User login
What’s Eating You? Human Body Lice (Pediculus humanus corporis)
Epidemiology and Transmission
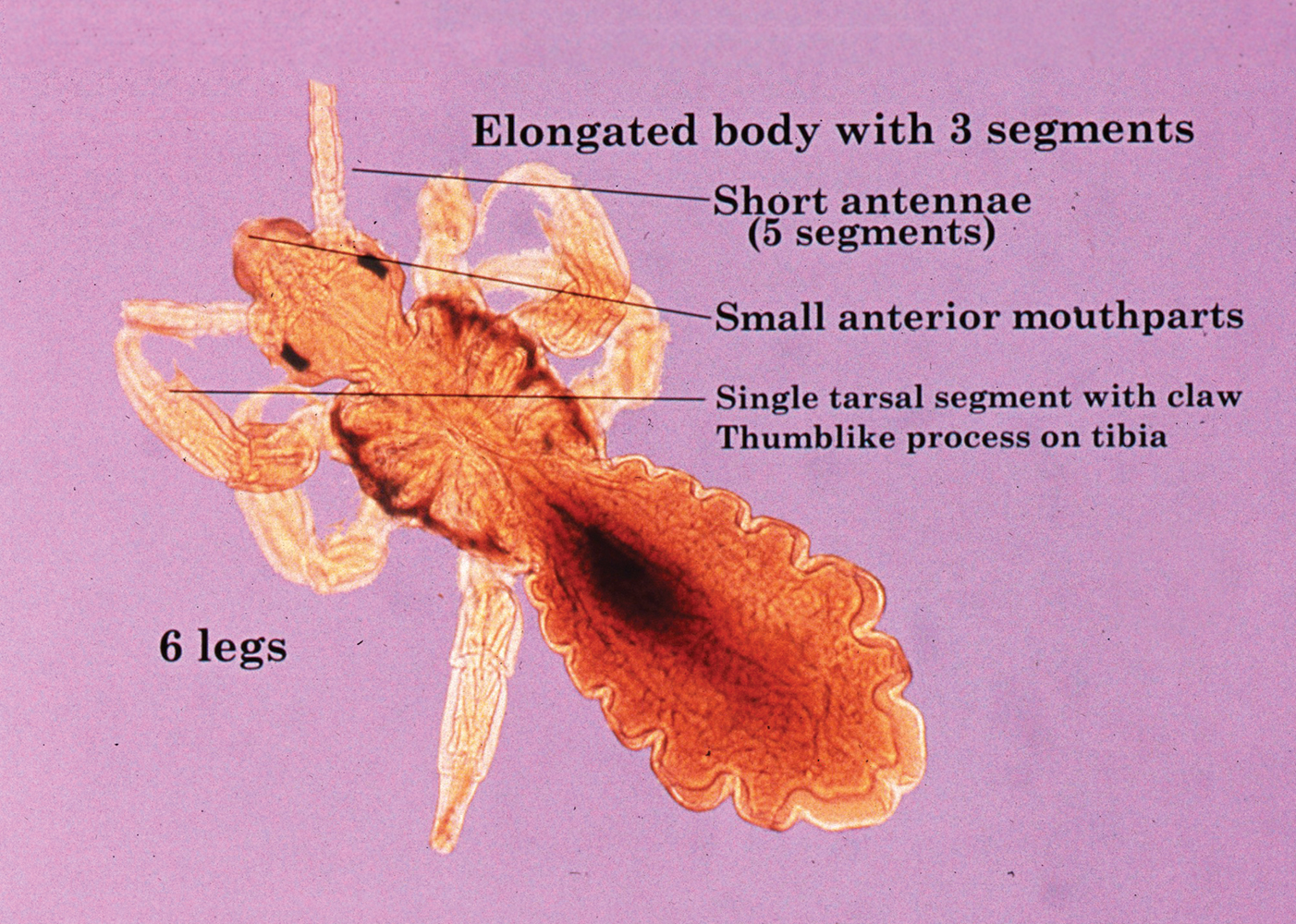
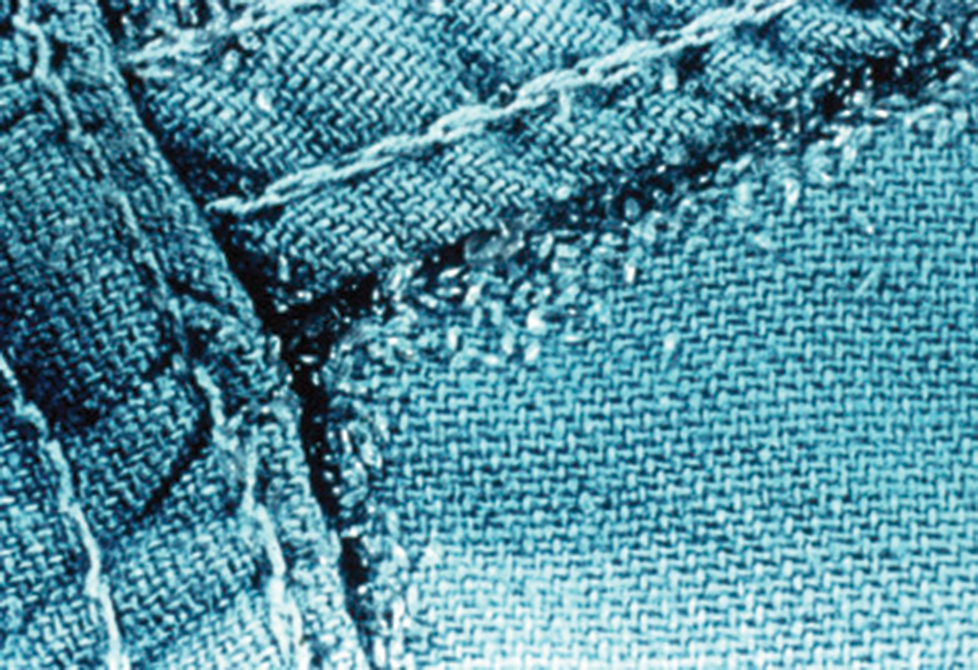
Pediculus humanus corporis, commonly known as the human body louse, is one in a family of 3 ectoparasites of the same suborder that also encompasses pubic lice (Phthirus pubis) and head lice (Pediculus humanus capitis). Adults are approximately 2 mm in size, with the same life cycle as head lice (Figure 1). They require blood meals roughly 5 times per day and cannot survive longer than 2 days without feeding.1 Although similar in structure to head lice, body lice differ behaviorally in that they do not reside on their human host’s body; instead, they infest the host’s clothing, localizing to seams (Figure 2), and migrate to the host for blood meals. In fact, based on this behavior, genetic analysis of early human body lice has been used to postulate when clothing was first used by humans as well as to determine early human migration patterns.2,3
Although clinicians in developed countries may be less familiar with body lice compared to their counterparts, body lice nevertheless remain a global health concern in impoverished, densely populated areas, as well as in homeless populations due to poor hygiene. Transmission frequently occurs via physical contact with an affected individual and his/her personal items (eg, linens) via fomites.4,5 Body louse infestation is more prevalent in homeless individuals who sleep outside vs in shelters; a history of pubic lice and lack of regular bathing have been reported as additional risk factors.6 Outbreaks have been noted in the wake of natural disasters, in the setting of political upheavals, and in refugee camps, as well as in individuals seeking political asylum.7 Unlike head and pubic lice, body lice can serve as vectors for infectious diseases including Rickettsia prowazekii (epidemic typhus), Borrelia recurrentis (louse-borne relapsing fever), Bartonella quintana (trench fever), and Yersinia pestis (plague).5,8,9 Several Acinetobacter species were isolated from nearly one-third of collected body louse specimens in a French study.10 Additionally, serology for B quintana was found to be positive in up to 30% of cases in one United States urban homeless population.4
Clinical Manifestations
Patients often present with generalized pruritus, usually considerably more severe than with P humanus capitis, with lesions concentrated on the trunk.11 In addition to often impetiginized, self-inflicted excoriations, feeding sites may present as erythematous macules (Figure 3), papules, or papular urticaria with a central hemorrhagic punctum. Extensive infestation also can manifest as the colloquial vagabond disease, characterized by postinflammatory hyperpigmentation and thickening of the involved skin. Remarkably, patients also may present with considerable iron-deficiency anemia secondary to high parasite load and large volume blood feeding. Multiple case reports have demonstrated associated morbidity.12-14 The differential diagnosis for pediculosis may include scabies, lichen simplex chronicus, and eczematous dermatitis, though the clinician should prudently consider whether both scabies and pediculosis may be present, as coexistence is possible.4,15

Diagnosis
Diagnosis can be reached by visualizing adult lice, nymphs, or viable nits on the body or more commonly within inner clothing seams; nits also fluoresce under Wood light.15 Although dermoscopy has proven useful for increased sensitivity and differentiation between viable and hatched nits, the insects also can be viewed with the unaided eye.16
Treatment: New Concerns and Strategies
The mainstay of treatment for body lice has long consisted of thorough washing and drying of all clothing and linens in a hot dryer. Treatment can be augmented with the addition of pharmacotherapy, plus antibiotics as warranted for louse-borne disease. Pharmacologic intervention often is used in cases of mass infestation and is similar to head lice.
Options for head lice include topical permethrin, malathion, lindane, spinosad, benzyl alcohol, and ivermectin. Pyrethroids, derived from the chrysanthemum, generally are considered safe for human use with a side-effect profile limited to irritation and allergy17; however, neurotoxicity and leukemia are clinical concerns, with an association more recently shown between large-volume use of pyrethroids and acute lymphoblastic leukemia.18,19 Use of lindane is not recommended due to a greater potential for central nervous system neurotoxicity, manifested by seizures, with repeated large surface application. Malathion is problematic due to the risk for mucosal irritation, flammability of some formulations, and theoretical organophosphate poisoning, as its mechanism of action involves inhibition of acetylcholinesterase.15 However, in the context of head lice treatment, a randomized controlled trial reported no incidence of acetylcholinesterase inhibition.20 Spinosad, manufactured from the soil bacterium Saccharopolyspora spinosa, functions similarly by interfering with the nicotinic acetylcholine receptor and also carries a risk for skin irritation.21 Among all the treatment options, we prefer benzyl alcohol, particularly in the context of resistance, as it is effective via a physical mechanism of action and lacks notable neurotoxic effects to the host. Use of benzyl alcohol is approved for patients as young as 6 months; it functions by asphyxiating the lice via paralysis of the respiratory spiracle with occlusion by inert ingredients. Itching, episodic numbness, and scalp or mucosal irritation are possible complications of treatment.22
Treatment resistance of body lice has increased in recent years, warranting exploration of additional management strategies. Moreover, developing resistance to lindane and malathion has been reported.23 Resistance to pyrethroids has been attributed to mutations in a voltage-gated sodium channel, one of which was universally present in the sampling of a single population.24 A randomized controlled trial showed that off-label oral ivermectin 400 μg/kg was superior to malathion lotion 0.5% in difficult-to-treat cases of head lice25; utility of oral ivermectin also has been reported in body lice.26 In vitro studies also have shown promise for pursuing synergistic treatment of body lice with both ivermectin and antibiotics.27
A novel primary prophylaxis approach for at-risk homeless individuals recently utilized permethrin-impregnated underwear. Although the intervention provided short-term infestation improvement, longer-term use did not show improvement from placebo and also increased prevalence of permethrin-resistant haplotypes.2
- Veracx A, Raoult D. Biology and genetics of human head and body lice. Trends Parasitol. 2012;28:563-571.
- Kittler R, Kayser M, Stoneking M. Molecular evolution of Pediculus humanus and the origin of clothing. Curr Biol. 2003;13:1414-1417.
- Drali R, Mumcuoglu KY, Yesilyurt G, et al. Studies of ancient lice reveal unsuspected past migrations of vectors. Am J Trop Med Hyg. 2015;93:623-625.
- Chosidow O. Scabies and pediculosis. Lancet. 2000;355:819-826.
- Feldmeier H, Heukelbach J. Epidermal parasitic skin diseases: a neglected category of poverty-associated plagues. Bull World Health Organ. 2009;87:152-159.
- Arnaud A, Chosidow O, Detrez MA, et al. Prevalence of scabies and Pediculosis corporis among homeless people in the Paris region: results from two randomized cross-sectional surveys (HYTPEAC study). Br J Dermatol. 2016;174:104-112.
- Hytonen J, Khawaja T, Gronroos JO, et al. Louse-borne relapsing fever in Finland in two asylum seekers from Somalia. APMIS. 2017;125:59-62.
- Nordmann T, Feldt T, Bosselmann M, et al. Outbreak of louse-borne relapsing fever among urban dwellers in Arsi Zone, Central Ethiopia, from July to November 2016. Am J Trop Med Hyg. 2018;98:1599-1602.
- Louni M, Mana N, Bitam I, et al. Body lice of homeless people reveal the presence of several emerging bacterial pathogens in northern Algeria. PLoS Negl Trop Dis. 2018;12:E0006397.
- Candy K, Amanzougaghene N, Izri A, et al. Molecular survey of head and body lice, Pediculus humanus, in France. Vector Borne Zoonotic Dis. 2018;18:243-251.
Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. Elsevier Limited; 2018. - Nara A, Nagai H, Yamaguchi R, et al. An unusual autopsy case of lethal hypothermia exacerbated by body lice-induced severe anemia. Int J Legal Med. 2016;130:765-769.
- Althomali SA, Alzubaidi LM, Alkhaldi DM. Severe iron deficiency anaemia associated with heavy lice infestation in a young woman [published online November 5, 2015]. BMJ Case Rep. doi:10.1136/bcr-2015-212207.
- Hau V, Muhi-Iddin N. A ghost covered in lice: a case of severe blood loss with long-standing heavy pediculosis capitis infestation [published online December 19, 2014]. BMJ Case Rep. doi:10.1136/bcr-2014-206623.
- Diaz JH. Lice (Pediculosis). In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 9th ed. New York, NY: Elsevier; 2020:3482-3486.
- Martins LG, Bernardes Filho F, Quaresma MV, et al. Dermoscopy applied to pediculosis corporis diagnosis. An Bras Dermatol. 2014;89:513-514.
- Devore CD, Schutze GE; Council on School Health and Committee on Infectious Diseases, American Academy of Pediatrics. Head lice. Pediatrics. 2015;135:E1355-E1365.
- Shafer TJ, Meyer DA, Crofton KM. Developmental neurotoxicity of pyrethroid insecticides: critical review and future research needs. Environ Health Perspect. 2005;113:123-136.
- Ding G, Shi R, Gao Y, et al. Pyrethroid pesticide exposure and risk of childhood acute lymphocytic leukemia in Shanghai. Environ Sci Technol. 2012;46:13480-13487.
- Meinking TL, Vicaria M, Eyerdam DH, et al. A randomized, investigator-blinded, time-ranging study of the comparative efficacy of 0.5% malathion gel versus Ovide Lotion (0.5% malathion) or Nix Crème Rinse (1% permethrin) used as labeled, for the treatment of head lice. Pediatr Dermatol. 2007;24:405-411.
- McCormack PL. Spinosad: in pediculosis capitis. Am J Clin Dermatol. 2011;12:349-353.
- Meinking TL, Villar ME, Vicaria M, et al. The clinical trials supporting benzyl alcohol lotion 5% (Ulesfia): a safe and effective topical treatment for head lice (pediculosis humanus capitis). Pediatr Dermatol. 2010;27:19-24.
- Lebwohl M, Clark L, Levitt J. Therapy for head lice based on life cycle, resistance, and safety considerations. Pediatrics. 2007;119:965-974
- Drali R, Benkouiten S, Badiaga S, et al. Detection of a knockdown resistance mutation associated with permethrin resistance in the body louse Pediculus humanus corporis by use of melting curve analysis genotyping. J Clin Microbiol. 2012;50:2229-2233.
- Chosidow O, Giraudeau B, Cottrell J, et al. Oral ivermectin versus malathion lotion for difficult-to-treat head lice. N Engl J Med. 2010;362:896-905.
- Foucault C, Ranque S, Badiaga S, et al. Oral ivermectin in the treatment of body lice. J Infect Dis. 2006;193:474-476.
- Sangaré AK, Doumbo OK, Raoult D. Management and treatment of human lice [published online July 27, 2016]. Biomed Res Int. doi:10.1155/2016/8962685.
- Benkouiten S, Drali R, Badiaga S, et al. Effect of permethrin-impregnated underwear on body lice in sheltered homeless persons: a randomized controlled trial. JAMA Dermatol. 2014;150:273-279.
Epidemiology and Transmission
Pediculus humanus corporis, commonly known as the human body louse, is one in a family of 3 ectoparasites of the same suborder that also encompasses pubic lice (Phthirus pubis) and head lice (Pediculus humanus capitis). Adults are approximately 2 mm in size, with the same life cycle as head lice (Figure 1). They require blood meals roughly 5 times per day and cannot survive longer than 2 days without feeding.1 Although similar in structure to head lice, body lice differ behaviorally in that they do not reside on their human host’s body; instead, they infest the host’s clothing, localizing to seams (Figure 2), and migrate to the host for blood meals. In fact, based on this behavior, genetic analysis of early human body lice has been used to postulate when clothing was first used by humans as well as to determine early human migration patterns.2,3
Although clinicians in developed countries may be less familiar with body lice compared to their counterparts, body lice nevertheless remain a global health concern in impoverished, densely populated areas, as well as in homeless populations due to poor hygiene. Transmission frequently occurs via physical contact with an affected individual and his/her personal items (eg, linens) via fomites.4,5 Body louse infestation is more prevalent in homeless individuals who sleep outside vs in shelters; a history of pubic lice and lack of regular bathing have been reported as additional risk factors.6 Outbreaks have been noted in the wake of natural disasters, in the setting of political upheavals, and in refugee camps, as well as in individuals seeking political asylum.7 Unlike head and pubic lice, body lice can serve as vectors for infectious diseases including Rickettsia prowazekii (epidemic typhus), Borrelia recurrentis (louse-borne relapsing fever), Bartonella quintana (trench fever), and Yersinia pestis (plague).5,8,9 Several Acinetobacter species were isolated from nearly one-third of collected body louse specimens in a French study.10 Additionally, serology for B quintana was found to be positive in up to 30% of cases in one United States urban homeless population.4
Clinical Manifestations
Patients often present with generalized pruritus, usually considerably more severe than with P humanus capitis, with lesions concentrated on the trunk.11 In addition to often impetiginized, self-inflicted excoriations, feeding sites may present as erythematous macules (Figure 3), papules, or papular urticaria with a central hemorrhagic punctum. Extensive infestation also can manifest as the colloquial vagabond disease, characterized by postinflammatory hyperpigmentation and thickening of the involved skin. Remarkably, patients also may present with considerable iron-deficiency anemia secondary to high parasite load and large volume blood feeding. Multiple case reports have demonstrated associated morbidity.12-14 The differential diagnosis for pediculosis may include scabies, lichen simplex chronicus, and eczematous dermatitis, though the clinician should prudently consider whether both scabies and pediculosis may be present, as coexistence is possible.4,15
Diagnosis
Diagnosis can be reached by visualizing adult lice, nymphs, or viable nits on the body or more commonly within inner clothing seams; nits also fluoresce under Wood light.15 Although dermoscopy has proven useful for increased sensitivity and differentiation between viable and hatched nits, the insects also can be viewed with the unaided eye.16
Treatment: New Concerns and Strategies
The mainstay of treatment for body lice has long consisted of thorough washing and drying of all clothing and linens in a hot dryer. Treatment can be augmented with the addition of pharmacotherapy, plus antibiotics as warranted for louse-borne disease. Pharmacologic intervention often is used in cases of mass infestation and is similar to head lice.
Options for head lice include topical permethrin, malathion, lindane, spinosad, benzyl alcohol, and ivermectin. Pyrethroids, derived from the chrysanthemum, generally are considered safe for human use with a side-effect profile limited to irritation and allergy17; however, neurotoxicity and leukemia are clinical concerns, with an association more recently shown between large-volume use of pyrethroids and acute lymphoblastic leukemia.18,19 Use of lindane is not recommended due to a greater potential for central nervous system neurotoxicity, manifested by seizures, with repeated large surface application. Malathion is problematic due to the risk for mucosal irritation, flammability of some formulations, and theoretical organophosphate poisoning, as its mechanism of action involves inhibition of acetylcholinesterase.15 However, in the context of head lice treatment, a randomized controlled trial reported no incidence of acetylcholinesterase inhibition.20 Spinosad, manufactured from the soil bacterium Saccharopolyspora spinosa, functions similarly by interfering with the nicotinic acetylcholine receptor and also carries a risk for skin irritation.21 Among all the treatment options, we prefer benzyl alcohol, particularly in the context of resistance, as it is effective via a physical mechanism of action and lacks notable neurotoxic effects to the host. Use of benzyl alcohol is approved for patients as young as 6 months; it functions by asphyxiating the lice via paralysis of the respiratory spiracle with occlusion by inert ingredients. Itching, episodic numbness, and scalp or mucosal irritation are possible complications of treatment.22
Treatment resistance of body lice has increased in recent years, warranting exploration of additional management strategies. Moreover, developing resistance to lindane and malathion has been reported.23 Resistance to pyrethroids has been attributed to mutations in a voltage-gated sodium channel, one of which was universally present in the sampling of a single population.24 A randomized controlled trial showed that off-label oral ivermectin 400 μg/kg was superior to malathion lotion 0.5% in difficult-to-treat cases of head lice25; utility of oral ivermectin also has been reported in body lice.26 In vitro studies also have shown promise for pursuing synergistic treatment of body lice with both ivermectin and antibiotics.27
A novel primary prophylaxis approach for at-risk homeless individuals recently utilized permethrin-impregnated underwear. Although the intervention provided short-term infestation improvement, longer-term use did not show improvement from placebo and also increased prevalence of permethrin-resistant haplotypes.2
Epidemiology and Transmission
Pediculus humanus corporis, commonly known as the human body louse, is one in a family of 3 ectoparasites of the same suborder that also encompasses pubic lice (Phthirus pubis) and head lice (Pediculus humanus capitis). Adults are approximately 2 mm in size, with the same life cycle as head lice (Figure 1). They require blood meals roughly 5 times per day and cannot survive longer than 2 days without feeding.1 Although similar in structure to head lice, body lice differ behaviorally in that they do not reside on their human host’s body; instead, they infest the host’s clothing, localizing to seams (Figure 2), and migrate to the host for blood meals. In fact, based on this behavior, genetic analysis of early human body lice has been used to postulate when clothing was first used by humans as well as to determine early human migration patterns.2,3
Although clinicians in developed countries may be less familiar with body lice compared to their counterparts, body lice nevertheless remain a global health concern in impoverished, densely populated areas, as well as in homeless populations due to poor hygiene. Transmission frequently occurs via physical contact with an affected individual and his/her personal items (eg, linens) via fomites.4,5 Body louse infestation is more prevalent in homeless individuals who sleep outside vs in shelters; a history of pubic lice and lack of regular bathing have been reported as additional risk factors.6 Outbreaks have been noted in the wake of natural disasters, in the setting of political upheavals, and in refugee camps, as well as in individuals seeking political asylum.7 Unlike head and pubic lice, body lice can serve as vectors for infectious diseases including Rickettsia prowazekii (epidemic typhus), Borrelia recurrentis (louse-borne relapsing fever), Bartonella quintana (trench fever), and Yersinia pestis (plague).5,8,9 Several Acinetobacter species were isolated from nearly one-third of collected body louse specimens in a French study.10 Additionally, serology for B quintana was found to be positive in up to 30% of cases in one United States urban homeless population.4
Clinical Manifestations
Patients often present with generalized pruritus, usually considerably more severe than with P humanus capitis, with lesions concentrated on the trunk.11 In addition to often impetiginized, self-inflicted excoriations, feeding sites may present as erythematous macules (Figure 3), papules, or papular urticaria with a central hemorrhagic punctum. Extensive infestation also can manifest as the colloquial vagabond disease, characterized by postinflammatory hyperpigmentation and thickening of the involved skin. Remarkably, patients also may present with considerable iron-deficiency anemia secondary to high parasite load and large volume blood feeding. Multiple case reports have demonstrated associated morbidity.12-14 The differential diagnosis for pediculosis may include scabies, lichen simplex chronicus, and eczematous dermatitis, though the clinician should prudently consider whether both scabies and pediculosis may be present, as coexistence is possible.4,15
Diagnosis
Diagnosis can be reached by visualizing adult lice, nymphs, or viable nits on the body or more commonly within inner clothing seams; nits also fluoresce under Wood light.15 Although dermoscopy has proven useful for increased sensitivity and differentiation between viable and hatched nits, the insects also can be viewed with the unaided eye.16
Treatment: New Concerns and Strategies
The mainstay of treatment for body lice has long consisted of thorough washing and drying of all clothing and linens in a hot dryer. Treatment can be augmented with the addition of pharmacotherapy, plus antibiotics as warranted for louse-borne disease. Pharmacologic intervention often is used in cases of mass infestation and is similar to head lice.
Options for head lice include topical permethrin, malathion, lindane, spinosad, benzyl alcohol, and ivermectin. Pyrethroids, derived from the chrysanthemum, generally are considered safe for human use with a side-effect profile limited to irritation and allergy17; however, neurotoxicity and leukemia are clinical concerns, with an association more recently shown between large-volume use of pyrethroids and acute lymphoblastic leukemia.18,19 Use of lindane is not recommended due to a greater potential for central nervous system neurotoxicity, manifested by seizures, with repeated large surface application. Malathion is problematic due to the risk for mucosal irritation, flammability of some formulations, and theoretical organophosphate poisoning, as its mechanism of action involves inhibition of acetylcholinesterase.15 However, in the context of head lice treatment, a randomized controlled trial reported no incidence of acetylcholinesterase inhibition.20 Spinosad, manufactured from the soil bacterium Saccharopolyspora spinosa, functions similarly by interfering with the nicotinic acetylcholine receptor and also carries a risk for skin irritation.21 Among all the treatment options, we prefer benzyl alcohol, particularly in the context of resistance, as it is effective via a physical mechanism of action and lacks notable neurotoxic effects to the host. Use of benzyl alcohol is approved for patients as young as 6 months; it functions by asphyxiating the lice via paralysis of the respiratory spiracle with occlusion by inert ingredients. Itching, episodic numbness, and scalp or mucosal irritation are possible complications of treatment.22
Treatment resistance of body lice has increased in recent years, warranting exploration of additional management strategies. Moreover, developing resistance to lindane and malathion has been reported.23 Resistance to pyrethroids has been attributed to mutations in a voltage-gated sodium channel, one of which was universally present in the sampling of a single population.24 A randomized controlled trial showed that off-label oral ivermectin 400 μg/kg was superior to malathion lotion 0.5% in difficult-to-treat cases of head lice25; utility of oral ivermectin also has been reported in body lice.26 In vitro studies also have shown promise for pursuing synergistic treatment of body lice with both ivermectin and antibiotics.27
A novel primary prophylaxis approach for at-risk homeless individuals recently utilized permethrin-impregnated underwear. Although the intervention provided short-term infestation improvement, longer-term use did not show improvement from placebo and also increased prevalence of permethrin-resistant haplotypes.2
- Veracx A, Raoult D. Biology and genetics of human head and body lice. Trends Parasitol. 2012;28:563-571.
- Kittler R, Kayser M, Stoneking M. Molecular evolution of Pediculus humanus and the origin of clothing. Curr Biol. 2003;13:1414-1417.
- Drali R, Mumcuoglu KY, Yesilyurt G, et al. Studies of ancient lice reveal unsuspected past migrations of vectors. Am J Trop Med Hyg. 2015;93:623-625.
- Chosidow O. Scabies and pediculosis. Lancet. 2000;355:819-826.
- Feldmeier H, Heukelbach J. Epidermal parasitic skin diseases: a neglected category of poverty-associated plagues. Bull World Health Organ. 2009;87:152-159.
- Arnaud A, Chosidow O, Detrez MA, et al. Prevalence of scabies and Pediculosis corporis among homeless people in the Paris region: results from two randomized cross-sectional surveys (HYTPEAC study). Br J Dermatol. 2016;174:104-112.
- Hytonen J, Khawaja T, Gronroos JO, et al. Louse-borne relapsing fever in Finland in two asylum seekers from Somalia. APMIS. 2017;125:59-62.
- Nordmann T, Feldt T, Bosselmann M, et al. Outbreak of louse-borne relapsing fever among urban dwellers in Arsi Zone, Central Ethiopia, from July to November 2016. Am J Trop Med Hyg. 2018;98:1599-1602.
- Louni M, Mana N, Bitam I, et al. Body lice of homeless people reveal the presence of several emerging bacterial pathogens in northern Algeria. PLoS Negl Trop Dis. 2018;12:E0006397.
- Candy K, Amanzougaghene N, Izri A, et al. Molecular survey of head and body lice, Pediculus humanus, in France. Vector Borne Zoonotic Dis. 2018;18:243-251.
Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. Elsevier Limited; 2018. - Nara A, Nagai H, Yamaguchi R, et al. An unusual autopsy case of lethal hypothermia exacerbated by body lice-induced severe anemia. Int J Legal Med. 2016;130:765-769.
- Althomali SA, Alzubaidi LM, Alkhaldi DM. Severe iron deficiency anaemia associated with heavy lice infestation in a young woman [published online November 5, 2015]. BMJ Case Rep. doi:10.1136/bcr-2015-212207.
- Hau V, Muhi-Iddin N. A ghost covered in lice: a case of severe blood loss with long-standing heavy pediculosis capitis infestation [published online December 19, 2014]. BMJ Case Rep. doi:10.1136/bcr-2014-206623.
- Diaz JH. Lice (Pediculosis). In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 9th ed. New York, NY: Elsevier; 2020:3482-3486.
- Martins LG, Bernardes Filho F, Quaresma MV, et al. Dermoscopy applied to pediculosis corporis diagnosis. An Bras Dermatol. 2014;89:513-514.
- Devore CD, Schutze GE; Council on School Health and Committee on Infectious Diseases, American Academy of Pediatrics. Head lice. Pediatrics. 2015;135:E1355-E1365.
- Shafer TJ, Meyer DA, Crofton KM. Developmental neurotoxicity of pyrethroid insecticides: critical review and future research needs. Environ Health Perspect. 2005;113:123-136.
- Ding G, Shi R, Gao Y, et al. Pyrethroid pesticide exposure and risk of childhood acute lymphocytic leukemia in Shanghai. Environ Sci Technol. 2012;46:13480-13487.
- Meinking TL, Vicaria M, Eyerdam DH, et al. A randomized, investigator-blinded, time-ranging study of the comparative efficacy of 0.5% malathion gel versus Ovide Lotion (0.5% malathion) or Nix Crème Rinse (1% permethrin) used as labeled, for the treatment of head lice. Pediatr Dermatol. 2007;24:405-411.
- McCormack PL. Spinosad: in pediculosis capitis. Am J Clin Dermatol. 2011;12:349-353.
- Meinking TL, Villar ME, Vicaria M, et al. The clinical trials supporting benzyl alcohol lotion 5% (Ulesfia): a safe and effective topical treatment for head lice (pediculosis humanus capitis). Pediatr Dermatol. 2010;27:19-24.
- Lebwohl M, Clark L, Levitt J. Therapy for head lice based on life cycle, resistance, and safety considerations. Pediatrics. 2007;119:965-974
- Drali R, Benkouiten S, Badiaga S, et al. Detection of a knockdown resistance mutation associated with permethrin resistance in the body louse Pediculus humanus corporis by use of melting curve analysis genotyping. J Clin Microbiol. 2012;50:2229-2233.
- Chosidow O, Giraudeau B, Cottrell J, et al. Oral ivermectin versus malathion lotion for difficult-to-treat head lice. N Engl J Med. 2010;362:896-905.
- Foucault C, Ranque S, Badiaga S, et al. Oral ivermectin in the treatment of body lice. J Infect Dis. 2006;193:474-476.
- Sangaré AK, Doumbo OK, Raoult D. Management and treatment of human lice [published online July 27, 2016]. Biomed Res Int. doi:10.1155/2016/8962685.
- Benkouiten S, Drali R, Badiaga S, et al. Effect of permethrin-impregnated underwear on body lice in sheltered homeless persons: a randomized controlled trial. JAMA Dermatol. 2014;150:273-279.
- Veracx A, Raoult D. Biology and genetics of human head and body lice. Trends Parasitol. 2012;28:563-571.
- Kittler R, Kayser M, Stoneking M. Molecular evolution of Pediculus humanus and the origin of clothing. Curr Biol. 2003;13:1414-1417.
- Drali R, Mumcuoglu KY, Yesilyurt G, et al. Studies of ancient lice reveal unsuspected past migrations of vectors. Am J Trop Med Hyg. 2015;93:623-625.
- Chosidow O. Scabies and pediculosis. Lancet. 2000;355:819-826.
- Feldmeier H, Heukelbach J. Epidermal parasitic skin diseases: a neglected category of poverty-associated plagues. Bull World Health Organ. 2009;87:152-159.
- Arnaud A, Chosidow O, Detrez MA, et al. Prevalence of scabies and Pediculosis corporis among homeless people in the Paris region: results from two randomized cross-sectional surveys (HYTPEAC study). Br J Dermatol. 2016;174:104-112.
- Hytonen J, Khawaja T, Gronroos JO, et al. Louse-borne relapsing fever in Finland in two asylum seekers from Somalia. APMIS. 2017;125:59-62.
- Nordmann T, Feldt T, Bosselmann M, et al. Outbreak of louse-borne relapsing fever among urban dwellers in Arsi Zone, Central Ethiopia, from July to November 2016. Am J Trop Med Hyg. 2018;98:1599-1602.
- Louni M, Mana N, Bitam I, et al. Body lice of homeless people reveal the presence of several emerging bacterial pathogens in northern Algeria. PLoS Negl Trop Dis. 2018;12:E0006397.
- Candy K, Amanzougaghene N, Izri A, et al. Molecular survey of head and body lice, Pediculus humanus, in France. Vector Borne Zoonotic Dis. 2018;18:243-251.
Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. Elsevier Limited; 2018. - Nara A, Nagai H, Yamaguchi R, et al. An unusual autopsy case of lethal hypothermia exacerbated by body lice-induced severe anemia. Int J Legal Med. 2016;130:765-769.
- Althomali SA, Alzubaidi LM, Alkhaldi DM. Severe iron deficiency anaemia associated with heavy lice infestation in a young woman [published online November 5, 2015]. BMJ Case Rep. doi:10.1136/bcr-2015-212207.
- Hau V, Muhi-Iddin N. A ghost covered in lice: a case of severe blood loss with long-standing heavy pediculosis capitis infestation [published online December 19, 2014]. BMJ Case Rep. doi:10.1136/bcr-2014-206623.
- Diaz JH. Lice (Pediculosis). In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 9th ed. New York, NY: Elsevier; 2020:3482-3486.
- Martins LG, Bernardes Filho F, Quaresma MV, et al. Dermoscopy applied to pediculosis corporis diagnosis. An Bras Dermatol. 2014;89:513-514.
- Devore CD, Schutze GE; Council on School Health and Committee on Infectious Diseases, American Academy of Pediatrics. Head lice. Pediatrics. 2015;135:E1355-E1365.
- Shafer TJ, Meyer DA, Crofton KM. Developmental neurotoxicity of pyrethroid insecticides: critical review and future research needs. Environ Health Perspect. 2005;113:123-136.
- Ding G, Shi R, Gao Y, et al. Pyrethroid pesticide exposure and risk of childhood acute lymphocytic leukemia in Shanghai. Environ Sci Technol. 2012;46:13480-13487.
- Meinking TL, Vicaria M, Eyerdam DH, et al. A randomized, investigator-blinded, time-ranging study of the comparative efficacy of 0.5% malathion gel versus Ovide Lotion (0.5% malathion) or Nix Crème Rinse (1% permethrin) used as labeled, for the treatment of head lice. Pediatr Dermatol. 2007;24:405-411.
- McCormack PL. Spinosad: in pediculosis capitis. Am J Clin Dermatol. 2011;12:349-353.
- Meinking TL, Villar ME, Vicaria M, et al. The clinical trials supporting benzyl alcohol lotion 5% (Ulesfia): a safe and effective topical treatment for head lice (pediculosis humanus capitis). Pediatr Dermatol. 2010;27:19-24.
- Lebwohl M, Clark L, Levitt J. Therapy for head lice based on life cycle, resistance, and safety considerations. Pediatrics. 2007;119:965-974
- Drali R, Benkouiten S, Badiaga S, et al. Detection of a knockdown resistance mutation associated with permethrin resistance in the body louse Pediculus humanus corporis by use of melting curve analysis genotyping. J Clin Microbiol. 2012;50:2229-2233.
- Chosidow O, Giraudeau B, Cottrell J, et al. Oral ivermectin versus malathion lotion for difficult-to-treat head lice. N Engl J Med. 2010;362:896-905.
- Foucault C, Ranque S, Badiaga S, et al. Oral ivermectin in the treatment of body lice. J Infect Dis. 2006;193:474-476.
- Sangaré AK, Doumbo OK, Raoult D. Management and treatment of human lice [published online July 27, 2016]. Biomed Res Int. doi:10.1155/2016/8962685.
- Benkouiten S, Drali R, Badiaga S, et al. Effect of permethrin-impregnated underwear on body lice in sheltered homeless persons: a randomized controlled trial. JAMA Dermatol. 2014;150:273-279.
Practice Points
- Body lice reside in clothing, particularly folds and seams, and migrate to the host for blood meals. To evaluate for infestation, the clinician should not only look at the skin but also closely examine the patient’s clothing. Clothes also are a target for treatment via washing in hot water.
- Due to observed and theoretical adverse effects of other chemical treatments, benzyl alcohol is the authors’ choice for treatment of head lice.
- Oral ivermectin is a promising future treatment for body lice.

Emollients didn’t prevent atopic dermatitis in high-risk infants
The use of including those at high risk, in two new clinical trials.
The BEEP (Barrier Enhancement for Eczema Prevention) study compared the rates of AD among infants identified as at risk of AD because of family history who had daily applications of emollients (Diprobase cream or Doublebase gel) for the first year of life, compared with a standard skin care group. PreventADALL (Preventing Atopic Dermatitis and Allergies in Children) is a randomized, primary-prevention study conducted in Norway and Sweden that randomized infants into one of four groups: controls whose parents followed regular skin care advice and nutrition guidelines; those who received skin emollients (the addition of emulsified oil to their bath and application of facial cream on at least 4 days a week from age 2 weeks to 8 months); those who received early complementary feeding of peanut, cow’s milk, wheat, and egg introduced between aged 12 and 16 weeks; and a group that combined both the emollient and diet interventions.
Neither of the studies, published in the Lancet, found statistically significant differences in AD rates between the intervention and control groups.
The results put a damper on hopes raised by previous studies that included two small pilot studies, which found that daily use of leave-on emollients in infants considered at high risk of AD prevented the development of AD (J Allergy Clin Immunol 2014 Oct;134:824-30.e6; J Allergy Clin Immunol Oct 2014;134:818-23).
“It was maybe a little bit overly hopeful to think that we could just moisturize and prevent such a complex disorder,” Robert Sidbury, MD, chief of dermatology at Seattle Children’s Hospital, said in an interview. He emphasized that the studies only addressed emollients as a preventative, and that “there’s no question that emollients are still critical for the therapy of eczema.”
Bruce Brod, MD, clinical professor of dermatology at the University of Pennsylvania, Philadelphia, suggested that homogeneous patient populations or insufficient numbers might explain the negative findings. PreventADALL drew patients from Norway and Sweden, while BEEP recruited from the United Kingdom. “They’re important studies, but I think they still lend themselves to further studies with different patient populations and larger groups of patients,” Dr. Brod said in an interview.
BEEP was headed by Joanne Chalmers, PhD, and Hywel Williams, DSc, of the Centre of Evidence-Based Dermatology at the University of Nottingham (England). Håvard Ove Skjerven, PhD, and Karin C Lødrup Carlsen, PhD, of Oslo University Hospital led the PreventADALL study.
The BEEP study randomized 1,394 newborns at 16 sites in the United Kingdom to daily emollient treatment with standard skin care, or standard skin care alone. At one year, compliance was 74% in the intervention group. At age 2, 23% of the intervention group had AD, compared with 25% of controls (hazard ratio, 0.95; P =.61). Skin infections were also higher in the treatment arm (mean, 0.23 per year vs. 0.15 per year; adjusted incidence ratio, 1.55; 95% confidence interval, 1.15-2.09).
“Our study does not support the use of emollients for preventing eczema in high-risk infants, a finding supported by PreventADALL, another large trial using a skin barrier enhancing intervention,” they concluded. Their data “relate only to prevention of eczema and do not directly challenge the practice of using emollients as first-line treatment for eczema.”
In the PreventADALL study, 2,397 newborn infants born between 2015 and 2017 were randomized to one of the four groups. Use of facial cream and emollients during bathing began at 2 weeks, and early complementary feeding of peanut, cow’s milk, wheat, and egg at 3-4 months. The frequency of AD at aged 12 months in the control group was 8%, compared with 11% in the skin-intervention group, 9% in the food-intervention group, and 5% in the combined-intervention group.
These differences were not statistically significant, and “the primary hypothesis that either skin intervention or food intervention reduced atopic dermatitis were not confirmed,” the authors wrote. Parental atopy did not influence the effects of the interventions. Their results were in line with the BEEP results, and the authors “cannot recommend these interventions as primary prevention strategies.”
The researchers will continue to follow children until age 3 years to evaluate the food allergy rates, if the combined-treatment group experiences a long-term benefit. Adherence to the protocol was poor, with 44% compliance with the facial cream application and 27% compliance with bathing emollients; 32% fully adhered to the diet protocols.
The studies were funded by the National Institute for Health Research Health Technology Assessment (BEEP); and a range of public and private funders (PreventADALL). One author of the PreventADALL study disclosed receiving honoraria for presentations from several pharmaceutical companies, and one author received honoraria for presentations from Thermo Fisher Scientific; the rest had no disclosures. Dr. Sidbury has been an investigator for Regeneron. Dr. Brod had no relevant financial disclosures.
SOURCES: Chalmers JR et al. Lancet. 2020 Feb 19. doi: 10.1016/S0140-6736(19)32984-8; Skjerven HO et al. Lancet. 2020 Feb 19. doi: 10.1016/S0140-6736(19)32983-6.
The “null findings” of these two studies were “unexpected,” Kirsten P. Perrett, MBBS, Phd, and Rachel L. Peters, PhD, of the department of population allergy at Murdoch Children’s Research Institute, Parkville, Australia, wrote in an accompanying editorial. They noted that emollients are used regularly in the management of atopic dermatitis, where they help maintain the skin barrier and reduce the need for anti-inflammatory therapies.
These two large prevention studies were “prompted” by the results of small, proof-of-concept pilot studies, which “provided strong efficacy signals for the hypothesis that daily emollient use could prevent atopic dermatitis,” they wrote. But the two studies “found no evidence that daily emollient use in either a population-based or high-risk cohort of infants during the first year of life could delay, suppress, or prevent atopic dermatitis.” The lower incidence of atopic dermatitis among those in the dietary and emollient combination, compared with controls (5% vs. 8%) in PreventADALL, could be a chance finding.
The large, randomized Prevention of Eczema by a Barrier Lipid Equilibrium Strategy (PEBBLES) trial is ongoing to confirm results from a small study suggesting the efficacy of a ceramide-dominant emollient. But the PreventADALL study showed low compliance, suggesting that this intervention, if effective, a twice-daily emollient regimen may be tough to implement. “At this stage, emollients should not be recommended for the primary prevention of atopic dermatitis in infants,” they concluded.
Dr. Perrett and Dr. Peters declared no competing interests. Their comments appeared in the Lancet (2020 Feb 19. doi: 10.1016/S0140-6736[19]33174-5).
The “null findings” of these two studies were “unexpected,” Kirsten P. Perrett, MBBS, Phd, and Rachel L. Peters, PhD, of the department of population allergy at Murdoch Children’s Research Institute, Parkville, Australia, wrote in an accompanying editorial. They noted that emollients are used regularly in the management of atopic dermatitis, where they help maintain the skin barrier and reduce the need for anti-inflammatory therapies.
These two large prevention studies were “prompted” by the results of small, proof-of-concept pilot studies, which “provided strong efficacy signals for the hypothesis that daily emollient use could prevent atopic dermatitis,” they wrote. But the two studies “found no evidence that daily emollient use in either a population-based or high-risk cohort of infants during the first year of life could delay, suppress, or prevent atopic dermatitis.” The lower incidence of atopic dermatitis among those in the dietary and emollient combination, compared with controls (5% vs. 8%) in PreventADALL, could be a chance finding.
The large, randomized Prevention of Eczema by a Barrier Lipid Equilibrium Strategy (PEBBLES) trial is ongoing to confirm results from a small study suggesting the efficacy of a ceramide-dominant emollient. But the PreventADALL study showed low compliance, suggesting that this intervention, if effective, a twice-daily emollient regimen may be tough to implement. “At this stage, emollients should not be recommended for the primary prevention of atopic dermatitis in infants,” they concluded.
Dr. Perrett and Dr. Peters declared no competing interests. Their comments appeared in the Lancet (2020 Feb 19. doi: 10.1016/S0140-6736[19]33174-5).
The “null findings” of these two studies were “unexpected,” Kirsten P. Perrett, MBBS, Phd, and Rachel L. Peters, PhD, of the department of population allergy at Murdoch Children’s Research Institute, Parkville, Australia, wrote in an accompanying editorial. They noted that emollients are used regularly in the management of atopic dermatitis, where they help maintain the skin barrier and reduce the need for anti-inflammatory therapies.
These two large prevention studies were “prompted” by the results of small, proof-of-concept pilot studies, which “provided strong efficacy signals for the hypothesis that daily emollient use could prevent atopic dermatitis,” they wrote. But the two studies “found no evidence that daily emollient use in either a population-based or high-risk cohort of infants during the first year of life could delay, suppress, or prevent atopic dermatitis.” The lower incidence of atopic dermatitis among those in the dietary and emollient combination, compared with controls (5% vs. 8%) in PreventADALL, could be a chance finding.
The large, randomized Prevention of Eczema by a Barrier Lipid Equilibrium Strategy (PEBBLES) trial is ongoing to confirm results from a small study suggesting the efficacy of a ceramide-dominant emollient. But the PreventADALL study showed low compliance, suggesting that this intervention, if effective, a twice-daily emollient regimen may be tough to implement. “At this stage, emollients should not be recommended for the primary prevention of atopic dermatitis in infants,” they concluded.
Dr. Perrett and Dr. Peters declared no competing interests. Their comments appeared in the Lancet (2020 Feb 19. doi: 10.1016/S0140-6736[19]33174-5).
The use of including those at high risk, in two new clinical trials.
The BEEP (Barrier Enhancement for Eczema Prevention) study compared the rates of AD among infants identified as at risk of AD because of family history who had daily applications of emollients (Diprobase cream or Doublebase gel) for the first year of life, compared with a standard skin care group. PreventADALL (Preventing Atopic Dermatitis and Allergies in Children) is a randomized, primary-prevention study conducted in Norway and Sweden that randomized infants into one of four groups: controls whose parents followed regular skin care advice and nutrition guidelines; those who received skin emollients (the addition of emulsified oil to their bath and application of facial cream on at least 4 days a week from age 2 weeks to 8 months); those who received early complementary feeding of peanut, cow’s milk, wheat, and egg introduced between aged 12 and 16 weeks; and a group that combined both the emollient and diet interventions.
Neither of the studies, published in the Lancet, found statistically significant differences in AD rates between the intervention and control groups.
The results put a damper on hopes raised by previous studies that included two small pilot studies, which found that daily use of leave-on emollients in infants considered at high risk of AD prevented the development of AD (J Allergy Clin Immunol 2014 Oct;134:824-30.e6; J Allergy Clin Immunol Oct 2014;134:818-23).
“It was maybe a little bit overly hopeful to think that we could just moisturize and prevent such a complex disorder,” Robert Sidbury, MD, chief of dermatology at Seattle Children’s Hospital, said in an interview. He emphasized that the studies only addressed emollients as a preventative, and that “there’s no question that emollients are still critical for the therapy of eczema.”
Bruce Brod, MD, clinical professor of dermatology at the University of Pennsylvania, Philadelphia, suggested that homogeneous patient populations or insufficient numbers might explain the negative findings. PreventADALL drew patients from Norway and Sweden, while BEEP recruited from the United Kingdom. “They’re important studies, but I think they still lend themselves to further studies with different patient populations and larger groups of patients,” Dr. Brod said in an interview.
BEEP was headed by Joanne Chalmers, PhD, and Hywel Williams, DSc, of the Centre of Evidence-Based Dermatology at the University of Nottingham (England). Håvard Ove Skjerven, PhD, and Karin C Lødrup Carlsen, PhD, of Oslo University Hospital led the PreventADALL study.
The BEEP study randomized 1,394 newborns at 16 sites in the United Kingdom to daily emollient treatment with standard skin care, or standard skin care alone. At one year, compliance was 74% in the intervention group. At age 2, 23% of the intervention group had AD, compared with 25% of controls (hazard ratio, 0.95; P =.61). Skin infections were also higher in the treatment arm (mean, 0.23 per year vs. 0.15 per year; adjusted incidence ratio, 1.55; 95% confidence interval, 1.15-2.09).
“Our study does not support the use of emollients for preventing eczema in high-risk infants, a finding supported by PreventADALL, another large trial using a skin barrier enhancing intervention,” they concluded. Their data “relate only to prevention of eczema and do not directly challenge the practice of using emollients as first-line treatment for eczema.”
In the PreventADALL study, 2,397 newborn infants born between 2015 and 2017 were randomized to one of the four groups. Use of facial cream and emollients during bathing began at 2 weeks, and early complementary feeding of peanut, cow’s milk, wheat, and egg at 3-4 months. The frequency of AD at aged 12 months in the control group was 8%, compared with 11% in the skin-intervention group, 9% in the food-intervention group, and 5% in the combined-intervention group.
These differences were not statistically significant, and “the primary hypothesis that either skin intervention or food intervention reduced atopic dermatitis were not confirmed,” the authors wrote. Parental atopy did not influence the effects of the interventions. Their results were in line with the BEEP results, and the authors “cannot recommend these interventions as primary prevention strategies.”
The researchers will continue to follow children until age 3 years to evaluate the food allergy rates, if the combined-treatment group experiences a long-term benefit. Adherence to the protocol was poor, with 44% compliance with the facial cream application and 27% compliance with bathing emollients; 32% fully adhered to the diet protocols.
The studies were funded by the National Institute for Health Research Health Technology Assessment (BEEP); and a range of public and private funders (PreventADALL). One author of the PreventADALL study disclosed receiving honoraria for presentations from several pharmaceutical companies, and one author received honoraria for presentations from Thermo Fisher Scientific; the rest had no disclosures. Dr. Sidbury has been an investigator for Regeneron. Dr. Brod had no relevant financial disclosures.
SOURCES: Chalmers JR et al. Lancet. 2020 Feb 19. doi: 10.1016/S0140-6736(19)32984-8; Skjerven HO et al. Lancet. 2020 Feb 19. doi: 10.1016/S0140-6736(19)32983-6.
The use of including those at high risk, in two new clinical trials.
The BEEP (Barrier Enhancement for Eczema Prevention) study compared the rates of AD among infants identified as at risk of AD because of family history who had daily applications of emollients (Diprobase cream or Doublebase gel) for the first year of life, compared with a standard skin care group. PreventADALL (Preventing Atopic Dermatitis and Allergies in Children) is a randomized, primary-prevention study conducted in Norway and Sweden that randomized infants into one of four groups: controls whose parents followed regular skin care advice and nutrition guidelines; those who received skin emollients (the addition of emulsified oil to their bath and application of facial cream on at least 4 days a week from age 2 weeks to 8 months); those who received early complementary feeding of peanut, cow’s milk, wheat, and egg introduced between aged 12 and 16 weeks; and a group that combined both the emollient and diet interventions.
Neither of the studies, published in the Lancet, found statistically significant differences in AD rates between the intervention and control groups.
The results put a damper on hopes raised by previous studies that included two small pilot studies, which found that daily use of leave-on emollients in infants considered at high risk of AD prevented the development of AD (J Allergy Clin Immunol 2014 Oct;134:824-30.e6; J Allergy Clin Immunol Oct 2014;134:818-23).
“It was maybe a little bit overly hopeful to think that we could just moisturize and prevent such a complex disorder,” Robert Sidbury, MD, chief of dermatology at Seattle Children’s Hospital, said in an interview. He emphasized that the studies only addressed emollients as a preventative, and that “there’s no question that emollients are still critical for the therapy of eczema.”
Bruce Brod, MD, clinical professor of dermatology at the University of Pennsylvania, Philadelphia, suggested that homogeneous patient populations or insufficient numbers might explain the negative findings. PreventADALL drew patients from Norway and Sweden, while BEEP recruited from the United Kingdom. “They’re important studies, but I think they still lend themselves to further studies with different patient populations and larger groups of patients,” Dr. Brod said in an interview.
BEEP was headed by Joanne Chalmers, PhD, and Hywel Williams, DSc, of the Centre of Evidence-Based Dermatology at the University of Nottingham (England). Håvard Ove Skjerven, PhD, and Karin C Lødrup Carlsen, PhD, of Oslo University Hospital led the PreventADALL study.
The BEEP study randomized 1,394 newborns at 16 sites in the United Kingdom to daily emollient treatment with standard skin care, or standard skin care alone. At one year, compliance was 74% in the intervention group. At age 2, 23% of the intervention group had AD, compared with 25% of controls (hazard ratio, 0.95; P =.61). Skin infections were also higher in the treatment arm (mean, 0.23 per year vs. 0.15 per year; adjusted incidence ratio, 1.55; 95% confidence interval, 1.15-2.09).
“Our study does not support the use of emollients for preventing eczema in high-risk infants, a finding supported by PreventADALL, another large trial using a skin barrier enhancing intervention,” they concluded. Their data “relate only to prevention of eczema and do not directly challenge the practice of using emollients as first-line treatment for eczema.”
In the PreventADALL study, 2,397 newborn infants born between 2015 and 2017 were randomized to one of the four groups. Use of facial cream and emollients during bathing began at 2 weeks, and early complementary feeding of peanut, cow’s milk, wheat, and egg at 3-4 months. The frequency of AD at aged 12 months in the control group was 8%, compared with 11% in the skin-intervention group, 9% in the food-intervention group, and 5% in the combined-intervention group.
These differences were not statistically significant, and “the primary hypothesis that either skin intervention or food intervention reduced atopic dermatitis were not confirmed,” the authors wrote. Parental atopy did not influence the effects of the interventions. Their results were in line with the BEEP results, and the authors “cannot recommend these interventions as primary prevention strategies.”
The researchers will continue to follow children until age 3 years to evaluate the food allergy rates, if the combined-treatment group experiences a long-term benefit. Adherence to the protocol was poor, with 44% compliance with the facial cream application and 27% compliance with bathing emollients; 32% fully adhered to the diet protocols.
The studies were funded by the National Institute for Health Research Health Technology Assessment (BEEP); and a range of public and private funders (PreventADALL). One author of the PreventADALL study disclosed receiving honoraria for presentations from several pharmaceutical companies, and one author received honoraria for presentations from Thermo Fisher Scientific; the rest had no disclosures. Dr. Sidbury has been an investigator for Regeneron. Dr. Brod had no relevant financial disclosures.
SOURCES: Chalmers JR et al. Lancet. 2020 Feb 19. doi: 10.1016/S0140-6736(19)32984-8; Skjerven HO et al. Lancet. 2020 Feb 19. doi: 10.1016/S0140-6736(19)32983-6.
FROM THE LANCET
Nail growth

The treatment failure with the terbinafine made onychomycosis unlikely, and the appearance of the finger did not suggest that this was a wart. So, the physician opted for a 4-mm punch biopsy of the lateral nail fold, which confirmed that this was a well-differentiated squamous cell carcinoma (SCC) of the fingertip.
Periungual SCC is twice as common in men as women. Lesions tend to appear as hyperkeratotic plaques or nodules, pushing the nail plate away from the nail bed. With onychomycosis, one would expect the nail to be more thickened and discolored. A wart would not be as keratotic as this lesion was, and there would be thrombosed capillaries on closer inspection.
SCC is the second most common skin cancer in humans. It is most common on sun-exposed areas but may present in sites not exposed to the sun. It has been hypothesized that high risk human papillomavirus (HPV) types—particularly HPV 16—may contribute to diseases of the fingertips and nail unit in older adults. (There was no known history of HPV in this patient.)
A surgical approach often is curative. Achieving appropriate margins occasionally requires partial amputation. Mohs micrographic surgery (MMS) offers the highest cure rate and spares as much uninvolved tissue as possible. Radiation therapy is another tissue-sparing technique. It requires 15 to 30 sessions over 3 to 6 weeks and has a lower cure rate than MMS.
In this case, the patient underwent MMS. Follow-up skin surveillance exams revealed other small nonmelanoma skin cancers at other sites. The patient also developed a dystrophic nail spicule near the surgical site that was re-excised and deemed benign.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
Riddel C, Rashid R, Thomas V. Ungual and periungual human papillomavirus-associated squamous cell carcinoma: a review. J Am Acad Dermatol. 2011 Jun;64:1147-1153.
The treatment failure with the terbinafine made onychomycosis unlikely, and the appearance of the finger did not suggest that this was a wart. So, the physician opted for a 4-mm punch biopsy of the lateral nail fold, which confirmed that this was a well-differentiated squamous cell carcinoma (SCC) of the fingertip.
Periungual SCC is twice as common in men as women. Lesions tend to appear as hyperkeratotic plaques or nodules, pushing the nail plate away from the nail bed. With onychomycosis, one would expect the nail to be more thickened and discolored. A wart would not be as keratotic as this lesion was, and there would be thrombosed capillaries on closer inspection.
SCC is the second most common skin cancer in humans. It is most common on sun-exposed areas but may present in sites not exposed to the sun. It has been hypothesized that high risk human papillomavirus (HPV) types—particularly HPV 16—may contribute to diseases of the fingertips and nail unit in older adults. (There was no known history of HPV in this patient.)
A surgical approach often is curative. Achieving appropriate margins occasionally requires partial amputation. Mohs micrographic surgery (MMS) offers the highest cure rate and spares as much uninvolved tissue as possible. Radiation therapy is another tissue-sparing technique. It requires 15 to 30 sessions over 3 to 6 weeks and has a lower cure rate than MMS.
In this case, the patient underwent MMS. Follow-up skin surveillance exams revealed other small nonmelanoma skin cancers at other sites. The patient also developed a dystrophic nail spicule near the surgical site that was re-excised and deemed benign.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
The treatment failure with the terbinafine made onychomycosis unlikely, and the appearance of the finger did not suggest that this was a wart. So, the physician opted for a 4-mm punch biopsy of the lateral nail fold, which confirmed that this was a well-differentiated squamous cell carcinoma (SCC) of the fingertip.
Periungual SCC is twice as common in men as women. Lesions tend to appear as hyperkeratotic plaques or nodules, pushing the nail plate away from the nail bed. With onychomycosis, one would expect the nail to be more thickened and discolored. A wart would not be as keratotic as this lesion was, and there would be thrombosed capillaries on closer inspection.
SCC is the second most common skin cancer in humans. It is most common on sun-exposed areas but may present in sites not exposed to the sun. It has been hypothesized that high risk human papillomavirus (HPV) types—particularly HPV 16—may contribute to diseases of the fingertips and nail unit in older adults. (There was no known history of HPV in this patient.)
A surgical approach often is curative. Achieving appropriate margins occasionally requires partial amputation. Mohs micrographic surgery (MMS) offers the highest cure rate and spares as much uninvolved tissue as possible. Radiation therapy is another tissue-sparing technique. It requires 15 to 30 sessions over 3 to 6 weeks and has a lower cure rate than MMS.
In this case, the patient underwent MMS. Follow-up skin surveillance exams revealed other small nonmelanoma skin cancers at other sites. The patient also developed a dystrophic nail spicule near the surgical site that was re-excised and deemed benign.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
Riddel C, Rashid R, Thomas V. Ungual and periungual human papillomavirus-associated squamous cell carcinoma: a review. J Am Acad Dermatol. 2011 Jun;64:1147-1153.
Riddel C, Rashid R, Thomas V. Ungual and periungual human papillomavirus-associated squamous cell carcinoma: a review. J Am Acad Dermatol. 2011 Jun;64:1147-1153.

Loneliness, social isolation in seniors need urgent attention
Health care systems need to take urgent action to address social isolation and loneliness among U.S. seniors, experts say.
A new report from the National Academies of Sciences, Engineering, and Medicine (NAS) points out that social isolation in this population is a major public health concern that contributes to heart disease, depression, and premature death.
The report authors note that the health care system remains an underused partner in preventing, identifying, and intervening in social isolation and loneliness among adults over age 50.
For seniors who are homebound, have no family, or do not belong to community or faith groups, a medical appointment or home health visit may be one of the few social interactions they have, the report notes.
Health care providers and systems may be “first responders” in recognizing lonely or socially isolated patients, committee chair Dan Blazer, MD, from Duke University School of Medicine, Durham, N.C., said during a press briefing.
As deadly as obesity, smoking
Committee member Julianne Holt-Lunstad, PhD, from Brigham Young University, Provo, Utah, noted that social isolation and loneliness are “distinctly different.”
Social isolation is defined as an objective lack of (or limited) social connections, while loneliness is a subjective perception of social isolation or the subjective feeling of being lonely.
Not all older adults are isolated or lonely, but they are more likely to face predisposing factors such as living alone and the loss of loved ones, she explained.
The issue may be compounded for LGBT, minority, and immigrant older adults, who may already face barriers to care, stigma, and discrimination. Social isolation and loneliness may also directly stem from chronic illness, hearing or vision loss, or mobility issues. In these cases, health care providers might be able to help prevent or reduce social isolation and loneliness by directly addressing the underlying health-related causes.
Holt-Lunstad told the briefing. The report offers a vision for how the health care system can identify people at risk of social isolation and loneliness, intervene, and engage other community partners.
It recommends that providers use validated tools to periodically assess patients who may be at risk for social isolation and loneliness and connect them to community resources for help.
The report also calls for greater education and training among health providers. Schools of health professions and training programs for direct care workers (eg, home health aides, nurse aides, and personal care aides) should incorporate social isolation and loneliness in their curricula, the report says.
It also offers recommendations for leveraging digital health and health technology, improving community partnerships, increasing funding for research, and creation of a national resource center under the Department of Health and Human Services.
Blazer said there remains “much to be learned” about what approaches to mitigating social isolation and loneliness work best in which populations.
The report, from the Committee on the Health and Medical Dimensions of Social Isolation and Loneliness in Older Adults, was sponsored by the AARP Foundation.
This article first appeared on Medscape.com.
Health care systems need to take urgent action to address social isolation and loneliness among U.S. seniors, experts say.
A new report from the National Academies of Sciences, Engineering, and Medicine (NAS) points out that social isolation in this population is a major public health concern that contributes to heart disease, depression, and premature death.
The report authors note that the health care system remains an underused partner in preventing, identifying, and intervening in social isolation and loneliness among adults over age 50.
For seniors who are homebound, have no family, or do not belong to community or faith groups, a medical appointment or home health visit may be one of the few social interactions they have, the report notes.
Health care providers and systems may be “first responders” in recognizing lonely or socially isolated patients, committee chair Dan Blazer, MD, from Duke University School of Medicine, Durham, N.C., said during a press briefing.
As deadly as obesity, smoking
Committee member Julianne Holt-Lunstad, PhD, from Brigham Young University, Provo, Utah, noted that social isolation and loneliness are “distinctly different.”
Social isolation is defined as an objective lack of (or limited) social connections, while loneliness is a subjective perception of social isolation or the subjective feeling of being lonely.
Not all older adults are isolated or lonely, but they are more likely to face predisposing factors such as living alone and the loss of loved ones, she explained.
The issue may be compounded for LGBT, minority, and immigrant older adults, who may already face barriers to care, stigma, and discrimination. Social isolation and loneliness may also directly stem from chronic illness, hearing or vision loss, or mobility issues. In these cases, health care providers might be able to help prevent or reduce social isolation and loneliness by directly addressing the underlying health-related causes.
Holt-Lunstad told the briefing. The report offers a vision for how the health care system can identify people at risk of social isolation and loneliness, intervene, and engage other community partners.
It recommends that providers use validated tools to periodically assess patients who may be at risk for social isolation and loneliness and connect them to community resources for help.
The report also calls for greater education and training among health providers. Schools of health professions and training programs for direct care workers (eg, home health aides, nurse aides, and personal care aides) should incorporate social isolation and loneliness in their curricula, the report says.
It also offers recommendations for leveraging digital health and health technology, improving community partnerships, increasing funding for research, and creation of a national resource center under the Department of Health and Human Services.
Blazer said there remains “much to be learned” about what approaches to mitigating social isolation and loneliness work best in which populations.
The report, from the Committee on the Health and Medical Dimensions of Social Isolation and Loneliness in Older Adults, was sponsored by the AARP Foundation.
This article first appeared on Medscape.com.
Health care systems need to take urgent action to address social isolation and loneliness among U.S. seniors, experts say.
A new report from the National Academies of Sciences, Engineering, and Medicine (NAS) points out that social isolation in this population is a major public health concern that contributes to heart disease, depression, and premature death.
The report authors note that the health care system remains an underused partner in preventing, identifying, and intervening in social isolation and loneliness among adults over age 50.
For seniors who are homebound, have no family, or do not belong to community or faith groups, a medical appointment or home health visit may be one of the few social interactions they have, the report notes.
Health care providers and systems may be “first responders” in recognizing lonely or socially isolated patients, committee chair Dan Blazer, MD, from Duke University School of Medicine, Durham, N.C., said during a press briefing.
As deadly as obesity, smoking
Committee member Julianne Holt-Lunstad, PhD, from Brigham Young University, Provo, Utah, noted that social isolation and loneliness are “distinctly different.”
Social isolation is defined as an objective lack of (or limited) social connections, while loneliness is a subjective perception of social isolation or the subjective feeling of being lonely.
Not all older adults are isolated or lonely, but they are more likely to face predisposing factors such as living alone and the loss of loved ones, she explained.
The issue may be compounded for LGBT, minority, and immigrant older adults, who may already face barriers to care, stigma, and discrimination. Social isolation and loneliness may also directly stem from chronic illness, hearing or vision loss, or mobility issues. In these cases, health care providers might be able to help prevent or reduce social isolation and loneliness by directly addressing the underlying health-related causes.
Holt-Lunstad told the briefing. The report offers a vision for how the health care system can identify people at risk of social isolation and loneliness, intervene, and engage other community partners.
It recommends that providers use validated tools to periodically assess patients who may be at risk for social isolation and loneliness and connect them to community resources for help.
The report also calls for greater education and training among health providers. Schools of health professions and training programs for direct care workers (eg, home health aides, nurse aides, and personal care aides) should incorporate social isolation and loneliness in their curricula, the report says.
It also offers recommendations for leveraging digital health and health technology, improving community partnerships, increasing funding for research, and creation of a national resource center under the Department of Health and Human Services.
Blazer said there remains “much to be learned” about what approaches to mitigating social isolation and loneliness work best in which populations.
The report, from the Committee on the Health and Medical Dimensions of Social Isolation and Loneliness in Older Adults, was sponsored by the AARP Foundation.
This article first appeared on Medscape.com.
Combined biopsy method improves diagnostic accuracy in prostate cancer
among men with MRI-visible lesions in a single-center study.
Compared with either method alone, a combination of the two biopsy methods resulted in 9.9% more prostate cancer diagnoses, explained study author Michael Ahdoot, MD, of the National Institutes of Health and colleagues. Their report was published in the New England Journal of Medicine.
“With the addition of MRI-targeted biopsy to systematic biopsy, we may have entered an era of increased diagnostic certainty in prostate cancer,” the researchers wrote.
Their single-center, comparative diagnostic study included 2,103 patients with MRI-visible prostate lesions who underwent both systematic and MRI-targeted biopsy. In cases of multiple biopsies, only the results of the initial biopsies were included.
Each individual specimen was assigned a Gleason score by a genitourinary pathologist and was subsequently categorized into a grade group on a scale of 1-5, with higher scores reflecting greater cancer risk. Grade group 1 was defined as clinically insignificant disease. Grade group 2 was defined as favorable intermediate-risk disease. Grade group 3 or higher was defined as unfavorable intermediate-risk disease or worse.
The primary endpoints were cancer detection rates for each biopsy method, based on grade group. “Among the men who underwent subsequent radical prostatectomy, upgrading and downgrading of grade group from biopsy to whole-mount histopathological analysis of surgical specimens [was also assessed],” the researchers explained.
Among patients who underwent combined biopsy, prostate cancer was identified in 62.4% of patients, and 19.2% underwent radical prostatectomy.
For grade groups 3-5, rates of cancer detection were significantly higher with MRI-targeted biopsy than with systematic biopsy (P less than .01 for all). For grade group 1, detection rates were significantly lower with MRI-targeted biopsy (P less than .01).
“Although many of [the] benefits resulted from MRI-targeted biopsy alone, omission of systematic biopsy would have led to missing the diagnosis of 8.8% of clinically significant cancers,” the researchers reported.
In addition, among patients who underwent radical prostatectomy, the rates of upgrading (grade group 3 or higher) on histopathological analysis were lower for combined biopsy (3.5%) than for MRI-targeted biopsy (8.7%) and systematic biopsy (16.8%).
The researchers acknowledged that a key limitation of this study was the single-center design. As a result, the findings may not be generalizable to other institutions.
However, the researchers concluded that “these findings suggest that combined biopsy provides improved diagnostic accuracy over either systematic or MRI-targeted biopsy alone and better predicts the results of final histopathological analysis.”
The study was funded by the National Institutes of Health, Philips, and the Dr. Mildred Scheel Foundation for Cancer Research. The authors disclosed financial affiliations with Philips, Biocompatibles UK, Boston Scientific, Celsion, and other companies.
SOURCE: Ahdoot M et al. N Engl J Med. 2020 Mar 4. doi: 10.1056/NEJMoa1910038.
among men with MRI-visible lesions in a single-center study.
Compared with either method alone, a combination of the two biopsy methods resulted in 9.9% more prostate cancer diagnoses, explained study author Michael Ahdoot, MD, of the National Institutes of Health and colleagues. Their report was published in the New England Journal of Medicine.
“With the addition of MRI-targeted biopsy to systematic biopsy, we may have entered an era of increased diagnostic certainty in prostate cancer,” the researchers wrote.
Their single-center, comparative diagnostic study included 2,103 patients with MRI-visible prostate lesions who underwent both systematic and MRI-targeted biopsy. In cases of multiple biopsies, only the results of the initial biopsies were included.
Each individual specimen was assigned a Gleason score by a genitourinary pathologist and was subsequently categorized into a grade group on a scale of 1-5, with higher scores reflecting greater cancer risk. Grade group 1 was defined as clinically insignificant disease. Grade group 2 was defined as favorable intermediate-risk disease. Grade group 3 or higher was defined as unfavorable intermediate-risk disease or worse.
The primary endpoints were cancer detection rates for each biopsy method, based on grade group. “Among the men who underwent subsequent radical prostatectomy, upgrading and downgrading of grade group from biopsy to whole-mount histopathological analysis of surgical specimens [was also assessed],” the researchers explained.
Among patients who underwent combined biopsy, prostate cancer was identified in 62.4% of patients, and 19.2% underwent radical prostatectomy.
For grade groups 3-5, rates of cancer detection were significantly higher with MRI-targeted biopsy than with systematic biopsy (P less than .01 for all). For grade group 1, detection rates were significantly lower with MRI-targeted biopsy (P less than .01).
“Although many of [the] benefits resulted from MRI-targeted biopsy alone, omission of systematic biopsy would have led to missing the diagnosis of 8.8% of clinically significant cancers,” the researchers reported.
In addition, among patients who underwent radical prostatectomy, the rates of upgrading (grade group 3 or higher) on histopathological analysis were lower for combined biopsy (3.5%) than for MRI-targeted biopsy (8.7%) and systematic biopsy (16.8%).
The researchers acknowledged that a key limitation of this study was the single-center design. As a result, the findings may not be generalizable to other institutions.
However, the researchers concluded that “these findings suggest that combined biopsy provides improved diagnostic accuracy over either systematic or MRI-targeted biopsy alone and better predicts the results of final histopathological analysis.”
The study was funded by the National Institutes of Health, Philips, and the Dr. Mildred Scheel Foundation for Cancer Research. The authors disclosed financial affiliations with Philips, Biocompatibles UK, Boston Scientific, Celsion, and other companies.
SOURCE: Ahdoot M et al. N Engl J Med. 2020 Mar 4. doi: 10.1056/NEJMoa1910038.
among men with MRI-visible lesions in a single-center study.
Compared with either method alone, a combination of the two biopsy methods resulted in 9.9% more prostate cancer diagnoses, explained study author Michael Ahdoot, MD, of the National Institutes of Health and colleagues. Their report was published in the New England Journal of Medicine.
“With the addition of MRI-targeted biopsy to systematic biopsy, we may have entered an era of increased diagnostic certainty in prostate cancer,” the researchers wrote.
Their single-center, comparative diagnostic study included 2,103 patients with MRI-visible prostate lesions who underwent both systematic and MRI-targeted biopsy. In cases of multiple biopsies, only the results of the initial biopsies were included.
Each individual specimen was assigned a Gleason score by a genitourinary pathologist and was subsequently categorized into a grade group on a scale of 1-5, with higher scores reflecting greater cancer risk. Grade group 1 was defined as clinically insignificant disease. Grade group 2 was defined as favorable intermediate-risk disease. Grade group 3 or higher was defined as unfavorable intermediate-risk disease or worse.
The primary endpoints were cancer detection rates for each biopsy method, based on grade group. “Among the men who underwent subsequent radical prostatectomy, upgrading and downgrading of grade group from biopsy to whole-mount histopathological analysis of surgical specimens [was also assessed],” the researchers explained.
Among patients who underwent combined biopsy, prostate cancer was identified in 62.4% of patients, and 19.2% underwent radical prostatectomy.
For grade groups 3-5, rates of cancer detection were significantly higher with MRI-targeted biopsy than with systematic biopsy (P less than .01 for all). For grade group 1, detection rates were significantly lower with MRI-targeted biopsy (P less than .01).
“Although many of [the] benefits resulted from MRI-targeted biopsy alone, omission of systematic biopsy would have led to missing the diagnosis of 8.8% of clinically significant cancers,” the researchers reported.
In addition, among patients who underwent radical prostatectomy, the rates of upgrading (grade group 3 or higher) on histopathological analysis were lower for combined biopsy (3.5%) than for MRI-targeted biopsy (8.7%) and systematic biopsy (16.8%).
The researchers acknowledged that a key limitation of this study was the single-center design. As a result, the findings may not be generalizable to other institutions.
However, the researchers concluded that “these findings suggest that combined biopsy provides improved diagnostic accuracy over either systematic or MRI-targeted biopsy alone and better predicts the results of final histopathological analysis.”
The study was funded by the National Institutes of Health, Philips, and the Dr. Mildred Scheel Foundation for Cancer Research. The authors disclosed financial affiliations with Philips, Biocompatibles UK, Boston Scientific, Celsion, and other companies.
SOURCE: Ahdoot M et al. N Engl J Med. 2020 Mar 4. doi: 10.1056/NEJMoa1910038.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Combining magnetic resonance imaging (MRI)–targeted and systematic biopsy improved detection of prostate cancer in patients with MRI-visible lesions.
Major finding: When compared with either method alone, combining the methods resulted in 9.9% more prostate cancer diagnoses.
Study details: A comparative diagnostic study of 2,103 men with MRI-visible prostate lesions.
Disclosures: The study was funded by the National Institutes of Health, Philips, and the Dr. Mildred Scheel Foundation for Cancer Research. The authors disclosed financial affiliations with Philips, Biocompatibles UK, Boston Scientific, Celsion, and other companies.
Source: Ahdoot M et al. N Engl J Med. 2020 Mar 4. doi: 10.1056/NEJMoa1910038.
Survey: 2020 will see more attacks on ACA
When physicians gaze into their crystal balls to predict what’s coming in 2020, they see continued efforts to defund the Affordable Care Act – meaning the ACA will still be around to be defunded – but they don’t see a lot of support for universal health care, according to health care market research company InCrowd.
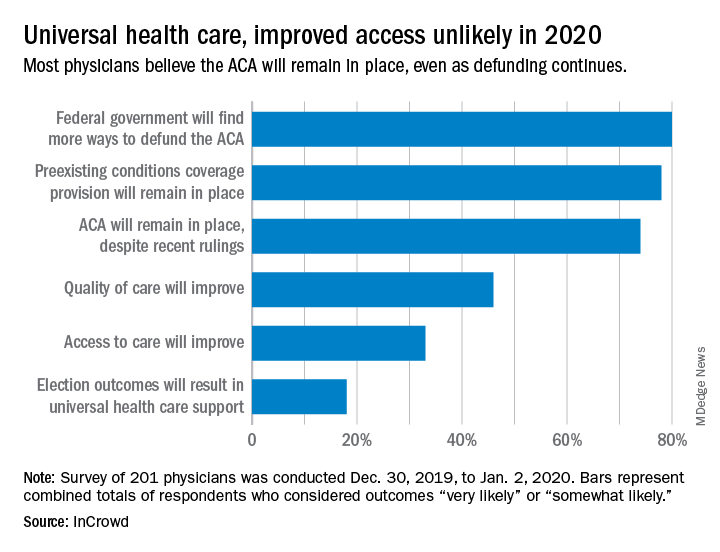
Expectations for universal health care came in at 18% of the 100 generalists and 101 specialists who responded to InCrowd’s fifth annual health care predictions survey, which left 82% who thought that “election outcomes will result in universal healthcare support” was somewhat or very unlikely in 2020.
One respondent, a specialist from California, commented that “the global data on universal healthcare for all shows that it results in overall improved population health. Unfortunately, we are so polarized in the US against universal healthcare driven by bias from health insurance companies and decision makers that are quick to ignore scientific data.”
This was the first time InCrowd asked physicians about universal health care, but ACA-related predictions have been included before, and all three scenarios presented were deemed to be increasingly likely, compared with 2019.
Respondents thought that federal government defunding was more likely to occur in 2020 (80%) than in 2019 (73%), but increased majorities also said that preexisting conditions coverage would continue (78% in 2020 vs. 70% in 2019) and that the ACA would remain in place (74% in 2020 vs. 60% in 2019), InCrowd reported after the survey, which was conducted from Dec. 30, 2019, to Jan. 2, 2020.
A respondent who thought the ACA will be eliminated said, “I have as many uninsured today as before the ACA. They are just different. Mainly younger patients who spend less in a year on healthcare than one month’s premium.” Another suggested that eliminateing it “will limit access to care and overload [emergency departments]. More people will die.”
Cost was addressed in a separate survey question that asked how physicians could help to reduce health care spending in 2020.
The leading answer, given by 37% of respondents, was for physicians to “inform themselves of costs and adapt cost-saving prescription practices.” Next came “limit use of expensive tests and scans” with 21%, followed by “prescribe generics when possible” at 20%, which was a substantial drop from the 38% it garnered in 2019, InCrowd noted.
“Participation in [shared savings] programs and risk-based incentive programs and pay-for-performance programs” would provide “better stewardship of resources,” a primary care physician from Michigan wrote.
When the survey turned to pharmaceutical industry predictions for 2020, cost was the major issue.
“What’s interesting about this year’s data is that we’re seeing less emphasis on the importance of bringing innovative, new therapies to market faster … versus expanding affordability, which was nearly a unanimous top priority for respondents,” Daniel S. Fitzgerald, InCrowd’s CEO and president, said in a separate statement.
When physicians gaze into their crystal balls to predict what’s coming in 2020, they see continued efforts to defund the Affordable Care Act – meaning the ACA will still be around to be defunded – but they don’t see a lot of support for universal health care, according to health care market research company InCrowd.
Expectations for universal health care came in at 18% of the 100 generalists and 101 specialists who responded to InCrowd’s fifth annual health care predictions survey, which left 82% who thought that “election outcomes will result in universal healthcare support” was somewhat or very unlikely in 2020.
One respondent, a specialist from California, commented that “the global data on universal healthcare for all shows that it results in overall improved population health. Unfortunately, we are so polarized in the US against universal healthcare driven by bias from health insurance companies and decision makers that are quick to ignore scientific data.”
This was the first time InCrowd asked physicians about universal health care, but ACA-related predictions have been included before, and all three scenarios presented were deemed to be increasingly likely, compared with 2019.
Respondents thought that federal government defunding was more likely to occur in 2020 (80%) than in 2019 (73%), but increased majorities also said that preexisting conditions coverage would continue (78% in 2020 vs. 70% in 2019) and that the ACA would remain in place (74% in 2020 vs. 60% in 2019), InCrowd reported after the survey, which was conducted from Dec. 30, 2019, to Jan. 2, 2020.
A respondent who thought the ACA will be eliminated said, “I have as many uninsured today as before the ACA. They are just different. Mainly younger patients who spend less in a year on healthcare than one month’s premium.” Another suggested that eliminateing it “will limit access to care and overload [emergency departments]. More people will die.”
Cost was addressed in a separate survey question that asked how physicians could help to reduce health care spending in 2020.
The leading answer, given by 37% of respondents, was for physicians to “inform themselves of costs and adapt cost-saving prescription practices.” Next came “limit use of expensive tests and scans” with 21%, followed by “prescribe generics when possible” at 20%, which was a substantial drop from the 38% it garnered in 2019, InCrowd noted.
“Participation in [shared savings] programs and risk-based incentive programs and pay-for-performance programs” would provide “better stewardship of resources,” a primary care physician from Michigan wrote.
When the survey turned to pharmaceutical industry predictions for 2020, cost was the major issue.
“What’s interesting about this year’s data is that we’re seeing less emphasis on the importance of bringing innovative, new therapies to market faster … versus expanding affordability, which was nearly a unanimous top priority for respondents,” Daniel S. Fitzgerald, InCrowd’s CEO and president, said in a separate statement.
When physicians gaze into their crystal balls to predict what’s coming in 2020, they see continued efforts to defund the Affordable Care Act – meaning the ACA will still be around to be defunded – but they don’t see a lot of support for universal health care, according to health care market research company InCrowd.
Expectations for universal health care came in at 18% of the 100 generalists and 101 specialists who responded to InCrowd’s fifth annual health care predictions survey, which left 82% who thought that “election outcomes will result in universal healthcare support” was somewhat or very unlikely in 2020.
One respondent, a specialist from California, commented that “the global data on universal healthcare for all shows that it results in overall improved population health. Unfortunately, we are so polarized in the US against universal healthcare driven by bias from health insurance companies and decision makers that are quick to ignore scientific data.”
This was the first time InCrowd asked physicians about universal health care, but ACA-related predictions have been included before, and all three scenarios presented were deemed to be increasingly likely, compared with 2019.
Respondents thought that federal government defunding was more likely to occur in 2020 (80%) than in 2019 (73%), but increased majorities also said that preexisting conditions coverage would continue (78% in 2020 vs. 70% in 2019) and that the ACA would remain in place (74% in 2020 vs. 60% in 2019), InCrowd reported after the survey, which was conducted from Dec. 30, 2019, to Jan. 2, 2020.
A respondent who thought the ACA will be eliminated said, “I have as many uninsured today as before the ACA. They are just different. Mainly younger patients who spend less in a year on healthcare than one month’s premium.” Another suggested that eliminateing it “will limit access to care and overload [emergency departments]. More people will die.”
Cost was addressed in a separate survey question that asked how physicians could help to reduce health care spending in 2020.
The leading answer, given by 37% of respondents, was for physicians to “inform themselves of costs and adapt cost-saving prescription practices.” Next came “limit use of expensive tests and scans” with 21%, followed by “prescribe generics when possible” at 20%, which was a substantial drop from the 38% it garnered in 2019, InCrowd noted.
“Participation in [shared savings] programs and risk-based incentive programs and pay-for-performance programs” would provide “better stewardship of resources,” a primary care physician from Michigan wrote.
When the survey turned to pharmaceutical industry predictions for 2020, cost was the major issue.
“What’s interesting about this year’s data is that we’re seeing less emphasis on the importance of bringing innovative, new therapies to market faster … versus expanding affordability, which was nearly a unanimous top priority for respondents,” Daniel S. Fitzgerald, InCrowd’s CEO and president, said in a separate statement.
Is telerheumatology the future of rheumatology?
MAUI, HAWAII – Alvin F. Wells, MD, PhD, believes he’s seen the future of rheumatology. So he’s taken a deep dive into telerheumatology, going all in.

“Whether you’re in academic, private, or hospital-based practice, in 2020 if you are not thinking about telerheumatology, you and your practice will not be able to compete with growing patient demands, expectations, and need for clinical monitoring. If you do not have a digital/virtual strategy, you do not have a health care strategy,” he asserted at the 2020 Rheumatology Winter Clinical Symposium.
“Begin now,” the rheumatologist advised.
In pursuit of his own telerheumatology strategy, he holds licenses to practice medicine in five states and has licensure pending in five others.
“My goal is to cover 20% of the U.S., so if the local guys can’t see the patients, I can see them virtually,” he explained. “The days of waiting 4-6 months to be seen by a rheumatologist are gone.”
Rheumatologists are already in short supply in most of the country, and a major shortage looms ahead as older practitioners retire. Telerheumatology can help fill that unmet need. But the specialty is behind the curve. In a survey that rated the medical specialties most engaged in telemedicine, the top three spots were held by radiology, psychiatry, and internal medicine. Rheumatology didn’t even crack the top 10, noted Dr. Wells, director of the Rheumatology and Immunotherapy Center in Franklin, Wisc., and a part-time faculty member at Duke University, the Medical College of Wisconsin, and the Karolinska Institute.
Yet telemedicine is primed for rheumatologic takeoff. Notably, the 2019 update of the American College of Rheumatology recommendations on rheumatoid arthritis disease activity measures incorporates the RAPID3 (Routine Assessment of Patient Index Data) as an endorsed three-question clinical assessment that doesn’t involve a physical exam or laboratory work. The ACR update is recognition that, while every rheumatology patient needs an initial physical exam along with follow-up physical exams at various rates, many patients with well-controlled disease don’t need a physical exam at every physician encounter, he said.
Telerheumatology saves time for both patient and physician. The patient saves travel time, doesn’t miss work, avoids having to arrange for child care in order to make a face-to-face clinic visit, and can schedule more frequent virtual follow-up visits. For the practitioner, telerheumatology means additional consults and – here’s the big one – “You never run behind,” according to Dr. Wells. “For a 15-minute appointment, the patient gets a 5-minute warning, then a 2-minute warning, and at 15 minutes the link is cut. If the fibromyalgia patients want 30 minutes, they pay for 30 minutes.”
He sees the strictly enforced, impersonally delivered electronic time limits as key to running an efficient practice.
“The patients with osteoarthritis who hate the nodules, the fibromyalgia patients because they’re hurting all over, the patients with back pain – you’ve really got to limit those patients because otherwise you’ll be running 30-40 minutes behind for a scheduled 15-minute visit,” he explained.
One rheumatologist’s telemedicine practice
Dr. Wells currently utilizes the Epic electronic health record integrated with a Zoom videoconferencing platform for real-time virtual patient encounters. But he noted that other virtual platforms are available, including Health Tap, American Well, MySpecialistMD, MDLIVE, and TelaDoc. The American Telemedicine Association is a valuable resource for state-by-state medicolegal, reimbursement, and how-to-do-it questions.
At present, he reserves two daily time slots for telerheumatology: one at 8:30-9:00 a.m., the other at 4:30-5:00 p.m. These can be filled with four 15-minute live consults or two 30-minute consults. His goal is to eventually make telerheumatology 20% of his patient load of about 100 patients per week.
His typical 15-minute virtual visit proceeds as follows: It begins with a 3-minute subjective patient assessment, followed by a 5-minute objective assessment which includes the RAPID3, a brief Health Assessment Questionnaire (HAQ) addressing the patient’s pain and overall satisfaction, a virtual joint inspection, the use of high-quality teleultrasound and other technology when warranted, and capture of relevant still photos. This is followed by 5 minutes to relay the treatment plan, and finally a 2-minute recap and summary.
“No niceties. We cut right to the chase,” he noted.
He documents the patient encounter as he goes, dictating his notes throughout the visit.
“When I walk out of the room, I’m done. It’s on to the next patient,” Dr. Wells said.
The reimbursement picture is improving, although major hurdles remain. At present, 48 states and the District of Columbia reimburse for live video telemedicine through Medicaid. And in January 2020, Aetna announced it covers reimbursement for telemedicine in all of its fully insured health plans via the Teladoc platform. Dr. Wells’ patients pay for their telerheumatology out of pocket if their insurance doesn’t cover it.
Telemedicine caveats
Dr. Wells shared his telerheumatology experience as the first half of a point/counterpoint session on telemedicine’s future in the specialty. His debate opponent, Orrin M. Troum, MD, announced at the outset that he is quite interested in getting into telerheumatology; however, while looking into it he has come across issues that for now give him pause and that other rheumatologists need to be aware of.

Legal risks. The telemedicine movement has gotten big enough to draw the scrutiny of federal prosecutors and regulatory enforcement officials. In April 2018, the Department of Health & Human Services Office of the Inspector General (OIG) issued a report that concluded that one-third of all examined telemedicine claims were improper.
“Just imagine who might come knocking on your door,” he said.
Among the most common offenses, according to the OIG, were claims for services outside the limited range currently covered; lack of the requisite HIPAA-compliant two-way audio and visual communication technology with fully encrypted data transmission; services billed by institutional providers not defined by Medicare as telemedicine-eligible; and claims for services received by patients who weren’t located in an officially designated Health Professional Shortage Area or in a rural county as determined by the U.S. Census Bureau.
Telemedicine is no panacea for out-of-control health care costs. A RAND study of participants in the California Public Employees’ Retirement System (CalPERS) concluded that only 12% of beneficiaries who used direct-to-consumer telemedicine did so to replace provider visits. The other 88% added on telemedicine as an additional service. So while telemedicine increased patient access to health care, it also increased the overall cost, observed Dr. Troum, a rheumatologist at the University of Southern California, Los Angeles, and in private practice in Santa Monica, Calif.
Talk to your attorney and malpractice insurer before embarking on telerheumatology. Physicians could potentially lose their medical malpractice insurance if they use telemedicine to treat patients located in states where they aren’t licensed to practice, even if through inadvertent error.
Telemedicine isn’t appropriate for all patients. Nearly a decade ago, rheumatologists at Dartmouth-Hitchcock Medical Center launched a telerheumatology service in order to bring specialty care to the largely rural populations of New Hampshire and Vermont. In a review of the experience that included interviews with both patients and providers, investigators concluded that telerheumatology successfully increased access to specialty care in underserved locations and got good satisfaction scores from both providers and beneficiaries. However, fully 19% of patients were found to be inappropriate for their telerheumatology visit, mainly because their disease was too complex or the underlying diagnosis was unclear.
“Almost one-fifth of their patients were inappropriate for telerheumatology. The question is, how are you supposed to know that ahead of time?” Dr. Troum asked.
Patient satisfaction. Dr. Troum’s reading of the literature on patient satisfaction with telerheumatology, coupled with his own extensive experience in clinical practice, makes him think that many of his younger patients with less disease activity might welcome a telerheumatology option, even with strict time boundaries. But his older patients with more disease activity are a different story.
“Typically my middle-aged and older patients won’t accept that without a lot of convincing,” he commented.
Dr. Wells and Dr. Troum had no relevant disclosures regarding their presentations.
MAUI, HAWAII – Alvin F. Wells, MD, PhD, believes he’s seen the future of rheumatology. So he’s taken a deep dive into telerheumatology, going all in.
“Whether you’re in academic, private, or hospital-based practice, in 2020 if you are not thinking about telerheumatology, you and your practice will not be able to compete with growing patient demands, expectations, and need for clinical monitoring. If you do not have a digital/virtual strategy, you do not have a health care strategy,” he asserted at the 2020 Rheumatology Winter Clinical Symposium.
“Begin now,” the rheumatologist advised.
In pursuit of his own telerheumatology strategy, he holds licenses to practice medicine in five states and has licensure pending in five others.
“My goal is to cover 20% of the U.S., so if the local guys can’t see the patients, I can see them virtually,” he explained. “The days of waiting 4-6 months to be seen by a rheumatologist are gone.”
Rheumatologists are already in short supply in most of the country, and a major shortage looms ahead as older practitioners retire. Telerheumatology can help fill that unmet need. But the specialty is behind the curve. In a survey that rated the medical specialties most engaged in telemedicine, the top three spots were held by radiology, psychiatry, and internal medicine. Rheumatology didn’t even crack the top 10, noted Dr. Wells, director of the Rheumatology and Immunotherapy Center in Franklin, Wisc., and a part-time faculty member at Duke University, the Medical College of Wisconsin, and the Karolinska Institute.
Yet telemedicine is primed for rheumatologic takeoff. Notably, the 2019 update of the American College of Rheumatology recommendations on rheumatoid arthritis disease activity measures incorporates the RAPID3 (Routine Assessment of Patient Index Data) as an endorsed three-question clinical assessment that doesn’t involve a physical exam or laboratory work. The ACR update is recognition that, while every rheumatology patient needs an initial physical exam along with follow-up physical exams at various rates, many patients with well-controlled disease don’t need a physical exam at every physician encounter, he said.
Telerheumatology saves time for both patient and physician. The patient saves travel time, doesn’t miss work, avoids having to arrange for child care in order to make a face-to-face clinic visit, and can schedule more frequent virtual follow-up visits. For the practitioner, telerheumatology means additional consults and – here’s the big one – “You never run behind,” according to Dr. Wells. “For a 15-minute appointment, the patient gets a 5-minute warning, then a 2-minute warning, and at 15 minutes the link is cut. If the fibromyalgia patients want 30 minutes, they pay for 30 minutes.”
He sees the strictly enforced, impersonally delivered electronic time limits as key to running an efficient practice.
“The patients with osteoarthritis who hate the nodules, the fibromyalgia patients because they’re hurting all over, the patients with back pain – you’ve really got to limit those patients because otherwise you’ll be running 30-40 minutes behind for a scheduled 15-minute visit,” he explained.
One rheumatologist’s telemedicine practice
Dr. Wells currently utilizes the Epic electronic health record integrated with a Zoom videoconferencing platform for real-time virtual patient encounters. But he noted that other virtual platforms are available, including Health Tap, American Well, MySpecialistMD, MDLIVE, and TelaDoc. The American Telemedicine Association is a valuable resource for state-by-state medicolegal, reimbursement, and how-to-do-it questions.
At present, he reserves two daily time slots for telerheumatology: one at 8:30-9:00 a.m., the other at 4:30-5:00 p.m. These can be filled with four 15-minute live consults or two 30-minute consults. His goal is to eventually make telerheumatology 20% of his patient load of about 100 patients per week.
His typical 15-minute virtual visit proceeds as follows: It begins with a 3-minute subjective patient assessment, followed by a 5-minute objective assessment which includes the RAPID3, a brief Health Assessment Questionnaire (HAQ) addressing the patient’s pain and overall satisfaction, a virtual joint inspection, the use of high-quality teleultrasound and other technology when warranted, and capture of relevant still photos. This is followed by 5 minutes to relay the treatment plan, and finally a 2-minute recap and summary.
“No niceties. We cut right to the chase,” he noted.
He documents the patient encounter as he goes, dictating his notes throughout the visit.
“When I walk out of the room, I’m done. It’s on to the next patient,” Dr. Wells said.
The reimbursement picture is improving, although major hurdles remain. At present, 48 states and the District of Columbia reimburse for live video telemedicine through Medicaid. And in January 2020, Aetna announced it covers reimbursement for telemedicine in all of its fully insured health plans via the Teladoc platform. Dr. Wells’ patients pay for their telerheumatology out of pocket if their insurance doesn’t cover it.
Telemedicine caveats
Dr. Wells shared his telerheumatology experience as the first half of a point/counterpoint session on telemedicine’s future in the specialty. His debate opponent, Orrin M. Troum, MD, announced at the outset that he is quite interested in getting into telerheumatology; however, while looking into it he has come across issues that for now give him pause and that other rheumatologists need to be aware of.
Legal risks. The telemedicine movement has gotten big enough to draw the scrutiny of federal prosecutors and regulatory enforcement officials. In April 2018, the Department of Health & Human Services Office of the Inspector General (OIG) issued a report that concluded that one-third of all examined telemedicine claims were improper.
“Just imagine who might come knocking on your door,” he said.
Among the most common offenses, according to the OIG, were claims for services outside the limited range currently covered; lack of the requisite HIPAA-compliant two-way audio and visual communication technology with fully encrypted data transmission; services billed by institutional providers not defined by Medicare as telemedicine-eligible; and claims for services received by patients who weren’t located in an officially designated Health Professional Shortage Area or in a rural county as determined by the U.S. Census Bureau.
Telemedicine is no panacea for out-of-control health care costs. A RAND study of participants in the California Public Employees’ Retirement System (CalPERS) concluded that only 12% of beneficiaries who used direct-to-consumer telemedicine did so to replace provider visits. The other 88% added on telemedicine as an additional service. So while telemedicine increased patient access to health care, it also increased the overall cost, observed Dr. Troum, a rheumatologist at the University of Southern California, Los Angeles, and in private practice in Santa Monica, Calif.
Talk to your attorney and malpractice insurer before embarking on telerheumatology. Physicians could potentially lose their medical malpractice insurance if they use telemedicine to treat patients located in states where they aren’t licensed to practice, even if through inadvertent error.
Telemedicine isn’t appropriate for all patients. Nearly a decade ago, rheumatologists at Dartmouth-Hitchcock Medical Center launched a telerheumatology service in order to bring specialty care to the largely rural populations of New Hampshire and Vermont. In a review of the experience that included interviews with both patients and providers, investigators concluded that telerheumatology successfully increased access to specialty care in underserved locations and got good satisfaction scores from both providers and beneficiaries. However, fully 19% of patients were found to be inappropriate for their telerheumatology visit, mainly because their disease was too complex or the underlying diagnosis was unclear.
“Almost one-fifth of their patients were inappropriate for telerheumatology. The question is, how are you supposed to know that ahead of time?” Dr. Troum asked.
Patient satisfaction. Dr. Troum’s reading of the literature on patient satisfaction with telerheumatology, coupled with his own extensive experience in clinical practice, makes him think that many of his younger patients with less disease activity might welcome a telerheumatology option, even with strict time boundaries. But his older patients with more disease activity are a different story.
“Typically my middle-aged and older patients won’t accept that without a lot of convincing,” he commented.
Dr. Wells and Dr. Troum had no relevant disclosures regarding their presentations.
MAUI, HAWAII – Alvin F. Wells, MD, PhD, believes he’s seen the future of rheumatology. So he’s taken a deep dive into telerheumatology, going all in.
“Whether you’re in academic, private, or hospital-based practice, in 2020 if you are not thinking about telerheumatology, you and your practice will not be able to compete with growing patient demands, expectations, and need for clinical monitoring. If you do not have a digital/virtual strategy, you do not have a health care strategy,” he asserted at the 2020 Rheumatology Winter Clinical Symposium.
“Begin now,” the rheumatologist advised.
In pursuit of his own telerheumatology strategy, he holds licenses to practice medicine in five states and has licensure pending in five others.
“My goal is to cover 20% of the U.S., so if the local guys can’t see the patients, I can see them virtually,” he explained. “The days of waiting 4-6 months to be seen by a rheumatologist are gone.”
Rheumatologists are already in short supply in most of the country, and a major shortage looms ahead as older practitioners retire. Telerheumatology can help fill that unmet need. But the specialty is behind the curve. In a survey that rated the medical specialties most engaged in telemedicine, the top three spots were held by radiology, psychiatry, and internal medicine. Rheumatology didn’t even crack the top 10, noted Dr. Wells, director of the Rheumatology and Immunotherapy Center in Franklin, Wisc., and a part-time faculty member at Duke University, the Medical College of Wisconsin, and the Karolinska Institute.
Yet telemedicine is primed for rheumatologic takeoff. Notably, the 2019 update of the American College of Rheumatology recommendations on rheumatoid arthritis disease activity measures incorporates the RAPID3 (Routine Assessment of Patient Index Data) as an endorsed three-question clinical assessment that doesn’t involve a physical exam or laboratory work. The ACR update is recognition that, while every rheumatology patient needs an initial physical exam along with follow-up physical exams at various rates, many patients with well-controlled disease don’t need a physical exam at every physician encounter, he said.
Telerheumatology saves time for both patient and physician. The patient saves travel time, doesn’t miss work, avoids having to arrange for child care in order to make a face-to-face clinic visit, and can schedule more frequent virtual follow-up visits. For the practitioner, telerheumatology means additional consults and – here’s the big one – “You never run behind,” according to Dr. Wells. “For a 15-minute appointment, the patient gets a 5-minute warning, then a 2-minute warning, and at 15 minutes the link is cut. If the fibromyalgia patients want 30 minutes, they pay for 30 minutes.”
He sees the strictly enforced, impersonally delivered electronic time limits as key to running an efficient practice.
“The patients with osteoarthritis who hate the nodules, the fibromyalgia patients because they’re hurting all over, the patients with back pain – you’ve really got to limit those patients because otherwise you’ll be running 30-40 minutes behind for a scheduled 15-minute visit,” he explained.
One rheumatologist’s telemedicine practice
Dr. Wells currently utilizes the Epic electronic health record integrated with a Zoom videoconferencing platform for real-time virtual patient encounters. But he noted that other virtual platforms are available, including Health Tap, American Well, MySpecialistMD, MDLIVE, and TelaDoc. The American Telemedicine Association is a valuable resource for state-by-state medicolegal, reimbursement, and how-to-do-it questions.
At present, he reserves two daily time slots for telerheumatology: one at 8:30-9:00 a.m., the other at 4:30-5:00 p.m. These can be filled with four 15-minute live consults or two 30-minute consults. His goal is to eventually make telerheumatology 20% of his patient load of about 100 patients per week.
His typical 15-minute virtual visit proceeds as follows: It begins with a 3-minute subjective patient assessment, followed by a 5-minute objective assessment which includes the RAPID3, a brief Health Assessment Questionnaire (HAQ) addressing the patient’s pain and overall satisfaction, a virtual joint inspection, the use of high-quality teleultrasound and other technology when warranted, and capture of relevant still photos. This is followed by 5 minutes to relay the treatment plan, and finally a 2-minute recap and summary.
“No niceties. We cut right to the chase,” he noted.
He documents the patient encounter as he goes, dictating his notes throughout the visit.
“When I walk out of the room, I’m done. It’s on to the next patient,” Dr. Wells said.
The reimbursement picture is improving, although major hurdles remain. At present, 48 states and the District of Columbia reimburse for live video telemedicine through Medicaid. And in January 2020, Aetna announced it covers reimbursement for telemedicine in all of its fully insured health plans via the Teladoc platform. Dr. Wells’ patients pay for their telerheumatology out of pocket if their insurance doesn’t cover it.
Telemedicine caveats
Dr. Wells shared his telerheumatology experience as the first half of a point/counterpoint session on telemedicine’s future in the specialty. His debate opponent, Orrin M. Troum, MD, announced at the outset that he is quite interested in getting into telerheumatology; however, while looking into it he has come across issues that for now give him pause and that other rheumatologists need to be aware of.
Legal risks. The telemedicine movement has gotten big enough to draw the scrutiny of federal prosecutors and regulatory enforcement officials. In April 2018, the Department of Health & Human Services Office of the Inspector General (OIG) issued a report that concluded that one-third of all examined telemedicine claims were improper.
“Just imagine who might come knocking on your door,” he said.
Among the most common offenses, according to the OIG, were claims for services outside the limited range currently covered; lack of the requisite HIPAA-compliant two-way audio and visual communication technology with fully encrypted data transmission; services billed by institutional providers not defined by Medicare as telemedicine-eligible; and claims for services received by patients who weren’t located in an officially designated Health Professional Shortage Area or in a rural county as determined by the U.S. Census Bureau.
Telemedicine is no panacea for out-of-control health care costs. A RAND study of participants in the California Public Employees’ Retirement System (CalPERS) concluded that only 12% of beneficiaries who used direct-to-consumer telemedicine did so to replace provider visits. The other 88% added on telemedicine as an additional service. So while telemedicine increased patient access to health care, it also increased the overall cost, observed Dr. Troum, a rheumatologist at the University of Southern California, Los Angeles, and in private practice in Santa Monica, Calif.
Talk to your attorney and malpractice insurer before embarking on telerheumatology. Physicians could potentially lose their medical malpractice insurance if they use telemedicine to treat patients located in states where they aren’t licensed to practice, even if through inadvertent error.
Telemedicine isn’t appropriate for all patients. Nearly a decade ago, rheumatologists at Dartmouth-Hitchcock Medical Center launched a telerheumatology service in order to bring specialty care to the largely rural populations of New Hampshire and Vermont. In a review of the experience that included interviews with both patients and providers, investigators concluded that telerheumatology successfully increased access to specialty care in underserved locations and got good satisfaction scores from both providers and beneficiaries. However, fully 19% of patients were found to be inappropriate for their telerheumatology visit, mainly because their disease was too complex or the underlying diagnosis was unclear.
“Almost one-fifth of their patients were inappropriate for telerheumatology. The question is, how are you supposed to know that ahead of time?” Dr. Troum asked.
Patient satisfaction. Dr. Troum’s reading of the literature on patient satisfaction with telerheumatology, coupled with his own extensive experience in clinical practice, makes him think that many of his younger patients with less disease activity might welcome a telerheumatology option, even with strict time boundaries. But his older patients with more disease activity are a different story.
“Typically my middle-aged and older patients won’t accept that without a lot of convincing,” he commented.
Dr. Wells and Dr. Troum had no relevant disclosures regarding their presentations.
REPORTING FROM RWCS 2020
AFib patients do best on a DOAC started 7-10 days post stroke
LOS ANGELES – When a patient with atrial fibrillation (AFib) has a cardioembolic stroke, the best blood thinner to start may be a direct-acting oral anticoagulant (DOAC), possibly beginning 7-10 days after the index stroke, according to an analysis of 90-day, observational outcomes data from nearly 1,300 patients.

The analysis also suggested that the use of “bridging” anticoagulant treatment by injection before a patient with atrial fibrillation (AFib) starts a daily oral anticoagulant regimen following a cardioembolic stroke is not a good idea. Patients who received bridging anticoagulation had a nearly threefold higher rate of symptomatic intracranial hemorrhage than did patients who did not, and their bridging treatment failed to protect them from recurrent ischemic events, Shadi Yaghi, MD, said at the International Stroke Conference, sponsored by the American Heart Association. The bridging regimens delivered either heparin or low-molecular-weight heparin.
Based on the findings, “it seems reasonable to avoid bridging unless absolutely necessary, to initiate a DOAC unless it’s contraindicated, and to start the DOAC on day 7-10 following the stroke in most patients,” said Dr. Yaghi, a vascular neurologist and director of stroke research at NYU Langone Health in New York.
“It’s been hard to develop a broad guideline on when to start oral anticoagulation” after a cardioembolic stroke in AFib patients. The best time “depends on a lot of variables and how the patient responded to acute treatment,” commented Alexis Simpkins, MD, a vascular and stroke neurologist at the University of Florida in Gainesville. “You want to start treatment before the patient has another stroke, but not so soon that the treatment causes symptomatic hemorrhagic transformation.”
Dr. Yaghi’s suggestion, based on his findings, to start treatment for most patients with a DOAC 7-10 days after their index stroke “shows consistency” with the prevailing guideline recommendation from the AHA/American Stroke Association to start oral anticoagulation in this patient population 4-14 days after the index stroke (Stroke. 2018 March;49[3]:e46-e99), she noted.

A recent article reviewed the uncertainty about the best time to start oral anticoagulation in AFib patients after a cardioembolic stroke and the subtle differences that distinguish various international medical groups that, like the ASA, have made recommendations (Lancet Neurol. 2019 Jan 1;18[1]:117-26). According to this review, a major limitation of these various recommendations has been the lack of actual evidence collected from AFib patients who began receiving a DOAC shortly after a cardioembolic stroke, although the article added that several studies in progress are collecting these data.
The study reported by Dr. Yaghi pooled data collected from 2,084 recent AFib patients with a cardioembolic stroke treated at any of eight comprehensive U.S. stroke centers. They excluded patients who died from causes unrelated to the primary endpoint, those who did not receive an anticoagulant or had incomplete data, and patients lost to follow-up, leaving 1,289 evaluable patients. During their 90-day follow-up, 10% of the patients had an ischemic event, a symptomatic intracranial hemorrhage, or an extracranial hemorrhage.
The study’s primary analysis showed no statistically significant difference in the incidence of recurrent ischemic events, symptomatic intracranial hemorrhage, or both based on when oral anticoagulant treatment began: 0-3 days, 4-14 days, or more than 14 days after the index stroke.
The investigators then subdivided patients into the subgroup that started treatment with a DOAC and the subgroup that started treatment with warfarin and also further subdivided the 4-14 day time window for starting treatment. Results of this analysis showed that patients who received a DOAC and began this treatment 7-10 days after their stroke had a 50% cut in their 90-day events compared with other patients, a difference that fell just short of statistical significance at P = .07. All the other combinations of oral anticoagulant and time of treatment initiation analyzed showed neutral effects that never came near statistical significance.
Secondary data analyses also showed that both patients with a history of a stroke prior to their index stroke and patients with ipsilateral atherosclerosis came close to having a statistically significant increased rate of a subsequent ischemic event during 90-day follow-up. Furthermore, women, patients with a history of hyperlipidemia, and patients who developed hemorrhagic transformation of their index stroke all had significantly increased rates of developing a symptomatic intracranial hemorrhage during 90-day follow-up. When the endpoint was limited to recurrent ischemic events only, patients who received a DOAC were 50% less likely to have an event than were patients treated with warfarin, a statistically significant difference.
Although starting a DOAC 7-10 days after the index stroke seems reasonable based on this analysis, the question needs a prospective, randomized study to create an appropriate evidence base, Dr. Yaghi said.
Dr. Yaghi disclosed a financial relationship with Medtronic. Dr. Simpkins had no disclosures.
SOURCE: Yaghi S et al. Stroke. 2020 Feb;51(suppl 1):A119.
LOS ANGELES – When a patient with atrial fibrillation (AFib) has a cardioembolic stroke, the best blood thinner to start may be a direct-acting oral anticoagulant (DOAC), possibly beginning 7-10 days after the index stroke, according to an analysis of 90-day, observational outcomes data from nearly 1,300 patients.
The analysis also suggested that the use of “bridging” anticoagulant treatment by injection before a patient with atrial fibrillation (AFib) starts a daily oral anticoagulant regimen following a cardioembolic stroke is not a good idea. Patients who received bridging anticoagulation had a nearly threefold higher rate of symptomatic intracranial hemorrhage than did patients who did not, and their bridging treatment failed to protect them from recurrent ischemic events, Shadi Yaghi, MD, said at the International Stroke Conference, sponsored by the American Heart Association. The bridging regimens delivered either heparin or low-molecular-weight heparin.
Based on the findings, “it seems reasonable to avoid bridging unless absolutely necessary, to initiate a DOAC unless it’s contraindicated, and to start the DOAC on day 7-10 following the stroke in most patients,” said Dr. Yaghi, a vascular neurologist and director of stroke research at NYU Langone Health in New York.
“It’s been hard to develop a broad guideline on when to start oral anticoagulation” after a cardioembolic stroke in AFib patients. The best time “depends on a lot of variables and how the patient responded to acute treatment,” commented Alexis Simpkins, MD, a vascular and stroke neurologist at the University of Florida in Gainesville. “You want to start treatment before the patient has another stroke, but not so soon that the treatment causes symptomatic hemorrhagic transformation.”
Dr. Yaghi’s suggestion, based on his findings, to start treatment for most patients with a DOAC 7-10 days after their index stroke “shows consistency” with the prevailing guideline recommendation from the AHA/American Stroke Association to start oral anticoagulation in this patient population 4-14 days after the index stroke (Stroke. 2018 March;49[3]:e46-e99), she noted.
A recent article reviewed the uncertainty about the best time to start oral anticoagulation in AFib patients after a cardioembolic stroke and the subtle differences that distinguish various international medical groups that, like the ASA, have made recommendations (Lancet Neurol. 2019 Jan 1;18[1]:117-26). According to this review, a major limitation of these various recommendations has been the lack of actual evidence collected from AFib patients who began receiving a DOAC shortly after a cardioembolic stroke, although the article added that several studies in progress are collecting these data.
The study reported by Dr. Yaghi pooled data collected from 2,084 recent AFib patients with a cardioembolic stroke treated at any of eight comprehensive U.S. stroke centers. They excluded patients who died from causes unrelated to the primary endpoint, those who did not receive an anticoagulant or had incomplete data, and patients lost to follow-up, leaving 1,289 evaluable patients. During their 90-day follow-up, 10% of the patients had an ischemic event, a symptomatic intracranial hemorrhage, or an extracranial hemorrhage.
The study’s primary analysis showed no statistically significant difference in the incidence of recurrent ischemic events, symptomatic intracranial hemorrhage, or both based on when oral anticoagulant treatment began: 0-3 days, 4-14 days, or more than 14 days after the index stroke.
The investigators then subdivided patients into the subgroup that started treatment with a DOAC and the subgroup that started treatment with warfarin and also further subdivided the 4-14 day time window for starting treatment. Results of this analysis showed that patients who received a DOAC and began this treatment 7-10 days after their stroke had a 50% cut in their 90-day events compared with other patients, a difference that fell just short of statistical significance at P = .07. All the other combinations of oral anticoagulant and time of treatment initiation analyzed showed neutral effects that never came near statistical significance.
Secondary data analyses also showed that both patients with a history of a stroke prior to their index stroke and patients with ipsilateral atherosclerosis came close to having a statistically significant increased rate of a subsequent ischemic event during 90-day follow-up. Furthermore, women, patients with a history of hyperlipidemia, and patients who developed hemorrhagic transformation of their index stroke all had significantly increased rates of developing a symptomatic intracranial hemorrhage during 90-day follow-up. When the endpoint was limited to recurrent ischemic events only, patients who received a DOAC were 50% less likely to have an event than were patients treated with warfarin, a statistically significant difference.
Although starting a DOAC 7-10 days after the index stroke seems reasonable based on this analysis, the question needs a prospective, randomized study to create an appropriate evidence base, Dr. Yaghi said.
Dr. Yaghi disclosed a financial relationship with Medtronic. Dr. Simpkins had no disclosures.
SOURCE: Yaghi S et al. Stroke. 2020 Feb;51(suppl 1):A119.
LOS ANGELES – When a patient with atrial fibrillation (AFib) has a cardioembolic stroke, the best blood thinner to start may be a direct-acting oral anticoagulant (DOAC), possibly beginning 7-10 days after the index stroke, according to an analysis of 90-day, observational outcomes data from nearly 1,300 patients.
The analysis also suggested that the use of “bridging” anticoagulant treatment by injection before a patient with atrial fibrillation (AFib) starts a daily oral anticoagulant regimen following a cardioembolic stroke is not a good idea. Patients who received bridging anticoagulation had a nearly threefold higher rate of symptomatic intracranial hemorrhage than did patients who did not, and their bridging treatment failed to protect them from recurrent ischemic events, Shadi Yaghi, MD, said at the International Stroke Conference, sponsored by the American Heart Association. The bridging regimens delivered either heparin or low-molecular-weight heparin.
Based on the findings, “it seems reasonable to avoid bridging unless absolutely necessary, to initiate a DOAC unless it’s contraindicated, and to start the DOAC on day 7-10 following the stroke in most patients,” said Dr. Yaghi, a vascular neurologist and director of stroke research at NYU Langone Health in New York.
“It’s been hard to develop a broad guideline on when to start oral anticoagulation” after a cardioembolic stroke in AFib patients. The best time “depends on a lot of variables and how the patient responded to acute treatment,” commented Alexis Simpkins, MD, a vascular and stroke neurologist at the University of Florida in Gainesville. “You want to start treatment before the patient has another stroke, but not so soon that the treatment causes symptomatic hemorrhagic transformation.”
Dr. Yaghi’s suggestion, based on his findings, to start treatment for most patients with a DOAC 7-10 days after their index stroke “shows consistency” with the prevailing guideline recommendation from the AHA/American Stroke Association to start oral anticoagulation in this patient population 4-14 days after the index stroke (Stroke. 2018 March;49[3]:e46-e99), she noted.
A recent article reviewed the uncertainty about the best time to start oral anticoagulation in AFib patients after a cardioembolic stroke and the subtle differences that distinguish various international medical groups that, like the ASA, have made recommendations (Lancet Neurol. 2019 Jan 1;18[1]:117-26). According to this review, a major limitation of these various recommendations has been the lack of actual evidence collected from AFib patients who began receiving a DOAC shortly after a cardioembolic stroke, although the article added that several studies in progress are collecting these data.
The study reported by Dr. Yaghi pooled data collected from 2,084 recent AFib patients with a cardioembolic stroke treated at any of eight comprehensive U.S. stroke centers. They excluded patients who died from causes unrelated to the primary endpoint, those who did not receive an anticoagulant or had incomplete data, and patients lost to follow-up, leaving 1,289 evaluable patients. During their 90-day follow-up, 10% of the patients had an ischemic event, a symptomatic intracranial hemorrhage, or an extracranial hemorrhage.
The study’s primary analysis showed no statistically significant difference in the incidence of recurrent ischemic events, symptomatic intracranial hemorrhage, or both based on when oral anticoagulant treatment began: 0-3 days, 4-14 days, or more than 14 days after the index stroke.
The investigators then subdivided patients into the subgroup that started treatment with a DOAC and the subgroup that started treatment with warfarin and also further subdivided the 4-14 day time window for starting treatment. Results of this analysis showed that patients who received a DOAC and began this treatment 7-10 days after their stroke had a 50% cut in their 90-day events compared with other patients, a difference that fell just short of statistical significance at P = .07. All the other combinations of oral anticoagulant and time of treatment initiation analyzed showed neutral effects that never came near statistical significance.
Secondary data analyses also showed that both patients with a history of a stroke prior to their index stroke and patients with ipsilateral atherosclerosis came close to having a statistically significant increased rate of a subsequent ischemic event during 90-day follow-up. Furthermore, women, patients with a history of hyperlipidemia, and patients who developed hemorrhagic transformation of their index stroke all had significantly increased rates of developing a symptomatic intracranial hemorrhage during 90-day follow-up. When the endpoint was limited to recurrent ischemic events only, patients who received a DOAC were 50% less likely to have an event than were patients treated with warfarin, a statistically significant difference.
Although starting a DOAC 7-10 days after the index stroke seems reasonable based on this analysis, the question needs a prospective, randomized study to create an appropriate evidence base, Dr. Yaghi said.
Dr. Yaghi disclosed a financial relationship with Medtronic. Dr. Simpkins had no disclosures.
SOURCE: Yaghi S et al. Stroke. 2020 Feb;51(suppl 1):A119.
REPORTING FROM ISC 2020
CLTX-CAR T cells exhibit preclinical activity and move on to a clinical trial
Chlorotoxin (CLTX)-directed chimeric antigen receptor (CAR) T cells demonstrated activity against glioblastoma in a preclinical study and will soon be tested in a clinical trial.
“We sought to develop a CAR T cell using chlorotoxin peptide as the tumor-targeting domain,” wrote Dongrui Wang, a PhD candidate at City of Hope National Medical Center in Duarte, Calif., and colleagues. Their report is in Science Translational Medicine.
“CLTX has been established to bind broadly and specifically to glioblastoma and other neuroectodermal tumors while showing minimal cross-reactivity with nonmalignant cells,” the researchers noted.
The team evaluated CLTX binding capacity in 23 tumor samples from 15 glioblastoma patients, in patient-derived glioblastoma cell lines, and in orthotopic mouse xenograft models. These experiments showed that CLTX could bind to a high percentage of patient tumors as well as to most glioblastoma cells within a tumor.
In the design phase, the researchers engineered a peptide-bearing CAR, which overcame previous barriers of other glioblastoma-directed CARs, including antigen escape and tumor heterogeneity.
The team evaluated the antitumor activity of CLTX-CAR T cells in two orthotopic mouse xenograft models. Intracranial administration of CLTX-CAR T cells controlled tumor growth and extended survival in both models. All mice originally bearing PBT106-TS tumors became tumor-free and remained so for more than 170 days. However, only a subset of mice bearing PBT003-4-TS tumors experienced similar long-term tumor-free survival.
The researchers assessed potential off-target effects of CLTX-CAR T cells in normal human cells. The team observed limited binding of CLTX-CAR T cells to embryonic kidney cells, peripheral blood mononuclear cells, and neural progenitor cells, suggesting minimal off-target activity.
Further toxicity experiments demonstrated that, even at high doses, CLTX-CAR T cells were tolerated in mouse models, suggesting high potency for tumor cells and low risk of systemic toxicity.
Additional preclinical experiments elucidated mechanisms of CLTX-CAR T-cell function, namely the essential role of matrix metalloproteinase 2 expression for cell activation.
The researchers acknowledged that a key limitation of this study was the use of glioblastoma xenograft models, which may not fully represent tumor activity in glioblastoma patients.
Nevertheless, the researchers concluded that “CLTX-CAR T cells present a strategic combination of selective yet ubiquitous tumor targeting and are a candidate for clinical development as anti-glioblastoma immunotherapy.”
In fact, City of Hope is now screening patients for a clinical trial of CLTX-CAR T cells for the treatment of recurrent or progressive glioblastoma (NCT04214392).
The preclinical research was funded by the Ben and Catherine Ivy Foundation and the National Institutes of Health. Two authors disclosed financial affiliations with Mustang Bio.
SOURCE: Wang D et al. Sci Transl Med. 2020 Mar 4. doi: 10.1126/scitranslmed.aaw2672.
Chlorotoxin (CLTX)-directed chimeric antigen receptor (CAR) T cells demonstrated activity against glioblastoma in a preclinical study and will soon be tested in a clinical trial.
“We sought to develop a CAR T cell using chlorotoxin peptide as the tumor-targeting domain,” wrote Dongrui Wang, a PhD candidate at City of Hope National Medical Center in Duarte, Calif., and colleagues. Their report is in Science Translational Medicine.
“CLTX has been established to bind broadly and specifically to glioblastoma and other neuroectodermal tumors while showing minimal cross-reactivity with nonmalignant cells,” the researchers noted.
The team evaluated CLTX binding capacity in 23 tumor samples from 15 glioblastoma patients, in patient-derived glioblastoma cell lines, and in orthotopic mouse xenograft models. These experiments showed that CLTX could bind to a high percentage of patient tumors as well as to most glioblastoma cells within a tumor.
In the design phase, the researchers engineered a peptide-bearing CAR, which overcame previous barriers of other glioblastoma-directed CARs, including antigen escape and tumor heterogeneity.
The team evaluated the antitumor activity of CLTX-CAR T cells in two orthotopic mouse xenograft models. Intracranial administration of CLTX-CAR T cells controlled tumor growth and extended survival in both models. All mice originally bearing PBT106-TS tumors became tumor-free and remained so for more than 170 days. However, only a subset of mice bearing PBT003-4-TS tumors experienced similar long-term tumor-free survival.
The researchers assessed potential off-target effects of CLTX-CAR T cells in normal human cells. The team observed limited binding of CLTX-CAR T cells to embryonic kidney cells, peripheral blood mononuclear cells, and neural progenitor cells, suggesting minimal off-target activity.
Further toxicity experiments demonstrated that, even at high doses, CLTX-CAR T cells were tolerated in mouse models, suggesting high potency for tumor cells and low risk of systemic toxicity.
Additional preclinical experiments elucidated mechanisms of CLTX-CAR T-cell function, namely the essential role of matrix metalloproteinase 2 expression for cell activation.
The researchers acknowledged that a key limitation of this study was the use of glioblastoma xenograft models, which may not fully represent tumor activity in glioblastoma patients.
Nevertheless, the researchers concluded that “CLTX-CAR T cells present a strategic combination of selective yet ubiquitous tumor targeting and are a candidate for clinical development as anti-glioblastoma immunotherapy.”
In fact, City of Hope is now screening patients for a clinical trial of CLTX-CAR T cells for the treatment of recurrent or progressive glioblastoma (NCT04214392).
The preclinical research was funded by the Ben and Catherine Ivy Foundation and the National Institutes of Health. Two authors disclosed financial affiliations with Mustang Bio.
SOURCE: Wang D et al. Sci Transl Med. 2020 Mar 4. doi: 10.1126/scitranslmed.aaw2672.
Chlorotoxin (CLTX)-directed chimeric antigen receptor (CAR) T cells demonstrated activity against glioblastoma in a preclinical study and will soon be tested in a clinical trial.
“We sought to develop a CAR T cell using chlorotoxin peptide as the tumor-targeting domain,” wrote Dongrui Wang, a PhD candidate at City of Hope National Medical Center in Duarte, Calif., and colleagues. Their report is in Science Translational Medicine.
“CLTX has been established to bind broadly and specifically to glioblastoma and other neuroectodermal tumors while showing minimal cross-reactivity with nonmalignant cells,” the researchers noted.
The team evaluated CLTX binding capacity in 23 tumor samples from 15 glioblastoma patients, in patient-derived glioblastoma cell lines, and in orthotopic mouse xenograft models. These experiments showed that CLTX could bind to a high percentage of patient tumors as well as to most glioblastoma cells within a tumor.
In the design phase, the researchers engineered a peptide-bearing CAR, which overcame previous barriers of other glioblastoma-directed CARs, including antigen escape and tumor heterogeneity.
The team evaluated the antitumor activity of CLTX-CAR T cells in two orthotopic mouse xenograft models. Intracranial administration of CLTX-CAR T cells controlled tumor growth and extended survival in both models. All mice originally bearing PBT106-TS tumors became tumor-free and remained so for more than 170 days. However, only a subset of mice bearing PBT003-4-TS tumors experienced similar long-term tumor-free survival.
The researchers assessed potential off-target effects of CLTX-CAR T cells in normal human cells. The team observed limited binding of CLTX-CAR T cells to embryonic kidney cells, peripheral blood mononuclear cells, and neural progenitor cells, suggesting minimal off-target activity.
Further toxicity experiments demonstrated that, even at high doses, CLTX-CAR T cells were tolerated in mouse models, suggesting high potency for tumor cells and low risk of systemic toxicity.
Additional preclinical experiments elucidated mechanisms of CLTX-CAR T-cell function, namely the essential role of matrix metalloproteinase 2 expression for cell activation.
The researchers acknowledged that a key limitation of this study was the use of glioblastoma xenograft models, which may not fully represent tumor activity in glioblastoma patients.
Nevertheless, the researchers concluded that “CLTX-CAR T cells present a strategic combination of selective yet ubiquitous tumor targeting and are a candidate for clinical development as anti-glioblastoma immunotherapy.”
In fact, City of Hope is now screening patients for a clinical trial of CLTX-CAR T cells for the treatment of recurrent or progressive glioblastoma (NCT04214392).
The preclinical research was funded by the Ben and Catherine Ivy Foundation and the National Institutes of Health. Two authors disclosed financial affiliations with Mustang Bio.
SOURCE: Wang D et al. Sci Transl Med. 2020 Mar 4. doi: 10.1126/scitranslmed.aaw2672.
FROM SCIENCE TRANSLATIONAL MEDICINE
COVID-19’s hairy conspiracy, and a Kardashian Kolonoscopy
Coronavirus conspiracy gets hairy
It was inevitable, of course. The government’s response to COVID-19 and the novel coronavirus has become an issue, and the increased scrutiny has now turned up a conspiracy.
This particular plot, recently uncovered by the Twitterverse and reported by Newsweek, is being perpetuated by the CDC against the American patriots who make up the bearded wings of the Men-ocratic and Republi-man parties.
Our story begins on Nov. 2, 2017, when the National Institute for Occupational Safety and Health posted “To Beard or not to Beard? That’s a good Question!” on its science blog, which was aimed at “workers who wear tight-fitting respirators.” Like the N95 face mask. More than 2 years before the coronavirus was “discovered” in China. Hmmm, interesting.
The NIOSH post claimed that beards, sideburns, and some mustaches “will interfere with respirators that rely on a tight facepiece seal to achieve maximum protection.” The agency further alleged that “research tells us that the presence of facial hair under the sealing surface causes 20 to 1,000 times more leakage, compared to clean-shaven individuals.” As if research ever proved anything.
The post’s pièce de résistance, however, was an infograph illustrating 36 types of facial hairstyles and whether they worked with a face mask/respirator. Did you know that beard styles such as the chin curtain, French fork, Garibaldi, and Hulihee get a thumbs down? Did you know there are beard styles called the chin curtain, French fork, Garibaldi, and Hulihee? [What? No ZZ Top beard?]
Most mustaches are okay, though, and therein lies the proof of a conspiracy. Among the approved mustache styles is the toothbrush. You’ll find it on the bottom row of the graph, third from the left. Notice anything?
It’s a Hitler mustache! The CDC put its seal of approval on a Hitler mustache!
Thus, by the transfollicular property of the High Castle corollary to the Boys from Brazil theorem, a government conspiracy must exist.
The coronavirus will now proceed to take over the world. Have a nice day.
Keeping up with the Kolonoscopies

Imagine owing your life to the Kardashians. It’s a bit tough to swallow, but a man from Ohio owes Kim and her Krew a life debt.
Gary Paine was just passing the time, watching some daytime “Keeping Up With the Kardashians” television in the doctor’s waiting room while his wife was getting a colonoscopy. We’ve all been there – we in the Bureau of LOTME have watched more waiting-room “Judge Judy” than we care to admit.
And just like us, Gary said he was getting bored while watching the Kardashians’ TV travails. Although he felt relatively healthy, he decided to distract himself the best way he knew how: making his own colonoscopy appointment. Anything’s better than getting sucked into an 8-hour Kardashian marathon, right?
During Gary’s Kim K–inspired colonoscopy, it was discovered that he had an irregularity in his heart. Eventually, doctors found two severely blocked arteries. Paine underwent immediate, lifesaving quadruple-bypass surgery.
He now urges people to be aware that checkups are essential, whether you’re showing symptoms of poor health or not.
Which leads us to wonder: Do Kris Jenner and her clan know they’re now officially more painful than a colonoscopy appointment?
(Crosswalks) Don’t stop me now

There’s always that one guy. You’re stuck in a long line behind a big slow tractor trailer going 10 under the speed limit, and there’s a flashy BMW practically living inside your trunk. A brief passing zone approaches, but there’s no point ... oh, of course they swerve around and cut you off, what did they even gain from doing that?
Point is, people who drive expensive cars have a bit of a reputation for being less than courteous behind the wheel, and thanks to a study published in the Journal of Transport & Health, there’s some science to back that up.
A group of four presumably well-paid volunteers were sent out to crosswalks and crossed in front of cars to see how many would yield. Results were less than encouraging: Only 28% of 461 cars yielded. The only factor that significantly predicted whether or not a car would yield was how expensive it was; for every $1,000 increase in the value of the car, the driver was 3% less likely to stop.
It’s not looking good for owners of expensive cars, especially when even the study authors suggest that these drivers were displaying increased entitlement and narcissism through their lack of yielding behavior.
Our suggestion? Clearly rich people are sick and need intensive psychotherapy, and the offending vehicles should be removed and redistributed to the rest of us. We wouldn’t mind a nice slightly used Corvette, in red preferably. Nope, no ulterior motive here.
Coronavirus conspiracy gets hairy
It was inevitable, of course. The government’s response to COVID-19 and the novel coronavirus has become an issue, and the increased scrutiny has now turned up a conspiracy.
This particular plot, recently uncovered by the Twitterverse and reported by Newsweek, is being perpetuated by the CDC against the American patriots who make up the bearded wings of the Men-ocratic and Republi-man parties.
Our story begins on Nov. 2, 2017, when the National Institute for Occupational Safety and Health posted “To Beard or not to Beard? That’s a good Question!” on its science blog, which was aimed at “workers who wear tight-fitting respirators.” Like the N95 face mask. More than 2 years before the coronavirus was “discovered” in China. Hmmm, interesting.
The NIOSH post claimed that beards, sideburns, and some mustaches “will interfere with respirators that rely on a tight facepiece seal to achieve maximum protection.” The agency further alleged that “research tells us that the presence of facial hair under the sealing surface causes 20 to 1,000 times more leakage, compared to clean-shaven individuals.” As if research ever proved anything.
The post’s pièce de résistance, however, was an infograph illustrating 36 types of facial hairstyles and whether they worked with a face mask/respirator. Did you know that beard styles such as the chin curtain, French fork, Garibaldi, and Hulihee get a thumbs down? Did you know there are beard styles called the chin curtain, French fork, Garibaldi, and Hulihee? [What? No ZZ Top beard?]
Most mustaches are okay, though, and therein lies the proof of a conspiracy. Among the approved mustache styles is the toothbrush. You’ll find it on the bottom row of the graph, third from the left. Notice anything?
It’s a Hitler mustache! The CDC put its seal of approval on a Hitler mustache!
Thus, by the transfollicular property of the High Castle corollary to the Boys from Brazil theorem, a government conspiracy must exist.
The coronavirus will now proceed to take over the world. Have a nice day.
Keeping up with the Kolonoscopies
Imagine owing your life to the Kardashians. It’s a bit tough to swallow, but a man from Ohio owes Kim and her Krew a life debt.
Gary Paine was just passing the time, watching some daytime “Keeping Up With the Kardashians” television in the doctor’s waiting room while his wife was getting a colonoscopy. We’ve all been there – we in the Bureau of LOTME have watched more waiting-room “Judge Judy” than we care to admit.
And just like us, Gary said he was getting bored while watching the Kardashians’ TV travails. Although he felt relatively healthy, he decided to distract himself the best way he knew how: making his own colonoscopy appointment. Anything’s better than getting sucked into an 8-hour Kardashian marathon, right?
During Gary’s Kim K–inspired colonoscopy, it was discovered that he had an irregularity in his heart. Eventually, doctors found two severely blocked arteries. Paine underwent immediate, lifesaving quadruple-bypass surgery.
He now urges people to be aware that checkups are essential, whether you’re showing symptoms of poor health or not.
Which leads us to wonder: Do Kris Jenner and her clan know they’re now officially more painful than a colonoscopy appointment?
(Crosswalks) Don’t stop me now
There’s always that one guy. You’re stuck in a long line behind a big slow tractor trailer going 10 under the speed limit, and there’s a flashy BMW practically living inside your trunk. A brief passing zone approaches, but there’s no point ... oh, of course they swerve around and cut you off, what did they even gain from doing that?
Point is, people who drive expensive cars have a bit of a reputation for being less than courteous behind the wheel, and thanks to a study published in the Journal of Transport & Health, there’s some science to back that up.
A group of four presumably well-paid volunteers were sent out to crosswalks and crossed in front of cars to see how many would yield. Results were less than encouraging: Only 28% of 461 cars yielded. The only factor that significantly predicted whether or not a car would yield was how expensive it was; for every $1,000 increase in the value of the car, the driver was 3% less likely to stop.
It’s not looking good for owners of expensive cars, especially when even the study authors suggest that these drivers were displaying increased entitlement and narcissism through their lack of yielding behavior.
Our suggestion? Clearly rich people are sick and need intensive psychotherapy, and the offending vehicles should be removed and redistributed to the rest of us. We wouldn’t mind a nice slightly used Corvette, in red preferably. Nope, no ulterior motive here.
Coronavirus conspiracy gets hairy
It was inevitable, of course. The government’s response to COVID-19 and the novel coronavirus has become an issue, and the increased scrutiny has now turned up a conspiracy.
This particular plot, recently uncovered by the Twitterverse and reported by Newsweek, is being perpetuated by the CDC against the American patriots who make up the bearded wings of the Men-ocratic and Republi-man parties.
Our story begins on Nov. 2, 2017, when the National Institute for Occupational Safety and Health posted “To Beard or not to Beard? That’s a good Question!” on its science blog, which was aimed at “workers who wear tight-fitting respirators.” Like the N95 face mask. More than 2 years before the coronavirus was “discovered” in China. Hmmm, interesting.
The NIOSH post claimed that beards, sideburns, and some mustaches “will interfere with respirators that rely on a tight facepiece seal to achieve maximum protection.” The agency further alleged that “research tells us that the presence of facial hair under the sealing surface causes 20 to 1,000 times more leakage, compared to clean-shaven individuals.” As if research ever proved anything.
The post’s pièce de résistance, however, was an infograph illustrating 36 types of facial hairstyles and whether they worked with a face mask/respirator. Did you know that beard styles such as the chin curtain, French fork, Garibaldi, and Hulihee get a thumbs down? Did you know there are beard styles called the chin curtain, French fork, Garibaldi, and Hulihee? [What? No ZZ Top beard?]
Most mustaches are okay, though, and therein lies the proof of a conspiracy. Among the approved mustache styles is the toothbrush. You’ll find it on the bottom row of the graph, third from the left. Notice anything?
It’s a Hitler mustache! The CDC put its seal of approval on a Hitler mustache!
Thus, by the transfollicular property of the High Castle corollary to the Boys from Brazil theorem, a government conspiracy must exist.
The coronavirus will now proceed to take over the world. Have a nice day.
Keeping up with the Kolonoscopies
Imagine owing your life to the Kardashians. It’s a bit tough to swallow, but a man from Ohio owes Kim and her Krew a life debt.
Gary Paine was just passing the time, watching some daytime “Keeping Up With the Kardashians” television in the doctor’s waiting room while his wife was getting a colonoscopy. We’ve all been there – we in the Bureau of LOTME have watched more waiting-room “Judge Judy” than we care to admit.
And just like us, Gary said he was getting bored while watching the Kardashians’ TV travails. Although he felt relatively healthy, he decided to distract himself the best way he knew how: making his own colonoscopy appointment. Anything’s better than getting sucked into an 8-hour Kardashian marathon, right?
During Gary’s Kim K–inspired colonoscopy, it was discovered that he had an irregularity in his heart. Eventually, doctors found two severely blocked arteries. Paine underwent immediate, lifesaving quadruple-bypass surgery.
He now urges people to be aware that checkups are essential, whether you’re showing symptoms of poor health or not.
Which leads us to wonder: Do Kris Jenner and her clan know they’re now officially more painful than a colonoscopy appointment?
(Crosswalks) Don’t stop me now
There’s always that one guy. You’re stuck in a long line behind a big slow tractor trailer going 10 under the speed limit, and there’s a flashy BMW practically living inside your trunk. A brief passing zone approaches, but there’s no point ... oh, of course they swerve around and cut you off, what did they even gain from doing that?
Point is, people who drive expensive cars have a bit of a reputation for being less than courteous behind the wheel, and thanks to a study published in the Journal of Transport & Health, there’s some science to back that up.
A group of four presumably well-paid volunteers were sent out to crosswalks and crossed in front of cars to see how many would yield. Results were less than encouraging: Only 28% of 461 cars yielded. The only factor that significantly predicted whether or not a car would yield was how expensive it was; for every $1,000 increase in the value of the car, the driver was 3% less likely to stop.
It’s not looking good for owners of expensive cars, especially when even the study authors suggest that these drivers were displaying increased entitlement and narcissism through their lack of yielding behavior.
Our suggestion? Clearly rich people are sick and need intensive psychotherapy, and the offending vehicles should be removed and redistributed to the rest of us. We wouldn’t mind a nice slightly used Corvette, in red preferably. Nope, no ulterior motive here.