User login
PCPs May Have a New Tool to Help Identify Autism in Young Children
Incorporating eye-tracking biomarkers into pediatric autism assessments may make identifying the condition easier, according to new findings published in JAMA Network Open.
Researchers created an artificial intelligence–based tool to help primary care clinicians and pediatricians spot potential cases of the neurological condition, according to Brandon Keehn, PhD, associate professor in the Department of Speech, Language, and Hearing Sciences at Purdue University in West Lafayette, Indiana, and an author of the study.
Most primary care clinicians do not receive specialized training in identifying autism, and around a third diagnose the condition with uncertainty, according to Dr. Keehn. The tool helps clinicians by incorporating their diagnosis and self-reported level of certainty with eye-tracking biomarkers. A clinical psychologist also assessed children, either verifying or confuting the earlier results.
The tool produced the same diagnosis as that from a psychologist in 90% of cases. When children were assessed using eye biomarkers alone, the diagnosis was aligned with that of a psychologist 77% of the time.
“This is the first step in demonstrating both that eye-tracking biomarkers are sensitive to autism and whether or not these biomarkers provide extra clinical information for primary care physicians to more accurately diagnose autism,” Dr. Keehn told this news organization.
The study took place between 2019 and 2022 and included 146 children between 14 and 48 months old who were treated at seven primary care practices in Indiana. Dr. Keehn and colleagues asked primary care clinicians to rate their level of certainty in their diagnosis.
During the biomarker test, toddlers watched cartoons while researchers tracked their eye movements. Six biomarkers included in the test were based on previous research linking eye movements to autism, according to Dr. Keehn.
These included whether toddlers looked more at images of people or geometric patterns and the speed and size of pupil dilation when exposed to bright light.
Most toddlers produced a positive result for autism in only one biomarker test. Dr. Keehn said this confirms that children should be tested for a variety of biomarkers because each patient’s condition manifests differently.
Dr. Keehn said his team is still a few steps away from determining how the model would work in a real clinical setting and that they are planning more research with a larger study population.
Alice Kuo, MD, a pediatrician specializing in autism at the University of California, Los Angeles (UCLA), said primary care clinicians should feel comfortable making an autism diagnosis.
“Any tool that helps them to do that can be useful, since wait times for a specialist can take years,” Dr. Kuo, also the director of the Autism Intervention Research Network on Physical Health at UCLA, said.
However, Dr. Kuo said she is concerned about the cases that were falsely identified as positive or negative.
“To be told your kid is autistic when he’s not, or to be told your kid is not when he clinically is, has huge ramifications,” she said.
The study was funded by the National Institute of Mental Health, the Riley Children’s Foundation, and the Indiana Clinical and Translational Sciences Institute. Dr. Keehn reported payments for workshops on the use of the Autism Diagnostic Observation Schedule.
A version of this article appeared on Medscape.com .
Incorporating eye-tracking biomarkers into pediatric autism assessments may make identifying the condition easier, according to new findings published in JAMA Network Open.
Researchers created an artificial intelligence–based tool to help primary care clinicians and pediatricians spot potential cases of the neurological condition, according to Brandon Keehn, PhD, associate professor in the Department of Speech, Language, and Hearing Sciences at Purdue University in West Lafayette, Indiana, and an author of the study.
Most primary care clinicians do not receive specialized training in identifying autism, and around a third diagnose the condition with uncertainty, according to Dr. Keehn. The tool helps clinicians by incorporating their diagnosis and self-reported level of certainty with eye-tracking biomarkers. A clinical psychologist also assessed children, either verifying or confuting the earlier results.
The tool produced the same diagnosis as that from a psychologist in 90% of cases. When children were assessed using eye biomarkers alone, the diagnosis was aligned with that of a psychologist 77% of the time.
“This is the first step in demonstrating both that eye-tracking biomarkers are sensitive to autism and whether or not these biomarkers provide extra clinical information for primary care physicians to more accurately diagnose autism,” Dr. Keehn told this news organization.
The study took place between 2019 and 2022 and included 146 children between 14 and 48 months old who were treated at seven primary care practices in Indiana. Dr. Keehn and colleagues asked primary care clinicians to rate their level of certainty in their diagnosis.
During the biomarker test, toddlers watched cartoons while researchers tracked their eye movements. Six biomarkers included in the test were based on previous research linking eye movements to autism, according to Dr. Keehn.
These included whether toddlers looked more at images of people or geometric patterns and the speed and size of pupil dilation when exposed to bright light.
Most toddlers produced a positive result for autism in only one biomarker test. Dr. Keehn said this confirms that children should be tested for a variety of biomarkers because each patient’s condition manifests differently.
Dr. Keehn said his team is still a few steps away from determining how the model would work in a real clinical setting and that they are planning more research with a larger study population.
Alice Kuo, MD, a pediatrician specializing in autism at the University of California, Los Angeles (UCLA), said primary care clinicians should feel comfortable making an autism diagnosis.
“Any tool that helps them to do that can be useful, since wait times for a specialist can take years,” Dr. Kuo, also the director of the Autism Intervention Research Network on Physical Health at UCLA, said.
However, Dr. Kuo said she is concerned about the cases that were falsely identified as positive or negative.
“To be told your kid is autistic when he’s not, or to be told your kid is not when he clinically is, has huge ramifications,” she said.
The study was funded by the National Institute of Mental Health, the Riley Children’s Foundation, and the Indiana Clinical and Translational Sciences Institute. Dr. Keehn reported payments for workshops on the use of the Autism Diagnostic Observation Schedule.
A version of this article appeared on Medscape.com .
Incorporating eye-tracking biomarkers into pediatric autism assessments may make identifying the condition easier, according to new findings published in JAMA Network Open.
Researchers created an artificial intelligence–based tool to help primary care clinicians and pediatricians spot potential cases of the neurological condition, according to Brandon Keehn, PhD, associate professor in the Department of Speech, Language, and Hearing Sciences at Purdue University in West Lafayette, Indiana, and an author of the study.
Most primary care clinicians do not receive specialized training in identifying autism, and around a third diagnose the condition with uncertainty, according to Dr. Keehn. The tool helps clinicians by incorporating their diagnosis and self-reported level of certainty with eye-tracking biomarkers. A clinical psychologist also assessed children, either verifying or confuting the earlier results.
The tool produced the same diagnosis as that from a psychologist in 90% of cases. When children were assessed using eye biomarkers alone, the diagnosis was aligned with that of a psychologist 77% of the time.
“This is the first step in demonstrating both that eye-tracking biomarkers are sensitive to autism and whether or not these biomarkers provide extra clinical information for primary care physicians to more accurately diagnose autism,” Dr. Keehn told this news organization.
The study took place between 2019 and 2022 and included 146 children between 14 and 48 months old who were treated at seven primary care practices in Indiana. Dr. Keehn and colleagues asked primary care clinicians to rate their level of certainty in their diagnosis.
During the biomarker test, toddlers watched cartoons while researchers tracked their eye movements. Six biomarkers included in the test were based on previous research linking eye movements to autism, according to Dr. Keehn.
These included whether toddlers looked more at images of people or geometric patterns and the speed and size of pupil dilation when exposed to bright light.
Most toddlers produced a positive result for autism in only one biomarker test. Dr. Keehn said this confirms that children should be tested for a variety of biomarkers because each patient’s condition manifests differently.
Dr. Keehn said his team is still a few steps away from determining how the model would work in a real clinical setting and that they are planning more research with a larger study population.
Alice Kuo, MD, a pediatrician specializing in autism at the University of California, Los Angeles (UCLA), said primary care clinicians should feel comfortable making an autism diagnosis.
“Any tool that helps them to do that can be useful, since wait times for a specialist can take years,” Dr. Kuo, also the director of the Autism Intervention Research Network on Physical Health at UCLA, said.
However, Dr. Kuo said she is concerned about the cases that were falsely identified as positive or negative.
“To be told your kid is autistic when he’s not, or to be told your kid is not when he clinically is, has huge ramifications,” she said.
The study was funded by the National Institute of Mental Health, the Riley Children’s Foundation, and the Indiana Clinical and Translational Sciences Institute. Dr. Keehn reported payments for workshops on the use of the Autism Diagnostic Observation Schedule.
A version of this article appeared on Medscape.com .
FROM JAMA NETWORK OPEN
Rethinking the Rebels
Each month I set out on an expedition to find a topic for this column. I came across a new book Rebel Health by Susannah Fox that I thought might be a good one. It’s both a treatise on the shortcomings of healthcare and a Baedeker for patients on how to find their way to being better served. Her argument is that many patients’ needs are unmet and their conditions are often invisible to us in mainstream healthcare. We fail to find solutions to help them. Patients would benefit from more open access to their records and more resources to take control of their own health, she argues. A few chapters in, I thought, “Oh, here we go, another diatribe on doctors and how we care most about how to keep patients in their rightful, subordinate place.” The “Rebel” title is provocative and implies patients need to overthrow the status quo. Well, I am part of the establishment. I stopped reading. This book doesn’t apply to me, I thought.
After all, I’m a healthcare progressive, right? My notes and results have been open for years. I encourage shared decision-making and try to empower patients as much as treat them. The idea that I or my colleagues are unwilling to do whatever is necessary to meet our patients’ needs was maddening. We dedicate our lives to it. My young daughter often greets me in the morning by asking if I’ll be working tonight. Most nights, I am — answering patient messages, collaborating with colleagues to help patients, keeping up with medical knowledge. I was angry at what felt like unjust criticism, especially that we’d neglect patients because their problems are not obvious or worse, there is not enough money to be made helping them. Harrumph.

That’s when I realized the best thing for me was to read the entire book and digest the arguments. I pride myself on being well-read, but I fall into a common trap: the podcasts I listen to, news I consume, and books I read mostly affirm my beliefs. It is a healthy choice to seek dispositive data and contrasting stories rather than always feeding our personal opinions.
Rebel Health was not written by Robespierre. It was penned by a thoughtful, articulate patient advocate with over 20 years experience. She has far more bona fides than I could achieve in two lifetimes. In the book, she reminds us that She describes four patient archetypes: seekers, networkers, solvers, and champions, and offers a four-quadrant model to visualize how some patients are unhelped by our current healthcare system. She advocates for frictionless, open access to health data and tries to inspire patients to connect, innovate, and create to fill the voids that exist in healthcare. We have come a long way from the immured system of a decade ago; much of that is the result of patient advocates. But healthcare is still too costly, too fragmented and too many patients unhelped. “Community is a superpower,” she writes. I agree, we should assemble all the heroes in the universe for this challenge.
Fox also tells stories of patients who solved diagnostic dilemmas through their own research and advocacy. I thought of my own contrasting experiences of patients whose DIY care was based on misinformation and how their false confidence led to poorer outcomes for them. I want to share with her readers how physicians feel hurt when patients question our competence or place the opinion of an adversarial Redditor over ours. Physicians are sometimes wrong and often in doubt. Most of us care deeply about our patients regardless of how visible their diagnosis or how easy they are to appease.
We don’t have time to engage back-and-forth on an insignificantly abnormal test they find in their open chart or why B12 and hormone testing would not be helpful for their disease. It’s also not the patients’ fault. Having unfettered access to their data might add work, but it also adds value. They are trying to learn and be active in their care. Physicians are frustrated mostly because we don’t have time to meet these unmet needs. Everyone is trying their best and we all want the same thing: patients to be satisfied and well.
As for learning the skill of being open-minded, an excellent reference is Adam Grant’s Think Again. It’s inspiring and instructive of how we can all be more open, including how to have productive arguments rather than fruitless fights. We live in divisive times. Perhaps if we all put in effort to be open-minded, push down righteous indignation, and advance more honest humility we’d all be a bit better off.
Patients are the primary audience for the Rebel Health book. Yet, as we care about them and we all want to make healthcare better, it is worth reading in its entirety. I told my daughter I don’t have to work tonight because I’ve written my article this month. When she’s a little older, I’ll tell her all about it. To be successful, she’ll have to be as open-minded as she is smart. She can learn both.
I have no conflict of interest in the book.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Each month I set out on an expedition to find a topic for this column. I came across a new book Rebel Health by Susannah Fox that I thought might be a good one. It’s both a treatise on the shortcomings of healthcare and a Baedeker for patients on how to find their way to being better served. Her argument is that many patients’ needs are unmet and their conditions are often invisible to us in mainstream healthcare. We fail to find solutions to help them. Patients would benefit from more open access to their records and more resources to take control of their own health, she argues. A few chapters in, I thought, “Oh, here we go, another diatribe on doctors and how we care most about how to keep patients in their rightful, subordinate place.” The “Rebel” title is provocative and implies patients need to overthrow the status quo. Well, I am part of the establishment. I stopped reading. This book doesn’t apply to me, I thought.
After all, I’m a healthcare progressive, right? My notes and results have been open for years. I encourage shared decision-making and try to empower patients as much as treat them. The idea that I or my colleagues are unwilling to do whatever is necessary to meet our patients’ needs was maddening. We dedicate our lives to it. My young daughter often greets me in the morning by asking if I’ll be working tonight. Most nights, I am — answering patient messages, collaborating with colleagues to help patients, keeping up with medical knowledge. I was angry at what felt like unjust criticism, especially that we’d neglect patients because their problems are not obvious or worse, there is not enough money to be made helping them. Harrumph.
That’s when I realized the best thing for me was to read the entire book and digest the arguments. I pride myself on being well-read, but I fall into a common trap: the podcasts I listen to, news I consume, and books I read mostly affirm my beliefs. It is a healthy choice to seek dispositive data and contrasting stories rather than always feeding our personal opinions.
Rebel Health was not written by Robespierre. It was penned by a thoughtful, articulate patient advocate with over 20 years experience. She has far more bona fides than I could achieve in two lifetimes. In the book, she reminds us that She describes four patient archetypes: seekers, networkers, solvers, and champions, and offers a four-quadrant model to visualize how some patients are unhelped by our current healthcare system. She advocates for frictionless, open access to health data and tries to inspire patients to connect, innovate, and create to fill the voids that exist in healthcare. We have come a long way from the immured system of a decade ago; much of that is the result of patient advocates. But healthcare is still too costly, too fragmented and too many patients unhelped. “Community is a superpower,” she writes. I agree, we should assemble all the heroes in the universe for this challenge.
Fox also tells stories of patients who solved diagnostic dilemmas through their own research and advocacy. I thought of my own contrasting experiences of patients whose DIY care was based on misinformation and how their false confidence led to poorer outcomes for them. I want to share with her readers how physicians feel hurt when patients question our competence or place the opinion of an adversarial Redditor over ours. Physicians are sometimes wrong and often in doubt. Most of us care deeply about our patients regardless of how visible their diagnosis or how easy they are to appease.
We don’t have time to engage back-and-forth on an insignificantly abnormal test they find in their open chart or why B12 and hormone testing would not be helpful for their disease. It’s also not the patients’ fault. Having unfettered access to their data might add work, but it also adds value. They are trying to learn and be active in their care. Physicians are frustrated mostly because we don’t have time to meet these unmet needs. Everyone is trying their best and we all want the same thing: patients to be satisfied and well.
As for learning the skill of being open-minded, an excellent reference is Adam Grant’s Think Again. It’s inspiring and instructive of how we can all be more open, including how to have productive arguments rather than fruitless fights. We live in divisive times. Perhaps if we all put in effort to be open-minded, push down righteous indignation, and advance more honest humility we’d all be a bit better off.
Patients are the primary audience for the Rebel Health book. Yet, as we care about them and we all want to make healthcare better, it is worth reading in its entirety. I told my daughter I don’t have to work tonight because I’ve written my article this month. When she’s a little older, I’ll tell her all about it. To be successful, she’ll have to be as open-minded as she is smart. She can learn both.
I have no conflict of interest in the book.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Each month I set out on an expedition to find a topic for this column. I came across a new book Rebel Health by Susannah Fox that I thought might be a good one. It’s both a treatise on the shortcomings of healthcare and a Baedeker for patients on how to find their way to being better served. Her argument is that many patients’ needs are unmet and their conditions are often invisible to us in mainstream healthcare. We fail to find solutions to help them. Patients would benefit from more open access to their records and more resources to take control of their own health, she argues. A few chapters in, I thought, “Oh, here we go, another diatribe on doctors and how we care most about how to keep patients in their rightful, subordinate place.” The “Rebel” title is provocative and implies patients need to overthrow the status quo. Well, I am part of the establishment. I stopped reading. This book doesn’t apply to me, I thought.
After all, I’m a healthcare progressive, right? My notes and results have been open for years. I encourage shared decision-making and try to empower patients as much as treat them. The idea that I or my colleagues are unwilling to do whatever is necessary to meet our patients’ needs was maddening. We dedicate our lives to it. My young daughter often greets me in the morning by asking if I’ll be working tonight. Most nights, I am — answering patient messages, collaborating with colleagues to help patients, keeping up with medical knowledge. I was angry at what felt like unjust criticism, especially that we’d neglect patients because their problems are not obvious or worse, there is not enough money to be made helping them. Harrumph.
That’s when I realized the best thing for me was to read the entire book and digest the arguments. I pride myself on being well-read, but I fall into a common trap: the podcasts I listen to, news I consume, and books I read mostly affirm my beliefs. It is a healthy choice to seek dispositive data and contrasting stories rather than always feeding our personal opinions.
Rebel Health was not written by Robespierre. It was penned by a thoughtful, articulate patient advocate with over 20 years experience. She has far more bona fides than I could achieve in two lifetimes. In the book, she reminds us that She describes four patient archetypes: seekers, networkers, solvers, and champions, and offers a four-quadrant model to visualize how some patients are unhelped by our current healthcare system. She advocates for frictionless, open access to health data and tries to inspire patients to connect, innovate, and create to fill the voids that exist in healthcare. We have come a long way from the immured system of a decade ago; much of that is the result of patient advocates. But healthcare is still too costly, too fragmented and too many patients unhelped. “Community is a superpower,” she writes. I agree, we should assemble all the heroes in the universe for this challenge.
Fox also tells stories of patients who solved diagnostic dilemmas through their own research and advocacy. I thought of my own contrasting experiences of patients whose DIY care was based on misinformation and how their false confidence led to poorer outcomes for them. I want to share with her readers how physicians feel hurt when patients question our competence or place the opinion of an adversarial Redditor over ours. Physicians are sometimes wrong and often in doubt. Most of us care deeply about our patients regardless of how visible their diagnosis or how easy they are to appease.
We don’t have time to engage back-and-forth on an insignificantly abnormal test they find in their open chart or why B12 and hormone testing would not be helpful for their disease. It’s also not the patients’ fault. Having unfettered access to their data might add work, but it also adds value. They are trying to learn and be active in their care. Physicians are frustrated mostly because we don’t have time to meet these unmet needs. Everyone is trying their best and we all want the same thing: patients to be satisfied and well.
As for learning the skill of being open-minded, an excellent reference is Adam Grant’s Think Again. It’s inspiring and instructive of how we can all be more open, including how to have productive arguments rather than fruitless fights. We live in divisive times. Perhaps if we all put in effort to be open-minded, push down righteous indignation, and advance more honest humility we’d all be a bit better off.
Patients are the primary audience for the Rebel Health book. Yet, as we care about them and we all want to make healthcare better, it is worth reading in its entirety. I told my daughter I don’t have to work tonight because I’ve written my article this month. When she’s a little older, I’ll tell her all about it. To be successful, she’ll have to be as open-minded as she is smart. She can learn both.
I have no conflict of interest in the book.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Commentary: Aspirin, Childbirth, and Everolimus in BC, June 2024

The postpartum period represents a possibly vulnerable time window for development of new cancers with metastatic potential. Studies in young-onset breast cancer have shown a postpartum diagnosis up to 10 years after childbirth associated with adverse breast cancer survival outcomes.4 Women with germline BRCA1/2 pathogenic variants have a higher risk of developing breast cancer at a younger age compared to the general population.5 A prospective cohort study that included 903 women with germline BRCA1/2 mutations diagnosed with stage I-III breast cancer at age ≤ 45 years investigated whether time since childbirth and time since breast cancer diagnosis were associated with mortality in this population (
The mechanisms involved in development of endocrine therapy (ET) resistance are complex and may include changes in hormone signaling, alterations in growth factor signaling pathway components, and appearance of resistant clonal populations.6 Prior studies have shown efficacy with the mammalian target of rapamycin (mTOR) inhibitor everolimus in combination with various ET backbones. However, the sequencing of these combinations in current clinical practice has shifted in light of significant therapeutic advancements in this space.7 A retrospective observational study including 161 patients with advanced hormone receptor–positive (HR+)/ human epidermal growth factor receptor–2 negative (HER2-) breast cancer treated with everolimus plus ET (exemestane, fulvestrant, tamoxifen) reported outcomes on the real-world use of these regimens after progression on cyclin-dependent kinase (CDK) 4/6 inhibitor therapy (Sánchez-Bayona et al). At a median follow-up of 15 months, the estimated median progression-free survival (PFS) was 6.0 months (95% CI 5.3-7.8 months); PFS was longer among those with previous CDK4/6 inhibitor use lasting >18 months (8.7 months; 95% CI 6.6-11.3 months), patients without visceral disease (8.0 months; 95% CI 5.8-10.5 months), and those who were chemotherapy-naive in the advanced setting (7.2 months; 95% CI 5.9-8.4 months). These data support a role for everolimus plus ET as a treatment option post–CDK4/6 inhibitor treatment for selected patient populations, including those whose tumors lack targetable somatic mutations (such as PIK3CA and ESR1 mutations), and may provide meaningful clinical benefit in this setting.
Additional References
- Rothwell PM, Wilson M, Price JF, et al. Effect of daily aspirin on risk of cancer metastasis: A study of incident cancers during randomised controlled trials. Lancet. 2012;379:1591-601. doi: 10.1016/S0140-6736(12)60209-8 Source
- Okada S, Morimoto T, Ogawa H, et al, and the JPAD Trial Investigators. Effect of aspirin on cancer chemoprevention in Japanese patients with type 2 diabetes: 10-year observational follow-up of a randomized controlled trial. Diabetes Care. 2018;41:1757-1764. doi: 10.2337/dc18-0368 Source
- Burn J, Sheth H, Elliott F, et al, on behalf of the CAPP2 Investigators. Cancer prevention with aspirin in hereditary colorectal cancer (Lynch syndrome), 10-year follow-up and registry-based 20-year data in the CAPP2 study: A double-blind, randomised, placebo-controlled trial. Lancet. 2020;395:1855-1863. doi: 10.1016/S0140-6736(20)30366-4 Source
- Shao C, Yu Z, Xiao J, et al. Prognosis of pregnancy-associated breast cancer: A meta-analysis. BMC Cancer. 2020;20:746. doi: 10.1186/s12885-020-07248-8 Source
- Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA. 2017;317:2402-2416. doi: 10.1001/jama.2017.7112 Source
- Hanker AB, Sudhan DR, Arteaga CL. Overcoming endocrine resistance in breast cancer. Cancer Cell. 2020;37:496-513. doi: 10.1016/j.ccell.2020.03.009 Source
- Kornblum N, Zhao F, Manola J, et al. Randomized phase II trial of fulvestrant plus everolimus or placebo in postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer resistant to aromatase inhibitor therapy: Results of PrE0102. J Clin Oncol. 2018;36:1556-1563. doi: 10.1200/JCO.2017.76.9331 Source
The postpartum period represents a possibly vulnerable time window for development of new cancers with metastatic potential. Studies in young-onset breast cancer have shown a postpartum diagnosis up to 10 years after childbirth associated with adverse breast cancer survival outcomes.4 Women with germline BRCA1/2 pathogenic variants have a higher risk of developing breast cancer at a younger age compared to the general population.5 A prospective cohort study that included 903 women with germline BRCA1/2 mutations diagnosed with stage I-III breast cancer at age ≤ 45 years investigated whether time since childbirth and time since breast cancer diagnosis were associated with mortality in this population (
The mechanisms involved in development of endocrine therapy (ET) resistance are complex and may include changes in hormone signaling, alterations in growth factor signaling pathway components, and appearance of resistant clonal populations.6 Prior studies have shown efficacy with the mammalian target of rapamycin (mTOR) inhibitor everolimus in combination with various ET backbones. However, the sequencing of these combinations in current clinical practice has shifted in light of significant therapeutic advancements in this space.7 A retrospective observational study including 161 patients with advanced hormone receptor–positive (HR+)/ human epidermal growth factor receptor–2 negative (HER2-) breast cancer treated with everolimus plus ET (exemestane, fulvestrant, tamoxifen) reported outcomes on the real-world use of these regimens after progression on cyclin-dependent kinase (CDK) 4/6 inhibitor therapy (Sánchez-Bayona et al). At a median follow-up of 15 months, the estimated median progression-free survival (PFS) was 6.0 months (95% CI 5.3-7.8 months); PFS was longer among those with previous CDK4/6 inhibitor use lasting >18 months (8.7 months; 95% CI 6.6-11.3 months), patients without visceral disease (8.0 months; 95% CI 5.8-10.5 months), and those who were chemotherapy-naive in the advanced setting (7.2 months; 95% CI 5.9-8.4 months). These data support a role for everolimus plus ET as a treatment option post–CDK4/6 inhibitor treatment for selected patient populations, including those whose tumors lack targetable somatic mutations (such as PIK3CA and ESR1 mutations), and may provide meaningful clinical benefit in this setting.
Additional References
- Rothwell PM, Wilson M, Price JF, et al. Effect of daily aspirin on risk of cancer metastasis: A study of incident cancers during randomised controlled trials. Lancet. 2012;379:1591-601. doi: 10.1016/S0140-6736(12)60209-8 Source
- Okada S, Morimoto T, Ogawa H, et al, and the JPAD Trial Investigators. Effect of aspirin on cancer chemoprevention in Japanese patients with type 2 diabetes: 10-year observational follow-up of a randomized controlled trial. Diabetes Care. 2018;41:1757-1764. doi: 10.2337/dc18-0368 Source
- Burn J, Sheth H, Elliott F, et al, on behalf of the CAPP2 Investigators. Cancer prevention with aspirin in hereditary colorectal cancer (Lynch syndrome), 10-year follow-up and registry-based 20-year data in the CAPP2 study: A double-blind, randomised, placebo-controlled trial. Lancet. 2020;395:1855-1863. doi: 10.1016/S0140-6736(20)30366-4 Source
- Shao C, Yu Z, Xiao J, et al. Prognosis of pregnancy-associated breast cancer: A meta-analysis. BMC Cancer. 2020;20:746. doi: 10.1186/s12885-020-07248-8 Source
- Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA. 2017;317:2402-2416. doi: 10.1001/jama.2017.7112 Source
- Hanker AB, Sudhan DR, Arteaga CL. Overcoming endocrine resistance in breast cancer. Cancer Cell. 2020;37:496-513. doi: 10.1016/j.ccell.2020.03.009 Source
- Kornblum N, Zhao F, Manola J, et al. Randomized phase II trial of fulvestrant plus everolimus or placebo in postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer resistant to aromatase inhibitor therapy: Results of PrE0102. J Clin Oncol. 2018;36:1556-1563. doi: 10.1200/JCO.2017.76.9331 Source
The postpartum period represents a possibly vulnerable time window for development of new cancers with metastatic potential. Studies in young-onset breast cancer have shown a postpartum diagnosis up to 10 years after childbirth associated with adverse breast cancer survival outcomes.4 Women with germline BRCA1/2 pathogenic variants have a higher risk of developing breast cancer at a younger age compared to the general population.5 A prospective cohort study that included 903 women with germline BRCA1/2 mutations diagnosed with stage I-III breast cancer at age ≤ 45 years investigated whether time since childbirth and time since breast cancer diagnosis were associated with mortality in this population (
The mechanisms involved in development of endocrine therapy (ET) resistance are complex and may include changes in hormone signaling, alterations in growth factor signaling pathway components, and appearance of resistant clonal populations.6 Prior studies have shown efficacy with the mammalian target of rapamycin (mTOR) inhibitor everolimus in combination with various ET backbones. However, the sequencing of these combinations in current clinical practice has shifted in light of significant therapeutic advancements in this space.7 A retrospective observational study including 161 patients with advanced hormone receptor–positive (HR+)/ human epidermal growth factor receptor–2 negative (HER2-) breast cancer treated with everolimus plus ET (exemestane, fulvestrant, tamoxifen) reported outcomes on the real-world use of these regimens after progression on cyclin-dependent kinase (CDK) 4/6 inhibitor therapy (Sánchez-Bayona et al). At a median follow-up of 15 months, the estimated median progression-free survival (PFS) was 6.0 months (95% CI 5.3-7.8 months); PFS was longer among those with previous CDK4/6 inhibitor use lasting >18 months (8.7 months; 95% CI 6.6-11.3 months), patients without visceral disease (8.0 months; 95% CI 5.8-10.5 months), and those who were chemotherapy-naive in the advanced setting (7.2 months; 95% CI 5.9-8.4 months). These data support a role for everolimus plus ET as a treatment option post–CDK4/6 inhibitor treatment for selected patient populations, including those whose tumors lack targetable somatic mutations (such as PIK3CA and ESR1 mutations), and may provide meaningful clinical benefit in this setting.
Additional References
- Rothwell PM, Wilson M, Price JF, et al. Effect of daily aspirin on risk of cancer metastasis: A study of incident cancers during randomised controlled trials. Lancet. 2012;379:1591-601. doi: 10.1016/S0140-6736(12)60209-8 Source
- Okada S, Morimoto T, Ogawa H, et al, and the JPAD Trial Investigators. Effect of aspirin on cancer chemoprevention in Japanese patients with type 2 diabetes: 10-year observational follow-up of a randomized controlled trial. Diabetes Care. 2018;41:1757-1764. doi: 10.2337/dc18-0368 Source
- Burn J, Sheth H, Elliott F, et al, on behalf of the CAPP2 Investigators. Cancer prevention with aspirin in hereditary colorectal cancer (Lynch syndrome), 10-year follow-up and registry-based 20-year data in the CAPP2 study: A double-blind, randomised, placebo-controlled trial. Lancet. 2020;395:1855-1863. doi: 10.1016/S0140-6736(20)30366-4 Source
- Shao C, Yu Z, Xiao J, et al. Prognosis of pregnancy-associated breast cancer: A meta-analysis. BMC Cancer. 2020;20:746. doi: 10.1186/s12885-020-07248-8 Source
- Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA. 2017;317:2402-2416. doi: 10.1001/jama.2017.7112 Source
- Hanker AB, Sudhan DR, Arteaga CL. Overcoming endocrine resistance in breast cancer. Cancer Cell. 2020;37:496-513. doi: 10.1016/j.ccell.2020.03.009 Source
- Kornblum N, Zhao F, Manola J, et al. Randomized phase II trial of fulvestrant plus everolimus or placebo in postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer resistant to aromatase inhibitor therapy: Results of PrE0102. J Clin Oncol. 2018;36:1556-1563. doi: 10.1200/JCO.2017.76.9331 Source
Ultraprocessed Foods May Be an Independent Risk Factor for Poor Brain Health
, new research suggests.
Observations from a large cohort of adults followed for more than 10 years suggested that eating more ultraprocessed foods (UPFs) may increase the risk for cognitive decline and stroke, while eating more unprocessed or minimally processed foods may lower the risk.
“The first key takeaway is that the type of food that we eat matters for brain health, but it’s equally important to think about how it’s made and handled when thinking about brain health,” said study investigator W. Taylor Kimberly, MD, PhD, with Massachusetts General Hospital in Boston.
“The second is that it’s not just all a bad news story because while increased consumption of ultra-processed foods is associated with a higher risk of cognitive impairment and stroke, unprocessed foods appear to be protective,” Dr. Kimberly added.
The study was published online on May 22 in Neurology.
Food Processing Matters
UPFs are highly manipulated, low in protein and fiber, and packed with added ingredients, including sugar, fat, and salt. Examples of UPFs are soft drinks, chips, chocolate, candy, ice cream, sweetened breakfast cereals, packaged soups, chicken nuggets, hot dogs, and fries.
Unprocessed or minimally processed foods include meats such as simple cuts of beef, pork, and chicken, and vegetables and fruits.
Research has shown associations between high UPF consumption and increased risk for metabolic and neurologic disorders.
As reported previously, in the ELSA-Brasil study, higher intake of UPFs was significantly associated with a faster rate of decline in executive and global cognitive function.
Yet, it’s unclear whether the extent of food processing contributes to the risk of adverse neurologic outcomes independent of dietary patterns.
Dr. Kimberly and colleagues examined the association of food processing levels with the risk for cognitive impairment and stroke in the long-running REGARDS study, a large prospective US cohort of Black and White adults aged 45 years and older.
Food processing levels were defined by the NOVA food classification system, which ranges from unprocessed or minimally processed foods (NOVA1) to UPFs (NOVA4). Dietary patterns were characterized based on food frequency questionnaires.
In the cognitive impairment cohort, 768 of 14,175 adults without evidence of impairment at baseline who underwent follow-up testing developed cognitive impairment.
Diet an Opportunity to Protect Brain Health
In multivariable Cox proportional hazards models adjusting for age, sex, high blood pressure, and other factors, a 10% increase in relative intake of UPFs was associated with a 16% higher risk for cognitive impairment (hazard ratio [HR], 1.16). Conversely, a higher intake of unprocessed or minimally processed foods correlated with a 12% lower risk for cognitive impairment (HR, 0.88).
In the stroke cohort, 1108 of 20,243 adults without a history of stroke had a stroke during the follow-up.
In multivariable Cox models, greater intake of UPFs was associated with an 8% increased risk for stroke (HR, 1.08), while greater intake of unprocessed or minimally processed foods correlated with a 9% lower risk for stroke (HR, 0.91).
The effect of UPFs on stroke risk was greater among Black than among White adults (UPF-by-race interaction HR, 1.15).
The associations between UPFs and both cognitive impairment and stroke were independent of adherence to the Mediterranean diet, the Dietary Approaches to Stop Hypertension (DASH) diet, and the Mediterranean-DASH Intervention for Neurodegenerative Delay diet.
These results “highlight the possibility that we have the capacity to maintain our brain health and prevent poor brain health outcomes by focusing on unprocessed foods in the long term,” Dr. Kimberly said.
He cautioned that this was “an observational study and not an interventional study, so we can’t say with certainty that substituting ultra-processed foods with unprocessed foods will definitively improve brain health,” Dr. Kimberly said. “That’s a clinical trial question that has not been done but our results certainly are provocative.”
Consider UPFs in National Guidelines?
The coauthors of an accompanying editorial said the “robust” results from Kimberly and colleagues highlight the “significant role of food processing levels and their relationship with adverse neurologic outcomes, independent of conventional dietary patterns.”
Peipei Gao, MS, with Harvard T.H. Chan School of Public Health, and Zhendong Mei, PhD, with Harvard Medical School, both in Boston, noted that the mechanisms underlying the impact of UPFs on adverse neurologic outcomes “can be attributed not only to their nutritional profiles,” including poor nutrient composition and high glycemic load, “but also to the presence of additives including emulsifiers, colorants, sweeteners, and nitrates/nitrites, which have been associated with disruptions in the gut microbial ecosystem and inflammation.
“Understanding how food processing levels are associated with human health offers a fresh take on the saying ‘you are what you eat,’ ” the editorialists wrote.
This new study, they noted, adds to the evidence by highlighting the link between UPFs and brain health, independent of traditional dietary patterns and “raises questions about whether considerations of UPFs should be included in dietary guidelines, as well as national and global public health policies for improving brain health.”
The editorialists called for large prospective population studies and randomized controlled trials to better understand the link between UPF consumption and brain health. “In addition, mechanistic studies are warranted to identify specific foods, detrimental processes, and additives that play a role in UPFs and their association with neurologic disorders,” they concluded.
Funding for the study was provided by the National Institute of Neurological Disorders and Stroke, the National Institute on Aging, National Institutes of Health, and Department of Health and Human Services. The authors and editorial writers had no relevant disclosures.
A version of this article appeared on Medscape.com.
, new research suggests.
Observations from a large cohort of adults followed for more than 10 years suggested that eating more ultraprocessed foods (UPFs) may increase the risk for cognitive decline and stroke, while eating more unprocessed or minimally processed foods may lower the risk.
“The first key takeaway is that the type of food that we eat matters for brain health, but it’s equally important to think about how it’s made and handled when thinking about brain health,” said study investigator W. Taylor Kimberly, MD, PhD, with Massachusetts General Hospital in Boston.
“The second is that it’s not just all a bad news story because while increased consumption of ultra-processed foods is associated with a higher risk of cognitive impairment and stroke, unprocessed foods appear to be protective,” Dr. Kimberly added.
The study was published online on May 22 in Neurology.
Food Processing Matters
UPFs are highly manipulated, low in protein and fiber, and packed with added ingredients, including sugar, fat, and salt. Examples of UPFs are soft drinks, chips, chocolate, candy, ice cream, sweetened breakfast cereals, packaged soups, chicken nuggets, hot dogs, and fries.
Unprocessed or minimally processed foods include meats such as simple cuts of beef, pork, and chicken, and vegetables and fruits.
Research has shown associations between high UPF consumption and increased risk for metabolic and neurologic disorders.
As reported previously, in the ELSA-Brasil study, higher intake of UPFs was significantly associated with a faster rate of decline in executive and global cognitive function.
Yet, it’s unclear whether the extent of food processing contributes to the risk of adverse neurologic outcomes independent of dietary patterns.
Dr. Kimberly and colleagues examined the association of food processing levels with the risk for cognitive impairment and stroke in the long-running REGARDS study, a large prospective US cohort of Black and White adults aged 45 years and older.
Food processing levels were defined by the NOVA food classification system, which ranges from unprocessed or minimally processed foods (NOVA1) to UPFs (NOVA4). Dietary patterns were characterized based on food frequency questionnaires.
In the cognitive impairment cohort, 768 of 14,175 adults without evidence of impairment at baseline who underwent follow-up testing developed cognitive impairment.
Diet an Opportunity to Protect Brain Health
In multivariable Cox proportional hazards models adjusting for age, sex, high blood pressure, and other factors, a 10% increase in relative intake of UPFs was associated with a 16% higher risk for cognitive impairment (hazard ratio [HR], 1.16). Conversely, a higher intake of unprocessed or minimally processed foods correlated with a 12% lower risk for cognitive impairment (HR, 0.88).
In the stroke cohort, 1108 of 20,243 adults without a history of stroke had a stroke during the follow-up.
In multivariable Cox models, greater intake of UPFs was associated with an 8% increased risk for stroke (HR, 1.08), while greater intake of unprocessed or minimally processed foods correlated with a 9% lower risk for stroke (HR, 0.91).
The effect of UPFs on stroke risk was greater among Black than among White adults (UPF-by-race interaction HR, 1.15).
The associations between UPFs and both cognitive impairment and stroke were independent of adherence to the Mediterranean diet, the Dietary Approaches to Stop Hypertension (DASH) diet, and the Mediterranean-DASH Intervention for Neurodegenerative Delay diet.
These results “highlight the possibility that we have the capacity to maintain our brain health and prevent poor brain health outcomes by focusing on unprocessed foods in the long term,” Dr. Kimberly said.
He cautioned that this was “an observational study and not an interventional study, so we can’t say with certainty that substituting ultra-processed foods with unprocessed foods will definitively improve brain health,” Dr. Kimberly said. “That’s a clinical trial question that has not been done but our results certainly are provocative.”
Consider UPFs in National Guidelines?
The coauthors of an accompanying editorial said the “robust” results from Kimberly and colleagues highlight the “significant role of food processing levels and their relationship with adverse neurologic outcomes, independent of conventional dietary patterns.”
Peipei Gao, MS, with Harvard T.H. Chan School of Public Health, and Zhendong Mei, PhD, with Harvard Medical School, both in Boston, noted that the mechanisms underlying the impact of UPFs on adverse neurologic outcomes “can be attributed not only to their nutritional profiles,” including poor nutrient composition and high glycemic load, “but also to the presence of additives including emulsifiers, colorants, sweeteners, and nitrates/nitrites, which have been associated with disruptions in the gut microbial ecosystem and inflammation.
“Understanding how food processing levels are associated with human health offers a fresh take on the saying ‘you are what you eat,’ ” the editorialists wrote.
This new study, they noted, adds to the evidence by highlighting the link between UPFs and brain health, independent of traditional dietary patterns and “raises questions about whether considerations of UPFs should be included in dietary guidelines, as well as national and global public health policies for improving brain health.”
The editorialists called for large prospective population studies and randomized controlled trials to better understand the link between UPF consumption and brain health. “In addition, mechanistic studies are warranted to identify specific foods, detrimental processes, and additives that play a role in UPFs and their association with neurologic disorders,” they concluded.
Funding for the study was provided by the National Institute of Neurological Disorders and Stroke, the National Institute on Aging, National Institutes of Health, and Department of Health and Human Services. The authors and editorial writers had no relevant disclosures.
A version of this article appeared on Medscape.com.
, new research suggests.
Observations from a large cohort of adults followed for more than 10 years suggested that eating more ultraprocessed foods (UPFs) may increase the risk for cognitive decline and stroke, while eating more unprocessed or minimally processed foods may lower the risk.
“The first key takeaway is that the type of food that we eat matters for brain health, but it’s equally important to think about how it’s made and handled when thinking about brain health,” said study investigator W. Taylor Kimberly, MD, PhD, with Massachusetts General Hospital in Boston.
“The second is that it’s not just all a bad news story because while increased consumption of ultra-processed foods is associated with a higher risk of cognitive impairment and stroke, unprocessed foods appear to be protective,” Dr. Kimberly added.
The study was published online on May 22 in Neurology.
Food Processing Matters
UPFs are highly manipulated, low in protein and fiber, and packed with added ingredients, including sugar, fat, and salt. Examples of UPFs are soft drinks, chips, chocolate, candy, ice cream, sweetened breakfast cereals, packaged soups, chicken nuggets, hot dogs, and fries.
Unprocessed or minimally processed foods include meats such as simple cuts of beef, pork, and chicken, and vegetables and fruits.
Research has shown associations between high UPF consumption and increased risk for metabolic and neurologic disorders.
As reported previously, in the ELSA-Brasil study, higher intake of UPFs was significantly associated with a faster rate of decline in executive and global cognitive function.
Yet, it’s unclear whether the extent of food processing contributes to the risk of adverse neurologic outcomes independent of dietary patterns.
Dr. Kimberly and colleagues examined the association of food processing levels with the risk for cognitive impairment and stroke in the long-running REGARDS study, a large prospective US cohort of Black and White adults aged 45 years and older.
Food processing levels were defined by the NOVA food classification system, which ranges from unprocessed or minimally processed foods (NOVA1) to UPFs (NOVA4). Dietary patterns were characterized based on food frequency questionnaires.
In the cognitive impairment cohort, 768 of 14,175 adults without evidence of impairment at baseline who underwent follow-up testing developed cognitive impairment.
Diet an Opportunity to Protect Brain Health
In multivariable Cox proportional hazards models adjusting for age, sex, high blood pressure, and other factors, a 10% increase in relative intake of UPFs was associated with a 16% higher risk for cognitive impairment (hazard ratio [HR], 1.16). Conversely, a higher intake of unprocessed or minimally processed foods correlated with a 12% lower risk for cognitive impairment (HR, 0.88).
In the stroke cohort, 1108 of 20,243 adults without a history of stroke had a stroke during the follow-up.
In multivariable Cox models, greater intake of UPFs was associated with an 8% increased risk for stroke (HR, 1.08), while greater intake of unprocessed or minimally processed foods correlated with a 9% lower risk for stroke (HR, 0.91).
The effect of UPFs on stroke risk was greater among Black than among White adults (UPF-by-race interaction HR, 1.15).
The associations between UPFs and both cognitive impairment and stroke were independent of adherence to the Mediterranean diet, the Dietary Approaches to Stop Hypertension (DASH) diet, and the Mediterranean-DASH Intervention for Neurodegenerative Delay diet.
These results “highlight the possibility that we have the capacity to maintain our brain health and prevent poor brain health outcomes by focusing on unprocessed foods in the long term,” Dr. Kimberly said.
He cautioned that this was “an observational study and not an interventional study, so we can’t say with certainty that substituting ultra-processed foods with unprocessed foods will definitively improve brain health,” Dr. Kimberly said. “That’s a clinical trial question that has not been done but our results certainly are provocative.”
Consider UPFs in National Guidelines?
The coauthors of an accompanying editorial said the “robust” results from Kimberly and colleagues highlight the “significant role of food processing levels and their relationship with adverse neurologic outcomes, independent of conventional dietary patterns.”
Peipei Gao, MS, with Harvard T.H. Chan School of Public Health, and Zhendong Mei, PhD, with Harvard Medical School, both in Boston, noted that the mechanisms underlying the impact of UPFs on adverse neurologic outcomes “can be attributed not only to their nutritional profiles,” including poor nutrient composition and high glycemic load, “but also to the presence of additives including emulsifiers, colorants, sweeteners, and nitrates/nitrites, which have been associated with disruptions in the gut microbial ecosystem and inflammation.
“Understanding how food processing levels are associated with human health offers a fresh take on the saying ‘you are what you eat,’ ” the editorialists wrote.
This new study, they noted, adds to the evidence by highlighting the link between UPFs and brain health, independent of traditional dietary patterns and “raises questions about whether considerations of UPFs should be included in dietary guidelines, as well as national and global public health policies for improving brain health.”
The editorialists called for large prospective population studies and randomized controlled trials to better understand the link between UPF consumption and brain health. “In addition, mechanistic studies are warranted to identify specific foods, detrimental processes, and additives that play a role in UPFs and their association with neurologic disorders,” they concluded.
Funding for the study was provided by the National Institute of Neurological Disorders and Stroke, the National Institute on Aging, National Institutes of Health, and Department of Health and Human Services. The authors and editorial writers had no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM NEUROLOGY
Access to Perinatal Mental Healthcare: What Exactly Are The Obstacles?
The first of May is marked as the World Maternal Mental Health Day, a time for patient groups, medical societies, clinicians, and other colleagues who care for women to highlight maternal mental health and to advocate for increased awareness, enhanced access to care, decrease in stigma, and development of the most effective treatments.
In this spirit, and within the context of greater mental health awareness, I wanted to highlight the ironic dichotomy we see in reproductive psychiatry today. Namely, although we have many useful treatments available in the field to treat maternal psychiatric illness, there are barriers to accessing mental healthcare that prevent women from receiving treatment and getting well.
Thinking back on the last few years from the other side of the pandemic, when COVID concerns turned the experience of motherhood on its side in so many ways, we can only acknowledge that it is an important time in the field of reproductive psychiatry. We have seen not only the development of new pharmacologic (neurosteroids) and nonpharmacologic therapies (transcranial magnetic stimulation, cognitive-behaviorial therapy for perinatal depression), but also the focus on new digital apps for perinatal depression that may be scalable and that may help bridge the voids in access to effective treatment from the most rural to the most urban settings.

In a previous column, I wrote about the potential difficulties of identifying at-risk women with postpartum psychiatric illness, particularly within the context of disparate data collection methods and management of data. Hospital systems that favor paper screening methods rather than digital platforms pose special problems. I also noted an even larger concern: namely, once screened, it can be very challenging to engage women with postpartum depression in treatment, and women may ultimately not navigate to care for a variety of reasons. These components are but one part of the so-called “perinatal treatment cascade.” When we look at access to care, patients would ideally move from depression screening as an example and, following endorsement of significant symptoms, would receive a referral, which would result in the patient being seen, followed up, and getting well. But that is not what is happening.
A recent preliminary study published as a short communication in the Archives of Women’s Mental Health highlighted this issue. The authors used the Edinburgh Postnatal Depression Scale (EPDS) to follow symptoms of depression in 145 pregnant women in ob.gyn. services, and found that there were low levels of adherence to psychiatric screenings and referrals in the perinatal period. Another study published in the Journal of Clinical Psychiatry found 30.8% of women with postpartum depression were identified clinically, 15.8% received treatment, and 3.2% achieved remission. That is the gulf, in 2024, that we have not managed to bridge.
The findings show the difficulty women experience accessing perinatal mental health resources. While we’ve known for a long time that the “perinatal treatment cascade” is real, what we don’t understand are the variables in the mix, particularly for patients in marginalized groups. We also do not know where women fall off the curve with regard to accessing care. In my mind, if we’re going to make a difference, we need to know the answer to that question.
Part of the issue is that the research into understanding why women fall off the curve is incomplete. You cannot simply hand a sheet to a woman with an EPDS score of 12 who’s depressed and has a newborn and expect her to navigate to care. What we should really be doing is investing in care navigation for women.
The situation is analogous to diagnosing and treating cardiac abnormalities in a catheterization laboratory. If a patient has a blocked coronary artery and needs a stent, then they need to go to the cath lab. We haven’t yet figured out the process in reproductive psychiatry to optimize the likelihood that patients will be screened and then referred to receive the best available treatment.
Some of our ob.gyn. colleagues have been working to improve access to perinatal mental health services, such as offering on-site services, and offering training and services to patients and providers on screening, assessment, and treatment. At the Center for Women’s Mental Health, we are conducting the Screening and Treatment Enhancement for Postpartum Depression study, which is a universal screening and referral program for women at our center. While some progress is being made, there are still far too many women who are falling through the cracks and not receiving the care they need.
It is both ironic and sad that the growing number of available treatments in reproductive psychiatry are scalable, yet we haven’t figured out how to facilitate access to care. While we should be excited about new treatments, we also need to take the time to understand what the barriers are for at-risk women accessing mental healthcare in the postpartum period.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. STEPS for PPD is funded by the Marriott Foundation. Full disclosure information for Dr. Cohen is available at womensmentalhealth.org. Email Dr. Cohen at [email protected].
The first of May is marked as the World Maternal Mental Health Day, a time for patient groups, medical societies, clinicians, and other colleagues who care for women to highlight maternal mental health and to advocate for increased awareness, enhanced access to care, decrease in stigma, and development of the most effective treatments.
In this spirit, and within the context of greater mental health awareness, I wanted to highlight the ironic dichotomy we see in reproductive psychiatry today. Namely, although we have many useful treatments available in the field to treat maternal psychiatric illness, there are barriers to accessing mental healthcare that prevent women from receiving treatment and getting well.
Thinking back on the last few years from the other side of the pandemic, when COVID concerns turned the experience of motherhood on its side in so many ways, we can only acknowledge that it is an important time in the field of reproductive psychiatry. We have seen not only the development of new pharmacologic (neurosteroids) and nonpharmacologic therapies (transcranial magnetic stimulation, cognitive-behaviorial therapy for perinatal depression), but also the focus on new digital apps for perinatal depression that may be scalable and that may help bridge the voids in access to effective treatment from the most rural to the most urban settings.
In a previous column, I wrote about the potential difficulties of identifying at-risk women with postpartum psychiatric illness, particularly within the context of disparate data collection methods and management of data. Hospital systems that favor paper screening methods rather than digital platforms pose special problems. I also noted an even larger concern: namely, once screened, it can be very challenging to engage women with postpartum depression in treatment, and women may ultimately not navigate to care for a variety of reasons. These components are but one part of the so-called “perinatal treatment cascade.” When we look at access to care, patients would ideally move from depression screening as an example and, following endorsement of significant symptoms, would receive a referral, which would result in the patient being seen, followed up, and getting well. But that is not what is happening.
A recent preliminary study published as a short communication in the Archives of Women’s Mental Health highlighted this issue. The authors used the Edinburgh Postnatal Depression Scale (EPDS) to follow symptoms of depression in 145 pregnant women in ob.gyn. services, and found that there were low levels of adherence to psychiatric screenings and referrals in the perinatal period. Another study published in the Journal of Clinical Psychiatry found 30.8% of women with postpartum depression were identified clinically, 15.8% received treatment, and 3.2% achieved remission. That is the gulf, in 2024, that we have not managed to bridge.
The findings show the difficulty women experience accessing perinatal mental health resources. While we’ve known for a long time that the “perinatal treatment cascade” is real, what we don’t understand are the variables in the mix, particularly for patients in marginalized groups. We also do not know where women fall off the curve with regard to accessing care. In my mind, if we’re going to make a difference, we need to know the answer to that question.
Part of the issue is that the research into understanding why women fall off the curve is incomplete. You cannot simply hand a sheet to a woman with an EPDS score of 12 who’s depressed and has a newborn and expect her to navigate to care. What we should really be doing is investing in care navigation for women.
The situation is analogous to diagnosing and treating cardiac abnormalities in a catheterization laboratory. If a patient has a blocked coronary artery and needs a stent, then they need to go to the cath lab. We haven’t yet figured out the process in reproductive psychiatry to optimize the likelihood that patients will be screened and then referred to receive the best available treatment.
Some of our ob.gyn. colleagues have been working to improve access to perinatal mental health services, such as offering on-site services, and offering training and services to patients and providers on screening, assessment, and treatment. At the Center for Women’s Mental Health, we are conducting the Screening and Treatment Enhancement for Postpartum Depression study, which is a universal screening and referral program for women at our center. While some progress is being made, there are still far too many women who are falling through the cracks and not receiving the care they need.
It is both ironic and sad that the growing number of available treatments in reproductive psychiatry are scalable, yet we haven’t figured out how to facilitate access to care. While we should be excited about new treatments, we also need to take the time to understand what the barriers are for at-risk women accessing mental healthcare in the postpartum period.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. STEPS for PPD is funded by the Marriott Foundation. Full disclosure information for Dr. Cohen is available at womensmentalhealth.org. Email Dr. Cohen at [email protected].
The first of May is marked as the World Maternal Mental Health Day, a time for patient groups, medical societies, clinicians, and other colleagues who care for women to highlight maternal mental health and to advocate for increased awareness, enhanced access to care, decrease in stigma, and development of the most effective treatments.
In this spirit, and within the context of greater mental health awareness, I wanted to highlight the ironic dichotomy we see in reproductive psychiatry today. Namely, although we have many useful treatments available in the field to treat maternal psychiatric illness, there are barriers to accessing mental healthcare that prevent women from receiving treatment and getting well.
Thinking back on the last few years from the other side of the pandemic, when COVID concerns turned the experience of motherhood on its side in so many ways, we can only acknowledge that it is an important time in the field of reproductive psychiatry. We have seen not only the development of new pharmacologic (neurosteroids) and nonpharmacologic therapies (transcranial magnetic stimulation, cognitive-behaviorial therapy for perinatal depression), but also the focus on new digital apps for perinatal depression that may be scalable and that may help bridge the voids in access to effective treatment from the most rural to the most urban settings.
In a previous column, I wrote about the potential difficulties of identifying at-risk women with postpartum psychiatric illness, particularly within the context of disparate data collection methods and management of data. Hospital systems that favor paper screening methods rather than digital platforms pose special problems. I also noted an even larger concern: namely, once screened, it can be very challenging to engage women with postpartum depression in treatment, and women may ultimately not navigate to care for a variety of reasons. These components are but one part of the so-called “perinatal treatment cascade.” When we look at access to care, patients would ideally move from depression screening as an example and, following endorsement of significant symptoms, would receive a referral, which would result in the patient being seen, followed up, and getting well. But that is not what is happening.
A recent preliminary study published as a short communication in the Archives of Women’s Mental Health highlighted this issue. The authors used the Edinburgh Postnatal Depression Scale (EPDS) to follow symptoms of depression in 145 pregnant women in ob.gyn. services, and found that there were low levels of adherence to psychiatric screenings and referrals in the perinatal period. Another study published in the Journal of Clinical Psychiatry found 30.8% of women with postpartum depression were identified clinically, 15.8% received treatment, and 3.2% achieved remission. That is the gulf, in 2024, that we have not managed to bridge.
The findings show the difficulty women experience accessing perinatal mental health resources. While we’ve known for a long time that the “perinatal treatment cascade” is real, what we don’t understand are the variables in the mix, particularly for patients in marginalized groups. We also do not know where women fall off the curve with regard to accessing care. In my mind, if we’re going to make a difference, we need to know the answer to that question.
Part of the issue is that the research into understanding why women fall off the curve is incomplete. You cannot simply hand a sheet to a woman with an EPDS score of 12 who’s depressed and has a newborn and expect her to navigate to care. What we should really be doing is investing in care navigation for women.
The situation is analogous to diagnosing and treating cardiac abnormalities in a catheterization laboratory. If a patient has a blocked coronary artery and needs a stent, then they need to go to the cath lab. We haven’t yet figured out the process in reproductive psychiatry to optimize the likelihood that patients will be screened and then referred to receive the best available treatment.
Some of our ob.gyn. colleagues have been working to improve access to perinatal mental health services, such as offering on-site services, and offering training and services to patients and providers on screening, assessment, and treatment. At the Center for Women’s Mental Health, we are conducting the Screening and Treatment Enhancement for Postpartum Depression study, which is a universal screening and referral program for women at our center. While some progress is being made, there are still far too many women who are falling through the cracks and not receiving the care they need.
It is both ironic and sad that the growing number of available treatments in reproductive psychiatry are scalable, yet we haven’t figured out how to facilitate access to care. While we should be excited about new treatments, we also need to take the time to understand what the barriers are for at-risk women accessing mental healthcare in the postpartum period.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. STEPS for PPD is funded by the Marriott Foundation. Full disclosure information for Dr. Cohen is available at womensmentalhealth.org. Email Dr. Cohen at [email protected].
Reimbursement for Mohs Surgery Not Keeping Up With Health Care Costs
PHOENIX — Medicare cuts, which are expected to continue, have exacerbated this issue even further.
“This ongoing downward trend in inflation-adjusted reimbursement may lead to delayed patient access to quality dermatology surgical care,” said lead study author Lily Park, DO, a resident in the Department of Dermatology, Larkin Community Hospital, Miami. “This trend will lead to reduced access.”
Dr. Park emphasized that reimbursement for Mohs surgery has also been further affected by the multiple surgery reduction rule, which is where Medicare pays less for the second and subsequent procedures performed during the same patient encounter. Reductions may be calculated in several ways, depending on what kind of procedure or service is involved.
“The Mohs surgery community needs to be aware of this financial trend and actively engage with healthcare policymakers to ensure the establishment of a sustainable payment infrastructure,” she said.
Dr. Park presented the study results at the annual meeting of the American College of Mohs Surgery.
The landscape of healthcare economics continues to evolve and has been further complicated by rising inflation. In addition, a 2% cut to the Medicare payment conversion factor was implemented in 2023, followed by a further 3.37% cut in early 2024 — which was cut by half in March 2024, with an additional cut expected this year, she noted. “This has presented more challenges for dermatologic surgeons who are already dealing with the rising healthcare costs.”
However, despite these financial challenges, there is a lack of research on physician reimbursement for dermatologic procedures, including surgery.
Decreased Reimbursement for All Procedures
Dr. Park and colleagues analyzed trends in Medicare reimbursement rates for Mohs micrographic surgery and several other common dermatologic procedures. Beginning with 2007, they calculated the inflation-adjusted values for each year’s non-facility prices for all codes except Current Procedural Terminology (CPT) codes 11102 and 11104. For those two codes, inflation-adjusted prices were based on the prices in 2019, the year when the codes were first introduced. The authors estimated the inflation adjusted value for each year based on the non-facility price for 2007, and the difference between the rate of inflation and the change in physician reimbursement over time was calculated.
The six most commonly performed procedures in 2023, ranked in descending order of frequency, were identified as CPT 17000, used for the removal of actinic keratosis; CPT 11102, used for biopsy of skin; CPT 17110, used for the destruction of benign lesions such as seborrheic keratoses and warts; CPT 17311, used for the destruction of malignant lesions (including Mohs surgery); CPT 11104, which is also related to biopsy of skin; and CPT 10060, used for incision and drainage of abscess.
Their analysis showed that all CPT codes experienced a decline when compared with their inflation-adjusted values. Both Mohs surgery (17311) and benign destruction of premalignant lesions (17000) showed a decrease of 46% in reimbursement during an inflation-adjusted 18-year time span between 2007 and 2024.
When adjusted for inflation, Dr. Park noted, reimbursement for CPT 17311 and 17000 should actually be increased by 42% and 41% in 2024, respectively. The greatest declines in reimbursement were seen during the last 4 years.
“Future legislation, such as H.R.2474, a bill proposing inflation-based updates to physician pay, would aid us in the future if implemented,” said Dr. Park.
Dangerous Trend
The finding that payments have declined for many common dermatologic procedures since 2007 “is particularly important given the rising cost of healthcare delivery,” said Jesse M. Lewin, MD, who was asked to comment on the study results. “The administrative burden of electronic medical records, filing, and following up insurance claims has necessitated the employment of more non-physician staff to support these tasks,” he told this news organization.
“Declining reimbursement for Mohs surgery and other cancer-related procedures is a dangerous trend, as the ultimate impact will be the effect it has on quality and accessibility of skin cancer care for patients,” added Dr. Lewin, chief of Mohs micrographic and dermatologic surgery and vice chair of surgical operations at the Icahn School of Medicine at Mount Sinai, New York City. “This is an important study that reinforces physician engagement in healthcare policy and legislation to advocate for our specialty and patients.”
The study was independently supported. Dr. Park and Dr. Lewin, who was not involved with the study, reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
PHOENIX — Medicare cuts, which are expected to continue, have exacerbated this issue even further.
“This ongoing downward trend in inflation-adjusted reimbursement may lead to delayed patient access to quality dermatology surgical care,” said lead study author Lily Park, DO, a resident in the Department of Dermatology, Larkin Community Hospital, Miami. “This trend will lead to reduced access.”
Dr. Park emphasized that reimbursement for Mohs surgery has also been further affected by the multiple surgery reduction rule, which is where Medicare pays less for the second and subsequent procedures performed during the same patient encounter. Reductions may be calculated in several ways, depending on what kind of procedure or service is involved.
“The Mohs surgery community needs to be aware of this financial trend and actively engage with healthcare policymakers to ensure the establishment of a sustainable payment infrastructure,” she said.
Dr. Park presented the study results at the annual meeting of the American College of Mohs Surgery.
The landscape of healthcare economics continues to evolve and has been further complicated by rising inflation. In addition, a 2% cut to the Medicare payment conversion factor was implemented in 2023, followed by a further 3.37% cut in early 2024 — which was cut by half in March 2024, with an additional cut expected this year, she noted. “This has presented more challenges for dermatologic surgeons who are already dealing with the rising healthcare costs.”
However, despite these financial challenges, there is a lack of research on physician reimbursement for dermatologic procedures, including surgery.
Decreased Reimbursement for All Procedures
Dr. Park and colleagues analyzed trends in Medicare reimbursement rates for Mohs micrographic surgery and several other common dermatologic procedures. Beginning with 2007, they calculated the inflation-adjusted values for each year’s non-facility prices for all codes except Current Procedural Terminology (CPT) codes 11102 and 11104. For those two codes, inflation-adjusted prices were based on the prices in 2019, the year when the codes were first introduced. The authors estimated the inflation adjusted value for each year based on the non-facility price for 2007, and the difference between the rate of inflation and the change in physician reimbursement over time was calculated.
The six most commonly performed procedures in 2023, ranked in descending order of frequency, were identified as CPT 17000, used for the removal of actinic keratosis; CPT 11102, used for biopsy of skin; CPT 17110, used for the destruction of benign lesions such as seborrheic keratoses and warts; CPT 17311, used for the destruction of malignant lesions (including Mohs surgery); CPT 11104, which is also related to biopsy of skin; and CPT 10060, used for incision and drainage of abscess.
Their analysis showed that all CPT codes experienced a decline when compared with their inflation-adjusted values. Both Mohs surgery (17311) and benign destruction of premalignant lesions (17000) showed a decrease of 46% in reimbursement during an inflation-adjusted 18-year time span between 2007 and 2024.
When adjusted for inflation, Dr. Park noted, reimbursement for CPT 17311 and 17000 should actually be increased by 42% and 41% in 2024, respectively. The greatest declines in reimbursement were seen during the last 4 years.
“Future legislation, such as H.R.2474, a bill proposing inflation-based updates to physician pay, would aid us in the future if implemented,” said Dr. Park.
Dangerous Trend
The finding that payments have declined for many common dermatologic procedures since 2007 “is particularly important given the rising cost of healthcare delivery,” said Jesse M. Lewin, MD, who was asked to comment on the study results. “The administrative burden of electronic medical records, filing, and following up insurance claims has necessitated the employment of more non-physician staff to support these tasks,” he told this news organization.
“Declining reimbursement for Mohs surgery and other cancer-related procedures is a dangerous trend, as the ultimate impact will be the effect it has on quality and accessibility of skin cancer care for patients,” added Dr. Lewin, chief of Mohs micrographic and dermatologic surgery and vice chair of surgical operations at the Icahn School of Medicine at Mount Sinai, New York City. “This is an important study that reinforces physician engagement in healthcare policy and legislation to advocate for our specialty and patients.”
The study was independently supported. Dr. Park and Dr. Lewin, who was not involved with the study, reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
PHOENIX — Medicare cuts, which are expected to continue, have exacerbated this issue even further.
“This ongoing downward trend in inflation-adjusted reimbursement may lead to delayed patient access to quality dermatology surgical care,” said lead study author Lily Park, DO, a resident in the Department of Dermatology, Larkin Community Hospital, Miami. “This trend will lead to reduced access.”
Dr. Park emphasized that reimbursement for Mohs surgery has also been further affected by the multiple surgery reduction rule, which is where Medicare pays less for the second and subsequent procedures performed during the same patient encounter. Reductions may be calculated in several ways, depending on what kind of procedure or service is involved.
“The Mohs surgery community needs to be aware of this financial trend and actively engage with healthcare policymakers to ensure the establishment of a sustainable payment infrastructure,” she said.
Dr. Park presented the study results at the annual meeting of the American College of Mohs Surgery.
The landscape of healthcare economics continues to evolve and has been further complicated by rising inflation. In addition, a 2% cut to the Medicare payment conversion factor was implemented in 2023, followed by a further 3.37% cut in early 2024 — which was cut by half in March 2024, with an additional cut expected this year, she noted. “This has presented more challenges for dermatologic surgeons who are already dealing with the rising healthcare costs.”
However, despite these financial challenges, there is a lack of research on physician reimbursement for dermatologic procedures, including surgery.
Decreased Reimbursement for All Procedures
Dr. Park and colleagues analyzed trends in Medicare reimbursement rates for Mohs micrographic surgery and several other common dermatologic procedures. Beginning with 2007, they calculated the inflation-adjusted values for each year’s non-facility prices for all codes except Current Procedural Terminology (CPT) codes 11102 and 11104. For those two codes, inflation-adjusted prices were based on the prices in 2019, the year when the codes were first introduced. The authors estimated the inflation adjusted value for each year based on the non-facility price for 2007, and the difference between the rate of inflation and the change in physician reimbursement over time was calculated.
The six most commonly performed procedures in 2023, ranked in descending order of frequency, were identified as CPT 17000, used for the removal of actinic keratosis; CPT 11102, used for biopsy of skin; CPT 17110, used for the destruction of benign lesions such as seborrheic keratoses and warts; CPT 17311, used for the destruction of malignant lesions (including Mohs surgery); CPT 11104, which is also related to biopsy of skin; and CPT 10060, used for incision and drainage of abscess.
Their analysis showed that all CPT codes experienced a decline when compared with their inflation-adjusted values. Both Mohs surgery (17311) and benign destruction of premalignant lesions (17000) showed a decrease of 46% in reimbursement during an inflation-adjusted 18-year time span between 2007 and 2024.
When adjusted for inflation, Dr. Park noted, reimbursement for CPT 17311 and 17000 should actually be increased by 42% and 41% in 2024, respectively. The greatest declines in reimbursement were seen during the last 4 years.
“Future legislation, such as H.R.2474, a bill proposing inflation-based updates to physician pay, would aid us in the future if implemented,” said Dr. Park.
Dangerous Trend
The finding that payments have declined for many common dermatologic procedures since 2007 “is particularly important given the rising cost of healthcare delivery,” said Jesse M. Lewin, MD, who was asked to comment on the study results. “The administrative burden of electronic medical records, filing, and following up insurance claims has necessitated the employment of more non-physician staff to support these tasks,” he told this news organization.
“Declining reimbursement for Mohs surgery and other cancer-related procedures is a dangerous trend, as the ultimate impact will be the effect it has on quality and accessibility of skin cancer care for patients,” added Dr. Lewin, chief of Mohs micrographic and dermatologic surgery and vice chair of surgical operations at the Icahn School of Medicine at Mount Sinai, New York City. “This is an important study that reinforces physician engagement in healthcare policy and legislation to advocate for our specialty and patients.”
The study was independently supported. Dr. Park and Dr. Lewin, who was not involved with the study, reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM ACMS 2024
Will the Federal Non-Compete Ban Take Effect?
(with very limited exceptions). The final rule will not go into effect until 120 days after its publication in the Federal Register, which took place on May 7, and numerous legal challenges appear to be on the horizon.
The principal components of the rule are as follows:
- After the effective date, most non-compete agreements (which prevent departing employees from signing with a new employer for a defined period within a specific geographic area) are banned nationwide.
- The rule exempts certain “senior executives,” ie individuals who earn more than $151,164 annually and serve in policy-making positions.
- There is another major exception for non-competes connected with a sale of a business.
- While not explicitly stated, the rule arguably exempts non-profits, tax-exempt hospitals, and other tax-exempt entities.
- Employers must provide verbal and written notice to employees regarding existing agreements, which would be voided under the rule.
The final rule is the latest skirmish in an ongoing, years-long debate. Twelve states have already put non-compete bans in place, according to a recent paper, and they may serve as a harbinger of things to come should the federal ban go into effect. Each state rule varies in its specifics as states respond to local market conditions. While some states ban all non-compete agreements outright, others limit them based on variables, such as income and employment circumstances. Of course, should the federal ban take effect, it will supersede whatever rules the individual states have in place.

In drafting the rule, the FTC reasoned that non-compete clauses constitute restraint of trade, and eliminating them could potentially increase worker earnings as well as lower health care costs by billions of dollars. In its statements on the proposed ban, the FTC claimed that it could lower health spending across the board by almost $150 billion per year and return $300 million to workers each year in earnings. The agency cited a large body of research that non-competes make it harder for workers to move between jobs and can raise prices for goods and services, while suppressing wages for workers and inhibiting the creation of new businesses.
Most physicians affected by non-compete agreements heavily favor the new rule, because it would give them more control over their careers and expand their practice and income opportunities. It would allow them to get a new job with a competing organization, bucking a long-standing trend that hospitals and health care systems have heavily relied on to keep staff in place.
The rule would, however, keep in place “non-solicitation” rules that many health care organizations have put in place. That means that if a physician leaves an employer, he or she cannot reach out to former patients and colleagues to bring them along or invite them to join him or her at the new employment venue.
Within that clause, however, the FTC has specified that if such non-solicitation agreement has the “equivalent effect” of a non-compete, the agency would deem it such. That means, even if that rule stands, it could be contested and may be interpreted as violating the non-compete provision. So, there is value in reading all the fine print should the rule move forward.
Physicians in independent practices who employ physician assistants and nurse practitioners have expressed concerns that their expensively trained employees might be tempted to accept a nearby, higher-paying position. The “non-solicitation” clause would theoretically prevent them from taking patients and co-workers with them — unless it were successfully contested. Many questions remain.
Further complicating the non-compete ban issue is how it might impact nonprofit institutions. Most hospitals structured as nonprofits would theoretically be exempt from the rule, although it is not specifically stated in the rule itself, because the FTC Act gives the Commission jurisdiction over for-profit companies only. This would obviously create an unfair advantage for nonprofits, who could continue writing non-compete clauses with impunity.
All of these questions may be moot, of course, because a number of powerful entities with deep pockets have lined up in opposition to the rule. Some of them have even questioned the FTC’s authority to pass the rule at all, on the grounds that Section 5 of the FTC Act does not give it the authority to police labor markets. A lawsuit has already been filed by the US Chamber of Commerce. Other large groups in opposition are the American Medical Group Association, the American Hospital Association, and numerous large hospital and healthcare networks.
Only time will tell whether this issue will be regulated on a national level or remain the purview of each individual state.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
(with very limited exceptions). The final rule will not go into effect until 120 days after its publication in the Federal Register, which took place on May 7, and numerous legal challenges appear to be on the horizon.
The principal components of the rule are as follows:
- After the effective date, most non-compete agreements (which prevent departing employees from signing with a new employer for a defined period within a specific geographic area) are banned nationwide.
- The rule exempts certain “senior executives,” ie individuals who earn more than $151,164 annually and serve in policy-making positions.
- There is another major exception for non-competes connected with a sale of a business.
- While not explicitly stated, the rule arguably exempts non-profits, tax-exempt hospitals, and other tax-exempt entities.
- Employers must provide verbal and written notice to employees regarding existing agreements, which would be voided under the rule.
The final rule is the latest skirmish in an ongoing, years-long debate. Twelve states have already put non-compete bans in place, according to a recent paper, and they may serve as a harbinger of things to come should the federal ban go into effect. Each state rule varies in its specifics as states respond to local market conditions. While some states ban all non-compete agreements outright, others limit them based on variables, such as income and employment circumstances. Of course, should the federal ban take effect, it will supersede whatever rules the individual states have in place.
In drafting the rule, the FTC reasoned that non-compete clauses constitute restraint of trade, and eliminating them could potentially increase worker earnings as well as lower health care costs by billions of dollars. In its statements on the proposed ban, the FTC claimed that it could lower health spending across the board by almost $150 billion per year and return $300 million to workers each year in earnings. The agency cited a large body of research that non-competes make it harder for workers to move between jobs and can raise prices for goods and services, while suppressing wages for workers and inhibiting the creation of new businesses.
Most physicians affected by non-compete agreements heavily favor the new rule, because it would give them more control over their careers and expand their practice and income opportunities. It would allow them to get a new job with a competing organization, bucking a long-standing trend that hospitals and health care systems have heavily relied on to keep staff in place.
The rule would, however, keep in place “non-solicitation” rules that many health care organizations have put in place. That means that if a physician leaves an employer, he or she cannot reach out to former patients and colleagues to bring them along or invite them to join him or her at the new employment venue.
Within that clause, however, the FTC has specified that if such non-solicitation agreement has the “equivalent effect” of a non-compete, the agency would deem it such. That means, even if that rule stands, it could be contested and may be interpreted as violating the non-compete provision. So, there is value in reading all the fine print should the rule move forward.
Physicians in independent practices who employ physician assistants and nurse practitioners have expressed concerns that their expensively trained employees might be tempted to accept a nearby, higher-paying position. The “non-solicitation” clause would theoretically prevent them from taking patients and co-workers with them — unless it were successfully contested. Many questions remain.
Further complicating the non-compete ban issue is how it might impact nonprofit institutions. Most hospitals structured as nonprofits would theoretically be exempt from the rule, although it is not specifically stated in the rule itself, because the FTC Act gives the Commission jurisdiction over for-profit companies only. This would obviously create an unfair advantage for nonprofits, who could continue writing non-compete clauses with impunity.
All of these questions may be moot, of course, because a number of powerful entities with deep pockets have lined up in opposition to the rule. Some of them have even questioned the FTC’s authority to pass the rule at all, on the grounds that Section 5 of the FTC Act does not give it the authority to police labor markets. A lawsuit has already been filed by the US Chamber of Commerce. Other large groups in opposition are the American Medical Group Association, the American Hospital Association, and numerous large hospital and healthcare networks.
Only time will tell whether this issue will be regulated on a national level or remain the purview of each individual state.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
(with very limited exceptions). The final rule will not go into effect until 120 days after its publication in the Federal Register, which took place on May 7, and numerous legal challenges appear to be on the horizon.
The principal components of the rule are as follows:
- After the effective date, most non-compete agreements (which prevent departing employees from signing with a new employer for a defined period within a specific geographic area) are banned nationwide.
- The rule exempts certain “senior executives,” ie individuals who earn more than $151,164 annually and serve in policy-making positions.
- There is another major exception for non-competes connected with a sale of a business.
- While not explicitly stated, the rule arguably exempts non-profits, tax-exempt hospitals, and other tax-exempt entities.
- Employers must provide verbal and written notice to employees regarding existing agreements, which would be voided under the rule.
The final rule is the latest skirmish in an ongoing, years-long debate. Twelve states have already put non-compete bans in place, according to a recent paper, and they may serve as a harbinger of things to come should the federal ban go into effect. Each state rule varies in its specifics as states respond to local market conditions. While some states ban all non-compete agreements outright, others limit them based on variables, such as income and employment circumstances. Of course, should the federal ban take effect, it will supersede whatever rules the individual states have in place.
In drafting the rule, the FTC reasoned that non-compete clauses constitute restraint of trade, and eliminating them could potentially increase worker earnings as well as lower health care costs by billions of dollars. In its statements on the proposed ban, the FTC claimed that it could lower health spending across the board by almost $150 billion per year and return $300 million to workers each year in earnings. The agency cited a large body of research that non-competes make it harder for workers to move between jobs and can raise prices for goods and services, while suppressing wages for workers and inhibiting the creation of new businesses.
Most physicians affected by non-compete agreements heavily favor the new rule, because it would give them more control over their careers and expand their practice and income opportunities. It would allow them to get a new job with a competing organization, bucking a long-standing trend that hospitals and health care systems have heavily relied on to keep staff in place.
The rule would, however, keep in place “non-solicitation” rules that many health care organizations have put in place. That means that if a physician leaves an employer, he or she cannot reach out to former patients and colleagues to bring them along or invite them to join him or her at the new employment venue.
Within that clause, however, the FTC has specified that if such non-solicitation agreement has the “equivalent effect” of a non-compete, the agency would deem it such. That means, even if that rule stands, it could be contested and may be interpreted as violating the non-compete provision. So, there is value in reading all the fine print should the rule move forward.
Physicians in independent practices who employ physician assistants and nurse practitioners have expressed concerns that their expensively trained employees might be tempted to accept a nearby, higher-paying position. The “non-solicitation” clause would theoretically prevent them from taking patients and co-workers with them — unless it were successfully contested. Many questions remain.
Further complicating the non-compete ban issue is how it might impact nonprofit institutions. Most hospitals structured as nonprofits would theoretically be exempt from the rule, although it is not specifically stated in the rule itself, because the FTC Act gives the Commission jurisdiction over for-profit companies only. This would obviously create an unfair advantage for nonprofits, who could continue writing non-compete clauses with impunity.
All of these questions may be moot, of course, because a number of powerful entities with deep pockets have lined up in opposition to the rule. Some of them have even questioned the FTC’s authority to pass the rule at all, on the grounds that Section 5 of the FTC Act does not give it the authority to police labor markets. A lawsuit has already been filed by the US Chamber of Commerce. Other large groups in opposition are the American Medical Group Association, the American Hospital Association, and numerous large hospital and healthcare networks.
Only time will tell whether this issue will be regulated on a national level or remain the purview of each individual state.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

Fluoride, Water, and Kids’ Brains: It’s Complicated
This transcript has been edited for clarity.
I recently looked back at my folder full of these medical study commentaries, this weekly video series we call Impact Factor, and realized that I’ve been doing this for a long time. More than 400 articles, believe it or not.
I’ve learned a lot in that time — about medicine, of course — but also about how people react to certain topics. If you’ve been with me this whole time, or even for just a chunk of it, you’ll know that I tend to take a measured approach to most topics. No one study is ever truly definitive, after all. But regardless of how even-keeled I may be, there are some topics that I just know in advance are going to be a bit divisive: studies about gun control; studies about vitamin D; and, of course, studies about fluoride.
Shall We Shake This Hornet’s Nest?
The fluoridation of the US water system began in 1945 with the goal of reducing cavities in the population. The CDC named water fluoridation one of the 10 great public health achievements of the 20th century, along with such inarguable achievements as the recognition of tobacco as a health hazard.
But fluoridation has never been without its detractors. One problem is that the spectrum of beliefs about the potential harm of fluoridation is huge. On one end, you have science-based concerns such as the recognition that excessive fluoride intake can cause fluorosis and stain tooth enamel. I’ll note that the EPA regulates fluoride levels — there is a fair amount of naturally occurring fluoride in water tables around the world — to prevent this. And, of course, on the other end of the spectrum, you have beliefs that are essentially conspiracy theories: “They” add fluoride to the water supply to control us.
The challenge for me is that when one “side” of a scientific debate includes the crazy theories, it can be hard to discuss that whole spectrum, since there are those who will see evidence of any adverse fluoride effect as confirmation that the conspiracy theory is true.
I can’t help this. So I’ll just say this up front: I am about to tell you about a study that shows some potential risk from fluoride exposure. I will tell you up front that there are some significant caveats to the study that call the results into question. And I will tell you up front that no one is controlling your mind, or my mind, with fluoride; they do it with social media.
Let’s Dive Into These Shark-Infested, Fluoridated Waters
We’re talking about the study, “Maternal Urinary Fluoride and Child Neurobehavior at Age 36 Months,” which appears in JAMA Network Open.
It’s a study of 229 mother-child pairs from the Los Angeles area. The moms had their urinary fluoride level measured once before 30 weeks of gestation. A neurobehavioral battery called the Preschool Child Behavior Checklist was administered to the children at age 36 months.
The main thing you’ll hear about this study — in headlines, Facebook posts, and manifestos locked in drawers somewhere — is the primary result: A 0.68-mg/L increase in urinary fluoride in the mothers, about 25 percentile points, was associated with a doubling of the risk for neurobehavioral problems in their kids when they were 3 years old.
Yikes.
But this is not a randomized trial. Researchers didn’t randomly assign some women to have high fluoride intake and some women to have low fluoride intake. They knew that other factors that might lead to neurobehavioral problems could also lead to higher fluoride intake. They represent these factors in what’s known as a directed acyclic graph, as seen here, and account for them statistically using a regression equation.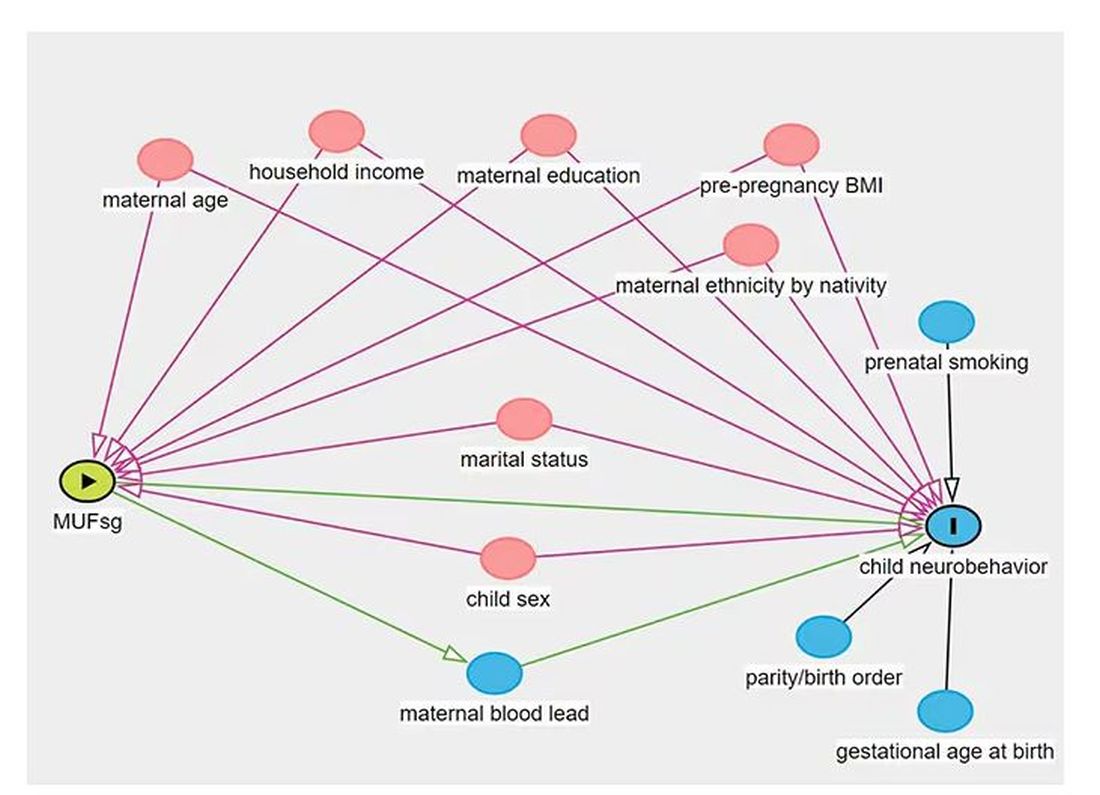
Not represented here are neighborhood characteristics. Los Angeles does not have uniformly fluoridated water, and neurobehavioral problems in kids are strongly linked to stressors in their environments. Fluoride level could be an innocent bystander.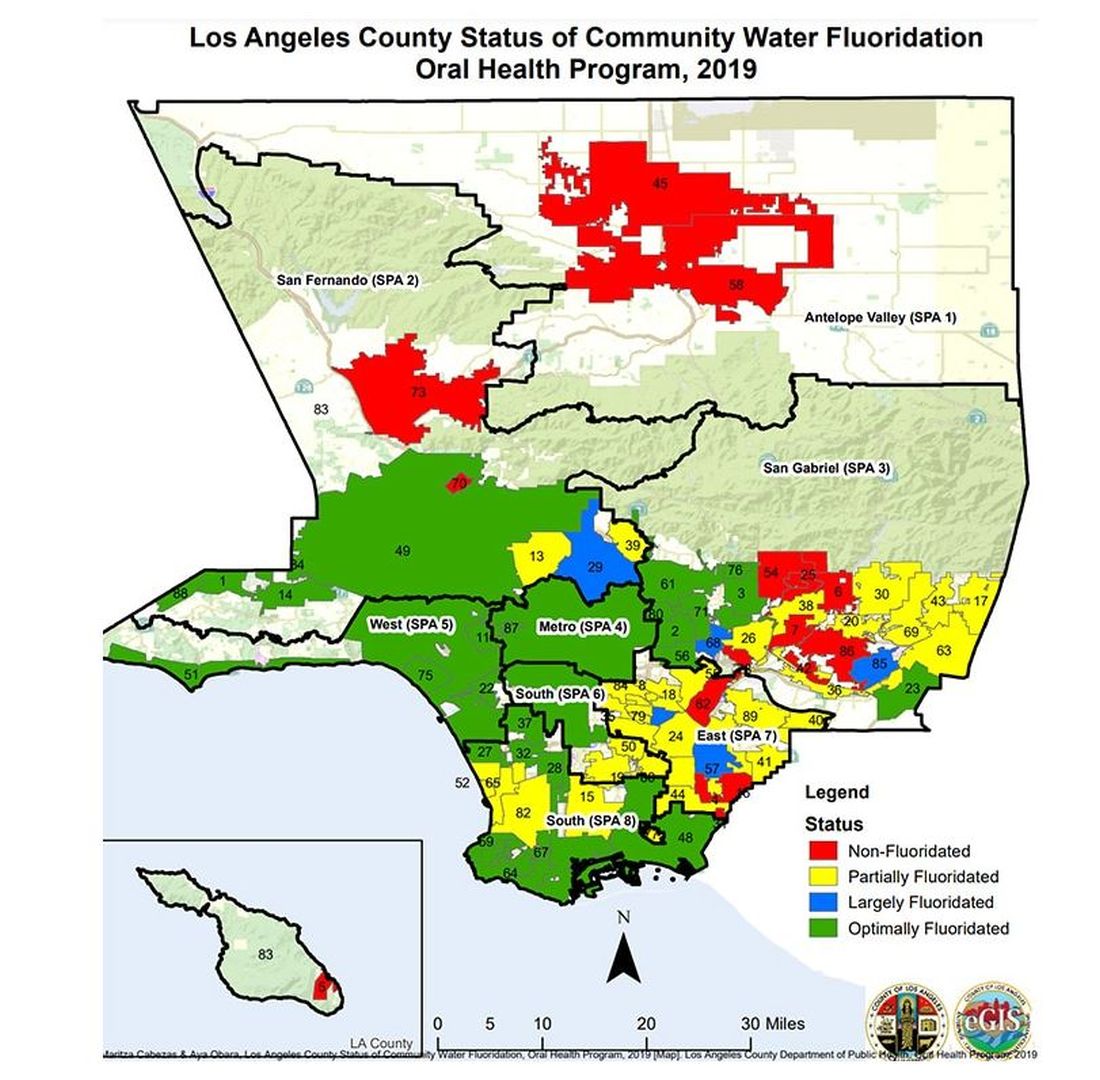
I’m really just describing the classic issue of correlation versus causation here, the bane of all observational research and — let’s be honest — a bit of a crutch that allows us to disregard the results of studies we don’t like, provided the study wasn’t a randomized trial.
But I have a deeper issue with this study than the old “failure to adjust for relevant confounders” thing, as important as that is.
The exposure of interest in this study is maternal urinary fluoride, as measured in a spot sample. It’s not often that I get to go deep on nephrology in this space, but let’s think about that for a second. Let’s assume for a moment that fluoride is toxic to the developing fetal brain, the main concern raised by the results of the study. How would that work? Presumably, mom would be ingesting fluoride from various sources (like the water supply), and that fluoride would get into her blood, and from her blood across the placenta to the baby’s blood, and into the baby’s brain.
Is Urinary Fluoride a Good Measure of Blood Fluoride?
It’s not great. Empirically, we have data that tell us that levels of urine fluoride are not all that similar to levels of serum fluoride. In 2014, a study investigated the correlation between urine and serum fluoride in a cohort of 60 schoolchildren and found a correlation coefficient of around 0.5.
Why isn’t urine fluoride a great proxy for serum fluoride? The most obvious reason is the urine concentration. Human urine concentration can range from about 50 mmol to 1200 mmol (a 24-fold difference) depending on hydration status. Over the course of 24 hours, for example, the amount of fluoride you put out in your urine may be fairly stable in relation to intake, but for a spot urine sample it would be wildly variable. The authors know this, of course, and so they divide the measured urine fluoride by the specific gravity of the urine to give a sort of “dilution adjusted” value. That’s what is actually used in this study. But specific gravity is, itself, an imperfect measure of how dilute the urine is.
This is something that comes up a lot in urinary biomarker research and it’s not that hard to get around. The best thing would be to just measure blood levels of fluoride. The second best option is 24-hour fluoride excretion. After that, the next best thing would be to adjust the spot concentration by other markers of urinary dilution — creatinine or osmolality — as sensitivity analyses. Any of these approaches would lend credence to the results of the study.
Urinary fluoride excretion is pH dependent. The more acidic the urine, the less fluoride is excreted. Many things — including, importantly, diet — affect urine pH. And it is not a stretch to think that diet may also affect the developing fetus. Neither urine pH nor dietary habits were accounted for in this study.
So, here we are. We have an observational study suggesting a harm that may be associated with fluoride. There may be a causal link here, in which case we need further studies to weigh the harm against the more well-established public health benefit. Or, this is all correlation — an illusion created by the limitations of observational data, and the unique challenges of estimating intake from a single urine sample. In other words, this study has something for everyone, fluoride boosters and skeptics alike. Let the arguments begin. But, if possible, leave me out of it.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I recently looked back at my folder full of these medical study commentaries, this weekly video series we call Impact Factor, and realized that I’ve been doing this for a long time. More than 400 articles, believe it or not.
I’ve learned a lot in that time — about medicine, of course — but also about how people react to certain topics. If you’ve been with me this whole time, or even for just a chunk of it, you’ll know that I tend to take a measured approach to most topics. No one study is ever truly definitive, after all. But regardless of how even-keeled I may be, there are some topics that I just know in advance are going to be a bit divisive: studies about gun control; studies about vitamin D; and, of course, studies about fluoride.
Shall We Shake This Hornet’s Nest?
The fluoridation of the US water system began in 1945 with the goal of reducing cavities in the population. The CDC named water fluoridation one of the 10 great public health achievements of the 20th century, along with such inarguable achievements as the recognition of tobacco as a health hazard.
But fluoridation has never been without its detractors. One problem is that the spectrum of beliefs about the potential harm of fluoridation is huge. On one end, you have science-based concerns such as the recognition that excessive fluoride intake can cause fluorosis and stain tooth enamel. I’ll note that the EPA regulates fluoride levels — there is a fair amount of naturally occurring fluoride in water tables around the world — to prevent this. And, of course, on the other end of the spectrum, you have beliefs that are essentially conspiracy theories: “They” add fluoride to the water supply to control us.
The challenge for me is that when one “side” of a scientific debate includes the crazy theories, it can be hard to discuss that whole spectrum, since there are those who will see evidence of any adverse fluoride effect as confirmation that the conspiracy theory is true.
I can’t help this. So I’ll just say this up front: I am about to tell you about a study that shows some potential risk from fluoride exposure. I will tell you up front that there are some significant caveats to the study that call the results into question. And I will tell you up front that no one is controlling your mind, or my mind, with fluoride; they do it with social media.
Let’s Dive Into These Shark-Infested, Fluoridated Waters
We’re talking about the study, “Maternal Urinary Fluoride and Child Neurobehavior at Age 36 Months,” which appears in JAMA Network Open.
It’s a study of 229 mother-child pairs from the Los Angeles area. The moms had their urinary fluoride level measured once before 30 weeks of gestation. A neurobehavioral battery called the Preschool Child Behavior Checklist was administered to the children at age 36 months.
The main thing you’ll hear about this study — in headlines, Facebook posts, and manifestos locked in drawers somewhere — is the primary result: A 0.68-mg/L increase in urinary fluoride in the mothers, about 25 percentile points, was associated with a doubling of the risk for neurobehavioral problems in their kids when they were 3 years old.
Yikes.
But this is not a randomized trial. Researchers didn’t randomly assign some women to have high fluoride intake and some women to have low fluoride intake. They knew that other factors that might lead to neurobehavioral problems could also lead to higher fluoride intake. They represent these factors in what’s known as a directed acyclic graph, as seen here, and account for them statistically using a regression equation.
Not represented here are neighborhood characteristics. Los Angeles does not have uniformly fluoridated water, and neurobehavioral problems in kids are strongly linked to stressors in their environments. Fluoride level could be an innocent bystander.
I’m really just describing the classic issue of correlation versus causation here, the bane of all observational research and — let’s be honest — a bit of a crutch that allows us to disregard the results of studies we don’t like, provided the study wasn’t a randomized trial.
But I have a deeper issue with this study than the old “failure to adjust for relevant confounders” thing, as important as that is.
The exposure of interest in this study is maternal urinary fluoride, as measured in a spot sample. It’s not often that I get to go deep on nephrology in this space, but let’s think about that for a second. Let’s assume for a moment that fluoride is toxic to the developing fetal brain, the main concern raised by the results of the study. How would that work? Presumably, mom would be ingesting fluoride from various sources (like the water supply), and that fluoride would get into her blood, and from her blood across the placenta to the baby’s blood, and into the baby’s brain.
Is Urinary Fluoride a Good Measure of Blood Fluoride?
It’s not great. Empirically, we have data that tell us that levels of urine fluoride are not all that similar to levels of serum fluoride. In 2014, a study investigated the correlation between urine and serum fluoride in a cohort of 60 schoolchildren and found a correlation coefficient of around 0.5.
Why isn’t urine fluoride a great proxy for serum fluoride? The most obvious reason is the urine concentration. Human urine concentration can range from about 50 mmol to 1200 mmol (a 24-fold difference) depending on hydration status. Over the course of 24 hours, for example, the amount of fluoride you put out in your urine may be fairly stable in relation to intake, but for a spot urine sample it would be wildly variable. The authors know this, of course, and so they divide the measured urine fluoride by the specific gravity of the urine to give a sort of “dilution adjusted” value. That’s what is actually used in this study. But specific gravity is, itself, an imperfect measure of how dilute the urine is.
This is something that comes up a lot in urinary biomarker research and it’s not that hard to get around. The best thing would be to just measure blood levels of fluoride. The second best option is 24-hour fluoride excretion. After that, the next best thing would be to adjust the spot concentration by other markers of urinary dilution — creatinine or osmolality — as sensitivity analyses. Any of these approaches would lend credence to the results of the study.
Urinary fluoride excretion is pH dependent. The more acidic the urine, the less fluoride is excreted. Many things — including, importantly, diet — affect urine pH. And it is not a stretch to think that diet may also affect the developing fetus. Neither urine pH nor dietary habits were accounted for in this study.
So, here we are. We have an observational study suggesting a harm that may be associated with fluoride. There may be a causal link here, in which case we need further studies to weigh the harm against the more well-established public health benefit. Or, this is all correlation — an illusion created by the limitations of observational data, and the unique challenges of estimating intake from a single urine sample. In other words, this study has something for everyone, fluoride boosters and skeptics alike. Let the arguments begin. But, if possible, leave me out of it.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I recently looked back at my folder full of these medical study commentaries, this weekly video series we call Impact Factor, and realized that I’ve been doing this for a long time. More than 400 articles, believe it or not.
I’ve learned a lot in that time — about medicine, of course — but also about how people react to certain topics. If you’ve been with me this whole time, or even for just a chunk of it, you’ll know that I tend to take a measured approach to most topics. No one study is ever truly definitive, after all. But regardless of how even-keeled I may be, there are some topics that I just know in advance are going to be a bit divisive: studies about gun control; studies about vitamin D; and, of course, studies about fluoride.
Shall We Shake This Hornet’s Nest?
The fluoridation of the US water system began in 1945 with the goal of reducing cavities in the population. The CDC named water fluoridation one of the 10 great public health achievements of the 20th century, along with such inarguable achievements as the recognition of tobacco as a health hazard.
But fluoridation has never been without its detractors. One problem is that the spectrum of beliefs about the potential harm of fluoridation is huge. On one end, you have science-based concerns such as the recognition that excessive fluoride intake can cause fluorosis and stain tooth enamel. I’ll note that the EPA regulates fluoride levels — there is a fair amount of naturally occurring fluoride in water tables around the world — to prevent this. And, of course, on the other end of the spectrum, you have beliefs that are essentially conspiracy theories: “They” add fluoride to the water supply to control us.
The challenge for me is that when one “side” of a scientific debate includes the crazy theories, it can be hard to discuss that whole spectrum, since there are those who will see evidence of any adverse fluoride effect as confirmation that the conspiracy theory is true.
I can’t help this. So I’ll just say this up front: I am about to tell you about a study that shows some potential risk from fluoride exposure. I will tell you up front that there are some significant caveats to the study that call the results into question. And I will tell you up front that no one is controlling your mind, or my mind, with fluoride; they do it with social media.
Let’s Dive Into These Shark-Infested, Fluoridated Waters
We’re talking about the study, “Maternal Urinary Fluoride and Child Neurobehavior at Age 36 Months,” which appears in JAMA Network Open.
It’s a study of 229 mother-child pairs from the Los Angeles area. The moms had their urinary fluoride level measured once before 30 weeks of gestation. A neurobehavioral battery called the Preschool Child Behavior Checklist was administered to the children at age 36 months.
The main thing you’ll hear about this study — in headlines, Facebook posts, and manifestos locked in drawers somewhere — is the primary result: A 0.68-mg/L increase in urinary fluoride in the mothers, about 25 percentile points, was associated with a doubling of the risk for neurobehavioral problems in their kids when they were 3 years old.
Yikes.
But this is not a randomized trial. Researchers didn’t randomly assign some women to have high fluoride intake and some women to have low fluoride intake. They knew that other factors that might lead to neurobehavioral problems could also lead to higher fluoride intake. They represent these factors in what’s known as a directed acyclic graph, as seen here, and account for them statistically using a regression equation.
Not represented here are neighborhood characteristics. Los Angeles does not have uniformly fluoridated water, and neurobehavioral problems in kids are strongly linked to stressors in their environments. Fluoride level could be an innocent bystander.
I’m really just describing the classic issue of correlation versus causation here, the bane of all observational research and — let’s be honest — a bit of a crutch that allows us to disregard the results of studies we don’t like, provided the study wasn’t a randomized trial.
But I have a deeper issue with this study than the old “failure to adjust for relevant confounders” thing, as important as that is.
The exposure of interest in this study is maternal urinary fluoride, as measured in a spot sample. It’s not often that I get to go deep on nephrology in this space, but let’s think about that for a second. Let’s assume for a moment that fluoride is toxic to the developing fetal brain, the main concern raised by the results of the study. How would that work? Presumably, mom would be ingesting fluoride from various sources (like the water supply), and that fluoride would get into her blood, and from her blood across the placenta to the baby’s blood, and into the baby’s brain.
Is Urinary Fluoride a Good Measure of Blood Fluoride?
It’s not great. Empirically, we have data that tell us that levels of urine fluoride are not all that similar to levels of serum fluoride. In 2014, a study investigated the correlation between urine and serum fluoride in a cohort of 60 schoolchildren and found a correlation coefficient of around 0.5.
Why isn’t urine fluoride a great proxy for serum fluoride? The most obvious reason is the urine concentration. Human urine concentration can range from about 50 mmol to 1200 mmol (a 24-fold difference) depending on hydration status. Over the course of 24 hours, for example, the amount of fluoride you put out in your urine may be fairly stable in relation to intake, but for a spot urine sample it would be wildly variable. The authors know this, of course, and so they divide the measured urine fluoride by the specific gravity of the urine to give a sort of “dilution adjusted” value. That’s what is actually used in this study. But specific gravity is, itself, an imperfect measure of how dilute the urine is.
This is something that comes up a lot in urinary biomarker research and it’s not that hard to get around. The best thing would be to just measure blood levels of fluoride. The second best option is 24-hour fluoride excretion. After that, the next best thing would be to adjust the spot concentration by other markers of urinary dilution — creatinine or osmolality — as sensitivity analyses. Any of these approaches would lend credence to the results of the study.
Urinary fluoride excretion is pH dependent. The more acidic the urine, the less fluoride is excreted. Many things — including, importantly, diet — affect urine pH. And it is not a stretch to think that diet may also affect the developing fetus. Neither urine pH nor dietary habits were accounted for in this study.
So, here we are. We have an observational study suggesting a harm that may be associated with fluoride. There may be a causal link here, in which case we need further studies to weigh the harm against the more well-established public health benefit. Or, this is all correlation — an illusion created by the limitations of observational data, and the unique challenges of estimating intake from a single urine sample. In other words, this study has something for everyone, fluoride boosters and skeptics alike. Let the arguments begin. But, if possible, leave me out of it.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Ob.Gyns. Can Help Patients Manage Weight With Anti-Obesity Medications
SAN FRANCISCO — An estimated two out of five adult women in the United States have obesity, and given the potential challenges of losing pregnancy weight postpartum or staving off the weight gain associated with menopause, women are likely to be receptive toward weight management help from their ob.gyns. A whole new armamentarium of anti-obesity medications has become available in the past decade, providing physicians and patients with more treatment options.
Ob.gyns. are therefore well-poised to offer counseling and treatment for obesity management for their patients, Johanna G. Finkle, MD, clinical assistant professor of obstetrics and gynecology and a weight management specialist at the University of Kansas Heath System, told attendees at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. Dr. Finkle provided an extensive overview of what ob.gyns. need to know if they are interested in prescribing anti-obesity medications or simply providing their patients with information about the available drugs.
Kitila S. Heyward, MD, an ob.gyn. at Atrium Health in Monroe, North Carolina, who attended the talk, tries to prescribe anti-obesity medications but has run into roadblocks that Dr. Finkle’s talk helped her understand how to overcome.
“I thought it was very helpful because [I] and one of my midwives, in practice, have been trying to get things prescribed, and we can’t figure out the loopholes,” Dr. Heyward said. “Also, the failure rates are really helpful to us so that we know how to counsel people.”
Even for clinicians who aren’t prescribing these medications, Dr. Heyward said the talk was illuminating. “It offered a better understanding of the medications that your patients are on and how it can affect things like birth control, management of surgery, pregnancy, and things along those lines from a clinical day-by-day standpoint,” she said.
Starting With the Basics
Dr. Finkle began by emphasizing the importance of using patient-first language in discussing obesity, which means using terms such as “weight, excess weight, overweight, body mass index,” and “affected by obesity” instead of “obese, morbidly obese, heaviness, or large.” She also cited the Obesity Medicine Association’s definition of obesity: “a chronic, relapsing and treatable multifactorial, neurobehavioral disease, wherein an increase in body fat promotes adipose tissue dysfunction and abnormal fat mass physical forces, resulting in adverse metabolic, biomechanical, and psychosocial health consequences.”
Though Dr. Finkle acknowledged the limitations of relying on BMI for defining obesity, it remains the standard tool in current practice, with a BMI of 25-29.9 defining overweight and a BMI of 30 or greater defining obesity. Other diagnostic criteria for obesity in women, however, include a percentage body fat over 32% or a waist circumference of more than 35 inches.
“Women are at risk for weight gain through their entire lifespan” Dr. Finkle said, and in women with polycystic ovarian syndrome, 60%-80% have pre-obesity or obesity. In menopause, the triple threat of decreased estrogen, decreased activity, and changes in diet all contribute to obesity risk and no evidence suggests that hormone therapy can prevent weight gain.
Healthy nutrition, physical activity, and behavioral modification remain key pillars of weight management, but interventions such as surgery or medications are also important tools, she said.
“One size does not fit all in terms of treatment,” Dr. Finkle said. ”When I talk to a patient, I think about other medical complications that I can treat with these medications.”
Women for whom anti-obesity medications may be indicated are those with a BMI of 30 or greater, and those with a BMI of at least 27 along with at least one obesity-related comorbidity, such as hypertension, high cholesterol, diabetes, or sleep apnea. The goal of treating obesity with medication is at least a 5%-10% reduction of body weight.
Three Pharmacotherapy Categories
Dr. Finkle reviewed three basic categories of anti-obesity medications: Food and Drug Administration–approved short-term and long-term medications and then off-label drugs that can also aid in healthy weight loss. Short-term options include phentermine, diethylpropion, phendimetrazine, and benzphetamine. Long-term options include orlistat, phentermine/topiramate ER, naltrexone HCl/bupropion HCl ER, and the three GLP-1 receptor agonist drugs, liraglutide, semaglutide, and tirzepatide.
The short-term medications are stimulants that increase satiety, but adverse effects can include tachycardia, hypertension, insomnia, dry mouth, constipation, and diarrhea.
These medications are contraindicated for anyone with uncontrolled hypertension, hyperthyroidism, cardiovascular disease, MAOI use, glaucoma, or history of substance use. The goal is a 5% weight loss in 3 months, and 3 months is the maximum prescribing term.
Then Dr. Finkle reviewed the side effects and contraindications for the oral long-term medications. Orlistat, which can aid in up to 5% weight loss, can result in oily stools and fecal incontinence and is contraindicated for people with chronic malabsorption or cholestasis.
Phentermine/topiramate ER, which can aid in up to 10% weight loss, can result in hypertension, paresthesia, or constipation, and is contraindicated for those with glaucoma, hyperthyroidism, and kidney stones. After the starting dose of 3.75 mg/23 mg, Dr. Finkle increases patients’ dose every 2 weeks, ”but if they’re not tolerating it, if they’re having significant side effects, or they’re losing weight, you do not increase the medication.”
Side effects of naltrexone HCl/bupropion HCl ER, which can lead to 5%-6% weight loss, can include hypertension, suicidal ideation, and glaucoma, and it’s contraindicated in those taking opioids or with a history of seizures or anorexia.
The GLP-1 Receptor Agonists
Next Dr. Finkle discussed the newest but most effective medications, the GLP-1 agonists liraglutide, semaglutide, and tirzepatide. The main contraindications for these drugs are a personal or family history of medullary thyroid cancer, multiple endocrine neoplasia type II syndrome, or any hypersensitivity to this drug class. The two main serious risks are pancreatitis — a 1% risk — and gallstones. Though Dr. Finkle included suicidal ideation as a potential risk of these drugs, the most recent evidence suggests there is no link between suicidal ideation and GLP-1 agonists. The most common side effects are nausea, vomiting, diarrhea, constipation, dyspepsia, and an increased heart rate, though these eventually resolve.
“We always start low with these medications,” Dr. Finkle said, and then titrate the dose up each week, “but if they are having awful side effects, just stay on that dose longer.”
The mechanisms of all three drugs for treating obesity are similar; they work to curb central satiety and slow gastric emptying, though they also have additional mechanisms with benefits for blood glucose levels and for the liver and heart.
- Liraglutide, the first of these drugs approved, is a daily subcutaneous injection that starts at a dose of 0.6 mg and goes up to 3 mg. Patients should lose 4% of weight in 16 weeks or else they are non-responders, Dr. Finkle said.
- Semaglutide, a GLP-1 agonist given as a weekly subcutaneous injection, starts at a dose of 0.25 mg and goes up to 2.4 mg; patients should expect a 5% weight loss in 16 weeks if they are responders. Long term, however, patients lose up to an average 15% of body weight with semaglutide; a third of patients lost more than 20% of body weight in clinical trials, compared with 7%-8% body weight loss with liraglutide. An additional benefit of semaglutide is a 20% reduction in risk of cardiovascular disease.
- Tirzepatide is a combined GLP-1 and GIP agonist, also delivered as a weekly subcutaneous injection, that should result in an estimated 5% weight loss in 16 weeks for responders. But tirzepatide is the most effective of the three, with 91% of patients losing at least 5% body weight and more than half of patients (56%) losing at least 20%.
The big drawbacks to the GLP-1 agonists, however, are their high cost, common lack of insurance coverage, and continued shortages. Dr. Finkle recommended using manufacturer coupons, comparison shopping on Good Rx, and appealing prior authorization requirements to help patients pay for the GLP-1 agonists.
“Drug availability is my second problem. There’s not enough drug,” she said, and her patients often have to call around to different pharmacies to find out which ones are carrying the drug and at what doses. She will sometimes switch their doses as needed based on availability.
It’s also important for physicians to be aware of guidance from the American Society of Anesthesiologists regarding GLP-1 agonist use prior to surgery because of their slowed gastric-emptying mechanism. To reduce the risk of aspiration, patients undergoing general anesthesia should not take liraglutide on the day of surgery, and semaglutide and tirzepatide should be held for 1 week prior to the procedure. New research in JAMA Surgery, however, suggests holding these medications for longer than a week may be wiser.
Getting Patients Started
All the short-term and long-term medications are contraindicated during pregnancy and breastfeeding, Dr. Finkle said. Animal studies with GLP-1 agonists suggest adverse fetal effects when used during pregnancy, but the limited data in human studies so far have not shown a risk of major malformations. Dr. Finkle said the recommendations for now are to stop all GLP-1 receptor agonist drugs 2 months before patients attempt to become pregnant and not to begin them again until after they are no longer breastfeeding.
Finally, Dr. Finkle reviewed off-label medications that can result in modest weight loss, including topiramate, phentermine (not to be used for longer than 12 weeks), bupropion, naltrexone, and metformin. Metformin is likely to result in only 2% weight loss, but it may enhance the effects of GLP-1s, she said.
For ob.gyns. who want to get their patients started on one of these medications, Dr. Finkle first recommends asking patients if it’s okay to discuss their weight. ”Studies show that if you just ask permission to discuss someone’s weight, they go on to lose weight and lose more than someone who has never been asked,” Dr. Finkle said. Then she takes a history.
”When I see a patient, I ask, ‘Tell me why you’re here today,’ ” Dr. Finkle said.
This gives me a lot of insight as to why they’re coming in and it helps me understand where they’re at in terms of other things, such as depression or anxiety with weight, and it helps me to tailor my treatment.”
A full medical history is important for learning about potential contraindications or picking medications that might help with other conditions, such as topiramate for migraines. Finally, Dr. Finkle advises a lab screening with a comprehensive metabolic panel, lipid panel, HbA1c, and vitamin D.
“The [comprehensive metabolic panel] allows me to know about creatinine and liver function,” she said. If these are elevated, she will still prescribe GLP-1s but will monitor the values more closely. “Then I discuss options with the patient. They may be eligible for bariatric surgery or medications. We talk about lifestyle behavioral management, and then I go through the medications and we set goals.”
Goals include nutrition and exercise; start modest and have them work their way up by doing activities they enjoy. In addition, patients taking GLP-1s need to eat enough protein — 80 to 100 grams a day, though she starts them at 60 grams — and do regular muscle strengthening since they can lose muscle mass.
Indications for referral to an obesity medicine specialist are a history of gastric bypass/sleeve surgery, having type 2 diabetes, having an eating disorder, or having failed one of these anti-obesity medications.
Finally, Dr. Finkle reviewed medications that can cause weight gain: medroxyprogesterone acetate for birth control; beta blockers for hypertension or migraine; the antidepressants amitriptyline, paroxetine, venlafaxine, and trazodone; the mood stabilizers gabapentin, lithium, valproate, and carbamazepine; and diphenhydramine and zolpidem for sleep.
No external funding was used for the talk. Dr. Finkle and Dr. Heyward had no disclosures.
SAN FRANCISCO — An estimated two out of five adult women in the United States have obesity, and given the potential challenges of losing pregnancy weight postpartum or staving off the weight gain associated with menopause, women are likely to be receptive toward weight management help from their ob.gyns. A whole new armamentarium of anti-obesity medications has become available in the past decade, providing physicians and patients with more treatment options.
Ob.gyns. are therefore well-poised to offer counseling and treatment for obesity management for their patients, Johanna G. Finkle, MD, clinical assistant professor of obstetrics and gynecology and a weight management specialist at the University of Kansas Heath System, told attendees at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. Dr. Finkle provided an extensive overview of what ob.gyns. need to know if they are interested in prescribing anti-obesity medications or simply providing their patients with information about the available drugs.
Kitila S. Heyward, MD, an ob.gyn. at Atrium Health in Monroe, North Carolina, who attended the talk, tries to prescribe anti-obesity medications but has run into roadblocks that Dr. Finkle’s talk helped her understand how to overcome.
“I thought it was very helpful because [I] and one of my midwives, in practice, have been trying to get things prescribed, and we can’t figure out the loopholes,” Dr. Heyward said. “Also, the failure rates are really helpful to us so that we know how to counsel people.”
Even for clinicians who aren’t prescribing these medications, Dr. Heyward said the talk was illuminating. “It offered a better understanding of the medications that your patients are on and how it can affect things like birth control, management of surgery, pregnancy, and things along those lines from a clinical day-by-day standpoint,” she said.
Starting With the Basics
Dr. Finkle began by emphasizing the importance of using patient-first language in discussing obesity, which means using terms such as “weight, excess weight, overweight, body mass index,” and “affected by obesity” instead of “obese, morbidly obese, heaviness, or large.” She also cited the Obesity Medicine Association’s definition of obesity: “a chronic, relapsing and treatable multifactorial, neurobehavioral disease, wherein an increase in body fat promotes adipose tissue dysfunction and abnormal fat mass physical forces, resulting in adverse metabolic, biomechanical, and psychosocial health consequences.”
Though Dr. Finkle acknowledged the limitations of relying on BMI for defining obesity, it remains the standard tool in current practice, with a BMI of 25-29.9 defining overweight and a BMI of 30 or greater defining obesity. Other diagnostic criteria for obesity in women, however, include a percentage body fat over 32% or a waist circumference of more than 35 inches.
“Women are at risk for weight gain through their entire lifespan” Dr. Finkle said, and in women with polycystic ovarian syndrome, 60%-80% have pre-obesity or obesity. In menopause, the triple threat of decreased estrogen, decreased activity, and changes in diet all contribute to obesity risk and no evidence suggests that hormone therapy can prevent weight gain.
Healthy nutrition, physical activity, and behavioral modification remain key pillars of weight management, but interventions such as surgery or medications are also important tools, she said.
“One size does not fit all in terms of treatment,” Dr. Finkle said. ”When I talk to a patient, I think about other medical complications that I can treat with these medications.”
Women for whom anti-obesity medications may be indicated are those with a BMI of 30 or greater, and those with a BMI of at least 27 along with at least one obesity-related comorbidity, such as hypertension, high cholesterol, diabetes, or sleep apnea. The goal of treating obesity with medication is at least a 5%-10% reduction of body weight.
Three Pharmacotherapy Categories
Dr. Finkle reviewed three basic categories of anti-obesity medications: Food and Drug Administration–approved short-term and long-term medications and then off-label drugs that can also aid in healthy weight loss. Short-term options include phentermine, diethylpropion, phendimetrazine, and benzphetamine. Long-term options include orlistat, phentermine/topiramate ER, naltrexone HCl/bupropion HCl ER, and the three GLP-1 receptor agonist drugs, liraglutide, semaglutide, and tirzepatide.
The short-term medications are stimulants that increase satiety, but adverse effects can include tachycardia, hypertension, insomnia, dry mouth, constipation, and diarrhea.
These medications are contraindicated for anyone with uncontrolled hypertension, hyperthyroidism, cardiovascular disease, MAOI use, glaucoma, or history of substance use. The goal is a 5% weight loss in 3 months, and 3 months is the maximum prescribing term.
Then Dr. Finkle reviewed the side effects and contraindications for the oral long-term medications. Orlistat, which can aid in up to 5% weight loss, can result in oily stools and fecal incontinence and is contraindicated for people with chronic malabsorption or cholestasis.
Phentermine/topiramate ER, which can aid in up to 10% weight loss, can result in hypertension, paresthesia, or constipation, and is contraindicated for those with glaucoma, hyperthyroidism, and kidney stones. After the starting dose of 3.75 mg/23 mg, Dr. Finkle increases patients’ dose every 2 weeks, ”but if they’re not tolerating it, if they’re having significant side effects, or they’re losing weight, you do not increase the medication.”
Side effects of naltrexone HCl/bupropion HCl ER, which can lead to 5%-6% weight loss, can include hypertension, suicidal ideation, and glaucoma, and it’s contraindicated in those taking opioids or with a history of seizures or anorexia.
The GLP-1 Receptor Agonists
Next Dr. Finkle discussed the newest but most effective medications, the GLP-1 agonists liraglutide, semaglutide, and tirzepatide. The main contraindications for these drugs are a personal or family history of medullary thyroid cancer, multiple endocrine neoplasia type II syndrome, or any hypersensitivity to this drug class. The two main serious risks are pancreatitis — a 1% risk — and gallstones. Though Dr. Finkle included suicidal ideation as a potential risk of these drugs, the most recent evidence suggests there is no link between suicidal ideation and GLP-1 agonists. The most common side effects are nausea, vomiting, diarrhea, constipation, dyspepsia, and an increased heart rate, though these eventually resolve.
“We always start low with these medications,” Dr. Finkle said, and then titrate the dose up each week, “but if they are having awful side effects, just stay on that dose longer.”
The mechanisms of all three drugs for treating obesity are similar; they work to curb central satiety and slow gastric emptying, though they also have additional mechanisms with benefits for blood glucose levels and for the liver and heart.
- Liraglutide, the first of these drugs approved, is a daily subcutaneous injection that starts at a dose of 0.6 mg and goes up to 3 mg. Patients should lose 4% of weight in 16 weeks or else they are non-responders, Dr. Finkle said.
- Semaglutide, a GLP-1 agonist given as a weekly subcutaneous injection, starts at a dose of 0.25 mg and goes up to 2.4 mg; patients should expect a 5% weight loss in 16 weeks if they are responders. Long term, however, patients lose up to an average 15% of body weight with semaglutide; a third of patients lost more than 20% of body weight in clinical trials, compared with 7%-8% body weight loss with liraglutide. An additional benefit of semaglutide is a 20% reduction in risk of cardiovascular disease.
- Tirzepatide is a combined GLP-1 and GIP agonist, also delivered as a weekly subcutaneous injection, that should result in an estimated 5% weight loss in 16 weeks for responders. But tirzepatide is the most effective of the three, with 91% of patients losing at least 5% body weight and more than half of patients (56%) losing at least 20%.
The big drawbacks to the GLP-1 agonists, however, are their high cost, common lack of insurance coverage, and continued shortages. Dr. Finkle recommended using manufacturer coupons, comparison shopping on Good Rx, and appealing prior authorization requirements to help patients pay for the GLP-1 agonists.
“Drug availability is my second problem. There’s not enough drug,” she said, and her patients often have to call around to different pharmacies to find out which ones are carrying the drug and at what doses. She will sometimes switch their doses as needed based on availability.
It’s also important for physicians to be aware of guidance from the American Society of Anesthesiologists regarding GLP-1 agonist use prior to surgery because of their slowed gastric-emptying mechanism. To reduce the risk of aspiration, patients undergoing general anesthesia should not take liraglutide on the day of surgery, and semaglutide and tirzepatide should be held for 1 week prior to the procedure. New research in JAMA Surgery, however, suggests holding these medications for longer than a week may be wiser.
Getting Patients Started
All the short-term and long-term medications are contraindicated during pregnancy and breastfeeding, Dr. Finkle said. Animal studies with GLP-1 agonists suggest adverse fetal effects when used during pregnancy, but the limited data in human studies so far have not shown a risk of major malformations. Dr. Finkle said the recommendations for now are to stop all GLP-1 receptor agonist drugs 2 months before patients attempt to become pregnant and not to begin them again until after they are no longer breastfeeding.
Finally, Dr. Finkle reviewed off-label medications that can result in modest weight loss, including topiramate, phentermine (not to be used for longer than 12 weeks), bupropion, naltrexone, and metformin. Metformin is likely to result in only 2% weight loss, but it may enhance the effects of GLP-1s, she said.
For ob.gyns. who want to get their patients started on one of these medications, Dr. Finkle first recommends asking patients if it’s okay to discuss their weight. ”Studies show that if you just ask permission to discuss someone’s weight, they go on to lose weight and lose more than someone who has never been asked,” Dr. Finkle said. Then she takes a history.
”When I see a patient, I ask, ‘Tell me why you’re here today,’ ” Dr. Finkle said.
This gives me a lot of insight as to why they’re coming in and it helps me understand where they’re at in terms of other things, such as depression or anxiety with weight, and it helps me to tailor my treatment.”
A full medical history is important for learning about potential contraindications or picking medications that might help with other conditions, such as topiramate for migraines. Finally, Dr. Finkle advises a lab screening with a comprehensive metabolic panel, lipid panel, HbA1c, and vitamin D.
“The [comprehensive metabolic panel] allows me to know about creatinine and liver function,” she said. If these are elevated, she will still prescribe GLP-1s but will monitor the values more closely. “Then I discuss options with the patient. They may be eligible for bariatric surgery or medications. We talk about lifestyle behavioral management, and then I go through the medications and we set goals.”
Goals include nutrition and exercise; start modest and have them work their way up by doing activities they enjoy. In addition, patients taking GLP-1s need to eat enough protein — 80 to 100 grams a day, though she starts them at 60 grams — and do regular muscle strengthening since they can lose muscle mass.
Indications for referral to an obesity medicine specialist are a history of gastric bypass/sleeve surgery, having type 2 diabetes, having an eating disorder, or having failed one of these anti-obesity medications.
Finally, Dr. Finkle reviewed medications that can cause weight gain: medroxyprogesterone acetate for birth control; beta blockers for hypertension or migraine; the antidepressants amitriptyline, paroxetine, venlafaxine, and trazodone; the mood stabilizers gabapentin, lithium, valproate, and carbamazepine; and diphenhydramine and zolpidem for sleep.
No external funding was used for the talk. Dr. Finkle and Dr. Heyward had no disclosures.
SAN FRANCISCO — An estimated two out of five adult women in the United States have obesity, and given the potential challenges of losing pregnancy weight postpartum or staving off the weight gain associated with menopause, women are likely to be receptive toward weight management help from their ob.gyns. A whole new armamentarium of anti-obesity medications has become available in the past decade, providing physicians and patients with more treatment options.
Ob.gyns. are therefore well-poised to offer counseling and treatment for obesity management for their patients, Johanna G. Finkle, MD, clinical assistant professor of obstetrics and gynecology and a weight management specialist at the University of Kansas Heath System, told attendees at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. Dr. Finkle provided an extensive overview of what ob.gyns. need to know if they are interested in prescribing anti-obesity medications or simply providing their patients with information about the available drugs.
Kitila S. Heyward, MD, an ob.gyn. at Atrium Health in Monroe, North Carolina, who attended the talk, tries to prescribe anti-obesity medications but has run into roadblocks that Dr. Finkle’s talk helped her understand how to overcome.
“I thought it was very helpful because [I] and one of my midwives, in practice, have been trying to get things prescribed, and we can’t figure out the loopholes,” Dr. Heyward said. “Also, the failure rates are really helpful to us so that we know how to counsel people.”
Even for clinicians who aren’t prescribing these medications, Dr. Heyward said the talk was illuminating. “It offered a better understanding of the medications that your patients are on and how it can affect things like birth control, management of surgery, pregnancy, and things along those lines from a clinical day-by-day standpoint,” she said.
Starting With the Basics
Dr. Finkle began by emphasizing the importance of using patient-first language in discussing obesity, which means using terms such as “weight, excess weight, overweight, body mass index,” and “affected by obesity” instead of “obese, morbidly obese, heaviness, or large.” She also cited the Obesity Medicine Association’s definition of obesity: “a chronic, relapsing and treatable multifactorial, neurobehavioral disease, wherein an increase in body fat promotes adipose tissue dysfunction and abnormal fat mass physical forces, resulting in adverse metabolic, biomechanical, and psychosocial health consequences.”
Though Dr. Finkle acknowledged the limitations of relying on BMI for defining obesity, it remains the standard tool in current practice, with a BMI of 25-29.9 defining overweight and a BMI of 30 or greater defining obesity. Other diagnostic criteria for obesity in women, however, include a percentage body fat over 32% or a waist circumference of more than 35 inches.
“Women are at risk for weight gain through their entire lifespan” Dr. Finkle said, and in women with polycystic ovarian syndrome, 60%-80% have pre-obesity or obesity. In menopause, the triple threat of decreased estrogen, decreased activity, and changes in diet all contribute to obesity risk and no evidence suggests that hormone therapy can prevent weight gain.
Healthy nutrition, physical activity, and behavioral modification remain key pillars of weight management, but interventions such as surgery or medications are also important tools, she said.
“One size does not fit all in terms of treatment,” Dr. Finkle said. ”When I talk to a patient, I think about other medical complications that I can treat with these medications.”
Women for whom anti-obesity medications may be indicated are those with a BMI of 30 or greater, and those with a BMI of at least 27 along with at least one obesity-related comorbidity, such as hypertension, high cholesterol, diabetes, or sleep apnea. The goal of treating obesity with medication is at least a 5%-10% reduction of body weight.
Three Pharmacotherapy Categories
Dr. Finkle reviewed three basic categories of anti-obesity medications: Food and Drug Administration–approved short-term and long-term medications and then off-label drugs that can also aid in healthy weight loss. Short-term options include phentermine, diethylpropion, phendimetrazine, and benzphetamine. Long-term options include orlistat, phentermine/topiramate ER, naltrexone HCl/bupropion HCl ER, and the three GLP-1 receptor agonist drugs, liraglutide, semaglutide, and tirzepatide.
The short-term medications are stimulants that increase satiety, but adverse effects can include tachycardia, hypertension, insomnia, dry mouth, constipation, and diarrhea.
These medications are contraindicated for anyone with uncontrolled hypertension, hyperthyroidism, cardiovascular disease, MAOI use, glaucoma, or history of substance use. The goal is a 5% weight loss in 3 months, and 3 months is the maximum prescribing term.
Then Dr. Finkle reviewed the side effects and contraindications for the oral long-term medications. Orlistat, which can aid in up to 5% weight loss, can result in oily stools and fecal incontinence and is contraindicated for people with chronic malabsorption or cholestasis.
Phentermine/topiramate ER, which can aid in up to 10% weight loss, can result in hypertension, paresthesia, or constipation, and is contraindicated for those with glaucoma, hyperthyroidism, and kidney stones. After the starting dose of 3.75 mg/23 mg, Dr. Finkle increases patients’ dose every 2 weeks, ”but if they’re not tolerating it, if they’re having significant side effects, or they’re losing weight, you do not increase the medication.”
Side effects of naltrexone HCl/bupropion HCl ER, which can lead to 5%-6% weight loss, can include hypertension, suicidal ideation, and glaucoma, and it’s contraindicated in those taking opioids or with a history of seizures or anorexia.
The GLP-1 Receptor Agonists
Next Dr. Finkle discussed the newest but most effective medications, the GLP-1 agonists liraglutide, semaglutide, and tirzepatide. The main contraindications for these drugs are a personal or family history of medullary thyroid cancer, multiple endocrine neoplasia type II syndrome, or any hypersensitivity to this drug class. The two main serious risks are pancreatitis — a 1% risk — and gallstones. Though Dr. Finkle included suicidal ideation as a potential risk of these drugs, the most recent evidence suggests there is no link between suicidal ideation and GLP-1 agonists. The most common side effects are nausea, vomiting, diarrhea, constipation, dyspepsia, and an increased heart rate, though these eventually resolve.
“We always start low with these medications,” Dr. Finkle said, and then titrate the dose up each week, “but if they are having awful side effects, just stay on that dose longer.”
The mechanisms of all three drugs for treating obesity are similar; they work to curb central satiety and slow gastric emptying, though they also have additional mechanisms with benefits for blood glucose levels and for the liver and heart.
- Liraglutide, the first of these drugs approved, is a daily subcutaneous injection that starts at a dose of 0.6 mg and goes up to 3 mg. Patients should lose 4% of weight in 16 weeks or else they are non-responders, Dr. Finkle said.
- Semaglutide, a GLP-1 agonist given as a weekly subcutaneous injection, starts at a dose of 0.25 mg and goes up to 2.4 mg; patients should expect a 5% weight loss in 16 weeks if they are responders. Long term, however, patients lose up to an average 15% of body weight with semaglutide; a third of patients lost more than 20% of body weight in clinical trials, compared with 7%-8% body weight loss with liraglutide. An additional benefit of semaglutide is a 20% reduction in risk of cardiovascular disease.
- Tirzepatide is a combined GLP-1 and GIP agonist, also delivered as a weekly subcutaneous injection, that should result in an estimated 5% weight loss in 16 weeks for responders. But tirzepatide is the most effective of the three, with 91% of patients losing at least 5% body weight and more than half of patients (56%) losing at least 20%.
The big drawbacks to the GLP-1 agonists, however, are their high cost, common lack of insurance coverage, and continued shortages. Dr. Finkle recommended using manufacturer coupons, comparison shopping on Good Rx, and appealing prior authorization requirements to help patients pay for the GLP-1 agonists.
“Drug availability is my second problem. There’s not enough drug,” she said, and her patients often have to call around to different pharmacies to find out which ones are carrying the drug and at what doses. She will sometimes switch their doses as needed based on availability.
It’s also important for physicians to be aware of guidance from the American Society of Anesthesiologists regarding GLP-1 agonist use prior to surgery because of their slowed gastric-emptying mechanism. To reduce the risk of aspiration, patients undergoing general anesthesia should not take liraglutide on the day of surgery, and semaglutide and tirzepatide should be held for 1 week prior to the procedure. New research in JAMA Surgery, however, suggests holding these medications for longer than a week may be wiser.
Getting Patients Started
All the short-term and long-term medications are contraindicated during pregnancy and breastfeeding, Dr. Finkle said. Animal studies with GLP-1 agonists suggest adverse fetal effects when used during pregnancy, but the limited data in human studies so far have not shown a risk of major malformations. Dr. Finkle said the recommendations for now are to stop all GLP-1 receptor agonist drugs 2 months before patients attempt to become pregnant and not to begin them again until after they are no longer breastfeeding.
Finally, Dr. Finkle reviewed off-label medications that can result in modest weight loss, including topiramate, phentermine (not to be used for longer than 12 weeks), bupropion, naltrexone, and metformin. Metformin is likely to result in only 2% weight loss, but it may enhance the effects of GLP-1s, she said.
For ob.gyns. who want to get their patients started on one of these medications, Dr. Finkle first recommends asking patients if it’s okay to discuss their weight. ”Studies show that if you just ask permission to discuss someone’s weight, they go on to lose weight and lose more than someone who has never been asked,” Dr. Finkle said. Then she takes a history.
”When I see a patient, I ask, ‘Tell me why you’re here today,’ ” Dr. Finkle said.
This gives me a lot of insight as to why they’re coming in and it helps me understand where they’re at in terms of other things, such as depression or anxiety with weight, and it helps me to tailor my treatment.”
A full medical history is important for learning about potential contraindications or picking medications that might help with other conditions, such as topiramate for migraines. Finally, Dr. Finkle advises a lab screening with a comprehensive metabolic panel, lipid panel, HbA1c, and vitamin D.
“The [comprehensive metabolic panel] allows me to know about creatinine and liver function,” she said. If these are elevated, she will still prescribe GLP-1s but will monitor the values more closely. “Then I discuss options with the patient. They may be eligible for bariatric surgery or medications. We talk about lifestyle behavioral management, and then I go through the medications and we set goals.”
Goals include nutrition and exercise; start modest and have them work their way up by doing activities they enjoy. In addition, patients taking GLP-1s need to eat enough protein — 80 to 100 grams a day, though she starts them at 60 grams — and do regular muscle strengthening since they can lose muscle mass.
Indications for referral to an obesity medicine specialist are a history of gastric bypass/sleeve surgery, having type 2 diabetes, having an eating disorder, or having failed one of these anti-obesity medications.
Finally, Dr. Finkle reviewed medications that can cause weight gain: medroxyprogesterone acetate for birth control; beta blockers for hypertension or migraine; the antidepressants amitriptyline, paroxetine, venlafaxine, and trazodone; the mood stabilizers gabapentin, lithium, valproate, and carbamazepine; and diphenhydramine and zolpidem for sleep.
No external funding was used for the talk. Dr. Finkle and Dr. Heyward had no disclosures.
FROM ACOG 2024
Recent Evidence for Home Phototherapy Benefits May Improve Access for Patients with Psoriasis
Supporters of home phototherapy for patients with plaque and guttate psoriasis had plenty to cheer about at the annual meeting of the American Academy of Dermatology (AAD) in March. There, Joel M. Gelfand, MD, professor of dermatology and epidemiology at the University of Pennsylvania in Philadelphia, presented results from the LITE study, a trial that tested the hypothesis that narrowband ultraviolet B phototherapy of psoriasis at home is noninferior to office treatment, based on outcomes that matter to patients, clinicians, and payers. While smaller studies have drawn similar conclusions,
The co-primary outcomes in the LITE study were a Physician’s Global Assessment (PGA) score of 0/1 (clear, almost clear) and a Dermatology Life Quality Index (DLQI) score of 5 or less (small, no effect on health-related quality of life).
Dr. Gelfand and colleagues at 42 sites in the United States enrolled 783 patients aged 12 years and older who had plaque or guttate psoriasis and were candidates for phototherapy at home or in an office setting. Following 12 weeks of treatment, 25.6% of patients in the office-based phototherapy group achieved a PGA score of 0/1 compared with 32.8% of patients in the home-based phototherapy group (P > .0001 for noninferiority, non-response imputation for missing data). Similarly, 33.6% of patients in the office-based phototherapy group achieved a DLQI score of 5 or less compared with 52.4% of patients in the home-based phototherapy group (P > .0001 for noninferiority, non-response imputation for missing data).

A Safe and Effective Option
“I think that it’s important for physicians, insurance companies, and patients with psoriasis to understand that this is a very safe and effective form of therapy,” Craig A. Elmets, MD, professor of dermatology at The University of Alabama at Birmingham, said in an interview. “For people who are not interested in systemic medications or who have contraindications to systemic medications, phototherapy would be ideal,” added Dr. Elmets, first author of the joint AAD–National Psoriasis Foundation (NPF) guidelines for the management and treatment of psoriasis with phototherapy, published in 2019.
Factors beyond efficacy support the role of home phototherapy, Dr. Gelfand said, including the fact that it costs 10-100 times less than biologics for psoriasis and that office-based phototherapy is not available in 90% of counties in the United States. However, insurance coverage of home phototherapy “is highly variable because until the LITE study, there was no large-scale US data to support its use,” he told this news organization.
“Also, insurance companies are broken up into two parts: Durable medical goods and the medical side such as pharmacy costs, and they are siloed. The durable medical goods side views phototherapy as expensive, while the pharmacy side views it as dirt cheap. This is part of the problem with our health system. A lot of things are siloed and don’t make any sense,” said Dr. Gelfand, director of the Psoriasis and Phototherapy Treatment Center at the University of Pennsylvania. By working with the NPF and payers, he added, “we’re hoping ... to transform the way insurance companies think about covering home phototherapy.”
In the meantime, he and Dr. Elmets shared practical ways to optimize access to home phototherapy for psoriasis patients:
Have the discussion. Patients “rarely bring this up as an option,” Dr. Elmets said, so the onus is on clinicians to talk about it. In his view, the ideal candidate “is averse to using systemic agents but whose disease is beyond the point where topical medicines alone will work. One of the advantages of phototherapy is that it doesn’t have immunosuppressive effects.”
Clinicians and patients can learn about the efficacy and safety of phototherapy for psoriasis, including home-based options, on the NPF’s web site and by reading the 2019 joint AAD-NPF guidelines.
Shared decision-making is key. “When a patient comes in, I’ll discuss what their treatment options are and [we] will decide upon a course of action based on their unique needs and preferences [and] if it’s medically appropriate, meaning they have the type of psoriasis likely to respond to phototherapy,” Dr. Gelfand said. A patient with psoriasis mainly on the fingernails or genitals “is not a good candidate for phototherapy. If it’s on the trunk or extremities, that patient would be a good candidate.”
Home phototherapy candidates also must be willing and able to operate a machine and have dedicated space in their dwelling for it (most units are about the size of a door). Patients also have to be reliable, follow directions, and come back in person for follow-up appointments “so we can assess their response to treatment and fine-tune things as necessary and make sure they’re not developing any skin damage,” Dr. Gelfand said.
Educate yourself about existing options. Home phototherapy units from manufacturers such as Daavlin, National Biological Corporation, and SolRx range between $1200 and $6000 in cost, Dr. Gelfand said. He and his colleagues used the Daavlin 7 series in the LITE study. That unit features an integrated dosimetry system that delivers the correct dose of energy based on parameters that the prescribing clinician recommends. Settings are based on the patient’s skin type and how much the prescriber wants to increase the dose for each treatment. “The machine does the rest,” he said. “It knows what dose to give, so they get the same dosing as they would in an office situation.”
Smaller home-based phototherapy units designed to treat the hands and feet are available. So are handheld units to treat the scalp. “These can be a nice option for patients who have a few spots, but if the disease is moderate to severe, then it’s going to be pretty laborious to [use them],” Dr. Elmets said.
Remember that phototherapy is not a cure-all. According to the joint AAD-NPF guidelines, most phototherapy regimens require treatments two to three times per week for 10-14 weeks. Once patients achieve their home phototherapy treatment goal, Dr. Elmets often recommends treatments one to two times per week for maintenance.
“Patients with psoriasis have a lifetime condition,” he noted. “There are certainly cases where people have gone on phototherapy, cleared, and then stopped for a period of time. If they flare up, they can always go back to phototherapy. Usually, people who are on phototherapy use some type of topical agents to touch up areas that are resistant.”
Expect pushback from insurers on coverage. While Medicare and some integrated health plans cover home phototherapy, expect to spend time writing letters or placing phone calls to insurance companies to convince them why they should cover home phototherapy for candidate psoriasis patients. “Usually there’s a lot of letter writing and a long delay in getting approval,” Dr. Elmets said.
Dr. Elmets and Dr. Gelfand reported no relevant financial relationships. The LITE study was funded by the Patient-Centered Outcomes Research Institute. Research partners included the National Psoriasis Foundation and Daavlin, which provided the home phototherapy machines and covered the cost of shipping the devices.
A version of this article appeared on Medscape.com.
Supporters of home phototherapy for patients with plaque and guttate psoriasis had plenty to cheer about at the annual meeting of the American Academy of Dermatology (AAD) in March. There, Joel M. Gelfand, MD, professor of dermatology and epidemiology at the University of Pennsylvania in Philadelphia, presented results from the LITE study, a trial that tested the hypothesis that narrowband ultraviolet B phototherapy of psoriasis at home is noninferior to office treatment, based on outcomes that matter to patients, clinicians, and payers. While smaller studies have drawn similar conclusions,
The co-primary outcomes in the LITE study were a Physician’s Global Assessment (PGA) score of 0/1 (clear, almost clear) and a Dermatology Life Quality Index (DLQI) score of 5 or less (small, no effect on health-related quality of life).
Dr. Gelfand and colleagues at 42 sites in the United States enrolled 783 patients aged 12 years and older who had plaque or guttate psoriasis and were candidates for phototherapy at home or in an office setting. Following 12 weeks of treatment, 25.6% of patients in the office-based phototherapy group achieved a PGA score of 0/1 compared with 32.8% of patients in the home-based phototherapy group (P > .0001 for noninferiority, non-response imputation for missing data). Similarly, 33.6% of patients in the office-based phototherapy group achieved a DLQI score of 5 or less compared with 52.4% of patients in the home-based phototherapy group (P > .0001 for noninferiority, non-response imputation for missing data).
A Safe and Effective Option
“I think that it’s important for physicians, insurance companies, and patients with psoriasis to understand that this is a very safe and effective form of therapy,” Craig A. Elmets, MD, professor of dermatology at The University of Alabama at Birmingham, said in an interview. “For people who are not interested in systemic medications or who have contraindications to systemic medications, phototherapy would be ideal,” added Dr. Elmets, first author of the joint AAD–National Psoriasis Foundation (NPF) guidelines for the management and treatment of psoriasis with phototherapy, published in 2019.
Factors beyond efficacy support the role of home phototherapy, Dr. Gelfand said, including the fact that it costs 10-100 times less than biologics for psoriasis and that office-based phototherapy is not available in 90% of counties in the United States. However, insurance coverage of home phototherapy “is highly variable because until the LITE study, there was no large-scale US data to support its use,” he told this news organization.
“Also, insurance companies are broken up into two parts: Durable medical goods and the medical side such as pharmacy costs, and they are siloed. The durable medical goods side views phototherapy as expensive, while the pharmacy side views it as dirt cheap. This is part of the problem with our health system. A lot of things are siloed and don’t make any sense,” said Dr. Gelfand, director of the Psoriasis and Phototherapy Treatment Center at the University of Pennsylvania. By working with the NPF and payers, he added, “we’re hoping ... to transform the way insurance companies think about covering home phototherapy.”
In the meantime, he and Dr. Elmets shared practical ways to optimize access to home phototherapy for psoriasis patients:
Have the discussion. Patients “rarely bring this up as an option,” Dr. Elmets said, so the onus is on clinicians to talk about it. In his view, the ideal candidate “is averse to using systemic agents but whose disease is beyond the point where topical medicines alone will work. One of the advantages of phototherapy is that it doesn’t have immunosuppressive effects.”
Clinicians and patients can learn about the efficacy and safety of phototherapy for psoriasis, including home-based options, on the NPF’s web site and by reading the 2019 joint AAD-NPF guidelines.
Shared decision-making is key. “When a patient comes in, I’ll discuss what their treatment options are and [we] will decide upon a course of action based on their unique needs and preferences [and] if it’s medically appropriate, meaning they have the type of psoriasis likely to respond to phototherapy,” Dr. Gelfand said. A patient with psoriasis mainly on the fingernails or genitals “is not a good candidate for phototherapy. If it’s on the trunk or extremities, that patient would be a good candidate.”
Home phototherapy candidates also must be willing and able to operate a machine and have dedicated space in their dwelling for it (most units are about the size of a door). Patients also have to be reliable, follow directions, and come back in person for follow-up appointments “so we can assess their response to treatment and fine-tune things as necessary and make sure they’re not developing any skin damage,” Dr. Gelfand said.
Educate yourself about existing options. Home phototherapy units from manufacturers such as Daavlin, National Biological Corporation, and SolRx range between $1200 and $6000 in cost, Dr. Gelfand said. He and his colleagues used the Daavlin 7 series in the LITE study. That unit features an integrated dosimetry system that delivers the correct dose of energy based on parameters that the prescribing clinician recommends. Settings are based on the patient’s skin type and how much the prescriber wants to increase the dose for each treatment. “The machine does the rest,” he said. “It knows what dose to give, so they get the same dosing as they would in an office situation.”
Smaller home-based phototherapy units designed to treat the hands and feet are available. So are handheld units to treat the scalp. “These can be a nice option for patients who have a few spots, but if the disease is moderate to severe, then it’s going to be pretty laborious to [use them],” Dr. Elmets said.
Remember that phototherapy is not a cure-all. According to the joint AAD-NPF guidelines, most phototherapy regimens require treatments two to three times per week for 10-14 weeks. Once patients achieve their home phototherapy treatment goal, Dr. Elmets often recommends treatments one to two times per week for maintenance.
“Patients with psoriasis have a lifetime condition,” he noted. “There are certainly cases where people have gone on phototherapy, cleared, and then stopped for a period of time. If they flare up, they can always go back to phototherapy. Usually, people who are on phototherapy use some type of topical agents to touch up areas that are resistant.”
Expect pushback from insurers on coverage. While Medicare and some integrated health plans cover home phototherapy, expect to spend time writing letters or placing phone calls to insurance companies to convince them why they should cover home phototherapy for candidate psoriasis patients. “Usually there’s a lot of letter writing and a long delay in getting approval,” Dr. Elmets said.
Dr. Elmets and Dr. Gelfand reported no relevant financial relationships. The LITE study was funded by the Patient-Centered Outcomes Research Institute. Research partners included the National Psoriasis Foundation and Daavlin, which provided the home phototherapy machines and covered the cost of shipping the devices.
A version of this article appeared on Medscape.com.
Supporters of home phototherapy for patients with plaque and guttate psoriasis had plenty to cheer about at the annual meeting of the American Academy of Dermatology (AAD) in March. There, Joel M. Gelfand, MD, professor of dermatology and epidemiology at the University of Pennsylvania in Philadelphia, presented results from the LITE study, a trial that tested the hypothesis that narrowband ultraviolet B phototherapy of psoriasis at home is noninferior to office treatment, based on outcomes that matter to patients, clinicians, and payers. While smaller studies have drawn similar conclusions,
The co-primary outcomes in the LITE study were a Physician’s Global Assessment (PGA) score of 0/1 (clear, almost clear) and a Dermatology Life Quality Index (DLQI) score of 5 or less (small, no effect on health-related quality of life).
Dr. Gelfand and colleagues at 42 sites in the United States enrolled 783 patients aged 12 years and older who had plaque or guttate psoriasis and were candidates for phototherapy at home or in an office setting. Following 12 weeks of treatment, 25.6% of patients in the office-based phototherapy group achieved a PGA score of 0/1 compared with 32.8% of patients in the home-based phototherapy group (P > .0001 for noninferiority, non-response imputation for missing data). Similarly, 33.6% of patients in the office-based phototherapy group achieved a DLQI score of 5 or less compared with 52.4% of patients in the home-based phototherapy group (P > .0001 for noninferiority, non-response imputation for missing data).
A Safe and Effective Option
“I think that it’s important for physicians, insurance companies, and patients with psoriasis to understand that this is a very safe and effective form of therapy,” Craig A. Elmets, MD, professor of dermatology at The University of Alabama at Birmingham, said in an interview. “For people who are not interested in systemic medications or who have contraindications to systemic medications, phototherapy would be ideal,” added Dr. Elmets, first author of the joint AAD–National Psoriasis Foundation (NPF) guidelines for the management and treatment of psoriasis with phototherapy, published in 2019.
Factors beyond efficacy support the role of home phototherapy, Dr. Gelfand said, including the fact that it costs 10-100 times less than biologics for psoriasis and that office-based phototherapy is not available in 90% of counties in the United States. However, insurance coverage of home phototherapy “is highly variable because until the LITE study, there was no large-scale US data to support its use,” he told this news organization.
“Also, insurance companies are broken up into two parts: Durable medical goods and the medical side such as pharmacy costs, and they are siloed. The durable medical goods side views phototherapy as expensive, while the pharmacy side views it as dirt cheap. This is part of the problem with our health system. A lot of things are siloed and don’t make any sense,” said Dr. Gelfand, director of the Psoriasis and Phototherapy Treatment Center at the University of Pennsylvania. By working with the NPF and payers, he added, “we’re hoping ... to transform the way insurance companies think about covering home phototherapy.”
In the meantime, he and Dr. Elmets shared practical ways to optimize access to home phototherapy for psoriasis patients:
Have the discussion. Patients “rarely bring this up as an option,” Dr. Elmets said, so the onus is on clinicians to talk about it. In his view, the ideal candidate “is averse to using systemic agents but whose disease is beyond the point where topical medicines alone will work. One of the advantages of phototherapy is that it doesn’t have immunosuppressive effects.”
Clinicians and patients can learn about the efficacy and safety of phototherapy for psoriasis, including home-based options, on the NPF’s web site and by reading the 2019 joint AAD-NPF guidelines.
Shared decision-making is key. “When a patient comes in, I’ll discuss what their treatment options are and [we] will decide upon a course of action based on their unique needs and preferences [and] if it’s medically appropriate, meaning they have the type of psoriasis likely to respond to phototherapy,” Dr. Gelfand said. A patient with psoriasis mainly on the fingernails or genitals “is not a good candidate for phototherapy. If it’s on the trunk or extremities, that patient would be a good candidate.”
Home phototherapy candidates also must be willing and able to operate a machine and have dedicated space in their dwelling for it (most units are about the size of a door). Patients also have to be reliable, follow directions, and come back in person for follow-up appointments “so we can assess their response to treatment and fine-tune things as necessary and make sure they’re not developing any skin damage,” Dr. Gelfand said.
Educate yourself about existing options. Home phototherapy units from manufacturers such as Daavlin, National Biological Corporation, and SolRx range between $1200 and $6000 in cost, Dr. Gelfand said. He and his colleagues used the Daavlin 7 series in the LITE study. That unit features an integrated dosimetry system that delivers the correct dose of energy based on parameters that the prescribing clinician recommends. Settings are based on the patient’s skin type and how much the prescriber wants to increase the dose for each treatment. “The machine does the rest,” he said. “It knows what dose to give, so they get the same dosing as they would in an office situation.”
Smaller home-based phototherapy units designed to treat the hands and feet are available. So are handheld units to treat the scalp. “These can be a nice option for patients who have a few spots, but if the disease is moderate to severe, then it’s going to be pretty laborious to [use them],” Dr. Elmets said.
Remember that phototherapy is not a cure-all. According to the joint AAD-NPF guidelines, most phototherapy regimens require treatments two to three times per week for 10-14 weeks. Once patients achieve their home phototherapy treatment goal, Dr. Elmets often recommends treatments one to two times per week for maintenance.
“Patients with psoriasis have a lifetime condition,” he noted. “There are certainly cases where people have gone on phototherapy, cleared, and then stopped for a period of time. If they flare up, they can always go back to phototherapy. Usually, people who are on phototherapy use some type of topical agents to touch up areas that are resistant.”
Expect pushback from insurers on coverage. While Medicare and some integrated health plans cover home phototherapy, expect to spend time writing letters or placing phone calls to insurance companies to convince them why they should cover home phototherapy for candidate psoriasis patients. “Usually there’s a lot of letter writing and a long delay in getting approval,” Dr. Elmets said.
Dr. Elmets and Dr. Gelfand reported no relevant financial relationships. The LITE study was funded by the Patient-Centered Outcomes Research Institute. Research partners included the National Psoriasis Foundation and Daavlin, which provided the home phototherapy machines and covered the cost of shipping the devices.
A version of this article appeared on Medscape.com.