User login
PCP Compensation, Part 4
I have already shared with you that healthcare systems value panel size and productivity when they are considering primary care physician compensation. Your employers also know that the market won’t bear a substantial price increase for the procedure-poor practice style typical of primary care. You know that the relative value unit (RVU) system for calculating complexity of service is time consuming and discourages the inclusion of customer-friendly short visits that could allow an efficient provider to see more patients. Unfortunately, there is little hope that RVUs will become more PCP-friendly in the near future.
However, before leaving the topic of value and moving on to a consideration of quality, I can’t resist sharing some thoughts about efficiency and time management.

First, it must be said that the inexpert development and the clumsy rollout of electronic medical records (EMRs) have struck the biggest blow to the compensation potential and mental health of even the most efficient PCPs. Until that chasm is filled, there will be little progress in improving the efficiency and, consequently, the fair compensation of PCPs.
However, there is a myth that there is a direct correlation between the time spent with the patient and the quality of care. Eighty-five percent of PCPs report they would like to spend more time to get to know their patients. On the other hand, in my experience, really getting to know a patient is a process best done over multiple visits — some long, many of them short. It is unrealistic and inefficient to gain an in-depth understanding of the patient in a single visit.
Yes, one often hears a patient complain “they only spent 5 minutes with me.” While the patient may be technically correct, I contend that the provider’s manner has a major influence on the patient’s perception of the time spent in the exam room.
Was the provider reasonably prompt? In other words did they value my time? Did they appear rushed? Were they aware of my relevant history and prepared to deal with the current situation? In other words, did they do their homework? Did they engage me visually and seem to know what they were talking about? But, most importantly, did they exude sympathy and seem to care? Was I treated in the same manner that they would like to have been treated? If the answer is YES to those questions, then likely the patient could care less about the time spent.
It may seem counterintuitive to some of you, but there is a simple strategy that a provider can employ that will give them more time with the patient and at the same time allow them to claim to the boss that they are lowering the overhead costs. Management consultants often lean heavily on delegation as a more efficient use of resources. However, when the provider takes the patient’s vital signs and gives the injections, this multitasking provides an excellent hands-on opportunity to take the history and get to know the patient better. And, by giving the immunizations the provider is making the clearest statement possible that these vaccines are so important that they administer them personally.
You may have been wondering why I haven’t included the quality of PCP care in a discussion of compensation. It is because I don’t believe anyone has figured out how to do it in a manner that makes sense and is fair. PCPs don’t do procedures on which their success rate can be measured. A PCP’s patient panel almost by definition is going to be a mix of ages with a broad variety of complaints. Do they see enough diabetics to use their panel’s hemoglobin A1cs as a metric, or enough asthmatics to use emergency department visits as a quality-of-care measurement? In pediatrics, the closest we can come to a valid measure may be the provider’s vaccine acceptance rate.
But, then how does one factor in the general health of the community? If I open a practice in an underserved community, can you measure the quality of my care based on how quickly I can improve the metrics when I have no control over the poverty and educational system?
Since we aren’t surgeons, outcomes can’t be used to judge our quality. I’m afraid the only way we can assure quality is to demand evidence of our efforts to keep abreast of the current knowledge in our field and hope that at some level CME credits accumulated translate to the care we provide. A recent study has demonstrated an association between board certification exam board scores and newly trained internists and the care they provide. The patients of the physicians with the top scores had a lower risk of being readmitted to the hospital and were less likely to die in the first seven days of hospitalization.
We now may have come full circle. The fact is that, like it or not, our value to the folks that pay us lies in the number of patients we can bring into the system. To keep our overhead down, we will always be encouraged to see as many patients as we can, or at least be efficient. Even if there were a way to quantify the quality of our care using outcome metrics, the patients will continue to select their providers based on availability, and the professional and consumer-friendly behavior of those providers. The patients’ perception of how good we are at making them feel better may be our strongest argument for better compensation.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
I have already shared with you that healthcare systems value panel size and productivity when they are considering primary care physician compensation. Your employers also know that the market won’t bear a substantial price increase for the procedure-poor practice style typical of primary care. You know that the relative value unit (RVU) system for calculating complexity of service is time consuming and discourages the inclusion of customer-friendly short visits that could allow an efficient provider to see more patients. Unfortunately, there is little hope that RVUs will become more PCP-friendly in the near future.
However, before leaving the topic of value and moving on to a consideration of quality, I can’t resist sharing some thoughts about efficiency and time management.
First, it must be said that the inexpert development and the clumsy rollout of electronic medical records (EMRs) have struck the biggest blow to the compensation potential and mental health of even the most efficient PCPs. Until that chasm is filled, there will be little progress in improving the efficiency and, consequently, the fair compensation of PCPs.
However, there is a myth that there is a direct correlation between the time spent with the patient and the quality of care. Eighty-five percent of PCPs report they would like to spend more time to get to know their patients. On the other hand, in my experience, really getting to know a patient is a process best done over multiple visits — some long, many of them short. It is unrealistic and inefficient to gain an in-depth understanding of the patient in a single visit.
Yes, one often hears a patient complain “they only spent 5 minutes with me.” While the patient may be technically correct, I contend that the provider’s manner has a major influence on the patient’s perception of the time spent in the exam room.
Was the provider reasonably prompt? In other words did they value my time? Did they appear rushed? Were they aware of my relevant history and prepared to deal with the current situation? In other words, did they do their homework? Did they engage me visually and seem to know what they were talking about? But, most importantly, did they exude sympathy and seem to care? Was I treated in the same manner that they would like to have been treated? If the answer is YES to those questions, then likely the patient could care less about the time spent.
It may seem counterintuitive to some of you, but there is a simple strategy that a provider can employ that will give them more time with the patient and at the same time allow them to claim to the boss that they are lowering the overhead costs. Management consultants often lean heavily on delegation as a more efficient use of resources. However, when the provider takes the patient’s vital signs and gives the injections, this multitasking provides an excellent hands-on opportunity to take the history and get to know the patient better. And, by giving the immunizations the provider is making the clearest statement possible that these vaccines are so important that they administer them personally.
You may have been wondering why I haven’t included the quality of PCP care in a discussion of compensation. It is because I don’t believe anyone has figured out how to do it in a manner that makes sense and is fair. PCPs don’t do procedures on which their success rate can be measured. A PCP’s patient panel almost by definition is going to be a mix of ages with a broad variety of complaints. Do they see enough diabetics to use their panel’s hemoglobin A1cs as a metric, or enough asthmatics to use emergency department visits as a quality-of-care measurement? In pediatrics, the closest we can come to a valid measure may be the provider’s vaccine acceptance rate.
But, then how does one factor in the general health of the community? If I open a practice in an underserved community, can you measure the quality of my care based on how quickly I can improve the metrics when I have no control over the poverty and educational system?
Since we aren’t surgeons, outcomes can’t be used to judge our quality. I’m afraid the only way we can assure quality is to demand evidence of our efforts to keep abreast of the current knowledge in our field and hope that at some level CME credits accumulated translate to the care we provide. A recent study has demonstrated an association between board certification exam board scores and newly trained internists and the care they provide. The patients of the physicians with the top scores had a lower risk of being readmitted to the hospital and were less likely to die in the first seven days of hospitalization.
We now may have come full circle. The fact is that, like it or not, our value to the folks that pay us lies in the number of patients we can bring into the system. To keep our overhead down, we will always be encouraged to see as many patients as we can, or at least be efficient. Even if there were a way to quantify the quality of our care using outcome metrics, the patients will continue to select their providers based on availability, and the professional and consumer-friendly behavior of those providers. The patients’ perception of how good we are at making them feel better may be our strongest argument for better compensation.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
I have already shared with you that healthcare systems value panel size and productivity when they are considering primary care physician compensation. Your employers also know that the market won’t bear a substantial price increase for the procedure-poor practice style typical of primary care. You know that the relative value unit (RVU) system for calculating complexity of service is time consuming and discourages the inclusion of customer-friendly short visits that could allow an efficient provider to see more patients. Unfortunately, there is little hope that RVUs will become more PCP-friendly in the near future.
However, before leaving the topic of value and moving on to a consideration of quality, I can’t resist sharing some thoughts about efficiency and time management.
First, it must be said that the inexpert development and the clumsy rollout of electronic medical records (EMRs) have struck the biggest blow to the compensation potential and mental health of even the most efficient PCPs. Until that chasm is filled, there will be little progress in improving the efficiency and, consequently, the fair compensation of PCPs.
However, there is a myth that there is a direct correlation between the time spent with the patient and the quality of care. Eighty-five percent of PCPs report they would like to spend more time to get to know their patients. On the other hand, in my experience, really getting to know a patient is a process best done over multiple visits — some long, many of them short. It is unrealistic and inefficient to gain an in-depth understanding of the patient in a single visit.
Yes, one often hears a patient complain “they only spent 5 minutes with me.” While the patient may be technically correct, I contend that the provider’s manner has a major influence on the patient’s perception of the time spent in the exam room.
Was the provider reasonably prompt? In other words did they value my time? Did they appear rushed? Were they aware of my relevant history and prepared to deal with the current situation? In other words, did they do their homework? Did they engage me visually and seem to know what they were talking about? But, most importantly, did they exude sympathy and seem to care? Was I treated in the same manner that they would like to have been treated? If the answer is YES to those questions, then likely the patient could care less about the time spent.
It may seem counterintuitive to some of you, but there is a simple strategy that a provider can employ that will give them more time with the patient and at the same time allow them to claim to the boss that they are lowering the overhead costs. Management consultants often lean heavily on delegation as a more efficient use of resources. However, when the provider takes the patient’s vital signs and gives the injections, this multitasking provides an excellent hands-on opportunity to take the history and get to know the patient better. And, by giving the immunizations the provider is making the clearest statement possible that these vaccines are so important that they administer them personally.
You may have been wondering why I haven’t included the quality of PCP care in a discussion of compensation. It is because I don’t believe anyone has figured out how to do it in a manner that makes sense and is fair. PCPs don’t do procedures on which their success rate can be measured. A PCP’s patient panel almost by definition is going to be a mix of ages with a broad variety of complaints. Do they see enough diabetics to use their panel’s hemoglobin A1cs as a metric, or enough asthmatics to use emergency department visits as a quality-of-care measurement? In pediatrics, the closest we can come to a valid measure may be the provider’s vaccine acceptance rate.
But, then how does one factor in the general health of the community? If I open a practice in an underserved community, can you measure the quality of my care based on how quickly I can improve the metrics when I have no control over the poverty and educational system?
Since we aren’t surgeons, outcomes can’t be used to judge our quality. I’m afraid the only way we can assure quality is to demand evidence of our efforts to keep abreast of the current knowledge in our field and hope that at some level CME credits accumulated translate to the care we provide. A recent study has demonstrated an association between board certification exam board scores and newly trained internists and the care they provide. The patients of the physicians with the top scores had a lower risk of being readmitted to the hospital and were less likely to die in the first seven days of hospitalization.
We now may have come full circle. The fact is that, like it or not, our value to the folks that pay us lies in the number of patients we can bring into the system. To keep our overhead down, we will always be encouraged to see as many patients as we can, or at least be efficient. Even if there were a way to quantify the quality of our care using outcome metrics, the patients will continue to select their providers based on availability, and the professional and consumer-friendly behavior of those providers. The patients’ perception of how good we are at making them feel better may be our strongest argument for better compensation.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Why Cardiac Biomarkers Don’t Help Predict Heart Disease
This transcript has been edited for clarity.
It’s the counterintuitive stuff in epidemiology that always really interests me. One intuition many of us have is that if a risk factor is significantly associated with an outcome, knowledge of that risk factor would help to predict that outcome. Makes sense. Feels right.
But it’s not right. Not always.
Here’s a fake example to illustrate my point. Let’s say we have 10,000 individuals who we follow for 10 years and 2000 of them die. (It’s been a rough decade.) At baseline, I measured a novel biomarker, the Perry Factor, in everyone. To keep it simple, the Perry Factor has only two values: 0 or 1.
I then do a standard associational analysis and find that individuals who are positive for the Perry Factor have a 40-fold higher odds of death than those who are negative for it. I am beginning to reconsider ascribing my good name to this biomarker. This is a highly statistically significant result — a P value <.001.
Clearly, knowledge of the Perry Factor should help me predict who will die in the cohort. I evaluate predictive power using a metric called the area under the receiver operating characteristic curve (AUC, referred to as the C-statistic in time-to-event studies). It tells you, given two people — one who dies and one who doesn’t — how frequently you “pick” the right person, given the knowledge of their Perry Factor.
A C-statistic of 0.5, or 50%, would mean the Perry Factor gives you no better results than a coin flip; it’s chance. A C-statistic of 1 is perfect prediction. So, what will the C-statistic be, given the incredibly strong association of the Perry Factor with outcomes? 0.9? 0.95?
0.5024. Almost useless.

Let’s figure out why strength of association and usefulness for prediction are not always the same thing.
I constructed my fake Perry Factor dataset quite carefully to illustrate this point. Let me show you what happened. What you see here is a breakdown of the patients in my fake study. You can see that just 11 of them were Perry Factor positive, but 10 of those 11 ended up dying.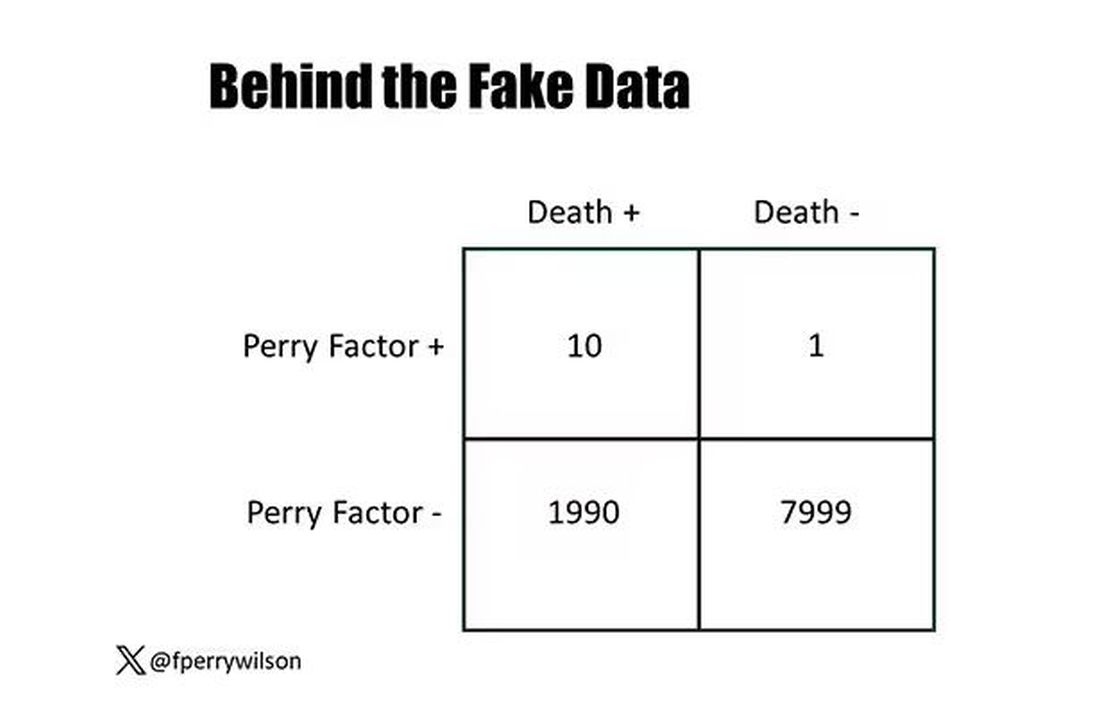
That’s quite unlikely by chance alone. It really does appear that if you have Perry Factor, your risk for death is much higher. But the reason that Perry Factor is a bad predictor is because it is so rare in the population. Sure, you can use it to correctly predict the outcome of 10 of the 11 people who have it, but the vast majority of people don’t have Perry Factor. It’s useless to distinguish who will die vs who will live in that population.
Why have I spent so much time trying to reverse our intuition that strength of association and strength of predictive power must be related? Because it helps to explain this paper, “Prognostic Value of Cardiovascular Biomarkers in the Population,” appearing in JAMA, which is a very nice piece of work trying to help us better predict cardiovascular disease.
I don’t need to tell you that cardiovascular disease is the number-one killer in this country and most of the world. I don’t need to tell you that we have really good preventive therapies and lifestyle interventions that can reduce the risk. But it would be nice to know in whom, specifically, we should use those interventions.
Cardiovascular risk scores, to date, are pretty simple. The most common one in use in the United States, the pooled cohort risk equation, has nine variables, two of which require a cholesterol panel and one a blood pressure test. It’s easy and it’s pretty accurate.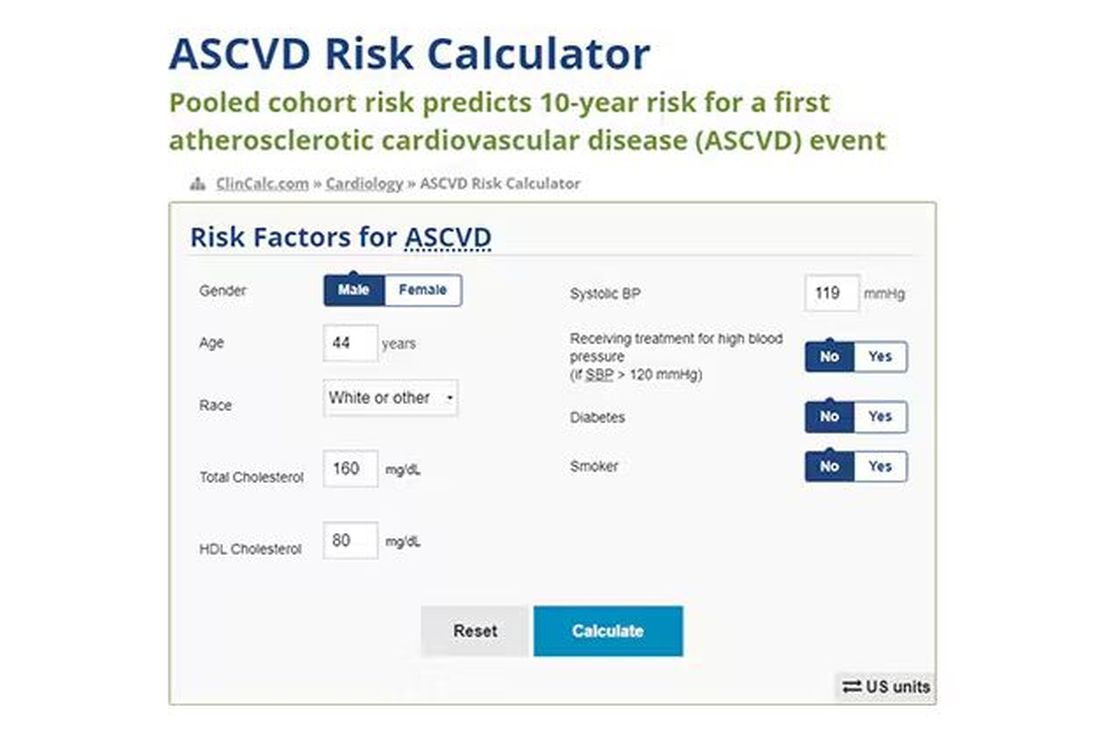
Using the score from the pooled cohort risk calculator, you get a C-statistic as high as 0.82 when applied to Black women, a low of 0.71 when applied to Black men. Non-Black individuals are in the middle. Not bad. But, clearly, not perfect.
And aren’t we in the era of big data, the era of personalized medicine? We have dozens, maybe hundreds, of quantifiable biomarkers that are associated with subsequent heart disease. Surely, by adding these biomarkers into the risk equation, we can improve prediction. Right?
The JAMA study includes 164,054 patients pooled from 28 cohort studies from 12 countries. All the studies measured various key biomarkers at baseline and followed their participants for cardiovascular events like heart attack, stroke, coronary revascularization, and so on.
The biomarkers in question are really the big guns in this space: troponin, a marker of stress on the heart muscle; NT-proBNP, a marker of stretch on the heart muscle; and C-reactive protein, a marker of inflammation. In every case, higher levels of these markers at baseline were associated with a higher risk for cardiovascular disease in the future.
Troponin T, shown here, has a basically linear risk with subsequent cardiovascular disease.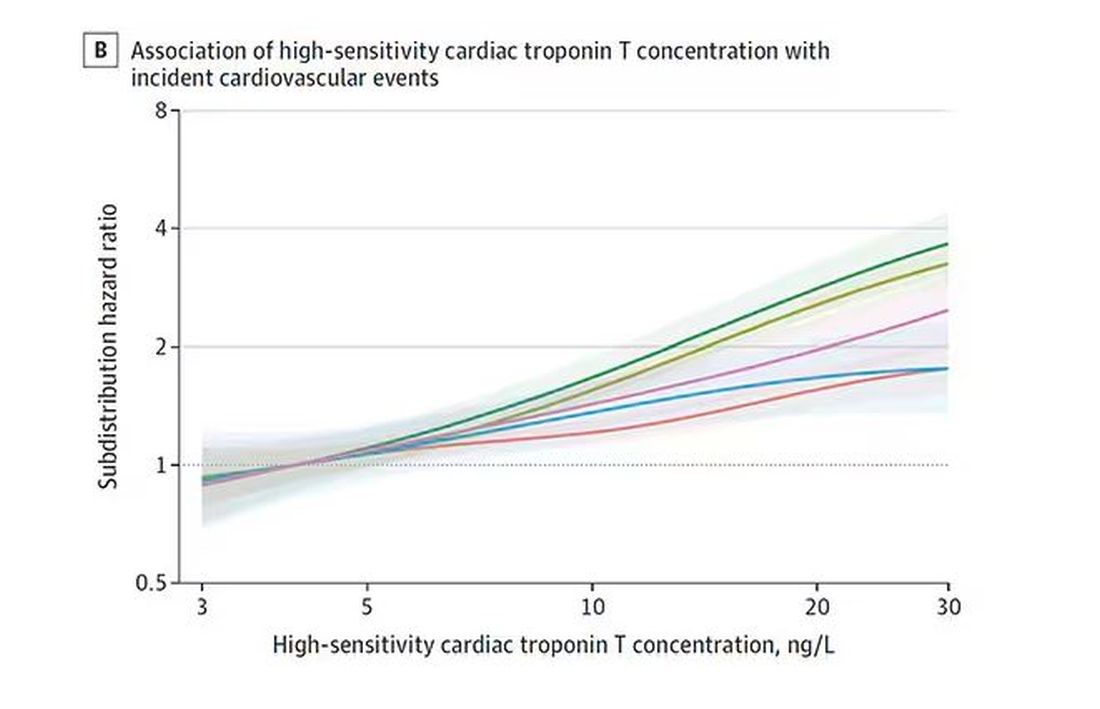
BNP seems to demonstrate more of a threshold effect, where levels above 60 start to associate with problems.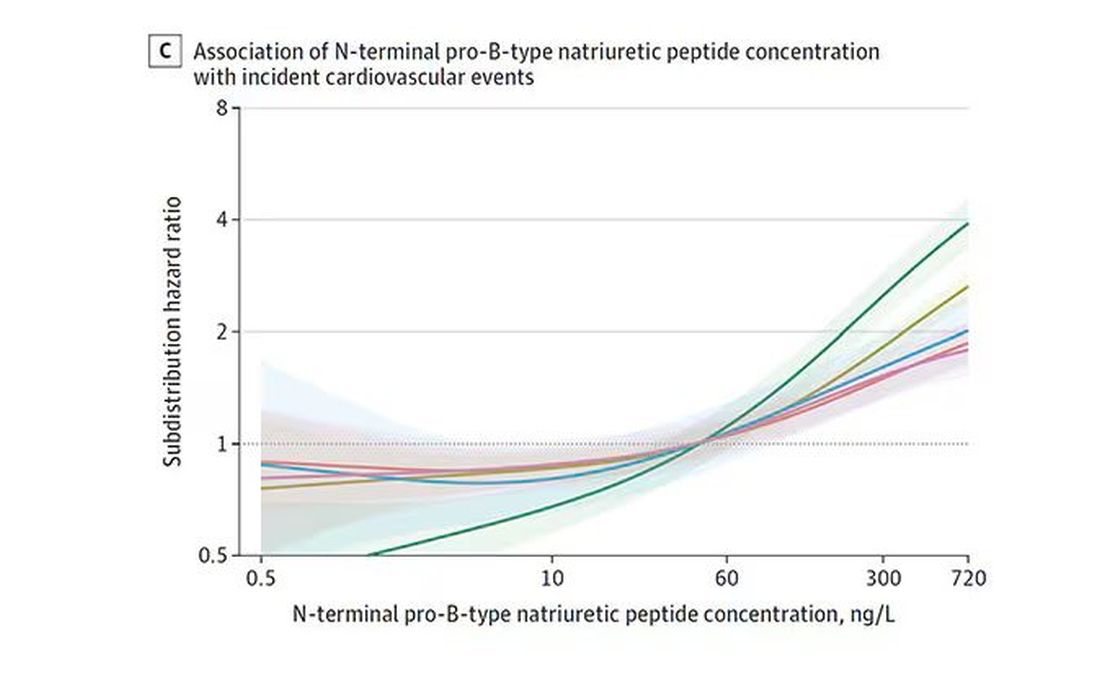
And CRP does a similar thing, with levels above 1.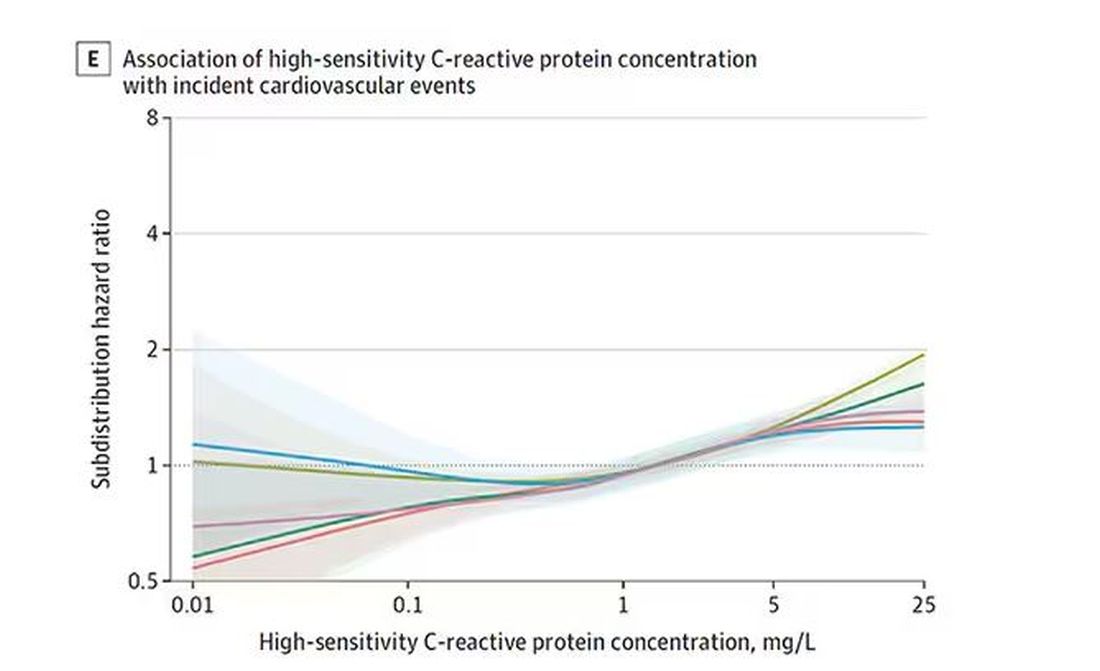
All of these findings were statistically significant. If you have higher levels of one or more of these biomarkers, you are more likely to have cardiovascular disease in the future.
Of course, our old friend the pooled cohort risk equation is still here — in the background — requiring just that one blood test and measurement of blood pressure. Let’s talk about predictive power.
The pooled cohort risk equation score, in this study, had a C-statistic of 0.812.
By adding troponin, BNP, and CRP to the equation, the new C-statistic is 0.819. Barely any change.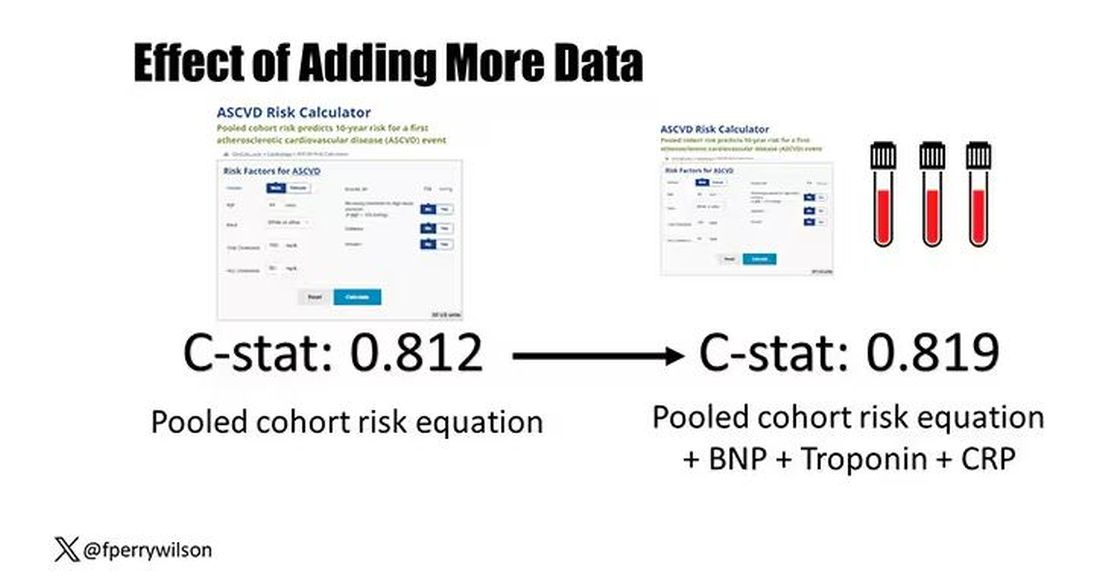
Now, the authors looked at different types of prediction here. The greatest improvement in the AUC was seen when they tried to predict heart failure within 1 year of measurement; there the AUC improved by 0.04. But the presence of BNP as a biomarker and the short time window of 1 year makes me wonder whether this is really prediction at all or whether they were essentially just diagnosing people with existing heart failure.
Why does this happen? Why do these promising biomarkers, clearly associated with bad outcomes, fail to improve our ability to predict the future? I already gave one example, which has to do with how the markers are distributed in the population. But even more relevant here is that the new markers will only improve prediction insofar as they are not already represented in the old predictive model.
Of course, BNP, for example, wasn’t in the old model. But smoking was. Diabetes was. Blood pressure was. All of that data might actually tell you something about the patient’s BNP through their mutual correlation. And improvement in prediction requires new information.
This is actually why I consider this a really successful study. We need to do studies like this to help us find what those new sources of information might be.
We will never get to a C-statistic of 1. Perfect prediction is the domain of palm readers and astrophysicists. But better prediction is always possible through data. The big question, of course, is which data?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It’s the counterintuitive stuff in epidemiology that always really interests me. One intuition many of us have is that if a risk factor is significantly associated with an outcome, knowledge of that risk factor would help to predict that outcome. Makes sense. Feels right.
But it’s not right. Not always.
Here’s a fake example to illustrate my point. Let’s say we have 10,000 individuals who we follow for 10 years and 2000 of them die. (It’s been a rough decade.) At baseline, I measured a novel biomarker, the Perry Factor, in everyone. To keep it simple, the Perry Factor has only two values: 0 or 1.
I then do a standard associational analysis and find that individuals who are positive for the Perry Factor have a 40-fold higher odds of death than those who are negative for it. I am beginning to reconsider ascribing my good name to this biomarker. This is a highly statistically significant result — a P value <.001.
Clearly, knowledge of the Perry Factor should help me predict who will die in the cohort. I evaluate predictive power using a metric called the area under the receiver operating characteristic curve (AUC, referred to as the C-statistic in time-to-event studies). It tells you, given two people — one who dies and one who doesn’t — how frequently you “pick” the right person, given the knowledge of their Perry Factor.
A C-statistic of 0.5, or 50%, would mean the Perry Factor gives you no better results than a coin flip; it’s chance. A C-statistic of 1 is perfect prediction. So, what will the C-statistic be, given the incredibly strong association of the Perry Factor with outcomes? 0.9? 0.95?
0.5024. Almost useless.
Let’s figure out why strength of association and usefulness for prediction are not always the same thing.
I constructed my fake Perry Factor dataset quite carefully to illustrate this point. Let me show you what happened. What you see here is a breakdown of the patients in my fake study. You can see that just 11 of them were Perry Factor positive, but 10 of those 11 ended up dying.
That’s quite unlikely by chance alone. It really does appear that if you have Perry Factor, your risk for death is much higher. But the reason that Perry Factor is a bad predictor is because it is so rare in the population. Sure, you can use it to correctly predict the outcome of 10 of the 11 people who have it, but the vast majority of people don’t have Perry Factor. It’s useless to distinguish who will die vs who will live in that population.
Why have I spent so much time trying to reverse our intuition that strength of association and strength of predictive power must be related? Because it helps to explain this paper, “Prognostic Value of Cardiovascular Biomarkers in the Population,” appearing in JAMA, which is a very nice piece of work trying to help us better predict cardiovascular disease.
I don’t need to tell you that cardiovascular disease is the number-one killer in this country and most of the world. I don’t need to tell you that we have really good preventive therapies and lifestyle interventions that can reduce the risk. But it would be nice to know in whom, specifically, we should use those interventions.
Cardiovascular risk scores, to date, are pretty simple. The most common one in use in the United States, the pooled cohort risk equation, has nine variables, two of which require a cholesterol panel and one a blood pressure test. It’s easy and it’s pretty accurate.
Using the score from the pooled cohort risk calculator, you get a C-statistic as high as 0.82 when applied to Black women, a low of 0.71 when applied to Black men. Non-Black individuals are in the middle. Not bad. But, clearly, not perfect.
And aren’t we in the era of big data, the era of personalized medicine? We have dozens, maybe hundreds, of quantifiable biomarkers that are associated with subsequent heart disease. Surely, by adding these biomarkers into the risk equation, we can improve prediction. Right?
The JAMA study includes 164,054 patients pooled from 28 cohort studies from 12 countries. All the studies measured various key biomarkers at baseline and followed their participants for cardiovascular events like heart attack, stroke, coronary revascularization, and so on.
The biomarkers in question are really the big guns in this space: troponin, a marker of stress on the heart muscle; NT-proBNP, a marker of stretch on the heart muscle; and C-reactive protein, a marker of inflammation. In every case, higher levels of these markers at baseline were associated with a higher risk for cardiovascular disease in the future.
Troponin T, shown here, has a basically linear risk with subsequent cardiovascular disease.
BNP seems to demonstrate more of a threshold effect, where levels above 60 start to associate with problems.
And CRP does a similar thing, with levels above 1.
All of these findings were statistically significant. If you have higher levels of one or more of these biomarkers, you are more likely to have cardiovascular disease in the future.
Of course, our old friend the pooled cohort risk equation is still here — in the background — requiring just that one blood test and measurement of blood pressure. Let’s talk about predictive power.
The pooled cohort risk equation score, in this study, had a C-statistic of 0.812.
By adding troponin, BNP, and CRP to the equation, the new C-statistic is 0.819. Barely any change.
Now, the authors looked at different types of prediction here. The greatest improvement in the AUC was seen when they tried to predict heart failure within 1 year of measurement; there the AUC improved by 0.04. But the presence of BNP as a biomarker and the short time window of 1 year makes me wonder whether this is really prediction at all or whether they were essentially just diagnosing people with existing heart failure.
Why does this happen? Why do these promising biomarkers, clearly associated with bad outcomes, fail to improve our ability to predict the future? I already gave one example, which has to do with how the markers are distributed in the population. But even more relevant here is that the new markers will only improve prediction insofar as they are not already represented in the old predictive model.
Of course, BNP, for example, wasn’t in the old model. But smoking was. Diabetes was. Blood pressure was. All of that data might actually tell you something about the patient’s BNP through their mutual correlation. And improvement in prediction requires new information.
This is actually why I consider this a really successful study. We need to do studies like this to help us find what those new sources of information might be.
We will never get to a C-statistic of 1. Perfect prediction is the domain of palm readers and astrophysicists. But better prediction is always possible through data. The big question, of course, is which data?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It’s the counterintuitive stuff in epidemiology that always really interests me. One intuition many of us have is that if a risk factor is significantly associated with an outcome, knowledge of that risk factor would help to predict that outcome. Makes sense. Feels right.
But it’s not right. Not always.
Here’s a fake example to illustrate my point. Let’s say we have 10,000 individuals who we follow for 10 years and 2000 of them die. (It’s been a rough decade.) At baseline, I measured a novel biomarker, the Perry Factor, in everyone. To keep it simple, the Perry Factor has only two values: 0 or 1.
I then do a standard associational analysis and find that individuals who are positive for the Perry Factor have a 40-fold higher odds of death than those who are negative for it. I am beginning to reconsider ascribing my good name to this biomarker. This is a highly statistically significant result — a P value <.001.
Clearly, knowledge of the Perry Factor should help me predict who will die in the cohort. I evaluate predictive power using a metric called the area under the receiver operating characteristic curve (AUC, referred to as the C-statistic in time-to-event studies). It tells you, given two people — one who dies and one who doesn’t — how frequently you “pick” the right person, given the knowledge of their Perry Factor.
A C-statistic of 0.5, or 50%, would mean the Perry Factor gives you no better results than a coin flip; it’s chance. A C-statistic of 1 is perfect prediction. So, what will the C-statistic be, given the incredibly strong association of the Perry Factor with outcomes? 0.9? 0.95?
0.5024. Almost useless.
Let’s figure out why strength of association and usefulness for prediction are not always the same thing.
I constructed my fake Perry Factor dataset quite carefully to illustrate this point. Let me show you what happened. What you see here is a breakdown of the patients in my fake study. You can see that just 11 of them were Perry Factor positive, but 10 of those 11 ended up dying.
That’s quite unlikely by chance alone. It really does appear that if you have Perry Factor, your risk for death is much higher. But the reason that Perry Factor is a bad predictor is because it is so rare in the population. Sure, you can use it to correctly predict the outcome of 10 of the 11 people who have it, but the vast majority of people don’t have Perry Factor. It’s useless to distinguish who will die vs who will live in that population.
Why have I spent so much time trying to reverse our intuition that strength of association and strength of predictive power must be related? Because it helps to explain this paper, “Prognostic Value of Cardiovascular Biomarkers in the Population,” appearing in JAMA, which is a very nice piece of work trying to help us better predict cardiovascular disease.
I don’t need to tell you that cardiovascular disease is the number-one killer in this country and most of the world. I don’t need to tell you that we have really good preventive therapies and lifestyle interventions that can reduce the risk. But it would be nice to know in whom, specifically, we should use those interventions.
Cardiovascular risk scores, to date, are pretty simple. The most common one in use in the United States, the pooled cohort risk equation, has nine variables, two of which require a cholesterol panel and one a blood pressure test. It’s easy and it’s pretty accurate.
Using the score from the pooled cohort risk calculator, you get a C-statistic as high as 0.82 when applied to Black women, a low of 0.71 when applied to Black men. Non-Black individuals are in the middle. Not bad. But, clearly, not perfect.
And aren’t we in the era of big data, the era of personalized medicine? We have dozens, maybe hundreds, of quantifiable biomarkers that are associated with subsequent heart disease. Surely, by adding these biomarkers into the risk equation, we can improve prediction. Right?
The JAMA study includes 164,054 patients pooled from 28 cohort studies from 12 countries. All the studies measured various key biomarkers at baseline and followed their participants for cardiovascular events like heart attack, stroke, coronary revascularization, and so on.
The biomarkers in question are really the big guns in this space: troponin, a marker of stress on the heart muscle; NT-proBNP, a marker of stretch on the heart muscle; and C-reactive protein, a marker of inflammation. In every case, higher levels of these markers at baseline were associated with a higher risk for cardiovascular disease in the future.
Troponin T, shown here, has a basically linear risk with subsequent cardiovascular disease.
BNP seems to demonstrate more of a threshold effect, where levels above 60 start to associate with problems.
And CRP does a similar thing, with levels above 1.
All of these findings were statistically significant. If you have higher levels of one or more of these biomarkers, you are more likely to have cardiovascular disease in the future.
Of course, our old friend the pooled cohort risk equation is still here — in the background — requiring just that one blood test and measurement of blood pressure. Let’s talk about predictive power.
The pooled cohort risk equation score, in this study, had a C-statistic of 0.812.
By adding troponin, BNP, and CRP to the equation, the new C-statistic is 0.819. Barely any change.
Now, the authors looked at different types of prediction here. The greatest improvement in the AUC was seen when they tried to predict heart failure within 1 year of measurement; there the AUC improved by 0.04. But the presence of BNP as a biomarker and the short time window of 1 year makes me wonder whether this is really prediction at all or whether they were essentially just diagnosing people with existing heart failure.
Why does this happen? Why do these promising biomarkers, clearly associated with bad outcomes, fail to improve our ability to predict the future? I already gave one example, which has to do with how the markers are distributed in the population. But even more relevant here is that the new markers will only improve prediction insofar as they are not already represented in the old predictive model.
Of course, BNP, for example, wasn’t in the old model. But smoking was. Diabetes was. Blood pressure was. All of that data might actually tell you something about the patient’s BNP through their mutual correlation. And improvement in prediction requires new information.
This is actually why I consider this a really successful study. We need to do studies like this to help us find what those new sources of information might be.
We will never get to a C-statistic of 1. Perfect prediction is the domain of palm readers and astrophysicists. But better prediction is always possible through data. The big question, of course, is which data?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Smart Use of Smartphones
Amid the declarations about the current mental health crisis among youth, it has become increasingly common to link rising rates of anxiety and depression among youth to screen time, and more specifically to hours spent on social media. But in truth, this matter is far from settled. The evidence linking mood and anxiety disorders to social media use is inconsistent. And where the evidence is stronger, causality has not been established. Does screen time precipitate an episode of depression or does a preteen at risk for depression, in the midst of a divorce or burdened by learning problems, use screen time excessively as a solution to these problems? There is also substantial variation across age groups, genders, and other factors that suggests that time spent on smartphone apps may not be the primary factor creating risk. Indeed, there is growing uncertainty about whether the climbing rates of anxiety and mood disorders among youth reflect yet to be identified factors increasing the burden of mental illness or the altered screening and tracking landscape in the United States after COVID and the Affordable Care Act. This uncertainty does not mean that we cannot make recommendations about how to guide patients and their families. Smartphones (and watches, glasses, etc) are here to stay.
Start by asking your patients how much time they spend on screens of all sorts and on social media in particular. Find out if there are rules at school or at home limiting screen time or social media. Are there disagreements about screen time? Are patients frustrated with their parents’ use of screens? What are their favorite apps to use? How much time do they think they spend on them? If they don’t know, point out how they can track it on their phone directly. Is it painful to be separated from their phone? Do they have interests or hobbies that are not screen-based? What would they do if the power or Wi-Fi was out for a week? These questions can be the start of an ongoing project for screen time and social media literacy.

Recognize That Apps Are Designed to Be Addictive
Smartphones are useful tools designed to help people stay connected, manage their bank accounts, keep up with current events, access entertainment, and much more. It is easy to spend more time than one intended on them. The applications developed for smartphones promise, and often deliver, efficiency and ease, including staying connected to friends and families. But social media applications have been developed to make their parent companies profit from ad revenue or selling user data. They are designed to encourage more and more use, and for some may become addictive. Start the literacy course with a clear statement of this fact. Remind teenagers that they are often the target audience for the corporations making money from these apps. They are especially sensitive to the likes and followers that can be the currency of social media. For every minute they spend on the apps, a corporation is profiting. It can be helpful to remind teenagers to bring their healthy skepticism of authority to their use of these corporate products.

Develop Awareness of Their Time, Energy, and Mood
Time is our most precious commodity, and most teenagers are stressed by not having enough of it. Ask your patients about the variety of things they need to do and want to do each day. Do they have enough time to do the things they want beyond their smartphones? Is the time on their smartphones more or less than they want? How do they feel when they finish with different activities? Energized? Engaged? Exhilarated? Drained? Irritable? Sad? Do they feel connected? Lonely? Loved? Left out? Suggest that they pay attention to how they feel after engaging in all kinds of activities (including homework, sports, hobbies, and time with friends), as these are the types of choices they will make throughout their adult lives. Some tasks are simply required (homework), some are relaxing (leaving us feeling calm and even sleepy), and some are recharging (leaving us feeling focused and energized). If an activity consistently leaves them drained and irritable, sad, and lonely or discouraged and insecure, they need to step back and ask themselves why they are making this choice and if that is the choice they want to make. Support their developing self-awareness, activating their sense of agency and independence in making choices that will serve them.
Develop Awareness of Their Sense of Connection to Others
As your patients are paying attention to their mood, focus, interest, and energy, they can also pay attention to these components of their social life. How do they feel with individual friends? With different groups? In different settings? How does this compare with how they feel when engaged with social media? In general, when technology is supporting strong connections with friends, it can enhance their health and well-being. When it helps youth isolated by interests or identity to become connected to supportive youth who are physically far away, it can be a social lifeline. But sometimes, social media exploits youth sensitivity to peer opinions and social comparison to keep their attention without the payoff of deepened or new relationships. Do they know the youth they are chatting with or following? Could they spend 2 hours with them offline? How do they feel after spending 2 hours “with” them online? Once again, the goal is to develop teens’ awareness of the quality of their relationships and of their control over how to manage this.
Acknowledge Their Own Vulnerabilities
Does your patient have attention-deficit/hyperactivity disorder (ADHD)? Are they being treated for depression? An anxiety disorder? An eating disorder? While we cannot say whether excessive use of social media can cause these problems, we know that it can be counterproductive to their treatment. Youth with ADHD have great difficulty switching their cognitive focus away from something rewarding, so are particularly prone to spending excessive time in addictive apps. Those with depression often have low energy and initiative alongside feelings of worthlessness that can make engaging in physical, in-person activities challenging. Those with anxiety disorders are prone to rumination and avoidance. The possibility of escaping into virtual social activities or distractions can be very hard to resist and counter-therapeutic for these youth (and adults). Those with eating disorders are vulnerable to comparing themselves with idealized (airbrushed) images online, which can intensify the body image distortion and competitiveness that are common in eating disorders. While there may be helpful information about diagnoses, treatment, and support, there is also troubling information about self-injury, restrictive eating, and even suicide that can increase the risk for these behaviors in vulnerable youth. You can help your patients cultivate awareness of how to take good care of themselves.
Create Habits That Support Sleep, Exercise, and Relationships
Talk with your patients and their parents about strategies to set habits that will make it easier for them to be smart users of their smartphones. Can they explore new apps or games together? Can they talk together about how each of them relaxes and recharges? Then they can work together on how this tool (and toy) can fit into a healthy life. The task is to prioritize sleep, exercise, and live, in-person social time, so virtual activities don’t take over the time needed for them. This can be as simple as consistent bed and waking times and ensuring that smartphones are not at the dining table or in bedrooms at night. Having dinner together as a family most nights (an especially positive habit), going for walks, runs, or hikes together, or doing activities that everyone enjoys (playing music or board games, making cookies or art, gardening) are beneficial for every family member’s physical and mental health and ensure that screen time is not at the expense of real connection. Invite your patients to tell you how they practice putting their smartphones away, getting their homework done, or making time for activities that matter to them. And find out how they relax and recharge beyond using their smartphones. Healthy habits evolve over a lifetime, and there will surely be new technologies that require new limits in the coming years. Helping your patients to make good choices will serve them well as they enter adulthood and throughout their lives.
Dr. Swick is physician in chief at Ohana Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (California) Peninsula. Dr. Michael S. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
Amid the declarations about the current mental health crisis among youth, it has become increasingly common to link rising rates of anxiety and depression among youth to screen time, and more specifically to hours spent on social media. But in truth, this matter is far from settled. The evidence linking mood and anxiety disorders to social media use is inconsistent. And where the evidence is stronger, causality has not been established. Does screen time precipitate an episode of depression or does a preteen at risk for depression, in the midst of a divorce or burdened by learning problems, use screen time excessively as a solution to these problems? There is also substantial variation across age groups, genders, and other factors that suggests that time spent on smartphone apps may not be the primary factor creating risk. Indeed, there is growing uncertainty about whether the climbing rates of anxiety and mood disorders among youth reflect yet to be identified factors increasing the burden of mental illness or the altered screening and tracking landscape in the United States after COVID and the Affordable Care Act. This uncertainty does not mean that we cannot make recommendations about how to guide patients and their families. Smartphones (and watches, glasses, etc) are here to stay.
Start by asking your patients how much time they spend on screens of all sorts and on social media in particular. Find out if there are rules at school or at home limiting screen time or social media. Are there disagreements about screen time? Are patients frustrated with their parents’ use of screens? What are their favorite apps to use? How much time do they think they spend on them? If they don’t know, point out how they can track it on their phone directly. Is it painful to be separated from their phone? Do they have interests or hobbies that are not screen-based? What would they do if the power or Wi-Fi was out for a week? These questions can be the start of an ongoing project for screen time and social media literacy.
Recognize That Apps Are Designed to Be Addictive
Smartphones are useful tools designed to help people stay connected, manage their bank accounts, keep up with current events, access entertainment, and much more. It is easy to spend more time than one intended on them. The applications developed for smartphones promise, and often deliver, efficiency and ease, including staying connected to friends and families. But social media applications have been developed to make their parent companies profit from ad revenue or selling user data. They are designed to encourage more and more use, and for some may become addictive. Start the literacy course with a clear statement of this fact. Remind teenagers that they are often the target audience for the corporations making money from these apps. They are especially sensitive to the likes and followers that can be the currency of social media. For every minute they spend on the apps, a corporation is profiting. It can be helpful to remind teenagers to bring their healthy skepticism of authority to their use of these corporate products.
Develop Awareness of Their Time, Energy, and Mood
Time is our most precious commodity, and most teenagers are stressed by not having enough of it. Ask your patients about the variety of things they need to do and want to do each day. Do they have enough time to do the things they want beyond their smartphones? Is the time on their smartphones more or less than they want? How do they feel when they finish with different activities? Energized? Engaged? Exhilarated? Drained? Irritable? Sad? Do they feel connected? Lonely? Loved? Left out? Suggest that they pay attention to how they feel after engaging in all kinds of activities (including homework, sports, hobbies, and time with friends), as these are the types of choices they will make throughout their adult lives. Some tasks are simply required (homework), some are relaxing (leaving us feeling calm and even sleepy), and some are recharging (leaving us feeling focused and energized). If an activity consistently leaves them drained and irritable, sad, and lonely or discouraged and insecure, they need to step back and ask themselves why they are making this choice and if that is the choice they want to make. Support their developing self-awareness, activating their sense of agency and independence in making choices that will serve them.
Develop Awareness of Their Sense of Connection to Others
As your patients are paying attention to their mood, focus, interest, and energy, they can also pay attention to these components of their social life. How do they feel with individual friends? With different groups? In different settings? How does this compare with how they feel when engaged with social media? In general, when technology is supporting strong connections with friends, it can enhance their health and well-being. When it helps youth isolated by interests or identity to become connected to supportive youth who are physically far away, it can be a social lifeline. But sometimes, social media exploits youth sensitivity to peer opinions and social comparison to keep their attention without the payoff of deepened or new relationships. Do they know the youth they are chatting with or following? Could they spend 2 hours with them offline? How do they feel after spending 2 hours “with” them online? Once again, the goal is to develop teens’ awareness of the quality of their relationships and of their control over how to manage this.
Acknowledge Their Own Vulnerabilities
Does your patient have attention-deficit/hyperactivity disorder (ADHD)? Are they being treated for depression? An anxiety disorder? An eating disorder? While we cannot say whether excessive use of social media can cause these problems, we know that it can be counterproductive to their treatment. Youth with ADHD have great difficulty switching their cognitive focus away from something rewarding, so are particularly prone to spending excessive time in addictive apps. Those with depression often have low energy and initiative alongside feelings of worthlessness that can make engaging in physical, in-person activities challenging. Those with anxiety disorders are prone to rumination and avoidance. The possibility of escaping into virtual social activities or distractions can be very hard to resist and counter-therapeutic for these youth (and adults). Those with eating disorders are vulnerable to comparing themselves with idealized (airbrushed) images online, which can intensify the body image distortion and competitiveness that are common in eating disorders. While there may be helpful information about diagnoses, treatment, and support, there is also troubling information about self-injury, restrictive eating, and even suicide that can increase the risk for these behaviors in vulnerable youth. You can help your patients cultivate awareness of how to take good care of themselves.
Create Habits That Support Sleep, Exercise, and Relationships
Talk with your patients and their parents about strategies to set habits that will make it easier for them to be smart users of their smartphones. Can they explore new apps or games together? Can they talk together about how each of them relaxes and recharges? Then they can work together on how this tool (and toy) can fit into a healthy life. The task is to prioritize sleep, exercise, and live, in-person social time, so virtual activities don’t take over the time needed for them. This can be as simple as consistent bed and waking times and ensuring that smartphones are not at the dining table or in bedrooms at night. Having dinner together as a family most nights (an especially positive habit), going for walks, runs, or hikes together, or doing activities that everyone enjoys (playing music or board games, making cookies or art, gardening) are beneficial for every family member’s physical and mental health and ensure that screen time is not at the expense of real connection. Invite your patients to tell you how they practice putting their smartphones away, getting their homework done, or making time for activities that matter to them. And find out how they relax and recharge beyond using their smartphones. Healthy habits evolve over a lifetime, and there will surely be new technologies that require new limits in the coming years. Helping your patients to make good choices will serve them well as they enter adulthood and throughout their lives.
Dr. Swick is physician in chief at Ohana Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (California) Peninsula. Dr. Michael S. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
Amid the declarations about the current mental health crisis among youth, it has become increasingly common to link rising rates of anxiety and depression among youth to screen time, and more specifically to hours spent on social media. But in truth, this matter is far from settled. The evidence linking mood and anxiety disorders to social media use is inconsistent. And where the evidence is stronger, causality has not been established. Does screen time precipitate an episode of depression or does a preteen at risk for depression, in the midst of a divorce or burdened by learning problems, use screen time excessively as a solution to these problems? There is also substantial variation across age groups, genders, and other factors that suggests that time spent on smartphone apps may not be the primary factor creating risk. Indeed, there is growing uncertainty about whether the climbing rates of anxiety and mood disorders among youth reflect yet to be identified factors increasing the burden of mental illness or the altered screening and tracking landscape in the United States after COVID and the Affordable Care Act. This uncertainty does not mean that we cannot make recommendations about how to guide patients and their families. Smartphones (and watches, glasses, etc) are here to stay.
Start by asking your patients how much time they spend on screens of all sorts and on social media in particular. Find out if there are rules at school or at home limiting screen time or social media. Are there disagreements about screen time? Are patients frustrated with their parents’ use of screens? What are their favorite apps to use? How much time do they think they spend on them? If they don’t know, point out how they can track it on their phone directly. Is it painful to be separated from their phone? Do they have interests or hobbies that are not screen-based? What would they do if the power or Wi-Fi was out for a week? These questions can be the start of an ongoing project for screen time and social media literacy.
Recognize That Apps Are Designed to Be Addictive
Smartphones are useful tools designed to help people stay connected, manage their bank accounts, keep up with current events, access entertainment, and much more. It is easy to spend more time than one intended on them. The applications developed for smartphones promise, and often deliver, efficiency and ease, including staying connected to friends and families. But social media applications have been developed to make their parent companies profit from ad revenue or selling user data. They are designed to encourage more and more use, and for some may become addictive. Start the literacy course with a clear statement of this fact. Remind teenagers that they are often the target audience for the corporations making money from these apps. They are especially sensitive to the likes and followers that can be the currency of social media. For every minute they spend on the apps, a corporation is profiting. It can be helpful to remind teenagers to bring their healthy skepticism of authority to their use of these corporate products.
Develop Awareness of Their Time, Energy, and Mood
Time is our most precious commodity, and most teenagers are stressed by not having enough of it. Ask your patients about the variety of things they need to do and want to do each day. Do they have enough time to do the things they want beyond their smartphones? Is the time on their smartphones more or less than they want? How do they feel when they finish with different activities? Energized? Engaged? Exhilarated? Drained? Irritable? Sad? Do they feel connected? Lonely? Loved? Left out? Suggest that they pay attention to how they feel after engaging in all kinds of activities (including homework, sports, hobbies, and time with friends), as these are the types of choices they will make throughout their adult lives. Some tasks are simply required (homework), some are relaxing (leaving us feeling calm and even sleepy), and some are recharging (leaving us feeling focused and energized). If an activity consistently leaves them drained and irritable, sad, and lonely or discouraged and insecure, they need to step back and ask themselves why they are making this choice and if that is the choice they want to make. Support their developing self-awareness, activating their sense of agency and independence in making choices that will serve them.
Develop Awareness of Their Sense of Connection to Others
As your patients are paying attention to their mood, focus, interest, and energy, they can also pay attention to these components of their social life. How do they feel with individual friends? With different groups? In different settings? How does this compare with how they feel when engaged with social media? In general, when technology is supporting strong connections with friends, it can enhance their health and well-being. When it helps youth isolated by interests or identity to become connected to supportive youth who are physically far away, it can be a social lifeline. But sometimes, social media exploits youth sensitivity to peer opinions and social comparison to keep their attention without the payoff of deepened or new relationships. Do they know the youth they are chatting with or following? Could they spend 2 hours with them offline? How do they feel after spending 2 hours “with” them online? Once again, the goal is to develop teens’ awareness of the quality of their relationships and of their control over how to manage this.
Acknowledge Their Own Vulnerabilities
Does your patient have attention-deficit/hyperactivity disorder (ADHD)? Are they being treated for depression? An anxiety disorder? An eating disorder? While we cannot say whether excessive use of social media can cause these problems, we know that it can be counterproductive to their treatment. Youth with ADHD have great difficulty switching their cognitive focus away from something rewarding, so are particularly prone to spending excessive time in addictive apps. Those with depression often have low energy and initiative alongside feelings of worthlessness that can make engaging in physical, in-person activities challenging. Those with anxiety disorders are prone to rumination and avoidance. The possibility of escaping into virtual social activities or distractions can be very hard to resist and counter-therapeutic for these youth (and adults). Those with eating disorders are vulnerable to comparing themselves with idealized (airbrushed) images online, which can intensify the body image distortion and competitiveness that are common in eating disorders. While there may be helpful information about diagnoses, treatment, and support, there is also troubling information about self-injury, restrictive eating, and even suicide that can increase the risk for these behaviors in vulnerable youth. You can help your patients cultivate awareness of how to take good care of themselves.
Create Habits That Support Sleep, Exercise, and Relationships
Talk with your patients and their parents about strategies to set habits that will make it easier for them to be smart users of their smartphones. Can they explore new apps or games together? Can they talk together about how each of them relaxes and recharges? Then they can work together on how this tool (and toy) can fit into a healthy life. The task is to prioritize sleep, exercise, and live, in-person social time, so virtual activities don’t take over the time needed for them. This can be as simple as consistent bed and waking times and ensuring that smartphones are not at the dining table or in bedrooms at night. Having dinner together as a family most nights (an especially positive habit), going for walks, runs, or hikes together, or doing activities that everyone enjoys (playing music or board games, making cookies or art, gardening) are beneficial for every family member’s physical and mental health and ensure that screen time is not at the expense of real connection. Invite your patients to tell you how they practice putting their smartphones away, getting their homework done, or making time for activities that matter to them. And find out how they relax and recharge beyond using their smartphones. Healthy habits evolve over a lifetime, and there will surely be new technologies that require new limits in the coming years. Helping your patients to make good choices will serve them well as they enter adulthood and throughout their lives.
Dr. Swick is physician in chief at Ohana Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (California) Peninsula. Dr. Michael S. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
What Does Natural Healing of ACL Ruptures Mean for Long-Term Outcomes?
VIENNA — Nearly one third of anterior cruciate ligament (ACL) injuries appear to heal without surgery, according to an analysis of three-dimensional MRI data taken from the NACOX study, presented as a late-breaking poster at the OARSI 2024 World Congress.
At 2 years after injury, three-dimensional MRI showed that 13 of 43 (30%) knees had evidence of normal, continuous ACL fibers. Moreover, a further 14 (33%) knees had a continuous ACL fiber structure following rehabilitation alone. ACL fibers were partly (16%) or completely (21%) ruptured in the remainder of cases.

“If you think of the ACL like a rope, when there is continuity, it means those fibers have rejoined,” study coauthor Stephanie Filbay, PhD, an associate professor at the University of Melbourne in Australia, told this news organization.
“Within that, there’s a few variations of healing that we’re seeing. Some look like they’ve never been injured, while some have rejoined but appear thinner or longer than a normal ACL,” Dr. Filbay said.
She added: “What all this research is showing is that it’s happening at a much higher rate than we thought possible. And in some of the studies, it looks like ACL healing is associated with very favorable outcomes.”
At OARSI 2024, Dr. Filbay presented additional data from her and others’ research on the relationships between ACL healing and long-term functional outcomes and osteoarthritis (OA) incidence in comparisons between patients’ treatment pathways: Early ACL surgery, rehabilitation followed by delayed surgery, or rehabilitation only.
Healing Without Surgery
The idea that the ACL can heal without surgery is relatively recent and perhaps still not widely accepted as a concept, as Dr. Filbay explained during a plenary lecture at the congress.
Dr. Filbay explained that the ideal management of ACL injury depends on the severity of knee injury and whether someone’s knee is stable after trying nonsurgical management. Results of the ACL SNNAP trial, for example, have suggested that surgical reconstruction is superior to a rehabilitation strategy for managing non-acute ACL injuries where there are persistent symptoms of instability.
However, there have been two trials — COMPARE performed in the Netherlands and KANON performed in Sweden — that found that early surgery was no better than a strategy of initial rehabilitation with the option of having a delayed ACL surgery if needed.
What Happens Long Term?
Posttraumatic OA is a well-known long-term consequence of ACL injury. According to a recent meta-analysis, there is a sevenfold increased risk for OA comparing people who have and have not had an ACL injury.
ACL injury also results in OA occurring at an earlier age than in people with OA who have not had an ACL injury. This has been shown to progress at a faster rate and be associated with a longer period of disability, Dr. Filbay said at the congress, sponsored by the Osteoarthritis Research Society International.
But does the ACL really heal? Dr. Filbay thinks that it does and has been involved in several studies that have used MRI to look at how the ACL may do so.
In a recently published paper, Dr. Filbay and colleagues reported the findings from a secondary analysis of the KANON trial and found that nearly one in three (30%) of the participants who had been randomized to optional delayed surgery had MRI evidence of healing at 2 years. But when they excluded people who had delayed surgery, 53% of people managed by rehabilitation alone had evidence of healing.
The evaluation also found that those who had a healed vs non-healed ligament had better results using the Knee Injury and Osteoarthritis Outcome Score (KOOS), and that there were better outcomes at 2 years among those with ACL healing vs those who had early or delayed ACL surgery.
ACL Continuity and Long-Term Outcomes
At OARSI 2024, Dr. Filbay and colleagues reported an even longer-term secondary analysis of the KANON trial on the relationship between ACL healing at 5 years and outcomes at 11 years. The results were first reported in NEJM Evidence.
Dr. Filbay reported that participants with ACL continuity on MRI at 5 years actually had worse patient-reported outcomes 11 years later than those who were managed with early or delayed ACL reconstruction.
“This does not align with previous findings suggesting better 2-year outcomes compared to the surgically managed groups,” Dr. Filbay said.
However, people with ACL continuity following rehabilitation did seem to show numerically similar or fewer signs of radiographic OA at 11 years vs the surgical groups.
Radiographic OA of the tibiofemoral joint (TFJ) or patellofemoral joint (PFJ) at 11 years was observed in a respective 14% and 21% of people with ACL continuity at 5 years (n = 14) and in 22% and 11% of people with ACL discontinuity at 5 years in the rehabilitation alone group.
By comparison, radiographic OA of the TFJ or PFJ at 11 years was seen in a respective 23% and 35% of people who had rehabilitation with delayed surgery (n = 26) and in 18% and 41% of those who had early surgery (n = 49).
These are descriptive results, Dr. Filbay said, because the numbers were too small to do a statistical analysis. Further, larger, longitudinal studies will be needed.
Posttraumatic OA After ACL Surgery
Elsewhere at OARSI 2024, Matthew Harkey, PhD, and colleagues from Michigan State University, East Lansing, Michigan, reported data showing that nearly two thirds of people who undergo surgical reconstruction have symptoms at 6 months that could be indicative of early knee OA.
Knee symptoms indicative of OA declined to 53% at 12 months and 45% at 24 months.
“It’s a bit complex — we can’t outright say arthritis is developing, but there’s a large group of patients whose symptoms linger long after surgery,” Dr. Harkey said in a press release.
“Often, clinicians assume that these postoperative symptoms will naturally improve as patients reengage with their usual activities. However, what we’re seeing suggests these symptoms persist and likely require a targeted approach to manage or improve them,” Dr. Harkey said.
The analysis used data on 3752 individuals aged 14-40 years who were enrolled in the New Zealand ACL Registry and who completed the KOOS at 6, 12, and 24 months after having ACL reconstruction.
Dr. Harkey and team reported that one in three people had persistent early OA symptoms at 2 years, while 23% had no early OA symptoms at any timepoint.
The studies were independently supported. Dr. Filbay and Dr. Harkey had no relevant financial relationships to report.
Dr. Filbay and colleagues have developed a treatment decision aid for individuals who have sustained an ACL injury. This provides information on the different treatment options available and how they compare.
A version of this article appeared on Medscape.com.
VIENNA — Nearly one third of anterior cruciate ligament (ACL) injuries appear to heal without surgery, according to an analysis of three-dimensional MRI data taken from the NACOX study, presented as a late-breaking poster at the OARSI 2024 World Congress.
At 2 years after injury, three-dimensional MRI showed that 13 of 43 (30%) knees had evidence of normal, continuous ACL fibers. Moreover, a further 14 (33%) knees had a continuous ACL fiber structure following rehabilitation alone. ACL fibers were partly (16%) or completely (21%) ruptured in the remainder of cases.
“If you think of the ACL like a rope, when there is continuity, it means those fibers have rejoined,” study coauthor Stephanie Filbay, PhD, an associate professor at the University of Melbourne in Australia, told this news organization.
“Within that, there’s a few variations of healing that we’re seeing. Some look like they’ve never been injured, while some have rejoined but appear thinner or longer than a normal ACL,” Dr. Filbay said.
She added: “What all this research is showing is that it’s happening at a much higher rate than we thought possible. And in some of the studies, it looks like ACL healing is associated with very favorable outcomes.”
At OARSI 2024, Dr. Filbay presented additional data from her and others’ research on the relationships between ACL healing and long-term functional outcomes and osteoarthritis (OA) incidence in comparisons between patients’ treatment pathways: Early ACL surgery, rehabilitation followed by delayed surgery, or rehabilitation only.
Healing Without Surgery
The idea that the ACL can heal without surgery is relatively recent and perhaps still not widely accepted as a concept, as Dr. Filbay explained during a plenary lecture at the congress.
Dr. Filbay explained that the ideal management of ACL injury depends on the severity of knee injury and whether someone’s knee is stable after trying nonsurgical management. Results of the ACL SNNAP trial, for example, have suggested that surgical reconstruction is superior to a rehabilitation strategy for managing non-acute ACL injuries where there are persistent symptoms of instability.
However, there have been two trials — COMPARE performed in the Netherlands and KANON performed in Sweden — that found that early surgery was no better than a strategy of initial rehabilitation with the option of having a delayed ACL surgery if needed.
What Happens Long Term?
Posttraumatic OA is a well-known long-term consequence of ACL injury. According to a recent meta-analysis, there is a sevenfold increased risk for OA comparing people who have and have not had an ACL injury.
ACL injury also results in OA occurring at an earlier age than in people with OA who have not had an ACL injury. This has been shown to progress at a faster rate and be associated with a longer period of disability, Dr. Filbay said at the congress, sponsored by the Osteoarthritis Research Society International.
But does the ACL really heal? Dr. Filbay thinks that it does and has been involved in several studies that have used MRI to look at how the ACL may do so.
In a recently published paper, Dr. Filbay and colleagues reported the findings from a secondary analysis of the KANON trial and found that nearly one in three (30%) of the participants who had been randomized to optional delayed surgery had MRI evidence of healing at 2 years. But when they excluded people who had delayed surgery, 53% of people managed by rehabilitation alone had evidence of healing.
The evaluation also found that those who had a healed vs non-healed ligament had better results using the Knee Injury and Osteoarthritis Outcome Score (KOOS), and that there were better outcomes at 2 years among those with ACL healing vs those who had early or delayed ACL surgery.
ACL Continuity and Long-Term Outcomes
At OARSI 2024, Dr. Filbay and colleagues reported an even longer-term secondary analysis of the KANON trial on the relationship between ACL healing at 5 years and outcomes at 11 years. The results were first reported in NEJM Evidence.
Dr. Filbay reported that participants with ACL continuity on MRI at 5 years actually had worse patient-reported outcomes 11 years later than those who were managed with early or delayed ACL reconstruction.
“This does not align with previous findings suggesting better 2-year outcomes compared to the surgically managed groups,” Dr. Filbay said.
However, people with ACL continuity following rehabilitation did seem to show numerically similar or fewer signs of radiographic OA at 11 years vs the surgical groups.
Radiographic OA of the tibiofemoral joint (TFJ) or patellofemoral joint (PFJ) at 11 years was observed in a respective 14% and 21% of people with ACL continuity at 5 years (n = 14) and in 22% and 11% of people with ACL discontinuity at 5 years in the rehabilitation alone group.
By comparison, radiographic OA of the TFJ or PFJ at 11 years was seen in a respective 23% and 35% of people who had rehabilitation with delayed surgery (n = 26) and in 18% and 41% of those who had early surgery (n = 49).
These are descriptive results, Dr. Filbay said, because the numbers were too small to do a statistical analysis. Further, larger, longitudinal studies will be needed.
Posttraumatic OA After ACL Surgery
Elsewhere at OARSI 2024, Matthew Harkey, PhD, and colleagues from Michigan State University, East Lansing, Michigan, reported data showing that nearly two thirds of people who undergo surgical reconstruction have symptoms at 6 months that could be indicative of early knee OA.
Knee symptoms indicative of OA declined to 53% at 12 months and 45% at 24 months.
“It’s a bit complex — we can’t outright say arthritis is developing, but there’s a large group of patients whose symptoms linger long after surgery,” Dr. Harkey said in a press release.
“Often, clinicians assume that these postoperative symptoms will naturally improve as patients reengage with their usual activities. However, what we’re seeing suggests these symptoms persist and likely require a targeted approach to manage or improve them,” Dr. Harkey said.
The analysis used data on 3752 individuals aged 14-40 years who were enrolled in the New Zealand ACL Registry and who completed the KOOS at 6, 12, and 24 months after having ACL reconstruction.
Dr. Harkey and team reported that one in three people had persistent early OA symptoms at 2 years, while 23% had no early OA symptoms at any timepoint.
The studies were independently supported. Dr. Filbay and Dr. Harkey had no relevant financial relationships to report.
Dr. Filbay and colleagues have developed a treatment decision aid for individuals who have sustained an ACL injury. This provides information on the different treatment options available and how they compare.
A version of this article appeared on Medscape.com.
VIENNA — Nearly one third of anterior cruciate ligament (ACL) injuries appear to heal without surgery, according to an analysis of three-dimensional MRI data taken from the NACOX study, presented as a late-breaking poster at the OARSI 2024 World Congress.
At 2 years after injury, three-dimensional MRI showed that 13 of 43 (30%) knees had evidence of normal, continuous ACL fibers. Moreover, a further 14 (33%) knees had a continuous ACL fiber structure following rehabilitation alone. ACL fibers were partly (16%) or completely (21%) ruptured in the remainder of cases.
“If you think of the ACL like a rope, when there is continuity, it means those fibers have rejoined,” study coauthor Stephanie Filbay, PhD, an associate professor at the University of Melbourne in Australia, told this news organization.
“Within that, there’s a few variations of healing that we’re seeing. Some look like they’ve never been injured, while some have rejoined but appear thinner or longer than a normal ACL,” Dr. Filbay said.
She added: “What all this research is showing is that it’s happening at a much higher rate than we thought possible. And in some of the studies, it looks like ACL healing is associated with very favorable outcomes.”
At OARSI 2024, Dr. Filbay presented additional data from her and others’ research on the relationships between ACL healing and long-term functional outcomes and osteoarthritis (OA) incidence in comparisons between patients’ treatment pathways: Early ACL surgery, rehabilitation followed by delayed surgery, or rehabilitation only.
Healing Without Surgery
The idea that the ACL can heal without surgery is relatively recent and perhaps still not widely accepted as a concept, as Dr. Filbay explained during a plenary lecture at the congress.
Dr. Filbay explained that the ideal management of ACL injury depends on the severity of knee injury and whether someone’s knee is stable after trying nonsurgical management. Results of the ACL SNNAP trial, for example, have suggested that surgical reconstruction is superior to a rehabilitation strategy for managing non-acute ACL injuries where there are persistent symptoms of instability.
However, there have been two trials — COMPARE performed in the Netherlands and KANON performed in Sweden — that found that early surgery was no better than a strategy of initial rehabilitation with the option of having a delayed ACL surgery if needed.
What Happens Long Term?
Posttraumatic OA is a well-known long-term consequence of ACL injury. According to a recent meta-analysis, there is a sevenfold increased risk for OA comparing people who have and have not had an ACL injury.
ACL injury also results in OA occurring at an earlier age than in people with OA who have not had an ACL injury. This has been shown to progress at a faster rate and be associated with a longer period of disability, Dr. Filbay said at the congress, sponsored by the Osteoarthritis Research Society International.
But does the ACL really heal? Dr. Filbay thinks that it does and has been involved in several studies that have used MRI to look at how the ACL may do so.
In a recently published paper, Dr. Filbay and colleagues reported the findings from a secondary analysis of the KANON trial and found that nearly one in three (30%) of the participants who had been randomized to optional delayed surgery had MRI evidence of healing at 2 years. But when they excluded people who had delayed surgery, 53% of people managed by rehabilitation alone had evidence of healing.
The evaluation also found that those who had a healed vs non-healed ligament had better results using the Knee Injury and Osteoarthritis Outcome Score (KOOS), and that there were better outcomes at 2 years among those with ACL healing vs those who had early or delayed ACL surgery.
ACL Continuity and Long-Term Outcomes
At OARSI 2024, Dr. Filbay and colleagues reported an even longer-term secondary analysis of the KANON trial on the relationship between ACL healing at 5 years and outcomes at 11 years. The results were first reported in NEJM Evidence.
Dr. Filbay reported that participants with ACL continuity on MRI at 5 years actually had worse patient-reported outcomes 11 years later than those who were managed with early or delayed ACL reconstruction.
“This does not align with previous findings suggesting better 2-year outcomes compared to the surgically managed groups,” Dr. Filbay said.
However, people with ACL continuity following rehabilitation did seem to show numerically similar or fewer signs of radiographic OA at 11 years vs the surgical groups.
Radiographic OA of the tibiofemoral joint (TFJ) or patellofemoral joint (PFJ) at 11 years was observed in a respective 14% and 21% of people with ACL continuity at 5 years (n = 14) and in 22% and 11% of people with ACL discontinuity at 5 years in the rehabilitation alone group.
By comparison, radiographic OA of the TFJ or PFJ at 11 years was seen in a respective 23% and 35% of people who had rehabilitation with delayed surgery (n = 26) and in 18% and 41% of those who had early surgery (n = 49).
These are descriptive results, Dr. Filbay said, because the numbers were too small to do a statistical analysis. Further, larger, longitudinal studies will be needed.
Posttraumatic OA After ACL Surgery
Elsewhere at OARSI 2024, Matthew Harkey, PhD, and colleagues from Michigan State University, East Lansing, Michigan, reported data showing that nearly two thirds of people who undergo surgical reconstruction have symptoms at 6 months that could be indicative of early knee OA.
Knee symptoms indicative of OA declined to 53% at 12 months and 45% at 24 months.
“It’s a bit complex — we can’t outright say arthritis is developing, but there’s a large group of patients whose symptoms linger long after surgery,” Dr. Harkey said in a press release.
“Often, clinicians assume that these postoperative symptoms will naturally improve as patients reengage with their usual activities. However, what we’re seeing suggests these symptoms persist and likely require a targeted approach to manage or improve them,” Dr. Harkey said.
The analysis used data on 3752 individuals aged 14-40 years who were enrolled in the New Zealand ACL Registry and who completed the KOOS at 6, 12, and 24 months after having ACL reconstruction.
Dr. Harkey and team reported that one in three people had persistent early OA symptoms at 2 years, while 23% had no early OA symptoms at any timepoint.
The studies were independently supported. Dr. Filbay and Dr. Harkey had no relevant financial relationships to report.
Dr. Filbay and colleagues have developed a treatment decision aid for individuals who have sustained an ACL injury. This provides information on the different treatment options available and how they compare.
A version of this article appeared on Medscape.com.
FROM OARSI 2024
Outside the Guidelines: Prostate Cancer Screening Overused in Older Men
In its most recent guidance, the US Preventive Services Task Force (USPSTF) revised a previous 2012 recommendation against routine screening for prostate cancer to instead endorse individual decision-making for men aged 55 to 69 years (grade C).
In the update guidance, which was published in 2018, the task force still recommended against PSA-based screening for prostate cancer in men 70 years and older (grade D) due to a range of potential risks and harms. Guidelines from the American Urological Association and American Cancer Society have echoed that recommendation, in general agreement that men over the age of 70 or with limited life expectancy show little benefit from the screening.
To take a closer look at how commonly men are being screened for prostate cancer, based not only on their age but their estimated life expectancy, Kevin H. Kensler, ScD, of Weill Cornell Medicine, and colleagues conducted a cross-sectional study using data from the 2020 Behavioral Risk Factor Surveillance System (BRFSS).
“Our findings indicate that many males aged 70 years and older or those with a high risk of death within 10 years undergo prostate cancer screening despite the recommendation against screening in these populations by current guidelines,” the authors wrote in their paper, published in JAMA Network Open. The results underscore that “enhancements to the shared decision-making process are needed to ensure that older males who undergo screening are those who may potentially benefit,” they noted.
For the study, the authors identified 57,397 men aged 60 and older without a history of prostate cancer who reported undergoing a screening PSA test in the prior 2 years.
Using a risk factor system, mortality risk was estimated based on the scales ranging from 5.5 or less to 10.0 or greater, corresponding to the estimated 10-year mortality of less than 30% to 71% or more, respectively.
Of the men, 19.2% were aged 70 to 74 years, 13.0% were aged 75 to 79 years, and 12.3% were aged 80 years or older. The rest were 69 years or younger.
While the estimated 2-year prostate cancer screening rates were 36.3% among those aged 60 to 64 years and 42.8% for those 65 to 69 years, the rates were even higher, at 47.1%, among those aged 70 to 74 years, and similar, at 42.7%, in the 75 to 79 years of age range. Among those aged 80 years and older, 30.4% had been screened.
While the screening frequency was 43.4% among males with the greatest estimated life expectancy, a fair percentage of men, 30.4%, with the lowest life expectancy, indicative of a 71% or greater risk of death within 10 years, received prostate cancer screening.
In fact, among those with lowest life expectancy, the screening rates were greater than 20% in all age groups.
Screening in Older Age: Benefit in Reducing Mortality Low
Autopsy research indicates that, in fact, as many as 50% of men do have prostate cancer at age 80; however, many of those tumors are low-risk and unlikely to affect the health of the men.
If detected early, as is the intention of screening, prostate cancer can take years to advance and the likelihood of receiving any mortality benefit from continued screening in older age is low.
Furthermore, screening in older age can have implications, including a higher risk of complications following a false positive prostate biopsy that may not have been necessary in the first place, the authors explained.
“Given the long natural history of prostate cancer and lead time associated with PSA-based screening, these males [aged 70 and older or with a high risk of death within 10 years] have a low likelihood of receiving any mortality benefit from continued screening,” the authors reported.
“Yet they face the potential harms of overdiagnosis, such as complications after prostate biopsy for a false-positive screening and psychological stress associated with a cancer diagnosis.”
Guideline Confusion, Habit, Among Reasons for Continued Screening
Among key reasons for the continued screening of men well into old age is the fluctuating history of the guidelines, Dr. Kensler said in an interview.
“There has been considerable variation in prostate cancer screening guidelines over time and across organizations that make screening recommendations, and this has inevitably led to some confusion among clinicians,” he explained.
However, the evidence of a lack of benefit over the age of 70 is strong enough that not performing PSA-based screening among men ages 70 or older is a Healthcare Effectiveness Data and Information Set (HEDIS) measure for quality of care, he noted.
Nevertheless, “I think the trends we found in our analysis reflect that it is difficult for patients and providers to stop providing screening once they have already started it,” Dr. Kensler said.
Another motivator may be an inclination by clinicians to err on the side of caution, he added.
“For clinicians, although they may be aware of the guidelines, they may perhaps fear that they will not have offered screening to one of the older individuals who would have benefited from it even though they recognize that most would not,” Dr. Kensler noted.
Too often, however, such screenings “can lead to a cascade of other events that end up harming the patient without extending their lifespan,” he said.
Difficult Discussions
Complicating matters is the task of informing patients that due to their life expectancy, screening is considered to not likely be worthwhile — which may not be an easy discussion.
“For patients, hearing that they are at a stage of life where they may not benefit from screening is an unpleasant message to receive,” Dr. Kensler said.
“Having an in-depth conversation on this topic is also difficult given the many other health topics that clinicians and patients must cover during a visit.”
Ultimately, “these and other factors lead to inertia, where it is easier to stick to the status quo of continuing screening.”
The challenges underscore the need for improvements to the shared decision-making process to make sure that older men who do undergo prostrate screening will benefit, Dr. Kensler argued.
“If the guidelines are going to recommend shared decision-making, we need to provide tools to help patients and clinicians navigate these potentially difficult conversations.
Life Expectancy Uncertainties
Commenting on the research in an interview, Kyle Richards, MD, associate professor with the Department of Urology at the University of Wisconsin School of Medicine and Public Health, in Madison, noted that, “while most urology experts agree that we should not screen for prostate cancer in men with less than 5-10 years life expectancy, the challenge is deciding which patients have a more limited life expectancy.”
Tools and calculators are available to try to calculate life expectancy, “but they can be cumbersome and difficult to incorporate into clinical practice,” he added.
Indeed, the difficulty in accurately estimating life expectancy is also a limitation of the study, he noted.
“The challenge with a study like this is it is very difficult to accurately estimate life expectancy,” he said. “It is easy to pick a cut point (i.e. age 70) but it is very difficult to calculate one’s life expectancy from survey data alone.”
Another limitation is that “screening PSA testing implies that the patient is not having any symptoms, and we do not know from this study if any of these men were getting PSA checks due to some urinary symptoms or other issues,” Dr. Richards added.
“So, while the study does raise some concern about screening PSA in older men, the data source makes it quite difficult to home in on this question.”
When it can be estimated, life expectancy can indeed provide a more useful guide in assessing the options if a patient is found to have prostate cancer, Dr. Richards noted.
“If a patient has a 5- to 10-year life expectancy, and they are diagnosed with a clinically significant prostate cancer, they absolutely may still benefit from treatment,” he said.
“If they have a clinically significant prostate cancer that is unrecognized, it could metastasize and cause symptoms or lead to death, as roughly 30,000 men die from prostate cancer each year in the USA.”
However, “if a patient has a limited life expectancy of less than 5 to 10 years, don’t screen for prostate cancer,” he advised. Proper guidance should furthermore be made loud and clear in guideline recommendations.
“I do think the USPSTF and AUA need to be the primary voices educating primary care and patients regarding prostate cancer screening,” Dr. Richards said.
“We need to be smart about whom to screen, when to screen, and how often to screen. And this message needs to be heard by the primary care providers that perform the screening.”
The study was supported by the Sandra and Edward Meyer Cancer Center and a grant from the National Cancer Institute of the National Institutes of Health.
Dr. Kensler and Dr. Richards had no disclosures to report.
In its most recent guidance, the US Preventive Services Task Force (USPSTF) revised a previous 2012 recommendation against routine screening for prostate cancer to instead endorse individual decision-making for men aged 55 to 69 years (grade C).
In the update guidance, which was published in 2018, the task force still recommended against PSA-based screening for prostate cancer in men 70 years and older (grade D) due to a range of potential risks and harms. Guidelines from the American Urological Association and American Cancer Society have echoed that recommendation, in general agreement that men over the age of 70 or with limited life expectancy show little benefit from the screening.
To take a closer look at how commonly men are being screened for prostate cancer, based not only on their age but their estimated life expectancy, Kevin H. Kensler, ScD, of Weill Cornell Medicine, and colleagues conducted a cross-sectional study using data from the 2020 Behavioral Risk Factor Surveillance System (BRFSS).
“Our findings indicate that many males aged 70 years and older or those with a high risk of death within 10 years undergo prostate cancer screening despite the recommendation against screening in these populations by current guidelines,” the authors wrote in their paper, published in JAMA Network Open. The results underscore that “enhancements to the shared decision-making process are needed to ensure that older males who undergo screening are those who may potentially benefit,” they noted.
For the study, the authors identified 57,397 men aged 60 and older without a history of prostate cancer who reported undergoing a screening PSA test in the prior 2 years.
Using a risk factor system, mortality risk was estimated based on the scales ranging from 5.5 or less to 10.0 or greater, corresponding to the estimated 10-year mortality of less than 30% to 71% or more, respectively.
Of the men, 19.2% were aged 70 to 74 years, 13.0% were aged 75 to 79 years, and 12.3% were aged 80 years or older. The rest were 69 years or younger.
While the estimated 2-year prostate cancer screening rates were 36.3% among those aged 60 to 64 years and 42.8% for those 65 to 69 years, the rates were even higher, at 47.1%, among those aged 70 to 74 years, and similar, at 42.7%, in the 75 to 79 years of age range. Among those aged 80 years and older, 30.4% had been screened.
While the screening frequency was 43.4% among males with the greatest estimated life expectancy, a fair percentage of men, 30.4%, with the lowest life expectancy, indicative of a 71% or greater risk of death within 10 years, received prostate cancer screening.
In fact, among those with lowest life expectancy, the screening rates were greater than 20% in all age groups.
Screening in Older Age: Benefit in Reducing Mortality Low
Autopsy research indicates that, in fact, as many as 50% of men do have prostate cancer at age 80; however, many of those tumors are low-risk and unlikely to affect the health of the men.
If detected early, as is the intention of screening, prostate cancer can take years to advance and the likelihood of receiving any mortality benefit from continued screening in older age is low.
Furthermore, screening in older age can have implications, including a higher risk of complications following a false positive prostate biopsy that may not have been necessary in the first place, the authors explained.
“Given the long natural history of prostate cancer and lead time associated with PSA-based screening, these males [aged 70 and older or with a high risk of death within 10 years] have a low likelihood of receiving any mortality benefit from continued screening,” the authors reported.
“Yet they face the potential harms of overdiagnosis, such as complications after prostate biopsy for a false-positive screening and psychological stress associated with a cancer diagnosis.”
Guideline Confusion, Habit, Among Reasons for Continued Screening
Among key reasons for the continued screening of men well into old age is the fluctuating history of the guidelines, Dr. Kensler said in an interview.
“There has been considerable variation in prostate cancer screening guidelines over time and across organizations that make screening recommendations, and this has inevitably led to some confusion among clinicians,” he explained.
However, the evidence of a lack of benefit over the age of 70 is strong enough that not performing PSA-based screening among men ages 70 or older is a Healthcare Effectiveness Data and Information Set (HEDIS) measure for quality of care, he noted.
Nevertheless, “I think the trends we found in our analysis reflect that it is difficult for patients and providers to stop providing screening once they have already started it,” Dr. Kensler said.
Another motivator may be an inclination by clinicians to err on the side of caution, he added.
“For clinicians, although they may be aware of the guidelines, they may perhaps fear that they will not have offered screening to one of the older individuals who would have benefited from it even though they recognize that most would not,” Dr. Kensler noted.
Too often, however, such screenings “can lead to a cascade of other events that end up harming the patient without extending their lifespan,” he said.
Difficult Discussions
Complicating matters is the task of informing patients that due to their life expectancy, screening is considered to not likely be worthwhile — which may not be an easy discussion.
“For patients, hearing that they are at a stage of life where they may not benefit from screening is an unpleasant message to receive,” Dr. Kensler said.
“Having an in-depth conversation on this topic is also difficult given the many other health topics that clinicians and patients must cover during a visit.”
Ultimately, “these and other factors lead to inertia, where it is easier to stick to the status quo of continuing screening.”
The challenges underscore the need for improvements to the shared decision-making process to make sure that older men who do undergo prostrate screening will benefit, Dr. Kensler argued.
“If the guidelines are going to recommend shared decision-making, we need to provide tools to help patients and clinicians navigate these potentially difficult conversations.
Life Expectancy Uncertainties
Commenting on the research in an interview, Kyle Richards, MD, associate professor with the Department of Urology at the University of Wisconsin School of Medicine and Public Health, in Madison, noted that, “while most urology experts agree that we should not screen for prostate cancer in men with less than 5-10 years life expectancy, the challenge is deciding which patients have a more limited life expectancy.”
Tools and calculators are available to try to calculate life expectancy, “but they can be cumbersome and difficult to incorporate into clinical practice,” he added.
Indeed, the difficulty in accurately estimating life expectancy is also a limitation of the study, he noted.
“The challenge with a study like this is it is very difficult to accurately estimate life expectancy,” he said. “It is easy to pick a cut point (i.e. age 70) but it is very difficult to calculate one’s life expectancy from survey data alone.”
Another limitation is that “screening PSA testing implies that the patient is not having any symptoms, and we do not know from this study if any of these men were getting PSA checks due to some urinary symptoms or other issues,” Dr. Richards added.
“So, while the study does raise some concern about screening PSA in older men, the data source makes it quite difficult to home in on this question.”
When it can be estimated, life expectancy can indeed provide a more useful guide in assessing the options if a patient is found to have prostate cancer, Dr. Richards noted.
“If a patient has a 5- to 10-year life expectancy, and they are diagnosed with a clinically significant prostate cancer, they absolutely may still benefit from treatment,” he said.
“If they have a clinically significant prostate cancer that is unrecognized, it could metastasize and cause symptoms or lead to death, as roughly 30,000 men die from prostate cancer each year in the USA.”
However, “if a patient has a limited life expectancy of less than 5 to 10 years, don’t screen for prostate cancer,” he advised. Proper guidance should furthermore be made loud and clear in guideline recommendations.
“I do think the USPSTF and AUA need to be the primary voices educating primary care and patients regarding prostate cancer screening,” Dr. Richards said.
“We need to be smart about whom to screen, when to screen, and how often to screen. And this message needs to be heard by the primary care providers that perform the screening.”
The study was supported by the Sandra and Edward Meyer Cancer Center and a grant from the National Cancer Institute of the National Institutes of Health.
Dr. Kensler and Dr. Richards had no disclosures to report.
In its most recent guidance, the US Preventive Services Task Force (USPSTF) revised a previous 2012 recommendation against routine screening for prostate cancer to instead endorse individual decision-making for men aged 55 to 69 years (grade C).
In the update guidance, which was published in 2018, the task force still recommended against PSA-based screening for prostate cancer in men 70 years and older (grade D) due to a range of potential risks and harms. Guidelines from the American Urological Association and American Cancer Society have echoed that recommendation, in general agreement that men over the age of 70 or with limited life expectancy show little benefit from the screening.
To take a closer look at how commonly men are being screened for prostate cancer, based not only on their age but their estimated life expectancy, Kevin H. Kensler, ScD, of Weill Cornell Medicine, and colleagues conducted a cross-sectional study using data from the 2020 Behavioral Risk Factor Surveillance System (BRFSS).
“Our findings indicate that many males aged 70 years and older or those with a high risk of death within 10 years undergo prostate cancer screening despite the recommendation against screening in these populations by current guidelines,” the authors wrote in their paper, published in JAMA Network Open. The results underscore that “enhancements to the shared decision-making process are needed to ensure that older males who undergo screening are those who may potentially benefit,” they noted.
For the study, the authors identified 57,397 men aged 60 and older without a history of prostate cancer who reported undergoing a screening PSA test in the prior 2 years.
Using a risk factor system, mortality risk was estimated based on the scales ranging from 5.5 or less to 10.0 or greater, corresponding to the estimated 10-year mortality of less than 30% to 71% or more, respectively.
Of the men, 19.2% were aged 70 to 74 years, 13.0% were aged 75 to 79 years, and 12.3% were aged 80 years or older. The rest were 69 years or younger.
While the estimated 2-year prostate cancer screening rates were 36.3% among those aged 60 to 64 years and 42.8% for those 65 to 69 years, the rates were even higher, at 47.1%, among those aged 70 to 74 years, and similar, at 42.7%, in the 75 to 79 years of age range. Among those aged 80 years and older, 30.4% had been screened.
While the screening frequency was 43.4% among males with the greatest estimated life expectancy, a fair percentage of men, 30.4%, with the lowest life expectancy, indicative of a 71% or greater risk of death within 10 years, received prostate cancer screening.
In fact, among those with lowest life expectancy, the screening rates were greater than 20% in all age groups.
Screening in Older Age: Benefit in Reducing Mortality Low
Autopsy research indicates that, in fact, as many as 50% of men do have prostate cancer at age 80; however, many of those tumors are low-risk and unlikely to affect the health of the men.
If detected early, as is the intention of screening, prostate cancer can take years to advance and the likelihood of receiving any mortality benefit from continued screening in older age is low.
Furthermore, screening in older age can have implications, including a higher risk of complications following a false positive prostate biopsy that may not have been necessary in the first place, the authors explained.
“Given the long natural history of prostate cancer and lead time associated with PSA-based screening, these males [aged 70 and older or with a high risk of death within 10 years] have a low likelihood of receiving any mortality benefit from continued screening,” the authors reported.
“Yet they face the potential harms of overdiagnosis, such as complications after prostate biopsy for a false-positive screening and psychological stress associated with a cancer diagnosis.”
Guideline Confusion, Habit, Among Reasons for Continued Screening
Among key reasons for the continued screening of men well into old age is the fluctuating history of the guidelines, Dr. Kensler said in an interview.
“There has been considerable variation in prostate cancer screening guidelines over time and across organizations that make screening recommendations, and this has inevitably led to some confusion among clinicians,” he explained.
However, the evidence of a lack of benefit over the age of 70 is strong enough that not performing PSA-based screening among men ages 70 or older is a Healthcare Effectiveness Data and Information Set (HEDIS) measure for quality of care, he noted.
Nevertheless, “I think the trends we found in our analysis reflect that it is difficult for patients and providers to stop providing screening once they have already started it,” Dr. Kensler said.
Another motivator may be an inclination by clinicians to err on the side of caution, he added.
“For clinicians, although they may be aware of the guidelines, they may perhaps fear that they will not have offered screening to one of the older individuals who would have benefited from it even though they recognize that most would not,” Dr. Kensler noted.
Too often, however, such screenings “can lead to a cascade of other events that end up harming the patient without extending their lifespan,” he said.
Difficult Discussions
Complicating matters is the task of informing patients that due to their life expectancy, screening is considered to not likely be worthwhile — which may not be an easy discussion.
“For patients, hearing that they are at a stage of life where they may not benefit from screening is an unpleasant message to receive,” Dr. Kensler said.
“Having an in-depth conversation on this topic is also difficult given the many other health topics that clinicians and patients must cover during a visit.”
Ultimately, “these and other factors lead to inertia, where it is easier to stick to the status quo of continuing screening.”
The challenges underscore the need for improvements to the shared decision-making process to make sure that older men who do undergo prostrate screening will benefit, Dr. Kensler argued.
“If the guidelines are going to recommend shared decision-making, we need to provide tools to help patients and clinicians navigate these potentially difficult conversations.
Life Expectancy Uncertainties
Commenting on the research in an interview, Kyle Richards, MD, associate professor with the Department of Urology at the University of Wisconsin School of Medicine and Public Health, in Madison, noted that, “while most urology experts agree that we should not screen for prostate cancer in men with less than 5-10 years life expectancy, the challenge is deciding which patients have a more limited life expectancy.”
Tools and calculators are available to try to calculate life expectancy, “but they can be cumbersome and difficult to incorporate into clinical practice,” he added.
Indeed, the difficulty in accurately estimating life expectancy is also a limitation of the study, he noted.
“The challenge with a study like this is it is very difficult to accurately estimate life expectancy,” he said. “It is easy to pick a cut point (i.e. age 70) but it is very difficult to calculate one’s life expectancy from survey data alone.”
Another limitation is that “screening PSA testing implies that the patient is not having any symptoms, and we do not know from this study if any of these men were getting PSA checks due to some urinary symptoms or other issues,” Dr. Richards added.
“So, while the study does raise some concern about screening PSA in older men, the data source makes it quite difficult to home in on this question.”
When it can be estimated, life expectancy can indeed provide a more useful guide in assessing the options if a patient is found to have prostate cancer, Dr. Richards noted.
“If a patient has a 5- to 10-year life expectancy, and they are diagnosed with a clinically significant prostate cancer, they absolutely may still benefit from treatment,” he said.
“If they have a clinically significant prostate cancer that is unrecognized, it could metastasize and cause symptoms or lead to death, as roughly 30,000 men die from prostate cancer each year in the USA.”
However, “if a patient has a limited life expectancy of less than 5 to 10 years, don’t screen for prostate cancer,” he advised. Proper guidance should furthermore be made loud and clear in guideline recommendations.
“I do think the USPSTF and AUA need to be the primary voices educating primary care and patients regarding prostate cancer screening,” Dr. Richards said.
“We need to be smart about whom to screen, when to screen, and how often to screen. And this message needs to be heard by the primary care providers that perform the screening.”
The study was supported by the Sandra and Edward Meyer Cancer Center and a grant from the National Cancer Institute of the National Institutes of Health.
Dr. Kensler and Dr. Richards had no disclosures to report.
Is Meningitis a Risk Factor for Trigeminal Neuralgia? New Data
In multivariate analysis, the odds of meningitis were threefold higher in patients admitted with trigeminal neuralgia than in matched controls without trigeminal neuralgia.
This is the first nationwide population-based study of the rare, chronic pain disorder to identify the prevalence of trigeminal neuralgia admissions in the United States and risk factors contributing to trigeminal neuralgia development.
“Our results affirm known associations between trigeminal neuralgia and comorbidities like multiple sclerosis, and they also identify meningitis as a novel risk factor for trigeminal neuralgia,” said investigator Megan Tang, BS, a medical student at the Icahn School of Medicine at Mount Sinai, New York City.
The findings were presented at the American Association of Neurological Surgeons (AANS) 2024 annual meeting.
Strong Clinical Risk Factors
Trigeminal neuralgia is a rare pain disorder involving neurovascular compression of the trigeminal nerve. Its etiology and risk factors are poorly understood. Current literature is based on limited datasets and reports inconsistent risk factors across studies.
To better understand the disorder, researchers used International Classification of Diseases (ICD)-9 codes to identify trigeminal neuralgia admissions in the National Inpatient Sample from 2016 to 2019, and then propensity matched them 1:1 to non-trigeminal neuralgia admissions based on demographics, socioeconomic status, and Charlson comorbidity index scores.
Univariate analysis identified 136,345 trigeminal neuralgia admissions or an overall prevalence of 0.096%.
Trigeminal neuralgia admissions had lower morbidity than non-trigeminal neuralgia admissions and a higher prevalence of non-White patients, private insurance, and prolonged length of stay, Ms. Tang said.
Patients admitted for trigeminal neuralgia also had a higher prevalence of several chronic conditions, including hypertension, hyperlipidemia, and osteoarthritis; inflammatory conditions like lupus, meningitis, rheumatoid arthritis, and inflammatory bowel disease; and neurologic conditions including multiple sclerosis, epilepsy, stroke, and neurovascular compression disorders.
In multivariate analysis, investigators identified meningitis as a previously unknown risk factor for trigeminal neuralgia (odds ratio [OR], 3.1; P < .001).
Other strong risk factors were neurovascular compression disorders (OR, 39.82; P < .001) and multiple sclerosis (OR, 12.41; P < .001). Non-White race (Black; OR, 1.09; Hispanic; OR, 1.23; Other; OR, 1.24) and use of Medicaid (OR, 1.07) and other insurance (OR, 1.17) were demographic risk factors for trigeminal neuralgia.
“This finding points us toward future work exploring the potential mechanisms of predictors, most notably inflammatory conditions in trigeminal neuralgia development,” Ms. Tang concluded.
She declined to comment further on the findings, noting the investigators are still finalizing the results and interpretation.
Ask About Meningitis, Fever
Commenting on the findings, Michael D. Staudt, MD, MSc, University Hospitals Cleveland Medical Center, said that many patients who present with classical trigeminal neuralgia will have a blood vessel on MRI that is pressing on the trigeminal nerve.
“Obviously, the nerve is bathed in cerebrospinal fluid. So, if there’s an inflammatory marker, inflammation, or infection that could be injuring the nerve in a way that we don’t yet understand, that could be something that could cause trigeminal neuralgia without having to see a blood vessel,” said Dr. Staudt, who was not involved in the study. “It makes sense, theoretically. Something that’s inflammatory, something that’s irritating, that’s novel.”
Currently, predictive markers include clinical history, response to classical medications such as carbamazepine, and MRI findings, Dr. Staudt noted.
“Someone shows up with symptoms and MRI, and it’s basically do they have a blood vessel or not,” he said. “Treatments are generally within the same categories, but we don’t think it’s the same sort of success rate as seeing a blood vessel.”
Further research is needed, but, in the meantime, Dr. Staudt said, “We can ask patients who show up with facial pain if they’ve ever had meningitis or some sort of fever that preceded their onset of pain.”
The study had no specific funding. Ms. Tang and coauthor Jack Y. Zhang, MS, reported no relevant financial disclosures. Dr. Staudt reported serving as a consultant for Abbott and as a scientific adviser and consultant for Boston Scientific.
A version of this article appeared on Medscape.com.
In multivariate analysis, the odds of meningitis were threefold higher in patients admitted with trigeminal neuralgia than in matched controls without trigeminal neuralgia.
This is the first nationwide population-based study of the rare, chronic pain disorder to identify the prevalence of trigeminal neuralgia admissions in the United States and risk factors contributing to trigeminal neuralgia development.
“Our results affirm known associations between trigeminal neuralgia and comorbidities like multiple sclerosis, and they also identify meningitis as a novel risk factor for trigeminal neuralgia,” said investigator Megan Tang, BS, a medical student at the Icahn School of Medicine at Mount Sinai, New York City.
The findings were presented at the American Association of Neurological Surgeons (AANS) 2024 annual meeting.
Strong Clinical Risk Factors
Trigeminal neuralgia is a rare pain disorder involving neurovascular compression of the trigeminal nerve. Its etiology and risk factors are poorly understood. Current literature is based on limited datasets and reports inconsistent risk factors across studies.
To better understand the disorder, researchers used International Classification of Diseases (ICD)-9 codes to identify trigeminal neuralgia admissions in the National Inpatient Sample from 2016 to 2019, and then propensity matched them 1:1 to non-trigeminal neuralgia admissions based on demographics, socioeconomic status, and Charlson comorbidity index scores.
Univariate analysis identified 136,345 trigeminal neuralgia admissions or an overall prevalence of 0.096%.
Trigeminal neuralgia admissions had lower morbidity than non-trigeminal neuralgia admissions and a higher prevalence of non-White patients, private insurance, and prolonged length of stay, Ms. Tang said.
Patients admitted for trigeminal neuralgia also had a higher prevalence of several chronic conditions, including hypertension, hyperlipidemia, and osteoarthritis; inflammatory conditions like lupus, meningitis, rheumatoid arthritis, and inflammatory bowel disease; and neurologic conditions including multiple sclerosis, epilepsy, stroke, and neurovascular compression disorders.
In multivariate analysis, investigators identified meningitis as a previously unknown risk factor for trigeminal neuralgia (odds ratio [OR], 3.1; P < .001).
Other strong risk factors were neurovascular compression disorders (OR, 39.82; P < .001) and multiple sclerosis (OR, 12.41; P < .001). Non-White race (Black; OR, 1.09; Hispanic; OR, 1.23; Other; OR, 1.24) and use of Medicaid (OR, 1.07) and other insurance (OR, 1.17) were demographic risk factors for trigeminal neuralgia.
“This finding points us toward future work exploring the potential mechanisms of predictors, most notably inflammatory conditions in trigeminal neuralgia development,” Ms. Tang concluded.
She declined to comment further on the findings, noting the investigators are still finalizing the results and interpretation.
Ask About Meningitis, Fever
Commenting on the findings, Michael D. Staudt, MD, MSc, University Hospitals Cleveland Medical Center, said that many patients who present with classical trigeminal neuralgia will have a blood vessel on MRI that is pressing on the trigeminal nerve.
“Obviously, the nerve is bathed in cerebrospinal fluid. So, if there’s an inflammatory marker, inflammation, or infection that could be injuring the nerve in a way that we don’t yet understand, that could be something that could cause trigeminal neuralgia without having to see a blood vessel,” said Dr. Staudt, who was not involved in the study. “It makes sense, theoretically. Something that’s inflammatory, something that’s irritating, that’s novel.”
Currently, predictive markers include clinical history, response to classical medications such as carbamazepine, and MRI findings, Dr. Staudt noted.
“Someone shows up with symptoms and MRI, and it’s basically do they have a blood vessel or not,” he said. “Treatments are generally within the same categories, but we don’t think it’s the same sort of success rate as seeing a blood vessel.”
Further research is needed, but, in the meantime, Dr. Staudt said, “We can ask patients who show up with facial pain if they’ve ever had meningitis or some sort of fever that preceded their onset of pain.”
The study had no specific funding. Ms. Tang and coauthor Jack Y. Zhang, MS, reported no relevant financial disclosures. Dr. Staudt reported serving as a consultant for Abbott and as a scientific adviser and consultant for Boston Scientific.
A version of this article appeared on Medscape.com.
In multivariate analysis, the odds of meningitis were threefold higher in patients admitted with trigeminal neuralgia than in matched controls without trigeminal neuralgia.
This is the first nationwide population-based study of the rare, chronic pain disorder to identify the prevalence of trigeminal neuralgia admissions in the United States and risk factors contributing to trigeminal neuralgia development.
“Our results affirm known associations between trigeminal neuralgia and comorbidities like multiple sclerosis, and they also identify meningitis as a novel risk factor for trigeminal neuralgia,” said investigator Megan Tang, BS, a medical student at the Icahn School of Medicine at Mount Sinai, New York City.
The findings were presented at the American Association of Neurological Surgeons (AANS) 2024 annual meeting.
Strong Clinical Risk Factors
Trigeminal neuralgia is a rare pain disorder involving neurovascular compression of the trigeminal nerve. Its etiology and risk factors are poorly understood. Current literature is based on limited datasets and reports inconsistent risk factors across studies.
To better understand the disorder, researchers used International Classification of Diseases (ICD)-9 codes to identify trigeminal neuralgia admissions in the National Inpatient Sample from 2016 to 2019, and then propensity matched them 1:1 to non-trigeminal neuralgia admissions based on demographics, socioeconomic status, and Charlson comorbidity index scores.
Univariate analysis identified 136,345 trigeminal neuralgia admissions or an overall prevalence of 0.096%.
Trigeminal neuralgia admissions had lower morbidity than non-trigeminal neuralgia admissions and a higher prevalence of non-White patients, private insurance, and prolonged length of stay, Ms. Tang said.
Patients admitted for trigeminal neuralgia also had a higher prevalence of several chronic conditions, including hypertension, hyperlipidemia, and osteoarthritis; inflammatory conditions like lupus, meningitis, rheumatoid arthritis, and inflammatory bowel disease; and neurologic conditions including multiple sclerosis, epilepsy, stroke, and neurovascular compression disorders.
In multivariate analysis, investigators identified meningitis as a previously unknown risk factor for trigeminal neuralgia (odds ratio [OR], 3.1; P < .001).
Other strong risk factors were neurovascular compression disorders (OR, 39.82; P < .001) and multiple sclerosis (OR, 12.41; P < .001). Non-White race (Black; OR, 1.09; Hispanic; OR, 1.23; Other; OR, 1.24) and use of Medicaid (OR, 1.07) and other insurance (OR, 1.17) were demographic risk factors for trigeminal neuralgia.
“This finding points us toward future work exploring the potential mechanisms of predictors, most notably inflammatory conditions in trigeminal neuralgia development,” Ms. Tang concluded.
She declined to comment further on the findings, noting the investigators are still finalizing the results and interpretation.
Ask About Meningitis, Fever
Commenting on the findings, Michael D. Staudt, MD, MSc, University Hospitals Cleveland Medical Center, said that many patients who present with classical trigeminal neuralgia will have a blood vessel on MRI that is pressing on the trigeminal nerve.
“Obviously, the nerve is bathed in cerebrospinal fluid. So, if there’s an inflammatory marker, inflammation, or infection that could be injuring the nerve in a way that we don’t yet understand, that could be something that could cause trigeminal neuralgia without having to see a blood vessel,” said Dr. Staudt, who was not involved in the study. “It makes sense, theoretically. Something that’s inflammatory, something that’s irritating, that’s novel.”
Currently, predictive markers include clinical history, response to classical medications such as carbamazepine, and MRI findings, Dr. Staudt noted.
“Someone shows up with symptoms and MRI, and it’s basically do they have a blood vessel or not,” he said. “Treatments are generally within the same categories, but we don’t think it’s the same sort of success rate as seeing a blood vessel.”
Further research is needed, but, in the meantime, Dr. Staudt said, “We can ask patients who show up with facial pain if they’ve ever had meningitis or some sort of fever that preceded their onset of pain.”
The study had no specific funding. Ms. Tang and coauthor Jack Y. Zhang, MS, reported no relevant financial disclosures. Dr. Staudt reported serving as a consultant for Abbott and as a scientific adviser and consultant for Boston Scientific.
A version of this article appeared on Medscape.com.
FROM AANS 2024
Will Diabetes Drugs Advance Osteoarthritis Management?
VIENNA — With the glucagon-like peptide (GLP) 1 receptor agonist semaglutide (Wegovy) recently shown to significantly induce weight loss in people with osteoarthritis (OA) and obesity in the STEP-9 trial, could drugs traditionally used to treat type 2 diabetes be the next big thing for OA management?
“Hormone-based weight loss drugs are a game changer” for obesity management, Sébastien Czernichow, MD, PhD, said during a plenary session at the OARSI 2024 World Congress.

Drugs such as semaglutide may also have a cardioprotective effect, reducing the risk for major adverse cardiovascular events by as much as 20% vs placebo, added Dr. Czernichow, professor of nutrition at Paris Cité University and head of the Department of Nutrition at the George Pompidou European Hospital in Paris, France.
“You have to keep in mind that the short-term side effects are mainly gastrointestinal and [are] manageable. The mid-term side effects are an increased gallbladder [disease] risk, and the long-term benefits and risks are not really well known yet,” Dr. Czernichow said. With regard to that, the effects of these drugs on lean body mass, bone health, and nutritional deficiencies need to be further evaluated and monitored.
Weight Loss Benefits
Weight loss is one of the cornerstones of OA management, and in addition to the weight loss seen with the GLP-1 receptor agonists, there have also been changes in body composition, Dr. Czernichow said.
In SURMOUNT-1, for example, the dual glucose-dependent insulinotropic polypeptide and GLP-1 receptor agonist tirzepatide (Zepbound) was shown to significantly reduce total fat mass with a smaller decrease in total lean mass in a subanalysis.
It has been argued that effects on body composition need to be considered when evaluating new weight loss drugs, and that focusing only on the degree of weight reduction is “encouraging inaccurate measures of medication efficacy for both patients and clinicians,” Dr. Czernichow said, citing a viewpoint published in JAMA Internal Medicine.
“The real question is: Are we able to fund these drugs for everyone? Or will only the richest patients be allocated to these drugs?” Dr. Czernichow said.
Weight Rebound
Tonia Vincent, MBBS, PhD, professor of musculoskeletal biology and an honorary rheumatologist at The Kennedy Institute of Rheumatology at University of Oxford in England, was concerned about rebound weight gain.
“We hear a lot about this, that people stopping drugs actually get worse weight gain than before they started, and that’s a concern about a drug that is going to have a huge pressure for supply,” Dr. Vincent said following Dr. Czernichow’s presentation.
Another delegate said that calling GLP-1 receptor agonists a “game changer” for weight loss in OA was premature because long-term results are needed.
“You mentioned that the double-digit weight loss is getting very close to the results from bariatric surgery, but bariatric surgery you do once, and for these drugs, to maintain the weight loss, you need to take them continuously,” she said.
Weight Loss Affects Bone
Yet another delegate cautioned on the potential effects of significant weight loss on bone and cartilage. There is evidence, he said, that weight loss of 5-10 kg can significantly affect bone turnover, increasing bone resorption and thus putting patients at a risk of becoming osteopenic. “Are we looking at a new population of osteoporosis patients who may then also be at risk for fractures?” he asked.
Separately at OARSI 2024, Anne C. Bay-Jensen, PhD, chief technology officer at Nordic Bioscience in Herlev, Denmark, and colleagues reported data showing that weight loss was associated with an increase in bone and cartilage degradation.
Although Dr. Bay-Jensen and colleagues found that losing weight was associated with improved patient outcomes, there was a 1.58-fold increase in the bone resorption marker CTX-I in people who had lost weight vs a 1.37-fold gain in those whose weight remained stable and 1.11-fold increase in those who gained weight.
Moreover, there was a 1.15-fold increase in the cartilage degradation marker C2M in the weight loss group and 0.84-fold decrease in the interstitial matrix degradation marker C3M.
GLP-1 and Bone Effects
Another question is whether GLP-1 receptor agonists might be having direct effects on the bone that may be beneficial in OA. They might, postdoctoral researcher Eda Çiftci, PhD, of AO Research Institute Davos in Switzerland, and collaborators, said during the poster sessions at OARSI 2024.
Dr. Çiftci and researchers reported the findings of an in vitro study that looked at whether liraglutide might have anti-inflammatory and anabolic effects on a human chondrocytes model that had been treated with interleukin (IL)-1-beta to “mimic an inflammatory OA condition.”
The release of the proinflammatory cytokines IL-6 and IL-8 was reduced by treatment with liraglutide when compared with control chondrocytes. Furthermore, the expression of the proteoglycan aggrecan — important for articular cartilage function — also was preserved.
These results suggest that liraglutide does indeed have anabolic and anti-inflammatory effects, Dr. Çiftci and fellow researchers concluded.
New Role for Dipeptidyl Transferase Inhibitors?
Researchers are also looking at the potential role for other diabetes medications in OA management, including the dipeptidyl peptidase (DPP) 4 inhibitors.
Although these drugs are considered “weight neutral,” in vitro studies have suggested that the DPP4 enzyme may have a role to play in chondrocyte survival and inflammation, Yu-Hsiu Chen, MD, of the Tri-Service General Hospital and the National Defense Medical Center in Taipei, Taiwan, told this news organization. The DPP4 enzyme inactivates GLP-1, so there is rationale there.
“Last year, we published a paper where we found the concentration of DPP4 in the synovial fluid was correlated with radiographic change in knee OA,” Dr. Chen said. This time, “we’re trying to see if a DPP4 inhibitor can be used as a treatment.”
For their analysis, they used data on people newly diagnosed with type 2 diabetes who were and were not using DPP4 inhibitors obtained from Taiwan’s National Health Insurance Research Database. This database contains information on 99% of the Taiwanese population, Dr. Chen said.
Matching 165,333 DPP4 inhibitor users with an equal number of nonusers showed that there was a significant 58% risk reduction for developing OA with DPP4 inhibitor use (hazard ratio, 0.42; 95% CI, 0.41-0.44).
DPP4 inhibitor use was also associated with a 58% risk lower risk for total knee replacement (TKR) and a 62% lower risk for total hip replacement.
Dr. Chen and colleagues concluded: “These results strongly indicate that DPP4 inhibitors could be considered as a viable treatment approach for individuals with type 2 [diabetes mellitus] who are at risk for developing OA or [who] already have OA.”
Could Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitors Be Beneficial?
So, what about SGLT2 inhibitors? Do they also have a potential role to play in managing people with OA, regardless of whether there is diabetes present? Perhaps, and their effect may be even greater than what’s been observed for GLP-1 receptor agonists, as data presented by epidemiologist S. Reza Jafarzadeh, DVM, PhD, suggested.
“While GLP-1 receptor agonist drugs have been reported to reduce OA risk, largely attributed to their weight loss effect, SGLT2 inhibitors may provide a greater protective effect on OA outcomes,” said Dr. Jafarzadeh, assistant professor at Boston University.

He presented data from a large analysis of new users of SGLT2 inhibitors and GLP-1 receptor agonists within two claims databases — Merative (n = 603,471) and TriNetX (n = 1,202,972) — showing that SGLT2 inhibitors were associated with significantly lower risks for OA and the need for TKR.
Comparing new users of SGLT2 inhibitors and GLP-1 receptor agonists in the Merative dataset, the relative risks and odds ratios for OA were a respective 0.96 and 0.80, and having a TKR, 0.88 and 0.76.
Similar results were seen using the TriNetX dataset, with respective relative risks and hazard ratios of 0.90 and 0.85 for OA, and 0.81 and 0.78 for TKR.
In an interview, Dr. Jafarzadeh said that the initial hypothesis was that because SGLT2 inhibitors have only a modest effect on weight loss, there would be no effect on OA outcomes.
“But we were surprised that it actually looked like they reduced the risk of OA outcomes even more than GLP-1 receptor agonists,” Dr. Jafarzadeh said.
Further work is needed to understand these data, but they could mean that SLGT2 inhibitors, like GLP-1 receptor agonists, may have a role to play outside their current use in type 2 diabetes.
The congress was sponsored by the Osteoarthritis Research Society International.
Dr. Czernichow disclosed ties with BariaTek Medical, Boehringer Ingelheim, Bristol Myers Squibb, Fresenius, Janssen, Jellynov, Lilly, Novo Nordisk, Novartis, and ViiV Healthcare. Dr. Vincent had no relevant disclosures. Dr. Bay-Jensen is the chief technology officer and director of immunoscience at Nordic Bioscience, which funded the work in the poster she presented at OARSI 2024. The work presented by Dr. Çiftci and colleagues was funded by the Eurostars-2 joint program with co-funding from the European Horizon 2020 research and innovation program. Dr. Çiftci had no personal disclosures to report. Dr. Chen’s work was supported by the government of Taiwan, and she had no financial conflicts of interest to disclose. Dr. Jafarzadeh had no conflicts of interest to disclose.
A version of this article appeared on Medscape.com .
VIENNA — With the glucagon-like peptide (GLP) 1 receptor agonist semaglutide (Wegovy) recently shown to significantly induce weight loss in people with osteoarthritis (OA) and obesity in the STEP-9 trial, could drugs traditionally used to treat type 2 diabetes be the next big thing for OA management?
“Hormone-based weight loss drugs are a game changer” for obesity management, Sébastien Czernichow, MD, PhD, said during a plenary session at the OARSI 2024 World Congress.
Drugs such as semaglutide may also have a cardioprotective effect, reducing the risk for major adverse cardiovascular events by as much as 20% vs placebo, added Dr. Czernichow, professor of nutrition at Paris Cité University and head of the Department of Nutrition at the George Pompidou European Hospital in Paris, France.
“You have to keep in mind that the short-term side effects are mainly gastrointestinal and [are] manageable. The mid-term side effects are an increased gallbladder [disease] risk, and the long-term benefits and risks are not really well known yet,” Dr. Czernichow said. With regard to that, the effects of these drugs on lean body mass, bone health, and nutritional deficiencies need to be further evaluated and monitored.
Weight Loss Benefits
Weight loss is one of the cornerstones of OA management, and in addition to the weight loss seen with the GLP-1 receptor agonists, there have also been changes in body composition, Dr. Czernichow said.
In SURMOUNT-1, for example, the dual glucose-dependent insulinotropic polypeptide and GLP-1 receptor agonist tirzepatide (Zepbound) was shown to significantly reduce total fat mass with a smaller decrease in total lean mass in a subanalysis.
It has been argued that effects on body composition need to be considered when evaluating new weight loss drugs, and that focusing only on the degree of weight reduction is “encouraging inaccurate measures of medication efficacy for both patients and clinicians,” Dr. Czernichow said, citing a viewpoint published in JAMA Internal Medicine.
“The real question is: Are we able to fund these drugs for everyone? Or will only the richest patients be allocated to these drugs?” Dr. Czernichow said.
Weight Rebound
Tonia Vincent, MBBS, PhD, professor of musculoskeletal biology and an honorary rheumatologist at The Kennedy Institute of Rheumatology at University of Oxford in England, was concerned about rebound weight gain.
“We hear a lot about this, that people stopping drugs actually get worse weight gain than before they started, and that’s a concern about a drug that is going to have a huge pressure for supply,” Dr. Vincent said following Dr. Czernichow’s presentation.
Another delegate said that calling GLP-1 receptor agonists a “game changer” for weight loss in OA was premature because long-term results are needed.
“You mentioned that the double-digit weight loss is getting very close to the results from bariatric surgery, but bariatric surgery you do once, and for these drugs, to maintain the weight loss, you need to take them continuously,” she said.
Weight Loss Affects Bone
Yet another delegate cautioned on the potential effects of significant weight loss on bone and cartilage. There is evidence, he said, that weight loss of 5-10 kg can significantly affect bone turnover, increasing bone resorption and thus putting patients at a risk of becoming osteopenic. “Are we looking at a new population of osteoporosis patients who may then also be at risk for fractures?” he asked.
Separately at OARSI 2024, Anne C. Bay-Jensen, PhD, chief technology officer at Nordic Bioscience in Herlev, Denmark, and colleagues reported data showing that weight loss was associated with an increase in bone and cartilage degradation.
Although Dr. Bay-Jensen and colleagues found that losing weight was associated with improved patient outcomes, there was a 1.58-fold increase in the bone resorption marker CTX-I in people who had lost weight vs a 1.37-fold gain in those whose weight remained stable and 1.11-fold increase in those who gained weight.
Moreover, there was a 1.15-fold increase in the cartilage degradation marker C2M in the weight loss group and 0.84-fold decrease in the interstitial matrix degradation marker C3M.
GLP-1 and Bone Effects
Another question is whether GLP-1 receptor agonists might be having direct effects on the bone that may be beneficial in OA. They might, postdoctoral researcher Eda Çiftci, PhD, of AO Research Institute Davos in Switzerland, and collaborators, said during the poster sessions at OARSI 2024.
Dr. Çiftci and researchers reported the findings of an in vitro study that looked at whether liraglutide might have anti-inflammatory and anabolic effects on a human chondrocytes model that had been treated with interleukin (IL)-1-beta to “mimic an inflammatory OA condition.”
The release of the proinflammatory cytokines IL-6 and IL-8 was reduced by treatment with liraglutide when compared with control chondrocytes. Furthermore, the expression of the proteoglycan aggrecan — important for articular cartilage function — also was preserved.
These results suggest that liraglutide does indeed have anabolic and anti-inflammatory effects, Dr. Çiftci and fellow researchers concluded.
New Role for Dipeptidyl Transferase Inhibitors?
Researchers are also looking at the potential role for other diabetes medications in OA management, including the dipeptidyl peptidase (DPP) 4 inhibitors.
Although these drugs are considered “weight neutral,” in vitro studies have suggested that the DPP4 enzyme may have a role to play in chondrocyte survival and inflammation, Yu-Hsiu Chen, MD, of the Tri-Service General Hospital and the National Defense Medical Center in Taipei, Taiwan, told this news organization. The DPP4 enzyme inactivates GLP-1, so there is rationale there.
“Last year, we published a paper where we found the concentration of DPP4 in the synovial fluid was correlated with radiographic change in knee OA,” Dr. Chen said. This time, “we’re trying to see if a DPP4 inhibitor can be used as a treatment.”
For their analysis, they used data on people newly diagnosed with type 2 diabetes who were and were not using DPP4 inhibitors obtained from Taiwan’s National Health Insurance Research Database. This database contains information on 99% of the Taiwanese population, Dr. Chen said.
Matching 165,333 DPP4 inhibitor users with an equal number of nonusers showed that there was a significant 58% risk reduction for developing OA with DPP4 inhibitor use (hazard ratio, 0.42; 95% CI, 0.41-0.44).
DPP4 inhibitor use was also associated with a 58% risk lower risk for total knee replacement (TKR) and a 62% lower risk for total hip replacement.
Dr. Chen and colleagues concluded: “These results strongly indicate that DPP4 inhibitors could be considered as a viable treatment approach for individuals with type 2 [diabetes mellitus] who are at risk for developing OA or [who] already have OA.”
Could Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitors Be Beneficial?
So, what about SGLT2 inhibitors? Do they also have a potential role to play in managing people with OA, regardless of whether there is diabetes present? Perhaps, and their effect may be even greater than what’s been observed for GLP-1 receptor agonists, as data presented by epidemiologist S. Reza Jafarzadeh, DVM, PhD, suggested.
“While GLP-1 receptor agonist drugs have been reported to reduce OA risk, largely attributed to their weight loss effect, SGLT2 inhibitors may provide a greater protective effect on OA outcomes,” said Dr. Jafarzadeh, assistant professor at Boston University.
He presented data from a large analysis of new users of SGLT2 inhibitors and GLP-1 receptor agonists within two claims databases — Merative (n = 603,471) and TriNetX (n = 1,202,972) — showing that SGLT2 inhibitors were associated with significantly lower risks for OA and the need for TKR.
Comparing new users of SGLT2 inhibitors and GLP-1 receptor agonists in the Merative dataset, the relative risks and odds ratios for OA were a respective 0.96 and 0.80, and having a TKR, 0.88 and 0.76.
Similar results were seen using the TriNetX dataset, with respective relative risks and hazard ratios of 0.90 and 0.85 for OA, and 0.81 and 0.78 for TKR.
In an interview, Dr. Jafarzadeh said that the initial hypothesis was that because SGLT2 inhibitors have only a modest effect on weight loss, there would be no effect on OA outcomes.
“But we were surprised that it actually looked like they reduced the risk of OA outcomes even more than GLP-1 receptor agonists,” Dr. Jafarzadeh said.
Further work is needed to understand these data, but they could mean that SLGT2 inhibitors, like GLP-1 receptor agonists, may have a role to play outside their current use in type 2 diabetes.
The congress was sponsored by the Osteoarthritis Research Society International.
Dr. Czernichow disclosed ties with BariaTek Medical, Boehringer Ingelheim, Bristol Myers Squibb, Fresenius, Janssen, Jellynov, Lilly, Novo Nordisk, Novartis, and ViiV Healthcare. Dr. Vincent had no relevant disclosures. Dr. Bay-Jensen is the chief technology officer and director of immunoscience at Nordic Bioscience, which funded the work in the poster she presented at OARSI 2024. The work presented by Dr. Çiftci and colleagues was funded by the Eurostars-2 joint program with co-funding from the European Horizon 2020 research and innovation program. Dr. Çiftci had no personal disclosures to report. Dr. Chen’s work was supported by the government of Taiwan, and she had no financial conflicts of interest to disclose. Dr. Jafarzadeh had no conflicts of interest to disclose.
A version of this article appeared on Medscape.com .
VIENNA — With the glucagon-like peptide (GLP) 1 receptor agonist semaglutide (Wegovy) recently shown to significantly induce weight loss in people with osteoarthritis (OA) and obesity in the STEP-9 trial, could drugs traditionally used to treat type 2 diabetes be the next big thing for OA management?
“Hormone-based weight loss drugs are a game changer” for obesity management, Sébastien Czernichow, MD, PhD, said during a plenary session at the OARSI 2024 World Congress.
Drugs such as semaglutide may also have a cardioprotective effect, reducing the risk for major adverse cardiovascular events by as much as 20% vs placebo, added Dr. Czernichow, professor of nutrition at Paris Cité University and head of the Department of Nutrition at the George Pompidou European Hospital in Paris, France.
“You have to keep in mind that the short-term side effects are mainly gastrointestinal and [are] manageable. The mid-term side effects are an increased gallbladder [disease] risk, and the long-term benefits and risks are not really well known yet,” Dr. Czernichow said. With regard to that, the effects of these drugs on lean body mass, bone health, and nutritional deficiencies need to be further evaluated and monitored.
Weight Loss Benefits
Weight loss is one of the cornerstones of OA management, and in addition to the weight loss seen with the GLP-1 receptor agonists, there have also been changes in body composition, Dr. Czernichow said.
In SURMOUNT-1, for example, the dual glucose-dependent insulinotropic polypeptide and GLP-1 receptor agonist tirzepatide (Zepbound) was shown to significantly reduce total fat mass with a smaller decrease in total lean mass in a subanalysis.
It has been argued that effects on body composition need to be considered when evaluating new weight loss drugs, and that focusing only on the degree of weight reduction is “encouraging inaccurate measures of medication efficacy for both patients and clinicians,” Dr. Czernichow said, citing a viewpoint published in JAMA Internal Medicine.
“The real question is: Are we able to fund these drugs for everyone? Or will only the richest patients be allocated to these drugs?” Dr. Czernichow said.
Weight Rebound
Tonia Vincent, MBBS, PhD, professor of musculoskeletal biology and an honorary rheumatologist at The Kennedy Institute of Rheumatology at University of Oxford in England, was concerned about rebound weight gain.
“We hear a lot about this, that people stopping drugs actually get worse weight gain than before they started, and that’s a concern about a drug that is going to have a huge pressure for supply,” Dr. Vincent said following Dr. Czernichow’s presentation.
Another delegate said that calling GLP-1 receptor agonists a “game changer” for weight loss in OA was premature because long-term results are needed.
“You mentioned that the double-digit weight loss is getting very close to the results from bariatric surgery, but bariatric surgery you do once, and for these drugs, to maintain the weight loss, you need to take them continuously,” she said.
Weight Loss Affects Bone
Yet another delegate cautioned on the potential effects of significant weight loss on bone and cartilage. There is evidence, he said, that weight loss of 5-10 kg can significantly affect bone turnover, increasing bone resorption and thus putting patients at a risk of becoming osteopenic. “Are we looking at a new population of osteoporosis patients who may then also be at risk for fractures?” he asked.
Separately at OARSI 2024, Anne C. Bay-Jensen, PhD, chief technology officer at Nordic Bioscience in Herlev, Denmark, and colleagues reported data showing that weight loss was associated with an increase in bone and cartilage degradation.
Although Dr. Bay-Jensen and colleagues found that losing weight was associated with improved patient outcomes, there was a 1.58-fold increase in the bone resorption marker CTX-I in people who had lost weight vs a 1.37-fold gain in those whose weight remained stable and 1.11-fold increase in those who gained weight.
Moreover, there was a 1.15-fold increase in the cartilage degradation marker C2M in the weight loss group and 0.84-fold decrease in the interstitial matrix degradation marker C3M.
GLP-1 and Bone Effects
Another question is whether GLP-1 receptor agonists might be having direct effects on the bone that may be beneficial in OA. They might, postdoctoral researcher Eda Çiftci, PhD, of AO Research Institute Davos in Switzerland, and collaborators, said during the poster sessions at OARSI 2024.
Dr. Çiftci and researchers reported the findings of an in vitro study that looked at whether liraglutide might have anti-inflammatory and anabolic effects on a human chondrocytes model that had been treated with interleukin (IL)-1-beta to “mimic an inflammatory OA condition.”
The release of the proinflammatory cytokines IL-6 and IL-8 was reduced by treatment with liraglutide when compared with control chondrocytes. Furthermore, the expression of the proteoglycan aggrecan — important for articular cartilage function — also was preserved.
These results suggest that liraglutide does indeed have anabolic and anti-inflammatory effects, Dr. Çiftci and fellow researchers concluded.
New Role for Dipeptidyl Transferase Inhibitors?
Researchers are also looking at the potential role for other diabetes medications in OA management, including the dipeptidyl peptidase (DPP) 4 inhibitors.
Although these drugs are considered “weight neutral,” in vitro studies have suggested that the DPP4 enzyme may have a role to play in chondrocyte survival and inflammation, Yu-Hsiu Chen, MD, of the Tri-Service General Hospital and the National Defense Medical Center in Taipei, Taiwan, told this news organization. The DPP4 enzyme inactivates GLP-1, so there is rationale there.
“Last year, we published a paper where we found the concentration of DPP4 in the synovial fluid was correlated with radiographic change in knee OA,” Dr. Chen said. This time, “we’re trying to see if a DPP4 inhibitor can be used as a treatment.”
For their analysis, they used data on people newly diagnosed with type 2 diabetes who were and were not using DPP4 inhibitors obtained from Taiwan’s National Health Insurance Research Database. This database contains information on 99% of the Taiwanese population, Dr. Chen said.
Matching 165,333 DPP4 inhibitor users with an equal number of nonusers showed that there was a significant 58% risk reduction for developing OA with DPP4 inhibitor use (hazard ratio, 0.42; 95% CI, 0.41-0.44).
DPP4 inhibitor use was also associated with a 58% risk lower risk for total knee replacement (TKR) and a 62% lower risk for total hip replacement.
Dr. Chen and colleagues concluded: “These results strongly indicate that DPP4 inhibitors could be considered as a viable treatment approach for individuals with type 2 [diabetes mellitus] who are at risk for developing OA or [who] already have OA.”
Could Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitors Be Beneficial?
So, what about SGLT2 inhibitors? Do they also have a potential role to play in managing people with OA, regardless of whether there is diabetes present? Perhaps, and their effect may be even greater than what’s been observed for GLP-1 receptor agonists, as data presented by epidemiologist S. Reza Jafarzadeh, DVM, PhD, suggested.
“While GLP-1 receptor agonist drugs have been reported to reduce OA risk, largely attributed to their weight loss effect, SGLT2 inhibitors may provide a greater protective effect on OA outcomes,” said Dr. Jafarzadeh, assistant professor at Boston University.
He presented data from a large analysis of new users of SGLT2 inhibitors and GLP-1 receptor agonists within two claims databases — Merative (n = 603,471) and TriNetX (n = 1,202,972) — showing that SGLT2 inhibitors were associated with significantly lower risks for OA and the need for TKR.
Comparing new users of SGLT2 inhibitors and GLP-1 receptor agonists in the Merative dataset, the relative risks and odds ratios for OA were a respective 0.96 and 0.80, and having a TKR, 0.88 and 0.76.
Similar results were seen using the TriNetX dataset, with respective relative risks and hazard ratios of 0.90 and 0.85 for OA, and 0.81 and 0.78 for TKR.
In an interview, Dr. Jafarzadeh said that the initial hypothesis was that because SGLT2 inhibitors have only a modest effect on weight loss, there would be no effect on OA outcomes.
“But we were surprised that it actually looked like they reduced the risk of OA outcomes even more than GLP-1 receptor agonists,” Dr. Jafarzadeh said.
Further work is needed to understand these data, but they could mean that SLGT2 inhibitors, like GLP-1 receptor agonists, may have a role to play outside their current use in type 2 diabetes.
The congress was sponsored by the Osteoarthritis Research Society International.
Dr. Czernichow disclosed ties with BariaTek Medical, Boehringer Ingelheim, Bristol Myers Squibb, Fresenius, Janssen, Jellynov, Lilly, Novo Nordisk, Novartis, and ViiV Healthcare. Dr. Vincent had no relevant disclosures. Dr. Bay-Jensen is the chief technology officer and director of immunoscience at Nordic Bioscience, which funded the work in the poster she presented at OARSI 2024. The work presented by Dr. Çiftci and colleagues was funded by the Eurostars-2 joint program with co-funding from the European Horizon 2020 research and innovation program. Dr. Çiftci had no personal disclosures to report. Dr. Chen’s work was supported by the government of Taiwan, and she had no financial conflicts of interest to disclose. Dr. Jafarzadeh had no conflicts of interest to disclose.
A version of this article appeared on Medscape.com .
FROM OARSI 2024
Vacationing Doctors Fight to Revive a Drowned Child
Emergencies happen anywhere, anytime, and sometimes, medical professionals find themselves in situations where they are the only ones who can help. Is There a Doctor in the House? is a series telling these stories.
Jennifer Suders, DO: We were in Florida with our 1-year-old daughter visiting my parents. They moved to an area called Hallandale Beach and live in a high-rise community with a few different pools and spas.
Dan and I were in the spa area at the gym. He was getting me to hurry up because we were supposed to meet my parents who were with our daughter. I was sort of moseying and taking my time.
We were walking by one of the pool decks to get into the building when I heard what sounded like a slap. My first thought was that maybe somebody was choking and someone was hitting their back. Choking has always been my biggest fear with our daughter.
I turned and saw some people who seemed frantic. I looked at Dan and started to ask, “Do you think they need help?” I don’t even think I got the whole sentence out before this mom whipped her head around. I’ll never forget her dark brown hair flying. She screamed, “HELP!”
Dan and I just ran. I let go of my backpack and iPad and water bottle. They scattered across the pool deck. I instantly had my phone in my hand dialing 911.
Daniel Suders, DO: That’s what they teach us, to call 911 first. I didn’t think of it in the moment, but Jenny did.
Jennifer Suders:
Dan and I got down on either side of the boy and checked for a pulse. We couldn’t feel anything. Dan started chest compressions. I was talking to the 911 operator, and then I gave two rescue breaths. We did a sternal rub.
I was kind of yelling in the boy’s face, trying to get him to respond. I tried English and Russian because there’s a big Russian community there, and my family speaks Russian. The grandma asked us if we knew what we were doing.
Daniel Suders: I think she asked if Jenny was a nurse.
Jennifer Suders: Common misconception. Suddenly, the boy started vomiting, and so much water poured out. We turned him on his side, and he had two or three more episodes of spitting up the water. After that, we could see the color start to come back into his face. His eyes started fluttering.
We thought he was probably coming back. But we were too scared to say that in case we were wrong, and he went back under. So, we just held him steady. We didn’t know what had happened, if he might have hit his head, so we needed to keep him still.
Daniel Suders: It was amazing when those eyes opened, and he started to wake up.
Jennifer Suders: It felt like my heart had stopped while I was waiting for his to start.
Daniel Suders: He was clutching his chest like it hurt and started calling for his mom. He was crying and wanting to get in his mom’s arms. We had to keep him from standing up and walking.
Jennifer Suders: He was clearly scared. There were all these strange faces around him. I kept looking at my phone, anxiously waiting for EMS to come. They got there about 8 or 9 minutes later.
At some point, the father walked in with their daughter, a baby under a year old. He was in shock, not knowing what was going on. The grandma explained that the boy had been jumping into the pool over and over with his brother. All of a sudden, they looked over, and he was just lying there, floating, face down. They were right there; they were watching him. It was just that quick.
Daniel Suders: They pulled him out right away, and that was a big thing on his side that it was caught so quickly. He didn’t have to wait long to start resuscitation.
Jennifer Suders: Once EMS got there and assessed him, they put him and his mom on the stretcher. I remember watching them wheel it through the double doors to get to the elevator. As soon as they were gone, I just turned around and broke down. I had been in doctor mode if you will. Straight to the point. No nonsense. Suddenly, I went back into civilian mode, and my emotions just bubbled up.
After we left, we went to meet my parents who had our kid. Dan just beelined toward her and scooped her up and wouldn’t let her go.
For the rest of the day, it was all I could think about. It took me a while to fall asleep that night, and it was the first thing I thought when I woke up the next morning. We were hopeful that the boy was going to be okay, but you never know. We didn’t call the hospital because with HIPAA, I didn’t know if they could tell us anything.
And then the next day — there they were. The family was back at the pool. The little boy was running around like nothing had happened. We were a little surprised. But I would hate for him to be scared of the pool for the rest of his life. His family was watching him like a hawk.
They told us that the boy and his mom had stayed overnight in the ER, but only as a precaution. He didn’t have any more vomiting. He was absolutely fine. They were incredibly grateful.
We got their names and exchanged numbers and took a picture. That’s all I wanted — a photo to remember them.
A day or so later, we saw them again at a nearby park. The boy was climbing trees and seemed completely normal. It was the best outcome we could have hoped for.
Daniel Suders: My biggest worry was any harm to his chest from the resuscitation, or of course how long he was without oxygen. But everyone says that kids are really resilient. I work with adults, so I don’t have a lot of experience.
As a hospitalist, we don’t always see a lot of success with CPR. It’s often an elderly person who just doesn’t have much of a chance. That same week before our vacation, I had lost a 90-year-old in the hospital. It was such a juxtaposition — a 3-year-old with their whole life in front of them. We were able to preserve that, and it was incredible.
Jennifer Suders: I’m a nephrologist, so my field is pretty calm. No big emergencies. We have patients on the floor, but if a code gets called, there’s a team that comes in from the intensive care unit. I always kind of wondered what I would do if I was presented with a scenario like this.
Daniel Suders: We have a lot of friends that do ER medicine, and I felt like those were the guys that really understood when we told them the story. One friend said to me, “By the time they get to us, they’re either in bad shape or they’re better already.” A lot depends on what happens in the field.
Jennifer Suders: I’m even more vigilant about pool safety now. I want to make sure parents know that drowning doesn›t look like flailing theatrics. It can be soundless. Three adults were right next to this little boy and didn›t realize until they looked down and saw him.
If we hadn’t been there, I don’t know if anyone would’ve been able to step in. No one else was medically trained. But I think the message is — you don’t have to be. Anyone can take a CPR class.
When I told my parents, my dad said, “Oh my gosh, I would’ve laid right down there next to that kid and passed out.” Without any training, it’s petrifying to see something like that.
I think about how we could have stayed in the gym longer and been too late. Or we could have gotten on the elevator earlier and been gone. Two minutes, and it would’ve been a story we heard later, not one we were a part of. It feels like we were at a true crossroads in that moment where that boy could have lived or died. And the stars aligned perfectly.
We had no medicine, no monitors, nothing but our hands and our breaths. And we helped a family continue their vacation rather than plan a funeral.
Jennifer Suders, DO, is a nephrologist at West Virginia University Medicine Wheeling Clinic. Daniel Suders, DO, is a hospitalist at West Virginia University Medicine Reynolds Memorial Hospital.
A version of this article appeared on Medscape.com .
Emergencies happen anywhere, anytime, and sometimes, medical professionals find themselves in situations where they are the only ones who can help. Is There a Doctor in the House? is a series telling these stories.
Jennifer Suders, DO: We were in Florida with our 1-year-old daughter visiting my parents. They moved to an area called Hallandale Beach and live in a high-rise community with a few different pools and spas.
Dan and I were in the spa area at the gym. He was getting me to hurry up because we were supposed to meet my parents who were with our daughter. I was sort of moseying and taking my time.
We were walking by one of the pool decks to get into the building when I heard what sounded like a slap. My first thought was that maybe somebody was choking and someone was hitting their back. Choking has always been my biggest fear with our daughter.
I turned and saw some people who seemed frantic. I looked at Dan and started to ask, “Do you think they need help?” I don’t even think I got the whole sentence out before this mom whipped her head around. I’ll never forget her dark brown hair flying. She screamed, “HELP!”
Dan and I just ran. I let go of my backpack and iPad and water bottle. They scattered across the pool deck. I instantly had my phone in my hand dialing 911.
Daniel Suders, DO: That’s what they teach us, to call 911 first. I didn’t think of it in the moment, but Jenny did.
Jennifer Suders:
Dan and I got down on either side of the boy and checked for a pulse. We couldn’t feel anything. Dan started chest compressions. I was talking to the 911 operator, and then I gave two rescue breaths. We did a sternal rub.
I was kind of yelling in the boy’s face, trying to get him to respond. I tried English and Russian because there’s a big Russian community there, and my family speaks Russian. The grandma asked us if we knew what we were doing.
Daniel Suders: I think she asked if Jenny was a nurse.
Jennifer Suders: Common misconception. Suddenly, the boy started vomiting, and so much water poured out. We turned him on his side, and he had two or three more episodes of spitting up the water. After that, we could see the color start to come back into his face. His eyes started fluttering.
We thought he was probably coming back. But we were too scared to say that in case we were wrong, and he went back under. So, we just held him steady. We didn’t know what had happened, if he might have hit his head, so we needed to keep him still.
Daniel Suders: It was amazing when those eyes opened, and he started to wake up.
Jennifer Suders: It felt like my heart had stopped while I was waiting for his to start.
Daniel Suders: He was clutching his chest like it hurt and started calling for his mom. He was crying and wanting to get in his mom’s arms. We had to keep him from standing up and walking.
Jennifer Suders: He was clearly scared. There were all these strange faces around him. I kept looking at my phone, anxiously waiting for EMS to come. They got there about 8 or 9 minutes later.
At some point, the father walked in with their daughter, a baby under a year old. He was in shock, not knowing what was going on. The grandma explained that the boy had been jumping into the pool over and over with his brother. All of a sudden, they looked over, and he was just lying there, floating, face down. They were right there; they were watching him. It was just that quick.
Daniel Suders: They pulled him out right away, and that was a big thing on his side that it was caught so quickly. He didn’t have to wait long to start resuscitation.
Jennifer Suders: Once EMS got there and assessed him, they put him and his mom on the stretcher. I remember watching them wheel it through the double doors to get to the elevator. As soon as they were gone, I just turned around and broke down. I had been in doctor mode if you will. Straight to the point. No nonsense. Suddenly, I went back into civilian mode, and my emotions just bubbled up.
After we left, we went to meet my parents who had our kid. Dan just beelined toward her and scooped her up and wouldn’t let her go.
For the rest of the day, it was all I could think about. It took me a while to fall asleep that night, and it was the first thing I thought when I woke up the next morning. We were hopeful that the boy was going to be okay, but you never know. We didn’t call the hospital because with HIPAA, I didn’t know if they could tell us anything.
And then the next day — there they were. The family was back at the pool. The little boy was running around like nothing had happened. We were a little surprised. But I would hate for him to be scared of the pool for the rest of his life. His family was watching him like a hawk.
They told us that the boy and his mom had stayed overnight in the ER, but only as a precaution. He didn’t have any more vomiting. He was absolutely fine. They were incredibly grateful.
We got their names and exchanged numbers and took a picture. That’s all I wanted — a photo to remember them.
A day or so later, we saw them again at a nearby park. The boy was climbing trees and seemed completely normal. It was the best outcome we could have hoped for.
Daniel Suders: My biggest worry was any harm to his chest from the resuscitation, or of course how long he was without oxygen. But everyone says that kids are really resilient. I work with adults, so I don’t have a lot of experience.
As a hospitalist, we don’t always see a lot of success with CPR. It’s often an elderly person who just doesn’t have much of a chance. That same week before our vacation, I had lost a 90-year-old in the hospital. It was such a juxtaposition — a 3-year-old with their whole life in front of them. We were able to preserve that, and it was incredible.
Jennifer Suders: I’m a nephrologist, so my field is pretty calm. No big emergencies. We have patients on the floor, but if a code gets called, there’s a team that comes in from the intensive care unit. I always kind of wondered what I would do if I was presented with a scenario like this.
Daniel Suders: We have a lot of friends that do ER medicine, and I felt like those were the guys that really understood when we told them the story. One friend said to me, “By the time they get to us, they’re either in bad shape or they’re better already.” A lot depends on what happens in the field.
Jennifer Suders: I’m even more vigilant about pool safety now. I want to make sure parents know that drowning doesn›t look like flailing theatrics. It can be soundless. Three adults were right next to this little boy and didn›t realize until they looked down and saw him.
If we hadn’t been there, I don’t know if anyone would’ve been able to step in. No one else was medically trained. But I think the message is — you don’t have to be. Anyone can take a CPR class.
When I told my parents, my dad said, “Oh my gosh, I would’ve laid right down there next to that kid and passed out.” Without any training, it’s petrifying to see something like that.
I think about how we could have stayed in the gym longer and been too late. Or we could have gotten on the elevator earlier and been gone. Two minutes, and it would’ve been a story we heard later, not one we were a part of. It feels like we were at a true crossroads in that moment where that boy could have lived or died. And the stars aligned perfectly.
We had no medicine, no monitors, nothing but our hands and our breaths. And we helped a family continue their vacation rather than plan a funeral.
Jennifer Suders, DO, is a nephrologist at West Virginia University Medicine Wheeling Clinic. Daniel Suders, DO, is a hospitalist at West Virginia University Medicine Reynolds Memorial Hospital.
A version of this article appeared on Medscape.com .
Emergencies happen anywhere, anytime, and sometimes, medical professionals find themselves in situations where they are the only ones who can help. Is There a Doctor in the House? is a series telling these stories.
Jennifer Suders, DO: We were in Florida with our 1-year-old daughter visiting my parents. They moved to an area called Hallandale Beach and live in a high-rise community with a few different pools and spas.
Dan and I were in the spa area at the gym. He was getting me to hurry up because we were supposed to meet my parents who were with our daughter. I was sort of moseying and taking my time.
We were walking by one of the pool decks to get into the building when I heard what sounded like a slap. My first thought was that maybe somebody was choking and someone was hitting their back. Choking has always been my biggest fear with our daughter.
I turned and saw some people who seemed frantic. I looked at Dan and started to ask, “Do you think they need help?” I don’t even think I got the whole sentence out before this mom whipped her head around. I’ll never forget her dark brown hair flying. She screamed, “HELP!”
Dan and I just ran. I let go of my backpack and iPad and water bottle. They scattered across the pool deck. I instantly had my phone in my hand dialing 911.
Daniel Suders, DO: That’s what they teach us, to call 911 first. I didn’t think of it in the moment, but Jenny did.
Jennifer Suders:
Dan and I got down on either side of the boy and checked for a pulse. We couldn’t feel anything. Dan started chest compressions. I was talking to the 911 operator, and then I gave two rescue breaths. We did a sternal rub.
I was kind of yelling in the boy’s face, trying to get him to respond. I tried English and Russian because there’s a big Russian community there, and my family speaks Russian. The grandma asked us if we knew what we were doing.
Daniel Suders: I think she asked if Jenny was a nurse.
Jennifer Suders: Common misconception. Suddenly, the boy started vomiting, and so much water poured out. We turned him on his side, and he had two or three more episodes of spitting up the water. After that, we could see the color start to come back into his face. His eyes started fluttering.
We thought he was probably coming back. But we were too scared to say that in case we were wrong, and he went back under. So, we just held him steady. We didn’t know what had happened, if he might have hit his head, so we needed to keep him still.
Daniel Suders: It was amazing when those eyes opened, and he started to wake up.
Jennifer Suders: It felt like my heart had stopped while I was waiting for his to start.
Daniel Suders: He was clutching his chest like it hurt and started calling for his mom. He was crying and wanting to get in his mom’s arms. We had to keep him from standing up and walking.
Jennifer Suders: He was clearly scared. There were all these strange faces around him. I kept looking at my phone, anxiously waiting for EMS to come. They got there about 8 or 9 minutes later.
At some point, the father walked in with their daughter, a baby under a year old. He was in shock, not knowing what was going on. The grandma explained that the boy had been jumping into the pool over and over with his brother. All of a sudden, they looked over, and he was just lying there, floating, face down. They were right there; they were watching him. It was just that quick.
Daniel Suders: They pulled him out right away, and that was a big thing on his side that it was caught so quickly. He didn’t have to wait long to start resuscitation.
Jennifer Suders: Once EMS got there and assessed him, they put him and his mom on the stretcher. I remember watching them wheel it through the double doors to get to the elevator. As soon as they were gone, I just turned around and broke down. I had been in doctor mode if you will. Straight to the point. No nonsense. Suddenly, I went back into civilian mode, and my emotions just bubbled up.
After we left, we went to meet my parents who had our kid. Dan just beelined toward her and scooped her up and wouldn’t let her go.
For the rest of the day, it was all I could think about. It took me a while to fall asleep that night, and it was the first thing I thought when I woke up the next morning. We were hopeful that the boy was going to be okay, but you never know. We didn’t call the hospital because with HIPAA, I didn’t know if they could tell us anything.
And then the next day — there they were. The family was back at the pool. The little boy was running around like nothing had happened. We were a little surprised. But I would hate for him to be scared of the pool for the rest of his life. His family was watching him like a hawk.
They told us that the boy and his mom had stayed overnight in the ER, but only as a precaution. He didn’t have any more vomiting. He was absolutely fine. They were incredibly grateful.
We got their names and exchanged numbers and took a picture. That’s all I wanted — a photo to remember them.
A day or so later, we saw them again at a nearby park. The boy was climbing trees and seemed completely normal. It was the best outcome we could have hoped for.
Daniel Suders: My biggest worry was any harm to his chest from the resuscitation, or of course how long he was without oxygen. But everyone says that kids are really resilient. I work with adults, so I don’t have a lot of experience.
As a hospitalist, we don’t always see a lot of success with CPR. It’s often an elderly person who just doesn’t have much of a chance. That same week before our vacation, I had lost a 90-year-old in the hospital. It was such a juxtaposition — a 3-year-old with their whole life in front of them. We were able to preserve that, and it was incredible.
Jennifer Suders: I’m a nephrologist, so my field is pretty calm. No big emergencies. We have patients on the floor, but if a code gets called, there’s a team that comes in from the intensive care unit. I always kind of wondered what I would do if I was presented with a scenario like this.
Daniel Suders: We have a lot of friends that do ER medicine, and I felt like those were the guys that really understood when we told them the story. One friend said to me, “By the time they get to us, they’re either in bad shape or they’re better already.” A lot depends on what happens in the field.
Jennifer Suders: I’m even more vigilant about pool safety now. I want to make sure parents know that drowning doesn›t look like flailing theatrics. It can be soundless. Three adults were right next to this little boy and didn›t realize until they looked down and saw him.
If we hadn’t been there, I don’t know if anyone would’ve been able to step in. No one else was medically trained. But I think the message is — you don’t have to be. Anyone can take a CPR class.
When I told my parents, my dad said, “Oh my gosh, I would’ve laid right down there next to that kid and passed out.” Without any training, it’s petrifying to see something like that.
I think about how we could have stayed in the gym longer and been too late. Or we could have gotten on the elevator earlier and been gone. Two minutes, and it would’ve been a story we heard later, not one we were a part of. It feels like we were at a true crossroads in that moment where that boy could have lived or died. And the stars aligned perfectly.
We had no medicine, no monitors, nothing but our hands and our breaths. And we helped a family continue their vacation rather than plan a funeral.
Jennifer Suders, DO, is a nephrologist at West Virginia University Medicine Wheeling Clinic. Daniel Suders, DO, is a hospitalist at West Virginia University Medicine Reynolds Memorial Hospital.
A version of this article appeared on Medscape.com .
Tackling Lean Mass Loss When Weight Loss is Successful
DENVER — In addition to the established gastrointestinal side effects common with the highly effective anti-obesity drugs, there is growing discussion around their potential to contribute to the loss of lean mass, necessary to keep the metabolic engine running full-steam.
And although measures should be recommended to prevent those effects, experts also want to remind clinicians that the loss of lean mass is indeed expected with most weight loss interventions — when they’re successful.
“The bottom line is if you’re successful with weight loss, it’s a normal process that you’re going to lose some lean mass,” Angela Fitch, MD, associate director of the Massachusetts General Hospital Weight Center in Boston, said during a presentation on the issue at Obesity Medicine 2024.
“It’s what we would expect to see if you successfully lost weight with bariatric surgery or with an intense lifestyle intervention,” said Dr. Fitch, past president of the Obesity Medicine Association.
“The difference is, there haven’t been nearly as many people being successful with weight loss with those other interventions,” she noted. “But with the popularity of the glucagon-like peptide 1 (GLP-1) medications, people are hearing this for the first time and saying, ‘Oh my gosh, 30% of the weight loss is muscle mass — that’s horrible.’ “
, which have been reported in clinical trials of the GLP-1s semaglutide and the dual glucose-dependent insulinotropic polypeptide tirzepatide to range from about 25% to 40%, respectively, of weight loss.
“Excess adiposity is what makes us sick — not our weight,” Dr. Fitch underscored. “The amount of fat that people are losing [with anti-obesity medications] is far more beneficial than maybe the potential that they’ve lost a little bit of lean mass,” she said.
She cited research suggesting that significant weight loss from bariatric surgery is linked to increases in life expectancy, cardiovascular risk reduction, cancer risk reduction, and a wide array of other positive effects — despite the loss of lean mass that occurs with the weight loss.
Opportunity for Awareness
The increased attention on issues of body composition accompanying weight loss importantly provides clinicians the chance to underscore to patients the importance of offsetting the loss of lean mass through strength training, nutritional choices, and other measures.
However, patients should be prepared that achieving these goals can be more challenging than expected, said Dr. Fitch.
“It can be very hard to be in an energy deficit (due to a weight loss regimen) and gain muscle mass,” she said. “When athletes are trying to gain muscle mass, they’re increasing their intake to do so. It doesn’t come naturally in today’s world.”
Nevertheless, patients can be reassured that the losses can be reversed with some effort, Dr. Fitch noted.
She cautioned that for those who succeed in building or rebuilding lean mass, the evidence may be reflected on the scale, with numbers going up, not down — something they may not wish to see.
“Patients tend to freak out when they see the scale going up after losing all of that weight, but you can reassure them that it’s okay — this is healthier weight gain.”
Special Considerations in Older Patients
Efforts at staving off lean mass loss are particularly important in older patients, who are already most vulnerable to experiencing it naturally with age, even if not on a weight loss regimen.
But Dr. Fitch offered that age does not necessarily have to be a barrier in tackling those effects.
She described two cases of treating patients in their mid-70s, a male and female, with GLP-1s for obesity. Not only were they able to achieve substantial reductions in body mass index over nearly a year on treatment, but they were also able to avoid skeletal muscle mass loss during a period when it would have likely naturally occurred.
She noted the need to augment strength training with protein intake to help build muscle, citing recommendations including consumption of 1.4-2.0 g of protein per kg of body weight for building muscle and maintaining muscle mass.
Importantly, “make sure patients aren’t too appetite suppressed so they can keep up with their nutrition,” Dr. Fitch said.
A key condition to watch for in these patients is sarcopenia. Definitions of sarcopenia vary, but it is distinguished by low skeletal muscle mass and either low muscle strength — measured, for instance, with hand grip — or low muscle performance, such as reduced walking speed or muscle power, Dr. Fitch said.
In such cases, patients may need special considerations, including avoiding significant caloric deficits and whether the risks of medication outweigh the benefits.
‘Super-Responders’ and Other Lean Mass Loss Scenarios
Further addressing the issues of body composition and weight loss at the meeting, Robert F. Kushner, MD, professor of medicine and medicine education at Northwestern University in Chicago, noted that one area of concern regarding lean mass loss is “super-responders” — patients who have exceptionally high weight loss on GLP-1s.
“We are concerned about individuals who experience very high weight loss responses to medication, [specifically] 25% or more weight loss, as well as individuals at higher risk of losing lean body mass [muscle mass], specifically people in their 50s, 60s, and 70s,” Dr. Kushner told this news organization.
“Lifestyle counseling, particularly regarding safety and body composition, is recommended in these patients,” he said, adding that in managing these patients, “the approach is to use close patient monitoring, dose reduction if needed, and emphasizing a high-protein diet accompanied by aerobic and resistance physical activity.”
Potentially dramatic lean mass loss can occur in obesity whether or not patients are on obesity medications. As evidence of this, Dr. Kushner cited a subanalysis of the Look AHEAD trial of 1019 overweight or obese patients who had a mean age of 58 years at baseline. Patients were randomized to either a physical activity and reduced calorie intervention group or simply education.
Although the results showed that fat losses in the intervention group were generally regained over 8 years, a striking, steady decline was observed in lean mass in both the intervention and control groups, including men and women.
Dr. Fitch disclosed ties to Eli Lilly, Novo Nordisk, Currax, Vivus, SideKick Health, Jenny Craig, Carmot, and Seca. Dr. Kushner is on the advisory boards of Novo Nordisk, Weight Watchers, Lilly, Boehringer Ingelheim, and Altimmune.
A version of this article appeared on Medscape.com.
DENVER — In addition to the established gastrointestinal side effects common with the highly effective anti-obesity drugs, there is growing discussion around their potential to contribute to the loss of lean mass, necessary to keep the metabolic engine running full-steam.
And although measures should be recommended to prevent those effects, experts also want to remind clinicians that the loss of lean mass is indeed expected with most weight loss interventions — when they’re successful.
“The bottom line is if you’re successful with weight loss, it’s a normal process that you’re going to lose some lean mass,” Angela Fitch, MD, associate director of the Massachusetts General Hospital Weight Center in Boston, said during a presentation on the issue at Obesity Medicine 2024.
“It’s what we would expect to see if you successfully lost weight with bariatric surgery or with an intense lifestyle intervention,” said Dr. Fitch, past president of the Obesity Medicine Association.
“The difference is, there haven’t been nearly as many people being successful with weight loss with those other interventions,” she noted. “But with the popularity of the glucagon-like peptide 1 (GLP-1) medications, people are hearing this for the first time and saying, ‘Oh my gosh, 30% of the weight loss is muscle mass — that’s horrible.’ “
, which have been reported in clinical trials of the GLP-1s semaglutide and the dual glucose-dependent insulinotropic polypeptide tirzepatide to range from about 25% to 40%, respectively, of weight loss.
“Excess adiposity is what makes us sick — not our weight,” Dr. Fitch underscored. “The amount of fat that people are losing [with anti-obesity medications] is far more beneficial than maybe the potential that they’ve lost a little bit of lean mass,” she said.
She cited research suggesting that significant weight loss from bariatric surgery is linked to increases in life expectancy, cardiovascular risk reduction, cancer risk reduction, and a wide array of other positive effects — despite the loss of lean mass that occurs with the weight loss.
Opportunity for Awareness
The increased attention on issues of body composition accompanying weight loss importantly provides clinicians the chance to underscore to patients the importance of offsetting the loss of lean mass through strength training, nutritional choices, and other measures.
However, patients should be prepared that achieving these goals can be more challenging than expected, said Dr. Fitch.
“It can be very hard to be in an energy deficit (due to a weight loss regimen) and gain muscle mass,” she said. “When athletes are trying to gain muscle mass, they’re increasing their intake to do so. It doesn’t come naturally in today’s world.”
Nevertheless, patients can be reassured that the losses can be reversed with some effort, Dr. Fitch noted.
She cautioned that for those who succeed in building or rebuilding lean mass, the evidence may be reflected on the scale, with numbers going up, not down — something they may not wish to see.
“Patients tend to freak out when they see the scale going up after losing all of that weight, but you can reassure them that it’s okay — this is healthier weight gain.”
Special Considerations in Older Patients
Efforts at staving off lean mass loss are particularly important in older patients, who are already most vulnerable to experiencing it naturally with age, even if not on a weight loss regimen.
But Dr. Fitch offered that age does not necessarily have to be a barrier in tackling those effects.
She described two cases of treating patients in their mid-70s, a male and female, with GLP-1s for obesity. Not only were they able to achieve substantial reductions in body mass index over nearly a year on treatment, but they were also able to avoid skeletal muscle mass loss during a period when it would have likely naturally occurred.
She noted the need to augment strength training with protein intake to help build muscle, citing recommendations including consumption of 1.4-2.0 g of protein per kg of body weight for building muscle and maintaining muscle mass.
Importantly, “make sure patients aren’t too appetite suppressed so they can keep up with their nutrition,” Dr. Fitch said.
A key condition to watch for in these patients is sarcopenia. Definitions of sarcopenia vary, but it is distinguished by low skeletal muscle mass and either low muscle strength — measured, for instance, with hand grip — or low muscle performance, such as reduced walking speed or muscle power, Dr. Fitch said.
In such cases, patients may need special considerations, including avoiding significant caloric deficits and whether the risks of medication outweigh the benefits.
‘Super-Responders’ and Other Lean Mass Loss Scenarios
Further addressing the issues of body composition and weight loss at the meeting, Robert F. Kushner, MD, professor of medicine and medicine education at Northwestern University in Chicago, noted that one area of concern regarding lean mass loss is “super-responders” — patients who have exceptionally high weight loss on GLP-1s.
“We are concerned about individuals who experience very high weight loss responses to medication, [specifically] 25% or more weight loss, as well as individuals at higher risk of losing lean body mass [muscle mass], specifically people in their 50s, 60s, and 70s,” Dr. Kushner told this news organization.
“Lifestyle counseling, particularly regarding safety and body composition, is recommended in these patients,” he said, adding that in managing these patients, “the approach is to use close patient monitoring, dose reduction if needed, and emphasizing a high-protein diet accompanied by aerobic and resistance physical activity.”
Potentially dramatic lean mass loss can occur in obesity whether or not patients are on obesity medications. As evidence of this, Dr. Kushner cited a subanalysis of the Look AHEAD trial of 1019 overweight or obese patients who had a mean age of 58 years at baseline. Patients were randomized to either a physical activity and reduced calorie intervention group or simply education.
Although the results showed that fat losses in the intervention group were generally regained over 8 years, a striking, steady decline was observed in lean mass in both the intervention and control groups, including men and women.
Dr. Fitch disclosed ties to Eli Lilly, Novo Nordisk, Currax, Vivus, SideKick Health, Jenny Craig, Carmot, and Seca. Dr. Kushner is on the advisory boards of Novo Nordisk, Weight Watchers, Lilly, Boehringer Ingelheim, and Altimmune.
A version of this article appeared on Medscape.com.
DENVER — In addition to the established gastrointestinal side effects common with the highly effective anti-obesity drugs, there is growing discussion around their potential to contribute to the loss of lean mass, necessary to keep the metabolic engine running full-steam.
And although measures should be recommended to prevent those effects, experts also want to remind clinicians that the loss of lean mass is indeed expected with most weight loss interventions — when they’re successful.
“The bottom line is if you’re successful with weight loss, it’s a normal process that you’re going to lose some lean mass,” Angela Fitch, MD, associate director of the Massachusetts General Hospital Weight Center in Boston, said during a presentation on the issue at Obesity Medicine 2024.
“It’s what we would expect to see if you successfully lost weight with bariatric surgery or with an intense lifestyle intervention,” said Dr. Fitch, past president of the Obesity Medicine Association.
“The difference is, there haven’t been nearly as many people being successful with weight loss with those other interventions,” she noted. “But with the popularity of the glucagon-like peptide 1 (GLP-1) medications, people are hearing this for the first time and saying, ‘Oh my gosh, 30% of the weight loss is muscle mass — that’s horrible.’ “
, which have been reported in clinical trials of the GLP-1s semaglutide and the dual glucose-dependent insulinotropic polypeptide tirzepatide to range from about 25% to 40%, respectively, of weight loss.
“Excess adiposity is what makes us sick — not our weight,” Dr. Fitch underscored. “The amount of fat that people are losing [with anti-obesity medications] is far more beneficial than maybe the potential that they’ve lost a little bit of lean mass,” she said.
She cited research suggesting that significant weight loss from bariatric surgery is linked to increases in life expectancy, cardiovascular risk reduction, cancer risk reduction, and a wide array of other positive effects — despite the loss of lean mass that occurs with the weight loss.
Opportunity for Awareness
The increased attention on issues of body composition accompanying weight loss importantly provides clinicians the chance to underscore to patients the importance of offsetting the loss of lean mass through strength training, nutritional choices, and other measures.
However, patients should be prepared that achieving these goals can be more challenging than expected, said Dr. Fitch.
“It can be very hard to be in an energy deficit (due to a weight loss regimen) and gain muscle mass,” she said. “When athletes are trying to gain muscle mass, they’re increasing their intake to do so. It doesn’t come naturally in today’s world.”
Nevertheless, patients can be reassured that the losses can be reversed with some effort, Dr. Fitch noted.
She cautioned that for those who succeed in building or rebuilding lean mass, the evidence may be reflected on the scale, with numbers going up, not down — something they may not wish to see.
“Patients tend to freak out when they see the scale going up after losing all of that weight, but you can reassure them that it’s okay — this is healthier weight gain.”
Special Considerations in Older Patients
Efforts at staving off lean mass loss are particularly important in older patients, who are already most vulnerable to experiencing it naturally with age, even if not on a weight loss regimen.
But Dr. Fitch offered that age does not necessarily have to be a barrier in tackling those effects.
She described two cases of treating patients in their mid-70s, a male and female, with GLP-1s for obesity. Not only were they able to achieve substantial reductions in body mass index over nearly a year on treatment, but they were also able to avoid skeletal muscle mass loss during a period when it would have likely naturally occurred.
She noted the need to augment strength training with protein intake to help build muscle, citing recommendations including consumption of 1.4-2.0 g of protein per kg of body weight for building muscle and maintaining muscle mass.
Importantly, “make sure patients aren’t too appetite suppressed so they can keep up with their nutrition,” Dr. Fitch said.
A key condition to watch for in these patients is sarcopenia. Definitions of sarcopenia vary, but it is distinguished by low skeletal muscle mass and either low muscle strength — measured, for instance, with hand grip — or low muscle performance, such as reduced walking speed or muscle power, Dr. Fitch said.
In such cases, patients may need special considerations, including avoiding significant caloric deficits and whether the risks of medication outweigh the benefits.
‘Super-Responders’ and Other Lean Mass Loss Scenarios
Further addressing the issues of body composition and weight loss at the meeting, Robert F. Kushner, MD, professor of medicine and medicine education at Northwestern University in Chicago, noted that one area of concern regarding lean mass loss is “super-responders” — patients who have exceptionally high weight loss on GLP-1s.
“We are concerned about individuals who experience very high weight loss responses to medication, [specifically] 25% or more weight loss, as well as individuals at higher risk of losing lean body mass [muscle mass], specifically people in their 50s, 60s, and 70s,” Dr. Kushner told this news organization.
“Lifestyle counseling, particularly regarding safety and body composition, is recommended in these patients,” he said, adding that in managing these patients, “the approach is to use close patient monitoring, dose reduction if needed, and emphasizing a high-protein diet accompanied by aerobic and resistance physical activity.”
Potentially dramatic lean mass loss can occur in obesity whether or not patients are on obesity medications. As evidence of this, Dr. Kushner cited a subanalysis of the Look AHEAD trial of 1019 overweight or obese patients who had a mean age of 58 years at baseline. Patients were randomized to either a physical activity and reduced calorie intervention group or simply education.
Although the results showed that fat losses in the intervention group were generally regained over 8 years, a striking, steady decline was observed in lean mass in both the intervention and control groups, including men and women.
Dr. Fitch disclosed ties to Eli Lilly, Novo Nordisk, Currax, Vivus, SideKick Health, Jenny Craig, Carmot, and Seca. Dr. Kushner is on the advisory boards of Novo Nordisk, Weight Watchers, Lilly, Boehringer Ingelheim, and Altimmune.
A version of this article appeared on Medscape.com.
Internet Use Good for Mental Well-Being?
Contrary to previous research that suggests internet use can have a deleterious effect on mental health, a new study of more than 2 million individuals suggested it can actually enhance well-being.
Between 2006 and 2021, investigators studied more than 2 million people between the ages of 15 and 99 years in 168 countries, focusing on their psychological well-being and their use of the internet. Many of the included countries have rarely or never been studied in this connection.
“We were surprised to find a positive correlation between well-being and internet use across the majority of the thousands of models we used for our analysis,” lead author Matti Vuorre, PhD, of Tilburg University, Tilburg, the Netherlands, and a research associate at Oxford Internet Institute in England, said in a news release.
The study was published online on May 13 in Technology, Mind, and Behavior.
A Global Phenomenon
Coauthor Andrew K. Przybylski, PhD, professor of human behavior and technology at Oxford Internet Institute, explained the motive for conducting the study.
“Whilst internet technologies and their platforms and their potential psychological consequences remain debated, research to date has been inconclusive and of limited geographic and demographic scope,” he said.
He noted that the “overwhelming majority” of studies have focused on the Global North and on younger people and “ignoring the fact that the penetration of the internet has been, and continues to be, a global phenomenon.”
The researchers set out to address this gap by analyzing “how internet access, mobility internet access, and active internet use might predict psychological well-being on a global level across the life stages,” Dr. Przybylski continued. “To our knowledge, no other research has directly grappled with these issues and addressed the worldwide scope of the debate.”
To study internet use, the investigators analyzed data from the 2022 Gallup World Poll, a nationally representative survey of each country’s civilian, non-institutionalized adult population (ie, aged ≥ 15 years), conducted between 2002 and 2022. The poll assessed well-being using face-to-face, as well as phone interviews, conducted by local interviewers in the respondents’ native languages.
The total sample size included 2,414,295 adults drawn from 186 countries (53.1% women), drawn from countries that included those located in Latin America, Asia, and Africa.
The researchers examined eight indicators of well-being: life satisfaction, daily negative and positive experiences, two indices of social well-being, physical well-being, community well-being, and experiences of purpose.
Covariates included respondents’ income, education, work, relationship status, the ability to meet basic needs (food and shelter), and whether they reported having health problems.
Greater Life Satisfaction
The researchers conducted a “multiverse” of 33,792 types of analyses, researching the average differences in well-being between individuals who had access to mobile internet or had used the internet in the past 7 days.
They found that for the average country, those who had access to the internet reported approximately 0.08 units greater life satisfaction, positive experiences, and social life satisfaction and 0.06 units lower negative experience than those without access.
They also reported approximately 0.08 units greater experiences of purpose and 0.1 unit greater physical, 0.02 units greater community, and 0.08 units greater social well-being than individuals without access.
Being an active internet user was associated with a 0.03- to 0.08-unit increase in life satisfaction, positive experiences, social well-being, and physical well-being and a 0.04-unit decrease in negative experiences. Access to a smartphone predicted increases of 0.06 and 0.07 units.
Although the standard deviations (SDs) of well-being outcomes were small (eg, the median life satisfaction difference was 0.36 SDs between individuals who did and did not have access to the internet), they were “not negligible.”
In fact, when the researchers examined the associations’ robustness across all analyses, they found that 84.9% resulted in positive and statistically significant associations between internet connectivity and well-being.
Of the 4.9% of associations between internet use and community well-being that were negative, most were observed among young women between the ages of 15 and 24 years.
While the researchers did not identify this as a causal relationship, they noted that this finding is consistent with previous reports of increased cyberbullying and negative associations between social media use and depressive symptoms in young women.
“Overall, we found that average associations were consistent across internet adoption predictors and well-being outcomes, with those who had access to or actively used the internet reporting meaningfully greater well-being than those who did not,” Dr. Przybylski said.
The study’s limitations included comparing individuals with each other, given that there “are likely myriad other feature of the human condition that are associated with both uptake of internet technologies and well-being in such a manner that they might case spurious associations or mask true associations,” the authors noted.
Moreover, longitudinal studies tracking participants over time can provide more information about the “contexts of how and why an individual might be affected by internet technologies and platforms.” In addition, the self-reported measures of technology might be “lacking.”
Dr. Przybylski hopes that the findings will “bring some greater context to the screen time debate; however, further work is still needed in this important area.”
He urged platform providers “to share their detailed data on user behavior with social scientists working in this field for transparent and independent scientific enquiry, to enable a more comprehensive understanding of internet technologies in our daily lives.”
A Starting Point
In a separate news release, Kevin McConway, PhD, MBA, emeritus professor of applied statistics, The Open University, Milton Keynes, England, noted that there has been “endless debate and considerable speculation on the possible effects of internet use on well-being, in general across all ages, but more specifically in relation to children and young people.”
The current study “certainly extends the available information beyond simple speculation and beyond previous studies that used participants mostly in relatively rich Northern countries,” noted Dr. McConway, who was not involved in the study.
However, he cautioned, the study is only “a starting point, and if nothing else, it casts very serious doubt on the view, held by some people, that the internet is bad for us all.”
In particular, the observational nature of the study meant that the positive associations between internet use and measure of well-being could have been caused by other factors and are not causative.
“It’s important to understand that none of the well-being measures used in this research has been properly validated by experts in psychological measurement,” said Dr. McConway.
No source of study funding was listed. Dr. Przybylski’s research is supported by the Huo Family Foundation and the Economic and Social Research Council. In the preceding 5 years, Dr. Przybylski has worked on research grants provided by the John Fell Fund, The Diana Award, and the children’s charity Barnardo’s. These research grants were paid to Dr. Przybylski’s employer, the Oxford Internet Institute. During this period, Dr. Przybylski has engaged unpaid consultations with several organizations including UNICEF, the Organization for Economic Co-operation and Development, Meta Inc., UKIE, UK Research and Innovation, The UK’s DCMS, The Office of the UK’s Chief Medical Officer, the Office of the US Surgeon General, The UK’s Academy of Medical Sciences, and the UK Parliament. There were no financial products or benefits resulting from these consultations. Dr. Vuorre reported no relevant financial relationships. Neither author reported any conflicts of interest. Dr. McConway is a trustee of the Science Media Center. However, his remarks are in the capacity of an independent professional statistician.
A version of this article appeared on Medscape.com.
Contrary to previous research that suggests internet use can have a deleterious effect on mental health, a new study of more than 2 million individuals suggested it can actually enhance well-being.
Between 2006 and 2021, investigators studied more than 2 million people between the ages of 15 and 99 years in 168 countries, focusing on their psychological well-being and their use of the internet. Many of the included countries have rarely or never been studied in this connection.
“We were surprised to find a positive correlation between well-being and internet use across the majority of the thousands of models we used for our analysis,” lead author Matti Vuorre, PhD, of Tilburg University, Tilburg, the Netherlands, and a research associate at Oxford Internet Institute in England, said in a news release.
The study was published online on May 13 in Technology, Mind, and Behavior.
A Global Phenomenon
Coauthor Andrew K. Przybylski, PhD, professor of human behavior and technology at Oxford Internet Institute, explained the motive for conducting the study.
“Whilst internet technologies and their platforms and their potential psychological consequences remain debated, research to date has been inconclusive and of limited geographic and demographic scope,” he said.
He noted that the “overwhelming majority” of studies have focused on the Global North and on younger people and “ignoring the fact that the penetration of the internet has been, and continues to be, a global phenomenon.”
The researchers set out to address this gap by analyzing “how internet access, mobility internet access, and active internet use might predict psychological well-being on a global level across the life stages,” Dr. Przybylski continued. “To our knowledge, no other research has directly grappled with these issues and addressed the worldwide scope of the debate.”
To study internet use, the investigators analyzed data from the 2022 Gallup World Poll, a nationally representative survey of each country’s civilian, non-institutionalized adult population (ie, aged ≥ 15 years), conducted between 2002 and 2022. The poll assessed well-being using face-to-face, as well as phone interviews, conducted by local interviewers in the respondents’ native languages.
The total sample size included 2,414,295 adults drawn from 186 countries (53.1% women), drawn from countries that included those located in Latin America, Asia, and Africa.
The researchers examined eight indicators of well-being: life satisfaction, daily negative and positive experiences, two indices of social well-being, physical well-being, community well-being, and experiences of purpose.
Covariates included respondents’ income, education, work, relationship status, the ability to meet basic needs (food and shelter), and whether they reported having health problems.
Greater Life Satisfaction
The researchers conducted a “multiverse” of 33,792 types of analyses, researching the average differences in well-being between individuals who had access to mobile internet or had used the internet in the past 7 days.
They found that for the average country, those who had access to the internet reported approximately 0.08 units greater life satisfaction, positive experiences, and social life satisfaction and 0.06 units lower negative experience than those without access.
They also reported approximately 0.08 units greater experiences of purpose and 0.1 unit greater physical, 0.02 units greater community, and 0.08 units greater social well-being than individuals without access.
Being an active internet user was associated with a 0.03- to 0.08-unit increase in life satisfaction, positive experiences, social well-being, and physical well-being and a 0.04-unit decrease in negative experiences. Access to a smartphone predicted increases of 0.06 and 0.07 units.
Although the standard deviations (SDs) of well-being outcomes were small (eg, the median life satisfaction difference was 0.36 SDs between individuals who did and did not have access to the internet), they were “not negligible.”
In fact, when the researchers examined the associations’ robustness across all analyses, they found that 84.9% resulted in positive and statistically significant associations between internet connectivity and well-being.
Of the 4.9% of associations between internet use and community well-being that were negative, most were observed among young women between the ages of 15 and 24 years.
While the researchers did not identify this as a causal relationship, they noted that this finding is consistent with previous reports of increased cyberbullying and negative associations between social media use and depressive symptoms in young women.
“Overall, we found that average associations were consistent across internet adoption predictors and well-being outcomes, with those who had access to or actively used the internet reporting meaningfully greater well-being than those who did not,” Dr. Przybylski said.
The study’s limitations included comparing individuals with each other, given that there “are likely myriad other feature of the human condition that are associated with both uptake of internet technologies and well-being in such a manner that they might case spurious associations or mask true associations,” the authors noted.
Moreover, longitudinal studies tracking participants over time can provide more information about the “contexts of how and why an individual might be affected by internet technologies and platforms.” In addition, the self-reported measures of technology might be “lacking.”
Dr. Przybylski hopes that the findings will “bring some greater context to the screen time debate; however, further work is still needed in this important area.”
He urged platform providers “to share their detailed data on user behavior with social scientists working in this field for transparent and independent scientific enquiry, to enable a more comprehensive understanding of internet technologies in our daily lives.”
A Starting Point
In a separate news release, Kevin McConway, PhD, MBA, emeritus professor of applied statistics, The Open University, Milton Keynes, England, noted that there has been “endless debate and considerable speculation on the possible effects of internet use on well-being, in general across all ages, but more specifically in relation to children and young people.”
The current study “certainly extends the available information beyond simple speculation and beyond previous studies that used participants mostly in relatively rich Northern countries,” noted Dr. McConway, who was not involved in the study.
However, he cautioned, the study is only “a starting point, and if nothing else, it casts very serious doubt on the view, held by some people, that the internet is bad for us all.”
In particular, the observational nature of the study meant that the positive associations between internet use and measure of well-being could have been caused by other factors and are not causative.
“It’s important to understand that none of the well-being measures used in this research has been properly validated by experts in psychological measurement,” said Dr. McConway.
No source of study funding was listed. Dr. Przybylski’s research is supported by the Huo Family Foundation and the Economic and Social Research Council. In the preceding 5 years, Dr. Przybylski has worked on research grants provided by the John Fell Fund, The Diana Award, and the children’s charity Barnardo’s. These research grants were paid to Dr. Przybylski’s employer, the Oxford Internet Institute. During this period, Dr. Przybylski has engaged unpaid consultations with several organizations including UNICEF, the Organization for Economic Co-operation and Development, Meta Inc., UKIE, UK Research and Innovation, The UK’s DCMS, The Office of the UK’s Chief Medical Officer, the Office of the US Surgeon General, The UK’s Academy of Medical Sciences, and the UK Parliament. There were no financial products or benefits resulting from these consultations. Dr. Vuorre reported no relevant financial relationships. Neither author reported any conflicts of interest. Dr. McConway is a trustee of the Science Media Center. However, his remarks are in the capacity of an independent professional statistician.
A version of this article appeared on Medscape.com.
Contrary to previous research that suggests internet use can have a deleterious effect on mental health, a new study of more than 2 million individuals suggested it can actually enhance well-being.
Between 2006 and 2021, investigators studied more than 2 million people between the ages of 15 and 99 years in 168 countries, focusing on their psychological well-being and their use of the internet. Many of the included countries have rarely or never been studied in this connection.
“We were surprised to find a positive correlation between well-being and internet use across the majority of the thousands of models we used for our analysis,” lead author Matti Vuorre, PhD, of Tilburg University, Tilburg, the Netherlands, and a research associate at Oxford Internet Institute in England, said in a news release.
The study was published online on May 13 in Technology, Mind, and Behavior.
A Global Phenomenon
Coauthor Andrew K. Przybylski, PhD, professor of human behavior and technology at Oxford Internet Institute, explained the motive for conducting the study.
“Whilst internet technologies and their platforms and their potential psychological consequences remain debated, research to date has been inconclusive and of limited geographic and demographic scope,” he said.
He noted that the “overwhelming majority” of studies have focused on the Global North and on younger people and “ignoring the fact that the penetration of the internet has been, and continues to be, a global phenomenon.”
The researchers set out to address this gap by analyzing “how internet access, mobility internet access, and active internet use might predict psychological well-being on a global level across the life stages,” Dr. Przybylski continued. “To our knowledge, no other research has directly grappled with these issues and addressed the worldwide scope of the debate.”
To study internet use, the investigators analyzed data from the 2022 Gallup World Poll, a nationally representative survey of each country’s civilian, non-institutionalized adult population (ie, aged ≥ 15 years), conducted between 2002 and 2022. The poll assessed well-being using face-to-face, as well as phone interviews, conducted by local interviewers in the respondents’ native languages.
The total sample size included 2,414,295 adults drawn from 186 countries (53.1% women), drawn from countries that included those located in Latin America, Asia, and Africa.
The researchers examined eight indicators of well-being: life satisfaction, daily negative and positive experiences, two indices of social well-being, physical well-being, community well-being, and experiences of purpose.
Covariates included respondents’ income, education, work, relationship status, the ability to meet basic needs (food and shelter), and whether they reported having health problems.
Greater Life Satisfaction
The researchers conducted a “multiverse” of 33,792 types of analyses, researching the average differences in well-being between individuals who had access to mobile internet or had used the internet in the past 7 days.
They found that for the average country, those who had access to the internet reported approximately 0.08 units greater life satisfaction, positive experiences, and social life satisfaction and 0.06 units lower negative experience than those without access.
They also reported approximately 0.08 units greater experiences of purpose and 0.1 unit greater physical, 0.02 units greater community, and 0.08 units greater social well-being than individuals without access.
Being an active internet user was associated with a 0.03- to 0.08-unit increase in life satisfaction, positive experiences, social well-being, and physical well-being and a 0.04-unit decrease in negative experiences. Access to a smartphone predicted increases of 0.06 and 0.07 units.
Although the standard deviations (SDs) of well-being outcomes were small (eg, the median life satisfaction difference was 0.36 SDs between individuals who did and did not have access to the internet), they were “not negligible.”
In fact, when the researchers examined the associations’ robustness across all analyses, they found that 84.9% resulted in positive and statistically significant associations between internet connectivity and well-being.
Of the 4.9% of associations between internet use and community well-being that were negative, most were observed among young women between the ages of 15 and 24 years.
While the researchers did not identify this as a causal relationship, they noted that this finding is consistent with previous reports of increased cyberbullying and negative associations between social media use and depressive symptoms in young women.
“Overall, we found that average associations were consistent across internet adoption predictors and well-being outcomes, with those who had access to or actively used the internet reporting meaningfully greater well-being than those who did not,” Dr. Przybylski said.
The study’s limitations included comparing individuals with each other, given that there “are likely myriad other feature of the human condition that are associated with both uptake of internet technologies and well-being in such a manner that they might case spurious associations or mask true associations,” the authors noted.
Moreover, longitudinal studies tracking participants over time can provide more information about the “contexts of how and why an individual might be affected by internet technologies and platforms.” In addition, the self-reported measures of technology might be “lacking.”
Dr. Przybylski hopes that the findings will “bring some greater context to the screen time debate; however, further work is still needed in this important area.”
He urged platform providers “to share their detailed data on user behavior with social scientists working in this field for transparent and independent scientific enquiry, to enable a more comprehensive understanding of internet technologies in our daily lives.”
A Starting Point
In a separate news release, Kevin McConway, PhD, MBA, emeritus professor of applied statistics, The Open University, Milton Keynes, England, noted that there has been “endless debate and considerable speculation on the possible effects of internet use on well-being, in general across all ages, but more specifically in relation to children and young people.”
The current study “certainly extends the available information beyond simple speculation and beyond previous studies that used participants mostly in relatively rich Northern countries,” noted Dr. McConway, who was not involved in the study.
However, he cautioned, the study is only “a starting point, and if nothing else, it casts very serious doubt on the view, held by some people, that the internet is bad for us all.”
In particular, the observational nature of the study meant that the positive associations between internet use and measure of well-being could have been caused by other factors and are not causative.
“It’s important to understand that none of the well-being measures used in this research has been properly validated by experts in psychological measurement,” said Dr. McConway.
No source of study funding was listed. Dr. Przybylski’s research is supported by the Huo Family Foundation and the Economic and Social Research Council. In the preceding 5 years, Dr. Przybylski has worked on research grants provided by the John Fell Fund, The Diana Award, and the children’s charity Barnardo’s. These research grants were paid to Dr. Przybylski’s employer, the Oxford Internet Institute. During this period, Dr. Przybylski has engaged unpaid consultations with several organizations including UNICEF, the Organization for Economic Co-operation and Development, Meta Inc., UKIE, UK Research and Innovation, The UK’s DCMS, The Office of the UK’s Chief Medical Officer, the Office of the US Surgeon General, The UK’s Academy of Medical Sciences, and the UK Parliament. There were no financial products or benefits resulting from these consultations. Dr. Vuorre reported no relevant financial relationships. Neither author reported any conflicts of interest. Dr. McConway is a trustee of the Science Media Center. However, his remarks are in the capacity of an independent professional statistician.
A version of this article appeared on Medscape.com.