User login
Recalcitrant Folliculitis Decalvans Treatment Outcomes With Biologics and Small Molecule Inhibitors
Folliculitis decalvans (FD) is classified as a rare primary neutrophilic cicatricial alopecia occurring predominantly in middle-aged adults. Although the true etiology is still unknown, the pathogenesis behind the inflammatory follicular lesions stems from possible Staphylococcus aureus infection and an impaired host immune system in response to released superantigens. 1 The clinical severity of this inflammatory scalp disorder can range from mild to severe and debilitating. Multiple treatment regimens have been developed with the goal of maintaining full remission. We provide a summary of tumor necrosis factor (TNF) inhibitors, Janus kinase (JAK) inhibitors, phosphodiesterase 4 (PDE4) inhibitors, and monoclonal antibodies being utilized for patients with therapy-recalcitrant FD.
Methods
We conducted a PubMed, Medline, and Google Scholar search for the terms refractory FD, recalcitrant FD, or therapy-resistant FD to identify articles published in English from 1998 to 2022. Articles that reported recalcitrant cases and subsequent therapy with TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies were included. Articles were excluded if recalcitrant cases were not clearly defined. Remission was defined as no recurrence in lesions or pustules or as a reduction in the inflammatory process with stabilization upon continuation or discontinuation of the therapy regimen. Two reviewers (T.F. and K.U.) independently searched for and screened each report.
Results
Treatment of recalcitrant FD with biologics or small molecule inhibitors was discussed in 9 studies with a combined total of 35 patients.2-10 The treatment regimens included TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies (Table).
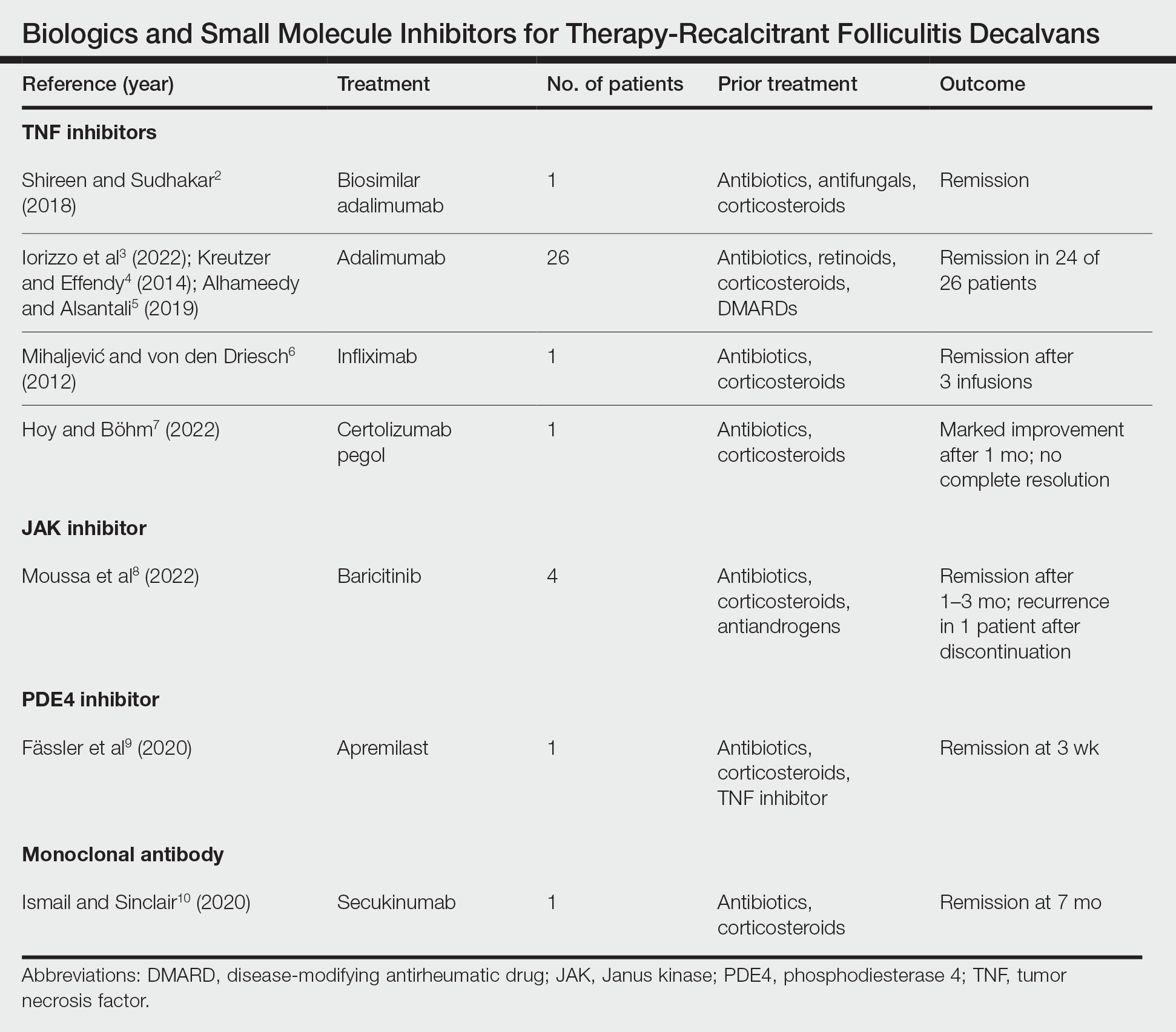
The TNF inhibitors were utilized in 6 reports with a combined total of 29 patients. Treatments included adalimumab or biosimilar adalimumab (27/29 patients), infliximab (1/29 patients), and certolizumab pegol (1/29 patients). Remission was reported in 26 of 29 cases. There were 2 nonresponders to adalimumab and marked improvement with certolizumab pegol without complete resolution. The use of the JAK inhibitor baricitinib in 4 patients resulted in remission. In all 4 patients, baricitinib was used with concurrent treatments, and remission was achieved in an average of 2.25 months. The use of a PDE4 inhibitor, apremilast, was reported in 1 case; remission was achieved in 3 weeks. Secukinumab, a monoclonal antibody that targets IL-17, was utilized in 1 patient. Marked improvement was seen after 2 months, with complete remission in 7 months.
Comment
Traditional treatment regimens for FD most often include a combination of topical and oral antibiotics; isotretinoin; and oral, topical, or intralesional corticosteroids. In the past, interventions typically were suppressive as opposed to curative; however, recent treatment advancements have shown promise in achieving lasting remission.
Most reports targeting treatment-resistant FD involved the use of TNF inhibitors, including adalimumab, biosimilar adalimumab, infliximab, and certolizumab pegol. Adalimumab was the most frequently used TNF inhibitor, with 24 of 26 treated patients achieving remission. Adalimumab may have been used the most in the treatment of FD because TNF is pronounced in other neutrophilic dermatoses that have been successfully treated with TNF inhibitors. It has been reported that adalimumab needs to be continued, as stoppage or interruption led to relapse.3
Although there are few reports of the use of JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies for FD, these treatment modalities show promise, as their use led to marked improvement or lasting remission with ongoing treatment. The use of the PDE4 inhibitor apremilast displayed the most rapid improvement of any of the reviewed treatments, with remission achieved in just 3 weeks.9 The rapid success of apremilast may be attributed to the inhibitory effect on neutrophils.
Miguel-Gómez et al11 provided a therapeutic protocol for FD based on the severity of disease (N=60). The protocol included rifampicin plus clindamycin for the treatment of severe disease, as 90.5% (19/21) of resistant cases showed clinical response, with remission of 5 months’ duration. Although this may be acceptable for some patients, others may require an alternative approach. Tietze et al12 showed that rifampicin and clindamycin had the lowest success rate for long-term remission, with 8 of 10 patients relapsing within 2 to 4 months. In addition, the emergence of antimicrobial resistance remains a major concern in the treatment of FD. Upon the review of the most recent reports of successful treatment of therapy-resistant FD, biologics and small molecule inhibitors have shown remission extending through a 12-month follow-up period. We suggest considering the addition of biologics and small molecule inhibitors to the treatment protocol for severe or resistant disease.
Limitations—In the articles reviewed, the definition of remission was inconsistent among authors—some characterized it as no recurrence in lesions or pustules and some as a reduction in the inflammatory process. True duration of remission was difficult to assess from case reports, as follow-up periods varied prior to publication. The studies included in this review consisted mainly of small sample sizes owing to the rarity of FD, and consequently, strength of evidence is lacking. Inherent to the nature of systematic reviews, publication bias may have occurred. Lastly, several studies were impacted by difficulty in obtaining optimal treatment due to financial hardship, and regimens were adjusted accordingly.
Conclusion
The relapsing nature of FD leads to frustration and poor quality of life for patients. There is a paucity of data to guide treatment when FD remains recalcitrant to traditional therapy. Therapies such as TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies have shown success in the treatment of this often difficult-to-treat disease. Small sample sizes in reports discussing treatment for resistant cases as well as conflicting results make it challenging to draw conclusions about treatment efficacy. Larger studies are needed to understand the long-term outcomes of treatment options. Regardless, disease severity, patient history, patient preferences, and treatment goals can guide the selection of therapeutic options.
- Otberg N, Kang H, Alzolibani AA, et al. Folliculitis decalvans. Dermatol Ther. 2008;21:238-244. doi:10.1111/j.1529-8019.2008.00204.x
- Shireen F, Sudhakar A. A case of isotretinoin therapy-refractory folliculitis decalvans treated successfully with biosimilar adalimumab (Exemptia). Int J Trichology. 2018;10:240-241.
- Iorizzo M, Starace M, Vano-Galvan S, et al. Refractory folliculitis decalvans treated with adalimumab: a case series of 23 patients. J Am Acad Dermatol. 2022;87:666-669. doi:10.1016/j.jaad.2022.02.044
- Kreutzer K, Effendy I. Therapy-resistant folliculitis decalvans and lichen planopilaris successfully treated with adalimumab. J Dtsch Dermatol Ges. 2014;12:74-76. doi:10.1111/ddg.12224
- Alhameedy MM, Alsantali AM. Therapy-recalcitrant folliculitis decalvans controlled successfully with adalimumab. Int J Trichology. 2019;11:241-243. doi:10.4103/ijt.ijt_92_19
- Mihaljevic´ N, von den Driesch P. Successful use of infliximab in a patient with recalcitrant folliculitis decalvans. J Dtsch Dermatol Ges. 2012;10:589-590. doi:10.1111/j.1610-0387.2012.07972.x
- Hoy M, Böhm M. Therapy-refractory folliculitis decalvans treated with certolizumab pegol. Int J Dermatol. 2022;61:e26-e28. doi:10.1111/ijd.15914
- Moussa A, Asfour L, Eisman S, et al. Successful treatment of folliculitis decalvans with baricitinib: a case series. Australas J Dermatol. 2022;63:279-281. doi:10.1111/ajd.13786
- Fässler M, Radonjic-Hoesli S, Feldmeyer L, et al. Successful treatment of refractory folliculitis decalvans with apremilast. JAAD Case Rep. 2020;6:1079-1081. doi:10.1016/j.jdcr.2020.08.019
- Ismail FF, Sinclair R. Successful treatment of refractory folliculitis decalvans with secukinumab. Australas J Dermatol. 2020;61:165-166. doi:10.1111/ajd.13190
- Miguel-Gómez L, Rodrigues-Barata AR, Molina-Ruiz A, et al. Folliculitis decalvans: effectiveness of therapies and prognostic factors in a multicenter series of 60 patients with long-term follow-up. J Am Acad Dermatol. 2018;79:878-883. doi:10.1016/j.jaad.2018.05.1240
- Tietze JK, Heppt MV, von Preußen A, et al. Oral isotretinoin as the most effective treatment in folliculitis decalvans: a retrospective comparison of different treatment regimens in 28 patients. J Eur Acad Dermatol Venereol. 2015;29:1816-1821. doi:10.1111/jdv.13052
Folliculitis decalvans (FD) is classified as a rare primary neutrophilic cicatricial alopecia occurring predominantly in middle-aged adults. Although the true etiology is still unknown, the pathogenesis behind the inflammatory follicular lesions stems from possible Staphylococcus aureus infection and an impaired host immune system in response to released superantigens. 1 The clinical severity of this inflammatory scalp disorder can range from mild to severe and debilitating. Multiple treatment regimens have been developed with the goal of maintaining full remission. We provide a summary of tumor necrosis factor (TNF) inhibitors, Janus kinase (JAK) inhibitors, phosphodiesterase 4 (PDE4) inhibitors, and monoclonal antibodies being utilized for patients with therapy-recalcitrant FD.
Methods
We conducted a PubMed, Medline, and Google Scholar search for the terms refractory FD, recalcitrant FD, or therapy-resistant FD to identify articles published in English from 1998 to 2022. Articles that reported recalcitrant cases and subsequent therapy with TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies were included. Articles were excluded if recalcitrant cases were not clearly defined. Remission was defined as no recurrence in lesions or pustules or as a reduction in the inflammatory process with stabilization upon continuation or discontinuation of the therapy regimen. Two reviewers (T.F. and K.U.) independently searched for and screened each report.
Results
Treatment of recalcitrant FD with biologics or small molecule inhibitors was discussed in 9 studies with a combined total of 35 patients.2-10 The treatment regimens included TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies (Table).
The TNF inhibitors were utilized in 6 reports with a combined total of 29 patients. Treatments included adalimumab or biosimilar adalimumab (27/29 patients), infliximab (1/29 patients), and certolizumab pegol (1/29 patients). Remission was reported in 26 of 29 cases. There were 2 nonresponders to adalimumab and marked improvement with certolizumab pegol without complete resolution. The use of the JAK inhibitor baricitinib in 4 patients resulted in remission. In all 4 patients, baricitinib was used with concurrent treatments, and remission was achieved in an average of 2.25 months. The use of a PDE4 inhibitor, apremilast, was reported in 1 case; remission was achieved in 3 weeks. Secukinumab, a monoclonal antibody that targets IL-17, was utilized in 1 patient. Marked improvement was seen after 2 months, with complete remission in 7 months.
Comment
Traditional treatment regimens for FD most often include a combination of topical and oral antibiotics; isotretinoin; and oral, topical, or intralesional corticosteroids. In the past, interventions typically were suppressive as opposed to curative; however, recent treatment advancements have shown promise in achieving lasting remission.
Most reports targeting treatment-resistant FD involved the use of TNF inhibitors, including adalimumab, biosimilar adalimumab, infliximab, and certolizumab pegol. Adalimumab was the most frequently used TNF inhibitor, with 24 of 26 treated patients achieving remission. Adalimumab may have been used the most in the treatment of FD because TNF is pronounced in other neutrophilic dermatoses that have been successfully treated with TNF inhibitors. It has been reported that adalimumab needs to be continued, as stoppage or interruption led to relapse.3
Although there are few reports of the use of JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies for FD, these treatment modalities show promise, as their use led to marked improvement or lasting remission with ongoing treatment. The use of the PDE4 inhibitor apremilast displayed the most rapid improvement of any of the reviewed treatments, with remission achieved in just 3 weeks.9 The rapid success of apremilast may be attributed to the inhibitory effect on neutrophils.
Miguel-Gómez et al11 provided a therapeutic protocol for FD based on the severity of disease (N=60). The protocol included rifampicin plus clindamycin for the treatment of severe disease, as 90.5% (19/21) of resistant cases showed clinical response, with remission of 5 months’ duration. Although this may be acceptable for some patients, others may require an alternative approach. Tietze et al12 showed that rifampicin and clindamycin had the lowest success rate for long-term remission, with 8 of 10 patients relapsing within 2 to 4 months. In addition, the emergence of antimicrobial resistance remains a major concern in the treatment of FD. Upon the review of the most recent reports of successful treatment of therapy-resistant FD, biologics and small molecule inhibitors have shown remission extending through a 12-month follow-up period. We suggest considering the addition of biologics and small molecule inhibitors to the treatment protocol for severe or resistant disease.
Limitations—In the articles reviewed, the definition of remission was inconsistent among authors—some characterized it as no recurrence in lesions or pustules and some as a reduction in the inflammatory process. True duration of remission was difficult to assess from case reports, as follow-up periods varied prior to publication. The studies included in this review consisted mainly of small sample sizes owing to the rarity of FD, and consequently, strength of evidence is lacking. Inherent to the nature of systematic reviews, publication bias may have occurred. Lastly, several studies were impacted by difficulty in obtaining optimal treatment due to financial hardship, and regimens were adjusted accordingly.
Conclusion
The relapsing nature of FD leads to frustration and poor quality of life for patients. There is a paucity of data to guide treatment when FD remains recalcitrant to traditional therapy. Therapies such as TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies have shown success in the treatment of this often difficult-to-treat disease. Small sample sizes in reports discussing treatment for resistant cases as well as conflicting results make it challenging to draw conclusions about treatment efficacy. Larger studies are needed to understand the long-term outcomes of treatment options. Regardless, disease severity, patient history, patient preferences, and treatment goals can guide the selection of therapeutic options.
Folliculitis decalvans (FD) is classified as a rare primary neutrophilic cicatricial alopecia occurring predominantly in middle-aged adults. Although the true etiology is still unknown, the pathogenesis behind the inflammatory follicular lesions stems from possible Staphylococcus aureus infection and an impaired host immune system in response to released superantigens. 1 The clinical severity of this inflammatory scalp disorder can range from mild to severe and debilitating. Multiple treatment regimens have been developed with the goal of maintaining full remission. We provide a summary of tumor necrosis factor (TNF) inhibitors, Janus kinase (JAK) inhibitors, phosphodiesterase 4 (PDE4) inhibitors, and monoclonal antibodies being utilized for patients with therapy-recalcitrant FD.
Methods
We conducted a PubMed, Medline, and Google Scholar search for the terms refractory FD, recalcitrant FD, or therapy-resistant FD to identify articles published in English from 1998 to 2022. Articles that reported recalcitrant cases and subsequent therapy with TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies were included. Articles were excluded if recalcitrant cases were not clearly defined. Remission was defined as no recurrence in lesions or pustules or as a reduction in the inflammatory process with stabilization upon continuation or discontinuation of the therapy regimen. Two reviewers (T.F. and K.U.) independently searched for and screened each report.
Results
Treatment of recalcitrant FD with biologics or small molecule inhibitors was discussed in 9 studies with a combined total of 35 patients.2-10 The treatment regimens included TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies (Table).
The TNF inhibitors were utilized in 6 reports with a combined total of 29 patients. Treatments included adalimumab or biosimilar adalimumab (27/29 patients), infliximab (1/29 patients), and certolizumab pegol (1/29 patients). Remission was reported in 26 of 29 cases. There were 2 nonresponders to adalimumab and marked improvement with certolizumab pegol without complete resolution. The use of the JAK inhibitor baricitinib in 4 patients resulted in remission. In all 4 patients, baricitinib was used with concurrent treatments, and remission was achieved in an average of 2.25 months. The use of a PDE4 inhibitor, apremilast, was reported in 1 case; remission was achieved in 3 weeks. Secukinumab, a monoclonal antibody that targets IL-17, was utilized in 1 patient. Marked improvement was seen after 2 months, with complete remission in 7 months.
Comment
Traditional treatment regimens for FD most often include a combination of topical and oral antibiotics; isotretinoin; and oral, topical, or intralesional corticosteroids. In the past, interventions typically were suppressive as opposed to curative; however, recent treatment advancements have shown promise in achieving lasting remission.
Most reports targeting treatment-resistant FD involved the use of TNF inhibitors, including adalimumab, biosimilar adalimumab, infliximab, and certolizumab pegol. Adalimumab was the most frequently used TNF inhibitor, with 24 of 26 treated patients achieving remission. Adalimumab may have been used the most in the treatment of FD because TNF is pronounced in other neutrophilic dermatoses that have been successfully treated with TNF inhibitors. It has been reported that adalimumab needs to be continued, as stoppage or interruption led to relapse.3
Although there are few reports of the use of JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies for FD, these treatment modalities show promise, as their use led to marked improvement or lasting remission with ongoing treatment. The use of the PDE4 inhibitor apremilast displayed the most rapid improvement of any of the reviewed treatments, with remission achieved in just 3 weeks.9 The rapid success of apremilast may be attributed to the inhibitory effect on neutrophils.
Miguel-Gómez et al11 provided a therapeutic protocol for FD based on the severity of disease (N=60). The protocol included rifampicin plus clindamycin for the treatment of severe disease, as 90.5% (19/21) of resistant cases showed clinical response, with remission of 5 months’ duration. Although this may be acceptable for some patients, others may require an alternative approach. Tietze et al12 showed that rifampicin and clindamycin had the lowest success rate for long-term remission, with 8 of 10 patients relapsing within 2 to 4 months. In addition, the emergence of antimicrobial resistance remains a major concern in the treatment of FD. Upon the review of the most recent reports of successful treatment of therapy-resistant FD, biologics and small molecule inhibitors have shown remission extending through a 12-month follow-up period. We suggest considering the addition of biologics and small molecule inhibitors to the treatment protocol for severe or resistant disease.
Limitations—In the articles reviewed, the definition of remission was inconsistent among authors—some characterized it as no recurrence in lesions or pustules and some as a reduction in the inflammatory process. True duration of remission was difficult to assess from case reports, as follow-up periods varied prior to publication. The studies included in this review consisted mainly of small sample sizes owing to the rarity of FD, and consequently, strength of evidence is lacking. Inherent to the nature of systematic reviews, publication bias may have occurred. Lastly, several studies were impacted by difficulty in obtaining optimal treatment due to financial hardship, and regimens were adjusted accordingly.
Conclusion
The relapsing nature of FD leads to frustration and poor quality of life for patients. There is a paucity of data to guide treatment when FD remains recalcitrant to traditional therapy. Therapies such as TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies have shown success in the treatment of this often difficult-to-treat disease. Small sample sizes in reports discussing treatment for resistant cases as well as conflicting results make it challenging to draw conclusions about treatment efficacy. Larger studies are needed to understand the long-term outcomes of treatment options. Regardless, disease severity, patient history, patient preferences, and treatment goals can guide the selection of therapeutic options.
- Otberg N, Kang H, Alzolibani AA, et al. Folliculitis decalvans. Dermatol Ther. 2008;21:238-244. doi:10.1111/j.1529-8019.2008.00204.x
- Shireen F, Sudhakar A. A case of isotretinoin therapy-refractory folliculitis decalvans treated successfully with biosimilar adalimumab (Exemptia). Int J Trichology. 2018;10:240-241.
- Iorizzo M, Starace M, Vano-Galvan S, et al. Refractory folliculitis decalvans treated with adalimumab: a case series of 23 patients. J Am Acad Dermatol. 2022;87:666-669. doi:10.1016/j.jaad.2022.02.044
- Kreutzer K, Effendy I. Therapy-resistant folliculitis decalvans and lichen planopilaris successfully treated with adalimumab. J Dtsch Dermatol Ges. 2014;12:74-76. doi:10.1111/ddg.12224
- Alhameedy MM, Alsantali AM. Therapy-recalcitrant folliculitis decalvans controlled successfully with adalimumab. Int J Trichology. 2019;11:241-243. doi:10.4103/ijt.ijt_92_19
- Mihaljevic´ N, von den Driesch P. Successful use of infliximab in a patient with recalcitrant folliculitis decalvans. J Dtsch Dermatol Ges. 2012;10:589-590. doi:10.1111/j.1610-0387.2012.07972.x
- Hoy M, Böhm M. Therapy-refractory folliculitis decalvans treated with certolizumab pegol. Int J Dermatol. 2022;61:e26-e28. doi:10.1111/ijd.15914
- Moussa A, Asfour L, Eisman S, et al. Successful treatment of folliculitis decalvans with baricitinib: a case series. Australas J Dermatol. 2022;63:279-281. doi:10.1111/ajd.13786
- Fässler M, Radonjic-Hoesli S, Feldmeyer L, et al. Successful treatment of refractory folliculitis decalvans with apremilast. JAAD Case Rep. 2020;6:1079-1081. doi:10.1016/j.jdcr.2020.08.019
- Ismail FF, Sinclair R. Successful treatment of refractory folliculitis decalvans with secukinumab. Australas J Dermatol. 2020;61:165-166. doi:10.1111/ajd.13190
- Miguel-Gómez L, Rodrigues-Barata AR, Molina-Ruiz A, et al. Folliculitis decalvans: effectiveness of therapies and prognostic factors in a multicenter series of 60 patients with long-term follow-up. J Am Acad Dermatol. 2018;79:878-883. doi:10.1016/j.jaad.2018.05.1240
- Tietze JK, Heppt MV, von Preußen A, et al. Oral isotretinoin as the most effective treatment in folliculitis decalvans: a retrospective comparison of different treatment regimens in 28 patients. J Eur Acad Dermatol Venereol. 2015;29:1816-1821. doi:10.1111/jdv.13052
- Otberg N, Kang H, Alzolibani AA, et al. Folliculitis decalvans. Dermatol Ther. 2008;21:238-244. doi:10.1111/j.1529-8019.2008.00204.x
- Shireen F, Sudhakar A. A case of isotretinoin therapy-refractory folliculitis decalvans treated successfully with biosimilar adalimumab (Exemptia). Int J Trichology. 2018;10:240-241.
- Iorizzo M, Starace M, Vano-Galvan S, et al. Refractory folliculitis decalvans treated with adalimumab: a case series of 23 patients. J Am Acad Dermatol. 2022;87:666-669. doi:10.1016/j.jaad.2022.02.044
- Kreutzer K, Effendy I. Therapy-resistant folliculitis decalvans and lichen planopilaris successfully treated with adalimumab. J Dtsch Dermatol Ges. 2014;12:74-76. doi:10.1111/ddg.12224
- Alhameedy MM, Alsantali AM. Therapy-recalcitrant folliculitis decalvans controlled successfully with adalimumab. Int J Trichology. 2019;11:241-243. doi:10.4103/ijt.ijt_92_19
- Mihaljevic´ N, von den Driesch P. Successful use of infliximab in a patient with recalcitrant folliculitis decalvans. J Dtsch Dermatol Ges. 2012;10:589-590. doi:10.1111/j.1610-0387.2012.07972.x
- Hoy M, Böhm M. Therapy-refractory folliculitis decalvans treated with certolizumab pegol. Int J Dermatol. 2022;61:e26-e28. doi:10.1111/ijd.15914
- Moussa A, Asfour L, Eisman S, et al. Successful treatment of folliculitis decalvans with baricitinib: a case series. Australas J Dermatol. 2022;63:279-281. doi:10.1111/ajd.13786
- Fässler M, Radonjic-Hoesli S, Feldmeyer L, et al. Successful treatment of refractory folliculitis decalvans with apremilast. JAAD Case Rep. 2020;6:1079-1081. doi:10.1016/j.jdcr.2020.08.019
- Ismail FF, Sinclair R. Successful treatment of refractory folliculitis decalvans with secukinumab. Australas J Dermatol. 2020;61:165-166. doi:10.1111/ajd.13190
- Miguel-Gómez L, Rodrigues-Barata AR, Molina-Ruiz A, et al. Folliculitis decalvans: effectiveness of therapies and prognostic factors in a multicenter series of 60 patients with long-term follow-up. J Am Acad Dermatol. 2018;79:878-883. doi:10.1016/j.jaad.2018.05.1240
- Tietze JK, Heppt MV, von Preußen A, et al. Oral isotretinoin as the most effective treatment in folliculitis decalvans: a retrospective comparison of different treatment regimens in 28 patients. J Eur Acad Dermatol Venereol. 2015;29:1816-1821. doi:10.1111/jdv.13052
Practice Points
- Tumor necrosis factor inhibitors, Janus kinase inhibitors, phosphodiesterase 4 inhibitors, and monoclonal antibodies have shown success in the treatment of folliculitis decalvans resistant to traditional therapies.
- The true etiology of folliculitis decalvans is still unknown, but possible factors include Staphylococcus aureus infection and an impaired host immune system, which may benefit from treatment with biologics and small molecule inhibitors.
Complementing, not competing
As we enter summer, it’s hard to believe that we’re halfway through my presidency. Registration for CHEST 2024 (October 6 to 9) is now open, and October will be here before we know it.
I’m happy to share that we received more than 4,000 abstract and case report submissions from clinicians at all stages of their careers, and, for the first year, we had a dedicated category to solicit submissions from physician assistants (PAs), nurse practitioners (NPs), respiratory therapists, and other members of the broader health care team.

In both my practice and my time as CHEST President, I’ve been reflecting on the benefits of the multidisciplinary team—especially in the ICU. Because this is a setting that relies heavily on a team aspect, every member of the care team is a great asset.
CHEST is working to ensure that all integral members of our professional health care teams have the resources they need to best serve our patients. We encourage advanced practice providers (APPs) to apply to serve on our committees during the current open call, and we recently launched a dedicated APP Intersection column, called APP Intersection, within this publication to elevate diverse perspectives. I anticipate more is on the horizon.
In my experience, I have seen tremendous success in partnering with and complementing each other, rather than competing for space when caring for a patient. Each and every one of us shares the same goal of providing the best patient care, and we each bring our own strengths.
Our future is ripe with opportunities to better serve the whole care team—MDs, PAs, NPs, and more—and it starts with recognizing the needs of everyone within the organization. To help CHEST better serve our members, I encourage you to take a short survey about your professional hurdles.
And please, do not hesitate to contact me ([email protected]) with suggestions or just to introduce yourself.
All the best,
Jack
As we enter summer, it’s hard to believe that we’re halfway through my presidency. Registration for CHEST 2024 (October 6 to 9) is now open, and October will be here before we know it.
I’m happy to share that we received more than 4,000 abstract and case report submissions from clinicians at all stages of their careers, and, for the first year, we had a dedicated category to solicit submissions from physician assistants (PAs), nurse practitioners (NPs), respiratory therapists, and other members of the broader health care team.
In both my practice and my time as CHEST President, I’ve been reflecting on the benefits of the multidisciplinary team—especially in the ICU. Because this is a setting that relies heavily on a team aspect, every member of the care team is a great asset.
CHEST is working to ensure that all integral members of our professional health care teams have the resources they need to best serve our patients. We encourage advanced practice providers (APPs) to apply to serve on our committees during the current open call, and we recently launched a dedicated APP Intersection column, called APP Intersection, within this publication to elevate diverse perspectives. I anticipate more is on the horizon.
In my experience, I have seen tremendous success in partnering with and complementing each other, rather than competing for space when caring for a patient. Each and every one of us shares the same goal of providing the best patient care, and we each bring our own strengths.
Our future is ripe with opportunities to better serve the whole care team—MDs, PAs, NPs, and more—and it starts with recognizing the needs of everyone within the organization. To help CHEST better serve our members, I encourage you to take a short survey about your professional hurdles.
And please, do not hesitate to contact me ([email protected]) with suggestions or just to introduce yourself.
All the best,
Jack
As we enter summer, it’s hard to believe that we’re halfway through my presidency. Registration for CHEST 2024 (October 6 to 9) is now open, and October will be here before we know it.
I’m happy to share that we received more than 4,000 abstract and case report submissions from clinicians at all stages of their careers, and, for the first year, we had a dedicated category to solicit submissions from physician assistants (PAs), nurse practitioners (NPs), respiratory therapists, and other members of the broader health care team.
In both my practice and my time as CHEST President, I’ve been reflecting on the benefits of the multidisciplinary team—especially in the ICU. Because this is a setting that relies heavily on a team aspect, every member of the care team is a great asset.
CHEST is working to ensure that all integral members of our professional health care teams have the resources they need to best serve our patients. We encourage advanced practice providers (APPs) to apply to serve on our committees during the current open call, and we recently launched a dedicated APP Intersection column, called APP Intersection, within this publication to elevate diverse perspectives. I anticipate more is on the horizon.
In my experience, I have seen tremendous success in partnering with and complementing each other, rather than competing for space when caring for a patient. Each and every one of us shares the same goal of providing the best patient care, and we each bring our own strengths.
Our future is ripe with opportunities to better serve the whole care team—MDs, PAs, NPs, and more—and it starts with recognizing the needs of everyone within the organization. To help CHEST better serve our members, I encourage you to take a short survey about your professional hurdles.
And please, do not hesitate to contact me ([email protected]) with suggestions or just to introduce yourself.
All the best,
Jack

Nurse practitioners as advocates for health policy and patient care
APP INTERSECTION
In the intricate tapestry of health care, the roles of advanced practice registered nurses, also known as nurse practitioners (NPs), have evolved beyond the confines of clinical settings.
The journey into the realm of nursing often begins with a passion for healing and caring for others. However, for many, this path frequently leads to overcoming barriers to patient care, restrictions to practice, and lengthy red tape in the face of care teams that do not fully understand the scope and role of the NP.

Delving into health policy intricacies, efforts focus on understanding how legislative decisions directly impact patient care. Involvement in advocacy aims to improve health care access, promote patient-centered policies, and reduce disparities in the workforce and patient care.
Achieving sound primary care for people with multiple comorbid conditions requires the skills and abilities of all members of the health care workforce, including NPs.1 NPs have assumed an increasing role in recent decades as primary care providers for people with chronic diseases, while national trends show few physicians entering and staying in primary care.2,3,4,5 NPs are the nation’s fastest-growing primary care workforce, with nearly 90% of them trained to deliver primary care.6,7 Yet, NPs continue to experience reduced reimbursement for services compared with their physician counterparts.
Barriers to practice reduce the productivity and capacity of these health care professionals. Not permitting NPs to practice to the full extent of their licensure and education decreases the types and amounts of health care services that can be provided for people who need care.8 As noted in the Future of Nursing 2020-2030 report, this restriction also has significant implications for addressing the disparities in access to health care between rural and urban areas. A recent systemic review revealed that full practice authority is associated with higher numbers of NPs in rural areas and in primary care where there is a shortage of physicians. Full practice authority is associated with increased access to care and utilization of health care services, lower cost of care, and no decrease in quality of care.9,10 As stated in the National Council of State Boards of Nursing 2022 Environmental Scan, regulators and nurse leaders are responsible for upholding rules and regulations of nursing practice as well as ensuring that standards of care are met and patients are protected.11
Of equal importance is regulator awareness of the degree to which barriers continue to impact NP practice and limit aspects of care that directly influence care quality and access. Nursing leaders can have a significant impact on removing nonregulatory barriers to practice, such as changing outdated hospital bylaws that restrict NP practice. In turn, regulators can support efforts to remove unnecessary barriers to NP practice.
Fueled by experience in reduced practice, NPs become catalysts for change, transcending the role of health care providers. At the core of the NP role lies a commitment to patient advocacy. Beyond diagnosing and treating illnesses, NPs champion patients’ rights, ensuring their voices in health care decision-making. Advocacy efforts range from expanding access to essential services to promoting preventive care and fighting discrimination. By embracing roles as caregivers and agents of change, NPs can help the health care system emerge equitable, accessible, and patient-centric.
Ms. Kavanaugh is Assistant Dean of Graduate Nursing, University of Mount Saint Vincent, Pulmonary Critical Care Nurse Practitioner, Stamford Hospital.
References
1. McMenamin, A., Turi, E., Schlak, A., & Poghosyan, L. (2023). A Systematic Review of Outcomes Related to Nurse Practitioner-Delivered Primary Care for Multiple Chronic Conditions. Medical care research and review: MCRR, 80(6), 563–581. https://doi.org/10.1177/10775587231186720
2. Fraze T, Briggs A, Whitcomb E, Peck K, & Meara E (2020). Role of nurse practitioners in caring for patients with complex health needs. Medical Care, 58(10), 853–860. 10.1097/mlr.0000000000001364
3. Xue Y, Goodwin J, Adhikari D, Raji M, & Kuo Y (2017). Trends in primary care provision to medicare beneficiaries by physicians, nurse practitioners, or physician assistants: 2008–2014. Journal of Primary Care & Community Health, 8(4), 256–263. 10.1177/2150131917736634
4. Buerhaus P (2018). Nurse practitioners: A solution to America’s primary care crisis. American Enterprise Institute. https://www.aei.org/research-products/report/nurse-practitioners-a-solution-to-americas-primary-care-crisis/
5. Xue Y, Goodwin J, Adhikari D, Raji M, & Kuo Y (2017). Trends in primary care provision to medicare beneficiaries by physicians, nurse practitioners, or physician assistants: 2008–2014. Journal of Primary Care & Community Health, 8(4), 256–263. 10.1177/2150131917736634
6. American Association of Nurse Practitioners. (2022). Nurse practitioners in primary care. https://www.aanp.org/advocacy/advocacy-resource/position-statements/nurse-practitioners-in-primary-care
7. Auerbach, D. I. (2012). Will the NP workforce grow in the future? New forecasts and implications for healthcare delivery. Medical Care, 50(7), 606-610. doi: http://dx.doi.org/10.1097/MLR.0b013e318249d6e7
8. National Academy of Medicine . The National Academies Press; 2021. The future of nursing 2020-2030: Charting a path to achieve health equity.
9. Yang BK, Trinkoff AM, Zito JM, Burcu M, Safer DJ, Storr CL, Johantgen ME, & Idzik S (2017). Nurse practitioner independent practice authority and mental health service delivery in U.S. Community Health Centers. Psychiatric Services, 68(10), 1032–1038. 10.1176/appi.ps.201600495
10. Xue Y., Kannan V., Greener E., Smith J.A., Brasch J., Johnson B.A., Spetz J. Full scope-of-practice regulation is associated with higher supply of nurse practitioners in rural and primary care health professional shortage counties. Journal of Nursing Regulation. 2018;8(4):5–13. doi: 10.1016/S2155-8256(17)30176-X.
11. National Council of State Boards of Nursing The NCSBN 2022 environmental scan: Resiliency, achievement, and public protection. Journal of Nursing Regulation. 2022;12:S3–S55. doi: 10.1016/S2155-8256(22)00015-1.
APP INTERSECTION
In the intricate tapestry of health care, the roles of advanced practice registered nurses, also known as nurse practitioners (NPs), have evolved beyond the confines of clinical settings.
The journey into the realm of nursing often begins with a passion for healing and caring for others. However, for many, this path frequently leads to overcoming barriers to patient care, restrictions to practice, and lengthy red tape in the face of care teams that do not fully understand the scope and role of the NP.
Delving into health policy intricacies, efforts focus on understanding how legislative decisions directly impact patient care. Involvement in advocacy aims to improve health care access, promote patient-centered policies, and reduce disparities in the workforce and patient care.
Achieving sound primary care for people with multiple comorbid conditions requires the skills and abilities of all members of the health care workforce, including NPs.1 NPs have assumed an increasing role in recent decades as primary care providers for people with chronic diseases, while national trends show few physicians entering and staying in primary care.2,3,4,5 NPs are the nation’s fastest-growing primary care workforce, with nearly 90% of them trained to deliver primary care.6,7 Yet, NPs continue to experience reduced reimbursement for services compared with their physician counterparts.
Barriers to practice reduce the productivity and capacity of these health care professionals. Not permitting NPs to practice to the full extent of their licensure and education decreases the types and amounts of health care services that can be provided for people who need care.8 As noted in the Future of Nursing 2020-2030 report, this restriction also has significant implications for addressing the disparities in access to health care between rural and urban areas. A recent systemic review revealed that full practice authority is associated with higher numbers of NPs in rural areas and in primary care where there is a shortage of physicians. Full practice authority is associated with increased access to care and utilization of health care services, lower cost of care, and no decrease in quality of care.9,10 As stated in the National Council of State Boards of Nursing 2022 Environmental Scan, regulators and nurse leaders are responsible for upholding rules and regulations of nursing practice as well as ensuring that standards of care are met and patients are protected.11
Of equal importance is regulator awareness of the degree to which barriers continue to impact NP practice and limit aspects of care that directly influence care quality and access. Nursing leaders can have a significant impact on removing nonregulatory barriers to practice, such as changing outdated hospital bylaws that restrict NP practice. In turn, regulators can support efforts to remove unnecessary barriers to NP practice.
Fueled by experience in reduced practice, NPs become catalysts for change, transcending the role of health care providers. At the core of the NP role lies a commitment to patient advocacy. Beyond diagnosing and treating illnesses, NPs champion patients’ rights, ensuring their voices in health care decision-making. Advocacy efforts range from expanding access to essential services to promoting preventive care and fighting discrimination. By embracing roles as caregivers and agents of change, NPs can help the health care system emerge equitable, accessible, and patient-centric.
Ms. Kavanaugh is Assistant Dean of Graduate Nursing, University of Mount Saint Vincent, Pulmonary Critical Care Nurse Practitioner, Stamford Hospital.
References
1. McMenamin, A., Turi, E., Schlak, A., & Poghosyan, L. (2023). A Systematic Review of Outcomes Related to Nurse Practitioner-Delivered Primary Care for Multiple Chronic Conditions. Medical care research and review: MCRR, 80(6), 563–581. https://doi.org/10.1177/10775587231186720
2. Fraze T, Briggs A, Whitcomb E, Peck K, & Meara E (2020). Role of nurse practitioners in caring for patients with complex health needs. Medical Care, 58(10), 853–860. 10.1097/mlr.0000000000001364
3. Xue Y, Goodwin J, Adhikari D, Raji M, & Kuo Y (2017). Trends in primary care provision to medicare beneficiaries by physicians, nurse practitioners, or physician assistants: 2008–2014. Journal of Primary Care & Community Health, 8(4), 256–263. 10.1177/2150131917736634
4. Buerhaus P (2018). Nurse practitioners: A solution to America’s primary care crisis. American Enterprise Institute. https://www.aei.org/research-products/report/nurse-practitioners-a-solution-to-americas-primary-care-crisis/
5. Xue Y, Goodwin J, Adhikari D, Raji M, & Kuo Y (2017). Trends in primary care provision to medicare beneficiaries by physicians, nurse practitioners, or physician assistants: 2008–2014. Journal of Primary Care & Community Health, 8(4), 256–263. 10.1177/2150131917736634
6. American Association of Nurse Practitioners. (2022). Nurse practitioners in primary care. https://www.aanp.org/advocacy/advocacy-resource/position-statements/nurse-practitioners-in-primary-care
7. Auerbach, D. I. (2012). Will the NP workforce grow in the future? New forecasts and implications for healthcare delivery. Medical Care, 50(7), 606-610. doi: http://dx.doi.org/10.1097/MLR.0b013e318249d6e7
8. National Academy of Medicine . The National Academies Press; 2021. The future of nursing 2020-2030: Charting a path to achieve health equity.
9. Yang BK, Trinkoff AM, Zito JM, Burcu M, Safer DJ, Storr CL, Johantgen ME, & Idzik S (2017). Nurse practitioner independent practice authority and mental health service delivery in U.S. Community Health Centers. Psychiatric Services, 68(10), 1032–1038. 10.1176/appi.ps.201600495
10. Xue Y., Kannan V., Greener E., Smith J.A., Brasch J., Johnson B.A., Spetz J. Full scope-of-practice regulation is associated with higher supply of nurse practitioners in rural and primary care health professional shortage counties. Journal of Nursing Regulation. 2018;8(4):5–13. doi: 10.1016/S2155-8256(17)30176-X.
11. National Council of State Boards of Nursing The NCSBN 2022 environmental scan: Resiliency, achievement, and public protection. Journal of Nursing Regulation. 2022;12:S3–S55. doi: 10.1016/S2155-8256(22)00015-1.
APP INTERSECTION
In the intricate tapestry of health care, the roles of advanced practice registered nurses, also known as nurse practitioners (NPs), have evolved beyond the confines of clinical settings.
The journey into the realm of nursing often begins with a passion for healing and caring for others. However, for many, this path frequently leads to overcoming barriers to patient care, restrictions to practice, and lengthy red tape in the face of care teams that do not fully understand the scope and role of the NP.
Delving into health policy intricacies, efforts focus on understanding how legislative decisions directly impact patient care. Involvement in advocacy aims to improve health care access, promote patient-centered policies, and reduce disparities in the workforce and patient care.
Achieving sound primary care for people with multiple comorbid conditions requires the skills and abilities of all members of the health care workforce, including NPs.1 NPs have assumed an increasing role in recent decades as primary care providers for people with chronic diseases, while national trends show few physicians entering and staying in primary care.2,3,4,5 NPs are the nation’s fastest-growing primary care workforce, with nearly 90% of them trained to deliver primary care.6,7 Yet, NPs continue to experience reduced reimbursement for services compared with their physician counterparts.
Barriers to practice reduce the productivity and capacity of these health care professionals. Not permitting NPs to practice to the full extent of their licensure and education decreases the types and amounts of health care services that can be provided for people who need care.8 As noted in the Future of Nursing 2020-2030 report, this restriction also has significant implications for addressing the disparities in access to health care between rural and urban areas. A recent systemic review revealed that full practice authority is associated with higher numbers of NPs in rural areas and in primary care where there is a shortage of physicians. Full practice authority is associated with increased access to care and utilization of health care services, lower cost of care, and no decrease in quality of care.9,10 As stated in the National Council of State Boards of Nursing 2022 Environmental Scan, regulators and nurse leaders are responsible for upholding rules and regulations of nursing practice as well as ensuring that standards of care are met and patients are protected.11
Of equal importance is regulator awareness of the degree to which barriers continue to impact NP practice and limit aspects of care that directly influence care quality and access. Nursing leaders can have a significant impact on removing nonregulatory barriers to practice, such as changing outdated hospital bylaws that restrict NP practice. In turn, regulators can support efforts to remove unnecessary barriers to NP practice.
Fueled by experience in reduced practice, NPs become catalysts for change, transcending the role of health care providers. At the core of the NP role lies a commitment to patient advocacy. Beyond diagnosing and treating illnesses, NPs champion patients’ rights, ensuring their voices in health care decision-making. Advocacy efforts range from expanding access to essential services to promoting preventive care and fighting discrimination. By embracing roles as caregivers and agents of change, NPs can help the health care system emerge equitable, accessible, and patient-centric.
Ms. Kavanaugh is Assistant Dean of Graduate Nursing, University of Mount Saint Vincent, Pulmonary Critical Care Nurse Practitioner, Stamford Hospital.
References
1. McMenamin, A., Turi, E., Schlak, A., & Poghosyan, L. (2023). A Systematic Review of Outcomes Related to Nurse Practitioner-Delivered Primary Care for Multiple Chronic Conditions. Medical care research and review: MCRR, 80(6), 563–581. https://doi.org/10.1177/10775587231186720
2. Fraze T, Briggs A, Whitcomb E, Peck K, & Meara E (2020). Role of nurse practitioners in caring for patients with complex health needs. Medical Care, 58(10), 853–860. 10.1097/mlr.0000000000001364
3. Xue Y, Goodwin J, Adhikari D, Raji M, & Kuo Y (2017). Trends in primary care provision to medicare beneficiaries by physicians, nurse practitioners, or physician assistants: 2008–2014. Journal of Primary Care & Community Health, 8(4), 256–263. 10.1177/2150131917736634
4. Buerhaus P (2018). Nurse practitioners: A solution to America’s primary care crisis. American Enterprise Institute. https://www.aei.org/research-products/report/nurse-practitioners-a-solution-to-americas-primary-care-crisis/
5. Xue Y, Goodwin J, Adhikari D, Raji M, & Kuo Y (2017). Trends in primary care provision to medicare beneficiaries by physicians, nurse practitioners, or physician assistants: 2008–2014. Journal of Primary Care & Community Health, 8(4), 256–263. 10.1177/2150131917736634
6. American Association of Nurse Practitioners. (2022). Nurse practitioners in primary care. https://www.aanp.org/advocacy/advocacy-resource/position-statements/nurse-practitioners-in-primary-care
7. Auerbach, D. I. (2012). Will the NP workforce grow in the future? New forecasts and implications for healthcare delivery. Medical Care, 50(7), 606-610. doi: http://dx.doi.org/10.1097/MLR.0b013e318249d6e7
8. National Academy of Medicine . The National Academies Press; 2021. The future of nursing 2020-2030: Charting a path to achieve health equity.
9. Yang BK, Trinkoff AM, Zito JM, Burcu M, Safer DJ, Storr CL, Johantgen ME, & Idzik S (2017). Nurse practitioner independent practice authority and mental health service delivery in U.S. Community Health Centers. Psychiatric Services, 68(10), 1032–1038. 10.1176/appi.ps.201600495
10. Xue Y., Kannan V., Greener E., Smith J.A., Brasch J., Johnson B.A., Spetz J. Full scope-of-practice regulation is associated with higher supply of nurse practitioners in rural and primary care health professional shortage counties. Journal of Nursing Regulation. 2018;8(4):5–13. doi: 10.1016/S2155-8256(17)30176-X.
11. National Council of State Boards of Nursing The NCSBN 2022 environmental scan: Resiliency, achievement, and public protection. Journal of Nursing Regulation. 2022;12:S3–S55. doi: 10.1016/S2155-8256(22)00015-1.

Military burn pits: Their evidence and implications for respiratory health
Military service is a hazard-ridden profession. It’s easy to recognize the direct dangers from warfighting, such as gunfire and explosions, but the risks from environmental, chemical, and other occupational exposures can be harder to see.
Combustion-based waste management systems, otherwise known as “burn pits,” were used in deployed environments by the US military from the 1990s to the early 2010s. These burn pits were commonly used to eliminate plastics, electronics, munitions, metals, wood, chemicals, and even human waste. At the height of the recent conflicts in Afghanistan, Iraq, and other southwest Asia locations, more than 70% of military installations employed at least one, and nearly 4 million service members were exposed to some degree to their emissions.

Reports of burn pits being related to organic disease have garnered widespread media attention. Initially, this came through anecdotal reports of post-deployment respiratory symptoms. Over time, the conditions attributed to burn pits expanded to include newly diagnosed respiratory diseases and malignancies.
Ultimately, Congress passed the 2022 Promise to Address Comprehensive Toxins (PACT) Act, presumptively linking more than 20 diagnoses to burn pits. The PACT Act provides countless veterans access to low-cost or free medical care for their respective conditions.
What do we know about burn pits and deployment-related respiratory disease?
Data from the Millennium Cohort Study noted an approximately 40% increase in respiratory symptoms among individuals returning from deployment but no increase in the frequency of diagnosed respiratory diseases.1 This study and others definitively established a temporal relationship between deployment and respiratory symptoms. Soon after, a retrospective, observational study of service members with post-deployment respiratory symptoms found a high prevalence of constrictive bronchiolitis (CB) identified by lung biopsy.2 Patients in this group reported exposure to burn pits and a sulfur mine fire in the Mosul area while deployed. Most had normal imaging and pulmonary function testing before biopsy, confounding the clinical significance of the CB finding. The publication of this report led to increased investigation of respiratory function during and after deployment.

In a series of prospective studies that included full pulmonary function testing, impulse oscillometry, cardiopulmonary exercise testing, bronchoscopy, and, occasionally, lung biopsy to evaluate post-deployment dyspnea, only a small minority received a diagnosis of clinically significant lung disease.3,4 Additionally, when comparing spirometry and impulse oscillometry results from before and after deployment, no decline in lung function was observed in a population of service members reporting regular burn pit exposure.5 These studies suggest that at the population level, deployment does not lead to abnormalities in the structure and function of the respiratory system.
The National Academies of Sciences published two separate reviews of burn pit exposure and outcomes in 2011 and 2020.6,7 They found insufficient evidence to support a causal relationship between burn pit exposure and pulmonary disease. They highlighted studies on the composition of emissions from the area surrounding the largest military burn pit in Iraq. Levels of particulate matter, volatile organic compounds, and polycyclic aromatic hydrocarbons were elevated when compared with those of a typical American city but were similar to the pollution levels seen in the region at the time. Given these findings, they suggested ambient air pollution may have contributed more to clinically significant disease than burn pit emissions.
How do we interpret this mixed data?
At the population level, we have yet to find conclusive data directly linking burn pit exposure to the development of any respiratory disease. Does this mean that burn pits are not harmful?
Not necessarily. Research on outcomes related to burn pit exposure is challenging given the heterogeneity in exposure volume. Much of the research is retrospective and subject to recall bias. Relationships may be distorted, and the precision of reported symptoms and exposure levels is altered. Given these challenges, it’s unsurprising that evidence of causality has yet to be proven. In addition, some portion of service members has been diagnosed with respiratory disease that could be related to burn pit exposure.
What is now indisputable is that deployment to southwest Asia leads to an increase in respiratory complaints. Whether veteran respiratory symptoms are due to burn pits, ambient pollution, environmental particulate matter, or dust storms is less clinically relevant. These symptoms require attention, investigation, and management.
What does this mean for the future medical care of service members and veterans?
Many veterans with post-deployment respiratory symptoms undergo extensive evaluations without obtaining a definitive diagnosis. A recent consensus statement on deployment-related respiratory symptoms provides a framework for evaluation in such cases.8 In keeping with that statement, we recommend veterans be referred to centers with expertise in this field, such as the Department of Veterans Affairs (VA) or military health centers, when deployment-related respiratory symptoms are reported. When the evaluation does not lead to a treatable diagnosis, these centers can provide multidisciplinary care to address the symptoms of dyspnea, cough, fatigue, and exercise intolerance to improve functional status.
Despite uncertainty in the evidence or challenges in diagnosis, both the Department of Defense (DoD) and VA remain fully committed to addressing the health concerns of service members and veterans. Notably, the VA has already screened more than 5 million veterans for toxic military exposures in accordance with the PACT Act and is providing ongoing screening and care for veterans with post-deployment respiratory symptoms. Furthermore, the DoD and VA have dedicated large portions of their research budgets to investigating the impacts of exposures during military service and optimizing the care of those with respiratory symptoms. With these commitments to patient care and research, our veterans’ respiratory health can now be optimized, and future risks can be mitigated.
Dr. Haynes is Fellow, Pulmonary and Critical Care Medicine, Walter Reed National Military Medical Center, Assistant Professor of Medicine, Uniformed Services University. Dr. Nations is Pulmonary and Critical Care Medicine, Deputy Chief of Staff for Operations, Washington DC VA Medical Center, Associate Professor of Medicine, Uniformed Services University.
References
1. Smith B, Wong CA, Smith TC, Boyko EJ, Gackstetter GD; Margaret A. K. Ryan for the Millennium Cohort Study Team. Newly reported respiratory symptoms and conditions among military personnel deployed to Iraq and Afghanistan: a prospective population-based study. Am J Epidemiol. 2009;170(11):1433-1442. Preprint. Posted online October 22, 2009. PMID: 19850627. doi: 10.1093/aje/kwp287
2. King MS, Eisenberg R, Newman JH, et al. Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan. N Engl J Med. 2011;365(3):222-230. Erratum in: N Engl J Med. 2011;365(18):1749. PMID: 21774710; PMCID: PMC3296566. doi: 10.1056/NEJMoa1101388
3. Morris MJ, Dodson DW, Lucero PF, et al. Study of active duty military for pulmonary disease related to environmental deployment exposures (STAMPEDE). Am J Respir Crit Care Med. 2014;190(1):77-84. PMID: 24922562. doi: 10.1164/rccm.201402-0372OC
4. Morris MJ, Walter RJ, McCann ET, et al. Clinical evaluation of deployed military personnel with chronic respiratory symptoms: study of active duty military for pulmonary disease related to environmental deployment exposures (STAMPEDE) III. Chest. 2020;157(6):1559-1567. Preprint. Posted online February 1, 2020. PMID: 32017933. doi: 10.1016/j.chest.2020.01.024
5. Morris MJ, Skabelund AJ, Rawlins FA 3rd, Gallup RA, Aden JK, Holley AB. Study of active duty military personnel for environmental deployment exposures: pre- and post-deployment spirometry (STAMPEDE II). Respir Care. 2019;64(5):536-544. Preprint. Posted online January 8, 2019.PMID: 30622173. doi: 10.4187/respcare.06396
6. Institute of Medicine. Long-Term Health Consequences of Exposure to Burn Pits in Iraq and Afghanistan. The National Academies Press; 2011. https://doi.org/10.17226/13209
7. National Academies of Sciences, Engineering, and Medicine. Respiratory Health Effects of Airborne Hazards Exposures in the Southwest Asia Theater of Military Operations. The National Academies Press; 2020. https://doi.org/10.17226/25837
8. Falvo MJ, Sotolongo AM, Osterholzer JJ, et al. Consensus statements on deployment-related respiratory disease, inclusive of constrictive bronchiolitis: a modified Delphi study. Chest. 2023;163(3):599-609. Preprint. Posted November 4, 2022. PMID: 36343686; PMCID: PMC10154857. doi: 10.1016/j.chest.2022.10.031
Military service is a hazard-ridden profession. It’s easy to recognize the direct dangers from warfighting, such as gunfire and explosions, but the risks from environmental, chemical, and other occupational exposures can be harder to see.
Combustion-based waste management systems, otherwise known as “burn pits,” were used in deployed environments by the US military from the 1990s to the early 2010s. These burn pits were commonly used to eliminate plastics, electronics, munitions, metals, wood, chemicals, and even human waste. At the height of the recent conflicts in Afghanistan, Iraq, and other southwest Asia locations, more than 70% of military installations employed at least one, and nearly 4 million service members were exposed to some degree to their emissions.
Reports of burn pits being related to organic disease have garnered widespread media attention. Initially, this came through anecdotal reports of post-deployment respiratory symptoms. Over time, the conditions attributed to burn pits expanded to include newly diagnosed respiratory diseases and malignancies.
Ultimately, Congress passed the 2022 Promise to Address Comprehensive Toxins (PACT) Act, presumptively linking more than 20 diagnoses to burn pits. The PACT Act provides countless veterans access to low-cost or free medical care for their respective conditions.
What do we know about burn pits and deployment-related respiratory disease?
Data from the Millennium Cohort Study noted an approximately 40% increase in respiratory symptoms among individuals returning from deployment but no increase in the frequency of diagnosed respiratory diseases.1 This study and others definitively established a temporal relationship between deployment and respiratory symptoms. Soon after, a retrospective, observational study of service members with post-deployment respiratory symptoms found a high prevalence of constrictive bronchiolitis (CB) identified by lung biopsy.2 Patients in this group reported exposure to burn pits and a sulfur mine fire in the Mosul area while deployed. Most had normal imaging and pulmonary function testing before biopsy, confounding the clinical significance of the CB finding. The publication of this report led to increased investigation of respiratory function during and after deployment.
In a series of prospective studies that included full pulmonary function testing, impulse oscillometry, cardiopulmonary exercise testing, bronchoscopy, and, occasionally, lung biopsy to evaluate post-deployment dyspnea, only a small minority received a diagnosis of clinically significant lung disease.3,4 Additionally, when comparing spirometry and impulse oscillometry results from before and after deployment, no decline in lung function was observed in a population of service members reporting regular burn pit exposure.5 These studies suggest that at the population level, deployment does not lead to abnormalities in the structure and function of the respiratory system.
The National Academies of Sciences published two separate reviews of burn pit exposure and outcomes in 2011 and 2020.6,7 They found insufficient evidence to support a causal relationship between burn pit exposure and pulmonary disease. They highlighted studies on the composition of emissions from the area surrounding the largest military burn pit in Iraq. Levels of particulate matter, volatile organic compounds, and polycyclic aromatic hydrocarbons were elevated when compared with those of a typical American city but were similar to the pollution levels seen in the region at the time. Given these findings, they suggested ambient air pollution may have contributed more to clinically significant disease than burn pit emissions.
How do we interpret this mixed data?
At the population level, we have yet to find conclusive data directly linking burn pit exposure to the development of any respiratory disease. Does this mean that burn pits are not harmful?
Not necessarily. Research on outcomes related to burn pit exposure is challenging given the heterogeneity in exposure volume. Much of the research is retrospective and subject to recall bias. Relationships may be distorted, and the precision of reported symptoms and exposure levels is altered. Given these challenges, it’s unsurprising that evidence of causality has yet to be proven. In addition, some portion of service members has been diagnosed with respiratory disease that could be related to burn pit exposure.
What is now indisputable is that deployment to southwest Asia leads to an increase in respiratory complaints. Whether veteran respiratory symptoms are due to burn pits, ambient pollution, environmental particulate matter, or dust storms is less clinically relevant. These symptoms require attention, investigation, and management.
What does this mean for the future medical care of service members and veterans?
Many veterans with post-deployment respiratory symptoms undergo extensive evaluations without obtaining a definitive diagnosis. A recent consensus statement on deployment-related respiratory symptoms provides a framework for evaluation in such cases.8 In keeping with that statement, we recommend veterans be referred to centers with expertise in this field, such as the Department of Veterans Affairs (VA) or military health centers, when deployment-related respiratory symptoms are reported. When the evaluation does not lead to a treatable diagnosis, these centers can provide multidisciplinary care to address the symptoms of dyspnea, cough, fatigue, and exercise intolerance to improve functional status.
Despite uncertainty in the evidence or challenges in diagnosis, both the Department of Defense (DoD) and VA remain fully committed to addressing the health concerns of service members and veterans. Notably, the VA has already screened more than 5 million veterans for toxic military exposures in accordance with the PACT Act and is providing ongoing screening and care for veterans with post-deployment respiratory symptoms. Furthermore, the DoD and VA have dedicated large portions of their research budgets to investigating the impacts of exposures during military service and optimizing the care of those with respiratory symptoms. With these commitments to patient care and research, our veterans’ respiratory health can now be optimized, and future risks can be mitigated.
Dr. Haynes is Fellow, Pulmonary and Critical Care Medicine, Walter Reed National Military Medical Center, Assistant Professor of Medicine, Uniformed Services University. Dr. Nations is Pulmonary and Critical Care Medicine, Deputy Chief of Staff for Operations, Washington DC VA Medical Center, Associate Professor of Medicine, Uniformed Services University.
References
1. Smith B, Wong CA, Smith TC, Boyko EJ, Gackstetter GD; Margaret A. K. Ryan for the Millennium Cohort Study Team. Newly reported respiratory symptoms and conditions among military personnel deployed to Iraq and Afghanistan: a prospective population-based study. Am J Epidemiol. 2009;170(11):1433-1442. Preprint. Posted online October 22, 2009. PMID: 19850627. doi: 10.1093/aje/kwp287
2. King MS, Eisenberg R, Newman JH, et al. Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan. N Engl J Med. 2011;365(3):222-230. Erratum in: N Engl J Med. 2011;365(18):1749. PMID: 21774710; PMCID: PMC3296566. doi: 10.1056/NEJMoa1101388
3. Morris MJ, Dodson DW, Lucero PF, et al. Study of active duty military for pulmonary disease related to environmental deployment exposures (STAMPEDE). Am J Respir Crit Care Med. 2014;190(1):77-84. PMID: 24922562. doi: 10.1164/rccm.201402-0372OC
4. Morris MJ, Walter RJ, McCann ET, et al. Clinical evaluation of deployed military personnel with chronic respiratory symptoms: study of active duty military for pulmonary disease related to environmental deployment exposures (STAMPEDE) III. Chest. 2020;157(6):1559-1567. Preprint. Posted online February 1, 2020. PMID: 32017933. doi: 10.1016/j.chest.2020.01.024
5. Morris MJ, Skabelund AJ, Rawlins FA 3rd, Gallup RA, Aden JK, Holley AB. Study of active duty military personnel for environmental deployment exposures: pre- and post-deployment spirometry (STAMPEDE II). Respir Care. 2019;64(5):536-544. Preprint. Posted online January 8, 2019.PMID: 30622173. doi: 10.4187/respcare.06396
6. Institute of Medicine. Long-Term Health Consequences of Exposure to Burn Pits in Iraq and Afghanistan. The National Academies Press; 2011. https://doi.org/10.17226/13209
7. National Academies of Sciences, Engineering, and Medicine. Respiratory Health Effects of Airborne Hazards Exposures in the Southwest Asia Theater of Military Operations. The National Academies Press; 2020. https://doi.org/10.17226/25837
8. Falvo MJ, Sotolongo AM, Osterholzer JJ, et al. Consensus statements on deployment-related respiratory disease, inclusive of constrictive bronchiolitis: a modified Delphi study. Chest. 2023;163(3):599-609. Preprint. Posted November 4, 2022. PMID: 36343686; PMCID: PMC10154857. doi: 10.1016/j.chest.2022.10.031
Military service is a hazard-ridden profession. It’s easy to recognize the direct dangers from warfighting, such as gunfire and explosions, but the risks from environmental, chemical, and other occupational exposures can be harder to see.
Combustion-based waste management systems, otherwise known as “burn pits,” were used in deployed environments by the US military from the 1990s to the early 2010s. These burn pits were commonly used to eliminate plastics, electronics, munitions, metals, wood, chemicals, and even human waste. At the height of the recent conflicts in Afghanistan, Iraq, and other southwest Asia locations, more than 70% of military installations employed at least one, and nearly 4 million service members were exposed to some degree to their emissions.
Reports of burn pits being related to organic disease have garnered widespread media attention. Initially, this came through anecdotal reports of post-deployment respiratory symptoms. Over time, the conditions attributed to burn pits expanded to include newly diagnosed respiratory diseases and malignancies.
Ultimately, Congress passed the 2022 Promise to Address Comprehensive Toxins (PACT) Act, presumptively linking more than 20 diagnoses to burn pits. The PACT Act provides countless veterans access to low-cost or free medical care for their respective conditions.
What do we know about burn pits and deployment-related respiratory disease?
Data from the Millennium Cohort Study noted an approximately 40% increase in respiratory symptoms among individuals returning from deployment but no increase in the frequency of diagnosed respiratory diseases.1 This study and others definitively established a temporal relationship between deployment and respiratory symptoms. Soon after, a retrospective, observational study of service members with post-deployment respiratory symptoms found a high prevalence of constrictive bronchiolitis (CB) identified by lung biopsy.2 Patients in this group reported exposure to burn pits and a sulfur mine fire in the Mosul area while deployed. Most had normal imaging and pulmonary function testing before biopsy, confounding the clinical significance of the CB finding. The publication of this report led to increased investigation of respiratory function during and after deployment.
In a series of prospective studies that included full pulmonary function testing, impulse oscillometry, cardiopulmonary exercise testing, bronchoscopy, and, occasionally, lung biopsy to evaluate post-deployment dyspnea, only a small minority received a diagnosis of clinically significant lung disease.3,4 Additionally, when comparing spirometry and impulse oscillometry results from before and after deployment, no decline in lung function was observed in a population of service members reporting regular burn pit exposure.5 These studies suggest that at the population level, deployment does not lead to abnormalities in the structure and function of the respiratory system.
The National Academies of Sciences published two separate reviews of burn pit exposure and outcomes in 2011 and 2020.6,7 They found insufficient evidence to support a causal relationship between burn pit exposure and pulmonary disease. They highlighted studies on the composition of emissions from the area surrounding the largest military burn pit in Iraq. Levels of particulate matter, volatile organic compounds, and polycyclic aromatic hydrocarbons were elevated when compared with those of a typical American city but were similar to the pollution levels seen in the region at the time. Given these findings, they suggested ambient air pollution may have contributed more to clinically significant disease than burn pit emissions.
How do we interpret this mixed data?
At the population level, we have yet to find conclusive data directly linking burn pit exposure to the development of any respiratory disease. Does this mean that burn pits are not harmful?
Not necessarily. Research on outcomes related to burn pit exposure is challenging given the heterogeneity in exposure volume. Much of the research is retrospective and subject to recall bias. Relationships may be distorted, and the precision of reported symptoms and exposure levels is altered. Given these challenges, it’s unsurprising that evidence of causality has yet to be proven. In addition, some portion of service members has been diagnosed with respiratory disease that could be related to burn pit exposure.
What is now indisputable is that deployment to southwest Asia leads to an increase in respiratory complaints. Whether veteran respiratory symptoms are due to burn pits, ambient pollution, environmental particulate matter, or dust storms is less clinically relevant. These symptoms require attention, investigation, and management.
What does this mean for the future medical care of service members and veterans?
Many veterans with post-deployment respiratory symptoms undergo extensive evaluations without obtaining a definitive diagnosis. A recent consensus statement on deployment-related respiratory symptoms provides a framework for evaluation in such cases.8 In keeping with that statement, we recommend veterans be referred to centers with expertise in this field, such as the Department of Veterans Affairs (VA) or military health centers, when deployment-related respiratory symptoms are reported. When the evaluation does not lead to a treatable diagnosis, these centers can provide multidisciplinary care to address the symptoms of dyspnea, cough, fatigue, and exercise intolerance to improve functional status.
Despite uncertainty in the evidence or challenges in diagnosis, both the Department of Defense (DoD) and VA remain fully committed to addressing the health concerns of service members and veterans. Notably, the VA has already screened more than 5 million veterans for toxic military exposures in accordance with the PACT Act and is providing ongoing screening and care for veterans with post-deployment respiratory symptoms. Furthermore, the DoD and VA have dedicated large portions of their research budgets to investigating the impacts of exposures during military service and optimizing the care of those with respiratory symptoms. With these commitments to patient care and research, our veterans’ respiratory health can now be optimized, and future risks can be mitigated.
Dr. Haynes is Fellow, Pulmonary and Critical Care Medicine, Walter Reed National Military Medical Center, Assistant Professor of Medicine, Uniformed Services University. Dr. Nations is Pulmonary and Critical Care Medicine, Deputy Chief of Staff for Operations, Washington DC VA Medical Center, Associate Professor of Medicine, Uniformed Services University.
References
1. Smith B, Wong CA, Smith TC, Boyko EJ, Gackstetter GD; Margaret A. K. Ryan for the Millennium Cohort Study Team. Newly reported respiratory symptoms and conditions among military personnel deployed to Iraq and Afghanistan: a prospective population-based study. Am J Epidemiol. 2009;170(11):1433-1442. Preprint. Posted online October 22, 2009. PMID: 19850627. doi: 10.1093/aje/kwp287
2. King MS, Eisenberg R, Newman JH, et al. Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan. N Engl J Med. 2011;365(3):222-230. Erratum in: N Engl J Med. 2011;365(18):1749. PMID: 21774710; PMCID: PMC3296566. doi: 10.1056/NEJMoa1101388
3. Morris MJ, Dodson DW, Lucero PF, et al. Study of active duty military for pulmonary disease related to environmental deployment exposures (STAMPEDE). Am J Respir Crit Care Med. 2014;190(1):77-84. PMID: 24922562. doi: 10.1164/rccm.201402-0372OC
4. Morris MJ, Walter RJ, McCann ET, et al. Clinical evaluation of deployed military personnel with chronic respiratory symptoms: study of active duty military for pulmonary disease related to environmental deployment exposures (STAMPEDE) III. Chest. 2020;157(6):1559-1567. Preprint. Posted online February 1, 2020. PMID: 32017933. doi: 10.1016/j.chest.2020.01.024
5. Morris MJ, Skabelund AJ, Rawlins FA 3rd, Gallup RA, Aden JK, Holley AB. Study of active duty military personnel for environmental deployment exposures: pre- and post-deployment spirometry (STAMPEDE II). Respir Care. 2019;64(5):536-544. Preprint. Posted online January 8, 2019.PMID: 30622173. doi: 10.4187/respcare.06396
6. Institute of Medicine. Long-Term Health Consequences of Exposure to Burn Pits in Iraq and Afghanistan. The National Academies Press; 2011. https://doi.org/10.17226/13209
7. National Academies of Sciences, Engineering, and Medicine. Respiratory Health Effects of Airborne Hazards Exposures in the Southwest Asia Theater of Military Operations. The National Academies Press; 2020. https://doi.org/10.17226/25837
8. Falvo MJ, Sotolongo AM, Osterholzer JJ, et al. Consensus statements on deployment-related respiratory disease, inclusive of constrictive bronchiolitis: a modified Delphi study. Chest. 2023;163(3):599-609. Preprint. Posted November 4, 2022. PMID: 36343686; PMCID: PMC10154857. doi: 10.1016/j.chest.2022.10.031
Hospital-onset sepsis: Why the brouhaha?
A 47-year-old woman with a history of cirrhosis is admitted with an acute kidney injury and altered mental status. On the initial workup, there are no signs of infection, and dehydration is determined to be the cause of the kidney injury. There are signs of improvement in the kidney injury with hydration. On hospital day 3, the patient develops a fever (101.9 o F) with accompanying leukocytosis to 14,000. Concerned for infection, the team starts empiric broad spectrum antibiotics for presumed spontaneous bacterial peritonitis. The next day (hospital day 4), a rapid response evaluation is activated as the patient is demonstrating increasing confusion, hypotension with a systolic blood pressure of 70 mm Hg, and elevated lactic acid. The patient receives 1 L of normal saline and transfers to the ICU. The new critical care fellow, who has just read up on sepsis early management bundles, and specifically the Severe Sepsis and Septic Shock Management Bundle (SEP-1), is reviewing the chart and notices a history of multidrug-resistant organisms in her urine cultures from an admission 2 months ago. They ask of the transferring team, “When was time zero, and was the 3-hour bundle completed?”
1 The excessive cost, both of human life and monetary, has led to the commitment of significant resources to sepsis care. Improved recognition and timely intervention for sepsis have led to noteworthy improvement in mortality. Most of this effort has been directed toward patients with sepsis diagnosed in the emergency department (ED) who are presenting with community-onset sepsis (COS). A new entity, called hospital-onset sepsis (HOS), has been described recently, defined by the Centers for Disease Control and Prevention (CDC) as both infection and organ dysfunction developing more than 48 hours after hospital admission.2

A systematic review of 51 studies found approximately 23.6% of all sepsis cases are HOS. The proportion of HOS is even higher (more than 45%) in patients admitted to the ICU with sepsis.3 The outcome for this group remains comparatively poor. The hospital mortality among patients with HOS is 35%, which increases to 52% with progression to septic shock compared with 25% with COS.3 Even after adjusting for baseline factors that make one prone to developing infection in the hospital, a patient developing HOS has three-times a higher risk of dying compared with a patient who never developed sepsis and two-times a higher risk of dying compared with patients with COS.4 Furthermore, HOS utilizes more resources with significantly longer ICU and hospital stays and has five-times the hospital cost compared with COS.4
The two most crucial factors in improving sepsis outcomes, as identified by the Surviving Sepsis Campaign guidelines, are: 1) prompt identification and treatment within the first few hours of onset and 2) regular reevaluation of the patient’s response to treatment.

Prompt identification
Diagnosing sepsis in the patient who is hospitalized is challenging. Patients admitted to the hospital often have competing comorbidities, have existing organ failure, or are in a postoperative/intervention state that clouds the application and interpretation of vital sign triggers customarily used to identify sepsis. The positive predictive value for all existing sepsis definitions and diagnostic criteria is dismally low. 5 And while automated electronic sepsis alerts may improve processes of care, they still have poor positive predictive value and have not impacted patient-centered outcomes (mortality or length of stay). Furthermore, the causative microorganisms often associated with hospital-acquired infections are complex, are drug-resistant, and can have courses which further delay identification. Finally, cognitive errors, such as anchoring biases or premature diagnosis closure, can contribute to provider-level identification delays that are only further exacerbated by system issues, such as capacity constraints, staffing issues, and differing paces between wards that tend to impede time-sensitive evaluations and interventions. 4,6,7
Management
The SEP-1 core measure uses a framework of early recognition of infection and completion of the sepsis bundles in a timely manner to improve outcomes. Patients with HOS are less likely than those with COS to receive Centers for Medicare & Medicaid Services SEP-1-compliant care, including timely blood culture collection, initial and repeat lactate testing, and fluid resuscitation.8 The Surviving Sepsis Campaign has explored barriers to managing HOS. Among caregivers, these include delay in recognition, poor communication regarding change in patient status, not prioritizing treatment for sepsis, failure to measure lactate, delayed or no antimicrobial administration, and inadequate fluid resuscitation. In one study, the adherence to SEP-1 for HOS was reported at 13% compared with 39.9% in COS. The differences in initial sepsis management included timing of antimicrobials and fluid resuscitation, which accounted for 23% of observed greater mortality risk among patients with HOS compared with COS.6,8 It remains unclear how these recommendations should be applied and whether some of these recommendations confer the same benefits for patients with HOS as for those with COS. For example, administration of fluids conferred no additional benefit to patients with HOS, while rapid antimicrobial administration was shown to be associated with improved mortality in patients with HOS. Although, the optimal timing for treatment initiation and microbial coverage has not been established.

The path forward
Effective HOS management requires both individual and systematic approaches. How clinicians identify a patient with sepsis must be context-dependent. Although standard criteria exist for defining sepsis, the approach to a patient presenting to the ED from home should differ from that of a patient who has been hospitalized for several days, is postoperative, or is in the ICU on multiple forms of life support. Clinical medicine is context-dependent, and the same principles apply to sepsis management. To address the diagnostic uncertainty of the syndrome, providers must remain vigilant and maintain a clinical “iterative urgency” in diagnosing and managing sepsis. While machine learning algorithms have potential, they still rely on human intervention and interaction to navigate the complexities of HOS diagnosis.
At the system level, survival from sepsis is determined by the speed with which complex medical care is delivered and the effectiveness with which resources and personnel are mobilized and coordinated. The Hospital Sepsis Program Core Elements, released by the CDC, serves as an initial playbook to aid hospitals in establishing comprehensive sepsis improvement programs.
A second invaluable resource for hospitals in sepsis management is the rapid response team (RRT). Studies have shown that resolute RRTs can enhance patient outcomes and compliance with sepsis bundles; though, the composition and scope of these teams are crucial to their effectiveness. Responding to in-hospital emergencies and urgencies without conflicting responsibilities is an essential feature of a successful RRT. Often, they are familiar with bundles, protocols, and documentation, and members of these teams can offer clinical and/or technical expertise as well as support active participation and reengagement with bedside staff, which fosters trust and collaboration. This partnership is key, as these interactions instill a common mission and foster a culture of sepsis improvement that is required to achieve sustained success and improved patient outcomes.
Dr. Dugar is Director, Point-of-Care Ultrasound, Department of Critical Care, Respiratory Institute, Assistant Professor, Cleveland Clinic Lerner College of Medicine, Cleveland, OH. Dr. Jayaprakash is Associate Medical Director, Quality, Emergency Medicine, Physician Lead, Henry Ford Health Sepsis Program. Dr. Reilkoff is Executive Medical Director of Critical Care, M Health Fairview Intensive Care Units, Director of Acting Internship in Critical Care, University of Minnesota Medical School, Associate Professor of Medicine and Surgery, University of Minnesota. Dr. Duggal is Vice-Chair, Department of Critical Care, Respiratory Institute, Director, Critical Care Clinical Research, Associate Professor, Cleveland Clinic Lerner College of Medicine, Cleveland, OH
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801-810.
2. Ginestra JC, Coz Yataco AO, Dugar SP, Dettmer MR. Hospital-onset sepsis warrants expanded investigation and consideration as a unique clinical entity. Chest. 2024;S0012-3692(24):00039-4.
3. Markwart R, Saito H, Harder T, et al. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med. 2020;46(8):1536-1551.
4. Rhee C, Wang R, Zhang Z, et al. Epidemiology of hospital-onset versus community-onset sepsis in U.S. hospitals and association with mortality: a retrospective analysis using electronic clinical data. Crit Care Med. 2019;47(9):1169-1176.
5. Wong A, Otles E, Donnelly JP, et al. External validation of a widely implemented proprietary sepsis prediction model in hospitalized patients. JAMA Intern Med. 2021;181(8):1065-1070.
6. Baghdadi JD, Brook RH, Uslan DZ, et al. Association of a care bundle for early sepsis management with mortality among patients with hospital-onset or community-onset sepsis. JAMA Intern Med. 2020;180(5):707-716.
7. Baghdadi JD, Wong MD, Uslan DZ, et al. Adherence to the SEP-1 sepsis bundle in hospital-onset v. community-onset sepsis: a multicenter retrospective cohort study. J Gen Intern Med. 2020;35(4):1153-1160.
8. Basheer A. Patients with hospital-onset sepsis are less likely to receive sepsis bundle care than those with community-onset sepsis. Evid Based Nurs. 2021;24(3):99.
A 47-year-old woman with a history of cirrhosis is admitted with an acute kidney injury and altered mental status. On the initial workup, there are no signs of infection, and dehydration is determined to be the cause of the kidney injury. There are signs of improvement in the kidney injury with hydration. On hospital day 3, the patient develops a fever (101.9 o F) with accompanying leukocytosis to 14,000. Concerned for infection, the team starts empiric broad spectrum antibiotics for presumed spontaneous bacterial peritonitis. The next day (hospital day 4), a rapid response evaluation is activated as the patient is demonstrating increasing confusion, hypotension with a systolic blood pressure of 70 mm Hg, and elevated lactic acid. The patient receives 1 L of normal saline and transfers to the ICU. The new critical care fellow, who has just read up on sepsis early management bundles, and specifically the Severe Sepsis and Septic Shock Management Bundle (SEP-1), is reviewing the chart and notices a history of multidrug-resistant organisms in her urine cultures from an admission 2 months ago. They ask of the transferring team, “When was time zero, and was the 3-hour bundle completed?”
1 The excessive cost, both of human life and monetary, has led to the commitment of significant resources to sepsis care. Improved recognition and timely intervention for sepsis have led to noteworthy improvement in mortality. Most of this effort has been directed toward patients with sepsis diagnosed in the emergency department (ED) who are presenting with community-onset sepsis (COS). A new entity, called hospital-onset sepsis (HOS), has been described recently, defined by the Centers for Disease Control and Prevention (CDC) as both infection and organ dysfunction developing more than 48 hours after hospital admission.2
A systematic review of 51 studies found approximately 23.6% of all sepsis cases are HOS. The proportion of HOS is even higher (more than 45%) in patients admitted to the ICU with sepsis.3 The outcome for this group remains comparatively poor. The hospital mortality among patients with HOS is 35%, which increases to 52% with progression to septic shock compared with 25% with COS.3 Even after adjusting for baseline factors that make one prone to developing infection in the hospital, a patient developing HOS has three-times a higher risk of dying compared with a patient who never developed sepsis and two-times a higher risk of dying compared with patients with COS.4 Furthermore, HOS utilizes more resources with significantly longer ICU and hospital stays and has five-times the hospital cost compared with COS.4
The two most crucial factors in improving sepsis outcomes, as identified by the Surviving Sepsis Campaign guidelines, are: 1) prompt identification and treatment within the first few hours of onset and 2) regular reevaluation of the patient’s response to treatment.
Prompt identification
Diagnosing sepsis in the patient who is hospitalized is challenging. Patients admitted to the hospital often have competing comorbidities, have existing organ failure, or are in a postoperative/intervention state that clouds the application and interpretation of vital sign triggers customarily used to identify sepsis. The positive predictive value for all existing sepsis definitions and diagnostic criteria is dismally low. 5 And while automated electronic sepsis alerts may improve processes of care, they still have poor positive predictive value and have not impacted patient-centered outcomes (mortality or length of stay). Furthermore, the causative microorganisms often associated with hospital-acquired infections are complex, are drug-resistant, and can have courses which further delay identification. Finally, cognitive errors, such as anchoring biases or premature diagnosis closure, can contribute to provider-level identification delays that are only further exacerbated by system issues, such as capacity constraints, staffing issues, and differing paces between wards that tend to impede time-sensitive evaluations and interventions. 4,6,7
Management
The SEP-1 core measure uses a framework of early recognition of infection and completion of the sepsis bundles in a timely manner to improve outcomes. Patients with HOS are less likely than those with COS to receive Centers for Medicare & Medicaid Services SEP-1-compliant care, including timely blood culture collection, initial and repeat lactate testing, and fluid resuscitation.8 The Surviving Sepsis Campaign has explored barriers to managing HOS. Among caregivers, these include delay in recognition, poor communication regarding change in patient status, not prioritizing treatment for sepsis, failure to measure lactate, delayed or no antimicrobial administration, and inadequate fluid resuscitation. In one study, the adherence to SEP-1 for HOS was reported at 13% compared with 39.9% in COS. The differences in initial sepsis management included timing of antimicrobials and fluid resuscitation, which accounted for 23% of observed greater mortality risk among patients with HOS compared with COS.6,8 It remains unclear how these recommendations should be applied and whether some of these recommendations confer the same benefits for patients with HOS as for those with COS. For example, administration of fluids conferred no additional benefit to patients with HOS, while rapid antimicrobial administration was shown to be associated with improved mortality in patients with HOS. Although, the optimal timing for treatment initiation and microbial coverage has not been established.
The path forward
Effective HOS management requires both individual and systematic approaches. How clinicians identify a patient with sepsis must be context-dependent. Although standard criteria exist for defining sepsis, the approach to a patient presenting to the ED from home should differ from that of a patient who has been hospitalized for several days, is postoperative, or is in the ICU on multiple forms of life support. Clinical medicine is context-dependent, and the same principles apply to sepsis management. To address the diagnostic uncertainty of the syndrome, providers must remain vigilant and maintain a clinical “iterative urgency” in diagnosing and managing sepsis. While machine learning algorithms have potential, they still rely on human intervention and interaction to navigate the complexities of HOS diagnosis.
At the system level, survival from sepsis is determined by the speed with which complex medical care is delivered and the effectiveness with which resources and personnel are mobilized and coordinated. The Hospital Sepsis Program Core Elements, released by the CDC, serves as an initial playbook to aid hospitals in establishing comprehensive sepsis improvement programs.
A second invaluable resource for hospitals in sepsis management is the rapid response team (RRT). Studies have shown that resolute RRTs can enhance patient outcomes and compliance with sepsis bundles; though, the composition and scope of these teams are crucial to their effectiveness. Responding to in-hospital emergencies and urgencies without conflicting responsibilities is an essential feature of a successful RRT. Often, they are familiar with bundles, protocols, and documentation, and members of these teams can offer clinical and/or technical expertise as well as support active participation and reengagement with bedside staff, which fosters trust and collaboration. This partnership is key, as these interactions instill a common mission and foster a culture of sepsis improvement that is required to achieve sustained success and improved patient outcomes.
Dr. Dugar is Director, Point-of-Care Ultrasound, Department of Critical Care, Respiratory Institute, Assistant Professor, Cleveland Clinic Lerner College of Medicine, Cleveland, OH. Dr. Jayaprakash is Associate Medical Director, Quality, Emergency Medicine, Physician Lead, Henry Ford Health Sepsis Program. Dr. Reilkoff is Executive Medical Director of Critical Care, M Health Fairview Intensive Care Units, Director of Acting Internship in Critical Care, University of Minnesota Medical School, Associate Professor of Medicine and Surgery, University of Minnesota. Dr. Duggal is Vice-Chair, Department of Critical Care, Respiratory Institute, Director, Critical Care Clinical Research, Associate Professor, Cleveland Clinic Lerner College of Medicine, Cleveland, OH
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801-810.
2. Ginestra JC, Coz Yataco AO, Dugar SP, Dettmer MR. Hospital-onset sepsis warrants expanded investigation and consideration as a unique clinical entity. Chest. 2024;S0012-3692(24):00039-4.
3. Markwart R, Saito H, Harder T, et al. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med. 2020;46(8):1536-1551.
4. Rhee C, Wang R, Zhang Z, et al. Epidemiology of hospital-onset versus community-onset sepsis in U.S. hospitals and association with mortality: a retrospective analysis using electronic clinical data. Crit Care Med. 2019;47(9):1169-1176.
5. Wong A, Otles E, Donnelly JP, et al. External validation of a widely implemented proprietary sepsis prediction model in hospitalized patients. JAMA Intern Med. 2021;181(8):1065-1070.
6. Baghdadi JD, Brook RH, Uslan DZ, et al. Association of a care bundle for early sepsis management with mortality among patients with hospital-onset or community-onset sepsis. JAMA Intern Med. 2020;180(5):707-716.
7. Baghdadi JD, Wong MD, Uslan DZ, et al. Adherence to the SEP-1 sepsis bundle in hospital-onset v. community-onset sepsis: a multicenter retrospective cohort study. J Gen Intern Med. 2020;35(4):1153-1160.
8. Basheer A. Patients with hospital-onset sepsis are less likely to receive sepsis bundle care than those with community-onset sepsis. Evid Based Nurs. 2021;24(3):99.
A 47-year-old woman with a history of cirrhosis is admitted with an acute kidney injury and altered mental status. On the initial workup, there are no signs of infection, and dehydration is determined to be the cause of the kidney injury. There are signs of improvement in the kidney injury with hydration. On hospital day 3, the patient develops a fever (101.9 o F) with accompanying leukocytosis to 14,000. Concerned for infection, the team starts empiric broad spectrum antibiotics for presumed spontaneous bacterial peritonitis. The next day (hospital day 4), a rapid response evaluation is activated as the patient is demonstrating increasing confusion, hypotension with a systolic blood pressure of 70 mm Hg, and elevated lactic acid. The patient receives 1 L of normal saline and transfers to the ICU. The new critical care fellow, who has just read up on sepsis early management bundles, and specifically the Severe Sepsis and Septic Shock Management Bundle (SEP-1), is reviewing the chart and notices a history of multidrug-resistant organisms in her urine cultures from an admission 2 months ago. They ask of the transferring team, “When was time zero, and was the 3-hour bundle completed?”
1 The excessive cost, both of human life and monetary, has led to the commitment of significant resources to sepsis care. Improved recognition and timely intervention for sepsis have led to noteworthy improvement in mortality. Most of this effort has been directed toward patients with sepsis diagnosed in the emergency department (ED) who are presenting with community-onset sepsis (COS). A new entity, called hospital-onset sepsis (HOS), has been described recently, defined by the Centers for Disease Control and Prevention (CDC) as both infection and organ dysfunction developing more than 48 hours after hospital admission.2
A systematic review of 51 studies found approximately 23.6% of all sepsis cases are HOS. The proportion of HOS is even higher (more than 45%) in patients admitted to the ICU with sepsis.3 The outcome for this group remains comparatively poor. The hospital mortality among patients with HOS is 35%, which increases to 52% with progression to septic shock compared with 25% with COS.3 Even after adjusting for baseline factors that make one prone to developing infection in the hospital, a patient developing HOS has three-times a higher risk of dying compared with a patient who never developed sepsis and two-times a higher risk of dying compared with patients with COS.4 Furthermore, HOS utilizes more resources with significantly longer ICU and hospital stays and has five-times the hospital cost compared with COS.4
The two most crucial factors in improving sepsis outcomes, as identified by the Surviving Sepsis Campaign guidelines, are: 1) prompt identification and treatment within the first few hours of onset and 2) regular reevaluation of the patient’s response to treatment.
Prompt identification
Diagnosing sepsis in the patient who is hospitalized is challenging. Patients admitted to the hospital often have competing comorbidities, have existing organ failure, or are in a postoperative/intervention state that clouds the application and interpretation of vital sign triggers customarily used to identify sepsis. The positive predictive value for all existing sepsis definitions and diagnostic criteria is dismally low. 5 And while automated electronic sepsis alerts may improve processes of care, they still have poor positive predictive value and have not impacted patient-centered outcomes (mortality or length of stay). Furthermore, the causative microorganisms often associated with hospital-acquired infections are complex, are drug-resistant, and can have courses which further delay identification. Finally, cognitive errors, such as anchoring biases or premature diagnosis closure, can contribute to provider-level identification delays that are only further exacerbated by system issues, such as capacity constraints, staffing issues, and differing paces between wards that tend to impede time-sensitive evaluations and interventions. 4,6,7
Management
The SEP-1 core measure uses a framework of early recognition of infection and completion of the sepsis bundles in a timely manner to improve outcomes. Patients with HOS are less likely than those with COS to receive Centers for Medicare & Medicaid Services SEP-1-compliant care, including timely blood culture collection, initial and repeat lactate testing, and fluid resuscitation.8 The Surviving Sepsis Campaign has explored barriers to managing HOS. Among caregivers, these include delay in recognition, poor communication regarding change in patient status, not prioritizing treatment for sepsis, failure to measure lactate, delayed or no antimicrobial administration, and inadequate fluid resuscitation. In one study, the adherence to SEP-1 for HOS was reported at 13% compared with 39.9% in COS. The differences in initial sepsis management included timing of antimicrobials and fluid resuscitation, which accounted for 23% of observed greater mortality risk among patients with HOS compared with COS.6,8 It remains unclear how these recommendations should be applied and whether some of these recommendations confer the same benefits for patients with HOS as for those with COS. For example, administration of fluids conferred no additional benefit to patients with HOS, while rapid antimicrobial administration was shown to be associated with improved mortality in patients with HOS. Although, the optimal timing for treatment initiation and microbial coverage has not been established.
The path forward
Effective HOS management requires both individual and systematic approaches. How clinicians identify a patient with sepsis must be context-dependent. Although standard criteria exist for defining sepsis, the approach to a patient presenting to the ED from home should differ from that of a patient who has been hospitalized for several days, is postoperative, or is in the ICU on multiple forms of life support. Clinical medicine is context-dependent, and the same principles apply to sepsis management. To address the diagnostic uncertainty of the syndrome, providers must remain vigilant and maintain a clinical “iterative urgency” in diagnosing and managing sepsis. While machine learning algorithms have potential, they still rely on human intervention and interaction to navigate the complexities of HOS diagnosis.
At the system level, survival from sepsis is determined by the speed with which complex medical care is delivered and the effectiveness with which resources and personnel are mobilized and coordinated. The Hospital Sepsis Program Core Elements, released by the CDC, serves as an initial playbook to aid hospitals in establishing comprehensive sepsis improvement programs.
A second invaluable resource for hospitals in sepsis management is the rapid response team (RRT). Studies have shown that resolute RRTs can enhance patient outcomes and compliance with sepsis bundles; though, the composition and scope of these teams are crucial to their effectiveness. Responding to in-hospital emergencies and urgencies without conflicting responsibilities is an essential feature of a successful RRT. Often, they are familiar with bundles, protocols, and documentation, and members of these teams can offer clinical and/or technical expertise as well as support active participation and reengagement with bedside staff, which fosters trust and collaboration. This partnership is key, as these interactions instill a common mission and foster a culture of sepsis improvement that is required to achieve sustained success and improved patient outcomes.
Dr. Dugar is Director, Point-of-Care Ultrasound, Department of Critical Care, Respiratory Institute, Assistant Professor, Cleveland Clinic Lerner College of Medicine, Cleveland, OH. Dr. Jayaprakash is Associate Medical Director, Quality, Emergency Medicine, Physician Lead, Henry Ford Health Sepsis Program. Dr. Reilkoff is Executive Medical Director of Critical Care, M Health Fairview Intensive Care Units, Director of Acting Internship in Critical Care, University of Minnesota Medical School, Associate Professor of Medicine and Surgery, University of Minnesota. Dr. Duggal is Vice-Chair, Department of Critical Care, Respiratory Institute, Director, Critical Care Clinical Research, Associate Professor, Cleveland Clinic Lerner College of Medicine, Cleveland, OH
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801-810.
2. Ginestra JC, Coz Yataco AO, Dugar SP, Dettmer MR. Hospital-onset sepsis warrants expanded investigation and consideration as a unique clinical entity. Chest. 2024;S0012-3692(24):00039-4.
3. Markwart R, Saito H, Harder T, et al. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med. 2020;46(8):1536-1551.
4. Rhee C, Wang R, Zhang Z, et al. Epidemiology of hospital-onset versus community-onset sepsis in U.S. hospitals and association with mortality: a retrospective analysis using electronic clinical data. Crit Care Med. 2019;47(9):1169-1176.
5. Wong A, Otles E, Donnelly JP, et al. External validation of a widely implemented proprietary sepsis prediction model in hospitalized patients. JAMA Intern Med. 2021;181(8):1065-1070.
6. Baghdadi JD, Brook RH, Uslan DZ, et al. Association of a care bundle for early sepsis management with mortality among patients with hospital-onset or community-onset sepsis. JAMA Intern Med. 2020;180(5):707-716.
7. Baghdadi JD, Wong MD, Uslan DZ, et al. Adherence to the SEP-1 sepsis bundle in hospital-onset v. community-onset sepsis: a multicenter retrospective cohort study. J Gen Intern Med. 2020;35(4):1153-1160.
8. Basheer A. Patients with hospital-onset sepsis are less likely to receive sepsis bundle care than those with community-onset sepsis. Evid Based Nurs. 2021;24(3):99.
AI Tools Could Change Pulmonological Imaging and Prognosis
MADRID — Artificial intelligence (AI) can enhance endobronchial ultrasound (EBUS) image processing and new techniques such as cryoEBUS to achieve significant diagnostic and prognostic breakthroughs in interventional pulmonology and general pulmonology.
Pulmonologists are witnessing a surge in new technologies for endoscopy and pulmonology in general. Some, such as AI, robotic bronchoscopy, radiomics, or improvements in electromagnetic bronchial navigation, are minimally invasive diagnostic techniques that significantly enhance the characterization of lung lesions, said Virginia Pajares, MD, a member of the Catalan Society of Pulmonology and coordinator of the Bronchoscopy Unit at Hospital de Sant Pau in Barcelona, Spain. She spoke at the XLI Pneumological Day of the Catalan Society of Pulmonology in Vilanova i la Geltrú, Spain.
Regarding AI, pulmonologists “already have platforms that enable the calculation of the malignancy risk of lung lesions and mediastinal adenopathies. In addition, some devices that allow for an initial radiological assessment of lung nodules are starting to be used,” said Dr. Pajares.
Radiomics: Histology and Markers
“At an endoscopic level, some studies have confirmed the ability of AI applied to imaging to differentiate between benign and malignant lesions, although currently the studies are limited and in the initial stages,” said Dr. Pajares. “AI in interventional pulmonology will be highly beneficial in image interpretation and patient assessment for those who require more invasive diagnostic techniques or for follow-up.”
Regarding the application of AI in medicine, “we lack knowledge and require specific training, especially concerning the learning curve of different technologies, such as electromagnetic navigation, cryoEBUS, or robotic bronchoscopy, which require significant training efforts,” said Dr. Pajares. “The use of AI without a specific goal, that is, creating a mathematical algorithm and feeding it with clinical patient data without control and validation, can lead to inaccurate conclusions. Additionally, we need to determine how to input patient data into these systems to avoid ethical issues, and, of course, legislation on this matter is essential.”
Electromagnetic Navigation
Bronchial electromagnetic navigation is a bronchoscopic technique that allows access to peripheral lung lesions. “It involves virtual route planning using the patient’s chest CT scan and subsequently performing bronchoscopy with navigation using a dirigible electromagnetic probe that allows access to the lesion,” Dr. Pajares explained. “Currently, we have navigators that can incorporate imaging techniques (fluoroscopy or cone-beam CT) to immediately correct discrepancies observed during navigation.”
These new technologies enable a greater number of precise diagnoses and may bring greater patient safety. Studies like NAVIGATE, which was published in 2022 by Folch and colleagues, confirm the diagnostic possibilities and performance of electromagnetic navigation.
In this prospective study, which followed patients for 24 months, the indications are broad. “Its most common use is as a diagnostic technique for peripheral lung nodules and for marking lung lesions for surgical resection or marking for radiotherapy field fiducial placement,” said Dr. Pajares. “Results are also beginning to be published on the treatment of lung lesions using electromagnetic navigation ablation, demonstrating its safety and efficacy in this area.”
Nonsolid Imaging
The challenges in navigation include “improving the diagnosis of lung lesions that are nonsolid, known as ground glass opacities, and verifying it as an additional treatment option for lung nodules in patients who are not candidates for surgical resection,” said Dr. Pajares.
Tess Kramer, PhD, of Amsterdam University Medical Center, Amsterdam, the Netherlands, advocates for the combined use of different technologies to have a beneficial impact on patients’ clinical outcomes.
Robotic bronchoscopy has been implemented in the United States for several years, enhancing the precision of lung nodule diagnosis. However, “currently, there are no clear differences in the diagnostic performance of robotic bronchoscopy compared with navigation in general. Soon, there will be studies to assess in which type of nodules one technique may be more cost-effective.” No centers in Spain have this technology yet, “although some are already evaluating the acquisition of robotic bronchoscopy; it’s only a matter of time,” said Dr. Pajares.
Improvements in echobronchoscopy technology include high-quality image processors and smaller device calibers with greater angulation to diagnose lesions and hard-to-reach adenopathies. From an imaging perspective, AI, combined with the creation of risk calculators, could enable the prediction of lymph node malignancy.
Moreover, the use of small-caliber cryoprobes (1.1 mm) for obtaining samples of adenopathies (cryoEBUS) has enhanced diagnosis by enabling larger tissue samples. Current studies are being conducted to confirm the utility of cryoEBUS in pathologies requiring extensive molecular and immunohistochemical studies for diagnosing lymphoproliferative syndromes or neoplasms.
In a different context, liquid biopsy, a recent laboratory technology unrelated to bronchoscopy, allows the analysis of blood/pleural fluid samples that were extracted using the aforementioned technologies to locate tumor cells and differentiate between malignancy and benignity.
The Challenge of Pneumonitis
Samantha Aso, MD, a pulmonologist, member of the Catalan Society of Pulmonology, and specialist at the Lung Unit of Bellvitge University Hospital in Barcelona, Spain, discussed the challenge of managing pneumonitis in oncology patients.
Pneumonitis is an inflammation of the lungs that can be secondary to treatments, such as oncological therapy, which is the leading cause in 15%-50% of cases. Most oncological treatments can result in this process, including chemotherapy, chest radiotherapy, targeted therapies, conjugated monoclonal antibodies, and monotherapy.
To date, there is no known idiosyncratic cause of this process, except for autoimmune diseases. Pulmonary fibrosis is believed to be a risk factor. “Patients with interstitial lung disease and pulmonary fibrosis have been found to have a higher mortality risk due to pneumonitis. Consequently, cancer treatment cannot be administered to these patients,” said Dr. Aso.
Pulmonologists face the challenge of managing pneumonitis secondary to monotherapy, which currently is treated with cortisone. Patients respond well to this medication, but after corticosteroid withdrawal, reinflammation may occur. “In pneumonitis patients, oncological treatment (monotherapy) should be suspended while pulmonologists manage the pneumonitis with corticosteroids. However, we are uncertain about how rapidly or slowly to reduce the dosage. We cannot taper these doses as quickly as desired because reinflammation may occur, and to date, there are no alternative treatments apart from corticosteroids,” said Dr. Aso.
She noted that excellent survival results are achieved with monotherapy, but further research is required on the safety of antineoplastic drugs as a secondary endpoint. “Suspending oncological treatment due to pneumonitis means that patients are not receiving adequate cancer treatment, which has a significant psychological impact that also needs to be addressed,” Dr. Aso concluded.
Dr. Pajares and Dr. Aso declared no relevant financial relationships.
This story was translated from the Medscape Spanish edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
MADRID — Artificial intelligence (AI) can enhance endobronchial ultrasound (EBUS) image processing and new techniques such as cryoEBUS to achieve significant diagnostic and prognostic breakthroughs in interventional pulmonology and general pulmonology.
Pulmonologists are witnessing a surge in new technologies for endoscopy and pulmonology in general. Some, such as AI, robotic bronchoscopy, radiomics, or improvements in electromagnetic bronchial navigation, are minimally invasive diagnostic techniques that significantly enhance the characterization of lung lesions, said Virginia Pajares, MD, a member of the Catalan Society of Pulmonology and coordinator of the Bronchoscopy Unit at Hospital de Sant Pau in Barcelona, Spain. She spoke at the XLI Pneumological Day of the Catalan Society of Pulmonology in Vilanova i la Geltrú, Spain.
Regarding AI, pulmonologists “already have platforms that enable the calculation of the malignancy risk of lung lesions and mediastinal adenopathies. In addition, some devices that allow for an initial radiological assessment of lung nodules are starting to be used,” said Dr. Pajares.
Radiomics: Histology and Markers
“At an endoscopic level, some studies have confirmed the ability of AI applied to imaging to differentiate between benign and malignant lesions, although currently the studies are limited and in the initial stages,” said Dr. Pajares. “AI in interventional pulmonology will be highly beneficial in image interpretation and patient assessment for those who require more invasive diagnostic techniques or for follow-up.”
Regarding the application of AI in medicine, “we lack knowledge and require specific training, especially concerning the learning curve of different technologies, such as electromagnetic navigation, cryoEBUS, or robotic bronchoscopy, which require significant training efforts,” said Dr. Pajares. “The use of AI without a specific goal, that is, creating a mathematical algorithm and feeding it with clinical patient data without control and validation, can lead to inaccurate conclusions. Additionally, we need to determine how to input patient data into these systems to avoid ethical issues, and, of course, legislation on this matter is essential.”
Electromagnetic Navigation
Bronchial electromagnetic navigation is a bronchoscopic technique that allows access to peripheral lung lesions. “It involves virtual route planning using the patient’s chest CT scan and subsequently performing bronchoscopy with navigation using a dirigible electromagnetic probe that allows access to the lesion,” Dr. Pajares explained. “Currently, we have navigators that can incorporate imaging techniques (fluoroscopy or cone-beam CT) to immediately correct discrepancies observed during navigation.”
These new technologies enable a greater number of precise diagnoses and may bring greater patient safety. Studies like NAVIGATE, which was published in 2022 by Folch and colleagues, confirm the diagnostic possibilities and performance of electromagnetic navigation.
In this prospective study, which followed patients for 24 months, the indications are broad. “Its most common use is as a diagnostic technique for peripheral lung nodules and for marking lung lesions for surgical resection or marking for radiotherapy field fiducial placement,” said Dr. Pajares. “Results are also beginning to be published on the treatment of lung lesions using electromagnetic navigation ablation, demonstrating its safety and efficacy in this area.”
Nonsolid Imaging
The challenges in navigation include “improving the diagnosis of lung lesions that are nonsolid, known as ground glass opacities, and verifying it as an additional treatment option for lung nodules in patients who are not candidates for surgical resection,” said Dr. Pajares.
Tess Kramer, PhD, of Amsterdam University Medical Center, Amsterdam, the Netherlands, advocates for the combined use of different technologies to have a beneficial impact on patients’ clinical outcomes.
Robotic bronchoscopy has been implemented in the United States for several years, enhancing the precision of lung nodule diagnosis. However, “currently, there are no clear differences in the diagnostic performance of robotic bronchoscopy compared with navigation in general. Soon, there will be studies to assess in which type of nodules one technique may be more cost-effective.” No centers in Spain have this technology yet, “although some are already evaluating the acquisition of robotic bronchoscopy; it’s only a matter of time,” said Dr. Pajares.
Improvements in echobronchoscopy technology include high-quality image processors and smaller device calibers with greater angulation to diagnose lesions and hard-to-reach adenopathies. From an imaging perspective, AI, combined with the creation of risk calculators, could enable the prediction of lymph node malignancy.
Moreover, the use of small-caliber cryoprobes (1.1 mm) for obtaining samples of adenopathies (cryoEBUS) has enhanced diagnosis by enabling larger tissue samples. Current studies are being conducted to confirm the utility of cryoEBUS in pathologies requiring extensive molecular and immunohistochemical studies for diagnosing lymphoproliferative syndromes or neoplasms.
In a different context, liquid biopsy, a recent laboratory technology unrelated to bronchoscopy, allows the analysis of blood/pleural fluid samples that were extracted using the aforementioned technologies to locate tumor cells and differentiate between malignancy and benignity.
The Challenge of Pneumonitis
Samantha Aso, MD, a pulmonologist, member of the Catalan Society of Pulmonology, and specialist at the Lung Unit of Bellvitge University Hospital in Barcelona, Spain, discussed the challenge of managing pneumonitis in oncology patients.
Pneumonitis is an inflammation of the lungs that can be secondary to treatments, such as oncological therapy, which is the leading cause in 15%-50% of cases. Most oncological treatments can result in this process, including chemotherapy, chest radiotherapy, targeted therapies, conjugated monoclonal antibodies, and monotherapy.
To date, there is no known idiosyncratic cause of this process, except for autoimmune diseases. Pulmonary fibrosis is believed to be a risk factor. “Patients with interstitial lung disease and pulmonary fibrosis have been found to have a higher mortality risk due to pneumonitis. Consequently, cancer treatment cannot be administered to these patients,” said Dr. Aso.
Pulmonologists face the challenge of managing pneumonitis secondary to monotherapy, which currently is treated with cortisone. Patients respond well to this medication, but after corticosteroid withdrawal, reinflammation may occur. “In pneumonitis patients, oncological treatment (monotherapy) should be suspended while pulmonologists manage the pneumonitis with corticosteroids. However, we are uncertain about how rapidly or slowly to reduce the dosage. We cannot taper these doses as quickly as desired because reinflammation may occur, and to date, there are no alternative treatments apart from corticosteroids,” said Dr. Aso.
She noted that excellent survival results are achieved with monotherapy, but further research is required on the safety of antineoplastic drugs as a secondary endpoint. “Suspending oncological treatment due to pneumonitis means that patients are not receiving adequate cancer treatment, which has a significant psychological impact that also needs to be addressed,” Dr. Aso concluded.
Dr. Pajares and Dr. Aso declared no relevant financial relationships.
This story was translated from the Medscape Spanish edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
MADRID — Artificial intelligence (AI) can enhance endobronchial ultrasound (EBUS) image processing and new techniques such as cryoEBUS to achieve significant diagnostic and prognostic breakthroughs in interventional pulmonology and general pulmonology.
Pulmonologists are witnessing a surge in new technologies for endoscopy and pulmonology in general. Some, such as AI, robotic bronchoscopy, radiomics, or improvements in electromagnetic bronchial navigation, are minimally invasive diagnostic techniques that significantly enhance the characterization of lung lesions, said Virginia Pajares, MD, a member of the Catalan Society of Pulmonology and coordinator of the Bronchoscopy Unit at Hospital de Sant Pau in Barcelona, Spain. She spoke at the XLI Pneumological Day of the Catalan Society of Pulmonology in Vilanova i la Geltrú, Spain.
Regarding AI, pulmonologists “already have platforms that enable the calculation of the malignancy risk of lung lesions and mediastinal adenopathies. In addition, some devices that allow for an initial radiological assessment of lung nodules are starting to be used,” said Dr. Pajares.
Radiomics: Histology and Markers
“At an endoscopic level, some studies have confirmed the ability of AI applied to imaging to differentiate between benign and malignant lesions, although currently the studies are limited and in the initial stages,” said Dr. Pajares. “AI in interventional pulmonology will be highly beneficial in image interpretation and patient assessment for those who require more invasive diagnostic techniques or for follow-up.”
Regarding the application of AI in medicine, “we lack knowledge and require specific training, especially concerning the learning curve of different technologies, such as electromagnetic navigation, cryoEBUS, or robotic bronchoscopy, which require significant training efforts,” said Dr. Pajares. “The use of AI without a specific goal, that is, creating a mathematical algorithm and feeding it with clinical patient data without control and validation, can lead to inaccurate conclusions. Additionally, we need to determine how to input patient data into these systems to avoid ethical issues, and, of course, legislation on this matter is essential.”
Electromagnetic Navigation
Bronchial electromagnetic navigation is a bronchoscopic technique that allows access to peripheral lung lesions. “It involves virtual route planning using the patient’s chest CT scan and subsequently performing bronchoscopy with navigation using a dirigible electromagnetic probe that allows access to the lesion,” Dr. Pajares explained. “Currently, we have navigators that can incorporate imaging techniques (fluoroscopy or cone-beam CT) to immediately correct discrepancies observed during navigation.”
These new technologies enable a greater number of precise diagnoses and may bring greater patient safety. Studies like NAVIGATE, which was published in 2022 by Folch and colleagues, confirm the diagnostic possibilities and performance of electromagnetic navigation.
In this prospective study, which followed patients for 24 months, the indications are broad. “Its most common use is as a diagnostic technique for peripheral lung nodules and for marking lung lesions for surgical resection or marking for radiotherapy field fiducial placement,” said Dr. Pajares. “Results are also beginning to be published on the treatment of lung lesions using electromagnetic navigation ablation, demonstrating its safety and efficacy in this area.”
Nonsolid Imaging
The challenges in navigation include “improving the diagnosis of lung lesions that are nonsolid, known as ground glass opacities, and verifying it as an additional treatment option for lung nodules in patients who are not candidates for surgical resection,” said Dr. Pajares.
Tess Kramer, PhD, of Amsterdam University Medical Center, Amsterdam, the Netherlands, advocates for the combined use of different technologies to have a beneficial impact on patients’ clinical outcomes.
Robotic bronchoscopy has been implemented in the United States for several years, enhancing the precision of lung nodule diagnosis. However, “currently, there are no clear differences in the diagnostic performance of robotic bronchoscopy compared with navigation in general. Soon, there will be studies to assess in which type of nodules one technique may be more cost-effective.” No centers in Spain have this technology yet, “although some are already evaluating the acquisition of robotic bronchoscopy; it’s only a matter of time,” said Dr. Pajares.
Improvements in echobronchoscopy technology include high-quality image processors and smaller device calibers with greater angulation to diagnose lesions and hard-to-reach adenopathies. From an imaging perspective, AI, combined with the creation of risk calculators, could enable the prediction of lymph node malignancy.
Moreover, the use of small-caliber cryoprobes (1.1 mm) for obtaining samples of adenopathies (cryoEBUS) has enhanced diagnosis by enabling larger tissue samples. Current studies are being conducted to confirm the utility of cryoEBUS in pathologies requiring extensive molecular and immunohistochemical studies for diagnosing lymphoproliferative syndromes or neoplasms.
In a different context, liquid biopsy, a recent laboratory technology unrelated to bronchoscopy, allows the analysis of blood/pleural fluid samples that were extracted using the aforementioned technologies to locate tumor cells and differentiate between malignancy and benignity.
The Challenge of Pneumonitis
Samantha Aso, MD, a pulmonologist, member of the Catalan Society of Pulmonology, and specialist at the Lung Unit of Bellvitge University Hospital in Barcelona, Spain, discussed the challenge of managing pneumonitis in oncology patients.
Pneumonitis is an inflammation of the lungs that can be secondary to treatments, such as oncological therapy, which is the leading cause in 15%-50% of cases. Most oncological treatments can result in this process, including chemotherapy, chest radiotherapy, targeted therapies, conjugated monoclonal antibodies, and monotherapy.
To date, there is no known idiosyncratic cause of this process, except for autoimmune diseases. Pulmonary fibrosis is believed to be a risk factor. “Patients with interstitial lung disease and pulmonary fibrosis have been found to have a higher mortality risk due to pneumonitis. Consequently, cancer treatment cannot be administered to these patients,” said Dr. Aso.
Pulmonologists face the challenge of managing pneumonitis secondary to monotherapy, which currently is treated with cortisone. Patients respond well to this medication, but after corticosteroid withdrawal, reinflammation may occur. “In pneumonitis patients, oncological treatment (monotherapy) should be suspended while pulmonologists manage the pneumonitis with corticosteroids. However, we are uncertain about how rapidly or slowly to reduce the dosage. We cannot taper these doses as quickly as desired because reinflammation may occur, and to date, there are no alternative treatments apart from corticosteroids,” said Dr. Aso.
She noted that excellent survival results are achieved with monotherapy, but further research is required on the safety of antineoplastic drugs as a secondary endpoint. “Suspending oncological treatment due to pneumonitis means that patients are not receiving adequate cancer treatment, which has a significant psychological impact that also needs to be addressed,” Dr. Aso concluded.
Dr. Pajares and Dr. Aso declared no relevant financial relationships.
This story was translated from the Medscape Spanish edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
NIH to Begin Long COVID Trial Focused on Sleep, Exercise
The National institutes of Health will soon start a clinical trial in an attempt to find potential treatments for symptoms of long COVID, focusing on sleep disturbances, problems with exercise, and post-exertional malaise.
“When people can’t get reliable sleep, can’t exert themselves and feel sick following tasks that used to be simple, the physical and mental anguish can lead to feelings of utter helplessness,” Walter J. Koroshetz, MD, director of the NIH’s National Institute of Neurological Disorders and Stroke, said in a statement. “We urgently need to come up with answers to help those struggling with long COVID feel whole again.”
The new trials will be part of the NIH’s Researching COVID to Enhance Recovery initiative, known as RECOVER. Since beginning enrollment in July 2023 for four trials, RECOVER now features eight trials across the country looking at all parts of long COVID. RECOVER is part of a $1.15 billion nationwide program that Congress approved in 2020 for the NIH to research and test treatments for long COVID.
While focused on sleep disturbances, the trial will test two Food and Drug Administration–approved drugs currently used to treat people with hypersomnia. There will also be a trial to test if melatonin helps people with long COVID-related sleep problems. Light therapy will also be tested.
The trials that deal with problems people have had with exercise will focus on personalized cardiopulmonary rehabilitation, where patients experiment with exercise training, strength and flexibility training, education, and social support.
Another trial will look at structured pacing, which is designed to help people with exercise problems identify, control, and ease long COVID symptoms.
A version of this article appeared on WebMD.com.
The National institutes of Health will soon start a clinical trial in an attempt to find potential treatments for symptoms of long COVID, focusing on sleep disturbances, problems with exercise, and post-exertional malaise.
“When people can’t get reliable sleep, can’t exert themselves and feel sick following tasks that used to be simple, the physical and mental anguish can lead to feelings of utter helplessness,” Walter J. Koroshetz, MD, director of the NIH’s National Institute of Neurological Disorders and Stroke, said in a statement. “We urgently need to come up with answers to help those struggling with long COVID feel whole again.”
The new trials will be part of the NIH’s Researching COVID to Enhance Recovery initiative, known as RECOVER. Since beginning enrollment in July 2023 for four trials, RECOVER now features eight trials across the country looking at all parts of long COVID. RECOVER is part of a $1.15 billion nationwide program that Congress approved in 2020 for the NIH to research and test treatments for long COVID.
While focused on sleep disturbances, the trial will test two Food and Drug Administration–approved drugs currently used to treat people with hypersomnia. There will also be a trial to test if melatonin helps people with long COVID-related sleep problems. Light therapy will also be tested.
The trials that deal with problems people have had with exercise will focus on personalized cardiopulmonary rehabilitation, where patients experiment with exercise training, strength and flexibility training, education, and social support.
Another trial will look at structured pacing, which is designed to help people with exercise problems identify, control, and ease long COVID symptoms.
A version of this article appeared on WebMD.com.
The National institutes of Health will soon start a clinical trial in an attempt to find potential treatments for symptoms of long COVID, focusing on sleep disturbances, problems with exercise, and post-exertional malaise.
“When people can’t get reliable sleep, can’t exert themselves and feel sick following tasks that used to be simple, the physical and mental anguish can lead to feelings of utter helplessness,” Walter J. Koroshetz, MD, director of the NIH’s National Institute of Neurological Disorders and Stroke, said in a statement. “We urgently need to come up with answers to help those struggling with long COVID feel whole again.”
The new trials will be part of the NIH’s Researching COVID to Enhance Recovery initiative, known as RECOVER. Since beginning enrollment in July 2023 for four trials, RECOVER now features eight trials across the country looking at all parts of long COVID. RECOVER is part of a $1.15 billion nationwide program that Congress approved in 2020 for the NIH to research and test treatments for long COVID.
While focused on sleep disturbances, the trial will test two Food and Drug Administration–approved drugs currently used to treat people with hypersomnia. There will also be a trial to test if melatonin helps people with long COVID-related sleep problems. Light therapy will also be tested.
The trials that deal with problems people have had with exercise will focus on personalized cardiopulmonary rehabilitation, where patients experiment with exercise training, strength and flexibility training, education, and social support.
Another trial will look at structured pacing, which is designed to help people with exercise problems identify, control, and ease long COVID symptoms.
A version of this article appeared on WebMD.com.
EASI, Other Instruments Recommended to Evaluate Patients With Atopic Dermatitis
recommended.
These include the Eczema Area and Severity Index (EASI), the Validated Investigator Global Assessment for AD (vIGAAD), and the Investigator’s Global Assessment (IGA) multiplied by or measured concurrently with a body surface area (BSA) assessment.
The recommendations are part of a consensus statement based on an updated systematic review conducted by the Harmonizing Outcome Measures for Eczema Clinical Practice (HOME-CP) initiative, whose goal is to identify validated, feasible outcome instruments designed to measure AD in the clinical setting. In the statement, which was published in JAMA Dermatology on May 22, 2024, corresponding author Eric L. Simpson, MD, MCR, professor of dermatology at Oregon Health & Science University, Portland, and coauthors described HOME-CP as “a ‘pick-and-choose’ list of valid and feasible OMIs [outcome measure instruments] that can be incorporated into the practice setting depending on the particular need of that clinic or health system.”
For the effort, the authors implemented a mixed methods design and incorporated systematic reviews and qualitative consensus methods modeled after the HOME core outcome set initiative, which developed a set of consensus-based core outcome sets for clinical trials and clinical practice. In October of 2022, a daylong in-person consensus exercise was held in Montreal, Canada, where attendees met to reach consensus on recommended instruments to measure AD clinical signs in clinical practice, based on an updated systematic review evaluating the validity of clinical signs instruments.
The review included 22 studies describing 16 instruments that assessed AD clinical signs and an additional 12 variants of instruments. The meeting was attended by 34 individuals from 13 countries, including patient and patient advocate research partners, health care professionals, researchers, methodologists, and industry representatives. Consensus was defined as less than 30% disagreement.
Following their daylong consensus exercise, the stakeholders reached consensus on recommendations to use the EASI, the vIGAAD, and an IGA multiplied or measured alongside a BSA measurement to measure the domain of clinical signs of AD in the clinical practice setting. “The use of multiple IGAs, most with insufficient validation, and the diverse methods used to assess BSA prevented participants from making specific recommendations for the exact IGA/BSA instrument,” the authors wrote. “We recommend that clinicians include at least one of the recommended instruments in their clinical practices and in documentation.”
They explained that the ideal method of measuring BSA was difficult to assess “because multiple techniques exist for its measurement, including regional percentages, the Rule of Nines, or the handprint method. Most studies did not report which method was performed, and to our knowledge, no studies have been performed in patients with AD that have formally compared them.”
During the consensus exercise, the authors noted, several clinicians “expressed concern whether the EASI was feasible for universal use in clinical practice given its complexity, long completion time, and documentation/calculation requirements.” But clinicians who commonly perform the EASI in clinical practice said that the time it takes to complete this measure “has dropped substantially and now is not a considerable burden,” they wrote, adding that, “studies have shown that with trained investigators, EASI completion times can be as low as nearly 2 minutes.”
The authors acknowledged certain limitations of their recommendations, including the lack of input from primary care clinicians. “It is unknown whether ClinROMs [clinician-reported outcome measures] for AD clinical signs are used in the primary care setting, especially given the large amount of conditions that are managed simultaneously and the ever-increasing number of primary care documentation requirements,” they wrote.
Robert Sidbury, MD, MPH, chief of the division of dermatology at Seattle Children’s Hospital, who was asked to comment on the consensus statement, said that with the advent of new, improved, and more expensive medications for AD, “it is ever more important that [the clinical] assessment is reliable and reproducible.”
Insurers “are understandably less willing to rubber-stamp approval of more expensive medications without a reliable standard by which to justify such decisions,” he added. “This is even more important in a disease state like atopic dermatitis that lacks a reliable biomarker. Therefore, one or several practical, reliable, validated severity metrics will help standardize and improve AD care.”
Dr. Sidbury, who cochaired the 2023 American Academy of Dermatology guidelines of care for the management of AD in adults with phototherapy and systemic therapies, added that the instruments evaluated in the review “can be challenging for anyone,” not just primary care providers. “The EASI isn’t that easy, and while there is a learning curve and it ultimately does, like anything, become more efficient in the gathering, it is unclear if non-AD researchers will be willing to invest the time” to routinely use it, he said.
Dr. Simpson and several coauthors reported receiving grants and personal fees from multiple pharmaceutical companies. Dr. Sidbury reported that he serves as an investigator for Regeneron, Galderma, UCB, Castle, and Pfizer; is a consultant for LEO, Lilly, Arcutis, Dermavant, and Pierre Fabre; and a speaker for Beiersdorf.
A version of this article appeared on Medscape.com .
recommended.
These include the Eczema Area and Severity Index (EASI), the Validated Investigator Global Assessment for AD (vIGAAD), and the Investigator’s Global Assessment (IGA) multiplied by or measured concurrently with a body surface area (BSA) assessment.
The recommendations are part of a consensus statement based on an updated systematic review conducted by the Harmonizing Outcome Measures for Eczema Clinical Practice (HOME-CP) initiative, whose goal is to identify validated, feasible outcome instruments designed to measure AD in the clinical setting. In the statement, which was published in JAMA Dermatology on May 22, 2024, corresponding author Eric L. Simpson, MD, MCR, professor of dermatology at Oregon Health & Science University, Portland, and coauthors described HOME-CP as “a ‘pick-and-choose’ list of valid and feasible OMIs [outcome measure instruments] that can be incorporated into the practice setting depending on the particular need of that clinic or health system.”
For the effort, the authors implemented a mixed methods design and incorporated systematic reviews and qualitative consensus methods modeled after the HOME core outcome set initiative, which developed a set of consensus-based core outcome sets for clinical trials and clinical practice. In October of 2022, a daylong in-person consensus exercise was held in Montreal, Canada, where attendees met to reach consensus on recommended instruments to measure AD clinical signs in clinical practice, based on an updated systematic review evaluating the validity of clinical signs instruments.
The review included 22 studies describing 16 instruments that assessed AD clinical signs and an additional 12 variants of instruments. The meeting was attended by 34 individuals from 13 countries, including patient and patient advocate research partners, health care professionals, researchers, methodologists, and industry representatives. Consensus was defined as less than 30% disagreement.
Following their daylong consensus exercise, the stakeholders reached consensus on recommendations to use the EASI, the vIGAAD, and an IGA multiplied or measured alongside a BSA measurement to measure the domain of clinical signs of AD in the clinical practice setting. “The use of multiple IGAs, most with insufficient validation, and the diverse methods used to assess BSA prevented participants from making specific recommendations for the exact IGA/BSA instrument,” the authors wrote. “We recommend that clinicians include at least one of the recommended instruments in their clinical practices and in documentation.”
They explained that the ideal method of measuring BSA was difficult to assess “because multiple techniques exist for its measurement, including regional percentages, the Rule of Nines, or the handprint method. Most studies did not report which method was performed, and to our knowledge, no studies have been performed in patients with AD that have formally compared them.”
During the consensus exercise, the authors noted, several clinicians “expressed concern whether the EASI was feasible for universal use in clinical practice given its complexity, long completion time, and documentation/calculation requirements.” But clinicians who commonly perform the EASI in clinical practice said that the time it takes to complete this measure “has dropped substantially and now is not a considerable burden,” they wrote, adding that, “studies have shown that with trained investigators, EASI completion times can be as low as nearly 2 minutes.”
The authors acknowledged certain limitations of their recommendations, including the lack of input from primary care clinicians. “It is unknown whether ClinROMs [clinician-reported outcome measures] for AD clinical signs are used in the primary care setting, especially given the large amount of conditions that are managed simultaneously and the ever-increasing number of primary care documentation requirements,” they wrote.
Robert Sidbury, MD, MPH, chief of the division of dermatology at Seattle Children’s Hospital, who was asked to comment on the consensus statement, said that with the advent of new, improved, and more expensive medications for AD, “it is ever more important that [the clinical] assessment is reliable and reproducible.”
Insurers “are understandably less willing to rubber-stamp approval of more expensive medications without a reliable standard by which to justify such decisions,” he added. “This is even more important in a disease state like atopic dermatitis that lacks a reliable biomarker. Therefore, one or several practical, reliable, validated severity metrics will help standardize and improve AD care.”
Dr. Sidbury, who cochaired the 2023 American Academy of Dermatology guidelines of care for the management of AD in adults with phototherapy and systemic therapies, added that the instruments evaluated in the review “can be challenging for anyone,” not just primary care providers. “The EASI isn’t that easy, and while there is a learning curve and it ultimately does, like anything, become more efficient in the gathering, it is unclear if non-AD researchers will be willing to invest the time” to routinely use it, he said.
Dr. Simpson and several coauthors reported receiving grants and personal fees from multiple pharmaceutical companies. Dr. Sidbury reported that he serves as an investigator for Regeneron, Galderma, UCB, Castle, and Pfizer; is a consultant for LEO, Lilly, Arcutis, Dermavant, and Pierre Fabre; and a speaker for Beiersdorf.
A version of this article appeared on Medscape.com .
recommended.
These include the Eczema Area and Severity Index (EASI), the Validated Investigator Global Assessment for AD (vIGAAD), and the Investigator’s Global Assessment (IGA) multiplied by or measured concurrently with a body surface area (BSA) assessment.
The recommendations are part of a consensus statement based on an updated systematic review conducted by the Harmonizing Outcome Measures for Eczema Clinical Practice (HOME-CP) initiative, whose goal is to identify validated, feasible outcome instruments designed to measure AD in the clinical setting. In the statement, which was published in JAMA Dermatology on May 22, 2024, corresponding author Eric L. Simpson, MD, MCR, professor of dermatology at Oregon Health & Science University, Portland, and coauthors described HOME-CP as “a ‘pick-and-choose’ list of valid and feasible OMIs [outcome measure instruments] that can be incorporated into the practice setting depending on the particular need of that clinic or health system.”
For the effort, the authors implemented a mixed methods design and incorporated systematic reviews and qualitative consensus methods modeled after the HOME core outcome set initiative, which developed a set of consensus-based core outcome sets for clinical trials and clinical practice. In October of 2022, a daylong in-person consensus exercise was held in Montreal, Canada, where attendees met to reach consensus on recommended instruments to measure AD clinical signs in clinical practice, based on an updated systematic review evaluating the validity of clinical signs instruments.
The review included 22 studies describing 16 instruments that assessed AD clinical signs and an additional 12 variants of instruments. The meeting was attended by 34 individuals from 13 countries, including patient and patient advocate research partners, health care professionals, researchers, methodologists, and industry representatives. Consensus was defined as less than 30% disagreement.
Following their daylong consensus exercise, the stakeholders reached consensus on recommendations to use the EASI, the vIGAAD, and an IGA multiplied or measured alongside a BSA measurement to measure the domain of clinical signs of AD in the clinical practice setting. “The use of multiple IGAs, most with insufficient validation, and the diverse methods used to assess BSA prevented participants from making specific recommendations for the exact IGA/BSA instrument,” the authors wrote. “We recommend that clinicians include at least one of the recommended instruments in their clinical practices and in documentation.”
They explained that the ideal method of measuring BSA was difficult to assess “because multiple techniques exist for its measurement, including regional percentages, the Rule of Nines, or the handprint method. Most studies did not report which method was performed, and to our knowledge, no studies have been performed in patients with AD that have formally compared them.”
During the consensus exercise, the authors noted, several clinicians “expressed concern whether the EASI was feasible for universal use in clinical practice given its complexity, long completion time, and documentation/calculation requirements.” But clinicians who commonly perform the EASI in clinical practice said that the time it takes to complete this measure “has dropped substantially and now is not a considerable burden,” they wrote, adding that, “studies have shown that with trained investigators, EASI completion times can be as low as nearly 2 minutes.”
The authors acknowledged certain limitations of their recommendations, including the lack of input from primary care clinicians. “It is unknown whether ClinROMs [clinician-reported outcome measures] for AD clinical signs are used in the primary care setting, especially given the large amount of conditions that are managed simultaneously and the ever-increasing number of primary care documentation requirements,” they wrote.
Robert Sidbury, MD, MPH, chief of the division of dermatology at Seattle Children’s Hospital, who was asked to comment on the consensus statement, said that with the advent of new, improved, and more expensive medications for AD, “it is ever more important that [the clinical] assessment is reliable and reproducible.”
Insurers “are understandably less willing to rubber-stamp approval of more expensive medications without a reliable standard by which to justify such decisions,” he added. “This is even more important in a disease state like atopic dermatitis that lacks a reliable biomarker. Therefore, one or several practical, reliable, validated severity metrics will help standardize and improve AD care.”
Dr. Sidbury, who cochaired the 2023 American Academy of Dermatology guidelines of care for the management of AD in adults with phototherapy and systemic therapies, added that the instruments evaluated in the review “can be challenging for anyone,” not just primary care providers. “The EASI isn’t that easy, and while there is a learning curve and it ultimately does, like anything, become more efficient in the gathering, it is unclear if non-AD researchers will be willing to invest the time” to routinely use it, he said.
Dr. Simpson and several coauthors reported receiving grants and personal fees from multiple pharmaceutical companies. Dr. Sidbury reported that he serves as an investigator for Regeneron, Galderma, UCB, Castle, and Pfizer; is a consultant for LEO, Lilly, Arcutis, Dermavant, and Pierre Fabre; and a speaker for Beiersdorf.
A version of this article appeared on Medscape.com .
FROM JAMA DERMATOLOGY
ASTRO Releases New EBRT Guideline for Symptomatic Bone Mets
The guideline was needed to update previous recommendations and incorporate new high-quality evidence for the management of symptomatic bone metastases, Sara Alcorn, MD, PhD, of the University of Minnesota, Minneapolis, and colleagues wrote in Practical Radiation Oncology.
The focus was on the efficacy of EBRT in reducing pain, improving skeletal function, and enhancing quality of life, they wrote in the clinical practice guideline.
In developing their recommendations, the ASTRO task force reviewed evidence from 53 randomized controlled trials (RCTs) and 31 nonrandomized studies, and considered clinical experience.
Indications for Palliative Radiation
EBRT is strongly recommended for reducing pain from osseous metastasis and improving ambulatory status, sphincter function, and reducing pain in patients with spinal metastases causing compression of the spinal cord or cauda equina.
For patients with symptomatic bone metastases and an anticipated life expectancy of at least 4 weeks, EBRT is conditionally recommended to improve quality of life.
Implementation of other Treatments Alongside Palliative Radiation
Instead of RT alone, surgery with postoperative RT is conditionally recommended for patients with compression of the spinal cord or cauda equina.
Postoperative RT is strongly recommended for patients who have undergone surgery for non-spine bone metastases or spine metastases without involving spinal cord or cauda equina compression.
For patients with spinal bone metastases compressing the spinal cord or cauda equina, combining RT with dexamethasone is strongly recommended over RT alone.
Techniques, Dose-Fractionation, and Dose-Constraints for Initial Palliative Radiation
For patients with symptomatic bone metastases undergoing conventional palliative RT, strongly recommended doses are 800 cGy in 1 fraction, 2000 cGy in 5 fractions, 2400 cGy in 6 fractions, or 3000 cGy in 10 fractions.
For patients with spinal bone metastases causing compression of the spinal cord or cauda equina who are not candidates for initial surgical decompression and are treated with conventional palliative RT, strongly recommended doses are 800 cGy in 1 fraction, 1600 cGy in 2 fractions, 2000 cGy in 5 fractions, or 3000 cGy in 10 fractions.
When selecting dose-fractionation, consider patient and disease factors such as prognosis and radiosensitivity, the authors wrote.
Highly conformal planning and delivery techniques, such as intensity-modulated radiation therapy, are conditionally recommended for patients with spinal bone metastases compressing the spinal cord or cauda equina who are receiving dose-escalated palliative RT.
The strongly recommended stereotactic body radiotherapy (SBRT) doses for patients with symptomatic bone metastases are 1200 to 1600 cGy in 1 fraction for non-spine metastases and 2400 cGy in 2 fractions for spine metastases. Other established SBRT dose and fractionation regimens with similar biologically effective doses may be considered based on patient tumor characteristics, normal tissue factors, and physician experience.
For patients with symptomatic bone metastases who have an ECOG PS of 0-2, are not undergoing surgical intervention, and have no neurological symptoms, SBRT is conditionally recommended over conventional palliative RT. Other factors to consider include life expectancy, tumor radiosensitivity, and metastatic disease burden, the guideline says.
Techniques, Dose-Fractionation, and Dose-Constraints for Palliative Reirradiation
For patients with spinal bone metastases requiring reirradiation to the same site, the strongly recommended conventional palliative RT regimens are 800 cGy in 1 fraction, 2000 cGy in 5 fractions, 2400 cGy in 6 fractions, or 2000 cGy in 8 fractions. When determining the RT dose-fractionation, consider the prior RT dose, time interval, and total spinal cord tolerance, the guideline says.
Treatment with SBRT is conditionally recommended for patients with spinal bone metastases needing reirradiation at the same site. When determining if SBRT is appropriate, consider patient factors such as urgency of treatment, prognosis, and radio-resistance. In addition, consider the prior RT dose, time interval, and total spinal cord tolerance when determining the RT dose-fractionation, the authors say.
The strongly recommended options for patients with symptomatic non-spine bone metastases needing reirradiation at the same site are single-fraction RT (800 cGy in 1 fraction) or multifraction conventional palliative RT (2000 cGy in 5 fractions or 2400 cGy in 6 fractions).
Impact of Techniques and Dose-fractionation on Quality of Life and Toxicity
For patients with bone metastases undergoing palliative radiation, it is strongly recommended to use a shared decision-making approach to determine the dose, fractionation, and supportive measures to optimize quality of life.
“Based on published data, the ASTRO task force’s recommendations inform best clinical practices on palliative RT for symptomatic bone metastases,” the guideline panelists said.
Limitations
While the guideline provides comprehensive recommendations, the panelists underscored the importance of individualized treatment approaches. Future research is needed to address gaps in evidence, particularly regarding advanced RT techniques and reirradiation strategies.
Guideline development was funded by ASTRO, with the systematic evidence review funded by the Patient-Centered Outcomes Research Institute. The panelists disclosed relationships with AstraZeneca, Elekta, Teladoc, and others.
The guideline was needed to update previous recommendations and incorporate new high-quality evidence for the management of symptomatic bone metastases, Sara Alcorn, MD, PhD, of the University of Minnesota, Minneapolis, and colleagues wrote in Practical Radiation Oncology.
The focus was on the efficacy of EBRT in reducing pain, improving skeletal function, and enhancing quality of life, they wrote in the clinical practice guideline.
In developing their recommendations, the ASTRO task force reviewed evidence from 53 randomized controlled trials (RCTs) and 31 nonrandomized studies, and considered clinical experience.
Indications for Palliative Radiation
EBRT is strongly recommended for reducing pain from osseous metastasis and improving ambulatory status, sphincter function, and reducing pain in patients with spinal metastases causing compression of the spinal cord or cauda equina.
For patients with symptomatic bone metastases and an anticipated life expectancy of at least 4 weeks, EBRT is conditionally recommended to improve quality of life.
Implementation of other Treatments Alongside Palliative Radiation
Instead of RT alone, surgery with postoperative RT is conditionally recommended for patients with compression of the spinal cord or cauda equina.
Postoperative RT is strongly recommended for patients who have undergone surgery for non-spine bone metastases or spine metastases without involving spinal cord or cauda equina compression.
For patients with spinal bone metastases compressing the spinal cord or cauda equina, combining RT with dexamethasone is strongly recommended over RT alone.
Techniques, Dose-Fractionation, and Dose-Constraints for Initial Palliative Radiation
For patients with symptomatic bone metastases undergoing conventional palliative RT, strongly recommended doses are 800 cGy in 1 fraction, 2000 cGy in 5 fractions, 2400 cGy in 6 fractions, or 3000 cGy in 10 fractions.
For patients with spinal bone metastases causing compression of the spinal cord or cauda equina who are not candidates for initial surgical decompression and are treated with conventional palliative RT, strongly recommended doses are 800 cGy in 1 fraction, 1600 cGy in 2 fractions, 2000 cGy in 5 fractions, or 3000 cGy in 10 fractions.
When selecting dose-fractionation, consider patient and disease factors such as prognosis and radiosensitivity, the authors wrote.
Highly conformal planning and delivery techniques, such as intensity-modulated radiation therapy, are conditionally recommended for patients with spinal bone metastases compressing the spinal cord or cauda equina who are receiving dose-escalated palliative RT.
The strongly recommended stereotactic body radiotherapy (SBRT) doses for patients with symptomatic bone metastases are 1200 to 1600 cGy in 1 fraction for non-spine metastases and 2400 cGy in 2 fractions for spine metastases. Other established SBRT dose and fractionation regimens with similar biologically effective doses may be considered based on patient tumor characteristics, normal tissue factors, and physician experience.
For patients with symptomatic bone metastases who have an ECOG PS of 0-2, are not undergoing surgical intervention, and have no neurological symptoms, SBRT is conditionally recommended over conventional palliative RT. Other factors to consider include life expectancy, tumor radiosensitivity, and metastatic disease burden, the guideline says.
Techniques, Dose-Fractionation, and Dose-Constraints for Palliative Reirradiation
For patients with spinal bone metastases requiring reirradiation to the same site, the strongly recommended conventional palliative RT regimens are 800 cGy in 1 fraction, 2000 cGy in 5 fractions, 2400 cGy in 6 fractions, or 2000 cGy in 8 fractions. When determining the RT dose-fractionation, consider the prior RT dose, time interval, and total spinal cord tolerance, the guideline says.
Treatment with SBRT is conditionally recommended for patients with spinal bone metastases needing reirradiation at the same site. When determining if SBRT is appropriate, consider patient factors such as urgency of treatment, prognosis, and radio-resistance. In addition, consider the prior RT dose, time interval, and total spinal cord tolerance when determining the RT dose-fractionation, the authors say.
The strongly recommended options for patients with symptomatic non-spine bone metastases needing reirradiation at the same site are single-fraction RT (800 cGy in 1 fraction) or multifraction conventional palliative RT (2000 cGy in 5 fractions or 2400 cGy in 6 fractions).
Impact of Techniques and Dose-fractionation on Quality of Life and Toxicity
For patients with bone metastases undergoing palliative radiation, it is strongly recommended to use a shared decision-making approach to determine the dose, fractionation, and supportive measures to optimize quality of life.
“Based on published data, the ASTRO task force’s recommendations inform best clinical practices on palliative RT for symptomatic bone metastases,” the guideline panelists said.
Limitations
While the guideline provides comprehensive recommendations, the panelists underscored the importance of individualized treatment approaches. Future research is needed to address gaps in evidence, particularly regarding advanced RT techniques and reirradiation strategies.
Guideline development was funded by ASTRO, with the systematic evidence review funded by the Patient-Centered Outcomes Research Institute. The panelists disclosed relationships with AstraZeneca, Elekta, Teladoc, and others.
The guideline was needed to update previous recommendations and incorporate new high-quality evidence for the management of symptomatic bone metastases, Sara Alcorn, MD, PhD, of the University of Minnesota, Minneapolis, and colleagues wrote in Practical Radiation Oncology.
The focus was on the efficacy of EBRT in reducing pain, improving skeletal function, and enhancing quality of life, they wrote in the clinical practice guideline.
In developing their recommendations, the ASTRO task force reviewed evidence from 53 randomized controlled trials (RCTs) and 31 nonrandomized studies, and considered clinical experience.
Indications for Palliative Radiation
EBRT is strongly recommended for reducing pain from osseous metastasis and improving ambulatory status, sphincter function, and reducing pain in patients with spinal metastases causing compression of the spinal cord or cauda equina.
For patients with symptomatic bone metastases and an anticipated life expectancy of at least 4 weeks, EBRT is conditionally recommended to improve quality of life.
Implementation of other Treatments Alongside Palliative Radiation
Instead of RT alone, surgery with postoperative RT is conditionally recommended for patients with compression of the spinal cord or cauda equina.
Postoperative RT is strongly recommended for patients who have undergone surgery for non-spine bone metastases or spine metastases without involving spinal cord or cauda equina compression.
For patients with spinal bone metastases compressing the spinal cord or cauda equina, combining RT with dexamethasone is strongly recommended over RT alone.
Techniques, Dose-Fractionation, and Dose-Constraints for Initial Palliative Radiation
For patients with symptomatic bone metastases undergoing conventional palliative RT, strongly recommended doses are 800 cGy in 1 fraction, 2000 cGy in 5 fractions, 2400 cGy in 6 fractions, or 3000 cGy in 10 fractions.
For patients with spinal bone metastases causing compression of the spinal cord or cauda equina who are not candidates for initial surgical decompression and are treated with conventional palliative RT, strongly recommended doses are 800 cGy in 1 fraction, 1600 cGy in 2 fractions, 2000 cGy in 5 fractions, or 3000 cGy in 10 fractions.
When selecting dose-fractionation, consider patient and disease factors such as prognosis and radiosensitivity, the authors wrote.
Highly conformal planning and delivery techniques, such as intensity-modulated radiation therapy, are conditionally recommended for patients with spinal bone metastases compressing the spinal cord or cauda equina who are receiving dose-escalated palliative RT.
The strongly recommended stereotactic body radiotherapy (SBRT) doses for patients with symptomatic bone metastases are 1200 to 1600 cGy in 1 fraction for non-spine metastases and 2400 cGy in 2 fractions for spine metastases. Other established SBRT dose and fractionation regimens with similar biologically effective doses may be considered based on patient tumor characteristics, normal tissue factors, and physician experience.
For patients with symptomatic bone metastases who have an ECOG PS of 0-2, are not undergoing surgical intervention, and have no neurological symptoms, SBRT is conditionally recommended over conventional palliative RT. Other factors to consider include life expectancy, tumor radiosensitivity, and metastatic disease burden, the guideline says.
Techniques, Dose-Fractionation, and Dose-Constraints for Palliative Reirradiation
For patients with spinal bone metastases requiring reirradiation to the same site, the strongly recommended conventional palliative RT regimens are 800 cGy in 1 fraction, 2000 cGy in 5 fractions, 2400 cGy in 6 fractions, or 2000 cGy in 8 fractions. When determining the RT dose-fractionation, consider the prior RT dose, time interval, and total spinal cord tolerance, the guideline says.
Treatment with SBRT is conditionally recommended for patients with spinal bone metastases needing reirradiation at the same site. When determining if SBRT is appropriate, consider patient factors such as urgency of treatment, prognosis, and radio-resistance. In addition, consider the prior RT dose, time interval, and total spinal cord tolerance when determining the RT dose-fractionation, the authors say.
The strongly recommended options for patients with symptomatic non-spine bone metastases needing reirradiation at the same site are single-fraction RT (800 cGy in 1 fraction) or multifraction conventional palliative RT (2000 cGy in 5 fractions or 2400 cGy in 6 fractions).
Impact of Techniques and Dose-fractionation on Quality of Life and Toxicity
For patients with bone metastases undergoing palliative radiation, it is strongly recommended to use a shared decision-making approach to determine the dose, fractionation, and supportive measures to optimize quality of life.
“Based on published data, the ASTRO task force’s recommendations inform best clinical practices on palliative RT for symptomatic bone metastases,” the guideline panelists said.
Limitations
While the guideline provides comprehensive recommendations, the panelists underscored the importance of individualized treatment approaches. Future research is needed to address gaps in evidence, particularly regarding advanced RT techniques and reirradiation strategies.
Guideline development was funded by ASTRO, with the systematic evidence review funded by the Patient-Centered Outcomes Research Institute. The panelists disclosed relationships with AstraZeneca, Elekta, Teladoc, and others.
FROM PRACTICAL RADIATION ONCOLOGY
High NSAID Use in Patients With Axial Spondyloarthritis May Not Raise Risk for Hypertension
TOPLINE:
Patients with axial spondyloarthritis (axSpA) who reported high nonsteroidal anti-inflammatory drug (NSAID) use did not have a higher risk for hypertension than those who reported low NSAID use.
METHODOLOGY:
- NSAIDs are first-line therapy for axSpA and are associated with a high risk for hypertension in the general population, but it’s unknown whether NSAID use increases the risk for hypertension in patients with axSpA, who are already at higher risk for cardiovascular disease and hypertension than the general population
- This study used the DESIR cohort, a multicenter cohort of patients with recent-onset axSpA in France, including 631 individuals aged 18-50 years who did not have hypertension at baseline and had 6 years of follow-up.
- NSAID use was evaluated at each follow-up visit, using the Assessment of Spondyloarthritis International Society NSAID index.
- A score ≥ 50 was categorized as high use, and a score < 50 was considered low use.
- The primary outcome was hypertension, defined by the use of antihypertensive medication, self-reported hypertension, and/or systolic blood pressure (BP) ≥ 140 mm Hg or diastolic BP ≥ 90 mm Hg on at least two visits.
TAKEAWAY:
- A total of 39% of patients were categorized as high NSAID users.
- Over 6 years of follow-up, 70 patients (11%) developed hypertension.
- There was no significant association between high NSAID use and the risk for hypertension.
IN PRACTICE:
The study is too preliminary to have practice application.
SOURCE:
The research was led and presented by Jose Meade-Aguilar, MD, of Boston University School of Medicine, at the Spondyloarthritis Research and Treatment Network (SPARTAN) 2024 annual meeting in Cleveland.
LIMITATIONS:
The study had a low number of hypertension events, which could be due to the younger age of participants and earlier disease stage. The study was observational, so residual or unmeasured confounding is possible.
DISCLOSURES:
The DESIR cohort study is financially supported by unrestricted grants from both the French Society for Rheumatology and Pfizer France. One coauthor reported receiving research grants and/or consultancy fees from AbbVie, Eli Lilly, Galapagos, Janssen, Merck Sharp & Dohme, Novartis, Pfizer, UCB, and Sanofi. Another coauthor reported receiving research grants from UCB and consulting fees from Eli Lilly, Novartis, Pfizer, and UCB. The remaining authors had no financial, relational, or commercial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Patients with axial spondyloarthritis (axSpA) who reported high nonsteroidal anti-inflammatory drug (NSAID) use did not have a higher risk for hypertension than those who reported low NSAID use.
METHODOLOGY:
- NSAIDs are first-line therapy for axSpA and are associated with a high risk for hypertension in the general population, but it’s unknown whether NSAID use increases the risk for hypertension in patients with axSpA, who are already at higher risk for cardiovascular disease and hypertension than the general population
- This study used the DESIR cohort, a multicenter cohort of patients with recent-onset axSpA in France, including 631 individuals aged 18-50 years who did not have hypertension at baseline and had 6 years of follow-up.
- NSAID use was evaluated at each follow-up visit, using the Assessment of Spondyloarthritis International Society NSAID index.
- A score ≥ 50 was categorized as high use, and a score < 50 was considered low use.
- The primary outcome was hypertension, defined by the use of antihypertensive medication, self-reported hypertension, and/or systolic blood pressure (BP) ≥ 140 mm Hg or diastolic BP ≥ 90 mm Hg on at least two visits.
TAKEAWAY:
- A total of 39% of patients were categorized as high NSAID users.
- Over 6 years of follow-up, 70 patients (11%) developed hypertension.
- There was no significant association between high NSAID use and the risk for hypertension.
IN PRACTICE:
The study is too preliminary to have practice application.
SOURCE:
The research was led and presented by Jose Meade-Aguilar, MD, of Boston University School of Medicine, at the Spondyloarthritis Research and Treatment Network (SPARTAN) 2024 annual meeting in Cleveland.
LIMITATIONS:
The study had a low number of hypertension events, which could be due to the younger age of participants and earlier disease stage. The study was observational, so residual or unmeasured confounding is possible.
DISCLOSURES:
The DESIR cohort study is financially supported by unrestricted grants from both the French Society for Rheumatology and Pfizer France. One coauthor reported receiving research grants and/or consultancy fees from AbbVie, Eli Lilly, Galapagos, Janssen, Merck Sharp & Dohme, Novartis, Pfizer, UCB, and Sanofi. Another coauthor reported receiving research grants from UCB and consulting fees from Eli Lilly, Novartis, Pfizer, and UCB. The remaining authors had no financial, relational, or commercial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Patients with axial spondyloarthritis (axSpA) who reported high nonsteroidal anti-inflammatory drug (NSAID) use did not have a higher risk for hypertension than those who reported low NSAID use.
METHODOLOGY:
- NSAIDs are first-line therapy for axSpA and are associated with a high risk for hypertension in the general population, but it’s unknown whether NSAID use increases the risk for hypertension in patients with axSpA, who are already at higher risk for cardiovascular disease and hypertension than the general population
- This study used the DESIR cohort, a multicenter cohort of patients with recent-onset axSpA in France, including 631 individuals aged 18-50 years who did not have hypertension at baseline and had 6 years of follow-up.
- NSAID use was evaluated at each follow-up visit, using the Assessment of Spondyloarthritis International Society NSAID index.
- A score ≥ 50 was categorized as high use, and a score < 50 was considered low use.
- The primary outcome was hypertension, defined by the use of antihypertensive medication, self-reported hypertension, and/or systolic blood pressure (BP) ≥ 140 mm Hg or diastolic BP ≥ 90 mm Hg on at least two visits.
TAKEAWAY:
- A total of 39% of patients were categorized as high NSAID users.
- Over 6 years of follow-up, 70 patients (11%) developed hypertension.
- There was no significant association between high NSAID use and the risk for hypertension.
IN PRACTICE:
The study is too preliminary to have practice application.
SOURCE:
The research was led and presented by Jose Meade-Aguilar, MD, of Boston University School of Medicine, at the Spondyloarthritis Research and Treatment Network (SPARTAN) 2024 annual meeting in Cleveland.
LIMITATIONS:
The study had a low number of hypertension events, which could be due to the younger age of participants and earlier disease stage. The study was observational, so residual or unmeasured confounding is possible.
DISCLOSURES:
The DESIR cohort study is financially supported by unrestricted grants from both the French Society for Rheumatology and Pfizer France. One coauthor reported receiving research grants and/or consultancy fees from AbbVie, Eli Lilly, Galapagos, Janssen, Merck Sharp & Dohme, Novartis, Pfizer, UCB, and Sanofi. Another coauthor reported receiving research grants from UCB and consulting fees from Eli Lilly, Novartis, Pfizer, and UCB. The remaining authors had no financial, relational, or commercial conflicts to disclose.
A version of this article appeared on Medscape.com.