User login
Atezolizumab fails to improve outcomes in postsurgery kidney cancer
Adjuvant immunotherapy with atezolizumab for patients with renal cell carcinoma who have had a nephrectomy with or without a metastasectomy, failed to improve clinical outcomes in a group of patients who are at high risk of recurrence, finds a new international study conducted across 28 countries.
The study, called IMmotion010 and published in The Lancet, was a randomized, double-blind, multicenter, phase 3 trial of 778 adult patients with renal cell carcinoma (RCC) with a clear cell or sarcomatoid component. The study failed to meet its primary endpoint which was defined as a statistically significant improvement in disease-free survival as compared with placebo.
“Our results add to an emerging body of literature around the role of adjuvant immunotherapy for renal cell carcinoma. With the longest duration of follow-up to date to our knowledge. We observed no evidence of clinical benefit in disease-free survival or overall survival with adjuvant atezolizumab in patients with high-risk localized or fully resected renal cell carcinoma,” wrote the authors who were led by Sumanta Kumar Pal, MD, of City of Hope Comprehensive Cancer Center, Duarte, Calif. “Given a growing list of trials that have not shown benefit with adjuvant immunotherapy, the results call for greater attention to patient selection with this approach.”
Dr. Pal and associates conducted the study to gain more insight into the potential role of adjuvant immunotherapy in patients with renal cell carcinoma who have undergone the standard treatment of nephrectomy with or without metastasectomy. Previous studies of anti-VEGF treatments have produced mixed results, including the large phase 3 ASSURE trial, the authors wrote. “Given these mixed results, use of adjuvant targeted therapy in renal cell carcinoma remains infrequent,” Dr. Pal and associates wrote.
However, pembrolizumab (Keytruda, Merck) a programmed death receptor-1–blocking antibody, is an immunotherapy which, in combination with axitinib, is approved as a first-line treatment for patients with advanced RCC.
Atezolizumab (Tecentriq, Genentech) is approved for treatment in urothelial carcinoma, non–small cell lung cancer (NSCLC), small cell lung cancer (SCLC), hepatocellular carcinoma (HCC), and melanoma. There are currently a number of ongoing studies that are exploring the use of atezolizumab as a treatment for renal cell carcinoma.
The study details
This new study was conducted between 2017 and 2019. It included 778 patients from 215 clinics in 28 countries who were assigned to the treatment arm (1,200 mg of IV atezolizumab (n = 390, 50%) once every 3 weeks for 16 cycles or 1 year, which ever came first – or, they were assigned to the placebo group (n = 388, 50%). The two groups were similar: average age 60-61, 72%-74% male, 78%-83% white, and 36%-37% based in North America. Most patients, (92%-93%) had clear cell cancer, and 64%-65% were at pathological disease stage T2 or T3a.
The 3-year disease-free survival rate at 36 months was 65.0% (95% confidence interval, 59.9-70.2) in the treatment group and 62.7% (95% CI, 57.5-67.9) in the placebo group. At follow-up at 44.7 months, there was no statistically significant difference in median disease-free survival between atezolizumab (57.2 months; 95% CI, 44.6 to not evaluable) and placebo (49.5 months; 95% CI, 47.4 to not evaluable).
While there were no deaths attributable to treatment, 69 (18%) patients who received atezolizumab and 46 (12%) patients who received placebo experienced a serious adverse event.
“. Future work will include exploration of clinical-based or biomarker-based subsets that might derive benefit from this approach,” the authors wrote.
The researchers acknowledge their findings contrast with those of the KEYNOTE-564 trial of adjuvant immunotherapy with pembrolizumab after nephrectomy in renal cell carcinoma. KEYNOTE-564 reported a disease-free survival benefit of over 24 months and in an analysis done at 30 months. But in KEYNOTE-564, the study comprised only 6% of patients with M1 no evidence of disease. And, it included only patients with synchronous metastases or metastases resected within 1 year of nephrectomy. In the new study, 14% of patients had M1 no evidence of disease, and it included both synchronous and metachronous disease with recurrence within 1year of surgery.
Adjuvant immunotherapy with pembrolizumab is considered optional for patients with intermediate-risk or high-risk operable clear cell renal cell carcinoma per European Society for Medical Oncology and European Association of Urology guidelines because of the lack of confirmed overall survival benefit and toxicity-related considerations associated with immunotherapy.
“These factors must be considered in the adjuvant setting as, following nephrectomy, patients are cancer free and might be cured by surgery alone. As such, additional trials are needed to clarify the role of adjuvant immunotherapy in this disease space,” the authors wrote.
What’s next? “Biomarker work is underway to determine whether tumor genomic characteristics or circulating biomarkers can identify patient populations who derive benefit from adjuvant atezolizumab,” Dr. Pal and associates wrote. “There is precedent for tissue-based adjuvant therapy selection in other diseases, such as HER2-based and endocrine receptor–based approaches in breast cancer and EGFR mutation–directed therapy in lung cancer.”
The study was funded by F Hoffmann-La Roche and Genentech. The academic authors of the study collaborated with F Hoffmann-La Roche and Genentech on all facets of the trial.
Adjuvant immunotherapy with atezolizumab for patients with renal cell carcinoma who have had a nephrectomy with or without a metastasectomy, failed to improve clinical outcomes in a group of patients who are at high risk of recurrence, finds a new international study conducted across 28 countries.
The study, called IMmotion010 and published in The Lancet, was a randomized, double-blind, multicenter, phase 3 trial of 778 adult patients with renal cell carcinoma (RCC) with a clear cell or sarcomatoid component. The study failed to meet its primary endpoint which was defined as a statistically significant improvement in disease-free survival as compared with placebo.
“Our results add to an emerging body of literature around the role of adjuvant immunotherapy for renal cell carcinoma. With the longest duration of follow-up to date to our knowledge. We observed no evidence of clinical benefit in disease-free survival or overall survival with adjuvant atezolizumab in patients with high-risk localized or fully resected renal cell carcinoma,” wrote the authors who were led by Sumanta Kumar Pal, MD, of City of Hope Comprehensive Cancer Center, Duarte, Calif. “Given a growing list of trials that have not shown benefit with adjuvant immunotherapy, the results call for greater attention to patient selection with this approach.”
Dr. Pal and associates conducted the study to gain more insight into the potential role of adjuvant immunotherapy in patients with renal cell carcinoma who have undergone the standard treatment of nephrectomy with or without metastasectomy. Previous studies of anti-VEGF treatments have produced mixed results, including the large phase 3 ASSURE trial, the authors wrote. “Given these mixed results, use of adjuvant targeted therapy in renal cell carcinoma remains infrequent,” Dr. Pal and associates wrote.
However, pembrolizumab (Keytruda, Merck) a programmed death receptor-1–blocking antibody, is an immunotherapy which, in combination with axitinib, is approved as a first-line treatment for patients with advanced RCC.
Atezolizumab (Tecentriq, Genentech) is approved for treatment in urothelial carcinoma, non–small cell lung cancer (NSCLC), small cell lung cancer (SCLC), hepatocellular carcinoma (HCC), and melanoma. There are currently a number of ongoing studies that are exploring the use of atezolizumab as a treatment for renal cell carcinoma.
The study details
This new study was conducted between 2017 and 2019. It included 778 patients from 215 clinics in 28 countries who were assigned to the treatment arm (1,200 mg of IV atezolizumab (n = 390, 50%) once every 3 weeks for 16 cycles or 1 year, which ever came first – or, they were assigned to the placebo group (n = 388, 50%). The two groups were similar: average age 60-61, 72%-74% male, 78%-83% white, and 36%-37% based in North America. Most patients, (92%-93%) had clear cell cancer, and 64%-65% were at pathological disease stage T2 or T3a.
The 3-year disease-free survival rate at 36 months was 65.0% (95% confidence interval, 59.9-70.2) in the treatment group and 62.7% (95% CI, 57.5-67.9) in the placebo group. At follow-up at 44.7 months, there was no statistically significant difference in median disease-free survival between atezolizumab (57.2 months; 95% CI, 44.6 to not evaluable) and placebo (49.5 months; 95% CI, 47.4 to not evaluable).
While there were no deaths attributable to treatment, 69 (18%) patients who received atezolizumab and 46 (12%) patients who received placebo experienced a serious adverse event.
“. Future work will include exploration of clinical-based or biomarker-based subsets that might derive benefit from this approach,” the authors wrote.
The researchers acknowledge their findings contrast with those of the KEYNOTE-564 trial of adjuvant immunotherapy with pembrolizumab after nephrectomy in renal cell carcinoma. KEYNOTE-564 reported a disease-free survival benefit of over 24 months and in an analysis done at 30 months. But in KEYNOTE-564, the study comprised only 6% of patients with M1 no evidence of disease. And, it included only patients with synchronous metastases or metastases resected within 1 year of nephrectomy. In the new study, 14% of patients had M1 no evidence of disease, and it included both synchronous and metachronous disease with recurrence within 1year of surgery.
Adjuvant immunotherapy with pembrolizumab is considered optional for patients with intermediate-risk or high-risk operable clear cell renal cell carcinoma per European Society for Medical Oncology and European Association of Urology guidelines because of the lack of confirmed overall survival benefit and toxicity-related considerations associated with immunotherapy.
“These factors must be considered in the adjuvant setting as, following nephrectomy, patients are cancer free and might be cured by surgery alone. As such, additional trials are needed to clarify the role of adjuvant immunotherapy in this disease space,” the authors wrote.
What’s next? “Biomarker work is underway to determine whether tumor genomic characteristics or circulating biomarkers can identify patient populations who derive benefit from adjuvant atezolizumab,” Dr. Pal and associates wrote. “There is precedent for tissue-based adjuvant therapy selection in other diseases, such as HER2-based and endocrine receptor–based approaches in breast cancer and EGFR mutation–directed therapy in lung cancer.”
The study was funded by F Hoffmann-La Roche and Genentech. The academic authors of the study collaborated with F Hoffmann-La Roche and Genentech on all facets of the trial.
Adjuvant immunotherapy with atezolizumab for patients with renal cell carcinoma who have had a nephrectomy with or without a metastasectomy, failed to improve clinical outcomes in a group of patients who are at high risk of recurrence, finds a new international study conducted across 28 countries.
The study, called IMmotion010 and published in The Lancet, was a randomized, double-blind, multicenter, phase 3 trial of 778 adult patients with renal cell carcinoma (RCC) with a clear cell or sarcomatoid component. The study failed to meet its primary endpoint which was defined as a statistically significant improvement in disease-free survival as compared with placebo.
“Our results add to an emerging body of literature around the role of adjuvant immunotherapy for renal cell carcinoma. With the longest duration of follow-up to date to our knowledge. We observed no evidence of clinical benefit in disease-free survival or overall survival with adjuvant atezolizumab in patients with high-risk localized or fully resected renal cell carcinoma,” wrote the authors who were led by Sumanta Kumar Pal, MD, of City of Hope Comprehensive Cancer Center, Duarte, Calif. “Given a growing list of trials that have not shown benefit with adjuvant immunotherapy, the results call for greater attention to patient selection with this approach.”
Dr. Pal and associates conducted the study to gain more insight into the potential role of adjuvant immunotherapy in patients with renal cell carcinoma who have undergone the standard treatment of nephrectomy with or without metastasectomy. Previous studies of anti-VEGF treatments have produced mixed results, including the large phase 3 ASSURE trial, the authors wrote. “Given these mixed results, use of adjuvant targeted therapy in renal cell carcinoma remains infrequent,” Dr. Pal and associates wrote.
However, pembrolizumab (Keytruda, Merck) a programmed death receptor-1–blocking antibody, is an immunotherapy which, in combination with axitinib, is approved as a first-line treatment for patients with advanced RCC.
Atezolizumab (Tecentriq, Genentech) is approved for treatment in urothelial carcinoma, non–small cell lung cancer (NSCLC), small cell lung cancer (SCLC), hepatocellular carcinoma (HCC), and melanoma. There are currently a number of ongoing studies that are exploring the use of atezolizumab as a treatment for renal cell carcinoma.
The study details
This new study was conducted between 2017 and 2019. It included 778 patients from 215 clinics in 28 countries who were assigned to the treatment arm (1,200 mg of IV atezolizumab (n = 390, 50%) once every 3 weeks for 16 cycles or 1 year, which ever came first – or, they were assigned to the placebo group (n = 388, 50%). The two groups were similar: average age 60-61, 72%-74% male, 78%-83% white, and 36%-37% based in North America. Most patients, (92%-93%) had clear cell cancer, and 64%-65% were at pathological disease stage T2 or T3a.
The 3-year disease-free survival rate at 36 months was 65.0% (95% confidence interval, 59.9-70.2) in the treatment group and 62.7% (95% CI, 57.5-67.9) in the placebo group. At follow-up at 44.7 months, there was no statistically significant difference in median disease-free survival between atezolizumab (57.2 months; 95% CI, 44.6 to not evaluable) and placebo (49.5 months; 95% CI, 47.4 to not evaluable).
While there were no deaths attributable to treatment, 69 (18%) patients who received atezolizumab and 46 (12%) patients who received placebo experienced a serious adverse event.
“. Future work will include exploration of clinical-based or biomarker-based subsets that might derive benefit from this approach,” the authors wrote.
The researchers acknowledge their findings contrast with those of the KEYNOTE-564 trial of adjuvant immunotherapy with pembrolizumab after nephrectomy in renal cell carcinoma. KEYNOTE-564 reported a disease-free survival benefit of over 24 months and in an analysis done at 30 months. But in KEYNOTE-564, the study comprised only 6% of patients with M1 no evidence of disease. And, it included only patients with synchronous metastases or metastases resected within 1 year of nephrectomy. In the new study, 14% of patients had M1 no evidence of disease, and it included both synchronous and metachronous disease with recurrence within 1year of surgery.
Adjuvant immunotherapy with pembrolizumab is considered optional for patients with intermediate-risk or high-risk operable clear cell renal cell carcinoma per European Society for Medical Oncology and European Association of Urology guidelines because of the lack of confirmed overall survival benefit and toxicity-related considerations associated with immunotherapy.
“These factors must be considered in the adjuvant setting as, following nephrectomy, patients are cancer free and might be cured by surgery alone. As such, additional trials are needed to clarify the role of adjuvant immunotherapy in this disease space,” the authors wrote.
What’s next? “Biomarker work is underway to determine whether tumor genomic characteristics or circulating biomarkers can identify patient populations who derive benefit from adjuvant atezolizumab,” Dr. Pal and associates wrote. “There is precedent for tissue-based adjuvant therapy selection in other diseases, such as HER2-based and endocrine receptor–based approaches in breast cancer and EGFR mutation–directed therapy in lung cancer.”
The study was funded by F Hoffmann-La Roche and Genentech. The academic authors of the study collaborated with F Hoffmann-La Roche and Genentech on all facets of the trial.
FROM THE LANCET
A new ultrabrief screening scale for pediatric OCD
Obsessive-compulsive disorder (OCD) affects 1-2% of the population. The disorder is characterized by recurrent intrusive unwanted thoughts (obsessions) that cause significant distress and anxiety, and behavioral or mental rituals (compulsions) that are performed to reduce distress stemming from obsessions. OCD may onset at any time in life, but most commonly begins in childhood or in early adulthood.

Cognitive behavioral therapy (CBT) with exposure and response prevention is an empirically based and highly effective treatment for OCD. However, most youth with OCD do not receive any treatment, which is related to a shortage of mental health care providers with expertise in assessment and treatment of the disorder, and misdiagnosis of the disorder is all too prevalent.

Aside from the subjective emotional toll associated with OCD, individuals living with this disorder frequently experience interpersonal, academic, and vocational impairments. Nevertheless, OCD is often overlooked or misdiagnosed. This may be more pronounced in youth with OCD, particularly in primary health care settings and large nonspecialized medical institutions. In fact, research indicates that pediatric OCD is often underrecognized even among mental health professionals. This situation is not new, and in fact the National Institute for Health and Care Excellence (NICE) in the United Kingdom stated that there is an urgent need to develop brief reliable screeners for OCD nearly 20 years ago.

Although there were several attempts to develop brief screening scales for adults and youth with OCD, none of them were found to be suitable for use as rapid screening tools in nonspecialized settings. One of the primary reasons is that OCD is associated with different “themes” or dimensions. For example, a child with OCD may engage in cleaning rituals because the context (or dimension) of their obsessions is contamination concerns. Another child with OCD, who may suffer from similar overall symptom severity, may primarily engage in checking rituals which are related with obsessions associated with fear of being responsible for harm. Therefore, one child with OCD may score very high on items assessing one dimension (e.g., contamination concerns), but very low on another dimension (e.g., harm obsessions).
This results in a known challenge in the assessment and psychometrics of self-report (as opposed to clinician administered) measures of OCD. Secondly, development of such measures requires very large carefully screened samples of individuals with OCD, with other disorders, and those without a known psychological disorder – which may be more challenging than requiring adult participants.
To accomplish this, we harmonized data from several sites that included three samples of carefully screened youths with OCD, with other disorders, and without known disorders who completed multiple self-report questionnaires, including the 21-item Obsessive-Compulsive Inventory – Child Version (OCI-CV).
Utilizing psychometric analyses including factor analyses, invariance analyses, and item response theory methodologies, we were able to develop an ultrabrief measure extracted from the OCI-CV: the 5-item Obsessive-Compulsive Inventory – Child Version (OCI-CV-5). This very brief self-report measure was found to have very good psychometric properties including a sensitive and specific clinical cutoff score. Youth who score at or above the cutoff score are nearly 21 times more likely to meet criteria for OCD.
This measure corresponds to a need to rapidly screen for OCD in children in nonspecialized settings, including community mental health clinics, primary care settings, and pediatric treatment facilities. However, it is important to note it is not a diagnostic measure. The measure is intended to identify youth who should be referred to a mental health care professional to conduct a diagnostic interview.
Dr. Abramovitch is a clinical psychologist and neuropsychologist based in Austin, Tex., and an associate professor at Texas State University. Dr. Abramowitz is professor and director of clinical training in the Anxiety and Stress Lab at University of North Carolina at Chapel Hill. Dr. McKay is professor of psychology at Fordham University, Bronx, N.Y.
Obsessive-compulsive disorder (OCD) affects 1-2% of the population. The disorder is characterized by recurrent intrusive unwanted thoughts (obsessions) that cause significant distress and anxiety, and behavioral or mental rituals (compulsions) that are performed to reduce distress stemming from obsessions. OCD may onset at any time in life, but most commonly begins in childhood or in early adulthood.
Cognitive behavioral therapy (CBT) with exposure and response prevention is an empirically based and highly effective treatment for OCD. However, most youth with OCD do not receive any treatment, which is related to a shortage of mental health care providers with expertise in assessment and treatment of the disorder, and misdiagnosis of the disorder is all too prevalent.
Aside from the subjective emotional toll associated with OCD, individuals living with this disorder frequently experience interpersonal, academic, and vocational impairments. Nevertheless, OCD is often overlooked or misdiagnosed. This may be more pronounced in youth with OCD, particularly in primary health care settings and large nonspecialized medical institutions. In fact, research indicates that pediatric OCD is often underrecognized even among mental health professionals. This situation is not new, and in fact the National Institute for Health and Care Excellence (NICE) in the United Kingdom stated that there is an urgent need to develop brief reliable screeners for OCD nearly 20 years ago.
Although there were several attempts to develop brief screening scales for adults and youth with OCD, none of them were found to be suitable for use as rapid screening tools in nonspecialized settings. One of the primary reasons is that OCD is associated with different “themes” or dimensions. For example, a child with OCD may engage in cleaning rituals because the context (or dimension) of their obsessions is contamination concerns. Another child with OCD, who may suffer from similar overall symptom severity, may primarily engage in checking rituals which are related with obsessions associated with fear of being responsible for harm. Therefore, one child with OCD may score very high on items assessing one dimension (e.g., contamination concerns), but very low on another dimension (e.g., harm obsessions).
This results in a known challenge in the assessment and psychometrics of self-report (as opposed to clinician administered) measures of OCD. Secondly, development of such measures requires very large carefully screened samples of individuals with OCD, with other disorders, and those without a known psychological disorder – which may be more challenging than requiring adult participants.
To accomplish this, we harmonized data from several sites that included three samples of carefully screened youths with OCD, with other disorders, and without known disorders who completed multiple self-report questionnaires, including the 21-item Obsessive-Compulsive Inventory – Child Version (OCI-CV).
Utilizing psychometric analyses including factor analyses, invariance analyses, and item response theory methodologies, we were able to develop an ultrabrief measure extracted from the OCI-CV: the 5-item Obsessive-Compulsive Inventory – Child Version (OCI-CV-5). This very brief self-report measure was found to have very good psychometric properties including a sensitive and specific clinical cutoff score. Youth who score at or above the cutoff score are nearly 21 times more likely to meet criteria for OCD.
This measure corresponds to a need to rapidly screen for OCD in children in nonspecialized settings, including community mental health clinics, primary care settings, and pediatric treatment facilities. However, it is important to note it is not a diagnostic measure. The measure is intended to identify youth who should be referred to a mental health care professional to conduct a diagnostic interview.
Dr. Abramovitch is a clinical psychologist and neuropsychologist based in Austin, Tex., and an associate professor at Texas State University. Dr. Abramowitz is professor and director of clinical training in the Anxiety and Stress Lab at University of North Carolina at Chapel Hill. Dr. McKay is professor of psychology at Fordham University, Bronx, N.Y.
Obsessive-compulsive disorder (OCD) affects 1-2% of the population. The disorder is characterized by recurrent intrusive unwanted thoughts (obsessions) that cause significant distress and anxiety, and behavioral or mental rituals (compulsions) that are performed to reduce distress stemming from obsessions. OCD may onset at any time in life, but most commonly begins in childhood or in early adulthood.
Cognitive behavioral therapy (CBT) with exposure and response prevention is an empirically based and highly effective treatment for OCD. However, most youth with OCD do not receive any treatment, which is related to a shortage of mental health care providers with expertise in assessment and treatment of the disorder, and misdiagnosis of the disorder is all too prevalent.
Aside from the subjective emotional toll associated with OCD, individuals living with this disorder frequently experience interpersonal, academic, and vocational impairments. Nevertheless, OCD is often overlooked or misdiagnosed. This may be more pronounced in youth with OCD, particularly in primary health care settings and large nonspecialized medical institutions. In fact, research indicates that pediatric OCD is often underrecognized even among mental health professionals. This situation is not new, and in fact the National Institute for Health and Care Excellence (NICE) in the United Kingdom stated that there is an urgent need to develop brief reliable screeners for OCD nearly 20 years ago.
Although there were several attempts to develop brief screening scales for adults and youth with OCD, none of them were found to be suitable for use as rapid screening tools in nonspecialized settings. One of the primary reasons is that OCD is associated with different “themes” or dimensions. For example, a child with OCD may engage in cleaning rituals because the context (or dimension) of their obsessions is contamination concerns. Another child with OCD, who may suffer from similar overall symptom severity, may primarily engage in checking rituals which are related with obsessions associated with fear of being responsible for harm. Therefore, one child with OCD may score very high on items assessing one dimension (e.g., contamination concerns), but very low on another dimension (e.g., harm obsessions).
This results in a known challenge in the assessment and psychometrics of self-report (as opposed to clinician administered) measures of OCD. Secondly, development of such measures requires very large carefully screened samples of individuals with OCD, with other disorders, and those without a known psychological disorder – which may be more challenging than requiring adult participants.
To accomplish this, we harmonized data from several sites that included three samples of carefully screened youths with OCD, with other disorders, and without known disorders who completed multiple self-report questionnaires, including the 21-item Obsessive-Compulsive Inventory – Child Version (OCI-CV).
Utilizing psychometric analyses including factor analyses, invariance analyses, and item response theory methodologies, we were able to develop an ultrabrief measure extracted from the OCI-CV: the 5-item Obsessive-Compulsive Inventory – Child Version (OCI-CV-5). This very brief self-report measure was found to have very good psychometric properties including a sensitive and specific clinical cutoff score. Youth who score at or above the cutoff score are nearly 21 times more likely to meet criteria for OCD.
This measure corresponds to a need to rapidly screen for OCD in children in nonspecialized settings, including community mental health clinics, primary care settings, and pediatric treatment facilities. However, it is important to note it is not a diagnostic measure. The measure is intended to identify youth who should be referred to a mental health care professional to conduct a diagnostic interview.
Dr. Abramovitch is a clinical psychologist and neuropsychologist based in Austin, Tex., and an associate professor at Texas State University. Dr. Abramowitz is professor and director of clinical training in the Anxiety and Stress Lab at University of North Carolina at Chapel Hill. Dr. McKay is professor of psychology at Fordham University, Bronx, N.Y.

No benefit of rivaroxaban in COVID outpatients: PREVENT-HD
A new U.S. randomized trial has failed to show benefit of a 35-day course of oral anticoagulation with rivaroxaban for the prevention of thrombotic events in outpatients with symptomatic COVID-19.
The PREVENT-HD trial was presented at the American Heart Association scientific sessions by Gregory Piazza, MD, Brigham and Women’s Hospital, Boston.
“With the caveat that the trial was underpowered to provide a definitive conclusion, these data do not support routine antithrombotic prophylaxis in nonhospitalized patients with symptomatic COVID-19,” Dr. Piazza concluded.

PREVENT-HD is the largest randomized study to look at anticoagulation in nonhospitalized COVID-19 patients and joins a long list of smaller trials that have also shown no benefit with this approach.
However, anticoagulation is recommended in patients who are hospitalized with COVID-19.
Dr. Piazza noted that the issue of anticoagulation in COVID-19 has focused mainly on hospitalized patients, but most COVID-19 cases are treated as outpatients, who are also suspected to be at risk for venous and arterial thrombotic events, especially if they have additional risk factors. Histopathological evidence also suggests that at least part of the deterioration in lung function leading to hospitalization may be attributable to in situ pulmonary artery thrombosis.
The PREVENT-HD trial explored the question of whether early initiation of thromboprophylaxis dosing of rivaroxaban in higher-risk outpatients with COVID-19 may lower the incidence of venous and arterial thrombotic events, reduce in situ pulmonary thrombosis and the worsening of pulmonary function that may lead to hospitalization, and reduce all-cause mortality.
The trial included 1,284 outpatients with a positive test for COVID-19 and who were within 14 days of symptom onset. They also had to have at least one of the following additional risk factors: age over 60 years; prior history of venous thromboembolism (VTE), thrombophilia, coronary artery disease, peripheral artery disease, cardiovascular disease or ischemic stroke, cancer, diabetes, heart failure, obesity (body mass index ≥ 35 kg/m2) or D-dimer > upper limit of normal. Around 35% of the study population had two or more of these risk factors.
Patients were randomized to rivaroxaban 10 mg daily for 35 days or placebo.
The primary efficacy endpoint was time to first occurrence of a composite of symptomatic VTE, myocardial infarction, ischemic stroke, acute limb ischemia, non–central nervous system systemic embolization, all-cause hospitalization, and all-cause mortality up to day 35.
The primary safety endpoint was time to first occurrence of International Society on Thrombosis and Hemostasis (ISTH) critical-site and fatal bleeding.
A modified intention-to-treat analysis (all participants taking at least one dose of study intervention) was also planned.
The trial was stopped early in April this year because of a lower than expected event incidence (3.2%), compared with the planned rate (8.5%), giving a very low likelihood of being able to achieve the required number of events.
Dr. Piazza said reasons contributing to the low event rate included a falling COVID-19 death and hospitalization rate nationwide, and increased use of effective vaccines.
Results of the main intention-to-treat analysis (in 1,284 patients) showed no significant difference in the primary efficacy composite endpoint, which occurred in 3.4% of the rivaroxaban group versus 3.0% of the placebo group.
In the modified intention-to-treat analysis (which included 1,197 patients who actually took at least one dose of the study medication) there was shift in the directionality of the point estimate (rivaroxaban 2.0% vs. placebo 2.7%), which Dr. Piazza said was related to a higher number of patients hospitalized before receiving study drug in the rivaroxaban group. However, the difference was still nonsignificant.
The first major secondary outcome of symptomatic VTE, arterial thrombotic events, and all-cause mortality occurred in 0.3% of rivaroxaban patients versus 1.1% of placebo patients, but this difference did not reach statistical significance.
However, a post hoc exploratory analysis did show a significant reduction in the outcome of symptomatic VTE and arterial thrombotic events.
In terms of safety, there were no fatal critical-site bleeding events, and there was no difference in ISTH major bleeding, which occurred in one patient in the rivaroxaban group versus no patients in the placebo group.
There was, however, a significant increase in nonmajor clinically relevant bleeding with rivaroxaban, which occurred in nine patients (1.5%) versus one patient (0.2%) in the placebo group.
Trivial bleeding was also increased in the rivaroxaban group, occurring in 17 patients (2.8%) versus 5 patients (0.8%) in the placebo group.

Discussant for the study, Renato Lopes, MD, Duke University Medical Center, Durham, N.C., noted that the relationship between COVID-19 and thrombosis has been an important issue since the beginning of the pandemic, with many proposed mechanisms to explain the COVID-19–associated coagulopathy, which is a major cause of death and disability.
While observational data at the beginning of the pandemic suggested patients with COVID-19 might benefit from anticoagulation, looking at all the different randomized trials that have tested anticoagulation in COVID-19 outpatients, there is no treatment effect on the various different primary outcomes in those studies and also no effect on all-cause mortality, Dr. Lopes said.
He pointed out that PREVENT-HD was stopped prematurely with only about one-third of the planned number of patients enrolled, “just like every other outpatient COVID-19 trial.”
He also drew attention to the low rates of vaccination in the trial population, which does not reflect the current vaccination rate in the United States, and said the different direction of the results between the main intention-to-treat and modified intention-to-treat analyses deserve further investigation.
However, Dr. Lopes concluded, “The results of this trial, in line with the body of evidence in this field, do not support the routine use of any antithrombotic therapy for outpatients with COVID-19.”
The PREVENT-HD trial was sponsored by Janssen. Dr. Piazza has reported receiving research support from Bristol-Myers Squibb/Pfizer Alliance, Bayer, Janssen, Alexion, Amgen, and Boston Scientific, and consulting fees from Bristol-Myers Squibb/Pfizer Alliance, Boston Scientific, Janssen, NAMSA, Prairie Education and Research Cooperative, Boston Clinical Research Institute, and Amgen.
A version of this article first appeared on Medscape.com.
A new U.S. randomized trial has failed to show benefit of a 35-day course of oral anticoagulation with rivaroxaban for the prevention of thrombotic events in outpatients with symptomatic COVID-19.
The PREVENT-HD trial was presented at the American Heart Association scientific sessions by Gregory Piazza, MD, Brigham and Women’s Hospital, Boston.
“With the caveat that the trial was underpowered to provide a definitive conclusion, these data do not support routine antithrombotic prophylaxis in nonhospitalized patients with symptomatic COVID-19,” Dr. Piazza concluded.
PREVENT-HD is the largest randomized study to look at anticoagulation in nonhospitalized COVID-19 patients and joins a long list of smaller trials that have also shown no benefit with this approach.
However, anticoagulation is recommended in patients who are hospitalized with COVID-19.
Dr. Piazza noted that the issue of anticoagulation in COVID-19 has focused mainly on hospitalized patients, but most COVID-19 cases are treated as outpatients, who are also suspected to be at risk for venous and arterial thrombotic events, especially if they have additional risk factors. Histopathological evidence also suggests that at least part of the deterioration in lung function leading to hospitalization may be attributable to in situ pulmonary artery thrombosis.
The PREVENT-HD trial explored the question of whether early initiation of thromboprophylaxis dosing of rivaroxaban in higher-risk outpatients with COVID-19 may lower the incidence of venous and arterial thrombotic events, reduce in situ pulmonary thrombosis and the worsening of pulmonary function that may lead to hospitalization, and reduce all-cause mortality.
The trial included 1,284 outpatients with a positive test for COVID-19 and who were within 14 days of symptom onset. They also had to have at least one of the following additional risk factors: age over 60 years; prior history of venous thromboembolism (VTE), thrombophilia, coronary artery disease, peripheral artery disease, cardiovascular disease or ischemic stroke, cancer, diabetes, heart failure, obesity (body mass index ≥ 35 kg/m2) or D-dimer > upper limit of normal. Around 35% of the study population had two or more of these risk factors.
Patients were randomized to rivaroxaban 10 mg daily for 35 days or placebo.
The primary efficacy endpoint was time to first occurrence of a composite of symptomatic VTE, myocardial infarction, ischemic stroke, acute limb ischemia, non–central nervous system systemic embolization, all-cause hospitalization, and all-cause mortality up to day 35.
The primary safety endpoint was time to first occurrence of International Society on Thrombosis and Hemostasis (ISTH) critical-site and fatal bleeding.
A modified intention-to-treat analysis (all participants taking at least one dose of study intervention) was also planned.
The trial was stopped early in April this year because of a lower than expected event incidence (3.2%), compared with the planned rate (8.5%), giving a very low likelihood of being able to achieve the required number of events.
Dr. Piazza said reasons contributing to the low event rate included a falling COVID-19 death and hospitalization rate nationwide, and increased use of effective vaccines.
Results of the main intention-to-treat analysis (in 1,284 patients) showed no significant difference in the primary efficacy composite endpoint, which occurred in 3.4% of the rivaroxaban group versus 3.0% of the placebo group.
In the modified intention-to-treat analysis (which included 1,197 patients who actually took at least one dose of the study medication) there was shift in the directionality of the point estimate (rivaroxaban 2.0% vs. placebo 2.7%), which Dr. Piazza said was related to a higher number of patients hospitalized before receiving study drug in the rivaroxaban group. However, the difference was still nonsignificant.
The first major secondary outcome of symptomatic VTE, arterial thrombotic events, and all-cause mortality occurred in 0.3% of rivaroxaban patients versus 1.1% of placebo patients, but this difference did not reach statistical significance.
However, a post hoc exploratory analysis did show a significant reduction in the outcome of symptomatic VTE and arterial thrombotic events.
In terms of safety, there were no fatal critical-site bleeding events, and there was no difference in ISTH major bleeding, which occurred in one patient in the rivaroxaban group versus no patients in the placebo group.
There was, however, a significant increase in nonmajor clinically relevant bleeding with rivaroxaban, which occurred in nine patients (1.5%) versus one patient (0.2%) in the placebo group.
Trivial bleeding was also increased in the rivaroxaban group, occurring in 17 patients (2.8%) versus 5 patients (0.8%) in the placebo group.
Discussant for the study, Renato Lopes, MD, Duke University Medical Center, Durham, N.C., noted that the relationship between COVID-19 and thrombosis has been an important issue since the beginning of the pandemic, with many proposed mechanisms to explain the COVID-19–associated coagulopathy, which is a major cause of death and disability.
While observational data at the beginning of the pandemic suggested patients with COVID-19 might benefit from anticoagulation, looking at all the different randomized trials that have tested anticoagulation in COVID-19 outpatients, there is no treatment effect on the various different primary outcomes in those studies and also no effect on all-cause mortality, Dr. Lopes said.
He pointed out that PREVENT-HD was stopped prematurely with only about one-third of the planned number of patients enrolled, “just like every other outpatient COVID-19 trial.”
He also drew attention to the low rates of vaccination in the trial population, which does not reflect the current vaccination rate in the United States, and said the different direction of the results between the main intention-to-treat and modified intention-to-treat analyses deserve further investigation.
However, Dr. Lopes concluded, “The results of this trial, in line with the body of evidence in this field, do not support the routine use of any antithrombotic therapy for outpatients with COVID-19.”
The PREVENT-HD trial was sponsored by Janssen. Dr. Piazza has reported receiving research support from Bristol-Myers Squibb/Pfizer Alliance, Bayer, Janssen, Alexion, Amgen, and Boston Scientific, and consulting fees from Bristol-Myers Squibb/Pfizer Alliance, Boston Scientific, Janssen, NAMSA, Prairie Education and Research Cooperative, Boston Clinical Research Institute, and Amgen.
A version of this article first appeared on Medscape.com.
A new U.S. randomized trial has failed to show benefit of a 35-day course of oral anticoagulation with rivaroxaban for the prevention of thrombotic events in outpatients with symptomatic COVID-19.
The PREVENT-HD trial was presented at the American Heart Association scientific sessions by Gregory Piazza, MD, Brigham and Women’s Hospital, Boston.
“With the caveat that the trial was underpowered to provide a definitive conclusion, these data do not support routine antithrombotic prophylaxis in nonhospitalized patients with symptomatic COVID-19,” Dr. Piazza concluded.
PREVENT-HD is the largest randomized study to look at anticoagulation in nonhospitalized COVID-19 patients and joins a long list of smaller trials that have also shown no benefit with this approach.
However, anticoagulation is recommended in patients who are hospitalized with COVID-19.
Dr. Piazza noted that the issue of anticoagulation in COVID-19 has focused mainly on hospitalized patients, but most COVID-19 cases are treated as outpatients, who are also suspected to be at risk for venous and arterial thrombotic events, especially if they have additional risk factors. Histopathological evidence also suggests that at least part of the deterioration in lung function leading to hospitalization may be attributable to in situ pulmonary artery thrombosis.
The PREVENT-HD trial explored the question of whether early initiation of thromboprophylaxis dosing of rivaroxaban in higher-risk outpatients with COVID-19 may lower the incidence of venous and arterial thrombotic events, reduce in situ pulmonary thrombosis and the worsening of pulmonary function that may lead to hospitalization, and reduce all-cause mortality.
The trial included 1,284 outpatients with a positive test for COVID-19 and who were within 14 days of symptom onset. They also had to have at least one of the following additional risk factors: age over 60 years; prior history of venous thromboembolism (VTE), thrombophilia, coronary artery disease, peripheral artery disease, cardiovascular disease or ischemic stroke, cancer, diabetes, heart failure, obesity (body mass index ≥ 35 kg/m2) or D-dimer > upper limit of normal. Around 35% of the study population had two or more of these risk factors.
Patients were randomized to rivaroxaban 10 mg daily for 35 days or placebo.
The primary efficacy endpoint was time to first occurrence of a composite of symptomatic VTE, myocardial infarction, ischemic stroke, acute limb ischemia, non–central nervous system systemic embolization, all-cause hospitalization, and all-cause mortality up to day 35.
The primary safety endpoint was time to first occurrence of International Society on Thrombosis and Hemostasis (ISTH) critical-site and fatal bleeding.
A modified intention-to-treat analysis (all participants taking at least one dose of study intervention) was also planned.
The trial was stopped early in April this year because of a lower than expected event incidence (3.2%), compared with the planned rate (8.5%), giving a very low likelihood of being able to achieve the required number of events.
Dr. Piazza said reasons contributing to the low event rate included a falling COVID-19 death and hospitalization rate nationwide, and increased use of effective vaccines.
Results of the main intention-to-treat analysis (in 1,284 patients) showed no significant difference in the primary efficacy composite endpoint, which occurred in 3.4% of the rivaroxaban group versus 3.0% of the placebo group.
In the modified intention-to-treat analysis (which included 1,197 patients who actually took at least one dose of the study medication) there was shift in the directionality of the point estimate (rivaroxaban 2.0% vs. placebo 2.7%), which Dr. Piazza said was related to a higher number of patients hospitalized before receiving study drug in the rivaroxaban group. However, the difference was still nonsignificant.
The first major secondary outcome of symptomatic VTE, arterial thrombotic events, and all-cause mortality occurred in 0.3% of rivaroxaban patients versus 1.1% of placebo patients, but this difference did not reach statistical significance.
However, a post hoc exploratory analysis did show a significant reduction in the outcome of symptomatic VTE and arterial thrombotic events.
In terms of safety, there were no fatal critical-site bleeding events, and there was no difference in ISTH major bleeding, which occurred in one patient in the rivaroxaban group versus no patients in the placebo group.
There was, however, a significant increase in nonmajor clinically relevant bleeding with rivaroxaban, which occurred in nine patients (1.5%) versus one patient (0.2%) in the placebo group.
Trivial bleeding was also increased in the rivaroxaban group, occurring in 17 patients (2.8%) versus 5 patients (0.8%) in the placebo group.
Discussant for the study, Renato Lopes, MD, Duke University Medical Center, Durham, N.C., noted that the relationship between COVID-19 and thrombosis has been an important issue since the beginning of the pandemic, with many proposed mechanisms to explain the COVID-19–associated coagulopathy, which is a major cause of death and disability.
While observational data at the beginning of the pandemic suggested patients with COVID-19 might benefit from anticoagulation, looking at all the different randomized trials that have tested anticoagulation in COVID-19 outpatients, there is no treatment effect on the various different primary outcomes in those studies and also no effect on all-cause mortality, Dr. Lopes said.
He pointed out that PREVENT-HD was stopped prematurely with only about one-third of the planned number of patients enrolled, “just like every other outpatient COVID-19 trial.”
He also drew attention to the low rates of vaccination in the trial population, which does not reflect the current vaccination rate in the United States, and said the different direction of the results between the main intention-to-treat and modified intention-to-treat analyses deserve further investigation.
However, Dr. Lopes concluded, “The results of this trial, in line with the body of evidence in this field, do not support the routine use of any antithrombotic therapy for outpatients with COVID-19.”
The PREVENT-HD trial was sponsored by Janssen. Dr. Piazza has reported receiving research support from Bristol-Myers Squibb/Pfizer Alliance, Bayer, Janssen, Alexion, Amgen, and Boston Scientific, and consulting fees from Bristol-Myers Squibb/Pfizer Alliance, Boston Scientific, Janssen, NAMSA, Prairie Education and Research Cooperative, Boston Clinical Research Institute, and Amgen.
A version of this article first appeared on Medscape.com.
FROM AHA 2022
Children from poorer ZIP codes often untreated for ear infections
Children from socially disadvantaged backgrounds are less likely to be treated for middle ear infections and are likely to experience serious complications from the condition – potentially with lifelong economic consequences – researchers have found.
Problems such as hearing loss and chronic ear infections were more common for children who lived in areas marked by difficult socioeconomic circumstances, according to the researchers, who linked the complications to a lack of adequate treatment in this population.
“We are treating socially disadvantaged kids differently than we are treating more advantaged kids,” said Jason Qian, MD, a resident in otolaryngology and head and neck surgery at Stanford (Calif.) University, who helped conduct the new study. “We have to think about social inequalities so we can ensure all kids are receiving the same level and type of care.”
In the United States, 80% of children will experience otitis media during their lifetime. Untreated ear infections can lead to symptoms ranging from mild discharge from the ear to life-threatening conditions like mastoiditis and intracranial abscesses.
For the new study, published online in JAMA Otolaryngology–Head & Neck Surgery, Dr. Qian and colleagues looked at 4.8 million children with private health insurance across the United States using a database with information on inpatient and outpatient visits and medication use. The researchers identified patients between January 2003 and March 2021 who received treatment for recurrent and suppurative otitis media, those who received tympanostomy tubes, and children who experienced severe complications from undertreated ear infections.
Social disadvantage was assessed using the Social Deprivation Index (SDI), a tool used to measure indicators of poverty throughout the United States based on seven demographic factors including level of educational attainment, the number of single-parent households, the share of people living in overcrowded homes, and other factors.
Every point increase in the SDI score was associated with a 14% lower likelihood of being treated for recurrent ear infections despite having them and a 28% greater chance of being hospitalized for severe ear infections, according to the researchers.
Previous research established that children with government health insurance or no coverage have more difficulty receiving proper treatment for ear infections. Although people with commercial insurance are generally wealthier than those without private coverage, Dr. Qian said, the new data indicate that significant social disparities in care exist even within this group.
Although some studies have found that wealthier children are more likely to develop otitis media, Dr. Qian’s group said that association likely reflects the better access to health care money affords.
“We found that socially disadvantaged children not only have a higher burden of otitis media but are also undertreated both medically and surgically for [ear infections]. Because chronic and complicated forms of otitis media can cause childhood hearing loss, which in turn limits academic and economic potential, undertreatment of [otitis media] in socially disadvantaged populations can contribute to generational cycles of poverty, unemployment, and low pay,” they write.
“The biggest take home is that we are not treating children equitably when it comes to ear infections,” Dr. Qian added. “In order to give children equal access to care, we as health care providers need to find strategies to do better.”
The study was supported by the Stanford Center for Population Health Science Data Core, which is supported by a grant from the National Institutes of Health and internal funding. Dr. Qian has reported receiving grant funding from Merck.
A version of this article first appeared on Medscape.com.
Children from socially disadvantaged backgrounds are less likely to be treated for middle ear infections and are likely to experience serious complications from the condition – potentially with lifelong economic consequences – researchers have found.
Problems such as hearing loss and chronic ear infections were more common for children who lived in areas marked by difficult socioeconomic circumstances, according to the researchers, who linked the complications to a lack of adequate treatment in this population.
“We are treating socially disadvantaged kids differently than we are treating more advantaged kids,” said Jason Qian, MD, a resident in otolaryngology and head and neck surgery at Stanford (Calif.) University, who helped conduct the new study. “We have to think about social inequalities so we can ensure all kids are receiving the same level and type of care.”
In the United States, 80% of children will experience otitis media during their lifetime. Untreated ear infections can lead to symptoms ranging from mild discharge from the ear to life-threatening conditions like mastoiditis and intracranial abscesses.
For the new study, published online in JAMA Otolaryngology–Head & Neck Surgery, Dr. Qian and colleagues looked at 4.8 million children with private health insurance across the United States using a database with information on inpatient and outpatient visits and medication use. The researchers identified patients between January 2003 and March 2021 who received treatment for recurrent and suppurative otitis media, those who received tympanostomy tubes, and children who experienced severe complications from undertreated ear infections.
Social disadvantage was assessed using the Social Deprivation Index (SDI), a tool used to measure indicators of poverty throughout the United States based on seven demographic factors including level of educational attainment, the number of single-parent households, the share of people living in overcrowded homes, and other factors.
Every point increase in the SDI score was associated with a 14% lower likelihood of being treated for recurrent ear infections despite having them and a 28% greater chance of being hospitalized for severe ear infections, according to the researchers.
Previous research established that children with government health insurance or no coverage have more difficulty receiving proper treatment for ear infections. Although people with commercial insurance are generally wealthier than those without private coverage, Dr. Qian said, the new data indicate that significant social disparities in care exist even within this group.
Although some studies have found that wealthier children are more likely to develop otitis media, Dr. Qian’s group said that association likely reflects the better access to health care money affords.
“We found that socially disadvantaged children not only have a higher burden of otitis media but are also undertreated both medically and surgically for [ear infections]. Because chronic and complicated forms of otitis media can cause childhood hearing loss, which in turn limits academic and economic potential, undertreatment of [otitis media] in socially disadvantaged populations can contribute to generational cycles of poverty, unemployment, and low pay,” they write.
“The biggest take home is that we are not treating children equitably when it comes to ear infections,” Dr. Qian added. “In order to give children equal access to care, we as health care providers need to find strategies to do better.”
The study was supported by the Stanford Center for Population Health Science Data Core, which is supported by a grant from the National Institutes of Health and internal funding. Dr. Qian has reported receiving grant funding from Merck.
A version of this article first appeared on Medscape.com.
Children from socially disadvantaged backgrounds are less likely to be treated for middle ear infections and are likely to experience serious complications from the condition – potentially with lifelong economic consequences – researchers have found.
Problems such as hearing loss and chronic ear infections were more common for children who lived in areas marked by difficult socioeconomic circumstances, according to the researchers, who linked the complications to a lack of adequate treatment in this population.
“We are treating socially disadvantaged kids differently than we are treating more advantaged kids,” said Jason Qian, MD, a resident in otolaryngology and head and neck surgery at Stanford (Calif.) University, who helped conduct the new study. “We have to think about social inequalities so we can ensure all kids are receiving the same level and type of care.”
In the United States, 80% of children will experience otitis media during their lifetime. Untreated ear infections can lead to symptoms ranging from mild discharge from the ear to life-threatening conditions like mastoiditis and intracranial abscesses.
For the new study, published online in JAMA Otolaryngology–Head & Neck Surgery, Dr. Qian and colleagues looked at 4.8 million children with private health insurance across the United States using a database with information on inpatient and outpatient visits and medication use. The researchers identified patients between January 2003 and March 2021 who received treatment for recurrent and suppurative otitis media, those who received tympanostomy tubes, and children who experienced severe complications from undertreated ear infections.
Social disadvantage was assessed using the Social Deprivation Index (SDI), a tool used to measure indicators of poverty throughout the United States based on seven demographic factors including level of educational attainment, the number of single-parent households, the share of people living in overcrowded homes, and other factors.
Every point increase in the SDI score was associated with a 14% lower likelihood of being treated for recurrent ear infections despite having them and a 28% greater chance of being hospitalized for severe ear infections, according to the researchers.
Previous research established that children with government health insurance or no coverage have more difficulty receiving proper treatment for ear infections. Although people with commercial insurance are generally wealthier than those without private coverage, Dr. Qian said, the new data indicate that significant social disparities in care exist even within this group.
Although some studies have found that wealthier children are more likely to develop otitis media, Dr. Qian’s group said that association likely reflects the better access to health care money affords.
“We found that socially disadvantaged children not only have a higher burden of otitis media but are also undertreated both medically and surgically for [ear infections]. Because chronic and complicated forms of otitis media can cause childhood hearing loss, which in turn limits academic and economic potential, undertreatment of [otitis media] in socially disadvantaged populations can contribute to generational cycles of poverty, unemployment, and low pay,” they write.
“The biggest take home is that we are not treating children equitably when it comes to ear infections,” Dr. Qian added. “In order to give children equal access to care, we as health care providers need to find strategies to do better.”
The study was supported by the Stanford Center for Population Health Science Data Core, which is supported by a grant from the National Institutes of Health and internal funding. Dr. Qian has reported receiving grant funding from Merck.
A version of this article first appeared on Medscape.com.
Monkeypox in children appears rare and relatively mild
Monkeypox virus infections in children and adolescents in the United States are rare, and young patients with known infections have all recovered, according to a study from the Centers for Disease Control and Prevention.
In addition, evidence suggests that secondary transmission in schools or childcare facilities may be unlikely.
The study was the first comprehensive study on the impact of monkeypox on children during the 2022 outbreak, according to a statement emailed to this news organization from the California Department of Public Health, one of the state health departments that partnered with the CDC to share information.
News of low infection rates and relatively mild disease was welcome to clinicians, who had braced for severe findings on the basis of sparse prior data, according to Peter Chin-Hong, MD, a professor of medicine and an infectious diseases physician at the University of California, San Francisco.
“We were on heightened alert that kids may do poorly,” said Dr. Chin-Hong, who was not involved in the study but who cared for monkeypox patients during the outbreak. “I think this study is reassuring.
“The other silver lining about it is that most of the kids got infected in the household setting from ways that you would expect them to get [infected],” Dr. Chin-Hong said in an interview.
However, Black and Hispanic children were more likely to contract the disease, underscoring troubling inequities.
“Early on, individuals of color were much less likely to be able to successfully access vaccination,” said first author Ian Hennessee, PhD, MPH, an epidemic intelligence service officer with the CDC and a member of the Special Case Investigation Unit of the Multinational Monkeypox Response Team at the CDC. “We think those kinds of structural inequities really trickled down towards the children and adolescents that have been affected by this outbreak.”
The study was published in Morbidity and Mortality Weekly Report.
A nationwide look at the data
The researchers discussed 83 children and adolescents with monkeypox who came to the CDC’s attention between May 17 and Sept. 24, 2022.
The 83 cases represent 0.3% of the 25,038 reported monkeypox cases in the United States over that period. Of the 28 children aged 12 years or younger, 18 (64%) were boys. Sixteen children were younger than 4 years.
Exposure data were available for 20 (71%) of those aged 0-12. In that group, 19 were exposed at home; 17 cases were due to routine skin-to-skin contact with a household caregiver; and one case was suspected to be caused by fomites (such as a shared towel). Exposure information was unavailable for the remaining case.
Most of the children experienced lesions on the trunk. No lesions were anogenital. Two patients in the youngest age group were hospitalized because of widespread rash that involved the eyelids, and a patient in the 5- to 12-year-old group was hospitalized because of periorbital cellulitis and conjunctivitis.
Among those aged 13-17, there were 55 cases. Of these patients, 89% were boys. Exposure data were available for 35 (64%). In 32 of these patients, the infection occurred from presumed sexual contact. Twenty-three of those adolescents reported male-to-male sexual contact. No case was found to be connected with sexual abuse.
Lesions in the adolescents were mostly truncal or anogenital. Six in this group were hospitalized, and all of them recovered. One adolescent was found to be HIV positive.
Black and Hispanic children accounted for 47% and 35% of all cases, respectively.
Eleven percent of all the children and adolescents were hospitalized, and none received intensive care.
Treatments, when given, included the antiviral drug tecovirimat, intravenous vaccinia immune globulin, and topical trifluridine. There were no deaths.
Ten symptomatic patients attended school or daycare. Among these patients, no secondary transmissions were found to have occurred. Some contacts were offered the JYNNEOS monkeypox vaccine as postexposure prophylaxis.
Limitations of the study included potentially overlooked cases. Data were collected through routine surveillance, children frequently experience rashes, and access to testing has been a challenge, Dr. Hennessee explained.
In addition, data on exposure characteristics were missing for some children.
Inequities and the risks of being judged
The outbreak in the United States has eased in recent months. However, though uncommon in children, monkeypox has affected some racial groups disproportionately.
“Especially in the later course of the outbreak, the majority of cases were among Black and Hispanic individuals,” said co-author Rachel E. Harold, MD, an infectious diseases specialist and supervisory medical officer with the District of Columbia Department of Health’s HIV/AIDS, Hepatitis, STDs, and TB Administration.
“Unfortunately, the pediatric cases do reflect the outbreak overall,” she told this news organization.
Dr. Harold noted there have been efforts in D.C. and other jurisdictions, as well as by the White House monkeypox response team, to reach populations at greatest risk and that they were “really trying to make vaccine available to people of color.”
Vaccination clinics often popped up in unexpected locations at short notice, and that made it hard for some people to get to them, Dr. Chin-Hong pointed out.
Another factor was “the public aspect of accessing diagnostics and vaccines and the way that that’s linked to potential judgment or sexual risk,” he added.
“Not everybody’s out,” Dr. Chin-Hong said, referring to members of the LGBTQ community. “In many communities of color, going to get a test or going to get a vaccine essentially means that you’re out.”
For clinicians who suspect monkeypox in a child, Dr. Harold suggests keeping a broad differential diagnosis, looking for an epidemiologic link, and contacting the CDC for assistance. Infected children should be encouraged to avoid touching their own eyes or mucous membranes, she added.
In addition, she said, tecovirimat is a reasonable treatment and is well tolerated by pediatric monkeypox patients with eczema, an underlying condition that could lead to severe disease.
For infected caregivers, Dr. Hennessee said, measures to prevent infecting children at home include isolation, contact precautions, and in some cases, postexposure prophylaxis via vaccination.
For sexually active adolescents, he advised that clinicians offer vaccination, education on sexual health, and testing for HIV and other sexually transmitted infections.
“It’s important to remember that adolescents may be sexually active, and clinicians should do a thorough and nonjudgmental sexual history,” Dr. Harold added. “That is always true, but especially if there is concern for [monkeypox].”
Dr. Hennessee, Dr. Chin-Hong, and Dr. Harold have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Monkeypox virus infections in children and adolescents in the United States are rare, and young patients with known infections have all recovered, according to a study from the Centers for Disease Control and Prevention.
In addition, evidence suggests that secondary transmission in schools or childcare facilities may be unlikely.
The study was the first comprehensive study on the impact of monkeypox on children during the 2022 outbreak, according to a statement emailed to this news organization from the California Department of Public Health, one of the state health departments that partnered with the CDC to share information.
News of low infection rates and relatively mild disease was welcome to clinicians, who had braced for severe findings on the basis of sparse prior data, according to Peter Chin-Hong, MD, a professor of medicine and an infectious diseases physician at the University of California, San Francisco.
“We were on heightened alert that kids may do poorly,” said Dr. Chin-Hong, who was not involved in the study but who cared for monkeypox patients during the outbreak. “I think this study is reassuring.
“The other silver lining about it is that most of the kids got infected in the household setting from ways that you would expect them to get [infected],” Dr. Chin-Hong said in an interview.
However, Black and Hispanic children were more likely to contract the disease, underscoring troubling inequities.
“Early on, individuals of color were much less likely to be able to successfully access vaccination,” said first author Ian Hennessee, PhD, MPH, an epidemic intelligence service officer with the CDC and a member of the Special Case Investigation Unit of the Multinational Monkeypox Response Team at the CDC. “We think those kinds of structural inequities really trickled down towards the children and adolescents that have been affected by this outbreak.”
The study was published in Morbidity and Mortality Weekly Report.
A nationwide look at the data
The researchers discussed 83 children and adolescents with monkeypox who came to the CDC’s attention between May 17 and Sept. 24, 2022.
The 83 cases represent 0.3% of the 25,038 reported monkeypox cases in the United States over that period. Of the 28 children aged 12 years or younger, 18 (64%) were boys. Sixteen children were younger than 4 years.
Exposure data were available for 20 (71%) of those aged 0-12. In that group, 19 were exposed at home; 17 cases were due to routine skin-to-skin contact with a household caregiver; and one case was suspected to be caused by fomites (such as a shared towel). Exposure information was unavailable for the remaining case.
Most of the children experienced lesions on the trunk. No lesions were anogenital. Two patients in the youngest age group were hospitalized because of widespread rash that involved the eyelids, and a patient in the 5- to 12-year-old group was hospitalized because of periorbital cellulitis and conjunctivitis.
Among those aged 13-17, there were 55 cases. Of these patients, 89% were boys. Exposure data were available for 35 (64%). In 32 of these patients, the infection occurred from presumed sexual contact. Twenty-three of those adolescents reported male-to-male sexual contact. No case was found to be connected with sexual abuse.
Lesions in the adolescents were mostly truncal or anogenital. Six in this group were hospitalized, and all of them recovered. One adolescent was found to be HIV positive.
Black and Hispanic children accounted for 47% and 35% of all cases, respectively.
Eleven percent of all the children and adolescents were hospitalized, and none received intensive care.
Treatments, when given, included the antiviral drug tecovirimat, intravenous vaccinia immune globulin, and topical trifluridine. There were no deaths.
Ten symptomatic patients attended school or daycare. Among these patients, no secondary transmissions were found to have occurred. Some contacts were offered the JYNNEOS monkeypox vaccine as postexposure prophylaxis.
Limitations of the study included potentially overlooked cases. Data were collected through routine surveillance, children frequently experience rashes, and access to testing has been a challenge, Dr. Hennessee explained.
In addition, data on exposure characteristics were missing for some children.
Inequities and the risks of being judged
The outbreak in the United States has eased in recent months. However, though uncommon in children, monkeypox has affected some racial groups disproportionately.
“Especially in the later course of the outbreak, the majority of cases were among Black and Hispanic individuals,” said co-author Rachel E. Harold, MD, an infectious diseases specialist and supervisory medical officer with the District of Columbia Department of Health’s HIV/AIDS, Hepatitis, STDs, and TB Administration.
“Unfortunately, the pediatric cases do reflect the outbreak overall,” she told this news organization.
Dr. Harold noted there have been efforts in D.C. and other jurisdictions, as well as by the White House monkeypox response team, to reach populations at greatest risk and that they were “really trying to make vaccine available to people of color.”
Vaccination clinics often popped up in unexpected locations at short notice, and that made it hard for some people to get to them, Dr. Chin-Hong pointed out.
Another factor was “the public aspect of accessing diagnostics and vaccines and the way that that’s linked to potential judgment or sexual risk,” he added.
“Not everybody’s out,” Dr. Chin-Hong said, referring to members of the LGBTQ community. “In many communities of color, going to get a test or going to get a vaccine essentially means that you’re out.”
For clinicians who suspect monkeypox in a child, Dr. Harold suggests keeping a broad differential diagnosis, looking for an epidemiologic link, and contacting the CDC for assistance. Infected children should be encouraged to avoid touching their own eyes or mucous membranes, she added.
In addition, she said, tecovirimat is a reasonable treatment and is well tolerated by pediatric monkeypox patients with eczema, an underlying condition that could lead to severe disease.
For infected caregivers, Dr. Hennessee said, measures to prevent infecting children at home include isolation, contact precautions, and in some cases, postexposure prophylaxis via vaccination.
For sexually active adolescents, he advised that clinicians offer vaccination, education on sexual health, and testing for HIV and other sexually transmitted infections.
“It’s important to remember that adolescents may be sexually active, and clinicians should do a thorough and nonjudgmental sexual history,” Dr. Harold added. “That is always true, but especially if there is concern for [monkeypox].”
Dr. Hennessee, Dr. Chin-Hong, and Dr. Harold have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Monkeypox virus infections in children and adolescents in the United States are rare, and young patients with known infections have all recovered, according to a study from the Centers for Disease Control and Prevention.
In addition, evidence suggests that secondary transmission in schools or childcare facilities may be unlikely.
The study was the first comprehensive study on the impact of monkeypox on children during the 2022 outbreak, according to a statement emailed to this news organization from the California Department of Public Health, one of the state health departments that partnered with the CDC to share information.
News of low infection rates and relatively mild disease was welcome to clinicians, who had braced for severe findings on the basis of sparse prior data, according to Peter Chin-Hong, MD, a professor of medicine and an infectious diseases physician at the University of California, San Francisco.
“We were on heightened alert that kids may do poorly,” said Dr. Chin-Hong, who was not involved in the study but who cared for monkeypox patients during the outbreak. “I think this study is reassuring.
“The other silver lining about it is that most of the kids got infected in the household setting from ways that you would expect them to get [infected],” Dr. Chin-Hong said in an interview.
However, Black and Hispanic children were more likely to contract the disease, underscoring troubling inequities.
“Early on, individuals of color were much less likely to be able to successfully access vaccination,” said first author Ian Hennessee, PhD, MPH, an epidemic intelligence service officer with the CDC and a member of the Special Case Investigation Unit of the Multinational Monkeypox Response Team at the CDC. “We think those kinds of structural inequities really trickled down towards the children and adolescents that have been affected by this outbreak.”
The study was published in Morbidity and Mortality Weekly Report.
A nationwide look at the data
The researchers discussed 83 children and adolescents with monkeypox who came to the CDC’s attention between May 17 and Sept. 24, 2022.
The 83 cases represent 0.3% of the 25,038 reported monkeypox cases in the United States over that period. Of the 28 children aged 12 years or younger, 18 (64%) were boys. Sixteen children were younger than 4 years.
Exposure data were available for 20 (71%) of those aged 0-12. In that group, 19 were exposed at home; 17 cases were due to routine skin-to-skin contact with a household caregiver; and one case was suspected to be caused by fomites (such as a shared towel). Exposure information was unavailable for the remaining case.
Most of the children experienced lesions on the trunk. No lesions were anogenital. Two patients in the youngest age group were hospitalized because of widespread rash that involved the eyelids, and a patient in the 5- to 12-year-old group was hospitalized because of periorbital cellulitis and conjunctivitis.
Among those aged 13-17, there were 55 cases. Of these patients, 89% were boys. Exposure data were available for 35 (64%). In 32 of these patients, the infection occurred from presumed sexual contact. Twenty-three of those adolescents reported male-to-male sexual contact. No case was found to be connected with sexual abuse.
Lesions in the adolescents were mostly truncal or anogenital. Six in this group were hospitalized, and all of them recovered. One adolescent was found to be HIV positive.
Black and Hispanic children accounted for 47% and 35% of all cases, respectively.
Eleven percent of all the children and adolescents were hospitalized, and none received intensive care.
Treatments, when given, included the antiviral drug tecovirimat, intravenous vaccinia immune globulin, and topical trifluridine. There were no deaths.
Ten symptomatic patients attended school or daycare. Among these patients, no secondary transmissions were found to have occurred. Some contacts were offered the JYNNEOS monkeypox vaccine as postexposure prophylaxis.
Limitations of the study included potentially overlooked cases. Data were collected through routine surveillance, children frequently experience rashes, and access to testing has been a challenge, Dr. Hennessee explained.
In addition, data on exposure characteristics were missing for some children.
Inequities and the risks of being judged
The outbreak in the United States has eased in recent months. However, though uncommon in children, monkeypox has affected some racial groups disproportionately.
“Especially in the later course of the outbreak, the majority of cases were among Black and Hispanic individuals,” said co-author Rachel E. Harold, MD, an infectious diseases specialist and supervisory medical officer with the District of Columbia Department of Health’s HIV/AIDS, Hepatitis, STDs, and TB Administration.
“Unfortunately, the pediatric cases do reflect the outbreak overall,” she told this news organization.
Dr. Harold noted there have been efforts in D.C. and other jurisdictions, as well as by the White House monkeypox response team, to reach populations at greatest risk and that they were “really trying to make vaccine available to people of color.”
Vaccination clinics often popped up in unexpected locations at short notice, and that made it hard for some people to get to them, Dr. Chin-Hong pointed out.
Another factor was “the public aspect of accessing diagnostics and vaccines and the way that that’s linked to potential judgment or sexual risk,” he added.
“Not everybody’s out,” Dr. Chin-Hong said, referring to members of the LGBTQ community. “In many communities of color, going to get a test or going to get a vaccine essentially means that you’re out.”
For clinicians who suspect monkeypox in a child, Dr. Harold suggests keeping a broad differential diagnosis, looking for an epidemiologic link, and contacting the CDC for assistance. Infected children should be encouraged to avoid touching their own eyes or mucous membranes, she added.
In addition, she said, tecovirimat is a reasonable treatment and is well tolerated by pediatric monkeypox patients with eczema, an underlying condition that could lead to severe disease.
For infected caregivers, Dr. Hennessee said, measures to prevent infecting children at home include isolation, contact precautions, and in some cases, postexposure prophylaxis via vaccination.
For sexually active adolescents, he advised that clinicians offer vaccination, education on sexual health, and testing for HIV and other sexually transmitted infections.
“It’s important to remember that adolescents may be sexually active, and clinicians should do a thorough and nonjudgmental sexual history,” Dr. Harold added. “That is always true, but especially if there is concern for [monkeypox].”
Dr. Hennessee, Dr. Chin-Hong, and Dr. Harold have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Glioblastoma spreading strategies discovered
Every year, around 7,000 people in Germany develop a brain tumor, and around half of those cases involve a glioblastoma, a particularly aggressive form of the disease. Glioblastomas are incurable, but advances are being made in both diagnostics and therapy.
This news organization spoke to Wolfgang Wick, MD, medical director of the neurologic clinic at UKHD, about how glioblastomas are treated; the role that vaccinations, recombinant proteins, and parvoviruses play; and what therapeutic approaches might be derived from the discovery of this method by which glioblastomas spread.
Question: Glioblastomas spread through the brain like a fungal network. So how would a glioblastoma currently be treated? The tumor can only be partially removed through surgery.
Answer: Nevertheless, glioblastoma would be operated on. This would have a significant effect. Relieving the strain of the main tumor mass, without generating a new deficit, is prognostically very good for the patient concerned. However, surgery on glioblastoma is never curative.
The reason a cure is not possible is down to the special form and spread of the glioblastoma. Nevertheless, an operation helps. This seems to be because removing the main tumor mass maybe has a positive immunological effect. But it may also be connected to the tumor’s network communication. The surgical intervention stimulates the network by increasing resistance.
If the main tumor mass is decreased through a surgical procedure, this results in an at least temporarily improved starting position for the patient until the mass regenerates. This could also be connected to the fact that tumor communication is not unregulated but is rather in accordance with a certain hierarchy and order, which requires a certain structure and mass.
The other aspect is that support can be requested via this communication. You can imagine that a cell connected to another cell via a conduit receives help from this other cell in the form of organelles by exchanging ions and that, for example, stress or toxicity can be much better balanced out in large networks than in small networks. That means that external attacks, such as a surgical intervention, can be much better balanced by a well-organized network than by isolated cells.
Resistance to chemotherapy
Q: How do irradiation and chemotherapy rank in the treatment of glioblastomas?
A: Irradiation is another therapeutic approach. It causes cells to be stuck in the growth phase of the cell cycle. The cells are not killed through radiation, but they are practically halted. And this arrest of the cell cycle is often sufficient to help people with glioblastomas for a very long time. But the same is true for irradiation as for surgery. This deep network of cells cannot be addressed.
Attempts have been made in the past to reduce the radiation dose to the extent that the brain is no longer damaged by it, but this low dose was then not sufficient to exert any control. If you want to control the tumor, the dose must be high and the volume must be correspondingly low, since there is a clear limit.
Every patient is offered alkylating chemotherapy. At the moment, just one substance is used here in the primary therapy: temozolomide. The problem with this is that two-thirds of tumors in all cells exhibit a resistance to this alkylating chemotherapy, which means that the efficacy of this therapy is highly limited in two-thirds of patients.
In the one-third of patients in whom this resistance is not present, the chemotherapy works fairly well. But even then, it is unfortunately only a matter of time until there is a relapse or disease progression. In my practice, this has always been the case, but there are people who have been living with this disease for 20 years now. There seem to be tumor cells that calmly and silently survive this phase of chemotherapy and then restart the cell cycle at some point.
Q: What do you think of alternating electric fields as a therapy option?
A: Therapy with alternating electric fields is currently being used and offered to patients. This means that patients who have survived well through radiochemotherapy should also be offered treatment with alternating electric fields.
However, what happens in this process is not as well understood as with other therapies. It is assumed that the cell cycle, i.e., cell division, is altered by disrupting the mitotic spindle. But you can imagine, and this is now speculation, but quite sound speculation I believe, that alternating electric fields also cause a certain amount of confusion in the previously described networks. But this still needs to be investigated in more detail.
It is not implausible. We know that such alternating electric fields disturb the organization of cell organelles. And we also know that for this communication, we need fairly good order and also organization. This would definitely be a starting point on the way to understanding why this therapy potentially shows a certain effect in some patients.
Nerve cell precursors
Q: Scientists from the UKHD and the DKFZ have discovered a new glioblastoma spreading strategy and have learned that the tumor cells imitate the properties and movement patterns of nerve cells. They are labeling the results a “milestone in the field of cancer neuroscience.” Could you explain a bit more?
A: Glioblastoma does not grow on its own as a solid mass, but instead, the entire brain is affected by the disease. The question of how the tumor’s individual cells move the main tumor mass from afar, how they get there, how they continue to be supplied, and what their interaction partners are – an entirely new light has been shed on all of this in our work.
The development of tumor cell mobility has been recognized as a remnant of brain development. The tumor cells have retained properties that the precursor cells for nervous-system development require for an organized nervous system to emerge from just a few cells. This means that the tumor cells copy or eventually retain properties of the nerve-cell precursors that, unlike mature nerve cells, are mobile to a fairly high degree.
Mobility here means that it can advance along a network, despite said network being very densely packed. This also means that certain processes, such as releasing and then continuing to move again, must function and that the communication regarding the original disease must be maintained.
First, we understand what the different glioblastoma cell types do, which molecular properties are associated with which behaviors, and which cell type (namely the swarming cells) is responsible for the invasive tumor growth. In contrast, the network-forming cell type, which only develops from these, is responsible for the resistance.
Interrupting communication
Q: Which starting points for new therapies do you see?
A: In terms of new therapies, these movement phenomena are one good starting point. The other starting point – I find this one much more interesting – is that the programming steps that these tumor cells use [are] no longer needed. This is because our mature nervous system no longer requires this program, which was necessary for the mobility of cells in development.
Our central nervous system exhibits little cell movement. This is to do with programs of nervous-system development that are switched off in the mature nervous system. But they are then reactivated or remain active in the tumor cells. This process reveals potential starting points for therapy.
Addressing the movement of cells, that has been investigated for the last 20 years, but it seems to have an extraordinarily high number of side effects, because these movement mechanisms are also important for other, healthy cells in the body. For example, digestive mechanisms and other proliferation mechanisms, on mucous membranes, in the blood system, in the bone marrow, are then affected and no longer function.
There is another possible approach: the more-or-less specific interaction between the nerve cells and the tumor cells also offers starting points for therapies, from our point of view. The key word is epilepsy treatment. We know that people with brain tumors suffer badly, or worse than usual, from epileptic seizures. This was often regarded purely as a pressure problem. There is a disruptive element in the brain, and this causes the electrical activity in the brain to become disorganized. For some people, this can lead to seizures in certain situations.
The communication between tumor cells and nerve cells takes place via transmission substances, e.g., through the neurotransmitter glutamate. Now you can consider whether a “surplus” of communication, such as an excessively strong stimulus, can trigger epileptic seizures.
In this work, we demonstrate that by interrupting this communication, we can also prevent the movement of these cells and the growth, the proliferation, of these cells.
Q: What is the significance of parvoviruses for therapy?
A: The major topic for cancer is immunotherapy. And one option for performing immunotherapies lies with viruses. Parvoviruses are a plausible therapy for proliferating cells.
Parvoviruses are usually administered locally. This means that a surgical cavity is infected with the viruses and the tumor cells that remain after an operation will then hopefully be killed off by these viruses.
This is the first step and the immediate effect of virus therapy. The attempt is made to kill off cells in the same way as with a medication. The advantage of viruses is the high specificity, i.e., only dividing cells will be attacked. In addition, parvoviruses are so small that they can also spread well and circulate through the brain.
The second reason for immunotherapy is that when killing off cells with viruses, antigens are often released that otherwise would not be, depending on the virus. But it’s the case with parvoviruses. They integrate with the virus’s genetic material. When cells rupture, certain proteins are then revealed, hybrids of viruses and the human genome, and these are attractive to the immune system.
There is a whole range of studies on this subject. However, there are currently no randomized studies that directly compare the therapies. But the expectation is that the use of parvoviruses could be a good addition to therapy.
One limitation that should be mentioned is that the use of viruses may be beneficial for some patients, but it will not have an effect in every patient. What is exciting about parvoviruses is that these viruses can be injected via the bloodstream and still achieve a good effect in the brain.
Protein APG101
Q: How relevant is the recombinant protein APG101 to therapy?
A: APG101 is a protein that simulates the cell-death receptor CD95 and binds with a stable antibody fragment. By doing so, it blocks the signaling pathway between CD95 ligand and receptor. The interaction between the CD95 ligand and the CD95 receptor activates an intracellular signaling pathway, which in turn stimulates the invasive growth and migration of tumor cells.
APG101 blocks the CD95 ligand and thereby prevents the activation of the CD95 signaling pathway, which leads to a reduction in the invasive cell growth and migration.
Apoptosis, programmed cell death, is a system we have used throughout our evolution to kill off the cell components we no longer need. During tumor development, this system is perverted, so to speak. Here, the stimulation of this system does not actually lead to cell death but rather to cell movement (i.e., to cell mobility). And in principle, APG101 blocks this mobility.
To date, I only know of three studies in which the medication has been used for tumors. One study was published 8 years ago. We demonstrated that we can achieve a relatively good effect with APG101 in connection with repeat irradiation, compared with repeat irradiation alone. We consider this effect to most likely be due to this influence on cell mobility.
There is a study on primary therapy: a four-arm study by the Neuro-Oncological Working Group. The results are still not available, however. In addition, a study on primary therapy with APG101 is currently being conducted in China. It is investigating whether the mechanism of action influences mobility. Whether it will be pushed through as therapy remains to be seen.
Vaccinations and antigens
Q: Vaccinations are of course a part of immunotherapy. What is their status?
A: We are looking at the IDH1 protein, which is present in mutated form in a group of brain tumors, as a very good target for a vaccine. The reason is that the protein is present in its mutated form in every cell of the tumor but not in healthy cells. That is a prerequisite for immunotherapy.
We started a study with peptides a few years ago. These peptides are injected under the skin on the stomach and leg. They cause an immune response systemically and in the brain tumor. This immune response may cause an inflammatory reaction (we can demonstrate this inflammatory reaction). And in this noncontrolled study, the approach was successful, at least compared to historical controls. There is no randomized study with treatment-naive control patients.
However, we are cautious because we know that peptide, unlike CAR T cells or RNA-based vaccines, for example, only triggers a relatively small immune response in many patients. The scale of the immune response is important, rather than the specificity. The scale is probably not large enough in most patients for a long-term effect to be expected.
But there are exceptions. Patients we vaccinated many years ago still have a very remarkable immune status. But we also have patients in whom an immune status cannot even be seen anymore, after just a short period of time.
Therefore, our aim is to perform the immune strategy with more effective, stronger measures – not more specific, but stronger. Unfortunately, it is often the case with glioblastomas that there is not a single antigen that can be vaccinated against. Instead, a relatively large cocktail is needed, which unfortunately also often varies from patient to patient. The conditions are difficult.
Q: You mentioned that glioblastomas can be classified into subgroups. Does this improve the prognosis?
A: Yes, in certain subgroups the prognosis improves. That is the case with those usually very small groups that are molecularly well defined. I believe that by better understanding the individual groups, we have succeeded in making major progress in those groups. But where there is light, there is also shadow. We know that there are many groups with which we have not achieved a great deal.
Fundamental research leads to a better understanding, and the next step in this is to be able to adapt the therapy. Instead of it being one therapy for everyone, it will become a part of various differing therapies for these quite different groups. We are making a lot of progress with individual groups. But unfortunately, we have not come quite as far as we want with many patients.
This article was translated from the Medscape German edition. A version of this article first appeared on Medscape.com.
Every year, around 7,000 people in Germany develop a brain tumor, and around half of those cases involve a glioblastoma, a particularly aggressive form of the disease. Glioblastomas are incurable, but advances are being made in both diagnostics and therapy.
This news organization spoke to Wolfgang Wick, MD, medical director of the neurologic clinic at UKHD, about how glioblastomas are treated; the role that vaccinations, recombinant proteins, and parvoviruses play; and what therapeutic approaches might be derived from the discovery of this method by which glioblastomas spread.
Question: Glioblastomas spread through the brain like a fungal network. So how would a glioblastoma currently be treated? The tumor can only be partially removed through surgery.
Answer: Nevertheless, glioblastoma would be operated on. This would have a significant effect. Relieving the strain of the main tumor mass, without generating a new deficit, is prognostically very good for the patient concerned. However, surgery on glioblastoma is never curative.
The reason a cure is not possible is down to the special form and spread of the glioblastoma. Nevertheless, an operation helps. This seems to be because removing the main tumor mass maybe has a positive immunological effect. But it may also be connected to the tumor’s network communication. The surgical intervention stimulates the network by increasing resistance.
If the main tumor mass is decreased through a surgical procedure, this results in an at least temporarily improved starting position for the patient until the mass regenerates. This could also be connected to the fact that tumor communication is not unregulated but is rather in accordance with a certain hierarchy and order, which requires a certain structure and mass.
The other aspect is that support can be requested via this communication. You can imagine that a cell connected to another cell via a conduit receives help from this other cell in the form of organelles by exchanging ions and that, for example, stress or toxicity can be much better balanced out in large networks than in small networks. That means that external attacks, such as a surgical intervention, can be much better balanced by a well-organized network than by isolated cells.
Resistance to chemotherapy
Q: How do irradiation and chemotherapy rank in the treatment of glioblastomas?
A: Irradiation is another therapeutic approach. It causes cells to be stuck in the growth phase of the cell cycle. The cells are not killed through radiation, but they are practically halted. And this arrest of the cell cycle is often sufficient to help people with glioblastomas for a very long time. But the same is true for irradiation as for surgery. This deep network of cells cannot be addressed.
Attempts have been made in the past to reduce the radiation dose to the extent that the brain is no longer damaged by it, but this low dose was then not sufficient to exert any control. If you want to control the tumor, the dose must be high and the volume must be correspondingly low, since there is a clear limit.
Every patient is offered alkylating chemotherapy. At the moment, just one substance is used here in the primary therapy: temozolomide. The problem with this is that two-thirds of tumors in all cells exhibit a resistance to this alkylating chemotherapy, which means that the efficacy of this therapy is highly limited in two-thirds of patients.
In the one-third of patients in whom this resistance is not present, the chemotherapy works fairly well. But even then, it is unfortunately only a matter of time until there is a relapse or disease progression. In my practice, this has always been the case, but there are people who have been living with this disease for 20 years now. There seem to be tumor cells that calmly and silently survive this phase of chemotherapy and then restart the cell cycle at some point.
Q: What do you think of alternating electric fields as a therapy option?
A: Therapy with alternating electric fields is currently being used and offered to patients. This means that patients who have survived well through radiochemotherapy should also be offered treatment with alternating electric fields.
However, what happens in this process is not as well understood as with other therapies. It is assumed that the cell cycle, i.e., cell division, is altered by disrupting the mitotic spindle. But you can imagine, and this is now speculation, but quite sound speculation I believe, that alternating electric fields also cause a certain amount of confusion in the previously described networks. But this still needs to be investigated in more detail.
It is not implausible. We know that such alternating electric fields disturb the organization of cell organelles. And we also know that for this communication, we need fairly good order and also organization. This would definitely be a starting point on the way to understanding why this therapy potentially shows a certain effect in some patients.
Nerve cell precursors
Q: Scientists from the UKHD and the DKFZ have discovered a new glioblastoma spreading strategy and have learned that the tumor cells imitate the properties and movement patterns of nerve cells. They are labeling the results a “milestone in the field of cancer neuroscience.” Could you explain a bit more?
A: Glioblastoma does not grow on its own as a solid mass, but instead, the entire brain is affected by the disease. The question of how the tumor’s individual cells move the main tumor mass from afar, how they get there, how they continue to be supplied, and what their interaction partners are – an entirely new light has been shed on all of this in our work.
The development of tumor cell mobility has been recognized as a remnant of brain development. The tumor cells have retained properties that the precursor cells for nervous-system development require for an organized nervous system to emerge from just a few cells. This means that the tumor cells copy or eventually retain properties of the nerve-cell precursors that, unlike mature nerve cells, are mobile to a fairly high degree.
Mobility here means that it can advance along a network, despite said network being very densely packed. This also means that certain processes, such as releasing and then continuing to move again, must function and that the communication regarding the original disease must be maintained.
First, we understand what the different glioblastoma cell types do, which molecular properties are associated with which behaviors, and which cell type (namely the swarming cells) is responsible for the invasive tumor growth. In contrast, the network-forming cell type, which only develops from these, is responsible for the resistance.
Interrupting communication
Q: Which starting points for new therapies do you see?
A: In terms of new therapies, these movement phenomena are one good starting point. The other starting point – I find this one much more interesting – is that the programming steps that these tumor cells use [are] no longer needed. This is because our mature nervous system no longer requires this program, which was necessary for the mobility of cells in development.
Our central nervous system exhibits little cell movement. This is to do with programs of nervous-system development that are switched off in the mature nervous system. But they are then reactivated or remain active in the tumor cells. This process reveals potential starting points for therapy.
Addressing the movement of cells, that has been investigated for the last 20 years, but it seems to have an extraordinarily high number of side effects, because these movement mechanisms are also important for other, healthy cells in the body. For example, digestive mechanisms and other proliferation mechanisms, on mucous membranes, in the blood system, in the bone marrow, are then affected and no longer function.
There is another possible approach: the more-or-less specific interaction between the nerve cells and the tumor cells also offers starting points for therapies, from our point of view. The key word is epilepsy treatment. We know that people with brain tumors suffer badly, or worse than usual, from epileptic seizures. This was often regarded purely as a pressure problem. There is a disruptive element in the brain, and this causes the electrical activity in the brain to become disorganized. For some people, this can lead to seizures in certain situations.
The communication between tumor cells and nerve cells takes place via transmission substances, e.g., through the neurotransmitter glutamate. Now you can consider whether a “surplus” of communication, such as an excessively strong stimulus, can trigger epileptic seizures.
In this work, we demonstrate that by interrupting this communication, we can also prevent the movement of these cells and the growth, the proliferation, of these cells.
Q: What is the significance of parvoviruses for therapy?
A: The major topic for cancer is immunotherapy. And one option for performing immunotherapies lies with viruses. Parvoviruses are a plausible therapy for proliferating cells.
Parvoviruses are usually administered locally. This means that a surgical cavity is infected with the viruses and the tumor cells that remain after an operation will then hopefully be killed off by these viruses.
This is the first step and the immediate effect of virus therapy. The attempt is made to kill off cells in the same way as with a medication. The advantage of viruses is the high specificity, i.e., only dividing cells will be attacked. In addition, parvoviruses are so small that they can also spread well and circulate through the brain.
The second reason for immunotherapy is that when killing off cells with viruses, antigens are often released that otherwise would not be, depending on the virus. But it’s the case with parvoviruses. They integrate with the virus’s genetic material. When cells rupture, certain proteins are then revealed, hybrids of viruses and the human genome, and these are attractive to the immune system.
There is a whole range of studies on this subject. However, there are currently no randomized studies that directly compare the therapies. But the expectation is that the use of parvoviruses could be a good addition to therapy.
One limitation that should be mentioned is that the use of viruses may be beneficial for some patients, but it will not have an effect in every patient. What is exciting about parvoviruses is that these viruses can be injected via the bloodstream and still achieve a good effect in the brain.
Protein APG101
Q: How relevant is the recombinant protein APG101 to therapy?
A: APG101 is a protein that simulates the cell-death receptor CD95 and binds with a stable antibody fragment. By doing so, it blocks the signaling pathway between CD95 ligand and receptor. The interaction between the CD95 ligand and the CD95 receptor activates an intracellular signaling pathway, which in turn stimulates the invasive growth and migration of tumor cells.
APG101 blocks the CD95 ligand and thereby prevents the activation of the CD95 signaling pathway, which leads to a reduction in the invasive cell growth and migration.
Apoptosis, programmed cell death, is a system we have used throughout our evolution to kill off the cell components we no longer need. During tumor development, this system is perverted, so to speak. Here, the stimulation of this system does not actually lead to cell death but rather to cell movement (i.e., to cell mobility). And in principle, APG101 blocks this mobility.
To date, I only know of three studies in which the medication has been used for tumors. One study was published 8 years ago. We demonstrated that we can achieve a relatively good effect with APG101 in connection with repeat irradiation, compared with repeat irradiation alone. We consider this effect to most likely be due to this influence on cell mobility.
There is a study on primary therapy: a four-arm study by the Neuro-Oncological Working Group. The results are still not available, however. In addition, a study on primary therapy with APG101 is currently being conducted in China. It is investigating whether the mechanism of action influences mobility. Whether it will be pushed through as therapy remains to be seen.
Vaccinations and antigens
Q: Vaccinations are of course a part of immunotherapy. What is their status?
A: We are looking at the IDH1 protein, which is present in mutated form in a group of brain tumors, as a very good target for a vaccine. The reason is that the protein is present in its mutated form in every cell of the tumor but not in healthy cells. That is a prerequisite for immunotherapy.
We started a study with peptides a few years ago. These peptides are injected under the skin on the stomach and leg. They cause an immune response systemically and in the brain tumor. This immune response may cause an inflammatory reaction (we can demonstrate this inflammatory reaction). And in this noncontrolled study, the approach was successful, at least compared to historical controls. There is no randomized study with treatment-naive control patients.
However, we are cautious because we know that peptide, unlike CAR T cells or RNA-based vaccines, for example, only triggers a relatively small immune response in many patients. The scale of the immune response is important, rather than the specificity. The scale is probably not large enough in most patients for a long-term effect to be expected.
But there are exceptions. Patients we vaccinated many years ago still have a very remarkable immune status. But we also have patients in whom an immune status cannot even be seen anymore, after just a short period of time.
Therefore, our aim is to perform the immune strategy with more effective, stronger measures – not more specific, but stronger. Unfortunately, it is often the case with glioblastomas that there is not a single antigen that can be vaccinated against. Instead, a relatively large cocktail is needed, which unfortunately also often varies from patient to patient. The conditions are difficult.
Q: You mentioned that glioblastomas can be classified into subgroups. Does this improve the prognosis?
A: Yes, in certain subgroups the prognosis improves. That is the case with those usually very small groups that are molecularly well defined. I believe that by better understanding the individual groups, we have succeeded in making major progress in those groups. But where there is light, there is also shadow. We know that there are many groups with which we have not achieved a great deal.
Fundamental research leads to a better understanding, and the next step in this is to be able to adapt the therapy. Instead of it being one therapy for everyone, it will become a part of various differing therapies for these quite different groups. We are making a lot of progress with individual groups. But unfortunately, we have not come quite as far as we want with many patients.
This article was translated from the Medscape German edition. A version of this article first appeared on Medscape.com.
Every year, around 7,000 people in Germany develop a brain tumor, and around half of those cases involve a glioblastoma, a particularly aggressive form of the disease. Glioblastomas are incurable, but advances are being made in both diagnostics and therapy.
This news organization spoke to Wolfgang Wick, MD, medical director of the neurologic clinic at UKHD, about how glioblastomas are treated; the role that vaccinations, recombinant proteins, and parvoviruses play; and what therapeutic approaches might be derived from the discovery of this method by which glioblastomas spread.
Question: Glioblastomas spread through the brain like a fungal network. So how would a glioblastoma currently be treated? The tumor can only be partially removed through surgery.
Answer: Nevertheless, glioblastoma would be operated on. This would have a significant effect. Relieving the strain of the main tumor mass, without generating a new deficit, is prognostically very good for the patient concerned. However, surgery on glioblastoma is never curative.
The reason a cure is not possible is down to the special form and spread of the glioblastoma. Nevertheless, an operation helps. This seems to be because removing the main tumor mass maybe has a positive immunological effect. But it may also be connected to the tumor’s network communication. The surgical intervention stimulates the network by increasing resistance.
If the main tumor mass is decreased through a surgical procedure, this results in an at least temporarily improved starting position for the patient until the mass regenerates. This could also be connected to the fact that tumor communication is not unregulated but is rather in accordance with a certain hierarchy and order, which requires a certain structure and mass.
The other aspect is that support can be requested via this communication. You can imagine that a cell connected to another cell via a conduit receives help from this other cell in the form of organelles by exchanging ions and that, for example, stress or toxicity can be much better balanced out in large networks than in small networks. That means that external attacks, such as a surgical intervention, can be much better balanced by a well-organized network than by isolated cells.
Resistance to chemotherapy
Q: How do irradiation and chemotherapy rank in the treatment of glioblastomas?
A: Irradiation is another therapeutic approach. It causes cells to be stuck in the growth phase of the cell cycle. The cells are not killed through radiation, but they are practically halted. And this arrest of the cell cycle is often sufficient to help people with glioblastomas for a very long time. But the same is true for irradiation as for surgery. This deep network of cells cannot be addressed.
Attempts have been made in the past to reduce the radiation dose to the extent that the brain is no longer damaged by it, but this low dose was then not sufficient to exert any control. If you want to control the tumor, the dose must be high and the volume must be correspondingly low, since there is a clear limit.
Every patient is offered alkylating chemotherapy. At the moment, just one substance is used here in the primary therapy: temozolomide. The problem with this is that two-thirds of tumors in all cells exhibit a resistance to this alkylating chemotherapy, which means that the efficacy of this therapy is highly limited in two-thirds of patients.
In the one-third of patients in whom this resistance is not present, the chemotherapy works fairly well. But even then, it is unfortunately only a matter of time until there is a relapse or disease progression. In my practice, this has always been the case, but there are people who have been living with this disease for 20 years now. There seem to be tumor cells that calmly and silently survive this phase of chemotherapy and then restart the cell cycle at some point.
Q: What do you think of alternating electric fields as a therapy option?
A: Therapy with alternating electric fields is currently being used and offered to patients. This means that patients who have survived well through radiochemotherapy should also be offered treatment with alternating electric fields.
However, what happens in this process is not as well understood as with other therapies. It is assumed that the cell cycle, i.e., cell division, is altered by disrupting the mitotic spindle. But you can imagine, and this is now speculation, but quite sound speculation I believe, that alternating electric fields also cause a certain amount of confusion in the previously described networks. But this still needs to be investigated in more detail.
It is not implausible. We know that such alternating electric fields disturb the organization of cell organelles. And we also know that for this communication, we need fairly good order and also organization. This would definitely be a starting point on the way to understanding why this therapy potentially shows a certain effect in some patients.
Nerve cell precursors
Q: Scientists from the UKHD and the DKFZ have discovered a new glioblastoma spreading strategy and have learned that the tumor cells imitate the properties and movement patterns of nerve cells. They are labeling the results a “milestone in the field of cancer neuroscience.” Could you explain a bit more?
A: Glioblastoma does not grow on its own as a solid mass, but instead, the entire brain is affected by the disease. The question of how the tumor’s individual cells move the main tumor mass from afar, how they get there, how they continue to be supplied, and what their interaction partners are – an entirely new light has been shed on all of this in our work.
The development of tumor cell mobility has been recognized as a remnant of brain development. The tumor cells have retained properties that the precursor cells for nervous-system development require for an organized nervous system to emerge from just a few cells. This means that the tumor cells copy or eventually retain properties of the nerve-cell precursors that, unlike mature nerve cells, are mobile to a fairly high degree.
Mobility here means that it can advance along a network, despite said network being very densely packed. This also means that certain processes, such as releasing and then continuing to move again, must function and that the communication regarding the original disease must be maintained.
First, we understand what the different glioblastoma cell types do, which molecular properties are associated with which behaviors, and which cell type (namely the swarming cells) is responsible for the invasive tumor growth. In contrast, the network-forming cell type, which only develops from these, is responsible for the resistance.
Interrupting communication
Q: Which starting points for new therapies do you see?
A: In terms of new therapies, these movement phenomena are one good starting point. The other starting point – I find this one much more interesting – is that the programming steps that these tumor cells use [are] no longer needed. This is because our mature nervous system no longer requires this program, which was necessary for the mobility of cells in development.
Our central nervous system exhibits little cell movement. This is to do with programs of nervous-system development that are switched off in the mature nervous system. But they are then reactivated or remain active in the tumor cells. This process reveals potential starting points for therapy.
Addressing the movement of cells, that has been investigated for the last 20 years, but it seems to have an extraordinarily high number of side effects, because these movement mechanisms are also important for other, healthy cells in the body. For example, digestive mechanisms and other proliferation mechanisms, on mucous membranes, in the blood system, in the bone marrow, are then affected and no longer function.
There is another possible approach: the more-or-less specific interaction between the nerve cells and the tumor cells also offers starting points for therapies, from our point of view. The key word is epilepsy treatment. We know that people with brain tumors suffer badly, or worse than usual, from epileptic seizures. This was often regarded purely as a pressure problem. There is a disruptive element in the brain, and this causes the electrical activity in the brain to become disorganized. For some people, this can lead to seizures in certain situations.
The communication between tumor cells and nerve cells takes place via transmission substances, e.g., through the neurotransmitter glutamate. Now you can consider whether a “surplus” of communication, such as an excessively strong stimulus, can trigger epileptic seizures.
In this work, we demonstrate that by interrupting this communication, we can also prevent the movement of these cells and the growth, the proliferation, of these cells.
Q: What is the significance of parvoviruses for therapy?
A: The major topic for cancer is immunotherapy. And one option for performing immunotherapies lies with viruses. Parvoviruses are a plausible therapy for proliferating cells.
Parvoviruses are usually administered locally. This means that a surgical cavity is infected with the viruses and the tumor cells that remain after an operation will then hopefully be killed off by these viruses.
This is the first step and the immediate effect of virus therapy. The attempt is made to kill off cells in the same way as with a medication. The advantage of viruses is the high specificity, i.e., only dividing cells will be attacked. In addition, parvoviruses are so small that they can also spread well and circulate through the brain.
The second reason for immunotherapy is that when killing off cells with viruses, antigens are often released that otherwise would not be, depending on the virus. But it’s the case with parvoviruses. They integrate with the virus’s genetic material. When cells rupture, certain proteins are then revealed, hybrids of viruses and the human genome, and these are attractive to the immune system.
There is a whole range of studies on this subject. However, there are currently no randomized studies that directly compare the therapies. But the expectation is that the use of parvoviruses could be a good addition to therapy.
One limitation that should be mentioned is that the use of viruses may be beneficial for some patients, but it will not have an effect in every patient. What is exciting about parvoviruses is that these viruses can be injected via the bloodstream and still achieve a good effect in the brain.
Protein APG101
Q: How relevant is the recombinant protein APG101 to therapy?
A: APG101 is a protein that simulates the cell-death receptor CD95 and binds with a stable antibody fragment. By doing so, it blocks the signaling pathway between CD95 ligand and receptor. The interaction between the CD95 ligand and the CD95 receptor activates an intracellular signaling pathway, which in turn stimulates the invasive growth and migration of tumor cells.
APG101 blocks the CD95 ligand and thereby prevents the activation of the CD95 signaling pathway, which leads to a reduction in the invasive cell growth and migration.
Apoptosis, programmed cell death, is a system we have used throughout our evolution to kill off the cell components we no longer need. During tumor development, this system is perverted, so to speak. Here, the stimulation of this system does not actually lead to cell death but rather to cell movement (i.e., to cell mobility). And in principle, APG101 blocks this mobility.
To date, I only know of three studies in which the medication has been used for tumors. One study was published 8 years ago. We demonstrated that we can achieve a relatively good effect with APG101 in connection with repeat irradiation, compared with repeat irradiation alone. We consider this effect to most likely be due to this influence on cell mobility.
There is a study on primary therapy: a four-arm study by the Neuro-Oncological Working Group. The results are still not available, however. In addition, a study on primary therapy with APG101 is currently being conducted in China. It is investigating whether the mechanism of action influences mobility. Whether it will be pushed through as therapy remains to be seen.
Vaccinations and antigens
Q: Vaccinations are of course a part of immunotherapy. What is their status?
A: We are looking at the IDH1 protein, which is present in mutated form in a group of brain tumors, as a very good target for a vaccine. The reason is that the protein is present in its mutated form in every cell of the tumor but not in healthy cells. That is a prerequisite for immunotherapy.
We started a study with peptides a few years ago. These peptides are injected under the skin on the stomach and leg. They cause an immune response systemically and in the brain tumor. This immune response may cause an inflammatory reaction (we can demonstrate this inflammatory reaction). And in this noncontrolled study, the approach was successful, at least compared to historical controls. There is no randomized study with treatment-naive control patients.
However, we are cautious because we know that peptide, unlike CAR T cells or RNA-based vaccines, for example, only triggers a relatively small immune response in many patients. The scale of the immune response is important, rather than the specificity. The scale is probably not large enough in most patients for a long-term effect to be expected.
But there are exceptions. Patients we vaccinated many years ago still have a very remarkable immune status. But we also have patients in whom an immune status cannot even be seen anymore, after just a short period of time.
Therefore, our aim is to perform the immune strategy with more effective, stronger measures – not more specific, but stronger. Unfortunately, it is often the case with glioblastomas that there is not a single antigen that can be vaccinated against. Instead, a relatively large cocktail is needed, which unfortunately also often varies from patient to patient. The conditions are difficult.
Q: You mentioned that glioblastomas can be classified into subgroups. Does this improve the prognosis?
A: Yes, in certain subgroups the prognosis improves. That is the case with those usually very small groups that are molecularly well defined. I believe that by better understanding the individual groups, we have succeeded in making major progress in those groups. But where there is light, there is also shadow. We know that there are many groups with which we have not achieved a great deal.
Fundamental research leads to a better understanding, and the next step in this is to be able to adapt the therapy. Instead of it being one therapy for everyone, it will become a part of various differing therapies for these quite different groups. We are making a lot of progress with individual groups. But unfortunately, we have not come quite as far as we want with many patients.
This article was translated from the Medscape German edition. A version of this article first appeared on Medscape.com.
Yellow Papules and Plaques on a Child
The Diagnosis: Tuberous Xanthoma
The skin biopsy revealed a nodular collection of foam cells (quiz image [bottom]). Tuberous xanthoma was the most likely diagnosis based on the patient’s history as well as the clinical and histologic findings. Tuberous xanthomas are flat or elevated nodules in the dermis and subcutaneous tissue, commonly occurring on the skin over the joints.1 Smaller nodules and papules often are referred to as tuberoeruptive xanthomas and exist on a continuum with the larger tuberous xanthomas. All xanthomas appear histologically similar, with collections of foam cells present within the dermis.2 Foam cells form when serum lipoproteins diffuse through capillary walls, deposit in the skin or tendons, and are scavenged by monocytes.3 Tuberous xanthomas, along with tendinous, eruptive, and planar xanthomas, are the most likely to be associated with hyperlipidemia.4 They may indicate an underlying disorder of lipid metabolism, such as familial hypercholesterolemia.1,3 This is the most common cause of inheritable cardiovascular disease, with a prevalence of approximately 1:250.2 Premature cardiovascular disease risk increases 2 to 4 times in patients with familial hypercholesterolemia and tendinous xanthomas,1 illustrating that recognition of cutaneous lesions can lead to earlier diagnosis and prevention of patient morbidity and mortality.
Juvenile xanthogranuloma typically presents as smooth yellow papules or nodules on the head and neck, with a characteristic “setting-sun” appearance (ie, yellow center with an erythematous halo) on dermoscopy.5 Histologically, juvenile xanthogranulomas are composed of foam cells and a mixed lymphohistiocytic infiltrate with eosinophils within the dermis. Giant cells with a ring of nuclei surrounded by cytoplasm containing lipid vacuoles (called Touton giant cells) are characteristic (Figure 1). In contrast to tuberous xanthomas, juvenile xanthogranulomas often present within the first year of life.6
. Reference bar indicates 50 mm.")
Keloid scars are more prevalent in patients with skin of color. They are characterized by eosinophilic keloidal collagen with a whorled proliferation of fibroblasts on histology (Figure 2).7 They occur spontaneously or at sites of injury and present as bluish-red or flesh-colored firm papules or nodules.8 In our patient, keloid scars were an unlikely diagnosis due to the lack of trauma and the absence of keloidal collagen on histology.
.")
Necrobiosis lipoidica diabeticorum typically presents as an erythematous, yellow-brown, circular plaque on the anterior lower leg in patients with diabetes mellitus; it rarely occurs in children.9 Microscopy shows palisaded granulomas surrounding necrobiotic collagen arranged horizontally in a layer cake–like fashion (Figure 3).9,10 The etiology of necrobiosis lipoidica diabeticorum currently is unknown, though immune complex deposition may contribute to its pathology. It has been associated with type 1 diabetes mellitus, though severity of the lesions is not associated with extent of glycemic control.10
.")
Rosai-Dorfman disease is an uncommon disorder characterized by a proliferation of histiocytes that most often presents as bilateral cervical lymphadenopathy in children and young adults but rarely can present with cutaneous lesions when extranodal involvement is present.11,12 The cutaneous form most commonly presents as red papules or nodules. On histology, the lesions exhibit a nodular dermal proliferation of histiocytes and smaller lymphocytoid cells with a marbled or starry sky–like appearance on low power (Figure 4). On higher magnification, the characteristic finding of emperipolesis can be seen.11 On immunohistochemistry, the histiocytes stain positively for CD68 and S-100. Although the pathogenesis currently is unknown, evidence of clonality indicates the disease may be related to a neoplastic process.12
.")
- Zak A, Zeman M, Slaby A, et al. Xanthomas: clinical and pathophysiological relations. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2014;158:181-188. doi:10.5507/bp.2014.016
- Ison HE, Clarke SL, Knowles JW. Familial hypercholesterolemia. In: Adam MP, Everman DB, Mirzaa GM, et al, eds. GeneReviews. University of Washington, Seattle; 1993-2022. https://www.ncbi.nlm.nih.gov/books/NBK174884/
- Sathiyakumar V, Jones SR, Martin SS. Xanthomas and lipoprotein disorders. In: Kang S, Amagai M, Bruckner AL, et al, eds. Fitzpatrick’s Dermatology. 9th ed. McGraw Hill; 2019.
- Massangale WT. Xanthomas. In: Bolognia JL, Schaffer JV, Cerroni L, et al, eds. Dermatology. Elsevier; 2018:1634-1643.
- Collie JS, Harper CD, Fillman EP. Juvenile xanthogranuloma. StatPearls. StatPearls Publishing; 2021. https://www.ncbi.nlm.nih.gov/books/NBK526103/
- Hernández-San Martín MJ, Vargas-Mora P, Aranibar L. Juvenile xanthogranuloma: an entity with a wide clinical spectrum. Actas Dermosifiliogr (Engl Ed). 2020;111:725-733. doi:10.1016/j.ad.2020.07.004
- Lee JY, Yang C, Chao S, et al. Histopathological differential diagnosis of keloid and hypertrophic scar. Am J Dermatopathology. 2004;26:379-384.
- Wolff K, Johnson R, Saavedra AP, et al. Benign neoplasms and hyperplasias. In: Wolff K, Johnson R, Saavedra AP, et al, eds. Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology. 8th ed. McGraw Hill; 2017:141-188.
- Bonura C, Frontino G, Rigamonti A, et al. Necrobiosis lipoidica diabeticorum: a pediatric case report. Dermatoendocrinol. 2014;6:E27790. doi:10.4161/derm.27790
- Lepe K, Riley CA, Salazar FJ. Necrobiosis lipoidica. StatPearls. StatPearls Publishing; 2021. https://www-ncbi-nlm-nih-gov.proxy.kumc.edu/books/NBK459318/
- Parrent T, Clark T, Hall D. Cutaneous Rosai-Dorfman disease. Cutis. 2012;90:237-238.
- Bruce-Brand C, Schneider JW, Schubert P. Rosai-Dorfman disease: an overview. J Clin Pathol. 2020;73:697-705. doi:10.1136/jclinpath-2020-206733
The Diagnosis: Tuberous Xanthoma
The skin biopsy revealed a nodular collection of foam cells (quiz image [bottom]). Tuberous xanthoma was the most likely diagnosis based on the patient’s history as well as the clinical and histologic findings. Tuberous xanthomas are flat or elevated nodules in the dermis and subcutaneous tissue, commonly occurring on the skin over the joints.1 Smaller nodules and papules often are referred to as tuberoeruptive xanthomas and exist on a continuum with the larger tuberous xanthomas. All xanthomas appear histologically similar, with collections of foam cells present within the dermis.2 Foam cells form when serum lipoproteins diffuse through capillary walls, deposit in the skin or tendons, and are scavenged by monocytes.3 Tuberous xanthomas, along with tendinous, eruptive, and planar xanthomas, are the most likely to be associated with hyperlipidemia.4 They may indicate an underlying disorder of lipid metabolism, such as familial hypercholesterolemia.1,3 This is the most common cause of inheritable cardiovascular disease, with a prevalence of approximately 1:250.2 Premature cardiovascular disease risk increases 2 to 4 times in patients with familial hypercholesterolemia and tendinous xanthomas,1 illustrating that recognition of cutaneous lesions can lead to earlier diagnosis and prevention of patient morbidity and mortality.
Juvenile xanthogranuloma typically presents as smooth yellow papules or nodules on the head and neck, with a characteristic “setting-sun” appearance (ie, yellow center with an erythematous halo) on dermoscopy.5 Histologically, juvenile xanthogranulomas are composed of foam cells and a mixed lymphohistiocytic infiltrate with eosinophils within the dermis. Giant cells with a ring of nuclei surrounded by cytoplasm containing lipid vacuoles (called Touton giant cells) are characteristic (Figure 1). In contrast to tuberous xanthomas, juvenile xanthogranulomas often present within the first year of life.6
Keloid scars are more prevalent in patients with skin of color. They are characterized by eosinophilic keloidal collagen with a whorled proliferation of fibroblasts on histology (Figure 2).7 They occur spontaneously or at sites of injury and present as bluish-red or flesh-colored firm papules or nodules.8 In our patient, keloid scars were an unlikely diagnosis due to the lack of trauma and the absence of keloidal collagen on histology.
Necrobiosis lipoidica diabeticorum typically presents as an erythematous, yellow-brown, circular plaque on the anterior lower leg in patients with diabetes mellitus; it rarely occurs in children.9 Microscopy shows palisaded granulomas surrounding necrobiotic collagen arranged horizontally in a layer cake–like fashion (Figure 3).9,10 The etiology of necrobiosis lipoidica diabeticorum currently is unknown, though immune complex deposition may contribute to its pathology. It has been associated with type 1 diabetes mellitus, though severity of the lesions is not associated with extent of glycemic control.10
Rosai-Dorfman disease is an uncommon disorder characterized by a proliferation of histiocytes that most often presents as bilateral cervical lymphadenopathy in children and young adults but rarely can present with cutaneous lesions when extranodal involvement is present.11,12 The cutaneous form most commonly presents as red papules or nodules. On histology, the lesions exhibit a nodular dermal proliferation of histiocytes and smaller lymphocytoid cells with a marbled or starry sky–like appearance on low power (Figure 4). On higher magnification, the characteristic finding of emperipolesis can be seen.11 On immunohistochemistry, the histiocytes stain positively for CD68 and S-100. Although the pathogenesis currently is unknown, evidence of clonality indicates the disease may be related to a neoplastic process.12
The Diagnosis: Tuberous Xanthoma
The skin biopsy revealed a nodular collection of foam cells (quiz image [bottom]). Tuberous xanthoma was the most likely diagnosis based on the patient’s history as well as the clinical and histologic findings. Tuberous xanthomas are flat or elevated nodules in the dermis and subcutaneous tissue, commonly occurring on the skin over the joints.1 Smaller nodules and papules often are referred to as tuberoeruptive xanthomas and exist on a continuum with the larger tuberous xanthomas. All xanthomas appear histologically similar, with collections of foam cells present within the dermis.2 Foam cells form when serum lipoproteins diffuse through capillary walls, deposit in the skin or tendons, and are scavenged by monocytes.3 Tuberous xanthomas, along with tendinous, eruptive, and planar xanthomas, are the most likely to be associated with hyperlipidemia.4 They may indicate an underlying disorder of lipid metabolism, such as familial hypercholesterolemia.1,3 This is the most common cause of inheritable cardiovascular disease, with a prevalence of approximately 1:250.2 Premature cardiovascular disease risk increases 2 to 4 times in patients with familial hypercholesterolemia and tendinous xanthomas,1 illustrating that recognition of cutaneous lesions can lead to earlier diagnosis and prevention of patient morbidity and mortality.
Juvenile xanthogranuloma typically presents as smooth yellow papules or nodules on the head and neck, with a characteristic “setting-sun” appearance (ie, yellow center with an erythematous halo) on dermoscopy.5 Histologically, juvenile xanthogranulomas are composed of foam cells and a mixed lymphohistiocytic infiltrate with eosinophils within the dermis. Giant cells with a ring of nuclei surrounded by cytoplasm containing lipid vacuoles (called Touton giant cells) are characteristic (Figure 1). In contrast to tuberous xanthomas, juvenile xanthogranulomas often present within the first year of life.6
Keloid scars are more prevalent in patients with skin of color. They are characterized by eosinophilic keloidal collagen with a whorled proliferation of fibroblasts on histology (Figure 2).7 They occur spontaneously or at sites of injury and present as bluish-red or flesh-colored firm papules or nodules.8 In our patient, keloid scars were an unlikely diagnosis due to the lack of trauma and the absence of keloidal collagen on histology.
Necrobiosis lipoidica diabeticorum typically presents as an erythematous, yellow-brown, circular plaque on the anterior lower leg in patients with diabetes mellitus; it rarely occurs in children.9 Microscopy shows palisaded granulomas surrounding necrobiotic collagen arranged horizontally in a layer cake–like fashion (Figure 3).9,10 The etiology of necrobiosis lipoidica diabeticorum currently is unknown, though immune complex deposition may contribute to its pathology. It has been associated with type 1 diabetes mellitus, though severity of the lesions is not associated with extent of glycemic control.10
Rosai-Dorfman disease is an uncommon disorder characterized by a proliferation of histiocytes that most often presents as bilateral cervical lymphadenopathy in children and young adults but rarely can present with cutaneous lesions when extranodal involvement is present.11,12 The cutaneous form most commonly presents as red papules or nodules. On histology, the lesions exhibit a nodular dermal proliferation of histiocytes and smaller lymphocytoid cells with a marbled or starry sky–like appearance on low power (Figure 4). On higher magnification, the characteristic finding of emperipolesis can be seen.11 On immunohistochemistry, the histiocytes stain positively for CD68 and S-100. Although the pathogenesis currently is unknown, evidence of clonality indicates the disease may be related to a neoplastic process.12
- Zak A, Zeman M, Slaby A, et al. Xanthomas: clinical and pathophysiological relations. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2014;158:181-188. doi:10.5507/bp.2014.016
- Ison HE, Clarke SL, Knowles JW. Familial hypercholesterolemia. In: Adam MP, Everman DB, Mirzaa GM, et al, eds. GeneReviews. University of Washington, Seattle; 1993-2022. https://www.ncbi.nlm.nih.gov/books/NBK174884/
- Sathiyakumar V, Jones SR, Martin SS. Xanthomas and lipoprotein disorders. In: Kang S, Amagai M, Bruckner AL, et al, eds. Fitzpatrick’s Dermatology. 9th ed. McGraw Hill; 2019.
- Massangale WT. Xanthomas. In: Bolognia JL, Schaffer JV, Cerroni L, et al, eds. Dermatology. Elsevier; 2018:1634-1643.
- Collie JS, Harper CD, Fillman EP. Juvenile xanthogranuloma. StatPearls. StatPearls Publishing; 2021. https://www.ncbi.nlm.nih.gov/books/NBK526103/
- Hernández-San Martín MJ, Vargas-Mora P, Aranibar L. Juvenile xanthogranuloma: an entity with a wide clinical spectrum. Actas Dermosifiliogr (Engl Ed). 2020;111:725-733. doi:10.1016/j.ad.2020.07.004
- Lee JY, Yang C, Chao S, et al. Histopathological differential diagnosis of keloid and hypertrophic scar. Am J Dermatopathology. 2004;26:379-384.
- Wolff K, Johnson R, Saavedra AP, et al. Benign neoplasms and hyperplasias. In: Wolff K, Johnson R, Saavedra AP, et al, eds. Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology. 8th ed. McGraw Hill; 2017:141-188.
- Bonura C, Frontino G, Rigamonti A, et al. Necrobiosis lipoidica diabeticorum: a pediatric case report. Dermatoendocrinol. 2014;6:E27790. doi:10.4161/derm.27790
- Lepe K, Riley CA, Salazar FJ. Necrobiosis lipoidica. StatPearls. StatPearls Publishing; 2021. https://www-ncbi-nlm-nih-gov.proxy.kumc.edu/books/NBK459318/
- Parrent T, Clark T, Hall D. Cutaneous Rosai-Dorfman disease. Cutis. 2012;90:237-238.
- Bruce-Brand C, Schneider JW, Schubert P. Rosai-Dorfman disease: an overview. J Clin Pathol. 2020;73:697-705. doi:10.1136/jclinpath-2020-206733
- Zak A, Zeman M, Slaby A, et al. Xanthomas: clinical and pathophysiological relations. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2014;158:181-188. doi:10.5507/bp.2014.016
- Ison HE, Clarke SL, Knowles JW. Familial hypercholesterolemia. In: Adam MP, Everman DB, Mirzaa GM, et al, eds. GeneReviews. University of Washington, Seattle; 1993-2022. https://www.ncbi.nlm.nih.gov/books/NBK174884/
- Sathiyakumar V, Jones SR, Martin SS. Xanthomas and lipoprotein disorders. In: Kang S, Amagai M, Bruckner AL, et al, eds. Fitzpatrick’s Dermatology. 9th ed. McGraw Hill; 2019.
- Massangale WT. Xanthomas. In: Bolognia JL, Schaffer JV, Cerroni L, et al, eds. Dermatology. Elsevier; 2018:1634-1643.
- Collie JS, Harper CD, Fillman EP. Juvenile xanthogranuloma. StatPearls. StatPearls Publishing; 2021. https://www.ncbi.nlm.nih.gov/books/NBK526103/
- Hernández-San Martín MJ, Vargas-Mora P, Aranibar L. Juvenile xanthogranuloma: an entity with a wide clinical spectrum. Actas Dermosifiliogr (Engl Ed). 2020;111:725-733. doi:10.1016/j.ad.2020.07.004
- Lee JY, Yang C, Chao S, et al. Histopathological differential diagnosis of keloid and hypertrophic scar. Am J Dermatopathology. 2004;26:379-384.
- Wolff K, Johnson R, Saavedra AP, et al. Benign neoplasms and hyperplasias. In: Wolff K, Johnson R, Saavedra AP, et al, eds. Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology. 8th ed. McGraw Hill; 2017:141-188.
- Bonura C, Frontino G, Rigamonti A, et al. Necrobiosis lipoidica diabeticorum: a pediatric case report. Dermatoendocrinol. 2014;6:E27790. doi:10.4161/derm.27790
- Lepe K, Riley CA, Salazar FJ. Necrobiosis lipoidica. StatPearls. StatPearls Publishing; 2021. https://www-ncbi-nlm-nih-gov.proxy.kumc.edu/books/NBK459318/
- Parrent T, Clark T, Hall D. Cutaneous Rosai-Dorfman disease. Cutis. 2012;90:237-238.
- Bruce-Brand C, Schneider JW, Schubert P. Rosai-Dorfman disease: an overview. J Clin Pathol. 2020;73:697-705. doi:10.1136/jclinpath-2020-206733
A 3-year-old girl presented with raised, firm, enlarging, asymptomatic, well-defined, subcutaneous papules, plaques, and nodules on the hands, knees, and posterior ankles of 1 year’s duration. The patient’s mother stated that the lesions began on the ankles (top), and she initially believed them to be due to friction from the child’s shoes until the more recent involvement of the knees and hands. The patient’s father, paternal grandfather, and paternal great-grandfather had a history of elevated cholesterol levels. A shave biopsy was performed (bottom).


. Reference bar indicates 50 mm.")
Novel co-admin of CAR T cells achieves 99% remission in leukemia
In this trial, the largest study to date of a CAR T-cell therapy for such patients, the researchers co-administered two CAR T-cell therapies, one targeting CD19 and the other targeting CD22.
The results showed that 192 of 194 patients (99%) achieved a complete remission.
The combined overall 12-month event-free survival was 73.5%.
The study was published online in the Journal of Clinical Oncology.
These results are better than what has been reported for CAR T cells that are already on the market. These products, which target CD19, have achieved complete remission in 85.5% of cases and a 12-month event-free survival of 52.4% in children with B-ALL.
“We do believe [this approach] will become standard of care,” said study author Ching-Hon Pui, MD, of the departments of oncology, pathology, and global pediatric medicine, St. Jude Children’s Research Hospital, Memphis.
He noted that this work builds on the huge success that has already been achieved in this field with CAR T-cell products directed at CD19. The first of these products to reach the market was tisagenlecleucel-T (Novartis).
“To put this study in context, the first child who received CAR T-cell therapy for B-ALL after multiple relapses has recently celebrated her 10-year cancer-free survival milestone, and we hope that our finding will result in many more such milestones,” he said.
These new results are very impressive, said Stephen P. Hunger, MD, an expert commenting for the American Society of Clinical Oncology, which highlighted the research in a press release. “They were also able to treat almost 200 patients in a relatively short time.”
Hunger pointed out that dual administration and targeting is not a new idea and is one of the strategies that is currently under investigation. But it is too early to consider this to be the standard of care, he said. “We want to see it replicated in other centers and to see longer follow-up,” said Dr. Hunger, who is Distinguished Chair in Pediatrics and director of the center for childhood cancer research at Children’s Hospital of Philadelphia. “We can establish this as a first step down the road, and we will see if others will achieve similar results.”
Strategy of dual targeting
Despite the success CAR T-cell therapy in childhood leukemia, the currently available products have limitations, Dr. Pui and colleagues note.
About half of patients treated with CD19 CAR T cells experience relapse within 1 year, owing either to loss of CAR T-cell persistence or to loss of CD19 antigen because of splice variants, acquired genetic mutations, or lineage switch.
With further treatment with CAR T cells directed against CD22, 70%-80% of patients who failed CD19 CAR T will achieve into complete remission. However, most will experience relapse.
Recent efforts in the field have turned to exploring the safety and feasibility of CAR T cells that target both CD19 and CD22. The results were not superior to those of the CD19 CAR T-cell therapy given alone, although sequential treatment has yielded promising response rates, the authors note.
They hypothesized that co-administration of CD19- and CD22-targeted CAR T cells would improve efficacy, as it could forestall the development of drug resistance.
Achieved 99% remission
Dr. Pui and colleagues conducted a phase 2 trial that included 225 evaluable patients aged 20 years or younger who were being treated at five urban hospitals in and near Shanghai, China. Of this group, 194 had refractory disease or hematologic relapse, and 31 patients had isolated extramedullary relapse.
A safety run-in stage to determine the recommended dose was initially conducted. An interim analysis of the first 30 patients who were treated (27 at the recommended dose) showed that the approach was safe and effective. Additional patients were then enrolled.
The 192 patients (of 194) who achieved complete remission attained negative minimal residual disease status.
At a median follow-up of 11 months, 43 patients experienced relapse (24 with CD191/CD221 relapse, 16 with CD19– /CD221, one with CD19– /CD22– , and two unknown), for a cumulative risk of 22.2%.
Transplant and relapse options
In an interview, Dr. Pui noted that various treatment options were available for the children who experienced relapse. “For patients who were in good clinical condition, we will treat them with molecular therapeutics, allogeneic CAR T cells from donor, or even repeated humanized CD19 and/or CD22 CAR T cells with or without CD20 CAR T cells in an attempt to induce a remission for allogeneic transplantation,” he said.
The site-specific 12-month event-free survival rate in the trial was 69.2% for patients who did not receive a transplant, 95% for those children who had an isolated relapse to the testicles, and 68.6% for those who had an isolated central nervous system relapse.
After censoring 78 patients for consolidative transplantation, the 12-month overall survival was 87.7%.
Consolidative transplantation was performed in 24 of the 37 patients with KMT2A-rearranged or ZNF384-rearranged ALL and in 54 patients because of parental request. The reason for this was that patients with these two genetic subtypes of leukemia (KMT2A-rearranged and ZNF384-rearranged), under the pressure of phenotype-specific treatment (such as CAR T cells or blinatumomab) are at risk of lineage switch and development of secondary acute myeloid leukemia, explained Dr. Pui. “That is an even more resistant form of leukemia, and up to 5%-10% of the patients have been reported to develop this complication.
“We performed consolidation transplantation in these patients to avoid the risk of lineage switch but would accept the parental request not to perform allogeneic transplant after they were clearly informed of the risk,” he told this news organization.
He also suggested that this approach of co-administration of two types of CAR T cells would be especially suitable for “patients with extramedullary involvement, because most of them will be spared of local irradiation so that they can preserve their neurocognitive function and fertility and avoid radiation-induced second cancer, such as brain tumor,” he said.
Lower toxicity
With regard to toxicity, the majority of patients (n = 98, 88%) developed cytokine release syndrome, which was grade ≥3 in 64 (28.4%) patients and fatal in one. Neurotoxicity occurred in 47 (20.9%) patients, was of grade ≥3 in 9 (4.0%) patients, and was fatal in 2 patients who received 12 x 106 and 5.6 x 106 CAR T cells/kg.
In addition, grade 3 or 4 seizure developed in 14.2% of the patients; it was more common in those who had presented with isolated or combined CNS leukemia. Grade 3 or 4 hypotension occurred in 40.9% of the patients. About three-quarters of the patients were treated with tocilizumab (n = 67, 74.2%), and 79 (35.1%) were treated with corticosteroids.
“In general, CD19 and CD22 CAR T cells were less toxic than CD19 CAR T cells, the historical controls, in our experience,” said Dr. Pui. “There were three fatal complications, a rate not excessive considering a large number of patients were treated.”
Future studies needed
The researchers note that in this trial, the CD22 CAR T cells did not expand as robustly or persist as long as did the CD19 CAR T cells, and they hope that future studies will elucidate whether enhancing CD22 CAR T-cell persistence and activity would further improve outcomes.
The study was supported in part by the National Natural Science Foundation of China, the Shanghai Collaborative Innovation Center for Translational Medicine, the Research Programs of Shanghai Science, the Technology Commission Foundation, the U.S. National Cancer Institute, the VIVA China Children’s Cancer Foundation, and the American Lebanese Syrian Associated Charities.
A version of this article first appeared on Medscape.com.
In this trial, the largest study to date of a CAR T-cell therapy for such patients, the researchers co-administered two CAR T-cell therapies, one targeting CD19 and the other targeting CD22.
The results showed that 192 of 194 patients (99%) achieved a complete remission.
The combined overall 12-month event-free survival was 73.5%.
The study was published online in the Journal of Clinical Oncology.
These results are better than what has been reported for CAR T cells that are already on the market. These products, which target CD19, have achieved complete remission in 85.5% of cases and a 12-month event-free survival of 52.4% in children with B-ALL.
“We do believe [this approach] will become standard of care,” said study author Ching-Hon Pui, MD, of the departments of oncology, pathology, and global pediatric medicine, St. Jude Children’s Research Hospital, Memphis.
He noted that this work builds on the huge success that has already been achieved in this field with CAR T-cell products directed at CD19. The first of these products to reach the market was tisagenlecleucel-T (Novartis).
“To put this study in context, the first child who received CAR T-cell therapy for B-ALL after multiple relapses has recently celebrated her 10-year cancer-free survival milestone, and we hope that our finding will result in many more such milestones,” he said.
These new results are very impressive, said Stephen P. Hunger, MD, an expert commenting for the American Society of Clinical Oncology, which highlighted the research in a press release. “They were also able to treat almost 200 patients in a relatively short time.”
Hunger pointed out that dual administration and targeting is not a new idea and is one of the strategies that is currently under investigation. But it is too early to consider this to be the standard of care, he said. “We want to see it replicated in other centers and to see longer follow-up,” said Dr. Hunger, who is Distinguished Chair in Pediatrics and director of the center for childhood cancer research at Children’s Hospital of Philadelphia. “We can establish this as a first step down the road, and we will see if others will achieve similar results.”
Strategy of dual targeting
Despite the success CAR T-cell therapy in childhood leukemia, the currently available products have limitations, Dr. Pui and colleagues note.
About half of patients treated with CD19 CAR T cells experience relapse within 1 year, owing either to loss of CAR T-cell persistence or to loss of CD19 antigen because of splice variants, acquired genetic mutations, or lineage switch.
With further treatment with CAR T cells directed against CD22, 70%-80% of patients who failed CD19 CAR T will achieve into complete remission. However, most will experience relapse.
Recent efforts in the field have turned to exploring the safety and feasibility of CAR T cells that target both CD19 and CD22. The results were not superior to those of the CD19 CAR T-cell therapy given alone, although sequential treatment has yielded promising response rates, the authors note.
They hypothesized that co-administration of CD19- and CD22-targeted CAR T cells would improve efficacy, as it could forestall the development of drug resistance.
Achieved 99% remission
Dr. Pui and colleagues conducted a phase 2 trial that included 225 evaluable patients aged 20 years or younger who were being treated at five urban hospitals in and near Shanghai, China. Of this group, 194 had refractory disease or hematologic relapse, and 31 patients had isolated extramedullary relapse.
A safety run-in stage to determine the recommended dose was initially conducted. An interim analysis of the first 30 patients who were treated (27 at the recommended dose) showed that the approach was safe and effective. Additional patients were then enrolled.
The 192 patients (of 194) who achieved complete remission attained negative minimal residual disease status.
At a median follow-up of 11 months, 43 patients experienced relapse (24 with CD191/CD221 relapse, 16 with CD19– /CD221, one with CD19– /CD22– , and two unknown), for a cumulative risk of 22.2%.
Transplant and relapse options
In an interview, Dr. Pui noted that various treatment options were available for the children who experienced relapse. “For patients who were in good clinical condition, we will treat them with molecular therapeutics, allogeneic CAR T cells from donor, or even repeated humanized CD19 and/or CD22 CAR T cells with or without CD20 CAR T cells in an attempt to induce a remission for allogeneic transplantation,” he said.
The site-specific 12-month event-free survival rate in the trial was 69.2% for patients who did not receive a transplant, 95% for those children who had an isolated relapse to the testicles, and 68.6% for those who had an isolated central nervous system relapse.
After censoring 78 patients for consolidative transplantation, the 12-month overall survival was 87.7%.
Consolidative transplantation was performed in 24 of the 37 patients with KMT2A-rearranged or ZNF384-rearranged ALL and in 54 patients because of parental request. The reason for this was that patients with these two genetic subtypes of leukemia (KMT2A-rearranged and ZNF384-rearranged), under the pressure of phenotype-specific treatment (such as CAR T cells or blinatumomab) are at risk of lineage switch and development of secondary acute myeloid leukemia, explained Dr. Pui. “That is an even more resistant form of leukemia, and up to 5%-10% of the patients have been reported to develop this complication.
“We performed consolidation transplantation in these patients to avoid the risk of lineage switch but would accept the parental request not to perform allogeneic transplant after they were clearly informed of the risk,” he told this news organization.
He also suggested that this approach of co-administration of two types of CAR T cells would be especially suitable for “patients with extramedullary involvement, because most of them will be spared of local irradiation so that they can preserve their neurocognitive function and fertility and avoid radiation-induced second cancer, such as brain tumor,” he said.
Lower toxicity
With regard to toxicity, the majority of patients (n = 98, 88%) developed cytokine release syndrome, which was grade ≥3 in 64 (28.4%) patients and fatal in one. Neurotoxicity occurred in 47 (20.9%) patients, was of grade ≥3 in 9 (4.0%) patients, and was fatal in 2 patients who received 12 x 106 and 5.6 x 106 CAR T cells/kg.
In addition, grade 3 or 4 seizure developed in 14.2% of the patients; it was more common in those who had presented with isolated or combined CNS leukemia. Grade 3 or 4 hypotension occurred in 40.9% of the patients. About three-quarters of the patients were treated with tocilizumab (n = 67, 74.2%), and 79 (35.1%) were treated with corticosteroids.
“In general, CD19 and CD22 CAR T cells were less toxic than CD19 CAR T cells, the historical controls, in our experience,” said Dr. Pui. “There were three fatal complications, a rate not excessive considering a large number of patients were treated.”
Future studies needed
The researchers note that in this trial, the CD22 CAR T cells did not expand as robustly or persist as long as did the CD19 CAR T cells, and they hope that future studies will elucidate whether enhancing CD22 CAR T-cell persistence and activity would further improve outcomes.
The study was supported in part by the National Natural Science Foundation of China, the Shanghai Collaborative Innovation Center for Translational Medicine, the Research Programs of Shanghai Science, the Technology Commission Foundation, the U.S. National Cancer Institute, the VIVA China Children’s Cancer Foundation, and the American Lebanese Syrian Associated Charities.
A version of this article first appeared on Medscape.com.
In this trial, the largest study to date of a CAR T-cell therapy for such patients, the researchers co-administered two CAR T-cell therapies, one targeting CD19 and the other targeting CD22.
The results showed that 192 of 194 patients (99%) achieved a complete remission.
The combined overall 12-month event-free survival was 73.5%.
The study was published online in the Journal of Clinical Oncology.
These results are better than what has been reported for CAR T cells that are already on the market. These products, which target CD19, have achieved complete remission in 85.5% of cases and a 12-month event-free survival of 52.4% in children with B-ALL.
“We do believe [this approach] will become standard of care,” said study author Ching-Hon Pui, MD, of the departments of oncology, pathology, and global pediatric medicine, St. Jude Children’s Research Hospital, Memphis.
He noted that this work builds on the huge success that has already been achieved in this field with CAR T-cell products directed at CD19. The first of these products to reach the market was tisagenlecleucel-T (Novartis).
“To put this study in context, the first child who received CAR T-cell therapy for B-ALL after multiple relapses has recently celebrated her 10-year cancer-free survival milestone, and we hope that our finding will result in many more such milestones,” he said.
These new results are very impressive, said Stephen P. Hunger, MD, an expert commenting for the American Society of Clinical Oncology, which highlighted the research in a press release. “They were also able to treat almost 200 patients in a relatively short time.”
Hunger pointed out that dual administration and targeting is not a new idea and is one of the strategies that is currently under investigation. But it is too early to consider this to be the standard of care, he said. “We want to see it replicated in other centers and to see longer follow-up,” said Dr. Hunger, who is Distinguished Chair in Pediatrics and director of the center for childhood cancer research at Children’s Hospital of Philadelphia. “We can establish this as a first step down the road, and we will see if others will achieve similar results.”
Strategy of dual targeting
Despite the success CAR T-cell therapy in childhood leukemia, the currently available products have limitations, Dr. Pui and colleagues note.
About half of patients treated with CD19 CAR T cells experience relapse within 1 year, owing either to loss of CAR T-cell persistence or to loss of CD19 antigen because of splice variants, acquired genetic mutations, or lineage switch.
With further treatment with CAR T cells directed against CD22, 70%-80% of patients who failed CD19 CAR T will achieve into complete remission. However, most will experience relapse.
Recent efforts in the field have turned to exploring the safety and feasibility of CAR T cells that target both CD19 and CD22. The results were not superior to those of the CD19 CAR T-cell therapy given alone, although sequential treatment has yielded promising response rates, the authors note.
They hypothesized that co-administration of CD19- and CD22-targeted CAR T cells would improve efficacy, as it could forestall the development of drug resistance.
Achieved 99% remission
Dr. Pui and colleagues conducted a phase 2 trial that included 225 evaluable patients aged 20 years or younger who were being treated at five urban hospitals in and near Shanghai, China. Of this group, 194 had refractory disease or hematologic relapse, and 31 patients had isolated extramedullary relapse.
A safety run-in stage to determine the recommended dose was initially conducted. An interim analysis of the first 30 patients who were treated (27 at the recommended dose) showed that the approach was safe and effective. Additional patients were then enrolled.
The 192 patients (of 194) who achieved complete remission attained negative minimal residual disease status.
At a median follow-up of 11 months, 43 patients experienced relapse (24 with CD191/CD221 relapse, 16 with CD19– /CD221, one with CD19– /CD22– , and two unknown), for a cumulative risk of 22.2%.
Transplant and relapse options
In an interview, Dr. Pui noted that various treatment options were available for the children who experienced relapse. “For patients who were in good clinical condition, we will treat them with molecular therapeutics, allogeneic CAR T cells from donor, or even repeated humanized CD19 and/or CD22 CAR T cells with or without CD20 CAR T cells in an attempt to induce a remission for allogeneic transplantation,” he said.
The site-specific 12-month event-free survival rate in the trial was 69.2% for patients who did not receive a transplant, 95% for those children who had an isolated relapse to the testicles, and 68.6% for those who had an isolated central nervous system relapse.
After censoring 78 patients for consolidative transplantation, the 12-month overall survival was 87.7%.
Consolidative transplantation was performed in 24 of the 37 patients with KMT2A-rearranged or ZNF384-rearranged ALL and in 54 patients because of parental request. The reason for this was that patients with these two genetic subtypes of leukemia (KMT2A-rearranged and ZNF384-rearranged), under the pressure of phenotype-specific treatment (such as CAR T cells or blinatumomab) are at risk of lineage switch and development of secondary acute myeloid leukemia, explained Dr. Pui. “That is an even more resistant form of leukemia, and up to 5%-10% of the patients have been reported to develop this complication.
“We performed consolidation transplantation in these patients to avoid the risk of lineage switch but would accept the parental request not to perform allogeneic transplant after they were clearly informed of the risk,” he told this news organization.
He also suggested that this approach of co-administration of two types of CAR T cells would be especially suitable for “patients with extramedullary involvement, because most of them will be spared of local irradiation so that they can preserve their neurocognitive function and fertility and avoid radiation-induced second cancer, such as brain tumor,” he said.
Lower toxicity
With regard to toxicity, the majority of patients (n = 98, 88%) developed cytokine release syndrome, which was grade ≥3 in 64 (28.4%) patients and fatal in one. Neurotoxicity occurred in 47 (20.9%) patients, was of grade ≥3 in 9 (4.0%) patients, and was fatal in 2 patients who received 12 x 106 and 5.6 x 106 CAR T cells/kg.
In addition, grade 3 or 4 seizure developed in 14.2% of the patients; it was more common in those who had presented with isolated or combined CNS leukemia. Grade 3 or 4 hypotension occurred in 40.9% of the patients. About three-quarters of the patients were treated with tocilizumab (n = 67, 74.2%), and 79 (35.1%) were treated with corticosteroids.
“In general, CD19 and CD22 CAR T cells were less toxic than CD19 CAR T cells, the historical controls, in our experience,” said Dr. Pui. “There were three fatal complications, a rate not excessive considering a large number of patients were treated.”
Future studies needed
The researchers note that in this trial, the CD22 CAR T cells did not expand as robustly or persist as long as did the CD19 CAR T cells, and they hope that future studies will elucidate whether enhancing CD22 CAR T-cell persistence and activity would further improve outcomes.
The study was supported in part by the National Natural Science Foundation of China, the Shanghai Collaborative Innovation Center for Translational Medicine, the Research Programs of Shanghai Science, the Technology Commission Foundation, the U.S. National Cancer Institute, the VIVA China Children’s Cancer Foundation, and the American Lebanese Syrian Associated Charities.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF CLINICAL ONCOLOGY
An adolescent male presents with an eroded bump on the temple
The correct answer is (D), molluscum contagiosum. Upon surgical excision, the pathology indicated the lesion was consistent with molluscum contagiosum.
Molluscum contagiosum is a benign skin disorder caused by a pox virus and is frequently seen in children. This disease is transmitted primarily through direct skin contact with an infected individual.1 Contaminated fomites have been suggested as another source of infection.2 The typical lesion appears dome-shaped, round, and pinkish-purple in color.1 The incubation period ranges from 2 weeks to 6 months and is typically self-limited in immunocompetent hosts; however, in immunocompromised persons, molluscum contagiosum lesions may present atypically such that they are larger in size and/or resemble malignancies, such as basal cell carcinoma or keratoacanthoma (for single lesions), or other infectious diseases, such as cryptococcosis and histoplasmosis (for more numerous lesions).3,4 A giant atypical molluscum contagiosum is rarely seen in healthy individuals.
What’s on the differential?
The recent episode of bleeding raises concern for other neoplastic processes of the skin including squamous cell carcinoma or basal cell carcinoma as well as cutaneous metastatic rhabdoid tumor, given the patient’s history.

Eruptive keratoacanthomas are also reported in patients taking nivolumab, an anti-PD-1 immunotherapy, which the patient has received for treatment of his recurrent metastatic rhabdoid tumor.5 More common entities such as a pyogenic granuloma or verruca are also included on the differential. The initial presentation of the lesion, however, is more consistent with the pearly umbilicated papules associated with molluscum contagiosum.
Comments from Dr. Eichenfield
This is a very hard diagnosis to make with the clinical findings and history.

Molluscum contagiosum infections are common, but with this patient’s medical history, biopsy and excision with pathologic examination was an appropriate approach to make a certain diagnosis.
Ms. Moyal is a research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego.
References
1. Brown J et al. Int J Dermatol. 2006 Feb;45(2):93-9.
2. Hanson D and Diven DG. Dermatol Online J. 2003 Mar;9(2).
3. Badri T and Gandhi GR. Molluscum contagiosum. 2022. In: StatPearls [Internet]. Treasure Island, Fla.: StatPearls Publishing.
4. Schwartz JJ and Myskowski PL. J Am Acad Dermatol. 1992 Oct 1;27(4):583-8.
5. Antonov NK et al. JAAD Case Rep. 2019 Apr 5;5(4):342-5.
The correct answer is (D), molluscum contagiosum. Upon surgical excision, the pathology indicated the lesion was consistent with molluscum contagiosum.
Molluscum contagiosum is a benign skin disorder caused by a pox virus and is frequently seen in children. This disease is transmitted primarily through direct skin contact with an infected individual.1 Contaminated fomites have been suggested as another source of infection.2 The typical lesion appears dome-shaped, round, and pinkish-purple in color.1 The incubation period ranges from 2 weeks to 6 months and is typically self-limited in immunocompetent hosts; however, in immunocompromised persons, molluscum contagiosum lesions may present atypically such that they are larger in size and/or resemble malignancies, such as basal cell carcinoma or keratoacanthoma (for single lesions), or other infectious diseases, such as cryptococcosis and histoplasmosis (for more numerous lesions).3,4 A giant atypical molluscum contagiosum is rarely seen in healthy individuals.
What’s on the differential?
The recent episode of bleeding raises concern for other neoplastic processes of the skin including squamous cell carcinoma or basal cell carcinoma as well as cutaneous metastatic rhabdoid tumor, given the patient’s history.
Eruptive keratoacanthomas are also reported in patients taking nivolumab, an anti-PD-1 immunotherapy, which the patient has received for treatment of his recurrent metastatic rhabdoid tumor.5 More common entities such as a pyogenic granuloma or verruca are also included on the differential. The initial presentation of the lesion, however, is more consistent with the pearly umbilicated papules associated with molluscum contagiosum.
Comments from Dr. Eichenfield
This is a very hard diagnosis to make with the clinical findings and history.
Molluscum contagiosum infections are common, but with this patient’s medical history, biopsy and excision with pathologic examination was an appropriate approach to make a certain diagnosis.
Ms. Moyal is a research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego.
References
1. Brown J et al. Int J Dermatol. 2006 Feb;45(2):93-9.
2. Hanson D and Diven DG. Dermatol Online J. 2003 Mar;9(2).
3. Badri T and Gandhi GR. Molluscum contagiosum. 2022. In: StatPearls [Internet]. Treasure Island, Fla.: StatPearls Publishing.
4. Schwartz JJ and Myskowski PL. J Am Acad Dermatol. 1992 Oct 1;27(4):583-8.
5. Antonov NK et al. JAAD Case Rep. 2019 Apr 5;5(4):342-5.
The correct answer is (D), molluscum contagiosum. Upon surgical excision, the pathology indicated the lesion was consistent with molluscum contagiosum.
Molluscum contagiosum is a benign skin disorder caused by a pox virus and is frequently seen in children. This disease is transmitted primarily through direct skin contact with an infected individual.1 Contaminated fomites have been suggested as another source of infection.2 The typical lesion appears dome-shaped, round, and pinkish-purple in color.1 The incubation period ranges from 2 weeks to 6 months and is typically self-limited in immunocompetent hosts; however, in immunocompromised persons, molluscum contagiosum lesions may present atypically such that they are larger in size and/or resemble malignancies, such as basal cell carcinoma or keratoacanthoma (for single lesions), or other infectious diseases, such as cryptococcosis and histoplasmosis (for more numerous lesions).3,4 A giant atypical molluscum contagiosum is rarely seen in healthy individuals.
What’s on the differential?
The recent episode of bleeding raises concern for other neoplastic processes of the skin including squamous cell carcinoma or basal cell carcinoma as well as cutaneous metastatic rhabdoid tumor, given the patient’s history.
Eruptive keratoacanthomas are also reported in patients taking nivolumab, an anti-PD-1 immunotherapy, which the patient has received for treatment of his recurrent metastatic rhabdoid tumor.5 More common entities such as a pyogenic granuloma or verruca are also included on the differential. The initial presentation of the lesion, however, is more consistent with the pearly umbilicated papules associated with molluscum contagiosum.
Comments from Dr. Eichenfield
This is a very hard diagnosis to make with the clinical findings and history.
Molluscum contagiosum infections are common, but with this patient’s medical history, biopsy and excision with pathologic examination was an appropriate approach to make a certain diagnosis.
Ms. Moyal is a research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego.
References
1. Brown J et al. Int J Dermatol. 2006 Feb;45(2):93-9.
2. Hanson D and Diven DG. Dermatol Online J. 2003 Mar;9(2).
3. Badri T and Gandhi GR. Molluscum contagiosum. 2022. In: StatPearls [Internet]. Treasure Island, Fla.: StatPearls Publishing.
4. Schwartz JJ and Myskowski PL. J Am Acad Dermatol. 1992 Oct 1;27(4):583-8.
5. Antonov NK et al. JAAD Case Rep. 2019 Apr 5;5(4):342-5.
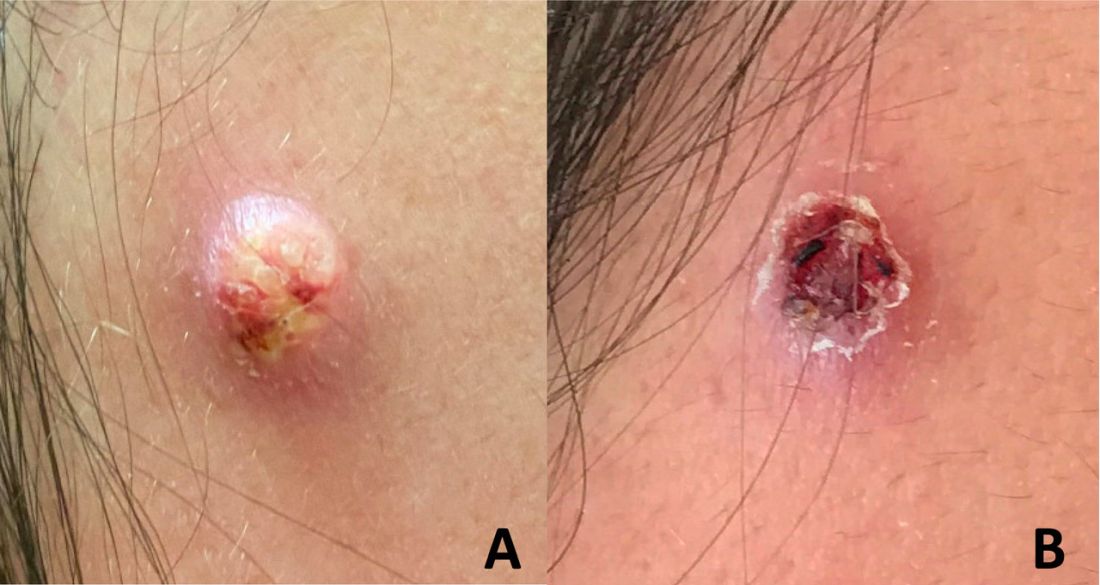
The clitoris steps into the spotlight with major scientific discovery
The patients of Jill Krapf, MD, are often too embarrassed to tell her about discomfort in their clitoris.
“I ask all of my patients about clitoral pain, and it is often the first time they have ever been asked about this,” says Dr. Krapf, the associate director of the Center for Vulvovaginal Disorders, a private clinic in Washington and New York.
Dr. Krapf is an ob.gyn. who specializes in female sexual pain that involves the pelvis, vagina, and vulva.
Many of the conditions Dr. Krapf treats don’t have outward symptoms that appear abnormal, but internally, there are damaged or irritated nerves that can result in hypersensitivity, unwanted arousal, or pain.
“Most recent research indicates that even a herniated disk or tear in the spine can lead to clitoral or vulvar symptoms, just like sciatica pain that shoots down the leg is related to issues in the spine,” Dr. Krapf says.
Dr. Krapf was excited to read of a new discovery: Dr. Krapf and other doctors are hopeful that the attention to the clitoris will spark more interest and comprehensive education among people in their field. They also hope it will empower patients to seek medical help if they are having issues with their clitoris.
“Female sexual health has historically been underfunded, especially compared with male sexual health, like erectile dysfunction,” Dr. Krapf says. “Optimizing vulvar and vaginal health is not only necessary for sexual well-being.”
Blair Peters, MD, a plastic surgeon who specializes in gender-affirming care, led the study, which was presented at the Sexual Medicine Society of North America conference in October. Dr. Peters says he hopes that the new information decreases stigma that the clitoris is not worthy of the same medical attention that other organs of the body receive.
When the clitoris doesn’t properly function, there can be harm to a person’s physical and mental health. Paying attention to discomfort in the clitoris, and seeking medical attention, can help catch and prevent some urinary and vaginal infections.
“The fact that it took until 2022 for someone to do this work speaks to how little attention the clitoris has received,” says Dr. Peters, an assistant professor of surgery at the Oregon Health and Science University School of Medicine, Portland.
What’s inside?
Dr. Peters and his colleagues completed the study by taking clitoral nerve tissue from seven adult transgender men who had received gender-affirming genital surgery. The tissues were dyed and magnified 1,000 times under a microscope so the researchers could count nerve fibers.
Dr. Peters says the finding is important because many surgeries take place in the groin region – like hip replacements, episiotomies during childbirth, and pelvic mesh procedures – and the revived attention to the clitoris may help health care providers know where nerves are so that injuries from medical mistakes are prevented.
“Nerves are at risk of damage if it’s not understood where they are at all times,” he says.
Dr. Peters hopes the new finding will help create new surgical techniques for nerve repair and offer insight for gender-affirming phalloplasty, which is the surgical construction of a penis often for transmasculine people.
Ownership of the body part
When it comes to the clitoris, no one type of doctor has specialized in the sex organ.
Urologists, gynecologists, plastic surgeons, and sex therapists all address potential problems that can arise with the clitoris and its surrounding body parts. But specialists like Dr. Krapf are few and far between.
It wasn’t until 2005 that Australian urologist Helen O’Connell found that the clitoris is filled with erectile and non-erectile tissues that are often hidden in anatomy drawings by fat and bone. And it wasn’t until the early 2000s that researchers began delving in earnest into the anatomy of the clitoris and how it functions.
And a 2018 study showed that if more doctors examined the clitoris, they could identify issues like adhesions or infections in the area, most of which can be treated without surgery.
A body part built for pleasure
Randi Levinson, a sex, marriage, and family therapist in Los Angeles, sees patients who have less sensation in the clitoris or pain while having sex, many of whom have recently given birth or are going through menopause.
Women often become embarrassed when they can’t orgasm, or have less sensation in the clitoris, but tend to avoid seeking medical advice, she says. Normalizing discussions about women’s pleasure and the vast anatomy that supports it may help some of her patients.
“The more normal it is to talk about and explore women’s pleasure, the less shame women will have when getting help when they aren’t experiencing pleasure,” Ms. Levinson says. “I have many ... clients who experience pain and discomfort with sex [after pregnancy] and no longer feel pleasure and are concerned that something is wrong with them.”
A version of this article first appeared on WebMD.com.
The patients of Jill Krapf, MD, are often too embarrassed to tell her about discomfort in their clitoris.
“I ask all of my patients about clitoral pain, and it is often the first time they have ever been asked about this,” says Dr. Krapf, the associate director of the Center for Vulvovaginal Disorders, a private clinic in Washington and New York.
Dr. Krapf is an ob.gyn. who specializes in female sexual pain that involves the pelvis, vagina, and vulva.
Many of the conditions Dr. Krapf treats don’t have outward symptoms that appear abnormal, but internally, there are damaged or irritated nerves that can result in hypersensitivity, unwanted arousal, or pain.
“Most recent research indicates that even a herniated disk or tear in the spine can lead to clitoral or vulvar symptoms, just like sciatica pain that shoots down the leg is related to issues in the spine,” Dr. Krapf says.
Dr. Krapf was excited to read of a new discovery: Dr. Krapf and other doctors are hopeful that the attention to the clitoris will spark more interest and comprehensive education among people in their field. They also hope it will empower patients to seek medical help if they are having issues with their clitoris.
“Female sexual health has historically been underfunded, especially compared with male sexual health, like erectile dysfunction,” Dr. Krapf says. “Optimizing vulvar and vaginal health is not only necessary for sexual well-being.”
Blair Peters, MD, a plastic surgeon who specializes in gender-affirming care, led the study, which was presented at the Sexual Medicine Society of North America conference in October. Dr. Peters says he hopes that the new information decreases stigma that the clitoris is not worthy of the same medical attention that other organs of the body receive.
When the clitoris doesn’t properly function, there can be harm to a person’s physical and mental health. Paying attention to discomfort in the clitoris, and seeking medical attention, can help catch and prevent some urinary and vaginal infections.
“The fact that it took until 2022 for someone to do this work speaks to how little attention the clitoris has received,” says Dr. Peters, an assistant professor of surgery at the Oregon Health and Science University School of Medicine, Portland.
What’s inside?
Dr. Peters and his colleagues completed the study by taking clitoral nerve tissue from seven adult transgender men who had received gender-affirming genital surgery. The tissues were dyed and magnified 1,000 times under a microscope so the researchers could count nerve fibers.
Dr. Peters says the finding is important because many surgeries take place in the groin region – like hip replacements, episiotomies during childbirth, and pelvic mesh procedures – and the revived attention to the clitoris may help health care providers know where nerves are so that injuries from medical mistakes are prevented.
“Nerves are at risk of damage if it’s not understood where they are at all times,” he says.
Dr. Peters hopes the new finding will help create new surgical techniques for nerve repair and offer insight for gender-affirming phalloplasty, which is the surgical construction of a penis often for transmasculine people.
Ownership of the body part
When it comes to the clitoris, no one type of doctor has specialized in the sex organ.
Urologists, gynecologists, plastic surgeons, and sex therapists all address potential problems that can arise with the clitoris and its surrounding body parts. But specialists like Dr. Krapf are few and far between.
It wasn’t until 2005 that Australian urologist Helen O’Connell found that the clitoris is filled with erectile and non-erectile tissues that are often hidden in anatomy drawings by fat and bone. And it wasn’t until the early 2000s that researchers began delving in earnest into the anatomy of the clitoris and how it functions.
And a 2018 study showed that if more doctors examined the clitoris, they could identify issues like adhesions or infections in the area, most of which can be treated without surgery.
A body part built for pleasure
Randi Levinson, a sex, marriage, and family therapist in Los Angeles, sees patients who have less sensation in the clitoris or pain while having sex, many of whom have recently given birth or are going through menopause.
Women often become embarrassed when they can’t orgasm, or have less sensation in the clitoris, but tend to avoid seeking medical advice, she says. Normalizing discussions about women’s pleasure and the vast anatomy that supports it may help some of her patients.
“The more normal it is to talk about and explore women’s pleasure, the less shame women will have when getting help when they aren’t experiencing pleasure,” Ms. Levinson says. “I have many ... clients who experience pain and discomfort with sex [after pregnancy] and no longer feel pleasure and are concerned that something is wrong with them.”
A version of this article first appeared on WebMD.com.
The patients of Jill Krapf, MD, are often too embarrassed to tell her about discomfort in their clitoris.
“I ask all of my patients about clitoral pain, and it is often the first time they have ever been asked about this,” says Dr. Krapf, the associate director of the Center for Vulvovaginal Disorders, a private clinic in Washington and New York.
Dr. Krapf is an ob.gyn. who specializes in female sexual pain that involves the pelvis, vagina, and vulva.
Many of the conditions Dr. Krapf treats don’t have outward symptoms that appear abnormal, but internally, there are damaged or irritated nerves that can result in hypersensitivity, unwanted arousal, or pain.
“Most recent research indicates that even a herniated disk or tear in the spine can lead to clitoral or vulvar symptoms, just like sciatica pain that shoots down the leg is related to issues in the spine,” Dr. Krapf says.
Dr. Krapf was excited to read of a new discovery: Dr. Krapf and other doctors are hopeful that the attention to the clitoris will spark more interest and comprehensive education among people in their field. They also hope it will empower patients to seek medical help if they are having issues with their clitoris.
“Female sexual health has historically been underfunded, especially compared with male sexual health, like erectile dysfunction,” Dr. Krapf says. “Optimizing vulvar and vaginal health is not only necessary for sexual well-being.”
Blair Peters, MD, a plastic surgeon who specializes in gender-affirming care, led the study, which was presented at the Sexual Medicine Society of North America conference in October. Dr. Peters says he hopes that the new information decreases stigma that the clitoris is not worthy of the same medical attention that other organs of the body receive.
When the clitoris doesn’t properly function, there can be harm to a person’s physical and mental health. Paying attention to discomfort in the clitoris, and seeking medical attention, can help catch and prevent some urinary and vaginal infections.
“The fact that it took until 2022 for someone to do this work speaks to how little attention the clitoris has received,” says Dr. Peters, an assistant professor of surgery at the Oregon Health and Science University School of Medicine, Portland.
What’s inside?
Dr. Peters and his colleagues completed the study by taking clitoral nerve tissue from seven adult transgender men who had received gender-affirming genital surgery. The tissues were dyed and magnified 1,000 times under a microscope so the researchers could count nerve fibers.
Dr. Peters says the finding is important because many surgeries take place in the groin region – like hip replacements, episiotomies during childbirth, and pelvic mesh procedures – and the revived attention to the clitoris may help health care providers know where nerves are so that injuries from medical mistakes are prevented.
“Nerves are at risk of damage if it’s not understood where they are at all times,” he says.
Dr. Peters hopes the new finding will help create new surgical techniques for nerve repair and offer insight for gender-affirming phalloplasty, which is the surgical construction of a penis often for transmasculine people.
Ownership of the body part
When it comes to the clitoris, no one type of doctor has specialized in the sex organ.
Urologists, gynecologists, plastic surgeons, and sex therapists all address potential problems that can arise with the clitoris and its surrounding body parts. But specialists like Dr. Krapf are few and far between.
It wasn’t until 2005 that Australian urologist Helen O’Connell found that the clitoris is filled with erectile and non-erectile tissues that are often hidden in anatomy drawings by fat and bone. And it wasn’t until the early 2000s that researchers began delving in earnest into the anatomy of the clitoris and how it functions.
And a 2018 study showed that if more doctors examined the clitoris, they could identify issues like adhesions or infections in the area, most of which can be treated without surgery.
A body part built for pleasure
Randi Levinson, a sex, marriage, and family therapist in Los Angeles, sees patients who have less sensation in the clitoris or pain while having sex, many of whom have recently given birth or are going through menopause.
Women often become embarrassed when they can’t orgasm, or have less sensation in the clitoris, but tend to avoid seeking medical advice, she says. Normalizing discussions about women’s pleasure and the vast anatomy that supports it may help some of her patients.
“The more normal it is to talk about and explore women’s pleasure, the less shame women will have when getting help when they aren’t experiencing pleasure,” Ms. Levinson says. “I have many ... clients who experience pain and discomfort with sex [after pregnancy] and no longer feel pleasure and are concerned that something is wrong with them.”
A version of this article first appeared on WebMD.com.