User login
DynamX Bioadaptor coronary stent shows promise in pilot study
The DynamX Bioadaptor – arguably the most original concept in coronary stent design to come along in 3 decades – demonstrated excellent safety and efficacy in a 12-month international, proof-of-concept study, Stefan Verheye, MD, said at the virtual annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
“There has been no fundamental change in stent design in over 30 years,” declared Dr. Verheye, codirector of the Antwerp (Belgium) Cardiovascular Center. “The DynamX Bioadaptor is a fundamental innovation in device design.”
The investigational device is a 71-mcm-thick, cobalt-chromium metal platform that elutes novolimus from a biodegradable polymer. Circumferential rings in low-stress sections of the device are held together by polymer connectors, and when the polymer erodes at about 6 months the stent segments are able to disengage from each other while maintaining longitudinal continuity. Dr. Verheye called this process “uncaging” the stented artery. The result is restoration of normal vessel angulation and compliance; the artery is no longer artificially straightened and constrained by a relatively stiff stent. Positive adaptive remodeling is preserved with enhanced vessel pulsatility and maintenance of lumenal area for good blood flow.
Dr. Verheye said the impetus for developing this outside-the-box novel stent platform lies in the recognition of a major unmet need for better drug-eluting stent (DES) performance. “Despite excellent acute outcomes, data with current-generation DES show long-term event rates are high and accrue at a rate of 2%-3% per year without a plateau.”
He was coprincipal investigator for the international study, which included 50 patients who received a DynamX Bioadaptor for a single de novo coronary artery lesion no more than 24 mm in length. The acute performance of the device was similar to that of second-generation DES, with a mean acute gain post procedure of 1.63 mm by quantitative coronary angiography and a mean late lumen loss of 0.12 mm when measured again at 9 or 12 months.
Intravascular ultrasound imaging showed a 3% increase in mean target vessel area and a 5% increase in the stented area from post procedure to 9 or 12 months’ follow-up, with no change in mean lumen area, all of which translates into maintenance of good blood flow over time. In contrast, what typically occurs following implantation of current DES is maintenance of target vessel and device areas, but with a loss in mean lumen area, the cardiologist noted.
There were two cardiac deaths but no cases of target lesion revascularization, device thrombosis, or strut fracture within 12 months of the procedure.
“The Bioadaptor performs similarly to second-generation DES in terms of implantation technique, deliverability, conformability, and radial strength during the healing phase, while showing the promise of mitigating the 2%-3% annualized event rate beyond 1 year,” Dr. Verheye concluded, adding, “Obviously, longer-term follow-up in comparative studies will be needed to show a reduction in the device-oriented events that have been observed with current DES.”
Session cochair Davide Capodanno, MD, PhD, of the University of Catania (Italy), declared: “This is an intriguing device because it’s metal, but it’s a kind of pulsatile metal after the biodegradation of the connectors. It’s something I’ve never seen.”

Discussant William Wijns, MD, PhD, said he was “thrilled” by the innovative aspect of the DynamX Bioadaptor, but he’s a long way from being persuaded that the device’s potential physiological advantages will translate into improved clinical outcomes relative to current DES.
“Don’t we all have a strange feeling of deja vu because all these anticipated benefits are the same as those we were told we would see with fully bioresorbable scaffolds? And we know so much after 10 years of experience with bioresorbable scaffolds that probably we will not accept this great story unless we get more and more evidence,” cautioned Dr. Wijns, professor of interventional cardiology at the National University of Ireland, Galway, and chairman of EuroPCR.
The claim regarding bioresorbable scaffolds was that, even though the acute results weren’t as good as with DES, that disadvantage would be outweighed by superior long-term clinical outcomes. But in fact the long-term outcomes turned out to be worse as well.
“We had to give up immediate results with the bioresorbable scaffolds. I don’t think we want to go that route again this time,” the cardiologist said.
Thus, the first thing that’s needed in order to make a convincing case for the Bioadaptor is evidence from a large, randomized, comparative trial demonstrating that the acute performance of the novel device is noninferior to that of current DES, including data on complex lesions. Such a study was supposed to be underway now but has been delayed by the COVID-19 pandemic, he noted.
Once there is evidence that the acute results with the Bioadaptor are truly comparable with those achieved with current DES, there will be a need for long-term data showing that the device reduces the 2%-3% annualized event rate seen with DES beyond 1 year, Dr. Wijns added.
Dr. Verheye reported receiving consultation fees from study sponsor Elixir Medical as well as from Biotronik. Dr. Wijns reported receiving research grants from MicroPort.
The DynamX Bioadaptor – arguably the most original concept in coronary stent design to come along in 3 decades – demonstrated excellent safety and efficacy in a 12-month international, proof-of-concept study, Stefan Verheye, MD, said at the virtual annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
“There has been no fundamental change in stent design in over 30 years,” declared Dr. Verheye, codirector of the Antwerp (Belgium) Cardiovascular Center. “The DynamX Bioadaptor is a fundamental innovation in device design.”
The investigational device is a 71-mcm-thick, cobalt-chromium metal platform that elutes novolimus from a biodegradable polymer. Circumferential rings in low-stress sections of the device are held together by polymer connectors, and when the polymer erodes at about 6 months the stent segments are able to disengage from each other while maintaining longitudinal continuity. Dr. Verheye called this process “uncaging” the stented artery. The result is restoration of normal vessel angulation and compliance; the artery is no longer artificially straightened and constrained by a relatively stiff stent. Positive adaptive remodeling is preserved with enhanced vessel pulsatility and maintenance of lumenal area for good blood flow.
Dr. Verheye said the impetus for developing this outside-the-box novel stent platform lies in the recognition of a major unmet need for better drug-eluting stent (DES) performance. “Despite excellent acute outcomes, data with current-generation DES show long-term event rates are high and accrue at a rate of 2%-3% per year without a plateau.”
He was coprincipal investigator for the international study, which included 50 patients who received a DynamX Bioadaptor for a single de novo coronary artery lesion no more than 24 mm in length. The acute performance of the device was similar to that of second-generation DES, with a mean acute gain post procedure of 1.63 mm by quantitative coronary angiography and a mean late lumen loss of 0.12 mm when measured again at 9 or 12 months.
Intravascular ultrasound imaging showed a 3% increase in mean target vessel area and a 5% increase in the stented area from post procedure to 9 or 12 months’ follow-up, with no change in mean lumen area, all of which translates into maintenance of good blood flow over time. In contrast, what typically occurs following implantation of current DES is maintenance of target vessel and device areas, but with a loss in mean lumen area, the cardiologist noted.
There were two cardiac deaths but no cases of target lesion revascularization, device thrombosis, or strut fracture within 12 months of the procedure.
“The Bioadaptor performs similarly to second-generation DES in terms of implantation technique, deliverability, conformability, and radial strength during the healing phase, while showing the promise of mitigating the 2%-3% annualized event rate beyond 1 year,” Dr. Verheye concluded, adding, “Obviously, longer-term follow-up in comparative studies will be needed to show a reduction in the device-oriented events that have been observed with current DES.”
Session cochair Davide Capodanno, MD, PhD, of the University of Catania (Italy), declared: “This is an intriguing device because it’s metal, but it’s a kind of pulsatile metal after the biodegradation of the connectors. It’s something I’ve never seen.”
Discussant William Wijns, MD, PhD, said he was “thrilled” by the innovative aspect of the DynamX Bioadaptor, but he’s a long way from being persuaded that the device’s potential physiological advantages will translate into improved clinical outcomes relative to current DES.
“Don’t we all have a strange feeling of deja vu because all these anticipated benefits are the same as those we were told we would see with fully bioresorbable scaffolds? And we know so much after 10 years of experience with bioresorbable scaffolds that probably we will not accept this great story unless we get more and more evidence,” cautioned Dr. Wijns, professor of interventional cardiology at the National University of Ireland, Galway, and chairman of EuroPCR.
The claim regarding bioresorbable scaffolds was that, even though the acute results weren’t as good as with DES, that disadvantage would be outweighed by superior long-term clinical outcomes. But in fact the long-term outcomes turned out to be worse as well.
“We had to give up immediate results with the bioresorbable scaffolds. I don’t think we want to go that route again this time,” the cardiologist said.
Thus, the first thing that’s needed in order to make a convincing case for the Bioadaptor is evidence from a large, randomized, comparative trial demonstrating that the acute performance of the novel device is noninferior to that of current DES, including data on complex lesions. Such a study was supposed to be underway now but has been delayed by the COVID-19 pandemic, he noted.
Once there is evidence that the acute results with the Bioadaptor are truly comparable with those achieved with current DES, there will be a need for long-term data showing that the device reduces the 2%-3% annualized event rate seen with DES beyond 1 year, Dr. Wijns added.
Dr. Verheye reported receiving consultation fees from study sponsor Elixir Medical as well as from Biotronik. Dr. Wijns reported receiving research grants from MicroPort.
The DynamX Bioadaptor – arguably the most original concept in coronary stent design to come along in 3 decades – demonstrated excellent safety and efficacy in a 12-month international, proof-of-concept study, Stefan Verheye, MD, said at the virtual annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
“There has been no fundamental change in stent design in over 30 years,” declared Dr. Verheye, codirector of the Antwerp (Belgium) Cardiovascular Center. “The DynamX Bioadaptor is a fundamental innovation in device design.”
The investigational device is a 71-mcm-thick, cobalt-chromium metal platform that elutes novolimus from a biodegradable polymer. Circumferential rings in low-stress sections of the device are held together by polymer connectors, and when the polymer erodes at about 6 months the stent segments are able to disengage from each other while maintaining longitudinal continuity. Dr. Verheye called this process “uncaging” the stented artery. The result is restoration of normal vessel angulation and compliance; the artery is no longer artificially straightened and constrained by a relatively stiff stent. Positive adaptive remodeling is preserved with enhanced vessel pulsatility and maintenance of lumenal area for good blood flow.
Dr. Verheye said the impetus for developing this outside-the-box novel stent platform lies in the recognition of a major unmet need for better drug-eluting stent (DES) performance. “Despite excellent acute outcomes, data with current-generation DES show long-term event rates are high and accrue at a rate of 2%-3% per year without a plateau.”
He was coprincipal investigator for the international study, which included 50 patients who received a DynamX Bioadaptor for a single de novo coronary artery lesion no more than 24 mm in length. The acute performance of the device was similar to that of second-generation DES, with a mean acute gain post procedure of 1.63 mm by quantitative coronary angiography and a mean late lumen loss of 0.12 mm when measured again at 9 or 12 months.
Intravascular ultrasound imaging showed a 3% increase in mean target vessel area and a 5% increase in the stented area from post procedure to 9 or 12 months’ follow-up, with no change in mean lumen area, all of which translates into maintenance of good blood flow over time. In contrast, what typically occurs following implantation of current DES is maintenance of target vessel and device areas, but with a loss in mean lumen area, the cardiologist noted.
There were two cardiac deaths but no cases of target lesion revascularization, device thrombosis, or strut fracture within 12 months of the procedure.
“The Bioadaptor performs similarly to second-generation DES in terms of implantation technique, deliverability, conformability, and radial strength during the healing phase, while showing the promise of mitigating the 2%-3% annualized event rate beyond 1 year,” Dr. Verheye concluded, adding, “Obviously, longer-term follow-up in comparative studies will be needed to show a reduction in the device-oriented events that have been observed with current DES.”
Session cochair Davide Capodanno, MD, PhD, of the University of Catania (Italy), declared: “This is an intriguing device because it’s metal, but it’s a kind of pulsatile metal after the biodegradation of the connectors. It’s something I’ve never seen.”
Discussant William Wijns, MD, PhD, said he was “thrilled” by the innovative aspect of the DynamX Bioadaptor, but he’s a long way from being persuaded that the device’s potential physiological advantages will translate into improved clinical outcomes relative to current DES.
“Don’t we all have a strange feeling of deja vu because all these anticipated benefits are the same as those we were told we would see with fully bioresorbable scaffolds? And we know so much after 10 years of experience with bioresorbable scaffolds that probably we will not accept this great story unless we get more and more evidence,” cautioned Dr. Wijns, professor of interventional cardiology at the National University of Ireland, Galway, and chairman of EuroPCR.
The claim regarding bioresorbable scaffolds was that, even though the acute results weren’t as good as with DES, that disadvantage would be outweighed by superior long-term clinical outcomes. But in fact the long-term outcomes turned out to be worse as well.
“We had to give up immediate results with the bioresorbable scaffolds. I don’t think we want to go that route again this time,” the cardiologist said.
Thus, the first thing that’s needed in order to make a convincing case for the Bioadaptor is evidence from a large, randomized, comparative trial demonstrating that the acute performance of the novel device is noninferior to that of current DES, including data on complex lesions. Such a study was supposed to be underway now but has been delayed by the COVID-19 pandemic, he noted.
Once there is evidence that the acute results with the Bioadaptor are truly comparable with those achieved with current DES, there will be a need for long-term data showing that the device reduces the 2%-3% annualized event rate seen with DES beyond 1 year, Dr. Wijns added.
Dr. Verheye reported receiving consultation fees from study sponsor Elixir Medical as well as from Biotronik. Dr. Wijns reported receiving research grants from MicroPort.
REPORTING FROM EUROPCR 2020
He Doesn’t Love It Warts and All
ANSWER
The correct answer is lichen planus (choice “c”).
DISCUSSION
Condyloma accuminata can demonstrate amazing lability, sometimes appearing decades after exposure. And spouses may not always be truthful when questioned about such exposure. To further confuse the issue, it's entirely possible that a patient may be unaware he or she has condyloma. So, this might well have been condyloma. But the differential for penile lesions would include this condition—and more.
Psoriasis (choice “a”) commonly affects the penis, manifesting as pinkish plaques and papules. But there is a good chance that examination would have revealed corroborative signs of this disease. Furthermore, the histologic results would have been entirely different.
While syphilis (choice “b”), especially in its primary stage, can present with nonhealing sores, in no way do they resemble the patient’s lesions. There is also no source for such an infection. And biopsy would have shown a predominately plasma cell infiltrate in an entirely different pattern.
Lichen sclerosus et atrophicus (choice “d”) is quite uncommon, especially on the penis, where it is usually known as balanitis xerotica obliterans (BXO). As its name suggests, BXO is usually atrophic—therefore macular—and whitish. Exclusive to uncircumcised men, it bears no resemblance to condyloma.
Though idiopathic, lichen planus is not contagious. Unless neglected, this condition seldom causes any suffering aside from mental anguish over its appearance. To make a more accurate diagnosis, it is always helpful for providers to consider a mnemonic device for “7 Ps” associated with lichen planus:
- Penile
- Pruritic
- Plaque-like
- Purple
- Papular
- Planar
- Puzzling.
TREATMENT
Fortunately, lichen planus affecting the penis responds readily to treatment with mid-strength topical steroid cream and the "tincture of time," which improves its appearance until it eventually disappears. For this patient, the PCP treated the affected area with triamcinolone 0.1% cream bid for 2 weeks. This was then applied once a day every other day for a month, which cleared the patient’s lesions.
ANSWER
The correct answer is lichen planus (choice “c”).
DISCUSSION
Condyloma accuminata can demonstrate amazing lability, sometimes appearing decades after exposure. And spouses may not always be truthful when questioned about such exposure. To further confuse the issue, it's entirely possible that a patient may be unaware he or she has condyloma. So, this might well have been condyloma. But the differential for penile lesions would include this condition—and more.
Psoriasis (choice “a”) commonly affects the penis, manifesting as pinkish plaques and papules. But there is a good chance that examination would have revealed corroborative signs of this disease. Furthermore, the histologic results would have been entirely different.
While syphilis (choice “b”), especially in its primary stage, can present with nonhealing sores, in no way do they resemble the patient’s lesions. There is also no source for such an infection. And biopsy would have shown a predominately plasma cell infiltrate in an entirely different pattern.
Lichen sclerosus et atrophicus (choice “d”) is quite uncommon, especially on the penis, where it is usually known as balanitis xerotica obliterans (BXO). As its name suggests, BXO is usually atrophic—therefore macular—and whitish. Exclusive to uncircumcised men, it bears no resemblance to condyloma.
Though idiopathic, lichen planus is not contagious. Unless neglected, this condition seldom causes any suffering aside from mental anguish over its appearance. To make a more accurate diagnosis, it is always helpful for providers to consider a mnemonic device for “7 Ps” associated with lichen planus:
- Penile
- Pruritic
- Plaque-like
- Purple
- Papular
- Planar
- Puzzling.
TREATMENT
Fortunately, lichen planus affecting the penis responds readily to treatment with mid-strength topical steroid cream and the "tincture of time," which improves its appearance until it eventually disappears. For this patient, the PCP treated the affected area with triamcinolone 0.1% cream bid for 2 weeks. This was then applied once a day every other day for a month, which cleared the patient’s lesions.
ANSWER
The correct answer is lichen planus (choice “c”).
DISCUSSION
Condyloma accuminata can demonstrate amazing lability, sometimes appearing decades after exposure. And spouses may not always be truthful when questioned about such exposure. To further confuse the issue, it's entirely possible that a patient may be unaware he or she has condyloma. So, this might well have been condyloma. But the differential for penile lesions would include this condition—and more.
Psoriasis (choice “a”) commonly affects the penis, manifesting as pinkish plaques and papules. But there is a good chance that examination would have revealed corroborative signs of this disease. Furthermore, the histologic results would have been entirely different.
While syphilis (choice “b”), especially in its primary stage, can present with nonhealing sores, in no way do they resemble the patient’s lesions. There is also no source for such an infection. And biopsy would have shown a predominately plasma cell infiltrate in an entirely different pattern.
Lichen sclerosus et atrophicus (choice “d”) is quite uncommon, especially on the penis, where it is usually known as balanitis xerotica obliterans (BXO). As its name suggests, BXO is usually atrophic—therefore macular—and whitish. Exclusive to uncircumcised men, it bears no resemblance to condyloma.
Though idiopathic, lichen planus is not contagious. Unless neglected, this condition seldom causes any suffering aside from mental anguish over its appearance. To make a more accurate diagnosis, it is always helpful for providers to consider a mnemonic device for “7 Ps” associated with lichen planus:
- Penile
- Pruritic
- Plaque-like
- Purple
- Papular
- Planar
- Puzzling.
TREATMENT
Fortunately, lichen planus affecting the penis responds readily to treatment with mid-strength topical steroid cream and the "tincture of time," which improves its appearance until it eventually disappears. For this patient, the PCP treated the affected area with triamcinolone 0.1% cream bid for 2 weeks. This was then applied once a day every other day for a month, which cleared the patient’s lesions.

A 41-year-old man is understandably upset when his primary care provider (PCP) diagnoses him with penile warts. Still, he is more than willing to allow his PCP to treat the area with liquid nitrogen, which clears the affected area. However, after about a month, the warts reappear in the same area, with the same appearance, and the patient decides to consult his PCP about additional treatment.
To his distress, his PCP suggests that the warts may continue to return despite treatment. This prompts the patient to ask a more upsetting question: How had he even acquired the warts? Neither he nor his wife of 20 years has had any other sexual contact. Prior to marriage, he had no sexual encounters by which he might have acquired human papillomavirus (HPV).
The patient is otherwise quite healthy, though anxious to have his warts treated again despite the possibility of recurrence. At no point have the warts been symptomatic. His wife's Pap smears have been completely normal.
Examination reveals 4 tiny, pink, planar (flat-topped), 2-to-4-mm papules in 2 locations on the penile shaft. Each has a soft shiny surface. There is also a soft, smooth, pink, annular, 2-cm plaque on the distal shaft that spills over onto the corona focally.
Shave biopsy of 1 lesion shows a brisk lymphocytic infiltrate, which obliterated the dermo-epidermal junction, imparting a jagged sawtooth pattern to its usually smooth wave-like pattern. There are no signs of HPV. The patient has no other remarkable lesions or changes on his elbows, knees, trunk, legs, nails, or scalp.

Radial artery beats saphenous vein grafting 10 years after CABG
With a median follow-up of 10 years after coronary artery bypass grafting (CABG), patients who received a radial artery graft rather than a saphenous vein graft as a second conduit were less likely to experience death, MI, or repeat revascularization, according to pooled data from five randomized trials.

The same result from the same set of data was produced after a median of 5 years, but the longer follow-up provides a more compelling case for the superiority of the radial artery graft, according to the authors of this meta-analysis, led by Mario F.L. Gaudino, MD, professor of cardiothoracic surgery at Weill Cornell Medicine, New York.
For the primary composite endpoint of death, MI, or repeat revascularization, the favorable hazard ratio at 5 years corresponded to a 33% risk reduction (HR, 0.67; P = .01), according to the previously published results (Gaudino M et al. N Engl J Med. 2018;378:2069-77).
The new data at 10 years show about the same risk reduction for the primary endpoint, but with more robust statistical significance (HR, 0.73; P < .001).
More importantly, because of the greater number of events by 10 years, the advantage of radial artery graft for the secondary composite outcome of death or MI has now reached statistical significance (HR, 0.77; P = .01).
In addition, there was a 27% reduction in risk of all-cause mortality (HR, 0.73; 95% confidence interval, 0.57-0.93) at 10 years associated with the radial artery graft. But this was not a prespecified endpoint, and so this is a hypothesis-generating post hoc finding.
The data was drawn from five randomized trials with a total of 1,036 patients. When used as an additional conduit to an internal thoracic artery in CABG, radial artery grafts relative to saphenous vein grafts were associated with a lower but nonsignificant risk of adverse outcomes in all five trials.
The advantage of radial artery grafts in the meta-analysis at 5 and now 10 years supports a series of observational studies that have also claimed better results with radial artery grafts.
The analysis was published July 14 in JAMA with essentially the same outcomes reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation in March.
However, a editorial that accompanied this meta-analysis in JAMA raised fundamental questions about revascularization.

“Intuitively, high-severity coronary lesions with significant ischemic burden, poor collateralization, and significant myocardium at risk may benefit from a durable revascularization option,” observed the editorial coauthors, Steven E. Nissen, MD, and Faisal G. Bakaeen, MD, both of the Cleveland Clinic. However, they cautioned that there is no definitive evidence that “any revascularization procedure reduces cardiovascular morbidity or mortality in patients with anatomically and physiologically stable coronary artery disease.”
They called the 10-year outcomes from the meta-analysis “the best available long-term data on the potential value of using the radial artery as a bypass conduit,” but warned that no randomized trial has confirmed that two or more conduits are superior to a single internal thoracic artery in CABG to for preventing death and major adverse cardiovascular events.
Such a trial, called ROMA, is now underway (Eur J Cardiothorac Surg. 2017;52:1031-40), but results are not expected until 2025.
In the meantime, placement of second conduits remains common in CABG procedures, about 400,000 of which are performed each year in the United States. According to Dr. Gaudino, there are indications and contraindications for second conduits, but radial artery should be the preferred standard when these are considered.
“Our data indicate that the radial artery graft should be used to complement the left internal thoracic artery in all patients who meet the indications for radial artery grafts,” he explained in an interview.
“Unfortunately, at the moment radial artery grafts are used in less than 10% of CABG cases in the U.S.,” he reported. “Hopefully, our data will lead to a larger use of this conduit by the surgical community.”
Dr. Gaudino, the principal investigator, reported no potential conflicts of interest relevant to this study.
SOURCE: Gaudino MFL et al. JAMA. 2020;324:179-87.
With a median follow-up of 10 years after coronary artery bypass grafting (CABG), patients who received a radial artery graft rather than a saphenous vein graft as a second conduit were less likely to experience death, MI, or repeat revascularization, according to pooled data from five randomized trials.
The same result from the same set of data was produced after a median of 5 years, but the longer follow-up provides a more compelling case for the superiority of the radial artery graft, according to the authors of this meta-analysis, led by Mario F.L. Gaudino, MD, professor of cardiothoracic surgery at Weill Cornell Medicine, New York.
For the primary composite endpoint of death, MI, or repeat revascularization, the favorable hazard ratio at 5 years corresponded to a 33% risk reduction (HR, 0.67; P = .01), according to the previously published results (Gaudino M et al. N Engl J Med. 2018;378:2069-77).
The new data at 10 years show about the same risk reduction for the primary endpoint, but with more robust statistical significance (HR, 0.73; P < .001).
More importantly, because of the greater number of events by 10 years, the advantage of radial artery graft for the secondary composite outcome of death or MI has now reached statistical significance (HR, 0.77; P = .01).
In addition, there was a 27% reduction in risk of all-cause mortality (HR, 0.73; 95% confidence interval, 0.57-0.93) at 10 years associated with the radial artery graft. But this was not a prespecified endpoint, and so this is a hypothesis-generating post hoc finding.
The data was drawn from five randomized trials with a total of 1,036 patients. When used as an additional conduit to an internal thoracic artery in CABG, radial artery grafts relative to saphenous vein grafts were associated with a lower but nonsignificant risk of adverse outcomes in all five trials.
The advantage of radial artery grafts in the meta-analysis at 5 and now 10 years supports a series of observational studies that have also claimed better results with radial artery grafts.
The analysis was published July 14 in JAMA with essentially the same outcomes reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation in March.
However, a editorial that accompanied this meta-analysis in JAMA raised fundamental questions about revascularization.
“Intuitively, high-severity coronary lesions with significant ischemic burden, poor collateralization, and significant myocardium at risk may benefit from a durable revascularization option,” observed the editorial coauthors, Steven E. Nissen, MD, and Faisal G. Bakaeen, MD, both of the Cleveland Clinic. However, they cautioned that there is no definitive evidence that “any revascularization procedure reduces cardiovascular morbidity or mortality in patients with anatomically and physiologically stable coronary artery disease.”
They called the 10-year outcomes from the meta-analysis “the best available long-term data on the potential value of using the radial artery as a bypass conduit,” but warned that no randomized trial has confirmed that two or more conduits are superior to a single internal thoracic artery in CABG to for preventing death and major adverse cardiovascular events.
Such a trial, called ROMA, is now underway (Eur J Cardiothorac Surg. 2017;52:1031-40), but results are not expected until 2025.
In the meantime, placement of second conduits remains common in CABG procedures, about 400,000 of which are performed each year in the United States. According to Dr. Gaudino, there are indications and contraindications for second conduits, but radial artery should be the preferred standard when these are considered.
“Our data indicate that the radial artery graft should be used to complement the left internal thoracic artery in all patients who meet the indications for radial artery grafts,” he explained in an interview.
“Unfortunately, at the moment radial artery grafts are used in less than 10% of CABG cases in the U.S.,” he reported. “Hopefully, our data will lead to a larger use of this conduit by the surgical community.”
Dr. Gaudino, the principal investigator, reported no potential conflicts of interest relevant to this study.
SOURCE: Gaudino MFL et al. JAMA. 2020;324:179-87.
With a median follow-up of 10 years after coronary artery bypass grafting (CABG), patients who received a radial artery graft rather than a saphenous vein graft as a second conduit were less likely to experience death, MI, or repeat revascularization, according to pooled data from five randomized trials.
The same result from the same set of data was produced after a median of 5 years, but the longer follow-up provides a more compelling case for the superiority of the radial artery graft, according to the authors of this meta-analysis, led by Mario F.L. Gaudino, MD, professor of cardiothoracic surgery at Weill Cornell Medicine, New York.
For the primary composite endpoint of death, MI, or repeat revascularization, the favorable hazard ratio at 5 years corresponded to a 33% risk reduction (HR, 0.67; P = .01), according to the previously published results (Gaudino M et al. N Engl J Med. 2018;378:2069-77).
The new data at 10 years show about the same risk reduction for the primary endpoint, but with more robust statistical significance (HR, 0.73; P < .001).
More importantly, because of the greater number of events by 10 years, the advantage of radial artery graft for the secondary composite outcome of death or MI has now reached statistical significance (HR, 0.77; P = .01).
In addition, there was a 27% reduction in risk of all-cause mortality (HR, 0.73; 95% confidence interval, 0.57-0.93) at 10 years associated with the radial artery graft. But this was not a prespecified endpoint, and so this is a hypothesis-generating post hoc finding.
The data was drawn from five randomized trials with a total of 1,036 patients. When used as an additional conduit to an internal thoracic artery in CABG, radial artery grafts relative to saphenous vein grafts were associated with a lower but nonsignificant risk of adverse outcomes in all five trials.
The advantage of radial artery grafts in the meta-analysis at 5 and now 10 years supports a series of observational studies that have also claimed better results with radial artery grafts.
The analysis was published July 14 in JAMA with essentially the same outcomes reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation in March.
However, a editorial that accompanied this meta-analysis in JAMA raised fundamental questions about revascularization.
“Intuitively, high-severity coronary lesions with significant ischemic burden, poor collateralization, and significant myocardium at risk may benefit from a durable revascularization option,” observed the editorial coauthors, Steven E. Nissen, MD, and Faisal G. Bakaeen, MD, both of the Cleveland Clinic. However, they cautioned that there is no definitive evidence that “any revascularization procedure reduces cardiovascular morbidity or mortality in patients with anatomically and physiologically stable coronary artery disease.”
They called the 10-year outcomes from the meta-analysis “the best available long-term data on the potential value of using the radial artery as a bypass conduit,” but warned that no randomized trial has confirmed that two or more conduits are superior to a single internal thoracic artery in CABG to for preventing death and major adverse cardiovascular events.
Such a trial, called ROMA, is now underway (Eur J Cardiothorac Surg. 2017;52:1031-40), but results are not expected until 2025.
In the meantime, placement of second conduits remains common in CABG procedures, about 400,000 of which are performed each year in the United States. According to Dr. Gaudino, there are indications and contraindications for second conduits, but radial artery should be the preferred standard when these are considered.
“Our data indicate that the radial artery graft should be used to complement the left internal thoracic artery in all patients who meet the indications for radial artery grafts,” he explained in an interview.
“Unfortunately, at the moment radial artery grafts are used in less than 10% of CABG cases in the U.S.,” he reported. “Hopefully, our data will lead to a larger use of this conduit by the surgical community.”
Dr. Gaudino, the principal investigator, reported no potential conflicts of interest relevant to this study.
SOURCE: Gaudino MFL et al. JAMA. 2020;324:179-87.
FROM JAMA
Pooled Testing for SARS-CoV-2 in Hospitalized Patients
Viral testing for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) of all patients admitted to the hospital is an appealing objective given the recognition of asymptomatic or minimally symptomatic infections. Yet such testing requires that all admitted patients be classified as persons under investigation (PUIs) until their test results are known. If an outside laboratory is used for the SARS-CoV-2 testing, the delay in obtaining results for these PUIs may cause significant personal protective equipment (PPE) use, postpone some care for non-coronavirus disease 2019 (COVID-19) conditions, block beds, and produce anxiety among staff and other patients. Rapid in-house testing of all admitted patients may resolve these issues but may be limited by the supply of reagents. To address this challenge, we piloted a pooled testing strategy for patients at low risk for SARS-CoV-2 admitted to a community hospital.
METHODS
From April 17, 2020, to May 11, 2020, we implemented a pooled testing strategy using the GeneXpert® System (Cepheid, Sunnyvale, California) at Saratoga Hospital, a 171-bed community hospital in upstate New York. Under normal procedures for this system, a single patient swab is placed in a vial containing viral transport media (VTM). An aliquot of this media is then transferred into a Xpert® Xpress SARS CoV-2 test cartridge and assayed on the GeneXpert® instrument in our laboratory. Obtaining immediate results allowed us to assign admitted patients to either a COVID-19 or a non–COVID-19 unit, improving the issues associated with PUIs. Unfortunately, we did not have enough test cartridges to sustain this strategy of rapid individual testing of all admitted patients, and supply lines have remained uncertain.
We sought to conserve our limited Xpert Xpress SARS CoV-2 test cartridges using the strategy of pooled testing, a technique reported in Germany and by the University of Nebraska.1,2 In this method, variable numbers of tests are pooled for a single analysis. If the test from the pooled vial is negative, these patients are all considered negative. If the pooled test is positive, all those patients need individual testing. This pooling method has been theorized to preserve test cartridges when the expected frequency of positive results is low.3
All patients admitted or placed on observation underwent SARS-CoV-2 PCR testing. The Emergency Department (ED) staff stratified patients into high or low risk to determine if they would be tested in a single send-out test (high risk) or a rapid in-house pooled group (low risk). High-risk patients were those with compatible history, physical exam, laboratory markers, and radiographic studies for COVID-19 disease. This often included increased supplemental oxygen requirement, multiple elevated inflammatory markers (including D-dimer, C-reactive protein, erythrocyte sedimentation rate, and ferritin levels), lymphopenia, and findings on chest radiograph or computed tomography scan including ground glass changes, multifocal pneumonia, or pneumonia. High-risk patients were admitted to the COVID unit or intensive care unit, had a send-out SARS-CoV-2 polymerase chain reaction (PCR) test, and were treated as a PUI until the results of their testing was known and correlated with their clinical course. Low-risk patients were those without complaints suggestive of COVID-19 infection and who may have had negative inflammatory markers, no significant lymphopenia, and negative imaging.
The samples from 3 admitted patients thought to be at low-risk for COVID-19 using the clinical judgement of our ED staff were pooled for testing. All samples were obtained using nasopharyngeal swabs by experienced staff. The swabs from these patients were placed into a single vial of 3 mL VTM, maintaining the recommended 1 swab per mL of VTM. An aliquot of this media was then transferred into an Xpert Xpress SARS CoV-2 test cartridge and assayed on the GeneXpert instrument in our laboratory following manufacturer’s instructions. Based on analytic laboratory studies of the Cepheid Xpert Express SARS-CoV-2 test,4 we assume a clinical performance comparable to other reverse-transcriptase PCR (RT-PCR) tests, which have so far demonstrated sensitivities of 60% to 80% and specificities of 95% to 99%.5
Validation studies were performed on pools made from samples obtained from admitted patients with previously known positive and negative samples tested at the New York State Department of Health, Wadsworth Center laboratory (Albany, New York). A total of 14 samples were used for the instrument validation study, including three samples for pooled testing. The cycle threshold (Ct) value is defined as the number of PCR cycles required for the signal to be detectable. Ct values for each nucleic acid target of a known positive sample tested singly and in the pool with known negative patients were compared. A small shift in Ct values was noted between single and pooled testing, demonstrating no decrease in analytic sensitivity and suggesting that we would experience no decrease in clinical sensitivity.
We selected the pooling of 3 samples into 1 cartridge for several reasons: (1) 3-sample pools are well within the appropriate pooling size for the percentage positive rate in the population being tested. The use of larger pool sizes results in the need for more repeat testing when a positive result is obtained; (2) Given our supply lines, the projected savings would allow us to continue this strategy; and (3) Holding 3 patients in the ED until a pool was ready was manageable given our rate of admissions and ED volume.
The strategy required patients being held in the ED until a pooled group of 3 could be tested. On select occasions when holding patients in the ED to obtain a pool of 3 was not practical, 2 patients were tested in the pool. These decisions required close coordination between the laboratory, ED, and nursing staff.
RESULTS
This strategy resulted in 530 unique patient tests in 179 cartridges (172 with three swabs and 7 with two swabs). We had 4 positive pooled tests, requiring the use of 11 additional cartridges, for a positive rate of 0.8% (4/530) in this low-risk population (patients without COVID-19–related symptoms). There were no patients from negative pools who developed evidence of COVID-19 disease or tested positive for SARS-CoV-2 during their hospitalization. The total number of cartridges used was 190 and the number saved was 340.
DISCUSSION
The strategy of pooled testing for SARS-CoV-2 in patients admitted to our community hospital allowed us to continue rapid testing of admitted patients at low risk for COVID-19 disease during a period when supplies would otherwise not have been sufficient. We believe this strategy conserved PPE, led to a marked reduction in staff and patient anxiety, and improved patient care. Our impression is that testing all admitted patients has also been reassuring to our community. Like many others, we have observed that public fear of entering the hospital during this pandemic has caused delays in patients seeking care for non–COVID-19 conditions. We believe this strategy will help reduce those fears.
This strategy may require modification as the pandemic progresses. Our ED physicians were able to identify patients who they felt to be low risk for having COVID-19 disease based on signs, symptoms, and clinical impression during a time when we had an 8% positive rate among symptomatic outpatients and an estimated community positive rate in the range of 1% to 2%. If the rate of positive tests in our community rises, the use of pooling may need to be limited or the pool size reduced. If our supply of reagents is further limited or patient testing demand increases, the pool size may need to be increased. This will need to be balanced with our ability to hold patients in the ED while waiting for the pool size to be reached.
CONCLUSION
The strategy of pooled testing for SARS-CoV-2 has allowed us to continue to immediately test all admitted patients, thus improving patient care. It has required close coordination between multiple members of our laboratory and clinical staff and may require adjustment as the pandemic progresses. We believe it is a valuable tool during a time of limited resources that may have application in testing other low-risk groups, including healthcare workers and clients of occupational medicine services.
Acknowledgment
The authors gratefully acknowledge the support of Kirsten St. George, MAppSc, PhD, Director, Virology Laboratory, Wadsworth, NYSDOH, and the services supplied by the Wadsworth laboratory to our region.
1. Corona ‘pool testing’ increases worldwide capacities many times over. January 4, 2020. Accessed April 20, 2020. https://healthcare-in-europe.com/en/news/corona-pool-testing-increases-worldwide-capacities-many-times-over.html
2. Abdalhamid B, Bilder CR, McCutchen EL, Hinrichs SH, Koepsell SA, Iwen PC. Assessment of specimen pooling to conserve SARS CoV-2 testing resources. Am J Clin Pathol. 2020;153(6):715-718. https://doi.org/10.1093/ajcp/aqaa064
3. Shani-Narkiss H, Gilday OD, Yayon N, Landau ID. Efficient and practical sample pooling for high-throughput PCR diagnosis of COVID-19. medRxiv. April 6, 2020. https://doi.org/10.1101/2020.04.06.20052159
4. Wolters F, van de Bovenkamp J, van den Bosch B, et al. Multi-center evaluation of Cepheid Xpert® Xpress SARS-CoV-2 point-of-care test during the SARS-CoV-2 pandemic. J Clin Virol. 2020;128:104426. https://doi.org/10.1016/j.jcv.2020.104426
5. Woloshin S, Patel N, Kesselheim AS. False negative tests for SARS-CoV-2 infection—challenges and implications. N Engl J Med. 2020. Online first. https://doi.org/10.1056/NEJMp2015897
Viral testing for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) of all patients admitted to the hospital is an appealing objective given the recognition of asymptomatic or minimally symptomatic infections. Yet such testing requires that all admitted patients be classified as persons under investigation (PUIs) until their test results are known. If an outside laboratory is used for the SARS-CoV-2 testing, the delay in obtaining results for these PUIs may cause significant personal protective equipment (PPE) use, postpone some care for non-coronavirus disease 2019 (COVID-19) conditions, block beds, and produce anxiety among staff and other patients. Rapid in-house testing of all admitted patients may resolve these issues but may be limited by the supply of reagents. To address this challenge, we piloted a pooled testing strategy for patients at low risk for SARS-CoV-2 admitted to a community hospital.
METHODS
From April 17, 2020, to May 11, 2020, we implemented a pooled testing strategy using the GeneXpert® System (Cepheid, Sunnyvale, California) at Saratoga Hospital, a 171-bed community hospital in upstate New York. Under normal procedures for this system, a single patient swab is placed in a vial containing viral transport media (VTM). An aliquot of this media is then transferred into a Xpert® Xpress SARS CoV-2 test cartridge and assayed on the GeneXpert® instrument in our laboratory. Obtaining immediate results allowed us to assign admitted patients to either a COVID-19 or a non–COVID-19 unit, improving the issues associated with PUIs. Unfortunately, we did not have enough test cartridges to sustain this strategy of rapid individual testing of all admitted patients, and supply lines have remained uncertain.
We sought to conserve our limited Xpert Xpress SARS CoV-2 test cartridges using the strategy of pooled testing, a technique reported in Germany and by the University of Nebraska.1,2 In this method, variable numbers of tests are pooled for a single analysis. If the test from the pooled vial is negative, these patients are all considered negative. If the pooled test is positive, all those patients need individual testing. This pooling method has been theorized to preserve test cartridges when the expected frequency of positive results is low.3
All patients admitted or placed on observation underwent SARS-CoV-2 PCR testing. The Emergency Department (ED) staff stratified patients into high or low risk to determine if they would be tested in a single send-out test (high risk) or a rapid in-house pooled group (low risk). High-risk patients were those with compatible history, physical exam, laboratory markers, and radiographic studies for COVID-19 disease. This often included increased supplemental oxygen requirement, multiple elevated inflammatory markers (including D-dimer, C-reactive protein, erythrocyte sedimentation rate, and ferritin levels), lymphopenia, and findings on chest radiograph or computed tomography scan including ground glass changes, multifocal pneumonia, or pneumonia. High-risk patients were admitted to the COVID unit or intensive care unit, had a send-out SARS-CoV-2 polymerase chain reaction (PCR) test, and were treated as a PUI until the results of their testing was known and correlated with their clinical course. Low-risk patients were those without complaints suggestive of COVID-19 infection and who may have had negative inflammatory markers, no significant lymphopenia, and negative imaging.
The samples from 3 admitted patients thought to be at low-risk for COVID-19 using the clinical judgement of our ED staff were pooled for testing. All samples were obtained using nasopharyngeal swabs by experienced staff. The swabs from these patients were placed into a single vial of 3 mL VTM, maintaining the recommended 1 swab per mL of VTM. An aliquot of this media was then transferred into an Xpert Xpress SARS CoV-2 test cartridge and assayed on the GeneXpert instrument in our laboratory following manufacturer’s instructions. Based on analytic laboratory studies of the Cepheid Xpert Express SARS-CoV-2 test,4 we assume a clinical performance comparable to other reverse-transcriptase PCR (RT-PCR) tests, which have so far demonstrated sensitivities of 60% to 80% and specificities of 95% to 99%.5
Validation studies were performed on pools made from samples obtained from admitted patients with previously known positive and negative samples tested at the New York State Department of Health, Wadsworth Center laboratory (Albany, New York). A total of 14 samples were used for the instrument validation study, including three samples for pooled testing. The cycle threshold (Ct) value is defined as the number of PCR cycles required for the signal to be detectable. Ct values for each nucleic acid target of a known positive sample tested singly and in the pool with known negative patients were compared. A small shift in Ct values was noted between single and pooled testing, demonstrating no decrease in analytic sensitivity and suggesting that we would experience no decrease in clinical sensitivity.
We selected the pooling of 3 samples into 1 cartridge for several reasons: (1) 3-sample pools are well within the appropriate pooling size for the percentage positive rate in the population being tested. The use of larger pool sizes results in the need for more repeat testing when a positive result is obtained; (2) Given our supply lines, the projected savings would allow us to continue this strategy; and (3) Holding 3 patients in the ED until a pool was ready was manageable given our rate of admissions and ED volume.
The strategy required patients being held in the ED until a pooled group of 3 could be tested. On select occasions when holding patients in the ED to obtain a pool of 3 was not practical, 2 patients were tested in the pool. These decisions required close coordination between the laboratory, ED, and nursing staff.
RESULTS
This strategy resulted in 530 unique patient tests in 179 cartridges (172 with three swabs and 7 with two swabs). We had 4 positive pooled tests, requiring the use of 11 additional cartridges, for a positive rate of 0.8% (4/530) in this low-risk population (patients without COVID-19–related symptoms). There were no patients from negative pools who developed evidence of COVID-19 disease or tested positive for SARS-CoV-2 during their hospitalization. The total number of cartridges used was 190 and the number saved was 340.
DISCUSSION
The strategy of pooled testing for SARS-CoV-2 in patients admitted to our community hospital allowed us to continue rapid testing of admitted patients at low risk for COVID-19 disease during a period when supplies would otherwise not have been sufficient. We believe this strategy conserved PPE, led to a marked reduction in staff and patient anxiety, and improved patient care. Our impression is that testing all admitted patients has also been reassuring to our community. Like many others, we have observed that public fear of entering the hospital during this pandemic has caused delays in patients seeking care for non–COVID-19 conditions. We believe this strategy will help reduce those fears.
This strategy may require modification as the pandemic progresses. Our ED physicians were able to identify patients who they felt to be low risk for having COVID-19 disease based on signs, symptoms, and clinical impression during a time when we had an 8% positive rate among symptomatic outpatients and an estimated community positive rate in the range of 1% to 2%. If the rate of positive tests in our community rises, the use of pooling may need to be limited or the pool size reduced. If our supply of reagents is further limited or patient testing demand increases, the pool size may need to be increased. This will need to be balanced with our ability to hold patients in the ED while waiting for the pool size to be reached.
CONCLUSION
The strategy of pooled testing for SARS-CoV-2 has allowed us to continue to immediately test all admitted patients, thus improving patient care. It has required close coordination between multiple members of our laboratory and clinical staff and may require adjustment as the pandemic progresses. We believe it is a valuable tool during a time of limited resources that may have application in testing other low-risk groups, including healthcare workers and clients of occupational medicine services.
Acknowledgment
The authors gratefully acknowledge the support of Kirsten St. George, MAppSc, PhD, Director, Virology Laboratory, Wadsworth, NYSDOH, and the services supplied by the Wadsworth laboratory to our region.
Viral testing for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) of all patients admitted to the hospital is an appealing objective given the recognition of asymptomatic or minimally symptomatic infections. Yet such testing requires that all admitted patients be classified as persons under investigation (PUIs) until their test results are known. If an outside laboratory is used for the SARS-CoV-2 testing, the delay in obtaining results for these PUIs may cause significant personal protective equipment (PPE) use, postpone some care for non-coronavirus disease 2019 (COVID-19) conditions, block beds, and produce anxiety among staff and other patients. Rapid in-house testing of all admitted patients may resolve these issues but may be limited by the supply of reagents. To address this challenge, we piloted a pooled testing strategy for patients at low risk for SARS-CoV-2 admitted to a community hospital.
METHODS
From April 17, 2020, to May 11, 2020, we implemented a pooled testing strategy using the GeneXpert® System (Cepheid, Sunnyvale, California) at Saratoga Hospital, a 171-bed community hospital in upstate New York. Under normal procedures for this system, a single patient swab is placed in a vial containing viral transport media (VTM). An aliquot of this media is then transferred into a Xpert® Xpress SARS CoV-2 test cartridge and assayed on the GeneXpert® instrument in our laboratory. Obtaining immediate results allowed us to assign admitted patients to either a COVID-19 or a non–COVID-19 unit, improving the issues associated with PUIs. Unfortunately, we did not have enough test cartridges to sustain this strategy of rapid individual testing of all admitted patients, and supply lines have remained uncertain.
We sought to conserve our limited Xpert Xpress SARS CoV-2 test cartridges using the strategy of pooled testing, a technique reported in Germany and by the University of Nebraska.1,2 In this method, variable numbers of tests are pooled for a single analysis. If the test from the pooled vial is negative, these patients are all considered negative. If the pooled test is positive, all those patients need individual testing. This pooling method has been theorized to preserve test cartridges when the expected frequency of positive results is low.3
All patients admitted or placed on observation underwent SARS-CoV-2 PCR testing. The Emergency Department (ED) staff stratified patients into high or low risk to determine if they would be tested in a single send-out test (high risk) or a rapid in-house pooled group (low risk). High-risk patients were those with compatible history, physical exam, laboratory markers, and radiographic studies for COVID-19 disease. This often included increased supplemental oxygen requirement, multiple elevated inflammatory markers (including D-dimer, C-reactive protein, erythrocyte sedimentation rate, and ferritin levels), lymphopenia, and findings on chest radiograph or computed tomography scan including ground glass changes, multifocal pneumonia, or pneumonia. High-risk patients were admitted to the COVID unit or intensive care unit, had a send-out SARS-CoV-2 polymerase chain reaction (PCR) test, and were treated as a PUI until the results of their testing was known and correlated with their clinical course. Low-risk patients were those without complaints suggestive of COVID-19 infection and who may have had negative inflammatory markers, no significant lymphopenia, and negative imaging.
The samples from 3 admitted patients thought to be at low-risk for COVID-19 using the clinical judgement of our ED staff were pooled for testing. All samples were obtained using nasopharyngeal swabs by experienced staff. The swabs from these patients were placed into a single vial of 3 mL VTM, maintaining the recommended 1 swab per mL of VTM. An aliquot of this media was then transferred into an Xpert Xpress SARS CoV-2 test cartridge and assayed on the GeneXpert instrument in our laboratory following manufacturer’s instructions. Based on analytic laboratory studies of the Cepheid Xpert Express SARS-CoV-2 test,4 we assume a clinical performance comparable to other reverse-transcriptase PCR (RT-PCR) tests, which have so far demonstrated sensitivities of 60% to 80% and specificities of 95% to 99%.5
Validation studies were performed on pools made from samples obtained from admitted patients with previously known positive and negative samples tested at the New York State Department of Health, Wadsworth Center laboratory (Albany, New York). A total of 14 samples were used for the instrument validation study, including three samples for pooled testing. The cycle threshold (Ct) value is defined as the number of PCR cycles required for the signal to be detectable. Ct values for each nucleic acid target of a known positive sample tested singly and in the pool with known negative patients were compared. A small shift in Ct values was noted between single and pooled testing, demonstrating no decrease in analytic sensitivity and suggesting that we would experience no decrease in clinical sensitivity.
We selected the pooling of 3 samples into 1 cartridge for several reasons: (1) 3-sample pools are well within the appropriate pooling size for the percentage positive rate in the population being tested. The use of larger pool sizes results in the need for more repeat testing when a positive result is obtained; (2) Given our supply lines, the projected savings would allow us to continue this strategy; and (3) Holding 3 patients in the ED until a pool was ready was manageable given our rate of admissions and ED volume.
The strategy required patients being held in the ED until a pooled group of 3 could be tested. On select occasions when holding patients in the ED to obtain a pool of 3 was not practical, 2 patients were tested in the pool. These decisions required close coordination between the laboratory, ED, and nursing staff.
RESULTS
This strategy resulted in 530 unique patient tests in 179 cartridges (172 with three swabs and 7 with two swabs). We had 4 positive pooled tests, requiring the use of 11 additional cartridges, for a positive rate of 0.8% (4/530) in this low-risk population (patients without COVID-19–related symptoms). There were no patients from negative pools who developed evidence of COVID-19 disease or tested positive for SARS-CoV-2 during their hospitalization. The total number of cartridges used was 190 and the number saved was 340.
DISCUSSION
The strategy of pooled testing for SARS-CoV-2 in patients admitted to our community hospital allowed us to continue rapid testing of admitted patients at low risk for COVID-19 disease during a period when supplies would otherwise not have been sufficient. We believe this strategy conserved PPE, led to a marked reduction in staff and patient anxiety, and improved patient care. Our impression is that testing all admitted patients has also been reassuring to our community. Like many others, we have observed that public fear of entering the hospital during this pandemic has caused delays in patients seeking care for non–COVID-19 conditions. We believe this strategy will help reduce those fears.
This strategy may require modification as the pandemic progresses. Our ED physicians were able to identify patients who they felt to be low risk for having COVID-19 disease based on signs, symptoms, and clinical impression during a time when we had an 8% positive rate among symptomatic outpatients and an estimated community positive rate in the range of 1% to 2%. If the rate of positive tests in our community rises, the use of pooling may need to be limited or the pool size reduced. If our supply of reagents is further limited or patient testing demand increases, the pool size may need to be increased. This will need to be balanced with our ability to hold patients in the ED while waiting for the pool size to be reached.
CONCLUSION
The strategy of pooled testing for SARS-CoV-2 has allowed us to continue to immediately test all admitted patients, thus improving patient care. It has required close coordination between multiple members of our laboratory and clinical staff and may require adjustment as the pandemic progresses. We believe it is a valuable tool during a time of limited resources that may have application in testing other low-risk groups, including healthcare workers and clients of occupational medicine services.
Acknowledgment
The authors gratefully acknowledge the support of Kirsten St. George, MAppSc, PhD, Director, Virology Laboratory, Wadsworth, NYSDOH, and the services supplied by the Wadsworth laboratory to our region.
1. Corona ‘pool testing’ increases worldwide capacities many times over. January 4, 2020. Accessed April 20, 2020. https://healthcare-in-europe.com/en/news/corona-pool-testing-increases-worldwide-capacities-many-times-over.html
2. Abdalhamid B, Bilder CR, McCutchen EL, Hinrichs SH, Koepsell SA, Iwen PC. Assessment of specimen pooling to conserve SARS CoV-2 testing resources. Am J Clin Pathol. 2020;153(6):715-718. https://doi.org/10.1093/ajcp/aqaa064
3. Shani-Narkiss H, Gilday OD, Yayon N, Landau ID. Efficient and practical sample pooling for high-throughput PCR diagnosis of COVID-19. medRxiv. April 6, 2020. https://doi.org/10.1101/2020.04.06.20052159
4. Wolters F, van de Bovenkamp J, van den Bosch B, et al. Multi-center evaluation of Cepheid Xpert® Xpress SARS-CoV-2 point-of-care test during the SARS-CoV-2 pandemic. J Clin Virol. 2020;128:104426. https://doi.org/10.1016/j.jcv.2020.104426
5. Woloshin S, Patel N, Kesselheim AS. False negative tests for SARS-CoV-2 infection—challenges and implications. N Engl J Med. 2020. Online first. https://doi.org/10.1056/NEJMp2015897
1. Corona ‘pool testing’ increases worldwide capacities many times over. January 4, 2020. Accessed April 20, 2020. https://healthcare-in-europe.com/en/news/corona-pool-testing-increases-worldwide-capacities-many-times-over.html
2. Abdalhamid B, Bilder CR, McCutchen EL, Hinrichs SH, Koepsell SA, Iwen PC. Assessment of specimen pooling to conserve SARS CoV-2 testing resources. Am J Clin Pathol. 2020;153(6):715-718. https://doi.org/10.1093/ajcp/aqaa064
3. Shani-Narkiss H, Gilday OD, Yayon N, Landau ID. Efficient and practical sample pooling for high-throughput PCR diagnosis of COVID-19. medRxiv. April 6, 2020. https://doi.org/10.1101/2020.04.06.20052159
4. Wolters F, van de Bovenkamp J, van den Bosch B, et al. Multi-center evaluation of Cepheid Xpert® Xpress SARS-CoV-2 point-of-care test during the SARS-CoV-2 pandemic. J Clin Virol. 2020;128:104426. https://doi.org/10.1016/j.jcv.2020.104426
5. Woloshin S, Patel N, Kesselheim AS. False negative tests for SARS-CoV-2 infection—challenges and implications. N Engl J Med. 2020. Online first. https://doi.org/10.1056/NEJMp2015897
© 2020 Society of Hospital Medicine
Collateral Damage: How COVID-19 Is Adversely Impacting Women Physicians
The coronavirus disease of 2019 (COVID-19) pandemic has affected every facet of our work and personal lives. While many hope we will return to “normal” with the pandemic’s passing, there is reason to believe medicine, and society, will experience irrevocable changes. Although the number of women pursuing and practicing medicine has increased, inequities remain in compensation, academic rank, and leadership positions.1,2 Within the workplace, women are more likely to be in frontline clinical positions, are more likely to be integral in promoting positive interpersonal relationships and collaborative work environments, and often are less represented in the high-level, decision-making roles in leadership or administration.3,4 These well-described issues may be exacerbated during this pandemic crisis. We describe how the current COVID-19 pandemic may intensify workplace inequities for women, and propose solutions for hospitalist groups, leaders, and administrators to ensure female hospitalists continue to prosper and thrive in these tenuous times.
HOW THE PANDEMIC MAY EXACERBATE EXISTING INEQUITIES
Increasing Demands at Home
Female physicians are more likely to have partners who are employed full-time and report spending more time on household activities including cleaning, cooking, and the care of children, compared with their male counterparts.5 With school and daycare closings, as well as stay-at-home orders in many US states, there has been an increase in household responsibilities and care needs for children remaining at home with a marked decrease in options for stable or emergency childcare.6 As compared with primary care and subspecialty colleagues who can provide a large percentage of their care through telemedicine, this is not the case for hospitalists who must be physically present to care for their patients. Therefore, hospitalists are unable to clinically “work from home” in the same way as many of their colleagues in other specialties. Increased childcare and schooling obligations, coupled with disproportionate household responsibilities and an inability to work from home, will likely result in female hospitalists struggling to meet family needs while pandemic-related work responsibilities are ramping up.7 In addition, women who are involved with administrative, leadership, or research activities may struggle to execute their responsibilities as a result of increased domestic duties.
Many hospitalists are also concerned about contracting COVID-19 and exposing their families to the illness given the high infection rate among healthcare workers and the shortage of personal protective equipment (PPE).8,9 Institutions and national organizations, including the Society of Hospital Medicine, have partnered with industry to provide discounted or complimentary hotel rooms for members to aid self-isolation while providing clinical care.10 One famous photo in popular and social media showed a pulmonary and critical care physician in a tent in his garage in order to self-isolate from his family.11 However, since women are often the primary caregivers for their children or other family members and may also be responsible for other important household activities, they may be unable or unwilling to remove themselves from their children and families. As a result, female hospitalists may encounter feelings of guilt or inadequacy if they’re unable to isolate in the same manner as male colleagues.8
Exaggerating Leadership Gap
One of the keys to a robust response to this pandemic is strong, thoughtful, and strategic leadership.12 Institutional, regional, and national leaders are at the forefront of designing the solutions to the many problems the COVID-19 pandemic has created. The paucity of women at high-level leadership positions in institutions across the United States, including university-based, community, public, and private institutions, means that there is a lack of female representation when institutional policy is being discussed and decided.4 This lack of representation may lead to policies and procedures that negatively affect female hospitalists or, at best, fail to consider the needs of or support female physicians. For example, leaders of a hospital medicine group may create mandatory “backup” coverage for night and weekend shifts for their group during surge periods of the pandemic without considering implications for childcare. Finding weekday, daytime coverage is challenging for many during this time when daycares and school are closed, and finding coverage during weekend or overnight hours will be even more challenging. With increased risks for older adults with high-risk medical conditions, grandparents or other friends or family members that previously would have assisted with childcare may no longer be an option. If a female hospitalist is not a member of the leadership group that helped design this coverage structure, there could be a lack of recognition of the undue strain this coverage model could create for women in the group. Even if not intentional, such policies may hinder women’s career stability and opportunities for further advancement, as well as their ability to adequately provide care for their families. Having women as a part of the leadership group that creates policies and schedules and makes pivotal decisions is imperative, especially regarding topics of providing access and compensation for “emergency childcare,” hazard pay, shift length, work conditions, job security, sick leave, workers compensation, advancement opportunities, and hiring practices.
Compensation
The gender pay gap in medicine has been consistently demonstrated among many specialties.13,14 The reasons for this inequity are multifactorial, and the COVID-19 pandemic has the potential to further widen this gap. With the unequal burden of unpaid care provided by women and their higher prevalence as frontline workers, they are at greater risk of needing to take unpaid leave to care for a sick family member or themselves.6,7 Similarly, without hazard pay, those with direct clinical responsibilities bear the risk of illness for themselves and their families without adequate compensation.
Impact on Physical and Mental Health
The overall well-being of the hospitalist workforce is critical to continue to provide the highest level of care for our patients. With higher workloads at home and at work, female hospitalists are at risk for increased burnout. Burnout has been linked to many negative outcomes including poor performance, depression, suicide, and leaving the profession.15 Burnout is documented to be higher in female physicians with several contributing factors that are aggravated by gender inequities, including having children at home, gender bias, and real or perceived lack of fairness in promotion and compensation.16 The COVID-19 pandemic has amplified the stress of having children in the home, as well as concerns around fair compensation as described above. The consequences of this have yet to be fully realized but may be dire.
PROPOSED RECOMMENDATIONS
We propose the following recommendations to help mitigate the effects of this epidemic and to continue to move our field forward on our path to equity.
1. Closely monitor the direct and indirect effects of COVID-19 on female hospitalists. While there has been a recent increase in scholarship on the pre–COVID-19 state of gender disparities, there is still much that is unknown. As we experience this upheaval in the way our institutions function, it is even more imperative to track gender deaggregated key indicators of wellness, burnout, and productivity. This includes the use of burnout inventories, salary equity reviews, procedures that track progress toward promotion, and even focus groups of female hospitalists.
2. Inquire about the needs of women in your organization and secure the support they need. This may take the form of including women on key task forces that address personal protective equipment allocation, design new processes, and prepare for surge capacity, as well as providing wellness initiatives, fostering collaborative social networks, or connecting them with emergency childcare resources.
3. Provide a mechanism to account for lack of academic productivity during this time. This period of decreased academic productivity may disproportionately derail progress toward promotion for women. Academic institutions should consider extending deadlines for promotion or tenure, as well as increasing flexibility in metrics used to determine appropriate progress in annual performance reviews.
4. Recognize and reward increased efforts in the areas of clinical or administrative contribution. In this time of crisis, women may be stepping up and leading efforts without titles or positions in ways that are significant and meaningful for their group or organization. Recognizing the ways women are contributing in a tangible and explicit way can provide an avenue for fair compensation, recognition, and career advancement. Female hospitalists should also “manage up” by speaking up and ensuring that leaders are aware of contributions. Amplification is another powerful technique whereby unrecognized contributions can be called out by other women or men.17
5. Support diversity, inclusion, and equity efforts. Keeping equity targets at the top of priority lists for goals moving forward will be imperative. Many institutions struggled to support strong diversity, inclusion, and equity efforts prior to COVID-19; however, the pandemic has highlighted the stark racial and socioeconomic disparities that exist in healthcare.18,19 As healthcare institutions and providers work to mitigate these disparities for patients, there would be no better time to look internally at how they pay, support, and promote their own employees. This would include actively identifying and mitigating any disparities that exist for employees by gender, race, religion, sexual orientation, ethnicity, age, or disability status.
6. Advocate for fair compensation for providers caring for COVID-19 patients. Frontline clinicians are bearing significant risks and increased workload during this crisis and should be compensated accordingly. Hazard pay, paid sick leave, medical and supplemental life insurance, and strong workers’ compensation protections for hospitalists who become ill at work are important for all clinicians, including women. Other long-term plans should include institutional interventions such as salary corrections and ongoing monitoring.20
SUMMARY
The COVID-19 pandemic will have long-term effects that are yet to be realized, including potentially widening gender disparities in medicine. With the current health and economic crises facing our institutions and nations, it can be tempting for diversity, equity, and inclusion initiatives to fall by the wayside. However, it is imperative that hospitalists, leaders, and institutions monitor the effects of the COVID-19 pandemic on women and proactively work to mitigate worsening disparities. Without this focus there is a risk that the recent gains in equity and advancement for women may be lost.
1. Association of American Medical Colleges. Table 13: US medical school faculty by sex, rank, and department, 2017-2018. December 31, 2019. Accessed January 16, 2020. https://www.aamc.org/download/486102/data/17table13.pdf
2. Spector ND, Asante PA, Marcelin JR, et al. Women in pediatrics: progress, barriers, and opportunities for equity, diversity, and inclusion. Pediatrics. 2019;144(5):e20192149. https://doi.org/10.1542/peds.2019-2149
3. Rouse LP, Nagy-Agren S, Gebhard RE, Bernstein WK. Women physicians: gender and the medical workplace. J Womens Health (Larchmt). 2020;29(3):297‐309. https://doi.org/10.1089/jwh.2018.7290
4. Burden M, Frank MG, Keniston A, et al. Gender disparities in leadership and scholarly productivity of academic hospitalists. J Hosp Med. 2015;10(8):481-485. https://doi.org/10.1002/jhm.2340
5. Starmer AJ, Frintner MP, Matos K, Somberg C, Freed G, Byrne BJ. Gender discrepancies related to pediatrician work-life balance and household responsibilities. Pediatrics. 2019;144(4):e20182926. https://doi.org/10.1542/peds.2018-2926
6. Alon TM, Doepke M, Olmstead-Rumsey J, Tertilt Ml. The impact of COVID-19 on gender equality. NBER Working Paper Series. 2020. https://doi.org/10.3386/w26947
7. Addati L, Cattaneo U, Esquivel V, Valarino I. Care work and care jobs for the future of decent work. Geneva: International Labour Office; 2018.
8. Maguire P. Should you steer clear of your own family? Hospitalists weigh living in isolation. Today’s Hospitalist. May 2020. Accessed May 4, 2020. https://www.todayshospitalist.com/treating-covid-patients/
9. Burrer SL, de Perio MA, Hughes MM, et al. Characteristics of health care personnel with COVID-19 — United States, February 12–April 9, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:477-481. DOI: http://dx.doi.org/10.15585/mmwr.mm6915e6
10. SHM Teams Up with Hilton and American Express to Provide Hotel Rooms for Members. SHM. April 13, 2020. Accessed May 7, 2020. https://www.hospitalmedicine.org/about/press-releases/SHM-One-Million-Beds-Hilton-AMEX/
11. Fichtel C, Kaufman S. Fearing COVID-19 spread to families, health care workers self-isolate at home. NBC News. March 31, 2020. Accessed May 7, 2020. https://www.nbcnews.com/health/health-news/fearing-covid-19-spread-families-health-care-workers-self-isolate-n1171726
12. Meier KA, Jerardi KE, Statile AM, Shah SS. Pediatric hospital medicine management, staffing, and well-being in the face of COVID-19. J Hosp Med. 2020;15(5):308‐310. https://doi.org/10.12788/jhm.3435
13. Frintner MP, Sisk B, Byrne BJ, Freed GL, Starmer AJ, Olson LM. Gender differences in earnings of early- and midcareer pediatricians. Pediatrics. 2019;144(4):e20183955. https://doi.org/10.1542/peds.2018-3955
14. Read S, Butkus R, Weissman A, Moyer DV. Compensation disparities by gender in internal medicine. Ann Intern Med. 2018;169(9):658-661. https://doi.org/10.7326/m18-0693
15. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516‐529. https://doi.org/10.1111/joim.12752
16. Templeton K, Halpern L, Jumper C, Carroll RG. Leading and sustaining curricular change: workshop proceedings from the 2018 Sex and Gender Health Education Summit. J Womens Health (Larchmt). 2019;28(12):1743-1747. https://doi.org/10.1089/jwh.2018.7387
17. Eilperin J. White House women want to be in the room where it happens. The Washington Post. September 13, 2016. Accessed April 24, 2020. https://www.washingtonpost.com/news/powerpost/wp/2016/09/13/white-house-women-are-now-in-the-room-where-it-happens/
18. Choo EK. COVID-19 fault lines. Lancet. 2020;395(10233):1333. https://doi.org/10.1016/s0140-6736(20)30812-6
19. Núñez A, Madison M, Schiavo R, Elk R, Prigerson HG. Responding to healthcare disparities and challenges with access to care during COVID-19. Health Equity. 2020;4(1):117-128. https://doi.org/10.1089/heq.2020.29000.rtl
20. Paturel A. Closing the gender pay gap in medicine. AAMC News. April 16, 2019. Accessed April 21, 2020. https://www.aamc.org/news-insights/closing-gender-pay-gap-medicine
The coronavirus disease of 2019 (COVID-19) pandemic has affected every facet of our work and personal lives. While many hope we will return to “normal” with the pandemic’s passing, there is reason to believe medicine, and society, will experience irrevocable changes. Although the number of women pursuing and practicing medicine has increased, inequities remain in compensation, academic rank, and leadership positions.1,2 Within the workplace, women are more likely to be in frontline clinical positions, are more likely to be integral in promoting positive interpersonal relationships and collaborative work environments, and often are less represented in the high-level, decision-making roles in leadership or administration.3,4 These well-described issues may be exacerbated during this pandemic crisis. We describe how the current COVID-19 pandemic may intensify workplace inequities for women, and propose solutions for hospitalist groups, leaders, and administrators to ensure female hospitalists continue to prosper and thrive in these tenuous times.
HOW THE PANDEMIC MAY EXACERBATE EXISTING INEQUITIES
Increasing Demands at Home
Female physicians are more likely to have partners who are employed full-time and report spending more time on household activities including cleaning, cooking, and the care of children, compared with their male counterparts.5 With school and daycare closings, as well as stay-at-home orders in many US states, there has been an increase in household responsibilities and care needs for children remaining at home with a marked decrease in options for stable or emergency childcare.6 As compared with primary care and subspecialty colleagues who can provide a large percentage of their care through telemedicine, this is not the case for hospitalists who must be physically present to care for their patients. Therefore, hospitalists are unable to clinically “work from home” in the same way as many of their colleagues in other specialties. Increased childcare and schooling obligations, coupled with disproportionate household responsibilities and an inability to work from home, will likely result in female hospitalists struggling to meet family needs while pandemic-related work responsibilities are ramping up.7 In addition, women who are involved with administrative, leadership, or research activities may struggle to execute their responsibilities as a result of increased domestic duties.
Many hospitalists are also concerned about contracting COVID-19 and exposing their families to the illness given the high infection rate among healthcare workers and the shortage of personal protective equipment (PPE).8,9 Institutions and national organizations, including the Society of Hospital Medicine, have partnered with industry to provide discounted or complimentary hotel rooms for members to aid self-isolation while providing clinical care.10 One famous photo in popular and social media showed a pulmonary and critical care physician in a tent in his garage in order to self-isolate from his family.11 However, since women are often the primary caregivers for their children or other family members and may also be responsible for other important household activities, they may be unable or unwilling to remove themselves from their children and families. As a result, female hospitalists may encounter feelings of guilt or inadequacy if they’re unable to isolate in the same manner as male colleagues.8
Exaggerating Leadership Gap
One of the keys to a robust response to this pandemic is strong, thoughtful, and strategic leadership.12 Institutional, regional, and national leaders are at the forefront of designing the solutions to the many problems the COVID-19 pandemic has created. The paucity of women at high-level leadership positions in institutions across the United States, including university-based, community, public, and private institutions, means that there is a lack of female representation when institutional policy is being discussed and decided.4 This lack of representation may lead to policies and procedures that negatively affect female hospitalists or, at best, fail to consider the needs of or support female physicians. For example, leaders of a hospital medicine group may create mandatory “backup” coverage for night and weekend shifts for their group during surge periods of the pandemic without considering implications for childcare. Finding weekday, daytime coverage is challenging for many during this time when daycares and school are closed, and finding coverage during weekend or overnight hours will be even more challenging. With increased risks for older adults with high-risk medical conditions, grandparents or other friends or family members that previously would have assisted with childcare may no longer be an option. If a female hospitalist is not a member of the leadership group that helped design this coverage structure, there could be a lack of recognition of the undue strain this coverage model could create for women in the group. Even if not intentional, such policies may hinder women’s career stability and opportunities for further advancement, as well as their ability to adequately provide care for their families. Having women as a part of the leadership group that creates policies and schedules and makes pivotal decisions is imperative, especially regarding topics of providing access and compensation for “emergency childcare,” hazard pay, shift length, work conditions, job security, sick leave, workers compensation, advancement opportunities, and hiring practices.
Compensation
The gender pay gap in medicine has been consistently demonstrated among many specialties.13,14 The reasons for this inequity are multifactorial, and the COVID-19 pandemic has the potential to further widen this gap. With the unequal burden of unpaid care provided by women and their higher prevalence as frontline workers, they are at greater risk of needing to take unpaid leave to care for a sick family member or themselves.6,7 Similarly, without hazard pay, those with direct clinical responsibilities bear the risk of illness for themselves and their families without adequate compensation.
Impact on Physical and Mental Health
The overall well-being of the hospitalist workforce is critical to continue to provide the highest level of care for our patients. With higher workloads at home and at work, female hospitalists are at risk for increased burnout. Burnout has been linked to many negative outcomes including poor performance, depression, suicide, and leaving the profession.15 Burnout is documented to be higher in female physicians with several contributing factors that are aggravated by gender inequities, including having children at home, gender bias, and real or perceived lack of fairness in promotion and compensation.16 The COVID-19 pandemic has amplified the stress of having children in the home, as well as concerns around fair compensation as described above. The consequences of this have yet to be fully realized but may be dire.
PROPOSED RECOMMENDATIONS
We propose the following recommendations to help mitigate the effects of this epidemic and to continue to move our field forward on our path to equity.
1. Closely monitor the direct and indirect effects of COVID-19 on female hospitalists. While there has been a recent increase in scholarship on the pre–COVID-19 state of gender disparities, there is still much that is unknown. As we experience this upheaval in the way our institutions function, it is even more imperative to track gender deaggregated key indicators of wellness, burnout, and productivity. This includes the use of burnout inventories, salary equity reviews, procedures that track progress toward promotion, and even focus groups of female hospitalists.
2. Inquire about the needs of women in your organization and secure the support they need. This may take the form of including women on key task forces that address personal protective equipment allocation, design new processes, and prepare for surge capacity, as well as providing wellness initiatives, fostering collaborative social networks, or connecting them with emergency childcare resources.
3. Provide a mechanism to account for lack of academic productivity during this time. This period of decreased academic productivity may disproportionately derail progress toward promotion for women. Academic institutions should consider extending deadlines for promotion or tenure, as well as increasing flexibility in metrics used to determine appropriate progress in annual performance reviews.
4. Recognize and reward increased efforts in the areas of clinical or administrative contribution. In this time of crisis, women may be stepping up and leading efforts without titles or positions in ways that are significant and meaningful for their group or organization. Recognizing the ways women are contributing in a tangible and explicit way can provide an avenue for fair compensation, recognition, and career advancement. Female hospitalists should also “manage up” by speaking up and ensuring that leaders are aware of contributions. Amplification is another powerful technique whereby unrecognized contributions can be called out by other women or men.17
5. Support diversity, inclusion, and equity efforts. Keeping equity targets at the top of priority lists for goals moving forward will be imperative. Many institutions struggled to support strong diversity, inclusion, and equity efforts prior to COVID-19; however, the pandemic has highlighted the stark racial and socioeconomic disparities that exist in healthcare.18,19 As healthcare institutions and providers work to mitigate these disparities for patients, there would be no better time to look internally at how they pay, support, and promote their own employees. This would include actively identifying and mitigating any disparities that exist for employees by gender, race, religion, sexual orientation, ethnicity, age, or disability status.
6. Advocate for fair compensation for providers caring for COVID-19 patients. Frontline clinicians are bearing significant risks and increased workload during this crisis and should be compensated accordingly. Hazard pay, paid sick leave, medical and supplemental life insurance, and strong workers’ compensation protections for hospitalists who become ill at work are important for all clinicians, including women. Other long-term plans should include institutional interventions such as salary corrections and ongoing monitoring.20
SUMMARY
The COVID-19 pandemic will have long-term effects that are yet to be realized, including potentially widening gender disparities in medicine. With the current health and economic crises facing our institutions and nations, it can be tempting for diversity, equity, and inclusion initiatives to fall by the wayside. However, it is imperative that hospitalists, leaders, and institutions monitor the effects of the COVID-19 pandemic on women and proactively work to mitigate worsening disparities. Without this focus there is a risk that the recent gains in equity and advancement for women may be lost.
The coronavirus disease of 2019 (COVID-19) pandemic has affected every facet of our work and personal lives. While many hope we will return to “normal” with the pandemic’s passing, there is reason to believe medicine, and society, will experience irrevocable changes. Although the number of women pursuing and practicing medicine has increased, inequities remain in compensation, academic rank, and leadership positions.1,2 Within the workplace, women are more likely to be in frontline clinical positions, are more likely to be integral in promoting positive interpersonal relationships and collaborative work environments, and often are less represented in the high-level, decision-making roles in leadership or administration.3,4 These well-described issues may be exacerbated during this pandemic crisis. We describe how the current COVID-19 pandemic may intensify workplace inequities for women, and propose solutions for hospitalist groups, leaders, and administrators to ensure female hospitalists continue to prosper and thrive in these tenuous times.
HOW THE PANDEMIC MAY EXACERBATE EXISTING INEQUITIES
Increasing Demands at Home
Female physicians are more likely to have partners who are employed full-time and report spending more time on household activities including cleaning, cooking, and the care of children, compared with their male counterparts.5 With school and daycare closings, as well as stay-at-home orders in many US states, there has been an increase in household responsibilities and care needs for children remaining at home with a marked decrease in options for stable or emergency childcare.6 As compared with primary care and subspecialty colleagues who can provide a large percentage of their care through telemedicine, this is not the case for hospitalists who must be physically present to care for their patients. Therefore, hospitalists are unable to clinically “work from home” in the same way as many of their colleagues in other specialties. Increased childcare and schooling obligations, coupled with disproportionate household responsibilities and an inability to work from home, will likely result in female hospitalists struggling to meet family needs while pandemic-related work responsibilities are ramping up.7 In addition, women who are involved with administrative, leadership, or research activities may struggle to execute their responsibilities as a result of increased domestic duties.
Many hospitalists are also concerned about contracting COVID-19 and exposing their families to the illness given the high infection rate among healthcare workers and the shortage of personal protective equipment (PPE).8,9 Institutions and national organizations, including the Society of Hospital Medicine, have partnered with industry to provide discounted or complimentary hotel rooms for members to aid self-isolation while providing clinical care.10 One famous photo in popular and social media showed a pulmonary and critical care physician in a tent in his garage in order to self-isolate from his family.11 However, since women are often the primary caregivers for their children or other family members and may also be responsible for other important household activities, they may be unable or unwilling to remove themselves from their children and families. As a result, female hospitalists may encounter feelings of guilt or inadequacy if they’re unable to isolate in the same manner as male colleagues.8
Exaggerating Leadership Gap
One of the keys to a robust response to this pandemic is strong, thoughtful, and strategic leadership.12 Institutional, regional, and national leaders are at the forefront of designing the solutions to the many problems the COVID-19 pandemic has created. The paucity of women at high-level leadership positions in institutions across the United States, including university-based, community, public, and private institutions, means that there is a lack of female representation when institutional policy is being discussed and decided.4 This lack of representation may lead to policies and procedures that negatively affect female hospitalists or, at best, fail to consider the needs of or support female physicians. For example, leaders of a hospital medicine group may create mandatory “backup” coverage for night and weekend shifts for their group during surge periods of the pandemic without considering implications for childcare. Finding weekday, daytime coverage is challenging for many during this time when daycares and school are closed, and finding coverage during weekend or overnight hours will be even more challenging. With increased risks for older adults with high-risk medical conditions, grandparents or other friends or family members that previously would have assisted with childcare may no longer be an option. If a female hospitalist is not a member of the leadership group that helped design this coverage structure, there could be a lack of recognition of the undue strain this coverage model could create for women in the group. Even if not intentional, such policies may hinder women’s career stability and opportunities for further advancement, as well as their ability to adequately provide care for their families. Having women as a part of the leadership group that creates policies and schedules and makes pivotal decisions is imperative, especially regarding topics of providing access and compensation for “emergency childcare,” hazard pay, shift length, work conditions, job security, sick leave, workers compensation, advancement opportunities, and hiring practices.
Compensation
The gender pay gap in medicine has been consistently demonstrated among many specialties.13,14 The reasons for this inequity are multifactorial, and the COVID-19 pandemic has the potential to further widen this gap. With the unequal burden of unpaid care provided by women and their higher prevalence as frontline workers, they are at greater risk of needing to take unpaid leave to care for a sick family member or themselves.6,7 Similarly, without hazard pay, those with direct clinical responsibilities bear the risk of illness for themselves and their families without adequate compensation.
Impact on Physical and Mental Health
The overall well-being of the hospitalist workforce is critical to continue to provide the highest level of care for our patients. With higher workloads at home and at work, female hospitalists are at risk for increased burnout. Burnout has been linked to many negative outcomes including poor performance, depression, suicide, and leaving the profession.15 Burnout is documented to be higher in female physicians with several contributing factors that are aggravated by gender inequities, including having children at home, gender bias, and real or perceived lack of fairness in promotion and compensation.16 The COVID-19 pandemic has amplified the stress of having children in the home, as well as concerns around fair compensation as described above. The consequences of this have yet to be fully realized but may be dire.
PROPOSED RECOMMENDATIONS
We propose the following recommendations to help mitigate the effects of this epidemic and to continue to move our field forward on our path to equity.
1. Closely monitor the direct and indirect effects of COVID-19 on female hospitalists. While there has been a recent increase in scholarship on the pre–COVID-19 state of gender disparities, there is still much that is unknown. As we experience this upheaval in the way our institutions function, it is even more imperative to track gender deaggregated key indicators of wellness, burnout, and productivity. This includes the use of burnout inventories, salary equity reviews, procedures that track progress toward promotion, and even focus groups of female hospitalists.
2. Inquire about the needs of women in your organization and secure the support they need. This may take the form of including women on key task forces that address personal protective equipment allocation, design new processes, and prepare for surge capacity, as well as providing wellness initiatives, fostering collaborative social networks, or connecting them with emergency childcare resources.
3. Provide a mechanism to account for lack of academic productivity during this time. This period of decreased academic productivity may disproportionately derail progress toward promotion for women. Academic institutions should consider extending deadlines for promotion or tenure, as well as increasing flexibility in metrics used to determine appropriate progress in annual performance reviews.
4. Recognize and reward increased efforts in the areas of clinical or administrative contribution. In this time of crisis, women may be stepping up and leading efforts without titles or positions in ways that are significant and meaningful for their group or organization. Recognizing the ways women are contributing in a tangible and explicit way can provide an avenue for fair compensation, recognition, and career advancement. Female hospitalists should also “manage up” by speaking up and ensuring that leaders are aware of contributions. Amplification is another powerful technique whereby unrecognized contributions can be called out by other women or men.17
5. Support diversity, inclusion, and equity efforts. Keeping equity targets at the top of priority lists for goals moving forward will be imperative. Many institutions struggled to support strong diversity, inclusion, and equity efforts prior to COVID-19; however, the pandemic has highlighted the stark racial and socioeconomic disparities that exist in healthcare.18,19 As healthcare institutions and providers work to mitigate these disparities for patients, there would be no better time to look internally at how they pay, support, and promote their own employees. This would include actively identifying and mitigating any disparities that exist for employees by gender, race, religion, sexual orientation, ethnicity, age, or disability status.
6. Advocate for fair compensation for providers caring for COVID-19 patients. Frontline clinicians are bearing significant risks and increased workload during this crisis and should be compensated accordingly. Hazard pay, paid sick leave, medical and supplemental life insurance, and strong workers’ compensation protections for hospitalists who become ill at work are important for all clinicians, including women. Other long-term plans should include institutional interventions such as salary corrections and ongoing monitoring.20
SUMMARY
The COVID-19 pandemic will have long-term effects that are yet to be realized, including potentially widening gender disparities in medicine. With the current health and economic crises facing our institutions and nations, it can be tempting for diversity, equity, and inclusion initiatives to fall by the wayside. However, it is imperative that hospitalists, leaders, and institutions monitor the effects of the COVID-19 pandemic on women and proactively work to mitigate worsening disparities. Without this focus there is a risk that the recent gains in equity and advancement for women may be lost.
1. Association of American Medical Colleges. Table 13: US medical school faculty by sex, rank, and department, 2017-2018. December 31, 2019. Accessed January 16, 2020. https://www.aamc.org/download/486102/data/17table13.pdf
2. Spector ND, Asante PA, Marcelin JR, et al. Women in pediatrics: progress, barriers, and opportunities for equity, diversity, and inclusion. Pediatrics. 2019;144(5):e20192149. https://doi.org/10.1542/peds.2019-2149
3. Rouse LP, Nagy-Agren S, Gebhard RE, Bernstein WK. Women physicians: gender and the medical workplace. J Womens Health (Larchmt). 2020;29(3):297‐309. https://doi.org/10.1089/jwh.2018.7290
4. Burden M, Frank MG, Keniston A, et al. Gender disparities in leadership and scholarly productivity of academic hospitalists. J Hosp Med. 2015;10(8):481-485. https://doi.org/10.1002/jhm.2340
5. Starmer AJ, Frintner MP, Matos K, Somberg C, Freed G, Byrne BJ. Gender discrepancies related to pediatrician work-life balance and household responsibilities. Pediatrics. 2019;144(4):e20182926. https://doi.org/10.1542/peds.2018-2926
6. Alon TM, Doepke M, Olmstead-Rumsey J, Tertilt Ml. The impact of COVID-19 on gender equality. NBER Working Paper Series. 2020. https://doi.org/10.3386/w26947
7. Addati L, Cattaneo U, Esquivel V, Valarino I. Care work and care jobs for the future of decent work. Geneva: International Labour Office; 2018.
8. Maguire P. Should you steer clear of your own family? Hospitalists weigh living in isolation. Today’s Hospitalist. May 2020. Accessed May 4, 2020. https://www.todayshospitalist.com/treating-covid-patients/
9. Burrer SL, de Perio MA, Hughes MM, et al. Characteristics of health care personnel with COVID-19 — United States, February 12–April 9, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:477-481. DOI: http://dx.doi.org/10.15585/mmwr.mm6915e6
10. SHM Teams Up with Hilton and American Express to Provide Hotel Rooms for Members. SHM. April 13, 2020. Accessed May 7, 2020. https://www.hospitalmedicine.org/about/press-releases/SHM-One-Million-Beds-Hilton-AMEX/
11. Fichtel C, Kaufman S. Fearing COVID-19 spread to families, health care workers self-isolate at home. NBC News. March 31, 2020. Accessed May 7, 2020. https://www.nbcnews.com/health/health-news/fearing-covid-19-spread-families-health-care-workers-self-isolate-n1171726
12. Meier KA, Jerardi KE, Statile AM, Shah SS. Pediatric hospital medicine management, staffing, and well-being in the face of COVID-19. J Hosp Med. 2020;15(5):308‐310. https://doi.org/10.12788/jhm.3435
13. Frintner MP, Sisk B, Byrne BJ, Freed GL, Starmer AJ, Olson LM. Gender differences in earnings of early- and midcareer pediatricians. Pediatrics. 2019;144(4):e20183955. https://doi.org/10.1542/peds.2018-3955
14. Read S, Butkus R, Weissman A, Moyer DV. Compensation disparities by gender in internal medicine. Ann Intern Med. 2018;169(9):658-661. https://doi.org/10.7326/m18-0693
15. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516‐529. https://doi.org/10.1111/joim.12752
16. Templeton K, Halpern L, Jumper C, Carroll RG. Leading and sustaining curricular change: workshop proceedings from the 2018 Sex and Gender Health Education Summit. J Womens Health (Larchmt). 2019;28(12):1743-1747. https://doi.org/10.1089/jwh.2018.7387
17. Eilperin J. White House women want to be in the room where it happens. The Washington Post. September 13, 2016. Accessed April 24, 2020. https://www.washingtonpost.com/news/powerpost/wp/2016/09/13/white-house-women-are-now-in-the-room-where-it-happens/
18. Choo EK. COVID-19 fault lines. Lancet. 2020;395(10233):1333. https://doi.org/10.1016/s0140-6736(20)30812-6
19. Núñez A, Madison M, Schiavo R, Elk R, Prigerson HG. Responding to healthcare disparities and challenges with access to care during COVID-19. Health Equity. 2020;4(1):117-128. https://doi.org/10.1089/heq.2020.29000.rtl
20. Paturel A. Closing the gender pay gap in medicine. AAMC News. April 16, 2019. Accessed April 21, 2020. https://www.aamc.org/news-insights/closing-gender-pay-gap-medicine
1. Association of American Medical Colleges. Table 13: US medical school faculty by sex, rank, and department, 2017-2018. December 31, 2019. Accessed January 16, 2020. https://www.aamc.org/download/486102/data/17table13.pdf
2. Spector ND, Asante PA, Marcelin JR, et al. Women in pediatrics: progress, barriers, and opportunities for equity, diversity, and inclusion. Pediatrics. 2019;144(5):e20192149. https://doi.org/10.1542/peds.2019-2149
3. Rouse LP, Nagy-Agren S, Gebhard RE, Bernstein WK. Women physicians: gender and the medical workplace. J Womens Health (Larchmt). 2020;29(3):297‐309. https://doi.org/10.1089/jwh.2018.7290
4. Burden M, Frank MG, Keniston A, et al. Gender disparities in leadership and scholarly productivity of academic hospitalists. J Hosp Med. 2015;10(8):481-485. https://doi.org/10.1002/jhm.2340
5. Starmer AJ, Frintner MP, Matos K, Somberg C, Freed G, Byrne BJ. Gender discrepancies related to pediatrician work-life balance and household responsibilities. Pediatrics. 2019;144(4):e20182926. https://doi.org/10.1542/peds.2018-2926
6. Alon TM, Doepke M, Olmstead-Rumsey J, Tertilt Ml. The impact of COVID-19 on gender equality. NBER Working Paper Series. 2020. https://doi.org/10.3386/w26947
7. Addati L, Cattaneo U, Esquivel V, Valarino I. Care work and care jobs for the future of decent work. Geneva: International Labour Office; 2018.
8. Maguire P. Should you steer clear of your own family? Hospitalists weigh living in isolation. Today’s Hospitalist. May 2020. Accessed May 4, 2020. https://www.todayshospitalist.com/treating-covid-patients/
9. Burrer SL, de Perio MA, Hughes MM, et al. Characteristics of health care personnel with COVID-19 — United States, February 12–April 9, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:477-481. DOI: http://dx.doi.org/10.15585/mmwr.mm6915e6
10. SHM Teams Up with Hilton and American Express to Provide Hotel Rooms for Members. SHM. April 13, 2020. Accessed May 7, 2020. https://www.hospitalmedicine.org/about/press-releases/SHM-One-Million-Beds-Hilton-AMEX/
11. Fichtel C, Kaufman S. Fearing COVID-19 spread to families, health care workers self-isolate at home. NBC News. March 31, 2020. Accessed May 7, 2020. https://www.nbcnews.com/health/health-news/fearing-covid-19-spread-families-health-care-workers-self-isolate-n1171726
12. Meier KA, Jerardi KE, Statile AM, Shah SS. Pediatric hospital medicine management, staffing, and well-being in the face of COVID-19. J Hosp Med. 2020;15(5):308‐310. https://doi.org/10.12788/jhm.3435
13. Frintner MP, Sisk B, Byrne BJ, Freed GL, Starmer AJ, Olson LM. Gender differences in earnings of early- and midcareer pediatricians. Pediatrics. 2019;144(4):e20183955. https://doi.org/10.1542/peds.2018-3955
14. Read S, Butkus R, Weissman A, Moyer DV. Compensation disparities by gender in internal medicine. Ann Intern Med. 2018;169(9):658-661. https://doi.org/10.7326/m18-0693
15. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516‐529. https://doi.org/10.1111/joim.12752
16. Templeton K, Halpern L, Jumper C, Carroll RG. Leading and sustaining curricular change: workshop proceedings from the 2018 Sex and Gender Health Education Summit. J Womens Health (Larchmt). 2019;28(12):1743-1747. https://doi.org/10.1089/jwh.2018.7387
17. Eilperin J. White House women want to be in the room where it happens. The Washington Post. September 13, 2016. Accessed April 24, 2020. https://www.washingtonpost.com/news/powerpost/wp/2016/09/13/white-house-women-are-now-in-the-room-where-it-happens/
18. Choo EK. COVID-19 fault lines. Lancet. 2020;395(10233):1333. https://doi.org/10.1016/s0140-6736(20)30812-6
19. Núñez A, Madison M, Schiavo R, Elk R, Prigerson HG. Responding to healthcare disparities and challenges with access to care during COVID-19. Health Equity. 2020;4(1):117-128. https://doi.org/10.1089/heq.2020.29000.rtl
20. Paturel A. Closing the gender pay gap in medicine. AAMC News. April 16, 2019. Accessed April 21, 2020. https://www.aamc.org/news-insights/closing-gender-pay-gap-medicine
© 2020 Society of Hospital Medicine
CRC: Mailing fecal test kits appears cost effective, boosts screening
Mailing fecal immunochemical testing (FIT) kits with colorectal cancer (CRC) screening reminders appears cost effective and may boost screening rates across a variety of payers and providers, according to investigators.
Cost savings, when compared with mailing reminders alone, would be greatest from a Medicaid and state government perspective, reported lead author Stephanie B. Wheeler, PhD, MPH, of the University of North Carolina at Chapel Hill and colleagues.
“As payers and providers endeavor to increase the proportion of age-eligible adults who are up to date with CRC screening, according to the National Colorectal Cancer Roundtable target of 80% screened, understanding the comparative value of mailed FIT-based programs in low-income populations is urgently needed,” the investigators wrote in Cancer.
To address this need, Dr. Wheeler and colleagues coupled a randomized clinical trial with a cost-effectiveness analysis.
The trial involved 2,144 North Carolina Medicaid enrollees between 52 and 64 years of age who were overdue for CRC screening. Participants were randomly assigned to receive either a mailed reminder with an FIT kit or a mailed reminder alone. Those who received the reminder alone were provided with information about how to get an FIT kit or undergo screening colonoscopy.
The screening rate was significantly higher in the combination mailer group than it was the reminder-only group, at 21.1% versus 12.3% (P less than .01). Based on data from previous research, the investigators estimated that a number of participants also underwent colonoscopy screenings because of the reminders; this resulted in an estimated 23.3% screening rate among those who received an FIT kit, compared with 15.8% among those who received a reminder alone.
For cost analysis, these rates were entered into a model involving 35,000 Medicaid enrollees. Annual costs were compared from two perspectives: Medicaid/state and health clinic/facility, the latter of which included primary care providers, integrated health care systems, county health departments, and federally qualified health centers. The model incorporated a number of costs, such as those associated with equipment, mailing supplies, FIT kits, colonoscopy screenings, and personnel.
From a Medicaid/state perspective, the estimated total population screening cost of mailing both an FIT kit and reminder was $1.40 million, compared with $1.45 million for a reminder alone. This translated to a total cost per person screened of $172 for the combination mailer versus $262 for the reminder alone.
“Notably, compared with the reminder-only alternative, the reminder + FIT alternative was cost-saving or dominant from this perspective because it yielded more screenings at lower cost,” the investigators wrote.
The cost analysis from a health clinic/facility perspective was more nuanced.
While the estimated total population screening cost of a combination mailer was more than the reminder alone ($927,000 vs. $624,000), sending test kits led to screening of 2,598 additional individuals (8,131 vs. 5,533). The incremental cost-effectiveness ratio (ICER) for the combination mailer was $116 per person screened.
“This ICER fell within the range of what decision makers typically would be willing to pay for an additional person screened for CRC, previously shown to include ICERs as high as several hundred dollars or more,” the investigators noted.
According to Beverly B. Green, MD, MPH, of Kaiser Permanente Washington, Seattle, and Richard T. Meenan, PhD, MPH, of Kaiser Permanente Northwest, Portland, Oregon, who wrote a simultaneously published editorial, the study “suggests that direct FIT mailing can be highly cost effective if not cost saving within the Medicaid population, similar to tobacco-cessation programs or diabetes prevention programs in the same context of a Medicaid population.”
Still, practical details need to be resolved prior to real-world application, they added.
“[T]he analysis by Wheeler et al. raises an important question: Who should pay for mailed FIT screening programs?”
The answer, they suggested, may be health plans, since prevention of CRC could mitigate greater costs of care down the line. Further motivation could come from a program such as the Medicare 5-star program, which rewards higher screening rates with bonuses such as longer enrollment periods and higher payments, according to Dr. Green and Dr. Meenan.
“Unsurprisingly, Medicare CRC screening rates have been steadily increasing and now are approaching 80%,” they noted, “whereas Medicaid CRC screening rates remain low.”
The study was supported by the University of North Carolina, the Cancer Prevention and Control Research Network, the Centers for Disease Control and Prevention, and the National Cancer Institute. Dr. Wheeler reported grant funding from Pfizer.
SOURCE: Wheeler SB et al. Cancer. 2020 Jul 20. doi: 10.1002/cncr.32992.
Mailing fecal immunochemical testing (FIT) kits with colorectal cancer (CRC) screening reminders appears cost effective and may boost screening rates across a variety of payers and providers, according to investigators.
Cost savings, when compared with mailing reminders alone, would be greatest from a Medicaid and state government perspective, reported lead author Stephanie B. Wheeler, PhD, MPH, of the University of North Carolina at Chapel Hill and colleagues.
“As payers and providers endeavor to increase the proportion of age-eligible adults who are up to date with CRC screening, according to the National Colorectal Cancer Roundtable target of 80% screened, understanding the comparative value of mailed FIT-based programs in low-income populations is urgently needed,” the investigators wrote in Cancer.
To address this need, Dr. Wheeler and colleagues coupled a randomized clinical trial with a cost-effectiveness analysis.
The trial involved 2,144 North Carolina Medicaid enrollees between 52 and 64 years of age who were overdue for CRC screening. Participants were randomly assigned to receive either a mailed reminder with an FIT kit or a mailed reminder alone. Those who received the reminder alone were provided with information about how to get an FIT kit or undergo screening colonoscopy.
The screening rate was significantly higher in the combination mailer group than it was the reminder-only group, at 21.1% versus 12.3% (P less than .01). Based on data from previous research, the investigators estimated that a number of participants also underwent colonoscopy screenings because of the reminders; this resulted in an estimated 23.3% screening rate among those who received an FIT kit, compared with 15.8% among those who received a reminder alone.
For cost analysis, these rates were entered into a model involving 35,000 Medicaid enrollees. Annual costs were compared from two perspectives: Medicaid/state and health clinic/facility, the latter of which included primary care providers, integrated health care systems, county health departments, and federally qualified health centers. The model incorporated a number of costs, such as those associated with equipment, mailing supplies, FIT kits, colonoscopy screenings, and personnel.
From a Medicaid/state perspective, the estimated total population screening cost of mailing both an FIT kit and reminder was $1.40 million, compared with $1.45 million for a reminder alone. This translated to a total cost per person screened of $172 for the combination mailer versus $262 for the reminder alone.
“Notably, compared with the reminder-only alternative, the reminder + FIT alternative was cost-saving or dominant from this perspective because it yielded more screenings at lower cost,” the investigators wrote.
The cost analysis from a health clinic/facility perspective was more nuanced.
While the estimated total population screening cost of a combination mailer was more than the reminder alone ($927,000 vs. $624,000), sending test kits led to screening of 2,598 additional individuals (8,131 vs. 5,533). The incremental cost-effectiveness ratio (ICER) for the combination mailer was $116 per person screened.
“This ICER fell within the range of what decision makers typically would be willing to pay for an additional person screened for CRC, previously shown to include ICERs as high as several hundred dollars or more,” the investigators noted.
According to Beverly B. Green, MD, MPH, of Kaiser Permanente Washington, Seattle, and Richard T. Meenan, PhD, MPH, of Kaiser Permanente Northwest, Portland, Oregon, who wrote a simultaneously published editorial, the study “suggests that direct FIT mailing can be highly cost effective if not cost saving within the Medicaid population, similar to tobacco-cessation programs or diabetes prevention programs in the same context of a Medicaid population.”
Still, practical details need to be resolved prior to real-world application, they added.
“[T]he analysis by Wheeler et al. raises an important question: Who should pay for mailed FIT screening programs?”
The answer, they suggested, may be health plans, since prevention of CRC could mitigate greater costs of care down the line. Further motivation could come from a program such as the Medicare 5-star program, which rewards higher screening rates with bonuses such as longer enrollment periods and higher payments, according to Dr. Green and Dr. Meenan.
“Unsurprisingly, Medicare CRC screening rates have been steadily increasing and now are approaching 80%,” they noted, “whereas Medicaid CRC screening rates remain low.”
The study was supported by the University of North Carolina, the Cancer Prevention and Control Research Network, the Centers for Disease Control and Prevention, and the National Cancer Institute. Dr. Wheeler reported grant funding from Pfizer.
SOURCE: Wheeler SB et al. Cancer. 2020 Jul 20. doi: 10.1002/cncr.32992.
Mailing fecal immunochemical testing (FIT) kits with colorectal cancer (CRC) screening reminders appears cost effective and may boost screening rates across a variety of payers and providers, according to investigators.
Cost savings, when compared with mailing reminders alone, would be greatest from a Medicaid and state government perspective, reported lead author Stephanie B. Wheeler, PhD, MPH, of the University of North Carolina at Chapel Hill and colleagues.
“As payers and providers endeavor to increase the proportion of age-eligible adults who are up to date with CRC screening, according to the National Colorectal Cancer Roundtable target of 80% screened, understanding the comparative value of mailed FIT-based programs in low-income populations is urgently needed,” the investigators wrote in Cancer.
To address this need, Dr. Wheeler and colleagues coupled a randomized clinical trial with a cost-effectiveness analysis.
The trial involved 2,144 North Carolina Medicaid enrollees between 52 and 64 years of age who were overdue for CRC screening. Participants were randomly assigned to receive either a mailed reminder with an FIT kit or a mailed reminder alone. Those who received the reminder alone were provided with information about how to get an FIT kit or undergo screening colonoscopy.
The screening rate was significantly higher in the combination mailer group than it was the reminder-only group, at 21.1% versus 12.3% (P less than .01). Based on data from previous research, the investigators estimated that a number of participants also underwent colonoscopy screenings because of the reminders; this resulted in an estimated 23.3% screening rate among those who received an FIT kit, compared with 15.8% among those who received a reminder alone.
For cost analysis, these rates were entered into a model involving 35,000 Medicaid enrollees. Annual costs were compared from two perspectives: Medicaid/state and health clinic/facility, the latter of which included primary care providers, integrated health care systems, county health departments, and federally qualified health centers. The model incorporated a number of costs, such as those associated with equipment, mailing supplies, FIT kits, colonoscopy screenings, and personnel.
From a Medicaid/state perspective, the estimated total population screening cost of mailing both an FIT kit and reminder was $1.40 million, compared with $1.45 million for a reminder alone. This translated to a total cost per person screened of $172 for the combination mailer versus $262 for the reminder alone.
“Notably, compared with the reminder-only alternative, the reminder + FIT alternative was cost-saving or dominant from this perspective because it yielded more screenings at lower cost,” the investigators wrote.
The cost analysis from a health clinic/facility perspective was more nuanced.
While the estimated total population screening cost of a combination mailer was more than the reminder alone ($927,000 vs. $624,000), sending test kits led to screening of 2,598 additional individuals (8,131 vs. 5,533). The incremental cost-effectiveness ratio (ICER) for the combination mailer was $116 per person screened.
“This ICER fell within the range of what decision makers typically would be willing to pay for an additional person screened for CRC, previously shown to include ICERs as high as several hundred dollars or more,” the investigators noted.
According to Beverly B. Green, MD, MPH, of Kaiser Permanente Washington, Seattle, and Richard T. Meenan, PhD, MPH, of Kaiser Permanente Northwest, Portland, Oregon, who wrote a simultaneously published editorial, the study “suggests that direct FIT mailing can be highly cost effective if not cost saving within the Medicaid population, similar to tobacco-cessation programs or diabetes prevention programs in the same context of a Medicaid population.”
Still, practical details need to be resolved prior to real-world application, they added.
“[T]he analysis by Wheeler et al. raises an important question: Who should pay for mailed FIT screening programs?”
The answer, they suggested, may be health plans, since prevention of CRC could mitigate greater costs of care down the line. Further motivation could come from a program such as the Medicare 5-star program, which rewards higher screening rates with bonuses such as longer enrollment periods and higher payments, according to Dr. Green and Dr. Meenan.
“Unsurprisingly, Medicare CRC screening rates have been steadily increasing and now are approaching 80%,” they noted, “whereas Medicaid CRC screening rates remain low.”
The study was supported by the University of North Carolina, the Cancer Prevention and Control Research Network, the Centers for Disease Control and Prevention, and the National Cancer Institute. Dr. Wheeler reported grant funding from Pfizer.
SOURCE: Wheeler SB et al. Cancer. 2020 Jul 20. doi: 10.1002/cncr.32992.
FROM CANCER
Key clinical point: Mailing fecal immunochemical testing (FIT) kits along with colorectal cancer screening reminders appears cost effective and may lead to higher screening rates than mailing reminders alone.
Major finding: Individuals who received a reminder and a fecal immunochemical testing (FIT) kit had an estimated 23.3% colorectal cancer screening rate, compared with 15.8% among those who received a reminder alone.
Study details: A cost-effectiveness analysis of a randomized clinical trial involving Medicaid enrollees between 52 and 64 years of age.
Disclosures: The study was supported by the University of North Carolina, the Cancer Prevention and Control Research Network, the Centers for Disease Control and Prevention, and the National Cancer Institute. Dr. Wheeler reported grant funding from Pfizer.
Source: Wheeler SB et al. Cancer. 2020 Jul 20. doi: 10.1002/cncr.32992.
Schools can reopen safely with precautions, experts say
The absence of in-person school has harmed children in ways beyond loss of academic learning, according to Josh Sharfstein, MD, vice dean for public health practice and community engagement at the Johns Hopkins Bloomberg School of Public Health, Baltimore. In addition to learning, school is a place where many children receive breakfast and lunch every day, as well as support services and the benefits of being in a safe and secure environment, Dr. Sharfstein said in a press briefing sponsored by Johns Hopkins University.
However, although it is an important priority for children to return to school, “we are in the midst of a pandemic that poses real risk,” he said.
In the press briefing, several experts shared ideas and considerations for safely reopening K-12 schools in the fall of 2020.
Data from other countries where schools have reopened, notably Austria and Denmark, have been reassuring about the lack of transmission of SARS-CoV-2 among children in a school setting, said Jennifer Nuzzo, DrPH, an epidemiologist at the Johns Hopkins Center for Health Security. However, other countries where schools have reopened successfully have reported low levels of viral transmission locally, and a responsible strategy for school reopening in the United States should follow a similar plan, she said. In areas where transmission and infection rates are increasing “it may not be safe to reopen,” but in areas where rates are declining or stable, schools could potentially reopen if they follow safety measures.
Dr. Nuzzo suggested that Considerations include protocols for handwashing and sanitation, and maintaining physical distance by creative use of outdoor classrooms (weather permitting) or other spaces within school buildings. Transportation to and from school also will be an issue to address, she noted.
None of the strategies being considered will completely eliminate risk of SARS-CoV-2 infection in school settings, so allowing parents and students to opt out and choose distance learning will be important as well, said Dr. Nuzzo. In addition, schools may need to consider alternative roles for teachers and staff who don’t feel comfortable being in contact with students and fellow staff members. “All of these things are going to be hard,” Dr. Nuzzo acknowledged. “Hard should not be a deterrent,” to reopening schools, but “we acknowledge the resources that schools will need in order to do this.”
At present, all 50 states and the District of Columbia have released some type of plan for reopening schools, said Megan Collins, MD, MPH, codirector the Johns Hopkins Consortium for School-Based Health Solutions.
Dr. Collins and colleagues have developed a school reopening tracker, which is “a national snapshot of current reopening plans that have been released,” she said. The tracker is being updated continuously as plans evolve. The eSchool+ K-12 School Reopening Tracker identifies 12 reopening categories that states could potentially address in the plans. These categories are divided into Operational and Ethics/Equity. The operational categories include:
- Core academics
- SARS-CoV-2 protection
- Before and after school programs
- School access and transportation
- Student health services
- Food and nutrition.
Ethics/equity categories include the following:
- Parent choice
- Teacher and staff choice
- Children of poverty and systemic disadvantage
- Children with special needs/English as second language/gifted and twice exceptional
- Privacy
- Engagement and transparency.
As of July 15, 2020, 16 states (Arizona, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, North Carolina, North Dakota, Ohio, Rhode Island, Tennessee, Texas, Virginia, Washington, and Wisconsin) had addressed all 12 categories in their reopening plans, Dr. Collins said.
School reopening plans must take equity issues into account, said Annette Anderson, PhD, of the Johns Hopkins University School of Education.
Specifically, developing learning plans for special education students and others at the most risk for learning loss will be essential. “The digital divide has become a digital canyon” in some areas, Dr. Anderson noted, and schools need to rethink eligibility and work to provide access to devices for online learning for all students.
In addition, schools need to convince parents that schools are safe. She recommended that schools consider inviting parents and families to visit buildings in advance of reopening so they can see the safety measures, such as space between desks, cleaning stations, and other protective strategies.
The message to pediatricians and health care professionals when counseling families about returning individual children to school is to consider the risk to the child and the family directly in the context of the local plans, Dr. Sharfstein said during a question and answer session. “One school system’s plan is one school system’s plan,” he said, and added that families who are concerned about the risk should have an online option. However, “if you see a thoughtful approach” to reopening, with safety steps taken and parents informed, with protocols such as keeping small groups of children together to reduce transmission, “it is a pretty good trade-off,” and that is why the American Academy of Pediatrics currently favors children returning to school, he said.
The briefing participants had no relevant financial conflicts to disclose.
The absence of in-person school has harmed children in ways beyond loss of academic learning, according to Josh Sharfstein, MD, vice dean for public health practice and community engagement at the Johns Hopkins Bloomberg School of Public Health, Baltimore. In addition to learning, school is a place where many children receive breakfast and lunch every day, as well as support services and the benefits of being in a safe and secure environment, Dr. Sharfstein said in a press briefing sponsored by Johns Hopkins University.
However, although it is an important priority for children to return to school, “we are in the midst of a pandemic that poses real risk,” he said.
In the press briefing, several experts shared ideas and considerations for safely reopening K-12 schools in the fall of 2020.
Data from other countries where schools have reopened, notably Austria and Denmark, have been reassuring about the lack of transmission of SARS-CoV-2 among children in a school setting, said Jennifer Nuzzo, DrPH, an epidemiologist at the Johns Hopkins Center for Health Security. However, other countries where schools have reopened successfully have reported low levels of viral transmission locally, and a responsible strategy for school reopening in the United States should follow a similar plan, she said. In areas where transmission and infection rates are increasing “it may not be safe to reopen,” but in areas where rates are declining or stable, schools could potentially reopen if they follow safety measures.
Dr. Nuzzo suggested that Considerations include protocols for handwashing and sanitation, and maintaining physical distance by creative use of outdoor classrooms (weather permitting) or other spaces within school buildings. Transportation to and from school also will be an issue to address, she noted.
None of the strategies being considered will completely eliminate risk of SARS-CoV-2 infection in school settings, so allowing parents and students to opt out and choose distance learning will be important as well, said Dr. Nuzzo. In addition, schools may need to consider alternative roles for teachers and staff who don’t feel comfortable being in contact with students and fellow staff members. “All of these things are going to be hard,” Dr. Nuzzo acknowledged. “Hard should not be a deterrent,” to reopening schools, but “we acknowledge the resources that schools will need in order to do this.”
At present, all 50 states and the District of Columbia have released some type of plan for reopening schools, said Megan Collins, MD, MPH, codirector the Johns Hopkins Consortium for School-Based Health Solutions.
Dr. Collins and colleagues have developed a school reopening tracker, which is “a national snapshot of current reopening plans that have been released,” she said. The tracker is being updated continuously as plans evolve. The eSchool+ K-12 School Reopening Tracker identifies 12 reopening categories that states could potentially address in the plans. These categories are divided into Operational and Ethics/Equity. The operational categories include:
- Core academics
- SARS-CoV-2 protection
- Before and after school programs
- School access and transportation
- Student health services
- Food and nutrition.
Ethics/equity categories include the following:
- Parent choice
- Teacher and staff choice
- Children of poverty and systemic disadvantage
- Children with special needs/English as second language/gifted and twice exceptional
- Privacy
- Engagement and transparency.
As of July 15, 2020, 16 states (Arizona, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, North Carolina, North Dakota, Ohio, Rhode Island, Tennessee, Texas, Virginia, Washington, and Wisconsin) had addressed all 12 categories in their reopening plans, Dr. Collins said.
School reopening plans must take equity issues into account, said Annette Anderson, PhD, of the Johns Hopkins University School of Education.
Specifically, developing learning plans for special education students and others at the most risk for learning loss will be essential. “The digital divide has become a digital canyon” in some areas, Dr. Anderson noted, and schools need to rethink eligibility and work to provide access to devices for online learning for all students.
In addition, schools need to convince parents that schools are safe. She recommended that schools consider inviting parents and families to visit buildings in advance of reopening so they can see the safety measures, such as space between desks, cleaning stations, and other protective strategies.
The message to pediatricians and health care professionals when counseling families about returning individual children to school is to consider the risk to the child and the family directly in the context of the local plans, Dr. Sharfstein said during a question and answer session. “One school system’s plan is one school system’s plan,” he said, and added that families who are concerned about the risk should have an online option. However, “if you see a thoughtful approach” to reopening, with safety steps taken and parents informed, with protocols such as keeping small groups of children together to reduce transmission, “it is a pretty good trade-off,” and that is why the American Academy of Pediatrics currently favors children returning to school, he said.
The briefing participants had no relevant financial conflicts to disclose.
The absence of in-person school has harmed children in ways beyond loss of academic learning, according to Josh Sharfstein, MD, vice dean for public health practice and community engagement at the Johns Hopkins Bloomberg School of Public Health, Baltimore. In addition to learning, school is a place where many children receive breakfast and lunch every day, as well as support services and the benefits of being in a safe and secure environment, Dr. Sharfstein said in a press briefing sponsored by Johns Hopkins University.
However, although it is an important priority for children to return to school, “we are in the midst of a pandemic that poses real risk,” he said.
In the press briefing, several experts shared ideas and considerations for safely reopening K-12 schools in the fall of 2020.
Data from other countries where schools have reopened, notably Austria and Denmark, have been reassuring about the lack of transmission of SARS-CoV-2 among children in a school setting, said Jennifer Nuzzo, DrPH, an epidemiologist at the Johns Hopkins Center for Health Security. However, other countries where schools have reopened successfully have reported low levels of viral transmission locally, and a responsible strategy for school reopening in the United States should follow a similar plan, she said. In areas where transmission and infection rates are increasing “it may not be safe to reopen,” but in areas where rates are declining or stable, schools could potentially reopen if they follow safety measures.
Dr. Nuzzo suggested that Considerations include protocols for handwashing and sanitation, and maintaining physical distance by creative use of outdoor classrooms (weather permitting) or other spaces within school buildings. Transportation to and from school also will be an issue to address, she noted.
None of the strategies being considered will completely eliminate risk of SARS-CoV-2 infection in school settings, so allowing parents and students to opt out and choose distance learning will be important as well, said Dr. Nuzzo. In addition, schools may need to consider alternative roles for teachers and staff who don’t feel comfortable being in contact with students and fellow staff members. “All of these things are going to be hard,” Dr. Nuzzo acknowledged. “Hard should not be a deterrent,” to reopening schools, but “we acknowledge the resources that schools will need in order to do this.”
At present, all 50 states and the District of Columbia have released some type of plan for reopening schools, said Megan Collins, MD, MPH, codirector the Johns Hopkins Consortium for School-Based Health Solutions.
Dr. Collins and colleagues have developed a school reopening tracker, which is “a national snapshot of current reopening plans that have been released,” she said. The tracker is being updated continuously as plans evolve. The eSchool+ K-12 School Reopening Tracker identifies 12 reopening categories that states could potentially address in the plans. These categories are divided into Operational and Ethics/Equity. The operational categories include:
- Core academics
- SARS-CoV-2 protection
- Before and after school programs
- School access and transportation
- Student health services
- Food and nutrition.
Ethics/equity categories include the following:
- Parent choice
- Teacher and staff choice
- Children of poverty and systemic disadvantage
- Children with special needs/English as second language/gifted and twice exceptional
- Privacy
- Engagement and transparency.
As of July 15, 2020, 16 states (Arizona, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, North Carolina, North Dakota, Ohio, Rhode Island, Tennessee, Texas, Virginia, Washington, and Wisconsin) had addressed all 12 categories in their reopening plans, Dr. Collins said.
School reopening plans must take equity issues into account, said Annette Anderson, PhD, of the Johns Hopkins University School of Education.
Specifically, developing learning plans for special education students and others at the most risk for learning loss will be essential. “The digital divide has become a digital canyon” in some areas, Dr. Anderson noted, and schools need to rethink eligibility and work to provide access to devices for online learning for all students.
In addition, schools need to convince parents that schools are safe. She recommended that schools consider inviting parents and families to visit buildings in advance of reopening so they can see the safety measures, such as space between desks, cleaning stations, and other protective strategies.
The message to pediatricians and health care professionals when counseling families about returning individual children to school is to consider the risk to the child and the family directly in the context of the local plans, Dr. Sharfstein said during a question and answer session. “One school system’s plan is one school system’s plan,” he said, and added that families who are concerned about the risk should have an online option. However, “if you see a thoughtful approach” to reopening, with safety steps taken and parents informed, with protocols such as keeping small groups of children together to reduce transmission, “it is a pretty good trade-off,” and that is why the American Academy of Pediatrics currently favors children returning to school, he said.
The briefing participants had no relevant financial conflicts to disclose.
Clinicians address psoriatic disease risk in the era of COVID-19
COVID-19 has posed serious questions for patients with psoriatic disease and the clinicians who treat them. Both have serious concerns over whether psoriasis or the medications used to treat it pose additional risk for contracting COVID-19 or experiencing worse outcomes with illness.
At the virtual annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis, experts gathered to discuss these concerns and what is known about the special risk factors for psoriatic disease patients.

Studies from a few registries have been done already among patients with autoimmune disease, and the results so far suggest that patients may be able to breathe a little easier. “I don’t see any data that suggests that use of immunosuppressives or having autoimmune disease increases your risk of acquiring it. I think most of the risk is driven by risk of exposure,” said Kevin Winthrop, MD, MPH, a professor of public health, infectious diseases, ophthalmology at Oregon Health & Science University, Portland, during a presentation.
That assertion was reinforced by data presented by Rebecca Haberman, MD, a rheumatologist at New York University Langone Health. Her group created the Web-Based Assessment of Autoimmune, Immune-Mediated, and Rheumatic Patients during the COVID-19 Pandemic (WARCOV) cohort study to address the question of whether patients with immune-mediated inflammatory disease (IMID), including inflammatory arthritis, psoriasis, or inflammatory bowel disease, should discontinue or modify their immunotherapy regimens in the face of potential exposure to COVID-19.
To date, the study has data on 1,122 patients; 604 with inflammatory arthritis, 128 of whom have tested positive for COVID-19. The team established a cohort using the first 86 IMID patients confirmed to have contracted COVID-19. The hospitalization rate was 16% overall, and use of corticosteroids was associated with increased hospitalization risk. A follow-up analysis looking at the first 103 inflammatory arthritis patients who contracted COVID-19 showed a hospitalization rate of 26% and a mortality of 4%. That hospitalization rate is similar to the general hospitalization rate estimated by the New York Department of Health, Dr. Haberman said in her presentation.
Risk factors associated with hospitalization included being older and having asthma or COPD, which is similar to the general population. Use of oral glucocorticoids was linked to a big increase in risk for hospitalization, even with doses less than 10 mg prednisone daily (odds ratio, 14.31; 95% confidence interval, 3.55-57.70). There were no links between use of any cytokine therapy and risk, but use of TNF inhibitors was associated with a reduced risk (OR, 0.35; 95% CI, 0.13-0.97), while use of JAK inhibitors was associated with greater risk (OR, 6.30; 95% CI, 1.68-23.69). The latter result is tentative because of a small sample size, and it was driven largely by the experiences of patients with psoriatic arthritis.

Another study, run by the COVID-19 Global Rheumatology Alliance, looked at 600 patients with rheumatic disease from 40 countries, and “found no smoking gun,” said Leonard Calabrese, DO, who leads the Cleveland Clinic’s section of clinical immunology, during his presentation. “People can develop this when they’re on hydroxychloroquine. They seem to do not remarkably bad or remarkably good. There is no adverse signal for biologics, but being on prednisone [at a dose of] more than 10 mg is not great,” said Dr. Calabrese, who also noted that other publications have supported these conclusions.
So given these findings, how should clinicians address patient concerns? In the absence of probable exposure, “we say it’s better to have a well-controlled IMID on therapy than a poorly-controlled IMID on submaximal therapy. We say stick to therapy and try to wean the prednisone down as low as possible,” Dr. Calabrese said.
More controversially, what should patients do if they have had a significant exposure, such as a close proximity, prolonged exposure encounter with an individual with documented COVID-19, or at high-risk of disease? Dr. Calabrese noted that the American College of Rheumatology (ACR) guidelines recommend that low-level immunomodulation can be continued, “with an asterisk if it’s hydroxychloroquine, and it is in most of our minds now that we know that it is not effective, and the toxicity in the COVID setting is still being worked out,” he said.
With respect to other immunosuppressants, the ACR recommends stopping them temporarily, although IL-6 inhibitors may be continued in select circumstances. Resumption of the therapeutics can resume after a negative COVID test or completion of a 2-week observation period.
When patients contract COVID-19, antimalarial medications can be continued because they have been studied. “But medium-level immunomodulators, in particular methotrexate, I have grave concerns about because it can inhibit the adaptive immune response and antibody formation,” he said. COVID-19 is a serious infection, and all serious biologics have a package insert saying to stop them in a serious infection. Again, IL-6 inhibitors may be considered an exception in the right circumstances. When to resume these medications remains unknown. “I think that’s a work in progress. Test-based versus clinic-based strategies are a matter of controversy,” Dr. Calabrese said.

Ultimately, the question of what to do with immunosuppressive therapies in this population will continue to be a challenge. “The only good answer is to follow the rules of social distancing and to wear a mask,” said Kristina Callis Duffin, MD, a cochair of the department of dermatology and associate professor of dermatology at the University of Utah, Salt Lake City.
COVID-19 has posed serious questions for patients with psoriatic disease and the clinicians who treat them. Both have serious concerns over whether psoriasis or the medications used to treat it pose additional risk for contracting COVID-19 or experiencing worse outcomes with illness.
At the virtual annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis, experts gathered to discuss these concerns and what is known about the special risk factors for psoriatic disease patients.
Studies from a few registries have been done already among patients with autoimmune disease, and the results so far suggest that patients may be able to breathe a little easier. “I don’t see any data that suggests that use of immunosuppressives or having autoimmune disease increases your risk of acquiring it. I think most of the risk is driven by risk of exposure,” said Kevin Winthrop, MD, MPH, a professor of public health, infectious diseases, ophthalmology at Oregon Health & Science University, Portland, during a presentation.
That assertion was reinforced by data presented by Rebecca Haberman, MD, a rheumatologist at New York University Langone Health. Her group created the Web-Based Assessment of Autoimmune, Immune-Mediated, and Rheumatic Patients during the COVID-19 Pandemic (WARCOV) cohort study to address the question of whether patients with immune-mediated inflammatory disease (IMID), including inflammatory arthritis, psoriasis, or inflammatory bowel disease, should discontinue or modify their immunotherapy regimens in the face of potential exposure to COVID-19.
To date, the study has data on 1,122 patients; 604 with inflammatory arthritis, 128 of whom have tested positive for COVID-19. The team established a cohort using the first 86 IMID patients confirmed to have contracted COVID-19. The hospitalization rate was 16% overall, and use of corticosteroids was associated with increased hospitalization risk. A follow-up analysis looking at the first 103 inflammatory arthritis patients who contracted COVID-19 showed a hospitalization rate of 26% and a mortality of 4%. That hospitalization rate is similar to the general hospitalization rate estimated by the New York Department of Health, Dr. Haberman said in her presentation.
Risk factors associated with hospitalization included being older and having asthma or COPD, which is similar to the general population. Use of oral glucocorticoids was linked to a big increase in risk for hospitalization, even with doses less than 10 mg prednisone daily (odds ratio, 14.31; 95% confidence interval, 3.55-57.70). There were no links between use of any cytokine therapy and risk, but use of TNF inhibitors was associated with a reduced risk (OR, 0.35; 95% CI, 0.13-0.97), while use of JAK inhibitors was associated with greater risk (OR, 6.30; 95% CI, 1.68-23.69). The latter result is tentative because of a small sample size, and it was driven largely by the experiences of patients with psoriatic arthritis.
Another study, run by the COVID-19 Global Rheumatology Alliance, looked at 600 patients with rheumatic disease from 40 countries, and “found no smoking gun,” said Leonard Calabrese, DO, who leads the Cleveland Clinic’s section of clinical immunology, during his presentation. “People can develop this when they’re on hydroxychloroquine. They seem to do not remarkably bad or remarkably good. There is no adverse signal for biologics, but being on prednisone [at a dose of] more than 10 mg is not great,” said Dr. Calabrese, who also noted that other publications have supported these conclusions.
So given these findings, how should clinicians address patient concerns? In the absence of probable exposure, “we say it’s better to have a well-controlled IMID on therapy than a poorly-controlled IMID on submaximal therapy. We say stick to therapy and try to wean the prednisone down as low as possible,” Dr. Calabrese said.
More controversially, what should patients do if they have had a significant exposure, such as a close proximity, prolonged exposure encounter with an individual with documented COVID-19, or at high-risk of disease? Dr. Calabrese noted that the American College of Rheumatology (ACR) guidelines recommend that low-level immunomodulation can be continued, “with an asterisk if it’s hydroxychloroquine, and it is in most of our minds now that we know that it is not effective, and the toxicity in the COVID setting is still being worked out,” he said.
With respect to other immunosuppressants, the ACR recommends stopping them temporarily, although IL-6 inhibitors may be continued in select circumstances. Resumption of the therapeutics can resume after a negative COVID test or completion of a 2-week observation period.
When patients contract COVID-19, antimalarial medications can be continued because they have been studied. “But medium-level immunomodulators, in particular methotrexate, I have grave concerns about because it can inhibit the adaptive immune response and antibody formation,” he said. COVID-19 is a serious infection, and all serious biologics have a package insert saying to stop them in a serious infection. Again, IL-6 inhibitors may be considered an exception in the right circumstances. When to resume these medications remains unknown. “I think that’s a work in progress. Test-based versus clinic-based strategies are a matter of controversy,” Dr. Calabrese said.
Ultimately, the question of what to do with immunosuppressive therapies in this population will continue to be a challenge. “The only good answer is to follow the rules of social distancing and to wear a mask,” said Kristina Callis Duffin, MD, a cochair of the department of dermatology and associate professor of dermatology at the University of Utah, Salt Lake City.
COVID-19 has posed serious questions for patients with psoriatic disease and the clinicians who treat them. Both have serious concerns over whether psoriasis or the medications used to treat it pose additional risk for contracting COVID-19 or experiencing worse outcomes with illness.
At the virtual annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis, experts gathered to discuss these concerns and what is known about the special risk factors for psoriatic disease patients.
Studies from a few registries have been done already among patients with autoimmune disease, and the results so far suggest that patients may be able to breathe a little easier. “I don’t see any data that suggests that use of immunosuppressives or having autoimmune disease increases your risk of acquiring it. I think most of the risk is driven by risk of exposure,” said Kevin Winthrop, MD, MPH, a professor of public health, infectious diseases, ophthalmology at Oregon Health & Science University, Portland, during a presentation.
That assertion was reinforced by data presented by Rebecca Haberman, MD, a rheumatologist at New York University Langone Health. Her group created the Web-Based Assessment of Autoimmune, Immune-Mediated, and Rheumatic Patients during the COVID-19 Pandemic (WARCOV) cohort study to address the question of whether patients with immune-mediated inflammatory disease (IMID), including inflammatory arthritis, psoriasis, or inflammatory bowel disease, should discontinue or modify their immunotherapy regimens in the face of potential exposure to COVID-19.
To date, the study has data on 1,122 patients; 604 with inflammatory arthritis, 128 of whom have tested positive for COVID-19. The team established a cohort using the first 86 IMID patients confirmed to have contracted COVID-19. The hospitalization rate was 16% overall, and use of corticosteroids was associated with increased hospitalization risk. A follow-up analysis looking at the first 103 inflammatory arthritis patients who contracted COVID-19 showed a hospitalization rate of 26% and a mortality of 4%. That hospitalization rate is similar to the general hospitalization rate estimated by the New York Department of Health, Dr. Haberman said in her presentation.
Risk factors associated with hospitalization included being older and having asthma or COPD, which is similar to the general population. Use of oral glucocorticoids was linked to a big increase in risk for hospitalization, even with doses less than 10 mg prednisone daily (odds ratio, 14.31; 95% confidence interval, 3.55-57.70). There were no links between use of any cytokine therapy and risk, but use of TNF inhibitors was associated with a reduced risk (OR, 0.35; 95% CI, 0.13-0.97), while use of JAK inhibitors was associated with greater risk (OR, 6.30; 95% CI, 1.68-23.69). The latter result is tentative because of a small sample size, and it was driven largely by the experiences of patients with psoriatic arthritis.
Another study, run by the COVID-19 Global Rheumatology Alliance, looked at 600 patients with rheumatic disease from 40 countries, and “found no smoking gun,” said Leonard Calabrese, DO, who leads the Cleveland Clinic’s section of clinical immunology, during his presentation. “People can develop this when they’re on hydroxychloroquine. They seem to do not remarkably bad or remarkably good. There is no adverse signal for biologics, but being on prednisone [at a dose of] more than 10 mg is not great,” said Dr. Calabrese, who also noted that other publications have supported these conclusions.
So given these findings, how should clinicians address patient concerns? In the absence of probable exposure, “we say it’s better to have a well-controlled IMID on therapy than a poorly-controlled IMID on submaximal therapy. We say stick to therapy and try to wean the prednisone down as low as possible,” Dr. Calabrese said.
More controversially, what should patients do if they have had a significant exposure, such as a close proximity, prolonged exposure encounter with an individual with documented COVID-19, or at high-risk of disease? Dr. Calabrese noted that the American College of Rheumatology (ACR) guidelines recommend that low-level immunomodulation can be continued, “with an asterisk if it’s hydroxychloroquine, and it is in most of our minds now that we know that it is not effective, and the toxicity in the COVID setting is still being worked out,” he said.
With respect to other immunosuppressants, the ACR recommends stopping them temporarily, although IL-6 inhibitors may be continued in select circumstances. Resumption of the therapeutics can resume after a negative COVID test or completion of a 2-week observation period.
When patients contract COVID-19, antimalarial medications can be continued because they have been studied. “But medium-level immunomodulators, in particular methotrexate, I have grave concerns about because it can inhibit the adaptive immune response and antibody formation,” he said. COVID-19 is a serious infection, and all serious biologics have a package insert saying to stop them in a serious infection. Again, IL-6 inhibitors may be considered an exception in the right circumstances. When to resume these medications remains unknown. “I think that’s a work in progress. Test-based versus clinic-based strategies are a matter of controversy,” Dr. Calabrese said.
Ultimately, the question of what to do with immunosuppressive therapies in this population will continue to be a challenge. “The only good answer is to follow the rules of social distancing and to wear a mask,” said Kristina Callis Duffin, MD, a cochair of the department of dermatology and associate professor of dermatology at the University of Utah, Salt Lake City.
FROM THE GRAPPA 2020 VIRTUAL ANNUAL MEETING
Don’t overlook treating older patients with acute promyelocytic leukemia, expert says
The estimated one third of patients with acute promyelocytic leukemia (APL) who are older than 60 years now enjoy a notably better prognosis than in years past, thanks to the introduction of all-trans retinoic acid (ATRA) and arsenic trioxide (ATO). However, such patients still require special management considerations, and can only benefit from treatment advantages if properly identified.
In a recently published set of recommendations, the International Society of Geriatric Oncology Task Force outlined the latest information on the treatment of APL in older patients. Medscape spoke with the lead author of the article, Heidi Klepin, MD, MS, professor in the section on hematology and oncology at Wake Forest School of Medicine in Winston Salem, N.C., who highlighted the key points that clinicians need to know about this often highly treatable subtype of acute myeloid leukemia (AML). This interview has been edited for length and clarity.
Medscape: How do the potential benefits of therapy for APL compare with other AML subtypes in older persons?
Dr. Klepin: Potential benefits of therapy are dramatically better for APL, compared with other AML subtypes. The use of non–chemotherapy based regimens with ATRA and ATO has substantially changed options for APL management. ATRA+ATO are associated with high remission and cure rates. The chance of cure with less toxicity extends the clinical benefit to adults of advanced age and, to some extent, with comorbidities.
How has the management strategy for this subgroup of patients with APL changed in recent years?
Management options have changed dramatically with the advent of non–chemotherapy-based regimens. The majority of treated older adults could be expected to achieve remissions that are durable, with less risk of major side effects during treatment. Adults with comorbid conditions, at advanced age, and with some functional limitations could also still benefit from treatment.
Does that management strategy change based on whether patients are considered low-risk or high-risk?
Clinical trials are lacking to provide best evidence for the optimal treatment for adults over age 70 years. However, based on available data and experience, the expert consensus provided in this report recommends that older adults regardless of age with low-risk disease should be offered ATRA+ATO–based therapy if available.
The optimal approach for patients with high-risk disease is less clear based on available studies. For fit older adults without cardiac disease, the use of single-drug anthracycline chemotherapy with ATRA plus/minus ATO is appropriate. However, treatment with ATRA+ATO may also provide a good response with less side-effect risk. For older patients with high-risk disease and comorbidity or poor functional status, the use of non-chemotherapy regimen ATRA+ATO is preferred.
What role does frailty have in making treatment decisions in this population?
Although frail older adults have not been specifically studied in clinical trials, it is reasonable to offer treatment with a non–chemotherapy based regimen for many of these patients, particularly if frailty may in part be related to disease burden. Frailty is a dynamic state. Rapid initiation of therapy can improve function and symptoms, potentially reversing the phenotype of frailty if driven largely by disease burden.
What is the role of consolidation and maintenance therapy in older patients with APL?
Consolidation therapy is recommended with ATRA+ATO as a standard consideration for most patients when available, although protocol-based treatments may vary. For those older adults treated with chemotherapy+ATRA for high-risk disease, decreased anthracycline [chemotherapy] exposure during consolidation results in less mortality risk. Maintenance therapy is not needed when ATRA+ATO are used for induction and consolidation and after achieving a molecular remission.
What other patient factors should influence treatment decisions?
In practice, older age, concurrent comorbid conditions [particularly cardiac disease], and physical function may all influence treatment decisions. Regarding the disease itself, a high white blood cell count at diagnosis, which is classified as higher-risk disease, directs choice of therapy, particularly for fit older adults. Cardiac disease can limit certain treatment options because of risk of side effects. In particular, the use of anthracycline chemotherapy is contraindicated for people with heart failure, and the use of ATO can increase risk of arrhythmia and is not used with certain EKG findings.
Special considerations in older patients with APL
How would you characterize older individuals’ involvement in clinical trials?
Older adults are underrepresented on clinical trials, with very limited inclusion of those over age 75 years. Some APL trials have had upper age exclusions, which is something we have advocated to remove.
Are there unique challenges in diagnosing older adults with APL?
The presentation of APL with low blood counts can look similar to other types of AML or myelodysplastic syndrome when reviewing routine lab results. If additional testing is not done quickly, the diagnosis will be missed, as well as the opportunity for effective treatment. Rapid diagnosis is essential in this disease.
Are there age-related differences in the presentation of APL?
There are no available data to support more-aggressive APL biology in older adults.
How does age impact the outcomes of patients with APL?
Although the outcomes in APL have improved, the survival difference between age groups has not decreased in recent years and the magnitude of improvement in survival in older patients still lags behind younger patients. Older age is also associated with worse outcomes driven largely by increased early death, with greater rates of infection and multiorgan failure leading to a decreased overall survival.
How important is a geriatric assessment for older patients with APL? What role does it play in management?
There are no data on the use of a geriatric assessment specifically in APL, although a geriatric assessment is recommended for older adults starting new chemotherapy in general. A geriatric assessment may help determine who is fit enough to be treated like a younger patient, which has the greatest implications for those with high-risk disease where chemotherapy would be added.
A geriatric assessment can also play an important role in management by identifying vulnerabilities that could be addressed to minimize complications during treatment regardless of the type of treatment given. An example would be identifying and addressing polypharmacy (commonly defined as ≥5 medications). One challenge faced when treating older patients is the use of multiple concomitant medications. Polypharmacy is common among older patients with cancer. Among older adults, each new drug increases the risk of adverse drug events by 10%. Drugs commonly used for the treatment of APL, such as ATRA and ATO, have many potential drug interactions, which must be carefully assessed by a pharmacist prior to and during treatment. Active deprescribing of medications that are not critical during treatment for APL should be done to minimize risks.
What is differentiation syndrome? What role does age appear to play in the risk of developing it and in strategies for managing it?
Differentiation syndrome is a serious side effect that may occur in patients with APL who have been treated with certain anticancer drugs. Differentiation syndrome usually occurs within a week or 2 of starting treatment. It is caused by a large, rapid release of cytokines [immune substances] from leukemia cells. The most common symptoms include fever; cough; shortness of breath; weight gain; swelling of the arms, legs, and neck; build-up of excess fluid around the heart and lungs; low blood pressure; and kidney failure. Differentiation syndrome can be life-threatening if not recognized and treated early.
Some evidence suggests older adults may be at a higher risk for developing differentiation syndrome and may be less likely to tolerate it. A risk factor is kidney dysfunction, which is more common in older adults.
It is not clear that management should differ by age, but vigilance is critical. The use of prophylactic steroids is considered for high-risk patients [high white cell count or kidney disease]. The treatment for differentiation syndrome involves rapid use of steroids.
Does the management of infections differ in older people with APL?
There is no clear data to support a different management of infection prevention for older adults, although preventive antibiotics can be considered as older adults are at a higher risk for infectious complications. However, drug interactions need to be carefully considered in this context.
Guiding clinicians toward better treatment of APL
Why did you decide to formulate these recommendations now?
It is particularly important to draw attention to the management of older adults with APL given the availability of effective non–chemotherapy based therapies and the large distinction between expected outcomes with APL vs. other types of acute leukemia in this population. This diagnosis should not be missed. Further, we highlight the importance of ensuring that older adults are included in trials to provide best evidence for both treatment choice and supportive care management.
How do you see these recommendations affecting clinical practice?
We want to emphasize that advanced age should not preclude treatment, which can have meaningful benefit with expectation of remission and quality time gained.
We hope that these recommendations provide a useful blueprint for guiding the management of older adults, particularly consolidating information to help inform treatment for those patients older than 75 years that can provide best estimates of side effects and benefits when making a decision with patients. We also hope that these recommendations will be used to educate providers on the importance of looking for this diagnosis in our older patients.
From a practical standpoint, it will be important that this information gets to those providers who are making the referrals to oncologists, which can include primary care physicians and emergency room providers, to ensure prompt diagnostic workup. Treatment decisions can only be made once a diagnosis has been recognized, and time is critical with this disease.
Dr. Klepin disclosed a consultancy for Genentech and Pfizer and is a contributor to UpToDate.
A version of this article originally appeared on Medscape.com.
The estimated one third of patients with acute promyelocytic leukemia (APL) who are older than 60 years now enjoy a notably better prognosis than in years past, thanks to the introduction of all-trans retinoic acid (ATRA) and arsenic trioxide (ATO). However, such patients still require special management considerations, and can only benefit from treatment advantages if properly identified.
In a recently published set of recommendations, the International Society of Geriatric Oncology Task Force outlined the latest information on the treatment of APL in older patients. Medscape spoke with the lead author of the article, Heidi Klepin, MD, MS, professor in the section on hematology and oncology at Wake Forest School of Medicine in Winston Salem, N.C., who highlighted the key points that clinicians need to know about this often highly treatable subtype of acute myeloid leukemia (AML). This interview has been edited for length and clarity.
Medscape: How do the potential benefits of therapy for APL compare with other AML subtypes in older persons?
Dr. Klepin: Potential benefits of therapy are dramatically better for APL, compared with other AML subtypes. The use of non–chemotherapy based regimens with ATRA and ATO has substantially changed options for APL management. ATRA+ATO are associated with high remission and cure rates. The chance of cure with less toxicity extends the clinical benefit to adults of advanced age and, to some extent, with comorbidities.
How has the management strategy for this subgroup of patients with APL changed in recent years?
Management options have changed dramatically with the advent of non–chemotherapy-based regimens. The majority of treated older adults could be expected to achieve remissions that are durable, with less risk of major side effects during treatment. Adults with comorbid conditions, at advanced age, and with some functional limitations could also still benefit from treatment.
Does that management strategy change based on whether patients are considered low-risk or high-risk?
Clinical trials are lacking to provide best evidence for the optimal treatment for adults over age 70 years. However, based on available data and experience, the expert consensus provided in this report recommends that older adults regardless of age with low-risk disease should be offered ATRA+ATO–based therapy if available.
The optimal approach for patients with high-risk disease is less clear based on available studies. For fit older adults without cardiac disease, the use of single-drug anthracycline chemotherapy with ATRA plus/minus ATO is appropriate. However, treatment with ATRA+ATO may also provide a good response with less side-effect risk. For older patients with high-risk disease and comorbidity or poor functional status, the use of non-chemotherapy regimen ATRA+ATO is preferred.
What role does frailty have in making treatment decisions in this population?
Although frail older adults have not been specifically studied in clinical trials, it is reasonable to offer treatment with a non–chemotherapy based regimen for many of these patients, particularly if frailty may in part be related to disease burden. Frailty is a dynamic state. Rapid initiation of therapy can improve function and symptoms, potentially reversing the phenotype of frailty if driven largely by disease burden.
What is the role of consolidation and maintenance therapy in older patients with APL?
Consolidation therapy is recommended with ATRA+ATO as a standard consideration for most patients when available, although protocol-based treatments may vary. For those older adults treated with chemotherapy+ATRA for high-risk disease, decreased anthracycline [chemotherapy] exposure during consolidation results in less mortality risk. Maintenance therapy is not needed when ATRA+ATO are used for induction and consolidation and after achieving a molecular remission.
What other patient factors should influence treatment decisions?
In practice, older age, concurrent comorbid conditions [particularly cardiac disease], and physical function may all influence treatment decisions. Regarding the disease itself, a high white blood cell count at diagnosis, which is classified as higher-risk disease, directs choice of therapy, particularly for fit older adults. Cardiac disease can limit certain treatment options because of risk of side effects. In particular, the use of anthracycline chemotherapy is contraindicated for people with heart failure, and the use of ATO can increase risk of arrhythmia and is not used with certain EKG findings.
Special considerations in older patients with APL
How would you characterize older individuals’ involvement in clinical trials?
Older adults are underrepresented on clinical trials, with very limited inclusion of those over age 75 years. Some APL trials have had upper age exclusions, which is something we have advocated to remove.
Are there unique challenges in diagnosing older adults with APL?
The presentation of APL with low blood counts can look similar to other types of AML or myelodysplastic syndrome when reviewing routine lab results. If additional testing is not done quickly, the diagnosis will be missed, as well as the opportunity for effective treatment. Rapid diagnosis is essential in this disease.
Are there age-related differences in the presentation of APL?
There are no available data to support more-aggressive APL biology in older adults.
How does age impact the outcomes of patients with APL?
Although the outcomes in APL have improved, the survival difference between age groups has not decreased in recent years and the magnitude of improvement in survival in older patients still lags behind younger patients. Older age is also associated with worse outcomes driven largely by increased early death, with greater rates of infection and multiorgan failure leading to a decreased overall survival.
How important is a geriatric assessment for older patients with APL? What role does it play in management?
There are no data on the use of a geriatric assessment specifically in APL, although a geriatric assessment is recommended for older adults starting new chemotherapy in general. A geriatric assessment may help determine who is fit enough to be treated like a younger patient, which has the greatest implications for those with high-risk disease where chemotherapy would be added.
A geriatric assessment can also play an important role in management by identifying vulnerabilities that could be addressed to minimize complications during treatment regardless of the type of treatment given. An example would be identifying and addressing polypharmacy (commonly defined as ≥5 medications). One challenge faced when treating older patients is the use of multiple concomitant medications. Polypharmacy is common among older patients with cancer. Among older adults, each new drug increases the risk of adverse drug events by 10%. Drugs commonly used for the treatment of APL, such as ATRA and ATO, have many potential drug interactions, which must be carefully assessed by a pharmacist prior to and during treatment. Active deprescribing of medications that are not critical during treatment for APL should be done to minimize risks.
What is differentiation syndrome? What role does age appear to play in the risk of developing it and in strategies for managing it?
Differentiation syndrome is a serious side effect that may occur in patients with APL who have been treated with certain anticancer drugs. Differentiation syndrome usually occurs within a week or 2 of starting treatment. It is caused by a large, rapid release of cytokines [immune substances] from leukemia cells. The most common symptoms include fever; cough; shortness of breath; weight gain; swelling of the arms, legs, and neck; build-up of excess fluid around the heart and lungs; low blood pressure; and kidney failure. Differentiation syndrome can be life-threatening if not recognized and treated early.
Some evidence suggests older adults may be at a higher risk for developing differentiation syndrome and may be less likely to tolerate it. A risk factor is kidney dysfunction, which is more common in older adults.
It is not clear that management should differ by age, but vigilance is critical. The use of prophylactic steroids is considered for high-risk patients [high white cell count or kidney disease]. The treatment for differentiation syndrome involves rapid use of steroids.
Does the management of infections differ in older people with APL?
There is no clear data to support a different management of infection prevention for older adults, although preventive antibiotics can be considered as older adults are at a higher risk for infectious complications. However, drug interactions need to be carefully considered in this context.
Guiding clinicians toward better treatment of APL
Why did you decide to formulate these recommendations now?
It is particularly important to draw attention to the management of older adults with APL given the availability of effective non–chemotherapy based therapies and the large distinction between expected outcomes with APL vs. other types of acute leukemia in this population. This diagnosis should not be missed. Further, we highlight the importance of ensuring that older adults are included in trials to provide best evidence for both treatment choice and supportive care management.
How do you see these recommendations affecting clinical practice?
We want to emphasize that advanced age should not preclude treatment, which can have meaningful benefit with expectation of remission and quality time gained.
We hope that these recommendations provide a useful blueprint for guiding the management of older adults, particularly consolidating information to help inform treatment for those patients older than 75 years that can provide best estimates of side effects and benefits when making a decision with patients. We also hope that these recommendations will be used to educate providers on the importance of looking for this diagnosis in our older patients.
From a practical standpoint, it will be important that this information gets to those providers who are making the referrals to oncologists, which can include primary care physicians and emergency room providers, to ensure prompt diagnostic workup. Treatment decisions can only be made once a diagnosis has been recognized, and time is critical with this disease.
Dr. Klepin disclosed a consultancy for Genentech and Pfizer and is a contributor to UpToDate.
A version of this article originally appeared on Medscape.com.
The estimated one third of patients with acute promyelocytic leukemia (APL) who are older than 60 years now enjoy a notably better prognosis than in years past, thanks to the introduction of all-trans retinoic acid (ATRA) and arsenic trioxide (ATO). However, such patients still require special management considerations, and can only benefit from treatment advantages if properly identified.
In a recently published set of recommendations, the International Society of Geriatric Oncology Task Force outlined the latest information on the treatment of APL in older patients. Medscape spoke with the lead author of the article, Heidi Klepin, MD, MS, professor in the section on hematology and oncology at Wake Forest School of Medicine in Winston Salem, N.C., who highlighted the key points that clinicians need to know about this often highly treatable subtype of acute myeloid leukemia (AML). This interview has been edited for length and clarity.
Medscape: How do the potential benefits of therapy for APL compare with other AML subtypes in older persons?
Dr. Klepin: Potential benefits of therapy are dramatically better for APL, compared with other AML subtypes. The use of non–chemotherapy based regimens with ATRA and ATO has substantially changed options for APL management. ATRA+ATO are associated with high remission and cure rates. The chance of cure with less toxicity extends the clinical benefit to adults of advanced age and, to some extent, with comorbidities.
How has the management strategy for this subgroup of patients with APL changed in recent years?
Management options have changed dramatically with the advent of non–chemotherapy-based regimens. The majority of treated older adults could be expected to achieve remissions that are durable, with less risk of major side effects during treatment. Adults with comorbid conditions, at advanced age, and with some functional limitations could also still benefit from treatment.
Does that management strategy change based on whether patients are considered low-risk or high-risk?
Clinical trials are lacking to provide best evidence for the optimal treatment for adults over age 70 years. However, based on available data and experience, the expert consensus provided in this report recommends that older adults regardless of age with low-risk disease should be offered ATRA+ATO–based therapy if available.
The optimal approach for patients with high-risk disease is less clear based on available studies. For fit older adults without cardiac disease, the use of single-drug anthracycline chemotherapy with ATRA plus/minus ATO is appropriate. However, treatment with ATRA+ATO may also provide a good response with less side-effect risk. For older patients with high-risk disease and comorbidity or poor functional status, the use of non-chemotherapy regimen ATRA+ATO is preferred.
What role does frailty have in making treatment decisions in this population?
Although frail older adults have not been specifically studied in clinical trials, it is reasonable to offer treatment with a non–chemotherapy based regimen for many of these patients, particularly if frailty may in part be related to disease burden. Frailty is a dynamic state. Rapid initiation of therapy can improve function and symptoms, potentially reversing the phenotype of frailty if driven largely by disease burden.
What is the role of consolidation and maintenance therapy in older patients with APL?
Consolidation therapy is recommended with ATRA+ATO as a standard consideration for most patients when available, although protocol-based treatments may vary. For those older adults treated with chemotherapy+ATRA for high-risk disease, decreased anthracycline [chemotherapy] exposure during consolidation results in less mortality risk. Maintenance therapy is not needed when ATRA+ATO are used for induction and consolidation and after achieving a molecular remission.
What other patient factors should influence treatment decisions?
In practice, older age, concurrent comorbid conditions [particularly cardiac disease], and physical function may all influence treatment decisions. Regarding the disease itself, a high white blood cell count at diagnosis, which is classified as higher-risk disease, directs choice of therapy, particularly for fit older adults. Cardiac disease can limit certain treatment options because of risk of side effects. In particular, the use of anthracycline chemotherapy is contraindicated for people with heart failure, and the use of ATO can increase risk of arrhythmia and is not used with certain EKG findings.
Special considerations in older patients with APL
How would you characterize older individuals’ involvement in clinical trials?
Older adults are underrepresented on clinical trials, with very limited inclusion of those over age 75 years. Some APL trials have had upper age exclusions, which is something we have advocated to remove.
Are there unique challenges in diagnosing older adults with APL?
The presentation of APL with low blood counts can look similar to other types of AML or myelodysplastic syndrome when reviewing routine lab results. If additional testing is not done quickly, the diagnosis will be missed, as well as the opportunity for effective treatment. Rapid diagnosis is essential in this disease.
Are there age-related differences in the presentation of APL?
There are no available data to support more-aggressive APL biology in older adults.
How does age impact the outcomes of patients with APL?
Although the outcomes in APL have improved, the survival difference between age groups has not decreased in recent years and the magnitude of improvement in survival in older patients still lags behind younger patients. Older age is also associated with worse outcomes driven largely by increased early death, with greater rates of infection and multiorgan failure leading to a decreased overall survival.
How important is a geriatric assessment for older patients with APL? What role does it play in management?
There are no data on the use of a geriatric assessment specifically in APL, although a geriatric assessment is recommended for older adults starting new chemotherapy in general. A geriatric assessment may help determine who is fit enough to be treated like a younger patient, which has the greatest implications for those with high-risk disease where chemotherapy would be added.
A geriatric assessment can also play an important role in management by identifying vulnerabilities that could be addressed to minimize complications during treatment regardless of the type of treatment given. An example would be identifying and addressing polypharmacy (commonly defined as ≥5 medications). One challenge faced when treating older patients is the use of multiple concomitant medications. Polypharmacy is common among older patients with cancer. Among older adults, each new drug increases the risk of adverse drug events by 10%. Drugs commonly used for the treatment of APL, such as ATRA and ATO, have many potential drug interactions, which must be carefully assessed by a pharmacist prior to and during treatment. Active deprescribing of medications that are not critical during treatment for APL should be done to minimize risks.
What is differentiation syndrome? What role does age appear to play in the risk of developing it and in strategies for managing it?
Differentiation syndrome is a serious side effect that may occur in patients with APL who have been treated with certain anticancer drugs. Differentiation syndrome usually occurs within a week or 2 of starting treatment. It is caused by a large, rapid release of cytokines [immune substances] from leukemia cells. The most common symptoms include fever; cough; shortness of breath; weight gain; swelling of the arms, legs, and neck; build-up of excess fluid around the heart and lungs; low blood pressure; and kidney failure. Differentiation syndrome can be life-threatening if not recognized and treated early.
Some evidence suggests older adults may be at a higher risk for developing differentiation syndrome and may be less likely to tolerate it. A risk factor is kidney dysfunction, which is more common in older adults.
It is not clear that management should differ by age, but vigilance is critical. The use of prophylactic steroids is considered for high-risk patients [high white cell count or kidney disease]. The treatment for differentiation syndrome involves rapid use of steroids.
Does the management of infections differ in older people with APL?
There is no clear data to support a different management of infection prevention for older adults, although preventive antibiotics can be considered as older adults are at a higher risk for infectious complications. However, drug interactions need to be carefully considered in this context.
Guiding clinicians toward better treatment of APL
Why did you decide to formulate these recommendations now?
It is particularly important to draw attention to the management of older adults with APL given the availability of effective non–chemotherapy based therapies and the large distinction between expected outcomes with APL vs. other types of acute leukemia in this population. This diagnosis should not be missed. Further, we highlight the importance of ensuring that older adults are included in trials to provide best evidence for both treatment choice and supportive care management.
How do you see these recommendations affecting clinical practice?
We want to emphasize that advanced age should not preclude treatment, which can have meaningful benefit with expectation of remission and quality time gained.
We hope that these recommendations provide a useful blueprint for guiding the management of older adults, particularly consolidating information to help inform treatment for those patients older than 75 years that can provide best estimates of side effects and benefits when making a decision with patients. We also hope that these recommendations will be used to educate providers on the importance of looking for this diagnosis in our older patients.
From a practical standpoint, it will be important that this information gets to those providers who are making the referrals to oncologists, which can include primary care physicians and emergency room providers, to ensure prompt diagnostic workup. Treatment decisions can only be made once a diagnosis has been recognized, and time is critical with this disease.
Dr. Klepin disclosed a consultancy for Genentech and Pfizer and is a contributor to UpToDate.
A version of this article originally appeared on Medscape.com.
Rupioid Psoriasis and Psoriatic Arthritis in a Patient With Skin of Color
To the Editor:
A 49-year-old black woman presented with multiple hyperkeratotic papules that progressed over the last 2 months to circular plaques with central thick black crust resembling eschar. She first noticed these lesions as firm, small, black papules on the legs and continued to develop new lesions that eventually evolved into large, coin-shaped, hyperkeratotic plaques. Her medical history was notable for stage III non-Hodgkin follicular lymphoma in remission after treatment with rituximab, cyclophosphamide, doxorubicin hydrochloride, vincristine sulfate, and prednisone 7 months earlier, and chronic hepatitis B infection being treated with entecavir. Her family history was not remarkable for psoriasis or inflammatory arthritis.
She initially was seen by internal medicine and was started on topical triamcinolone with no improvement of the lesions. At presentation to dermatology, physical examination revealed firm, small, black, hyperkeratotic papules (Figure 1A) and circular plaques with a rim of erythema and central thick, smooth, black crust resembling eschar (Figure 1B). No other skin changes were noted at the time. The bilateral metacarpophalangeal, bilateral proximal interphalangeal, left wrist, and bilateral ankle joints were remarkable for tenderness, swelling, and reduced range of motion. She noted concomitant arthralgia and stiffness but denied fever. She had no other systemic symptoms including night sweats, weight loss, fatigue, malaise, sun sensitivity, oral ulcers, or hair loss. A radiograph of the hand was negative for erosive changes but showed mild periarticular osteopenia and fusiform soft tissue swelling of the third digit. Given the central appearance of eschar in the larger lesions, the initial differential diagnosis included Sweet syndrome, invasive fungal infection, vasculitis, and recurrent lymphoma.

A 4-mm punch biopsy specimen of a representative lesion on the right leg revealed psoriasiform epidermal hyperplasia, parakeratosis, neutrophils in the stratum corneum and spinosum, elongation of the rete ridges, and superficial vascular ectasia, which favored a diagnosis of psoriasis (Figure 2). A periodic acid-Schiff stain was negative for fungal hyphae. Fungal culture, bacterial tissue culture, and acid-fast bacilli smear were negative. Absence of deep dermal inflammation precluded a diagnosis of Sweet syndrome. Further notable laboratory studies included negative human immunodeficiency virus (HIV) antibody, rapid plasma reagin, hepatitis C antibody, and rheumatoid factor.
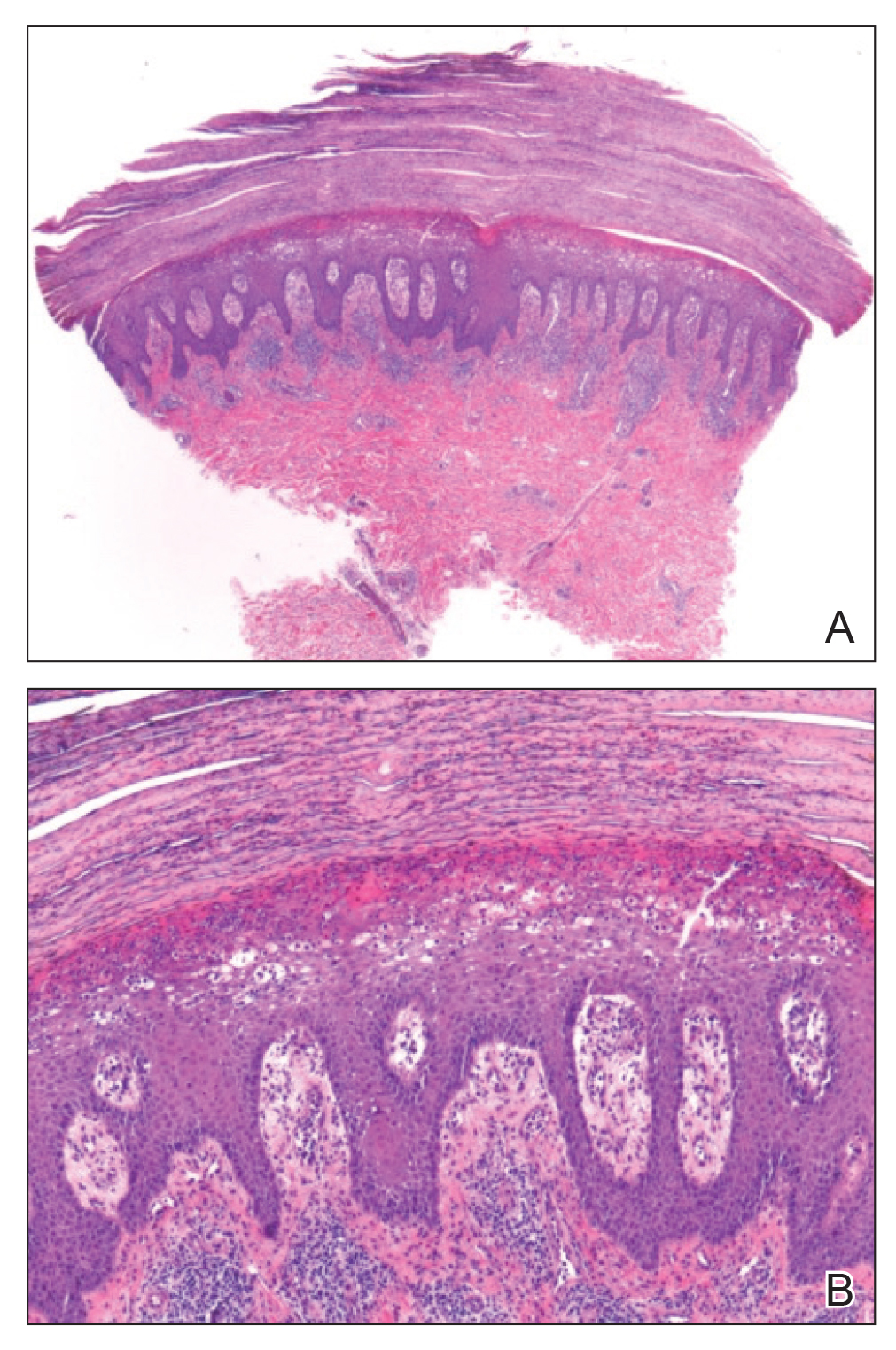
At follow-up 2 weeks later, the initial lesions were still present, and she had developed new widespread, well-demarcated, erythematous plaques with silver scale along the scalp, back, chest, and abdomen that were more typical of psoriasis. Oil spots were noted on several fingernails and toenails. Based on the clinicopathologic findings, nail changes, and asymmetric inflammatory arthritis, a diagnosis of rupioid psoriasis with psoriatic arthritis (PsA) was established. Treatment with clobetasol ointment 0.05% twice daily to active lesions was started. Initiation of systemic therapy with a steroid-sparing agent was deferred in anticipation of care coordination with rheumatology, hepatology, and hematology/oncology due to the patient's history of follicular lymphoma and chronic hepatitis B. Although attempts were made to avoid systemic corticosteroids due to the risk for a psoriasis flare upon discontinuation, because of the severity of arthralgia she was started on oral prednisone 20 mg daily by rheumatology with plans for a slow taper once an alternative systemic agent was started.1
At 10-week follow-up, the patient had marked improvement of psoriatic plaques with no active lesions while only on prednisone 20 mg daily. In consultation with her care team, she subsequently was started on methotrexate 10 mg weekly for 2 weeks followed by titration to 15 mg weekly. Plans were to start a prednisone taper after a month of methotrexate to allow her new treatment time for therapeutic effect. Notably, the patient chose to discontinue prednisone 2 weeks into methotrexate therapy after only two 10-mg doses of methotrexate weekly and well before therapeutic levels were achieved. Despite stopping prednisone early and without a taper, she did not experience a relapse in psoriatic skin lesions. Three months following initiation of methotrexate, she sustained resolution of the cutaneous lesions with only residual postinflammatory hyperpigmentation.
Psoriasis is a common chronic inflammatory skin disorder with multiple clinical presentations. There are several variants of psoriasis that are classified by their morphologic appearance including chronic plaque, guttate, erythrodermic, and pustular, with more than 90% of cases representing the plaque variant. Less common clinical presentations of psoriasis include rupioid, ostraceous, inverse, elephantine, and HIV associated.2 Rupioid psoriasis is a rare variant that presents with cone-shaped, limpetlike lesions.3,4 Similar to the limited epidemiological and clinical data pertaining to psoriasis in nonwhite racial groups, there also is a paucity of documented reports of rupioid psoriasis in skin of color.
Rupioid comes from the Greek word rhupos, meaning dirt or filth, and is used to describe well-demarcated lesions with thick, yellow, dirty-appearing, adherent crusts resembling oyster shells with a surrounding rim of erythema.5 Rupioid psoriasis initially was reported in 1948 and remains an uncommon and infrequently reported variant.6 The majority of reported cases have been associated with arthropathy, similar to our patient.3,4 Rupioid lesions also have been observed in an array of other diseases, such as secondary syphilis, crusted scabies, disseminated histoplasmosis, HIV, reactive arthritis, and aminoaciduria.7-11
Diagnosis of rupioid psoriasis can be confirmed with a skin biopsy, which demonstrates characteristic histopathologic findings of psoriasis.3 Laboratory analysis should be performed to rule out other causes of rupioid lesions, and PsA should be differentiated from rheumatoid arthritis if arthropathy is present. In our case, serum rapid plasma reagin, anti-HIV antibody, rheumatoid factor, and fungal cultures were negative. Usin0)g clinical findings, histopathology, laboratory analyses, and radiograph findings, the diagnosis of rupioid psoriasis with PsA was confirmed in our patient.
Psoriasis was not originally suspected in our patient due to the noncharacteristic lesions with smooth black crust--similar appearing to eschar--and the patient's complicated medical history. Variations in the presentation of psoriasis among white individuals and those with skin of color have been reported in the literature.12,13 Psoriatic lesions in darker skin tones may appear more violaceous or hyperpigmented with more conspicuous erythema and thicker plaques. Our patient lacked the classic rupioid appearance of concentric circular layers of dirty, yellow, oysterlike scale, and instead had thick, lamellate, black crust. A PubMed search of articles indexed for MEDLINE using the terms rupioid, coral reef psoriasis, rupioides, and rhupus revealed no other cases of rupioid psoriasis reported in black patients and no cases detailing the variations of rupioid lesions in skin of color. A case of rupioid psoriasis has been reported in a Hispanic patient, but the described psoriatic lesions were more characteristic of the dirty-appearing, conic plaques previously reported.14 Our case highlights a unique example of the variable presentations of cutaneous disorders in skin of color and black patients.
Our patient's case of rupioid psoriasis with PsA presented unique challenges for systemic treatment due to her multiple comorbidities. Rupioid psoriasis most often is treated with combination topical and systemic therapy, with agents such as methotrexate and cyclosporine having prior success.3,4 This variant of psoriasis is highly responsive to treatment, and marked improvement of lesions has been achieved with topical steroids alone with proper adherence.15 Our patient was started on clobetasol ointment 0.05% while a systemic agent was debated for her PsA. Although she did not have improvement with topical therapy alone, she experienced rapid resolution of the skin lesions after initiation of low-dose prednisone 20 mg daily. Interestingly, our patient did not experience a flare of the skin lesions upon discontinuation of systemic steroids despite the lack of an appropriate taper and methotrexate not having reached therapeutic levels.
The clinical nuances of rupioid psoriasis in skin of color have not yet been described and remain an important diagnostic consideration. Our patient achieved remission of skin lesions with sequential treatment of topical clobetasol, a low-dose systemic steroid, and methotrexate. Based on available reports, rupioid psoriasis may represent a variant of psoriasis that is highly responsive to treatment.
- Mrowietz U, Domm S. Systemic steroids in the treatment of psoriasis: what is fact, what is fiction? J Eur Acad Dermatol Venereol. 2013;27:1022-1025.
- Goldsmith LA, Katz SI, Gilchrest BA, eds. Fitzpatrick's Dermatology in General Medicine. 8th ed. New York, NY: The McGraw-Hill Companies; 2012.
- Wang JL, Yang JH. Rupioid psoriasis associated with arthropathy. J Dermatol. 1997;24:46-49.
- Murakami T, Ohtsuki M, Nakagawa H. Rupioid psoriasis with arthropathy. Clin Exp Dermatol. 2000;25:409-412.
- Chung HJ, Marley-Kemp D, Keller M. Rupioid psoriasis and other skin diseases with rupioid manifestations. Cutis. 2014;94:119-121.
- Salamon M, Omulecki A, Sysa-Jedrzejowska A, et al. Psoriasisrupioides: a rare variant of a common disease. Cutis. 2011;88:135-137.
- Krase IZ, Cavanaugh K, Curiel-Lewandrowski C. A case of rupioid syphilis. JAAD Case Rep. 2016;2:141-143.
- Garofalo V, Saraceno R, Milana M, et al. Crusted scabies in a liver transplant patient mimicking rupioid psoriasis. Eur J Dermatol. 2016;26:495-496.
- Corti M, Villafane MF, Palmieri O, et al. Rupioid histoplasmosis: first case reported in an AIDS patient in Argentina. Rev Inst Med Trop Sao Paulo. 2010;52:279-280.
- Sehgal VN, Koranne RV, Shyam Prasad AL. Unusual manifestations of Reiter's disease in a child. Dermatologica. 1985;170:77-79.
- Haim S, Gilhar A, Cohen A. Cutaneous manifestations associated with aminoaciduria. report of two cases. Dermatologica. 1978;156:244-250.
- McMichael AJ, Vachiramon V, Guzman-Sanchez DA, et al. Psoriasis in African-Americans: a caregivers' survey. J Drugs Dermatol. 2012;11:478-482.
- Alexis AF, Blackcloud P. Psoriasis in skin of color: epidemiology, genetics, clinical presentation, and treatment nuances. J Clin Aesthet Dermatol. 2014;7:16-24.
- Posligua A, Maldonado C, Gonzalez MG. Rupioid psoriasis preceded by varicella presenting as Koebner phenomenon. J Am Acad Dermatol. 2016;74(5 suppl 1):AB268.
- Feldman SR, Feldman S, Brown K, et al. "Coral reef" psoriasis: a marker of resistance to topical treatment. J Dermatolog Treat. 2008;19:257-258.
To the Editor:
A 49-year-old black woman presented with multiple hyperkeratotic papules that progressed over the last 2 months to circular plaques with central thick black crust resembling eschar. She first noticed these lesions as firm, small, black papules on the legs and continued to develop new lesions that eventually evolved into large, coin-shaped, hyperkeratotic plaques. Her medical history was notable for stage III non-Hodgkin follicular lymphoma in remission after treatment with rituximab, cyclophosphamide, doxorubicin hydrochloride, vincristine sulfate, and prednisone 7 months earlier, and chronic hepatitis B infection being treated with entecavir. Her family history was not remarkable for psoriasis or inflammatory arthritis.
She initially was seen by internal medicine and was started on topical triamcinolone with no improvement of the lesions. At presentation to dermatology, physical examination revealed firm, small, black, hyperkeratotic papules (Figure 1A) and circular plaques with a rim of erythema and central thick, smooth, black crust resembling eschar (Figure 1B). No other skin changes were noted at the time. The bilateral metacarpophalangeal, bilateral proximal interphalangeal, left wrist, and bilateral ankle joints were remarkable for tenderness, swelling, and reduced range of motion. She noted concomitant arthralgia and stiffness but denied fever. She had no other systemic symptoms including night sweats, weight loss, fatigue, malaise, sun sensitivity, oral ulcers, or hair loss. A radiograph of the hand was negative for erosive changes but showed mild periarticular osteopenia and fusiform soft tissue swelling of the third digit. Given the central appearance of eschar in the larger lesions, the initial differential diagnosis included Sweet syndrome, invasive fungal infection, vasculitis, and recurrent lymphoma.
A 4-mm punch biopsy specimen of a representative lesion on the right leg revealed psoriasiform epidermal hyperplasia, parakeratosis, neutrophils in the stratum corneum and spinosum, elongation of the rete ridges, and superficial vascular ectasia, which favored a diagnosis of psoriasis (Figure 2). A periodic acid-Schiff stain was negative for fungal hyphae. Fungal culture, bacterial tissue culture, and acid-fast bacilli smear were negative. Absence of deep dermal inflammation precluded a diagnosis of Sweet syndrome. Further notable laboratory studies included negative human immunodeficiency virus (HIV) antibody, rapid plasma reagin, hepatitis C antibody, and rheumatoid factor.
At follow-up 2 weeks later, the initial lesions were still present, and she had developed new widespread, well-demarcated, erythematous plaques with silver scale along the scalp, back, chest, and abdomen that were more typical of psoriasis. Oil spots were noted on several fingernails and toenails. Based on the clinicopathologic findings, nail changes, and asymmetric inflammatory arthritis, a diagnosis of rupioid psoriasis with psoriatic arthritis (PsA) was established. Treatment with clobetasol ointment 0.05% twice daily to active lesions was started. Initiation of systemic therapy with a steroid-sparing agent was deferred in anticipation of care coordination with rheumatology, hepatology, and hematology/oncology due to the patient's history of follicular lymphoma and chronic hepatitis B. Although attempts were made to avoid systemic corticosteroids due to the risk for a psoriasis flare upon discontinuation, because of the severity of arthralgia she was started on oral prednisone 20 mg daily by rheumatology with plans for a slow taper once an alternative systemic agent was started.1
At 10-week follow-up, the patient had marked improvement of psoriatic plaques with no active lesions while only on prednisone 20 mg daily. In consultation with her care team, she subsequently was started on methotrexate 10 mg weekly for 2 weeks followed by titration to 15 mg weekly. Plans were to start a prednisone taper after a month of methotrexate to allow her new treatment time for therapeutic effect. Notably, the patient chose to discontinue prednisone 2 weeks into methotrexate therapy after only two 10-mg doses of methotrexate weekly and well before therapeutic levels were achieved. Despite stopping prednisone early and without a taper, she did not experience a relapse in psoriatic skin lesions. Three months following initiation of methotrexate, she sustained resolution of the cutaneous lesions with only residual postinflammatory hyperpigmentation.
Psoriasis is a common chronic inflammatory skin disorder with multiple clinical presentations. There are several variants of psoriasis that are classified by their morphologic appearance including chronic plaque, guttate, erythrodermic, and pustular, with more than 90% of cases representing the plaque variant. Less common clinical presentations of psoriasis include rupioid, ostraceous, inverse, elephantine, and HIV associated.2 Rupioid psoriasis is a rare variant that presents with cone-shaped, limpetlike lesions.3,4 Similar to the limited epidemiological and clinical data pertaining to psoriasis in nonwhite racial groups, there also is a paucity of documented reports of rupioid psoriasis in skin of color.
Rupioid comes from the Greek word rhupos, meaning dirt or filth, and is used to describe well-demarcated lesions with thick, yellow, dirty-appearing, adherent crusts resembling oyster shells with a surrounding rim of erythema.5 Rupioid psoriasis initially was reported in 1948 and remains an uncommon and infrequently reported variant.6 The majority of reported cases have been associated with arthropathy, similar to our patient.3,4 Rupioid lesions also have been observed in an array of other diseases, such as secondary syphilis, crusted scabies, disseminated histoplasmosis, HIV, reactive arthritis, and aminoaciduria.7-11
Diagnosis of rupioid psoriasis can be confirmed with a skin biopsy, which demonstrates characteristic histopathologic findings of psoriasis.3 Laboratory analysis should be performed to rule out other causes of rupioid lesions, and PsA should be differentiated from rheumatoid arthritis if arthropathy is present. In our case, serum rapid plasma reagin, anti-HIV antibody, rheumatoid factor, and fungal cultures were negative. Usin0)g clinical findings, histopathology, laboratory analyses, and radiograph findings, the diagnosis of rupioid psoriasis with PsA was confirmed in our patient.
Psoriasis was not originally suspected in our patient due to the noncharacteristic lesions with smooth black crust--similar appearing to eschar--and the patient's complicated medical history. Variations in the presentation of psoriasis among white individuals and those with skin of color have been reported in the literature.12,13 Psoriatic lesions in darker skin tones may appear more violaceous or hyperpigmented with more conspicuous erythema and thicker plaques. Our patient lacked the classic rupioid appearance of concentric circular layers of dirty, yellow, oysterlike scale, and instead had thick, lamellate, black crust. A PubMed search of articles indexed for MEDLINE using the terms rupioid, coral reef psoriasis, rupioides, and rhupus revealed no other cases of rupioid psoriasis reported in black patients and no cases detailing the variations of rupioid lesions in skin of color. A case of rupioid psoriasis has been reported in a Hispanic patient, but the described psoriatic lesions were more characteristic of the dirty-appearing, conic plaques previously reported.14 Our case highlights a unique example of the variable presentations of cutaneous disorders in skin of color and black patients.
Our patient's case of rupioid psoriasis with PsA presented unique challenges for systemic treatment due to her multiple comorbidities. Rupioid psoriasis most often is treated with combination topical and systemic therapy, with agents such as methotrexate and cyclosporine having prior success.3,4 This variant of psoriasis is highly responsive to treatment, and marked improvement of lesions has been achieved with topical steroids alone with proper adherence.15 Our patient was started on clobetasol ointment 0.05% while a systemic agent was debated for her PsA. Although she did not have improvement with topical therapy alone, she experienced rapid resolution of the skin lesions after initiation of low-dose prednisone 20 mg daily. Interestingly, our patient did not experience a flare of the skin lesions upon discontinuation of systemic steroids despite the lack of an appropriate taper and methotrexate not having reached therapeutic levels.
The clinical nuances of rupioid psoriasis in skin of color have not yet been described and remain an important diagnostic consideration. Our patient achieved remission of skin lesions with sequential treatment of topical clobetasol, a low-dose systemic steroid, and methotrexate. Based on available reports, rupioid psoriasis may represent a variant of psoriasis that is highly responsive to treatment.
To the Editor:
A 49-year-old black woman presented with multiple hyperkeratotic papules that progressed over the last 2 months to circular plaques with central thick black crust resembling eschar. She first noticed these lesions as firm, small, black papules on the legs and continued to develop new lesions that eventually evolved into large, coin-shaped, hyperkeratotic plaques. Her medical history was notable for stage III non-Hodgkin follicular lymphoma in remission after treatment with rituximab, cyclophosphamide, doxorubicin hydrochloride, vincristine sulfate, and prednisone 7 months earlier, and chronic hepatitis B infection being treated with entecavir. Her family history was not remarkable for psoriasis or inflammatory arthritis.
She initially was seen by internal medicine and was started on topical triamcinolone with no improvement of the lesions. At presentation to dermatology, physical examination revealed firm, small, black, hyperkeratotic papules (Figure 1A) and circular plaques with a rim of erythema and central thick, smooth, black crust resembling eschar (Figure 1B). No other skin changes were noted at the time. The bilateral metacarpophalangeal, bilateral proximal interphalangeal, left wrist, and bilateral ankle joints were remarkable for tenderness, swelling, and reduced range of motion. She noted concomitant arthralgia and stiffness but denied fever. She had no other systemic symptoms including night sweats, weight loss, fatigue, malaise, sun sensitivity, oral ulcers, or hair loss. A radiograph of the hand was negative for erosive changes but showed mild periarticular osteopenia and fusiform soft tissue swelling of the third digit. Given the central appearance of eschar in the larger lesions, the initial differential diagnosis included Sweet syndrome, invasive fungal infection, vasculitis, and recurrent lymphoma.
A 4-mm punch biopsy specimen of a representative lesion on the right leg revealed psoriasiform epidermal hyperplasia, parakeratosis, neutrophils in the stratum corneum and spinosum, elongation of the rete ridges, and superficial vascular ectasia, which favored a diagnosis of psoriasis (Figure 2). A periodic acid-Schiff stain was negative for fungal hyphae. Fungal culture, bacterial tissue culture, and acid-fast bacilli smear were negative. Absence of deep dermal inflammation precluded a diagnosis of Sweet syndrome. Further notable laboratory studies included negative human immunodeficiency virus (HIV) antibody, rapid plasma reagin, hepatitis C antibody, and rheumatoid factor.
At follow-up 2 weeks later, the initial lesions were still present, and she had developed new widespread, well-demarcated, erythematous plaques with silver scale along the scalp, back, chest, and abdomen that were more typical of psoriasis. Oil spots were noted on several fingernails and toenails. Based on the clinicopathologic findings, nail changes, and asymmetric inflammatory arthritis, a diagnosis of rupioid psoriasis with psoriatic arthritis (PsA) was established. Treatment with clobetasol ointment 0.05% twice daily to active lesions was started. Initiation of systemic therapy with a steroid-sparing agent was deferred in anticipation of care coordination with rheumatology, hepatology, and hematology/oncology due to the patient's history of follicular lymphoma and chronic hepatitis B. Although attempts were made to avoid systemic corticosteroids due to the risk for a psoriasis flare upon discontinuation, because of the severity of arthralgia she was started on oral prednisone 20 mg daily by rheumatology with plans for a slow taper once an alternative systemic agent was started.1
At 10-week follow-up, the patient had marked improvement of psoriatic plaques with no active lesions while only on prednisone 20 mg daily. In consultation with her care team, she subsequently was started on methotrexate 10 mg weekly for 2 weeks followed by titration to 15 mg weekly. Plans were to start a prednisone taper after a month of methotrexate to allow her new treatment time for therapeutic effect. Notably, the patient chose to discontinue prednisone 2 weeks into methotrexate therapy after only two 10-mg doses of methotrexate weekly and well before therapeutic levels were achieved. Despite stopping prednisone early and without a taper, she did not experience a relapse in psoriatic skin lesions. Three months following initiation of methotrexate, she sustained resolution of the cutaneous lesions with only residual postinflammatory hyperpigmentation.
Psoriasis is a common chronic inflammatory skin disorder with multiple clinical presentations. There are several variants of psoriasis that are classified by their morphologic appearance including chronic plaque, guttate, erythrodermic, and pustular, with more than 90% of cases representing the plaque variant. Less common clinical presentations of psoriasis include rupioid, ostraceous, inverse, elephantine, and HIV associated.2 Rupioid psoriasis is a rare variant that presents with cone-shaped, limpetlike lesions.3,4 Similar to the limited epidemiological and clinical data pertaining to psoriasis in nonwhite racial groups, there also is a paucity of documented reports of rupioid psoriasis in skin of color.
Rupioid comes from the Greek word rhupos, meaning dirt or filth, and is used to describe well-demarcated lesions with thick, yellow, dirty-appearing, adherent crusts resembling oyster shells with a surrounding rim of erythema.5 Rupioid psoriasis initially was reported in 1948 and remains an uncommon and infrequently reported variant.6 The majority of reported cases have been associated with arthropathy, similar to our patient.3,4 Rupioid lesions also have been observed in an array of other diseases, such as secondary syphilis, crusted scabies, disseminated histoplasmosis, HIV, reactive arthritis, and aminoaciduria.7-11
Diagnosis of rupioid psoriasis can be confirmed with a skin biopsy, which demonstrates characteristic histopathologic findings of psoriasis.3 Laboratory analysis should be performed to rule out other causes of rupioid lesions, and PsA should be differentiated from rheumatoid arthritis if arthropathy is present. In our case, serum rapid plasma reagin, anti-HIV antibody, rheumatoid factor, and fungal cultures were negative. Usin0)g clinical findings, histopathology, laboratory analyses, and radiograph findings, the diagnosis of rupioid psoriasis with PsA was confirmed in our patient.
Psoriasis was not originally suspected in our patient due to the noncharacteristic lesions with smooth black crust--similar appearing to eschar--and the patient's complicated medical history. Variations in the presentation of psoriasis among white individuals and those with skin of color have been reported in the literature.12,13 Psoriatic lesions in darker skin tones may appear more violaceous or hyperpigmented with more conspicuous erythema and thicker plaques. Our patient lacked the classic rupioid appearance of concentric circular layers of dirty, yellow, oysterlike scale, and instead had thick, lamellate, black crust. A PubMed search of articles indexed for MEDLINE using the terms rupioid, coral reef psoriasis, rupioides, and rhupus revealed no other cases of rupioid psoriasis reported in black patients and no cases detailing the variations of rupioid lesions in skin of color. A case of rupioid psoriasis has been reported in a Hispanic patient, but the described psoriatic lesions were more characteristic of the dirty-appearing, conic plaques previously reported.14 Our case highlights a unique example of the variable presentations of cutaneous disorders in skin of color and black patients.
Our patient's case of rupioid psoriasis with PsA presented unique challenges for systemic treatment due to her multiple comorbidities. Rupioid psoriasis most often is treated with combination topical and systemic therapy, with agents such as methotrexate and cyclosporine having prior success.3,4 This variant of psoriasis is highly responsive to treatment, and marked improvement of lesions has been achieved with topical steroids alone with proper adherence.15 Our patient was started on clobetasol ointment 0.05% while a systemic agent was debated for her PsA. Although she did not have improvement with topical therapy alone, she experienced rapid resolution of the skin lesions after initiation of low-dose prednisone 20 mg daily. Interestingly, our patient did not experience a flare of the skin lesions upon discontinuation of systemic steroids despite the lack of an appropriate taper and methotrexate not having reached therapeutic levels.
The clinical nuances of rupioid psoriasis in skin of color have not yet been described and remain an important diagnostic consideration. Our patient achieved remission of skin lesions with sequential treatment of topical clobetasol, a low-dose systemic steroid, and methotrexate. Based on available reports, rupioid psoriasis may represent a variant of psoriasis that is highly responsive to treatment.
- Mrowietz U, Domm S. Systemic steroids in the treatment of psoriasis: what is fact, what is fiction? J Eur Acad Dermatol Venereol. 2013;27:1022-1025.
- Goldsmith LA, Katz SI, Gilchrest BA, eds. Fitzpatrick's Dermatology in General Medicine. 8th ed. New York, NY: The McGraw-Hill Companies; 2012.
- Wang JL, Yang JH. Rupioid psoriasis associated with arthropathy. J Dermatol. 1997;24:46-49.
- Murakami T, Ohtsuki M, Nakagawa H. Rupioid psoriasis with arthropathy. Clin Exp Dermatol. 2000;25:409-412.
- Chung HJ, Marley-Kemp D, Keller M. Rupioid psoriasis and other skin diseases with rupioid manifestations. Cutis. 2014;94:119-121.
- Salamon M, Omulecki A, Sysa-Jedrzejowska A, et al. Psoriasisrupioides: a rare variant of a common disease. Cutis. 2011;88:135-137.
- Krase IZ, Cavanaugh K, Curiel-Lewandrowski C. A case of rupioid syphilis. JAAD Case Rep. 2016;2:141-143.
- Garofalo V, Saraceno R, Milana M, et al. Crusted scabies in a liver transplant patient mimicking rupioid psoriasis. Eur J Dermatol. 2016;26:495-496.
- Corti M, Villafane MF, Palmieri O, et al. Rupioid histoplasmosis: first case reported in an AIDS patient in Argentina. Rev Inst Med Trop Sao Paulo. 2010;52:279-280.
- Sehgal VN, Koranne RV, Shyam Prasad AL. Unusual manifestations of Reiter's disease in a child. Dermatologica. 1985;170:77-79.
- Haim S, Gilhar A, Cohen A. Cutaneous manifestations associated with aminoaciduria. report of two cases. Dermatologica. 1978;156:244-250.
- McMichael AJ, Vachiramon V, Guzman-Sanchez DA, et al. Psoriasis in African-Americans: a caregivers' survey. J Drugs Dermatol. 2012;11:478-482.
- Alexis AF, Blackcloud P. Psoriasis in skin of color: epidemiology, genetics, clinical presentation, and treatment nuances. J Clin Aesthet Dermatol. 2014;7:16-24.
- Posligua A, Maldonado C, Gonzalez MG. Rupioid psoriasis preceded by varicella presenting as Koebner phenomenon. J Am Acad Dermatol. 2016;74(5 suppl 1):AB268.
- Feldman SR, Feldman S, Brown K, et al. "Coral reef" psoriasis: a marker of resistance to topical treatment. J Dermatolog Treat. 2008;19:257-258.
- Mrowietz U, Domm S. Systemic steroids in the treatment of psoriasis: what is fact, what is fiction? J Eur Acad Dermatol Venereol. 2013;27:1022-1025.
- Goldsmith LA, Katz SI, Gilchrest BA, eds. Fitzpatrick's Dermatology in General Medicine. 8th ed. New York, NY: The McGraw-Hill Companies; 2012.
- Wang JL, Yang JH. Rupioid psoriasis associated with arthropathy. J Dermatol. 1997;24:46-49.
- Murakami T, Ohtsuki M, Nakagawa H. Rupioid psoriasis with arthropathy. Clin Exp Dermatol. 2000;25:409-412.
- Chung HJ, Marley-Kemp D, Keller M. Rupioid psoriasis and other skin diseases with rupioid manifestations. Cutis. 2014;94:119-121.
- Salamon M, Omulecki A, Sysa-Jedrzejowska A, et al. Psoriasisrupioides: a rare variant of a common disease. Cutis. 2011;88:135-137.
- Krase IZ, Cavanaugh K, Curiel-Lewandrowski C. A case of rupioid syphilis. JAAD Case Rep. 2016;2:141-143.
- Garofalo V, Saraceno R, Milana M, et al. Crusted scabies in a liver transplant patient mimicking rupioid psoriasis. Eur J Dermatol. 2016;26:495-496.
- Corti M, Villafane MF, Palmieri O, et al. Rupioid histoplasmosis: first case reported in an AIDS patient in Argentina. Rev Inst Med Trop Sao Paulo. 2010;52:279-280.
- Sehgal VN, Koranne RV, Shyam Prasad AL. Unusual manifestations of Reiter's disease in a child. Dermatologica. 1985;170:77-79.
- Haim S, Gilhar A, Cohen A. Cutaneous manifestations associated with aminoaciduria. report of two cases. Dermatologica. 1978;156:244-250.
- McMichael AJ, Vachiramon V, Guzman-Sanchez DA, et al. Psoriasis in African-Americans: a caregivers' survey. J Drugs Dermatol. 2012;11:478-482.
- Alexis AF, Blackcloud P. Psoriasis in skin of color: epidemiology, genetics, clinical presentation, and treatment nuances. J Clin Aesthet Dermatol. 2014;7:16-24.
- Posligua A, Maldonado C, Gonzalez MG. Rupioid psoriasis preceded by varicella presenting as Koebner phenomenon. J Am Acad Dermatol. 2016;74(5 suppl 1):AB268.
- Feldman SR, Feldman S, Brown K, et al. "Coral reef" psoriasis: a marker of resistance to topical treatment. J Dermatolog Treat. 2008;19:257-258.
Practice Points
- Rupioid psoriasis in skin of color may present a diagnostic challenge for health care providers.
- Rupioid psoriasis may represent a psoriasis variant that is highly responsive to treatment.
