User login
Weight Loss Surgery Yields Long-Term BP Control in Obesity
For adults with obesity and uncontrolled hypertension, bariatric surgery is an effective and durable strategy to control high blood pressure (BP), final, 5-year follow-up data from the GATEWAY trial suggested.
In the trial, those who underwent bariatric surgery had lower body mass index (BMI) and were on fewer antihypertensive medications after 5 years while maintaining normal BP than those who only used antihypertensive medications.
The results show that “bariatric and metabolic surgery can be very effective in the treatment of patients with obesity and hypertension in the long term,” chief investigator Carlos Aurelio Schiavon, MD, with the Research Institute, Heart Hospital, São Paulo, Brazil, told this news organization.
“The most important clinical implication of this trial is that we must treat obesity to accomplish success when treating patients with cardiovascular diseases, such as hypertension and obesity,” Dr. Schiavon said.
The study was published online on February 5, 2024, in the Journal of the American College of Cardiology.
A Gateway to Lasting BP Control
GATEWAY enrolled 100 adults (76% women) with grade 1/2 obesity (BMI, 30 to < 40 kg/m2; mean, 37 kg/m2) who were on at least two antihypertensive medications at maximum doses at baseline.
Half were randomly allocated to laparoscopic Roux-en-Y gastric-bypass surgery (RYGB) plus medications and half to medication alone. The primary outcome was at least a 30% reduction of antihypertensive medications while maintaining BP < 140/90 mm Hg. Five-year results were based on 37 patients in the surgery group and 32 in the medication only group.
After 5 years, BMI was 28.01 kg/m2 for those who had surgery vs 36.40 kg/m2 for those on medication alone (P < .001).
Patients who underwent RYGB had an 80.7% reduction in the number of antihypertensive medications they were taking while maintaining BP < 140/90 mm Hg compared with a 13.7% reduction in those on medication alone.
After 5 years, surgery patients were taking a mean of 0.80 antihypertensive medications vs 2.97 in the medication only group to control BP at or below the target.
Despite using less antihypertensive medications in the RYGB, ambulatory BP monitoring data revealed similar 24-hour, daytime, and nighttime BP profiles compared with medication alone.
The rate of hypertension remission (controlled BP without medication) was nearly 20-fold higher in the surgery group than in the medication only group (46.9% vs 2.4%; P < .001).
In addition, the rate of apparent resistant hypertension was lower with than without surgery (0% vs 15.2%). The surgery group also showed evidence of less atrial remodeling.
The 5-year results were consistent with the 1-year GATEWAY results Dr. Schiavon presented at the American Heart Association 2017 scientific sessions, as reported by this news organization. They also mirrored the results reported at 3 years.
Limitations of the study include its single-center, open-label design with a small sample size and loss of follow-up in some patients.
“Taken together, these results support the long-term effective role of bariatric surgery in reducing the burden of hypertension and related polypharmacy, which is frequently observed in patients with obesity and is a cause of concern for them,” the authors wrote.
“In clinical practice, obesity is an overlooked condition. As a consequence, there is a frequent failure in approaching obesity as a crucial step for mitigating the risk of important cardiovascular risk factors including hypertension. Our results underscore the importance of approaching obesity in reducing hypertension rates,” they added.
Important Data, Lingering Questions
The coauthors of an accompanying editorial said this study provides “important long-term data on the benefits of gastric bypass on weight loss and blood pressure control, but questions remain.”
Yet, Michael Hall, MD, MSc, with University of Mississippi Medical Center in Jackson, and coauthors noted that the study only included patients undergoing RYGB; it remains unclear if other bariatric surgery procedures would have the same long-term results.
“Sleeve gastrectomy has become more common than RYGB because it is less complex and has earlier recovery and similar effectiveness for treating obesity and type 2 diabetes,” they pointed out. “Further comparative randomized controlled trials are needed to determine whether sleeve gastrectomy is as effective as RYGB for long-term BP control.”
As reported previously by this news organization, in SLEEVEPASS, there was greater weight loss and higher likelihood of hypertension remission with RYGB than with sleeve gastrectomy (24% vs 8%; P = .04), although BP control was not the primary outcome.
The GATEWAY study was supported by a grant from Ethicon. Dr. Schiavon received a research grant from Ethicon and has received lecture fees from Ethicon and Medtronic. The editorial writers had no relevant disclosures.
A version of this article appeared on Medscape.com.
For adults with obesity and uncontrolled hypertension, bariatric surgery is an effective and durable strategy to control high blood pressure (BP), final, 5-year follow-up data from the GATEWAY trial suggested.
In the trial, those who underwent bariatric surgery had lower body mass index (BMI) and were on fewer antihypertensive medications after 5 years while maintaining normal BP than those who only used antihypertensive medications.
The results show that “bariatric and metabolic surgery can be very effective in the treatment of patients with obesity and hypertension in the long term,” chief investigator Carlos Aurelio Schiavon, MD, with the Research Institute, Heart Hospital, São Paulo, Brazil, told this news organization.
“The most important clinical implication of this trial is that we must treat obesity to accomplish success when treating patients with cardiovascular diseases, such as hypertension and obesity,” Dr. Schiavon said.
The study was published online on February 5, 2024, in the Journal of the American College of Cardiology.
A Gateway to Lasting BP Control
GATEWAY enrolled 100 adults (76% women) with grade 1/2 obesity (BMI, 30 to < 40 kg/m2; mean, 37 kg/m2) who were on at least two antihypertensive medications at maximum doses at baseline.
Half were randomly allocated to laparoscopic Roux-en-Y gastric-bypass surgery (RYGB) plus medications and half to medication alone. The primary outcome was at least a 30% reduction of antihypertensive medications while maintaining BP < 140/90 mm Hg. Five-year results were based on 37 patients in the surgery group and 32 in the medication only group.
After 5 years, BMI was 28.01 kg/m2 for those who had surgery vs 36.40 kg/m2 for those on medication alone (P < .001).
Patients who underwent RYGB had an 80.7% reduction in the number of antihypertensive medications they were taking while maintaining BP < 140/90 mm Hg compared with a 13.7% reduction in those on medication alone.
After 5 years, surgery patients were taking a mean of 0.80 antihypertensive medications vs 2.97 in the medication only group to control BP at or below the target.
Despite using less antihypertensive medications in the RYGB, ambulatory BP monitoring data revealed similar 24-hour, daytime, and nighttime BP profiles compared with medication alone.
The rate of hypertension remission (controlled BP without medication) was nearly 20-fold higher in the surgery group than in the medication only group (46.9% vs 2.4%; P < .001).
In addition, the rate of apparent resistant hypertension was lower with than without surgery (0% vs 15.2%). The surgery group also showed evidence of less atrial remodeling.
The 5-year results were consistent with the 1-year GATEWAY results Dr. Schiavon presented at the American Heart Association 2017 scientific sessions, as reported by this news organization. They also mirrored the results reported at 3 years.
Limitations of the study include its single-center, open-label design with a small sample size and loss of follow-up in some patients.
“Taken together, these results support the long-term effective role of bariatric surgery in reducing the burden of hypertension and related polypharmacy, which is frequently observed in patients with obesity and is a cause of concern for them,” the authors wrote.
“In clinical practice, obesity is an overlooked condition. As a consequence, there is a frequent failure in approaching obesity as a crucial step for mitigating the risk of important cardiovascular risk factors including hypertension. Our results underscore the importance of approaching obesity in reducing hypertension rates,” they added.
Important Data, Lingering Questions
The coauthors of an accompanying editorial said this study provides “important long-term data on the benefits of gastric bypass on weight loss and blood pressure control, but questions remain.”
Yet, Michael Hall, MD, MSc, with University of Mississippi Medical Center in Jackson, and coauthors noted that the study only included patients undergoing RYGB; it remains unclear if other bariatric surgery procedures would have the same long-term results.
“Sleeve gastrectomy has become more common than RYGB because it is less complex and has earlier recovery and similar effectiveness for treating obesity and type 2 diabetes,” they pointed out. “Further comparative randomized controlled trials are needed to determine whether sleeve gastrectomy is as effective as RYGB for long-term BP control.”
As reported previously by this news organization, in SLEEVEPASS, there was greater weight loss and higher likelihood of hypertension remission with RYGB than with sleeve gastrectomy (24% vs 8%; P = .04), although BP control was not the primary outcome.
The GATEWAY study was supported by a grant from Ethicon. Dr. Schiavon received a research grant from Ethicon and has received lecture fees from Ethicon and Medtronic. The editorial writers had no relevant disclosures.
A version of this article appeared on Medscape.com.
For adults with obesity and uncontrolled hypertension, bariatric surgery is an effective and durable strategy to control high blood pressure (BP), final, 5-year follow-up data from the GATEWAY trial suggested.
In the trial, those who underwent bariatric surgery had lower body mass index (BMI) and were on fewer antihypertensive medications after 5 years while maintaining normal BP than those who only used antihypertensive medications.
The results show that “bariatric and metabolic surgery can be very effective in the treatment of patients with obesity and hypertension in the long term,” chief investigator Carlos Aurelio Schiavon, MD, with the Research Institute, Heart Hospital, São Paulo, Brazil, told this news organization.
“The most important clinical implication of this trial is that we must treat obesity to accomplish success when treating patients with cardiovascular diseases, such as hypertension and obesity,” Dr. Schiavon said.
The study was published online on February 5, 2024, in the Journal of the American College of Cardiology.
A Gateway to Lasting BP Control
GATEWAY enrolled 100 adults (76% women) with grade 1/2 obesity (BMI, 30 to < 40 kg/m2; mean, 37 kg/m2) who were on at least two antihypertensive medications at maximum doses at baseline.
Half were randomly allocated to laparoscopic Roux-en-Y gastric-bypass surgery (RYGB) plus medications and half to medication alone. The primary outcome was at least a 30% reduction of antihypertensive medications while maintaining BP < 140/90 mm Hg. Five-year results were based on 37 patients in the surgery group and 32 in the medication only group.
After 5 years, BMI was 28.01 kg/m2 for those who had surgery vs 36.40 kg/m2 for those on medication alone (P < .001).
Patients who underwent RYGB had an 80.7% reduction in the number of antihypertensive medications they were taking while maintaining BP < 140/90 mm Hg compared with a 13.7% reduction in those on medication alone.
After 5 years, surgery patients were taking a mean of 0.80 antihypertensive medications vs 2.97 in the medication only group to control BP at or below the target.
Despite using less antihypertensive medications in the RYGB, ambulatory BP monitoring data revealed similar 24-hour, daytime, and nighttime BP profiles compared with medication alone.
The rate of hypertension remission (controlled BP without medication) was nearly 20-fold higher in the surgery group than in the medication only group (46.9% vs 2.4%; P < .001).
In addition, the rate of apparent resistant hypertension was lower with than without surgery (0% vs 15.2%). The surgery group also showed evidence of less atrial remodeling.
The 5-year results were consistent with the 1-year GATEWAY results Dr. Schiavon presented at the American Heart Association 2017 scientific sessions, as reported by this news organization. They also mirrored the results reported at 3 years.
Limitations of the study include its single-center, open-label design with a small sample size and loss of follow-up in some patients.
“Taken together, these results support the long-term effective role of bariatric surgery in reducing the burden of hypertension and related polypharmacy, which is frequently observed in patients with obesity and is a cause of concern for them,” the authors wrote.
“In clinical practice, obesity is an overlooked condition. As a consequence, there is a frequent failure in approaching obesity as a crucial step for mitigating the risk of important cardiovascular risk factors including hypertension. Our results underscore the importance of approaching obesity in reducing hypertension rates,” they added.
Important Data, Lingering Questions
The coauthors of an accompanying editorial said this study provides “important long-term data on the benefits of gastric bypass on weight loss and blood pressure control, but questions remain.”
Yet, Michael Hall, MD, MSc, with University of Mississippi Medical Center in Jackson, and coauthors noted that the study only included patients undergoing RYGB; it remains unclear if other bariatric surgery procedures would have the same long-term results.
“Sleeve gastrectomy has become more common than RYGB because it is less complex and has earlier recovery and similar effectiveness for treating obesity and type 2 diabetes,” they pointed out. “Further comparative randomized controlled trials are needed to determine whether sleeve gastrectomy is as effective as RYGB for long-term BP control.”
As reported previously by this news organization, in SLEEVEPASS, there was greater weight loss and higher likelihood of hypertension remission with RYGB than with sleeve gastrectomy (24% vs 8%; P = .04), although BP control was not the primary outcome.
The GATEWAY study was supported by a grant from Ethicon. Dr. Schiavon received a research grant from Ethicon and has received lecture fees from Ethicon and Medtronic. The editorial writers had no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
How to Avoid the $400,000 Med School Debt Mistakes I Made
It’s not always great to be tops among your peers.
, according to Medscape Medical News’ 2023 Residents Salary and Debt Report.
I’m smack in that upper percentile. I amassed nearly a half million dollars in student debt and currently stand at roughly $400,000. Yay me.
As a naive twentysomething making a major life decision, I never thought my loans would amount to this inconceivable figure, the proverbial “mortgage without a roof” you hear student debt experts talk about.
This isn’t a story about how the student loan industry needs to be reformed or how education has become increasingly expensive or regrets about going to medical school.
It’s also not a story about how you should be handling basics like consolidating and refinancing and paying extra toward your principal.
It’s about my experience as a physician 13 years after signing that first promissory note. In short: I completely miscalculated the impact loans would have on my life.
I bought money to go to school. I can’t undo that. But over the past decade, I have learned a lot, particularly how those with their own mountain of debt — or who will inevitably wind up with one — can manage things better than I have.
Mistake #1: Loan Forgiveness Is More Complicated Than it Seems
My parents and I were aware of the Public Service Loan Forgiveness (PSLF) program which began in 2007 shortly before I started exploring medical school options. I wanted to help people, so working in the nonprofit sector sounded like a no-brainer. Making 120 payments while practicing at a qualifying institution didn’t sound hard.
Newsflash: Not all healthcare organizations are 501(c)3 programs that qualify as nonprofit for the PSLF program. You can’t just snap your fingers and land at one. I graduated from fellowship just as the COVID-19 pandemic began, which meant I was launching my medical career in the midst of hiring freezes and an overnight disappearance of job opportunities.
I had to take a 2-year hiatus from the nonprofit sector and found a part-time position with a local private practice group. It still stings. Had I been working for a qualified employer, I could have benefited from the student loan payment pause and been closer to applying for loan forgiveness.
Avoid it: Be brutally honest with yourself about what kind of medicine you want to practice — especially within the opportunities you have on hand. Private practice is very different from working for the nonprofit sector. I didn›t know that. When weighing career choices, immediately ask, “How will this impact how I pay my loans?” You may not like the answer, but you›ll always know where you stand financially.
Mistake #2: I Forgot to Factor in Life Goals
To be fair, some things were out of my control: Not getting into a state school with cheaper tuition rates, graduating at the start of a once-in-a-lifetime global pandemic. I wasn’t prepared for a changing job landscape. But there were also “expected” life events like getting married, developing a geographical preference, and having a child. I didn’t consider those either.
How about the “expected” goal of buying a home? For years I didn’t feel financially comfortable enough to take on a mortgage. For so long, my attitude has been don’t take on any more debt. (A special shout-out to my 6.8% interest rate which has contributed over a third of my total loan amount.)
This even affected how my husband and I would talk about what a future home might look like. There’s always a giant unwelcome guest casting a shadow over my thoughts.
Avoid it: Don’t compartmentalize your personal and professional lives. Your student loans will hang over both, and you need to be honest with yourself about what “upward mobility” really means to you while in debt. There’s a reason people say “live like a resident” until your loans are paid off. My husband and I finally worked our numbers to where we bought our first home this past year — a moment years in the making. I still drive around in my beloved Honda CR-V like it’s a Mercedes G-Wagon.
Mistake #3: I Didn’t Ask Questions
I regret not talking to a practicing physician about their experience with student loans. I didn’t know any. There weren’t any physicians in my extended family or my community network. I was a first-generation Pakistani American kid trying to figure it out.
It’s difficult because even today, many physicians aren’t comfortable discussing their financial circumstances. The lack of financial transparency and even financial literacy is astounding among young medical professionals. We live in a medical culture where no one talks about the money. I was too diffident and nervous to even try.
Avoid it: Don’t be afraid to have uncomfortable conversations about money. Don’t allow yourself to make even one passive decision. It’s your life.
If you can’t find someone in medicine to talk to about their financial journey, there are plenty of credible resources. Medscape Medical News has a Physician Business Academy with hot topics like personal finance. The White Coat Investor is literally bookmarked on all my electronic devices. KevinMD.com has a ton of resources and articles answering common financial questions about retirement, savings, and house buying. And Travis Hornsby with www.studentloanplanner.com has wonderful advice on all kinds of different loans.
There are no stupid questions. Just ask. You might be surprised by what people are willing to share.
Mistake #4: Playing it Casual With My Lenders
If $400,000 in debt doesn’t sound bad enough, imagine lots more. It turns out my loan carrier had me at a much higher loan balance because they’d inadvertently duplicated one of my loans in the total. I didn’t know that until I transferred my loans to another handler and it came to light.
Imagine my relief at having a lower total. Imagine my anger at myself for not checking sooner.
Avoid it: Do a thorough self-audit on all your loans more than once a year. Pretend they’re a patient with odd symptoms you can’t pin down and you have the luxury of doing every diagnostic test available. It’s not fun studying your own debt, but it’s the only way to really know how much you have.
Mistake #5: Not Leaving Room to Change My Mind
I underestimated how I would evolve and how my goals would change after having the letters “MD” after my name. I never dreamed that a nonprofit salary might not be enough.
A lot of us assume that the bedside is where we will find professional satisfaction. But you might be surprised. In a climate where we’re constantly being pushed to do more in a broken healthcare system, a landscape where misinformation and technology are forcing medicine to change, there might be little joy in working clinically full time. Then what do you do?
Because I elected to go the PSLF route, I’m tied to this decision. And while it still makes the most economic sense for me personally, it now limits my professional exploration and freedom.
Avoid it: Consider how much time you really want to spend in clinical medicine. Be mindful that you have to work at least 0.8 full time equivalent to qualify for the PSLF program. It’s very hard to predict the future, let alone your future, but just know you›ll have moments where you ask, “Do I really want to stay on this career track?” Will you be able to pivot? Can you live with it if the answer is no?
Looking Ahead
Let me be clear about one thing. Despite all the negativity I feel toward my student loans — guilt about the burden I brought to my marriage and my adult life, disappointment about the cost of becoming a successful physician, and frustration that this has turned out to be the most influential factor shaping my professional and personal choices — the one thing I don’t feel is shame.
I worked hard to get to this point in my life. I am proud of being a physician.
My student loan burden will follow me to the grave. But progress is also possible. I have friends that have paid their loans down by hustling, working hard, and dropping every penny toward them.
I also have friends that have had their loans forgiven. There are options. Everyone’s experience looks a little different. But don’t be naive: Student loans will color every financial decision you make.
I’m finding solace now in recently moving and finding work at a nonprofit institution. I’m back at it; 77 payments made, and 43 to go.
Well, technically I’ve made 93 payments. I’m still waiting for my loan servicer to get around to updating my account.
You really have to stay on top of those folks.
A version of this article appeared on Medscape.com.
It’s not always great to be tops among your peers.
, according to Medscape Medical News’ 2023 Residents Salary and Debt Report.
I’m smack in that upper percentile. I amassed nearly a half million dollars in student debt and currently stand at roughly $400,000. Yay me.
As a naive twentysomething making a major life decision, I never thought my loans would amount to this inconceivable figure, the proverbial “mortgage without a roof” you hear student debt experts talk about.
This isn’t a story about how the student loan industry needs to be reformed or how education has become increasingly expensive or regrets about going to medical school.
It’s also not a story about how you should be handling basics like consolidating and refinancing and paying extra toward your principal.
It’s about my experience as a physician 13 years after signing that first promissory note. In short: I completely miscalculated the impact loans would have on my life.
I bought money to go to school. I can’t undo that. But over the past decade, I have learned a lot, particularly how those with their own mountain of debt — or who will inevitably wind up with one — can manage things better than I have.
Mistake #1: Loan Forgiveness Is More Complicated Than it Seems
My parents and I were aware of the Public Service Loan Forgiveness (PSLF) program which began in 2007 shortly before I started exploring medical school options. I wanted to help people, so working in the nonprofit sector sounded like a no-brainer. Making 120 payments while practicing at a qualifying institution didn’t sound hard.
Newsflash: Not all healthcare organizations are 501(c)3 programs that qualify as nonprofit for the PSLF program. You can’t just snap your fingers and land at one. I graduated from fellowship just as the COVID-19 pandemic began, which meant I was launching my medical career in the midst of hiring freezes and an overnight disappearance of job opportunities.
I had to take a 2-year hiatus from the nonprofit sector and found a part-time position with a local private practice group. It still stings. Had I been working for a qualified employer, I could have benefited from the student loan payment pause and been closer to applying for loan forgiveness.
Avoid it: Be brutally honest with yourself about what kind of medicine you want to practice — especially within the opportunities you have on hand. Private practice is very different from working for the nonprofit sector. I didn›t know that. When weighing career choices, immediately ask, “How will this impact how I pay my loans?” You may not like the answer, but you›ll always know where you stand financially.
Mistake #2: I Forgot to Factor in Life Goals
To be fair, some things were out of my control: Not getting into a state school with cheaper tuition rates, graduating at the start of a once-in-a-lifetime global pandemic. I wasn’t prepared for a changing job landscape. But there were also “expected” life events like getting married, developing a geographical preference, and having a child. I didn’t consider those either.
How about the “expected” goal of buying a home? For years I didn’t feel financially comfortable enough to take on a mortgage. For so long, my attitude has been don’t take on any more debt. (A special shout-out to my 6.8% interest rate which has contributed over a third of my total loan amount.)
This even affected how my husband and I would talk about what a future home might look like. There’s always a giant unwelcome guest casting a shadow over my thoughts.
Avoid it: Don’t compartmentalize your personal and professional lives. Your student loans will hang over both, and you need to be honest with yourself about what “upward mobility” really means to you while in debt. There’s a reason people say “live like a resident” until your loans are paid off. My husband and I finally worked our numbers to where we bought our first home this past year — a moment years in the making. I still drive around in my beloved Honda CR-V like it’s a Mercedes G-Wagon.
Mistake #3: I Didn’t Ask Questions
I regret not talking to a practicing physician about their experience with student loans. I didn’t know any. There weren’t any physicians in my extended family or my community network. I was a first-generation Pakistani American kid trying to figure it out.
It’s difficult because even today, many physicians aren’t comfortable discussing their financial circumstances. The lack of financial transparency and even financial literacy is astounding among young medical professionals. We live in a medical culture where no one talks about the money. I was too diffident and nervous to even try.
Avoid it: Don’t be afraid to have uncomfortable conversations about money. Don’t allow yourself to make even one passive decision. It’s your life.
If you can’t find someone in medicine to talk to about their financial journey, there are plenty of credible resources. Medscape Medical News has a Physician Business Academy with hot topics like personal finance. The White Coat Investor is literally bookmarked on all my electronic devices. KevinMD.com has a ton of resources and articles answering common financial questions about retirement, savings, and house buying. And Travis Hornsby with www.studentloanplanner.com has wonderful advice on all kinds of different loans.
There are no stupid questions. Just ask. You might be surprised by what people are willing to share.
Mistake #4: Playing it Casual With My Lenders
If $400,000 in debt doesn’t sound bad enough, imagine lots more. It turns out my loan carrier had me at a much higher loan balance because they’d inadvertently duplicated one of my loans in the total. I didn’t know that until I transferred my loans to another handler and it came to light.
Imagine my relief at having a lower total. Imagine my anger at myself for not checking sooner.
Avoid it: Do a thorough self-audit on all your loans more than once a year. Pretend they’re a patient with odd symptoms you can’t pin down and you have the luxury of doing every diagnostic test available. It’s not fun studying your own debt, but it’s the only way to really know how much you have.
Mistake #5: Not Leaving Room to Change My Mind
I underestimated how I would evolve and how my goals would change after having the letters “MD” after my name. I never dreamed that a nonprofit salary might not be enough.
A lot of us assume that the bedside is where we will find professional satisfaction. But you might be surprised. In a climate where we’re constantly being pushed to do more in a broken healthcare system, a landscape where misinformation and technology are forcing medicine to change, there might be little joy in working clinically full time. Then what do you do?
Because I elected to go the PSLF route, I’m tied to this decision. And while it still makes the most economic sense for me personally, it now limits my professional exploration and freedom.
Avoid it: Consider how much time you really want to spend in clinical medicine. Be mindful that you have to work at least 0.8 full time equivalent to qualify for the PSLF program. It’s very hard to predict the future, let alone your future, but just know you›ll have moments where you ask, “Do I really want to stay on this career track?” Will you be able to pivot? Can you live with it if the answer is no?
Looking Ahead
Let me be clear about one thing. Despite all the negativity I feel toward my student loans — guilt about the burden I brought to my marriage and my adult life, disappointment about the cost of becoming a successful physician, and frustration that this has turned out to be the most influential factor shaping my professional and personal choices — the one thing I don’t feel is shame.
I worked hard to get to this point in my life. I am proud of being a physician.
My student loan burden will follow me to the grave. But progress is also possible. I have friends that have paid their loans down by hustling, working hard, and dropping every penny toward them.
I also have friends that have had their loans forgiven. There are options. Everyone’s experience looks a little different. But don’t be naive: Student loans will color every financial decision you make.
I’m finding solace now in recently moving and finding work at a nonprofit institution. I’m back at it; 77 payments made, and 43 to go.
Well, technically I’ve made 93 payments. I’m still waiting for my loan servicer to get around to updating my account.
You really have to stay on top of those folks.
A version of this article appeared on Medscape.com.
It’s not always great to be tops among your peers.
, according to Medscape Medical News’ 2023 Residents Salary and Debt Report.
I’m smack in that upper percentile. I amassed nearly a half million dollars in student debt and currently stand at roughly $400,000. Yay me.
As a naive twentysomething making a major life decision, I never thought my loans would amount to this inconceivable figure, the proverbial “mortgage without a roof” you hear student debt experts talk about.
This isn’t a story about how the student loan industry needs to be reformed or how education has become increasingly expensive or regrets about going to medical school.
It’s also not a story about how you should be handling basics like consolidating and refinancing and paying extra toward your principal.
It’s about my experience as a physician 13 years after signing that first promissory note. In short: I completely miscalculated the impact loans would have on my life.
I bought money to go to school. I can’t undo that. But over the past decade, I have learned a lot, particularly how those with their own mountain of debt — or who will inevitably wind up with one — can manage things better than I have.
Mistake #1: Loan Forgiveness Is More Complicated Than it Seems
My parents and I were aware of the Public Service Loan Forgiveness (PSLF) program which began in 2007 shortly before I started exploring medical school options. I wanted to help people, so working in the nonprofit sector sounded like a no-brainer. Making 120 payments while practicing at a qualifying institution didn’t sound hard.
Newsflash: Not all healthcare organizations are 501(c)3 programs that qualify as nonprofit for the PSLF program. You can’t just snap your fingers and land at one. I graduated from fellowship just as the COVID-19 pandemic began, which meant I was launching my medical career in the midst of hiring freezes and an overnight disappearance of job opportunities.
I had to take a 2-year hiatus from the nonprofit sector and found a part-time position with a local private practice group. It still stings. Had I been working for a qualified employer, I could have benefited from the student loan payment pause and been closer to applying for loan forgiveness.
Avoid it: Be brutally honest with yourself about what kind of medicine you want to practice — especially within the opportunities you have on hand. Private practice is very different from working for the nonprofit sector. I didn›t know that. When weighing career choices, immediately ask, “How will this impact how I pay my loans?” You may not like the answer, but you›ll always know where you stand financially.
Mistake #2: I Forgot to Factor in Life Goals
To be fair, some things were out of my control: Not getting into a state school with cheaper tuition rates, graduating at the start of a once-in-a-lifetime global pandemic. I wasn’t prepared for a changing job landscape. But there were also “expected” life events like getting married, developing a geographical preference, and having a child. I didn’t consider those either.
How about the “expected” goal of buying a home? For years I didn’t feel financially comfortable enough to take on a mortgage. For so long, my attitude has been don’t take on any more debt. (A special shout-out to my 6.8% interest rate which has contributed over a third of my total loan amount.)
This even affected how my husband and I would talk about what a future home might look like. There’s always a giant unwelcome guest casting a shadow over my thoughts.
Avoid it: Don’t compartmentalize your personal and professional lives. Your student loans will hang over both, and you need to be honest with yourself about what “upward mobility” really means to you while in debt. There’s a reason people say “live like a resident” until your loans are paid off. My husband and I finally worked our numbers to where we bought our first home this past year — a moment years in the making. I still drive around in my beloved Honda CR-V like it’s a Mercedes G-Wagon.
Mistake #3: I Didn’t Ask Questions
I regret not talking to a practicing physician about their experience with student loans. I didn’t know any. There weren’t any physicians in my extended family or my community network. I was a first-generation Pakistani American kid trying to figure it out.
It’s difficult because even today, many physicians aren’t comfortable discussing their financial circumstances. The lack of financial transparency and even financial literacy is astounding among young medical professionals. We live in a medical culture where no one talks about the money. I was too diffident and nervous to even try.
Avoid it: Don’t be afraid to have uncomfortable conversations about money. Don’t allow yourself to make even one passive decision. It’s your life.
If you can’t find someone in medicine to talk to about their financial journey, there are plenty of credible resources. Medscape Medical News has a Physician Business Academy with hot topics like personal finance. The White Coat Investor is literally bookmarked on all my electronic devices. KevinMD.com has a ton of resources and articles answering common financial questions about retirement, savings, and house buying. And Travis Hornsby with www.studentloanplanner.com has wonderful advice on all kinds of different loans.
There are no stupid questions. Just ask. You might be surprised by what people are willing to share.
Mistake #4: Playing it Casual With My Lenders
If $400,000 in debt doesn’t sound bad enough, imagine lots more. It turns out my loan carrier had me at a much higher loan balance because they’d inadvertently duplicated one of my loans in the total. I didn’t know that until I transferred my loans to another handler and it came to light.
Imagine my relief at having a lower total. Imagine my anger at myself for not checking sooner.
Avoid it: Do a thorough self-audit on all your loans more than once a year. Pretend they’re a patient with odd symptoms you can’t pin down and you have the luxury of doing every diagnostic test available. It’s not fun studying your own debt, but it’s the only way to really know how much you have.
Mistake #5: Not Leaving Room to Change My Mind
I underestimated how I would evolve and how my goals would change after having the letters “MD” after my name. I never dreamed that a nonprofit salary might not be enough.
A lot of us assume that the bedside is where we will find professional satisfaction. But you might be surprised. In a climate where we’re constantly being pushed to do more in a broken healthcare system, a landscape where misinformation and technology are forcing medicine to change, there might be little joy in working clinically full time. Then what do you do?
Because I elected to go the PSLF route, I’m tied to this decision. And while it still makes the most economic sense for me personally, it now limits my professional exploration and freedom.
Avoid it: Consider how much time you really want to spend in clinical medicine. Be mindful that you have to work at least 0.8 full time equivalent to qualify for the PSLF program. It’s very hard to predict the future, let alone your future, but just know you›ll have moments where you ask, “Do I really want to stay on this career track?” Will you be able to pivot? Can you live with it if the answer is no?
Looking Ahead
Let me be clear about one thing. Despite all the negativity I feel toward my student loans — guilt about the burden I brought to my marriage and my adult life, disappointment about the cost of becoming a successful physician, and frustration that this has turned out to be the most influential factor shaping my professional and personal choices — the one thing I don’t feel is shame.
I worked hard to get to this point in my life. I am proud of being a physician.
My student loan burden will follow me to the grave. But progress is also possible. I have friends that have paid their loans down by hustling, working hard, and dropping every penny toward them.
I also have friends that have had their loans forgiven. There are options. Everyone’s experience looks a little different. But don’t be naive: Student loans will color every financial decision you make.
I’m finding solace now in recently moving and finding work at a nonprofit institution. I’m back at it; 77 payments made, and 43 to go.
Well, technically I’ve made 93 payments. I’m still waiting for my loan servicer to get around to updating my account.
You really have to stay on top of those folks.
A version of this article appeared on Medscape.com.
Coma Due to Poisoning: Caution Urged in Intubation
Tracheal intubation is recommended for comatose patients, but its use in individuals with altered consciousness due to acute poisoning remains uncertain. A French team conducted a large randomized trial to assess the risk–benefit ratio of a conservative approach in this context.
Patients with altered consciousness are at high risk for respiratory distress and pneumonia. Acute poisoning, whether from alcohol, drugs, or medications, is a nontraumatic cause of altered consciousness that often leads to intubation. In the United States alone, 20,000 patients with acute poisoning are intubated annually. While this practice aims to prevent the inhalation of gastric content and, consequently, pneumonia, intubation itself can cause hemodynamic instability, hypoxia, difficulties during tube insertion, or dental injuries. Until now, no study had attempted to evaluate the risk–benefit ratio of this practice in cases of toxic coma.
A Randomized Trial
The randomized trial conducted with a parallel, nonblinded design aimed to determine whether abstaining from intubation was equivalent to standard practice in certain situations. The study took place in 20 French emergency services and one intensive care unit. Participants were at least 18 years old with suspected acute poisoning and a Glasgow Coma Scale (GCS) score of less than 9. Pregnant women; prisoners; those requiring immediate intubation because of respiratory distress, cerebral edema, or other critical conditions; and those using cardiotoxic drugs or drugs that could be rapidly antagonized, such as opioids or sedatives, were excluded. Participants were randomized in a 1:1 ratio after hospital stratification. In the control group, the decision to intubate was at the discretion of the attending practitioner.
In the nonintubated by default group (the intervention group), a procedure could be performed later in case of respiratory distress, vomiting, or other complications. If abstaining, patients were closely monitored through oximetry, heart rate, GCS, etc. If intubation was required, it was performed under sedation (sedatives or hypnotics) and succinylcholine or rocuronium, after appropriate preoxygenation. In addition, capnography was recommended later to ensure proper endotracheal tube placement.
The primary outcome was a hierarchical composite outcome combining in-hospital death, duration of stay in the intensive care unit (ICU), and overall hospital stay (up to the 28th day). Secondary outcomes included, besides the aforementioned individual outcomes, the number of patients requiring mechanical ventilation, the proportion of admissions to the ICU, the incidence of pneumonia, and iatrogenic effects related to intubation itself.
Noninvasive Strategy’s Advantages
The primary analysis included 225 participants, and 116 were in the intervention arm. The average age was 33 years, and 38% were women. The median GCS at inclusion was 6. Alcohol was the most frequently implicated toxin, accounting for 67% of observations. Fewer intubations were observed in the intervention group: 19 (16.4%) versus 63 (57.8%). Of the 19 patients eventually intubated in the intervention group, 16 had met at least one emergency intubation criterion. No deaths were recorded across the entire cohort.
In the intervention group, the median duration of stay in the ICU was 0 hours compared with 24.0 hours in the control group, resulting in a relative risk of 0.39. Hospitalization duration was 21.5 hours in the intervention group, compared with 37.0 hours, yielding a relative risk of 0.74. The win ratio (a method of analyzing composite parameters that prioritizes the most clinically significant event) for the composite criterion was 1.85 (P < .001). In a prespecified subgroup analysis, this ratio was 1.70 (P = .02) when the GCS was below 7. It was 1.42 when poisoning was caused by alcohol, benzodiazepines, gamma-hydroxybutyric acid, or gamma-butyrolactone.
It is essential to note, however, that this trial was not conducted blindly, and the Hawthorne effect may have influenced the physician’s decision to intubate or not. Conversely, the study’s strengths include a substantial cohort (225 patients), consideration of various parameters beyond pneumonia from aspiration, with a relative risk reduction of 53%. In addition, the etiology of toxic coma was not established in all cases. Finally, in cases of intubation, the use of a video laryngoscope or stylets was not specified.
In conclusion, for comatose patients with suspected acute poisoning, a conservative strategy aiming to avoid intubation as much as possible is associated with superior clinical benefits, in terms of the composite outcome of in-hospital mortality, duration of stay in intensive care or the hospital, and a decrease in adverse events.
This article was translated from JIM, which is part of the Medscape Professional Network. A version of this article appeared on Medscape.com.
Tracheal intubation is recommended for comatose patients, but its use in individuals with altered consciousness due to acute poisoning remains uncertain. A French team conducted a large randomized trial to assess the risk–benefit ratio of a conservative approach in this context.
Patients with altered consciousness are at high risk for respiratory distress and pneumonia. Acute poisoning, whether from alcohol, drugs, or medications, is a nontraumatic cause of altered consciousness that often leads to intubation. In the United States alone, 20,000 patients with acute poisoning are intubated annually. While this practice aims to prevent the inhalation of gastric content and, consequently, pneumonia, intubation itself can cause hemodynamic instability, hypoxia, difficulties during tube insertion, or dental injuries. Until now, no study had attempted to evaluate the risk–benefit ratio of this practice in cases of toxic coma.
A Randomized Trial
The randomized trial conducted with a parallel, nonblinded design aimed to determine whether abstaining from intubation was equivalent to standard practice in certain situations. The study took place in 20 French emergency services and one intensive care unit. Participants were at least 18 years old with suspected acute poisoning and a Glasgow Coma Scale (GCS) score of less than 9. Pregnant women; prisoners; those requiring immediate intubation because of respiratory distress, cerebral edema, or other critical conditions; and those using cardiotoxic drugs or drugs that could be rapidly antagonized, such as opioids or sedatives, were excluded. Participants were randomized in a 1:1 ratio after hospital stratification. In the control group, the decision to intubate was at the discretion of the attending practitioner.
In the nonintubated by default group (the intervention group), a procedure could be performed later in case of respiratory distress, vomiting, or other complications. If abstaining, patients were closely monitored through oximetry, heart rate, GCS, etc. If intubation was required, it was performed under sedation (sedatives or hypnotics) and succinylcholine or rocuronium, after appropriate preoxygenation. In addition, capnography was recommended later to ensure proper endotracheal tube placement.
The primary outcome was a hierarchical composite outcome combining in-hospital death, duration of stay in the intensive care unit (ICU), and overall hospital stay (up to the 28th day). Secondary outcomes included, besides the aforementioned individual outcomes, the number of patients requiring mechanical ventilation, the proportion of admissions to the ICU, the incidence of pneumonia, and iatrogenic effects related to intubation itself.
Noninvasive Strategy’s Advantages
The primary analysis included 225 participants, and 116 were in the intervention arm. The average age was 33 years, and 38% were women. The median GCS at inclusion was 6. Alcohol was the most frequently implicated toxin, accounting for 67% of observations. Fewer intubations were observed in the intervention group: 19 (16.4%) versus 63 (57.8%). Of the 19 patients eventually intubated in the intervention group, 16 had met at least one emergency intubation criterion. No deaths were recorded across the entire cohort.
In the intervention group, the median duration of stay in the ICU was 0 hours compared with 24.0 hours in the control group, resulting in a relative risk of 0.39. Hospitalization duration was 21.5 hours in the intervention group, compared with 37.0 hours, yielding a relative risk of 0.74. The win ratio (a method of analyzing composite parameters that prioritizes the most clinically significant event) for the composite criterion was 1.85 (P < .001). In a prespecified subgroup analysis, this ratio was 1.70 (P = .02) when the GCS was below 7. It was 1.42 when poisoning was caused by alcohol, benzodiazepines, gamma-hydroxybutyric acid, or gamma-butyrolactone.
It is essential to note, however, that this trial was not conducted blindly, and the Hawthorne effect may have influenced the physician’s decision to intubate or not. Conversely, the study’s strengths include a substantial cohort (225 patients), consideration of various parameters beyond pneumonia from aspiration, with a relative risk reduction of 53%. In addition, the etiology of toxic coma was not established in all cases. Finally, in cases of intubation, the use of a video laryngoscope or stylets was not specified.
In conclusion, for comatose patients with suspected acute poisoning, a conservative strategy aiming to avoid intubation as much as possible is associated with superior clinical benefits, in terms of the composite outcome of in-hospital mortality, duration of stay in intensive care or the hospital, and a decrease in adverse events.
This article was translated from JIM, which is part of the Medscape Professional Network. A version of this article appeared on Medscape.com.
Tracheal intubation is recommended for comatose patients, but its use in individuals with altered consciousness due to acute poisoning remains uncertain. A French team conducted a large randomized trial to assess the risk–benefit ratio of a conservative approach in this context.
Patients with altered consciousness are at high risk for respiratory distress and pneumonia. Acute poisoning, whether from alcohol, drugs, or medications, is a nontraumatic cause of altered consciousness that often leads to intubation. In the United States alone, 20,000 patients with acute poisoning are intubated annually. While this practice aims to prevent the inhalation of gastric content and, consequently, pneumonia, intubation itself can cause hemodynamic instability, hypoxia, difficulties during tube insertion, or dental injuries. Until now, no study had attempted to evaluate the risk–benefit ratio of this practice in cases of toxic coma.
A Randomized Trial
The randomized trial conducted with a parallel, nonblinded design aimed to determine whether abstaining from intubation was equivalent to standard practice in certain situations. The study took place in 20 French emergency services and one intensive care unit. Participants were at least 18 years old with suspected acute poisoning and a Glasgow Coma Scale (GCS) score of less than 9. Pregnant women; prisoners; those requiring immediate intubation because of respiratory distress, cerebral edema, or other critical conditions; and those using cardiotoxic drugs or drugs that could be rapidly antagonized, such as opioids or sedatives, were excluded. Participants were randomized in a 1:1 ratio after hospital stratification. In the control group, the decision to intubate was at the discretion of the attending practitioner.
In the nonintubated by default group (the intervention group), a procedure could be performed later in case of respiratory distress, vomiting, or other complications. If abstaining, patients were closely monitored through oximetry, heart rate, GCS, etc. If intubation was required, it was performed under sedation (sedatives or hypnotics) and succinylcholine or rocuronium, after appropriate preoxygenation. In addition, capnography was recommended later to ensure proper endotracheal tube placement.
The primary outcome was a hierarchical composite outcome combining in-hospital death, duration of stay in the intensive care unit (ICU), and overall hospital stay (up to the 28th day). Secondary outcomes included, besides the aforementioned individual outcomes, the number of patients requiring mechanical ventilation, the proportion of admissions to the ICU, the incidence of pneumonia, and iatrogenic effects related to intubation itself.
Noninvasive Strategy’s Advantages
The primary analysis included 225 participants, and 116 were in the intervention arm. The average age was 33 years, and 38% were women. The median GCS at inclusion was 6. Alcohol was the most frequently implicated toxin, accounting for 67% of observations. Fewer intubations were observed in the intervention group: 19 (16.4%) versus 63 (57.8%). Of the 19 patients eventually intubated in the intervention group, 16 had met at least one emergency intubation criterion. No deaths were recorded across the entire cohort.
In the intervention group, the median duration of stay in the ICU was 0 hours compared with 24.0 hours in the control group, resulting in a relative risk of 0.39. Hospitalization duration was 21.5 hours in the intervention group, compared with 37.0 hours, yielding a relative risk of 0.74. The win ratio (a method of analyzing composite parameters that prioritizes the most clinically significant event) for the composite criterion was 1.85 (P < .001). In a prespecified subgroup analysis, this ratio was 1.70 (P = .02) when the GCS was below 7. It was 1.42 when poisoning was caused by alcohol, benzodiazepines, gamma-hydroxybutyric acid, or gamma-butyrolactone.
It is essential to note, however, that this trial was not conducted blindly, and the Hawthorne effect may have influenced the physician’s decision to intubate or not. Conversely, the study’s strengths include a substantial cohort (225 patients), consideration of various parameters beyond pneumonia from aspiration, with a relative risk reduction of 53%. In addition, the etiology of toxic coma was not established in all cases. Finally, in cases of intubation, the use of a video laryngoscope or stylets was not specified.
In conclusion, for comatose patients with suspected acute poisoning, a conservative strategy aiming to avoid intubation as much as possible is associated with superior clinical benefits, in terms of the composite outcome of in-hospital mortality, duration of stay in intensive care or the hospital, and a decrease in adverse events.
This article was translated from JIM, which is part of the Medscape Professional Network. A version of this article appeared on Medscape.com.
FROM JAMA
Meta-Analysis Highlights Litany of MASLD-Associated Complications, Encouraging New Treatment Targets
, based on a large-scale meta-analysis of longitudinal data.
These findings emphasize the multisystemic nature of MASLD, suggesting that broader treatment targets are needed to reduce systemic events and end organ complications, reported lead author Kai En Chan, MBBS, of the National University of Singapore, and colleagues.
“[D]espite the substantial impact of MASLD, with direct medical costs estimated to reach $103 billion in the United States alone, a comprehensive umbrella meta-analysis of the longitudinal complications associated with MASLD has yet to be conducted,” the investigators wrote in Clinical Gastroenterology and Hepatology, noting that key outcomes associated with sex and disease severity have yet to be elucidated. “A comprehensive understanding of the spectrum of clinical complications associated with MASLD is thus crucial in developing effective disease management strategies and optimizing the allocation of limited healthcare resources.”
To this end, the investigators analyzed data from 129 studies reporting longitudinal risks of clinical outcomes among adults with MASLD. Assessed complications spanned a broad array of organ systems and pathologies. Cardiovascular and oncologic conditions predominated, while chronic kidney disease, liver-related outcomes, gallstone formation, dementia, and reflux esophagitis were also considered.
The analysis revealed significant associations between MASLD and — in ascending level of risk — chronic kidney disease (hazard ratio [HR], 1.38), cardiovascular diseases (HR, 1.43), cancer (HR, 1.54), prediabetes (HR, 1.69), hypertension (HR, 1.75), diabetes (HR, 2.56), and metabolic syndrome (HR, 2.57).
Across cardiovascular diseases, MASLD raised risk of hypertension the most, by 75%. Among cancer types, MASLD increased risk of hepatocellular carcinoma to the greatest degree, by more than fourfold.
No significant sex-specific differences in MASLD-associated risk were detected for cancer, chronic kidney disease, diabetes, or cardiovascular disease, although the investigators urged a cautious interpretation of these findings, since relevant data were scarce.
“It is imperative to understand that MASLD is a complex and multifaceted condition that requires a comprehensive approach to recognition and treatment beyond that of the hepatologist alone,” the investigators wrote.
They also suggested that the link between MASLD and cancer deserves particular attention.
“Although the mechanism by which MASLD gives rise to cardiovascular disease and diabetes has been thoroughly researched, the pathophysiology of MASLD leading to extrahepatic carcinogenesis is less well understood and has been postulated to be linked to chronic inflammation and dysregulation of the gut microbiome in MASLD,” they wrote.
Lastly, considering the multiprong association between MASLD and so many complications, the investigators recommended broader clinical metrics for measuring outcomes in patients with MASLD.
“With the synergistic increases of metabolic diseases globally, treatment targets should in turn act beyond the resolution of fibrosis but also to reduce systemic end organ complications,” they concluded.The investigators disclosed relationships with AbbVie, Echosens, Gilead Sciences, and others.
In a massive meta-analysis of 129 studies that included over 6 million participants, Chan and colleagues evaluated the associations of MASLD with incident hepatic and extrahepatic outcomes. They report numerous associations for MASLD with metabolic, cardiovascular, and renal events as well as with gastrointestinal, hepatobiliary, and other types of cancers.

The unimpeded pace of the obesity pandemic remains a steady driver of the rise in the burden of metabolic syndrome and its components, including MASLD. Thus, approaches to tackle the rising burden of metabolic diseases including MASLD should start with the root driver, obesity. It is also imperative to consider addressing the cardiometabolic milieu in any approach designed to specifically target MASLD/MASH. Lifestyle modifications that include weight loss, smoking cessation, and avoidance of alcohol use may help reduce risks of cardiovascular disease and cancer, the leading causes of death in patients with MASLD. Anticipated pharmacologic therapies for MASH should not only improve liver endpoints but also have a beneficial or, at minimum, neutral extrahepatic effects on coexisting cardiometabolic conditions.
Samer Gawrieh, MD, is professor of clinical medicine in the Division of Gastroenterology and Hepatology at Indiana University School of Medicine, Indianapolis, where he serves as the Director of Hepatology Research and Clinical Fellowship Program. He receives funding for the National Institute of Diabetes and Digestive and Kidney Diseases and the National Institute on Alcohol Abuse and Alcoholism, and research grant support from Zydus and Viking, and serves on safety committees with TransMedics, Pfizer and Spruce.
In a massive meta-analysis of 129 studies that included over 6 million participants, Chan and colleagues evaluated the associations of MASLD with incident hepatic and extrahepatic outcomes. They report numerous associations for MASLD with metabolic, cardiovascular, and renal events as well as with gastrointestinal, hepatobiliary, and other types of cancers.
The unimpeded pace of the obesity pandemic remains a steady driver of the rise in the burden of metabolic syndrome and its components, including MASLD. Thus, approaches to tackle the rising burden of metabolic diseases including MASLD should start with the root driver, obesity. It is also imperative to consider addressing the cardiometabolic milieu in any approach designed to specifically target MASLD/MASH. Lifestyle modifications that include weight loss, smoking cessation, and avoidance of alcohol use may help reduce risks of cardiovascular disease and cancer, the leading causes of death in patients with MASLD. Anticipated pharmacologic therapies for MASH should not only improve liver endpoints but also have a beneficial or, at minimum, neutral extrahepatic effects on coexisting cardiometabolic conditions.
Samer Gawrieh, MD, is professor of clinical medicine in the Division of Gastroenterology and Hepatology at Indiana University School of Medicine, Indianapolis, where he serves as the Director of Hepatology Research and Clinical Fellowship Program. He receives funding for the National Institute of Diabetes and Digestive and Kidney Diseases and the National Institute on Alcohol Abuse and Alcoholism, and research grant support from Zydus and Viking, and serves on safety committees with TransMedics, Pfizer and Spruce.
In a massive meta-analysis of 129 studies that included over 6 million participants, Chan and colleagues evaluated the associations of MASLD with incident hepatic and extrahepatic outcomes. They report numerous associations for MASLD with metabolic, cardiovascular, and renal events as well as with gastrointestinal, hepatobiliary, and other types of cancers.
The unimpeded pace of the obesity pandemic remains a steady driver of the rise in the burden of metabolic syndrome and its components, including MASLD. Thus, approaches to tackle the rising burden of metabolic diseases including MASLD should start with the root driver, obesity. It is also imperative to consider addressing the cardiometabolic milieu in any approach designed to specifically target MASLD/MASH. Lifestyle modifications that include weight loss, smoking cessation, and avoidance of alcohol use may help reduce risks of cardiovascular disease and cancer, the leading causes of death in patients with MASLD. Anticipated pharmacologic therapies for MASH should not only improve liver endpoints but also have a beneficial or, at minimum, neutral extrahepatic effects on coexisting cardiometabolic conditions.
Samer Gawrieh, MD, is professor of clinical medicine in the Division of Gastroenterology and Hepatology at Indiana University School of Medicine, Indianapolis, where he serves as the Director of Hepatology Research and Clinical Fellowship Program. He receives funding for the National Institute of Diabetes and Digestive and Kidney Diseases and the National Institute on Alcohol Abuse and Alcoholism, and research grant support from Zydus and Viking, and serves on safety committees with TransMedics, Pfizer and Spruce.
, based on a large-scale meta-analysis of longitudinal data.
These findings emphasize the multisystemic nature of MASLD, suggesting that broader treatment targets are needed to reduce systemic events and end organ complications, reported lead author Kai En Chan, MBBS, of the National University of Singapore, and colleagues.
“[D]espite the substantial impact of MASLD, with direct medical costs estimated to reach $103 billion in the United States alone, a comprehensive umbrella meta-analysis of the longitudinal complications associated with MASLD has yet to be conducted,” the investigators wrote in Clinical Gastroenterology and Hepatology, noting that key outcomes associated with sex and disease severity have yet to be elucidated. “A comprehensive understanding of the spectrum of clinical complications associated with MASLD is thus crucial in developing effective disease management strategies and optimizing the allocation of limited healthcare resources.”
To this end, the investigators analyzed data from 129 studies reporting longitudinal risks of clinical outcomes among adults with MASLD. Assessed complications spanned a broad array of organ systems and pathologies. Cardiovascular and oncologic conditions predominated, while chronic kidney disease, liver-related outcomes, gallstone formation, dementia, and reflux esophagitis were also considered.
The analysis revealed significant associations between MASLD and — in ascending level of risk — chronic kidney disease (hazard ratio [HR], 1.38), cardiovascular diseases (HR, 1.43), cancer (HR, 1.54), prediabetes (HR, 1.69), hypertension (HR, 1.75), diabetes (HR, 2.56), and metabolic syndrome (HR, 2.57).
Across cardiovascular diseases, MASLD raised risk of hypertension the most, by 75%. Among cancer types, MASLD increased risk of hepatocellular carcinoma to the greatest degree, by more than fourfold.
No significant sex-specific differences in MASLD-associated risk were detected for cancer, chronic kidney disease, diabetes, or cardiovascular disease, although the investigators urged a cautious interpretation of these findings, since relevant data were scarce.
“It is imperative to understand that MASLD is a complex and multifaceted condition that requires a comprehensive approach to recognition and treatment beyond that of the hepatologist alone,” the investigators wrote.
They also suggested that the link between MASLD and cancer deserves particular attention.
“Although the mechanism by which MASLD gives rise to cardiovascular disease and diabetes has been thoroughly researched, the pathophysiology of MASLD leading to extrahepatic carcinogenesis is less well understood and has been postulated to be linked to chronic inflammation and dysregulation of the gut microbiome in MASLD,” they wrote.
Lastly, considering the multiprong association between MASLD and so many complications, the investigators recommended broader clinical metrics for measuring outcomes in patients with MASLD.
“With the synergistic increases of metabolic diseases globally, treatment targets should in turn act beyond the resolution of fibrosis but also to reduce systemic end organ complications,” they concluded.The investigators disclosed relationships with AbbVie, Echosens, Gilead Sciences, and others.
, based on a large-scale meta-analysis of longitudinal data.
These findings emphasize the multisystemic nature of MASLD, suggesting that broader treatment targets are needed to reduce systemic events and end organ complications, reported lead author Kai En Chan, MBBS, of the National University of Singapore, and colleagues.
“[D]espite the substantial impact of MASLD, with direct medical costs estimated to reach $103 billion in the United States alone, a comprehensive umbrella meta-analysis of the longitudinal complications associated with MASLD has yet to be conducted,” the investigators wrote in Clinical Gastroenterology and Hepatology, noting that key outcomes associated with sex and disease severity have yet to be elucidated. “A comprehensive understanding of the spectrum of clinical complications associated with MASLD is thus crucial in developing effective disease management strategies and optimizing the allocation of limited healthcare resources.”
To this end, the investigators analyzed data from 129 studies reporting longitudinal risks of clinical outcomes among adults with MASLD. Assessed complications spanned a broad array of organ systems and pathologies. Cardiovascular and oncologic conditions predominated, while chronic kidney disease, liver-related outcomes, gallstone formation, dementia, and reflux esophagitis were also considered.
The analysis revealed significant associations between MASLD and — in ascending level of risk — chronic kidney disease (hazard ratio [HR], 1.38), cardiovascular diseases (HR, 1.43), cancer (HR, 1.54), prediabetes (HR, 1.69), hypertension (HR, 1.75), diabetes (HR, 2.56), and metabolic syndrome (HR, 2.57).
Across cardiovascular diseases, MASLD raised risk of hypertension the most, by 75%. Among cancer types, MASLD increased risk of hepatocellular carcinoma to the greatest degree, by more than fourfold.
No significant sex-specific differences in MASLD-associated risk were detected for cancer, chronic kidney disease, diabetes, or cardiovascular disease, although the investigators urged a cautious interpretation of these findings, since relevant data were scarce.
“It is imperative to understand that MASLD is a complex and multifaceted condition that requires a comprehensive approach to recognition and treatment beyond that of the hepatologist alone,” the investigators wrote.
They also suggested that the link between MASLD and cancer deserves particular attention.
“Although the mechanism by which MASLD gives rise to cardiovascular disease and diabetes has been thoroughly researched, the pathophysiology of MASLD leading to extrahepatic carcinogenesis is less well understood and has been postulated to be linked to chronic inflammation and dysregulation of the gut microbiome in MASLD,” they wrote.
Lastly, considering the multiprong association between MASLD and so many complications, the investigators recommended broader clinical metrics for measuring outcomes in patients with MASLD.
“With the synergistic increases of metabolic diseases globally, treatment targets should in turn act beyond the resolution of fibrosis but also to reduce systemic end organ complications,” they concluded.The investigators disclosed relationships with AbbVie, Echosens, Gilead Sciences, and others.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
New, Updated Guidelines for Comprehensive Epilepsy Care
The guidelines — the first from the National Association of Epilepsy Centers (NAEC) in a decade — describe the comprehensive services and resources specialized epilepsy centers should provide to improve quality of care for people living with epilepsy.
“In addition to advances in medicine, there has been a shift toward addressing overall well-being beyond seizure management,” Fred A. Lado, MD, PhD, NAEC president and guideline panel cochair, said in a news release. “This includes care for comorbid conditions like anxiety and depression, enhanced communication between the patient and care team, and addressing health disparities in the epilepsy community.
The guidance was developed by a panel of multidisciplinary experts, which is the first time that the NAEC has gone beyond the field of neurology to seek input from other medical specialists and allied health personnel, the panel noted.
“Expanded guidelines are also sorely needed to help centers and hospitals obtain the resources to provide this level of comprehensive care,” said Dr. Lado, regional director of epilepsy and professor of neurology at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York.
An executive summary of the guidelines was published online in Neurology.
A Multidisciplinary Approach
Epilepsy is one of the most common chronic neurologic conditions worldwide, affecting an estimated 3.4 million people in the United States alone. Recurring seizures can be debilitating and, in some cases, life-threatening.
To update epilepsy care guidelines, an expert panel of 41 stakeholders with diverse expertise evaluated the latest evidence and reached consensus on 52 recommendations spanning a range of services that make up high-quality epilepsy care.
“This is exhibited in a greater emphasis on multidisciplinary care conferences, screening for comorbidities of epilepsy, and providing access to other specialty services in addition to the core epilepsy center components of outpatient care, diagnostic procedures, and epilepsy surgery,” they wrote.
For the first time, the guidelines advise specialized epilepsy centers to offer genetic testing and counseling, provide more education and communication for patients, give greater attention to special-needs populations, employ a care coordinator to organize and facilitate multidisciplinary care, provide mental health screening, and address health disparities and inequities.
“All recommendations quickly reached consensus despite there being such a diverse panel of stakeholders, which emphasizes that the recommendations reflect the important elements of healthcare services that should be in place for an epilepsy center to provide the highest quality of care,” said Susan Arnold, MD, guideline panel co-chair and a pediatric epileptologist at Yale University School of Medicine, New Haven, Connecticut.
“But epilepsy centers will need the resources to provide this comprehensive level of care. We hope the guidelines will help increase health insurer and institutional support and recognition of these recommendations,” Dr. Arnold added.
The guidelines were funded by NAEC. Dr. Lado has no relevant disclosures. Dr. Arnold holds stock in Pfizer. A complete list of disclosures for the guideline panel is available with the original article.
A version of this article appeared on Medscape.com.
The guidelines — the first from the National Association of Epilepsy Centers (NAEC) in a decade — describe the comprehensive services and resources specialized epilepsy centers should provide to improve quality of care for people living with epilepsy.
“In addition to advances in medicine, there has been a shift toward addressing overall well-being beyond seizure management,” Fred A. Lado, MD, PhD, NAEC president and guideline panel cochair, said in a news release. “This includes care for comorbid conditions like anxiety and depression, enhanced communication between the patient and care team, and addressing health disparities in the epilepsy community.
The guidance was developed by a panel of multidisciplinary experts, which is the first time that the NAEC has gone beyond the field of neurology to seek input from other medical specialists and allied health personnel, the panel noted.
“Expanded guidelines are also sorely needed to help centers and hospitals obtain the resources to provide this level of comprehensive care,” said Dr. Lado, regional director of epilepsy and professor of neurology at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York.
An executive summary of the guidelines was published online in Neurology.
A Multidisciplinary Approach
Epilepsy is one of the most common chronic neurologic conditions worldwide, affecting an estimated 3.4 million people in the United States alone. Recurring seizures can be debilitating and, in some cases, life-threatening.
To update epilepsy care guidelines, an expert panel of 41 stakeholders with diverse expertise evaluated the latest evidence and reached consensus on 52 recommendations spanning a range of services that make up high-quality epilepsy care.
“This is exhibited in a greater emphasis on multidisciplinary care conferences, screening for comorbidities of epilepsy, and providing access to other specialty services in addition to the core epilepsy center components of outpatient care, diagnostic procedures, and epilepsy surgery,” they wrote.
For the first time, the guidelines advise specialized epilepsy centers to offer genetic testing and counseling, provide more education and communication for patients, give greater attention to special-needs populations, employ a care coordinator to organize and facilitate multidisciplinary care, provide mental health screening, and address health disparities and inequities.
“All recommendations quickly reached consensus despite there being such a diverse panel of stakeholders, which emphasizes that the recommendations reflect the important elements of healthcare services that should be in place for an epilepsy center to provide the highest quality of care,” said Susan Arnold, MD, guideline panel co-chair and a pediatric epileptologist at Yale University School of Medicine, New Haven, Connecticut.
“But epilepsy centers will need the resources to provide this comprehensive level of care. We hope the guidelines will help increase health insurer and institutional support and recognition of these recommendations,” Dr. Arnold added.
The guidelines were funded by NAEC. Dr. Lado has no relevant disclosures. Dr. Arnold holds stock in Pfizer. A complete list of disclosures for the guideline panel is available with the original article.
A version of this article appeared on Medscape.com.
The guidelines — the first from the National Association of Epilepsy Centers (NAEC) in a decade — describe the comprehensive services and resources specialized epilepsy centers should provide to improve quality of care for people living with epilepsy.
“In addition to advances in medicine, there has been a shift toward addressing overall well-being beyond seizure management,” Fred A. Lado, MD, PhD, NAEC president and guideline panel cochair, said in a news release. “This includes care for comorbid conditions like anxiety and depression, enhanced communication between the patient and care team, and addressing health disparities in the epilepsy community.
The guidance was developed by a panel of multidisciplinary experts, which is the first time that the NAEC has gone beyond the field of neurology to seek input from other medical specialists and allied health personnel, the panel noted.
“Expanded guidelines are also sorely needed to help centers and hospitals obtain the resources to provide this level of comprehensive care,” said Dr. Lado, regional director of epilepsy and professor of neurology at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York.
An executive summary of the guidelines was published online in Neurology.
A Multidisciplinary Approach
Epilepsy is one of the most common chronic neurologic conditions worldwide, affecting an estimated 3.4 million people in the United States alone. Recurring seizures can be debilitating and, in some cases, life-threatening.
To update epilepsy care guidelines, an expert panel of 41 stakeholders with diverse expertise evaluated the latest evidence and reached consensus on 52 recommendations spanning a range of services that make up high-quality epilepsy care.
“This is exhibited in a greater emphasis on multidisciplinary care conferences, screening for comorbidities of epilepsy, and providing access to other specialty services in addition to the core epilepsy center components of outpatient care, diagnostic procedures, and epilepsy surgery,” they wrote.
For the first time, the guidelines advise specialized epilepsy centers to offer genetic testing and counseling, provide more education and communication for patients, give greater attention to special-needs populations, employ a care coordinator to organize and facilitate multidisciplinary care, provide mental health screening, and address health disparities and inequities.
“All recommendations quickly reached consensus despite there being such a diverse panel of stakeholders, which emphasizes that the recommendations reflect the important elements of healthcare services that should be in place for an epilepsy center to provide the highest quality of care,” said Susan Arnold, MD, guideline panel co-chair and a pediatric epileptologist at Yale University School of Medicine, New Haven, Connecticut.
“But epilepsy centers will need the resources to provide this comprehensive level of care. We hope the guidelines will help increase health insurer and institutional support and recognition of these recommendations,” Dr. Arnold added.
The guidelines were funded by NAEC. Dr. Lado has no relevant disclosures. Dr. Arnold holds stock in Pfizer. A complete list of disclosures for the guideline panel is available with the original article.
A version of this article appeared on Medscape.com.
FROM NEUROLOGY
Diagnosis and Treatment Options for Polycythemia Vera

Dr. Richard: The first thing we as physicians are worried about is patients with PV developing thrombosis. We start prophylaxis with aspirin, as aspirin remains the best treatment for reducing this risk. It is essential to make sure patients with PV understand the importance of taking an aspirin, even at a low dosage.
The second step is trying to control patients’ red blood cell counts. Phlebotomy has been used for this purpose for many decades and continues to be effective. You will find some experts in the field who consider phlebotomy to be the mainstay of treatment for patients with PV, and that it has benefits in and of itself.
However, despite the benefits, phlebotomy can be a little tough on patients. For instance, patients with PV cannot donate blood at a traditional blood center such as Red Cross, and therefore need to go to an actual infusion center. They also must stop their day and travel to a site to receive therapeutic phlebotomy treatment, which is most effective for patients with a blood disorder. I work in Seattle taking care of patients throughout the Northwest, and it is not always easy to find a close location to send patients for phlebotomy. Nevertheless, phlebotomy should be part of the treatment options for patients with PV, especially patients in the high-risk range who have high hemoglobin and hematocrit values.
The third step is controlling hemoglobin and hematocrit levels. Hydroxyurea is our standard of care with strong beneficial data for this purpose.
These are the 3 approaches to treatment we initially discuss with our patients during their first visit. These 3 strategies can improve a patient's life and reduce their risk for thrombosis.
Which treatment do you recommend depending on the patient’s symptoms?
Dr. Richard: The treatment that we offer can vary. The first thing I want to know is how their symptoms respond to aspirin. For instance, symptoms such as erythromelalgia oftentimes respond beautifully to aspirin. Most patients do not have massive splenomegaly—that would give me a high suspicion for myelofibrosis—but they can develop and present with some level of splenomegaly.
If the symptoms are bothersome to the patient, I will probably want to get them on some kind of cytoreduction to see if that is effective. Hydroxyurea, although not as effective as aspirin and associated with adverse effects in some patients, is a good medication to start cytoreductive therapy. The National Comprehensive Cancer Network® (NCCN®) Guidelines suggest that if a patient taking hydroxyurea experiences severe gastrointestinal (GI) toxicity, go ahead and move to a Janus kinase 2 (JAK2) inhibitor or try interferon. JAK2 inhibition with ruxolitinib, in this case, is effective, at least initially for treating splenomegaly. Unfortunately, symptoms sometimes get confused with effects from the medications. You have to use an individualized treatment approach and see what works for each patient.
What are some of the common adverse effects of treatment?
Dr. Richard: As you probably can tell, I never skip aspirin since it is such an important part of treatment for patients with PV. However, I do talk to patients about GI upset and the bleeding risks, such as the potential for GI bleed. Obviously, clotting is what causes an increase in morbidity and mortality, but bleeding can be an important adverse effect with platelets that do not function, or for other issues.
Hydroxyurea is generally well tolerated, but some patients can develop skin issues or ulcers due to GI toxicity. I have a lot of confidence in the use of hydroxyurea, and I use it without hesitation. However, you may have a patient who already has a relatively low neutrophil count or has some level of thrombocytopenia from either liver disease or some other issue, and they just cannot tolerate hydroxyurea. Some other bothersome symptoms include change of taste, skin changes, and brittle nails. It can be tricky. I will attempt hydroxyurea, if needed, but sometimes they just cannot tolerate it.
What happens when a patient cannot tolerate one or all the medications you mentioned?
Dr. Richard: Now that we have JAK2 inhibitors, ruxolitinib is generally my choice for patients who cannot tolerate hydroxyurea, which is more common than maybe we would like. Other problems with hydroxyurea include that it might not work, or phlebotomy combined with hydroxyurea results in cytopenias, or patients have a particularly aggressive form of PV.
There are numerous other JAK2 drug inhibitors on the market for myelofibrosis. The assumption is they probably work as well as ruxolitinib for PV, but right now ruxolitinib is what is approved by the US Food and Drug Administration for these patients.
The other drug that we do not use much is interferon, or now, pegylated interferon. It is a drug that has been around for a long time and worked well in chronic myelogenous leukemia before we had the tyrosine kinase inhibitors. Pegylated interferon is a well-tolerated drug that can be used for patients with PV who are pregnant or could get pregnant. It is not the interferon of our parents or grandparents. We now have options for controlling the disease and its complications, but the hardest thing is to tell patients that none of these treatments are going to cure them or reverse the overproduction of red blood cells in their bone marrow. There has always been discussion about whether there could be some effect of interferon on the actual tumor burden, but that remains to be proven.
Can you go a little bit more into your recommended approach to managing newly diagnosed patients with PV in your day-to-day practice?
Dr. Richard: Oftentimes these patients are identified through our consultation service. It can be hard on the primary care physician to identify whether a patient has secondary or primary PV.
We are lucky now that JAK2 has been identified. The JAK2-V617F and the other exon 12 mutations were identified back in 2006 by several groups and is a great test. With JAK2 along with an erythropoietin test, you can feel confident whether you have identified PV.
PV encompasses a wide variety of syndromes. Patients can come into the office with terrible symptoms, including aquagenic pruritus or erythromelalgia. I have seen young people in their 30s who happen to have a slightly elevated hematocrit and a positive JAK2 test. When this occurs, you try to understand how much the disease is affecting their life, whether they are going to be in a high-risk category or a low-risk category, whether they have had thrombosis, and how their age figures into all of it. To try to figure out this high-risk versus low-risk factor, we use a simple staging system to help determine whether they are going to need cytoreductive therapy or whether you can just start with phlebotomy and see how they do.
Oftentimes in the first visit, I recommend a bone marrow study. Is that going to be true 5 years from now? I am not sure. You know, next-generation sequencing (NGS) is turning into such an important part of determining prognosis in these patients. It helps if you have a great colleague down in hematopathology who can look at the bone marrow as it relates to megakaryocyte morphology, or whether there is early fibrosis.
Although these techniques may not be as prominent in practice today for determining diagnosis, they help us understand the prognosis. A bone marrow study or NGS is particularly useful when you have patients who you are convinced have PV, but it turns out they already have extensive fibrosis and are actually moving more toward the post-polycythemia phase a little faster than you think. While we do not use an allogeneic transplant often, in this scenario we may recommend it. Our primary goal at this point is to try to determine which patients would benefit from a transplant early on and to prepare the patient for this option.
What socioeconomic disparities have you observed in newly diagnosed patients?
Dr. Richard: There are definitely social disparities for people who have low income. I work in a veteran’s hospital where we take care of a lot of people who do not have health insurance, but who come to the VA because they do have benefits. If they are in our system, they get identified and their care is great. However, if they have been out in the regular system without health insurance, oftentimes they get diagnosed late. Identifying and treating patients from low socioeconomic backgrounds is an issue. I think everyone can agree with that.
We have a delicate situation with women veterans. Something that is incredibly painful that I think people should be aware of is the amount of military sexual trauma (MST) that has occurred over the years. These patients are in a unique place of trust with their care providers. They have spent a lot of time not being listened to in a variety of arenas. I see this in young military women who no one expects to have a stem cell disorder. We as health care providers do them a disservice if their complaints lead to referral to a psychotherapist or being prescribed a nonsteroidal anti-inflammatory drug or something like that. As health care providers, we are in a unique position to listen to and accurately evaluate these patients. We have a large population of veterans and, increasingly more women veterans, but I think we can all agree that they need better care, especially if they have suffered from MST. That is what I see in my patient population.
When I was a resident in Baltimore, it was Black people with lower income who did not trust doctors. We still have a lot of work to do.
Dr. Richard: The first thing we as physicians are worried about is patients with PV developing thrombosis. We start prophylaxis with aspirin, as aspirin remains the best treatment for reducing this risk. It is essential to make sure patients with PV understand the importance of taking an aspirin, even at a low dosage.
The second step is trying to control patients’ red blood cell counts. Phlebotomy has been used for this purpose for many decades and continues to be effective. You will find some experts in the field who consider phlebotomy to be the mainstay of treatment for patients with PV, and that it has benefits in and of itself.
However, despite the benefits, phlebotomy can be a little tough on patients. For instance, patients with PV cannot donate blood at a traditional blood center such as Red Cross, and therefore need to go to an actual infusion center. They also must stop their day and travel to a site to receive therapeutic phlebotomy treatment, which is most effective for patients with a blood disorder. I work in Seattle taking care of patients throughout the Northwest, and it is not always easy to find a close location to send patients for phlebotomy. Nevertheless, phlebotomy should be part of the treatment options for patients with PV, especially patients in the high-risk range who have high hemoglobin and hematocrit values.
The third step is controlling hemoglobin and hematocrit levels. Hydroxyurea is our standard of care with strong beneficial data for this purpose.
These are the 3 approaches to treatment we initially discuss with our patients during their first visit. These 3 strategies can improve a patient's life and reduce their risk for thrombosis.
Which treatment do you recommend depending on the patient’s symptoms?
Dr. Richard: The treatment that we offer can vary. The first thing I want to know is how their symptoms respond to aspirin. For instance, symptoms such as erythromelalgia oftentimes respond beautifully to aspirin. Most patients do not have massive splenomegaly—that would give me a high suspicion for myelofibrosis—but they can develop and present with some level of splenomegaly.
If the symptoms are bothersome to the patient, I will probably want to get them on some kind of cytoreduction to see if that is effective. Hydroxyurea, although not as effective as aspirin and associated with adverse effects in some patients, is a good medication to start cytoreductive therapy. The National Comprehensive Cancer Network® (NCCN®) Guidelines suggest that if a patient taking hydroxyurea experiences severe gastrointestinal (GI) toxicity, go ahead and move to a Janus kinase 2 (JAK2) inhibitor or try interferon. JAK2 inhibition with ruxolitinib, in this case, is effective, at least initially for treating splenomegaly. Unfortunately, symptoms sometimes get confused with effects from the medications. You have to use an individualized treatment approach and see what works for each patient.
What are some of the common adverse effects of treatment?
Dr. Richard: As you probably can tell, I never skip aspirin since it is such an important part of treatment for patients with PV. However, I do talk to patients about GI upset and the bleeding risks, such as the potential for GI bleed. Obviously, clotting is what causes an increase in morbidity and mortality, but bleeding can be an important adverse effect with platelets that do not function, or for other issues.
Hydroxyurea is generally well tolerated, but some patients can develop skin issues or ulcers due to GI toxicity. I have a lot of confidence in the use of hydroxyurea, and I use it without hesitation. However, you may have a patient who already has a relatively low neutrophil count or has some level of thrombocytopenia from either liver disease or some other issue, and they just cannot tolerate hydroxyurea. Some other bothersome symptoms include change of taste, skin changes, and brittle nails. It can be tricky. I will attempt hydroxyurea, if needed, but sometimes they just cannot tolerate it.
What happens when a patient cannot tolerate one or all the medications you mentioned?
Dr. Richard: Now that we have JAK2 inhibitors, ruxolitinib is generally my choice for patients who cannot tolerate hydroxyurea, which is more common than maybe we would like. Other problems with hydroxyurea include that it might not work, or phlebotomy combined with hydroxyurea results in cytopenias, or patients have a particularly aggressive form of PV.
There are numerous other JAK2 drug inhibitors on the market for myelofibrosis. The assumption is they probably work as well as ruxolitinib for PV, but right now ruxolitinib is what is approved by the US Food and Drug Administration for these patients.
The other drug that we do not use much is interferon, or now, pegylated interferon. It is a drug that has been around for a long time and worked well in chronic myelogenous leukemia before we had the tyrosine kinase inhibitors. Pegylated interferon is a well-tolerated drug that can be used for patients with PV who are pregnant or could get pregnant. It is not the interferon of our parents or grandparents. We now have options for controlling the disease and its complications, but the hardest thing is to tell patients that none of these treatments are going to cure them or reverse the overproduction of red blood cells in their bone marrow. There has always been discussion about whether there could be some effect of interferon on the actual tumor burden, but that remains to be proven.
Can you go a little bit more into your recommended approach to managing newly diagnosed patients with PV in your day-to-day practice?
Dr. Richard: Oftentimes these patients are identified through our consultation service. It can be hard on the primary care physician to identify whether a patient has secondary or primary PV.
We are lucky now that JAK2 has been identified. The JAK2-V617F and the other exon 12 mutations were identified back in 2006 by several groups and is a great test. With JAK2 along with an erythropoietin test, you can feel confident whether you have identified PV.
PV encompasses a wide variety of syndromes. Patients can come into the office with terrible symptoms, including aquagenic pruritus or erythromelalgia. I have seen young people in their 30s who happen to have a slightly elevated hematocrit and a positive JAK2 test. When this occurs, you try to understand how much the disease is affecting their life, whether they are going to be in a high-risk category or a low-risk category, whether they have had thrombosis, and how their age figures into all of it. To try to figure out this high-risk versus low-risk factor, we use a simple staging system to help determine whether they are going to need cytoreductive therapy or whether you can just start with phlebotomy and see how they do.
Oftentimes in the first visit, I recommend a bone marrow study. Is that going to be true 5 years from now? I am not sure. You know, next-generation sequencing (NGS) is turning into such an important part of determining prognosis in these patients. It helps if you have a great colleague down in hematopathology who can look at the bone marrow as it relates to megakaryocyte morphology, or whether there is early fibrosis.
Although these techniques may not be as prominent in practice today for determining diagnosis, they help us understand the prognosis. A bone marrow study or NGS is particularly useful when you have patients who you are convinced have PV, but it turns out they already have extensive fibrosis and are actually moving more toward the post-polycythemia phase a little faster than you think. While we do not use an allogeneic transplant often, in this scenario we may recommend it. Our primary goal at this point is to try to determine which patients would benefit from a transplant early on and to prepare the patient for this option.
What socioeconomic disparities have you observed in newly diagnosed patients?
Dr. Richard: There are definitely social disparities for people who have low income. I work in a veteran’s hospital where we take care of a lot of people who do not have health insurance, but who come to the VA because they do have benefits. If they are in our system, they get identified and their care is great. However, if they have been out in the regular system without health insurance, oftentimes they get diagnosed late. Identifying and treating patients from low socioeconomic backgrounds is an issue. I think everyone can agree with that.
We have a delicate situation with women veterans. Something that is incredibly painful that I think people should be aware of is the amount of military sexual trauma (MST) that has occurred over the years. These patients are in a unique place of trust with their care providers. They have spent a lot of time not being listened to in a variety of arenas. I see this in young military women who no one expects to have a stem cell disorder. We as health care providers do them a disservice if their complaints lead to referral to a psychotherapist or being prescribed a nonsteroidal anti-inflammatory drug or something like that. As health care providers, we are in a unique position to listen to and accurately evaluate these patients. We have a large population of veterans and, increasingly more women veterans, but I think we can all agree that they need better care, especially if they have suffered from MST. That is what I see in my patient population.
When I was a resident in Baltimore, it was Black people with lower income who did not trust doctors. We still have a lot of work to do.
Dr. Richard: The first thing we as physicians are worried about is patients with PV developing thrombosis. We start prophylaxis with aspirin, as aspirin remains the best treatment for reducing this risk. It is essential to make sure patients with PV understand the importance of taking an aspirin, even at a low dosage.
The second step is trying to control patients’ red blood cell counts. Phlebotomy has been used for this purpose for many decades and continues to be effective. You will find some experts in the field who consider phlebotomy to be the mainstay of treatment for patients with PV, and that it has benefits in and of itself.
However, despite the benefits, phlebotomy can be a little tough on patients. For instance, patients with PV cannot donate blood at a traditional blood center such as Red Cross, and therefore need to go to an actual infusion center. They also must stop their day and travel to a site to receive therapeutic phlebotomy treatment, which is most effective for patients with a blood disorder. I work in Seattle taking care of patients throughout the Northwest, and it is not always easy to find a close location to send patients for phlebotomy. Nevertheless, phlebotomy should be part of the treatment options for patients with PV, especially patients in the high-risk range who have high hemoglobin and hematocrit values.
The third step is controlling hemoglobin and hematocrit levels. Hydroxyurea is our standard of care with strong beneficial data for this purpose.
These are the 3 approaches to treatment we initially discuss with our patients during their first visit. These 3 strategies can improve a patient's life and reduce their risk for thrombosis.
Which treatment do you recommend depending on the patient’s symptoms?
Dr. Richard: The treatment that we offer can vary. The first thing I want to know is how their symptoms respond to aspirin. For instance, symptoms such as erythromelalgia oftentimes respond beautifully to aspirin. Most patients do not have massive splenomegaly—that would give me a high suspicion for myelofibrosis—but they can develop and present with some level of splenomegaly.
If the symptoms are bothersome to the patient, I will probably want to get them on some kind of cytoreduction to see if that is effective. Hydroxyurea, although not as effective as aspirin and associated with adverse effects in some patients, is a good medication to start cytoreductive therapy. The National Comprehensive Cancer Network® (NCCN®) Guidelines suggest that if a patient taking hydroxyurea experiences severe gastrointestinal (GI) toxicity, go ahead and move to a Janus kinase 2 (JAK2) inhibitor or try interferon. JAK2 inhibition with ruxolitinib, in this case, is effective, at least initially for treating splenomegaly. Unfortunately, symptoms sometimes get confused with effects from the medications. You have to use an individualized treatment approach and see what works for each patient.
What are some of the common adverse effects of treatment?
Dr. Richard: As you probably can tell, I never skip aspirin since it is such an important part of treatment for patients with PV. However, I do talk to patients about GI upset and the bleeding risks, such as the potential for GI bleed. Obviously, clotting is what causes an increase in morbidity and mortality, but bleeding can be an important adverse effect with platelets that do not function, or for other issues.
Hydroxyurea is generally well tolerated, but some patients can develop skin issues or ulcers due to GI toxicity. I have a lot of confidence in the use of hydroxyurea, and I use it without hesitation. However, you may have a patient who already has a relatively low neutrophil count or has some level of thrombocytopenia from either liver disease or some other issue, and they just cannot tolerate hydroxyurea. Some other bothersome symptoms include change of taste, skin changes, and brittle nails. It can be tricky. I will attempt hydroxyurea, if needed, but sometimes they just cannot tolerate it.
What happens when a patient cannot tolerate one or all the medications you mentioned?
Dr. Richard: Now that we have JAK2 inhibitors, ruxolitinib is generally my choice for patients who cannot tolerate hydroxyurea, which is more common than maybe we would like. Other problems with hydroxyurea include that it might not work, or phlebotomy combined with hydroxyurea results in cytopenias, or patients have a particularly aggressive form of PV.
There are numerous other JAK2 drug inhibitors on the market for myelofibrosis. The assumption is they probably work as well as ruxolitinib for PV, but right now ruxolitinib is what is approved by the US Food and Drug Administration for these patients.
The other drug that we do not use much is interferon, or now, pegylated interferon. It is a drug that has been around for a long time and worked well in chronic myelogenous leukemia before we had the tyrosine kinase inhibitors. Pegylated interferon is a well-tolerated drug that can be used for patients with PV who are pregnant or could get pregnant. It is not the interferon of our parents or grandparents. We now have options for controlling the disease and its complications, but the hardest thing is to tell patients that none of these treatments are going to cure them or reverse the overproduction of red blood cells in their bone marrow. There has always been discussion about whether there could be some effect of interferon on the actual tumor burden, but that remains to be proven.
Can you go a little bit more into your recommended approach to managing newly diagnosed patients with PV in your day-to-day practice?
Dr. Richard: Oftentimes these patients are identified through our consultation service. It can be hard on the primary care physician to identify whether a patient has secondary or primary PV.
We are lucky now that JAK2 has been identified. The JAK2-V617F and the other exon 12 mutations were identified back in 2006 by several groups and is a great test. With JAK2 along with an erythropoietin test, you can feel confident whether you have identified PV.
PV encompasses a wide variety of syndromes. Patients can come into the office with terrible symptoms, including aquagenic pruritus or erythromelalgia. I have seen young people in their 30s who happen to have a slightly elevated hematocrit and a positive JAK2 test. When this occurs, you try to understand how much the disease is affecting their life, whether they are going to be in a high-risk category or a low-risk category, whether they have had thrombosis, and how their age figures into all of it. To try to figure out this high-risk versus low-risk factor, we use a simple staging system to help determine whether they are going to need cytoreductive therapy or whether you can just start with phlebotomy and see how they do.
Oftentimes in the first visit, I recommend a bone marrow study. Is that going to be true 5 years from now? I am not sure. You know, next-generation sequencing (NGS) is turning into such an important part of determining prognosis in these patients. It helps if you have a great colleague down in hematopathology who can look at the bone marrow as it relates to megakaryocyte morphology, or whether there is early fibrosis.
Although these techniques may not be as prominent in practice today for determining diagnosis, they help us understand the prognosis. A bone marrow study or NGS is particularly useful when you have patients who you are convinced have PV, but it turns out they already have extensive fibrosis and are actually moving more toward the post-polycythemia phase a little faster than you think. While we do not use an allogeneic transplant often, in this scenario we may recommend it. Our primary goal at this point is to try to determine which patients would benefit from a transplant early on and to prepare the patient for this option.
What socioeconomic disparities have you observed in newly diagnosed patients?
Dr. Richard: There are definitely social disparities for people who have low income. I work in a veteran’s hospital where we take care of a lot of people who do not have health insurance, but who come to the VA because they do have benefits. If they are in our system, they get identified and their care is great. However, if they have been out in the regular system without health insurance, oftentimes they get diagnosed late. Identifying and treating patients from low socioeconomic backgrounds is an issue. I think everyone can agree with that.
We have a delicate situation with women veterans. Something that is incredibly painful that I think people should be aware of is the amount of military sexual trauma (MST) that has occurred over the years. These patients are in a unique place of trust with their care providers. They have spent a lot of time not being listened to in a variety of arenas. I see this in young military women who no one expects to have a stem cell disorder. We as health care providers do them a disservice if their complaints lead to referral to a psychotherapist or being prescribed a nonsteroidal anti-inflammatory drug or something like that. As health care providers, we are in a unique position to listen to and accurately evaluate these patients. We have a large population of veterans and, increasingly more women veterans, but I think we can all agree that they need better care, especially if they have suffered from MST. That is what I see in my patient population.
When I was a resident in Baltimore, it was Black people with lower income who did not trust doctors. We still have a lot of work to do.
AGA Gives Guidance on Subepithelial Lesions
The new guidance document, authored by Lionel S. D’Souza, MD, of Stony Brook University Hospital, Stony Brook, New York, and colleagues, offers a framework for deciding between various EFTR techniques based on lesion histology, size, and location.
“EFTR has emerged as a novel treatment option for select SELs,” the update panelists wrote in Gastroenterology. “In this commentary, we reviewed the different techniques and uses of EFTR for the management of SELs.”

They noted that all patients with SELs should first undergo multidisciplinary evaluation in accordance with a separate AGA guidance document on SELs.
The present update focuses specifically on EFTR, first by distinguishing between exposed and nonexposed techniques. While the former involves resection of the mucosa and all other layers of the wall, the latter relies upon a ‘close first, then cut’ method to prevent perforation, or preservation of an overlying flap of mucosa.
The new guidance calls for a nonexposed technique unless the exposed approach is necessary.
“In our opinion, the exposed EFTR technique should be considered for lesions in which other methods (i.e., endoscopic mucosal resection, endoscopic submucosal dissection, and nonexposed EFTR) cannot reliably and completely excise SELs due to larger size or difficult location of the lesion,” the update panelists wrote. “The exposed EFTR technique may be best suited for gastric lesions and as an alternative to other endoscopic approaches for SELs in the rectum. The exposed technique should be avoided in the esophagus and duodenum, as the clinical consequences of a leak can be devastating and endoscopic closure is notoriously challenging.”
Dr. D’Souza and colleagues went on to discuss various nonexposed techniques, including submucosal tunneling and endoscopic resection and peroral endoscopic tunnel resection (STER/POET), device-assisted endoscopic full-thickness resection, and full-thickness resection with an over-the-scope clip with integrated snare (FTRD).
They highlighted how STER/POET encourages traction on the lesion and scope stability while limiting extravasation of luminal contents, and closure tends to be easier than with exposed EFTR. This approach should be reserved for tumors smaller than approximately 3-4 cm, however, with the update noting that lesions larger than 2 cm may present increased risk of incomplete resection. Similarly, device-assisted endoscopic full-thickness resection, which involves pulling or suctioning the lesion into the device, is also limited by lesion size, although fewer data are available to guide size thresholds.
FTRD, which involves “a 23-mm deep cap with a specially designed over-the-scope clip and integrated cautery snare,” also lacks a broad evidence base.
“Although there has been reasonable clinical success reported in most case series, several factors should be considered with the use of the FTRD for SELs,” the update cautions.
Specifically, a recent Dutch and German registry study of FTRD had an adverse event rate of 11.3%, with an approximate 1% perforation rate. More than half of the perforations were due to technical or procedural issues.
“This adverse event rate may improve as individual experience with the device is gained; however, data on this are lacking,” the panelists wrote, also noting that lesions 1.5 cm or larger may carry a higher risk of incomplete resection.
Ultimately, the clinical practice update calls for a personalized approach to EFTR decision-making that considers factors extending beyond the lesion.
“The ‘ideal’ technique will depend on various patient and lesion characteristics, as well as the endoscopist’s preference and available expertise,” Dr. D’Souza and colleagues concluded. “Further research into the efficacy of these resection techniques and the long-term outcomes in patients after endoscopic resection of SELs will be essential in standardizing appropriate resection algorithms.”
This clinical practice update was commissioned and approved by AGA Institute. The investigators disclosed relationships with Olympus, Fujifilm, Apollo Endosurgery, and others.
The new guidance document, authored by Lionel S. D’Souza, MD, of Stony Brook University Hospital, Stony Brook, New York, and colleagues, offers a framework for deciding between various EFTR techniques based on lesion histology, size, and location.
“EFTR has emerged as a novel treatment option for select SELs,” the update panelists wrote in Gastroenterology. “In this commentary, we reviewed the different techniques and uses of EFTR for the management of SELs.”
They noted that all patients with SELs should first undergo multidisciplinary evaluation in accordance with a separate AGA guidance document on SELs.
The present update focuses specifically on EFTR, first by distinguishing between exposed and nonexposed techniques. While the former involves resection of the mucosa and all other layers of the wall, the latter relies upon a ‘close first, then cut’ method to prevent perforation, or preservation of an overlying flap of mucosa.
The new guidance calls for a nonexposed technique unless the exposed approach is necessary.
“In our opinion, the exposed EFTR technique should be considered for lesions in which other methods (i.e., endoscopic mucosal resection, endoscopic submucosal dissection, and nonexposed EFTR) cannot reliably and completely excise SELs due to larger size or difficult location of the lesion,” the update panelists wrote. “The exposed EFTR technique may be best suited for gastric lesions and as an alternative to other endoscopic approaches for SELs in the rectum. The exposed technique should be avoided in the esophagus and duodenum, as the clinical consequences of a leak can be devastating and endoscopic closure is notoriously challenging.”
Dr. D’Souza and colleagues went on to discuss various nonexposed techniques, including submucosal tunneling and endoscopic resection and peroral endoscopic tunnel resection (STER/POET), device-assisted endoscopic full-thickness resection, and full-thickness resection with an over-the-scope clip with integrated snare (FTRD).
They highlighted how STER/POET encourages traction on the lesion and scope stability while limiting extravasation of luminal contents, and closure tends to be easier than with exposed EFTR. This approach should be reserved for tumors smaller than approximately 3-4 cm, however, with the update noting that lesions larger than 2 cm may present increased risk of incomplete resection. Similarly, device-assisted endoscopic full-thickness resection, which involves pulling or suctioning the lesion into the device, is also limited by lesion size, although fewer data are available to guide size thresholds.
FTRD, which involves “a 23-mm deep cap with a specially designed over-the-scope clip and integrated cautery snare,” also lacks a broad evidence base.
“Although there has been reasonable clinical success reported in most case series, several factors should be considered with the use of the FTRD for SELs,” the update cautions.
Specifically, a recent Dutch and German registry study of FTRD had an adverse event rate of 11.3%, with an approximate 1% perforation rate. More than half of the perforations were due to technical or procedural issues.
“This adverse event rate may improve as individual experience with the device is gained; however, data on this are lacking,” the panelists wrote, also noting that lesions 1.5 cm or larger may carry a higher risk of incomplete resection.
Ultimately, the clinical practice update calls for a personalized approach to EFTR decision-making that considers factors extending beyond the lesion.
“The ‘ideal’ technique will depend on various patient and lesion characteristics, as well as the endoscopist’s preference and available expertise,” Dr. D’Souza and colleagues concluded. “Further research into the efficacy of these resection techniques and the long-term outcomes in patients after endoscopic resection of SELs will be essential in standardizing appropriate resection algorithms.”
This clinical practice update was commissioned and approved by AGA Institute. The investigators disclosed relationships with Olympus, Fujifilm, Apollo Endosurgery, and others.
The new guidance document, authored by Lionel S. D’Souza, MD, of Stony Brook University Hospital, Stony Brook, New York, and colleagues, offers a framework for deciding between various EFTR techniques based on lesion histology, size, and location.
“EFTR has emerged as a novel treatment option for select SELs,” the update panelists wrote in Gastroenterology. “In this commentary, we reviewed the different techniques and uses of EFTR for the management of SELs.”
They noted that all patients with SELs should first undergo multidisciplinary evaluation in accordance with a separate AGA guidance document on SELs.
The present update focuses specifically on EFTR, first by distinguishing between exposed and nonexposed techniques. While the former involves resection of the mucosa and all other layers of the wall, the latter relies upon a ‘close first, then cut’ method to prevent perforation, or preservation of an overlying flap of mucosa.
The new guidance calls for a nonexposed technique unless the exposed approach is necessary.
“In our opinion, the exposed EFTR technique should be considered for lesions in which other methods (i.e., endoscopic mucosal resection, endoscopic submucosal dissection, and nonexposed EFTR) cannot reliably and completely excise SELs due to larger size or difficult location of the lesion,” the update panelists wrote. “The exposed EFTR technique may be best suited for gastric lesions and as an alternative to other endoscopic approaches for SELs in the rectum. The exposed technique should be avoided in the esophagus and duodenum, as the clinical consequences of a leak can be devastating and endoscopic closure is notoriously challenging.”
Dr. D’Souza and colleagues went on to discuss various nonexposed techniques, including submucosal tunneling and endoscopic resection and peroral endoscopic tunnel resection (STER/POET), device-assisted endoscopic full-thickness resection, and full-thickness resection with an over-the-scope clip with integrated snare (FTRD).
They highlighted how STER/POET encourages traction on the lesion and scope stability while limiting extravasation of luminal contents, and closure tends to be easier than with exposed EFTR. This approach should be reserved for tumors smaller than approximately 3-4 cm, however, with the update noting that lesions larger than 2 cm may present increased risk of incomplete resection. Similarly, device-assisted endoscopic full-thickness resection, which involves pulling or suctioning the lesion into the device, is also limited by lesion size, although fewer data are available to guide size thresholds.
FTRD, which involves “a 23-mm deep cap with a specially designed over-the-scope clip and integrated cautery snare,” also lacks a broad evidence base.
“Although there has been reasonable clinical success reported in most case series, several factors should be considered with the use of the FTRD for SELs,” the update cautions.
Specifically, a recent Dutch and German registry study of FTRD had an adverse event rate of 11.3%, with an approximate 1% perforation rate. More than half of the perforations were due to technical or procedural issues.
“This adverse event rate may improve as individual experience with the device is gained; however, data on this are lacking,” the panelists wrote, also noting that lesions 1.5 cm or larger may carry a higher risk of incomplete resection.
Ultimately, the clinical practice update calls for a personalized approach to EFTR decision-making that considers factors extending beyond the lesion.
“The ‘ideal’ technique will depend on various patient and lesion characteristics, as well as the endoscopist’s preference and available expertise,” Dr. D’Souza and colleagues concluded. “Further research into the efficacy of these resection techniques and the long-term outcomes in patients after endoscopic resection of SELs will be essential in standardizing appropriate resection algorithms.”
This clinical practice update was commissioned and approved by AGA Institute. The investigators disclosed relationships with Olympus, Fujifilm, Apollo Endosurgery, and others.
FROM GASTROENTEROLOGY
Telephone Best for Switching Patients to New Colonoscopy Intervals
In an article published in Clinical Gastroenterology and Hepatology, a group led by Jeffrey K. Lee, MD, MPH, a gastroenterologist at Kaiser Permanente Medical Center in San Francisco, reported the following 60-day response rates for the three contact methods in potentially transitioning more than 600 post-polypectomy patients to the new interval:
- Telephone: 64.5%
- Secure messaging: 51.7%
- Mailed letter: 31.3%
Compared with letter outreach, overall rate differences were significant for telephone (18.1%) and secure message outreach (13.1%).
Such interventions are widely used, the authors noted , but have not been compared for efficacy terms of communicating updated colonoscopy intervals.

The trial’s aim was to inform low-risk patients of the recommended interval update from 5 years — used since the 1990s — to 7-10 years. Given a choice, more patients opted to transition to the 10-year surveillance interval in the telephone (37%) and secure messaging arms (32.%) compared with mailed-letter arm (18.9%).
In addition to telephone and secure messaging outreach, factors positively associated with adoption of the 10-year interval were a positive fecal immunochemical test–based index colonoscopy and increasing age. Patients with these characteristics may be biased toward avoiding colonoscopy if not medically necessary, the authors conjectured.
Inversely associated factors included Asian or Pacific Islander race (odds ratio .58), Hispanic ethnicity (OR .40), and a higher Charlson comorbidity score of 2 vs 0 (OR .43).
Possible explanations for the race and ethnicity associations include gaps in culturally component care, lack of engagement with the English-based outreach approaches, and medical mistrust, the authors said.
“In this study, we gave all our patients an option to either extend their surveillance interval to current guideline recommendations or continue with their old interval, and some chose to do that,” Dr. Lee said in an interview. “Patients really appreciated having a choice and to be informed about the latest guideline changes.”
“A critical challenge to health systems is how to effectively de-implement outdated surveillance recommendations for low-risk patients who have a 5-year follow-up interval and potentially transition them to the recommended 7- to 10-year interval,” Dr. Lee and colleagues wrote.
More than 5 million surveillance colonoscopies are performed annually in US patients with a history of adenomas, the main precursor lesion for colorectal cancer, the authors noted.
With the recent guidelines issued in 2020 by the US Multi-Society Task Force on Colorectal Cancer lengthening the follow-up interval to 7-10 years , physicians are being advised to reevaluate low-risk patients previously scheduled with 5-year surveillance and provide an updated recommendation for follow-up.
Study Details
The three-arm pragmatic randomized trial was conducted in low-risk patients 54-70 years of age with one or two small (< 10 mm) tubular adenomas at baseline colonoscopy. Participants due for 5-year surveillance in 2022 were randomly assigned to one of three outreach arms: telephone (n = 200], secure messaging (n = 203), and mailed letter (n = 201). Stratified by age, sex, race, and ethnicity, participants could change their assigned interval to 10 years or continue with their previously scheduled 5-year interval.
As to economic considerations, the authors said that telephone may be the costliest form of outreach in terms of staffing resources. “We don’t know because we did not conduct a formal cost-effectiveness analysis,” Dr. Lee said. “However, we do know phone outreach requires a lot of personnel effort, which is why we also explored the less costly option of secure messaging/email.”
But based on the findings, telephone outreach would be a reasonable approach to update patients on post-polypectomy surveillance guideline changes if secure messaging or text messaging isn’t available, he added.
Downsides to Retroactive Changes?
Commenting on the study but not involved in it, Nabil M. Mansour, MD, an assistant professor and director of the McNair General GI Clinic at Baylor College of Medicine in Houston, noted that unlike Kaiser Permanente, his center decided against an overall effort to switch patients colonoscopied before the release of the new guidelines over to the new interval.

“Several of our physicians may have chosen to recommend a 5-year interval specifically for a variety of reasons and we felt going back, and making a blanket change to everyone’s interval retrospectively might create confusion and frustration and might actually delay the colonoscopies of some patients for which their doctors had a very good, legitimate reason to recommend a 5-year interval,” he said in an interview.
Dr. Mansour added that no difficulties were encountered in getting patients to agree to a 10-year interval. In his view telephone communication or in-person clinic visits are likely the most effective ways but both are more labor-intensive than automated patient portal messages. “I do not think traditional snail mail is effective.” His clinic uses automatic EMR reminders.
Offering another perspective on the study, Aditya Sreenivasan, MD, a gastroenterologist at Northwell Health in New York City, said his center has not reached out to correct the old intervals. “When I see a patient who previously had a colonoscopy with another physician, I always follow the previous recommendation for when the next colonoscopy should be, regardless of whether or not it technically meets guideline recommendations,” he told this news organization. “I do this because I was not there during the procedure and am not aware of any circumstances that would require a shorter interval that may not be apparent from the report.”

While he agrees with the new guidelines, Dr. Sreenivasan is “not sure if retroactively changing intervals is beneficial to patients, as the presence of guidelines may subconsciously influence the behavior of the endoscopist at the time of the procedure. For example, if a patient has a technically challenging colonoscopy and the endoscopist is running late, the endoscopist may drop their guard once they find a polyp and miss 1-2 additional small polyps that they would have spent more time looking for if they knew their next one would be in 10 years instead of 5.”
As for notification method, despite the logistical downside of taking dedicated staff time to make telephone calls, Dr. Sreenivasan said, “I think having a conversation with the patient directly is a much better way to communicate this information as it allows the patient to ask and answer questions. Things like tone of voice can provide reassurance that one cannot get via email.” Looking to the future, the study authors acknowledged that combinations of initial and reminder outreach approaches — for example, a mailed letter followed by secure message or telephone call — could potentially yield higher response rates and/or adoption rates than they observed. And a longer follow-up period with additional reminders may have produced higher yields. Additional studies are needed to optimize outreach approaches and to understand patient barriers to adopting the new guideline recommendations in different healthcare settings.
The study was supported by a Delivery Science grant from the Kaiser Permanente Northern California.
The authors disclosed no conflicts of interest. Dr. Mansour and Dr. Sreenivasan disclosed no conflicts of interest relevant to their comments.
In an article published in Clinical Gastroenterology and Hepatology, a group led by Jeffrey K. Lee, MD, MPH, a gastroenterologist at Kaiser Permanente Medical Center in San Francisco, reported the following 60-day response rates for the three contact methods in potentially transitioning more than 600 post-polypectomy patients to the new interval:
- Telephone: 64.5%
- Secure messaging: 51.7%
- Mailed letter: 31.3%
Compared with letter outreach, overall rate differences were significant for telephone (18.1%) and secure message outreach (13.1%).
Such interventions are widely used, the authors noted , but have not been compared for efficacy terms of communicating updated colonoscopy intervals.
The trial’s aim was to inform low-risk patients of the recommended interval update from 5 years — used since the 1990s — to 7-10 years. Given a choice, more patients opted to transition to the 10-year surveillance interval in the telephone (37%) and secure messaging arms (32.%) compared with mailed-letter arm (18.9%).
In addition to telephone and secure messaging outreach, factors positively associated with adoption of the 10-year interval were a positive fecal immunochemical test–based index colonoscopy and increasing age. Patients with these characteristics may be biased toward avoiding colonoscopy if not medically necessary, the authors conjectured.
Inversely associated factors included Asian or Pacific Islander race (odds ratio .58), Hispanic ethnicity (OR .40), and a higher Charlson comorbidity score of 2 vs 0 (OR .43).
Possible explanations for the race and ethnicity associations include gaps in culturally component care, lack of engagement with the English-based outreach approaches, and medical mistrust, the authors said.
“In this study, we gave all our patients an option to either extend their surveillance interval to current guideline recommendations or continue with their old interval, and some chose to do that,” Dr. Lee said in an interview. “Patients really appreciated having a choice and to be informed about the latest guideline changes.”
“A critical challenge to health systems is how to effectively de-implement outdated surveillance recommendations for low-risk patients who have a 5-year follow-up interval and potentially transition them to the recommended 7- to 10-year interval,” Dr. Lee and colleagues wrote.
More than 5 million surveillance colonoscopies are performed annually in US patients with a history of adenomas, the main precursor lesion for colorectal cancer, the authors noted.
With the recent guidelines issued in 2020 by the US Multi-Society Task Force on Colorectal Cancer lengthening the follow-up interval to 7-10 years , physicians are being advised to reevaluate low-risk patients previously scheduled with 5-year surveillance and provide an updated recommendation for follow-up.
Study Details
The three-arm pragmatic randomized trial was conducted in low-risk patients 54-70 years of age with one or two small (< 10 mm) tubular adenomas at baseline colonoscopy. Participants due for 5-year surveillance in 2022 were randomly assigned to one of three outreach arms: telephone (n = 200], secure messaging (n = 203), and mailed letter (n = 201). Stratified by age, sex, race, and ethnicity, participants could change their assigned interval to 10 years or continue with their previously scheduled 5-year interval.
As to economic considerations, the authors said that telephone may be the costliest form of outreach in terms of staffing resources. “We don’t know because we did not conduct a formal cost-effectiveness analysis,” Dr. Lee said. “However, we do know phone outreach requires a lot of personnel effort, which is why we also explored the less costly option of secure messaging/email.”
But based on the findings, telephone outreach would be a reasonable approach to update patients on post-polypectomy surveillance guideline changes if secure messaging or text messaging isn’t available, he added.
Downsides to Retroactive Changes?
Commenting on the study but not involved in it, Nabil M. Mansour, MD, an assistant professor and director of the McNair General GI Clinic at Baylor College of Medicine in Houston, noted that unlike Kaiser Permanente, his center decided against an overall effort to switch patients colonoscopied before the release of the new guidelines over to the new interval.
“Several of our physicians may have chosen to recommend a 5-year interval specifically for a variety of reasons and we felt going back, and making a blanket change to everyone’s interval retrospectively might create confusion and frustration and might actually delay the colonoscopies of some patients for which their doctors had a very good, legitimate reason to recommend a 5-year interval,” he said in an interview.
Dr. Mansour added that no difficulties were encountered in getting patients to agree to a 10-year interval. In his view telephone communication or in-person clinic visits are likely the most effective ways but both are more labor-intensive than automated patient portal messages. “I do not think traditional snail mail is effective.” His clinic uses automatic EMR reminders.
Offering another perspective on the study, Aditya Sreenivasan, MD, a gastroenterologist at Northwell Health in New York City, said his center has not reached out to correct the old intervals. “When I see a patient who previously had a colonoscopy with another physician, I always follow the previous recommendation for when the next colonoscopy should be, regardless of whether or not it technically meets guideline recommendations,” he told this news organization. “I do this because I was not there during the procedure and am not aware of any circumstances that would require a shorter interval that may not be apparent from the report.”
While he agrees with the new guidelines, Dr. Sreenivasan is “not sure if retroactively changing intervals is beneficial to patients, as the presence of guidelines may subconsciously influence the behavior of the endoscopist at the time of the procedure. For example, if a patient has a technically challenging colonoscopy and the endoscopist is running late, the endoscopist may drop their guard once they find a polyp and miss 1-2 additional small polyps that they would have spent more time looking for if they knew their next one would be in 10 years instead of 5.”
As for notification method, despite the logistical downside of taking dedicated staff time to make telephone calls, Dr. Sreenivasan said, “I think having a conversation with the patient directly is a much better way to communicate this information as it allows the patient to ask and answer questions. Things like tone of voice can provide reassurance that one cannot get via email.” Looking to the future, the study authors acknowledged that combinations of initial and reminder outreach approaches — for example, a mailed letter followed by secure message or telephone call — could potentially yield higher response rates and/or adoption rates than they observed. And a longer follow-up period with additional reminders may have produced higher yields. Additional studies are needed to optimize outreach approaches and to understand patient barriers to adopting the new guideline recommendations in different healthcare settings.
The study was supported by a Delivery Science grant from the Kaiser Permanente Northern California.
The authors disclosed no conflicts of interest. Dr. Mansour and Dr. Sreenivasan disclosed no conflicts of interest relevant to their comments.
In an article published in Clinical Gastroenterology and Hepatology, a group led by Jeffrey K. Lee, MD, MPH, a gastroenterologist at Kaiser Permanente Medical Center in San Francisco, reported the following 60-day response rates for the three contact methods in potentially transitioning more than 600 post-polypectomy patients to the new interval:
- Telephone: 64.5%
- Secure messaging: 51.7%
- Mailed letter: 31.3%
Compared with letter outreach, overall rate differences were significant for telephone (18.1%) and secure message outreach (13.1%).
Such interventions are widely used, the authors noted , but have not been compared for efficacy terms of communicating updated colonoscopy intervals.
The trial’s aim was to inform low-risk patients of the recommended interval update from 5 years — used since the 1990s — to 7-10 years. Given a choice, more patients opted to transition to the 10-year surveillance interval in the telephone (37%) and secure messaging arms (32.%) compared with mailed-letter arm (18.9%).
In addition to telephone and secure messaging outreach, factors positively associated with adoption of the 10-year interval were a positive fecal immunochemical test–based index colonoscopy and increasing age. Patients with these characteristics may be biased toward avoiding colonoscopy if not medically necessary, the authors conjectured.
Inversely associated factors included Asian or Pacific Islander race (odds ratio .58), Hispanic ethnicity (OR .40), and a higher Charlson comorbidity score of 2 vs 0 (OR .43).
Possible explanations for the race and ethnicity associations include gaps in culturally component care, lack of engagement with the English-based outreach approaches, and medical mistrust, the authors said.
“In this study, we gave all our patients an option to either extend their surveillance interval to current guideline recommendations or continue with their old interval, and some chose to do that,” Dr. Lee said in an interview. “Patients really appreciated having a choice and to be informed about the latest guideline changes.”
“A critical challenge to health systems is how to effectively de-implement outdated surveillance recommendations for low-risk patients who have a 5-year follow-up interval and potentially transition them to the recommended 7- to 10-year interval,” Dr. Lee and colleagues wrote.
More than 5 million surveillance colonoscopies are performed annually in US patients with a history of adenomas, the main precursor lesion for colorectal cancer, the authors noted.
With the recent guidelines issued in 2020 by the US Multi-Society Task Force on Colorectal Cancer lengthening the follow-up interval to 7-10 years , physicians are being advised to reevaluate low-risk patients previously scheduled with 5-year surveillance and provide an updated recommendation for follow-up.
Study Details
The three-arm pragmatic randomized trial was conducted in low-risk patients 54-70 years of age with one or two small (< 10 mm) tubular adenomas at baseline colonoscopy. Participants due for 5-year surveillance in 2022 were randomly assigned to one of three outreach arms: telephone (n = 200], secure messaging (n = 203), and mailed letter (n = 201). Stratified by age, sex, race, and ethnicity, participants could change their assigned interval to 10 years or continue with their previously scheduled 5-year interval.
As to economic considerations, the authors said that telephone may be the costliest form of outreach in terms of staffing resources. “We don’t know because we did not conduct a formal cost-effectiveness analysis,” Dr. Lee said. “However, we do know phone outreach requires a lot of personnel effort, which is why we also explored the less costly option of secure messaging/email.”
But based on the findings, telephone outreach would be a reasonable approach to update patients on post-polypectomy surveillance guideline changes if secure messaging or text messaging isn’t available, he added.
Downsides to Retroactive Changes?
Commenting on the study but not involved in it, Nabil M. Mansour, MD, an assistant professor and director of the McNair General GI Clinic at Baylor College of Medicine in Houston, noted that unlike Kaiser Permanente, his center decided against an overall effort to switch patients colonoscopied before the release of the new guidelines over to the new interval.
“Several of our physicians may have chosen to recommend a 5-year interval specifically for a variety of reasons and we felt going back, and making a blanket change to everyone’s interval retrospectively might create confusion and frustration and might actually delay the colonoscopies of some patients for which their doctors had a very good, legitimate reason to recommend a 5-year interval,” he said in an interview.
Dr. Mansour added that no difficulties were encountered in getting patients to agree to a 10-year interval. In his view telephone communication or in-person clinic visits are likely the most effective ways but both are more labor-intensive than automated patient portal messages. “I do not think traditional snail mail is effective.” His clinic uses automatic EMR reminders.
Offering another perspective on the study, Aditya Sreenivasan, MD, a gastroenterologist at Northwell Health in New York City, said his center has not reached out to correct the old intervals. “When I see a patient who previously had a colonoscopy with another physician, I always follow the previous recommendation for when the next colonoscopy should be, regardless of whether or not it technically meets guideline recommendations,” he told this news organization. “I do this because I was not there during the procedure and am not aware of any circumstances that would require a shorter interval that may not be apparent from the report.”
While he agrees with the new guidelines, Dr. Sreenivasan is “not sure if retroactively changing intervals is beneficial to patients, as the presence of guidelines may subconsciously influence the behavior of the endoscopist at the time of the procedure. For example, if a patient has a technically challenging colonoscopy and the endoscopist is running late, the endoscopist may drop their guard once they find a polyp and miss 1-2 additional small polyps that they would have spent more time looking for if they knew their next one would be in 10 years instead of 5.”
As for notification method, despite the logistical downside of taking dedicated staff time to make telephone calls, Dr. Sreenivasan said, “I think having a conversation with the patient directly is a much better way to communicate this information as it allows the patient to ask and answer questions. Things like tone of voice can provide reassurance that one cannot get via email.” Looking to the future, the study authors acknowledged that combinations of initial and reminder outreach approaches — for example, a mailed letter followed by secure message or telephone call — could potentially yield higher response rates and/or adoption rates than they observed. And a longer follow-up period with additional reminders may have produced higher yields. Additional studies are needed to optimize outreach approaches and to understand patient barriers to adopting the new guideline recommendations in different healthcare settings.
The study was supported by a Delivery Science grant from the Kaiser Permanente Northern California.
The authors disclosed no conflicts of interest. Dr. Mansour and Dr. Sreenivasan disclosed no conflicts of interest relevant to their comments.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Obesity and lung disease in the era of GLP-1 agonists
Now is the time for pulmonary clinicians to become comfortable counseling patients about and treating obesity. By 2030, half of the US population will have obesity, a quarter of which will be severe (Ward et al. NEJM. 2019;2440-2450).
Many pulmonary diseases, including asthma, COPD, and interstitial pulmonary fibrosis (IPF) are linked to and made worse by obesity with increased exacerbations, patient-reported decreased quality of life, and resistance to therapy (Ray et al. Am Rev Respir Dis. 1983;501-6). Asthma is even recognized as an obesity-related comorbid condition by both the American Society Metabolic and Bariatric Surgery (ASMBS) and the American Association of Clinical Endocrinologists (AACE) when considering indications for early or more aggressive treatment of obesity (Eisenberg et al. Obesity Surg. 2023;3-14) (Garvey et al. Endocr Pract. 2016;1-203).
Obesity has multiple negative effects on pulmonary function due to the physical forces of extra weight on the lungs and inflammation related to adipose tissue (see Figure 1) (Zerah et al. Chest. 1993;1470-6).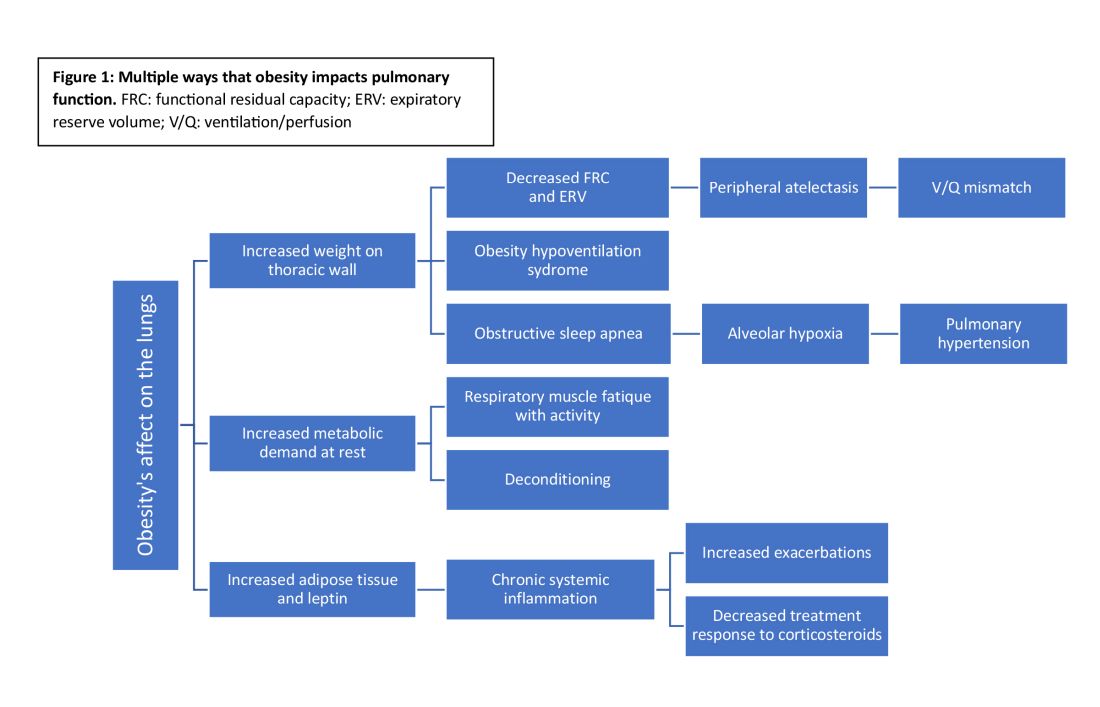
Obesity-related respiratory changes include reduced lung compliance, functional residual capacity (FRC), and expiratory reserve volume (ERV). These changes lead to peripheral atelectasis and V/Q mismatch and increased metabolic demands placed on the respiratory system (Parameswaran et al. Can Respir J. 2006;203-10). The increased weight supported by the thoracic cage alters the equilibrium between the chest wall and lung tissue decreasing FRC and ERV. This reduces lung compliance and increases stiffness by promoting areas of atelectasis and increased alveolar surface tension (Dixon et al. Expert Rev Respir Med. 2018;755-67).

Another biomechanical cost of obesity on respiratory function is the increased consumption of oxygen to sustain ventilation at rest (Koenig SM, Am J Med Sci. 2001;249-79). This can lead to early respiratory muscle fatigue when respiratory rate and tidal volume increase with activity. Patients with obesity are more likely to develop obstructive sleep apnea and obesity hypoventilation syndrome. The resulting alveolar hypoxemia is thought to contribute to the increase in pulmonary hypertension observed in patients with obesity (Shah et al. Breathe. 2023;19[1]). In addition to the biomechanical consequences of obesity, increased adipose tissue can lead to chronic, systemic inflammation that can exacerbate or unmask underlying respiratory disease. Increased leptin and downregulation of adiponectin have been shown to increase systemic cytokine production (Ray et al. Am Rev Respir Dis. 1983;501-6). This inflammatory process contributes to increased airway resistance and an altered response to corticosteroids (inhaled or systemic) in obese patients treated for bronchial hyperresponsiveness. This perhaps reflects the Th2-low phenotype seen in patients with obesity and metabolic syndrome-related asthma (Shah et al. Breathe. 2023;19[1]) (Kanwar et al. Cureus. 2022 Oct 28. doi: 10.7759/cureus.30812).

Multiple studies have demonstrated weight loss through lifestyle changes, medical therapy, and obesity surgery result benefits pulmonary disease (Forno et al. PloS One. 2019;14[4]) (Ardila-Gatas et al. Surg Endosc. 2019;1952-8). Benefits include decreased exacerbation frequency, improved functional testing, and improved patient-reported quality of life. Pulmonary clinicians should be empowered to address obesity as a comorbid condition and treat with appropriate referrals for obesity surgery and initiation of medications when indicated.
GLP-1 receptor agonists
In the past year, glucagon-like peptide receptor agonists (GLP-1RAs) have garnered attention in the medical literature and popular news outlets. GLP-1RAs, including semaglutide, liraglutide, and tirzepatide, are currently FDA approved for the treatment of obesity in patients with a body mass index (BMI) greater than or equal to 30 or a BMI greater than or equal to 27 in the setting of an obesity-related comorbidity, including asthma.
This class of medications acts by increasing the physiologic insulin response to a glucose load, delaying gastric emptying, and reducing production of glucagon. In a phase III study, semaglutide resulted in greater than 15% weight reduction from baseline (Wadden et al. JAMA. 2021;1403-13). In clinical trials, these medications have not only resulted in significant, sustained weight loss but also improved lipid profiles, decreased A1c, and reduced major cardiovascular events (Lincoff et al. N Engl J Med. 2023;389[23]:2221-32) (Verma et al. Circulation. 2018;138[25]:2884-94).
GLP-1RAs and lung disease
GLP-1RAs are associated with ranges of weight loss that lead to symptom improvement. Beyond the anticipated benefits for pulmonary health, there is interest in whether GLP-1RAs may improve specific lung diseases. GLP-1 receptors are found throughout the body (eg, gastrointestinal tract, kidneys, and heart) with the largest proportion located in the lungs (Wu AY and Peebles RS. Expert Rev Clin Immunol. 2021;1053-7). In addition to their known effect on insulin response, GLP-1RAs are hypothesized to reduce proinflammatory cytokine signaling and alter surfactant production potentially improving both airway resistance and lung compliance (Kanwar et al. Cureus. 2022 Oct 28. doi: 10.7759/cureus.30812). Animal models suggest an antifibrotic effect with delay in the endothelial-mesenchymal transition. If further substantiated, this could impact both acute and chronic lung injury.
Early clinical studies of GLP-1RAs in patients with respiratory diseases have demonstrated improved symptoms and pulmonary function (Kanwar et al. Cureus. 2022 Oct 28. doi: 10.7759/cureus.30812). Even modest weight loss (2.5 kg in a year) with GLP-1RAs leads to improved symptoms and a reduction in asthma exacerbations. Other asthma literature shows GLP-1RAs improve symptoms and reduce exacerbations independent of changes in weight, supporting the hypothesis that the benefit of GLP-1RAs may be more than biomechanical improvement from weight loss alone (Foer et al. Am J Respir Crit Care Med. 2021;831-40).
GLP-1RAs reduce the proinflammatory cytokine signaling in both TH2-high and TH2-low asthma phenotypes and alter surfactant production, airway resistance, and perhaps even pulmonary vascular resistance (Altintas Dogan et al. Int J Chron Obstruct Pulmon Dis. 2022,405-14). GATA-3 is an ongoing clinical trial examining whether GLP-1RAs reduce airway inflammation via direct effects on of the respiratory tract (NCT05254314).
Drugs developed to treat one condition are often found to impact others during validation studies or postmarketing observation. Some examples are aspirin, sildenafil, minoxidil, hydroxychloroquine, and SGLT-2 inhibitors. Will GLP-1RAs be the latest medication to affect a broad array of physiologic process and end up improving not just metabolic but also lung health?
Now is the time for pulmonary clinicians to become comfortable counseling patients about and treating obesity. By 2030, half of the US population will have obesity, a quarter of which will be severe (Ward et al. NEJM. 2019;2440-2450).
Many pulmonary diseases, including asthma, COPD, and interstitial pulmonary fibrosis (IPF) are linked to and made worse by obesity with increased exacerbations, patient-reported decreased quality of life, and resistance to therapy (Ray et al. Am Rev Respir Dis. 1983;501-6). Asthma is even recognized as an obesity-related comorbid condition by both the American Society Metabolic and Bariatric Surgery (ASMBS) and the American Association of Clinical Endocrinologists (AACE) when considering indications for early or more aggressive treatment of obesity (Eisenberg et al. Obesity Surg. 2023;3-14) (Garvey et al. Endocr Pract. 2016;1-203).
Obesity has multiple negative effects on pulmonary function due to the physical forces of extra weight on the lungs and inflammation related to adipose tissue (see Figure 1) (Zerah et al. Chest. 1993;1470-6).
Obesity-related respiratory changes include reduced lung compliance, functional residual capacity (FRC), and expiratory reserve volume (ERV). These changes lead to peripheral atelectasis and V/Q mismatch and increased metabolic demands placed on the respiratory system (Parameswaran et al. Can Respir J. 2006;203-10). The increased weight supported by the thoracic cage alters the equilibrium between the chest wall and lung tissue decreasing FRC and ERV. This reduces lung compliance and increases stiffness by promoting areas of atelectasis and increased alveolar surface tension (Dixon et al. Expert Rev Respir Med. 2018;755-67).
Another biomechanical cost of obesity on respiratory function is the increased consumption of oxygen to sustain ventilation at rest (Koenig SM, Am J Med Sci. 2001;249-79). This can lead to early respiratory muscle fatigue when respiratory rate and tidal volume increase with activity. Patients with obesity are more likely to develop obstructive sleep apnea and obesity hypoventilation syndrome. The resulting alveolar hypoxemia is thought to contribute to the increase in pulmonary hypertension observed in patients with obesity (Shah et al. Breathe. 2023;19[1]). In addition to the biomechanical consequences of obesity, increased adipose tissue can lead to chronic, systemic inflammation that can exacerbate or unmask underlying respiratory disease. Increased leptin and downregulation of adiponectin have been shown to increase systemic cytokine production (Ray et al. Am Rev Respir Dis. 1983;501-6). This inflammatory process contributes to increased airway resistance and an altered response to corticosteroids (inhaled or systemic) in obese patients treated for bronchial hyperresponsiveness. This perhaps reflects the Th2-low phenotype seen in patients with obesity and metabolic syndrome-related asthma (Shah et al. Breathe. 2023;19[1]) (Kanwar et al. Cureus. 2022 Oct 28. doi: 10.7759/cureus.30812).
Multiple studies have demonstrated weight loss through lifestyle changes, medical therapy, and obesity surgery result benefits pulmonary disease (Forno et al. PloS One. 2019;14[4]) (Ardila-Gatas et al. Surg Endosc. 2019;1952-8). Benefits include decreased exacerbation frequency, improved functional testing, and improved patient-reported quality of life. Pulmonary clinicians should be empowered to address obesity as a comorbid condition and treat with appropriate referrals for obesity surgery and initiation of medications when indicated.
GLP-1 receptor agonists
In the past year, glucagon-like peptide receptor agonists (GLP-1RAs) have garnered attention in the medical literature and popular news outlets. GLP-1RAs, including semaglutide, liraglutide, and tirzepatide, are currently FDA approved for the treatment of obesity in patients with a body mass index (BMI) greater than or equal to 30 or a BMI greater than or equal to 27 in the setting of an obesity-related comorbidity, including asthma.
This class of medications acts by increasing the physiologic insulin response to a glucose load, delaying gastric emptying, and reducing production of glucagon. In a phase III study, semaglutide resulted in greater than 15% weight reduction from baseline (Wadden et al. JAMA. 2021;1403-13). In clinical trials, these medications have not only resulted in significant, sustained weight loss but also improved lipid profiles, decreased A1c, and reduced major cardiovascular events (Lincoff et al. N Engl J Med. 2023;389[23]:2221-32) (Verma et al. Circulation. 2018;138[25]:2884-94).
GLP-1RAs and lung disease
GLP-1RAs are associated with ranges of weight loss that lead to symptom improvement. Beyond the anticipated benefits for pulmonary health, there is interest in whether GLP-1RAs may improve specific lung diseases. GLP-1 receptors are found throughout the body (eg, gastrointestinal tract, kidneys, and heart) with the largest proportion located in the lungs (Wu AY and Peebles RS. Expert Rev Clin Immunol. 2021;1053-7). In addition to their known effect on insulin response, GLP-1RAs are hypothesized to reduce proinflammatory cytokine signaling and alter surfactant production potentially improving both airway resistance and lung compliance (Kanwar et al. Cureus. 2022 Oct 28. doi: 10.7759/cureus.30812). Animal models suggest an antifibrotic effect with delay in the endothelial-mesenchymal transition. If further substantiated, this could impact both acute and chronic lung injury.
Early clinical studies of GLP-1RAs in patients with respiratory diseases have demonstrated improved symptoms and pulmonary function (Kanwar et al. Cureus. 2022 Oct 28. doi: 10.7759/cureus.30812). Even modest weight loss (2.5 kg in a year) with GLP-1RAs leads to improved symptoms and a reduction in asthma exacerbations. Other asthma literature shows GLP-1RAs improve symptoms and reduce exacerbations independent of changes in weight, supporting the hypothesis that the benefit of GLP-1RAs may be more than biomechanical improvement from weight loss alone (Foer et al. Am J Respir Crit Care Med. 2021;831-40).
GLP-1RAs reduce the proinflammatory cytokine signaling in both TH2-high and TH2-low asthma phenotypes and alter surfactant production, airway resistance, and perhaps even pulmonary vascular resistance (Altintas Dogan et al. Int J Chron Obstruct Pulmon Dis. 2022,405-14). GATA-3 is an ongoing clinical trial examining whether GLP-1RAs reduce airway inflammation via direct effects on of the respiratory tract (NCT05254314).
Drugs developed to treat one condition are often found to impact others during validation studies or postmarketing observation. Some examples are aspirin, sildenafil, minoxidil, hydroxychloroquine, and SGLT-2 inhibitors. Will GLP-1RAs be the latest medication to affect a broad array of physiologic process and end up improving not just metabolic but also lung health?
Now is the time for pulmonary clinicians to become comfortable counseling patients about and treating obesity. By 2030, half of the US population will have obesity, a quarter of which will be severe (Ward et al. NEJM. 2019;2440-2450).
Many pulmonary diseases, including asthma, COPD, and interstitial pulmonary fibrosis (IPF) are linked to and made worse by obesity with increased exacerbations, patient-reported decreased quality of life, and resistance to therapy (Ray et al. Am Rev Respir Dis. 1983;501-6). Asthma is even recognized as an obesity-related comorbid condition by both the American Society Metabolic and Bariatric Surgery (ASMBS) and the American Association of Clinical Endocrinologists (AACE) when considering indications for early or more aggressive treatment of obesity (Eisenberg et al. Obesity Surg. 2023;3-14) (Garvey et al. Endocr Pract. 2016;1-203).
Obesity has multiple negative effects on pulmonary function due to the physical forces of extra weight on the lungs and inflammation related to adipose tissue (see Figure 1) (Zerah et al. Chest. 1993;1470-6).
Obesity-related respiratory changes include reduced lung compliance, functional residual capacity (FRC), and expiratory reserve volume (ERV). These changes lead to peripheral atelectasis and V/Q mismatch and increased metabolic demands placed on the respiratory system (Parameswaran et al. Can Respir J. 2006;203-10). The increased weight supported by the thoracic cage alters the equilibrium between the chest wall and lung tissue decreasing FRC and ERV. This reduces lung compliance and increases stiffness by promoting areas of atelectasis and increased alveolar surface tension (Dixon et al. Expert Rev Respir Med. 2018;755-67).
Another biomechanical cost of obesity on respiratory function is the increased consumption of oxygen to sustain ventilation at rest (Koenig SM, Am J Med Sci. 2001;249-79). This can lead to early respiratory muscle fatigue when respiratory rate and tidal volume increase with activity. Patients with obesity are more likely to develop obstructive sleep apnea and obesity hypoventilation syndrome. The resulting alveolar hypoxemia is thought to contribute to the increase in pulmonary hypertension observed in patients with obesity (Shah et al. Breathe. 2023;19[1]). In addition to the biomechanical consequences of obesity, increased adipose tissue can lead to chronic, systemic inflammation that can exacerbate or unmask underlying respiratory disease. Increased leptin and downregulation of adiponectin have been shown to increase systemic cytokine production (Ray et al. Am Rev Respir Dis. 1983;501-6). This inflammatory process contributes to increased airway resistance and an altered response to corticosteroids (inhaled or systemic) in obese patients treated for bronchial hyperresponsiveness. This perhaps reflects the Th2-low phenotype seen in patients with obesity and metabolic syndrome-related asthma (Shah et al. Breathe. 2023;19[1]) (Kanwar et al. Cureus. 2022 Oct 28. doi: 10.7759/cureus.30812).
Multiple studies have demonstrated weight loss through lifestyle changes, medical therapy, and obesity surgery result benefits pulmonary disease (Forno et al. PloS One. 2019;14[4]) (Ardila-Gatas et al. Surg Endosc. 2019;1952-8). Benefits include decreased exacerbation frequency, improved functional testing, and improved patient-reported quality of life. Pulmonary clinicians should be empowered to address obesity as a comorbid condition and treat with appropriate referrals for obesity surgery and initiation of medications when indicated.
GLP-1 receptor agonists
In the past year, glucagon-like peptide receptor agonists (GLP-1RAs) have garnered attention in the medical literature and popular news outlets. GLP-1RAs, including semaglutide, liraglutide, and tirzepatide, are currently FDA approved for the treatment of obesity in patients with a body mass index (BMI) greater than or equal to 30 or a BMI greater than or equal to 27 in the setting of an obesity-related comorbidity, including asthma.
This class of medications acts by increasing the physiologic insulin response to a glucose load, delaying gastric emptying, and reducing production of glucagon. In a phase III study, semaglutide resulted in greater than 15% weight reduction from baseline (Wadden et al. JAMA. 2021;1403-13). In clinical trials, these medications have not only resulted in significant, sustained weight loss but also improved lipid profiles, decreased A1c, and reduced major cardiovascular events (Lincoff et al. N Engl J Med. 2023;389[23]:2221-32) (Verma et al. Circulation. 2018;138[25]:2884-94).
GLP-1RAs and lung disease
GLP-1RAs are associated with ranges of weight loss that lead to symptom improvement. Beyond the anticipated benefits for pulmonary health, there is interest in whether GLP-1RAs may improve specific lung diseases. GLP-1 receptors are found throughout the body (eg, gastrointestinal tract, kidneys, and heart) with the largest proportion located in the lungs (Wu AY and Peebles RS. Expert Rev Clin Immunol. 2021;1053-7). In addition to their known effect on insulin response, GLP-1RAs are hypothesized to reduce proinflammatory cytokine signaling and alter surfactant production potentially improving both airway resistance and lung compliance (Kanwar et al. Cureus. 2022 Oct 28. doi: 10.7759/cureus.30812). Animal models suggest an antifibrotic effect with delay in the endothelial-mesenchymal transition. If further substantiated, this could impact both acute and chronic lung injury.
Early clinical studies of GLP-1RAs in patients with respiratory diseases have demonstrated improved symptoms and pulmonary function (Kanwar et al. Cureus. 2022 Oct 28. doi: 10.7759/cureus.30812). Even modest weight loss (2.5 kg in a year) with GLP-1RAs leads to improved symptoms and a reduction in asthma exacerbations. Other asthma literature shows GLP-1RAs improve symptoms and reduce exacerbations independent of changes in weight, supporting the hypothesis that the benefit of GLP-1RAs may be more than biomechanical improvement from weight loss alone (Foer et al. Am J Respir Crit Care Med. 2021;831-40).
GLP-1RAs reduce the proinflammatory cytokine signaling in both TH2-high and TH2-low asthma phenotypes and alter surfactant production, airway resistance, and perhaps even pulmonary vascular resistance (Altintas Dogan et al. Int J Chron Obstruct Pulmon Dis. 2022,405-14). GATA-3 is an ongoing clinical trial examining whether GLP-1RAs reduce airway inflammation via direct effects on of the respiratory tract (NCT05254314).
Drugs developed to treat one condition are often found to impact others during validation studies or postmarketing observation. Some examples are aspirin, sildenafil, minoxidil, hydroxychloroquine, and SGLT-2 inhibitors. Will GLP-1RAs be the latest medication to affect a broad array of physiologic process and end up improving not just metabolic but also lung health?
New age of CHEST philanthropy to focus on education, impact, community
In a time echoing with the constant call for transformation, CHEST delved deep into its essence, questioning its potential for impact. This pivotal introspection led to a crucial inquiry…
Are we harnessing every opportunity to make a difference?
It’s a familiar question, yet its resonance urged a deeper evaluation.
Philanthropy has long been entwined in CHEST’s identity. Commemorating 25 years of the CHEST Foundation at CHEST 2022 spotlighted our history of generosity. Stories of transformative community initiatives and pivotal clinical research grants narrated a tale of empowered change and fostering healthier communities worldwide.

However, amid these achievements, more pressing inquiries surfaced:
- What unique role can CHEST play?
- Where do unmet needs persist?
- Which causes deeply resonate within our community?
CHEST’s leadership and dedicated staff embarked on a comprehensive review, scrutinizing past triumphs, donor commitments, and the evolving aspirations of our members. Themes of social responsibility, professional diversity, community impact, and expanded partnerships emerged as pivotal points. This extensive process, spanning nearly a year, resembled a reflective pause amid the rapid cadence of change.
Achieving these aspirations meant reimagining our approach, thereby streamlining efforts for maximal impact by…
- Integrating philanthropy as an integral facet of our mission, and amplifying the culture of giving within CHEST
- Consolidating philanthropic initiatives under CHEST to maximize resources for direct, substantial impact
- Defining clear avenues for giving that deeply resonate with our members
With endorsement from the Board of Regents, the CHEST Foundation seamlessly merged into CHEST, inaugurating a new chapter in our philanthropic endeavors.
Central to this transformative shift is the crystallization of our giving strategy, fortified by four pillars: Clinical Research, Community Impact, Support to the Profession, and Dedication to Education. These pillars encapsulate our commitment to nurturing clinicians, supporting trainees, and enhancing patient care.
Clinical Research emerges as the cornerstone, transcending boundaries to empower researchers in their pursuit of groundbreaking insights. Through strategic grants, we embolden early career investigators to delve into uncharted territories, unraveling mysteries that underpin advancements in chest medicine. The ripple effect extends beyond labs; it traverses communities, amplifying equitable health care solutions and bridging disparities in patient care. Our commitment to nurturing this pillar springs from the belief that every breakthrough, regardless of scale, is a catalyst for transformative change.
Community Impact extends CHEST’s reach far beyond clinical settings, fostering alliances with local organizations. Together, we forge a tapestry of collaboration, weaving essential services and imparting knowledge on crucial lung health issues into the fabric of diverse communities. This engagement not only elevates awareness but also empowers individuals and communities to take charge of their respiratory well-being. It’s the grassroots unity that amplifies our impact, creating enduring shifts in local landscapes.
Support of the Profession epitomizes our dedication to fortifying the backbone of pulmonary, critical care, and sleep medicine. By offering unparalleled clinical education and mentorship, we empower emerging clinicians from diverse backgrounds with the latest knowledge and resources. Fueling their professional growth is pivotal to nurturing a robust and inclusive cadre of health care professionals, ensuring comprehensive and culturally sensitive care for patients worldwide.
Dedication to Education isn’t just a commitment—it’s a bridge spanning the gap between knowledge and application, patient and clinician. Strengthening this connection involves equipping clinicians with tools for effective communication and partnering with patient-centered organizations. Our focus transcends textbooks; it embodies a relentless pursuit to refine patient-clinician interactions, enhancing patient understanding and, ultimately, elevating their quality of life.
CHEST’s philanthropic evolution signifies not just growth but a resolute commitment to effecting tangible change in chest medicine and patient care. These pillars stand as guiding beacons, steering us toward a future that mirrors our mission, vision, and values. Each pillar represents a pathway to meaningful, enduring change within chest medicine, ensuring a lasting impact on patient well-being.
In a time echoing with the constant call for transformation, CHEST delved deep into its essence, questioning its potential for impact. This pivotal introspection led to a crucial inquiry…
Are we harnessing every opportunity to make a difference?
It’s a familiar question, yet its resonance urged a deeper evaluation.
Philanthropy has long been entwined in CHEST’s identity. Commemorating 25 years of the CHEST Foundation at CHEST 2022 spotlighted our history of generosity. Stories of transformative community initiatives and pivotal clinical research grants narrated a tale of empowered change and fostering healthier communities worldwide.
However, amid these achievements, more pressing inquiries surfaced:
- What unique role can CHEST play?
- Where do unmet needs persist?
- Which causes deeply resonate within our community?
CHEST’s leadership and dedicated staff embarked on a comprehensive review, scrutinizing past triumphs, donor commitments, and the evolving aspirations of our members. Themes of social responsibility, professional diversity, community impact, and expanded partnerships emerged as pivotal points. This extensive process, spanning nearly a year, resembled a reflective pause amid the rapid cadence of change.
Achieving these aspirations meant reimagining our approach, thereby streamlining efforts for maximal impact by…
- Integrating philanthropy as an integral facet of our mission, and amplifying the culture of giving within CHEST
- Consolidating philanthropic initiatives under CHEST to maximize resources for direct, substantial impact
- Defining clear avenues for giving that deeply resonate with our members
With endorsement from the Board of Regents, the CHEST Foundation seamlessly merged into CHEST, inaugurating a new chapter in our philanthropic endeavors.
Central to this transformative shift is the crystallization of our giving strategy, fortified by four pillars: Clinical Research, Community Impact, Support to the Profession, and Dedication to Education. These pillars encapsulate our commitment to nurturing clinicians, supporting trainees, and enhancing patient care.
Clinical Research emerges as the cornerstone, transcending boundaries to empower researchers in their pursuit of groundbreaking insights. Through strategic grants, we embolden early career investigators to delve into uncharted territories, unraveling mysteries that underpin advancements in chest medicine. The ripple effect extends beyond labs; it traverses communities, amplifying equitable health care solutions and bridging disparities in patient care. Our commitment to nurturing this pillar springs from the belief that every breakthrough, regardless of scale, is a catalyst for transformative change.
Community Impact extends CHEST’s reach far beyond clinical settings, fostering alliances with local organizations. Together, we forge a tapestry of collaboration, weaving essential services and imparting knowledge on crucial lung health issues into the fabric of diverse communities. This engagement not only elevates awareness but also empowers individuals and communities to take charge of their respiratory well-being. It’s the grassroots unity that amplifies our impact, creating enduring shifts in local landscapes.
Support of the Profession epitomizes our dedication to fortifying the backbone of pulmonary, critical care, and sleep medicine. By offering unparalleled clinical education and mentorship, we empower emerging clinicians from diverse backgrounds with the latest knowledge and resources. Fueling their professional growth is pivotal to nurturing a robust and inclusive cadre of health care professionals, ensuring comprehensive and culturally sensitive care for patients worldwide.
Dedication to Education isn’t just a commitment—it’s a bridge spanning the gap between knowledge and application, patient and clinician. Strengthening this connection involves equipping clinicians with tools for effective communication and partnering with patient-centered organizations. Our focus transcends textbooks; it embodies a relentless pursuit to refine patient-clinician interactions, enhancing patient understanding and, ultimately, elevating their quality of life.
CHEST’s philanthropic evolution signifies not just growth but a resolute commitment to effecting tangible change in chest medicine and patient care. These pillars stand as guiding beacons, steering us toward a future that mirrors our mission, vision, and values. Each pillar represents a pathway to meaningful, enduring change within chest medicine, ensuring a lasting impact on patient well-being.
In a time echoing with the constant call for transformation, CHEST delved deep into its essence, questioning its potential for impact. This pivotal introspection led to a crucial inquiry…
Are we harnessing every opportunity to make a difference?
It’s a familiar question, yet its resonance urged a deeper evaluation.
Philanthropy has long been entwined in CHEST’s identity. Commemorating 25 years of the CHEST Foundation at CHEST 2022 spotlighted our history of generosity. Stories of transformative community initiatives and pivotal clinical research grants narrated a tale of empowered change and fostering healthier communities worldwide.
However, amid these achievements, more pressing inquiries surfaced:
- What unique role can CHEST play?
- Where do unmet needs persist?
- Which causes deeply resonate within our community?
CHEST’s leadership and dedicated staff embarked on a comprehensive review, scrutinizing past triumphs, donor commitments, and the evolving aspirations of our members. Themes of social responsibility, professional diversity, community impact, and expanded partnerships emerged as pivotal points. This extensive process, spanning nearly a year, resembled a reflective pause amid the rapid cadence of change.
Achieving these aspirations meant reimagining our approach, thereby streamlining efforts for maximal impact by…
- Integrating philanthropy as an integral facet of our mission, and amplifying the culture of giving within CHEST
- Consolidating philanthropic initiatives under CHEST to maximize resources for direct, substantial impact
- Defining clear avenues for giving that deeply resonate with our members
With endorsement from the Board of Regents, the CHEST Foundation seamlessly merged into CHEST, inaugurating a new chapter in our philanthropic endeavors.
Central to this transformative shift is the crystallization of our giving strategy, fortified by four pillars: Clinical Research, Community Impact, Support to the Profession, and Dedication to Education. These pillars encapsulate our commitment to nurturing clinicians, supporting trainees, and enhancing patient care.
Clinical Research emerges as the cornerstone, transcending boundaries to empower researchers in their pursuit of groundbreaking insights. Through strategic grants, we embolden early career investigators to delve into uncharted territories, unraveling mysteries that underpin advancements in chest medicine. The ripple effect extends beyond labs; it traverses communities, amplifying equitable health care solutions and bridging disparities in patient care. Our commitment to nurturing this pillar springs from the belief that every breakthrough, regardless of scale, is a catalyst for transformative change.
Community Impact extends CHEST’s reach far beyond clinical settings, fostering alliances with local organizations. Together, we forge a tapestry of collaboration, weaving essential services and imparting knowledge on crucial lung health issues into the fabric of diverse communities. This engagement not only elevates awareness but also empowers individuals and communities to take charge of their respiratory well-being. It’s the grassroots unity that amplifies our impact, creating enduring shifts in local landscapes.
Support of the Profession epitomizes our dedication to fortifying the backbone of pulmonary, critical care, and sleep medicine. By offering unparalleled clinical education and mentorship, we empower emerging clinicians from diverse backgrounds with the latest knowledge and resources. Fueling their professional growth is pivotal to nurturing a robust and inclusive cadre of health care professionals, ensuring comprehensive and culturally sensitive care for patients worldwide.
Dedication to Education isn’t just a commitment—it’s a bridge spanning the gap between knowledge and application, patient and clinician. Strengthening this connection involves equipping clinicians with tools for effective communication and partnering with patient-centered organizations. Our focus transcends textbooks; it embodies a relentless pursuit to refine patient-clinician interactions, enhancing patient understanding and, ultimately, elevating their quality of life.
CHEST’s philanthropic evolution signifies not just growth but a resolute commitment to effecting tangible change in chest medicine and patient care. These pillars stand as guiding beacons, steering us toward a future that mirrors our mission, vision, and values. Each pillar represents a pathway to meaningful, enduring change within chest medicine, ensuring a lasting impact on patient well-being.