User login
No Added Weight-Loss Benefits From Switching Healthy Diets?
TOPLINE:
Individuals with overweight and obesity who reach a weight-loss plateau at around 6 months on a healthy weight-loss diet may not achieve further weight reduction after switching to a different weight-loss diet.
METHODOLOGY:
- Dietary and lifestyle interventions initially result in rapid weight loss, followed by a weight-loss plateau after a few months and weight regain within a year or two, and diet fatigue has been proposed as a cause but not studied.
- This secondary analysis of a randomized trial assessed weight-loss trajectories before and after switching from a healthy low-carbohydrate (LC) diet to a healthy low-fat (LF) diet (or vice versa) in individuals with overweight and obesity.
- Overall, 42 participants (mean age, 42 years; 64% women; 87% White individuals) recruited from a local community in Palo Alto, California, were assigned to the LF or LC diet for the first 6 months, after which they were switched to the other diet for the remaining 6 months.
- Data from the DIETFITS trial, wherein participants remained either on the LF or LC diet for 12 months, were used as historical control.
The primary outcome was percent weight change at 3-6 months vs that observed at 6-9 months.
TAKEAWAY:
- The combined average weight loss was 7% (95% CI, 8%-6%) during the first 3 months, declining to 2% (95% CI, 3%-1%) between 3 and 6 months. On switching diets, the weight loss further slowed to 1% (95% CI, 2%-0.4%) between 6 and 9 months, with a modest increase in weight of 0.6% (95% CI, −0.1% to 1.3%) between 9 and 12 months.
- By diet order, participants in the LF first arm did not plateau and experienced a similar weight loss from 6 to 9 months as they had experienced from 3 to 6 months (relative change, −0.1%; 95% CI, −1.5% to 1.3%), while the LC first arm essentially nullified the 3-6 month weight loss during the 6-9 month LF phase (relative change, 2.2%; 95% CI, 0.7%-3.6%).
- For the LC first arm, low-density lipoprotein increased at 3 months and decreased when the participants switched to LF at 6 months, whereas the opposite effect was seen for the transition from LF to LC. Triglyceride levels decreased in both intervention arms.
- Insulin levels decreased in both dietary intervention arms between baseline and 6 months and plateaued following the 6-month dietary switch.
IN PRACTICE:
“This suggests that the weight-loss plateau typically seen at 6 months is physiological and cannot be overcome by simply switching to a different weight-loss diet,” wrote the authors. “As a person transitions from a weight loss to weight maintenance phase, a shift in the approach used may be required.”
SOURCE:
The study, led by Matthew J. Landry, Stanford Prevention Research Center, School of Medicine, Stanford University, California, was published in Scientific Reports.
LIMITATIONS:
The study results showed some possible differential trends but also highlighted the small sample size and large variability. Participants may have been unable to provide accurate estimates of self-reported energy intake. The authors also acknowledged that regular physical activity may have contributed to the maintenance of weight loss observed in this study.
DISCLOSURES:
The study was supported by the Hass Avocado Board; Human Health Service grant (General Clinical Research Centers and National Center for Research Resources, National Institutes of Health); National Heart, Lung, and Blood Institute; and Stanford Diabetes Research Center. The authors declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
Individuals with overweight and obesity who reach a weight-loss plateau at around 6 months on a healthy weight-loss diet may not achieve further weight reduction after switching to a different weight-loss diet.
METHODOLOGY:
- Dietary and lifestyle interventions initially result in rapid weight loss, followed by a weight-loss plateau after a few months and weight regain within a year or two, and diet fatigue has been proposed as a cause but not studied.
- This secondary analysis of a randomized trial assessed weight-loss trajectories before and after switching from a healthy low-carbohydrate (LC) diet to a healthy low-fat (LF) diet (or vice versa) in individuals with overweight and obesity.
- Overall, 42 participants (mean age, 42 years; 64% women; 87% White individuals) recruited from a local community in Palo Alto, California, were assigned to the LF or LC diet for the first 6 months, after which they were switched to the other diet for the remaining 6 months.
- Data from the DIETFITS trial, wherein participants remained either on the LF or LC diet for 12 months, were used as historical control.
The primary outcome was percent weight change at 3-6 months vs that observed at 6-9 months.
TAKEAWAY:
- The combined average weight loss was 7% (95% CI, 8%-6%) during the first 3 months, declining to 2% (95% CI, 3%-1%) between 3 and 6 months. On switching diets, the weight loss further slowed to 1% (95% CI, 2%-0.4%) between 6 and 9 months, with a modest increase in weight of 0.6% (95% CI, −0.1% to 1.3%) between 9 and 12 months.
- By diet order, participants in the LF first arm did not plateau and experienced a similar weight loss from 6 to 9 months as they had experienced from 3 to 6 months (relative change, −0.1%; 95% CI, −1.5% to 1.3%), while the LC first arm essentially nullified the 3-6 month weight loss during the 6-9 month LF phase (relative change, 2.2%; 95% CI, 0.7%-3.6%).
- For the LC first arm, low-density lipoprotein increased at 3 months and decreased when the participants switched to LF at 6 months, whereas the opposite effect was seen for the transition from LF to LC. Triglyceride levels decreased in both intervention arms.
- Insulin levels decreased in both dietary intervention arms between baseline and 6 months and plateaued following the 6-month dietary switch.
IN PRACTICE:
“This suggests that the weight-loss plateau typically seen at 6 months is physiological and cannot be overcome by simply switching to a different weight-loss diet,” wrote the authors. “As a person transitions from a weight loss to weight maintenance phase, a shift in the approach used may be required.”
SOURCE:
The study, led by Matthew J. Landry, Stanford Prevention Research Center, School of Medicine, Stanford University, California, was published in Scientific Reports.
LIMITATIONS:
The study results showed some possible differential trends but also highlighted the small sample size and large variability. Participants may have been unable to provide accurate estimates of self-reported energy intake. The authors also acknowledged that regular physical activity may have contributed to the maintenance of weight loss observed in this study.
DISCLOSURES:
The study was supported by the Hass Avocado Board; Human Health Service grant (General Clinical Research Centers and National Center for Research Resources, National Institutes of Health); National Heart, Lung, and Blood Institute; and Stanford Diabetes Research Center. The authors declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
Individuals with overweight and obesity who reach a weight-loss plateau at around 6 months on a healthy weight-loss diet may not achieve further weight reduction after switching to a different weight-loss diet.
METHODOLOGY:
- Dietary and lifestyle interventions initially result in rapid weight loss, followed by a weight-loss plateau after a few months and weight regain within a year or two, and diet fatigue has been proposed as a cause but not studied.
- This secondary analysis of a randomized trial assessed weight-loss trajectories before and after switching from a healthy low-carbohydrate (LC) diet to a healthy low-fat (LF) diet (or vice versa) in individuals with overweight and obesity.
- Overall, 42 participants (mean age, 42 years; 64% women; 87% White individuals) recruited from a local community in Palo Alto, California, were assigned to the LF or LC diet for the first 6 months, after which they were switched to the other diet for the remaining 6 months.
- Data from the DIETFITS trial, wherein participants remained either on the LF or LC diet for 12 months, were used as historical control.
The primary outcome was percent weight change at 3-6 months vs that observed at 6-9 months.
TAKEAWAY:
- The combined average weight loss was 7% (95% CI, 8%-6%) during the first 3 months, declining to 2% (95% CI, 3%-1%) between 3 and 6 months. On switching diets, the weight loss further slowed to 1% (95% CI, 2%-0.4%) between 6 and 9 months, with a modest increase in weight of 0.6% (95% CI, −0.1% to 1.3%) between 9 and 12 months.
- By diet order, participants in the LF first arm did not plateau and experienced a similar weight loss from 6 to 9 months as they had experienced from 3 to 6 months (relative change, −0.1%; 95% CI, −1.5% to 1.3%), while the LC first arm essentially nullified the 3-6 month weight loss during the 6-9 month LF phase (relative change, 2.2%; 95% CI, 0.7%-3.6%).
- For the LC first arm, low-density lipoprotein increased at 3 months and decreased when the participants switched to LF at 6 months, whereas the opposite effect was seen for the transition from LF to LC. Triglyceride levels decreased in both intervention arms.
- Insulin levels decreased in both dietary intervention arms between baseline and 6 months and plateaued following the 6-month dietary switch.
IN PRACTICE:
“This suggests that the weight-loss plateau typically seen at 6 months is physiological and cannot be overcome by simply switching to a different weight-loss diet,” wrote the authors. “As a person transitions from a weight loss to weight maintenance phase, a shift in the approach used may be required.”
SOURCE:
The study, led by Matthew J. Landry, Stanford Prevention Research Center, School of Medicine, Stanford University, California, was published in Scientific Reports.
LIMITATIONS:
The study results showed some possible differential trends but also highlighted the small sample size and large variability. Participants may have been unable to provide accurate estimates of self-reported energy intake. The authors also acknowledged that regular physical activity may have contributed to the maintenance of weight loss observed in this study.
DISCLOSURES:
The study was supported by the Hass Avocado Board; Human Health Service grant (General Clinical Research Centers and National Center for Research Resources, National Institutes of Health); National Heart, Lung, and Blood Institute; and Stanford Diabetes Research Center. The authors declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
Psychiatric Comorbidity Prevalent in Eating Disorders
NEW YORK — Psychiatric comorbidities are highly prevalent in patients with eating disorders (EDs), a large study showed.
In a propensity-matched cohort of young adults with and without EDs, a wide variety of psychiatric disorders including depression and anxiety, as well as cannabis and alcohol use disorders, were more common in those with EDs, investigators found.
Comorbid psychiatric disorders should be “top of mind when working with someone with an eating disorder. If you are able to treat the comorbid psychiatric conditions, they might have a better recovery from the eating disorder,” study investigator Angela Liu, MD, with Northwell Health at Zucker Hillside Hospital, Glen Oaks, New York, told this news organization.
The findings were presented at the annual meeting of the American Psychiatric Association.
Data Gap
As previously reported by this news organization, more than one in five children worldwide are at risk for an ED and US medical admissions for adolescents with restrictive EDs more than doubled during the pandemic.
Yet there remains a “gap in the literature” about the prevalence of comorbid psychiatric conditions in people with EDs, specifically in young people, Dr. Liu explained.
“To our knowledge, this is the first study using a real-world, multistate administrative dataset to estimate the prevalence of psychiatric comorbidities in young people diagnosed with an eating disorder,” Dr. Liu said.
Using the TriNetX database, the researchers identified through ICD-10 codes 14,524 individuals with EDs (mean age, 15.9 years; 79% women) and 110,051 without EDs who were receiving antidepressants (mean age, 17.8 years; 65% women).
“There was a much higher prevalence of almost all other psychiatric conditions in those with an eating disorder compared to the general psychiatry population,” coinvestigator Binx Y. Lin, MD, MSc, with Virginia Tech Carilion School of Medicine in Roanoke, Virginia, told this news organization.
In the baseline comparison (before matching), psychiatric disorders seen more often in adults with than in those without EDs included (but were not limited to) mood disorders (51% vs 23%), generalized anxiety disorder (GAD; 30% vs 8%), posttraumatic stress disorder (PTSD; 10% vs 2%), obsessive-compulsive disorder (OCD; 8% vs 1%), panic disorder (6% vs 2%), substance use disorder (8% vs 5%), and adjustment disorders (5% vs 2%).
The results held after propensity score matching, with numerous psychiatric conditions significantly (P < .001) more prevalent in the ED cohort.
Understanding the burden of comorbid psychiatric disorders in young people with EDs is important to design comprehensive, evidence-based interventions, the researchers said.
Providing perspective on this topic, Petros Levounis, MD, professor and chair, Department of Psychiatry, Rutgers New Jersey Medical School, Newark, New Jersey, noted that “comorbidity between substance use disorders and other psychiatric disorders has both been grossly underestimated and grossly overestimated.
“I go around the country and see rehab programs, and there are people that very strongly believe that if you stop using the drugs, you won’t have problems with depression or anxiety or whatever,” Dr. Levounis, immediate past president of the APA, shared with this news organization.
“Others say they have never seen somebody who’s addicted to something that doesn’t also have some other psychiatric disorders and if you just scratch the surface, you always find some other psychological or psychiatric problem lying behind. Neither of them are true,” he cautioned.
Dr. Levounis said it’s important to recognize that “some people with addiction will also have another psychiatric disorder. But clearly there are people who just have a mental illness without addiction, and there are clearly people who will just have addiction without other mental illness.”
This research had no commercial funding and was supported in part by the American Psychiatric Association Research Fellowship. Dr. Liu, Dr. Lin, and Dr. Levounis had no relevant disclosures.
A version of this article appeared on Medscape.com .
NEW YORK — Psychiatric comorbidities are highly prevalent in patients with eating disorders (EDs), a large study showed.
In a propensity-matched cohort of young adults with and without EDs, a wide variety of psychiatric disorders including depression and anxiety, as well as cannabis and alcohol use disorders, were more common in those with EDs, investigators found.
Comorbid psychiatric disorders should be “top of mind when working with someone with an eating disorder. If you are able to treat the comorbid psychiatric conditions, they might have a better recovery from the eating disorder,” study investigator Angela Liu, MD, with Northwell Health at Zucker Hillside Hospital, Glen Oaks, New York, told this news organization.
The findings were presented at the annual meeting of the American Psychiatric Association.
Data Gap
As previously reported by this news organization, more than one in five children worldwide are at risk for an ED and US medical admissions for adolescents with restrictive EDs more than doubled during the pandemic.
Yet there remains a “gap in the literature” about the prevalence of comorbid psychiatric conditions in people with EDs, specifically in young people, Dr. Liu explained.
“To our knowledge, this is the first study using a real-world, multistate administrative dataset to estimate the prevalence of psychiatric comorbidities in young people diagnosed with an eating disorder,” Dr. Liu said.
Using the TriNetX database, the researchers identified through ICD-10 codes 14,524 individuals with EDs (mean age, 15.9 years; 79% women) and 110,051 without EDs who were receiving antidepressants (mean age, 17.8 years; 65% women).
“There was a much higher prevalence of almost all other psychiatric conditions in those with an eating disorder compared to the general psychiatry population,” coinvestigator Binx Y. Lin, MD, MSc, with Virginia Tech Carilion School of Medicine in Roanoke, Virginia, told this news organization.
In the baseline comparison (before matching), psychiatric disorders seen more often in adults with than in those without EDs included (but were not limited to) mood disorders (51% vs 23%), generalized anxiety disorder (GAD; 30% vs 8%), posttraumatic stress disorder (PTSD; 10% vs 2%), obsessive-compulsive disorder (OCD; 8% vs 1%), panic disorder (6% vs 2%), substance use disorder (8% vs 5%), and adjustment disorders (5% vs 2%).
The results held after propensity score matching, with numerous psychiatric conditions significantly (P < .001) more prevalent in the ED cohort.
Understanding the burden of comorbid psychiatric disorders in young people with EDs is important to design comprehensive, evidence-based interventions, the researchers said.
Providing perspective on this topic, Petros Levounis, MD, professor and chair, Department of Psychiatry, Rutgers New Jersey Medical School, Newark, New Jersey, noted that “comorbidity between substance use disorders and other psychiatric disorders has both been grossly underestimated and grossly overestimated.
“I go around the country and see rehab programs, and there are people that very strongly believe that if you stop using the drugs, you won’t have problems with depression or anxiety or whatever,” Dr. Levounis, immediate past president of the APA, shared with this news organization.
“Others say they have never seen somebody who’s addicted to something that doesn’t also have some other psychiatric disorders and if you just scratch the surface, you always find some other psychological or psychiatric problem lying behind. Neither of them are true,” he cautioned.
Dr. Levounis said it’s important to recognize that “some people with addiction will also have another psychiatric disorder. But clearly there are people who just have a mental illness without addiction, and there are clearly people who will just have addiction without other mental illness.”
This research had no commercial funding and was supported in part by the American Psychiatric Association Research Fellowship. Dr. Liu, Dr. Lin, and Dr. Levounis had no relevant disclosures.
A version of this article appeared on Medscape.com .
NEW YORK — Psychiatric comorbidities are highly prevalent in patients with eating disorders (EDs), a large study showed.
In a propensity-matched cohort of young adults with and without EDs, a wide variety of psychiatric disorders including depression and anxiety, as well as cannabis and alcohol use disorders, were more common in those with EDs, investigators found.
Comorbid psychiatric disorders should be “top of mind when working with someone with an eating disorder. If you are able to treat the comorbid psychiatric conditions, they might have a better recovery from the eating disorder,” study investigator Angela Liu, MD, with Northwell Health at Zucker Hillside Hospital, Glen Oaks, New York, told this news organization.
The findings were presented at the annual meeting of the American Psychiatric Association.
Data Gap
As previously reported by this news organization, more than one in five children worldwide are at risk for an ED and US medical admissions for adolescents with restrictive EDs more than doubled during the pandemic.
Yet there remains a “gap in the literature” about the prevalence of comorbid psychiatric conditions in people with EDs, specifically in young people, Dr. Liu explained.
“To our knowledge, this is the first study using a real-world, multistate administrative dataset to estimate the prevalence of psychiatric comorbidities in young people diagnosed with an eating disorder,” Dr. Liu said.
Using the TriNetX database, the researchers identified through ICD-10 codes 14,524 individuals with EDs (mean age, 15.9 years; 79% women) and 110,051 without EDs who were receiving antidepressants (mean age, 17.8 years; 65% women).
“There was a much higher prevalence of almost all other psychiatric conditions in those with an eating disorder compared to the general psychiatry population,” coinvestigator Binx Y. Lin, MD, MSc, with Virginia Tech Carilion School of Medicine in Roanoke, Virginia, told this news organization.
In the baseline comparison (before matching), psychiatric disorders seen more often in adults with than in those without EDs included (but were not limited to) mood disorders (51% vs 23%), generalized anxiety disorder (GAD; 30% vs 8%), posttraumatic stress disorder (PTSD; 10% vs 2%), obsessive-compulsive disorder (OCD; 8% vs 1%), panic disorder (6% vs 2%), substance use disorder (8% vs 5%), and adjustment disorders (5% vs 2%).
The results held after propensity score matching, with numerous psychiatric conditions significantly (P < .001) more prevalent in the ED cohort.
Understanding the burden of comorbid psychiatric disorders in young people with EDs is important to design comprehensive, evidence-based interventions, the researchers said.
Providing perspective on this topic, Petros Levounis, MD, professor and chair, Department of Psychiatry, Rutgers New Jersey Medical School, Newark, New Jersey, noted that “comorbidity between substance use disorders and other psychiatric disorders has both been grossly underestimated and grossly overestimated.
“I go around the country and see rehab programs, and there are people that very strongly believe that if you stop using the drugs, you won’t have problems with depression or anxiety or whatever,” Dr. Levounis, immediate past president of the APA, shared with this news organization.
“Others say they have never seen somebody who’s addicted to something that doesn’t also have some other psychiatric disorders and if you just scratch the surface, you always find some other psychological or psychiatric problem lying behind. Neither of them are true,” he cautioned.
Dr. Levounis said it’s important to recognize that “some people with addiction will also have another psychiatric disorder. But clearly there are people who just have a mental illness without addiction, and there are clearly people who will just have addiction without other mental illness.”
This research had no commercial funding and was supported in part by the American Psychiatric Association Research Fellowship. Dr. Liu, Dr. Lin, and Dr. Levounis had no relevant disclosures.
A version of this article appeared on Medscape.com .
Endoscopic Procedure Targets ‘Hunger Hormone’ for Weight Loss
WASHINGTON — .
“Patients reported a decrease in hunger, appetite, and cravings and an increase in control over [their] eating,” said senior study investigator Christopher McGowan, MD, AGAF, a gastroenterologist in private practice and medical director of True You Weight Loss in Cary, North Carolina.

“They generally described that their relationship with food had changed,” Dr. McGowan said at a May 8 press briefing during which his research (Abstract 516) was previewed for Digestive Disease Week® (DDW).
Researchers targeted the gastric fundus because its mucosal lining contains 80%-90% of the cells that produce ghrelin. When a person diets and/or loses weight, ghrelin levels increase, making the person hungrier and preventing sustained weight loss, Dr. McGowan said.
Previously, the only proven way to reduce ghrelin was to surgically remove or bypass the fundus. Weight-loss medications like Wegovy, Zepbound, and Ozempic target a different hormonal pathway, glucagon-like peptide 1 (GLP-1).
“What we’ve learned from the GLP-1 medications is the profound impact of reducing hunger,” Dr. McGowan said. “That’s what patients describe quite often — that it really changes their life and their quality of life. That’s really, really important.”
Major Findings
In the trial, 10 women (mean age, 38 years; mean body mass index, 40.2) underwent endoscopic fundic mucosal ablation via hybrid argon plasma coagulation in an ambulatory setting under general anesthesia from November 1, 2022, to April 14, 2023. The procedure took less than an hour on average, and the technique gave them easy access to the fundus, Dr. McGowan said.
Compared with baseline, there were multiple beneficial outcomes at 6 months:
- 45% less circulating ghrelin in the blood.
- 53% drop in ghrelin-producing cells in the fundus.
- 42% reduction in stomach capacity.
- 43% decrease in hunger, appetite, and cravings.
- 7.7% body weight loss.
Over the 6 months of the study, mean ghrelin concentrations dropped from 461.6 pg/mL at baseline to 254.8 pg/mL (P = .006).
It is fascinating that the hormone ghrelin decreased just by ablating, said Loren Laine, MD, AGAF, professor of medicine (digestive diseases) at Yale School of Medicine and chair of DDW 2024. “They used the same device that we use to treat bleeding ulcers or lesions in the stomach and applied it broadly over the whole upper part of the stomach.”

In a standard nutrient drink test, the maximum tolerated volume among participants dropped from a mean 27.3 oz at baseline to 15.8 oz at 6-month follow-up (P = .004).
Participants also completed three questionnaires. From baseline to 6 months, their DAILY EATS mean hunger score decreased from 6.2 to 4 (P = .002), mean Eating Drivers Index score dropped from 7 to 4 (P < .001), and WEL-SF score improved from 47.7 to 62.4 (P = .001).
Repeat endoscopy at 6 months showed that the gastric fundus contracted and healed. An unexpected and beneficial finding was fibrotic tissue, which made the fundus less able to expand, Dr. McGowan said. A smaller fundus “is critical for feeling full.”
No serious adverse events were reported. Participants described gas pressure, mild nausea, and cramping, all of which lasted 1-3 days, he said.
“The key here is preserving safety. This is why we use the technique of injecting a fluid cushion prior to ablating, so we’re not entering any deeper layers of the stomach,” Dr. McGowan said. “Importantly, there are no nerve receptors within the lining of the stomach, so there’s no pain from this procedure.”
Another Anti-Obesity Tool?
“We’re all familiar with the epidemic that is obesity affecting nearly one in two adults, and the profound impact that it has on patients’ health, their quality of life, as well as the healthcare system,” Dr. McGowan said. “It’s clear that we need every tool possible to address this because we know that obesity is not a matter of willpower. It’s a disease.”
Gastric fundus ablation “may represent, and frankly should represent, a treatment option for the greater than 100 million US adults with obesity,” he added.
Not every patient wants to or can access GLP-1 medications, Dr. McGowan said. Also, “there’s a difference between taking a medication long-term, requiring an injection every week, vs a single intervention in time that carries forward.”
Ablation could also help people transition after they stop GLP-1 medications to help them maintain their weight loss, he said.
Weight loss is the endpoint you care about the most, said Dr. Laine, who co-moderated the press briefing.
Though the weight loss of 7.7% was not a large percentage, it was only 10 patients. We will have to see whether the total body weight loss is different when they do the procedure in more patients or if they can combine different mechanisms, Dr. Laine said.
It remains unclear whether gastric fundus ablation would be a stand-alone procedure or used in combination with another endoscopic weight-management intervention, bariatric surgery, or medication.
The endoscopic sleeve, which is a stomach-reducing procedure, is very effective, but it doesn’t diminish hunger, Dr. McGowan said. Combining it with ablation may be “a best-of-both-worlds scenario.”
Dr. Laine added that another open question is whether the gastric fundal accommodation will be associated with any side effects such as dyspepsia.
Dr. McGowan reported consulting for Boston Scientific and Apollo Endosurgery. Dr. Laine reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
WASHINGTON — .
“Patients reported a decrease in hunger, appetite, and cravings and an increase in control over [their] eating,” said senior study investigator Christopher McGowan, MD, AGAF, a gastroenterologist in private practice and medical director of True You Weight Loss in Cary, North Carolina.
“They generally described that their relationship with food had changed,” Dr. McGowan said at a May 8 press briefing during which his research (Abstract 516) was previewed for Digestive Disease Week® (DDW).
Researchers targeted the gastric fundus because its mucosal lining contains 80%-90% of the cells that produce ghrelin. When a person diets and/or loses weight, ghrelin levels increase, making the person hungrier and preventing sustained weight loss, Dr. McGowan said.
Previously, the only proven way to reduce ghrelin was to surgically remove or bypass the fundus. Weight-loss medications like Wegovy, Zepbound, and Ozempic target a different hormonal pathway, glucagon-like peptide 1 (GLP-1).
“What we’ve learned from the GLP-1 medications is the profound impact of reducing hunger,” Dr. McGowan said. “That’s what patients describe quite often — that it really changes their life and their quality of life. That’s really, really important.”
Major Findings
In the trial, 10 women (mean age, 38 years; mean body mass index, 40.2) underwent endoscopic fundic mucosal ablation via hybrid argon plasma coagulation in an ambulatory setting under general anesthesia from November 1, 2022, to April 14, 2023. The procedure took less than an hour on average, and the technique gave them easy access to the fundus, Dr. McGowan said.
Compared with baseline, there were multiple beneficial outcomes at 6 months:
- 45% less circulating ghrelin in the blood.
- 53% drop in ghrelin-producing cells in the fundus.
- 42% reduction in stomach capacity.
- 43% decrease in hunger, appetite, and cravings.
- 7.7% body weight loss.
Over the 6 months of the study, mean ghrelin concentrations dropped from 461.6 pg/mL at baseline to 254.8 pg/mL (P = .006).
It is fascinating that the hormone ghrelin decreased just by ablating, said Loren Laine, MD, AGAF, professor of medicine (digestive diseases) at Yale School of Medicine and chair of DDW 2024. “They used the same device that we use to treat bleeding ulcers or lesions in the stomach and applied it broadly over the whole upper part of the stomach.”
In a standard nutrient drink test, the maximum tolerated volume among participants dropped from a mean 27.3 oz at baseline to 15.8 oz at 6-month follow-up (P = .004).
Participants also completed three questionnaires. From baseline to 6 months, their DAILY EATS mean hunger score decreased from 6.2 to 4 (P = .002), mean Eating Drivers Index score dropped from 7 to 4 (P < .001), and WEL-SF score improved from 47.7 to 62.4 (P = .001).
Repeat endoscopy at 6 months showed that the gastric fundus contracted and healed. An unexpected and beneficial finding was fibrotic tissue, which made the fundus less able to expand, Dr. McGowan said. A smaller fundus “is critical for feeling full.”
No serious adverse events were reported. Participants described gas pressure, mild nausea, and cramping, all of which lasted 1-3 days, he said.
“The key here is preserving safety. This is why we use the technique of injecting a fluid cushion prior to ablating, so we’re not entering any deeper layers of the stomach,” Dr. McGowan said. “Importantly, there are no nerve receptors within the lining of the stomach, so there’s no pain from this procedure.”
Another Anti-Obesity Tool?
“We’re all familiar with the epidemic that is obesity affecting nearly one in two adults, and the profound impact that it has on patients’ health, their quality of life, as well as the healthcare system,” Dr. McGowan said. “It’s clear that we need every tool possible to address this because we know that obesity is not a matter of willpower. It’s a disease.”
Gastric fundus ablation “may represent, and frankly should represent, a treatment option for the greater than 100 million US adults with obesity,” he added.
Not every patient wants to or can access GLP-1 medications, Dr. McGowan said. Also, “there’s a difference between taking a medication long-term, requiring an injection every week, vs a single intervention in time that carries forward.”
Ablation could also help people transition after they stop GLP-1 medications to help them maintain their weight loss, he said.
Weight loss is the endpoint you care about the most, said Dr. Laine, who co-moderated the press briefing.
Though the weight loss of 7.7% was not a large percentage, it was only 10 patients. We will have to see whether the total body weight loss is different when they do the procedure in more patients or if they can combine different mechanisms, Dr. Laine said.
It remains unclear whether gastric fundus ablation would be a stand-alone procedure or used in combination with another endoscopic weight-management intervention, bariatric surgery, or medication.
The endoscopic sleeve, which is a stomach-reducing procedure, is very effective, but it doesn’t diminish hunger, Dr. McGowan said. Combining it with ablation may be “a best-of-both-worlds scenario.”
Dr. Laine added that another open question is whether the gastric fundal accommodation will be associated with any side effects such as dyspepsia.
Dr. McGowan reported consulting for Boston Scientific and Apollo Endosurgery. Dr. Laine reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
WASHINGTON — .
“Patients reported a decrease in hunger, appetite, and cravings and an increase in control over [their] eating,” said senior study investigator Christopher McGowan, MD, AGAF, a gastroenterologist in private practice and medical director of True You Weight Loss in Cary, North Carolina.
“They generally described that their relationship with food had changed,” Dr. McGowan said at a May 8 press briefing during which his research (Abstract 516) was previewed for Digestive Disease Week® (DDW).
Researchers targeted the gastric fundus because its mucosal lining contains 80%-90% of the cells that produce ghrelin. When a person diets and/or loses weight, ghrelin levels increase, making the person hungrier and preventing sustained weight loss, Dr. McGowan said.
Previously, the only proven way to reduce ghrelin was to surgically remove or bypass the fundus. Weight-loss medications like Wegovy, Zepbound, and Ozempic target a different hormonal pathway, glucagon-like peptide 1 (GLP-1).
“What we’ve learned from the GLP-1 medications is the profound impact of reducing hunger,” Dr. McGowan said. “That’s what patients describe quite often — that it really changes their life and their quality of life. That’s really, really important.”
Major Findings
In the trial, 10 women (mean age, 38 years; mean body mass index, 40.2) underwent endoscopic fundic mucosal ablation via hybrid argon plasma coagulation in an ambulatory setting under general anesthesia from November 1, 2022, to April 14, 2023. The procedure took less than an hour on average, and the technique gave them easy access to the fundus, Dr. McGowan said.
Compared with baseline, there were multiple beneficial outcomes at 6 months:
- 45% less circulating ghrelin in the blood.
- 53% drop in ghrelin-producing cells in the fundus.
- 42% reduction in stomach capacity.
- 43% decrease in hunger, appetite, and cravings.
- 7.7% body weight loss.
Over the 6 months of the study, mean ghrelin concentrations dropped from 461.6 pg/mL at baseline to 254.8 pg/mL (P = .006).
It is fascinating that the hormone ghrelin decreased just by ablating, said Loren Laine, MD, AGAF, professor of medicine (digestive diseases) at Yale School of Medicine and chair of DDW 2024. “They used the same device that we use to treat bleeding ulcers or lesions in the stomach and applied it broadly over the whole upper part of the stomach.”
In a standard nutrient drink test, the maximum tolerated volume among participants dropped from a mean 27.3 oz at baseline to 15.8 oz at 6-month follow-up (P = .004).
Participants also completed three questionnaires. From baseline to 6 months, their DAILY EATS mean hunger score decreased from 6.2 to 4 (P = .002), mean Eating Drivers Index score dropped from 7 to 4 (P < .001), and WEL-SF score improved from 47.7 to 62.4 (P = .001).
Repeat endoscopy at 6 months showed that the gastric fundus contracted and healed. An unexpected and beneficial finding was fibrotic tissue, which made the fundus less able to expand, Dr. McGowan said. A smaller fundus “is critical for feeling full.”
No serious adverse events were reported. Participants described gas pressure, mild nausea, and cramping, all of which lasted 1-3 days, he said.
“The key here is preserving safety. This is why we use the technique of injecting a fluid cushion prior to ablating, so we’re not entering any deeper layers of the stomach,” Dr. McGowan said. “Importantly, there are no nerve receptors within the lining of the stomach, so there’s no pain from this procedure.”
Another Anti-Obesity Tool?
“We’re all familiar with the epidemic that is obesity affecting nearly one in two adults, and the profound impact that it has on patients’ health, their quality of life, as well as the healthcare system,” Dr. McGowan said. “It’s clear that we need every tool possible to address this because we know that obesity is not a matter of willpower. It’s a disease.”
Gastric fundus ablation “may represent, and frankly should represent, a treatment option for the greater than 100 million US adults with obesity,” he added.
Not every patient wants to or can access GLP-1 medications, Dr. McGowan said. Also, “there’s a difference between taking a medication long-term, requiring an injection every week, vs a single intervention in time that carries forward.”
Ablation could also help people transition after they stop GLP-1 medications to help them maintain their weight loss, he said.
Weight loss is the endpoint you care about the most, said Dr. Laine, who co-moderated the press briefing.
Though the weight loss of 7.7% was not a large percentage, it was only 10 patients. We will have to see whether the total body weight loss is different when they do the procedure in more patients or if they can combine different mechanisms, Dr. Laine said.
It remains unclear whether gastric fundus ablation would be a stand-alone procedure or used in combination with another endoscopic weight-management intervention, bariatric surgery, or medication.
The endoscopic sleeve, which is a stomach-reducing procedure, is very effective, but it doesn’t diminish hunger, Dr. McGowan said. Combining it with ablation may be “a best-of-both-worlds scenario.”
Dr. Laine added that another open question is whether the gastric fundal accommodation will be associated with any side effects such as dyspepsia.
Dr. McGowan reported consulting for Boston Scientific and Apollo Endosurgery. Dr. Laine reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM DDW 2024
Resource Menu Gives Choice to Caregivers Struggling to Meet Basic Needs
Screenings may not be the way to get needed resources to children and their caregivers, according to new research presented at the annual meeting of the Pediatric Academic Societies (PAS).
Caregivers and parents who were asked if they wanted assistance in several areas of need, including transportation and childcare, were nearly twice as likely to say they wanted such help than those who received a screening on current hardships. Generally, each questionnaire is administered in front of their children in primary care or pediatric hospital settings.
“Families have a lot of concern about being seen a different way by their healthcare team, being seen as unfit, and having child protective services involved in their childcare for issues related to poverty,” said Danielle Cullen, MD, a pediatric emergency medicine specialist at Children’s Hospital of Philadelphia (CHOP) and assistant professor of pediatrics at the University of Pennsylvania in Philadelphia.
Dr. Cullen and her colleagues analyzed data from nearly 4000 caregivers of children up to age 21 at emergency departments or primary care clinics at CHOP between 2021 and 2023.
Caregivers were randomly assigned to one of three arms — screening with a version of WE CARE (Well Child Care, Evaluation, Community Resources, Advocacy, Referral, Education), use of an online menu of options for help in areas like housing, or neither approach.
Caregivers in all three arms received a map of resources and a follow-up text from a resource navigator to assist them as needed.
Nearly 40% of caregivers who presented with the digital menu said they wanted resources compared with 29% of those who were screened (P < .001). Non-native English speakers given the menu were 2.5 times more likely to say yes to resources compared with those who were screened.
“We need to be thoughtful about these mandates to screen for social determinants of health: It’s not that straightforward,” said Esther K. Chung, MD, a pediatrician and professor of pediatrics at the University of Washington Medicine in Seattle, who was not involved in the study. “What we’re getting from this study is that patients want choice, and the menu provides them choice.”
Dr. Cullen said the menu option allows caregivers to make choices based on their priorities and not on whether they meet the screening thresholds for need.
While some health clinics utilize tablet forms for screenings to offer more privacy with questions, asking direct questions about income, food insecurity, and housing stability can be stigmatizing, Dr. Cullen said.
“Screening positive for social risk doesn’t mean that you actually want resources, and on the flip side, the literature shows that about half of the people who screen negative want resources,” she said.
Dr. Cullen and her team also conducted follow-up interviews with caregivers and found many feared that their clinician would assume a medical condition was connected to living conditions. They also had concerns about insurance companies gaining access to the data and using it to deny coverage or raise costs.
Spanish-speaking caregivers cited fears about their immigration status, experiences of discrimination, and language barriers when trying to access resources.
Participants said a few key strategies could make screening less intimidating, such as abstaining from screening during a serious medical visit, asking for consent to record answers in medical records, and communicating in an empathetic manner.
“Some families are a bit surprised when we ask about things like housing and food insecurity, but I think as long as we contextualize it, we can minimize the stigma associated with it,” Dr. Chung said. “That takes quite a bit of nuance and skill.”
The study was funded by the William T. Grant Foundation and the Emergency Medicine Foundation. The authors reported no disclosures.
A version of this article appeared on Medscape.com.
Screenings may not be the way to get needed resources to children and their caregivers, according to new research presented at the annual meeting of the Pediatric Academic Societies (PAS).
Caregivers and parents who were asked if they wanted assistance in several areas of need, including transportation and childcare, were nearly twice as likely to say they wanted such help than those who received a screening on current hardships. Generally, each questionnaire is administered in front of their children in primary care or pediatric hospital settings.
“Families have a lot of concern about being seen a different way by their healthcare team, being seen as unfit, and having child protective services involved in their childcare for issues related to poverty,” said Danielle Cullen, MD, a pediatric emergency medicine specialist at Children’s Hospital of Philadelphia (CHOP) and assistant professor of pediatrics at the University of Pennsylvania in Philadelphia.
Dr. Cullen and her colleagues analyzed data from nearly 4000 caregivers of children up to age 21 at emergency departments or primary care clinics at CHOP between 2021 and 2023.
Caregivers were randomly assigned to one of three arms — screening with a version of WE CARE (Well Child Care, Evaluation, Community Resources, Advocacy, Referral, Education), use of an online menu of options for help in areas like housing, or neither approach.
Caregivers in all three arms received a map of resources and a follow-up text from a resource navigator to assist them as needed.
Nearly 40% of caregivers who presented with the digital menu said they wanted resources compared with 29% of those who were screened (P < .001). Non-native English speakers given the menu were 2.5 times more likely to say yes to resources compared with those who were screened.
“We need to be thoughtful about these mandates to screen for social determinants of health: It’s not that straightforward,” said Esther K. Chung, MD, a pediatrician and professor of pediatrics at the University of Washington Medicine in Seattle, who was not involved in the study. “What we’re getting from this study is that patients want choice, and the menu provides them choice.”
Dr. Cullen said the menu option allows caregivers to make choices based on their priorities and not on whether they meet the screening thresholds for need.
While some health clinics utilize tablet forms for screenings to offer more privacy with questions, asking direct questions about income, food insecurity, and housing stability can be stigmatizing, Dr. Cullen said.
“Screening positive for social risk doesn’t mean that you actually want resources, and on the flip side, the literature shows that about half of the people who screen negative want resources,” she said.
Dr. Cullen and her team also conducted follow-up interviews with caregivers and found many feared that their clinician would assume a medical condition was connected to living conditions. They also had concerns about insurance companies gaining access to the data and using it to deny coverage or raise costs.
Spanish-speaking caregivers cited fears about their immigration status, experiences of discrimination, and language barriers when trying to access resources.
Participants said a few key strategies could make screening less intimidating, such as abstaining from screening during a serious medical visit, asking for consent to record answers in medical records, and communicating in an empathetic manner.
“Some families are a bit surprised when we ask about things like housing and food insecurity, but I think as long as we contextualize it, we can minimize the stigma associated with it,” Dr. Chung said. “That takes quite a bit of nuance and skill.”
The study was funded by the William T. Grant Foundation and the Emergency Medicine Foundation. The authors reported no disclosures.
A version of this article appeared on Medscape.com.
Screenings may not be the way to get needed resources to children and their caregivers, according to new research presented at the annual meeting of the Pediatric Academic Societies (PAS).
Caregivers and parents who were asked if they wanted assistance in several areas of need, including transportation and childcare, were nearly twice as likely to say they wanted such help than those who received a screening on current hardships. Generally, each questionnaire is administered in front of their children in primary care or pediatric hospital settings.
“Families have a lot of concern about being seen a different way by their healthcare team, being seen as unfit, and having child protective services involved in their childcare for issues related to poverty,” said Danielle Cullen, MD, a pediatric emergency medicine specialist at Children’s Hospital of Philadelphia (CHOP) and assistant professor of pediatrics at the University of Pennsylvania in Philadelphia.
Dr. Cullen and her colleagues analyzed data from nearly 4000 caregivers of children up to age 21 at emergency departments or primary care clinics at CHOP between 2021 and 2023.
Caregivers were randomly assigned to one of three arms — screening with a version of WE CARE (Well Child Care, Evaluation, Community Resources, Advocacy, Referral, Education), use of an online menu of options for help in areas like housing, or neither approach.
Caregivers in all three arms received a map of resources and a follow-up text from a resource navigator to assist them as needed.
Nearly 40% of caregivers who presented with the digital menu said they wanted resources compared with 29% of those who were screened (P < .001). Non-native English speakers given the menu were 2.5 times more likely to say yes to resources compared with those who were screened.
“We need to be thoughtful about these mandates to screen for social determinants of health: It’s not that straightforward,” said Esther K. Chung, MD, a pediatrician and professor of pediatrics at the University of Washington Medicine in Seattle, who was not involved in the study. “What we’re getting from this study is that patients want choice, and the menu provides them choice.”
Dr. Cullen said the menu option allows caregivers to make choices based on their priorities and not on whether they meet the screening thresholds for need.
While some health clinics utilize tablet forms for screenings to offer more privacy with questions, asking direct questions about income, food insecurity, and housing stability can be stigmatizing, Dr. Cullen said.
“Screening positive for social risk doesn’t mean that you actually want resources, and on the flip side, the literature shows that about half of the people who screen negative want resources,” she said.
Dr. Cullen and her team also conducted follow-up interviews with caregivers and found many feared that their clinician would assume a medical condition was connected to living conditions. They also had concerns about insurance companies gaining access to the data and using it to deny coverage or raise costs.
Spanish-speaking caregivers cited fears about their immigration status, experiences of discrimination, and language barriers when trying to access resources.
Participants said a few key strategies could make screening less intimidating, such as abstaining from screening during a serious medical visit, asking for consent to record answers in medical records, and communicating in an empathetic manner.
“Some families are a bit surprised when we ask about things like housing and food insecurity, but I think as long as we contextualize it, we can minimize the stigma associated with it,” Dr. Chung said. “That takes quite a bit of nuance and skill.”
The study was funded by the William T. Grant Foundation and the Emergency Medicine Foundation. The authors reported no disclosures.
A version of this article appeared on Medscape.com.
FROM PAS 2024
FDA Approves Tarlatamab for Extensive-Stage Small Cell Lung Cancer
Tarlatamab is a first-in-class bispecific T-cell engager (BiTE) that binds delta-like ligand 3 on the surface of cells, including tumor cells, and CD3 expressed on the surface of T cells. It causes T-cell activation, release of inflammatory cytokines, and lysis of DLL3-expressing cells, according to labeling.
Approval was based on data from 99 patients in the DeLLphi-301 trial with relapsed/refractory extensive-stage SCLC who had progressed after platinum-based chemotherapy. Patients with symptomatic brain metastases, interstitial lung disease, noninfectious pneumonitis, and active immunodeficiency were excluded.
The overall response rate was 40%, and median duration of response 9.7 months. The overall response rate was 52% in 27 patients with platinum-resistant SCLC and 31% in 42 with platinum-sensitive disease.
Continued approval may depend on verification of clinical benefit in a confirmatory trial.
Labeling includes a box warning of serious or life-threatening cytokine release syndrome and neurologic toxicity, including immune effector cell–associated neurotoxicity syndrome.
The most common adverse events, occurring in 20% or more of patients, were cytokine release syndrome, fatigue, pyrexia, dysgeusia, decreased appetite, musculoskeletal pain, constipation, anemia, and nausea.
The most common grade 3 or 4 laboratory abnormalities included decreased lymphocytes, decreased sodium, increased uric acid, decreased total neutrophils, decreased hemoglobin, increased activated partial thromboplastin time, and decreased potassium.
The starting dose is 1 mg given intravenously over 1 hour on the first day of the first cycle followed by 10 mg on day 8 and day 15 of the first cycle, then every 2 weeks until disease progression or unacceptable toxicity.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award-winning medical journalist who worked for several major news outlets before joining Medscape. Alex is also an MIT Knight Science Journalism fellow. Email: [email protected]
A version of this article appeared on Medscape.com.
Tarlatamab is a first-in-class bispecific T-cell engager (BiTE) that binds delta-like ligand 3 on the surface of cells, including tumor cells, and CD3 expressed on the surface of T cells. It causes T-cell activation, release of inflammatory cytokines, and lysis of DLL3-expressing cells, according to labeling.
Approval was based on data from 99 patients in the DeLLphi-301 trial with relapsed/refractory extensive-stage SCLC who had progressed after platinum-based chemotherapy. Patients with symptomatic brain metastases, interstitial lung disease, noninfectious pneumonitis, and active immunodeficiency were excluded.
The overall response rate was 40%, and median duration of response 9.7 months. The overall response rate was 52% in 27 patients with platinum-resistant SCLC and 31% in 42 with platinum-sensitive disease.
Continued approval may depend on verification of clinical benefit in a confirmatory trial.
Labeling includes a box warning of serious or life-threatening cytokine release syndrome and neurologic toxicity, including immune effector cell–associated neurotoxicity syndrome.
The most common adverse events, occurring in 20% or more of patients, were cytokine release syndrome, fatigue, pyrexia, dysgeusia, decreased appetite, musculoskeletal pain, constipation, anemia, and nausea.
The most common grade 3 or 4 laboratory abnormalities included decreased lymphocytes, decreased sodium, increased uric acid, decreased total neutrophils, decreased hemoglobin, increased activated partial thromboplastin time, and decreased potassium.
The starting dose is 1 mg given intravenously over 1 hour on the first day of the first cycle followed by 10 mg on day 8 and day 15 of the first cycle, then every 2 weeks until disease progression or unacceptable toxicity.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award-winning medical journalist who worked for several major news outlets before joining Medscape. Alex is also an MIT Knight Science Journalism fellow. Email: [email protected]
A version of this article appeared on Medscape.com.
Tarlatamab is a first-in-class bispecific T-cell engager (BiTE) that binds delta-like ligand 3 on the surface of cells, including tumor cells, and CD3 expressed on the surface of T cells. It causes T-cell activation, release of inflammatory cytokines, and lysis of DLL3-expressing cells, according to labeling.
Approval was based on data from 99 patients in the DeLLphi-301 trial with relapsed/refractory extensive-stage SCLC who had progressed after platinum-based chemotherapy. Patients with symptomatic brain metastases, interstitial lung disease, noninfectious pneumonitis, and active immunodeficiency were excluded.
The overall response rate was 40%, and median duration of response 9.7 months. The overall response rate was 52% in 27 patients with platinum-resistant SCLC and 31% in 42 with platinum-sensitive disease.
Continued approval may depend on verification of clinical benefit in a confirmatory trial.
Labeling includes a box warning of serious or life-threatening cytokine release syndrome and neurologic toxicity, including immune effector cell–associated neurotoxicity syndrome.
The most common adverse events, occurring in 20% or more of patients, were cytokine release syndrome, fatigue, pyrexia, dysgeusia, decreased appetite, musculoskeletal pain, constipation, anemia, and nausea.
The most common grade 3 or 4 laboratory abnormalities included decreased lymphocytes, decreased sodium, increased uric acid, decreased total neutrophils, decreased hemoglobin, increased activated partial thromboplastin time, and decreased potassium.
The starting dose is 1 mg given intravenously over 1 hour on the first day of the first cycle followed by 10 mg on day 8 and day 15 of the first cycle, then every 2 weeks until disease progression or unacceptable toxicity.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award-winning medical journalist who worked for several major news outlets before joining Medscape. Alex is also an MIT Knight Science Journalism fellow. Email: [email protected]
A version of this article appeared on Medscape.com.
No Improvement in OS With Atezolizumab in Early Relapsing TNBC
Our results “highlight the importance of recognizing TNBC heterogeneity, especially in the first-line setting” said Rebecca A. Dent, MD, MSc, National Cancer Center Singapore and Duke-NUS Medical School, Singapore, who presented the study at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress.
“These patients have a dismal prognosis and represent a high unmet need,” she added.
The current findings follow those from the IMpassion130 trial, which showed that the combination of atezolizumab with nab-paclitaxel chemotherapy offered no survival benefit in previously untreated locally advanced or metastatic TNBC despite a progression-free survival benefit on interim analysis.
Rapidly relapsing TNBC “represents one of most challenging clinical situations” because it is aggressive and “intrinsically resistant to standard therapies,” said Dr. Dent. It is also more common in younger patients with large primary tumors and no BRCA alterations.
“Most importantly, however, is that most trials actually exclude these patients,” she noted, “posing a real challenge for us in clinical practice.”
IMpassion132 enrolled 594 patients with unresectable locally advanced or metastatic TNBC who had experienced disease progression more than 12 months after their last treatment for early TNBC with curative intent.
Patients had received prior anthracycline and taxane therapy for but no prior chemotherapy for advanced disease.
Study participants were randomly assigned to chemotherapy with carboplatin-gemcitabine or capecitabine plus atezolizumab or placebo, with treatment continued until disease progression or unacceptable toxicity. The primary endpoint was overall survival.
Initially, all patients with TNBC who met the study criteria were enrolled in the randomized, phase 3, double-blinded trial; however, the trial was then amended to include only PD-L1–positive patients after the results of IMpassion130 “clearly showed us that the benefits of immune checkpoint inhibition were largely driven by those patients,” Dr. Dent explained.
The 354 patients with PD-L1–positive disease were “young,” she added, with a median age of 48 years. The youngest was 23 years old.
The majority (66%-69%) had a disease-free interval of less than 6 months after treatment with curative intent. Lung and/or liver metastases were present in 60%-62% of patients, and 18% had previously received platinum-based chemotherapy.
After a median follow-up of 9.8 months, overall survival was a median of 12.1 months in the atezolizumab group vs 11.2 months with placebo, at a hazard ratio of 0.93 (P = .59).
A similar result was seen when looking at the modified intention-to-treat population, and when stratifying the patients by prespecified subgroup.
Dr. Dent pointed out that in the placebo group, patients treated with capecitabine had a median overall survival of 12.6 months vs 9.9 months in those given carboplatin-gemcitabine , which she described as “hypothesis generating” because “prior therapy may trigger a variety of resistance mechanisms.”
The disease-free interval also seemed to play a role in the placebo group. Patients who had a disease-free interval of 6 or more months prior to study enrollment had a median overall survival of 12.8 months vs 9.4 months in those with an interval of less than 6 months.
There were no significant differences in progression-free survival or duration of overall response between the atezolizumab and placebo groups.
“In terms of the safety data, clearly we’re getting better at identifying immune checkpoint inhibition toxicities and initiating therapies for these toxicities earlier,” Dr. Dent said, because there were “no new safety signals.”
The rate of treatment-related grade 3 or 4 adverse events was similar between patients given atezolizumab and those assigned to placebo, at 65% vs 62%. Rates of grade 5 events were identical, at 1%.
Commenting on the study, Sara M. Tolaney, MD, MPH, chief, Division of Breast Oncology, Susan F. Smith Center for Women’s Cancers, Dana-Farber Cancer Institute, Boston, questioned the role for immunotherapy in patients with TNBC who experience early relapse.
This is not the first trial to fail to show a benefit in this space, she said. Collectively, these results make “me think that these tumors are pretty immunologically cold, making them less likely to benefit from checkpoint inhibition.”
The patients that do relapse, “have highly treatment refractory disease,” and “we need to think about other novel therapeutic strategies for this population,” she told this news organization.
IMpassion132 nevertheless represents a “unique opportunity to better understand the biology of these rapidly relapsing tumors, and hopefully use this information to develop more novel treatment approaches for this population,” she said.
“That being said, I do think that this is going to become an even more challenging area,” Dr. Tolaney said. “In the modern era, these patients are receiving multi-agent chemotherapy with preoperative checkpoint inhibition, and many then go on to receive additional systemic treatment in the adjuvant setting.”
The study was sponsored by Hoffmann-La Roche.
Dr. Dent declares relationships with AstraZeneca, Roche, Eisai, Lilly, MSD, Novartis, and Pfizer. Dr. Tolaney declares relationships with Novartis, Pfizer, Merck, Lilly, AstraZeneca, Genentech/Roche, Eisai, Sanofi, Bristol Myers Squib, Seattle Genetics, CytomX Therapeutics, Daiichi Sankyo, Gilead, Ellipses Pharma, 4D Pharma, OncoSec Medical Inc, BeyondSpring Pharmaceuticals, OncXerna, Zymeworks, Zentalis, Blueprint Medicines, Reveal Genomics, ARC Therapeutics, Myovant, Zetagen, Umoja Biopharma, Menarini/Stemline, Aadi Biopharma, Bayer, Jazz Pharmaceuticals, Exelixis, Novartis, Nanonstring, and Cyclacel.
A version of this article appeared on Medscape.com .
Our results “highlight the importance of recognizing TNBC heterogeneity, especially in the first-line setting” said Rebecca A. Dent, MD, MSc, National Cancer Center Singapore and Duke-NUS Medical School, Singapore, who presented the study at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress.
“These patients have a dismal prognosis and represent a high unmet need,” she added.
The current findings follow those from the IMpassion130 trial, which showed that the combination of atezolizumab with nab-paclitaxel chemotherapy offered no survival benefit in previously untreated locally advanced or metastatic TNBC despite a progression-free survival benefit on interim analysis.
Rapidly relapsing TNBC “represents one of most challenging clinical situations” because it is aggressive and “intrinsically resistant to standard therapies,” said Dr. Dent. It is also more common in younger patients with large primary tumors and no BRCA alterations.
“Most importantly, however, is that most trials actually exclude these patients,” she noted, “posing a real challenge for us in clinical practice.”
IMpassion132 enrolled 594 patients with unresectable locally advanced or metastatic TNBC who had experienced disease progression more than 12 months after their last treatment for early TNBC with curative intent.
Patients had received prior anthracycline and taxane therapy for but no prior chemotherapy for advanced disease.
Study participants were randomly assigned to chemotherapy with carboplatin-gemcitabine or capecitabine plus atezolizumab or placebo, with treatment continued until disease progression or unacceptable toxicity. The primary endpoint was overall survival.
Initially, all patients with TNBC who met the study criteria were enrolled in the randomized, phase 3, double-blinded trial; however, the trial was then amended to include only PD-L1–positive patients after the results of IMpassion130 “clearly showed us that the benefits of immune checkpoint inhibition were largely driven by those patients,” Dr. Dent explained.
The 354 patients with PD-L1–positive disease were “young,” she added, with a median age of 48 years. The youngest was 23 years old.
The majority (66%-69%) had a disease-free interval of less than 6 months after treatment with curative intent. Lung and/or liver metastases were present in 60%-62% of patients, and 18% had previously received platinum-based chemotherapy.
After a median follow-up of 9.8 months, overall survival was a median of 12.1 months in the atezolizumab group vs 11.2 months with placebo, at a hazard ratio of 0.93 (P = .59).
A similar result was seen when looking at the modified intention-to-treat population, and when stratifying the patients by prespecified subgroup.
Dr. Dent pointed out that in the placebo group, patients treated with capecitabine had a median overall survival of 12.6 months vs 9.9 months in those given carboplatin-gemcitabine , which she described as “hypothesis generating” because “prior therapy may trigger a variety of resistance mechanisms.”
The disease-free interval also seemed to play a role in the placebo group. Patients who had a disease-free interval of 6 or more months prior to study enrollment had a median overall survival of 12.8 months vs 9.4 months in those with an interval of less than 6 months.
There were no significant differences in progression-free survival or duration of overall response between the atezolizumab and placebo groups.
“In terms of the safety data, clearly we’re getting better at identifying immune checkpoint inhibition toxicities and initiating therapies for these toxicities earlier,” Dr. Dent said, because there were “no new safety signals.”
The rate of treatment-related grade 3 or 4 adverse events was similar between patients given atezolizumab and those assigned to placebo, at 65% vs 62%. Rates of grade 5 events were identical, at 1%.
Commenting on the study, Sara M. Tolaney, MD, MPH, chief, Division of Breast Oncology, Susan F. Smith Center for Women’s Cancers, Dana-Farber Cancer Institute, Boston, questioned the role for immunotherapy in patients with TNBC who experience early relapse.
This is not the first trial to fail to show a benefit in this space, she said. Collectively, these results make “me think that these tumors are pretty immunologically cold, making them less likely to benefit from checkpoint inhibition.”
The patients that do relapse, “have highly treatment refractory disease,” and “we need to think about other novel therapeutic strategies for this population,” she told this news organization.
IMpassion132 nevertheless represents a “unique opportunity to better understand the biology of these rapidly relapsing tumors, and hopefully use this information to develop more novel treatment approaches for this population,” she said.
“That being said, I do think that this is going to become an even more challenging area,” Dr. Tolaney said. “In the modern era, these patients are receiving multi-agent chemotherapy with preoperative checkpoint inhibition, and many then go on to receive additional systemic treatment in the adjuvant setting.”
The study was sponsored by Hoffmann-La Roche.
Dr. Dent declares relationships with AstraZeneca, Roche, Eisai, Lilly, MSD, Novartis, and Pfizer. Dr. Tolaney declares relationships with Novartis, Pfizer, Merck, Lilly, AstraZeneca, Genentech/Roche, Eisai, Sanofi, Bristol Myers Squib, Seattle Genetics, CytomX Therapeutics, Daiichi Sankyo, Gilead, Ellipses Pharma, 4D Pharma, OncoSec Medical Inc, BeyondSpring Pharmaceuticals, OncXerna, Zymeworks, Zentalis, Blueprint Medicines, Reveal Genomics, ARC Therapeutics, Myovant, Zetagen, Umoja Biopharma, Menarini/Stemline, Aadi Biopharma, Bayer, Jazz Pharmaceuticals, Exelixis, Novartis, Nanonstring, and Cyclacel.
A version of this article appeared on Medscape.com .
Our results “highlight the importance of recognizing TNBC heterogeneity, especially in the first-line setting” said Rebecca A. Dent, MD, MSc, National Cancer Center Singapore and Duke-NUS Medical School, Singapore, who presented the study at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress.
“These patients have a dismal prognosis and represent a high unmet need,” she added.
The current findings follow those from the IMpassion130 trial, which showed that the combination of atezolizumab with nab-paclitaxel chemotherapy offered no survival benefit in previously untreated locally advanced or metastatic TNBC despite a progression-free survival benefit on interim analysis.
Rapidly relapsing TNBC “represents one of most challenging clinical situations” because it is aggressive and “intrinsically resistant to standard therapies,” said Dr. Dent. It is also more common in younger patients with large primary tumors and no BRCA alterations.
“Most importantly, however, is that most trials actually exclude these patients,” she noted, “posing a real challenge for us in clinical practice.”
IMpassion132 enrolled 594 patients with unresectable locally advanced or metastatic TNBC who had experienced disease progression more than 12 months after their last treatment for early TNBC with curative intent.
Patients had received prior anthracycline and taxane therapy for but no prior chemotherapy for advanced disease.
Study participants were randomly assigned to chemotherapy with carboplatin-gemcitabine or capecitabine plus atezolizumab or placebo, with treatment continued until disease progression or unacceptable toxicity. The primary endpoint was overall survival.
Initially, all patients with TNBC who met the study criteria were enrolled in the randomized, phase 3, double-blinded trial; however, the trial was then amended to include only PD-L1–positive patients after the results of IMpassion130 “clearly showed us that the benefits of immune checkpoint inhibition were largely driven by those patients,” Dr. Dent explained.
The 354 patients with PD-L1–positive disease were “young,” she added, with a median age of 48 years. The youngest was 23 years old.
The majority (66%-69%) had a disease-free interval of less than 6 months after treatment with curative intent. Lung and/or liver metastases were present in 60%-62% of patients, and 18% had previously received platinum-based chemotherapy.
After a median follow-up of 9.8 months, overall survival was a median of 12.1 months in the atezolizumab group vs 11.2 months with placebo, at a hazard ratio of 0.93 (P = .59).
A similar result was seen when looking at the modified intention-to-treat population, and when stratifying the patients by prespecified subgroup.
Dr. Dent pointed out that in the placebo group, patients treated with capecitabine had a median overall survival of 12.6 months vs 9.9 months in those given carboplatin-gemcitabine , which she described as “hypothesis generating” because “prior therapy may trigger a variety of resistance mechanisms.”
The disease-free interval also seemed to play a role in the placebo group. Patients who had a disease-free interval of 6 or more months prior to study enrollment had a median overall survival of 12.8 months vs 9.4 months in those with an interval of less than 6 months.
There were no significant differences in progression-free survival or duration of overall response between the atezolizumab and placebo groups.
“In terms of the safety data, clearly we’re getting better at identifying immune checkpoint inhibition toxicities and initiating therapies for these toxicities earlier,” Dr. Dent said, because there were “no new safety signals.”
The rate of treatment-related grade 3 or 4 adverse events was similar between patients given atezolizumab and those assigned to placebo, at 65% vs 62%. Rates of grade 5 events were identical, at 1%.
Commenting on the study, Sara M. Tolaney, MD, MPH, chief, Division of Breast Oncology, Susan F. Smith Center for Women’s Cancers, Dana-Farber Cancer Institute, Boston, questioned the role for immunotherapy in patients with TNBC who experience early relapse.
This is not the first trial to fail to show a benefit in this space, she said. Collectively, these results make “me think that these tumors are pretty immunologically cold, making them less likely to benefit from checkpoint inhibition.”
The patients that do relapse, “have highly treatment refractory disease,” and “we need to think about other novel therapeutic strategies for this population,” she told this news organization.
IMpassion132 nevertheless represents a “unique opportunity to better understand the biology of these rapidly relapsing tumors, and hopefully use this information to develop more novel treatment approaches for this population,” she said.
“That being said, I do think that this is going to become an even more challenging area,” Dr. Tolaney said. “In the modern era, these patients are receiving multi-agent chemotherapy with preoperative checkpoint inhibition, and many then go on to receive additional systemic treatment in the adjuvant setting.”
The study was sponsored by Hoffmann-La Roche.
Dr. Dent declares relationships with AstraZeneca, Roche, Eisai, Lilly, MSD, Novartis, and Pfizer. Dr. Tolaney declares relationships with Novartis, Pfizer, Merck, Lilly, AstraZeneca, Genentech/Roche, Eisai, Sanofi, Bristol Myers Squib, Seattle Genetics, CytomX Therapeutics, Daiichi Sankyo, Gilead, Ellipses Pharma, 4D Pharma, OncoSec Medical Inc, BeyondSpring Pharmaceuticals, OncXerna, Zymeworks, Zentalis, Blueprint Medicines, Reveal Genomics, ARC Therapeutics, Myovant, Zetagen, Umoja Biopharma, Menarini/Stemline, Aadi Biopharma, Bayer, Jazz Pharmaceuticals, Exelixis, Novartis, Nanonstring, and Cyclacel.
A version of this article appeared on Medscape.com .
FROM ESMO BREAST CANCER 2024
Little Less Talk and a Lot More Action
No matter where one looks for the statistics, no matter what words one chooses to describe it, this country has a child and adolescent mental health crisis. Almost 20% of young people in the 3-17 age bracket have a mental, emotional, developmental, or behavioral disorder. COVID-19 has certainly exacerbated the problem, but the downward trend in the mental health of this nation has been going on for decades.
The voices calling for more services to address the problem are getting more numerous and louder. But, what exactly should those services look like and who should be delivering them?

When considered together, two recent research papers suggest that we should be venturing well beyond the usual mental health strategies if we are going to be successful in addressing the current crisis.
The first paper is an analysis by two psychologists who contend that our efforts to raise the awareness of mental issues may be contributing to the increase in reported mental health problems. The authors agree that more attention paid to mental health conditions can result in “more accurate reporting of previous under-recognized symptoms” and would seem to be a positive. However, the investigators also observe that when exposed to this flood of information, some individuals who are only experiencing minor distress may report their symptoms as mental problems. The authors of the paper have coined the term for this phenomenon as “prevalence inflation.” Their preliminary investigation suggests it may be much more common than once believed and they present numerous situations in which prevalence inflation seems to have occurred.
A New York Times article about this hypothesis reports on a British study in which nearly 30,000 teenagers were instructed by their teachers to “direct their attentions to the present moment” and utilize other mindfulness strategies. The educators had hoped that after 8 years of this indoctrination, the students’ mental health would have improved. The bottom line was that this mindfulness-based program was of no help and may have actually made things worse for a subgroup of students who were at greatest risk for mental health challenges.
Dr. Jack Andrews, one of the authors, feels that mindfulness training may encourage what he calls “co-rumination,” which he describes as “the kind of long, unresolved group discussion that churns up problems without finding solutions.” One has to wonder if “prevalence inflation” and “co-rumination,” if they do exist, may be playing a role in the hotly debated phenomenon some have termed “late-onset gender dysphoria.”
Never having been a fan of mindfulness training as an effective strategy, I am relieved to learn that serious investigators are finding evidence that supports my gut reaction.
If raising awareness, “education,” and group discussion aren’t working, and in some cases are actually contributing to the crisis, or at least making the data difficult to interpret, what should we be doing to turn this foundering ship around?
A second paper, coming from Taiwan, may provide an answer. Huey-Ling Chiang and fellow investigators have reported on a study of nearly two million children and adolescents in which they found improved performance in a variety of physical fitness challenges “was linked with a lower risk of mental health disorder.” The dose-dependent effect resulted in less anxiety and depressive disorders as well as less attention-deficit/hyperactivity disorder when cardio-respiratory, muscle endurance, and power indices improved.
There have been other observers who have suggested a link between physical fitness and improved mental health, but this Taiwanese study is by far one of the largest. And, the discovery of a dose-dependent effect makes it particularly convincing.
As I reviewed these two papers, I became increasingly frustrated because this is another example in which one of the answers is staring us in the face and we continue to do nothing more than talk about it.
We already know that physically active people are healthier both physically and mentally, but we do little more than talk. It may be helpful for some people to become a bit more self-aware. However, it is becoming increasingly clear that you can’t talk yourself into being mentally healthy without a concurrent effort to actually do the things that can improve your overall health, such as being physically active and adopting healthy sleep habits. A political advisor once said, “It’s the economy, stupid.” As a community interested in the health of our children and the adults they will become, we need to remind ourselves again, “It’s the old Mind-Body Thing, Stupid.” Our children need a little less talk and a lot more action.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
No matter where one looks for the statistics, no matter what words one chooses to describe it, this country has a child and adolescent mental health crisis. Almost 20% of young people in the 3-17 age bracket have a mental, emotional, developmental, or behavioral disorder. COVID-19 has certainly exacerbated the problem, but the downward trend in the mental health of this nation has been going on for decades.
The voices calling for more services to address the problem are getting more numerous and louder. But, what exactly should those services look like and who should be delivering them?
When considered together, two recent research papers suggest that we should be venturing well beyond the usual mental health strategies if we are going to be successful in addressing the current crisis.
The first paper is an analysis by two psychologists who contend that our efforts to raise the awareness of mental issues may be contributing to the increase in reported mental health problems. The authors agree that more attention paid to mental health conditions can result in “more accurate reporting of previous under-recognized symptoms” and would seem to be a positive. However, the investigators also observe that when exposed to this flood of information, some individuals who are only experiencing minor distress may report their symptoms as mental problems. The authors of the paper have coined the term for this phenomenon as “prevalence inflation.” Their preliminary investigation suggests it may be much more common than once believed and they present numerous situations in which prevalence inflation seems to have occurred.
A New York Times article about this hypothesis reports on a British study in which nearly 30,000 teenagers were instructed by their teachers to “direct their attentions to the present moment” and utilize other mindfulness strategies. The educators had hoped that after 8 years of this indoctrination, the students’ mental health would have improved. The bottom line was that this mindfulness-based program was of no help and may have actually made things worse for a subgroup of students who were at greatest risk for mental health challenges.
Dr. Jack Andrews, one of the authors, feels that mindfulness training may encourage what he calls “co-rumination,” which he describes as “the kind of long, unresolved group discussion that churns up problems without finding solutions.” One has to wonder if “prevalence inflation” and “co-rumination,” if they do exist, may be playing a role in the hotly debated phenomenon some have termed “late-onset gender dysphoria.”
Never having been a fan of mindfulness training as an effective strategy, I am relieved to learn that serious investigators are finding evidence that supports my gut reaction.
If raising awareness, “education,” and group discussion aren’t working, and in some cases are actually contributing to the crisis, or at least making the data difficult to interpret, what should we be doing to turn this foundering ship around?
A second paper, coming from Taiwan, may provide an answer. Huey-Ling Chiang and fellow investigators have reported on a study of nearly two million children and adolescents in which they found improved performance in a variety of physical fitness challenges “was linked with a lower risk of mental health disorder.” The dose-dependent effect resulted in less anxiety and depressive disorders as well as less attention-deficit/hyperactivity disorder when cardio-respiratory, muscle endurance, and power indices improved.
There have been other observers who have suggested a link between physical fitness and improved mental health, but this Taiwanese study is by far one of the largest. And, the discovery of a dose-dependent effect makes it particularly convincing.
As I reviewed these two papers, I became increasingly frustrated because this is another example in which one of the answers is staring us in the face and we continue to do nothing more than talk about it.
We already know that physically active people are healthier both physically and mentally, but we do little more than talk. It may be helpful for some people to become a bit more self-aware. However, it is becoming increasingly clear that you can’t talk yourself into being mentally healthy without a concurrent effort to actually do the things that can improve your overall health, such as being physically active and adopting healthy sleep habits. A political advisor once said, “It’s the economy, stupid.” As a community interested in the health of our children and the adults they will become, we need to remind ourselves again, “It’s the old Mind-Body Thing, Stupid.” Our children need a little less talk and a lot more action.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
No matter where one looks for the statistics, no matter what words one chooses to describe it, this country has a child and adolescent mental health crisis. Almost 20% of young people in the 3-17 age bracket have a mental, emotional, developmental, or behavioral disorder. COVID-19 has certainly exacerbated the problem, but the downward trend in the mental health of this nation has been going on for decades.
The voices calling for more services to address the problem are getting more numerous and louder. But, what exactly should those services look like and who should be delivering them?
When considered together, two recent research papers suggest that we should be venturing well beyond the usual mental health strategies if we are going to be successful in addressing the current crisis.
The first paper is an analysis by two psychologists who contend that our efforts to raise the awareness of mental issues may be contributing to the increase in reported mental health problems. The authors agree that more attention paid to mental health conditions can result in “more accurate reporting of previous under-recognized symptoms” and would seem to be a positive. However, the investigators also observe that when exposed to this flood of information, some individuals who are only experiencing minor distress may report their symptoms as mental problems. The authors of the paper have coined the term for this phenomenon as “prevalence inflation.” Their preliminary investigation suggests it may be much more common than once believed and they present numerous situations in which prevalence inflation seems to have occurred.
A New York Times article about this hypothesis reports on a British study in which nearly 30,000 teenagers were instructed by their teachers to “direct their attentions to the present moment” and utilize other mindfulness strategies. The educators had hoped that after 8 years of this indoctrination, the students’ mental health would have improved. The bottom line was that this mindfulness-based program was of no help and may have actually made things worse for a subgroup of students who were at greatest risk for mental health challenges.
Dr. Jack Andrews, one of the authors, feels that mindfulness training may encourage what he calls “co-rumination,” which he describes as “the kind of long, unresolved group discussion that churns up problems without finding solutions.” One has to wonder if “prevalence inflation” and “co-rumination,” if they do exist, may be playing a role in the hotly debated phenomenon some have termed “late-onset gender dysphoria.”
Never having been a fan of mindfulness training as an effective strategy, I am relieved to learn that serious investigators are finding evidence that supports my gut reaction.
If raising awareness, “education,” and group discussion aren’t working, and in some cases are actually contributing to the crisis, or at least making the data difficult to interpret, what should we be doing to turn this foundering ship around?
A second paper, coming from Taiwan, may provide an answer. Huey-Ling Chiang and fellow investigators have reported on a study of nearly two million children and adolescents in which they found improved performance in a variety of physical fitness challenges “was linked with a lower risk of mental health disorder.” The dose-dependent effect resulted in less anxiety and depressive disorders as well as less attention-deficit/hyperactivity disorder when cardio-respiratory, muscle endurance, and power indices improved.
There have been other observers who have suggested a link between physical fitness and improved mental health, but this Taiwanese study is by far one of the largest. And, the discovery of a dose-dependent effect makes it particularly convincing.
As I reviewed these two papers, I became increasingly frustrated because this is another example in which one of the answers is staring us in the face and we continue to do nothing more than talk about it.
We already know that physically active people are healthier both physically and mentally, but we do little more than talk. It may be helpful for some people to become a bit more self-aware. However, it is becoming increasingly clear that you can’t talk yourself into being mentally healthy without a concurrent effort to actually do the things that can improve your overall health, such as being physically active and adopting healthy sleep habits. A political advisor once said, “It’s the economy, stupid.” As a community interested in the health of our children and the adults they will become, we need to remind ourselves again, “It’s the old Mind-Body Thing, Stupid.” Our children need a little less talk and a lot more action.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Hypopigmented Cutaneous Langerhans Cell Histiocytosis in a Hispanic Infant
To the Editor:
Langerhans cell histiocytosis (LCH) is a rare inflammatory neoplasia caused by accumulation of clonal Langerhans cells in 1 or more organs. The clinical spectrum is diverse, ranging from mild, single-organ involvement that may resolve spontaneously to severe progressive multisystem disease that can be fatal. It is most prevalent in children, affecting an estimated 4 to 5 children for every 1 million annually, with male predominance.1 The pathogenesis is driven by activating mutations in the mitogen-activated protein kinase pathway, with the BRAF V600E mutation detected in most LCH patients, resulting in proliferation of pathologic Langerhans cells and dysregulated expression of inflammatory cytokines in LCH lesions.2 A biopsy of lesional tissue is required for definitive diagnosis. Histopathology reveals a mixed inflammatory infiltrate and characteristic mononuclear cells with reniform nuclei that are positive for CD1a and CD207 proteins on immunohistochemical staining.3
Langerhans cell histiocytosis is categorized by the extent of organ involvement. It commonly affects the bones, skin, pituitary gland, liver, lungs, bone marrow, and lymph nodes.4 Single-system LCH involves a single organ with unifocal or multifocal lesions; multisystem LCH involves 2 or more organs and has a worse prognosis if risk organs (eg, liver, spleen, bone marrow) are involved.4
Skin lesions are reported in more than half of LCH cases and are the most common initial manifestation in patients younger than 2 years.4 Cutaneous findings are highly variable, which poses a diagnostic challenge. Common morphologies include erythematous papules, pustules, papulovesicles, scaly plaques, erosions, and petechiae. Lesions can be solitary or widespread and favor the trunk, head, and face.4 We describe an atypical case of hypopigmented cutaneous LCH and review the literature on this morphology in patients with skin of color.
A 7-month-old Hispanic male infant who was otherwise healthy presented with numerous hypopigmented macules and pink papules on the trunk and groin that had progressed since birth. A review of systems was unremarkable. Physical examination revealed 1- to 3-mm, discrete, hypopigmented macules intermixed with 1- to 2-mm pearly pink papules scattered on the back, chest, abdomen, and inguinal folds (Figure 1). Some lesions appeared koebnerized; however, the parents denied a history of scratching or trauma.
Histopathology of a lesion in the inguinal fold showed aggregates of mononuclear cells with reniform nuclei and abundant amphophilic cytoplasm in the papillary dermis, with focal extension into the epidermis. Scattered eosinophils and multinucleated giant cells were present in the dermal inflammatory infiltrate (Figure 2). Immunohistochemical staining was positive for CD1a (Figure 3) and S-100 protein (Figure 4). Although epidermal Langerhans cell collections also can be seen in allergic contact dermatitis,5 predominant involvement of the papillary dermis and the presence of multinucleated giant cells are characteristic of LCH.4 Given these findings, which were consistent with LCH, the dermatopathology deemed BRAF V600E immunostaining unnecessary for diagnostic purposes.

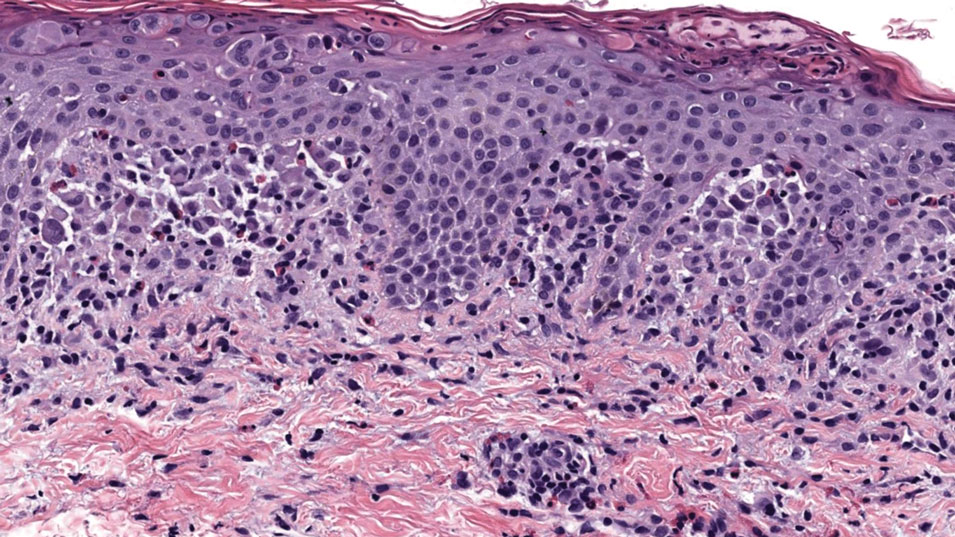
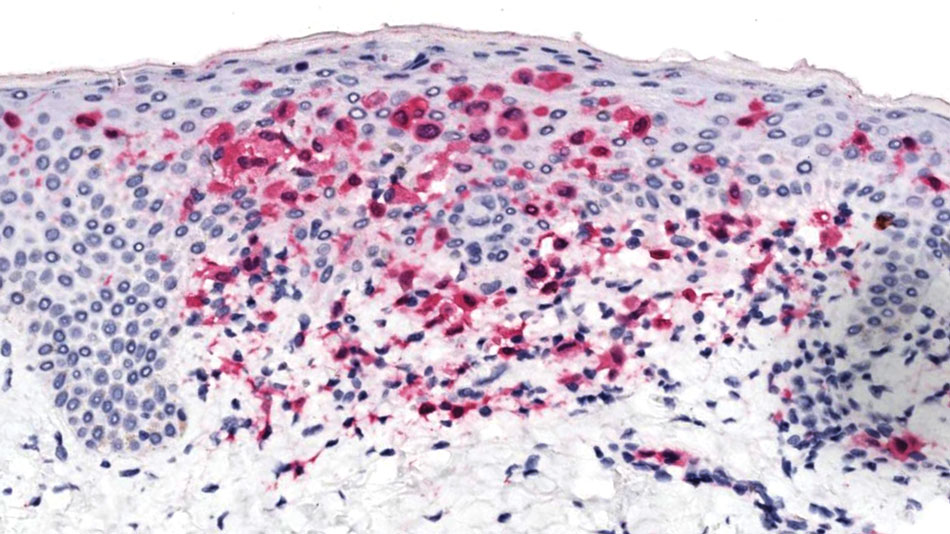
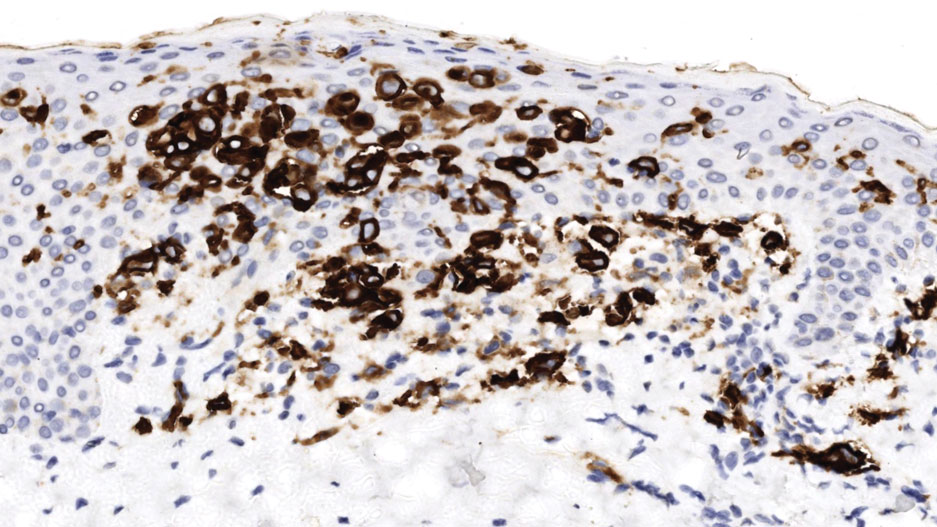
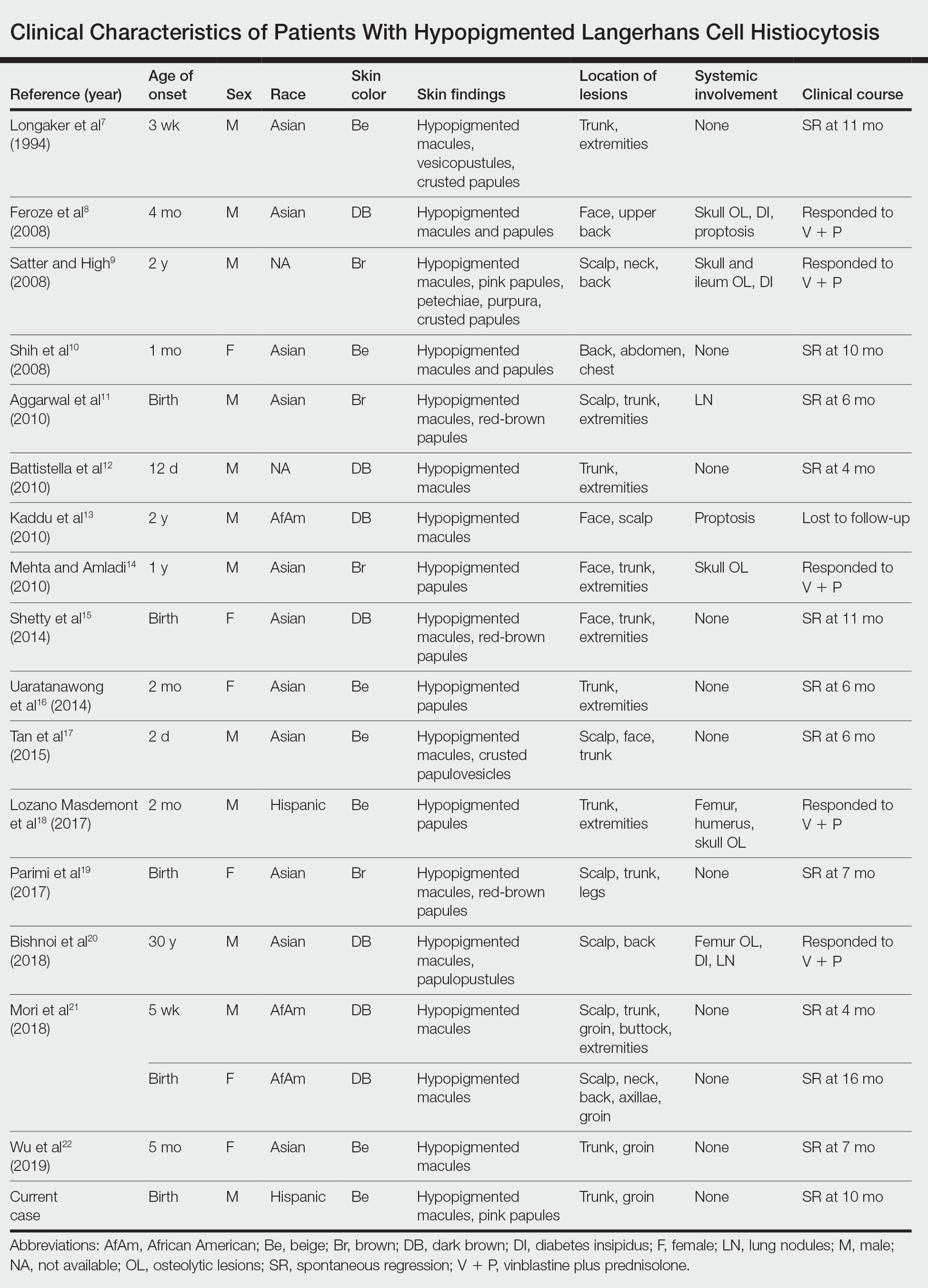
The patient was referred to the hematology and oncology department to undergo thorough evaluation for extracutaneous involvement. The workup included a complete blood cell count, liver function testing, electrolyte assessment, skeletal survey, chest radiography, and ultrasonography of the liver and spleen. All results were negative, suggesting a diagnosis of single-system cutaneous LCH.
Three months later, the patient presented to dermatology with spontaneous regression of all skin lesions. Continued follow-up—every 6 months for 5 years—was recommended to monitor for disease recurrence or progression to multisystem disease.
Cutaneous LCH is a clinically heterogeneous disease with the potential for multisystem involvement and long-term sequelae; therefore, timely diagnosis is paramount to optimize outcomes. However, delayed diagnosis is common because of the spectrum of skin findings that can mimic common pediatric dermatoses, such as seborrheic dermatitis, atopic dermatitis, and diaper dermatitis.4 In one study, the median time from onset of skin lesions to diagnostic biopsy was longer than 3 months (maximum, 5 years).6 Our patient was referred to dermatology 7 months after onset of hypopigmented macules, a rarely reported cutaneous manifestation of LCH.
A PubMed search of articles indexed for MEDLINE from 1994 to 2019 using the terms Langerhans cell histiocytotis and hypopigmented yielded 17 cases of LCH presenting as hypopigmented skin lesions (Table).7-22 All cases occurred in patients with skin of color (ie, patients of Asian, Hispanic, or African descent). Hypopigmented macules were the only cutaneous manifestation in 10 (59%) cases. Lesions most commonly were distributed on the trunk (16/17 [94%]) and extremities (8/17 [47%]). The median age of onset was 1 month; 76% (13/17) of patients developed skin lesions before 1 year of age, indicating that this morphology may be more common in newborns. In most patients, the diagnosis was single-system cutaneous LCH; they exhibited spontaneous regression by 8 months of age on average, suggesting that this variant may be associated with a better prognosis. Mori and colleagues21 hypothesized that hypopigmented lesions may represent the resolving stage of active LCH based on histopathologic findings of dermal pallor and fibrosis in a hypopigmented LCH lesion. However, systemic involvement was reported in 7 cases of hypopigmented LCH, highlighting the importance of assessing for multisystem disease regardless of cutaneous morphology.21Langerhans cell histiocytosis should be considered in the differential diagnosis when evaluating hypopigmented skin eruptions in infants with darker skin types. Prompt diagnosis of this atypical variant requires a higher index of suspicion because of its rarity and the polymorphic nature of cutaneous LCH. This morphology may go undiagnosed in the setting of mild or spontaneously resolving disease; notwithstanding, accurate diagnosis and longitudinal surveillance are necessary given the potential for progressive systemic involvement.
1. Guyot-Goubin A, Donadieu J, Barkaoui M, et al. Descriptive epidemiology of childhood Langerhans cell histiocytosis in France, 2000–2004. Pediatr Blood Cancer. 2008;51:71-75. doi:10.1002/pbc.21498
2. Badalian-Very G, Vergilio J-A, Degar BA, et al. Recurrent BRAF mutations in Langerhans cell histiocytosis. Blood. 2010;116:1919-1923. doi:10.1182/blood-2010-04-279083
3. Haupt R, Minkov M, Astigarraga I, et al; Euro Histio Network. Langerhans cell histiocytosis (LCH): guidelines for diagnosis, clinical work‐up, and treatment for patients till the age of 18 years. Pediatr Blood Cancer. 2013;60:175-184. doi:10.1002/pbc.24367
4. Krooks J, Minkov M, Weatherall AG. Langerhans cell histiocytosis in children: history, classification, pathobiology, clinical manifestations, and prognosis. J Am Acad Dermatol. 2018;78:1035-1044. doi:10.1016/j.jaad.2017.05.059
5. Rosa G, Fernandez AP, Vij A, et al. Langerhans cell collections, but not eosinophils, are clues to a diagnosis of allergic contact dermatitis in appropriate skin biopsies. J Cutan Pathol. 2016;43:498-504. doi:10.1111/cup.12707
6. Simko SJ, Garmezy B, Abhyankar H, et al. Differentiating skin-limited and multisystem Langerhans cell histiocytosis. J Pediatr. 2014;165:990-996. doi:10.1016/j.jpeds.2014.07.063
7. Longaker MA, Frieden IJ, LeBoit PE, et al. Congenital “self-healing” Langerhans cell histiocytosis: the need for long-term follow-up. J Am Acad Dermatol. 1994;31(5, pt 2):910-916. doi:10.1016/s0190-9622(94)70258-6
8. Feroze K, Unni M, Jayasree MG, et al. Langerhans cell histiocytosis presenting with hypopigmented macules. Indian J Dermatol Venereol Leprol. 2008;74:670-672. doi:10.4103/0378-6323.45128
9. Satter EK, High WA. Langerhans cell histiocytosis: a case report and summary of the current recommendations of the Histiocyte Society. Dermatol Online J. 2008;14:3.
10. Chang SL, Shih IH, Kuo TT, et al. Congenital self-healing reticulohistiocytosis presenting as hypopigmented macules and papules in a neonate. Dermatologica Sinica 2008;26:80-84.
11. Aggarwal V, Seth A, Jain M, et al. Congenital Langerhans cell histiocytosis with skin and lung involvement: spontaneous regression. Indian J Pediatr. 2010;77:811-812.
12. Battistella M, Fraitag S, Teillac DH, et al. Neonatal and early infantile cutaneous Langerhans cell histiocytosis: comparison of self-regressive and non-self-regressive forms. Arch Dermatol. 2010;146:149-156. doi:10.1001/archdermatol.2009.360
13. Kaddu S, Mulyowa G, Kovarik C. Hypopigmented scaly, scalp and facial lesions and disfiguring exopthalmus. Clin Exp Dermatol. 2010;3:E52-E53. doi:10.1111/j.1365-2230.2009.03336.x
14. Mehta B, Amladi S. Langerhans cell histiocytosis presenting as hypopigmented papules. Pediatr Dermatol. 2010;27:215-217. doi:10.1111/j.1525-1470.2010.01104.x
15. Shetty S, Monappa V, Pai K, et al. Congenital self-healing reticulohistiocytosis: a case report. Our Dermatol Online. 2014;5:264-266.
16. Uaratanawong R, Kootiratrakarn T, Sudtikoonaseth P, et al. Congenital self-healing reticulohistiocytosis presented with multiple hypopigmented flat-topped papules: a case report and review of literatures. J Med Assoc Thai. 2014;97:993-997.
17. Tan Q, Gan LQ, Wang H. Congenital self-healing Langerhans cell histiocytosis in a male neonate. Indian J Dermatol Venereol Leprol. 2015;81:75-77. doi:10.4103/0378-6323.148587
18. Lozano Masdemont B, Gómez‐Recuero Muñoz L, Villanueva Álvarez‐Santullano A, et al. Langerhans cell histiocytosis mimicking lichen nitidus with bone involvement. Australas J Dermatol. 2017;58:231-233. doi:10.1111/ajd.12467
19. Parimi LR, You J, Hong L, et al. Congenital self-healing reticulohistiocytosis with spontaneous regression. An Bras Dermatol. 2017;92:553-555. doi:10.1590/abd1806-4841.20175432
20. Bishnoi A, De D, Khullar G, et al. Hypopigmented and acneiform lesions: an unusual initial presentation of adult-onset multisystem Langerhans cell histiocytosis. Indian J Dermatol Venereol Leprol. 2018;84:621-626. doi:10.4103/ijdvl.IJDVL_639_17
21. Mori S, Adar T, Kazlouskaya V, et al. Cutaneous Langerhans cell histiocytosis presenting with hypopigmented lesions: report of two cases and review of literature. Pediatr Dermatol. 2018;35:502-506. doi:10.1111/pde.13509
22. Wu X, Huang J, Jiang L, et al. Congenital self‐healing reticulohistiocytosis with BRAF V600E mutation in an infant. Clin Exp Dermatol. 2019;44:647-650. doi:10.1111/ced.13880
To the Editor:
Langerhans cell histiocytosis (LCH) is a rare inflammatory neoplasia caused by accumulation of clonal Langerhans cells in 1 or more organs. The clinical spectrum is diverse, ranging from mild, single-organ involvement that may resolve spontaneously to severe progressive multisystem disease that can be fatal. It is most prevalent in children, affecting an estimated 4 to 5 children for every 1 million annually, with male predominance.1 The pathogenesis is driven by activating mutations in the mitogen-activated protein kinase pathway, with the BRAF V600E mutation detected in most LCH patients, resulting in proliferation of pathologic Langerhans cells and dysregulated expression of inflammatory cytokines in LCH lesions.2 A biopsy of lesional tissue is required for definitive diagnosis. Histopathology reveals a mixed inflammatory infiltrate and characteristic mononuclear cells with reniform nuclei that are positive for CD1a and CD207 proteins on immunohistochemical staining.3
Langerhans cell histiocytosis is categorized by the extent of organ involvement. It commonly affects the bones, skin, pituitary gland, liver, lungs, bone marrow, and lymph nodes.4 Single-system LCH involves a single organ with unifocal or multifocal lesions; multisystem LCH involves 2 or more organs and has a worse prognosis if risk organs (eg, liver, spleen, bone marrow) are involved.4
Skin lesions are reported in more than half of LCH cases and are the most common initial manifestation in patients younger than 2 years.4 Cutaneous findings are highly variable, which poses a diagnostic challenge. Common morphologies include erythematous papules, pustules, papulovesicles, scaly plaques, erosions, and petechiae. Lesions can be solitary or widespread and favor the trunk, head, and face.4 We describe an atypical case of hypopigmented cutaneous LCH and review the literature on this morphology in patients with skin of color.
A 7-month-old Hispanic male infant who was otherwise healthy presented with numerous hypopigmented macules and pink papules on the trunk and groin that had progressed since birth. A review of systems was unremarkable. Physical examination revealed 1- to 3-mm, discrete, hypopigmented macules intermixed with 1- to 2-mm pearly pink papules scattered on the back, chest, abdomen, and inguinal folds (Figure 1). Some lesions appeared koebnerized; however, the parents denied a history of scratching or trauma.
Histopathology of a lesion in the inguinal fold showed aggregates of mononuclear cells with reniform nuclei and abundant amphophilic cytoplasm in the papillary dermis, with focal extension into the epidermis. Scattered eosinophils and multinucleated giant cells were present in the dermal inflammatory infiltrate (Figure 2). Immunohistochemical staining was positive for CD1a (Figure 3) and S-100 protein (Figure 4). Although epidermal Langerhans cell collections also can be seen in allergic contact dermatitis,5 predominant involvement of the papillary dermis and the presence of multinucleated giant cells are characteristic of LCH.4 Given these findings, which were consistent with LCH, the dermatopathology deemed BRAF V600E immunostaining unnecessary for diagnostic purposes.
The patient was referred to the hematology and oncology department to undergo thorough evaluation for extracutaneous involvement. The workup included a complete blood cell count, liver function testing, electrolyte assessment, skeletal survey, chest radiography, and ultrasonography of the liver and spleen. All results were negative, suggesting a diagnosis of single-system cutaneous LCH.
Three months later, the patient presented to dermatology with spontaneous regression of all skin lesions. Continued follow-up—every 6 months for 5 years—was recommended to monitor for disease recurrence or progression to multisystem disease.
Cutaneous LCH is a clinically heterogeneous disease with the potential for multisystem involvement and long-term sequelae; therefore, timely diagnosis is paramount to optimize outcomes. However, delayed diagnosis is common because of the spectrum of skin findings that can mimic common pediatric dermatoses, such as seborrheic dermatitis, atopic dermatitis, and diaper dermatitis.4 In one study, the median time from onset of skin lesions to diagnostic biopsy was longer than 3 months (maximum, 5 years).6 Our patient was referred to dermatology 7 months after onset of hypopigmented macules, a rarely reported cutaneous manifestation of LCH.
A PubMed search of articles indexed for MEDLINE from 1994 to 2019 using the terms Langerhans cell histiocytotis and hypopigmented yielded 17 cases of LCH presenting as hypopigmented skin lesions (Table).7-22 All cases occurred in patients with skin of color (ie, patients of Asian, Hispanic, or African descent). Hypopigmented macules were the only cutaneous manifestation in 10 (59%) cases. Lesions most commonly were distributed on the trunk (16/17 [94%]) and extremities (8/17 [47%]). The median age of onset was 1 month; 76% (13/17) of patients developed skin lesions before 1 year of age, indicating that this morphology may be more common in newborns. In most patients, the diagnosis was single-system cutaneous LCH; they exhibited spontaneous regression by 8 months of age on average, suggesting that this variant may be associated with a better prognosis. Mori and colleagues21 hypothesized that hypopigmented lesions may represent the resolving stage of active LCH based on histopathologic findings of dermal pallor and fibrosis in a hypopigmented LCH lesion. However, systemic involvement was reported in 7 cases of hypopigmented LCH, highlighting the importance of assessing for multisystem disease regardless of cutaneous morphology.21Langerhans cell histiocytosis should be considered in the differential diagnosis when evaluating hypopigmented skin eruptions in infants with darker skin types. Prompt diagnosis of this atypical variant requires a higher index of suspicion because of its rarity and the polymorphic nature of cutaneous LCH. This morphology may go undiagnosed in the setting of mild or spontaneously resolving disease; notwithstanding, accurate diagnosis and longitudinal surveillance are necessary given the potential for progressive systemic involvement.
To the Editor:
Langerhans cell histiocytosis (LCH) is a rare inflammatory neoplasia caused by accumulation of clonal Langerhans cells in 1 or more organs. The clinical spectrum is diverse, ranging from mild, single-organ involvement that may resolve spontaneously to severe progressive multisystem disease that can be fatal. It is most prevalent in children, affecting an estimated 4 to 5 children for every 1 million annually, with male predominance.1 The pathogenesis is driven by activating mutations in the mitogen-activated protein kinase pathway, with the BRAF V600E mutation detected in most LCH patients, resulting in proliferation of pathologic Langerhans cells and dysregulated expression of inflammatory cytokines in LCH lesions.2 A biopsy of lesional tissue is required for definitive diagnosis. Histopathology reveals a mixed inflammatory infiltrate and characteristic mononuclear cells with reniform nuclei that are positive for CD1a and CD207 proteins on immunohistochemical staining.3
Langerhans cell histiocytosis is categorized by the extent of organ involvement. It commonly affects the bones, skin, pituitary gland, liver, lungs, bone marrow, and lymph nodes.4 Single-system LCH involves a single organ with unifocal or multifocal lesions; multisystem LCH involves 2 or more organs and has a worse prognosis if risk organs (eg, liver, spleen, bone marrow) are involved.4
Skin lesions are reported in more than half of LCH cases and are the most common initial manifestation in patients younger than 2 years.4 Cutaneous findings are highly variable, which poses a diagnostic challenge. Common morphologies include erythematous papules, pustules, papulovesicles, scaly plaques, erosions, and petechiae. Lesions can be solitary or widespread and favor the trunk, head, and face.4 We describe an atypical case of hypopigmented cutaneous LCH and review the literature on this morphology in patients with skin of color.
A 7-month-old Hispanic male infant who was otherwise healthy presented with numerous hypopigmented macules and pink papules on the trunk and groin that had progressed since birth. A review of systems was unremarkable. Physical examination revealed 1- to 3-mm, discrete, hypopigmented macules intermixed with 1- to 2-mm pearly pink papules scattered on the back, chest, abdomen, and inguinal folds (Figure 1). Some lesions appeared koebnerized; however, the parents denied a history of scratching or trauma.
Histopathology of a lesion in the inguinal fold showed aggregates of mononuclear cells with reniform nuclei and abundant amphophilic cytoplasm in the papillary dermis, with focal extension into the epidermis. Scattered eosinophils and multinucleated giant cells were present in the dermal inflammatory infiltrate (Figure 2). Immunohistochemical staining was positive for CD1a (Figure 3) and S-100 protein (Figure 4). Although epidermal Langerhans cell collections also can be seen in allergic contact dermatitis,5 predominant involvement of the papillary dermis and the presence of multinucleated giant cells are characteristic of LCH.4 Given these findings, which were consistent with LCH, the dermatopathology deemed BRAF V600E immunostaining unnecessary for diagnostic purposes.
The patient was referred to the hematology and oncology department to undergo thorough evaluation for extracutaneous involvement. The workup included a complete blood cell count, liver function testing, electrolyte assessment, skeletal survey, chest radiography, and ultrasonography of the liver and spleen. All results were negative, suggesting a diagnosis of single-system cutaneous LCH.
Three months later, the patient presented to dermatology with spontaneous regression of all skin lesions. Continued follow-up—every 6 months for 5 years—was recommended to monitor for disease recurrence or progression to multisystem disease.
Cutaneous LCH is a clinically heterogeneous disease with the potential for multisystem involvement and long-term sequelae; therefore, timely diagnosis is paramount to optimize outcomes. However, delayed diagnosis is common because of the spectrum of skin findings that can mimic common pediatric dermatoses, such as seborrheic dermatitis, atopic dermatitis, and diaper dermatitis.4 In one study, the median time from onset of skin lesions to diagnostic biopsy was longer than 3 months (maximum, 5 years).6 Our patient was referred to dermatology 7 months after onset of hypopigmented macules, a rarely reported cutaneous manifestation of LCH.
A PubMed search of articles indexed for MEDLINE from 1994 to 2019 using the terms Langerhans cell histiocytotis and hypopigmented yielded 17 cases of LCH presenting as hypopigmented skin lesions (Table).7-22 All cases occurred in patients with skin of color (ie, patients of Asian, Hispanic, or African descent). Hypopigmented macules were the only cutaneous manifestation in 10 (59%) cases. Lesions most commonly were distributed on the trunk (16/17 [94%]) and extremities (8/17 [47%]). The median age of onset was 1 month; 76% (13/17) of patients developed skin lesions before 1 year of age, indicating that this morphology may be more common in newborns. In most patients, the diagnosis was single-system cutaneous LCH; they exhibited spontaneous regression by 8 months of age on average, suggesting that this variant may be associated with a better prognosis. Mori and colleagues21 hypothesized that hypopigmented lesions may represent the resolving stage of active LCH based on histopathologic findings of dermal pallor and fibrosis in a hypopigmented LCH lesion. However, systemic involvement was reported in 7 cases of hypopigmented LCH, highlighting the importance of assessing for multisystem disease regardless of cutaneous morphology.21Langerhans cell histiocytosis should be considered in the differential diagnosis when evaluating hypopigmented skin eruptions in infants with darker skin types. Prompt diagnosis of this atypical variant requires a higher index of suspicion because of its rarity and the polymorphic nature of cutaneous LCH. This morphology may go undiagnosed in the setting of mild or spontaneously resolving disease; notwithstanding, accurate diagnosis and longitudinal surveillance are necessary given the potential for progressive systemic involvement.
1. Guyot-Goubin A, Donadieu J, Barkaoui M, et al. Descriptive epidemiology of childhood Langerhans cell histiocytosis in France, 2000–2004. Pediatr Blood Cancer. 2008;51:71-75. doi:10.1002/pbc.21498
2. Badalian-Very G, Vergilio J-A, Degar BA, et al. Recurrent BRAF mutations in Langerhans cell histiocytosis. Blood. 2010;116:1919-1923. doi:10.1182/blood-2010-04-279083
3. Haupt R, Minkov M, Astigarraga I, et al; Euro Histio Network. Langerhans cell histiocytosis (LCH): guidelines for diagnosis, clinical work‐up, and treatment for patients till the age of 18 years. Pediatr Blood Cancer. 2013;60:175-184. doi:10.1002/pbc.24367
4. Krooks J, Minkov M, Weatherall AG. Langerhans cell histiocytosis in children: history, classification, pathobiology, clinical manifestations, and prognosis. J Am Acad Dermatol. 2018;78:1035-1044. doi:10.1016/j.jaad.2017.05.059
5. Rosa G, Fernandez AP, Vij A, et al. Langerhans cell collections, but not eosinophils, are clues to a diagnosis of allergic contact dermatitis in appropriate skin biopsies. J Cutan Pathol. 2016;43:498-504. doi:10.1111/cup.12707
6. Simko SJ, Garmezy B, Abhyankar H, et al. Differentiating skin-limited and multisystem Langerhans cell histiocytosis. J Pediatr. 2014;165:990-996. doi:10.1016/j.jpeds.2014.07.063
7. Longaker MA, Frieden IJ, LeBoit PE, et al. Congenital “self-healing” Langerhans cell histiocytosis: the need for long-term follow-up. J Am Acad Dermatol. 1994;31(5, pt 2):910-916. doi:10.1016/s0190-9622(94)70258-6
8. Feroze K, Unni M, Jayasree MG, et al. Langerhans cell histiocytosis presenting with hypopigmented macules. Indian J Dermatol Venereol Leprol. 2008;74:670-672. doi:10.4103/0378-6323.45128
9. Satter EK, High WA. Langerhans cell histiocytosis: a case report and summary of the current recommendations of the Histiocyte Society. Dermatol Online J. 2008;14:3.
10. Chang SL, Shih IH, Kuo TT, et al. Congenital self-healing reticulohistiocytosis presenting as hypopigmented macules and papules in a neonate. Dermatologica Sinica 2008;26:80-84.
11. Aggarwal V, Seth A, Jain M, et al. Congenital Langerhans cell histiocytosis with skin and lung involvement: spontaneous regression. Indian J Pediatr. 2010;77:811-812.
12. Battistella M, Fraitag S, Teillac DH, et al. Neonatal and early infantile cutaneous Langerhans cell histiocytosis: comparison of self-regressive and non-self-regressive forms. Arch Dermatol. 2010;146:149-156. doi:10.1001/archdermatol.2009.360
13. Kaddu S, Mulyowa G, Kovarik C. Hypopigmented scaly, scalp and facial lesions and disfiguring exopthalmus. Clin Exp Dermatol. 2010;3:E52-E53. doi:10.1111/j.1365-2230.2009.03336.x
14. Mehta B, Amladi S. Langerhans cell histiocytosis presenting as hypopigmented papules. Pediatr Dermatol. 2010;27:215-217. doi:10.1111/j.1525-1470.2010.01104.x
15. Shetty S, Monappa V, Pai K, et al. Congenital self-healing reticulohistiocytosis: a case report. Our Dermatol Online. 2014;5:264-266.
16. Uaratanawong R, Kootiratrakarn T, Sudtikoonaseth P, et al. Congenital self-healing reticulohistiocytosis presented with multiple hypopigmented flat-topped papules: a case report and review of literatures. J Med Assoc Thai. 2014;97:993-997.
17. Tan Q, Gan LQ, Wang H. Congenital self-healing Langerhans cell histiocytosis in a male neonate. Indian J Dermatol Venereol Leprol. 2015;81:75-77. doi:10.4103/0378-6323.148587
18. Lozano Masdemont B, Gómez‐Recuero Muñoz L, Villanueva Álvarez‐Santullano A, et al. Langerhans cell histiocytosis mimicking lichen nitidus with bone involvement. Australas J Dermatol. 2017;58:231-233. doi:10.1111/ajd.12467
19. Parimi LR, You J, Hong L, et al. Congenital self-healing reticulohistiocytosis with spontaneous regression. An Bras Dermatol. 2017;92:553-555. doi:10.1590/abd1806-4841.20175432
20. Bishnoi A, De D, Khullar G, et al. Hypopigmented and acneiform lesions: an unusual initial presentation of adult-onset multisystem Langerhans cell histiocytosis. Indian J Dermatol Venereol Leprol. 2018;84:621-626. doi:10.4103/ijdvl.IJDVL_639_17
21. Mori S, Adar T, Kazlouskaya V, et al. Cutaneous Langerhans cell histiocytosis presenting with hypopigmented lesions: report of two cases and review of literature. Pediatr Dermatol. 2018;35:502-506. doi:10.1111/pde.13509
22. Wu X, Huang J, Jiang L, et al. Congenital self‐healing reticulohistiocytosis with BRAF V600E mutation in an infant. Clin Exp Dermatol. 2019;44:647-650. doi:10.1111/ced.13880
1. Guyot-Goubin A, Donadieu J, Barkaoui M, et al. Descriptive epidemiology of childhood Langerhans cell histiocytosis in France, 2000–2004. Pediatr Blood Cancer. 2008;51:71-75. doi:10.1002/pbc.21498
2. Badalian-Very G, Vergilio J-A, Degar BA, et al. Recurrent BRAF mutations in Langerhans cell histiocytosis. Blood. 2010;116:1919-1923. doi:10.1182/blood-2010-04-279083
3. Haupt R, Minkov M, Astigarraga I, et al; Euro Histio Network. Langerhans cell histiocytosis (LCH): guidelines for diagnosis, clinical work‐up, and treatment for patients till the age of 18 years. Pediatr Blood Cancer. 2013;60:175-184. doi:10.1002/pbc.24367
4. Krooks J, Minkov M, Weatherall AG. Langerhans cell histiocytosis in children: history, classification, pathobiology, clinical manifestations, and prognosis. J Am Acad Dermatol. 2018;78:1035-1044. doi:10.1016/j.jaad.2017.05.059
5. Rosa G, Fernandez AP, Vij A, et al. Langerhans cell collections, but not eosinophils, are clues to a diagnosis of allergic contact dermatitis in appropriate skin biopsies. J Cutan Pathol. 2016;43:498-504. doi:10.1111/cup.12707
6. Simko SJ, Garmezy B, Abhyankar H, et al. Differentiating skin-limited and multisystem Langerhans cell histiocytosis. J Pediatr. 2014;165:990-996. doi:10.1016/j.jpeds.2014.07.063
7. Longaker MA, Frieden IJ, LeBoit PE, et al. Congenital “self-healing” Langerhans cell histiocytosis: the need for long-term follow-up. J Am Acad Dermatol. 1994;31(5, pt 2):910-916. doi:10.1016/s0190-9622(94)70258-6
8. Feroze K, Unni M, Jayasree MG, et al. Langerhans cell histiocytosis presenting with hypopigmented macules. Indian J Dermatol Venereol Leprol. 2008;74:670-672. doi:10.4103/0378-6323.45128
9. Satter EK, High WA. Langerhans cell histiocytosis: a case report and summary of the current recommendations of the Histiocyte Society. Dermatol Online J. 2008;14:3.
10. Chang SL, Shih IH, Kuo TT, et al. Congenital self-healing reticulohistiocytosis presenting as hypopigmented macules and papules in a neonate. Dermatologica Sinica 2008;26:80-84.
11. Aggarwal V, Seth A, Jain M, et al. Congenital Langerhans cell histiocytosis with skin and lung involvement: spontaneous regression. Indian J Pediatr. 2010;77:811-812.
12. Battistella M, Fraitag S, Teillac DH, et al. Neonatal and early infantile cutaneous Langerhans cell histiocytosis: comparison of self-regressive and non-self-regressive forms. Arch Dermatol. 2010;146:149-156. doi:10.1001/archdermatol.2009.360
13. Kaddu S, Mulyowa G, Kovarik C. Hypopigmented scaly, scalp and facial lesions and disfiguring exopthalmus. Clin Exp Dermatol. 2010;3:E52-E53. doi:10.1111/j.1365-2230.2009.03336.x
14. Mehta B, Amladi S. Langerhans cell histiocytosis presenting as hypopigmented papules. Pediatr Dermatol. 2010;27:215-217. doi:10.1111/j.1525-1470.2010.01104.x
15. Shetty S, Monappa V, Pai K, et al. Congenital self-healing reticulohistiocytosis: a case report. Our Dermatol Online. 2014;5:264-266.
16. Uaratanawong R, Kootiratrakarn T, Sudtikoonaseth P, et al. Congenital self-healing reticulohistiocytosis presented with multiple hypopigmented flat-topped papules: a case report and review of literatures. J Med Assoc Thai. 2014;97:993-997.
17. Tan Q, Gan LQ, Wang H. Congenital self-healing Langerhans cell histiocytosis in a male neonate. Indian J Dermatol Venereol Leprol. 2015;81:75-77. doi:10.4103/0378-6323.148587
18. Lozano Masdemont B, Gómez‐Recuero Muñoz L, Villanueva Álvarez‐Santullano A, et al. Langerhans cell histiocytosis mimicking lichen nitidus with bone involvement. Australas J Dermatol. 2017;58:231-233. doi:10.1111/ajd.12467
19. Parimi LR, You J, Hong L, et al. Congenital self-healing reticulohistiocytosis with spontaneous regression. An Bras Dermatol. 2017;92:553-555. doi:10.1590/abd1806-4841.20175432
20. Bishnoi A, De D, Khullar G, et al. Hypopigmented and acneiform lesions: an unusual initial presentation of adult-onset multisystem Langerhans cell histiocytosis. Indian J Dermatol Venereol Leprol. 2018;84:621-626. doi:10.4103/ijdvl.IJDVL_639_17
21. Mori S, Adar T, Kazlouskaya V, et al. Cutaneous Langerhans cell histiocytosis presenting with hypopigmented lesions: report of two cases and review of literature. Pediatr Dermatol. 2018;35:502-506. doi:10.1111/pde.13509
22. Wu X, Huang J, Jiang L, et al. Congenital self‐healing reticulohistiocytosis with BRAF V600E mutation in an infant. Clin Exp Dermatol. 2019;44:647-650. doi:10.1111/ced.13880
Practice Points
- Dermatologists should be aware of the hypopigmented variant of cutaneous Langerhans cell histiocytosis (LCH), which has been reported exclusively in patients with skin of color.
- Langerhans cell histiocytosis should be included in the differential diagnosis of hypopigmented macules, which may be the only cutaneous manifestation or may coincide with typical lesions of LCH.
- Hypopigmented cutaneous LCH may be more common in newborns and associated with a better prognosis.

Arthroscopy Doesn’t Delay Total Knee Replacement in Knee Osteoarthritis
TOPLINE:
Adding arthroscopic surgery to nonoperative management neither delays nor accelerates the timing of total knee arthroplasty (TKA) in patients with knee osteoarthritis (OA).
METHODOLOGY:
- Some case series show that arthroscopic surgery for knee OA may delay more invasive procedures, such as TKA or osteotomy, while longitudinal cohort studies often contradict this. Current OA guidelines are yet to address this issue.
- This secondary analysis of a randomized trial compared the long-term incidence of TKA in 178 patients (mean age, 59 years; 64.3% women) with knee OA who were referred for potential arthroscopic surgery at a tertiary care center in Canada.
- The patients received nonoperative care with or without additional arthroscopic surgery.
- Patients in the arthroscopic surgery group had specific knee procedures (resection of degenerative knee tissues) along with nonoperative management (physical therapy plus medications as required), while the control group received nonoperative management alone.
- The primary outcome was TKA on the knee being studied, and the secondary outcome was TKA or osteotomy on either knee.
TAKEAWAY:
- During a median follow-up of 13.8 years, 37.6% of patients underwent TKA, with comparable proportions of patients in the arthroscopic surgery and control groups undergoing TKA (adjusted hazard ratio [aHR], 0.85; 95% CI, 0.52-1.40).
- The rates of TKA or osteotomy on either knee were similar in both groups (aHR, 0.91; 95% CI, 0.59-1.41).
- A time-stratified analysis done for 0-5 years, 5-10 years, and beyond 10 years of follow-up also showed a consistent interpretation.
- When patients with crossover to arthroscopic surgery during the follow-up were included, the results remained similar for both the primary (HR, 0.88; 95% CI, 0.53-1.44) and secondary (HR, 1.08; 95% CI, 0.69-1.68) outcomes.
IN PRACTICE:
“Our study findings do not support the use of arthroscopic surgery for OA of the knee.” “Arthroscopic surgery does not provide additional benefit to nonoperative management for improving pain, stiffness, and function and is likely not cost-effective at 2 years of follow-up,” the authors wrote.
SOURCE:
This study was led by Trevor B. Birmingham, PhD, Fowler Kennedy Sport Medicine Clinic, University of Western Ontario, London, Ontario, Canada. It was published online in JAMA Network Open
LIMITATIONS:
The study was designed to assess differences in 2-year patient-reported outcomes rather than long-term TKA incidence. Factors influencing decisions to undergo TKA or osteotomy were not considered. Moreover, the effects observed in this study should be evaluated considering the estimated confidence intervals.
DISCLOSURES:
This study was supported by the ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care. Some authors declared consulting, performing contracted services, or receiving grant funding, royalties, and nonfinancial support from various sources.
A version of this article appeared on Medscape.com.
TOPLINE:
Adding arthroscopic surgery to nonoperative management neither delays nor accelerates the timing of total knee arthroplasty (TKA) in patients with knee osteoarthritis (OA).
METHODOLOGY:
- Some case series show that arthroscopic surgery for knee OA may delay more invasive procedures, such as TKA or osteotomy, while longitudinal cohort studies often contradict this. Current OA guidelines are yet to address this issue.
- This secondary analysis of a randomized trial compared the long-term incidence of TKA in 178 patients (mean age, 59 years; 64.3% women) with knee OA who were referred for potential arthroscopic surgery at a tertiary care center in Canada.
- The patients received nonoperative care with or without additional arthroscopic surgery.
- Patients in the arthroscopic surgery group had specific knee procedures (resection of degenerative knee tissues) along with nonoperative management (physical therapy plus medications as required), while the control group received nonoperative management alone.
- The primary outcome was TKA on the knee being studied, and the secondary outcome was TKA or osteotomy on either knee.
TAKEAWAY:
- During a median follow-up of 13.8 years, 37.6% of patients underwent TKA, with comparable proportions of patients in the arthroscopic surgery and control groups undergoing TKA (adjusted hazard ratio [aHR], 0.85; 95% CI, 0.52-1.40).
- The rates of TKA or osteotomy on either knee were similar in both groups (aHR, 0.91; 95% CI, 0.59-1.41).
- A time-stratified analysis done for 0-5 years, 5-10 years, and beyond 10 years of follow-up also showed a consistent interpretation.
- When patients with crossover to arthroscopic surgery during the follow-up were included, the results remained similar for both the primary (HR, 0.88; 95% CI, 0.53-1.44) and secondary (HR, 1.08; 95% CI, 0.69-1.68) outcomes.
IN PRACTICE:
“Our study findings do not support the use of arthroscopic surgery for OA of the knee.” “Arthroscopic surgery does not provide additional benefit to nonoperative management for improving pain, stiffness, and function and is likely not cost-effective at 2 years of follow-up,” the authors wrote.
SOURCE:
This study was led by Trevor B. Birmingham, PhD, Fowler Kennedy Sport Medicine Clinic, University of Western Ontario, London, Ontario, Canada. It was published online in JAMA Network Open
LIMITATIONS:
The study was designed to assess differences in 2-year patient-reported outcomes rather than long-term TKA incidence. Factors influencing decisions to undergo TKA or osteotomy were not considered. Moreover, the effects observed in this study should be evaluated considering the estimated confidence intervals.
DISCLOSURES:
This study was supported by the ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care. Some authors declared consulting, performing contracted services, or receiving grant funding, royalties, and nonfinancial support from various sources.
A version of this article appeared on Medscape.com.
TOPLINE:
Adding arthroscopic surgery to nonoperative management neither delays nor accelerates the timing of total knee arthroplasty (TKA) in patients with knee osteoarthritis (OA).
METHODOLOGY:
- Some case series show that arthroscopic surgery for knee OA may delay more invasive procedures, such as TKA or osteotomy, while longitudinal cohort studies often contradict this. Current OA guidelines are yet to address this issue.
- This secondary analysis of a randomized trial compared the long-term incidence of TKA in 178 patients (mean age, 59 years; 64.3% women) with knee OA who were referred for potential arthroscopic surgery at a tertiary care center in Canada.
- The patients received nonoperative care with or without additional arthroscopic surgery.
- Patients in the arthroscopic surgery group had specific knee procedures (resection of degenerative knee tissues) along with nonoperative management (physical therapy plus medications as required), while the control group received nonoperative management alone.
- The primary outcome was TKA on the knee being studied, and the secondary outcome was TKA or osteotomy on either knee.
TAKEAWAY:
- During a median follow-up of 13.8 years, 37.6% of patients underwent TKA, with comparable proportions of patients in the arthroscopic surgery and control groups undergoing TKA (adjusted hazard ratio [aHR], 0.85; 95% CI, 0.52-1.40).
- The rates of TKA or osteotomy on either knee were similar in both groups (aHR, 0.91; 95% CI, 0.59-1.41).
- A time-stratified analysis done for 0-5 years, 5-10 years, and beyond 10 years of follow-up also showed a consistent interpretation.
- When patients with crossover to arthroscopic surgery during the follow-up were included, the results remained similar for both the primary (HR, 0.88; 95% CI, 0.53-1.44) and secondary (HR, 1.08; 95% CI, 0.69-1.68) outcomes.
IN PRACTICE:
“Our study findings do not support the use of arthroscopic surgery for OA of the knee.” “Arthroscopic surgery does not provide additional benefit to nonoperative management for improving pain, stiffness, and function and is likely not cost-effective at 2 years of follow-up,” the authors wrote.
SOURCE:
This study was led by Trevor B. Birmingham, PhD, Fowler Kennedy Sport Medicine Clinic, University of Western Ontario, London, Ontario, Canada. It was published online in JAMA Network Open
LIMITATIONS:
The study was designed to assess differences in 2-year patient-reported outcomes rather than long-term TKA incidence. Factors influencing decisions to undergo TKA or osteotomy were not considered. Moreover, the effects observed in this study should be evaluated considering the estimated confidence intervals.
DISCLOSURES:
This study was supported by the ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care. Some authors declared consulting, performing contracted services, or receiving grant funding, royalties, and nonfinancial support from various sources.
A version of this article appeared on Medscape.com.
Vigilance Needed in Gout Treatment to Reduce CVD Risks
NEW YORK — Urate, the culprit of gout, affects the vasculature in multiple ways that can raise cardiovascular risk (CV) in an individual with gout, and following guidelines for gout treatment, including the use of colchicine, can be the key to reducing those risks.
“Guideline-concordant gout treatment, which is essentially an anti-inflammatory urate-lowering strategy, at least improves arterial physiology and likely reduces cardiovascular risk,” Michael H. Pillinger, MD, told attendees at the 4th Annual Cardiometabolic Risk in Inflammatory Conditions conference. Dr. Pillinger is professor of medicine and biochemistry and molecular pharmacology at New York University Grossman School of Medicine, New York City, who has published multiple studies on gout.

He cited evidence that has shown soluble urate stimulates the production of C-reactive protein (CRP), which is a predictor of cardiovascular disease (CVD). Another study, in which Dr. Pillinger participated, demonstrated that gout patients have impaired vascular endothelial function associated with a chronic, low-level inflammatory state, he said.
“There’s good evidence that urate itself affects the vasculature in multiple ways, and I suspect this may be a model for other metabolic effects on vasculature,” Dr. Pillinger said. “Patients with gout have abnormal endothelium in ways that really convey vascular risk.”
Gout, Inflammation, and CVD
However, for rheumatologists to study the association between gout-related inflammation and CVD is “very, very hard,” Dr. Pillinger added. “But I do think that the mechanisms by which gout induces biological changes in the vasculature may provide insights into cardiovascular disease in general.”
One way to evaluate the effects of gout on the endothelium in the clinic is to measure flow-mediated dilation. This technique involves placing an ultrasound probe over the brachial artery and measuring the baseline artery diameter. Then, with the blood pressure cuff over the forearm, inflate it to reduce flow, then release the cuff and measure the brachial artery diameter after the endothelium releases vasodilators.
Dr. Pillinger and colleagues evaluated this technique in 34 patients with gout and 64 controls and found that patients with gout had an almost 50% decrease in flow-mediated dilation, he said. “Interestingly, the higher the urate, the worse the flow; the more the inflammation, the worse the flow, so seemingly corresponding with the severity of the gout,” he said. That raised an obvious question, Dr. Pillinger continued: “If you can treat the gout, can you improve the flow-mediated dilation?”
His group answered that question with a study in 38 previously untreated patients with gout, giving them colchicine 0.6 mg twice daily for a month plus a urate-lowering xanthine oxidase inhibitor (allopurinol or febuxostat) to treat them to a target urate level of < 6 mg/dL. “We saw an increase in endothelial function, and it normalized,” Dr. Pillinger said.
However, some study participants didn’t respond. “They were people with well-established other cardiovascular comorbidities — hypertension, hyperlipidemia,” he said. “I think some people just have vessels that are too damaged to get at them just by fixing their gout problem or their inflammation.”
That means patients with gout need to be treated with colchicine early on to avoid CV problems, Dr. Pillinger added. “We ought to get to them before they have the other problems,” he said.
Managing gout, and the concomitant CV problems, requires vigilance both during and in between flares, Dr. Pillinger said after his presentation.
“We have always taught that patients between flares basically look like people with no gout, but we do know now that patients with gout between flares tend to have what you might call ‘subclinical’ inflammation: CRPs and ESRs [erythrocyte sedimentation rates] that are higher than those of the general population, though not so excessive that they might grab attention,” he said. “We also know that many, if not all, patients between flares have urate deposited in or around their joints, but how these two relate is not fully established.”
Better treatment within 3 months of an acute gout flare may reduce the risk for CV events, he said, but that’s based on speculation more so than clinical data.
Potential Benefits of Targeting Inflammation
“More chronically, we know from the cardiologists’ studies that anti-inflammatory therapy should reduce risk in the high-risk general population,” Dr. Pillinger said. “There are no prospective studies confirming that this approach will work among gout patients, but there is no reason why it shouldn’t work — except perhaps that gout patients may have higher inflammation than the general population and also have more comorbidities, so they could perhaps be more resistant.”
Dr. Pillinger said that his group’s studies and another led by Daniel Solomon, MD, at Brigham and Women’s Hospital in Boston, have indicated that anti-inflammatory strategies in gout will lower CV risk.
“And interestingly,” he added, “our data suggest that colchicine use may lower risk not only in high-risk gout patients but also in gout patients who start with no CAD [coronary artery disease] but who seem to have less incident CAD on colchicine. I see this as identifying that gout patients are intrinsically at high risk for CAD, even if they don’t actually have any, so they represent a population for whom lowering chronic inflammation may help prevent incident disease.”
Dr. Pillinger provided more evidence that the understanding of the relationship between gout, gout flares, and CV risk is evolving, said Michael S. Garshick, MD, who attended the conference and is head of the Cardio-Rheumatology Program at NYU Langone, New York City.

“There’s epidemiologic evidence supporting the association,” Dr. Garshick told this news organization after the conference. “We think that most conditions with immune system activation do tend to have an increased risk of some form of cardiovascular disease, but I think the relationship with gout has been highly underpublicized.”
Many patients with gout tend to have a higher prevalence of traditional cardiometabolic issues, which may compound the relationship, Dr. Garshick added. “However, I would argue that with this patient subset that it doesn’t matter because gout patients have a higher risk of traditional risk factors, and you have to [treat-to-target] those traditional risk factors.”
While the clinical evidence of a link between gout and atherosclerosis may not be conclusive, enough circumstantial evidence exists to believe that treating gout will reduce CV risks, he said. “Some of the imaging techniques do suggest that gouty crystals [are] in the atherosclerotic plaque of gout patients,” Dr. Garshick added. Dr. Pillinger’s work, he said, “is showing us that there are different pathways to develop atherosclerosis.”
Dr. Pillinger disclosed relationships with Federation Bio, Fortress Biotech, Amgen, Scilex, Hikma Pharmaceuticals, LG Chem, and Olatec Therapeutics. Dr. Garshick disclosed relationships with Kiniksa Pharmaceuticals, Agepha Pharma, Bristol Myers Squibb, and Horizon Therapeutics.
A version of this article appeared on Medscape.com.
NEW YORK — Urate, the culprit of gout, affects the vasculature in multiple ways that can raise cardiovascular risk (CV) in an individual with gout, and following guidelines for gout treatment, including the use of colchicine, can be the key to reducing those risks.
“Guideline-concordant gout treatment, which is essentially an anti-inflammatory urate-lowering strategy, at least improves arterial physiology and likely reduces cardiovascular risk,” Michael H. Pillinger, MD, told attendees at the 4th Annual Cardiometabolic Risk in Inflammatory Conditions conference. Dr. Pillinger is professor of medicine and biochemistry and molecular pharmacology at New York University Grossman School of Medicine, New York City, who has published multiple studies on gout.
He cited evidence that has shown soluble urate stimulates the production of C-reactive protein (CRP), which is a predictor of cardiovascular disease (CVD). Another study, in which Dr. Pillinger participated, demonstrated that gout patients have impaired vascular endothelial function associated with a chronic, low-level inflammatory state, he said.
“There’s good evidence that urate itself affects the vasculature in multiple ways, and I suspect this may be a model for other metabolic effects on vasculature,” Dr. Pillinger said. “Patients with gout have abnormal endothelium in ways that really convey vascular risk.”
Gout, Inflammation, and CVD
However, for rheumatologists to study the association between gout-related inflammation and CVD is “very, very hard,” Dr. Pillinger added. “But I do think that the mechanisms by which gout induces biological changes in the vasculature may provide insights into cardiovascular disease in general.”
One way to evaluate the effects of gout on the endothelium in the clinic is to measure flow-mediated dilation. This technique involves placing an ultrasound probe over the brachial artery and measuring the baseline artery diameter. Then, with the blood pressure cuff over the forearm, inflate it to reduce flow, then release the cuff and measure the brachial artery diameter after the endothelium releases vasodilators.
Dr. Pillinger and colleagues evaluated this technique in 34 patients with gout and 64 controls and found that patients with gout had an almost 50% decrease in flow-mediated dilation, he said. “Interestingly, the higher the urate, the worse the flow; the more the inflammation, the worse the flow, so seemingly corresponding with the severity of the gout,” he said. That raised an obvious question, Dr. Pillinger continued: “If you can treat the gout, can you improve the flow-mediated dilation?”
His group answered that question with a study in 38 previously untreated patients with gout, giving them colchicine 0.6 mg twice daily for a month plus a urate-lowering xanthine oxidase inhibitor (allopurinol or febuxostat) to treat them to a target urate level of < 6 mg/dL. “We saw an increase in endothelial function, and it normalized,” Dr. Pillinger said.
However, some study participants didn’t respond. “They were people with well-established other cardiovascular comorbidities — hypertension, hyperlipidemia,” he said. “I think some people just have vessels that are too damaged to get at them just by fixing their gout problem or their inflammation.”
That means patients with gout need to be treated with colchicine early on to avoid CV problems, Dr. Pillinger added. “We ought to get to them before they have the other problems,” he said.
Managing gout, and the concomitant CV problems, requires vigilance both during and in between flares, Dr. Pillinger said after his presentation.
“We have always taught that patients between flares basically look like people with no gout, but we do know now that patients with gout between flares tend to have what you might call ‘subclinical’ inflammation: CRPs and ESRs [erythrocyte sedimentation rates] that are higher than those of the general population, though not so excessive that they might grab attention,” he said. “We also know that many, if not all, patients between flares have urate deposited in or around their joints, but how these two relate is not fully established.”
Better treatment within 3 months of an acute gout flare may reduce the risk for CV events, he said, but that’s based on speculation more so than clinical data.
Potential Benefits of Targeting Inflammation
“More chronically, we know from the cardiologists’ studies that anti-inflammatory therapy should reduce risk in the high-risk general population,” Dr. Pillinger said. “There are no prospective studies confirming that this approach will work among gout patients, but there is no reason why it shouldn’t work — except perhaps that gout patients may have higher inflammation than the general population and also have more comorbidities, so they could perhaps be more resistant.”
Dr. Pillinger said that his group’s studies and another led by Daniel Solomon, MD, at Brigham and Women’s Hospital in Boston, have indicated that anti-inflammatory strategies in gout will lower CV risk.
“And interestingly,” he added, “our data suggest that colchicine use may lower risk not only in high-risk gout patients but also in gout patients who start with no CAD [coronary artery disease] but who seem to have less incident CAD on colchicine. I see this as identifying that gout patients are intrinsically at high risk for CAD, even if they don’t actually have any, so they represent a population for whom lowering chronic inflammation may help prevent incident disease.”
Dr. Pillinger provided more evidence that the understanding of the relationship between gout, gout flares, and CV risk is evolving, said Michael S. Garshick, MD, who attended the conference and is head of the Cardio-Rheumatology Program at NYU Langone, New York City.
“There’s epidemiologic evidence supporting the association,” Dr. Garshick told this news organization after the conference. “We think that most conditions with immune system activation do tend to have an increased risk of some form of cardiovascular disease, but I think the relationship with gout has been highly underpublicized.”
Many patients with gout tend to have a higher prevalence of traditional cardiometabolic issues, which may compound the relationship, Dr. Garshick added. “However, I would argue that with this patient subset that it doesn’t matter because gout patients have a higher risk of traditional risk factors, and you have to [treat-to-target] those traditional risk factors.”
While the clinical evidence of a link between gout and atherosclerosis may not be conclusive, enough circumstantial evidence exists to believe that treating gout will reduce CV risks, he said. “Some of the imaging techniques do suggest that gouty crystals [are] in the atherosclerotic plaque of gout patients,” Dr. Garshick added. Dr. Pillinger’s work, he said, “is showing us that there are different pathways to develop atherosclerosis.”
Dr. Pillinger disclosed relationships with Federation Bio, Fortress Biotech, Amgen, Scilex, Hikma Pharmaceuticals, LG Chem, and Olatec Therapeutics. Dr. Garshick disclosed relationships with Kiniksa Pharmaceuticals, Agepha Pharma, Bristol Myers Squibb, and Horizon Therapeutics.
A version of this article appeared on Medscape.com.
NEW YORK — Urate, the culprit of gout, affects the vasculature in multiple ways that can raise cardiovascular risk (CV) in an individual with gout, and following guidelines for gout treatment, including the use of colchicine, can be the key to reducing those risks.
“Guideline-concordant gout treatment, which is essentially an anti-inflammatory urate-lowering strategy, at least improves arterial physiology and likely reduces cardiovascular risk,” Michael H. Pillinger, MD, told attendees at the 4th Annual Cardiometabolic Risk in Inflammatory Conditions conference. Dr. Pillinger is professor of medicine and biochemistry and molecular pharmacology at New York University Grossman School of Medicine, New York City, who has published multiple studies on gout.
He cited evidence that has shown soluble urate stimulates the production of C-reactive protein (CRP), which is a predictor of cardiovascular disease (CVD). Another study, in which Dr. Pillinger participated, demonstrated that gout patients have impaired vascular endothelial function associated with a chronic, low-level inflammatory state, he said.
“There’s good evidence that urate itself affects the vasculature in multiple ways, and I suspect this may be a model for other metabolic effects on vasculature,” Dr. Pillinger said. “Patients with gout have abnormal endothelium in ways that really convey vascular risk.”
Gout, Inflammation, and CVD
However, for rheumatologists to study the association between gout-related inflammation and CVD is “very, very hard,” Dr. Pillinger added. “But I do think that the mechanisms by which gout induces biological changes in the vasculature may provide insights into cardiovascular disease in general.”
One way to evaluate the effects of gout on the endothelium in the clinic is to measure flow-mediated dilation. This technique involves placing an ultrasound probe over the brachial artery and measuring the baseline artery diameter. Then, with the blood pressure cuff over the forearm, inflate it to reduce flow, then release the cuff and measure the brachial artery diameter after the endothelium releases vasodilators.
Dr. Pillinger and colleagues evaluated this technique in 34 patients with gout and 64 controls and found that patients with gout had an almost 50% decrease in flow-mediated dilation, he said. “Interestingly, the higher the urate, the worse the flow; the more the inflammation, the worse the flow, so seemingly corresponding with the severity of the gout,” he said. That raised an obvious question, Dr. Pillinger continued: “If you can treat the gout, can you improve the flow-mediated dilation?”
His group answered that question with a study in 38 previously untreated patients with gout, giving them colchicine 0.6 mg twice daily for a month plus a urate-lowering xanthine oxidase inhibitor (allopurinol or febuxostat) to treat them to a target urate level of < 6 mg/dL. “We saw an increase in endothelial function, and it normalized,” Dr. Pillinger said.
However, some study participants didn’t respond. “They were people with well-established other cardiovascular comorbidities — hypertension, hyperlipidemia,” he said. “I think some people just have vessels that are too damaged to get at them just by fixing their gout problem or their inflammation.”
That means patients with gout need to be treated with colchicine early on to avoid CV problems, Dr. Pillinger added. “We ought to get to them before they have the other problems,” he said.
Managing gout, and the concomitant CV problems, requires vigilance both during and in between flares, Dr. Pillinger said after his presentation.
“We have always taught that patients between flares basically look like people with no gout, but we do know now that patients with gout between flares tend to have what you might call ‘subclinical’ inflammation: CRPs and ESRs [erythrocyte sedimentation rates] that are higher than those of the general population, though not so excessive that they might grab attention,” he said. “We also know that many, if not all, patients between flares have urate deposited in or around their joints, but how these two relate is not fully established.”
Better treatment within 3 months of an acute gout flare may reduce the risk for CV events, he said, but that’s based on speculation more so than clinical data.
Potential Benefits of Targeting Inflammation
“More chronically, we know from the cardiologists’ studies that anti-inflammatory therapy should reduce risk in the high-risk general population,” Dr. Pillinger said. “There are no prospective studies confirming that this approach will work among gout patients, but there is no reason why it shouldn’t work — except perhaps that gout patients may have higher inflammation than the general population and also have more comorbidities, so they could perhaps be more resistant.”
Dr. Pillinger said that his group’s studies and another led by Daniel Solomon, MD, at Brigham and Women’s Hospital in Boston, have indicated that anti-inflammatory strategies in gout will lower CV risk.
“And interestingly,” he added, “our data suggest that colchicine use may lower risk not only in high-risk gout patients but also in gout patients who start with no CAD [coronary artery disease] but who seem to have less incident CAD on colchicine. I see this as identifying that gout patients are intrinsically at high risk for CAD, even if they don’t actually have any, so they represent a population for whom lowering chronic inflammation may help prevent incident disease.”
Dr. Pillinger provided more evidence that the understanding of the relationship between gout, gout flares, and CV risk is evolving, said Michael S. Garshick, MD, who attended the conference and is head of the Cardio-Rheumatology Program at NYU Langone, New York City.
“There’s epidemiologic evidence supporting the association,” Dr. Garshick told this news organization after the conference. “We think that most conditions with immune system activation do tend to have an increased risk of some form of cardiovascular disease, but I think the relationship with gout has been highly underpublicized.”
Many patients with gout tend to have a higher prevalence of traditional cardiometabolic issues, which may compound the relationship, Dr. Garshick added. “However, I would argue that with this patient subset that it doesn’t matter because gout patients have a higher risk of traditional risk factors, and you have to [treat-to-target] those traditional risk factors.”
While the clinical evidence of a link between gout and atherosclerosis may not be conclusive, enough circumstantial evidence exists to believe that treating gout will reduce CV risks, he said. “Some of the imaging techniques do suggest that gouty crystals [are] in the atherosclerotic plaque of gout patients,” Dr. Garshick added. Dr. Pillinger’s work, he said, “is showing us that there are different pathways to develop atherosclerosis.”
Dr. Pillinger disclosed relationships with Federation Bio, Fortress Biotech, Amgen, Scilex, Hikma Pharmaceuticals, LG Chem, and Olatec Therapeutics. Dr. Garshick disclosed relationships with Kiniksa Pharmaceuticals, Agepha Pharma, Bristol Myers Squibb, and Horizon Therapeutics.
A version of this article appeared on Medscape.com.