User login
Are computers and AI prompting us to think less?
The collection of vast amounts of data and the use of more sophisticated algorithms seem beneficial in all fields. However, I have deep concerns about the “other side of the coin” when it comes to artificial intelligence (AI) as discussed in “An FP’s guide to AI-enabled clinical decision support” (J Fam Pract. 2019;68:486-492).
Years ago, when I worked in urgent care, one of my colleagues would log in to her favorite Web site to search for the appropriate diagnosis for almost all of her patients. Surely this physician was able to memorize and regurgitate enough information to get through medical school and pass the boards, but was she able to think, in the sense of using/applying the information she stored away? My answer is, “No!”
Certainly, having a computer helps one to get through medical school. However, while we use terms such as “AI,” I would argue that none of these machines do more than duplicate the algorithmic functioning of the brain. Which leads me to the other side of the coin: Are computers, of which we ask questions and expect legitimate answers in return, helping us to think? Or are they leading us to think less?
In other words, are we inadvertently “dumbing down” as physicians (and as a species)? And do we want a physician who seems less capable of actually processing the sum total of a patient’s complaints, symptoms, and findings in trying to understand the patient’s problem?
While we cannot go back and disconnect from computers, we can make sure that we do not become totally dependent on them. We need to acknowledge this possible blind spot in the evolution of technology (particularly AI)—the potential to reinforce “not thinking”—especially within the medical school environment. There needs to be an awareness of, and a conscious effort to counter, an overreliance on computers thinking for us.
As individual physicians, we owe it to our patients and ourselves, each and every working day, to use our brains to apply our education, training, and accumulated data to help diagnose and treat our patients effectively.
Barry Marged, DO, ABD, MA
Mansfield, OH
The collection of vast amounts of data and the use of more sophisticated algorithms seem beneficial in all fields. However, I have deep concerns about the “other side of the coin” when it comes to artificial intelligence (AI) as discussed in “An FP’s guide to AI-enabled clinical decision support” (J Fam Pract. 2019;68:486-492).
Years ago, when I worked in urgent care, one of my colleagues would log in to her favorite Web site to search for the appropriate diagnosis for almost all of her patients. Surely this physician was able to memorize and regurgitate enough information to get through medical school and pass the boards, but was she able to think, in the sense of using/applying the information she stored away? My answer is, “No!”
Certainly, having a computer helps one to get through medical school. However, while we use terms such as “AI,” I would argue that none of these machines do more than duplicate the algorithmic functioning of the brain. Which leads me to the other side of the coin: Are computers, of which we ask questions and expect legitimate answers in return, helping us to think? Or are they leading us to think less?
In other words, are we inadvertently “dumbing down” as physicians (and as a species)? And do we want a physician who seems less capable of actually processing the sum total of a patient’s complaints, symptoms, and findings in trying to understand the patient’s problem?
While we cannot go back and disconnect from computers, we can make sure that we do not become totally dependent on them. We need to acknowledge this possible blind spot in the evolution of technology (particularly AI)—the potential to reinforce “not thinking”—especially within the medical school environment. There needs to be an awareness of, and a conscious effort to counter, an overreliance on computers thinking for us.
As individual physicians, we owe it to our patients and ourselves, each and every working day, to use our brains to apply our education, training, and accumulated data to help diagnose and treat our patients effectively.
Barry Marged, DO, ABD, MA
Mansfield, OH
The collection of vast amounts of data and the use of more sophisticated algorithms seem beneficial in all fields. However, I have deep concerns about the “other side of the coin” when it comes to artificial intelligence (AI) as discussed in “An FP’s guide to AI-enabled clinical decision support” (J Fam Pract. 2019;68:486-492).
Years ago, when I worked in urgent care, one of my colleagues would log in to her favorite Web site to search for the appropriate diagnosis for almost all of her patients. Surely this physician was able to memorize and regurgitate enough information to get through medical school and pass the boards, but was she able to think, in the sense of using/applying the information she stored away? My answer is, “No!”
Certainly, having a computer helps one to get through medical school. However, while we use terms such as “AI,” I would argue that none of these machines do more than duplicate the algorithmic functioning of the brain. Which leads me to the other side of the coin: Are computers, of which we ask questions and expect legitimate answers in return, helping us to think? Or are they leading us to think less?
In other words, are we inadvertently “dumbing down” as physicians (and as a species)? And do we want a physician who seems less capable of actually processing the sum total of a patient’s complaints, symptoms, and findings in trying to understand the patient’s problem?
While we cannot go back and disconnect from computers, we can make sure that we do not become totally dependent on them. We need to acknowledge this possible blind spot in the evolution of technology (particularly AI)—the potential to reinforce “not thinking”—especially within the medical school environment. There needs to be an awareness of, and a conscious effort to counter, an overreliance on computers thinking for us.
As individual physicians, we owe it to our patients and ourselves, each and every working day, to use our brains to apply our education, training, and accumulated data to help diagnose and treat our patients effectively.
Barry Marged, DO, ABD, MA
Mansfield, OH
A rarely discussed aspect of the opioid crisis
Your article, “A patient-centered approach to tapering opioids” (J Fam Pract. 2019;68:548-556) by Davis et al is the most thoughtful article I have seen on opioids. The patient-centered ap-proach takes this article to a place that is rarely discussed in the opioid crisis.
If we could really understand and treat chronic psychic and physical pain better, we might begin to have a real impact on this crisis. I completely agree that evidence-based intensive trauma treatment is generally unavailable in the United States. I have been working with women in a residential chemical dependency treatment program for the past 15 years and more than 90% of them were sexually abused. Trauma can lead to all forms of addiction, and trauma induced hyperalgesia is not the same as nociceptive pain.
We have so many unaddressed mental health issues in our country and your article emphasized the importance of understanding people and their mental health issues rather than taking a formulaic approach and replacing one opioid with another. It is clear to me that we will not win this battle with medication-assisted treatment alone.
Richard Usatine, MD
San Antonio, TX
Associate Editor, The Journal of Family Practice
Your article, “A patient-centered approach to tapering opioids” (J Fam Pract. 2019;68:548-556) by Davis et al is the most thoughtful article I have seen on opioids. The patient-centered ap-proach takes this article to a place that is rarely discussed in the opioid crisis.
If we could really understand and treat chronic psychic and physical pain better, we might begin to have a real impact on this crisis. I completely agree that evidence-based intensive trauma treatment is generally unavailable in the United States. I have been working with women in a residential chemical dependency treatment program for the past 15 years and more than 90% of them were sexually abused. Trauma can lead to all forms of addiction, and trauma induced hyperalgesia is not the same as nociceptive pain.
We have so many unaddressed mental health issues in our country and your article emphasized the importance of understanding people and their mental health issues rather than taking a formulaic approach and replacing one opioid with another. It is clear to me that we will not win this battle with medication-assisted treatment alone.
Richard Usatine, MD
San Antonio, TX
Associate Editor, The Journal of Family Practice
Your article, “A patient-centered approach to tapering opioids” (J Fam Pract. 2019;68:548-556) by Davis et al is the most thoughtful article I have seen on opioids. The patient-centered ap-proach takes this article to a place that is rarely discussed in the opioid crisis.
If we could really understand and treat chronic psychic and physical pain better, we might begin to have a real impact on this crisis. I completely agree that evidence-based intensive trauma treatment is generally unavailable in the United States. I have been working with women in a residential chemical dependency treatment program for the past 15 years and more than 90% of them were sexually abused. Trauma can lead to all forms of addiction, and trauma induced hyperalgesia is not the same as nociceptive pain.
We have so many unaddressed mental health issues in our country and your article emphasized the importance of understanding people and their mental health issues rather than taking a formulaic approach and replacing one opioid with another. It is clear to me that we will not win this battle with medication-assisted treatment alone.
Richard Usatine, MD
San Antonio, TX
Associate Editor, The Journal of Family Practice
MACE benefits with dapagliflozin improve with disease duration
Treatment with the sodium-glucose transporter 2 inhibitor dapagliflozin reduced the risk for cardiovascular disease or hospitalization for heart failure (CVD/HHF) in patients with diabetes, regardless of the duration of the disease, but had a greater protective benefit against major adverse cardiovascular events (MACE) and renal events in patients with longer disease duration, according to new findings from a post hoc analysis of the DECLARE-TIMI 58 trial.
The positive effect of dapagliflozin in patients with MACE – which includes myocardial infarction (MI), CVD, and ischemic stroke – may have been driven by lower rates of MI and ischemic stroke with the drug, compared with placebo, in patients with longer disease duration, wrote Harpreet S. Bajaj, MD, and colleagues. Their report is in Diabetes, Obesity and Metabolism (2020 Feb 23. doi: 10.1111/dom.14011).
It has been previously reported that the risk for complications in diabetes increases with increasing duration of the disease. Recent studies with SGLT-2 inhibitors have shown that the drugs improve cardiovascular and renal outcomes in diabetes, and they are recommended by the American Diabetes Association as second-line therapy in patients with atherosclerotic cardiovascular disease, chronic kidney disease, or heart failure. The European Society of Cardiology and the European Association for the Study of Diabetes recommend that patients with diabetes patients who have three or more risk factors, or those with a disease duration of more than 20 years, should be deemed very high risk and be considered for early treatment with SGLT2 inhibitors.
“The MACE benefit observed with dapagliflozin in this study in patients with diabetes duration of [more than] 20 years, clearly supports that notion,” the authors wrote.
In DECLARE-TIMI 58, 17,160 patients with type 2 diabetes received dapagliflozin or placebo and were followed for a median of 4.2 years. Of those patients, 22.4% had a disease duration of fewer than 5 years; 27.6%, a duration of 5-10 years; 23.0%, 10-15 years; 14.2%, 10-15 years; and 12.9%, more than 20 years. The median duration of disease was 11 years.
Patients in all the age groups had similar reductions in CVD/HHF, compared with placebo, with hazard ratios of 0.79 (disease duration of 5 or fewer years), 0.86, 0.92, 0.81, and 0.75 (duration of 20 years), respectively (interaction trend P = .760).
Treatment with dapagliflozin reduced the incidence of MACE, but the benefit was more apparent in patients with longer-term disease: HR, 1.08; 1.02; 0.94; 0.92; and 0.67, respectively (interaction trend P = .004). Similar trends were seen with MI (interaction trend P = .019) and ischemic stroke (interaction trend P = .015).
The researchers also reported improved benefits in renal-specific outcome with increasing disease duration, with HRs ranging from 0.79 in patients with diabetes duration of fewer than 5 years, to 0.42 in those with a duration of more than 20 years (interaction trend P = .084).
Limitations of the study include the fact that the information about diabetes duration relied on patient reports, and that the original trial was not powered for all subgroup interactions. This authors emphasized that this was a post hoc analysis and as such, should be considered hypothesis generating.
All but two of the authors reported relationships with Astra Zeneca, which funded the study, and other drug companies.
SOURCE: Bajaj HS et al. Diabetes Obes Metab. 2020 Feb 23. doi: 10.1111/dom.14011.
Treatment with the sodium-glucose transporter 2 inhibitor dapagliflozin reduced the risk for cardiovascular disease or hospitalization for heart failure (CVD/HHF) in patients with diabetes, regardless of the duration of the disease, but had a greater protective benefit against major adverse cardiovascular events (MACE) and renal events in patients with longer disease duration, according to new findings from a post hoc analysis of the DECLARE-TIMI 58 trial.
The positive effect of dapagliflozin in patients with MACE – which includes myocardial infarction (MI), CVD, and ischemic stroke – may have been driven by lower rates of MI and ischemic stroke with the drug, compared with placebo, in patients with longer disease duration, wrote Harpreet S. Bajaj, MD, and colleagues. Their report is in Diabetes, Obesity and Metabolism (2020 Feb 23. doi: 10.1111/dom.14011).
It has been previously reported that the risk for complications in diabetes increases with increasing duration of the disease. Recent studies with SGLT-2 inhibitors have shown that the drugs improve cardiovascular and renal outcomes in diabetes, and they are recommended by the American Diabetes Association as second-line therapy in patients with atherosclerotic cardiovascular disease, chronic kidney disease, or heart failure. The European Society of Cardiology and the European Association for the Study of Diabetes recommend that patients with diabetes patients who have three or more risk factors, or those with a disease duration of more than 20 years, should be deemed very high risk and be considered for early treatment with SGLT2 inhibitors.
“The MACE benefit observed with dapagliflozin in this study in patients with diabetes duration of [more than] 20 years, clearly supports that notion,” the authors wrote.
In DECLARE-TIMI 58, 17,160 patients with type 2 diabetes received dapagliflozin or placebo and were followed for a median of 4.2 years. Of those patients, 22.4% had a disease duration of fewer than 5 years; 27.6%, a duration of 5-10 years; 23.0%, 10-15 years; 14.2%, 10-15 years; and 12.9%, more than 20 years. The median duration of disease was 11 years.
Patients in all the age groups had similar reductions in CVD/HHF, compared with placebo, with hazard ratios of 0.79 (disease duration of 5 or fewer years), 0.86, 0.92, 0.81, and 0.75 (duration of 20 years), respectively (interaction trend P = .760).
Treatment with dapagliflozin reduced the incidence of MACE, but the benefit was more apparent in patients with longer-term disease: HR, 1.08; 1.02; 0.94; 0.92; and 0.67, respectively (interaction trend P = .004). Similar trends were seen with MI (interaction trend P = .019) and ischemic stroke (interaction trend P = .015).
The researchers also reported improved benefits in renal-specific outcome with increasing disease duration, with HRs ranging from 0.79 in patients with diabetes duration of fewer than 5 years, to 0.42 in those with a duration of more than 20 years (interaction trend P = .084).
Limitations of the study include the fact that the information about diabetes duration relied on patient reports, and that the original trial was not powered for all subgroup interactions. This authors emphasized that this was a post hoc analysis and as such, should be considered hypothesis generating.
All but two of the authors reported relationships with Astra Zeneca, which funded the study, and other drug companies.
SOURCE: Bajaj HS et al. Diabetes Obes Metab. 2020 Feb 23. doi: 10.1111/dom.14011.
Treatment with the sodium-glucose transporter 2 inhibitor dapagliflozin reduced the risk for cardiovascular disease or hospitalization for heart failure (CVD/HHF) in patients with diabetes, regardless of the duration of the disease, but had a greater protective benefit against major adverse cardiovascular events (MACE) and renal events in patients with longer disease duration, according to new findings from a post hoc analysis of the DECLARE-TIMI 58 trial.
The positive effect of dapagliflozin in patients with MACE – which includes myocardial infarction (MI), CVD, and ischemic stroke – may have been driven by lower rates of MI and ischemic stroke with the drug, compared with placebo, in patients with longer disease duration, wrote Harpreet S. Bajaj, MD, and colleagues. Their report is in Diabetes, Obesity and Metabolism (2020 Feb 23. doi: 10.1111/dom.14011).
It has been previously reported that the risk for complications in diabetes increases with increasing duration of the disease. Recent studies with SGLT-2 inhibitors have shown that the drugs improve cardiovascular and renal outcomes in diabetes, and they are recommended by the American Diabetes Association as second-line therapy in patients with atherosclerotic cardiovascular disease, chronic kidney disease, or heart failure. The European Society of Cardiology and the European Association for the Study of Diabetes recommend that patients with diabetes patients who have three or more risk factors, or those with a disease duration of more than 20 years, should be deemed very high risk and be considered for early treatment with SGLT2 inhibitors.
“The MACE benefit observed with dapagliflozin in this study in patients with diabetes duration of [more than] 20 years, clearly supports that notion,” the authors wrote.
In DECLARE-TIMI 58, 17,160 patients with type 2 diabetes received dapagliflozin or placebo and were followed for a median of 4.2 years. Of those patients, 22.4% had a disease duration of fewer than 5 years; 27.6%, a duration of 5-10 years; 23.0%, 10-15 years; 14.2%, 10-15 years; and 12.9%, more than 20 years. The median duration of disease was 11 years.
Patients in all the age groups had similar reductions in CVD/HHF, compared with placebo, with hazard ratios of 0.79 (disease duration of 5 or fewer years), 0.86, 0.92, 0.81, and 0.75 (duration of 20 years), respectively (interaction trend P = .760).
Treatment with dapagliflozin reduced the incidence of MACE, but the benefit was more apparent in patients with longer-term disease: HR, 1.08; 1.02; 0.94; 0.92; and 0.67, respectively (interaction trend P = .004). Similar trends were seen with MI (interaction trend P = .019) and ischemic stroke (interaction trend P = .015).
The researchers also reported improved benefits in renal-specific outcome with increasing disease duration, with HRs ranging from 0.79 in patients with diabetes duration of fewer than 5 years, to 0.42 in those with a duration of more than 20 years (interaction trend P = .084).
Limitations of the study include the fact that the information about diabetes duration relied on patient reports, and that the original trial was not powered for all subgroup interactions. This authors emphasized that this was a post hoc analysis and as such, should be considered hypothesis generating.
All but two of the authors reported relationships with Astra Zeneca, which funded the study, and other drug companies.
SOURCE: Bajaj HS et al. Diabetes Obes Metab. 2020 Feb 23. doi: 10.1111/dom.14011.
FROM DIABETES, OBESITY AND METABOLISM
Preoperative chemoradiotherapy failed to boost overall survival in pancreatic cancer
, according to findings from a phase 3 trial.
On the other hand, preoperative chemoradiotherapy improved disease-free survival, locoregional failure-free interval, and other secondary endpoints, according to study author Eva Versteijne, MD, of the University of Amsterdam, and colleagues. Their findings were published in the Journal of Clinical Oncology.
The randomized, phase 3 study included 246 patients with borderline or resectable pancreatic ductal adenocarcinoma without distant metastases. Patients were randomized to receive preoperative chemoradiotherapy (n = 119) or immediate surgery (n = 127).
Patients in the preoperative chemoradiotherapy arm received three courses of gemcitabine at 1,000 mg/m2, combined with 15 fractions of radiotherapy at 2.4 Gy during the second course. Explorative laparotomy with subsequent resection followed, in addition to four 4-week cycles of adjuvant gemcitabine at 1,000 mg/m2. Following resection in the immediate surgery arm, patients received six 4-week cycles of adjuvant gemcitabine at the same dose.
The primary outcome was median overall survival in the intention-to-treat population. The median overall survival was 16.0 months in the preoperative chemoradiotherapy arm and 14.3 months in the immediate surgery arm (hazard ratio, 0.78; P = .096).
Secondary outcomes included disease-free survival, resection rate, R0 resection rate, and locoregional failure-free interval, among others.
The resection rate was 61% in the preoperative chemoradiotherapy arm and 72% in the immediate surgery arm (odds ratio, 0.58; P = .058). The R0 resection rates were 71% and 40%, respectively (OR, 3.61; P less than .001).
The median disease-free survival was 8.1 months in the preoperative chemoradiotherapy arm and 7.7 months in the immediate surgery arm (HR, 0.73; P = .032). The median locoregional failure-free interval was not reached and 13.4 months, respectively (HR, 0.56; P = .0034). The rate of serious adverse events was 52% and 41%, respectively (OR, 1.57; P = .096).
“Preoperative chemoradiotherapy was associated with significantly better [disease-free survival] and [locoregional failure-free interval] as well as with significantly lower rates of pathologic lymph nodes, perineural invasion, and venous invasion,” the researchers noted.
They acknowledged that some findings, particularly the median overall survival in patients assigned to immediate surgery, require further investigation, as these data suggest the trial may have been underpowered.
“The consistent benefits for most secondary endpoints and the better compliance with preoperative chemoradiotherapy compared with postoperative adjuvant chemotherapy suggest superiority of the neoadjuvant approach,” the researchers concluded.
The study was funded by the Dutch Cancer Society. The authors disclosed financial affiliations with Bristol-Myers Squibb, Eisai, Ipsen, Merck Serono, and several other companies.
SOURCE: Versteijne E et al. J Clin Oncol. 2020 Feb 27. doi: 10.1200/JCO.19.02274.
, according to findings from a phase 3 trial.
On the other hand, preoperative chemoradiotherapy improved disease-free survival, locoregional failure-free interval, and other secondary endpoints, according to study author Eva Versteijne, MD, of the University of Amsterdam, and colleagues. Their findings were published in the Journal of Clinical Oncology.
The randomized, phase 3 study included 246 patients with borderline or resectable pancreatic ductal adenocarcinoma without distant metastases. Patients were randomized to receive preoperative chemoradiotherapy (n = 119) or immediate surgery (n = 127).
Patients in the preoperative chemoradiotherapy arm received three courses of gemcitabine at 1,000 mg/m2, combined with 15 fractions of radiotherapy at 2.4 Gy during the second course. Explorative laparotomy with subsequent resection followed, in addition to four 4-week cycles of adjuvant gemcitabine at 1,000 mg/m2. Following resection in the immediate surgery arm, patients received six 4-week cycles of adjuvant gemcitabine at the same dose.
The primary outcome was median overall survival in the intention-to-treat population. The median overall survival was 16.0 months in the preoperative chemoradiotherapy arm and 14.3 months in the immediate surgery arm (hazard ratio, 0.78; P = .096).
Secondary outcomes included disease-free survival, resection rate, R0 resection rate, and locoregional failure-free interval, among others.
The resection rate was 61% in the preoperative chemoradiotherapy arm and 72% in the immediate surgery arm (odds ratio, 0.58; P = .058). The R0 resection rates were 71% and 40%, respectively (OR, 3.61; P less than .001).
The median disease-free survival was 8.1 months in the preoperative chemoradiotherapy arm and 7.7 months in the immediate surgery arm (HR, 0.73; P = .032). The median locoregional failure-free interval was not reached and 13.4 months, respectively (HR, 0.56; P = .0034). The rate of serious adverse events was 52% and 41%, respectively (OR, 1.57; P = .096).
“Preoperative chemoradiotherapy was associated with significantly better [disease-free survival] and [locoregional failure-free interval] as well as with significantly lower rates of pathologic lymph nodes, perineural invasion, and venous invasion,” the researchers noted.
They acknowledged that some findings, particularly the median overall survival in patients assigned to immediate surgery, require further investigation, as these data suggest the trial may have been underpowered.
“The consistent benefits for most secondary endpoints and the better compliance with preoperative chemoradiotherapy compared with postoperative adjuvant chemotherapy suggest superiority of the neoadjuvant approach,” the researchers concluded.
The study was funded by the Dutch Cancer Society. The authors disclosed financial affiliations with Bristol-Myers Squibb, Eisai, Ipsen, Merck Serono, and several other companies.
SOURCE: Versteijne E et al. J Clin Oncol. 2020 Feb 27. doi: 10.1200/JCO.19.02274.
, according to findings from a phase 3 trial.
On the other hand, preoperative chemoradiotherapy improved disease-free survival, locoregional failure-free interval, and other secondary endpoints, according to study author Eva Versteijne, MD, of the University of Amsterdam, and colleagues. Their findings were published in the Journal of Clinical Oncology.
The randomized, phase 3 study included 246 patients with borderline or resectable pancreatic ductal adenocarcinoma without distant metastases. Patients were randomized to receive preoperative chemoradiotherapy (n = 119) or immediate surgery (n = 127).
Patients in the preoperative chemoradiotherapy arm received three courses of gemcitabine at 1,000 mg/m2, combined with 15 fractions of radiotherapy at 2.4 Gy during the second course. Explorative laparotomy with subsequent resection followed, in addition to four 4-week cycles of adjuvant gemcitabine at 1,000 mg/m2. Following resection in the immediate surgery arm, patients received six 4-week cycles of adjuvant gemcitabine at the same dose.
The primary outcome was median overall survival in the intention-to-treat population. The median overall survival was 16.0 months in the preoperative chemoradiotherapy arm and 14.3 months in the immediate surgery arm (hazard ratio, 0.78; P = .096).
Secondary outcomes included disease-free survival, resection rate, R0 resection rate, and locoregional failure-free interval, among others.
The resection rate was 61% in the preoperative chemoradiotherapy arm and 72% in the immediate surgery arm (odds ratio, 0.58; P = .058). The R0 resection rates were 71% and 40%, respectively (OR, 3.61; P less than .001).
The median disease-free survival was 8.1 months in the preoperative chemoradiotherapy arm and 7.7 months in the immediate surgery arm (HR, 0.73; P = .032). The median locoregional failure-free interval was not reached and 13.4 months, respectively (HR, 0.56; P = .0034). The rate of serious adverse events was 52% and 41%, respectively (OR, 1.57; P = .096).
“Preoperative chemoradiotherapy was associated with significantly better [disease-free survival] and [locoregional failure-free interval] as well as with significantly lower rates of pathologic lymph nodes, perineural invasion, and venous invasion,” the researchers noted.
They acknowledged that some findings, particularly the median overall survival in patients assigned to immediate surgery, require further investigation, as these data suggest the trial may have been underpowered.
“The consistent benefits for most secondary endpoints and the better compliance with preoperative chemoradiotherapy compared with postoperative adjuvant chemotherapy suggest superiority of the neoadjuvant approach,” the researchers concluded.
The study was funded by the Dutch Cancer Society. The authors disclosed financial affiliations with Bristol-Myers Squibb, Eisai, Ipsen, Merck Serono, and several other companies.
SOURCE: Versteijne E et al. J Clin Oncol. 2020 Feb 27. doi: 10.1200/JCO.19.02274.
FROM JOURNAL OF CLINICAL ONCOLOGY
In a public health crisis, obstetric collaboration is mission-critical
With the novel coronavirus (COVID-19) monopolizing the news cycle, fear and misinformation are at an all-time high. Public health officials and physicians are accelerating education outreach to the public to address misinformation, and identify and care for patients who may have been exposed to the virus.

In times of public health crises, pregnant women have unique and pressing concerns about their personal health and the health of their unborn children. While not often mentioned in major news coverage, obstetricians play a critical role during health crises because of their uniquely personal role with patients during all stages of pregnancy, providing this vulnerable population with the most up-to-date information and following the latest guidelines for recommended care.
Unfortunately, COVID-19 is breaking unfamiliar new ground. We know that pregnant women are at higher risk for viral infection – annually, influenza is a grim reminder that pregnant women are more immunocompromised than the general public – but we do not yet have data to confirm or refute that pregnant women have a higher susceptibility to COVID-19 than the rest of the adult population. We also do not know enough about COVID-19 transmission, including whether the virus can cross the transplacental barrier to affect a fetus, or whether it can be transmitted through breast milk.
As private practice community obstetricians work to protect their patients during this public health crisis, Ob hospitalists can play an important role in supporting them in the provision of patient care.
First, Ob hospitalists are highly-trained specialists who can help ensure that pregnant patients who seek care at the hospital – either with viral symptoms or with separate pregnancy-related concerns – are protected during triage until the treating community obstetrician can take the reins.
When a pregnant woman presents at a hospital, in most cases she will bypass the ED and instead be sent directly to the labor and delivery (L&D) unit. During a viral outbreak, there are two major concerns with this approach. For one thing, it means an immunocompromised woman is being sent through the hospital to get to L&D, and along the path, is exposed to every airborne pathogen in the facility (and, if she is already infected, exposes others along the way). In addition, in hospitals without an Ob hospitalist on site, the patient generally is not immediately triaged by a physician, physician’s assistant, or nurse practitioner upon arrival because those clinicians are not consistently on site in L&D.
In times of viral pandemics, new approaches are warranted. For hospitals with contracted L&D management with hospitalists, hospitalists work closely with department heads to implement protocols loosely based on the Emergency Severity Index (ESI) model established by the Agency for Healthcare Research and Quality. Just as the ESI algorithm guides clinical stratification of patients, in times of reported viral outbreaks, L&D should consider triage of all pregnant women at higher levels of acuity, regardless of presentation status. In particular, if they show clinical symptoms, they should be masked, accompanied to the L&D unit by protected personnel, separated from other patients in areas of forced proximity such as hallways and elevators, and triaged in a secure single-patient room with a closed door (ideally at negative pressure relative to the surrounding areas).
If the patient has traveled to an area of outbreak, reports exposure to travelers who have visited high-risk areas, has had contact with individuals who tested positive for COVID-19, or exhibits any clinical symptoms of COVID-19 (fever, dry cough, fatigue, etc.), her care management should adhere to standing hospital emergency protocols. Following consultation with the assigned community obstetrician, the Ob hospitalist and hospital staff should contact their local/state health departments immediately for all cases of patients who show symptoms to determine if the patient meets requirements for a person under investigation (PUI) for COVID-19. The state/local health department will work with clinicians to collect, store, and ship clinical specimens appropriately. Very ill patients may need to be treated in an intensive care setting where respiratory status can be closely monitored.
At Ob Hospitalist Group, our body of evidence from our large national footprint has informed the development of standard sets of protocols for delivery complications such as preeclampsia and postpartum hemorrhage, as well as a cesarean section reduction toolkit to combat medically unnecessary cesarean sections. OB hospitalists therefore can assist with refining COVID-19 protocols specifically for the L&D setting, using evidence-based data to tailor protocols to address public health emergencies as they evolve.
The second way that Ob hospitalists can support their colleagues is by covering L&D 24/7 so that community obstetricians can focus on other pressing medical needs. From our experience with other outbreaks such as severe acute respiratory syndrome (SARS) and influenza, we anticipate that obstetricians in private practice likely will have their hands full juggling a regular patient load, fielding calls from concerned patients, and caring for infected or ill patients who are being treated in an outpatient setting. Adding to that plate the need to rush to the hospital to clinically assess a patient for COVID-19 or for a delivery only compounds stress and exhaustion. At Ob Hospitalist Group, our hospitalist programs provide coverage and support to community obstetricians until they can arrive at the hospital or when the woman has no assigned obstetrician, reducing the pressure on community obstetricians to rush through their schedules.
Diagnostic and pharmaceutical companies are collaborating with public health officials to expedite diagnostic testing staff, hospital treatment capacity, vaccines, and even early therapies that may help to minimize severity. But right now, as clinicians work to protect their vulnerable patients, a close collaboration between community obstetricians and Ob hospitalists will help to keep patients and health care personnel safe and healthy – a goal that should apply not only to public health crises, but to the provision of maternal care every day.
Dr. Simon is chief medical officer at Ob Hospitalist Group (OBHG), is a board-certified ob.gyn., and former head of the department of obstetrics and gynecology for a U.S. hospital. He has no relevant conflicts of interest or financial disclosures. Email him at [email protected].
With the novel coronavirus (COVID-19) monopolizing the news cycle, fear and misinformation are at an all-time high. Public health officials and physicians are accelerating education outreach to the public to address misinformation, and identify and care for patients who may have been exposed to the virus.
In times of public health crises, pregnant women have unique and pressing concerns about their personal health and the health of their unborn children. While not often mentioned in major news coverage, obstetricians play a critical role during health crises because of their uniquely personal role with patients during all stages of pregnancy, providing this vulnerable population with the most up-to-date information and following the latest guidelines for recommended care.
Unfortunately, COVID-19 is breaking unfamiliar new ground. We know that pregnant women are at higher risk for viral infection – annually, influenza is a grim reminder that pregnant women are more immunocompromised than the general public – but we do not yet have data to confirm or refute that pregnant women have a higher susceptibility to COVID-19 than the rest of the adult population. We also do not know enough about COVID-19 transmission, including whether the virus can cross the transplacental barrier to affect a fetus, or whether it can be transmitted through breast milk.
As private practice community obstetricians work to protect their patients during this public health crisis, Ob hospitalists can play an important role in supporting them in the provision of patient care.
First, Ob hospitalists are highly-trained specialists who can help ensure that pregnant patients who seek care at the hospital – either with viral symptoms or with separate pregnancy-related concerns – are protected during triage until the treating community obstetrician can take the reins.
When a pregnant woman presents at a hospital, in most cases she will bypass the ED and instead be sent directly to the labor and delivery (L&D) unit. During a viral outbreak, there are two major concerns with this approach. For one thing, it means an immunocompromised woman is being sent through the hospital to get to L&D, and along the path, is exposed to every airborne pathogen in the facility (and, if she is already infected, exposes others along the way). In addition, in hospitals without an Ob hospitalist on site, the patient generally is not immediately triaged by a physician, physician’s assistant, or nurse practitioner upon arrival because those clinicians are not consistently on site in L&D.
In times of viral pandemics, new approaches are warranted. For hospitals with contracted L&D management with hospitalists, hospitalists work closely with department heads to implement protocols loosely based on the Emergency Severity Index (ESI) model established by the Agency for Healthcare Research and Quality. Just as the ESI algorithm guides clinical stratification of patients, in times of reported viral outbreaks, L&D should consider triage of all pregnant women at higher levels of acuity, regardless of presentation status. In particular, if they show clinical symptoms, they should be masked, accompanied to the L&D unit by protected personnel, separated from other patients in areas of forced proximity such as hallways and elevators, and triaged in a secure single-patient room with a closed door (ideally at negative pressure relative to the surrounding areas).
If the patient has traveled to an area of outbreak, reports exposure to travelers who have visited high-risk areas, has had contact with individuals who tested positive for COVID-19, or exhibits any clinical symptoms of COVID-19 (fever, dry cough, fatigue, etc.), her care management should adhere to standing hospital emergency protocols. Following consultation with the assigned community obstetrician, the Ob hospitalist and hospital staff should contact their local/state health departments immediately for all cases of patients who show symptoms to determine if the patient meets requirements for a person under investigation (PUI) for COVID-19. The state/local health department will work with clinicians to collect, store, and ship clinical specimens appropriately. Very ill patients may need to be treated in an intensive care setting where respiratory status can be closely monitored.
At Ob Hospitalist Group, our body of evidence from our large national footprint has informed the development of standard sets of protocols for delivery complications such as preeclampsia and postpartum hemorrhage, as well as a cesarean section reduction toolkit to combat medically unnecessary cesarean sections. OB hospitalists therefore can assist with refining COVID-19 protocols specifically for the L&D setting, using evidence-based data to tailor protocols to address public health emergencies as they evolve.
The second way that Ob hospitalists can support their colleagues is by covering L&D 24/7 so that community obstetricians can focus on other pressing medical needs. From our experience with other outbreaks such as severe acute respiratory syndrome (SARS) and influenza, we anticipate that obstetricians in private practice likely will have their hands full juggling a regular patient load, fielding calls from concerned patients, and caring for infected or ill patients who are being treated in an outpatient setting. Adding to that plate the need to rush to the hospital to clinically assess a patient for COVID-19 or for a delivery only compounds stress and exhaustion. At Ob Hospitalist Group, our hospitalist programs provide coverage and support to community obstetricians until they can arrive at the hospital or when the woman has no assigned obstetrician, reducing the pressure on community obstetricians to rush through their schedules.
Diagnostic and pharmaceutical companies are collaborating with public health officials to expedite diagnostic testing staff, hospital treatment capacity, vaccines, and even early therapies that may help to minimize severity. But right now, as clinicians work to protect their vulnerable patients, a close collaboration between community obstetricians and Ob hospitalists will help to keep patients and health care personnel safe and healthy – a goal that should apply not only to public health crises, but to the provision of maternal care every day.
Dr. Simon is chief medical officer at Ob Hospitalist Group (OBHG), is a board-certified ob.gyn., and former head of the department of obstetrics and gynecology for a U.S. hospital. He has no relevant conflicts of interest or financial disclosures. Email him at [email protected].
With the novel coronavirus (COVID-19) monopolizing the news cycle, fear and misinformation are at an all-time high. Public health officials and physicians are accelerating education outreach to the public to address misinformation, and identify and care for patients who may have been exposed to the virus.
In times of public health crises, pregnant women have unique and pressing concerns about their personal health and the health of their unborn children. While not often mentioned in major news coverage, obstetricians play a critical role during health crises because of their uniquely personal role with patients during all stages of pregnancy, providing this vulnerable population with the most up-to-date information and following the latest guidelines for recommended care.
Unfortunately, COVID-19 is breaking unfamiliar new ground. We know that pregnant women are at higher risk for viral infection – annually, influenza is a grim reminder that pregnant women are more immunocompromised than the general public – but we do not yet have data to confirm or refute that pregnant women have a higher susceptibility to COVID-19 than the rest of the adult population. We also do not know enough about COVID-19 transmission, including whether the virus can cross the transplacental barrier to affect a fetus, or whether it can be transmitted through breast milk.
As private practice community obstetricians work to protect their patients during this public health crisis, Ob hospitalists can play an important role in supporting them in the provision of patient care.
First, Ob hospitalists are highly-trained specialists who can help ensure that pregnant patients who seek care at the hospital – either with viral symptoms or with separate pregnancy-related concerns – are protected during triage until the treating community obstetrician can take the reins.
When a pregnant woman presents at a hospital, in most cases she will bypass the ED and instead be sent directly to the labor and delivery (L&D) unit. During a viral outbreak, there are two major concerns with this approach. For one thing, it means an immunocompromised woman is being sent through the hospital to get to L&D, and along the path, is exposed to every airborne pathogen in the facility (and, if she is already infected, exposes others along the way). In addition, in hospitals without an Ob hospitalist on site, the patient generally is not immediately triaged by a physician, physician’s assistant, or nurse practitioner upon arrival because those clinicians are not consistently on site in L&D.
In times of viral pandemics, new approaches are warranted. For hospitals with contracted L&D management with hospitalists, hospitalists work closely with department heads to implement protocols loosely based on the Emergency Severity Index (ESI) model established by the Agency for Healthcare Research and Quality. Just as the ESI algorithm guides clinical stratification of patients, in times of reported viral outbreaks, L&D should consider triage of all pregnant women at higher levels of acuity, regardless of presentation status. In particular, if they show clinical symptoms, they should be masked, accompanied to the L&D unit by protected personnel, separated from other patients in areas of forced proximity such as hallways and elevators, and triaged in a secure single-patient room with a closed door (ideally at negative pressure relative to the surrounding areas).
If the patient has traveled to an area of outbreak, reports exposure to travelers who have visited high-risk areas, has had contact with individuals who tested positive for COVID-19, or exhibits any clinical symptoms of COVID-19 (fever, dry cough, fatigue, etc.), her care management should adhere to standing hospital emergency protocols. Following consultation with the assigned community obstetrician, the Ob hospitalist and hospital staff should contact their local/state health departments immediately for all cases of patients who show symptoms to determine if the patient meets requirements for a person under investigation (PUI) for COVID-19. The state/local health department will work with clinicians to collect, store, and ship clinical specimens appropriately. Very ill patients may need to be treated in an intensive care setting where respiratory status can be closely monitored.
At Ob Hospitalist Group, our body of evidence from our large national footprint has informed the development of standard sets of protocols for delivery complications such as preeclampsia and postpartum hemorrhage, as well as a cesarean section reduction toolkit to combat medically unnecessary cesarean sections. OB hospitalists therefore can assist with refining COVID-19 protocols specifically for the L&D setting, using evidence-based data to tailor protocols to address public health emergencies as they evolve.
The second way that Ob hospitalists can support their colleagues is by covering L&D 24/7 so that community obstetricians can focus on other pressing medical needs. From our experience with other outbreaks such as severe acute respiratory syndrome (SARS) and influenza, we anticipate that obstetricians in private practice likely will have their hands full juggling a regular patient load, fielding calls from concerned patients, and caring for infected or ill patients who are being treated in an outpatient setting. Adding to that plate the need to rush to the hospital to clinically assess a patient for COVID-19 or for a delivery only compounds stress and exhaustion. At Ob Hospitalist Group, our hospitalist programs provide coverage and support to community obstetricians until they can arrive at the hospital or when the woman has no assigned obstetrician, reducing the pressure on community obstetricians to rush through their schedules.
Diagnostic and pharmaceutical companies are collaborating with public health officials to expedite diagnostic testing staff, hospital treatment capacity, vaccines, and even early therapies that may help to minimize severity. But right now, as clinicians work to protect their vulnerable patients, a close collaboration between community obstetricians and Ob hospitalists will help to keep patients and health care personnel safe and healthy – a goal that should apply not only to public health crises, but to the provision of maternal care every day.
Dr. Simon is chief medical officer at Ob Hospitalist Group (OBHG), is a board-certified ob.gyn., and former head of the department of obstetrics and gynecology for a U.S. hospital. He has no relevant conflicts of interest or financial disclosures. Email him at [email protected].
DAPT may benefit symptomatic carotid endarterectomy patients
LOS ANGELES –

The only patients who benefited from postsurgical treatment with dual antiplatelet therapy (DAPT) were those who were symptomatic (had a stroke or transient ischemic attack) prior to their carotid endarterectomy surgery, a minority of the more than 17,000 matched U.S. patients who underwent carotid endarterectomy during 2003-2018 and were part of this analysis, Nathan Belkin, MD, said at the International Stroke Conference, sponsored by the American Heart Association.
Among patients with symptoms prior to their carotid endarterectomy, DAPT at the time of hospital discharge was associated with a 2-year follow-up rate of stroke, transient ischemic attack (TIA), or death of about 8%, compared with a rate of about 11% among similar patients discharged on aspirin only, a statistically significant difference. In contrast, among patients who were asymptomatic prior to their carotid endarterectomy, discharge treatment with aspirin only was associated with a 2-year event rate similar to the rate among patients discharged on DAPT.
Based in part on this finding, Dr. Belkin and associates at the University of Pennsylvania, Philadelphia, now start symptomatic patients scheduled for carotid endarterectomy on DAPT with aspirin plus clopidogrel (Plavix) about 2 weeks before surgery, and then continue the combined regimen long term after surgery. A prospective, randomized study is needed to fully resolve the optimal use of DAPT in patients with significant carotid artery disease scheduled for carotid endarterectomy, but until then, “we’re individualizing DAPT” to patients at high risk because of a prior stroke or TIA who also have no evidence of an elevated bleeding risk, said Dr. Belkin, a vascular surgeon.
“We hypothesize that patients with systemic carotid disease have a systemic disease process and more activated platelets,” which suggests a potential benefit from DAPT, he explained. But the data that Dr. Belkin reported also indicated that recent U.S. use of DAPT in patients undergoing carotid endarterectomy has moved beyond this subgroup. The U.S. national data set that Dr. Belkin used for the analysis, the Vascular Quality Initiative registry maintained by the Society for Vascular Surgery, included 87,074 patients who underwent carotid endarterectomy during 2003-2018. During the entire 16-year period, 30% of patients overall received a prescription for DAPT at hospital discharge, but this level went steadily up during those years. In 2003, the rate of DAPT prescriptions at discharge was below 10% of patients but then rose incrementally over the following years and by 2018 had increased to about 44% despite a prevalence of symptomatic carotid disease closer to about a third of patients.

“It’s surprising that so many patients received DAPT for carotid disease” in recent years, commented Mai N. Nguyen-Huynh, MD, a vascular neurologist with Kaiser Permanente Northern California in Oakland. “It’s been thought that DAPT, and especially clopidogrel, was more beneficial for patients with intracranial atherosclerotic disease, but not so much for patients with carotid disease,” she said in an interview. “We don’t always see systemic atherosclerotic disease in patients with carotid artery disease. It’s not standard practice to look for systemic atherosclerotic disease in patients with carotid disease,” unless something in the patient’s presentation suggests wider vascular-disease progression.
The primary analysis that Dr. Belkin and associates ran removed about 16% of the patients who underwent carotid endarterectomy from the database: those who received no antiplatelet drug, those who received only clopidogrel, and those who went home from surgery on an anticoagulant. Among the remaining 72,122 patients, 35% received DAPT at discharge and 65% received aspirin only. The patients averaged 70 years old, 61% were men, 37% had a history of stroke or TIA, and their overall 2-year incidence of stroke, TIA, or death was 7.3%. To adjust for many baseline differences between the patients discharged on DAPT and those who got only aspirin, the researchers used propensity-score sorting to identify 17,398 matched patients from the two treatment subgroups, 24% of the total population. Comparison of these DAPT and aspirin-only subgroups showed no difference in the overall, 2-year rate of stroke, TIA, or death.
However, when the analysis divided the patients into asymptomatic and symptomatic subgroups, those discharged on DAPT showed a statistically significant lower rate of stroke, TIA, or death during 2 years of follow-up. The same symptomatic subgroup also showed a statistically significant lower rate of total mortality during 5 years of follow-up when treated with DAPT compared with aspirin only, again an absolute, between-group difference of about 3 percentage points that was statistically significant, a difference not seen in the asymptomatic patients. The type of treatment that symptomatic patients received had no relationship to their 2-year incidence of stroke or TIA.
To confirm these findings, Dr. Belkin and coworkers ran a multivariate logistic regression analysis on the data collected from all 72,122 patients who underwent carotid endarterectomy and subsequently received either DAPT or aspirin only. The only statistically significant association between treatment and outcome was among the symptomatic patients who received DAPT, who had a significant reduction in their 5-year mortality, compared with symptomatic patients who received only aspirin at hospital discharge.
Ideally, a comparison of DAPT and aspirin-only treatment should also assess the incidence and severity of bleeding events associated with these treatments, but bleeding data were not available in the database, Dr. Belkin said.
Dr. Belkin and Dr. Nguyen-Huynh had no relevant disclosures.
SOURCE: Belkin N et al. Stroke. 2020 Feb;51(suppl 1): Abstract 67.
LOS ANGELES –
The only patients who benefited from postsurgical treatment with dual antiplatelet therapy (DAPT) were those who were symptomatic (had a stroke or transient ischemic attack) prior to their carotid endarterectomy surgery, a minority of the more than 17,000 matched U.S. patients who underwent carotid endarterectomy during 2003-2018 and were part of this analysis, Nathan Belkin, MD, said at the International Stroke Conference, sponsored by the American Heart Association.
Among patients with symptoms prior to their carotid endarterectomy, DAPT at the time of hospital discharge was associated with a 2-year follow-up rate of stroke, transient ischemic attack (TIA), or death of about 8%, compared with a rate of about 11% among similar patients discharged on aspirin only, a statistically significant difference. In contrast, among patients who were asymptomatic prior to their carotid endarterectomy, discharge treatment with aspirin only was associated with a 2-year event rate similar to the rate among patients discharged on DAPT.
Based in part on this finding, Dr. Belkin and associates at the University of Pennsylvania, Philadelphia, now start symptomatic patients scheduled for carotid endarterectomy on DAPT with aspirin plus clopidogrel (Plavix) about 2 weeks before surgery, and then continue the combined regimen long term after surgery. A prospective, randomized study is needed to fully resolve the optimal use of DAPT in patients with significant carotid artery disease scheduled for carotid endarterectomy, but until then, “we’re individualizing DAPT” to patients at high risk because of a prior stroke or TIA who also have no evidence of an elevated bleeding risk, said Dr. Belkin, a vascular surgeon.
“We hypothesize that patients with systemic carotid disease have a systemic disease process and more activated platelets,” which suggests a potential benefit from DAPT, he explained. But the data that Dr. Belkin reported also indicated that recent U.S. use of DAPT in patients undergoing carotid endarterectomy has moved beyond this subgroup. The U.S. national data set that Dr. Belkin used for the analysis, the Vascular Quality Initiative registry maintained by the Society for Vascular Surgery, included 87,074 patients who underwent carotid endarterectomy during 2003-2018. During the entire 16-year period, 30% of patients overall received a prescription for DAPT at hospital discharge, but this level went steadily up during those years. In 2003, the rate of DAPT prescriptions at discharge was below 10% of patients but then rose incrementally over the following years and by 2018 had increased to about 44% despite a prevalence of symptomatic carotid disease closer to about a third of patients.
“It’s surprising that so many patients received DAPT for carotid disease” in recent years, commented Mai N. Nguyen-Huynh, MD, a vascular neurologist with Kaiser Permanente Northern California in Oakland. “It’s been thought that DAPT, and especially clopidogrel, was more beneficial for patients with intracranial atherosclerotic disease, but not so much for patients with carotid disease,” she said in an interview. “We don’t always see systemic atherosclerotic disease in patients with carotid artery disease. It’s not standard practice to look for systemic atherosclerotic disease in patients with carotid disease,” unless something in the patient’s presentation suggests wider vascular-disease progression.
The primary analysis that Dr. Belkin and associates ran removed about 16% of the patients who underwent carotid endarterectomy from the database: those who received no antiplatelet drug, those who received only clopidogrel, and those who went home from surgery on an anticoagulant. Among the remaining 72,122 patients, 35% received DAPT at discharge and 65% received aspirin only. The patients averaged 70 years old, 61% were men, 37% had a history of stroke or TIA, and their overall 2-year incidence of stroke, TIA, or death was 7.3%. To adjust for many baseline differences between the patients discharged on DAPT and those who got only aspirin, the researchers used propensity-score sorting to identify 17,398 matched patients from the two treatment subgroups, 24% of the total population. Comparison of these DAPT and aspirin-only subgroups showed no difference in the overall, 2-year rate of stroke, TIA, or death.
However, when the analysis divided the patients into asymptomatic and symptomatic subgroups, those discharged on DAPT showed a statistically significant lower rate of stroke, TIA, or death during 2 years of follow-up. The same symptomatic subgroup also showed a statistically significant lower rate of total mortality during 5 years of follow-up when treated with DAPT compared with aspirin only, again an absolute, between-group difference of about 3 percentage points that was statistically significant, a difference not seen in the asymptomatic patients. The type of treatment that symptomatic patients received had no relationship to their 2-year incidence of stroke or TIA.
To confirm these findings, Dr. Belkin and coworkers ran a multivariate logistic regression analysis on the data collected from all 72,122 patients who underwent carotid endarterectomy and subsequently received either DAPT or aspirin only. The only statistically significant association between treatment and outcome was among the symptomatic patients who received DAPT, who had a significant reduction in their 5-year mortality, compared with symptomatic patients who received only aspirin at hospital discharge.
Ideally, a comparison of DAPT and aspirin-only treatment should also assess the incidence and severity of bleeding events associated with these treatments, but bleeding data were not available in the database, Dr. Belkin said.
Dr. Belkin and Dr. Nguyen-Huynh had no relevant disclosures.
SOURCE: Belkin N et al. Stroke. 2020 Feb;51(suppl 1): Abstract 67.
LOS ANGELES –
The only patients who benefited from postsurgical treatment with dual antiplatelet therapy (DAPT) were those who were symptomatic (had a stroke or transient ischemic attack) prior to their carotid endarterectomy surgery, a minority of the more than 17,000 matched U.S. patients who underwent carotid endarterectomy during 2003-2018 and were part of this analysis, Nathan Belkin, MD, said at the International Stroke Conference, sponsored by the American Heart Association.
Among patients with symptoms prior to their carotid endarterectomy, DAPT at the time of hospital discharge was associated with a 2-year follow-up rate of stroke, transient ischemic attack (TIA), or death of about 8%, compared with a rate of about 11% among similar patients discharged on aspirin only, a statistically significant difference. In contrast, among patients who were asymptomatic prior to their carotid endarterectomy, discharge treatment with aspirin only was associated with a 2-year event rate similar to the rate among patients discharged on DAPT.
Based in part on this finding, Dr. Belkin and associates at the University of Pennsylvania, Philadelphia, now start symptomatic patients scheduled for carotid endarterectomy on DAPT with aspirin plus clopidogrel (Plavix) about 2 weeks before surgery, and then continue the combined regimen long term after surgery. A prospective, randomized study is needed to fully resolve the optimal use of DAPT in patients with significant carotid artery disease scheduled for carotid endarterectomy, but until then, “we’re individualizing DAPT” to patients at high risk because of a prior stroke or TIA who also have no evidence of an elevated bleeding risk, said Dr. Belkin, a vascular surgeon.
“We hypothesize that patients with systemic carotid disease have a systemic disease process and more activated platelets,” which suggests a potential benefit from DAPT, he explained. But the data that Dr. Belkin reported also indicated that recent U.S. use of DAPT in patients undergoing carotid endarterectomy has moved beyond this subgroup. The U.S. national data set that Dr. Belkin used for the analysis, the Vascular Quality Initiative registry maintained by the Society for Vascular Surgery, included 87,074 patients who underwent carotid endarterectomy during 2003-2018. During the entire 16-year period, 30% of patients overall received a prescription for DAPT at hospital discharge, but this level went steadily up during those years. In 2003, the rate of DAPT prescriptions at discharge was below 10% of patients but then rose incrementally over the following years and by 2018 had increased to about 44% despite a prevalence of symptomatic carotid disease closer to about a third of patients.
“It’s surprising that so many patients received DAPT for carotid disease” in recent years, commented Mai N. Nguyen-Huynh, MD, a vascular neurologist with Kaiser Permanente Northern California in Oakland. “It’s been thought that DAPT, and especially clopidogrel, was more beneficial for patients with intracranial atherosclerotic disease, but not so much for patients with carotid disease,” she said in an interview. “We don’t always see systemic atherosclerotic disease in patients with carotid artery disease. It’s not standard practice to look for systemic atherosclerotic disease in patients with carotid disease,” unless something in the patient’s presentation suggests wider vascular-disease progression.
The primary analysis that Dr. Belkin and associates ran removed about 16% of the patients who underwent carotid endarterectomy from the database: those who received no antiplatelet drug, those who received only clopidogrel, and those who went home from surgery on an anticoagulant. Among the remaining 72,122 patients, 35% received DAPT at discharge and 65% received aspirin only. The patients averaged 70 years old, 61% were men, 37% had a history of stroke or TIA, and their overall 2-year incidence of stroke, TIA, or death was 7.3%. To adjust for many baseline differences between the patients discharged on DAPT and those who got only aspirin, the researchers used propensity-score sorting to identify 17,398 matched patients from the two treatment subgroups, 24% of the total population. Comparison of these DAPT and aspirin-only subgroups showed no difference in the overall, 2-year rate of stroke, TIA, or death.
However, when the analysis divided the patients into asymptomatic and symptomatic subgroups, those discharged on DAPT showed a statistically significant lower rate of stroke, TIA, or death during 2 years of follow-up. The same symptomatic subgroup also showed a statistically significant lower rate of total mortality during 5 years of follow-up when treated with DAPT compared with aspirin only, again an absolute, between-group difference of about 3 percentage points that was statistically significant, a difference not seen in the asymptomatic patients. The type of treatment that symptomatic patients received had no relationship to their 2-year incidence of stroke or TIA.
To confirm these findings, Dr. Belkin and coworkers ran a multivariate logistic regression analysis on the data collected from all 72,122 patients who underwent carotid endarterectomy and subsequently received either DAPT or aspirin only. The only statistically significant association between treatment and outcome was among the symptomatic patients who received DAPT, who had a significant reduction in their 5-year mortality, compared with symptomatic patients who received only aspirin at hospital discharge.
Ideally, a comparison of DAPT and aspirin-only treatment should also assess the incidence and severity of bleeding events associated with these treatments, but bleeding data were not available in the database, Dr. Belkin said.
Dr. Belkin and Dr. Nguyen-Huynh had no relevant disclosures.
SOURCE: Belkin N et al. Stroke. 2020 Feb;51(suppl 1): Abstract 67.
REPORTING FROM ISC 2020
Firm Abdominal Papule
The Diagnosis: Cutaneous Metastatic Gastric Carcinoma
Cutaneous metastasis of primary gastric carcinoma is a rare occurrence, with the more common metastatic sites being the lymph nodes, liver, and peritoneal cavity. The incidence of visceral neoplasm metastasis to the skin ranges from 0.7% to 9% and is less than 1% for upper digestive tract carcinomas.1 Cutaneous metastases make up 2% of all tumors of the skin and commonly are located near the site of the primary tumor.2 The most common cutaneous metastasis sites for gastric carcinoma include the neck, chest, and head.3 One of the more typical sites of cutaneous metastasis from gastric cancer is the umbilicus (ie, Sister Mary Joseph nodule). Cutaneous metastases from gastric carcinoma commonly present as asymptomatic hyperpigmented nodules.1,3
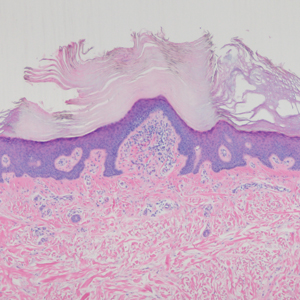
In our patient, histopathologic sections showed diffuse infiltration of the dermis by atypical polygonal/round cells arranged in cords and small aggregates. Some of the neoplastic cells had signet ring morphology (Figure). Tumor cells demonstrated positive immunostaining for CDX2, villin, CAM 5.2, and epithelial membrane antigen; they were negative for S-100, MART-1 (melanoma-associated antigen recognized by T cells 1), leukocyte common antigen, gross cystic disease fluid protein 15, estrogen and progesterone receptor, and HER2/neu (human epidermal growth factor receptor 2).
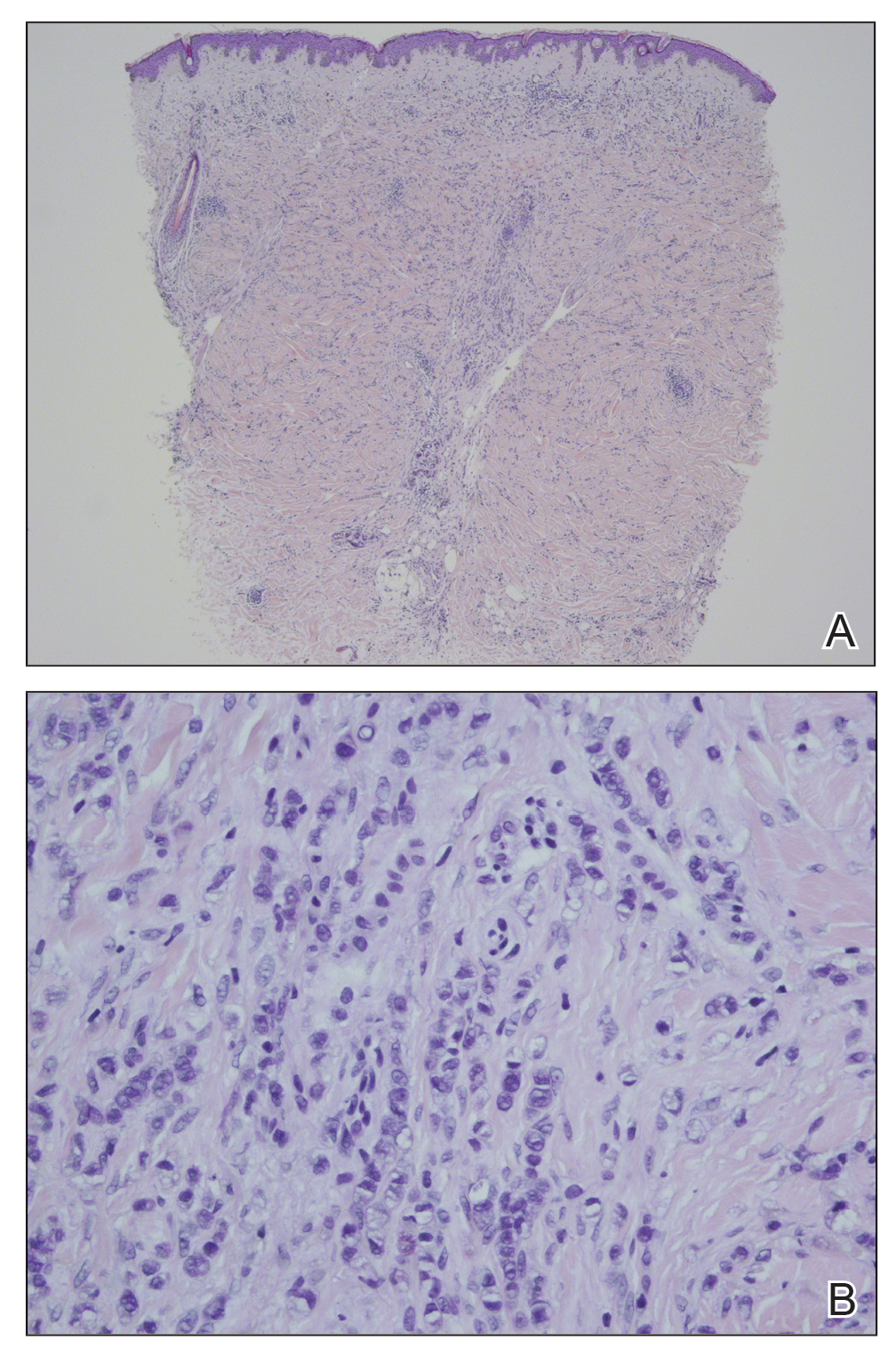
Our patient's presentation was rare in that she developed an asymptomatic erythematous papule on the skin of the abdomen. However, her history of stage IIIB gastric adenocarcinoma in conjunction with the clinical picture and microscopic findings were most consistent with metastatic carcinoma of gastrointestinal origin. The histologic hallmarks of cutaneous metastatic gastric carcinoma include aggregates of neoplastic cells arranged in cords, sometimes forming glands, embedded in a fibrous stroma. Tumor cells may demonstrate signet ring morphology. These unique histologic findings, as well as positive immunostaining for CDX2, villin, CAM 5.2, and epithelial membrane antigen, rule out other potential diagnoses for an asymptomatic solitary papule.
Dermatofibrosarcoma protuberans presents as an asymptomatic, slow-growing, indurated papule or plaque that develops into a red or brownish nodule. Histologically, dermatofibrosarcoma protuberans is characterized by spindled cells, few mitotic figures, infiltration of the subcutaneous tissue in a honeycomblike pattern, and obliteration of the adnexal structures.4
Cutaneous B-cell lymphoma (CBCL) can present as single or multiple red papules or nodules located on the trunk, face, or extremities. Histologically, CBCL would show a nodular or diffuse infiltrate throughout the dermis, frequently with accentuation in the deep reticular dermis, sparing of the epidermis, and the presence of a grenz zone. The infiltrate in CBCL consists of CD20+, CD19+, and CD79a+ B cells. Identification of a monoclonal B-cell population either by immunohistochemistry or polymerase chain reaction would further support a diagnosis of CBCL.4 These specific histologic findings and the immunohistochemical staining pattern helped rule out CBCL as the diagnosis in our patient.
Amelanotic melanomas present as flesh-colored to light pink papules, making them especially challenging to diagnose clinically. Asymmetrical, poorly circumscribed nests of atypical melanocytes as well as single melanocytes within the epidermis and dermis are seen histologically; mitotic figures are common. Immunohistochemical staining for melanoma includes S-100, human melanoma black 45, MART-1/Melan-A, tyrosinase, and microphthalmia-associated transcription factor 1.4
Neurothekeomas can present as asymptomatic, solitary, flesh-colored papules located on the head, neck, and upper trunk. Histologically, neurothekeomas have a distinct appearance consisting of a well-defined mass composed of variable-sized lobules of spindled and epithelioid cells dispersed in a myxoid stroma within the reticular dermis.4 These specific histologic findings helped rule out neurothekeoma in our patient.
Following the diagnosis of cutaneous metastatic gastric carcinoma in our patient, positron emission tomography and computed tomography of the chest, abdomen, and pelvis were unremarkable for distant disease. Subsequently, the patient underwent surgical excision of the papule with clear margins, followed by a short course of radiation therapy. She currently is under close monitoring but remains in remission with no new cutaneous manifestations of the gastric carcinoma.
- Erdemir A, Atilganoglu U, Onsun N, et al. Cutaneous metastases from gastric adenocarcinoma. Indian J Dermatol. 2011;56:236-237.
- Junqueira AL, Corbett AM, Oliveira Filho Jd, et al. Cutaneous metastasis from gastrointestinal adenocarcinoma of unknown primary origin. An Bras Dermatol. 2015;90:564-566.
- Cesaretti M, Malerba M, Basso V, et al. Cutaneous metastasis from primary gastric cancer: a case report and review of the literature. Cutis. 2014;93:E9-E13.
- Bolognia J, Jorizzo JL, Schaffer JV. Dermatology. Philadelphia, PA: Elsevier Saunders; 2012.
The Diagnosis: Cutaneous Metastatic Gastric Carcinoma
Cutaneous metastasis of primary gastric carcinoma is a rare occurrence, with the more common metastatic sites being the lymph nodes, liver, and peritoneal cavity. The incidence of visceral neoplasm metastasis to the skin ranges from 0.7% to 9% and is less than 1% for upper digestive tract carcinomas.1 Cutaneous metastases make up 2% of all tumors of the skin and commonly are located near the site of the primary tumor.2 The most common cutaneous metastasis sites for gastric carcinoma include the neck, chest, and head.3 One of the more typical sites of cutaneous metastasis from gastric cancer is the umbilicus (ie, Sister Mary Joseph nodule). Cutaneous metastases from gastric carcinoma commonly present as asymptomatic hyperpigmented nodules.1,3
In our patient, histopathologic sections showed diffuse infiltration of the dermis by atypical polygonal/round cells arranged in cords and small aggregates. Some of the neoplastic cells had signet ring morphology (Figure). Tumor cells demonstrated positive immunostaining for CDX2, villin, CAM 5.2, and epithelial membrane antigen; they were negative for S-100, MART-1 (melanoma-associated antigen recognized by T cells 1), leukocyte common antigen, gross cystic disease fluid protein 15, estrogen and progesterone receptor, and HER2/neu (human epidermal growth factor receptor 2).
Our patient's presentation was rare in that she developed an asymptomatic erythematous papule on the skin of the abdomen. However, her history of stage IIIB gastric adenocarcinoma in conjunction with the clinical picture and microscopic findings were most consistent with metastatic carcinoma of gastrointestinal origin. The histologic hallmarks of cutaneous metastatic gastric carcinoma include aggregates of neoplastic cells arranged in cords, sometimes forming glands, embedded in a fibrous stroma. Tumor cells may demonstrate signet ring morphology. These unique histologic findings, as well as positive immunostaining for CDX2, villin, CAM 5.2, and epithelial membrane antigen, rule out other potential diagnoses for an asymptomatic solitary papule.
Dermatofibrosarcoma protuberans presents as an asymptomatic, slow-growing, indurated papule or plaque that develops into a red or brownish nodule. Histologically, dermatofibrosarcoma protuberans is characterized by spindled cells, few mitotic figures, infiltration of the subcutaneous tissue in a honeycomblike pattern, and obliteration of the adnexal structures.4
Cutaneous B-cell lymphoma (CBCL) can present as single or multiple red papules or nodules located on the trunk, face, or extremities. Histologically, CBCL would show a nodular or diffuse infiltrate throughout the dermis, frequently with accentuation in the deep reticular dermis, sparing of the epidermis, and the presence of a grenz zone. The infiltrate in CBCL consists of CD20+, CD19+, and CD79a+ B cells. Identification of a monoclonal B-cell population either by immunohistochemistry or polymerase chain reaction would further support a diagnosis of CBCL.4 These specific histologic findings and the immunohistochemical staining pattern helped rule out CBCL as the diagnosis in our patient.
Amelanotic melanomas present as flesh-colored to light pink papules, making them especially challenging to diagnose clinically. Asymmetrical, poorly circumscribed nests of atypical melanocytes as well as single melanocytes within the epidermis and dermis are seen histologically; mitotic figures are common. Immunohistochemical staining for melanoma includes S-100, human melanoma black 45, MART-1/Melan-A, tyrosinase, and microphthalmia-associated transcription factor 1.4
Neurothekeomas can present as asymptomatic, solitary, flesh-colored papules located on the head, neck, and upper trunk. Histologically, neurothekeomas have a distinct appearance consisting of a well-defined mass composed of variable-sized lobules of spindled and epithelioid cells dispersed in a myxoid stroma within the reticular dermis.4 These specific histologic findings helped rule out neurothekeoma in our patient.
Following the diagnosis of cutaneous metastatic gastric carcinoma in our patient, positron emission tomography and computed tomography of the chest, abdomen, and pelvis were unremarkable for distant disease. Subsequently, the patient underwent surgical excision of the papule with clear margins, followed by a short course of radiation therapy. She currently is under close monitoring but remains in remission with no new cutaneous manifestations of the gastric carcinoma.
The Diagnosis: Cutaneous Metastatic Gastric Carcinoma
Cutaneous metastasis of primary gastric carcinoma is a rare occurrence, with the more common metastatic sites being the lymph nodes, liver, and peritoneal cavity. The incidence of visceral neoplasm metastasis to the skin ranges from 0.7% to 9% and is less than 1% for upper digestive tract carcinomas.1 Cutaneous metastases make up 2% of all tumors of the skin and commonly are located near the site of the primary tumor.2 The most common cutaneous metastasis sites for gastric carcinoma include the neck, chest, and head.3 One of the more typical sites of cutaneous metastasis from gastric cancer is the umbilicus (ie, Sister Mary Joseph nodule). Cutaneous metastases from gastric carcinoma commonly present as asymptomatic hyperpigmented nodules.1,3
In our patient, histopathologic sections showed diffuse infiltration of the dermis by atypical polygonal/round cells arranged in cords and small aggregates. Some of the neoplastic cells had signet ring morphology (Figure). Tumor cells demonstrated positive immunostaining for CDX2, villin, CAM 5.2, and epithelial membrane antigen; they were negative for S-100, MART-1 (melanoma-associated antigen recognized by T cells 1), leukocyte common antigen, gross cystic disease fluid protein 15, estrogen and progesterone receptor, and HER2/neu (human epidermal growth factor receptor 2).
Our patient's presentation was rare in that she developed an asymptomatic erythematous papule on the skin of the abdomen. However, her history of stage IIIB gastric adenocarcinoma in conjunction with the clinical picture and microscopic findings were most consistent with metastatic carcinoma of gastrointestinal origin. The histologic hallmarks of cutaneous metastatic gastric carcinoma include aggregates of neoplastic cells arranged in cords, sometimes forming glands, embedded in a fibrous stroma. Tumor cells may demonstrate signet ring morphology. These unique histologic findings, as well as positive immunostaining for CDX2, villin, CAM 5.2, and epithelial membrane antigen, rule out other potential diagnoses for an asymptomatic solitary papule.
Dermatofibrosarcoma protuberans presents as an asymptomatic, slow-growing, indurated papule or plaque that develops into a red or brownish nodule. Histologically, dermatofibrosarcoma protuberans is characterized by spindled cells, few mitotic figures, infiltration of the subcutaneous tissue in a honeycomblike pattern, and obliteration of the adnexal structures.4
Cutaneous B-cell lymphoma (CBCL) can present as single or multiple red papules or nodules located on the trunk, face, or extremities. Histologically, CBCL would show a nodular or diffuse infiltrate throughout the dermis, frequently with accentuation in the deep reticular dermis, sparing of the epidermis, and the presence of a grenz zone. The infiltrate in CBCL consists of CD20+, CD19+, and CD79a+ B cells. Identification of a monoclonal B-cell population either by immunohistochemistry or polymerase chain reaction would further support a diagnosis of CBCL.4 These specific histologic findings and the immunohistochemical staining pattern helped rule out CBCL as the diagnosis in our patient.
Amelanotic melanomas present as flesh-colored to light pink papules, making them especially challenging to diagnose clinically. Asymmetrical, poorly circumscribed nests of atypical melanocytes as well as single melanocytes within the epidermis and dermis are seen histologically; mitotic figures are common. Immunohistochemical staining for melanoma includes S-100, human melanoma black 45, MART-1/Melan-A, tyrosinase, and microphthalmia-associated transcription factor 1.4
Neurothekeomas can present as asymptomatic, solitary, flesh-colored papules located on the head, neck, and upper trunk. Histologically, neurothekeomas have a distinct appearance consisting of a well-defined mass composed of variable-sized lobules of spindled and epithelioid cells dispersed in a myxoid stroma within the reticular dermis.4 These specific histologic findings helped rule out neurothekeoma in our patient.
Following the diagnosis of cutaneous metastatic gastric carcinoma in our patient, positron emission tomography and computed tomography of the chest, abdomen, and pelvis were unremarkable for distant disease. Subsequently, the patient underwent surgical excision of the papule with clear margins, followed by a short course of radiation therapy. She currently is under close monitoring but remains in remission with no new cutaneous manifestations of the gastric carcinoma.
- Erdemir A, Atilganoglu U, Onsun N, et al. Cutaneous metastases from gastric adenocarcinoma. Indian J Dermatol. 2011;56:236-237.
- Junqueira AL, Corbett AM, Oliveira Filho Jd, et al. Cutaneous metastasis from gastrointestinal adenocarcinoma of unknown primary origin. An Bras Dermatol. 2015;90:564-566.
- Cesaretti M, Malerba M, Basso V, et al. Cutaneous metastasis from primary gastric cancer: a case report and review of the literature. Cutis. 2014;93:E9-E13.
- Bolognia J, Jorizzo JL, Schaffer JV. Dermatology. Philadelphia, PA: Elsevier Saunders; 2012.
- Erdemir A, Atilganoglu U, Onsun N, et al. Cutaneous metastases from gastric adenocarcinoma. Indian J Dermatol. 2011;56:236-237.
- Junqueira AL, Corbett AM, Oliveira Filho Jd, et al. Cutaneous metastasis from gastrointestinal adenocarcinoma of unknown primary origin. An Bras Dermatol. 2015;90:564-566.
- Cesaretti M, Malerba M, Basso V, et al. Cutaneous metastasis from primary gastric cancer: a case report and review of the literature. Cutis. 2014;93:E9-E13.
- Bolognia J, Jorizzo JL, Schaffer JV. Dermatology. Philadelphia, PA: Elsevier Saunders; 2012.
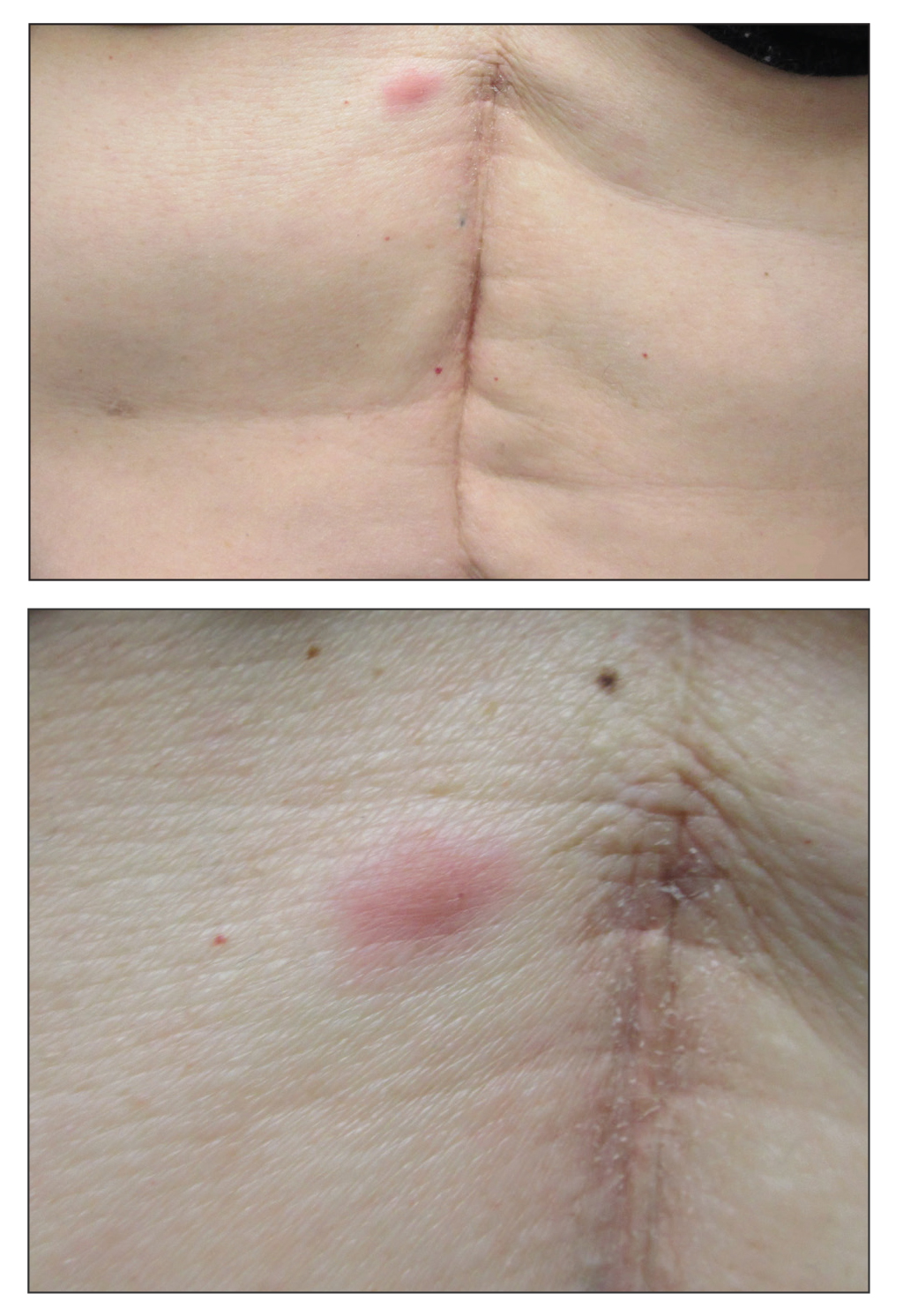
A 53-year-old woman with a history of melanoma on the right thigh, stage II Hodgkin lymphoma, and stage IIIB gastric adenocarcinoma treated with a distal gastrectomy presented with an asymptomatic but persistent skin lesion on the abdomen of 2 months' duration. The lesion arose spontaneously 6 months prior and had increased in size during that time. Physical examination revealed a 6-mm, solitary, firm, erythematous papule on the skin of the right upper quadrant of the abdomen. The patient was otherwise healthy, and a review of systems did not reveal any abnormalities. A punch biopsy was submitted for histopathologic review.

Does screening by primary care providers effectively detect melanoma and other skin cancers?
EVIDENCE SUMMARY
No trials have directly assessed skin cancer morbidity associated with physician visual skin screening. A 2018 ecologic cohort study found no difference in melanoma mortality in a population undergoing a national screening program, although screening was associated with 41% more diagnoses of skin cancer.1 A 2012 cohort study found a reduction in melanoma mortality over 7 years associated with a population-based visual skin cancer screening program compared with similar populations that didn’t undergo specific screening.2 At 12-year follow-up, however, there was no longer a difference in mortality.
Primary care visual screening doesn’t decrease melanoma mortality
German researchers trained 1673 non-dermatologists (64% of general practitioners, obstetrician-gynecologists, and urologists in that region of Germany) and 116 dermatologists (98% in the region) to recognize skin cancer through whole-body visual inspection.1 They recruited and screened 360,000 adults (19% of the population older than 20 years; 74% women) and followed age- and sex-adjusted melanoma mortality over the next 10 years. Non-dermatologists performed most screening exams (77%); 37% of screened positive patients were lost to follow-up.
Melanoma mortality ultimately didn’t change in the screened region, compared with populations in other European countries without national screening programs. Screening detected approximately half of melanoma cases (585/1169) in the region and was associated with 41% greater detection of skin cancers compared with other countries.
Researchers recorded age-adjusted increases in incidence per 100,000 of melanoma from 14.2 (95% confidence interval [CI], 13.3-15.1) to 18 (95% CI, 16.6-19.4), melanoma in situ from 5.8 (95% CI, 5.2-6.4) to 8.5 (95% CI, 7.5-9.5), squamous cell carcinoma from 11.2 (95% CI, 10.6-11.8) to 12.9 (95% CI, 12.0-13.8), and basal cell carcinoma from 60.5 (95% CI, 59.0-62.1) to 78.4 (95% CI, 75.9-80.8).
Visual screening by primary care providers vs screening by dermatologists
A cohort study of 16,383 Australian adults found that visual screening by primary care physicians detected melanoma over 3 years with a sensitivity of 40.2% (95% CIs not supplied) and specificity of 86.1% (95% CI, 85.6-86.6%; positive predictive value = 1.4%).3
A second cohort study, enrolling 7436 adults, that evaluated visual screening by dermatologists and plastic surgeons over 2 years found a sensitivity for melanoma of 49% (95% CI, 34.4-63.7%) and a specificity of 97.6% (95% CI, 97.2-97.9%) with a positive predictive value of 11.9% (95% CI, 7.8-17.2%).4
Visual screening more often detects thinner melanomas
A 3-year case-control study (3762 cases, 3824 controls) that examined the association between visual skin screening by a physician (type of physician not specified) and thickness of melanomas detected found that thin melanomas (≤ 0.75 mm) were more common among screened patients compared with unscreened patients (odds ratio [OR] = 1.38; 95% CI, 1.22-1.56) and thicker melanomas (≥ 0.75 mm) were less common (OR = 0.86; 95% CI, 0.75-0.98).5
Continue to: A systematic review...
A systematic review of 8 observational cohort studies with a total of 200,000 patients found a consistent linear increase in melanoma mortality with increasing tumor thickness.6 The largest study (68,495 patients), which compared melanoma mortality for thinner (< 1 mm) and thicker lesions, reported risk ratios of 2.89 for lesion thicknesses of 1.01 to 2 mm (95% CI, 2.62-3.18); 4.69 for thicknesses of 2.01 to 4 mm (95% CI, 4.24-5.02); and 5.71 for thicknesses > 4 mm (95% CI, 5.10-6.39).
The downside of visual screening: False-positives
The 2012 cohort study, which reported outcomes from 16,000 biopsies performed following visual screening exams, found that 28 biopsies were performed for each diagnosis of melanoma and 9 to 10 biopsies for each basal cell carcinoma.2 Diagnosis rates (number of skin biopsies performed for each case of cancer diagnosed) were equal in men and women for both types of cancer. However, researchers observed more biopsies for each diagnosis of squamous cell carcinoma in women than men (56 vs 28 biopsies per case).
Younger patients underwent more biopsies than older patients for each diagnosis of skin cancer. Women 20 to 34 years of age underwent more biopsies than women 65 years or older for each diagnosis of melanoma (19 additional excisions) and basal cell carcinoma (134 additional excisions). Women 35 to 49 years of age underwent 565 more biopsies for each diagnosis of squamous cell carcinoma than women 65 years or older. Similar patterns applied to men 20 to 34 years of age compared with men 65 years or older (24 additional biopsies per melanoma, 109 per basal cell carcinoma, and 898 per squamous cell carcinoma).
RECOMMENDATIONS
The US Preventive Services Task Force recommendations, based on a systematic review of mostly cohort studies, state that the current evidence is insufficient to assess the balance of benefits and harms of clinician visual skin cancer screening.7,8
The American Academy of Dermatology states that skin cancer screening can save lives and supports research on the benefits and harms of screening in the primary care setting.9
Continue to: Editor's Takeaway
Editor’s Takeaway
Skin cancer screening by primary care physicians is associated with increased detection of skin cancers, including melanomas—even though we have no confirmation that it changes melanoma mortality. It is unclear what the appropriate rate of false-positive screening tests should be, but wider adoption of noninvasive diagnostic techniques such as dermoscopy might reduce unwarranted biopsies.
1. Kaiser M, Schiller J, Schreckenberger C. The effectiveness of a population-based skin cancer screening program: evidence from Germany. Eur J Health Econ. 2018:19:355-367.
2. Waldmann A, Nolte S, Weinstock MA, et al. Skin cancer screening participation and impact on melanoma incidence in Germany—an observational study on incidence trends in regions with and without population-based screening. Br J Cancer. 2012;106:970-974.
3. Aitken JF, Janda M, Elwood M, et al. Clinical outcomes from skin screening clinics within a community-based melanoma screening program. J Am Acad Dermatol. 2006:54:105-114.
4. Fritschi L, Dye SA, Katris P. Validity of melanoma diagnosis in a community-based screening program. Am J Epidemiol. 2006:164:385-390.
5. Aitken JF, Elwood M, Baade PD, et al. Clinical whole-body skin examination reduces the incidence of thick melanomas. Int J Cancer. 2010:126:450-458.
6. Wernli KJ, Henrikson NB, Morrison CC, et al. Screening for Skin Cancer in Adults: An Updated Systematic Evidence Review for the US Preventive Services Task Force. Rockville, MD: Agency for Healthcare Research and Quality; 2016. Evidence Synthesis 137.
7. Waldmann A, Nolte S, Geller AC, et al. Frequency of excisions and yields of malignant skin tumors in a population-based screening intervention of 360,288 whole-body examinations. Arch Dermatol. 2012:148:903-910.
8. US Preventive Services Task Force. Screening for Skin Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2016;316:429-435.
9. Torres A. AAD statement on USPSTF recommendation on skin cancer screening. July 2016. https://www.aad.org/media/news-releases/aad-statement-on-uspstf 26. Accessed May 2018.
EVIDENCE SUMMARY
No trials have directly assessed skin cancer morbidity associated with physician visual skin screening. A 2018 ecologic cohort study found no difference in melanoma mortality in a population undergoing a national screening program, although screening was associated with 41% more diagnoses of skin cancer.1 A 2012 cohort study found a reduction in melanoma mortality over 7 years associated with a population-based visual skin cancer screening program compared with similar populations that didn’t undergo specific screening.2 At 12-year follow-up, however, there was no longer a difference in mortality.
Primary care visual screening doesn’t decrease melanoma mortality
German researchers trained 1673 non-dermatologists (64% of general practitioners, obstetrician-gynecologists, and urologists in that region of Germany) and 116 dermatologists (98% in the region) to recognize skin cancer through whole-body visual inspection.1 They recruited and screened 360,000 adults (19% of the population older than 20 years; 74% women) and followed age- and sex-adjusted melanoma mortality over the next 10 years. Non-dermatologists performed most screening exams (77%); 37% of screened positive patients were lost to follow-up.
Melanoma mortality ultimately didn’t change in the screened region, compared with populations in other European countries without national screening programs. Screening detected approximately half of melanoma cases (585/1169) in the region and was associated with 41% greater detection of skin cancers compared with other countries.
Researchers recorded age-adjusted increases in incidence per 100,000 of melanoma from 14.2 (95% confidence interval [CI], 13.3-15.1) to 18 (95% CI, 16.6-19.4), melanoma in situ from 5.8 (95% CI, 5.2-6.4) to 8.5 (95% CI, 7.5-9.5), squamous cell carcinoma from 11.2 (95% CI, 10.6-11.8) to 12.9 (95% CI, 12.0-13.8), and basal cell carcinoma from 60.5 (95% CI, 59.0-62.1) to 78.4 (95% CI, 75.9-80.8).
Visual screening by primary care providers vs screening by dermatologists
A cohort study of 16,383 Australian adults found that visual screening by primary care physicians detected melanoma over 3 years with a sensitivity of 40.2% (95% CIs not supplied) and specificity of 86.1% (95% CI, 85.6-86.6%; positive predictive value = 1.4%).3
A second cohort study, enrolling 7436 adults, that evaluated visual screening by dermatologists and plastic surgeons over 2 years found a sensitivity for melanoma of 49% (95% CI, 34.4-63.7%) and a specificity of 97.6% (95% CI, 97.2-97.9%) with a positive predictive value of 11.9% (95% CI, 7.8-17.2%).4
Visual screening more often detects thinner melanomas
A 3-year case-control study (3762 cases, 3824 controls) that examined the association between visual skin screening by a physician (type of physician not specified) and thickness of melanomas detected found that thin melanomas (≤ 0.75 mm) were more common among screened patients compared with unscreened patients (odds ratio [OR] = 1.38; 95% CI, 1.22-1.56) and thicker melanomas (≥ 0.75 mm) were less common (OR = 0.86; 95% CI, 0.75-0.98).5
Continue to: A systematic review...
A systematic review of 8 observational cohort studies with a total of 200,000 patients found a consistent linear increase in melanoma mortality with increasing tumor thickness.6 The largest study (68,495 patients), which compared melanoma mortality for thinner (< 1 mm) and thicker lesions, reported risk ratios of 2.89 for lesion thicknesses of 1.01 to 2 mm (95% CI, 2.62-3.18); 4.69 for thicknesses of 2.01 to 4 mm (95% CI, 4.24-5.02); and 5.71 for thicknesses > 4 mm (95% CI, 5.10-6.39).
The downside of visual screening: False-positives
The 2012 cohort study, which reported outcomes from 16,000 biopsies performed following visual screening exams, found that 28 biopsies were performed for each diagnosis of melanoma and 9 to 10 biopsies for each basal cell carcinoma.2 Diagnosis rates (number of skin biopsies performed for each case of cancer diagnosed) were equal in men and women for both types of cancer. However, researchers observed more biopsies for each diagnosis of squamous cell carcinoma in women than men (56 vs 28 biopsies per case).
Younger patients underwent more biopsies than older patients for each diagnosis of skin cancer. Women 20 to 34 years of age underwent more biopsies than women 65 years or older for each diagnosis of melanoma (19 additional excisions) and basal cell carcinoma (134 additional excisions). Women 35 to 49 years of age underwent 565 more biopsies for each diagnosis of squamous cell carcinoma than women 65 years or older. Similar patterns applied to men 20 to 34 years of age compared with men 65 years or older (24 additional biopsies per melanoma, 109 per basal cell carcinoma, and 898 per squamous cell carcinoma).
RECOMMENDATIONS
The US Preventive Services Task Force recommendations, based on a systematic review of mostly cohort studies, state that the current evidence is insufficient to assess the balance of benefits and harms of clinician visual skin cancer screening.7,8
The American Academy of Dermatology states that skin cancer screening can save lives and supports research on the benefits and harms of screening in the primary care setting.9
Continue to: Editor's Takeaway
Editor’s Takeaway
Skin cancer screening by primary care physicians is associated with increased detection of skin cancers, including melanomas—even though we have no confirmation that it changes melanoma mortality. It is unclear what the appropriate rate of false-positive screening tests should be, but wider adoption of noninvasive diagnostic techniques such as dermoscopy might reduce unwarranted biopsies.
EVIDENCE SUMMARY
No trials have directly assessed skin cancer morbidity associated with physician visual skin screening. A 2018 ecologic cohort study found no difference in melanoma mortality in a population undergoing a national screening program, although screening was associated with 41% more diagnoses of skin cancer.1 A 2012 cohort study found a reduction in melanoma mortality over 7 years associated with a population-based visual skin cancer screening program compared with similar populations that didn’t undergo specific screening.2 At 12-year follow-up, however, there was no longer a difference in mortality.
Primary care visual screening doesn’t decrease melanoma mortality
German researchers trained 1673 non-dermatologists (64% of general practitioners, obstetrician-gynecologists, and urologists in that region of Germany) and 116 dermatologists (98% in the region) to recognize skin cancer through whole-body visual inspection.1 They recruited and screened 360,000 adults (19% of the population older than 20 years; 74% women) and followed age- and sex-adjusted melanoma mortality over the next 10 years. Non-dermatologists performed most screening exams (77%); 37% of screened positive patients were lost to follow-up.
Melanoma mortality ultimately didn’t change in the screened region, compared with populations in other European countries without national screening programs. Screening detected approximately half of melanoma cases (585/1169) in the region and was associated with 41% greater detection of skin cancers compared with other countries.
Researchers recorded age-adjusted increases in incidence per 100,000 of melanoma from 14.2 (95% confidence interval [CI], 13.3-15.1) to 18 (95% CI, 16.6-19.4), melanoma in situ from 5.8 (95% CI, 5.2-6.4) to 8.5 (95% CI, 7.5-9.5), squamous cell carcinoma from 11.2 (95% CI, 10.6-11.8) to 12.9 (95% CI, 12.0-13.8), and basal cell carcinoma from 60.5 (95% CI, 59.0-62.1) to 78.4 (95% CI, 75.9-80.8).
Visual screening by primary care providers vs screening by dermatologists
A cohort study of 16,383 Australian adults found that visual screening by primary care physicians detected melanoma over 3 years with a sensitivity of 40.2% (95% CIs not supplied) and specificity of 86.1% (95% CI, 85.6-86.6%; positive predictive value = 1.4%).3
A second cohort study, enrolling 7436 adults, that evaluated visual screening by dermatologists and plastic surgeons over 2 years found a sensitivity for melanoma of 49% (95% CI, 34.4-63.7%) and a specificity of 97.6% (95% CI, 97.2-97.9%) with a positive predictive value of 11.9% (95% CI, 7.8-17.2%).4
Visual screening more often detects thinner melanomas
A 3-year case-control study (3762 cases, 3824 controls) that examined the association between visual skin screening by a physician (type of physician not specified) and thickness of melanomas detected found that thin melanomas (≤ 0.75 mm) were more common among screened patients compared with unscreened patients (odds ratio [OR] = 1.38; 95% CI, 1.22-1.56) and thicker melanomas (≥ 0.75 mm) were less common (OR = 0.86; 95% CI, 0.75-0.98).5
Continue to: A systematic review...
A systematic review of 8 observational cohort studies with a total of 200,000 patients found a consistent linear increase in melanoma mortality with increasing tumor thickness.6 The largest study (68,495 patients), which compared melanoma mortality for thinner (< 1 mm) and thicker lesions, reported risk ratios of 2.89 for lesion thicknesses of 1.01 to 2 mm (95% CI, 2.62-3.18); 4.69 for thicknesses of 2.01 to 4 mm (95% CI, 4.24-5.02); and 5.71 for thicknesses > 4 mm (95% CI, 5.10-6.39).
The downside of visual screening: False-positives
The 2012 cohort study, which reported outcomes from 16,000 biopsies performed following visual screening exams, found that 28 biopsies were performed for each diagnosis of melanoma and 9 to 10 biopsies for each basal cell carcinoma.2 Diagnosis rates (number of skin biopsies performed for each case of cancer diagnosed) were equal in men and women for both types of cancer. However, researchers observed more biopsies for each diagnosis of squamous cell carcinoma in women than men (56 vs 28 biopsies per case).
Younger patients underwent more biopsies than older patients for each diagnosis of skin cancer. Women 20 to 34 years of age underwent more biopsies than women 65 years or older for each diagnosis of melanoma (19 additional excisions) and basal cell carcinoma (134 additional excisions). Women 35 to 49 years of age underwent 565 more biopsies for each diagnosis of squamous cell carcinoma than women 65 years or older. Similar patterns applied to men 20 to 34 years of age compared with men 65 years or older (24 additional biopsies per melanoma, 109 per basal cell carcinoma, and 898 per squamous cell carcinoma).
RECOMMENDATIONS
The US Preventive Services Task Force recommendations, based on a systematic review of mostly cohort studies, state that the current evidence is insufficient to assess the balance of benefits and harms of clinician visual skin cancer screening.7,8
The American Academy of Dermatology states that skin cancer screening can save lives and supports research on the benefits and harms of screening in the primary care setting.9
Continue to: Editor's Takeaway
Editor’s Takeaway
Skin cancer screening by primary care physicians is associated with increased detection of skin cancers, including melanomas—even though we have no confirmation that it changes melanoma mortality. It is unclear what the appropriate rate of false-positive screening tests should be, but wider adoption of noninvasive diagnostic techniques such as dermoscopy might reduce unwarranted biopsies.
1. Kaiser M, Schiller J, Schreckenberger C. The effectiveness of a population-based skin cancer screening program: evidence from Germany. Eur J Health Econ. 2018:19:355-367.
2. Waldmann A, Nolte S, Weinstock MA, et al. Skin cancer screening participation and impact on melanoma incidence in Germany—an observational study on incidence trends in regions with and without population-based screening. Br J Cancer. 2012;106:970-974.
3. Aitken JF, Janda M, Elwood M, et al. Clinical outcomes from skin screening clinics within a community-based melanoma screening program. J Am Acad Dermatol. 2006:54:105-114.
4. Fritschi L, Dye SA, Katris P. Validity of melanoma diagnosis in a community-based screening program. Am J Epidemiol. 2006:164:385-390.
5. Aitken JF, Elwood M, Baade PD, et al. Clinical whole-body skin examination reduces the incidence of thick melanomas. Int J Cancer. 2010:126:450-458.
6. Wernli KJ, Henrikson NB, Morrison CC, et al. Screening for Skin Cancer in Adults: An Updated Systematic Evidence Review for the US Preventive Services Task Force. Rockville, MD: Agency for Healthcare Research and Quality; 2016. Evidence Synthesis 137.
7. Waldmann A, Nolte S, Geller AC, et al. Frequency of excisions and yields of malignant skin tumors in a population-based screening intervention of 360,288 whole-body examinations. Arch Dermatol. 2012:148:903-910.
8. US Preventive Services Task Force. Screening for Skin Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2016;316:429-435.
9. Torres A. AAD statement on USPSTF recommendation on skin cancer screening. July 2016. https://www.aad.org/media/news-releases/aad-statement-on-uspstf 26. Accessed May 2018.
1. Kaiser M, Schiller J, Schreckenberger C. The effectiveness of a population-based skin cancer screening program: evidence from Germany. Eur J Health Econ. 2018:19:355-367.
2. Waldmann A, Nolte S, Weinstock MA, et al. Skin cancer screening participation and impact on melanoma incidence in Germany—an observational study on incidence trends in regions with and without population-based screening. Br J Cancer. 2012;106:970-974.
3. Aitken JF, Janda M, Elwood M, et al. Clinical outcomes from skin screening clinics within a community-based melanoma screening program. J Am Acad Dermatol. 2006:54:105-114.
4. Fritschi L, Dye SA, Katris P. Validity of melanoma diagnosis in a community-based screening program. Am J Epidemiol. 2006:164:385-390.
5. Aitken JF, Elwood M, Baade PD, et al. Clinical whole-body skin examination reduces the incidence of thick melanomas. Int J Cancer. 2010:126:450-458.
6. Wernli KJ, Henrikson NB, Morrison CC, et al. Screening for Skin Cancer in Adults: An Updated Systematic Evidence Review for the US Preventive Services Task Force. Rockville, MD: Agency for Healthcare Research and Quality; 2016. Evidence Synthesis 137.
7. Waldmann A, Nolte S, Geller AC, et al. Frequency of excisions and yields of malignant skin tumors in a population-based screening intervention of 360,288 whole-body examinations. Arch Dermatol. 2012:148:903-910.
8. US Preventive Services Task Force. Screening for Skin Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2016;316:429-435.
9. Torres A. AAD statement on USPSTF recommendation on skin cancer screening. July 2016. https://www.aad.org/media/news-releases/aad-statement-on-uspstf 26. Accessed May 2018.
EVIDENCE-BASED ANSWER:
Possibly. No trials have directly assessed detection of melanoma and other skin cancers by primary care providers.
Training a group comprised largely of primary care physicians to perform skin cancer screening was associated with a 41% increase in skin cancer diagnoses but no change in melanoma mortality.
Visual screening for melanoma by primary care physicians is 40% sensitive and 86% specific (compared with 49% and 98%, respectively, for dermatologists and plastic surgeons).
Melanomas found by visual screening are 38% more likely to be thin (≤ 0.75 mm) than melanomas discovered without screening, which correlates with improved outcomes.
Visual skin cancer screening overall is associated with false-positive rates as follows: 28 biopsies for each melanoma detected, 9 to 10 biopsies for each basal cell carcinoma, and 28 to 56 biopsies for squamous cell carcinoma. False-positive rates are higher for women—as much as double the rate for men—and younger patients—as much as 20-fold the rate for older patients (strength of recommendations for all foregoing statements: B, cohort studies).

DoD ‘Taking all Necessary Precautions’ Against COVID-19
In late February, a soldier stationed at Camp Carroll near Daegu, South Korea, was the first military member to test positive for the coronavirus (COVID-19). Before being diagnosed, he visited other areas, including Camp Walker in Daegu, according to a statement released by US Forces Korea. More than 75,000 troops are stationed in countries with virus outbreaks, including Japan, Italy, and Bahrain.
Military research laboratories are working “feverishly around the horn” to come up with a vaccine, Joint Chiefs of Staff Chairman Gen. Mark A. Milley said in a March 2, 2020, news conference. At the same conference, Defense Secretary Mark T. Esper, MD, said US Department of Defense (DoD) civilian and military leadership are working together to prepare for short-and long-term scenarios.
The US Northern Command is the “global integrator,” Esper said, with the DoD communicating regularly with operational commanders to assess how the virus might impact exercises and ongoing operations around the world. For example, a command post exercise in South Korea has been postponed; Exercise Cobra Gold in Thailand is continuing.
Commanders are taking all necessary precautions because the virus is unique to every situation and every location, Esper said: “We’re relying on them to make good judgments.”
He emphasized that commanders at all levels have the authority and guidance they need to operate. In a late February video teleconference, Esper had told commanders deployed overseas that he wanted them to give him a heads-up before making decisions related to protecting their troops, according to The New York Times.
The New York Times article cited an exchange in which Gen. Robert Abrams, commander of American forces in South Korea, where > 4,000 coronavirus cases have been confirmed, discussed his options to protect American military personnel against the virus. Esper said he wanted advance notice, according to an official briefed on the call and quoted in the Times article. Gen. Abrams said although he would try to give Sec. Esper advance warning, he might have to make urgent health decisions before receiving final approval from Washington.
In a statement responding to the Times article, Jonathan Hoffman, Assistant to the Secretary of Defense for Public Affairs, said the Secretary of Defense has given the Global Combatant Commanders the “clear and unequivocal authority” to take any and all actions necessary to ensure the health and safety of US service members, civilian DoD personnel, families, and dependents.
In the video teleconference, Hoffman said, Secretary Espers “directed commanders to take all force health protection measures, and to notify their chain of command when actions are taken so that DoD leadership can inform the interagency—including US Department of Health and Human Services, the Centers for Disease Control and Prevention (CDC), the Department of Homeland Security, the State Department, and the White House—and the American people.” Esper “explicitly did not direct them to ‘clear’ their force health decisions in advance,” Hoffman said. “[T]hat is a dangerous and inaccurate mischaracterization.”
In January, the Office of the Under Secretary of Defense released a memorandum on force health protection guidance for the coronavirus outbreak. The DoD, it says, will follow the CDC guidance and will “closely coordinate with interagency partners to ensure accurate and timely information is available.”
“An informed, common-sense approach minimizes the chances of getting sick,” military health officials say. But, “due to the dynamic nature of this outbreak,” people should frequently check the CDC website for additional updates. Related Military Health System information and links to the CDC are available at https://www.health.mil/News/In-the-Spotlight/Coronavirus.
The CDC provides a summary of its latest recommendations and DoD health care providers can access COVID-19–specific guidance, including information on evaluating “persons under investigation,” at https://www.cdc.gov/coronavirus/2019-nCoV/clinical-criteria.html.
Sec. Esper, in the Monday news conference, said, “My number-one priority remains to protect our forces and their families; second is to safeguard our mission capabilities and third [is] to support the interagency whole-of-government’s approach. We will continue to take all necessary precautions to ensure that our people are safe and able to continue their very important mission.”
In late February, a soldier stationed at Camp Carroll near Daegu, South Korea, was the first military member to test positive for the coronavirus (COVID-19). Before being diagnosed, he visited other areas, including Camp Walker in Daegu, according to a statement released by US Forces Korea. More than 75,000 troops are stationed in countries with virus outbreaks, including Japan, Italy, and Bahrain.
Military research laboratories are working “feverishly around the horn” to come up with a vaccine, Joint Chiefs of Staff Chairman Gen. Mark A. Milley said in a March 2, 2020, news conference. At the same conference, Defense Secretary Mark T. Esper, MD, said US Department of Defense (DoD) civilian and military leadership are working together to prepare for short-and long-term scenarios.
The US Northern Command is the “global integrator,” Esper said, with the DoD communicating regularly with operational commanders to assess how the virus might impact exercises and ongoing operations around the world. For example, a command post exercise in South Korea has been postponed; Exercise Cobra Gold in Thailand is continuing.
Commanders are taking all necessary precautions because the virus is unique to every situation and every location, Esper said: “We’re relying on them to make good judgments.”
He emphasized that commanders at all levels have the authority and guidance they need to operate. In a late February video teleconference, Esper had told commanders deployed overseas that he wanted them to give him a heads-up before making decisions related to protecting their troops, according to The New York Times.
The New York Times article cited an exchange in which Gen. Robert Abrams, commander of American forces in South Korea, where > 4,000 coronavirus cases have been confirmed, discussed his options to protect American military personnel against the virus. Esper said he wanted advance notice, according to an official briefed on the call and quoted in the Times article. Gen. Abrams said although he would try to give Sec. Esper advance warning, he might have to make urgent health decisions before receiving final approval from Washington.
In a statement responding to the Times article, Jonathan Hoffman, Assistant to the Secretary of Defense for Public Affairs, said the Secretary of Defense has given the Global Combatant Commanders the “clear and unequivocal authority” to take any and all actions necessary to ensure the health and safety of US service members, civilian DoD personnel, families, and dependents.
In the video teleconference, Hoffman said, Secretary Espers “directed commanders to take all force health protection measures, and to notify their chain of command when actions are taken so that DoD leadership can inform the interagency—including US Department of Health and Human Services, the Centers for Disease Control and Prevention (CDC), the Department of Homeland Security, the State Department, and the White House—and the American people.” Esper “explicitly did not direct them to ‘clear’ their force health decisions in advance,” Hoffman said. “[T]hat is a dangerous and inaccurate mischaracterization.”
In January, the Office of the Under Secretary of Defense released a memorandum on force health protection guidance for the coronavirus outbreak. The DoD, it says, will follow the CDC guidance and will “closely coordinate with interagency partners to ensure accurate and timely information is available.”
“An informed, common-sense approach minimizes the chances of getting sick,” military health officials say. But, “due to the dynamic nature of this outbreak,” people should frequently check the CDC website for additional updates. Related Military Health System information and links to the CDC are available at https://www.health.mil/News/In-the-Spotlight/Coronavirus.
The CDC provides a summary of its latest recommendations and DoD health care providers can access COVID-19–specific guidance, including information on evaluating “persons under investigation,” at https://www.cdc.gov/coronavirus/2019-nCoV/clinical-criteria.html.
Sec. Esper, in the Monday news conference, said, “My number-one priority remains to protect our forces and their families; second is to safeguard our mission capabilities and third [is] to support the interagency whole-of-government’s approach. We will continue to take all necessary precautions to ensure that our people are safe and able to continue their very important mission.”
In late February, a soldier stationed at Camp Carroll near Daegu, South Korea, was the first military member to test positive for the coronavirus (COVID-19). Before being diagnosed, he visited other areas, including Camp Walker in Daegu, according to a statement released by US Forces Korea. More than 75,000 troops are stationed in countries with virus outbreaks, including Japan, Italy, and Bahrain.
Military research laboratories are working “feverishly around the horn” to come up with a vaccine, Joint Chiefs of Staff Chairman Gen. Mark A. Milley said in a March 2, 2020, news conference. At the same conference, Defense Secretary Mark T. Esper, MD, said US Department of Defense (DoD) civilian and military leadership are working together to prepare for short-and long-term scenarios.
The US Northern Command is the “global integrator,” Esper said, with the DoD communicating regularly with operational commanders to assess how the virus might impact exercises and ongoing operations around the world. For example, a command post exercise in South Korea has been postponed; Exercise Cobra Gold in Thailand is continuing.
Commanders are taking all necessary precautions because the virus is unique to every situation and every location, Esper said: “We’re relying on them to make good judgments.”
He emphasized that commanders at all levels have the authority and guidance they need to operate. In a late February video teleconference, Esper had told commanders deployed overseas that he wanted them to give him a heads-up before making decisions related to protecting their troops, according to The New York Times.
The New York Times article cited an exchange in which Gen. Robert Abrams, commander of American forces in South Korea, where > 4,000 coronavirus cases have been confirmed, discussed his options to protect American military personnel against the virus. Esper said he wanted advance notice, according to an official briefed on the call and quoted in the Times article. Gen. Abrams said although he would try to give Sec. Esper advance warning, he might have to make urgent health decisions before receiving final approval from Washington.
In a statement responding to the Times article, Jonathan Hoffman, Assistant to the Secretary of Defense for Public Affairs, said the Secretary of Defense has given the Global Combatant Commanders the “clear and unequivocal authority” to take any and all actions necessary to ensure the health and safety of US service members, civilian DoD personnel, families, and dependents.
In the video teleconference, Hoffman said, Secretary Espers “directed commanders to take all force health protection measures, and to notify their chain of command when actions are taken so that DoD leadership can inform the interagency—including US Department of Health and Human Services, the Centers for Disease Control and Prevention (CDC), the Department of Homeland Security, the State Department, and the White House—and the American people.” Esper “explicitly did not direct them to ‘clear’ their force health decisions in advance,” Hoffman said. “[T]hat is a dangerous and inaccurate mischaracterization.”
In January, the Office of the Under Secretary of Defense released a memorandum on force health protection guidance for the coronavirus outbreak. The DoD, it says, will follow the CDC guidance and will “closely coordinate with interagency partners to ensure accurate and timely information is available.”
“An informed, common-sense approach minimizes the chances of getting sick,” military health officials say. But, “due to the dynamic nature of this outbreak,” people should frequently check the CDC website for additional updates. Related Military Health System information and links to the CDC are available at https://www.health.mil/News/In-the-Spotlight/Coronavirus.
The CDC provides a summary of its latest recommendations and DoD health care providers can access COVID-19–specific guidance, including information on evaluating “persons under investigation,” at https://www.cdc.gov/coronavirus/2019-nCoV/clinical-criteria.html.
Sec. Esper, in the Monday news conference, said, “My number-one priority remains to protect our forces and their families; second is to safeguard our mission capabilities and third [is] to support the interagency whole-of-government’s approach. We will continue to take all necessary precautions to ensure that our people are safe and able to continue their very important mission.”
Spiky Papules on the Dorsal Feet
The Diagnosis: Hyperkeratosis Lenticularis Perstans (Flegel Disease)
Hyperkeratosis lenticularis perstans, also known as Flegel disease, is a rare dermatosis first described by Flegel1 in 1958. This benign disorder is characterized by multiple asymptomatic 1- to 5-mm keratotic papules in a symmetric distribution favoring the dorsal aspects of the feet and distal extremities in adults. An autosomal-dominant inheritance pattern has been postulated, though many cases sporadically occur.2 The characteristic spiky papules typically appear during mid to late adulthood and tend to persist. Treatment options are lacking, with reports of partial or no response to topical calcipotriol, topical 5-fluorouracil, cryotherapy, and topical and oral retinoids.3,4
The histopathology of hyperkeratosis lenticularis perstans is distinct, showing a central discrete area of orthohyperkeratosis with patchy parakeratosis flanked by a normal stratum corneum. The underlying epidermis typically shows effacement of the rete ridge pattern with subtle basal zone vacuolization and rare necrotic keratinocytes with an underlying lichenoid infiltrate within the papillary dermis comprised of lymphomononuclear cells.
In contrast, punctate porokeratosis clinically tends to involve the palms and soles, though the arms and legs also may be involved. This entity tends to occur during adolescence. A raised hyperkeratotic papule clinically is present. Histopathologically, the epidermis has a cup-shaped depression filled with hyperkeratosis and a column of parakeratosis (coronoid lamellae)(Figure 1).
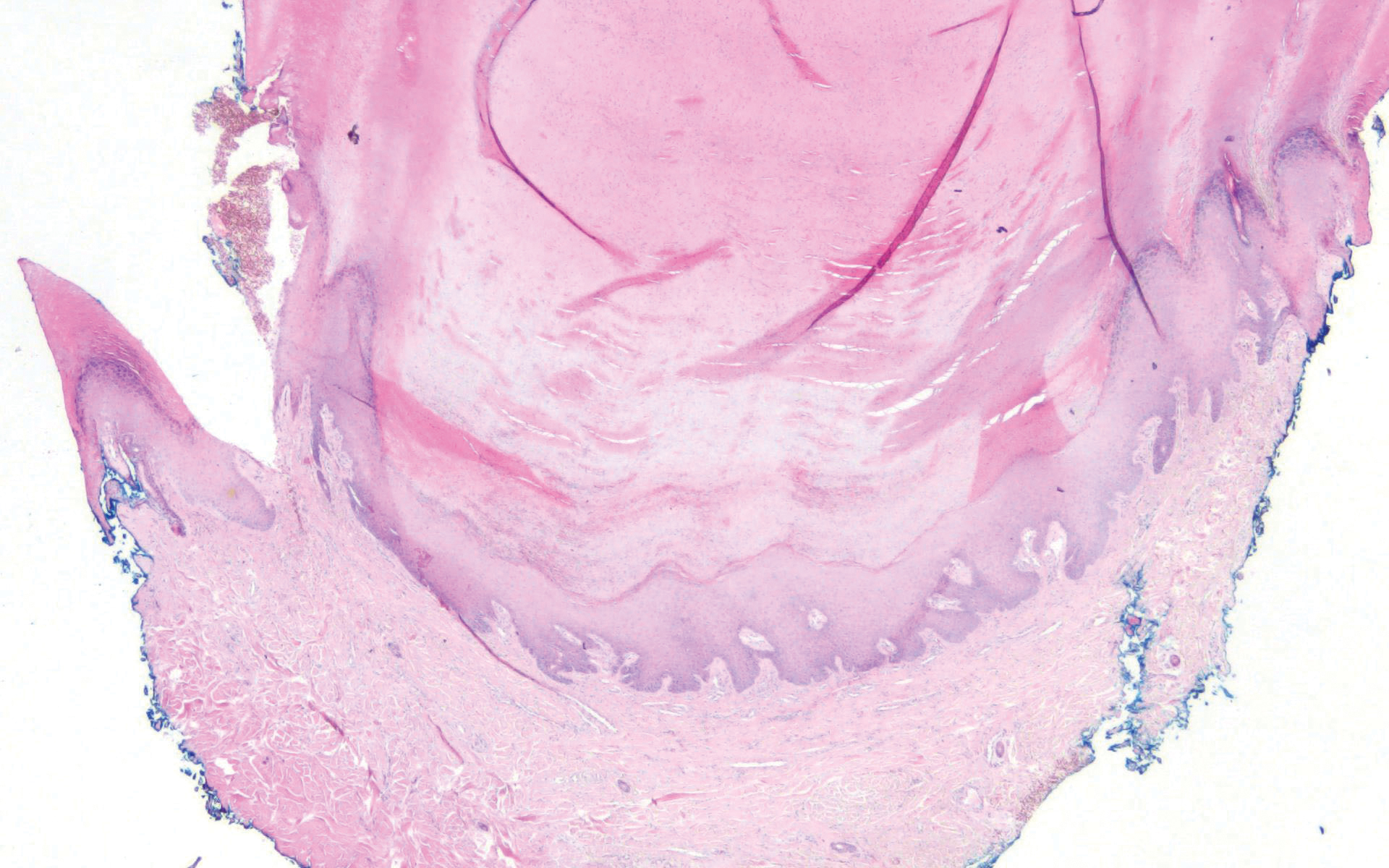
Acrokeratosis verruciformis of Hopf clinically appears on the dorsal aspects of the hands and feet as small warty papules in association with Darier disease. It typically presents during early childhood. Histopathology shows tiered hyperkeratosis, papillomatosis, and acanthosis (Figure 2).
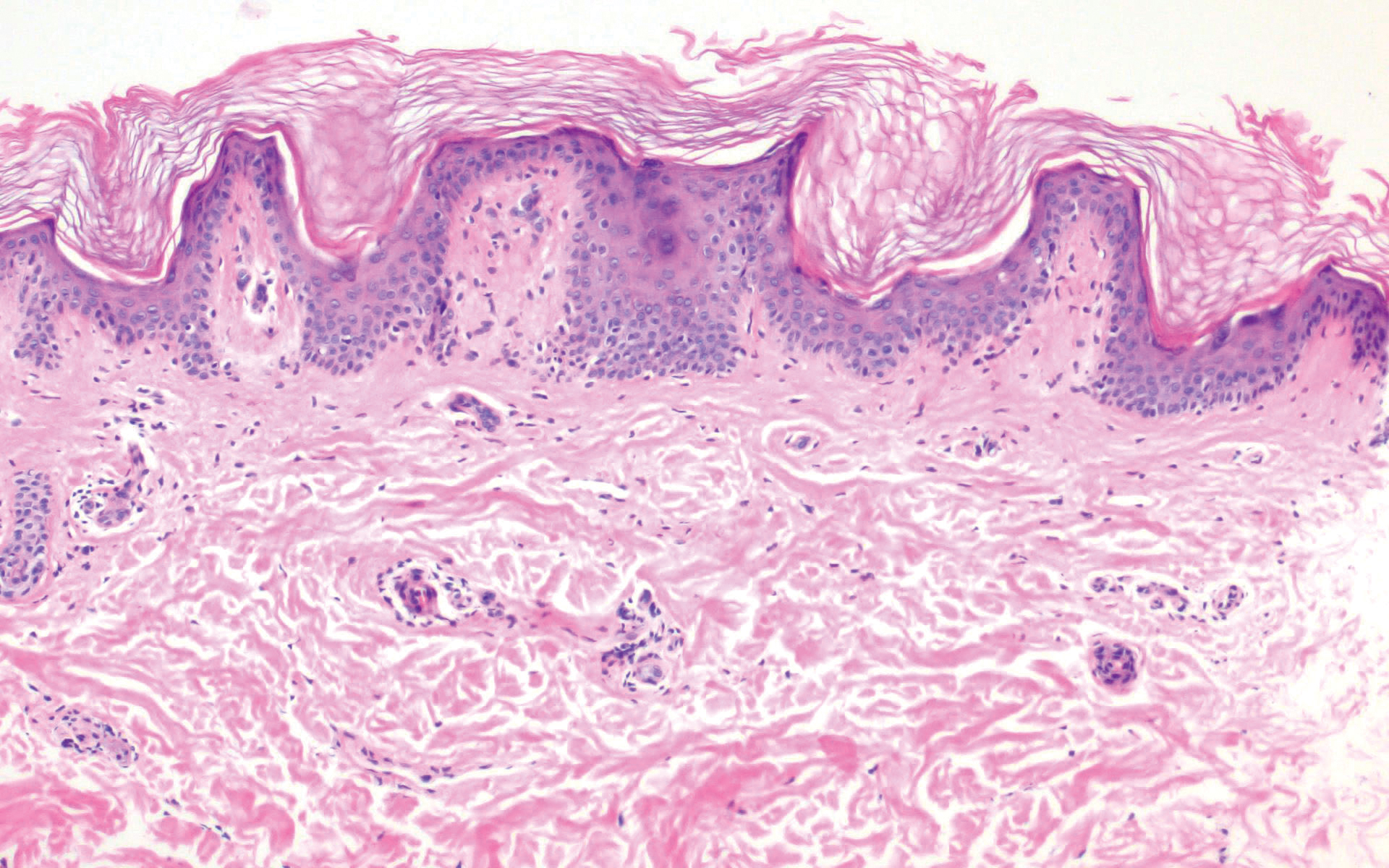
Perforating granuloma annulare presents on the dorsal aspects of the hands and fingers as scaly papules with either central umbilication or keratotic plugs. Histopathology shows transepidermal elimination of degenerated collagen (Figure 3).
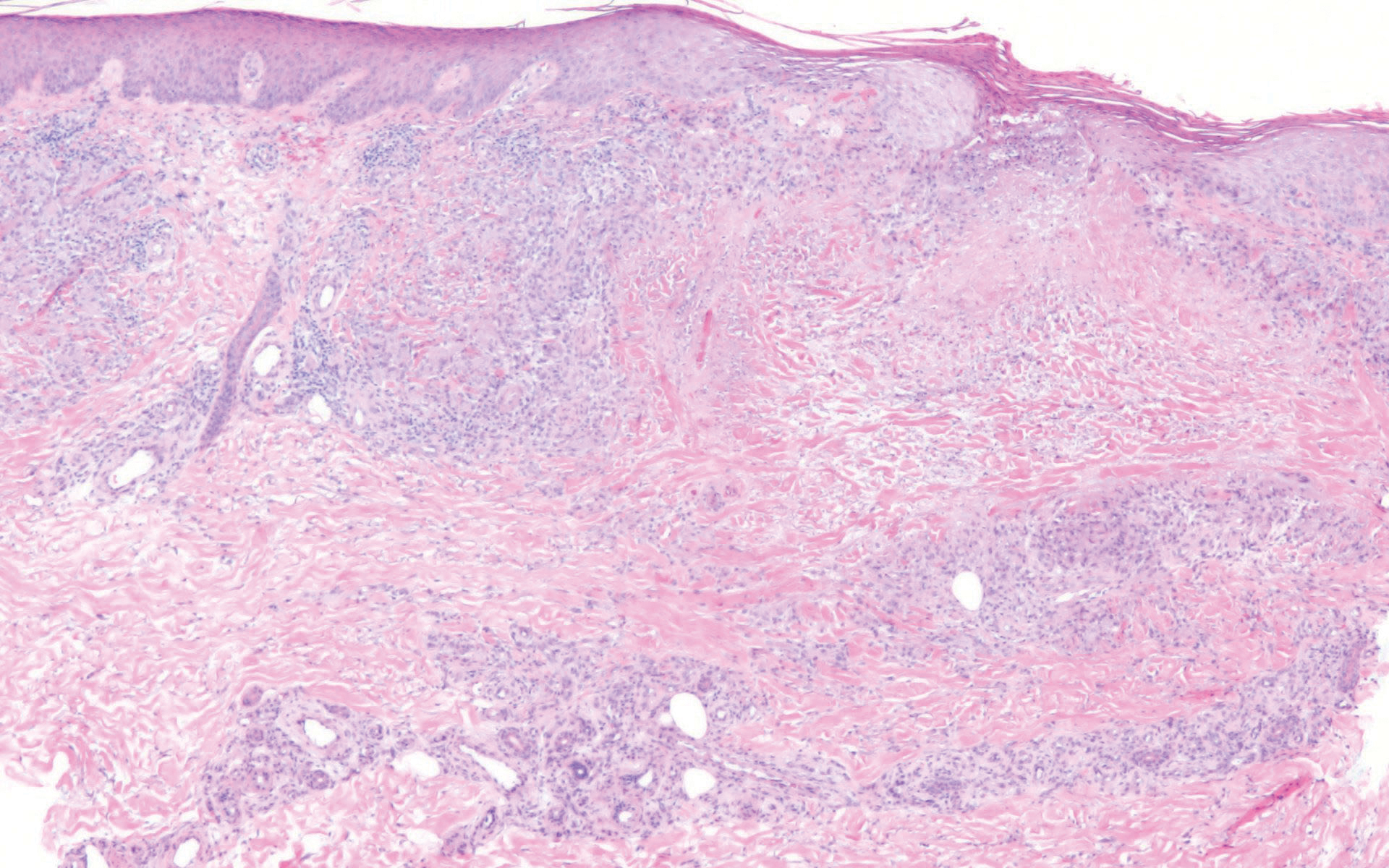
Stucco keratoses present on the dorsal aspects of the feet and ankles but are waxy smooth papules as opposed to hyperkeratotic spiky papules. Histologically, they are characterized by retention hyperkeratosis with lack of parakeratosis and regular acanthosis with a "string sign" indicating that the lesion extends to a uniform depth. (Figure 4).
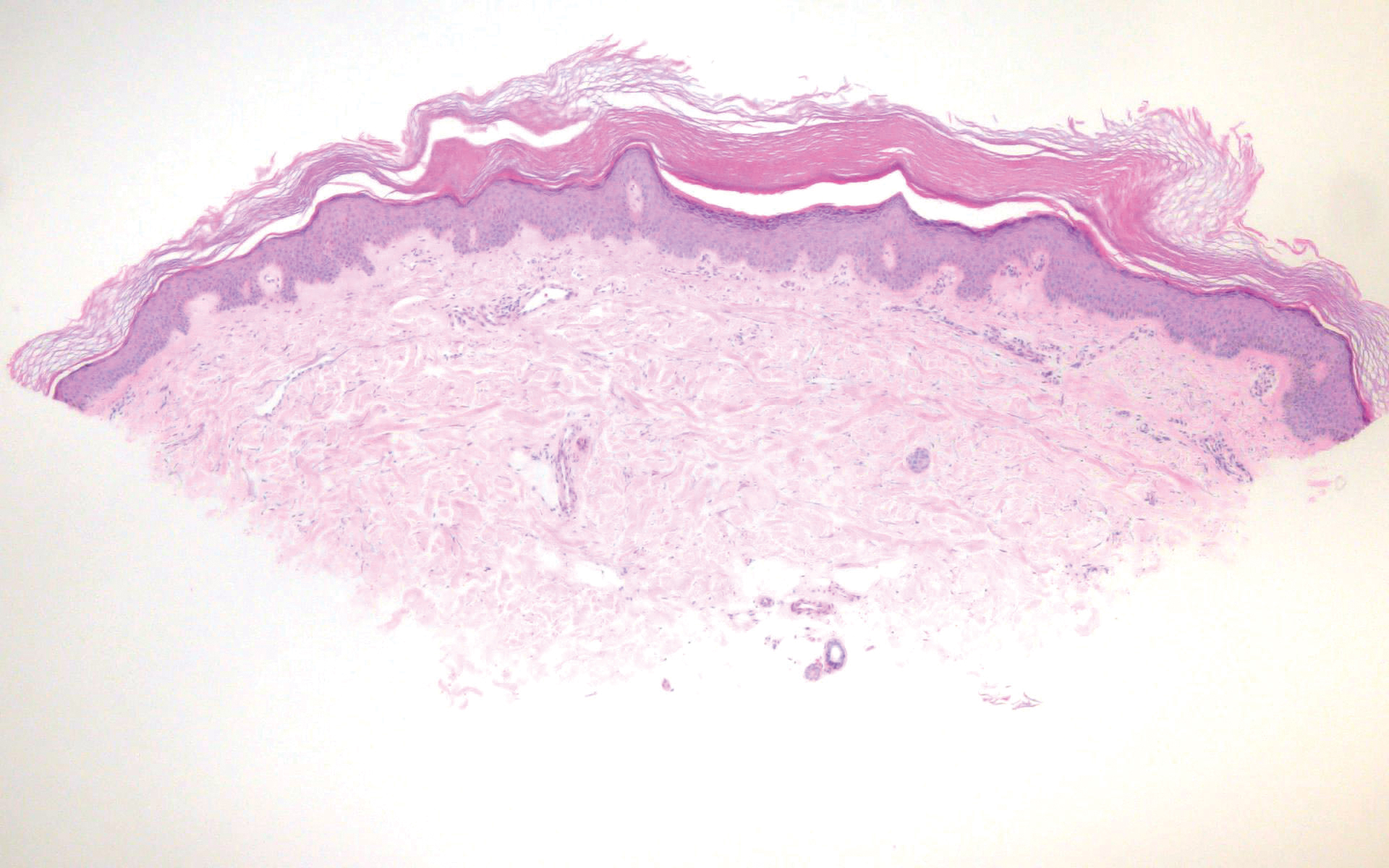
- Flegel H. Hyperkeratosis lenticularis perstans. Hautzarzt. 1958;9:363-364.
- Ando K, Hattori H, Yamauchi Y. Histopathological differences between early and old lesions of hyperkeratosis lenticularis perstans (Flegel's disease). Am J Dermatopathol. 2006;28:122-126.
- Langer K, Zonzits E, Konrad K. Hyperkeratosis lenticularis perstans (Flegel's disease). ultrastructural study of lesional and perilesional skin and therapeutic trial of topical tretinoin versus 5-fluorouracil. J Am Acad Dermatol. 1992;27:812-816.
- Blaheta HJ, Metzler G, Rassner G, et al. Hyperkeratosis lenticularis perstans (Flegel's disease)--lack of response to treatment with tacalcitol and calcipotriol. Dermatology. 2001;202:255-258.
The Diagnosis: Hyperkeratosis Lenticularis Perstans (Flegel Disease)
Hyperkeratosis lenticularis perstans, also known as Flegel disease, is a rare dermatosis first described by Flegel1 in 1958. This benign disorder is characterized by multiple asymptomatic 1- to 5-mm keratotic papules in a symmetric distribution favoring the dorsal aspects of the feet and distal extremities in adults. An autosomal-dominant inheritance pattern has been postulated, though many cases sporadically occur.2 The characteristic spiky papules typically appear during mid to late adulthood and tend to persist. Treatment options are lacking, with reports of partial or no response to topical calcipotriol, topical 5-fluorouracil, cryotherapy, and topical and oral retinoids.3,4
The histopathology of hyperkeratosis lenticularis perstans is distinct, showing a central discrete area of orthohyperkeratosis with patchy parakeratosis flanked by a normal stratum corneum. The underlying epidermis typically shows effacement of the rete ridge pattern with subtle basal zone vacuolization and rare necrotic keratinocytes with an underlying lichenoid infiltrate within the papillary dermis comprised of lymphomononuclear cells.
In contrast, punctate porokeratosis clinically tends to involve the palms and soles, though the arms and legs also may be involved. This entity tends to occur during adolescence. A raised hyperkeratotic papule clinically is present. Histopathologically, the epidermis has a cup-shaped depression filled with hyperkeratosis and a column of parakeratosis (coronoid lamellae)(Figure 1).
Acrokeratosis verruciformis of Hopf clinically appears on the dorsal aspects of the hands and feet as small warty papules in association with Darier disease. It typically presents during early childhood. Histopathology shows tiered hyperkeratosis, papillomatosis, and acanthosis (Figure 2).
Perforating granuloma annulare presents on the dorsal aspects of the hands and fingers as scaly papules with either central umbilication or keratotic plugs. Histopathology shows transepidermal elimination of degenerated collagen (Figure 3).
Stucco keratoses present on the dorsal aspects of the feet and ankles but are waxy smooth papules as opposed to hyperkeratotic spiky papules. Histologically, they are characterized by retention hyperkeratosis with lack of parakeratosis and regular acanthosis with a "string sign" indicating that the lesion extends to a uniform depth. (Figure 4).
The Diagnosis: Hyperkeratosis Lenticularis Perstans (Flegel Disease)
Hyperkeratosis lenticularis perstans, also known as Flegel disease, is a rare dermatosis first described by Flegel1 in 1958. This benign disorder is characterized by multiple asymptomatic 1- to 5-mm keratotic papules in a symmetric distribution favoring the dorsal aspects of the feet and distal extremities in adults. An autosomal-dominant inheritance pattern has been postulated, though many cases sporadically occur.2 The characteristic spiky papules typically appear during mid to late adulthood and tend to persist. Treatment options are lacking, with reports of partial or no response to topical calcipotriol, topical 5-fluorouracil, cryotherapy, and topical and oral retinoids.3,4
The histopathology of hyperkeratosis lenticularis perstans is distinct, showing a central discrete area of orthohyperkeratosis with patchy parakeratosis flanked by a normal stratum corneum. The underlying epidermis typically shows effacement of the rete ridge pattern with subtle basal zone vacuolization and rare necrotic keratinocytes with an underlying lichenoid infiltrate within the papillary dermis comprised of lymphomononuclear cells.
In contrast, punctate porokeratosis clinically tends to involve the palms and soles, though the arms and legs also may be involved. This entity tends to occur during adolescence. A raised hyperkeratotic papule clinically is present. Histopathologically, the epidermis has a cup-shaped depression filled with hyperkeratosis and a column of parakeratosis (coronoid lamellae)(Figure 1).
Acrokeratosis verruciformis of Hopf clinically appears on the dorsal aspects of the hands and feet as small warty papules in association with Darier disease. It typically presents during early childhood. Histopathology shows tiered hyperkeratosis, papillomatosis, and acanthosis (Figure 2).
Perforating granuloma annulare presents on the dorsal aspects of the hands and fingers as scaly papules with either central umbilication or keratotic plugs. Histopathology shows transepidermal elimination of degenerated collagen (Figure 3).
Stucco keratoses present on the dorsal aspects of the feet and ankles but are waxy smooth papules as opposed to hyperkeratotic spiky papules. Histologically, they are characterized by retention hyperkeratosis with lack of parakeratosis and regular acanthosis with a "string sign" indicating that the lesion extends to a uniform depth. (Figure 4).
- Flegel H. Hyperkeratosis lenticularis perstans. Hautzarzt. 1958;9:363-364.
- Ando K, Hattori H, Yamauchi Y. Histopathological differences between early and old lesions of hyperkeratosis lenticularis perstans (Flegel's disease). Am J Dermatopathol. 2006;28:122-126.
- Langer K, Zonzits E, Konrad K. Hyperkeratosis lenticularis perstans (Flegel's disease). ultrastructural study of lesional and perilesional skin and therapeutic trial of topical tretinoin versus 5-fluorouracil. J Am Acad Dermatol. 1992;27:812-816.
- Blaheta HJ, Metzler G, Rassner G, et al. Hyperkeratosis lenticularis perstans (Flegel's disease)--lack of response to treatment with tacalcitol and calcipotriol. Dermatology. 2001;202:255-258.
- Flegel H. Hyperkeratosis lenticularis perstans. Hautzarzt. 1958;9:363-364.
- Ando K, Hattori H, Yamauchi Y. Histopathological differences between early and old lesions of hyperkeratosis lenticularis perstans (Flegel's disease). Am J Dermatopathol. 2006;28:122-126.
- Langer K, Zonzits E, Konrad K. Hyperkeratosis lenticularis perstans (Flegel's disease). ultrastructural study of lesional and perilesional skin and therapeutic trial of topical tretinoin versus 5-fluorouracil. J Am Acad Dermatol. 1992;27:812-816.
- Blaheta HJ, Metzler G, Rassner G, et al. Hyperkeratosis lenticularis perstans (Flegel's disease)--lack of response to treatment with tacalcitol and calcipotriol. Dermatology. 2001;202:255-258.
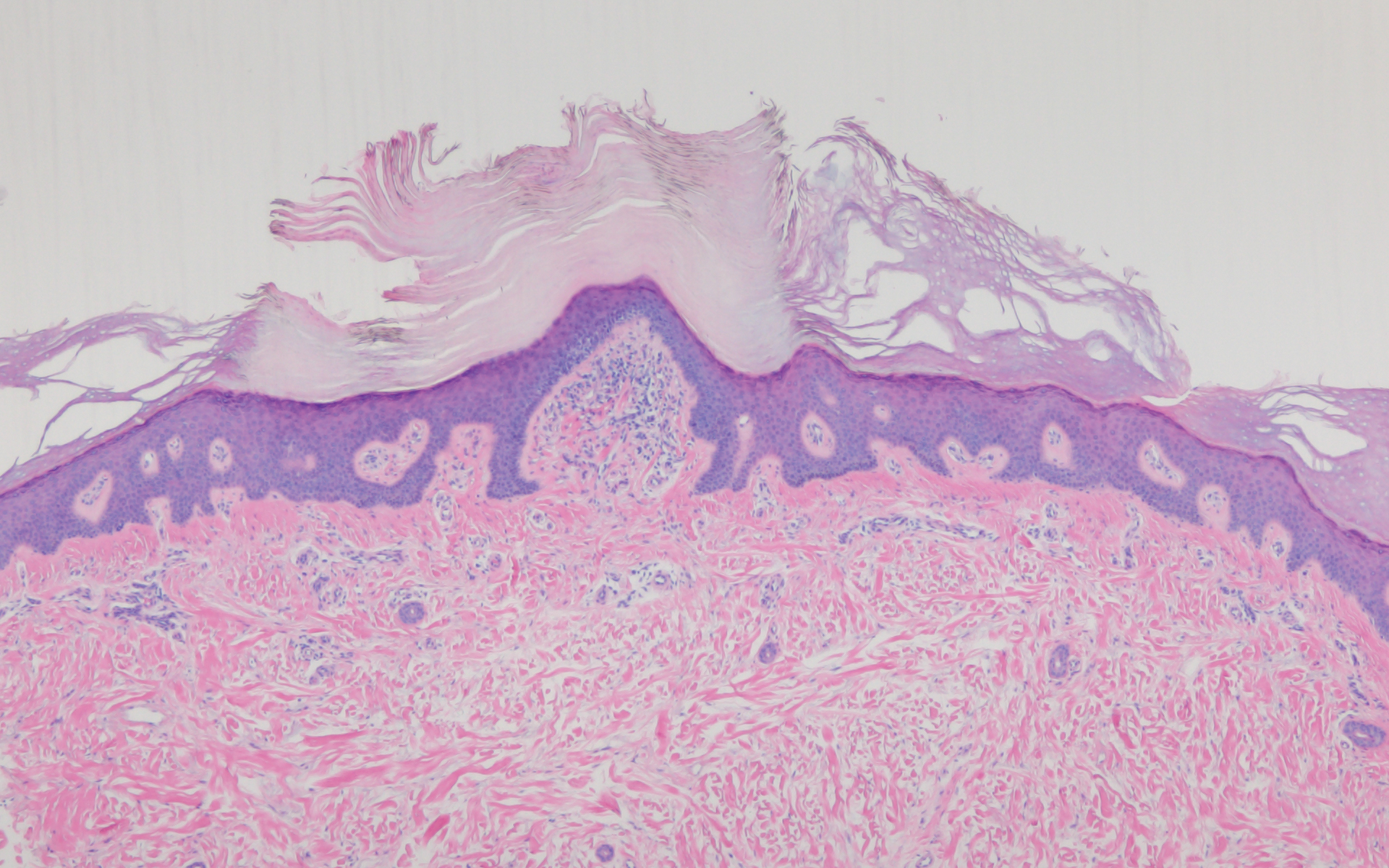
A 54-year-old man who was otherwise healthy presented with asymptomatic, discrete, rough, red-brown, hyperkeratotic papules on the dorsal aspects of the feet of several years' duration. The lesions spared the soles of the feet and hands. A diagnosis of eczema previously was made by his general practitioner, and he was using moisturizer. No prescription treatments were pursued, and no other rashes or lesions were noted on physical examination. A punch biopsy of a spiky papule was performed.