User login
Diagnosing Mild Hidradenitis Suppurativa: Early Stage Can Mimic Other Diseases
, such as an infection, folliculitis, and acne.
According to 2019 guidelines from the United States and Canadian hidradenitis suppurativa foundations, the diagnostic criteria for HS in general are the presence of typical lesions such as abscesses, nodules, and tunnels in classic locations such as underarms, groins, and buttocks that recur over the course of at least 6 months. “There is no need for additional testing or imaging to make the diagnosis,” said Dr. Sayed, co-chair of the 2019 guidelines work group, who sees patients at the HS and Follicular Disorders Clinic at the University of North Carolina, Chapel Hill. “In many ways, the diagnosis should be very simple since the presentation is classic in most cases, though it can be confusing in the first 6 months or so.”

Persistence, Recurrence Major Clues
Prior to being diagnosed with Hurley stage I HS — characterized by recurrent nodules and abscesses with minimal scars, according to the guidelines — most people figure they’ve been getting recurrent Staphylococcus aureus infections or are having trouble with ingrown hairs from shaving, he continued. They may also say they get “boils” without an understanding of what has been causing them.
“Early HS can mimic an intense folliculitis or furuncles that can sometimes be caused by Staphylococcus infections, but the history of persistence or recurrence for months, despite treatment that should cover something like a Staph infection is a major clue,” Dr. Sayed said. “Thanks to improved resources on the internet, more patients, compared to several years ago, come in asking about HS after they’ve done their own research. As public awareness improves, hopefully this trend will grow, and patients will be diagnosed and treated earlier.” Family history is also a strong predictor of HS, since about half of patients have first-degree relatives who have a history of HS, he noted.

Clinicians can use the Hurley staging system to characterize the extent of disease and the Dermatology Life Quality Index to measure the impact of HS on quality of life. “We perform these assessments in our specialty clinic at each visit, but they are not necessary for diagnosis,” Dr. Sayed told this news organization.
The ‘2-2-6 Rule’
When she sees a patient who might have HS, Jennifer L. Hsiao, MD, a dermatologist who directs the HS clinic at the University of Southern California, Los Angeles, follows the “2-2-6 rule,” which involves asking patients if they have had 2 episodes of 2 or more abscesses in 6 months. “If the patient answers yes, there’s a high likelihood that person has HS,” she said.
Hurley stage I HS is defined as nodules and abscesses without sinus tracts (tunnels) or scarring. But in Dr. Hsiao’s opinion, the Hurley staging system “is not the best way to characterize disease activity” because some patients meet criteria for Hurley stage I disease, meaning they do not have any scars or sinus tracts/tunnels, “but they have high disease activity with several inflammatory nodules and large painful abscesses that are limiting their quality of life and ability to function.”

Most cases of early-stage HS can be diagnosed in a single clinic visit, but some patients may present with a limited history of disease. For example, they may report having only had one episode of an axillary abscess or one episode of a few folliculitis-like papules in the groin. “In the absence of other physical exam findings suggestive of HS, such as open or double-headed comedones in flexural regions, I tell the patient that it is too early to call their condition HS, and I recommend that if they have another episode to call the office for an appointment for evaluation,” Dr. Hsiao said in an interview.
“What sets HS apart from an isolated incidence of a Staphylococcus aureus furuncle is the history of recurrence,” she added. To better characterize HS disease severity, she uses the six-point HS Physician Global Assessment score, a scale from 0 to 5, which classifies a patient as having moderate HS if they have five or more inflammatory nodules, or one abscess and one or more inflammatory nodule(s), without the requirement of demonstrating a scar or tunnel on a physical exam.
To help guide management decisions, Dr. Hsiao also considers asking patients with early-stage HS the following questions:
- Do you have a primary care provider (PCP)? PCPs are important care partners for patients with HS doctor to help screen for the comorbidities associated with the condition.
- What seems to make your HS worse? This can help identify potential triggers to avoid.
- What other medical conditions do you have?
- How would you describe the impact HS has on your quality of life?
- For women: Does your HS get worse around your period? “This can help to identify a potential hormonal trigger,” she said. “If the patient answers ‘yes,’ I would strongly consider a combined oral contraceptive pill and/or spironolactone as part of the patient’s treatment regimen.”
‘Window of Opportunity’ to Intervene
According to Dr. Hsiao, there has been a paradigm shift in the approach to HS management that emphasizes a “window of opportunity,” where earlier initiation of appropriate long-term immunomodulator therapy is recommended to try to mitigate disease progression. The development of tunnels and scars is a telltale sign that permanent tissue destruction is occurring, and the patient’s HS is no longer mild.
Ideally, a conversation about adalimumab, a tumor necrosis factor inhibitor, and secukinumab, an interleukin-17A antagonist (the two currently Food and Drug Administration–approved medications for HS, for moderate to severe disease/Hurley stage II/III) will have already been started with patients prior to development of a high tunnel or scar burden, signs of later-stage disease.
“Medications like this have the potential to slow and prevent that progression and reduce the surgical burden patients face over time, which is a major priority,” Dr. Sayed said. He noted that while comfort level with managing HS can vary among clinicians, “I’d encourage dermatologists to stay engaged with these patients because our training in the medical and surgical management of complex diseases like this is unmatched among other specialties,” he said. “Education of colleagues in other specialties should also be a big priority, especially for those in urgent care, emergency medicine, surgery, and ob.gyn. who often encounter these patients and may be less familiar” with HS.
Besides the North American clinical management guidelines for HS, which are expected to be updated in the next 18-24 months, as well as comorbidity screening recommendations for HS published in 2022, another resource Dr. Sayed and Dr. Hsiao recommend is the HS Foundation website, which features a link to Continuing Medical Education video lectures. The foundation also hosts an annual Symposium on HS Advances. This year’s event is scheduled in November in Austin, Texas.
Dr. Sayed disclosed that he is secretary of the HS Foundation and a member of the European HS Foundation. He has served as a consultant for AbbVie, Alumis, AstraZeneca, Incyte, InflaRx, Novartis, Sanofi, Sonoma Biotherapeutics, and UCB; as a speaker for AbbVie, Novartis, and UCB; and as an investigator for Chemocentryx, Incyte, InflaRx, Novartis, and UCB. Dr. Hsiao disclosed that she is a member of the board of directors for the HS Foundation and has served as a consultant for AbbVie, Aclaris, Boehringer Ingelheim, Incyte, Novartis, and UCB; as a speaker for AbbVie, Novartis, Sanofi Regeneron, and UCB; and as an investigator for Amgen, Boehringer Ingelheim, and Incyte.
A version of this article first appeared on Medscape.com.
, such as an infection, folliculitis, and acne.
According to 2019 guidelines from the United States and Canadian hidradenitis suppurativa foundations, the diagnostic criteria for HS in general are the presence of typical lesions such as abscesses, nodules, and tunnels in classic locations such as underarms, groins, and buttocks that recur over the course of at least 6 months. “There is no need for additional testing or imaging to make the diagnosis,” said Dr. Sayed, co-chair of the 2019 guidelines work group, who sees patients at the HS and Follicular Disorders Clinic at the University of North Carolina, Chapel Hill. “In many ways, the diagnosis should be very simple since the presentation is classic in most cases, though it can be confusing in the first 6 months or so.”
Persistence, Recurrence Major Clues
Prior to being diagnosed with Hurley stage I HS — characterized by recurrent nodules and abscesses with minimal scars, according to the guidelines — most people figure they’ve been getting recurrent Staphylococcus aureus infections or are having trouble with ingrown hairs from shaving, he continued. They may also say they get “boils” without an understanding of what has been causing them.
“Early HS can mimic an intense folliculitis or furuncles that can sometimes be caused by Staphylococcus infections, but the history of persistence or recurrence for months, despite treatment that should cover something like a Staph infection is a major clue,” Dr. Sayed said. “Thanks to improved resources on the internet, more patients, compared to several years ago, come in asking about HS after they’ve done their own research. As public awareness improves, hopefully this trend will grow, and patients will be diagnosed and treated earlier.” Family history is also a strong predictor of HS, since about half of patients have first-degree relatives who have a history of HS, he noted.
Clinicians can use the Hurley staging system to characterize the extent of disease and the Dermatology Life Quality Index to measure the impact of HS on quality of life. “We perform these assessments in our specialty clinic at each visit, but they are not necessary for diagnosis,” Dr. Sayed told this news organization.
The ‘2-2-6 Rule’
When she sees a patient who might have HS, Jennifer L. Hsiao, MD, a dermatologist who directs the HS clinic at the University of Southern California, Los Angeles, follows the “2-2-6 rule,” which involves asking patients if they have had 2 episodes of 2 or more abscesses in 6 months. “If the patient answers yes, there’s a high likelihood that person has HS,” she said.
Hurley stage I HS is defined as nodules and abscesses without sinus tracts (tunnels) or scarring. But in Dr. Hsiao’s opinion, the Hurley staging system “is not the best way to characterize disease activity” because some patients meet criteria for Hurley stage I disease, meaning they do not have any scars or sinus tracts/tunnels, “but they have high disease activity with several inflammatory nodules and large painful abscesses that are limiting their quality of life and ability to function.”
Most cases of early-stage HS can be diagnosed in a single clinic visit, but some patients may present with a limited history of disease. For example, they may report having only had one episode of an axillary abscess or one episode of a few folliculitis-like papules in the groin. “In the absence of other physical exam findings suggestive of HS, such as open or double-headed comedones in flexural regions, I tell the patient that it is too early to call their condition HS, and I recommend that if they have another episode to call the office for an appointment for evaluation,” Dr. Hsiao said in an interview.
“What sets HS apart from an isolated incidence of a Staphylococcus aureus furuncle is the history of recurrence,” she added. To better characterize HS disease severity, she uses the six-point HS Physician Global Assessment score, a scale from 0 to 5, which classifies a patient as having moderate HS if they have five or more inflammatory nodules, or one abscess and one or more inflammatory nodule(s), without the requirement of demonstrating a scar or tunnel on a physical exam.
To help guide management decisions, Dr. Hsiao also considers asking patients with early-stage HS the following questions:
- Do you have a primary care provider (PCP)? PCPs are important care partners for patients with HS doctor to help screen for the comorbidities associated with the condition.
- What seems to make your HS worse? This can help identify potential triggers to avoid.
- What other medical conditions do you have?
- How would you describe the impact HS has on your quality of life?
- For women: Does your HS get worse around your period? “This can help to identify a potential hormonal trigger,” she said. “If the patient answers ‘yes,’ I would strongly consider a combined oral contraceptive pill and/or spironolactone as part of the patient’s treatment regimen.”
‘Window of Opportunity’ to Intervene
According to Dr. Hsiao, there has been a paradigm shift in the approach to HS management that emphasizes a “window of opportunity,” where earlier initiation of appropriate long-term immunomodulator therapy is recommended to try to mitigate disease progression. The development of tunnels and scars is a telltale sign that permanent tissue destruction is occurring, and the patient’s HS is no longer mild.
Ideally, a conversation about adalimumab, a tumor necrosis factor inhibitor, and secukinumab, an interleukin-17A antagonist (the two currently Food and Drug Administration–approved medications for HS, for moderate to severe disease/Hurley stage II/III) will have already been started with patients prior to development of a high tunnel or scar burden, signs of later-stage disease.
“Medications like this have the potential to slow and prevent that progression and reduce the surgical burden patients face over time, which is a major priority,” Dr. Sayed said. He noted that while comfort level with managing HS can vary among clinicians, “I’d encourage dermatologists to stay engaged with these patients because our training in the medical and surgical management of complex diseases like this is unmatched among other specialties,” he said. “Education of colleagues in other specialties should also be a big priority, especially for those in urgent care, emergency medicine, surgery, and ob.gyn. who often encounter these patients and may be less familiar” with HS.
Besides the North American clinical management guidelines for HS, which are expected to be updated in the next 18-24 months, as well as comorbidity screening recommendations for HS published in 2022, another resource Dr. Sayed and Dr. Hsiao recommend is the HS Foundation website, which features a link to Continuing Medical Education video lectures. The foundation also hosts an annual Symposium on HS Advances. This year’s event is scheduled in November in Austin, Texas.
Dr. Sayed disclosed that he is secretary of the HS Foundation and a member of the European HS Foundation. He has served as a consultant for AbbVie, Alumis, AstraZeneca, Incyte, InflaRx, Novartis, Sanofi, Sonoma Biotherapeutics, and UCB; as a speaker for AbbVie, Novartis, and UCB; and as an investigator for Chemocentryx, Incyte, InflaRx, Novartis, and UCB. Dr. Hsiao disclosed that she is a member of the board of directors for the HS Foundation and has served as a consultant for AbbVie, Aclaris, Boehringer Ingelheim, Incyte, Novartis, and UCB; as a speaker for AbbVie, Novartis, Sanofi Regeneron, and UCB; and as an investigator for Amgen, Boehringer Ingelheim, and Incyte.
A version of this article first appeared on Medscape.com.
, such as an infection, folliculitis, and acne.
According to 2019 guidelines from the United States and Canadian hidradenitis suppurativa foundations, the diagnostic criteria for HS in general are the presence of typical lesions such as abscesses, nodules, and tunnels in classic locations such as underarms, groins, and buttocks that recur over the course of at least 6 months. “There is no need for additional testing or imaging to make the diagnosis,” said Dr. Sayed, co-chair of the 2019 guidelines work group, who sees patients at the HS and Follicular Disorders Clinic at the University of North Carolina, Chapel Hill. “In many ways, the diagnosis should be very simple since the presentation is classic in most cases, though it can be confusing in the first 6 months or so.”
Persistence, Recurrence Major Clues
Prior to being diagnosed with Hurley stage I HS — characterized by recurrent nodules and abscesses with minimal scars, according to the guidelines — most people figure they’ve been getting recurrent Staphylococcus aureus infections or are having trouble with ingrown hairs from shaving, he continued. They may also say they get “boils” without an understanding of what has been causing them.
“Early HS can mimic an intense folliculitis or furuncles that can sometimes be caused by Staphylococcus infections, but the history of persistence or recurrence for months, despite treatment that should cover something like a Staph infection is a major clue,” Dr. Sayed said. “Thanks to improved resources on the internet, more patients, compared to several years ago, come in asking about HS after they’ve done their own research. As public awareness improves, hopefully this trend will grow, and patients will be diagnosed and treated earlier.” Family history is also a strong predictor of HS, since about half of patients have first-degree relatives who have a history of HS, he noted.
Clinicians can use the Hurley staging system to characterize the extent of disease and the Dermatology Life Quality Index to measure the impact of HS on quality of life. “We perform these assessments in our specialty clinic at each visit, but they are not necessary for diagnosis,” Dr. Sayed told this news organization.
The ‘2-2-6 Rule’
When she sees a patient who might have HS, Jennifer L. Hsiao, MD, a dermatologist who directs the HS clinic at the University of Southern California, Los Angeles, follows the “2-2-6 rule,” which involves asking patients if they have had 2 episodes of 2 or more abscesses in 6 months. “If the patient answers yes, there’s a high likelihood that person has HS,” she said.
Hurley stage I HS is defined as nodules and abscesses without sinus tracts (tunnels) or scarring. But in Dr. Hsiao’s opinion, the Hurley staging system “is not the best way to characterize disease activity” because some patients meet criteria for Hurley stage I disease, meaning they do not have any scars or sinus tracts/tunnels, “but they have high disease activity with several inflammatory nodules and large painful abscesses that are limiting their quality of life and ability to function.”
Most cases of early-stage HS can be diagnosed in a single clinic visit, but some patients may present with a limited history of disease. For example, they may report having only had one episode of an axillary abscess or one episode of a few folliculitis-like papules in the groin. “In the absence of other physical exam findings suggestive of HS, such as open or double-headed comedones in flexural regions, I tell the patient that it is too early to call their condition HS, and I recommend that if they have another episode to call the office for an appointment for evaluation,” Dr. Hsiao said in an interview.
“What sets HS apart from an isolated incidence of a Staphylococcus aureus furuncle is the history of recurrence,” she added. To better characterize HS disease severity, she uses the six-point HS Physician Global Assessment score, a scale from 0 to 5, which classifies a patient as having moderate HS if they have five or more inflammatory nodules, or one abscess and one or more inflammatory nodule(s), without the requirement of demonstrating a scar or tunnel on a physical exam.
To help guide management decisions, Dr. Hsiao also considers asking patients with early-stage HS the following questions:
- Do you have a primary care provider (PCP)? PCPs are important care partners for patients with HS doctor to help screen for the comorbidities associated with the condition.
- What seems to make your HS worse? This can help identify potential triggers to avoid.
- What other medical conditions do you have?
- How would you describe the impact HS has on your quality of life?
- For women: Does your HS get worse around your period? “This can help to identify a potential hormonal trigger,” she said. “If the patient answers ‘yes,’ I would strongly consider a combined oral contraceptive pill and/or spironolactone as part of the patient’s treatment regimen.”
‘Window of Opportunity’ to Intervene
According to Dr. Hsiao, there has been a paradigm shift in the approach to HS management that emphasizes a “window of opportunity,” where earlier initiation of appropriate long-term immunomodulator therapy is recommended to try to mitigate disease progression. The development of tunnels and scars is a telltale sign that permanent tissue destruction is occurring, and the patient’s HS is no longer mild.
Ideally, a conversation about adalimumab, a tumor necrosis factor inhibitor, and secukinumab, an interleukin-17A antagonist (the two currently Food and Drug Administration–approved medications for HS, for moderate to severe disease/Hurley stage II/III) will have already been started with patients prior to development of a high tunnel or scar burden, signs of later-stage disease.
“Medications like this have the potential to slow and prevent that progression and reduce the surgical burden patients face over time, which is a major priority,” Dr. Sayed said. He noted that while comfort level with managing HS can vary among clinicians, “I’d encourage dermatologists to stay engaged with these patients because our training in the medical and surgical management of complex diseases like this is unmatched among other specialties,” he said. “Education of colleagues in other specialties should also be a big priority, especially for those in urgent care, emergency medicine, surgery, and ob.gyn. who often encounter these patients and may be less familiar” with HS.
Besides the North American clinical management guidelines for HS, which are expected to be updated in the next 18-24 months, as well as comorbidity screening recommendations for HS published in 2022, another resource Dr. Sayed and Dr. Hsiao recommend is the HS Foundation website, which features a link to Continuing Medical Education video lectures. The foundation also hosts an annual Symposium on HS Advances. This year’s event is scheduled in November in Austin, Texas.
Dr. Sayed disclosed that he is secretary of the HS Foundation and a member of the European HS Foundation. He has served as a consultant for AbbVie, Alumis, AstraZeneca, Incyte, InflaRx, Novartis, Sanofi, Sonoma Biotherapeutics, and UCB; as a speaker for AbbVie, Novartis, and UCB; and as an investigator for Chemocentryx, Incyte, InflaRx, Novartis, and UCB. Dr. Hsiao disclosed that she is a member of the board of directors for the HS Foundation and has served as a consultant for AbbVie, Aclaris, Boehringer Ingelheim, Incyte, Novartis, and UCB; as a speaker for AbbVie, Novartis, Sanofi Regeneron, and UCB; and as an investigator for Amgen, Boehringer Ingelheim, and Incyte.
A version of this article first appeared on Medscape.com.
The Lure of Specialty Medicine Pulls Nurse Practitioners From Primary Care
For many patients, seeing a nurse practitioner has become a routine part of primary care, in which these “NPs” often perform the same tasks that patients have relied on doctors for.
But NPs in specialty care? That’s not routine, at least not yet. Increasingly, though, nurse practitioners and physician assistants are joining cardiology, dermatology, and other specialty practices, broadening their skills and increasing their income.
This development worries some people who track the health workforce, because current trends suggest primary care, which has counted on nurse practitioners to backstop physician shortages, soon might not be able to rely on them to the same extent.
“They’re succumbing to the same challenges that we have with physicians,” said Atul Grover, MD, PhD, executive director of the Research and Action Institute at the Association of American Medical Colleges. The rates NPs can command in a specialty practice “are quite a bit higher” than practice salaries in primary care, he said.
When nurse practitioner programs began to proliferate in the 1970s, “at first it looked great, producing all these nurse practitioners that go to work with primary care physicians,” said Yalda Jabbarpour, MD, director of the American Academy of Family Physicians’ Robert Graham Center for Policy Studies. “But now only 30% are going into primary care.”
Dr. Jabbarpour was referring to the 2024 primary care scorecard by the Milbank Memorial Fund, which found that from 2016 to 2021 the proportion of nurse practitioners who worked in primary care practices hovered between 32% and 34%, even though their numbers grew rapidly. The proportion of physician assistants, also known as physician associates, in primary care ranged from 27% to 30%, the study found.
Both nurse practitioners and physician assistants are advanced practice clinicians who, in addition to graduate degrees, must complete distinct education, training, and certification steps. NPs can practice without a doctor’s supervision in more than two dozen states, while PAs have similar independence in only a handful of states.
About 88% of nurse practitioners are certified in an area of primary care, according to the American Association of Nurse Practitioners. But it is difficult to track exactly how many work in primary care or in specialty practices. Unlike physicians, they’re generally not required to be endorsed by a national standard-setting body to practice in specialties like oncology or cardiology, for example. The AANP declined to answer questions about its annual workforce survey or the extent to which primary care NPs are moving toward specialties.
Though data tracking the change is sparse, specialty practices are adding these advanced practice clinicians at almost the same rate as primary care practices, according to frequently cited research published in 2018.
The clearest evidence of the shift: From 2008 to 2016, there was a 22% increase in the number of specialty practices that employed nurse practitioners and physician assistants, according to that study. The increase in the number of primary care practices that employed these professionals was 24%.
Once more, the most recent projections by the Association of American Medical Colleges predict a dearth of at least 20,200 primary care physicians by 2036. There will also be a shortfall of non-primary care specialists, including a deficiency of at least 10,100 surgical physicians and up to 25,000 physicians in other specialties.
When it comes to the actual work performed, the lines between primary and specialty care are often blurred, said Candice Chen, MD, MPH, associate professor of health policy and management at George Washington University.
“You might be a nurse practitioner working in a gastroenterology clinic or cardiology clinic, but the scope of what you do is starting to overlap with primary care,” she said.
Nurse practitioners’ salaries vary widely by location, type of facility, and experience. Still, according to data from health care recruiter AMN Healthcare Physician Solutions, formerly known as Merritt Hawkins, the total annual average starting compensation, including signing bonus, for nurse practitioners and physician assistants in specialty practice was $172,544 in the year that ended March 31, slightly higher than the $166,544 for those in primary care.
According to forecasts from the federal Bureau of Labor Statistics, nurse practitioner jobs will increase faster than jobs in almost any other occupation in the decade leading up to 2032, growing by 123,600 jobs or 45%. (Wind turbine service technician is the only other occupation projected to grow as fast.) The growth rate for physician assistants is also much faster than average, at 27%. There are more than twice as many nurse practitioners as physician assistants, however: 323,900 versus 148,000, in 2022.
To Dr. Grover of the AAMC, numbers like this signal that there will probably be enough NPs, PAs, and physicians to meet primary care needs. At the same time, “expect more NPs and PAs to also flow out into other specialties,” he said.
When Pamela Ograbisz started working as a registered nurse 27 years ago, she worked in a cardiothoracic intensive care unit. After she became a family nurse practitioner a few years later, she found a job with a similar specialty practice, which trained her to take on a bigger role, first running their outpatient clinic, then working on the floor, and later in the intensive care unit.
If nurse practitioners want to specialize, often “the doctors mentor them just like they would with a physician residency,” said Ms. Ograbisz, now vice president of clinical operations at temporary placement recruiter LocumTenens.com.
If physician assistants want to specialize, they also can do so through mentoring, or they can receive “certificates of added qualifications” in 10 specialties to demonstrate their expertise. Most employers don’t “encourage or require” these certificates, however, said Jennifer Orozco, DMSc, PA-C, DFAAPA, chief medical officer at the American Academy of Physician Associates.
There are a number of training programs for family nurse practitioners who want to develop skills in other areas.
Raina Hoebelheinrich, 40, a family nurse practitioner at a regional medical center in Yankton, South Dakota, recently enrolled in a three-semester post-master’s endocrinology training program at Mount Marty University. She lives on a farm in nearby northeastern Nebraska with her husband and five sons.
Ms. Hoebelheinrich’s new skills could be helpful in her current hospital job, in which she sees a lot of patients with acute diabetes, or in a clinic setting like the one in Sioux Falls, South Dakota, where she is doing her clinical endocrinology training.
Lack of access to endocrinology care in rural areas is a real problem, and many people may travel hundreds of miles to see a specialist.
“There aren’t a lot of options,” she said.
A version of this article first appeared on Medscape.com.
For many patients, seeing a nurse practitioner has become a routine part of primary care, in which these “NPs” often perform the same tasks that patients have relied on doctors for.
But NPs in specialty care? That’s not routine, at least not yet. Increasingly, though, nurse practitioners and physician assistants are joining cardiology, dermatology, and other specialty practices, broadening their skills and increasing their income.
This development worries some people who track the health workforce, because current trends suggest primary care, which has counted on nurse practitioners to backstop physician shortages, soon might not be able to rely on them to the same extent.
“They’re succumbing to the same challenges that we have with physicians,” said Atul Grover, MD, PhD, executive director of the Research and Action Institute at the Association of American Medical Colleges. The rates NPs can command in a specialty practice “are quite a bit higher” than practice salaries in primary care, he said.
When nurse practitioner programs began to proliferate in the 1970s, “at first it looked great, producing all these nurse practitioners that go to work with primary care physicians,” said Yalda Jabbarpour, MD, director of the American Academy of Family Physicians’ Robert Graham Center for Policy Studies. “But now only 30% are going into primary care.”
Dr. Jabbarpour was referring to the 2024 primary care scorecard by the Milbank Memorial Fund, which found that from 2016 to 2021 the proportion of nurse practitioners who worked in primary care practices hovered between 32% and 34%, even though their numbers grew rapidly. The proportion of physician assistants, also known as physician associates, in primary care ranged from 27% to 30%, the study found.
Both nurse practitioners and physician assistants are advanced practice clinicians who, in addition to graduate degrees, must complete distinct education, training, and certification steps. NPs can practice without a doctor’s supervision in more than two dozen states, while PAs have similar independence in only a handful of states.
About 88% of nurse practitioners are certified in an area of primary care, according to the American Association of Nurse Practitioners. But it is difficult to track exactly how many work in primary care or in specialty practices. Unlike physicians, they’re generally not required to be endorsed by a national standard-setting body to practice in specialties like oncology or cardiology, for example. The AANP declined to answer questions about its annual workforce survey or the extent to which primary care NPs are moving toward specialties.
Though data tracking the change is sparse, specialty practices are adding these advanced practice clinicians at almost the same rate as primary care practices, according to frequently cited research published in 2018.
The clearest evidence of the shift: From 2008 to 2016, there was a 22% increase in the number of specialty practices that employed nurse practitioners and physician assistants, according to that study. The increase in the number of primary care practices that employed these professionals was 24%.
Once more, the most recent projections by the Association of American Medical Colleges predict a dearth of at least 20,200 primary care physicians by 2036. There will also be a shortfall of non-primary care specialists, including a deficiency of at least 10,100 surgical physicians and up to 25,000 physicians in other specialties.
When it comes to the actual work performed, the lines between primary and specialty care are often blurred, said Candice Chen, MD, MPH, associate professor of health policy and management at George Washington University.
“You might be a nurse practitioner working in a gastroenterology clinic or cardiology clinic, but the scope of what you do is starting to overlap with primary care,” she said.
Nurse practitioners’ salaries vary widely by location, type of facility, and experience. Still, according to data from health care recruiter AMN Healthcare Physician Solutions, formerly known as Merritt Hawkins, the total annual average starting compensation, including signing bonus, for nurse practitioners and physician assistants in specialty practice was $172,544 in the year that ended March 31, slightly higher than the $166,544 for those in primary care.
According to forecasts from the federal Bureau of Labor Statistics, nurse practitioner jobs will increase faster than jobs in almost any other occupation in the decade leading up to 2032, growing by 123,600 jobs or 45%. (Wind turbine service technician is the only other occupation projected to grow as fast.) The growth rate for physician assistants is also much faster than average, at 27%. There are more than twice as many nurse practitioners as physician assistants, however: 323,900 versus 148,000, in 2022.
To Dr. Grover of the AAMC, numbers like this signal that there will probably be enough NPs, PAs, and physicians to meet primary care needs. At the same time, “expect more NPs and PAs to also flow out into other specialties,” he said.
When Pamela Ograbisz started working as a registered nurse 27 years ago, she worked in a cardiothoracic intensive care unit. After she became a family nurse practitioner a few years later, she found a job with a similar specialty practice, which trained her to take on a bigger role, first running their outpatient clinic, then working on the floor, and later in the intensive care unit.
If nurse practitioners want to specialize, often “the doctors mentor them just like they would with a physician residency,” said Ms. Ograbisz, now vice president of clinical operations at temporary placement recruiter LocumTenens.com.
If physician assistants want to specialize, they also can do so through mentoring, or they can receive “certificates of added qualifications” in 10 specialties to demonstrate their expertise. Most employers don’t “encourage or require” these certificates, however, said Jennifer Orozco, DMSc, PA-C, DFAAPA, chief medical officer at the American Academy of Physician Associates.
There are a number of training programs for family nurse practitioners who want to develop skills in other areas.
Raina Hoebelheinrich, 40, a family nurse practitioner at a regional medical center in Yankton, South Dakota, recently enrolled in a three-semester post-master’s endocrinology training program at Mount Marty University. She lives on a farm in nearby northeastern Nebraska with her husband and five sons.
Ms. Hoebelheinrich’s new skills could be helpful in her current hospital job, in which she sees a lot of patients with acute diabetes, or in a clinic setting like the one in Sioux Falls, South Dakota, where she is doing her clinical endocrinology training.
Lack of access to endocrinology care in rural areas is a real problem, and many people may travel hundreds of miles to see a specialist.
“There aren’t a lot of options,” she said.
A version of this article first appeared on Medscape.com.
For many patients, seeing a nurse practitioner has become a routine part of primary care, in which these “NPs” often perform the same tasks that patients have relied on doctors for.
But NPs in specialty care? That’s not routine, at least not yet. Increasingly, though, nurse practitioners and physician assistants are joining cardiology, dermatology, and other specialty practices, broadening their skills and increasing their income.
This development worries some people who track the health workforce, because current trends suggest primary care, which has counted on nurse practitioners to backstop physician shortages, soon might not be able to rely on them to the same extent.
“They’re succumbing to the same challenges that we have with physicians,” said Atul Grover, MD, PhD, executive director of the Research and Action Institute at the Association of American Medical Colleges. The rates NPs can command in a specialty practice “are quite a bit higher” than practice salaries in primary care, he said.
When nurse practitioner programs began to proliferate in the 1970s, “at first it looked great, producing all these nurse practitioners that go to work with primary care physicians,” said Yalda Jabbarpour, MD, director of the American Academy of Family Physicians’ Robert Graham Center for Policy Studies. “But now only 30% are going into primary care.”
Dr. Jabbarpour was referring to the 2024 primary care scorecard by the Milbank Memorial Fund, which found that from 2016 to 2021 the proportion of nurse practitioners who worked in primary care practices hovered between 32% and 34%, even though their numbers grew rapidly. The proportion of physician assistants, also known as physician associates, in primary care ranged from 27% to 30%, the study found.
Both nurse practitioners and physician assistants are advanced practice clinicians who, in addition to graduate degrees, must complete distinct education, training, and certification steps. NPs can practice without a doctor’s supervision in more than two dozen states, while PAs have similar independence in only a handful of states.
About 88% of nurse practitioners are certified in an area of primary care, according to the American Association of Nurse Practitioners. But it is difficult to track exactly how many work in primary care or in specialty practices. Unlike physicians, they’re generally not required to be endorsed by a national standard-setting body to practice in specialties like oncology or cardiology, for example. The AANP declined to answer questions about its annual workforce survey or the extent to which primary care NPs are moving toward specialties.
Though data tracking the change is sparse, specialty practices are adding these advanced practice clinicians at almost the same rate as primary care practices, according to frequently cited research published in 2018.
The clearest evidence of the shift: From 2008 to 2016, there was a 22% increase in the number of specialty practices that employed nurse practitioners and physician assistants, according to that study. The increase in the number of primary care practices that employed these professionals was 24%.
Once more, the most recent projections by the Association of American Medical Colleges predict a dearth of at least 20,200 primary care physicians by 2036. There will also be a shortfall of non-primary care specialists, including a deficiency of at least 10,100 surgical physicians and up to 25,000 physicians in other specialties.
When it comes to the actual work performed, the lines between primary and specialty care are often blurred, said Candice Chen, MD, MPH, associate professor of health policy and management at George Washington University.
“You might be a nurse practitioner working in a gastroenterology clinic or cardiology clinic, but the scope of what you do is starting to overlap with primary care,” she said.
Nurse practitioners’ salaries vary widely by location, type of facility, and experience. Still, according to data from health care recruiter AMN Healthcare Physician Solutions, formerly known as Merritt Hawkins, the total annual average starting compensation, including signing bonus, for nurse practitioners and physician assistants in specialty practice was $172,544 in the year that ended March 31, slightly higher than the $166,544 for those in primary care.
According to forecasts from the federal Bureau of Labor Statistics, nurse practitioner jobs will increase faster than jobs in almost any other occupation in the decade leading up to 2032, growing by 123,600 jobs or 45%. (Wind turbine service technician is the only other occupation projected to grow as fast.) The growth rate for physician assistants is also much faster than average, at 27%. There are more than twice as many nurse practitioners as physician assistants, however: 323,900 versus 148,000, in 2022.
To Dr. Grover of the AAMC, numbers like this signal that there will probably be enough NPs, PAs, and physicians to meet primary care needs. At the same time, “expect more NPs and PAs to also flow out into other specialties,” he said.
When Pamela Ograbisz started working as a registered nurse 27 years ago, she worked in a cardiothoracic intensive care unit. After she became a family nurse practitioner a few years later, she found a job with a similar specialty practice, which trained her to take on a bigger role, first running their outpatient clinic, then working on the floor, and later in the intensive care unit.
If nurse practitioners want to specialize, often “the doctors mentor them just like they would with a physician residency,” said Ms. Ograbisz, now vice president of clinical operations at temporary placement recruiter LocumTenens.com.
If physician assistants want to specialize, they also can do so through mentoring, or they can receive “certificates of added qualifications” in 10 specialties to demonstrate their expertise. Most employers don’t “encourage or require” these certificates, however, said Jennifer Orozco, DMSc, PA-C, DFAAPA, chief medical officer at the American Academy of Physician Associates.
There are a number of training programs for family nurse practitioners who want to develop skills in other areas.
Raina Hoebelheinrich, 40, a family nurse practitioner at a regional medical center in Yankton, South Dakota, recently enrolled in a three-semester post-master’s endocrinology training program at Mount Marty University. She lives on a farm in nearby northeastern Nebraska with her husband and five sons.
Ms. Hoebelheinrich’s new skills could be helpful in her current hospital job, in which she sees a lot of patients with acute diabetes, or in a clinic setting like the one in Sioux Falls, South Dakota, where she is doing her clinical endocrinology training.
Lack of access to endocrinology care in rural areas is a real problem, and many people may travel hundreds of miles to see a specialist.
“There aren’t a lot of options,” she said.
A version of this article first appeared on Medscape.com.
Severe Maternal Morbidity Can Adversely Affect Mental Health
TOPLINE:
Individuals with severe maternal morbidity (SMM) are at an increased risk for mental health condition–related hospitalization or emergency department (ED) visits up to 13 years after delivery.
METHODOLOGY:
- This retrospective cohort study compared mental health hospitalizations and ED visits in postpartum individuals with and without SMM over 13 years after delivery from April 2008 to March 2021.
- The study analyzed 1,579,392 individuals aged 18-55 years with a first recorded liveborn or stillborn delivery from a pregnancy lasting 20-43 weeks, of which 35,825 (2.3%) had exposure to SMM.
- The SMM exposure was analyzed for events occurring after 20 weeks’ gestation and up to 42 days after delivery hospital discharge in the first recorded birth; those without SMM were considered unexposed.
- The main outcome was a combination of mental health hospitalizations or ED visits occurring at least 43 days after the index birth hospitalization.
TAKEAWAY:
- Individuals with SMM had a 1.3-fold increased risk of mental health hospitalizations or ED visits.
- The hospital or ED visits per 10,000 person-years were 59.2 for mood and anxiety disorders, 17.1 for substance abuse and related disorders, 4.8 for suicidality or self-harm, and 4.1 for schizophrenia spectrum or other psychotic disorders.
- Following SMM, an elevated risk was observed for all mental health outcomes except one (schizophrenia spectrum and other psychotic disorders), with the highest risk seen for suicidality and self-harm (aHR, 1.54).
IN PRACTICE:
“Knowledge of the short- and long-term risks of serious mental health conditions after SMM and its subtypes could inform the need for enhanced postpartum supportive resources,” the authors wrote.
SOURCE:
This study was led by Asia Blackman, MSc, Department of Epidemiology, Biostatistics and Occupational Health, McGill University, Montreal, Québec, Canada. It was published online in JAMA Network Open.
LIMITATIONS:
The study is limited by its observational design, missing data, and misclassification bias.
DISCLOSURES:
This study was supported by funding from the Canadian Institutes of Health Research. Three authors reported receiving personal fees or grants outside the submitted work. No other conflicts of interest were reported.
A version of this article first appeared on Medscape.com.
TOPLINE:
Individuals with severe maternal morbidity (SMM) are at an increased risk for mental health condition–related hospitalization or emergency department (ED) visits up to 13 years after delivery.
METHODOLOGY:
- This retrospective cohort study compared mental health hospitalizations and ED visits in postpartum individuals with and without SMM over 13 years after delivery from April 2008 to March 2021.
- The study analyzed 1,579,392 individuals aged 18-55 years with a first recorded liveborn or stillborn delivery from a pregnancy lasting 20-43 weeks, of which 35,825 (2.3%) had exposure to SMM.
- The SMM exposure was analyzed for events occurring after 20 weeks’ gestation and up to 42 days after delivery hospital discharge in the first recorded birth; those without SMM were considered unexposed.
- The main outcome was a combination of mental health hospitalizations or ED visits occurring at least 43 days after the index birth hospitalization.
TAKEAWAY:
- Individuals with SMM had a 1.3-fold increased risk of mental health hospitalizations or ED visits.
- The hospital or ED visits per 10,000 person-years were 59.2 for mood and anxiety disorders, 17.1 for substance abuse and related disorders, 4.8 for suicidality or self-harm, and 4.1 for schizophrenia spectrum or other psychotic disorders.
- Following SMM, an elevated risk was observed for all mental health outcomes except one (schizophrenia spectrum and other psychotic disorders), with the highest risk seen for suicidality and self-harm (aHR, 1.54).
IN PRACTICE:
“Knowledge of the short- and long-term risks of serious mental health conditions after SMM and its subtypes could inform the need for enhanced postpartum supportive resources,” the authors wrote.
SOURCE:
This study was led by Asia Blackman, MSc, Department of Epidemiology, Biostatistics and Occupational Health, McGill University, Montreal, Québec, Canada. It was published online in JAMA Network Open.
LIMITATIONS:
The study is limited by its observational design, missing data, and misclassification bias.
DISCLOSURES:
This study was supported by funding from the Canadian Institutes of Health Research. Three authors reported receiving personal fees or grants outside the submitted work. No other conflicts of interest were reported.
A version of this article first appeared on Medscape.com.
TOPLINE:
Individuals with severe maternal morbidity (SMM) are at an increased risk for mental health condition–related hospitalization or emergency department (ED) visits up to 13 years after delivery.
METHODOLOGY:
- This retrospective cohort study compared mental health hospitalizations and ED visits in postpartum individuals with and without SMM over 13 years after delivery from April 2008 to March 2021.
- The study analyzed 1,579,392 individuals aged 18-55 years with a first recorded liveborn or stillborn delivery from a pregnancy lasting 20-43 weeks, of which 35,825 (2.3%) had exposure to SMM.
- The SMM exposure was analyzed for events occurring after 20 weeks’ gestation and up to 42 days after delivery hospital discharge in the first recorded birth; those without SMM were considered unexposed.
- The main outcome was a combination of mental health hospitalizations or ED visits occurring at least 43 days after the index birth hospitalization.
TAKEAWAY:
- Individuals with SMM had a 1.3-fold increased risk of mental health hospitalizations or ED visits.
- The hospital or ED visits per 10,000 person-years were 59.2 for mood and anxiety disorders, 17.1 for substance abuse and related disorders, 4.8 for suicidality or self-harm, and 4.1 for schizophrenia spectrum or other psychotic disorders.
- Following SMM, an elevated risk was observed for all mental health outcomes except one (schizophrenia spectrum and other psychotic disorders), with the highest risk seen for suicidality and self-harm (aHR, 1.54).
IN PRACTICE:
“Knowledge of the short- and long-term risks of serious mental health conditions after SMM and its subtypes could inform the need for enhanced postpartum supportive resources,” the authors wrote.
SOURCE:
This study was led by Asia Blackman, MSc, Department of Epidemiology, Biostatistics and Occupational Health, McGill University, Montreal, Québec, Canada. It was published online in JAMA Network Open.
LIMITATIONS:
The study is limited by its observational design, missing data, and misclassification bias.
DISCLOSURES:
This study was supported by funding from the Canadian Institutes of Health Research. Three authors reported receiving personal fees or grants outside the submitted work. No other conflicts of interest were reported.
A version of this article first appeared on Medscape.com.
Statin Use May Extend Life for Early Breast Cancer Patients
Previous research examining the association between cholesterol and breast cancer metabolism suggests that cholesterol-lowering medications such as statins may improve outcomes in breast cancer patients, Sixten Harborg, a medical student and PhD student at Aarhus University, Denmark, said in a presentation at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress.
In addition, cardiovascular-related death is the second most common cause of death for breast cancer survivors, and given the survival rates in early breast cancer, there is a demand for cardioprotective initiatives and maintenance of cardioprotective drugs after diagnosis, he said in an interview.
What Is Known About Statins and Breast Cancer?
Statins are the most common drugs used to lower cholesterol and may deprive tumor cells of the cholesterol needed for cell membrane synthesis, Mr. Harborg said in his presentation.
Data from a randomized trial published in the Journal of Clinical Oncology in 2017 showed significantly improved disease-free survival, breast cancer–free interval, and distant recurrence–free interval in early stage breast cancer patients randomized to cholesterol-lowering medication vs. those who did not receive cholesterol-lowering medication.
The 2017 study prompted the creation of the MASTER study, a randomized, multicenter, double-blind, placebo-controlled trial comparing standard adjuvant therapy plus placebo to standard adjuvant therapy plus atorvastatin in patients with early breast cancer (NCT04601116), Mr. Harborg said. The MASTER trial is currently recruiting patients in Denmark.
How Was the Current Study Designed?
To provide preliminary analysis, Mr. Harborg and colleagues used an emulation trial design based on electronic health care data from 110,160 females with a diagnosis of stage I, II, or III breast cancer who were part of the Danish Breast Cancer Group, a national clinical registry in Denmark, between 2000 and 2020.
As defined in the European Journal of Epidemiology in 2017, target trial emulation involves application of randomized trial designs to observational data with the goal of improving the quality of observational epidemiology when a comparator trial is not yet available.
The researchers created a cohort of patients based on electronic health care data to simulate a target trial of the use of atorvastatin after breast cancer diagnosis. Patients were randomized to one of two treatment strategies: starting to use statins within 36 months of diagnosis, or not using statins. The primary outcome was death from breast cancer. The follow-up for the MASTER study starts with inclusion and ends with death, emigration from Denmark, end of clinical follow-up, or 10 years of follow-up (whichever comes first); the follow-up was the same in the current study.
The researchers calculated hazard ratios (HR) of breast cancer mortality in statin users vs. non–statin users and used a technique known as inverse-probability of censoring-weighting (IPCW) to estimate the effects of statin use based on prognostic factors.
What Did the Results Show?
The results favored statin use for improved survival in early breast cancer patients, Mr. Harborg said. Overall, the hazard ratio for breast cancer mortality was 0.96 in statin users compared with non–statin users, and was similar in both a Cox regression analysis (HR 0.81), and in a 10-year landmark analysis (HR 0.86).
The difference in mortality between statin and non–statin users was even stronger in patients who were receiving adjuvant chemotherapy (HR 0.94, 0.64, and 0.76 on the IPCW, Cox, and landmark analyses, respectively).
The results were in line with previous reports of statins’ effect on breast cancer survival, Mr. Harborg said in an interview.
“We believe the results encourage the continuous effort of the currently enrolling MASTER trial,” he said.
The results also suggest that deprescribing statins at the time of breast cancer diagnosis is not recommended, and that statin treatment can safely be prescribed to breast cancer patients with increased cardiovascular disease risk and/or dyslipidemia, Mr. Harborg said in the interview.
What Is the Takeaway Message for Clinical Practice?
“The clinical takeaway from our study is that statin use is associated with reduced risk of dying from breast cancer, but that it is not possible to determine the true effect of statins on breast cancer survival without a randomized, placebo-controlled trial,” Mr. Harborg told this publication. “Statins are inexpensive and well-tolerated drugs and may have a beneficial effect in terms of survival for breast cancer patients. However, with the current level of evidence [because the MASTER study is ongoing], we still cannot recommend that oncologists prescribe statins to prevent mortality from breast cancer,” he said.
What Are the Next Steps for Research?
The findings were limited by the study design, and real-world data are needed, Dr. Harborg said. Other limitations include the presence of residual bias, and the use of data based on prescription codes, but these were not considered to have an effect on the main conclusion of the study, Mr. Harborg said in the interview.
However, the results suggest that the addition of statins may improve outcomes for early breast cancer patients, especially when used with chemotherapy, and support the value of the ongoing MASTER study, he concluded.
Ultimately, the MASTER study will provide a more definitive answer to the question of whether statins should be added to the adjuvant treatment regimen of breast cancer to improve breast cancer outcomes, he said.
What Do Clinicians Think of the Study?
The current study is timely and highlights the need for phase 3 trials to examine the potential of statin use for breast cancer outcomes, Malinda T. West, MD, a medical oncologist and breast oncologist at the University of Wisconsin Carbone Cancer Center, Madison, said in an interview.
Questions for future research include whether statins can be used in combination with adjuvant abemaciclib if indicated, or how to best sequence these agents, said Dr. West, who was not involved in the study. Other questions raised by the current study include whether other cholesterol-lowering agents have a potential adjuvant benefit in reducing breast cancer recurrent and/or mortality, and whether the addition of statins would benefit subgroups such as HER2+ and triple negative breast cancer, she said.
“I was not surprised to see another study reporting benefit with statins and reduced risk of breast cancer recurrence and/or mortality, but I think the larger question is defining the subgroups who benefit the most, and identifying predictors for benefit or resistance,” Dr. West said in an interview.
Previous studies have shown that cholesterol elevation, specifically LDL levels, can be linked to increased tumor growth in breast cancer, so the lower mortality risk associated with lipid-lowering therapies in the current study was consistent, Peyton L. Reves, MD, a hematology/oncology fellow, also at the University of Wisconsin, said in an interview. In practice, data from the current study and previous research could be especially useful for patients with elevated LDL levels, said Dr. Reves, who was not involved in the study.
“These results could impact clinical practice in many ways, including leading to routine cholesterol monitoring in breast cancer patients on adjuvant therapy as well as the addition of lipid-lowering therapy with statins in these patients,” Dr. Reves said.
The findings showing particular benefit for patients on adjuvant chemotherapy highlight the need for more research on this specific population and the effect of statins on overall breast cancer mortality, to explore the extent to which the results of the current study were driven by the benefit seen in patients receiving adjuvant chemotherapy, Dr. Reves said.
The study was supported by Director Michael Hermann Nielsen’s Memorial Grant, Manufacturer Einar Willumsen’s Memorial Grant, Astrid Thaysen’s Grant for Medical Basic Research, Eva and Henry Fraenkel’s Memorial Fund, and the Novo Nordisk Foundation.
The researchers had no financial conflicts to disclose. Dr. West and Dr. Reves had no financial conflicts to disclose.
Previous research examining the association between cholesterol and breast cancer metabolism suggests that cholesterol-lowering medications such as statins may improve outcomes in breast cancer patients, Sixten Harborg, a medical student and PhD student at Aarhus University, Denmark, said in a presentation at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress.
In addition, cardiovascular-related death is the second most common cause of death for breast cancer survivors, and given the survival rates in early breast cancer, there is a demand for cardioprotective initiatives and maintenance of cardioprotective drugs after diagnosis, he said in an interview.
What Is Known About Statins and Breast Cancer?
Statins are the most common drugs used to lower cholesterol and may deprive tumor cells of the cholesterol needed for cell membrane synthesis, Mr. Harborg said in his presentation.
Data from a randomized trial published in the Journal of Clinical Oncology in 2017 showed significantly improved disease-free survival, breast cancer–free interval, and distant recurrence–free interval in early stage breast cancer patients randomized to cholesterol-lowering medication vs. those who did not receive cholesterol-lowering medication.
The 2017 study prompted the creation of the MASTER study, a randomized, multicenter, double-blind, placebo-controlled trial comparing standard adjuvant therapy plus placebo to standard adjuvant therapy plus atorvastatin in patients with early breast cancer (NCT04601116), Mr. Harborg said. The MASTER trial is currently recruiting patients in Denmark.
How Was the Current Study Designed?
To provide preliminary analysis, Mr. Harborg and colleagues used an emulation trial design based on electronic health care data from 110,160 females with a diagnosis of stage I, II, or III breast cancer who were part of the Danish Breast Cancer Group, a national clinical registry in Denmark, between 2000 and 2020.
As defined in the European Journal of Epidemiology in 2017, target trial emulation involves application of randomized trial designs to observational data with the goal of improving the quality of observational epidemiology when a comparator trial is not yet available.
The researchers created a cohort of patients based on electronic health care data to simulate a target trial of the use of atorvastatin after breast cancer diagnosis. Patients were randomized to one of two treatment strategies: starting to use statins within 36 months of diagnosis, or not using statins. The primary outcome was death from breast cancer. The follow-up for the MASTER study starts with inclusion and ends with death, emigration from Denmark, end of clinical follow-up, or 10 years of follow-up (whichever comes first); the follow-up was the same in the current study.
The researchers calculated hazard ratios (HR) of breast cancer mortality in statin users vs. non–statin users and used a technique known as inverse-probability of censoring-weighting (IPCW) to estimate the effects of statin use based on prognostic factors.
What Did the Results Show?
The results favored statin use for improved survival in early breast cancer patients, Mr. Harborg said. Overall, the hazard ratio for breast cancer mortality was 0.96 in statin users compared with non–statin users, and was similar in both a Cox regression analysis (HR 0.81), and in a 10-year landmark analysis (HR 0.86).
The difference in mortality between statin and non–statin users was even stronger in patients who were receiving adjuvant chemotherapy (HR 0.94, 0.64, and 0.76 on the IPCW, Cox, and landmark analyses, respectively).
The results were in line with previous reports of statins’ effect on breast cancer survival, Mr. Harborg said in an interview.
“We believe the results encourage the continuous effort of the currently enrolling MASTER trial,” he said.
The results also suggest that deprescribing statins at the time of breast cancer diagnosis is not recommended, and that statin treatment can safely be prescribed to breast cancer patients with increased cardiovascular disease risk and/or dyslipidemia, Mr. Harborg said in the interview.
What Is the Takeaway Message for Clinical Practice?
“The clinical takeaway from our study is that statin use is associated with reduced risk of dying from breast cancer, but that it is not possible to determine the true effect of statins on breast cancer survival without a randomized, placebo-controlled trial,” Mr. Harborg told this publication. “Statins are inexpensive and well-tolerated drugs and may have a beneficial effect in terms of survival for breast cancer patients. However, with the current level of evidence [because the MASTER study is ongoing], we still cannot recommend that oncologists prescribe statins to prevent mortality from breast cancer,” he said.
What Are the Next Steps for Research?
The findings were limited by the study design, and real-world data are needed, Dr. Harborg said. Other limitations include the presence of residual bias, and the use of data based on prescription codes, but these were not considered to have an effect on the main conclusion of the study, Mr. Harborg said in the interview.
However, the results suggest that the addition of statins may improve outcomes for early breast cancer patients, especially when used with chemotherapy, and support the value of the ongoing MASTER study, he concluded.
Ultimately, the MASTER study will provide a more definitive answer to the question of whether statins should be added to the adjuvant treatment regimen of breast cancer to improve breast cancer outcomes, he said.
What Do Clinicians Think of the Study?
The current study is timely and highlights the need for phase 3 trials to examine the potential of statin use for breast cancer outcomes, Malinda T. West, MD, a medical oncologist and breast oncologist at the University of Wisconsin Carbone Cancer Center, Madison, said in an interview.
Questions for future research include whether statins can be used in combination with adjuvant abemaciclib if indicated, or how to best sequence these agents, said Dr. West, who was not involved in the study. Other questions raised by the current study include whether other cholesterol-lowering agents have a potential adjuvant benefit in reducing breast cancer recurrent and/or mortality, and whether the addition of statins would benefit subgroups such as HER2+ and triple negative breast cancer, she said.
“I was not surprised to see another study reporting benefit with statins and reduced risk of breast cancer recurrence and/or mortality, but I think the larger question is defining the subgroups who benefit the most, and identifying predictors for benefit or resistance,” Dr. West said in an interview.
Previous studies have shown that cholesterol elevation, specifically LDL levels, can be linked to increased tumor growth in breast cancer, so the lower mortality risk associated with lipid-lowering therapies in the current study was consistent, Peyton L. Reves, MD, a hematology/oncology fellow, also at the University of Wisconsin, said in an interview. In practice, data from the current study and previous research could be especially useful for patients with elevated LDL levels, said Dr. Reves, who was not involved in the study.
“These results could impact clinical practice in many ways, including leading to routine cholesterol monitoring in breast cancer patients on adjuvant therapy as well as the addition of lipid-lowering therapy with statins in these patients,” Dr. Reves said.
The findings showing particular benefit for patients on adjuvant chemotherapy highlight the need for more research on this specific population and the effect of statins on overall breast cancer mortality, to explore the extent to which the results of the current study were driven by the benefit seen in patients receiving adjuvant chemotherapy, Dr. Reves said.
The study was supported by Director Michael Hermann Nielsen’s Memorial Grant, Manufacturer Einar Willumsen’s Memorial Grant, Astrid Thaysen’s Grant for Medical Basic Research, Eva and Henry Fraenkel’s Memorial Fund, and the Novo Nordisk Foundation.
The researchers had no financial conflicts to disclose. Dr. West and Dr. Reves had no financial conflicts to disclose.
Previous research examining the association between cholesterol and breast cancer metabolism suggests that cholesterol-lowering medications such as statins may improve outcomes in breast cancer patients, Sixten Harborg, a medical student and PhD student at Aarhus University, Denmark, said in a presentation at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress.
In addition, cardiovascular-related death is the second most common cause of death for breast cancer survivors, and given the survival rates in early breast cancer, there is a demand for cardioprotective initiatives and maintenance of cardioprotective drugs after diagnosis, he said in an interview.
What Is Known About Statins and Breast Cancer?
Statins are the most common drugs used to lower cholesterol and may deprive tumor cells of the cholesterol needed for cell membrane synthesis, Mr. Harborg said in his presentation.
Data from a randomized trial published in the Journal of Clinical Oncology in 2017 showed significantly improved disease-free survival, breast cancer–free interval, and distant recurrence–free interval in early stage breast cancer patients randomized to cholesterol-lowering medication vs. those who did not receive cholesterol-lowering medication.
The 2017 study prompted the creation of the MASTER study, a randomized, multicenter, double-blind, placebo-controlled trial comparing standard adjuvant therapy plus placebo to standard adjuvant therapy plus atorvastatin in patients with early breast cancer (NCT04601116), Mr. Harborg said. The MASTER trial is currently recruiting patients in Denmark.
How Was the Current Study Designed?
To provide preliminary analysis, Mr. Harborg and colleagues used an emulation trial design based on electronic health care data from 110,160 females with a diagnosis of stage I, II, or III breast cancer who were part of the Danish Breast Cancer Group, a national clinical registry in Denmark, between 2000 and 2020.
As defined in the European Journal of Epidemiology in 2017, target trial emulation involves application of randomized trial designs to observational data with the goal of improving the quality of observational epidemiology when a comparator trial is not yet available.
The researchers created a cohort of patients based on electronic health care data to simulate a target trial of the use of atorvastatin after breast cancer diagnosis. Patients were randomized to one of two treatment strategies: starting to use statins within 36 months of diagnosis, or not using statins. The primary outcome was death from breast cancer. The follow-up for the MASTER study starts with inclusion and ends with death, emigration from Denmark, end of clinical follow-up, or 10 years of follow-up (whichever comes first); the follow-up was the same in the current study.
The researchers calculated hazard ratios (HR) of breast cancer mortality in statin users vs. non–statin users and used a technique known as inverse-probability of censoring-weighting (IPCW) to estimate the effects of statin use based on prognostic factors.
What Did the Results Show?
The results favored statin use for improved survival in early breast cancer patients, Mr. Harborg said. Overall, the hazard ratio for breast cancer mortality was 0.96 in statin users compared with non–statin users, and was similar in both a Cox regression analysis (HR 0.81), and in a 10-year landmark analysis (HR 0.86).
The difference in mortality between statin and non–statin users was even stronger in patients who were receiving adjuvant chemotherapy (HR 0.94, 0.64, and 0.76 on the IPCW, Cox, and landmark analyses, respectively).
The results were in line with previous reports of statins’ effect on breast cancer survival, Mr. Harborg said in an interview.
“We believe the results encourage the continuous effort of the currently enrolling MASTER trial,” he said.
The results also suggest that deprescribing statins at the time of breast cancer diagnosis is not recommended, and that statin treatment can safely be prescribed to breast cancer patients with increased cardiovascular disease risk and/or dyslipidemia, Mr. Harborg said in the interview.
What Is the Takeaway Message for Clinical Practice?
“The clinical takeaway from our study is that statin use is associated with reduced risk of dying from breast cancer, but that it is not possible to determine the true effect of statins on breast cancer survival without a randomized, placebo-controlled trial,” Mr. Harborg told this publication. “Statins are inexpensive and well-tolerated drugs and may have a beneficial effect in terms of survival for breast cancer patients. However, with the current level of evidence [because the MASTER study is ongoing], we still cannot recommend that oncologists prescribe statins to prevent mortality from breast cancer,” he said.
What Are the Next Steps for Research?
The findings were limited by the study design, and real-world data are needed, Dr. Harborg said. Other limitations include the presence of residual bias, and the use of data based on prescription codes, but these were not considered to have an effect on the main conclusion of the study, Mr. Harborg said in the interview.
However, the results suggest that the addition of statins may improve outcomes for early breast cancer patients, especially when used with chemotherapy, and support the value of the ongoing MASTER study, he concluded.
Ultimately, the MASTER study will provide a more definitive answer to the question of whether statins should be added to the adjuvant treatment regimen of breast cancer to improve breast cancer outcomes, he said.
What Do Clinicians Think of the Study?
The current study is timely and highlights the need for phase 3 trials to examine the potential of statin use for breast cancer outcomes, Malinda T. West, MD, a medical oncologist and breast oncologist at the University of Wisconsin Carbone Cancer Center, Madison, said in an interview.
Questions for future research include whether statins can be used in combination with adjuvant abemaciclib if indicated, or how to best sequence these agents, said Dr. West, who was not involved in the study. Other questions raised by the current study include whether other cholesterol-lowering agents have a potential adjuvant benefit in reducing breast cancer recurrent and/or mortality, and whether the addition of statins would benefit subgroups such as HER2+ and triple negative breast cancer, she said.
“I was not surprised to see another study reporting benefit with statins and reduced risk of breast cancer recurrence and/or mortality, but I think the larger question is defining the subgroups who benefit the most, and identifying predictors for benefit or resistance,” Dr. West said in an interview.
Previous studies have shown that cholesterol elevation, specifically LDL levels, can be linked to increased tumor growth in breast cancer, so the lower mortality risk associated with lipid-lowering therapies in the current study was consistent, Peyton L. Reves, MD, a hematology/oncology fellow, also at the University of Wisconsin, said in an interview. In practice, data from the current study and previous research could be especially useful for patients with elevated LDL levels, said Dr. Reves, who was not involved in the study.
“These results could impact clinical practice in many ways, including leading to routine cholesterol monitoring in breast cancer patients on adjuvant therapy as well as the addition of lipid-lowering therapy with statins in these patients,” Dr. Reves said.
The findings showing particular benefit for patients on adjuvant chemotherapy highlight the need for more research on this specific population and the effect of statins on overall breast cancer mortality, to explore the extent to which the results of the current study were driven by the benefit seen in patients receiving adjuvant chemotherapy, Dr. Reves said.
The study was supported by Director Michael Hermann Nielsen’s Memorial Grant, Manufacturer Einar Willumsen’s Memorial Grant, Astrid Thaysen’s Grant for Medical Basic Research, Eva and Henry Fraenkel’s Memorial Fund, and the Novo Nordisk Foundation.
The researchers had no financial conflicts to disclose. Dr. West and Dr. Reves had no financial conflicts to disclose.
FROM ESMO BREAST CANCER 2024
Do You Really Know a UTI When You See It?
An updated clinical approach to diagnosing urinary tract infections (UTIs) that considers five potential phenotype categories instead of the usual three could aid clinical management and better center patient needs, according to the authors of a new study in The Journal of Urology.
The current diagnostic paradigm includes UTI, asymptomatic bacteriuria (ASB), or not UTI, but the researchers believe these categories exclude for more ambiguous clinical cases, such as patients whose bacteria counts are low but who are symptomatic, or when nonspecific symptoms make it difficult to determine whether treatment with antibiotics is appropriate.
“Our findings suggest the need to reframe our conceptual model of UTI vs ASB to recognize clinical uncertainty and reflect the full spectrum of clinical presentations,” Sonali D. Advani, MBBS, MPH, an associate professor of medicine in infectious disease at Duke University School of Medicine, in Durham, North Carolina, and her colleagues wrote. “Recent data suggest that UTI may present as a bidirectional continuum from asymptomatic bladder colonization to a symptomatic bladder infection,” and some populations may lack the signs or symptoms specific to urinary tract or have chronic lower urinary tract symptoms (LUTS) that make it difficult to distinguish between ASB and UTI, they wrote.
Nitya E. Abraham, MD, an associate professor of urology at Albert Einstein College of Medicine and Montefiore Einstein in New York City, agreed the current paradigm has room for refinement.
“The current classification system doesn’t account for certain patients such as patients who have bothersome urinary symptoms, but urine testing comes back negative, or patients with positive urine testing, but who aren’t able to report the presence or absence of symptoms,” Dr. Abraham, who was not involved in the new research, told this news organization.
Boback Berookhim, MD, a urologist at Northwell Health in New Hyde Park, New York, who was also not involved in the research, said the goal with this study appears to be better identifying who will need antibiotics.
“I think this is more of a forward-looking study in terms of trying to identify patients who currently may not be treated or may be over treated and better identifying subsets,” Dr. Berookhim told this news organization.
However, he said the relevance of the work is far greater in hospitals than in outpatient settings.
“I think it’s much more relevant in inpatient environments where a patient is in hospital and whatever antibiotics are being written are going to be overseen and you’re going to see higher resistance patterns,” Dr. Berookhim said. “For the average doctor who’s seeing patients in the office and writing them prescriptions in the office, this doesn’t really affect them.”
Antibiotic Dilemma
A key issue in determining the best approach to UTI diagnosis is assessing the appropriateness of antibiotic treatment. Up to half of hospitalized patients have ASB, for which current practice guidelines advise against antibiotics, Dr. Advani and her colleagues noted. Yet many of these patients receive antibiotics regardless, and research has shown links between treatment and longer length of stay, antibiotic resistance, and infection with Clostridioides difficile.
The challenge comes with patients who do not fit easily into the existing categories. One includes patients who have positive urine cultures but whose symptoms, such as hypotension or fever, are not specific to the genitourinary tract.
While current guidelines advise against treating these patients with antibiotics, the patients are often older adults with cognitive impairment or delirium, and frontline physicians may err on the side of prescribing antibiotics because of their clinical uncertainty. That treatment can lead to tension with hospital antibiotic stewardship teams that recommend withholding antibiotics for those patients.
“These clinical scenarios highlight differences between the frontline clinicians’ and antibiotic stewardship teams’ definitions of ‘asymptomatic,’ highlighting the ambiguity of the term ‘asymptomatic bacteriuria,’” Dr. Advani and her colleagues wrote.
A fever, for example, could signal a viral or bacterial infection or result from a nonurinary source, Dr. Abraham said. “The antibiotic stewardship team likely prefers to observe the clinical course and wait for more data to demonstrate need for antibiotics,” she said. “Hence, there are conflicting priorities and confusion of when to treat with antibiotics for this common dilemma in patients presenting to the ER or urgent care.”
Meanwhile, other patients, particularly women, may present with urinary symptoms and pyuria but have lab results revealing a colony count below the 100,000 CFU/mL threshold that would indicate antibiotic treatment.
“Some of these women are likely suffering from a UTI and may not receive treatment if clinicians focus primarily on the urine culture results,” Dr. Abraham said. She pointed out the existence of other options than urine culture for better identifying UTI, such as urinary cell-free DNA or next-generation DNA testing of the urine. But she also said the 100,000 CFU/mL threshold should not be absolute.
“For example, I will treat patients for UTI with 10,000-50,000 CFU/mL if they also have UTI symptoms like blood in the urine, burning with urination, bladder pain, increased urgency or frequency, and the urinalysis shows a high white blood cell count,” Dr. Abraham said.
Dr. Abraham also noted a third group outside the scope of the new study: People with urinary symptoms who don’t undergo urine tests or who are treated empirically with antibiotics. “It is unclear whether those in this group truly have a UTI, but it is a common scenario that patients are unable to get urine tests and are treated with over-the-phone prescriptions to expedite treatment,” she said.
Get on the BUS
The researchers conducted a retrospective study across one academic medical center and four community hospitals in three states to assess the feasibility of using five categories of UTI diagnosis: The three existing ones plus LUTS/other urologic symptoms (OUS) and bacteriuria of unclear significance (BUS). These additional categories arose out of an hour-long discussion with a focus group of experts across several disciplines.
The analysis covered the charts of 3392 randomly selected encounters out of 220,531 total inpatient or emergency department encounters between January 2017 and December 2019 in which adults received a urinalysis and urine culture order within the same 24-hour period. The patients’ median age was 67 years, over half (59.6%) were women, and nearly a quarter (24.2%) had an underlying immunocompromising condition.
Most of the cultures were obtained from inpatients. Nearly a third (30.6%) were negative for culture, while 42.1% grew at least 100,000 CFU/mL of bacteria and 17% grew mixed flora.
Based on current criteria, 21.3% of the patients had a UTI, 20.8% had ASB, and 47.6% had no UTI. The remaining 10.3% had culture growth under 100,000 CFU/mL and, therefore, did not fit in any of these categories, “as there is no consistent guidance on whether to classify them as no UTI or ASB or contamination,” the authors wrote.
When the researchers applied the new criteria, more than half of the cases of ASB (68%) were reclassified as BUS, and 28.9% of the no-UTI cases were reclassified as LUTS/OUS.
In a sensitivity analysis that examined samples with bacteriuria below the 100,000 CFU/mL threshold, nearly half the unclassified cases (43.3%) were reassigned as a UTI, increasing the proportion of patients with a diagnosed UTI from 21.3% to 25.8% of the total population. Of the remaining patients who had originally been unclassified, 14.2% were newly defined as ASB, and 42.5% became BUS.
Dr. Abraham said the addition of the BUS and LUTS/OUS categories has the potential to improve and individualize patient care. Clinicians can consider nonantibiotic therapies for the patients who had LUTS/OUS while they look into possible causes, while the BUS cases enable frontline clinicians and antibiotic stewardship teams to “meet in the middle” by monitoring those patients more closely in case symptoms worsen, she said.
The authors highlighted three key takeaways from their study, starting with the fact that nearly two thirds of patients who underwent testing for a UTI did not have signs or symptoms localized to the urinary tract — the ones reclassified as BUS.
“Hence, reclassifying patients as BUS may provide an opportunity to acknowledge diagnostic uncertainty and need for additional monitoring than ASB patients so as to promote a nuanced and patient-centered approach to diagnosis and management,” the authors wrote.
Second, a third of patients initially classified as not having a UTI were reclassified into the new LUTS/OUS category because of their symptoms, such as a poor or intermittent stream, dribbling, hesitancy, frequency, urge incontinence, and nocturia. These patients would need further workup to determine the best approach to management.
Finally, the sensitivity analysis “suggested that lowering the bacterial threshold in some symptomatic patients may capture additional patients with UTI whose symptoms may be dismissed due to concern for contamination or attributed to LUTS rather than infection.” Given that the 100,000 CFU/mL threshold is based on a single study in 1956, the authors suggested more research may help define better CFU thresholds to improve clinical care.
Dr. Berookhim said the study authors took a reasonable and thorough approach in how they tried to consider the best way to update the current diagnostic classification schema.
“I think using this as a jumping off point to look deeper is worthwhile,” such as conducting randomized controlled trials to assess the use of new categories, he said. “Getting more granular than this, I think, would just muddy the waters and make it more difficult to make clinical decisions.”
The research was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Advani reported consulting fees from Locus Biosciences, Sysmex America, GlaxoSmithKline, and bioMérieux. Dr. Abraham and Dr. Berookhim reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
An updated clinical approach to diagnosing urinary tract infections (UTIs) that considers five potential phenotype categories instead of the usual three could aid clinical management and better center patient needs, according to the authors of a new study in The Journal of Urology.
The current diagnostic paradigm includes UTI, asymptomatic bacteriuria (ASB), or not UTI, but the researchers believe these categories exclude for more ambiguous clinical cases, such as patients whose bacteria counts are low but who are symptomatic, or when nonspecific symptoms make it difficult to determine whether treatment with antibiotics is appropriate.
“Our findings suggest the need to reframe our conceptual model of UTI vs ASB to recognize clinical uncertainty and reflect the full spectrum of clinical presentations,” Sonali D. Advani, MBBS, MPH, an associate professor of medicine in infectious disease at Duke University School of Medicine, in Durham, North Carolina, and her colleagues wrote. “Recent data suggest that UTI may present as a bidirectional continuum from asymptomatic bladder colonization to a symptomatic bladder infection,” and some populations may lack the signs or symptoms specific to urinary tract or have chronic lower urinary tract symptoms (LUTS) that make it difficult to distinguish between ASB and UTI, they wrote.
Nitya E. Abraham, MD, an associate professor of urology at Albert Einstein College of Medicine and Montefiore Einstein in New York City, agreed the current paradigm has room for refinement.
“The current classification system doesn’t account for certain patients such as patients who have bothersome urinary symptoms, but urine testing comes back negative, or patients with positive urine testing, but who aren’t able to report the presence or absence of symptoms,” Dr. Abraham, who was not involved in the new research, told this news organization.
Boback Berookhim, MD, a urologist at Northwell Health in New Hyde Park, New York, who was also not involved in the research, said the goal with this study appears to be better identifying who will need antibiotics.
“I think this is more of a forward-looking study in terms of trying to identify patients who currently may not be treated or may be over treated and better identifying subsets,” Dr. Berookhim told this news organization.
However, he said the relevance of the work is far greater in hospitals than in outpatient settings.
“I think it’s much more relevant in inpatient environments where a patient is in hospital and whatever antibiotics are being written are going to be overseen and you’re going to see higher resistance patterns,” Dr. Berookhim said. “For the average doctor who’s seeing patients in the office and writing them prescriptions in the office, this doesn’t really affect them.”
Antibiotic Dilemma
A key issue in determining the best approach to UTI diagnosis is assessing the appropriateness of antibiotic treatment. Up to half of hospitalized patients have ASB, for which current practice guidelines advise against antibiotics, Dr. Advani and her colleagues noted. Yet many of these patients receive antibiotics regardless, and research has shown links between treatment and longer length of stay, antibiotic resistance, and infection with Clostridioides difficile.
The challenge comes with patients who do not fit easily into the existing categories. One includes patients who have positive urine cultures but whose symptoms, such as hypotension or fever, are not specific to the genitourinary tract.
While current guidelines advise against treating these patients with antibiotics, the patients are often older adults with cognitive impairment or delirium, and frontline physicians may err on the side of prescribing antibiotics because of their clinical uncertainty. That treatment can lead to tension with hospital antibiotic stewardship teams that recommend withholding antibiotics for those patients.
“These clinical scenarios highlight differences between the frontline clinicians’ and antibiotic stewardship teams’ definitions of ‘asymptomatic,’ highlighting the ambiguity of the term ‘asymptomatic bacteriuria,’” Dr. Advani and her colleagues wrote.
A fever, for example, could signal a viral or bacterial infection or result from a nonurinary source, Dr. Abraham said. “The antibiotic stewardship team likely prefers to observe the clinical course and wait for more data to demonstrate need for antibiotics,” she said. “Hence, there are conflicting priorities and confusion of when to treat with antibiotics for this common dilemma in patients presenting to the ER or urgent care.”
Meanwhile, other patients, particularly women, may present with urinary symptoms and pyuria but have lab results revealing a colony count below the 100,000 CFU/mL threshold that would indicate antibiotic treatment.
“Some of these women are likely suffering from a UTI and may not receive treatment if clinicians focus primarily on the urine culture results,” Dr. Abraham said. She pointed out the existence of other options than urine culture for better identifying UTI, such as urinary cell-free DNA or next-generation DNA testing of the urine. But she also said the 100,000 CFU/mL threshold should not be absolute.
“For example, I will treat patients for UTI with 10,000-50,000 CFU/mL if they also have UTI symptoms like blood in the urine, burning with urination, bladder pain, increased urgency or frequency, and the urinalysis shows a high white blood cell count,” Dr. Abraham said.
Dr. Abraham also noted a third group outside the scope of the new study: People with urinary symptoms who don’t undergo urine tests or who are treated empirically with antibiotics. “It is unclear whether those in this group truly have a UTI, but it is a common scenario that patients are unable to get urine tests and are treated with over-the-phone prescriptions to expedite treatment,” she said.
Get on the BUS
The researchers conducted a retrospective study across one academic medical center and four community hospitals in three states to assess the feasibility of using five categories of UTI diagnosis: The three existing ones plus LUTS/other urologic symptoms (OUS) and bacteriuria of unclear significance (BUS). These additional categories arose out of an hour-long discussion with a focus group of experts across several disciplines.
The analysis covered the charts of 3392 randomly selected encounters out of 220,531 total inpatient or emergency department encounters between January 2017 and December 2019 in which adults received a urinalysis and urine culture order within the same 24-hour period. The patients’ median age was 67 years, over half (59.6%) were women, and nearly a quarter (24.2%) had an underlying immunocompromising condition.
Most of the cultures were obtained from inpatients. Nearly a third (30.6%) were negative for culture, while 42.1% grew at least 100,000 CFU/mL of bacteria and 17% grew mixed flora.
Based on current criteria, 21.3% of the patients had a UTI, 20.8% had ASB, and 47.6% had no UTI. The remaining 10.3% had culture growth under 100,000 CFU/mL and, therefore, did not fit in any of these categories, “as there is no consistent guidance on whether to classify them as no UTI or ASB or contamination,” the authors wrote.
When the researchers applied the new criteria, more than half of the cases of ASB (68%) were reclassified as BUS, and 28.9% of the no-UTI cases were reclassified as LUTS/OUS.
In a sensitivity analysis that examined samples with bacteriuria below the 100,000 CFU/mL threshold, nearly half the unclassified cases (43.3%) were reassigned as a UTI, increasing the proportion of patients with a diagnosed UTI from 21.3% to 25.8% of the total population. Of the remaining patients who had originally been unclassified, 14.2% were newly defined as ASB, and 42.5% became BUS.
Dr. Abraham said the addition of the BUS and LUTS/OUS categories has the potential to improve and individualize patient care. Clinicians can consider nonantibiotic therapies for the patients who had LUTS/OUS while they look into possible causes, while the BUS cases enable frontline clinicians and antibiotic stewardship teams to “meet in the middle” by monitoring those patients more closely in case symptoms worsen, she said.
The authors highlighted three key takeaways from their study, starting with the fact that nearly two thirds of patients who underwent testing for a UTI did not have signs or symptoms localized to the urinary tract — the ones reclassified as BUS.
“Hence, reclassifying patients as BUS may provide an opportunity to acknowledge diagnostic uncertainty and need for additional monitoring than ASB patients so as to promote a nuanced and patient-centered approach to diagnosis and management,” the authors wrote.
Second, a third of patients initially classified as not having a UTI were reclassified into the new LUTS/OUS category because of their symptoms, such as a poor or intermittent stream, dribbling, hesitancy, frequency, urge incontinence, and nocturia. These patients would need further workup to determine the best approach to management.
Finally, the sensitivity analysis “suggested that lowering the bacterial threshold in some symptomatic patients may capture additional patients with UTI whose symptoms may be dismissed due to concern for contamination or attributed to LUTS rather than infection.” Given that the 100,000 CFU/mL threshold is based on a single study in 1956, the authors suggested more research may help define better CFU thresholds to improve clinical care.
Dr. Berookhim said the study authors took a reasonable and thorough approach in how they tried to consider the best way to update the current diagnostic classification schema.
“I think using this as a jumping off point to look deeper is worthwhile,” such as conducting randomized controlled trials to assess the use of new categories, he said. “Getting more granular than this, I think, would just muddy the waters and make it more difficult to make clinical decisions.”
The research was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Advani reported consulting fees from Locus Biosciences, Sysmex America, GlaxoSmithKline, and bioMérieux. Dr. Abraham and Dr. Berookhim reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
An updated clinical approach to diagnosing urinary tract infections (UTIs) that considers five potential phenotype categories instead of the usual three could aid clinical management and better center patient needs, according to the authors of a new study in The Journal of Urology.
The current diagnostic paradigm includes UTI, asymptomatic bacteriuria (ASB), or not UTI, but the researchers believe these categories exclude for more ambiguous clinical cases, such as patients whose bacteria counts are low but who are symptomatic, or when nonspecific symptoms make it difficult to determine whether treatment with antibiotics is appropriate.
“Our findings suggest the need to reframe our conceptual model of UTI vs ASB to recognize clinical uncertainty and reflect the full spectrum of clinical presentations,” Sonali D. Advani, MBBS, MPH, an associate professor of medicine in infectious disease at Duke University School of Medicine, in Durham, North Carolina, and her colleagues wrote. “Recent data suggest that UTI may present as a bidirectional continuum from asymptomatic bladder colonization to a symptomatic bladder infection,” and some populations may lack the signs or symptoms specific to urinary tract or have chronic lower urinary tract symptoms (LUTS) that make it difficult to distinguish between ASB and UTI, they wrote.
Nitya E. Abraham, MD, an associate professor of urology at Albert Einstein College of Medicine and Montefiore Einstein in New York City, agreed the current paradigm has room for refinement.
“The current classification system doesn’t account for certain patients such as patients who have bothersome urinary symptoms, but urine testing comes back negative, or patients with positive urine testing, but who aren’t able to report the presence or absence of symptoms,” Dr. Abraham, who was not involved in the new research, told this news organization.
Boback Berookhim, MD, a urologist at Northwell Health in New Hyde Park, New York, who was also not involved in the research, said the goal with this study appears to be better identifying who will need antibiotics.
“I think this is more of a forward-looking study in terms of trying to identify patients who currently may not be treated or may be over treated and better identifying subsets,” Dr. Berookhim told this news organization.
However, he said the relevance of the work is far greater in hospitals than in outpatient settings.
“I think it’s much more relevant in inpatient environments where a patient is in hospital and whatever antibiotics are being written are going to be overseen and you’re going to see higher resistance patterns,” Dr. Berookhim said. “For the average doctor who’s seeing patients in the office and writing them prescriptions in the office, this doesn’t really affect them.”
Antibiotic Dilemma
A key issue in determining the best approach to UTI diagnosis is assessing the appropriateness of antibiotic treatment. Up to half of hospitalized patients have ASB, for which current practice guidelines advise against antibiotics, Dr. Advani and her colleagues noted. Yet many of these patients receive antibiotics regardless, and research has shown links between treatment and longer length of stay, antibiotic resistance, and infection with Clostridioides difficile.
The challenge comes with patients who do not fit easily into the existing categories. One includes patients who have positive urine cultures but whose symptoms, such as hypotension or fever, are not specific to the genitourinary tract.
While current guidelines advise against treating these patients with antibiotics, the patients are often older adults with cognitive impairment or delirium, and frontline physicians may err on the side of prescribing antibiotics because of their clinical uncertainty. That treatment can lead to tension with hospital antibiotic stewardship teams that recommend withholding antibiotics for those patients.
“These clinical scenarios highlight differences between the frontline clinicians’ and antibiotic stewardship teams’ definitions of ‘asymptomatic,’ highlighting the ambiguity of the term ‘asymptomatic bacteriuria,’” Dr. Advani and her colleagues wrote.
A fever, for example, could signal a viral or bacterial infection or result from a nonurinary source, Dr. Abraham said. “The antibiotic stewardship team likely prefers to observe the clinical course and wait for more data to demonstrate need for antibiotics,” she said. “Hence, there are conflicting priorities and confusion of when to treat with antibiotics for this common dilemma in patients presenting to the ER or urgent care.”
Meanwhile, other patients, particularly women, may present with urinary symptoms and pyuria but have lab results revealing a colony count below the 100,000 CFU/mL threshold that would indicate antibiotic treatment.
“Some of these women are likely suffering from a UTI and may not receive treatment if clinicians focus primarily on the urine culture results,” Dr. Abraham said. She pointed out the existence of other options than urine culture for better identifying UTI, such as urinary cell-free DNA or next-generation DNA testing of the urine. But she also said the 100,000 CFU/mL threshold should not be absolute.
“For example, I will treat patients for UTI with 10,000-50,000 CFU/mL if they also have UTI symptoms like blood in the urine, burning with urination, bladder pain, increased urgency or frequency, and the urinalysis shows a high white blood cell count,” Dr. Abraham said.
Dr. Abraham also noted a third group outside the scope of the new study: People with urinary symptoms who don’t undergo urine tests or who are treated empirically with antibiotics. “It is unclear whether those in this group truly have a UTI, but it is a common scenario that patients are unable to get urine tests and are treated with over-the-phone prescriptions to expedite treatment,” she said.
Get on the BUS
The researchers conducted a retrospective study across one academic medical center and four community hospitals in three states to assess the feasibility of using five categories of UTI diagnosis: The three existing ones plus LUTS/other urologic symptoms (OUS) and bacteriuria of unclear significance (BUS). These additional categories arose out of an hour-long discussion with a focus group of experts across several disciplines.
The analysis covered the charts of 3392 randomly selected encounters out of 220,531 total inpatient or emergency department encounters between January 2017 and December 2019 in which adults received a urinalysis and urine culture order within the same 24-hour period. The patients’ median age was 67 years, over half (59.6%) were women, and nearly a quarter (24.2%) had an underlying immunocompromising condition.
Most of the cultures were obtained from inpatients. Nearly a third (30.6%) were negative for culture, while 42.1% grew at least 100,000 CFU/mL of bacteria and 17% grew mixed flora.
Based on current criteria, 21.3% of the patients had a UTI, 20.8% had ASB, and 47.6% had no UTI. The remaining 10.3% had culture growth under 100,000 CFU/mL and, therefore, did not fit in any of these categories, “as there is no consistent guidance on whether to classify them as no UTI or ASB or contamination,” the authors wrote.
When the researchers applied the new criteria, more than half of the cases of ASB (68%) were reclassified as BUS, and 28.9% of the no-UTI cases were reclassified as LUTS/OUS.
In a sensitivity analysis that examined samples with bacteriuria below the 100,000 CFU/mL threshold, nearly half the unclassified cases (43.3%) were reassigned as a UTI, increasing the proportion of patients with a diagnosed UTI from 21.3% to 25.8% of the total population. Of the remaining patients who had originally been unclassified, 14.2% were newly defined as ASB, and 42.5% became BUS.
Dr. Abraham said the addition of the BUS and LUTS/OUS categories has the potential to improve and individualize patient care. Clinicians can consider nonantibiotic therapies for the patients who had LUTS/OUS while they look into possible causes, while the BUS cases enable frontline clinicians and antibiotic stewardship teams to “meet in the middle” by monitoring those patients more closely in case symptoms worsen, she said.
The authors highlighted three key takeaways from their study, starting with the fact that nearly two thirds of patients who underwent testing for a UTI did not have signs or symptoms localized to the urinary tract — the ones reclassified as BUS.
“Hence, reclassifying patients as BUS may provide an opportunity to acknowledge diagnostic uncertainty and need for additional monitoring than ASB patients so as to promote a nuanced and patient-centered approach to diagnosis and management,” the authors wrote.
Second, a third of patients initially classified as not having a UTI were reclassified into the new LUTS/OUS category because of their symptoms, such as a poor or intermittent stream, dribbling, hesitancy, frequency, urge incontinence, and nocturia. These patients would need further workup to determine the best approach to management.
Finally, the sensitivity analysis “suggested that lowering the bacterial threshold in some symptomatic patients may capture additional patients with UTI whose symptoms may be dismissed due to concern for contamination or attributed to LUTS rather than infection.” Given that the 100,000 CFU/mL threshold is based on a single study in 1956, the authors suggested more research may help define better CFU thresholds to improve clinical care.
Dr. Berookhim said the study authors took a reasonable and thorough approach in how they tried to consider the best way to update the current diagnostic classification schema.
“I think using this as a jumping off point to look deeper is worthwhile,” such as conducting randomized controlled trials to assess the use of new categories, he said. “Getting more granular than this, I think, would just muddy the waters and make it more difficult to make clinical decisions.”
The research was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Advani reported consulting fees from Locus Biosciences, Sysmex America, GlaxoSmithKline, and bioMérieux. Dr. Abraham and Dr. Berookhim reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
FROM THE JOURNAL OF UROLOGY
Former UCLA Doctor Receives $14 Million in Gender Discrimination Retrial
A California jury has awarded $14 million to a former University of California, Los Angeles (UCLA) oncologist who claimed she was paid thousands less than her male colleagues and wrongfully terminated after her complaints of gender-based harassment and intimidation were ignored by program leadership.
The decision comes after a lengthy 8-year legal battle in which an appellate judge reversed a previous jury decision in her favor.
Lauren Pinter-Brown, MD, a hematologic oncologist, was hired in 2005 by the University of California, Los Angeles School of Medicine — now called UCLA’s David Geffen School of Medicine. As the school’s lymphoma program director, she conducted clinical research alongside other oncology doctors, including Sven de Vos, MD.
She claimed that her professional relationship with Dr. de Vos became contentious after he demonstrated “oppositional” and “disrespectful” behavior at team meetings, such as talking over her and turning his chair so Dr. Pinter-Brown faced his back. Court documents indicated that Dr. de Vos refused to use Dr. Pinter-Brown’s title in front of colleagues despite doing so for male counterparts.
Dr. Pinter-Brown argued that she was treated as the “butt of a joke” by Dr. de Vos and other male colleagues. In 2016, she sued Dr. de Vos, the university, and its governing body, the Board of Regents, for wrongful termination.
She was awarded a $13 million verdict in 2018. However, the California Court of Appeals overturned it in 2020 after concluding that several mistakes during the court proceedings impeded the school’s right to a fair and impartial trial. The case was retried, culminating in the even higher award of $14 million issued on May 9.
“Two juries have come to virtually identical findings showing multiple problems at UCLA involving gender discrimination,” Dr. Pinter-Brown’s attorney, Carney R. Shegerian, JD, told this news organization.
A spokesperson from UCLA’s David Geffen School of Medicine said administrators are carefully reviewing the new decision.
The spokesperson told this news organization that the medical school and its health system remain “deeply committed to maintaining a workplace free from discrimination, intimidation, retaliation, or harassment of any kind” and fostering a “respectful and inclusive environment ... in research, medical education, and patient care.”
Gender Pay Disparities Persist in Medicine
The gender pay gap in medicine is well documented. The 2024 Medscape Physician Compensation Report found that male doctors earn about 29% more than their female counterparts, with the disparity growing larger among specialists. In addition, a recent JAMA Health Forum study found that male physicians earned 21%-24% more per hour than female physicians.
Dr. Pinter-Brown, who now works at the University of California, Irvine, alleged that she was paid $200,000 less annually, on average, than her male colleagues.
That’s not surprising, says Martha Gulati, MD, professor and director of preventive cardiology at Cedars-Sinai Smidt Heart Institute, Los Angeles. She coauthored a commentary about gender disparities in JAMA Network Open. Dr. Gulati told this news organization that even a “small” pay disparity of $100,000 annually adds up.
“Let’s say the [male physician] invests it at 3% and adds to it yearly. Even without a raise, in 20 years, that is approximately $3 million,” Dr. Gulati explained. “Once you find out you are paid less than your male colleagues, you are upset. Your sense of value and self-worth disappears.”
Eileen Barrett, MD, MPH, president-elect of the American Medical Women’s Association, said that gender discrimination is likely more prevalent than research indicates. She told this news organization that self-doubt and fear of retaliation keep many from exposing the mistreatment.
Although more women are entering medicine, too few rise to the highest positions, Dr. Barrett said.
“Unfortunately, many are pulled and pushed into specialties and subspecialties that have lower compensation and are not promoted to leadership, so just having numbers isn’t enough to achieve equity,” Dr. Barrett said.
Dr. Pinter-Brown claimed she was repeatedly harassed and intimidated by Dr. de Vos from 2008 to 2015. Despite voicing concerns multiple times about the discriminatory behavior, the only resolutions offered by the male-dominated program leadership were for her to separate from the group and conduct lymphoma research independently or to avoid interacting with Dr. de Vos, court records said.
Even the school’s male Title IX officer, Jan Tillisch, MD, who handled gender-based discrimination complaints, reportedly made sexist comments. When Dr. Pinter-Brown sought his help, he allegedly told her that she had a reputation as an “angry woman” and “diva,” court records showed.
According to court documents, Dr. Pinter-Brown endured nitpicking and research audits as retaliation for speaking out, temporarily suspending her research privileges. She said she was subsequently removed from the director position and replaced by Dr. de Vos.
Female physicians who report discriminatory behavior often have unfavorable outcomes and risk future career prospects, Dr. Gulati said.
To shift this dynamic, she said institutions must increase transparency and practices that support female doctors receiving “equal pay for equal work.”
A version of this article appeared on Medscape.com.
A California jury has awarded $14 million to a former University of California, Los Angeles (UCLA) oncologist who claimed she was paid thousands less than her male colleagues and wrongfully terminated after her complaints of gender-based harassment and intimidation were ignored by program leadership.
The decision comes after a lengthy 8-year legal battle in which an appellate judge reversed a previous jury decision in her favor.
Lauren Pinter-Brown, MD, a hematologic oncologist, was hired in 2005 by the University of California, Los Angeles School of Medicine — now called UCLA’s David Geffen School of Medicine. As the school’s lymphoma program director, she conducted clinical research alongside other oncology doctors, including Sven de Vos, MD.
She claimed that her professional relationship with Dr. de Vos became contentious after he demonstrated “oppositional” and “disrespectful” behavior at team meetings, such as talking over her and turning his chair so Dr. Pinter-Brown faced his back. Court documents indicated that Dr. de Vos refused to use Dr. Pinter-Brown’s title in front of colleagues despite doing so for male counterparts.
Dr. Pinter-Brown argued that she was treated as the “butt of a joke” by Dr. de Vos and other male colleagues. In 2016, she sued Dr. de Vos, the university, and its governing body, the Board of Regents, for wrongful termination.
She was awarded a $13 million verdict in 2018. However, the California Court of Appeals overturned it in 2020 after concluding that several mistakes during the court proceedings impeded the school’s right to a fair and impartial trial. The case was retried, culminating in the even higher award of $14 million issued on May 9.
“Two juries have come to virtually identical findings showing multiple problems at UCLA involving gender discrimination,” Dr. Pinter-Brown’s attorney, Carney R. Shegerian, JD, told this news organization.
A spokesperson from UCLA’s David Geffen School of Medicine said administrators are carefully reviewing the new decision.
The spokesperson told this news organization that the medical school and its health system remain “deeply committed to maintaining a workplace free from discrimination, intimidation, retaliation, or harassment of any kind” and fostering a “respectful and inclusive environment ... in research, medical education, and patient care.”
Gender Pay Disparities Persist in Medicine
The gender pay gap in medicine is well documented. The 2024 Medscape Physician Compensation Report found that male doctors earn about 29% more than their female counterparts, with the disparity growing larger among specialists. In addition, a recent JAMA Health Forum study found that male physicians earned 21%-24% more per hour than female physicians.
Dr. Pinter-Brown, who now works at the University of California, Irvine, alleged that she was paid $200,000 less annually, on average, than her male colleagues.
That’s not surprising, says Martha Gulati, MD, professor and director of preventive cardiology at Cedars-Sinai Smidt Heart Institute, Los Angeles. She coauthored a commentary about gender disparities in JAMA Network Open. Dr. Gulati told this news organization that even a “small” pay disparity of $100,000 annually adds up.
“Let’s say the [male physician] invests it at 3% and adds to it yearly. Even without a raise, in 20 years, that is approximately $3 million,” Dr. Gulati explained. “Once you find out you are paid less than your male colleagues, you are upset. Your sense of value and self-worth disappears.”
Eileen Barrett, MD, MPH, president-elect of the American Medical Women’s Association, said that gender discrimination is likely more prevalent than research indicates. She told this news organization that self-doubt and fear of retaliation keep many from exposing the mistreatment.
Although more women are entering medicine, too few rise to the highest positions, Dr. Barrett said.
“Unfortunately, many are pulled and pushed into specialties and subspecialties that have lower compensation and are not promoted to leadership, so just having numbers isn’t enough to achieve equity,” Dr. Barrett said.
Dr. Pinter-Brown claimed she was repeatedly harassed and intimidated by Dr. de Vos from 2008 to 2015. Despite voicing concerns multiple times about the discriminatory behavior, the only resolutions offered by the male-dominated program leadership were for her to separate from the group and conduct lymphoma research independently or to avoid interacting with Dr. de Vos, court records said.
Even the school’s male Title IX officer, Jan Tillisch, MD, who handled gender-based discrimination complaints, reportedly made sexist comments. When Dr. Pinter-Brown sought his help, he allegedly told her that she had a reputation as an “angry woman” and “diva,” court records showed.
According to court documents, Dr. Pinter-Brown endured nitpicking and research audits as retaliation for speaking out, temporarily suspending her research privileges. She said she was subsequently removed from the director position and replaced by Dr. de Vos.
Female physicians who report discriminatory behavior often have unfavorable outcomes and risk future career prospects, Dr. Gulati said.
To shift this dynamic, she said institutions must increase transparency and practices that support female doctors receiving “equal pay for equal work.”
A version of this article appeared on Medscape.com.
A California jury has awarded $14 million to a former University of California, Los Angeles (UCLA) oncologist who claimed she was paid thousands less than her male colleagues and wrongfully terminated after her complaints of gender-based harassment and intimidation were ignored by program leadership.
The decision comes after a lengthy 8-year legal battle in which an appellate judge reversed a previous jury decision in her favor.
Lauren Pinter-Brown, MD, a hematologic oncologist, was hired in 2005 by the University of California, Los Angeles School of Medicine — now called UCLA’s David Geffen School of Medicine. As the school’s lymphoma program director, she conducted clinical research alongside other oncology doctors, including Sven de Vos, MD.
She claimed that her professional relationship with Dr. de Vos became contentious after he demonstrated “oppositional” and “disrespectful” behavior at team meetings, such as talking over her and turning his chair so Dr. Pinter-Brown faced his back. Court documents indicated that Dr. de Vos refused to use Dr. Pinter-Brown’s title in front of colleagues despite doing so for male counterparts.
Dr. Pinter-Brown argued that she was treated as the “butt of a joke” by Dr. de Vos and other male colleagues. In 2016, she sued Dr. de Vos, the university, and its governing body, the Board of Regents, for wrongful termination.
She was awarded a $13 million verdict in 2018. However, the California Court of Appeals overturned it in 2020 after concluding that several mistakes during the court proceedings impeded the school’s right to a fair and impartial trial. The case was retried, culminating in the even higher award of $14 million issued on May 9.
“Two juries have come to virtually identical findings showing multiple problems at UCLA involving gender discrimination,” Dr. Pinter-Brown’s attorney, Carney R. Shegerian, JD, told this news organization.
A spokesperson from UCLA’s David Geffen School of Medicine said administrators are carefully reviewing the new decision.
The spokesperson told this news organization that the medical school and its health system remain “deeply committed to maintaining a workplace free from discrimination, intimidation, retaliation, or harassment of any kind” and fostering a “respectful and inclusive environment ... in research, medical education, and patient care.”
Gender Pay Disparities Persist in Medicine
The gender pay gap in medicine is well documented. The 2024 Medscape Physician Compensation Report found that male doctors earn about 29% more than their female counterparts, with the disparity growing larger among specialists. In addition, a recent JAMA Health Forum study found that male physicians earned 21%-24% more per hour than female physicians.
Dr. Pinter-Brown, who now works at the University of California, Irvine, alleged that she was paid $200,000 less annually, on average, than her male colleagues.
That’s not surprising, says Martha Gulati, MD, professor and director of preventive cardiology at Cedars-Sinai Smidt Heart Institute, Los Angeles. She coauthored a commentary about gender disparities in JAMA Network Open. Dr. Gulati told this news organization that even a “small” pay disparity of $100,000 annually adds up.
“Let’s say the [male physician] invests it at 3% and adds to it yearly. Even without a raise, in 20 years, that is approximately $3 million,” Dr. Gulati explained. “Once you find out you are paid less than your male colleagues, you are upset. Your sense of value and self-worth disappears.”
Eileen Barrett, MD, MPH, president-elect of the American Medical Women’s Association, said that gender discrimination is likely more prevalent than research indicates. She told this news organization that self-doubt and fear of retaliation keep many from exposing the mistreatment.
Although more women are entering medicine, too few rise to the highest positions, Dr. Barrett said.
“Unfortunately, many are pulled and pushed into specialties and subspecialties that have lower compensation and are not promoted to leadership, so just having numbers isn’t enough to achieve equity,” Dr. Barrett said.
Dr. Pinter-Brown claimed she was repeatedly harassed and intimidated by Dr. de Vos from 2008 to 2015. Despite voicing concerns multiple times about the discriminatory behavior, the only resolutions offered by the male-dominated program leadership were for her to separate from the group and conduct lymphoma research independently or to avoid interacting with Dr. de Vos, court records said.
Even the school’s male Title IX officer, Jan Tillisch, MD, who handled gender-based discrimination complaints, reportedly made sexist comments. When Dr. Pinter-Brown sought his help, he allegedly told her that she had a reputation as an “angry woman” and “diva,” court records showed.
According to court documents, Dr. Pinter-Brown endured nitpicking and research audits as retaliation for speaking out, temporarily suspending her research privileges. She said she was subsequently removed from the director position and replaced by Dr. de Vos.
Female physicians who report discriminatory behavior often have unfavorable outcomes and risk future career prospects, Dr. Gulati said.
To shift this dynamic, she said institutions must increase transparency and practices that support female doctors receiving “equal pay for equal work.”
A version of this article appeared on Medscape.com.
Transient Symmetric Blanching Macules on a Background of Reticulate Erythema
The Diagnosis: BASCULE Syndrome
The patient had previously been thought to have livedo reticularis by primary care. Repeat antinuclear antibody (ANA) testing was positive (1:1280 homogeneous [reflexive titers all negative]). However, upon dermatologic evaluation, the manifestation of the rash in addition to onset occurring with postural changes challenged the livedo reticularis diagnosis. Extensive research and consultation with dermatologic colleagues led to the diagnosis of the rare entity BASCULE syndrome. BASCULE (Bier anemic spots, cyanosis, and urticarialike eruption) syndrome was described by Bessis et al1 in 2016. It is a rare condition but may be underreported.2 It is a benign pediatric disorder in the vascular acrosyndrome family that is characterized by underlying vasomotor dysfunction in distal regions of the body. Raynaud phenomenon is a widely known member of this family. As seen in our patient, it typically presents on the distal legs and feet with numerous irregular hypopigmented macules on a cyanotic background. Red-orange papules may appear on the hypopigmented macules and often are pruritic. Lesions on the distal upper extremities are less common, and a case involving the trunk has been reported.3 Onset generally begins within a couple of minutes of standing or mechanical compression of the lower legs, with full reversal of symptoms occurring within minutes of laying down or walking. Commonly reported associated symptoms include tenderness, pruritus, edema, and pain; however, the cutaneous lesions may be asymptomatic. The condition tends to affect adolescents, as seen in our patient; however, there have been reports in infants as young as 3 months to adults aged 19 years.2
The pathophysiology behind BASCULE syndrome remains unclear but is believed to be centered around the role of physiologic venous stasis that occurs when standing. The hypoxia secondary to stasis is thought to induce amplified vasoconstriction of arterioles. These responses are further exaggerated due to absence of venoarteriolar reflexes in dermal ascending arterioles, leading to Bier spots.2 The role of mast cells and eosinophils remains unclear. It is a clinical diagnosis without clear histologic findings; therefore, biopsy was not pursued in our patient.
Although BASCULE syndrome is a benign entity, it is imperative that it be recognized to avoid a time consuming, expensive, and anxiety-producing diagnostic workup, as occurred in our patient. Although not a manifestation of systemic disease, BASCULE syndrome may be associated with orthostatic hypotension in up to 20% of cases.2,4 Therefore, these patients should undergo orthostatic testing, including the tilt table test. In our patient, these manifestations were not appreciated.
There are no current guidelines for effective treatment of BASCULE syndrome. Given the possible role of mast cells in the condition, H1 antihistamines are proposed as first-line treatment. Desloratadine (10 mg/d for 7 days) has been found to be associated with improvement of pruritus. However, a recent literature review found little evidence to support the use of H1 antihistamines for resolution of other symptoms.2
The differential diagnosis includes livedo reticularis, Bier spots, Sneddon syndrome, and urticarial vasculitis. Livedo reticularis presents as distinct, netlike, blue-erythematousviolaceous discoloration, which differs from the distinct orange-red macules in BASCULE syndrome.5 In addition to distinct variances in dermatologic presentation, livedo reticularis typically is associated with cold exposure as a causative agent, with cold avoidance as the treatment for this benign and often transient condition.6 This phenomenon was not appreciated in our patient. Livedo reticularis commonly occurs with antiphospholipid syndrome.5 This association in combination with our patient's positive ANA findings and her mother's history of miscarriages resulted in the misdiagnosis as livedo reticularis.
Bier spots manifest as white macules with surrounding erythema and typically present in young adults. When first described in the literature, it was debated if BASCULE syndrome was simply another manifestation of Bier spots or postural orthostatic intolerance,4 as there was a large consensus that postural orthostatic intolerance was associated with BASCULE syndrome, with the majority of patients not meeting criteria for the condition. Heymann4 addressed the differences in BASCULE manifestations vs typical Bier spots. The author extended the syndrome to include cyanosis, an urticarialike eruption of red-orange macules with central papules located centrally, pruritus, tenderness, and partial or diffuse edema, in addition to Bier spots.4
Sneddon syndrome is a rare progressive disorder that affects small- to medium-sized blood vessels resulting in multiple episodes of ischemia in the brain. Skin manifestations of these repeated strokes are similar to livedo reticularis, typically manifesting as livedo racemosa—irregular reticular patterns of skin mottling with reddish-blue hues.6 However, Sneddon syndrome is more generalized and widespread and differs from BASCULE syndrome in shape and histologic findings. Our patient presented with findings on the legs, which is more characteristic of livedo reticularis vs livedo racemosa. Our patient experienced resolution upon laying down and sitting, and Sneddon syndrome persists beyond postural changes. Furthermore, patients with Sneddon syndrome present with neurologic symptoms such as prodromal headaches.6
Urticarial vasculitis was ruled out in our patient because of the duration of symptoms as well as the spatial changes. Urticarial vasculitis is a rare skin condition characterized by chronic recurring urticarial lesions that may persist for more than a day. This condition typically presents in middle-aged women and rarely in children. Urticarial vasculitis is thought to be immune-complex mediated, but its cause is largely unknown. It is a common manifestation of underlying conditions such as systemic lupus erythematosus.6 Our patient had a positive ANA and possible autoimmune history from her mother; however, urticarial vasculitis does not present transiently on the legs or in the rash pattern appreciated in our patient.
- Bessis D, Jeziorski E, Rigau V, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome: a new entity? Br J Dermatol. 2016;175:218-220. doi:10.1111/bjd.14589
- Baurens N, Briand C, Giovannini-Chami L, et al. Case report, practices survey and literature review of an under-recognized pediatric vascular disorder: the BASCULE syndrome. Front Pediatr. 2022;10:849914. doi:10.3389/fped.2022.849914
- Jiménez-Gallo D, Collantes-Rodríguez C, Ossorio-García L, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome on trunk and upper limbs. Pediatr Dermatol. 2018;35:E313-E315. doi:10.1111/pde.13558
- Heymann WR. BASCULE syndrome: is something brewing with Bier spots? Dermatology World Insights and Inquiries. September 7, 2022. https://www.aad.org/dw/dw-insights-and-inquiries/archive/2022/bascule-syndrome
- Sajjan VV, Lunge S, Swamy MB, et al. Livedo reticularis: a review of the literature. Indian Dermatol Online J. 2015;6:315-321. doi:10.4103/2229-5178.164493
- Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. 2021;7:290-297. doi:10.1016/j.ijwd.2021.01.021
The Diagnosis: BASCULE Syndrome
The patient had previously been thought to have livedo reticularis by primary care. Repeat antinuclear antibody (ANA) testing was positive (1:1280 homogeneous [reflexive titers all negative]). However, upon dermatologic evaluation, the manifestation of the rash in addition to onset occurring with postural changes challenged the livedo reticularis diagnosis. Extensive research and consultation with dermatologic colleagues led to the diagnosis of the rare entity BASCULE syndrome. BASCULE (Bier anemic spots, cyanosis, and urticarialike eruption) syndrome was described by Bessis et al1 in 2016. It is a rare condition but may be underreported.2 It is a benign pediatric disorder in the vascular acrosyndrome family that is characterized by underlying vasomotor dysfunction in distal regions of the body. Raynaud phenomenon is a widely known member of this family. As seen in our patient, it typically presents on the distal legs and feet with numerous irregular hypopigmented macules on a cyanotic background. Red-orange papules may appear on the hypopigmented macules and often are pruritic. Lesions on the distal upper extremities are less common, and a case involving the trunk has been reported.3 Onset generally begins within a couple of minutes of standing or mechanical compression of the lower legs, with full reversal of symptoms occurring within minutes of laying down or walking. Commonly reported associated symptoms include tenderness, pruritus, edema, and pain; however, the cutaneous lesions may be asymptomatic. The condition tends to affect adolescents, as seen in our patient; however, there have been reports in infants as young as 3 months to adults aged 19 years.2
The pathophysiology behind BASCULE syndrome remains unclear but is believed to be centered around the role of physiologic venous stasis that occurs when standing. The hypoxia secondary to stasis is thought to induce amplified vasoconstriction of arterioles. These responses are further exaggerated due to absence of venoarteriolar reflexes in dermal ascending arterioles, leading to Bier spots.2 The role of mast cells and eosinophils remains unclear. It is a clinical diagnosis without clear histologic findings; therefore, biopsy was not pursued in our patient.
Although BASCULE syndrome is a benign entity, it is imperative that it be recognized to avoid a time consuming, expensive, and anxiety-producing diagnostic workup, as occurred in our patient. Although not a manifestation of systemic disease, BASCULE syndrome may be associated with orthostatic hypotension in up to 20% of cases.2,4 Therefore, these patients should undergo orthostatic testing, including the tilt table test. In our patient, these manifestations were not appreciated.
There are no current guidelines for effective treatment of BASCULE syndrome. Given the possible role of mast cells in the condition, H1 antihistamines are proposed as first-line treatment. Desloratadine (10 mg/d for 7 days) has been found to be associated with improvement of pruritus. However, a recent literature review found little evidence to support the use of H1 antihistamines for resolution of other symptoms.2
The differential diagnosis includes livedo reticularis, Bier spots, Sneddon syndrome, and urticarial vasculitis. Livedo reticularis presents as distinct, netlike, blue-erythematousviolaceous discoloration, which differs from the distinct orange-red macules in BASCULE syndrome.5 In addition to distinct variances in dermatologic presentation, livedo reticularis typically is associated with cold exposure as a causative agent, with cold avoidance as the treatment for this benign and often transient condition.6 This phenomenon was not appreciated in our patient. Livedo reticularis commonly occurs with antiphospholipid syndrome.5 This association in combination with our patient's positive ANA findings and her mother's history of miscarriages resulted in the misdiagnosis as livedo reticularis.
Bier spots manifest as white macules with surrounding erythema and typically present in young adults. When first described in the literature, it was debated if BASCULE syndrome was simply another manifestation of Bier spots or postural orthostatic intolerance,4 as there was a large consensus that postural orthostatic intolerance was associated with BASCULE syndrome, with the majority of patients not meeting criteria for the condition. Heymann4 addressed the differences in BASCULE manifestations vs typical Bier spots. The author extended the syndrome to include cyanosis, an urticarialike eruption of red-orange macules with central papules located centrally, pruritus, tenderness, and partial or diffuse edema, in addition to Bier spots.4
Sneddon syndrome is a rare progressive disorder that affects small- to medium-sized blood vessels resulting in multiple episodes of ischemia in the brain. Skin manifestations of these repeated strokes are similar to livedo reticularis, typically manifesting as livedo racemosa—irregular reticular patterns of skin mottling with reddish-blue hues.6 However, Sneddon syndrome is more generalized and widespread and differs from BASCULE syndrome in shape and histologic findings. Our patient presented with findings on the legs, which is more characteristic of livedo reticularis vs livedo racemosa. Our patient experienced resolution upon laying down and sitting, and Sneddon syndrome persists beyond postural changes. Furthermore, patients with Sneddon syndrome present with neurologic symptoms such as prodromal headaches.6
Urticarial vasculitis was ruled out in our patient because of the duration of symptoms as well as the spatial changes. Urticarial vasculitis is a rare skin condition characterized by chronic recurring urticarial lesions that may persist for more than a day. This condition typically presents in middle-aged women and rarely in children. Urticarial vasculitis is thought to be immune-complex mediated, but its cause is largely unknown. It is a common manifestation of underlying conditions such as systemic lupus erythematosus.6 Our patient had a positive ANA and possible autoimmune history from her mother; however, urticarial vasculitis does not present transiently on the legs or in the rash pattern appreciated in our patient.
The Diagnosis: BASCULE Syndrome
The patient had previously been thought to have livedo reticularis by primary care. Repeat antinuclear antibody (ANA) testing was positive (1:1280 homogeneous [reflexive titers all negative]). However, upon dermatologic evaluation, the manifestation of the rash in addition to onset occurring with postural changes challenged the livedo reticularis diagnosis. Extensive research and consultation with dermatologic colleagues led to the diagnosis of the rare entity BASCULE syndrome. BASCULE (Bier anemic spots, cyanosis, and urticarialike eruption) syndrome was described by Bessis et al1 in 2016. It is a rare condition but may be underreported.2 It is a benign pediatric disorder in the vascular acrosyndrome family that is characterized by underlying vasomotor dysfunction in distal regions of the body. Raynaud phenomenon is a widely known member of this family. As seen in our patient, it typically presents on the distal legs and feet with numerous irregular hypopigmented macules on a cyanotic background. Red-orange papules may appear on the hypopigmented macules and often are pruritic. Lesions on the distal upper extremities are less common, and a case involving the trunk has been reported.3 Onset generally begins within a couple of minutes of standing or mechanical compression of the lower legs, with full reversal of symptoms occurring within minutes of laying down or walking. Commonly reported associated symptoms include tenderness, pruritus, edema, and pain; however, the cutaneous lesions may be asymptomatic. The condition tends to affect adolescents, as seen in our patient; however, there have been reports in infants as young as 3 months to adults aged 19 years.2
The pathophysiology behind BASCULE syndrome remains unclear but is believed to be centered around the role of physiologic venous stasis that occurs when standing. The hypoxia secondary to stasis is thought to induce amplified vasoconstriction of arterioles. These responses are further exaggerated due to absence of venoarteriolar reflexes in dermal ascending arterioles, leading to Bier spots.2 The role of mast cells and eosinophils remains unclear. It is a clinical diagnosis without clear histologic findings; therefore, biopsy was not pursued in our patient.
Although BASCULE syndrome is a benign entity, it is imperative that it be recognized to avoid a time consuming, expensive, and anxiety-producing diagnostic workup, as occurred in our patient. Although not a manifestation of systemic disease, BASCULE syndrome may be associated with orthostatic hypotension in up to 20% of cases.2,4 Therefore, these patients should undergo orthostatic testing, including the tilt table test. In our patient, these manifestations were not appreciated.
There are no current guidelines for effective treatment of BASCULE syndrome. Given the possible role of mast cells in the condition, H1 antihistamines are proposed as first-line treatment. Desloratadine (10 mg/d for 7 days) has been found to be associated with improvement of pruritus. However, a recent literature review found little evidence to support the use of H1 antihistamines for resolution of other symptoms.2
The differential diagnosis includes livedo reticularis, Bier spots, Sneddon syndrome, and urticarial vasculitis. Livedo reticularis presents as distinct, netlike, blue-erythematousviolaceous discoloration, which differs from the distinct orange-red macules in BASCULE syndrome.5 In addition to distinct variances in dermatologic presentation, livedo reticularis typically is associated with cold exposure as a causative agent, with cold avoidance as the treatment for this benign and often transient condition.6 This phenomenon was not appreciated in our patient. Livedo reticularis commonly occurs with antiphospholipid syndrome.5 This association in combination with our patient's positive ANA findings and her mother's history of miscarriages resulted in the misdiagnosis as livedo reticularis.
Bier spots manifest as white macules with surrounding erythema and typically present in young adults. When first described in the literature, it was debated if BASCULE syndrome was simply another manifestation of Bier spots or postural orthostatic intolerance,4 as there was a large consensus that postural orthostatic intolerance was associated with BASCULE syndrome, with the majority of patients not meeting criteria for the condition. Heymann4 addressed the differences in BASCULE manifestations vs typical Bier spots. The author extended the syndrome to include cyanosis, an urticarialike eruption of red-orange macules with central papules located centrally, pruritus, tenderness, and partial or diffuse edema, in addition to Bier spots.4
Sneddon syndrome is a rare progressive disorder that affects small- to medium-sized blood vessels resulting in multiple episodes of ischemia in the brain. Skin manifestations of these repeated strokes are similar to livedo reticularis, typically manifesting as livedo racemosa—irregular reticular patterns of skin mottling with reddish-blue hues.6 However, Sneddon syndrome is more generalized and widespread and differs from BASCULE syndrome in shape and histologic findings. Our patient presented with findings on the legs, which is more characteristic of livedo reticularis vs livedo racemosa. Our patient experienced resolution upon laying down and sitting, and Sneddon syndrome persists beyond postural changes. Furthermore, patients with Sneddon syndrome present with neurologic symptoms such as prodromal headaches.6
Urticarial vasculitis was ruled out in our patient because of the duration of symptoms as well as the spatial changes. Urticarial vasculitis is a rare skin condition characterized by chronic recurring urticarial lesions that may persist for more than a day. This condition typically presents in middle-aged women and rarely in children. Urticarial vasculitis is thought to be immune-complex mediated, but its cause is largely unknown. It is a common manifestation of underlying conditions such as systemic lupus erythematosus.6 Our patient had a positive ANA and possible autoimmune history from her mother; however, urticarial vasculitis does not present transiently on the legs or in the rash pattern appreciated in our patient.
- Bessis D, Jeziorski E, Rigau V, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome: a new entity? Br J Dermatol. 2016;175:218-220. doi:10.1111/bjd.14589
- Baurens N, Briand C, Giovannini-Chami L, et al. Case report, practices survey and literature review of an under-recognized pediatric vascular disorder: the BASCULE syndrome. Front Pediatr. 2022;10:849914. doi:10.3389/fped.2022.849914
- Jiménez-Gallo D, Collantes-Rodríguez C, Ossorio-García L, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome on trunk and upper limbs. Pediatr Dermatol. 2018;35:E313-E315. doi:10.1111/pde.13558
- Heymann WR. BASCULE syndrome: is something brewing with Bier spots? Dermatology World Insights and Inquiries. September 7, 2022. https://www.aad.org/dw/dw-insights-and-inquiries/archive/2022/bascule-syndrome
- Sajjan VV, Lunge S, Swamy MB, et al. Livedo reticularis: a review of the literature. Indian Dermatol Online J. 2015;6:315-321. doi:10.4103/2229-5178.164493
- Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. 2021;7:290-297. doi:10.1016/j.ijwd.2021.01.021
- Bessis D, Jeziorski E, Rigau V, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome: a new entity? Br J Dermatol. 2016;175:218-220. doi:10.1111/bjd.14589
- Baurens N, Briand C, Giovannini-Chami L, et al. Case report, practices survey and literature review of an under-recognized pediatric vascular disorder: the BASCULE syndrome. Front Pediatr. 2022;10:849914. doi:10.3389/fped.2022.849914
- Jiménez-Gallo D, Collantes-Rodríguez C, Ossorio-García L, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome on trunk and upper limbs. Pediatr Dermatol. 2018;35:E313-E315. doi:10.1111/pde.13558
- Heymann WR. BASCULE syndrome: is something brewing with Bier spots? Dermatology World Insights and Inquiries. September 7, 2022. https://www.aad.org/dw/dw-insights-and-inquiries/archive/2022/bascule-syndrome
- Sajjan VV, Lunge S, Swamy MB, et al. Livedo reticularis: a review of the literature. Indian Dermatol Online J. 2015;6:315-321. doi:10.4103/2229-5178.164493
- Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. 2021;7:290-297. doi:10.1016/j.ijwd.2021.01.021
An 11-year-old girl was referred to the dermatology clinic for evaluation of a rash on the legs and feet of 1 year’s duration. The rash appeared every time she was standing for longer than 10 to 15 minutes and resolved when sitting or laying down. After the initial onset, the rash did not spread to other body areas but became more prominent in appearance. The patient endorsed intense pruritus associated with the rash. A review of systems was negative for fever, headaches, history of blood clots, and joint pain. She did not have any known medical conditions or take any medications. The patient’s mother reported that the patient experienced episodes of leg numbness while sitting in vehicles from 6 to 10 years of age. There was no family history of rheumatologic, hematologic, or cardiac conditions. The patient’s mother had experienced 2 miscarriages but denied any other obstetric complications. The patient had 1 sibling who was unaffected. Physical examination revealed reticulate erythema on the calves with scattered regions of blanching and evanescent pink macules as well as dermatographism.
One month prior to presenting to dermatology, the patient was evaluated by rheumatology, endocrinology, and hematology. Laboratory workup completed at age 3 years included antinuclear antibody, anticardiolipin antibody, and antithrombin III activity; factor V Leiden; cryoglobulins; quantitation (human chorionic gonadotropin); proteins S and C activity; antineutrophil cytoplasmic antibody screen; thyroid studies; prothrombin time; and partial thromboplastin time. All laboratory results were within reference range.
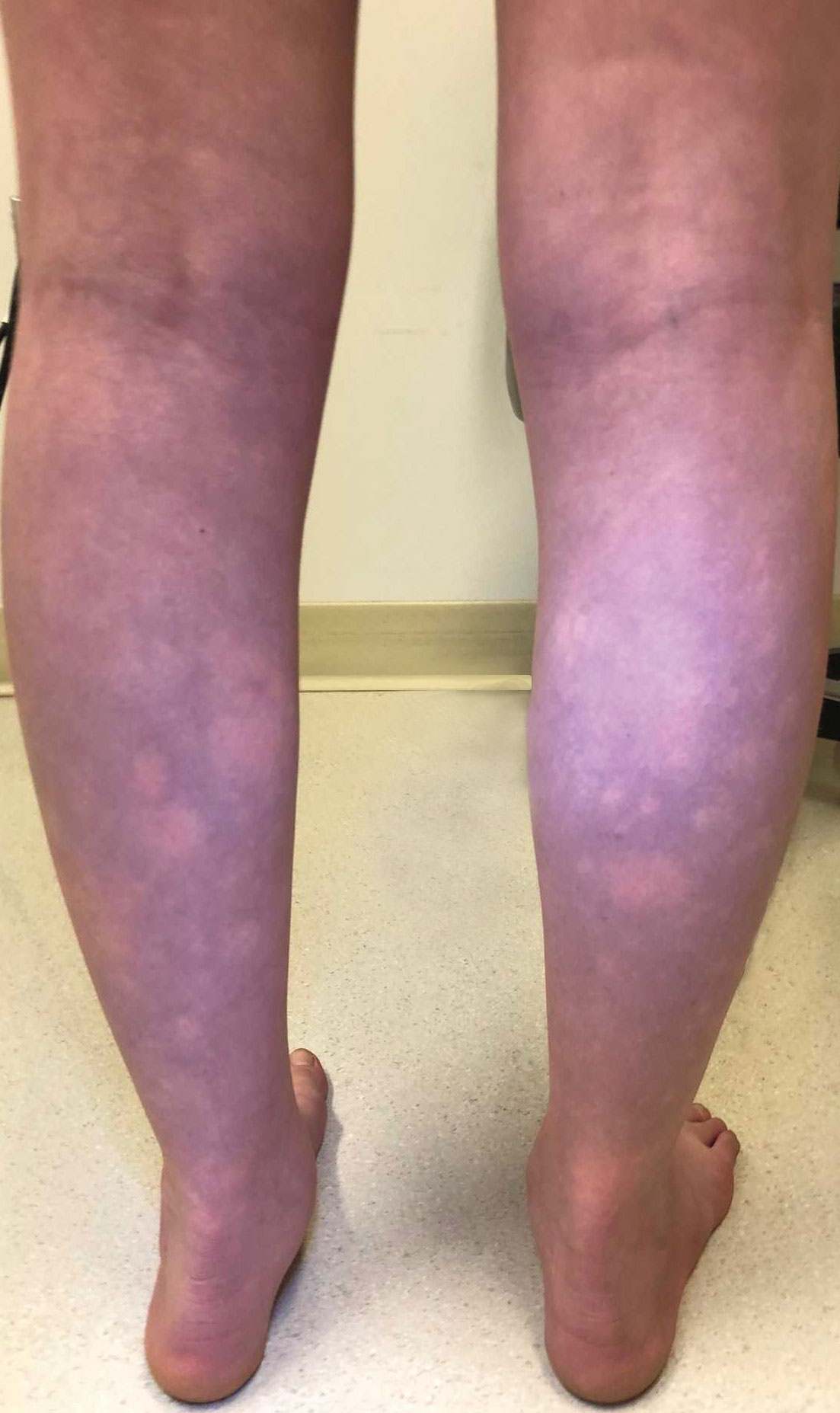

Does Eating Food With Emulsifiers Increase T2D Risk?
TOPLINE:
Various food additive emulsifiers, including total carrageenans, carrageenan gum, tripotassium phosphate, sodium citrate, and guar gum, can increase the risk for type 2 diabetes (T2D), showed a recent study.
METHODOLOGY:
- Food emulsifiers, which are extensively used to enhance the texture and improve the shelf life of various ultraprocessed food items, have been shown to increase the risk for cardiovascular disease and cancer.
- In this study, the dietary intake data of 104,139 adults (79.2% women; mean age, 42.7 years) enrolled in the French NutriNet-Santé prospective cohort study from May 2009 to April 2023 were assessed for 24 hours on 3 nonconsecutive days at inclusion and every 6 months thereafter to determine the risk for T2D.
- The dietary records of participants, which were linked to food composition databases, were used to quantify the food additive intake.
- T2D cases were identified using a multisource approach encompassing self-reports, health questionnaires, national health insurance system databases, and/or mortality registries.
TAKEAWAY:
- During a mean follow-up period of 6.8 years, 1056 incident cases of T2D were reported.
- Almost all (99.7%) participants were exposed to at least one food additive emulsifier, with the main contributors being ultraprocessed fruits and vegetables (18.5%), cakes and biscuits (14.7%), and dairy products (10.0%).
- The intake of the following emulsifiers increased the risk for T2D:
- Total carrageenans and carrageenan gum (3% increased risk per increment of 100 mg/d; P < .001)
- Tripotassium phosphate (15% increased risk per increment of 500 mg/d; P = .023)
- Acetyl tartaric acid esters of monoglycerides and diglycerides of fatty acids (4% increased risk per increment of 100 mg/d; P = .042)
- Sodium citrate (4% increased risk per increment of 500 mg/d; P = .008)
- Guar gum (11% increased risk per increment of 500 mg/d; P < .0001)
- Gum arabic (3% increased risk per increment of 1000 mg/d; P = .013)
- Xanthan gum (8% increased risk per increment of 500 mg/d; P = .013)
IN PRACTICE:
In an accompanying commentary, experts postulated that “findings from this and other studies could prompt regulatory agencies and policymakers to reconsider the rules governing the use of emulsifiers and other additives by the food industry such as setting limits and requiring better disclosure of food additive contents to help consumers make more informed choices.”
SOURCE:
Clara Salame, PhD, Université Sorbonne Paris Nord and Université Paris Cité, INSERM, INRAE, CNAM, Center of Research in Epidemiology and Statistics, Nutritional Epidemiology Research Team, Paris, France, led this study, which was published online in The Lancet Diabetes & Endocrinology.
LIMITATIONS:
The observational nature of this study is not sufficient to establish causality relationships. There may have been measurement errors in emulsifier exposure, particularly in products exempted from labeling requirements. This cohort’s demographics, which included a higher percentage of women and a health-conscious population, may affect the generalizability of the study’s findings.
DISCLOSURES:
This study received funding from the European Research Council, and the NutriNet-Santé study was supported by many public institutions such as the Ministère de la Santé, Santé publique France, Université Sorbonne Paris Nord, and others. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Various food additive emulsifiers, including total carrageenans, carrageenan gum, tripotassium phosphate, sodium citrate, and guar gum, can increase the risk for type 2 diabetes (T2D), showed a recent study.
METHODOLOGY:
- Food emulsifiers, which are extensively used to enhance the texture and improve the shelf life of various ultraprocessed food items, have been shown to increase the risk for cardiovascular disease and cancer.
- In this study, the dietary intake data of 104,139 adults (79.2% women; mean age, 42.7 years) enrolled in the French NutriNet-Santé prospective cohort study from May 2009 to April 2023 were assessed for 24 hours on 3 nonconsecutive days at inclusion and every 6 months thereafter to determine the risk for T2D.
- The dietary records of participants, which were linked to food composition databases, were used to quantify the food additive intake.
- T2D cases were identified using a multisource approach encompassing self-reports, health questionnaires, national health insurance system databases, and/or mortality registries.
TAKEAWAY:
- During a mean follow-up period of 6.8 years, 1056 incident cases of T2D were reported.
- Almost all (99.7%) participants were exposed to at least one food additive emulsifier, with the main contributors being ultraprocessed fruits and vegetables (18.5%), cakes and biscuits (14.7%), and dairy products (10.0%).
- The intake of the following emulsifiers increased the risk for T2D:
- Total carrageenans and carrageenan gum (3% increased risk per increment of 100 mg/d; P < .001)
- Tripotassium phosphate (15% increased risk per increment of 500 mg/d; P = .023)
- Acetyl tartaric acid esters of monoglycerides and diglycerides of fatty acids (4% increased risk per increment of 100 mg/d; P = .042)
- Sodium citrate (4% increased risk per increment of 500 mg/d; P = .008)
- Guar gum (11% increased risk per increment of 500 mg/d; P < .0001)
- Gum arabic (3% increased risk per increment of 1000 mg/d; P = .013)
- Xanthan gum (8% increased risk per increment of 500 mg/d; P = .013)
IN PRACTICE:
In an accompanying commentary, experts postulated that “findings from this and other studies could prompt regulatory agencies and policymakers to reconsider the rules governing the use of emulsifiers and other additives by the food industry such as setting limits and requiring better disclosure of food additive contents to help consumers make more informed choices.”
SOURCE:
Clara Salame, PhD, Université Sorbonne Paris Nord and Université Paris Cité, INSERM, INRAE, CNAM, Center of Research in Epidemiology and Statistics, Nutritional Epidemiology Research Team, Paris, France, led this study, which was published online in The Lancet Diabetes & Endocrinology.
LIMITATIONS:
The observational nature of this study is not sufficient to establish causality relationships. There may have been measurement errors in emulsifier exposure, particularly in products exempted from labeling requirements. This cohort’s demographics, which included a higher percentage of women and a health-conscious population, may affect the generalizability of the study’s findings.
DISCLOSURES:
This study received funding from the European Research Council, and the NutriNet-Santé study was supported by many public institutions such as the Ministère de la Santé, Santé publique France, Université Sorbonne Paris Nord, and others. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Various food additive emulsifiers, including total carrageenans, carrageenan gum, tripotassium phosphate, sodium citrate, and guar gum, can increase the risk for type 2 diabetes (T2D), showed a recent study.
METHODOLOGY:
- Food emulsifiers, which are extensively used to enhance the texture and improve the shelf life of various ultraprocessed food items, have been shown to increase the risk for cardiovascular disease and cancer.
- In this study, the dietary intake data of 104,139 adults (79.2% women; mean age, 42.7 years) enrolled in the French NutriNet-Santé prospective cohort study from May 2009 to April 2023 were assessed for 24 hours on 3 nonconsecutive days at inclusion and every 6 months thereafter to determine the risk for T2D.
- The dietary records of participants, which were linked to food composition databases, were used to quantify the food additive intake.
- T2D cases were identified using a multisource approach encompassing self-reports, health questionnaires, national health insurance system databases, and/or mortality registries.
TAKEAWAY:
- During a mean follow-up period of 6.8 years, 1056 incident cases of T2D were reported.
- Almost all (99.7%) participants were exposed to at least one food additive emulsifier, with the main contributors being ultraprocessed fruits and vegetables (18.5%), cakes and biscuits (14.7%), and dairy products (10.0%).
- The intake of the following emulsifiers increased the risk for T2D:
- Total carrageenans and carrageenan gum (3% increased risk per increment of 100 mg/d; P < .001)
- Tripotassium phosphate (15% increased risk per increment of 500 mg/d; P = .023)
- Acetyl tartaric acid esters of monoglycerides and diglycerides of fatty acids (4% increased risk per increment of 100 mg/d; P = .042)
- Sodium citrate (4% increased risk per increment of 500 mg/d; P = .008)
- Guar gum (11% increased risk per increment of 500 mg/d; P < .0001)
- Gum arabic (3% increased risk per increment of 1000 mg/d; P = .013)
- Xanthan gum (8% increased risk per increment of 500 mg/d; P = .013)
IN PRACTICE:
In an accompanying commentary, experts postulated that “findings from this and other studies could prompt regulatory agencies and policymakers to reconsider the rules governing the use of emulsifiers and other additives by the food industry such as setting limits and requiring better disclosure of food additive contents to help consumers make more informed choices.”
SOURCE:
Clara Salame, PhD, Université Sorbonne Paris Nord and Université Paris Cité, INSERM, INRAE, CNAM, Center of Research in Epidemiology and Statistics, Nutritional Epidemiology Research Team, Paris, France, led this study, which was published online in The Lancet Diabetes & Endocrinology.
LIMITATIONS:
The observational nature of this study is not sufficient to establish causality relationships. There may have been measurement errors in emulsifier exposure, particularly in products exempted from labeling requirements. This cohort’s demographics, which included a higher percentage of women and a health-conscious population, may affect the generalizability of the study’s findings.
DISCLOSURES:
This study received funding from the European Research Council, and the NutriNet-Santé study was supported by many public institutions such as the Ministère de la Santé, Santé publique France, Université Sorbonne Paris Nord, and others. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
Novel ENV-101 associated with improved lung function in IPF
SAN DIEGO —
Early efficacy data from a phase 2a safety trial suggest that the novel oral agent, dubbed ENV-101, is associated with improvements in forced vital capacity (FVC) and other measures of lung function, and may be a disease-modifying therapy for IPF, according to Toby M. Maher, MD, PhD, director of the interstitial lung disease program at Keck School of Medicine, University of Southern California, Los Angeles. Dr. Maher presented the results at the American Thoracic Society’s international conference.
“Historically we’ve not been seeing improvements in FVC, which is what we’ve been seeing [with ENV-101], and I think it’s conceivable that you can get remodeling of early areas of fibrosis in the lung,” Dr. Maher said in an interview with Chest Physician.
“We know from histology studies that if you look at IPF lungs you’ll see areas of end-stage fibrosis, but even in advanced disease you’ll see areas where the lung is relatively well preserved and there’s early fibrosis, so I think it’s conceivable that there is remodeling of some of those early areas of fibrosis,” he said.
Vital pathway
The Hedgehog pathway is highly conserved in evolution. The cell-signaling pathway is active embryogenesis, tissue proliferation, and organ development. There is also evidence to suggest that in adult the pathway becomes reactivated following tissue injury, as can occur in lung epithelia, Dr. Maher explained.
Although as the word “idiopathic” in IPF indicates the etiology of the disease is unknown, investigators have found that in IPF repetitive epithelial injury to lung tissue leads to activation of the Hedgehog pathway. Hedgehog signaling in turn induces formation and activation of myofibroblasts that lay down fibrotic matrix and contract lung tissue, leading to significant impairments in gas exchange, Dr. Maher said.
ENV-101 blocks Hedgehog from binding to the PTCH1 receptor, preventing release of the zinc-finger protein GLI1 from the kinase complex into the cell cytoplasm. With signaling blocked, myofibroblasts undergo apoptosis instead of initiating wound repair as they normally would, thereby eliminating an evident mechanism of IPF pathology, he explained.
Study details
In the phase 2a trial, investigators enrolled patients with IPF who were not taking antifibrotic agents and who had a percent predicted FVC greater than 50%, percent predicted diffusing capacity for carbon monoxide (DLCO) of at least 35%, and life expectancy of more than 1 year.
The patients were randomized to receive 200 mg oral ENV-101 daily (18 patients) or placebo (15 patients) for 12 weeks.
The primary endpoint of the trial was safety of the experimental agent. A previous phase 1b study of a different Hedgehog inhibitor — vismodegib (Erivedge), in combination with the antifibrotic agent pirfenidone (Pirespa) — in patients with IPF was discontinued because of poor tolerability.
In the current study, the most common treatment-related adverse events were dysgeusia in 57% of patients who received the drug, alopecia in 52%, and muscle spasms in 43%. The spasms were generally less severe than those seen in the vismodegib/pirfenidone trial mentioned above.
Seven patients (33%) had treatment-emergent events leading to dose interruption. Five patients discontinued treatment: one who withdrew because of taste alterations, one who was lost to follow-up after an IPF exacerbation, and three who withdrew consent.
There were no treatment-related deaths, and no clinically significant findings on labs, vital signs, electrocardiograms, or physical exam.
Efficacy endpoints
An analysis of the secondary efficacy endpoints showed a 1.9% mean improvement in FVC from baseline among patients assigned to ENV-101, compared with a mean decline of 1.3% of patients assigned to placebo (P = .035).
Patients on the active drug also had a 200-mL mean increase in total lung capacity, compared with a mean decline of 56 mL for patients on placebo (P = .005).
In addition, high-resolution CR studies showed a 9.4% absolute decrease from baseline in quantitative interstitial lung disease with ENV-101, vs. a 1.1% increase among controls, a 2% absolute decline from baseline in quantitative lung fibrosis compared with a 0.87% increase with placebo, and a 4.6% absolute decrease from baseline in quantitative ground glass, compared with an increase of 0.29% with placebo.
Bad taste a good sign?
Reinoud Gosens PhD, University of Groningen, the Netherlands, who co-moderated the session but was not involved in the study, questioned whether the dysgeusia seen in patients who received ENV-101 might be related to the dysgeusia seen in clinical trials of P2X3 receptor antagonists for cough.
“I was wondering if there would be a mechanistic overlap between Hedgehog inhibition and cough, which would be quite relevant for IPF,” he said in an interview.
The increase in FVC seen with ENV-101 and with the investigational agent buloxibutid, a novel angiotensin II type 2 receptor agonist described in a separate presentation by Dr. Maher, suggests that these drugs may have the ability to help remodel damaged lungs, Dr. Gosens said.
Investigators are currently planning a phase 2 dose-ranging trial (WHISTLE-PF) in patients with IPF or progressive pulmonary fibrosis.
The phase 2a trial was supported by Endeavor BioMedicines. Dr. Maher disclosed consultancy or speaker fees from Endeavor and others. Dr. Gosens had no relevant disclosures.
SAN DIEGO —
Early efficacy data from a phase 2a safety trial suggest that the novel oral agent, dubbed ENV-101, is associated with improvements in forced vital capacity (FVC) and other measures of lung function, and may be a disease-modifying therapy for IPF, according to Toby M. Maher, MD, PhD, director of the interstitial lung disease program at Keck School of Medicine, University of Southern California, Los Angeles. Dr. Maher presented the results at the American Thoracic Society’s international conference.
“Historically we’ve not been seeing improvements in FVC, which is what we’ve been seeing [with ENV-101], and I think it’s conceivable that you can get remodeling of early areas of fibrosis in the lung,” Dr. Maher said in an interview with Chest Physician.
“We know from histology studies that if you look at IPF lungs you’ll see areas of end-stage fibrosis, but even in advanced disease you’ll see areas where the lung is relatively well preserved and there’s early fibrosis, so I think it’s conceivable that there is remodeling of some of those early areas of fibrosis,” he said.
Vital pathway
The Hedgehog pathway is highly conserved in evolution. The cell-signaling pathway is active embryogenesis, tissue proliferation, and organ development. There is also evidence to suggest that in adult the pathway becomes reactivated following tissue injury, as can occur in lung epithelia, Dr. Maher explained.
Although as the word “idiopathic” in IPF indicates the etiology of the disease is unknown, investigators have found that in IPF repetitive epithelial injury to lung tissue leads to activation of the Hedgehog pathway. Hedgehog signaling in turn induces formation and activation of myofibroblasts that lay down fibrotic matrix and contract lung tissue, leading to significant impairments in gas exchange, Dr. Maher said.
ENV-101 blocks Hedgehog from binding to the PTCH1 receptor, preventing release of the zinc-finger protein GLI1 from the kinase complex into the cell cytoplasm. With signaling blocked, myofibroblasts undergo apoptosis instead of initiating wound repair as they normally would, thereby eliminating an evident mechanism of IPF pathology, he explained.
Study details
In the phase 2a trial, investigators enrolled patients with IPF who were not taking antifibrotic agents and who had a percent predicted FVC greater than 50%, percent predicted diffusing capacity for carbon monoxide (DLCO) of at least 35%, and life expectancy of more than 1 year.
The patients were randomized to receive 200 mg oral ENV-101 daily (18 patients) or placebo (15 patients) for 12 weeks.
The primary endpoint of the trial was safety of the experimental agent. A previous phase 1b study of a different Hedgehog inhibitor — vismodegib (Erivedge), in combination with the antifibrotic agent pirfenidone (Pirespa) — in patients with IPF was discontinued because of poor tolerability.
In the current study, the most common treatment-related adverse events were dysgeusia in 57% of patients who received the drug, alopecia in 52%, and muscle spasms in 43%. The spasms were generally less severe than those seen in the vismodegib/pirfenidone trial mentioned above.
Seven patients (33%) had treatment-emergent events leading to dose interruption. Five patients discontinued treatment: one who withdrew because of taste alterations, one who was lost to follow-up after an IPF exacerbation, and three who withdrew consent.
There were no treatment-related deaths, and no clinically significant findings on labs, vital signs, electrocardiograms, or physical exam.
Efficacy endpoints
An analysis of the secondary efficacy endpoints showed a 1.9% mean improvement in FVC from baseline among patients assigned to ENV-101, compared with a mean decline of 1.3% of patients assigned to placebo (P = .035).
Patients on the active drug also had a 200-mL mean increase in total lung capacity, compared with a mean decline of 56 mL for patients on placebo (P = .005).
In addition, high-resolution CR studies showed a 9.4% absolute decrease from baseline in quantitative interstitial lung disease with ENV-101, vs. a 1.1% increase among controls, a 2% absolute decline from baseline in quantitative lung fibrosis compared with a 0.87% increase with placebo, and a 4.6% absolute decrease from baseline in quantitative ground glass, compared with an increase of 0.29% with placebo.
Bad taste a good sign?
Reinoud Gosens PhD, University of Groningen, the Netherlands, who co-moderated the session but was not involved in the study, questioned whether the dysgeusia seen in patients who received ENV-101 might be related to the dysgeusia seen in clinical trials of P2X3 receptor antagonists for cough.
“I was wondering if there would be a mechanistic overlap between Hedgehog inhibition and cough, which would be quite relevant for IPF,” he said in an interview.
The increase in FVC seen with ENV-101 and with the investigational agent buloxibutid, a novel angiotensin II type 2 receptor agonist described in a separate presentation by Dr. Maher, suggests that these drugs may have the ability to help remodel damaged lungs, Dr. Gosens said.
Investigators are currently planning a phase 2 dose-ranging trial (WHISTLE-PF) in patients with IPF or progressive pulmonary fibrosis.
The phase 2a trial was supported by Endeavor BioMedicines. Dr. Maher disclosed consultancy or speaker fees from Endeavor and others. Dr. Gosens had no relevant disclosures.
SAN DIEGO —
Early efficacy data from a phase 2a safety trial suggest that the novel oral agent, dubbed ENV-101, is associated with improvements in forced vital capacity (FVC) and other measures of lung function, and may be a disease-modifying therapy for IPF, according to Toby M. Maher, MD, PhD, director of the interstitial lung disease program at Keck School of Medicine, University of Southern California, Los Angeles. Dr. Maher presented the results at the American Thoracic Society’s international conference.
“Historically we’ve not been seeing improvements in FVC, which is what we’ve been seeing [with ENV-101], and I think it’s conceivable that you can get remodeling of early areas of fibrosis in the lung,” Dr. Maher said in an interview with Chest Physician.
“We know from histology studies that if you look at IPF lungs you’ll see areas of end-stage fibrosis, but even in advanced disease you’ll see areas where the lung is relatively well preserved and there’s early fibrosis, so I think it’s conceivable that there is remodeling of some of those early areas of fibrosis,” he said.
Vital pathway
The Hedgehog pathway is highly conserved in evolution. The cell-signaling pathway is active embryogenesis, tissue proliferation, and organ development. There is also evidence to suggest that in adult the pathway becomes reactivated following tissue injury, as can occur in lung epithelia, Dr. Maher explained.
Although as the word “idiopathic” in IPF indicates the etiology of the disease is unknown, investigators have found that in IPF repetitive epithelial injury to lung tissue leads to activation of the Hedgehog pathway. Hedgehog signaling in turn induces formation and activation of myofibroblasts that lay down fibrotic matrix and contract lung tissue, leading to significant impairments in gas exchange, Dr. Maher said.
ENV-101 blocks Hedgehog from binding to the PTCH1 receptor, preventing release of the zinc-finger protein GLI1 from the kinase complex into the cell cytoplasm. With signaling blocked, myofibroblasts undergo apoptosis instead of initiating wound repair as they normally would, thereby eliminating an evident mechanism of IPF pathology, he explained.
Study details
In the phase 2a trial, investigators enrolled patients with IPF who were not taking antifibrotic agents and who had a percent predicted FVC greater than 50%, percent predicted diffusing capacity for carbon monoxide (DLCO) of at least 35%, and life expectancy of more than 1 year.
The patients were randomized to receive 200 mg oral ENV-101 daily (18 patients) or placebo (15 patients) for 12 weeks.
The primary endpoint of the trial was safety of the experimental agent. A previous phase 1b study of a different Hedgehog inhibitor — vismodegib (Erivedge), in combination with the antifibrotic agent pirfenidone (Pirespa) — in patients with IPF was discontinued because of poor tolerability.
In the current study, the most common treatment-related adverse events were dysgeusia in 57% of patients who received the drug, alopecia in 52%, and muscle spasms in 43%. The spasms were generally less severe than those seen in the vismodegib/pirfenidone trial mentioned above.
Seven patients (33%) had treatment-emergent events leading to dose interruption. Five patients discontinued treatment: one who withdrew because of taste alterations, one who was lost to follow-up after an IPF exacerbation, and three who withdrew consent.
There were no treatment-related deaths, and no clinically significant findings on labs, vital signs, electrocardiograms, or physical exam.
Efficacy endpoints
An analysis of the secondary efficacy endpoints showed a 1.9% mean improvement in FVC from baseline among patients assigned to ENV-101, compared with a mean decline of 1.3% of patients assigned to placebo (P = .035).
Patients on the active drug also had a 200-mL mean increase in total lung capacity, compared with a mean decline of 56 mL for patients on placebo (P = .005).
In addition, high-resolution CR studies showed a 9.4% absolute decrease from baseline in quantitative interstitial lung disease with ENV-101, vs. a 1.1% increase among controls, a 2% absolute decline from baseline in quantitative lung fibrosis compared with a 0.87% increase with placebo, and a 4.6% absolute decrease from baseline in quantitative ground glass, compared with an increase of 0.29% with placebo.
Bad taste a good sign?
Reinoud Gosens PhD, University of Groningen, the Netherlands, who co-moderated the session but was not involved in the study, questioned whether the dysgeusia seen in patients who received ENV-101 might be related to the dysgeusia seen in clinical trials of P2X3 receptor antagonists for cough.
“I was wondering if there would be a mechanistic overlap between Hedgehog inhibition and cough, which would be quite relevant for IPF,” he said in an interview.
The increase in FVC seen with ENV-101 and with the investigational agent buloxibutid, a novel angiotensin II type 2 receptor agonist described in a separate presentation by Dr. Maher, suggests that these drugs may have the ability to help remodel damaged lungs, Dr. Gosens said.
Investigators are currently planning a phase 2 dose-ranging trial (WHISTLE-PF) in patients with IPF or progressive pulmonary fibrosis.
The phase 2a trial was supported by Endeavor BioMedicines. Dr. Maher disclosed consultancy or speaker fees from Endeavor and others. Dr. Gosens had no relevant disclosures.
FROM ATS 2024
Lilly’s Once-Weekly Insulin Top-Line Results Show Benefit
Eli Lilly has announced positive phase 3 top-line results for its once-weekly insulin efsitora alfa (efsitora) in insulin-naive adults with type 2 diabetes and those who require multiple daily insulin injections.
The new data come from the company’s QWINT-2 and QWINT-4 phase 3 clinical trials. In both, efsitora was noninferior to daily basal insulin in lowering A1c. The comparator was once-daily degludec in QUINT-2 and glargine in QUINT-4.
These results come days before the once-weekly competitor, Novo Nordisk’s insulin icodec, will be discussed by the US Food and Drug Administration’s Endocrinologic and Metabolic Drugs Advisory Committee. On May 24, 2024, the panel will review safety and efficacy of icodec for the proposed indication of improving glycemic control in adults with diabetes.
Hypoglycemia and Affordability Are Concerns
Asked to comment, Anne L. Peters, MD, director of the University of Southern California Westside Center for Diabetes, Los Angeles, told this news organization that she’s “cautiously optimistic” about once-weekly insulin. “I honestly think it’s going to have an important role in diabetes. … And I’m looking forward to learning how it’s going to help my patients.”
However, Dr. Peters also said she’s concerned about the possible risk for hypoglycemia with long-acting insulin, particularly in patients with variable schedules. “The real fear they have and I have is hypoglycemia. That being said, I think that it will be great for some patients where hypoglycemia is less of a concern, and they’re in a more stable environment. … I think there are patients who will really benefit but I have to figure out who those patients are.”
Dr. Peters, who takes care of many low-income patients, also pointed out that once approved, these newer insulins may not be affordable for those who could most benefit from them in terms of improved adherence. Insurance plans may not cover them initially, especially given that the data thus far show noninferiority, not superiority, to daily basal. “The patients in whom I would like to use it most are the patients who have the most trouble with social determinants of health and other issues. I really think it could really make a difference for them, but it won’t get there for a while.”
And, she noted, titrating doses of once-weekly insulin will likely come with a learning curve. “Having spent a lifetime adjusting basal insulin on a daily basis to suddenly do it on a weekly basis, as a diabetologist I’m going to have to get used to what that feels like.”
Topline Data Show Noninferiority to Daily Basal Insulin
In QWINT-2, efficacy and safety of once-weekly efsitora was compared with those of once-daily insulin degludec for 52 weeks. Study participants were all new to using insulin, but some were using glucagon-like peptide 1 receptor agonists.
The treat-to-target trial met its primary noninferiority endpoint for hemoglobin A1c reduction at week 52. A1c values were lowered by 1.34 percentage points with efsitora compared with 1.26 for insulin degludec, resulting in non–significantly different A1c values of 6.87% and 6.95%, respectively.
In QWINT-4, efficacy and safety of once-weekly efsitora was compared with those of daily insulin glargine for 26 weeks in adults with type 2 diabetes who had previously been treated with basal insulin and at least two injections of premeal insulin per day. Participants were randomized to receive efsitora once weekly or insulin glargine once daily, and both groups used lispro before meals.
This trial also met its primary endpoint, with both reducing A1c by 1.07 percentage points at 26 weeks, resulting in levels of 7.12% and 7.11%, respectively.
The full results for QWINT-2 will be presented at the European Association for the Study of Diabetes meeting this September.
Dr. Peters served on the advisory board for Abbott Diabetes Care; Becton Dickinson; Boehringer Ingelheim Pharmaceuticals, Inc.; Eli Lilly and Company; Lexicon Pharmaceuticals, Inc.; Livongo; Medscape Medical News; Merck & Co., Inc.; Novo Nordisk; Omada Health; OptumHealth; Sanofi; and Zafgen. She received research support from Dexcom, MannKind Corporation, and Astra Zeneca and served as a member of a speakers bureau for Novo Nordisk.
A version of this article first appeared on Medscape.com.
Eli Lilly has announced positive phase 3 top-line results for its once-weekly insulin efsitora alfa (efsitora) in insulin-naive adults with type 2 diabetes and those who require multiple daily insulin injections.
The new data come from the company’s QWINT-2 and QWINT-4 phase 3 clinical trials. In both, efsitora was noninferior to daily basal insulin in lowering A1c. The comparator was once-daily degludec in QUINT-2 and glargine in QUINT-4.
These results come days before the once-weekly competitor, Novo Nordisk’s insulin icodec, will be discussed by the US Food and Drug Administration’s Endocrinologic and Metabolic Drugs Advisory Committee. On May 24, 2024, the panel will review safety and efficacy of icodec for the proposed indication of improving glycemic control in adults with diabetes.
Hypoglycemia and Affordability Are Concerns
Asked to comment, Anne L. Peters, MD, director of the University of Southern California Westside Center for Diabetes, Los Angeles, told this news organization that she’s “cautiously optimistic” about once-weekly insulin. “I honestly think it’s going to have an important role in diabetes. … And I’m looking forward to learning how it’s going to help my patients.”
However, Dr. Peters also said she’s concerned about the possible risk for hypoglycemia with long-acting insulin, particularly in patients with variable schedules. “The real fear they have and I have is hypoglycemia. That being said, I think that it will be great for some patients where hypoglycemia is less of a concern, and they’re in a more stable environment. … I think there are patients who will really benefit but I have to figure out who those patients are.”
Dr. Peters, who takes care of many low-income patients, also pointed out that once approved, these newer insulins may not be affordable for those who could most benefit from them in terms of improved adherence. Insurance plans may not cover them initially, especially given that the data thus far show noninferiority, not superiority, to daily basal. “The patients in whom I would like to use it most are the patients who have the most trouble with social determinants of health and other issues. I really think it could really make a difference for them, but it won’t get there for a while.”
And, she noted, titrating doses of once-weekly insulin will likely come with a learning curve. “Having spent a lifetime adjusting basal insulin on a daily basis to suddenly do it on a weekly basis, as a diabetologist I’m going to have to get used to what that feels like.”
Topline Data Show Noninferiority to Daily Basal Insulin
In QWINT-2, efficacy and safety of once-weekly efsitora was compared with those of once-daily insulin degludec for 52 weeks. Study participants were all new to using insulin, but some were using glucagon-like peptide 1 receptor agonists.
The treat-to-target trial met its primary noninferiority endpoint for hemoglobin A1c reduction at week 52. A1c values were lowered by 1.34 percentage points with efsitora compared with 1.26 for insulin degludec, resulting in non–significantly different A1c values of 6.87% and 6.95%, respectively.
In QWINT-4, efficacy and safety of once-weekly efsitora was compared with those of daily insulin glargine for 26 weeks in adults with type 2 diabetes who had previously been treated with basal insulin and at least two injections of premeal insulin per day. Participants were randomized to receive efsitora once weekly or insulin glargine once daily, and both groups used lispro before meals.
This trial also met its primary endpoint, with both reducing A1c by 1.07 percentage points at 26 weeks, resulting in levels of 7.12% and 7.11%, respectively.
The full results for QWINT-2 will be presented at the European Association for the Study of Diabetes meeting this September.
Dr. Peters served on the advisory board for Abbott Diabetes Care; Becton Dickinson; Boehringer Ingelheim Pharmaceuticals, Inc.; Eli Lilly and Company; Lexicon Pharmaceuticals, Inc.; Livongo; Medscape Medical News; Merck & Co., Inc.; Novo Nordisk; Omada Health; OptumHealth; Sanofi; and Zafgen. She received research support from Dexcom, MannKind Corporation, and Astra Zeneca and served as a member of a speakers bureau for Novo Nordisk.
A version of this article first appeared on Medscape.com.
Eli Lilly has announced positive phase 3 top-line results for its once-weekly insulin efsitora alfa (efsitora) in insulin-naive adults with type 2 diabetes and those who require multiple daily insulin injections.
The new data come from the company’s QWINT-2 and QWINT-4 phase 3 clinical trials. In both, efsitora was noninferior to daily basal insulin in lowering A1c. The comparator was once-daily degludec in QUINT-2 and glargine in QUINT-4.
These results come days before the once-weekly competitor, Novo Nordisk’s insulin icodec, will be discussed by the US Food and Drug Administration’s Endocrinologic and Metabolic Drugs Advisory Committee. On May 24, 2024, the panel will review safety and efficacy of icodec for the proposed indication of improving glycemic control in adults with diabetes.
Hypoglycemia and Affordability Are Concerns
Asked to comment, Anne L. Peters, MD, director of the University of Southern California Westside Center for Diabetes, Los Angeles, told this news organization that she’s “cautiously optimistic” about once-weekly insulin. “I honestly think it’s going to have an important role in diabetes. … And I’m looking forward to learning how it’s going to help my patients.”
However, Dr. Peters also said she’s concerned about the possible risk for hypoglycemia with long-acting insulin, particularly in patients with variable schedules. “The real fear they have and I have is hypoglycemia. That being said, I think that it will be great for some patients where hypoglycemia is less of a concern, and they’re in a more stable environment. … I think there are patients who will really benefit but I have to figure out who those patients are.”
Dr. Peters, who takes care of many low-income patients, also pointed out that once approved, these newer insulins may not be affordable for those who could most benefit from them in terms of improved adherence. Insurance plans may not cover them initially, especially given that the data thus far show noninferiority, not superiority, to daily basal. “The patients in whom I would like to use it most are the patients who have the most trouble with social determinants of health and other issues. I really think it could really make a difference for them, but it won’t get there for a while.”
And, she noted, titrating doses of once-weekly insulin will likely come with a learning curve. “Having spent a lifetime adjusting basal insulin on a daily basis to suddenly do it on a weekly basis, as a diabetologist I’m going to have to get used to what that feels like.”
Topline Data Show Noninferiority to Daily Basal Insulin
In QWINT-2, efficacy and safety of once-weekly efsitora was compared with those of once-daily insulin degludec for 52 weeks. Study participants were all new to using insulin, but some were using glucagon-like peptide 1 receptor agonists.
The treat-to-target trial met its primary noninferiority endpoint for hemoglobin A1c reduction at week 52. A1c values were lowered by 1.34 percentage points with efsitora compared with 1.26 for insulin degludec, resulting in non–significantly different A1c values of 6.87% and 6.95%, respectively.
In QWINT-4, efficacy and safety of once-weekly efsitora was compared with those of daily insulin glargine for 26 weeks in adults with type 2 diabetes who had previously been treated with basal insulin and at least two injections of premeal insulin per day. Participants were randomized to receive efsitora once weekly or insulin glargine once daily, and both groups used lispro before meals.
This trial also met its primary endpoint, with both reducing A1c by 1.07 percentage points at 26 weeks, resulting in levels of 7.12% and 7.11%, respectively.
The full results for QWINT-2 will be presented at the European Association for the Study of Diabetes meeting this September.
Dr. Peters served on the advisory board for Abbott Diabetes Care; Becton Dickinson; Boehringer Ingelheim Pharmaceuticals, Inc.; Eli Lilly and Company; Lexicon Pharmaceuticals, Inc.; Livongo; Medscape Medical News; Merck & Co., Inc.; Novo Nordisk; Omada Health; OptumHealth; Sanofi; and Zafgen. She received research support from Dexcom, MannKind Corporation, and Astra Zeneca and served as a member of a speakers bureau for Novo Nordisk.
A version of this article first appeared on Medscape.com.