User login
Concomitant emicizumab, ITI shows promise in severe hemophilia A
Concomitant emicizumab prophylaxis and immune tolerance induction (ITI) may be suitable for bleeding prevention in pediatric patients with severe hemophilia A and inhibitors, according to a retrospective analysis.
“The primary objective of this study [was] to review a case series of pediatric patients with hemophilia A and inhibitors at our institution who have received emicizumab concurrently with ITI,” wrote Glaivy Batsuli, MD, of Emory University in Atlanta, and her colleagues. The results of the study were reported in Haemophilia.
The case series included seven pediatric patients with severe hemophilia A who received concurrent emicizumab for bleeding prevention and ITI for inhibitor eradication. Data were collected from electronic medical records at a single hemophilia treatment center from Aug. 1 to Dec. 1, 2018.
The researchers included male patients from 0 to 21 years old who had titres greater than 0.6 chromogenic Bethesda units (CBU) per mL on two instances more than 2 weeks apart.
The treatment protocol, termed the “Atlanta Protocol,” used a novel dosing regimen, established using provider consensus, for the concomitant use of ITI and emicizumab.
After analysis, the researchers found that three patients attained a negative inhibitor titer of less than 0.6 CBU/mL, and two patients had a normal factor VIII recovery of greater than or equal to 66%.
In total, nine bleeding events were observed in four patients; however, no thrombotic events were reported. All patients continued on concomitant therapy at the point of data analysis.
The researchers reported that six patients used three different recombinant factor VIII products at 100 IU/kg, three times each week. The remaining patient used a plasma‐derived factor VIII product at an initial dose of 50 IU/kg, three times each week.
The small sample size, retrospective design, and short follow‐up period were key limitations of the study.
“Prospective studies will be necessary to compare treatment outcomes of ITI and emicizumab to other ITI regimens and to investigate whether emicizumab modifies the immunologic response to FVIII,” the researchers wrote.
No funding sources were reported. The authors reported financial affiliations with Bayer, Bioverativ, CSL Behring, Catalyst Biosciences, Genentech, HEMA Biologics, Novo Nordisk, Octapharma, and several others.
SOURCE: Batsuli G et al. Haemophilia. 2019 Aug 2. doi: 10.1111/hae.13819.
Concomitant emicizumab prophylaxis and immune tolerance induction (ITI) may be suitable for bleeding prevention in pediatric patients with severe hemophilia A and inhibitors, according to a retrospective analysis.
“The primary objective of this study [was] to review a case series of pediatric patients with hemophilia A and inhibitors at our institution who have received emicizumab concurrently with ITI,” wrote Glaivy Batsuli, MD, of Emory University in Atlanta, and her colleagues. The results of the study were reported in Haemophilia.
The case series included seven pediatric patients with severe hemophilia A who received concurrent emicizumab for bleeding prevention and ITI for inhibitor eradication. Data were collected from electronic medical records at a single hemophilia treatment center from Aug. 1 to Dec. 1, 2018.
The researchers included male patients from 0 to 21 years old who had titres greater than 0.6 chromogenic Bethesda units (CBU) per mL on two instances more than 2 weeks apart.
The treatment protocol, termed the “Atlanta Protocol,” used a novel dosing regimen, established using provider consensus, for the concomitant use of ITI and emicizumab.
After analysis, the researchers found that three patients attained a negative inhibitor titer of less than 0.6 CBU/mL, and two patients had a normal factor VIII recovery of greater than or equal to 66%.
In total, nine bleeding events were observed in four patients; however, no thrombotic events were reported. All patients continued on concomitant therapy at the point of data analysis.
The researchers reported that six patients used three different recombinant factor VIII products at 100 IU/kg, three times each week. The remaining patient used a plasma‐derived factor VIII product at an initial dose of 50 IU/kg, three times each week.
The small sample size, retrospective design, and short follow‐up period were key limitations of the study.
“Prospective studies will be necessary to compare treatment outcomes of ITI and emicizumab to other ITI regimens and to investigate whether emicizumab modifies the immunologic response to FVIII,” the researchers wrote.
No funding sources were reported. The authors reported financial affiliations with Bayer, Bioverativ, CSL Behring, Catalyst Biosciences, Genentech, HEMA Biologics, Novo Nordisk, Octapharma, and several others.
SOURCE: Batsuli G et al. Haemophilia. 2019 Aug 2. doi: 10.1111/hae.13819.
Concomitant emicizumab prophylaxis and immune tolerance induction (ITI) may be suitable for bleeding prevention in pediatric patients with severe hemophilia A and inhibitors, according to a retrospective analysis.
“The primary objective of this study [was] to review a case series of pediatric patients with hemophilia A and inhibitors at our institution who have received emicizumab concurrently with ITI,” wrote Glaivy Batsuli, MD, of Emory University in Atlanta, and her colleagues. The results of the study were reported in Haemophilia.
The case series included seven pediatric patients with severe hemophilia A who received concurrent emicizumab for bleeding prevention and ITI for inhibitor eradication. Data were collected from electronic medical records at a single hemophilia treatment center from Aug. 1 to Dec. 1, 2018.
The researchers included male patients from 0 to 21 years old who had titres greater than 0.6 chromogenic Bethesda units (CBU) per mL on two instances more than 2 weeks apart.
The treatment protocol, termed the “Atlanta Protocol,” used a novel dosing regimen, established using provider consensus, for the concomitant use of ITI and emicizumab.
After analysis, the researchers found that three patients attained a negative inhibitor titer of less than 0.6 CBU/mL, and two patients had a normal factor VIII recovery of greater than or equal to 66%.
In total, nine bleeding events were observed in four patients; however, no thrombotic events were reported. All patients continued on concomitant therapy at the point of data analysis.
The researchers reported that six patients used three different recombinant factor VIII products at 100 IU/kg, three times each week. The remaining patient used a plasma‐derived factor VIII product at an initial dose of 50 IU/kg, three times each week.
The small sample size, retrospective design, and short follow‐up period were key limitations of the study.
“Prospective studies will be necessary to compare treatment outcomes of ITI and emicizumab to other ITI regimens and to investigate whether emicizumab modifies the immunologic response to FVIII,” the researchers wrote.
No funding sources were reported. The authors reported financial affiliations with Bayer, Bioverativ, CSL Behring, Catalyst Biosciences, Genentech, HEMA Biologics, Novo Nordisk, Octapharma, and several others.
SOURCE: Batsuli G et al. Haemophilia. 2019 Aug 2. doi: 10.1111/hae.13819.
FROM HAEMOPHILIA
Dabrafenib plus trametinib yields long-term benefit in melanoma patients
Dabrafenib plus trametinib treatment was associated with a 5-year overall survival rate of 34% in patients with melanoma harboring a BRAF V600E or V600K mutation, according to a combined analysis of two trials.
The 5-year progression-free survival rate was 19% in the long-term, pooled analysis of the COMBI-d and COMBI-v trials, which included at total of 563 patients with previously untreated, unresectable or metastatic melanoma who received combined treatment with the BRAF inhibitor dabrafenib and the MEK inhibitor trametinib.
Previously reported 5-year progression-free survival rates for patients treated with anti–programmed death-1 checkpoint inhibitors, either nivolumab or pembrolizumab, “appear to be similar” to these results for dabrafenib plus trametinib, investigators said in a report on the analysis appearing in the New England Journal of Medicine.
To date, however, 5-year survival data have not been reported for other BRAF-targeted therapies, according to the investigators, who were led by Caroline Robert, MD, PhD, of Institut Gustave Roussy and Paris-Sud-Paris-Saclay University, Villejuif, France.
“These data will be critical to assess the potential of therapy to exert long-term disease control through analysis of survival plateaus and to understand factors predictive of long-term survival,” Dr. Robert and coauthors wrote in their report.
A total of 211 patients in the COMBI-d trial were randomly allocated to receive the combination of dabrafenib plus trametinib, while in COMBI-v, 352 received this combination therapy, according to investigators.
Notably, the survival curves for dabrafenib plus trametinib appear to plateau starting at 3 years, investigators reported. In a previously published report on pooled COMBI-d and COMBI-v data, the 3-year progression-free survival rate was 23%, and the 3-year overall survival rate was 44%.
In this more recent analysis, progression-free survival rates were 21% at 4 years and 19% at 5 years, while overall survival rates were 37% at 4 years and 34% at 5 years.
“This finding suggests stabilization of rates of progression-free survival and overall survival over time in this population,” Dr. Robert and colleagues wrote.
Survival rates were higher in patients with normal lactate dehydrogenase (LDH) levels at baseline, and they were especially high in those with normal LDH and three or fewer disease sites at baseline, according to the report. Specifically, the reported 5-year rates of progression-free and overall survival were 31% and 55%, respectively.
Other factors associated with prolonged progression-free survival included female sex, older age, better performance status, and BRAF V600E genotype, according to results of a multivariate analysis that investigators said confirmed findings from the previously reported 3-year data.
The study was supported by GlaxoSmithKline and Novartis. Dr. Robert provided disclosures related to BMS, Pierre Fabre, Novartis, Amgen, Merck, Roche, MSD, and Sanofi.
SOURCE: Robert C et al. N Engl J Med. 2019 Aug 15. doi: 10.1056/NEJMoa1904059
Dabrafenib plus trametinib treatment was associated with a 5-year overall survival rate of 34% in patients with melanoma harboring a BRAF V600E or V600K mutation, according to a combined analysis of two trials.
The 5-year progression-free survival rate was 19% in the long-term, pooled analysis of the COMBI-d and COMBI-v trials, which included at total of 563 patients with previously untreated, unresectable or metastatic melanoma who received combined treatment with the BRAF inhibitor dabrafenib and the MEK inhibitor trametinib.
Previously reported 5-year progression-free survival rates for patients treated with anti–programmed death-1 checkpoint inhibitors, either nivolumab or pembrolizumab, “appear to be similar” to these results for dabrafenib plus trametinib, investigators said in a report on the analysis appearing in the New England Journal of Medicine.
To date, however, 5-year survival data have not been reported for other BRAF-targeted therapies, according to the investigators, who were led by Caroline Robert, MD, PhD, of Institut Gustave Roussy and Paris-Sud-Paris-Saclay University, Villejuif, France.
“These data will be critical to assess the potential of therapy to exert long-term disease control through analysis of survival plateaus and to understand factors predictive of long-term survival,” Dr. Robert and coauthors wrote in their report.
A total of 211 patients in the COMBI-d trial were randomly allocated to receive the combination of dabrafenib plus trametinib, while in COMBI-v, 352 received this combination therapy, according to investigators.
Notably, the survival curves for dabrafenib plus trametinib appear to plateau starting at 3 years, investigators reported. In a previously published report on pooled COMBI-d and COMBI-v data, the 3-year progression-free survival rate was 23%, and the 3-year overall survival rate was 44%.
In this more recent analysis, progression-free survival rates were 21% at 4 years and 19% at 5 years, while overall survival rates were 37% at 4 years and 34% at 5 years.
“This finding suggests stabilization of rates of progression-free survival and overall survival over time in this population,” Dr. Robert and colleagues wrote.
Survival rates were higher in patients with normal lactate dehydrogenase (LDH) levels at baseline, and they were especially high in those with normal LDH and three or fewer disease sites at baseline, according to the report. Specifically, the reported 5-year rates of progression-free and overall survival were 31% and 55%, respectively.
Other factors associated with prolonged progression-free survival included female sex, older age, better performance status, and BRAF V600E genotype, according to results of a multivariate analysis that investigators said confirmed findings from the previously reported 3-year data.
The study was supported by GlaxoSmithKline and Novartis. Dr. Robert provided disclosures related to BMS, Pierre Fabre, Novartis, Amgen, Merck, Roche, MSD, and Sanofi.
SOURCE: Robert C et al. N Engl J Med. 2019 Aug 15. doi: 10.1056/NEJMoa1904059
Dabrafenib plus trametinib treatment was associated with a 5-year overall survival rate of 34% in patients with melanoma harboring a BRAF V600E or V600K mutation, according to a combined analysis of two trials.
The 5-year progression-free survival rate was 19% in the long-term, pooled analysis of the COMBI-d and COMBI-v trials, which included at total of 563 patients with previously untreated, unresectable or metastatic melanoma who received combined treatment with the BRAF inhibitor dabrafenib and the MEK inhibitor trametinib.
Previously reported 5-year progression-free survival rates for patients treated with anti–programmed death-1 checkpoint inhibitors, either nivolumab or pembrolizumab, “appear to be similar” to these results for dabrafenib plus trametinib, investigators said in a report on the analysis appearing in the New England Journal of Medicine.
To date, however, 5-year survival data have not been reported for other BRAF-targeted therapies, according to the investigators, who were led by Caroline Robert, MD, PhD, of Institut Gustave Roussy and Paris-Sud-Paris-Saclay University, Villejuif, France.
“These data will be critical to assess the potential of therapy to exert long-term disease control through analysis of survival plateaus and to understand factors predictive of long-term survival,” Dr. Robert and coauthors wrote in their report.
A total of 211 patients in the COMBI-d trial were randomly allocated to receive the combination of dabrafenib plus trametinib, while in COMBI-v, 352 received this combination therapy, according to investigators.
Notably, the survival curves for dabrafenib plus trametinib appear to plateau starting at 3 years, investigators reported. In a previously published report on pooled COMBI-d and COMBI-v data, the 3-year progression-free survival rate was 23%, and the 3-year overall survival rate was 44%.
In this more recent analysis, progression-free survival rates were 21% at 4 years and 19% at 5 years, while overall survival rates were 37% at 4 years and 34% at 5 years.
“This finding suggests stabilization of rates of progression-free survival and overall survival over time in this population,” Dr. Robert and colleagues wrote.
Survival rates were higher in patients with normal lactate dehydrogenase (LDH) levels at baseline, and they were especially high in those with normal LDH and three or fewer disease sites at baseline, according to the report. Specifically, the reported 5-year rates of progression-free and overall survival were 31% and 55%, respectively.
Other factors associated with prolonged progression-free survival included female sex, older age, better performance status, and BRAF V600E genotype, according to results of a multivariate analysis that investigators said confirmed findings from the previously reported 3-year data.
The study was supported by GlaxoSmithKline and Novartis. Dr. Robert provided disclosures related to BMS, Pierre Fabre, Novartis, Amgen, Merck, Roche, MSD, and Sanofi.
SOURCE: Robert C et al. N Engl J Med. 2019 Aug 15. doi: 10.1056/NEJMoa1904059
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: A long-term survival benefit was seen in about a third of patients with metastatic or unresectable melanoma who underwent first-line treatment with dabrafenib and trametinib.
Major finding: The 5-year rates of progression-free survival and overall survival were 19% and 34%, respectively.
Study details: Pooled analysis including 563 patients randomly allocated to the combination treatment in two randomized trials (COMBI-d and COMBI-v).
Disclosures: The study was supported by GlaxoSmithKline and Novartis. The first author provided disclosures related to BMS, Pierre Fabre, Novartis, Amgen, Merck, Roche, MSD, and Sanofi.
Source: Robert C et al. N Engl J Med. 2019 Aug 15. doi: 10.1056/NEJMoa1904059
FDA approves drug combo to treat highly resistant TB
The U.S. Food and Drug Administration granted special approval to a new drug combo intended for the treatment of “a limited and specific population of adult patients with extensively drug resistant, treatment-intolerant or nonresponsive multidrug-resistant pulmonary” tuberculosis, according to an FDA news release.

The effectiveness of the combination treatment of pretomanid tablets with bedaquiline and linezolid was shown in a clinical study of patients with extensively drug-resistant, treatment-intolerant, or nonresponsive multidrug-resistant pulmonary tuberculosis of the lungs. Of 107 infected patients who were evaluated 6 months after the end of therapy, 95 (89%) were deemed successes, which significantly exceeded the historical success rates for treatment of extensively drug-resistant TB, the FDA reported. The trial is sponsored by the Global Alliance for TB Drug Development.
The most common adverse effects reported included peripheral neuropathy, anemia, nausea, vomiting, headache, increased liver enzymes, dyspepsia, rash, visual impairment, low blood sugar, and diarrhea, according to the release.
“Multidrug-resistant TB and extensively drug-resistant TB are public health threats due to limited treatment options. New treatments are important to meet patient national and global health needs,” stated FDA Principal Deputy Commissioner Amy Abernethy, MD, PhD, in the release. She also explained that the approval marked the second time a drug was approved under the “Limited Population Pathway for Antibacterial and Antifungal Drugs, a pathway advanced by Congress to spur development of drugs targeting infections that lack effective therapies.”
In 2016, the World Health Organization reported that there were an estimated 490,000 new cases of multidrug-resistant TB worldwide, with a smaller portion of cases of extensively drug-resistant TB, according to the release, demonstrating the need for new therapeutics.
SOURCE: U.S. Food and Drug Administration. Aug. 14, 2019. News release.
The U.S. Food and Drug Administration granted special approval to a new drug combo intended for the treatment of “a limited and specific population of adult patients with extensively drug resistant, treatment-intolerant or nonresponsive multidrug-resistant pulmonary” tuberculosis, according to an FDA news release.
The effectiveness of the combination treatment of pretomanid tablets with bedaquiline and linezolid was shown in a clinical study of patients with extensively drug-resistant, treatment-intolerant, or nonresponsive multidrug-resistant pulmonary tuberculosis of the lungs. Of 107 infected patients who were evaluated 6 months after the end of therapy, 95 (89%) were deemed successes, which significantly exceeded the historical success rates for treatment of extensively drug-resistant TB, the FDA reported. The trial is sponsored by the Global Alliance for TB Drug Development.
The most common adverse effects reported included peripheral neuropathy, anemia, nausea, vomiting, headache, increased liver enzymes, dyspepsia, rash, visual impairment, low blood sugar, and diarrhea, according to the release.
“Multidrug-resistant TB and extensively drug-resistant TB are public health threats due to limited treatment options. New treatments are important to meet patient national and global health needs,” stated FDA Principal Deputy Commissioner Amy Abernethy, MD, PhD, in the release. She also explained that the approval marked the second time a drug was approved under the “Limited Population Pathway for Antibacterial and Antifungal Drugs, a pathway advanced by Congress to spur development of drugs targeting infections that lack effective therapies.”
In 2016, the World Health Organization reported that there were an estimated 490,000 new cases of multidrug-resistant TB worldwide, with a smaller portion of cases of extensively drug-resistant TB, according to the release, demonstrating the need for new therapeutics.
SOURCE: U.S. Food and Drug Administration. Aug. 14, 2019. News release.
The U.S. Food and Drug Administration granted special approval to a new drug combo intended for the treatment of “a limited and specific population of adult patients with extensively drug resistant, treatment-intolerant or nonresponsive multidrug-resistant pulmonary” tuberculosis, according to an FDA news release.
The effectiveness of the combination treatment of pretomanid tablets with bedaquiline and linezolid was shown in a clinical study of patients with extensively drug-resistant, treatment-intolerant, or nonresponsive multidrug-resistant pulmonary tuberculosis of the lungs. Of 107 infected patients who were evaluated 6 months after the end of therapy, 95 (89%) were deemed successes, which significantly exceeded the historical success rates for treatment of extensively drug-resistant TB, the FDA reported. The trial is sponsored by the Global Alliance for TB Drug Development.
The most common adverse effects reported included peripheral neuropathy, anemia, nausea, vomiting, headache, increased liver enzymes, dyspepsia, rash, visual impairment, low blood sugar, and diarrhea, according to the release.
“Multidrug-resistant TB and extensively drug-resistant TB are public health threats due to limited treatment options. New treatments are important to meet patient national and global health needs,” stated FDA Principal Deputy Commissioner Amy Abernethy, MD, PhD, in the release. She also explained that the approval marked the second time a drug was approved under the “Limited Population Pathway for Antibacterial and Antifungal Drugs, a pathway advanced by Congress to spur development of drugs targeting infections that lack effective therapies.”
In 2016, the World Health Organization reported that there were an estimated 490,000 new cases of multidrug-resistant TB worldwide, with a smaller portion of cases of extensively drug-resistant TB, according to the release, demonstrating the need for new therapeutics.
SOURCE: U.S. Food and Drug Administration. Aug. 14, 2019. News release.
NEWS FROM THE FDA
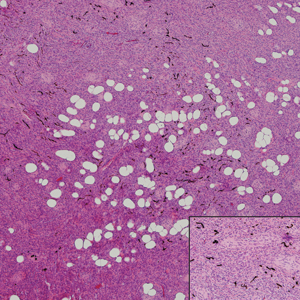
Pigmented Mass on the Shoulder
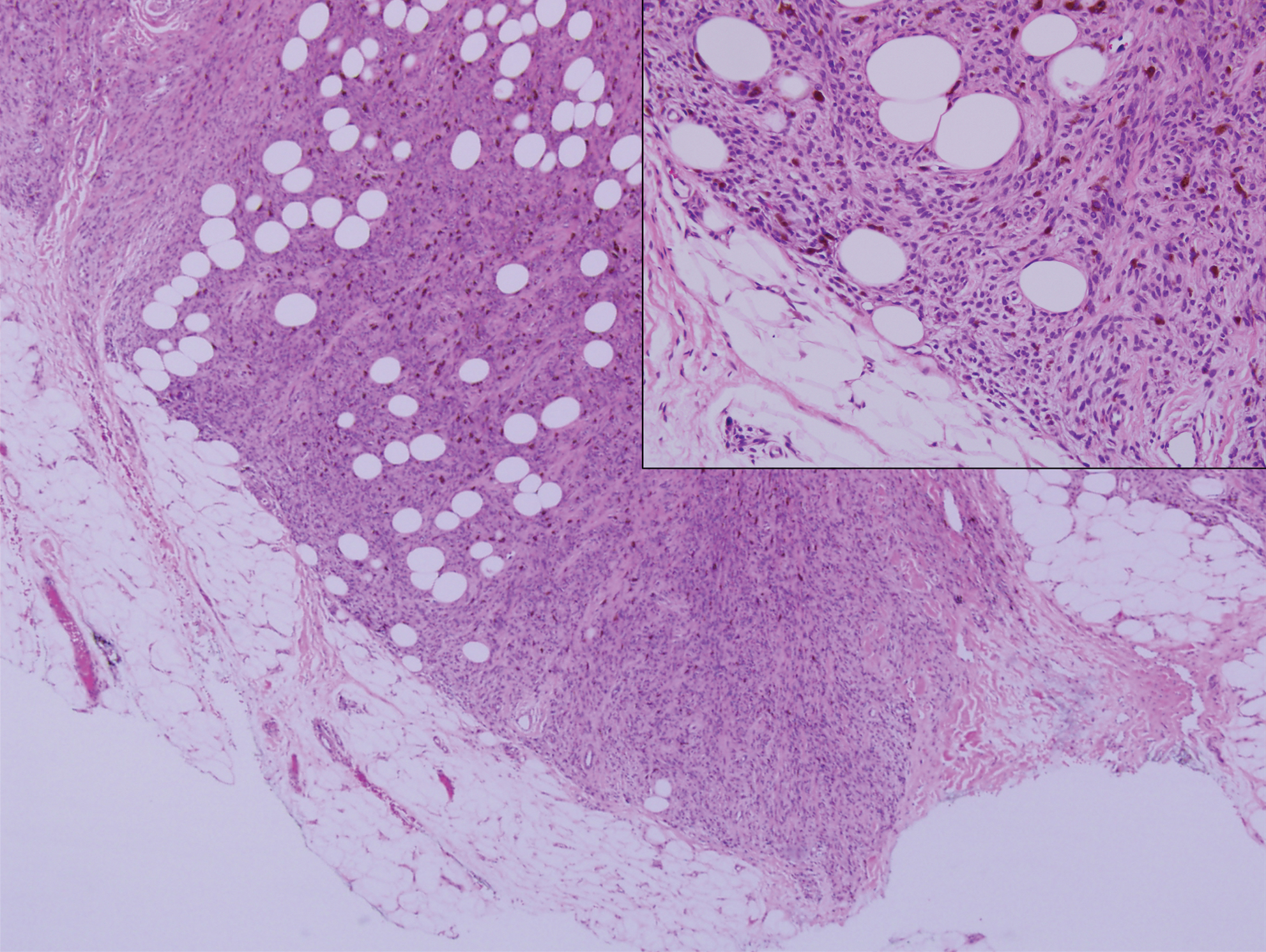
The Diagnosis: Pigmented Dermatofibrosarcoma Protuberans
Pigmented dermatofibrosarcoma protuberans (PDFSP), also known as Bednar tumor, is an uncommon variant of dermatofibrosarcoma protuberans (DFSP). Pigmented dermatofibrosarcoma protuberans constitutes 1% to 5% of all DFSP cases and most commonly is seen in nonwhite adults in the fourth decade of life, with occasional cases seen in pediatric patients, including some congenital cases. Typical sites of involvement include the shoulders, trunk, arms, legs, head, and neck.1,2 It also has been reported at sites of prior immunization, trauma, and insect bites.3
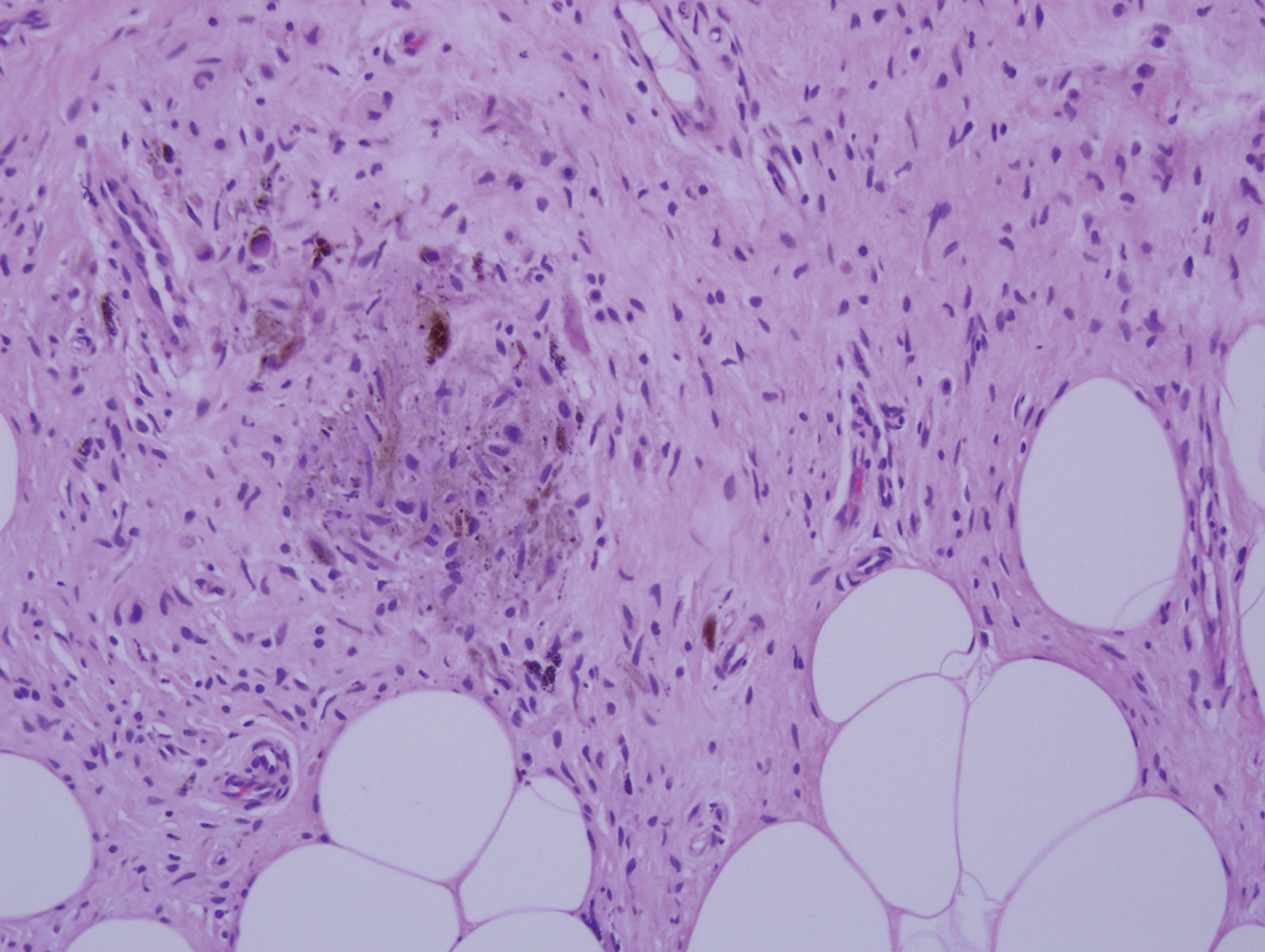
Histopathologic examination of our patient's shoulder nodule revealed an infiltrative neoplasm in the dermis and subcutaneous tissue composed of spindled cells with a storiform pattern and foci of scattered elongated dendritic pigmented cells. A narrow grenz zone separated the tumor from the epidermis, and characteristic honeycomb infiltration by tumor cells was noted in the subcutaneous fat. The nuclei were bland and monomorphous with areas of neuroid differentiation containing whorls and nerve cord-like structures (quiz image). The tumor cells were diffusely CD34 and vimentin positive, while S-100, SOX-10, neurofilament, smooth muscle actin, desmin, epithelial membrane antigen, and cytokeratins were negative. The immunophenotype excluded the possibility of neurogenic, pericytic, myofibroblastic, and myoid differentiation.
Wang and Yang4 previously reported a case of PDFSP with prominent meningothelial-like whorls focally resembling extracranial meningioma; however, the tumor cells were CD34 positive and epithelial membrane antigen negative, weighing against a diagnosis of meningioma. Most cases of PDFSP demonstrate the COL1A1-PDGFB (collagen type I α; 1/platelet-derived growth factor B-chain) fusion protein caused by the translocation t(17;22)(q22;q13), as in classic DFSP.5
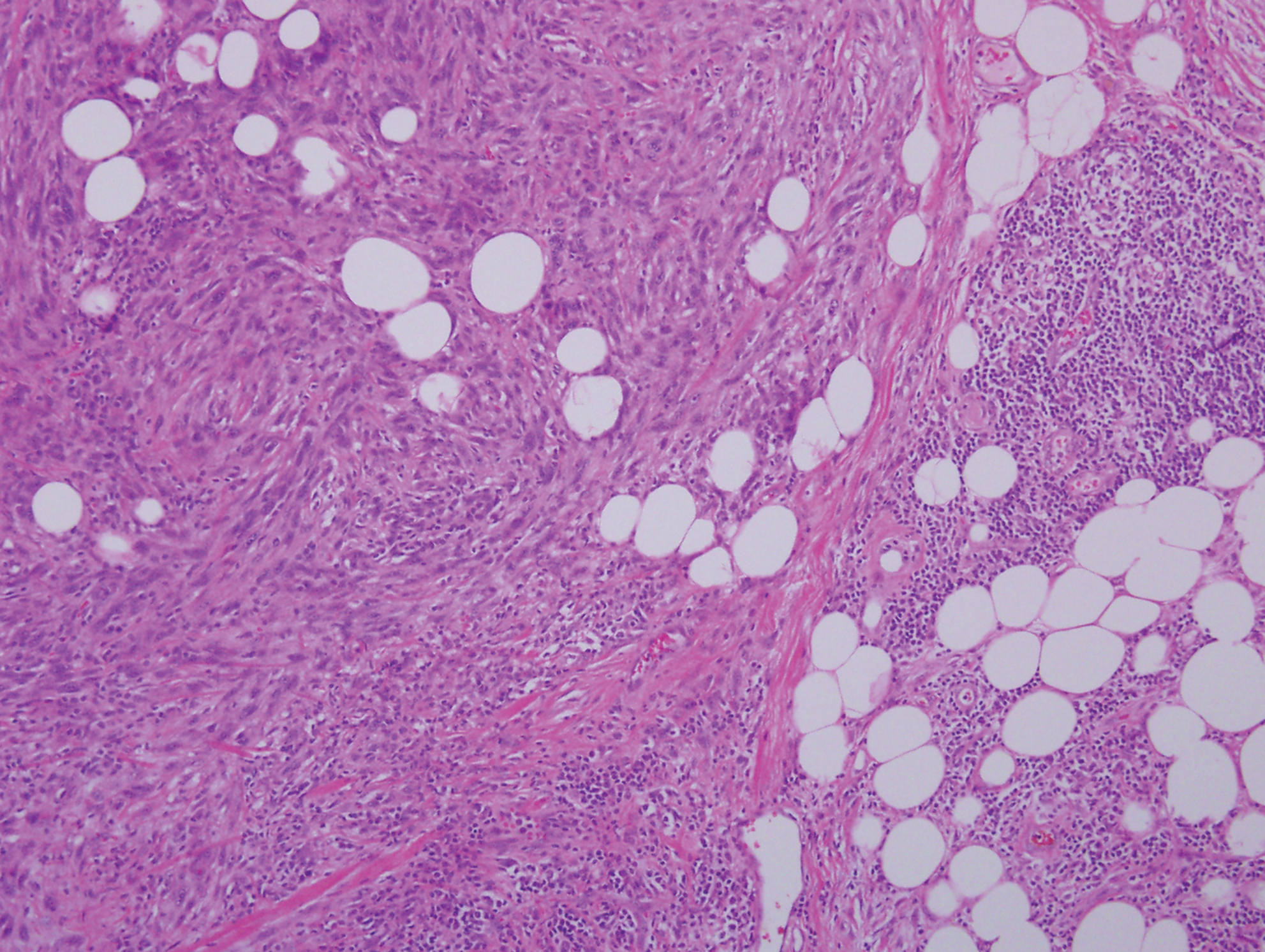
Cellular blue nevus (CBN) is a benign melanocytic neoplasm that can present at any age and often occurs on the buttocks and in the sacrococcygeal region. Clinically, CBN presents as a firm, bluish black to bluish gray, dome-shaped nodule. The size varies from a few millimeters to several centimeters.6,7 Histologically, CBN is located completely in the dermis, extending along the adnexae into the subcutaneous tissue with a dumbbell-shaped outline (Figure 1).6-8 The tumor demonstrates oval epithelioid melanocytes with vesicular nuclei and prominent nucleoli. Immunohistochemically, tumor cells stain positively for melanocytic markers such as S-100, SOX-10, MART-1, and human melanoma black 45. CD34 expression rarely is reported in a subset of CBN.9
Pigmented neurofibroma is a rare variant of neurofibroma that produces melanin pigment and has a strong association with neurofibromatosis.10 It occurs most frequently in dark-skinned populations (Fitzpatrick skin types IV-VI). The most common location is the head and neck region.11,12 Histologically, pigmented neurofibroma resembles a diffuse neurofibroma admixed with melanin-producing cells (Figure 2).12 Immunostaining shows positivity for S-100 in both pigmented and Schwann cells; however, the pigmented cells stain positively for human melanoma black 45, Melan-A, and tyrosinase.10 CD34 can be fingerprint positive in neurofibroma, but a distinction from DFSP can be made by S-100 and SOX-10 immunostaining.13
Desmoplastic melanoma (DM) is an uncommon variant of malignant melanoma and has a higher tendency for persistent local growth and less frequent metastases than other variants of melanoma. It has a predilection for chronically sun-exposed areas such as the head and neck and occurs later in life. Clinically, DM appears as nonspecific, often amelanotic nodules or plaques or as scarlike lesions.14 Histologically, DM can be classified as mixed or pure based on the degree of desmoplasia and cellularity. A paucicellular proliferation of malignant spindled melanocytes within a densely fibrotic stroma with lymphoid nodules in the dermis is characteristic (Figure 3); perineural involvement is common.14,15 The most reliable confirmative stains are S-100 and SOX-10.16
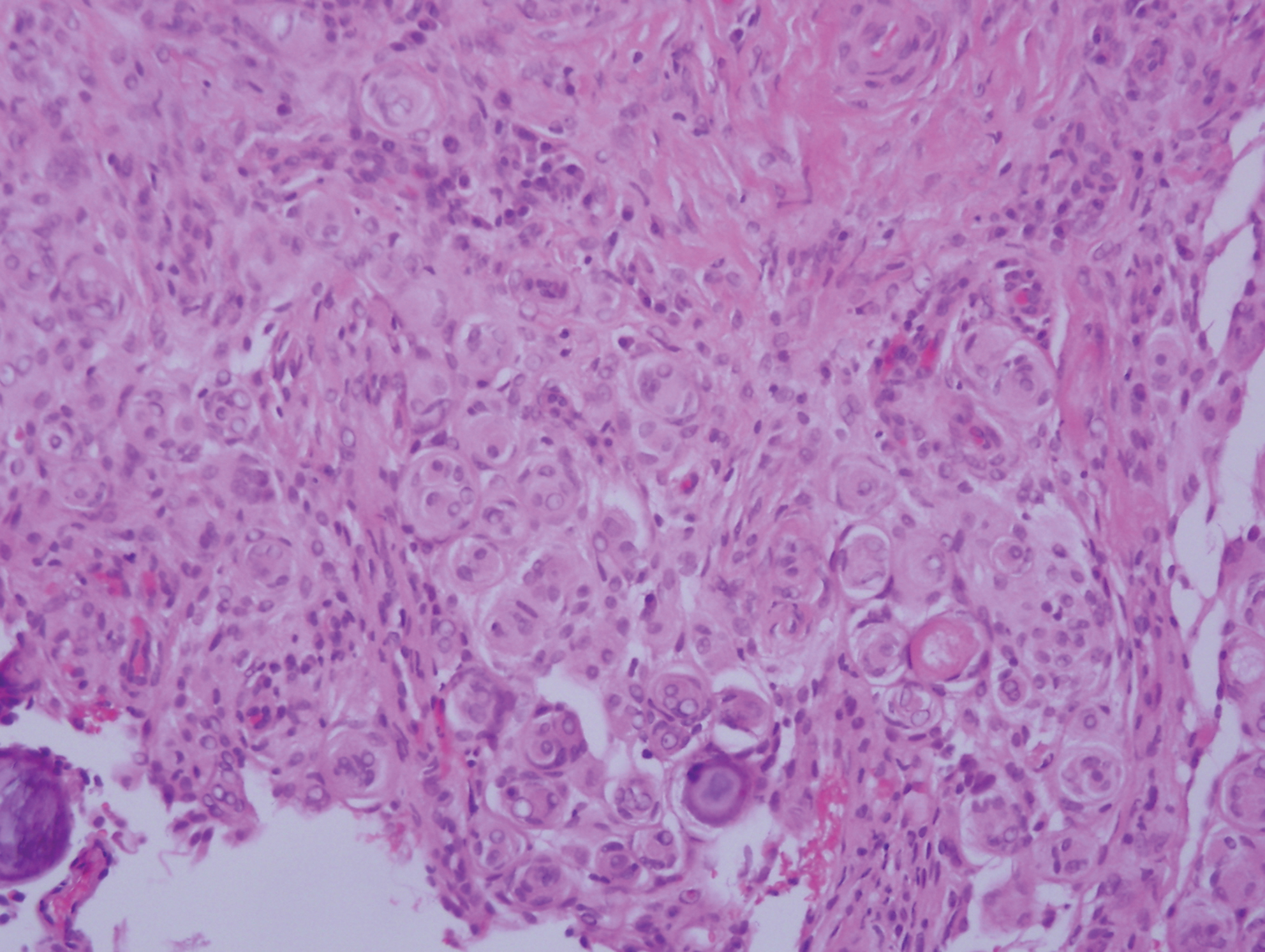
Cutaneous meningioma is a rare tumor and could be subtyped into 3 groups. Type I is primary cutaneous meningioma and usually is present at birth on the scalp and paravertebral regions with a relatively good prognosis. Type II is ectopic soft-tissue meningioma that extends into the skin from around the sensory organs on the face. Type III is local invasion or true metastasis from a central nervous system meningioma. Types II and III develop later in life and the prognosis is poor.17,18 Clinically, lesions present as firm subcutaneous nodules or swellings. Cutaneous meningioma has several histopathologic variants. The classic presentation reveals concentric wrapping of tumor cells with round-oval nuclei containing delicate chromatin. Psammoma bodies are a common finding (Figure 4). Immunohistochemically, tumor cells are diffusely positive for epithelial membrane antigen and vimentin.18,19
- Amonkar GP, Rupani A, Shah A, et al. Bednar tumor: an uncommon entity. Dermatopathology (Basel). 2016;3:36-38.
- El Hachem M, Diociaiuti A, Latella E, et al. Congenital myxoid and pigmented dermatofibrosarcoma protuberans: a case report. Pediatr Dermatol. 2013;30:E74-E77.
- Anon-Requena MJ, Pico-Valimana M, Munoz-Arias G. Bednar tumor (pigmented dermatofibrosarcoma protuberans). Actas Dermosifiliogr. 2016;107:618-620.
- Wang J, Yang W. Pigmented dermatofibrosarcoma protuberans with prominent meningothelial-like whorls. J Cutan Pathol. 2008;35(suppl 1):65-69.
- Zardawi IM, Kattampallil J, Rode J. An unusual pigmented skin tumour. Bednar tumour, dorsum of left foot (pigmented dermatofibrosarcoma protuberans). Pathology. 2004;36:358-361.
- Sugianto JZ, Ralston JS, Metcalf JS, et al. Blue nevus and "malignant blue nevus": a concise review. Semin Diagn Pathol. 2016;33:219-224.
- Zembowicz A. Blue nevi and related tumors. Clin Lab Med. 2017;37:401-415.
- Zembowicz A, Granter SR, McKee PH, et al. Amelanotic cellular blue nevus: a hypopigmented variant of the cellular blue nevus: clinicopathologic analysis of 20 cases. Am J Surg Pathol. 2002;26:1493-1500.
- Smith K, Germain M, Williams J, et al. CD34-positive cellular blue nevi. J Cutan Pathol. 2001;28:145-150.
- Inaba M, Yamamoto T, Minami R, et al. Pigmented neurofibroma: report of two cases and literature review. Pathol Int. 2001;51:565-569.
- Fetsch JF, Michal M, Miettinen M. Pigmented (melanotic) neurofibroma: a clinicopathologic and immunohistochemical analysis of 19 lesions from 17 patients. Am J Surg Pathol. 2000;24:331-343.
- Motoi T, Ishida T, Kawato A, et al. Pigmented neurofibroma: review of Japanese patients with an analysis of melanogenesis demonstrating coexpression of c-met protooncogene and microphthalmia-associated transcription factor. Hum Pathol. 2005;36:871-877.
- Yeh I, McCalmont TH. Distinguishing neurofibroma from desmoplastic melanoma: the value of the CD34 fingerprint. J Cutan Pathol. 2011;38:625-630.
- Chen LL, Jaimes N, Barker CA, et al. Desmoplastic melanoma: a review. J Am Acad Dermatol. 2013;68:825-833.
- Busam KJ. Desmoplastic melanoma. Clin Lab Med. 2011;31:321-330.
- Schleich C, Ferringer T. Desmoplastic melanoma. Cutis. 2015;96:306, 313-314, 335.
- Lopez DA, Silvers DN, Helwig EB. Cutaneous meningiomas--a clinicopathologic study. Cancer. 1974;34:728-744.
- Miedema JR, Zedek D. Cutaneous meningioma. Arch Pathol Lab Med. 2012;136:208-211.
- Bhanusali DG, Heath C, Gur D, et al. Metastatic meningioma of the scalp. Cutis. 2018;101:386-389.
The Diagnosis: Pigmented Dermatofibrosarcoma Protuberans
Pigmented dermatofibrosarcoma protuberans (PDFSP), also known as Bednar tumor, is an uncommon variant of dermatofibrosarcoma protuberans (DFSP). Pigmented dermatofibrosarcoma protuberans constitutes 1% to 5% of all DFSP cases and most commonly is seen in nonwhite adults in the fourth decade of life, with occasional cases seen in pediatric patients, including some congenital cases. Typical sites of involvement include the shoulders, trunk, arms, legs, head, and neck.1,2 It also has been reported at sites of prior immunization, trauma, and insect bites.3
Histopathologic examination of our patient's shoulder nodule revealed an infiltrative neoplasm in the dermis and subcutaneous tissue composed of spindled cells with a storiform pattern and foci of scattered elongated dendritic pigmented cells. A narrow grenz zone separated the tumor from the epidermis, and characteristic honeycomb infiltration by tumor cells was noted in the subcutaneous fat. The nuclei were bland and monomorphous with areas of neuroid differentiation containing whorls and nerve cord-like structures (quiz image). The tumor cells were diffusely CD34 and vimentin positive, while S-100, SOX-10, neurofilament, smooth muscle actin, desmin, epithelial membrane antigen, and cytokeratins were negative. The immunophenotype excluded the possibility of neurogenic, pericytic, myofibroblastic, and myoid differentiation.
Wang and Yang4 previously reported a case of PDFSP with prominent meningothelial-like whorls focally resembling extracranial meningioma; however, the tumor cells were CD34 positive and epithelial membrane antigen negative, weighing against a diagnosis of meningioma. Most cases of PDFSP demonstrate the COL1A1-PDGFB (collagen type I α; 1/platelet-derived growth factor B-chain) fusion protein caused by the translocation t(17;22)(q22;q13), as in classic DFSP.5
Cellular blue nevus (CBN) is a benign melanocytic neoplasm that can present at any age and often occurs on the buttocks and in the sacrococcygeal region. Clinically, CBN presents as a firm, bluish black to bluish gray, dome-shaped nodule. The size varies from a few millimeters to several centimeters.6,7 Histologically, CBN is located completely in the dermis, extending along the adnexae into the subcutaneous tissue with a dumbbell-shaped outline (Figure 1).6-8 The tumor demonstrates oval epithelioid melanocytes with vesicular nuclei and prominent nucleoli. Immunohistochemically, tumor cells stain positively for melanocytic markers such as S-100, SOX-10, MART-1, and human melanoma black 45. CD34 expression rarely is reported in a subset of CBN.9
Pigmented neurofibroma is a rare variant of neurofibroma that produces melanin pigment and has a strong association with neurofibromatosis.10 It occurs most frequently in dark-skinned populations (Fitzpatrick skin types IV-VI). The most common location is the head and neck region.11,12 Histologically, pigmented neurofibroma resembles a diffuse neurofibroma admixed with melanin-producing cells (Figure 2).12 Immunostaining shows positivity for S-100 in both pigmented and Schwann cells; however, the pigmented cells stain positively for human melanoma black 45, Melan-A, and tyrosinase.10 CD34 can be fingerprint positive in neurofibroma, but a distinction from DFSP can be made by S-100 and SOX-10 immunostaining.13
Desmoplastic melanoma (DM) is an uncommon variant of malignant melanoma and has a higher tendency for persistent local growth and less frequent metastases than other variants of melanoma. It has a predilection for chronically sun-exposed areas such as the head and neck and occurs later in life. Clinically, DM appears as nonspecific, often amelanotic nodules or plaques or as scarlike lesions.14 Histologically, DM can be classified as mixed or pure based on the degree of desmoplasia and cellularity. A paucicellular proliferation of malignant spindled melanocytes within a densely fibrotic stroma with lymphoid nodules in the dermis is characteristic (Figure 3); perineural involvement is common.14,15 The most reliable confirmative stains are S-100 and SOX-10.16
Cutaneous meningioma is a rare tumor and could be subtyped into 3 groups. Type I is primary cutaneous meningioma and usually is present at birth on the scalp and paravertebral regions with a relatively good prognosis. Type II is ectopic soft-tissue meningioma that extends into the skin from around the sensory organs on the face. Type III is local invasion or true metastasis from a central nervous system meningioma. Types II and III develop later in life and the prognosis is poor.17,18 Clinically, lesions present as firm subcutaneous nodules or swellings. Cutaneous meningioma has several histopathologic variants. The classic presentation reveals concentric wrapping of tumor cells with round-oval nuclei containing delicate chromatin. Psammoma bodies are a common finding (Figure 4). Immunohistochemically, tumor cells are diffusely positive for epithelial membrane antigen and vimentin.18,19
The Diagnosis: Pigmented Dermatofibrosarcoma Protuberans
Pigmented dermatofibrosarcoma protuberans (PDFSP), also known as Bednar tumor, is an uncommon variant of dermatofibrosarcoma protuberans (DFSP). Pigmented dermatofibrosarcoma protuberans constitutes 1% to 5% of all DFSP cases and most commonly is seen in nonwhite adults in the fourth decade of life, with occasional cases seen in pediatric patients, including some congenital cases. Typical sites of involvement include the shoulders, trunk, arms, legs, head, and neck.1,2 It also has been reported at sites of prior immunization, trauma, and insect bites.3
Histopathologic examination of our patient's shoulder nodule revealed an infiltrative neoplasm in the dermis and subcutaneous tissue composed of spindled cells with a storiform pattern and foci of scattered elongated dendritic pigmented cells. A narrow grenz zone separated the tumor from the epidermis, and characteristic honeycomb infiltration by tumor cells was noted in the subcutaneous fat. The nuclei were bland and monomorphous with areas of neuroid differentiation containing whorls and nerve cord-like structures (quiz image). The tumor cells were diffusely CD34 and vimentin positive, while S-100, SOX-10, neurofilament, smooth muscle actin, desmin, epithelial membrane antigen, and cytokeratins were negative. The immunophenotype excluded the possibility of neurogenic, pericytic, myofibroblastic, and myoid differentiation.
Wang and Yang4 previously reported a case of PDFSP with prominent meningothelial-like whorls focally resembling extracranial meningioma; however, the tumor cells were CD34 positive and epithelial membrane antigen negative, weighing against a diagnosis of meningioma. Most cases of PDFSP demonstrate the COL1A1-PDGFB (collagen type I α; 1/platelet-derived growth factor B-chain) fusion protein caused by the translocation t(17;22)(q22;q13), as in classic DFSP.5
Cellular blue nevus (CBN) is a benign melanocytic neoplasm that can present at any age and often occurs on the buttocks and in the sacrococcygeal region. Clinically, CBN presents as a firm, bluish black to bluish gray, dome-shaped nodule. The size varies from a few millimeters to several centimeters.6,7 Histologically, CBN is located completely in the dermis, extending along the adnexae into the subcutaneous tissue with a dumbbell-shaped outline (Figure 1).6-8 The tumor demonstrates oval epithelioid melanocytes with vesicular nuclei and prominent nucleoli. Immunohistochemically, tumor cells stain positively for melanocytic markers such as S-100, SOX-10, MART-1, and human melanoma black 45. CD34 expression rarely is reported in a subset of CBN.9
Pigmented neurofibroma is a rare variant of neurofibroma that produces melanin pigment and has a strong association with neurofibromatosis.10 It occurs most frequently in dark-skinned populations (Fitzpatrick skin types IV-VI). The most common location is the head and neck region.11,12 Histologically, pigmented neurofibroma resembles a diffuse neurofibroma admixed with melanin-producing cells (Figure 2).12 Immunostaining shows positivity for S-100 in both pigmented and Schwann cells; however, the pigmented cells stain positively for human melanoma black 45, Melan-A, and tyrosinase.10 CD34 can be fingerprint positive in neurofibroma, but a distinction from DFSP can be made by S-100 and SOX-10 immunostaining.13
Desmoplastic melanoma (DM) is an uncommon variant of malignant melanoma and has a higher tendency for persistent local growth and less frequent metastases than other variants of melanoma. It has a predilection for chronically sun-exposed areas such as the head and neck and occurs later in life. Clinically, DM appears as nonspecific, often amelanotic nodules or plaques or as scarlike lesions.14 Histologically, DM can be classified as mixed or pure based on the degree of desmoplasia and cellularity. A paucicellular proliferation of malignant spindled melanocytes within a densely fibrotic stroma with lymphoid nodules in the dermis is characteristic (Figure 3); perineural involvement is common.14,15 The most reliable confirmative stains are S-100 and SOX-10.16
Cutaneous meningioma is a rare tumor and could be subtyped into 3 groups. Type I is primary cutaneous meningioma and usually is present at birth on the scalp and paravertebral regions with a relatively good prognosis. Type II is ectopic soft-tissue meningioma that extends into the skin from around the sensory organs on the face. Type III is local invasion or true metastasis from a central nervous system meningioma. Types II and III develop later in life and the prognosis is poor.17,18 Clinically, lesions present as firm subcutaneous nodules or swellings. Cutaneous meningioma has several histopathologic variants. The classic presentation reveals concentric wrapping of tumor cells with round-oval nuclei containing delicate chromatin. Psammoma bodies are a common finding (Figure 4). Immunohistochemically, tumor cells are diffusely positive for epithelial membrane antigen and vimentin.18,19
- Amonkar GP, Rupani A, Shah A, et al. Bednar tumor: an uncommon entity. Dermatopathology (Basel). 2016;3:36-38.
- El Hachem M, Diociaiuti A, Latella E, et al. Congenital myxoid and pigmented dermatofibrosarcoma protuberans: a case report. Pediatr Dermatol. 2013;30:E74-E77.
- Anon-Requena MJ, Pico-Valimana M, Munoz-Arias G. Bednar tumor (pigmented dermatofibrosarcoma protuberans). Actas Dermosifiliogr. 2016;107:618-620.
- Wang J, Yang W. Pigmented dermatofibrosarcoma protuberans with prominent meningothelial-like whorls. J Cutan Pathol. 2008;35(suppl 1):65-69.
- Zardawi IM, Kattampallil J, Rode J. An unusual pigmented skin tumour. Bednar tumour, dorsum of left foot (pigmented dermatofibrosarcoma protuberans). Pathology. 2004;36:358-361.
- Sugianto JZ, Ralston JS, Metcalf JS, et al. Blue nevus and "malignant blue nevus": a concise review. Semin Diagn Pathol. 2016;33:219-224.
- Zembowicz A. Blue nevi and related tumors. Clin Lab Med. 2017;37:401-415.
- Zembowicz A, Granter SR, McKee PH, et al. Amelanotic cellular blue nevus: a hypopigmented variant of the cellular blue nevus: clinicopathologic analysis of 20 cases. Am J Surg Pathol. 2002;26:1493-1500.
- Smith K, Germain M, Williams J, et al. CD34-positive cellular blue nevi. J Cutan Pathol. 2001;28:145-150.
- Inaba M, Yamamoto T, Minami R, et al. Pigmented neurofibroma: report of two cases and literature review. Pathol Int. 2001;51:565-569.
- Fetsch JF, Michal M, Miettinen M. Pigmented (melanotic) neurofibroma: a clinicopathologic and immunohistochemical analysis of 19 lesions from 17 patients. Am J Surg Pathol. 2000;24:331-343.
- Motoi T, Ishida T, Kawato A, et al. Pigmented neurofibroma: review of Japanese patients with an analysis of melanogenesis demonstrating coexpression of c-met protooncogene and microphthalmia-associated transcription factor. Hum Pathol. 2005;36:871-877.
- Yeh I, McCalmont TH. Distinguishing neurofibroma from desmoplastic melanoma: the value of the CD34 fingerprint. J Cutan Pathol. 2011;38:625-630.
- Chen LL, Jaimes N, Barker CA, et al. Desmoplastic melanoma: a review. J Am Acad Dermatol. 2013;68:825-833.
- Busam KJ. Desmoplastic melanoma. Clin Lab Med. 2011;31:321-330.
- Schleich C, Ferringer T. Desmoplastic melanoma. Cutis. 2015;96:306, 313-314, 335.
- Lopez DA, Silvers DN, Helwig EB. Cutaneous meningiomas--a clinicopathologic study. Cancer. 1974;34:728-744.
- Miedema JR, Zedek D. Cutaneous meningioma. Arch Pathol Lab Med. 2012;136:208-211.
- Bhanusali DG, Heath C, Gur D, et al. Metastatic meningioma of the scalp. Cutis. 2018;101:386-389.
- Amonkar GP, Rupani A, Shah A, et al. Bednar tumor: an uncommon entity. Dermatopathology (Basel). 2016;3:36-38.
- El Hachem M, Diociaiuti A, Latella E, et al. Congenital myxoid and pigmented dermatofibrosarcoma protuberans: a case report. Pediatr Dermatol. 2013;30:E74-E77.
- Anon-Requena MJ, Pico-Valimana M, Munoz-Arias G. Bednar tumor (pigmented dermatofibrosarcoma protuberans). Actas Dermosifiliogr. 2016;107:618-620.
- Wang J, Yang W. Pigmented dermatofibrosarcoma protuberans with prominent meningothelial-like whorls. J Cutan Pathol. 2008;35(suppl 1):65-69.
- Zardawi IM, Kattampallil J, Rode J. An unusual pigmented skin tumour. Bednar tumour, dorsum of left foot (pigmented dermatofibrosarcoma protuberans). Pathology. 2004;36:358-361.
- Sugianto JZ, Ralston JS, Metcalf JS, et al. Blue nevus and "malignant blue nevus": a concise review. Semin Diagn Pathol. 2016;33:219-224.
- Zembowicz A. Blue nevi and related tumors. Clin Lab Med. 2017;37:401-415.
- Zembowicz A, Granter SR, McKee PH, et al. Amelanotic cellular blue nevus: a hypopigmented variant of the cellular blue nevus: clinicopathologic analysis of 20 cases. Am J Surg Pathol. 2002;26:1493-1500.
- Smith K, Germain M, Williams J, et al. CD34-positive cellular blue nevi. J Cutan Pathol. 2001;28:145-150.
- Inaba M, Yamamoto T, Minami R, et al. Pigmented neurofibroma: report of two cases and literature review. Pathol Int. 2001;51:565-569.
- Fetsch JF, Michal M, Miettinen M. Pigmented (melanotic) neurofibroma: a clinicopathologic and immunohistochemical analysis of 19 lesions from 17 patients. Am J Surg Pathol. 2000;24:331-343.
- Motoi T, Ishida T, Kawato A, et al. Pigmented neurofibroma: review of Japanese patients with an analysis of melanogenesis demonstrating coexpression of c-met protooncogene and microphthalmia-associated transcription factor. Hum Pathol. 2005;36:871-877.
- Yeh I, McCalmont TH. Distinguishing neurofibroma from desmoplastic melanoma: the value of the CD34 fingerprint. J Cutan Pathol. 2011;38:625-630.
- Chen LL, Jaimes N, Barker CA, et al. Desmoplastic melanoma: a review. J Am Acad Dermatol. 2013;68:825-833.
- Busam KJ. Desmoplastic melanoma. Clin Lab Med. 2011;31:321-330.
- Schleich C, Ferringer T. Desmoplastic melanoma. Cutis. 2015;96:306, 313-314, 335.
- Lopez DA, Silvers DN, Helwig EB. Cutaneous meningiomas--a clinicopathologic study. Cancer. 1974;34:728-744.
- Miedema JR, Zedek D. Cutaneous meningioma. Arch Pathol Lab Med. 2012;136:208-211.
- Bhanusali DG, Heath C, Gur D, et al. Metastatic meningioma of the scalp. Cutis. 2018;101:386-389.

A 37-year-old woman presented with an asymptomatic, indurated, pigmented, subcutaneous nodule on the right shoulder of more than 3 years' duration. The lesion had gradually increased in size with no associated symptoms. The patient had a history of endometrial adenocarcinoma and papillary thyroid carcinoma, which had been treated by hysterectomy-oophorectomy and right thyroidectomy, respectively. She had no other notable systemic abnormalities, and there was no family history of genetic disease or cancer. Physical examination demonstrated a 1.2×1.8-cm nontender, pigmented, subcutaneous nodule with a rough surface and indistinct borders. An excisional biopsy was performed.
Self-reported adherence fails to line up with objective measures in hemophilia
Considerable differences may exist between objective and subjective measures of adherence to prophylaxis in patients with hemophilia, according to a cross-sectional study.
The results highlight the effect of social desirability bias in self-reported measures of adherence and differences in conceptual understanding of adherence between hemophilia experts and patients.
Vanessa Giroto Guedes, MPH, of the Federal University of Rio de Janeiro and colleagues studied 29 male patients with hemophilia who received prophylactic treatment between August 2015 and January 2016. The study was conducted at two hemophilia treatment centers in São Paulo.
Self-perceived adherence, measured using the estimated number of clotting factor concentrate doses missed over the previous dispensing interval, was compared with an objective estimate of adherence, measured using the number of vials returned by study participants. The findings were published in Haemophilia.
Patient interviews were conducted during regularly scheduled visits to the treatment facility. The team collected self-perceived adherence data using a 5-point Likert scale, scored from very poor to very good adherence.
After analysis, the researchers found no significant correlation between the objective categorization of adherence and self-perceived extent of adherence (correlation coefficient, 0.10; 95% confidence interval, –0.28 to 0.46; P = .61).
Additionally, there was no significant correlation between the categorization of adherence measured using the proportion of missed doses evaluated objectively and using participants’ self‐reports (correlation coefficient, 0.32; 95% CI, –0.01 to 0.59; P = .11).
“Participants’ self-reported perception of adherence was almost three times more likely to be rated as very good or good than it was for the objective assessment of adherence to be classified as adherent or suboptimally adherent,” the researchers wrote.
No funding sources were reported. One coauthor reported providing consultancy services for manufacturers of therapies for hemophilia. The others reported no conflicts of interest.
SOURCE: Guedes VG et al. Haemophilia. 2019 Jul 19. doi: 10.1111/hae.13811.
Considerable differences may exist between objective and subjective measures of adherence to prophylaxis in patients with hemophilia, according to a cross-sectional study.
The results highlight the effect of social desirability bias in self-reported measures of adherence and differences in conceptual understanding of adherence between hemophilia experts and patients.
Vanessa Giroto Guedes, MPH, of the Federal University of Rio de Janeiro and colleagues studied 29 male patients with hemophilia who received prophylactic treatment between August 2015 and January 2016. The study was conducted at two hemophilia treatment centers in São Paulo.
Self-perceived adherence, measured using the estimated number of clotting factor concentrate doses missed over the previous dispensing interval, was compared with an objective estimate of adherence, measured using the number of vials returned by study participants. The findings were published in Haemophilia.
Patient interviews were conducted during regularly scheduled visits to the treatment facility. The team collected self-perceived adherence data using a 5-point Likert scale, scored from very poor to very good adherence.
After analysis, the researchers found no significant correlation between the objective categorization of adherence and self-perceived extent of adherence (correlation coefficient, 0.10; 95% confidence interval, –0.28 to 0.46; P = .61).
Additionally, there was no significant correlation between the categorization of adherence measured using the proportion of missed doses evaluated objectively and using participants’ self‐reports (correlation coefficient, 0.32; 95% CI, –0.01 to 0.59; P = .11).
“Participants’ self-reported perception of adherence was almost three times more likely to be rated as very good or good than it was for the objective assessment of adherence to be classified as adherent or suboptimally adherent,” the researchers wrote.
No funding sources were reported. One coauthor reported providing consultancy services for manufacturers of therapies for hemophilia. The others reported no conflicts of interest.
SOURCE: Guedes VG et al. Haemophilia. 2019 Jul 19. doi: 10.1111/hae.13811.
Considerable differences may exist between objective and subjective measures of adherence to prophylaxis in patients with hemophilia, according to a cross-sectional study.
The results highlight the effect of social desirability bias in self-reported measures of adherence and differences in conceptual understanding of adherence between hemophilia experts and patients.
Vanessa Giroto Guedes, MPH, of the Federal University of Rio de Janeiro and colleagues studied 29 male patients with hemophilia who received prophylactic treatment between August 2015 and January 2016. The study was conducted at two hemophilia treatment centers in São Paulo.
Self-perceived adherence, measured using the estimated number of clotting factor concentrate doses missed over the previous dispensing interval, was compared with an objective estimate of adherence, measured using the number of vials returned by study participants. The findings were published in Haemophilia.
Patient interviews were conducted during regularly scheduled visits to the treatment facility. The team collected self-perceived adherence data using a 5-point Likert scale, scored from very poor to very good adherence.
After analysis, the researchers found no significant correlation between the objective categorization of adherence and self-perceived extent of adherence (correlation coefficient, 0.10; 95% confidence interval, –0.28 to 0.46; P = .61).
Additionally, there was no significant correlation between the categorization of adherence measured using the proportion of missed doses evaluated objectively and using participants’ self‐reports (correlation coefficient, 0.32; 95% CI, –0.01 to 0.59; P = .11).
“Participants’ self-reported perception of adherence was almost three times more likely to be rated as very good or good than it was for the objective assessment of adherence to be classified as adherent or suboptimally adherent,” the researchers wrote.
No funding sources were reported. One coauthor reported providing consultancy services for manufacturers of therapies for hemophilia. The others reported no conflicts of interest.
SOURCE: Guedes VG et al. Haemophilia. 2019 Jul 19. doi: 10.1111/hae.13811.
FROM HAEMOPHILIA
Drug-inducible gene therapy unlocks IL-12 for glioblastoma
For patients with recurrent, high-grade glioblastoma, localized, drug-inducible gene therapy could unlock the anticancer potential of interleukin-12, based on a phase 1 trial.
In 31 patients who had their tumors excised, intraoperative site injection with an IL-12 vector followed by postoperative administration of veledimex, an oral activator of the transgene, increased IL-12 levels in the brain and appeared to improve overall survival, reported E. Antonio Chiocca, MD, PhD, Harvey W. Cushing Professor of Neurosurgery at Harvard Medical School, Boston, and colleagues. Although some serious adverse events were encountered, the investigators noted that these were less common with lower doses of veledimex and were reversible upon discontinuation. These findings mark a turning point in IL-12 cancer research, which previously encountered prohibitive safety obstacles.
“There was interest in the use of recombinant IL-12 in humans with cancer, and clinical trials of systemic IL-12 were undertaken but had to be stopped because the cytokine, administered as a recombinant soluble protein, was poorly tolerated,” the investigators wrote in Science Translational Medicine.
To overcome this issue, a novel treatment approach was developed. “With the objective of minimizing systemic toxicity, a ligand-inducible expression switch [RheoSwitch Therapeutic System] was developed to locally control production of IL-12 in the tumor microenvironment. In this system, transcription of the IL-12 transgene occurs only in the presence of the activator ligand, veledimex,” they noted.
The primary aim of the study was to evaluate safety and determine the optimal dose of veledimex; four dose levels were tested: 10, 20, 30, and 40 mg. Survival outcomes also were reported.
The protocol-defined maximum tolerated dose was not reached; however, the 20-mg dose was chosen, based on observed tolerability. At this dose level, the most common grade 3 or higher adverse events were lymphopenia (20.3%), thrombocytopenia (13.3%), and hyponatremia (13.3%). Specifically for grade 3 or higher neurologic adverse events, headache was most common, occurring in 13.3% of patients. Grade 2 cytokine release syndrome occurred in about one-fourth of patients (26.7%), whereas grade 3 cytokine release syndrome occurred about half as frequently (13.3%). All adverse events, including cytokine release syndrome, were reversible upon discontinuation of veledimex.
After a mean follow-up of 13.1 months, the median overall survival among patients receiving the 20-mg dose was 12.7 months. The investigators pointed out that this compared favorably with historical controls, who had a weighted median overall survival of 8.1 months. Those who received 30- or 40-mg doses had the poorest survival, which the investigators attributed to intolerability and other subgroup factors.
Data analysis also revealed a negative correlation between dexamethasone use and survival. Among patients in the 20-mg veledimex group who received 20 mg or less of dexamethasone during active veledimex dosing, median overall survival was extended to 17.8 months. The investigators speculated that this was because of reduced immune suppression, although dexamethasone could have induced cytochrome P450 3A4, which may have increased elimination of veledimex.
“In summary, this phase 1 trial reports the use of a transcriptional switch to safely control dosing of [IL-12], highlighting that this can be accomplished across the [blood-brain barrier] to remodel the tumor microenvironment with an influx of activated immune cells,” the investigators wrote.
They noted that this strategy could potentially be applied to other types of cancer, particularly those that are immunologically cold. “These data contribute to our understanding of IL-12 as a ‘master regulator’ of the immune system and highlight that even the transient production of this cytokine may function as a match to turn tumors from cold to hot.”
The study was funded by Ziopharm Oncology and the National Institutes of Health. The investigators reported additional relationships with Advantagene, Stemgen, Sigilon Therapeutics, and others.
SOURCE: Chiocca EA et al. Sci Transl Med. 2019 Aug 14. doi: 10.1126/scitranslmed.aaw5680.
For patients with recurrent, high-grade glioblastoma, localized, drug-inducible gene therapy could unlock the anticancer potential of interleukin-12, based on a phase 1 trial.
In 31 patients who had their tumors excised, intraoperative site injection with an IL-12 vector followed by postoperative administration of veledimex, an oral activator of the transgene, increased IL-12 levels in the brain and appeared to improve overall survival, reported E. Antonio Chiocca, MD, PhD, Harvey W. Cushing Professor of Neurosurgery at Harvard Medical School, Boston, and colleagues. Although some serious adverse events were encountered, the investigators noted that these were less common with lower doses of veledimex and were reversible upon discontinuation. These findings mark a turning point in IL-12 cancer research, which previously encountered prohibitive safety obstacles.
“There was interest in the use of recombinant IL-12 in humans with cancer, and clinical trials of systemic IL-12 were undertaken but had to be stopped because the cytokine, administered as a recombinant soluble protein, was poorly tolerated,” the investigators wrote in Science Translational Medicine.
To overcome this issue, a novel treatment approach was developed. “With the objective of minimizing systemic toxicity, a ligand-inducible expression switch [RheoSwitch Therapeutic System] was developed to locally control production of IL-12 in the tumor microenvironment. In this system, transcription of the IL-12 transgene occurs only in the presence of the activator ligand, veledimex,” they noted.
The primary aim of the study was to evaluate safety and determine the optimal dose of veledimex; four dose levels were tested: 10, 20, 30, and 40 mg. Survival outcomes also were reported.
The protocol-defined maximum tolerated dose was not reached; however, the 20-mg dose was chosen, based on observed tolerability. At this dose level, the most common grade 3 or higher adverse events were lymphopenia (20.3%), thrombocytopenia (13.3%), and hyponatremia (13.3%). Specifically for grade 3 or higher neurologic adverse events, headache was most common, occurring in 13.3% of patients. Grade 2 cytokine release syndrome occurred in about one-fourth of patients (26.7%), whereas grade 3 cytokine release syndrome occurred about half as frequently (13.3%). All adverse events, including cytokine release syndrome, were reversible upon discontinuation of veledimex.
After a mean follow-up of 13.1 months, the median overall survival among patients receiving the 20-mg dose was 12.7 months. The investigators pointed out that this compared favorably with historical controls, who had a weighted median overall survival of 8.1 months. Those who received 30- or 40-mg doses had the poorest survival, which the investigators attributed to intolerability and other subgroup factors.
Data analysis also revealed a negative correlation between dexamethasone use and survival. Among patients in the 20-mg veledimex group who received 20 mg or less of dexamethasone during active veledimex dosing, median overall survival was extended to 17.8 months. The investigators speculated that this was because of reduced immune suppression, although dexamethasone could have induced cytochrome P450 3A4, which may have increased elimination of veledimex.
“In summary, this phase 1 trial reports the use of a transcriptional switch to safely control dosing of [IL-12], highlighting that this can be accomplished across the [blood-brain barrier] to remodel the tumor microenvironment with an influx of activated immune cells,” the investigators wrote.
They noted that this strategy could potentially be applied to other types of cancer, particularly those that are immunologically cold. “These data contribute to our understanding of IL-12 as a ‘master regulator’ of the immune system and highlight that even the transient production of this cytokine may function as a match to turn tumors from cold to hot.”
The study was funded by Ziopharm Oncology and the National Institutes of Health. The investigators reported additional relationships with Advantagene, Stemgen, Sigilon Therapeutics, and others.
SOURCE: Chiocca EA et al. Sci Transl Med. 2019 Aug 14. doi: 10.1126/scitranslmed.aaw5680.
For patients with recurrent, high-grade glioblastoma, localized, drug-inducible gene therapy could unlock the anticancer potential of interleukin-12, based on a phase 1 trial.
In 31 patients who had their tumors excised, intraoperative site injection with an IL-12 vector followed by postoperative administration of veledimex, an oral activator of the transgene, increased IL-12 levels in the brain and appeared to improve overall survival, reported E. Antonio Chiocca, MD, PhD, Harvey W. Cushing Professor of Neurosurgery at Harvard Medical School, Boston, and colleagues. Although some serious adverse events were encountered, the investigators noted that these were less common with lower doses of veledimex and were reversible upon discontinuation. These findings mark a turning point in IL-12 cancer research, which previously encountered prohibitive safety obstacles.
“There was interest in the use of recombinant IL-12 in humans with cancer, and clinical trials of systemic IL-12 were undertaken but had to be stopped because the cytokine, administered as a recombinant soluble protein, was poorly tolerated,” the investigators wrote in Science Translational Medicine.
To overcome this issue, a novel treatment approach was developed. “With the objective of minimizing systemic toxicity, a ligand-inducible expression switch [RheoSwitch Therapeutic System] was developed to locally control production of IL-12 in the tumor microenvironment. In this system, transcription of the IL-12 transgene occurs only in the presence of the activator ligand, veledimex,” they noted.
The primary aim of the study was to evaluate safety and determine the optimal dose of veledimex; four dose levels were tested: 10, 20, 30, and 40 mg. Survival outcomes also were reported.
The protocol-defined maximum tolerated dose was not reached; however, the 20-mg dose was chosen, based on observed tolerability. At this dose level, the most common grade 3 or higher adverse events were lymphopenia (20.3%), thrombocytopenia (13.3%), and hyponatremia (13.3%). Specifically for grade 3 or higher neurologic adverse events, headache was most common, occurring in 13.3% of patients. Grade 2 cytokine release syndrome occurred in about one-fourth of patients (26.7%), whereas grade 3 cytokine release syndrome occurred about half as frequently (13.3%). All adverse events, including cytokine release syndrome, were reversible upon discontinuation of veledimex.
After a mean follow-up of 13.1 months, the median overall survival among patients receiving the 20-mg dose was 12.7 months. The investigators pointed out that this compared favorably with historical controls, who had a weighted median overall survival of 8.1 months. Those who received 30- or 40-mg doses had the poorest survival, which the investigators attributed to intolerability and other subgroup factors.
Data analysis also revealed a negative correlation between dexamethasone use and survival. Among patients in the 20-mg veledimex group who received 20 mg or less of dexamethasone during active veledimex dosing, median overall survival was extended to 17.8 months. The investigators speculated that this was because of reduced immune suppression, although dexamethasone could have induced cytochrome P450 3A4, which may have increased elimination of veledimex.
“In summary, this phase 1 trial reports the use of a transcriptional switch to safely control dosing of [IL-12], highlighting that this can be accomplished across the [blood-brain barrier] to remodel the tumor microenvironment with an influx of activated immune cells,” the investigators wrote.
They noted that this strategy could potentially be applied to other types of cancer, particularly those that are immunologically cold. “These data contribute to our understanding of IL-12 as a ‘master regulator’ of the immune system and highlight that even the transient production of this cytokine may function as a match to turn tumors from cold to hot.”
The study was funded by Ziopharm Oncology and the National Institutes of Health. The investigators reported additional relationships with Advantagene, Stemgen, Sigilon Therapeutics, and others.
SOURCE: Chiocca EA et al. Sci Transl Med. 2019 Aug 14. doi: 10.1126/scitranslmed.aaw5680.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point: For patients with recurrent, high-grade glioblastoma, localized, drug-inducible gene therapy could unlock the anticancer potential of interleukin-12.
Major finding: After 13.1 months of follow-up, median overall survival was 12.7 months, compared with a weighted median overall survival among historical controls of 8.1 months.
Study details: A phase 1 trial involving 31 patients with recurrent glioblastoma.
Disclosures: The study was funded by Ziopharm Oncology and the National Institutes of Health. The investigators reported additional relationships with Advantagene, Stemgen, Sigilon Therapeutics, and others.
Source: Chiocca EA et al. Sci Transl Med. 2019 Aug 14. doi: 10.1126/scitranslmed.aaw5680.
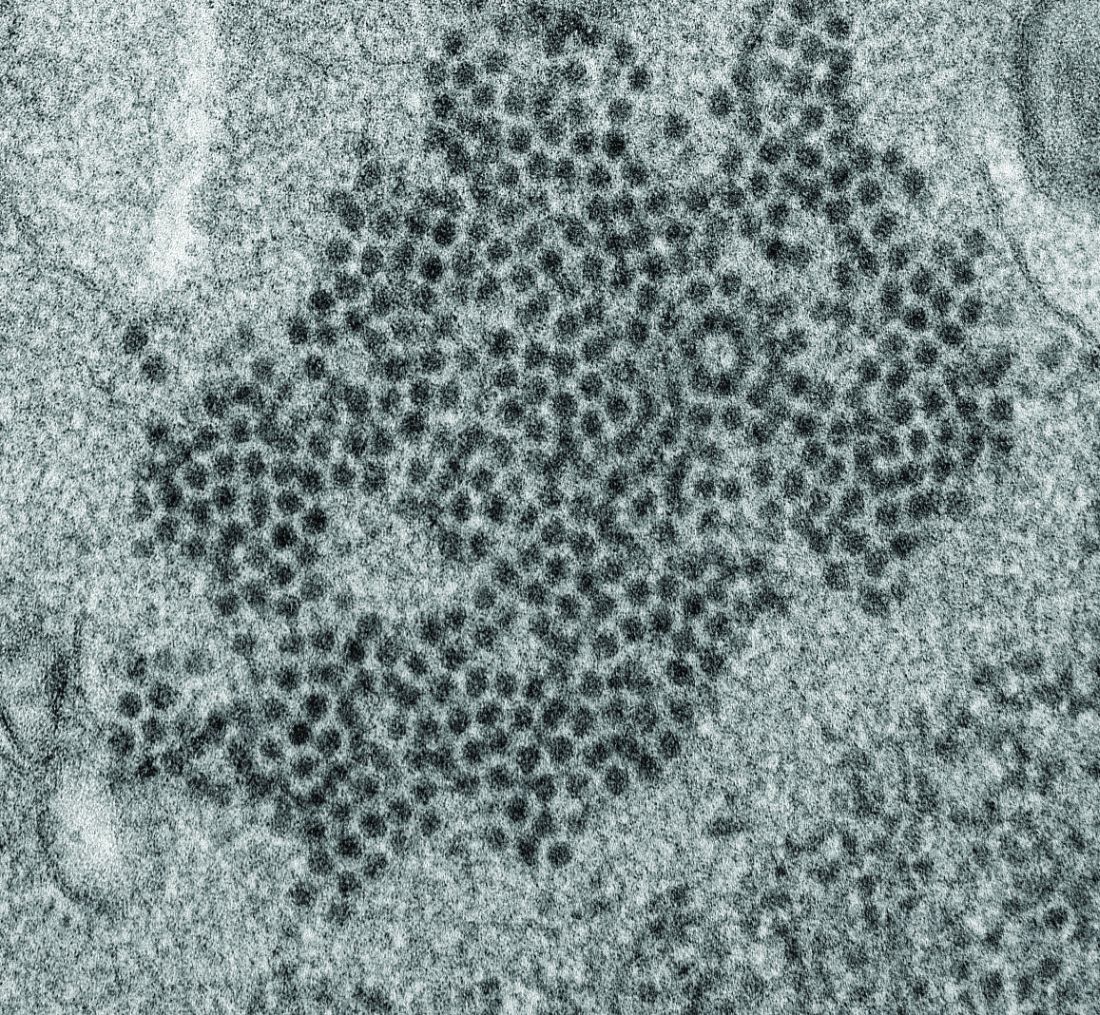
Possible role of enterovirus infection in acute flaccid myelitis cases detected
High levels of enterovirus (EV) peptides were found in the cerebrospinal fluid (CSF) and serum samples of individuals with acute flaccid myelitis (AFM) that were not present in a variety of control individuals, according to the results of a small study of patients with and without AFM published online in mBio.
In 2018, CSF samples from AFM patients were investigated by viral-capture high-throughput sequencing. These CSF and serum samples, as well as those from multiple controls, were tested for antibodies to human EVs using peptide microarrays, according to Nischay Mishra, PhD, of Columbia University, New York, and colleagues.
Although EV RNA was confirmed in CSF from only 1 adult AFM case and 1 non-AFM case, antibodies to EV peptides were present in 11 of 14 AFM patients (79%), which was a significantly higher rate than in control groups, including non-AFM patients (1 of 5, or 20%), children with Kawasaki disease (0 of 10), and adults with non-AFM CNS diseases (2 of 11, 18%), according to the authors.
In addition, 6 of 14 (43%) CSF samples and 8 of 11 (73%) serum samples from AFM patients were immunoreactive to an EV-D68–specific peptide, whereas samples from the three control groups were not immunoreactive in either CSF or sera. Previous studies have suggested that infection with EV-D68 and EV-A71 may contribute to AFM.
“There have been 570 confirmed cases since CDC began tracking AFM in August 2014. AFM outbreaks were reported to the CDC in 2014, 2016, and 2018. AFM affects the spinal cord and is characterized by the sudden onset of muscle weakness in one or more limbs. Spikes in AFM cases, primarily in children, have coincided in time and location with outbreaks of EV-D68 and a related enterovirus, EV-A71,” according to an NIH media advisory discussing the article.
In particular, as the study authors point out, a potential link to EV-D68 has also been based on the presence of viral RNA in some respiratory and stool specimens and the observation that EV-D68 infection can result in spinal cord infection.
“While other etiologies of AFM continue to be investigated, our study provides further evidence that EV infection may be a factor in AFM. In the absence of direct detection of a pathogen, antibody evidence of pathogen exposure within the CNS can be an important indicator of the underlying cause of disease,” Dr. Mishra and his colleagues added.
“These initial results may provide avenues to further explore how exposure to EV may contribute to AFM as well as the development of diagnostic tools and treatments,” the researchers concluded.
The study was funded by the National Institutes of Health. The authors reported that they had no competing financial interests.
SOURCE: Mishra N et al. mBio. 2019 Aug;10(4):e01903-19.
High levels of enterovirus (EV) peptides were found in the cerebrospinal fluid (CSF) and serum samples of individuals with acute flaccid myelitis (AFM) that were not present in a variety of control individuals, according to the results of a small study of patients with and without AFM published online in mBio.
In 2018, CSF samples from AFM patients were investigated by viral-capture high-throughput sequencing. These CSF and serum samples, as well as those from multiple controls, were tested for antibodies to human EVs using peptide microarrays, according to Nischay Mishra, PhD, of Columbia University, New York, and colleagues.
Although EV RNA was confirmed in CSF from only 1 adult AFM case and 1 non-AFM case, antibodies to EV peptides were present in 11 of 14 AFM patients (79%), which was a significantly higher rate than in control groups, including non-AFM patients (1 of 5, or 20%), children with Kawasaki disease (0 of 10), and adults with non-AFM CNS diseases (2 of 11, 18%), according to the authors.
In addition, 6 of 14 (43%) CSF samples and 8 of 11 (73%) serum samples from AFM patients were immunoreactive to an EV-D68–specific peptide, whereas samples from the three control groups were not immunoreactive in either CSF or sera. Previous studies have suggested that infection with EV-D68 and EV-A71 may contribute to AFM.
“There have been 570 confirmed cases since CDC began tracking AFM in August 2014. AFM outbreaks were reported to the CDC in 2014, 2016, and 2018. AFM affects the spinal cord and is characterized by the sudden onset of muscle weakness in one or more limbs. Spikes in AFM cases, primarily in children, have coincided in time and location with outbreaks of EV-D68 and a related enterovirus, EV-A71,” according to an NIH media advisory discussing the article.
In particular, as the study authors point out, a potential link to EV-D68 has also been based on the presence of viral RNA in some respiratory and stool specimens and the observation that EV-D68 infection can result in spinal cord infection.
“While other etiologies of AFM continue to be investigated, our study provides further evidence that EV infection may be a factor in AFM. In the absence of direct detection of a pathogen, antibody evidence of pathogen exposure within the CNS can be an important indicator of the underlying cause of disease,” Dr. Mishra and his colleagues added.
“These initial results may provide avenues to further explore how exposure to EV may contribute to AFM as well as the development of diagnostic tools and treatments,” the researchers concluded.
The study was funded by the National Institutes of Health. The authors reported that they had no competing financial interests.
SOURCE: Mishra N et al. mBio. 2019 Aug;10(4):e01903-19.
High levels of enterovirus (EV) peptides were found in the cerebrospinal fluid (CSF) and serum samples of individuals with acute flaccid myelitis (AFM) that were not present in a variety of control individuals, according to the results of a small study of patients with and without AFM published online in mBio.
In 2018, CSF samples from AFM patients were investigated by viral-capture high-throughput sequencing. These CSF and serum samples, as well as those from multiple controls, were tested for antibodies to human EVs using peptide microarrays, according to Nischay Mishra, PhD, of Columbia University, New York, and colleagues.
Although EV RNA was confirmed in CSF from only 1 adult AFM case and 1 non-AFM case, antibodies to EV peptides were present in 11 of 14 AFM patients (79%), which was a significantly higher rate than in control groups, including non-AFM patients (1 of 5, or 20%), children with Kawasaki disease (0 of 10), and adults with non-AFM CNS diseases (2 of 11, 18%), according to the authors.
In addition, 6 of 14 (43%) CSF samples and 8 of 11 (73%) serum samples from AFM patients were immunoreactive to an EV-D68–specific peptide, whereas samples from the three control groups were not immunoreactive in either CSF or sera. Previous studies have suggested that infection with EV-D68 and EV-A71 may contribute to AFM.
“There have been 570 confirmed cases since CDC began tracking AFM in August 2014. AFM outbreaks were reported to the CDC in 2014, 2016, and 2018. AFM affects the spinal cord and is characterized by the sudden onset of muscle weakness in one or more limbs. Spikes in AFM cases, primarily in children, have coincided in time and location with outbreaks of EV-D68 and a related enterovirus, EV-A71,” according to an NIH media advisory discussing the article.
In particular, as the study authors point out, a potential link to EV-D68 has also been based on the presence of viral RNA in some respiratory and stool specimens and the observation that EV-D68 infection can result in spinal cord infection.
“While other etiologies of AFM continue to be investigated, our study provides further evidence that EV infection may be a factor in AFM. In the absence of direct detection of a pathogen, antibody evidence of pathogen exposure within the CNS can be an important indicator of the underlying cause of disease,” Dr. Mishra and his colleagues added.
“These initial results may provide avenues to further explore how exposure to EV may contribute to AFM as well as the development of diagnostic tools and treatments,” the researchers concluded.
The study was funded by the National Institutes of Health. The authors reported that they had no competing financial interests.
SOURCE: Mishra N et al. mBio. 2019 Aug;10(4):e01903-19.
FROM MBIO
Key clinical point:
Major finding: EV peptide antibodies were present in 11 of 14 AFM patients (79%), significantly higher than in controls.
Study details: A peptide microarray analysis was performed on CSF and sera from 14 AFM patients, as well as three control groups of 5 pediatric and adult patients with a non-AFM CNS diseases, 10 children with Kawasaki disease, and 10 adult patients with non-AFM CNS diseases.
Disclosures: The study was funded by the National Institutes of Health. The authors reported that they had no conflicts.
Source: Mishra N et al. mBio. 2019 Aug;10(4):e01903-19.
Low benefits spur alternative drug cost proposals
It’s no secret that cancer drugs are among the most expensive medical treatments in the United States, and now, new research reveals some high-priced cancer drugs may yield little benefit for patients.
A recent analysis of 71 oncology indications approved by the Food and Drug Administration between 2011 and 2017 found that overall survival gains were marginal for drugs approved by the FDA based on overall survival (OS) data. The majority of the 71 indications (75%) demonstrated no statistically significant improvement in patient-reported outcomes (PROs), according to the study (JAMA Oncol. 2019 Jul 3 doi: 10.1001/jamaoncol.2019.1760).
More than half of the indications evaluated demonstrated neither an OS benefit nor a PRO improvement post approval, the study found.
While the researchers did not analyze cost, a number of the cancer drugs that demonstrated little benefit come with a high price tag. Cabozantinib (Cabometyx) for example, approved for the treatment of medullary thyroid carcinoma and advanced renal cell carcinoma (RCC) during the study period, did not demonstrate an overall survival benefit post approval, findings showed. Cabometyx, approved based on survival data, had a 2016 wholesale acquisition cost of $13,750 for a 1-month supply. Olaparib (Lynparza) meanwhile, approved for the treatment of advanced ovarian cancer during the study period, also showed no overall survival benefit post approval. The 2017 wholesale acquisition cost for olaparib was $13,482 for a 30-day supply.
Investigators noted in the study that evaluation of OS can be challenging or unfeasible in some instances and is complicated by factors such as use of crossover trial design.
The findings emphasize the need for a sharper eye on how regulatory authorities approve drugs, said Chadi Nabhan, MD, senior author of the study and chief medical officer at Aptitude Health based in Chicago.

“We all want our patients to receive the best and the latest and the most important and innovative drug they can possible get, as long as these drugs show a benefit,” said Dr. Nabhan, a hematologist and medical oncologist. “We need to look critically at making sure drugs getting approved are truly helping patients by extending their lives or improving their quality of life.”
Growing questions about the benefits of some cancer drugs come as a push to reconsider the pricing of medications to better account for value gains momentum. A number of proposals have recently emerged that would revamp the current payment structure for prescription drugs with the aim of lowering costs and improving access. Value-based pricing proposals are not without challenges, namely defining what value truly means, said Leonard Saltz, MD, a medical oncologist at Memorial Sloan Kettering Cancer Center in New York.
“We’re all quite clear there is a huge absence of connection between cost and value,” Dr. Saltz said in an interview. “There is also a real absence of the definition of, ‘What is value?’ I think that ultimately we have to rely on defining value by its absence. By that I mean, where do we say, this is insufficient value?”
Many drugs show little benefit
The JAMA Oncology study builds on other data that raise doubts about how the FDA determines value when making approval decisions for cancer drugs.
Overall survival is the most direct measure of clinical benefit used to determine value. But OS as an endpoint in clinical trials generally requires larger patient numbers and increased time for follow-up, thereby delaying approvals. This is likely why the use of surrogate endpoints to approve drugs has increased. Dr. Nabhan’s study found the use of surrogate endpoints during trials grew from 67% during the period of 2008 through 2012 to 76% during the period of 2011 through 2017. Surrogate endpoints can include tumor shrinkage, time to progression, or time to reappearance of disease.
The use of surrogate endpoints to determine value however, has long come under scrutiny. A 2019 analysis published in JAMA Internal Medicine found that most cancer drugs approved by the FDA based on response rate (RR) – the percentage of patients who experience tumor shrinkage – have less than transformational response rates, and that such indications do not have confirmed clinical benefit.
Of 59 oncology drugs with 85 unique indications, most had a response rate ranging from 20% to 59%. Of 81 available indications, the median complete response rate – defined as the percentage of patients with no visible disease and normalization of lymph nodes – was 6%. (Complete response data were not reported for four drug indications.) Investigators also reported that many of the drugs have remained on the market for years without subsequent confirmatory data.
In addition, a 2018 review of randomized clinical trials published in JAMA Internal Medicine that analyzed progression-free survival in cancer patients found the endpoint did not improve patients’ lives. A quantitative analysis of 52 articles that covered 38 randomized clinical trials involving 13,979 patients across 12 cancer types found no significant association between progression-free survival and health-related quality of life.
“These findings raise questions regarding the assumption that interventions prolonging [progression-free survival] also improve [health-related quality of life] in patients with cancer,” the study authors wrote. “Therefore, to ensure that patients are truly obtaining important benefit from cancer therapies, clinical trial investigators should measure [health-related quality of life] directly and accurately, ensuring adequate duration and follow-up.
PROs, which can encompass health-related quality of life, is a measure the FDA has encouraged investigators to use during trials – when the benefit exists. In the analysis by Dr. Nabhan, trials evaluated PROs during pivotal studies supporting initial approval in 50 of the 71 indications. Before approval, 14 drugs demonstrated a statistically significant improvement in at least one PRO, but only 1 of the 14 – ruxolitinib – was granted a PRO labeling claim at the time of approval. Post approval, a statistically significant improvement in PROs was shown for only 18 of the 71 (25%) initial indications.
Meanwhile, although overall survival is considered the optimal yardstick with which to measure drug benefit, the value of longevity – and how it should be weighted – poses further questions. A number of new oncology drugs approved based on survival data lengthen lives by a very short time, Dr. Saltz noted. In the study of 71 indications for example, the median OS gain for drugs approved based on survival data was 1.7 months.
“We crossed the absurdity boundary a long time ago with drugs in the range of $10,000 to $20,000 a month with median survival benefits of less than 2 months,” Dr. Saltz said. “That’s not very much. Then we get into a rather circuitous argument that doesn’t settle anything as to whether it’s ‘worth it or not.’ The question becomes to whom is it worth what, and who’s paying for it?”
Proposals aim to lower cost
Recent cost ideas that center on value-pricing seek to answer some of those questions. Outcomes-based contracts is one such proposal. Under the approach, a drug manufacturer and a payer reach an agreement that ties reimbursement to observed outcomes in patients. Rather than a payer covering all prescriptions at a single price, the initial price remains in place if a certain volume of patients achieves the agreed-upon outcome. If the threshold is not met, the drugmaker refunds some of the original price to the payer.
Outcomes-based contracting sounds like a promising approach because various parties involved in the sale have a stake in the result, Dr. Nabhan said. “If you are a manufacturer, you want to make sure the outcomes are actually good,” he said. “If you’re a physician, you want to maximize monitoring your patient and managing adverse events. If you are the payer, you want to make sure your patient stays adherent to therapy, and you want to make sure you provide access to the doctor’s office, and to the hospital when needed. There’s more skin in the game when we look at outcomes-based contracting.”
Another idea gaining popularity is long-term financing for some drugs, particularly curative treatments. The idea has various models, but generally entails a financing arrangement, such as a loan mechanism for payers or a contractual annuitization that commits payers to pay costs over time. Such financing proposals are gaining speed in response to the high-cost of new gene therapies, according to a summary in Health Affairs. The payment agreements could be augmented by government funds such as government bonds or subsidies and/or efforts to promote risk-pooling across payers.
Peter B. Bach, MD, however, believes neither long-term financing nor outcomes-based contracting are good ideas. In January 2019 testimony to the U.S. Senate Committee on Finance, Dr. Bach, director of the Center for Health Policy and Outcomes at Memorial Sloan Kettering Cancer Center, New York, outlined why both value-based proposals are faulty. Outcomes-based contracting does not guarantee that prices are value based, he said, because it leaves untouched how much a drug costs when it does work. In addition, the long-term financing approach only pushes drug costs into future years, he testified.
“Financing does not reduce total spending, it just changes current obligations,” Dr. Bach said during testimony. “It is also relevant to appreciate that, whether for student loans or home mortgages, long-term payment arrangements are inflationary.”
Dr. Bach, a health policy expert whose work focuses on the cost and value of cancer drugs, and his colleagues at Memorial Sloan Kettering Cancer Center have spent the last few years fine-tuning an interactive drug-pricing tool that Dr. Bach says has distinct advantages over alternative drug-pricing proposals when it comes to considering value. The tool, called the DrugAbacus, integrates objective information about cancer drugs while empowering users to define what value means to them. For example, the DrugAbacus allows users to choose a dollar amount for each additional year of life the drug provides and lets them decide how much to discount the price for side effects, according to a summary of the tool by Dr. Bach published in the New England Journal of Medicine Catalyst. The price can be adjusted for factors such as treating a rare disease or having a novel action mechanism. The final result reveals the user’s self-valued DrugAbacus price and compares the cost with the drug’s initial market price.
“[DrugAbacus] provides a template for how we need to start thinking about value in drug pricing – by capturing some of the inherent complexity of value-based decisions without making the fundamentally flawed assumptions that are embedded in other drug-pricing proposals,” Dr. Bach wrote in the summary.
He declined to comment for this story.
A three-tiered approach
Another novel idea would link drug prices to value, but allow costs to change with new information. The proposal would create a three-part pricing model where prices vary over fixed time intervals, according to an article published in the New England Journal of Medicine Catalyst.
First, drugmakers would agree to launch a drug with a low price, with a potentially significant increase after a specified period to observe performance. During a second period, the price would be adjusted up or down based on newly emergent evidence. After a window of higher prices to reward innovation, the cost would then decline in a third period to ensure long-term access.
The advantage is access to truly miraculous therapies in a very short time – from 3 to 5 years earlier than the current system, said Luca Pani, MD, a coauthor of the paper and professor of psychiatry at the University of Miami.

“Another advantage emerges when it comes to drugs that treat patient populations with inaccurate epidemiology, in which we do not know exactly how many patients we have,” Dr. Pani said. “The model in this case allows to reduce the economic impact of this uncertainty.”
The main challenge would be finding a drug manufacturer that would agree to the arrangement, said Erik Snowberg, PhD, a coauthor of the study and a research associate for the National Bureau of Economic Research.

“There’s a lot of uncertainty right now,” Dr. Snowberg said. “The big challenge would be to find a drugmaker that would think about implementing this and finding the right payer for whom this would solve a pressing need.”
Despite the barriers to the idea, Dr. Pani said a more cost-effective drug cost structure is imperative, especially as the rapid rate of new therapies continues.
“We have a moral obligation to find alternative models that allow access and that are not only scientifically and economically sound and sustainable but also realistic and logical to implement,” he said.
It’s no secret that cancer drugs are among the most expensive medical treatments in the United States, and now, new research reveals some high-priced cancer drugs may yield little benefit for patients.
A recent analysis of 71 oncology indications approved by the Food and Drug Administration between 2011 and 2017 found that overall survival gains were marginal for drugs approved by the FDA based on overall survival (OS) data. The majority of the 71 indications (75%) demonstrated no statistically significant improvement in patient-reported outcomes (PROs), according to the study (JAMA Oncol. 2019 Jul 3 doi: 10.1001/jamaoncol.2019.1760).
More than half of the indications evaluated demonstrated neither an OS benefit nor a PRO improvement post approval, the study found.
While the researchers did not analyze cost, a number of the cancer drugs that demonstrated little benefit come with a high price tag. Cabozantinib (Cabometyx) for example, approved for the treatment of medullary thyroid carcinoma and advanced renal cell carcinoma (RCC) during the study period, did not demonstrate an overall survival benefit post approval, findings showed. Cabometyx, approved based on survival data, had a 2016 wholesale acquisition cost of $13,750 for a 1-month supply. Olaparib (Lynparza) meanwhile, approved for the treatment of advanced ovarian cancer during the study period, also showed no overall survival benefit post approval. The 2017 wholesale acquisition cost for olaparib was $13,482 for a 30-day supply.
Investigators noted in the study that evaluation of OS can be challenging or unfeasible in some instances and is complicated by factors such as use of crossover trial design.
The findings emphasize the need for a sharper eye on how regulatory authorities approve drugs, said Chadi Nabhan, MD, senior author of the study and chief medical officer at Aptitude Health based in Chicago.
“We all want our patients to receive the best and the latest and the most important and innovative drug they can possible get, as long as these drugs show a benefit,” said Dr. Nabhan, a hematologist and medical oncologist. “We need to look critically at making sure drugs getting approved are truly helping patients by extending their lives or improving their quality of life.”
Growing questions about the benefits of some cancer drugs come as a push to reconsider the pricing of medications to better account for value gains momentum. A number of proposals have recently emerged that would revamp the current payment structure for prescription drugs with the aim of lowering costs and improving access. Value-based pricing proposals are not without challenges, namely defining what value truly means, said Leonard Saltz, MD, a medical oncologist at Memorial Sloan Kettering Cancer Center in New York.
“We’re all quite clear there is a huge absence of connection between cost and value,” Dr. Saltz said in an interview. “There is also a real absence of the definition of, ‘What is value?’ I think that ultimately we have to rely on defining value by its absence. By that I mean, where do we say, this is insufficient value?”
Many drugs show little benefit
The JAMA Oncology study builds on other data that raise doubts about how the FDA determines value when making approval decisions for cancer drugs.
Overall survival is the most direct measure of clinical benefit used to determine value. But OS as an endpoint in clinical trials generally requires larger patient numbers and increased time for follow-up, thereby delaying approvals. This is likely why the use of surrogate endpoints to approve drugs has increased. Dr. Nabhan’s study found the use of surrogate endpoints during trials grew from 67% during the period of 2008 through 2012 to 76% during the period of 2011 through 2017. Surrogate endpoints can include tumor shrinkage, time to progression, or time to reappearance of disease.
The use of surrogate endpoints to determine value however, has long come under scrutiny. A 2019 analysis published in JAMA Internal Medicine found that most cancer drugs approved by the FDA based on response rate (RR) – the percentage of patients who experience tumor shrinkage – have less than transformational response rates, and that such indications do not have confirmed clinical benefit.
Of 59 oncology drugs with 85 unique indications, most had a response rate ranging from 20% to 59%. Of 81 available indications, the median complete response rate – defined as the percentage of patients with no visible disease and normalization of lymph nodes – was 6%. (Complete response data were not reported for four drug indications.) Investigators also reported that many of the drugs have remained on the market for years without subsequent confirmatory data.
In addition, a 2018 review of randomized clinical trials published in JAMA Internal Medicine that analyzed progression-free survival in cancer patients found the endpoint did not improve patients’ lives. A quantitative analysis of 52 articles that covered 38 randomized clinical trials involving 13,979 patients across 12 cancer types found no significant association between progression-free survival and health-related quality of life.
“These findings raise questions regarding the assumption that interventions prolonging [progression-free survival] also improve [health-related quality of life] in patients with cancer,” the study authors wrote. “Therefore, to ensure that patients are truly obtaining important benefit from cancer therapies, clinical trial investigators should measure [health-related quality of life] directly and accurately, ensuring adequate duration and follow-up.
PROs, which can encompass health-related quality of life, is a measure the FDA has encouraged investigators to use during trials – when the benefit exists. In the analysis by Dr. Nabhan, trials evaluated PROs during pivotal studies supporting initial approval in 50 of the 71 indications. Before approval, 14 drugs demonstrated a statistically significant improvement in at least one PRO, but only 1 of the 14 – ruxolitinib – was granted a PRO labeling claim at the time of approval. Post approval, a statistically significant improvement in PROs was shown for only 18 of the 71 (25%) initial indications.
Meanwhile, although overall survival is considered the optimal yardstick with which to measure drug benefit, the value of longevity – and how it should be weighted – poses further questions. A number of new oncology drugs approved based on survival data lengthen lives by a very short time, Dr. Saltz noted. In the study of 71 indications for example, the median OS gain for drugs approved based on survival data was 1.7 months.
“We crossed the absurdity boundary a long time ago with drugs in the range of $10,000 to $20,000 a month with median survival benefits of less than 2 months,” Dr. Saltz said. “That’s not very much. Then we get into a rather circuitous argument that doesn’t settle anything as to whether it’s ‘worth it or not.’ The question becomes to whom is it worth what, and who’s paying for it?”
Proposals aim to lower cost
Recent cost ideas that center on value-pricing seek to answer some of those questions. Outcomes-based contracts is one such proposal. Under the approach, a drug manufacturer and a payer reach an agreement that ties reimbursement to observed outcomes in patients. Rather than a payer covering all prescriptions at a single price, the initial price remains in place if a certain volume of patients achieves the agreed-upon outcome. If the threshold is not met, the drugmaker refunds some of the original price to the payer.
Outcomes-based contracting sounds like a promising approach because various parties involved in the sale have a stake in the result, Dr. Nabhan said. “If you are a manufacturer, you want to make sure the outcomes are actually good,” he said. “If you’re a physician, you want to maximize monitoring your patient and managing adverse events. If you are the payer, you want to make sure your patient stays adherent to therapy, and you want to make sure you provide access to the doctor’s office, and to the hospital when needed. There’s more skin in the game when we look at outcomes-based contracting.”
Another idea gaining popularity is long-term financing for some drugs, particularly curative treatments. The idea has various models, but generally entails a financing arrangement, such as a loan mechanism for payers or a contractual annuitization that commits payers to pay costs over time. Such financing proposals are gaining speed in response to the high-cost of new gene therapies, according to a summary in Health Affairs. The payment agreements could be augmented by government funds such as government bonds or subsidies and/or efforts to promote risk-pooling across payers.
Peter B. Bach, MD, however, believes neither long-term financing nor outcomes-based contracting are good ideas. In January 2019 testimony to the U.S. Senate Committee on Finance, Dr. Bach, director of the Center for Health Policy and Outcomes at Memorial Sloan Kettering Cancer Center, New York, outlined why both value-based proposals are faulty. Outcomes-based contracting does not guarantee that prices are value based, he said, because it leaves untouched how much a drug costs when it does work. In addition, the long-term financing approach only pushes drug costs into future years, he testified.
“Financing does not reduce total spending, it just changes current obligations,” Dr. Bach said during testimony. “It is also relevant to appreciate that, whether for student loans or home mortgages, long-term payment arrangements are inflationary.”
Dr. Bach, a health policy expert whose work focuses on the cost and value of cancer drugs, and his colleagues at Memorial Sloan Kettering Cancer Center have spent the last few years fine-tuning an interactive drug-pricing tool that Dr. Bach says has distinct advantages over alternative drug-pricing proposals when it comes to considering value. The tool, called the DrugAbacus, integrates objective information about cancer drugs while empowering users to define what value means to them. For example, the DrugAbacus allows users to choose a dollar amount for each additional year of life the drug provides and lets them decide how much to discount the price for side effects, according to a summary of the tool by Dr. Bach published in the New England Journal of Medicine Catalyst. The price can be adjusted for factors such as treating a rare disease or having a novel action mechanism. The final result reveals the user’s self-valued DrugAbacus price and compares the cost with the drug’s initial market price.
“[DrugAbacus] provides a template for how we need to start thinking about value in drug pricing – by capturing some of the inherent complexity of value-based decisions without making the fundamentally flawed assumptions that are embedded in other drug-pricing proposals,” Dr. Bach wrote in the summary.
He declined to comment for this story.
A three-tiered approach
Another novel idea would link drug prices to value, but allow costs to change with new information. The proposal would create a three-part pricing model where prices vary over fixed time intervals, according to an article published in the New England Journal of Medicine Catalyst.
First, drugmakers would agree to launch a drug with a low price, with a potentially significant increase after a specified period to observe performance. During a second period, the price would be adjusted up or down based on newly emergent evidence. After a window of higher prices to reward innovation, the cost would then decline in a third period to ensure long-term access.
The advantage is access to truly miraculous therapies in a very short time – from 3 to 5 years earlier than the current system, said Luca Pani, MD, a coauthor of the paper and professor of psychiatry at the University of Miami.
“Another advantage emerges when it comes to drugs that treat patient populations with inaccurate epidemiology, in which we do not know exactly how many patients we have,” Dr. Pani said. “The model in this case allows to reduce the economic impact of this uncertainty.”
The main challenge would be finding a drug manufacturer that would agree to the arrangement, said Erik Snowberg, PhD, a coauthor of the study and a research associate for the National Bureau of Economic Research.
“There’s a lot of uncertainty right now,” Dr. Snowberg said. “The big challenge would be to find a drugmaker that would think about implementing this and finding the right payer for whom this would solve a pressing need.”
Despite the barriers to the idea, Dr. Pani said a more cost-effective drug cost structure is imperative, especially as the rapid rate of new therapies continues.
“We have a moral obligation to find alternative models that allow access and that are not only scientifically and economically sound and sustainable but also realistic and logical to implement,” he said.
It’s no secret that cancer drugs are among the most expensive medical treatments in the United States, and now, new research reveals some high-priced cancer drugs may yield little benefit for patients.
A recent analysis of 71 oncology indications approved by the Food and Drug Administration between 2011 and 2017 found that overall survival gains were marginal for drugs approved by the FDA based on overall survival (OS) data. The majority of the 71 indications (75%) demonstrated no statistically significant improvement in patient-reported outcomes (PROs), according to the study (JAMA Oncol. 2019 Jul 3 doi: 10.1001/jamaoncol.2019.1760).
More than half of the indications evaluated demonstrated neither an OS benefit nor a PRO improvement post approval, the study found.
While the researchers did not analyze cost, a number of the cancer drugs that demonstrated little benefit come with a high price tag. Cabozantinib (Cabometyx) for example, approved for the treatment of medullary thyroid carcinoma and advanced renal cell carcinoma (RCC) during the study period, did not demonstrate an overall survival benefit post approval, findings showed. Cabometyx, approved based on survival data, had a 2016 wholesale acquisition cost of $13,750 for a 1-month supply. Olaparib (Lynparza) meanwhile, approved for the treatment of advanced ovarian cancer during the study period, also showed no overall survival benefit post approval. The 2017 wholesale acquisition cost for olaparib was $13,482 for a 30-day supply.
Investigators noted in the study that evaluation of OS can be challenging or unfeasible in some instances and is complicated by factors such as use of crossover trial design.
The findings emphasize the need for a sharper eye on how regulatory authorities approve drugs, said Chadi Nabhan, MD, senior author of the study and chief medical officer at Aptitude Health based in Chicago.
“We all want our patients to receive the best and the latest and the most important and innovative drug they can possible get, as long as these drugs show a benefit,” said Dr. Nabhan, a hematologist and medical oncologist. “We need to look critically at making sure drugs getting approved are truly helping patients by extending their lives or improving their quality of life.”
Growing questions about the benefits of some cancer drugs come as a push to reconsider the pricing of medications to better account for value gains momentum. A number of proposals have recently emerged that would revamp the current payment structure for prescription drugs with the aim of lowering costs and improving access. Value-based pricing proposals are not without challenges, namely defining what value truly means, said Leonard Saltz, MD, a medical oncologist at Memorial Sloan Kettering Cancer Center in New York.
“We’re all quite clear there is a huge absence of connection between cost and value,” Dr. Saltz said in an interview. “There is also a real absence of the definition of, ‘What is value?’ I think that ultimately we have to rely on defining value by its absence. By that I mean, where do we say, this is insufficient value?”
Many drugs show little benefit
The JAMA Oncology study builds on other data that raise doubts about how the FDA determines value when making approval decisions for cancer drugs.
Overall survival is the most direct measure of clinical benefit used to determine value. But OS as an endpoint in clinical trials generally requires larger patient numbers and increased time for follow-up, thereby delaying approvals. This is likely why the use of surrogate endpoints to approve drugs has increased. Dr. Nabhan’s study found the use of surrogate endpoints during trials grew from 67% during the period of 2008 through 2012 to 76% during the period of 2011 through 2017. Surrogate endpoints can include tumor shrinkage, time to progression, or time to reappearance of disease.
The use of surrogate endpoints to determine value however, has long come under scrutiny. A 2019 analysis published in JAMA Internal Medicine found that most cancer drugs approved by the FDA based on response rate (RR) – the percentage of patients who experience tumor shrinkage – have less than transformational response rates, and that such indications do not have confirmed clinical benefit.
Of 59 oncology drugs with 85 unique indications, most had a response rate ranging from 20% to 59%. Of 81 available indications, the median complete response rate – defined as the percentage of patients with no visible disease and normalization of lymph nodes – was 6%. (Complete response data were not reported for four drug indications.) Investigators also reported that many of the drugs have remained on the market for years without subsequent confirmatory data.
In addition, a 2018 review of randomized clinical trials published in JAMA Internal Medicine that analyzed progression-free survival in cancer patients found the endpoint did not improve patients’ lives. A quantitative analysis of 52 articles that covered 38 randomized clinical trials involving 13,979 patients across 12 cancer types found no significant association between progression-free survival and health-related quality of life.
“These findings raise questions regarding the assumption that interventions prolonging [progression-free survival] also improve [health-related quality of life] in patients with cancer,” the study authors wrote. “Therefore, to ensure that patients are truly obtaining important benefit from cancer therapies, clinical trial investigators should measure [health-related quality of life] directly and accurately, ensuring adequate duration and follow-up.
PROs, which can encompass health-related quality of life, is a measure the FDA has encouraged investigators to use during trials – when the benefit exists. In the analysis by Dr. Nabhan, trials evaluated PROs during pivotal studies supporting initial approval in 50 of the 71 indications. Before approval, 14 drugs demonstrated a statistically significant improvement in at least one PRO, but only 1 of the 14 – ruxolitinib – was granted a PRO labeling claim at the time of approval. Post approval, a statistically significant improvement in PROs was shown for only 18 of the 71 (25%) initial indications.
Meanwhile, although overall survival is considered the optimal yardstick with which to measure drug benefit, the value of longevity – and how it should be weighted – poses further questions. A number of new oncology drugs approved based on survival data lengthen lives by a very short time, Dr. Saltz noted. In the study of 71 indications for example, the median OS gain for drugs approved based on survival data was 1.7 months.
“We crossed the absurdity boundary a long time ago with drugs in the range of $10,000 to $20,000 a month with median survival benefits of less than 2 months,” Dr. Saltz said. “That’s not very much. Then we get into a rather circuitous argument that doesn’t settle anything as to whether it’s ‘worth it or not.’ The question becomes to whom is it worth what, and who’s paying for it?”
Proposals aim to lower cost
Recent cost ideas that center on value-pricing seek to answer some of those questions. Outcomes-based contracts is one such proposal. Under the approach, a drug manufacturer and a payer reach an agreement that ties reimbursement to observed outcomes in patients. Rather than a payer covering all prescriptions at a single price, the initial price remains in place if a certain volume of patients achieves the agreed-upon outcome. If the threshold is not met, the drugmaker refunds some of the original price to the payer.
Outcomes-based contracting sounds like a promising approach because various parties involved in the sale have a stake in the result, Dr. Nabhan said. “If you are a manufacturer, you want to make sure the outcomes are actually good,” he said. “If you’re a physician, you want to maximize monitoring your patient and managing adverse events. If you are the payer, you want to make sure your patient stays adherent to therapy, and you want to make sure you provide access to the doctor’s office, and to the hospital when needed. There’s more skin in the game when we look at outcomes-based contracting.”
Another idea gaining popularity is long-term financing for some drugs, particularly curative treatments. The idea has various models, but generally entails a financing arrangement, such as a loan mechanism for payers or a contractual annuitization that commits payers to pay costs over time. Such financing proposals are gaining speed in response to the high-cost of new gene therapies, according to a summary in Health Affairs. The payment agreements could be augmented by government funds such as government bonds or subsidies and/or efforts to promote risk-pooling across payers.
Peter B. Bach, MD, however, believes neither long-term financing nor outcomes-based contracting are good ideas. In January 2019 testimony to the U.S. Senate Committee on Finance, Dr. Bach, director of the Center for Health Policy and Outcomes at Memorial Sloan Kettering Cancer Center, New York, outlined why both value-based proposals are faulty. Outcomes-based contracting does not guarantee that prices are value based, he said, because it leaves untouched how much a drug costs when it does work. In addition, the long-term financing approach only pushes drug costs into future years, he testified.
“Financing does not reduce total spending, it just changes current obligations,” Dr. Bach said during testimony. “It is also relevant to appreciate that, whether for student loans or home mortgages, long-term payment arrangements are inflationary.”
Dr. Bach, a health policy expert whose work focuses on the cost and value of cancer drugs, and his colleagues at Memorial Sloan Kettering Cancer Center have spent the last few years fine-tuning an interactive drug-pricing tool that Dr. Bach says has distinct advantages over alternative drug-pricing proposals when it comes to considering value. The tool, called the DrugAbacus, integrates objective information about cancer drugs while empowering users to define what value means to them. For example, the DrugAbacus allows users to choose a dollar amount for each additional year of life the drug provides and lets them decide how much to discount the price for side effects, according to a summary of the tool by Dr. Bach published in the New England Journal of Medicine Catalyst. The price can be adjusted for factors such as treating a rare disease or having a novel action mechanism. The final result reveals the user’s self-valued DrugAbacus price and compares the cost with the drug’s initial market price.
“[DrugAbacus] provides a template for how we need to start thinking about value in drug pricing – by capturing some of the inherent complexity of value-based decisions without making the fundamentally flawed assumptions that are embedded in other drug-pricing proposals,” Dr. Bach wrote in the summary.
He declined to comment for this story.
A three-tiered approach
Another novel idea would link drug prices to value, but allow costs to change with new information. The proposal would create a three-part pricing model where prices vary over fixed time intervals, according to an article published in the New England Journal of Medicine Catalyst.
First, drugmakers would agree to launch a drug with a low price, with a potentially significant increase after a specified period to observe performance. During a second period, the price would be adjusted up or down based on newly emergent evidence. After a window of higher prices to reward innovation, the cost would then decline in a third period to ensure long-term access.
The advantage is access to truly miraculous therapies in a very short time – from 3 to 5 years earlier than the current system, said Luca Pani, MD, a coauthor of the paper and professor of psychiatry at the University of Miami.
“Another advantage emerges when it comes to drugs that treat patient populations with inaccurate epidemiology, in which we do not know exactly how many patients we have,” Dr. Pani said. “The model in this case allows to reduce the economic impact of this uncertainty.”
The main challenge would be finding a drug manufacturer that would agree to the arrangement, said Erik Snowberg, PhD, a coauthor of the study and a research associate for the National Bureau of Economic Research.
“There’s a lot of uncertainty right now,” Dr. Snowberg said. “The big challenge would be to find a drugmaker that would think about implementing this and finding the right payer for whom this would solve a pressing need.”
Despite the barriers to the idea, Dr. Pani said a more cost-effective drug cost structure is imperative, especially as the rapid rate of new therapies continues.
“We have a moral obligation to find alternative models that allow access and that are not only scientifically and economically sound and sustainable but also realistic and logical to implement,” he said.
Serum neurofilament light chain level may indicate MS disease activity
according to an investigation published online August 12 in JAMA Neurology. Furthermore, changes in sNfL levels are associated with disability worsening, and sNfL levels may be influenced by treatment. These data support the potential of sNfL as an objective surrogate of ongoing MS disease activity, according to the researchers.
Neuronal and axonal loss increase levels of NfL in cerebrospinal fluid (CSF) in patients with MS. Previous research indicated that sNfL levels are correlated with CSF levels of NfL and are associated with clinical and imaging measures of disease activity. For the purpose of repeated sampling, collecting blood from patients would be more practical than performing lumbar punctures, said the investigators. No long-term studies of sNfL concentrations and their associations with MS disease outcomes had been performed, however.
Ester Cantó, PhD, of the University of California, San Francisco (UCSF), and colleagues examined data from the prospective Expression, Proteomics, Imaging, Clinical (EPIC) study to assess sNfL as a biomarker of MS disease activity and progression. The ongoing EPIC study is being conducted at UCSF. Dr. Cantó and colleagues analyzed data collected from July 1, 2004, through August 31, 2017, for 607 patients with MS. Participants underwent clinical examinations and serum sample collections annually for 5 years, then at various time points for as long as 12 years. The median follow-up duration was 10 years. The researchers measured sNfL levels with a sensitive single-molecule array platform and compared them with clinical and MRI variables using univariable and multivariable analyses. Dr. Cantó and colleagues chose disability progression, defined as clinically significant worsening on the Expanded Disability Status Scale (EDSS) score, and brain fraction atrophy as their primary outcomes.
The population’s mean age was 42.5 years. About 70% of participants were women, and all were of non-Hispanic European descent. At baseline, sNfL levels were significantly associated with EDSS score, MS subtype, and treatment status.
Dr. Cantó and colleagues found a significant interaction between EDSS worsening and change in levels of sNfL over time. Baseline sNfL levels were associated with approximately 11.6% of the variance in participants’ brain fraction atrophy at year 10. When the investigators controlled for sex, age, and disease duration, they found that baseline sNfL levels were associated with 18% of the variance in brain fraction atrophy at year 10. After 5 years’ follow-up, active treatment was associated with lower levels of sNfL. High-efficacy treatments were associated with greater decreases in sNfL levels, compared with platform therapies.
More frequent sample acquisition could provide greater detail about changes in sNfL levels, wrote Dr. Cantó and colleagues. They acknowledged that their study had insufficient power for the researchers to assess the outcomes of individual MS therapies. Other limitations included the lack of data on NfL stability and the lack of a group of healthy controls.
“For an individual patient, the biomarker prognostic power of sNfL level for clinical and MRI outcomes was limited,” said the investigators. “Further prospective studies are necessary to assess the assay’s utility for decision making in individual patients.”
The National Institutes of Health and the U.S. National MS Society supported the study. Several of the investigators received compensation from Novartis, which provided funds for the reagents needed for the single-molecule array assay.
SOURCE: Cantó E et al. JAMA Neurol. 2019 Aug. 12. doi: 10.1001/jamaneurol.2019.2137.
according to an investigation published online August 12 in JAMA Neurology. Furthermore, changes in sNfL levels are associated with disability worsening, and sNfL levels may be influenced by treatment. These data support the potential of sNfL as an objective surrogate of ongoing MS disease activity, according to the researchers.
Neuronal and axonal loss increase levels of NfL in cerebrospinal fluid (CSF) in patients with MS. Previous research indicated that sNfL levels are correlated with CSF levels of NfL and are associated with clinical and imaging measures of disease activity. For the purpose of repeated sampling, collecting blood from patients would be more practical than performing lumbar punctures, said the investigators. No long-term studies of sNfL concentrations and their associations with MS disease outcomes had been performed, however.
Ester Cantó, PhD, of the University of California, San Francisco (UCSF), and colleagues examined data from the prospective Expression, Proteomics, Imaging, Clinical (EPIC) study to assess sNfL as a biomarker of MS disease activity and progression. The ongoing EPIC study is being conducted at UCSF. Dr. Cantó and colleagues analyzed data collected from July 1, 2004, through August 31, 2017, for 607 patients with MS. Participants underwent clinical examinations and serum sample collections annually for 5 years, then at various time points for as long as 12 years. The median follow-up duration was 10 years. The researchers measured sNfL levels with a sensitive single-molecule array platform and compared them with clinical and MRI variables using univariable and multivariable analyses. Dr. Cantó and colleagues chose disability progression, defined as clinically significant worsening on the Expanded Disability Status Scale (EDSS) score, and brain fraction atrophy as their primary outcomes.
The population’s mean age was 42.5 years. About 70% of participants were women, and all were of non-Hispanic European descent. At baseline, sNfL levels were significantly associated with EDSS score, MS subtype, and treatment status.
Dr. Cantó and colleagues found a significant interaction between EDSS worsening and change in levels of sNfL over time. Baseline sNfL levels were associated with approximately 11.6% of the variance in participants’ brain fraction atrophy at year 10. When the investigators controlled for sex, age, and disease duration, they found that baseline sNfL levels were associated with 18% of the variance in brain fraction atrophy at year 10. After 5 years’ follow-up, active treatment was associated with lower levels of sNfL. High-efficacy treatments were associated with greater decreases in sNfL levels, compared with platform therapies.
More frequent sample acquisition could provide greater detail about changes in sNfL levels, wrote Dr. Cantó and colleagues. They acknowledged that their study had insufficient power for the researchers to assess the outcomes of individual MS therapies. Other limitations included the lack of data on NfL stability and the lack of a group of healthy controls.
“For an individual patient, the biomarker prognostic power of sNfL level for clinical and MRI outcomes was limited,” said the investigators. “Further prospective studies are necessary to assess the assay’s utility for decision making in individual patients.”
The National Institutes of Health and the U.S. National MS Society supported the study. Several of the investigators received compensation from Novartis, which provided funds for the reagents needed for the single-molecule array assay.
SOURCE: Cantó E et al. JAMA Neurol. 2019 Aug. 12. doi: 10.1001/jamaneurol.2019.2137.
according to an investigation published online August 12 in JAMA Neurology. Furthermore, changes in sNfL levels are associated with disability worsening, and sNfL levels may be influenced by treatment. These data support the potential of sNfL as an objective surrogate of ongoing MS disease activity, according to the researchers.
Neuronal and axonal loss increase levels of NfL in cerebrospinal fluid (CSF) in patients with MS. Previous research indicated that sNfL levels are correlated with CSF levels of NfL and are associated with clinical and imaging measures of disease activity. For the purpose of repeated sampling, collecting blood from patients would be more practical than performing lumbar punctures, said the investigators. No long-term studies of sNfL concentrations and their associations with MS disease outcomes had been performed, however.
Ester Cantó, PhD, of the University of California, San Francisco (UCSF), and colleagues examined data from the prospective Expression, Proteomics, Imaging, Clinical (EPIC) study to assess sNfL as a biomarker of MS disease activity and progression. The ongoing EPIC study is being conducted at UCSF. Dr. Cantó and colleagues analyzed data collected from July 1, 2004, through August 31, 2017, for 607 patients with MS. Participants underwent clinical examinations and serum sample collections annually for 5 years, then at various time points for as long as 12 years. The median follow-up duration was 10 years. The researchers measured sNfL levels with a sensitive single-molecule array platform and compared them with clinical and MRI variables using univariable and multivariable analyses. Dr. Cantó and colleagues chose disability progression, defined as clinically significant worsening on the Expanded Disability Status Scale (EDSS) score, and brain fraction atrophy as their primary outcomes.
The population’s mean age was 42.5 years. About 70% of participants were women, and all were of non-Hispanic European descent. At baseline, sNfL levels were significantly associated with EDSS score, MS subtype, and treatment status.
Dr. Cantó and colleagues found a significant interaction between EDSS worsening and change in levels of sNfL over time. Baseline sNfL levels were associated with approximately 11.6% of the variance in participants’ brain fraction atrophy at year 10. When the investigators controlled for sex, age, and disease duration, they found that baseline sNfL levels were associated with 18% of the variance in brain fraction atrophy at year 10. After 5 years’ follow-up, active treatment was associated with lower levels of sNfL. High-efficacy treatments were associated with greater decreases in sNfL levels, compared with platform therapies.
More frequent sample acquisition could provide greater detail about changes in sNfL levels, wrote Dr. Cantó and colleagues. They acknowledged that their study had insufficient power for the researchers to assess the outcomes of individual MS therapies. Other limitations included the lack of data on NfL stability and the lack of a group of healthy controls.
“For an individual patient, the biomarker prognostic power of sNfL level for clinical and MRI outcomes was limited,” said the investigators. “Further prospective studies are necessary to assess the assay’s utility for decision making in individual patients.”
The National Institutes of Health and the U.S. National MS Society supported the study. Several of the investigators received compensation from Novartis, which provided funds for the reagents needed for the single-molecule array assay.
SOURCE: Cantó E et al. JAMA Neurol. 2019 Aug. 12. doi: 10.1001/jamaneurol.2019.2137.
FROM JAMA NEUROLOGY
Key clinical point: Serum neurofilament light chain level has potential as a surrogate of ongoing MS disease activity.
Major finding: Serum neurofilament light chain level is associated with brain fraction atrophy.
Study details: An ongoing, prospective, observational study of 607 patients with MS.
Disclosures: The National Institutes of Health and the U.S. National MS Society supported the study. Several of the investigators received compensation from Novartis, which provided funds for the reagents needed for the single-molecule array assay.
Source: Cantó E et al. JAMA Neurol. 2019 Aug 12. doi: 10.1001/jamaneurol.2019.2137.
Midlife hypertension is associated with subsequent risk of dementia
Uncontrolled hypertension among individuals aged 45-65 years of age is associated with an increased risk of subsequent dementia, according to a relatively large prospective population-based cohort study that followed patients for almost 30 years.

Even though previously published studies have not conclusively linked blood pressure control with a reduction in dementia risk, a second study, published simultaneously, did link blood pressure control with a smaller increase in white matter lesions, which are a marker of dementia risk. However, a reduction in total brain volume that accompanied this protection raised concern.
In the first of the two reports published Aug. 13 in JAMA, individuals 45-65 years of age participating in the Atherosclerosis Risk in Communities (ARIC) study were followed for cognitive function in relation to blood pressure. The baseline visit took place in 1987-1989. Cognitive function was also evaluated at the fifth visit, which took place in 2011-2013, and the sixth visit, which took place in 2016-2017.
At the sixth visit, the incidence of dementia among patients who were normotensive at baseline and also normotensive at the fifth visit was 1.31 per 100 person-years. For those with hypertension (greater than 140/90 mm Hg) at the fifth visit but normotensive at baseline, the incidence was 1.99 per 100 patient-years. For those with hypertension at both time points, the incidence was 4.26 per 100 patient-years.
When translated into hazard ratios, those with midlife and late-life hypertension were nearly 50% more likely to develop dementia (HR, 1.49) relative to those who remained normotensive. For those who had only midlife hypertension, the risk was also significantly increased (HR, 1.41) relative to those who remained normotensive at both time points.
Those with midlife hypertension but late-life hypotension were also found to be at greater risk of dementia (HR, 1.62) relative to those who remained normotensive.
These data support the premise that uncontrolled midlife hypertension increases risk of dementia but do not touch on whether blood pressure reductions reduce this risk. However, a second study published simultaneously provided at least some evidence that blood pressure control might offer some protection.
In this report, which is a substudy of the previously published Systolic Blood Pressure Intervention Trial (SPRINT) MIND trial, brain volume changes were evaluated via MRI in 449 of the more than 2,000 patients included in the previously published trial (Williamson JD et al. JAMA. 2019;321[6]:553-61).
After a median 3.4 years of follow-up, mean white matter lesion volume increased only 0.92 cm3 in patients receiving intensive systolic blood pressure control, defined as less than 120 mm Hg, versus 1.45 cm3 in those with higher systolic blood pressures.
These substudy data are encouraging, but it is important to recognize that the previously published and larger SPRINT MIND trial did not achieve its endpoint. In that study, the protection against dementia was nonsignificant (HR, 0.83; 95% confidence interval, 0.67-1.04).
In addition, the lower loss in white matter volume with intensive blood pressure lowering in the MRI substudy was accompanied with a greater loss in total brain volume (–30.6 vs. –26.9 cm3), which is considered a potentially negative effect.
As a result, the picture for risk management remains unclear, according to an editorial that accompanied publication of both studies.
“The important clinical question is whether changes of a few cubic millimeters in white matter hyperintensity volume or brain make a difference on brain function,” observed the author of the editorial, Shyam Prabhakaran, MD, of the department of neurology at the University of Chicago.
He believes that there are several findings from both studies that are “encouraging” in regard to blood pressure control for the prevention of dementia, but he also listed many unanswered questions, including why benefits observed to date have been so modest. He speculated that meaningful clinical benefits might depend on a multimodal approach that includes modification of other vascular risk factors, such as elevated lipids.
He also suggested that many issues regarding intensive blood pressure control for preventing dementia are unresolved, suggesting the need for more studies.
Not least, “later blood-pressure lowering interventions require careful monitoring for the potential cognitive harm associated with late-life hypotension,” Dr. Prabhakaran noted. Calling the effects of blood pressure control on brain health “nuanced,” he concluded that there is an opportunity for blood pressure modifications to prevent dementia, but stressed that optimal blood pressure targets for the purposes of preventing dementia are unknown.
The ARIC and SPRINT studies are supported by the National Institutes of Health. Several authors reported relationships with industry but no conflicts of interest relevant to this study.
SOURCES: Walker KA et al. JAMA. 2019;322(6):535-45; SPRINT MIND investigators. JAMA. 2019;322(6):524-34; Prabhakaran S. JAMA. 2019;322(6):512-3
Uncontrolled hypertension among individuals aged 45-65 years of age is associated with an increased risk of subsequent dementia, according to a relatively large prospective population-based cohort study that followed patients for almost 30 years.
Even though previously published studies have not conclusively linked blood pressure control with a reduction in dementia risk, a second study, published simultaneously, did link blood pressure control with a smaller increase in white matter lesions, which are a marker of dementia risk. However, a reduction in total brain volume that accompanied this protection raised concern.
In the first of the two reports published Aug. 13 in JAMA, individuals 45-65 years of age participating in the Atherosclerosis Risk in Communities (ARIC) study were followed for cognitive function in relation to blood pressure. The baseline visit took place in 1987-1989. Cognitive function was also evaluated at the fifth visit, which took place in 2011-2013, and the sixth visit, which took place in 2016-2017.
At the sixth visit, the incidence of dementia among patients who were normotensive at baseline and also normotensive at the fifth visit was 1.31 per 100 person-years. For those with hypertension (greater than 140/90 mm Hg) at the fifth visit but normotensive at baseline, the incidence was 1.99 per 100 patient-years. For those with hypertension at both time points, the incidence was 4.26 per 100 patient-years.
When translated into hazard ratios, those with midlife and late-life hypertension were nearly 50% more likely to develop dementia (HR, 1.49) relative to those who remained normotensive. For those who had only midlife hypertension, the risk was also significantly increased (HR, 1.41) relative to those who remained normotensive at both time points.
Those with midlife hypertension but late-life hypotension were also found to be at greater risk of dementia (HR, 1.62) relative to those who remained normotensive.
These data support the premise that uncontrolled midlife hypertension increases risk of dementia but do not touch on whether blood pressure reductions reduce this risk. However, a second study published simultaneously provided at least some evidence that blood pressure control might offer some protection.
In this report, which is a substudy of the previously published Systolic Blood Pressure Intervention Trial (SPRINT) MIND trial, brain volume changes were evaluated via MRI in 449 of the more than 2,000 patients included in the previously published trial (Williamson JD et al. JAMA. 2019;321[6]:553-61).
After a median 3.4 years of follow-up, mean white matter lesion volume increased only 0.92 cm3 in patients receiving intensive systolic blood pressure control, defined as less than 120 mm Hg, versus 1.45 cm3 in those with higher systolic blood pressures.
These substudy data are encouraging, but it is important to recognize that the previously published and larger SPRINT MIND trial did not achieve its endpoint. In that study, the protection against dementia was nonsignificant (HR, 0.83; 95% confidence interval, 0.67-1.04).
In addition, the lower loss in white matter volume with intensive blood pressure lowering in the MRI substudy was accompanied with a greater loss in total brain volume (–30.6 vs. –26.9 cm3), which is considered a potentially negative effect.
As a result, the picture for risk management remains unclear, according to an editorial that accompanied publication of both studies.
“The important clinical question is whether changes of a few cubic millimeters in white matter hyperintensity volume or brain make a difference on brain function,” observed the author of the editorial, Shyam Prabhakaran, MD, of the department of neurology at the University of Chicago.
He believes that there are several findings from both studies that are “encouraging” in regard to blood pressure control for the prevention of dementia, but he also listed many unanswered questions, including why benefits observed to date have been so modest. He speculated that meaningful clinical benefits might depend on a multimodal approach that includes modification of other vascular risk factors, such as elevated lipids.
He also suggested that many issues regarding intensive blood pressure control for preventing dementia are unresolved, suggesting the need for more studies.
Not least, “later blood-pressure lowering interventions require careful monitoring for the potential cognitive harm associated with late-life hypotension,” Dr. Prabhakaran noted. Calling the effects of blood pressure control on brain health “nuanced,” he concluded that there is an opportunity for blood pressure modifications to prevent dementia, but stressed that optimal blood pressure targets for the purposes of preventing dementia are unknown.
The ARIC and SPRINT studies are supported by the National Institutes of Health. Several authors reported relationships with industry but no conflicts of interest relevant to this study.
SOURCES: Walker KA et al. JAMA. 2019;322(6):535-45; SPRINT MIND investigators. JAMA. 2019;322(6):524-34; Prabhakaran S. JAMA. 2019;322(6):512-3
Uncontrolled hypertension among individuals aged 45-65 years of age is associated with an increased risk of subsequent dementia, according to a relatively large prospective population-based cohort study that followed patients for almost 30 years.
Even though previously published studies have not conclusively linked blood pressure control with a reduction in dementia risk, a second study, published simultaneously, did link blood pressure control with a smaller increase in white matter lesions, which are a marker of dementia risk. However, a reduction in total brain volume that accompanied this protection raised concern.
In the first of the two reports published Aug. 13 in JAMA, individuals 45-65 years of age participating in the Atherosclerosis Risk in Communities (ARIC) study were followed for cognitive function in relation to blood pressure. The baseline visit took place in 1987-1989. Cognitive function was also evaluated at the fifth visit, which took place in 2011-2013, and the sixth visit, which took place in 2016-2017.
At the sixth visit, the incidence of dementia among patients who were normotensive at baseline and also normotensive at the fifth visit was 1.31 per 100 person-years. For those with hypertension (greater than 140/90 mm Hg) at the fifth visit but normotensive at baseline, the incidence was 1.99 per 100 patient-years. For those with hypertension at both time points, the incidence was 4.26 per 100 patient-years.
When translated into hazard ratios, those with midlife and late-life hypertension were nearly 50% more likely to develop dementia (HR, 1.49) relative to those who remained normotensive. For those who had only midlife hypertension, the risk was also significantly increased (HR, 1.41) relative to those who remained normotensive at both time points.
Those with midlife hypertension but late-life hypotension were also found to be at greater risk of dementia (HR, 1.62) relative to those who remained normotensive.
These data support the premise that uncontrolled midlife hypertension increases risk of dementia but do not touch on whether blood pressure reductions reduce this risk. However, a second study published simultaneously provided at least some evidence that blood pressure control might offer some protection.
In this report, which is a substudy of the previously published Systolic Blood Pressure Intervention Trial (SPRINT) MIND trial, brain volume changes were evaluated via MRI in 449 of the more than 2,000 patients included in the previously published trial (Williamson JD et al. JAMA. 2019;321[6]:553-61).
After a median 3.4 years of follow-up, mean white matter lesion volume increased only 0.92 cm3 in patients receiving intensive systolic blood pressure control, defined as less than 120 mm Hg, versus 1.45 cm3 in those with higher systolic blood pressures.
These substudy data are encouraging, but it is important to recognize that the previously published and larger SPRINT MIND trial did not achieve its endpoint. In that study, the protection against dementia was nonsignificant (HR, 0.83; 95% confidence interval, 0.67-1.04).
In addition, the lower loss in white matter volume with intensive blood pressure lowering in the MRI substudy was accompanied with a greater loss in total brain volume (–30.6 vs. –26.9 cm3), which is considered a potentially negative effect.
As a result, the picture for risk management remains unclear, according to an editorial that accompanied publication of both studies.
“The important clinical question is whether changes of a few cubic millimeters in white matter hyperintensity volume or brain make a difference on brain function,” observed the author of the editorial, Shyam Prabhakaran, MD, of the department of neurology at the University of Chicago.
He believes that there are several findings from both studies that are “encouraging” in regard to blood pressure control for the prevention of dementia, but he also listed many unanswered questions, including why benefits observed to date have been so modest. He speculated that meaningful clinical benefits might depend on a multimodal approach that includes modification of other vascular risk factors, such as elevated lipids.
He also suggested that many issues regarding intensive blood pressure control for preventing dementia are unresolved, suggesting the need for more studies.
Not least, “later blood-pressure lowering interventions require careful monitoring for the potential cognitive harm associated with late-life hypotension,” Dr. Prabhakaran noted. Calling the effects of blood pressure control on brain health “nuanced,” he concluded that there is an opportunity for blood pressure modifications to prevent dementia, but stressed that optimal blood pressure targets for the purposes of preventing dementia are unknown.
The ARIC and SPRINT studies are supported by the National Institutes of Health. Several authors reported relationships with industry but no conflicts of interest relevant to this study.
SOURCES: Walker KA et al. JAMA. 2019;322(6):535-45; SPRINT MIND investigators. JAMA. 2019;322(6):524-34; Prabhakaran S. JAMA. 2019;322(6):512-3
FROM JAMA