User login
Child suicides drive Colorado hospital to declare state of emergency
On May 25, Jena Hausmann, CEO of Children’s Hospital Colorado, Aurora, declared a state of emergency in youth mental health in response to an astronomical increase in pediatric mental health cases, including suicide, which has overwhelmed the institution.

From April 2019 to April 2021, the demand for pediatric behavioral health treatment at the hospital system increased by 90%. In Colorado, suicide is now the number one cause of death among youth and occurs in children as young as 10 years of age.
“Now we are seeing our pediatric emergency departments and our inpatient units overrun with kids attempting suicide and suffering from other forms of major mental health illness,” Dr. Hausmann said in a press release.
“We had to draw attention to what we’re seeing in our hospital and our community on an everyday basis – an unprecedented number of suicidal children who need acute treatment for behavioral health problems – and when I say ‘unprecedented,’ I’m serious – I’ve been in pediatrics for two decades and have never seen anything like this before,” David Brumbaugh, MD, a pediatric gastroenterologist and chief medical officer for Children’s Colorado, told this news organization.
Christine Crawford, MD, associate medical director of the National Alliance on Mental Illness, stated in an interview that she “commends the CEO of the hospital for making this announcement, because it is outrageous to see what is happening with more and more children with significant psychiatric symptoms who are not getting adequate care.”
Jenna Glover, PhD, child psychologist and director of psychology training at Children’s Hospital, said that during the past decade, there has been a steady increase in depression, anxiety, and suicide among youth in Colorado. Suicide, she added, is now the number one cause of death in youth, “so we were already in a state of crisis.” She added that COVID-19 was “the straw that broke the camel’s back.”
“In January to April of this year, behavioral health ED visits to Children’s Hospital were 72% higher than they were 2 years ago at this time,” she said. “Colorado Springs had a 145% increase for ED behavioral health visits during the first 4 months of 2021, compared to the first 4 months of 2020.”
COVID’s impact
Other problems that have been “skyrocketing” in youth are self-harm, substance use, and eating disorders. Younger children are experiencing an increase in behavioral problems, including developmental regression, such as tantrums, and problems with sleeping, toileting, and eating, Dr. Glover noted.

The youth mental health crisis has mushroomed, although social distancing requirements are now beginning to ease and we are in the “home stretch of the pandemic,” Dr. Brumbaugh said.
One possible reason “is that we took kids out of their normal routines, social circles, friendships, etc., for 12 months, and that was the limit of their physiological or mental resistance, and they got to the end of their rope,” he speculated.
Dr. Glover said, “Kids are burned out, and although they’re asking to return to their life, they don’t feel they have the resources. They feel so behind; they don’t know how to catch up.”
Dr. Brumbaugh said that there are not enough child psychiatrists to provide outpatient services or enough inpatient beds for children in crisis.
“This is an unacceptable situation. We would never allow a child with leukemia or appendicitis to go several weeks without treatment,” he said.
Community donors have come forward, enabling an anticipated 50% increase in Children’s Hospital’s mental health outpatient, inpatient, and day services by March 2022.
“On a hospital level, we are continuing to do things to expand access to care, like opening units that provide different levels of care for patients with psychiatric problems, as well as expanding into areas that are more rural,” Dr. Glover said.
However, the “blueprint is not in action yet, and a lot of money still needs to be allocated. A workforce has to be created, because there are not enough clinicians to fill these roles,” she added.
Chronic underfunding
Dr. Brumbaugh said Colorado has always had a “relatively underfunded behavioral health system for kids.” A 2021 report by

However, Dr. Glover noted that Colorado is “not exceptional.” The increased vulnerability to youth mental illness and suicide is characteristic of other mountain states, which have larger rural areas, less access to care, and increased access to guns, she said.
Mass shootings may have amped up stress levels. “For some kids, this is happening in their schools or towns, and they feel traumatized and unsafe,” Dr. Glover added.
Dr. Crawford, who is an assistant professor of psychiatry at Boston University, also pointed out that the mental health crisis in youth is not unique to Colorado.
“Throughout the country, we’ve seen these colliding pandemics – inadequate mental health resources for children and COVID-19, which exacerbated the existing mental health crisis,” she said.
“The pandemic led to an increase in telehealth services, making individual and group psychotherapy available to kids in areas that never had access to these before, which is a ‘silver lining’ of the pandemic,” Dr. Glover said.
Dr. Crawford is “encouraged that we are having more conversations about pediatric mental health, because the pandemic amplified what was already going on and made it impossible to ignore.”
Screening is essential
Screening for mental health problems should be at the top of the mind of pediatricians and other clinicians who work with children, Dr. Glover said.
“Pediatricians are in the best place to catch potentially suicidal kids, because they are more likely to see these kids than therapists,” she noted.
She suggested using a rapid screen for depression, such as the Patient Health Questionnaire-9 (PHQ-9) modified for adolescents. Parents can also fill out a PHQ-9 for younger children and even for themselves.
“Depression, anxiety, and suicidality affect the whole family, so screening for these conditions in adults will benefit the children too,” she said. Teachers should also “be aware of what depression and anxiety symptoms look like in kids, because sometimes they can manifest more as irritability,” Dr. Glover added.
Policymakers and insurers need to prioritize pediatric mental health when determining allocation of health care, said Dr. Crawford.
“Financial incentives should be provided for hospitals to want to reserve beds for psychiatric patients, and in the outpatient setting, we also need to look at the payment structure of psychiatric visits,” she added.
Many psychiatrists do not want to accept insurance because of the increased bureaucracy and low reimbursement rates of insurance companies, and families cannot afford to pay out of pocket, “so we really need to look at the insurance issue at a policy level,” Dr. Crawford said.
Dr. Brumbaugh, Dr. Glover, and Dr. Crawford have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
On May 25, Jena Hausmann, CEO of Children’s Hospital Colorado, Aurora, declared a state of emergency in youth mental health in response to an astronomical increase in pediatric mental health cases, including suicide, which has overwhelmed the institution.
From April 2019 to April 2021, the demand for pediatric behavioral health treatment at the hospital system increased by 90%. In Colorado, suicide is now the number one cause of death among youth and occurs in children as young as 10 years of age.
“Now we are seeing our pediatric emergency departments and our inpatient units overrun with kids attempting suicide and suffering from other forms of major mental health illness,” Dr. Hausmann said in a press release.
“We had to draw attention to what we’re seeing in our hospital and our community on an everyday basis – an unprecedented number of suicidal children who need acute treatment for behavioral health problems – and when I say ‘unprecedented,’ I’m serious – I’ve been in pediatrics for two decades and have never seen anything like this before,” David Brumbaugh, MD, a pediatric gastroenterologist and chief medical officer for Children’s Colorado, told this news organization.
Christine Crawford, MD, associate medical director of the National Alliance on Mental Illness, stated in an interview that she “commends the CEO of the hospital for making this announcement, because it is outrageous to see what is happening with more and more children with significant psychiatric symptoms who are not getting adequate care.”
Jenna Glover, PhD, child psychologist and director of psychology training at Children’s Hospital, said that during the past decade, there has been a steady increase in depression, anxiety, and suicide among youth in Colorado. Suicide, she added, is now the number one cause of death in youth, “so we were already in a state of crisis.” She added that COVID-19 was “the straw that broke the camel’s back.”
“In January to April of this year, behavioral health ED visits to Children’s Hospital were 72% higher than they were 2 years ago at this time,” she said. “Colorado Springs had a 145% increase for ED behavioral health visits during the first 4 months of 2021, compared to the first 4 months of 2020.”
COVID’s impact
Other problems that have been “skyrocketing” in youth are self-harm, substance use, and eating disorders. Younger children are experiencing an increase in behavioral problems, including developmental regression, such as tantrums, and problems with sleeping, toileting, and eating, Dr. Glover noted.
The youth mental health crisis has mushroomed, although social distancing requirements are now beginning to ease and we are in the “home stretch of the pandemic,” Dr. Brumbaugh said.
One possible reason “is that we took kids out of their normal routines, social circles, friendships, etc., for 12 months, and that was the limit of their physiological or mental resistance, and they got to the end of their rope,” he speculated.
Dr. Glover said, “Kids are burned out, and although they’re asking to return to their life, they don’t feel they have the resources. They feel so behind; they don’t know how to catch up.”
Dr. Brumbaugh said that there are not enough child psychiatrists to provide outpatient services or enough inpatient beds for children in crisis.
“This is an unacceptable situation. We would never allow a child with leukemia or appendicitis to go several weeks without treatment,” he said.
Community donors have come forward, enabling an anticipated 50% increase in Children’s Hospital’s mental health outpatient, inpatient, and day services by March 2022.
“On a hospital level, we are continuing to do things to expand access to care, like opening units that provide different levels of care for patients with psychiatric problems, as well as expanding into areas that are more rural,” Dr. Glover said.
However, the “blueprint is not in action yet, and a lot of money still needs to be allocated. A workforce has to be created, because there are not enough clinicians to fill these roles,” she added.
Chronic underfunding
Dr. Brumbaugh said Colorado has always had a “relatively underfunded behavioral health system for kids.” A 2021 report by
However, Dr. Glover noted that Colorado is “not exceptional.” The increased vulnerability to youth mental illness and suicide is characteristic of other mountain states, which have larger rural areas, less access to care, and increased access to guns, she said.
Mass shootings may have amped up stress levels. “For some kids, this is happening in their schools or towns, and they feel traumatized and unsafe,” Dr. Glover added.
Dr. Crawford, who is an assistant professor of psychiatry at Boston University, also pointed out that the mental health crisis in youth is not unique to Colorado.
“Throughout the country, we’ve seen these colliding pandemics – inadequate mental health resources for children and COVID-19, which exacerbated the existing mental health crisis,” she said.
“The pandemic led to an increase in telehealth services, making individual and group psychotherapy available to kids in areas that never had access to these before, which is a ‘silver lining’ of the pandemic,” Dr. Glover said.
Dr. Crawford is “encouraged that we are having more conversations about pediatric mental health, because the pandemic amplified what was already going on and made it impossible to ignore.”
Screening is essential
Screening for mental health problems should be at the top of the mind of pediatricians and other clinicians who work with children, Dr. Glover said.
“Pediatricians are in the best place to catch potentially suicidal kids, because they are more likely to see these kids than therapists,” she noted.
She suggested using a rapid screen for depression, such as the Patient Health Questionnaire-9 (PHQ-9) modified for adolescents. Parents can also fill out a PHQ-9 for younger children and even for themselves.
“Depression, anxiety, and suicidality affect the whole family, so screening for these conditions in adults will benefit the children too,” she said. Teachers should also “be aware of what depression and anxiety symptoms look like in kids, because sometimes they can manifest more as irritability,” Dr. Glover added.
Policymakers and insurers need to prioritize pediatric mental health when determining allocation of health care, said Dr. Crawford.
“Financial incentives should be provided for hospitals to want to reserve beds for psychiatric patients, and in the outpatient setting, we also need to look at the payment structure of psychiatric visits,” she added.
Many psychiatrists do not want to accept insurance because of the increased bureaucracy and low reimbursement rates of insurance companies, and families cannot afford to pay out of pocket, “so we really need to look at the insurance issue at a policy level,” Dr. Crawford said.
Dr. Brumbaugh, Dr. Glover, and Dr. Crawford have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
On May 25, Jena Hausmann, CEO of Children’s Hospital Colorado, Aurora, declared a state of emergency in youth mental health in response to an astronomical increase in pediatric mental health cases, including suicide, which has overwhelmed the institution.
From April 2019 to April 2021, the demand for pediatric behavioral health treatment at the hospital system increased by 90%. In Colorado, suicide is now the number one cause of death among youth and occurs in children as young as 10 years of age.
“Now we are seeing our pediatric emergency departments and our inpatient units overrun with kids attempting suicide and suffering from other forms of major mental health illness,” Dr. Hausmann said in a press release.
“We had to draw attention to what we’re seeing in our hospital and our community on an everyday basis – an unprecedented number of suicidal children who need acute treatment for behavioral health problems – and when I say ‘unprecedented,’ I’m serious – I’ve been in pediatrics for two decades and have never seen anything like this before,” David Brumbaugh, MD, a pediatric gastroenterologist and chief medical officer for Children’s Colorado, told this news organization.
Christine Crawford, MD, associate medical director of the National Alliance on Mental Illness, stated in an interview that she “commends the CEO of the hospital for making this announcement, because it is outrageous to see what is happening with more and more children with significant psychiatric symptoms who are not getting adequate care.”
Jenna Glover, PhD, child psychologist and director of psychology training at Children’s Hospital, said that during the past decade, there has been a steady increase in depression, anxiety, and suicide among youth in Colorado. Suicide, she added, is now the number one cause of death in youth, “so we were already in a state of crisis.” She added that COVID-19 was “the straw that broke the camel’s back.”
“In January to April of this year, behavioral health ED visits to Children’s Hospital were 72% higher than they were 2 years ago at this time,” she said. “Colorado Springs had a 145% increase for ED behavioral health visits during the first 4 months of 2021, compared to the first 4 months of 2020.”
COVID’s impact
Other problems that have been “skyrocketing” in youth are self-harm, substance use, and eating disorders. Younger children are experiencing an increase in behavioral problems, including developmental regression, such as tantrums, and problems with sleeping, toileting, and eating, Dr. Glover noted.
The youth mental health crisis has mushroomed, although social distancing requirements are now beginning to ease and we are in the “home stretch of the pandemic,” Dr. Brumbaugh said.
One possible reason “is that we took kids out of their normal routines, social circles, friendships, etc., for 12 months, and that was the limit of their physiological or mental resistance, and they got to the end of their rope,” he speculated.
Dr. Glover said, “Kids are burned out, and although they’re asking to return to their life, they don’t feel they have the resources. They feel so behind; they don’t know how to catch up.”
Dr. Brumbaugh said that there are not enough child psychiatrists to provide outpatient services or enough inpatient beds for children in crisis.
“This is an unacceptable situation. We would never allow a child with leukemia or appendicitis to go several weeks without treatment,” he said.
Community donors have come forward, enabling an anticipated 50% increase in Children’s Hospital’s mental health outpatient, inpatient, and day services by March 2022.
“On a hospital level, we are continuing to do things to expand access to care, like opening units that provide different levels of care for patients with psychiatric problems, as well as expanding into areas that are more rural,” Dr. Glover said.
However, the “blueprint is not in action yet, and a lot of money still needs to be allocated. A workforce has to be created, because there are not enough clinicians to fill these roles,” she added.
Chronic underfunding
Dr. Brumbaugh said Colorado has always had a “relatively underfunded behavioral health system for kids.” A 2021 report by
However, Dr. Glover noted that Colorado is “not exceptional.” The increased vulnerability to youth mental illness and suicide is characteristic of other mountain states, which have larger rural areas, less access to care, and increased access to guns, she said.
Mass shootings may have amped up stress levels. “For some kids, this is happening in their schools or towns, and they feel traumatized and unsafe,” Dr. Glover added.
Dr. Crawford, who is an assistant professor of psychiatry at Boston University, also pointed out that the mental health crisis in youth is not unique to Colorado.
“Throughout the country, we’ve seen these colliding pandemics – inadequate mental health resources for children and COVID-19, which exacerbated the existing mental health crisis,” she said.
“The pandemic led to an increase in telehealth services, making individual and group psychotherapy available to kids in areas that never had access to these before, which is a ‘silver lining’ of the pandemic,” Dr. Glover said.
Dr. Crawford is “encouraged that we are having more conversations about pediatric mental health, because the pandemic amplified what was already going on and made it impossible to ignore.”
Screening is essential
Screening for mental health problems should be at the top of the mind of pediatricians and other clinicians who work with children, Dr. Glover said.
“Pediatricians are in the best place to catch potentially suicidal kids, because they are more likely to see these kids than therapists,” she noted.
She suggested using a rapid screen for depression, such as the Patient Health Questionnaire-9 (PHQ-9) modified for adolescents. Parents can also fill out a PHQ-9 for younger children and even for themselves.
“Depression, anxiety, and suicidality affect the whole family, so screening for these conditions in adults will benefit the children too,” she said. Teachers should also “be aware of what depression and anxiety symptoms look like in kids, because sometimes they can manifest more as irritability,” Dr. Glover added.
Policymakers and insurers need to prioritize pediatric mental health when determining allocation of health care, said Dr. Crawford.
“Financial incentives should be provided for hospitals to want to reserve beds for psychiatric patients, and in the outpatient setting, we also need to look at the payment structure of psychiatric visits,” she added.
Many psychiatrists do not want to accept insurance because of the increased bureaucracy and low reimbursement rates of insurance companies, and families cannot afford to pay out of pocket, “so we really need to look at the insurance issue at a policy level,” Dr. Crawford said.
Dr. Brumbaugh, Dr. Glover, and Dr. Crawford have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Relationship-Centered Care in the Physician-Patient Interaction: Improving Your Understanding of Metacognitive Interventions
Communication and relationships cannot be taken for granted, particularly in the physician-patient relationship, where life-altering diagnoses may be given. With one diagnosis, someone’s life may be changed, and both physicians and patients need to be cognizant of the importance of a strong relationship and clear communication.
In the current US health care system, both physicians and patients often are not getting their needs met, and studies that include factors of race, ethnicity, and socioeconomic status suggest that physician-patient relationship barriers contribute to racial disparities in health care.1,2 Although patient-centered care is a widely recognized and upheld model, relationship-centered care between physician and patient involves focusing on the patient and the physician-patient relationship through recognizing personhood, affect (being empathic), and reciprocal influence.3,4 Although it is not necessarily intuitive because it can appear to be yet another task for busy physicians, relationship-centered care improves health care delivery for both physicians and patients through decreased physician burnout, reduced medical errors, and better patient outcomes and satisfaction.5,6
Every physician, patient, and physician-patient relationship is different; unlike the standard questions directed at a routine patient history focused on gathering data, there is no one-size-fits-all relationship-centered conversation.7-10 As with any successful interaction between 2 people, there is a certain amount of necessary self-awareness (Table 1)11 that allows for improvisation and appropriate responsiveness to what is seen, heard, and felt. Rather than attending solely to disease states, the focus of relationship-centered care is on patients, interpersonal interaction, and promoting health and well-being.15
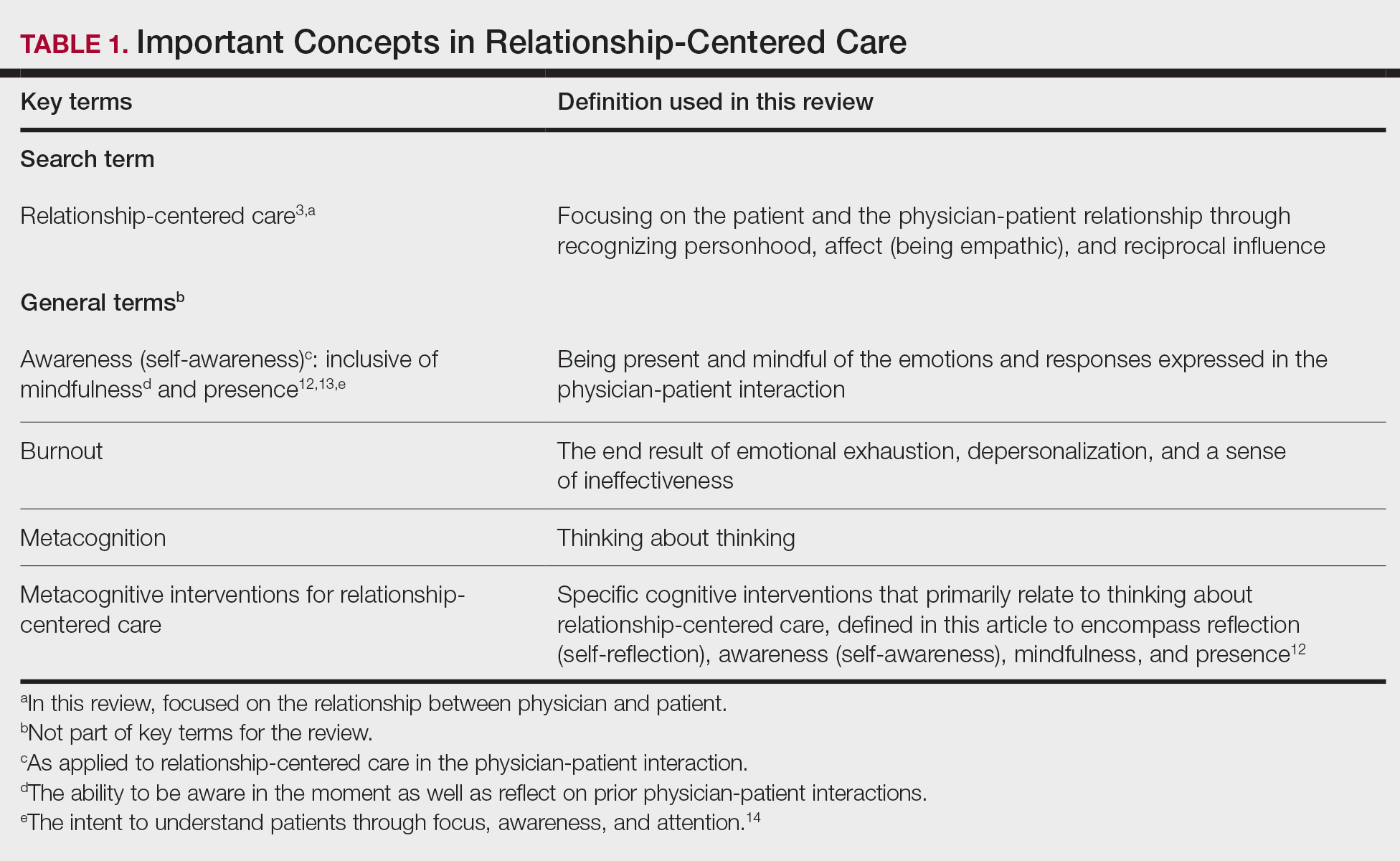
This review summarizes the existing literature on relationship-centered care, introduces the use of metacognition (Table 1), and suggests creating simple habits to promote such care. The following databases were searched from inception through November 23, 2020, using the term relationship-centered care: MEDLINE (Ovid), EMBASE (Ovid), APA PsycInfo (Ovid), Scopus, Web of Science Core Collection, CINAHL Complete (EBSCO), Academic Search Premier (EBSCOhost), and ERIC (ProQuest). A total of 1772 records were retrieved through searches, and after deduplication of 1116 studies, 350 records were screened through a 2-part process. Articles were first screened by title and abstract for relevance to the relationship between physician and patient, with 185 studies deemed irrelevant (eg, pertaining to the relationship of veterinarian to animal). The remaining 165 studies were assessed for eligibility, with 69 further studies excluded for various reasons. The screening process resulted in 96 articles considered in this review.
Definitions/key terms, as used in this article, are listed in Table 1.
Background of Relationship-Centered Care
Given time constraints, the diagnosis and treatment of medical problems often are the focus of physicians. Although proper medical diagnosis and treatment are important, and their delivery is made possible by the physician having the appropriate knowledge, a physician-patient relationship that focuses solely on disease without acknowledging the patient creates a system that ultimately neglects both patients and physicians.15 This prevailing physician-patient relationship paradigm is suboptimal, and a proposed remedy is relationship-centered care, which focuses on relationships among the human beings in health care interactions.3 Relationship-centered care has 4 principles: (1) the personhood of each party must be recognized, (2) emotion is part of relationships, (3) relationships are reciprocal and not just one way, and (4) creating these types of relationships is morally valuable3 and beneficial to patient care.16
Assessment of the Need for Relationship-Centered Care
Relationship-centered care has been studied in physician-patient interactions in various health care settings.17-23 For at least 2 decades, relationship-centered care has been set forth as a model,4,24,25 but there are challenges. Physicians tend to overrate or underrate their communication skills in patient interactions.26,27 A given physician’s preferences often still seem to supersede those of the patient.3,28,29 The impetus to develop relationship-centered care skills generally needs to be internally driven,4,30 as, ultimately, physicians and patients have varying needs.4,31 However, providing physicians with a potential structure is helpful.32
A Solution: Metacognition in the Physician-Patient Interaction
Metacognition is important to integrating basic science knowledge into medical learning and practice,33,34 and it is no less important in translating interpersonal knowledge to the physician-patient interaction. Decreased metacognitive effort35 may underpin the decline in empathy seen with increasing medical training.36,37 Understanding how metacognitive practices foster relationship-centered care is important for teaching, developing, and maintaining that care.
Metacognition is already embedded in the fabric of the physician-patient interaction.33,34 The complex interplay of the physician-patient interview, patient examination, and integration of physical as well as ancillary data requires higher-order thinking and the ability to parse out that thinking successfully. As a concrete example, coming to a diagnosis requires thinking about what has been presented during the physician-patient interaction and considering what supports and suggests the disease while a list of potential differential diagnosis alternatives is being generated. Physicians are trained to apply this clinical reasoning approach to their patient care.
Conversely, although communication skills are a key component of doctoring,38 both between physician and patient as well as among other colleagues and staff, many physicians have never received formal training in communication skills,26,32,39 though it is now an integral part of medical school curricula.40 When such training is mandatory, less than 1% of physicians continue to believe that there was no benefit, even from a single 8-hour communications skills training session.41 Communication cannot be taught comprehensively in 8 hours; thus, the benefit of such training may be the end result of metacognition and increased self-awareness (Table 1).42,43
Building Relationship-Centered Care Through Metacognitive Attention
Metacognition as manifested by such self-awareness can build relationship-centered care.4 Self-awareness can be taught through mentorship or role models.44 Journaling,40 meditation, and appreciation of beauty and the arts45 can contribute, as well as more formal training programs,32,38,42 as offered by the Academy of Communication in Healthcare. Creating opportunities for patient empowerment also supports relationship-centered care, as does applying knowledge of implicit bias.46
Even without formal training, relationship-centered care can be built through attention to cues9—visual (eg, sitting down, other body language),47,48 auditory (eg, knocking, language, tone, conversational flow),48,49 and emotional (eg, clinical empathy, emotional intelligence)(Table 2). Such attention is familiar to everyone, not just physicians or patients, through interactions outside of health care; inattention may be due to the hidden curriculum or culture of medicine40 as well as real-time changes, such as the introduction of the electronic health record.51 Inattention to these cues also may be a result of context-specific knowledge, in which a physician’s real-life communication skills are not applied to the unique context of patient care.
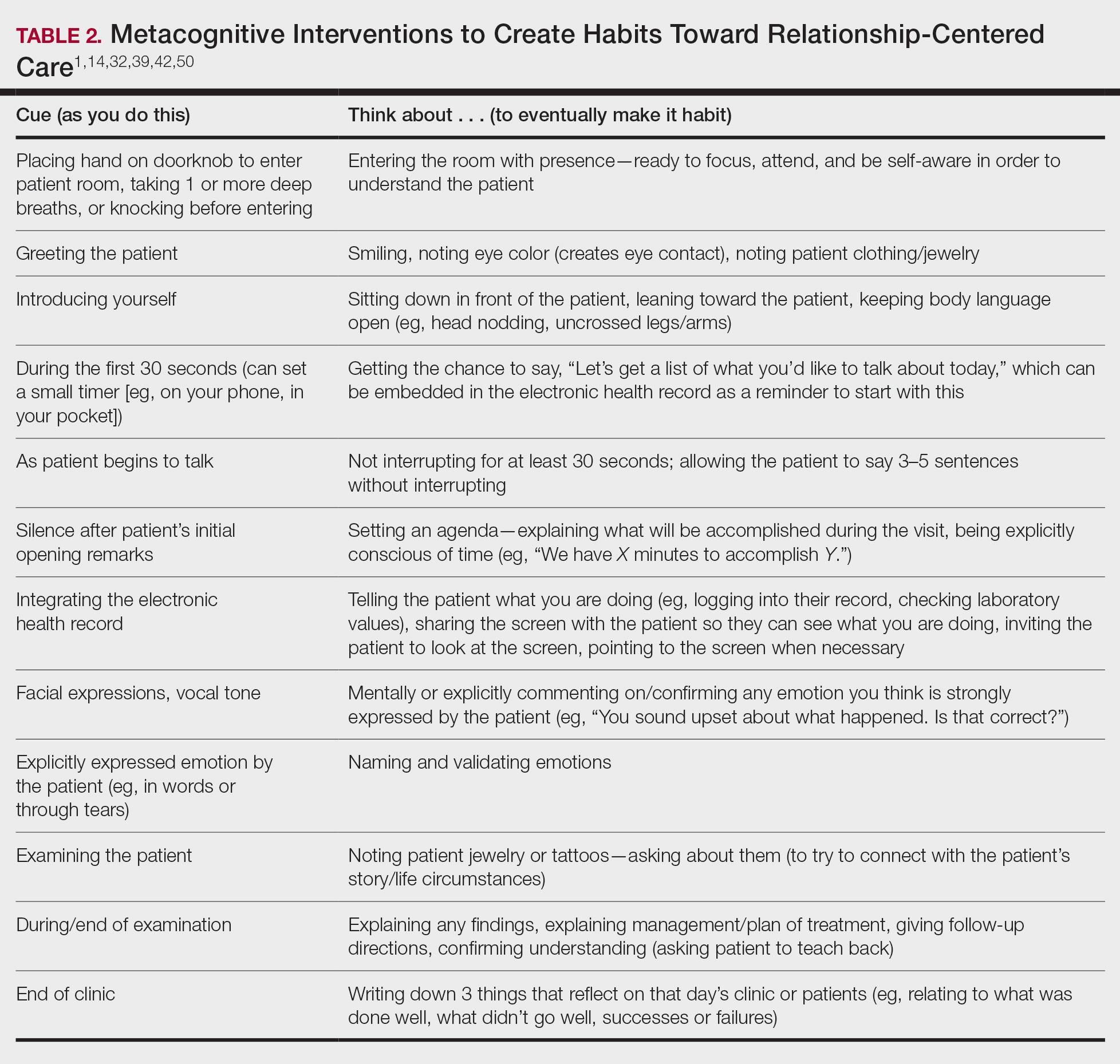
Although the theoretical foundation of relationship-centered care is relatively complex,9 a simple formula that has improved patient experience is “The Big 3,” which entails (1) simply knocking before entering the examination room, (2) sitting, and (3) asking, “What is your main concern?”30 Another relatively simple technique would be to involve the patient with the electronic health record by sharing the screen with them.52 Learning about narrative medicine and developing skills to appreciate each patient’s story is another method to increase relationship-centered care,40,53 as is emotional intelligence.54 These interventions are simple to implement, and good relationship-centered care will save time, help manage patient visits more effectively, and aid in avoiding the urgent new concern that the patient adds at the end of the visit.55 The positive effect of these different interventions highlights that small changes (Table 2) can shift the prevailing culture of medicine to become more relationship centered.56
Metacognitive Attention Can Generate Habit
Taking metacognition a step further, these small interventions can become habit11,14,39 through self-awareness, deliberate practice, and feedback.43 Habit is generated by linking a given intervention to another defined cue. For example, placing a hand on a doorknob to enter an examination room can be the cue to generate a habit of entering with presence.14 Alternatively, before entering an examination room, taking 3 deep breaths can be the cue to trigger presence.14 Habits can be created in just 3 weeks,57 and other proposed cues to generate habits toward relationship-centered care are listed in Table 2. By creating habit through metacognitive attention, relationship-centered care will become something that happens subconsciously without further burdening physicians with another task. Asking patients for permission to record video of an interaction also can create opportunities for self-awareness and self-evaluation through rewatching the video.58
Final Thoughts
Physicians already have the tools to create relationship-centered care in physician-patient interactions. A critical mental shift is to develop habits and apply thinking patterns toward understanding and responding appropriately to patients of all ethnicities and their emotions in the physician-patient interaction. This shift is aided by metacognitive awareness (Table 1) and the development of useful habits (Table 2).
- Sanders L, Fortin AH VI, Schiff GD. Connecting with patients—the missing links. JAMA. 2020;323:33-34.
- Peck BM, Denney M. Disparities in the conduct of the medical encounter: the effects of physician and patient race and gender. SAGE Open. 2012;2:1-14.
- Beach MC, Inui T. Relationship-centered care. a constructive reframing. J Gen Intern Med. 2006;21(suppl 1):S3-S8.
- Tresolini CP, Pew-Fetzer Task Force. Health Professions Education and Relationship-Centered Care. Pew Health Professions Commission; 1994.
- Hojat M. Empathy in Health Professions Education and Patient Care. Springer; 2016.
- Wilkinson H, Whittington R, Perry L, et al. Examining the relationship between burnout and empathy in healthcare professionals: a systematic review. Burn Res. 2017;6:18-29.
- Frankel RM, Quill T. Integrating biopsychosocial and relationship-centered care into mainstream medical practice: a challenge that continues to produce positive results. Fam Syst Health. 2005;23:413-421.
- Frankel RM. Relationship-centered care and the patient-physician relationship. J Gen Intern Med. 2004;19:1163-1165.
- Ventres WB, Frankel RM. Shared presence in physician-patient communication: a graphic representation. Fam Syst Health. 2015;33:270-279.
- Cooper LA, Beach MC, Johnson RL, et al. Delving below the surface: understanding how race and ethnicity influence relationships in health care. J Gen Intern Med. 2006;21(suppl 1):S21-S27.
- Epstein RM. Mindful practice. JAMA. 1999;282:833-839.
- Dobie S. Viewpoint: reflections on a well-traveled path: self-awareness, mindful practice, and relationship-centered care as foundations for medical education. Acad Med. 2007;82:422-427.
- Rabow MW. Meaning and relationship-centered care: recommendations for clinicians attending to the spiritual distress of patients at the end of life. Ethics Med Public Health. 2019;9:57-62.
- Zulman DM, Haverfield MC, Shaw JG, et al. Practices to foster physician presence and connection with patients in the clinical encounter. JAMA. 2020;323:70-81.
- Rakel DP, Guerrera MP, Bayles BP, et al. CAM education: promoting a salutogenic focus in health care. J Altern Complement Med. 2008;14:87-93.
- Olaisen RH, Schluchter MD, Flocke SA, et al. Assessing the longitudinal impact of physician-patient relationship on functional health. Ann Fam Med. 2020;18:422-429.
- Berg GM, Ekengren F, Lee FA, et al. Patient satisfaction with surgeons in a trauma population: testing a structural equation model using perceptions of interpersonal and technical care. J Trauma Acute Care Surg. 2012;72:1316-1322.
- Nassar A, Weimer-Elder B, Kline M, et al. Developing an inpatient relationship-centered communication curriculum for surgical teams: pilot study. J Am Coll Surg. 2019;229(4 suppl 2):E48.
- Caldicott CV, Dunn KA, Frankel RM. Can patients tell when they are unwanted? “turfing” in residency training. Patient Educ Couns. 2005;56:104-111.
- Tucker Edmonds B, Mogul M, Shea JA. Understanding low-income African American women’s expectations, preferences, and priorities in prenatal care. Fam Community Health. 2015;38:149-157.
- Sundstrom B, Szabo C, Dempsey A. “My body. my choice:” a qualitative study of the influence of trust and locus of control on postpartum contraceptive choice. J Health Commun. 2018;23:162-169.
- Block S, Billings JA. Nurturing humanism through teaching palliative care. Acad Med. 1998;73:763-765.
- Hebert RS, Schulz R, Copeland VC, et al. Preparing family caregivers for death and bereavement. insights from caregivers of terminally ill patients. J Pain Symptom Manage. 2009;37:3-12.
- Nundy S, Oswald J. Relationship-centered care: a new paradigm for population health management. Healthc (Amst). 2014;2:216-219.
- Sprague S. Relationship centered care. J S C Med Assoc. 2009;105:135-136.
- Roter DL, Frankel RM, Hall JA, et al. The expression of emotion through nonverbal behavior in medical visits. mechanisms and outcomes. J Gen Intern Med. 2006;21(suppl 1):S28-S34.
- Kenny DA, Veldhuijzen W, van der Weijden T, et al. Interpersonal perception in the context of doctor-patient relationships: a dyadic analysis of doctor-patient communication. Soc Sci Med. 2010;70:763-768.
- Tarzian AJ, Neal MT, O’Neil JA. Attitudes, experiences, and beliefs affecting end-of-life decision-making among homeless individuals. J Palliat Med. 2005;8:36-48.
- Roter D. The enduring and evolving nature of the patient-physician relationship. Patient Educ Couns. 2000;39:5-15.
- Sharieff GQ. MD to MD coaching: improving physician-patient experience scores: what works, what doesn’t. J Patient Exp. 2017;4:210-212.
- Duggan AP, Bradshaw YS, Swergold N, et al. When rapport building extends beyond affiliation: communication overaccommodation toward patients with disabilities. Perm J. 2011;15:23-30.
- Hirschmann K, Rosler G, Fortin AH VI. “For me, this has been transforming”: a qualitative analysis of interprofessional relationship-centered communication skills training. J Patient Exp. 2020;7:1007-1014.
- Hennrikus EF, Skolka MP, Hennrikus N. Applying metacognition through patient encounters and illness scripts to create a conceptual framework for basic science integration, storage, and retrieval. J Med Educ Curric Dev. 2018;5:2382120518777770.
- Eichbaum QG. Thinking about thinking and emotion: the metacognitive approach to the medical humanities that integrates the humanities with the basic and clinical sciences. Perm J. 2014;18:64-75.
- Stansfield RB, Schwartz A, O’Brien CL, et al. Development of a metacognitive effort construct of empathy during clinical training: a longitudinal study of the factor structure of the Jefferson Scale of Empathy. Adv Health Sci Educ Theory Pract. 2016;21:5-17.
- Hojat M, Vergare MJ, Maxwell K, et al. The devil is in the third year: a longitudinal study of erosion of empathy in medical school. Acad Med. 2009;84:1182-1191.
- Neumann M, Edelhäuser F, Tauschel D, et al. Empathy decline and its reasons: a systematic review of studies with medical students and residents. Acad Med. 2011;86:996-1009.
- Chou CL, Hirschmann K, Fortin AHT, et al. The impact of a faculty learning community on professional and personal development: the facilitator training program of the American Academy on Communication in Healthcare. Acad Med. 2014;89:1051-1056.
- Rider EA. Advanced communication strategies for relationship-centered care. Pediatr Ann. 2011;40:447-453.
- Reichman JAH. Narrative competence, mindfulness,and relationship-centered care in medical education: an innovative approach to teaching medical interviewing. Dissertation Abstracts International Section A: Humanities and Social Sciences. 2015;75(8-A(E)).
- Boissy A, Windover AK, Bokar D, et al. Communication skills training for physicians improves patient satisfaction. J Gen Intern Med. 2016;31:755-761.
- Hatem DS, Barrett SV, Hewson M, et al. Teaching the medical interview: methods and key learning issues in a faculty development course. J Gen Intern Med. 2007;22:1718-1724.
- Gilligan TD, Baile WF. ASCO patient-clinician communication guideline: fostering relationship-centered care. ASCO Connection. November 20, 2017. Accessed March 5, 2021. https://connection.asco.org/blogs/asco-patient-clinician-communication-guideline-fostering-relationship-centered-care
- Haidet P, Stein HF. The role of the student-teacher relationship in the formation of physicians. The hidden curriculum as process. J Gen Intern Med. 2006;(suppl 1):S16-S20.
- Puchalski CM, Guenther M. Restoration and re-creation: spirituality in the lives of healthcare professionals. Curr Opin Support Palliat Care. 2012;6:254-258.
- Williams SW, Hanson LC, Boyd C, et al. Communication, decision making, and cancer: what African Americans want physicians to know. J Palliative Med. 2008;11:1221-1226.
- Lindsley I, Woodhead S, Micallef C, et al. The concept of body language in the medical consultation. Psychiatr Danub. 2015;27(suppl 1):S41-S47.
- Hall JA, Harrigan JA, Rosenthal R. Nonverbal behavior in clinician-patient interaction. Appl Prev Psychol. 1995;4:21-37.
- Ness DE, Kiesling SF. Language and connectedness in the medical and psychiatric interview. Patient Educ Couns. 2007;68:139-144.
- Miller WL. The clinical hand: a curricular map for relationship-centered care. Fam Med. 2004;36:330-335.
- Wald HS, George P, Reis SP, et al. Electronic health record training in undergraduate medical education: bridging theory to practice with curricula for empowering patient- and relationship-centered care in the computerized setting. Acad Med. 2014;89:380-386.
- Silverman H, Ho YX, Kaib S, et al. A novel approach to supporting relationship-centered care through electronic health record ergonomic training in preclerkship medical education. Acad Med. 2014;89:1230-1234.
- Weiss T, Swede MJ. Transforming preprofessional health education through relationship-centered care and narrative medicine. Teach Learn Med. 2019;31:222-233.
- Blanch-Hartigan D. An effective training to increase accurate recognition of patient emotion cues. Patient Educ Couns. 2012;89:274-280.
- White J, Levinson W, Roter D. “Oh, by the way ...”: the closing moments of the medical visit. J Gen Intern Med. 1994;9:24-28.
- Suchman AL, Williamson PR, Litzelman DK, et al. Toward an informal curriculum that teaches professionalism. Transforming the social environment of a medical school. J Gen Intern Med. 2004;19:501-504.
- Lally P, van Jaarsveld CHM, Potts HWW, et al. How are habits formed: modelling habit formation in the real world. Eur J Soc Psychol. 2010;40:998-1009.
- Little P, White P, Kelly J, et al. Randomised controlled trial of a brief intervention targeting predominantly non-verbal communication in general practice consultations. Br J Gen Pract. 2015;65:E351-E356.
Communication and relationships cannot be taken for granted, particularly in the physician-patient relationship, where life-altering diagnoses may be given. With one diagnosis, someone’s life may be changed, and both physicians and patients need to be cognizant of the importance of a strong relationship and clear communication.
In the current US health care system, both physicians and patients often are not getting their needs met, and studies that include factors of race, ethnicity, and socioeconomic status suggest that physician-patient relationship barriers contribute to racial disparities in health care.1,2 Although patient-centered care is a widely recognized and upheld model, relationship-centered care between physician and patient involves focusing on the patient and the physician-patient relationship through recognizing personhood, affect (being empathic), and reciprocal influence.3,4 Although it is not necessarily intuitive because it can appear to be yet another task for busy physicians, relationship-centered care improves health care delivery for both physicians and patients through decreased physician burnout, reduced medical errors, and better patient outcomes and satisfaction.5,6
Every physician, patient, and physician-patient relationship is different; unlike the standard questions directed at a routine patient history focused on gathering data, there is no one-size-fits-all relationship-centered conversation.7-10 As with any successful interaction between 2 people, there is a certain amount of necessary self-awareness (Table 1)11 that allows for improvisation and appropriate responsiveness to what is seen, heard, and felt. Rather than attending solely to disease states, the focus of relationship-centered care is on patients, interpersonal interaction, and promoting health and well-being.15
This review summarizes the existing literature on relationship-centered care, introduces the use of metacognition (Table 1), and suggests creating simple habits to promote such care. The following databases were searched from inception through November 23, 2020, using the term relationship-centered care: MEDLINE (Ovid), EMBASE (Ovid), APA PsycInfo (Ovid), Scopus, Web of Science Core Collection, CINAHL Complete (EBSCO), Academic Search Premier (EBSCOhost), and ERIC (ProQuest). A total of 1772 records were retrieved through searches, and after deduplication of 1116 studies, 350 records were screened through a 2-part process. Articles were first screened by title and abstract for relevance to the relationship between physician and patient, with 185 studies deemed irrelevant (eg, pertaining to the relationship of veterinarian to animal). The remaining 165 studies were assessed for eligibility, with 69 further studies excluded for various reasons. The screening process resulted in 96 articles considered in this review.
Definitions/key terms, as used in this article, are listed in Table 1.
Background of Relationship-Centered Care
Given time constraints, the diagnosis and treatment of medical problems often are the focus of physicians. Although proper medical diagnosis and treatment are important, and their delivery is made possible by the physician having the appropriate knowledge, a physician-patient relationship that focuses solely on disease without acknowledging the patient creates a system that ultimately neglects both patients and physicians.15 This prevailing physician-patient relationship paradigm is suboptimal, and a proposed remedy is relationship-centered care, which focuses on relationships among the human beings in health care interactions.3 Relationship-centered care has 4 principles: (1) the personhood of each party must be recognized, (2) emotion is part of relationships, (3) relationships are reciprocal and not just one way, and (4) creating these types of relationships is morally valuable3 and beneficial to patient care.16
Assessment of the Need for Relationship-Centered Care
Relationship-centered care has been studied in physician-patient interactions in various health care settings.17-23 For at least 2 decades, relationship-centered care has been set forth as a model,4,24,25 but there are challenges. Physicians tend to overrate or underrate their communication skills in patient interactions.26,27 A given physician’s preferences often still seem to supersede those of the patient.3,28,29 The impetus to develop relationship-centered care skills generally needs to be internally driven,4,30 as, ultimately, physicians and patients have varying needs.4,31 However, providing physicians with a potential structure is helpful.32
A Solution: Metacognition in the Physician-Patient Interaction
Metacognition is important to integrating basic science knowledge into medical learning and practice,33,34 and it is no less important in translating interpersonal knowledge to the physician-patient interaction. Decreased metacognitive effort35 may underpin the decline in empathy seen with increasing medical training.36,37 Understanding how metacognitive practices foster relationship-centered care is important for teaching, developing, and maintaining that care.
Metacognition is already embedded in the fabric of the physician-patient interaction.33,34 The complex interplay of the physician-patient interview, patient examination, and integration of physical as well as ancillary data requires higher-order thinking and the ability to parse out that thinking successfully. As a concrete example, coming to a diagnosis requires thinking about what has been presented during the physician-patient interaction and considering what supports and suggests the disease while a list of potential differential diagnosis alternatives is being generated. Physicians are trained to apply this clinical reasoning approach to their patient care.
Conversely, although communication skills are a key component of doctoring,38 both between physician and patient as well as among other colleagues and staff, many physicians have never received formal training in communication skills,26,32,39 though it is now an integral part of medical school curricula.40 When such training is mandatory, less than 1% of physicians continue to believe that there was no benefit, even from a single 8-hour communications skills training session.41 Communication cannot be taught comprehensively in 8 hours; thus, the benefit of such training may be the end result of metacognition and increased self-awareness (Table 1).42,43
Building Relationship-Centered Care Through Metacognitive Attention
Metacognition as manifested by such self-awareness can build relationship-centered care.4 Self-awareness can be taught through mentorship or role models.44 Journaling,40 meditation, and appreciation of beauty and the arts45 can contribute, as well as more formal training programs,32,38,42 as offered by the Academy of Communication in Healthcare. Creating opportunities for patient empowerment also supports relationship-centered care, as does applying knowledge of implicit bias.46
Even without formal training, relationship-centered care can be built through attention to cues9—visual (eg, sitting down, other body language),47,48 auditory (eg, knocking, language, tone, conversational flow),48,49 and emotional (eg, clinical empathy, emotional intelligence)(Table 2). Such attention is familiar to everyone, not just physicians or patients, through interactions outside of health care; inattention may be due to the hidden curriculum or culture of medicine40 as well as real-time changes, such as the introduction of the electronic health record.51 Inattention to these cues also may be a result of context-specific knowledge, in which a physician’s real-life communication skills are not applied to the unique context of patient care.
Although the theoretical foundation of relationship-centered care is relatively complex,9 a simple formula that has improved patient experience is “The Big 3,” which entails (1) simply knocking before entering the examination room, (2) sitting, and (3) asking, “What is your main concern?”30 Another relatively simple technique would be to involve the patient with the electronic health record by sharing the screen with them.52 Learning about narrative medicine and developing skills to appreciate each patient’s story is another method to increase relationship-centered care,40,53 as is emotional intelligence.54 These interventions are simple to implement, and good relationship-centered care will save time, help manage patient visits more effectively, and aid in avoiding the urgent new concern that the patient adds at the end of the visit.55 The positive effect of these different interventions highlights that small changes (Table 2) can shift the prevailing culture of medicine to become more relationship centered.56
Metacognitive Attention Can Generate Habit
Taking metacognition a step further, these small interventions can become habit11,14,39 through self-awareness, deliberate practice, and feedback.43 Habit is generated by linking a given intervention to another defined cue. For example, placing a hand on a doorknob to enter an examination room can be the cue to generate a habit of entering with presence.14 Alternatively, before entering an examination room, taking 3 deep breaths can be the cue to trigger presence.14 Habits can be created in just 3 weeks,57 and other proposed cues to generate habits toward relationship-centered care are listed in Table 2. By creating habit through metacognitive attention, relationship-centered care will become something that happens subconsciously without further burdening physicians with another task. Asking patients for permission to record video of an interaction also can create opportunities for self-awareness and self-evaluation through rewatching the video.58
Final Thoughts
Physicians already have the tools to create relationship-centered care in physician-patient interactions. A critical mental shift is to develop habits and apply thinking patterns toward understanding and responding appropriately to patients of all ethnicities and their emotions in the physician-patient interaction. This shift is aided by metacognitive awareness (Table 1) and the development of useful habits (Table 2).
Communication and relationships cannot be taken for granted, particularly in the physician-patient relationship, where life-altering diagnoses may be given. With one diagnosis, someone’s life may be changed, and both physicians and patients need to be cognizant of the importance of a strong relationship and clear communication.
In the current US health care system, both physicians and patients often are not getting their needs met, and studies that include factors of race, ethnicity, and socioeconomic status suggest that physician-patient relationship barriers contribute to racial disparities in health care.1,2 Although patient-centered care is a widely recognized and upheld model, relationship-centered care between physician and patient involves focusing on the patient and the physician-patient relationship through recognizing personhood, affect (being empathic), and reciprocal influence.3,4 Although it is not necessarily intuitive because it can appear to be yet another task for busy physicians, relationship-centered care improves health care delivery for both physicians and patients through decreased physician burnout, reduced medical errors, and better patient outcomes and satisfaction.5,6
Every physician, patient, and physician-patient relationship is different; unlike the standard questions directed at a routine patient history focused on gathering data, there is no one-size-fits-all relationship-centered conversation.7-10 As with any successful interaction between 2 people, there is a certain amount of necessary self-awareness (Table 1)11 that allows for improvisation and appropriate responsiveness to what is seen, heard, and felt. Rather than attending solely to disease states, the focus of relationship-centered care is on patients, interpersonal interaction, and promoting health and well-being.15
This review summarizes the existing literature on relationship-centered care, introduces the use of metacognition (Table 1), and suggests creating simple habits to promote such care. The following databases were searched from inception through November 23, 2020, using the term relationship-centered care: MEDLINE (Ovid), EMBASE (Ovid), APA PsycInfo (Ovid), Scopus, Web of Science Core Collection, CINAHL Complete (EBSCO), Academic Search Premier (EBSCOhost), and ERIC (ProQuest). A total of 1772 records were retrieved through searches, and after deduplication of 1116 studies, 350 records were screened through a 2-part process. Articles were first screened by title and abstract for relevance to the relationship between physician and patient, with 185 studies deemed irrelevant (eg, pertaining to the relationship of veterinarian to animal). The remaining 165 studies were assessed for eligibility, with 69 further studies excluded for various reasons. The screening process resulted in 96 articles considered in this review.
Definitions/key terms, as used in this article, are listed in Table 1.
Background of Relationship-Centered Care
Given time constraints, the diagnosis and treatment of medical problems often are the focus of physicians. Although proper medical diagnosis and treatment are important, and their delivery is made possible by the physician having the appropriate knowledge, a physician-patient relationship that focuses solely on disease without acknowledging the patient creates a system that ultimately neglects both patients and physicians.15 This prevailing physician-patient relationship paradigm is suboptimal, and a proposed remedy is relationship-centered care, which focuses on relationships among the human beings in health care interactions.3 Relationship-centered care has 4 principles: (1) the personhood of each party must be recognized, (2) emotion is part of relationships, (3) relationships are reciprocal and not just one way, and (4) creating these types of relationships is morally valuable3 and beneficial to patient care.16
Assessment of the Need for Relationship-Centered Care
Relationship-centered care has been studied in physician-patient interactions in various health care settings.17-23 For at least 2 decades, relationship-centered care has been set forth as a model,4,24,25 but there are challenges. Physicians tend to overrate or underrate their communication skills in patient interactions.26,27 A given physician’s preferences often still seem to supersede those of the patient.3,28,29 The impetus to develop relationship-centered care skills generally needs to be internally driven,4,30 as, ultimately, physicians and patients have varying needs.4,31 However, providing physicians with a potential structure is helpful.32
A Solution: Metacognition in the Physician-Patient Interaction
Metacognition is important to integrating basic science knowledge into medical learning and practice,33,34 and it is no less important in translating interpersonal knowledge to the physician-patient interaction. Decreased metacognitive effort35 may underpin the decline in empathy seen with increasing medical training.36,37 Understanding how metacognitive practices foster relationship-centered care is important for teaching, developing, and maintaining that care.
Metacognition is already embedded in the fabric of the physician-patient interaction.33,34 The complex interplay of the physician-patient interview, patient examination, and integration of physical as well as ancillary data requires higher-order thinking and the ability to parse out that thinking successfully. As a concrete example, coming to a diagnosis requires thinking about what has been presented during the physician-patient interaction and considering what supports and suggests the disease while a list of potential differential diagnosis alternatives is being generated. Physicians are trained to apply this clinical reasoning approach to their patient care.
Conversely, although communication skills are a key component of doctoring,38 both between physician and patient as well as among other colleagues and staff, many physicians have never received formal training in communication skills,26,32,39 though it is now an integral part of medical school curricula.40 When such training is mandatory, less than 1% of physicians continue to believe that there was no benefit, even from a single 8-hour communications skills training session.41 Communication cannot be taught comprehensively in 8 hours; thus, the benefit of such training may be the end result of metacognition and increased self-awareness (Table 1).42,43
Building Relationship-Centered Care Through Metacognitive Attention
Metacognition as manifested by such self-awareness can build relationship-centered care.4 Self-awareness can be taught through mentorship or role models.44 Journaling,40 meditation, and appreciation of beauty and the arts45 can contribute, as well as more formal training programs,32,38,42 as offered by the Academy of Communication in Healthcare. Creating opportunities for patient empowerment also supports relationship-centered care, as does applying knowledge of implicit bias.46
Even without formal training, relationship-centered care can be built through attention to cues9—visual (eg, sitting down, other body language),47,48 auditory (eg, knocking, language, tone, conversational flow),48,49 and emotional (eg, clinical empathy, emotional intelligence)(Table 2). Such attention is familiar to everyone, not just physicians or patients, through interactions outside of health care; inattention may be due to the hidden curriculum or culture of medicine40 as well as real-time changes, such as the introduction of the electronic health record.51 Inattention to these cues also may be a result of context-specific knowledge, in which a physician’s real-life communication skills are not applied to the unique context of patient care.
Although the theoretical foundation of relationship-centered care is relatively complex,9 a simple formula that has improved patient experience is “The Big 3,” which entails (1) simply knocking before entering the examination room, (2) sitting, and (3) asking, “What is your main concern?”30 Another relatively simple technique would be to involve the patient with the electronic health record by sharing the screen with them.52 Learning about narrative medicine and developing skills to appreciate each patient’s story is another method to increase relationship-centered care,40,53 as is emotional intelligence.54 These interventions are simple to implement, and good relationship-centered care will save time, help manage patient visits more effectively, and aid in avoiding the urgent new concern that the patient adds at the end of the visit.55 The positive effect of these different interventions highlights that small changes (Table 2) can shift the prevailing culture of medicine to become more relationship centered.56
Metacognitive Attention Can Generate Habit
Taking metacognition a step further, these small interventions can become habit11,14,39 through self-awareness, deliberate practice, and feedback.43 Habit is generated by linking a given intervention to another defined cue. For example, placing a hand on a doorknob to enter an examination room can be the cue to generate a habit of entering with presence.14 Alternatively, before entering an examination room, taking 3 deep breaths can be the cue to trigger presence.14 Habits can be created in just 3 weeks,57 and other proposed cues to generate habits toward relationship-centered care are listed in Table 2. By creating habit through metacognitive attention, relationship-centered care will become something that happens subconsciously without further burdening physicians with another task. Asking patients for permission to record video of an interaction also can create opportunities for self-awareness and self-evaluation through rewatching the video.58
Final Thoughts
Physicians already have the tools to create relationship-centered care in physician-patient interactions. A critical mental shift is to develop habits and apply thinking patterns toward understanding and responding appropriately to patients of all ethnicities and their emotions in the physician-patient interaction. This shift is aided by metacognitive awareness (Table 1) and the development of useful habits (Table 2).
- Sanders L, Fortin AH VI, Schiff GD. Connecting with patients—the missing links. JAMA. 2020;323:33-34.
- Peck BM, Denney M. Disparities in the conduct of the medical encounter: the effects of physician and patient race and gender. SAGE Open. 2012;2:1-14.
- Beach MC, Inui T. Relationship-centered care. a constructive reframing. J Gen Intern Med. 2006;21(suppl 1):S3-S8.
- Tresolini CP, Pew-Fetzer Task Force. Health Professions Education and Relationship-Centered Care. Pew Health Professions Commission; 1994.
- Hojat M. Empathy in Health Professions Education and Patient Care. Springer; 2016.
- Wilkinson H, Whittington R, Perry L, et al. Examining the relationship between burnout and empathy in healthcare professionals: a systematic review. Burn Res. 2017;6:18-29.
- Frankel RM, Quill T. Integrating biopsychosocial and relationship-centered care into mainstream medical practice: a challenge that continues to produce positive results. Fam Syst Health. 2005;23:413-421.
- Frankel RM. Relationship-centered care and the patient-physician relationship. J Gen Intern Med. 2004;19:1163-1165.
- Ventres WB, Frankel RM. Shared presence in physician-patient communication: a graphic representation. Fam Syst Health. 2015;33:270-279.
- Cooper LA, Beach MC, Johnson RL, et al. Delving below the surface: understanding how race and ethnicity influence relationships in health care. J Gen Intern Med. 2006;21(suppl 1):S21-S27.
- Epstein RM. Mindful practice. JAMA. 1999;282:833-839.
- Dobie S. Viewpoint: reflections on a well-traveled path: self-awareness, mindful practice, and relationship-centered care as foundations for medical education. Acad Med. 2007;82:422-427.
- Rabow MW. Meaning and relationship-centered care: recommendations for clinicians attending to the spiritual distress of patients at the end of life. Ethics Med Public Health. 2019;9:57-62.
- Zulman DM, Haverfield MC, Shaw JG, et al. Practices to foster physician presence and connection with patients in the clinical encounter. JAMA. 2020;323:70-81.
- Rakel DP, Guerrera MP, Bayles BP, et al. CAM education: promoting a salutogenic focus in health care. J Altern Complement Med. 2008;14:87-93.
- Olaisen RH, Schluchter MD, Flocke SA, et al. Assessing the longitudinal impact of physician-patient relationship on functional health. Ann Fam Med. 2020;18:422-429.
- Berg GM, Ekengren F, Lee FA, et al. Patient satisfaction with surgeons in a trauma population: testing a structural equation model using perceptions of interpersonal and technical care. J Trauma Acute Care Surg. 2012;72:1316-1322.
- Nassar A, Weimer-Elder B, Kline M, et al. Developing an inpatient relationship-centered communication curriculum for surgical teams: pilot study. J Am Coll Surg. 2019;229(4 suppl 2):E48.
- Caldicott CV, Dunn KA, Frankel RM. Can patients tell when they are unwanted? “turfing” in residency training. Patient Educ Couns. 2005;56:104-111.
- Tucker Edmonds B, Mogul M, Shea JA. Understanding low-income African American women’s expectations, preferences, and priorities in prenatal care. Fam Community Health. 2015;38:149-157.
- Sundstrom B, Szabo C, Dempsey A. “My body. my choice:” a qualitative study of the influence of trust and locus of control on postpartum contraceptive choice. J Health Commun. 2018;23:162-169.
- Block S, Billings JA. Nurturing humanism through teaching palliative care. Acad Med. 1998;73:763-765.
- Hebert RS, Schulz R, Copeland VC, et al. Preparing family caregivers for death and bereavement. insights from caregivers of terminally ill patients. J Pain Symptom Manage. 2009;37:3-12.
- Nundy S, Oswald J. Relationship-centered care: a new paradigm for population health management. Healthc (Amst). 2014;2:216-219.
- Sprague S. Relationship centered care. J S C Med Assoc. 2009;105:135-136.
- Roter DL, Frankel RM, Hall JA, et al. The expression of emotion through nonverbal behavior in medical visits. mechanisms and outcomes. J Gen Intern Med. 2006;21(suppl 1):S28-S34.
- Kenny DA, Veldhuijzen W, van der Weijden T, et al. Interpersonal perception in the context of doctor-patient relationships: a dyadic analysis of doctor-patient communication. Soc Sci Med. 2010;70:763-768.
- Tarzian AJ, Neal MT, O’Neil JA. Attitudes, experiences, and beliefs affecting end-of-life decision-making among homeless individuals. J Palliat Med. 2005;8:36-48.
- Roter D. The enduring and evolving nature of the patient-physician relationship. Patient Educ Couns. 2000;39:5-15.
- Sharieff GQ. MD to MD coaching: improving physician-patient experience scores: what works, what doesn’t. J Patient Exp. 2017;4:210-212.
- Duggan AP, Bradshaw YS, Swergold N, et al. When rapport building extends beyond affiliation: communication overaccommodation toward patients with disabilities. Perm J. 2011;15:23-30.
- Hirschmann K, Rosler G, Fortin AH VI. “For me, this has been transforming”: a qualitative analysis of interprofessional relationship-centered communication skills training. J Patient Exp. 2020;7:1007-1014.
- Hennrikus EF, Skolka MP, Hennrikus N. Applying metacognition through patient encounters and illness scripts to create a conceptual framework for basic science integration, storage, and retrieval. J Med Educ Curric Dev. 2018;5:2382120518777770.
- Eichbaum QG. Thinking about thinking and emotion: the metacognitive approach to the medical humanities that integrates the humanities with the basic and clinical sciences. Perm J. 2014;18:64-75.
- Stansfield RB, Schwartz A, O’Brien CL, et al. Development of a metacognitive effort construct of empathy during clinical training: a longitudinal study of the factor structure of the Jefferson Scale of Empathy. Adv Health Sci Educ Theory Pract. 2016;21:5-17.
- Hojat M, Vergare MJ, Maxwell K, et al. The devil is in the third year: a longitudinal study of erosion of empathy in medical school. Acad Med. 2009;84:1182-1191.
- Neumann M, Edelhäuser F, Tauschel D, et al. Empathy decline and its reasons: a systematic review of studies with medical students and residents. Acad Med. 2011;86:996-1009.
- Chou CL, Hirschmann K, Fortin AHT, et al. The impact of a faculty learning community on professional and personal development: the facilitator training program of the American Academy on Communication in Healthcare. Acad Med. 2014;89:1051-1056.
- Rider EA. Advanced communication strategies for relationship-centered care. Pediatr Ann. 2011;40:447-453.
- Reichman JAH. Narrative competence, mindfulness,and relationship-centered care in medical education: an innovative approach to teaching medical interviewing. Dissertation Abstracts International Section A: Humanities and Social Sciences. 2015;75(8-A(E)).
- Boissy A, Windover AK, Bokar D, et al. Communication skills training for physicians improves patient satisfaction. J Gen Intern Med. 2016;31:755-761.
- Hatem DS, Barrett SV, Hewson M, et al. Teaching the medical interview: methods and key learning issues in a faculty development course. J Gen Intern Med. 2007;22:1718-1724.
- Gilligan TD, Baile WF. ASCO patient-clinician communication guideline: fostering relationship-centered care. ASCO Connection. November 20, 2017. Accessed March 5, 2021. https://connection.asco.org/blogs/asco-patient-clinician-communication-guideline-fostering-relationship-centered-care
- Haidet P, Stein HF. The role of the student-teacher relationship in the formation of physicians. The hidden curriculum as process. J Gen Intern Med. 2006;(suppl 1):S16-S20.
- Puchalski CM, Guenther M. Restoration and re-creation: spirituality in the lives of healthcare professionals. Curr Opin Support Palliat Care. 2012;6:254-258.
- Williams SW, Hanson LC, Boyd C, et al. Communication, decision making, and cancer: what African Americans want physicians to know. J Palliative Med. 2008;11:1221-1226.
- Lindsley I, Woodhead S, Micallef C, et al. The concept of body language in the medical consultation. Psychiatr Danub. 2015;27(suppl 1):S41-S47.
- Hall JA, Harrigan JA, Rosenthal R. Nonverbal behavior in clinician-patient interaction. Appl Prev Psychol. 1995;4:21-37.
- Ness DE, Kiesling SF. Language and connectedness in the medical and psychiatric interview. Patient Educ Couns. 2007;68:139-144.
- Miller WL. The clinical hand: a curricular map for relationship-centered care. Fam Med. 2004;36:330-335.
- Wald HS, George P, Reis SP, et al. Electronic health record training in undergraduate medical education: bridging theory to practice with curricula for empowering patient- and relationship-centered care in the computerized setting. Acad Med. 2014;89:380-386.
- Silverman H, Ho YX, Kaib S, et al. A novel approach to supporting relationship-centered care through electronic health record ergonomic training in preclerkship medical education. Acad Med. 2014;89:1230-1234.
- Weiss T, Swede MJ. Transforming preprofessional health education through relationship-centered care and narrative medicine. Teach Learn Med. 2019;31:222-233.
- Blanch-Hartigan D. An effective training to increase accurate recognition of patient emotion cues. Patient Educ Couns. 2012;89:274-280.
- White J, Levinson W, Roter D. “Oh, by the way ...”: the closing moments of the medical visit. J Gen Intern Med. 1994;9:24-28.
- Suchman AL, Williamson PR, Litzelman DK, et al. Toward an informal curriculum that teaches professionalism. Transforming the social environment of a medical school. J Gen Intern Med. 2004;19:501-504.
- Lally P, van Jaarsveld CHM, Potts HWW, et al. How are habits formed: modelling habit formation in the real world. Eur J Soc Psychol. 2010;40:998-1009.
- Little P, White P, Kelly J, et al. Randomised controlled trial of a brief intervention targeting predominantly non-verbal communication in general practice consultations. Br J Gen Pract. 2015;65:E351-E356.
- Sanders L, Fortin AH VI, Schiff GD. Connecting with patients—the missing links. JAMA. 2020;323:33-34.
- Peck BM, Denney M. Disparities in the conduct of the medical encounter: the effects of physician and patient race and gender. SAGE Open. 2012;2:1-14.
- Beach MC, Inui T. Relationship-centered care. a constructive reframing. J Gen Intern Med. 2006;21(suppl 1):S3-S8.
- Tresolini CP, Pew-Fetzer Task Force. Health Professions Education and Relationship-Centered Care. Pew Health Professions Commission; 1994.
- Hojat M. Empathy in Health Professions Education and Patient Care. Springer; 2016.
- Wilkinson H, Whittington R, Perry L, et al. Examining the relationship between burnout and empathy in healthcare professionals: a systematic review. Burn Res. 2017;6:18-29.
- Frankel RM, Quill T. Integrating biopsychosocial and relationship-centered care into mainstream medical practice: a challenge that continues to produce positive results. Fam Syst Health. 2005;23:413-421.
- Frankel RM. Relationship-centered care and the patient-physician relationship. J Gen Intern Med. 2004;19:1163-1165.
- Ventres WB, Frankel RM. Shared presence in physician-patient communication: a graphic representation. Fam Syst Health. 2015;33:270-279.
- Cooper LA, Beach MC, Johnson RL, et al. Delving below the surface: understanding how race and ethnicity influence relationships in health care. J Gen Intern Med. 2006;21(suppl 1):S21-S27.
- Epstein RM. Mindful practice. JAMA. 1999;282:833-839.
- Dobie S. Viewpoint: reflections on a well-traveled path: self-awareness, mindful practice, and relationship-centered care as foundations for medical education. Acad Med. 2007;82:422-427.
- Rabow MW. Meaning and relationship-centered care: recommendations for clinicians attending to the spiritual distress of patients at the end of life. Ethics Med Public Health. 2019;9:57-62.
- Zulman DM, Haverfield MC, Shaw JG, et al. Practices to foster physician presence and connection with patients in the clinical encounter. JAMA. 2020;323:70-81.
- Rakel DP, Guerrera MP, Bayles BP, et al. CAM education: promoting a salutogenic focus in health care. J Altern Complement Med. 2008;14:87-93.
- Olaisen RH, Schluchter MD, Flocke SA, et al. Assessing the longitudinal impact of physician-patient relationship on functional health. Ann Fam Med. 2020;18:422-429.
- Berg GM, Ekengren F, Lee FA, et al. Patient satisfaction with surgeons in a trauma population: testing a structural equation model using perceptions of interpersonal and technical care. J Trauma Acute Care Surg. 2012;72:1316-1322.
- Nassar A, Weimer-Elder B, Kline M, et al. Developing an inpatient relationship-centered communication curriculum for surgical teams: pilot study. J Am Coll Surg. 2019;229(4 suppl 2):E48.
- Caldicott CV, Dunn KA, Frankel RM. Can patients tell when they are unwanted? “turfing” in residency training. Patient Educ Couns. 2005;56:104-111.
- Tucker Edmonds B, Mogul M, Shea JA. Understanding low-income African American women’s expectations, preferences, and priorities in prenatal care. Fam Community Health. 2015;38:149-157.
- Sundstrom B, Szabo C, Dempsey A. “My body. my choice:” a qualitative study of the influence of trust and locus of control on postpartum contraceptive choice. J Health Commun. 2018;23:162-169.
- Block S, Billings JA. Nurturing humanism through teaching palliative care. Acad Med. 1998;73:763-765.
- Hebert RS, Schulz R, Copeland VC, et al. Preparing family caregivers for death and bereavement. insights from caregivers of terminally ill patients. J Pain Symptom Manage. 2009;37:3-12.
- Nundy S, Oswald J. Relationship-centered care: a new paradigm for population health management. Healthc (Amst). 2014;2:216-219.
- Sprague S. Relationship centered care. J S C Med Assoc. 2009;105:135-136.
- Roter DL, Frankel RM, Hall JA, et al. The expression of emotion through nonverbal behavior in medical visits. mechanisms and outcomes. J Gen Intern Med. 2006;21(suppl 1):S28-S34.
- Kenny DA, Veldhuijzen W, van der Weijden T, et al. Interpersonal perception in the context of doctor-patient relationships: a dyadic analysis of doctor-patient communication. Soc Sci Med. 2010;70:763-768.
- Tarzian AJ, Neal MT, O’Neil JA. Attitudes, experiences, and beliefs affecting end-of-life decision-making among homeless individuals. J Palliat Med. 2005;8:36-48.
- Roter D. The enduring and evolving nature of the patient-physician relationship. Patient Educ Couns. 2000;39:5-15.
- Sharieff GQ. MD to MD coaching: improving physician-patient experience scores: what works, what doesn’t. J Patient Exp. 2017;4:210-212.
- Duggan AP, Bradshaw YS, Swergold N, et al. When rapport building extends beyond affiliation: communication overaccommodation toward patients with disabilities. Perm J. 2011;15:23-30.
- Hirschmann K, Rosler G, Fortin AH VI. “For me, this has been transforming”: a qualitative analysis of interprofessional relationship-centered communication skills training. J Patient Exp. 2020;7:1007-1014.
- Hennrikus EF, Skolka MP, Hennrikus N. Applying metacognition through patient encounters and illness scripts to create a conceptual framework for basic science integration, storage, and retrieval. J Med Educ Curric Dev. 2018;5:2382120518777770.
- Eichbaum QG. Thinking about thinking and emotion: the metacognitive approach to the medical humanities that integrates the humanities with the basic and clinical sciences. Perm J. 2014;18:64-75.
- Stansfield RB, Schwartz A, O’Brien CL, et al. Development of a metacognitive effort construct of empathy during clinical training: a longitudinal study of the factor structure of the Jefferson Scale of Empathy. Adv Health Sci Educ Theory Pract. 2016;21:5-17.
- Hojat M, Vergare MJ, Maxwell K, et al. The devil is in the third year: a longitudinal study of erosion of empathy in medical school. Acad Med. 2009;84:1182-1191.
- Neumann M, Edelhäuser F, Tauschel D, et al. Empathy decline and its reasons: a systematic review of studies with medical students and residents. Acad Med. 2011;86:996-1009.
- Chou CL, Hirschmann K, Fortin AHT, et al. The impact of a faculty learning community on professional and personal development: the facilitator training program of the American Academy on Communication in Healthcare. Acad Med. 2014;89:1051-1056.
- Rider EA. Advanced communication strategies for relationship-centered care. Pediatr Ann. 2011;40:447-453.
- Reichman JAH. Narrative competence, mindfulness,and relationship-centered care in medical education: an innovative approach to teaching medical interviewing. Dissertation Abstracts International Section A: Humanities and Social Sciences. 2015;75(8-A(E)).
- Boissy A, Windover AK, Bokar D, et al. Communication skills training for physicians improves patient satisfaction. J Gen Intern Med. 2016;31:755-761.
- Hatem DS, Barrett SV, Hewson M, et al. Teaching the medical interview: methods and key learning issues in a faculty development course. J Gen Intern Med. 2007;22:1718-1724.
- Gilligan TD, Baile WF. ASCO patient-clinician communication guideline: fostering relationship-centered care. ASCO Connection. November 20, 2017. Accessed March 5, 2021. https://connection.asco.org/blogs/asco-patient-clinician-communication-guideline-fostering-relationship-centered-care
- Haidet P, Stein HF. The role of the student-teacher relationship in the formation of physicians. The hidden curriculum as process. J Gen Intern Med. 2006;(suppl 1):S16-S20.
- Puchalski CM, Guenther M. Restoration and re-creation: spirituality in the lives of healthcare professionals. Curr Opin Support Palliat Care. 2012;6:254-258.
- Williams SW, Hanson LC, Boyd C, et al. Communication, decision making, and cancer: what African Americans want physicians to know. J Palliative Med. 2008;11:1221-1226.
- Lindsley I, Woodhead S, Micallef C, et al. The concept of body language in the medical consultation. Psychiatr Danub. 2015;27(suppl 1):S41-S47.
- Hall JA, Harrigan JA, Rosenthal R. Nonverbal behavior in clinician-patient interaction. Appl Prev Psychol. 1995;4:21-37.
- Ness DE, Kiesling SF. Language and connectedness in the medical and psychiatric interview. Patient Educ Couns. 2007;68:139-144.
- Miller WL. The clinical hand: a curricular map for relationship-centered care. Fam Med. 2004;36:330-335.
- Wald HS, George P, Reis SP, et al. Electronic health record training in undergraduate medical education: bridging theory to practice with curricula for empowering patient- and relationship-centered care in the computerized setting. Acad Med. 2014;89:380-386.
- Silverman H, Ho YX, Kaib S, et al. A novel approach to supporting relationship-centered care through electronic health record ergonomic training in preclerkship medical education. Acad Med. 2014;89:1230-1234.
- Weiss T, Swede MJ. Transforming preprofessional health education through relationship-centered care and narrative medicine. Teach Learn Med. 2019;31:222-233.
- Blanch-Hartigan D. An effective training to increase accurate recognition of patient emotion cues. Patient Educ Couns. 2012;89:274-280.
- White J, Levinson W, Roter D. “Oh, by the way ...”: the closing moments of the medical visit. J Gen Intern Med. 1994;9:24-28.
- Suchman AL, Williamson PR, Litzelman DK, et al. Toward an informal curriculum that teaches professionalism. Transforming the social environment of a medical school. J Gen Intern Med. 2004;19:501-504.
- Lally P, van Jaarsveld CHM, Potts HWW, et al. How are habits formed: modelling habit formation in the real world. Eur J Soc Psychol. 2010;40:998-1009.
- Little P, White P, Kelly J, et al. Randomised controlled trial of a brief intervention targeting predominantly non-verbal communication in general practice consultations. Br J Gen Pract. 2015;65:E351-E356.
Practice Points
- Relationship-centered care emphasizes that all relationships in health care are important, including not only relationships between physicians and patients but also among physicians and colleagues, staff, students, community, and self.
- The physician-patient relationship can be complex, and metacognition can lead to habitual practice of simple techniques to optimize the interaction

In acute lower GI bleeding, there may be no benefit to early colonoscopy
Background: Current U.S. guidelines recommend colonoscopy within 24 hours for patients presenting with high-risk or severe acute lower gastrointestinal bleeding. However, prior meta-analyses of the timing of colonoscopy relied primarily on observational studies, and a recent multicenter randomized, controlled trial suggests no substantial benefit for early colonoscopy.
Study design: Systematic review and meta-analysis of randomized, clinical trials.
Setting: English language literature search from MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials, performed in July 2019.
Synopsis: The authors identified four randomized, controlled trials that compared early colonoscopy (defined as within 24 hours) with elective colonoscopy (defined as beyond 24 hours) and/or other diagnostic tests for patients presenting with acute lower GI bleeding. They performed a meta-analysis, including 463 patients, which showed no significant difference in risk of persistent or recurrent bleeding for early versus elective colonoscopy. The authors also found no significant differences in secondary outcomes of mortality, endoscopic intervention, primary hemostatic intervention, or identification of bleeding source. Limitations of this research include the relatively small number of studies included, and potential for selection bias in the original studies. Notably two of the four studies included were prematurely terminated before their planned sample sizes were reached.
Bottom line: In patients hospitalized with acute lower GI bleeding, colonoscopy within 24 hours may not reduce further bleeding or mortality when compared with elective colonoscopy.
Citation: Tsay C et al. Early colonoscopy does not improve outcomes of patients with lower gastrointestinal bleeding: Systematic review of randomized trials. Clin Gastroenterol Hepatol. 2019 Dec 13. doi: 10.1016/j.cgh.2019.11.061.
Dr. Hu is a hospitalist at Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, both in Boston.
Background: Current U.S. guidelines recommend colonoscopy within 24 hours for patients presenting with high-risk or severe acute lower gastrointestinal bleeding. However, prior meta-analyses of the timing of colonoscopy relied primarily on observational studies, and a recent multicenter randomized, controlled trial suggests no substantial benefit for early colonoscopy.
Study design: Systematic review and meta-analysis of randomized, clinical trials.
Setting: English language literature search from MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials, performed in July 2019.
Synopsis: The authors identified four randomized, controlled trials that compared early colonoscopy (defined as within 24 hours) with elective colonoscopy (defined as beyond 24 hours) and/or other diagnostic tests for patients presenting with acute lower GI bleeding. They performed a meta-analysis, including 463 patients, which showed no significant difference in risk of persistent or recurrent bleeding for early versus elective colonoscopy. The authors also found no significant differences in secondary outcomes of mortality, endoscopic intervention, primary hemostatic intervention, or identification of bleeding source. Limitations of this research include the relatively small number of studies included, and potential for selection bias in the original studies. Notably two of the four studies included were prematurely terminated before their planned sample sizes were reached.
Bottom line: In patients hospitalized with acute lower GI bleeding, colonoscopy within 24 hours may not reduce further bleeding or mortality when compared with elective colonoscopy.
Citation: Tsay C et al. Early colonoscopy does not improve outcomes of patients with lower gastrointestinal bleeding: Systematic review of randomized trials. Clin Gastroenterol Hepatol. 2019 Dec 13. doi: 10.1016/j.cgh.2019.11.061.
Dr. Hu is a hospitalist at Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, both in Boston.
Background: Current U.S. guidelines recommend colonoscopy within 24 hours for patients presenting with high-risk or severe acute lower gastrointestinal bleeding. However, prior meta-analyses of the timing of colonoscopy relied primarily on observational studies, and a recent multicenter randomized, controlled trial suggests no substantial benefit for early colonoscopy.
Study design: Systematic review and meta-analysis of randomized, clinical trials.
Setting: English language literature search from MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials, performed in July 2019.
Synopsis: The authors identified four randomized, controlled trials that compared early colonoscopy (defined as within 24 hours) with elective colonoscopy (defined as beyond 24 hours) and/or other diagnostic tests for patients presenting with acute lower GI bleeding. They performed a meta-analysis, including 463 patients, which showed no significant difference in risk of persistent or recurrent bleeding for early versus elective colonoscopy. The authors also found no significant differences in secondary outcomes of mortality, endoscopic intervention, primary hemostatic intervention, or identification of bleeding source. Limitations of this research include the relatively small number of studies included, and potential for selection bias in the original studies. Notably two of the four studies included were prematurely terminated before their planned sample sizes were reached.
Bottom line: In patients hospitalized with acute lower GI bleeding, colonoscopy within 24 hours may not reduce further bleeding or mortality when compared with elective colonoscopy.
Citation: Tsay C et al. Early colonoscopy does not improve outcomes of patients with lower gastrointestinal bleeding: Systematic review of randomized trials. Clin Gastroenterol Hepatol. 2019 Dec 13. doi: 10.1016/j.cgh.2019.11.061.
Dr. Hu is a hospitalist at Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, both in Boston.
Not your ordinary neuropathy
She has had a diagnosis of type 2 diabetes for the past 4 years. She initially presented with polyuria/polydipsia and a hemoglobin A1c level of 9.5. She has previously not tolerated metformin, and did not want to take any subsequent medications. She was seen 4 months ago and at that time had an A1c level of 12.5. She decided she wanted to really treat her diabetes as well as she could. She started consuming a low carbohydrate diet, restarted metformin and began using a continuous glucose monitor. She also started taking nighttime glargine insulin, and mealtime insulin apart. She reports she lost 20 pounds over the past 4 months, her blood sugars now run between 100-120 fasting, and up to 180 before meals. She has had a severe, sharp pain in both of her feet over the past month that is interfering with sleep and makes walking painful for her. An exam reveals hyperesthesia of both feet, and her A1c level is 7.5. What is the most likely cause of her neuropathic symptoms?

A. Vitamin B12 deficiency
B. Diabetic neuropathy
C. Insulin neuritis
D. Charcot-Marie-Tooth disease
The most likely cause
In this case, certainly considering vitamin B12 deficiency is reasonable. It is highly unlikely though, given the rapidity of onset of symptoms, and that the patient has been on metformin for a very short period of time. Chronic metformin use is associated with low B12 levels, and the American Diabetes Association has advised that regular monitoring of vitamin B12 levels should be done on patients who are on long-term metformin.1
Diabetic neuropathy is also unlikely, given the rapidity of symptoms in this patient. What is most likely in this patient is treatment-induced neuropathy (TIN), first described with the name “insulin neuritis”.
Research on TIN
Gibbons and colleagues evaluated 16 patients with diabetes with recent marked, rapid improvement in glycemic control who developed a sudden, painful neuropathy.2 All developed symptoms within 8 weeks of intensive glucose control, with 69% having autonomic dysfunction as well, and all developing worsening retinopathy.
Gibbons and Freeman did a retrospective study of patients referred to a diabetic neuropathy clinic over a 5-year period to try to understand how prevalent TIN is.3
A total of 954 patients were evaluated for diabetic neuropathy. Treatment induced neuropathy was defined as a painful neuropathy and/or autonomic dysfunction occurring within 8 weeks of intensified treatment and a drop of the A1c level greater than 2 over a 3-month period.
A total of 104 patients (10.9%) met the criteria for treatment induced neuropathy. Patients who had a decrease in A1c had a much greater chance of developing a painful or autonomic neuropathy than patients who had no change in A1c (P < .0001). The same patients had a much higher risk of developing retinopathy (P < .001). The greater the reduction in A1c, the greater the risk. Patients whose A1c decreased by 2%-3% over 3 months had an absolute risk of 20%, whereas those with a A1c decease of greater than 4% had an 80% absolute risk.
Siddique and colleagues reported on three cases with very different clinical presentations of TIN.4 One patient had an acute third nerve palsy, another patient had a lumbosacral radiculoplexus neuropathy, and the third patient presented with a diffuse painful sensory neuropathy and postural hypotension.
Most patients improve over time from their neuropathic symptoms, with better recovery in patients with type 1 diabetes.2
Pearl
Strongly consider treatment induced neuropathy in your patients with diabetes who present with acute painful neuropathy and/or autonomic dysfunction in the setting of rapid improvement of glucose control.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. American Diabetes Association. Diabetes Care. 2019 Jan;42(Suppl 1):S90-102.
2. Gibbons CH and Freeman R. Ann Neurol 2010; 67:534–41.
3. Gibbons CH and Freeman R. Brain. 2015;138:43-52.
4. Siddique N et al. Endocrinol Diabetes Metab Case Rep. 2020 Feb 26;2020:19-0140.
She has had a diagnosis of type 2 diabetes for the past 4 years. She initially presented with polyuria/polydipsia and a hemoglobin A1c level of 9.5. She has previously not tolerated metformin, and did not want to take any subsequent medications. She was seen 4 months ago and at that time had an A1c level of 12.5. She decided she wanted to really treat her diabetes as well as she could. She started consuming a low carbohydrate diet, restarted metformin and began using a continuous glucose monitor. She also started taking nighttime glargine insulin, and mealtime insulin apart. She reports she lost 20 pounds over the past 4 months, her blood sugars now run between 100-120 fasting, and up to 180 before meals. She has had a severe, sharp pain in both of her feet over the past month that is interfering with sleep and makes walking painful for her. An exam reveals hyperesthesia of both feet, and her A1c level is 7.5. What is the most likely cause of her neuropathic symptoms?
A. Vitamin B12 deficiency
B. Diabetic neuropathy
C. Insulin neuritis
D. Charcot-Marie-Tooth disease
The most likely cause
In this case, certainly considering vitamin B12 deficiency is reasonable. It is highly unlikely though, given the rapidity of onset of symptoms, and that the patient has been on metformin for a very short period of time. Chronic metformin use is associated with low B12 levels, and the American Diabetes Association has advised that regular monitoring of vitamin B12 levels should be done on patients who are on long-term metformin.1
Diabetic neuropathy is also unlikely, given the rapidity of symptoms in this patient. What is most likely in this patient is treatment-induced neuropathy (TIN), first described with the name “insulin neuritis”.
Research on TIN
Gibbons and colleagues evaluated 16 patients with diabetes with recent marked, rapid improvement in glycemic control who developed a sudden, painful neuropathy.2 All developed symptoms within 8 weeks of intensive glucose control, with 69% having autonomic dysfunction as well, and all developing worsening retinopathy.
Gibbons and Freeman did a retrospective study of patients referred to a diabetic neuropathy clinic over a 5-year period to try to understand how prevalent TIN is.3
A total of 954 patients were evaluated for diabetic neuropathy. Treatment induced neuropathy was defined as a painful neuropathy and/or autonomic dysfunction occurring within 8 weeks of intensified treatment and a drop of the A1c level greater than 2 over a 3-month period.
A total of 104 patients (10.9%) met the criteria for treatment induced neuropathy. Patients who had a decrease in A1c had a much greater chance of developing a painful or autonomic neuropathy than patients who had no change in A1c (P < .0001). The same patients had a much higher risk of developing retinopathy (P < .001). The greater the reduction in A1c, the greater the risk. Patients whose A1c decreased by 2%-3% over 3 months had an absolute risk of 20%, whereas those with a A1c decease of greater than 4% had an 80% absolute risk.
Siddique and colleagues reported on three cases with very different clinical presentations of TIN.4 One patient had an acute third nerve palsy, another patient had a lumbosacral radiculoplexus neuropathy, and the third patient presented with a diffuse painful sensory neuropathy and postural hypotension.
Most patients improve over time from their neuropathic symptoms, with better recovery in patients with type 1 diabetes.2
Pearl
Strongly consider treatment induced neuropathy in your patients with diabetes who present with acute painful neuropathy and/or autonomic dysfunction in the setting of rapid improvement of glucose control.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. American Diabetes Association. Diabetes Care. 2019 Jan;42(Suppl 1):S90-102.
2. Gibbons CH and Freeman R. Ann Neurol 2010; 67:534–41.
3. Gibbons CH and Freeman R. Brain. 2015;138:43-52.
4. Siddique N et al. Endocrinol Diabetes Metab Case Rep. 2020 Feb 26;2020:19-0140.
She has had a diagnosis of type 2 diabetes for the past 4 years. She initially presented with polyuria/polydipsia and a hemoglobin A1c level of 9.5. She has previously not tolerated metformin, and did not want to take any subsequent medications. She was seen 4 months ago and at that time had an A1c level of 12.5. She decided she wanted to really treat her diabetes as well as she could. She started consuming a low carbohydrate diet, restarted metformin and began using a continuous glucose monitor. She also started taking nighttime glargine insulin, and mealtime insulin apart. She reports she lost 20 pounds over the past 4 months, her blood sugars now run between 100-120 fasting, and up to 180 before meals. She has had a severe, sharp pain in both of her feet over the past month that is interfering with sleep and makes walking painful for her. An exam reveals hyperesthesia of both feet, and her A1c level is 7.5. What is the most likely cause of her neuropathic symptoms?
A. Vitamin B12 deficiency
B. Diabetic neuropathy
C. Insulin neuritis
D. Charcot-Marie-Tooth disease
The most likely cause
In this case, certainly considering vitamin B12 deficiency is reasonable. It is highly unlikely though, given the rapidity of onset of symptoms, and that the patient has been on metformin for a very short period of time. Chronic metformin use is associated with low B12 levels, and the American Diabetes Association has advised that regular monitoring of vitamin B12 levels should be done on patients who are on long-term metformin.1
Diabetic neuropathy is also unlikely, given the rapidity of symptoms in this patient. What is most likely in this patient is treatment-induced neuropathy (TIN), first described with the name “insulin neuritis”.
Research on TIN
Gibbons and colleagues evaluated 16 patients with diabetes with recent marked, rapid improvement in glycemic control who developed a sudden, painful neuropathy.2 All developed symptoms within 8 weeks of intensive glucose control, with 69% having autonomic dysfunction as well, and all developing worsening retinopathy.
Gibbons and Freeman did a retrospective study of patients referred to a diabetic neuropathy clinic over a 5-year period to try to understand how prevalent TIN is.3
A total of 954 patients were evaluated for diabetic neuropathy. Treatment induced neuropathy was defined as a painful neuropathy and/or autonomic dysfunction occurring within 8 weeks of intensified treatment and a drop of the A1c level greater than 2 over a 3-month period.
A total of 104 patients (10.9%) met the criteria for treatment induced neuropathy. Patients who had a decrease in A1c had a much greater chance of developing a painful or autonomic neuropathy than patients who had no change in A1c (P < .0001). The same patients had a much higher risk of developing retinopathy (P < .001). The greater the reduction in A1c, the greater the risk. Patients whose A1c decreased by 2%-3% over 3 months had an absolute risk of 20%, whereas those with a A1c decease of greater than 4% had an 80% absolute risk.
Siddique and colleagues reported on three cases with very different clinical presentations of TIN.4 One patient had an acute third nerve palsy, another patient had a lumbosacral radiculoplexus neuropathy, and the third patient presented with a diffuse painful sensory neuropathy and postural hypotension.
Most patients improve over time from their neuropathic symptoms, with better recovery in patients with type 1 diabetes.2
Pearl
Strongly consider treatment induced neuropathy in your patients with diabetes who present with acute painful neuropathy and/or autonomic dysfunction in the setting of rapid improvement of glucose control.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. American Diabetes Association. Diabetes Care. 2019 Jan;42(Suppl 1):S90-102.
2. Gibbons CH and Freeman R. Ann Neurol 2010; 67:534–41.
3. Gibbons CH and Freeman R. Brain. 2015;138:43-52.
4. Siddique N et al. Endocrinol Diabetes Metab Case Rep. 2020 Feb 26;2020:19-0140.
Upper GI bleed guidelines say endoscopy within 24 hours of bleed
Updated guidelines from the American College of Gastroenterology address upper gastrointestinal and ulcer bleeding. Many recommendations are similar to the 2012 version, but some important changes place an emphasis on risk-stratification tools to reduce hospitalization in low-risk patients, and the timing of endoscopy for patients who are admitted to the hospital.
The guidelines were published in the American Journal of Gastroenterology.
One key change was the expansion of the Glasgow-Blatchford score (GBS) that could be used to identify patients at very low risk for a hospital intervention, from 0 in the 2012 guidelines to 0-1 in the current version. That expands the group of patients that could be discharged with outpatient follow-up.
A cutoff score of 0 identifies very few people, said Neil Sengupta, MD, who is an assistant professor of medicine at University of Chicago Medicine. Although expanding the qualification to 0-1 can increase the number of patients sent home, “which is certainly a good thing,” Dr. Sengupta said, it may be difficult to put into practice – especially in EDs. In most situations, GBS requires manual inputs. A few hospital systems have implemented automatic calculation of GBS from medical records, but the practice is not widespread.
“No. 1, the compliance of measuring the score is pretty low. No. 2, it’s difficult for an emergency room physician to discharge a patient with upper GI bleeding if patients don’t have good social support, or if they don’t have a good follow-up plan. So it’s hard to know whether this will really make a difference in terms of the number of people being discharged,” said Dr. Sengupta, who served as a monitor for the ACG committee that produced this guideline, and will become chair of the ACG guideline committee in October.
Another key message in the updated guidelines centers around timing of endoscopy. The 2012 guidelines recommended considering endoscopy within 12 hours for patients with high-risk clinical features. The new guidelines recommend that all patients should undergo endoscopy within 24 hours, and they do not specifically recommend endoscopy within 12 hours. Earlier endoscopy can lead to a more accurate prognosis, but can also cause mortality or complications if resuscitation and management of active comorbidities is insufficient, and outcomes can be worse during after-hours endoscopies. The change is based on a recent randomized, controlled trial that showed no 30-day mortality benefit to endoscopy performed within 6 hours of a consult, versus endoscopy performed between 6 and 24 hours.
That change still leaves uncertainty, because there may be some patients who would potentially benefit from earlier endoscopy. “I think that’s kind of the unknown: Whether there’s a subset of people who may benefit from going in very early and limiting the amount of resuscitation they get,” Dr. Sengupta said.
Another important message in the new guideline addresses proton pump inhibitor (PPI) therapy before endoscopy. Although the 2012 guidelines recommended considering pre-endoscopy PPI infusions, the new version states that there is no clear benefit for clinical outcomes. The authors of the guidelines did not recommend against it, either, because it is associated with a modest reduction in the need to perform endoscopic therapy. “And there’s a theoretical possibility that PPIs may benefit a minority of patients in whom endoscopy may not be possible in a timely fashion,” he said.
This advice may generate some controversy, since PPI use is very common prior to endoscopy, and in some places in the world, it might not be possible to complete an endoscopy within 24 hours. “As such, a lot of providers use PPIs routinely prior to endoscopy. It’s a little challenging just because this is such a common clinical scenario, and PPI use is so widespread that I don’t think it’s likely that practice is going to change based on this guideline,” Dr. Sengupta said. He did suggest that the benefit of PPIs after endoscopic therapy is well established, “so it’s going to be important to identify people who are at high risk (after an endoscopic treatment).
“The other the other thing is that you don’t really have too much guidance on whether there’s a benefit of using a continuous intravenous PPI versus intermittent PPI [either oral or intravenous] after endoscopy in high-risk patients, primarily [because of] the lack of high-quality data,” Dr. Sengupta said.
There is also good evidence that patients with ulcers and high-risk stigmata should receive endoscopic therapy, and these patients can benefit from posttherapy high-dose PPIs for 3 days.
Some guideline authors reported relationships with Phathom Pharmaceuticals, Olympus, and Cook. Dr. Sengupta is the upcoming chair of the ACG Practice Parameters Committees, which oversees the commissioning, updating, and review of all ACG clinical practice guidelines.
Updated guidelines from the American College of Gastroenterology address upper gastrointestinal and ulcer bleeding. Many recommendations are similar to the 2012 version, but some important changes place an emphasis on risk-stratification tools to reduce hospitalization in low-risk patients, and the timing of endoscopy for patients who are admitted to the hospital.
The guidelines were published in the American Journal of Gastroenterology.
One key change was the expansion of the Glasgow-Blatchford score (GBS) that could be used to identify patients at very low risk for a hospital intervention, from 0 in the 2012 guidelines to 0-1 in the current version. That expands the group of patients that could be discharged with outpatient follow-up.
A cutoff score of 0 identifies very few people, said Neil Sengupta, MD, who is an assistant professor of medicine at University of Chicago Medicine. Although expanding the qualification to 0-1 can increase the number of patients sent home, “which is certainly a good thing,” Dr. Sengupta said, it may be difficult to put into practice – especially in EDs. In most situations, GBS requires manual inputs. A few hospital systems have implemented automatic calculation of GBS from medical records, but the practice is not widespread.
“No. 1, the compliance of measuring the score is pretty low. No. 2, it’s difficult for an emergency room physician to discharge a patient with upper GI bleeding if patients don’t have good social support, or if they don’t have a good follow-up plan. So it’s hard to know whether this will really make a difference in terms of the number of people being discharged,” said Dr. Sengupta, who served as a monitor for the ACG committee that produced this guideline, and will become chair of the ACG guideline committee in October.
Another key message in the updated guidelines centers around timing of endoscopy. The 2012 guidelines recommended considering endoscopy within 12 hours for patients with high-risk clinical features. The new guidelines recommend that all patients should undergo endoscopy within 24 hours, and they do not specifically recommend endoscopy within 12 hours. Earlier endoscopy can lead to a more accurate prognosis, but can also cause mortality or complications if resuscitation and management of active comorbidities is insufficient, and outcomes can be worse during after-hours endoscopies. The change is based on a recent randomized, controlled trial that showed no 30-day mortality benefit to endoscopy performed within 6 hours of a consult, versus endoscopy performed between 6 and 24 hours.
That change still leaves uncertainty, because there may be some patients who would potentially benefit from earlier endoscopy. “I think that’s kind of the unknown: Whether there’s a subset of people who may benefit from going in very early and limiting the amount of resuscitation they get,” Dr. Sengupta said.
Another important message in the new guideline addresses proton pump inhibitor (PPI) therapy before endoscopy. Although the 2012 guidelines recommended considering pre-endoscopy PPI infusions, the new version states that there is no clear benefit for clinical outcomes. The authors of the guidelines did not recommend against it, either, because it is associated with a modest reduction in the need to perform endoscopic therapy. “And there’s a theoretical possibility that PPIs may benefit a minority of patients in whom endoscopy may not be possible in a timely fashion,” he said.
This advice may generate some controversy, since PPI use is very common prior to endoscopy, and in some places in the world, it might not be possible to complete an endoscopy within 24 hours. “As such, a lot of providers use PPIs routinely prior to endoscopy. It’s a little challenging just because this is such a common clinical scenario, and PPI use is so widespread that I don’t think it’s likely that practice is going to change based on this guideline,” Dr. Sengupta said. He did suggest that the benefit of PPIs after endoscopic therapy is well established, “so it’s going to be important to identify people who are at high risk (after an endoscopic treatment).
“The other the other thing is that you don’t really have too much guidance on whether there’s a benefit of using a continuous intravenous PPI versus intermittent PPI [either oral or intravenous] after endoscopy in high-risk patients, primarily [because of] the lack of high-quality data,” Dr. Sengupta said.
There is also good evidence that patients with ulcers and high-risk stigmata should receive endoscopic therapy, and these patients can benefit from posttherapy high-dose PPIs for 3 days.
Some guideline authors reported relationships with Phathom Pharmaceuticals, Olympus, and Cook. Dr. Sengupta is the upcoming chair of the ACG Practice Parameters Committees, which oversees the commissioning, updating, and review of all ACG clinical practice guidelines.
Updated guidelines from the American College of Gastroenterology address upper gastrointestinal and ulcer bleeding. Many recommendations are similar to the 2012 version, but some important changes place an emphasis on risk-stratification tools to reduce hospitalization in low-risk patients, and the timing of endoscopy for patients who are admitted to the hospital.
The guidelines were published in the American Journal of Gastroenterology.
One key change was the expansion of the Glasgow-Blatchford score (GBS) that could be used to identify patients at very low risk for a hospital intervention, from 0 in the 2012 guidelines to 0-1 in the current version. That expands the group of patients that could be discharged with outpatient follow-up.
A cutoff score of 0 identifies very few people, said Neil Sengupta, MD, who is an assistant professor of medicine at University of Chicago Medicine. Although expanding the qualification to 0-1 can increase the number of patients sent home, “which is certainly a good thing,” Dr. Sengupta said, it may be difficult to put into practice – especially in EDs. In most situations, GBS requires manual inputs. A few hospital systems have implemented automatic calculation of GBS from medical records, but the practice is not widespread.
“No. 1, the compliance of measuring the score is pretty low. No. 2, it’s difficult for an emergency room physician to discharge a patient with upper GI bleeding if patients don’t have good social support, or if they don’t have a good follow-up plan. So it’s hard to know whether this will really make a difference in terms of the number of people being discharged,” said Dr. Sengupta, who served as a monitor for the ACG committee that produced this guideline, and will become chair of the ACG guideline committee in October.
Another key message in the updated guidelines centers around timing of endoscopy. The 2012 guidelines recommended considering endoscopy within 12 hours for patients with high-risk clinical features. The new guidelines recommend that all patients should undergo endoscopy within 24 hours, and they do not specifically recommend endoscopy within 12 hours. Earlier endoscopy can lead to a more accurate prognosis, but can also cause mortality or complications if resuscitation and management of active comorbidities is insufficient, and outcomes can be worse during after-hours endoscopies. The change is based on a recent randomized, controlled trial that showed no 30-day mortality benefit to endoscopy performed within 6 hours of a consult, versus endoscopy performed between 6 and 24 hours.
That change still leaves uncertainty, because there may be some patients who would potentially benefit from earlier endoscopy. “I think that’s kind of the unknown: Whether there’s a subset of people who may benefit from going in very early and limiting the amount of resuscitation they get,” Dr. Sengupta said.
Another important message in the new guideline addresses proton pump inhibitor (PPI) therapy before endoscopy. Although the 2012 guidelines recommended considering pre-endoscopy PPI infusions, the new version states that there is no clear benefit for clinical outcomes. The authors of the guidelines did not recommend against it, either, because it is associated with a modest reduction in the need to perform endoscopic therapy. “And there’s a theoretical possibility that PPIs may benefit a minority of patients in whom endoscopy may not be possible in a timely fashion,” he said.
This advice may generate some controversy, since PPI use is very common prior to endoscopy, and in some places in the world, it might not be possible to complete an endoscopy within 24 hours. “As such, a lot of providers use PPIs routinely prior to endoscopy. It’s a little challenging just because this is such a common clinical scenario, and PPI use is so widespread that I don’t think it’s likely that practice is going to change based on this guideline,” Dr. Sengupta said. He did suggest that the benefit of PPIs after endoscopic therapy is well established, “so it’s going to be important to identify people who are at high risk (after an endoscopic treatment).
“The other the other thing is that you don’t really have too much guidance on whether there’s a benefit of using a continuous intravenous PPI versus intermittent PPI [either oral or intravenous] after endoscopy in high-risk patients, primarily [because of] the lack of high-quality data,” Dr. Sengupta said.
There is also good evidence that patients with ulcers and high-risk stigmata should receive endoscopic therapy, and these patients can benefit from posttherapy high-dose PPIs for 3 days.
Some guideline authors reported relationships with Phathom Pharmaceuticals, Olympus, and Cook. Dr. Sengupta is the upcoming chair of the ACG Practice Parameters Committees, which oversees the commissioning, updating, and review of all ACG clinical practice guidelines.
FROM THE AMERICAN JOURNAL OF GASTROENTEROLOGY
Better ways to handle in-hospital conflicts
Imagine a hospitalist, part of a group with 35 hospitalists, is in her second year of practice and is caring for a 55-year-old woman with a history of congestive heart failure and cirrhosis from hepatitis C due to heroin use. The patient was hospitalized with acute back pain and found to have vertebral osteomyelitis confirmed on MRI.
The hospitalist calls a surgeon to get a biopsy so that antibiotic therapy can be chosen. The surgeon says it’s the second time the patient has been hospitalized for this condition, and asks, “Why do you need me to see this patient?” He says the hospitalist should just give IV antibiotics and consult infectious disease.
The hospitalist says, “The patient needs this biopsy. I’ll just call your chair.”
In the course of a busy day, conflicts arise all the time in the hospital – between clinicians, between patients and clinicians, and as internal battles when clinicians face uncertain situations. There are ways to make these conflicts less tense and more in tune with patient care, panelists said recently during a session at SHM Converge, the annual conference of the Society of Hospital Medicine.
In the case of vertebral osteomyelitis, for instance, the hospitalist was using a “position-based” strategy to deal with the conflict with the surgeon – she came in knowing she wanted a biopsy – rather than an “interest-based” strategy, or what is in the patient’s interest, said Patrick Rendon, MD, FHM, assistant professor in the hospital medicine division at the University of New Mexico, Albuquerque.

“What we really need to do is realign the thinking from both the hospitalist as well as the consult perspective,” Dr. Rendon said. “It is not us versus the consultant or the consult versus us. It should be both, together, versus the problem.”
Instead of saying something like, “I need this biopsy,” it might be better to ask for an evaluation, he said.
Handling conflicts better can improve patient care but can also benefit the clinicians themselves. While hospitalists say they routinely experience “pushback” when making a request of a consultant, they also say that they prefer to receive instruction when consulting about a case. Dr. Rendon said that hospitalists also say they want this teaching done “in the right way,” and consultants routinely say that their instruction, when they give it, is often met with resistance.
“The idea here is to open up perspectives,” Dr. Rendon said.
Emily Gottenborg, MD, hospitalist and assistant professor of medicine at the University of Colorado, discussed the case of an intern caring for a patient who says something offensive.
Conflicts, she said, come in all sorts – intimidation, harassment, bias. And they can be based on race, gender, disability, and hierarchy, she said. When on the receiving end of offensive remarks from patients, it’s important for a clinician to set boundaries and quickly move on, with responses such as, “I care about you as a person, but I will not tolerate offensive behavior. Let’s focus on how I can help you today.”
“Practice that behavior so that you have a script in your mind and then use it when needed so that you can nip this behavior in the bud,” Dr. Gottenborg said.
In her hypothetical case, the intern asks for help from her program, and monthly morbidity and mortality workshops on bias and harassment are scheduled. She also receives counseling, and faculty and staff receive discrimination and bias training. Getting help from the institution can help systematically reduce these problems, Dr. Gottenborg said.
Ernie Esquivel, MD, SFHM, hospitalist and assistant professor of clinical medicine at Weill Cornell Medicine, New York, said internal conflicts test physicians routinely – and this has been especially true during the COVID-19 pandemic, in which urgent clinical situations arose with no clear answers.
“In the past year, physicians have experienced an incredible amount of anxiety and stress,” he said. “Tolerating uncertainty is probably one of the most mature skills that we need to learn as a physician.”
The culture of medicine, to a large degree, promotes the opposite tendency: value is placed on nailing down the diagnosis or achieving certainty. Confidence levels of physicians tend not to waver, even in the face of difficult cases full of uncertainty, Dr. Esquivel said.
He urged physicians to practice “deliberate clinical inertia” – to resist a quick response and to think more deeply and systematically about a situation. To show the importance of this, he asks residents to rank diagnoses, using sticky notes, as information about a case is provided. By the fourth round, when much more information is available, the diagnoses have changed dramatically.
Dr. Esquivel suggested physicians switch from thinking in terms of “diagnoses” to thinking in terms of “hypotheses.” That approach can help clinicians tolerate uncertainty, because it reinforces the idea that they are dealing with an “iterative process.”
“There may not be one diagnosis to consider,” he said, “but several in play at once.”
A version of this article first appeared on Medscape.com.
Imagine a hospitalist, part of a group with 35 hospitalists, is in her second year of practice and is caring for a 55-year-old woman with a history of congestive heart failure and cirrhosis from hepatitis C due to heroin use. The patient was hospitalized with acute back pain and found to have vertebral osteomyelitis confirmed on MRI.
The hospitalist calls a surgeon to get a biopsy so that antibiotic therapy can be chosen. The surgeon says it’s the second time the patient has been hospitalized for this condition, and asks, “Why do you need me to see this patient?” He says the hospitalist should just give IV antibiotics and consult infectious disease.
The hospitalist says, “The patient needs this biopsy. I’ll just call your chair.”
In the course of a busy day, conflicts arise all the time in the hospital – between clinicians, between patients and clinicians, and as internal battles when clinicians face uncertain situations. There are ways to make these conflicts less tense and more in tune with patient care, panelists said recently during a session at SHM Converge, the annual conference of the Society of Hospital Medicine.
In the case of vertebral osteomyelitis, for instance, the hospitalist was using a “position-based” strategy to deal with the conflict with the surgeon – she came in knowing she wanted a biopsy – rather than an “interest-based” strategy, or what is in the patient’s interest, said Patrick Rendon, MD, FHM, assistant professor in the hospital medicine division at the University of New Mexico, Albuquerque.
“What we really need to do is realign the thinking from both the hospitalist as well as the consult perspective,” Dr. Rendon said. “It is not us versus the consultant or the consult versus us. It should be both, together, versus the problem.”
Instead of saying something like, “I need this biopsy,” it might be better to ask for an evaluation, he said.
Handling conflicts better can improve patient care but can also benefit the clinicians themselves. While hospitalists say they routinely experience “pushback” when making a request of a consultant, they also say that they prefer to receive instruction when consulting about a case. Dr. Rendon said that hospitalists also say they want this teaching done “in the right way,” and consultants routinely say that their instruction, when they give it, is often met with resistance.
“The idea here is to open up perspectives,” Dr. Rendon said.
Emily Gottenborg, MD, hospitalist and assistant professor of medicine at the University of Colorado, discussed the case of an intern caring for a patient who says something offensive.
Conflicts, she said, come in all sorts – intimidation, harassment, bias. And they can be based on race, gender, disability, and hierarchy, she said. When on the receiving end of offensive remarks from patients, it’s important for a clinician to set boundaries and quickly move on, with responses such as, “I care about you as a person, but I will not tolerate offensive behavior. Let’s focus on how I can help you today.”
“Practice that behavior so that you have a script in your mind and then use it when needed so that you can nip this behavior in the bud,” Dr. Gottenborg said.
In her hypothetical case, the intern asks for help from her program, and monthly morbidity and mortality workshops on bias and harassment are scheduled. She also receives counseling, and faculty and staff receive discrimination and bias training. Getting help from the institution can help systematically reduce these problems, Dr. Gottenborg said.
Ernie Esquivel, MD, SFHM, hospitalist and assistant professor of clinical medicine at Weill Cornell Medicine, New York, said internal conflicts test physicians routinely – and this has been especially true during the COVID-19 pandemic, in which urgent clinical situations arose with no clear answers.
“In the past year, physicians have experienced an incredible amount of anxiety and stress,” he said. “Tolerating uncertainty is probably one of the most mature skills that we need to learn as a physician.”
The culture of medicine, to a large degree, promotes the opposite tendency: value is placed on nailing down the diagnosis or achieving certainty. Confidence levels of physicians tend not to waver, even in the face of difficult cases full of uncertainty, Dr. Esquivel said.
He urged physicians to practice “deliberate clinical inertia” – to resist a quick response and to think more deeply and systematically about a situation. To show the importance of this, he asks residents to rank diagnoses, using sticky notes, as information about a case is provided. By the fourth round, when much more information is available, the diagnoses have changed dramatically.
Dr. Esquivel suggested physicians switch from thinking in terms of “diagnoses” to thinking in terms of “hypotheses.” That approach can help clinicians tolerate uncertainty, because it reinforces the idea that they are dealing with an “iterative process.”
“There may not be one diagnosis to consider,” he said, “but several in play at once.”
A version of this article first appeared on Medscape.com.
Imagine a hospitalist, part of a group with 35 hospitalists, is in her second year of practice and is caring for a 55-year-old woman with a history of congestive heart failure and cirrhosis from hepatitis C due to heroin use. The patient was hospitalized with acute back pain and found to have vertebral osteomyelitis confirmed on MRI.
The hospitalist calls a surgeon to get a biopsy so that antibiotic therapy can be chosen. The surgeon says it’s the second time the patient has been hospitalized for this condition, and asks, “Why do you need me to see this patient?” He says the hospitalist should just give IV antibiotics and consult infectious disease.
The hospitalist says, “The patient needs this biopsy. I’ll just call your chair.”
In the course of a busy day, conflicts arise all the time in the hospital – between clinicians, between patients and clinicians, and as internal battles when clinicians face uncertain situations. There are ways to make these conflicts less tense and more in tune with patient care, panelists said recently during a session at SHM Converge, the annual conference of the Society of Hospital Medicine.
In the case of vertebral osteomyelitis, for instance, the hospitalist was using a “position-based” strategy to deal with the conflict with the surgeon – she came in knowing she wanted a biopsy – rather than an “interest-based” strategy, or what is in the patient’s interest, said Patrick Rendon, MD, FHM, assistant professor in the hospital medicine division at the University of New Mexico, Albuquerque.
“What we really need to do is realign the thinking from both the hospitalist as well as the consult perspective,” Dr. Rendon said. “It is not us versus the consultant or the consult versus us. It should be both, together, versus the problem.”
Instead of saying something like, “I need this biopsy,” it might be better to ask for an evaluation, he said.
Handling conflicts better can improve patient care but can also benefit the clinicians themselves. While hospitalists say they routinely experience “pushback” when making a request of a consultant, they also say that they prefer to receive instruction when consulting about a case. Dr. Rendon said that hospitalists also say they want this teaching done “in the right way,” and consultants routinely say that their instruction, when they give it, is often met with resistance.
“The idea here is to open up perspectives,” Dr. Rendon said.
Emily Gottenborg, MD, hospitalist and assistant professor of medicine at the University of Colorado, discussed the case of an intern caring for a patient who says something offensive.
Conflicts, she said, come in all sorts – intimidation, harassment, bias. And they can be based on race, gender, disability, and hierarchy, she said. When on the receiving end of offensive remarks from patients, it’s important for a clinician to set boundaries and quickly move on, with responses such as, “I care about you as a person, but I will not tolerate offensive behavior. Let’s focus on how I can help you today.”
“Practice that behavior so that you have a script in your mind and then use it when needed so that you can nip this behavior in the bud,” Dr. Gottenborg said.
In her hypothetical case, the intern asks for help from her program, and monthly morbidity and mortality workshops on bias and harassment are scheduled. She also receives counseling, and faculty and staff receive discrimination and bias training. Getting help from the institution can help systematically reduce these problems, Dr. Gottenborg said.
Ernie Esquivel, MD, SFHM, hospitalist and assistant professor of clinical medicine at Weill Cornell Medicine, New York, said internal conflicts test physicians routinely – and this has been especially true during the COVID-19 pandemic, in which urgent clinical situations arose with no clear answers.
“In the past year, physicians have experienced an incredible amount of anxiety and stress,” he said. “Tolerating uncertainty is probably one of the most mature skills that we need to learn as a physician.”
The culture of medicine, to a large degree, promotes the opposite tendency: value is placed on nailing down the diagnosis or achieving certainty. Confidence levels of physicians tend not to waver, even in the face of difficult cases full of uncertainty, Dr. Esquivel said.
He urged physicians to practice “deliberate clinical inertia” – to resist a quick response and to think more deeply and systematically about a situation. To show the importance of this, he asks residents to rank diagnoses, using sticky notes, as information about a case is provided. By the fourth round, when much more information is available, the diagnoses have changed dramatically.
Dr. Esquivel suggested physicians switch from thinking in terms of “diagnoses” to thinking in terms of “hypotheses.” That approach can help clinicians tolerate uncertainty, because it reinforces the idea that they are dealing with an “iterative process.”
“There may not be one diagnosis to consider,” he said, “but several in play at once.”
A version of this article first appeared on Medscape.com.
FROM SHM CONVERGE 2021
Deep brain stimulation is effective over the long haul
, new research indicates.
“Subthalamic nucleus stimulation is a well recognized treatment used for improving motor conditions and quality of life in people with Parkinson’s disease. Our study, for the first time, supports its efficacy in the very long term – 15 years after surgery and 25 years since the Parkinson’s disease diagnosis,” said Elena Moro, MD, PhD, Grenoble Alpes University, Grenoble, France.
“This information is relevant for physicians, patients, and their families when they need to decide about the surgical option to deal with Parkinson’s disease,” said Dr. Moro.
The study was published online June 2 in Neurology.
‘Don’t delay’
The findings are based on 51 patients with Parkinson’s disease who underwent treatment with bilateral STN-DBS for an average of 17 years (range, 15-24 years). Their average age at diagnosis was 40 years, and the average age at device implantation was 51 years.
The results demonstrate that STN-DBS continues to be effective for motor complications for longer than 15 years, reducing time spent with dyskinesia by 75% and time spent in the off-state by 58.7%. This is similar to the amount of improvement seen 1 year after surgery.
Doses of dopaminergic medications continued to be low at long-term follow-up; dosing was reduced by 50.6% compared with baseline.
There was also continued improvement in quality of life. Scores on the Parkinson’s Disease Quality of Life Questionnaire in the very long term were 13.8% better compared with baseline.
“Few and mostly manageable device-related adverse events were observed during the follow-up,” the authors reported in their article.
“Deep brain stimulation is already recommended when a patient’s conditions are not optimized by medical treatment. Patients with Parkinson’s disease without dementia and in good general health conditions are the best candidates for this surgery,” said Dr. Moro.
“Taking into account our results and the data available in the literature, DBS surgery should not be delayed when motor conditions and quality of life decline despite medical treatment, if patients meet the inclusion criteria,” she added.
A revolutionary treatment
The authors of an accompanying editorial say these results, which indicate better motor outcomes with less medication, “reinforce why STN-DBS has revolutionized treatment for advanced Parkinson’s disease.”
Kelvin Chou, MD, of the University of Michigan, Ann Arbor, and David Charles, MD, of Vanderbilt University, Nashville, Tenn., pointed out that longer disease duration is associated with an increase in the likelihood of cognitive impairment and psychosis, both of which are risk factors for nursing home placement, and they limit the ability to use dopaminergic medications.
Although many of the patients in this cohort experienced hallucinations and psychosis over the long follow-up period, “one can imagine that the number and severity would be higher without DBS therapy,” they wrote.
Key caveats, said Dr. Chou and Dr. Charles, are that the results are based on a highly selected cohort and that the patients were managed by experts in the field of movement disorders and DBS.
Additionally, the patients’ conditions were highly responsive to levodopa; there was a 75.3% baseline improvement in Unified Parkinson’s Disease Rating Scale motor scores from the off-state to the on-state. In general, most DBS centers consider a levodopa response of approximately 30% as an acceptable cutoff for moving forward with STN-DBS, they noted.
Despite these caveats and limitations, the results of the study are important with respect to counseling potential candidates for DBS, Dr. Chou and Dr. Charles said.
“A common question that patients have is, ‘How long do the benefits of DBS last?’ We can now reassure them that, at least for STN-DBS, improvement in motor complications lasts beyond 15 years and is often accompanied by improvement in quality of life. In other words, with STN-DBS, we can uncomplicate their motor complications for the long haul,” the editorial writers concluded.
The research had no targeted funding. Moro has received honoraria from Medtronic and Abbott for consulting and lecturing and an educational grant from Boston and Newronika. A complete list of disclosures is available with the original articles.
A version of this article first appeared on Medscape.com.
, new research indicates.
“Subthalamic nucleus stimulation is a well recognized treatment used for improving motor conditions and quality of life in people with Parkinson’s disease. Our study, for the first time, supports its efficacy in the very long term – 15 years after surgery and 25 years since the Parkinson’s disease diagnosis,” said Elena Moro, MD, PhD, Grenoble Alpes University, Grenoble, France.
“This information is relevant for physicians, patients, and their families when they need to decide about the surgical option to deal with Parkinson’s disease,” said Dr. Moro.
The study was published online June 2 in Neurology.
‘Don’t delay’
The findings are based on 51 patients with Parkinson’s disease who underwent treatment with bilateral STN-DBS for an average of 17 years (range, 15-24 years). Their average age at diagnosis was 40 years, and the average age at device implantation was 51 years.
The results demonstrate that STN-DBS continues to be effective for motor complications for longer than 15 years, reducing time spent with dyskinesia by 75% and time spent in the off-state by 58.7%. This is similar to the amount of improvement seen 1 year after surgery.
Doses of dopaminergic medications continued to be low at long-term follow-up; dosing was reduced by 50.6% compared with baseline.
There was also continued improvement in quality of life. Scores on the Parkinson’s Disease Quality of Life Questionnaire in the very long term were 13.8% better compared with baseline.
“Few and mostly manageable device-related adverse events were observed during the follow-up,” the authors reported in their article.
“Deep brain stimulation is already recommended when a patient’s conditions are not optimized by medical treatment. Patients with Parkinson’s disease without dementia and in good general health conditions are the best candidates for this surgery,” said Dr. Moro.
“Taking into account our results and the data available in the literature, DBS surgery should not be delayed when motor conditions and quality of life decline despite medical treatment, if patients meet the inclusion criteria,” she added.
A revolutionary treatment
The authors of an accompanying editorial say these results, which indicate better motor outcomes with less medication, “reinforce why STN-DBS has revolutionized treatment for advanced Parkinson’s disease.”
Kelvin Chou, MD, of the University of Michigan, Ann Arbor, and David Charles, MD, of Vanderbilt University, Nashville, Tenn., pointed out that longer disease duration is associated with an increase in the likelihood of cognitive impairment and psychosis, both of which are risk factors for nursing home placement, and they limit the ability to use dopaminergic medications.
Although many of the patients in this cohort experienced hallucinations and psychosis over the long follow-up period, “one can imagine that the number and severity would be higher without DBS therapy,” they wrote.
Key caveats, said Dr. Chou and Dr. Charles, are that the results are based on a highly selected cohort and that the patients were managed by experts in the field of movement disorders and DBS.
Additionally, the patients’ conditions were highly responsive to levodopa; there was a 75.3% baseline improvement in Unified Parkinson’s Disease Rating Scale motor scores from the off-state to the on-state. In general, most DBS centers consider a levodopa response of approximately 30% as an acceptable cutoff for moving forward with STN-DBS, they noted.
Despite these caveats and limitations, the results of the study are important with respect to counseling potential candidates for DBS, Dr. Chou and Dr. Charles said.
“A common question that patients have is, ‘How long do the benefits of DBS last?’ We can now reassure them that, at least for STN-DBS, improvement in motor complications lasts beyond 15 years and is often accompanied by improvement in quality of life. In other words, with STN-DBS, we can uncomplicate their motor complications for the long haul,” the editorial writers concluded.
The research had no targeted funding. Moro has received honoraria from Medtronic and Abbott for consulting and lecturing and an educational grant from Boston and Newronika. A complete list of disclosures is available with the original articles.
A version of this article first appeared on Medscape.com.
, new research indicates.
“Subthalamic nucleus stimulation is a well recognized treatment used for improving motor conditions and quality of life in people with Parkinson’s disease. Our study, for the first time, supports its efficacy in the very long term – 15 years after surgery and 25 years since the Parkinson’s disease diagnosis,” said Elena Moro, MD, PhD, Grenoble Alpes University, Grenoble, France.
“This information is relevant for physicians, patients, and their families when they need to decide about the surgical option to deal with Parkinson’s disease,” said Dr. Moro.
The study was published online June 2 in Neurology.
‘Don’t delay’
The findings are based on 51 patients with Parkinson’s disease who underwent treatment with bilateral STN-DBS for an average of 17 years (range, 15-24 years). Their average age at diagnosis was 40 years, and the average age at device implantation was 51 years.
The results demonstrate that STN-DBS continues to be effective for motor complications for longer than 15 years, reducing time spent with dyskinesia by 75% and time spent in the off-state by 58.7%. This is similar to the amount of improvement seen 1 year after surgery.
Doses of dopaminergic medications continued to be low at long-term follow-up; dosing was reduced by 50.6% compared with baseline.
There was also continued improvement in quality of life. Scores on the Parkinson’s Disease Quality of Life Questionnaire in the very long term were 13.8% better compared with baseline.
“Few and mostly manageable device-related adverse events were observed during the follow-up,” the authors reported in their article.
“Deep brain stimulation is already recommended when a patient’s conditions are not optimized by medical treatment. Patients with Parkinson’s disease without dementia and in good general health conditions are the best candidates for this surgery,” said Dr. Moro.
“Taking into account our results and the data available in the literature, DBS surgery should not be delayed when motor conditions and quality of life decline despite medical treatment, if patients meet the inclusion criteria,” she added.
A revolutionary treatment
The authors of an accompanying editorial say these results, which indicate better motor outcomes with less medication, “reinforce why STN-DBS has revolutionized treatment for advanced Parkinson’s disease.”
Kelvin Chou, MD, of the University of Michigan, Ann Arbor, and David Charles, MD, of Vanderbilt University, Nashville, Tenn., pointed out that longer disease duration is associated with an increase in the likelihood of cognitive impairment and psychosis, both of which are risk factors for nursing home placement, and they limit the ability to use dopaminergic medications.
Although many of the patients in this cohort experienced hallucinations and psychosis over the long follow-up period, “one can imagine that the number and severity would be higher without DBS therapy,” they wrote.
Key caveats, said Dr. Chou and Dr. Charles, are that the results are based on a highly selected cohort and that the patients were managed by experts in the field of movement disorders and DBS.
Additionally, the patients’ conditions were highly responsive to levodopa; there was a 75.3% baseline improvement in Unified Parkinson’s Disease Rating Scale motor scores from the off-state to the on-state. In general, most DBS centers consider a levodopa response of approximately 30% as an acceptable cutoff for moving forward with STN-DBS, they noted.
Despite these caveats and limitations, the results of the study are important with respect to counseling potential candidates for DBS, Dr. Chou and Dr. Charles said.
“A common question that patients have is, ‘How long do the benefits of DBS last?’ We can now reassure them that, at least for STN-DBS, improvement in motor complications lasts beyond 15 years and is often accompanied by improvement in quality of life. In other words, with STN-DBS, we can uncomplicate their motor complications for the long haul,” the editorial writers concluded.
The research had no targeted funding. Moro has received honoraria from Medtronic and Abbott for consulting and lecturing and an educational grant from Boston and Newronika. A complete list of disclosures is available with the original articles.
A version of this article first appeared on Medscape.com.
From Neurology
Pregnant women with PsA at risk for adverse maternal outcomes
Key clinical point: Psoriatic arthritis (PsA) adversely affected maternal outcomes in pregnant women; however, there was no adverse effect on neonatal outcomes.
Major finding: The risk for cesarean delivery (odds ratio [OR], 1.45; 95% confidence interval [CI], 1.27-1.66), preterm birth (OR, 1.48; 95% CI, 1.24-1.78), preeclampsia (OR, 1.45; 95% CI, 1.13-1.85), and gestational hypertension (OR, 1.49; 95% CI, 1.09-2.06) was significantly higher in pregnant women with PsA vs. general population. However, no statistically increased risk for fetal complications was observed in women with PsA.
Study details: Findings are from a meta-analysis of 16 observational studies including more than 46,909 cases of psoriasis/PsA with over 53,541 pregnancies and more than 4,771,352 healthy controls with over 8,044,996 pregnancies.
Disclosures: This study was funded by the National Natural Science Foundation of China. All authors declared no conflicts of interest.
Source: Xie W et al. Rheumatology (Oxford). 2021 Apr 20. doi: 10.1093/rheumatology/keab357.
Key clinical point: Psoriatic arthritis (PsA) adversely affected maternal outcomes in pregnant women; however, there was no adverse effect on neonatal outcomes.
Major finding: The risk for cesarean delivery (odds ratio [OR], 1.45; 95% confidence interval [CI], 1.27-1.66), preterm birth (OR, 1.48; 95% CI, 1.24-1.78), preeclampsia (OR, 1.45; 95% CI, 1.13-1.85), and gestational hypertension (OR, 1.49; 95% CI, 1.09-2.06) was significantly higher in pregnant women with PsA vs. general population. However, no statistically increased risk for fetal complications was observed in women with PsA.
Study details: Findings are from a meta-analysis of 16 observational studies including more than 46,909 cases of psoriasis/PsA with over 53,541 pregnancies and more than 4,771,352 healthy controls with over 8,044,996 pregnancies.
Disclosures: This study was funded by the National Natural Science Foundation of China. All authors declared no conflicts of interest.
Source: Xie W et al. Rheumatology (Oxford). 2021 Apr 20. doi: 10.1093/rheumatology/keab357.
Key clinical point: Psoriatic arthritis (PsA) adversely affected maternal outcomes in pregnant women; however, there was no adverse effect on neonatal outcomes.
Major finding: The risk for cesarean delivery (odds ratio [OR], 1.45; 95% confidence interval [CI], 1.27-1.66), preterm birth (OR, 1.48; 95% CI, 1.24-1.78), preeclampsia (OR, 1.45; 95% CI, 1.13-1.85), and gestational hypertension (OR, 1.49; 95% CI, 1.09-2.06) was significantly higher in pregnant women with PsA vs. general population. However, no statistically increased risk for fetal complications was observed in women with PsA.
Study details: Findings are from a meta-analysis of 16 observational studies including more than 46,909 cases of psoriasis/PsA with over 53,541 pregnancies and more than 4,771,352 healthy controls with over 8,044,996 pregnancies.
Disclosures: This study was funded by the National Natural Science Foundation of China. All authors declared no conflicts of interest.
Source: Xie W et al. Rheumatology (Oxford). 2021 Apr 20. doi: 10.1093/rheumatology/keab357.
Tender joints in active PsA poorly reflect inflammation indicated by ultrasound and MRI
Key clinical point: Joint tenderness showed poor association with imaging signs of inflammation in patients with psoriatic arthritis (PsA).
Major finding: Tender or swollen joint count showed no significant correlations with imaging inflammation sum-scores. Negligible to weak correlation (rho, −0.31 to 0.38) was observed between imaging inflammation sum-scores and the respective clinical joint counts, patient-reported outcomes, and composite scores with no consistently significant results.
Study details: This was a cross-sectional study of 41 patients with active PsA assessed by ultrasound and magnetic resonance imaging (MRI) for joint swelling.
Disclosures: The study was financially supported by AbbVie. Some of the authors reported receiving research grants, consulting fees, and speaker fees from various sources including AbbVie.
Source: Felbo SK et al. Rheumatology (Oxford). 2021 Apr 24. doi: 10.1093/rheumatology/keab384.
Key clinical point: Joint tenderness showed poor association with imaging signs of inflammation in patients with psoriatic arthritis (PsA).
Major finding: Tender or swollen joint count showed no significant correlations with imaging inflammation sum-scores. Negligible to weak correlation (rho, −0.31 to 0.38) was observed between imaging inflammation sum-scores and the respective clinical joint counts, patient-reported outcomes, and composite scores with no consistently significant results.
Study details: This was a cross-sectional study of 41 patients with active PsA assessed by ultrasound and magnetic resonance imaging (MRI) for joint swelling.
Disclosures: The study was financially supported by AbbVie. Some of the authors reported receiving research grants, consulting fees, and speaker fees from various sources including AbbVie.
Source: Felbo SK et al. Rheumatology (Oxford). 2021 Apr 24. doi: 10.1093/rheumatology/keab384.
Key clinical point: Joint tenderness showed poor association with imaging signs of inflammation in patients with psoriatic arthritis (PsA).
Major finding: Tender or swollen joint count showed no significant correlations with imaging inflammation sum-scores. Negligible to weak correlation (rho, −0.31 to 0.38) was observed between imaging inflammation sum-scores and the respective clinical joint counts, patient-reported outcomes, and composite scores with no consistently significant results.
Study details: This was a cross-sectional study of 41 patients with active PsA assessed by ultrasound and magnetic resonance imaging (MRI) for joint swelling.
Disclosures: The study was financially supported by AbbVie. Some of the authors reported receiving research grants, consulting fees, and speaker fees from various sources including AbbVie.
Source: Felbo SK et al. Rheumatology (Oxford). 2021 Apr 24. doi: 10.1093/rheumatology/keab384.
Once-weekly oral antipsychotic for schizophrenia on the horizon
A novel, ultra–long-acting oral formulation of the antipsychotic risperidone (Risperdal) only needs to be taken once weekly and appears to be safe and effective, results of a new phase 2 study suggest.

The new formulation, LYN-005 (Lyndra Therapeutics), quickly reached therapeutic levels in patients, provided sustained exposure to risperidone active moiety over 7 days, and reduced peak drug exposure.
“This novel formulation has the potential to improve treatment adherence and quality of life in patients with schizophrenia or schizoaffective disorder,” study investigator David Walling, PhD, chief clinical officer for the Collaborative NeuroScience Network, Long Beach, Calif., said in an interview.
The findings were presented at the 2021 American Society of Clinical Psychopharmacology annual meeting.
Adherence is key
About 50% of patients don’t take medications as prescribed, creating a significant relapse risk, Dr. Walling noted.
“Here we have the possibility of having a once-weekly oral medication, which means patients don’t have to struggle with the issue of taking the medication daily. Right now, all we have on the market for long-acting medications for schizophrenia are injectables, where the patient has to go get a shot every month or every 2 weeks in order to have the medication in their system for a longer period of time,” he added.
The study included 32 clinically stable patients with a primary diagnosis of schizophrenia or schizoaffective disorder.
Patients received immediate-release (IR) risperidone at 2 mg or 4 mg, based on their current antipsychotic dose, for 13 days.
They were then randomly assigned 3:1 to receive either IR risperidone-matched placebo and LYN-005 at 14 mg or 28 mg risperidone (12 patients per group), or to LYN-005 matched placebo and IR risperidone, 2 mg or 4 mg, (4 patients per group) for 3 weeks.
LYN-05 was administered once weekly for a total of three doses. IR risperidone was administered once daily.
The study’s primary endpoints were pharmacokinetics after LYN-005 and IR risperidone and the incidence of adverse events.
Following LYN-005 administration, systemic exposure to risperidone active moiety (risperidone and 9-hydroxyrisperidone combined) increased with the increasing dose. Peak concentration occurred within the first 3 days of dosing and peak exposures from LYN-005 were lower than with IR risperidone.
“Steady state was achieved around day 15. It didn’t take 3 weeks of dosing for patients to achieve steady state. We achieved that around day 15,” Dr. Walling said.
LYN-005 was well tolerated in the 85% of study participants who received all three doses.
Adverse events occurred in 18 (75%) patients who received LYN-005. Of these, 10 were with the 14-mg dose, and 8 with the 28-mg dose.
The most common AEs were gastrointestinal, which occurred in 13 (54%) patients receiving LYN-005, with a higher incidence in the 28-mg group than in the 14 mg group.
Additionally, nine patients had abdominal pain, discomfort, or tenderness, and five patients (21%) had nausea.
Overall, the incidence of adverse events was higher for LYN-005, compared with IR risperidone, but they were judged to be mild and transitory, with fewer AEs reported with subsequent LYN-005 dosing. After the first dose, 58% of patients reported an AE; this dropped to 18% after the third dose.
An important development
Commenting on the findings, Ira D. Glick, MD, professor emeritus, Stanford (Calif.) University, said: “The major problem with schizophrenia is getting adherence.”
“The better the adherence, the better the outcome, the worst the adherence, the worse the outcome, so being able to take a preparation less often is a very important advance in the field,” said Dr. Glick, who was not involved in the research
Long-acting preparations for chronic mental illness represent a significant advance, he said.
“The future of the treatment of schizophrenia is long-acting injectables. That is the trend,” Dr. Glick explained. “The oral once-a-week preparation may be useful in a group of patients who are phobic about needles, but with the injections, you can be sure that the patient has received their medication. With the oral, there is more of a chance to be noncompliant.
“That said, having an effective, longer-acting oral for those who refuse injections is helpful. to ensure adherence to treatment. We know treatment works, we know it is going to save lives, and that’s what this ultra–long-acting formulation is promoting.”
Dr. Glick has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A novel, ultra–long-acting oral formulation of the antipsychotic risperidone (Risperdal) only needs to be taken once weekly and appears to be safe and effective, results of a new phase 2 study suggest.
The new formulation, LYN-005 (Lyndra Therapeutics), quickly reached therapeutic levels in patients, provided sustained exposure to risperidone active moiety over 7 days, and reduced peak drug exposure.
“This novel formulation has the potential to improve treatment adherence and quality of life in patients with schizophrenia or schizoaffective disorder,” study investigator David Walling, PhD, chief clinical officer for the Collaborative NeuroScience Network, Long Beach, Calif., said in an interview.
The findings were presented at the 2021 American Society of Clinical Psychopharmacology annual meeting.
Adherence is key
About 50% of patients don’t take medications as prescribed, creating a significant relapse risk, Dr. Walling noted.
“Here we have the possibility of having a once-weekly oral medication, which means patients don’t have to struggle with the issue of taking the medication daily. Right now, all we have on the market for long-acting medications for schizophrenia are injectables, where the patient has to go get a shot every month or every 2 weeks in order to have the medication in their system for a longer period of time,” he added.
The study included 32 clinically stable patients with a primary diagnosis of schizophrenia or schizoaffective disorder.
Patients received immediate-release (IR) risperidone at 2 mg or 4 mg, based on their current antipsychotic dose, for 13 days.
They were then randomly assigned 3:1 to receive either IR risperidone-matched placebo and LYN-005 at 14 mg or 28 mg risperidone (12 patients per group), or to LYN-005 matched placebo and IR risperidone, 2 mg or 4 mg, (4 patients per group) for 3 weeks.
LYN-05 was administered once weekly for a total of three doses. IR risperidone was administered once daily.
The study’s primary endpoints were pharmacokinetics after LYN-005 and IR risperidone and the incidence of adverse events.
Following LYN-005 administration, systemic exposure to risperidone active moiety (risperidone and 9-hydroxyrisperidone combined) increased with the increasing dose. Peak concentration occurred within the first 3 days of dosing and peak exposures from LYN-005 were lower than with IR risperidone.
“Steady state was achieved around day 15. It didn’t take 3 weeks of dosing for patients to achieve steady state. We achieved that around day 15,” Dr. Walling said.
LYN-005 was well tolerated in the 85% of study participants who received all three doses.
Adverse events occurred in 18 (75%) patients who received LYN-005. Of these, 10 were with the 14-mg dose, and 8 with the 28-mg dose.
The most common AEs were gastrointestinal, which occurred in 13 (54%) patients receiving LYN-005, with a higher incidence in the 28-mg group than in the 14 mg group.
Additionally, nine patients had abdominal pain, discomfort, or tenderness, and five patients (21%) had nausea.
Overall, the incidence of adverse events was higher for LYN-005, compared with IR risperidone, but they were judged to be mild and transitory, with fewer AEs reported with subsequent LYN-005 dosing. After the first dose, 58% of patients reported an AE; this dropped to 18% after the third dose.
An important development
Commenting on the findings, Ira D. Glick, MD, professor emeritus, Stanford (Calif.) University, said: “The major problem with schizophrenia is getting adherence.”
“The better the adherence, the better the outcome, the worst the adherence, the worse the outcome, so being able to take a preparation less often is a very important advance in the field,” said Dr. Glick, who was not involved in the research
Long-acting preparations for chronic mental illness represent a significant advance, he said.
“The future of the treatment of schizophrenia is long-acting injectables. That is the trend,” Dr. Glick explained. “The oral once-a-week preparation may be useful in a group of patients who are phobic about needles, but with the injections, you can be sure that the patient has received their medication. With the oral, there is more of a chance to be noncompliant.
“That said, having an effective, longer-acting oral for those who refuse injections is helpful. to ensure adherence to treatment. We know treatment works, we know it is going to save lives, and that’s what this ultra–long-acting formulation is promoting.”
Dr. Glick has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A novel, ultra–long-acting oral formulation of the antipsychotic risperidone (Risperdal) only needs to be taken once weekly and appears to be safe and effective, results of a new phase 2 study suggest.
The new formulation, LYN-005 (Lyndra Therapeutics), quickly reached therapeutic levels in patients, provided sustained exposure to risperidone active moiety over 7 days, and reduced peak drug exposure.
“This novel formulation has the potential to improve treatment adherence and quality of life in patients with schizophrenia or schizoaffective disorder,” study investigator David Walling, PhD, chief clinical officer for the Collaborative NeuroScience Network, Long Beach, Calif., said in an interview.
The findings were presented at the 2021 American Society of Clinical Psychopharmacology annual meeting.
Adherence is key
About 50% of patients don’t take medications as prescribed, creating a significant relapse risk, Dr. Walling noted.
“Here we have the possibility of having a once-weekly oral medication, which means patients don’t have to struggle with the issue of taking the medication daily. Right now, all we have on the market for long-acting medications for schizophrenia are injectables, where the patient has to go get a shot every month or every 2 weeks in order to have the medication in their system for a longer period of time,” he added.
The study included 32 clinically stable patients with a primary diagnosis of schizophrenia or schizoaffective disorder.
Patients received immediate-release (IR) risperidone at 2 mg or 4 mg, based on their current antipsychotic dose, for 13 days.
They were then randomly assigned 3:1 to receive either IR risperidone-matched placebo and LYN-005 at 14 mg or 28 mg risperidone (12 patients per group), or to LYN-005 matched placebo and IR risperidone, 2 mg or 4 mg, (4 patients per group) for 3 weeks.
LYN-05 was administered once weekly for a total of three doses. IR risperidone was administered once daily.
The study’s primary endpoints were pharmacokinetics after LYN-005 and IR risperidone and the incidence of adverse events.
Following LYN-005 administration, systemic exposure to risperidone active moiety (risperidone and 9-hydroxyrisperidone combined) increased with the increasing dose. Peak concentration occurred within the first 3 days of dosing and peak exposures from LYN-005 were lower than with IR risperidone.
“Steady state was achieved around day 15. It didn’t take 3 weeks of dosing for patients to achieve steady state. We achieved that around day 15,” Dr. Walling said.
LYN-005 was well tolerated in the 85% of study participants who received all three doses.
Adverse events occurred in 18 (75%) patients who received LYN-005. Of these, 10 were with the 14-mg dose, and 8 with the 28-mg dose.
The most common AEs were gastrointestinal, which occurred in 13 (54%) patients receiving LYN-005, with a higher incidence in the 28-mg group than in the 14 mg group.
Additionally, nine patients had abdominal pain, discomfort, or tenderness, and five patients (21%) had nausea.
Overall, the incidence of adverse events was higher for LYN-005, compared with IR risperidone, but they were judged to be mild and transitory, with fewer AEs reported with subsequent LYN-005 dosing. After the first dose, 58% of patients reported an AE; this dropped to 18% after the third dose.
An important development
Commenting on the findings, Ira D. Glick, MD, professor emeritus, Stanford (Calif.) University, said: “The major problem with schizophrenia is getting adherence.”
“The better the adherence, the better the outcome, the worst the adherence, the worse the outcome, so being able to take a preparation less often is a very important advance in the field,” said Dr. Glick, who was not involved in the research
Long-acting preparations for chronic mental illness represent a significant advance, he said.
“The future of the treatment of schizophrenia is long-acting injectables. That is the trend,” Dr. Glick explained. “The oral once-a-week preparation may be useful in a group of patients who are phobic about needles, but with the injections, you can be sure that the patient has received their medication. With the oral, there is more of a chance to be noncompliant.
“That said, having an effective, longer-acting oral for those who refuse injections is helpful. to ensure adherence to treatment. We know treatment works, we know it is going to save lives, and that’s what this ultra–long-acting formulation is promoting.”
Dr. Glick has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.