User login
-
Black race linked to poorer survival in AML
Black race is the most important risk factor for patients with acute myeloid leukemia (AML) and is associated with poor survival, according to new findings.
Among patients with AML younger than 60 years, the rate of overall 3-year survival was significantly less among Black patients than White patients (34% vs. 43%). The risk for death was 27% higher for Black patients compared with White patients.
“Our study demonstrates the delicate interplay between a variety of factors that influence survival disparities, particularly for younger Black AML patients,” said first author Bhavana Bhatnagar, DO, of the Ohio State University’s Comprehensive Cancer Center, Columbus. “We were able to confirm the impact of socioeconomic factors while also demonstrating that being Black is, in and of itself, an independent poor prognostic variable for survival.”
She noted that the persistently poor outcomes of young Black patients that were seen despite similar treatments in clinical trials strongly suggest that additional factors have a bearing on their survival.
The findings of the study were presented during the plenary session of the annual meeting of the American Society of Hematology, which was held online this year. The study was simultaneously published in Cancer Discovery.
Racial disparities in cancer outcomes remain a challenge. The term “health disparities” describes the differences of health outcomes among different groups, said Chancellor Donald, MD, of Tulane University, New Orleans, who introduced the article at the meeting. “Racial health disparities usually result from an unequal distribution of power and resources, not genetics.
“The examination of health disparities is certainly a worthwhile endeavor,” he continued. “For generations, differences in key health outcomes have negatively impacted the quality of life and shortened the life span of countless individuals. As scientists, clinicians, and invested members of our shared society, we are obligated to obtain a profound understanding of the mechanisms and impact of this morbid reality.”
Black race a risk factor
For their study, Dr. Bhatnagar and colleagues conducted a nationwide population analysis using data from the Surveillance Epidemiology End Results (SEER) Program of the National Cancer Institute to identify 11,190 adults aged 18-60 years who were diagnosed with AML between 1986 and 2015.
To characterize molecular features, they conducted targeted sequencing of 81 genes in 1,339 patients with AML who were treated on frontline Cancer and Leukemia Group B/Alliance for Clinical Trials in Oncology (Alliance) protocols based on standard-intensity cytarabine/anthracycline induction followed by consolidation between 1986 and 2016. None of these patients received an allogeneic stem cell transplant when they achieved complete remission.
Although overall survival has improved during the past 3 decades, survival disparities between Black and White patients has widened over time (P < .001). The authors found a nonstatistically significant difference in survival between 1986 and 1995 (White patients, n = 1,365; Black patients, n = 160; P = .19). However, the difference was significant between 1996 and 2005 (White patients, n = 2,994; Black patients, n = 480; P = .004). “And it became even more noticeable in the most recent decade,” said Dr. Bhatnagar. “Furthermore, younger Black AML patients were found to have worse survival compared with younger White AML patients.”
Results from the second analysis of patients treated on Alliance protocols did not show any significant differences in early death rates (10% vs. 46%; P = .02) and complete remission rates (71% vs. 71%; P = 1.00). “While relapse rates were slightly higher in Black compared to White patients, this difference did not reach statistical significance,” said Dr. Bhatnagar. “There was also no significant difference in the number of cycles of consolidation chemotherapy administered to these patients.”
However, both disease-free and overall survival were significantly worse for Black patients, suggesting that factors other than treatment selection were likely at play in influencing the survival disparity. The median disease-free survival for Black patients was 0.8 years, vs. 1.4 years for White patients (P = .02). Overall survival was 1.2 years vs. 1.8 years (P = .02).
Relapse rates were slightly higher in Black patients than in White patients, at 71% vs. 59%, but this difference did not reach statistical significance (P = .14).
Differences in biomarkers
With regard to underlying molecular differences between Black and White patients, the investigators found that the most common mutations were in NPM1, FLT3-ITD, and DNM3TA. Mutations were detected in more than 20% of Black patients. Other commonly mutated genes were IDH2, NRAS, TET2, IDH1, and TP53, which were mutated in more than 10% of patients. “All of these genes are established commonly mutated genes in AML,” said Bhatnagar.
On univariable and multivariable outcome analyses, which were used to identify clinical or molecular features that had a bearing on outcome, FLT3-ITD and IDH2 mutations were the only mutations associated with a higher risk for death among Black patients.
“This is actually a very important finding, as both FLT3 and IDH2 are now targetable with small-molecule inhibitors,” said Dr. Bhatnagar. “In addition, it is also worth noting that other gene mutations that have known prognostic significance in AML, such as NPM1, as well as RUNX1 and TP53, did not remain in the final statistical model.
“Importantly, our study provides powerful evidence that suggests differences in underlying disease biology between young Black and White AML patients, as evidenced by differences in the frequencies of recurrent gene mutations, “ she said.
Understudied disparities
Although the study showed that Black patients had worse outcomes, “surprisingly, the authors found these outcomes hold even when the patients are participating in clinical trials,” noted Elisa Weiss, PhD, senior vice president of education, services, and health research for the Leukemia and Lymphoma Society.
“The study makes clear that the medical and science community need to do more to better understand the social, economic, environmental, and biological causes of these disparities,” she said in an interview. “In fact, the findings suggest that there are myriad complex and understudied causes of the identified disparities, and they are likely to lie at the intersection of all levels of the social ecology that impact an individual’s ability to access timely and unbiased care, maintain their mental and physical health, and receive needed social support and resources.”
She noted that the Leukemia and Lymphoma Society has an Equity in Access research program that aims to “advance study of underlying causes of inequitable access to care and identify policies, strategies, and interventions that have the potential to reduce inequities and increase access to health care, services, and programs for blood cancer patients and survivors.”
The research was supported in part by the National Cancer Institute of the National Institutes of Health, other institutions, and through several scholar awards. Dr. Bhatnagar has received advisory board honoraria from Novartis, Kite Pharma, Celgene, Astellas, and Cell Therapeutics. Dr. Weiss has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Black race is the most important risk factor for patients with acute myeloid leukemia (AML) and is associated with poor survival, according to new findings.
Among patients with AML younger than 60 years, the rate of overall 3-year survival was significantly less among Black patients than White patients (34% vs. 43%). The risk for death was 27% higher for Black patients compared with White patients.
“Our study demonstrates the delicate interplay between a variety of factors that influence survival disparities, particularly for younger Black AML patients,” said first author Bhavana Bhatnagar, DO, of the Ohio State University’s Comprehensive Cancer Center, Columbus. “We were able to confirm the impact of socioeconomic factors while also demonstrating that being Black is, in and of itself, an independent poor prognostic variable for survival.”
She noted that the persistently poor outcomes of young Black patients that were seen despite similar treatments in clinical trials strongly suggest that additional factors have a bearing on their survival.
The findings of the study were presented during the plenary session of the annual meeting of the American Society of Hematology, which was held online this year. The study was simultaneously published in Cancer Discovery.
Racial disparities in cancer outcomes remain a challenge. The term “health disparities” describes the differences of health outcomes among different groups, said Chancellor Donald, MD, of Tulane University, New Orleans, who introduced the article at the meeting. “Racial health disparities usually result from an unequal distribution of power and resources, not genetics.
“The examination of health disparities is certainly a worthwhile endeavor,” he continued. “For generations, differences in key health outcomes have negatively impacted the quality of life and shortened the life span of countless individuals. As scientists, clinicians, and invested members of our shared society, we are obligated to obtain a profound understanding of the mechanisms and impact of this morbid reality.”
Black race a risk factor
For their study, Dr. Bhatnagar and colleagues conducted a nationwide population analysis using data from the Surveillance Epidemiology End Results (SEER) Program of the National Cancer Institute to identify 11,190 adults aged 18-60 years who were diagnosed with AML between 1986 and 2015.
To characterize molecular features, they conducted targeted sequencing of 81 genes in 1,339 patients with AML who were treated on frontline Cancer and Leukemia Group B/Alliance for Clinical Trials in Oncology (Alliance) protocols based on standard-intensity cytarabine/anthracycline induction followed by consolidation between 1986 and 2016. None of these patients received an allogeneic stem cell transplant when they achieved complete remission.
Although overall survival has improved during the past 3 decades, survival disparities between Black and White patients has widened over time (P < .001). The authors found a nonstatistically significant difference in survival between 1986 and 1995 (White patients, n = 1,365; Black patients, n = 160; P = .19). However, the difference was significant between 1996 and 2005 (White patients, n = 2,994; Black patients, n = 480; P = .004). “And it became even more noticeable in the most recent decade,” said Dr. Bhatnagar. “Furthermore, younger Black AML patients were found to have worse survival compared with younger White AML patients.”
Results from the second analysis of patients treated on Alliance protocols did not show any significant differences in early death rates (10% vs. 46%; P = .02) and complete remission rates (71% vs. 71%; P = 1.00). “While relapse rates were slightly higher in Black compared to White patients, this difference did not reach statistical significance,” said Dr. Bhatnagar. “There was also no significant difference in the number of cycles of consolidation chemotherapy administered to these patients.”
However, both disease-free and overall survival were significantly worse for Black patients, suggesting that factors other than treatment selection were likely at play in influencing the survival disparity. The median disease-free survival for Black patients was 0.8 years, vs. 1.4 years for White patients (P = .02). Overall survival was 1.2 years vs. 1.8 years (P = .02).
Relapse rates were slightly higher in Black patients than in White patients, at 71% vs. 59%, but this difference did not reach statistical significance (P = .14).
Differences in biomarkers
With regard to underlying molecular differences between Black and White patients, the investigators found that the most common mutations were in NPM1, FLT3-ITD, and DNM3TA. Mutations were detected in more than 20% of Black patients. Other commonly mutated genes were IDH2, NRAS, TET2, IDH1, and TP53, which were mutated in more than 10% of patients. “All of these genes are established commonly mutated genes in AML,” said Bhatnagar.
On univariable and multivariable outcome analyses, which were used to identify clinical or molecular features that had a bearing on outcome, FLT3-ITD and IDH2 mutations were the only mutations associated with a higher risk for death among Black patients.
“This is actually a very important finding, as both FLT3 and IDH2 are now targetable with small-molecule inhibitors,” said Dr. Bhatnagar. “In addition, it is also worth noting that other gene mutations that have known prognostic significance in AML, such as NPM1, as well as RUNX1 and TP53, did not remain in the final statistical model.
“Importantly, our study provides powerful evidence that suggests differences in underlying disease biology between young Black and White AML patients, as evidenced by differences in the frequencies of recurrent gene mutations, “ she said.
Understudied disparities
Although the study showed that Black patients had worse outcomes, “surprisingly, the authors found these outcomes hold even when the patients are participating in clinical trials,” noted Elisa Weiss, PhD, senior vice president of education, services, and health research for the Leukemia and Lymphoma Society.
“The study makes clear that the medical and science community need to do more to better understand the social, economic, environmental, and biological causes of these disparities,” she said in an interview. “In fact, the findings suggest that there are myriad complex and understudied causes of the identified disparities, and they are likely to lie at the intersection of all levels of the social ecology that impact an individual’s ability to access timely and unbiased care, maintain their mental and physical health, and receive needed social support and resources.”
She noted that the Leukemia and Lymphoma Society has an Equity in Access research program that aims to “advance study of underlying causes of inequitable access to care and identify policies, strategies, and interventions that have the potential to reduce inequities and increase access to health care, services, and programs for blood cancer patients and survivors.”
The research was supported in part by the National Cancer Institute of the National Institutes of Health, other institutions, and through several scholar awards. Dr. Bhatnagar has received advisory board honoraria from Novartis, Kite Pharma, Celgene, Astellas, and Cell Therapeutics. Dr. Weiss has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Black race is the most important risk factor for patients with acute myeloid leukemia (AML) and is associated with poor survival, according to new findings.
Among patients with AML younger than 60 years, the rate of overall 3-year survival was significantly less among Black patients than White patients (34% vs. 43%). The risk for death was 27% higher for Black patients compared with White patients.
“Our study demonstrates the delicate interplay between a variety of factors that influence survival disparities, particularly for younger Black AML patients,” said first author Bhavana Bhatnagar, DO, of the Ohio State University’s Comprehensive Cancer Center, Columbus. “We were able to confirm the impact of socioeconomic factors while also demonstrating that being Black is, in and of itself, an independent poor prognostic variable for survival.”
She noted that the persistently poor outcomes of young Black patients that were seen despite similar treatments in clinical trials strongly suggest that additional factors have a bearing on their survival.
The findings of the study were presented during the plenary session of the annual meeting of the American Society of Hematology, which was held online this year. The study was simultaneously published in Cancer Discovery.
Racial disparities in cancer outcomes remain a challenge. The term “health disparities” describes the differences of health outcomes among different groups, said Chancellor Donald, MD, of Tulane University, New Orleans, who introduced the article at the meeting. “Racial health disparities usually result from an unequal distribution of power and resources, not genetics.
“The examination of health disparities is certainly a worthwhile endeavor,” he continued. “For generations, differences in key health outcomes have negatively impacted the quality of life and shortened the life span of countless individuals. As scientists, clinicians, and invested members of our shared society, we are obligated to obtain a profound understanding of the mechanisms and impact of this morbid reality.”
Black race a risk factor
For their study, Dr. Bhatnagar and colleagues conducted a nationwide population analysis using data from the Surveillance Epidemiology End Results (SEER) Program of the National Cancer Institute to identify 11,190 adults aged 18-60 years who were diagnosed with AML between 1986 and 2015.
To characterize molecular features, they conducted targeted sequencing of 81 genes in 1,339 patients with AML who were treated on frontline Cancer and Leukemia Group B/Alliance for Clinical Trials in Oncology (Alliance) protocols based on standard-intensity cytarabine/anthracycline induction followed by consolidation between 1986 and 2016. None of these patients received an allogeneic stem cell transplant when they achieved complete remission.
Although overall survival has improved during the past 3 decades, survival disparities between Black and White patients has widened over time (P < .001). The authors found a nonstatistically significant difference in survival between 1986 and 1995 (White patients, n = 1,365; Black patients, n = 160; P = .19). However, the difference was significant between 1996 and 2005 (White patients, n = 2,994; Black patients, n = 480; P = .004). “And it became even more noticeable in the most recent decade,” said Dr. Bhatnagar. “Furthermore, younger Black AML patients were found to have worse survival compared with younger White AML patients.”
Results from the second analysis of patients treated on Alliance protocols did not show any significant differences in early death rates (10% vs. 46%; P = .02) and complete remission rates (71% vs. 71%; P = 1.00). “While relapse rates were slightly higher in Black compared to White patients, this difference did not reach statistical significance,” said Dr. Bhatnagar. “There was also no significant difference in the number of cycles of consolidation chemotherapy administered to these patients.”
However, both disease-free and overall survival were significantly worse for Black patients, suggesting that factors other than treatment selection were likely at play in influencing the survival disparity. The median disease-free survival for Black patients was 0.8 years, vs. 1.4 years for White patients (P = .02). Overall survival was 1.2 years vs. 1.8 years (P = .02).
Relapse rates were slightly higher in Black patients than in White patients, at 71% vs. 59%, but this difference did not reach statistical significance (P = .14).
Differences in biomarkers
With regard to underlying molecular differences between Black and White patients, the investigators found that the most common mutations were in NPM1, FLT3-ITD, and DNM3TA. Mutations were detected in more than 20% of Black patients. Other commonly mutated genes were IDH2, NRAS, TET2, IDH1, and TP53, which were mutated in more than 10% of patients. “All of these genes are established commonly mutated genes in AML,” said Bhatnagar.
On univariable and multivariable outcome analyses, which were used to identify clinical or molecular features that had a bearing on outcome, FLT3-ITD and IDH2 mutations were the only mutations associated with a higher risk for death among Black patients.
“This is actually a very important finding, as both FLT3 and IDH2 are now targetable with small-molecule inhibitors,” said Dr. Bhatnagar. “In addition, it is also worth noting that other gene mutations that have known prognostic significance in AML, such as NPM1, as well as RUNX1 and TP53, did not remain in the final statistical model.
“Importantly, our study provides powerful evidence that suggests differences in underlying disease biology between young Black and White AML patients, as evidenced by differences in the frequencies of recurrent gene mutations, “ she said.
Understudied disparities
Although the study showed that Black patients had worse outcomes, “surprisingly, the authors found these outcomes hold even when the patients are participating in clinical trials,” noted Elisa Weiss, PhD, senior vice president of education, services, and health research for the Leukemia and Lymphoma Society.
“The study makes clear that the medical and science community need to do more to better understand the social, economic, environmental, and biological causes of these disparities,” she said in an interview. “In fact, the findings suggest that there are myriad complex and understudied causes of the identified disparities, and they are likely to lie at the intersection of all levels of the social ecology that impact an individual’s ability to access timely and unbiased care, maintain their mental and physical health, and receive needed social support and resources.”
She noted that the Leukemia and Lymphoma Society has an Equity in Access research program that aims to “advance study of underlying causes of inequitable access to care and identify policies, strategies, and interventions that have the potential to reduce inequities and increase access to health care, services, and programs for blood cancer patients and survivors.”
The research was supported in part by the National Cancer Institute of the National Institutes of Health, other institutions, and through several scholar awards. Dr. Bhatnagar has received advisory board honoraria from Novartis, Kite Pharma, Celgene, Astellas, and Cell Therapeutics. Dr. Weiss has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Upper GI bleeds in COVID-19 not related to increased mortality
A Spanish survey of COVID-19 patients suggests that upper gastrointestinal bleeding (UGB) does not affect in-hospital mortality. It also found that fewer COVID-19–positive patients underwent endoscopies, but there was no statistically significant difference in in-hospital mortality outcome as a result of delays.
“In-hospital mortality in COVID-19 patients with upper-GI bleeding seemed to be more influenced by COVID-19 than by upper-GI bleeding, and that’s something I think is important for us to know,” Gyanprakash Ketwaroo, MD, associate professor at Baylor College of Medicine, Houston, said in an interview. Dr. Ketwaroo was not involved in the study.
The results weren’t a surprise, but they do provide some reassurance. “It’s probably what I expected. Initially, we thought there might be some COVID-19 related (GI) lesions, but that didn’t seem to be borne out. So we thought the bleeding was related to (the patient) being in a hospital or the typical reasons for bleeding. It’s also what I expected that less endoscopies would be performed in these patients, and even though fewer endoscopies were performed, the outcomes were still similar. I think it’s what most people expected,” said Dr. Ketwaroo.
The study was published online Nov. 25 in the Journal of Clinical Gastroenterology, and led by Rebeca González González, MD, of Severo Ochoa University Hospital in Leganés, Madrid, and Pascual Piñera-Salmerón, MD, of Reina Sofia University General Hospital in Murcia, Spain. The researchers retrospectively analyzed data on 71,904 COVID-19 patients at 62 emergency departments in Spain, and compared 83 patients who had COVID-19 and UGB to two control groups: 249 randomly selected COVID-19 patients without UGB, and 249 randomly selected non-COVID-19 patients with UGB.
They found that 1.11% of COVID-19 patients presented with UGB, compared with 1.78% of non-COVID-19 patients at emergency departments. In patients with COVID-19, risk of UGB was associated with hemoglobin values < 10 g/L (odds ratio [OR], 34.255, 95% confidence interval [CI], 12.752-92.021), abdominal pain (OR, 11.4; 95% CI, 5.092-25.944), and systolic blood pressure < 90 mm Hg (OR, 11.096; 95% CI, 2.975-41.390).
Compared with non-COVID-19 patients with UGB, those COVID-19 patients with UGB were more likely to have interstitial lung infiltrates (OR, 66.42; 95% CI, 15.364-287.223) and ground-glass opacities (OR, 21.27; 95% CI, 9.720-46.567) in chest radiograph, as well as fever (OR, 34.67; 95% CI, 11.719-102.572) and cough (OR, 26.4; 95% CI, 8.845-78.806).
Gastroscopy and endoscopic procedures were lower in patients with COVID-19 than in the general population (gastroscopy OR, 0.269; 95% CI, 0.160-0.453: endoscopy OR, 0.26; 95% CI, 0.165-0.623). There was no difference between the two groups with respect to endoscopic findings. After adjustment for age and sex, the only significant difference between COVID-19 patients with UGB and COVID-19 patients without UGB was a higher rate of intensive care unit admission (OR, 2.98; 95% CI, 1.16-7.65). Differences between COVID-19 patients with UGB and non–COVID-19 patients with UGB included higher rates of ICU admission (OR, 3.29; 95% CI, 1.28-8.47), prolonged hospitalizations (OR, 2.02; 95% CI, 1.15-3.55), and in-hospital mortality (OR, 2.05; 95% CI, 1.09-3.86).
UGB development was not associated with increased in-hospital mortality in COVID-19 patients (OR, 1.14; 95% CI, 0.59-2.19).
A limitation to the study it was that it was performed in Spain, where endoscopies are performed in the emergency department, and where there are different thresholds for admission to the intensive care unit than in the United States.
The authors did not report a funding source. Dr. Ketwaroo has no relevant financial disclosures.
SOURCE: González González R et al. J Clin Gastroenterol. 10.1097/MCG.0000000000001465.
A Spanish survey of COVID-19 patients suggests that upper gastrointestinal bleeding (UGB) does not affect in-hospital mortality. It also found that fewer COVID-19–positive patients underwent endoscopies, but there was no statistically significant difference in in-hospital mortality outcome as a result of delays.
“In-hospital mortality in COVID-19 patients with upper-GI bleeding seemed to be more influenced by COVID-19 than by upper-GI bleeding, and that’s something I think is important for us to know,” Gyanprakash Ketwaroo, MD, associate professor at Baylor College of Medicine, Houston, said in an interview. Dr. Ketwaroo was not involved in the study.
The results weren’t a surprise, but they do provide some reassurance. “It’s probably what I expected. Initially, we thought there might be some COVID-19 related (GI) lesions, but that didn’t seem to be borne out. So we thought the bleeding was related to (the patient) being in a hospital or the typical reasons for bleeding. It’s also what I expected that less endoscopies would be performed in these patients, and even though fewer endoscopies were performed, the outcomes were still similar. I think it’s what most people expected,” said Dr. Ketwaroo.
The study was published online Nov. 25 in the Journal of Clinical Gastroenterology, and led by Rebeca González González, MD, of Severo Ochoa University Hospital in Leganés, Madrid, and Pascual Piñera-Salmerón, MD, of Reina Sofia University General Hospital in Murcia, Spain. The researchers retrospectively analyzed data on 71,904 COVID-19 patients at 62 emergency departments in Spain, and compared 83 patients who had COVID-19 and UGB to two control groups: 249 randomly selected COVID-19 patients without UGB, and 249 randomly selected non-COVID-19 patients with UGB.
They found that 1.11% of COVID-19 patients presented with UGB, compared with 1.78% of non-COVID-19 patients at emergency departments. In patients with COVID-19, risk of UGB was associated with hemoglobin values < 10 g/L (odds ratio [OR], 34.255, 95% confidence interval [CI], 12.752-92.021), abdominal pain (OR, 11.4; 95% CI, 5.092-25.944), and systolic blood pressure < 90 mm Hg (OR, 11.096; 95% CI, 2.975-41.390).
Compared with non-COVID-19 patients with UGB, those COVID-19 patients with UGB were more likely to have interstitial lung infiltrates (OR, 66.42; 95% CI, 15.364-287.223) and ground-glass opacities (OR, 21.27; 95% CI, 9.720-46.567) in chest radiograph, as well as fever (OR, 34.67; 95% CI, 11.719-102.572) and cough (OR, 26.4; 95% CI, 8.845-78.806).
Gastroscopy and endoscopic procedures were lower in patients with COVID-19 than in the general population (gastroscopy OR, 0.269; 95% CI, 0.160-0.453: endoscopy OR, 0.26; 95% CI, 0.165-0.623). There was no difference between the two groups with respect to endoscopic findings. After adjustment for age and sex, the only significant difference between COVID-19 patients with UGB and COVID-19 patients without UGB was a higher rate of intensive care unit admission (OR, 2.98; 95% CI, 1.16-7.65). Differences between COVID-19 patients with UGB and non–COVID-19 patients with UGB included higher rates of ICU admission (OR, 3.29; 95% CI, 1.28-8.47), prolonged hospitalizations (OR, 2.02; 95% CI, 1.15-3.55), and in-hospital mortality (OR, 2.05; 95% CI, 1.09-3.86).
UGB development was not associated with increased in-hospital mortality in COVID-19 patients (OR, 1.14; 95% CI, 0.59-2.19).
A limitation to the study it was that it was performed in Spain, where endoscopies are performed in the emergency department, and where there are different thresholds for admission to the intensive care unit than in the United States.
The authors did not report a funding source. Dr. Ketwaroo has no relevant financial disclosures.
SOURCE: González González R et al. J Clin Gastroenterol. 10.1097/MCG.0000000000001465.
A Spanish survey of COVID-19 patients suggests that upper gastrointestinal bleeding (UGB) does not affect in-hospital mortality. It also found that fewer COVID-19–positive patients underwent endoscopies, but there was no statistically significant difference in in-hospital mortality outcome as a result of delays.
“In-hospital mortality in COVID-19 patients with upper-GI bleeding seemed to be more influenced by COVID-19 than by upper-GI bleeding, and that’s something I think is important for us to know,” Gyanprakash Ketwaroo, MD, associate professor at Baylor College of Medicine, Houston, said in an interview. Dr. Ketwaroo was not involved in the study.
The results weren’t a surprise, but they do provide some reassurance. “It’s probably what I expected. Initially, we thought there might be some COVID-19 related (GI) lesions, but that didn’t seem to be borne out. So we thought the bleeding was related to (the patient) being in a hospital or the typical reasons for bleeding. It’s also what I expected that less endoscopies would be performed in these patients, and even though fewer endoscopies were performed, the outcomes were still similar. I think it’s what most people expected,” said Dr. Ketwaroo.
The study was published online Nov. 25 in the Journal of Clinical Gastroenterology, and led by Rebeca González González, MD, of Severo Ochoa University Hospital in Leganés, Madrid, and Pascual Piñera-Salmerón, MD, of Reina Sofia University General Hospital in Murcia, Spain. The researchers retrospectively analyzed data on 71,904 COVID-19 patients at 62 emergency departments in Spain, and compared 83 patients who had COVID-19 and UGB to two control groups: 249 randomly selected COVID-19 patients without UGB, and 249 randomly selected non-COVID-19 patients with UGB.
They found that 1.11% of COVID-19 patients presented with UGB, compared with 1.78% of non-COVID-19 patients at emergency departments. In patients with COVID-19, risk of UGB was associated with hemoglobin values < 10 g/L (odds ratio [OR], 34.255, 95% confidence interval [CI], 12.752-92.021), abdominal pain (OR, 11.4; 95% CI, 5.092-25.944), and systolic blood pressure < 90 mm Hg (OR, 11.096; 95% CI, 2.975-41.390).
Compared with non-COVID-19 patients with UGB, those COVID-19 patients with UGB were more likely to have interstitial lung infiltrates (OR, 66.42; 95% CI, 15.364-287.223) and ground-glass opacities (OR, 21.27; 95% CI, 9.720-46.567) in chest radiograph, as well as fever (OR, 34.67; 95% CI, 11.719-102.572) and cough (OR, 26.4; 95% CI, 8.845-78.806).
Gastroscopy and endoscopic procedures were lower in patients with COVID-19 than in the general population (gastroscopy OR, 0.269; 95% CI, 0.160-0.453: endoscopy OR, 0.26; 95% CI, 0.165-0.623). There was no difference between the two groups with respect to endoscopic findings. After adjustment for age and sex, the only significant difference between COVID-19 patients with UGB and COVID-19 patients without UGB was a higher rate of intensive care unit admission (OR, 2.98; 95% CI, 1.16-7.65). Differences between COVID-19 patients with UGB and non–COVID-19 patients with UGB included higher rates of ICU admission (OR, 3.29; 95% CI, 1.28-8.47), prolonged hospitalizations (OR, 2.02; 95% CI, 1.15-3.55), and in-hospital mortality (OR, 2.05; 95% CI, 1.09-3.86).
UGB development was not associated with increased in-hospital mortality in COVID-19 patients (OR, 1.14; 95% CI, 0.59-2.19).
A limitation to the study it was that it was performed in Spain, where endoscopies are performed in the emergency department, and where there are different thresholds for admission to the intensive care unit than in the United States.
The authors did not report a funding source. Dr. Ketwaroo has no relevant financial disclosures.
SOURCE: González González R et al. J Clin Gastroenterol. 10.1097/MCG.0000000000001465.
FROM THE JOURNAL OF CLINICAL GASTROENTEROLOGY
Medical societies waive fees, weigh other options during pandemic
COVID-19’s toll on member facilities pushed the American Academy of Sleep Medicine (AASM) recently to take a sizable gamble.
AASM announced in September that it would waive facility fees at all 2,648 AASM-accredited sleep facilities for 2021.
At $1,800-$2,600 for each facility, that will mean lost revenue of between $4.8 million and $6.9 million, but it’s a risk the academy felt it had to take.
AASM President Kannan Ramar, MBBS, MD, said in an interview that they are betting on the future of the field.
An internal survey of members, he said, found that nearly half (46%) of the 551 respondents thought they might have to close by the end of the year.
In addition, 66% reported a lower patient volume in the past month, and 36% reported that their practice or facility had to apply for loans or other financial assistance because of COVID-19, AASM said in its press release.
“We are hoping that if we help our members through this, they will be there for our patients,” Dr. Ramar said.
Other medical societies also are weighing options, straddling the line between needing income to provide resources for members but being acutely aware of the financial toll the pandemic is taking, according to one sampling.
As previously reported, primary care practices are projected to lose more than $68,000 in revenue per full-time physician in 2020, after steep drops in office visits and the collection of fees from March to May, according to a study led by researchers in the Blavatnik Institute at Harvard Medical School, Boston.
Those losses were calculated without considering a potential second wave of COVID-19 this year, the authors noted.
‘We can survive this’
Although AASM waived fees for its member facilities, individual physician fees have not been reduced so far. But the group is looking for more ways to help lower the economic burden on members, Dr. Ramar said.
“I don’t think we’ve ever been in this situation in the 45 years of the academy. This is a once-in-a-lifetime event for challenges we’re going through,” he said. “The board and the leadership realized that, if we’re going to do something, this is the time to do it.”
In addition to waiving the fees, AASM and the AASM Foundation are offering relief funding to state and regional sleep societies and research award recipients through programs created in response to COVID-19.
Some societies said they are not making changes to their dues or fees, some are forgoing cost-of-living fee increases, and some are waiving registration fees for annual meetings.
The American College of Allergy, Asthma and Immunology (ACAAI) waived most members’ registration fees for its annual meeting in November. Typically, that fee would be $500-$800 per member, plus charges for some premium sessions, Michael Blaiss, MD, ACAAI executive medical director, said.
Dr. Blaiss said in an interview that the college thought offering its 6,000 members essentially 25 free hours of CME would benefit them more than waiving annual membership dues, which are about $425 for physicians in the United States.
If the pandemic stretches through 2021, Dr. Blaiss said, “We can survive this. I’m not worried about that at all.”
But he acknowledged the painful effect on medical societies.
“I don’t think any organization would tell you it’s not having an effect on their income,” he said. “I know it is for us and for virtually any medical organization. A high percentage of income comes from the annual meeting.”
Waiving dues has not been a high priority among members in communications so far, Blaiss said.
American Academy of Dermatology President Bruce H. Thiers, MD, said in an interview that there will be no cost-of-living increase for 2021 dues, and AAD members can request a reduction in dues, which will be considered on a case-by-case basis.
“We understand that many members will have to make tough financial decisions,” he said.
In addition, AAD, which has more than 20,000 members, is exploring payment options to help members spread out the cost of membership.
ACP extends membership
The American College of Physicians, whose membership cycle starts in July, did not reduce dues but extended membership at no cost for 3 months through September to its 163,000 members, Phil Masters, MD, ACP’s vice president of membership, said in an interview.
It also expanded its educational offerings related to the pandemic, including webinars on physician wellness and issues regarding telemedicine.
He said expanding educational resources rather than waiving dues was an intentional decision after much discussion because “we’re primarily a services resource organization.”
Membership data are still being calculated, but early indications are that membership is not increasing this year, after seeing annual growth of about 2%-2.5%, Dr. Masters said. He noted that income is down “by several percent.” Annual membership dues average about $500 for physicians who have been practicing for 10 years.
“We’re well positioned to tolerate the ups and downs,” he said, but he acknowledged that “there’s no question the financial impact has been devastating on some practices.”
Like some other associations, ACP decided to cancel this year’s annual meeting, which had been planned for April. The 2021 annual meeting will be conducted online from April 29 to May 1.
Smaller organizations that rely heavily on income from the annual meeting will be severely challenged the longer the pandemic continues, Dr. Masters said.
The decision is not as simple as whether to reduce or eliminate dues, he noted. Organizations will have to reexamine their missions and structure their fees and offerings according to the needs of members.
“It’s a balance in doing things for the community at large and balancing the need to be sensitive to financial implications,” Dr. Masters said.
This article first appeared on Medscape.com.
COVID-19’s toll on member facilities pushed the American Academy of Sleep Medicine (AASM) recently to take a sizable gamble.
AASM announced in September that it would waive facility fees at all 2,648 AASM-accredited sleep facilities for 2021.
At $1,800-$2,600 for each facility, that will mean lost revenue of between $4.8 million and $6.9 million, but it’s a risk the academy felt it had to take.
AASM President Kannan Ramar, MBBS, MD, said in an interview that they are betting on the future of the field.
An internal survey of members, he said, found that nearly half (46%) of the 551 respondents thought they might have to close by the end of the year.
In addition, 66% reported a lower patient volume in the past month, and 36% reported that their practice or facility had to apply for loans or other financial assistance because of COVID-19, AASM said in its press release.
“We are hoping that if we help our members through this, they will be there for our patients,” Dr. Ramar said.
Other medical societies also are weighing options, straddling the line between needing income to provide resources for members but being acutely aware of the financial toll the pandemic is taking, according to one sampling.
As previously reported, primary care practices are projected to lose more than $68,000 in revenue per full-time physician in 2020, after steep drops in office visits and the collection of fees from March to May, according to a study led by researchers in the Blavatnik Institute at Harvard Medical School, Boston.
Those losses were calculated without considering a potential second wave of COVID-19 this year, the authors noted.
‘We can survive this’
Although AASM waived fees for its member facilities, individual physician fees have not been reduced so far. But the group is looking for more ways to help lower the economic burden on members, Dr. Ramar said.
“I don’t think we’ve ever been in this situation in the 45 years of the academy. This is a once-in-a-lifetime event for challenges we’re going through,” he said. “The board and the leadership realized that, if we’re going to do something, this is the time to do it.”
In addition to waiving the fees, AASM and the AASM Foundation are offering relief funding to state and regional sleep societies and research award recipients through programs created in response to COVID-19.
Some societies said they are not making changes to their dues or fees, some are forgoing cost-of-living fee increases, and some are waiving registration fees for annual meetings.
The American College of Allergy, Asthma and Immunology (ACAAI) waived most members’ registration fees for its annual meeting in November. Typically, that fee would be $500-$800 per member, plus charges for some premium sessions, Michael Blaiss, MD, ACAAI executive medical director, said.
Dr. Blaiss said in an interview that the college thought offering its 6,000 members essentially 25 free hours of CME would benefit them more than waiving annual membership dues, which are about $425 for physicians in the United States.
If the pandemic stretches through 2021, Dr. Blaiss said, “We can survive this. I’m not worried about that at all.”
But he acknowledged the painful effect on medical societies.
“I don’t think any organization would tell you it’s not having an effect on their income,” he said. “I know it is for us and for virtually any medical organization. A high percentage of income comes from the annual meeting.”
Waiving dues has not been a high priority among members in communications so far, Blaiss said.
American Academy of Dermatology President Bruce H. Thiers, MD, said in an interview that there will be no cost-of-living increase for 2021 dues, and AAD members can request a reduction in dues, which will be considered on a case-by-case basis.
“We understand that many members will have to make tough financial decisions,” he said.
In addition, AAD, which has more than 20,000 members, is exploring payment options to help members spread out the cost of membership.
ACP extends membership
The American College of Physicians, whose membership cycle starts in July, did not reduce dues but extended membership at no cost for 3 months through September to its 163,000 members, Phil Masters, MD, ACP’s vice president of membership, said in an interview.
It also expanded its educational offerings related to the pandemic, including webinars on physician wellness and issues regarding telemedicine.
He said expanding educational resources rather than waiving dues was an intentional decision after much discussion because “we’re primarily a services resource organization.”
Membership data are still being calculated, but early indications are that membership is not increasing this year, after seeing annual growth of about 2%-2.5%, Dr. Masters said. He noted that income is down “by several percent.” Annual membership dues average about $500 for physicians who have been practicing for 10 years.
“We’re well positioned to tolerate the ups and downs,” he said, but he acknowledged that “there’s no question the financial impact has been devastating on some practices.”
Like some other associations, ACP decided to cancel this year’s annual meeting, which had been planned for April. The 2021 annual meeting will be conducted online from April 29 to May 1.
Smaller organizations that rely heavily on income from the annual meeting will be severely challenged the longer the pandemic continues, Dr. Masters said.
The decision is not as simple as whether to reduce or eliminate dues, he noted. Organizations will have to reexamine their missions and structure their fees and offerings according to the needs of members.
“It’s a balance in doing things for the community at large and balancing the need to be sensitive to financial implications,” Dr. Masters said.
This article first appeared on Medscape.com.
COVID-19’s toll on member facilities pushed the American Academy of Sleep Medicine (AASM) recently to take a sizable gamble.
AASM announced in September that it would waive facility fees at all 2,648 AASM-accredited sleep facilities for 2021.
At $1,800-$2,600 for each facility, that will mean lost revenue of between $4.8 million and $6.9 million, but it’s a risk the academy felt it had to take.
AASM President Kannan Ramar, MBBS, MD, said in an interview that they are betting on the future of the field.
An internal survey of members, he said, found that nearly half (46%) of the 551 respondents thought they might have to close by the end of the year.
In addition, 66% reported a lower patient volume in the past month, and 36% reported that their practice or facility had to apply for loans or other financial assistance because of COVID-19, AASM said in its press release.
“We are hoping that if we help our members through this, they will be there for our patients,” Dr. Ramar said.
Other medical societies also are weighing options, straddling the line between needing income to provide resources for members but being acutely aware of the financial toll the pandemic is taking, according to one sampling.
As previously reported, primary care practices are projected to lose more than $68,000 in revenue per full-time physician in 2020, after steep drops in office visits and the collection of fees from March to May, according to a study led by researchers in the Blavatnik Institute at Harvard Medical School, Boston.
Those losses were calculated without considering a potential second wave of COVID-19 this year, the authors noted.
‘We can survive this’
Although AASM waived fees for its member facilities, individual physician fees have not been reduced so far. But the group is looking for more ways to help lower the economic burden on members, Dr. Ramar said.
“I don’t think we’ve ever been in this situation in the 45 years of the academy. This is a once-in-a-lifetime event for challenges we’re going through,” he said. “The board and the leadership realized that, if we’re going to do something, this is the time to do it.”
In addition to waiving the fees, AASM and the AASM Foundation are offering relief funding to state and regional sleep societies and research award recipients through programs created in response to COVID-19.
Some societies said they are not making changes to their dues or fees, some are forgoing cost-of-living fee increases, and some are waiving registration fees for annual meetings.
The American College of Allergy, Asthma and Immunology (ACAAI) waived most members’ registration fees for its annual meeting in November. Typically, that fee would be $500-$800 per member, plus charges for some premium sessions, Michael Blaiss, MD, ACAAI executive medical director, said.
Dr. Blaiss said in an interview that the college thought offering its 6,000 members essentially 25 free hours of CME would benefit them more than waiving annual membership dues, which are about $425 for physicians in the United States.
If the pandemic stretches through 2021, Dr. Blaiss said, “We can survive this. I’m not worried about that at all.”
But he acknowledged the painful effect on medical societies.
“I don’t think any organization would tell you it’s not having an effect on their income,” he said. “I know it is for us and for virtually any medical organization. A high percentage of income comes from the annual meeting.”
Waiving dues has not been a high priority among members in communications so far, Blaiss said.
American Academy of Dermatology President Bruce H. Thiers, MD, said in an interview that there will be no cost-of-living increase for 2021 dues, and AAD members can request a reduction in dues, which will be considered on a case-by-case basis.
“We understand that many members will have to make tough financial decisions,” he said.
In addition, AAD, which has more than 20,000 members, is exploring payment options to help members spread out the cost of membership.
ACP extends membership
The American College of Physicians, whose membership cycle starts in July, did not reduce dues but extended membership at no cost for 3 months through September to its 163,000 members, Phil Masters, MD, ACP’s vice president of membership, said in an interview.
It also expanded its educational offerings related to the pandemic, including webinars on physician wellness and issues regarding telemedicine.
He said expanding educational resources rather than waiving dues was an intentional decision after much discussion because “we’re primarily a services resource organization.”
Membership data are still being calculated, but early indications are that membership is not increasing this year, after seeing annual growth of about 2%-2.5%, Dr. Masters said. He noted that income is down “by several percent.” Annual membership dues average about $500 for physicians who have been practicing for 10 years.
“We’re well positioned to tolerate the ups and downs,” he said, but he acknowledged that “there’s no question the financial impact has been devastating on some practices.”
Like some other associations, ACP decided to cancel this year’s annual meeting, which had been planned for April. The 2021 annual meeting will be conducted online from April 29 to May 1.
Smaller organizations that rely heavily on income from the annual meeting will be severely challenged the longer the pandemic continues, Dr. Masters said.
The decision is not as simple as whether to reduce or eliminate dues, he noted. Organizations will have to reexamine their missions and structure their fees and offerings according to the needs of members.
“It’s a balance in doing things for the community at large and balancing the need to be sensitive to financial implications,” Dr. Masters said.
This article first appeared on Medscape.com.
Prioritize COVID-19 vaccination in both types of diabetes, say docs
The risk for increased COVID-19 severity in people with type 1 diabetes appears similar to that of type 2 diabetes, contrary to some official advice from the Centers for Disease Control and Prevention. The new finding indicates that people with both types should be priority for receiving a vaccine, investigators say.
The study is the first to prospectively evaluate both inpatients and outpatients and to examine COVID-19 severity factors in addition to death in people with type 1 and type 2 diabetes separately, and was published online Dec. 2 in Diabetes Care.
Among the patients, who were seen at Vanderbilt University Medical Center in Nashville, Tenn., between March and August of 2020, those with both type 1 and type 2 diabetes had between a three- and fourfold greater risk for COVID-19 hospitalization and greater illness severity compared with people without diabetes after adjustments for age, race, and a number of other risk factors.
This finding is important since as of Dec. 1, 2020, the CDC has classified the diabetes types differently in terms of underlying medical conditions that increase the risk for severe COVID-19.
Adults of any age with type 2 diabetes are considered “at increased risk of severe illness” from the virus that causes COVID-19 whereas the CDC says those with type 1 “might be at an increased risk.”
Lead author of the new paper Justin M. Gregory, MD, said in an interview: “I think this needs revision based on the current evidence. I think the data presented in our study and that of Barron et al. in Lancet Endocrinology 2020 indicate the need to place type 1 diabetes at parity with type 2 diabetes.
“These studies indicate both conditions carry an adjusted odds ratio of three to four when compared with people without diabetes for hospitalization, illness severity, and mortality,” he stressed.
Vaccines look promising for patients with diabetes
There were no phase 3 vaccine data available for the vaccine at the time that Dr. Gregory, of the Ian M. Burr Division of Pediatric Endocrinology and Diabetes, Vanderbilt University, Nashville, Tenn., and colleagues were writing their manuscript in late summer, so the article does not mention this.
But now, Dr. Gregory said, “Based on the initial press releases from Pfizer and Moderna, I am now optimistic that these vaccines might mitigate the excess morbidity and mortality from COVID-19 experienced by patients with diabetes.
“I am eager to see what we learn on December 10 and 17 [the scheduled dates for the meetings of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee to review the Pfizer and Moderna vaccines, respectively].”
But with the winter pandemic surge in the meantime, “Our investigation suggests that as COVID-19 hospitalizations rise, patients with both type 1 and 2 diabetes will comprise a disproportionately higher number of those admissions and, once hospitalized, demonstrate a greater degree of illness severity,” he and his colleagues said.
“In light of these data, we call on our colleagues to emphasize the importance of social distancing measures and hand hygiene, with particular emphasis on patients with diabetes, including those in the most vulnerable communities whom our study affirms will face the most severe impact.”
After adjustments, excess severity risk similar for both diabetes types
The new study data came from electronic health records at Vanderbilt University Medical Center, comprising 137 primary care, urgent care, and hospital facilities where patients were tested for SARS-CoV-2 regardless of the reason for their visit.
Between March 17 and August 7, 2020, 6,451 patients tested positive for COVID-19. Of those, 273 had type 2 diabetes and 40 had type 1 diabetes.
Children younger than 18 years accounted for 20% of those with type 1 diabetes and 9.4% of those without diabetes, but none of the type 2 group. The group with type 2 diabetes was considerably older than the type 1 diabetes and no-diabetes groups, 58 years versus 37 and 33 years, respectively.
Before adjustment for baseline characteristics that differed between groups, patients with type 1 diabetes appeared to have a risk for hospitalization and greater illness severity that was intermediate between the group with no diabetes and the group with type 2 diabetes, the researchers said.
But after adjustment for age, race, sex, hypertension, smoking, and body mass index, people with type 1 diabetes had odds ratios of 3.90 for hospitalization and 3.35 for greater illness severity, which was similar to risk in type 2 diabetes (3.36 and 3.42, respectively), compared to those without diabetes.
Deep dive explores COVID-19 severity risk factors in type 1 diabetes
The investigators then conducted a detailed chart review for 37 of the 40 patients with type 1 diabetes and phone surveys with 15 of them.
The majority (28) had not been hospitalized, and only one was hospitalized for diabetic ketoacidosis (DKA) within 14 days of positive SARS-CoV-2 testing.
This contrasts with a report from the T1D Exchange, in which nearly half of 33 patients with type 1 diabetes and COVID-19 had been hospitalized with DKA. The reason for the discrepancy may be that more severe patients would more likely be referred to the T1D Exchange Registry, Dr. Gregory and colleagues hypothesized.
Clinical factors associated with COVID-19 severity (P < .05) in their study included a prior hypertension diagnosis, higher hemoglobin A1c, at least one prior DKA admission in the past year, and not using a continuous glucose monitor (CGM).
Hospitalizations were twice as likely and illness severity nearly twice as great among those with type 1 diabetes who were Black versus White. Just 8% of those with private insurance were hospitalized, compared with 60% of those with public insurance and 67% with no insurance (P = .001).
“Whereas previous reports have indicated proportionally higher rates of hospitalizations from COVID-19 among Black patients and those with public insurance, this study is the first to show a similar finding in the population with type 1 diabetes,” Dr. Gregory and colleagues wrote.
Only 9% of patients using a CGM were hospitalized versus 47% who used blood glucose meters (P < .016). Similarly, hospitalizations occurred in 6% using an insulin pump versus 33% using multiple daily injections (P < .085).
“Our analysis cannot exclude the possibility that greater amounts of diabetes technology use are a surrogate for higher socioeconomic status,” they noted.
This research was supported by the National Institute of Diabetes and Digestive and Kidney Diseases, JDRF, and the Appleby Foundation. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
The risk for increased COVID-19 severity in people with type 1 diabetes appears similar to that of type 2 diabetes, contrary to some official advice from the Centers for Disease Control and Prevention. The new finding indicates that people with both types should be priority for receiving a vaccine, investigators say.
The study is the first to prospectively evaluate both inpatients and outpatients and to examine COVID-19 severity factors in addition to death in people with type 1 and type 2 diabetes separately, and was published online Dec. 2 in Diabetes Care.
Among the patients, who were seen at Vanderbilt University Medical Center in Nashville, Tenn., between March and August of 2020, those with both type 1 and type 2 diabetes had between a three- and fourfold greater risk for COVID-19 hospitalization and greater illness severity compared with people without diabetes after adjustments for age, race, and a number of other risk factors.
This finding is important since as of Dec. 1, 2020, the CDC has classified the diabetes types differently in terms of underlying medical conditions that increase the risk for severe COVID-19.
Adults of any age with type 2 diabetes are considered “at increased risk of severe illness” from the virus that causes COVID-19 whereas the CDC says those with type 1 “might be at an increased risk.”
Lead author of the new paper Justin M. Gregory, MD, said in an interview: “I think this needs revision based on the current evidence. I think the data presented in our study and that of Barron et al. in Lancet Endocrinology 2020 indicate the need to place type 1 diabetes at parity with type 2 diabetes.
“These studies indicate both conditions carry an adjusted odds ratio of three to four when compared with people without diabetes for hospitalization, illness severity, and mortality,” he stressed.
Vaccines look promising for patients with diabetes
There were no phase 3 vaccine data available for the vaccine at the time that Dr. Gregory, of the Ian M. Burr Division of Pediatric Endocrinology and Diabetes, Vanderbilt University, Nashville, Tenn., and colleagues were writing their manuscript in late summer, so the article does not mention this.
But now, Dr. Gregory said, “Based on the initial press releases from Pfizer and Moderna, I am now optimistic that these vaccines might mitigate the excess morbidity and mortality from COVID-19 experienced by patients with diabetes.
“I am eager to see what we learn on December 10 and 17 [the scheduled dates for the meetings of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee to review the Pfizer and Moderna vaccines, respectively].”
But with the winter pandemic surge in the meantime, “Our investigation suggests that as COVID-19 hospitalizations rise, patients with both type 1 and 2 diabetes will comprise a disproportionately higher number of those admissions and, once hospitalized, demonstrate a greater degree of illness severity,” he and his colleagues said.
“In light of these data, we call on our colleagues to emphasize the importance of social distancing measures and hand hygiene, with particular emphasis on patients with diabetes, including those in the most vulnerable communities whom our study affirms will face the most severe impact.”
After adjustments, excess severity risk similar for both diabetes types
The new study data came from electronic health records at Vanderbilt University Medical Center, comprising 137 primary care, urgent care, and hospital facilities where patients were tested for SARS-CoV-2 regardless of the reason for their visit.
Between March 17 and August 7, 2020, 6,451 patients tested positive for COVID-19. Of those, 273 had type 2 diabetes and 40 had type 1 diabetes.
Children younger than 18 years accounted for 20% of those with type 1 diabetes and 9.4% of those without diabetes, but none of the type 2 group. The group with type 2 diabetes was considerably older than the type 1 diabetes and no-diabetes groups, 58 years versus 37 and 33 years, respectively.
Before adjustment for baseline characteristics that differed between groups, patients with type 1 diabetes appeared to have a risk for hospitalization and greater illness severity that was intermediate between the group with no diabetes and the group with type 2 diabetes, the researchers said.
But after adjustment for age, race, sex, hypertension, smoking, and body mass index, people with type 1 diabetes had odds ratios of 3.90 for hospitalization and 3.35 for greater illness severity, which was similar to risk in type 2 diabetes (3.36 and 3.42, respectively), compared to those without diabetes.
Deep dive explores COVID-19 severity risk factors in type 1 diabetes
The investigators then conducted a detailed chart review for 37 of the 40 patients with type 1 diabetes and phone surveys with 15 of them.
The majority (28) had not been hospitalized, and only one was hospitalized for diabetic ketoacidosis (DKA) within 14 days of positive SARS-CoV-2 testing.
This contrasts with a report from the T1D Exchange, in which nearly half of 33 patients with type 1 diabetes and COVID-19 had been hospitalized with DKA. The reason for the discrepancy may be that more severe patients would more likely be referred to the T1D Exchange Registry, Dr. Gregory and colleagues hypothesized.
Clinical factors associated with COVID-19 severity (P < .05) in their study included a prior hypertension diagnosis, higher hemoglobin A1c, at least one prior DKA admission in the past year, and not using a continuous glucose monitor (CGM).
Hospitalizations were twice as likely and illness severity nearly twice as great among those with type 1 diabetes who were Black versus White. Just 8% of those with private insurance were hospitalized, compared with 60% of those with public insurance and 67% with no insurance (P = .001).
“Whereas previous reports have indicated proportionally higher rates of hospitalizations from COVID-19 among Black patients and those with public insurance, this study is the first to show a similar finding in the population with type 1 diabetes,” Dr. Gregory and colleagues wrote.
Only 9% of patients using a CGM were hospitalized versus 47% who used blood glucose meters (P < .016). Similarly, hospitalizations occurred in 6% using an insulin pump versus 33% using multiple daily injections (P < .085).
“Our analysis cannot exclude the possibility that greater amounts of diabetes technology use are a surrogate for higher socioeconomic status,” they noted.
This research was supported by the National Institute of Diabetes and Digestive and Kidney Diseases, JDRF, and the Appleby Foundation. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
The risk for increased COVID-19 severity in people with type 1 diabetes appears similar to that of type 2 diabetes, contrary to some official advice from the Centers for Disease Control and Prevention. The new finding indicates that people with both types should be priority for receiving a vaccine, investigators say.
The study is the first to prospectively evaluate both inpatients and outpatients and to examine COVID-19 severity factors in addition to death in people with type 1 and type 2 diabetes separately, and was published online Dec. 2 in Diabetes Care.
Among the patients, who were seen at Vanderbilt University Medical Center in Nashville, Tenn., between March and August of 2020, those with both type 1 and type 2 diabetes had between a three- and fourfold greater risk for COVID-19 hospitalization and greater illness severity compared with people without diabetes after adjustments for age, race, and a number of other risk factors.
This finding is important since as of Dec. 1, 2020, the CDC has classified the diabetes types differently in terms of underlying medical conditions that increase the risk for severe COVID-19.
Adults of any age with type 2 diabetes are considered “at increased risk of severe illness” from the virus that causes COVID-19 whereas the CDC says those with type 1 “might be at an increased risk.”
Lead author of the new paper Justin M. Gregory, MD, said in an interview: “I think this needs revision based on the current evidence. I think the data presented in our study and that of Barron et al. in Lancet Endocrinology 2020 indicate the need to place type 1 diabetes at parity with type 2 diabetes.
“These studies indicate both conditions carry an adjusted odds ratio of three to four when compared with people without diabetes for hospitalization, illness severity, and mortality,” he stressed.
Vaccines look promising for patients with diabetes
There were no phase 3 vaccine data available for the vaccine at the time that Dr. Gregory, of the Ian M. Burr Division of Pediatric Endocrinology and Diabetes, Vanderbilt University, Nashville, Tenn., and colleagues were writing their manuscript in late summer, so the article does not mention this.
But now, Dr. Gregory said, “Based on the initial press releases from Pfizer and Moderna, I am now optimistic that these vaccines might mitigate the excess morbidity and mortality from COVID-19 experienced by patients with diabetes.
“I am eager to see what we learn on December 10 and 17 [the scheduled dates for the meetings of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee to review the Pfizer and Moderna vaccines, respectively].”
But with the winter pandemic surge in the meantime, “Our investigation suggests that as COVID-19 hospitalizations rise, patients with both type 1 and 2 diabetes will comprise a disproportionately higher number of those admissions and, once hospitalized, demonstrate a greater degree of illness severity,” he and his colleagues said.
“In light of these data, we call on our colleagues to emphasize the importance of social distancing measures and hand hygiene, with particular emphasis on patients with diabetes, including those in the most vulnerable communities whom our study affirms will face the most severe impact.”
After adjustments, excess severity risk similar for both diabetes types
The new study data came from electronic health records at Vanderbilt University Medical Center, comprising 137 primary care, urgent care, and hospital facilities where patients were tested for SARS-CoV-2 regardless of the reason for their visit.
Between March 17 and August 7, 2020, 6,451 patients tested positive for COVID-19. Of those, 273 had type 2 diabetes and 40 had type 1 diabetes.
Children younger than 18 years accounted for 20% of those with type 1 diabetes and 9.4% of those without diabetes, but none of the type 2 group. The group with type 2 diabetes was considerably older than the type 1 diabetes and no-diabetes groups, 58 years versus 37 and 33 years, respectively.
Before adjustment for baseline characteristics that differed between groups, patients with type 1 diabetes appeared to have a risk for hospitalization and greater illness severity that was intermediate between the group with no diabetes and the group with type 2 diabetes, the researchers said.
But after adjustment for age, race, sex, hypertension, smoking, and body mass index, people with type 1 diabetes had odds ratios of 3.90 for hospitalization and 3.35 for greater illness severity, which was similar to risk in type 2 diabetes (3.36 and 3.42, respectively), compared to those without diabetes.
Deep dive explores COVID-19 severity risk factors in type 1 diabetes
The investigators then conducted a detailed chart review for 37 of the 40 patients with type 1 diabetes and phone surveys with 15 of them.
The majority (28) had not been hospitalized, and only one was hospitalized for diabetic ketoacidosis (DKA) within 14 days of positive SARS-CoV-2 testing.
This contrasts with a report from the T1D Exchange, in which nearly half of 33 patients with type 1 diabetes and COVID-19 had been hospitalized with DKA. The reason for the discrepancy may be that more severe patients would more likely be referred to the T1D Exchange Registry, Dr. Gregory and colleagues hypothesized.
Clinical factors associated with COVID-19 severity (P < .05) in their study included a prior hypertension diagnosis, higher hemoglobin A1c, at least one prior DKA admission in the past year, and not using a continuous glucose monitor (CGM).
Hospitalizations were twice as likely and illness severity nearly twice as great among those with type 1 diabetes who were Black versus White. Just 8% of those with private insurance were hospitalized, compared with 60% of those with public insurance and 67% with no insurance (P = .001).
“Whereas previous reports have indicated proportionally higher rates of hospitalizations from COVID-19 among Black patients and those with public insurance, this study is the first to show a similar finding in the population with type 1 diabetes,” Dr. Gregory and colleagues wrote.
Only 9% of patients using a CGM were hospitalized versus 47% who used blood glucose meters (P < .016). Similarly, hospitalizations occurred in 6% using an insulin pump versus 33% using multiple daily injections (P < .085).
“Our analysis cannot exclude the possibility that greater amounts of diabetes technology use are a surrogate for higher socioeconomic status,” they noted.
This research was supported by the National Institute of Diabetes and Digestive and Kidney Diseases, JDRF, and the Appleby Foundation. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Five-minute SC injection of daratumumab in RRMM
Data from the Apollo study provide proof for the subcutaneous administration (SC) of daratumumab (Darzalex Faspro) in combination with pomalidomide (Pomalyst) and dexamethasone (Pd) for patients with relapsed or refractory multiple myeloma (RRMM).
The SC formulation of daratumumab (with hyaluronidase) was approved in the United States in May, and is administered by injection into the abdomen over 3-5 minutes. Previously the drug was available only as an intravenous infusion.
“The appeal of subcutaneous daratumumab is the 5 minutes it needs for administering, cutting down considerable on ‘chair/clinic’ time. Intravenous daratumumab is given over several hours,” said Joseph Mikhael, MD, MEd, chief medical officer of the International Myeloma Foundation. He also highlighted the low rates of infusion reactions seen with the subcutaneous daratumumab triplet.
“In the COVID era the subcutaneous route may be the way to go,” he said in an interview.
“This is an effective combination with a predictable safety profile that allows for the use of SC daratumumab along with oral pomalidomide and dexamethasone for patients who have received at least one prior line of therapy that included lenalidomide [Revlimid] and a proteasome inhibitor,” commented lead author Meletios A. Dimopoulos, MD, of the National and Kapodistrian University of Athens.
The triplet combination was associated with a 37% reduced risk for progression or death, compared with the two-drug combination of pomalidomide and dexamethasone.
He presented the results from the Apollo trial at the annual meeting of the American Society of Hematology.
Treatment landscape of RRMM
Dr. Mikhael, who is also professor in the applied cancer research and drug discovery division at the Translational Genomics Research Institute, Phoenix, provided his insights into Apollo as well as how this triplet fits into the treatment landscape of RRMM.
Daratumumab is approved for use in both RRMM and newly diagnosed MM, either alone or in combination with standard-of-care regimens. The drug already has eight specific indications for the intravenous formulation, and five indications for the SC formulation of daratumumab, Dr. Mikhael noted. The Apollo study “will likely provide the subcutaneous approval for the daratumumab triplet in MM.”
According to Dr. Mikhael, the triplet of daratumumab with pomalidomide and dexamethasone is the most commonly used combination at first relapse, and this phase 3 study provides confirmatory evidence for its initial approval. The initial approval for intravenous daratumumab and Pd was based on a phase 1b study, he noted.
“The Apollo study is the first randomized trial comparing the triplet of D-Pd to Pd,” Noopur Raje, MD, of the Massachusetts General Hospital, Boston, said in an interview. She explained that the majority of patients included in Apollo were refractory to lenalidomide, which is the patient population typically seen at the time of first relapse. “This regimen will be adopted at either first or second relapse in the majority of patients,” Dr. Raje said.
“In keeping with strategy in MM, we use the best triplet first and do not save the best for last,” Dr. Mikhael said. The triplet of the proteasome inhibitor bortezomib (Velcade), lenalidomide, and dexamethasone is used in first-line MM. “Most patients meet the criteria for using D-Pd at first relapse,” he added, noting that all patients in the study have received a proteasome inhibitor and lenalidomide as first-line therapy and had relapsed with or were refractory to these agents.
“The short administration time and significantly low rates of infusion-site reactions are two important considerations for using this triplet with the subcutaneous formulation of daratumumab [at first relapse],” he said.
In the treatment landscape of MM, the triplet of isatuximab (Sarclisa), pomalidomide, and dexamethasone has recently been approved for RRMM based on data from the ICARIA study. Isatuximab and daratumumab are both CD38-directed antibodies. Dr. Mikhael pointed out that the datasets from ICARIA and Apollo with respect to progression-free survival (PFS) and hazard ratios overlapped and were remarkably similar. However, daratumumab now has an advantage in being available as an SC formulation.
The landscape of MM treatment has been changing rapidly in recent years, and more changes may be afoot. Dr. Mikhael suggested that the quartet of daratumumab, bortezomib, lenalidomide, and dexamethasone is likely to move into the first-line setting for MM based on data from the GRIFFIN study (trial update in Abstract 3243), and then the choice of drugs to use in first relapse would also change.
Apollo study details
Apollo was an open-label, phase 3 study that randomly assigned patients with RRMM to receive SC daratumumab in combination with pomalidomide and low-dose dexamethasone (D-Pd; n = 151) or the two-drug combination of Pd (n = 153).
Approximately 80% of the patients were refractory to lenalidomide and half were refractory to a proteasome inhibitor.
Median duration of SC daratumumab administration was 5 minutes. Median duration of study treatment was longer for patients on D-Pd (11.5 months vs. 6.6 months for Pd).
For the primary endpoint, at a median follow up of 16.9 months, median PFS was 12.4 months for patients receiving D-Pd and 6.9 months for those receiving Pd. One-year PFS was 52% for patients receiving the triplet combination and 35% for those receiving Pd. Treatment effect was generally consistent across subgroups examined, Dr. Dimopoulos reported.
Depth of response was significantly higher for patients on D-Pd. Stringent complete remission or CR was seen in 25% of patients on D-Pd versus 4% on Pd. Overall response rate was 69% for patients on D-Pd and 45% for patients on Pd alone (P < .0001). Minimal residual disease negativity was more than four times higher with D-Pd (9% vs. 2% for Pd; P = .0102).
The safety profile of D-Pd was consistent with the known safety profile of SC daratumumab and Pd. Infusion-site reactions were grade 1-2 and occurred in 5% of patients; in addition, only grade 1 injection-site reactions were seen and occurred in 2% of patients. The most serious treatment-emergent adverse events in patients on D-Pd were pneumonia (15% vs. 8% for Pd) and lower respiratory tract infection (12% vs. 9% for Pd). Incidence of secondary primary malignancy was 2% for each group.
Apollo results were ‘no surprise’
“These results are of no surprise and further support the current practice of using a three-drug combination in the relapsed setting,” Henry Fung, MD, chair of the department of bone marrow transplant and cellular therapies at Fox Chase Cancer Center, Philadelphia, said in an interview.
Although Dr. Fung agreed that the triplet of a proteasome inhibitor, an immunomodulating drug such as lenalidomide, and the steroid dexamethasone is becoming the standard of care for newly diagnosed MM, D-Pd should be considered an excellent option for patients who have limited choices in the relapsed/refractory setting.
However, he said that the median PFS of 12.4 months for patients receiving D-Pd after a median of two prior regimens is not satisfactory.
“The impact on the natural history of the disease will be limited and the duration of responses decline with each treatment regimen, and the true impact on the disease will be an effective frontline strategy.” Dr. Fung said. “This will not be a practice-changing trial. We need to find out which three-drug regimen works best and what biomarkers can predict the response to individual regimen.”
Dr. Dimopoulos reported receiving honoraria from Beigene, Bristol-Myers Squibb, Amgen, Takeda, Celgene, and Janssen. Dr. Mikhael reported receiving honoraria from Amgen, GlaxoSmithKline, Janssen, Karyopharm, Sanofi, Takeda; consulting with Celgene; and receiving research funding from Celgene and Sanofi. Dr. Fung is on the speakers’ bureau of Apollo and receives honoraria from Jansen Oncology and Celgene/Bristol-Myers Squibb. Dr. Raje is a consultant for Bristol-Myers Squibb and Janssen.
A version of this article originally appeared on Medscape.com.
Data from the Apollo study provide proof for the subcutaneous administration (SC) of daratumumab (Darzalex Faspro) in combination with pomalidomide (Pomalyst) and dexamethasone (Pd) for patients with relapsed or refractory multiple myeloma (RRMM).
The SC formulation of daratumumab (with hyaluronidase) was approved in the United States in May, and is administered by injection into the abdomen over 3-5 minutes. Previously the drug was available only as an intravenous infusion.
“The appeal of subcutaneous daratumumab is the 5 minutes it needs for administering, cutting down considerable on ‘chair/clinic’ time. Intravenous daratumumab is given over several hours,” said Joseph Mikhael, MD, MEd, chief medical officer of the International Myeloma Foundation. He also highlighted the low rates of infusion reactions seen with the subcutaneous daratumumab triplet.
“In the COVID era the subcutaneous route may be the way to go,” he said in an interview.
“This is an effective combination with a predictable safety profile that allows for the use of SC daratumumab along with oral pomalidomide and dexamethasone for patients who have received at least one prior line of therapy that included lenalidomide [Revlimid] and a proteasome inhibitor,” commented lead author Meletios A. Dimopoulos, MD, of the National and Kapodistrian University of Athens.
The triplet combination was associated with a 37% reduced risk for progression or death, compared with the two-drug combination of pomalidomide and dexamethasone.
He presented the results from the Apollo trial at the annual meeting of the American Society of Hematology.
Treatment landscape of RRMM
Dr. Mikhael, who is also professor in the applied cancer research and drug discovery division at the Translational Genomics Research Institute, Phoenix, provided his insights into Apollo as well as how this triplet fits into the treatment landscape of RRMM.
Daratumumab is approved for use in both RRMM and newly diagnosed MM, either alone or in combination with standard-of-care regimens. The drug already has eight specific indications for the intravenous formulation, and five indications for the SC formulation of daratumumab, Dr. Mikhael noted. The Apollo study “will likely provide the subcutaneous approval for the daratumumab triplet in MM.”
According to Dr. Mikhael, the triplet of daratumumab with pomalidomide and dexamethasone is the most commonly used combination at first relapse, and this phase 3 study provides confirmatory evidence for its initial approval. The initial approval for intravenous daratumumab and Pd was based on a phase 1b study, he noted.
“The Apollo study is the first randomized trial comparing the triplet of D-Pd to Pd,” Noopur Raje, MD, of the Massachusetts General Hospital, Boston, said in an interview. She explained that the majority of patients included in Apollo were refractory to lenalidomide, which is the patient population typically seen at the time of first relapse. “This regimen will be adopted at either first or second relapse in the majority of patients,” Dr. Raje said.
“In keeping with strategy in MM, we use the best triplet first and do not save the best for last,” Dr. Mikhael said. The triplet of the proteasome inhibitor bortezomib (Velcade), lenalidomide, and dexamethasone is used in first-line MM. “Most patients meet the criteria for using D-Pd at first relapse,” he added, noting that all patients in the study have received a proteasome inhibitor and lenalidomide as first-line therapy and had relapsed with or were refractory to these agents.
“The short administration time and significantly low rates of infusion-site reactions are two important considerations for using this triplet with the subcutaneous formulation of daratumumab [at first relapse],” he said.
In the treatment landscape of MM, the triplet of isatuximab (Sarclisa), pomalidomide, and dexamethasone has recently been approved for RRMM based on data from the ICARIA study. Isatuximab and daratumumab are both CD38-directed antibodies. Dr. Mikhael pointed out that the datasets from ICARIA and Apollo with respect to progression-free survival (PFS) and hazard ratios overlapped and were remarkably similar. However, daratumumab now has an advantage in being available as an SC formulation.
The landscape of MM treatment has been changing rapidly in recent years, and more changes may be afoot. Dr. Mikhael suggested that the quartet of daratumumab, bortezomib, lenalidomide, and dexamethasone is likely to move into the first-line setting for MM based on data from the GRIFFIN study (trial update in Abstract 3243), and then the choice of drugs to use in first relapse would also change.
Apollo study details
Apollo was an open-label, phase 3 study that randomly assigned patients with RRMM to receive SC daratumumab in combination with pomalidomide and low-dose dexamethasone (D-Pd; n = 151) or the two-drug combination of Pd (n = 153).
Approximately 80% of the patients were refractory to lenalidomide and half were refractory to a proteasome inhibitor.
Median duration of SC daratumumab administration was 5 minutes. Median duration of study treatment was longer for patients on D-Pd (11.5 months vs. 6.6 months for Pd).
For the primary endpoint, at a median follow up of 16.9 months, median PFS was 12.4 months for patients receiving D-Pd and 6.9 months for those receiving Pd. One-year PFS was 52% for patients receiving the triplet combination and 35% for those receiving Pd. Treatment effect was generally consistent across subgroups examined, Dr. Dimopoulos reported.
Depth of response was significantly higher for patients on D-Pd. Stringent complete remission or CR was seen in 25% of patients on D-Pd versus 4% on Pd. Overall response rate was 69% for patients on D-Pd and 45% for patients on Pd alone (P < .0001). Minimal residual disease negativity was more than four times higher with D-Pd (9% vs. 2% for Pd; P = .0102).
The safety profile of D-Pd was consistent with the known safety profile of SC daratumumab and Pd. Infusion-site reactions were grade 1-2 and occurred in 5% of patients; in addition, only grade 1 injection-site reactions were seen and occurred in 2% of patients. The most serious treatment-emergent adverse events in patients on D-Pd were pneumonia (15% vs. 8% for Pd) and lower respiratory tract infection (12% vs. 9% for Pd). Incidence of secondary primary malignancy was 2% for each group.
Apollo results were ‘no surprise’
“These results are of no surprise and further support the current practice of using a three-drug combination in the relapsed setting,” Henry Fung, MD, chair of the department of bone marrow transplant and cellular therapies at Fox Chase Cancer Center, Philadelphia, said in an interview.
Although Dr. Fung agreed that the triplet of a proteasome inhibitor, an immunomodulating drug such as lenalidomide, and the steroid dexamethasone is becoming the standard of care for newly diagnosed MM, D-Pd should be considered an excellent option for patients who have limited choices in the relapsed/refractory setting.
However, he said that the median PFS of 12.4 months for patients receiving D-Pd after a median of two prior regimens is not satisfactory.
“The impact on the natural history of the disease will be limited and the duration of responses decline with each treatment regimen, and the true impact on the disease will be an effective frontline strategy.” Dr. Fung said. “This will not be a practice-changing trial. We need to find out which three-drug regimen works best and what biomarkers can predict the response to individual regimen.”
Dr. Dimopoulos reported receiving honoraria from Beigene, Bristol-Myers Squibb, Amgen, Takeda, Celgene, and Janssen. Dr. Mikhael reported receiving honoraria from Amgen, GlaxoSmithKline, Janssen, Karyopharm, Sanofi, Takeda; consulting with Celgene; and receiving research funding from Celgene and Sanofi. Dr. Fung is on the speakers’ bureau of Apollo and receives honoraria from Jansen Oncology and Celgene/Bristol-Myers Squibb. Dr. Raje is a consultant for Bristol-Myers Squibb and Janssen.
A version of this article originally appeared on Medscape.com.
Data from the Apollo study provide proof for the subcutaneous administration (SC) of daratumumab (Darzalex Faspro) in combination with pomalidomide (Pomalyst) and dexamethasone (Pd) for patients with relapsed or refractory multiple myeloma (RRMM).
The SC formulation of daratumumab (with hyaluronidase) was approved in the United States in May, and is administered by injection into the abdomen over 3-5 minutes. Previously the drug was available only as an intravenous infusion.
“The appeal of subcutaneous daratumumab is the 5 minutes it needs for administering, cutting down considerable on ‘chair/clinic’ time. Intravenous daratumumab is given over several hours,” said Joseph Mikhael, MD, MEd, chief medical officer of the International Myeloma Foundation. He also highlighted the low rates of infusion reactions seen with the subcutaneous daratumumab triplet.
“In the COVID era the subcutaneous route may be the way to go,” he said in an interview.
“This is an effective combination with a predictable safety profile that allows for the use of SC daratumumab along with oral pomalidomide and dexamethasone for patients who have received at least one prior line of therapy that included lenalidomide [Revlimid] and a proteasome inhibitor,” commented lead author Meletios A. Dimopoulos, MD, of the National and Kapodistrian University of Athens.
The triplet combination was associated with a 37% reduced risk for progression or death, compared with the two-drug combination of pomalidomide and dexamethasone.
He presented the results from the Apollo trial at the annual meeting of the American Society of Hematology.
Treatment landscape of RRMM
Dr. Mikhael, who is also professor in the applied cancer research and drug discovery division at the Translational Genomics Research Institute, Phoenix, provided his insights into Apollo as well as how this triplet fits into the treatment landscape of RRMM.
Daratumumab is approved for use in both RRMM and newly diagnosed MM, either alone or in combination with standard-of-care regimens. The drug already has eight specific indications for the intravenous formulation, and five indications for the SC formulation of daratumumab, Dr. Mikhael noted. The Apollo study “will likely provide the subcutaneous approval for the daratumumab triplet in MM.”
According to Dr. Mikhael, the triplet of daratumumab with pomalidomide and dexamethasone is the most commonly used combination at first relapse, and this phase 3 study provides confirmatory evidence for its initial approval. The initial approval for intravenous daratumumab and Pd was based on a phase 1b study, he noted.
“The Apollo study is the first randomized trial comparing the triplet of D-Pd to Pd,” Noopur Raje, MD, of the Massachusetts General Hospital, Boston, said in an interview. She explained that the majority of patients included in Apollo were refractory to lenalidomide, which is the patient population typically seen at the time of first relapse. “This regimen will be adopted at either first or second relapse in the majority of patients,” Dr. Raje said.
“In keeping with strategy in MM, we use the best triplet first and do not save the best for last,” Dr. Mikhael said. The triplet of the proteasome inhibitor bortezomib (Velcade), lenalidomide, and dexamethasone is used in first-line MM. “Most patients meet the criteria for using D-Pd at first relapse,” he added, noting that all patients in the study have received a proteasome inhibitor and lenalidomide as first-line therapy and had relapsed with or were refractory to these agents.
“The short administration time and significantly low rates of infusion-site reactions are two important considerations for using this triplet with the subcutaneous formulation of daratumumab [at first relapse],” he said.
In the treatment landscape of MM, the triplet of isatuximab (Sarclisa), pomalidomide, and dexamethasone has recently been approved for RRMM based on data from the ICARIA study. Isatuximab and daratumumab are both CD38-directed antibodies. Dr. Mikhael pointed out that the datasets from ICARIA and Apollo with respect to progression-free survival (PFS) and hazard ratios overlapped and were remarkably similar. However, daratumumab now has an advantage in being available as an SC formulation.
The landscape of MM treatment has been changing rapidly in recent years, and more changes may be afoot. Dr. Mikhael suggested that the quartet of daratumumab, bortezomib, lenalidomide, and dexamethasone is likely to move into the first-line setting for MM based on data from the GRIFFIN study (trial update in Abstract 3243), and then the choice of drugs to use in first relapse would also change.
Apollo study details
Apollo was an open-label, phase 3 study that randomly assigned patients with RRMM to receive SC daratumumab in combination with pomalidomide and low-dose dexamethasone (D-Pd; n = 151) or the two-drug combination of Pd (n = 153).
Approximately 80% of the patients were refractory to lenalidomide and half were refractory to a proteasome inhibitor.
Median duration of SC daratumumab administration was 5 minutes. Median duration of study treatment was longer for patients on D-Pd (11.5 months vs. 6.6 months for Pd).
For the primary endpoint, at a median follow up of 16.9 months, median PFS was 12.4 months for patients receiving D-Pd and 6.9 months for those receiving Pd. One-year PFS was 52% for patients receiving the triplet combination and 35% for those receiving Pd. Treatment effect was generally consistent across subgroups examined, Dr. Dimopoulos reported.
Depth of response was significantly higher for patients on D-Pd. Stringent complete remission or CR was seen in 25% of patients on D-Pd versus 4% on Pd. Overall response rate was 69% for patients on D-Pd and 45% for patients on Pd alone (P < .0001). Minimal residual disease negativity was more than four times higher with D-Pd (9% vs. 2% for Pd; P = .0102).
The safety profile of D-Pd was consistent with the known safety profile of SC daratumumab and Pd. Infusion-site reactions were grade 1-2 and occurred in 5% of patients; in addition, only grade 1 injection-site reactions were seen and occurred in 2% of patients. The most serious treatment-emergent adverse events in patients on D-Pd were pneumonia (15% vs. 8% for Pd) and lower respiratory tract infection (12% vs. 9% for Pd). Incidence of secondary primary malignancy was 2% for each group.
Apollo results were ‘no surprise’
“These results are of no surprise and further support the current practice of using a three-drug combination in the relapsed setting,” Henry Fung, MD, chair of the department of bone marrow transplant and cellular therapies at Fox Chase Cancer Center, Philadelphia, said in an interview.
Although Dr. Fung agreed that the triplet of a proteasome inhibitor, an immunomodulating drug such as lenalidomide, and the steroid dexamethasone is becoming the standard of care for newly diagnosed MM, D-Pd should be considered an excellent option for patients who have limited choices in the relapsed/refractory setting.
However, he said that the median PFS of 12.4 months for patients receiving D-Pd after a median of two prior regimens is not satisfactory.
“The impact on the natural history of the disease will be limited and the duration of responses decline with each treatment regimen, and the true impact on the disease will be an effective frontline strategy.” Dr. Fung said. “This will not be a practice-changing trial. We need to find out which three-drug regimen works best and what biomarkers can predict the response to individual regimen.”
Dr. Dimopoulos reported receiving honoraria from Beigene, Bristol-Myers Squibb, Amgen, Takeda, Celgene, and Janssen. Dr. Mikhael reported receiving honoraria from Amgen, GlaxoSmithKline, Janssen, Karyopharm, Sanofi, Takeda; consulting with Celgene; and receiving research funding from Celgene and Sanofi. Dr. Fung is on the speakers’ bureau of Apollo and receives honoraria from Jansen Oncology and Celgene/Bristol-Myers Squibb. Dr. Raje is a consultant for Bristol-Myers Squibb and Janssen.
A version of this article originally appeared on Medscape.com.
FDA safety alert: Face masks with metal can burn during MRI
After a patient’s face was burned in the outline of a mask worn during a 3-Tesla MRI neck scan, the US Food and Drug Administration (FDA) cautioned that face masks containing metal can heat to unsafe temperatures during scanning.
Clinicians have known for years to ask patients to remove all metal jewelry and other objects prior to an MRI. The widespread wearing of face masks during the COVID-19 pandemic, however, adds one more consideration to the list.
The FDA’s December 7 safety communication applies to surgical and nonsurgical face masks and respirators.
The injury risk relates to rapid heating of metal components. Many face masks contain a nose wire or metal clip that helps the product conform to the face. Some masks contain metal nanoparticles, while others feature antimicrobial coatings with silver or copper. Each of these products should be avoided during MRI scanning. Also watch out for staples on headbands, the FDA warned.
If the metal content of a face mask is unknown, the FDA suggests providing the patient with a facial covering that is known not to contain any metal.
Robert E. Watson Jr, MD, PhD, chair of the American College of Radiology (ACR) Committee on MR Safety, agreed. He recommended that facilities “provide patients with masks known to be MRI-safe and not permit patient-owned masks in the MRI.”
Watson suggested this strategy at a time when face masks are required.
“COVID-19 safety protocols require that patients wear masks when being scanned, to decrease infection risk to MRI staff, decrease risk of contaminating the MRI scanner, and to protect themselves from infection,” he told Medscape Medical News. “Any conducting metal that enters the MRI machine is at risk of heating due to the radiofrequency fields inherent to image generation.”
Adverse events related to the metal components of a face mask should be reported to the FDA using the MedWatch voluntary reporting form. In addition, healthcare providers subject to the FDA user facility reporting requirements should follow procedures at their facilities to report such events.
This article first appeared on Medscape.com.
After a patient’s face was burned in the outline of a mask worn during a 3-Tesla MRI neck scan, the US Food and Drug Administration (FDA) cautioned that face masks containing metal can heat to unsafe temperatures during scanning.
Clinicians have known for years to ask patients to remove all metal jewelry and other objects prior to an MRI. The widespread wearing of face masks during the COVID-19 pandemic, however, adds one more consideration to the list.
The FDA’s December 7 safety communication applies to surgical and nonsurgical face masks and respirators.
The injury risk relates to rapid heating of metal components. Many face masks contain a nose wire or metal clip that helps the product conform to the face. Some masks contain metal nanoparticles, while others feature antimicrobial coatings with silver or copper. Each of these products should be avoided during MRI scanning. Also watch out for staples on headbands, the FDA warned.
If the metal content of a face mask is unknown, the FDA suggests providing the patient with a facial covering that is known not to contain any metal.
Robert E. Watson Jr, MD, PhD, chair of the American College of Radiology (ACR) Committee on MR Safety, agreed. He recommended that facilities “provide patients with masks known to be MRI-safe and not permit patient-owned masks in the MRI.”
Watson suggested this strategy at a time when face masks are required.
“COVID-19 safety protocols require that patients wear masks when being scanned, to decrease infection risk to MRI staff, decrease risk of contaminating the MRI scanner, and to protect themselves from infection,” he told Medscape Medical News. “Any conducting metal that enters the MRI machine is at risk of heating due to the radiofrequency fields inherent to image generation.”
Adverse events related to the metal components of a face mask should be reported to the FDA using the MedWatch voluntary reporting form. In addition, healthcare providers subject to the FDA user facility reporting requirements should follow procedures at their facilities to report such events.
This article first appeared on Medscape.com.
After a patient’s face was burned in the outline of a mask worn during a 3-Tesla MRI neck scan, the US Food and Drug Administration (FDA) cautioned that face masks containing metal can heat to unsafe temperatures during scanning.
Clinicians have known for years to ask patients to remove all metal jewelry and other objects prior to an MRI. The widespread wearing of face masks during the COVID-19 pandemic, however, adds one more consideration to the list.
The FDA’s December 7 safety communication applies to surgical and nonsurgical face masks and respirators.
The injury risk relates to rapid heating of metal components. Many face masks contain a nose wire or metal clip that helps the product conform to the face. Some masks contain metal nanoparticles, while others feature antimicrobial coatings with silver or copper. Each of these products should be avoided during MRI scanning. Also watch out for staples on headbands, the FDA warned.
If the metal content of a face mask is unknown, the FDA suggests providing the patient with a facial covering that is known not to contain any metal.
Robert E. Watson Jr, MD, PhD, chair of the American College of Radiology (ACR) Committee on MR Safety, agreed. He recommended that facilities “provide patients with masks known to be MRI-safe and not permit patient-owned masks in the MRI.”
Watson suggested this strategy at a time when face masks are required.
“COVID-19 safety protocols require that patients wear masks when being scanned, to decrease infection risk to MRI staff, decrease risk of contaminating the MRI scanner, and to protect themselves from infection,” he told Medscape Medical News. “Any conducting metal that enters the MRI machine is at risk of heating due to the radiofrequency fields inherent to image generation.”
Adverse events related to the metal components of a face mask should be reported to the FDA using the MedWatch voluntary reporting form. In addition, healthcare providers subject to the FDA user facility reporting requirements should follow procedures at their facilities to report such events.
This article first appeared on Medscape.com.
Emotions, worse attention linked to pain-related health care use in SCD
The cognitive and emotional status of children with sickle cell disease (SCD) appears to have a significant effect on how they cope with pain and use health care resources, investigators have found.
Results of a retrospective study of 112 children and adolescents with SCD, the majority of whom had sickle cell anemia, showed that ED visits and hospitalizations were significantly lower among children with SCD who performed better on an attention task, as well as those who were better able to cope emotionally with having SCD and pain, reported Zaria Williams, a second-year medical student at Howard University, Washington, and colleagues.
“Since I started learning more about sickle cell disease, I’ve been very concerned about the great disease burden that this condition can place on pediatric patients, particularly those who suffer from pain,” Ms. Williams said in an oral abstract presented at the annual meeting of the American Society of Hematology.
Although many children and adolescents with SCD can have their pain effectively managed at home with opioids and other medications, some require ED visits and potentially hospitalizations for pain management.
“There is great variability in health care utilization among patients with sickle cell disease, with some having to come to the ED and be admit to the hospital more than others. In searching for reasons why this might be the case, we thought about cognitive function and emotional differences between children with sickle cell disease as potentially affecting disease management,” she said.
Anxiety and catastrophizing
Children with SCD are known to be susceptible to affective comorbidities such as anxiety and catastrophizing, and to conditions that have the potential for deleterious effects on executive function, attention, and working memory. To determine whether cognitive and emotional factors affect the disease self-management in children and adolescents with SCD, Ms. Williams and coinvestigators looked at a cohort of 112 SCD patients aged 7-16 years treated at Children’s National Hospital in Washington, D.C.
The patients had participated in a previous pilot study of computerized working memory training. The authors reviewed charts for data on health care utilization, focusing on ED visits and hospitalization for pain 1 and 3 years after enrollment in the study.
They collected data on SCD genotype, disease-related variables, psychosocial information, and measures of cognition and emotion from the dataset. The information included socioeconomic status, parent education level, household income, and number of adults in the household.
Cognitive measures included the Weschler Intelligence Scale for Children full scale IQ, and the Cogstate computerized cognitive assessment system, which measures attention, executive function, and working memory.
Emotional measures were captured from the Pediatric Quality of Life Inventory Sickle Cell Disease module, including questions about worrying and emotions such as anger regarding SCD and pain.
The mean age of participants was 10.61 years. Of the 112 children/adolescents in the study, 65 (58%) were female, and 83 (74%) had sickle cell anemia (either HbSS or HbSβ0 thalassemia).
The participants had a median number of ED visits for pain of one within a year of enrollment, and a median of three within 3 years of enrollment,
The median number of hospital admissions for pain was zero and one, respectively.
Attention, emotions linked to higher use
Factors significantly associated with ED visits for pain within the first year were higher (worse) scores for attention (P = .001) and self-reported emotion (P = .049). ED visits within 3 years of enrollment were associated with attention (P = .003) and working memory (P = .039).
Similarly, hospitalizations for pain within the first year were significantly associated with worse attention scores (P = .009) and child-reported emotion (P = .013). Hospitalizations for pain within 3 years of enrollment were also significantly associated with attention deficits (P = .006) and with worse emotional function as reported by a parent (P = .020).
There was no significant effect of SCD genotype or socioeconomic status on either pain-related ED visits or hospitalizations, however.
The investigators theorized that poor attention may make it difficult to distract children from focusing on their pain, and could also hamper disease self-management strategies such as medication adherence and avoiding pain triggers.
Age-related differences?
In the question-and-answer session following her presentation, comoderator Susanna A Curtis, MD, from Yale New Haven (Conn.) Hospital, commented that “some previous work has shown that adolescents and young adults with sickle cell disease have higher utilization as compared to their younger counterparts,” and asked whether the investigators found differences between cognition and utilization among different age groups within the cohort.
“We didn’t find a significant association with age, but I’m also very interested in that as well, especially considering that maybe there is more or less parent involvement, considering how old the child is,” Ms. Williams said.
Dr. Curtis noted that many of the comorbidities of sickle cell disease such as stroke or degree of anemia can affect cognitive function, but can also have an effect on health care utilization as well, asked whether the investigators were able to look at the potential confounding effects of comorbidities.
Ms. Williams said that, although they have not looked at potential confounders as yet, they hope to do so in future research.
Asked by another audience member whether the authors had considered using the Pain Catastrophizing Scale for children and/or their parents, in addition to other markers, Ms. Williams replied that “I definitely have considered it. Under recommendations from my mentors, we just focused on the quality-of-life scale first, but catastrophizing is something I’m very interested in. Especially, I would love to have the parent factors as well, so along the journey I hope to include that.”
The study was sponsored in part by a grant from the Doris Duke Charitable Foundation. Ms Williams is the recipient of an ASH Minority Medical Student Award. Dr. Curtis and Ms. Williams both reported no relevant conflicts of interest to disclose.
SOURCE: Williams Z et al. ASH 2020, Abstract 366
The cognitive and emotional status of children with sickle cell disease (SCD) appears to have a significant effect on how they cope with pain and use health care resources, investigators have found.
Results of a retrospective study of 112 children and adolescents with SCD, the majority of whom had sickle cell anemia, showed that ED visits and hospitalizations were significantly lower among children with SCD who performed better on an attention task, as well as those who were better able to cope emotionally with having SCD and pain, reported Zaria Williams, a second-year medical student at Howard University, Washington, and colleagues.
“Since I started learning more about sickle cell disease, I’ve been very concerned about the great disease burden that this condition can place on pediatric patients, particularly those who suffer from pain,” Ms. Williams said in an oral abstract presented at the annual meeting of the American Society of Hematology.
Although many children and adolescents with SCD can have their pain effectively managed at home with opioids and other medications, some require ED visits and potentially hospitalizations for pain management.
“There is great variability in health care utilization among patients with sickle cell disease, with some having to come to the ED and be admit to the hospital more than others. In searching for reasons why this might be the case, we thought about cognitive function and emotional differences between children with sickle cell disease as potentially affecting disease management,” she said.
Anxiety and catastrophizing
Children with SCD are known to be susceptible to affective comorbidities such as anxiety and catastrophizing, and to conditions that have the potential for deleterious effects on executive function, attention, and working memory. To determine whether cognitive and emotional factors affect the disease self-management in children and adolescents with SCD, Ms. Williams and coinvestigators looked at a cohort of 112 SCD patients aged 7-16 years treated at Children’s National Hospital in Washington, D.C.
The patients had participated in a previous pilot study of computerized working memory training. The authors reviewed charts for data on health care utilization, focusing on ED visits and hospitalization for pain 1 and 3 years after enrollment in the study.
They collected data on SCD genotype, disease-related variables, psychosocial information, and measures of cognition and emotion from the dataset. The information included socioeconomic status, parent education level, household income, and number of adults in the household.
Cognitive measures included the Weschler Intelligence Scale for Children full scale IQ, and the Cogstate computerized cognitive assessment system, which measures attention, executive function, and working memory.
Emotional measures were captured from the Pediatric Quality of Life Inventory Sickle Cell Disease module, including questions about worrying and emotions such as anger regarding SCD and pain.
The mean age of participants was 10.61 years. Of the 112 children/adolescents in the study, 65 (58%) were female, and 83 (74%) had sickle cell anemia (either HbSS or HbSβ0 thalassemia).
The participants had a median number of ED visits for pain of one within a year of enrollment, and a median of three within 3 years of enrollment,
The median number of hospital admissions for pain was zero and one, respectively.
Attention, emotions linked to higher use
Factors significantly associated with ED visits for pain within the first year were higher (worse) scores for attention (P = .001) and self-reported emotion (P = .049). ED visits within 3 years of enrollment were associated with attention (P = .003) and working memory (P = .039).
Similarly, hospitalizations for pain within the first year were significantly associated with worse attention scores (P = .009) and child-reported emotion (P = .013). Hospitalizations for pain within 3 years of enrollment were also significantly associated with attention deficits (P = .006) and with worse emotional function as reported by a parent (P = .020).
There was no significant effect of SCD genotype or socioeconomic status on either pain-related ED visits or hospitalizations, however.
The investigators theorized that poor attention may make it difficult to distract children from focusing on their pain, and could also hamper disease self-management strategies such as medication adherence and avoiding pain triggers.
Age-related differences?
In the question-and-answer session following her presentation, comoderator Susanna A Curtis, MD, from Yale New Haven (Conn.) Hospital, commented that “some previous work has shown that adolescents and young adults with sickle cell disease have higher utilization as compared to their younger counterparts,” and asked whether the investigators found differences between cognition and utilization among different age groups within the cohort.
“We didn’t find a significant association with age, but I’m also very interested in that as well, especially considering that maybe there is more or less parent involvement, considering how old the child is,” Ms. Williams said.
Dr. Curtis noted that many of the comorbidities of sickle cell disease such as stroke or degree of anemia can affect cognitive function, but can also have an effect on health care utilization as well, asked whether the investigators were able to look at the potential confounding effects of comorbidities.
Ms. Williams said that, although they have not looked at potential confounders as yet, they hope to do so in future research.
Asked by another audience member whether the authors had considered using the Pain Catastrophizing Scale for children and/or their parents, in addition to other markers, Ms. Williams replied that “I definitely have considered it. Under recommendations from my mentors, we just focused on the quality-of-life scale first, but catastrophizing is something I’m very interested in. Especially, I would love to have the parent factors as well, so along the journey I hope to include that.”
The study was sponsored in part by a grant from the Doris Duke Charitable Foundation. Ms Williams is the recipient of an ASH Minority Medical Student Award. Dr. Curtis and Ms. Williams both reported no relevant conflicts of interest to disclose.
SOURCE: Williams Z et al. ASH 2020, Abstract 366
The cognitive and emotional status of children with sickle cell disease (SCD) appears to have a significant effect on how they cope with pain and use health care resources, investigators have found.
Results of a retrospective study of 112 children and adolescents with SCD, the majority of whom had sickle cell anemia, showed that ED visits and hospitalizations were significantly lower among children with SCD who performed better on an attention task, as well as those who were better able to cope emotionally with having SCD and pain, reported Zaria Williams, a second-year medical student at Howard University, Washington, and colleagues.
“Since I started learning more about sickle cell disease, I’ve been very concerned about the great disease burden that this condition can place on pediatric patients, particularly those who suffer from pain,” Ms. Williams said in an oral abstract presented at the annual meeting of the American Society of Hematology.
Although many children and adolescents with SCD can have their pain effectively managed at home with opioids and other medications, some require ED visits and potentially hospitalizations for pain management.
“There is great variability in health care utilization among patients with sickle cell disease, with some having to come to the ED and be admit to the hospital more than others. In searching for reasons why this might be the case, we thought about cognitive function and emotional differences between children with sickle cell disease as potentially affecting disease management,” she said.
Anxiety and catastrophizing
Children with SCD are known to be susceptible to affective comorbidities such as anxiety and catastrophizing, and to conditions that have the potential for deleterious effects on executive function, attention, and working memory. To determine whether cognitive and emotional factors affect the disease self-management in children and adolescents with SCD, Ms. Williams and coinvestigators looked at a cohort of 112 SCD patients aged 7-16 years treated at Children’s National Hospital in Washington, D.C.
The patients had participated in a previous pilot study of computerized working memory training. The authors reviewed charts for data on health care utilization, focusing on ED visits and hospitalization for pain 1 and 3 years after enrollment in the study.
They collected data on SCD genotype, disease-related variables, psychosocial information, and measures of cognition and emotion from the dataset. The information included socioeconomic status, parent education level, household income, and number of adults in the household.
Cognitive measures included the Weschler Intelligence Scale for Children full scale IQ, and the Cogstate computerized cognitive assessment system, which measures attention, executive function, and working memory.
Emotional measures were captured from the Pediatric Quality of Life Inventory Sickle Cell Disease module, including questions about worrying and emotions such as anger regarding SCD and pain.
The mean age of participants was 10.61 years. Of the 112 children/adolescents in the study, 65 (58%) were female, and 83 (74%) had sickle cell anemia (either HbSS or HbSβ0 thalassemia).
The participants had a median number of ED visits for pain of one within a year of enrollment, and a median of three within 3 years of enrollment,
The median number of hospital admissions for pain was zero and one, respectively.
Attention, emotions linked to higher use
Factors significantly associated with ED visits for pain within the first year were higher (worse) scores for attention (P = .001) and self-reported emotion (P = .049). ED visits within 3 years of enrollment were associated with attention (P = .003) and working memory (P = .039).
Similarly, hospitalizations for pain within the first year were significantly associated with worse attention scores (P = .009) and child-reported emotion (P = .013). Hospitalizations for pain within 3 years of enrollment were also significantly associated with attention deficits (P = .006) and with worse emotional function as reported by a parent (P = .020).
There was no significant effect of SCD genotype or socioeconomic status on either pain-related ED visits or hospitalizations, however.
The investigators theorized that poor attention may make it difficult to distract children from focusing on their pain, and could also hamper disease self-management strategies such as medication adherence and avoiding pain triggers.
Age-related differences?
In the question-and-answer session following her presentation, comoderator Susanna A Curtis, MD, from Yale New Haven (Conn.) Hospital, commented that “some previous work has shown that adolescents and young adults with sickle cell disease have higher utilization as compared to their younger counterparts,” and asked whether the investigators found differences between cognition and utilization among different age groups within the cohort.
“We didn’t find a significant association with age, but I’m also very interested in that as well, especially considering that maybe there is more or less parent involvement, considering how old the child is,” Ms. Williams said.
Dr. Curtis noted that many of the comorbidities of sickle cell disease such as stroke or degree of anemia can affect cognitive function, but can also have an effect on health care utilization as well, asked whether the investigators were able to look at the potential confounding effects of comorbidities.
Ms. Williams said that, although they have not looked at potential confounders as yet, they hope to do so in future research.
Asked by another audience member whether the authors had considered using the Pain Catastrophizing Scale for children and/or their parents, in addition to other markers, Ms. Williams replied that “I definitely have considered it. Under recommendations from my mentors, we just focused on the quality-of-life scale first, but catastrophizing is something I’m very interested in. Especially, I would love to have the parent factors as well, so along the journey I hope to include that.”
The study was sponsored in part by a grant from the Doris Duke Charitable Foundation. Ms Williams is the recipient of an ASH Minority Medical Student Award. Dr. Curtis and Ms. Williams both reported no relevant conflicts of interest to disclose.
SOURCE: Williams Z et al. ASH 2020, Abstract 366
FROM ASH 2020
Demand for COVID vaccines expected to get heated – and fast
Americans have made no secret of their skepticism of COVID-19 vaccines this year, with fears of political interference and a “warp speed” timeline blunting confidence in the shots. As recently as September, nearly half of U.S. adults said they didn’t intend to be inoculated.
But with two promising vaccines primed for release, likely within weeks, experts in ethics and immunization behavior say they expect attitudes to shift quickly from widespread hesitancy to urgent, even heated demand.
“People talk about the antivaccine people being able to kind of squelch uptake. I don’t see that happening,” Dr. Paul Offit, MD, a vaccinologist with Children’s Hospital of Philadelphia, told viewers of a recent JAMA Network webinar. “This, to me, is more like the Beanie Baby phenomenon. The attractiveness of a limited edition.”
Reports that vaccines produced by drugmakers Pfizer and BioNTech and Moderna appear to be safe and effective, along with the deliberate emphasis on science-based guidance from the incoming Biden administration, are likely to reverse uncertainty in a big way, said Arthur Caplan, PhD, director of the division of medical ethics at New York University.
“I think that’s going to flip the trust issue,” he said.
The shift is already apparent. A new poll by the Pew Research Center found that by the end of November 60% of Americans said they would get a vaccine for the coronavirus. This month, even as a federal advisory group met to hash out guidelines for vaccine distribution, a long list of advocacy groups – from those representing home-based health workers and community health centers to patients with kidney disease – were lobbying state and federal officials in hopes their constituents would be prioritized for the first scarce doses.
“As we get closer to the vaccine being a reality, there’s a lot of jockeying, to be sure,” said Katie Smith Sloan, chief executive of LeadingAge, a nonprofit organization pushing for staff and patients at long-term care centers to be included in the highest-priority category.
Certainly, some consumers remain wary, said Rupali Limaye, PhD, a social and behavioral health scientist at the Johns Hopkins Bloomberg School of Public Health, Baltimore. Fears that drugmakers and regulators might cut corners to speed a vaccine linger, even as details of the trials become public and the review process is made more transparent. Some health care workers, who are at the front of the line for the shots, are not eager to go first.
“There will be people who will say, ‘I will wait a little bit more for safety data,” Dr. Limaye said.
But those doubts likely will recede once the vaccines are approved for use and begin to circulate broadly, said Dr. Offit, who sits on the Food and Drug Administration advisory panel set to review the requests for emergency authorization Pfizer and Moderna have submitted.
He predicted demand for the COVID vaccines could rival the clamor that occurred in 2004, when production problems caused a severe shortage of flu shots just as influenza season began. That led to long lines, rationed doses and ethical debates over distribution.
“That was a highly desired vaccine,” Dr. Offit said. “I think in many ways that might happen here.”
Initially, vaccine supplies will be tight, with federal officials planning to ship 6.4 million doses within 24 hours of FDA authorization and up to 40 million doses by the end of the year. The CDC panel recommended that the first shots go to the 21 million health care workers in the United States and 3 million nursing home staff and residents, before being rolled out to other groups based on a hierarchy of risk factors.
Even before any vaccine is available, some people are trying to boost their chances of access, said Allison Kempe, MD, a professor of pediatrics at the University of Coloradoat Denver, Aurora, and expert in vaccine dissemination. “People have called me and said, ‘How can I get the vaccine?’” she said. “I think that not everyone will be happy to wait, that’s for sure. I don’t think there will be rioting in the streets, but there may be pressure brought to bear.”
That likely will include emotional debates over how, when, and to whom next doses should be distributed, said Dr. Caplan. Under the CDC recommendations, vulnerable groups next in line include 87 million workers whose jobs are deemed “essential” – a broad and ill-defined category – as well as 53 million adults age 65 and older.
“We’re going to have some fights about high-risk groups,” Dr. Caplan said.
The conversations will be complicated. Should prisoners, who have little control over their COVID exposure, get vaccine priority? How about professional sports teams, whose performance could bolster society’s overall morale? And what about residents of facilities providing care for people with intellectual and developmental disabilities, who are three times more likely to die from COVID-19 than the general population?
Control over vaccination allocation rests with the states, so that’s where the biggest conflicts will occur, Dr. Caplan said. “It’s a short fight, I hope, in the sense in which it gets done in a few months, but I think it will be pretty vocal.”
Once vaccine supplies become more plentiful, perhaps by May or June, another consideration is sure to boost demand: requirements for proof of COVID vaccination for work and travel.
“It’s inevitable that you’re going to see immunity passports or that you’re required to show a certificate on the train, airplane, bus, or subway,” Dr. Caplan predicted. “Probably also to enter certain hospitals, probably to enter certain restaurants and government facilities.”
But with a grueling winter surge ahead, and new predictions that COVID-19 will fell as many as 450,000 Americans by February, the tragic reality of the disease will no doubt fuel ample demand for vaccination.
“People now know someone who has gotten COVID, who has been hospitalized or has unfortunately died,” Dr. Limaye said.
“We’re all seeing this now,” said Dr. Kempe. “Even deniers are beginning to see what this illness can do.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Americans have made no secret of their skepticism of COVID-19 vaccines this year, with fears of political interference and a “warp speed” timeline blunting confidence in the shots. As recently as September, nearly half of U.S. adults said they didn’t intend to be inoculated.
But with two promising vaccines primed for release, likely within weeks, experts in ethics and immunization behavior say they expect attitudes to shift quickly from widespread hesitancy to urgent, even heated demand.
“People talk about the antivaccine people being able to kind of squelch uptake. I don’t see that happening,” Dr. Paul Offit, MD, a vaccinologist with Children’s Hospital of Philadelphia, told viewers of a recent JAMA Network webinar. “This, to me, is more like the Beanie Baby phenomenon. The attractiveness of a limited edition.”
Reports that vaccines produced by drugmakers Pfizer and BioNTech and Moderna appear to be safe and effective, along with the deliberate emphasis on science-based guidance from the incoming Biden administration, are likely to reverse uncertainty in a big way, said Arthur Caplan, PhD, director of the division of medical ethics at New York University.
“I think that’s going to flip the trust issue,” he said.
The shift is already apparent. A new poll by the Pew Research Center found that by the end of November 60% of Americans said they would get a vaccine for the coronavirus. This month, even as a federal advisory group met to hash out guidelines for vaccine distribution, a long list of advocacy groups – from those representing home-based health workers and community health centers to patients with kidney disease – were lobbying state and federal officials in hopes their constituents would be prioritized for the first scarce doses.
“As we get closer to the vaccine being a reality, there’s a lot of jockeying, to be sure,” said Katie Smith Sloan, chief executive of LeadingAge, a nonprofit organization pushing for staff and patients at long-term care centers to be included in the highest-priority category.
Certainly, some consumers remain wary, said Rupali Limaye, PhD, a social and behavioral health scientist at the Johns Hopkins Bloomberg School of Public Health, Baltimore. Fears that drugmakers and regulators might cut corners to speed a vaccine linger, even as details of the trials become public and the review process is made more transparent. Some health care workers, who are at the front of the line for the shots, are not eager to go first.
“There will be people who will say, ‘I will wait a little bit more for safety data,” Dr. Limaye said.
But those doubts likely will recede once the vaccines are approved for use and begin to circulate broadly, said Dr. Offit, who sits on the Food and Drug Administration advisory panel set to review the requests for emergency authorization Pfizer and Moderna have submitted.
He predicted demand for the COVID vaccines could rival the clamor that occurred in 2004, when production problems caused a severe shortage of flu shots just as influenza season began. That led to long lines, rationed doses and ethical debates over distribution.
“That was a highly desired vaccine,” Dr. Offit said. “I think in many ways that might happen here.”
Initially, vaccine supplies will be tight, with federal officials planning to ship 6.4 million doses within 24 hours of FDA authorization and up to 40 million doses by the end of the year. The CDC panel recommended that the first shots go to the 21 million health care workers in the United States and 3 million nursing home staff and residents, before being rolled out to other groups based on a hierarchy of risk factors.
Even before any vaccine is available, some people are trying to boost their chances of access, said Allison Kempe, MD, a professor of pediatrics at the University of Coloradoat Denver, Aurora, and expert in vaccine dissemination. “People have called me and said, ‘How can I get the vaccine?’” she said. “I think that not everyone will be happy to wait, that’s for sure. I don’t think there will be rioting in the streets, but there may be pressure brought to bear.”
That likely will include emotional debates over how, when, and to whom next doses should be distributed, said Dr. Caplan. Under the CDC recommendations, vulnerable groups next in line include 87 million workers whose jobs are deemed “essential” – a broad and ill-defined category – as well as 53 million adults age 65 and older.
“We’re going to have some fights about high-risk groups,” Dr. Caplan said.
The conversations will be complicated. Should prisoners, who have little control over their COVID exposure, get vaccine priority? How about professional sports teams, whose performance could bolster society’s overall morale? And what about residents of facilities providing care for people with intellectual and developmental disabilities, who are three times more likely to die from COVID-19 than the general population?
Control over vaccination allocation rests with the states, so that’s where the biggest conflicts will occur, Dr. Caplan said. “It’s a short fight, I hope, in the sense in which it gets done in a few months, but I think it will be pretty vocal.”
Once vaccine supplies become more plentiful, perhaps by May or June, another consideration is sure to boost demand: requirements for proof of COVID vaccination for work and travel.
“It’s inevitable that you’re going to see immunity passports or that you’re required to show a certificate on the train, airplane, bus, or subway,” Dr. Caplan predicted. “Probably also to enter certain hospitals, probably to enter certain restaurants and government facilities.”
But with a grueling winter surge ahead, and new predictions that COVID-19 will fell as many as 450,000 Americans by February, the tragic reality of the disease will no doubt fuel ample demand for vaccination.
“People now know someone who has gotten COVID, who has been hospitalized or has unfortunately died,” Dr. Limaye said.
“We’re all seeing this now,” said Dr. Kempe. “Even deniers are beginning to see what this illness can do.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Americans have made no secret of their skepticism of COVID-19 vaccines this year, with fears of political interference and a “warp speed” timeline blunting confidence in the shots. As recently as September, nearly half of U.S. adults said they didn’t intend to be inoculated.
But with two promising vaccines primed for release, likely within weeks, experts in ethics and immunization behavior say they expect attitudes to shift quickly from widespread hesitancy to urgent, even heated demand.
“People talk about the antivaccine people being able to kind of squelch uptake. I don’t see that happening,” Dr. Paul Offit, MD, a vaccinologist with Children’s Hospital of Philadelphia, told viewers of a recent JAMA Network webinar. “This, to me, is more like the Beanie Baby phenomenon. The attractiveness of a limited edition.”
Reports that vaccines produced by drugmakers Pfizer and BioNTech and Moderna appear to be safe and effective, along with the deliberate emphasis on science-based guidance from the incoming Biden administration, are likely to reverse uncertainty in a big way, said Arthur Caplan, PhD, director of the division of medical ethics at New York University.
“I think that’s going to flip the trust issue,” he said.
The shift is already apparent. A new poll by the Pew Research Center found that by the end of November 60% of Americans said they would get a vaccine for the coronavirus. This month, even as a federal advisory group met to hash out guidelines for vaccine distribution, a long list of advocacy groups – from those representing home-based health workers and community health centers to patients with kidney disease – were lobbying state and federal officials in hopes their constituents would be prioritized for the first scarce doses.
“As we get closer to the vaccine being a reality, there’s a lot of jockeying, to be sure,” said Katie Smith Sloan, chief executive of LeadingAge, a nonprofit organization pushing for staff and patients at long-term care centers to be included in the highest-priority category.
Certainly, some consumers remain wary, said Rupali Limaye, PhD, a social and behavioral health scientist at the Johns Hopkins Bloomberg School of Public Health, Baltimore. Fears that drugmakers and regulators might cut corners to speed a vaccine linger, even as details of the trials become public and the review process is made more transparent. Some health care workers, who are at the front of the line for the shots, are not eager to go first.
“There will be people who will say, ‘I will wait a little bit more for safety data,” Dr. Limaye said.
But those doubts likely will recede once the vaccines are approved for use and begin to circulate broadly, said Dr. Offit, who sits on the Food and Drug Administration advisory panel set to review the requests for emergency authorization Pfizer and Moderna have submitted.
He predicted demand for the COVID vaccines could rival the clamor that occurred in 2004, when production problems caused a severe shortage of flu shots just as influenza season began. That led to long lines, rationed doses and ethical debates over distribution.
“That was a highly desired vaccine,” Dr. Offit said. “I think in many ways that might happen here.”
Initially, vaccine supplies will be tight, with federal officials planning to ship 6.4 million doses within 24 hours of FDA authorization and up to 40 million doses by the end of the year. The CDC panel recommended that the first shots go to the 21 million health care workers in the United States and 3 million nursing home staff and residents, before being rolled out to other groups based on a hierarchy of risk factors.
Even before any vaccine is available, some people are trying to boost their chances of access, said Allison Kempe, MD, a professor of pediatrics at the University of Coloradoat Denver, Aurora, and expert in vaccine dissemination. “People have called me and said, ‘How can I get the vaccine?’” she said. “I think that not everyone will be happy to wait, that’s for sure. I don’t think there will be rioting in the streets, but there may be pressure brought to bear.”
That likely will include emotional debates over how, when, and to whom next doses should be distributed, said Dr. Caplan. Under the CDC recommendations, vulnerable groups next in line include 87 million workers whose jobs are deemed “essential” – a broad and ill-defined category – as well as 53 million adults age 65 and older.
“We’re going to have some fights about high-risk groups,” Dr. Caplan said.
The conversations will be complicated. Should prisoners, who have little control over their COVID exposure, get vaccine priority? How about professional sports teams, whose performance could bolster society’s overall morale? And what about residents of facilities providing care for people with intellectual and developmental disabilities, who are three times more likely to die from COVID-19 than the general population?
Control over vaccination allocation rests with the states, so that’s where the biggest conflicts will occur, Dr. Caplan said. “It’s a short fight, I hope, in the sense in which it gets done in a few months, but I think it will be pretty vocal.”
Once vaccine supplies become more plentiful, perhaps by May or June, another consideration is sure to boost demand: requirements for proof of COVID vaccination for work and travel.
“It’s inevitable that you’re going to see immunity passports or that you’re required to show a certificate on the train, airplane, bus, or subway,” Dr. Caplan predicted. “Probably also to enter certain hospitals, probably to enter certain restaurants and government facilities.”
But with a grueling winter surge ahead, and new predictions that COVID-19 will fell as many as 450,000 Americans by February, the tragic reality of the disease will no doubt fuel ample demand for vaccination.
“People now know someone who has gotten COVID, who has been hospitalized or has unfortunately died,” Dr. Limaye said.
“We’re all seeing this now,” said Dr. Kempe. “Even deniers are beginning to see what this illness can do.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
‘Practice changing’: Ruxolitinib as second-line in chronic GVHD
When chronic graft-versus-host disease (cGVHD) develops as a complication of allogeneic hematopoietic stem cell transplant (alloHSCT), treatment options are limited. New findings show that ruxolitinib (Jakafi) was superior to standard therapy in reducing symptoms of cGVHD in the second-line setting, and the results are potentially practice changing.
The new data, from the REACH3 trial, were presented at the annual meeting of the American Society of Hematology, held virtually this year.
This trial is “almost certainly a practice changer,” Robert Brodsky, MD, ASH secretary, said during a press preview webinar.
Chronic GVHD occurs in approximately 30%-70% of patients who undergo alloSCT, and “has been really hard to treat,” said Dr. Brodsky, of Johns Hopkins University, Baltimore. “Steroids are the first-line treatment, but after that, nothing else has shown any improvement and even steroids don’t work that well.”
Of the patients assessed, 50% of those who received ruxolitinib responded to therapy compared with only 25% who received standard therapies.
“This is the first multicenter randomized controlled trial for chronic GVHD that is positive,” said senior study author Robert Zeiser, PhD, of University Medical Center, Freiburg, Germany. “It shows a significant advantage for ruxolitinib. It is likely that this trial will lead to approval for this indication and change the guidelines for the treatment of this disease.”
Ruxolitinib, a JAK inhibitor first marketed for use in myelofibrosis, is already approved for acute GVHD. The Food and Drug Administration approved that indication last year on the basis of data from two previous trials, REACH 1 and REACH 2. The trials found that ruxolitinib was superior to best available therapy for treating patients with acute GVHD.
Superior to best available therapy
In the current REACH 3 study, Dr. Zeiser and colleagues compared ruxolitinib with best available therapy in 329 patients with moderate-to-severe cGVHD (both steroid dependent and steroid resistant).
All patients had undergone alloSCT and were randomly assigned to ruxolitinib (10 mg twice daily) for six 28-day cycles or investigator-selected best available therapy (BAT), of which there were 10 options. Patients continued receiving their regimen of corticosteroids, and viral prophylaxis and antibiotics were allowed as needed for infection prevention and treatment.
The study permitted crossover: Patients on BAT were allowed to start on ruxolitinib on or after cycle 7 day 1 for those who did not achieve or maintain a response, developed toxicity to BAT, or had a cGVHD flare.
The study met its primary endpoint of overall response rate (ORR), with a clear and substantial improvement among patients taking ruxolitinib (50% vs 26%; odds ratio, 2.99; P < .0001a), Dr. Zeiser noted. The complete response rate was also higher (7% vs. 3%).
Both key secondary endpoints also showed that ruxolitinib was superior to BAT. Failure-free survival was significantly longer in the ruxolitinib group (median not reached vs 5.7 months; hazard ratio, 0.370; P < .0001). There was also an improvement in symptoms based on changes in the modified Lee symptom score (mLSS; 0 [no symptoms] to 100 [worst symptoms]) at cycle 7 day 1; the results show that the mLSS responder rate was higher in patients on ruxolitinib (24% vs. 11%; odds ratio, 2.62; P = .0011).
A total of 31 patients in the ruxolitinib group died (19%) along with 27 in the BAT group (16%), with the cGVHD as the main cause of death.
Adverse events were comparable in both groups (ruxolitinib 98% [grade ≥ 3, 57%]; BAT, 92% [grade ≥ 3, 58%], with the most common being anemia (29% vs. 13%), hypertension (16% vs. 13%), pyrexia (16% vs. 9%), and ALT increase (15% vs 4%).
More options for patients
“The addition of ruxolitinib is definitely practice changing for this very difficult to treat population,” said James Essell, MD, medical director of the Blood Cancer Center at Mercy Health, Cincinnati, who was not involved in the study.
However, he added, “more options are still required, as evidenced by the continued deaths of patients despite this new option.”
Dr. Essell pointed out that ibrutinib (Imbruvica) is already approved for the treatment of cGVHD. “Ruxolitinib offers another option for treating this group of patients,” he said, and predicted that “it will be used frequently and has a different toxicity profile, ultimately improving the care for patients with cGVHD.”
It is likely that ruxolitinib will be considered earlier in the treatment of cGVHD to avoid the toxicity of chronic steroid use, he added, but price is a consideration. “The cost of ruxolitinib is over 200 times more than prednisone, limiting the adoption front line without a clinical trial.”
Another expert approached for comment was enthusiastic. “The abstract gave good evidence and efficacy with chronic GVHD,” said Ryotaro Nakamura, MD, associate professor of hematology & hematopoietic cell transplantation at City of Hope, Duarte, Calif. He noted that there have been two previous REACH trials which showed a benefit for ruxolitinib in acute GVHD.
What this means is that there is now global evidence that ruxolitinib is better than anything else so far, he said, and this latest trial is just part of the “practice-changing data,” from the three studies. “It is practice changing in that it is providing options now for these patients,” he said.
Dr. Zeiser has disclosed relationships with Incyte, Novartis and Mallinckrodt; other authors disclosed relationships with industry as noted in the abstract. Dr. Essell and Dr. Nakamura have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
When chronic graft-versus-host disease (cGVHD) develops as a complication of allogeneic hematopoietic stem cell transplant (alloHSCT), treatment options are limited. New findings show that ruxolitinib (Jakafi) was superior to standard therapy in reducing symptoms of cGVHD in the second-line setting, and the results are potentially practice changing.
The new data, from the REACH3 trial, were presented at the annual meeting of the American Society of Hematology, held virtually this year.
This trial is “almost certainly a practice changer,” Robert Brodsky, MD, ASH secretary, said during a press preview webinar.
Chronic GVHD occurs in approximately 30%-70% of patients who undergo alloSCT, and “has been really hard to treat,” said Dr. Brodsky, of Johns Hopkins University, Baltimore. “Steroids are the first-line treatment, but after that, nothing else has shown any improvement and even steroids don’t work that well.”
Of the patients assessed, 50% of those who received ruxolitinib responded to therapy compared with only 25% who received standard therapies.
“This is the first multicenter randomized controlled trial for chronic GVHD that is positive,” said senior study author Robert Zeiser, PhD, of University Medical Center, Freiburg, Germany. “It shows a significant advantage for ruxolitinib. It is likely that this trial will lead to approval for this indication and change the guidelines for the treatment of this disease.”
Ruxolitinib, a JAK inhibitor first marketed for use in myelofibrosis, is already approved for acute GVHD. The Food and Drug Administration approved that indication last year on the basis of data from two previous trials, REACH 1 and REACH 2. The trials found that ruxolitinib was superior to best available therapy for treating patients with acute GVHD.
Superior to best available therapy
In the current REACH 3 study, Dr. Zeiser and colleagues compared ruxolitinib with best available therapy in 329 patients with moderate-to-severe cGVHD (both steroid dependent and steroid resistant).
All patients had undergone alloSCT and were randomly assigned to ruxolitinib (10 mg twice daily) for six 28-day cycles or investigator-selected best available therapy (BAT), of which there were 10 options. Patients continued receiving their regimen of corticosteroids, and viral prophylaxis and antibiotics were allowed as needed for infection prevention and treatment.
The study permitted crossover: Patients on BAT were allowed to start on ruxolitinib on or after cycle 7 day 1 for those who did not achieve or maintain a response, developed toxicity to BAT, or had a cGVHD flare.
The study met its primary endpoint of overall response rate (ORR), with a clear and substantial improvement among patients taking ruxolitinib (50% vs 26%; odds ratio, 2.99; P < .0001a), Dr. Zeiser noted. The complete response rate was also higher (7% vs. 3%).
Both key secondary endpoints also showed that ruxolitinib was superior to BAT. Failure-free survival was significantly longer in the ruxolitinib group (median not reached vs 5.7 months; hazard ratio, 0.370; P < .0001). There was also an improvement in symptoms based on changes in the modified Lee symptom score (mLSS; 0 [no symptoms] to 100 [worst symptoms]) at cycle 7 day 1; the results show that the mLSS responder rate was higher in patients on ruxolitinib (24% vs. 11%; odds ratio, 2.62; P = .0011).
A total of 31 patients in the ruxolitinib group died (19%) along with 27 in the BAT group (16%), with the cGVHD as the main cause of death.
Adverse events were comparable in both groups (ruxolitinib 98% [grade ≥ 3, 57%]; BAT, 92% [grade ≥ 3, 58%], with the most common being anemia (29% vs. 13%), hypertension (16% vs. 13%), pyrexia (16% vs. 9%), and ALT increase (15% vs 4%).
More options for patients
“The addition of ruxolitinib is definitely practice changing for this very difficult to treat population,” said James Essell, MD, medical director of the Blood Cancer Center at Mercy Health, Cincinnati, who was not involved in the study.
However, he added, “more options are still required, as evidenced by the continued deaths of patients despite this new option.”
Dr. Essell pointed out that ibrutinib (Imbruvica) is already approved for the treatment of cGVHD. “Ruxolitinib offers another option for treating this group of patients,” he said, and predicted that “it will be used frequently and has a different toxicity profile, ultimately improving the care for patients with cGVHD.”
It is likely that ruxolitinib will be considered earlier in the treatment of cGVHD to avoid the toxicity of chronic steroid use, he added, but price is a consideration. “The cost of ruxolitinib is over 200 times more than prednisone, limiting the adoption front line without a clinical trial.”
Another expert approached for comment was enthusiastic. “The abstract gave good evidence and efficacy with chronic GVHD,” said Ryotaro Nakamura, MD, associate professor of hematology & hematopoietic cell transplantation at City of Hope, Duarte, Calif. He noted that there have been two previous REACH trials which showed a benefit for ruxolitinib in acute GVHD.
What this means is that there is now global evidence that ruxolitinib is better than anything else so far, he said, and this latest trial is just part of the “practice-changing data,” from the three studies. “It is practice changing in that it is providing options now for these patients,” he said.
Dr. Zeiser has disclosed relationships with Incyte, Novartis and Mallinckrodt; other authors disclosed relationships with industry as noted in the abstract. Dr. Essell and Dr. Nakamura have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
When chronic graft-versus-host disease (cGVHD) develops as a complication of allogeneic hematopoietic stem cell transplant (alloHSCT), treatment options are limited. New findings show that ruxolitinib (Jakafi) was superior to standard therapy in reducing symptoms of cGVHD in the second-line setting, and the results are potentially practice changing.
The new data, from the REACH3 trial, were presented at the annual meeting of the American Society of Hematology, held virtually this year.
This trial is “almost certainly a practice changer,” Robert Brodsky, MD, ASH secretary, said during a press preview webinar.
Chronic GVHD occurs in approximately 30%-70% of patients who undergo alloSCT, and “has been really hard to treat,” said Dr. Brodsky, of Johns Hopkins University, Baltimore. “Steroids are the first-line treatment, but after that, nothing else has shown any improvement and even steroids don’t work that well.”
Of the patients assessed, 50% of those who received ruxolitinib responded to therapy compared with only 25% who received standard therapies.
“This is the first multicenter randomized controlled trial for chronic GVHD that is positive,” said senior study author Robert Zeiser, PhD, of University Medical Center, Freiburg, Germany. “It shows a significant advantage for ruxolitinib. It is likely that this trial will lead to approval for this indication and change the guidelines for the treatment of this disease.”
Ruxolitinib, a JAK inhibitor first marketed for use in myelofibrosis, is already approved for acute GVHD. The Food and Drug Administration approved that indication last year on the basis of data from two previous trials, REACH 1 and REACH 2. The trials found that ruxolitinib was superior to best available therapy for treating patients with acute GVHD.
Superior to best available therapy
In the current REACH 3 study, Dr. Zeiser and colleagues compared ruxolitinib with best available therapy in 329 patients with moderate-to-severe cGVHD (both steroid dependent and steroid resistant).
All patients had undergone alloSCT and were randomly assigned to ruxolitinib (10 mg twice daily) for six 28-day cycles or investigator-selected best available therapy (BAT), of which there were 10 options. Patients continued receiving their regimen of corticosteroids, and viral prophylaxis and antibiotics were allowed as needed for infection prevention and treatment.
The study permitted crossover: Patients on BAT were allowed to start on ruxolitinib on or after cycle 7 day 1 for those who did not achieve or maintain a response, developed toxicity to BAT, or had a cGVHD flare.
The study met its primary endpoint of overall response rate (ORR), with a clear and substantial improvement among patients taking ruxolitinib (50% vs 26%; odds ratio, 2.99; P < .0001a), Dr. Zeiser noted. The complete response rate was also higher (7% vs. 3%).
Both key secondary endpoints also showed that ruxolitinib was superior to BAT. Failure-free survival was significantly longer in the ruxolitinib group (median not reached vs 5.7 months; hazard ratio, 0.370; P < .0001). There was also an improvement in symptoms based on changes in the modified Lee symptom score (mLSS; 0 [no symptoms] to 100 [worst symptoms]) at cycle 7 day 1; the results show that the mLSS responder rate was higher in patients on ruxolitinib (24% vs. 11%; odds ratio, 2.62; P = .0011).
A total of 31 patients in the ruxolitinib group died (19%) along with 27 in the BAT group (16%), with the cGVHD as the main cause of death.
Adverse events were comparable in both groups (ruxolitinib 98% [grade ≥ 3, 57%]; BAT, 92% [grade ≥ 3, 58%], with the most common being anemia (29% vs. 13%), hypertension (16% vs. 13%), pyrexia (16% vs. 9%), and ALT increase (15% vs 4%).
More options for patients
“The addition of ruxolitinib is definitely practice changing for this very difficult to treat population,” said James Essell, MD, medical director of the Blood Cancer Center at Mercy Health, Cincinnati, who was not involved in the study.
However, he added, “more options are still required, as evidenced by the continued deaths of patients despite this new option.”
Dr. Essell pointed out that ibrutinib (Imbruvica) is already approved for the treatment of cGVHD. “Ruxolitinib offers another option for treating this group of patients,” he said, and predicted that “it will be used frequently and has a different toxicity profile, ultimately improving the care for patients with cGVHD.”
It is likely that ruxolitinib will be considered earlier in the treatment of cGVHD to avoid the toxicity of chronic steroid use, he added, but price is a consideration. “The cost of ruxolitinib is over 200 times more than prednisone, limiting the adoption front line without a clinical trial.”
Another expert approached for comment was enthusiastic. “The abstract gave good evidence and efficacy with chronic GVHD,” said Ryotaro Nakamura, MD, associate professor of hematology & hematopoietic cell transplantation at City of Hope, Duarte, Calif. He noted that there have been two previous REACH trials which showed a benefit for ruxolitinib in acute GVHD.
What this means is that there is now global evidence that ruxolitinib is better than anything else so far, he said, and this latest trial is just part of the “practice-changing data,” from the three studies. “It is practice changing in that it is providing options now for these patients,” he said.
Dr. Zeiser has disclosed relationships with Incyte, Novartis and Mallinckrodt; other authors disclosed relationships with industry as noted in the abstract. Dr. Essell and Dr. Nakamura have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
COVID-19 and risk of clotting: ‘Be proactive about prevention’
The risk of arterial and venous thrombosis in patients with COVID-19 has been a major issue throughout the pandemic, and how best to manage this risk is the subject of a new review article.

The article, by Gregory Dr. Piazza, MD, and David A. Morrow, MD, Brigham and Women’s Hospital, Boston, was published online in JAMA on Nov. 23.
“Basically we’re saying: ‘Be proactive about prevention,’” Dr. Piazza told this news organization.
There is growing recognition among those on the frontline that there is an increased risk of thrombosis in COVID-19 patients, Dr. Piazza said. The risk is highest in patients in the intensive care unit, but the risk is also increased in patients hospitalized with COVID-19, even those not in ICU.
“We don’t really know what the risk is in nonhospitalized COVID-19 patients, but we think it’s much lower than in those who are hospitalized,” he said. “We are waiting for data on the optimal way of managing this increased risk of thrombosis in COVID patients, but for the time being, we believe a systematic way of addressing this risk is best, with every patient hospitalized with COVID-19 receiving some type of thromboprophylaxis. This would mainly be with anticoagulation, but in patients in whom anticoagulation is contraindicated, then mechanical methods could be used, such as pneumatic compression boots or compression stockings.”
The authors report thrombotic complication rates of 2.6% in noncritically ill hospitalized patients with COVID-19 and 35.3% in critically ill patients from a recent U.S. registry study.
Autopsy findings of microthrombi in multiple organ systems, including the lungs, heart, and kidneys, suggest that thrombosis may contribute to multisystem organ dysfunction in severe COVID-19, they note. Although the pathophysiology is not fully defined, prothrombotic abnormalities have been identified in patients with COVID-19, including elevated levels of D-dimer, fibrinogen, and factor VIII, they add.
“There are several major questions about which COVID-19 patients to treat with thromboprophylaxis, how to treat them in term of levels of anticoagulation, and there are many ongoing clinical trials to try and answer these questions,” Dr. Piazza commented. “We need results from these randomized trials to provide a better compass for COVID-19 patients at risk of clotting.”
At present, clinicians can follow two different sets of guidelines on the issue, one from the American College of Chest Physicians and the other from the International Society on Thrombosis and Hemostasis, the authors note.
“The ACCP guidelines are very conservative and basically follow the evidence base for medical patients, while the ISTH guidelines are more aggressive and recommend increased levels of anticoagulation in both ICU and hospitalized non-ICU patients and also extend prophylaxis after discharge,” Dr. Piazza said.
“There is quite a difference between the two sets of guidelines, which can be a point of confusion,” he added.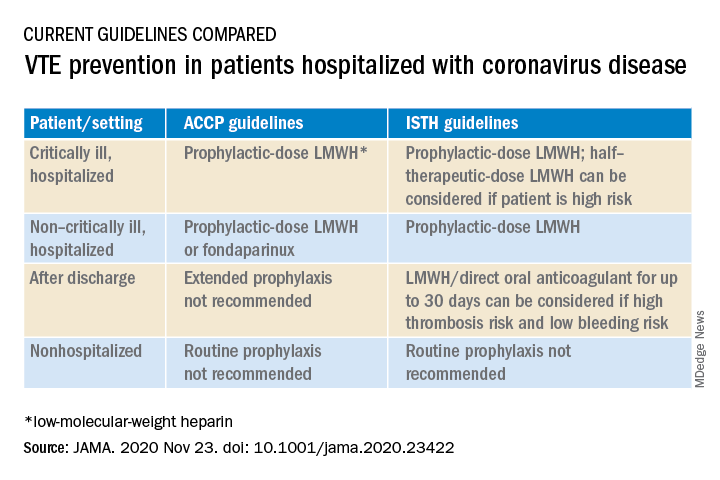
Dr. Piazza notes that at his center every hospitalized COVID patient who does not have a contraindication to anticoagulation receives a standard prophylactic dose of a once-daily low-molecular-weight heparin (for example, enoxaparin 40 mg). A once-daily product is used to minimize infection risk to staff.
While all COVID patients in the ICU should automatically receive some anticoagulation, the optimal dose is an area of active investigation, he explained. “There were several early reports of ICU patients developing blood clots despite receiving standard thromboprophylaxis so perhaps we need to use higher doses. There are trials underway looking at this, and we would advise enrolling patients into these trials.”
If patients can’t be enrolled into trials, and clinicians feel higher anticoagulation levels are needed, Dr. Piazza advises following the ISTH guidance, which allows an intermediate dose of low-molecular-weight heparin (up to 1 mg/kg enoxaparin).
“Some experts are suggesting even higher doses may be needed in some ICU patients, such as the full therapeutic dose, but I worry about the risk of bleeding with such a strategy,” he said.
Dr. Piazza says they do not routinely give anticoagulation after discharge, but if this is desired then patients could be switched to an oral agent, and some of the direct-acting oral anticoagulants are approved for prophylactic use in medically ill patients.
Dr. Piazza points out that whether thromboprophylaxis should be used for nonhospitalized COVID patients who have risk factors for clotting such as a prior history of thrombosis or obesity is a pressing question, and he encourages clinicians to enroll these patients in clinical trials evaluating this issue, such as the PREVENT-HD trial.
“If they can’t enroll patents in a trial, then they have to make a decision whether the patient is high-enough risk to justify off-label use of anticoagulant. There is a case to be made for this, but there is no evidence for or against such action at present,” he noted.
At this time, neither the ISTH nor ACCP recommend measuring D-dimer to screen for venous thromboembolism or to determine intensity of prophylaxis or treatment, the authors note.
“Ongoing investigation will determine optimal preventive regimens in COVID-19 in the intensive care unit, at hospital discharge, and in nonhospitalized patients at high risk for thrombosis,” they conclude.
Dr. Piazza reported grants from Bayer, Bristol Myers Squibb, Boston Scientific, Janssen, and Portola, and personal fees from Agile, Amgen, Pfizer, and the Prairie Education and Research Cooperative outside the submitted work. Dr. Morrow reported grants from Abbott Laboratories, Amgen, Anthos Therapeutics, Esai, GlaxoSmithKline, Takeda, and The Medicines Company; grants and personal fees from AstraZeneca, Merck, Novartis, and Roche Diagnostics; and personal fees from Bayer Pharma and InCarda outside the submitted work.
A version of this article originally appeared on Medscape.com.
The risk of arterial and venous thrombosis in patients with COVID-19 has been a major issue throughout the pandemic, and how best to manage this risk is the subject of a new review article.
The article, by Gregory Dr. Piazza, MD, and David A. Morrow, MD, Brigham and Women’s Hospital, Boston, was published online in JAMA on Nov. 23.
“Basically we’re saying: ‘Be proactive about prevention,’” Dr. Piazza told this news organization.
There is growing recognition among those on the frontline that there is an increased risk of thrombosis in COVID-19 patients, Dr. Piazza said. The risk is highest in patients in the intensive care unit, but the risk is also increased in patients hospitalized with COVID-19, even those not in ICU.
“We don’t really know what the risk is in nonhospitalized COVID-19 patients, but we think it’s much lower than in those who are hospitalized,” he said. “We are waiting for data on the optimal way of managing this increased risk of thrombosis in COVID patients, but for the time being, we believe a systematic way of addressing this risk is best, with every patient hospitalized with COVID-19 receiving some type of thromboprophylaxis. This would mainly be with anticoagulation, but in patients in whom anticoagulation is contraindicated, then mechanical methods could be used, such as pneumatic compression boots or compression stockings.”
The authors report thrombotic complication rates of 2.6% in noncritically ill hospitalized patients with COVID-19 and 35.3% in critically ill patients from a recent U.S. registry study.
Autopsy findings of microthrombi in multiple organ systems, including the lungs, heart, and kidneys, suggest that thrombosis may contribute to multisystem organ dysfunction in severe COVID-19, they note. Although the pathophysiology is not fully defined, prothrombotic abnormalities have been identified in patients with COVID-19, including elevated levels of D-dimer, fibrinogen, and factor VIII, they add.
“There are several major questions about which COVID-19 patients to treat with thromboprophylaxis, how to treat them in term of levels of anticoagulation, and there are many ongoing clinical trials to try and answer these questions,” Dr. Piazza commented. “We need results from these randomized trials to provide a better compass for COVID-19 patients at risk of clotting.”
At present, clinicians can follow two different sets of guidelines on the issue, one from the American College of Chest Physicians and the other from the International Society on Thrombosis and Hemostasis, the authors note.
“The ACCP guidelines are very conservative and basically follow the evidence base for medical patients, while the ISTH guidelines are more aggressive and recommend increased levels of anticoagulation in both ICU and hospitalized non-ICU patients and also extend prophylaxis after discharge,” Dr. Piazza said.
“There is quite a difference between the two sets of guidelines, which can be a point of confusion,” he added.
Dr. Piazza notes that at his center every hospitalized COVID patient who does not have a contraindication to anticoagulation receives a standard prophylactic dose of a once-daily low-molecular-weight heparin (for example, enoxaparin 40 mg). A once-daily product is used to minimize infection risk to staff.
While all COVID patients in the ICU should automatically receive some anticoagulation, the optimal dose is an area of active investigation, he explained. “There were several early reports of ICU patients developing blood clots despite receiving standard thromboprophylaxis so perhaps we need to use higher doses. There are trials underway looking at this, and we would advise enrolling patients into these trials.”
If patients can’t be enrolled into trials, and clinicians feel higher anticoagulation levels are needed, Dr. Piazza advises following the ISTH guidance, which allows an intermediate dose of low-molecular-weight heparin (up to 1 mg/kg enoxaparin).
“Some experts are suggesting even higher doses may be needed in some ICU patients, such as the full therapeutic dose, but I worry about the risk of bleeding with such a strategy,” he said.
Dr. Piazza says they do not routinely give anticoagulation after discharge, but if this is desired then patients could be switched to an oral agent, and some of the direct-acting oral anticoagulants are approved for prophylactic use in medically ill patients.
Dr. Piazza points out that whether thromboprophylaxis should be used for nonhospitalized COVID patients who have risk factors for clotting such as a prior history of thrombosis or obesity is a pressing question, and he encourages clinicians to enroll these patients in clinical trials evaluating this issue, such as the PREVENT-HD trial.
“If they can’t enroll patents in a trial, then they have to make a decision whether the patient is high-enough risk to justify off-label use of anticoagulant. There is a case to be made for this, but there is no evidence for or against such action at present,” he noted.
At this time, neither the ISTH nor ACCP recommend measuring D-dimer to screen for venous thromboembolism or to determine intensity of prophylaxis or treatment, the authors note.
“Ongoing investigation will determine optimal preventive regimens in COVID-19 in the intensive care unit, at hospital discharge, and in nonhospitalized patients at high risk for thrombosis,” they conclude.
Dr. Piazza reported grants from Bayer, Bristol Myers Squibb, Boston Scientific, Janssen, and Portola, and personal fees from Agile, Amgen, Pfizer, and the Prairie Education and Research Cooperative outside the submitted work. Dr. Morrow reported grants from Abbott Laboratories, Amgen, Anthos Therapeutics, Esai, GlaxoSmithKline, Takeda, and The Medicines Company; grants and personal fees from AstraZeneca, Merck, Novartis, and Roche Diagnostics; and personal fees from Bayer Pharma and InCarda outside the submitted work.
A version of this article originally appeared on Medscape.com.
The risk of arterial and venous thrombosis in patients with COVID-19 has been a major issue throughout the pandemic, and how best to manage this risk is the subject of a new review article.
The article, by Gregory Dr. Piazza, MD, and David A. Morrow, MD, Brigham and Women’s Hospital, Boston, was published online in JAMA on Nov. 23.
“Basically we’re saying: ‘Be proactive about prevention,’” Dr. Piazza told this news organization.
There is growing recognition among those on the frontline that there is an increased risk of thrombosis in COVID-19 patients, Dr. Piazza said. The risk is highest in patients in the intensive care unit, but the risk is also increased in patients hospitalized with COVID-19, even those not in ICU.
“We don’t really know what the risk is in nonhospitalized COVID-19 patients, but we think it’s much lower than in those who are hospitalized,” he said. “We are waiting for data on the optimal way of managing this increased risk of thrombosis in COVID patients, but for the time being, we believe a systematic way of addressing this risk is best, with every patient hospitalized with COVID-19 receiving some type of thromboprophylaxis. This would mainly be with anticoagulation, but in patients in whom anticoagulation is contraindicated, then mechanical methods could be used, such as pneumatic compression boots or compression stockings.”
The authors report thrombotic complication rates of 2.6% in noncritically ill hospitalized patients with COVID-19 and 35.3% in critically ill patients from a recent U.S. registry study.
Autopsy findings of microthrombi in multiple organ systems, including the lungs, heart, and kidneys, suggest that thrombosis may contribute to multisystem organ dysfunction in severe COVID-19, they note. Although the pathophysiology is not fully defined, prothrombotic abnormalities have been identified in patients with COVID-19, including elevated levels of D-dimer, fibrinogen, and factor VIII, they add.
“There are several major questions about which COVID-19 patients to treat with thromboprophylaxis, how to treat them in term of levels of anticoagulation, and there are many ongoing clinical trials to try and answer these questions,” Dr. Piazza commented. “We need results from these randomized trials to provide a better compass for COVID-19 patients at risk of clotting.”
At present, clinicians can follow two different sets of guidelines on the issue, one from the American College of Chest Physicians and the other from the International Society on Thrombosis and Hemostasis, the authors note.
“The ACCP guidelines are very conservative and basically follow the evidence base for medical patients, while the ISTH guidelines are more aggressive and recommend increased levels of anticoagulation in both ICU and hospitalized non-ICU patients and also extend prophylaxis after discharge,” Dr. Piazza said.
“There is quite a difference between the two sets of guidelines, which can be a point of confusion,” he added.
Dr. Piazza notes that at his center every hospitalized COVID patient who does not have a contraindication to anticoagulation receives a standard prophylactic dose of a once-daily low-molecular-weight heparin (for example, enoxaparin 40 mg). A once-daily product is used to minimize infection risk to staff.
While all COVID patients in the ICU should automatically receive some anticoagulation, the optimal dose is an area of active investigation, he explained. “There were several early reports of ICU patients developing blood clots despite receiving standard thromboprophylaxis so perhaps we need to use higher doses. There are trials underway looking at this, and we would advise enrolling patients into these trials.”
If patients can’t be enrolled into trials, and clinicians feel higher anticoagulation levels are needed, Dr. Piazza advises following the ISTH guidance, which allows an intermediate dose of low-molecular-weight heparin (up to 1 mg/kg enoxaparin).
“Some experts are suggesting even higher doses may be needed in some ICU patients, such as the full therapeutic dose, but I worry about the risk of bleeding with such a strategy,” he said.
Dr. Piazza says they do not routinely give anticoagulation after discharge, but if this is desired then patients could be switched to an oral agent, and some of the direct-acting oral anticoagulants are approved for prophylactic use in medically ill patients.
Dr. Piazza points out that whether thromboprophylaxis should be used for nonhospitalized COVID patients who have risk factors for clotting such as a prior history of thrombosis or obesity is a pressing question, and he encourages clinicians to enroll these patients in clinical trials evaluating this issue, such as the PREVENT-HD trial.
“If they can’t enroll patents in a trial, then they have to make a decision whether the patient is high-enough risk to justify off-label use of anticoagulant. There is a case to be made for this, but there is no evidence for or against such action at present,” he noted.
At this time, neither the ISTH nor ACCP recommend measuring D-dimer to screen for venous thromboembolism or to determine intensity of prophylaxis or treatment, the authors note.
“Ongoing investigation will determine optimal preventive regimens in COVID-19 in the intensive care unit, at hospital discharge, and in nonhospitalized patients at high risk for thrombosis,” they conclude.
Dr. Piazza reported grants from Bayer, Bristol Myers Squibb, Boston Scientific, Janssen, and Portola, and personal fees from Agile, Amgen, Pfizer, and the Prairie Education and Research Cooperative outside the submitted work. Dr. Morrow reported grants from Abbott Laboratories, Amgen, Anthos Therapeutics, Esai, GlaxoSmithKline, Takeda, and The Medicines Company; grants and personal fees from AstraZeneca, Merck, Novartis, and Roche Diagnostics; and personal fees from Bayer Pharma and InCarda outside the submitted work.
A version of this article originally appeared on Medscape.com.