User login
It Sure Looks Like Cannabis Is Bad for the Heart, Doesn’t It?
This transcript has been edited for clarity.
If you’re an epidemiologist trying to explore whether some exposure is a risk factor for a disease, you can run into a tough problem when your exposure of interest is highly correlated with another risk factor for the disease. For decades, this stymied investigations into the link, if any, between marijuana use and cardiovascular disease because, for decades, most people who used marijuana in some way also smoked cigarettes — which is a very clear risk factor for heart disease.
But the times they are a-changing.
Thanks to the legalization of marijuana for recreational use in many states, and even broader social trends, there is now a large population of people who use marijuana but do not use cigarettes. That means we can start to determine whether marijuana use is an independent risk factor for heart disease.
And this week, we have the largest study yet to attempt to answer that question, though, as I’ll explain momentarily, the smoke hasn’t entirely cleared yet.
The centerpiece of the study we are discussing this week, “Association of Cannabis Use With Cardiovascular Outcomes Among US Adults,” which appeared in the Journal of the American Heart Association, is the Behavioral Risk Factor Surveillance System, an annual telephone survey conducted by the Centers for Disease Control and Prevention since 1984 that gathers data on all sorts of stuff that we do to ourselves: our drinking habits, our smoking habits, and, more recently, our marijuana habits.
The paper combines annual data from 2016 to 2020 representing 27 states and two US territories for a total sample size of more than 430,000 individuals. The key exposure? Marijuana use, which was coded as the number of days of marijuana use in the past 30 days. The key outcome? Coronary heart disease, collected through questions such as “Has a doctor, nurse, or other health professional ever told you that you had a heart attack?”
Right away you might detect a couple of problems here. But let me show you the results before we worry about what they mean.
You can see the rates of the major cardiovascular outcomes here, stratified by daily use of marijuana, nondaily use, and no use. Broadly speaking, the risk was highest for daily users, lowest for occasional users, and in the middle for non-users.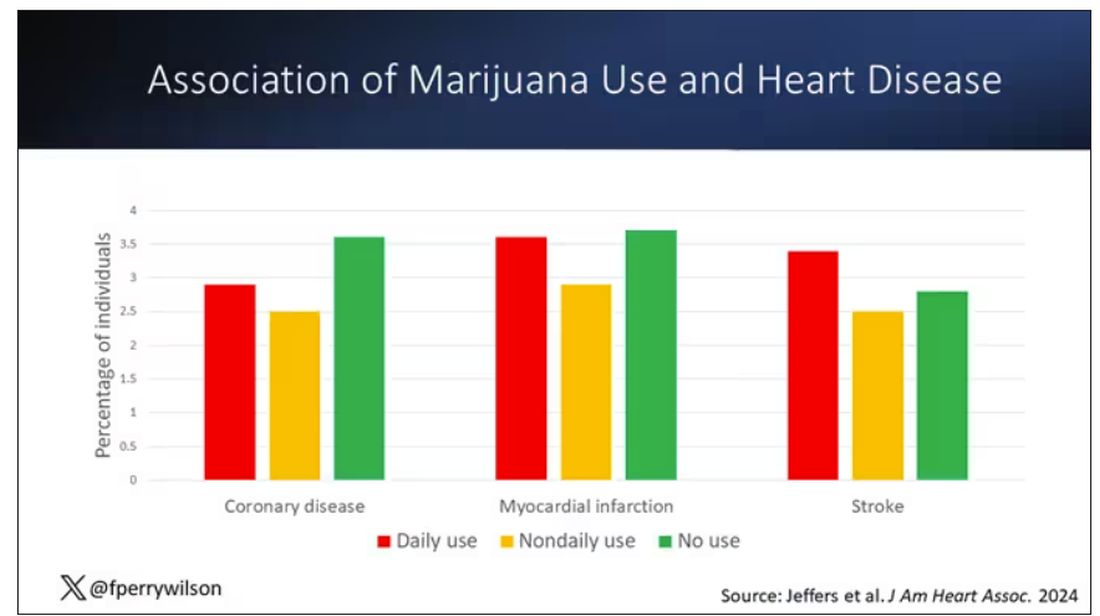
Of course, non-users and users are different in lots of other ways; non-users were quite a bit older, for example. Adjusting for all those factors showed that, independent of age, smoking status, the presence of diabetes, and so on, there was an independently increased risk for cardiovascular outcomes in people who used marijuana.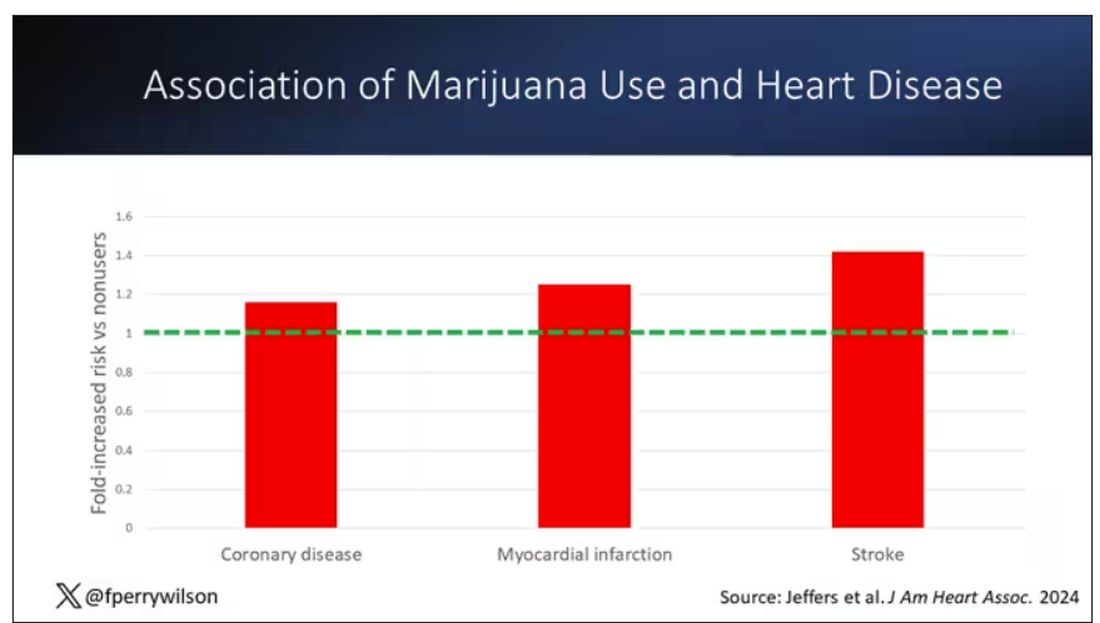
Importantly, 60% of people in this study were never smokers, and the results in that group looked pretty similar to the results overall.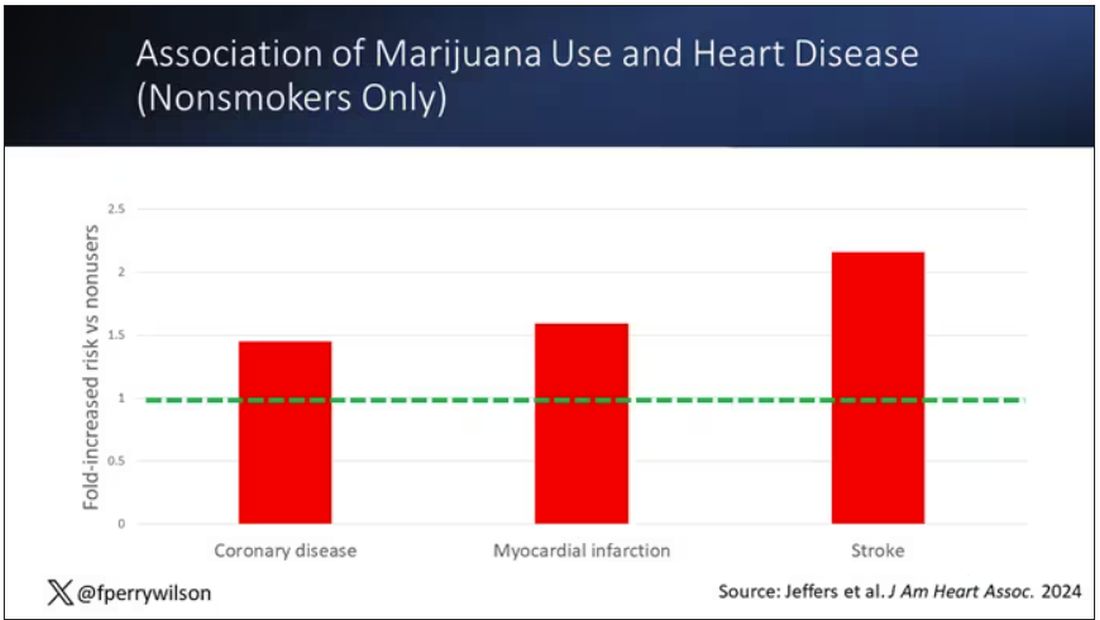
But I said there were a couple of problems, so let’s dig into those a bit.
First, like most survey studies, this one requires honest and accurate reporting from its subjects. There was no verification of heart disease using electronic health records or of marijuana usage based on biosamples. Broadly, miscategorization of exposure and outcomes in surveys tends to bias the results toward the null hypothesis, toward concluding that there is no link between exposure and outcome, so perhaps this is okay.
The bigger problem is the fact that this is a cross-sectional design. If you really wanted to know whether marijuana led to heart disease, you’d do a longitudinal study following users and non-users for some number of decades and see who developed heart disease and who didn’t. (For the pedants out there, I suppose you’d actually want to randomize people to use marijuana or not and then see who had a heart attack, but the IRB keeps rejecting my protocol when I submit it.)
Here, though, we literally can’t tell whether people who use marijuana have more heart attacks or whether people who have heart attacks use more marijuana. The authors argue that there are no data that show that people are more likely to use marijuana after a heart attack or stroke, but at the time the survey was conducted, they had already had their heart attack or stroke.
The authors also imply that they found a dose-response relationship between marijuana use and these cardiovascular outcomes. This is an important statement because dose response is one factor that we use to determine whether a risk factor may actually be causative as opposed to just correlative.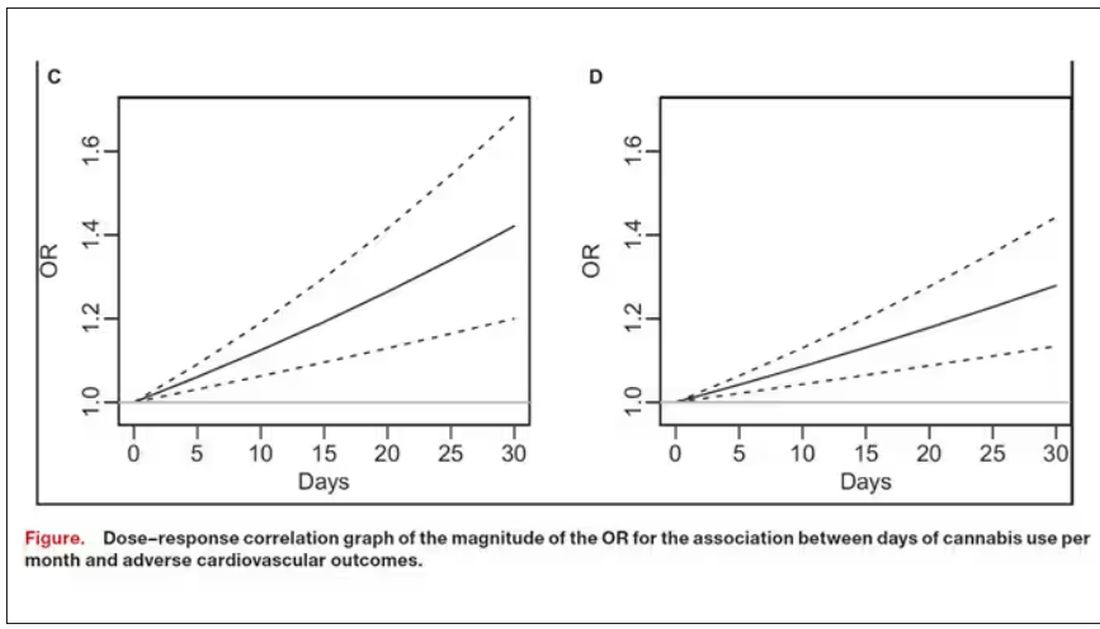
But I take issue with the dose-response language here. The model used to make these graphs classifies marijuana use as a single continuous variable ranging from 0 (no days of use in the past 30 days) to 1 (30 days of use in the past 30 days). The model is thus constrained to monotonically increase or decrease with respect to the outcome. To prove a dose response, you have to give the model the option to find something that isn’t a dose response — for example, by classifying marijuana use into discrete, independent categories rather than a single continuous number.
Am I arguing here that marijuana use is good for you? Of course not. Nor am I even arguing that it has no effect on the cardiovascular system. There are endocannabinoid receptors all over your vasculature. But a cross-sectional survey study, while a good start, is not quite the right way to answer the question. So, while the jury is still out, it’s high time for more research.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
If you’re an epidemiologist trying to explore whether some exposure is a risk factor for a disease, you can run into a tough problem when your exposure of interest is highly correlated with another risk factor for the disease. For decades, this stymied investigations into the link, if any, between marijuana use and cardiovascular disease because, for decades, most people who used marijuana in some way also smoked cigarettes — which is a very clear risk factor for heart disease.
But the times they are a-changing.
Thanks to the legalization of marijuana for recreational use in many states, and even broader social trends, there is now a large population of people who use marijuana but do not use cigarettes. That means we can start to determine whether marijuana use is an independent risk factor for heart disease.
And this week, we have the largest study yet to attempt to answer that question, though, as I’ll explain momentarily, the smoke hasn’t entirely cleared yet.
The centerpiece of the study we are discussing this week, “Association of Cannabis Use With Cardiovascular Outcomes Among US Adults,” which appeared in the Journal of the American Heart Association, is the Behavioral Risk Factor Surveillance System, an annual telephone survey conducted by the Centers for Disease Control and Prevention since 1984 that gathers data on all sorts of stuff that we do to ourselves: our drinking habits, our smoking habits, and, more recently, our marijuana habits.
The paper combines annual data from 2016 to 2020 representing 27 states and two US territories for a total sample size of more than 430,000 individuals. The key exposure? Marijuana use, which was coded as the number of days of marijuana use in the past 30 days. The key outcome? Coronary heart disease, collected through questions such as “Has a doctor, nurse, or other health professional ever told you that you had a heart attack?”
Right away you might detect a couple of problems here. But let me show you the results before we worry about what they mean.
You can see the rates of the major cardiovascular outcomes here, stratified by daily use of marijuana, nondaily use, and no use. Broadly speaking, the risk was highest for daily users, lowest for occasional users, and in the middle for non-users.
Of course, non-users and users are different in lots of other ways; non-users were quite a bit older, for example. Adjusting for all those factors showed that, independent of age, smoking status, the presence of diabetes, and so on, there was an independently increased risk for cardiovascular outcomes in people who used marijuana.
Importantly, 60% of people in this study were never smokers, and the results in that group looked pretty similar to the results overall.
But I said there were a couple of problems, so let’s dig into those a bit.
First, like most survey studies, this one requires honest and accurate reporting from its subjects. There was no verification of heart disease using electronic health records or of marijuana usage based on biosamples. Broadly, miscategorization of exposure and outcomes in surveys tends to bias the results toward the null hypothesis, toward concluding that there is no link between exposure and outcome, so perhaps this is okay.
The bigger problem is the fact that this is a cross-sectional design. If you really wanted to know whether marijuana led to heart disease, you’d do a longitudinal study following users and non-users for some number of decades and see who developed heart disease and who didn’t. (For the pedants out there, I suppose you’d actually want to randomize people to use marijuana or not and then see who had a heart attack, but the IRB keeps rejecting my protocol when I submit it.)
Here, though, we literally can’t tell whether people who use marijuana have more heart attacks or whether people who have heart attacks use more marijuana. The authors argue that there are no data that show that people are more likely to use marijuana after a heart attack or stroke, but at the time the survey was conducted, they had already had their heart attack or stroke.
The authors also imply that they found a dose-response relationship between marijuana use and these cardiovascular outcomes. This is an important statement because dose response is one factor that we use to determine whether a risk factor may actually be causative as opposed to just correlative.
But I take issue with the dose-response language here. The model used to make these graphs classifies marijuana use as a single continuous variable ranging from 0 (no days of use in the past 30 days) to 1 (30 days of use in the past 30 days). The model is thus constrained to monotonically increase or decrease with respect to the outcome. To prove a dose response, you have to give the model the option to find something that isn’t a dose response — for example, by classifying marijuana use into discrete, independent categories rather than a single continuous number.
Am I arguing here that marijuana use is good for you? Of course not. Nor am I even arguing that it has no effect on the cardiovascular system. There are endocannabinoid receptors all over your vasculature. But a cross-sectional survey study, while a good start, is not quite the right way to answer the question. So, while the jury is still out, it’s high time for more research.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
If you’re an epidemiologist trying to explore whether some exposure is a risk factor for a disease, you can run into a tough problem when your exposure of interest is highly correlated with another risk factor for the disease. For decades, this stymied investigations into the link, if any, between marijuana use and cardiovascular disease because, for decades, most people who used marijuana in some way also smoked cigarettes — which is a very clear risk factor for heart disease.
But the times they are a-changing.
Thanks to the legalization of marijuana for recreational use in many states, and even broader social trends, there is now a large population of people who use marijuana but do not use cigarettes. That means we can start to determine whether marijuana use is an independent risk factor for heart disease.
And this week, we have the largest study yet to attempt to answer that question, though, as I’ll explain momentarily, the smoke hasn’t entirely cleared yet.
The centerpiece of the study we are discussing this week, “Association of Cannabis Use With Cardiovascular Outcomes Among US Adults,” which appeared in the Journal of the American Heart Association, is the Behavioral Risk Factor Surveillance System, an annual telephone survey conducted by the Centers for Disease Control and Prevention since 1984 that gathers data on all sorts of stuff that we do to ourselves: our drinking habits, our smoking habits, and, more recently, our marijuana habits.
The paper combines annual data from 2016 to 2020 representing 27 states and two US territories for a total sample size of more than 430,000 individuals. The key exposure? Marijuana use, which was coded as the number of days of marijuana use in the past 30 days. The key outcome? Coronary heart disease, collected through questions such as “Has a doctor, nurse, or other health professional ever told you that you had a heart attack?”
Right away you might detect a couple of problems here. But let me show you the results before we worry about what they mean.
You can see the rates of the major cardiovascular outcomes here, stratified by daily use of marijuana, nondaily use, and no use. Broadly speaking, the risk was highest for daily users, lowest for occasional users, and in the middle for non-users.
Of course, non-users and users are different in lots of other ways; non-users were quite a bit older, for example. Adjusting for all those factors showed that, independent of age, smoking status, the presence of diabetes, and so on, there was an independently increased risk for cardiovascular outcomes in people who used marijuana.
Importantly, 60% of people in this study were never smokers, and the results in that group looked pretty similar to the results overall.
But I said there were a couple of problems, so let’s dig into those a bit.
First, like most survey studies, this one requires honest and accurate reporting from its subjects. There was no verification of heart disease using electronic health records or of marijuana usage based on biosamples. Broadly, miscategorization of exposure and outcomes in surveys tends to bias the results toward the null hypothesis, toward concluding that there is no link between exposure and outcome, so perhaps this is okay.
The bigger problem is the fact that this is a cross-sectional design. If you really wanted to know whether marijuana led to heart disease, you’d do a longitudinal study following users and non-users for some number of decades and see who developed heart disease and who didn’t. (For the pedants out there, I suppose you’d actually want to randomize people to use marijuana or not and then see who had a heart attack, but the IRB keeps rejecting my protocol when I submit it.)
Here, though, we literally can’t tell whether people who use marijuana have more heart attacks or whether people who have heart attacks use more marijuana. The authors argue that there are no data that show that people are more likely to use marijuana after a heart attack or stroke, but at the time the survey was conducted, they had already had their heart attack or stroke.
The authors also imply that they found a dose-response relationship between marijuana use and these cardiovascular outcomes. This is an important statement because dose response is one factor that we use to determine whether a risk factor may actually be causative as opposed to just correlative.
But I take issue with the dose-response language here. The model used to make these graphs classifies marijuana use as a single continuous variable ranging from 0 (no days of use in the past 30 days) to 1 (30 days of use in the past 30 days). The model is thus constrained to monotonically increase or decrease with respect to the outcome. To prove a dose response, you have to give the model the option to find something that isn’t a dose response — for example, by classifying marijuana use into discrete, independent categories rather than a single continuous number.
Am I arguing here that marijuana use is good for you? Of course not. Nor am I even arguing that it has no effect on the cardiovascular system. There are endocannabinoid receptors all over your vasculature. But a cross-sectional survey study, while a good start, is not quite the right way to answer the question. So, while the jury is still out, it’s high time for more research.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Galantamine Supplements Found Mislabeled, Contaminated
TOPLINE:
Galantamine purchased as a dietary supplement may be more likely to contain bacterial contaminants and an incorrect amount of the product vs when it is prescribed as a generic drug, new research showed.
METHODOLOGY:
- Galantamine, a plant alkaloid, is approved for treating mild to moderate Alzheimer’s dementia but is also marketed as a dietary supplement for cognitive enhancement.
- In June 2023, researchers purchased all 10 galantamine dietary supplements available on Amazon.com that had a Supplement Facts panel.
- In September 2023, they acquired all 11 generic immediate-release formulations of prescription galantamine available in the United States.
- They analyzed the content of galantamine in each product using ultrahigh-performance liquid chromatography-mass spectrometry and quantified any microorganisms present.
TAKEAWAY:
- Generic galantamine drugs were found to contain 97.5%-104.2% of the labeled content, with no microbial contamination.
- , according to the authors of the study.
IN PRACTICE:
“Clinicians should query patients with memory concerns about the use of dietary supplements and advise patients not to use galantamine supplements,” the researchers wrote.
SOURCE:
The corresponding author of the study was Pieter A. Cohen, MD, with Broadway Clinic, Cambridge Health Alliance, in Somerville, Massachusetts. The paper was published online as a research letter in JAMA.
LIMITATIONS:
The products were purchased at a single point in time and may not reflect current options, the researchers noted. The generalizability of the findings to other supplement ingredients or generic drugs is unknown.
DISCLOSURES:
Dr. Cohen has received grants from the Consumers Union and PEW Charitable Trust and personal fees from UpToDate and the Centers for Disease Control and Prevention. He has been sued by a supplement company in a case where the jury found in his favor.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article appeared on Medscape.com.
TOPLINE:
Galantamine purchased as a dietary supplement may be more likely to contain bacterial contaminants and an incorrect amount of the product vs when it is prescribed as a generic drug, new research showed.
METHODOLOGY:
- Galantamine, a plant alkaloid, is approved for treating mild to moderate Alzheimer’s dementia but is also marketed as a dietary supplement for cognitive enhancement.
- In June 2023, researchers purchased all 10 galantamine dietary supplements available on Amazon.com that had a Supplement Facts panel.
- In September 2023, they acquired all 11 generic immediate-release formulations of prescription galantamine available in the United States.
- They analyzed the content of galantamine in each product using ultrahigh-performance liquid chromatography-mass spectrometry and quantified any microorganisms present.
TAKEAWAY:
- Generic galantamine drugs were found to contain 97.5%-104.2% of the labeled content, with no microbial contamination.
- , according to the authors of the study.
IN PRACTICE:
“Clinicians should query patients with memory concerns about the use of dietary supplements and advise patients not to use galantamine supplements,” the researchers wrote.
SOURCE:
The corresponding author of the study was Pieter A. Cohen, MD, with Broadway Clinic, Cambridge Health Alliance, in Somerville, Massachusetts. The paper was published online as a research letter in JAMA.
LIMITATIONS:
The products were purchased at a single point in time and may not reflect current options, the researchers noted. The generalizability of the findings to other supplement ingredients or generic drugs is unknown.
DISCLOSURES:
Dr. Cohen has received grants from the Consumers Union and PEW Charitable Trust and personal fees from UpToDate and the Centers for Disease Control and Prevention. He has been sued by a supplement company in a case where the jury found in his favor.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article appeared on Medscape.com.
TOPLINE:
Galantamine purchased as a dietary supplement may be more likely to contain bacterial contaminants and an incorrect amount of the product vs when it is prescribed as a generic drug, new research showed.
METHODOLOGY:
- Galantamine, a plant alkaloid, is approved for treating mild to moderate Alzheimer’s dementia but is also marketed as a dietary supplement for cognitive enhancement.
- In June 2023, researchers purchased all 10 galantamine dietary supplements available on Amazon.com that had a Supplement Facts panel.
- In September 2023, they acquired all 11 generic immediate-release formulations of prescription galantamine available in the United States.
- They analyzed the content of galantamine in each product using ultrahigh-performance liquid chromatography-mass spectrometry and quantified any microorganisms present.
TAKEAWAY:
- Generic galantamine drugs were found to contain 97.5%-104.2% of the labeled content, with no microbial contamination.
- , according to the authors of the study.
IN PRACTICE:
“Clinicians should query patients with memory concerns about the use of dietary supplements and advise patients not to use galantamine supplements,” the researchers wrote.
SOURCE:
The corresponding author of the study was Pieter A. Cohen, MD, with Broadway Clinic, Cambridge Health Alliance, in Somerville, Massachusetts. The paper was published online as a research letter in JAMA.
LIMITATIONS:
The products were purchased at a single point in time and may not reflect current options, the researchers noted. The generalizability of the findings to other supplement ingredients or generic drugs is unknown.
DISCLOSURES:
Dr. Cohen has received grants from the Consumers Union and PEW Charitable Trust and personal fees from UpToDate and the Centers for Disease Control and Prevention. He has been sued by a supplement company in a case where the jury found in his favor.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article appeared on Medscape.com.
New Trials in Leukemia and Lymphoma: Could Your Patient Benefit?
Several clinical trials in leukemia and lymphoma have started enrolling recently. Maybe one of your patients could benefit from taking part?
run by the Center for International Blood and Bone Marrow Transplant Research.
The purpose of the study is to test whether cyclophosphamide, which is given to prevent a dreaded complication of stem cell transplantation called graft-versus-host disease, can be safely reduced without increasing infection or reducing protection. All participants will receive cyclophosphamide on days 3 and 4 post transplant. One group will receive a reduced dose of cyclophosphamide (25 mg/kg per dose), and the other will be given a usual dose (37.5 mg/kg).
Sites in Michigan, Missouri, Oregon, Virginia, and Washington started recruiting for 190 participants in December 2023. Study centers in Florida, Massachusetts, New York, and Wisconsin are also planned. Infection-free survival is the primary endpoint, and overall survival is a secondary measure. Quality of life (QoL) is not recorded. More details at clinicaltrials.gov.
Untreated chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL). Adults who are newly diagnosed with this type of cancer and have active disease may wish to consider a randomized, open-label, phase 3 trial testing an experimental Bruton tyrosine kinase (BTK) inhibitor, nemtabrutinib (from Merck Sharp & Dohme), against standard-of-care BTK inhibitors ibrutinib (Imbruvica) and acalabrutinib (Calquence).
BTK inhibitors target B-cell proliferation in B-cell cancers such as CLL/SLL and allow for chemotherapy-free treatment of some hematological malignancies. In this study, until disease progression, unacceptable toxicity, or another reason for discontinuation occurs, participants will take daily oral nemtabrutinib, ibrutinib, or acalabrutinib.
The study opened in December 2023 in Pennsylvania, Washington, Taiwan, Israel, and the United Kingdom seeking 1200 participants. The primary outcomes are objective response rate and progression-free survival. Overall survival is a secondary outcome, and QoL is not measured. More details at clinicaltrials.gov.
Relapsed or refractory leukemia with a KMT2A-gene rearrangement (KMT2A-r). Children aged 1 month to younger than 6 years with this diagnosis may be able to join an open-label, nonrandomized, Children’s Oncology Group phase 2 study to determine the most tolerable and/or effective dose of an experimental oral drug called revumenib when added to chemotherapy.
KMT2A-gene alterations are associated with a poor prognosis in leukemia. These alterations cause blood cells to dedifferentiate and start proliferating uncontrollably as leukemia cells. The expression of the damaged KMT2A gene relies on a protein called menin. Revumenib, from Syndax Pharmaceuticals, blocks menin and prevents expression of KMT2A.
Children in the study will receive two different regimens of revumenib in combination with chemotherapy for up to a year, or until disease progression or unacceptable toxicity, and will then be followed for up to 5 years. Trial centers in 12 US states opened their doors in January 2024 looking for 78 participants. Toxicities and minimal residual disease are the primary outcomes; overall survival is a secondary outcome, and QoL is not assessed. More details at clinicaltrials.gov.
Previously untreated follicular lymphoma or diffuse large B-cell lymphoma. Adults with one of these types of lymphoma may be eligible for one of three open-label, randomized, phase 3 trials testing odronextamab (from Regeneron). This bispecific antibody is designed to ‘lock together’ CD20 on cancer cells with CD3-expressing cancer-killing T cells. It has shown anti-lymphoma activity in heavily pretreated patients.
Late in 2023, three phase 3 trials turned the spotlight on treatment-naive patients and started recruiting 2115 participants to assess odronextamab in this setting. The trial OLYMPIA-1 will compare odronextamab with standard-of-care rituximab (Rituxan) plus chemotherapy in follicular lymphoma. OLYMPIA-2 will test the drug in combination with chemotherapy, also in follicular lymphoma. OLYMPIA-3 will evaluate odronextamab plus chemotherapy against rituximab and chemotherapy in people with large B-cell lymphoma.
All study drugs, including odronextamab, will be administered by intravenous infusion, and participants will be followed for up to 5 years. Research centers across eight US states and Australia, Czechia, France, Italy, Poland, Spain, Turkey, and Thailand are currently accepting participants for the three trials. The primary outcomes are various measures of toxicity and complete response at 30 months in the follicular lymphoma studies and toxicity and progression-free survival in large B-cell lymphoma. All three trials are measuring overall survival and QoL as secondary endpoints.
Previously untreated stage II, III, or IV follicular lymphoma. Adults with this type of cancer may be eligible to participate in a randomized, open-label, phase 3 study testing whether an experimental therapy called epcoritamab (from AbbVie) improves disease response and is tolerable when added to standard therapy. For up to 120 weeks, one group of participants will receive a combination of intravenous rituximab and oral lenalidomide (Revlimid), while a second group will also receive subcutaneous injections of epcoritamab. Some participants may be offered investigators’ choice of chemotherapy as well.
Sites across Iowa, Maryland, Missouri, Ohio, Washington, and Montana started welcoming their 900 participants in February 2024. The primary outcome is complete response at 30 months. Overall survival and QoL are secondary outcomes. More details at clinicaltrials.gov.
Relapsed or refractory mantle cell lymphoma. Adults facing one of these clinical scenarios can join an Academic and Community Cancer Research United open label, phase 2 trial examining the effectiveness of combining tafasitamab (Monjuvi), lenalidomide, and venetoclax (Venclexta) for such patients.
Frontline therapy does not cure mantle cell lymphoma, and continued relapses are common. In this situation, treatments can include acalabrutinib, ibrutinib, stem cell transplantation, venetoclax, lenalidomide, and rituximab.
In this study, participants will take venetoclax and lenalidomide daily and receive intravenous tafasitamab every 2 weeks after an initial ramp-up period as per clinic standards. Participants will be followed for 5 years after entering the trial. The Mayo Clinic in Rochester, Minnesota, began recruiting the planned 100 trial participants in January 2024. The primary outcome is objective response rate; overall survival is a secondary outcome, and QoL will not be tracked. More details at clinicaltrials.gov.
All trial information is from the National Institutes of Health US National Library of Medicine (online at clinicaltrials.gov).
A version of this article appeared on Medscape.com .
Several clinical trials in leukemia and lymphoma have started enrolling recently. Maybe one of your patients could benefit from taking part?
run by the Center for International Blood and Bone Marrow Transplant Research.
The purpose of the study is to test whether cyclophosphamide, which is given to prevent a dreaded complication of stem cell transplantation called graft-versus-host disease, can be safely reduced without increasing infection or reducing protection. All participants will receive cyclophosphamide on days 3 and 4 post transplant. One group will receive a reduced dose of cyclophosphamide (25 mg/kg per dose), and the other will be given a usual dose (37.5 mg/kg).
Sites in Michigan, Missouri, Oregon, Virginia, and Washington started recruiting for 190 participants in December 2023. Study centers in Florida, Massachusetts, New York, and Wisconsin are also planned. Infection-free survival is the primary endpoint, and overall survival is a secondary measure. Quality of life (QoL) is not recorded. More details at clinicaltrials.gov.
Untreated chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL). Adults who are newly diagnosed with this type of cancer and have active disease may wish to consider a randomized, open-label, phase 3 trial testing an experimental Bruton tyrosine kinase (BTK) inhibitor, nemtabrutinib (from Merck Sharp & Dohme), against standard-of-care BTK inhibitors ibrutinib (Imbruvica) and acalabrutinib (Calquence).
BTK inhibitors target B-cell proliferation in B-cell cancers such as CLL/SLL and allow for chemotherapy-free treatment of some hematological malignancies. In this study, until disease progression, unacceptable toxicity, or another reason for discontinuation occurs, participants will take daily oral nemtabrutinib, ibrutinib, or acalabrutinib.
The study opened in December 2023 in Pennsylvania, Washington, Taiwan, Israel, and the United Kingdom seeking 1200 participants. The primary outcomes are objective response rate and progression-free survival. Overall survival is a secondary outcome, and QoL is not measured. More details at clinicaltrials.gov.
Relapsed or refractory leukemia with a KMT2A-gene rearrangement (KMT2A-r). Children aged 1 month to younger than 6 years with this diagnosis may be able to join an open-label, nonrandomized, Children’s Oncology Group phase 2 study to determine the most tolerable and/or effective dose of an experimental oral drug called revumenib when added to chemotherapy.
KMT2A-gene alterations are associated with a poor prognosis in leukemia. These alterations cause blood cells to dedifferentiate and start proliferating uncontrollably as leukemia cells. The expression of the damaged KMT2A gene relies on a protein called menin. Revumenib, from Syndax Pharmaceuticals, blocks menin and prevents expression of KMT2A.
Children in the study will receive two different regimens of revumenib in combination with chemotherapy for up to a year, or until disease progression or unacceptable toxicity, and will then be followed for up to 5 years. Trial centers in 12 US states opened their doors in January 2024 looking for 78 participants. Toxicities and minimal residual disease are the primary outcomes; overall survival is a secondary outcome, and QoL is not assessed. More details at clinicaltrials.gov.
Previously untreated follicular lymphoma or diffuse large B-cell lymphoma. Adults with one of these types of lymphoma may be eligible for one of three open-label, randomized, phase 3 trials testing odronextamab (from Regeneron). This bispecific antibody is designed to ‘lock together’ CD20 on cancer cells with CD3-expressing cancer-killing T cells. It has shown anti-lymphoma activity in heavily pretreated patients.
Late in 2023, three phase 3 trials turned the spotlight on treatment-naive patients and started recruiting 2115 participants to assess odronextamab in this setting. The trial OLYMPIA-1 will compare odronextamab with standard-of-care rituximab (Rituxan) plus chemotherapy in follicular lymphoma. OLYMPIA-2 will test the drug in combination with chemotherapy, also in follicular lymphoma. OLYMPIA-3 will evaluate odronextamab plus chemotherapy against rituximab and chemotherapy in people with large B-cell lymphoma.
All study drugs, including odronextamab, will be administered by intravenous infusion, and participants will be followed for up to 5 years. Research centers across eight US states and Australia, Czechia, France, Italy, Poland, Spain, Turkey, and Thailand are currently accepting participants for the three trials. The primary outcomes are various measures of toxicity and complete response at 30 months in the follicular lymphoma studies and toxicity and progression-free survival in large B-cell lymphoma. All three trials are measuring overall survival and QoL as secondary endpoints.
Previously untreated stage II, III, or IV follicular lymphoma. Adults with this type of cancer may be eligible to participate in a randomized, open-label, phase 3 study testing whether an experimental therapy called epcoritamab (from AbbVie) improves disease response and is tolerable when added to standard therapy. For up to 120 weeks, one group of participants will receive a combination of intravenous rituximab and oral lenalidomide (Revlimid), while a second group will also receive subcutaneous injections of epcoritamab. Some participants may be offered investigators’ choice of chemotherapy as well.
Sites across Iowa, Maryland, Missouri, Ohio, Washington, and Montana started welcoming their 900 participants in February 2024. The primary outcome is complete response at 30 months. Overall survival and QoL are secondary outcomes. More details at clinicaltrials.gov.
Relapsed or refractory mantle cell lymphoma. Adults facing one of these clinical scenarios can join an Academic and Community Cancer Research United open label, phase 2 trial examining the effectiveness of combining tafasitamab (Monjuvi), lenalidomide, and venetoclax (Venclexta) for such patients.
Frontline therapy does not cure mantle cell lymphoma, and continued relapses are common. In this situation, treatments can include acalabrutinib, ibrutinib, stem cell transplantation, venetoclax, lenalidomide, and rituximab.
In this study, participants will take venetoclax and lenalidomide daily and receive intravenous tafasitamab every 2 weeks after an initial ramp-up period as per clinic standards. Participants will be followed for 5 years after entering the trial. The Mayo Clinic in Rochester, Minnesota, began recruiting the planned 100 trial participants in January 2024. The primary outcome is objective response rate; overall survival is a secondary outcome, and QoL will not be tracked. More details at clinicaltrials.gov.
All trial information is from the National Institutes of Health US National Library of Medicine (online at clinicaltrials.gov).
A version of this article appeared on Medscape.com .
Several clinical trials in leukemia and lymphoma have started enrolling recently. Maybe one of your patients could benefit from taking part?
run by the Center for International Blood and Bone Marrow Transplant Research.
The purpose of the study is to test whether cyclophosphamide, which is given to prevent a dreaded complication of stem cell transplantation called graft-versus-host disease, can be safely reduced without increasing infection or reducing protection. All participants will receive cyclophosphamide on days 3 and 4 post transplant. One group will receive a reduced dose of cyclophosphamide (25 mg/kg per dose), and the other will be given a usual dose (37.5 mg/kg).
Sites in Michigan, Missouri, Oregon, Virginia, and Washington started recruiting for 190 participants in December 2023. Study centers in Florida, Massachusetts, New York, and Wisconsin are also planned. Infection-free survival is the primary endpoint, and overall survival is a secondary measure. Quality of life (QoL) is not recorded. More details at clinicaltrials.gov.
Untreated chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL). Adults who are newly diagnosed with this type of cancer and have active disease may wish to consider a randomized, open-label, phase 3 trial testing an experimental Bruton tyrosine kinase (BTK) inhibitor, nemtabrutinib (from Merck Sharp & Dohme), against standard-of-care BTK inhibitors ibrutinib (Imbruvica) and acalabrutinib (Calquence).
BTK inhibitors target B-cell proliferation in B-cell cancers such as CLL/SLL and allow for chemotherapy-free treatment of some hematological malignancies. In this study, until disease progression, unacceptable toxicity, or another reason for discontinuation occurs, participants will take daily oral nemtabrutinib, ibrutinib, or acalabrutinib.
The study opened in December 2023 in Pennsylvania, Washington, Taiwan, Israel, and the United Kingdom seeking 1200 participants. The primary outcomes are objective response rate and progression-free survival. Overall survival is a secondary outcome, and QoL is not measured. More details at clinicaltrials.gov.
Relapsed or refractory leukemia with a KMT2A-gene rearrangement (KMT2A-r). Children aged 1 month to younger than 6 years with this diagnosis may be able to join an open-label, nonrandomized, Children’s Oncology Group phase 2 study to determine the most tolerable and/or effective dose of an experimental oral drug called revumenib when added to chemotherapy.
KMT2A-gene alterations are associated with a poor prognosis in leukemia. These alterations cause blood cells to dedifferentiate and start proliferating uncontrollably as leukemia cells. The expression of the damaged KMT2A gene relies on a protein called menin. Revumenib, from Syndax Pharmaceuticals, blocks menin and prevents expression of KMT2A.
Children in the study will receive two different regimens of revumenib in combination with chemotherapy for up to a year, or until disease progression or unacceptable toxicity, and will then be followed for up to 5 years. Trial centers in 12 US states opened their doors in January 2024 looking for 78 participants. Toxicities and minimal residual disease are the primary outcomes; overall survival is a secondary outcome, and QoL is not assessed. More details at clinicaltrials.gov.
Previously untreated follicular lymphoma or diffuse large B-cell lymphoma. Adults with one of these types of lymphoma may be eligible for one of three open-label, randomized, phase 3 trials testing odronextamab (from Regeneron). This bispecific antibody is designed to ‘lock together’ CD20 on cancer cells with CD3-expressing cancer-killing T cells. It has shown anti-lymphoma activity in heavily pretreated patients.
Late in 2023, three phase 3 trials turned the spotlight on treatment-naive patients and started recruiting 2115 participants to assess odronextamab in this setting. The trial OLYMPIA-1 will compare odronextamab with standard-of-care rituximab (Rituxan) plus chemotherapy in follicular lymphoma. OLYMPIA-2 will test the drug in combination with chemotherapy, also in follicular lymphoma. OLYMPIA-3 will evaluate odronextamab plus chemotherapy against rituximab and chemotherapy in people with large B-cell lymphoma.
All study drugs, including odronextamab, will be administered by intravenous infusion, and participants will be followed for up to 5 years. Research centers across eight US states and Australia, Czechia, France, Italy, Poland, Spain, Turkey, and Thailand are currently accepting participants for the three trials. The primary outcomes are various measures of toxicity and complete response at 30 months in the follicular lymphoma studies and toxicity and progression-free survival in large B-cell lymphoma. All three trials are measuring overall survival and QoL as secondary endpoints.
Previously untreated stage II, III, or IV follicular lymphoma. Adults with this type of cancer may be eligible to participate in a randomized, open-label, phase 3 study testing whether an experimental therapy called epcoritamab (from AbbVie) improves disease response and is tolerable when added to standard therapy. For up to 120 weeks, one group of participants will receive a combination of intravenous rituximab and oral lenalidomide (Revlimid), while a second group will also receive subcutaneous injections of epcoritamab. Some participants may be offered investigators’ choice of chemotherapy as well.
Sites across Iowa, Maryland, Missouri, Ohio, Washington, and Montana started welcoming their 900 participants in February 2024. The primary outcome is complete response at 30 months. Overall survival and QoL are secondary outcomes. More details at clinicaltrials.gov.
Relapsed or refractory mantle cell lymphoma. Adults facing one of these clinical scenarios can join an Academic and Community Cancer Research United open label, phase 2 trial examining the effectiveness of combining tafasitamab (Monjuvi), lenalidomide, and venetoclax (Venclexta) for such patients.
Frontline therapy does not cure mantle cell lymphoma, and continued relapses are common. In this situation, treatments can include acalabrutinib, ibrutinib, stem cell transplantation, venetoclax, lenalidomide, and rituximab.
In this study, participants will take venetoclax and lenalidomide daily and receive intravenous tafasitamab every 2 weeks after an initial ramp-up period as per clinic standards. Participants will be followed for 5 years after entering the trial. The Mayo Clinic in Rochester, Minnesota, began recruiting the planned 100 trial participants in January 2024. The primary outcome is objective response rate; overall survival is a secondary outcome, and QoL will not be tracked. More details at clinicaltrials.gov.
All trial information is from the National Institutes of Health US National Library of Medicine (online at clinicaltrials.gov).
A version of this article appeared on Medscape.com .
Myasthenia Gravis: Treating the Whole Patient
In the dynamic field of myasthenia gravis (MG) treatment, characterized by recent therapeutic advancements and a promising pipeline, Nicholas J. Silvestri, MD, advises early-career professionals to approach the whole patient, considering not only the disease manifestations but also its broader impact on their lives, including work and family.
Emphasizing the importance of tailoring therapies based on individual needs, Dr Silvestri encourages early and aggressive intervention, citing evidence supporting better long-term outcomes, and underscores the significance of treating the whole patient rather than just the disease.
In the dynamic field of myasthenia gravis (MG) treatment, characterized by recent therapeutic advancements and a promising pipeline, Nicholas J. Silvestri, MD, advises early-career professionals to approach the whole patient, considering not only the disease manifestations but also its broader impact on their lives, including work and family.
Emphasizing the importance of tailoring therapies based on individual needs, Dr Silvestri encourages early and aggressive intervention, citing evidence supporting better long-term outcomes, and underscores the significance of treating the whole patient rather than just the disease.
In the dynamic field of myasthenia gravis (MG) treatment, characterized by recent therapeutic advancements and a promising pipeline, Nicholas J. Silvestri, MD, advises early-career professionals to approach the whole patient, considering not only the disease manifestations but also its broader impact on their lives, including work and family.
Emphasizing the importance of tailoring therapies based on individual needs, Dr Silvestri encourages early and aggressive intervention, citing evidence supporting better long-term outcomes, and underscores the significance of treating the whole patient rather than just the disease.



Myasthenia Gravis: 3 Tips to Improve Patient-Centered Care
Kelly G. Gwathmey, MD, offers three key tips for clinicians early in their careers regarding myasthenia gravis (MG): First, prioritize listening to patients, as their experiences may not always align with clinical observations. Second, advocate for shared decision-making when starting or changing treatments, considering individual patient preferences and medical conditions. Third, understand the significance of ongoing monitoring using patient-reported outcome measures and MG scales to assess treatment response and optimize care for patients with MG.
Kelly G. Gwathmey, MD, offers three key tips for clinicians early in their careers regarding myasthenia gravis (MG): First, prioritize listening to patients, as their experiences may not always align with clinical observations. Second, advocate for shared decision-making when starting or changing treatments, considering individual patient preferences and medical conditions. Third, understand the significance of ongoing monitoring using patient-reported outcome measures and MG scales to assess treatment response and optimize care for patients with MG.
Kelly G. Gwathmey, MD, offers three key tips for clinicians early in their careers regarding myasthenia gravis (MG): First, prioritize listening to patients, as their experiences may not always align with clinical observations. Second, advocate for shared decision-making when starting or changing treatments, considering individual patient preferences and medical conditions. Third, understand the significance of ongoing monitoring using patient-reported outcome measures and MG scales to assess treatment response and optimize care for patients with MG.

Myasthenia Gravis: Reflections on Past Challenges and Evolving Strategies
Nicholas J. Silvestri, MD, recounts a memorable experience with a patient with myasthenia gravis (MG) during early neurology residency, detailing the diagnostic process and initial treatment with standard therapies. Despite the patient's positive response in terms of efficacy, tolerability issues and side effects posed challenges.
Dr Silvestri highlights the evolution in MG treatment, emphasizing the availability of newer, well-tolerated options with proven efficacy, suggesting a more balanced approach between effectiveness and patient safety in contemporary MG management.
Nicholas J. Silvestri, MD, recounts a memorable experience with a patient with myasthenia gravis (MG) during early neurology residency, detailing the diagnostic process and initial treatment with standard therapies. Despite the patient's positive response in terms of efficacy, tolerability issues and side effects posed challenges.
Dr Silvestri highlights the evolution in MG treatment, emphasizing the availability of newer, well-tolerated options with proven efficacy, suggesting a more balanced approach between effectiveness and patient safety in contemporary MG management.
Nicholas J. Silvestri, MD, recounts a memorable experience with a patient with myasthenia gravis (MG) during early neurology residency, detailing the diagnostic process and initial treatment with standard therapies. Despite the patient's positive response in terms of efficacy, tolerability issues and side effects posed challenges.
Dr Silvestri highlights the evolution in MG treatment, emphasizing the availability of newer, well-tolerated options with proven efficacy, suggesting a more balanced approach between effectiveness and patient safety in contemporary MG management.

Inspiring Encounters in the Treatment of Myasthenia Gravis
Kelly G. Gwathmey, MD, recounts shadowing a neurologist during an early phase of academic training and how witnessing examinations of patients with conditions like myasthenia gravis and amyotrophic lateral sclerosis inspired a career path in neuromuscular medicine.
Dr Gwathmey also reflects on the evolution of myasthenia gravis treatment over the past two decades, noting the introduction of new medications like eculizumab, complement inhibitors, and FcRn inhibitors — offering more targeted options and hope for patients with fewer side effects — and anticipates further advancements in treatment leading to improved disease control.
Kelly G. Gwathmey, MD, recounts shadowing a neurologist during an early phase of academic training and how witnessing examinations of patients with conditions like myasthenia gravis and amyotrophic lateral sclerosis inspired a career path in neuromuscular medicine.
Dr Gwathmey also reflects on the evolution of myasthenia gravis treatment over the past two decades, noting the introduction of new medications like eculizumab, complement inhibitors, and FcRn inhibitors — offering more targeted options and hope for patients with fewer side effects — and anticipates further advancements in treatment leading to improved disease control.
Kelly G. Gwathmey, MD, recounts shadowing a neurologist during an early phase of academic training and how witnessing examinations of patients with conditions like myasthenia gravis and amyotrophic lateral sclerosis inspired a career path in neuromuscular medicine.
Dr Gwathmey also reflects on the evolution of myasthenia gravis treatment over the past two decades, noting the introduction of new medications like eculizumab, complement inhibitors, and FcRn inhibitors — offering more targeted options and hope for patients with fewer side effects — and anticipates further advancements in treatment leading to improved disease control.
Myasthenia Gravis: Lessons on a Comprehensive Approach to Patient Care
Nicholas J. Silvestri, MD, expresses gratitude for the impactful relationships and mentorship in the field of myasthenia gravis. Dr Chip Howard at the University of North Carolina is distinguished as a humble and inclusive mentor, considered influential in the field.
Dr Howard's influence goes beyond the efficacy of medications, emphasizing the importance of considering patient care comprehensively, including side effects and overall safety. This perspective has significantly shaped Dr Silvestri’s treatment approach, leading to a more holistic and patient-centered care paradigm for individuals with myasthenia gravis.
Nicholas J. Silvestri, MD, expresses gratitude for the impactful relationships and mentorship in the field of myasthenia gravis. Dr Chip Howard at the University of North Carolina is distinguished as a humble and inclusive mentor, considered influential in the field.
Dr Howard's influence goes beyond the efficacy of medications, emphasizing the importance of considering patient care comprehensively, including side effects and overall safety. This perspective has significantly shaped Dr Silvestri’s treatment approach, leading to a more holistic and patient-centered care paradigm for individuals with myasthenia gravis.
Nicholas J. Silvestri, MD, expresses gratitude for the impactful relationships and mentorship in the field of myasthenia gravis. Dr Chip Howard at the University of North Carolina is distinguished as a humble and inclusive mentor, considered influential in the field.
Dr Howard's influence goes beyond the efficacy of medications, emphasizing the importance of considering patient care comprehensively, including side effects and overall safety. This perspective has significantly shaped Dr Silvestri’s treatment approach, leading to a more holistic and patient-centered care paradigm for individuals with myasthenia gravis.

Myasthenia Gravis: A Mentor's Emphasis on Patient-Centered Outcomes
During her time in training at the University of Virginia, Kelly G. Gwathmey, MD, gained invaluable insights into myasthenia gravis (MG) care and research from the late Dr Ted Burns and Dr Larry Phillips. Dr Burns, a renowned leader in MG research, emphasized patient-centric approaches, fostering the development of crucial outcome measures like the MG composite scale and MG-QOL-15.
Burns' dedication to listening to patients' experiences shaped the development of health-related quality-of-life instruments used in MG clinical trials. For Dr Gwathmey, learning under Dr Burns underscored the significance of patient experiences in treatment decisions and highlighted the importance of incorporating patient perspectives in clinical care and research endeavors.
During her time in training at the University of Virginia, Kelly G. Gwathmey, MD, gained invaluable insights into myasthenia gravis (MG) care and research from the late Dr Ted Burns and Dr Larry Phillips. Dr Burns, a renowned leader in MG research, emphasized patient-centric approaches, fostering the development of crucial outcome measures like the MG composite scale and MG-QOL-15.
Burns' dedication to listening to patients' experiences shaped the development of health-related quality-of-life instruments used in MG clinical trials. For Dr Gwathmey, learning under Dr Burns underscored the significance of patient experiences in treatment decisions and highlighted the importance of incorporating patient perspectives in clinical care and research endeavors.
During her time in training at the University of Virginia, Kelly G. Gwathmey, MD, gained invaluable insights into myasthenia gravis (MG) care and research from the late Dr Ted Burns and Dr Larry Phillips. Dr Burns, a renowned leader in MG research, emphasized patient-centric approaches, fostering the development of crucial outcome measures like the MG composite scale and MG-QOL-15.
Burns' dedication to listening to patients' experiences shaped the development of health-related quality-of-life instruments used in MG clinical trials. For Dr Gwathmey, learning under Dr Burns underscored the significance of patient experiences in treatment decisions and highlighted the importance of incorporating patient perspectives in clinical care and research endeavors.

AML: Genetic Testing Unlocks Hope
For adult patients, “we’ve seen a series of remarkable and well-overdue advances in a space that had not changed much over the prior decades,” hematologist/oncologist Thomas William LeBlanc, MD, associate professor of medicine at Duke University School of Medicine, Durham, North Carolina, said in an interview.
According to the National Cancer Institute, AML will be newly diagnosed in 20,800 patients in 2024, at a median age of 69, and will cause 11,220 deaths. As many as 70% of adult patients will reach complete remission, and 45% of those will live for more than 3 years and potentially be cured. As for children, the Leukemia & Lymphoma Society says the 5-year survival rate from 2012-2018 was 69% for those under 15 years old.
As the American Cancer Society notes, the goal of AML treatment “is to put the leukemia into complete remission (the bone marrow and blood cell counts return to normal), preferably a complete molecular remission (no signs of leukemia in the bone marrow, even using sensitive lab tests), and to keep it that way.”
Chemotherapy Strategies Shift Over Time
In terms of the treatment of adults with AML, “targeted therapies, in addition to the expanding role of venetoclax, has really altered our approach to AML from diagnosis, including after relapse, and later in the disease,” hematologist/oncologist Andrew M. Brunner, MD, of Harvard Medical School and Massachusetts General Hospital, Boston, said in an interview. “The ability to explore these options as monotherapy and in novel combinations has dramatically expanded our treatment options.”
Much depends on the underlying genetic profile of the disease, he said. “There certainly have been gains in patient survival in AML, but those improvements remain fairly heterogeneous and dependent on the underlying genetic profile of the disease. For instance, advances in FLT3- and IDH1/2-mutated AML are a direct result of the improvements in targeted therapies directed at these mutations. Similarly, some molecular and cytogenetic subtypes of AML are particularly responsive to venetoclax-based regimens, and these regimens have been expanded to previously undertreated populations, particularly those over age 60.”
Specifically, Dr. LeBlanc said, the Food and Drug Administration has approved “3 different FLT3 inhibitors, 2 IDH1 inhibitors, 1 IDH2 inhibitor, a BCL-2 inhibitor, a smoothened/hedgehog pathway inhibitor, an oral maintenance chemotherapy/hypomethylating agent (CC-486/oral azacitidine), a CD33-targeting antibody-drug conjugate, and even a novel formulation of two older chemotherapies that improves efficacy in a poor prognosis subgroup (CPX-351/liposomal daunorubicin and cytarabine).”
There’s also been a shift in treatment protocols for patients who were not fit for intensive chemotherapy. In the past, he said, it was standard “to give single-agent hypomethylating chemotherapy with azacitidine or decitabine, or in some contexts, low-dose chemotherapy with cytarabine. Today, many patients who are older and/or more frail are receiving novel therapies either alone or in combination, with greater efficacy and longer duration of response than previously seen with chemotherapy alone.”
Outcomes Improve but Remain Grim in High-Risk Cases
As a result, Dr. LeBlanc said, “we’re definitely seeing much better outcomes in AML overall. It takes some time to prove this via outcomes data assessments in a large population, but I expect that registries will show significant improvements in overall survival in the coming years, owing to the many new FDA approvals in AML”
Dr. LeBlanc highlighted national data from 2013-2019 showing that the 5-year relative survival rate from AML is 31.7%. That’s up from 26% just a few years ago, and the numbers “always lag several years behind the current year of practice,” he said. However, “the major area where we still have relatively poor outcomes and significant unmet needs remains the ‘adverse risk’ group of patients, particularly those who are older and/or not candidates for hematopoietic stem cell transplantation, which generally is the only potentially curative option for adverse-risk AML.”
He went on to say that “this risk grouping includes those with TP53 mutations, most of which confer a particularly poor prognosis. Exciting therapies that many of us were hoping would prove effective in this subgroup have unfortunately failed in recent clinical trials. We still have a lot of work to do in adverse-risk AML particularly, and also for those whose leukemia has relapsed.”
Mikkael Sekeres, MD, MS, chief of the Division of Hematology at the University of Miami Miller School of Medicine/Sylvester Comprehensive Cancer Center, agreed that more progress is needed, since survival rates are low even as lifespans improve. One key will be “better identifying subtypes of acute myeloid leukemia, and identifying the therapies that will benefit those people most,” he said in an interview. On the other side, it’s important to identify “when aggressive therapies aren’t going to work in somebody and maybe turn toward less-aggressive approaches so we can maximize that person’s quality of life.”
What advice do AML experts have for their colleagues? Dr. LeBlanc said “older patients are not often enough considered for allogeneic stem cell transplantation, which could potentially cure their AML when given as a consolidation treatment for those in remission. I have several patients who are healthy and in their 70s who have enormously benefited from transplants and are now being several years out from transplant with adverse risk AML and without relapse. They’ve had no significant impairments of their quality of life, including no significant graft vs. host disease.”
Dr. Sekeres highlighted the American Society of Hematology’s guidelines for treating older adults with AML, which are currently being updated. It’s crucial to order genetic testing “up front,” he said. “I’m often pleasantly surprised when genetic testing returns and reveals that I have other treatment options.”
However, it’s crucial to understand a patient’s priorities. “I’ve had patients who are 75 who say to me, ‘Do everything under the sun to get rid of my leukemia, I want to live as long as possible.’ And I’ve had patients who say, ‘I want to see as little of doctors and nurses as I can. I want you to maximize my quality of life and keep me out of the hospital.’ ”
Dr. Sekeres also noted that insurers may not cover some pill-based AML treatments such as venetoclax. “We work with our patients and assistance programs. For the most part, we’re pretty successful at getting these drugs for our patients,” he said.
In Pediatrics, Clinical Trials Are Crucial
AML in children is less well-known than in adults, since the number of cases is so small. The disease is diagnosed in about 500 children a year in the United States, according to St. Jude Children’s Research Hospital, adding, however, that AML is “the most common second cancer among children treated for other cancers.”
AML in children gained attention earlier this year when the 2-year-old daughter of a Boston Herald NFL reporter died of the disease following a bone marrow transplant and chemotherapy. Despite the agonies of her treatment, reporter Doug Kyed told a reporter that his daughter Hallie “was still able to find joy every day.”
In an interview, hematologist/oncologist Sarah K. Tasian, MD, of Children’s Hospital of Philadelphia, said researchers are discovering that pediatric AML is significantly different on from a biological perspective from adult AML. “We’ve come to understand a lot more about who these patients are, what makes these leukemias tick, and what their Achilles’ heels are. Then we can align that with the clinical trials outcome data that we have.”
About 80%-90% of pediatric patients with AML nationwide are enrolled in clinical trials, Dr. Tasian said, and an international consortium called the Children’s Oncology Group gathers data about genetics. About 60%-70% of patients will be cured, she added.
However, “we’ve kind of been stuck for about the last 20 years,” she said. “A lot of improving the survival of patients has not been because we’ve been better at chemotherapy or using new chemo, but because we’ve gotten better at supportive care, at treating infections that can be fatal.”
There haven’t been major conflicts with insurers over coverage, she said, although drug shortages are a problem, especially in relapsed AML.
As for advice to colleagues, Dr. Tasian counseled them to understand the importance of genetic testing and the expanding role of stem cell transplants. “We are now transplanting somewhere between 30% and 50% of children with AML, which is a higher rate than we used to do,” she said. The number is up thanks to genetic testing that reveals which patients are most likely to benefit.
Also, she noted, “the chemotherapy that we get to these patients is really strong, and patients have a lot of complications. Really pay attention to supportive care.”
Dr. LeBlanc reported ties with AbbVie, Agios/Servier, Astellas, BMS/Celgene, Genentech, Pfizer, Incyte, Rige, Deverra, GSK, Jazz, and Seattle Genetics. Dr. Sekeres discloses relationships with BMS and Kurome. Dr. Tasian serves as the Leukemia & Lymphoma Society Pediatric Acute Leukemia consortium clinical trials leader and works with pharmaceutical companies on clinical trials under confidentiality agreements. Dr. Brunner has no disclosures.
For adult patients, “we’ve seen a series of remarkable and well-overdue advances in a space that had not changed much over the prior decades,” hematologist/oncologist Thomas William LeBlanc, MD, associate professor of medicine at Duke University School of Medicine, Durham, North Carolina, said in an interview.
According to the National Cancer Institute, AML will be newly diagnosed in 20,800 patients in 2024, at a median age of 69, and will cause 11,220 deaths. As many as 70% of adult patients will reach complete remission, and 45% of those will live for more than 3 years and potentially be cured. As for children, the Leukemia & Lymphoma Society says the 5-year survival rate from 2012-2018 was 69% for those under 15 years old.
As the American Cancer Society notes, the goal of AML treatment “is to put the leukemia into complete remission (the bone marrow and blood cell counts return to normal), preferably a complete molecular remission (no signs of leukemia in the bone marrow, even using sensitive lab tests), and to keep it that way.”
Chemotherapy Strategies Shift Over Time
In terms of the treatment of adults with AML, “targeted therapies, in addition to the expanding role of venetoclax, has really altered our approach to AML from diagnosis, including after relapse, and later in the disease,” hematologist/oncologist Andrew M. Brunner, MD, of Harvard Medical School and Massachusetts General Hospital, Boston, said in an interview. “The ability to explore these options as monotherapy and in novel combinations has dramatically expanded our treatment options.”
Much depends on the underlying genetic profile of the disease, he said. “There certainly have been gains in patient survival in AML, but those improvements remain fairly heterogeneous and dependent on the underlying genetic profile of the disease. For instance, advances in FLT3- and IDH1/2-mutated AML are a direct result of the improvements in targeted therapies directed at these mutations. Similarly, some molecular and cytogenetic subtypes of AML are particularly responsive to venetoclax-based regimens, and these regimens have been expanded to previously undertreated populations, particularly those over age 60.”
Specifically, Dr. LeBlanc said, the Food and Drug Administration has approved “3 different FLT3 inhibitors, 2 IDH1 inhibitors, 1 IDH2 inhibitor, a BCL-2 inhibitor, a smoothened/hedgehog pathway inhibitor, an oral maintenance chemotherapy/hypomethylating agent (CC-486/oral azacitidine), a CD33-targeting antibody-drug conjugate, and even a novel formulation of two older chemotherapies that improves efficacy in a poor prognosis subgroup (CPX-351/liposomal daunorubicin and cytarabine).”
There’s also been a shift in treatment protocols for patients who were not fit for intensive chemotherapy. In the past, he said, it was standard “to give single-agent hypomethylating chemotherapy with azacitidine or decitabine, or in some contexts, low-dose chemotherapy with cytarabine. Today, many patients who are older and/or more frail are receiving novel therapies either alone or in combination, with greater efficacy and longer duration of response than previously seen with chemotherapy alone.”
Outcomes Improve but Remain Grim in High-Risk Cases
As a result, Dr. LeBlanc said, “we’re definitely seeing much better outcomes in AML overall. It takes some time to prove this via outcomes data assessments in a large population, but I expect that registries will show significant improvements in overall survival in the coming years, owing to the many new FDA approvals in AML”
Dr. LeBlanc highlighted national data from 2013-2019 showing that the 5-year relative survival rate from AML is 31.7%. That’s up from 26% just a few years ago, and the numbers “always lag several years behind the current year of practice,” he said. However, “the major area where we still have relatively poor outcomes and significant unmet needs remains the ‘adverse risk’ group of patients, particularly those who are older and/or not candidates for hematopoietic stem cell transplantation, which generally is the only potentially curative option for adverse-risk AML.”
He went on to say that “this risk grouping includes those with TP53 mutations, most of which confer a particularly poor prognosis. Exciting therapies that many of us were hoping would prove effective in this subgroup have unfortunately failed in recent clinical trials. We still have a lot of work to do in adverse-risk AML particularly, and also for those whose leukemia has relapsed.”
Mikkael Sekeres, MD, MS, chief of the Division of Hematology at the University of Miami Miller School of Medicine/Sylvester Comprehensive Cancer Center, agreed that more progress is needed, since survival rates are low even as lifespans improve. One key will be “better identifying subtypes of acute myeloid leukemia, and identifying the therapies that will benefit those people most,” he said in an interview. On the other side, it’s important to identify “when aggressive therapies aren’t going to work in somebody and maybe turn toward less-aggressive approaches so we can maximize that person’s quality of life.”
What advice do AML experts have for their colleagues? Dr. LeBlanc said “older patients are not often enough considered for allogeneic stem cell transplantation, which could potentially cure their AML when given as a consolidation treatment for those in remission. I have several patients who are healthy and in their 70s who have enormously benefited from transplants and are now being several years out from transplant with adverse risk AML and without relapse. They’ve had no significant impairments of their quality of life, including no significant graft vs. host disease.”
Dr. Sekeres highlighted the American Society of Hematology’s guidelines for treating older adults with AML, which are currently being updated. It’s crucial to order genetic testing “up front,” he said. “I’m often pleasantly surprised when genetic testing returns and reveals that I have other treatment options.”
However, it’s crucial to understand a patient’s priorities. “I’ve had patients who are 75 who say to me, ‘Do everything under the sun to get rid of my leukemia, I want to live as long as possible.’ And I’ve had patients who say, ‘I want to see as little of doctors and nurses as I can. I want you to maximize my quality of life and keep me out of the hospital.’ ”
Dr. Sekeres also noted that insurers may not cover some pill-based AML treatments such as venetoclax. “We work with our patients and assistance programs. For the most part, we’re pretty successful at getting these drugs for our patients,” he said.
In Pediatrics, Clinical Trials Are Crucial
AML in children is less well-known than in adults, since the number of cases is so small. The disease is diagnosed in about 500 children a year in the United States, according to St. Jude Children’s Research Hospital, adding, however, that AML is “the most common second cancer among children treated for other cancers.”
AML in children gained attention earlier this year when the 2-year-old daughter of a Boston Herald NFL reporter died of the disease following a bone marrow transplant and chemotherapy. Despite the agonies of her treatment, reporter Doug Kyed told a reporter that his daughter Hallie “was still able to find joy every day.”
In an interview, hematologist/oncologist Sarah K. Tasian, MD, of Children’s Hospital of Philadelphia, said researchers are discovering that pediatric AML is significantly different on from a biological perspective from adult AML. “We’ve come to understand a lot more about who these patients are, what makes these leukemias tick, and what their Achilles’ heels are. Then we can align that with the clinical trials outcome data that we have.”
About 80%-90% of pediatric patients with AML nationwide are enrolled in clinical trials, Dr. Tasian said, and an international consortium called the Children’s Oncology Group gathers data about genetics. About 60%-70% of patients will be cured, she added.
However, “we’ve kind of been stuck for about the last 20 years,” she said. “A lot of improving the survival of patients has not been because we’ve been better at chemotherapy or using new chemo, but because we’ve gotten better at supportive care, at treating infections that can be fatal.”
There haven’t been major conflicts with insurers over coverage, she said, although drug shortages are a problem, especially in relapsed AML.
As for advice to colleagues, Dr. Tasian counseled them to understand the importance of genetic testing and the expanding role of stem cell transplants. “We are now transplanting somewhere between 30% and 50% of children with AML, which is a higher rate than we used to do,” she said. The number is up thanks to genetic testing that reveals which patients are most likely to benefit.
Also, she noted, “the chemotherapy that we get to these patients is really strong, and patients have a lot of complications. Really pay attention to supportive care.”
Dr. LeBlanc reported ties with AbbVie, Agios/Servier, Astellas, BMS/Celgene, Genentech, Pfizer, Incyte, Rige, Deverra, GSK, Jazz, and Seattle Genetics. Dr. Sekeres discloses relationships with BMS and Kurome. Dr. Tasian serves as the Leukemia & Lymphoma Society Pediatric Acute Leukemia consortium clinical trials leader and works with pharmaceutical companies on clinical trials under confidentiality agreements. Dr. Brunner has no disclosures.
For adult patients, “we’ve seen a series of remarkable and well-overdue advances in a space that had not changed much over the prior decades,” hematologist/oncologist Thomas William LeBlanc, MD, associate professor of medicine at Duke University School of Medicine, Durham, North Carolina, said in an interview.
According to the National Cancer Institute, AML will be newly diagnosed in 20,800 patients in 2024, at a median age of 69, and will cause 11,220 deaths. As many as 70% of adult patients will reach complete remission, and 45% of those will live for more than 3 years and potentially be cured. As for children, the Leukemia & Lymphoma Society says the 5-year survival rate from 2012-2018 was 69% for those under 15 years old.
As the American Cancer Society notes, the goal of AML treatment “is to put the leukemia into complete remission (the bone marrow and blood cell counts return to normal), preferably a complete molecular remission (no signs of leukemia in the bone marrow, even using sensitive lab tests), and to keep it that way.”
Chemotherapy Strategies Shift Over Time
In terms of the treatment of adults with AML, “targeted therapies, in addition to the expanding role of venetoclax, has really altered our approach to AML from diagnosis, including after relapse, and later in the disease,” hematologist/oncologist Andrew M. Brunner, MD, of Harvard Medical School and Massachusetts General Hospital, Boston, said in an interview. “The ability to explore these options as monotherapy and in novel combinations has dramatically expanded our treatment options.”
Much depends on the underlying genetic profile of the disease, he said. “There certainly have been gains in patient survival in AML, but those improvements remain fairly heterogeneous and dependent on the underlying genetic profile of the disease. For instance, advances in FLT3- and IDH1/2-mutated AML are a direct result of the improvements in targeted therapies directed at these mutations. Similarly, some molecular and cytogenetic subtypes of AML are particularly responsive to venetoclax-based regimens, and these regimens have been expanded to previously undertreated populations, particularly those over age 60.”
Specifically, Dr. LeBlanc said, the Food and Drug Administration has approved “3 different FLT3 inhibitors, 2 IDH1 inhibitors, 1 IDH2 inhibitor, a BCL-2 inhibitor, a smoothened/hedgehog pathway inhibitor, an oral maintenance chemotherapy/hypomethylating agent (CC-486/oral azacitidine), a CD33-targeting antibody-drug conjugate, and even a novel formulation of two older chemotherapies that improves efficacy in a poor prognosis subgroup (CPX-351/liposomal daunorubicin and cytarabine).”
There’s also been a shift in treatment protocols for patients who were not fit for intensive chemotherapy. In the past, he said, it was standard “to give single-agent hypomethylating chemotherapy with azacitidine or decitabine, or in some contexts, low-dose chemotherapy with cytarabine. Today, many patients who are older and/or more frail are receiving novel therapies either alone or in combination, with greater efficacy and longer duration of response than previously seen with chemotherapy alone.”
Outcomes Improve but Remain Grim in High-Risk Cases
As a result, Dr. LeBlanc said, “we’re definitely seeing much better outcomes in AML overall. It takes some time to prove this via outcomes data assessments in a large population, but I expect that registries will show significant improvements in overall survival in the coming years, owing to the many new FDA approvals in AML”
Dr. LeBlanc highlighted national data from 2013-2019 showing that the 5-year relative survival rate from AML is 31.7%. That’s up from 26% just a few years ago, and the numbers “always lag several years behind the current year of practice,” he said. However, “the major area where we still have relatively poor outcomes and significant unmet needs remains the ‘adverse risk’ group of patients, particularly those who are older and/or not candidates for hematopoietic stem cell transplantation, which generally is the only potentially curative option for adverse-risk AML.”
He went on to say that “this risk grouping includes those with TP53 mutations, most of which confer a particularly poor prognosis. Exciting therapies that many of us were hoping would prove effective in this subgroup have unfortunately failed in recent clinical trials. We still have a lot of work to do in adverse-risk AML particularly, and also for those whose leukemia has relapsed.”
Mikkael Sekeres, MD, MS, chief of the Division of Hematology at the University of Miami Miller School of Medicine/Sylvester Comprehensive Cancer Center, agreed that more progress is needed, since survival rates are low even as lifespans improve. One key will be “better identifying subtypes of acute myeloid leukemia, and identifying the therapies that will benefit those people most,” he said in an interview. On the other side, it’s important to identify “when aggressive therapies aren’t going to work in somebody and maybe turn toward less-aggressive approaches so we can maximize that person’s quality of life.”
What advice do AML experts have for their colleagues? Dr. LeBlanc said “older patients are not often enough considered for allogeneic stem cell transplantation, which could potentially cure their AML when given as a consolidation treatment for those in remission. I have several patients who are healthy and in their 70s who have enormously benefited from transplants and are now being several years out from transplant with adverse risk AML and without relapse. They’ve had no significant impairments of their quality of life, including no significant graft vs. host disease.”
Dr. Sekeres highlighted the American Society of Hematology’s guidelines for treating older adults with AML, which are currently being updated. It’s crucial to order genetic testing “up front,” he said. “I’m often pleasantly surprised when genetic testing returns and reveals that I have other treatment options.”
However, it’s crucial to understand a patient’s priorities. “I’ve had patients who are 75 who say to me, ‘Do everything under the sun to get rid of my leukemia, I want to live as long as possible.’ And I’ve had patients who say, ‘I want to see as little of doctors and nurses as I can. I want you to maximize my quality of life and keep me out of the hospital.’ ”
Dr. Sekeres also noted that insurers may not cover some pill-based AML treatments such as venetoclax. “We work with our patients and assistance programs. For the most part, we’re pretty successful at getting these drugs for our patients,” he said.
In Pediatrics, Clinical Trials Are Crucial
AML in children is less well-known than in adults, since the number of cases is so small. The disease is diagnosed in about 500 children a year in the United States, according to St. Jude Children’s Research Hospital, adding, however, that AML is “the most common second cancer among children treated for other cancers.”
AML in children gained attention earlier this year when the 2-year-old daughter of a Boston Herald NFL reporter died of the disease following a bone marrow transplant and chemotherapy. Despite the agonies of her treatment, reporter Doug Kyed told a reporter that his daughter Hallie “was still able to find joy every day.”
In an interview, hematologist/oncologist Sarah K. Tasian, MD, of Children’s Hospital of Philadelphia, said researchers are discovering that pediatric AML is significantly different on from a biological perspective from adult AML. “We’ve come to understand a lot more about who these patients are, what makes these leukemias tick, and what their Achilles’ heels are. Then we can align that with the clinical trials outcome data that we have.”
About 80%-90% of pediatric patients with AML nationwide are enrolled in clinical trials, Dr. Tasian said, and an international consortium called the Children’s Oncology Group gathers data about genetics. About 60%-70% of patients will be cured, she added.
However, “we’ve kind of been stuck for about the last 20 years,” she said. “A lot of improving the survival of patients has not been because we’ve been better at chemotherapy or using new chemo, but because we’ve gotten better at supportive care, at treating infections that can be fatal.”
There haven’t been major conflicts with insurers over coverage, she said, although drug shortages are a problem, especially in relapsed AML.
As for advice to colleagues, Dr. Tasian counseled them to understand the importance of genetic testing and the expanding role of stem cell transplants. “We are now transplanting somewhere between 30% and 50% of children with AML, which is a higher rate than we used to do,” she said. The number is up thanks to genetic testing that reveals which patients are most likely to benefit.
Also, she noted, “the chemotherapy that we get to these patients is really strong, and patients have a lot of complications. Really pay attention to supportive care.”
Dr. LeBlanc reported ties with AbbVie, Agios/Servier, Astellas, BMS/Celgene, Genentech, Pfizer, Incyte, Rige, Deverra, GSK, Jazz, and Seattle Genetics. Dr. Sekeres discloses relationships with BMS and Kurome. Dr. Tasian serves as the Leukemia & Lymphoma Society Pediatric Acute Leukemia consortium clinical trials leader and works with pharmaceutical companies on clinical trials under confidentiality agreements. Dr. Brunner has no disclosures.