User login
Cost is the main hurdle to broad use of caplacizumab for TTP
As hematologists debated the role of the anti–von Willebrand factor agent caplacizumab for acquired thrombotic thrombocytopenic purpura (TTP), an investigator on the phase 3 trial that led to its approval had a message.
,” said hematologist Spero Cataland, MD, of the department of internal medicine at Ohio State University in Columbus.
If cost is going to be a factor, and it “has to be in our world these days, it’s more of a discussion,” he said during his presentation at the 2020 Update in Nonneoplastic Hematology virtual conference.
The HERCULES trial Dr. Cataland helped conduct found a median time to platelet count normalization of 2.69 days when caplacizumab was started during plasma exchange versus 2.88 days for placebo; 12% of patients had a TTP recurrence while they continued caplacizumab for 30 days past their last exchange and were followed for an additional 28 days versus 38% randomized to placebo. Caplacizumab subjects needed an average of 5.8 days of plasma exchange versus 9.4 days in the placebo arm (N Engl J Med. 2019 Jan 24;380(4):335-46).
Based on the results, the Food and Drug Administration approved the agent for acquired TTP in combination with plasma exchange and immunosuppressives in Feb. 2019 for 30 days beyond the last plasma exchange, with up to 28 additional days if ADAMTS13 activity remains suppressed. Labeling notes a risk of severe bleeding.
“The data on refractory disease and mortality aren’t quite there yet, but there’s a suggestion [caplacizumab] might impact that as well,” Dr. Cataland said. In its recent TTP guidelines, the International Society on Thrombosis and Haemostasis gave the agent only a conditional recommendation, in part because it’s backed up only by HERCULES and a phase 2 trial.
Also, the group noted that in the phase 2 study caplacizumab patients had a clinically and statistically significant increase in the number of relapses at 12 months: 31% versus 8% placebo. “Caplacizumab may leave patients prone to experience a later recurrence owing to the unresolved ADAMTS13 deficiency and inhibitors,” Dr. Cataland said.
“We do see some early recurrence” when caplacizumab is stopped, suggesting that when the agent’s “protective effect is removed, the risk is still there,” said Dr. Cataland, who was also an author on the ISTH guidelines, as well as the phase 2 trial.
It raises the question of how long patients should be kept on caplacizumab. There are few data on the issue, “but the consensus has been to stop caplacizumab when two consecutive ADAMTS13 measurements show 20% or greater activity,” or perhaps with one reading above 20% in a patient trending in the right direction. “With a bleeding complication, you might stop it sooner,” he said.
Dr. Cataland anticipates TTP management will eventually move away from plasma exchange to more directed therapies, including caplacizumab and perhaps recombinant ADAMTS13, which is in development.
There have been a few reports of TTP patients who refuse plasma exchange on religious grounds being successfully treated with caplacizumab. Dr. Cataland also noted a patient of his with relapsing TTP who didn’t want to be admitted yet again for plasma exchange and steroids at the start of a new episode.
“We managed her with caplacizumab and rituximab, and in a couple weeks she had recovered her ADAMTS13 activity and was able to stop the caplacizumab.” She was a motivated, knowledgeable person, “someone I trusted, so I was comfortable with the approach. I think that may be where we are headed in the future, hopefully,” he said.
Dr. Cataland disclosed research funding and consulting fees from Alexion, caplacizumab’s maker, Sanofi Genzyme, and Takeda,. The conference was sponsored by MedscapeLive. MedscapeLive and this news organization are owned by the same parent company.
As hematologists debated the role of the anti–von Willebrand factor agent caplacizumab for acquired thrombotic thrombocytopenic purpura (TTP), an investigator on the phase 3 trial that led to its approval had a message.
,” said hematologist Spero Cataland, MD, of the department of internal medicine at Ohio State University in Columbus.
If cost is going to be a factor, and it “has to be in our world these days, it’s more of a discussion,” he said during his presentation at the 2020 Update in Nonneoplastic Hematology virtual conference.
The HERCULES trial Dr. Cataland helped conduct found a median time to platelet count normalization of 2.69 days when caplacizumab was started during plasma exchange versus 2.88 days for placebo; 12% of patients had a TTP recurrence while they continued caplacizumab for 30 days past their last exchange and were followed for an additional 28 days versus 38% randomized to placebo. Caplacizumab subjects needed an average of 5.8 days of plasma exchange versus 9.4 days in the placebo arm (N Engl J Med. 2019 Jan 24;380(4):335-46).
Based on the results, the Food and Drug Administration approved the agent for acquired TTP in combination with plasma exchange and immunosuppressives in Feb. 2019 for 30 days beyond the last plasma exchange, with up to 28 additional days if ADAMTS13 activity remains suppressed. Labeling notes a risk of severe bleeding.
“The data on refractory disease and mortality aren’t quite there yet, but there’s a suggestion [caplacizumab] might impact that as well,” Dr. Cataland said. In its recent TTP guidelines, the International Society on Thrombosis and Haemostasis gave the agent only a conditional recommendation, in part because it’s backed up only by HERCULES and a phase 2 trial.
Also, the group noted that in the phase 2 study caplacizumab patients had a clinically and statistically significant increase in the number of relapses at 12 months: 31% versus 8% placebo. “Caplacizumab may leave patients prone to experience a later recurrence owing to the unresolved ADAMTS13 deficiency and inhibitors,” Dr. Cataland said.
“We do see some early recurrence” when caplacizumab is stopped, suggesting that when the agent’s “protective effect is removed, the risk is still there,” said Dr. Cataland, who was also an author on the ISTH guidelines, as well as the phase 2 trial.
It raises the question of how long patients should be kept on caplacizumab. There are few data on the issue, “but the consensus has been to stop caplacizumab when two consecutive ADAMTS13 measurements show 20% or greater activity,” or perhaps with one reading above 20% in a patient trending in the right direction. “With a bleeding complication, you might stop it sooner,” he said.
Dr. Cataland anticipates TTP management will eventually move away from plasma exchange to more directed therapies, including caplacizumab and perhaps recombinant ADAMTS13, which is in development.
There have been a few reports of TTP patients who refuse plasma exchange on religious grounds being successfully treated with caplacizumab. Dr. Cataland also noted a patient of his with relapsing TTP who didn’t want to be admitted yet again for plasma exchange and steroids at the start of a new episode.
“We managed her with caplacizumab and rituximab, and in a couple weeks she had recovered her ADAMTS13 activity and was able to stop the caplacizumab.” She was a motivated, knowledgeable person, “someone I trusted, so I was comfortable with the approach. I think that may be where we are headed in the future, hopefully,” he said.
Dr. Cataland disclosed research funding and consulting fees from Alexion, caplacizumab’s maker, Sanofi Genzyme, and Takeda,. The conference was sponsored by MedscapeLive. MedscapeLive and this news organization are owned by the same parent company.
As hematologists debated the role of the anti–von Willebrand factor agent caplacizumab for acquired thrombotic thrombocytopenic purpura (TTP), an investigator on the phase 3 trial that led to its approval had a message.
,” said hematologist Spero Cataland, MD, of the department of internal medicine at Ohio State University in Columbus.
If cost is going to be a factor, and it “has to be in our world these days, it’s more of a discussion,” he said during his presentation at the 2020 Update in Nonneoplastic Hematology virtual conference.
The HERCULES trial Dr. Cataland helped conduct found a median time to platelet count normalization of 2.69 days when caplacizumab was started during plasma exchange versus 2.88 days for placebo; 12% of patients had a TTP recurrence while they continued caplacizumab for 30 days past their last exchange and were followed for an additional 28 days versus 38% randomized to placebo. Caplacizumab subjects needed an average of 5.8 days of plasma exchange versus 9.4 days in the placebo arm (N Engl J Med. 2019 Jan 24;380(4):335-46).
Based on the results, the Food and Drug Administration approved the agent for acquired TTP in combination with plasma exchange and immunosuppressives in Feb. 2019 for 30 days beyond the last plasma exchange, with up to 28 additional days if ADAMTS13 activity remains suppressed. Labeling notes a risk of severe bleeding.
“The data on refractory disease and mortality aren’t quite there yet, but there’s a suggestion [caplacizumab] might impact that as well,” Dr. Cataland said. In its recent TTP guidelines, the International Society on Thrombosis and Haemostasis gave the agent only a conditional recommendation, in part because it’s backed up only by HERCULES and a phase 2 trial.
Also, the group noted that in the phase 2 study caplacizumab patients had a clinically and statistically significant increase in the number of relapses at 12 months: 31% versus 8% placebo. “Caplacizumab may leave patients prone to experience a later recurrence owing to the unresolved ADAMTS13 deficiency and inhibitors,” Dr. Cataland said.
“We do see some early recurrence” when caplacizumab is stopped, suggesting that when the agent’s “protective effect is removed, the risk is still there,” said Dr. Cataland, who was also an author on the ISTH guidelines, as well as the phase 2 trial.
It raises the question of how long patients should be kept on caplacizumab. There are few data on the issue, “but the consensus has been to stop caplacizumab when two consecutive ADAMTS13 measurements show 20% or greater activity,” or perhaps with one reading above 20% in a patient trending in the right direction. “With a bleeding complication, you might stop it sooner,” he said.
Dr. Cataland anticipates TTP management will eventually move away from plasma exchange to more directed therapies, including caplacizumab and perhaps recombinant ADAMTS13, which is in development.
There have been a few reports of TTP patients who refuse plasma exchange on religious grounds being successfully treated with caplacizumab. Dr. Cataland also noted a patient of his with relapsing TTP who didn’t want to be admitted yet again for plasma exchange and steroids at the start of a new episode.
“We managed her with caplacizumab and rituximab, and in a couple weeks she had recovered her ADAMTS13 activity and was able to stop the caplacizumab.” She was a motivated, knowledgeable person, “someone I trusted, so I was comfortable with the approach. I think that may be where we are headed in the future, hopefully,” he said.
Dr. Cataland disclosed research funding and consulting fees from Alexion, caplacizumab’s maker, Sanofi Genzyme, and Takeda,. The conference was sponsored by MedscapeLive. MedscapeLive and this news organization are owned by the same parent company.
FROM 2020 UNNH
NHS England starts pilot trial of blood test for many cancers
“Early detection, particularly for hard-to-treat conditions like ovarian and pancreatic cancer, has the potential to save many lives,” said NHS Chief Executive Sir Simon Stevens in a statement.
The pilot trial will use the Galleri blood test, developed by Grail. Sir Stevens described the blood test as “promising” and said it could “be a game changer in cancer care, helping thousands more people to get successful treatment.”
However, some clinicians have expressed concerns over the potential for false-positive results with the test.
Results of a study of the Galleri blood test, published earlier this year, showed that the test detected 50 types of cancer with a specificity of 99.3% and a false positive rate of 0.7%.
It also correctly identified the originating tissue in 90% of cases. However, the sensitivity was lower, at 67%, for the 12 most common cancers, as reported at the time.
The senior author of that study, Michael Seiden, MD, PhD, president of the U.S. Oncology Network, The Woodlands, Tex., noted that it was not a screening study: the test had been used in patients with cancer and in healthy volunteers. He said the test “is intended to be complementary to, and not replace, existing guideline-recommended screening tests and might provide new avenues of investigation for cancers that don’t currently have screening tests.”
The Galleri test uses next-generation sequencing to analyze the arrangement of methyl groups on circulating cell-free DNA in a blood sample.
Several other blood tests for cancer are under development, including the CancerSEEK test, which has been reported to be able to identify eight common cancers. It measures circulating tumor DNA from 16 genes and eight protein biomarkers and then uses machine learning to analyze the data.
Improving early detection rates
The pilot trial of the blood test is due to start in mid-2021 and will involve 165,000 people.
The trial will include 140,000 individuals aged 50-79 years who were identified through their health records and who have no cancer symptoms. They will undergo blood tests annually for 3 years and will be referred for investigation if a test result is positive.
A second group will include 25,000 people with potential cancer symptoms. These patients will be offered the blood test to speed up their diagnosis after referral to a hospital via the normal channels.
The results of the pilot are expected in 2023. If successful, the test will be rolled out to 1 million individuals from 2024 to 2025.
The pilot trial is part of the NHS Long Term Plan, which aims to increase early detection of cancer. At present, around half of cancers in England are diagnosed in stage I or II; the NHS aims to increase this to 75% by 2028.
“The NHS has set itself an ambitious target,” commented Peter Johnson, MD, PhD, national clinical director for cancer at NHS England and Improvement.
“Tests like this may help us get there far faster, and I am excited to see how this cutting-edge technology will work out as we test it in clinics across the NHS,” he added.
Lord David Prior, chair of NHS England, noted that almost 200,000 people die from cancer in the United Kingdom every year and that “many of these people are diagnosed too late for treatment to be effective.
“This collaboration between the NHS and Grail offers the chance for a wide range of cancers to be diagnosed much earlier and could fundamentally change the outlook for people with cancer,” he said.
However, some clinicians raised potential concerns.
Stephen Duffy, PhD, Center for Cancer Prevention, Queen Mary University of London, described the pilot as “very exciting,” but cautioned: “We will need to find out just how early the test detects cancers and whether it can it be used in a way which minimizes anxiety from false positives.”
Yong-Jie Lu, MD, PhD, also at Queen Mary University of London, said: “It is not clear how early it aims to catch cancer. For a cancer screen test, it needs very high specificity (>99%), otherwise it may end up in a similar situation as the PSA [prostate-specific antigen] test for prostate cancer, or even worse.”
Mangesh Thorat, MD, Cancer Prevention Trials Unit, King’s College London, warned: “It is likely that for every testing round ... there will be about 1,000 false-positive results, and the test may not be able to pinpoint the location of cancer in 3%-4% of those with a true positive result, necessitating a range of imaging and other investigations in these participants.”
No funding for the study has been declared. The investigators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
“Early detection, particularly for hard-to-treat conditions like ovarian and pancreatic cancer, has the potential to save many lives,” said NHS Chief Executive Sir Simon Stevens in a statement.
The pilot trial will use the Galleri blood test, developed by Grail. Sir Stevens described the blood test as “promising” and said it could “be a game changer in cancer care, helping thousands more people to get successful treatment.”
However, some clinicians have expressed concerns over the potential for false-positive results with the test.
Results of a study of the Galleri blood test, published earlier this year, showed that the test detected 50 types of cancer with a specificity of 99.3% and a false positive rate of 0.7%.
It also correctly identified the originating tissue in 90% of cases. However, the sensitivity was lower, at 67%, for the 12 most common cancers, as reported at the time.
The senior author of that study, Michael Seiden, MD, PhD, president of the U.S. Oncology Network, The Woodlands, Tex., noted that it was not a screening study: the test had been used in patients with cancer and in healthy volunteers. He said the test “is intended to be complementary to, and not replace, existing guideline-recommended screening tests and might provide new avenues of investigation for cancers that don’t currently have screening tests.”
The Galleri test uses next-generation sequencing to analyze the arrangement of methyl groups on circulating cell-free DNA in a blood sample.
Several other blood tests for cancer are under development, including the CancerSEEK test, which has been reported to be able to identify eight common cancers. It measures circulating tumor DNA from 16 genes and eight protein biomarkers and then uses machine learning to analyze the data.
Improving early detection rates
The pilot trial of the blood test is due to start in mid-2021 and will involve 165,000 people.
The trial will include 140,000 individuals aged 50-79 years who were identified through their health records and who have no cancer symptoms. They will undergo blood tests annually for 3 years and will be referred for investigation if a test result is positive.
A second group will include 25,000 people with potential cancer symptoms. These patients will be offered the blood test to speed up their diagnosis after referral to a hospital via the normal channels.
The results of the pilot are expected in 2023. If successful, the test will be rolled out to 1 million individuals from 2024 to 2025.
The pilot trial is part of the NHS Long Term Plan, which aims to increase early detection of cancer. At present, around half of cancers in England are diagnosed in stage I or II; the NHS aims to increase this to 75% by 2028.
“The NHS has set itself an ambitious target,” commented Peter Johnson, MD, PhD, national clinical director for cancer at NHS England and Improvement.
“Tests like this may help us get there far faster, and I am excited to see how this cutting-edge technology will work out as we test it in clinics across the NHS,” he added.
Lord David Prior, chair of NHS England, noted that almost 200,000 people die from cancer in the United Kingdom every year and that “many of these people are diagnosed too late for treatment to be effective.
“This collaboration between the NHS and Grail offers the chance for a wide range of cancers to be diagnosed much earlier and could fundamentally change the outlook for people with cancer,” he said.
However, some clinicians raised potential concerns.
Stephen Duffy, PhD, Center for Cancer Prevention, Queen Mary University of London, described the pilot as “very exciting,” but cautioned: “We will need to find out just how early the test detects cancers and whether it can it be used in a way which minimizes anxiety from false positives.”
Yong-Jie Lu, MD, PhD, also at Queen Mary University of London, said: “It is not clear how early it aims to catch cancer. For a cancer screen test, it needs very high specificity (>99%), otherwise it may end up in a similar situation as the PSA [prostate-specific antigen] test for prostate cancer, or even worse.”
Mangesh Thorat, MD, Cancer Prevention Trials Unit, King’s College London, warned: “It is likely that for every testing round ... there will be about 1,000 false-positive results, and the test may not be able to pinpoint the location of cancer in 3%-4% of those with a true positive result, necessitating a range of imaging and other investigations in these participants.”
No funding for the study has been declared. The investigators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
“Early detection, particularly for hard-to-treat conditions like ovarian and pancreatic cancer, has the potential to save many lives,” said NHS Chief Executive Sir Simon Stevens in a statement.
The pilot trial will use the Galleri blood test, developed by Grail. Sir Stevens described the blood test as “promising” and said it could “be a game changer in cancer care, helping thousands more people to get successful treatment.”
However, some clinicians have expressed concerns over the potential for false-positive results with the test.
Results of a study of the Galleri blood test, published earlier this year, showed that the test detected 50 types of cancer with a specificity of 99.3% and a false positive rate of 0.7%.
It also correctly identified the originating tissue in 90% of cases. However, the sensitivity was lower, at 67%, for the 12 most common cancers, as reported at the time.
The senior author of that study, Michael Seiden, MD, PhD, president of the U.S. Oncology Network, The Woodlands, Tex., noted that it was not a screening study: the test had been used in patients with cancer and in healthy volunteers. He said the test “is intended to be complementary to, and not replace, existing guideline-recommended screening tests and might provide new avenues of investigation for cancers that don’t currently have screening tests.”
The Galleri test uses next-generation sequencing to analyze the arrangement of methyl groups on circulating cell-free DNA in a blood sample.
Several other blood tests for cancer are under development, including the CancerSEEK test, which has been reported to be able to identify eight common cancers. It measures circulating tumor DNA from 16 genes and eight protein biomarkers and then uses machine learning to analyze the data.
Improving early detection rates
The pilot trial of the blood test is due to start in mid-2021 and will involve 165,000 people.
The trial will include 140,000 individuals aged 50-79 years who were identified through their health records and who have no cancer symptoms. They will undergo blood tests annually for 3 years and will be referred for investigation if a test result is positive.
A second group will include 25,000 people with potential cancer symptoms. These patients will be offered the blood test to speed up their diagnosis after referral to a hospital via the normal channels.
The results of the pilot are expected in 2023. If successful, the test will be rolled out to 1 million individuals from 2024 to 2025.
The pilot trial is part of the NHS Long Term Plan, which aims to increase early detection of cancer. At present, around half of cancers in England are diagnosed in stage I or II; the NHS aims to increase this to 75% by 2028.
“The NHS has set itself an ambitious target,” commented Peter Johnson, MD, PhD, national clinical director for cancer at NHS England and Improvement.
“Tests like this may help us get there far faster, and I am excited to see how this cutting-edge technology will work out as we test it in clinics across the NHS,” he added.
Lord David Prior, chair of NHS England, noted that almost 200,000 people die from cancer in the United Kingdom every year and that “many of these people are diagnosed too late for treatment to be effective.
“This collaboration between the NHS and Grail offers the chance for a wide range of cancers to be diagnosed much earlier and could fundamentally change the outlook for people with cancer,” he said.
However, some clinicians raised potential concerns.
Stephen Duffy, PhD, Center for Cancer Prevention, Queen Mary University of London, described the pilot as “very exciting,” but cautioned: “We will need to find out just how early the test detects cancers and whether it can it be used in a way which minimizes anxiety from false positives.”
Yong-Jie Lu, MD, PhD, also at Queen Mary University of London, said: “It is not clear how early it aims to catch cancer. For a cancer screen test, it needs very high specificity (>99%), otherwise it may end up in a similar situation as the PSA [prostate-specific antigen] test for prostate cancer, or even worse.”
Mangesh Thorat, MD, Cancer Prevention Trials Unit, King’s College London, warned: “It is likely that for every testing round ... there will be about 1,000 false-positive results, and the test may not be able to pinpoint the location of cancer in 3%-4% of those with a true positive result, necessitating a range of imaging and other investigations in these participants.”
No funding for the study has been declared. The investigators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
No benefit from tranexamic acid prophylaxis in blood cancers
Despite being routinely used in clinical settings, prophylactic use of tranexamic acid, an antifibrinolytic agent administered with platelet transfusions, did not reduce bleeding among patients with blood cancers and severe thrombocytopenia, according to a new study.
The study compared tranexamic acid to placebo and found no significant differences in terms of the number of bleeding events, the number of red blood cell transfusions, or the number of platelet transfusions that were required.
However, the rate of occlusions in the central venous line was significantly higher for patients in the tranexamic acid group, although there was no difference between groups for other types of thrombotic events.
The findings were presented at the annual meeting of the American Society of Hematology, which was held online.
The study was highlighted as potentially practice changing at a press preview webinar by ASH Secretary Robert Brodsky, MD.
“They found absolutely no difference in bleeding or need for transfusion,” said Brodsky. “What they did find was more catheter-associated blood clots in the tranexamic acid group. This is a practice changer in that it probably should not be given prophylactically to patients with thrombocytopenia.”
Senior author Terry B. Gernsheimer, MD, of the University of Washington, Seattle, noted that tranexamic acid has been found to be effective in the treatment of bleeding related to childbirth, surgery, and inherited blood disorders.
It is also used for patients with blood cancers and severe thrombocytopenia. There is little evidence to support this use, which is why the researchers decided to investigate.
“Clearly patients with low platelet counts and blood cancers have a different kind of bleeding than the bleeding experienced by patients who have suffered some kind of trauma or surgery,” Dr. Gernsheimer said in a statement.
“Their bleeding likely is due to endothelial damage – damage to the lining of blood vessels – that tranexamic acid would not treat,” she added.
“To prevent bleeding in these patients, we may need to look at ways to speed the healing of the endothelium that occurs with chemotherapy, radiation, and graft-vs-host disease in patients receiving a transplant,” Dr. Gernsheimer commented.
Temper enthusiasm
“Overall, I think these results will temper enthusiasm for using tranexamic acid in this setting,” said Mitul Gandhi, MD, a medical oncologist with Virginia Cancer Specialists, who was approached for comment.
These data do not support the routine use of prophylactic tranexamic acid in chemotherapy-induced thrombocytopenia for patients with platelet counts lower than 30,000/μL, he added.
“The primary objective was not met, and there was an observed increased rate of catheter-associated thrombosis,” he said. “Continued use of judicious transfusion support and correction of a concomitant coagulopathy remains the main clinical approach to these patients.”
Dr. Gandhi commented that tranexamic acid “remains a potentially useful adjunct agent in certain cases of recalcitrant bleeding related to thrombocytopenia or coagulopathy.
“While there is no uniform scenario, it is typically reserved on a case-by-case basis after addressing vascular defects, utilization of platelet, fresh frozen plasma, cryoprecipitate transfusions, vitamin K repletion, and of course excluding any antiplatelet or anticoagulant therapy,» he told this news organization. “For persistent bleeding in spite of all corrective measures or hemorrhage into noncompressible vascular beds, such as with intracranial bleeds, antifibrinolytic therapy may assist in mitigating further blood loss.”
However, this has to be balanced with the potential increased risk for thrombosis after correction of the hemostatic insult.
At present, tranexamic acid “only has an FDA indication for uterine bleeding, but it is frequently used in trauma settings and obstetrical emergencies,” said Douglas Tremblay, MD, an internist at the Icahn School of Medicine at Mount Sinai, New York, who was also approached for comment.
“There is evidence from prior studies that were done 20 or 30 years ago that it may help in this setting, so it is used in some institutions, although we don’t give it prophylactically for patients with a hematologic malignancy.”
Although this was a negative study, Dr. Tremblay pointed out that one thing that may come out of it is that there may be subgroups who can benefit from the prophylactic use of tranexamic acid. “There is very wide inclusion criteria for the study – any type of hematologic malignancy in patients undergoing chemotherapy or stem cell transplant,” he said in an interview. “Even among chemotherapy and transplant patients, there are different risks for bleeding.”
For example, patients undergoing induction chemotherapy for acute myeloid leukemia are at an increased risk of bleeding in comparison with patients with other hematologic malignancies, and those undergoing allogeneic transplant are at an increased risk of bleeding in comparison with patients undergoing autologous transplant. “So while its unclear if a subgroup may benefit from this strategy, lumped together, it doesn’t appear it is of any benefit and potentially harmful, in terms of line occlusions,” he said. “While that may seem to be a nuisance, it can delay chemotherapy or supportive infusions, and that can be a big deal.”
No evidence of benefit
Dr. Gernsheimer and colleagues conducted the American Trial Using Tranexamic Acid in Thrombocytopenia (A-TREAT), which evaluated the effects of prophylactic tranexamic acid as an adjunct to routine transfusion therapy on bleeding and transfusion requirements.
A total of 330 patients were randomly assigned to receive either tranexamic acid 1,000 mg IV or 1,300 mg or placebo. Randomization was stratified by site and therapy: chemotherapy, allogeneic transplant, or autologous transplant. It was anticipated that all patients had hypoproliferative thrombocytopenia (expected platelet count, 10,000/µL for at least 5 days).
Treatment continued for 30 days or platelet count recovery (>30,000/µL), diagnosis of thrombosis or veno-occlusive disease, recurrent line occlusion, visible hematuria, or physician or patient request.
The primary endpoint of the study was the proportion of patients with bleeding of World Health Organization grade 2 or above over 30 days after beginning therapy. Secondary endpoints included the number of transfusions and the number of days alive without WHO grade 2+ bleeding during the first 30 days post activation of study drug.
The time to first WHO 2+ bleeding was “remarkably similar” between the tranexamic acid groups and the placebo group, said Dr. Gernsheimer.
In the cohort as a whole, 48.8% in the placebo group experienced a grade 2+ bleed vs. 45.4% in the tranexamic group (odds ratio, 0.86).
Similar results were observed across subgroups: allogeneic transplant, 57.3% vs. 58.8% (OR, 0.94); autologous transplant, 19.9% vs. 24.7% ( OR, 0.71); or chemotherapy, 48% vs. 52.1% (OR, 0.84).
There were no significant differences in mean number of transfusions (difference, 0.1; 95% confidence interval, –1.9 to 2) or days alive without grade 2 or higher bleeding (difference, 0.1; 95% CI, –1.4 to 1.5).
“A post hoc analysis of WHO 3+ bleeding showed these events to be rare and without any improvement with tranexamic acid,” she said.
A higher percentage of patients in the tranexamic acid group experienced thrombotic events (19.5% vs. 11%). “But importantly, in both groups, it was primarily due to central line occlusions without an associated thrombus,” said Dr. Gernsheimer. “This was statistically significant.”
Fewer non–catheter related thrombotic events occurred in the tranexamic acid group (3.7% vs. 5.5%), but the difference was not statistically significant.
There was also no significant difference between groups in veno-occlusive disease after 30 days (1.8% vs. 1.2%) or all-cause mortality at 30 days (2.4% vs. 3%) or 100 days (11.5% vs. 11.5%). No deaths associated with thrombosis had occurred in either group at 120 days.
The study was supported by the University of Washington and the National Heart, Lung, and Blood Institute. Dr. Gernsheimer has relationships with Amgen, Cellphire, Dova Pharmaceuticals, Novartis, Principia, Rigel, Sanofi, and Vertex. Dr. Tremblay and Dr. Gandhi have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Despite being routinely used in clinical settings, prophylactic use of tranexamic acid, an antifibrinolytic agent administered with platelet transfusions, did not reduce bleeding among patients with blood cancers and severe thrombocytopenia, according to a new study.
The study compared tranexamic acid to placebo and found no significant differences in terms of the number of bleeding events, the number of red blood cell transfusions, or the number of platelet transfusions that were required.
However, the rate of occlusions in the central venous line was significantly higher for patients in the tranexamic acid group, although there was no difference between groups for other types of thrombotic events.
The findings were presented at the annual meeting of the American Society of Hematology, which was held online.
The study was highlighted as potentially practice changing at a press preview webinar by ASH Secretary Robert Brodsky, MD.
“They found absolutely no difference in bleeding or need for transfusion,” said Brodsky. “What they did find was more catheter-associated blood clots in the tranexamic acid group. This is a practice changer in that it probably should not be given prophylactically to patients with thrombocytopenia.”
Senior author Terry B. Gernsheimer, MD, of the University of Washington, Seattle, noted that tranexamic acid has been found to be effective in the treatment of bleeding related to childbirth, surgery, and inherited blood disorders.
It is also used for patients with blood cancers and severe thrombocytopenia. There is little evidence to support this use, which is why the researchers decided to investigate.
“Clearly patients with low platelet counts and blood cancers have a different kind of bleeding than the bleeding experienced by patients who have suffered some kind of trauma or surgery,” Dr. Gernsheimer said in a statement.
“Their bleeding likely is due to endothelial damage – damage to the lining of blood vessels – that tranexamic acid would not treat,” she added.
“To prevent bleeding in these patients, we may need to look at ways to speed the healing of the endothelium that occurs with chemotherapy, radiation, and graft-vs-host disease in patients receiving a transplant,” Dr. Gernsheimer commented.
Temper enthusiasm
“Overall, I think these results will temper enthusiasm for using tranexamic acid in this setting,” said Mitul Gandhi, MD, a medical oncologist with Virginia Cancer Specialists, who was approached for comment.
These data do not support the routine use of prophylactic tranexamic acid in chemotherapy-induced thrombocytopenia for patients with platelet counts lower than 30,000/μL, he added.
“The primary objective was not met, and there was an observed increased rate of catheter-associated thrombosis,” he said. “Continued use of judicious transfusion support and correction of a concomitant coagulopathy remains the main clinical approach to these patients.”
Dr. Gandhi commented that tranexamic acid “remains a potentially useful adjunct agent in certain cases of recalcitrant bleeding related to thrombocytopenia or coagulopathy.
“While there is no uniform scenario, it is typically reserved on a case-by-case basis after addressing vascular defects, utilization of platelet, fresh frozen plasma, cryoprecipitate transfusions, vitamin K repletion, and of course excluding any antiplatelet or anticoagulant therapy,» he told this news organization. “For persistent bleeding in spite of all corrective measures or hemorrhage into noncompressible vascular beds, such as with intracranial bleeds, antifibrinolytic therapy may assist in mitigating further blood loss.”
However, this has to be balanced with the potential increased risk for thrombosis after correction of the hemostatic insult.
At present, tranexamic acid “only has an FDA indication for uterine bleeding, but it is frequently used in trauma settings and obstetrical emergencies,” said Douglas Tremblay, MD, an internist at the Icahn School of Medicine at Mount Sinai, New York, who was also approached for comment.
“There is evidence from prior studies that were done 20 or 30 years ago that it may help in this setting, so it is used in some institutions, although we don’t give it prophylactically for patients with a hematologic malignancy.”
Although this was a negative study, Dr. Tremblay pointed out that one thing that may come out of it is that there may be subgroups who can benefit from the prophylactic use of tranexamic acid. “There is very wide inclusion criteria for the study – any type of hematologic malignancy in patients undergoing chemotherapy or stem cell transplant,” he said in an interview. “Even among chemotherapy and transplant patients, there are different risks for bleeding.”
For example, patients undergoing induction chemotherapy for acute myeloid leukemia are at an increased risk of bleeding in comparison with patients with other hematologic malignancies, and those undergoing allogeneic transplant are at an increased risk of bleeding in comparison with patients undergoing autologous transplant. “So while its unclear if a subgroup may benefit from this strategy, lumped together, it doesn’t appear it is of any benefit and potentially harmful, in terms of line occlusions,” he said. “While that may seem to be a nuisance, it can delay chemotherapy or supportive infusions, and that can be a big deal.”
No evidence of benefit
Dr. Gernsheimer and colleagues conducted the American Trial Using Tranexamic Acid in Thrombocytopenia (A-TREAT), which evaluated the effects of prophylactic tranexamic acid as an adjunct to routine transfusion therapy on bleeding and transfusion requirements.
A total of 330 patients were randomly assigned to receive either tranexamic acid 1,000 mg IV or 1,300 mg or placebo. Randomization was stratified by site and therapy: chemotherapy, allogeneic transplant, or autologous transplant. It was anticipated that all patients had hypoproliferative thrombocytopenia (expected platelet count, 10,000/µL for at least 5 days).
Treatment continued for 30 days or platelet count recovery (>30,000/µL), diagnosis of thrombosis or veno-occlusive disease, recurrent line occlusion, visible hematuria, or physician or patient request.
The primary endpoint of the study was the proportion of patients with bleeding of World Health Organization grade 2 or above over 30 days after beginning therapy. Secondary endpoints included the number of transfusions and the number of days alive without WHO grade 2+ bleeding during the first 30 days post activation of study drug.
The time to first WHO 2+ bleeding was “remarkably similar” between the tranexamic acid groups and the placebo group, said Dr. Gernsheimer.
In the cohort as a whole, 48.8% in the placebo group experienced a grade 2+ bleed vs. 45.4% in the tranexamic group (odds ratio, 0.86).
Similar results were observed across subgroups: allogeneic transplant, 57.3% vs. 58.8% (OR, 0.94); autologous transplant, 19.9% vs. 24.7% ( OR, 0.71); or chemotherapy, 48% vs. 52.1% (OR, 0.84).
There were no significant differences in mean number of transfusions (difference, 0.1; 95% confidence interval, –1.9 to 2) or days alive without grade 2 or higher bleeding (difference, 0.1; 95% CI, –1.4 to 1.5).
“A post hoc analysis of WHO 3+ bleeding showed these events to be rare and without any improvement with tranexamic acid,” she said.
A higher percentage of patients in the tranexamic acid group experienced thrombotic events (19.5% vs. 11%). “But importantly, in both groups, it was primarily due to central line occlusions without an associated thrombus,” said Dr. Gernsheimer. “This was statistically significant.”
Fewer non–catheter related thrombotic events occurred in the tranexamic acid group (3.7% vs. 5.5%), but the difference was not statistically significant.
There was also no significant difference between groups in veno-occlusive disease after 30 days (1.8% vs. 1.2%) or all-cause mortality at 30 days (2.4% vs. 3%) or 100 days (11.5% vs. 11.5%). No deaths associated with thrombosis had occurred in either group at 120 days.
The study was supported by the University of Washington and the National Heart, Lung, and Blood Institute. Dr. Gernsheimer has relationships with Amgen, Cellphire, Dova Pharmaceuticals, Novartis, Principia, Rigel, Sanofi, and Vertex. Dr. Tremblay and Dr. Gandhi have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Despite being routinely used in clinical settings, prophylactic use of tranexamic acid, an antifibrinolytic agent administered with platelet transfusions, did not reduce bleeding among patients with blood cancers and severe thrombocytopenia, according to a new study.
The study compared tranexamic acid to placebo and found no significant differences in terms of the number of bleeding events, the number of red blood cell transfusions, or the number of platelet transfusions that were required.
However, the rate of occlusions in the central venous line was significantly higher for patients in the tranexamic acid group, although there was no difference between groups for other types of thrombotic events.
The findings were presented at the annual meeting of the American Society of Hematology, which was held online.
The study was highlighted as potentially practice changing at a press preview webinar by ASH Secretary Robert Brodsky, MD.
“They found absolutely no difference in bleeding or need for transfusion,” said Brodsky. “What they did find was more catheter-associated blood clots in the tranexamic acid group. This is a practice changer in that it probably should not be given prophylactically to patients with thrombocytopenia.”
Senior author Terry B. Gernsheimer, MD, of the University of Washington, Seattle, noted that tranexamic acid has been found to be effective in the treatment of bleeding related to childbirth, surgery, and inherited blood disorders.
It is also used for patients with blood cancers and severe thrombocytopenia. There is little evidence to support this use, which is why the researchers decided to investigate.
“Clearly patients with low platelet counts and blood cancers have a different kind of bleeding than the bleeding experienced by patients who have suffered some kind of trauma or surgery,” Dr. Gernsheimer said in a statement.
“Their bleeding likely is due to endothelial damage – damage to the lining of blood vessels – that tranexamic acid would not treat,” she added.
“To prevent bleeding in these patients, we may need to look at ways to speed the healing of the endothelium that occurs with chemotherapy, radiation, and graft-vs-host disease in patients receiving a transplant,” Dr. Gernsheimer commented.
Temper enthusiasm
“Overall, I think these results will temper enthusiasm for using tranexamic acid in this setting,” said Mitul Gandhi, MD, a medical oncologist with Virginia Cancer Specialists, who was approached for comment.
These data do not support the routine use of prophylactic tranexamic acid in chemotherapy-induced thrombocytopenia for patients with platelet counts lower than 30,000/μL, he added.
“The primary objective was not met, and there was an observed increased rate of catheter-associated thrombosis,” he said. “Continued use of judicious transfusion support and correction of a concomitant coagulopathy remains the main clinical approach to these patients.”
Dr. Gandhi commented that tranexamic acid “remains a potentially useful adjunct agent in certain cases of recalcitrant bleeding related to thrombocytopenia or coagulopathy.
“While there is no uniform scenario, it is typically reserved on a case-by-case basis after addressing vascular defects, utilization of platelet, fresh frozen plasma, cryoprecipitate transfusions, vitamin K repletion, and of course excluding any antiplatelet or anticoagulant therapy,» he told this news organization. “For persistent bleeding in spite of all corrective measures or hemorrhage into noncompressible vascular beds, such as with intracranial bleeds, antifibrinolytic therapy may assist in mitigating further blood loss.”
However, this has to be balanced with the potential increased risk for thrombosis after correction of the hemostatic insult.
At present, tranexamic acid “only has an FDA indication for uterine bleeding, but it is frequently used in trauma settings and obstetrical emergencies,” said Douglas Tremblay, MD, an internist at the Icahn School of Medicine at Mount Sinai, New York, who was also approached for comment.
“There is evidence from prior studies that were done 20 or 30 years ago that it may help in this setting, so it is used in some institutions, although we don’t give it prophylactically for patients with a hematologic malignancy.”
Although this was a negative study, Dr. Tremblay pointed out that one thing that may come out of it is that there may be subgroups who can benefit from the prophylactic use of tranexamic acid. “There is very wide inclusion criteria for the study – any type of hematologic malignancy in patients undergoing chemotherapy or stem cell transplant,” he said in an interview. “Even among chemotherapy and transplant patients, there are different risks for bleeding.”
For example, patients undergoing induction chemotherapy for acute myeloid leukemia are at an increased risk of bleeding in comparison with patients with other hematologic malignancies, and those undergoing allogeneic transplant are at an increased risk of bleeding in comparison with patients undergoing autologous transplant. “So while its unclear if a subgroup may benefit from this strategy, lumped together, it doesn’t appear it is of any benefit and potentially harmful, in terms of line occlusions,” he said. “While that may seem to be a nuisance, it can delay chemotherapy or supportive infusions, and that can be a big deal.”
No evidence of benefit
Dr. Gernsheimer and colleagues conducted the American Trial Using Tranexamic Acid in Thrombocytopenia (A-TREAT), which evaluated the effects of prophylactic tranexamic acid as an adjunct to routine transfusion therapy on bleeding and transfusion requirements.
A total of 330 patients were randomly assigned to receive either tranexamic acid 1,000 mg IV or 1,300 mg or placebo. Randomization was stratified by site and therapy: chemotherapy, allogeneic transplant, or autologous transplant. It was anticipated that all patients had hypoproliferative thrombocytopenia (expected platelet count, 10,000/µL for at least 5 days).
Treatment continued for 30 days or platelet count recovery (>30,000/µL), diagnosis of thrombosis or veno-occlusive disease, recurrent line occlusion, visible hematuria, or physician or patient request.
The primary endpoint of the study was the proportion of patients with bleeding of World Health Organization grade 2 or above over 30 days after beginning therapy. Secondary endpoints included the number of transfusions and the number of days alive without WHO grade 2+ bleeding during the first 30 days post activation of study drug.
The time to first WHO 2+ bleeding was “remarkably similar” between the tranexamic acid groups and the placebo group, said Dr. Gernsheimer.
In the cohort as a whole, 48.8% in the placebo group experienced a grade 2+ bleed vs. 45.4% in the tranexamic group (odds ratio, 0.86).
Similar results were observed across subgroups: allogeneic transplant, 57.3% vs. 58.8% (OR, 0.94); autologous transplant, 19.9% vs. 24.7% ( OR, 0.71); or chemotherapy, 48% vs. 52.1% (OR, 0.84).
There were no significant differences in mean number of transfusions (difference, 0.1; 95% confidence interval, –1.9 to 2) or days alive without grade 2 or higher bleeding (difference, 0.1; 95% CI, –1.4 to 1.5).
“A post hoc analysis of WHO 3+ bleeding showed these events to be rare and without any improvement with tranexamic acid,” she said.
A higher percentage of patients in the tranexamic acid group experienced thrombotic events (19.5% vs. 11%). “But importantly, in both groups, it was primarily due to central line occlusions without an associated thrombus,” said Dr. Gernsheimer. “This was statistically significant.”
Fewer non–catheter related thrombotic events occurred in the tranexamic acid group (3.7% vs. 5.5%), but the difference was not statistically significant.
There was also no significant difference between groups in veno-occlusive disease after 30 days (1.8% vs. 1.2%) or all-cause mortality at 30 days (2.4% vs. 3%) or 100 days (11.5% vs. 11.5%). No deaths associated with thrombosis had occurred in either group at 120 days.
The study was supported by the University of Washington and the National Heart, Lung, and Blood Institute. Dr. Gernsheimer has relationships with Amgen, Cellphire, Dova Pharmaceuticals, Novartis, Principia, Rigel, Sanofi, and Vertex. Dr. Tremblay and Dr. Gandhi have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Childhood Hodgkin survivors have neurocognitive impairment
More than 2 decades on, adult survivors of childhood Hodgkin lymphoma report significantly more neurocognitive impairment than their siblings, but the differences may be related to risk factors in adulthood rather than to treatment in childhood, investigators say.
Among adults with a history of childhood Hodgkin lymphoma and their siblings as controls, the survivors reported significantly worse functioning than their brothers or sisters in four domains of neurocognitive functioning.
In multivariate analysis, however, while sex, race, activity level and smoking status were all significant predictors for worse neurocognitive impairment, there were no significant associations between chemotherapy drugs or chest radiation and neurocognitive impairment, said Annalynn M. Williams, PhD, from St. Jude Children’s Research Hospital in Memphis.
“Hodgkin lymphoma is the most common cancer diagnosed in adolescents, and for many years we’ve had high cure rates, resulting in a growing population of survivors who are now, unfortunately, at an increased risk for cardiovascular, respiratory, endocrine and neurologic late morbidity. The neurocognitive morbidity in this population, however, is unknown,” she said in oral abstract presented at the annual meeting of the American Society of Hematology.
Survivors and sibs
To better characterize the potential late neurocognitive effects of intensive Hodgkin lymphoma therapy in childhood, Dr. Williams and colleagues polled survivors of childhood Hodgkin lymphoma and randomly selected sibling controls who were participants in the Childhood Cancer Survivor Study (CCSS).
Participants were asked to complete questionnaires regarding four domains of neurocognitive impairment: task efficiency, emotional regulation, organization, and memory. The investigators defined impairment in each domain as a score lower than that of the 90th percentile of community controls from the St. Jude Lifetime Cohort.
A total of 1,564 survivors and 725 controls completed the questionnaires and were included in the study.
The median age at follow-up was slightly higher among survivors, at 37 versus 32 years. The median age at diagnosis was 14, and the median time since diagnosis was 23 years.
In all, 10.8% of survivors reported impaired task efficiency, compared with 7.7% of controls. Problems with emotional regulation were reported by 16.6% of survivors versus 11.5% of siblings, and difficulties with organization and memory were reported by 12.1% versus10.3%, and 8.1% versus 5.7%, respectively.
In a model adjusted for age, sex, and race, the relative risks for neurocognitive impairment among survivors versus siblings, were as follows: task efficiency (RR,1.37); emotional regulation (RR, 1.56); organization (RR, 1.32); memory (RR, 1.72) (all significant by confidence interval).
In a model adjusted for sex, race, smoking status, exercise, age, time since diagnosis, and treatment exposures, risk factors for neurocognitive impairment among survivors included female versus male sex (significant for emotional regulation and memory deficits); non-White versus White (significant for task efficiency); former smoker versus never (significant for all domains except organization); current smoker versus never (significant for task efficiency and emotional regulation); and meeting Centers for Disease Control and Prevention exercise criteria versus not (negatively significant for task efficiency and organization); (P < .05 for all above comparisons).
However, in a model adjusted for relapse, second malignancy, treatment exposures, age, sex, race, time since diagnosis, smoking status and physical activity, only relapse or second malignancy – surrogates for additional treatment exposures – were significantly associated with neurocognitive impairment, and then only in the domain of task efficiency.
Chronic conditions significantly associated with risk for impairment included cardiovascular disease (significant across all domains), respiratory comorbidities (significant for task efficiency), endocrine disorders (significant for task efficiency), and neurologic disorders (significant in all domains except organization).
“While these analyses give us a sense of the presence of neurocognitive impairment in a large sample of Hodgkin lymphoma survivors from across the U.S., these analyses are limited by the self-reported nature of the data,” Dr. Williams acknowledged.
“Because survivors self-report impairments, these likely represent overt, symptomatic neurocognitive impairments. Many more survivors may experience more subtle neurocognitive impairments, and additional research with objective measures of both chronic health conditions and neurocognitive functioning are warranted,” she added.
Smoking gun?
In the question-and-answer session following the presentation, session comoderator Pallawi Torka, MD, from Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., who was not involved in the research, commented that the finding regarding a link between current and former smoking as risk factors for neurocognitive impairment was “intriguing.”
“Do you think that smoking is a cause or an effect of having that impairment in childhood survivors of Hodgkin lymphoma?” she asked.
“That’s a great question, and actually one we have spent a great deal of time discussing, and we’re still trying to tease that apart. We’re still not really sure where that association is coming from,” Dr. Williams replied.
She noted that, in a different sample of CCSS participants from whom biospecimens were collected, the investigators plan to see whether smoking drives inflammation and oxidative stress mechanisms that may be contributing to neurocognitive impairment, or whether smoking is a coping mechanism related to anxiety and depression, which have also been seen in survivors.
Kara Kelly, MD, a pediatric oncologist at Roswell Park, commented that some survivors report symptoms of cognitive dysfunction shortly after treatment, and asked whether there might be a relationship to Hodgkin-specific factors such as B symptoms, in which cytokine-mediated inflammation may play a role.
Dr. Williams said that, “unfortunately, in CCSS these survivors had to be at least 5 years from diagnosis, but in many cases were recruited years after their diagnosis and treatment, so we don’t have data on B symptoms.”
The CCSS is funded by the National Cancer Institute. Dr. Williams, Dr. Palawi, and Dr. Kelly all reported no relevant conflicts of interest to disclose.
SOURCE: Williams AM et al. ASH 2020, Abstract 370.
More than 2 decades on, adult survivors of childhood Hodgkin lymphoma report significantly more neurocognitive impairment than their siblings, but the differences may be related to risk factors in adulthood rather than to treatment in childhood, investigators say.
Among adults with a history of childhood Hodgkin lymphoma and their siblings as controls, the survivors reported significantly worse functioning than their brothers or sisters in four domains of neurocognitive functioning.
In multivariate analysis, however, while sex, race, activity level and smoking status were all significant predictors for worse neurocognitive impairment, there were no significant associations between chemotherapy drugs or chest radiation and neurocognitive impairment, said Annalynn M. Williams, PhD, from St. Jude Children’s Research Hospital in Memphis.
“Hodgkin lymphoma is the most common cancer diagnosed in adolescents, and for many years we’ve had high cure rates, resulting in a growing population of survivors who are now, unfortunately, at an increased risk for cardiovascular, respiratory, endocrine and neurologic late morbidity. The neurocognitive morbidity in this population, however, is unknown,” she said in oral abstract presented at the annual meeting of the American Society of Hematology.
Survivors and sibs
To better characterize the potential late neurocognitive effects of intensive Hodgkin lymphoma therapy in childhood, Dr. Williams and colleagues polled survivors of childhood Hodgkin lymphoma and randomly selected sibling controls who were participants in the Childhood Cancer Survivor Study (CCSS).
Participants were asked to complete questionnaires regarding four domains of neurocognitive impairment: task efficiency, emotional regulation, organization, and memory. The investigators defined impairment in each domain as a score lower than that of the 90th percentile of community controls from the St. Jude Lifetime Cohort.
A total of 1,564 survivors and 725 controls completed the questionnaires and were included in the study.
The median age at follow-up was slightly higher among survivors, at 37 versus 32 years. The median age at diagnosis was 14, and the median time since diagnosis was 23 years.
In all, 10.8% of survivors reported impaired task efficiency, compared with 7.7% of controls. Problems with emotional regulation were reported by 16.6% of survivors versus 11.5% of siblings, and difficulties with organization and memory were reported by 12.1% versus10.3%, and 8.1% versus 5.7%, respectively.
In a model adjusted for age, sex, and race, the relative risks for neurocognitive impairment among survivors versus siblings, were as follows: task efficiency (RR,1.37); emotional regulation (RR, 1.56); organization (RR, 1.32); memory (RR, 1.72) (all significant by confidence interval).
In a model adjusted for sex, race, smoking status, exercise, age, time since diagnosis, and treatment exposures, risk factors for neurocognitive impairment among survivors included female versus male sex (significant for emotional regulation and memory deficits); non-White versus White (significant for task efficiency); former smoker versus never (significant for all domains except organization); current smoker versus never (significant for task efficiency and emotional regulation); and meeting Centers for Disease Control and Prevention exercise criteria versus not (negatively significant for task efficiency and organization); (P < .05 for all above comparisons).
However, in a model adjusted for relapse, second malignancy, treatment exposures, age, sex, race, time since diagnosis, smoking status and physical activity, only relapse or second malignancy – surrogates for additional treatment exposures – were significantly associated with neurocognitive impairment, and then only in the domain of task efficiency.
Chronic conditions significantly associated with risk for impairment included cardiovascular disease (significant across all domains), respiratory comorbidities (significant for task efficiency), endocrine disorders (significant for task efficiency), and neurologic disorders (significant in all domains except organization).
“While these analyses give us a sense of the presence of neurocognitive impairment in a large sample of Hodgkin lymphoma survivors from across the U.S., these analyses are limited by the self-reported nature of the data,” Dr. Williams acknowledged.
“Because survivors self-report impairments, these likely represent overt, symptomatic neurocognitive impairments. Many more survivors may experience more subtle neurocognitive impairments, and additional research with objective measures of both chronic health conditions and neurocognitive functioning are warranted,” she added.
Smoking gun?
In the question-and-answer session following the presentation, session comoderator Pallawi Torka, MD, from Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., who was not involved in the research, commented that the finding regarding a link between current and former smoking as risk factors for neurocognitive impairment was “intriguing.”
“Do you think that smoking is a cause or an effect of having that impairment in childhood survivors of Hodgkin lymphoma?” she asked.
“That’s a great question, and actually one we have spent a great deal of time discussing, and we’re still trying to tease that apart. We’re still not really sure where that association is coming from,” Dr. Williams replied.
She noted that, in a different sample of CCSS participants from whom biospecimens were collected, the investigators plan to see whether smoking drives inflammation and oxidative stress mechanisms that may be contributing to neurocognitive impairment, or whether smoking is a coping mechanism related to anxiety and depression, which have also been seen in survivors.
Kara Kelly, MD, a pediatric oncologist at Roswell Park, commented that some survivors report symptoms of cognitive dysfunction shortly after treatment, and asked whether there might be a relationship to Hodgkin-specific factors such as B symptoms, in which cytokine-mediated inflammation may play a role.
Dr. Williams said that, “unfortunately, in CCSS these survivors had to be at least 5 years from diagnosis, but in many cases were recruited years after their diagnosis and treatment, so we don’t have data on B symptoms.”
The CCSS is funded by the National Cancer Institute. Dr. Williams, Dr. Palawi, and Dr. Kelly all reported no relevant conflicts of interest to disclose.
SOURCE: Williams AM et al. ASH 2020, Abstract 370.
More than 2 decades on, adult survivors of childhood Hodgkin lymphoma report significantly more neurocognitive impairment than their siblings, but the differences may be related to risk factors in adulthood rather than to treatment in childhood, investigators say.
Among adults with a history of childhood Hodgkin lymphoma and their siblings as controls, the survivors reported significantly worse functioning than their brothers or sisters in four domains of neurocognitive functioning.
In multivariate analysis, however, while sex, race, activity level and smoking status were all significant predictors for worse neurocognitive impairment, there were no significant associations between chemotherapy drugs or chest radiation and neurocognitive impairment, said Annalynn M. Williams, PhD, from St. Jude Children’s Research Hospital in Memphis.
“Hodgkin lymphoma is the most common cancer diagnosed in adolescents, and for many years we’ve had high cure rates, resulting in a growing population of survivors who are now, unfortunately, at an increased risk for cardiovascular, respiratory, endocrine and neurologic late morbidity. The neurocognitive morbidity in this population, however, is unknown,” she said in oral abstract presented at the annual meeting of the American Society of Hematology.
Survivors and sibs
To better characterize the potential late neurocognitive effects of intensive Hodgkin lymphoma therapy in childhood, Dr. Williams and colleagues polled survivors of childhood Hodgkin lymphoma and randomly selected sibling controls who were participants in the Childhood Cancer Survivor Study (CCSS).
Participants were asked to complete questionnaires regarding four domains of neurocognitive impairment: task efficiency, emotional regulation, organization, and memory. The investigators defined impairment in each domain as a score lower than that of the 90th percentile of community controls from the St. Jude Lifetime Cohort.
A total of 1,564 survivors and 725 controls completed the questionnaires and were included in the study.
The median age at follow-up was slightly higher among survivors, at 37 versus 32 years. The median age at diagnosis was 14, and the median time since diagnosis was 23 years.
In all, 10.8% of survivors reported impaired task efficiency, compared with 7.7% of controls. Problems with emotional regulation were reported by 16.6% of survivors versus 11.5% of siblings, and difficulties with organization and memory were reported by 12.1% versus10.3%, and 8.1% versus 5.7%, respectively.
In a model adjusted for age, sex, and race, the relative risks for neurocognitive impairment among survivors versus siblings, were as follows: task efficiency (RR,1.37); emotional regulation (RR, 1.56); organization (RR, 1.32); memory (RR, 1.72) (all significant by confidence interval).
In a model adjusted for sex, race, smoking status, exercise, age, time since diagnosis, and treatment exposures, risk factors for neurocognitive impairment among survivors included female versus male sex (significant for emotional regulation and memory deficits); non-White versus White (significant for task efficiency); former smoker versus never (significant for all domains except organization); current smoker versus never (significant for task efficiency and emotional regulation); and meeting Centers for Disease Control and Prevention exercise criteria versus not (negatively significant for task efficiency and organization); (P < .05 for all above comparisons).
However, in a model adjusted for relapse, second malignancy, treatment exposures, age, sex, race, time since diagnosis, smoking status and physical activity, only relapse or second malignancy – surrogates for additional treatment exposures – were significantly associated with neurocognitive impairment, and then only in the domain of task efficiency.
Chronic conditions significantly associated with risk for impairment included cardiovascular disease (significant across all domains), respiratory comorbidities (significant for task efficiency), endocrine disorders (significant for task efficiency), and neurologic disorders (significant in all domains except organization).
“While these analyses give us a sense of the presence of neurocognitive impairment in a large sample of Hodgkin lymphoma survivors from across the U.S., these analyses are limited by the self-reported nature of the data,” Dr. Williams acknowledged.
“Because survivors self-report impairments, these likely represent overt, symptomatic neurocognitive impairments. Many more survivors may experience more subtle neurocognitive impairments, and additional research with objective measures of both chronic health conditions and neurocognitive functioning are warranted,” she added.
Smoking gun?
In the question-and-answer session following the presentation, session comoderator Pallawi Torka, MD, from Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., who was not involved in the research, commented that the finding regarding a link between current and former smoking as risk factors for neurocognitive impairment was “intriguing.”
“Do you think that smoking is a cause or an effect of having that impairment in childhood survivors of Hodgkin lymphoma?” she asked.
“That’s a great question, and actually one we have spent a great deal of time discussing, and we’re still trying to tease that apart. We’re still not really sure where that association is coming from,” Dr. Williams replied.
She noted that, in a different sample of CCSS participants from whom biospecimens were collected, the investigators plan to see whether smoking drives inflammation and oxidative stress mechanisms that may be contributing to neurocognitive impairment, or whether smoking is a coping mechanism related to anxiety and depression, which have also been seen in survivors.
Kara Kelly, MD, a pediatric oncologist at Roswell Park, commented that some survivors report symptoms of cognitive dysfunction shortly after treatment, and asked whether there might be a relationship to Hodgkin-specific factors such as B symptoms, in which cytokine-mediated inflammation may play a role.
Dr. Williams said that, “unfortunately, in CCSS these survivors had to be at least 5 years from diagnosis, but in many cases were recruited years after their diagnosis and treatment, so we don’t have data on B symptoms.”
The CCSS is funded by the National Cancer Institute. Dr. Williams, Dr. Palawi, and Dr. Kelly all reported no relevant conflicts of interest to disclose.
SOURCE: Williams AM et al. ASH 2020, Abstract 370.
FROM ASH 2020
PPE shortage crisis continues at most hospitals, survey shows
A majority of hospitals and health care facilities surveyed report operating according to “crisis standards of care” as they struggle to provide sufficient personal protective equipment (PPE).
For example, in a national survey, 73% of 1,083 infection prevention experts said respirator shortages related to care for patients with COVID-19 drove their facility to move beyond conventional standards of care. Furthermore, 69% of facilities are using crisis standards of care (CSC) to provide masks, and 76% are apportioning face shields or eye protection.
Almost 76% of respondents who report reusing respirators said their facility allows them to use each respirator either five times or as many times as possible before replacement; 74% allow similar reuse of masks.
Although the majority of institutions remain in this crisis mode, many health care providers have better access to PPE than they did in the spring 2020, the Association for Professionals in Infection Control and Epidemiology (APIC) noted in its latest national survey.
“It is disheartening to see our healthcare system strained and implementing PPE crisis standards of care more than eight months into the pandemic,” APIC President Connie Steed, MSN, RN, said in a December 3 news release.
The association surveyed experts online between Oct. 22 and Nov. 5. The survey was timed to gauge the extent of resource shortages as COVID-19 cases increase and the 2020-2021 flu season begins.
“Many of us on the front lines are waiting for the other shoe to drop. With the upcoming flu season, we implore people to do what they can to keep safe, protect our healthcare personnel, and lessen the strain on our health care system,” Ms. Steed said.
COVID-19 linked to more infections, too
APIC also asked infection prevention specialists about changes in health care–associated infection rates since the onset of the pandemic. The experts reported an almost 28% increase in central line–associated bloodstream infections and 21% more catheter-associated urinary tract infections. They also reported an 18% rise in ventilator-associated pneumonia or ventilator-associated events, compared with before the COVID-19 pandemic.
This is the second PPE survey the APIC has conducted during the pandemic. The organization first reported a dire situation in March. For example, the initial survey found that 48% of facilities were almost out or were out of respirators used to care for patients with COVID-19.
This article first appeared on Medscape.com.
A majority of hospitals and health care facilities surveyed report operating according to “crisis standards of care” as they struggle to provide sufficient personal protective equipment (PPE).
For example, in a national survey, 73% of 1,083 infection prevention experts said respirator shortages related to care for patients with COVID-19 drove their facility to move beyond conventional standards of care. Furthermore, 69% of facilities are using crisis standards of care (CSC) to provide masks, and 76% are apportioning face shields or eye protection.
Almost 76% of respondents who report reusing respirators said their facility allows them to use each respirator either five times or as many times as possible before replacement; 74% allow similar reuse of masks.
Although the majority of institutions remain in this crisis mode, many health care providers have better access to PPE than they did in the spring 2020, the Association for Professionals in Infection Control and Epidemiology (APIC) noted in its latest national survey.
“It is disheartening to see our healthcare system strained and implementing PPE crisis standards of care more than eight months into the pandemic,” APIC President Connie Steed, MSN, RN, said in a December 3 news release.
The association surveyed experts online between Oct. 22 and Nov. 5. The survey was timed to gauge the extent of resource shortages as COVID-19 cases increase and the 2020-2021 flu season begins.
“Many of us on the front lines are waiting for the other shoe to drop. With the upcoming flu season, we implore people to do what they can to keep safe, protect our healthcare personnel, and lessen the strain on our health care system,” Ms. Steed said.
COVID-19 linked to more infections, too
APIC also asked infection prevention specialists about changes in health care–associated infection rates since the onset of the pandemic. The experts reported an almost 28% increase in central line–associated bloodstream infections and 21% more catheter-associated urinary tract infections. They also reported an 18% rise in ventilator-associated pneumonia or ventilator-associated events, compared with before the COVID-19 pandemic.
This is the second PPE survey the APIC has conducted during the pandemic. The organization first reported a dire situation in March. For example, the initial survey found that 48% of facilities were almost out or were out of respirators used to care for patients with COVID-19.
This article first appeared on Medscape.com.
A majority of hospitals and health care facilities surveyed report operating according to “crisis standards of care” as they struggle to provide sufficient personal protective equipment (PPE).
For example, in a national survey, 73% of 1,083 infection prevention experts said respirator shortages related to care for patients with COVID-19 drove their facility to move beyond conventional standards of care. Furthermore, 69% of facilities are using crisis standards of care (CSC) to provide masks, and 76% are apportioning face shields or eye protection.
Almost 76% of respondents who report reusing respirators said their facility allows them to use each respirator either five times or as many times as possible before replacement; 74% allow similar reuse of masks.
Although the majority of institutions remain in this crisis mode, many health care providers have better access to PPE than they did in the spring 2020, the Association for Professionals in Infection Control and Epidemiology (APIC) noted in its latest national survey.
“It is disheartening to see our healthcare system strained and implementing PPE crisis standards of care more than eight months into the pandemic,” APIC President Connie Steed, MSN, RN, said in a December 3 news release.
The association surveyed experts online between Oct. 22 and Nov. 5. The survey was timed to gauge the extent of resource shortages as COVID-19 cases increase and the 2020-2021 flu season begins.
“Many of us on the front lines are waiting for the other shoe to drop. With the upcoming flu season, we implore people to do what they can to keep safe, protect our healthcare personnel, and lessen the strain on our health care system,” Ms. Steed said.
COVID-19 linked to more infections, too
APIC also asked infection prevention specialists about changes in health care–associated infection rates since the onset of the pandemic. The experts reported an almost 28% increase in central line–associated bloodstream infections and 21% more catheter-associated urinary tract infections. They also reported an 18% rise in ventilator-associated pneumonia or ventilator-associated events, compared with before the COVID-19 pandemic.
This is the second PPE survey the APIC has conducted during the pandemic. The organization first reported a dire situation in March. For example, the initial survey found that 48% of facilities were almost out or were out of respirators used to care for patients with COVID-19.
This article first appeared on Medscape.com.
Higher 10-day mortality of lower-acuity patients during times of increased ED crowding
Background: Studies have assessed mortality effect from ED crowding on high-acuity patients, but limited evidence exists for how this affects lower-acuity patients who are discharged home.

Study design: Retrospective cohort study.
Setting: Emergency department, Karolinska University Hospital, Solna, Sweden.
Synopsis: During 2009-2016, 705,813 encounters seen in the ED, triaged to lower-acuity levels 3-5 and discharged without further hospitalization needs were identified. A total of 623 patients died within 10 days of the initial ED visit (0.09%). The study evaluated the association of 10-day mortality with mean ED length of stay and ED-occupancy ratio.
The study demonstrated an increased 10-day mortality for mean ED length of stay of 8 hours or more vs. less than 2 hours (adjusted odds ratio, 5.86; 95% CI, 2.15-15.94). It also found an increased mortality rate for occupancy ratio quartiles with an aOR for quartiles 2, 3, and 4 vs. quartile 1 of 1.48 (95% CI, 1.14-1.92), 1.63 (95% CI, 1.24-2.14), and 1.53 (95% CI, 1.15-2.03), respectively.
While this suggests increased 10-day mortality in this patient population, additional studies should be conducted to determine if this risk is caused by ED crowding and length of stay or by current limitations in triage scoring.
Bottom line: There is an increased 10-day mortality rate for lower-acuity triaged patients who were discharged from the ED without hospitalization experiencing increased ED length of stay and during times of ED crowding.
Citation: Berg L et al. Associations between crowding and 10-day mortality among patients allocated lower triage acuity levels without need of acute hospital care on departure from the emergency department. Ann Emerg Med. 2019 Sep;74(3):345-56.
Dr. Merando is a hospitalist and assistant professor of internal medicine at St. Louis University School of Medicine.
Background: Studies have assessed mortality effect from ED crowding on high-acuity patients, but limited evidence exists for how this affects lower-acuity patients who are discharged home.
Study design: Retrospective cohort study.
Setting: Emergency department, Karolinska University Hospital, Solna, Sweden.
Synopsis: During 2009-2016, 705,813 encounters seen in the ED, triaged to lower-acuity levels 3-5 and discharged without further hospitalization needs were identified. A total of 623 patients died within 10 days of the initial ED visit (0.09%). The study evaluated the association of 10-day mortality with mean ED length of stay and ED-occupancy ratio.
The study demonstrated an increased 10-day mortality for mean ED length of stay of 8 hours or more vs. less than 2 hours (adjusted odds ratio, 5.86; 95% CI, 2.15-15.94). It also found an increased mortality rate for occupancy ratio quartiles with an aOR for quartiles 2, 3, and 4 vs. quartile 1 of 1.48 (95% CI, 1.14-1.92), 1.63 (95% CI, 1.24-2.14), and 1.53 (95% CI, 1.15-2.03), respectively.
While this suggests increased 10-day mortality in this patient population, additional studies should be conducted to determine if this risk is caused by ED crowding and length of stay or by current limitations in triage scoring.
Bottom line: There is an increased 10-day mortality rate for lower-acuity triaged patients who were discharged from the ED without hospitalization experiencing increased ED length of stay and during times of ED crowding.
Citation: Berg L et al. Associations between crowding and 10-day mortality among patients allocated lower triage acuity levels without need of acute hospital care on departure from the emergency department. Ann Emerg Med. 2019 Sep;74(3):345-56.
Dr. Merando is a hospitalist and assistant professor of internal medicine at St. Louis University School of Medicine.
Background: Studies have assessed mortality effect from ED crowding on high-acuity patients, but limited evidence exists for how this affects lower-acuity patients who are discharged home.
Study design: Retrospective cohort study.
Setting: Emergency department, Karolinska University Hospital, Solna, Sweden.
Synopsis: During 2009-2016, 705,813 encounters seen in the ED, triaged to lower-acuity levels 3-5 and discharged without further hospitalization needs were identified. A total of 623 patients died within 10 days of the initial ED visit (0.09%). The study evaluated the association of 10-day mortality with mean ED length of stay and ED-occupancy ratio.
The study demonstrated an increased 10-day mortality for mean ED length of stay of 8 hours or more vs. less than 2 hours (adjusted odds ratio, 5.86; 95% CI, 2.15-15.94). It also found an increased mortality rate for occupancy ratio quartiles with an aOR for quartiles 2, 3, and 4 vs. quartile 1 of 1.48 (95% CI, 1.14-1.92), 1.63 (95% CI, 1.24-2.14), and 1.53 (95% CI, 1.15-2.03), respectively.
While this suggests increased 10-day mortality in this patient population, additional studies should be conducted to determine if this risk is caused by ED crowding and length of stay or by current limitations in triage scoring.
Bottom line: There is an increased 10-day mortality rate for lower-acuity triaged patients who were discharged from the ED without hospitalization experiencing increased ED length of stay and during times of ED crowding.
Citation: Berg L et al. Associations between crowding and 10-day mortality among patients allocated lower triage acuity levels without need of acute hospital care on departure from the emergency department. Ann Emerg Med. 2019 Sep;74(3):345-56.
Dr. Merando is a hospitalist and assistant professor of internal medicine at St. Louis University School of Medicine.

Herpes Zoster May Be a Marker for COVID-19 Infection During Pregnancy
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the most recently identified member of the zoonotic pathogens of coronaviruses. It caused an outbreak of pneumonia in December 2019 in Wuhan, China.1 Among all related acute respiratory syndromes (SARS-CoV, Middle East respiratory syndrome coronavirus), SARS-CoV-2 remains to be the most infectious, has the highest potential for human transmission, and can eventually result in acute respiratory distress syndrome.2,3
Only 15% of coronavirus disease 2019 (COVID-19) cases progress to pneumonia, and approximately 5% of these cases develop acute respiratory distress syndrome, septic shock, and/or multiple organ failure. The majority of cases only exhibit mild to moderate symptoms.4,5 A wide array of skin manifestations in COVID-19 infection have been reported, including maculopapular eruptions, morbilliform rashes, urticaria, chickenpoxlike lesions, livedo reticularis, COVID toes, erythema multiforme, pityriasis rosea, and several other patterns.6 We report a case of herpes zoster (HZ) complication in a COVID-19–positive woman who was 27 weeks pregnant.
Case Report
A 36-year-old woman who was 27 weeks pregnant was referred by her obstetrician to the dermatology clinic. She presented with a low-grade fever and a vesicular painful rash. Physical examination revealed painful, itchy, dysesthetic papules and vesicles on the left side of the forehead along with mild edema of the left upper eyelid but no watering of the eye or photophobia. She reported episodes of fever (temperature, 38.9°C), fatigue, and myalgia over the last week. She had bouts of dyspnea and tachycardia that she thought were related to being in the late second trimester of pregnancy. The area surrounding the vesicular eruption was tender to touch. No dry cough or any gastrointestinal or urinary tract symptoms were noted. She reported a burning sensation when splashing water on the face or when exposed to air currents. One week following the initial symptoms, she experienced a painful vesicular rash along the upper left forehead (Figure) associated with eyelid edema. Oral and ocular mucosae were free of any presentations. She had no relevant history and had not experienced any complications during pregnancy. A diagnosis of HZ was made, and she was prescribed valacyclovir 1 g 3 times daily for 7 days, acetaminophen for the fever, and calamine lotion. We recommended COVID-19 testing based on her symptoms. A chest radiograph and a positive nasopharyngeal smear were consistent with COVID-19 infection. She reported via telephone follow-up 1 week after presentation that her skin condition had improved following the treatment course and that the vesicles eventually dried, leaving a crusting appearance after 5 to 7 days. Regarding her SARS-CoV-2 condition, her oxygen saturation was 95% at presentation; she self-quarantined at home; and she was treated with oseltamivir 75 mg orally every 12 hours for 5 days, azithromycin 500 mg orally daily, acetaminophen, and vitamin C. Electronic fetal heart rate monitoring and ultrasound examinations were performed to assess the condition of the fetus and were reported normal. At the time of writing this article, she was 32 weeks pregnant and tested negative to 2 consecutive nasopharyngeal swabs for COVID-19 and was in good general condition. She continued her pregnancy according to her obstetrician’s recommendations.

Comment
The incubation time of COVID-19 can be up to 14 days. Fever, dry cough, fatigue, and diarrhea have been speculated to be clinical symptoms; however, many cases may be asymptomatic. Aside from a medical or travel history at risk for COVID-19, diagnosis can be confirmed by detection of viral RNA by reverse transcriptase–polymerase chain reaction for nasopharyngeal swabs or bronchoalveolar fluid. Patients who are immunocompromised, older, or male or who have a history of cardiovascular conditions or debilitating chronic conditions are at an increased risk for severe disease and poor outcome compared to younger healthy individuals.7
The vesicular rash of COVID-19 has been reported to have different forms of presentation. A diffuse widespread pattern resembling hand-foot-and-mouth disease and a localized monomorphic pattern resembling chickenpox but with predilection to the trunk has been described.8
Physiologic changes in the immune and cardiopulmonary systems during pregnancy (eg, diaphragm elevation, increased oxygen consumption, edema of the respiratory tract mucosae) make pregnant women intolerant to hypoxia. The mortality rate of the 1918 influenza pandemic was 2.6% in the overall population but 37% among pregnant women.9 In 2009, pregnant women were reported to be at an increased risk for complications from the H1N1 influenza virus pandemic, with a higher estimated rate of hospital admission than the general population.10 In 2003, approximately 50% of pregnant women who received a diagnosis of SARS-CoV were admitted to the intensive care unit, approximately 33% of pregnant women with SARS-CoV required mechanical ventilation, and the mortality rate was as high as 25% for these women.11 To date, data on the effects of COVID-19 in pregnancy are limited to small case series.12-15
It was confirmed that COVID-19 infection is accompanied by a reduction in lymphocytes, monocytes, and eosinophils, along with a notable reduction of CD4/CD8 T cells, B cells, and natural killer cells. It was further revealed that nonsurvivor COVID-19 patients continued to show a decrease in lymphocyte counts along the course of their disease until death.16-18
Different mechanisms for lymphocyte depletion and deficiency were speculated among COVID-19 patients and include direct lymphocyte death through coronavirus angiotensin-converting enzyme 2–lymphocyte-expressed receptors; direct damage to lymphatic organs, such as the thymus and spleen, but this theory needs to be further investigated; direct lymphocyte apoptosis mediated by tumor necrosis factor α, IL-6, and other proinflammatory cytokines; and direct inhibition of lymphocytes by metabolic upset, such as acidosis.19,20
These causes may precipitate lymphopenia and impaired antiviral responses.21 It also has been postulated that the functional damage of CD4+ T cells may predispose patients with COVID-19 to severe disease.22 Such immune changes can render a patient more susceptible to developing shingles by reactivating varicella-zoster virus, which could be a sign of undiagnosed COVID-19 infection in younger age groups.
Two earlier reports discussed HZ among COVID-19–diagnosed patients. Shors23 presented a case of a patient who developed varicella-zoster virus reactivation of the V2 dermatome during the course of COVID-19 infection. In addition, the patient developed severe acute herpetic neuralgia despite the early initiation of antiviral therapy.23 Elsaie et al24 described 2 cases of patients during the pandemic who first presented with HZ before later being diagnosed with COVID-19 infection.
New information and cutaneous manifestations possibly related to COVID-19 are emerging every day. We report a pregnant female presenting with HZ during the course of COVID-19 infection, which suggests that the clinical presentation of HZ at the time of the current pandemic, especially if associated with other signs of COVID-19 infection, should be carefully monitored and reported for further assessment.
Acknowledgment
The authors would like to thank all the health care workers who have been fighting COVID-19 in Egypt and worldwide.
- Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020;382:1199-1207.
- Zhang YZ, Holes EC. A genomic perspective on the origin and emergence of sars-cov-2. Cell. 2020;181:223-227.
- Prompetchara E, Ketloy C, Palaga T. Immune responses in COVID-19 and potential vaccines: lessons learned from SARS and MERS epidemic. Asian Pac J Allergy Immunol. 2020;38:1‐9.
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan0, China. Lancet. 2020;395:497-506.
- Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8:420-422.
- Wollina U, Karadag˘ AS, Rowland-Payne C, et al. Cutaneous signs in COVID-19 patients: a review. Dermatol Ther. 2020;33:e13549.
- Lauer SA, Grantz KH, Bi Q, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med. 2020;172:577‐582.
- Fernandez-Nieto D, Ortega-Quijano D, Jimenez-Cauhe J, et al. Clinical and histological characterization of vesicular COVID-19 rashes: a prospective study in a tertiary care hospital. Clin Exp Dermatol. 2020;45:872-875.
- Gottfredsson M. The Spanish flu in Iceland 1918. Lessons in medicine and history [in Icelandic]. Laeknabladid. 2008;94:737-745.
- Jamieson D, Honein M, Rasmussen S, et al. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet. 2009;374:451-458.
- Ksiazek TG, Erdman D, Goldsmith CS. A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med. 2003;348:1953-1966.
- Chen H, Guo J, Wang C, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020;395:809‐815.
- Zhu H, Wang L, Fang C, et al. Clinical analysis of 10 neonates born to mothers with 2019-nCov pneumonia. Transl Pediatr. 2020;9:51-60.
- Liu Y, Chen H, Tang K, et al. Clinical manifestations and outcome of SARS-CoV-2 infection during pregnancy [published online March 4, 2020]. J Infect. doi:10.1016/j.jinf.2020.02.028.
- Zhang L, Jiang Y, Wei M, et al. Analysis of the pregnancy outcomes in pregnant women with COVID-19 in Hubei Province [in Chinese]. Zhonghua Fu Chan Ke Za Zhi. 2020;55:166-171.
- Henry BM, de Oliveira MHS, Benoit S, et al. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): a meta-analysis. Clin Chem Lab Med. 2020;58:1021-1028.
- Cai Q, Huang D, Ou P, et al. COVID-19 in a designated infectious diseases hospital outside Hubei Province, China. Allergy. 2020;75:1742-1752.
- Ruan Q, Yang K, Wang W, et al. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020;46:846-884.
- Kumar A, Anil A, Sharma P, et al. Clinical features of COVID-19 and factors associated with severe clinical course: a systematic review and meta-analysis [preprint]. SSRN. doi:10.2139/ssrn.3566166.
- Xu H, Zhong L, Deng J, et al. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Sci. 2020;12. https://doi.org/10.1038/s41368-020-0074-x.
- Li H, Liu L, Zhang D, et al. SARS-CoV-2 and viral sepsis: observations and hypotheses. Lancet. 2020;395:1517-1520.
- Zheng M, Gao Y, Wang G, et al. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell Mol Immunol. 2020;17:533-535.
- Shors AR. Herpes zoster and severe acute herpetic neuralgia as a complication of COVID-19 infection. JAAD Case Rep. 2020;6:656-657.
- Elsaie ML, Youssef EA, Nada HA. Herpes zoster might be an indicator for latent COVID 19 infection [published online May 23, 2020]. Dermatol Ther. doi:10.1111/dth.13666.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the most recently identified member of the zoonotic pathogens of coronaviruses. It caused an outbreak of pneumonia in December 2019 in Wuhan, China.1 Among all related acute respiratory syndromes (SARS-CoV, Middle East respiratory syndrome coronavirus), SARS-CoV-2 remains to be the most infectious, has the highest potential for human transmission, and can eventually result in acute respiratory distress syndrome.2,3
Only 15% of coronavirus disease 2019 (COVID-19) cases progress to pneumonia, and approximately 5% of these cases develop acute respiratory distress syndrome, septic shock, and/or multiple organ failure. The majority of cases only exhibit mild to moderate symptoms.4,5 A wide array of skin manifestations in COVID-19 infection have been reported, including maculopapular eruptions, morbilliform rashes, urticaria, chickenpoxlike lesions, livedo reticularis, COVID toes, erythema multiforme, pityriasis rosea, and several other patterns.6 We report a case of herpes zoster (HZ) complication in a COVID-19–positive woman who was 27 weeks pregnant.
Case Report
A 36-year-old woman who was 27 weeks pregnant was referred by her obstetrician to the dermatology clinic. She presented with a low-grade fever and a vesicular painful rash. Physical examination revealed painful, itchy, dysesthetic papules and vesicles on the left side of the forehead along with mild edema of the left upper eyelid but no watering of the eye or photophobia. She reported episodes of fever (temperature, 38.9°C), fatigue, and myalgia over the last week. She had bouts of dyspnea and tachycardia that she thought were related to being in the late second trimester of pregnancy. The area surrounding the vesicular eruption was tender to touch. No dry cough or any gastrointestinal or urinary tract symptoms were noted. She reported a burning sensation when splashing water on the face or when exposed to air currents. One week following the initial symptoms, she experienced a painful vesicular rash along the upper left forehead (Figure) associated with eyelid edema. Oral and ocular mucosae were free of any presentations. She had no relevant history and had not experienced any complications during pregnancy. A diagnosis of HZ was made, and she was prescribed valacyclovir 1 g 3 times daily for 7 days, acetaminophen for the fever, and calamine lotion. We recommended COVID-19 testing based on her symptoms. A chest radiograph and a positive nasopharyngeal smear were consistent with COVID-19 infection. She reported via telephone follow-up 1 week after presentation that her skin condition had improved following the treatment course and that the vesicles eventually dried, leaving a crusting appearance after 5 to 7 days. Regarding her SARS-CoV-2 condition, her oxygen saturation was 95% at presentation; she self-quarantined at home; and she was treated with oseltamivir 75 mg orally every 12 hours for 5 days, azithromycin 500 mg orally daily, acetaminophen, and vitamin C. Electronic fetal heart rate monitoring and ultrasound examinations were performed to assess the condition of the fetus and were reported normal. At the time of writing this article, she was 32 weeks pregnant and tested negative to 2 consecutive nasopharyngeal swabs for COVID-19 and was in good general condition. She continued her pregnancy according to her obstetrician’s recommendations.
Comment
The incubation time of COVID-19 can be up to 14 days. Fever, dry cough, fatigue, and diarrhea have been speculated to be clinical symptoms; however, many cases may be asymptomatic. Aside from a medical or travel history at risk for COVID-19, diagnosis can be confirmed by detection of viral RNA by reverse transcriptase–polymerase chain reaction for nasopharyngeal swabs or bronchoalveolar fluid. Patients who are immunocompromised, older, or male or who have a history of cardiovascular conditions or debilitating chronic conditions are at an increased risk for severe disease and poor outcome compared to younger healthy individuals.7
The vesicular rash of COVID-19 has been reported to have different forms of presentation. A diffuse widespread pattern resembling hand-foot-and-mouth disease and a localized monomorphic pattern resembling chickenpox but with predilection to the trunk has been described.8
Physiologic changes in the immune and cardiopulmonary systems during pregnancy (eg, diaphragm elevation, increased oxygen consumption, edema of the respiratory tract mucosae) make pregnant women intolerant to hypoxia. The mortality rate of the 1918 influenza pandemic was 2.6% in the overall population but 37% among pregnant women.9 In 2009, pregnant women were reported to be at an increased risk for complications from the H1N1 influenza virus pandemic, with a higher estimated rate of hospital admission than the general population.10 In 2003, approximately 50% of pregnant women who received a diagnosis of SARS-CoV were admitted to the intensive care unit, approximately 33% of pregnant women with SARS-CoV required mechanical ventilation, and the mortality rate was as high as 25% for these women.11 To date, data on the effects of COVID-19 in pregnancy are limited to small case series.12-15
It was confirmed that COVID-19 infection is accompanied by a reduction in lymphocytes, monocytes, and eosinophils, along with a notable reduction of CD4/CD8 T cells, B cells, and natural killer cells. It was further revealed that nonsurvivor COVID-19 patients continued to show a decrease in lymphocyte counts along the course of their disease until death.16-18
Different mechanisms for lymphocyte depletion and deficiency were speculated among COVID-19 patients and include direct lymphocyte death through coronavirus angiotensin-converting enzyme 2–lymphocyte-expressed receptors; direct damage to lymphatic organs, such as the thymus and spleen, but this theory needs to be further investigated; direct lymphocyte apoptosis mediated by tumor necrosis factor α, IL-6, and other proinflammatory cytokines; and direct inhibition of lymphocytes by metabolic upset, such as acidosis.19,20
These causes may precipitate lymphopenia and impaired antiviral responses.21 It also has been postulated that the functional damage of CD4+ T cells may predispose patients with COVID-19 to severe disease.22 Such immune changes can render a patient more susceptible to developing shingles by reactivating varicella-zoster virus, which could be a sign of undiagnosed COVID-19 infection in younger age groups.
Two earlier reports discussed HZ among COVID-19–diagnosed patients. Shors23 presented a case of a patient who developed varicella-zoster virus reactivation of the V2 dermatome during the course of COVID-19 infection. In addition, the patient developed severe acute herpetic neuralgia despite the early initiation of antiviral therapy.23 Elsaie et al24 described 2 cases of patients during the pandemic who first presented with HZ before later being diagnosed with COVID-19 infection.
New information and cutaneous manifestations possibly related to COVID-19 are emerging every day. We report a pregnant female presenting with HZ during the course of COVID-19 infection, which suggests that the clinical presentation of HZ at the time of the current pandemic, especially if associated with other signs of COVID-19 infection, should be carefully monitored and reported for further assessment.
Acknowledgment
The authors would like to thank all the health care workers who have been fighting COVID-19 in Egypt and worldwide.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the most recently identified member of the zoonotic pathogens of coronaviruses. It caused an outbreak of pneumonia in December 2019 in Wuhan, China.1 Among all related acute respiratory syndromes (SARS-CoV, Middle East respiratory syndrome coronavirus), SARS-CoV-2 remains to be the most infectious, has the highest potential for human transmission, and can eventually result in acute respiratory distress syndrome.2,3
Only 15% of coronavirus disease 2019 (COVID-19) cases progress to pneumonia, and approximately 5% of these cases develop acute respiratory distress syndrome, septic shock, and/or multiple organ failure. The majority of cases only exhibit mild to moderate symptoms.4,5 A wide array of skin manifestations in COVID-19 infection have been reported, including maculopapular eruptions, morbilliform rashes, urticaria, chickenpoxlike lesions, livedo reticularis, COVID toes, erythema multiforme, pityriasis rosea, and several other patterns.6 We report a case of herpes zoster (HZ) complication in a COVID-19–positive woman who was 27 weeks pregnant.
Case Report
A 36-year-old woman who was 27 weeks pregnant was referred by her obstetrician to the dermatology clinic. She presented with a low-grade fever and a vesicular painful rash. Physical examination revealed painful, itchy, dysesthetic papules and vesicles on the left side of the forehead along with mild edema of the left upper eyelid but no watering of the eye or photophobia. She reported episodes of fever (temperature, 38.9°C), fatigue, and myalgia over the last week. She had bouts of dyspnea and tachycardia that she thought were related to being in the late second trimester of pregnancy. The area surrounding the vesicular eruption was tender to touch. No dry cough or any gastrointestinal or urinary tract symptoms were noted. She reported a burning sensation when splashing water on the face or when exposed to air currents. One week following the initial symptoms, she experienced a painful vesicular rash along the upper left forehead (Figure) associated with eyelid edema. Oral and ocular mucosae were free of any presentations. She had no relevant history and had not experienced any complications during pregnancy. A diagnosis of HZ was made, and she was prescribed valacyclovir 1 g 3 times daily for 7 days, acetaminophen for the fever, and calamine lotion. We recommended COVID-19 testing based on her symptoms. A chest radiograph and a positive nasopharyngeal smear were consistent with COVID-19 infection. She reported via telephone follow-up 1 week after presentation that her skin condition had improved following the treatment course and that the vesicles eventually dried, leaving a crusting appearance after 5 to 7 days. Regarding her SARS-CoV-2 condition, her oxygen saturation was 95% at presentation; she self-quarantined at home; and she was treated with oseltamivir 75 mg orally every 12 hours for 5 days, azithromycin 500 mg orally daily, acetaminophen, and vitamin C. Electronic fetal heart rate monitoring and ultrasound examinations were performed to assess the condition of the fetus and were reported normal. At the time of writing this article, she was 32 weeks pregnant and tested negative to 2 consecutive nasopharyngeal swabs for COVID-19 and was in good general condition. She continued her pregnancy according to her obstetrician’s recommendations.
Comment
The incubation time of COVID-19 can be up to 14 days. Fever, dry cough, fatigue, and diarrhea have been speculated to be clinical symptoms; however, many cases may be asymptomatic. Aside from a medical or travel history at risk for COVID-19, diagnosis can be confirmed by detection of viral RNA by reverse transcriptase–polymerase chain reaction for nasopharyngeal swabs or bronchoalveolar fluid. Patients who are immunocompromised, older, or male or who have a history of cardiovascular conditions or debilitating chronic conditions are at an increased risk for severe disease and poor outcome compared to younger healthy individuals.7
The vesicular rash of COVID-19 has been reported to have different forms of presentation. A diffuse widespread pattern resembling hand-foot-and-mouth disease and a localized monomorphic pattern resembling chickenpox but with predilection to the trunk has been described.8
Physiologic changes in the immune and cardiopulmonary systems during pregnancy (eg, diaphragm elevation, increased oxygen consumption, edema of the respiratory tract mucosae) make pregnant women intolerant to hypoxia. The mortality rate of the 1918 influenza pandemic was 2.6% in the overall population but 37% among pregnant women.9 In 2009, pregnant women were reported to be at an increased risk for complications from the H1N1 influenza virus pandemic, with a higher estimated rate of hospital admission than the general population.10 In 2003, approximately 50% of pregnant women who received a diagnosis of SARS-CoV were admitted to the intensive care unit, approximately 33% of pregnant women with SARS-CoV required mechanical ventilation, and the mortality rate was as high as 25% for these women.11 To date, data on the effects of COVID-19 in pregnancy are limited to small case series.12-15
It was confirmed that COVID-19 infection is accompanied by a reduction in lymphocytes, monocytes, and eosinophils, along with a notable reduction of CD4/CD8 T cells, B cells, and natural killer cells. It was further revealed that nonsurvivor COVID-19 patients continued to show a decrease in lymphocyte counts along the course of their disease until death.16-18
Different mechanisms for lymphocyte depletion and deficiency were speculated among COVID-19 patients and include direct lymphocyte death through coronavirus angiotensin-converting enzyme 2–lymphocyte-expressed receptors; direct damage to lymphatic organs, such as the thymus and spleen, but this theory needs to be further investigated; direct lymphocyte apoptosis mediated by tumor necrosis factor α, IL-6, and other proinflammatory cytokines; and direct inhibition of lymphocytes by metabolic upset, such as acidosis.19,20
These causes may precipitate lymphopenia and impaired antiviral responses.21 It also has been postulated that the functional damage of CD4+ T cells may predispose patients with COVID-19 to severe disease.22 Such immune changes can render a patient more susceptible to developing shingles by reactivating varicella-zoster virus, which could be a sign of undiagnosed COVID-19 infection in younger age groups.
Two earlier reports discussed HZ among COVID-19–diagnosed patients. Shors23 presented a case of a patient who developed varicella-zoster virus reactivation of the V2 dermatome during the course of COVID-19 infection. In addition, the patient developed severe acute herpetic neuralgia despite the early initiation of antiviral therapy.23 Elsaie et al24 described 2 cases of patients during the pandemic who first presented with HZ before later being diagnosed with COVID-19 infection.
New information and cutaneous manifestations possibly related to COVID-19 are emerging every day. We report a pregnant female presenting with HZ during the course of COVID-19 infection, which suggests that the clinical presentation of HZ at the time of the current pandemic, especially if associated with other signs of COVID-19 infection, should be carefully monitored and reported for further assessment.
Acknowledgment
The authors would like to thank all the health care workers who have been fighting COVID-19 in Egypt and worldwide.
- Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020;382:1199-1207.
- Zhang YZ, Holes EC. A genomic perspective on the origin and emergence of sars-cov-2. Cell. 2020;181:223-227.
- Prompetchara E, Ketloy C, Palaga T. Immune responses in COVID-19 and potential vaccines: lessons learned from SARS and MERS epidemic. Asian Pac J Allergy Immunol. 2020;38:1‐9.
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan0, China. Lancet. 2020;395:497-506.
- Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8:420-422.
- Wollina U, Karadag˘ AS, Rowland-Payne C, et al. Cutaneous signs in COVID-19 patients: a review. Dermatol Ther. 2020;33:e13549.
- Lauer SA, Grantz KH, Bi Q, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med. 2020;172:577‐582.
- Fernandez-Nieto D, Ortega-Quijano D, Jimenez-Cauhe J, et al. Clinical and histological characterization of vesicular COVID-19 rashes: a prospective study in a tertiary care hospital. Clin Exp Dermatol. 2020;45:872-875.
- Gottfredsson M. The Spanish flu in Iceland 1918. Lessons in medicine and history [in Icelandic]. Laeknabladid. 2008;94:737-745.
- Jamieson D, Honein M, Rasmussen S, et al. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet. 2009;374:451-458.
- Ksiazek TG, Erdman D, Goldsmith CS. A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med. 2003;348:1953-1966.
- Chen H, Guo J, Wang C, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020;395:809‐815.
- Zhu H, Wang L, Fang C, et al. Clinical analysis of 10 neonates born to mothers with 2019-nCov pneumonia. Transl Pediatr. 2020;9:51-60.
- Liu Y, Chen H, Tang K, et al. Clinical manifestations and outcome of SARS-CoV-2 infection during pregnancy [published online March 4, 2020]. J Infect. doi:10.1016/j.jinf.2020.02.028.
- Zhang L, Jiang Y, Wei M, et al. Analysis of the pregnancy outcomes in pregnant women with COVID-19 in Hubei Province [in Chinese]. Zhonghua Fu Chan Ke Za Zhi. 2020;55:166-171.
- Henry BM, de Oliveira MHS, Benoit S, et al. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): a meta-analysis. Clin Chem Lab Med. 2020;58:1021-1028.
- Cai Q, Huang D, Ou P, et al. COVID-19 in a designated infectious diseases hospital outside Hubei Province, China. Allergy. 2020;75:1742-1752.
- Ruan Q, Yang K, Wang W, et al. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020;46:846-884.
- Kumar A, Anil A, Sharma P, et al. Clinical features of COVID-19 and factors associated with severe clinical course: a systematic review and meta-analysis [preprint]. SSRN. doi:10.2139/ssrn.3566166.
- Xu H, Zhong L, Deng J, et al. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Sci. 2020;12. https://doi.org/10.1038/s41368-020-0074-x.
- Li H, Liu L, Zhang D, et al. SARS-CoV-2 and viral sepsis: observations and hypotheses. Lancet. 2020;395:1517-1520.
- Zheng M, Gao Y, Wang G, et al. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell Mol Immunol. 2020;17:533-535.
- Shors AR. Herpes zoster and severe acute herpetic neuralgia as a complication of COVID-19 infection. JAAD Case Rep. 2020;6:656-657.
- Elsaie ML, Youssef EA, Nada HA. Herpes zoster might be an indicator for latent COVID 19 infection [published online May 23, 2020]. Dermatol Ther. doi:10.1111/dth.13666.
- Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020;382:1199-1207.
- Zhang YZ, Holes EC. A genomic perspective on the origin and emergence of sars-cov-2. Cell. 2020;181:223-227.
- Prompetchara E, Ketloy C, Palaga T. Immune responses in COVID-19 and potential vaccines: lessons learned from SARS and MERS epidemic. Asian Pac J Allergy Immunol. 2020;38:1‐9.
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan0, China. Lancet. 2020;395:497-506.
- Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8:420-422.
- Wollina U, Karadag˘ AS, Rowland-Payne C, et al. Cutaneous signs in COVID-19 patients: a review. Dermatol Ther. 2020;33:e13549.
- Lauer SA, Grantz KH, Bi Q, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med. 2020;172:577‐582.
- Fernandez-Nieto D, Ortega-Quijano D, Jimenez-Cauhe J, et al. Clinical and histological characterization of vesicular COVID-19 rashes: a prospective study in a tertiary care hospital. Clin Exp Dermatol. 2020;45:872-875.
- Gottfredsson M. The Spanish flu in Iceland 1918. Lessons in medicine and history [in Icelandic]. Laeknabladid. 2008;94:737-745.
- Jamieson D, Honein M, Rasmussen S, et al. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet. 2009;374:451-458.
- Ksiazek TG, Erdman D, Goldsmith CS. A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med. 2003;348:1953-1966.
- Chen H, Guo J, Wang C, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020;395:809‐815.
- Zhu H, Wang L, Fang C, et al. Clinical analysis of 10 neonates born to mothers with 2019-nCov pneumonia. Transl Pediatr. 2020;9:51-60.
- Liu Y, Chen H, Tang K, et al. Clinical manifestations and outcome of SARS-CoV-2 infection during pregnancy [published online March 4, 2020]. J Infect. doi:10.1016/j.jinf.2020.02.028.
- Zhang L, Jiang Y, Wei M, et al. Analysis of the pregnancy outcomes in pregnant women with COVID-19 in Hubei Province [in Chinese]. Zhonghua Fu Chan Ke Za Zhi. 2020;55:166-171.
- Henry BM, de Oliveira MHS, Benoit S, et al. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): a meta-analysis. Clin Chem Lab Med. 2020;58:1021-1028.
- Cai Q, Huang D, Ou P, et al. COVID-19 in a designated infectious diseases hospital outside Hubei Province, China. Allergy. 2020;75:1742-1752.
- Ruan Q, Yang K, Wang W, et al. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020;46:846-884.
- Kumar A, Anil A, Sharma P, et al. Clinical features of COVID-19 and factors associated with severe clinical course: a systematic review and meta-analysis [preprint]. SSRN. doi:10.2139/ssrn.3566166.
- Xu H, Zhong L, Deng J, et al. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Sci. 2020;12. https://doi.org/10.1038/s41368-020-0074-x.
- Li H, Liu L, Zhang D, et al. SARS-CoV-2 and viral sepsis: observations and hypotheses. Lancet. 2020;395:1517-1520.
- Zheng M, Gao Y, Wang G, et al. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell Mol Immunol. 2020;17:533-535.
- Shors AR. Herpes zoster and severe acute herpetic neuralgia as a complication of COVID-19 infection. JAAD Case Rep. 2020;6:656-657.
- Elsaie ML, Youssef EA, Nada HA. Herpes zoster might be an indicator for latent COVID 19 infection [published online May 23, 2020]. Dermatol Ther. doi:10.1111/dth.13666.
Practice Points
- The vesicular rash of coronavirus disease 2019 (COVID-19) has been reported to have different forms of presentation.
- Pregnant women appear to be at increased risk for complications from COVID-19 infection.
- The clinical presentation of herpes zoster should be carefully monitored and reported for further assessment, especially if associated with other signs of COVID-19 infection.

Racial Disparities in Dermatology Training: The Impact on Black Patients
Although physicians commit themselves to providing equitable treatment to all patients, significant disparities remain in the dermatologic care of Black patients, who constitute 13% of the US population, which continues to grow increasingly diverse.1 Despite these changes in the population, the literature demonstrates that dermatologic training does not adequately focus on unique presentations of cutaneous pathology in the Black population.2,3 Accordingly, medical students lack proper training in how skin disorders manifest in people of color. Compounding the problem, only 3% of dermatologists are Black, creating a cultural barrier that can compromise care for Black patients.2,4 Racial disparities in dermatology training can compromise treatment, patient satisfaction, and outcomes.3
Issues in Medical Education Training and Resources
Lack of diversity in the resources used for dermatology training in medical schools affects diagnosis and treatment, as skin manifestations such as hypersensitivity reactions, rashes, and cancer can appear differently on different skin tones.5 A study of medical students’ ability to diagnose common dermatologic pathologies found that when trainees were presented with photographs of dark skin, their accuracy in identifying urticaria, squamous cell carcinoma, and even atopic dermatitis was reduced, despite these diseases being more prevalent in children of African American ancestry.4,6
Dermatologic diseases also can have different distributions in different races; for example, on non–sun-exposed sites, squamous cell carcinoma in Black patients occurs at 8.5 times the frequency of White patients.7 Failure to identify diseases accurately due to insufficient training can have grave consequences for patients. Although skin cancer is less common in individuals with skin of color, it is associated with greater morbidity and mortality, in part due to delayed diagnosis.7
Inadequate research, reporting, and instruction on dermatologic findings in patients with darker complexions further compound racial disparities in dermatology. A 2006 study of the representation of darker skin in major dermatology educational resources found that only 2% of teaching events at American Academy of Dermatology annual meetings focused on skin of color. Furthermore, the study determined that many common diseases in patients with dark skin, such as acne vulgaris and pityriasis rosea, were completely absent or limited in dermatology textbooks.8
Impact on the Black Patient Experience
Patients’ therapeutic relationship with their physician also is damaged by limitations in training in diverse skin color. A study that assessed Black patients seen in a skin of color clinic (SOCC) compared to Black patients seen in a non-SOCC found that non-SOCC patients reported a lower degree of respect, dignity, understanding, and trust compared to the patients seen in a SOCC. Black patients expressed specific concerns about non-SOCC dermatologists’ knowledge of abnormalities that present in darker skin and Black hair.3 These findings are compounded by reports suggesting that, independent of care, structural racism contributes to dermatologic disease severity by influencing patient education level, household income, and degree of exposure to harmful environmental irritants.6
Racial disparities continue to be seen in the makeup of the universe of dermatologists and skin researchers. As of 2016, only 3% of dermatologists were Black, making dermatology one of the least diverse medical specialties.2 Increasing the diversity of the dermatology workforce is important to improve patient satisfaction and treatment, both for minority and nonminority patients. Compared to race-discordant medical visits, race-concordant visits were shown to have a higher rate of satisfaction and better shared decision-making.9 Also, minority physicians are more likely to practice health care in areas that are traditionally underserved and to care for patients who do not have health insurance, making their participation essential in addressing some of the baseline disparities Black patients face in securing quality dermatologic care.1
Structural Racism in Medicine
Changing dermatology training to ensure improved treatment of Black patients requires not only increased attention to differences in disease presentation but also heightened awareness of underlying genetic, environmental, and structural factors that contribute to the disease course.6 For example, there is evidence suggesting that structural racism in the form of residential segregation, lower socioeconomic status, and lower educational attainment contribute to disease severity in conditions such as atopic dermatitis. There is additional evidence suggesting that White patients are more readily offered therapeutic options than Black patients. A study of racial disparities in psoriasis treatment found that Black patients with moderate to severe psoriasis were 70% less likely to receive treatment with a biologic than White patients, independent of socioeconomic factors, comorbidities, and insurance plans.10
Moving Forward
Although research continues to underscore racial disparities in dermatology, some leaders in the field are actively combating these problems. A recent study that looked at representations of dark skin images in medical educational resources found far greater representation of dark pigmented skin in web-based resources than in traditional printed texts. Specifically, the online resource VisualDx (https://www.visualdx.com/) features 28.5% dark skin images compared to 10.3% (on average) in printed dermatology books.11 There also is increasing public awareness of these issues, with organizations such as the Skin of Color Society (http://skinofcolorsociety.org/) helping to promote interest in racial disparities in dermatology. Physicians also have created textbooks and social media accounts focused on dermatologic manifestations in skin of color.12 The Instagram account Brown Skin Matters (@brownskinmatters) has created a publicly accessible online resource where physicians and patients can see and post dermatologic diseases in skin of color.5
Final Thoughts
It is critical that physicians be trained to identify skin and hair manifestations of disease and disorders in Black patients. Training can be improved by including more images of skin manifestations in dark skin, both in medical school curricula and in new editions of dermatology textbooks. Training also must teach students about hair in Black individuals and how to properly treat it as well as related conditions of the hair and scalp.13 More research also is needed to better understand how dermatologists can improve the patient experience for Black patients. Residency programs must work to increase diversity among dermatology trainees.
Lastly, dermatology education should increasingly be supplemented with newer, web-based resources that show dermatologic manifestations across the spectrum of skin tones. Dermatology training must be adapted to better account for diverse patient populations and increase its focus on the systems that produce baseline disparities in disease morbidity and mortality.
- Pandya AG, Alexis AF, Berger TG, et al. Increasing racial and ethnic diversity in dermatology: a call to action. J Am Acad Dermatol. 2016;74:584-587.
- Gallegos A. Dermatology lacks diversity. Dermatology News. June 1, 2016. Accessed November 18, 2020. https://www.mdedge.com/dermatology/article/108920/practice-management/dermatology-lacks-diversity.
- Gorbatenko-Roth K, Prose N, Kundu RV, et al. Assessment of black patients’ perception of their dermatology care. JAMA Dermatol. 2019;155:1129-1134.
- Fenton A, Elliott E, Shahbandi A, et al. Medical students’ ability to diagnose common dermatologic conditions in skin of color. J Am Acad Dermatol. 2020;83:957-958.
- Prichep D. Diagnostic gaps: skin comes in many shades and so do rashes. NPR website. November 14, 2019. Accessed November 19, 2020. https://www.npr.org/sections/health-shots/2019/11/04/774910915/diagnostic-gaps-skin-comes-in-many-shades-and-so-do-rashes.
- Tackett KJ, Jenkins F, Morrell DS, et al. Structural racism and its influence on the severity of atopic dermatitis in African American children. Pediatr Dermatol. 2020;37:142-146.
- Gloster HM, Neal K. Skin cancer in skin of color. J Am Acad Dermatol. 2006;55:741-760.
- Ebede T, Papier A. Disparities in dermatology educational resources. J Am Acad Dermatol. 2006;55:687-690.
- Cooper LA, Roter DL, Johnson RL, et al. Patient-centered communication, ratings of care, and concordance of patient and physician race. Ann Intern Med. 2003;139:907-915.
- Takeshita J, Eriksen WT, Raziano VT, et al. Racial differences in perceptions of psoriasis therapies: implications for racial disparities in psoriasis treatment. J Invest Dermatol. 2019;139:1672-1679.e1.
- Alvarado SM, Feng H. Representation of dark skin images of common dermatologic conditions in educational resources: a cross-sectional analysis [published online June 18, 2020]. J Am Acad Dermatol. doi:10.1016/j.jaad.2020.06.041.
- Rabin RC. Dermatology has a problem with skin color. The New York Times. August 30, 2020. http://www.nytimes.com/2020/08/30/health/skin-diseases-black-hispanic.html. Accessed November 19, 2020.
- Bosley RE, Daveluy S. A primer to natural hair care practices in black patients. Cutis. 2015;95:78-80.
Although physicians commit themselves to providing equitable treatment to all patients, significant disparities remain in the dermatologic care of Black patients, who constitute 13% of the US population, which continues to grow increasingly diverse.1 Despite these changes in the population, the literature demonstrates that dermatologic training does not adequately focus on unique presentations of cutaneous pathology in the Black population.2,3 Accordingly, medical students lack proper training in how skin disorders manifest in people of color. Compounding the problem, only 3% of dermatologists are Black, creating a cultural barrier that can compromise care for Black patients.2,4 Racial disparities in dermatology training can compromise treatment, patient satisfaction, and outcomes.3
Issues in Medical Education Training and Resources
Lack of diversity in the resources used for dermatology training in medical schools affects diagnosis and treatment, as skin manifestations such as hypersensitivity reactions, rashes, and cancer can appear differently on different skin tones.5 A study of medical students’ ability to diagnose common dermatologic pathologies found that when trainees were presented with photographs of dark skin, their accuracy in identifying urticaria, squamous cell carcinoma, and even atopic dermatitis was reduced, despite these diseases being more prevalent in children of African American ancestry.4,6
Dermatologic diseases also can have different distributions in different races; for example, on non–sun-exposed sites, squamous cell carcinoma in Black patients occurs at 8.5 times the frequency of White patients.7 Failure to identify diseases accurately due to insufficient training can have grave consequences for patients. Although skin cancer is less common in individuals with skin of color, it is associated with greater morbidity and mortality, in part due to delayed diagnosis.7
Inadequate research, reporting, and instruction on dermatologic findings in patients with darker complexions further compound racial disparities in dermatology. A 2006 study of the representation of darker skin in major dermatology educational resources found that only 2% of teaching events at American Academy of Dermatology annual meetings focused on skin of color. Furthermore, the study determined that many common diseases in patients with dark skin, such as acne vulgaris and pityriasis rosea, were completely absent or limited in dermatology textbooks.8
Impact on the Black Patient Experience
Patients’ therapeutic relationship with their physician also is damaged by limitations in training in diverse skin color. A study that assessed Black patients seen in a skin of color clinic (SOCC) compared to Black patients seen in a non-SOCC found that non-SOCC patients reported a lower degree of respect, dignity, understanding, and trust compared to the patients seen in a SOCC. Black patients expressed specific concerns about non-SOCC dermatologists’ knowledge of abnormalities that present in darker skin and Black hair.3 These findings are compounded by reports suggesting that, independent of care, structural racism contributes to dermatologic disease severity by influencing patient education level, household income, and degree of exposure to harmful environmental irritants.6
Racial disparities continue to be seen in the makeup of the universe of dermatologists and skin researchers. As of 2016, only 3% of dermatologists were Black, making dermatology one of the least diverse medical specialties.2 Increasing the diversity of the dermatology workforce is important to improve patient satisfaction and treatment, both for minority and nonminority patients. Compared to race-discordant medical visits, race-concordant visits were shown to have a higher rate of satisfaction and better shared decision-making.9 Also, minority physicians are more likely to practice health care in areas that are traditionally underserved and to care for patients who do not have health insurance, making their participation essential in addressing some of the baseline disparities Black patients face in securing quality dermatologic care.1
Structural Racism in Medicine
Changing dermatology training to ensure improved treatment of Black patients requires not only increased attention to differences in disease presentation but also heightened awareness of underlying genetic, environmental, and structural factors that contribute to the disease course.6 For example, there is evidence suggesting that structural racism in the form of residential segregation, lower socioeconomic status, and lower educational attainment contribute to disease severity in conditions such as atopic dermatitis. There is additional evidence suggesting that White patients are more readily offered therapeutic options than Black patients. A study of racial disparities in psoriasis treatment found that Black patients with moderate to severe psoriasis were 70% less likely to receive treatment with a biologic than White patients, independent of socioeconomic factors, comorbidities, and insurance plans.10
Moving Forward
Although research continues to underscore racial disparities in dermatology, some leaders in the field are actively combating these problems. A recent study that looked at representations of dark skin images in medical educational resources found far greater representation of dark pigmented skin in web-based resources than in traditional printed texts. Specifically, the online resource VisualDx (https://www.visualdx.com/) features 28.5% dark skin images compared to 10.3% (on average) in printed dermatology books.11 There also is increasing public awareness of these issues, with organizations such as the Skin of Color Society (http://skinofcolorsociety.org/) helping to promote interest in racial disparities in dermatology. Physicians also have created textbooks and social media accounts focused on dermatologic manifestations in skin of color.12 The Instagram account Brown Skin Matters (@brownskinmatters) has created a publicly accessible online resource where physicians and patients can see and post dermatologic diseases in skin of color.5
Final Thoughts
It is critical that physicians be trained to identify skin and hair manifestations of disease and disorders in Black patients. Training can be improved by including more images of skin manifestations in dark skin, both in medical school curricula and in new editions of dermatology textbooks. Training also must teach students about hair in Black individuals and how to properly treat it as well as related conditions of the hair and scalp.13 More research also is needed to better understand how dermatologists can improve the patient experience for Black patients. Residency programs must work to increase diversity among dermatology trainees.
Lastly, dermatology education should increasingly be supplemented with newer, web-based resources that show dermatologic manifestations across the spectrum of skin tones. Dermatology training must be adapted to better account for diverse patient populations and increase its focus on the systems that produce baseline disparities in disease morbidity and mortality.
Although physicians commit themselves to providing equitable treatment to all patients, significant disparities remain in the dermatologic care of Black patients, who constitute 13% of the US population, which continues to grow increasingly diverse.1 Despite these changes in the population, the literature demonstrates that dermatologic training does not adequately focus on unique presentations of cutaneous pathology in the Black population.2,3 Accordingly, medical students lack proper training in how skin disorders manifest in people of color. Compounding the problem, only 3% of dermatologists are Black, creating a cultural barrier that can compromise care for Black patients.2,4 Racial disparities in dermatology training can compromise treatment, patient satisfaction, and outcomes.3
Issues in Medical Education Training and Resources
Lack of diversity in the resources used for dermatology training in medical schools affects diagnosis and treatment, as skin manifestations such as hypersensitivity reactions, rashes, and cancer can appear differently on different skin tones.5 A study of medical students’ ability to diagnose common dermatologic pathologies found that when trainees were presented with photographs of dark skin, their accuracy in identifying urticaria, squamous cell carcinoma, and even atopic dermatitis was reduced, despite these diseases being more prevalent in children of African American ancestry.4,6
Dermatologic diseases also can have different distributions in different races; for example, on non–sun-exposed sites, squamous cell carcinoma in Black patients occurs at 8.5 times the frequency of White patients.7 Failure to identify diseases accurately due to insufficient training can have grave consequences for patients. Although skin cancer is less common in individuals with skin of color, it is associated with greater morbidity and mortality, in part due to delayed diagnosis.7
Inadequate research, reporting, and instruction on dermatologic findings in patients with darker complexions further compound racial disparities in dermatology. A 2006 study of the representation of darker skin in major dermatology educational resources found that only 2% of teaching events at American Academy of Dermatology annual meetings focused on skin of color. Furthermore, the study determined that many common diseases in patients with dark skin, such as acne vulgaris and pityriasis rosea, were completely absent or limited in dermatology textbooks.8
Impact on the Black Patient Experience
Patients’ therapeutic relationship with their physician also is damaged by limitations in training in diverse skin color. A study that assessed Black patients seen in a skin of color clinic (SOCC) compared to Black patients seen in a non-SOCC found that non-SOCC patients reported a lower degree of respect, dignity, understanding, and trust compared to the patients seen in a SOCC. Black patients expressed specific concerns about non-SOCC dermatologists’ knowledge of abnormalities that present in darker skin and Black hair.3 These findings are compounded by reports suggesting that, independent of care, structural racism contributes to dermatologic disease severity by influencing patient education level, household income, and degree of exposure to harmful environmental irritants.6
Racial disparities continue to be seen in the makeup of the universe of dermatologists and skin researchers. As of 2016, only 3% of dermatologists were Black, making dermatology one of the least diverse medical specialties.2 Increasing the diversity of the dermatology workforce is important to improve patient satisfaction and treatment, both for minority and nonminority patients. Compared to race-discordant medical visits, race-concordant visits were shown to have a higher rate of satisfaction and better shared decision-making.9 Also, minority physicians are more likely to practice health care in areas that are traditionally underserved and to care for patients who do not have health insurance, making their participation essential in addressing some of the baseline disparities Black patients face in securing quality dermatologic care.1
Structural Racism in Medicine
Changing dermatology training to ensure improved treatment of Black patients requires not only increased attention to differences in disease presentation but also heightened awareness of underlying genetic, environmental, and structural factors that contribute to the disease course.6 For example, there is evidence suggesting that structural racism in the form of residential segregation, lower socioeconomic status, and lower educational attainment contribute to disease severity in conditions such as atopic dermatitis. There is additional evidence suggesting that White patients are more readily offered therapeutic options than Black patients. A study of racial disparities in psoriasis treatment found that Black patients with moderate to severe psoriasis were 70% less likely to receive treatment with a biologic than White patients, independent of socioeconomic factors, comorbidities, and insurance plans.10
Moving Forward
Although research continues to underscore racial disparities in dermatology, some leaders in the field are actively combating these problems. A recent study that looked at representations of dark skin images in medical educational resources found far greater representation of dark pigmented skin in web-based resources than in traditional printed texts. Specifically, the online resource VisualDx (https://www.visualdx.com/) features 28.5% dark skin images compared to 10.3% (on average) in printed dermatology books.11 There also is increasing public awareness of these issues, with organizations such as the Skin of Color Society (http://skinofcolorsociety.org/) helping to promote interest in racial disparities in dermatology. Physicians also have created textbooks and social media accounts focused on dermatologic manifestations in skin of color.12 The Instagram account Brown Skin Matters (@brownskinmatters) has created a publicly accessible online resource where physicians and patients can see and post dermatologic diseases in skin of color.5
Final Thoughts
It is critical that physicians be trained to identify skin and hair manifestations of disease and disorders in Black patients. Training can be improved by including more images of skin manifestations in dark skin, both in medical school curricula and in new editions of dermatology textbooks. Training also must teach students about hair in Black individuals and how to properly treat it as well as related conditions of the hair and scalp.13 More research also is needed to better understand how dermatologists can improve the patient experience for Black patients. Residency programs must work to increase diversity among dermatology trainees.
Lastly, dermatology education should increasingly be supplemented with newer, web-based resources that show dermatologic manifestations across the spectrum of skin tones. Dermatology training must be adapted to better account for diverse patient populations and increase its focus on the systems that produce baseline disparities in disease morbidity and mortality.
- Pandya AG, Alexis AF, Berger TG, et al. Increasing racial and ethnic diversity in dermatology: a call to action. J Am Acad Dermatol. 2016;74:584-587.
- Gallegos A. Dermatology lacks diversity. Dermatology News. June 1, 2016. Accessed November 18, 2020. https://www.mdedge.com/dermatology/article/108920/practice-management/dermatology-lacks-diversity.
- Gorbatenko-Roth K, Prose N, Kundu RV, et al. Assessment of black patients’ perception of their dermatology care. JAMA Dermatol. 2019;155:1129-1134.
- Fenton A, Elliott E, Shahbandi A, et al. Medical students’ ability to diagnose common dermatologic conditions in skin of color. J Am Acad Dermatol. 2020;83:957-958.
- Prichep D. Diagnostic gaps: skin comes in many shades and so do rashes. NPR website. November 14, 2019. Accessed November 19, 2020. https://www.npr.org/sections/health-shots/2019/11/04/774910915/diagnostic-gaps-skin-comes-in-many-shades-and-so-do-rashes.
- Tackett KJ, Jenkins F, Morrell DS, et al. Structural racism and its influence on the severity of atopic dermatitis in African American children. Pediatr Dermatol. 2020;37:142-146.
- Gloster HM, Neal K. Skin cancer in skin of color. J Am Acad Dermatol. 2006;55:741-760.
- Ebede T, Papier A. Disparities in dermatology educational resources. J Am Acad Dermatol. 2006;55:687-690.
- Cooper LA, Roter DL, Johnson RL, et al. Patient-centered communication, ratings of care, and concordance of patient and physician race. Ann Intern Med. 2003;139:907-915.
- Takeshita J, Eriksen WT, Raziano VT, et al. Racial differences in perceptions of psoriasis therapies: implications for racial disparities in psoriasis treatment. J Invest Dermatol. 2019;139:1672-1679.e1.
- Alvarado SM, Feng H. Representation of dark skin images of common dermatologic conditions in educational resources: a cross-sectional analysis [published online June 18, 2020]. J Am Acad Dermatol. doi:10.1016/j.jaad.2020.06.041.
- Rabin RC. Dermatology has a problem with skin color. The New York Times. August 30, 2020. http://www.nytimes.com/2020/08/30/health/skin-diseases-black-hispanic.html. Accessed November 19, 2020.
- Bosley RE, Daveluy S. A primer to natural hair care practices in black patients. Cutis. 2015;95:78-80.
- Pandya AG, Alexis AF, Berger TG, et al. Increasing racial and ethnic diversity in dermatology: a call to action. J Am Acad Dermatol. 2016;74:584-587.
- Gallegos A. Dermatology lacks diversity. Dermatology News. June 1, 2016. Accessed November 18, 2020. https://www.mdedge.com/dermatology/article/108920/practice-management/dermatology-lacks-diversity.
- Gorbatenko-Roth K, Prose N, Kundu RV, et al. Assessment of black patients’ perception of their dermatology care. JAMA Dermatol. 2019;155:1129-1134.
- Fenton A, Elliott E, Shahbandi A, et al. Medical students’ ability to diagnose common dermatologic conditions in skin of color. J Am Acad Dermatol. 2020;83:957-958.
- Prichep D. Diagnostic gaps: skin comes in many shades and so do rashes. NPR website. November 14, 2019. Accessed November 19, 2020. https://www.npr.org/sections/health-shots/2019/11/04/774910915/diagnostic-gaps-skin-comes-in-many-shades-and-so-do-rashes.
- Tackett KJ, Jenkins F, Morrell DS, et al. Structural racism and its influence on the severity of atopic dermatitis in African American children. Pediatr Dermatol. 2020;37:142-146.
- Gloster HM, Neal K. Skin cancer in skin of color. J Am Acad Dermatol. 2006;55:741-760.
- Ebede T, Papier A. Disparities in dermatology educational resources. J Am Acad Dermatol. 2006;55:687-690.
- Cooper LA, Roter DL, Johnson RL, et al. Patient-centered communication, ratings of care, and concordance of patient and physician race. Ann Intern Med. 2003;139:907-915.
- Takeshita J, Eriksen WT, Raziano VT, et al. Racial differences in perceptions of psoriasis therapies: implications for racial disparities in psoriasis treatment. J Invest Dermatol. 2019;139:1672-1679.e1.
- Alvarado SM, Feng H. Representation of dark skin images of common dermatologic conditions in educational resources: a cross-sectional analysis [published online June 18, 2020]. J Am Acad Dermatol. doi:10.1016/j.jaad.2020.06.041.
- Rabin RC. Dermatology has a problem with skin color. The New York Times. August 30, 2020. http://www.nytimes.com/2020/08/30/health/skin-diseases-black-hispanic.html. Accessed November 19, 2020.
- Bosley RE, Daveluy S. A primer to natural hair care practices in black patients. Cutis. 2015;95:78-80.
Practice Points
- Dermatologists should be aware of the existing health disparities in dermatology training, including lack of representation among dermatologists, treatment, patient satisfaction, and outcomes.
- Dermatologic diseases can present differently in different skin tones, and current dermatology training does not reflect these differences.
- We must continue to work toward increasing diversity of the dermatology workforce, including a diverse range of skin tones in images used in dermatology training, and teaching trainees how diseases present differently in different skin tones.
Blood pressure changes with alemtuzumab infusion in MS
Key clinical point: This study found significant increases in blood pressure (BP) during alemtuzumab infusions in patients with multiple sclerosis (MS).
Major finding: For cycle 1, systolic BP (SBP) increased by 19.2 ± 9.4 mmHg during first infusion, with comparable percentage over the next 5 infusions (16%, 22%, 17%, 11%, and 13%), respectively. Diastolic BP (DBP) increased by 6.2 ± 3.8 mmHg with similar percentage increase as well (8.4%, 11.5%, 5.5%, 7%, and 3%). Second cycle (12 months later) showed similar increases in SBP and DBP as the first cycle. Third cycle (at variable follow-up times) showed similar trends with increased SBP and DBP. Overall, 54.8% of patients had increasing BP reading by 20% or more from baseline, while 29% had increased by at least 20 mmHg from baseline.
Study details: The data come from a retrospective study of SBP and DBP in MS patients treated with alemtuzumab at the London MS Clinic (n = 31; 64.5% females; mean age, 35.2 years).
Disclosures: No study sponsor was identified. Eslam Shosha and Christine Tomkinson reported no disclosures. Sarah Morrow and Courtney Casserly reported relationships with multiple pharmaceutical companies.
Source: Shosha E et al. Eur J Neurol. 2020 Nov 11. doi: 10.1111/ene.14633.
Key clinical point: This study found significant increases in blood pressure (BP) during alemtuzumab infusions in patients with multiple sclerosis (MS).
Major finding: For cycle 1, systolic BP (SBP) increased by 19.2 ± 9.4 mmHg during first infusion, with comparable percentage over the next 5 infusions (16%, 22%, 17%, 11%, and 13%), respectively. Diastolic BP (DBP) increased by 6.2 ± 3.8 mmHg with similar percentage increase as well (8.4%, 11.5%, 5.5%, 7%, and 3%). Second cycle (12 months later) showed similar increases in SBP and DBP as the first cycle. Third cycle (at variable follow-up times) showed similar trends with increased SBP and DBP. Overall, 54.8% of patients had increasing BP reading by 20% or more from baseline, while 29% had increased by at least 20 mmHg from baseline.
Study details: The data come from a retrospective study of SBP and DBP in MS patients treated with alemtuzumab at the London MS Clinic (n = 31; 64.5% females; mean age, 35.2 years).
Disclosures: No study sponsor was identified. Eslam Shosha and Christine Tomkinson reported no disclosures. Sarah Morrow and Courtney Casserly reported relationships with multiple pharmaceutical companies.
Source: Shosha E et al. Eur J Neurol. 2020 Nov 11. doi: 10.1111/ene.14633.
Key clinical point: This study found significant increases in blood pressure (BP) during alemtuzumab infusions in patients with multiple sclerosis (MS).
Major finding: For cycle 1, systolic BP (SBP) increased by 19.2 ± 9.4 mmHg during first infusion, with comparable percentage over the next 5 infusions (16%, 22%, 17%, 11%, and 13%), respectively. Diastolic BP (DBP) increased by 6.2 ± 3.8 mmHg with similar percentage increase as well (8.4%, 11.5%, 5.5%, 7%, and 3%). Second cycle (12 months later) showed similar increases in SBP and DBP as the first cycle. Third cycle (at variable follow-up times) showed similar trends with increased SBP and DBP. Overall, 54.8% of patients had increasing BP reading by 20% or more from baseline, while 29% had increased by at least 20 mmHg from baseline.
Study details: The data come from a retrospective study of SBP and DBP in MS patients treated with alemtuzumab at the London MS Clinic (n = 31; 64.5% females; mean age, 35.2 years).
Disclosures: No study sponsor was identified. Eslam Shosha and Christine Tomkinson reported no disclosures. Sarah Morrow and Courtney Casserly reported relationships with multiple pharmaceutical companies.
Source: Shosha E et al. Eur J Neurol. 2020 Nov 11. doi: 10.1111/ene.14633.
Prescribing Patterns of Onychomycosis Therapies in the United States
To the Editor:
Onychomycosis is the most common nail disorder, affecting approximately 5.5% of the world’s population.1 There are a limited number of topical and systemic therapies approved by the US Food and Drug Administration (FDA), but no consensus guidelines exist for the management of onychomycosis. Therefore, we hypothesized that prescribing patterns would vary among different groups.
We examined data from the Centers for Medicare & Medicaid Services’ Part D Prescriber Public Use Files for 2013 to 2016.2 Prescribing patterns were assessed for dermatologists, nurse practitioners, physician assistants, and podiatrists prescribing systemic (ie, terbinafine, itraconazole) or topical (ie, efinaconazole, tavaborole, ciclopirox) therapies. A cut-off of systemic therapy lasting 84 days or more (reflecting FDA-approved treatment regimens for toenail onychomycosis) was used to exclude prescriptions for other fungal conditions that require shorter treatment courses. Statistical analysis with χ2 tests identified differences among specialties’ prescribing patterns.
Overall, onychomycosis medications accounted for $85.4 million in expenditures from 2013 to 2016, with spending increasing at a rate of 21.2% annually (Table 1). The greatest single-year increase was observed from 2014 to 2015, with a 40.6% surge in overall expenditures for onychomycosis medications—increasing from $17.8 million to $25.0 million in spending. Dermatologists’ prescriptions accounted for 14.8% of all claims for onychomycosis medications and 18.3% of total expenditures during the study period, totaling $15.7 million in costs. Dermatologists’ claims increased at a rate of 7.4% annually, while expenditures increased at 15.4% annually. A greater proportion of dermatologists (96.4%) prescribed topicals for onychomycosis relative to nurse practitioners (90.2%) and podiatrists (91.3%)(P<.01)(Table 2). No significant difference was observed in the prescribing patterns of dermatologists and physician assistants (P=.99).
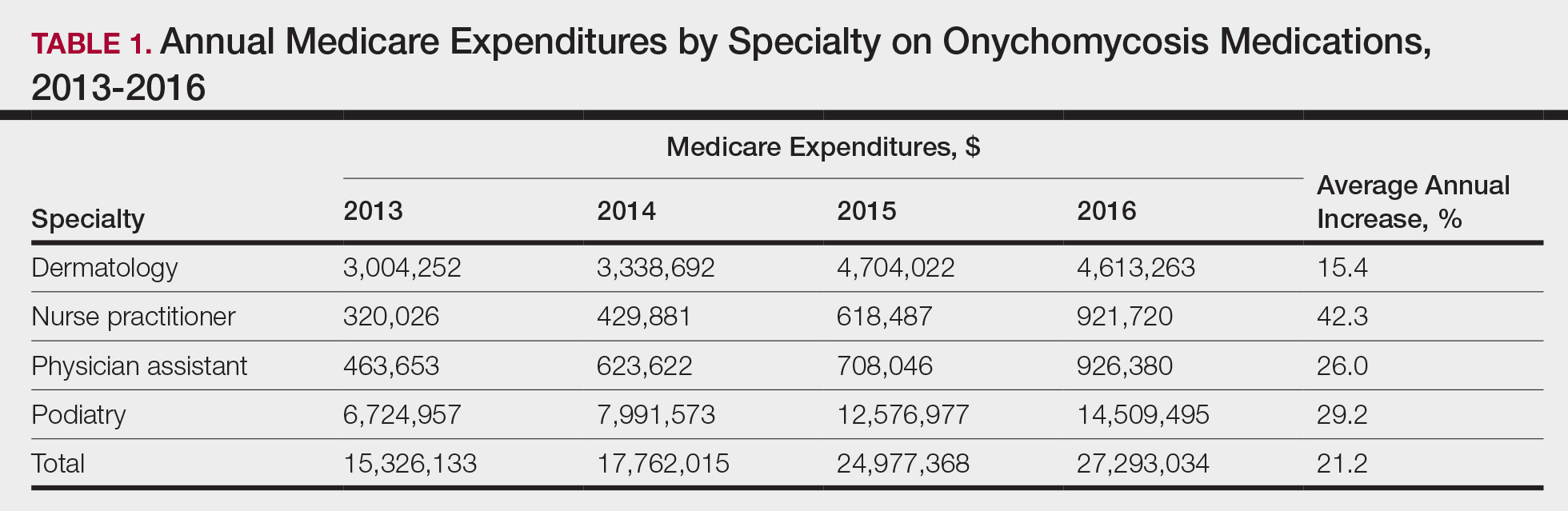
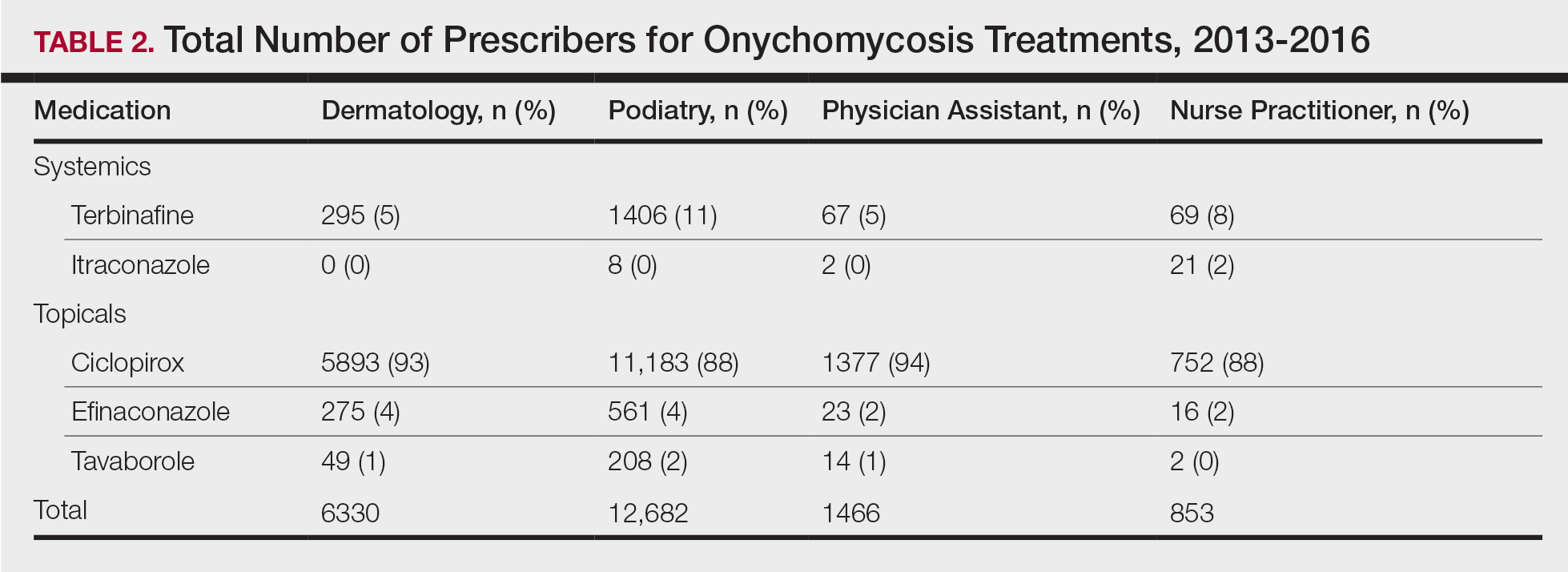
Per-claim spending for treating onychomycosis increased 7.4% annually for dermatologists, second only to podiatrists at 17.2% annually. Each analyzed group reported at least a 7% annual increase in the amount of topicals prescribed for onychomycosis. Following their FDA approvals in 2014, tavaborole and efinaconazole accounted for 0.9% and 2.3% of onychomycosis claims in 2016, respectively, and 15.0% and 25.1% of total Medicare expenditures on onychomycosis treatments that same year, respectively. Itraconazole also disproportionately contributed to expenditures, accounting for 1.3% of onychomycosis claims in 2016 while accounting for 9.5% of total expenditures.
The introduction of efinaconazole and tavaborole in 2014 resulted in large increases in Medicare spending for onychomycosis. Limited manufacturer competition due to patents may contribute to increased spending on these topicals in the future.3 A prior analysis demonstrated that podiatrists prescribe topicals more often than other clinicians,4 but after adjusting for the number of dermatologists managing onychomycosis, we found that a greater proportion of dermatologists (96.4%) are prescribing topicals for onychomycosis than other clinicians. This includes these newly approved, high-cost topicals, thus disproportionately contributing to the cost burden of onychomycosis treatment.
Ciclopirox is the most commonly prescribed therapy for onychomycosis across all groups, prescribed by more than 88% of prescribers in all studied specialties. Although ciclopirox is one of the least expensive treatment options available for onychomycosis, it has the lowest relative cure rate.5 Onychomycosis management requires understanding of drug efficacy and disease severity.6 Inappropriate treatment selection may result in prolonged treatment courses and increased costs. Consensus guidelines for onychomycosis therapies across specialties may yield more cost-effective treatment for this common nail condition.
Acknowledgment
The authors thank Paul J. Christos, DrPH, MS (New York, New York), for his advisement regarding statistical analysis for this manuscript.
- Lipner SR, Scher RK. Onychomycosis: clinical overview and diagnosis. J Am Acad Dermatol. 2019;80:835-851.
- Medicare provider utilization and payment data: part D prescriber. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Medicare-Provider-Charge-Data/Part-D-Prescriber. Updated November 27, 2019. Accessed November 22, 2020.
- Yang EJ, Lipner SR. Pharmacy costs of medications for the treatment of onychomycosis in the United States. J Am Acad Dermatol. 2019;81:276-278.
- Singh P, Silverberg JI. Trends in utilization and expenditure for onychomycosis treatments in the United States in 2013-2016. Am J Clin Dermatol. 2019;20:311-313.
- Lipner SR, Scher RK. Onychomycosis: treatment and prevention of recurrence. J Am Acad Dermatol. 2019;80:853-867.
- Lipner SR. Pharmacotherapy for onychomycosis: new and emerging treatments. Expert Opin Pharmacother. 2019;20:725-735.
To the Editor:
Onychomycosis is the most common nail disorder, affecting approximately 5.5% of the world’s population.1 There are a limited number of topical and systemic therapies approved by the US Food and Drug Administration (FDA), but no consensus guidelines exist for the management of onychomycosis. Therefore, we hypothesized that prescribing patterns would vary among different groups.
We examined data from the Centers for Medicare & Medicaid Services’ Part D Prescriber Public Use Files for 2013 to 2016.2 Prescribing patterns were assessed for dermatologists, nurse practitioners, physician assistants, and podiatrists prescribing systemic (ie, terbinafine, itraconazole) or topical (ie, efinaconazole, tavaborole, ciclopirox) therapies. A cut-off of systemic therapy lasting 84 days or more (reflecting FDA-approved treatment regimens for toenail onychomycosis) was used to exclude prescriptions for other fungal conditions that require shorter treatment courses. Statistical analysis with χ2 tests identified differences among specialties’ prescribing patterns.
Overall, onychomycosis medications accounted for $85.4 million in expenditures from 2013 to 2016, with spending increasing at a rate of 21.2% annually (Table 1). The greatest single-year increase was observed from 2014 to 2015, with a 40.6% surge in overall expenditures for onychomycosis medications—increasing from $17.8 million to $25.0 million in spending. Dermatologists’ prescriptions accounted for 14.8% of all claims for onychomycosis medications and 18.3% of total expenditures during the study period, totaling $15.7 million in costs. Dermatologists’ claims increased at a rate of 7.4% annually, while expenditures increased at 15.4% annually. A greater proportion of dermatologists (96.4%) prescribed topicals for onychomycosis relative to nurse practitioners (90.2%) and podiatrists (91.3%)(P<.01)(Table 2). No significant difference was observed in the prescribing patterns of dermatologists and physician assistants (P=.99).
Per-claim spending for treating onychomycosis increased 7.4% annually for dermatologists, second only to podiatrists at 17.2% annually. Each analyzed group reported at least a 7% annual increase in the amount of topicals prescribed for onychomycosis. Following their FDA approvals in 2014, tavaborole and efinaconazole accounted for 0.9% and 2.3% of onychomycosis claims in 2016, respectively, and 15.0% and 25.1% of total Medicare expenditures on onychomycosis treatments that same year, respectively. Itraconazole also disproportionately contributed to expenditures, accounting for 1.3% of onychomycosis claims in 2016 while accounting for 9.5% of total expenditures.
The introduction of efinaconazole and tavaborole in 2014 resulted in large increases in Medicare spending for onychomycosis. Limited manufacturer competition due to patents may contribute to increased spending on these topicals in the future.3 A prior analysis demonstrated that podiatrists prescribe topicals more often than other clinicians,4 but after adjusting for the number of dermatologists managing onychomycosis, we found that a greater proportion of dermatologists (96.4%) are prescribing topicals for onychomycosis than other clinicians. This includes these newly approved, high-cost topicals, thus disproportionately contributing to the cost burden of onychomycosis treatment.
Ciclopirox is the most commonly prescribed therapy for onychomycosis across all groups, prescribed by more than 88% of prescribers in all studied specialties. Although ciclopirox is one of the least expensive treatment options available for onychomycosis, it has the lowest relative cure rate.5 Onychomycosis management requires understanding of drug efficacy and disease severity.6 Inappropriate treatment selection may result in prolonged treatment courses and increased costs. Consensus guidelines for onychomycosis therapies across specialties may yield more cost-effective treatment for this common nail condition.
Acknowledgment
The authors thank Paul J. Christos, DrPH, MS (New York, New York), for his advisement regarding statistical analysis for this manuscript.
To the Editor:
Onychomycosis is the most common nail disorder, affecting approximately 5.5% of the world’s population.1 There are a limited number of topical and systemic therapies approved by the US Food and Drug Administration (FDA), but no consensus guidelines exist for the management of onychomycosis. Therefore, we hypothesized that prescribing patterns would vary among different groups.
We examined data from the Centers for Medicare & Medicaid Services’ Part D Prescriber Public Use Files for 2013 to 2016.2 Prescribing patterns were assessed for dermatologists, nurse practitioners, physician assistants, and podiatrists prescribing systemic (ie, terbinafine, itraconazole) or topical (ie, efinaconazole, tavaborole, ciclopirox) therapies. A cut-off of systemic therapy lasting 84 days or more (reflecting FDA-approved treatment regimens for toenail onychomycosis) was used to exclude prescriptions for other fungal conditions that require shorter treatment courses. Statistical analysis with χ2 tests identified differences among specialties’ prescribing patterns.
Overall, onychomycosis medications accounted for $85.4 million in expenditures from 2013 to 2016, with spending increasing at a rate of 21.2% annually (Table 1). The greatest single-year increase was observed from 2014 to 2015, with a 40.6% surge in overall expenditures for onychomycosis medications—increasing from $17.8 million to $25.0 million in spending. Dermatologists’ prescriptions accounted for 14.8% of all claims for onychomycosis medications and 18.3% of total expenditures during the study period, totaling $15.7 million in costs. Dermatologists’ claims increased at a rate of 7.4% annually, while expenditures increased at 15.4% annually. A greater proportion of dermatologists (96.4%) prescribed topicals for onychomycosis relative to nurse practitioners (90.2%) and podiatrists (91.3%)(P<.01)(Table 2). No significant difference was observed in the prescribing patterns of dermatologists and physician assistants (P=.99).
Per-claim spending for treating onychomycosis increased 7.4% annually for dermatologists, second only to podiatrists at 17.2% annually. Each analyzed group reported at least a 7% annual increase in the amount of topicals prescribed for onychomycosis. Following their FDA approvals in 2014, tavaborole and efinaconazole accounted for 0.9% and 2.3% of onychomycosis claims in 2016, respectively, and 15.0% and 25.1% of total Medicare expenditures on onychomycosis treatments that same year, respectively. Itraconazole also disproportionately contributed to expenditures, accounting for 1.3% of onychomycosis claims in 2016 while accounting for 9.5% of total expenditures.
The introduction of efinaconazole and tavaborole in 2014 resulted in large increases in Medicare spending for onychomycosis. Limited manufacturer competition due to patents may contribute to increased spending on these topicals in the future.3 A prior analysis demonstrated that podiatrists prescribe topicals more often than other clinicians,4 but after adjusting for the number of dermatologists managing onychomycosis, we found that a greater proportion of dermatologists (96.4%) are prescribing topicals for onychomycosis than other clinicians. This includes these newly approved, high-cost topicals, thus disproportionately contributing to the cost burden of onychomycosis treatment.
Ciclopirox is the most commonly prescribed therapy for onychomycosis across all groups, prescribed by more than 88% of prescribers in all studied specialties. Although ciclopirox is one of the least expensive treatment options available for onychomycosis, it has the lowest relative cure rate.5 Onychomycosis management requires understanding of drug efficacy and disease severity.6 Inappropriate treatment selection may result in prolonged treatment courses and increased costs. Consensus guidelines for onychomycosis therapies across specialties may yield more cost-effective treatment for this common nail condition.
Acknowledgment
The authors thank Paul J. Christos, DrPH, MS (New York, New York), for his advisement regarding statistical analysis for this manuscript.
- Lipner SR, Scher RK. Onychomycosis: clinical overview and diagnosis. J Am Acad Dermatol. 2019;80:835-851.
- Medicare provider utilization and payment data: part D prescriber. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Medicare-Provider-Charge-Data/Part-D-Prescriber. Updated November 27, 2019. Accessed November 22, 2020.
- Yang EJ, Lipner SR. Pharmacy costs of medications for the treatment of onychomycosis in the United States. J Am Acad Dermatol. 2019;81:276-278.
- Singh P, Silverberg JI. Trends in utilization and expenditure for onychomycosis treatments in the United States in 2013-2016. Am J Clin Dermatol. 2019;20:311-313.
- Lipner SR, Scher RK. Onychomycosis: treatment and prevention of recurrence. J Am Acad Dermatol. 2019;80:853-867.
- Lipner SR. Pharmacotherapy for onychomycosis: new and emerging treatments. Expert Opin Pharmacother. 2019;20:725-735.
- Lipner SR, Scher RK. Onychomycosis: clinical overview and diagnosis. J Am Acad Dermatol. 2019;80:835-851.
- Medicare provider utilization and payment data: part D prescriber. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Medicare-Provider-Charge-Data/Part-D-Prescriber. Updated November 27, 2019. Accessed November 22, 2020.
- Yang EJ, Lipner SR. Pharmacy costs of medications for the treatment of onychomycosis in the United States. J Am Acad Dermatol. 2019;81:276-278.
- Singh P, Silverberg JI. Trends in utilization and expenditure for onychomycosis treatments in the United States in 2013-2016. Am J Clin Dermatol. 2019;20:311-313.
- Lipner SR, Scher RK. Onychomycosis: treatment and prevention of recurrence. J Am Acad Dermatol. 2019;80:853-867.
- Lipner SR. Pharmacotherapy for onychomycosis: new and emerging treatments. Expert Opin Pharmacother. 2019;20:725-735.
Practice Points
- Dermatologists should consider efficacy and cost of onychomycosis therapies, as inappropriate treatment selection results in longer treatment courses and increased costs.
- Creation of consensus guidelines for the management of onychomycosis may decrease the costs of treating this difficult-to-manage disease.
