary services (e.g., lab and pathology services, in-office infusions, dietary and weight loss management) that are more typically seen in larger practices. Patients may find this fragmentation of care burdensome when they have to go to several providers for treatment.
The difficulties of implementing and maintaining information technology, EHRs, and patient-engagement tools are often inversely related to group size. In addition, the ability and effectiveness of a group to negotiate with hospital systems and insurance companies can be easier for larger practices, although other local factors will also come into play.
Beyond the administrative aspects of running a small group practice, your views about work-life balance should also be an important consideration when choosing a career path. Understandably, issues of call coverage and time off can be more restrictive in small groups.
Is bigger better?
The consolidation seen in hospital systems and multispecialty groups has found its way into single specialty practices. Many urban areas now have GI group practices of 10 or more physicians. There are now approximately 15 groups with 40 or more gastroenterologists, including a few GI practices with 100 or more physicians.
Increasing the size of a practice has obvious potential advantages, including less burdensome on-call requirements and a lower per-physician cost of maintaining and operating the practice. Larger groups often have dedicated software development and IT support staff. Patients are engaged and can connect with their providers through all manner of social media.
Large practice size also can make it possible to enable physicians who may choose to focus on single areas of gastroenterology. This means that a physician who wants to subspecialize in areas such as inflammatory bowel disease, hepatology, woman’s health, and advanced therapeutic endoscopy, would have the requisite large patient base, through internal practice referral, to support subspecialization. Larger groups can also integrate ancillary services into their practice such as pathology, infusion therapy, and nonhospital-based endoscopy services.
However, there can be disadvantages to choosing a larger practice. As in other larger institutions, physicians practicing in larger-sized groups may feel somewhat removed from practice management decisions. It may take several years to become a partner in a large practice – if you are more interested in the opportunity to be involved in practice decisions, a smaller group may be right for you.
New trends in practice groups
Physicians are continuously looking for ways to practice effectively and efficiently while expanding the range of services offered (think obesity management). Independent practice physicians are finding it increasingly difficult to grow and manage successful organizations while they care for their patients. Larger practices now typically include areas such as nursing, information technology, human resources, billing, and practice administration. I trained to treat patients, not run a business – there was much I’ve learned along the way. Many schools now offer joint MD/MBA programs. This may help blend the clinical, operational, and business components of practice.
In a newly developing trend, practice groups are exploring strategic partnerships with private equity/venture capital, practice management companies, national ambulatory surgery center companies, and even managed care insurance companies. This creates the opportunity to forge partnerships with these various health care–focused groups, and results in investment in GI practices seeking experienced business leadership and management while remaining independent of a health system. Already well established in dermatology, ophthalmology, and anesthesia, this phenomenon is now beginning in gastroenterology.
There are many things to consider when choosing a career path. Independent practice in gastroenterology continues as a vitally important component of care delivery, and it’s my hope that the new generation of gastroenterologists finds their journey as rewarding and personally satisfying as mine has been.
Fred B. Rosenberg, MD, is a board-certified gastroenterologist and the medical director of the North Shore Endoscopy Center in Lake Bluff, Ill., the founding president of Illinois Gastroenterology Group, and immediate past president of DHPA.
Editor’s note: It is my pleasure to introduce this new quarterly column in The New Gastroenterologist that will be dedicated to addressing important topics for early-career GIs who are either considering a career or starting a career as an independent GI physician in practice. This column is a collaboration between the AGA’s The New Gastroenterologist and the Digestive Health Physicians Association (DHPA), a national advocacy organization of more than 1,800 gastroenterologists in 79 member practices, which is focused exclusively on policies that promote and protect the high-quality, cost-efficient care provided to patients in the independent GI-practice setting.
Bryson W. Katona, MD, PhD
Editor in Chief, The New Gastroenterologist
Educating and training for your life’s work has likely occupied much of the past 10 years including medical school, residency, and fellowship. When it comes to deciding the next steps, the options can seem daunting.
As a long-standing private practice gastroenterologist, I think it is important for early-career GIs to understand the different private practice options and the new challenges and opportunities that private practitioners are experiencing.
According to recent data, there are approximately 12,500 clinical gastroenterologists divided among private gastroenterology practice models, hospital-based employees, and large multispecialty groups. There are nearly 6,000 private practice gastroenterologists.
There has been ongoing dialogue among all health care system stakeholders and the public regarding health care delivery, access, and financing. For the past several years, private practice advocacy groups, including DHPA, have been urging the elimination of the Medicare “site of service” differential between hospital and nonhospital settings, which typically results in substantially higher costs for hospital-based services.
In the 2015 Balanced Budget Act, Congress mandated that patient services provided in off-campus locations acquired by hospitals after Nov.1, 2015, be paid at the nonhospital rate. The 2019 Medicare Outpatient Prospective Payment System/Ambulatory Surgical Center proposed rule takes additional steps in achieving site neutrality and will likely have the effect of tamping down hospitals’ incentives to acquire independent physician practices.
This is a positive step forward in preserving the cost-efficient, high-quality care provided in the independent GI medical setting. And, with the growing health needs of an aging population and an aging GI physician workforce (nearly half of gastroenterologists are older than 55 years old), there is sure to be an ongoing high demand for providers in our specialty.
Selecting the career path that best fits your goals, ambitions, and lifestyle can be challenging. But, our professional training has taught us that the best method for arriving at the correct course of action is to first understand the questions and then seek the answers – let’s get to it.
Private practice models: What are the options?
A lot has changed since I completed my fellowship training in 1978. But the most dramatic changes have happened in the past decade, including the trend of smaller practices consolidating into larger groups.
Traditionally, physicians and patients have favored individual and very-small-group practices. Patients view small-group practices as highly personalized. They come to appreciate knowing all the physicians and staff in a practice. These long-standing “family type” relationships among patients and providers that often develop in this clinical care setting engenders in both the patient and provider a high level of satisfaction with the type and experience of care provided.
New physicians who are part of a small group practice often have the opportunity to take an earlier and more active role within the leadership of the practice. Small groups typically look to new physicians to function as “innovators” who can introduce into the practice those cutting-edge treatments and procedures learned during fellowship.
In the past decade, however, the trend toward the disappearance of solo and very-small-group practices has accelerated. Today, very small groups face several challenges. Providing all the “necessities” that are now part of today’s medical practice can be daunting. Small-sized practices are less likely to integrate ancillary services (e.g., lab and pathology services, in-office infusions, dietary and weight loss management) that are more typically seen in larger practices. Patients may find this fragmentation of care burdensome when they have to go to several providers for treatment.
The difficulties of implementing and maintaining information technology, EHRs, and patient-engagement tools are often inversely related to group size. In addition, the ability and effectiveness of a group to negotiate with hospital systems and insurance companies can be easier for larger practices, although other local factors will also come into play.
Beyond the administrative aspects of running a small group practice, your views about work-life balance should also be an important consideration when choosing a career path. Understandably, issues of call coverage and time off can be more restrictive in small groups.
Is bigger better?
The consolidation seen in hospital systems and multispecialty groups has found its way into single specialty practices. Many urban areas now have GI group practices of 10 or more physicians. There are now approximately 15 groups with 40 or more gastroenterologists, including a few GI practices with 100 or more physicians.
Increasing the size of a practice has obvious potential advantages, including less burdensome on-call requirements and a lower per-physician cost of maintaining and operating the practice. Larger groups often have dedicated software development and IT support staff. Patients are engaged and can connect with their providers through all manner of social media.
Large practice size also can make it possible to enable physicians who may choose to focus on single areas of gastroenterology. This means that a physician who wants to subspecialize in areas such as inflammatory bowel disease, hepatology, woman’s health, and advanced therapeutic endoscopy, would have the requisite large patient base, through internal practice referral, to support subspecialization. Larger groups can also integrate ancillary services into their practice such as pathology, infusion therapy, and nonhospital-based endoscopy services.
However, there can be disadvantages to choosing a larger practice. As in other larger institutions, physicians practicing in larger-sized groups may feel somewhat removed from practice management decisions. It may take several years to become a partner in a large practice – if you are more interested in the opportunity to be involved in practice decisions, a smaller group may be right for you.
New trends in practice groups
Physicians are continuously looking for ways to practice effectively and efficiently while expanding the range of services offered (think obesity management). Independent practice physicians are finding it increasingly difficult to grow and manage successful organizations while they care for their patients. Larger practices now typically include areas such as nursing, information technology, human resources, billing, and practice administration. I trained to treat patients, not run a business – there was much I’ve learned along the way. Many schools now offer joint MD/MBA programs. This may help blend the clinical, operational, and business components of practice.
In a newly developing trend, practice groups are exploring strategic partnerships with private equity/venture capital, practice management companies, national ambulatory surgery center companies, and even managed care insurance companies. This creates the opportunity to forge partnerships with these various health care–focused groups, and results in investment in GI practices seeking experienced business leadership and management while remaining independent of a health system. Already well established in dermatology, ophthalmology, and anesthesia, this phenomenon is now beginning in gastroenterology.
There are many things to consider when choosing a career path. Independent practice in gastroenterology continues as a vitally important component of care delivery, and it’s my hope that the new generation of gastroenterologists finds their journey as rewarding and personally satisfying as mine has been.
Fred B. Rosenberg, MD, is a board-certified gastroenterologist and the medical director of the North Shore Endoscopy Center in Lake Bluff, Ill., the founding president of Illinois Gastroenterology Group, and immediate past president of DHPA.
Editor’s note: It is my pleasure to introduce this new quarterly column in The New Gastroenterologist that will be dedicated to addressing important topics for early-career GIs who are either considering a career or starting a career as an independent GI physician in practice. This column is a collaboration between the AGA’s The New Gastroenterologist and the Digestive Health Physicians Association (DHPA), a national advocacy organization of more than 1,800 gastroenterologists in 79 member practices, which is focused exclusively on policies that promote and protect the high-quality, cost-efficient care provided to patients in the independent GI-practice setting.
Bryson W. Katona, MD, PhD
Editor in Chief, The New Gastroenterologist
Educating and training for your life’s work has likely occupied much of the past 10 years including medical school, residency, and fellowship. When it comes to deciding the next steps, the options can seem daunting.
As a long-standing private practice gastroenterologist, I think it is important for early-career GIs to understand the different private practice options and the new challenges and opportunities that private practitioners are experiencing.
According to recent data, there are approximately 12,500 clinical gastroenterologists divided among private gastroenterology practice models, hospital-based employees, and large multispecialty groups. There are nearly 6,000 private practice gastroenterologists.
There has been ongoing dialogue among all health care system stakeholders and the public regarding health care delivery, access, and financing. For the past several years, private practice advocacy groups, including DHPA, have been urging the elimination of the Medicare “site of service” differential between hospital and nonhospital settings, which typically results in substantially higher costs for hospital-based services.
In the 2015 Balanced Budget Act, Congress mandated that patient services provided in off-campus locations acquired by hospitals after Nov.1, 2015, be paid at the nonhospital rate. The 2019 Medicare Outpatient Prospective Payment System/Ambulatory Surgical Center proposed rule takes additional steps in achieving site neutrality and will likely have the effect of tamping down hospitals’ incentives to acquire independent physician practices.
This is a positive step forward in preserving the cost-efficient, high-quality care provided in the independent GI medical setting. And, with the growing health needs of an aging population and an aging GI physician workforce (nearly half of gastroenterologists are older than 55 years old), there is sure to be an ongoing high demand for providers in our specialty.
Selecting the career path that best fits your goals, ambitions, and lifestyle can be challenging. But, our professional training has taught us that the best method for arriving at the correct course of action is to first understand the questions and then seek the answers – let’s get to it.
Private practice models: What are the options?
A lot has changed since I completed my fellowship training in 1978. But the most dramatic changes have happened in the past decade, including the trend of smaller practices consolidating into larger groups.
Traditionally, physicians and patients have favored individual and very-small-group practices. Patients view small-group practices as highly personalized. They come to appreciate knowing all the physicians and staff in a practice. These long-standing “family type” relationships among patients and providers that often develop in this clinical care setting engenders in both the patient and provider a high level of satisfaction with the type and experience of care provided.
New physicians who are part of a small group practice often have the opportunity to take an earlier and more active role within the leadership of the practice. Small groups typically look to new physicians to function as “innovators” who can introduce into the practice those cutting-edge treatments and procedures learned during fellowship.
In the past decade, however, the trend toward the disappearance of solo and very-small-group practices has accelerated. Today, very small groups face several challenges. Providing all the “necessities” that are now part of today’s medical practice can be daunting. Small-sized practices are less likely to integrate ancillary services (e.g., lab and pathology services, in-office infusions, dietary and weight loss management) that are more typically seen in larger practices. Patients may find this fragmentation of care burdensome when they have to go to several providers for treatment.
The difficulties of implementing and maintaining information technology, EHRs, and patient-engagement tools are often inversely related to group size. In addition, the ability and effectiveness of a group to negotiate with hospital systems and insurance companies can be easier for larger practices, although other local factors will also come into play.
Beyond the administrative aspects of running a small group practice, your views about work-life balance should also be an important consideration when choosing a career path. Understandably, issues of call coverage and time off can be more restrictive in small groups.
Is bigger better?
The consolidation seen in hospital systems and multispecialty groups has found its way into single specialty practices. Many urban areas now have GI group practices of 10 or more physicians. There are now approximately 15 groups with 40 or more gastroenterologists, including a few GI practices with 100 or more physicians.
Increasing the size of a practice has obvious potential advantages, including less burdensome on-call requirements and a lower per-physician cost of maintaining and operating the practice. Larger groups often have dedicated software development and IT support staff. Patients are engaged and can connect with their providers through all manner of social media.
Large practice size also can make it possible to enable physicians who may choose to focus on single areas of gastroenterology. This means that a physician who wants to subspecialize in areas such as inflammatory bowel disease, hepatology, woman’s health, and advanced therapeutic endoscopy, would have the requisite large patient base, through internal practice referral, to support subspecialization. Larger groups can also integrate ancillary services into their practice such as pathology, infusion therapy, and nonhospital-based endoscopy services.
However, there can be disadvantages to choosing a larger practice. As in other larger institutions, physicians practicing in larger-sized groups may feel somewhat removed from practice management decisions. It may take several years to become a partner in a large practice – if you are more interested in the opportunity to be involved in practice decisions, a smaller group may be right for you.
New trends in practice groups
Physicians are continuously looking for ways to practice effectively and efficiently while expanding the range of services offered (think obesity management). Independent practice physicians are finding it increasingly difficult to grow and manage successful organizations while they care for their patients. Larger practices now typically include areas such as nursing, information technology, human resources, billing, and practice administration. I trained to treat patients, not run a business – there was much I’ve learned along the way. Many schools now offer joint MD/MBA programs. This may help blend the clinical, operational, and business components of practice.
In a newly developing trend, practice groups are exploring strategic partnerships with private equity/venture capital, practice management companies, national ambulatory surgery center companies, and even managed care insurance companies. This creates the opportunity to forge partnerships with these various health care–focused groups, and results in investment in GI practices seeking experienced business leadership and management while remaining independent of a health system. Already well established in dermatology, ophthalmology, and anesthesia, this phenomenon is now beginning in gastroenterology.
There are many things to consider when choosing a career path. Independent practice in gastroenterology continues as a vitally important component of care delivery, and it’s my hope that the new generation of gastroenterologists finds their journey as rewarding and personally satisfying as mine has been.
Fred B. Rosenberg, MD, is a board-certified gastroenterologist and the medical director of the North Shore Endoscopy Center in Lake Bluff, Ill., the founding president of Illinois Gastroenterology Group, and immediate past president of DHPA.
Drug overdose deaths down since late 2017
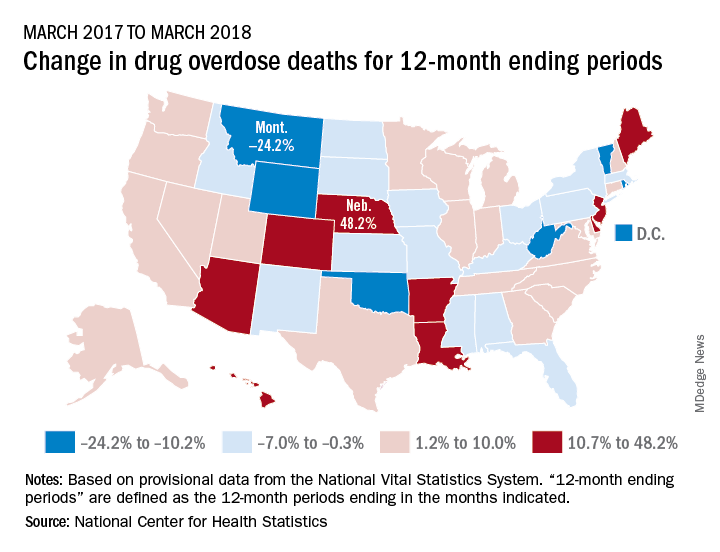
Longer-term data, however, show an increase over the year from March 2017 to March 2018, as the short-term decrease was not enough to overcome the previous year’s increase. The provisional 12-month ending count – deaths during the 12-month period ending in the month indicated – went from 66,859 in March 2017 to 68,690 in March 2018, an increase of 2.7%, the NCHS reported.
That year-long increase was not spread evenly among the states. Nebraska’s 12-month ending count jumped over 48% from March 2017 to March 2018, more than twice as much as second-place Hawaii’s 20.9%. Montana had the largest drop over that year, –24.2%, with Wyoming next at –20.7% and the District of Columbia third at –14.8%, data from the National Vital Statistics System show.
“Provisional drug overdose death data are often incomplete,” the NCHS noted, “and the degree of completeness varies by jurisdiction and 12-month ending period. Consequently, the numbers of drug overdose deaths are underestimated, based on provisional data relative to final data and are subject to random variation.”
Longer-term data, however, show an increase over the year from March 2017 to March 2018, as the short-term decrease was not enough to overcome the previous year’s increase. The provisional 12-month ending count – deaths during the 12-month period ending in the month indicated – went from 66,859 in March 2017 to 68,690 in March 2018, an increase of 2.7%, the NCHS reported.
That year-long increase was not spread evenly among the states. Nebraska’s 12-month ending count jumped over 48% from March 2017 to March 2018, more than twice as much as second-place Hawaii’s 20.9%. Montana had the largest drop over that year, –24.2%, with Wyoming next at –20.7% and the District of Columbia third at –14.8%, data from the National Vital Statistics System show.
“Provisional drug overdose death data are often incomplete,” the NCHS noted, “and the degree of completeness varies by jurisdiction and 12-month ending period. Consequently, the numbers of drug overdose deaths are underestimated, based on provisional data relative to final data and are subject to random variation.”
Longer-term data, however, show an increase over the year from March 2017 to March 2018, as the short-term decrease was not enough to overcome the previous year’s increase. The provisional 12-month ending count – deaths during the 12-month period ending in the month indicated – went from 66,859 in March 2017 to 68,690 in March 2018, an increase of 2.7%, the NCHS reported.
That year-long increase was not spread evenly among the states. Nebraska’s 12-month ending count jumped over 48% from March 2017 to March 2018, more than twice as much as second-place Hawaii’s 20.9%. Montana had the largest drop over that year, –24.2%, with Wyoming next at –20.7% and the District of Columbia third at –14.8%, data from the National Vital Statistics System show.
“Provisional drug overdose death data are often incomplete,” the NCHS noted, “and the degree of completeness varies by jurisdiction and 12-month ending period. Consequently, the numbers of drug overdose deaths are underestimated, based on provisional data relative to final data and are subject to random variation.”
Calendar
For more information about upcoming events and award deadlines, please visit http://agau.gastro.org and http://www.gastro.org/research-funding.
UPCOMING EVENTS
Dec. 10-11, 12-13, 2018; Jan. 16-17, 22-23, 23-24, 2019; Feb. 20-21, 2019
Two-Day, In-Depth Coding Seminar by McVey Associates, Inc
.Become a certified GI coder with a two-day, in-depth training course provided by McVey Associates, Inc.
Tampa, FL (12/10-11), Dallas, TX (12/12-13), Houston, TX (1/16-17), New Orleans, LA (1/22-23), Pittsburgh, PA (1/23-24), 2/20 (Hartford, CT)
Jan. 17-19, 2019
2019 GI Cancers Symposium
Join colleagues from across the globe in San Francisco to discover and share groundbreaking research in treating gastrointestinal cancers.
San Francisco, CA

Feb. 7–9, 2019
Crohn’s & Colitis Congress™ (A Partnership of the Crohn’s & Colitis Foundation and American Gastroenterological Association)
Expand your knowledge, network with IBD leaders, spark innovative research and get inspired to improve patient care.
Las Vegas, NV
March 8-9, 2019
2019 Women’s Leadership Conference
The conference is specifically designed for women looking to advance their careers, further professional goals, enhance personal growth and effectively network.
Bethesda, MD
March 8-10, 2019
FORWARD Program
AGA’s Fostering Opportunities Resulting in Workforce and Research Diversity (FORWARD) Program is a new initiative funded by NIH, supporting the career entry and development for underrepresented minority physician scientists in gastroenterology. The program provides concrete leadership and skill development that includes scientific manuscript and grant writing, research development, executive coaching and more.
Bethesda, MD
March 8-10, 2019
Future Leaders Program
The Future Leaders Program provides a pathway within the organization to network, connect with mentors, develop leadership skills and learn about AGA’s governance and operations while advancing your career and supporting the profession.
Bethesda, MD
March 23–24, 2019
2019 Gut Microbiota for Health World Summit
The 2019 program will present the latest evidence on the interaction between diet, nutrition and the gut microbiome. Learn how diet and nutrition are being used in concert with traditional therapies to manage GI disorders.
Miami, FL
May 18-21, 2019
Digestive Disease Week (DDW)®
DDW® is the world’s leading educational forum for academicians, clinicians, researchers, students and trainees working in gastroenterology, hepatology, GI endoscopy, gastrointestinal surgery and related fields. Whether you work in patient care, research, education or administration, the DDW program offers something for you. DDW is co-sponsored by AGA, AASLD, ASGE and SSAT.
San Diego, CA
AWARDS APPLICATION DEADLINES
AGA-Rady Children’s Institute for Genomic Medicine Research Scholar Award in Pediatric Genomics
This award provides $90,000 per year for three years (totaling $270,000) to a young investigator, instructor, research associate or equivalent working toward an independent career in gastroenterology, hepatology or related areas. The proposed research may be basic, translational or clinical and must use genomics as an approach to enhance understanding of pediatric digestive diseases toward prevention, treatment and/or cure of such diseases. The funded research must be conducted full-time at the Rady Children’s Institute for Genomic Medicine in San Diego, California, or at Rady Children’s Hospital – San Diego.
Application Deadline: Dec. 14, 2018
AGA-Bern Schwartz Family Fund Research Scholar Award in Pancreatic Cancer
This award provides $100,000 per year for three years (total $300,000) to early career faculty (i.e., investigator, instructor, research associate or equivalent) working toward an independent career in pancreatic cancer research.
Application Deadline: Dec. 14, 2018
AGA Research Scholar Award (RSA)
This award provides $90,000 per year for three years (total $270,000) to a young investigator, instructor, research associate or equivalent working toward an independent career in gastroenterology, hepatology or related areas.
Application Deadline: Dec. 14, 2018
AGA-Shire Research Scholar Award in Functional GI and Motility Disorders
This award provides $90,000 per year for three years (total $270,000) to a young investigator, instructor, research associate or equivalent working toward an independent career in functional GI and motility disorders research.
Application Deadline: Dec. 14, 2018
AGA-Takeda Pharmaceuticals Research Scholar Award in Inflammatory Bowel Disease
This award provides $90,000 per year for three years (total $270,000) to a young investigator, instructor, research associate or equivalent working toward an independent career in inflammatory bowel disease research.
Application Deadline: Dec. 14, 2018
AGA Fellow Abstract Award
This travel award provides nine $500 and one $1,000 prize to recipients who are MD, PhD or equivalent fellows presenting posters/oral sessions at Digestive Disease Week® (DDW).
Application Deadline: Feb. 15, 2019
AGA Moti L. & Kamla Rustgi International Travel Awards
This travel award provides two $750 prizes to recipients who are young basic, translational or clinical investigators residing outside North America to support travel and related expenses to attend Digestive Disease Week® (DDW).
Application Deadline: Feb. 15, 2019
AGA Student Abstract Award
This travel award provides nine $500 and one $1,000 prize to recipients who are high school, undergraduate, graduate, or medical students or residents (residents up to year three postgraduate) presenting posters/oral sessions at Digestive Disease Week® (DDW).
Application Deadline: Feb. 15, 2019
For more information about upcoming events and award deadlines, please visit http://agau.gastro.org and http://www.gastro.org/research-funding.
UPCOMING EVENTS
Dec. 10-11, 12-13, 2018; Jan. 16-17, 22-23, 23-24, 2019; Feb. 20-21, 2019
Two-Day, In-Depth Coding Seminar by McVey Associates, Inc
.Become a certified GI coder with a two-day, in-depth training course provided by McVey Associates, Inc.
Tampa, FL (12/10-11), Dallas, TX (12/12-13), Houston, TX (1/16-17), New Orleans, LA (1/22-23), Pittsburgh, PA (1/23-24), 2/20 (Hartford, CT)
Jan. 17-19, 2019
2019 GI Cancers Symposium
Join colleagues from across the globe in San Francisco to discover and share groundbreaking research in treating gastrointestinal cancers.
San Francisco, CA
Feb. 7–9, 2019
Crohn’s & Colitis Congress™ (A Partnership of the Crohn’s & Colitis Foundation and American Gastroenterological Association)
Expand your knowledge, network with IBD leaders, spark innovative research and get inspired to improve patient care.
Las Vegas, NV
March 8-9, 2019
2019 Women’s Leadership Conference
The conference is specifically designed for women looking to advance their careers, further professional goals, enhance personal growth and effectively network.
Bethesda, MD
March 8-10, 2019
FORWARD Program
AGA’s Fostering Opportunities Resulting in Workforce and Research Diversity (FORWARD) Program is a new initiative funded by NIH, supporting the career entry and development for underrepresented minority physician scientists in gastroenterology. The program provides concrete leadership and skill development that includes scientific manuscript and grant writing, research development, executive coaching and more.
Bethesda, MD
March 8-10, 2019
Future Leaders Program
The Future Leaders Program provides a pathway within the organization to network, connect with mentors, develop leadership skills and learn about AGA’s governance and operations while advancing your career and supporting the profession.
Bethesda, MD
March 23–24, 2019
2019 Gut Microbiota for Health World Summit
The 2019 program will present the latest evidence on the interaction between diet, nutrition and the gut microbiome. Learn how diet and nutrition are being used in concert with traditional therapies to manage GI disorders.
Miami, FL
May 18-21, 2019
Digestive Disease Week (DDW)®
DDW® is the world’s leading educational forum for academicians, clinicians, researchers, students and trainees working in gastroenterology, hepatology, GI endoscopy, gastrointestinal surgery and related fields. Whether you work in patient care, research, education or administration, the DDW program offers something for you. DDW is co-sponsored by AGA, AASLD, ASGE and SSAT.
San Diego, CA
AWARDS APPLICATION DEADLINES
AGA-Rady Children’s Institute for Genomic Medicine Research Scholar Award in Pediatric Genomics
This award provides $90,000 per year for three years (totaling $270,000) to a young investigator, instructor, research associate or equivalent working toward an independent career in gastroenterology, hepatology or related areas. The proposed research may be basic, translational or clinical and must use genomics as an approach to enhance understanding of pediatric digestive diseases toward prevention, treatment and/or cure of such diseases. The funded research must be conducted full-time at the Rady Children’s Institute for Genomic Medicine in San Diego, California, or at Rady Children’s Hospital – San Diego.
Application Deadline: Dec. 14, 2018
AGA-Bern Schwartz Family Fund Research Scholar Award in Pancreatic Cancer
This award provides $100,000 per year for three years (total $300,000) to early career faculty (i.e., investigator, instructor, research associate or equivalent) working toward an independent career in pancreatic cancer research.
Application Deadline: Dec. 14, 2018
AGA Research Scholar Award (RSA)
This award provides $90,000 per year for three years (total $270,000) to a young investigator, instructor, research associate or equivalent working toward an independent career in gastroenterology, hepatology or related areas.
Application Deadline: Dec. 14, 2018
AGA-Shire Research Scholar Award in Functional GI and Motility Disorders
This award provides $90,000 per year for three years (total $270,000) to a young investigator, instructor, research associate or equivalent working toward an independent career in functional GI and motility disorders research.
Application Deadline: Dec. 14, 2018
AGA-Takeda Pharmaceuticals Research Scholar Award in Inflammatory Bowel Disease
This award provides $90,000 per year for three years (total $270,000) to a young investigator, instructor, research associate or equivalent working toward an independent career in inflammatory bowel disease research.
Application Deadline: Dec. 14, 2018
AGA Fellow Abstract Award
This travel award provides nine $500 and one $1,000 prize to recipients who are MD, PhD or equivalent fellows presenting posters/oral sessions at Digestive Disease Week® (DDW).
Application Deadline: Feb. 15, 2019
AGA Moti L. & Kamla Rustgi International Travel Awards
This travel award provides two $750 prizes to recipients who are young basic, translational or clinical investigators residing outside North America to support travel and related expenses to attend Digestive Disease Week® (DDW).
Application Deadline: Feb. 15, 2019
AGA Student Abstract Award
This travel award provides nine $500 and one $1,000 prize to recipients who are high school, undergraduate, graduate, or medical students or residents (residents up to year three postgraduate) presenting posters/oral sessions at Digestive Disease Week® (DDW).
Application Deadline: Feb. 15, 2019
For more information about upcoming events and award deadlines, please visit http://agau.gastro.org and http://www.gastro.org/research-funding.
UPCOMING EVENTS
Dec. 10-11, 12-13, 2018; Jan. 16-17, 22-23, 23-24, 2019; Feb. 20-21, 2019
Two-Day, In-Depth Coding Seminar by McVey Associates, Inc
.Become a certified GI coder with a two-day, in-depth training course provided by McVey Associates, Inc.
Tampa, FL (12/10-11), Dallas, TX (12/12-13), Houston, TX (1/16-17), New Orleans, LA (1/22-23), Pittsburgh, PA (1/23-24), 2/20 (Hartford, CT)
Jan. 17-19, 2019
2019 GI Cancers Symposium
Join colleagues from across the globe in San Francisco to discover and share groundbreaking research in treating gastrointestinal cancers.
San Francisco, CA
Feb. 7–9, 2019
Crohn’s & Colitis Congress™ (A Partnership of the Crohn’s & Colitis Foundation and American Gastroenterological Association)
Expand your knowledge, network with IBD leaders, spark innovative research and get inspired to improve patient care.
Las Vegas, NV
March 8-9, 2019
2019 Women’s Leadership Conference
The conference is specifically designed for women looking to advance their careers, further professional goals, enhance personal growth and effectively network.
Bethesda, MD
March 8-10, 2019
FORWARD Program
AGA’s Fostering Opportunities Resulting in Workforce and Research Diversity (FORWARD) Program is a new initiative funded by NIH, supporting the career entry and development for underrepresented minority physician scientists in gastroenterology. The program provides concrete leadership and skill development that includes scientific manuscript and grant writing, research development, executive coaching and more.
Bethesda, MD
March 8-10, 2019
Future Leaders Program
The Future Leaders Program provides a pathway within the organization to network, connect with mentors, develop leadership skills and learn about AGA’s governance and operations while advancing your career and supporting the profession.
Bethesda, MD
March 23–24, 2019
2019 Gut Microbiota for Health World Summit
The 2019 program will present the latest evidence on the interaction between diet, nutrition and the gut microbiome. Learn how diet and nutrition are being used in concert with traditional therapies to manage GI disorders.
Miami, FL
May 18-21, 2019
Digestive Disease Week (DDW)®
DDW® is the world’s leading educational forum for academicians, clinicians, researchers, students and trainees working in gastroenterology, hepatology, GI endoscopy, gastrointestinal surgery and related fields. Whether you work in patient care, research, education or administration, the DDW program offers something for you. DDW is co-sponsored by AGA, AASLD, ASGE and SSAT.
San Diego, CA
AWARDS APPLICATION DEADLINES
AGA-Rady Children’s Institute for Genomic Medicine Research Scholar Award in Pediatric Genomics
This award provides $90,000 per year for three years (totaling $270,000) to a young investigator, instructor, research associate or equivalent working toward an independent career in gastroenterology, hepatology or related areas. The proposed research may be basic, translational or clinical and must use genomics as an approach to enhance understanding of pediatric digestive diseases toward prevention, treatment and/or cure of such diseases. The funded research must be conducted full-time at the Rady Children’s Institute for Genomic Medicine in San Diego, California, or at Rady Children’s Hospital – San Diego.
Application Deadline: Dec. 14, 2018
AGA-Bern Schwartz Family Fund Research Scholar Award in Pancreatic Cancer
This award provides $100,000 per year for three years (total $300,000) to early career faculty (i.e., investigator, instructor, research associate or equivalent) working toward an independent career in pancreatic cancer research.
Application Deadline: Dec. 14, 2018
AGA Research Scholar Award (RSA)
This award provides $90,000 per year for three years (total $270,000) to a young investigator, instructor, research associate or equivalent working toward an independent career in gastroenterology, hepatology or related areas.
Application Deadline: Dec. 14, 2018
AGA-Shire Research Scholar Award in Functional GI and Motility Disorders
This award provides $90,000 per year for three years (total $270,000) to a young investigator, instructor, research associate or equivalent working toward an independent career in functional GI and motility disorders research.
Application Deadline: Dec. 14, 2018
AGA-Takeda Pharmaceuticals Research Scholar Award in Inflammatory Bowel Disease
This award provides $90,000 per year for three years (total $270,000) to a young investigator, instructor, research associate or equivalent working toward an independent career in inflammatory bowel disease research.
Application Deadline: Dec. 14, 2018
AGA Fellow Abstract Award
This travel award provides nine $500 and one $1,000 prize to recipients who are MD, PhD or equivalent fellows presenting posters/oral sessions at Digestive Disease Week® (DDW).
Application Deadline: Feb. 15, 2019
AGA Moti L. & Kamla Rustgi International Travel Awards
This travel award provides two $750 prizes to recipients who are young basic, translational or clinical investigators residing outside North America to support travel and related expenses to attend Digestive Disease Week® (DDW).
Application Deadline: Feb. 15, 2019
AGA Student Abstract Award
This travel award provides nine $500 and one $1,000 prize to recipients who are high school, undergraduate, graduate, or medical students or residents (residents up to year three postgraduate) presenting posters/oral sessions at Digestive Disease Week® (DDW).
Application Deadline: Feb. 15, 2019
