User login
The pandemic experience through the eyes of APPs
The evolution of hospitalist advanced practice providers
Throughout the chaos of the COVID-19 pandemic, advanced practice providers (APPs) – physician assistants (PAs) and nurse practitioners (NPs) – have become an integral component of the hospitalist response. As many physicians began shifting into telemedicine and away from direct patient care, APPs have been eagerly jumping in to fill the gaps. Their work has been changing almost as dramatically and quickly as the pandemic itself, bringing with it expected challenges but bestowing hugely satisfying, often unanticipated, rewards.
APPs on the rise
As the coronavirus pandemic evolves, the role of APPs is evolving right alongside it. With the current relaxation of hospital bylaw restrictions on APPs, their utilization has increased, said Tracy Cardin, ACNP-BC, SFHM, a nurse practitioner and vice president of advanced practice providers at Sound Physicians. “We have not really furloughed any advanced practice providers,” Ms. Cardin said. “In fact, I consider them to be, within hospital medicine, a key lever to finding more cost-effective care delivery models.”

Ms. Cardin said APPs have been working more independently since COVID-19 started, seeing patients on their own and using physician consultation and backup via telemedicine or telephone as needed. With the reduction in elective surgeries and patient volumes at many hospitals, APP-led care also saves money. Because one of the biggest costs is labor, Ms. Cardin said, offering this high-quality care delivery model using APPs in collaboration with physician providers helps defray some of that cost. “We’re hoping that advanced practice providers are really a solution to some of these financial pressures in a lot of different ways,” she said.
“COVID … forced us to expedite conversations about how to maximize caseloads using APPs,” said Alicia Sheffer, AGAC-AGPC NP, a nurse practitioner and Great Lakes regional director of advanced practice providers at Sound Physicians in Cincinnati. Some of those staffing model changes have included using APPs while transitioning ICUs and med-surg units to COVID cohort units, APP-led COVID cohorts, and APP-led ICUs.
“At first the hospital system had ideas about bringing in telemedicine as an alternative to seeing patients, rather than just putting APPs on the front lines and having them go in and see patients,” said Jessica Drane, APRN, PhD, DNP FNP-C, a nurse practitioner and regional director of advanced practice provider services and hospital medicine at Sound Physicians in San Antonio. In Texas at the beginning of the pandemic, hospital numbers were so low that Dr. Drane did not work at all in April. “We were all afraid we were going to lose our jobs,” she said. Then the state got slammed and APPs have been desperately needed.
Ilaria Gadalla, DMSc, PA-C, a PA at Treasure Coast Hospitalists in Port St. Lucie, Fla., and the PA program director at South University, West Palm Beach, Fla., noted that many of her APP colleagues have pivoted fluidly from other specialties to the hospitalist realm as the need for frontline workers has increased. “Hospitalists have shined through this and their value has been recognized even more than previously as a result of COVID-19,” Dr. Gadalla said.
“I don’t think it’s any surprise that hospitalists became a pillar of the COVID pandemic,” said Bridget McGrath, PA-C, a physician assistant and director of the NP/PAs service line for the section of hospital medicine at the University of Chicago. “There are just some innate traits that hospitalists have, such as the ability to be flexible, to problem solve, and to be the solution to the problem.”
Building team camaraderie

Ms. Cardin says that the need for APPs has led to an evolving integration between physicians and APPs. The growing teamwork and bonding between colleagues have been some of the most rewarding aspects of the pandemic for Dr. Gadalla. “We rely even more on each other and there isn’t really a line of, ‘I’m a physician versus an NP or PA or nurse.’ We’re all working together with the same goal,” she said.
Ms. McGrath said she has been learning what it means to lead a team during a challenging time. It has been gratifying for her to watch mentors get down to the bare bones of patient care and see everyone unify, putting aside roles and titles and coming together to care for their patients in innovative ways.
“This pandemic has really opened up a lot of doors for us because up until now, we were used almost like scribes for physicians,” Dr. Drane said. She has seen even the most resistant hospital systems beginning to rely on APPs as the pandemic has progressed. “They have become pleasantly surprised at what an APP can do.”
Work challenges
Obviously, challenges abound. Dr. Gadalla listed hers as visiting restrictions that invariably lead to slower patient visits thanks to obligatory phone calls, constantly fluctuating patient censuses, sporadic elective surgeries, watching colleagues become furloughed, and trying to balance external perceptions with what’s actually happening in the hospital.
Overall, though, “There have been a lot more rewards than barriers,” added Dr. Drane.
One of the biggest obstacles for health care workers navigating a pandemic is balancing work and home life, not to mention having time to unwind while working long hours. “Finding time for my family has been very limited. My kids feel really neglected,” said Dr. Gadalla. Some days, she gets up extra early to exercise to help clear her head, but other times she’s just too exhausted to even move.
Dr. Drane agreed that the work can get overwhelming. “We’re changing the way we practice almost every week, which can make you doubt yourself as an educator, as a practitioner. You constantly feel like you’re not sure what you’re doing, and people trust you to heal them,” she said. “Today is my first day off in 24 days. I only got it off because I said I needed a moment.”
Ms. Sheffer’s crazy days were at the beginning of the pandemic when she had to self-quarantine from her family and was working nonstop. “I would come home and sleep and work and wake up in the middle of the night and double check and triple check and go back to sleep and work, and that consumed me for several months,” she said.
The biggest challenge for Ms. Sheffer has been coping with public fear. “No matter how logical our medical approach has been, I think the constant feeling of the public threat of COVID has had this insidious effect on how patients approach their health,” she said. “We’re spending a lot more time shaping our approach to best address their fears first and not to politicize COVID so we can actually deal with the health issue at hand.”
Complications of COVID
With all the restrictions, caring for patients these days has meant learning to interact with them in different ways that aren’t as personal, Ms. McGrath said. It has been difficult to lose “that humanity of medicine, the usual ways that you interact with your patients that are going through a vulnerable time,” she noted.

Additionally, students in the medical field are being held back from graduation because they cannot participate in direct patient care. This is particularly problematic for PAs and medical students who must touch patients to graduate, Dr. Gadalla said. “All of this is slowing down future providers. We’re going to have trouble catching up. Who’s going to relieve us? That’s a huge problem and no one is finding solutions for that yet,” she said.
At the University of Chicago, Ms. McGrath explained, they created virtual rotations so that PA students could continue to do them at the university. Not only has the experience reminded Ms. McGrath how much she loves being a medical educator and fighting for the education of PA students, but she was surprised to find that her patients came to appreciate the time they spent with her students on the virtual platform as well.
“It’s isolating for patients to be in the hospital in a vulnerable state and with no support system,” she said. “I think being a part of [the PA students’] education gave some meaning to their hospitalization and highlighted that collaboration and connection is a human need.”
Despite everything, there’s a noticeable emphasis on the flowering buds of hope, unity, compassion, and pride that have been quietly blooming from the daily hardships. As Ms. Cardin puts it, “It’s so cliché to say that there’s a crisis. The other word is ‘opportunity,’ and it’s true, there are opportunities here.”
Taking care of each other
Creating resources for providers has been a priority at the University of Chicago, according to Ms. McGrath. “As hospitalists, we’re used to taking care of a variety of patients, but our section leadership and providers on the front lines quickly realized that COVID patients are more akin to trauma patients with their quick changes in health, as well as their isolation, fear, and unexpected deterioration,” she said. Her facility has implemented wellness initiatives to help prevent burnout and mental health problems in COVID providers so they can continue to give the best care to their patients.
Both Ms. Sheffer and Dr. Drane say that they have a peer network of APPs at Sound Physicians to call on for questions and support. And it’s encouraging to know you’re not alone and to keep tabs on how colleagues in other states are doing, Ms. Sheffer noted.
“The peer support system has been helpful,” Dr. Drane said. “This job, right now, takes pieces of you every day. Sometimes it’s so emotional that you can’t put it into words. You just have to cry and get it out so that you can go be with your family.”
Getting back to basics
The changes in patient care have turned into something Ms. McGrath said she appreciates. “This pandemic has really stripped away the extra fluff of medicine and brought us back to the reason why many of us have gotten into the field, because it became about the patients again,” she says. “You quickly learn your strengths and weaknesses as a provider and as a leader, and that flows into the decisions you’re making for your team and for your patients.”
Ms. Sheffer acknowledged that it is difficult to deal with patients’ family members who don’t understand that they can’t visit their sick relatives, but she said the flip side is that frontline workers become surrogate family members, an outcome she considers to be an honor.
“You step into the emotion with the family or with the patient because you’re all they have. That is a beautiful, honorable role, but it’s also tremendously emotional and sometimes devastating,” she said. “But to me, it’s one of the most beautiful things I’ve been able to offer in a time where we don’t even know what to do with COVID.”
Limited resources mixed with a healthy dose of fear can stifle creativity, Dr. Drane said. Right away, she noticed that despite the abundance of incentive spirometers at her hospital, they were not being utilized. She came in 2 hours early for 3 days to pass one out to every patient under investigation or COVID-positive patient and enlisted the help of her chief nursing officer, CEO, and regional medical director to get everyone on board.
Dr. Drane’s out-of-the-box thinking has enabled people to go home without oxygen 2 days earlier and cut the hospital’s length of stay by 5%. “It’s something so small, but it has such a great end reward,” she said. “I’m proud of this project because it didn’t take money; it was getting creative with what we already have.”
Renewed pride and passion
Dr. Drane is intensely proud of being an NP and working on the front lines. She sees that the pandemic has encouraged her and other APPs to expand their horizons.
“For me, it’s made me work to get dual certified,” she said. “APPs can be all-inclusive. I feel like I’m doing what I was meant to do and it’s not just a job anymore.”
Ms. McGrath is even more passionate about being a hospitalist now, as she has realized how valuable their unique skill sets are. “I think other people have also been able to realize that our ability to see the patient as a whole has allowed us to take care of this pandemic, because this disease impacts all organ systems and has a trickle-down effect that we as hospitalists are well versed to manage,” she said.
Ms. Cardin’s work involves communicating with APPs all around the country. Recently she had a phone exchange with an APP who needed to vent.
“She was weeping, and I thought she was going to say, ‘I can’t do this anymore, I need to go home,’ ” said Ms. Cardin. “Instead, she said, ‘I just want to make a difference in one of these people’s lives.’ And that is who the advanced practice providers are. They’re willing to go into those COVID units. They’re willing to be in the front lines. They are dedicated. They’re just intensely inspirational to me.”
The evolution of hospitalist advanced practice providers
The evolution of hospitalist advanced practice providers
Throughout the chaos of the COVID-19 pandemic, advanced practice providers (APPs) – physician assistants (PAs) and nurse practitioners (NPs) – have become an integral component of the hospitalist response. As many physicians began shifting into telemedicine and away from direct patient care, APPs have been eagerly jumping in to fill the gaps. Their work has been changing almost as dramatically and quickly as the pandemic itself, bringing with it expected challenges but bestowing hugely satisfying, often unanticipated, rewards.
APPs on the rise
As the coronavirus pandemic evolves, the role of APPs is evolving right alongside it. With the current relaxation of hospital bylaw restrictions on APPs, their utilization has increased, said Tracy Cardin, ACNP-BC, SFHM, a nurse practitioner and vice president of advanced practice providers at Sound Physicians. “We have not really furloughed any advanced practice providers,” Ms. Cardin said. “In fact, I consider them to be, within hospital medicine, a key lever to finding more cost-effective care delivery models.”
Ms. Cardin said APPs have been working more independently since COVID-19 started, seeing patients on their own and using physician consultation and backup via telemedicine or telephone as needed. With the reduction in elective surgeries and patient volumes at many hospitals, APP-led care also saves money. Because one of the biggest costs is labor, Ms. Cardin said, offering this high-quality care delivery model using APPs in collaboration with physician providers helps defray some of that cost. “We’re hoping that advanced practice providers are really a solution to some of these financial pressures in a lot of different ways,” she said.
“COVID … forced us to expedite conversations about how to maximize caseloads using APPs,” said Alicia Sheffer, AGAC-AGPC NP, a nurse practitioner and Great Lakes regional director of advanced practice providers at Sound Physicians in Cincinnati. Some of those staffing model changes have included using APPs while transitioning ICUs and med-surg units to COVID cohort units, APP-led COVID cohorts, and APP-led ICUs.
“At first the hospital system had ideas about bringing in telemedicine as an alternative to seeing patients, rather than just putting APPs on the front lines and having them go in and see patients,” said Jessica Drane, APRN, PhD, DNP FNP-C, a nurse practitioner and regional director of advanced practice provider services and hospital medicine at Sound Physicians in San Antonio. In Texas at the beginning of the pandemic, hospital numbers were so low that Dr. Drane did not work at all in April. “We were all afraid we were going to lose our jobs,” she said. Then the state got slammed and APPs have been desperately needed.
Ilaria Gadalla, DMSc, PA-C, a PA at Treasure Coast Hospitalists in Port St. Lucie, Fla., and the PA program director at South University, West Palm Beach, Fla., noted that many of her APP colleagues have pivoted fluidly from other specialties to the hospitalist realm as the need for frontline workers has increased. “Hospitalists have shined through this and their value has been recognized even more than previously as a result of COVID-19,” Dr. Gadalla said.
“I don’t think it’s any surprise that hospitalists became a pillar of the COVID pandemic,” said Bridget McGrath, PA-C, a physician assistant and director of the NP/PAs service line for the section of hospital medicine at the University of Chicago. “There are just some innate traits that hospitalists have, such as the ability to be flexible, to problem solve, and to be the solution to the problem.”
Building team camaraderie
Ms. Cardin says that the need for APPs has led to an evolving integration between physicians and APPs. The growing teamwork and bonding between colleagues have been some of the most rewarding aspects of the pandemic for Dr. Gadalla. “We rely even more on each other and there isn’t really a line of, ‘I’m a physician versus an NP or PA or nurse.’ We’re all working together with the same goal,” she said.
Ms. McGrath said she has been learning what it means to lead a team during a challenging time. It has been gratifying for her to watch mentors get down to the bare bones of patient care and see everyone unify, putting aside roles and titles and coming together to care for their patients in innovative ways.
“This pandemic has really opened up a lot of doors for us because up until now, we were used almost like scribes for physicians,” Dr. Drane said. She has seen even the most resistant hospital systems beginning to rely on APPs as the pandemic has progressed. “They have become pleasantly surprised at what an APP can do.”
Work challenges
Obviously, challenges abound. Dr. Gadalla listed hers as visiting restrictions that invariably lead to slower patient visits thanks to obligatory phone calls, constantly fluctuating patient censuses, sporadic elective surgeries, watching colleagues become furloughed, and trying to balance external perceptions with what’s actually happening in the hospital.
Overall, though, “There have been a lot more rewards than barriers,” added Dr. Drane.
One of the biggest obstacles for health care workers navigating a pandemic is balancing work and home life, not to mention having time to unwind while working long hours. “Finding time for my family has been very limited. My kids feel really neglected,” said Dr. Gadalla. Some days, she gets up extra early to exercise to help clear her head, but other times she’s just too exhausted to even move.
Dr. Drane agreed that the work can get overwhelming. “We’re changing the way we practice almost every week, which can make you doubt yourself as an educator, as a practitioner. You constantly feel like you’re not sure what you’re doing, and people trust you to heal them,” she said. “Today is my first day off in 24 days. I only got it off because I said I needed a moment.”
Ms. Sheffer’s crazy days were at the beginning of the pandemic when she had to self-quarantine from her family and was working nonstop. “I would come home and sleep and work and wake up in the middle of the night and double check and triple check and go back to sleep and work, and that consumed me for several months,” she said.
The biggest challenge for Ms. Sheffer has been coping with public fear. “No matter how logical our medical approach has been, I think the constant feeling of the public threat of COVID has had this insidious effect on how patients approach their health,” she said. “We’re spending a lot more time shaping our approach to best address their fears first and not to politicize COVID so we can actually deal with the health issue at hand.”
Complications of COVID
With all the restrictions, caring for patients these days has meant learning to interact with them in different ways that aren’t as personal, Ms. McGrath said. It has been difficult to lose “that humanity of medicine, the usual ways that you interact with your patients that are going through a vulnerable time,” she noted.
Additionally, students in the medical field are being held back from graduation because they cannot participate in direct patient care. This is particularly problematic for PAs and medical students who must touch patients to graduate, Dr. Gadalla said. “All of this is slowing down future providers. We’re going to have trouble catching up. Who’s going to relieve us? That’s a huge problem and no one is finding solutions for that yet,” she said.
At the University of Chicago, Ms. McGrath explained, they created virtual rotations so that PA students could continue to do them at the university. Not only has the experience reminded Ms. McGrath how much she loves being a medical educator and fighting for the education of PA students, but she was surprised to find that her patients came to appreciate the time they spent with her students on the virtual platform as well.
“It’s isolating for patients to be in the hospital in a vulnerable state and with no support system,” she said. “I think being a part of [the PA students’] education gave some meaning to their hospitalization and highlighted that collaboration and connection is a human need.”
Despite everything, there’s a noticeable emphasis on the flowering buds of hope, unity, compassion, and pride that have been quietly blooming from the daily hardships. As Ms. Cardin puts it, “It’s so cliché to say that there’s a crisis. The other word is ‘opportunity,’ and it’s true, there are opportunities here.”
Taking care of each other
Creating resources for providers has been a priority at the University of Chicago, according to Ms. McGrath. “As hospitalists, we’re used to taking care of a variety of patients, but our section leadership and providers on the front lines quickly realized that COVID patients are more akin to trauma patients with their quick changes in health, as well as their isolation, fear, and unexpected deterioration,” she said. Her facility has implemented wellness initiatives to help prevent burnout and mental health problems in COVID providers so they can continue to give the best care to their patients.
Both Ms. Sheffer and Dr. Drane say that they have a peer network of APPs at Sound Physicians to call on for questions and support. And it’s encouraging to know you’re not alone and to keep tabs on how colleagues in other states are doing, Ms. Sheffer noted.
“The peer support system has been helpful,” Dr. Drane said. “This job, right now, takes pieces of you every day. Sometimes it’s so emotional that you can’t put it into words. You just have to cry and get it out so that you can go be with your family.”
Getting back to basics
The changes in patient care have turned into something Ms. McGrath said she appreciates. “This pandemic has really stripped away the extra fluff of medicine and brought us back to the reason why many of us have gotten into the field, because it became about the patients again,” she says. “You quickly learn your strengths and weaknesses as a provider and as a leader, and that flows into the decisions you’re making for your team and for your patients.”
Ms. Sheffer acknowledged that it is difficult to deal with patients’ family members who don’t understand that they can’t visit their sick relatives, but she said the flip side is that frontline workers become surrogate family members, an outcome she considers to be an honor.
“You step into the emotion with the family or with the patient because you’re all they have. That is a beautiful, honorable role, but it’s also tremendously emotional and sometimes devastating,” she said. “But to me, it’s one of the most beautiful things I’ve been able to offer in a time where we don’t even know what to do with COVID.”
Limited resources mixed with a healthy dose of fear can stifle creativity, Dr. Drane said. Right away, she noticed that despite the abundance of incentive spirometers at her hospital, they were not being utilized. She came in 2 hours early for 3 days to pass one out to every patient under investigation or COVID-positive patient and enlisted the help of her chief nursing officer, CEO, and regional medical director to get everyone on board.
Dr. Drane’s out-of-the-box thinking has enabled people to go home without oxygen 2 days earlier and cut the hospital’s length of stay by 5%. “It’s something so small, but it has such a great end reward,” she said. “I’m proud of this project because it didn’t take money; it was getting creative with what we already have.”
Renewed pride and passion
Dr. Drane is intensely proud of being an NP and working on the front lines. She sees that the pandemic has encouraged her and other APPs to expand their horizons.
“For me, it’s made me work to get dual certified,” she said. “APPs can be all-inclusive. I feel like I’m doing what I was meant to do and it’s not just a job anymore.”
Ms. McGrath is even more passionate about being a hospitalist now, as she has realized how valuable their unique skill sets are. “I think other people have also been able to realize that our ability to see the patient as a whole has allowed us to take care of this pandemic, because this disease impacts all organ systems and has a trickle-down effect that we as hospitalists are well versed to manage,” she said.
Ms. Cardin’s work involves communicating with APPs all around the country. Recently she had a phone exchange with an APP who needed to vent.
“She was weeping, and I thought she was going to say, ‘I can’t do this anymore, I need to go home,’ ” said Ms. Cardin. “Instead, she said, ‘I just want to make a difference in one of these people’s lives.’ And that is who the advanced practice providers are. They’re willing to go into those COVID units. They’re willing to be in the front lines. They are dedicated. They’re just intensely inspirational to me.”
Throughout the chaos of the COVID-19 pandemic, advanced practice providers (APPs) – physician assistants (PAs) and nurse practitioners (NPs) – have become an integral component of the hospitalist response. As many physicians began shifting into telemedicine and away from direct patient care, APPs have been eagerly jumping in to fill the gaps. Their work has been changing almost as dramatically and quickly as the pandemic itself, bringing with it expected challenges but bestowing hugely satisfying, often unanticipated, rewards.
APPs on the rise
As the coronavirus pandemic evolves, the role of APPs is evolving right alongside it. With the current relaxation of hospital bylaw restrictions on APPs, their utilization has increased, said Tracy Cardin, ACNP-BC, SFHM, a nurse practitioner and vice president of advanced practice providers at Sound Physicians. “We have not really furloughed any advanced practice providers,” Ms. Cardin said. “In fact, I consider them to be, within hospital medicine, a key lever to finding more cost-effective care delivery models.”
Ms. Cardin said APPs have been working more independently since COVID-19 started, seeing patients on their own and using physician consultation and backup via telemedicine or telephone as needed. With the reduction in elective surgeries and patient volumes at many hospitals, APP-led care also saves money. Because one of the biggest costs is labor, Ms. Cardin said, offering this high-quality care delivery model using APPs in collaboration with physician providers helps defray some of that cost. “We’re hoping that advanced practice providers are really a solution to some of these financial pressures in a lot of different ways,” she said.
“COVID … forced us to expedite conversations about how to maximize caseloads using APPs,” said Alicia Sheffer, AGAC-AGPC NP, a nurse practitioner and Great Lakes regional director of advanced practice providers at Sound Physicians in Cincinnati. Some of those staffing model changes have included using APPs while transitioning ICUs and med-surg units to COVID cohort units, APP-led COVID cohorts, and APP-led ICUs.
“At first the hospital system had ideas about bringing in telemedicine as an alternative to seeing patients, rather than just putting APPs on the front lines and having them go in and see patients,” said Jessica Drane, APRN, PhD, DNP FNP-C, a nurse practitioner and regional director of advanced practice provider services and hospital medicine at Sound Physicians in San Antonio. In Texas at the beginning of the pandemic, hospital numbers were so low that Dr. Drane did not work at all in April. “We were all afraid we were going to lose our jobs,” she said. Then the state got slammed and APPs have been desperately needed.
Ilaria Gadalla, DMSc, PA-C, a PA at Treasure Coast Hospitalists in Port St. Lucie, Fla., and the PA program director at South University, West Palm Beach, Fla., noted that many of her APP colleagues have pivoted fluidly from other specialties to the hospitalist realm as the need for frontline workers has increased. “Hospitalists have shined through this and their value has been recognized even more than previously as a result of COVID-19,” Dr. Gadalla said.
“I don’t think it’s any surprise that hospitalists became a pillar of the COVID pandemic,” said Bridget McGrath, PA-C, a physician assistant and director of the NP/PAs service line for the section of hospital medicine at the University of Chicago. “There are just some innate traits that hospitalists have, such as the ability to be flexible, to problem solve, and to be the solution to the problem.”
Building team camaraderie
Ms. Cardin says that the need for APPs has led to an evolving integration between physicians and APPs. The growing teamwork and bonding between colleagues have been some of the most rewarding aspects of the pandemic for Dr. Gadalla. “We rely even more on each other and there isn’t really a line of, ‘I’m a physician versus an NP or PA or nurse.’ We’re all working together with the same goal,” she said.
Ms. McGrath said she has been learning what it means to lead a team during a challenging time. It has been gratifying for her to watch mentors get down to the bare bones of patient care and see everyone unify, putting aside roles and titles and coming together to care for their patients in innovative ways.
“This pandemic has really opened up a lot of doors for us because up until now, we were used almost like scribes for physicians,” Dr. Drane said. She has seen even the most resistant hospital systems beginning to rely on APPs as the pandemic has progressed. “They have become pleasantly surprised at what an APP can do.”
Work challenges
Obviously, challenges abound. Dr. Gadalla listed hers as visiting restrictions that invariably lead to slower patient visits thanks to obligatory phone calls, constantly fluctuating patient censuses, sporadic elective surgeries, watching colleagues become furloughed, and trying to balance external perceptions with what’s actually happening in the hospital.
Overall, though, “There have been a lot more rewards than barriers,” added Dr. Drane.
One of the biggest obstacles for health care workers navigating a pandemic is balancing work and home life, not to mention having time to unwind while working long hours. “Finding time for my family has been very limited. My kids feel really neglected,” said Dr. Gadalla. Some days, she gets up extra early to exercise to help clear her head, but other times she’s just too exhausted to even move.
Dr. Drane agreed that the work can get overwhelming. “We’re changing the way we practice almost every week, which can make you doubt yourself as an educator, as a practitioner. You constantly feel like you’re not sure what you’re doing, and people trust you to heal them,” she said. “Today is my first day off in 24 days. I only got it off because I said I needed a moment.”
Ms. Sheffer’s crazy days were at the beginning of the pandemic when she had to self-quarantine from her family and was working nonstop. “I would come home and sleep and work and wake up in the middle of the night and double check and triple check and go back to sleep and work, and that consumed me for several months,” she said.
The biggest challenge for Ms. Sheffer has been coping with public fear. “No matter how logical our medical approach has been, I think the constant feeling of the public threat of COVID has had this insidious effect on how patients approach their health,” she said. “We’re spending a lot more time shaping our approach to best address their fears first and not to politicize COVID so we can actually deal with the health issue at hand.”
Complications of COVID
With all the restrictions, caring for patients these days has meant learning to interact with them in different ways that aren’t as personal, Ms. McGrath said. It has been difficult to lose “that humanity of medicine, the usual ways that you interact with your patients that are going through a vulnerable time,” she noted.
Additionally, students in the medical field are being held back from graduation because they cannot participate in direct patient care. This is particularly problematic for PAs and medical students who must touch patients to graduate, Dr. Gadalla said. “All of this is slowing down future providers. We’re going to have trouble catching up. Who’s going to relieve us? That’s a huge problem and no one is finding solutions for that yet,” she said.
At the University of Chicago, Ms. McGrath explained, they created virtual rotations so that PA students could continue to do them at the university. Not only has the experience reminded Ms. McGrath how much she loves being a medical educator and fighting for the education of PA students, but she was surprised to find that her patients came to appreciate the time they spent with her students on the virtual platform as well.
“It’s isolating for patients to be in the hospital in a vulnerable state and with no support system,” she said. “I think being a part of [the PA students’] education gave some meaning to their hospitalization and highlighted that collaboration and connection is a human need.”
Despite everything, there’s a noticeable emphasis on the flowering buds of hope, unity, compassion, and pride that have been quietly blooming from the daily hardships. As Ms. Cardin puts it, “It’s so cliché to say that there’s a crisis. The other word is ‘opportunity,’ and it’s true, there are opportunities here.”
Taking care of each other
Creating resources for providers has been a priority at the University of Chicago, according to Ms. McGrath. “As hospitalists, we’re used to taking care of a variety of patients, but our section leadership and providers on the front lines quickly realized that COVID patients are more akin to trauma patients with their quick changes in health, as well as their isolation, fear, and unexpected deterioration,” she said. Her facility has implemented wellness initiatives to help prevent burnout and mental health problems in COVID providers so they can continue to give the best care to their patients.
Both Ms. Sheffer and Dr. Drane say that they have a peer network of APPs at Sound Physicians to call on for questions and support. And it’s encouraging to know you’re not alone and to keep tabs on how colleagues in other states are doing, Ms. Sheffer noted.
“The peer support system has been helpful,” Dr. Drane said. “This job, right now, takes pieces of you every day. Sometimes it’s so emotional that you can’t put it into words. You just have to cry and get it out so that you can go be with your family.”
Getting back to basics
The changes in patient care have turned into something Ms. McGrath said she appreciates. “This pandemic has really stripped away the extra fluff of medicine and brought us back to the reason why many of us have gotten into the field, because it became about the patients again,” she says. “You quickly learn your strengths and weaknesses as a provider and as a leader, and that flows into the decisions you’re making for your team and for your patients.”
Ms. Sheffer acknowledged that it is difficult to deal with patients’ family members who don’t understand that they can’t visit their sick relatives, but she said the flip side is that frontline workers become surrogate family members, an outcome she considers to be an honor.
“You step into the emotion with the family or with the patient because you’re all they have. That is a beautiful, honorable role, but it’s also tremendously emotional and sometimes devastating,” she said. “But to me, it’s one of the most beautiful things I’ve been able to offer in a time where we don’t even know what to do with COVID.”
Limited resources mixed with a healthy dose of fear can stifle creativity, Dr. Drane said. Right away, she noticed that despite the abundance of incentive spirometers at her hospital, they were not being utilized. She came in 2 hours early for 3 days to pass one out to every patient under investigation or COVID-positive patient and enlisted the help of her chief nursing officer, CEO, and regional medical director to get everyone on board.
Dr. Drane’s out-of-the-box thinking has enabled people to go home without oxygen 2 days earlier and cut the hospital’s length of stay by 5%. “It’s something so small, but it has such a great end reward,” she said. “I’m proud of this project because it didn’t take money; it was getting creative with what we already have.”
Renewed pride and passion
Dr. Drane is intensely proud of being an NP and working on the front lines. She sees that the pandemic has encouraged her and other APPs to expand their horizons.
“For me, it’s made me work to get dual certified,” she said. “APPs can be all-inclusive. I feel like I’m doing what I was meant to do and it’s not just a job anymore.”
Ms. McGrath is even more passionate about being a hospitalist now, as she has realized how valuable their unique skill sets are. “I think other people have also been able to realize that our ability to see the patient as a whole has allowed us to take care of this pandemic, because this disease impacts all organ systems and has a trickle-down effect that we as hospitalists are well versed to manage,” she said.
Ms. Cardin’s work involves communicating with APPs all around the country. Recently she had a phone exchange with an APP who needed to vent.
“She was weeping, and I thought she was going to say, ‘I can’t do this anymore, I need to go home,’ ” said Ms. Cardin. “Instead, she said, ‘I just want to make a difference in one of these people’s lives.’ And that is who the advanced practice providers are. They’re willing to go into those COVID units. They’re willing to be in the front lines. They are dedicated. They’re just intensely inspirational to me.”
HCC rates slow in cities, continue to climb in rural areas
The incidence rate of hepatocellular carcinoma in urban areas of the United States began to slow in 2009, but the rate in rural areas of the nation continued to rise at a steady pace, especially among non-Hispanic Whites and Blacks, investigators have found.
Although overall hepatocellular carcinoma (HCC) incidence rates were consistently lower among people living in nonmetro (rural) versus metro (urban) areas, the average annual percentage change in urban areas began to slow from 5.3% for the period of 1995 through 2009 to 2.7% thereafter. In contrast, the average annual percentage change in rural areas remained steady at 5.7%, a disparity that remained even after adjusting for differences among subgroups, reported Christina Gainey, MD, a third-year resident in internal medicine at the University of Southern California Medical Center, Los Angeles.
“We found that there are striking urban-rural disparities in HCC incidence trends that vary by race and ethnicity, and these disparities are growing over time,” she said during the virtual annual meeting of the American Association for the Study of Liver Diseases.
“Our study really highlights a critical public health issue that’s disproportionately affecting rural Americans. They already face considerable health inequities when it comes to access to care, health outcomes, and public health infrastructure and resources, and as of now we still don’t know why cases of HCC continue to rise in these areas,” she said.
Dr. Gainey noted that HCC is the fastest-growing cancer in the United States, according to the 2020 Annual Report to the Nation on the Status of Cancer, issued jointly by the Centers for Disease Control and Prevention, the North American Association of Central Cancer Registries, the American Cancer Society, and the National Cancer Institute.
Previous studies have identified disparities between urban and rural regions in care of patients with cervical cancer, colorectal cancer, and other malignancies, but there are very few data on urban-rural differences in HCC incidence, she said.
Incidence trends
To better understand whether such differences exists, the investigators compared trends in age-adjusted incidence rates of HCC in both rural and urban areas of the United States from 1995 to 2016, with stratification of trends by race/ethnicity and other demographic factors.
They drew from the NAACR database, which captures 93% of the U.S. population, in contrast to the CDC’s Surveillance, Epidemiology, and End Results (SEER) database which samples just 18% of the population.
Patients with HCC were defined by diagnostic codes, with diagnoses of intrahepatic bile duct cancers excluded.
They used 2013 U.S. Department of Agriculture Rural-Urban Continuum Codes to identify rural areas (regions of open countryside with town populations fewer than 2,500 people) and urban areas (populations ranging from 2,500 to 49,999, but not part of a larger labor market area).
The investigators identified a total of 310,635 HCC cases, 85% in urban areas and 15% in rural areas. Three-fourths of the patients (77%) were male. The median age ranged from 55-59 years.
There were notable demographic differences between the regions with non-Hispanic Whites comprising only 57% of the urban sample, but 82% of the rural sample. The urban sample included 16% non-Hispanic Blacks, 10% Asian/Pacific Islanders, and 17% Hispanics. The respective proportions in the rural areas were 8%, 2%, and 8%.
As noted before, age-adjusted incidence rates (adjusted to the year 2000 U.S. population) were lower in rural areas, at 4.9 per 100,000 population, compared with 6.9/100,000 in urban areas.
But when they looked at the average annual percentage changes using jointpoint regression, they saw that beginning in 2009 the AAPC in urban areas began to slow, from 5.3% for the period prior to 2009 to 2.7% thereafter, while the average annual percentage change in urban areas remained steady at 5.7%.
The largest increase in incidence over the course of the study was among rural non-Hispanic Whites, with an AAPC of 5.7%. Among urban non-Hispanic Blacks, the AAPC rose by 6.6% from 1995 to 2009, but slowed thereafter.
In contrast, among rural non-Hispanic Blacks the AAPC remained steady, at 5.4%.
The only group to see a decline in incidence was urban Asians/Pacific Islanders, who had an overall decline of 1%.
Among all groups, rural Hispanics had the highest age-adjusted incidence rates, at 14.9 per 100,000 in 2016.
Awareness gap?
Lewis R. Roberts, MB, ChB, PhD, a hepatobiliary cancer researcher at the Mayo Clinic in Rochester, Minn., who was not involved in the study, said in an interview that the difference in incidence rates between cities and the country may be attributable to a number of factors, including the opioid crisis, which can lead to an increase in injectable drug use or sexual behaviors resulting in increases in chronic hepatitis C infections and cirrhosis, known risk factors for HCC, as well as a lack of awareness of infections as a risk factor.
“In order for people to find these diseases, they have to be looking, and many of these are hidden diseases in our community,” he said. “What the study made me wonder was whether it just happens to be that they are in some ways more hidden in a rural community than they are in an urban community.”
He noted that clinicians in urban communities are more accustomed to treating more diverse populations who may have higher susceptibility to viral hepatitis, for example, and that screening and treatment for hepatitis C may be more common in urban areas than rural areas, he said.
No funding source for the study was reported. Dr. Gainey and Dr. Roberts reported having no conflicts of interest to disclose.
SOURCE: Gainey C et al. Liver Meeting 2020, Abstract 136.
The incidence rate of hepatocellular carcinoma in urban areas of the United States began to slow in 2009, but the rate in rural areas of the nation continued to rise at a steady pace, especially among non-Hispanic Whites and Blacks, investigators have found.
Although overall hepatocellular carcinoma (HCC) incidence rates were consistently lower among people living in nonmetro (rural) versus metro (urban) areas, the average annual percentage change in urban areas began to slow from 5.3% for the period of 1995 through 2009 to 2.7% thereafter. In contrast, the average annual percentage change in rural areas remained steady at 5.7%, a disparity that remained even after adjusting for differences among subgroups, reported Christina Gainey, MD, a third-year resident in internal medicine at the University of Southern California Medical Center, Los Angeles.
“We found that there are striking urban-rural disparities in HCC incidence trends that vary by race and ethnicity, and these disparities are growing over time,” she said during the virtual annual meeting of the American Association for the Study of Liver Diseases.
“Our study really highlights a critical public health issue that’s disproportionately affecting rural Americans. They already face considerable health inequities when it comes to access to care, health outcomes, and public health infrastructure and resources, and as of now we still don’t know why cases of HCC continue to rise in these areas,” she said.
Dr. Gainey noted that HCC is the fastest-growing cancer in the United States, according to the 2020 Annual Report to the Nation on the Status of Cancer, issued jointly by the Centers for Disease Control and Prevention, the North American Association of Central Cancer Registries, the American Cancer Society, and the National Cancer Institute.
Previous studies have identified disparities between urban and rural regions in care of patients with cervical cancer, colorectal cancer, and other malignancies, but there are very few data on urban-rural differences in HCC incidence, she said.
Incidence trends
To better understand whether such differences exists, the investigators compared trends in age-adjusted incidence rates of HCC in both rural and urban areas of the United States from 1995 to 2016, with stratification of trends by race/ethnicity and other demographic factors.
They drew from the NAACR database, which captures 93% of the U.S. population, in contrast to the CDC’s Surveillance, Epidemiology, and End Results (SEER) database which samples just 18% of the population.
Patients with HCC were defined by diagnostic codes, with diagnoses of intrahepatic bile duct cancers excluded.
They used 2013 U.S. Department of Agriculture Rural-Urban Continuum Codes to identify rural areas (regions of open countryside with town populations fewer than 2,500 people) and urban areas (populations ranging from 2,500 to 49,999, but not part of a larger labor market area).
The investigators identified a total of 310,635 HCC cases, 85% in urban areas and 15% in rural areas. Three-fourths of the patients (77%) were male. The median age ranged from 55-59 years.
There were notable demographic differences between the regions with non-Hispanic Whites comprising only 57% of the urban sample, but 82% of the rural sample. The urban sample included 16% non-Hispanic Blacks, 10% Asian/Pacific Islanders, and 17% Hispanics. The respective proportions in the rural areas were 8%, 2%, and 8%.
As noted before, age-adjusted incidence rates (adjusted to the year 2000 U.S. population) were lower in rural areas, at 4.9 per 100,000 population, compared with 6.9/100,000 in urban areas.
But when they looked at the average annual percentage changes using jointpoint regression, they saw that beginning in 2009 the AAPC in urban areas began to slow, from 5.3% for the period prior to 2009 to 2.7% thereafter, while the average annual percentage change in urban areas remained steady at 5.7%.
The largest increase in incidence over the course of the study was among rural non-Hispanic Whites, with an AAPC of 5.7%. Among urban non-Hispanic Blacks, the AAPC rose by 6.6% from 1995 to 2009, but slowed thereafter.
In contrast, among rural non-Hispanic Blacks the AAPC remained steady, at 5.4%.
The only group to see a decline in incidence was urban Asians/Pacific Islanders, who had an overall decline of 1%.
Among all groups, rural Hispanics had the highest age-adjusted incidence rates, at 14.9 per 100,000 in 2016.
Awareness gap?
Lewis R. Roberts, MB, ChB, PhD, a hepatobiliary cancer researcher at the Mayo Clinic in Rochester, Minn., who was not involved in the study, said in an interview that the difference in incidence rates between cities and the country may be attributable to a number of factors, including the opioid crisis, which can lead to an increase in injectable drug use or sexual behaviors resulting in increases in chronic hepatitis C infections and cirrhosis, known risk factors for HCC, as well as a lack of awareness of infections as a risk factor.
“In order for people to find these diseases, they have to be looking, and many of these are hidden diseases in our community,” he said. “What the study made me wonder was whether it just happens to be that they are in some ways more hidden in a rural community than they are in an urban community.”
He noted that clinicians in urban communities are more accustomed to treating more diverse populations who may have higher susceptibility to viral hepatitis, for example, and that screening and treatment for hepatitis C may be more common in urban areas than rural areas, he said.
No funding source for the study was reported. Dr. Gainey and Dr. Roberts reported having no conflicts of interest to disclose.
SOURCE: Gainey C et al. Liver Meeting 2020, Abstract 136.
The incidence rate of hepatocellular carcinoma in urban areas of the United States began to slow in 2009, but the rate in rural areas of the nation continued to rise at a steady pace, especially among non-Hispanic Whites and Blacks, investigators have found.
Although overall hepatocellular carcinoma (HCC) incidence rates were consistently lower among people living in nonmetro (rural) versus metro (urban) areas, the average annual percentage change in urban areas began to slow from 5.3% for the period of 1995 through 2009 to 2.7% thereafter. In contrast, the average annual percentage change in rural areas remained steady at 5.7%, a disparity that remained even after adjusting for differences among subgroups, reported Christina Gainey, MD, a third-year resident in internal medicine at the University of Southern California Medical Center, Los Angeles.
“We found that there are striking urban-rural disparities in HCC incidence trends that vary by race and ethnicity, and these disparities are growing over time,” she said during the virtual annual meeting of the American Association for the Study of Liver Diseases.
“Our study really highlights a critical public health issue that’s disproportionately affecting rural Americans. They already face considerable health inequities when it comes to access to care, health outcomes, and public health infrastructure and resources, and as of now we still don’t know why cases of HCC continue to rise in these areas,” she said.
Dr. Gainey noted that HCC is the fastest-growing cancer in the United States, according to the 2020 Annual Report to the Nation on the Status of Cancer, issued jointly by the Centers for Disease Control and Prevention, the North American Association of Central Cancer Registries, the American Cancer Society, and the National Cancer Institute.
Previous studies have identified disparities between urban and rural regions in care of patients with cervical cancer, colorectal cancer, and other malignancies, but there are very few data on urban-rural differences in HCC incidence, she said.
Incidence trends
To better understand whether such differences exists, the investigators compared trends in age-adjusted incidence rates of HCC in both rural and urban areas of the United States from 1995 to 2016, with stratification of trends by race/ethnicity and other demographic factors.
They drew from the NAACR database, which captures 93% of the U.S. population, in contrast to the CDC’s Surveillance, Epidemiology, and End Results (SEER) database which samples just 18% of the population.
Patients with HCC were defined by diagnostic codes, with diagnoses of intrahepatic bile duct cancers excluded.
They used 2013 U.S. Department of Agriculture Rural-Urban Continuum Codes to identify rural areas (regions of open countryside with town populations fewer than 2,500 people) and urban areas (populations ranging from 2,500 to 49,999, but not part of a larger labor market area).
The investigators identified a total of 310,635 HCC cases, 85% in urban areas and 15% in rural areas. Three-fourths of the patients (77%) were male. The median age ranged from 55-59 years.
There were notable demographic differences between the regions with non-Hispanic Whites comprising only 57% of the urban sample, but 82% of the rural sample. The urban sample included 16% non-Hispanic Blacks, 10% Asian/Pacific Islanders, and 17% Hispanics. The respective proportions in the rural areas were 8%, 2%, and 8%.
As noted before, age-adjusted incidence rates (adjusted to the year 2000 U.S. population) were lower in rural areas, at 4.9 per 100,000 population, compared with 6.9/100,000 in urban areas.
But when they looked at the average annual percentage changes using jointpoint regression, they saw that beginning in 2009 the AAPC in urban areas began to slow, from 5.3% for the period prior to 2009 to 2.7% thereafter, while the average annual percentage change in urban areas remained steady at 5.7%.
The largest increase in incidence over the course of the study was among rural non-Hispanic Whites, with an AAPC of 5.7%. Among urban non-Hispanic Blacks, the AAPC rose by 6.6% from 1995 to 2009, but slowed thereafter.
In contrast, among rural non-Hispanic Blacks the AAPC remained steady, at 5.4%.
The only group to see a decline in incidence was urban Asians/Pacific Islanders, who had an overall decline of 1%.
Among all groups, rural Hispanics had the highest age-adjusted incidence rates, at 14.9 per 100,000 in 2016.
Awareness gap?
Lewis R. Roberts, MB, ChB, PhD, a hepatobiliary cancer researcher at the Mayo Clinic in Rochester, Minn., who was not involved in the study, said in an interview that the difference in incidence rates between cities and the country may be attributable to a number of factors, including the opioid crisis, which can lead to an increase in injectable drug use or sexual behaviors resulting in increases in chronic hepatitis C infections and cirrhosis, known risk factors for HCC, as well as a lack of awareness of infections as a risk factor.
“In order for people to find these diseases, they have to be looking, and many of these are hidden diseases in our community,” he said. “What the study made me wonder was whether it just happens to be that they are in some ways more hidden in a rural community than they are in an urban community.”
He noted that clinicians in urban communities are more accustomed to treating more diverse populations who may have higher susceptibility to viral hepatitis, for example, and that screening and treatment for hepatitis C may be more common in urban areas than rural areas, he said.
No funding source for the study was reported. Dr. Gainey and Dr. Roberts reported having no conflicts of interest to disclose.
SOURCE: Gainey C et al. Liver Meeting 2020, Abstract 136.
FROM THE LIVER MEETING DIGITAL EXPERIENCE
Hemophilia, von Willebrand disease do not increase postop complications for ACL reconstruction
Patients with hemophilia A or von Willebrand disease undergoing anterior cruciate ligament (ACL) reconstruction had rates of postoperative complications and ACL reinjuries that were not significantly different from those control patients. However, the cost of health care utilization was significantly greater for the hemophilia A and von Willebrand disease patients, according to a large retrospective database study published online in The Knee.
All patients who underwent an ACL reconstruction from 2010 to 2014 in a large commercial database were assessed. Patients with hemophilia A, hemophilia B, and von Willebrand disease were identified. Patient demographics, cost of surgery, blood product use, concomitant injuries, repeat ACL injury, complications, and various operative variables were collected.
A total of 33 patients with hemophilia A, 3 with hemophilia B patients, 63 with von Willebrand disease and 103,478 control patients who had ACL reconstruction were compared, according to Connor Zale, MD, and colleagues at Penn State Hershey (Pa.) Medical Center.
Similar outcomes, higher costs
Complications – including length of hospital stay, postoperative hemorrhage within 14 days after surgery, infection rates within 90 days of surgery, lysis of adhesions or manipulation under anesthesia within 90 days of surgery, concomitant injuries to the knee, additional ACL injury within 1 year of surgery, deep-vein thrombosis, and pulmonary embolism – were not statistically different between the hemophilia/von Willebrand cohorts and the control group, according to the researchers.
However, surgery and postoperative care were costlier in the hemophilia A and von Willebrand cohorts. Total health care utilization within 30 days of ACL reconstruction was significantly more expensive for patients with hemophilia A ($25,982) and those with von Willebrand disease ($16,445), compared with those among controls ($12,887). In addition, the total health care utilization costs within 90 days of ACL reconstruction were significantly higher for patients with hemophilia A ($30,310) and those with von Willebrand disease ($20,355), compared with those among controls ($14,564), with all P values less than .001.
None of the patients with hemophilia A or those with von Willebrand received blood products perioperatively, had a known major hemarthrosis, or were readmitted within 30 or 90 days, the authors noted, adding that this finding differs from previous studies. The authors speculated that, since no blood products were administered and there was no significant difference in postoperative hemorrhage, the patients with hemophilia A were preoperatively optimized for an acceptable prothrombin time and international normalized ratio and/or were more effectively managed postoperatively.
“Many surgeons may be fearful of performing an ACL reconstruction on those with hemophilia A, hemophilia B, and von Willebrand disease due to concerns over risk of a major hemarthrosis and other complications postoperatively. This study observed that hemophilia A and von Willebrand disease patients who underwent an ACL reconstruction had rates of postoperative complications that were not statistically different than those who underwent ACL reconstructions and did not have a known hypocoagulable condition,” the researchers concluded.
The authors reported that they had no potential conflicts of interest to disclose.
SOURCE: Zale C et al. Knee. 2020;27(6):1729-34.
Patients with hemophilia A or von Willebrand disease undergoing anterior cruciate ligament (ACL) reconstruction had rates of postoperative complications and ACL reinjuries that were not significantly different from those control patients. However, the cost of health care utilization was significantly greater for the hemophilia A and von Willebrand disease patients, according to a large retrospective database study published online in The Knee.
All patients who underwent an ACL reconstruction from 2010 to 2014 in a large commercial database were assessed. Patients with hemophilia A, hemophilia B, and von Willebrand disease were identified. Patient demographics, cost of surgery, blood product use, concomitant injuries, repeat ACL injury, complications, and various operative variables were collected.
A total of 33 patients with hemophilia A, 3 with hemophilia B patients, 63 with von Willebrand disease and 103,478 control patients who had ACL reconstruction were compared, according to Connor Zale, MD, and colleagues at Penn State Hershey (Pa.) Medical Center.
Similar outcomes, higher costs
Complications – including length of hospital stay, postoperative hemorrhage within 14 days after surgery, infection rates within 90 days of surgery, lysis of adhesions or manipulation under anesthesia within 90 days of surgery, concomitant injuries to the knee, additional ACL injury within 1 year of surgery, deep-vein thrombosis, and pulmonary embolism – were not statistically different between the hemophilia/von Willebrand cohorts and the control group, according to the researchers.
However, surgery and postoperative care were costlier in the hemophilia A and von Willebrand cohorts. Total health care utilization within 30 days of ACL reconstruction was significantly more expensive for patients with hemophilia A ($25,982) and those with von Willebrand disease ($16,445), compared with those among controls ($12,887). In addition, the total health care utilization costs within 90 days of ACL reconstruction were significantly higher for patients with hemophilia A ($30,310) and those with von Willebrand disease ($20,355), compared with those among controls ($14,564), with all P values less than .001.
None of the patients with hemophilia A or those with von Willebrand received blood products perioperatively, had a known major hemarthrosis, or were readmitted within 30 or 90 days, the authors noted, adding that this finding differs from previous studies. The authors speculated that, since no blood products were administered and there was no significant difference in postoperative hemorrhage, the patients with hemophilia A were preoperatively optimized for an acceptable prothrombin time and international normalized ratio and/or were more effectively managed postoperatively.
“Many surgeons may be fearful of performing an ACL reconstruction on those with hemophilia A, hemophilia B, and von Willebrand disease due to concerns over risk of a major hemarthrosis and other complications postoperatively. This study observed that hemophilia A and von Willebrand disease patients who underwent an ACL reconstruction had rates of postoperative complications that were not statistically different than those who underwent ACL reconstructions and did not have a known hypocoagulable condition,” the researchers concluded.
The authors reported that they had no potential conflicts of interest to disclose.
SOURCE: Zale C et al. Knee. 2020;27(6):1729-34.
Patients with hemophilia A or von Willebrand disease undergoing anterior cruciate ligament (ACL) reconstruction had rates of postoperative complications and ACL reinjuries that were not significantly different from those control patients. However, the cost of health care utilization was significantly greater for the hemophilia A and von Willebrand disease patients, according to a large retrospective database study published online in The Knee.
All patients who underwent an ACL reconstruction from 2010 to 2014 in a large commercial database were assessed. Patients with hemophilia A, hemophilia B, and von Willebrand disease were identified. Patient demographics, cost of surgery, blood product use, concomitant injuries, repeat ACL injury, complications, and various operative variables were collected.
A total of 33 patients with hemophilia A, 3 with hemophilia B patients, 63 with von Willebrand disease and 103,478 control patients who had ACL reconstruction were compared, according to Connor Zale, MD, and colleagues at Penn State Hershey (Pa.) Medical Center.
Similar outcomes, higher costs
Complications – including length of hospital stay, postoperative hemorrhage within 14 days after surgery, infection rates within 90 days of surgery, lysis of adhesions or manipulation under anesthesia within 90 days of surgery, concomitant injuries to the knee, additional ACL injury within 1 year of surgery, deep-vein thrombosis, and pulmonary embolism – were not statistically different between the hemophilia/von Willebrand cohorts and the control group, according to the researchers.
However, surgery and postoperative care were costlier in the hemophilia A and von Willebrand cohorts. Total health care utilization within 30 days of ACL reconstruction was significantly more expensive for patients with hemophilia A ($25,982) and those with von Willebrand disease ($16,445), compared with those among controls ($12,887). In addition, the total health care utilization costs within 90 days of ACL reconstruction were significantly higher for patients with hemophilia A ($30,310) and those with von Willebrand disease ($20,355), compared with those among controls ($14,564), with all P values less than .001.
None of the patients with hemophilia A or those with von Willebrand received blood products perioperatively, had a known major hemarthrosis, or were readmitted within 30 or 90 days, the authors noted, adding that this finding differs from previous studies. The authors speculated that, since no blood products were administered and there was no significant difference in postoperative hemorrhage, the patients with hemophilia A were preoperatively optimized for an acceptable prothrombin time and international normalized ratio and/or were more effectively managed postoperatively.
“Many surgeons may be fearful of performing an ACL reconstruction on those with hemophilia A, hemophilia B, and von Willebrand disease due to concerns over risk of a major hemarthrosis and other complications postoperatively. This study observed that hemophilia A and von Willebrand disease patients who underwent an ACL reconstruction had rates of postoperative complications that were not statistically different than those who underwent ACL reconstructions and did not have a known hypocoagulable condition,” the researchers concluded.
The authors reported that they had no potential conflicts of interest to disclose.
SOURCE: Zale C et al. Knee. 2020;27(6):1729-34.
FROM THE KNEE
Key clinical point:
Major finding: Total health care utilization within 30 days of ACL reconstruction was significantly greater for hemophilia A ($25,982) and von Willebrand disease ($16,445) patients, compared with controls ($12,887).
Study details: A retrospective study of 33 patients with hemophilia A, 3 with hemophilia B, and 63 with von Willebrand factor, as well as 103,478 controls, who all underwent ACL reconstruction.
Disclosures: The authors reported that they had no potential conflicts of interest to disclose.
Source: Zale C et al. Knee. 2020;27(6):1729-34.
@GiJournal: An online platform to discuss the latest gastroenterology and hepatology publications
The last decade has seen an increased focus on the use of social media for medical education. Twitter, with over 330 million active users, is the most popular social media platform for medical education. We describe here our recent initiative to establish a weekly online gastroenterology-focused journal club on Twitter.
How was the idea conceived?
Sultan Mahmood, MD (@SultanMahmoodMD)

I joined #GITwitter at the end of 2019 and started following some of the leading experts in the field of gastroenterology and hepatology. It was a pleasant surprise to see how easy it was to engage with them and get expert opinions from across the world in real time. #MondayNightIBD, led by Aline Charabaty, MD, had become a phenomenon in the GI community and changed the perception of medical education in the digital world. There were online journal clubs for different medical subspecialties, including #NephroJC, #HOJournalClub, and #DermJC, but none for gastroenterology. Realizing this opportunity, and with guidance from Dr. Charabaty, we started @GiJournal in December of 2019 with weekly discussions.
@GiJournal started off as an informal discussion in which we would post a summary of the article and invite an expert in the field to comment. However, the interest in the journal club quickly took off as we gained more followers and a worldwide audience joined our journal club discussions on a weekly basis. As the COVID-19 pandemic took hold and endoscopy suites around the word closed, interest in online medical education grew. @GIJournal provided a platform for trainees and practicing physicians alike to stay up to date with the latest publications from the comfort of their homes. Needless to say, the journal club has evolved since its inception in that we now work with a team of experts and trainees who run the journal club on a rotating basis.
How does @GiJournal work?
Ijlal Akbar Ali, MD (@IjlalAkbar)
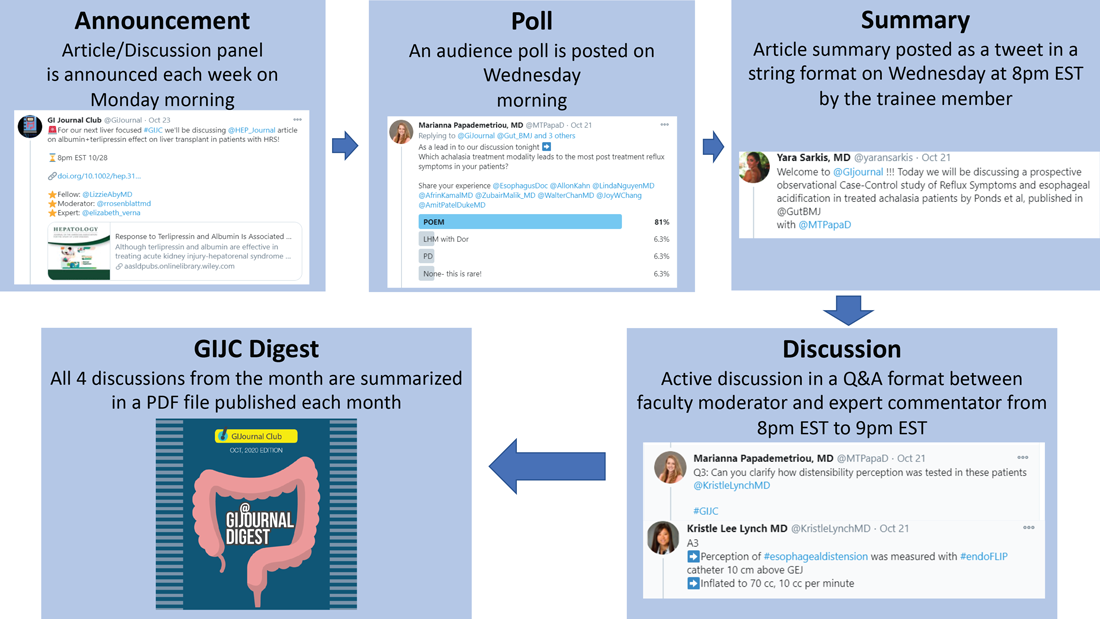
We have a large editorial board with volunteer faculty and trainees, all divided into four special interest groups (general GI/inflammatory bowel disease, interventional endoscopy/bariatric endoscopy, hepatology, and esophageal/motility disorders). Each week, a faculty member and a trainee pick a recently published article from a high-impact GI-focused journal. We also try to invite an expert of international repute (often the authors of the article themselves!) to engage as well. The faculty moderator and invited expert then work with the trainee to plan the session content. We post the topic and article on Monday. At 8 p.m. EST on Wednesday, the trainee posts a series of six to eight tweets summarizing the article. The faculty then asks the invited expert (and audience at large) a series of predetermined questions. Anyone can respond, share their opinion, and direct their own questions toward the moderator and expert who continually check their notifications and respond in real time. This brews into an hour-long discussion which covers not only the methodologic aspects of the article, but clinical practice in general. Discussions often trickle into the next day as people from different time zones participate. Everyone uses #GIJC at the end of their tweets which assists those following the article and facilitates indexing for future review. For those who miss or want to review sessions, we conveniently summarize all articles and corresponding discussions in a monthly publication, @GiJournal Digest, that is posted on Twitter for anyone to download, read and enjoy (Figure 1).
How is this different from any other journal club?
Atoosa Rabiee, MD (@AtoosaRabiee)

@GiJournal is unique in that it provides trainees and practicing gastroenterologists access to interactive discussions with both authors and world-renowned experts in the field. Online journal clubs operate with a flattened hierarchy; as such, they inherently break down access barriers to both the researchers who performed the study and key opinion leaders who commonly participate. There is no boundary as far as institutions or even countries. As a result, our platform has uncovered an unexpected degree of interest in live online discussion, and we have enjoyed collaborating and learning from experts from all over the world. @GiJournal also differs from conventional journal clubs by allowing trainees the opportunity to collaborate and engage with mentors from other institutions. As such, trainees develop relationships with experts in the field outside their home institutions, experts with whom they may not have had contact otherwise.
Although worldwide participation is a key strength of the online @GiJournal platform, it may be challenging for some members to attend the live discussion based on time difference. We account for this in two ways. First, participants are encouraged to continue with comments and questions afterward at their convenience, which allows experts and moderators to continue the conversation, often for several days. Second, to promote inclusivity, we have created a unique, customized publication to summarize and present the key points of conversation for each session. This asynchronous access is a quality not found in more traditional journal club formats. Finally, studies have shown that articles shared on social media tend to have increased citations and higher Altmetric scores.
What are the opportunities for trainees and recent graduates?
Sunil Amin, MD, MPH (@SunilAminMD)

Our surveys have shown that 30%-45% of the @GiJournal discussion participants are trainees. Both gastroenterology fellows and internal medicine residents from around the world are an integral part of each specialty panel for the weekly @GIjournal discussions. Trainees are paired up with a specific faculty mentor and together they choose an article for discussion, create a summary, informal twitter poll, and questions for the discussion. This direct access provides an opportunity for trainees to interact, ask questions, and learn from faculty in an informal atmosphere.
We have heard from multiple trainees who have developed long-term relationships with the experts and faculty mentors they worked with and are now also working on research projects. Additionally, trainees can bring the expertise they have now acquired back to their home institutions to pick articles, add specific teaching points, and enrich their local journal club discussions. Finally, trainees who present on the @GiJournal platform are given unique visibility to the many faculty members and opinion leaders participating in each discussion. This may facilitate future networking opportunities and enhance their CVs for future fellowship or employment applications.
Plans for the future?
Allon Kahn, MD (@AllonKahn)

Despite significant evolution and growth in @GiJournal over the past year, we are still actively working to expand our platform. Modes of online medical education, specifically Twitter-based GI journal club discussions, remain in their infancy. We see this @GiJournal as an opportunity for innovation as we plan for the year ahead. Our top priority for the upcoming year includes obtaining CME approval, which we are currently developing with Integrity CE (an Accreditation Council for Continuing Medical Education–accredited provider of CME for health care professionals). This will give an opportunity for the participants to be awarded CME credit when they participate in our weekly discussions. Other options being explored include starting a podcast and translation of @GiJournal Digest in different languages to reach a wider international audience. Furthermore, with the continued expansion of GI leaders and experts joining and engaging in Twitter, our options for unique and multidisciplinary discussion topics will continue to grow.
How can you join the @GiJournal discussions?
@SultanMahmoodMD
Joining the journal club discussion is easy. Just follow the @GiJournal handle on Twitter and turn on the notifications icon. Although we encourage everyone to “actively” participate in the discussion by asking questions or sharing your personal experience, joining the discussion as an “observer” is also a great way to learn. The discussion starts at 8 p.m. EST every Wednesday. Follow the #GIJC and the @GiJournal handle as questions are posted by the faculty moderator and answered by the experts. Even if you miss the discussion, the @GiJournal Digest is a great way to recap the discussions in an easy-to-read PDF format. The @GiJournal Digest is a monthly publication that archives the four @GiJournal club discussions in the previous month. Follow the link below to access the recent publications: http://ow.ly/uu2550C3RXX
Conclusion
In summary, we believe Twitter-based journal clubs offer an engaging way of virtual learning from the comfort of one’s home and a convenient way to directly interact with the experts. The success of @GiJournal highlights the importance of social media for medical education in the field of gastroenterology and hepatology and we look forward to developing this endeavor further.
Dr. Mahmood is clinical assistant professor of medicine, co–program director of the GI fellowship program, UB division of gastroenterology, hepatology & nutrition, State University of New York at Buffalo; Dr. Rabiee is assistant professor of medicine, director of hepatology, division of gastroenterology and hepatology, Washington DC VA Medical Center, Washington; Dr. Amin is assistant professor of medicine, director of endoscopy, The Lennar Foundation Medical Center, division of digestive health and liver disease, department of medicine, University of Miami; Dr. Kahn is assistant professor of medicine, division of gastroenterology & hepatology, Mayo Clinic, Scottsdale, Ariz.; and Dr. Akbar Ali is a gastroenterology fellow in the division of digestive diseases and nutrition, University of Oklahoma Health Sciences Center, Oklahoma City.
The last decade has seen an increased focus on the use of social media for medical education. Twitter, with over 330 million active users, is the most popular social media platform for medical education. We describe here our recent initiative to establish a weekly online gastroenterology-focused journal club on Twitter.
How was the idea conceived?
Sultan Mahmood, MD (@SultanMahmoodMD)
I joined #GITwitter at the end of 2019 and started following some of the leading experts in the field of gastroenterology and hepatology. It was a pleasant surprise to see how easy it was to engage with them and get expert opinions from across the world in real time. #MondayNightIBD, led by Aline Charabaty, MD, had become a phenomenon in the GI community and changed the perception of medical education in the digital world. There were online journal clubs for different medical subspecialties, including #NephroJC, #HOJournalClub, and #DermJC, but none for gastroenterology. Realizing this opportunity, and with guidance from Dr. Charabaty, we started @GiJournal in December of 2019 with weekly discussions.
@GiJournal started off as an informal discussion in which we would post a summary of the article and invite an expert in the field to comment. However, the interest in the journal club quickly took off as we gained more followers and a worldwide audience joined our journal club discussions on a weekly basis. As the COVID-19 pandemic took hold and endoscopy suites around the word closed, interest in online medical education grew. @GIJournal provided a platform for trainees and practicing physicians alike to stay up to date with the latest publications from the comfort of their homes. Needless to say, the journal club has evolved since its inception in that we now work with a team of experts and trainees who run the journal club on a rotating basis.
How does @GiJournal work?
Ijlal Akbar Ali, MD (@IjlalAkbar)
We have a large editorial board with volunteer faculty and trainees, all divided into four special interest groups (general GI/inflammatory bowel disease, interventional endoscopy/bariatric endoscopy, hepatology, and esophageal/motility disorders). Each week, a faculty member and a trainee pick a recently published article from a high-impact GI-focused journal. We also try to invite an expert of international repute (often the authors of the article themselves!) to engage as well. The faculty moderator and invited expert then work with the trainee to plan the session content. We post the topic and article on Monday. At 8 p.m. EST on Wednesday, the trainee posts a series of six to eight tweets summarizing the article. The faculty then asks the invited expert (and audience at large) a series of predetermined questions. Anyone can respond, share their opinion, and direct their own questions toward the moderator and expert who continually check their notifications and respond in real time. This brews into an hour-long discussion which covers not only the methodologic aspects of the article, but clinical practice in general. Discussions often trickle into the next day as people from different time zones participate. Everyone uses #GIJC at the end of their tweets which assists those following the article and facilitates indexing for future review. For those who miss or want to review sessions, we conveniently summarize all articles and corresponding discussions in a monthly publication, @GiJournal Digest, that is posted on Twitter for anyone to download, read and enjoy (Figure 1).
How is this different from any other journal club?
Atoosa Rabiee, MD (@AtoosaRabiee)
@GiJournal is unique in that it provides trainees and practicing gastroenterologists access to interactive discussions with both authors and world-renowned experts in the field. Online journal clubs operate with a flattened hierarchy; as such, they inherently break down access barriers to both the researchers who performed the study and key opinion leaders who commonly participate. There is no boundary as far as institutions or even countries. As a result, our platform has uncovered an unexpected degree of interest in live online discussion, and we have enjoyed collaborating and learning from experts from all over the world. @GiJournal also differs from conventional journal clubs by allowing trainees the opportunity to collaborate and engage with mentors from other institutions. As such, trainees develop relationships with experts in the field outside their home institutions, experts with whom they may not have had contact otherwise.
Although worldwide participation is a key strength of the online @GiJournal platform, it may be challenging for some members to attend the live discussion based on time difference. We account for this in two ways. First, participants are encouraged to continue with comments and questions afterward at their convenience, which allows experts and moderators to continue the conversation, often for several days. Second, to promote inclusivity, we have created a unique, customized publication to summarize and present the key points of conversation for each session. This asynchronous access is a quality not found in more traditional journal club formats. Finally, studies have shown that articles shared on social media tend to have increased citations and higher Altmetric scores.
What are the opportunities for trainees and recent graduates?
Sunil Amin, MD, MPH (@SunilAminMD)
Our surveys have shown that 30%-45% of the @GiJournal discussion participants are trainees. Both gastroenterology fellows and internal medicine residents from around the world are an integral part of each specialty panel for the weekly @GIjournal discussions. Trainees are paired up with a specific faculty mentor and together they choose an article for discussion, create a summary, informal twitter poll, and questions for the discussion. This direct access provides an opportunity for trainees to interact, ask questions, and learn from faculty in an informal atmosphere.
We have heard from multiple trainees who have developed long-term relationships with the experts and faculty mentors they worked with and are now also working on research projects. Additionally, trainees can bring the expertise they have now acquired back to their home institutions to pick articles, add specific teaching points, and enrich their local journal club discussions. Finally, trainees who present on the @GiJournal platform are given unique visibility to the many faculty members and opinion leaders participating in each discussion. This may facilitate future networking opportunities and enhance their CVs for future fellowship or employment applications.
Plans for the future?
Allon Kahn, MD (@AllonKahn)
Despite significant evolution and growth in @GiJournal over the past year, we are still actively working to expand our platform. Modes of online medical education, specifically Twitter-based GI journal club discussions, remain in their infancy. We see this @GiJournal as an opportunity for innovation as we plan for the year ahead. Our top priority for the upcoming year includes obtaining CME approval, which we are currently developing with Integrity CE (an Accreditation Council for Continuing Medical Education–accredited provider of CME for health care professionals). This will give an opportunity for the participants to be awarded CME credit when they participate in our weekly discussions. Other options being explored include starting a podcast and translation of @GiJournal Digest in different languages to reach a wider international audience. Furthermore, with the continued expansion of GI leaders and experts joining and engaging in Twitter, our options for unique and multidisciplinary discussion topics will continue to grow.
How can you join the @GiJournal discussions?
@SultanMahmoodMD
Joining the journal club discussion is easy. Just follow the @GiJournal handle on Twitter and turn on the notifications icon. Although we encourage everyone to “actively” participate in the discussion by asking questions or sharing your personal experience, joining the discussion as an “observer” is also a great way to learn. The discussion starts at 8 p.m. EST every Wednesday. Follow the #GIJC and the @GiJournal handle as questions are posted by the faculty moderator and answered by the experts. Even if you miss the discussion, the @GiJournal Digest is a great way to recap the discussions in an easy-to-read PDF format. The @GiJournal Digest is a monthly publication that archives the four @GiJournal club discussions in the previous month. Follow the link below to access the recent publications: http://ow.ly/uu2550C3RXX
Conclusion
In summary, we believe Twitter-based journal clubs offer an engaging way of virtual learning from the comfort of one’s home and a convenient way to directly interact with the experts. The success of @GiJournal highlights the importance of social media for medical education in the field of gastroenterology and hepatology and we look forward to developing this endeavor further.
Dr. Mahmood is clinical assistant professor of medicine, co–program director of the GI fellowship program, UB division of gastroenterology, hepatology & nutrition, State University of New York at Buffalo; Dr. Rabiee is assistant professor of medicine, director of hepatology, division of gastroenterology and hepatology, Washington DC VA Medical Center, Washington; Dr. Amin is assistant professor of medicine, director of endoscopy, The Lennar Foundation Medical Center, division of digestive health and liver disease, department of medicine, University of Miami; Dr. Kahn is assistant professor of medicine, division of gastroenterology & hepatology, Mayo Clinic, Scottsdale, Ariz.; and Dr. Akbar Ali is a gastroenterology fellow in the division of digestive diseases and nutrition, University of Oklahoma Health Sciences Center, Oklahoma City.
The last decade has seen an increased focus on the use of social media for medical education. Twitter, with over 330 million active users, is the most popular social media platform for medical education. We describe here our recent initiative to establish a weekly online gastroenterology-focused journal club on Twitter.
How was the idea conceived?
Sultan Mahmood, MD (@SultanMahmoodMD)
I joined #GITwitter at the end of 2019 and started following some of the leading experts in the field of gastroenterology and hepatology. It was a pleasant surprise to see how easy it was to engage with them and get expert opinions from across the world in real time. #MondayNightIBD, led by Aline Charabaty, MD, had become a phenomenon in the GI community and changed the perception of medical education in the digital world. There were online journal clubs for different medical subspecialties, including #NephroJC, #HOJournalClub, and #DermJC, but none for gastroenterology. Realizing this opportunity, and with guidance from Dr. Charabaty, we started @GiJournal in December of 2019 with weekly discussions.
@GiJournal started off as an informal discussion in which we would post a summary of the article and invite an expert in the field to comment. However, the interest in the journal club quickly took off as we gained more followers and a worldwide audience joined our journal club discussions on a weekly basis. As the COVID-19 pandemic took hold and endoscopy suites around the word closed, interest in online medical education grew. @GIJournal provided a platform for trainees and practicing physicians alike to stay up to date with the latest publications from the comfort of their homes. Needless to say, the journal club has evolved since its inception in that we now work with a team of experts and trainees who run the journal club on a rotating basis.
How does @GiJournal work?
Ijlal Akbar Ali, MD (@IjlalAkbar)
We have a large editorial board with volunteer faculty and trainees, all divided into four special interest groups (general GI/inflammatory bowel disease, interventional endoscopy/bariatric endoscopy, hepatology, and esophageal/motility disorders). Each week, a faculty member and a trainee pick a recently published article from a high-impact GI-focused journal. We also try to invite an expert of international repute (often the authors of the article themselves!) to engage as well. The faculty moderator and invited expert then work with the trainee to plan the session content. We post the topic and article on Monday. At 8 p.m. EST on Wednesday, the trainee posts a series of six to eight tweets summarizing the article. The faculty then asks the invited expert (and audience at large) a series of predetermined questions. Anyone can respond, share their opinion, and direct their own questions toward the moderator and expert who continually check their notifications and respond in real time. This brews into an hour-long discussion which covers not only the methodologic aspects of the article, but clinical practice in general. Discussions often trickle into the next day as people from different time zones participate. Everyone uses #GIJC at the end of their tweets which assists those following the article and facilitates indexing for future review. For those who miss or want to review sessions, we conveniently summarize all articles and corresponding discussions in a monthly publication, @GiJournal Digest, that is posted on Twitter for anyone to download, read and enjoy (Figure 1).
How is this different from any other journal club?
Atoosa Rabiee, MD (@AtoosaRabiee)
@GiJournal is unique in that it provides trainees and practicing gastroenterologists access to interactive discussions with both authors and world-renowned experts in the field. Online journal clubs operate with a flattened hierarchy; as such, they inherently break down access barriers to both the researchers who performed the study and key opinion leaders who commonly participate. There is no boundary as far as institutions or even countries. As a result, our platform has uncovered an unexpected degree of interest in live online discussion, and we have enjoyed collaborating and learning from experts from all over the world. @GiJournal also differs from conventional journal clubs by allowing trainees the opportunity to collaborate and engage with mentors from other institutions. As such, trainees develop relationships with experts in the field outside their home institutions, experts with whom they may not have had contact otherwise.
Although worldwide participation is a key strength of the online @GiJournal platform, it may be challenging for some members to attend the live discussion based on time difference. We account for this in two ways. First, participants are encouraged to continue with comments and questions afterward at their convenience, which allows experts and moderators to continue the conversation, often for several days. Second, to promote inclusivity, we have created a unique, customized publication to summarize and present the key points of conversation for each session. This asynchronous access is a quality not found in more traditional journal club formats. Finally, studies have shown that articles shared on social media tend to have increased citations and higher Altmetric scores.
What are the opportunities for trainees and recent graduates?
Sunil Amin, MD, MPH (@SunilAminMD)
Our surveys have shown that 30%-45% of the @GiJournal discussion participants are trainees. Both gastroenterology fellows and internal medicine residents from around the world are an integral part of each specialty panel for the weekly @GIjournal discussions. Trainees are paired up with a specific faculty mentor and together they choose an article for discussion, create a summary, informal twitter poll, and questions for the discussion. This direct access provides an opportunity for trainees to interact, ask questions, and learn from faculty in an informal atmosphere.
We have heard from multiple trainees who have developed long-term relationships with the experts and faculty mentors they worked with and are now also working on research projects. Additionally, trainees can bring the expertise they have now acquired back to their home institutions to pick articles, add specific teaching points, and enrich their local journal club discussions. Finally, trainees who present on the @GiJournal platform are given unique visibility to the many faculty members and opinion leaders participating in each discussion. This may facilitate future networking opportunities and enhance their CVs for future fellowship or employment applications.
Plans for the future?
Allon Kahn, MD (@AllonKahn)
Despite significant evolution and growth in @GiJournal over the past year, we are still actively working to expand our platform. Modes of online medical education, specifically Twitter-based GI journal club discussions, remain in their infancy. We see this @GiJournal as an opportunity for innovation as we plan for the year ahead. Our top priority for the upcoming year includes obtaining CME approval, which we are currently developing with Integrity CE (an Accreditation Council for Continuing Medical Education–accredited provider of CME for health care professionals). This will give an opportunity for the participants to be awarded CME credit when they participate in our weekly discussions. Other options being explored include starting a podcast and translation of @GiJournal Digest in different languages to reach a wider international audience. Furthermore, with the continued expansion of GI leaders and experts joining and engaging in Twitter, our options for unique and multidisciplinary discussion topics will continue to grow.
How can you join the @GiJournal discussions?
@SultanMahmoodMD
Joining the journal club discussion is easy. Just follow the @GiJournal handle on Twitter and turn on the notifications icon. Although we encourage everyone to “actively” participate in the discussion by asking questions or sharing your personal experience, joining the discussion as an “observer” is also a great way to learn. The discussion starts at 8 p.m. EST every Wednesday. Follow the #GIJC and the @GiJournal handle as questions are posted by the faculty moderator and answered by the experts. Even if you miss the discussion, the @GiJournal Digest is a great way to recap the discussions in an easy-to-read PDF format. The @GiJournal Digest is a monthly publication that archives the four @GiJournal club discussions in the previous month. Follow the link below to access the recent publications: http://ow.ly/uu2550C3RXX
Conclusion
In summary, we believe Twitter-based journal clubs offer an engaging way of virtual learning from the comfort of one’s home and a convenient way to directly interact with the experts. The success of @GiJournal highlights the importance of social media for medical education in the field of gastroenterology and hepatology and we look forward to developing this endeavor further.
Dr. Mahmood is clinical assistant professor of medicine, co–program director of the GI fellowship program, UB division of gastroenterology, hepatology & nutrition, State University of New York at Buffalo; Dr. Rabiee is assistant professor of medicine, director of hepatology, division of gastroenterology and hepatology, Washington DC VA Medical Center, Washington; Dr. Amin is assistant professor of medicine, director of endoscopy, The Lennar Foundation Medical Center, division of digestive health and liver disease, department of medicine, University of Miami; Dr. Kahn is assistant professor of medicine, division of gastroenterology & hepatology, Mayo Clinic, Scottsdale, Ariz.; and Dr. Akbar Ali is a gastroenterology fellow in the division of digestive diseases and nutrition, University of Oklahoma Health Sciences Center, Oklahoma City.
Mitotic rate makes comeback as melanoma prognosticator
at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medical Education.

Dr. Kashani-Sabet, a dermatologist, director of the melanoma research program, and senior scientist at the California Pacific Medical Center Research Institute, San Francisco, was first author of a large recently published study that made a strong case for reincorporation of mitotic index into the American Joint Cancer Committee (AJCC) melanoma staging system.
Mitotic index was included in the 7th edition of the AJCC classification system, but was dropped from the current 8th edition in part because of concern it could potentially lead to overtreatment of patients with very thin melanomas of less than 0.5-mm thickness.
However, mitotic rate, like tumor thickness, is a continuous variable. And like tumor thickness, mitotic rate has a nonlinear relationship with survival. That’s why the AJCC staging system utilizes unequally spaced tumor thickness cut points of 1, 2, and 4 mm to define T1-T4 disease. But until the study led by Dr. Kashani-Sabet, optimal cut points for mitotic rate hadn’t been defined.
He and his coinvestigators at Melanoma Institute Australia collected a dataset comprising 5,050 patients with primary cutaneous melanoma in Australia and Northern California, all of whom either died of metastatic melanoma or remained distant metastasis–free for at least 8 years of follow-up. Median follow-up of the cohort was 9.5 years.
The investigators developed computer-generated cut points for mitotic rate and its impact on survival for each melanoma T category, then assessed their value in randomly split training and validation sets from their large cohort. For T1 melanoma, the optimal cut point proved to be 2 mitoses/mm2; more than two was independently associated with increased mortality risk. For T2 disease, the optimal cut point was 4, for T3 it was 6, and for T4 it was 7 mitoses/mm2.
A key study finding: In a multivariate regression analysis, tumor thickness was associated with survival, with an odds ratio of 1.58, ulceration had an odds ratio of 1.55, and mitotic rate by cut point had an odds ratio of 5.38. Each of these three characteristics was independently associated with survival (P < .00005). Dr. Kashani-Sabet said that, despite the more than threefold greater odds ratio for mitotic rate, compared with ulceration, in a Kaplan-Meier analysis, the survival impact of ulceration being present was “virtually identical” to an elevated mitotic rate in each T category.
He and his coinvestigators proposed a revised T-category system which incorporates this new insight. There is no change in tumor thickness to define T1-T4 melanoma: T1 is less than 1.0 mm, T2 is greater than 1-2.0 mm, T3 is greater than 2.01-4.0 mm, and T4 is greater than 4.0 mm. But now, within each T category the proposal is that the “a” designation indicates neither ulceration nor an elevated mitotic rate is present, while “b” means ulceration and/or an elevated mitotic rate using the optimal cut point for that T category is present. In their Australian/Northern California dataset, these new T categories showed a distinct separation in cumulative survival.
Dr. Kashani-Sabet and coworkers have submitted a proposal to validate their results using the AJCC database. Based upon a first look at the numbers, “We think it’s really very likely that these observations can be reproduced in this most important of datasets,” he predicted.

During a panel discussion, Sancy Leachman, MD, PhD, offered a recent example from her own practice where an elevated mitotic index as defined by Dr. Kashani-Sabet and coworkers served as a red flag.
“I had a patient with a 0.3-mm melanoma with three mitoses. I did a sentinel lymph node biopsy on the patient, and she was positive,” said Dr. Leachman, professor and chair of the department of dermatology at Oregon Health & Science University, Portland.
Dr. Kashani-Sabet commented that, while an elevated mitotic index is clearly not an absolute requirement for metastasis, when present it’s a prognostically important finding.
Moreover, as adjuvant therapies of proven value in node-positive disease increasingly come under study in node-negative melanoma, it will be critical to identify the high-risk node-negative subgroup for whom such therapies should be targeted.
“While T4 tumors and ulcerated melanomas are clearly high risk, they’re not going to capture every patient who has a very high risk of distant metastases and death. I think mitotic rate is another pathway to identify patients who very well might benefit and should be candidates for inclusion in those adjuvant therapy trials as we’re moving more into node-negative patients,” according to Dr. Kashani-Sabet.
He reported having no financial conflicts of interest regarding his presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medical Education.
Dr. Kashani-Sabet, a dermatologist, director of the melanoma research program, and senior scientist at the California Pacific Medical Center Research Institute, San Francisco, was first author of a large recently published study that made a strong case for reincorporation of mitotic index into the American Joint Cancer Committee (AJCC) melanoma staging system.
Mitotic index was included in the 7th edition of the AJCC classification system, but was dropped from the current 8th edition in part because of concern it could potentially lead to overtreatment of patients with very thin melanomas of less than 0.5-mm thickness.
However, mitotic rate, like tumor thickness, is a continuous variable. And like tumor thickness, mitotic rate has a nonlinear relationship with survival. That’s why the AJCC staging system utilizes unequally spaced tumor thickness cut points of 1, 2, and 4 mm to define T1-T4 disease. But until the study led by Dr. Kashani-Sabet, optimal cut points for mitotic rate hadn’t been defined.
He and his coinvestigators at Melanoma Institute Australia collected a dataset comprising 5,050 patients with primary cutaneous melanoma in Australia and Northern California, all of whom either died of metastatic melanoma or remained distant metastasis–free for at least 8 years of follow-up. Median follow-up of the cohort was 9.5 years.
The investigators developed computer-generated cut points for mitotic rate and its impact on survival for each melanoma T category, then assessed their value in randomly split training and validation sets from their large cohort. For T1 melanoma, the optimal cut point proved to be 2 mitoses/mm2; more than two was independently associated with increased mortality risk. For T2 disease, the optimal cut point was 4, for T3 it was 6, and for T4 it was 7 mitoses/mm2.
A key study finding: In a multivariate regression analysis, tumor thickness was associated with survival, with an odds ratio of 1.58, ulceration had an odds ratio of 1.55, and mitotic rate by cut point had an odds ratio of 5.38. Each of these three characteristics was independently associated with survival (P < .00005). Dr. Kashani-Sabet said that, despite the more than threefold greater odds ratio for mitotic rate, compared with ulceration, in a Kaplan-Meier analysis, the survival impact of ulceration being present was “virtually identical” to an elevated mitotic rate in each T category.
He and his coinvestigators proposed a revised T-category system which incorporates this new insight. There is no change in tumor thickness to define T1-T4 melanoma: T1 is less than 1.0 mm, T2 is greater than 1-2.0 mm, T3 is greater than 2.01-4.0 mm, and T4 is greater than 4.0 mm. But now, within each T category the proposal is that the “a” designation indicates neither ulceration nor an elevated mitotic rate is present, while “b” means ulceration and/or an elevated mitotic rate using the optimal cut point for that T category is present. In their Australian/Northern California dataset, these new T categories showed a distinct separation in cumulative survival.
Dr. Kashani-Sabet and coworkers have submitted a proposal to validate their results using the AJCC database. Based upon a first look at the numbers, “We think it’s really very likely that these observations can be reproduced in this most important of datasets,” he predicted.
During a panel discussion, Sancy Leachman, MD, PhD, offered a recent example from her own practice where an elevated mitotic index as defined by Dr. Kashani-Sabet and coworkers served as a red flag.
“I had a patient with a 0.3-mm melanoma with three mitoses. I did a sentinel lymph node biopsy on the patient, and she was positive,” said Dr. Leachman, professor and chair of the department of dermatology at Oregon Health & Science University, Portland.
Dr. Kashani-Sabet commented that, while an elevated mitotic index is clearly not an absolute requirement for metastasis, when present it’s a prognostically important finding.
Moreover, as adjuvant therapies of proven value in node-positive disease increasingly come under study in node-negative melanoma, it will be critical to identify the high-risk node-negative subgroup for whom such therapies should be targeted.
“While T4 tumors and ulcerated melanomas are clearly high risk, they’re not going to capture every patient who has a very high risk of distant metastases and death. I think mitotic rate is another pathway to identify patients who very well might benefit and should be candidates for inclusion in those adjuvant therapy trials as we’re moving more into node-negative patients,” according to Dr. Kashani-Sabet.
He reported having no financial conflicts of interest regarding his presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medical Education.
Dr. Kashani-Sabet, a dermatologist, director of the melanoma research program, and senior scientist at the California Pacific Medical Center Research Institute, San Francisco, was first author of a large recently published study that made a strong case for reincorporation of mitotic index into the American Joint Cancer Committee (AJCC) melanoma staging system.
Mitotic index was included in the 7th edition of the AJCC classification system, but was dropped from the current 8th edition in part because of concern it could potentially lead to overtreatment of patients with very thin melanomas of less than 0.5-mm thickness.
However, mitotic rate, like tumor thickness, is a continuous variable. And like tumor thickness, mitotic rate has a nonlinear relationship with survival. That’s why the AJCC staging system utilizes unequally spaced tumor thickness cut points of 1, 2, and 4 mm to define T1-T4 disease. But until the study led by Dr. Kashani-Sabet, optimal cut points for mitotic rate hadn’t been defined.
He and his coinvestigators at Melanoma Institute Australia collected a dataset comprising 5,050 patients with primary cutaneous melanoma in Australia and Northern California, all of whom either died of metastatic melanoma or remained distant metastasis–free for at least 8 years of follow-up. Median follow-up of the cohort was 9.5 years.
The investigators developed computer-generated cut points for mitotic rate and its impact on survival for each melanoma T category, then assessed their value in randomly split training and validation sets from their large cohort. For T1 melanoma, the optimal cut point proved to be 2 mitoses/mm2; more than two was independently associated with increased mortality risk. For T2 disease, the optimal cut point was 4, for T3 it was 6, and for T4 it was 7 mitoses/mm2.
A key study finding: In a multivariate regression analysis, tumor thickness was associated with survival, with an odds ratio of 1.58, ulceration had an odds ratio of 1.55, and mitotic rate by cut point had an odds ratio of 5.38. Each of these three characteristics was independently associated with survival (P < .00005). Dr. Kashani-Sabet said that, despite the more than threefold greater odds ratio for mitotic rate, compared with ulceration, in a Kaplan-Meier analysis, the survival impact of ulceration being present was “virtually identical” to an elevated mitotic rate in each T category.
He and his coinvestigators proposed a revised T-category system which incorporates this new insight. There is no change in tumor thickness to define T1-T4 melanoma: T1 is less than 1.0 mm, T2 is greater than 1-2.0 mm, T3 is greater than 2.01-4.0 mm, and T4 is greater than 4.0 mm. But now, within each T category the proposal is that the “a” designation indicates neither ulceration nor an elevated mitotic rate is present, while “b” means ulceration and/or an elevated mitotic rate using the optimal cut point for that T category is present. In their Australian/Northern California dataset, these new T categories showed a distinct separation in cumulative survival.
Dr. Kashani-Sabet and coworkers have submitted a proposal to validate their results using the AJCC database. Based upon a first look at the numbers, “We think it’s really very likely that these observations can be reproduced in this most important of datasets,” he predicted.
During a panel discussion, Sancy Leachman, MD, PhD, offered a recent example from her own practice where an elevated mitotic index as defined by Dr. Kashani-Sabet and coworkers served as a red flag.
“I had a patient with a 0.3-mm melanoma with three mitoses. I did a sentinel lymph node biopsy on the patient, and she was positive,” said Dr. Leachman, professor and chair of the department of dermatology at Oregon Health & Science University, Portland.
Dr. Kashani-Sabet commented that, while an elevated mitotic index is clearly not an absolute requirement for metastasis, when present it’s a prognostically important finding.
Moreover, as adjuvant therapies of proven value in node-positive disease increasingly come under study in node-negative melanoma, it will be critical to identify the high-risk node-negative subgroup for whom such therapies should be targeted.
“While T4 tumors and ulcerated melanomas are clearly high risk, they’re not going to capture every patient who has a very high risk of distant metastases and death. I think mitotic rate is another pathway to identify patients who very well might benefit and should be candidates for inclusion in those adjuvant therapy trials as we’re moving more into node-negative patients,” according to Dr. Kashani-Sabet.
He reported having no financial conflicts of interest regarding his presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
FROM THE CUTANEOUS MALIGNANCIES FORUM
Harnessing the HIV care continuum model to improve HCV treatment success
Better linkage to care with providers who are familiar with both the HCV and HIV treatment cascade may not only improve access to HCV treatment, but it may also support patient retention, treatment adherence, and achievement of sustained virologic response (SVR) and viral suppression, said Stephanie LaMoy, CAN Community Health, North Point, Florida. She presented the results of a pilot study at the virtual Association of Nurses in AIDS Care 2020 Annual Meeting.
In an effort to identify strategies most important for improving care access among their patients with HCV, LaMoy and her colleagues assessed 12-month patient data collected from three of their clinics. These data were evaluated for HCV treatment access, engagement, and outcomes.
The pilot study included 126 patients who were reactive and another 24 HCV-positive patients who were referred from other sources. Active HCV infections requiring treatment were reported in 144 patients.
A total of 59 patients were linked to care but did not initiate treatment for their active infection. LaMoy said there were multiple causes, including homelessness, substance abuse, and inability to maintain contact.
In contrast, 85 patients with HCV infection started treatment, but 35 of these patients did not complete their regimen. Out of the 50 patients who reported completing treatment, 30 did not return to the clinic to confirm sustained viral suppression.
According to LaMoy, this raised a red flag, causing the investigators to consider a different approach to care.
HIV care continuum model and its role in HCV
To improve the rate at which patients with HCV infection complete treatment within their clinics, the researchers formed a panel to determine necessary interventions that could reduce barriers to care.
The HIV care continuum came into play. They chose this model based on knowledge that HCV and HIV share the same care continuum with similar goals in diagnosis, linkage to care, retention, and suppression.
Based on the consensus of the panel and consideration of the HIV care continuum model, they identified a number of interventions needed to mitigate HCV treatment barriers. These included the incorporation of peer navigators or linkage-to-care (LCC) coordinators, use of the mobile medical unit, greater implementation of onsite lab visits, and medication-assisted treatment.
The LCC coordinators proved to be particularly important, as these team members helped assist patients with social and financial support to address challenges with access to treatment. These coordinators can also help patients gain access to specialized providers, ultimately improving the chance of successful HCV management.
Additionally, LCC coordinators may help identify and reduce barriers associated with housing, transportation, and nutrition. Frequent patient contact by the LCC coordinators can encourage adherence and promote risk reduction education, such as providing referrals to needle exchange services.
“Linking individuals to care with providers who are familiar with the treatment cascade could help improve retention and should be a top priority for those involved in HCV screening and treatment,” said LaMoy. “An environment with knowledge, lack of judgment, and a tenacious need to heal the community that welcomes those with barriers to care is exactly what is needed for the patients in our program.”
National, community challenges fuel barriers to HCV treatment access
Substance use, trauma histories, and mental health problems can negatively affect care engagement and must be addressed before the benefits of HCV therapy can be realized.
Addressing these issues isn’t always easy, said Kathleen Bernock, FNP-BC, AACRN, AAHIVS, of the Bedford-Stuyvesant Family Health Center in New York City, in an email to Medscape Medical News. She pointed out that several states have harsh restrictions on who is able to access HCV treatment, and some states will not approve certain medications for people who actively use drugs.
“Even for states without these restrictions, many health systems are difficult to navigate and may not be welcoming to persons actively using,” said Bernock. Trauma-informed care can also be difficult to translate into clinics, she added.
“Decentralizing care to the communities most affected would greatly help mitigate these barriers,” suggested Bernock. Decentralization, she explained, might include co-locating services such as syringe exchanges, utilizing community health workers and patient navigators, and expanding capacity-to-treat to community-based providers.
“[And] with the expansion of telehealth services in the US,” said Bernock, “we now have even more avenues to reach people that we never had before.”
LaMoy and Bernock have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Better linkage to care with providers who are familiar with both the HCV and HIV treatment cascade may not only improve access to HCV treatment, but it may also support patient retention, treatment adherence, and achievement of sustained virologic response (SVR) and viral suppression, said Stephanie LaMoy, CAN Community Health, North Point, Florida. She presented the results of a pilot study at the virtual Association of Nurses in AIDS Care 2020 Annual Meeting.
In an effort to identify strategies most important for improving care access among their patients with HCV, LaMoy and her colleagues assessed 12-month patient data collected from three of their clinics. These data were evaluated for HCV treatment access, engagement, and outcomes.
The pilot study included 126 patients who were reactive and another 24 HCV-positive patients who were referred from other sources. Active HCV infections requiring treatment were reported in 144 patients.
A total of 59 patients were linked to care but did not initiate treatment for their active infection. LaMoy said there were multiple causes, including homelessness, substance abuse, and inability to maintain contact.
In contrast, 85 patients with HCV infection started treatment, but 35 of these patients did not complete their regimen. Out of the 50 patients who reported completing treatment, 30 did not return to the clinic to confirm sustained viral suppression.
According to LaMoy, this raised a red flag, causing the investigators to consider a different approach to care.
HIV care continuum model and its role in HCV
To improve the rate at which patients with HCV infection complete treatment within their clinics, the researchers formed a panel to determine necessary interventions that could reduce barriers to care.
The HIV care continuum came into play. They chose this model based on knowledge that HCV and HIV share the same care continuum with similar goals in diagnosis, linkage to care, retention, and suppression.
Based on the consensus of the panel and consideration of the HIV care continuum model, they identified a number of interventions needed to mitigate HCV treatment barriers. These included the incorporation of peer navigators or linkage-to-care (LCC) coordinators, use of the mobile medical unit, greater implementation of onsite lab visits, and medication-assisted treatment.
The LCC coordinators proved to be particularly important, as these team members helped assist patients with social and financial support to address challenges with access to treatment. These coordinators can also help patients gain access to specialized providers, ultimately improving the chance of successful HCV management.
Additionally, LCC coordinators may help identify and reduce barriers associated with housing, transportation, and nutrition. Frequent patient contact by the LCC coordinators can encourage adherence and promote risk reduction education, such as providing referrals to needle exchange services.
“Linking individuals to care with providers who are familiar with the treatment cascade could help improve retention and should be a top priority for those involved in HCV screening and treatment,” said LaMoy. “An environment with knowledge, lack of judgment, and a tenacious need to heal the community that welcomes those with barriers to care is exactly what is needed for the patients in our program.”
National, community challenges fuel barriers to HCV treatment access
Substance use, trauma histories, and mental health problems can negatively affect care engagement and must be addressed before the benefits of HCV therapy can be realized.
Addressing these issues isn’t always easy, said Kathleen Bernock, FNP-BC, AACRN, AAHIVS, of the Bedford-Stuyvesant Family Health Center in New York City, in an email to Medscape Medical News. She pointed out that several states have harsh restrictions on who is able to access HCV treatment, and some states will not approve certain medications for people who actively use drugs.
“Even for states without these restrictions, many health systems are difficult to navigate and may not be welcoming to persons actively using,” said Bernock. Trauma-informed care can also be difficult to translate into clinics, she added.
“Decentralizing care to the communities most affected would greatly help mitigate these barriers,” suggested Bernock. Decentralization, she explained, might include co-locating services such as syringe exchanges, utilizing community health workers and patient navigators, and expanding capacity-to-treat to community-based providers.
“[And] with the expansion of telehealth services in the US,” said Bernock, “we now have even more avenues to reach people that we never had before.”
LaMoy and Bernock have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Better linkage to care with providers who are familiar with both the HCV and HIV treatment cascade may not only improve access to HCV treatment, but it may also support patient retention, treatment adherence, and achievement of sustained virologic response (SVR) and viral suppression, said Stephanie LaMoy, CAN Community Health, North Point, Florida. She presented the results of a pilot study at the virtual Association of Nurses in AIDS Care 2020 Annual Meeting.
In an effort to identify strategies most important for improving care access among their patients with HCV, LaMoy and her colleagues assessed 12-month patient data collected from three of their clinics. These data were evaluated for HCV treatment access, engagement, and outcomes.
The pilot study included 126 patients who were reactive and another 24 HCV-positive patients who were referred from other sources. Active HCV infections requiring treatment were reported in 144 patients.
A total of 59 patients were linked to care but did not initiate treatment for their active infection. LaMoy said there were multiple causes, including homelessness, substance abuse, and inability to maintain contact.
In contrast, 85 patients with HCV infection started treatment, but 35 of these patients did not complete their regimen. Out of the 50 patients who reported completing treatment, 30 did not return to the clinic to confirm sustained viral suppression.
According to LaMoy, this raised a red flag, causing the investigators to consider a different approach to care.
HIV care continuum model and its role in HCV
To improve the rate at which patients with HCV infection complete treatment within their clinics, the researchers formed a panel to determine necessary interventions that could reduce barriers to care.
The HIV care continuum came into play. They chose this model based on knowledge that HCV and HIV share the same care continuum with similar goals in diagnosis, linkage to care, retention, and suppression.
Based on the consensus of the panel and consideration of the HIV care continuum model, they identified a number of interventions needed to mitigate HCV treatment barriers. These included the incorporation of peer navigators or linkage-to-care (LCC) coordinators, use of the mobile medical unit, greater implementation of onsite lab visits, and medication-assisted treatment.
The LCC coordinators proved to be particularly important, as these team members helped assist patients with social and financial support to address challenges with access to treatment. These coordinators can also help patients gain access to specialized providers, ultimately improving the chance of successful HCV management.
Additionally, LCC coordinators may help identify and reduce barriers associated with housing, transportation, and nutrition. Frequent patient contact by the LCC coordinators can encourage adherence and promote risk reduction education, such as providing referrals to needle exchange services.
“Linking individuals to care with providers who are familiar with the treatment cascade could help improve retention and should be a top priority for those involved in HCV screening and treatment,” said LaMoy. “An environment with knowledge, lack of judgment, and a tenacious need to heal the community that welcomes those with barriers to care is exactly what is needed for the patients in our program.”
National, community challenges fuel barriers to HCV treatment access
Substance use, trauma histories, and mental health problems can negatively affect care engagement and must be addressed before the benefits of HCV therapy can be realized.
Addressing these issues isn’t always easy, said Kathleen Bernock, FNP-BC, AACRN, AAHIVS, of the Bedford-Stuyvesant Family Health Center in New York City, in an email to Medscape Medical News. She pointed out that several states have harsh restrictions on who is able to access HCV treatment, and some states will not approve certain medications for people who actively use drugs.
“Even for states without these restrictions, many health systems are difficult to navigate and may not be welcoming to persons actively using,” said Bernock. Trauma-informed care can also be difficult to translate into clinics, she added.
“Decentralizing care to the communities most affected would greatly help mitigate these barriers,” suggested Bernock. Decentralization, she explained, might include co-locating services such as syringe exchanges, utilizing community health workers and patient navigators, and expanding capacity-to-treat to community-based providers.
“[And] with the expansion of telehealth services in the US,” said Bernock, “we now have even more avenues to reach people that we never had before.”
LaMoy and Bernock have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Abnormal anal paps in people with HIV can go more than a year without follow-up
That delay “revealed missed opportunities for a better experience on the patient, clinic, and provider level,” Jessica Wells, PhD, research assistant professor at the Nell Hodgson Woodruff School of Nursing at Emory University, Atlanta, said in an interview. After all, “a lot can happen in that 1 year,” including early development of human papillomavirus (HPV)–associated anal cancer.
Although it’s too soon to say how significant that delay is with respect to the natural history of anal cancer, Dr. Wells said the data are a potential signal of disparities.
“The findings from my study may foreshadow potential disparities if we don’t have the necessary resources in place to promote follow-up care after an abnormal Pap test, similar to the disparities that we see in cervical cancer,” she said during the virtual Association of Nurses in AIDS Care 2020 Annual Meeting.
Single-center study
In the United States, people living with HIV are 19 times more likely to develop anal cancer than the general population, according to a 2018 article in the Journal of Clinical Oncology. Another single-center study from Yale University found that, in minority communities, anal cancer rates were 75% higher than in White communities. Anal cancer rates were 72% higher in communities with greater poverty. As a result, many clinics are beginning to administer Pap tests to determine early signs of HPV infection and associated changes.
In Dr. Wells’ study, which was conducted from 2012 to 2015, 150 adults with HIV who were aged 21 and older were recruited from Grady Ponce De Leon Center in Atlanta. According to a 2018 study from that center, a large minority of participants had late-stage HIV and suppressed immune systems.
All participants had been referred for HRA after a recent abnormal anal Pap test. Participants filled out questionnaires on sociodemographics, internalized HIV-related stigma, depression, risk behaviors, social support, and knowledge about HPV and anal cancer.
Participants were disproportionately older (mean age, 50.9 years); cisgender (86.7%), Black (78%); and gay, lesbian, or bisexual (84.3%). Slightly more than 1 in 10 participants (11.3%) were transgender women.
Although for 6% of participants, Pap test results indicated high-grade squamous intraepithelial lesions (HSIL), an additional 8% had atypical Pap findings that couldn’t exclude HSIL – the kinds of results that are one step away from a cancer diagnosis. More than 80% of participants had low-grade or inconclusive results. Nearly half (44%) of participants’ Pap tests revealed low-grade squamous cell intraepithelial cell lesions (LSIL); 42% indicated atypical squamous cells of undetermined significance.
When Dr. Wells looked at how long participants had waited to undergo HRA, she found something that surprised her: although some participants underwent follow-up assessment in 17 days, for many, it took much longer. The longest wait was 2,350 days – more than 6 years.
“There were quite a few patients who had follow-up beyond 1,000-plus days,” Dr. Wells said in an interview. “I didn›t think the delays were that long — at most, I would say that patients will get scheduled and come back within a few weeks or months.”
What’s more, she discovered through the HPV knowledge questionnaire that many participants did not understand why they were having a follow-up appointment. Anecdotally, some confused HPV with HIV.
“There’s education to be done to inform this target population that those living with HIV are more prone or at increased risk of this virus causing cancer later,” she said. “There are a lot of campaigns around women living with HIV, that they need to do cervical cancer screening. I think we need to really expand this campaign to include that HPV can also cause anal cancer.”
Dr. Wells had planned to primarily investigate the impact of psychosocial factors on wait time to follow-up, but none of those factors were associated with longer wait times.
Systems-level factors
That led Ann Gakumo, PhD, chair of nursing at the College of Nursing and Health Sciences of the University of Massachusetts, Boston, to ask what other factors could account for the delay.
There were several, Dr. Wells said. Precarious housing, for example, could have influenced this lag in follow-up. About one in four participants were in transient housing, and one participant reported having been incarcerated. She gathered street addresses and plans to analyze that data to see whether the cases occurred in clusters in specific neighborhoods, as the Yale data indicated.
In addition, the anoscopy clinic was only available to receive patients one day a week and was staffed with only one clinician who was trained to perform HRA. Wait times could stretch for hours. Sometimes, participants had to leave the clinic to attend to other business, and their appointments needed to be rescheduled, Wells said.
In addition to the sometimes poor understanding of the importance of the follow-up test, Dr. Wells said, “we start to see a layering of these barriers. That’s where we start seeing breakdowns. So I’m hoping in a larger study I can address some of these barriers on a multilevel approach.”
This resonated with Dr. Gakumo.
“Oftentimes, we put so much of the responsibility for this on the part of the client and not enough on the part of the provider or on the systems level,” she said.
Guiding guidelines
Guidelines on follow-up for abnormal anal Pap test results are scarce, mostly because, unlike cervical cancer, the natural history of HPV-related anal cancers hasn’t been established. The HIV Medical Association does recommend anal Pap tests, but only in cases in which “access to appropriate referral for follow-up, including high-resolution anoscopy, is available.”
In an interview, Cecile Lahiri, MD, assistant professor of infectious disease at Emory University, said that, at Ponce De Leon Center, they recommend an anal Pap for women with HIV who have a history of cervical dysplasia.
There is a reliable association between high-grade abnormal Pap tests and cervical cancer, although low-grade changes can resolve on their own. In the case of anal cancer, especially in patients with HIV, low-grade cell changes are predictive; moreover, for such patients, anal cancer is more likely to recur and is harder to treat, Dr. Lahiri said.
“The cervical environment and the anal environment are very different,” said Dr. Lahiri, who works at the Grady Ponce De Leon Center but was not involved in Dr. Wells’ study. Dr. Lahiri is also a coinvestigator of the multisite, randomized, controlled Anal Cancer HSIL Outcomes Research (ANCHOR) study, which seeks to establish whether early treatment of high-grade anal Pap changes is better than a watch-and-wait approach.
Dr. Lahiri said that when the results of that trial become available, they are more likely to know how important early anoscopy and treatment are. The findings should inform guidelines and insurance coverage of anal Pap tests and anoscopy.
In the meantime, she said, she suspected that, with the ANCHOR trial in 2015, many sites’ capacity for anoscopy may have increased, and the wait times may have gone down.
“One of the most important pieces of the study is actually the time period in which it was conducted,” said Dr. Lahiri, who in 2015 became the clinic’s second physician trained in anoscopy. Currently, more than 200 people at the Ponce De Leon Center are enrolled in the ANCHOR trial. In addition, the general capacity for performing anoscopies has gone up nationwide as a result of the trial, which required that more providers learn how to properly perform an HRA. Many clinicians are not routinely trained in performing HRA, including gastroenterologists and surgeons, Dr. Lahiri said.
“It would be interesting to look at the differences, with the start of ANCHOR being the time point for before and after,” she said.
This article first appeared on Medscape.com.
That delay “revealed missed opportunities for a better experience on the patient, clinic, and provider level,” Jessica Wells, PhD, research assistant professor at the Nell Hodgson Woodruff School of Nursing at Emory University, Atlanta, said in an interview. After all, “a lot can happen in that 1 year,” including early development of human papillomavirus (HPV)–associated anal cancer.
Although it’s too soon to say how significant that delay is with respect to the natural history of anal cancer, Dr. Wells said the data are a potential signal of disparities.
“The findings from my study may foreshadow potential disparities if we don’t have the necessary resources in place to promote follow-up care after an abnormal Pap test, similar to the disparities that we see in cervical cancer,” she said during the virtual Association of Nurses in AIDS Care 2020 Annual Meeting.
Single-center study
In the United States, people living with HIV are 19 times more likely to develop anal cancer than the general population, according to a 2018 article in the Journal of Clinical Oncology. Another single-center study from Yale University found that, in minority communities, anal cancer rates were 75% higher than in White communities. Anal cancer rates were 72% higher in communities with greater poverty. As a result, many clinics are beginning to administer Pap tests to determine early signs of HPV infection and associated changes.
In Dr. Wells’ study, which was conducted from 2012 to 2015, 150 adults with HIV who were aged 21 and older were recruited from Grady Ponce De Leon Center in Atlanta. According to a 2018 study from that center, a large minority of participants had late-stage HIV and suppressed immune systems.
All participants had been referred for HRA after a recent abnormal anal Pap test. Participants filled out questionnaires on sociodemographics, internalized HIV-related stigma, depression, risk behaviors, social support, and knowledge about HPV and anal cancer.
Participants were disproportionately older (mean age, 50.9 years); cisgender (86.7%), Black (78%); and gay, lesbian, or bisexual (84.3%). Slightly more than 1 in 10 participants (11.3%) were transgender women.
Although for 6% of participants, Pap test results indicated high-grade squamous intraepithelial lesions (HSIL), an additional 8% had atypical Pap findings that couldn’t exclude HSIL – the kinds of results that are one step away from a cancer diagnosis. More than 80% of participants had low-grade or inconclusive results. Nearly half (44%) of participants’ Pap tests revealed low-grade squamous cell intraepithelial cell lesions (LSIL); 42% indicated atypical squamous cells of undetermined significance.
When Dr. Wells looked at how long participants had waited to undergo HRA, she found something that surprised her: although some participants underwent follow-up assessment in 17 days, for many, it took much longer. The longest wait was 2,350 days – more than 6 years.
“There were quite a few patients who had follow-up beyond 1,000-plus days,” Dr. Wells said in an interview. “I didn›t think the delays were that long — at most, I would say that patients will get scheduled and come back within a few weeks or months.”
What’s more, she discovered through the HPV knowledge questionnaire that many participants did not understand why they were having a follow-up appointment. Anecdotally, some confused HPV with HIV.
“There’s education to be done to inform this target population that those living with HIV are more prone or at increased risk of this virus causing cancer later,” she said. “There are a lot of campaigns around women living with HIV, that they need to do cervical cancer screening. I think we need to really expand this campaign to include that HPV can also cause anal cancer.”
Dr. Wells had planned to primarily investigate the impact of psychosocial factors on wait time to follow-up, but none of those factors were associated with longer wait times.
Systems-level factors
That led Ann Gakumo, PhD, chair of nursing at the College of Nursing and Health Sciences of the University of Massachusetts, Boston, to ask what other factors could account for the delay.
There were several, Dr. Wells said. Precarious housing, for example, could have influenced this lag in follow-up. About one in four participants were in transient housing, and one participant reported having been incarcerated. She gathered street addresses and plans to analyze that data to see whether the cases occurred in clusters in specific neighborhoods, as the Yale data indicated.
In addition, the anoscopy clinic was only available to receive patients one day a week and was staffed with only one clinician who was trained to perform HRA. Wait times could stretch for hours. Sometimes, participants had to leave the clinic to attend to other business, and their appointments needed to be rescheduled, Wells said.
In addition to the sometimes poor understanding of the importance of the follow-up test, Dr. Wells said, “we start to see a layering of these barriers. That’s where we start seeing breakdowns. So I’m hoping in a larger study I can address some of these barriers on a multilevel approach.”
This resonated with Dr. Gakumo.
“Oftentimes, we put so much of the responsibility for this on the part of the client and not enough on the part of the provider or on the systems level,” she said.
Guiding guidelines
Guidelines on follow-up for abnormal anal Pap test results are scarce, mostly because, unlike cervical cancer, the natural history of HPV-related anal cancers hasn’t been established. The HIV Medical Association does recommend anal Pap tests, but only in cases in which “access to appropriate referral for follow-up, including high-resolution anoscopy, is available.”
In an interview, Cecile Lahiri, MD, assistant professor of infectious disease at Emory University, said that, at Ponce De Leon Center, they recommend an anal Pap for women with HIV who have a history of cervical dysplasia.
There is a reliable association between high-grade abnormal Pap tests and cervical cancer, although low-grade changes can resolve on their own. In the case of anal cancer, especially in patients with HIV, low-grade cell changes are predictive; moreover, for such patients, anal cancer is more likely to recur and is harder to treat, Dr. Lahiri said.
“The cervical environment and the anal environment are very different,” said Dr. Lahiri, who works at the Grady Ponce De Leon Center but was not involved in Dr. Wells’ study. Dr. Lahiri is also a coinvestigator of the multisite, randomized, controlled Anal Cancer HSIL Outcomes Research (ANCHOR) study, which seeks to establish whether early treatment of high-grade anal Pap changes is better than a watch-and-wait approach.
Dr. Lahiri said that when the results of that trial become available, they are more likely to know how important early anoscopy and treatment are. The findings should inform guidelines and insurance coverage of anal Pap tests and anoscopy.
In the meantime, she said, she suspected that, with the ANCHOR trial in 2015, many sites’ capacity for anoscopy may have increased, and the wait times may have gone down.
“One of the most important pieces of the study is actually the time period in which it was conducted,” said Dr. Lahiri, who in 2015 became the clinic’s second physician trained in anoscopy. Currently, more than 200 people at the Ponce De Leon Center are enrolled in the ANCHOR trial. In addition, the general capacity for performing anoscopies has gone up nationwide as a result of the trial, which required that more providers learn how to properly perform an HRA. Many clinicians are not routinely trained in performing HRA, including gastroenterologists and surgeons, Dr. Lahiri said.
“It would be interesting to look at the differences, with the start of ANCHOR being the time point for before and after,” she said.
This article first appeared on Medscape.com.
That delay “revealed missed opportunities for a better experience on the patient, clinic, and provider level,” Jessica Wells, PhD, research assistant professor at the Nell Hodgson Woodruff School of Nursing at Emory University, Atlanta, said in an interview. After all, “a lot can happen in that 1 year,” including early development of human papillomavirus (HPV)–associated anal cancer.
Although it’s too soon to say how significant that delay is with respect to the natural history of anal cancer, Dr. Wells said the data are a potential signal of disparities.
“The findings from my study may foreshadow potential disparities if we don’t have the necessary resources in place to promote follow-up care after an abnormal Pap test, similar to the disparities that we see in cervical cancer,” she said during the virtual Association of Nurses in AIDS Care 2020 Annual Meeting.
Single-center study
In the United States, people living with HIV are 19 times more likely to develop anal cancer than the general population, according to a 2018 article in the Journal of Clinical Oncology. Another single-center study from Yale University found that, in minority communities, anal cancer rates were 75% higher than in White communities. Anal cancer rates were 72% higher in communities with greater poverty. As a result, many clinics are beginning to administer Pap tests to determine early signs of HPV infection and associated changes.
In Dr. Wells’ study, which was conducted from 2012 to 2015, 150 adults with HIV who were aged 21 and older were recruited from Grady Ponce De Leon Center in Atlanta. According to a 2018 study from that center, a large minority of participants had late-stage HIV and suppressed immune systems.
All participants had been referred for HRA after a recent abnormal anal Pap test. Participants filled out questionnaires on sociodemographics, internalized HIV-related stigma, depression, risk behaviors, social support, and knowledge about HPV and anal cancer.
Participants were disproportionately older (mean age, 50.9 years); cisgender (86.7%), Black (78%); and gay, lesbian, or bisexual (84.3%). Slightly more than 1 in 10 participants (11.3%) were transgender women.
Although for 6% of participants, Pap test results indicated high-grade squamous intraepithelial lesions (HSIL), an additional 8% had atypical Pap findings that couldn’t exclude HSIL – the kinds of results that are one step away from a cancer diagnosis. More than 80% of participants had low-grade or inconclusive results. Nearly half (44%) of participants’ Pap tests revealed low-grade squamous cell intraepithelial cell lesions (LSIL); 42% indicated atypical squamous cells of undetermined significance.
When Dr. Wells looked at how long participants had waited to undergo HRA, she found something that surprised her: although some participants underwent follow-up assessment in 17 days, for many, it took much longer. The longest wait was 2,350 days – more than 6 years.
“There were quite a few patients who had follow-up beyond 1,000-plus days,” Dr. Wells said in an interview. “I didn›t think the delays were that long — at most, I would say that patients will get scheduled and come back within a few weeks or months.”
What’s more, she discovered through the HPV knowledge questionnaire that many participants did not understand why they were having a follow-up appointment. Anecdotally, some confused HPV with HIV.
“There’s education to be done to inform this target population that those living with HIV are more prone or at increased risk of this virus causing cancer later,” she said. “There are a lot of campaigns around women living with HIV, that they need to do cervical cancer screening. I think we need to really expand this campaign to include that HPV can also cause anal cancer.”
Dr. Wells had planned to primarily investigate the impact of psychosocial factors on wait time to follow-up, but none of those factors were associated with longer wait times.
Systems-level factors
That led Ann Gakumo, PhD, chair of nursing at the College of Nursing and Health Sciences of the University of Massachusetts, Boston, to ask what other factors could account for the delay.
There were several, Dr. Wells said. Precarious housing, for example, could have influenced this lag in follow-up. About one in four participants were in transient housing, and one participant reported having been incarcerated. She gathered street addresses and plans to analyze that data to see whether the cases occurred in clusters in specific neighborhoods, as the Yale data indicated.
In addition, the anoscopy clinic was only available to receive patients one day a week and was staffed with only one clinician who was trained to perform HRA. Wait times could stretch for hours. Sometimes, participants had to leave the clinic to attend to other business, and their appointments needed to be rescheduled, Wells said.
In addition to the sometimes poor understanding of the importance of the follow-up test, Dr. Wells said, “we start to see a layering of these barriers. That’s where we start seeing breakdowns. So I’m hoping in a larger study I can address some of these barriers on a multilevel approach.”
This resonated with Dr. Gakumo.
“Oftentimes, we put so much of the responsibility for this on the part of the client and not enough on the part of the provider or on the systems level,” she said.
Guiding guidelines
Guidelines on follow-up for abnormal anal Pap test results are scarce, mostly because, unlike cervical cancer, the natural history of HPV-related anal cancers hasn’t been established. The HIV Medical Association does recommend anal Pap tests, but only in cases in which “access to appropriate referral for follow-up, including high-resolution anoscopy, is available.”
In an interview, Cecile Lahiri, MD, assistant professor of infectious disease at Emory University, said that, at Ponce De Leon Center, they recommend an anal Pap for women with HIV who have a history of cervical dysplasia.
There is a reliable association between high-grade abnormal Pap tests and cervical cancer, although low-grade changes can resolve on their own. In the case of anal cancer, especially in patients with HIV, low-grade cell changes are predictive; moreover, for such patients, anal cancer is more likely to recur and is harder to treat, Dr. Lahiri said.
“The cervical environment and the anal environment are very different,” said Dr. Lahiri, who works at the Grady Ponce De Leon Center but was not involved in Dr. Wells’ study. Dr. Lahiri is also a coinvestigator of the multisite, randomized, controlled Anal Cancer HSIL Outcomes Research (ANCHOR) study, which seeks to establish whether early treatment of high-grade anal Pap changes is better than a watch-and-wait approach.
Dr. Lahiri said that when the results of that trial become available, they are more likely to know how important early anoscopy and treatment are. The findings should inform guidelines and insurance coverage of anal Pap tests and anoscopy.
In the meantime, she said, she suspected that, with the ANCHOR trial in 2015, many sites’ capacity for anoscopy may have increased, and the wait times may have gone down.
“One of the most important pieces of the study is actually the time period in which it was conducted,” said Dr. Lahiri, who in 2015 became the clinic’s second physician trained in anoscopy. Currently, more than 200 people at the Ponce De Leon Center are enrolled in the ANCHOR trial. In addition, the general capacity for performing anoscopies has gone up nationwide as a result of the trial, which required that more providers learn how to properly perform an HRA. Many clinicians are not routinely trained in performing HRA, including gastroenterologists and surgeons, Dr. Lahiri said.
“It would be interesting to look at the differences, with the start of ANCHOR being the time point for before and after,” she said.
This article first appeared on Medscape.com.
‘Smart’ insulin pen with CGM first to launch in emerging field
Medtronic’s launch of a new version of its smart insulin pen with integrated continuous glucose monitoring (CGM) is the first such device for use by people with diabetes who use multiple daily injections (MDI) of insulin.
Initially launched by Companion Medical in 2017, the InPen system is a reusable insulin injector pen combined with a smartphone app that provides insulin dose calculation information and tracking.
Medtronic acquired Companion in September 2020 and now the new version, the InPen with Real-Time Guardian Connect CGM Data, allows users to view glucose readings and insulin dose information in the same app.
The InPen, a so-called “connected delivery device,” also provides reports that aggregate insulin, glucose, and carbohydrate information into graphical displays. As with other current CGM systems, the information can be sent wirelessly to a clinician. And as with insulin pumps, the pens are programmed with target blood glucose levels, insulin-to-carb ratios, and insulin sensitivity parameters. The device tracks “insulin on board” and delivers reminders for basal and bolus doses.
InPen delivers only short-acting insulin from cartridges, all the three major brands. Patients who need long-acting insulin still need to inject that separately.
Barry H. Ginsberg, MD, PhD, of Diabetes Technology Consultants, Arlington, Va., said in an interview, “People using pumps have had data integration for a while now. This is an excellent first step in data integration for people doing MDI and I am sure it will improve blood glucose control.”
Asked about comparative costs, Medtronic spokeswoman Pamela Reese said in an interview, “While insurance costs will vary, the smart pen is less expensive than the insulin pump.”
Smart pens: How large is the market?
Speaking on Nov. 14 at the Diabetes Technology Society conference, diabetes care and education specialist Hope Warshaw, RD, gave an overview of the current smart pen/connected delivery device landscape.
She noted that the patient population who might benefit from smart pens, those using MDI, which is defined as injecting both long-acting insulin and short-acting insulin before meals, may be larger than appreciated. There are about 1.6 million U.S. patients with type 1 diabetes, of whom just 30%-40% currently use insulin pumps. In addition, of the 5.8 million with type 2 diabetes who take insulin, about 29%, or 1.7 million, use MDI.
Among those with type 1 diabetes, she said that smart pens might be a good option for “people who don’t want to wear the physical pump. They can deal with the sensor, but for psychological reasons or they have dermatologic issues, they just can’t wear a pump.”
But, Ms. Warshaw stressed, the type 2 diabetes population shouldn’t be overlooked. “More and more people with type 2 diabetes are on MDI. ... In fact, there are more who use MDI than the entire population with type 1 diabetes. ... This is happening because people with type 2 are getting it earlier and living longer.”
Dr. Ginsberg views smart pens as a bridge between simple pen injectors to automated insulin delivery (AID) systems, those that link insulin pumps with CGMs.
Regarding patients with type 1 diabetes, he said, “I see pen users on MDI slowly moving to integrated systems and then, when comfortable with the technology, moving to AID, finances allowing.”
As for those with type 2 diabetes, he said that they “are less computer literate and less likely to move to integrated systems, but they will, over time.”
In all, Dr. Ginsberg said, “I see integrated pens as increasing, not decreasing, the AID market.”
Emerging field: “I think they’re here to stay”
The new Medtronic InPen system can still display information from other compatible CGM systems, but on a 3-hour delay. This is important since the Guardian is not currently approved for determining insulin doses. In order to do that, users must still either use readings from another CGM system on a separate app or perform fingerstick blood glucose measurements.
The InPen is the first CGM-integrated pen device but is not likely to be the last. Similar technologies are being pursued by all three of the major insulin manufacturers and some other companies.
Eli Lilly’s Humalog Tempo Pen, a modified version of KwikPen, is integrated with the Dexcom CGM. The pen itself has been cleared by the U.S. Food and Drug Administration, but some of the component parts await authorization.
Novo Nordisk is expected to file with the FDA in 2021 for its NovoPen Echo Plus.
For its part, in December 2019, Sanofi teamed up with Bioport to fit its SoloStar insulin pens with their technology called Mallya, which had received CE Mark in June 2019. That device, which clips onto the top and the button of most major pens, adds smart pen capacity via Bluetooth. BioCorp also has teamed up with other manufacturers including Roche and AgaMatrix.
Another major player, Bigfoot Biomedical, has filed with the FDA for its connected pen that works with the Abbott FreeStyle Libre 2 CGM.
Ms. Warshaw advised, “We need to start talking more about the ways that peoples’ wants, needs, and desires change and evolve over the person’s life as their diabetes evolves and as all this technology evolves.
“Time will tell how many people will be on the very expensive [AID] systems. ... Pens are cheaper. The main cost is insulin. I think they’re here to stay. The big insulin makers wouldn’t be doing it otherwise.”
Dr. Ginsberg has no disclosures. Ms. Warshaw is a consultant and writer for Companion Medical/Medtronic and a faculty member of LifeScan Diabetes Institute.
A version of this article originally appeared on Medscape.com.
Medtronic’s launch of a new version of its smart insulin pen with integrated continuous glucose monitoring (CGM) is the first such device for use by people with diabetes who use multiple daily injections (MDI) of insulin.
Initially launched by Companion Medical in 2017, the InPen system is a reusable insulin injector pen combined with a smartphone app that provides insulin dose calculation information and tracking.
Medtronic acquired Companion in September 2020 and now the new version, the InPen with Real-Time Guardian Connect CGM Data, allows users to view glucose readings and insulin dose information in the same app.
The InPen, a so-called “connected delivery device,” also provides reports that aggregate insulin, glucose, and carbohydrate information into graphical displays. As with other current CGM systems, the information can be sent wirelessly to a clinician. And as with insulin pumps, the pens are programmed with target blood glucose levels, insulin-to-carb ratios, and insulin sensitivity parameters. The device tracks “insulin on board” and delivers reminders for basal and bolus doses.
InPen delivers only short-acting insulin from cartridges, all the three major brands. Patients who need long-acting insulin still need to inject that separately.
Barry H. Ginsberg, MD, PhD, of Diabetes Technology Consultants, Arlington, Va., said in an interview, “People using pumps have had data integration for a while now. This is an excellent first step in data integration for people doing MDI and I am sure it will improve blood glucose control.”
Asked about comparative costs, Medtronic spokeswoman Pamela Reese said in an interview, “While insurance costs will vary, the smart pen is less expensive than the insulin pump.”
Smart pens: How large is the market?
Speaking on Nov. 14 at the Diabetes Technology Society conference, diabetes care and education specialist Hope Warshaw, RD, gave an overview of the current smart pen/connected delivery device landscape.
She noted that the patient population who might benefit from smart pens, those using MDI, which is defined as injecting both long-acting insulin and short-acting insulin before meals, may be larger than appreciated. There are about 1.6 million U.S. patients with type 1 diabetes, of whom just 30%-40% currently use insulin pumps. In addition, of the 5.8 million with type 2 diabetes who take insulin, about 29%, or 1.7 million, use MDI.
Among those with type 1 diabetes, she said that smart pens might be a good option for “people who don’t want to wear the physical pump. They can deal with the sensor, but for psychological reasons or they have dermatologic issues, they just can’t wear a pump.”
But, Ms. Warshaw stressed, the type 2 diabetes population shouldn’t be overlooked. “More and more people with type 2 diabetes are on MDI. ... In fact, there are more who use MDI than the entire population with type 1 diabetes. ... This is happening because people with type 2 are getting it earlier and living longer.”
Dr. Ginsberg views smart pens as a bridge between simple pen injectors to automated insulin delivery (AID) systems, those that link insulin pumps with CGMs.
Regarding patients with type 1 diabetes, he said, “I see pen users on MDI slowly moving to integrated systems and then, when comfortable with the technology, moving to AID, finances allowing.”
As for those with type 2 diabetes, he said that they “are less computer literate and less likely to move to integrated systems, but they will, over time.”
In all, Dr. Ginsberg said, “I see integrated pens as increasing, not decreasing, the AID market.”
Emerging field: “I think they’re here to stay”
The new Medtronic InPen system can still display information from other compatible CGM systems, but on a 3-hour delay. This is important since the Guardian is not currently approved for determining insulin doses. In order to do that, users must still either use readings from another CGM system on a separate app or perform fingerstick blood glucose measurements.
The InPen is the first CGM-integrated pen device but is not likely to be the last. Similar technologies are being pursued by all three of the major insulin manufacturers and some other companies.
Eli Lilly’s Humalog Tempo Pen, a modified version of KwikPen, is integrated with the Dexcom CGM. The pen itself has been cleared by the U.S. Food and Drug Administration, but some of the component parts await authorization.
Novo Nordisk is expected to file with the FDA in 2021 for its NovoPen Echo Plus.
For its part, in December 2019, Sanofi teamed up with Bioport to fit its SoloStar insulin pens with their technology called Mallya, which had received CE Mark in June 2019. That device, which clips onto the top and the button of most major pens, adds smart pen capacity via Bluetooth. BioCorp also has teamed up with other manufacturers including Roche and AgaMatrix.
Another major player, Bigfoot Biomedical, has filed with the FDA for its connected pen that works with the Abbott FreeStyle Libre 2 CGM.
Ms. Warshaw advised, “We need to start talking more about the ways that peoples’ wants, needs, and desires change and evolve over the person’s life as their diabetes evolves and as all this technology evolves.
“Time will tell how many people will be on the very expensive [AID] systems. ... Pens are cheaper. The main cost is insulin. I think they’re here to stay. The big insulin makers wouldn’t be doing it otherwise.”
Dr. Ginsberg has no disclosures. Ms. Warshaw is a consultant and writer for Companion Medical/Medtronic and a faculty member of LifeScan Diabetes Institute.
A version of this article originally appeared on Medscape.com.
Medtronic’s launch of a new version of its smart insulin pen with integrated continuous glucose monitoring (CGM) is the first such device for use by people with diabetes who use multiple daily injections (MDI) of insulin.
Initially launched by Companion Medical in 2017, the InPen system is a reusable insulin injector pen combined with a smartphone app that provides insulin dose calculation information and tracking.
Medtronic acquired Companion in September 2020 and now the new version, the InPen with Real-Time Guardian Connect CGM Data, allows users to view glucose readings and insulin dose information in the same app.
The InPen, a so-called “connected delivery device,” also provides reports that aggregate insulin, glucose, and carbohydrate information into graphical displays. As with other current CGM systems, the information can be sent wirelessly to a clinician. And as with insulin pumps, the pens are programmed with target blood glucose levels, insulin-to-carb ratios, and insulin sensitivity parameters. The device tracks “insulin on board” and delivers reminders for basal and bolus doses.
InPen delivers only short-acting insulin from cartridges, all the three major brands. Patients who need long-acting insulin still need to inject that separately.
Barry H. Ginsberg, MD, PhD, of Diabetes Technology Consultants, Arlington, Va., said in an interview, “People using pumps have had data integration for a while now. This is an excellent first step in data integration for people doing MDI and I am sure it will improve blood glucose control.”
Asked about comparative costs, Medtronic spokeswoman Pamela Reese said in an interview, “While insurance costs will vary, the smart pen is less expensive than the insulin pump.”
Smart pens: How large is the market?
Speaking on Nov. 14 at the Diabetes Technology Society conference, diabetes care and education specialist Hope Warshaw, RD, gave an overview of the current smart pen/connected delivery device landscape.
She noted that the patient population who might benefit from smart pens, those using MDI, which is defined as injecting both long-acting insulin and short-acting insulin before meals, may be larger than appreciated. There are about 1.6 million U.S. patients with type 1 diabetes, of whom just 30%-40% currently use insulin pumps. In addition, of the 5.8 million with type 2 diabetes who take insulin, about 29%, or 1.7 million, use MDI.
Among those with type 1 diabetes, she said that smart pens might be a good option for “people who don’t want to wear the physical pump. They can deal with the sensor, but for psychological reasons or they have dermatologic issues, they just can’t wear a pump.”
But, Ms. Warshaw stressed, the type 2 diabetes population shouldn’t be overlooked. “More and more people with type 2 diabetes are on MDI. ... In fact, there are more who use MDI than the entire population with type 1 diabetes. ... This is happening because people with type 2 are getting it earlier and living longer.”
Dr. Ginsberg views smart pens as a bridge between simple pen injectors to automated insulin delivery (AID) systems, those that link insulin pumps with CGMs.
Regarding patients with type 1 diabetes, he said, “I see pen users on MDI slowly moving to integrated systems and then, when comfortable with the technology, moving to AID, finances allowing.”
As for those with type 2 diabetes, he said that they “are less computer literate and less likely to move to integrated systems, but they will, over time.”
In all, Dr. Ginsberg said, “I see integrated pens as increasing, not decreasing, the AID market.”
Emerging field: “I think they’re here to stay”
The new Medtronic InPen system can still display information from other compatible CGM systems, but on a 3-hour delay. This is important since the Guardian is not currently approved for determining insulin doses. In order to do that, users must still either use readings from another CGM system on a separate app or perform fingerstick blood glucose measurements.
The InPen is the first CGM-integrated pen device but is not likely to be the last. Similar technologies are being pursued by all three of the major insulin manufacturers and some other companies.
Eli Lilly’s Humalog Tempo Pen, a modified version of KwikPen, is integrated with the Dexcom CGM. The pen itself has been cleared by the U.S. Food and Drug Administration, but some of the component parts await authorization.
Novo Nordisk is expected to file with the FDA in 2021 for its NovoPen Echo Plus.
For its part, in December 2019, Sanofi teamed up with Bioport to fit its SoloStar insulin pens with their technology called Mallya, which had received CE Mark in June 2019. That device, which clips onto the top and the button of most major pens, adds smart pen capacity via Bluetooth. BioCorp also has teamed up with other manufacturers including Roche and AgaMatrix.
Another major player, Bigfoot Biomedical, has filed with the FDA for its connected pen that works with the Abbott FreeStyle Libre 2 CGM.
Ms. Warshaw advised, “We need to start talking more about the ways that peoples’ wants, needs, and desires change and evolve over the person’s life as their diabetes evolves and as all this technology evolves.
“Time will tell how many people will be on the very expensive [AID] systems. ... Pens are cheaper. The main cost is insulin. I think they’re here to stay. The big insulin makers wouldn’t be doing it otherwise.”
Dr. Ginsberg has no disclosures. Ms. Warshaw is a consultant and writer for Companion Medical/Medtronic and a faculty member of LifeScan Diabetes Institute.
A version of this article originally appeared on Medscape.com.
Do general neurologists fall victim to a plethora of treatment options?
In 1993 I graduated from medical school. That same year Betaseron (interferon beta-1b) came to market as the first treatment specifically approved for multiple sclerosis (MS). This was a groundbreaker at the time, as there’d been little besides steroids and other potent immunosuppressants to try. Now we had a real drug to offer patients.

The demand for Betaseron was huge, so much so that a lottery system was used to determine which patients would get it first, as there simply wasn’t enough to go around. In the next several years a few more agents jumped into the ring – Avonex (interferon beta-1a), Copaxone (glatiramer acetate), Novantrone (mitoxantrone), and Rebif (interferon beta-1a) – before things went quiet for a while.
In 2006 the first monoclonal antibody for MS – Tysabri (natalizumab) – came out, then almost just as quickly vanished again, not returning until 2009.
Since then we’ve had a gradual explosion of new treatments for MS – like watching kernels become popcorn – first one, then two, then a deluge filling up the basket.
So here we are, approaching the end of 2020, with a remarkable collection of monoclonal antibodies, S1P modulators, fumarates, immunosuppressants, and one symptomatic treatment, many of which weren’t even imagined in 1993. Not to mention the original ABCR (Avonex, Betaseron, Copaxone, Rebif) agents, though they’re riding into the sunset.
A friend and I were talking about this remarkable success story. MS certainly hasn’t been cured, but its treatments have had a dramatic improvement in efficacy over the last quarter century.
He made a point though: that this selection of treatments may be relegating MS from the province of a general neurologist to that of the fellowship-trained MS subspecialist.
Not that that is such a bad thing, as MS is a very challenging disease. But the point is well taken. As treatments become increasingly complicated, and numerous, it becomes harder to know which one is best. Most of us likely choose orals first and monoclonal antibodies second, but the question of “which one?” arises for each category. They each have their own risks, side effects, initiation protocols, and peculiarities. In a disease of heterogeneous presentations and courses, there are no clear data on which agent to start first for what patient type. To a general neurologist, also juggling migraines, strokes, Parkinson’s disease, dementia, and neuropathy (and many other disorders) in the course of a day, it becomes tricky to keep up on such.
At some point do general neurologists become a victim of this success? Maybe, but probably not. Just as there are more general practitioners than neurologists, there are more general neurologists than MS subspecialists. Their knowledge and training should be reserved for those patients not responding to our first- (and second-) line treatments, presentations that are atypical, and more complex issues outside the scope of those of us practicing whatever-comes-to-the-door neurology.
It would, however, be nice to have a good consensus on how to best use this array of treatments. Solid guidelines, breaking disease subtypes and treatments down by patient types, drugs, and mechanisms of action, would help those of us on the neurology frontlines to better care for those who need us.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
In 1993 I graduated from medical school. That same year Betaseron (interferon beta-1b) came to market as the first treatment specifically approved for multiple sclerosis (MS). This was a groundbreaker at the time, as there’d been little besides steroids and other potent immunosuppressants to try. Now we had a real drug to offer patients.
The demand for Betaseron was huge, so much so that a lottery system was used to determine which patients would get it first, as there simply wasn’t enough to go around. In the next several years a few more agents jumped into the ring – Avonex (interferon beta-1a), Copaxone (glatiramer acetate), Novantrone (mitoxantrone), and Rebif (interferon beta-1a) – before things went quiet for a while.
In 2006 the first monoclonal antibody for MS – Tysabri (natalizumab) – came out, then almost just as quickly vanished again, not returning until 2009.
Since then we’ve had a gradual explosion of new treatments for MS – like watching kernels become popcorn – first one, then two, then a deluge filling up the basket.
So here we are, approaching the end of 2020, with a remarkable collection of monoclonal antibodies, S1P modulators, fumarates, immunosuppressants, and one symptomatic treatment, many of which weren’t even imagined in 1993. Not to mention the original ABCR (Avonex, Betaseron, Copaxone, Rebif) agents, though they’re riding into the sunset.
A friend and I were talking about this remarkable success story. MS certainly hasn’t been cured, but its treatments have had a dramatic improvement in efficacy over the last quarter century.
He made a point though: that this selection of treatments may be relegating MS from the province of a general neurologist to that of the fellowship-trained MS subspecialist.
Not that that is such a bad thing, as MS is a very challenging disease. But the point is well taken. As treatments become increasingly complicated, and numerous, it becomes harder to know which one is best. Most of us likely choose orals first and monoclonal antibodies second, but the question of “which one?” arises for each category. They each have their own risks, side effects, initiation protocols, and peculiarities. In a disease of heterogeneous presentations and courses, there are no clear data on which agent to start first for what patient type. To a general neurologist, also juggling migraines, strokes, Parkinson’s disease, dementia, and neuropathy (and many other disorders) in the course of a day, it becomes tricky to keep up on such.
At some point do general neurologists become a victim of this success? Maybe, but probably not. Just as there are more general practitioners than neurologists, there are more general neurologists than MS subspecialists. Their knowledge and training should be reserved for those patients not responding to our first- (and second-) line treatments, presentations that are atypical, and more complex issues outside the scope of those of us practicing whatever-comes-to-the-door neurology.
It would, however, be nice to have a good consensus on how to best use this array of treatments. Solid guidelines, breaking disease subtypes and treatments down by patient types, drugs, and mechanisms of action, would help those of us on the neurology frontlines to better care for those who need us.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
In 1993 I graduated from medical school. That same year Betaseron (interferon beta-1b) came to market as the first treatment specifically approved for multiple sclerosis (MS). This was a groundbreaker at the time, as there’d been little besides steroids and other potent immunosuppressants to try. Now we had a real drug to offer patients.
The demand for Betaseron was huge, so much so that a lottery system was used to determine which patients would get it first, as there simply wasn’t enough to go around. In the next several years a few more agents jumped into the ring – Avonex (interferon beta-1a), Copaxone (glatiramer acetate), Novantrone (mitoxantrone), and Rebif (interferon beta-1a) – before things went quiet for a while.
In 2006 the first monoclonal antibody for MS – Tysabri (natalizumab) – came out, then almost just as quickly vanished again, not returning until 2009.
Since then we’ve had a gradual explosion of new treatments for MS – like watching kernels become popcorn – first one, then two, then a deluge filling up the basket.
So here we are, approaching the end of 2020, with a remarkable collection of monoclonal antibodies, S1P modulators, fumarates, immunosuppressants, and one symptomatic treatment, many of which weren’t even imagined in 1993. Not to mention the original ABCR (Avonex, Betaseron, Copaxone, Rebif) agents, though they’re riding into the sunset.
A friend and I were talking about this remarkable success story. MS certainly hasn’t been cured, but its treatments have had a dramatic improvement in efficacy over the last quarter century.
He made a point though: that this selection of treatments may be relegating MS from the province of a general neurologist to that of the fellowship-trained MS subspecialist.
Not that that is such a bad thing, as MS is a very challenging disease. But the point is well taken. As treatments become increasingly complicated, and numerous, it becomes harder to know which one is best. Most of us likely choose orals first and monoclonal antibodies second, but the question of “which one?” arises for each category. They each have their own risks, side effects, initiation protocols, and peculiarities. In a disease of heterogeneous presentations and courses, there are no clear data on which agent to start first for what patient type. To a general neurologist, also juggling migraines, strokes, Parkinson’s disease, dementia, and neuropathy (and many other disorders) in the course of a day, it becomes tricky to keep up on such.
At some point do general neurologists become a victim of this success? Maybe, but probably not. Just as there are more general practitioners than neurologists, there are more general neurologists than MS subspecialists. Their knowledge and training should be reserved for those patients not responding to our first- (and second-) line treatments, presentations that are atypical, and more complex issues outside the scope of those of us practicing whatever-comes-to-the-door neurology.
It would, however, be nice to have a good consensus on how to best use this array of treatments. Solid guidelines, breaking disease subtypes and treatments down by patient types, drugs, and mechanisms of action, would help those of us on the neurology frontlines to better care for those who need us.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
‘Uptake is only the first step’ for effective HIV PrEP protection
To Amanda Allmacher, DNP, RN, nurse practitioner at the Detroit Public Health STD Clinic, that means that same-day PrEP prescribing works and is acceptable. But there’s more work to do on the clinic and pharmacy side to make HIV protection a reality for most of her patients. Allmacher presented her data at the Association of Nurses in AIDS Care 2020 virtual annual meeting.
Dawn K. Smith, MD, epidemiologist and medical officer in the Division of HIV/AIDS Prevention at the Centers for Disease Control and Prevention’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, said this adds to other data to show that we’re now entering the next phase of PrEP implementation.
“Our original focus was on uptake — informing folks what PrEP is, why they might benefit from its use, and then prescribing it if accepted,” Smith told Medscape Medical News via email. “Whether standard or same-day [PrEP prescribing], it is clear that uptake is only the first step.”
Nurses help navigate
Patients who attended the Detroit Public Health STD Clinic are more likely to be younger, have no insurance, and otherwise “have little to no contact with the healthcare system,” Allmacher said in her presentation. They also tend to come from communities that bear the greatest burden of HIV in the US — in other words, they are often the people most missed in PrEP rollouts thus far.
In response, the clinic implemented a same-day PrEP protocol, in which registered nurses trained in HIV risk assessment identify clients who might most benefit from PrEP. Criteria often include the presence of other STIs. Once the nurse explains what PrEP is and how it works, if the patient is interested, clients meet with a nurse practitioner right then to get the prescription for PrEP. The clinic also does labs to rule out current HIV infection, hepatitis B, metabolic issues, and other STI screening.
But it doesn’t stop there. The clinic used grant funding to offer PrEP navigation and financial counseling services, which help clients navigate the sometimes-thorny process of paying for PrEP. Payment comes either through Medicaid, which in Michigan charges $3 a month for a PrEP prescription, through patient assistance programs, or through private insurance. With clients under age 18 who are interested in PrEP, the clinic works to find a way to access PrEP without having to inform their parents. These same navigators schedule follow-up appointments, offer appointment reminders, and contact clients when they miss an appointment.
“Our navigators and financial counselors are a huge support for our same-day PrEP starts, helping with financial assistance, prior authorization, navigating different plans, and helping patients apply for Medicaid when appropriate,” she said.
The clinic also offers community outreach and incentives, which can include gift cards, bus passes, and pill containers, among other things.
This was a key lesson in setting up the program, Allmacher told Medscape Medical News.
“Starting PrEP at that initial visit allows for clinicians to meet patients where they are and administer care in a more equitable manner,” Allmacher said via email. “Use all available resources and funding sources. We have a versatile team working together to increase access for patients and promote HIV prevention and risk reduction.”
Script vs. follow-up
This approach is common, used in places like New York City and San Francisco. So once it was set up Allmacher sat back and waited to see how the program helped clients protect themselves from HIV.
Of the 451 clients eligible for PrEP in 2019, 336 were gay and bisexual men, 6 were transgender women, 61 were heterosexual, cisgender men, and 48 were cisgender women. One transgender man also screened as eligible. Allmacher did not break down data by race.
Uptake was high: 70% of all eligible clients did receive a prescription for PrEP, either generic tenofovir disoproxil fumarate/emtricitabine (Truvada) or tenofovir alafenamide/emtricitabine (Descovy). And uptake was high among people most at risk: 80% of gay and bisexual men who were eligible got a prescription, 60% of eligible cisgender women, 50% of the small number of transgender women, and 32.7% of heterosexual cisgender men did as well. The 1 transgender man also received a prescription.
This is a higher rate than found in a recent PrEP demonstration project, which found that despite gay and bisexual men, transgender adults, and Black people having the highest risk for HIV in the US, state health departments were more likely to refer heterosexual adults for PrEP.
That high uptake rate is encouraging, but follow-up? Not so much. After initial intake, clients are meant to return in a month to double-check their labs, ask about side effects, and start their 90-day supply of the medication. But just 40% showed up for their 30-day appointment, Allmacher said. And only one third of those showed up for the follow-up in 90 days.
By the end of 2019, just 73 of the original 451 clients screened were still taking PrEP.
“It was surprising to see just how significant the follow-up dropped off after that first visit, when the patient initially accepted the prescription,” Allmacher said.
And while it’s possible that some clients get their follow-up care from their primary care providers, “our clinic serves individuals regardless of insurance status and many do not identify having access to primary care for any type of service, PrEP or otherwise,” she said.
5 HIV acquisitions
In addition, the program review identified five clients who had been offered PrEP or had taken PrEP briefly who later acquired HIV. Those clients were offered same-day antiretroviral treatment, Allmacher said.
“So we’re finding people who are at high risk for HIV and we can prevent them, but we’re still not quite doing enough,” Allmacher said of those acquisitions. “Clearly we have a lot of work to do to focus on HIV prevention, and we are looking to create a more formal follow-up process” from the clinic’s side.
For instance, clinic staff call clients 1 week after their initial visit to share lab results. “This was identified as a missed opportunity for us to ask about their status, whether they filled their prescription, or if they need further assistance,” she said. “This is an area where our registered nurses are going to be taking on a greater role moving forward.”
Allmacher and team also discovered that, despite PrEP navigators arranging insurance coverage for clients on the day they receive their prescription, sometimes there were still barriers when the client showed up at the pharmacy to pick up their meds. The clinic does not have an in-house pharmacy and does not currently have the funding that would allow them to hand patients a bottle of the appropriate medication when they leave the clinic.
“Navigating the copays and the insurance coverage and using financial assistance through the drug manufacturer — even though we have the support in the clinic, it seems like there’s a disconnect between our clinic and getting to the pharmacy. Not every pharmacy is super familiar with navigating those,” she said. “So we have started to identify some area pharmacies near our clinic that are great at navigating these, and we really try to get our patients to go to places we know can give them assistance.”
A version of this story originally appeared on Medscape.com.
To Amanda Allmacher, DNP, RN, nurse practitioner at the Detroit Public Health STD Clinic, that means that same-day PrEP prescribing works and is acceptable. But there’s more work to do on the clinic and pharmacy side to make HIV protection a reality for most of her patients. Allmacher presented her data at the Association of Nurses in AIDS Care 2020 virtual annual meeting.
Dawn K. Smith, MD, epidemiologist and medical officer in the Division of HIV/AIDS Prevention at the Centers for Disease Control and Prevention’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, said this adds to other data to show that we’re now entering the next phase of PrEP implementation.
“Our original focus was on uptake — informing folks what PrEP is, why they might benefit from its use, and then prescribing it if accepted,” Smith told Medscape Medical News via email. “Whether standard or same-day [PrEP prescribing], it is clear that uptake is only the first step.”
Nurses help navigate
Patients who attended the Detroit Public Health STD Clinic are more likely to be younger, have no insurance, and otherwise “have little to no contact with the healthcare system,” Allmacher said in her presentation. They also tend to come from communities that bear the greatest burden of HIV in the US — in other words, they are often the people most missed in PrEP rollouts thus far.
In response, the clinic implemented a same-day PrEP protocol, in which registered nurses trained in HIV risk assessment identify clients who might most benefit from PrEP. Criteria often include the presence of other STIs. Once the nurse explains what PrEP is and how it works, if the patient is interested, clients meet with a nurse practitioner right then to get the prescription for PrEP. The clinic also does labs to rule out current HIV infection, hepatitis B, metabolic issues, and other STI screening.
But it doesn’t stop there. The clinic used grant funding to offer PrEP navigation and financial counseling services, which help clients navigate the sometimes-thorny process of paying for PrEP. Payment comes either through Medicaid, which in Michigan charges $3 a month for a PrEP prescription, through patient assistance programs, or through private insurance. With clients under age 18 who are interested in PrEP, the clinic works to find a way to access PrEP without having to inform their parents. These same navigators schedule follow-up appointments, offer appointment reminders, and contact clients when they miss an appointment.
“Our navigators and financial counselors are a huge support for our same-day PrEP starts, helping with financial assistance, prior authorization, navigating different plans, and helping patients apply for Medicaid when appropriate,” she said.
The clinic also offers community outreach and incentives, which can include gift cards, bus passes, and pill containers, among other things.
This was a key lesson in setting up the program, Allmacher told Medscape Medical News.
“Starting PrEP at that initial visit allows for clinicians to meet patients where they are and administer care in a more equitable manner,” Allmacher said via email. “Use all available resources and funding sources. We have a versatile team working together to increase access for patients and promote HIV prevention and risk reduction.”
Script vs. follow-up
This approach is common, used in places like New York City and San Francisco. So once it was set up Allmacher sat back and waited to see how the program helped clients protect themselves from HIV.
Of the 451 clients eligible for PrEP in 2019, 336 were gay and bisexual men, 6 were transgender women, 61 were heterosexual, cisgender men, and 48 were cisgender women. One transgender man also screened as eligible. Allmacher did not break down data by race.
Uptake was high: 70% of all eligible clients did receive a prescription for PrEP, either generic tenofovir disoproxil fumarate/emtricitabine (Truvada) or tenofovir alafenamide/emtricitabine (Descovy). And uptake was high among people most at risk: 80% of gay and bisexual men who were eligible got a prescription, 60% of eligible cisgender women, 50% of the small number of transgender women, and 32.7% of heterosexual cisgender men did as well. The 1 transgender man also received a prescription.
This is a higher rate than found in a recent PrEP demonstration project, which found that despite gay and bisexual men, transgender adults, and Black people having the highest risk for HIV in the US, state health departments were more likely to refer heterosexual adults for PrEP.
That high uptake rate is encouraging, but follow-up? Not so much. After initial intake, clients are meant to return in a month to double-check their labs, ask about side effects, and start their 90-day supply of the medication. But just 40% showed up for their 30-day appointment, Allmacher said. And only one third of those showed up for the follow-up in 90 days.
By the end of 2019, just 73 of the original 451 clients screened were still taking PrEP.
“It was surprising to see just how significant the follow-up dropped off after that first visit, when the patient initially accepted the prescription,” Allmacher said.
And while it’s possible that some clients get their follow-up care from their primary care providers, “our clinic serves individuals regardless of insurance status and many do not identify having access to primary care for any type of service, PrEP or otherwise,” she said.
5 HIV acquisitions
In addition, the program review identified five clients who had been offered PrEP or had taken PrEP briefly who later acquired HIV. Those clients were offered same-day antiretroviral treatment, Allmacher said.
“So we’re finding people who are at high risk for HIV and we can prevent them, but we’re still not quite doing enough,” Allmacher said of those acquisitions. “Clearly we have a lot of work to do to focus on HIV prevention, and we are looking to create a more formal follow-up process” from the clinic’s side.
For instance, clinic staff call clients 1 week after their initial visit to share lab results. “This was identified as a missed opportunity for us to ask about their status, whether they filled their prescription, or if they need further assistance,” she said. “This is an area where our registered nurses are going to be taking on a greater role moving forward.”
Allmacher and team also discovered that, despite PrEP navigators arranging insurance coverage for clients on the day they receive their prescription, sometimes there were still barriers when the client showed up at the pharmacy to pick up their meds. The clinic does not have an in-house pharmacy and does not currently have the funding that would allow them to hand patients a bottle of the appropriate medication when they leave the clinic.
“Navigating the copays and the insurance coverage and using financial assistance through the drug manufacturer — even though we have the support in the clinic, it seems like there’s a disconnect between our clinic and getting to the pharmacy. Not every pharmacy is super familiar with navigating those,” she said. “So we have started to identify some area pharmacies near our clinic that are great at navigating these, and we really try to get our patients to go to places we know can give them assistance.”
A version of this story originally appeared on Medscape.com.
To Amanda Allmacher, DNP, RN, nurse practitioner at the Detroit Public Health STD Clinic, that means that same-day PrEP prescribing works and is acceptable. But there’s more work to do on the clinic and pharmacy side to make HIV protection a reality for most of her patients. Allmacher presented her data at the Association of Nurses in AIDS Care 2020 virtual annual meeting.
Dawn K. Smith, MD, epidemiologist and medical officer in the Division of HIV/AIDS Prevention at the Centers for Disease Control and Prevention’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, said this adds to other data to show that we’re now entering the next phase of PrEP implementation.
“Our original focus was on uptake — informing folks what PrEP is, why they might benefit from its use, and then prescribing it if accepted,” Smith told Medscape Medical News via email. “Whether standard or same-day [PrEP prescribing], it is clear that uptake is only the first step.”
Nurses help navigate
Patients who attended the Detroit Public Health STD Clinic are more likely to be younger, have no insurance, and otherwise “have little to no contact with the healthcare system,” Allmacher said in her presentation. They also tend to come from communities that bear the greatest burden of HIV in the US — in other words, they are often the people most missed in PrEP rollouts thus far.
In response, the clinic implemented a same-day PrEP protocol, in which registered nurses trained in HIV risk assessment identify clients who might most benefit from PrEP. Criteria often include the presence of other STIs. Once the nurse explains what PrEP is and how it works, if the patient is interested, clients meet with a nurse practitioner right then to get the prescription for PrEP. The clinic also does labs to rule out current HIV infection, hepatitis B, metabolic issues, and other STI screening.
But it doesn’t stop there. The clinic used grant funding to offer PrEP navigation and financial counseling services, which help clients navigate the sometimes-thorny process of paying for PrEP. Payment comes either through Medicaid, which in Michigan charges $3 a month for a PrEP prescription, through patient assistance programs, or through private insurance. With clients under age 18 who are interested in PrEP, the clinic works to find a way to access PrEP without having to inform their parents. These same navigators schedule follow-up appointments, offer appointment reminders, and contact clients when they miss an appointment.
“Our navigators and financial counselors are a huge support for our same-day PrEP starts, helping with financial assistance, prior authorization, navigating different plans, and helping patients apply for Medicaid when appropriate,” she said.
The clinic also offers community outreach and incentives, which can include gift cards, bus passes, and pill containers, among other things.
This was a key lesson in setting up the program, Allmacher told Medscape Medical News.
“Starting PrEP at that initial visit allows for clinicians to meet patients where they are and administer care in a more equitable manner,” Allmacher said via email. “Use all available resources and funding sources. We have a versatile team working together to increase access for patients and promote HIV prevention and risk reduction.”
Script vs. follow-up
This approach is common, used in places like New York City and San Francisco. So once it was set up Allmacher sat back and waited to see how the program helped clients protect themselves from HIV.
Of the 451 clients eligible for PrEP in 2019, 336 were gay and bisexual men, 6 were transgender women, 61 were heterosexual, cisgender men, and 48 were cisgender women. One transgender man also screened as eligible. Allmacher did not break down data by race.
Uptake was high: 70% of all eligible clients did receive a prescription for PrEP, either generic tenofovir disoproxil fumarate/emtricitabine (Truvada) or tenofovir alafenamide/emtricitabine (Descovy). And uptake was high among people most at risk: 80% of gay and bisexual men who were eligible got a prescription, 60% of eligible cisgender women, 50% of the small number of transgender women, and 32.7% of heterosexual cisgender men did as well. The 1 transgender man also received a prescription.
This is a higher rate than found in a recent PrEP demonstration project, which found that despite gay and bisexual men, transgender adults, and Black people having the highest risk for HIV in the US, state health departments were more likely to refer heterosexual adults for PrEP.
That high uptake rate is encouraging, but follow-up? Not so much. After initial intake, clients are meant to return in a month to double-check their labs, ask about side effects, and start their 90-day supply of the medication. But just 40% showed up for their 30-day appointment, Allmacher said. And only one third of those showed up for the follow-up in 90 days.
By the end of 2019, just 73 of the original 451 clients screened were still taking PrEP.
“It was surprising to see just how significant the follow-up dropped off after that first visit, when the patient initially accepted the prescription,” Allmacher said.
And while it’s possible that some clients get their follow-up care from their primary care providers, “our clinic serves individuals regardless of insurance status and many do not identify having access to primary care for any type of service, PrEP or otherwise,” she said.
5 HIV acquisitions
In addition, the program review identified five clients who had been offered PrEP or had taken PrEP briefly who later acquired HIV. Those clients were offered same-day antiretroviral treatment, Allmacher said.
“So we’re finding people who are at high risk for HIV and we can prevent them, but we’re still not quite doing enough,” Allmacher said of those acquisitions. “Clearly we have a lot of work to do to focus on HIV prevention, and we are looking to create a more formal follow-up process” from the clinic’s side.
For instance, clinic staff call clients 1 week after their initial visit to share lab results. “This was identified as a missed opportunity for us to ask about their status, whether they filled their prescription, or if they need further assistance,” she said. “This is an area where our registered nurses are going to be taking on a greater role moving forward.”
Allmacher and team also discovered that, despite PrEP navigators arranging insurance coverage for clients on the day they receive their prescription, sometimes there were still barriers when the client showed up at the pharmacy to pick up their meds. The clinic does not have an in-house pharmacy and does not currently have the funding that would allow them to hand patients a bottle of the appropriate medication when they leave the clinic.
“Navigating the copays and the insurance coverage and using financial assistance through the drug manufacturer — even though we have the support in the clinic, it seems like there’s a disconnect between our clinic and getting to the pharmacy. Not every pharmacy is super familiar with navigating those,” she said. “So we have started to identify some area pharmacies near our clinic that are great at navigating these, and we really try to get our patients to go to places we know can give them assistance.”
A version of this story originally appeared on Medscape.com.