User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Unleashing Our Immune Response to Quash Cancer
This article was originally published on February 10 in Eric Topol’s substack “Ground Truths.”
It’s astounding how devious cancer cells and tumor tissue can be. This week in Science we learned how certain lung cancer cells can function like “Catch Me If You Can” — changing their driver mutation and cell identity to escape targeted therapy. This histologic transformation, as seen in an experimental model, is just one of so many cancer tricks that we are learning about.
Recently, as shown by single-cell sequencing, cancer cells can steal the mitochondria from T cells, a double whammy that turbocharges cancer cells with the hijacked fuel supply and, at the same time, dismantles the immune response.
Last week, we saw how tumor cells can release a virus-like protein that unleashes a vicious autoimmune response.
And then there’s the finding that cancer cell spread predominantly is occurring while we sleep.
As I previously reviewed, the ability for cancer cells to hijack neurons and neural circuits is now well established, no less their ability to reprogram neurons to become adrenergic and stimulate tumor progression, and interfere with the immune response. Stay tuned on that for a new Ground Truths podcast with Prof Michelle Monje, a leader in cancer neuroscience, which will post soon.
Add advancing age’s immunosenescence as yet another challenge to the long and growing list of formidable ways that cancer cells, and the tumor microenvironment, evade our immune response.
An Ever-Expanding Armamentarium
Immune Checkpoint Inhibitors
The field of immunotherapies took off with the immune checkpoint inhibitors, first approved by the FDA in 2011, that take the brakes off of T cells, with the programmed death-1 (PD-1), PD-ligand1, and anti-CTLA-4 monoclonal antibodies.
But we’re clearly learning they are not enough to prevail over cancer with common recurrences, only short term success in most patients, with some notable exceptions. Adding other immune response strategies, such as a vaccine, or antibody-drug conjugates, or engineered T cells, are showing improved chances for success.
Therapeutic Cancer Vaccines
There are many therapeutic cancer vaccines in the works, as reviewed in depth here.
Here’s a list of ongoing clinical trials of cancer vaccines. You’ll note most of these are on top of a checkpoint inhibitor and use personalized neoantigens (cancer cell surface proteins) derived from sequencing (whole-exome or whole genome, RNA-sequencing and HLA-profiling) the patient’s tumor.
An example of positive findings is with the combination of an mRNA-nanoparticle vaccine with up to 34 personalized neoantigens and pembrolizumab (Keytruda) vs pembrolizumab alone in advanced melanoma after resection, with improved outcomes at 3-year follow-up, cutting death or relapse rate in half.
{kind=link}
Antibody-Drug Conjugates (ADC)
There is considerable excitement about antibody-drug conjugates (ADC) whereby a linker is used to attach a chemotherapy agent to the checkpoint inhibitor antibody, specifically targeting the cancer cell and facilitating entry of the chemotherapy into the cell. Akin to these are bispecific antibodies (BiTEs, binding to a tumor antigen and T cell receptor simultaneously), both of these conjugates acting as “biologic” or “guided” missiles.
A very good example of the potency of an ADC was seen in a “HER2-low” breast cancer randomized trial. The absence or very low expression or amplification of the HER2 receptor is common in breast cancer and successful treatment has been elusive. A randomized trial of an ADC (trastuzumab deruxtecan) compared to physician’s choice therapy demonstrated a marked success for progression-free survival in HER2-low patients, which was characterized as “unheard-of success” by media coverage.
This strategy is being used to target some of the most difficult cancer driver mutations such as TP53 and KRAS.
{kind=link}
Oncolytic Viruses
Modifying viruses to infect the tumor and make it more visible to the immune system, potentiating anti-tumor responses, known as oncolytic viruses, have been proposed as a way to rev up the immune response for a long time but without positive Phase 3 clinical trials.
After decades of failure, a recent trial in refractory bladder cancer showed marked success, along with others, summarized here, now providing very encouraging results. It looks like oncolytic viruses are on a comeback path.
Engineering T Cells (Chimeric Antigen Receptor [CAR-T])
As I recently reviewed, there are over 500 ongoing clinical trials to build on the success of the first CAR-T approval for leukemia 7 years ago. I won’t go through that all again here, but to reiterate most of the success to date has been in “liquid” blood (leukemia and lymphoma) cancer tumors. This week in Nature is the discovery of a T cell cancer mutation, a gene fusion CARD11-PIK3R3, from a T cell lymphoma that can potentially be used to augment CAR-T efficacy. It has pronounced and prolonged effects in the experimental model. Instead of 1 million cells needed for treatment, even 20,000 were enough to melt the tumor. This is a noteworthy discovery since CAR-T work to date has largely not exploited such naturally occurring mutations, while instead concentrating on those seen in the patient’s set of key tumor mutations.
As currently conceived, CAR-T, and what is being referred to more broadly as adoptive cell therapies, involves removing T cells from the patient’s body and engineering their activation, then reintroducing them back to the patient. This is laborious, technically difficult, and very expensive. Recently, the idea of achieving all of this via an injection of virus that specifically infects T cells and inserts the genes needed, was advanced by two biotech companies with preclinical results, one in non-human primates.
Gearing up to meet the challenge of solid tumor CAR-T intervention, there’s more work using CRISPR genome editing of T cell receptors. A.I. is increasingly being exploited to process the data from sequencing and identify optimal neoantigens.
Instead of just CAR-T, we’re seeing the emergence of CAR-macrophage and CAR-natural killer (NK) cells strategies, and rapidly expanding potential combinations of all the strategies I’ve mentioned. No less, there’s been maturation of on-off suicide switches programmed in, to limit cytokine release and promote safety of these interventions. Overall, major side effects of immunotherapies are not only cytokine release syndromes, but also include interstitial pneumonitis and neurotoxicity.
Summary
Given the multitude of ways cancer cells and tumor tissue can evade our immune response, durably successful treatment remains a daunting challenge. But the ingenuity of so many different approaches to unleash our immune response, and their combinations, provides considerable hope that we’ll increasingly meet the challenge in the years ahead. We have clearly learned that combining different immunotherapy strategies will be essential for many patients with the most resilient solid tumors.
Of concern, as noted by a recent editorial in The Lancet, entitled “Cancer Research Equity: Innovations For The Many, Not The Few,” is that these individualized, sophisticated strategies are not scalable; they will have limited reach and benefit. The movement towards “off the shelf” CAR-T and inexpensive, orally active checkpoint inhibitors may help mitigate this issue.
Notwithstanding this important concern, we’re seeing an array of diverse and potent immunotherapy strategies that are providing highly encouraging results, engendering more excitement than we’ve seen in this space for some time. These should propel substantial improvements in outcomes for patients in the years ahead. It can’t happen soon enough.
Thanks for reading this edition of Ground Truths. If you found it informative, please share it with your colleagues.
Dr. Topol has disclosed the following relevant financial relationships: Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for Dexcom; Illumina; Molecular Stethoscope; Quest Diagnostics; Blue Cross Blue Shield Association. Received research grant from National Institutes of Health.
A version of this article appeared on Medscape.com.
This article was originally published on February 10 in Eric Topol’s substack “Ground Truths.”
It’s astounding how devious cancer cells and tumor tissue can be. This week in Science we learned how certain lung cancer cells can function like “Catch Me If You Can” — changing their driver mutation and cell identity to escape targeted therapy. This histologic transformation, as seen in an experimental model, is just one of so many cancer tricks that we are learning about.
Recently, as shown by single-cell sequencing, cancer cells can steal the mitochondria from T cells, a double whammy that turbocharges cancer cells with the hijacked fuel supply and, at the same time, dismantles the immune response.
Last week, we saw how tumor cells can release a virus-like protein that unleashes a vicious autoimmune response.
And then there’s the finding that cancer cell spread predominantly is occurring while we sleep.
As I previously reviewed, the ability for cancer cells to hijack neurons and neural circuits is now well established, no less their ability to reprogram neurons to become adrenergic and stimulate tumor progression, and interfere with the immune response. Stay tuned on that for a new Ground Truths podcast with Prof Michelle Monje, a leader in cancer neuroscience, which will post soon.
Add advancing age’s immunosenescence as yet another challenge to the long and growing list of formidable ways that cancer cells, and the tumor microenvironment, evade our immune response.
An Ever-Expanding Armamentarium
Immune Checkpoint Inhibitors
The field of immunotherapies took off with the immune checkpoint inhibitors, first approved by the FDA in 2011, that take the brakes off of T cells, with the programmed death-1 (PD-1), PD-ligand1, and anti-CTLA-4 monoclonal antibodies.
But we’re clearly learning they are not enough to prevail over cancer with common recurrences, only short term success in most patients, with some notable exceptions. Adding other immune response strategies, such as a vaccine, or antibody-drug conjugates, or engineered T cells, are showing improved chances for success.
Therapeutic Cancer Vaccines
There are many therapeutic cancer vaccines in the works, as reviewed in depth here.
Here’s a list of ongoing clinical trials of cancer vaccines. You’ll note most of these are on top of a checkpoint inhibitor and use personalized neoantigens (cancer cell surface proteins) derived from sequencing (whole-exome or whole genome, RNA-sequencing and HLA-profiling) the patient’s tumor.
An example of positive findings is with the combination of an mRNA-nanoparticle vaccine with up to 34 personalized neoantigens and pembrolizumab (Keytruda) vs pembrolizumab alone in advanced melanoma after resection, with improved outcomes at 3-year follow-up, cutting death or relapse rate in half.
Antibody-Drug Conjugates (ADC)
There is considerable excitement about antibody-drug conjugates (ADC) whereby a linker is used to attach a chemotherapy agent to the checkpoint inhibitor antibody, specifically targeting the cancer cell and facilitating entry of the chemotherapy into the cell. Akin to these are bispecific antibodies (BiTEs, binding to a tumor antigen and T cell receptor simultaneously), both of these conjugates acting as “biologic” or “guided” missiles.
A very good example of the potency of an ADC was seen in a “HER2-low” breast cancer randomized trial. The absence or very low expression or amplification of the HER2 receptor is common in breast cancer and successful treatment has been elusive. A randomized trial of an ADC (trastuzumab deruxtecan) compared to physician’s choice therapy demonstrated a marked success for progression-free survival in HER2-low patients, which was characterized as “unheard-of success” by media coverage.
This strategy is being used to target some of the most difficult cancer driver mutations such as TP53 and KRAS.
Oncolytic Viruses
Modifying viruses to infect the tumor and make it more visible to the immune system, potentiating anti-tumor responses, known as oncolytic viruses, have been proposed as a way to rev up the immune response for a long time but without positive Phase 3 clinical trials.
After decades of failure, a recent trial in refractory bladder cancer showed marked success, along with others, summarized here, now providing very encouraging results. It looks like oncolytic viruses are on a comeback path.
Engineering T Cells (Chimeric Antigen Receptor [CAR-T])
As I recently reviewed, there are over 500 ongoing clinical trials to build on the success of the first CAR-T approval for leukemia 7 years ago. I won’t go through that all again here, but to reiterate most of the success to date has been in “liquid” blood (leukemia and lymphoma) cancer tumors. This week in Nature is the discovery of a T cell cancer mutation, a gene fusion CARD11-PIK3R3, from a T cell lymphoma that can potentially be used to augment CAR-T efficacy. It has pronounced and prolonged effects in the experimental model. Instead of 1 million cells needed for treatment, even 20,000 were enough to melt the tumor. This is a noteworthy discovery since CAR-T work to date has largely not exploited such naturally occurring mutations, while instead concentrating on those seen in the patient’s set of key tumor mutations.
As currently conceived, CAR-T, and what is being referred to more broadly as adoptive cell therapies, involves removing T cells from the patient’s body and engineering their activation, then reintroducing them back to the patient. This is laborious, technically difficult, and very expensive. Recently, the idea of achieving all of this via an injection of virus that specifically infects T cells and inserts the genes needed, was advanced by two biotech companies with preclinical results, one in non-human primates.
Gearing up to meet the challenge of solid tumor CAR-T intervention, there’s more work using CRISPR genome editing of T cell receptors. A.I. is increasingly being exploited to process the data from sequencing and identify optimal neoantigens.
Instead of just CAR-T, we’re seeing the emergence of CAR-macrophage and CAR-natural killer (NK) cells strategies, and rapidly expanding potential combinations of all the strategies I’ve mentioned. No less, there’s been maturation of on-off suicide switches programmed in, to limit cytokine release and promote safety of these interventions. Overall, major side effects of immunotherapies are not only cytokine release syndromes, but also include interstitial pneumonitis and neurotoxicity.
Summary
Given the multitude of ways cancer cells and tumor tissue can evade our immune response, durably successful treatment remains a daunting challenge. But the ingenuity of so many different approaches to unleash our immune response, and their combinations, provides considerable hope that we’ll increasingly meet the challenge in the years ahead. We have clearly learned that combining different immunotherapy strategies will be essential for many patients with the most resilient solid tumors.
Of concern, as noted by a recent editorial in The Lancet, entitled “Cancer Research Equity: Innovations For The Many, Not The Few,” is that these individualized, sophisticated strategies are not scalable; they will have limited reach and benefit. The movement towards “off the shelf” CAR-T and inexpensive, orally active checkpoint inhibitors may help mitigate this issue.
Notwithstanding this important concern, we’re seeing an array of diverse and potent immunotherapy strategies that are providing highly encouraging results, engendering more excitement than we’ve seen in this space for some time. These should propel substantial improvements in outcomes for patients in the years ahead. It can’t happen soon enough.
Thanks for reading this edition of Ground Truths. If you found it informative, please share it with your colleagues.
Dr. Topol has disclosed the following relevant financial relationships: Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for Dexcom; Illumina; Molecular Stethoscope; Quest Diagnostics; Blue Cross Blue Shield Association. Received research grant from National Institutes of Health.
A version of this article appeared on Medscape.com.
This article was originally published on February 10 in Eric Topol’s substack “Ground Truths.”
It’s astounding how devious cancer cells and tumor tissue can be. This week in Science we learned how certain lung cancer cells can function like “Catch Me If You Can” — changing their driver mutation and cell identity to escape targeted therapy. This histologic transformation, as seen in an experimental model, is just one of so many cancer tricks that we are learning about.
Recently, as shown by single-cell sequencing, cancer cells can steal the mitochondria from T cells, a double whammy that turbocharges cancer cells with the hijacked fuel supply and, at the same time, dismantles the immune response.
Last week, we saw how tumor cells can release a virus-like protein that unleashes a vicious autoimmune response.
And then there’s the finding that cancer cell spread predominantly is occurring while we sleep.
As I previously reviewed, the ability for cancer cells to hijack neurons and neural circuits is now well established, no less their ability to reprogram neurons to become adrenergic and stimulate tumor progression, and interfere with the immune response. Stay tuned on that for a new Ground Truths podcast with Prof Michelle Monje, a leader in cancer neuroscience, which will post soon.
Add advancing age’s immunosenescence as yet another challenge to the long and growing list of formidable ways that cancer cells, and the tumor microenvironment, evade our immune response.
An Ever-Expanding Armamentarium
Immune Checkpoint Inhibitors
The field of immunotherapies took off with the immune checkpoint inhibitors, first approved by the FDA in 2011, that take the brakes off of T cells, with the programmed death-1 (PD-1), PD-ligand1, and anti-CTLA-4 monoclonal antibodies.
But we’re clearly learning they are not enough to prevail over cancer with common recurrences, only short term success in most patients, with some notable exceptions. Adding other immune response strategies, such as a vaccine, or antibody-drug conjugates, or engineered T cells, are showing improved chances for success.
Therapeutic Cancer Vaccines
There are many therapeutic cancer vaccines in the works, as reviewed in depth here.
Here’s a list of ongoing clinical trials of cancer vaccines. You’ll note most of these are on top of a checkpoint inhibitor and use personalized neoantigens (cancer cell surface proteins) derived from sequencing (whole-exome or whole genome, RNA-sequencing and HLA-profiling) the patient’s tumor.
An example of positive findings is with the combination of an mRNA-nanoparticle vaccine with up to 34 personalized neoantigens and pembrolizumab (Keytruda) vs pembrolizumab alone in advanced melanoma after resection, with improved outcomes at 3-year follow-up, cutting death or relapse rate in half.
Antibody-Drug Conjugates (ADC)
There is considerable excitement about antibody-drug conjugates (ADC) whereby a linker is used to attach a chemotherapy agent to the checkpoint inhibitor antibody, specifically targeting the cancer cell and facilitating entry of the chemotherapy into the cell. Akin to these are bispecific antibodies (BiTEs, binding to a tumor antigen and T cell receptor simultaneously), both of these conjugates acting as “biologic” or “guided” missiles.
A very good example of the potency of an ADC was seen in a “HER2-low” breast cancer randomized trial. The absence or very low expression or amplification of the HER2 receptor is common in breast cancer and successful treatment has been elusive. A randomized trial of an ADC (trastuzumab deruxtecan) compared to physician’s choice therapy demonstrated a marked success for progression-free survival in HER2-low patients, which was characterized as “unheard-of success” by media coverage.
This strategy is being used to target some of the most difficult cancer driver mutations such as TP53 and KRAS.
Oncolytic Viruses
Modifying viruses to infect the tumor and make it more visible to the immune system, potentiating anti-tumor responses, known as oncolytic viruses, have been proposed as a way to rev up the immune response for a long time but without positive Phase 3 clinical trials.
After decades of failure, a recent trial in refractory bladder cancer showed marked success, along with others, summarized here, now providing very encouraging results. It looks like oncolytic viruses are on a comeback path.
Engineering T Cells (Chimeric Antigen Receptor [CAR-T])
As I recently reviewed, there are over 500 ongoing clinical trials to build on the success of the first CAR-T approval for leukemia 7 years ago. I won’t go through that all again here, but to reiterate most of the success to date has been in “liquid” blood (leukemia and lymphoma) cancer tumors. This week in Nature is the discovery of a T cell cancer mutation, a gene fusion CARD11-PIK3R3, from a T cell lymphoma that can potentially be used to augment CAR-T efficacy. It has pronounced and prolonged effects in the experimental model. Instead of 1 million cells needed for treatment, even 20,000 were enough to melt the tumor. This is a noteworthy discovery since CAR-T work to date has largely not exploited such naturally occurring mutations, while instead concentrating on those seen in the patient’s set of key tumor mutations.
As currently conceived, CAR-T, and what is being referred to more broadly as adoptive cell therapies, involves removing T cells from the patient’s body and engineering their activation, then reintroducing them back to the patient. This is laborious, technically difficult, and very expensive. Recently, the idea of achieving all of this via an injection of virus that specifically infects T cells and inserts the genes needed, was advanced by two biotech companies with preclinical results, one in non-human primates.
Gearing up to meet the challenge of solid tumor CAR-T intervention, there’s more work using CRISPR genome editing of T cell receptors. A.I. is increasingly being exploited to process the data from sequencing and identify optimal neoantigens.
Instead of just CAR-T, we’re seeing the emergence of CAR-macrophage and CAR-natural killer (NK) cells strategies, and rapidly expanding potential combinations of all the strategies I’ve mentioned. No less, there’s been maturation of on-off suicide switches programmed in, to limit cytokine release and promote safety of these interventions. Overall, major side effects of immunotherapies are not only cytokine release syndromes, but also include interstitial pneumonitis and neurotoxicity.
Summary
Given the multitude of ways cancer cells and tumor tissue can evade our immune response, durably successful treatment remains a daunting challenge. But the ingenuity of so many different approaches to unleash our immune response, and their combinations, provides considerable hope that we’ll increasingly meet the challenge in the years ahead. We have clearly learned that combining different immunotherapy strategies will be essential for many patients with the most resilient solid tumors.
Of concern, as noted by a recent editorial in The Lancet, entitled “Cancer Research Equity: Innovations For The Many, Not The Few,” is that these individualized, sophisticated strategies are not scalable; they will have limited reach and benefit. The movement towards “off the shelf” CAR-T and inexpensive, orally active checkpoint inhibitors may help mitigate this issue.
Notwithstanding this important concern, we’re seeing an array of diverse and potent immunotherapy strategies that are providing highly encouraging results, engendering more excitement than we’ve seen in this space for some time. These should propel substantial improvements in outcomes for patients in the years ahead. It can’t happen soon enough.
Thanks for reading this edition of Ground Truths. If you found it informative, please share it with your colleagues.
Dr. Topol has disclosed the following relevant financial relationships: Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for Dexcom; Illumina; Molecular Stethoscope; Quest Diagnostics; Blue Cross Blue Shield Association. Received research grant from National Institutes of Health.
A version of this article appeared on Medscape.com.
High Niacin Levels Linked to Major CV Events
TOPLINE:
Two breakdown products from excess niacin, called 2PY and 4PY, were strongly associated with myocardial infarction, stroke, and other adverse cardiac events, suggesting that niacin supplementation may require a more “nuanced, titrated approach,” researchers said.
METHODOLOGY:
- Investigators performed an untargeted metabolomics analysis of fasting plasma from stable cardiac patients in a prospective discovery cohort of 1162 individuals (36% women).
- Additional analyses were performed in a US validation cohort, including measurement of soluble vascular adhesion molecule-1 (sVCAM-1), and on archival fasting samples from patients in a European validation cohort undergoing diagnostic coronary angiography.
- Genetic analyses of samples from the UK Biobank were used to test the association with sVCAM-1 levels of a genetic variant, rs10496731, which was significantly associated with both N1-methyl-2-pyridone-5-carboxamide (2 PY) and N1-methyl-4-pyridone-3-carboxamide (4PY) levels.
TAKEAWAY:
- Plasma levels of the terminal metabolites of excess niacin, 2PY and 4PY, were associated with increased 3-year MACE risk in two validation cohorts (US: 2331 total, 33% women; European: 832 total, 30% women), with adjusted hazard ratios for 2PY of 1.64 and 2.02, respectively, and for 4PY, 1.89 and 1.99.
- The genetic variant rs10496731 was significantly associated with levels of sVCAM-1.
- Treatment with physiological levels of 4PY, but not 2PY, induced expression of VCAM-1 and leukocyte adherence to vascular endothelium in mice, suggesting an inflammation-dependent mechanism underlying the clinical association of 4PY, in particular, with MACE.
- In functional testing, a physiological level of 4PY, but not 2PY, provoked messenger RNA and protein expression of VCAM-1 on human endothelial cells.
IN PRACTICE:
“Total niacin consumption in the US averaged 48 mg/d from 2017 to 2020 — more than triple the Recommended Daily Allowance — and 2PY and 4PY were also increased by nicotinamideriboside and nicotinamide mononucleotide, both of which are commonly sold supplements with claimed antiaging benefits,” the authors noted.
“The present studies suggest that niacin pool supplementation may optimally require a more nuanced, titrated approach to achieve intended health benefits,” while not fostering excess 4PY generation.
SOURCE:
Stanley Hazen, MD, PhD, of Cleveland Clinic, Cleveland, Ohio, was the principal author of the study, published online in Nature Medicine.
LIMITATIONS:
Measurement of 2PY and 4PY in the validation cohorts was performed only once, whereas serial measures might have provided enhanced prognostic value for incident cardiovascular disease (CVD) risks. Cohorts were recruited at quaternary referral centers and showed a high prevalence of CVD and cardiometabolic disease risk factors. Although the meta-analysis of the community-based genomic (Biobank) studies showed a link between 4PY and VCAM-1 expression in multiple ethnic groups, the clinical studies linking 4PY to CVD events were based on high-risk European ancestry populations in the US and European cohorts.
DISCLOSURES:
The study was supported by grants from the National Institutes of Health (NIH; both the National Heart, Lung, and Blood Institute and the Office of Dietary Supplements: A), Pilot Project Programs of the USC Center for Genetic Epidemiology and Southern California Environmental Health Sciences Center, and the Deutsche Forschungsgemeinschaft. One co-author was supported, in part, by NIH training grants; another was a participant in the BIH-Charité Advanced Clinician Scientist Program funded by Charité – Universitätsmedizin Berlin and the Berlin Institute of Health. The LipidCardio study [validation cohort] was partially supported by Sanofi-Aventis Deutschland GmbH. The UK Biobank Resource provided access to their data. Dr. Hazen and a co-author reported being coinventors on pending and issued patents held by the Cleveland Clinic relating to cardiovascular diagnostics and therapeutics, and Dr. Hazen and two co-authors received funds from industry.
A version of the article appeared on Medscape.com.
TOPLINE:
Two breakdown products from excess niacin, called 2PY and 4PY, were strongly associated with myocardial infarction, stroke, and other adverse cardiac events, suggesting that niacin supplementation may require a more “nuanced, titrated approach,” researchers said.
METHODOLOGY:
- Investigators performed an untargeted metabolomics analysis of fasting plasma from stable cardiac patients in a prospective discovery cohort of 1162 individuals (36% women).
- Additional analyses were performed in a US validation cohort, including measurement of soluble vascular adhesion molecule-1 (sVCAM-1), and on archival fasting samples from patients in a European validation cohort undergoing diagnostic coronary angiography.
- Genetic analyses of samples from the UK Biobank were used to test the association with sVCAM-1 levels of a genetic variant, rs10496731, which was significantly associated with both N1-methyl-2-pyridone-5-carboxamide (2 PY) and N1-methyl-4-pyridone-3-carboxamide (4PY) levels.
TAKEAWAY:
- Plasma levels of the terminal metabolites of excess niacin, 2PY and 4PY, were associated with increased 3-year MACE risk in two validation cohorts (US: 2331 total, 33% women; European: 832 total, 30% women), with adjusted hazard ratios for 2PY of 1.64 and 2.02, respectively, and for 4PY, 1.89 and 1.99.
- The genetic variant rs10496731 was significantly associated with levels of sVCAM-1.
- Treatment with physiological levels of 4PY, but not 2PY, induced expression of VCAM-1 and leukocyte adherence to vascular endothelium in mice, suggesting an inflammation-dependent mechanism underlying the clinical association of 4PY, in particular, with MACE.
- In functional testing, a physiological level of 4PY, but not 2PY, provoked messenger RNA and protein expression of VCAM-1 on human endothelial cells.
IN PRACTICE:
“Total niacin consumption in the US averaged 48 mg/d from 2017 to 2020 — more than triple the Recommended Daily Allowance — and 2PY and 4PY were also increased by nicotinamideriboside and nicotinamide mononucleotide, both of which are commonly sold supplements with claimed antiaging benefits,” the authors noted.
“The present studies suggest that niacin pool supplementation may optimally require a more nuanced, titrated approach to achieve intended health benefits,” while not fostering excess 4PY generation.
SOURCE:
Stanley Hazen, MD, PhD, of Cleveland Clinic, Cleveland, Ohio, was the principal author of the study, published online in Nature Medicine.
LIMITATIONS:
Measurement of 2PY and 4PY in the validation cohorts was performed only once, whereas serial measures might have provided enhanced prognostic value for incident cardiovascular disease (CVD) risks. Cohorts were recruited at quaternary referral centers and showed a high prevalence of CVD and cardiometabolic disease risk factors. Although the meta-analysis of the community-based genomic (Biobank) studies showed a link between 4PY and VCAM-1 expression in multiple ethnic groups, the clinical studies linking 4PY to CVD events were based on high-risk European ancestry populations in the US and European cohorts.
DISCLOSURES:
The study was supported by grants from the National Institutes of Health (NIH; both the National Heart, Lung, and Blood Institute and the Office of Dietary Supplements: A), Pilot Project Programs of the USC Center for Genetic Epidemiology and Southern California Environmental Health Sciences Center, and the Deutsche Forschungsgemeinschaft. One co-author was supported, in part, by NIH training grants; another was a participant in the BIH-Charité Advanced Clinician Scientist Program funded by Charité – Universitätsmedizin Berlin and the Berlin Institute of Health. The LipidCardio study [validation cohort] was partially supported by Sanofi-Aventis Deutschland GmbH. The UK Biobank Resource provided access to their data. Dr. Hazen and a co-author reported being coinventors on pending and issued patents held by the Cleveland Clinic relating to cardiovascular diagnostics and therapeutics, and Dr. Hazen and two co-authors received funds from industry.
A version of the article appeared on Medscape.com.
TOPLINE:
Two breakdown products from excess niacin, called 2PY and 4PY, were strongly associated with myocardial infarction, stroke, and other adverse cardiac events, suggesting that niacin supplementation may require a more “nuanced, titrated approach,” researchers said.
METHODOLOGY:
- Investigators performed an untargeted metabolomics analysis of fasting plasma from stable cardiac patients in a prospective discovery cohort of 1162 individuals (36% women).
- Additional analyses were performed in a US validation cohort, including measurement of soluble vascular adhesion molecule-1 (sVCAM-1), and on archival fasting samples from patients in a European validation cohort undergoing diagnostic coronary angiography.
- Genetic analyses of samples from the UK Biobank were used to test the association with sVCAM-1 levels of a genetic variant, rs10496731, which was significantly associated with both N1-methyl-2-pyridone-5-carboxamide (2 PY) and N1-methyl-4-pyridone-3-carboxamide (4PY) levels.
TAKEAWAY:
- Plasma levels of the terminal metabolites of excess niacin, 2PY and 4PY, were associated with increased 3-year MACE risk in two validation cohorts (US: 2331 total, 33% women; European: 832 total, 30% women), with adjusted hazard ratios for 2PY of 1.64 and 2.02, respectively, and for 4PY, 1.89 and 1.99.
- The genetic variant rs10496731 was significantly associated with levels of sVCAM-1.
- Treatment with physiological levels of 4PY, but not 2PY, induced expression of VCAM-1 and leukocyte adherence to vascular endothelium in mice, suggesting an inflammation-dependent mechanism underlying the clinical association of 4PY, in particular, with MACE.
- In functional testing, a physiological level of 4PY, but not 2PY, provoked messenger RNA and protein expression of VCAM-1 on human endothelial cells.
IN PRACTICE:
“Total niacin consumption in the US averaged 48 mg/d from 2017 to 2020 — more than triple the Recommended Daily Allowance — and 2PY and 4PY were also increased by nicotinamideriboside and nicotinamide mononucleotide, both of which are commonly sold supplements with claimed antiaging benefits,” the authors noted.
“The present studies suggest that niacin pool supplementation may optimally require a more nuanced, titrated approach to achieve intended health benefits,” while not fostering excess 4PY generation.
SOURCE:
Stanley Hazen, MD, PhD, of Cleveland Clinic, Cleveland, Ohio, was the principal author of the study, published online in Nature Medicine.
LIMITATIONS:
Measurement of 2PY and 4PY in the validation cohorts was performed only once, whereas serial measures might have provided enhanced prognostic value for incident cardiovascular disease (CVD) risks. Cohorts were recruited at quaternary referral centers and showed a high prevalence of CVD and cardiometabolic disease risk factors. Although the meta-analysis of the community-based genomic (Biobank) studies showed a link between 4PY and VCAM-1 expression in multiple ethnic groups, the clinical studies linking 4PY to CVD events were based on high-risk European ancestry populations in the US and European cohorts.
DISCLOSURES:
The study was supported by grants from the National Institutes of Health (NIH; both the National Heart, Lung, and Blood Institute and the Office of Dietary Supplements: A), Pilot Project Programs of the USC Center for Genetic Epidemiology and Southern California Environmental Health Sciences Center, and the Deutsche Forschungsgemeinschaft. One co-author was supported, in part, by NIH training grants; another was a participant in the BIH-Charité Advanced Clinician Scientist Program funded by Charité – Universitätsmedizin Berlin and the Berlin Institute of Health. The LipidCardio study [validation cohort] was partially supported by Sanofi-Aventis Deutschland GmbH. The UK Biobank Resource provided access to their data. Dr. Hazen and a co-author reported being coinventors on pending and issued patents held by the Cleveland Clinic relating to cardiovascular diagnostics and therapeutics, and Dr. Hazen and two co-authors received funds from industry.
A version of the article appeared on Medscape.com.
Most Sudden Infant Deaths Occur in Shared Sleep Space
, according to new data published online in Pediatrics.
SUID occur in infants less than 1 year old. The deaths happen without an obvious cause before investigation and account for 3,400 deaths per year in the United States.
Alexa B. Erck Lambert, MPH, Maternal and Infant Health Branch of the Centers for Disease Control and Prevention (CDC), led the study that examined 7,595 such deaths in 23 US jurisdictions from 2011 to 2020, using data from the CDC’s SUID Case Registry.
The researchers reported that the prevalence of surface sharing ranges from 34% to 64% among living infants and about 50% among SUID.
Common Factors
They found common factors when infants share sleep space compared with infants who did not. Those who shared space, for example, were often 0-3 months old; publicly insured; non-Hispanic Black; found in an adult bed, couch, or chair; exposed to maternal cigarette smoking prenatally; and supervised by a parent when they died or had a supervisor who was impaired by drugs or alcohol at the time of death.
Having a supervisor who was impaired by drugs or alcohol was much more common among sharing (16.3%) than nonsharing infants (4.7%).
The American Academy of Pediatrics (AAP) guidance says a safe sleep environment for infants includes a place to sleep on a nonshared sleep surface (in a crib or bassinet) without soft bedding, and lying on the back facing up.
Most Who Died had Multiple Unsafe Sleep Factors
At least 76% of all SUID had multiple unsafe sleep factors present, regardless of whether the infants shared sleep space. Unsafe sleep factors include an inclined or soft sleep surface, sleeping on the side or stomach, sleeping with soft or loose bedding or objects, not breastfeeding, prenatal or environmental exposure to cigarette smoke, and overheating.
Sharing sleep space combined with parents’ smoking and maternal alcohol or drug use greatly increases risk of sudden infant death, the authors noted.
Sharing More Common With Multiples
Among SUID, surface sharing was more common among multiples than singletons and more common in an adult bed than in the same crib. The authors noted that parents often cite financial reasons for such arrangements.
However, AAP recommends multiples sleep on separate surfaces. The authors say pediatricians and other healthcare providers should be aware of free crib distribution programs. A study by Hauck et al. found “crib distribution and safe sleep education positively influence knowledge and practices about safe sleep.”
Robin Haynes, PhD, who studies causes underlying the pathology of SIDS at Boston Children’s Hospital, pointed to the Cribs for Kids website as a place for parents and clinicians to start for help with providing separate sleeping surfaces.
Dr. Haynes said the large number of infants included is a strength of the study. The findings help confirm the risk of sharing a sleep surface, she said, but the details on characteristics of sleep-sharing environments provide “novel insight into this problem,” she said.
“For basic researchers,” Dr. Haynes said, “it reiterates that most cases of sudden and unexpected infant deaths are exposed to multiple risk factors. It also highlights the role that young infant age and maternal smoking have as risk factors that contribute to biological vulnerabilities in infants.”
The results also give clinicians more information on characteristics of bedsharing families and some of the factors related to bedsharing, including socioeconomic and behavioral factors, she said. She highlighted the higher risk of SUID when drug or alcohol impairment is involved while bedsharing.
“All of this information is really important and helps clinicians shape the safe sleep messages to families,” she said.
The study authors and Dr. Haynes report no relevant financial relationships.
, according to new data published online in Pediatrics.
SUID occur in infants less than 1 year old. The deaths happen without an obvious cause before investigation and account for 3,400 deaths per year in the United States.
Alexa B. Erck Lambert, MPH, Maternal and Infant Health Branch of the Centers for Disease Control and Prevention (CDC), led the study that examined 7,595 such deaths in 23 US jurisdictions from 2011 to 2020, using data from the CDC’s SUID Case Registry.
The researchers reported that the prevalence of surface sharing ranges from 34% to 64% among living infants and about 50% among SUID.
Common Factors
They found common factors when infants share sleep space compared with infants who did not. Those who shared space, for example, were often 0-3 months old; publicly insured; non-Hispanic Black; found in an adult bed, couch, or chair; exposed to maternal cigarette smoking prenatally; and supervised by a parent when they died or had a supervisor who was impaired by drugs or alcohol at the time of death.
Having a supervisor who was impaired by drugs or alcohol was much more common among sharing (16.3%) than nonsharing infants (4.7%).
The American Academy of Pediatrics (AAP) guidance says a safe sleep environment for infants includes a place to sleep on a nonshared sleep surface (in a crib or bassinet) without soft bedding, and lying on the back facing up.
Most Who Died had Multiple Unsafe Sleep Factors
At least 76% of all SUID had multiple unsafe sleep factors present, regardless of whether the infants shared sleep space. Unsafe sleep factors include an inclined or soft sleep surface, sleeping on the side or stomach, sleeping with soft or loose bedding or objects, not breastfeeding, prenatal or environmental exposure to cigarette smoke, and overheating.
Sharing sleep space combined with parents’ smoking and maternal alcohol or drug use greatly increases risk of sudden infant death, the authors noted.
Sharing More Common With Multiples
Among SUID, surface sharing was more common among multiples than singletons and more common in an adult bed than in the same crib. The authors noted that parents often cite financial reasons for such arrangements.
However, AAP recommends multiples sleep on separate surfaces. The authors say pediatricians and other healthcare providers should be aware of free crib distribution programs. A study by Hauck et al. found “crib distribution and safe sleep education positively influence knowledge and practices about safe sleep.”
Robin Haynes, PhD, who studies causes underlying the pathology of SIDS at Boston Children’s Hospital, pointed to the Cribs for Kids website as a place for parents and clinicians to start for help with providing separate sleeping surfaces.
Dr. Haynes said the large number of infants included is a strength of the study. The findings help confirm the risk of sharing a sleep surface, she said, but the details on characteristics of sleep-sharing environments provide “novel insight into this problem,” she said.
“For basic researchers,” Dr. Haynes said, “it reiterates that most cases of sudden and unexpected infant deaths are exposed to multiple risk factors. It also highlights the role that young infant age and maternal smoking have as risk factors that contribute to biological vulnerabilities in infants.”
The results also give clinicians more information on characteristics of bedsharing families and some of the factors related to bedsharing, including socioeconomic and behavioral factors, she said. She highlighted the higher risk of SUID when drug or alcohol impairment is involved while bedsharing.
“All of this information is really important and helps clinicians shape the safe sleep messages to families,” she said.
The study authors and Dr. Haynes report no relevant financial relationships.
, according to new data published online in Pediatrics.
SUID occur in infants less than 1 year old. The deaths happen without an obvious cause before investigation and account for 3,400 deaths per year in the United States.
Alexa B. Erck Lambert, MPH, Maternal and Infant Health Branch of the Centers for Disease Control and Prevention (CDC), led the study that examined 7,595 such deaths in 23 US jurisdictions from 2011 to 2020, using data from the CDC’s SUID Case Registry.
The researchers reported that the prevalence of surface sharing ranges from 34% to 64% among living infants and about 50% among SUID.
Common Factors
They found common factors when infants share sleep space compared with infants who did not. Those who shared space, for example, were often 0-3 months old; publicly insured; non-Hispanic Black; found in an adult bed, couch, or chair; exposed to maternal cigarette smoking prenatally; and supervised by a parent when they died or had a supervisor who was impaired by drugs or alcohol at the time of death.
Having a supervisor who was impaired by drugs or alcohol was much more common among sharing (16.3%) than nonsharing infants (4.7%).
The American Academy of Pediatrics (AAP) guidance says a safe sleep environment for infants includes a place to sleep on a nonshared sleep surface (in a crib or bassinet) without soft bedding, and lying on the back facing up.
Most Who Died had Multiple Unsafe Sleep Factors
At least 76% of all SUID had multiple unsafe sleep factors present, regardless of whether the infants shared sleep space. Unsafe sleep factors include an inclined or soft sleep surface, sleeping on the side or stomach, sleeping with soft or loose bedding or objects, not breastfeeding, prenatal or environmental exposure to cigarette smoke, and overheating.
Sharing sleep space combined with parents’ smoking and maternal alcohol or drug use greatly increases risk of sudden infant death, the authors noted.
Sharing More Common With Multiples
Among SUID, surface sharing was more common among multiples than singletons and more common in an adult bed than in the same crib. The authors noted that parents often cite financial reasons for such arrangements.
However, AAP recommends multiples sleep on separate surfaces. The authors say pediatricians and other healthcare providers should be aware of free crib distribution programs. A study by Hauck et al. found “crib distribution and safe sleep education positively influence knowledge and practices about safe sleep.”
Robin Haynes, PhD, who studies causes underlying the pathology of SIDS at Boston Children’s Hospital, pointed to the Cribs for Kids website as a place for parents and clinicians to start for help with providing separate sleeping surfaces.
Dr. Haynes said the large number of infants included is a strength of the study. The findings help confirm the risk of sharing a sleep surface, she said, but the details on characteristics of sleep-sharing environments provide “novel insight into this problem,” she said.
“For basic researchers,” Dr. Haynes said, “it reiterates that most cases of sudden and unexpected infant deaths are exposed to multiple risk factors. It also highlights the role that young infant age and maternal smoking have as risk factors that contribute to biological vulnerabilities in infants.”
The results also give clinicians more information on characteristics of bedsharing families and some of the factors related to bedsharing, including socioeconomic and behavioral factors, she said. She highlighted the higher risk of SUID when drug or alcohol impairment is involved while bedsharing.
“All of this information is really important and helps clinicians shape the safe sleep messages to families,” she said.
The study authors and Dr. Haynes report no relevant financial relationships.
FROM PEDIATRICS
New Marker of Cardiovascular Risk Discovered in T2D
, according to a new publication. Nicolas Venteclef, PhD, director of an Inserm institute for diabetes research at Necker Enfants Malades Hospital in Paris, France, led the research.
Quantifying Inflammation
Patients with type 2 diabetes have about twice the risk for a cardiovascular event associated with atherosclerosis, such as a heart attack or stroke, during their lifetimes. “Predicting these complications in diabetic patients is usually very difficult,” Dr. Venteclef told this news organization.
“They are strongly associated with inflammation in these patients. Therefore, we sought to quantify this inflammation in the blood.” To do this, his team focused on monocytes, a category of white blood cells circulating in the blood. They measured the blood concentration of monocytes and the subtypes present in patients with type 2 diabetes.
The results were published in Circulation Research.
Dysfunctional Monocytes
The team worked with three cohorts of patients. The first, named AngioSafe-2, consisting of 672 patients with type 2 diabetes, was recruited from the diabetology departments of Lariboisière and Bichat Claude Bernard hospitals in France. This cohort allowed researchers to demonstrate that the higher the number of circulating monocytes, the greater the risk for cardiovascular events, independent of age and duration of diabetes. This observation was confirmed through a second cohort, GLUTADIAB, that comprised 279 patients with type 2 diabetes. Scientists complemented their work with molecular analysis of circulating monocytes in these two cohorts, which revealed certain predominant monocyte subtypes in patients with type 2 diabetes at high cardiovascular risk. “These monocytes are dysfunctional because they have a mitochondrial problem,” Dr. Venteclef explained.
To better understand how these results could be used to predict cardiovascular risk, the team collaborated with colleagues from the University Hospital of Nantes on a cohort called SURDIAGENE, which included 757 patients with type 2 diabetes. “We conducted a longitudinal study by following these patients for 10 years and quantifying cardiovascular events and deaths,” said Dr. Venteclef. Circulating monocyte levels were correlated with the occurrence of heart attacks or strokes. The researchers observed that patients with type 2 diabetes with a monocyte count above a certain threshold (0.5 × 109/L) had a five- to seven-times higher risk for cardiovascular events over 10 years than those with a monocyte count below this threshold.
A patent was filed at the end of 2023 to protect this discovery. “Our next step is to develop a sensor to quantify monocytes more easily and avoid blood draws,” said Dr. Venteclef. “As part of a European project, we will also launch a trial with an anti-inflammatory drug in diabetics, with the hope of interrupting the inflammatory trajectory and preventing complications.”
This story was translated from the Medscape French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
, according to a new publication. Nicolas Venteclef, PhD, director of an Inserm institute for diabetes research at Necker Enfants Malades Hospital in Paris, France, led the research.
Quantifying Inflammation
Patients with type 2 diabetes have about twice the risk for a cardiovascular event associated with atherosclerosis, such as a heart attack or stroke, during their lifetimes. “Predicting these complications in diabetic patients is usually very difficult,” Dr. Venteclef told this news organization.
“They are strongly associated with inflammation in these patients. Therefore, we sought to quantify this inflammation in the blood.” To do this, his team focused on monocytes, a category of white blood cells circulating in the blood. They measured the blood concentration of monocytes and the subtypes present in patients with type 2 diabetes.
The results were published in Circulation Research.
Dysfunctional Monocytes
The team worked with three cohorts of patients. The first, named AngioSafe-2, consisting of 672 patients with type 2 diabetes, was recruited from the diabetology departments of Lariboisière and Bichat Claude Bernard hospitals in France. This cohort allowed researchers to demonstrate that the higher the number of circulating monocytes, the greater the risk for cardiovascular events, independent of age and duration of diabetes. This observation was confirmed through a second cohort, GLUTADIAB, that comprised 279 patients with type 2 diabetes. Scientists complemented their work with molecular analysis of circulating monocytes in these two cohorts, which revealed certain predominant monocyte subtypes in patients with type 2 diabetes at high cardiovascular risk. “These monocytes are dysfunctional because they have a mitochondrial problem,” Dr. Venteclef explained.
To better understand how these results could be used to predict cardiovascular risk, the team collaborated with colleagues from the University Hospital of Nantes on a cohort called SURDIAGENE, which included 757 patients with type 2 diabetes. “We conducted a longitudinal study by following these patients for 10 years and quantifying cardiovascular events and deaths,” said Dr. Venteclef. Circulating monocyte levels were correlated with the occurrence of heart attacks or strokes. The researchers observed that patients with type 2 diabetes with a monocyte count above a certain threshold (0.5 × 109/L) had a five- to seven-times higher risk for cardiovascular events over 10 years than those with a monocyte count below this threshold.
A patent was filed at the end of 2023 to protect this discovery. “Our next step is to develop a sensor to quantify monocytes more easily and avoid blood draws,” said Dr. Venteclef. “As part of a European project, we will also launch a trial with an anti-inflammatory drug in diabetics, with the hope of interrupting the inflammatory trajectory and preventing complications.”
This story was translated from the Medscape French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
, according to a new publication. Nicolas Venteclef, PhD, director of an Inserm institute for diabetes research at Necker Enfants Malades Hospital in Paris, France, led the research.
Quantifying Inflammation
Patients with type 2 diabetes have about twice the risk for a cardiovascular event associated with atherosclerosis, such as a heart attack or stroke, during their lifetimes. “Predicting these complications in diabetic patients is usually very difficult,” Dr. Venteclef told this news organization.
“They are strongly associated with inflammation in these patients. Therefore, we sought to quantify this inflammation in the blood.” To do this, his team focused on monocytes, a category of white blood cells circulating in the blood. They measured the blood concentration of monocytes and the subtypes present in patients with type 2 diabetes.
The results were published in Circulation Research.
Dysfunctional Monocytes
The team worked with three cohorts of patients. The first, named AngioSafe-2, consisting of 672 patients with type 2 diabetes, was recruited from the diabetology departments of Lariboisière and Bichat Claude Bernard hospitals in France. This cohort allowed researchers to demonstrate that the higher the number of circulating monocytes, the greater the risk for cardiovascular events, independent of age and duration of diabetes. This observation was confirmed through a second cohort, GLUTADIAB, that comprised 279 patients with type 2 diabetes. Scientists complemented their work with molecular analysis of circulating monocytes in these two cohorts, which revealed certain predominant monocyte subtypes in patients with type 2 diabetes at high cardiovascular risk. “These monocytes are dysfunctional because they have a mitochondrial problem,” Dr. Venteclef explained.
To better understand how these results could be used to predict cardiovascular risk, the team collaborated with colleagues from the University Hospital of Nantes on a cohort called SURDIAGENE, which included 757 patients with type 2 diabetes. “We conducted a longitudinal study by following these patients for 10 years and quantifying cardiovascular events and deaths,” said Dr. Venteclef. Circulating monocyte levels were correlated with the occurrence of heart attacks or strokes. The researchers observed that patients with type 2 diabetes with a monocyte count above a certain threshold (0.5 × 109/L) had a five- to seven-times higher risk for cardiovascular events over 10 years than those with a monocyte count below this threshold.
A patent was filed at the end of 2023 to protect this discovery. “Our next step is to develop a sensor to quantify monocytes more easily and avoid blood draws,” said Dr. Venteclef. “As part of a European project, we will also launch a trial with an anti-inflammatory drug in diabetics, with the hope of interrupting the inflammatory trajectory and preventing complications.”
This story was translated from the Medscape French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
FDA Approves Drug to Reduce Accidental Food Allergies
The US Food and Drug Administration (FDA) has approved omalizumab (Xolair, Genentech) for reducing allergic reactions to foods in adults and most children. The drug is meant to be taken regularly by patients with food allergies to reduce the risk for reactions, including anaphylaxis, in case of accidental exposure to one or more allergens. The injection is not approved for emergency treatment of an allergic reaction.
Omalizumab first was approved for persistent allergic asthma in 2003. It also is approved for chronic spontaneous urticaria and chronic rhinosinusitis with nasal polyps.
, the FDA said. Peanut-allergen powder (Palforzia) can reduce reactions to peanut, but its benefits are limited to that allergy.
“While it will not eliminate food allergies or allow patients to consume food allergens freely, its repeated use will help reduce the health impact if accidental exposure occurs,” said Kelly Stone, MD, PhD, associate director of the division of pulmonology, allergy, and critical care in the FDA’s Center for Drug Evaluation and Research, in a news release.
The safety and efficacy of the monoclonal antibody in reducing allergic reactions was studied in a double-blind, placebo-controlled study of 168 children and adults who were allergic to peanut and at least two other foods, including milk, egg, wheat, cashew, hazelnut, or walnut. Patients received omalizumab or placebo for 16-20 weeks. At the end of the study, patients consumed peanut protein (equivalent to 2.5 peanuts). Of those who received the drug, 68% were able to consume peanut without moderate or severe allergic symptoms, versus 6% in the placebo group.
More patients who received the medication also avoided moderate or severe reactions to cashews (42% vs 3%), milk (66% vs 11%), and eggs (67% vs 0%).
The most common side effects of omalizumab included injection site reactions and fever. The drug’s label includes warnings and precautions about anaphylaxis, cancer, fever, joint pain, rash, parasitic (worm) infection, and abnormal laboratory tests. Omalizumab comes with a boxed warning for anaphylaxis and should be started only in a healthcare setting equipped to manage anaphylaxis, according to the FDA.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved omalizumab (Xolair, Genentech) for reducing allergic reactions to foods in adults and most children. The drug is meant to be taken regularly by patients with food allergies to reduce the risk for reactions, including anaphylaxis, in case of accidental exposure to one or more allergens. The injection is not approved for emergency treatment of an allergic reaction.
Omalizumab first was approved for persistent allergic asthma in 2003. It also is approved for chronic spontaneous urticaria and chronic rhinosinusitis with nasal polyps.
, the FDA said. Peanut-allergen powder (Palforzia) can reduce reactions to peanut, but its benefits are limited to that allergy.
“While it will not eliminate food allergies or allow patients to consume food allergens freely, its repeated use will help reduce the health impact if accidental exposure occurs,” said Kelly Stone, MD, PhD, associate director of the division of pulmonology, allergy, and critical care in the FDA’s Center for Drug Evaluation and Research, in a news release.
The safety and efficacy of the monoclonal antibody in reducing allergic reactions was studied in a double-blind, placebo-controlled study of 168 children and adults who were allergic to peanut and at least two other foods, including milk, egg, wheat, cashew, hazelnut, or walnut. Patients received omalizumab or placebo for 16-20 weeks. At the end of the study, patients consumed peanut protein (equivalent to 2.5 peanuts). Of those who received the drug, 68% were able to consume peanut without moderate or severe allergic symptoms, versus 6% in the placebo group.
More patients who received the medication also avoided moderate or severe reactions to cashews (42% vs 3%), milk (66% vs 11%), and eggs (67% vs 0%).
The most common side effects of omalizumab included injection site reactions and fever. The drug’s label includes warnings and precautions about anaphylaxis, cancer, fever, joint pain, rash, parasitic (worm) infection, and abnormal laboratory tests. Omalizumab comes with a boxed warning for anaphylaxis and should be started only in a healthcare setting equipped to manage anaphylaxis, according to the FDA.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved omalizumab (Xolair, Genentech) for reducing allergic reactions to foods in adults and most children. The drug is meant to be taken regularly by patients with food allergies to reduce the risk for reactions, including anaphylaxis, in case of accidental exposure to one or more allergens. The injection is not approved for emergency treatment of an allergic reaction.
Omalizumab first was approved for persistent allergic asthma in 2003. It also is approved for chronic spontaneous urticaria and chronic rhinosinusitis with nasal polyps.
, the FDA said. Peanut-allergen powder (Palforzia) can reduce reactions to peanut, but its benefits are limited to that allergy.
“While it will not eliminate food allergies or allow patients to consume food allergens freely, its repeated use will help reduce the health impact if accidental exposure occurs,” said Kelly Stone, MD, PhD, associate director of the division of pulmonology, allergy, and critical care in the FDA’s Center for Drug Evaluation and Research, in a news release.
The safety and efficacy of the monoclonal antibody in reducing allergic reactions was studied in a double-blind, placebo-controlled study of 168 children and adults who were allergic to peanut and at least two other foods, including milk, egg, wheat, cashew, hazelnut, or walnut. Patients received omalizumab or placebo for 16-20 weeks. At the end of the study, patients consumed peanut protein (equivalent to 2.5 peanuts). Of those who received the drug, 68% were able to consume peanut without moderate or severe allergic symptoms, versus 6% in the placebo group.
More patients who received the medication also avoided moderate or severe reactions to cashews (42% vs 3%), milk (66% vs 11%), and eggs (67% vs 0%).
The most common side effects of omalizumab included injection site reactions and fever. The drug’s label includes warnings and precautions about anaphylaxis, cancer, fever, joint pain, rash, parasitic (worm) infection, and abnormal laboratory tests. Omalizumab comes with a boxed warning for anaphylaxis and should be started only in a healthcare setting equipped to manage anaphylaxis, according to the FDA.
A version of this article appeared on Medscape.com.
Urologist Sues Health System Over Noncompete Clause
The lawsuit brings renewed attention to the ongoing public discourse around restrictive covenants for physicians as more state and federal legislators signal plans to limit or ban the practice.
According to a civil suit filed on January 30 in the Court of Common Pleas, Scranton, Pennsylvania, Eric Rottenberg, MD, signed a 3-year employment agreement with Commonwealth Health Physician Network (CPN) in November 2022. He worked for the health system from May to November 2023, seeing patients at several of its locations, including Wilkes-Barre General Hospital and other facilities throughout northeast and central Pennsylvania.
Although Dr. Rottenberg previously practiced in Albany, New York, court records state he did not bring a significant referral or patient base to the new role, receive any specialized training, or have knowledge of CPN’s trade secrets during his tenure.
Instead, he was a “9-to-5 practitioner,” or a physician-employee like a “locum tenens whose replacement would not cost the employer more than his traditional compensation,” the complaint said. Dr. Rottenberg only treated patients assigned to him by CPN and its parent company, Commonwealth Health Systems, and did not take a patient base with him upon his departure from CPN.
Commonwealth Health spokesperson Annmarie Poslock declined to comment on pending litigation.
After becoming frustrated by “restrictions on his ability to practice medicine” at CPN, Dr. Rottenberg submitted the required 90-day written notice to terminate the employment agreement. He subsequently received a letter from Simon Ratliff, CPN’s chief executive officer, confirming that his last day of employment would be February 11, 2024. Ratliff also reiterated that the noncompete clause would be enforced, essentially banning Dr. Rottenberg from practicing within a 20-mile radius of his previous CPN locations for the next 2 years, court documents said.
Dr. Rottenberg was recruited by Lehigh Valley Physician Group (LVPG), part of Lehigh Valley Health Network, in December 2023 for a urology position at its Dickson City and Scranton locations — some of which are within 20 miles of CPN facilities, the complaint said.
Employers often include noncompete terms in physician contracts because they want to keep the departing physician’s patients from following them to a competitor. However, about a dozen states and the District of Columbia have passed legislation that allows physicians and other clinicians to more easily exit contracts and change jobs.
For example, an Indiana law took effect on July 1 that prohibits employers from entering a noncompete agreement with primary care physicians. Minnesota legislators also banned new noncompete agreements for all employees effective July 1.
“There’s actually been a long-standing push for bans on physician noncompetes going back to some of the first states to pass them, like Colorado, Delaware, and Massachusetts, in the late 1970s and early 1980s,” said Evan Starr, PhD, associate professor of management and organization at the Robert H. Smith School of Business at the University of Maryland.
Although New York Governor Kathy Hochul recently vetoed a bill that would have outlawed restrictive covenants, more states may consider passing laws that limit or ban noncompetes amid increasing patient equity and care access concerns. Dr. Starr told this news organization that one reason to eliminate restrictive covenants is because they can cause “third-party harm” to patients. “The patient doesn’t get the choice to sign a noncompete, but they’re going to be impacted by that agreement if the physician has to leave the area,” he said.
Interestingly, one profession — lawyers — is the only occupation in the US for which noncompete agreements are banned, says Dr. Starr. “Basically, the American Medical Association (AMA) and other physician governing bodies haven’t made the same policies to exempt themselves that the lawyers have.”
That may be changing. In June, the AMA’s House of Delegates adopted policies to support the prohibition of noncompete contracts for employed physicians. The change came several months after the Federal Trade Commission (FTC) proposed a new rule that could more broadly ban companies from enforcing noncompete clauses.
Despite Rottenberg’s attorney, Ryan Campbell, Esq, claiming that the noncompete is unenforceable without a protectable business interest, CPN would not release him from the agreement and opted to move forward with litigation, court records said. The suit cites several other cases where Pennsylvania judges have released physicians from similar restrictive covenants.
Mr. Campbell told this news organization that he and his client are “working diligently with CPN and its counsel to resolve the matter amicably and without further litigation.”
As employers await the FTC’s final rule, Dr. Starr says they could take steps to eliminate noncompete agreements altogether in favor of other stipulations. Contract terms prohibiting physicians from soliciting former patients could protect business interests and still allow patients to seek their preferred physician on their own accord.
A version of this article appeared on Medscape.com .
The lawsuit brings renewed attention to the ongoing public discourse around restrictive covenants for physicians as more state and federal legislators signal plans to limit or ban the practice.
According to a civil suit filed on January 30 in the Court of Common Pleas, Scranton, Pennsylvania, Eric Rottenberg, MD, signed a 3-year employment agreement with Commonwealth Health Physician Network (CPN) in November 2022. He worked for the health system from May to November 2023, seeing patients at several of its locations, including Wilkes-Barre General Hospital and other facilities throughout northeast and central Pennsylvania.
Although Dr. Rottenberg previously practiced in Albany, New York, court records state he did not bring a significant referral or patient base to the new role, receive any specialized training, or have knowledge of CPN’s trade secrets during his tenure.
Instead, he was a “9-to-5 practitioner,” or a physician-employee like a “locum tenens whose replacement would not cost the employer more than his traditional compensation,” the complaint said. Dr. Rottenberg only treated patients assigned to him by CPN and its parent company, Commonwealth Health Systems, and did not take a patient base with him upon his departure from CPN.
Commonwealth Health spokesperson Annmarie Poslock declined to comment on pending litigation.
After becoming frustrated by “restrictions on his ability to practice medicine” at CPN, Dr. Rottenberg submitted the required 90-day written notice to terminate the employment agreement. He subsequently received a letter from Simon Ratliff, CPN’s chief executive officer, confirming that his last day of employment would be February 11, 2024. Ratliff also reiterated that the noncompete clause would be enforced, essentially banning Dr. Rottenberg from practicing within a 20-mile radius of his previous CPN locations for the next 2 years, court documents said.
Dr. Rottenberg was recruited by Lehigh Valley Physician Group (LVPG), part of Lehigh Valley Health Network, in December 2023 for a urology position at its Dickson City and Scranton locations — some of which are within 20 miles of CPN facilities, the complaint said.
Employers often include noncompete terms in physician contracts because they want to keep the departing physician’s patients from following them to a competitor. However, about a dozen states and the District of Columbia have passed legislation that allows physicians and other clinicians to more easily exit contracts and change jobs.
For example, an Indiana law took effect on July 1 that prohibits employers from entering a noncompete agreement with primary care physicians. Minnesota legislators also banned new noncompete agreements for all employees effective July 1.
“There’s actually been a long-standing push for bans on physician noncompetes going back to some of the first states to pass them, like Colorado, Delaware, and Massachusetts, in the late 1970s and early 1980s,” said Evan Starr, PhD, associate professor of management and organization at the Robert H. Smith School of Business at the University of Maryland.
Although New York Governor Kathy Hochul recently vetoed a bill that would have outlawed restrictive covenants, more states may consider passing laws that limit or ban noncompetes amid increasing patient equity and care access concerns. Dr. Starr told this news organization that one reason to eliminate restrictive covenants is because they can cause “third-party harm” to patients. “The patient doesn’t get the choice to sign a noncompete, but they’re going to be impacted by that agreement if the physician has to leave the area,” he said.
Interestingly, one profession — lawyers — is the only occupation in the US for which noncompete agreements are banned, says Dr. Starr. “Basically, the American Medical Association (AMA) and other physician governing bodies haven’t made the same policies to exempt themselves that the lawyers have.”
That may be changing. In June, the AMA’s House of Delegates adopted policies to support the prohibition of noncompete contracts for employed physicians. The change came several months after the Federal Trade Commission (FTC) proposed a new rule that could more broadly ban companies from enforcing noncompete clauses.
Despite Rottenberg’s attorney, Ryan Campbell, Esq, claiming that the noncompete is unenforceable without a protectable business interest, CPN would not release him from the agreement and opted to move forward with litigation, court records said. The suit cites several other cases where Pennsylvania judges have released physicians from similar restrictive covenants.
Mr. Campbell told this news organization that he and his client are “working diligently with CPN and its counsel to resolve the matter amicably and without further litigation.”
As employers await the FTC’s final rule, Dr. Starr says they could take steps to eliminate noncompete agreements altogether in favor of other stipulations. Contract terms prohibiting physicians from soliciting former patients could protect business interests and still allow patients to seek their preferred physician on their own accord.
A version of this article appeared on Medscape.com .
The lawsuit brings renewed attention to the ongoing public discourse around restrictive covenants for physicians as more state and federal legislators signal plans to limit or ban the practice.
According to a civil suit filed on January 30 in the Court of Common Pleas, Scranton, Pennsylvania, Eric Rottenberg, MD, signed a 3-year employment agreement with Commonwealth Health Physician Network (CPN) in November 2022. He worked for the health system from May to November 2023, seeing patients at several of its locations, including Wilkes-Barre General Hospital and other facilities throughout northeast and central Pennsylvania.
Although Dr. Rottenberg previously practiced in Albany, New York, court records state he did not bring a significant referral or patient base to the new role, receive any specialized training, or have knowledge of CPN’s trade secrets during his tenure.
Instead, he was a “9-to-5 practitioner,” or a physician-employee like a “locum tenens whose replacement would not cost the employer more than his traditional compensation,” the complaint said. Dr. Rottenberg only treated patients assigned to him by CPN and its parent company, Commonwealth Health Systems, and did not take a patient base with him upon his departure from CPN.
Commonwealth Health spokesperson Annmarie Poslock declined to comment on pending litigation.
After becoming frustrated by “restrictions on his ability to practice medicine” at CPN, Dr. Rottenberg submitted the required 90-day written notice to terminate the employment agreement. He subsequently received a letter from Simon Ratliff, CPN’s chief executive officer, confirming that his last day of employment would be February 11, 2024. Ratliff also reiterated that the noncompete clause would be enforced, essentially banning Dr. Rottenberg from practicing within a 20-mile radius of his previous CPN locations for the next 2 years, court documents said.
Dr. Rottenberg was recruited by Lehigh Valley Physician Group (LVPG), part of Lehigh Valley Health Network, in December 2023 for a urology position at its Dickson City and Scranton locations — some of which are within 20 miles of CPN facilities, the complaint said.
Employers often include noncompete terms in physician contracts because they want to keep the departing physician’s patients from following them to a competitor. However, about a dozen states and the District of Columbia have passed legislation that allows physicians and other clinicians to more easily exit contracts and change jobs.
For example, an Indiana law took effect on July 1 that prohibits employers from entering a noncompete agreement with primary care physicians. Minnesota legislators also banned new noncompete agreements for all employees effective July 1.
“There’s actually been a long-standing push for bans on physician noncompetes going back to some of the first states to pass them, like Colorado, Delaware, and Massachusetts, in the late 1970s and early 1980s,” said Evan Starr, PhD, associate professor of management and organization at the Robert H. Smith School of Business at the University of Maryland.
Although New York Governor Kathy Hochul recently vetoed a bill that would have outlawed restrictive covenants, more states may consider passing laws that limit or ban noncompetes amid increasing patient equity and care access concerns. Dr. Starr told this news organization that one reason to eliminate restrictive covenants is because they can cause “third-party harm” to patients. “The patient doesn’t get the choice to sign a noncompete, but they’re going to be impacted by that agreement if the physician has to leave the area,” he said.
Interestingly, one profession — lawyers — is the only occupation in the US for which noncompete agreements are banned, says Dr. Starr. “Basically, the American Medical Association (AMA) and other physician governing bodies haven’t made the same policies to exempt themselves that the lawyers have.”
That may be changing. In June, the AMA’s House of Delegates adopted policies to support the prohibition of noncompete contracts for employed physicians. The change came several months after the Federal Trade Commission (FTC) proposed a new rule that could more broadly ban companies from enforcing noncompete clauses.
Despite Rottenberg’s attorney, Ryan Campbell, Esq, claiming that the noncompete is unenforceable without a protectable business interest, CPN would not release him from the agreement and opted to move forward with litigation, court records said. The suit cites several other cases where Pennsylvania judges have released physicians from similar restrictive covenants.
Mr. Campbell told this news organization that he and his client are “working diligently with CPN and its counsel to resolve the matter amicably and without further litigation.”
As employers await the FTC’s final rule, Dr. Starr says they could take steps to eliminate noncompete agreements altogether in favor of other stipulations. Contract terms prohibiting physicians from soliciting former patients could protect business interests and still allow patients to seek their preferred physician on their own accord.
A version of this article appeared on Medscape.com .
Postinfectious Cough: Are Treatments Ever Warranted?
Lingering postinfectious cough has been a concern across Canada this winter. , according to an overview published on February 12 in the Canadian Medical Association Journal
“It’s something a lot of patients are worried about: That lingering cough after a common cold or flu,” lead author Kevin Liang, MD, of the Department of Family Medicine at The University of British Columbia in Vancouver, British Columbia, Canada, told this news organization. He added that some studies show that as much as a quarter of adult patients have this complaint.
Dr. Liang and his colleagues emphasized that the diagnosis of postinfectious cough is one of exclusion. It relies on the absence of concerning physical examination findings and other “subacute cough mimics” such as asthma, chronic obstructive pulmonary disease (COPD), gastroesophageal reflux disease, or use of angiotensin-converting enzyme inhibitors.
“Pertussis should be considered in patients with a paroxysmal cough, post-tussive vomiting, and inspiratory whoop,” they added. Coughs that persist beyond 8 weeks warrant further workup such as a pulmonary function test to rule out asthma or COPD. Coughs accompanied by hemoptysis, systemic symptoms, dysphagia, excessive dyspnea, or hoarseness also warrant further workup, they added. And patients with a history of smoking or recurrent pneumonia should be followed more closely.
In the absence of red flags, Dr. Liang and coauthors advised that there is no evidence supporting pharmacologic treatment, “which is associated with harms,” such as medication adverse effects, cost, strain on the medical supply chain, and the fact that pressurized metered-dose inhalers emit powerful greenhouse gases. “A lot of patients come in looking for solutions, but really, all the evidence says the over-the-counter cough syrup just doesn’t work. Or I see clinicians prescribing inhalers or different medication that can cost hundreds of dollars, and their efficacy, at least from the literature, shows that there’s really no improvement. Time and patience are the two keys to solving this,” Dr. Liang told this news organization.
Moreover, there is a distinct absence of guidelines on this topic. The College of Family Physicians of Canada’s recent literature review cited limited data supporting a trial of inhaled corticosteroids, a bronchodilator such as ipratropium-salbutamol, or an intranasal steroid if postnasal drip is suspected. However, “there’s a high risk of bias in the study they cite from using the short-acting bronchodilators, and what it ultimately says is that in most cases, this is self-resolving by around the 20-day mark,” said Dr. Liang. “Our advice is just to err on the side of caution and just provide that information piece to the patient.”
‘Significant Nuance’
Imran Satia, MD, assistant professor of respirology at McMaster University in Hamilton, Ontario, Canada, agreed that “most people who get a viral or bacterial upper or lower respiratory tract infection will get better with time, and there is very little evidence that giving steroids, antibiotics, or cough suppressants is better than waiting it out.” There is “significant nuance” in how to manage this situation, however.
“In some patients with underlying lung disease like asthma or COPD, increasing the frequency of regular inhaled steroids, bronchodilators, oral steroids, antibiotics, and chest imaging with breathing tests may be clinically warranted, and many physicians will do this,” he told this news organization. “In some patients with refractory chronic cough, there is no underlying identifiable disease, despite completing the necessary investigations. Or coughing persists despite trials of treatment for lung diseases, nasal diseases, and stomach reflux disease. This is commonly described as cough hypersensitivity syndrome, for which therapies targeting the neuronal pathways that control coughing are needed.”
Physicians should occasionally consider trying a temporary course of a short-acting bronchodilator inhaler, said Nicholas Vozoris, MD, assistant professor and clinician investigator in respirology at the University of Toronto, Toronto, Ontario, Canada. “I think that would be a reasonable first step in a case of really bad postinfectious cough,” he told this news organization. “But in general, drug treatments are not indicated.”
Environmental Concerns
Yet some things should raise clinicians’ suspicion of more complex issues.
“A pattern of recurrent colds or bronchitis with protracted coughing afterward raises strong suspicion for asthma, which can present as repeated, prolonged respiratory exacerbations,” he said. “Unless asthma is treated with appropriate inhaler therapy on a regular basis, it will unlikely come under control.”
Dr. Vozoris added that the environmental concerns over the use of metered dose inhalers (MDIs) are minimal compared with the other sources of pollution and the risks for undertreatment. “The authors are overplaying the environmental impact of MDI, in my opinion,” he said. “Physicians already have to deal with the challenging issue of suboptimal patient adherence to inhalers, and I fear that such comments may further drive that up. Furthermore, there is also an environmental footprint with not using inhalers, as patients can then experience suboptimally controlled lung disease as a result — and then present to the ER and get admitted to hospital for exacerbations of disease, where more resources and medications are used up.”
“In addition, in patients who are immunocompromised, protracted coughing after what was thought to be a cold may be associated with an “atypical” respiratory infection, such as tuberculosis, that will require special medical treatment,” Dr. Vozoris concluded.
No funding for the review of postinfectious cough was reported. Dr. Liang and Dr. Vozoris disclosed no competing interests. Dr. Satia reported receiving funding from the ERS Respire 3 Fellowship Award, BMA James Trust Award, North-West Lung Centre Charity (Manchester), NIHR CRF Manchester, Merck MSD, AstraZeneca, and GSK. Dr. Satia also has received consulting fees from Merck MSD, Genentech, and Respiplus; as well as speaker fees from AstraZeneca, GSK, Merck MSD, Sanofi-Regeneron. Satia has served on the following task force committees: Chronic Cough (ERS), Asthma Diagnosis and Management (ERS), NEUROCOUGH (ERS CRC), and the CTS Chronic Cough working group.
A version of this article appeared on Medscape.com.
Lingering postinfectious cough has been a concern across Canada this winter. , according to an overview published on February 12 in the Canadian Medical Association Journal
“It’s something a lot of patients are worried about: That lingering cough after a common cold or flu,” lead author Kevin Liang, MD, of the Department of Family Medicine at The University of British Columbia in Vancouver, British Columbia, Canada, told this news organization. He added that some studies show that as much as a quarter of adult patients have this complaint.
Dr. Liang and his colleagues emphasized that the diagnosis of postinfectious cough is one of exclusion. It relies on the absence of concerning physical examination findings and other “subacute cough mimics” such as asthma, chronic obstructive pulmonary disease (COPD), gastroesophageal reflux disease, or use of angiotensin-converting enzyme inhibitors.
“Pertussis should be considered in patients with a paroxysmal cough, post-tussive vomiting, and inspiratory whoop,” they added. Coughs that persist beyond 8 weeks warrant further workup such as a pulmonary function test to rule out asthma or COPD. Coughs accompanied by hemoptysis, systemic symptoms, dysphagia, excessive dyspnea, or hoarseness also warrant further workup, they added. And patients with a history of smoking or recurrent pneumonia should be followed more closely.
In the absence of red flags, Dr. Liang and coauthors advised that there is no evidence supporting pharmacologic treatment, “which is associated with harms,” such as medication adverse effects, cost, strain on the medical supply chain, and the fact that pressurized metered-dose inhalers emit powerful greenhouse gases. “A lot of patients come in looking for solutions, but really, all the evidence says the over-the-counter cough syrup just doesn’t work. Or I see clinicians prescribing inhalers or different medication that can cost hundreds of dollars, and their efficacy, at least from the literature, shows that there’s really no improvement. Time and patience are the two keys to solving this,” Dr. Liang told this news organization.
Moreover, there is a distinct absence of guidelines on this topic. The College of Family Physicians of Canada’s recent literature review cited limited data supporting a trial of inhaled corticosteroids, a bronchodilator such as ipratropium-salbutamol, or an intranasal steroid if postnasal drip is suspected. However, “there’s a high risk of bias in the study they cite from using the short-acting bronchodilators, and what it ultimately says is that in most cases, this is self-resolving by around the 20-day mark,” said Dr. Liang. “Our advice is just to err on the side of caution and just provide that information piece to the patient.”
‘Significant Nuance’
Imran Satia, MD, assistant professor of respirology at McMaster University in Hamilton, Ontario, Canada, agreed that “most people who get a viral or bacterial upper or lower respiratory tract infection will get better with time, and there is very little evidence that giving steroids, antibiotics, or cough suppressants is better than waiting it out.” There is “significant nuance” in how to manage this situation, however.
“In some patients with underlying lung disease like asthma or COPD, increasing the frequency of regular inhaled steroids, bronchodilators, oral steroids, antibiotics, and chest imaging with breathing tests may be clinically warranted, and many physicians will do this,” he told this news organization. “In some patients with refractory chronic cough, there is no underlying identifiable disease, despite completing the necessary investigations. Or coughing persists despite trials of treatment for lung diseases, nasal diseases, and stomach reflux disease. This is commonly described as cough hypersensitivity syndrome, for which therapies targeting the neuronal pathways that control coughing are needed.”
Physicians should occasionally consider trying a temporary course of a short-acting bronchodilator inhaler, said Nicholas Vozoris, MD, assistant professor and clinician investigator in respirology at the University of Toronto, Toronto, Ontario, Canada. “I think that would be a reasonable first step in a case of really bad postinfectious cough,” he told this news organization. “But in general, drug treatments are not indicated.”
Environmental Concerns
Yet some things should raise clinicians’ suspicion of more complex issues.
“A pattern of recurrent colds or bronchitis with protracted coughing afterward raises strong suspicion for asthma, which can present as repeated, prolonged respiratory exacerbations,” he said. “Unless asthma is treated with appropriate inhaler therapy on a regular basis, it will unlikely come under control.”
Dr. Vozoris added that the environmental concerns over the use of metered dose inhalers (MDIs) are minimal compared with the other sources of pollution and the risks for undertreatment. “The authors are overplaying the environmental impact of MDI, in my opinion,” he said. “Physicians already have to deal with the challenging issue of suboptimal patient adherence to inhalers, and I fear that such comments may further drive that up. Furthermore, there is also an environmental footprint with not using inhalers, as patients can then experience suboptimally controlled lung disease as a result — and then present to the ER and get admitted to hospital for exacerbations of disease, where more resources and medications are used up.”
“In addition, in patients who are immunocompromised, protracted coughing after what was thought to be a cold may be associated with an “atypical” respiratory infection, such as tuberculosis, that will require special medical treatment,” Dr. Vozoris concluded.
No funding for the review of postinfectious cough was reported. Dr. Liang and Dr. Vozoris disclosed no competing interests. Dr. Satia reported receiving funding from the ERS Respire 3 Fellowship Award, BMA James Trust Award, North-West Lung Centre Charity (Manchester), NIHR CRF Manchester, Merck MSD, AstraZeneca, and GSK. Dr. Satia also has received consulting fees from Merck MSD, Genentech, and Respiplus; as well as speaker fees from AstraZeneca, GSK, Merck MSD, Sanofi-Regeneron. Satia has served on the following task force committees: Chronic Cough (ERS), Asthma Diagnosis and Management (ERS), NEUROCOUGH (ERS CRC), and the CTS Chronic Cough working group.
A version of this article appeared on Medscape.com.
Lingering postinfectious cough has been a concern across Canada this winter. , according to an overview published on February 12 in the Canadian Medical Association Journal
“It’s something a lot of patients are worried about: That lingering cough after a common cold or flu,” lead author Kevin Liang, MD, of the Department of Family Medicine at The University of British Columbia in Vancouver, British Columbia, Canada, told this news organization. He added that some studies show that as much as a quarter of adult patients have this complaint.
Dr. Liang and his colleagues emphasized that the diagnosis of postinfectious cough is one of exclusion. It relies on the absence of concerning physical examination findings and other “subacute cough mimics” such as asthma, chronic obstructive pulmonary disease (COPD), gastroesophageal reflux disease, or use of angiotensin-converting enzyme inhibitors.
“Pertussis should be considered in patients with a paroxysmal cough, post-tussive vomiting, and inspiratory whoop,” they added. Coughs that persist beyond 8 weeks warrant further workup such as a pulmonary function test to rule out asthma or COPD. Coughs accompanied by hemoptysis, systemic symptoms, dysphagia, excessive dyspnea, or hoarseness also warrant further workup, they added. And patients with a history of smoking or recurrent pneumonia should be followed more closely.
In the absence of red flags, Dr. Liang and coauthors advised that there is no evidence supporting pharmacologic treatment, “which is associated with harms,” such as medication adverse effects, cost, strain on the medical supply chain, and the fact that pressurized metered-dose inhalers emit powerful greenhouse gases. “A lot of patients come in looking for solutions, but really, all the evidence says the over-the-counter cough syrup just doesn’t work. Or I see clinicians prescribing inhalers or different medication that can cost hundreds of dollars, and their efficacy, at least from the literature, shows that there’s really no improvement. Time and patience are the two keys to solving this,” Dr. Liang told this news organization.
Moreover, there is a distinct absence of guidelines on this topic. The College of Family Physicians of Canada’s recent literature review cited limited data supporting a trial of inhaled corticosteroids, a bronchodilator such as ipratropium-salbutamol, or an intranasal steroid if postnasal drip is suspected. However, “there’s a high risk of bias in the study they cite from using the short-acting bronchodilators, and what it ultimately says is that in most cases, this is self-resolving by around the 20-day mark,” said Dr. Liang. “Our advice is just to err on the side of caution and just provide that information piece to the patient.”
‘Significant Nuance’
Imran Satia, MD, assistant professor of respirology at McMaster University in Hamilton, Ontario, Canada, agreed that “most people who get a viral or bacterial upper or lower respiratory tract infection will get better with time, and there is very little evidence that giving steroids, antibiotics, or cough suppressants is better than waiting it out.” There is “significant nuance” in how to manage this situation, however.
“In some patients with underlying lung disease like asthma or COPD, increasing the frequency of regular inhaled steroids, bronchodilators, oral steroids, antibiotics, and chest imaging with breathing tests may be clinically warranted, and many physicians will do this,” he told this news organization. “In some patients with refractory chronic cough, there is no underlying identifiable disease, despite completing the necessary investigations. Or coughing persists despite trials of treatment for lung diseases, nasal diseases, and stomach reflux disease. This is commonly described as cough hypersensitivity syndrome, for which therapies targeting the neuronal pathways that control coughing are needed.”
Physicians should occasionally consider trying a temporary course of a short-acting bronchodilator inhaler, said Nicholas Vozoris, MD, assistant professor and clinician investigator in respirology at the University of Toronto, Toronto, Ontario, Canada. “I think that would be a reasonable first step in a case of really bad postinfectious cough,” he told this news organization. “But in general, drug treatments are not indicated.”
Environmental Concerns
Yet some things should raise clinicians’ suspicion of more complex issues.
“A pattern of recurrent colds or bronchitis with protracted coughing afterward raises strong suspicion for asthma, which can present as repeated, prolonged respiratory exacerbations,” he said. “Unless asthma is treated with appropriate inhaler therapy on a regular basis, it will unlikely come under control.”
Dr. Vozoris added that the environmental concerns over the use of metered dose inhalers (MDIs) are minimal compared with the other sources of pollution and the risks for undertreatment. “The authors are overplaying the environmental impact of MDI, in my opinion,” he said. “Physicians already have to deal with the challenging issue of suboptimal patient adherence to inhalers, and I fear that such comments may further drive that up. Furthermore, there is also an environmental footprint with not using inhalers, as patients can then experience suboptimally controlled lung disease as a result — and then present to the ER and get admitted to hospital for exacerbations of disease, where more resources and medications are used up.”
“In addition, in patients who are immunocompromised, protracted coughing after what was thought to be a cold may be associated with an “atypical” respiratory infection, such as tuberculosis, that will require special medical treatment,” Dr. Vozoris concluded.
No funding for the review of postinfectious cough was reported. Dr. Liang and Dr. Vozoris disclosed no competing interests. Dr. Satia reported receiving funding from the ERS Respire 3 Fellowship Award, BMA James Trust Award, North-West Lung Centre Charity (Manchester), NIHR CRF Manchester, Merck MSD, AstraZeneca, and GSK. Dr. Satia also has received consulting fees from Merck MSD, Genentech, and Respiplus; as well as speaker fees from AstraZeneca, GSK, Merck MSD, Sanofi-Regeneron. Satia has served on the following task force committees: Chronic Cough (ERS), Asthma Diagnosis and Management (ERS), NEUROCOUGH (ERS CRC), and the CTS Chronic Cough working group.
A version of this article appeared on Medscape.com.
FROM THE CANADIAN MEDICAL ASSOCIATION JOURNAL
5 Things to Know About the Future of Obesity Medicine
As more and more treatments for obesity become available, what does the future hold for these patients? Here are five things that clinicians need to know.
1. Public health officials will prioritize dietary quality over quantity.
Dietitians, healthcare providers, and scientists are already prioritizing the quality of calories, and now policymakers are aligning with this goal, with calls for more research on ultraprocessed foods (UPFs) to answer the key question, “Why do UPFs cause people to eat 500 more calories per day compared with unprocessed foods?” The food industry has taken notice of the potential “Ozempic effect” associated with reduced spending on groceries and is responding with product lines “designed to complement” glucagon-like peptide-1 receptor agonists (GLP-1 RAs) while simultaneously lobbying against any UPF reform. However, with emerging data on how sugar taxes may reduce sales and Congress honing in on the diabetes epidemic, we are hopeful that change is coming in 2024.
2. Antiobesity medications will target fat loss instead of weight loss.
The focus on weight has been long-standing, but with highly effective medications like tirzepatide causing about 20% weight loss, attention is shifting to body composition — namely, how do we optimize fat loss while preserving muscle? We are seeing this transition in the research community. Bimagrumab, for example, a once-monthly injection that increases muscle mass and decreases fat mass, is being tested in a phase 3 clinical trial alongside semaglutide. Agents initially designed for spinal muscular atrophy, like apitegromab and taldefgrobep alfa, are being repurposed for obesity. Watch for results of these phase 2 trials in 2024.
3. Increasing energy expenditure is the holy grail of obesity research.
The success of GLP-1 RAs, and the even greater success of dual- and triple-target agents like tirzepatide and retatrutide, tells us that obesity is, indeed, a hormone problem. These medications primarily cause weight loss by suppressing appetite and reducing caloric intake. As scientists develop more therapeutics to normalize appetite regulation, attention will shift to optimizing energy expenditure. Researchers are already investigating brown fat, mitochondrial uncouplers, and skeletal muscle metabolism, but no agent thus far has been proven to be both safe and effective in increasing energy expenditure. Of these, keep an eye on clinical trials involving brown fat and the excitement over the anti-inflammatory cytokine growth differentiating factor 15 (GDF15).
4. Chronic disease without chronic medications.
Obesity is a chronic disease, just like hypertension or diabetes. Similarly, medications that treat chronic diseases are expected to be taken long-term because discontinuation often results in disease recurrence. However, obesity research is getting closer and closer to options that require less frequent administration. Bimagrumab, for example, is a once-monthly injection. In endocrinology, the premier example is osteoporosis: Osteoporosis can be treated with just 3 years of an annual injection and never require treatment again. In obesity, anticipate more basic science discoveries aimed at developing safe and specific treatments that are truly disease-modifying — ones that reverse appetitive dysregulation, reduce proinflammatory adiposity, and optimize anabolic metabolism.
5. Barriers to access are barriers to progress.
The biggest challenge to obesity treatment today is access: drug shortages, medication costs, and lack of obesity medicine providers. Shortages of medications like semaglutide 2.4 mg are being driven by high “demand”; in other words, manufacturers failed to anticipate the massive interest in antiobesity medications.
Medicare and most state Medicaid programs don’t cover these medications; commercial payers are refusing, reversing, or limiting coverage. An out-of-pocket monthly cost over $1000 limits affordability for the majority of Americans.
Seeking care from an obesity medicine doctor is a challenge as well. Over 40% of US adults have obesity, but less than 1% of doctors are certified in obesity medicine. Meanwhile, private equity is eager to address the lack of access through compounding pharmacies, medispas, or telemedicine services, but the quality of care varies greatly. Some companies purposely avoid the term “patient,” preferring ethics-free labels like “consumers” or “members.”
The $100 billion–dollar weight loss industry unfortunately has created financial incentives that drive obesity commerce over obesity care. Because of these barriers, the epidemic of obesity, with a prevalence projected to be 50% by 2030, will not be solved or slowed despite the scientific progress in obesity treatment. A single silver lining exists among policymakers who are aiming to correct our costly sick-care system in steps, starting with pharmacy benefit manager reform. Five of these bills are the ones to track in 2024: Pharmacy Benefit Manager Reform Act, Pharmacy Benefits Manager Accountability Act, Pharmacy Benefit Manager Sunshine and Accountability Act, Pharmacy Benefit Manager Transparency Act of 2023, and Lower Costs, More Transparency Act.
I believe that these five things will have the most impact on the treatment of our patients with obesity. Stay tuned throughout the year as I share updates in obesity research, pharmacotherapy, and public policy.
Dr. Tchang is Assistant Professor, Clinical Medicine, Division of Endocrinology, Diabetes, and Metabolism, Weill Cornell Medicine; Physician, Department of Medicine, Iris Cantor Women’s Health Center, Comprehensive Weight Control Center, New York, NY. She disclosed ties with Gelesis and Novo Nordisk.
A version of this article appeared on Medscape.com.
As more and more treatments for obesity become available, what does the future hold for these patients? Here are five things that clinicians need to know.
1. Public health officials will prioritize dietary quality over quantity.
Dietitians, healthcare providers, and scientists are already prioritizing the quality of calories, and now policymakers are aligning with this goal, with calls for more research on ultraprocessed foods (UPFs) to answer the key question, “Why do UPFs cause people to eat 500 more calories per day compared with unprocessed foods?” The food industry has taken notice of the potential “Ozempic effect” associated with reduced spending on groceries and is responding with product lines “designed to complement” glucagon-like peptide-1 receptor agonists (GLP-1 RAs) while simultaneously lobbying against any UPF reform. However, with emerging data on how sugar taxes may reduce sales and Congress honing in on the diabetes epidemic, we are hopeful that change is coming in 2024.
2. Antiobesity medications will target fat loss instead of weight loss.
The focus on weight has been long-standing, but with highly effective medications like tirzepatide causing about 20% weight loss, attention is shifting to body composition — namely, how do we optimize fat loss while preserving muscle? We are seeing this transition in the research community. Bimagrumab, for example, a once-monthly injection that increases muscle mass and decreases fat mass, is being tested in a phase 3 clinical trial alongside semaglutide. Agents initially designed for spinal muscular atrophy, like apitegromab and taldefgrobep alfa, are being repurposed for obesity. Watch for results of these phase 2 trials in 2024.
3. Increasing energy expenditure is the holy grail of obesity research.
The success of GLP-1 RAs, and the even greater success of dual- and triple-target agents like tirzepatide and retatrutide, tells us that obesity is, indeed, a hormone problem. These medications primarily cause weight loss by suppressing appetite and reducing caloric intake. As scientists develop more therapeutics to normalize appetite regulation, attention will shift to optimizing energy expenditure. Researchers are already investigating brown fat, mitochondrial uncouplers, and skeletal muscle metabolism, but no agent thus far has been proven to be both safe and effective in increasing energy expenditure. Of these, keep an eye on clinical trials involving brown fat and the excitement over the anti-inflammatory cytokine growth differentiating factor 15 (GDF15).
4. Chronic disease without chronic medications.
Obesity is a chronic disease, just like hypertension or diabetes. Similarly, medications that treat chronic diseases are expected to be taken long-term because discontinuation often results in disease recurrence. However, obesity research is getting closer and closer to options that require less frequent administration. Bimagrumab, for example, is a once-monthly injection. In endocrinology, the premier example is osteoporosis: Osteoporosis can be treated with just 3 years of an annual injection and never require treatment again. In obesity, anticipate more basic science discoveries aimed at developing safe and specific treatments that are truly disease-modifying — ones that reverse appetitive dysregulation, reduce proinflammatory adiposity, and optimize anabolic metabolism.
5. Barriers to access are barriers to progress.
The biggest challenge to obesity treatment today is access: drug shortages, medication costs, and lack of obesity medicine providers. Shortages of medications like semaglutide 2.4 mg are being driven by high “demand”; in other words, manufacturers failed to anticipate the massive interest in antiobesity medications.
Medicare and most state Medicaid programs don’t cover these medications; commercial payers are refusing, reversing, or limiting coverage. An out-of-pocket monthly cost over $1000 limits affordability for the majority of Americans.
Seeking care from an obesity medicine doctor is a challenge as well. Over 40% of US adults have obesity, but less than 1% of doctors are certified in obesity medicine. Meanwhile, private equity is eager to address the lack of access through compounding pharmacies, medispas, or telemedicine services, but the quality of care varies greatly. Some companies purposely avoid the term “patient,” preferring ethics-free labels like “consumers” or “members.”
The $100 billion–dollar weight loss industry unfortunately has created financial incentives that drive obesity commerce over obesity care. Because of these barriers, the epidemic of obesity, with a prevalence projected to be 50% by 2030, will not be solved or slowed despite the scientific progress in obesity treatment. A single silver lining exists among policymakers who are aiming to correct our costly sick-care system in steps, starting with pharmacy benefit manager reform. Five of these bills are the ones to track in 2024: Pharmacy Benefit Manager Reform Act, Pharmacy Benefits Manager Accountability Act, Pharmacy Benefit Manager Sunshine and Accountability Act, Pharmacy Benefit Manager Transparency Act of 2023, and Lower Costs, More Transparency Act.
I believe that these five things will have the most impact on the treatment of our patients with obesity. Stay tuned throughout the year as I share updates in obesity research, pharmacotherapy, and public policy.
Dr. Tchang is Assistant Professor, Clinical Medicine, Division of Endocrinology, Diabetes, and Metabolism, Weill Cornell Medicine; Physician, Department of Medicine, Iris Cantor Women’s Health Center, Comprehensive Weight Control Center, New York, NY. She disclosed ties with Gelesis and Novo Nordisk.
A version of this article appeared on Medscape.com.
As more and more treatments for obesity become available, what does the future hold for these patients? Here are five things that clinicians need to know.
1. Public health officials will prioritize dietary quality over quantity.
Dietitians, healthcare providers, and scientists are already prioritizing the quality of calories, and now policymakers are aligning with this goal, with calls for more research on ultraprocessed foods (UPFs) to answer the key question, “Why do UPFs cause people to eat 500 more calories per day compared with unprocessed foods?” The food industry has taken notice of the potential “Ozempic effect” associated with reduced spending on groceries and is responding with product lines “designed to complement” glucagon-like peptide-1 receptor agonists (GLP-1 RAs) while simultaneously lobbying against any UPF reform. However, with emerging data on how sugar taxes may reduce sales and Congress honing in on the diabetes epidemic, we are hopeful that change is coming in 2024.
2. Antiobesity medications will target fat loss instead of weight loss.
The focus on weight has been long-standing, but with highly effective medications like tirzepatide causing about 20% weight loss, attention is shifting to body composition — namely, how do we optimize fat loss while preserving muscle? We are seeing this transition in the research community. Bimagrumab, for example, a once-monthly injection that increases muscle mass and decreases fat mass, is being tested in a phase 3 clinical trial alongside semaglutide. Agents initially designed for spinal muscular atrophy, like apitegromab and taldefgrobep alfa, are being repurposed for obesity. Watch for results of these phase 2 trials in 2024.
3. Increasing energy expenditure is the holy grail of obesity research.
The success of GLP-1 RAs, and the even greater success of dual- and triple-target agents like tirzepatide and retatrutide, tells us that obesity is, indeed, a hormone problem. These medications primarily cause weight loss by suppressing appetite and reducing caloric intake. As scientists develop more therapeutics to normalize appetite regulation, attention will shift to optimizing energy expenditure. Researchers are already investigating brown fat, mitochondrial uncouplers, and skeletal muscle metabolism, but no agent thus far has been proven to be both safe and effective in increasing energy expenditure. Of these, keep an eye on clinical trials involving brown fat and the excitement over the anti-inflammatory cytokine growth differentiating factor 15 (GDF15).
4. Chronic disease without chronic medications.
Obesity is a chronic disease, just like hypertension or diabetes. Similarly, medications that treat chronic diseases are expected to be taken long-term because discontinuation often results in disease recurrence. However, obesity research is getting closer and closer to options that require less frequent administration. Bimagrumab, for example, is a once-monthly injection. In endocrinology, the premier example is osteoporosis: Osteoporosis can be treated with just 3 years of an annual injection and never require treatment again. In obesity, anticipate more basic science discoveries aimed at developing safe and specific treatments that are truly disease-modifying — ones that reverse appetitive dysregulation, reduce proinflammatory adiposity, and optimize anabolic metabolism.
5. Barriers to access are barriers to progress.
The biggest challenge to obesity treatment today is access: drug shortages, medication costs, and lack of obesity medicine providers. Shortages of medications like semaglutide 2.4 mg are being driven by high “demand”; in other words, manufacturers failed to anticipate the massive interest in antiobesity medications.
Medicare and most state Medicaid programs don’t cover these medications; commercial payers are refusing, reversing, or limiting coverage. An out-of-pocket monthly cost over $1000 limits affordability for the majority of Americans.
Seeking care from an obesity medicine doctor is a challenge as well. Over 40% of US adults have obesity, but less than 1% of doctors are certified in obesity medicine. Meanwhile, private equity is eager to address the lack of access through compounding pharmacies, medispas, or telemedicine services, but the quality of care varies greatly. Some companies purposely avoid the term “patient,” preferring ethics-free labels like “consumers” or “members.”
The $100 billion–dollar weight loss industry unfortunately has created financial incentives that drive obesity commerce over obesity care. Because of these barriers, the epidemic of obesity, with a prevalence projected to be 50% by 2030, will not be solved or slowed despite the scientific progress in obesity treatment. A single silver lining exists among policymakers who are aiming to correct our costly sick-care system in steps, starting with pharmacy benefit manager reform. Five of these bills are the ones to track in 2024: Pharmacy Benefit Manager Reform Act, Pharmacy Benefits Manager Accountability Act, Pharmacy Benefit Manager Sunshine and Accountability Act, Pharmacy Benefit Manager Transparency Act of 2023, and Lower Costs, More Transparency Act.
I believe that these five things will have the most impact on the treatment of our patients with obesity. Stay tuned throughout the year as I share updates in obesity research, pharmacotherapy, and public policy.
Dr. Tchang is Assistant Professor, Clinical Medicine, Division of Endocrinology, Diabetes, and Metabolism, Weill Cornell Medicine; Physician, Department of Medicine, Iris Cantor Women’s Health Center, Comprehensive Weight Control Center, New York, NY. She disclosed ties with Gelesis and Novo Nordisk.
A version of this article appeared on Medscape.com.
Virus and Booster Apathy Could Be Fueling Long COVID
A celebrity makeup artist, the 55-year-old New Yorker had been boosted and vaccinated at every opportunity since vaccines were approved at the end of 2020, until the fall of 2023, when she skipped the shot.
“I really started subscribing to the mindset that you have an immune system and your immune system is supposed to work for you,” she said. “That was the stupidest thing I’ve ever done.”
Maio was not the only person to skip the latest booster: A recent study reported that while nearly 80% of adults in the United States said they’d received their first series of vaccines, barely 20% were up to date on boosters. Nor was Maio alone in getting long COVID 4 years after the start of the deadliest pandemic in a century.
It’s tempting, this far out from the shutdowns of 2020, to think the virus is over, that we’re immune, and nobody’s going to get sick anymore. But while fewer people are getting COVID, it is still very much a part of our lives. And as Maio and others are learning the hard way, long COVID is, too — and it can be deadly.
For those who have recently contracted long COVID, it can feel as if the whole world has moved on from the pandemic, and they are being left behind.
Too Easy to Let Our Guard Down
“It’s really difficult to prevent exposure to COVID no matter how careful you are and no matter how many times you are vaccinated,” said Akiko Iwasaki, an immunology professor at Yale School of Medicine, New Haven, Connecticut, and pioneer in long COVID research. Iwasaki was quick to point out that “we should never blame anybody for getting long COVID because there is no bulletproof way of preventing long COVID from happening” — although research shows you can increase your protection through vaccination, masking, and increasing ventilation indoors.
Also, just because you didn’t get long COVID after catching the virus once, doesn’t mean you’ll dodge the bullet if you get sick again, as Maio has now learned twice. She had long COVID in 2022 after her second bout with the virus, with breathing problems and brain fog that lasted for several months.
Subsequent long COVID experiences won’t necessarily mimic previous ones. Although Maio developed brain fog again, this time she didn’t have the breathing problems that plagued her in 2022. Instead, she had headaches so excruciating she thought she was dying of a brain aneurysm.
A Journal of the American Medical Association study released in May identified the 37 most common symptoms of long COVID, including symptom subgroups that occurred in 80% of the nearly 10,000 study participants. But the symptoms that patients with long COVID are experiencing now are slightly different from earlier in the pandemic or at least that’s what doctors are finding at the Post-COVID Recovery Clinic affiliated with the University of Pittsburgh Medical Center.
Michael Risbano, MD, the clinic’s codirector, said fewer patients have pulmonary or lung damage now than in the past, but a steady stream report problems with brain fog, forgetfulness, exercise intolerance (shortness of breath and fatigue with exercise and difficulty performing any kind of exertional activity), and post-exertional malaise (feeling wiped out or fatigued for hours or even days after physical or mental activity).
Long COVID Treatments Showing Improvement — Slowly
“There still isn’t a great way to treat any of this,” said Risbano, whose clinic is involved with the National Institute of Health’s RECOVER-VITAL trial, which is evaluating potential treatments including Paxlovid and exercise to treat autonomic dysfunction with similarities to myalgic encephalomyelitis/chronic fatigue syndrome and POTS, exercise intolerance, and neurocognitive effects such as brain fog.
Risbano and colleagues have found that physical therapy and exercise training have helped patients with exercise intolerance and neurocognitive problems. “It’s not a quick thing where they go through one visit and are better the next day,” he stressed. “It takes a little bit of time, a little bit of effort, a little bit of homework — there are no silver bullets, no magic medications.”
A quick fix was definitely not in the cards for Dean Jones, PhD, who could barely move when he developed long COVID in May 2023. A 74-year-old biochemist and professor of medicine at Emory University in Atlanta, Georgia, he’d recovered fully the first time he had COVID, in August 2022, but had a completely different experience the second time. He had been vaccinated four times when he began experiencing chronic fatigue, intense exertion-induced migraines, severe airway congestion, brain fog, and shortness of breath. The symptoms began after Memorial Day and worsened over the next month.
His resting heart rate began racing even when he was sleeping, jumping from 53 to 70 beats per minute. “It was almost as though the virus had hit my heart rather than the lungs alone,” he said.
Doctors prescribed multiple inhalers and glucocorticoids to calm Jones’s immune system. The worst symptoms began to abate after a few weeks. The bad ones continued for fully 2 months, severely limiting Jones’s activity. Although he no longer slept all day, just walking from one room to another was exhausting. A dedicated scientist who typically worked 10-15 hours a day before getting sick, he was lucky to focus on work-related tasks for a fraction of that time.
Although the migraines went away early on, the headaches remained until well into the fall. Jones’s energy level gradually returned, and by Christmas, he was beginning to feel as healthy as he had before getting COVID in May.
Still, he’s not complaining that it took so long to get better. “At 74, there’s a lot of colleagues who have already passed away,” he said. “I respect the realities of my age. There are so many people who died from COVID that I’m thankful I had those vaccines. I’m thankful that I pulled through it and was able to rebound.”
Time Helps Healing — But Prompt Care Still Needed
Recovery is the case for most patients with long COVID, said Lisa Sanders, MD, medical director of the Yale New Haven Health Systems Long COVID Consultation Clinic, which opened in March 2023. Although the clinic has a small segment of patients who have had the condition since 2020, “people who recover, who are most people, move on,” she said. “Even the patients who sometimes have to wait a month or so to see me, some of them say, ‘I’m already starting to get better. I wasn’t sure I should come.’”
Maio, too, is recovering but only after multiple visits to the emergency room and a neurologist in late December and early January. The third emergency room trip was prompted after a brief episode in which she lost the feeling in her legs, which began convulsing. A CAT scan showed severely constricted blood vessels in her brain, leading the medical team to speculate she might have reversible cerebral vasoconstriction syndrome (RCVS), which can trigger the thunderclap headaches that had been causing her such misery.
After her third such headache prompted a fourth emergency room visit, further tests confirmed RCVS, which doctors said was related to inflammation caused by COVID. Maio was then admitted to the hospital, where she spent 4 days starting on a regimen of blood pressure medication, magnesium for the headaches, and oxycodone for pain management.
The TV show Maio works on went back into production after the holidays. She went back at the end of January. She’s still having headaches, though they’re less intense, and she’s still taking medication. She was scheduled for another test to look at her blood vessels in February.
Maio has yet to forgive herself for skipping the last booster, even though there’s no guarantee it would have prevented her from getting sick. Her message for others: it’s better to be safe than to be as sorry as she is.
“I’ll never, ever be persuaded by people who don’t believe in vaccines because I believe in science, and I believe in vaccines — that’s why people don’t die at the age of 30 anymore,” she said. “I really think that people need to know about this and what to expect. Because it is horrendous. It is very painful. I would never want anyone to go through this. Ever.”
A version of this article appeared on Medscape.com.
A celebrity makeup artist, the 55-year-old New Yorker had been boosted and vaccinated at every opportunity since vaccines were approved at the end of 2020, until the fall of 2023, when she skipped the shot.
“I really started subscribing to the mindset that you have an immune system and your immune system is supposed to work for you,” she said. “That was the stupidest thing I’ve ever done.”
Maio was not the only person to skip the latest booster: A recent study reported that while nearly 80% of adults in the United States said they’d received their first series of vaccines, barely 20% were up to date on boosters. Nor was Maio alone in getting long COVID 4 years after the start of the deadliest pandemic in a century.
It’s tempting, this far out from the shutdowns of 2020, to think the virus is over, that we’re immune, and nobody’s going to get sick anymore. But while fewer people are getting COVID, it is still very much a part of our lives. And as Maio and others are learning the hard way, long COVID is, too — and it can be deadly.
For those who have recently contracted long COVID, it can feel as if the whole world has moved on from the pandemic, and they are being left behind.
Too Easy to Let Our Guard Down
“It’s really difficult to prevent exposure to COVID no matter how careful you are and no matter how many times you are vaccinated,” said Akiko Iwasaki, an immunology professor at Yale School of Medicine, New Haven, Connecticut, and pioneer in long COVID research. Iwasaki was quick to point out that “we should never blame anybody for getting long COVID because there is no bulletproof way of preventing long COVID from happening” — although research shows you can increase your protection through vaccination, masking, and increasing ventilation indoors.
Also, just because you didn’t get long COVID after catching the virus once, doesn’t mean you’ll dodge the bullet if you get sick again, as Maio has now learned twice. She had long COVID in 2022 after her second bout with the virus, with breathing problems and brain fog that lasted for several months.
Subsequent long COVID experiences won’t necessarily mimic previous ones. Although Maio developed brain fog again, this time she didn’t have the breathing problems that plagued her in 2022. Instead, she had headaches so excruciating she thought she was dying of a brain aneurysm.
A Journal of the American Medical Association study released in May identified the 37 most common symptoms of long COVID, including symptom subgroups that occurred in 80% of the nearly 10,000 study participants. But the symptoms that patients with long COVID are experiencing now are slightly different from earlier in the pandemic or at least that’s what doctors are finding at the Post-COVID Recovery Clinic affiliated with the University of Pittsburgh Medical Center.
Michael Risbano, MD, the clinic’s codirector, said fewer patients have pulmonary or lung damage now than in the past, but a steady stream report problems with brain fog, forgetfulness, exercise intolerance (shortness of breath and fatigue with exercise and difficulty performing any kind of exertional activity), and post-exertional malaise (feeling wiped out or fatigued for hours or even days after physical or mental activity).
Long COVID Treatments Showing Improvement — Slowly
“There still isn’t a great way to treat any of this,” said Risbano, whose clinic is involved with the National Institute of Health’s RECOVER-VITAL trial, which is evaluating potential treatments including Paxlovid and exercise to treat autonomic dysfunction with similarities to myalgic encephalomyelitis/chronic fatigue syndrome and POTS, exercise intolerance, and neurocognitive effects such as brain fog.
Risbano and colleagues have found that physical therapy and exercise training have helped patients with exercise intolerance and neurocognitive problems. “It’s not a quick thing where they go through one visit and are better the next day,” he stressed. “It takes a little bit of time, a little bit of effort, a little bit of homework — there are no silver bullets, no magic medications.”
A quick fix was definitely not in the cards for Dean Jones, PhD, who could barely move when he developed long COVID in May 2023. A 74-year-old biochemist and professor of medicine at Emory University in Atlanta, Georgia, he’d recovered fully the first time he had COVID, in August 2022, but had a completely different experience the second time. He had been vaccinated four times when he began experiencing chronic fatigue, intense exertion-induced migraines, severe airway congestion, brain fog, and shortness of breath. The symptoms began after Memorial Day and worsened over the next month.
His resting heart rate began racing even when he was sleeping, jumping from 53 to 70 beats per minute. “It was almost as though the virus had hit my heart rather than the lungs alone,” he said.
Doctors prescribed multiple inhalers and glucocorticoids to calm Jones’s immune system. The worst symptoms began to abate after a few weeks. The bad ones continued for fully 2 months, severely limiting Jones’s activity. Although he no longer slept all day, just walking from one room to another was exhausting. A dedicated scientist who typically worked 10-15 hours a day before getting sick, he was lucky to focus on work-related tasks for a fraction of that time.
Although the migraines went away early on, the headaches remained until well into the fall. Jones’s energy level gradually returned, and by Christmas, he was beginning to feel as healthy as he had before getting COVID in May.
Still, he’s not complaining that it took so long to get better. “At 74, there’s a lot of colleagues who have already passed away,” he said. “I respect the realities of my age. There are so many people who died from COVID that I’m thankful I had those vaccines. I’m thankful that I pulled through it and was able to rebound.”
Time Helps Healing — But Prompt Care Still Needed
Recovery is the case for most patients with long COVID, said Lisa Sanders, MD, medical director of the Yale New Haven Health Systems Long COVID Consultation Clinic, which opened in March 2023. Although the clinic has a small segment of patients who have had the condition since 2020, “people who recover, who are most people, move on,” she said. “Even the patients who sometimes have to wait a month or so to see me, some of them say, ‘I’m already starting to get better. I wasn’t sure I should come.’”
Maio, too, is recovering but only after multiple visits to the emergency room and a neurologist in late December and early January. The third emergency room trip was prompted after a brief episode in which she lost the feeling in her legs, which began convulsing. A CAT scan showed severely constricted blood vessels in her brain, leading the medical team to speculate she might have reversible cerebral vasoconstriction syndrome (RCVS), which can trigger the thunderclap headaches that had been causing her such misery.
After her third such headache prompted a fourth emergency room visit, further tests confirmed RCVS, which doctors said was related to inflammation caused by COVID. Maio was then admitted to the hospital, where she spent 4 days starting on a regimen of blood pressure medication, magnesium for the headaches, and oxycodone for pain management.
The TV show Maio works on went back into production after the holidays. She went back at the end of January. She’s still having headaches, though they’re less intense, and she’s still taking medication. She was scheduled for another test to look at her blood vessels in February.
Maio has yet to forgive herself for skipping the last booster, even though there’s no guarantee it would have prevented her from getting sick. Her message for others: it’s better to be safe than to be as sorry as she is.
“I’ll never, ever be persuaded by people who don’t believe in vaccines because I believe in science, and I believe in vaccines — that’s why people don’t die at the age of 30 anymore,” she said. “I really think that people need to know about this and what to expect. Because it is horrendous. It is very painful. I would never want anyone to go through this. Ever.”
A version of this article appeared on Medscape.com.
A celebrity makeup artist, the 55-year-old New Yorker had been boosted and vaccinated at every opportunity since vaccines were approved at the end of 2020, until the fall of 2023, when she skipped the shot.
“I really started subscribing to the mindset that you have an immune system and your immune system is supposed to work for you,” she said. “That was the stupidest thing I’ve ever done.”
Maio was not the only person to skip the latest booster: A recent study reported that while nearly 80% of adults in the United States said they’d received their first series of vaccines, barely 20% were up to date on boosters. Nor was Maio alone in getting long COVID 4 years after the start of the deadliest pandemic in a century.
It’s tempting, this far out from the shutdowns of 2020, to think the virus is over, that we’re immune, and nobody’s going to get sick anymore. But while fewer people are getting COVID, it is still very much a part of our lives. And as Maio and others are learning the hard way, long COVID is, too — and it can be deadly.
For those who have recently contracted long COVID, it can feel as if the whole world has moved on from the pandemic, and they are being left behind.
Too Easy to Let Our Guard Down
“It’s really difficult to prevent exposure to COVID no matter how careful you are and no matter how many times you are vaccinated,” said Akiko Iwasaki, an immunology professor at Yale School of Medicine, New Haven, Connecticut, and pioneer in long COVID research. Iwasaki was quick to point out that “we should never blame anybody for getting long COVID because there is no bulletproof way of preventing long COVID from happening” — although research shows you can increase your protection through vaccination, masking, and increasing ventilation indoors.
Also, just because you didn’t get long COVID after catching the virus once, doesn’t mean you’ll dodge the bullet if you get sick again, as Maio has now learned twice. She had long COVID in 2022 after her second bout with the virus, with breathing problems and brain fog that lasted for several months.
Subsequent long COVID experiences won’t necessarily mimic previous ones. Although Maio developed brain fog again, this time she didn’t have the breathing problems that plagued her in 2022. Instead, she had headaches so excruciating she thought she was dying of a brain aneurysm.
A Journal of the American Medical Association study released in May identified the 37 most common symptoms of long COVID, including symptom subgroups that occurred in 80% of the nearly 10,000 study participants. But the symptoms that patients with long COVID are experiencing now are slightly different from earlier in the pandemic or at least that’s what doctors are finding at the Post-COVID Recovery Clinic affiliated with the University of Pittsburgh Medical Center.
Michael Risbano, MD, the clinic’s codirector, said fewer patients have pulmonary or lung damage now than in the past, but a steady stream report problems with brain fog, forgetfulness, exercise intolerance (shortness of breath and fatigue with exercise and difficulty performing any kind of exertional activity), and post-exertional malaise (feeling wiped out or fatigued for hours or even days after physical or mental activity).
Long COVID Treatments Showing Improvement — Slowly
“There still isn’t a great way to treat any of this,” said Risbano, whose clinic is involved with the National Institute of Health’s RECOVER-VITAL trial, which is evaluating potential treatments including Paxlovid and exercise to treat autonomic dysfunction with similarities to myalgic encephalomyelitis/chronic fatigue syndrome and POTS, exercise intolerance, and neurocognitive effects such as brain fog.
Risbano and colleagues have found that physical therapy and exercise training have helped patients with exercise intolerance and neurocognitive problems. “It’s not a quick thing where they go through one visit and are better the next day,” he stressed. “It takes a little bit of time, a little bit of effort, a little bit of homework — there are no silver bullets, no magic medications.”
A quick fix was definitely not in the cards for Dean Jones, PhD, who could barely move when he developed long COVID in May 2023. A 74-year-old biochemist and professor of medicine at Emory University in Atlanta, Georgia, he’d recovered fully the first time he had COVID, in August 2022, but had a completely different experience the second time. He had been vaccinated four times when he began experiencing chronic fatigue, intense exertion-induced migraines, severe airway congestion, brain fog, and shortness of breath. The symptoms began after Memorial Day and worsened over the next month.
His resting heart rate began racing even when he was sleeping, jumping from 53 to 70 beats per minute. “It was almost as though the virus had hit my heart rather than the lungs alone,” he said.
Doctors prescribed multiple inhalers and glucocorticoids to calm Jones’s immune system. The worst symptoms began to abate after a few weeks. The bad ones continued for fully 2 months, severely limiting Jones’s activity. Although he no longer slept all day, just walking from one room to another was exhausting. A dedicated scientist who typically worked 10-15 hours a day before getting sick, he was lucky to focus on work-related tasks for a fraction of that time.
Although the migraines went away early on, the headaches remained until well into the fall. Jones’s energy level gradually returned, and by Christmas, he was beginning to feel as healthy as he had before getting COVID in May.
Still, he’s not complaining that it took so long to get better. “At 74, there’s a lot of colleagues who have already passed away,” he said. “I respect the realities of my age. There are so many people who died from COVID that I’m thankful I had those vaccines. I’m thankful that I pulled through it and was able to rebound.”
Time Helps Healing — But Prompt Care Still Needed
Recovery is the case for most patients with long COVID, said Lisa Sanders, MD, medical director of the Yale New Haven Health Systems Long COVID Consultation Clinic, which opened in March 2023. Although the clinic has a small segment of patients who have had the condition since 2020, “people who recover, who are most people, move on,” she said. “Even the patients who sometimes have to wait a month or so to see me, some of them say, ‘I’m already starting to get better. I wasn’t sure I should come.’”
Maio, too, is recovering but only after multiple visits to the emergency room and a neurologist in late December and early January. The third emergency room trip was prompted after a brief episode in which she lost the feeling in her legs, which began convulsing. A CAT scan showed severely constricted blood vessels in her brain, leading the medical team to speculate she might have reversible cerebral vasoconstriction syndrome (RCVS), which can trigger the thunderclap headaches that had been causing her such misery.
After her third such headache prompted a fourth emergency room visit, further tests confirmed RCVS, which doctors said was related to inflammation caused by COVID. Maio was then admitted to the hospital, where she spent 4 days starting on a regimen of blood pressure medication, magnesium for the headaches, and oxycodone for pain management.
The TV show Maio works on went back into production after the holidays. She went back at the end of January. She’s still having headaches, though they’re less intense, and she’s still taking medication. She was scheduled for another test to look at her blood vessels in February.
Maio has yet to forgive herself for skipping the last booster, even though there’s no guarantee it would have prevented her from getting sick. Her message for others: it’s better to be safe than to be as sorry as she is.
“I’ll never, ever be persuaded by people who don’t believe in vaccines because I believe in science, and I believe in vaccines — that’s why people don’t die at the age of 30 anymore,” she said. “I really think that people need to know about this and what to expect. Because it is horrendous. It is very painful. I would never want anyone to go through this. Ever.”
A version of this article appeared on Medscape.com.
Bivalent Vaccines Protect Even Children Who’ve Had COVID
This transcript has been edited for clarity.
It was only 3 years ago when we called the pathogen we now refer to as the coronavirus “nCOV-19.” It was, in many ways, more descriptive than what we have today. The little “n” there stood for “novel” — and it was really that little “n” that caused us all the trouble.
You see, coronaviruses themselves were not really new to us. Understudied, perhaps, but with four strains running around the globe at any time giving rise to the common cold, these were viruses our bodies understood.
But Instead of acting like a cold, it acted like nothing we had seen before, at least in our lifetime. The story of the pandemic is very much a bildungsroman of our immune systems — a story of how our immunity grew up.
The difference between the start of 2020 and now, when infections with the coronavirus remain common but not as deadly, can be measured in terms of immune education. Some of our immune systems were educated by infection, some by vaccination, and many by both.
When the first vaccines emerged in December 2020, the opportunity to educate our immune systems was still huge. Though, at the time, an estimated 20 million had been infected in the US and 350,000 had died, there was a large population that remained immunologically naive. I was one of them.
If 2020 into early 2021 was the era of immune education, the postvaccine period was the era of the variant. From one COVID strain to two, to five, to innumerable, our immune memory — trained on a specific version of the virus or its spike protein — became imperfect again. Not naive; these variants were not “novel” in the way COVID-19 was novel, but they were different. And different enough to cause infection.
Following the playbook of another virus that loves to come dressed up in different outfits, the flu virus, we find ourselves in the booster era — a world where yearly doses of a vaccine, ideally matched to the variants circulating when the vaccine is given, are the recommendation if not the norm.
But questions remain about the vaccination program, particularly around who should get it. And two populations with big question marks over their heads are (1) people who have already been infected and (2) kids, because their risk for bad outcomes is so much lower.
This week, we finally have some evidence that can shed light on these questions. The study under the spotlight is this one, appearing in JAMA, which tries to analyze the ability of the bivalent vaccine — that’s the second one to come out, around September 2022 — to protect kids from COVID-19.
Now, right off the bat, this was not a randomized trial. The studies that established the viability of the mRNA vaccine platform were; they happened before the vaccine was authorized. But trials of the bivalent vaccine were mostly limited to proving immune response, not protection from disease.
Nevertheless, with some good observational methods and some statistics, we can try to tease out whether bivalent vaccines in kids worked.
The study combines three prospective cohort studies. The details are in the paper, but what you need to know is that the special sauce of these studies was that the kids were tested for COVID-19 on a weekly basis, whether they had symptoms or not. This is critical because asymptomatic infections can transmit COVID-19.
Let’s do the variables of interest. First and foremost, the bivalent vaccine. Some of these kids got the bivalent vaccine, some didn’t. Other key variables include prior vaccination with the monovalent vaccine. Some had been vaccinated with the monovalent vaccine before, some hadn’t. And, of course, prior infection. Some had been infected before (based on either nasal swabs or blood tests).
Let’s focus first on the primary exposure of interest: getting that bivalent vaccine. Again, this was not randomly assigned; kids who got the bivalent vaccine were different from those who did not. In general, they lived in smaller households, they were more likely to be White, less likely to have had a prior COVID infection, and quite a bit more likely to have at least one chronic condition.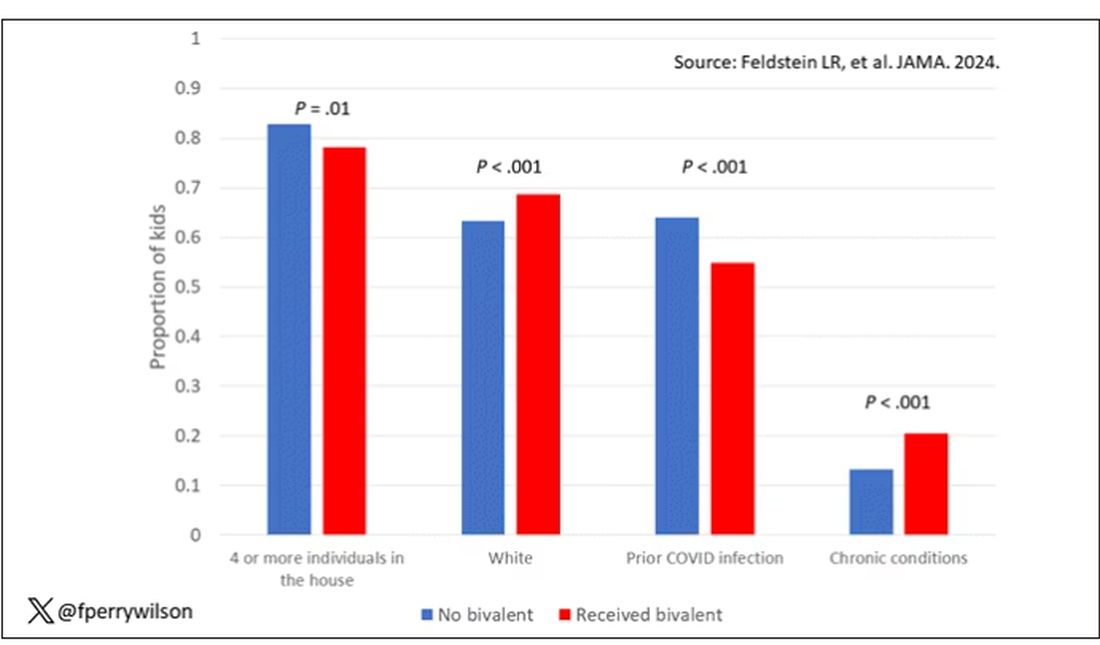
To me, this constellation of factors describes a slightly higher-risk group; it makes sense that they were more likely to get the second vaccine.
Given those factors, what were the rates of COVID infection? After nearly a year of follow-up, around 15% of the kids who hadn’t received the bivalent vaccine got infected compared with 5% of the vaccinated kids. Symptomatic infections represented roughly half of all infections in both groups.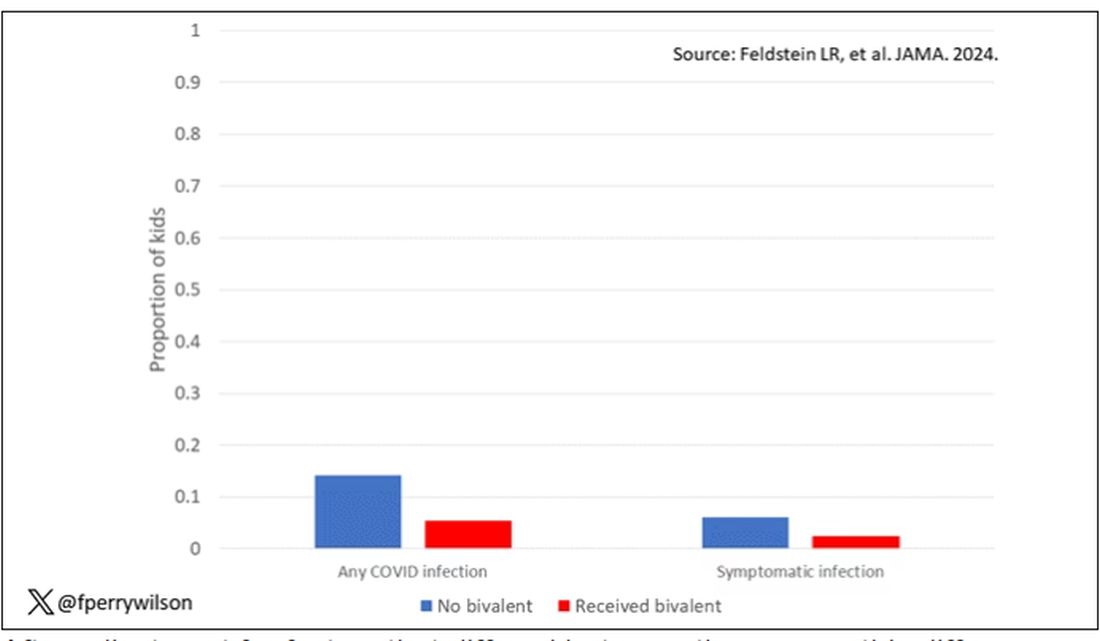
After adjustment for factors that differed between the groups, this difference translated into a vaccine efficacy of about 50% in this population. That’s our first data point. Yes, the bivalent vaccine worked. Not amazingly, of course. But it worked.
What about the kids who had had a prior COVID infection? Somewhat surprisingly, the vaccine was just as effective in this population, despite the fact that their immune systems already had some knowledge of COVID. Ten percent of unvaccinated kids got infected, even though they had been infected before. Just 2.5% of kids who received the bivalent vaccine got infected, suggesting some synergy between prior infection and vaccination.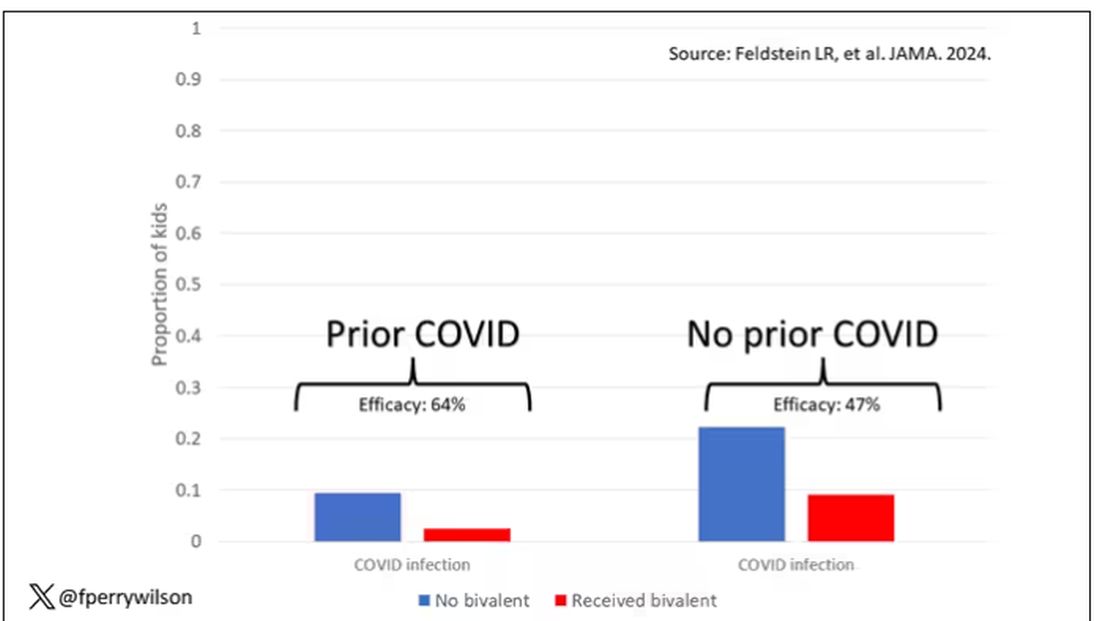
These data suggest that the bivalent vaccine did reduce the risk for COVID infection in kids. All good. But the piece still missing is how severe these infections were. It doesn’t appear that any of the 426 infections documented in this study resulted in hospitalization or death, fortunately. And no data are presented on the incidence of multisystem inflammatory syndrome of children, though given the rarity, I’d be surprised if any of these kids have this either.
So where are we? Well, it seems that the narrative out there that says “the vaccines don’t work” or “the vaccines don’t work if you’ve already been infected” is probably not true. They do work. This study and others in adults show that. If they work to reduce infections, as this study shows, they will also work to reduce deaths. It’s just that death is fortunately so rare in children that the number needed to vaccinate to prevent one death is very large. In that situation, the decision to vaccinate comes down to the risks associated with vaccination. So far, those risk seem very minimal.
Perhaps falling into a flu-like yearly vaccination schedule is not simply the result of old habits dying hard. Maybe it’s actually not a bad idea.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It was only 3 years ago when we called the pathogen we now refer to as the coronavirus “nCOV-19.” It was, in many ways, more descriptive than what we have today. The little “n” there stood for “novel” — and it was really that little “n” that caused us all the trouble.
You see, coronaviruses themselves were not really new to us. Understudied, perhaps, but with four strains running around the globe at any time giving rise to the common cold, these were viruses our bodies understood.
But Instead of acting like a cold, it acted like nothing we had seen before, at least in our lifetime. The story of the pandemic is very much a bildungsroman of our immune systems — a story of how our immunity grew up.
The difference between the start of 2020 and now, when infections with the coronavirus remain common but not as deadly, can be measured in terms of immune education. Some of our immune systems were educated by infection, some by vaccination, and many by both.
When the first vaccines emerged in December 2020, the opportunity to educate our immune systems was still huge. Though, at the time, an estimated 20 million had been infected in the US and 350,000 had died, there was a large population that remained immunologically naive. I was one of them.
If 2020 into early 2021 was the era of immune education, the postvaccine period was the era of the variant. From one COVID strain to two, to five, to innumerable, our immune memory — trained on a specific version of the virus or its spike protein — became imperfect again. Not naive; these variants were not “novel” in the way COVID-19 was novel, but they were different. And different enough to cause infection.
Following the playbook of another virus that loves to come dressed up in different outfits, the flu virus, we find ourselves in the booster era — a world where yearly doses of a vaccine, ideally matched to the variants circulating when the vaccine is given, are the recommendation if not the norm.
But questions remain about the vaccination program, particularly around who should get it. And two populations with big question marks over their heads are (1) people who have already been infected and (2) kids, because their risk for bad outcomes is so much lower.
This week, we finally have some evidence that can shed light on these questions. The study under the spotlight is this one, appearing in JAMA, which tries to analyze the ability of the bivalent vaccine — that’s the second one to come out, around September 2022 — to protect kids from COVID-19.
Now, right off the bat, this was not a randomized trial. The studies that established the viability of the mRNA vaccine platform were; they happened before the vaccine was authorized. But trials of the bivalent vaccine were mostly limited to proving immune response, not protection from disease.
Nevertheless, with some good observational methods and some statistics, we can try to tease out whether bivalent vaccines in kids worked.
The study combines three prospective cohort studies. The details are in the paper, but what you need to know is that the special sauce of these studies was that the kids were tested for COVID-19 on a weekly basis, whether they had symptoms or not. This is critical because asymptomatic infections can transmit COVID-19.
Let’s do the variables of interest. First and foremost, the bivalent vaccine. Some of these kids got the bivalent vaccine, some didn’t. Other key variables include prior vaccination with the monovalent vaccine. Some had been vaccinated with the monovalent vaccine before, some hadn’t. And, of course, prior infection. Some had been infected before (based on either nasal swabs or blood tests).
Let’s focus first on the primary exposure of interest: getting that bivalent vaccine. Again, this was not randomly assigned; kids who got the bivalent vaccine were different from those who did not. In general, they lived in smaller households, they were more likely to be White, less likely to have had a prior COVID infection, and quite a bit more likely to have at least one chronic condition.
To me, this constellation of factors describes a slightly higher-risk group; it makes sense that they were more likely to get the second vaccine.
Given those factors, what were the rates of COVID infection? After nearly a year of follow-up, around 15% of the kids who hadn’t received the bivalent vaccine got infected compared with 5% of the vaccinated kids. Symptomatic infections represented roughly half of all infections in both groups.
After adjustment for factors that differed between the groups, this difference translated into a vaccine efficacy of about 50% in this population. That’s our first data point. Yes, the bivalent vaccine worked. Not amazingly, of course. But it worked.
What about the kids who had had a prior COVID infection? Somewhat surprisingly, the vaccine was just as effective in this population, despite the fact that their immune systems already had some knowledge of COVID. Ten percent of unvaccinated kids got infected, even though they had been infected before. Just 2.5% of kids who received the bivalent vaccine got infected, suggesting some synergy between prior infection and vaccination.
These data suggest that the bivalent vaccine did reduce the risk for COVID infection in kids. All good. But the piece still missing is how severe these infections were. It doesn’t appear that any of the 426 infections documented in this study resulted in hospitalization or death, fortunately. And no data are presented on the incidence of multisystem inflammatory syndrome of children, though given the rarity, I’d be surprised if any of these kids have this either.
So where are we? Well, it seems that the narrative out there that says “the vaccines don’t work” or “the vaccines don’t work if you’ve already been infected” is probably not true. They do work. This study and others in adults show that. If they work to reduce infections, as this study shows, they will also work to reduce deaths. It’s just that death is fortunately so rare in children that the number needed to vaccinate to prevent one death is very large. In that situation, the decision to vaccinate comes down to the risks associated with vaccination. So far, those risk seem very minimal.
Perhaps falling into a flu-like yearly vaccination schedule is not simply the result of old habits dying hard. Maybe it’s actually not a bad idea.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It was only 3 years ago when we called the pathogen we now refer to as the coronavirus “nCOV-19.” It was, in many ways, more descriptive than what we have today. The little “n” there stood for “novel” — and it was really that little “n” that caused us all the trouble.
You see, coronaviruses themselves were not really new to us. Understudied, perhaps, but with four strains running around the globe at any time giving rise to the common cold, these were viruses our bodies understood.
But Instead of acting like a cold, it acted like nothing we had seen before, at least in our lifetime. The story of the pandemic is very much a bildungsroman of our immune systems — a story of how our immunity grew up.
The difference between the start of 2020 and now, when infections with the coronavirus remain common but not as deadly, can be measured in terms of immune education. Some of our immune systems were educated by infection, some by vaccination, and many by both.
When the first vaccines emerged in December 2020, the opportunity to educate our immune systems was still huge. Though, at the time, an estimated 20 million had been infected in the US and 350,000 had died, there was a large population that remained immunologically naive. I was one of them.
If 2020 into early 2021 was the era of immune education, the postvaccine period was the era of the variant. From one COVID strain to two, to five, to innumerable, our immune memory — trained on a specific version of the virus or its spike protein — became imperfect again. Not naive; these variants were not “novel” in the way COVID-19 was novel, but they were different. And different enough to cause infection.
Following the playbook of another virus that loves to come dressed up in different outfits, the flu virus, we find ourselves in the booster era — a world where yearly doses of a vaccine, ideally matched to the variants circulating when the vaccine is given, are the recommendation if not the norm.
But questions remain about the vaccination program, particularly around who should get it. And two populations with big question marks over their heads are (1) people who have already been infected and (2) kids, because their risk for bad outcomes is so much lower.
This week, we finally have some evidence that can shed light on these questions. The study under the spotlight is this one, appearing in JAMA, which tries to analyze the ability of the bivalent vaccine — that’s the second one to come out, around September 2022 — to protect kids from COVID-19.
Now, right off the bat, this was not a randomized trial. The studies that established the viability of the mRNA vaccine platform were; they happened before the vaccine was authorized. But trials of the bivalent vaccine were mostly limited to proving immune response, not protection from disease.
Nevertheless, with some good observational methods and some statistics, we can try to tease out whether bivalent vaccines in kids worked.
The study combines three prospective cohort studies. The details are in the paper, but what you need to know is that the special sauce of these studies was that the kids were tested for COVID-19 on a weekly basis, whether they had symptoms or not. This is critical because asymptomatic infections can transmit COVID-19.
Let’s do the variables of interest. First and foremost, the bivalent vaccine. Some of these kids got the bivalent vaccine, some didn’t. Other key variables include prior vaccination with the monovalent vaccine. Some had been vaccinated with the monovalent vaccine before, some hadn’t. And, of course, prior infection. Some had been infected before (based on either nasal swabs or blood tests).
Let’s focus first on the primary exposure of interest: getting that bivalent vaccine. Again, this was not randomly assigned; kids who got the bivalent vaccine were different from those who did not. In general, they lived in smaller households, they were more likely to be White, less likely to have had a prior COVID infection, and quite a bit more likely to have at least one chronic condition.
To me, this constellation of factors describes a slightly higher-risk group; it makes sense that they were more likely to get the second vaccine.
Given those factors, what were the rates of COVID infection? After nearly a year of follow-up, around 15% of the kids who hadn’t received the bivalent vaccine got infected compared with 5% of the vaccinated kids. Symptomatic infections represented roughly half of all infections in both groups.
After adjustment for factors that differed between the groups, this difference translated into a vaccine efficacy of about 50% in this population. That’s our first data point. Yes, the bivalent vaccine worked. Not amazingly, of course. But it worked.
What about the kids who had had a prior COVID infection? Somewhat surprisingly, the vaccine was just as effective in this population, despite the fact that their immune systems already had some knowledge of COVID. Ten percent of unvaccinated kids got infected, even though they had been infected before. Just 2.5% of kids who received the bivalent vaccine got infected, suggesting some synergy between prior infection and vaccination.
These data suggest that the bivalent vaccine did reduce the risk for COVID infection in kids. All good. But the piece still missing is how severe these infections were. It doesn’t appear that any of the 426 infections documented in this study resulted in hospitalization or death, fortunately. And no data are presented on the incidence of multisystem inflammatory syndrome of children, though given the rarity, I’d be surprised if any of these kids have this either.
So where are we? Well, it seems that the narrative out there that says “the vaccines don’t work” or “the vaccines don’t work if you’ve already been infected” is probably not true. They do work. This study and others in adults show that. If they work to reduce infections, as this study shows, they will also work to reduce deaths. It’s just that death is fortunately so rare in children that the number needed to vaccinate to prevent one death is very large. In that situation, the decision to vaccinate comes down to the risks associated with vaccination. So far, those risk seem very minimal.
Perhaps falling into a flu-like yearly vaccination schedule is not simply the result of old habits dying hard. Maybe it’s actually not a bad idea.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.