User login
Experts: EPA should assess risk of sunscreens’ UV filters
The , an expert panel of the National Academies of Sciences, Engineering, and Medicine (NAS) said on Aug. 9.
The assessment is urgently needed, the experts said, and the results should be shared with the Food and Drug Administration, which oversees sunscreens.
In its 400-page report, titled the Review of Fate, Exposure, and Effects of Sunscreens in Aquatic Environments and Implications for Sunscreen Usage and Human Health, the panel does not make recommendations but suggests that such an EPA risk assessment should highlight gaps in knowledge.
“We are teeing up the critical information that will be used to take on the challenge of risk assessment,” Charles A. Menzie, PhD, chair of the committee that wrote the report, said at a media briefing Aug. 9 when the report was released. Dr. Menzie is a principal at Exponent, Inc., an engineering and scientific consulting firm. He is former executive director of the Society of Environmental Toxicology and Chemistry.
The EPA sponsored the study, which was conducted by a committee of the National Academy of Sciences, a nonprofit, nongovernmental organization authorized by Congress that studies issues related to science, technology, and medicine.
Balancing aquatic, human health concerns
Such an EPA assessment, Dr. Menzie said in a statement, will help inform efforts to understand the environmental effects of UV filters as well as clarify a path forward for managing sunscreens. For years, concerns have been raised about the potential toxicity of sunscreens regarding many marine and freshwater aquatic organisms, especially coral. That concern, however, must be balanced against the benefits of sunscreens, which are known to protect against skin cancer. A low percentage of people use sunscreen regularly, Dr. Menzie and other panel members said.
“Only about a third of the U.S. population regularly uses sunscreen,” Mark Cullen, MD, vice chair of the NAS committee and former director of the Center for Population Health Sciences, Stanford (Calif.) University, said at the briefing. About 70% or 80% of people use it at the beach or outdoors, he said.
Report background, details
UV filters are the active ingredients in physical as well as chemical sunscreen products. They decrease the amount of UV radiation that reaches the skin. They have been found in water, sediments, and marine organisms, both saltwater and freshwater.
Currently, 17 UV filters are used in U.S. sunscreens; 15 of those are organic, such as oxybenzone and avobenzone, and are used in chemical sunscreens. They work by absorbing the rays before they damage the skin. In addition, two inorganic filters, which are used in physical sunscreens, sit on the skin and as a shield to block the rays.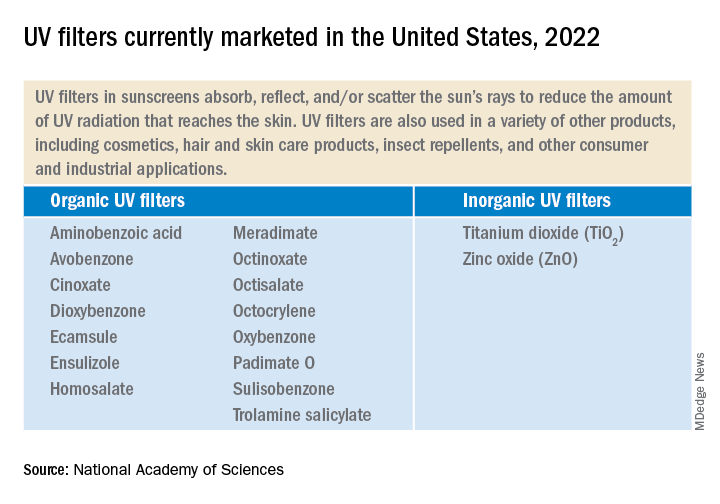
UV filters enter bodies of water by direct release, as when sunscreens rinse off people while swimming or while engaging in other water activities. They also enter bodies of water in storm water runoff and wastewater.
Lab toxicity tests, which are the most widely used, provide effects data for ecologic risk assessment. The tests are more often used in the study of short-term, not long-term exposure. Test results have shown that in high enough concentrations, some UV filters can be toxic to algal, invertebrate, and fish species.
But much information is lacking, the experts said. Toxicity data for many species, for instance, are limited. There are few studies on the longer-term environmental effects of UV filter exposure. Not enough is known about the rate at which the filters degrade in the environment. The filters accumulate in higher amounts in different areas. Recreational water areas have higher concentrations.
The recommendations
The panel is urging the EPA to complete a formal risk assessment of the UV filters “with some urgency,” Dr. Cullen said. That will enable decisions to be made about the use of the products. The risks to aquatic life must be balanced against the need for sun protection to reduce skin cancer risk.
The experts made two recommendations:
- The EPA should conduct ecologic risk assessments for all the UV filters now marketed and for all new ones. The assessment should evaluate the filters individually as well as the risk from co-occurring filters. The assessments should take into account the different exposure scenarios.
- The EPA, along with partner agencies, and sunscreen and UV filter manufacturers should fund, support, and conduct research and share data. Research should include study of human health outcomes if usage and availability of sunscreens change.
Dermatologists should “continue to emphasize the importance of protection from UV radiation in every way that can be done,” Dr. Cullen said, including the use of sunscreen as well as other protective practices, such as wearing long sleeves and hats, seeking shade, and avoiding the sun during peak hours.
A dermatologist’s perspective
“I applaud their scientific curiosity to know one way or the other whether this is an issue,” said Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, DC. “I welcome this investigation.”

The multitude of studies, Dr. Friedman said, don’t always agree about whether the filters pose dangers. He noted that the concentration of UV filters detected in water is often lower than the concentrations found to be harmful in a lab setting to marine life, specifically coral.
However, he said, “these studies are snapshots.” For that reason, calling for more assessment of risk is desirable, Dr. Friedman said, but “I want to be sure the call to do more research is not an admission of guilt. It’s very easy to vilify sunscreens – but the facts we know are that UV light causes skin cancer and aging, and sunscreen protects us against this.”
Dr. Friedman has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The , an expert panel of the National Academies of Sciences, Engineering, and Medicine (NAS) said on Aug. 9.
The assessment is urgently needed, the experts said, and the results should be shared with the Food and Drug Administration, which oversees sunscreens.
In its 400-page report, titled the Review of Fate, Exposure, and Effects of Sunscreens in Aquatic Environments and Implications for Sunscreen Usage and Human Health, the panel does not make recommendations but suggests that such an EPA risk assessment should highlight gaps in knowledge.
“We are teeing up the critical information that will be used to take on the challenge of risk assessment,” Charles A. Menzie, PhD, chair of the committee that wrote the report, said at a media briefing Aug. 9 when the report was released. Dr. Menzie is a principal at Exponent, Inc., an engineering and scientific consulting firm. He is former executive director of the Society of Environmental Toxicology and Chemistry.
The EPA sponsored the study, which was conducted by a committee of the National Academy of Sciences, a nonprofit, nongovernmental organization authorized by Congress that studies issues related to science, technology, and medicine.
Balancing aquatic, human health concerns
Such an EPA assessment, Dr. Menzie said in a statement, will help inform efforts to understand the environmental effects of UV filters as well as clarify a path forward for managing sunscreens. For years, concerns have been raised about the potential toxicity of sunscreens regarding many marine and freshwater aquatic organisms, especially coral. That concern, however, must be balanced against the benefits of sunscreens, which are known to protect against skin cancer. A low percentage of people use sunscreen regularly, Dr. Menzie and other panel members said.
“Only about a third of the U.S. population regularly uses sunscreen,” Mark Cullen, MD, vice chair of the NAS committee and former director of the Center for Population Health Sciences, Stanford (Calif.) University, said at the briefing. About 70% or 80% of people use it at the beach or outdoors, he said.
Report background, details
UV filters are the active ingredients in physical as well as chemical sunscreen products. They decrease the amount of UV radiation that reaches the skin. They have been found in water, sediments, and marine organisms, both saltwater and freshwater.
Currently, 17 UV filters are used in U.S. sunscreens; 15 of those are organic, such as oxybenzone and avobenzone, and are used in chemical sunscreens. They work by absorbing the rays before they damage the skin. In addition, two inorganic filters, which are used in physical sunscreens, sit on the skin and as a shield to block the rays.
UV filters enter bodies of water by direct release, as when sunscreens rinse off people while swimming or while engaging in other water activities. They also enter bodies of water in storm water runoff and wastewater.
Lab toxicity tests, which are the most widely used, provide effects data for ecologic risk assessment. The tests are more often used in the study of short-term, not long-term exposure. Test results have shown that in high enough concentrations, some UV filters can be toxic to algal, invertebrate, and fish species.
But much information is lacking, the experts said. Toxicity data for many species, for instance, are limited. There are few studies on the longer-term environmental effects of UV filter exposure. Not enough is known about the rate at which the filters degrade in the environment. The filters accumulate in higher amounts in different areas. Recreational water areas have higher concentrations.
The recommendations
The panel is urging the EPA to complete a formal risk assessment of the UV filters “with some urgency,” Dr. Cullen said. That will enable decisions to be made about the use of the products. The risks to aquatic life must be balanced against the need for sun protection to reduce skin cancer risk.
The experts made two recommendations:
- The EPA should conduct ecologic risk assessments for all the UV filters now marketed and for all new ones. The assessment should evaluate the filters individually as well as the risk from co-occurring filters. The assessments should take into account the different exposure scenarios.
- The EPA, along with partner agencies, and sunscreen and UV filter manufacturers should fund, support, and conduct research and share data. Research should include study of human health outcomes if usage and availability of sunscreens change.
Dermatologists should “continue to emphasize the importance of protection from UV radiation in every way that can be done,” Dr. Cullen said, including the use of sunscreen as well as other protective practices, such as wearing long sleeves and hats, seeking shade, and avoiding the sun during peak hours.
A dermatologist’s perspective
“I applaud their scientific curiosity to know one way or the other whether this is an issue,” said Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, DC. “I welcome this investigation.”
The multitude of studies, Dr. Friedman said, don’t always agree about whether the filters pose dangers. He noted that the concentration of UV filters detected in water is often lower than the concentrations found to be harmful in a lab setting to marine life, specifically coral.
However, he said, “these studies are snapshots.” For that reason, calling for more assessment of risk is desirable, Dr. Friedman said, but “I want to be sure the call to do more research is not an admission of guilt. It’s very easy to vilify sunscreens – but the facts we know are that UV light causes skin cancer and aging, and sunscreen protects us against this.”
Dr. Friedman has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The , an expert panel of the National Academies of Sciences, Engineering, and Medicine (NAS) said on Aug. 9.
The assessment is urgently needed, the experts said, and the results should be shared with the Food and Drug Administration, which oversees sunscreens.
In its 400-page report, titled the Review of Fate, Exposure, and Effects of Sunscreens in Aquatic Environments and Implications for Sunscreen Usage and Human Health, the panel does not make recommendations but suggests that such an EPA risk assessment should highlight gaps in knowledge.
“We are teeing up the critical information that will be used to take on the challenge of risk assessment,” Charles A. Menzie, PhD, chair of the committee that wrote the report, said at a media briefing Aug. 9 when the report was released. Dr. Menzie is a principal at Exponent, Inc., an engineering and scientific consulting firm. He is former executive director of the Society of Environmental Toxicology and Chemistry.
The EPA sponsored the study, which was conducted by a committee of the National Academy of Sciences, a nonprofit, nongovernmental organization authorized by Congress that studies issues related to science, technology, and medicine.
Balancing aquatic, human health concerns
Such an EPA assessment, Dr. Menzie said in a statement, will help inform efforts to understand the environmental effects of UV filters as well as clarify a path forward for managing sunscreens. For years, concerns have been raised about the potential toxicity of sunscreens regarding many marine and freshwater aquatic organisms, especially coral. That concern, however, must be balanced against the benefits of sunscreens, which are known to protect against skin cancer. A low percentage of people use sunscreen regularly, Dr. Menzie and other panel members said.
“Only about a third of the U.S. population regularly uses sunscreen,” Mark Cullen, MD, vice chair of the NAS committee and former director of the Center for Population Health Sciences, Stanford (Calif.) University, said at the briefing. About 70% or 80% of people use it at the beach or outdoors, he said.
Report background, details
UV filters are the active ingredients in physical as well as chemical sunscreen products. They decrease the amount of UV radiation that reaches the skin. They have been found in water, sediments, and marine organisms, both saltwater and freshwater.
Currently, 17 UV filters are used in U.S. sunscreens; 15 of those are organic, such as oxybenzone and avobenzone, and are used in chemical sunscreens. They work by absorbing the rays before they damage the skin. In addition, two inorganic filters, which are used in physical sunscreens, sit on the skin and as a shield to block the rays.
UV filters enter bodies of water by direct release, as when sunscreens rinse off people while swimming or while engaging in other water activities. They also enter bodies of water in storm water runoff and wastewater.
Lab toxicity tests, which are the most widely used, provide effects data for ecologic risk assessment. The tests are more often used in the study of short-term, not long-term exposure. Test results have shown that in high enough concentrations, some UV filters can be toxic to algal, invertebrate, and fish species.
But much information is lacking, the experts said. Toxicity data for many species, for instance, are limited. There are few studies on the longer-term environmental effects of UV filter exposure. Not enough is known about the rate at which the filters degrade in the environment. The filters accumulate in higher amounts in different areas. Recreational water areas have higher concentrations.
The recommendations
The panel is urging the EPA to complete a formal risk assessment of the UV filters “with some urgency,” Dr. Cullen said. That will enable decisions to be made about the use of the products. The risks to aquatic life must be balanced against the need for sun protection to reduce skin cancer risk.
The experts made two recommendations:
- The EPA should conduct ecologic risk assessments for all the UV filters now marketed and for all new ones. The assessment should evaluate the filters individually as well as the risk from co-occurring filters. The assessments should take into account the different exposure scenarios.
- The EPA, along with partner agencies, and sunscreen and UV filter manufacturers should fund, support, and conduct research and share data. Research should include study of human health outcomes if usage and availability of sunscreens change.
Dermatologists should “continue to emphasize the importance of protection from UV radiation in every way that can be done,” Dr. Cullen said, including the use of sunscreen as well as other protective practices, such as wearing long sleeves and hats, seeking shade, and avoiding the sun during peak hours.
A dermatologist’s perspective
“I applaud their scientific curiosity to know one way or the other whether this is an issue,” said Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, DC. “I welcome this investigation.”
The multitude of studies, Dr. Friedman said, don’t always agree about whether the filters pose dangers. He noted that the concentration of UV filters detected in water is often lower than the concentrations found to be harmful in a lab setting to marine life, specifically coral.
However, he said, “these studies are snapshots.” For that reason, calling for more assessment of risk is desirable, Dr. Friedman said, but “I want to be sure the call to do more research is not an admission of guilt. It’s very easy to vilify sunscreens – but the facts we know are that UV light causes skin cancer and aging, and sunscreen protects us against this.”
Dr. Friedman has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In RA, tofacitinib shows higher infection rate than TNF inhibitors
Patients with rheumatoid arthritis treated with tofacitinib (Xeljanz) are more likely to develop infections than are those who take a tumor necrosis factor inhibitor (TNFi), results of an industry-sponsored randomized controlled trial suggest.
The Janus kinase (JAK) inhibitor tofacitinib and TNFi biologics are common RA treatments that, along with factors including age, disease activity, and comorbidities, can put patients with RA at increased risk for infections.

“In this secondary analysis of the ORAL Surveillance trial, infections were increased with tofacitinib, compared with TNFi,” study coauthor Deepak L. Bhatt, MD, MPH, professor of medicine at Harvard Medical School and executive director of interventional cardiovascular programs at Brigham and Women’s Hospital, both in Boston, explained in an interview.
As reported in Annals of the Rheumatic Diseases, Dr. Bhatt and colleagues performed a subanalysis of the final dataset from the phase 3b/4 open-label safety trial of tofacitinib in RA conducted between March 2014 and July 2020, in 345 study locations worldwide.
Study participants were 50 years of age or older with moderate to severe RA who were taking methotrexate but having inadequate symptom control. They had at least one cardiovascular risk factor such as being a current smoker or having hypertension, past heart attack, family history of coronary heart disease, high cholesterol, diabetes mellitus, or extra-articular RA. Patients with current or recent infection, clinically significant laboratory abnormalities, or pregnancy, were excluded from the study.
In the study, 1,455 participants received oral tofacitinib 5 mg twice per day; 1,456 received oral tofacitinib 10 mg twice per day; and 1,451 were treated with subcutaneous TNFi (40 mg subcutaneous adalimumab [Humira] injection every 2 weeks in the United States, Puerto Rico, and Canada; and 50 mg subcutaneous etanercept [Enbrel] injection every week in all other countries. Participants continued their prestudy stable dose of methotrexate if clinically indicated.
The researchers calculated incidence rates and hazard ratios for infections, overall and by age (50-64 years, compared with 65 years and older). They calculated probabilities of infection using Kaplan-Meier estimates and identified infection risk factors through Cox modeling.
They found higher infection rates, serious infection events (SIEs), and nonserious infections (NSIs) with tofacitinib than with TNFi, including:
- Patients taking tofacitinib 5 mg (HR, 1.17; 95% confidence interval, 0.92-1.50) and 10 mg (HR, 1.48; 95% CI, 1.17-1.87) were at greater risk for SIEs.
- Patients older than 65 who were taking tofacitinib 10 mg had increased IRs and HRs for all infections and for SIEs, compared with those aged 50-64.
- The probability of a SIE rose from month 18 onward in participants taking tofacitinib 5 mg, as well as before month 6 in those taking tofacitinib 10 mg.
- In both tofacitinib groups, the probability of NSI increased before month 6.
The most common risk factors for SIEs were higher age, baseline opioid use, history of chronic lung disease, and time-dependent oral corticosteroid use. Risk factors for NSIs were female sex, history of chronic lung disease or infection, history of smoking, as well as time-dependent higher Disease Activity Score in 28 joints and C-reactive protein score.
‘Best information to date’
Michael George, MD, MSCE, assistant professor of medicine and epidemiology at the University of Pennsylvania, Philadelphia, welcomed the study’s results.

“This study provides the best information to date on the risk of infection with the JAK inhibitor tofacitinib, compared to a TNF inhibitor,” Dr. George, who was not involved in the study, said in an interview. “It is rare to have such a large randomized trial with an active comparator focused on safety. This is a major strength.
“Being able to quantify the amount of increased risk will help with shared decision-making when counseling patients,” he added.
Dr. George said that, while the small overall risk may not be clinically meaningful for younger, healthier patients, trying biologics such as TNFi before tofacitinib may be optimal for high-risk patients who are older or have comorbidities.
Dr. Bhatt agreed.
“In deciding on appropriate therapies for RA (or other conditions where tofacitinib is used), it is important for the prescribing physician to explain the risks to the patient and weigh them against the potential benefits,” he advised.
Dr. Bhatt noted that increased infection is not the first risk that’s been linked with tofacitinib.
“ORAL Surveillance was designed primarily to assess cardiovascular safety and showed higher rates of cardiovascular events such as myocardial infarction and pulmonary embolism, as well as cancer, with tofacitinib,” he explained.
He recommended further related research.
“Randomized trials are needed to determine the best ways to treat conditions such as RA while trying to minimize cardiovascular, cancer, and infectious risks,” he said.
The study was sponsored by Pfizer. All authors reported financial involvements with Pfizer; most have financial involvements with other pharmaceutical companies as well; four authors are employees of Pfizer and three are also stockholders in the company. Dr. George reported involvements with the pharmaceutical industry.
Patients with rheumatoid arthritis treated with tofacitinib (Xeljanz) are more likely to develop infections than are those who take a tumor necrosis factor inhibitor (TNFi), results of an industry-sponsored randomized controlled trial suggest.
The Janus kinase (JAK) inhibitor tofacitinib and TNFi biologics are common RA treatments that, along with factors including age, disease activity, and comorbidities, can put patients with RA at increased risk for infections.
“In this secondary analysis of the ORAL Surveillance trial, infections were increased with tofacitinib, compared with TNFi,” study coauthor Deepak L. Bhatt, MD, MPH, professor of medicine at Harvard Medical School and executive director of interventional cardiovascular programs at Brigham and Women’s Hospital, both in Boston, explained in an interview.
As reported in Annals of the Rheumatic Diseases, Dr. Bhatt and colleagues performed a subanalysis of the final dataset from the phase 3b/4 open-label safety trial of tofacitinib in RA conducted between March 2014 and July 2020, in 345 study locations worldwide.
Study participants were 50 years of age or older with moderate to severe RA who were taking methotrexate but having inadequate symptom control. They had at least one cardiovascular risk factor such as being a current smoker or having hypertension, past heart attack, family history of coronary heart disease, high cholesterol, diabetes mellitus, or extra-articular RA. Patients with current or recent infection, clinically significant laboratory abnormalities, or pregnancy, were excluded from the study.
In the study, 1,455 participants received oral tofacitinib 5 mg twice per day; 1,456 received oral tofacitinib 10 mg twice per day; and 1,451 were treated with subcutaneous TNFi (40 mg subcutaneous adalimumab [Humira] injection every 2 weeks in the United States, Puerto Rico, and Canada; and 50 mg subcutaneous etanercept [Enbrel] injection every week in all other countries. Participants continued their prestudy stable dose of methotrexate if clinically indicated.
The researchers calculated incidence rates and hazard ratios for infections, overall and by age (50-64 years, compared with 65 years and older). They calculated probabilities of infection using Kaplan-Meier estimates and identified infection risk factors through Cox modeling.
They found higher infection rates, serious infection events (SIEs), and nonserious infections (NSIs) with tofacitinib than with TNFi, including:
- Patients taking tofacitinib 5 mg (HR, 1.17; 95% confidence interval, 0.92-1.50) and 10 mg (HR, 1.48; 95% CI, 1.17-1.87) were at greater risk for SIEs.
- Patients older than 65 who were taking tofacitinib 10 mg had increased IRs and HRs for all infections and for SIEs, compared with those aged 50-64.
- The probability of a SIE rose from month 18 onward in participants taking tofacitinib 5 mg, as well as before month 6 in those taking tofacitinib 10 mg.
- In both tofacitinib groups, the probability of NSI increased before month 6.
The most common risk factors for SIEs were higher age, baseline opioid use, history of chronic lung disease, and time-dependent oral corticosteroid use. Risk factors for NSIs were female sex, history of chronic lung disease or infection, history of smoking, as well as time-dependent higher Disease Activity Score in 28 joints and C-reactive protein score.
‘Best information to date’
Michael George, MD, MSCE, assistant professor of medicine and epidemiology at the University of Pennsylvania, Philadelphia, welcomed the study’s results.
“This study provides the best information to date on the risk of infection with the JAK inhibitor tofacitinib, compared to a TNF inhibitor,” Dr. George, who was not involved in the study, said in an interview. “It is rare to have such a large randomized trial with an active comparator focused on safety. This is a major strength.
“Being able to quantify the amount of increased risk will help with shared decision-making when counseling patients,” he added.
Dr. George said that, while the small overall risk may not be clinically meaningful for younger, healthier patients, trying biologics such as TNFi before tofacitinib may be optimal for high-risk patients who are older or have comorbidities.
Dr. Bhatt agreed.
“In deciding on appropriate therapies for RA (or other conditions where tofacitinib is used), it is important for the prescribing physician to explain the risks to the patient and weigh them against the potential benefits,” he advised.
Dr. Bhatt noted that increased infection is not the first risk that’s been linked with tofacitinib.
“ORAL Surveillance was designed primarily to assess cardiovascular safety and showed higher rates of cardiovascular events such as myocardial infarction and pulmonary embolism, as well as cancer, with tofacitinib,” he explained.
He recommended further related research.
“Randomized trials are needed to determine the best ways to treat conditions such as RA while trying to minimize cardiovascular, cancer, and infectious risks,” he said.
The study was sponsored by Pfizer. All authors reported financial involvements with Pfizer; most have financial involvements with other pharmaceutical companies as well; four authors are employees of Pfizer and three are also stockholders in the company. Dr. George reported involvements with the pharmaceutical industry.
Patients with rheumatoid arthritis treated with tofacitinib (Xeljanz) are more likely to develop infections than are those who take a tumor necrosis factor inhibitor (TNFi), results of an industry-sponsored randomized controlled trial suggest.
The Janus kinase (JAK) inhibitor tofacitinib and TNFi biologics are common RA treatments that, along with factors including age, disease activity, and comorbidities, can put patients with RA at increased risk for infections.
“In this secondary analysis of the ORAL Surveillance trial, infections were increased with tofacitinib, compared with TNFi,” study coauthor Deepak L. Bhatt, MD, MPH, professor of medicine at Harvard Medical School and executive director of interventional cardiovascular programs at Brigham and Women’s Hospital, both in Boston, explained in an interview.
As reported in Annals of the Rheumatic Diseases, Dr. Bhatt and colleagues performed a subanalysis of the final dataset from the phase 3b/4 open-label safety trial of tofacitinib in RA conducted between March 2014 and July 2020, in 345 study locations worldwide.
Study participants were 50 years of age or older with moderate to severe RA who were taking methotrexate but having inadequate symptom control. They had at least one cardiovascular risk factor such as being a current smoker or having hypertension, past heart attack, family history of coronary heart disease, high cholesterol, diabetes mellitus, or extra-articular RA. Patients with current or recent infection, clinically significant laboratory abnormalities, or pregnancy, were excluded from the study.
In the study, 1,455 participants received oral tofacitinib 5 mg twice per day; 1,456 received oral tofacitinib 10 mg twice per day; and 1,451 were treated with subcutaneous TNFi (40 mg subcutaneous adalimumab [Humira] injection every 2 weeks in the United States, Puerto Rico, and Canada; and 50 mg subcutaneous etanercept [Enbrel] injection every week in all other countries. Participants continued their prestudy stable dose of methotrexate if clinically indicated.
The researchers calculated incidence rates and hazard ratios for infections, overall and by age (50-64 years, compared with 65 years and older). They calculated probabilities of infection using Kaplan-Meier estimates and identified infection risk factors through Cox modeling.
They found higher infection rates, serious infection events (SIEs), and nonserious infections (NSIs) with tofacitinib than with TNFi, including:
- Patients taking tofacitinib 5 mg (HR, 1.17; 95% confidence interval, 0.92-1.50) and 10 mg (HR, 1.48; 95% CI, 1.17-1.87) were at greater risk for SIEs.
- Patients older than 65 who were taking tofacitinib 10 mg had increased IRs and HRs for all infections and for SIEs, compared with those aged 50-64.
- The probability of a SIE rose from month 18 onward in participants taking tofacitinib 5 mg, as well as before month 6 in those taking tofacitinib 10 mg.
- In both tofacitinib groups, the probability of NSI increased before month 6.
The most common risk factors for SIEs were higher age, baseline opioid use, history of chronic lung disease, and time-dependent oral corticosteroid use. Risk factors for NSIs were female sex, history of chronic lung disease or infection, history of smoking, as well as time-dependent higher Disease Activity Score in 28 joints and C-reactive protein score.
‘Best information to date’
Michael George, MD, MSCE, assistant professor of medicine and epidemiology at the University of Pennsylvania, Philadelphia, welcomed the study’s results.
“This study provides the best information to date on the risk of infection with the JAK inhibitor tofacitinib, compared to a TNF inhibitor,” Dr. George, who was not involved in the study, said in an interview. “It is rare to have such a large randomized trial with an active comparator focused on safety. This is a major strength.
“Being able to quantify the amount of increased risk will help with shared decision-making when counseling patients,” he added.
Dr. George said that, while the small overall risk may not be clinically meaningful for younger, healthier patients, trying biologics such as TNFi before tofacitinib may be optimal for high-risk patients who are older or have comorbidities.
Dr. Bhatt agreed.
“In deciding on appropriate therapies for RA (or other conditions where tofacitinib is used), it is important for the prescribing physician to explain the risks to the patient and weigh them against the potential benefits,” he advised.
Dr. Bhatt noted that increased infection is not the first risk that’s been linked with tofacitinib.
“ORAL Surveillance was designed primarily to assess cardiovascular safety and showed higher rates of cardiovascular events such as myocardial infarction and pulmonary embolism, as well as cancer, with tofacitinib,” he explained.
He recommended further related research.
“Randomized trials are needed to determine the best ways to treat conditions such as RA while trying to minimize cardiovascular, cancer, and infectious risks,” he said.
The study was sponsored by Pfizer. All authors reported financial involvements with Pfizer; most have financial involvements with other pharmaceutical companies as well; four authors are employees of Pfizer and three are also stockholders in the company. Dr. George reported involvements with the pharmaceutical industry.
FROM ANNALS OF THE RHEUMATIC DISEASES
Weight-loss surgery has a big effect on marriage
Kristal was only in her mid-30s when she decided to have surgery. Her doctor said it was too early. But the Oregon mom of three had found herself in the hospital twice for obesity-related lung complications before her 35th birthday. So she got the gastric sleeve.
And at first it seemed like the best decision for her and her family. She was losing weight – 100 pounds in 16 months – and so was her husband. The whole family was more active and seemed to have more energy. But then her husband’s weight began to creep back up.
While she joined a running group and signed up for half-marathons, her husband’s depression and drinking worsened. The healthier lifestyle they’d shared was now an unspoken wedge between them.
And the added attention Kristal was getting from men and women because of her thinner size only added to the tension. After 30 years together and 22 years of marriage, the high school sweethearts divorced in June 2021. Kristal’s weight loss wasn’t the only problem, but she and her ex-husband believe it was the beginning of the end.
An unexpected outcome?
New research from the University of Pittsburgh found that Kristal’s experience is a common one. The study looked at data from 1,441 bariatric surgery patients and found that never-married patients were over 50% more likely to get married, and married patients were more than twice as likely to get divorced, compared to the general U.S. population.
This U.S. data follows two Scandinavian studies from 2018 and 2020 that found similar relationship changes after bariatric surgery. But the postsurgery divorce rate in the United States was only about half that found in the Danish and Swedish studies, according to the new study published in Annals of Surgery.
It’s important to note that even with an increase in the divorce rate, most marriages in the study were unchanged, said epidemiologist and lead author Wendy King, PhD. In fact, 81% of couples were still married 5 years after surgery. But where the U.S. population has a divorce rate of 3.5%, bariatric patients in the study had an 8% divorce rate. Likewise, those who’d never been married before the surgery had a marriage rate of 18%, compared to 7% in the U.S. population.
Surgery certainly isn’t a death sentence for a patient’s love life. But the uptick in marriage and divorce suggests bariatric surgery significantly impacts how people engage in relationships.
“It makes sense,” said clinical psychologist Rachel Goldman, PhD, who specializes in health and wellness issues and bariatric surgery cases in New York City. “People are changing their lifestyle.” And those changes don’t start or stop the day of surgery, they begin as soon as someone decides to have surgery and continue as a lifelong process, she said.
For some patients, these healthy habits may offer a “new lease on life,” said Dr. King. According to the study, patients who had better physical health after surgery were more likely to get married.
But the continual lifestyle changes can dramatically impact the rituals of existing relationships, said Dr. Goldman. Maybe a couple loved to go out and enjoy an extravagant meal before surgery, or they had ice cream and watched a movie every Friday. The habit changes that come with bariatric surgery can require one partner to focus less on those rituals.
These sorts of changes may leave one or both people feeling like their partner is turning away from them, said Don Cole, DMin, a relationship therapist and clinical director at the Gottman Institute in Seattle, a think tank focused on the science of relationships. The person who had surgery may feel unsupported in the new journey if the partner keeps advocating for unhealthy habits, he said. And the person who didn’t have surgery may feel cast aside by the partner’s new health priorities.
Changes, even those that are positive and healthy, create a kind of crisis for relationships, Dr. Cole said. It’s not just bariatric surgery. Bringing a baby into the home, infertility treatments, and substance abuse recovery are all considered positive changes that are also predictors of relationship dissatisfaction and divorce, he said.
A couple could have a range of emotions after one partner gets bariatric surgery, Dr. Cole said. Unfortunately, “my experience as a therapist says they aren’t that good [at talking about it],” he said.
But bariatric surgery isn’t the only thing at play in these relationship changes, according to the study. Married patients had a much lower chance of separation or divorce (13%) than patients who were unmarried but living together (44%) by 5 years after surgery. Similarly, most people who were already separated either got divorced or resumed being married. It’s as if the surgery and lifestyle changes served as a catalyst for people who already had one foot out of (or in) the door, Dr. Goldman said.
A high sexual desire after surgery was also a predictor of divorce. In fact, there were more things before surgery that impacted divorce than surgery-related changes. It’s possible that many of these patients are “on the path toward change already,” Dr. King said. “Who knows how much the surgery had to do with it.”
Dr. Goldman recalled a patient who, before surgery, had very low self-worth. She wasn’t satisfied with her relationship but admitted to staying because she didn’t believe she could do any better than her current partner. After surgery, her perspective radically changed. She started to get healthier, invested in her education, and changed jobs. And when her partner refused to join her in making changes, she left. Maybe some of these patients “were already thinking about leaving but just didn’t have the confidence,” Dr. Goldman said.
Still, it’s critical that patients receive more counseling on how choosing to have bariatric surgery can impact their relationship before and after their weight loss procedure, Dr. King said. It should be the standard of care.
Currently, relationship-specific counseling isn’t required, Dr. Goldman said. Most programs do require a psychosocial evaluation before surgery, “but they are quite varied.” And even in programs where relationships are mentioned, there often isn’t a psychologist or licensed mental health professional on the team.
Since Dr. King’s previous research on substance abuse after bariatric surgery changed common practice in the field, Dr. Goldman said she hopes the new data will have a similar influence and relationship counseling will become the norm.
Dr. Cole actually had bariatric surgery. He recalled potential relationship issues were briefly mentioned. Someone at the clinic said if his marriage felt challenged, he should seek help from a professional, and that was it.
For Dr. Cole, there were unexpected negative feelings of shame and disappointment after surgery. He felt the extreme weight loss was all his colleagues could talk about and was very disappointed when there was no change in his chronic pain, a primary reason he had the procedure.
Fortunately, he could talk to his wife – also is a relationship therapist at Gottman – about the range of emotions. “One of the things that we know that creates a deep sense of trust is [when] I know my partner is there for me when I’m not well,” Dr. Cole said.
But these negative emotions can be the very things that feel most difficult to talk about or hear from a partner. It’s hard to share our own negative feelings and to hear someone else’s, Dr. Cole said.
He advises creating a new “ritual of connection: moments in time when you plan to turn toward one another.”
That could be a daily walk, where you intentionally talk about the surgery-related changes that both of you have had. Dr. Cole said to ask yourself, “Are we intentional about turning toward one another in those [challenging] moments?”
A version of this article first appeared on WebMD.com.
Kristal was only in her mid-30s when she decided to have surgery. Her doctor said it was too early. But the Oregon mom of three had found herself in the hospital twice for obesity-related lung complications before her 35th birthday. So she got the gastric sleeve.
And at first it seemed like the best decision for her and her family. She was losing weight – 100 pounds in 16 months – and so was her husband. The whole family was more active and seemed to have more energy. But then her husband’s weight began to creep back up.
While she joined a running group and signed up for half-marathons, her husband’s depression and drinking worsened. The healthier lifestyle they’d shared was now an unspoken wedge between them.
And the added attention Kristal was getting from men and women because of her thinner size only added to the tension. After 30 years together and 22 years of marriage, the high school sweethearts divorced in June 2021. Kristal’s weight loss wasn’t the only problem, but she and her ex-husband believe it was the beginning of the end.
An unexpected outcome?
New research from the University of Pittsburgh found that Kristal’s experience is a common one. The study looked at data from 1,441 bariatric surgery patients and found that never-married patients were over 50% more likely to get married, and married patients were more than twice as likely to get divorced, compared to the general U.S. population.
This U.S. data follows two Scandinavian studies from 2018 and 2020 that found similar relationship changes after bariatric surgery. But the postsurgery divorce rate in the United States was only about half that found in the Danish and Swedish studies, according to the new study published in Annals of Surgery.
It’s important to note that even with an increase in the divorce rate, most marriages in the study were unchanged, said epidemiologist and lead author Wendy King, PhD. In fact, 81% of couples were still married 5 years after surgery. But where the U.S. population has a divorce rate of 3.5%, bariatric patients in the study had an 8% divorce rate. Likewise, those who’d never been married before the surgery had a marriage rate of 18%, compared to 7% in the U.S. population.
Surgery certainly isn’t a death sentence for a patient’s love life. But the uptick in marriage and divorce suggests bariatric surgery significantly impacts how people engage in relationships.
“It makes sense,” said clinical psychologist Rachel Goldman, PhD, who specializes in health and wellness issues and bariatric surgery cases in New York City. “People are changing their lifestyle.” And those changes don’t start or stop the day of surgery, they begin as soon as someone decides to have surgery and continue as a lifelong process, she said.
For some patients, these healthy habits may offer a “new lease on life,” said Dr. King. According to the study, patients who had better physical health after surgery were more likely to get married.
But the continual lifestyle changes can dramatically impact the rituals of existing relationships, said Dr. Goldman. Maybe a couple loved to go out and enjoy an extravagant meal before surgery, or they had ice cream and watched a movie every Friday. The habit changes that come with bariatric surgery can require one partner to focus less on those rituals.
These sorts of changes may leave one or both people feeling like their partner is turning away from them, said Don Cole, DMin, a relationship therapist and clinical director at the Gottman Institute in Seattle, a think tank focused on the science of relationships. The person who had surgery may feel unsupported in the new journey if the partner keeps advocating for unhealthy habits, he said. And the person who didn’t have surgery may feel cast aside by the partner’s new health priorities.
Changes, even those that are positive and healthy, create a kind of crisis for relationships, Dr. Cole said. It’s not just bariatric surgery. Bringing a baby into the home, infertility treatments, and substance abuse recovery are all considered positive changes that are also predictors of relationship dissatisfaction and divorce, he said.
A couple could have a range of emotions after one partner gets bariatric surgery, Dr. Cole said. Unfortunately, “my experience as a therapist says they aren’t that good [at talking about it],” he said.
But bariatric surgery isn’t the only thing at play in these relationship changes, according to the study. Married patients had a much lower chance of separation or divorce (13%) than patients who were unmarried but living together (44%) by 5 years after surgery. Similarly, most people who were already separated either got divorced or resumed being married. It’s as if the surgery and lifestyle changes served as a catalyst for people who already had one foot out of (or in) the door, Dr. Goldman said.
A high sexual desire after surgery was also a predictor of divorce. In fact, there were more things before surgery that impacted divorce than surgery-related changes. It’s possible that many of these patients are “on the path toward change already,” Dr. King said. “Who knows how much the surgery had to do with it.”
Dr. Goldman recalled a patient who, before surgery, had very low self-worth. She wasn’t satisfied with her relationship but admitted to staying because she didn’t believe she could do any better than her current partner. After surgery, her perspective radically changed. She started to get healthier, invested in her education, and changed jobs. And when her partner refused to join her in making changes, she left. Maybe some of these patients “were already thinking about leaving but just didn’t have the confidence,” Dr. Goldman said.
Still, it’s critical that patients receive more counseling on how choosing to have bariatric surgery can impact their relationship before and after their weight loss procedure, Dr. King said. It should be the standard of care.
Currently, relationship-specific counseling isn’t required, Dr. Goldman said. Most programs do require a psychosocial evaluation before surgery, “but they are quite varied.” And even in programs where relationships are mentioned, there often isn’t a psychologist or licensed mental health professional on the team.
Since Dr. King’s previous research on substance abuse after bariatric surgery changed common practice in the field, Dr. Goldman said she hopes the new data will have a similar influence and relationship counseling will become the norm.
Dr. Cole actually had bariatric surgery. He recalled potential relationship issues were briefly mentioned. Someone at the clinic said if his marriage felt challenged, he should seek help from a professional, and that was it.
For Dr. Cole, there were unexpected negative feelings of shame and disappointment after surgery. He felt the extreme weight loss was all his colleagues could talk about and was very disappointed when there was no change in his chronic pain, a primary reason he had the procedure.
Fortunately, he could talk to his wife – also is a relationship therapist at Gottman – about the range of emotions. “One of the things that we know that creates a deep sense of trust is [when] I know my partner is there for me when I’m not well,” Dr. Cole said.
But these negative emotions can be the very things that feel most difficult to talk about or hear from a partner. It’s hard to share our own negative feelings and to hear someone else’s, Dr. Cole said.
He advises creating a new “ritual of connection: moments in time when you plan to turn toward one another.”
That could be a daily walk, where you intentionally talk about the surgery-related changes that both of you have had. Dr. Cole said to ask yourself, “Are we intentional about turning toward one another in those [challenging] moments?”
A version of this article first appeared on WebMD.com.
Kristal was only in her mid-30s when she decided to have surgery. Her doctor said it was too early. But the Oregon mom of three had found herself in the hospital twice for obesity-related lung complications before her 35th birthday. So she got the gastric sleeve.
And at first it seemed like the best decision for her and her family. She was losing weight – 100 pounds in 16 months – and so was her husband. The whole family was more active and seemed to have more energy. But then her husband’s weight began to creep back up.
While she joined a running group and signed up for half-marathons, her husband’s depression and drinking worsened. The healthier lifestyle they’d shared was now an unspoken wedge between them.
And the added attention Kristal was getting from men and women because of her thinner size only added to the tension. After 30 years together and 22 years of marriage, the high school sweethearts divorced in June 2021. Kristal’s weight loss wasn’t the only problem, but she and her ex-husband believe it was the beginning of the end.
An unexpected outcome?
New research from the University of Pittsburgh found that Kristal’s experience is a common one. The study looked at data from 1,441 bariatric surgery patients and found that never-married patients were over 50% more likely to get married, and married patients were more than twice as likely to get divorced, compared to the general U.S. population.
This U.S. data follows two Scandinavian studies from 2018 and 2020 that found similar relationship changes after bariatric surgery. But the postsurgery divorce rate in the United States was only about half that found in the Danish and Swedish studies, according to the new study published in Annals of Surgery.
It’s important to note that even with an increase in the divorce rate, most marriages in the study were unchanged, said epidemiologist and lead author Wendy King, PhD. In fact, 81% of couples were still married 5 years after surgery. But where the U.S. population has a divorce rate of 3.5%, bariatric patients in the study had an 8% divorce rate. Likewise, those who’d never been married before the surgery had a marriage rate of 18%, compared to 7% in the U.S. population.
Surgery certainly isn’t a death sentence for a patient’s love life. But the uptick in marriage and divorce suggests bariatric surgery significantly impacts how people engage in relationships.
“It makes sense,” said clinical psychologist Rachel Goldman, PhD, who specializes in health and wellness issues and bariatric surgery cases in New York City. “People are changing their lifestyle.” And those changes don’t start or stop the day of surgery, they begin as soon as someone decides to have surgery and continue as a lifelong process, she said.
For some patients, these healthy habits may offer a “new lease on life,” said Dr. King. According to the study, patients who had better physical health after surgery were more likely to get married.
But the continual lifestyle changes can dramatically impact the rituals of existing relationships, said Dr. Goldman. Maybe a couple loved to go out and enjoy an extravagant meal before surgery, or they had ice cream and watched a movie every Friday. The habit changes that come with bariatric surgery can require one partner to focus less on those rituals.
These sorts of changes may leave one or both people feeling like their partner is turning away from them, said Don Cole, DMin, a relationship therapist and clinical director at the Gottman Institute in Seattle, a think tank focused on the science of relationships. The person who had surgery may feel unsupported in the new journey if the partner keeps advocating for unhealthy habits, he said. And the person who didn’t have surgery may feel cast aside by the partner’s new health priorities.
Changes, even those that are positive and healthy, create a kind of crisis for relationships, Dr. Cole said. It’s not just bariatric surgery. Bringing a baby into the home, infertility treatments, and substance abuse recovery are all considered positive changes that are also predictors of relationship dissatisfaction and divorce, he said.
A couple could have a range of emotions after one partner gets bariatric surgery, Dr. Cole said. Unfortunately, “my experience as a therapist says they aren’t that good [at talking about it],” he said.
But bariatric surgery isn’t the only thing at play in these relationship changes, according to the study. Married patients had a much lower chance of separation or divorce (13%) than patients who were unmarried but living together (44%) by 5 years after surgery. Similarly, most people who were already separated either got divorced or resumed being married. It’s as if the surgery and lifestyle changes served as a catalyst for people who already had one foot out of (or in) the door, Dr. Goldman said.
A high sexual desire after surgery was also a predictor of divorce. In fact, there were more things before surgery that impacted divorce than surgery-related changes. It’s possible that many of these patients are “on the path toward change already,” Dr. King said. “Who knows how much the surgery had to do with it.”
Dr. Goldman recalled a patient who, before surgery, had very low self-worth. She wasn’t satisfied with her relationship but admitted to staying because she didn’t believe she could do any better than her current partner. After surgery, her perspective radically changed. She started to get healthier, invested in her education, and changed jobs. And when her partner refused to join her in making changes, she left. Maybe some of these patients “were already thinking about leaving but just didn’t have the confidence,” Dr. Goldman said.
Still, it’s critical that patients receive more counseling on how choosing to have bariatric surgery can impact their relationship before and after their weight loss procedure, Dr. King said. It should be the standard of care.
Currently, relationship-specific counseling isn’t required, Dr. Goldman said. Most programs do require a psychosocial evaluation before surgery, “but they are quite varied.” And even in programs where relationships are mentioned, there often isn’t a psychologist or licensed mental health professional on the team.
Since Dr. King’s previous research on substance abuse after bariatric surgery changed common practice in the field, Dr. Goldman said she hopes the new data will have a similar influence and relationship counseling will become the norm.
Dr. Cole actually had bariatric surgery. He recalled potential relationship issues were briefly mentioned. Someone at the clinic said if his marriage felt challenged, he should seek help from a professional, and that was it.
For Dr. Cole, there were unexpected negative feelings of shame and disappointment after surgery. He felt the extreme weight loss was all his colleagues could talk about and was very disappointed when there was no change in his chronic pain, a primary reason he had the procedure.
Fortunately, he could talk to his wife – also is a relationship therapist at Gottman – about the range of emotions. “One of the things that we know that creates a deep sense of trust is [when] I know my partner is there for me when I’m not well,” Dr. Cole said.
But these negative emotions can be the very things that feel most difficult to talk about or hear from a partner. It’s hard to share our own negative feelings and to hear someone else’s, Dr. Cole said.
He advises creating a new “ritual of connection: moments in time when you plan to turn toward one another.”
That could be a daily walk, where you intentionally talk about the surgery-related changes that both of you have had. Dr. Cole said to ask yourself, “Are we intentional about turning toward one another in those [challenging] moments?”
A version of this article first appeared on WebMD.com.
FROM ANNALS OF SURGERY
Young adults who learn how to cook eat more veggies
Obesity remains a significant risk factor for numerous diseases, and is often a problem in young adults, who often fall back on fast food and other less-healthy meals associated with a lower quality diet, lead author Carol S. O’Neal, PhD, of the University of Louisville (Ky.), said in an interview.
Previous research involving Social Cognitive Theory and goal-setting to promote self-efficacy and behavior changes has shown success in improving eating habits in young adults, but adding video technology for an additional education element has not been well studied, Dr. O’Neal and colleagues wrote in the Journal of Nutrition Education and Behavior.
Methods and results
In the study, 138 college students aged 18-40 years participated in a 15-week pilot intervention course at a large, metropolitan university. The course included lectures on a topic, such as carbohydrates, and included skill-based activities, such as how to read an ingredient list, and discussion of how these skills could improve healthier eating and meet nutrition goals, such as eating more whole grains.
A total of 77 completed the study in person, and 61 participated online. The majority (59%) were college sophomores, 74% were White, and 82% were female.
The course engaged the students in weekly food challenges to apply their knowledge and develop better eating habits and behaviors. The challenges were accompanied by cooking videos related to each week’s topic, such as how to make overnight oats for the healthy carbohydrates/whole grains week.
Students also selected two goals each week, such as choosing whole grain foods to increase fiber consumption, from a list of 10-15 goals, and were required to write weekly reflections to track their progress toward these goals. Goal-setting was based on the strategy of creating goals that are specific, measurable, attainable, realistic, and time-bound (the SMART method).
The main outcomes were increased consumption of fruits and vegetables, improved skills in cooking and healthy eating, and improved attitudes about healthy cooking and eating. The researchers surveyed the students to determine whether these outcomes were met.
Students participating in the study indicated that they met the goal of eating at least five servings of fruits and vegetables per day more often after the course than before, the researchers wrote.
By the course’s end, the students showed significant increases in consumption of fruits and vegetables (P < .001 for both), and in the self-efficacy related to consumption of produce (P = .004); cooking (P = .002;, and using more fruits, vegetables, and seasonings rather than salt in cooking (P = .001).
A review of the students’ written reflections illustrated positive behavior changes such as planning meals before shopping, preparing meals in advance on weekends, taking lunch to school, and using herbs and spices, the researchers noted.
“Self-directed SMART goals set you up for success by making goals specific, measurable, achievable, realistic, and timely,” Dr. O’Neal said in an interview. “The SMART method helps push you further, gives you a sense of direction, and helps you organize and reach your goals,” but self-monitoring and social support are also needed for success. The takeaway message for clinicians is that use of a self-directed goal-setting strategy may be more effective at changing dietary behaviors and promoting self-efficacy than a traditional dietary prescription.
In addition, “this model could be used to address a variety of health outcomes in dietetics, health education and community health programs,” said Dr. O’Neal. “I think the key components of this intervention are teaching SMART goal setting, self-monitoring, and social support of successes. I see time as a main barrier, but this barrier could be reduced for populations who are able to use online learning. Our intervention was successful for in-person and online learning.”
Other areas for future research include evaluation of progress that combines quantitative data and qualitative reflections, she said.
Real-world applications
“Clinicians have limited time to address behavioral counseling, and this study offers an opportunity to reach patients not only in class sessions, but virtually,” M. Susan Jay, MD, of the Medical College of Wisconsin, Milwaukee, said in an interview.
Although the findings from the study are not new, the knowledge can be used by clinicians to help promote behavior change. The study also showcased the use of additional tools, such as weekly food challenges, to impact college students who often consume high-fat diets in nonmedical settings, Dr. Jay said.
For consumers, the real-world implications are exciting, Dr. Jay said.
“People are increasingly attempting to “eat healthy” and despite clinicians wanting to impact healthy eating, limited office visits may not be conducive to behavioral change,” she said.
The current study was important as a way to identify tactics to improve the diet and nutrition of young adults, Margaret Thew, DNP, FNP-BC, medical director of adolescent medicine at the University of Wisconsin–Madison, said in an interview.
The study findings of increased fruit and vegetable consumption were not surprising, as the study population may have been more highly motivated to improve their diets, Dr. Thew said. However, she was surprised to see the significant improvement in cooking attitudes and cooking self-efficiency after the intervention. “This tells me that we need to offer more opportunities to educate young adults on how to cook to improve diet outcomes.”
The message for clinicians is to encourage and support young adults to learn cooking skills to promote healthier eating, said Dr. Thew.
“When patients have confidence in their ability to cook, they will explore more food options and consequently improve their diets,” she emphasized. “As clinicians, we need to advocate for nutrition education and promote cooking classes that are accessible to all if we hope to reduce obesity and improve our patients’ diets.”
Limitations
The study findings were limited by several factors including the use of a convenience sample that might not represent all college students, the reliance on self-reports, the inability to account for the impact of demographic factors, and the lack of a control group, the researchers wrote.
“Larger prospective studies are needed,” given the limitations of the pilot design and short study period, Dr. Jay noted.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Jay and Dr. Thew had no financial conflicts to disclose.
Obesity remains a significant risk factor for numerous diseases, and is often a problem in young adults, who often fall back on fast food and other less-healthy meals associated with a lower quality diet, lead author Carol S. O’Neal, PhD, of the University of Louisville (Ky.), said in an interview.
Previous research involving Social Cognitive Theory and goal-setting to promote self-efficacy and behavior changes has shown success in improving eating habits in young adults, but adding video technology for an additional education element has not been well studied, Dr. O’Neal and colleagues wrote in the Journal of Nutrition Education and Behavior.
Methods and results
In the study, 138 college students aged 18-40 years participated in a 15-week pilot intervention course at a large, metropolitan university. The course included lectures on a topic, such as carbohydrates, and included skill-based activities, such as how to read an ingredient list, and discussion of how these skills could improve healthier eating and meet nutrition goals, such as eating more whole grains.
A total of 77 completed the study in person, and 61 participated online. The majority (59%) were college sophomores, 74% were White, and 82% were female.
The course engaged the students in weekly food challenges to apply their knowledge and develop better eating habits and behaviors. The challenges were accompanied by cooking videos related to each week’s topic, such as how to make overnight oats for the healthy carbohydrates/whole grains week.
Students also selected two goals each week, such as choosing whole grain foods to increase fiber consumption, from a list of 10-15 goals, and were required to write weekly reflections to track their progress toward these goals. Goal-setting was based on the strategy of creating goals that are specific, measurable, attainable, realistic, and time-bound (the SMART method).
The main outcomes were increased consumption of fruits and vegetables, improved skills in cooking and healthy eating, and improved attitudes about healthy cooking and eating. The researchers surveyed the students to determine whether these outcomes were met.
Students participating in the study indicated that they met the goal of eating at least five servings of fruits and vegetables per day more often after the course than before, the researchers wrote.
By the course’s end, the students showed significant increases in consumption of fruits and vegetables (P < .001 for both), and in the self-efficacy related to consumption of produce (P = .004); cooking (P = .002;, and using more fruits, vegetables, and seasonings rather than salt in cooking (P = .001).
A review of the students’ written reflections illustrated positive behavior changes such as planning meals before shopping, preparing meals in advance on weekends, taking lunch to school, and using herbs and spices, the researchers noted.
“Self-directed SMART goals set you up for success by making goals specific, measurable, achievable, realistic, and timely,” Dr. O’Neal said in an interview. “The SMART method helps push you further, gives you a sense of direction, and helps you organize and reach your goals,” but self-monitoring and social support are also needed for success. The takeaway message for clinicians is that use of a self-directed goal-setting strategy may be more effective at changing dietary behaviors and promoting self-efficacy than a traditional dietary prescription.
In addition, “this model could be used to address a variety of health outcomes in dietetics, health education and community health programs,” said Dr. O’Neal. “I think the key components of this intervention are teaching SMART goal setting, self-monitoring, and social support of successes. I see time as a main barrier, but this barrier could be reduced for populations who are able to use online learning. Our intervention was successful for in-person and online learning.”
Other areas for future research include evaluation of progress that combines quantitative data and qualitative reflections, she said.
Real-world applications
“Clinicians have limited time to address behavioral counseling, and this study offers an opportunity to reach patients not only in class sessions, but virtually,” M. Susan Jay, MD, of the Medical College of Wisconsin, Milwaukee, said in an interview.
Although the findings from the study are not new, the knowledge can be used by clinicians to help promote behavior change. The study also showcased the use of additional tools, such as weekly food challenges, to impact college students who often consume high-fat diets in nonmedical settings, Dr. Jay said.
For consumers, the real-world implications are exciting, Dr. Jay said.
“People are increasingly attempting to “eat healthy” and despite clinicians wanting to impact healthy eating, limited office visits may not be conducive to behavioral change,” she said.
The current study was important as a way to identify tactics to improve the diet and nutrition of young adults, Margaret Thew, DNP, FNP-BC, medical director of adolescent medicine at the University of Wisconsin–Madison, said in an interview.
The study findings of increased fruit and vegetable consumption were not surprising, as the study population may have been more highly motivated to improve their diets, Dr. Thew said. However, she was surprised to see the significant improvement in cooking attitudes and cooking self-efficiency after the intervention. “This tells me that we need to offer more opportunities to educate young adults on how to cook to improve diet outcomes.”
The message for clinicians is to encourage and support young adults to learn cooking skills to promote healthier eating, said Dr. Thew.
“When patients have confidence in their ability to cook, they will explore more food options and consequently improve their diets,” she emphasized. “As clinicians, we need to advocate for nutrition education and promote cooking classes that are accessible to all if we hope to reduce obesity and improve our patients’ diets.”
Limitations
The study findings were limited by several factors including the use of a convenience sample that might not represent all college students, the reliance on self-reports, the inability to account for the impact of demographic factors, and the lack of a control group, the researchers wrote.
“Larger prospective studies are needed,” given the limitations of the pilot design and short study period, Dr. Jay noted.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Jay and Dr. Thew had no financial conflicts to disclose.
Obesity remains a significant risk factor for numerous diseases, and is often a problem in young adults, who often fall back on fast food and other less-healthy meals associated with a lower quality diet, lead author Carol S. O’Neal, PhD, of the University of Louisville (Ky.), said in an interview.
Previous research involving Social Cognitive Theory and goal-setting to promote self-efficacy and behavior changes has shown success in improving eating habits in young adults, but adding video technology for an additional education element has not been well studied, Dr. O’Neal and colleagues wrote in the Journal of Nutrition Education and Behavior.
Methods and results
In the study, 138 college students aged 18-40 years participated in a 15-week pilot intervention course at a large, metropolitan university. The course included lectures on a topic, such as carbohydrates, and included skill-based activities, such as how to read an ingredient list, and discussion of how these skills could improve healthier eating and meet nutrition goals, such as eating more whole grains.
A total of 77 completed the study in person, and 61 participated online. The majority (59%) were college sophomores, 74% were White, and 82% were female.
The course engaged the students in weekly food challenges to apply their knowledge and develop better eating habits and behaviors. The challenges were accompanied by cooking videos related to each week’s topic, such as how to make overnight oats for the healthy carbohydrates/whole grains week.
Students also selected two goals each week, such as choosing whole grain foods to increase fiber consumption, from a list of 10-15 goals, and were required to write weekly reflections to track their progress toward these goals. Goal-setting was based on the strategy of creating goals that are specific, measurable, attainable, realistic, and time-bound (the SMART method).
The main outcomes were increased consumption of fruits and vegetables, improved skills in cooking and healthy eating, and improved attitudes about healthy cooking and eating. The researchers surveyed the students to determine whether these outcomes were met.
Students participating in the study indicated that they met the goal of eating at least five servings of fruits and vegetables per day more often after the course than before, the researchers wrote.
By the course’s end, the students showed significant increases in consumption of fruits and vegetables (P < .001 for both), and in the self-efficacy related to consumption of produce (P = .004); cooking (P = .002;, and using more fruits, vegetables, and seasonings rather than salt in cooking (P = .001).
A review of the students’ written reflections illustrated positive behavior changes such as planning meals before shopping, preparing meals in advance on weekends, taking lunch to school, and using herbs and spices, the researchers noted.
“Self-directed SMART goals set you up for success by making goals specific, measurable, achievable, realistic, and timely,” Dr. O’Neal said in an interview. “The SMART method helps push you further, gives you a sense of direction, and helps you organize and reach your goals,” but self-monitoring and social support are also needed for success. The takeaway message for clinicians is that use of a self-directed goal-setting strategy may be more effective at changing dietary behaviors and promoting self-efficacy than a traditional dietary prescription.
In addition, “this model could be used to address a variety of health outcomes in dietetics, health education and community health programs,” said Dr. O’Neal. “I think the key components of this intervention are teaching SMART goal setting, self-monitoring, and social support of successes. I see time as a main barrier, but this barrier could be reduced for populations who are able to use online learning. Our intervention was successful for in-person and online learning.”
Other areas for future research include evaluation of progress that combines quantitative data and qualitative reflections, she said.
Real-world applications
“Clinicians have limited time to address behavioral counseling, and this study offers an opportunity to reach patients not only in class sessions, but virtually,” M. Susan Jay, MD, of the Medical College of Wisconsin, Milwaukee, said in an interview.
Although the findings from the study are not new, the knowledge can be used by clinicians to help promote behavior change. The study also showcased the use of additional tools, such as weekly food challenges, to impact college students who often consume high-fat diets in nonmedical settings, Dr. Jay said.
For consumers, the real-world implications are exciting, Dr. Jay said.
“People are increasingly attempting to “eat healthy” and despite clinicians wanting to impact healthy eating, limited office visits may not be conducive to behavioral change,” she said.
The current study was important as a way to identify tactics to improve the diet and nutrition of young adults, Margaret Thew, DNP, FNP-BC, medical director of adolescent medicine at the University of Wisconsin–Madison, said in an interview.
The study findings of increased fruit and vegetable consumption were not surprising, as the study population may have been more highly motivated to improve their diets, Dr. Thew said. However, she was surprised to see the significant improvement in cooking attitudes and cooking self-efficiency after the intervention. “This tells me that we need to offer more opportunities to educate young adults on how to cook to improve diet outcomes.”
The message for clinicians is to encourage and support young adults to learn cooking skills to promote healthier eating, said Dr. Thew.
“When patients have confidence in their ability to cook, they will explore more food options and consequently improve their diets,” she emphasized. “As clinicians, we need to advocate for nutrition education and promote cooking classes that are accessible to all if we hope to reduce obesity and improve our patients’ diets.”
Limitations
The study findings were limited by several factors including the use of a convenience sample that might not represent all college students, the reliance on self-reports, the inability to account for the impact of demographic factors, and the lack of a control group, the researchers wrote.
“Larger prospective studies are needed,” given the limitations of the pilot design and short study period, Dr. Jay noted.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Jay and Dr. Thew had no financial conflicts to disclose.
FROM THE JOURNAL OF NUTRITION EDUCATION AND BEHAVIOR
Federal Health Care Data Trends 2022
Federal Health Care Data Trends (click to view the digital edition) is a special supplement to Federal Practitioner highlighting the latest research and study outcomes related to the health of veteran and active-duty populations.
In this issue:
- Vaccinations
- Mental Health and Related Disorders
- LGBTQ+ Veterans
- Military Sexual Trauma
- Sleep Disorders
- Respiratory Illnesses
- HIV Care in the VA
- Rheumatologic Diseases
- The Cancer-Obesity Connection
- Skin Health for Active-Duty Personnel
- Contraception
- Chronic Kidney Disease
- Cardiovascular Diseases
- Neurologic Disorders
- Hearing, Vision, and Balance
Federal Practitioner would like to thank the following experts for their review of content and helpful guidance in developing this issue:
Kelvin N.V. Bush, MD, FACC, CCDS; Sonya Borrero, MD, MS; Kenneth L. Cameron, PhD, MPH, ATC, FNATA; Jason DeViva, PhD; Ellen Lockard Edens, MD; Leonard E. Egede, MD, MS; Amy Justice, MD, PhD; Stephanie Knudson, MD; Willis H. Lyford, MD; Sarah O. Meadows, PhD; Tamara Schult, PhD, MPH; Eric L. Singman, MD, PhD; Art Wallace, MD, PhD; Elizabeth Waterhouse, MD, FAAN
Federal Health Care Data Trends (click to view the digital edition) is a special supplement to Federal Practitioner highlighting the latest research and study outcomes related to the health of veteran and active-duty populations.
In this issue:
- Vaccinations
- Mental Health and Related Disorders
- LGBTQ+ Veterans
- Military Sexual Trauma
- Sleep Disorders
- Respiratory Illnesses
- HIV Care in the VA
- Rheumatologic Diseases
- The Cancer-Obesity Connection
- Skin Health for Active-Duty Personnel
- Contraception
- Chronic Kidney Disease
- Cardiovascular Diseases
- Neurologic Disorders
- Hearing, Vision, and Balance
Federal Practitioner would like to thank the following experts for their review of content and helpful guidance in developing this issue:
Kelvin N.V. Bush, MD, FACC, CCDS; Sonya Borrero, MD, MS; Kenneth L. Cameron, PhD, MPH, ATC, FNATA; Jason DeViva, PhD; Ellen Lockard Edens, MD; Leonard E. Egede, MD, MS; Amy Justice, MD, PhD; Stephanie Knudson, MD; Willis H. Lyford, MD; Sarah O. Meadows, PhD; Tamara Schult, PhD, MPH; Eric L. Singman, MD, PhD; Art Wallace, MD, PhD; Elizabeth Waterhouse, MD, FAAN
Federal Health Care Data Trends (click to view the digital edition) is a special supplement to Federal Practitioner highlighting the latest research and study outcomes related to the health of veteran and active-duty populations.
In this issue:
- Vaccinations
- Mental Health and Related Disorders
- LGBTQ+ Veterans
- Military Sexual Trauma
- Sleep Disorders
- Respiratory Illnesses
- HIV Care in the VA
- Rheumatologic Diseases
- The Cancer-Obesity Connection
- Skin Health for Active-Duty Personnel
- Contraception
- Chronic Kidney Disease
- Cardiovascular Diseases
- Neurologic Disorders
- Hearing, Vision, and Balance
Federal Practitioner would like to thank the following experts for their review of content and helpful guidance in developing this issue:
Kelvin N.V. Bush, MD, FACC, CCDS; Sonya Borrero, MD, MS; Kenneth L. Cameron, PhD, MPH, ATC, FNATA; Jason DeViva, PhD; Ellen Lockard Edens, MD; Leonard E. Egede, MD, MS; Amy Justice, MD, PhD; Stephanie Knudson, MD; Willis H. Lyford, MD; Sarah O. Meadows, PhD; Tamara Schult, PhD, MPH; Eric L. Singman, MD, PhD; Art Wallace, MD, PhD; Elizabeth Waterhouse, MD, FAAN
Regular fasting linked to less severe COVID: Study
, according to the findings of a new study.
The study was done on men and women in Utah who were, on average, in their 60s and got COVID before vaccines were available.
Roughly one in three people in Utah fast from time to time – higher than in other states. This is partly because more than 60% of people in Utah belong to the Church of Jesus Christ of Latter-day Saints, and roughly 40% of them fast – typically skipping two meals in a row.
Those who fasted, on average, for a day a month over the past 40 years were not less likely to get COVID, but they were less likely to be hospitalized or die from the virus.
“Intermittent fasting has already shown to lower inflammation and improve cardiovascular health,” lead study author Benjamin Horne, PhD, of Intermountain Medical Center Heart Institute in Salt Lake City, said in a statement.
“In this study, we’re finding additional benefits when it comes to battling an infection of COVID-19 in patients who have been fasting for decades,” he said.
The study was published in BMJ Nutrition, Prevention & Health.
Intermittent fasting not a substitute for a COVID-19 vaccine
Importantly, intermittent fasting shouldn’t be seen as a substitute for getting a COVID vaccine, the researchers stressed. Rather, periodic fasting might be a health habit to consider, since it is also linked to a lower risk of diabetes and heart disease, for example.
But anyone who wants to consider intermittent fasting should consult their doctor first, Dr. Horne stressed, especially if they are elderly, pregnant, or have diabetes, heart disease, or kidney disease.
Fasting didn’t prevent COVID-19 but made it less severe
In their study, the team looked at data from 1,524 adults who were seen in the cardiac catheterization lab at Intermountain Medical Center Heart Institute, completed a survey, and had a test for the virus that causes COVID-19 from March 16, 2020, to Feb. 25, 2021.
Of these patients, 205 tested positive for COVID, and of these, 73 reported that they had fasted regularly at least once a month.
Similar numbers of patients got COVID-19 whether they had, or had not, fasted regularly (14%, versus 13%).
But among those who tested positive for the virus, fewer patients were hospitalized for COVID or died during the study follow-up if they had fasted regularly (11%) than if they had not fasted regularly (29%).
Even when the analyses were adjusted for age, smoking, alcohol use, ethnicity, history of heart disease, and other factors, periodic fasting was still an independent predictor of a lower risk of hospitalization or death.
Several things may explain the findings, the researchers suggested.
A loss of appetite is a typical response to infection, they noted.
Fasting reduces inflammation, and after 12-14 hours of fasting, the body switches from using glucose in the blood to using ketones, including linoleic acid.
“There’s a pocket on the surface of SARS-CoV-2 that linoleic acid fits into – and can make the virus less able to attach to other cells,” Dr. Horne said.
Intermittent fasting also promotes autophagy, he noted, which is “the body’s recycling system that helps your body destroy and recycle damaged and infected cells.”
The researchers concluded that intermittent fasting plans should be investigated in further research “as a complementary therapy to vaccines to reduce COVID-19 severity, both during the pandemic and post pandemic, since repeat vaccinations cannot be performed every few months indefinitely for the entire world and vaccine access is limited in many nations.”
A version of this article first appeared on WebMD.com.
, according to the findings of a new study.
The study was done on men and women in Utah who were, on average, in their 60s and got COVID before vaccines were available.
Roughly one in three people in Utah fast from time to time – higher than in other states. This is partly because more than 60% of people in Utah belong to the Church of Jesus Christ of Latter-day Saints, and roughly 40% of them fast – typically skipping two meals in a row.
Those who fasted, on average, for a day a month over the past 40 years were not less likely to get COVID, but they were less likely to be hospitalized or die from the virus.
“Intermittent fasting has already shown to lower inflammation and improve cardiovascular health,” lead study author Benjamin Horne, PhD, of Intermountain Medical Center Heart Institute in Salt Lake City, said in a statement.
“In this study, we’re finding additional benefits when it comes to battling an infection of COVID-19 in patients who have been fasting for decades,” he said.
The study was published in BMJ Nutrition, Prevention & Health.
Intermittent fasting not a substitute for a COVID-19 vaccine
Importantly, intermittent fasting shouldn’t be seen as a substitute for getting a COVID vaccine, the researchers stressed. Rather, periodic fasting might be a health habit to consider, since it is also linked to a lower risk of diabetes and heart disease, for example.
But anyone who wants to consider intermittent fasting should consult their doctor first, Dr. Horne stressed, especially if they are elderly, pregnant, or have diabetes, heart disease, or kidney disease.
Fasting didn’t prevent COVID-19 but made it less severe
In their study, the team looked at data from 1,524 adults who were seen in the cardiac catheterization lab at Intermountain Medical Center Heart Institute, completed a survey, and had a test for the virus that causes COVID-19 from March 16, 2020, to Feb. 25, 2021.
Of these patients, 205 tested positive for COVID, and of these, 73 reported that they had fasted regularly at least once a month.
Similar numbers of patients got COVID-19 whether they had, or had not, fasted regularly (14%, versus 13%).
But among those who tested positive for the virus, fewer patients were hospitalized for COVID or died during the study follow-up if they had fasted regularly (11%) than if they had not fasted regularly (29%).
Even when the analyses were adjusted for age, smoking, alcohol use, ethnicity, history of heart disease, and other factors, periodic fasting was still an independent predictor of a lower risk of hospitalization or death.
Several things may explain the findings, the researchers suggested.
A loss of appetite is a typical response to infection, they noted.
Fasting reduces inflammation, and after 12-14 hours of fasting, the body switches from using glucose in the blood to using ketones, including linoleic acid.
“There’s a pocket on the surface of SARS-CoV-2 that linoleic acid fits into – and can make the virus less able to attach to other cells,” Dr. Horne said.
Intermittent fasting also promotes autophagy, he noted, which is “the body’s recycling system that helps your body destroy and recycle damaged and infected cells.”
The researchers concluded that intermittent fasting plans should be investigated in further research “as a complementary therapy to vaccines to reduce COVID-19 severity, both during the pandemic and post pandemic, since repeat vaccinations cannot be performed every few months indefinitely for the entire world and vaccine access is limited in many nations.”
A version of this article first appeared on WebMD.com.
, according to the findings of a new study.
The study was done on men and women in Utah who were, on average, in their 60s and got COVID before vaccines were available.
Roughly one in three people in Utah fast from time to time – higher than in other states. This is partly because more than 60% of people in Utah belong to the Church of Jesus Christ of Latter-day Saints, and roughly 40% of them fast – typically skipping two meals in a row.
Those who fasted, on average, for a day a month over the past 40 years were not less likely to get COVID, but they were less likely to be hospitalized or die from the virus.
“Intermittent fasting has already shown to lower inflammation and improve cardiovascular health,” lead study author Benjamin Horne, PhD, of Intermountain Medical Center Heart Institute in Salt Lake City, said in a statement.
“In this study, we’re finding additional benefits when it comes to battling an infection of COVID-19 in patients who have been fasting for decades,” he said.
The study was published in BMJ Nutrition, Prevention & Health.
Intermittent fasting not a substitute for a COVID-19 vaccine
Importantly, intermittent fasting shouldn’t be seen as a substitute for getting a COVID vaccine, the researchers stressed. Rather, periodic fasting might be a health habit to consider, since it is also linked to a lower risk of diabetes and heart disease, for example.
But anyone who wants to consider intermittent fasting should consult their doctor first, Dr. Horne stressed, especially if they are elderly, pregnant, or have diabetes, heart disease, or kidney disease.
Fasting didn’t prevent COVID-19 but made it less severe
In their study, the team looked at data from 1,524 adults who were seen in the cardiac catheterization lab at Intermountain Medical Center Heart Institute, completed a survey, and had a test for the virus that causes COVID-19 from March 16, 2020, to Feb. 25, 2021.
Of these patients, 205 tested positive for COVID, and of these, 73 reported that they had fasted regularly at least once a month.
Similar numbers of patients got COVID-19 whether they had, or had not, fasted regularly (14%, versus 13%).
But among those who tested positive for the virus, fewer patients were hospitalized for COVID or died during the study follow-up if they had fasted regularly (11%) than if they had not fasted regularly (29%).
Even when the analyses were adjusted for age, smoking, alcohol use, ethnicity, history of heart disease, and other factors, periodic fasting was still an independent predictor of a lower risk of hospitalization or death.
Several things may explain the findings, the researchers suggested.
A loss of appetite is a typical response to infection, they noted.
Fasting reduces inflammation, and after 12-14 hours of fasting, the body switches from using glucose in the blood to using ketones, including linoleic acid.
“There’s a pocket on the surface of SARS-CoV-2 that linoleic acid fits into – and can make the virus less able to attach to other cells,” Dr. Horne said.
Intermittent fasting also promotes autophagy, he noted, which is “the body’s recycling system that helps your body destroy and recycle damaged and infected cells.”
The researchers concluded that intermittent fasting plans should be investigated in further research “as a complementary therapy to vaccines to reduce COVID-19 severity, both during the pandemic and post pandemic, since repeat vaccinations cannot be performed every few months indefinitely for the entire world and vaccine access is limited in many nations.”
A version of this article first appeared on WebMD.com.
FROM BMJ NUTRITION, PREVENTION & HEALTH
Dermatologist arrested for allegedly poisoning radiologist husband
It is a story that has quickly gone viral around the world:
Yue Yu, MD, aged 45, was booked into the Orange County Jail on Aug. 4, after Irvine Police had been called to her residence that day by her husband, Jack Chen, MD, 53, a radiologist. Dr. Chen provided the police with video evidence that he said showed Dr. Yu pouring a drain-opening chemical into his hot lemonade drink.
“The victim sustained significant internal injuries but is expected to recover,” the Irvine police department said in a statement.
Dr. Yu was released after paying a $30,000 bond and has not been formally charged, according to the New York Post.
In a statement to the court on Aug. 5, Dr. Chen said he and the couple’s two children had long suffered verbal abuse from his wife and her mother, according to the Post. Multiple news organizations reported that Dr. Chen filed for divorce and also for a restraining order against Dr. Yu on that day.
After feeling ill for months – and being diagnosed with ulcers and esophageal inflammation – Dr. Chen reportedly set up video cameras in the couple’s house. He said he caught Dr. Yu on camera pouring something into his drink on several occasions in July.
According to NBC News, Dr. Yu’s attorney, David E. Wohl, said that Dr. Yu “vehemently and unequivocally denies ever attempting to poison her husband or anyone else.”
Dr. Yu received her medical degree from Washington University in St. Louis in 2006 and has no disciplinary actions against her, according to the Medical Board of California. She was head of dermatology at Mission Heritage Medical Group, but her name and information have been scrubbed from that group’s website. Mission Heritage is affiliated with Providence Mission Hospital. A spokesperson for the hospital told NBC News that it is cooperating with the police investigation and that no patients are in danger.
The dermatologist is due to report back to court in November, NBC News said.
A version of this article first appeared on Medscape.com.
It is a story that has quickly gone viral around the world:
Yue Yu, MD, aged 45, was booked into the Orange County Jail on Aug. 4, after Irvine Police had been called to her residence that day by her husband, Jack Chen, MD, 53, a radiologist. Dr. Chen provided the police with video evidence that he said showed Dr. Yu pouring a drain-opening chemical into his hot lemonade drink.
“The victim sustained significant internal injuries but is expected to recover,” the Irvine police department said in a statement.
Dr. Yu was released after paying a $30,000 bond and has not been formally charged, according to the New York Post.
In a statement to the court on Aug. 5, Dr. Chen said he and the couple’s two children had long suffered verbal abuse from his wife and her mother, according to the Post. Multiple news organizations reported that Dr. Chen filed for divorce and also for a restraining order against Dr. Yu on that day.
After feeling ill for months – and being diagnosed with ulcers and esophageal inflammation – Dr. Chen reportedly set up video cameras in the couple’s house. He said he caught Dr. Yu on camera pouring something into his drink on several occasions in July.
According to NBC News, Dr. Yu’s attorney, David E. Wohl, said that Dr. Yu “vehemently and unequivocally denies ever attempting to poison her husband or anyone else.”
Dr. Yu received her medical degree from Washington University in St. Louis in 2006 and has no disciplinary actions against her, according to the Medical Board of California. She was head of dermatology at Mission Heritage Medical Group, but her name and information have been scrubbed from that group’s website. Mission Heritage is affiliated with Providence Mission Hospital. A spokesperson for the hospital told NBC News that it is cooperating with the police investigation and that no patients are in danger.
The dermatologist is due to report back to court in November, NBC News said.
A version of this article first appeared on Medscape.com.
It is a story that has quickly gone viral around the world:
Yue Yu, MD, aged 45, was booked into the Orange County Jail on Aug. 4, after Irvine Police had been called to her residence that day by her husband, Jack Chen, MD, 53, a radiologist. Dr. Chen provided the police with video evidence that he said showed Dr. Yu pouring a drain-opening chemical into his hot lemonade drink.
“The victim sustained significant internal injuries but is expected to recover,” the Irvine police department said in a statement.
Dr. Yu was released after paying a $30,000 bond and has not been formally charged, according to the New York Post.
In a statement to the court on Aug. 5, Dr. Chen said he and the couple’s two children had long suffered verbal abuse from his wife and her mother, according to the Post. Multiple news organizations reported that Dr. Chen filed for divorce and also for a restraining order against Dr. Yu on that day.
After feeling ill for months – and being diagnosed with ulcers and esophageal inflammation – Dr. Chen reportedly set up video cameras in the couple’s house. He said he caught Dr. Yu on camera pouring something into his drink on several occasions in July.
According to NBC News, Dr. Yu’s attorney, David E. Wohl, said that Dr. Yu “vehemently and unequivocally denies ever attempting to poison her husband or anyone else.”
Dr. Yu received her medical degree from Washington University in St. Louis in 2006 and has no disciplinary actions against her, according to the Medical Board of California. She was head of dermatology at Mission Heritage Medical Group, but her name and information have been scrubbed from that group’s website. Mission Heritage is affiliated with Providence Mission Hospital. A spokesperson for the hospital told NBC News that it is cooperating with the police investigation and that no patients are in danger.
The dermatologist is due to report back to court in November, NBC News said.
A version of this article first appeared on Medscape.com.
Long COVID’s grip will likely tighten as infections continue
COVID-19 is far from done in the United States, with more than 111,000 new cases being recorded a day in the second week of August, according to Johns Hopkins University, and 625 deaths being reported every day. , a condition that already has affected between 7.7 million and 23 million Americans, according to U.S. government estimates.
“It is evident that long COVID is real, that it already impacts a substantial number of people, and that this number may continue to grow as new infections occur,” the U.S. Department of Health and Human Services (HHS) said in a research action plan released Aug. 4.
“We are heading towards a big problem on our hands,” says Ziyad Al-Aly, MD, chief of research and development at the Veterans Affairs Hospital in St. Louis. “It’s like if we are falling in a plane, hurtling towards the ground. It doesn’t matter at what speed we are falling; what matters is that we are all falling, and falling fast. It’s a real problem. We needed to bring attention to this, yesterday,” he said.
Bryan Lau, PhD, professor of epidemiology at Johns Hopkins Bloomberg School of Public Health, Baltimore, and co-lead of a long COVID study there, says whether it’s 5% of the 92 million officially recorded U.S. COVID-19 cases, or 30% – on the higher end of estimates – that means anywhere between 4.5 million and 27 million Americans will have the effects of long COVID.
Other experts put the estimates even higher.
“If we conservatively assume 100 million working-age adults have been infected, that implies 10 to 33 million may have long COVID,” Alice Burns, PhD, associate director for the Kaiser Family Foundation’s Program on Medicaid and the Uninsured, wrote in an analysis.
And even the Centers for Disease Control and Prevention says only a fraction of cases have been recorded.
That, in turn, means tens of millions of people who struggle to work, to get to school, and to take care of their families – and who will be making demands on an already stressed U.S. health care system.
The HHS said in its Aug. 4 report that long COVID could keep 1 million people a day out of work, with a loss of $50 billion in annual pay.
Dr. Lau said health workers and policymakers are woefully unprepared.
“If you have a family unit, and the mom or dad can’t work, or has trouble taking their child to activities, where does the question of support come into play? Where is there potential for food issues, or housing issues?” he asked. “I see the potential for the burden to be extremely large in that capacity.”
Dr. Lau said he has yet to see any strong estimates of how many cases of long COVID might develop. Because a person has to get COVID-19 to ultimately get long COVID, the two are linked. In other words, as COVID-19 cases rise, so will cases of long COVID, and vice versa.
Evidence from the Kaiser Family Foundation analysis suggests a significant impact on employment: Surveys showed more than half of adults with long COVID who worked before becoming infected are either out of work or working fewer hours. Conditions associated with long COVID – such as fatigue, malaise, or problems concentrating – limit people’s ability to work, even if they have jobs that allow for accommodations.
Two surveys of people with long COVID who had worked before becoming infected showed that between 22% and 27% of them were out of work after getting long COVID. In comparison, among all working-age adults in 2019, only 7% were out of work. Given the sheer number of working-age adults with long COVID, the effects on employment may be profound and are likely to involve more people over time. One study estimates that long COVID already accounts for 15% of unfilled jobs.
The most severe symptoms of long COVID include brain fog and heart complications, known to persist for weeks for months after a COVID-19 infection.
A study from the University of Norway published in Open Forum Infectious Diseases found 53% of people tested had at least one symptom of thinking problems 13 months after infection with COVID-19. According to the HHS’ latest report on long COVID, people with thinking problems, heart conditions, mobility issues, and other symptoms are going to need a considerable amount of care. Many will need lengthy periods of rehabilitation.
Dr. Al-Aly worries that long COVID has already severely affected the labor force and the job market, all while burdening the country’s health care system.
“While there are variations in how individuals respond and cope with long COVID, the unifying thread is that with the level of disability it causes, more people will be struggling to keep up with the demands of the workforce and more people will be out on disability than ever before,” he said.
Studies from Johns Hopkins and the University of Washington estimate that 5%-30% of people could get long COVID in the future. Projections beyond that are hazy.
“So far, all the studies we have done on long COVID have been reactionary. Much of the activism around long COVID has been patient led. We are seeing more and more people with lasting symptoms. We need our research to catch up,” Dr. Lau said.
Theo Vos, MD, PhD, professor of health sciences at University of Washington, Seattle, said the main reasons for the huge range of predictions are the variety of methods used, as well as differences in sample size. Also, much long COVID data is self-reported, making it difficult for epidemiologists to track.
“With self-reported data, you can’t plug people into a machine and say this is what they have or this is what they don’t have. At the population level, the only thing you can do is ask questions. There is no systematic way to define long COVID,” he said.
Dr. Vos’s most recent study, which is being peer-reviewed and revised, found that most people with long COVID have symptoms similar to those seen in other autoimmune diseases. But sometimes the immune system can overreact, causing the more severe symptoms, such as brain fog and heart problems, associated with long COVID.
One reason that researchers struggle to come up with numbers, said Dr. Al-Aly, is the rapid rise of new variants. These variants appear to sometimes cause less severe disease than previous ones, but it’s not clear whether that means different risks for long COVID.
“There’s a wide diversity in severity. Someone can have long COVID and be fully functional, while others are not functional at all. We still have a long way to go before we figure out why,” Dr. Lau said.
A version of this article first appeared on WebMD.com.
COVID-19 is far from done in the United States, with more than 111,000 new cases being recorded a day in the second week of August, according to Johns Hopkins University, and 625 deaths being reported every day. , a condition that already has affected between 7.7 million and 23 million Americans, according to U.S. government estimates.
“It is evident that long COVID is real, that it already impacts a substantial number of people, and that this number may continue to grow as new infections occur,” the U.S. Department of Health and Human Services (HHS) said in a research action plan released Aug. 4.
“We are heading towards a big problem on our hands,” says Ziyad Al-Aly, MD, chief of research and development at the Veterans Affairs Hospital in St. Louis. “It’s like if we are falling in a plane, hurtling towards the ground. It doesn’t matter at what speed we are falling; what matters is that we are all falling, and falling fast. It’s a real problem. We needed to bring attention to this, yesterday,” he said.
Bryan Lau, PhD, professor of epidemiology at Johns Hopkins Bloomberg School of Public Health, Baltimore, and co-lead of a long COVID study there, says whether it’s 5% of the 92 million officially recorded U.S. COVID-19 cases, or 30% – on the higher end of estimates – that means anywhere between 4.5 million and 27 million Americans will have the effects of long COVID.
Other experts put the estimates even higher.
“If we conservatively assume 100 million working-age adults have been infected, that implies 10 to 33 million may have long COVID,” Alice Burns, PhD, associate director for the Kaiser Family Foundation’s Program on Medicaid and the Uninsured, wrote in an analysis.
And even the Centers for Disease Control and Prevention says only a fraction of cases have been recorded.
That, in turn, means tens of millions of people who struggle to work, to get to school, and to take care of their families – and who will be making demands on an already stressed U.S. health care system.
The HHS said in its Aug. 4 report that long COVID could keep 1 million people a day out of work, with a loss of $50 billion in annual pay.
Dr. Lau said health workers and policymakers are woefully unprepared.
“If you have a family unit, and the mom or dad can’t work, or has trouble taking their child to activities, where does the question of support come into play? Where is there potential for food issues, or housing issues?” he asked. “I see the potential for the burden to be extremely large in that capacity.”
Dr. Lau said he has yet to see any strong estimates of how many cases of long COVID might develop. Because a person has to get COVID-19 to ultimately get long COVID, the two are linked. In other words, as COVID-19 cases rise, so will cases of long COVID, and vice versa.
Evidence from the Kaiser Family Foundation analysis suggests a significant impact on employment: Surveys showed more than half of adults with long COVID who worked before becoming infected are either out of work or working fewer hours. Conditions associated with long COVID – such as fatigue, malaise, or problems concentrating – limit people’s ability to work, even if they have jobs that allow for accommodations.
Two surveys of people with long COVID who had worked before becoming infected showed that between 22% and 27% of them were out of work after getting long COVID. In comparison, among all working-age adults in 2019, only 7% were out of work. Given the sheer number of working-age adults with long COVID, the effects on employment may be profound and are likely to involve more people over time. One study estimates that long COVID already accounts for 15% of unfilled jobs.
The most severe symptoms of long COVID include brain fog and heart complications, known to persist for weeks for months after a COVID-19 infection.
A study from the University of Norway published in Open Forum Infectious Diseases found 53% of people tested had at least one symptom of thinking problems 13 months after infection with COVID-19. According to the HHS’ latest report on long COVID, people with thinking problems, heart conditions, mobility issues, and other symptoms are going to need a considerable amount of care. Many will need lengthy periods of rehabilitation.
Dr. Al-Aly worries that long COVID has already severely affected the labor force and the job market, all while burdening the country’s health care system.
“While there are variations in how individuals respond and cope with long COVID, the unifying thread is that with the level of disability it causes, more people will be struggling to keep up with the demands of the workforce and more people will be out on disability than ever before,” he said.
Studies from Johns Hopkins and the University of Washington estimate that 5%-30% of people could get long COVID in the future. Projections beyond that are hazy.
“So far, all the studies we have done on long COVID have been reactionary. Much of the activism around long COVID has been patient led. We are seeing more and more people with lasting symptoms. We need our research to catch up,” Dr. Lau said.
Theo Vos, MD, PhD, professor of health sciences at University of Washington, Seattle, said the main reasons for the huge range of predictions are the variety of methods used, as well as differences in sample size. Also, much long COVID data is self-reported, making it difficult for epidemiologists to track.
“With self-reported data, you can’t plug people into a machine and say this is what they have or this is what they don’t have. At the population level, the only thing you can do is ask questions. There is no systematic way to define long COVID,” he said.
Dr. Vos’s most recent study, which is being peer-reviewed and revised, found that most people with long COVID have symptoms similar to those seen in other autoimmune diseases. But sometimes the immune system can overreact, causing the more severe symptoms, such as brain fog and heart problems, associated with long COVID.
One reason that researchers struggle to come up with numbers, said Dr. Al-Aly, is the rapid rise of new variants. These variants appear to sometimes cause less severe disease than previous ones, but it’s not clear whether that means different risks for long COVID.
“There’s a wide diversity in severity. Someone can have long COVID and be fully functional, while others are not functional at all. We still have a long way to go before we figure out why,” Dr. Lau said.
A version of this article first appeared on WebMD.com.
COVID-19 is far from done in the United States, with more than 111,000 new cases being recorded a day in the second week of August, according to Johns Hopkins University, and 625 deaths being reported every day. , a condition that already has affected between 7.7 million and 23 million Americans, according to U.S. government estimates.
“It is evident that long COVID is real, that it already impacts a substantial number of people, and that this number may continue to grow as new infections occur,” the U.S. Department of Health and Human Services (HHS) said in a research action plan released Aug. 4.
“We are heading towards a big problem on our hands,” says Ziyad Al-Aly, MD, chief of research and development at the Veterans Affairs Hospital in St. Louis. “It’s like if we are falling in a plane, hurtling towards the ground. It doesn’t matter at what speed we are falling; what matters is that we are all falling, and falling fast. It’s a real problem. We needed to bring attention to this, yesterday,” he said.
Bryan Lau, PhD, professor of epidemiology at Johns Hopkins Bloomberg School of Public Health, Baltimore, and co-lead of a long COVID study there, says whether it’s 5% of the 92 million officially recorded U.S. COVID-19 cases, or 30% – on the higher end of estimates – that means anywhere between 4.5 million and 27 million Americans will have the effects of long COVID.
Other experts put the estimates even higher.
“If we conservatively assume 100 million working-age adults have been infected, that implies 10 to 33 million may have long COVID,” Alice Burns, PhD, associate director for the Kaiser Family Foundation’s Program on Medicaid and the Uninsured, wrote in an analysis.
And even the Centers for Disease Control and Prevention says only a fraction of cases have been recorded.
That, in turn, means tens of millions of people who struggle to work, to get to school, and to take care of their families – and who will be making demands on an already stressed U.S. health care system.
The HHS said in its Aug. 4 report that long COVID could keep 1 million people a day out of work, with a loss of $50 billion in annual pay.
Dr. Lau said health workers and policymakers are woefully unprepared.
“If you have a family unit, and the mom or dad can’t work, or has trouble taking their child to activities, where does the question of support come into play? Where is there potential for food issues, or housing issues?” he asked. “I see the potential for the burden to be extremely large in that capacity.”
Dr. Lau said he has yet to see any strong estimates of how many cases of long COVID might develop. Because a person has to get COVID-19 to ultimately get long COVID, the two are linked. In other words, as COVID-19 cases rise, so will cases of long COVID, and vice versa.
Evidence from the Kaiser Family Foundation analysis suggests a significant impact on employment: Surveys showed more than half of adults with long COVID who worked before becoming infected are either out of work or working fewer hours. Conditions associated with long COVID – such as fatigue, malaise, or problems concentrating – limit people’s ability to work, even if they have jobs that allow for accommodations.
Two surveys of people with long COVID who had worked before becoming infected showed that between 22% and 27% of them were out of work after getting long COVID. In comparison, among all working-age adults in 2019, only 7% were out of work. Given the sheer number of working-age adults with long COVID, the effects on employment may be profound and are likely to involve more people over time. One study estimates that long COVID already accounts for 15% of unfilled jobs.
The most severe symptoms of long COVID include brain fog and heart complications, known to persist for weeks for months after a COVID-19 infection.
A study from the University of Norway published in Open Forum Infectious Diseases found 53% of people tested had at least one symptom of thinking problems 13 months after infection with COVID-19. According to the HHS’ latest report on long COVID, people with thinking problems, heart conditions, mobility issues, and other symptoms are going to need a considerable amount of care. Many will need lengthy periods of rehabilitation.
Dr. Al-Aly worries that long COVID has already severely affected the labor force and the job market, all while burdening the country’s health care system.
“While there are variations in how individuals respond and cope with long COVID, the unifying thread is that with the level of disability it causes, more people will be struggling to keep up with the demands of the workforce and more people will be out on disability than ever before,” he said.
Studies from Johns Hopkins and the University of Washington estimate that 5%-30% of people could get long COVID in the future. Projections beyond that are hazy.
“So far, all the studies we have done on long COVID have been reactionary. Much of the activism around long COVID has been patient led. We are seeing more and more people with lasting symptoms. We need our research to catch up,” Dr. Lau said.
Theo Vos, MD, PhD, professor of health sciences at University of Washington, Seattle, said the main reasons for the huge range of predictions are the variety of methods used, as well as differences in sample size. Also, much long COVID data is self-reported, making it difficult for epidemiologists to track.
“With self-reported data, you can’t plug people into a machine and say this is what they have or this is what they don’t have. At the population level, the only thing you can do is ask questions. There is no systematic way to define long COVID,” he said.
Dr. Vos’s most recent study, which is being peer-reviewed and revised, found that most people with long COVID have symptoms similar to those seen in other autoimmune diseases. But sometimes the immune system can overreact, causing the more severe symptoms, such as brain fog and heart problems, associated with long COVID.
One reason that researchers struggle to come up with numbers, said Dr. Al-Aly, is the rapid rise of new variants. These variants appear to sometimes cause less severe disease than previous ones, but it’s not clear whether that means different risks for long COVID.
“There’s a wide diversity in severity. Someone can have long COVID and be fully functional, while others are not functional at all. We still have a long way to go before we figure out why,” Dr. Lau said.
A version of this article first appeared on WebMD.com.
Federal Health Care Data Trends 2022: Hearing, Vision, and Balance
- Lucas JW, Zelaya CE. Hearing difficulty, vision trouble, and balance problems among male veterans and nonveterans. Natl Health Stat Report. 2020;(142):1-8. Accessed March 30, 2020. https://www.cdc.gov/nchs/data/nhsr/nhsr142-508.pdf
- Shrauner W, Lord EM, Nguyen XMT, et al. Frailty and cardiovascular mortality in more than 3 million US veterans. Eur Heart J. 2022;43(8):818-826. https://doi.org/10.1093/eurheartj/ehab850
- Defense Health Agency, Vision Center of Excellence (email, March 23, 2022).
- Frick KD, Singman EL. Cost of military eye injury and vision impairment related to traumatic brain injury: 2001–2017. Mil Med. 2019;184(5-6):e338. http://doi.org/10.1093/milmed/usy420
- Hussain SF, Raza Z, Cash ATG, et al. Traumatic brain injury and sight loss in military and veteran populations – a review. Mil Med Res. 2021;8(1):42. http://doi.org/10.1186/s40779-021-00334-3
- Lucas JW, Zelaya CE. Hearing difficulty, vision trouble, and balance problems among male veterans and nonveterans. Natl Health Stat Report. 2020;(142):1-8. Accessed March 30, 2020. https://www.cdc.gov/nchs/data/nhsr/nhsr142-508.pdf
- Shrauner W, Lord EM, Nguyen XMT, et al. Frailty and cardiovascular mortality in more than 3 million US veterans. Eur Heart J. 2022;43(8):818-826. https://doi.org/10.1093/eurheartj/ehab850
- Defense Health Agency, Vision Center of Excellence (email, March 23, 2022).
- Frick KD, Singman EL. Cost of military eye injury and vision impairment related to traumatic brain injury: 2001–2017. Mil Med. 2019;184(5-6):e338. http://doi.org/10.1093/milmed/usy420
- Hussain SF, Raza Z, Cash ATG, et al. Traumatic brain injury and sight loss in military and veteran populations – a review. Mil Med Res. 2021;8(1):42. http://doi.org/10.1186/s40779-021-00334-3
- Lucas JW, Zelaya CE. Hearing difficulty, vision trouble, and balance problems among male veterans and nonveterans. Natl Health Stat Report. 2020;(142):1-8. Accessed March 30, 2020. https://www.cdc.gov/nchs/data/nhsr/nhsr142-508.pdf
- Shrauner W, Lord EM, Nguyen XMT, et al. Frailty and cardiovascular mortality in more than 3 million US veterans. Eur Heart J. 2022;43(8):818-826. https://doi.org/10.1093/eurheartj/ehab850
- Defense Health Agency, Vision Center of Excellence (email, March 23, 2022).
- Frick KD, Singman EL. Cost of military eye injury and vision impairment related to traumatic brain injury: 2001–2017. Mil Med. 2019;184(5-6):e338. http://doi.org/10.1093/milmed/usy420
- Hussain SF, Raza Z, Cash ATG, et al. Traumatic brain injury and sight loss in military and veteran populations – a review. Mil Med Res. 2021;8(1):42. http://doi.org/10.1186/s40779-021-00334-3
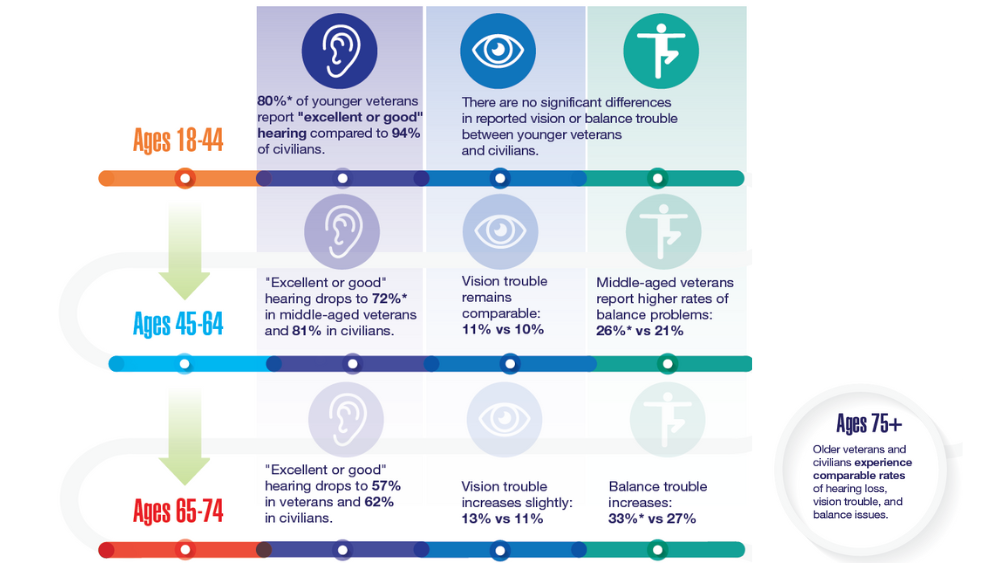



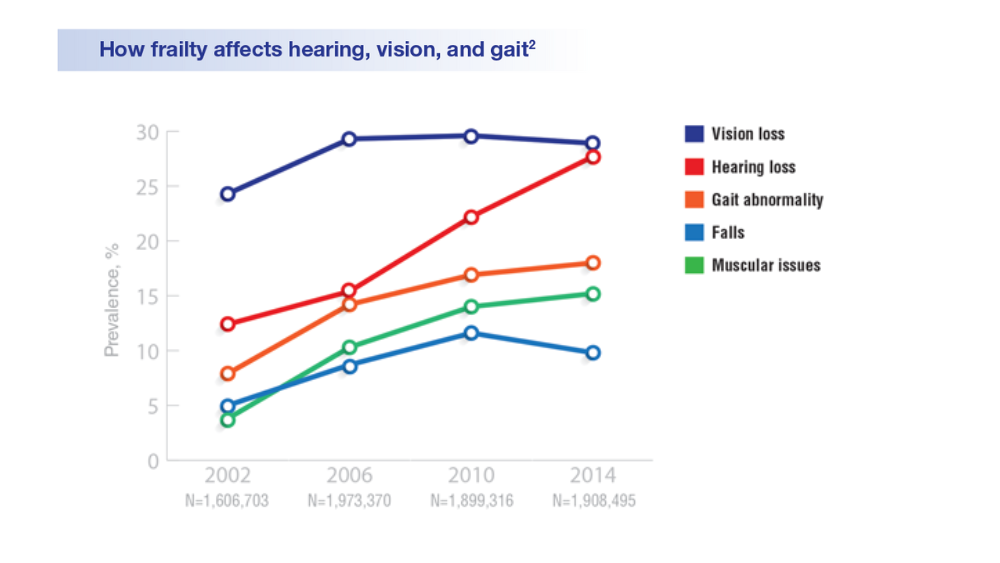
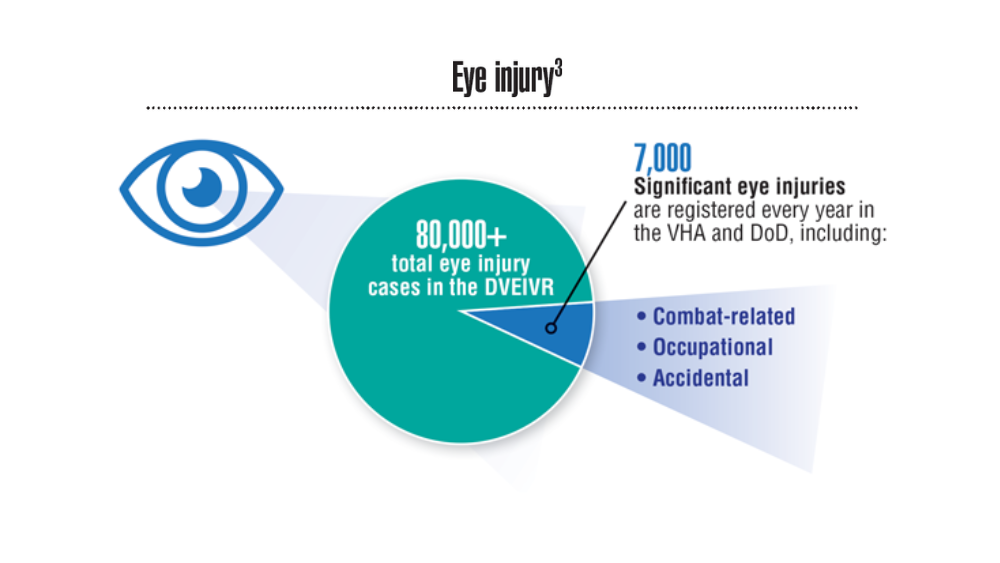

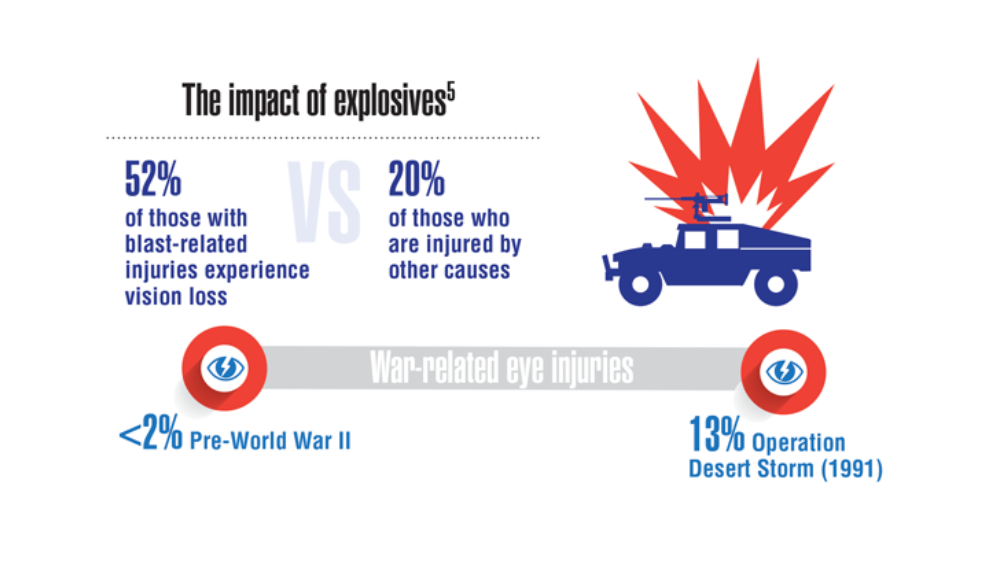
‘Shocking’ and persistent gap in treatment for opioid addiction
The vast majority of Americans with opioid use disorder (OUD) do not receive potentially lifesaving medications.
Drugs such as methadone, buprenorphine, and extended-release naltrexone have been shown to reduce opioid overdoses by more than 50%. Yet a new analysis shows that only about 1 in 10 people living with OUD receive these medications.
“Even though it’s not especially surprising, it’s still disturbing and shocking in a way that we have just made such little progress on this huge issue,” study investigator Noa Krawczyk, PhD, with the Center for Opioid Epidemiology and Policy, department of population health, NYU Langone, told this news organization.

The study was published online in the International Journal of Drug Policy.
Increased urgency
Despite efforts to increase capacity for OUD treatment in the United States, how receipt of treatment compares to need for treatment remains unclear.
Dr. Krawczyk and colleagues examined the gap between new estimates of OUD prevalence and treatment at the national and state levels from 2010 through 2019.
“,” the investigators write.
Adjusted estimates suggest that past-year OUD affected roughly 7.63 million individuals in the United States (2,773 per 100,000), yet only about 1.02 million received medication (365 per 100,000), they note.
Overall, there was a 106% increase in receipt of medications for OUD across the United States from 2010 to 2019 and a 5% increase from 2018 to 2019.
Yet, as of 2019, 87% of people with OUD were not receiving medication.
“While the number of people getting treatment doubled over the last decade, it’s nowhere near the amount of people who are still struggling with an opioid use disorder, and the urgency of the problem has become much worse because of the worsening fentanyl crisis and the lethality of the drug supply,” said Dr. Krawczyk.
The study also showed wide variation in past-year OUD prevalence and treatment across the United States.
Past-year OUD rates were highest in Washington, D.C., and lowest in Minnesota. Receipt of treatment was lowest in South Dakota and highest in Vermont.
However, in all 50 states and Washington, D.C., past-year OUD prevalence was greater than rates of medication use. As of 2019, the largest treatment gaps were in Iowa, North Dakota, and Washington, D.C. The smallest treatment gaps were in Connecticut, Maryland, and Rhode Island.
Long road ahead
“Even in states with the smallest treatment gaps, at least 50% of people who could benefit from medications for opioid use disorder are still not receiving them,” senior author Magdalena Cerdá, DrPH, director of the Center for Opioid Epidemiology and Policy in the department of population health at NYU Langone Health, said in a statement.
“We have a long way to go in reducing stigma surrounding treatment and in devising the types of policies and programs we need to ensure these medications reach the people who need them the most,” Dr. Cerdá added.
Access to OUD treatment is an ongoing problem in the United States.
“A lot of areas don’t have specialty treatment programs that provide methadone, or they might not have addiction-trained providers who are willing to prescribe buprenorphine or have a waiver to prescribe buprenorphine, so a lot places are really struggling with where people can get treatment,” said Dr. Krawczyk.
Recent data show that 46% of counties lack an OUD medication provider, and 32% have no specialty programs to treat substance use disorders.
Dr. Krawczyk and colleagues note that COVID-19–related policy changes and recently proposed legislation to allow more flexible and convenient access to OUD treatment may be a first step toward expanding access to this lifesaving treatment.
But improving initial access to medication for OUD is “only the first step – our research and health systems have a long way to go in addressing the needs of people with OUD to support retention in treatment and services to effectively reduce overdose and improve long-term health and well-being,” the researchers write.
The study was supported by the NYU Center for Epidemiology and Policy. Dr. Krawczyk has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The vast majority of Americans with opioid use disorder (OUD) do not receive potentially lifesaving medications.
Drugs such as methadone, buprenorphine, and extended-release naltrexone have been shown to reduce opioid overdoses by more than 50%. Yet a new analysis shows that only about 1 in 10 people living with OUD receive these medications.
“Even though it’s not especially surprising, it’s still disturbing and shocking in a way that we have just made such little progress on this huge issue,” study investigator Noa Krawczyk, PhD, with the Center for Opioid Epidemiology and Policy, department of population health, NYU Langone, told this news organization.
The study was published online in the International Journal of Drug Policy.
Increased urgency
Despite efforts to increase capacity for OUD treatment in the United States, how receipt of treatment compares to need for treatment remains unclear.
Dr. Krawczyk and colleagues examined the gap between new estimates of OUD prevalence and treatment at the national and state levels from 2010 through 2019.
“,” the investigators write.
Adjusted estimates suggest that past-year OUD affected roughly 7.63 million individuals in the United States (2,773 per 100,000), yet only about 1.02 million received medication (365 per 100,000), they note.
Overall, there was a 106% increase in receipt of medications for OUD across the United States from 2010 to 2019 and a 5% increase from 2018 to 2019.
Yet, as of 2019, 87% of people with OUD were not receiving medication.
“While the number of people getting treatment doubled over the last decade, it’s nowhere near the amount of people who are still struggling with an opioid use disorder, and the urgency of the problem has become much worse because of the worsening fentanyl crisis and the lethality of the drug supply,” said Dr. Krawczyk.
The study also showed wide variation in past-year OUD prevalence and treatment across the United States.
Past-year OUD rates were highest in Washington, D.C., and lowest in Minnesota. Receipt of treatment was lowest in South Dakota and highest in Vermont.
However, in all 50 states and Washington, D.C., past-year OUD prevalence was greater than rates of medication use. As of 2019, the largest treatment gaps were in Iowa, North Dakota, and Washington, D.C. The smallest treatment gaps were in Connecticut, Maryland, and Rhode Island.
Long road ahead
“Even in states with the smallest treatment gaps, at least 50% of people who could benefit from medications for opioid use disorder are still not receiving them,” senior author Magdalena Cerdá, DrPH, director of the Center for Opioid Epidemiology and Policy in the department of population health at NYU Langone Health, said in a statement.
“We have a long way to go in reducing stigma surrounding treatment and in devising the types of policies and programs we need to ensure these medications reach the people who need them the most,” Dr. Cerdá added.
Access to OUD treatment is an ongoing problem in the United States.
“A lot of areas don’t have specialty treatment programs that provide methadone, or they might not have addiction-trained providers who are willing to prescribe buprenorphine or have a waiver to prescribe buprenorphine, so a lot places are really struggling with where people can get treatment,” said Dr. Krawczyk.
Recent data show that 46% of counties lack an OUD medication provider, and 32% have no specialty programs to treat substance use disorders.
Dr. Krawczyk and colleagues note that COVID-19–related policy changes and recently proposed legislation to allow more flexible and convenient access to OUD treatment may be a first step toward expanding access to this lifesaving treatment.
But improving initial access to medication for OUD is “only the first step – our research and health systems have a long way to go in addressing the needs of people with OUD to support retention in treatment and services to effectively reduce overdose and improve long-term health and well-being,” the researchers write.
The study was supported by the NYU Center for Epidemiology and Policy. Dr. Krawczyk has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The vast majority of Americans with opioid use disorder (OUD) do not receive potentially lifesaving medications.
Drugs such as methadone, buprenorphine, and extended-release naltrexone have been shown to reduce opioid overdoses by more than 50%. Yet a new analysis shows that only about 1 in 10 people living with OUD receive these medications.
“Even though it’s not especially surprising, it’s still disturbing and shocking in a way that we have just made such little progress on this huge issue,” study investigator Noa Krawczyk, PhD, with the Center for Opioid Epidemiology and Policy, department of population health, NYU Langone, told this news organization.
The study was published online in the International Journal of Drug Policy.
Increased urgency
Despite efforts to increase capacity for OUD treatment in the United States, how receipt of treatment compares to need for treatment remains unclear.
Dr. Krawczyk and colleagues examined the gap between new estimates of OUD prevalence and treatment at the national and state levels from 2010 through 2019.
“,” the investigators write.
Adjusted estimates suggest that past-year OUD affected roughly 7.63 million individuals in the United States (2,773 per 100,000), yet only about 1.02 million received medication (365 per 100,000), they note.
Overall, there was a 106% increase in receipt of medications for OUD across the United States from 2010 to 2019 and a 5% increase from 2018 to 2019.
Yet, as of 2019, 87% of people with OUD were not receiving medication.
“While the number of people getting treatment doubled over the last decade, it’s nowhere near the amount of people who are still struggling with an opioid use disorder, and the urgency of the problem has become much worse because of the worsening fentanyl crisis and the lethality of the drug supply,” said Dr. Krawczyk.
The study also showed wide variation in past-year OUD prevalence and treatment across the United States.
Past-year OUD rates were highest in Washington, D.C., and lowest in Minnesota. Receipt of treatment was lowest in South Dakota and highest in Vermont.
However, in all 50 states and Washington, D.C., past-year OUD prevalence was greater than rates of medication use. As of 2019, the largest treatment gaps were in Iowa, North Dakota, and Washington, D.C. The smallest treatment gaps were in Connecticut, Maryland, and Rhode Island.
Long road ahead
“Even in states with the smallest treatment gaps, at least 50% of people who could benefit from medications for opioid use disorder are still not receiving them,” senior author Magdalena Cerdá, DrPH, director of the Center for Opioid Epidemiology and Policy in the department of population health at NYU Langone Health, said in a statement.
“We have a long way to go in reducing stigma surrounding treatment and in devising the types of policies and programs we need to ensure these medications reach the people who need them the most,” Dr. Cerdá added.
Access to OUD treatment is an ongoing problem in the United States.
“A lot of areas don’t have specialty treatment programs that provide methadone, or they might not have addiction-trained providers who are willing to prescribe buprenorphine or have a waiver to prescribe buprenorphine, so a lot places are really struggling with where people can get treatment,” said Dr. Krawczyk.
Recent data show that 46% of counties lack an OUD medication provider, and 32% have no specialty programs to treat substance use disorders.
Dr. Krawczyk and colleagues note that COVID-19–related policy changes and recently proposed legislation to allow more flexible and convenient access to OUD treatment may be a first step toward expanding access to this lifesaving treatment.
But improving initial access to medication for OUD is “only the first step – our research and health systems have a long way to go in addressing the needs of people with OUD to support retention in treatment and services to effectively reduce overdose and improve long-term health and well-being,” the researchers write.
The study was supported by the NYU Center for Epidemiology and Policy. Dr. Krawczyk has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE INTERNATIONAL JOURNAL OF DRUG POLICY