User login
Retinal thinning in aquaporin-4-positive NMOSD may occur without optic neuritis
BERLIN – Retinal thinning related to ganglion loss may be independent of optic neuritis attacks in patients with neuromyelitis optica spectrum disorders who have anti–aquaporin-4 antibodies.
These eyes exhibited an annual retinal volume loss of about 0.6 micrometers – 80 times higher than that of normal controls – even though they did not have a history of optic neuritis (ON), Frederike C. Oertel said at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis.
“The most likely explanation for this seems to be a disease-related primary retinopathy due to the high density of astrocytic cells in the retina and the afferent visual system,” said Ms. Oertel, a doctoral student at NeuroCure Clinical Research Center, Berlin.
The study appeared in the Journal of Neurology, Neurosurgery & Psychiatry (J Neurol Neurosurg Psychiatry. 2018 Jun 19. doi: 10.1136/jnnp-2018-318382).
A previous cross-sectional study by her group found retinal thinning and an alteration of foveal shape in anti–aquaporin-4 (anti-AQP4) positive patients with neuromyelitis optica spectrum disorders (NMOSD) independent of whether they had experienced a clinical attack of optic neuritis (Neurol Neuroimmunol Neuroinflamm. 2017 May;4[3]:e334). In these patients, the fovea changed shape from a characteristic steeply angled “V” to a broader, flatter “U” shape, she said.
In that 2017 paper, Ms. Oertel and her colleagues theorized that the relationship between the water-channel regulator AQP4 and astrocytes could be the root cause of these microstructural alterations.
“The parafoveal area is characterized by a high density of retinal astrocytic Müller cells, which express AQP4 and may thus serve as retinal targets in NMOSD,” they wrote. “Müller cells regulate the retinal water balance and have a relevant role in neurotransmitter and photopigment recycling, as well as in energy and lipid metabolism. Müller cell dysfunction or degeneration could thus lead to impaired retinal function including changes in water homeostasis. Of interest, both the initial cohort and the confirmatory cohort showed a mild increase of peripapillary retinal nerve fiber layer thickness, which could indicate tissue swelling. These findings are supported by animal studies showing retraction of astrocytic end feet in some and astrocyte death in other cases, suggesting a primary astrocytoma in NMOSD also outside acute lesions.”
The study Ms. Oertel presented at ECTRIMS looked at full retinal thickness using the same imaging tool, optical coherence tomography (OCT). The longitudinal cohort comprised 94 eyes in 51 anti–AQP4-IgG seropositive patients who had NMOSD; 60 of these eyes had experienced an optic neuritis attack and 34 had not. Most of the patients were female; the mean age was 47 years. They were compared against 28 age- and sex-matched healthy controls.
OCT measured combined ganglion cell and inner plexiform layer (GCIP), the peripapillary retinal nerve fiber layer (pRNFL), fovea thickness (FT), inner nuclear layer (INL), and total macular volume (TMV).
At baseline, ON eyes already displayed reduced GCIP, FT, and TMV, compared with healthy controls – but so had eyes that had not had ON. Over the follow-up period, eyes without ON continued to show thinning, even in the absence of a clinical attack. Although visual acuity didn’t change over time, the retinas continued to thin, losing an average of 0.6 micrometers each year, a rate 80 times greater than that seen in the control group.
“We saw this significant loss of the ganglion cell layer volume independent of ON, suggesting that retinal neurodegeneration is not dependent on ON in these patients,” Ms. Oertel said.
The results fit well into the group’s prior theory of astrocytic involvement. However, she added, “We still have to think about an alternative theory of drug-induced neuroaxonal damage and retrograde neuroaxonal degeneration.”
The project was supported with grants from the German Ministry for Education and Research. Ms. Oertel had no financial disclosures relevant to the work, but many coauthors reported financial relationships with industry.
BERLIN – Retinal thinning related to ganglion loss may be independent of optic neuritis attacks in patients with neuromyelitis optica spectrum disorders who have anti–aquaporin-4 antibodies.
These eyes exhibited an annual retinal volume loss of about 0.6 micrometers – 80 times higher than that of normal controls – even though they did not have a history of optic neuritis (ON), Frederike C. Oertel said at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis.
“The most likely explanation for this seems to be a disease-related primary retinopathy due to the high density of astrocytic cells in the retina and the afferent visual system,” said Ms. Oertel, a doctoral student at NeuroCure Clinical Research Center, Berlin.
The study appeared in the Journal of Neurology, Neurosurgery & Psychiatry (J Neurol Neurosurg Psychiatry. 2018 Jun 19. doi: 10.1136/jnnp-2018-318382).
A previous cross-sectional study by her group found retinal thinning and an alteration of foveal shape in anti–aquaporin-4 (anti-AQP4) positive patients with neuromyelitis optica spectrum disorders (NMOSD) independent of whether they had experienced a clinical attack of optic neuritis (Neurol Neuroimmunol Neuroinflamm. 2017 May;4[3]:e334). In these patients, the fovea changed shape from a characteristic steeply angled “V” to a broader, flatter “U” shape, she said.
In that 2017 paper, Ms. Oertel and her colleagues theorized that the relationship between the water-channel regulator AQP4 and astrocytes could be the root cause of these microstructural alterations.
“The parafoveal area is characterized by a high density of retinal astrocytic Müller cells, which express AQP4 and may thus serve as retinal targets in NMOSD,” they wrote. “Müller cells regulate the retinal water balance and have a relevant role in neurotransmitter and photopigment recycling, as well as in energy and lipid metabolism. Müller cell dysfunction or degeneration could thus lead to impaired retinal function including changes in water homeostasis. Of interest, both the initial cohort and the confirmatory cohort showed a mild increase of peripapillary retinal nerve fiber layer thickness, which could indicate tissue swelling. These findings are supported by animal studies showing retraction of astrocytic end feet in some and astrocyte death in other cases, suggesting a primary astrocytoma in NMOSD also outside acute lesions.”
The study Ms. Oertel presented at ECTRIMS looked at full retinal thickness using the same imaging tool, optical coherence tomography (OCT). The longitudinal cohort comprised 94 eyes in 51 anti–AQP4-IgG seropositive patients who had NMOSD; 60 of these eyes had experienced an optic neuritis attack and 34 had not. Most of the patients were female; the mean age was 47 years. They were compared against 28 age- and sex-matched healthy controls.
OCT measured combined ganglion cell and inner plexiform layer (GCIP), the peripapillary retinal nerve fiber layer (pRNFL), fovea thickness (FT), inner nuclear layer (INL), and total macular volume (TMV).
At baseline, ON eyes already displayed reduced GCIP, FT, and TMV, compared with healthy controls – but so had eyes that had not had ON. Over the follow-up period, eyes without ON continued to show thinning, even in the absence of a clinical attack. Although visual acuity didn’t change over time, the retinas continued to thin, losing an average of 0.6 micrometers each year, a rate 80 times greater than that seen in the control group.
“We saw this significant loss of the ganglion cell layer volume independent of ON, suggesting that retinal neurodegeneration is not dependent on ON in these patients,” Ms. Oertel said.
The results fit well into the group’s prior theory of astrocytic involvement. However, she added, “We still have to think about an alternative theory of drug-induced neuroaxonal damage and retrograde neuroaxonal degeneration.”
The project was supported with grants from the German Ministry for Education and Research. Ms. Oertel had no financial disclosures relevant to the work, but many coauthors reported financial relationships with industry.
BERLIN – Retinal thinning related to ganglion loss may be independent of optic neuritis attacks in patients with neuromyelitis optica spectrum disorders who have anti–aquaporin-4 antibodies.
These eyes exhibited an annual retinal volume loss of about 0.6 micrometers – 80 times higher than that of normal controls – even though they did not have a history of optic neuritis (ON), Frederike C. Oertel said at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis.
“The most likely explanation for this seems to be a disease-related primary retinopathy due to the high density of astrocytic cells in the retina and the afferent visual system,” said Ms. Oertel, a doctoral student at NeuroCure Clinical Research Center, Berlin.
The study appeared in the Journal of Neurology, Neurosurgery & Psychiatry (J Neurol Neurosurg Psychiatry. 2018 Jun 19. doi: 10.1136/jnnp-2018-318382).
A previous cross-sectional study by her group found retinal thinning and an alteration of foveal shape in anti–aquaporin-4 (anti-AQP4) positive patients with neuromyelitis optica spectrum disorders (NMOSD) independent of whether they had experienced a clinical attack of optic neuritis (Neurol Neuroimmunol Neuroinflamm. 2017 May;4[3]:e334). In these patients, the fovea changed shape from a characteristic steeply angled “V” to a broader, flatter “U” shape, she said.
In that 2017 paper, Ms. Oertel and her colleagues theorized that the relationship between the water-channel regulator AQP4 and astrocytes could be the root cause of these microstructural alterations.
“The parafoveal area is characterized by a high density of retinal astrocytic Müller cells, which express AQP4 and may thus serve as retinal targets in NMOSD,” they wrote. “Müller cells regulate the retinal water balance and have a relevant role in neurotransmitter and photopigment recycling, as well as in energy and lipid metabolism. Müller cell dysfunction or degeneration could thus lead to impaired retinal function including changes in water homeostasis. Of interest, both the initial cohort and the confirmatory cohort showed a mild increase of peripapillary retinal nerve fiber layer thickness, which could indicate tissue swelling. These findings are supported by animal studies showing retraction of astrocytic end feet in some and astrocyte death in other cases, suggesting a primary astrocytoma in NMOSD also outside acute lesions.”
The study Ms. Oertel presented at ECTRIMS looked at full retinal thickness using the same imaging tool, optical coherence tomography (OCT). The longitudinal cohort comprised 94 eyes in 51 anti–AQP4-IgG seropositive patients who had NMOSD; 60 of these eyes had experienced an optic neuritis attack and 34 had not. Most of the patients were female; the mean age was 47 years. They were compared against 28 age- and sex-matched healthy controls.
OCT measured combined ganglion cell and inner plexiform layer (GCIP), the peripapillary retinal nerve fiber layer (pRNFL), fovea thickness (FT), inner nuclear layer (INL), and total macular volume (TMV).
At baseline, ON eyes already displayed reduced GCIP, FT, and TMV, compared with healthy controls – but so had eyes that had not had ON. Over the follow-up period, eyes without ON continued to show thinning, even in the absence of a clinical attack. Although visual acuity didn’t change over time, the retinas continued to thin, losing an average of 0.6 micrometers each year, a rate 80 times greater than that seen in the control group.
“We saw this significant loss of the ganglion cell layer volume independent of ON, suggesting that retinal neurodegeneration is not dependent on ON in these patients,” Ms. Oertel said.
The results fit well into the group’s prior theory of astrocytic involvement. However, she added, “We still have to think about an alternative theory of drug-induced neuroaxonal damage and retrograde neuroaxonal degeneration.”
The project was supported with grants from the German Ministry for Education and Research. Ms. Oertel had no financial disclosures relevant to the work, but many coauthors reported financial relationships with industry.
REPORTING FROM ECTRIMS 2018
Key clinical point:
Major finding: Over 2.5 years retinas thinned an average of 0.6 micrometers annually.
Study details: The longitudinal study comprised 94 eyes.
Disclosures: The project was supported with grants from the German Ministry for Education and Research. Dr. Oertel had no conflicts of interest, but many coauthors reported financial relationships with industry.
Source: Oertel FC et al. ECTRIMS 2018, Abstract 212.
High-dose flu vaccine in RA patients beats standard dose
CHICAGO – The administration of high-dose vs. standard-dose influenza vaccine provided substantially better immune responses in seropositive rheumatoid arthritis patients in a randomized, active-controlled trial.
High-dose trivalent influenza vaccine is known to improve immune responses in the elderly, but the current findings, which were presented at the annual meeting of the American College of Rheumatology, are the first to document a successful intervention to enhance vaccine responses in immunocompromised patients, according to Inés Colmegna, MD, of McGill University, Montreal.
Dr. Colmegna and her colleagues assessed antibody responses to either standard-dose (15 mcg of hemagglutinin per strain) quadrivalent inactivated influenza vaccine (SD-QIV) or high-dose (60 mcg of hemagglutinin per strain) trivalent inactivated influenza vaccine (HD-TIV) in 140 and 139 patients, respectively.
Seroprotection rates prior to vaccination were comparable in the two groups, but the high-dose recipients had consistently higher overall responses to vaccination.
Seroconversion rates were 22.3% vs. 8.6% (odds ratio, 2.93) for the H3N2 strain (A/HongKong/4801/2014), and 44.6% vs. 28.6% (OR, 1.93) for the B Victoria Lin strain (B/Brisbane/60/2008). For the H1N1 strain A/California/7/2009 in 2016-2017 and closely related A/Michigan/45/2015 in 2017-2018, the seroconversion rates were 51.1% vs. 30.0% (OR, 2.91) and 46.4% vs. 24.6% (OR, 2.79), respectively. Seroprotection rates for the H3N2 strain were 48.5% vs. 30.9%, and for the B Victoria Lin strain, 60.0% vs. 50.7%. The seroprotection rates for the H1N1 strains together were and 80.4% vs. 73.5%, Dr. Colmegna said.
Seroconversion was defined as at least a fourfold serum hemagglutination inhibition (HI) antibody increase from prevaccination level (day 0), and seroprotection was defined as percent with HI titers of 1:40 or greater at postvaccination day 28.
After the researchers controlled for age, vaccine type, treatment type in the 3 months prior to vaccination and during the study period, Charlson comorbidity index, and RA duration, the only significant predictors of vaccine seroresponse were vaccine dose and age.
The findings are notable because RA patients have a nearly threefold increase in the risk of contracting influenza infection or related illness, compared with age-matched healthy controls, because of “inherent immune dysfunction associated with RA, comorbidities, the age of our patients, and immunosuppressive therapy,” Dr. Colmegna said.
For this reason, RA patients are a priority group for annual vaccination. However, while vaccination remains the most effective method for preventing influenza and its associated complications, vaccine-induced antibody responses and protection in RA are suboptimal, she explained, noting that this puts them at increased risk for severe influenza.
“There is a high priority to develop new approaches to try to decrease this risk,” she said.
It was unknown whether HD-TIV – the only currently available high-dose influenza vaccine – would safely enhance antibody production in RA as it does in the elderly, so she and her colleagues recruited patients from a tertiary care center during the 2016-2017 and 2017-2018 Northern Hemisphere influenza seasons for this study.
The mean age of the patients was 61 years, and 80% were women. All were on stable treatment with either disease-modifying antirheumatic drugs (DMARDs) or biologics for at least 3 months prior to vaccination; treatment types included DMARDs in 138 patients (49.5%), anticytokine therapy in 92 patients (33%), and anti-B-cell therapy and small molecules in 49 patients (17.6%). An analysis by treatment type showed a possible reduction in the rate of seroconversion in patients who received anti-B-cell therapy and small molecules, but the number of patients in the group was too small to make definitive conclusions, Dr. Colmegna said.
Treatment in all groups was safe, with no differences in adverse events between those receiving high- or standard-dose vaccine, and none of the adverse events were related to treatment.
Further, the high-dose vaccine was not associated with an increase in disease activity.
“We believe that these results will likely change clinical practice,” she concluded.
Dr. Colmegna reported having no disclosures.
SOURCE: Colmegna I et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 837.
CHICAGO – The administration of high-dose vs. standard-dose influenza vaccine provided substantially better immune responses in seropositive rheumatoid arthritis patients in a randomized, active-controlled trial.
High-dose trivalent influenza vaccine is known to improve immune responses in the elderly, but the current findings, which were presented at the annual meeting of the American College of Rheumatology, are the first to document a successful intervention to enhance vaccine responses in immunocompromised patients, according to Inés Colmegna, MD, of McGill University, Montreal.
Dr. Colmegna and her colleagues assessed antibody responses to either standard-dose (15 mcg of hemagglutinin per strain) quadrivalent inactivated influenza vaccine (SD-QIV) or high-dose (60 mcg of hemagglutinin per strain) trivalent inactivated influenza vaccine (HD-TIV) in 140 and 139 patients, respectively.
Seroprotection rates prior to vaccination were comparable in the two groups, but the high-dose recipients had consistently higher overall responses to vaccination.
Seroconversion rates were 22.3% vs. 8.6% (odds ratio, 2.93) for the H3N2 strain (A/HongKong/4801/2014), and 44.6% vs. 28.6% (OR, 1.93) for the B Victoria Lin strain (B/Brisbane/60/2008). For the H1N1 strain A/California/7/2009 in 2016-2017 and closely related A/Michigan/45/2015 in 2017-2018, the seroconversion rates were 51.1% vs. 30.0% (OR, 2.91) and 46.4% vs. 24.6% (OR, 2.79), respectively. Seroprotection rates for the H3N2 strain were 48.5% vs. 30.9%, and for the B Victoria Lin strain, 60.0% vs. 50.7%. The seroprotection rates for the H1N1 strains together were and 80.4% vs. 73.5%, Dr. Colmegna said.
Seroconversion was defined as at least a fourfold serum hemagglutination inhibition (HI) antibody increase from prevaccination level (day 0), and seroprotection was defined as percent with HI titers of 1:40 or greater at postvaccination day 28.
After the researchers controlled for age, vaccine type, treatment type in the 3 months prior to vaccination and during the study period, Charlson comorbidity index, and RA duration, the only significant predictors of vaccine seroresponse were vaccine dose and age.
The findings are notable because RA patients have a nearly threefold increase in the risk of contracting influenza infection or related illness, compared with age-matched healthy controls, because of “inherent immune dysfunction associated with RA, comorbidities, the age of our patients, and immunosuppressive therapy,” Dr. Colmegna said.
For this reason, RA patients are a priority group for annual vaccination. However, while vaccination remains the most effective method for preventing influenza and its associated complications, vaccine-induced antibody responses and protection in RA are suboptimal, she explained, noting that this puts them at increased risk for severe influenza.
“There is a high priority to develop new approaches to try to decrease this risk,” she said.
It was unknown whether HD-TIV – the only currently available high-dose influenza vaccine – would safely enhance antibody production in RA as it does in the elderly, so she and her colleagues recruited patients from a tertiary care center during the 2016-2017 and 2017-2018 Northern Hemisphere influenza seasons for this study.
The mean age of the patients was 61 years, and 80% were women. All were on stable treatment with either disease-modifying antirheumatic drugs (DMARDs) or biologics for at least 3 months prior to vaccination; treatment types included DMARDs in 138 patients (49.5%), anticytokine therapy in 92 patients (33%), and anti-B-cell therapy and small molecules in 49 patients (17.6%). An analysis by treatment type showed a possible reduction in the rate of seroconversion in patients who received anti-B-cell therapy and small molecules, but the number of patients in the group was too small to make definitive conclusions, Dr. Colmegna said.
Treatment in all groups was safe, with no differences in adverse events between those receiving high- or standard-dose vaccine, and none of the adverse events were related to treatment.
Further, the high-dose vaccine was not associated with an increase in disease activity.
“We believe that these results will likely change clinical practice,” she concluded.
Dr. Colmegna reported having no disclosures.
SOURCE: Colmegna I et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 837.
CHICAGO – The administration of high-dose vs. standard-dose influenza vaccine provided substantially better immune responses in seropositive rheumatoid arthritis patients in a randomized, active-controlled trial.
High-dose trivalent influenza vaccine is known to improve immune responses in the elderly, but the current findings, which were presented at the annual meeting of the American College of Rheumatology, are the first to document a successful intervention to enhance vaccine responses in immunocompromised patients, according to Inés Colmegna, MD, of McGill University, Montreal.
Dr. Colmegna and her colleagues assessed antibody responses to either standard-dose (15 mcg of hemagglutinin per strain) quadrivalent inactivated influenza vaccine (SD-QIV) or high-dose (60 mcg of hemagglutinin per strain) trivalent inactivated influenza vaccine (HD-TIV) in 140 and 139 patients, respectively.
Seroprotection rates prior to vaccination were comparable in the two groups, but the high-dose recipients had consistently higher overall responses to vaccination.
Seroconversion rates were 22.3% vs. 8.6% (odds ratio, 2.93) for the H3N2 strain (A/HongKong/4801/2014), and 44.6% vs. 28.6% (OR, 1.93) for the B Victoria Lin strain (B/Brisbane/60/2008). For the H1N1 strain A/California/7/2009 in 2016-2017 and closely related A/Michigan/45/2015 in 2017-2018, the seroconversion rates were 51.1% vs. 30.0% (OR, 2.91) and 46.4% vs. 24.6% (OR, 2.79), respectively. Seroprotection rates for the H3N2 strain were 48.5% vs. 30.9%, and for the B Victoria Lin strain, 60.0% vs. 50.7%. The seroprotection rates for the H1N1 strains together were and 80.4% vs. 73.5%, Dr. Colmegna said.
Seroconversion was defined as at least a fourfold serum hemagglutination inhibition (HI) antibody increase from prevaccination level (day 0), and seroprotection was defined as percent with HI titers of 1:40 or greater at postvaccination day 28.
After the researchers controlled for age, vaccine type, treatment type in the 3 months prior to vaccination and during the study period, Charlson comorbidity index, and RA duration, the only significant predictors of vaccine seroresponse were vaccine dose and age.
The findings are notable because RA patients have a nearly threefold increase in the risk of contracting influenza infection or related illness, compared with age-matched healthy controls, because of “inherent immune dysfunction associated with RA, comorbidities, the age of our patients, and immunosuppressive therapy,” Dr. Colmegna said.
For this reason, RA patients are a priority group for annual vaccination. However, while vaccination remains the most effective method for preventing influenza and its associated complications, vaccine-induced antibody responses and protection in RA are suboptimal, she explained, noting that this puts them at increased risk for severe influenza.
“There is a high priority to develop new approaches to try to decrease this risk,” she said.
It was unknown whether HD-TIV – the only currently available high-dose influenza vaccine – would safely enhance antibody production in RA as it does in the elderly, so she and her colleagues recruited patients from a tertiary care center during the 2016-2017 and 2017-2018 Northern Hemisphere influenza seasons for this study.
The mean age of the patients was 61 years, and 80% were women. All were on stable treatment with either disease-modifying antirheumatic drugs (DMARDs) or biologics for at least 3 months prior to vaccination; treatment types included DMARDs in 138 patients (49.5%), anticytokine therapy in 92 patients (33%), and anti-B-cell therapy and small molecules in 49 patients (17.6%). An analysis by treatment type showed a possible reduction in the rate of seroconversion in patients who received anti-B-cell therapy and small molecules, but the number of patients in the group was too small to make definitive conclusions, Dr. Colmegna said.
Treatment in all groups was safe, with no differences in adverse events between those receiving high- or standard-dose vaccine, and none of the adverse events were related to treatment.
Further, the high-dose vaccine was not associated with an increase in disease activity.
“We believe that these results will likely change clinical practice,” she concluded.
Dr. Colmegna reported having no disclosures.
SOURCE: Colmegna I et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 837.
REPORTING FROM THE ACR ANNUAL MEETING
Key clinical point: High- vs. standard-dose flu vaccine improves immune responses in RA patients.
Major finding: High-dose trivalent inactivated influenza vaccine was associated with greater odds of H3N2, B Victoria Lin, and H1N1 seroconversion.
Study details: A randomized, active-controlled trial of 279 RA patients
Disclosures: Dr. Colmegna reported having no disclosures.
Source: Colmegna I et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 837.

Chinese American man with high risk of psychosis
Editors’ Note: Curbside Consult is an occasional column aimed at helping psychiatrists think through family and cultural considerations when treating patients. It examines case vignettes and is written by two Group for the Advancement of Psychiatry (GAP) committees – the Committee on Family Psychiatry and the Committee on Cultural Psychiatry. The contributors have revised selected patient details to shield the identities of the patients/cases and to comply with HIPAA requirements.
Case vignette
Bill is a 25-year-old man of Chinese descent who sought psychiatric evaluation of his psychosis risk. His parents emigrated from China to Canada more than 30 years ago; Bill was born in Canada, and moved to the United States with his parents and two siblings at age 7.
His family has a strong history of mental illness. His older sister was diagnosed with schizophrenia; she frequently got into verbal altercations with her parents. When Bill was 15, she walked out of the house after a fight with the family and never returned. Bill’s family thinks his father has had paranoid delusions. In the past, he attempted to call the police multiple times because he suspected the neighbors had planted a listening device in his front yard. The family stopped him from making the actual calls. However, the family never brought him to psychiatric evaluation because of perceived stigma and social discrimination in their community. He also was emotionally and physically abusive to Bill during his childhood by calling him names and hitting him with a belt. As an adult, Bill still has posttraumatic stress disorder symptoms including flashbacks, nightmares, and avoidance when thinking about his father.
Bill identifies himself as Chinese American and speaks English only. He often perceives himself as a newcomer to U.S. society, making comments such as: “I guess I should live my life like this to fulfill the American dream.” Bill’s parents placed a strong emphasis on academic success, often at the expense of their children’s social interaction and playtime activities. Bill describes himself as a “loner” with few friends. He maintained high academic achievement during high school and was accepted by a prestigious college. Although he was interested in music composition, Bill was “forced” by his parents to major in courses deemed good preparation for law school.
During college, he suffered severe depression with insomnia, low energy, hopelessness, anhedonia, social withdrawal, poor appetite with weight loss, and ruminative thoughts but without delusional thoughts or perceptual disturbances. He had one near-lethal suicide attempt, during which he impulsively took the contents of an entire bottle of Tylenol in the context of family conflicts, resulting in psychiatric hospitalization. Bill recalled with animosity the inpatient psychiatrists who put him on psychotropic medications during a 3-day hospitalization. He was not adherent to the medication and did not follow up with postdischarge outpatient care. He did not remember the medication trial he had during the hospitalization, nor did he give consent to obtain medical records from there. Bill withdrew from college in sophomore year, because of his declining academic performance secondary to his mental illness. He currently works at a gas station.
Over the last year, Bill’s interpersonal communication has become disorganized in both work and social settings, and he has developed thought blocking, causing him substantial distress. He intermittently hears voices of strangers in the background; these have gradually become more frequent, now occurring 3-4 times a week. Bill also is more depressed, with frequent crying episodes and worsening social isolation. He often thinks that life is not worth living, but he has no active suicidal plans or intent.
Bill’s supervisor and coworkers strongly suggested that he seek medical evaluation. As an outpatient, Bill started weekly cognitive-behavioral therapy (CBT) and biweekly medication sessions for early psychosis symptoms, receiving low-dose risperidone (1 mg b.i.d.) and fluoxetine (20 mg daily). Despite initial improvement, he was very skeptical about continuing the medications because of concern that they will cause a “change in his identity” by altering his body chemistry. His parents have been reluctant to join family meetings, because they were ambivalent about Bill’s ongoing psychiatric treatment.
Treatment team’s impressions
Clinical high risk (CHR) syndrome refers to the prodromal phase before a full psychotic disorder. As one of the three subcategories of CHR, genetic risk and deterioration (GRD) prodromal syndrome is defined by having a genetic risk for psychosis (first-degree relative with a psychotic disorder or meeting criteria for schizotypal personality disorder) and a recent decline in daily functioning equivalent to a 30% drop in Global Assessment of Functioning rating.1 Due to Bill’s family history of psychosis, new difficulties in self-care, psychotic-spectrum symptoms, and declining social/executive function, he meets criteria for GRD prodromal syndrome. In addition, major depressive disorder should be considered on his differential diagnosis.

Bill has not received a diagnosis of acute psychosis, and instead is judged to be in the CHR spectrum for psychosis, because of his level of insight that the occasional perceptual disturbance and abnormal thought content are in his own mind. Since 26% of individuals with CHR in mainland China2 and 35% in the general U.S. population develop fully psychotic symptoms within 2-3 years, Bill’s current presentation warrants secondary preventive care (early intervention) to promote improved clinical outcomes. Given the high rates of comorbid depressive and anxiety disorders among individuals with CHR, Bill’s mood symptoms and passive suicidality also require psychiatric intervention. The treatment team raised three questions, which are answered below.
1. How can we understand Bill’s and his family’s resistance to mental health treatment?
Chinese Americans tend to access mental health services at a lower rate than that of the general U.S. population.3 They also tend to exhibit elevated discontinuation from mental health care, compared with non-Latino whites.4 Since first- and second-generation Chinese Americans have similar use rates, it is likely the barriers to care are not immigration specific but also related to factors that endure across generations, including culture-related aspects. These include cultural concepts of illness and how to interpret prodromal symptoms such as Bill’s, stigma and interpersonal shame regarding mental illness and psychiatric treatment, and value orientations such as self-reliance, avoidance of direct expressions of interpersonal conflict, and family privacy.

For example, Chinese Americans tend to emphasize the physical-symptom components of psychiatric problems, partly because of mind-body holism – which combines physical and psychological symptoms into cultural syndromes and idioms of distress – and partly because of concerns about stigma and shame regarding mental health symptoms. Hence, they are more likely to seek help from primary care clinicians for psychological distress before any mental health provider. Many Chinese Americans interpret mild to moderate psychological distress as “mental weakness” or “excessive thinking” (xiang tai duo), which does not require clinical evaluation. In this view, only alarmingly bizarre or disruptive behaviors warrant formal psychiatric treatment.

Some Chinese parents perceive psychosocial stressors, including hardships, interpersonal conflicts, and academic burdens, as understandable triggers for symptoms that clinicians would classify as schizophrenia or attenuated psychosis syndrome.5 Those views of illness can be associated in the Chinese American community with delayed diagnosis and intervention for emerging psychiatric disorders.
Social stigma regarding mental illness is pervasive in many Chinese American communities. Stigma hinders service use, to avoid shame and save the family’s “face.” Although many Chinese Americans acknowledge the efficacy of biomedical treatments for mental illness, they also remain concerned about enduring shame in their communities if they access those services.6 In line with collectivistic values traditionally held by many Chinese Americans, individuals tend to turn to relatives for help first and keep mental illness confidential within the family group to avoid disgracing the family name.7 Hence, social stigma in the Chinese community can be a key barrier to early detection and early intervention for youth at high risk of psychosis.

Culturally influenced cognitions, emotions, and values also might contribute to underuse of formal mental health services in this population. Many Chinese Americans perceive the roots of mental illness in a lack of willpower and the unwise indulgence of morbid thoughts. In these communities, direct communication of strong emotions can be discouraged – in the name of maintaining harmony, collective interests, and tolerance.8 Hence, many Chinese Americans find Western models of psychotherapy that focus on intrapsychic conflicts and/or intense interpersonal emotions incongruous with their treatment expectations. Psychiatric interview processes that explore gloomy or disturbing thoughts can be perceived as disquieting and antithetical to the goals of treatment. In addition, some individuals rooted in collectivist communities would rather keep personal psychological problems private within the family than seek counseling from an expert who is an out-group stranger.
2. How does Bill’s cultural and social context affect his prognosis?
Individuals with psychosis and their close relatives are generally vulnerable to stigma and discrimination. Mental health stigma has a substantial effect on the lives of patients with psychosis and their family members. The magnitude of the perceived stigma tends to be greater if the patient has more severe positive symptoms, is more educated, or resides in a highly urbanized area.
Acutely ill patients usually face more negative community responses than do milder cases, since their close relatives are blamed for failing to uphold the moral and legal responsibility of ensuring that the patients control their behavior. The effect of stigma in Chinese society also is greater among male patients with early-onset illness, because of the expectation that men marry and become the family breadwinner to attain higher social status. Hence, young males who are unable to achieve these socially determined adult milestones can be considered socially inferior, and suffer more community discrimination and exclusion, which are risk factors for clinical deterioration and functional impairment.
Social stigma can intensify relationship conflicts within the family and magnify expressed emotion (EE), which is defined as caregivers’ attitude toward a person with mental illness as reflected by their comments and interaction patterns. “High EE” comprises three behavioral patterns: criticism, hostility, and emotional overinvolvement. High EE is associated with psychiatric symptom relapse among individuals with schizophrenia and other disorders.9
Currently, most of the literature on EE is limited to white samples in Western countries. Some researchers have studied the relationship between the EE index of emotional overinvolvement and schizophrenia relapse among Hispanic populations.10 However, there are limited data on cultural congruence of EE research in Asian populations. Therefore, clinicians should carefully evaluate the contribution of high EE to Bill’s family’s situation during his course of treatment.
Higher education often is associated with greater levels of EE and can result in anxious and fearful responses to the person’s illness.11 This may be attributable to more negative reactions to actual or feared stigma and discrimination, possibly because relatives feel they have more to lose regarding the family’s social status, especially in densely populated urban areas where it might be harder to keep the patient’s mental illness as a “family secret.”
On the other hand, certain explanatory models of psychosis can modulate Chinese community members’ perceptions and allow ill individuals to remain socially integrated. Cultural idioms such as “excessive thinking” (xiang tai duo), “taking things too hard” (xiang bu kai), and “narrow-mindedness” (xiao xin yan) promote socially accommodating behaviors that facilitate acceptance of mildly to moderately ill individuals as full-status community members.12
Another important contributor to psychosis risk is Bill’s acculturative stress about his cultural identity. Linguistic challenges, limited social support, perceived discrimination, and an acculturation gap between parents and children are major sources of acculturative stress among Chinese American college students.13 Greater acculturative stress elevates the risk of mental illness and symptom deterioration. However, highly acculturated Chinese Americans with above-average bicultural self-efficacy tend to express more positive attitudes toward mental health services.
3. Are there culturally appropriate interventions that can help Bill and his family?
A major predictor among Chinese Americans of the intent to use services is the perceived credibility of the treatment and the provider. Ethnic-specific services staffed by bicultural/bilingual mental health clinicians delivering culturally responsive interventions are increasingly available in many metropolitan areas with major Asian communities. These programs have shown clinical efficacy in encouraging service use and promoting treatment persistence. Bill and his family may benefit from referral to ethnic-specific services, where they can obtain culturally sensitive psychoeducation about his mental illness and treatment plan.
Other services that might be useful for Bill and his family include family psychoeducation programs and supportive groups specifically designed for Chinese American families; these can improve the entire family’s psychosocial health, promote medication adherence, and reduce the risk of symptom relapse through family-centered intervention models.14 Connecting with local National Alliance on Mental Illness (NAMI) programs might help Bill’s parents obtain social support from Chinese American families with similar caregiver experiences.
However, services that are not designed specifically for Chinese-origin patients also can provide excellent care for these patients, and be perceived as credible and effective. A thorough cultural assessment is necessary, as well as inclusion of the information obtained in the treatment plan. As described in the DSM-5 Outline for Cultural Formulation and operationalized in the Cultural Formulation Interview, clinicians should assess possible cultural differences among Bill, his family, his community, and his clinicians regarding their cultural concepts of distress and illness and expectations of care in order to formulate a treatment plan acceptable to patient and family. Practical cultural barriers should be addressed, such as Bill’s parents’ limited English proficiency, in which case a bilingual clinician or trained interpreter should be included in the treatment team.
With Bill’s consent, the treatment team also should consider reaching out to his parents, especially his mother, to understand and empathize with their cultural concepts of distress and illness as well as expectations for care. In addition to providing psychoeducation, the clinicians should validate the parents’ experience of shame, fear, and worry about their son. Bill’s brother, for example, might be a useful bridge in communicating with the parents given his higher acculturation and potentially greater acceptance of psychiatric care. He might help alleviate the tension between Bill and his parents and encourage them to seek family-based help.
Take-home points
- Clinical training programs should offer cultural competency training about underserved populations, including communities of color.
- Certain key concepts, such as traditional idioms of distress and explanatory models, social stigma, and acculturative stress, should be included in these trainings and evaluated in a comprehensive psychosocial assessment.
- High expressed emotion among family caregivers is associated with higher rates of psychiatric symptom relapse, whereas families with above-average bicultural self-efficacy have more positive attitudes toward mental health services.
- Clinicians should incorporate culturally appropriate educational materials (for example, CHR warning signs) and interventions to engage underserved patients and their families in mental health treatment.
Contributors
Emily Wu, MD – Harvard Medical School, Boston
Francis Lu, MD – University of California, Davis
John Sargent, MD – Tufts Medical Center, Boston
Roberto Lewis-Fernández, MD – Columbia College of Physicians & Surgeons, New York
If you would like to a submit case in which your understanding and treatment are affected by challenging cultural and family values, send it to [email protected]. We will then write back with our best answers about how one might proceed in such a case. Your case and our response will then be published at mdedge.com/psychiatry. This column is meant to be educational and does not constitute medical advice. The opinions expressed are those of the contributors and do not represent those of the organizations they are employed by or affiliated with or the Group for the Advancement of Psychiatry.
References
1. J Nerv Ment Dis. 2013 Jun;20(6);484-9.
2. Schizophr Res. 2014 Feb;152(2-3):391-9.
3. Perspect Psychiatr Care. 2013;49(4):288-92.
4. Ment Health Serv Res. 2001 Dec;3(4):201-14.
5. Br J Psychiatry. 2000 Jul;177;20-5.
6. Cultr Divers Ethnic Minor Psychol. 2008 Jan;14(1):10-8.
7. Couns Psychol. 2003 May1;31:343-61.
8. Emotion. 2002 Dec;2(4):341-60.
9. Am J Psychiatry. 1986 Nov;143(11):1361-73.
10. J Nerv Ment Dis. 2013 Oct;201(10):833-40.
11. Schizophr Bull. 1981;7(1):43-4.
12. Schizophr Bull. 2010 Jul;36(4):836-45.
13. Am J Orthopsychiatry. 2011 Oct;81(4):489-97.
14. Patient Educ Couns. 2009 Apr;75(1):67-76.
Editors’ Note: Curbside Consult is an occasional column aimed at helping psychiatrists think through family and cultural considerations when treating patients. It examines case vignettes and is written by two Group for the Advancement of Psychiatry (GAP) committees – the Committee on Family Psychiatry and the Committee on Cultural Psychiatry. The contributors have revised selected patient details to shield the identities of the patients/cases and to comply with HIPAA requirements.
Case vignette
Bill is a 25-year-old man of Chinese descent who sought psychiatric evaluation of his psychosis risk. His parents emigrated from China to Canada more than 30 years ago; Bill was born in Canada, and moved to the United States with his parents and two siblings at age 7.
His family has a strong history of mental illness. His older sister was diagnosed with schizophrenia; she frequently got into verbal altercations with her parents. When Bill was 15, she walked out of the house after a fight with the family and never returned. Bill’s family thinks his father has had paranoid delusions. In the past, he attempted to call the police multiple times because he suspected the neighbors had planted a listening device in his front yard. The family stopped him from making the actual calls. However, the family never brought him to psychiatric evaluation because of perceived stigma and social discrimination in their community. He also was emotionally and physically abusive to Bill during his childhood by calling him names and hitting him with a belt. As an adult, Bill still has posttraumatic stress disorder symptoms including flashbacks, nightmares, and avoidance when thinking about his father.
Bill identifies himself as Chinese American and speaks English only. He often perceives himself as a newcomer to U.S. society, making comments such as: “I guess I should live my life like this to fulfill the American dream.” Bill’s parents placed a strong emphasis on academic success, often at the expense of their children’s social interaction and playtime activities. Bill describes himself as a “loner” with few friends. He maintained high academic achievement during high school and was accepted by a prestigious college. Although he was interested in music composition, Bill was “forced” by his parents to major in courses deemed good preparation for law school.
During college, he suffered severe depression with insomnia, low energy, hopelessness, anhedonia, social withdrawal, poor appetite with weight loss, and ruminative thoughts but without delusional thoughts or perceptual disturbances. He had one near-lethal suicide attempt, during which he impulsively took the contents of an entire bottle of Tylenol in the context of family conflicts, resulting in psychiatric hospitalization. Bill recalled with animosity the inpatient psychiatrists who put him on psychotropic medications during a 3-day hospitalization. He was not adherent to the medication and did not follow up with postdischarge outpatient care. He did not remember the medication trial he had during the hospitalization, nor did he give consent to obtain medical records from there. Bill withdrew from college in sophomore year, because of his declining academic performance secondary to his mental illness. He currently works at a gas station.
Over the last year, Bill’s interpersonal communication has become disorganized in both work and social settings, and he has developed thought blocking, causing him substantial distress. He intermittently hears voices of strangers in the background; these have gradually become more frequent, now occurring 3-4 times a week. Bill also is more depressed, with frequent crying episodes and worsening social isolation. He often thinks that life is not worth living, but he has no active suicidal plans or intent.
Bill’s supervisor and coworkers strongly suggested that he seek medical evaluation. As an outpatient, Bill started weekly cognitive-behavioral therapy (CBT) and biweekly medication sessions for early psychosis symptoms, receiving low-dose risperidone (1 mg b.i.d.) and fluoxetine (20 mg daily). Despite initial improvement, he was very skeptical about continuing the medications because of concern that they will cause a “change in his identity” by altering his body chemistry. His parents have been reluctant to join family meetings, because they were ambivalent about Bill’s ongoing psychiatric treatment.
Treatment team’s impressions
Clinical high risk (CHR) syndrome refers to the prodromal phase before a full psychotic disorder. As one of the three subcategories of CHR, genetic risk and deterioration (GRD) prodromal syndrome is defined by having a genetic risk for psychosis (first-degree relative with a psychotic disorder or meeting criteria for schizotypal personality disorder) and a recent decline in daily functioning equivalent to a 30% drop in Global Assessment of Functioning rating.1 Due to Bill’s family history of psychosis, new difficulties in self-care, psychotic-spectrum symptoms, and declining social/executive function, he meets criteria for GRD prodromal syndrome. In addition, major depressive disorder should be considered on his differential diagnosis.
Bill has not received a diagnosis of acute psychosis, and instead is judged to be in the CHR spectrum for psychosis, because of his level of insight that the occasional perceptual disturbance and abnormal thought content are in his own mind. Since 26% of individuals with CHR in mainland China2 and 35% in the general U.S. population develop fully psychotic symptoms within 2-3 years, Bill’s current presentation warrants secondary preventive care (early intervention) to promote improved clinical outcomes. Given the high rates of comorbid depressive and anxiety disorders among individuals with CHR, Bill’s mood symptoms and passive suicidality also require psychiatric intervention. The treatment team raised three questions, which are answered below.
1. How can we understand Bill’s and his family’s resistance to mental health treatment?
Chinese Americans tend to access mental health services at a lower rate than that of the general U.S. population.3 They also tend to exhibit elevated discontinuation from mental health care, compared with non-Latino whites.4 Since first- and second-generation Chinese Americans have similar use rates, it is likely the barriers to care are not immigration specific but also related to factors that endure across generations, including culture-related aspects. These include cultural concepts of illness and how to interpret prodromal symptoms such as Bill’s, stigma and interpersonal shame regarding mental illness and psychiatric treatment, and value orientations such as self-reliance, avoidance of direct expressions of interpersonal conflict, and family privacy.
For example, Chinese Americans tend to emphasize the physical-symptom components of psychiatric problems, partly because of mind-body holism – which combines physical and psychological symptoms into cultural syndromes and idioms of distress – and partly because of concerns about stigma and shame regarding mental health symptoms. Hence, they are more likely to seek help from primary care clinicians for psychological distress before any mental health provider. Many Chinese Americans interpret mild to moderate psychological distress as “mental weakness” or “excessive thinking” (xiang tai duo), which does not require clinical evaluation. In this view, only alarmingly bizarre or disruptive behaviors warrant formal psychiatric treatment.
Some Chinese parents perceive psychosocial stressors, including hardships, interpersonal conflicts, and academic burdens, as understandable triggers for symptoms that clinicians would classify as schizophrenia or attenuated psychosis syndrome.5 Those views of illness can be associated in the Chinese American community with delayed diagnosis and intervention for emerging psychiatric disorders.
Social stigma regarding mental illness is pervasive in many Chinese American communities. Stigma hinders service use, to avoid shame and save the family’s “face.” Although many Chinese Americans acknowledge the efficacy of biomedical treatments for mental illness, they also remain concerned about enduring shame in their communities if they access those services.6 In line with collectivistic values traditionally held by many Chinese Americans, individuals tend to turn to relatives for help first and keep mental illness confidential within the family group to avoid disgracing the family name.7 Hence, social stigma in the Chinese community can be a key barrier to early detection and early intervention for youth at high risk of psychosis.
Culturally influenced cognitions, emotions, and values also might contribute to underuse of formal mental health services in this population. Many Chinese Americans perceive the roots of mental illness in a lack of willpower and the unwise indulgence of morbid thoughts. In these communities, direct communication of strong emotions can be discouraged – in the name of maintaining harmony, collective interests, and tolerance.8 Hence, many Chinese Americans find Western models of psychotherapy that focus on intrapsychic conflicts and/or intense interpersonal emotions incongruous with their treatment expectations. Psychiatric interview processes that explore gloomy or disturbing thoughts can be perceived as disquieting and antithetical to the goals of treatment. In addition, some individuals rooted in collectivist communities would rather keep personal psychological problems private within the family than seek counseling from an expert who is an out-group stranger.
2. How does Bill’s cultural and social context affect his prognosis?
Individuals with psychosis and their close relatives are generally vulnerable to stigma and discrimination. Mental health stigma has a substantial effect on the lives of patients with psychosis and their family members. The magnitude of the perceived stigma tends to be greater if the patient has more severe positive symptoms, is more educated, or resides in a highly urbanized area.
Acutely ill patients usually face more negative community responses than do milder cases, since their close relatives are blamed for failing to uphold the moral and legal responsibility of ensuring that the patients control their behavior. The effect of stigma in Chinese society also is greater among male patients with early-onset illness, because of the expectation that men marry and become the family breadwinner to attain higher social status. Hence, young males who are unable to achieve these socially determined adult milestones can be considered socially inferior, and suffer more community discrimination and exclusion, which are risk factors for clinical deterioration and functional impairment.
Social stigma can intensify relationship conflicts within the family and magnify expressed emotion (EE), which is defined as caregivers’ attitude toward a person with mental illness as reflected by their comments and interaction patterns. “High EE” comprises three behavioral patterns: criticism, hostility, and emotional overinvolvement. High EE is associated with psychiatric symptom relapse among individuals with schizophrenia and other disorders.9
Currently, most of the literature on EE is limited to white samples in Western countries. Some researchers have studied the relationship between the EE index of emotional overinvolvement and schizophrenia relapse among Hispanic populations.10 However, there are limited data on cultural congruence of EE research in Asian populations. Therefore, clinicians should carefully evaluate the contribution of high EE to Bill’s family’s situation during his course of treatment.
Higher education often is associated with greater levels of EE and can result in anxious and fearful responses to the person’s illness.11 This may be attributable to more negative reactions to actual or feared stigma and discrimination, possibly because relatives feel they have more to lose regarding the family’s social status, especially in densely populated urban areas where it might be harder to keep the patient’s mental illness as a “family secret.”
On the other hand, certain explanatory models of psychosis can modulate Chinese community members’ perceptions and allow ill individuals to remain socially integrated. Cultural idioms such as “excessive thinking” (xiang tai duo), “taking things too hard” (xiang bu kai), and “narrow-mindedness” (xiao xin yan) promote socially accommodating behaviors that facilitate acceptance of mildly to moderately ill individuals as full-status community members.12
Another important contributor to psychosis risk is Bill’s acculturative stress about his cultural identity. Linguistic challenges, limited social support, perceived discrimination, and an acculturation gap between parents and children are major sources of acculturative stress among Chinese American college students.13 Greater acculturative stress elevates the risk of mental illness and symptom deterioration. However, highly acculturated Chinese Americans with above-average bicultural self-efficacy tend to express more positive attitudes toward mental health services.
3. Are there culturally appropriate interventions that can help Bill and his family?
A major predictor among Chinese Americans of the intent to use services is the perceived credibility of the treatment and the provider. Ethnic-specific services staffed by bicultural/bilingual mental health clinicians delivering culturally responsive interventions are increasingly available in many metropolitan areas with major Asian communities. These programs have shown clinical efficacy in encouraging service use and promoting treatment persistence. Bill and his family may benefit from referral to ethnic-specific services, where they can obtain culturally sensitive psychoeducation about his mental illness and treatment plan.
Other services that might be useful for Bill and his family include family psychoeducation programs and supportive groups specifically designed for Chinese American families; these can improve the entire family’s psychosocial health, promote medication adherence, and reduce the risk of symptom relapse through family-centered intervention models.14 Connecting with local National Alliance on Mental Illness (NAMI) programs might help Bill’s parents obtain social support from Chinese American families with similar caregiver experiences.
However, services that are not designed specifically for Chinese-origin patients also can provide excellent care for these patients, and be perceived as credible and effective. A thorough cultural assessment is necessary, as well as inclusion of the information obtained in the treatment plan. As described in the DSM-5 Outline for Cultural Formulation and operationalized in the Cultural Formulation Interview, clinicians should assess possible cultural differences among Bill, his family, his community, and his clinicians regarding their cultural concepts of distress and illness and expectations of care in order to formulate a treatment plan acceptable to patient and family. Practical cultural barriers should be addressed, such as Bill’s parents’ limited English proficiency, in which case a bilingual clinician or trained interpreter should be included in the treatment team.
With Bill’s consent, the treatment team also should consider reaching out to his parents, especially his mother, to understand and empathize with their cultural concepts of distress and illness as well as expectations for care. In addition to providing psychoeducation, the clinicians should validate the parents’ experience of shame, fear, and worry about their son. Bill’s brother, for example, might be a useful bridge in communicating with the parents given his higher acculturation and potentially greater acceptance of psychiatric care. He might help alleviate the tension between Bill and his parents and encourage them to seek family-based help.
Take-home points
- Clinical training programs should offer cultural competency training about underserved populations, including communities of color.
- Certain key concepts, such as traditional idioms of distress and explanatory models, social stigma, and acculturative stress, should be included in these trainings and evaluated in a comprehensive psychosocial assessment.
- High expressed emotion among family caregivers is associated with higher rates of psychiatric symptom relapse, whereas families with above-average bicultural self-efficacy have more positive attitudes toward mental health services.
- Clinicians should incorporate culturally appropriate educational materials (for example, CHR warning signs) and interventions to engage underserved patients and their families in mental health treatment.
Contributors
Emily Wu, MD – Harvard Medical School, Boston
Francis Lu, MD – University of California, Davis
John Sargent, MD – Tufts Medical Center, Boston
Roberto Lewis-Fernández, MD – Columbia College of Physicians & Surgeons, New York
If you would like to a submit case in which your understanding and treatment are affected by challenging cultural and family values, send it to [email protected]. We will then write back with our best answers about how one might proceed in such a case. Your case and our response will then be published at mdedge.com/psychiatry. This column is meant to be educational and does not constitute medical advice. The opinions expressed are those of the contributors and do not represent those of the organizations they are employed by or affiliated with or the Group for the Advancement of Psychiatry.
References
1. J Nerv Ment Dis. 2013 Jun;20(6);484-9.
2. Schizophr Res. 2014 Feb;152(2-3):391-9.
3. Perspect Psychiatr Care. 2013;49(4):288-92.
4. Ment Health Serv Res. 2001 Dec;3(4):201-14.
5. Br J Psychiatry. 2000 Jul;177;20-5.
6. Cultr Divers Ethnic Minor Psychol. 2008 Jan;14(1):10-8.
7. Couns Psychol. 2003 May1;31:343-61.
8. Emotion. 2002 Dec;2(4):341-60.
9. Am J Psychiatry. 1986 Nov;143(11):1361-73.
10. J Nerv Ment Dis. 2013 Oct;201(10):833-40.
11. Schizophr Bull. 1981;7(1):43-4.
12. Schizophr Bull. 2010 Jul;36(4):836-45.
13. Am J Orthopsychiatry. 2011 Oct;81(4):489-97.
14. Patient Educ Couns. 2009 Apr;75(1):67-76.
Editors’ Note: Curbside Consult is an occasional column aimed at helping psychiatrists think through family and cultural considerations when treating patients. It examines case vignettes and is written by two Group for the Advancement of Psychiatry (GAP) committees – the Committee on Family Psychiatry and the Committee on Cultural Psychiatry. The contributors have revised selected patient details to shield the identities of the patients/cases and to comply with HIPAA requirements.
Case vignette
Bill is a 25-year-old man of Chinese descent who sought psychiatric evaluation of his psychosis risk. His parents emigrated from China to Canada more than 30 years ago; Bill was born in Canada, and moved to the United States with his parents and two siblings at age 7.
His family has a strong history of mental illness. His older sister was diagnosed with schizophrenia; she frequently got into verbal altercations with her parents. When Bill was 15, she walked out of the house after a fight with the family and never returned. Bill’s family thinks his father has had paranoid delusions. In the past, he attempted to call the police multiple times because he suspected the neighbors had planted a listening device in his front yard. The family stopped him from making the actual calls. However, the family never brought him to psychiatric evaluation because of perceived stigma and social discrimination in their community. He also was emotionally and physically abusive to Bill during his childhood by calling him names and hitting him with a belt. As an adult, Bill still has posttraumatic stress disorder symptoms including flashbacks, nightmares, and avoidance when thinking about his father.
Bill identifies himself as Chinese American and speaks English only. He often perceives himself as a newcomer to U.S. society, making comments such as: “I guess I should live my life like this to fulfill the American dream.” Bill’s parents placed a strong emphasis on academic success, often at the expense of their children’s social interaction and playtime activities. Bill describes himself as a “loner” with few friends. He maintained high academic achievement during high school and was accepted by a prestigious college. Although he was interested in music composition, Bill was “forced” by his parents to major in courses deemed good preparation for law school.
During college, he suffered severe depression with insomnia, low energy, hopelessness, anhedonia, social withdrawal, poor appetite with weight loss, and ruminative thoughts but without delusional thoughts or perceptual disturbances. He had one near-lethal suicide attempt, during which he impulsively took the contents of an entire bottle of Tylenol in the context of family conflicts, resulting in psychiatric hospitalization. Bill recalled with animosity the inpatient psychiatrists who put him on psychotropic medications during a 3-day hospitalization. He was not adherent to the medication and did not follow up with postdischarge outpatient care. He did not remember the medication trial he had during the hospitalization, nor did he give consent to obtain medical records from there. Bill withdrew from college in sophomore year, because of his declining academic performance secondary to his mental illness. He currently works at a gas station.
Over the last year, Bill’s interpersonal communication has become disorganized in both work and social settings, and he has developed thought blocking, causing him substantial distress. He intermittently hears voices of strangers in the background; these have gradually become more frequent, now occurring 3-4 times a week. Bill also is more depressed, with frequent crying episodes and worsening social isolation. He often thinks that life is not worth living, but he has no active suicidal plans or intent.
Bill’s supervisor and coworkers strongly suggested that he seek medical evaluation. As an outpatient, Bill started weekly cognitive-behavioral therapy (CBT) and biweekly medication sessions for early psychosis symptoms, receiving low-dose risperidone (1 mg b.i.d.) and fluoxetine (20 mg daily). Despite initial improvement, he was very skeptical about continuing the medications because of concern that they will cause a “change in his identity” by altering his body chemistry. His parents have been reluctant to join family meetings, because they were ambivalent about Bill’s ongoing psychiatric treatment.
Treatment team’s impressions
Clinical high risk (CHR) syndrome refers to the prodromal phase before a full psychotic disorder. As one of the three subcategories of CHR, genetic risk and deterioration (GRD) prodromal syndrome is defined by having a genetic risk for psychosis (first-degree relative with a psychotic disorder or meeting criteria for schizotypal personality disorder) and a recent decline in daily functioning equivalent to a 30% drop in Global Assessment of Functioning rating.1 Due to Bill’s family history of psychosis, new difficulties in self-care, psychotic-spectrum symptoms, and declining social/executive function, he meets criteria for GRD prodromal syndrome. In addition, major depressive disorder should be considered on his differential diagnosis.
Bill has not received a diagnosis of acute psychosis, and instead is judged to be in the CHR spectrum for psychosis, because of his level of insight that the occasional perceptual disturbance and abnormal thought content are in his own mind. Since 26% of individuals with CHR in mainland China2 and 35% in the general U.S. population develop fully psychotic symptoms within 2-3 years, Bill’s current presentation warrants secondary preventive care (early intervention) to promote improved clinical outcomes. Given the high rates of comorbid depressive and anxiety disorders among individuals with CHR, Bill’s mood symptoms and passive suicidality also require psychiatric intervention. The treatment team raised three questions, which are answered below.
1. How can we understand Bill’s and his family’s resistance to mental health treatment?
Chinese Americans tend to access mental health services at a lower rate than that of the general U.S. population.3 They also tend to exhibit elevated discontinuation from mental health care, compared with non-Latino whites.4 Since first- and second-generation Chinese Americans have similar use rates, it is likely the barriers to care are not immigration specific but also related to factors that endure across generations, including culture-related aspects. These include cultural concepts of illness and how to interpret prodromal symptoms such as Bill’s, stigma and interpersonal shame regarding mental illness and psychiatric treatment, and value orientations such as self-reliance, avoidance of direct expressions of interpersonal conflict, and family privacy.
For example, Chinese Americans tend to emphasize the physical-symptom components of psychiatric problems, partly because of mind-body holism – which combines physical and psychological symptoms into cultural syndromes and idioms of distress – and partly because of concerns about stigma and shame regarding mental health symptoms. Hence, they are more likely to seek help from primary care clinicians for psychological distress before any mental health provider. Many Chinese Americans interpret mild to moderate psychological distress as “mental weakness” or “excessive thinking” (xiang tai duo), which does not require clinical evaluation. In this view, only alarmingly bizarre or disruptive behaviors warrant formal psychiatric treatment.
Some Chinese parents perceive psychosocial stressors, including hardships, interpersonal conflicts, and academic burdens, as understandable triggers for symptoms that clinicians would classify as schizophrenia or attenuated psychosis syndrome.5 Those views of illness can be associated in the Chinese American community with delayed diagnosis and intervention for emerging psychiatric disorders.
Social stigma regarding mental illness is pervasive in many Chinese American communities. Stigma hinders service use, to avoid shame and save the family’s “face.” Although many Chinese Americans acknowledge the efficacy of biomedical treatments for mental illness, they also remain concerned about enduring shame in their communities if they access those services.6 In line with collectivistic values traditionally held by many Chinese Americans, individuals tend to turn to relatives for help first and keep mental illness confidential within the family group to avoid disgracing the family name.7 Hence, social stigma in the Chinese community can be a key barrier to early detection and early intervention for youth at high risk of psychosis.
Culturally influenced cognitions, emotions, and values also might contribute to underuse of formal mental health services in this population. Many Chinese Americans perceive the roots of mental illness in a lack of willpower and the unwise indulgence of morbid thoughts. In these communities, direct communication of strong emotions can be discouraged – in the name of maintaining harmony, collective interests, and tolerance.8 Hence, many Chinese Americans find Western models of psychotherapy that focus on intrapsychic conflicts and/or intense interpersonal emotions incongruous with their treatment expectations. Psychiatric interview processes that explore gloomy or disturbing thoughts can be perceived as disquieting and antithetical to the goals of treatment. In addition, some individuals rooted in collectivist communities would rather keep personal psychological problems private within the family than seek counseling from an expert who is an out-group stranger.
2. How does Bill’s cultural and social context affect his prognosis?
Individuals with psychosis and their close relatives are generally vulnerable to stigma and discrimination. Mental health stigma has a substantial effect on the lives of patients with psychosis and their family members. The magnitude of the perceived stigma tends to be greater if the patient has more severe positive symptoms, is more educated, or resides in a highly urbanized area.
Acutely ill patients usually face more negative community responses than do milder cases, since their close relatives are blamed for failing to uphold the moral and legal responsibility of ensuring that the patients control their behavior. The effect of stigma in Chinese society also is greater among male patients with early-onset illness, because of the expectation that men marry and become the family breadwinner to attain higher social status. Hence, young males who are unable to achieve these socially determined adult milestones can be considered socially inferior, and suffer more community discrimination and exclusion, which are risk factors for clinical deterioration and functional impairment.
Social stigma can intensify relationship conflicts within the family and magnify expressed emotion (EE), which is defined as caregivers’ attitude toward a person with mental illness as reflected by their comments and interaction patterns. “High EE” comprises three behavioral patterns: criticism, hostility, and emotional overinvolvement. High EE is associated with psychiatric symptom relapse among individuals with schizophrenia and other disorders.9
Currently, most of the literature on EE is limited to white samples in Western countries. Some researchers have studied the relationship between the EE index of emotional overinvolvement and schizophrenia relapse among Hispanic populations.10 However, there are limited data on cultural congruence of EE research in Asian populations. Therefore, clinicians should carefully evaluate the contribution of high EE to Bill’s family’s situation during his course of treatment.
Higher education often is associated with greater levels of EE and can result in anxious and fearful responses to the person’s illness.11 This may be attributable to more negative reactions to actual or feared stigma and discrimination, possibly because relatives feel they have more to lose regarding the family’s social status, especially in densely populated urban areas where it might be harder to keep the patient’s mental illness as a “family secret.”
On the other hand, certain explanatory models of psychosis can modulate Chinese community members’ perceptions and allow ill individuals to remain socially integrated. Cultural idioms such as “excessive thinking” (xiang tai duo), “taking things too hard” (xiang bu kai), and “narrow-mindedness” (xiao xin yan) promote socially accommodating behaviors that facilitate acceptance of mildly to moderately ill individuals as full-status community members.12
Another important contributor to psychosis risk is Bill’s acculturative stress about his cultural identity. Linguistic challenges, limited social support, perceived discrimination, and an acculturation gap between parents and children are major sources of acculturative stress among Chinese American college students.13 Greater acculturative stress elevates the risk of mental illness and symptom deterioration. However, highly acculturated Chinese Americans with above-average bicultural self-efficacy tend to express more positive attitudes toward mental health services.
3. Are there culturally appropriate interventions that can help Bill and his family?
A major predictor among Chinese Americans of the intent to use services is the perceived credibility of the treatment and the provider. Ethnic-specific services staffed by bicultural/bilingual mental health clinicians delivering culturally responsive interventions are increasingly available in many metropolitan areas with major Asian communities. These programs have shown clinical efficacy in encouraging service use and promoting treatment persistence. Bill and his family may benefit from referral to ethnic-specific services, where they can obtain culturally sensitive psychoeducation about his mental illness and treatment plan.
Other services that might be useful for Bill and his family include family psychoeducation programs and supportive groups specifically designed for Chinese American families; these can improve the entire family’s psychosocial health, promote medication adherence, and reduce the risk of symptom relapse through family-centered intervention models.14 Connecting with local National Alliance on Mental Illness (NAMI) programs might help Bill’s parents obtain social support from Chinese American families with similar caregiver experiences.
However, services that are not designed specifically for Chinese-origin patients also can provide excellent care for these patients, and be perceived as credible and effective. A thorough cultural assessment is necessary, as well as inclusion of the information obtained in the treatment plan. As described in the DSM-5 Outline for Cultural Formulation and operationalized in the Cultural Formulation Interview, clinicians should assess possible cultural differences among Bill, his family, his community, and his clinicians regarding their cultural concepts of distress and illness and expectations of care in order to formulate a treatment plan acceptable to patient and family. Practical cultural barriers should be addressed, such as Bill’s parents’ limited English proficiency, in which case a bilingual clinician or trained interpreter should be included in the treatment team.
With Bill’s consent, the treatment team also should consider reaching out to his parents, especially his mother, to understand and empathize with their cultural concepts of distress and illness as well as expectations for care. In addition to providing psychoeducation, the clinicians should validate the parents’ experience of shame, fear, and worry about their son. Bill’s brother, for example, might be a useful bridge in communicating with the parents given his higher acculturation and potentially greater acceptance of psychiatric care. He might help alleviate the tension between Bill and his parents and encourage them to seek family-based help.
Take-home points
- Clinical training programs should offer cultural competency training about underserved populations, including communities of color.
- Certain key concepts, such as traditional idioms of distress and explanatory models, social stigma, and acculturative stress, should be included in these trainings and evaluated in a comprehensive psychosocial assessment.
- High expressed emotion among family caregivers is associated with higher rates of psychiatric symptom relapse, whereas families with above-average bicultural self-efficacy have more positive attitudes toward mental health services.
- Clinicians should incorporate culturally appropriate educational materials (for example, CHR warning signs) and interventions to engage underserved patients and their families in mental health treatment.
Contributors
Emily Wu, MD – Harvard Medical School, Boston
Francis Lu, MD – University of California, Davis
John Sargent, MD – Tufts Medical Center, Boston
Roberto Lewis-Fernández, MD – Columbia College of Physicians & Surgeons, New York
If you would like to a submit case in which your understanding and treatment are affected by challenging cultural and family values, send it to [email protected]. We will then write back with our best answers about how one might proceed in such a case. Your case and our response will then be published at mdedge.com/psychiatry. This column is meant to be educational and does not constitute medical advice. The opinions expressed are those of the contributors and do not represent those of the organizations they are employed by or affiliated with or the Group for the Advancement of Psychiatry.
References
1. J Nerv Ment Dis. 2013 Jun;20(6);484-9.
2. Schizophr Res. 2014 Feb;152(2-3):391-9.
3. Perspect Psychiatr Care. 2013;49(4):288-92.
4. Ment Health Serv Res. 2001 Dec;3(4):201-14.
5. Br J Psychiatry. 2000 Jul;177;20-5.
6. Cultr Divers Ethnic Minor Psychol. 2008 Jan;14(1):10-8.
7. Couns Psychol. 2003 May1;31:343-61.
8. Emotion. 2002 Dec;2(4):341-60.
9. Am J Psychiatry. 1986 Nov;143(11):1361-73.
10. J Nerv Ment Dis. 2013 Oct;201(10):833-40.
11. Schizophr Bull. 1981;7(1):43-4.
12. Schizophr Bull. 2010 Jul;36(4):836-45.
13. Am J Orthopsychiatry. 2011 Oct;81(4):489-97.
14. Patient Educ Couns. 2009 Apr;75(1):67-76.
About 20% of penalties from EMTALA violations linked to psychiatric emergencies
SAN DIEGO – Between 2002 and April 2018, about one in five civil monetary penalty payments linked to Emergency Medical Treatment and Labor Act (EMTALA) violations involved psychiatric emergencies, an analysis of national data found.
“Penalties were twice as high for psychiatric cases as for nonpsychiatric cases, with failure to stabilize being more common,” Sophie Terp, MD, MPH, said at the annual meeting of the American College of Emergency Physicians. “Recent large penalties suggest the need to improve care for psychiatric emergencies.”
In an effort to characterize U.S. Office of Inspector General (OIG) penalties resulting from EMTALA violations involving psychiatric emergencies, Dr. Terp, of the department of emergency medicine at the University of Southern California, Los Angeles, and her colleagues reviewed all OIG penalties between 2002 and April 2018. Characteristics of penalties involving psychiatric emergencies were described and compared with other penalties.
Of the 229 civil monetary penalties levied during the study period, 44 (19%) were related to psychiatric emergencies and the average fine was $85,488, which was significantly higher than the average fine of $32,042 for nonpsychiatric-related civil monetary penalties (P = .004). The three largest penalties during the study period were all related to psychiatric emergencies, including one for $360,000 in 2012, one for $1,295,000 in 2017, and one for $200,000 in 2018.
“Settlements have been particularly high in recent years,” Dr. Terp said. By comparison, the largest civil monetary penalty for a nonpsychiatric case was $170,000.
Failure to provide a medical screening exam was the most common reason for civil monetary settlements in both psychiatric and nonpsychiatric cases (84% vs. 74%; P = .147), but “failure to stabilize” occurred in a significantly greater proportion of psychiatric versus nonpsychiatric cases (68% vs. 51%; P = .041). About one-third of all psychiatric cases occurred in Centers for Medicare & Medicaid Services Region 4, “which is a region known to have a very high rate of EMTALA enforcement overall,” Dr. Terp said. “About half of those cases occurred in Florida, and another 20% occurred in South Carolina. About 20% occurred in CMS Region 6, and about half of those were in Texas. But the overall proportions of psychiatric versus nonpsychiatric cases that distributed over the CMS regions did not significantly differ.”
Dr. Terp reported having no financial disclosures.
SOURCE: Terp S et al. ACEP18, Abstract 46.
SAN DIEGO – Between 2002 and April 2018, about one in five civil monetary penalty payments linked to Emergency Medical Treatment and Labor Act (EMTALA) violations involved psychiatric emergencies, an analysis of national data found.
“Penalties were twice as high for psychiatric cases as for nonpsychiatric cases, with failure to stabilize being more common,” Sophie Terp, MD, MPH, said at the annual meeting of the American College of Emergency Physicians. “Recent large penalties suggest the need to improve care for psychiatric emergencies.”
In an effort to characterize U.S. Office of Inspector General (OIG) penalties resulting from EMTALA violations involving psychiatric emergencies, Dr. Terp, of the department of emergency medicine at the University of Southern California, Los Angeles, and her colleagues reviewed all OIG penalties between 2002 and April 2018. Characteristics of penalties involving psychiatric emergencies were described and compared with other penalties.
Of the 229 civil monetary penalties levied during the study period, 44 (19%) were related to psychiatric emergencies and the average fine was $85,488, which was significantly higher than the average fine of $32,042 for nonpsychiatric-related civil monetary penalties (P = .004). The three largest penalties during the study period were all related to psychiatric emergencies, including one for $360,000 in 2012, one for $1,295,000 in 2017, and one for $200,000 in 2018.
“Settlements have been particularly high in recent years,” Dr. Terp said. By comparison, the largest civil monetary penalty for a nonpsychiatric case was $170,000.
Failure to provide a medical screening exam was the most common reason for civil monetary settlements in both psychiatric and nonpsychiatric cases (84% vs. 74%; P = .147), but “failure to stabilize” occurred in a significantly greater proportion of psychiatric versus nonpsychiatric cases (68% vs. 51%; P = .041). About one-third of all psychiatric cases occurred in Centers for Medicare & Medicaid Services Region 4, “which is a region known to have a very high rate of EMTALA enforcement overall,” Dr. Terp said. “About half of those cases occurred in Florida, and another 20% occurred in South Carolina. About 20% occurred in CMS Region 6, and about half of those were in Texas. But the overall proportions of psychiatric versus nonpsychiatric cases that distributed over the CMS regions did not significantly differ.”
Dr. Terp reported having no financial disclosures.
SOURCE: Terp S et al. ACEP18, Abstract 46.
SAN DIEGO – Between 2002 and April 2018, about one in five civil monetary penalty payments linked to Emergency Medical Treatment and Labor Act (EMTALA) violations involved psychiatric emergencies, an analysis of national data found.
“Penalties were twice as high for psychiatric cases as for nonpsychiatric cases, with failure to stabilize being more common,” Sophie Terp, MD, MPH, said at the annual meeting of the American College of Emergency Physicians. “Recent large penalties suggest the need to improve care for psychiatric emergencies.”
In an effort to characterize U.S. Office of Inspector General (OIG) penalties resulting from EMTALA violations involving psychiatric emergencies, Dr. Terp, of the department of emergency medicine at the University of Southern California, Los Angeles, and her colleagues reviewed all OIG penalties between 2002 and April 2018. Characteristics of penalties involving psychiatric emergencies were described and compared with other penalties.
Of the 229 civil monetary penalties levied during the study period, 44 (19%) were related to psychiatric emergencies and the average fine was $85,488, which was significantly higher than the average fine of $32,042 for nonpsychiatric-related civil monetary penalties (P = .004). The three largest penalties during the study period were all related to psychiatric emergencies, including one for $360,000 in 2012, one for $1,295,000 in 2017, and one for $200,000 in 2018.
“Settlements have been particularly high in recent years,” Dr. Terp said. By comparison, the largest civil monetary penalty for a nonpsychiatric case was $170,000.
Failure to provide a medical screening exam was the most common reason for civil monetary settlements in both psychiatric and nonpsychiatric cases (84% vs. 74%; P = .147), but “failure to stabilize” occurred in a significantly greater proportion of psychiatric versus nonpsychiatric cases (68% vs. 51%; P = .041). About one-third of all psychiatric cases occurred in Centers for Medicare & Medicaid Services Region 4, “which is a region known to have a very high rate of EMTALA enforcement overall,” Dr. Terp said. “About half of those cases occurred in Florida, and another 20% occurred in South Carolina. About 20% occurred in CMS Region 6, and about half of those were in Texas. But the overall proportions of psychiatric versus nonpsychiatric cases that distributed over the CMS regions did not significantly differ.”
Dr. Terp reported having no financial disclosures.
SOURCE: Terp S et al. ACEP18, Abstract 46.
REPORTING FROM ACEP18
Key clinical point: Nearly one in five settlements related to Emergency Medical Treatment and Labor Act violations involved psychiatric emergencies.
Major finding: Of the civil monetary penalties levied during the study period, 19% were related to psychiatric emergencies and the average fine was $85,488.
Study details: An analysis of 229 civil monetary penalties levied by the Office of Inspector General related to violations of EMTALA between 2002 and April 2018.
Disclosures: Dr. Terp reported having no financial disclosures.
Source: Terp S et al. ACEP18, Abstract 46.
Cardiomyopathy could be under recognized in lupus
Also today, low bone mineral density and spinal syndesmophytes predict radiographic progression in axial spondyloarthritis, sensory feedback modalities tackle gait and balance problems in Parkinson’s disease, and clinically meaningful change is determined for RAPID-3 in active RA.
Amazon Alexa
Apple Podcasts
Spotify
Also today, low bone mineral density and spinal syndesmophytes predict radiographic progression in axial spondyloarthritis, sensory feedback modalities tackle gait and balance problems in Parkinson’s disease, and clinically meaningful change is determined for RAPID-3 in active RA.
Amazon Alexa
Apple Podcasts
Spotify
Also today, low bone mineral density and spinal syndesmophytes predict radiographic progression in axial spondyloarthritis, sensory feedback modalities tackle gait and balance problems in Parkinson’s disease, and clinically meaningful change is determined for RAPID-3 in active RA.
Amazon Alexa
Apple Podcasts
Spotify

An Overview of Pharmacotherapy Options for Alcohol Use Disorder
Alcohol use disorder (AUD) is a relatively common condition characterized by a pattern of problematic alcohol consumption. According to the 2016 National Survey on Drug Use and Health (NSDUH) approximately 14.6 million Americans aged > 18 years had a diagnosis of AUD.1 This same survey also found that 26.2% of individuals over the age of 18 years reported engaging in binge drinking, which is ≥ 5 drinks in males or ≥ 4 drinks in females on the same occasion in the past month. Of those surveyed, 6.6% reported engaging in heavy drinking (binge drinking on 5 or more days in the past month).1
Military and veteran populations have a higher prevalence of alcohol misuse compared with that of the general population.2 Two out of 5 US veterans screen positive for lifetime AUD, which is higher than the prevalence of AUD in the general population.3 A number of studies have found that excessive alcohol use is common among military personnel.2,4,5 One study suggested that the average active-duty military member engages in approximately 30 binge drinking episodes per person per year.4 Military veterans may continue with a similar drinking pattern when transitioning to civilian life, explaining the high prevalence of AUD in the veteran population.6 Furthermore, since alcohol use provides temporary relief of posttraumatic stress disorder(PTSD) symptoms, a diagnosis of PTSD may also contribute to hazardous drinking in this population.7
Excessive alcohol consumption is associated with a number of negative outcomes, including increased motor-vehicle accidents, decreased medication adherence, and therefore, decreased efficacy, increased health care costs, and increased morbidity and mortality.8-13 Additionally, alcohol use is associated with a number of medical and psychiatric comorbidities.14,15 Compared with veterans without AUD, those with a diagnosis of AUD were 2.6 times more likely to have current depression and 2.8 times more likely to have generalized anxiety.3 Veterans with AUD also are 2.1 times more likely to have current suicidal ideation and 4.1 times more likely to have had a suicide attempt compared with veterans without AUD.3
Given the high prevalence and the associated risks, alcohol misuse should be properly addressed and treated. Pharmacotherapy for AUD has demonstrated efficacy in decreasing heavy drinking and prolonging periods of abstinence.16 Despite the proven benefits of available pharmacotherapy, these medications still are drastically underutilized in both the nonveteran and veteran populations. In fiscal year 2012, there were 444,000 veterans with a documented diagnosis of AUD; however, only 5.8% received evidence-based pharmacotherapy.17 The potential barriers for the utilization of AUD pharmacotherapy includes perceived low patient demand, lack of skill or knowledge about addiction, and lack of health care provider (HCP) confidence in efficacy.18 This article will provide a thorough overview of the pharmacotherapy options for the treatment of AUD and the evidence that supports the use of pharmacotherapy. We will then conclude with the recommended treatment approach for specialized patient populations.
FDA-Approved Pharmacotherapies
Naltrexone
Naltrexone was the second FDA-approved medication for the treatment of AUD and is considered a first-line agent by the Department of Veterans Affairs (VA).19,20 Unlike its predecessor, disulfiram, naltrexone significantly reduces cravings.21 During alcohol consumption endogenous opioid activity is greatly enhanced, leading to the rewarding effects of alcohol. By antagonizing the µ-opioid receptor, naltrexone mediates endorphin release during alcohol consumption, explaining the efficacy of naltrexone in AUD.21-28 Since cravings are reduced, patients are able to abstain from drinking for longer periods of time, and since pleasure is reduced, heavy drinking is also reduced.21,25
When compared with other pharmacotherapy options for AUD, naltrexone is less effective for abstinence and more effective for decreasing the time and frequency of heavy drinking days and average number of drinks consumed.29 A meta-analysis of 19 clinical trials found that naltrexone significantly reduced relapse rates in patients with AUD compared with those of placebo.30 This analysis also found that naltrexone reduced both the number of alcoholic beverages consumed and the risk of relapse to heavy drinking while increasing the total number of days of abstinence.30 The COMBINE study also found that patients receiving oral naltrexone in combination with medical treatment had a 28% reduced risk of having a heavy-drinking day.31
Dosing and Formulations
Naltrexone is available as a tablet or a long-acting injectable. The tablet is often dosed as 50 mg daily; although some studies suggest that daily doses up to 150 mg are safe and efficacious.21,25,32 The initial and maintenance dose for most patients is 50 mg daily. 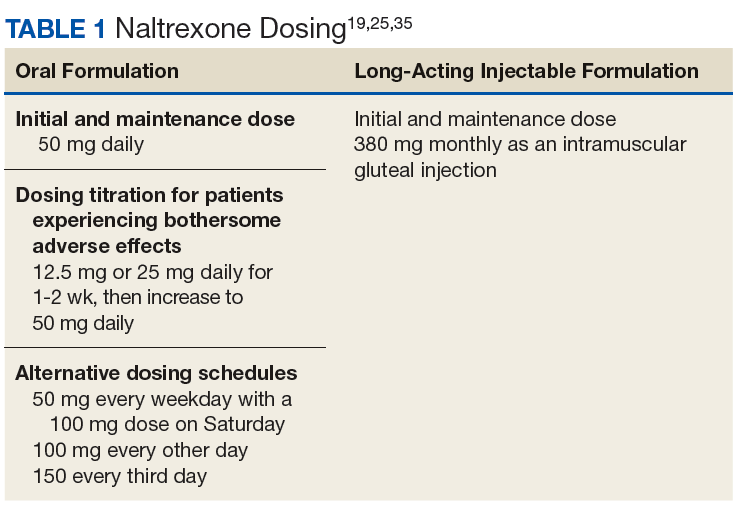
Nonadherence to the oral formulation of naltrexone is a significant barrier to the treatment of AUD. The long-acting injectable formulation is an option for patients who may have difficulty with adhering to oral naltrexone. As with the oral formulation, the long-acting naltrexone injection significantly reduces drinking days and increases abstinence.33 It was also found to be superior to oral naltrexone, acamprosate, and disulfiram in preventing discontinuation of AUD treatment.34 The long-acting injectable should be administered as an intramuscular gluteal injection at a dose of 380 mg monthly.35
Ideally, naltrexone should be initiated following the cessation of alcohol withdrawal symptoms. However, naltrexone can be safely administered in patients who are actively withdrawing from alcohol or in patients who continue to consume alcohol.25
Warnings, Precautions, and AEs
Naltrexone carries a US Food and Drug Administration (FDA) boxed warning for reversible hepatotoxicity. The risk of hepatotoxicity is increased in patients who receive higher doses (100-300 mg daily).21 A safety study demonstrated that the administration of 50 mg daily or less is not associated with significant hepatotoxicity.21,31 It is contraindicated in patients with acute hepatitis or liver failure and should be avoided in patients with liver function tests > 5 times the upper limit of normal.
Since naltrexone is a µ-opioid receptor antagonist, it is contraindicated in patients who are actively taking opioids or patients who have used opioids within the past 7 days. Co-administration with an opioid can lead to precipitated opioid withdrawal.21 Therefore, opioids should not be administered within 7 to 10 days of initiating naltrexone and 2 to 3 days after discontinuation of oral naltrexone.21 For patients receiving the long-acting injectable form of naltrexone, opioids should be avoided at least 1 month after the injection.25
To ensure that a patient is opioid free, HCPs can perform a toxicology screening prior to the initiation of naltrexone. Some HCPs may also perform a naloxone challenge to test whether a patient is at risk for precipitated opioid withdrawal prior to prescribing naltrexone. 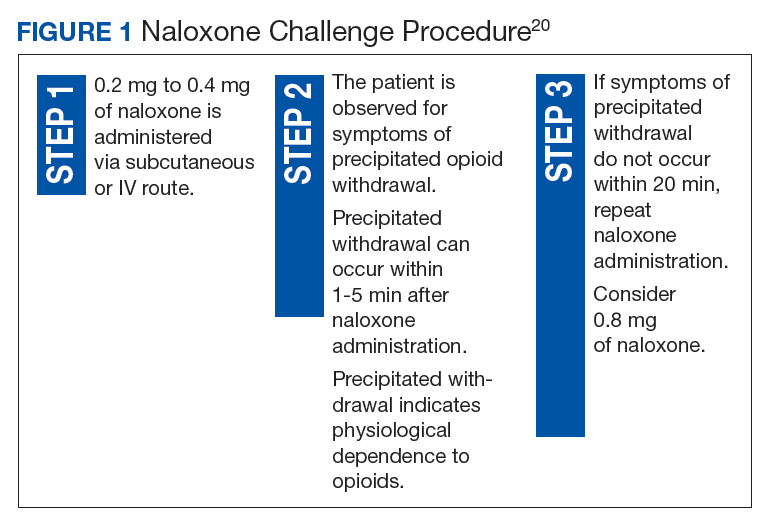
The adverse effects (AEs) of naltrexone are transient and include nausea, vomiting, anorexia, dizziness, and fatigue.19,35 Injection site reactions can be experienced with the long-acting naltrexone injection. Liver transaminases, such as the alanine aminotransferase and aspartate transaminase, should be monitored at baseline, 6 months after initiation, and annually during the course of treatment (Table 2). 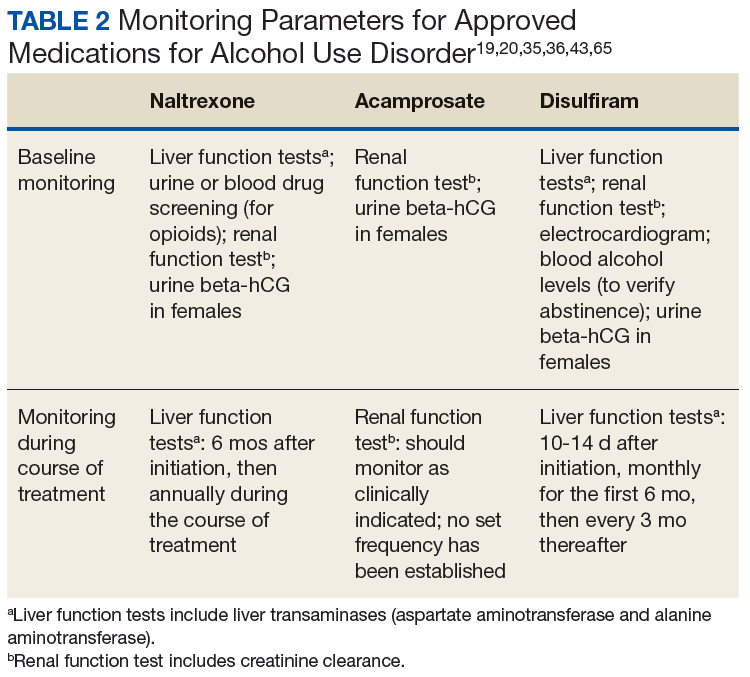
Acamprosate
The FDA approved acamprosate for the treatment of AUD in 2004, and it is also considered a first-line agent for AUD by the VA.20 It is approved for the maintenance of abstinence from alcohol use and is most efficacious when initiated in patients who are abstinent prior to treatment.29,36 Patients with AUD typically have a disruption in the balance between the inhibitory neurotransmitter, gamma-aminobutyric acid (GABA), and the excitatory neurotransmitter, glutamate. While its mechanism of action remains unknown, acamprosate is thought to increase the activity of GABA and to decrease the activity of glutamate at the N-methyl-D-aspartate (NMDA) receptors in the central nervous system. In essence, it is thought to restores the balance between GABA and glutamate in patients with AUD.36
Acamprosate has been found to effectively prevent relapse. Three randomized, double-blind, placebo-controlled European clinical trials evaluated the efficacy of acamprosate in combination with psychotherapy. The results demonstrated that patients taking acamprosate had longer durations of abstinence compared with that of placebo, improved rates of complete abstinence, and a prolonged time to first drink.37-39 A meta-analysis evaluated the use of acamprosate in AUD showed that acamprosate was more effective at maintaining abstinence in patients who had been abstinent prior to the initiation of therapy.29 These patients also had better abstinence rates if they had been abstinent for a longer duration prior to treatment initiation.30 Studies also showed that acamprosate significantly assisted with maintaining abstinence, improved rates of abstinence, and led to more days of abstinence.40,41 Of note, there also have been studies that have shown no significant benefit with acamprosate compared with placebo in the treatment of AUD.42
Dosing and Formulations
Acamprosate is available as a 333 mg delayed-release tablet. The recommended dose is 666 mg 3 times daily.36 The dose can be decreased to 333 mg 3 times a day in patients with moderate renal impairment (CrCl-30-50 mL/min).
Since acamprosate has been proven more effective in patients who are abstinent prior to initiation, acamprosate is typically initiated 5 days following alcohol cessation.25 However, it may be safely administered with alcohol and can continue to be administered in the event of a relapse.36
Warnings, Precautions, and AEs
Acamprosate is safe to use in patients with hepatic and mild-to-moderate renal impairment; however, it is contraindicated in patients with severe renal impairment (creatinine clearance [CrCl] ≤ 30 mL/min).36 Serum creatinine levels should be monitored at baseline and during treatment.
Acamprosate has a number of related AEs. The most common is diarrhea. Less common AEs include insomnia, anxiety, and depression. Due to its possible potential to increase suicidality, HCPs should monitor for the emergence of mood changes.36
Disulfiram
Disulfiram is an aldehyde dehydrogenase inhibitor that is FDA approved for the management of AUD.43 When ingested, ethanol is typically metabolized to acetaldehyde, which is further metabolized to acetic acid by aldehyde dehydrogenase.44 Disulfiram inhibits aldehyde dehydrogenase, leading to a rapid accumulation of acetaldehyde within the plasma (outlined in Figure 2). 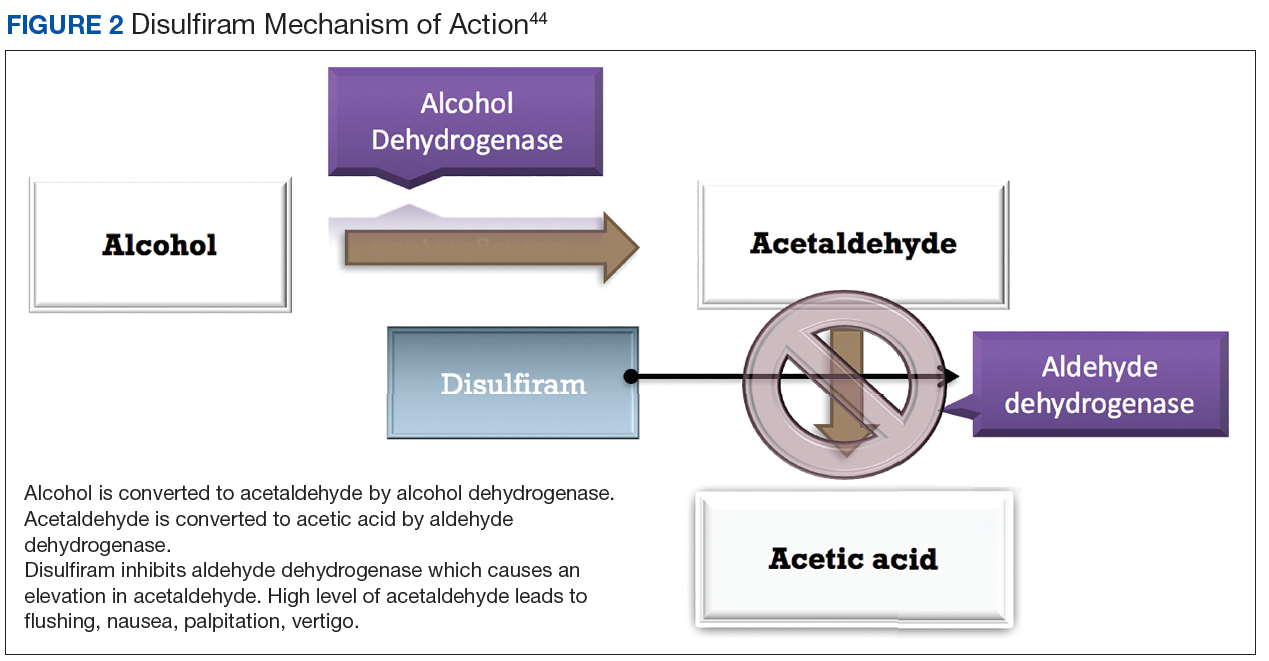
There are limited studies that prove the efficacy of disulfiram. In a randomized trial comparing disulfiram, acamprosate, and naltrexone, patients treated with disulfiram had fewer heavy drinking days, lower rates of weekly alcohol consumption, and a longer period of abstinence compared to other medications.45 Additionally, a 2014 meta-analysis showed that in open-label studies, disulfiram was more beneficial in preventing alcohol consumption when compared with acamprosate, naltrexone, and placebo. This result was not seen in blinded studies.46 Disulfiram does not reduce alcohol cravings, and adherence is a significant issue. It is most effective between 2 and 12 months, when taken under supervised administration.47
Dosing and Formulations
Disulfiram is only available as a tablet. The recommended starting dose is up to 500 mg for the first 2 weeks. However, the maintenance dose can range from 125 to 500 mg daily.43 Patients must be abstinent from alcohol at least 12 to 24 hours prior to the initiation of disulfiram.25 A blood alcohol level can be obtained in order to confirm abstinence.25
Warnings, Precautions, and AEs
Disulfiram is contraindicated in patients with severe myocardial disease or coronary occlusion and severe hepatic impairment.43 Other contraindications are outlined in Table 3. 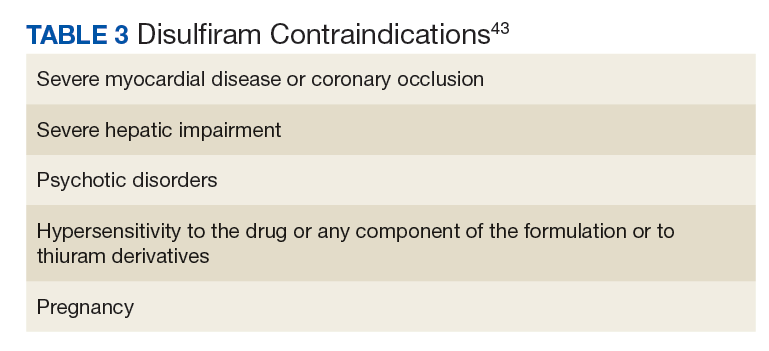
Common AEs include somnolence, a metallic after-taste, and peripheral neuropathy.43 Patients should be informed that they could experience a disulfiram reaction with even small amounts of alcohol; all foods, drinks, and medications containing alcohol should be avoided. Due to the potential of disulfiram potential to cause hepatotoxicity, liver transaminases should be monitored at baseline, 2 weeks after initiation, and monthly for the first 6 months of therapy, and every 3 months thereafter (Table 2).25
Off-Label Pharmacotherapies
Topiramate
Although not approved for AUD, topiramate has been used off-label for this indication as it has proven efficacy in clinical trials.48-56 While its mechanism of action for AUD is unclear, it has been theorized that topiramate antagonizes glutamate receptors, thereby reducing dopamine release in the nucleus accumbens upon alcohol consumption, and potentiates the inhibitory neurotransmitter GABA.50,51,57-60
In clinical trials, topiramate has demonstrated significant efficacy in reducing cravings, the risk of relapse, and the number of drinks consumed daily, while increasing abstinence.51,53,60 Batki and colleagues report that the administration of topiramate in veterans with co-occurring AUD and PTSD reduced alcohol consumption, cravings, and the severity of their PTSD symptoms.61
Dosing and Formulations
Topiramate is available in a number of formulations; however, only the immediate-release formulation is recommended for the treatment of AUD. The extended-release formulation is contraindicated in the setting of alcohol consumption and is therefore not used for the treatment of AUD.62 Doses should be initiated at 25 mg daily and can be titrated in 25 to 50 mg weekly increments. To minimize AEs and to reduce the risk of patients discontinuing therapy, the dose may be slowly titrated over 8 weeks.53,59 An effective dose can range from 75 to 300 mg in divided doses; however, AEs often limit the tolerability of increased doses.48,50,63,64 The VA/DoD Practice Guideline for the Management of Substance Use Disorders recommends titrating topiramate to a target dose of 100 mg twice daily.65
Warnings, Precautions, and AEs
Common AEs include memory impairment, anorexia, fatigue, paresthesias, and somnolence.62 There is an increased risk of nephrolithiasis with topiramate administration; therefore, adequate hydration is crucial.49,59 Titration of topiramate to the target dose is suggested to limit AEs.35
Prior to initiating topiramate, the patient’s renal function should be assessed. In those with a CrCl < 70 mL/min the dose should be decreased by 50% and titrated more slowly.62
Gabapentin
Gabapentin is prescribed for the treatment of partial seizures and postherpetic neuralgia. In recent years, it has shown efficacy for treating other conditions, such as AUD. While its mechanism for this indication remains unclear, the inhibition of excitatory alpha-2-delta calcium channels and stimulation of inhibitory GABAA receptors by gabapentin is believed to decrease alcohol cravings, reduce anxiety, and increase abstinence.66
A 12-week, double-blind, randomized controlled trial demonstrated that oral gabapentin was more efficacious than was placebo for improving rates of abstinence, decreasing heavy drinking, and reducing alcohol cravings.67 Gabapentin may also serve as a good adjunctive option to naltrexone therapy either when naltrexone monotherapy fails or if a patient is complaining of sleep and mood disturbances with abstinence.67,68
Dosing and Formulations
Gabapentin should be titrated slowly to minimize AEs. It can be initiated at 300 mgon day 1 and increase by 300-mg increments. Doses of 900 to 1,800 mg per day have proven to be efficacious for the treatment of AUD.66,67 These proposed doses can be safely administered to most patients, but caution should be observed in elderly and patients with renal impairment.69,70
Warnings, Precautions, and AEs
The most common AEs for gabapentin include drowsiness, dizziness, and fatigue.69 Since it is renally cleared, renal function should be monitored at baseline and periodically during treatment. Gabapentin is not metabolized by liver enzymes and does not significantly interact with drugs that require hepatic metabolism.
Baclofen
Baclofen has generated attention as an unconventional treatment option for alcohol dependence. Its unique mechanism of action, which involves the activation of GABAB receptors and the subsequent inhibition of dopaminergic neurons, makes it useful for the treatment of AUD.71
A 12-week study evaluating the effectiveness and safety of baclofen for the maintenance of alcohol abstinence demonstrated that baclofen was more efficacious than placebo for increasing abstinence in patients with liver cirrhosis. In addition, there were more cumulative days of abstinence with baclofen use (62.8 days) vs placebo (30.8 days) in cirrhotic patients.72
Dosing and Formulations
There has been a range of doses studied for baclofen in the treatment of AUD. Studies indicate that initiating baclofen at 30 mg daily and increasing doses based on the patient’s clinical response is most effective.72 As a result, doses as high as 275 mg per day have been used for some patients.73 Baclofen is renally cleared; therefore, the dose should be adjusted in patients with renal impairment.74
Warnings, Precautions, and AEs
Some of the common AEs of baclofen include drowsiness, confusion, headache, and nausea. Due to its CNS depressant effects, baclofen should be used with caution in the elderly. Also, due to its potential to cause withdrawal symptoms, baclofen should not be discontinued abruptly.74,75 Baclofen is a safe option for patients with severe liver disease, due to its minimal hepatic metabolism.76
Ondansetron
Ondansetron is approved for both prophylactic and therapeutic use as an antiemetic agent for chemotherapy and anesthesia-induced nausea and vomiting.77As a highly selective and competitive 5-HT3 receptor antagonist, ondansetron has demonstrated efficacy in reducing serotonin-mediated dopaminergic effects in AUD.78,79 The lowering of these dopaminergic effects is associated with a reduction in alcohol-induced gratification and consumption.
In a 12-week, randomized controlled trial, 271 patients diagnosed with AUD received ondansetron twice daily or placebo, combined with weekly cognitive behavioral therapy (CBT). There was a statistically significant decrease in alcohol consumption in patients treated with ondansetron compared with those who received placebo. Additionally, ondansetron was superior to placebo for increasing the percentage and total amount of days abstinent.80 These results were primarily observed in participants diagnosed with early-onset AUD (defined as onset at 25 years or younger), which may suggest the presence of genetically predisposed serotonin dysfunctions.80,81 In contrast, there were no significant differences observed in participants with late-onset AUD (onset after age 25 years) in either study group.80
Dosing and Formulations
Given its modest efficacy for the treatment of AUD, ondansetron has demonstrated clinical benefits at doses of 0.001 to 0.016 mg/kg twice daily. Additionally, 1 study reported that low-dose ondansetron (0.25 mg twice daily) was effective in reducing alcohol consumption when compared with placebo or high-dose ondansetron, which was considered 2 mg twice daily.82
Warnings, Precautions, and AEs
The most commonly reported AEs with ondansetron include fatigue, headache, anxiety, and serotonin syndrome when used concomitantly with other serotonergic agents.77 Also, serious cardiovascular complications, such as QTc prolongation, angina pectoris, atrial fibrillation, and arrhythmias have been observed with IV administration.77,81,83 Consequently, patients with electrolyte imbalances (eg, hypokalemia, hypomagnesemia), a history of congestive heart failure, or concomitant medications associated with QTc prolongation, should be monitored with an electrocardiogram (ECG) or switched to another agent.77
Treatment Approach with AUD Pharmacotherapy
There is insufficient evidence to support the use of 1 medication for AUD over the others.16,46,84 Instead, the choice of therapy largely depends on the patient’s comorbidities, renal and hepatic function, and on the patient’s established goals, whether abstinence or reduction in alcohol consumption (Table 4). 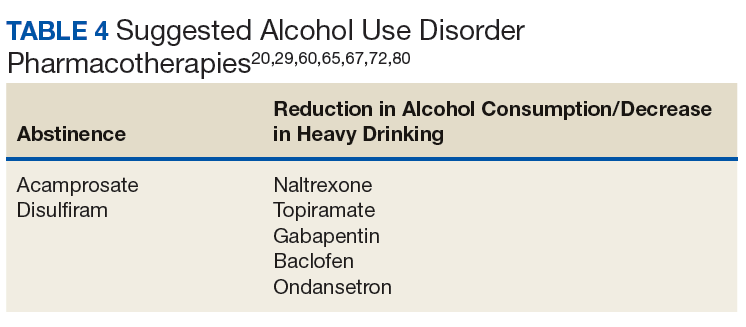
There is much debate over the appropriate duration of treatment for AUD pharmacotherapy. It is recommended that patients remain on these medications for at least 3 months. Pharmacotherapy can be continued for 6 to 12 months as the risk for relapse is highest during this time frame.85,86 The National Institute for Health and Care Excellence guidelines recommend discontinuing AUD pharmacotherapy if alcohol consumption persists 4 to 6 weeks after initiation.86
Comorbid Liver Disease
Due to the negative effects of heavy alcohol consumption on the liver, patients with AUD may develop liver disease. Health care providers should be aware of the appropriate pharmacotherapy options for patients with comorbid liver disease. Acamprosate is mostly excreted unchanged by the kidneys, therefore is an option for patients with liver disease whose goal is complete abstinence. Topiramate is another option for use in patients with liver impairment. Unlike acamprosate, topiramate would be a better option in patients who may not completely abstain from alcohol consumption but would like to decrease the amount of heavy drinking days.87
Gabapentin, baclofen, and ondansetron are also options for those with liver disease. Baclofen in particular has been studied in those with advanced liver disease, and it was found to be safe and effective.88,89
Comorbid Renal Disease
Naltrexone is an option for patients with mild renal impairment. Naltrexone and its major metabolite, 6-ß-naltrexol, are renally excreted; however, urinary excretion of unchanged naltrexone accounts for < 2% of the oral dose.19 Even with its low potential for accumulation, HCPs should carefully monitor for AEs in patients with moderate-to-severe renal impairment. Disulfiram is another pharmacotherapy option, since it is mostly metabolized by the liver.
Gabapentin, baclofen, and ondansetron are also possible options; however, their doses should be renally adjusted. Overall, there are limited studies on the use of these medications treating AUD in patients with renal impairment.
Pregnancy
Alcohol consumption during pregnancy can result in a wide range of birth defects to the unborn fetus. Due to the negative effects of alcohol consumption on the fetus, pregnant females should be referred to a professional alcohol treatment program. Although AUD pharmacotherapy may be considered in pregnant females, there have been no human studies that have examined the efficacy and safety in this patient population. All evidence comes from animal studies, case reports, and case series.90
Naltrexone is the most widely used medication for AUD in pregnancy. It is considered pregnancy category C and 1 study in particular did not detect any gross abnormalities in fetal development in pregnancy.19, 90 Disulfiram, acamprosate, and topiramate have all been shown to cause harm to either animal or human fetuses and are generally not recommended.36,44,63 Similar to naltrexone, gabapentin and baclofen are also pregnancy category C.69,77 Ondansetron is pregnancy category B, but it should still be used with caution since its use in pregnancy for the treatment of AUD has not been studied.77,90
Psychosocial Interventions
It is recommended that AUD pharmacotherapy be used in conjunction with a psychosocial intervention, such as CBT or medical management. Many of the studies evaluating the efficacy of AUD pharmacotherapy combined psychosocial interventions with medications. The literature suggests that when combined with CBT or medical management therapy, pharmacotherapy used for AUD results in better alcohol consumption outcomes.31,91 It has also been suggested that psychosocial interventions may improve patient adherence to AUD pharmacotherapy.25
Barriers
Inadequate HCP training on the use of AUD pharmacotherapy has been found to be a major barrier to the utilization of AUD pharmacotherapy, along with a lack of confidence in the effectiveness of these medications.18 Increasing HCP education on the use and benefits of these agents may increase the overall confidence of HCPs in prescribing pharmacotherapy for the treatment of AUD, especially in the primary care setting. One aspect that has been found to improve education and the prescribing of pharmacotherapy for AUD within the Veterans Health Administration has been the use of academic detailing programs.92 Academic detailing is a multifaceted educational outreach program that is used to assist with HCP education. Additionally, clinical pharmacists can be consulted to help develop a safe and effective AUD pharmacotherapy treatment regimen.
Conclusion
There is a major disparity in the prevalence of AUD between the general population and the military and veteran populations. Many clinical trials have found a number of pharmacotherapy options to be effective for the treatment of AUD. Despite the need and the proven benefits, the utilization of AUD pharmacotherapy still remains low in both the general and veteran populations. Increasing provider education and addressing other potential barriers for the use of pharmacotherapy for AUD can have a positive impact on prescribing patterns, which can ultimately improve alcohol consumption outcomes in patients with a diagnosis of AUD.
1. Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. Results from the 2016 National Survey on Drug Use and Health: detailed tables. Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2016/NSDUH-DetTabs-2016.pdf. Published September 7, 2017. Accessed September 13, 2018.
2. Jones E, Fear NT. Alcohol use and misuse within the military: a review. Int Rev Psychiatry. 2011;23(2):166-172.
3. Fuehrlein BS, Mota N, Arias AJ, et al. The burden of alcohol use disorders in US military veterans: results from the National Health and Resilience in Veterans Study. Addiction. 2016;111(10):1786-1794.
4. Stahre MA, Brewer RD, Fonseca VP, Naimi TS. Binge drinking among US active-duty military personnel. Am J Prev Med. 2009;36(3):208-217.
5. Institute of Medicine. Substance use disorders in the U.S. armed forces. https://www.nap.edu/resource/13441/SUD_rb.pdf. Published September 2012. Accessed September 12, 2018.
6. McDevitt-Murphy ME, Murphy JG, Williams JL, Monahan CJ, Bracken-Minor KL. Brief intervention to reduce hazardous drinking and enhance coping among OEF/OIF/OND veterans. Prof Psychol Res Pr. 2015;46(2):83-89.
7. Jacobson IG, Ryan MA, Hooper TI, et al. Alcohol use and alcohol-related problems before and after military combat deployment. JAMA. 2008;300(6):663-675.
8. Chou SP, Dawson DA, Stinson FS, et al. The prevalence of drinking and driving in the United States, 2001-2002: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Drug Alcohol Depend. 2006;83(2):137-146.
9. Bazargan-Hejazi S, Bazargan M, Hardin E, Bing EG. Alcohol use and adherence to prescribed therapy among under-served Latino and African-American patients using emergency department services. Ethn Dis. 2005;15(2):267-275.
10. Kamali M, Kelly BD, Clarke M, et al. A prospective evaluation of adherence to medication in first episode of schizophrenia. Eur Psychiatry. 2006;21(1):29-33.
11. Tucker JS, Burnam MA, Sherbourne CD, Kung FY, Gifford AL. Substance abuse and mental health correlates of nonadherence to antiretroviral medications in a sample of patients with human immunodeficiency virus infection. Am J Med. 2003;114(7):573-580.
12. Rehm J, Room R, Graham K, Monteiro M, Gmel G, Sempos CT. The relationship of average volume of alcohol consumption and patterns of drinking to burden of disease: an overview. Addiction. 2003;98(9):1209-1228.
13. Kendler KS, Ohlsson H, Sundquist J, Sundquist K. Alcohol use disorder and mortality across the lifespan: a longitudinal cohort and co-relative analysis. JAMA Psychiatry. 2016;73(6):575-581.
14. Hasin DS, Stinson FS, Ogburn E, Grant BF. Prevalence, correlates, disability, and comorbidity of DSM-IV alcohol abuse and dependence in the United States. Arch Gen Psychiatry. 2007;64(7):830-842.
15. Grant BF, Stinson FS, Dawson DA, et al. Prevalence and co-occurrence of substance use disorders and independent mood and anxiety disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2004;61(8):807-816.
16. Jonas DE, Amick HR, Feltner C, et al. Pharmacotherapy for adults with alcohol use disorders in outpatient settings: a systematic review and meta-analysis. JAMA. 2014;311(18):1889-1900.
17. Del Re AC, Gordon AJ, Lembke A, Harris AH. Prescription of topiramate to treat alcohol use disorders in the Veterans Health Administration. Addict Sci Clin Pract. 2013;8:12.
18. Harris AH, Ellerbe L, Reeder RN, et al. Pharmacotherapy for alcohol dependence: perceived treatment barriers and action strategies among Veterans Health Administration service providers. Psychol Serv. 2013;10(4):410-419.
19. ReVia [package insert]. Pomona, NY: Duramed Pharmaceuticals; 2013.
20. US Department of Veterans Affairs, Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives. Alcohol use disorder pharmacotherapy: naltrexone, acamprosate, and disulfiram recommendations for use. https://www.pbm.va.gov/PBM/clinicalguidance/clinicalrecommendations/Alcohol_Use_Disorder_Pharmacotherapy_Acamprosate_Naltrexone_Disulfiram_Recommendations_for_Use.docx. Published December 2013. Accessed September 17, 2018.
21. Anton RF. Naltrexone for the management of alcohol dependence. N Engl J Med. 2008;359(7):715-721.
22. O’Malley SS, Rounsaville BJ, Farren C, et al. Initial and maintenance naltrexone treatment for alcohol dependence using primary care vs specialty care: a nested sequence of 3 randomized trials. Arch Intern Med. 2003;163(14):1695-1704.
23. O’Brien CP. A range of research-based pharmacotherapies for addiction. Science. 1997;278(5335):66-70.
24. Swift RM. Effect of naltrexone on human alcohol consumption. J Clin Psychiatry. 1995;56 (suppl 7):24-29.
25. Center for Substance Abuse Treatment. Incorporating Alcohol Pharmacotherapies into Medical Practice. Treatment Improvement Protocol (TIP) Series 49. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2009.
26. Spanagel R, Zieglgänsberger W. Anti-craving compounds for ethanol: new pharmacological tools to study addictive processes. Trends Pharmacol Sci. 1997;18(2):54-59.
27. Herz A. Endogenous opioid systems and alcohol addiction. Psychopharmacology (Berl). 1997;129(2):99-111.
28. Miller NS. The integration of pharmacological and nonpharmacological treatments in drug/alcohol addiction. J Addict Dis. 1997;16(4):1-5.
 29. Maisel NC, Blodgett JC, Wilbourne PL, Humphreys K, Finney JW. Meta-analysis of naltrexone and acamprosate for treating alcohol use disorders: when are these medications most helpful? Addiction. 2013;108(2):275-293.
29. Maisel NC, Blodgett JC, Wilbourne PL, Humphreys K, Finney JW. Meta-analysis of naltrexone and acamprosate for treating alcohol use disorders: when are these medications most helpful? Addiction. 2013;108(2):275-293.
30. Bouza C, Angeles M, Muñoz A, Amate JM. Efficacy and safety of naltrexone and acamprosate in the treatment of alcohol dependence: a systematic review. Addiction. 2004;99(7):811-828.
31. Anton RF, O’Malley SS, Ciraulo DA, et al; COMBINE Study Research Group. Combined pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE study: a randomized controlled trial. JAMA. 2006;295(17):2003-2017.
32. Oslin DW, Pettinati HM, Volpicelli JR, Wolf AL, Kampman KM, O’Brien CP. The effects of naltrexone on alcohol and cocaine use in dually addicted patients. J Subst Abuse Treat. 1999;16(2):163-167.
33. Kranzler HR, Wesson DR, Billot L; DrugAbuse Sciences Naltrexone Depot Study Group. Naltrexone depot for treatment of alcohol dependence: a multicenter, randomized, placebo-controlled clinical trial. Alcohol Clin Exp Res. 2004;28(7):1051-1059.
34. Bryson WC, McConnell J, Korthuis PT, McCarty D. Extended-release naltrexone for alcohol dependence: persistence and healthcare costs and utilization. Am J Manag Care. 2011;17 (suppl 8):S222-S234.
35. Vivitrol [package insert]. Waltham, MA: Alkermes, Inc.; 2010.
36. Campral [package insert]. St. Louis, MO: Forest Laboratories Inc; 2012.
37. Paille F, Guelfi J, Perkins AC, Royer RJ, Steru L, Parot P. Double-blind randomized multicentre trial of acamprosate in maintaining abstinence from alcohol. Alcohol. 1995;30(2):239-247.
38. Pelc I, Verbanck P, Le Bon O, Gavrilovic M, Lion K, Lehert P. Efficacy and safety of acamprosate in the treatment of detoxified alcohol-dependent patients. A 90-day placebo-controlled dose-finding study. Br J Psychiatry. 1997;171:73-77.
39. Sass H, Soyka M, Mann K, Zieglgänsberger W. Relapse prevention by acamprosate. Results from a placebo-controlled study on alcohol dependence. Arch Gen Psychiatry. 1996;53(8):673-680.
40. Mann K, Lehert P, Morgan MY. The efficacy of acamprosate in the maintenance of abstinence in alcohol-dependent individuals: results of a meta-analysis. Alcohol Clin Exp Res. 2004;28(1):51-63.
41. Mason BJ, Lehert P. Acamprosate for alcohol dependence: a sex-specific meta-analysis based on individual patient data. Alcohol Clin Exp Res. 2012;36(3):497-508.
42. Richardson K, Baillie A, Reid S, et al. Do acamprosate or naltrexone have an effect on daily drinking by reducing craving for alcohol? Addiction. 2008;103(6):953-959.
43. Antabuse [package insert]. North Wales, PA: Teva Pharmaceuticals; 2015.
44. Ait-Daoud N, Johnson BA. Medications for the treatment of alcoholism. In: Johnson BA, Ruiz P, Galanter M, eds. Handbook of Clinical Alcoholism Treatment. Lippincott Williams & Wilkins, Baltimore; 2003
45. Laaksonen E, Koski-Jännes A, Salaspuro M, Ahtinen H, Alho H. A randomized, multicentre, open-label, comparative trial of disulfiram, naltrexone and acamprosate in the treatment of alcohol dependence. Alcohol Alcohol. 2008;43(1):53-61.
46. Skinner MD, Lahmek P, Pham H, Aubin HJ. Disulfiram efficacy in the treatment of alcohol dependence: a meta-analysis. PLoS One. 2014;9(2):e87366.
47. Jørgensen CH, Pedersen B, Tønnesen H. The efficacy of disulfiram for the treatment of alcohol use disorder. Alcohol Clin Exp Res. 2011;35(10):1749-1758.
48. Arbaizar B, Diersen-Sotos T, Gómez-Acebo I, Llorca J. Topiramate in the treatment of alcohol dependence: a meta-analysis. [Article in English, Spanish] Actas Esp Psiquiatr. 2010;38(1):8-12.
49. Johnson BA, Ait-Daoud N. Topiramate in the new generation of drugs: efficacy in the treatment of alcoholic patients. Curr Pharm Des. 2010;16(19):2103-2112.
50. Paparrigopoulos T, Tzavellas E, Karaiskos D, Kourlaba G, Liappas I. Treatment of alcohol dependence with low-dose topiramate: an open-label controlled study. BMC Psychiatry. 2011;11:41.
51. Johnson BA, Ait-Daoud N, Bowden CL, et al. Oral topiramate for treatment of alcohol dependence: a randomised controlled trial. Lancet. 2003;361(9370):1677-1685.
52. Johnson BA, Ait-Daoud N, Akhtar FZ, Ma JZ. Oral topiramate reduces the consequences of drinking and improves the quality of life of alcohol-dependent individuals: a randomized controlled trial. Arch Gen Psychiatry. 2004;61(9):905-912.
53. Johnson BA, Rosenthal N, Capece JA, et al; Topiramate for Alcoholism Advisory Board; Topiramate for Alcoholism Study Group. Topiramate for treating alcohol dependence: a randomized controlled trial. JAMA. 2007;298(14):1641-1651.
54. Flórez G, García-Portilla P, Alvarez S, Saiz PA, Nogueiras L, Bobes J. Using topiramate or naltrexone for the treatment of alcohol-dependent patients. Alcohol Clin Exp Res. 2008;32(7):1251-1259.
55. Flórez G, Saiz PA, Garcia-Portilla P, Alvarez S, Nogueiras L, Bobes J. Topiramate for the treatment of alcohol dependence: comparison with naltrexone. Eur Addict Res. 2011;17(1):29-36.
56. Baltieri DA, Daró FR, Ribeiro PL, de Andrade AG. Comparing topiramate with naltrexone in the treatment of alcohol dependence. Addiction. 2008;103(12):2035-2044.
57. White HS, Brown SD, Woodhead JH, Skeen GA, Wolf HH. Topiramate modulates GABA-evoked currents in murine cortical neurons by a nonbenzodiazepine mechanism. Epilepsia. 2000;41(suppl 1):S17-S20.
58. White HS, Brown SD, Woodhead JH, Skeen GA, Wolf HH. Topiramate enhances GABA-mediated chloride flux and GABA-evoked chloride currents in murine brain neurons and increases seizure threshold. Epilepsy Res. 1997;28(3):167-179.
59. Guglielmo R, Martinotti G, Quatrale M, et al. Topiramate in alcohol use disorders: review and update. CNS Drugs. 2015;29(5):383-395.
60. Kranzler HR, Covault J, Feinn R, et al. Topiramate treatment for heavy drinkers: moderation by a GRIK1 polymorphism. Am J Psychiatry. 2014;171(4):445-452.
61. Batki SL, Pennington DL, Lasher B, et al. Topiramate treatment of alcohol use disorder in veterans with posttraumatic stress disorder: a randomized controlled pilot trial. Alcohol Clin Exp Res. 2014;38(8):2169-2177.
62. Topamax [package insert]. Titusville, NJ: Janssen Pharmaceuticals Inc; 2017.
63. Meador KJ. Cognitive effects of levetiracetam versus topiramate. Epilepsy Curr. 2008;8(3):64-65.
64. Luykx JJ, Carpay JA. Nervous system adverse responses to topiramate in the treatment of neuropsychiatric disorders. Expert Opin Drug Saf. 2010;9(4):623-631.
65. The Management of Substance Use Disorder Work Group; US Department of Veteran Affairs, US Department of Defense. VA/DoD clinical practice guideline for the management of substance use disorders. https://www.healthquality.va.gov/guidelines/MH/sud/VADODSUDCPGRevised22216.pdf. Published December 2015. Accessed September 12, 2018.
66. Sills GJ. The mechanism of action of gabapentin and pregabalin. Curr Opin Pharmacol. 2006;6(1):108-113.
67. Mason BJ, Quello S, Goodell V, Shandan F, Kyle M, Begovic A. Gabapentin treatment for alcohol dependence: a randomized clinical trial. JAMA Intern Med. 2014;174(1):70-77.
68. Anton RF, Myrick H, Wright TM, et al. Gabapentin combined with naltrexone for the treatment of alcohol dependence. Am J Psychiatry. 2011;168(7):709-717.
69. Neurontin [package insert]. New York, NY: Pfizer; 2017.
70. American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American Geriatrics Society 2015 updated Beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2015;63(11):2227-2246.
71. Addolorato G, Leggio L. Safety and efficacy of baclofen in the treatment of alcohol-dependent patients. Curr Pharm Des. 2010;16(19):2113-2117.
72. Addolorato G, Leggio L, Ferrulli A, et al. Effectiveness and safety of baclofen for maintenance of alcohol abstinence in alcohol-dependent patients with liver cirrhosis: a randomized, double-blind, controlled study. Lancet. 2007;370(9603):1915-1922.
73. Dore GM, Lo K, Juckes L, Bezyan S, Latt N. Clinical experience with baclofen in the management of alcohol-dependent patients with psychiatric comorbidity: a selected cases series. Alcohol Alcohol. 2011;46(6):714-720.
74. Baclofen tablet [package insert]. Pulaski, TN: AvKare Inc; 2018.
75. Hansel DE, Hansel CR, Shindle MK, et al. Oral baclofen in cerebral palsy: possible seizure potentiation? Pediatr Neurol. 2003;29(3):203-206.
76. Leggio L, Ferrulli A, Zambon A, et al. Baclofen promotes alcohol abstinence in alcohol dependent cirrhotic patients with hepatitis C virus (HCV) infection. Addict Behav. 2012;37(4):561-564.
77. Zofran [package insert]. East Hanover, NJ: Norvartis Pharmaceuticals; 2017.
78. Barnes NM, Sharp T. A review of central 5-HT receptors and their function. Neuropharmacology. 1999;38(8):1083-1152.
79. Johnson BA, Campling GM, Griffiths P, Cowen PJ. Attenuation of some alcohol-induced mood changes and the desire to drink by 5-HT3 receptor blockade: a preliminary study in health male volunteers. Psychopharmacology (Berl). 1993;112(1):142-144.
80. Johnson B, Roache J, Javors M, et al. Ondansetron for reduction of drinking among biologically predisposed alcoholic patients: a randomized controlled trial. JAMA. 2000;284(8):963-971.
81. Kasinath NS, Malak O, Tetzlaff J. Atrial fibrillation after ondansetron for the prevention and treatment of postoperative nausea and vomiting: a case report. Can J Anaesth. 2003;50(3):229-231.
82. Sellers EM, Toneatto T, Romach MK, Somer GR, Sobell LC, Sobell MB. Clinical efficacy of the 5-HT3 antagonist ondansetron in alcohol abuse and dependence. Alcohol Clin Exp Res. 1994;18(4):879-885.
83. Havrilla PL, Kane-Gill SL, Verrico MM, Seybert AL, Reis SE. Coronary vasospasm and atrial fibrillation associated with ondansetron therapy. Ann Pharmacother. 2009;43(3):532-536.
84. Donoghue K, Elzerbi C, Saunders R, Whittington C, Pilling S, Drummond C. The efficacy of acamprosate and naltrexone in the treatment alcohol dependence, Europe versus the rest of the world: a meta-analysis. Addiction. 2015;110(6):920-930.
85. National Institute for Health and Care Excellence. Alcohol-use disorder: diagnosis, assessment and management of harmful drinking and alcohol dependence. Clinical guideline [CG115]. https://www.nice.org.uk/guidance/cg115. Published February 2011. Accessed September 12, 2018.
86. U.S. Department of Health and Human Services, National Institutes of Health, National Institute on Alcohol Abuse and Alcoholism. Helping patients who drink too much a clinician’s guide. https://www.niaaa.nih.gov/guide. Accessed September 12, 2018.
87. Blodgett JC, Del Re AC, Maisel NC, Finney JW. A meta-analysis of topiramate’s effects for individuals with alcohol use disorders. Alcohol Clin Exp Res. 2014;38(6):1481-1488.
88. Müller CA, Geisel O, Pelz P, et al. High-dose baclofen for the treatment of alcohol dependence (BACLAD study): a randomized, placebo-controlled trial. Eur Neuropsychopharmacol. 2015;25(8):1167-1177.
89. Beraha EM, Salemink E, Goudriaan AE, et al. Efficacy and safety of high-dose baclofen for the treatment of alcohol dependence: a multicentre, randomized, double-blind controlled trial. Eur Neuropsychopharmacol. 2016;26(12):1950-1959.
90. DeVido J, Bogunovic O, Weiss RD. Alcohol use disorders in pregnancy. Harv Rev Psychiatry. 2015;23(2)112-121.
91. Anton RF, Moak DH, Latham P, et al. Naltrexone combined with either cognitive behavioral or motivational enhancement therapy for alcohol dependence. J Clin Psychopharmacol. 2005;25(4):349-357.
92. Harris AHS, Bowe T, Hagedorn H, et al. Multifaceted academic detailing program to increase pharmacotherapy for alcohol use disorder: interrupted time series evaluation of effectiveness. Addict Sci Clin Pract. 2016;11(1):15.
Alcohol use disorder (AUD) is a relatively common condition characterized by a pattern of problematic alcohol consumption. According to the 2016 National Survey on Drug Use and Health (NSDUH) approximately 14.6 million Americans aged > 18 years had a diagnosis of AUD.1 This same survey also found that 26.2% of individuals over the age of 18 years reported engaging in binge drinking, which is ≥ 5 drinks in males or ≥ 4 drinks in females on the same occasion in the past month. Of those surveyed, 6.6% reported engaging in heavy drinking (binge drinking on 5 or more days in the past month).1
Military and veteran populations have a higher prevalence of alcohol misuse compared with that of the general population.2 Two out of 5 US veterans screen positive for lifetime AUD, which is higher than the prevalence of AUD in the general population.3 A number of studies have found that excessive alcohol use is common among military personnel.2,4,5 One study suggested that the average active-duty military member engages in approximately 30 binge drinking episodes per person per year.4 Military veterans may continue with a similar drinking pattern when transitioning to civilian life, explaining the high prevalence of AUD in the veteran population.6 Furthermore, since alcohol use provides temporary relief of posttraumatic stress disorder(PTSD) symptoms, a diagnosis of PTSD may also contribute to hazardous drinking in this population.7
Excessive alcohol consumption is associated with a number of negative outcomes, including increased motor-vehicle accidents, decreased medication adherence, and therefore, decreased efficacy, increased health care costs, and increased morbidity and mortality.8-13 Additionally, alcohol use is associated with a number of medical and psychiatric comorbidities.14,15 Compared with veterans without AUD, those with a diagnosis of AUD were 2.6 times more likely to have current depression and 2.8 times more likely to have generalized anxiety.3 Veterans with AUD also are 2.1 times more likely to have current suicidal ideation and 4.1 times more likely to have had a suicide attempt compared with veterans without AUD.3
Given the high prevalence and the associated risks, alcohol misuse should be properly addressed and treated. Pharmacotherapy for AUD has demonstrated efficacy in decreasing heavy drinking and prolonging periods of abstinence.16 Despite the proven benefits of available pharmacotherapy, these medications still are drastically underutilized in both the nonveteran and veteran populations. In fiscal year 2012, there were 444,000 veterans with a documented diagnosis of AUD; however, only 5.8% received evidence-based pharmacotherapy.17 The potential barriers for the utilization of AUD pharmacotherapy includes perceived low patient demand, lack of skill or knowledge about addiction, and lack of health care provider (HCP) confidence in efficacy.18 This article will provide a thorough overview of the pharmacotherapy options for the treatment of AUD and the evidence that supports the use of pharmacotherapy. We will then conclude with the recommended treatment approach for specialized patient populations.
FDA-Approved Pharmacotherapies
Naltrexone
Naltrexone was the second FDA-approved medication for the treatment of AUD and is considered a first-line agent by the Department of Veterans Affairs (VA).19,20 Unlike its predecessor, disulfiram, naltrexone significantly reduces cravings.21 During alcohol consumption endogenous opioid activity is greatly enhanced, leading to the rewarding effects of alcohol. By antagonizing the µ-opioid receptor, naltrexone mediates endorphin release during alcohol consumption, explaining the efficacy of naltrexone in AUD.21-28 Since cravings are reduced, patients are able to abstain from drinking for longer periods of time, and since pleasure is reduced, heavy drinking is also reduced.21,25
When compared with other pharmacotherapy options for AUD, naltrexone is less effective for abstinence and more effective for decreasing the time and frequency of heavy drinking days and average number of drinks consumed.29 A meta-analysis of 19 clinical trials found that naltrexone significantly reduced relapse rates in patients with AUD compared with those of placebo.30 This analysis also found that naltrexone reduced both the number of alcoholic beverages consumed and the risk of relapse to heavy drinking while increasing the total number of days of abstinence.30 The COMBINE study also found that patients receiving oral naltrexone in combination with medical treatment had a 28% reduced risk of having a heavy-drinking day.31
Dosing and Formulations
Naltrexone is available as a tablet or a long-acting injectable. The tablet is often dosed as 50 mg daily; although some studies suggest that daily doses up to 150 mg are safe and efficacious.21,25,32 The initial and maintenance dose for most patients is 50 mg daily.
Nonadherence to the oral formulation of naltrexone is a significant barrier to the treatment of AUD. The long-acting injectable formulation is an option for patients who may have difficulty with adhering to oral naltrexone. As with the oral formulation, the long-acting naltrexone injection significantly reduces drinking days and increases abstinence.33 It was also found to be superior to oral naltrexone, acamprosate, and disulfiram in preventing discontinuation of AUD treatment.34 The long-acting injectable should be administered as an intramuscular gluteal injection at a dose of 380 mg monthly.35
Ideally, naltrexone should be initiated following the cessation of alcohol withdrawal symptoms. However, naltrexone can be safely administered in patients who are actively withdrawing from alcohol or in patients who continue to consume alcohol.25
Warnings, Precautions, and AEs
Naltrexone carries a US Food and Drug Administration (FDA) boxed warning for reversible hepatotoxicity. The risk of hepatotoxicity is increased in patients who receive higher doses (100-300 mg daily).21 A safety study demonstrated that the administration of 50 mg daily or less is not associated with significant hepatotoxicity.21,31 It is contraindicated in patients with acute hepatitis or liver failure and should be avoided in patients with liver function tests > 5 times the upper limit of normal.
Since naltrexone is a µ-opioid receptor antagonist, it is contraindicated in patients who are actively taking opioids or patients who have used opioids within the past 7 days. Co-administration with an opioid can lead to precipitated opioid withdrawal.21 Therefore, opioids should not be administered within 7 to 10 days of initiating naltrexone and 2 to 3 days after discontinuation of oral naltrexone.21 For patients receiving the long-acting injectable form of naltrexone, opioids should be avoided at least 1 month after the injection.25
To ensure that a patient is opioid free, HCPs can perform a toxicology screening prior to the initiation of naltrexone. Some HCPs may also perform a naloxone challenge to test whether a patient is at risk for precipitated opioid withdrawal prior to prescribing naltrexone.
The adverse effects (AEs) of naltrexone are transient and include nausea, vomiting, anorexia, dizziness, and fatigue.19,35 Injection site reactions can be experienced with the long-acting naltrexone injection. Liver transaminases, such as the alanine aminotransferase and aspartate transaminase, should be monitored at baseline, 6 months after initiation, and annually during the course of treatment (Table 2).
Acamprosate
The FDA approved acamprosate for the treatment of AUD in 2004, and it is also considered a first-line agent for AUD by the VA.20 It is approved for the maintenance of abstinence from alcohol use and is most efficacious when initiated in patients who are abstinent prior to treatment.29,36 Patients with AUD typically have a disruption in the balance between the inhibitory neurotransmitter, gamma-aminobutyric acid (GABA), and the excitatory neurotransmitter, glutamate. While its mechanism of action remains unknown, acamprosate is thought to increase the activity of GABA and to decrease the activity of glutamate at the N-methyl-D-aspartate (NMDA) receptors in the central nervous system. In essence, it is thought to restores the balance between GABA and glutamate in patients with AUD.36
Acamprosate has been found to effectively prevent relapse. Three randomized, double-blind, placebo-controlled European clinical trials evaluated the efficacy of acamprosate in combination with psychotherapy. The results demonstrated that patients taking acamprosate had longer durations of abstinence compared with that of placebo, improved rates of complete abstinence, and a prolonged time to first drink.37-39 A meta-analysis evaluated the use of acamprosate in AUD showed that acamprosate was more effective at maintaining abstinence in patients who had been abstinent prior to the initiation of therapy.29 These patients also had better abstinence rates if they had been abstinent for a longer duration prior to treatment initiation.30 Studies also showed that acamprosate significantly assisted with maintaining abstinence, improved rates of abstinence, and led to more days of abstinence.40,41 Of note, there also have been studies that have shown no significant benefit with acamprosate compared with placebo in the treatment of AUD.42
Dosing and Formulations
Acamprosate is available as a 333 mg delayed-release tablet. The recommended dose is 666 mg 3 times daily.36 The dose can be decreased to 333 mg 3 times a day in patients with moderate renal impairment (CrCl-30-50 mL/min).
Since acamprosate has been proven more effective in patients who are abstinent prior to initiation, acamprosate is typically initiated 5 days following alcohol cessation.25 However, it may be safely administered with alcohol and can continue to be administered in the event of a relapse.36
Warnings, Precautions, and AEs
Acamprosate is safe to use in patients with hepatic and mild-to-moderate renal impairment; however, it is contraindicated in patients with severe renal impairment (creatinine clearance [CrCl] ≤ 30 mL/min).36 Serum creatinine levels should be monitored at baseline and during treatment.
Acamprosate has a number of related AEs. The most common is diarrhea. Less common AEs include insomnia, anxiety, and depression. Due to its possible potential to increase suicidality, HCPs should monitor for the emergence of mood changes.36
Disulfiram
Disulfiram is an aldehyde dehydrogenase inhibitor that is FDA approved for the management of AUD.43 When ingested, ethanol is typically metabolized to acetaldehyde, which is further metabolized to acetic acid by aldehyde dehydrogenase.44 Disulfiram inhibits aldehyde dehydrogenase, leading to a rapid accumulation of acetaldehyde within the plasma (outlined in Figure 2).
There are limited studies that prove the efficacy of disulfiram. In a randomized trial comparing disulfiram, acamprosate, and naltrexone, patients treated with disulfiram had fewer heavy drinking days, lower rates of weekly alcohol consumption, and a longer period of abstinence compared to other medications.45 Additionally, a 2014 meta-analysis showed that in open-label studies, disulfiram was more beneficial in preventing alcohol consumption when compared with acamprosate, naltrexone, and placebo. This result was not seen in blinded studies.46 Disulfiram does not reduce alcohol cravings, and adherence is a significant issue. It is most effective between 2 and 12 months, when taken under supervised administration.47
Dosing and Formulations
Disulfiram is only available as a tablet. The recommended starting dose is up to 500 mg for the first 2 weeks. However, the maintenance dose can range from 125 to 500 mg daily.43 Patients must be abstinent from alcohol at least 12 to 24 hours prior to the initiation of disulfiram.25 A blood alcohol level can be obtained in order to confirm abstinence.25
Warnings, Precautions, and AEs
Disulfiram is contraindicated in patients with severe myocardial disease or coronary occlusion and severe hepatic impairment.43 Other contraindications are outlined in Table 3.
Common AEs include somnolence, a metallic after-taste, and peripheral neuropathy.43 Patients should be informed that they could experience a disulfiram reaction with even small amounts of alcohol; all foods, drinks, and medications containing alcohol should be avoided. Due to the potential of disulfiram potential to cause hepatotoxicity, liver transaminases should be monitored at baseline, 2 weeks after initiation, and monthly for the first 6 months of therapy, and every 3 months thereafter (Table 2).25
Off-Label Pharmacotherapies
Topiramate
Although not approved for AUD, topiramate has been used off-label for this indication as it has proven efficacy in clinical trials.48-56 While its mechanism of action for AUD is unclear, it has been theorized that topiramate antagonizes glutamate receptors, thereby reducing dopamine release in the nucleus accumbens upon alcohol consumption, and potentiates the inhibitory neurotransmitter GABA.50,51,57-60
In clinical trials, topiramate has demonstrated significant efficacy in reducing cravings, the risk of relapse, and the number of drinks consumed daily, while increasing abstinence.51,53,60 Batki and colleagues report that the administration of topiramate in veterans with co-occurring AUD and PTSD reduced alcohol consumption, cravings, and the severity of their PTSD symptoms.61
Dosing and Formulations
Topiramate is available in a number of formulations; however, only the immediate-release formulation is recommended for the treatment of AUD. The extended-release formulation is contraindicated in the setting of alcohol consumption and is therefore not used for the treatment of AUD.62 Doses should be initiated at 25 mg daily and can be titrated in 25 to 50 mg weekly increments. To minimize AEs and to reduce the risk of patients discontinuing therapy, the dose may be slowly titrated over 8 weeks.53,59 An effective dose can range from 75 to 300 mg in divided doses; however, AEs often limit the tolerability of increased doses.48,50,63,64 The VA/DoD Practice Guideline for the Management of Substance Use Disorders recommends titrating topiramate to a target dose of 100 mg twice daily.65
Warnings, Precautions, and AEs
Common AEs include memory impairment, anorexia, fatigue, paresthesias, and somnolence.62 There is an increased risk of nephrolithiasis with topiramate administration; therefore, adequate hydration is crucial.49,59 Titration of topiramate to the target dose is suggested to limit AEs.35
Prior to initiating topiramate, the patient’s renal function should be assessed. In those with a CrCl < 70 mL/min the dose should be decreased by 50% and titrated more slowly.62
Gabapentin
Gabapentin is prescribed for the treatment of partial seizures and postherpetic neuralgia. In recent years, it has shown efficacy for treating other conditions, such as AUD. While its mechanism for this indication remains unclear, the inhibition of excitatory alpha-2-delta calcium channels and stimulation of inhibitory GABAA receptors by gabapentin is believed to decrease alcohol cravings, reduce anxiety, and increase abstinence.66
A 12-week, double-blind, randomized controlled trial demonstrated that oral gabapentin was more efficacious than was placebo for improving rates of abstinence, decreasing heavy drinking, and reducing alcohol cravings.67 Gabapentin may also serve as a good adjunctive option to naltrexone therapy either when naltrexone monotherapy fails or if a patient is complaining of sleep and mood disturbances with abstinence.67,68
Dosing and Formulations
Gabapentin should be titrated slowly to minimize AEs. It can be initiated at 300 mgon day 1 and increase by 300-mg increments. Doses of 900 to 1,800 mg per day have proven to be efficacious for the treatment of AUD.66,67 These proposed doses can be safely administered to most patients, but caution should be observed in elderly and patients with renal impairment.69,70
Warnings, Precautions, and AEs
The most common AEs for gabapentin include drowsiness, dizziness, and fatigue.69 Since it is renally cleared, renal function should be monitored at baseline and periodically during treatment. Gabapentin is not metabolized by liver enzymes and does not significantly interact with drugs that require hepatic metabolism.
Baclofen
Baclofen has generated attention as an unconventional treatment option for alcohol dependence. Its unique mechanism of action, which involves the activation of GABAB receptors and the subsequent inhibition of dopaminergic neurons, makes it useful for the treatment of AUD.71
A 12-week study evaluating the effectiveness and safety of baclofen for the maintenance of alcohol abstinence demonstrated that baclofen was more efficacious than placebo for increasing abstinence in patients with liver cirrhosis. In addition, there were more cumulative days of abstinence with baclofen use (62.8 days) vs placebo (30.8 days) in cirrhotic patients.72
Dosing and Formulations
There has been a range of doses studied for baclofen in the treatment of AUD. Studies indicate that initiating baclofen at 30 mg daily and increasing doses based on the patient’s clinical response is most effective.72 As a result, doses as high as 275 mg per day have been used for some patients.73 Baclofen is renally cleared; therefore, the dose should be adjusted in patients with renal impairment.74
Warnings, Precautions, and AEs
Some of the common AEs of baclofen include drowsiness, confusion, headache, and nausea. Due to its CNS depressant effects, baclofen should be used with caution in the elderly. Also, due to its potential to cause withdrawal symptoms, baclofen should not be discontinued abruptly.74,75 Baclofen is a safe option for patients with severe liver disease, due to its minimal hepatic metabolism.76
Ondansetron
Ondansetron is approved for both prophylactic and therapeutic use as an antiemetic agent for chemotherapy and anesthesia-induced nausea and vomiting.77As a highly selective and competitive 5-HT3 receptor antagonist, ondansetron has demonstrated efficacy in reducing serotonin-mediated dopaminergic effects in AUD.78,79 The lowering of these dopaminergic effects is associated with a reduction in alcohol-induced gratification and consumption.
In a 12-week, randomized controlled trial, 271 patients diagnosed with AUD received ondansetron twice daily or placebo, combined with weekly cognitive behavioral therapy (CBT). There was a statistically significant decrease in alcohol consumption in patients treated with ondansetron compared with those who received placebo. Additionally, ondansetron was superior to placebo for increasing the percentage and total amount of days abstinent.80 These results were primarily observed in participants diagnosed with early-onset AUD (defined as onset at 25 years or younger), which may suggest the presence of genetically predisposed serotonin dysfunctions.80,81 In contrast, there were no significant differences observed in participants with late-onset AUD (onset after age 25 years) in either study group.80
Dosing and Formulations
Given its modest efficacy for the treatment of AUD, ondansetron has demonstrated clinical benefits at doses of 0.001 to 0.016 mg/kg twice daily. Additionally, 1 study reported that low-dose ondansetron (0.25 mg twice daily) was effective in reducing alcohol consumption when compared with placebo or high-dose ondansetron, which was considered 2 mg twice daily.82
Warnings, Precautions, and AEs
The most commonly reported AEs with ondansetron include fatigue, headache, anxiety, and serotonin syndrome when used concomitantly with other serotonergic agents.77 Also, serious cardiovascular complications, such as QTc prolongation, angina pectoris, atrial fibrillation, and arrhythmias have been observed with IV administration.77,81,83 Consequently, patients with electrolyte imbalances (eg, hypokalemia, hypomagnesemia), a history of congestive heart failure, or concomitant medications associated with QTc prolongation, should be monitored with an electrocardiogram (ECG) or switched to another agent.77
Treatment Approach with AUD Pharmacotherapy
There is insufficient evidence to support the use of 1 medication for AUD over the others.16,46,84 Instead, the choice of therapy largely depends on the patient’s comorbidities, renal and hepatic function, and on the patient’s established goals, whether abstinence or reduction in alcohol consumption (Table 4).
There is much debate over the appropriate duration of treatment for AUD pharmacotherapy. It is recommended that patients remain on these medications for at least 3 months. Pharmacotherapy can be continued for 6 to 12 months as the risk for relapse is highest during this time frame.85,86 The National Institute for Health and Care Excellence guidelines recommend discontinuing AUD pharmacotherapy if alcohol consumption persists 4 to 6 weeks after initiation.86
Comorbid Liver Disease
Due to the negative effects of heavy alcohol consumption on the liver, patients with AUD may develop liver disease. Health care providers should be aware of the appropriate pharmacotherapy options for patients with comorbid liver disease. Acamprosate is mostly excreted unchanged by the kidneys, therefore is an option for patients with liver disease whose goal is complete abstinence. Topiramate is another option for use in patients with liver impairment. Unlike acamprosate, topiramate would be a better option in patients who may not completely abstain from alcohol consumption but would like to decrease the amount of heavy drinking days.87
Gabapentin, baclofen, and ondansetron are also options for those with liver disease. Baclofen in particular has been studied in those with advanced liver disease, and it was found to be safe and effective.88,89
Comorbid Renal Disease
Naltrexone is an option for patients with mild renal impairment. Naltrexone and its major metabolite, 6-ß-naltrexol, are renally excreted; however, urinary excretion of unchanged naltrexone accounts for < 2% of the oral dose.19 Even with its low potential for accumulation, HCPs should carefully monitor for AEs in patients with moderate-to-severe renal impairment. Disulfiram is another pharmacotherapy option, since it is mostly metabolized by the liver.
Gabapentin, baclofen, and ondansetron are also possible options; however, their doses should be renally adjusted. Overall, there are limited studies on the use of these medications treating AUD in patients with renal impairment.
Pregnancy
Alcohol consumption during pregnancy can result in a wide range of birth defects to the unborn fetus. Due to the negative effects of alcohol consumption on the fetus, pregnant females should be referred to a professional alcohol treatment program. Although AUD pharmacotherapy may be considered in pregnant females, there have been no human studies that have examined the efficacy and safety in this patient population. All evidence comes from animal studies, case reports, and case series.90
Naltrexone is the most widely used medication for AUD in pregnancy. It is considered pregnancy category C and 1 study in particular did not detect any gross abnormalities in fetal development in pregnancy.19, 90 Disulfiram, acamprosate, and topiramate have all been shown to cause harm to either animal or human fetuses and are generally not recommended.36,44,63 Similar to naltrexone, gabapentin and baclofen are also pregnancy category C.69,77 Ondansetron is pregnancy category B, but it should still be used with caution since its use in pregnancy for the treatment of AUD has not been studied.77,90
Psychosocial Interventions
It is recommended that AUD pharmacotherapy be used in conjunction with a psychosocial intervention, such as CBT or medical management. Many of the studies evaluating the efficacy of AUD pharmacotherapy combined psychosocial interventions with medications. The literature suggests that when combined with CBT or medical management therapy, pharmacotherapy used for AUD results in better alcohol consumption outcomes.31,91 It has also been suggested that psychosocial interventions may improve patient adherence to AUD pharmacotherapy.25
Barriers
Inadequate HCP training on the use of AUD pharmacotherapy has been found to be a major barrier to the utilization of AUD pharmacotherapy, along with a lack of confidence in the effectiveness of these medications.18 Increasing HCP education on the use and benefits of these agents may increase the overall confidence of HCPs in prescribing pharmacotherapy for the treatment of AUD, especially in the primary care setting. One aspect that has been found to improve education and the prescribing of pharmacotherapy for AUD within the Veterans Health Administration has been the use of academic detailing programs.92 Academic detailing is a multifaceted educational outreach program that is used to assist with HCP education. Additionally, clinical pharmacists can be consulted to help develop a safe and effective AUD pharmacotherapy treatment regimen.
Conclusion
There is a major disparity in the prevalence of AUD between the general population and the military and veteran populations. Many clinical trials have found a number of pharmacotherapy options to be effective for the treatment of AUD. Despite the need and the proven benefits, the utilization of AUD pharmacotherapy still remains low in both the general and veteran populations. Increasing provider education and addressing other potential barriers for the use of pharmacotherapy for AUD can have a positive impact on prescribing patterns, which can ultimately improve alcohol consumption outcomes in patients with a diagnosis of AUD.
Alcohol use disorder (AUD) is a relatively common condition characterized by a pattern of problematic alcohol consumption. According to the 2016 National Survey on Drug Use and Health (NSDUH) approximately 14.6 million Americans aged > 18 years had a diagnosis of AUD.1 This same survey also found that 26.2% of individuals over the age of 18 years reported engaging in binge drinking, which is ≥ 5 drinks in males or ≥ 4 drinks in females on the same occasion in the past month. Of those surveyed, 6.6% reported engaging in heavy drinking (binge drinking on 5 or more days in the past month).1
Military and veteran populations have a higher prevalence of alcohol misuse compared with that of the general population.2 Two out of 5 US veterans screen positive for lifetime AUD, which is higher than the prevalence of AUD in the general population.3 A number of studies have found that excessive alcohol use is common among military personnel.2,4,5 One study suggested that the average active-duty military member engages in approximately 30 binge drinking episodes per person per year.4 Military veterans may continue with a similar drinking pattern when transitioning to civilian life, explaining the high prevalence of AUD in the veteran population.6 Furthermore, since alcohol use provides temporary relief of posttraumatic stress disorder(PTSD) symptoms, a diagnosis of PTSD may also contribute to hazardous drinking in this population.7
Excessive alcohol consumption is associated with a number of negative outcomes, including increased motor-vehicle accidents, decreased medication adherence, and therefore, decreased efficacy, increased health care costs, and increased morbidity and mortality.8-13 Additionally, alcohol use is associated with a number of medical and psychiatric comorbidities.14,15 Compared with veterans without AUD, those with a diagnosis of AUD were 2.6 times more likely to have current depression and 2.8 times more likely to have generalized anxiety.3 Veterans with AUD also are 2.1 times more likely to have current suicidal ideation and 4.1 times more likely to have had a suicide attempt compared with veterans without AUD.3
Given the high prevalence and the associated risks, alcohol misuse should be properly addressed and treated. Pharmacotherapy for AUD has demonstrated efficacy in decreasing heavy drinking and prolonging periods of abstinence.16 Despite the proven benefits of available pharmacotherapy, these medications still are drastically underutilized in both the nonveteran and veteran populations. In fiscal year 2012, there were 444,000 veterans with a documented diagnosis of AUD; however, only 5.8% received evidence-based pharmacotherapy.17 The potential barriers for the utilization of AUD pharmacotherapy includes perceived low patient demand, lack of skill or knowledge about addiction, and lack of health care provider (HCP) confidence in efficacy.18 This article will provide a thorough overview of the pharmacotherapy options for the treatment of AUD and the evidence that supports the use of pharmacotherapy. We will then conclude with the recommended treatment approach for specialized patient populations.
FDA-Approved Pharmacotherapies
Naltrexone
Naltrexone was the second FDA-approved medication for the treatment of AUD and is considered a first-line agent by the Department of Veterans Affairs (VA).19,20 Unlike its predecessor, disulfiram, naltrexone significantly reduces cravings.21 During alcohol consumption endogenous opioid activity is greatly enhanced, leading to the rewarding effects of alcohol. By antagonizing the µ-opioid receptor, naltrexone mediates endorphin release during alcohol consumption, explaining the efficacy of naltrexone in AUD.21-28 Since cravings are reduced, patients are able to abstain from drinking for longer periods of time, and since pleasure is reduced, heavy drinking is also reduced.21,25
When compared with other pharmacotherapy options for AUD, naltrexone is less effective for abstinence and more effective for decreasing the time and frequency of heavy drinking days and average number of drinks consumed.29 A meta-analysis of 19 clinical trials found that naltrexone significantly reduced relapse rates in patients with AUD compared with those of placebo.30 This analysis also found that naltrexone reduced both the number of alcoholic beverages consumed and the risk of relapse to heavy drinking while increasing the total number of days of abstinence.30 The COMBINE study also found that patients receiving oral naltrexone in combination with medical treatment had a 28% reduced risk of having a heavy-drinking day.31
Dosing and Formulations
Naltrexone is available as a tablet or a long-acting injectable. The tablet is often dosed as 50 mg daily; although some studies suggest that daily doses up to 150 mg are safe and efficacious.21,25,32 The initial and maintenance dose for most patients is 50 mg daily.
Nonadherence to the oral formulation of naltrexone is a significant barrier to the treatment of AUD. The long-acting injectable formulation is an option for patients who may have difficulty with adhering to oral naltrexone. As with the oral formulation, the long-acting naltrexone injection significantly reduces drinking days and increases abstinence.33 It was also found to be superior to oral naltrexone, acamprosate, and disulfiram in preventing discontinuation of AUD treatment.34 The long-acting injectable should be administered as an intramuscular gluteal injection at a dose of 380 mg monthly.35
Ideally, naltrexone should be initiated following the cessation of alcohol withdrawal symptoms. However, naltrexone can be safely administered in patients who are actively withdrawing from alcohol or in patients who continue to consume alcohol.25
Warnings, Precautions, and AEs
Naltrexone carries a US Food and Drug Administration (FDA) boxed warning for reversible hepatotoxicity. The risk of hepatotoxicity is increased in patients who receive higher doses (100-300 mg daily).21 A safety study demonstrated that the administration of 50 mg daily or less is not associated with significant hepatotoxicity.21,31 It is contraindicated in patients with acute hepatitis or liver failure and should be avoided in patients with liver function tests > 5 times the upper limit of normal.
Since naltrexone is a µ-opioid receptor antagonist, it is contraindicated in patients who are actively taking opioids or patients who have used opioids within the past 7 days. Co-administration with an opioid can lead to precipitated opioid withdrawal.21 Therefore, opioids should not be administered within 7 to 10 days of initiating naltrexone and 2 to 3 days after discontinuation of oral naltrexone.21 For patients receiving the long-acting injectable form of naltrexone, opioids should be avoided at least 1 month after the injection.25
To ensure that a patient is opioid free, HCPs can perform a toxicology screening prior to the initiation of naltrexone. Some HCPs may also perform a naloxone challenge to test whether a patient is at risk for precipitated opioid withdrawal prior to prescribing naltrexone.
The adverse effects (AEs) of naltrexone are transient and include nausea, vomiting, anorexia, dizziness, and fatigue.19,35 Injection site reactions can be experienced with the long-acting naltrexone injection. Liver transaminases, such as the alanine aminotransferase and aspartate transaminase, should be monitored at baseline, 6 months after initiation, and annually during the course of treatment (Table 2).
Acamprosate
The FDA approved acamprosate for the treatment of AUD in 2004, and it is also considered a first-line agent for AUD by the VA.20 It is approved for the maintenance of abstinence from alcohol use and is most efficacious when initiated in patients who are abstinent prior to treatment.29,36 Patients with AUD typically have a disruption in the balance between the inhibitory neurotransmitter, gamma-aminobutyric acid (GABA), and the excitatory neurotransmitter, glutamate. While its mechanism of action remains unknown, acamprosate is thought to increase the activity of GABA and to decrease the activity of glutamate at the N-methyl-D-aspartate (NMDA) receptors in the central nervous system. In essence, it is thought to restores the balance between GABA and glutamate in patients with AUD.36
Acamprosate has been found to effectively prevent relapse. Three randomized, double-blind, placebo-controlled European clinical trials evaluated the efficacy of acamprosate in combination with psychotherapy. The results demonstrated that patients taking acamprosate had longer durations of abstinence compared with that of placebo, improved rates of complete abstinence, and a prolonged time to first drink.37-39 A meta-analysis evaluated the use of acamprosate in AUD showed that acamprosate was more effective at maintaining abstinence in patients who had been abstinent prior to the initiation of therapy.29 These patients also had better abstinence rates if they had been abstinent for a longer duration prior to treatment initiation.30 Studies also showed that acamprosate significantly assisted with maintaining abstinence, improved rates of abstinence, and led to more days of abstinence.40,41 Of note, there also have been studies that have shown no significant benefit with acamprosate compared with placebo in the treatment of AUD.42
Dosing and Formulations
Acamprosate is available as a 333 mg delayed-release tablet. The recommended dose is 666 mg 3 times daily.36 The dose can be decreased to 333 mg 3 times a day in patients with moderate renal impairment (CrCl-30-50 mL/min).
Since acamprosate has been proven more effective in patients who are abstinent prior to initiation, acamprosate is typically initiated 5 days following alcohol cessation.25 However, it may be safely administered with alcohol and can continue to be administered in the event of a relapse.36
Warnings, Precautions, and AEs
Acamprosate is safe to use in patients with hepatic and mild-to-moderate renal impairment; however, it is contraindicated in patients with severe renal impairment (creatinine clearance [CrCl] ≤ 30 mL/min).36 Serum creatinine levels should be monitored at baseline and during treatment.
Acamprosate has a number of related AEs. The most common is diarrhea. Less common AEs include insomnia, anxiety, and depression. Due to its possible potential to increase suicidality, HCPs should monitor for the emergence of mood changes.36
Disulfiram
Disulfiram is an aldehyde dehydrogenase inhibitor that is FDA approved for the management of AUD.43 When ingested, ethanol is typically metabolized to acetaldehyde, which is further metabolized to acetic acid by aldehyde dehydrogenase.44 Disulfiram inhibits aldehyde dehydrogenase, leading to a rapid accumulation of acetaldehyde within the plasma (outlined in Figure 2).
There are limited studies that prove the efficacy of disulfiram. In a randomized trial comparing disulfiram, acamprosate, and naltrexone, patients treated with disulfiram had fewer heavy drinking days, lower rates of weekly alcohol consumption, and a longer period of abstinence compared to other medications.45 Additionally, a 2014 meta-analysis showed that in open-label studies, disulfiram was more beneficial in preventing alcohol consumption when compared with acamprosate, naltrexone, and placebo. This result was not seen in blinded studies.46 Disulfiram does not reduce alcohol cravings, and adherence is a significant issue. It is most effective between 2 and 12 months, when taken under supervised administration.47
Dosing and Formulations
Disulfiram is only available as a tablet. The recommended starting dose is up to 500 mg for the first 2 weeks. However, the maintenance dose can range from 125 to 500 mg daily.43 Patients must be abstinent from alcohol at least 12 to 24 hours prior to the initiation of disulfiram.25 A blood alcohol level can be obtained in order to confirm abstinence.25
Warnings, Precautions, and AEs
Disulfiram is contraindicated in patients with severe myocardial disease or coronary occlusion and severe hepatic impairment.43 Other contraindications are outlined in Table 3.
Common AEs include somnolence, a metallic after-taste, and peripheral neuropathy.43 Patients should be informed that they could experience a disulfiram reaction with even small amounts of alcohol; all foods, drinks, and medications containing alcohol should be avoided. Due to the potential of disulfiram potential to cause hepatotoxicity, liver transaminases should be monitored at baseline, 2 weeks after initiation, and monthly for the first 6 months of therapy, and every 3 months thereafter (Table 2).25
Off-Label Pharmacotherapies
Topiramate
Although not approved for AUD, topiramate has been used off-label for this indication as it has proven efficacy in clinical trials.48-56 While its mechanism of action for AUD is unclear, it has been theorized that topiramate antagonizes glutamate receptors, thereby reducing dopamine release in the nucleus accumbens upon alcohol consumption, and potentiates the inhibitory neurotransmitter GABA.50,51,57-60
In clinical trials, topiramate has demonstrated significant efficacy in reducing cravings, the risk of relapse, and the number of drinks consumed daily, while increasing abstinence.51,53,60 Batki and colleagues report that the administration of topiramate in veterans with co-occurring AUD and PTSD reduced alcohol consumption, cravings, and the severity of their PTSD symptoms.61
Dosing and Formulations
Topiramate is available in a number of formulations; however, only the immediate-release formulation is recommended for the treatment of AUD. The extended-release formulation is contraindicated in the setting of alcohol consumption and is therefore not used for the treatment of AUD.62 Doses should be initiated at 25 mg daily and can be titrated in 25 to 50 mg weekly increments. To minimize AEs and to reduce the risk of patients discontinuing therapy, the dose may be slowly titrated over 8 weeks.53,59 An effective dose can range from 75 to 300 mg in divided doses; however, AEs often limit the tolerability of increased doses.48,50,63,64 The VA/DoD Practice Guideline for the Management of Substance Use Disorders recommends titrating topiramate to a target dose of 100 mg twice daily.65
Warnings, Precautions, and AEs
Common AEs include memory impairment, anorexia, fatigue, paresthesias, and somnolence.62 There is an increased risk of nephrolithiasis with topiramate administration; therefore, adequate hydration is crucial.49,59 Titration of topiramate to the target dose is suggested to limit AEs.35
Prior to initiating topiramate, the patient’s renal function should be assessed. In those with a CrCl < 70 mL/min the dose should be decreased by 50% and titrated more slowly.62
Gabapentin
Gabapentin is prescribed for the treatment of partial seizures and postherpetic neuralgia. In recent years, it has shown efficacy for treating other conditions, such as AUD. While its mechanism for this indication remains unclear, the inhibition of excitatory alpha-2-delta calcium channels and stimulation of inhibitory GABAA receptors by gabapentin is believed to decrease alcohol cravings, reduce anxiety, and increase abstinence.66
A 12-week, double-blind, randomized controlled trial demonstrated that oral gabapentin was more efficacious than was placebo for improving rates of abstinence, decreasing heavy drinking, and reducing alcohol cravings.67 Gabapentin may also serve as a good adjunctive option to naltrexone therapy either when naltrexone monotherapy fails or if a patient is complaining of sleep and mood disturbances with abstinence.67,68
Dosing and Formulations
Gabapentin should be titrated slowly to minimize AEs. It can be initiated at 300 mgon day 1 and increase by 300-mg increments. Doses of 900 to 1,800 mg per day have proven to be efficacious for the treatment of AUD.66,67 These proposed doses can be safely administered to most patients, but caution should be observed in elderly and patients with renal impairment.69,70
Warnings, Precautions, and AEs
The most common AEs for gabapentin include drowsiness, dizziness, and fatigue.69 Since it is renally cleared, renal function should be monitored at baseline and periodically during treatment. Gabapentin is not metabolized by liver enzymes and does not significantly interact with drugs that require hepatic metabolism.
Baclofen
Baclofen has generated attention as an unconventional treatment option for alcohol dependence. Its unique mechanism of action, which involves the activation of GABAB receptors and the subsequent inhibition of dopaminergic neurons, makes it useful for the treatment of AUD.71
A 12-week study evaluating the effectiveness and safety of baclofen for the maintenance of alcohol abstinence demonstrated that baclofen was more efficacious than placebo for increasing abstinence in patients with liver cirrhosis. In addition, there were more cumulative days of abstinence with baclofen use (62.8 days) vs placebo (30.8 days) in cirrhotic patients.72
Dosing and Formulations
There has been a range of doses studied for baclofen in the treatment of AUD. Studies indicate that initiating baclofen at 30 mg daily and increasing doses based on the patient’s clinical response is most effective.72 As a result, doses as high as 275 mg per day have been used for some patients.73 Baclofen is renally cleared; therefore, the dose should be adjusted in patients with renal impairment.74
Warnings, Precautions, and AEs
Some of the common AEs of baclofen include drowsiness, confusion, headache, and nausea. Due to its CNS depressant effects, baclofen should be used with caution in the elderly. Also, due to its potential to cause withdrawal symptoms, baclofen should not be discontinued abruptly.74,75 Baclofen is a safe option for patients with severe liver disease, due to its minimal hepatic metabolism.76
Ondansetron
Ondansetron is approved for both prophylactic and therapeutic use as an antiemetic agent for chemotherapy and anesthesia-induced nausea and vomiting.77As a highly selective and competitive 5-HT3 receptor antagonist, ondansetron has demonstrated efficacy in reducing serotonin-mediated dopaminergic effects in AUD.78,79 The lowering of these dopaminergic effects is associated with a reduction in alcohol-induced gratification and consumption.
In a 12-week, randomized controlled trial, 271 patients diagnosed with AUD received ondansetron twice daily or placebo, combined with weekly cognitive behavioral therapy (CBT). There was a statistically significant decrease in alcohol consumption in patients treated with ondansetron compared with those who received placebo. Additionally, ondansetron was superior to placebo for increasing the percentage and total amount of days abstinent.80 These results were primarily observed in participants diagnosed with early-onset AUD (defined as onset at 25 years or younger), which may suggest the presence of genetically predisposed serotonin dysfunctions.80,81 In contrast, there were no significant differences observed in participants with late-onset AUD (onset after age 25 years) in either study group.80
Dosing and Formulations
Given its modest efficacy for the treatment of AUD, ondansetron has demonstrated clinical benefits at doses of 0.001 to 0.016 mg/kg twice daily. Additionally, 1 study reported that low-dose ondansetron (0.25 mg twice daily) was effective in reducing alcohol consumption when compared with placebo or high-dose ondansetron, which was considered 2 mg twice daily.82
Warnings, Precautions, and AEs
The most commonly reported AEs with ondansetron include fatigue, headache, anxiety, and serotonin syndrome when used concomitantly with other serotonergic agents.77 Also, serious cardiovascular complications, such as QTc prolongation, angina pectoris, atrial fibrillation, and arrhythmias have been observed with IV administration.77,81,83 Consequently, patients with electrolyte imbalances (eg, hypokalemia, hypomagnesemia), a history of congestive heart failure, or concomitant medications associated with QTc prolongation, should be monitored with an electrocardiogram (ECG) or switched to another agent.77
Treatment Approach with AUD Pharmacotherapy
There is insufficient evidence to support the use of 1 medication for AUD over the others.16,46,84 Instead, the choice of therapy largely depends on the patient’s comorbidities, renal and hepatic function, and on the patient’s established goals, whether abstinence or reduction in alcohol consumption (Table 4).
There is much debate over the appropriate duration of treatment for AUD pharmacotherapy. It is recommended that patients remain on these medications for at least 3 months. Pharmacotherapy can be continued for 6 to 12 months as the risk for relapse is highest during this time frame.85,86 The National Institute for Health and Care Excellence guidelines recommend discontinuing AUD pharmacotherapy if alcohol consumption persists 4 to 6 weeks after initiation.86
Comorbid Liver Disease
Due to the negative effects of heavy alcohol consumption on the liver, patients with AUD may develop liver disease. Health care providers should be aware of the appropriate pharmacotherapy options for patients with comorbid liver disease. Acamprosate is mostly excreted unchanged by the kidneys, therefore is an option for patients with liver disease whose goal is complete abstinence. Topiramate is another option for use in patients with liver impairment. Unlike acamprosate, topiramate would be a better option in patients who may not completely abstain from alcohol consumption but would like to decrease the amount of heavy drinking days.87
Gabapentin, baclofen, and ondansetron are also options for those with liver disease. Baclofen in particular has been studied in those with advanced liver disease, and it was found to be safe and effective.88,89
Comorbid Renal Disease
Naltrexone is an option for patients with mild renal impairment. Naltrexone and its major metabolite, 6-ß-naltrexol, are renally excreted; however, urinary excretion of unchanged naltrexone accounts for < 2% of the oral dose.19 Even with its low potential for accumulation, HCPs should carefully monitor for AEs in patients with moderate-to-severe renal impairment. Disulfiram is another pharmacotherapy option, since it is mostly metabolized by the liver.
Gabapentin, baclofen, and ondansetron are also possible options; however, their doses should be renally adjusted. Overall, there are limited studies on the use of these medications treating AUD in patients with renal impairment.
Pregnancy
Alcohol consumption during pregnancy can result in a wide range of birth defects to the unborn fetus. Due to the negative effects of alcohol consumption on the fetus, pregnant females should be referred to a professional alcohol treatment program. Although AUD pharmacotherapy may be considered in pregnant females, there have been no human studies that have examined the efficacy and safety in this patient population. All evidence comes from animal studies, case reports, and case series.90
Naltrexone is the most widely used medication for AUD in pregnancy. It is considered pregnancy category C and 1 study in particular did not detect any gross abnormalities in fetal development in pregnancy.19, 90 Disulfiram, acamprosate, and topiramate have all been shown to cause harm to either animal or human fetuses and are generally not recommended.36,44,63 Similar to naltrexone, gabapentin and baclofen are also pregnancy category C.69,77 Ondansetron is pregnancy category B, but it should still be used with caution since its use in pregnancy for the treatment of AUD has not been studied.77,90
Psychosocial Interventions
It is recommended that AUD pharmacotherapy be used in conjunction with a psychosocial intervention, such as CBT or medical management. Many of the studies evaluating the efficacy of AUD pharmacotherapy combined psychosocial interventions with medications. The literature suggests that when combined with CBT or medical management therapy, pharmacotherapy used for AUD results in better alcohol consumption outcomes.31,91 It has also been suggested that psychosocial interventions may improve patient adherence to AUD pharmacotherapy.25
Barriers
Inadequate HCP training on the use of AUD pharmacotherapy has been found to be a major barrier to the utilization of AUD pharmacotherapy, along with a lack of confidence in the effectiveness of these medications.18 Increasing HCP education on the use and benefits of these agents may increase the overall confidence of HCPs in prescribing pharmacotherapy for the treatment of AUD, especially in the primary care setting. One aspect that has been found to improve education and the prescribing of pharmacotherapy for AUD within the Veterans Health Administration has been the use of academic detailing programs.92 Academic detailing is a multifaceted educational outreach program that is used to assist with HCP education. Additionally, clinical pharmacists can be consulted to help develop a safe and effective AUD pharmacotherapy treatment regimen.
Conclusion
There is a major disparity in the prevalence of AUD between the general population and the military and veteran populations. Many clinical trials have found a number of pharmacotherapy options to be effective for the treatment of AUD. Despite the need and the proven benefits, the utilization of AUD pharmacotherapy still remains low in both the general and veteran populations. Increasing provider education and addressing other potential barriers for the use of pharmacotherapy for AUD can have a positive impact on prescribing patterns, which can ultimately improve alcohol consumption outcomes in patients with a diagnosis of AUD.
1. Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. Results from the 2016 National Survey on Drug Use and Health: detailed tables. Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2016/NSDUH-DetTabs-2016.pdf. Published September 7, 2017. Accessed September 13, 2018.
2. Jones E, Fear NT. Alcohol use and misuse within the military: a review. Int Rev Psychiatry. 2011;23(2):166-172.
3. Fuehrlein BS, Mota N, Arias AJ, et al. The burden of alcohol use disorders in US military veterans: results from the National Health and Resilience in Veterans Study. Addiction. 2016;111(10):1786-1794.
4. Stahre MA, Brewer RD, Fonseca VP, Naimi TS. Binge drinking among US active-duty military personnel. Am J Prev Med. 2009;36(3):208-217.
5. Institute of Medicine. Substance use disorders in the U.S. armed forces. https://www.nap.edu/resource/13441/SUD_rb.pdf. Published September 2012. Accessed September 12, 2018.
6. McDevitt-Murphy ME, Murphy JG, Williams JL, Monahan CJ, Bracken-Minor KL. Brief intervention to reduce hazardous drinking and enhance coping among OEF/OIF/OND veterans. Prof Psychol Res Pr. 2015;46(2):83-89.
7. Jacobson IG, Ryan MA, Hooper TI, et al. Alcohol use and alcohol-related problems before and after military combat deployment. JAMA. 2008;300(6):663-675.
8. Chou SP, Dawson DA, Stinson FS, et al. The prevalence of drinking and driving in the United States, 2001-2002: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Drug Alcohol Depend. 2006;83(2):137-146.
9. Bazargan-Hejazi S, Bazargan M, Hardin E, Bing EG. Alcohol use and adherence to prescribed therapy among under-served Latino and African-American patients using emergency department services. Ethn Dis. 2005;15(2):267-275.
10. Kamali M, Kelly BD, Clarke M, et al. A prospective evaluation of adherence to medication in first episode of schizophrenia. Eur Psychiatry. 2006;21(1):29-33.
11. Tucker JS, Burnam MA, Sherbourne CD, Kung FY, Gifford AL. Substance abuse and mental health correlates of nonadherence to antiretroviral medications in a sample of patients with human immunodeficiency virus infection. Am J Med. 2003;114(7):573-580.
12. Rehm J, Room R, Graham K, Monteiro M, Gmel G, Sempos CT. The relationship of average volume of alcohol consumption and patterns of drinking to burden of disease: an overview. Addiction. 2003;98(9):1209-1228.
13. Kendler KS, Ohlsson H, Sundquist J, Sundquist K. Alcohol use disorder and mortality across the lifespan: a longitudinal cohort and co-relative analysis. JAMA Psychiatry. 2016;73(6):575-581.
14. Hasin DS, Stinson FS, Ogburn E, Grant BF. Prevalence, correlates, disability, and comorbidity of DSM-IV alcohol abuse and dependence in the United States. Arch Gen Psychiatry. 2007;64(7):830-842.
15. Grant BF, Stinson FS, Dawson DA, et al. Prevalence and co-occurrence of substance use disorders and independent mood and anxiety disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2004;61(8):807-816.
16. Jonas DE, Amick HR, Feltner C, et al. Pharmacotherapy for adults with alcohol use disorders in outpatient settings: a systematic review and meta-analysis. JAMA. 2014;311(18):1889-1900.
17. Del Re AC, Gordon AJ, Lembke A, Harris AH. Prescription of topiramate to treat alcohol use disorders in the Veterans Health Administration. Addict Sci Clin Pract. 2013;8:12.
18. Harris AH, Ellerbe L, Reeder RN, et al. Pharmacotherapy for alcohol dependence: perceived treatment barriers and action strategies among Veterans Health Administration service providers. Psychol Serv. 2013;10(4):410-419.
19. ReVia [package insert]. Pomona, NY: Duramed Pharmaceuticals; 2013.
20. US Department of Veterans Affairs, Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives. Alcohol use disorder pharmacotherapy: naltrexone, acamprosate, and disulfiram recommendations for use. https://www.pbm.va.gov/PBM/clinicalguidance/clinicalrecommendations/Alcohol_Use_Disorder_Pharmacotherapy_Acamprosate_Naltrexone_Disulfiram_Recommendations_for_Use.docx. Published December 2013. Accessed September 17, 2018.
21. Anton RF. Naltrexone for the management of alcohol dependence. N Engl J Med. 2008;359(7):715-721.
22. O’Malley SS, Rounsaville BJ, Farren C, et al. Initial and maintenance naltrexone treatment for alcohol dependence using primary care vs specialty care: a nested sequence of 3 randomized trials. Arch Intern Med. 2003;163(14):1695-1704.
23. O’Brien CP. A range of research-based pharmacotherapies for addiction. Science. 1997;278(5335):66-70.
24. Swift RM. Effect of naltrexone on human alcohol consumption. J Clin Psychiatry. 1995;56 (suppl 7):24-29.
25. Center for Substance Abuse Treatment. Incorporating Alcohol Pharmacotherapies into Medical Practice. Treatment Improvement Protocol (TIP) Series 49. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2009.
26. Spanagel R, Zieglgänsberger W. Anti-craving compounds for ethanol: new pharmacological tools to study addictive processes. Trends Pharmacol Sci. 1997;18(2):54-59.
27. Herz A. Endogenous opioid systems and alcohol addiction. Psychopharmacology (Berl). 1997;129(2):99-111.
28. Miller NS. The integration of pharmacological and nonpharmacological treatments in drug/alcohol addiction. J Addict Dis. 1997;16(4):1-5.
29. Maisel NC, Blodgett JC, Wilbourne PL, Humphreys K, Finney JW. Meta-analysis of naltrexone and acamprosate for treating alcohol use disorders: when are these medications most helpful? Addiction. 2013;108(2):275-293.
30. Bouza C, Angeles M, Muñoz A, Amate JM. Efficacy and safety of naltrexone and acamprosate in the treatment of alcohol dependence: a systematic review. Addiction. 2004;99(7):811-828.
31. Anton RF, O’Malley SS, Ciraulo DA, et al; COMBINE Study Research Group. Combined pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE study: a randomized controlled trial. JAMA. 2006;295(17):2003-2017.
32. Oslin DW, Pettinati HM, Volpicelli JR, Wolf AL, Kampman KM, O’Brien CP. The effects of naltrexone on alcohol and cocaine use in dually addicted patients. J Subst Abuse Treat. 1999;16(2):163-167.
33. Kranzler HR, Wesson DR, Billot L; DrugAbuse Sciences Naltrexone Depot Study Group. Naltrexone depot for treatment of alcohol dependence: a multicenter, randomized, placebo-controlled clinical trial. Alcohol Clin Exp Res. 2004;28(7):1051-1059.
34. Bryson WC, McConnell J, Korthuis PT, McCarty D. Extended-release naltrexone for alcohol dependence: persistence and healthcare costs and utilization. Am J Manag Care. 2011;17 (suppl 8):S222-S234.
35. Vivitrol [package insert]. Waltham, MA: Alkermes, Inc.; 2010.
36. Campral [package insert]. St. Louis, MO: Forest Laboratories Inc; 2012.
37. Paille F, Guelfi J, Perkins AC, Royer RJ, Steru L, Parot P. Double-blind randomized multicentre trial of acamprosate in maintaining abstinence from alcohol. Alcohol. 1995;30(2):239-247.
38. Pelc I, Verbanck P, Le Bon O, Gavrilovic M, Lion K, Lehert P. Efficacy and safety of acamprosate in the treatment of detoxified alcohol-dependent patients. A 90-day placebo-controlled dose-finding study. Br J Psychiatry. 1997;171:73-77.
39. Sass H, Soyka M, Mann K, Zieglgänsberger W. Relapse prevention by acamprosate. Results from a placebo-controlled study on alcohol dependence. Arch Gen Psychiatry. 1996;53(8):673-680.
40. Mann K, Lehert P, Morgan MY. The efficacy of acamprosate in the maintenance of abstinence in alcohol-dependent individuals: results of a meta-analysis. Alcohol Clin Exp Res. 2004;28(1):51-63.
41. Mason BJ, Lehert P. Acamprosate for alcohol dependence: a sex-specific meta-analysis based on individual patient data. Alcohol Clin Exp Res. 2012;36(3):497-508.
42. Richardson K, Baillie A, Reid S, et al. Do acamprosate or naltrexone have an effect on daily drinking by reducing craving for alcohol? Addiction. 2008;103(6):953-959.
43. Antabuse [package insert]. North Wales, PA: Teva Pharmaceuticals; 2015.
44. Ait-Daoud N, Johnson BA. Medications for the treatment of alcoholism. In: Johnson BA, Ruiz P, Galanter M, eds. Handbook of Clinical Alcoholism Treatment. Lippincott Williams & Wilkins, Baltimore; 2003
45. Laaksonen E, Koski-Jännes A, Salaspuro M, Ahtinen H, Alho H. A randomized, multicentre, open-label, comparative trial of disulfiram, naltrexone and acamprosate in the treatment of alcohol dependence. Alcohol Alcohol. 2008;43(1):53-61.
46. Skinner MD, Lahmek P, Pham H, Aubin HJ. Disulfiram efficacy in the treatment of alcohol dependence: a meta-analysis. PLoS One. 2014;9(2):e87366.
47. Jørgensen CH, Pedersen B, Tønnesen H. The efficacy of disulfiram for the treatment of alcohol use disorder. Alcohol Clin Exp Res. 2011;35(10):1749-1758.
48. Arbaizar B, Diersen-Sotos T, Gómez-Acebo I, Llorca J. Topiramate in the treatment of alcohol dependence: a meta-analysis. [Article in English, Spanish] Actas Esp Psiquiatr. 2010;38(1):8-12.
49. Johnson BA, Ait-Daoud N. Topiramate in the new generation of drugs: efficacy in the treatment of alcoholic patients. Curr Pharm Des. 2010;16(19):2103-2112.
50. Paparrigopoulos T, Tzavellas E, Karaiskos D, Kourlaba G, Liappas I. Treatment of alcohol dependence with low-dose topiramate: an open-label controlled study. BMC Psychiatry. 2011;11:41.
51. Johnson BA, Ait-Daoud N, Bowden CL, et al. Oral topiramate for treatment of alcohol dependence: a randomised controlled trial. Lancet. 2003;361(9370):1677-1685.
52. Johnson BA, Ait-Daoud N, Akhtar FZ, Ma JZ. Oral topiramate reduces the consequences of drinking and improves the quality of life of alcohol-dependent individuals: a randomized controlled trial. Arch Gen Psychiatry. 2004;61(9):905-912.
53. Johnson BA, Rosenthal N, Capece JA, et al; Topiramate for Alcoholism Advisory Board; Topiramate for Alcoholism Study Group. Topiramate for treating alcohol dependence: a randomized controlled trial. JAMA. 2007;298(14):1641-1651.
54. Flórez G, García-Portilla P, Alvarez S, Saiz PA, Nogueiras L, Bobes J. Using topiramate or naltrexone for the treatment of alcohol-dependent patients. Alcohol Clin Exp Res. 2008;32(7):1251-1259.
55. Flórez G, Saiz PA, Garcia-Portilla P, Alvarez S, Nogueiras L, Bobes J. Topiramate for the treatment of alcohol dependence: comparison with naltrexone. Eur Addict Res. 2011;17(1):29-36.
56. Baltieri DA, Daró FR, Ribeiro PL, de Andrade AG. Comparing topiramate with naltrexone in the treatment of alcohol dependence. Addiction. 2008;103(12):2035-2044.
57. White HS, Brown SD, Woodhead JH, Skeen GA, Wolf HH. Topiramate modulates GABA-evoked currents in murine cortical neurons by a nonbenzodiazepine mechanism. Epilepsia. 2000;41(suppl 1):S17-S20.
58. White HS, Brown SD, Woodhead JH, Skeen GA, Wolf HH. Topiramate enhances GABA-mediated chloride flux and GABA-evoked chloride currents in murine brain neurons and increases seizure threshold. Epilepsy Res. 1997;28(3):167-179.
59. Guglielmo R, Martinotti G, Quatrale M, et al. Topiramate in alcohol use disorders: review and update. CNS Drugs. 2015;29(5):383-395.
60. Kranzler HR, Covault J, Feinn R, et al. Topiramate treatment for heavy drinkers: moderation by a GRIK1 polymorphism. Am J Psychiatry. 2014;171(4):445-452.
61. Batki SL, Pennington DL, Lasher B, et al. Topiramate treatment of alcohol use disorder in veterans with posttraumatic stress disorder: a randomized controlled pilot trial. Alcohol Clin Exp Res. 2014;38(8):2169-2177.
62. Topamax [package insert]. Titusville, NJ: Janssen Pharmaceuticals Inc; 2017.
63. Meador KJ. Cognitive effects of levetiracetam versus topiramate. Epilepsy Curr. 2008;8(3):64-65.
64. Luykx JJ, Carpay JA. Nervous system adverse responses to topiramate in the treatment of neuropsychiatric disorders. Expert Opin Drug Saf. 2010;9(4):623-631.
65. The Management of Substance Use Disorder Work Group; US Department of Veteran Affairs, US Department of Defense. VA/DoD clinical practice guideline for the management of substance use disorders. https://www.healthquality.va.gov/guidelines/MH/sud/VADODSUDCPGRevised22216.pdf. Published December 2015. Accessed September 12, 2018.
66. Sills GJ. The mechanism of action of gabapentin and pregabalin. Curr Opin Pharmacol. 2006;6(1):108-113.
67. Mason BJ, Quello S, Goodell V, Shandan F, Kyle M, Begovic A. Gabapentin treatment for alcohol dependence: a randomized clinical trial. JAMA Intern Med. 2014;174(1):70-77.
68. Anton RF, Myrick H, Wright TM, et al. Gabapentin combined with naltrexone for the treatment of alcohol dependence. Am J Psychiatry. 2011;168(7):709-717.
69. Neurontin [package insert]. New York, NY: Pfizer; 2017.
70. American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American Geriatrics Society 2015 updated Beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2015;63(11):2227-2246.
71. Addolorato G, Leggio L. Safety and efficacy of baclofen in the treatment of alcohol-dependent patients. Curr Pharm Des. 2010;16(19):2113-2117.
72. Addolorato G, Leggio L, Ferrulli A, et al. Effectiveness and safety of baclofen for maintenance of alcohol abstinence in alcohol-dependent patients with liver cirrhosis: a randomized, double-blind, controlled study. Lancet. 2007;370(9603):1915-1922.
73. Dore GM, Lo K, Juckes L, Bezyan S, Latt N. Clinical experience with baclofen in the management of alcohol-dependent patients with psychiatric comorbidity: a selected cases series. Alcohol Alcohol. 2011;46(6):714-720.
74. Baclofen tablet [package insert]. Pulaski, TN: AvKare Inc; 2018.
75. Hansel DE, Hansel CR, Shindle MK, et al. Oral baclofen in cerebral palsy: possible seizure potentiation? Pediatr Neurol. 2003;29(3):203-206.
76. Leggio L, Ferrulli A, Zambon A, et al. Baclofen promotes alcohol abstinence in alcohol dependent cirrhotic patients with hepatitis C virus (HCV) infection. Addict Behav. 2012;37(4):561-564.
77. Zofran [package insert]. East Hanover, NJ: Norvartis Pharmaceuticals; 2017.
78. Barnes NM, Sharp T. A review of central 5-HT receptors and their function. Neuropharmacology. 1999;38(8):1083-1152.
79. Johnson BA, Campling GM, Griffiths P, Cowen PJ. Attenuation of some alcohol-induced mood changes and the desire to drink by 5-HT3 receptor blockade: a preliminary study in health male volunteers. Psychopharmacology (Berl). 1993;112(1):142-144.
80. Johnson B, Roache J, Javors M, et al. Ondansetron for reduction of drinking among biologically predisposed alcoholic patients: a randomized controlled trial. JAMA. 2000;284(8):963-971.
81. Kasinath NS, Malak O, Tetzlaff J. Atrial fibrillation after ondansetron for the prevention and treatment of postoperative nausea and vomiting: a case report. Can J Anaesth. 2003;50(3):229-231.
82. Sellers EM, Toneatto T, Romach MK, Somer GR, Sobell LC, Sobell MB. Clinical efficacy of the 5-HT3 antagonist ondansetron in alcohol abuse and dependence. Alcohol Clin Exp Res. 1994;18(4):879-885.
83. Havrilla PL, Kane-Gill SL, Verrico MM, Seybert AL, Reis SE. Coronary vasospasm and atrial fibrillation associated with ondansetron therapy. Ann Pharmacother. 2009;43(3):532-536.
84. Donoghue K, Elzerbi C, Saunders R, Whittington C, Pilling S, Drummond C. The efficacy of acamprosate and naltrexone in the treatment alcohol dependence, Europe versus the rest of the world: a meta-analysis. Addiction. 2015;110(6):920-930.
85. National Institute for Health and Care Excellence. Alcohol-use disorder: diagnosis, assessment and management of harmful drinking and alcohol dependence. Clinical guideline [CG115]. https://www.nice.org.uk/guidance/cg115. Published February 2011. Accessed September 12, 2018.
86. U.S. Department of Health and Human Services, National Institutes of Health, National Institute on Alcohol Abuse and Alcoholism. Helping patients who drink too much a clinician’s guide. https://www.niaaa.nih.gov/guide. Accessed September 12, 2018.
87. Blodgett JC, Del Re AC, Maisel NC, Finney JW. A meta-analysis of topiramate’s effects for individuals with alcohol use disorders. Alcohol Clin Exp Res. 2014;38(6):1481-1488.
88. Müller CA, Geisel O, Pelz P, et al. High-dose baclofen for the treatment of alcohol dependence (BACLAD study): a randomized, placebo-controlled trial. Eur Neuropsychopharmacol. 2015;25(8):1167-1177.
89. Beraha EM, Salemink E, Goudriaan AE, et al. Efficacy and safety of high-dose baclofen for the treatment of alcohol dependence: a multicentre, randomized, double-blind controlled trial. Eur Neuropsychopharmacol. 2016;26(12):1950-1959.
90. DeVido J, Bogunovic O, Weiss RD. Alcohol use disorders in pregnancy. Harv Rev Psychiatry. 2015;23(2)112-121.
91. Anton RF, Moak DH, Latham P, et al. Naltrexone combined with either cognitive behavioral or motivational enhancement therapy for alcohol dependence. J Clin Psychopharmacol. 2005;25(4):349-357.
92. Harris AHS, Bowe T, Hagedorn H, et al. Multifaceted academic detailing program to increase pharmacotherapy for alcohol use disorder: interrupted time series evaluation of effectiveness. Addict Sci Clin Pract. 2016;11(1):15.
1. Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. Results from the 2016 National Survey on Drug Use and Health: detailed tables. Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2016/NSDUH-DetTabs-2016.pdf. Published September 7, 2017. Accessed September 13, 2018.
2. Jones E, Fear NT. Alcohol use and misuse within the military: a review. Int Rev Psychiatry. 2011;23(2):166-172.
3. Fuehrlein BS, Mota N, Arias AJ, et al. The burden of alcohol use disorders in US military veterans: results from the National Health and Resilience in Veterans Study. Addiction. 2016;111(10):1786-1794.
4. Stahre MA, Brewer RD, Fonseca VP, Naimi TS. Binge drinking among US active-duty military personnel. Am J Prev Med. 2009;36(3):208-217.
5. Institute of Medicine. Substance use disorders in the U.S. armed forces. https://www.nap.edu/resource/13441/SUD_rb.pdf. Published September 2012. Accessed September 12, 2018.
6. McDevitt-Murphy ME, Murphy JG, Williams JL, Monahan CJ, Bracken-Minor KL. Brief intervention to reduce hazardous drinking and enhance coping among OEF/OIF/OND veterans. Prof Psychol Res Pr. 2015;46(2):83-89.
7. Jacobson IG, Ryan MA, Hooper TI, et al. Alcohol use and alcohol-related problems before and after military combat deployment. JAMA. 2008;300(6):663-675.
8. Chou SP, Dawson DA, Stinson FS, et al. The prevalence of drinking and driving in the United States, 2001-2002: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Drug Alcohol Depend. 2006;83(2):137-146.
9. Bazargan-Hejazi S, Bazargan M, Hardin E, Bing EG. Alcohol use and adherence to prescribed therapy among under-served Latino and African-American patients using emergency department services. Ethn Dis. 2005;15(2):267-275.
10. Kamali M, Kelly BD, Clarke M, et al. A prospective evaluation of adherence to medication in first episode of schizophrenia. Eur Psychiatry. 2006;21(1):29-33.
11. Tucker JS, Burnam MA, Sherbourne CD, Kung FY, Gifford AL. Substance abuse and mental health correlates of nonadherence to antiretroviral medications in a sample of patients with human immunodeficiency virus infection. Am J Med. 2003;114(7):573-580.
12. Rehm J, Room R, Graham K, Monteiro M, Gmel G, Sempos CT. The relationship of average volume of alcohol consumption and patterns of drinking to burden of disease: an overview. Addiction. 2003;98(9):1209-1228.
13. Kendler KS, Ohlsson H, Sundquist J, Sundquist K. Alcohol use disorder and mortality across the lifespan: a longitudinal cohort and co-relative analysis. JAMA Psychiatry. 2016;73(6):575-581.
14. Hasin DS, Stinson FS, Ogburn E, Grant BF. Prevalence, correlates, disability, and comorbidity of DSM-IV alcohol abuse and dependence in the United States. Arch Gen Psychiatry. 2007;64(7):830-842.
15. Grant BF, Stinson FS, Dawson DA, et al. Prevalence and co-occurrence of substance use disorders and independent mood and anxiety disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2004;61(8):807-816.
16. Jonas DE, Amick HR, Feltner C, et al. Pharmacotherapy for adults with alcohol use disorders in outpatient settings: a systematic review and meta-analysis. JAMA. 2014;311(18):1889-1900.
17. Del Re AC, Gordon AJ, Lembke A, Harris AH. Prescription of topiramate to treat alcohol use disorders in the Veterans Health Administration. Addict Sci Clin Pract. 2013;8:12.
18. Harris AH, Ellerbe L, Reeder RN, et al. Pharmacotherapy for alcohol dependence: perceived treatment barriers and action strategies among Veterans Health Administration service providers. Psychol Serv. 2013;10(4):410-419.
19. ReVia [package insert]. Pomona, NY: Duramed Pharmaceuticals; 2013.
20. US Department of Veterans Affairs, Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives. Alcohol use disorder pharmacotherapy: naltrexone, acamprosate, and disulfiram recommendations for use. https://www.pbm.va.gov/PBM/clinicalguidance/clinicalrecommendations/Alcohol_Use_Disorder_Pharmacotherapy_Acamprosate_Naltrexone_Disulfiram_Recommendations_for_Use.docx. Published December 2013. Accessed September 17, 2018.
21. Anton RF. Naltrexone for the management of alcohol dependence. N Engl J Med. 2008;359(7):715-721.
22. O’Malley SS, Rounsaville BJ, Farren C, et al. Initial and maintenance naltrexone treatment for alcohol dependence using primary care vs specialty care: a nested sequence of 3 randomized trials. Arch Intern Med. 2003;163(14):1695-1704.
23. O’Brien CP. A range of research-based pharmacotherapies for addiction. Science. 1997;278(5335):66-70.
24. Swift RM. Effect of naltrexone on human alcohol consumption. J Clin Psychiatry. 1995;56 (suppl 7):24-29.
25. Center for Substance Abuse Treatment. Incorporating Alcohol Pharmacotherapies into Medical Practice. Treatment Improvement Protocol (TIP) Series 49. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2009.
26. Spanagel R, Zieglgänsberger W. Anti-craving compounds for ethanol: new pharmacological tools to study addictive processes. Trends Pharmacol Sci. 1997;18(2):54-59.
27. Herz A. Endogenous opioid systems and alcohol addiction. Psychopharmacology (Berl). 1997;129(2):99-111.
28. Miller NS. The integration of pharmacological and nonpharmacological treatments in drug/alcohol addiction. J Addict Dis. 1997;16(4):1-5.
29. Maisel NC, Blodgett JC, Wilbourne PL, Humphreys K, Finney JW. Meta-analysis of naltrexone and acamprosate for treating alcohol use disorders: when are these medications most helpful? Addiction. 2013;108(2):275-293.
30. Bouza C, Angeles M, Muñoz A, Amate JM. Efficacy and safety of naltrexone and acamprosate in the treatment of alcohol dependence: a systematic review. Addiction. 2004;99(7):811-828.
31. Anton RF, O’Malley SS, Ciraulo DA, et al; COMBINE Study Research Group. Combined pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE study: a randomized controlled trial. JAMA. 2006;295(17):2003-2017.
32. Oslin DW, Pettinati HM, Volpicelli JR, Wolf AL, Kampman KM, O’Brien CP. The effects of naltrexone on alcohol and cocaine use in dually addicted patients. J Subst Abuse Treat. 1999;16(2):163-167.
33. Kranzler HR, Wesson DR, Billot L; DrugAbuse Sciences Naltrexone Depot Study Group. Naltrexone depot for treatment of alcohol dependence: a multicenter, randomized, placebo-controlled clinical trial. Alcohol Clin Exp Res. 2004;28(7):1051-1059.
34. Bryson WC, McConnell J, Korthuis PT, McCarty D. Extended-release naltrexone for alcohol dependence: persistence and healthcare costs and utilization. Am J Manag Care. 2011;17 (suppl 8):S222-S234.
35. Vivitrol [package insert]. Waltham, MA: Alkermes, Inc.; 2010.
36. Campral [package insert]. St. Louis, MO: Forest Laboratories Inc; 2012.
37. Paille F, Guelfi J, Perkins AC, Royer RJ, Steru L, Parot P. Double-blind randomized multicentre trial of acamprosate in maintaining abstinence from alcohol. Alcohol. 1995;30(2):239-247.
38. Pelc I, Verbanck P, Le Bon O, Gavrilovic M, Lion K, Lehert P. Efficacy and safety of acamprosate in the treatment of detoxified alcohol-dependent patients. A 90-day placebo-controlled dose-finding study. Br J Psychiatry. 1997;171:73-77.
39. Sass H, Soyka M, Mann K, Zieglgänsberger W. Relapse prevention by acamprosate. Results from a placebo-controlled study on alcohol dependence. Arch Gen Psychiatry. 1996;53(8):673-680.
40. Mann K, Lehert P, Morgan MY. The efficacy of acamprosate in the maintenance of abstinence in alcohol-dependent individuals: results of a meta-analysis. Alcohol Clin Exp Res. 2004;28(1):51-63.
41. Mason BJ, Lehert P. Acamprosate for alcohol dependence: a sex-specific meta-analysis based on individual patient data. Alcohol Clin Exp Res. 2012;36(3):497-508.
42. Richardson K, Baillie A, Reid S, et al. Do acamprosate or naltrexone have an effect on daily drinking by reducing craving for alcohol? Addiction. 2008;103(6):953-959.
43. Antabuse [package insert]. North Wales, PA: Teva Pharmaceuticals; 2015.
44. Ait-Daoud N, Johnson BA. Medications for the treatment of alcoholism. In: Johnson BA, Ruiz P, Galanter M, eds. Handbook of Clinical Alcoholism Treatment. Lippincott Williams & Wilkins, Baltimore; 2003
45. Laaksonen E, Koski-Jännes A, Salaspuro M, Ahtinen H, Alho H. A randomized, multicentre, open-label, comparative trial of disulfiram, naltrexone and acamprosate in the treatment of alcohol dependence. Alcohol Alcohol. 2008;43(1):53-61.
46. Skinner MD, Lahmek P, Pham H, Aubin HJ. Disulfiram efficacy in the treatment of alcohol dependence: a meta-analysis. PLoS One. 2014;9(2):e87366.
47. Jørgensen CH, Pedersen B, Tønnesen H. The efficacy of disulfiram for the treatment of alcohol use disorder. Alcohol Clin Exp Res. 2011;35(10):1749-1758.
48. Arbaizar B, Diersen-Sotos T, Gómez-Acebo I, Llorca J. Topiramate in the treatment of alcohol dependence: a meta-analysis. [Article in English, Spanish] Actas Esp Psiquiatr. 2010;38(1):8-12.
49. Johnson BA, Ait-Daoud N. Topiramate in the new generation of drugs: efficacy in the treatment of alcoholic patients. Curr Pharm Des. 2010;16(19):2103-2112.
50. Paparrigopoulos T, Tzavellas E, Karaiskos D, Kourlaba G, Liappas I. Treatment of alcohol dependence with low-dose topiramate: an open-label controlled study. BMC Psychiatry. 2011;11:41.
51. Johnson BA, Ait-Daoud N, Bowden CL, et al. Oral topiramate for treatment of alcohol dependence: a randomised controlled trial. Lancet. 2003;361(9370):1677-1685.
52. Johnson BA, Ait-Daoud N, Akhtar FZ, Ma JZ. Oral topiramate reduces the consequences of drinking and improves the quality of life of alcohol-dependent individuals: a randomized controlled trial. Arch Gen Psychiatry. 2004;61(9):905-912.
53. Johnson BA, Rosenthal N, Capece JA, et al; Topiramate for Alcoholism Advisory Board; Topiramate for Alcoholism Study Group. Topiramate for treating alcohol dependence: a randomized controlled trial. JAMA. 2007;298(14):1641-1651.
54. Flórez G, García-Portilla P, Alvarez S, Saiz PA, Nogueiras L, Bobes J. Using topiramate or naltrexone for the treatment of alcohol-dependent patients. Alcohol Clin Exp Res. 2008;32(7):1251-1259.
55. Flórez G, Saiz PA, Garcia-Portilla P, Alvarez S, Nogueiras L, Bobes J. Topiramate for the treatment of alcohol dependence: comparison with naltrexone. Eur Addict Res. 2011;17(1):29-36.
56. Baltieri DA, Daró FR, Ribeiro PL, de Andrade AG. Comparing topiramate with naltrexone in the treatment of alcohol dependence. Addiction. 2008;103(12):2035-2044.
57. White HS, Brown SD, Woodhead JH, Skeen GA, Wolf HH. Topiramate modulates GABA-evoked currents in murine cortical neurons by a nonbenzodiazepine mechanism. Epilepsia. 2000;41(suppl 1):S17-S20.
58. White HS, Brown SD, Woodhead JH, Skeen GA, Wolf HH. Topiramate enhances GABA-mediated chloride flux and GABA-evoked chloride currents in murine brain neurons and increases seizure threshold. Epilepsy Res. 1997;28(3):167-179.
59. Guglielmo R, Martinotti G, Quatrale M, et al. Topiramate in alcohol use disorders: review and update. CNS Drugs. 2015;29(5):383-395.
60. Kranzler HR, Covault J, Feinn R, et al. Topiramate treatment for heavy drinkers: moderation by a GRIK1 polymorphism. Am J Psychiatry. 2014;171(4):445-452.
61. Batki SL, Pennington DL, Lasher B, et al. Topiramate treatment of alcohol use disorder in veterans with posttraumatic stress disorder: a randomized controlled pilot trial. Alcohol Clin Exp Res. 2014;38(8):2169-2177.
62. Topamax [package insert]. Titusville, NJ: Janssen Pharmaceuticals Inc; 2017.
63. Meador KJ. Cognitive effects of levetiracetam versus topiramate. Epilepsy Curr. 2008;8(3):64-65.
64. Luykx JJ, Carpay JA. Nervous system adverse responses to topiramate in the treatment of neuropsychiatric disorders. Expert Opin Drug Saf. 2010;9(4):623-631.
65. The Management of Substance Use Disorder Work Group; US Department of Veteran Affairs, US Department of Defense. VA/DoD clinical practice guideline for the management of substance use disorders. https://www.healthquality.va.gov/guidelines/MH/sud/VADODSUDCPGRevised22216.pdf. Published December 2015. Accessed September 12, 2018.
66. Sills GJ. The mechanism of action of gabapentin and pregabalin. Curr Opin Pharmacol. 2006;6(1):108-113.
67. Mason BJ, Quello S, Goodell V, Shandan F, Kyle M, Begovic A. Gabapentin treatment for alcohol dependence: a randomized clinical trial. JAMA Intern Med. 2014;174(1):70-77.
68. Anton RF, Myrick H, Wright TM, et al. Gabapentin combined with naltrexone for the treatment of alcohol dependence. Am J Psychiatry. 2011;168(7):709-717.
69. Neurontin [package insert]. New York, NY: Pfizer; 2017.
70. American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American Geriatrics Society 2015 updated Beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2015;63(11):2227-2246.
71. Addolorato G, Leggio L. Safety and efficacy of baclofen in the treatment of alcohol-dependent patients. Curr Pharm Des. 2010;16(19):2113-2117.
72. Addolorato G, Leggio L, Ferrulli A, et al. Effectiveness and safety of baclofen for maintenance of alcohol abstinence in alcohol-dependent patients with liver cirrhosis: a randomized, double-blind, controlled study. Lancet. 2007;370(9603):1915-1922.
73. Dore GM, Lo K, Juckes L, Bezyan S, Latt N. Clinical experience with baclofen in the management of alcohol-dependent patients with psychiatric comorbidity: a selected cases series. Alcohol Alcohol. 2011;46(6):714-720.
74. Baclofen tablet [package insert]. Pulaski, TN: AvKare Inc; 2018.
75. Hansel DE, Hansel CR, Shindle MK, et al. Oral baclofen in cerebral palsy: possible seizure potentiation? Pediatr Neurol. 2003;29(3):203-206.
76. Leggio L, Ferrulli A, Zambon A, et al. Baclofen promotes alcohol abstinence in alcohol dependent cirrhotic patients with hepatitis C virus (HCV) infection. Addict Behav. 2012;37(4):561-564.
77. Zofran [package insert]. East Hanover, NJ: Norvartis Pharmaceuticals; 2017.
78. Barnes NM, Sharp T. A review of central 5-HT receptors and their function. Neuropharmacology. 1999;38(8):1083-1152.
79. Johnson BA, Campling GM, Griffiths P, Cowen PJ. Attenuation of some alcohol-induced mood changes and the desire to drink by 5-HT3 receptor blockade: a preliminary study in health male volunteers. Psychopharmacology (Berl). 1993;112(1):142-144.
80. Johnson B, Roache J, Javors M, et al. Ondansetron for reduction of drinking among biologically predisposed alcoholic patients: a randomized controlled trial. JAMA. 2000;284(8):963-971.
81. Kasinath NS, Malak O, Tetzlaff J. Atrial fibrillation after ondansetron for the prevention and treatment of postoperative nausea and vomiting: a case report. Can J Anaesth. 2003;50(3):229-231.
82. Sellers EM, Toneatto T, Romach MK, Somer GR, Sobell LC, Sobell MB. Clinical efficacy of the 5-HT3 antagonist ondansetron in alcohol abuse and dependence. Alcohol Clin Exp Res. 1994;18(4):879-885.
83. Havrilla PL, Kane-Gill SL, Verrico MM, Seybert AL, Reis SE. Coronary vasospasm and atrial fibrillation associated with ondansetron therapy. Ann Pharmacother. 2009;43(3):532-536.
84. Donoghue K, Elzerbi C, Saunders R, Whittington C, Pilling S, Drummond C. The efficacy of acamprosate and naltrexone in the treatment alcohol dependence, Europe versus the rest of the world: a meta-analysis. Addiction. 2015;110(6):920-930.
85. National Institute for Health and Care Excellence. Alcohol-use disorder: diagnosis, assessment and management of harmful drinking and alcohol dependence. Clinical guideline [CG115]. https://www.nice.org.uk/guidance/cg115. Published February 2011. Accessed September 12, 2018.
86. U.S. Department of Health and Human Services, National Institutes of Health, National Institute on Alcohol Abuse and Alcoholism. Helping patients who drink too much a clinician’s guide. https://www.niaaa.nih.gov/guide. Accessed September 12, 2018.
87. Blodgett JC, Del Re AC, Maisel NC, Finney JW. A meta-analysis of topiramate’s effects for individuals with alcohol use disorders. Alcohol Clin Exp Res. 2014;38(6):1481-1488.
88. Müller CA, Geisel O, Pelz P, et al. High-dose baclofen for the treatment of alcohol dependence (BACLAD study): a randomized, placebo-controlled trial. Eur Neuropsychopharmacol. 2015;25(8):1167-1177.
89. Beraha EM, Salemink E, Goudriaan AE, et al. Efficacy and safety of high-dose baclofen for the treatment of alcohol dependence: a multicentre, randomized, double-blind controlled trial. Eur Neuropsychopharmacol. 2016;26(12):1950-1959.
90. DeVido J, Bogunovic O, Weiss RD. Alcohol use disorders in pregnancy. Harv Rev Psychiatry. 2015;23(2)112-121.
91. Anton RF, Moak DH, Latham P, et al. Naltrexone combined with either cognitive behavioral or motivational enhancement therapy for alcohol dependence. J Clin Psychopharmacol. 2005;25(4):349-357.
92. Harris AHS, Bowe T, Hagedorn H, et al. Multifaceted academic detailing program to increase pharmacotherapy for alcohol use disorder: interrupted time series evaluation of effectiveness. Addict Sci Clin Pract. 2016;11(1):15.
Inhibitor could improve HSC donation and transplant

Preclinical research suggests a small-molecule inhibitor could potentially improve the donation and transplant of hematopoietic stem cells (HSCs).
One study showed that the inhibitor, CASIN, could improve HSC yields from murine transplant donors.
Another study showed that CASIN could be used as conditioning, with or without fludarabine, in murine transplant recipients.
Yi Zheng, PhD, of Cincinnati Children’s Cancer and Blood Diseases Institute in Ohio, and his colleagues conducted both studies and reported the results in Leukemia.
Previous research had shown that genetic ablation of CDC42 in HSCs mobilizes the cells without affecting their survival. CDC42 is a Rho family small GTPase that helps regulate HSC maintenance.
Dr. Zheng and his colleagues expanded upon this finding with two studies.
In the first study, the researchers identified CASIN, a small-molecule inhibitor of CDC42. The team tested CASIN in mice and found the inhibitor can effectively mobilize HSCs.
In fact, CASIN and plerixafor mobilized a similar number of phenotypic HSCs. However, HSCs harvested from CASIN-treated donor mice had better long-term reconstitution potential after transplant than HSCs harvested from plerixafor-treated mice.
In the second study, Dr. Zheng and his colleagues used CASIN to condition mice that were receiving HSC transplants.
The team found that CASIN reduced the number of phenotypic long-term HSCs in the bone marrow, starting 2 hours after CASIN administration and ending within 24 hours.
The researchers also found that CASIN synergized with fludarabine. Engraftment of transplanted HSCs was significantly higher in mice that received conditioning with CASIN and fludarabine than in mice that received either CASIN or fludarabine alone.
“Our data demonstrate that the new regimen of CASIN application has the potential to improve both sides of the transplant practice,” Dr. Zheng said. “It mobilizes higher quality donor HSCs during stem cell harvest, and it would condition transplant patients beforehand to increase engraftment efficiency.”
“This would be a major step forward, especially for the most vulnerable patients who cannot withstand the toxicity of chemotherapy conditioning regimens or are non-responsive to current [HSC] mobilization regimens.”
Both of these studies were funded, in part, by the National Institutes of Health. The authors declared no conflicts of interest.
Preclinical research suggests a small-molecule inhibitor could potentially improve the donation and transplant of hematopoietic stem cells (HSCs).
One study showed that the inhibitor, CASIN, could improve HSC yields from murine transplant donors.
Another study showed that CASIN could be used as conditioning, with or without fludarabine, in murine transplant recipients.
Yi Zheng, PhD, of Cincinnati Children’s Cancer and Blood Diseases Institute in Ohio, and his colleagues conducted both studies and reported the results in Leukemia.
Previous research had shown that genetic ablation of CDC42 in HSCs mobilizes the cells without affecting their survival. CDC42 is a Rho family small GTPase that helps regulate HSC maintenance.
Dr. Zheng and his colleagues expanded upon this finding with two studies.
In the first study, the researchers identified CASIN, a small-molecule inhibitor of CDC42. The team tested CASIN in mice and found the inhibitor can effectively mobilize HSCs.
In fact, CASIN and plerixafor mobilized a similar number of phenotypic HSCs. However, HSCs harvested from CASIN-treated donor mice had better long-term reconstitution potential after transplant than HSCs harvested from plerixafor-treated mice.
In the second study, Dr. Zheng and his colleagues used CASIN to condition mice that were receiving HSC transplants.
The team found that CASIN reduced the number of phenotypic long-term HSCs in the bone marrow, starting 2 hours after CASIN administration and ending within 24 hours.
The researchers also found that CASIN synergized with fludarabine. Engraftment of transplanted HSCs was significantly higher in mice that received conditioning with CASIN and fludarabine than in mice that received either CASIN or fludarabine alone.
“Our data demonstrate that the new regimen of CASIN application has the potential to improve both sides of the transplant practice,” Dr. Zheng said. “It mobilizes higher quality donor HSCs during stem cell harvest, and it would condition transplant patients beforehand to increase engraftment efficiency.”
“This would be a major step forward, especially for the most vulnerable patients who cannot withstand the toxicity of chemotherapy conditioning regimens or are non-responsive to current [HSC] mobilization regimens.”
Both of these studies were funded, in part, by the National Institutes of Health. The authors declared no conflicts of interest.
Preclinical research suggests a small-molecule inhibitor could potentially improve the donation and transplant of hematopoietic stem cells (HSCs).
One study showed that the inhibitor, CASIN, could improve HSC yields from murine transplant donors.
Another study showed that CASIN could be used as conditioning, with or without fludarabine, in murine transplant recipients.
Yi Zheng, PhD, of Cincinnati Children’s Cancer and Blood Diseases Institute in Ohio, and his colleagues conducted both studies and reported the results in Leukemia.
Previous research had shown that genetic ablation of CDC42 in HSCs mobilizes the cells without affecting their survival. CDC42 is a Rho family small GTPase that helps regulate HSC maintenance.
Dr. Zheng and his colleagues expanded upon this finding with two studies.
In the first study, the researchers identified CASIN, a small-molecule inhibitor of CDC42. The team tested CASIN in mice and found the inhibitor can effectively mobilize HSCs.
In fact, CASIN and plerixafor mobilized a similar number of phenotypic HSCs. However, HSCs harvested from CASIN-treated donor mice had better long-term reconstitution potential after transplant than HSCs harvested from plerixafor-treated mice.
In the second study, Dr. Zheng and his colleagues used CASIN to condition mice that were receiving HSC transplants.
The team found that CASIN reduced the number of phenotypic long-term HSCs in the bone marrow, starting 2 hours after CASIN administration and ending within 24 hours.
The researchers also found that CASIN synergized with fludarabine. Engraftment of transplanted HSCs was significantly higher in mice that received conditioning with CASIN and fludarabine than in mice that received either CASIN or fludarabine alone.
“Our data demonstrate that the new regimen of CASIN application has the potential to improve both sides of the transplant practice,” Dr. Zheng said. “It mobilizes higher quality donor HSCs during stem cell harvest, and it would condition transplant patients beforehand to increase engraftment efficiency.”
“This would be a major step forward, especially for the most vulnerable patients who cannot withstand the toxicity of chemotherapy conditioning regimens or are non-responsive to current [HSC] mobilization regimens.”
Both of these studies were funded, in part, by the National Institutes of Health. The authors declared no conflicts of interest.
Cost-effectiveness of CAR T-cell therapy

Tisagenlecleucel has the potential to be cost-effective for pediatric B-cell acute lymphoblastic leukemia (B-ALL) patients in the United States, according to researchers.
The group found evidence to suggest the chimeric antigen receptor (CAR) T-cell therapy—which has a list price of $475,000—may prove cost-effective if long-term survival benefits are realized.
An analysis indicated that the incremental cost-effectiveness ratio for tisagenlecleucel compared to clofarabine ranged from $37,000 to $78,000 per quality-adjusted life year (QALY) gained.
Melanie D. Whittington, PhD, of the University of Colorado at Denver, Aurora, and her colleagues described this work in JAMA Pediatrics.
For this study, the researchers used a decision analytic model that extrapolated the evidence from clinical trials over a patient’s lifetime to assess life-years gained, QALYs gained, and incremental costs per life-year and QALY gained. The researchers compared tisagenlecleucel to the antineoplastic agent clofarabine.
While tisagenlecleucel has a list price of $475,000, researchers discounted the price by 3% and added several additional costs, such as hospital administration, pretreatment, and potential adverse events, to get to a total discounted cost of about $667,000.
The team estimated that 42.6% of B-ALL patients would be long-term survivors with tisagenlecleucel, 10.34 life-years would be gained, and 9.28 QALYs would be gained.
In comparison, clofarabine had a total discounted cost of approximately $337,000, which included an initial discounted price of $164,000 plus additional treatment and administrative costs.
With clofarabine, 10.8% of B-ALL patients were long-term survivors, 2.43 life-years were gained, and 2.10 QALYs were gained in the model.
Overall, the mean incremental cost-effectiveness ratio was about $46,000 per QALY gained in this base-case model.
In analyses of different scenarios, such as a deeper discount, a different treatment start, or a different calculation of future treatment costs, the cost-effectiveness ratio varied from $37,000 to $78,000 per QALY gained.
The researchers noted that clinical trial evidence for tisagenlecleucel came from single-arm trials, which made the selection of a comparator challenging. Clofarabine was chosen because it had the most similar baseline population characteristics, but the researchers acknowledged that blinatumomab is also frequently used as a treatment for these patients.
“We suspect that tisagenlecleucel would remain cost-effective compared with blinatumomab,” the researchers wrote in JAMA Pediatrics. “A study conducted by other researchers found the incremental cost-effectiveness ratio of tisagenlecleucel versus blinatumomab was similar to the incremental cost-effectiveness ratio of tisagenlecleucel versus clofarabine [i.e., $3,000 more per QALY].”
The researchers suggested that uncertainties in the evidence should be considered as payers are negotiating coverage and payment for tisagenlecleucel.
This study was funded by the Institute for Clinical and Economic Review, which receives some funding from the pharmaceutical industry. Four study authors are employees of the Institute for Clinical and Economic Review.
Tisagenlecleucel has the potential to be cost-effective for pediatric B-cell acute lymphoblastic leukemia (B-ALL) patients in the United States, according to researchers.
The group found evidence to suggest the chimeric antigen receptor (CAR) T-cell therapy—which has a list price of $475,000—may prove cost-effective if long-term survival benefits are realized.
An analysis indicated that the incremental cost-effectiveness ratio for tisagenlecleucel compared to clofarabine ranged from $37,000 to $78,000 per quality-adjusted life year (QALY) gained.
Melanie D. Whittington, PhD, of the University of Colorado at Denver, Aurora, and her colleagues described this work in JAMA Pediatrics.
For this study, the researchers used a decision analytic model that extrapolated the evidence from clinical trials over a patient’s lifetime to assess life-years gained, QALYs gained, and incremental costs per life-year and QALY gained. The researchers compared tisagenlecleucel to the antineoplastic agent clofarabine.
While tisagenlecleucel has a list price of $475,000, researchers discounted the price by 3% and added several additional costs, such as hospital administration, pretreatment, and potential adverse events, to get to a total discounted cost of about $667,000.
The team estimated that 42.6% of B-ALL patients would be long-term survivors with tisagenlecleucel, 10.34 life-years would be gained, and 9.28 QALYs would be gained.
In comparison, clofarabine had a total discounted cost of approximately $337,000, which included an initial discounted price of $164,000 plus additional treatment and administrative costs.
With clofarabine, 10.8% of B-ALL patients were long-term survivors, 2.43 life-years were gained, and 2.10 QALYs were gained in the model.
Overall, the mean incremental cost-effectiveness ratio was about $46,000 per QALY gained in this base-case model.
In analyses of different scenarios, such as a deeper discount, a different treatment start, or a different calculation of future treatment costs, the cost-effectiveness ratio varied from $37,000 to $78,000 per QALY gained.
The researchers noted that clinical trial evidence for tisagenlecleucel came from single-arm trials, which made the selection of a comparator challenging. Clofarabine was chosen because it had the most similar baseline population characteristics, but the researchers acknowledged that blinatumomab is also frequently used as a treatment for these patients.
“We suspect that tisagenlecleucel would remain cost-effective compared with blinatumomab,” the researchers wrote in JAMA Pediatrics. “A study conducted by other researchers found the incremental cost-effectiveness ratio of tisagenlecleucel versus blinatumomab was similar to the incremental cost-effectiveness ratio of tisagenlecleucel versus clofarabine [i.e., $3,000 more per QALY].”
The researchers suggested that uncertainties in the evidence should be considered as payers are negotiating coverage and payment for tisagenlecleucel.
This study was funded by the Institute for Clinical and Economic Review, which receives some funding from the pharmaceutical industry. Four study authors are employees of the Institute for Clinical and Economic Review.
Tisagenlecleucel has the potential to be cost-effective for pediatric B-cell acute lymphoblastic leukemia (B-ALL) patients in the United States, according to researchers.
The group found evidence to suggest the chimeric antigen receptor (CAR) T-cell therapy—which has a list price of $475,000—may prove cost-effective if long-term survival benefits are realized.
An analysis indicated that the incremental cost-effectiveness ratio for tisagenlecleucel compared to clofarabine ranged from $37,000 to $78,000 per quality-adjusted life year (QALY) gained.
Melanie D. Whittington, PhD, of the University of Colorado at Denver, Aurora, and her colleagues described this work in JAMA Pediatrics.
For this study, the researchers used a decision analytic model that extrapolated the evidence from clinical trials over a patient’s lifetime to assess life-years gained, QALYs gained, and incremental costs per life-year and QALY gained. The researchers compared tisagenlecleucel to the antineoplastic agent clofarabine.
While tisagenlecleucel has a list price of $475,000, researchers discounted the price by 3% and added several additional costs, such as hospital administration, pretreatment, and potential adverse events, to get to a total discounted cost of about $667,000.
The team estimated that 42.6% of B-ALL patients would be long-term survivors with tisagenlecleucel, 10.34 life-years would be gained, and 9.28 QALYs would be gained.
In comparison, clofarabine had a total discounted cost of approximately $337,000, which included an initial discounted price of $164,000 plus additional treatment and administrative costs.
With clofarabine, 10.8% of B-ALL patients were long-term survivors, 2.43 life-years were gained, and 2.10 QALYs were gained in the model.
Overall, the mean incremental cost-effectiveness ratio was about $46,000 per QALY gained in this base-case model.
In analyses of different scenarios, such as a deeper discount, a different treatment start, or a different calculation of future treatment costs, the cost-effectiveness ratio varied from $37,000 to $78,000 per QALY gained.
The researchers noted that clinical trial evidence for tisagenlecleucel came from single-arm trials, which made the selection of a comparator challenging. Clofarabine was chosen because it had the most similar baseline population characteristics, but the researchers acknowledged that blinatumomab is also frequently used as a treatment for these patients.
“We suspect that tisagenlecleucel would remain cost-effective compared with blinatumomab,” the researchers wrote in JAMA Pediatrics. “A study conducted by other researchers found the incremental cost-effectiveness ratio of tisagenlecleucel versus blinatumomab was similar to the incremental cost-effectiveness ratio of tisagenlecleucel versus clofarabine [i.e., $3,000 more per QALY].”
The researchers suggested that uncertainties in the evidence should be considered as payers are negotiating coverage and payment for tisagenlecleucel.
This study was funded by the Institute for Clinical and Economic Review, which receives some funding from the pharmaceutical industry. Four study authors are employees of the Institute for Clinical and Economic Review.
Better PFS may not mean better HRQOL

Cancer treatments that prolong progression-free survival (PFS) may not improve health-related quality of life (HRQOL), researchers reported in JAMA Internal Medicine.
The researchers failed to find a significant association between PFS and HRQOL in an analysis of cancer clinical trials.
“There are only two reasons to use progression-free survival as a valid endpoint in oncology,” said study author Feng Xie, PhD, of McMaster University in Hamilton, Ontario, Canada.
“One is that it is a valid surrogate marker for overall survival. The second is the assumption that patients who live longer without disease progression will have better health-related quality of life, even without longer survival.”
“Given the increased use of progression-free survival as the primary outcome in new oncology drug trials, and uncertainty of overall survival, it remains possible that patients are receiving toxic and/or expensive treatments without experiencing important benefit.”
With this in mind, Dr. Xie and his colleagues conducted a review and meta-analysis of 52 articles reporting on 38 randomized clinical trials. The trials included 13,979 patients with 12 types of cancer, including 1 trial of patients with multiple myeloma.
The median follow-up in these trials ranged from 10.5 months to 66.0 months.
The median PFS of patients who received the trial interventions ranged from 1.8 months to 33.7 months.
For 28 of the trials (74%), patients who received the trial intervention had better PFS than patients who received the comparator. Overall, the mean difference in median PFS between the intervention and comparator arms was 1.91 months.
HRQOL was measured with 6 different instruments* across the trials, and the types of HRQOL measured varied. Thirty trials included global HRQOL, 20 included physical, and 13 included emotional HRQOL. The duration of reported or measured HRQOL ranged from 1 month to 34 months.
Improved global HRQOL was reported in 53% of trials (16/30), improved physical HRQOL was reported in 55% (11/20), and improved emotional HRQOL was reported in 62% (8/13). The mean difference in change of HRQOL adjusted to per-month values was −0.39 for global, 0.26 for physical, and 1.08 for emotional HRQOL.
The slope of the association between the difference in median PFS and the difference in HRQOL change was:
- 0.12 (95% confidence interval [CI], −0.27 to 0.52) for global HRQOL
- −0.20 (95% CI,−0.62 to 0.23) for physical HRQOL
- 0.78 (95% CI, −0.05 to 1.60) for emotional HRQOL.
Dr. Xie and his colleagues said these results suggest there is no significant association between PFS and HRQOL, so interventions prolonging PFS may not improve HRQOL.
“Therefore, to ensure patients are truly obtaining important benefit from cancer therapies, clinical trial investigators should measure health-related quality of life directly and accurately, ensuring adequate duration and follow-up, and publish it,” Dr. Xie said.
He also argued for the need to “revisit this issue of using surrogate outcomes to measure the safety and efficacy of new oncology drugs.”
Dr. Xie and his colleagues did not report any conflicts of interest. One study author (Marcin Waligora, PhD) reported funding from the National Science Centre in Poland.
*EORTC-QLQ-C30, FACT-G19, Lung Cancer Symptom Scale, EQ-5D, 8-item linear analog self-assessment (LASA) questionnaire, and clinician-reported Karnofsky score
Cancer treatments that prolong progression-free survival (PFS) may not improve health-related quality of life (HRQOL), researchers reported in JAMA Internal Medicine.
The researchers failed to find a significant association between PFS and HRQOL in an analysis of cancer clinical trials.
“There are only two reasons to use progression-free survival as a valid endpoint in oncology,” said study author Feng Xie, PhD, of McMaster University in Hamilton, Ontario, Canada.
“One is that it is a valid surrogate marker for overall survival. The second is the assumption that patients who live longer without disease progression will have better health-related quality of life, even without longer survival.”
“Given the increased use of progression-free survival as the primary outcome in new oncology drug trials, and uncertainty of overall survival, it remains possible that patients are receiving toxic and/or expensive treatments without experiencing important benefit.”
With this in mind, Dr. Xie and his colleagues conducted a review and meta-analysis of 52 articles reporting on 38 randomized clinical trials. The trials included 13,979 patients with 12 types of cancer, including 1 trial of patients with multiple myeloma.
The median follow-up in these trials ranged from 10.5 months to 66.0 months.
The median PFS of patients who received the trial interventions ranged from 1.8 months to 33.7 months.
For 28 of the trials (74%), patients who received the trial intervention had better PFS than patients who received the comparator. Overall, the mean difference in median PFS between the intervention and comparator arms was 1.91 months.
HRQOL was measured with 6 different instruments* across the trials, and the types of HRQOL measured varied. Thirty trials included global HRQOL, 20 included physical, and 13 included emotional HRQOL. The duration of reported or measured HRQOL ranged from 1 month to 34 months.
Improved global HRQOL was reported in 53% of trials (16/30), improved physical HRQOL was reported in 55% (11/20), and improved emotional HRQOL was reported in 62% (8/13). The mean difference in change of HRQOL adjusted to per-month values was −0.39 for global, 0.26 for physical, and 1.08 for emotional HRQOL.
The slope of the association between the difference in median PFS and the difference in HRQOL change was:
- 0.12 (95% confidence interval [CI], −0.27 to 0.52) for global HRQOL
- −0.20 (95% CI,−0.62 to 0.23) for physical HRQOL
- 0.78 (95% CI, −0.05 to 1.60) for emotional HRQOL.
Dr. Xie and his colleagues said these results suggest there is no significant association between PFS and HRQOL, so interventions prolonging PFS may not improve HRQOL.
“Therefore, to ensure patients are truly obtaining important benefit from cancer therapies, clinical trial investigators should measure health-related quality of life directly and accurately, ensuring adequate duration and follow-up, and publish it,” Dr. Xie said.
He also argued for the need to “revisit this issue of using surrogate outcomes to measure the safety and efficacy of new oncology drugs.”
Dr. Xie and his colleagues did not report any conflicts of interest. One study author (Marcin Waligora, PhD) reported funding from the National Science Centre in Poland.
*EORTC-QLQ-C30, FACT-G19, Lung Cancer Symptom Scale, EQ-5D, 8-item linear analog self-assessment (LASA) questionnaire, and clinician-reported Karnofsky score
Cancer treatments that prolong progression-free survival (PFS) may not improve health-related quality of life (HRQOL), researchers reported in JAMA Internal Medicine.
The researchers failed to find a significant association between PFS and HRQOL in an analysis of cancer clinical trials.
“There are only two reasons to use progression-free survival as a valid endpoint in oncology,” said study author Feng Xie, PhD, of McMaster University in Hamilton, Ontario, Canada.
“One is that it is a valid surrogate marker for overall survival. The second is the assumption that patients who live longer without disease progression will have better health-related quality of life, even without longer survival.”
“Given the increased use of progression-free survival as the primary outcome in new oncology drug trials, and uncertainty of overall survival, it remains possible that patients are receiving toxic and/or expensive treatments without experiencing important benefit.”
With this in mind, Dr. Xie and his colleagues conducted a review and meta-analysis of 52 articles reporting on 38 randomized clinical trials. The trials included 13,979 patients with 12 types of cancer, including 1 trial of patients with multiple myeloma.
The median follow-up in these trials ranged from 10.5 months to 66.0 months.
The median PFS of patients who received the trial interventions ranged from 1.8 months to 33.7 months.
For 28 of the trials (74%), patients who received the trial intervention had better PFS than patients who received the comparator. Overall, the mean difference in median PFS between the intervention and comparator arms was 1.91 months.
HRQOL was measured with 6 different instruments* across the trials, and the types of HRQOL measured varied. Thirty trials included global HRQOL, 20 included physical, and 13 included emotional HRQOL. The duration of reported or measured HRQOL ranged from 1 month to 34 months.
Improved global HRQOL was reported in 53% of trials (16/30), improved physical HRQOL was reported in 55% (11/20), and improved emotional HRQOL was reported in 62% (8/13). The mean difference in change of HRQOL adjusted to per-month values was −0.39 for global, 0.26 for physical, and 1.08 for emotional HRQOL.
The slope of the association between the difference in median PFS and the difference in HRQOL change was:
- 0.12 (95% confidence interval [CI], −0.27 to 0.52) for global HRQOL
- −0.20 (95% CI,−0.62 to 0.23) for physical HRQOL
- 0.78 (95% CI, −0.05 to 1.60) for emotional HRQOL.
Dr. Xie and his colleagues said these results suggest there is no significant association between PFS and HRQOL, so interventions prolonging PFS may not improve HRQOL.
“Therefore, to ensure patients are truly obtaining important benefit from cancer therapies, clinical trial investigators should measure health-related quality of life directly and accurately, ensuring adequate duration and follow-up, and publish it,” Dr. Xie said.
He also argued for the need to “revisit this issue of using surrogate outcomes to measure the safety and efficacy of new oncology drugs.”
Dr. Xie and his colleagues did not report any conflicts of interest. One study author (Marcin Waligora, PhD) reported funding from the National Science Centre in Poland.
*EORTC-QLQ-C30, FACT-G19, Lung Cancer Symptom Scale, EQ-5D, 8-item linear analog self-assessment (LASA) questionnaire, and clinician-reported Karnofsky score
Synthetic HCV glycoproteins elicit narrow, but not widely effective antibodies
Immunization with two synthetic consensus constructs of hepatitis C virus (HCV) glycoproteins was found to elicit narrow, but not widely effective, virus-neutralizing antibodies in guinea pigs, according to the results of a model study published in the journal Antiviral Research.

Researchers created two novel synthetic E2 glycoprotein immunogens (NotC1 and NotC2) using consensus nucleotide sequences deduced from samples of circulating genotype 1 HCV strains, according to Alexander W. Tarr, PhD, of the Nottingham (England) University Hospitals NHS Trust, and his colleagues.
Expression of these constructs in Drosophila melanogaster cells resulted in high yields of correctly folded, monomeric E2 proteins, which were used to immunize guinea pigs. Both proteins generated antibodies capable of neutralizing the H77 strain of HCV, although NotC1 elicited antibodies that were more potent at neutralizing virus entry. The two sets of glycoprotein-induced antibodies neutralized some HCV strains representing genotype 1, but not those strains representing genotype 2 or genotype 3.
“The broader objective of eliciting antibodies that neutralize patient strains representing multiple genotypes will require further refinement of immunization protocols. A vaccine construct comprising the consensus of a minimal CD81 binding domain might be able to focus the antibody response to conserved epitopes on E2. Additionally, boosting immunized animals with glycoproteins representing different strains might be required to focus the antibody response on to conserved conformational epitopes,” the researchers concluded.
The research was funded by the Medical Research Council, the NIHR Nottingham Biomedical Research Centre, and the European Union. Disclosures were not reported.
SOURCE: Tarr AW et al. Antiviral Research 2018;160:25-37.
Immunization with two synthetic consensus constructs of hepatitis C virus (HCV) glycoproteins was found to elicit narrow, but not widely effective, virus-neutralizing antibodies in guinea pigs, according to the results of a model study published in the journal Antiviral Research.
Researchers created two novel synthetic E2 glycoprotein immunogens (NotC1 and NotC2) using consensus nucleotide sequences deduced from samples of circulating genotype 1 HCV strains, according to Alexander W. Tarr, PhD, of the Nottingham (England) University Hospitals NHS Trust, and his colleagues.
Expression of these constructs in Drosophila melanogaster cells resulted in high yields of correctly folded, monomeric E2 proteins, which were used to immunize guinea pigs. Both proteins generated antibodies capable of neutralizing the H77 strain of HCV, although NotC1 elicited antibodies that were more potent at neutralizing virus entry. The two sets of glycoprotein-induced antibodies neutralized some HCV strains representing genotype 1, but not those strains representing genotype 2 or genotype 3.
“The broader objective of eliciting antibodies that neutralize patient strains representing multiple genotypes will require further refinement of immunization protocols. A vaccine construct comprising the consensus of a minimal CD81 binding domain might be able to focus the antibody response to conserved epitopes on E2. Additionally, boosting immunized animals with glycoproteins representing different strains might be required to focus the antibody response on to conserved conformational epitopes,” the researchers concluded.
The research was funded by the Medical Research Council, the NIHR Nottingham Biomedical Research Centre, and the European Union. Disclosures were not reported.
SOURCE: Tarr AW et al. Antiviral Research 2018;160:25-37.
Immunization with two synthetic consensus constructs of hepatitis C virus (HCV) glycoproteins was found to elicit narrow, but not widely effective, virus-neutralizing antibodies in guinea pigs, according to the results of a model study published in the journal Antiviral Research.
Researchers created two novel synthetic E2 glycoprotein immunogens (NotC1 and NotC2) using consensus nucleotide sequences deduced from samples of circulating genotype 1 HCV strains, according to Alexander W. Tarr, PhD, of the Nottingham (England) University Hospitals NHS Trust, and his colleagues.
Expression of these constructs in Drosophila melanogaster cells resulted in high yields of correctly folded, monomeric E2 proteins, which were used to immunize guinea pigs. Both proteins generated antibodies capable of neutralizing the H77 strain of HCV, although NotC1 elicited antibodies that were more potent at neutralizing virus entry. The two sets of glycoprotein-induced antibodies neutralized some HCV strains representing genotype 1, but not those strains representing genotype 2 or genotype 3.
“The broader objective of eliciting antibodies that neutralize patient strains representing multiple genotypes will require further refinement of immunization protocols. A vaccine construct comprising the consensus of a minimal CD81 binding domain might be able to focus the antibody response to conserved epitopes on E2. Additionally, boosting immunized animals with glycoproteins representing different strains might be required to focus the antibody response on to conserved conformational epitopes,” the researchers concluded.
The research was funded by the Medical Research Council, the NIHR Nottingham Biomedical Research Centre, and the European Union. Disclosures were not reported.
SOURCE: Tarr AW et al. Antiviral Research 2018;160:25-37.
FROM ANTIVIRAL RESEARCH