User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Watch, but don’t worry yet, about new Omicron subvariant
In the meantime, it’s worth watching BA.2, the World Health Organization said. The subvariant has been identified across at least 40 countries, including three cases reported in Houston and several in Washington state.
BA.2 accounts for only a small minority of reported cases so far, including 5% in India, 4% of those in the United Kingdom, and 2% each of cases in Sweden and Singapore.
The one exception is Denmark, a country with robust genetic sequencing abilities, where estimates range from 50% to 81% of cases.
The news throws a little more uncertainty into an already uncertain situation, including how close the world might be to a less life-altering infectious disease.
For example, the world is at an ideal point for a new variant to emerge, WHO Director General Tedros Adhanom Ghebreyesus, PhD, said during a Jan. 24 meeting of the WHO executive board. He also said it’s too early to call an “end game” to the pandemic.
Similarly, Anthony S. Fauci, MD, said on Jan. 19 that it remained “an open question” whether the Omicron variant could hasten endemic COVID-19, a situation where the virus still circulates but is much less disruptive to everyday life.
No Pi for you
This could be the first time a coronavirus subvariant rises to the level of a household name, or – if previous variants of the moment have shown us – it could recede from the spotlight.
For example, a lot of focus on the potential of the Mu variant to wreak havoc fizzled out a few weeks after the WHO listed it as a variant of interest on Aug. 30.
Subvariants can feature mutations and other small differences but are not distinct enough from an existing strain to be called a variant on their own and be named after the next letter in the Greek alphabet. That’s why BA.2 is not called the “Pi variant.”
Predicting what’s next for the coronavirus has puzzled many experts throughout the pandemic. That is why many public health officials wait for the WHO to officially designate a strain as a variant of interest or variant of concern before taking action.
At the moment with BA.2, it seems close monitoring is warranted.
Because it’s too early to call, expert predictions about BA.2 vary widely, from worry to cautious optimism.
For example, early data indicates that BA.2 could be more worrisome than original Omicron, Eric Feigl-Ding, ScD, an epidemiologist and health economist, said on Twitter.
Information from Denmark seems to show BA.2 either has “much faster transmission or it evades immunity even more,” he said.
The same day, Jan. 23, Dr. Feigl-Ding tweeted that other data shows the subvariant can spread twice as fast as Omicron, which was already much more contagious than previous versions of the virus.
At the same time, other experts appear less concerned. Robert Garry, PhD, a virologist at Tulane University, New Orleans, told the Washington Post that there is no reason to think BA.2 will be any worse than the original Omicron strain.
So which expert predictions will come closer to BA.2’s potential? For now, it’s just a watch-and-see situation.
For updated information, the website outbreak.info tracks BA.2’s average daily and cumulative prevalence in the United States and in other locations.
Also, if and when WHO experts decide to elevate BA.2 to a variant of interest or a variant of concern, it will be noted on its coronavirus variant tracking website.
A version of this article first appeared on WebMD.com.
In the meantime, it’s worth watching BA.2, the World Health Organization said. The subvariant has been identified across at least 40 countries, including three cases reported in Houston and several in Washington state.
BA.2 accounts for only a small minority of reported cases so far, including 5% in India, 4% of those in the United Kingdom, and 2% each of cases in Sweden and Singapore.
The one exception is Denmark, a country with robust genetic sequencing abilities, where estimates range from 50% to 81% of cases.
The news throws a little more uncertainty into an already uncertain situation, including how close the world might be to a less life-altering infectious disease.
For example, the world is at an ideal point for a new variant to emerge, WHO Director General Tedros Adhanom Ghebreyesus, PhD, said during a Jan. 24 meeting of the WHO executive board. He also said it’s too early to call an “end game” to the pandemic.
Similarly, Anthony S. Fauci, MD, said on Jan. 19 that it remained “an open question” whether the Omicron variant could hasten endemic COVID-19, a situation where the virus still circulates but is much less disruptive to everyday life.
No Pi for you
This could be the first time a coronavirus subvariant rises to the level of a household name, or – if previous variants of the moment have shown us – it could recede from the spotlight.
For example, a lot of focus on the potential of the Mu variant to wreak havoc fizzled out a few weeks after the WHO listed it as a variant of interest on Aug. 30.
Subvariants can feature mutations and other small differences but are not distinct enough from an existing strain to be called a variant on their own and be named after the next letter in the Greek alphabet. That’s why BA.2 is not called the “Pi variant.”
Predicting what’s next for the coronavirus has puzzled many experts throughout the pandemic. That is why many public health officials wait for the WHO to officially designate a strain as a variant of interest or variant of concern before taking action.
At the moment with BA.2, it seems close monitoring is warranted.
Because it’s too early to call, expert predictions about BA.2 vary widely, from worry to cautious optimism.
For example, early data indicates that BA.2 could be more worrisome than original Omicron, Eric Feigl-Ding, ScD, an epidemiologist and health economist, said on Twitter.
Information from Denmark seems to show BA.2 either has “much faster transmission or it evades immunity even more,” he said.
The same day, Jan. 23, Dr. Feigl-Ding tweeted that other data shows the subvariant can spread twice as fast as Omicron, which was already much more contagious than previous versions of the virus.
At the same time, other experts appear less concerned. Robert Garry, PhD, a virologist at Tulane University, New Orleans, told the Washington Post that there is no reason to think BA.2 will be any worse than the original Omicron strain.
So which expert predictions will come closer to BA.2’s potential? For now, it’s just a watch-and-see situation.
For updated information, the website outbreak.info tracks BA.2’s average daily and cumulative prevalence in the United States and in other locations.
Also, if and when WHO experts decide to elevate BA.2 to a variant of interest or a variant of concern, it will be noted on its coronavirus variant tracking website.
A version of this article first appeared on WebMD.com.
In the meantime, it’s worth watching BA.2, the World Health Organization said. The subvariant has been identified across at least 40 countries, including three cases reported in Houston and several in Washington state.
BA.2 accounts for only a small minority of reported cases so far, including 5% in India, 4% of those in the United Kingdom, and 2% each of cases in Sweden and Singapore.
The one exception is Denmark, a country with robust genetic sequencing abilities, where estimates range from 50% to 81% of cases.
The news throws a little more uncertainty into an already uncertain situation, including how close the world might be to a less life-altering infectious disease.
For example, the world is at an ideal point for a new variant to emerge, WHO Director General Tedros Adhanom Ghebreyesus, PhD, said during a Jan. 24 meeting of the WHO executive board. He also said it’s too early to call an “end game” to the pandemic.
Similarly, Anthony S. Fauci, MD, said on Jan. 19 that it remained “an open question” whether the Omicron variant could hasten endemic COVID-19, a situation where the virus still circulates but is much less disruptive to everyday life.
No Pi for you
This could be the first time a coronavirus subvariant rises to the level of a household name, or – if previous variants of the moment have shown us – it could recede from the spotlight.
For example, a lot of focus on the potential of the Mu variant to wreak havoc fizzled out a few weeks after the WHO listed it as a variant of interest on Aug. 30.
Subvariants can feature mutations and other small differences but are not distinct enough from an existing strain to be called a variant on their own and be named after the next letter in the Greek alphabet. That’s why BA.2 is not called the “Pi variant.”
Predicting what’s next for the coronavirus has puzzled many experts throughout the pandemic. That is why many public health officials wait for the WHO to officially designate a strain as a variant of interest or variant of concern before taking action.
At the moment with BA.2, it seems close monitoring is warranted.
Because it’s too early to call, expert predictions about BA.2 vary widely, from worry to cautious optimism.
For example, early data indicates that BA.2 could be more worrisome than original Omicron, Eric Feigl-Ding, ScD, an epidemiologist and health economist, said on Twitter.
Information from Denmark seems to show BA.2 either has “much faster transmission or it evades immunity even more,” he said.
The same day, Jan. 23, Dr. Feigl-Ding tweeted that other data shows the subvariant can spread twice as fast as Omicron, which was already much more contagious than previous versions of the virus.
At the same time, other experts appear less concerned. Robert Garry, PhD, a virologist at Tulane University, New Orleans, told the Washington Post that there is no reason to think BA.2 will be any worse than the original Omicron strain.
So which expert predictions will come closer to BA.2’s potential? For now, it’s just a watch-and-see situation.
For updated information, the website outbreak.info tracks BA.2’s average daily and cumulative prevalence in the United States and in other locations.
Also, if and when WHO experts decide to elevate BA.2 to a variant of interest or a variant of concern, it will be noted on its coronavirus variant tracking website.
A version of this article first appeared on WebMD.com.
Ways to make sure 2022 doesn’t stink for docs
Depending on the data you’re looking at, 40%-60% of physicians are burned out.
Research studies and the eye test reveal the painfully obvious: Colleagues are tired, winded, spent, and at times way past burned out. People aren’t asking me if they’re burned out. They know they’re burned out; heck, they can even recite the Maslach burnout inventory, forward and backward, in a mask, or while completing a COVID quarantine. A fair share of people know the key steps to prevent burnout and promote recovery.
What I’m starting to see more of is, “Why should I even bother to recover from this? Why pick myself up again just to get another occupational stress injury (burnout, demoralization, moral injury, etc.)?” In other words, it’s not just simply about negating burnout; it’s about supporting and facilitating the motivation to work.
We’ve been through so much with COVID that it might be challenging to remember when you saw a truly engaged work environment. No doubt, we have outstanding professionals across medicine who answer the bell every day. However, if you’ve been looking closely, many teams/units have lost a bit of the zip and pep. The synergy and trust aren’t as smooth, and at noon, everyone counts the hours to the end of the shift.
You may be thinking, Well, of course, they are; we’re still amid a pandemic, and people have been through hell. Your observation would be correct, except I’ve personally seen some teams weather the pandemic storm and still remain engaged (some even more involved).
The No. 1 consult result for the GW Resiliency and Well-Being Center, where I work, has been on lectures for burnout. The R&WC has given so many of these lectures that my dreams take the form of a PowerPoint presentation. Overall the talks have gone very well. We’ve added skills sections on practices of whole-person care. We’ve blitzed the daylights out of restorative sleep, yet I know we are still searching for the correct narrative.
Motivated staff, faculty, and students will genuinely take in the information and follow the recommendations; however, they still struggle to find that drive and zest for work. Yes, moving from burnout to neutral is reasonable but likely won’t move the needle of your professional or personal life. We need to have the emotional energy and the clear desire to utilize that energy for a meaningful purpose.
Talking about burnout in specific ways is straightforward and, in my opinion, much easier than talking about engagement. Part of the challenge when trying to discuss engagement is that people can feel invalidated or that you’re telling them to be stoic. Or worse yet, that the problem of burnout primarily lies with them. It’s essential to recognize the role of an organizational factor in burnout (approximately 80%, depending on the study); still, even if you address burnout, people may not be miserable, but it doesn’t mean they will stay at their current job (please cue intro music for the Great Resignation).
Engagement models have existed for some time and certainly have gained much more attention in health care settings over the past 2 decades. Engagement can be described as having three components: dedication, vigor, and absorption. When a person is filling all three of these components over time, presto – you get the much-sought-after state of the supremely engaged professional.
These models definitely give us excellent starting points to approach engagement from a pre-COVID era. In COVID and beyond, I’m not sure how these models will stand up in a hybrid work environment, where autonomy and flexibility could be more valued than ever. Personally, COVID revealed some things I was missing in my work pre-COVID:
- Time to think and process. This was one of the great things about being a consultation-liaison psychiatrist; it was literally feast or famine.
- Doing what I’m talented at and really enjoy.
- Time is short, and I want to be more present in the life of my family.
The list above isn’t exhaustive, but I’ve found them to be my own personal recipe for being engaged. Over the next series of articles, I’m going to focus on engagement and factors related to key resilience. These articles will be informed by a front-line view from my colleagues, and hopefully start to separate the myth from reality on the subject of health professional engagement and resilience.
Everyone be safe and well!
A version of this article first appeared on Medscape.com.
Depending on the data you’re looking at, 40%-60% of physicians are burned out.
Research studies and the eye test reveal the painfully obvious: Colleagues are tired, winded, spent, and at times way past burned out. People aren’t asking me if they’re burned out. They know they’re burned out; heck, they can even recite the Maslach burnout inventory, forward and backward, in a mask, or while completing a COVID quarantine. A fair share of people know the key steps to prevent burnout and promote recovery.
What I’m starting to see more of is, “Why should I even bother to recover from this? Why pick myself up again just to get another occupational stress injury (burnout, demoralization, moral injury, etc.)?” In other words, it’s not just simply about negating burnout; it’s about supporting and facilitating the motivation to work.
We’ve been through so much with COVID that it might be challenging to remember when you saw a truly engaged work environment. No doubt, we have outstanding professionals across medicine who answer the bell every day. However, if you’ve been looking closely, many teams/units have lost a bit of the zip and pep. The synergy and trust aren’t as smooth, and at noon, everyone counts the hours to the end of the shift.
You may be thinking, Well, of course, they are; we’re still amid a pandemic, and people have been through hell. Your observation would be correct, except I’ve personally seen some teams weather the pandemic storm and still remain engaged (some even more involved).
The No. 1 consult result for the GW Resiliency and Well-Being Center, where I work, has been on lectures for burnout. The R&WC has given so many of these lectures that my dreams take the form of a PowerPoint presentation. Overall the talks have gone very well. We’ve added skills sections on practices of whole-person care. We’ve blitzed the daylights out of restorative sleep, yet I know we are still searching for the correct narrative.
Motivated staff, faculty, and students will genuinely take in the information and follow the recommendations; however, they still struggle to find that drive and zest for work. Yes, moving from burnout to neutral is reasonable but likely won’t move the needle of your professional or personal life. We need to have the emotional energy and the clear desire to utilize that energy for a meaningful purpose.
Talking about burnout in specific ways is straightforward and, in my opinion, much easier than talking about engagement. Part of the challenge when trying to discuss engagement is that people can feel invalidated or that you’re telling them to be stoic. Or worse yet, that the problem of burnout primarily lies with them. It’s essential to recognize the role of an organizational factor in burnout (approximately 80%, depending on the study); still, even if you address burnout, people may not be miserable, but it doesn’t mean they will stay at their current job (please cue intro music for the Great Resignation).
Engagement models have existed for some time and certainly have gained much more attention in health care settings over the past 2 decades. Engagement can be described as having three components: dedication, vigor, and absorption. When a person is filling all three of these components over time, presto – you get the much-sought-after state of the supremely engaged professional.
These models definitely give us excellent starting points to approach engagement from a pre-COVID era. In COVID and beyond, I’m not sure how these models will stand up in a hybrid work environment, where autonomy and flexibility could be more valued than ever. Personally, COVID revealed some things I was missing in my work pre-COVID:
- Time to think and process. This was one of the great things about being a consultation-liaison psychiatrist; it was literally feast or famine.
- Doing what I’m talented at and really enjoy.
- Time is short, and I want to be more present in the life of my family.
The list above isn’t exhaustive, but I’ve found them to be my own personal recipe for being engaged. Over the next series of articles, I’m going to focus on engagement and factors related to key resilience. These articles will be informed by a front-line view from my colleagues, and hopefully start to separate the myth from reality on the subject of health professional engagement and resilience.
Everyone be safe and well!
A version of this article first appeared on Medscape.com.
Depending on the data you’re looking at, 40%-60% of physicians are burned out.
Research studies and the eye test reveal the painfully obvious: Colleagues are tired, winded, spent, and at times way past burned out. People aren’t asking me if they’re burned out. They know they’re burned out; heck, they can even recite the Maslach burnout inventory, forward and backward, in a mask, or while completing a COVID quarantine. A fair share of people know the key steps to prevent burnout and promote recovery.
What I’m starting to see more of is, “Why should I even bother to recover from this? Why pick myself up again just to get another occupational stress injury (burnout, demoralization, moral injury, etc.)?” In other words, it’s not just simply about negating burnout; it’s about supporting and facilitating the motivation to work.
We’ve been through so much with COVID that it might be challenging to remember when you saw a truly engaged work environment. No doubt, we have outstanding professionals across medicine who answer the bell every day. However, if you’ve been looking closely, many teams/units have lost a bit of the zip and pep. The synergy and trust aren’t as smooth, and at noon, everyone counts the hours to the end of the shift.
You may be thinking, Well, of course, they are; we’re still amid a pandemic, and people have been through hell. Your observation would be correct, except I’ve personally seen some teams weather the pandemic storm and still remain engaged (some even more involved).
The No. 1 consult result for the GW Resiliency and Well-Being Center, where I work, has been on lectures for burnout. The R&WC has given so many of these lectures that my dreams take the form of a PowerPoint presentation. Overall the talks have gone very well. We’ve added skills sections on practices of whole-person care. We’ve blitzed the daylights out of restorative sleep, yet I know we are still searching for the correct narrative.
Motivated staff, faculty, and students will genuinely take in the information and follow the recommendations; however, they still struggle to find that drive and zest for work. Yes, moving from burnout to neutral is reasonable but likely won’t move the needle of your professional or personal life. We need to have the emotional energy and the clear desire to utilize that energy for a meaningful purpose.
Talking about burnout in specific ways is straightforward and, in my opinion, much easier than talking about engagement. Part of the challenge when trying to discuss engagement is that people can feel invalidated or that you’re telling them to be stoic. Or worse yet, that the problem of burnout primarily lies with them. It’s essential to recognize the role of an organizational factor in burnout (approximately 80%, depending on the study); still, even if you address burnout, people may not be miserable, but it doesn’t mean they will stay at their current job (please cue intro music for the Great Resignation).
Engagement models have existed for some time and certainly have gained much more attention in health care settings over the past 2 decades. Engagement can be described as having three components: dedication, vigor, and absorption. When a person is filling all three of these components over time, presto – you get the much-sought-after state of the supremely engaged professional.
These models definitely give us excellent starting points to approach engagement from a pre-COVID era. In COVID and beyond, I’m not sure how these models will stand up in a hybrid work environment, where autonomy and flexibility could be more valued than ever. Personally, COVID revealed some things I was missing in my work pre-COVID:
- Time to think and process. This was one of the great things about being a consultation-liaison psychiatrist; it was literally feast or famine.
- Doing what I’m talented at and really enjoy.
- Time is short, and I want to be more present in the life of my family.
The list above isn’t exhaustive, but I’ve found them to be my own personal recipe for being engaged. Over the next series of articles, I’m going to focus on engagement and factors related to key resilience. These articles will be informed by a front-line view from my colleagues, and hopefully start to separate the myth from reality on the subject of health professional engagement and resilience.
Everyone be safe and well!
A version of this article first appeared on Medscape.com.
No amount of alcohol safe for the heart: WHF
The widely held notion that consuming small to moderate amounts of alcohol is good for cardiovascular health is not supported by the data, the World Heart Federation says in a new policy brief.
In fact, the evidence is clear that any level of drinking can contribute to loss of a healthy life, the organization says.
“Over the past several decades, the prevalence of cardiovascular disease has nearly doubled, and alcohol has played a major role in the incidence of much of it,” the WHF said in the brief.
“The portrayal of alcohol as necessary for a vibrant social life has diverted attention from the harms of alcohol use, as have the frequent and widely publicized claims that moderate drinking, such as a glass of red wine a day, can offer protection against cardiovascular disease,” Monika Arora, PhD, member of the WHF advocacy committee and coauthor of the brief, said in a news release.
“These claims are at best misinformed and at worst an attempt by the alcohol industry to mislead the public about the danger of their product,” Dr. Arora added.
The WHF conclusions follow a report in the Lancet based on the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD), which found that there is no safe level of alcohol consumption.
In 2019, nearly 2.4 million deaths were attributed to alcohol, accounting for 4.3% of all deaths globally and 12.6% of deaths in men 15 to 49 years of age.
Even small amounts of alcohol have been shown to raise the risk for cardiovascular disease, including coronary disease, stroke, heart failure, hypertensive heart disease, cardiomyopathy, atrial fibrillation, and aneurysm, the WHF notes.
Studies that claim otherwise are largely based on purely observational research, which fails to account for relevant cofactors, the organization writes.
Based on their summary of the evidence to date, there is no reliable correlation between moderate alcohol consumption and a lower risk for cardiovascular disease.
Alcohol use is also a “major avoidable risk factor” for cancer, digestive diseases, intentional and unintentional injuries, and several infectious diseases, the WHF says.
Alcohol use also has significant economic and social costs, which include costs to individuals and health systems, productivity losses, as well as the increased risk for violence, homelessness, and criminal activity.
The WHF policy brief calls for “urgent and decisive action” to tackle the unprecedented rise in alcohol-related death and disability worldwide.
Recommended actions include boosting restrictions on alcohol availability; advancing and enforcing drinking and driving countermeasures; increasing access to screening, brief interventions, and treatment for alcohol use disorder; enforcing bans on alcohol advertising; establishing a uniform minimum legal drinking age; and mandating health warnings on alcohol products.
A version of this article first appeared on Medscape.com.
The widely held notion that consuming small to moderate amounts of alcohol is good for cardiovascular health is not supported by the data, the World Heart Federation says in a new policy brief.
In fact, the evidence is clear that any level of drinking can contribute to loss of a healthy life, the organization says.
“Over the past several decades, the prevalence of cardiovascular disease has nearly doubled, and alcohol has played a major role in the incidence of much of it,” the WHF said in the brief.
“The portrayal of alcohol as necessary for a vibrant social life has diverted attention from the harms of alcohol use, as have the frequent and widely publicized claims that moderate drinking, such as a glass of red wine a day, can offer protection against cardiovascular disease,” Monika Arora, PhD, member of the WHF advocacy committee and coauthor of the brief, said in a news release.
“These claims are at best misinformed and at worst an attempt by the alcohol industry to mislead the public about the danger of their product,” Dr. Arora added.
The WHF conclusions follow a report in the Lancet based on the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD), which found that there is no safe level of alcohol consumption.
In 2019, nearly 2.4 million deaths were attributed to alcohol, accounting for 4.3% of all deaths globally and 12.6% of deaths in men 15 to 49 years of age.
Even small amounts of alcohol have been shown to raise the risk for cardiovascular disease, including coronary disease, stroke, heart failure, hypertensive heart disease, cardiomyopathy, atrial fibrillation, and aneurysm, the WHF notes.
Studies that claim otherwise are largely based on purely observational research, which fails to account for relevant cofactors, the organization writes.
Based on their summary of the evidence to date, there is no reliable correlation between moderate alcohol consumption and a lower risk for cardiovascular disease.
Alcohol use is also a “major avoidable risk factor” for cancer, digestive diseases, intentional and unintentional injuries, and several infectious diseases, the WHF says.
Alcohol use also has significant economic and social costs, which include costs to individuals and health systems, productivity losses, as well as the increased risk for violence, homelessness, and criminal activity.
The WHF policy brief calls for “urgent and decisive action” to tackle the unprecedented rise in alcohol-related death and disability worldwide.
Recommended actions include boosting restrictions on alcohol availability; advancing and enforcing drinking and driving countermeasures; increasing access to screening, brief interventions, and treatment for alcohol use disorder; enforcing bans on alcohol advertising; establishing a uniform minimum legal drinking age; and mandating health warnings on alcohol products.
A version of this article first appeared on Medscape.com.
The widely held notion that consuming small to moderate amounts of alcohol is good for cardiovascular health is not supported by the data, the World Heart Federation says in a new policy brief.
In fact, the evidence is clear that any level of drinking can contribute to loss of a healthy life, the organization says.
“Over the past several decades, the prevalence of cardiovascular disease has nearly doubled, and alcohol has played a major role in the incidence of much of it,” the WHF said in the brief.
“The portrayal of alcohol as necessary for a vibrant social life has diverted attention from the harms of alcohol use, as have the frequent and widely publicized claims that moderate drinking, such as a glass of red wine a day, can offer protection against cardiovascular disease,” Monika Arora, PhD, member of the WHF advocacy committee and coauthor of the brief, said in a news release.
“These claims are at best misinformed and at worst an attempt by the alcohol industry to mislead the public about the danger of their product,” Dr. Arora added.
The WHF conclusions follow a report in the Lancet based on the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD), which found that there is no safe level of alcohol consumption.
In 2019, nearly 2.4 million deaths were attributed to alcohol, accounting for 4.3% of all deaths globally and 12.6% of deaths in men 15 to 49 years of age.
Even small amounts of alcohol have been shown to raise the risk for cardiovascular disease, including coronary disease, stroke, heart failure, hypertensive heart disease, cardiomyopathy, atrial fibrillation, and aneurysm, the WHF notes.
Studies that claim otherwise are largely based on purely observational research, which fails to account for relevant cofactors, the organization writes.
Based on their summary of the evidence to date, there is no reliable correlation between moderate alcohol consumption and a lower risk for cardiovascular disease.
Alcohol use is also a “major avoidable risk factor” for cancer, digestive diseases, intentional and unintentional injuries, and several infectious diseases, the WHF says.
Alcohol use also has significant economic and social costs, which include costs to individuals and health systems, productivity losses, as well as the increased risk for violence, homelessness, and criminal activity.
The WHF policy brief calls for “urgent and decisive action” to tackle the unprecedented rise in alcohol-related death and disability worldwide.
Recommended actions include boosting restrictions on alcohol availability; advancing and enforcing drinking and driving countermeasures; increasing access to screening, brief interventions, and treatment for alcohol use disorder; enforcing bans on alcohol advertising; establishing a uniform minimum legal drinking age; and mandating health warnings on alcohol products.
A version of this article first appeared on Medscape.com.
Gut bacteria linked with long COVID
While links have been found between the gut’s microbiome and COVID-19, as well as other diseases, this is the first published research to show a link specifically to COVID’s long-term effects, the investigators, based at the Chinese University of Hong Kong, wrote in Gut.

“To our knowledge, this is the first study to show that altered gut microbiome composition is strongly associated with persistent symptoms in patients with COVID-19 up to 6 months after clearance of SARS-CoV-2 virus,” said Siew Ng, MBBS, PhD, associate director at the university’s Center for Gut Microbiota Research.
At three hospitals, the researchers enrolled 106 patients with COVID-19 from February to August 2020 with stool samples at admission and at 1 month and 6 months after discharge, and compared them with people who did not have COVID, recruited in 2019. The severity of COVID in the enrolled patients was mostly mild to moderate.
At 3 months, 86 of the patients with COVID had post–acute COVID-19 syndrome (PACS) – defined as at least one persistent, otherwise unexplained symptom 4 weeks after clearance of the virus. And 81 patients had PACS at 6 months, most commonly fatigue, poor memory, hair loss, anxiety, and trouble sleeping.
Using stool samples for their analysis, the researchers found that, broadly, the diversity of the types of bacteria, and the abundance of these bacteria, were significantly lower at 6 months for those with PACS, compared with those without PACS and with controls (P < .05 and P < .0001, respectively). Among those with PACS, 28 bacteria species were diminished and 14 were enriched, both at baseline and follow-up. Those patients who had COVID but not PACS showed just 25 alterations of bacteria species at the time of hospital admission, and they all normalized by 6 months.
Having respiratory symptoms at 6 months was linked with higher levels of opportunistic pathogens such as Streptococcus anginosus and S. vestibularis. Neuropsychiatric symptoms and fatigue were associated with nosocomial pathogens that are linked to opportunistic infections, such as Clostridium innocuum and Actinomyces naeslundii (P < .05).
Bacteria known for producing butyrate, a beneficial fatty acid, were significantly depleted in those patients with hair loss. And certain of these bacteria, including Bifidobacterium pseudocatenulatum and Faecalibacterium prausnitzii, had the largest inverse correlations with PACS at 6 months (P < .05), the researchers found.
“Particular gut microbial profiles may indicate heightened susceptibility,” Dr. Ng said.
Although the findings were drawn from patients with earlier strains of the COVID-19 virus, the findings still apply to new variants, including Omicron, since these pose the same problem of persistent disruption of the immune system, Dr. Ng said.
Her group is conducting trials to look at how modulating the microbiome might prevent long COVID and boost antibodies after vaccination in high-risk people, she said.
“Gut microbiota influences the health of the host,” Dr. Ng said. “It provides crucial benefits in the form of immune system development, prevention of infections, nutrient acquisition, and brain and nervous system functionality. Considering the millions of people infected during the ongoing pandemic, our findings are a strong impetus for consideration of microbiota modulation to facilitate timely recovery and reduce the burden of post–acute COVID-19 syndrome.”

John Haran, MD, PhD, associate professor of microbiology and physiological systems and emergency medicine at the University of Massachusetts, Worcester, said the research adds to the evidence base on the gut microbiome’s links to COVID, but there was likely be no clinical impact yet. Still, he said the findings linking specific species to specific symptoms was particularly interesting.
“Very early on during hospitalization, [the researchers] saw these differences and correlated out with people who have longer symptoms, and especially different groups of people that have longer symptoms, too,” said Dr. Haran, who has done research on the topic. “It’s very different if you have different symptoms, for example, you keep coughing for months versus you have brain fog and fatigue, or other debilitating symptoms.”
Dr. Haran noted that the findings didn’t identify bacteria types especially linked to COVID, but rather species that have already been found to be associated with a “bad” microbiome. He also pointed out that the patients enrolled in the study were not vaccinated, because vaccines weren’t available at the time. Still, further study to see whether modulation of gut bacteria can be a therapy seems worthwhile.
“Microbiome modulation is pretty safe, and that’s really the next big step that needs to be taken in this,” he said.
For now, the findings don’t give the clinician much new ammunition for treatment.
“We’re not there yet,” he added. “It’s not as if clinicians are going to tell their COVID patients: ‘Go out and buy some kale.’ ”
Eugene Chang, MD, professor of medicine at the University of Chicago, who has studied the gut microbiome and gastrointestinal disease, said it’s “too preliminary” to say whether the findings could lead to a clinical impact. The measures used merely identify the microbes present, but not what they are doing.
“These measures are unlikely to perform well enough to be useful for risk assessment or predicting clinical outcomes,” he said. “That being said, advances in technology are being made where next generations of metrics could be developed and useful as stratifiers and predictors of risk.”
Seeing shifting patterns associated with certain symptoms, he said, is “notable because it suggests that the disturbances of the gut microbiota in PACS are significant.”
But he said it’s important to know whether these changes are a cause of PACS in some way or just an effect of it.
“If causative or contributory – this has to be proven – then ‘microbiota modulation’ would make sense and could be a priority for development,” he said. “If merely an effect, these metrics and better ones to come could be useful as predictors or measures of the patient’s general state of health.”
As seen in his group’s work and other work, he said, “the gut microbiota is highly sensitive to changes in their ecosystem, which is influenced by the health state of the patient.”
Dr. Ng, Dr. Haran, and Dr. Chang reported no relevant disclosures.
This article was updated Jan. 27, 2022.
While links have been found between the gut’s microbiome and COVID-19, as well as other diseases, this is the first published research to show a link specifically to COVID’s long-term effects, the investigators, based at the Chinese University of Hong Kong, wrote in Gut.
“To our knowledge, this is the first study to show that altered gut microbiome composition is strongly associated with persistent symptoms in patients with COVID-19 up to 6 months after clearance of SARS-CoV-2 virus,” said Siew Ng, MBBS, PhD, associate director at the university’s Center for Gut Microbiota Research.
At three hospitals, the researchers enrolled 106 patients with COVID-19 from February to August 2020 with stool samples at admission and at 1 month and 6 months after discharge, and compared them with people who did not have COVID, recruited in 2019. The severity of COVID in the enrolled patients was mostly mild to moderate.
At 3 months, 86 of the patients with COVID had post–acute COVID-19 syndrome (PACS) – defined as at least one persistent, otherwise unexplained symptom 4 weeks after clearance of the virus. And 81 patients had PACS at 6 months, most commonly fatigue, poor memory, hair loss, anxiety, and trouble sleeping.
Using stool samples for their analysis, the researchers found that, broadly, the diversity of the types of bacteria, and the abundance of these bacteria, were significantly lower at 6 months for those with PACS, compared with those without PACS and with controls (P < .05 and P < .0001, respectively). Among those with PACS, 28 bacteria species were diminished and 14 were enriched, both at baseline and follow-up. Those patients who had COVID but not PACS showed just 25 alterations of bacteria species at the time of hospital admission, and they all normalized by 6 months.
Having respiratory symptoms at 6 months was linked with higher levels of opportunistic pathogens such as Streptococcus anginosus and S. vestibularis. Neuropsychiatric symptoms and fatigue were associated with nosocomial pathogens that are linked to opportunistic infections, such as Clostridium innocuum and Actinomyces naeslundii (P < .05).
Bacteria known for producing butyrate, a beneficial fatty acid, were significantly depleted in those patients with hair loss. And certain of these bacteria, including Bifidobacterium pseudocatenulatum and Faecalibacterium prausnitzii, had the largest inverse correlations with PACS at 6 months (P < .05), the researchers found.
“Particular gut microbial profiles may indicate heightened susceptibility,” Dr. Ng said.
Although the findings were drawn from patients with earlier strains of the COVID-19 virus, the findings still apply to new variants, including Omicron, since these pose the same problem of persistent disruption of the immune system, Dr. Ng said.
Her group is conducting trials to look at how modulating the microbiome might prevent long COVID and boost antibodies after vaccination in high-risk people, she said.
“Gut microbiota influences the health of the host,” Dr. Ng said. “It provides crucial benefits in the form of immune system development, prevention of infections, nutrient acquisition, and brain and nervous system functionality. Considering the millions of people infected during the ongoing pandemic, our findings are a strong impetus for consideration of microbiota modulation to facilitate timely recovery and reduce the burden of post–acute COVID-19 syndrome.”
John Haran, MD, PhD, associate professor of microbiology and physiological systems and emergency medicine at the University of Massachusetts, Worcester, said the research adds to the evidence base on the gut microbiome’s links to COVID, but there was likely be no clinical impact yet. Still, he said the findings linking specific species to specific symptoms was particularly interesting.
“Very early on during hospitalization, [the researchers] saw these differences and correlated out with people who have longer symptoms, and especially different groups of people that have longer symptoms, too,” said Dr. Haran, who has done research on the topic. “It’s very different if you have different symptoms, for example, you keep coughing for months versus you have brain fog and fatigue, or other debilitating symptoms.”
Dr. Haran noted that the findings didn’t identify bacteria types especially linked to COVID, but rather species that have already been found to be associated with a “bad” microbiome. He also pointed out that the patients enrolled in the study were not vaccinated, because vaccines weren’t available at the time. Still, further study to see whether modulation of gut bacteria can be a therapy seems worthwhile.
“Microbiome modulation is pretty safe, and that’s really the next big step that needs to be taken in this,” he said.
For now, the findings don’t give the clinician much new ammunition for treatment.
“We’re not there yet,” he added. “It’s not as if clinicians are going to tell their COVID patients: ‘Go out and buy some kale.’ ”
Eugene Chang, MD, professor of medicine at the University of Chicago, who has studied the gut microbiome and gastrointestinal disease, said it’s “too preliminary” to say whether the findings could lead to a clinical impact. The measures used merely identify the microbes present, but not what they are doing.
“These measures are unlikely to perform well enough to be useful for risk assessment or predicting clinical outcomes,” he said. “That being said, advances in technology are being made where next generations of metrics could be developed and useful as stratifiers and predictors of risk.”
Seeing shifting patterns associated with certain symptoms, he said, is “notable because it suggests that the disturbances of the gut microbiota in PACS are significant.”
But he said it’s important to know whether these changes are a cause of PACS in some way or just an effect of it.
“If causative or contributory – this has to be proven – then ‘microbiota modulation’ would make sense and could be a priority for development,” he said. “If merely an effect, these metrics and better ones to come could be useful as predictors or measures of the patient’s general state of health.”
As seen in his group’s work and other work, he said, “the gut microbiota is highly sensitive to changes in their ecosystem, which is influenced by the health state of the patient.”
Dr. Ng, Dr. Haran, and Dr. Chang reported no relevant disclosures.
This article was updated Jan. 27, 2022.
While links have been found between the gut’s microbiome and COVID-19, as well as other diseases, this is the first published research to show a link specifically to COVID’s long-term effects, the investigators, based at the Chinese University of Hong Kong, wrote in Gut.
“To our knowledge, this is the first study to show that altered gut microbiome composition is strongly associated with persistent symptoms in patients with COVID-19 up to 6 months after clearance of SARS-CoV-2 virus,” said Siew Ng, MBBS, PhD, associate director at the university’s Center for Gut Microbiota Research.
At three hospitals, the researchers enrolled 106 patients with COVID-19 from February to August 2020 with stool samples at admission and at 1 month and 6 months after discharge, and compared them with people who did not have COVID, recruited in 2019. The severity of COVID in the enrolled patients was mostly mild to moderate.
At 3 months, 86 of the patients with COVID had post–acute COVID-19 syndrome (PACS) – defined as at least one persistent, otherwise unexplained symptom 4 weeks after clearance of the virus. And 81 patients had PACS at 6 months, most commonly fatigue, poor memory, hair loss, anxiety, and trouble sleeping.
Using stool samples for their analysis, the researchers found that, broadly, the diversity of the types of bacteria, and the abundance of these bacteria, were significantly lower at 6 months for those with PACS, compared with those without PACS and with controls (P < .05 and P < .0001, respectively). Among those with PACS, 28 bacteria species were diminished and 14 were enriched, both at baseline and follow-up. Those patients who had COVID but not PACS showed just 25 alterations of bacteria species at the time of hospital admission, and they all normalized by 6 months.
Having respiratory symptoms at 6 months was linked with higher levels of opportunistic pathogens such as Streptococcus anginosus and S. vestibularis. Neuropsychiatric symptoms and fatigue were associated with nosocomial pathogens that are linked to opportunistic infections, such as Clostridium innocuum and Actinomyces naeslundii (P < .05).
Bacteria known for producing butyrate, a beneficial fatty acid, were significantly depleted in those patients with hair loss. And certain of these bacteria, including Bifidobacterium pseudocatenulatum and Faecalibacterium prausnitzii, had the largest inverse correlations with PACS at 6 months (P < .05), the researchers found.
“Particular gut microbial profiles may indicate heightened susceptibility,” Dr. Ng said.
Although the findings were drawn from patients with earlier strains of the COVID-19 virus, the findings still apply to new variants, including Omicron, since these pose the same problem of persistent disruption of the immune system, Dr. Ng said.
Her group is conducting trials to look at how modulating the microbiome might prevent long COVID and boost antibodies after vaccination in high-risk people, she said.
“Gut microbiota influences the health of the host,” Dr. Ng said. “It provides crucial benefits in the form of immune system development, prevention of infections, nutrient acquisition, and brain and nervous system functionality. Considering the millions of people infected during the ongoing pandemic, our findings are a strong impetus for consideration of microbiota modulation to facilitate timely recovery and reduce the burden of post–acute COVID-19 syndrome.”
John Haran, MD, PhD, associate professor of microbiology and physiological systems and emergency medicine at the University of Massachusetts, Worcester, said the research adds to the evidence base on the gut microbiome’s links to COVID, but there was likely be no clinical impact yet. Still, he said the findings linking specific species to specific symptoms was particularly interesting.
“Very early on during hospitalization, [the researchers] saw these differences and correlated out with people who have longer symptoms, and especially different groups of people that have longer symptoms, too,” said Dr. Haran, who has done research on the topic. “It’s very different if you have different symptoms, for example, you keep coughing for months versus you have brain fog and fatigue, or other debilitating symptoms.”
Dr. Haran noted that the findings didn’t identify bacteria types especially linked to COVID, but rather species that have already been found to be associated with a “bad” microbiome. He also pointed out that the patients enrolled in the study were not vaccinated, because vaccines weren’t available at the time. Still, further study to see whether modulation of gut bacteria can be a therapy seems worthwhile.
“Microbiome modulation is pretty safe, and that’s really the next big step that needs to be taken in this,” he said.
For now, the findings don’t give the clinician much new ammunition for treatment.
“We’re not there yet,” he added. “It’s not as if clinicians are going to tell their COVID patients: ‘Go out and buy some kale.’ ”
Eugene Chang, MD, professor of medicine at the University of Chicago, who has studied the gut microbiome and gastrointestinal disease, said it’s “too preliminary” to say whether the findings could lead to a clinical impact. The measures used merely identify the microbes present, but not what they are doing.
“These measures are unlikely to perform well enough to be useful for risk assessment or predicting clinical outcomes,” he said. “That being said, advances in technology are being made where next generations of metrics could be developed and useful as stratifiers and predictors of risk.”
Seeing shifting patterns associated with certain symptoms, he said, is “notable because it suggests that the disturbances of the gut microbiota in PACS are significant.”
But he said it’s important to know whether these changes are a cause of PACS in some way or just an effect of it.
“If causative or contributory – this has to be proven – then ‘microbiota modulation’ would make sense and could be a priority for development,” he said. “If merely an effect, these metrics and better ones to come could be useful as predictors or measures of the patient’s general state of health.”
As seen in his group’s work and other work, he said, “the gut microbiota is highly sensitive to changes in their ecosystem, which is influenced by the health state of the patient.”
Dr. Ng, Dr. Haran, and Dr. Chang reported no relevant disclosures.
This article was updated Jan. 27, 2022.
FROM GUT
‘Post-truth era’ hurts COVID-19 response, trust in science
Can you tell which of the following statements are true and which are false?
COVID-19 is not a threat to younger people, and only those who have other medical conditions are dying from it.
The mRNA vaccines developed to prevent the coronavirus alter your genes, can make your body “magnetic,” and are killing more people than the virus itself.
President Joe Biden’s climate change plan calls for a ban on meat consumption to cut greenhouse gas emissions.
The 2020 presidential election was rigged and stolen.
If you guessed that all of these claims are false, you’re right – take a bow. Not a single one of these statements has any factual support, according to scientific research, legal rulings, and legitimate government authorities.
And yet public opinion surveys show millions of Americans, and others around the world, believe some of these falsehoods are true and can’t be convinced otherwise.
Social media, politicians and partisan websites, TV programs, and commentators have widely circulated these and other unfounded claims so frequently that many people say they simply can’t tell what’s objectively true and not anymore.
So much so,
The new study – The Rise and Fall of Rationality in Language, published in the Proceedings of the National Academy of Sciences – found that facts have become less important in public discourse.
As a result, unsupported beliefs have taken precedent over readily identifiable truths in discussions of health, science, and politics. The upshot: “Feelings trump facts” in social media, news reports, books, and other sources of information.
And here’s the kicker: The trend did not begin with the rise of former President Donald Trump, the COVID-19 pandemic, or the advent of social media; in fact, it has been growing for much longer than you might think.
“While the current ‘post-truth era’ has taken many by surprise, the study shows that over the past 40 years, public interest has undergone an accelerating shift from the collective to the individual, and from rationality towards emotion,” concluded the researchers from Indiana University and Wageningen University & Research in the Netherlands.
“Our work suggests that the societal balance between emotion and reason has shifted back to what it used to be around 150 years ago,” says lead researcher Marten Scheffer, PhD, a professor in the department of environmental sciences at WUR. “This implies that scientists, experts, and policymakers will have to think about the best way to respond to that social change.”
Researchers surprised by findings
The findings are based on a very detailed analysis of language from millions of books, newspaper articles, Google searches, TV reports, social media posts, and other sources dating back to 1850.
The researchers analyzed how often the 5,000 most used words appeared over the past 170 years and found that the use of those having to do with facts and reasoning, such as “determine” and “conclusion,” has fallen dramatically since 1980. Meanwhile, the use of words related to human emotion, such as “feel” and “believe,” have skyrocketed.
Dr. Scheffer notes rapid developments in science and technology from 1850 to 1980 had profound social and economic benefits that helped boost the status of the scientific approach. That shift in public attitudes had ripple effects on culture, society, education, politics, and religion – and “the role of spiritualism dwindled” in the modern world, he says.
But since 1980, that trend has seen a major reversal, with beliefs becoming more important than facts to many people, he says. At the same time, trust in science and scientists has fallen.
Dr. Scheffer says the researchers expected to find some evidence of a swing toward more belief-based sentiments during the Trump era but were surprised to discover how strong it is and that the trend has actually been a long time coming.
“The shift in interest from rational to intuitive/emotional is pretty obvious now in the post-truth political and social media discussion,” he says. “However, our work shows that it already started in the 1980s. For me personally, that went under the radar, except perhaps for the rise of alternative (to religion) forms of spirituality.
“We were especially struck by how strong the patterns are and how universal they appear across languages, nonfiction and fiction, and even in The New York Times.”
In the political world, the implications are significant enough – impacting policies and politicians on both sides of the aisle and across the globe. Just look at the deepening political divisions during the Trump presidency.
But for health and science, the spread of misinformation and falsehoods can be matters of life or death, as we have seen in the politically charged debates over how best to combat COVID-19 and global climate change.
“Our public debate seems increasingly driven by what people want to be true rather than what is actually true. As a scientist, that worries me,” says study co-author Johan Bollen, PhD, a professor of informatics at Indiana University.
“As a society, we are now faced with major collective problems that we need to approach from a pragmatic, rational, and objective perspective to be successful,” he says. “After all, global warming doesn’t care about whether you believe in it or not … but we will all suffer as a society if we fail to take adequate measures.”
For WUR co-researcher Ingrid van de Leemput, the trend isn’t merely academic; she’s seen it play out in her personal life.
“I do speak to people that, for instance, think the vaccines are poison,” she says. “I’m also on Twitter, and there, I’m every day surprised about how easily many people form their opinions, based on feelings, on what others say, or on some unfounded source.”
Public health experts say the embrace of personal beliefs over facts is one reason only 63% of Americans have been vaccinated against COVID-19. The result: millions of preventable infections among those who downplay the risks of the virus and reject the strong scientific evidence of vaccine safety and effectiveness.
“None of this really surprises me,” Johns Hopkins University social and behavioral scientist Rupali Limaye, PhD, says of the new study findings. Dr. Limaye coauthored a paper in 2016 in JAMA Pediatrics about how to talk to parents about vaccine hesitancy and the fact that we’re living in what they called “this post-truth era.”
Dr. Limaye says the trend has made it difficult for doctors, scientists, and health authorities to make fact-based arguments for COVID-19 vaccination, mask-wearing, social distancing, and other measures to control the virus.
“It’s been really hard being a scientist to hear people say, ‘Well, that’s not true’ when we say something very basic that I think all of us can agree on – like the grass is green,” she says. “To be honest, I worry that a lot of scientists are going to quit being in science because they’re exhausted.”
What’s driving the trend?
So, what’s behind the embrace of “alternative facts,” as former White House counselor Kellyanne Conway put it so brazenly in 2017, in defending the White House’s false claims that Trump’s inauguration crowd was the largest ever?
Dr. Scheffer and colleagues identified a handful of things that have encouraged the embrace of falsehoods over facts in recent years.
- The Internet: Its rise in the late 1980s, and its growing role as a primary source of news and information, has allowed more belief-based misinformation to flourish and spread like wildfire.
- Social media: The new study found the use of sentiment- and intuition-related words accelerated around 2007, along with a global surge in social media that catapulted Facebook, Twitter, and others into the mainstream, replacing more traditional fact-based media (i.e., newspapers and magazines).
- The 2007 financial crisis: The downturn in the global economy meant more people were dealing with job stress, investment losses, and other problems that fed the interest in belief-based, anti-establishment social media posts.
- Conspiracy theories: Falsehoods involving hidden political agendas, shadow “elites,” and wealthy people with dark motives tend to thrive during times of crisis and societal anxiety. “Conspiracy theories originate particularly in times of uncertainty and crisis and generally depict established institutions as hiding the truth and sustaining an unfair situation,” the researchers noted. “As a result, they may find fertile grounds on social media platforms promulgating a sense of unfairness, subsequently feeding anti-system sentiments.”
Dr. Scheffer says that growing political divisions during the Trump era have widened the fact-vs.-fiction divide. The ex-president voiced many anti-science views on global climate change, for instance, and spread so many falsehoods about COVID-19 and the 2020 election that Facebook, Twitter, and YouTube suspended his accounts.
Yet Trump remains a popular figure among Republicans, with most saying in a December poll they believe his baseless claims that the 2020 election was “rigged” and “stolen,” despite all credible, easily accessible evidence that it was secure, according to a recent poll by the University of Massachusetts at Amherst.
More than 60 courts have rejected Trump’s lawsuits seeking to overturn the election results. All 50 states, the District of Columbia, and both branches of Congress have certified the election results, giving Biden the White House. Even Trump’s own Justice Department confirmed that the 2020 election was free and fair.
Nevertheless, the University of Massachusetts survey found that most Republicans believe one or more conspiracy theories floated by the former president and those pushing his “big lie” that Democrats rigged the election to elect Biden.
Ed Berliner, an Emmy Award-winning broadcast journalist and media consultant, suggests something else is driving the spread of misinformation: the pursuit of ratings by cable TV and media companies to boost ad and subscriber revenues.
As a former executive producer and syndicated cable TV show host, he says he has seen firsthand how facts are often lost in opinion-driven news programs, even on network programs claiming to offer “fair and balanced” journalism.
“Propaganda is the new currency in America, and those who do not fight back against it are doomed to be overrun by the misinformation,” says Mr. Berliner, host of The Man in the Arena and CEO of Entourage Media LLC.
“The broadcast news media has to stop this incessant ‘infotainment’ prattle, stop trying to nuzzle up to a soft side, and bear down on hard facts, exposing the lies and refusing to back down.”
Public health implications
Public health and media experts alike say the PNAS study findings are disheartening but underscore the need for doctors and scientists to do a better job of communicating about COVID-19 and other pressing issues.
Dr. Limaye, from Johns Hopkins, is particularly concerned about the rise in conspiracy theories that has led to COVID-19 vaccine hesitancy.
“When we speak to individuals about getting the COVID vaccine…the types of concerns that come up now are very different than they were 8 years ago,” she says. “The comments we used to hear were much more related to vaccine safety. [People] would say, ‘I’m worried about an ingredient in the vaccine’ or ‘I’m worried that my kiddo has to get three different shots within 6 months to have a series dose completed.’”
But now, a lot of comments they receive are about government and pharma conspiracies.
What that means is doctors and scientists must do more than simply say “here are the facts” and “trust me, I’m a doctor or a scientist,” she says. And these approaches don’t only apply to public health.
“It’s funny, because when we talk to climate change scientists, as vaccine [specialists], we’ll say we can’t believe that people think COVID is a hoax,” she says. “And they’re like, ‘Hold my beer, we’ve been dealing with this for 20 years. Hello, it’s just your guys’ turn to deal with this public denial of science.’”
Dr. Limaye is also concerned about the impacts on funding for scientific research.
“There’s always been a really strong bipartisan effort with regards to funding for science, when you look at Congress and when you look at appropriations,” she says. “But what ended up happening, especially with the Trump administration, was that there was a real shift in that. We’ve never really seen that before in past generations.”
So, what’s the big take-home message?
Dr. Limaye believes doctors and public health experts must show more empathy – and not be combative or arrogant – in communicating science in one-on-one conversations. This month, she’s launching a new course for parents, school administrators, and nurses on how to do precisely that.
“It’s really all about how to have hard conversations with people who might be anti-science,” she says. “It’s being empathetic and not being dismissive. But it’s hard work, and I think a lot of people are just not cut out for it and just don’t have the time for it…You can’t just say, ‘Well, this is science, and I’m a doctor’ – that doesn’t work anymore.”
Brendan Nyhan, PhD, a Dartmouth College political scientist, echoes those sentiments in a separate paper recently published in the Proceedings of the National Academy of Sciences. In fact, he suggests that providing accurate, fact-based information to counter false claims may actually backfire and reinforce some people’s unfounded beliefs.
“One response to the prevalence of mistaken beliefs is to try to set the record straight by providing accurate information – for instance, by providing evidence of the scientific consensus on climate change,” he writes. “The failures of this approach, which is sometimes referred to as the ‘deficit model’ in science communication, are well-known.”
Dr. Nyhan argues two things make some people more prone to believe falsehoods:
What scientists call “ingrouping,” a kind of tribal mentality that makes some people choose social identity or politics over truth-seeking and demonize others who don’t agree with their views
The rise of high-profile political figures, such as Trump, who encourage their followers to indulge in their desire for “identify-affirming misinformation”
Dr. Scheffer says the most important thing for doctors, health experts, and scientists to recognize is that it’s crucial to gain the trust of someone who may believe fictions over facts to make any persuasive argument on COVID-19 or any other issue.
He also has a standard response to those who present falsehoods to him as facts that he suggests anyone can use: “That is interesting. Would you mind helping me understand how you came to that opinion?”
A version of this article first appeared on WebMD.com.
Can you tell which of the following statements are true and which are false?
COVID-19 is not a threat to younger people, and only those who have other medical conditions are dying from it.
The mRNA vaccines developed to prevent the coronavirus alter your genes, can make your body “magnetic,” and are killing more people than the virus itself.
President Joe Biden’s climate change plan calls for a ban on meat consumption to cut greenhouse gas emissions.
The 2020 presidential election was rigged and stolen.
If you guessed that all of these claims are false, you’re right – take a bow. Not a single one of these statements has any factual support, according to scientific research, legal rulings, and legitimate government authorities.
And yet public opinion surveys show millions of Americans, and others around the world, believe some of these falsehoods are true and can’t be convinced otherwise.
Social media, politicians and partisan websites, TV programs, and commentators have widely circulated these and other unfounded claims so frequently that many people say they simply can’t tell what’s objectively true and not anymore.
So much so,
The new study – The Rise and Fall of Rationality in Language, published in the Proceedings of the National Academy of Sciences – found that facts have become less important in public discourse.
As a result, unsupported beliefs have taken precedent over readily identifiable truths in discussions of health, science, and politics. The upshot: “Feelings trump facts” in social media, news reports, books, and other sources of information.
And here’s the kicker: The trend did not begin with the rise of former President Donald Trump, the COVID-19 pandemic, or the advent of social media; in fact, it has been growing for much longer than you might think.
“While the current ‘post-truth era’ has taken many by surprise, the study shows that over the past 40 years, public interest has undergone an accelerating shift from the collective to the individual, and from rationality towards emotion,” concluded the researchers from Indiana University and Wageningen University & Research in the Netherlands.
“Our work suggests that the societal balance between emotion and reason has shifted back to what it used to be around 150 years ago,” says lead researcher Marten Scheffer, PhD, a professor in the department of environmental sciences at WUR. “This implies that scientists, experts, and policymakers will have to think about the best way to respond to that social change.”
Researchers surprised by findings
The findings are based on a very detailed analysis of language from millions of books, newspaper articles, Google searches, TV reports, social media posts, and other sources dating back to 1850.
The researchers analyzed how often the 5,000 most used words appeared over the past 170 years and found that the use of those having to do with facts and reasoning, such as “determine” and “conclusion,” has fallen dramatically since 1980. Meanwhile, the use of words related to human emotion, such as “feel” and “believe,” have skyrocketed.
Dr. Scheffer notes rapid developments in science and technology from 1850 to 1980 had profound social and economic benefits that helped boost the status of the scientific approach. That shift in public attitudes had ripple effects on culture, society, education, politics, and religion – and “the role of spiritualism dwindled” in the modern world, he says.
But since 1980, that trend has seen a major reversal, with beliefs becoming more important than facts to many people, he says. At the same time, trust in science and scientists has fallen.
Dr. Scheffer says the researchers expected to find some evidence of a swing toward more belief-based sentiments during the Trump era but were surprised to discover how strong it is and that the trend has actually been a long time coming.
“The shift in interest from rational to intuitive/emotional is pretty obvious now in the post-truth political and social media discussion,” he says. “However, our work shows that it already started in the 1980s. For me personally, that went under the radar, except perhaps for the rise of alternative (to religion) forms of spirituality.
“We were especially struck by how strong the patterns are and how universal they appear across languages, nonfiction and fiction, and even in The New York Times.”
In the political world, the implications are significant enough – impacting policies and politicians on both sides of the aisle and across the globe. Just look at the deepening political divisions during the Trump presidency.
But for health and science, the spread of misinformation and falsehoods can be matters of life or death, as we have seen in the politically charged debates over how best to combat COVID-19 and global climate change.
“Our public debate seems increasingly driven by what people want to be true rather than what is actually true. As a scientist, that worries me,” says study co-author Johan Bollen, PhD, a professor of informatics at Indiana University.
“As a society, we are now faced with major collective problems that we need to approach from a pragmatic, rational, and objective perspective to be successful,” he says. “After all, global warming doesn’t care about whether you believe in it or not … but we will all suffer as a society if we fail to take adequate measures.”
For WUR co-researcher Ingrid van de Leemput, the trend isn’t merely academic; she’s seen it play out in her personal life.
“I do speak to people that, for instance, think the vaccines are poison,” she says. “I’m also on Twitter, and there, I’m every day surprised about how easily many people form their opinions, based on feelings, on what others say, or on some unfounded source.”
Public health experts say the embrace of personal beliefs over facts is one reason only 63% of Americans have been vaccinated against COVID-19. The result: millions of preventable infections among those who downplay the risks of the virus and reject the strong scientific evidence of vaccine safety and effectiveness.
“None of this really surprises me,” Johns Hopkins University social and behavioral scientist Rupali Limaye, PhD, says of the new study findings. Dr. Limaye coauthored a paper in 2016 in JAMA Pediatrics about how to talk to parents about vaccine hesitancy and the fact that we’re living in what they called “this post-truth era.”
Dr. Limaye says the trend has made it difficult for doctors, scientists, and health authorities to make fact-based arguments for COVID-19 vaccination, mask-wearing, social distancing, and other measures to control the virus.
“It’s been really hard being a scientist to hear people say, ‘Well, that’s not true’ when we say something very basic that I think all of us can agree on – like the grass is green,” she says. “To be honest, I worry that a lot of scientists are going to quit being in science because they’re exhausted.”
What’s driving the trend?
So, what’s behind the embrace of “alternative facts,” as former White House counselor Kellyanne Conway put it so brazenly in 2017, in defending the White House’s false claims that Trump’s inauguration crowd was the largest ever?
Dr. Scheffer and colleagues identified a handful of things that have encouraged the embrace of falsehoods over facts in recent years.
- The Internet: Its rise in the late 1980s, and its growing role as a primary source of news and information, has allowed more belief-based misinformation to flourish and spread like wildfire.
- Social media: The new study found the use of sentiment- and intuition-related words accelerated around 2007, along with a global surge in social media that catapulted Facebook, Twitter, and others into the mainstream, replacing more traditional fact-based media (i.e., newspapers and magazines).
- The 2007 financial crisis: The downturn in the global economy meant more people were dealing with job stress, investment losses, and other problems that fed the interest in belief-based, anti-establishment social media posts.
- Conspiracy theories: Falsehoods involving hidden political agendas, shadow “elites,” and wealthy people with dark motives tend to thrive during times of crisis and societal anxiety. “Conspiracy theories originate particularly in times of uncertainty and crisis and generally depict established institutions as hiding the truth and sustaining an unfair situation,” the researchers noted. “As a result, they may find fertile grounds on social media platforms promulgating a sense of unfairness, subsequently feeding anti-system sentiments.”
Dr. Scheffer says that growing political divisions during the Trump era have widened the fact-vs.-fiction divide. The ex-president voiced many anti-science views on global climate change, for instance, and spread so many falsehoods about COVID-19 and the 2020 election that Facebook, Twitter, and YouTube suspended his accounts.
Yet Trump remains a popular figure among Republicans, with most saying in a December poll they believe his baseless claims that the 2020 election was “rigged” and “stolen,” despite all credible, easily accessible evidence that it was secure, according to a recent poll by the University of Massachusetts at Amherst.
More than 60 courts have rejected Trump’s lawsuits seeking to overturn the election results. All 50 states, the District of Columbia, and both branches of Congress have certified the election results, giving Biden the White House. Even Trump’s own Justice Department confirmed that the 2020 election was free and fair.
Nevertheless, the University of Massachusetts survey found that most Republicans believe one or more conspiracy theories floated by the former president and those pushing his “big lie” that Democrats rigged the election to elect Biden.
Ed Berliner, an Emmy Award-winning broadcast journalist and media consultant, suggests something else is driving the spread of misinformation: the pursuit of ratings by cable TV and media companies to boost ad and subscriber revenues.
As a former executive producer and syndicated cable TV show host, he says he has seen firsthand how facts are often lost in opinion-driven news programs, even on network programs claiming to offer “fair and balanced” journalism.
“Propaganda is the new currency in America, and those who do not fight back against it are doomed to be overrun by the misinformation,” says Mr. Berliner, host of The Man in the Arena and CEO of Entourage Media LLC.
“The broadcast news media has to stop this incessant ‘infotainment’ prattle, stop trying to nuzzle up to a soft side, and bear down on hard facts, exposing the lies and refusing to back down.”
Public health implications
Public health and media experts alike say the PNAS study findings are disheartening but underscore the need for doctors and scientists to do a better job of communicating about COVID-19 and other pressing issues.
Dr. Limaye, from Johns Hopkins, is particularly concerned about the rise in conspiracy theories that has led to COVID-19 vaccine hesitancy.
“When we speak to individuals about getting the COVID vaccine…the types of concerns that come up now are very different than they were 8 years ago,” she says. “The comments we used to hear were much more related to vaccine safety. [People] would say, ‘I’m worried about an ingredient in the vaccine’ or ‘I’m worried that my kiddo has to get three different shots within 6 months to have a series dose completed.’”
But now, a lot of comments they receive are about government and pharma conspiracies.
What that means is doctors and scientists must do more than simply say “here are the facts” and “trust me, I’m a doctor or a scientist,” she says. And these approaches don’t only apply to public health.
“It’s funny, because when we talk to climate change scientists, as vaccine [specialists], we’ll say we can’t believe that people think COVID is a hoax,” she says. “And they’re like, ‘Hold my beer, we’ve been dealing with this for 20 years. Hello, it’s just your guys’ turn to deal with this public denial of science.’”
Dr. Limaye is also concerned about the impacts on funding for scientific research.
“There’s always been a really strong bipartisan effort with regards to funding for science, when you look at Congress and when you look at appropriations,” she says. “But what ended up happening, especially with the Trump administration, was that there was a real shift in that. We’ve never really seen that before in past generations.”
So, what’s the big take-home message?
Dr. Limaye believes doctors and public health experts must show more empathy – and not be combative or arrogant – in communicating science in one-on-one conversations. This month, she’s launching a new course for parents, school administrators, and nurses on how to do precisely that.
“It’s really all about how to have hard conversations with people who might be anti-science,” she says. “It’s being empathetic and not being dismissive. But it’s hard work, and I think a lot of people are just not cut out for it and just don’t have the time for it…You can’t just say, ‘Well, this is science, and I’m a doctor’ – that doesn’t work anymore.”
Brendan Nyhan, PhD, a Dartmouth College political scientist, echoes those sentiments in a separate paper recently published in the Proceedings of the National Academy of Sciences. In fact, he suggests that providing accurate, fact-based information to counter false claims may actually backfire and reinforce some people’s unfounded beliefs.
“One response to the prevalence of mistaken beliefs is to try to set the record straight by providing accurate information – for instance, by providing evidence of the scientific consensus on climate change,” he writes. “The failures of this approach, which is sometimes referred to as the ‘deficit model’ in science communication, are well-known.”
Dr. Nyhan argues two things make some people more prone to believe falsehoods:
What scientists call “ingrouping,” a kind of tribal mentality that makes some people choose social identity or politics over truth-seeking and demonize others who don’t agree with their views
The rise of high-profile political figures, such as Trump, who encourage their followers to indulge in their desire for “identify-affirming misinformation”
Dr. Scheffer says the most important thing for doctors, health experts, and scientists to recognize is that it’s crucial to gain the trust of someone who may believe fictions over facts to make any persuasive argument on COVID-19 or any other issue.
He also has a standard response to those who present falsehoods to him as facts that he suggests anyone can use: “That is interesting. Would you mind helping me understand how you came to that opinion?”
A version of this article first appeared on WebMD.com.
Can you tell which of the following statements are true and which are false?
COVID-19 is not a threat to younger people, and only those who have other medical conditions are dying from it.
The mRNA vaccines developed to prevent the coronavirus alter your genes, can make your body “magnetic,” and are killing more people than the virus itself.
President Joe Biden’s climate change plan calls for a ban on meat consumption to cut greenhouse gas emissions.
The 2020 presidential election was rigged and stolen.
If you guessed that all of these claims are false, you’re right – take a bow. Not a single one of these statements has any factual support, according to scientific research, legal rulings, and legitimate government authorities.
And yet public opinion surveys show millions of Americans, and others around the world, believe some of these falsehoods are true and can’t be convinced otherwise.
Social media, politicians and partisan websites, TV programs, and commentators have widely circulated these and other unfounded claims so frequently that many people say they simply can’t tell what’s objectively true and not anymore.
So much so,
The new study – The Rise and Fall of Rationality in Language, published in the Proceedings of the National Academy of Sciences – found that facts have become less important in public discourse.
As a result, unsupported beliefs have taken precedent over readily identifiable truths in discussions of health, science, and politics. The upshot: “Feelings trump facts” in social media, news reports, books, and other sources of information.
And here’s the kicker: The trend did not begin with the rise of former President Donald Trump, the COVID-19 pandemic, or the advent of social media; in fact, it has been growing for much longer than you might think.
“While the current ‘post-truth era’ has taken many by surprise, the study shows that over the past 40 years, public interest has undergone an accelerating shift from the collective to the individual, and from rationality towards emotion,” concluded the researchers from Indiana University and Wageningen University & Research in the Netherlands.
“Our work suggests that the societal balance between emotion and reason has shifted back to what it used to be around 150 years ago,” says lead researcher Marten Scheffer, PhD, a professor in the department of environmental sciences at WUR. “This implies that scientists, experts, and policymakers will have to think about the best way to respond to that social change.”
Researchers surprised by findings
The findings are based on a very detailed analysis of language from millions of books, newspaper articles, Google searches, TV reports, social media posts, and other sources dating back to 1850.
The researchers analyzed how often the 5,000 most used words appeared over the past 170 years and found that the use of those having to do with facts and reasoning, such as “determine” and “conclusion,” has fallen dramatically since 1980. Meanwhile, the use of words related to human emotion, such as “feel” and “believe,” have skyrocketed.
Dr. Scheffer notes rapid developments in science and technology from 1850 to 1980 had profound social and economic benefits that helped boost the status of the scientific approach. That shift in public attitudes had ripple effects on culture, society, education, politics, and religion – and “the role of spiritualism dwindled” in the modern world, he says.
But since 1980, that trend has seen a major reversal, with beliefs becoming more important than facts to many people, he says. At the same time, trust in science and scientists has fallen.
Dr. Scheffer says the researchers expected to find some evidence of a swing toward more belief-based sentiments during the Trump era but were surprised to discover how strong it is and that the trend has actually been a long time coming.
“The shift in interest from rational to intuitive/emotional is pretty obvious now in the post-truth political and social media discussion,” he says. “However, our work shows that it already started in the 1980s. For me personally, that went under the radar, except perhaps for the rise of alternative (to religion) forms of spirituality.
“We were especially struck by how strong the patterns are and how universal they appear across languages, nonfiction and fiction, and even in The New York Times.”
In the political world, the implications are significant enough – impacting policies and politicians on both sides of the aisle and across the globe. Just look at the deepening political divisions during the Trump presidency.
But for health and science, the spread of misinformation and falsehoods can be matters of life or death, as we have seen in the politically charged debates over how best to combat COVID-19 and global climate change.
“Our public debate seems increasingly driven by what people want to be true rather than what is actually true. As a scientist, that worries me,” says study co-author Johan Bollen, PhD, a professor of informatics at Indiana University.
“As a society, we are now faced with major collective problems that we need to approach from a pragmatic, rational, and objective perspective to be successful,” he says. “After all, global warming doesn’t care about whether you believe in it or not … but we will all suffer as a society if we fail to take adequate measures.”
For WUR co-researcher Ingrid van de Leemput, the trend isn’t merely academic; she’s seen it play out in her personal life.
“I do speak to people that, for instance, think the vaccines are poison,” she says. “I’m also on Twitter, and there, I’m every day surprised about how easily many people form their opinions, based on feelings, on what others say, or on some unfounded source.”
Public health experts say the embrace of personal beliefs over facts is one reason only 63% of Americans have been vaccinated against COVID-19. The result: millions of preventable infections among those who downplay the risks of the virus and reject the strong scientific evidence of vaccine safety and effectiveness.
“None of this really surprises me,” Johns Hopkins University social and behavioral scientist Rupali Limaye, PhD, says of the new study findings. Dr. Limaye coauthored a paper in 2016 in JAMA Pediatrics about how to talk to parents about vaccine hesitancy and the fact that we’re living in what they called “this post-truth era.”
Dr. Limaye says the trend has made it difficult for doctors, scientists, and health authorities to make fact-based arguments for COVID-19 vaccination, mask-wearing, social distancing, and other measures to control the virus.
“It’s been really hard being a scientist to hear people say, ‘Well, that’s not true’ when we say something very basic that I think all of us can agree on – like the grass is green,” she says. “To be honest, I worry that a lot of scientists are going to quit being in science because they’re exhausted.”
What’s driving the trend?
So, what’s behind the embrace of “alternative facts,” as former White House counselor Kellyanne Conway put it so brazenly in 2017, in defending the White House’s false claims that Trump’s inauguration crowd was the largest ever?
Dr. Scheffer and colleagues identified a handful of things that have encouraged the embrace of falsehoods over facts in recent years.
- The Internet: Its rise in the late 1980s, and its growing role as a primary source of news and information, has allowed more belief-based misinformation to flourish and spread like wildfire.
- Social media: The new study found the use of sentiment- and intuition-related words accelerated around 2007, along with a global surge in social media that catapulted Facebook, Twitter, and others into the mainstream, replacing more traditional fact-based media (i.e., newspapers and magazines).
- The 2007 financial crisis: The downturn in the global economy meant more people were dealing with job stress, investment losses, and other problems that fed the interest in belief-based, anti-establishment social media posts.
- Conspiracy theories: Falsehoods involving hidden political agendas, shadow “elites,” and wealthy people with dark motives tend to thrive during times of crisis and societal anxiety. “Conspiracy theories originate particularly in times of uncertainty and crisis and generally depict established institutions as hiding the truth and sustaining an unfair situation,” the researchers noted. “As a result, they may find fertile grounds on social media platforms promulgating a sense of unfairness, subsequently feeding anti-system sentiments.”
Dr. Scheffer says that growing political divisions during the Trump era have widened the fact-vs.-fiction divide. The ex-president voiced many anti-science views on global climate change, for instance, and spread so many falsehoods about COVID-19 and the 2020 election that Facebook, Twitter, and YouTube suspended his accounts.
Yet Trump remains a popular figure among Republicans, with most saying in a December poll they believe his baseless claims that the 2020 election was “rigged” and “stolen,” despite all credible, easily accessible evidence that it was secure, according to a recent poll by the University of Massachusetts at Amherst.
More than 60 courts have rejected Trump’s lawsuits seeking to overturn the election results. All 50 states, the District of Columbia, and both branches of Congress have certified the election results, giving Biden the White House. Even Trump’s own Justice Department confirmed that the 2020 election was free and fair.
Nevertheless, the University of Massachusetts survey found that most Republicans believe one or more conspiracy theories floated by the former president and those pushing his “big lie” that Democrats rigged the election to elect Biden.
Ed Berliner, an Emmy Award-winning broadcast journalist and media consultant, suggests something else is driving the spread of misinformation: the pursuit of ratings by cable TV and media companies to boost ad and subscriber revenues.
As a former executive producer and syndicated cable TV show host, he says he has seen firsthand how facts are often lost in opinion-driven news programs, even on network programs claiming to offer “fair and balanced” journalism.
“Propaganda is the new currency in America, and those who do not fight back against it are doomed to be overrun by the misinformation,” says Mr. Berliner, host of The Man in the Arena and CEO of Entourage Media LLC.
“The broadcast news media has to stop this incessant ‘infotainment’ prattle, stop trying to nuzzle up to a soft side, and bear down on hard facts, exposing the lies and refusing to back down.”
Public health implications
Public health and media experts alike say the PNAS study findings are disheartening but underscore the need for doctors and scientists to do a better job of communicating about COVID-19 and other pressing issues.
Dr. Limaye, from Johns Hopkins, is particularly concerned about the rise in conspiracy theories that has led to COVID-19 vaccine hesitancy.
“When we speak to individuals about getting the COVID vaccine…the types of concerns that come up now are very different than they were 8 years ago,” she says. “The comments we used to hear were much more related to vaccine safety. [People] would say, ‘I’m worried about an ingredient in the vaccine’ or ‘I’m worried that my kiddo has to get three different shots within 6 months to have a series dose completed.’”
But now, a lot of comments they receive are about government and pharma conspiracies.
What that means is doctors and scientists must do more than simply say “here are the facts” and “trust me, I’m a doctor or a scientist,” she says. And these approaches don’t only apply to public health.
“It’s funny, because when we talk to climate change scientists, as vaccine [specialists], we’ll say we can’t believe that people think COVID is a hoax,” she says. “And they’re like, ‘Hold my beer, we’ve been dealing with this for 20 years. Hello, it’s just your guys’ turn to deal with this public denial of science.’”
Dr. Limaye is also concerned about the impacts on funding for scientific research.
“There’s always been a really strong bipartisan effort with regards to funding for science, when you look at Congress and when you look at appropriations,” she says. “But what ended up happening, especially with the Trump administration, was that there was a real shift in that. We’ve never really seen that before in past generations.”
So, what’s the big take-home message?
Dr. Limaye believes doctors and public health experts must show more empathy – and not be combative or arrogant – in communicating science in one-on-one conversations. This month, she’s launching a new course for parents, school administrators, and nurses on how to do precisely that.
“It’s really all about how to have hard conversations with people who might be anti-science,” she says. “It’s being empathetic and not being dismissive. But it’s hard work, and I think a lot of people are just not cut out for it and just don’t have the time for it…You can’t just say, ‘Well, this is science, and I’m a doctor’ – that doesn’t work anymore.”
Brendan Nyhan, PhD, a Dartmouth College political scientist, echoes those sentiments in a separate paper recently published in the Proceedings of the National Academy of Sciences. In fact, he suggests that providing accurate, fact-based information to counter false claims may actually backfire and reinforce some people’s unfounded beliefs.
“One response to the prevalence of mistaken beliefs is to try to set the record straight by providing accurate information – for instance, by providing evidence of the scientific consensus on climate change,” he writes. “The failures of this approach, which is sometimes referred to as the ‘deficit model’ in science communication, are well-known.”
Dr. Nyhan argues two things make some people more prone to believe falsehoods:
What scientists call “ingrouping,” a kind of tribal mentality that makes some people choose social identity or politics over truth-seeking and demonize others who don’t agree with their views
The rise of high-profile political figures, such as Trump, who encourage their followers to indulge in their desire for “identify-affirming misinformation”
Dr. Scheffer says the most important thing for doctors, health experts, and scientists to recognize is that it’s crucial to gain the trust of someone who may believe fictions over facts to make any persuasive argument on COVID-19 or any other issue.
He also has a standard response to those who present falsehoods to him as facts that he suggests anyone can use: “That is interesting. Would you mind helping me understand how you came to that opinion?”
A version of this article first appeared on WebMD.com.
Physician burnout, depression compounded by COVID: Survey
In 2020, it was hard to imagine that the situation could get worse for doctors.
But 2021 presented a new set of challenges. As quarantines lifted and physicians tried to get back to work, they were forced to deal with reduced staff, continuing COVID stress, and pandemic-related anxieties about family and loved ones.
Medscape’s National Burnout and Depression Report 2022 asked more than 13,000 physicians from 29 specialties to share details about their lives and struggles with burnout and depression in 2021. The results paint a picture of physicians trying to fulfill their mission to care for patients, but struggling to maintain their own well-being amid a global pandemic.
Burnout bump
In 2021’s report, 42% of physicians said they were burned out. In 2022, that number increased to 47%. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, increasing from 43% to 60%. Critical care (56%), ob.gyn. (53%), and infectious disease and family medicine (both at 51%) rounded out the top five specialties with doctors experiencing burnout in 2021.
Burnout has typically been a greater problem for women than men physicians, and the pandemic hasn’t changed that. “There’s no question that women have reported far more role strain during the pandemic than men,” says Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at the Albert Einstein College of Medicine, both in New York. And indeed, 56% of women and 41% of men reported burnout in the 2022 survey.
The causes, however, weren’t especially pandemic related – or at least not directly. As in previous surveys, the major contributing factor to burnout was too much paperwork (60%), such as charting and other bureaucratic tasks. Treating COVID-19 patients was cited as the major source of stress by 10% of respondents. About 34% said too many hours at work was the biggest contributing factor to burnout.
The nature of the beast
What is burnout like for these doctors? One described the conditions that lead to burnout like this: “I barely spend enough time with most patients, just running from one to the next; and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk.” Another said: “Where’s the relationships with patients that used to make this worthwhile?” Others fingered staffing shortages at work or an overwhelming home life: “Staff calls in sick; we’re all running around trying to find things and get things done. It never ends.”
Of those who do experience burnout, the problem reaches beyond the workplace, with 54% saying that their burnout has a strong/severe impact on life and 68% reporting that burnout affects their relationships. One respondent said: “I’m always tired; I have trouble concentrating, no time for the children, more arguments with my hubby.” Another put it this way: “Home is just as busy and chaotic as work. I can never relax.”
It doesn’t help matters that physicians are likely to think they’re the only professionals experiencing job burnout. For example, only 36% of respondents believe teachers experience comparable burnout, yet more than 41% of teachers leave the profession within 5 years of starting – often because of burnout.
When it comes to methods for coping with burnout, exercise is the clear favorite, with 63% of respondents saying exercise helps maintain their mental health. About 41% talk with family members or close friends. However, less healthy coping mechanisms were cited as well, such as isolating themselves from others (45%), sleeping (41%), and eating junk food (35%) or drinking alcohol (24%).
When it comes to trying to alleviate burnout, 29% have tried meditation or similar stress-reduction techniques, while others have reduced their work hours (29%) or changed their work settings (19%).
‘Now I feel like there’s no hope’
About a fifth of physicians (21%) said they suffered from clinical depression, and 64% reported feeling “blue, down, or sad.” One physician characterized their depression this way: “I used to think my life would be great. Now I feel like there’s no hope, this will never get better, I’ll never be happy.”
Of doctors reporting depression, 53% said their illness did not affect their interactions with patients, while 34% said depression caused them to be more easily exasperated by patients.
When asked about seeking help for depression, about half (49%) said they believed they could deal with emotional stress on their own. Unfortunately, fear of medical boards finding out keeps 43% of physicians from reaching out for help, according to the survey.
A version of this article first appeared on Medscape.com.
In 2020, it was hard to imagine that the situation could get worse for doctors.
But 2021 presented a new set of challenges. As quarantines lifted and physicians tried to get back to work, they were forced to deal with reduced staff, continuing COVID stress, and pandemic-related anxieties about family and loved ones.
Medscape’s National Burnout and Depression Report 2022 asked more than 13,000 physicians from 29 specialties to share details about their lives and struggles with burnout and depression in 2021. The results paint a picture of physicians trying to fulfill their mission to care for patients, but struggling to maintain their own well-being amid a global pandemic.
Burnout bump
In 2021’s report, 42% of physicians said they were burned out. In 2022, that number increased to 47%. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, increasing from 43% to 60%. Critical care (56%), ob.gyn. (53%), and infectious disease and family medicine (both at 51%) rounded out the top five specialties with doctors experiencing burnout in 2021.
Burnout has typically been a greater problem for women than men physicians, and the pandemic hasn’t changed that. “There’s no question that women have reported far more role strain during the pandemic than men,” says Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at the Albert Einstein College of Medicine, both in New York. And indeed, 56% of women and 41% of men reported burnout in the 2022 survey.
The causes, however, weren’t especially pandemic related – or at least not directly. As in previous surveys, the major contributing factor to burnout was too much paperwork (60%), such as charting and other bureaucratic tasks. Treating COVID-19 patients was cited as the major source of stress by 10% of respondents. About 34% said too many hours at work was the biggest contributing factor to burnout.
The nature of the beast
What is burnout like for these doctors? One described the conditions that lead to burnout like this: “I barely spend enough time with most patients, just running from one to the next; and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk.” Another said: “Where’s the relationships with patients that used to make this worthwhile?” Others fingered staffing shortages at work or an overwhelming home life: “Staff calls in sick; we’re all running around trying to find things and get things done. It never ends.”
Of those who do experience burnout, the problem reaches beyond the workplace, with 54% saying that their burnout has a strong/severe impact on life and 68% reporting that burnout affects their relationships. One respondent said: “I’m always tired; I have trouble concentrating, no time for the children, more arguments with my hubby.” Another put it this way: “Home is just as busy and chaotic as work. I can never relax.”
It doesn’t help matters that physicians are likely to think they’re the only professionals experiencing job burnout. For example, only 36% of respondents believe teachers experience comparable burnout, yet more than 41% of teachers leave the profession within 5 years of starting – often because of burnout.
When it comes to methods for coping with burnout, exercise is the clear favorite, with 63% of respondents saying exercise helps maintain their mental health. About 41% talk with family members or close friends. However, less healthy coping mechanisms were cited as well, such as isolating themselves from others (45%), sleeping (41%), and eating junk food (35%) or drinking alcohol (24%).
When it comes to trying to alleviate burnout, 29% have tried meditation or similar stress-reduction techniques, while others have reduced their work hours (29%) or changed their work settings (19%).
‘Now I feel like there’s no hope’
About a fifth of physicians (21%) said they suffered from clinical depression, and 64% reported feeling “blue, down, or sad.” One physician characterized their depression this way: “I used to think my life would be great. Now I feel like there’s no hope, this will never get better, I’ll never be happy.”
Of doctors reporting depression, 53% said their illness did not affect their interactions with patients, while 34% said depression caused them to be more easily exasperated by patients.
When asked about seeking help for depression, about half (49%) said they believed they could deal with emotional stress on their own. Unfortunately, fear of medical boards finding out keeps 43% of physicians from reaching out for help, according to the survey.
A version of this article first appeared on Medscape.com.
In 2020, it was hard to imagine that the situation could get worse for doctors.
But 2021 presented a new set of challenges. As quarantines lifted and physicians tried to get back to work, they were forced to deal with reduced staff, continuing COVID stress, and pandemic-related anxieties about family and loved ones.
Medscape’s National Burnout and Depression Report 2022 asked more than 13,000 physicians from 29 specialties to share details about their lives and struggles with burnout and depression in 2021. The results paint a picture of physicians trying to fulfill their mission to care for patients, but struggling to maintain their own well-being amid a global pandemic.
Burnout bump
In 2021’s report, 42% of physicians said they were burned out. In 2022, that number increased to 47%. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, increasing from 43% to 60%. Critical care (56%), ob.gyn. (53%), and infectious disease and family medicine (both at 51%) rounded out the top five specialties with doctors experiencing burnout in 2021.
Burnout has typically been a greater problem for women than men physicians, and the pandemic hasn’t changed that. “There’s no question that women have reported far more role strain during the pandemic than men,” says Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at the Albert Einstein College of Medicine, both in New York. And indeed, 56% of women and 41% of men reported burnout in the 2022 survey.
The causes, however, weren’t especially pandemic related – or at least not directly. As in previous surveys, the major contributing factor to burnout was too much paperwork (60%), such as charting and other bureaucratic tasks. Treating COVID-19 patients was cited as the major source of stress by 10% of respondents. About 34% said too many hours at work was the biggest contributing factor to burnout.
The nature of the beast
What is burnout like for these doctors? One described the conditions that lead to burnout like this: “I barely spend enough time with most patients, just running from one to the next; and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk.” Another said: “Where’s the relationships with patients that used to make this worthwhile?” Others fingered staffing shortages at work or an overwhelming home life: “Staff calls in sick; we’re all running around trying to find things and get things done. It never ends.”
Of those who do experience burnout, the problem reaches beyond the workplace, with 54% saying that their burnout has a strong/severe impact on life and 68% reporting that burnout affects their relationships. One respondent said: “I’m always tired; I have trouble concentrating, no time for the children, more arguments with my hubby.” Another put it this way: “Home is just as busy and chaotic as work. I can never relax.”
It doesn’t help matters that physicians are likely to think they’re the only professionals experiencing job burnout. For example, only 36% of respondents believe teachers experience comparable burnout, yet more than 41% of teachers leave the profession within 5 years of starting – often because of burnout.
When it comes to methods for coping with burnout, exercise is the clear favorite, with 63% of respondents saying exercise helps maintain their mental health. About 41% talk with family members or close friends. However, less healthy coping mechanisms were cited as well, such as isolating themselves from others (45%), sleeping (41%), and eating junk food (35%) or drinking alcohol (24%).
When it comes to trying to alleviate burnout, 29% have tried meditation or similar stress-reduction techniques, while others have reduced their work hours (29%) or changed their work settings (19%).
‘Now I feel like there’s no hope’
About a fifth of physicians (21%) said they suffered from clinical depression, and 64% reported feeling “blue, down, or sad.” One physician characterized their depression this way: “I used to think my life would be great. Now I feel like there’s no hope, this will never get better, I’ll never be happy.”
Of doctors reporting depression, 53% said their illness did not affect their interactions with patients, while 34% said depression caused them to be more easily exasperated by patients.
When asked about seeking help for depression, about half (49%) said they believed they could deal with emotional stress on their own. Unfortunately, fear of medical boards finding out keeps 43% of physicians from reaching out for help, according to the survey.
A version of this article first appeared on Medscape.com.
Expert views diverge on adding chemotherapy to EGFR TKIs in EGFR-mutant NSCLC
One affirms single-agent EGFR TKI treatment, such as with osimertinib, as the current standard of care for first-line advanced metastatic EGFR-positive mNSCLC, and the other affirms clear benefits for first-generation EGFR TKIs combined with either chemotherapy or VEGF monoclonal antibodies.
In the analysis supporting combination therapy for mNSCLC, Sara Moore, MD, and Paul Wheatley-Price MD, wrote that while targeted therapy with EGFR TKIs is highly effective initially, resistance inevitably develops.
Recent data, they stated, have demonstrated that combination strategies can delay development of resistance and improve outcomes for mNSCLC populations. Combining first-generation EGFR TKIs with either chemotherapy or VEGF monoclonal antibodies has led to consistent improvement in progression-free survival (PFS) and overall survival (OS) in some cases. In the NEJ009 trial, the combination of chemotherapy (carboplatin and pemetrexed, with pemetrexed maintenance) plus gefitinib versus gefitinib alone improved response rate (84% vs. 67%, P < 0.001), PFS (median, 20.9 months vs. 11.2 months; P < .001), and OS (median, 50.9 months vs. 38.8 months; P = .021). An increase in adverse events in the chemotherapy arm led to a decrease in quality of life.
Another clinical trial (by Noronha and colleagues) conducted in India of the same combination found benefit for combination therapy in response rate (75% vs. 63%), PFS (median, 16 months vs. 8 months), and OS (not reached vs. 17 months). Grade 3 or higher adverse event rates were higher with the combination (51% vs. 25%) with quality of life was not yet reported.
While both trials have been criticized owing to a lack of standard T790M resistance testing and low use of osimertinib in subsequent lines of therapy, Dr. Moore and Dr. Wheatley-Price pointed out: “Even with the use of first-line osimertinib monotherapy, patients may still be exposed to chemotherapy with later lines of treatment. Therefore, combination therapy does not expose patients to new toxicity, it simply changes when they will be exposed to that toxicity during their treatment course.”
The importance of using combination therapy in the first-line setting, they stated, is underscored by the consistent drop-off in patients who receive second-line combination therapy. In the phase 3 FLAURA trial of first-line osimertinib monotherapy, of the patients who discontinued osimertinib, the most common reason for not receiving subsequent therapy was death (60% went on to receive further systemic therapy). This highlights the need to use the most effective treatments up front, Dr. Moore and Dr. Wheatley-Price wrote.
The four large trials of VEGF-targeted therapy with either monoclonal antibodies or TKIs added to first-generation EGFR TKIs have consistently shown improved PFS. Increased toxicities led to discontinuation of VEGF-targeted therapy in 20%-30%.
In the RELAY trial, however, despite more toxicities, quality of life was not diminished. In general, the authors concluded that long-term detriments to quality of life have not been demonstrated. Ongoing studies of osimertinib in combination with VEGF inhibition include a phase 1/2 trial with bevacizumab in previously untreated patients showing an 80% response rate (median PFS, 18.4 months) with no unexpected toxicity.
Chemotherapy-based treatment for mNSCLC with third-generation EGFR TKIs, in appropriately selected patients, the authors concluded, “can offer an additional standard-of-care option as first-line treatment of EGFR-mutant lung cancer.”
Since the introduction of EGFR TKIs, Sophie Stock-Martineau, MD and Frances A. Shepherd, MD noted in their analysis, researchers have aimed to improve their efficacy through combining them with other agents. The authors review research on the addition of chemo- or immunotherapy and agents targeting major resistance mechanisms such as MET. Their review of the same NEJ009 trial focuses, however, on the 65.3% (EGFR TKI plus chemotherapy) versus 31.0% (gefitinib alone) grade 3 adverse event rate, and the 51% versus 25% grade 3 adverse event rate in a similar trial by Noronha and colleagues. The review by Dr. Stock-Martineau and Dr. Shepherd further found that, while adding antiangiogenic agents to an EGFR TKI “mildly” prolongs PFS, survival benefits have not been demonstrated. The added costs, not just in toxicity, were a “far from negligible” $120,000 above the cost of bevacizumab alone for 16 treatments. Data from trials of immune checkpoint inhibitors added to EGFR TKIs reveal heightened toxicities and limited efficacy. Trials of EGFR monoclonal antibodies with an EGFR TKI showed no PFS or OS benefit and were terminated early. Similarly, evidence to date shows no benefit beyond that shown for EGFR TKI monotherapy with the addition of a MET inhibitor.
“Adding virtually all agents to EGFR TKIs has been associated with more toxicity to patients and a significant financial burden to the health care system,” Dr. Stock-Martineau and Dr. Shepherd concluded, further observing that combinations, given their heightened toxicity profiles, could potentially also worsen quality of life.
No conflicts of interest were reported by the authors of either study.
One affirms single-agent EGFR TKI treatment, such as with osimertinib, as the current standard of care for first-line advanced metastatic EGFR-positive mNSCLC, and the other affirms clear benefits for first-generation EGFR TKIs combined with either chemotherapy or VEGF monoclonal antibodies.
In the analysis supporting combination therapy for mNSCLC, Sara Moore, MD, and Paul Wheatley-Price MD, wrote that while targeted therapy with EGFR TKIs is highly effective initially, resistance inevitably develops.
Recent data, they stated, have demonstrated that combination strategies can delay development of resistance and improve outcomes for mNSCLC populations. Combining first-generation EGFR TKIs with either chemotherapy or VEGF monoclonal antibodies has led to consistent improvement in progression-free survival (PFS) and overall survival (OS) in some cases. In the NEJ009 trial, the combination of chemotherapy (carboplatin and pemetrexed, with pemetrexed maintenance) plus gefitinib versus gefitinib alone improved response rate (84% vs. 67%, P < 0.001), PFS (median, 20.9 months vs. 11.2 months; P < .001), and OS (median, 50.9 months vs. 38.8 months; P = .021). An increase in adverse events in the chemotherapy arm led to a decrease in quality of life.
Another clinical trial (by Noronha and colleagues) conducted in India of the same combination found benefit for combination therapy in response rate (75% vs. 63%), PFS (median, 16 months vs. 8 months), and OS (not reached vs. 17 months). Grade 3 or higher adverse event rates were higher with the combination (51% vs. 25%) with quality of life was not yet reported.
While both trials have been criticized owing to a lack of standard T790M resistance testing and low use of osimertinib in subsequent lines of therapy, Dr. Moore and Dr. Wheatley-Price pointed out: “Even with the use of first-line osimertinib monotherapy, patients may still be exposed to chemotherapy with later lines of treatment. Therefore, combination therapy does not expose patients to new toxicity, it simply changes when they will be exposed to that toxicity during their treatment course.”
The importance of using combination therapy in the first-line setting, they stated, is underscored by the consistent drop-off in patients who receive second-line combination therapy. In the phase 3 FLAURA trial of first-line osimertinib monotherapy, of the patients who discontinued osimertinib, the most common reason for not receiving subsequent therapy was death (60% went on to receive further systemic therapy). This highlights the need to use the most effective treatments up front, Dr. Moore and Dr. Wheatley-Price wrote.
The four large trials of VEGF-targeted therapy with either monoclonal antibodies or TKIs added to first-generation EGFR TKIs have consistently shown improved PFS. Increased toxicities led to discontinuation of VEGF-targeted therapy in 20%-30%.
In the RELAY trial, however, despite more toxicities, quality of life was not diminished. In general, the authors concluded that long-term detriments to quality of life have not been demonstrated. Ongoing studies of osimertinib in combination with VEGF inhibition include a phase 1/2 trial with bevacizumab in previously untreated patients showing an 80% response rate (median PFS, 18.4 months) with no unexpected toxicity.
Chemotherapy-based treatment for mNSCLC with third-generation EGFR TKIs, in appropriately selected patients, the authors concluded, “can offer an additional standard-of-care option as first-line treatment of EGFR-mutant lung cancer.”
Since the introduction of EGFR TKIs, Sophie Stock-Martineau, MD and Frances A. Shepherd, MD noted in their analysis, researchers have aimed to improve their efficacy through combining them with other agents. The authors review research on the addition of chemo- or immunotherapy and agents targeting major resistance mechanisms such as MET. Their review of the same NEJ009 trial focuses, however, on the 65.3% (EGFR TKI plus chemotherapy) versus 31.0% (gefitinib alone) grade 3 adverse event rate, and the 51% versus 25% grade 3 adverse event rate in a similar trial by Noronha and colleagues. The review by Dr. Stock-Martineau and Dr. Shepherd further found that, while adding antiangiogenic agents to an EGFR TKI “mildly” prolongs PFS, survival benefits have not been demonstrated. The added costs, not just in toxicity, were a “far from negligible” $120,000 above the cost of bevacizumab alone for 16 treatments. Data from trials of immune checkpoint inhibitors added to EGFR TKIs reveal heightened toxicities and limited efficacy. Trials of EGFR monoclonal antibodies with an EGFR TKI showed no PFS or OS benefit and were terminated early. Similarly, evidence to date shows no benefit beyond that shown for EGFR TKI monotherapy with the addition of a MET inhibitor.
“Adding virtually all agents to EGFR TKIs has been associated with more toxicity to patients and a significant financial burden to the health care system,” Dr. Stock-Martineau and Dr. Shepherd concluded, further observing that combinations, given their heightened toxicity profiles, could potentially also worsen quality of life.
No conflicts of interest were reported by the authors of either study.
One affirms single-agent EGFR TKI treatment, such as with osimertinib, as the current standard of care for first-line advanced metastatic EGFR-positive mNSCLC, and the other affirms clear benefits for first-generation EGFR TKIs combined with either chemotherapy or VEGF monoclonal antibodies.
In the analysis supporting combination therapy for mNSCLC, Sara Moore, MD, and Paul Wheatley-Price MD, wrote that while targeted therapy with EGFR TKIs is highly effective initially, resistance inevitably develops.
Recent data, they stated, have demonstrated that combination strategies can delay development of resistance and improve outcomes for mNSCLC populations. Combining first-generation EGFR TKIs with either chemotherapy or VEGF monoclonal antibodies has led to consistent improvement in progression-free survival (PFS) and overall survival (OS) in some cases. In the NEJ009 trial, the combination of chemotherapy (carboplatin and pemetrexed, with pemetrexed maintenance) plus gefitinib versus gefitinib alone improved response rate (84% vs. 67%, P < 0.001), PFS (median, 20.9 months vs. 11.2 months; P < .001), and OS (median, 50.9 months vs. 38.8 months; P = .021). An increase in adverse events in the chemotherapy arm led to a decrease in quality of life.
Another clinical trial (by Noronha and colleagues) conducted in India of the same combination found benefit for combination therapy in response rate (75% vs. 63%), PFS (median, 16 months vs. 8 months), and OS (not reached vs. 17 months). Grade 3 or higher adverse event rates were higher with the combination (51% vs. 25%) with quality of life was not yet reported.
While both trials have been criticized owing to a lack of standard T790M resistance testing and low use of osimertinib in subsequent lines of therapy, Dr. Moore and Dr. Wheatley-Price pointed out: “Even with the use of first-line osimertinib monotherapy, patients may still be exposed to chemotherapy with later lines of treatment. Therefore, combination therapy does not expose patients to new toxicity, it simply changes when they will be exposed to that toxicity during their treatment course.”
The importance of using combination therapy in the first-line setting, they stated, is underscored by the consistent drop-off in patients who receive second-line combination therapy. In the phase 3 FLAURA trial of first-line osimertinib monotherapy, of the patients who discontinued osimertinib, the most common reason for not receiving subsequent therapy was death (60% went on to receive further systemic therapy). This highlights the need to use the most effective treatments up front, Dr. Moore and Dr. Wheatley-Price wrote.
The four large trials of VEGF-targeted therapy with either monoclonal antibodies or TKIs added to first-generation EGFR TKIs have consistently shown improved PFS. Increased toxicities led to discontinuation of VEGF-targeted therapy in 20%-30%.
In the RELAY trial, however, despite more toxicities, quality of life was not diminished. In general, the authors concluded that long-term detriments to quality of life have not been demonstrated. Ongoing studies of osimertinib in combination with VEGF inhibition include a phase 1/2 trial with bevacizumab in previously untreated patients showing an 80% response rate (median PFS, 18.4 months) with no unexpected toxicity.
Chemotherapy-based treatment for mNSCLC with third-generation EGFR TKIs, in appropriately selected patients, the authors concluded, “can offer an additional standard-of-care option as first-line treatment of EGFR-mutant lung cancer.”
Since the introduction of EGFR TKIs, Sophie Stock-Martineau, MD and Frances A. Shepherd, MD noted in their analysis, researchers have aimed to improve their efficacy through combining them with other agents. The authors review research on the addition of chemo- or immunotherapy and agents targeting major resistance mechanisms such as MET. Their review of the same NEJ009 trial focuses, however, on the 65.3% (EGFR TKI plus chemotherapy) versus 31.0% (gefitinib alone) grade 3 adverse event rate, and the 51% versus 25% grade 3 adverse event rate in a similar trial by Noronha and colleagues. The review by Dr. Stock-Martineau and Dr. Shepherd further found that, while adding antiangiogenic agents to an EGFR TKI “mildly” prolongs PFS, survival benefits have not been demonstrated. The added costs, not just in toxicity, were a “far from negligible” $120,000 above the cost of bevacizumab alone for 16 treatments. Data from trials of immune checkpoint inhibitors added to EGFR TKIs reveal heightened toxicities and limited efficacy. Trials of EGFR monoclonal antibodies with an EGFR TKI showed no PFS or OS benefit and were terminated early. Similarly, evidence to date shows no benefit beyond that shown for EGFR TKI monotherapy with the addition of a MET inhibitor.
“Adding virtually all agents to EGFR TKIs has been associated with more toxicity to patients and a significant financial burden to the health care system,” Dr. Stock-Martineau and Dr. Shepherd concluded, further observing that combinations, given their heightened toxicity profiles, could potentially also worsen quality of life.
No conflicts of interest were reported by the authors of either study.
FROM THE JOURNAL OF THORACIC ONCOLOGY
Abraxane still in short supply for cancer patients
forcing physicians to find alternatives for a drug once lauded for being easier to tolerate.
Abraxane (Bristol-Myers Squibb) is a paclitaxel albumin-bound injectable. It is different from alternative chemotherapy treatments like Taxol (paclitaxel) because it doesn’t use the solvents that can make Taxol difficult to tolerate. It was described as a “next-generation taxane” because it didn’t rely on solvents. It was approved in 2005 for metastatic breast cancer, then in 2012 for advanced non–small cell lung cancer, in 2013 for late-stage pancreatic cancer and in 2019 for people with PD-L1–positive metastatic triple-negative breast cancer.
The shortage, which was announced on Oct. 5, 2021, by the Food and Drug Administration, has led to some difficult decisions for patients and physicians. How long the shortage will last isn’t clear.
“I printed out [an] allotment sheet 2 days ago, and all it says [for Abraxane] is allocated,” said Kathy Oubre, MS, CEO of Pontchartrain Cancer Center, Hammond, La. “Everyone is keeping what they’ve got for their own patients, so there really isn’t anything available.”
The Pontchartrain Cancer Center sent two patients to the University of Texas MD Anderson Cancer Center, Houston, for continued treatment with Abraxane, but that option is costly and time consuming for patients. The two patients had the means to travel, but Ms. Oubre said that many others cannot afford to travel for treatment. “Everyone has patients who are living paycheck to paycheck who certainly couldn’t afford to do that. There are going to be patients across the nation that are not going to be able to have care as a result of these things.”
The supply problems are causing difficult decisions for physicians, who may have to switch a patient from an unavailable drug to an alternative that isn’t as effective, Ms. Oubre said. “I can’t imagine the stress and the sadness that the physicians have to feel when they have to go explain that to a patient. That runs counter to everything they are as physicians.”
Other strategies include chemo holidays and rounding down doses in patients with metastatic cancer, according to Camille Hill, PharmD, vice president of oncology pharmacy services, West Cancer Center, Germantown, Tenn.
Shortages and allocations are growing at an alarming rate, Ms. Oubre said. In her 15 years of working in the industry, “I don’t recall it ever being this challenging.” During a Zoom interview, she held up a lengthy list of drugs on allocation or unavailable that her pharmacy group purchasing organization sent her the previous week. “I don’t ever recall getting this kind of list. Every 3 days, I’m getting this. If it were just that one product, I can live with that. We figure it out. But it’s bigger than that.”
Worker shortages are exacerbating the issue. Ms. Oubre received a letter from a drug company describing its employee issues, which included chemists, plant workers, and loading dock staff. On top of that, delivery companies are experiencing staff shortages, which can result in more delays and complicate matters further. “It’s just compounding. These things can get really difficult very quickly. I don’t want to say we’re in crisis, and we’re not rationing care. We’re not in those buckets yet. But I would say that if these things don’t get better, it’s the first time in my work career that we are having those conversations of: ‘How we are going to plan for that it does come to that?’ ” she said.
“In general, with the pandemic, we have seen all sorts of just disruptions to the supply chain. So, I think you just do your best, you find alternatives for those patients that you can, and you come up with strategies. I don’t know that for Abraxane, or any other product, that I’d be particularly confident that we may not see another shortage,” Dr. Hill said.
forcing physicians to find alternatives for a drug once lauded for being easier to tolerate.
Abraxane (Bristol-Myers Squibb) is a paclitaxel albumin-bound injectable. It is different from alternative chemotherapy treatments like Taxol (paclitaxel) because it doesn’t use the solvents that can make Taxol difficult to tolerate. It was described as a “next-generation taxane” because it didn’t rely on solvents. It was approved in 2005 for metastatic breast cancer, then in 2012 for advanced non–small cell lung cancer, in 2013 for late-stage pancreatic cancer and in 2019 for people with PD-L1–positive metastatic triple-negative breast cancer.
The shortage, which was announced on Oct. 5, 2021, by the Food and Drug Administration, has led to some difficult decisions for patients and physicians. How long the shortage will last isn’t clear.
“I printed out [an] allotment sheet 2 days ago, and all it says [for Abraxane] is allocated,” said Kathy Oubre, MS, CEO of Pontchartrain Cancer Center, Hammond, La. “Everyone is keeping what they’ve got for their own patients, so there really isn’t anything available.”
The Pontchartrain Cancer Center sent two patients to the University of Texas MD Anderson Cancer Center, Houston, for continued treatment with Abraxane, but that option is costly and time consuming for patients. The two patients had the means to travel, but Ms. Oubre said that many others cannot afford to travel for treatment. “Everyone has patients who are living paycheck to paycheck who certainly couldn’t afford to do that. There are going to be patients across the nation that are not going to be able to have care as a result of these things.”
The supply problems are causing difficult decisions for physicians, who may have to switch a patient from an unavailable drug to an alternative that isn’t as effective, Ms. Oubre said. “I can’t imagine the stress and the sadness that the physicians have to feel when they have to go explain that to a patient. That runs counter to everything they are as physicians.”
Other strategies include chemo holidays and rounding down doses in patients with metastatic cancer, according to Camille Hill, PharmD, vice president of oncology pharmacy services, West Cancer Center, Germantown, Tenn.
Shortages and allocations are growing at an alarming rate, Ms. Oubre said. In her 15 years of working in the industry, “I don’t recall it ever being this challenging.” During a Zoom interview, she held up a lengthy list of drugs on allocation or unavailable that her pharmacy group purchasing organization sent her the previous week. “I don’t ever recall getting this kind of list. Every 3 days, I’m getting this. If it were just that one product, I can live with that. We figure it out. But it’s bigger than that.”
Worker shortages are exacerbating the issue. Ms. Oubre received a letter from a drug company describing its employee issues, which included chemists, plant workers, and loading dock staff. On top of that, delivery companies are experiencing staff shortages, which can result in more delays and complicate matters further. “It’s just compounding. These things can get really difficult very quickly. I don’t want to say we’re in crisis, and we’re not rationing care. We’re not in those buckets yet. But I would say that if these things don’t get better, it’s the first time in my work career that we are having those conversations of: ‘How we are going to plan for that it does come to that?’ ” she said.
“In general, with the pandemic, we have seen all sorts of just disruptions to the supply chain. So, I think you just do your best, you find alternatives for those patients that you can, and you come up with strategies. I don’t know that for Abraxane, or any other product, that I’d be particularly confident that we may not see another shortage,” Dr. Hill said.
forcing physicians to find alternatives for a drug once lauded for being easier to tolerate.
Abraxane (Bristol-Myers Squibb) is a paclitaxel albumin-bound injectable. It is different from alternative chemotherapy treatments like Taxol (paclitaxel) because it doesn’t use the solvents that can make Taxol difficult to tolerate. It was described as a “next-generation taxane” because it didn’t rely on solvents. It was approved in 2005 for metastatic breast cancer, then in 2012 for advanced non–small cell lung cancer, in 2013 for late-stage pancreatic cancer and in 2019 for people with PD-L1–positive metastatic triple-negative breast cancer.
The shortage, which was announced on Oct. 5, 2021, by the Food and Drug Administration, has led to some difficult decisions for patients and physicians. How long the shortage will last isn’t clear.
“I printed out [an] allotment sheet 2 days ago, and all it says [for Abraxane] is allocated,” said Kathy Oubre, MS, CEO of Pontchartrain Cancer Center, Hammond, La. “Everyone is keeping what they’ve got for their own patients, so there really isn’t anything available.”
The Pontchartrain Cancer Center sent two patients to the University of Texas MD Anderson Cancer Center, Houston, for continued treatment with Abraxane, but that option is costly and time consuming for patients. The two patients had the means to travel, but Ms. Oubre said that many others cannot afford to travel for treatment. “Everyone has patients who are living paycheck to paycheck who certainly couldn’t afford to do that. There are going to be patients across the nation that are not going to be able to have care as a result of these things.”
The supply problems are causing difficult decisions for physicians, who may have to switch a patient from an unavailable drug to an alternative that isn’t as effective, Ms. Oubre said. “I can’t imagine the stress and the sadness that the physicians have to feel when they have to go explain that to a patient. That runs counter to everything they are as physicians.”
Other strategies include chemo holidays and rounding down doses in patients with metastatic cancer, according to Camille Hill, PharmD, vice president of oncology pharmacy services, West Cancer Center, Germantown, Tenn.
Shortages and allocations are growing at an alarming rate, Ms. Oubre said. In her 15 years of working in the industry, “I don’t recall it ever being this challenging.” During a Zoom interview, she held up a lengthy list of drugs on allocation or unavailable that her pharmacy group purchasing organization sent her the previous week. “I don’t ever recall getting this kind of list. Every 3 days, I’m getting this. If it were just that one product, I can live with that. We figure it out. But it’s bigger than that.”
Worker shortages are exacerbating the issue. Ms. Oubre received a letter from a drug company describing its employee issues, which included chemists, plant workers, and loading dock staff. On top of that, delivery companies are experiencing staff shortages, which can result in more delays and complicate matters further. “It’s just compounding. These things can get really difficult very quickly. I don’t want to say we’re in crisis, and we’re not rationing care. We’re not in those buckets yet. But I would say that if these things don’t get better, it’s the first time in my work career that we are having those conversations of: ‘How we are going to plan for that it does come to that?’ ” she said.
“In general, with the pandemic, we have seen all sorts of just disruptions to the supply chain. So, I think you just do your best, you find alternatives for those patients that you can, and you come up with strategies. I don’t know that for Abraxane, or any other product, that I’d be particularly confident that we may not see another shortage,” Dr. Hill said.
Peanut oral immunotherapy is safe and effective in toddlers in large placebo-controlled trial
In a large, blinded study of peanut-allergic toddlers published in The Lancet, 71% of treated participants could safely consume 5,000 mg of peanut protein – equivalent to nearly 17 peanuts – after 2½ years on oral immunotherapy. Even after stopping maintenance dosing for the next 6 months, more than 1 in 5 maintained that level of protection, and nearly 3 in 5 still met the 600-mg benchmark (about 2 peanuts) set by the phase 3 PALISADE trial of the FDA-approved peanut-flour product, Palforzia.
About 2% of children in the United States are allergic to peanuts, and most will not outgrow this allergy. In addition, other research suggests that the immune system is more malleable during early childhood.
Consistent with this idea, prior research showed that toddlers can succeed with peanut oral immunotherapy (OIT) – a regimen that builds tolerance through small amounts of the allergen consumed daily for months. However, that trial (DEVIL) was small, was conducted at a single site, and had no placebo group.
In contrast, the Peanut Oral Immunotherapy in Children Trial (IMPACT) enrolled 146 children aged 1-3 years at five academic medical centers in the United States – the first placebo-controlled study of OIT in this younger age group.
“This is a well done study,” Jaclyn Bjelac, MD, associate director of the Food Allergy Center of Excellence at the Cleveland Clinic, told this news organization. “We have seen improved outcomes in OIT, both in our own experience and other published studies, so while this is no surprise, the outcomes and large number of participants contribute to this being a really exciting publication.”
The trial was long and demanding for families. Toddlers who reacted to 500 mg or less of peanut protein in an entry food challenge were randomized in a 2:1 ratio to receive daily peanut flour or oat flour placebo. After initial dose escalation (from 0.1 mg to 6 mg) and biweekly buildup to a 2,000-mg target dose by week 30, participants continued with 20,00-mg daily maintenance dosing through week 134 – at which point they underwent a food challenge. They then went off treatment for 26 weeks and had another food challenge (week 160). In addition, participants came in for skin-prick and blood tests at baseline and at weeks 30, 82, 134, and 160.
In the placebo group, only 23 of 50 participants (46%) completed the study. “If you did 2½ years of this and then bombed the food challenge, you probably can guess that you were not on the real thing. And they were still asked to come back in 6 months and do it again. So, sure enough, a big chunk of those people chose not to continue, and you can’t blame them,” said Lancet co-author Edwin Kim, MD, in an interview. Dr. Kim directs the UNC Food Allergy Initiative at the University of North Carolina School of Medicine, Chapel Hill.
There was attrition in the treatment group as well. Among 96 children initially assigned to this arm, 68 (71%) passed the 5,000-mg peanut challenge at week 134 – but 11 withdrew in the study’s off-treatment phase. “It was a very tough decision. How much do you give toward science?” said Dr. Kim. “When push came to shove, some of the families couldn’t pull the trigger to potentially give up what they worked so hard for.”
In the intention-to-treat analysis, 20 of 96 treated participants (21%) could still tolerate 5,000 mg of peanut protein after going off therapy for 6 months. That translates to a 29% remission rate in the per-protocol subset (n = 70) who completed the study. Forty (57%) of these completers safely consumed at least 1,755 mg of peanut (cumulative dose). By comparison, the PALISADE trial of Palforzia used a 10,430-mg cumulative peanut dose to measure treatment efficacy.
On safety, 98% of treated participants – but also 80% of the placebo group – reported reactions, of which 35 were treated with epinephrine in 21 children receiving peanut OIT.
While some have noted that epinephrine use seemed high, Dr. Kim said, “we’re actually OK with that, because we’d much rather they overtreat and make sure that 1-year-old is safe than take any chances.” Overall, the safety profile looks similar to prior OIT studies of older children. “I think it suggests that, yeah, side effects will happen, [but] they’re all manageable, and people are not anaphylaxing left and right.”
On remission and immunologic parameters, benefits seemed stronger in the youngest subset (12 to 24 months), particularly those with lower peanut-specific IgE at baseline. These trends require further analyses, though, given the limited number of participants under 24 months.
Another noteworthy observation from longitudinal peanut-specific IgE trends in the placebo group: “Avoidance may not be benign,” Dr. Kim said. “If you look at their labs, they don’t stay flat. They actually go up.” The results jibe with the long-held idea of an early window of opportunity while a child’s immune system is maturing. “If you can grab this kid when his IgE is 10, versus next year when it might be 50, maybe you’ll get a different treatment effect,” Dr. Kim said. “We don’t know that for sure, but the placebo labs kind of point toward that.”
Beyond the science, there are practical advantages to starting OIT early. “Trying to convince a 9-year-old who’s been petrified of peanuts for their whole life to start doing this every day is not an easy task,” whereas with a 1- or 2-year-old, “you build it into their routine,” Dr. Kim said.
Plus, some say there’s no need for families to wait for regulatory approval of additional commercial products for very young children. Though some have advocated against the use of “grocery store” products, most peanut OIT research “has used the same 12% light roast defatted peanut flour used in IMPACT,” noted Marcus S. Shaker, MD, professor of pediatrics and of medicine at the Dartmouth Geisel School of Medicine and a physician at the Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire. The commercial product (Palforzia) and grocery-store products “come from the exact same source in the U.S.,” he said in an interview. “Both are an option for parents to consider, but a commercial product is not, nor has [it] ever been, a necessity.”
Dr. Bjelac reports no relevant financial relationships. Dr. Kim reports consultancy with Aimmune Therapeutics, Allako, AllerGenis, Belhaven Pharma, DBV Technologies, Duke Clinical Research Institute, and Nutricia; advisory board membership with ALK, DBV Technologies, Kenota Health, and Ukko; and grant support from the NIH’s National Institute of Allergy and Infectious Diseases, National Center for Complementary and Integrative Health and Immune Tolerance Network, Food Allergy Research and Education, and the Wallace Research Foundation. Dr. Shaker has participated in research funded by DBV, is cochair of the AAAAI/ACAAI Joint Task Force on Practice Parameters, is an associate editor at the Annals of Allergy, Asthma, and Immunology, and is an editorial board member of the Journal of Allergy and Clinical Immunology in Practice.
A version of this article first appeared on Medscape.com.
In a large, blinded study of peanut-allergic toddlers published in The Lancet, 71% of treated participants could safely consume 5,000 mg of peanut protein – equivalent to nearly 17 peanuts – after 2½ years on oral immunotherapy. Even after stopping maintenance dosing for the next 6 months, more than 1 in 5 maintained that level of protection, and nearly 3 in 5 still met the 600-mg benchmark (about 2 peanuts) set by the phase 3 PALISADE trial of the FDA-approved peanut-flour product, Palforzia.
About 2% of children in the United States are allergic to peanuts, and most will not outgrow this allergy. In addition, other research suggests that the immune system is more malleable during early childhood.
Consistent with this idea, prior research showed that toddlers can succeed with peanut oral immunotherapy (OIT) – a regimen that builds tolerance through small amounts of the allergen consumed daily for months. However, that trial (DEVIL) was small, was conducted at a single site, and had no placebo group.
In contrast, the Peanut Oral Immunotherapy in Children Trial (IMPACT) enrolled 146 children aged 1-3 years at five academic medical centers in the United States – the first placebo-controlled study of OIT in this younger age group.
“This is a well done study,” Jaclyn Bjelac, MD, associate director of the Food Allergy Center of Excellence at the Cleveland Clinic, told this news organization. “We have seen improved outcomes in OIT, both in our own experience and other published studies, so while this is no surprise, the outcomes and large number of participants contribute to this being a really exciting publication.”
The trial was long and demanding for families. Toddlers who reacted to 500 mg or less of peanut protein in an entry food challenge were randomized in a 2:1 ratio to receive daily peanut flour or oat flour placebo. After initial dose escalation (from 0.1 mg to 6 mg) and biweekly buildup to a 2,000-mg target dose by week 30, participants continued with 20,00-mg daily maintenance dosing through week 134 – at which point they underwent a food challenge. They then went off treatment for 26 weeks and had another food challenge (week 160). In addition, participants came in for skin-prick and blood tests at baseline and at weeks 30, 82, 134, and 160.
In the placebo group, only 23 of 50 participants (46%) completed the study. “If you did 2½ years of this and then bombed the food challenge, you probably can guess that you were not on the real thing. And they were still asked to come back in 6 months and do it again. So, sure enough, a big chunk of those people chose not to continue, and you can’t blame them,” said Lancet co-author Edwin Kim, MD, in an interview. Dr. Kim directs the UNC Food Allergy Initiative at the University of North Carolina School of Medicine, Chapel Hill.
There was attrition in the treatment group as well. Among 96 children initially assigned to this arm, 68 (71%) passed the 5,000-mg peanut challenge at week 134 – but 11 withdrew in the study’s off-treatment phase. “It was a very tough decision. How much do you give toward science?” said Dr. Kim. “When push came to shove, some of the families couldn’t pull the trigger to potentially give up what they worked so hard for.”
In the intention-to-treat analysis, 20 of 96 treated participants (21%) could still tolerate 5,000 mg of peanut protein after going off therapy for 6 months. That translates to a 29% remission rate in the per-protocol subset (n = 70) who completed the study. Forty (57%) of these completers safely consumed at least 1,755 mg of peanut (cumulative dose). By comparison, the PALISADE trial of Palforzia used a 10,430-mg cumulative peanut dose to measure treatment efficacy.
On safety, 98% of treated participants – but also 80% of the placebo group – reported reactions, of which 35 were treated with epinephrine in 21 children receiving peanut OIT.
While some have noted that epinephrine use seemed high, Dr. Kim said, “we’re actually OK with that, because we’d much rather they overtreat and make sure that 1-year-old is safe than take any chances.” Overall, the safety profile looks similar to prior OIT studies of older children. “I think it suggests that, yeah, side effects will happen, [but] they’re all manageable, and people are not anaphylaxing left and right.”
On remission and immunologic parameters, benefits seemed stronger in the youngest subset (12 to 24 months), particularly those with lower peanut-specific IgE at baseline. These trends require further analyses, though, given the limited number of participants under 24 months.
Another noteworthy observation from longitudinal peanut-specific IgE trends in the placebo group: “Avoidance may not be benign,” Dr. Kim said. “If you look at their labs, they don’t stay flat. They actually go up.” The results jibe with the long-held idea of an early window of opportunity while a child’s immune system is maturing. “If you can grab this kid when his IgE is 10, versus next year when it might be 50, maybe you’ll get a different treatment effect,” Dr. Kim said. “We don’t know that for sure, but the placebo labs kind of point toward that.”
Beyond the science, there are practical advantages to starting OIT early. “Trying to convince a 9-year-old who’s been petrified of peanuts for their whole life to start doing this every day is not an easy task,” whereas with a 1- or 2-year-old, “you build it into their routine,” Dr. Kim said.
Plus, some say there’s no need for families to wait for regulatory approval of additional commercial products for very young children. Though some have advocated against the use of “grocery store” products, most peanut OIT research “has used the same 12% light roast defatted peanut flour used in IMPACT,” noted Marcus S. Shaker, MD, professor of pediatrics and of medicine at the Dartmouth Geisel School of Medicine and a physician at the Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire. The commercial product (Palforzia) and grocery-store products “come from the exact same source in the U.S.,” he said in an interview. “Both are an option for parents to consider, but a commercial product is not, nor has [it] ever been, a necessity.”
Dr. Bjelac reports no relevant financial relationships. Dr. Kim reports consultancy with Aimmune Therapeutics, Allako, AllerGenis, Belhaven Pharma, DBV Technologies, Duke Clinical Research Institute, and Nutricia; advisory board membership with ALK, DBV Technologies, Kenota Health, and Ukko; and grant support from the NIH’s National Institute of Allergy and Infectious Diseases, National Center for Complementary and Integrative Health and Immune Tolerance Network, Food Allergy Research and Education, and the Wallace Research Foundation. Dr. Shaker has participated in research funded by DBV, is cochair of the AAAAI/ACAAI Joint Task Force on Practice Parameters, is an associate editor at the Annals of Allergy, Asthma, and Immunology, and is an editorial board member of the Journal of Allergy and Clinical Immunology in Practice.
A version of this article first appeared on Medscape.com.
In a large, blinded study of peanut-allergic toddlers published in The Lancet, 71% of treated participants could safely consume 5,000 mg of peanut protein – equivalent to nearly 17 peanuts – after 2½ years on oral immunotherapy. Even after stopping maintenance dosing for the next 6 months, more than 1 in 5 maintained that level of protection, and nearly 3 in 5 still met the 600-mg benchmark (about 2 peanuts) set by the phase 3 PALISADE trial of the FDA-approved peanut-flour product, Palforzia.
About 2% of children in the United States are allergic to peanuts, and most will not outgrow this allergy. In addition, other research suggests that the immune system is more malleable during early childhood.
Consistent with this idea, prior research showed that toddlers can succeed with peanut oral immunotherapy (OIT) – a regimen that builds tolerance through small amounts of the allergen consumed daily for months. However, that trial (DEVIL) was small, was conducted at a single site, and had no placebo group.
In contrast, the Peanut Oral Immunotherapy in Children Trial (IMPACT) enrolled 146 children aged 1-3 years at five academic medical centers in the United States – the first placebo-controlled study of OIT in this younger age group.
“This is a well done study,” Jaclyn Bjelac, MD, associate director of the Food Allergy Center of Excellence at the Cleveland Clinic, told this news organization. “We have seen improved outcomes in OIT, both in our own experience and other published studies, so while this is no surprise, the outcomes and large number of participants contribute to this being a really exciting publication.”
The trial was long and demanding for families. Toddlers who reacted to 500 mg or less of peanut protein in an entry food challenge were randomized in a 2:1 ratio to receive daily peanut flour or oat flour placebo. After initial dose escalation (from 0.1 mg to 6 mg) and biweekly buildup to a 2,000-mg target dose by week 30, participants continued with 20,00-mg daily maintenance dosing through week 134 – at which point they underwent a food challenge. They then went off treatment for 26 weeks and had another food challenge (week 160). In addition, participants came in for skin-prick and blood tests at baseline and at weeks 30, 82, 134, and 160.
In the placebo group, only 23 of 50 participants (46%) completed the study. “If you did 2½ years of this and then bombed the food challenge, you probably can guess that you were not on the real thing. And they were still asked to come back in 6 months and do it again. So, sure enough, a big chunk of those people chose not to continue, and you can’t blame them,” said Lancet co-author Edwin Kim, MD, in an interview. Dr. Kim directs the UNC Food Allergy Initiative at the University of North Carolina School of Medicine, Chapel Hill.
There was attrition in the treatment group as well. Among 96 children initially assigned to this arm, 68 (71%) passed the 5,000-mg peanut challenge at week 134 – but 11 withdrew in the study’s off-treatment phase. “It was a very tough decision. How much do you give toward science?” said Dr. Kim. “When push came to shove, some of the families couldn’t pull the trigger to potentially give up what they worked so hard for.”
In the intention-to-treat analysis, 20 of 96 treated participants (21%) could still tolerate 5,000 mg of peanut protein after going off therapy for 6 months. That translates to a 29% remission rate in the per-protocol subset (n = 70) who completed the study. Forty (57%) of these completers safely consumed at least 1,755 mg of peanut (cumulative dose). By comparison, the PALISADE trial of Palforzia used a 10,430-mg cumulative peanut dose to measure treatment efficacy.
On safety, 98% of treated participants – but also 80% of the placebo group – reported reactions, of which 35 were treated with epinephrine in 21 children receiving peanut OIT.
While some have noted that epinephrine use seemed high, Dr. Kim said, “we’re actually OK with that, because we’d much rather they overtreat and make sure that 1-year-old is safe than take any chances.” Overall, the safety profile looks similar to prior OIT studies of older children. “I think it suggests that, yeah, side effects will happen, [but] they’re all manageable, and people are not anaphylaxing left and right.”
On remission and immunologic parameters, benefits seemed stronger in the youngest subset (12 to 24 months), particularly those with lower peanut-specific IgE at baseline. These trends require further analyses, though, given the limited number of participants under 24 months.
Another noteworthy observation from longitudinal peanut-specific IgE trends in the placebo group: “Avoidance may not be benign,” Dr. Kim said. “If you look at their labs, they don’t stay flat. They actually go up.” The results jibe with the long-held idea of an early window of opportunity while a child’s immune system is maturing. “If you can grab this kid when his IgE is 10, versus next year when it might be 50, maybe you’ll get a different treatment effect,” Dr. Kim said. “We don’t know that for sure, but the placebo labs kind of point toward that.”
Beyond the science, there are practical advantages to starting OIT early. “Trying to convince a 9-year-old who’s been petrified of peanuts for their whole life to start doing this every day is not an easy task,” whereas with a 1- or 2-year-old, “you build it into their routine,” Dr. Kim said.
Plus, some say there’s no need for families to wait for regulatory approval of additional commercial products for very young children. Though some have advocated against the use of “grocery store” products, most peanut OIT research “has used the same 12% light roast defatted peanut flour used in IMPACT,” noted Marcus S. Shaker, MD, professor of pediatrics and of medicine at the Dartmouth Geisel School of Medicine and a physician at the Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire. The commercial product (Palforzia) and grocery-store products “come from the exact same source in the U.S.,” he said in an interview. “Both are an option for parents to consider, but a commercial product is not, nor has [it] ever been, a necessity.”
Dr. Bjelac reports no relevant financial relationships. Dr. Kim reports consultancy with Aimmune Therapeutics, Allako, AllerGenis, Belhaven Pharma, DBV Technologies, Duke Clinical Research Institute, and Nutricia; advisory board membership with ALK, DBV Technologies, Kenota Health, and Ukko; and grant support from the NIH’s National Institute of Allergy and Infectious Diseases, National Center for Complementary and Integrative Health and Immune Tolerance Network, Food Allergy Research and Education, and the Wallace Research Foundation. Dr. Shaker has participated in research funded by DBV, is cochair of the AAAAI/ACAAI Joint Task Force on Practice Parameters, is an associate editor at the Annals of Allergy, Asthma, and Immunology, and is an editorial board member of the Journal of Allergy and Clinical Immunology in Practice.
A version of this article first appeared on Medscape.com.
Antimicrobial resistance linked to 1.2 million global deaths in 2019
More than HIV, more than malaria.
In terms of preventable deaths, 1.27 million people could have been saved if drug-resistant infections were replaced with infections susceptible to current antibiotics. Furthermore, 4.95 million fewer people would have died if drug-resistant infections were replaced by no infections, researchers estimated.
Although the COVID-19 pandemic took some focus off the AMR burden worldwide over the past 2 years, the urgency to address risk to public health did not ebb. In fact, based on the findings, the researchers noted that AMR is now a leading cause of death worldwide.
“If left unchecked, the spread of AMR could make many bacterial pathogens much more lethal in the future than they are today,” the researchers noted in the study, published online Jan. 20, 2022, in The Lancet.
“These findings are a warning signal that antibiotic resistance is placing pressure on health care systems and leading to significant health loss,” study author Kevin Ikuta, MD, MPH, told this news organization.
“We need to continue to adhere to and support infection prevention and control programs, be thoughtful about our antibiotic use, and advocate for increased funding to vaccine discovery and the antibiotic development pipeline,” added Dr. Ikuta, health sciences assistant clinical professor of medicine at the University of California, Los Angeles.
Although many investigators have studied AMR, this study is the largest in scope, covering 204 countries and territories and incorporating data on a comprehensive range of pathogens and pathogen-drug combinations.
Dr. Ikuta, lead author Christopher J.L. Murray, DPhil, and colleagues estimated the global burden of AMR using the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019. They specifically looked at rates of death directly attributed to and separately those associated with resistance.
Regional differences
Broken down by 21 regions, Australasia had 6.5 deaths per 100,000 people attributable to AMR, the lowest rate reported. This region also had 28 deaths per 100,000 associated with AMR.
Researchers found the highest rates in western sub-Saharan Africa. Deaths attributable to AMR were 27.3 per 100,000 and associated death rate was 114.8 per 100,000.
Lower- and middle-income regions had the highest AMR death rates, although resistance remains a high-priority issue for high-income countries as well.
“It’s important to take a global perspective on resistant infections because we can learn about regions and countries that are experiencing the greatest burden, information that was previously unknown,” Dr. Ikuta said. “With these estimates policy makers can prioritize regions that are hotspots and would most benefit from additional interventions.”
Furthermore, the study emphasized the global nature of AMR. “We’ve seen over the last 2 years with COVID-19 that this sort of problem doesn’t respect country borders, and high rates of resistance in one location can spread across a region or spread globally pretty quickly,” Dr. Ikuta said.
Leading resistant infections
Lower respiratory and thorax infections, bloodstream infections, and intra-abdominal infections together accounted for almost 79% of such deaths linked to AMR.
The six leading pathogens are likely household names among infectious disease specialists. The researchers found Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa, each responsible for more than 250,000 AMR-associated deaths.
The study also revealed that resistance to several first-line antibiotic agents often used empirically to treat infections accounted for more than 70% of the AMR-attributable deaths. These included fluoroquinolones and beta-lactam antibiotics such as carbapenems, cephalosporins, and penicillins.
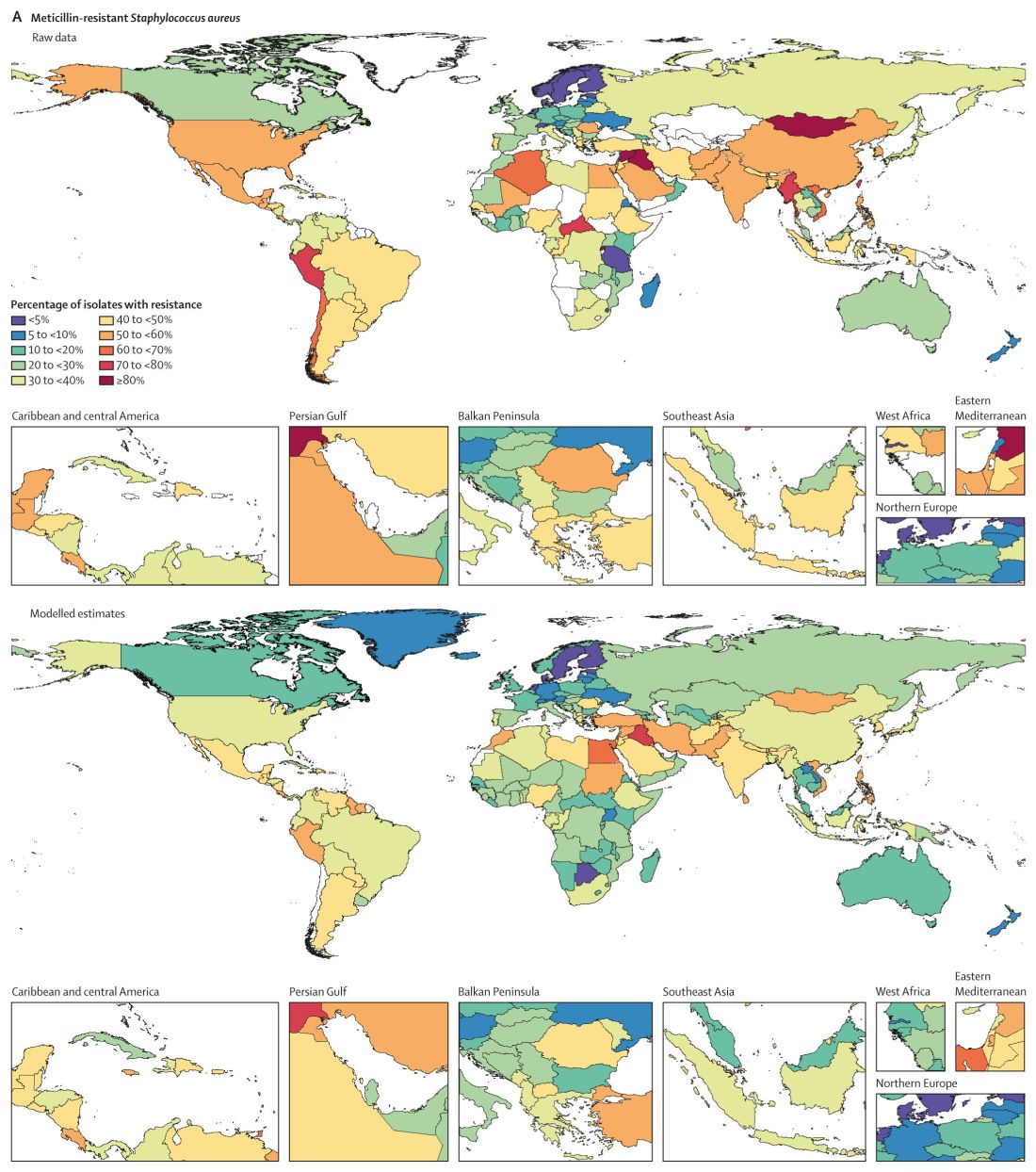
Consistent with previous studies, MRSA stood out as a major cause of mortality. Of 88 different pathogen-drug combinations evaluated, MRSA was responsible for the most mortality: more than 100,000 deaths and 3·5 million disability-adjusted life-years.
The current study findings on MRSA “being a particularly nasty culprit” in AMR infections validates previous work that reported similar results, Vance Fowler, MD, told this news organization when asked to comment on the research. “That is reassuring.”
Potential solutions offered
Dr. Murray and colleagues outlined five strategies to address the challenge of bacterial AMR:
- Infection prevention and control remain paramount in minimizing infections in general and AMR infections in particular.
- More vaccines are needed to reduce the need for antibiotics. “Vaccines are available for only one of the six leading pathogens (S. pneumoniae), although new vaccine programs are underway for S. aureus, E. coli, and others,” the researchers wrote.
- Reduce antibiotic use unrelated to treatment of human disease.
- Avoid using antibiotics for viral infections and other unnecessary indications.
- Invest in new antibiotic development and ensure access to second-line agents in areas without widespread access.
“Identifying strategies that can work to reduce the burden of bacterial AMR – either across a wide range of settings or those that are specifically tailored to the resources available and leading pathogen-drug combinations in a particular setting – is an urgent priority,” the researchers noted.
Admirable AMR research
The results of the study are “startling, but not surprising,” said Dr. Fowler, professor of medicine at Duke University, Durham, N.C.
The authors did a “nice job” of addressing both deaths attributable and associated with AMR, Dr. Fowler added. “Those two categories unlock applications, not just in terms of how you interpret it but also what you do about it.”
The deaths attributable to AMR show that there is more work to be done regarding infection control and prevention, Dr. Fowler said, including in areas of the world like lower- and middle-income countries where infection resistance is most pronounced.
The deaths associated with AMR can be more challenging to calculate – people with infections can die for multiple reasons. However, Dr. Fowler applauded the researchers for doing “as good a job as you can” in estimating the extent of associated mortality.
‘The overlooked pandemic of antimicrobial resistance’
In an accompanying editorial in The Lancet, Ramanan Laxminarayan, PhD, MPH, wrote: “As COVID-19 rages on, the pandemic of antimicrobial resistance continues in the shadows. The toll taken by AMR on patients and their families is largely invisible but is reflected in prolonged bacterial infections that extend hospital stays and cause needless deaths.”
Dr. Laxminarayan pointed out an irony with AMR in different regions. Some of the AMR burden in sub-Saharan Africa is “probably due to inadequate access to antibiotics and high infection levels, albeit at low levels of resistance, whereas in south Asia and Latin America, it is because of high resistance even with good access to antibiotics.”
More funding to address AMR is needed, Dr. Laxminarayan noted. “Even the lower end of 911,000 deaths estimated by Murray and colleagues is higher than the number of deaths from HIV, which attracts close to U.S. $50 billion each year. However, global spending on addressing AMR is probably much lower than that.” Dr. Laxminarayan is an economist and epidemiologist affiliated with the Center for Disease Dynamics, Economics & Policy in Washington, D.C., and the Global Antibiotic Research and Development Partnership in Geneva.
An overlap with COVID-19
The Lancet report is likely “to bring more attention to AMR, especially since so many people have been distracted by COVID, and rightly so,” Dr. Fowler predicted. “The world has had its hands full with COVID.”
The two infections interact in direct ways, Dr. Fowler added. For example, some people hospitalized for COVID-19 for an extended time could develop progressively drug-resistant bacteria – leading to a superinfection.
The overlap could be illustrated by a Venn diagram, he said. A yellow circle could illustrate people with COVID-19 who are asymptomatic or who remain outpatients. Next to that would be a blue circle showing people who develop AMR infections. Where the two circles overlap would be green for those hospitalized who – because of receiving steroids, being on a ventilator, or getting a central line – develop a superinfection.
Official guidance continues
The study comes in the context of recent guidance and federal action on AMR. For example, the Infectious Diseases Society of America released new guidelines for AMR in November 2021 as part of ongoing advice on prevention and treatment of this “ongoing crisis.”
This most recent IDSA guidance addresses three pathogens in particular: AmpC beta-lactamase–producing Enterobacterales, carbapenem-resistant A. baumannii, and Stenotrophomonas maltophilia.
Also in November, the World Health Organization released an updated fact sheet on antimicrobial resistance. The WHO declared AMR one of the world’s top 10 global public health threats. The agency emphasized that misuse and overuse of antimicrobials are the main drivers in the development of drug-resistant pathogens. The WHO also pointed out that lack of clean water and sanitation in many areas of the world contribute to spread of microbes, including those resistant to current treatment options.
In September 2021, the Biden administration acknowledged the threat of AMR with allocation of more than $2 billion of the American Rescue Plan money for prevention and treatment of these infections.
Asked if there are any reasons for hope or optimism at this point, Dr. Ikuta said: “Definitely. We know what needs to be done to combat the spread of resistance. COVID-19 has demonstrated the importance of global commitment to infection control measures, such as hand washing and surveillance, and rapid investments in treatments, which can all be applied to antimicrobial resistance.”
The Bill & Melinda Gates Foundation, the Wellcome Trust, and the U.K. Department of Health and Social Care using U.K. aid funding managed by the Fleming Fund and other organizations provided funding for the study. Dr. Ikuta and Dr. Laxminarayan have disclosed no relevant financial relationships. Dr. Fowler reported receiving grants or honoraria, as well as serving as a consultant, for numerous sources. He also reported a patent pending in sepsis diagnostics and serving as chair of the V710 Scientific Advisory Committee (Merck).
A version of this article first appeared on Medscape.com.
More than HIV, more than malaria.
In terms of preventable deaths, 1.27 million people could have been saved if drug-resistant infections were replaced with infections susceptible to current antibiotics. Furthermore, 4.95 million fewer people would have died if drug-resistant infections were replaced by no infections, researchers estimated.
Although the COVID-19 pandemic took some focus off the AMR burden worldwide over the past 2 years, the urgency to address risk to public health did not ebb. In fact, based on the findings, the researchers noted that AMR is now a leading cause of death worldwide.
“If left unchecked, the spread of AMR could make many bacterial pathogens much more lethal in the future than they are today,” the researchers noted in the study, published online Jan. 20, 2022, in The Lancet.
“These findings are a warning signal that antibiotic resistance is placing pressure on health care systems and leading to significant health loss,” study author Kevin Ikuta, MD, MPH, told this news organization.
“We need to continue to adhere to and support infection prevention and control programs, be thoughtful about our antibiotic use, and advocate for increased funding to vaccine discovery and the antibiotic development pipeline,” added Dr. Ikuta, health sciences assistant clinical professor of medicine at the University of California, Los Angeles.
Although many investigators have studied AMR, this study is the largest in scope, covering 204 countries and territories and incorporating data on a comprehensive range of pathogens and pathogen-drug combinations.
Dr. Ikuta, lead author Christopher J.L. Murray, DPhil, and colleagues estimated the global burden of AMR using the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019. They specifically looked at rates of death directly attributed to and separately those associated with resistance.
Regional differences
Broken down by 21 regions, Australasia had 6.5 deaths per 100,000 people attributable to AMR, the lowest rate reported. This region also had 28 deaths per 100,000 associated with AMR.
Researchers found the highest rates in western sub-Saharan Africa. Deaths attributable to AMR were 27.3 per 100,000 and associated death rate was 114.8 per 100,000.
Lower- and middle-income regions had the highest AMR death rates, although resistance remains a high-priority issue for high-income countries as well.
“It’s important to take a global perspective on resistant infections because we can learn about regions and countries that are experiencing the greatest burden, information that was previously unknown,” Dr. Ikuta said. “With these estimates policy makers can prioritize regions that are hotspots and would most benefit from additional interventions.”
Furthermore, the study emphasized the global nature of AMR. “We’ve seen over the last 2 years with COVID-19 that this sort of problem doesn’t respect country borders, and high rates of resistance in one location can spread across a region or spread globally pretty quickly,” Dr. Ikuta said.
Leading resistant infections
Lower respiratory and thorax infections, bloodstream infections, and intra-abdominal infections together accounted for almost 79% of such deaths linked to AMR.
The six leading pathogens are likely household names among infectious disease specialists. The researchers found Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa, each responsible for more than 250,000 AMR-associated deaths.
The study also revealed that resistance to several first-line antibiotic agents often used empirically to treat infections accounted for more than 70% of the AMR-attributable deaths. These included fluoroquinolones and beta-lactam antibiotics such as carbapenems, cephalosporins, and penicillins.
Consistent with previous studies, MRSA stood out as a major cause of mortality. Of 88 different pathogen-drug combinations evaluated, MRSA was responsible for the most mortality: more than 100,000 deaths and 3·5 million disability-adjusted life-years.
The current study findings on MRSA “being a particularly nasty culprit” in AMR infections validates previous work that reported similar results, Vance Fowler, MD, told this news organization when asked to comment on the research. “That is reassuring.”
Potential solutions offered
Dr. Murray and colleagues outlined five strategies to address the challenge of bacterial AMR:
- Infection prevention and control remain paramount in minimizing infections in general and AMR infections in particular.
- More vaccines are needed to reduce the need for antibiotics. “Vaccines are available for only one of the six leading pathogens (S. pneumoniae), although new vaccine programs are underway for S. aureus, E. coli, and others,” the researchers wrote.
- Reduce antibiotic use unrelated to treatment of human disease.
- Avoid using antibiotics for viral infections and other unnecessary indications.
- Invest in new antibiotic development and ensure access to second-line agents in areas without widespread access.
“Identifying strategies that can work to reduce the burden of bacterial AMR – either across a wide range of settings or those that are specifically tailored to the resources available and leading pathogen-drug combinations in a particular setting – is an urgent priority,” the researchers noted.
Admirable AMR research
The results of the study are “startling, but not surprising,” said Dr. Fowler, professor of medicine at Duke University, Durham, N.C.
The authors did a “nice job” of addressing both deaths attributable and associated with AMR, Dr. Fowler added. “Those two categories unlock applications, not just in terms of how you interpret it but also what you do about it.”
The deaths attributable to AMR show that there is more work to be done regarding infection control and prevention, Dr. Fowler said, including in areas of the world like lower- and middle-income countries where infection resistance is most pronounced.
The deaths associated with AMR can be more challenging to calculate – people with infections can die for multiple reasons. However, Dr. Fowler applauded the researchers for doing “as good a job as you can” in estimating the extent of associated mortality.
‘The overlooked pandemic of antimicrobial resistance’
In an accompanying editorial in The Lancet, Ramanan Laxminarayan, PhD, MPH, wrote: “As COVID-19 rages on, the pandemic of antimicrobial resistance continues in the shadows. The toll taken by AMR on patients and their families is largely invisible but is reflected in prolonged bacterial infections that extend hospital stays and cause needless deaths.”
Dr. Laxminarayan pointed out an irony with AMR in different regions. Some of the AMR burden in sub-Saharan Africa is “probably due to inadequate access to antibiotics and high infection levels, albeit at low levels of resistance, whereas in south Asia and Latin America, it is because of high resistance even with good access to antibiotics.”
More funding to address AMR is needed, Dr. Laxminarayan noted. “Even the lower end of 911,000 deaths estimated by Murray and colleagues is higher than the number of deaths from HIV, which attracts close to U.S. $50 billion each year. However, global spending on addressing AMR is probably much lower than that.” Dr. Laxminarayan is an economist and epidemiologist affiliated with the Center for Disease Dynamics, Economics & Policy in Washington, D.C., and the Global Antibiotic Research and Development Partnership in Geneva.
An overlap with COVID-19
The Lancet report is likely “to bring more attention to AMR, especially since so many people have been distracted by COVID, and rightly so,” Dr. Fowler predicted. “The world has had its hands full with COVID.”
The two infections interact in direct ways, Dr. Fowler added. For example, some people hospitalized for COVID-19 for an extended time could develop progressively drug-resistant bacteria – leading to a superinfection.
The overlap could be illustrated by a Venn diagram, he said. A yellow circle could illustrate people with COVID-19 who are asymptomatic or who remain outpatients. Next to that would be a blue circle showing people who develop AMR infections. Where the two circles overlap would be green for those hospitalized who – because of receiving steroids, being on a ventilator, or getting a central line – develop a superinfection.
Official guidance continues
The study comes in the context of recent guidance and federal action on AMR. For example, the Infectious Diseases Society of America released new guidelines for AMR in November 2021 as part of ongoing advice on prevention and treatment of this “ongoing crisis.”
This most recent IDSA guidance addresses three pathogens in particular: AmpC beta-lactamase–producing Enterobacterales, carbapenem-resistant A. baumannii, and Stenotrophomonas maltophilia.
Also in November, the World Health Organization released an updated fact sheet on antimicrobial resistance. The WHO declared AMR one of the world’s top 10 global public health threats. The agency emphasized that misuse and overuse of antimicrobials are the main drivers in the development of drug-resistant pathogens. The WHO also pointed out that lack of clean water and sanitation in many areas of the world contribute to spread of microbes, including those resistant to current treatment options.
In September 2021, the Biden administration acknowledged the threat of AMR with allocation of more than $2 billion of the American Rescue Plan money for prevention and treatment of these infections.
Asked if there are any reasons for hope or optimism at this point, Dr. Ikuta said: “Definitely. We know what needs to be done to combat the spread of resistance. COVID-19 has demonstrated the importance of global commitment to infection control measures, such as hand washing and surveillance, and rapid investments in treatments, which can all be applied to antimicrobial resistance.”
The Bill & Melinda Gates Foundation, the Wellcome Trust, and the U.K. Department of Health and Social Care using U.K. aid funding managed by the Fleming Fund and other organizations provided funding for the study. Dr. Ikuta and Dr. Laxminarayan have disclosed no relevant financial relationships. Dr. Fowler reported receiving grants or honoraria, as well as serving as a consultant, for numerous sources. He also reported a patent pending in sepsis diagnostics and serving as chair of the V710 Scientific Advisory Committee (Merck).
A version of this article first appeared on Medscape.com.
More than HIV, more than malaria.
In terms of preventable deaths, 1.27 million people could have been saved if drug-resistant infections were replaced with infections susceptible to current antibiotics. Furthermore, 4.95 million fewer people would have died if drug-resistant infections were replaced by no infections, researchers estimated.
Although the COVID-19 pandemic took some focus off the AMR burden worldwide over the past 2 years, the urgency to address risk to public health did not ebb. In fact, based on the findings, the researchers noted that AMR is now a leading cause of death worldwide.
“If left unchecked, the spread of AMR could make many bacterial pathogens much more lethal in the future than they are today,” the researchers noted in the study, published online Jan. 20, 2022, in The Lancet.
“These findings are a warning signal that antibiotic resistance is placing pressure on health care systems and leading to significant health loss,” study author Kevin Ikuta, MD, MPH, told this news organization.
“We need to continue to adhere to and support infection prevention and control programs, be thoughtful about our antibiotic use, and advocate for increased funding to vaccine discovery and the antibiotic development pipeline,” added Dr. Ikuta, health sciences assistant clinical professor of medicine at the University of California, Los Angeles.
Although many investigators have studied AMR, this study is the largest in scope, covering 204 countries and territories and incorporating data on a comprehensive range of pathogens and pathogen-drug combinations.
Dr. Ikuta, lead author Christopher J.L. Murray, DPhil, and colleagues estimated the global burden of AMR using the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019. They specifically looked at rates of death directly attributed to and separately those associated with resistance.
Regional differences
Broken down by 21 regions, Australasia had 6.5 deaths per 100,000 people attributable to AMR, the lowest rate reported. This region also had 28 deaths per 100,000 associated with AMR.
Researchers found the highest rates in western sub-Saharan Africa. Deaths attributable to AMR were 27.3 per 100,000 and associated death rate was 114.8 per 100,000.
Lower- and middle-income regions had the highest AMR death rates, although resistance remains a high-priority issue for high-income countries as well.
“It’s important to take a global perspective on resistant infections because we can learn about regions and countries that are experiencing the greatest burden, information that was previously unknown,” Dr. Ikuta said. “With these estimates policy makers can prioritize regions that are hotspots and would most benefit from additional interventions.”
Furthermore, the study emphasized the global nature of AMR. “We’ve seen over the last 2 years with COVID-19 that this sort of problem doesn’t respect country borders, and high rates of resistance in one location can spread across a region or spread globally pretty quickly,” Dr. Ikuta said.
Leading resistant infections
Lower respiratory and thorax infections, bloodstream infections, and intra-abdominal infections together accounted for almost 79% of such deaths linked to AMR.
The six leading pathogens are likely household names among infectious disease specialists. The researchers found Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa, each responsible for more than 250,000 AMR-associated deaths.
The study also revealed that resistance to several first-line antibiotic agents often used empirically to treat infections accounted for more than 70% of the AMR-attributable deaths. These included fluoroquinolones and beta-lactam antibiotics such as carbapenems, cephalosporins, and penicillins.
Consistent with previous studies, MRSA stood out as a major cause of mortality. Of 88 different pathogen-drug combinations evaluated, MRSA was responsible for the most mortality: more than 100,000 deaths and 3·5 million disability-adjusted life-years.
The current study findings on MRSA “being a particularly nasty culprit” in AMR infections validates previous work that reported similar results, Vance Fowler, MD, told this news organization when asked to comment on the research. “That is reassuring.”
Potential solutions offered
Dr. Murray and colleagues outlined five strategies to address the challenge of bacterial AMR:
- Infection prevention and control remain paramount in minimizing infections in general and AMR infections in particular.
- More vaccines are needed to reduce the need for antibiotics. “Vaccines are available for only one of the six leading pathogens (S. pneumoniae), although new vaccine programs are underway for S. aureus, E. coli, and others,” the researchers wrote.
- Reduce antibiotic use unrelated to treatment of human disease.
- Avoid using antibiotics for viral infections and other unnecessary indications.
- Invest in new antibiotic development and ensure access to second-line agents in areas without widespread access.
“Identifying strategies that can work to reduce the burden of bacterial AMR – either across a wide range of settings or those that are specifically tailored to the resources available and leading pathogen-drug combinations in a particular setting – is an urgent priority,” the researchers noted.
Admirable AMR research
The results of the study are “startling, but not surprising,” said Dr. Fowler, professor of medicine at Duke University, Durham, N.C.
The authors did a “nice job” of addressing both deaths attributable and associated with AMR, Dr. Fowler added. “Those two categories unlock applications, not just in terms of how you interpret it but also what you do about it.”
The deaths attributable to AMR show that there is more work to be done regarding infection control and prevention, Dr. Fowler said, including in areas of the world like lower- and middle-income countries where infection resistance is most pronounced.
The deaths associated with AMR can be more challenging to calculate – people with infections can die for multiple reasons. However, Dr. Fowler applauded the researchers for doing “as good a job as you can” in estimating the extent of associated mortality.
‘The overlooked pandemic of antimicrobial resistance’
In an accompanying editorial in The Lancet, Ramanan Laxminarayan, PhD, MPH, wrote: “As COVID-19 rages on, the pandemic of antimicrobial resistance continues in the shadows. The toll taken by AMR on patients and their families is largely invisible but is reflected in prolonged bacterial infections that extend hospital stays and cause needless deaths.”
Dr. Laxminarayan pointed out an irony with AMR in different regions. Some of the AMR burden in sub-Saharan Africa is “probably due to inadequate access to antibiotics and high infection levels, albeit at low levels of resistance, whereas in south Asia and Latin America, it is because of high resistance even with good access to antibiotics.”
More funding to address AMR is needed, Dr. Laxminarayan noted. “Even the lower end of 911,000 deaths estimated by Murray and colleagues is higher than the number of deaths from HIV, which attracts close to U.S. $50 billion each year. However, global spending on addressing AMR is probably much lower than that.” Dr. Laxminarayan is an economist and epidemiologist affiliated with the Center for Disease Dynamics, Economics & Policy in Washington, D.C., and the Global Antibiotic Research and Development Partnership in Geneva.
An overlap with COVID-19
The Lancet report is likely “to bring more attention to AMR, especially since so many people have been distracted by COVID, and rightly so,” Dr. Fowler predicted. “The world has had its hands full with COVID.”
The two infections interact in direct ways, Dr. Fowler added. For example, some people hospitalized for COVID-19 for an extended time could develop progressively drug-resistant bacteria – leading to a superinfection.
The overlap could be illustrated by a Venn diagram, he said. A yellow circle could illustrate people with COVID-19 who are asymptomatic or who remain outpatients. Next to that would be a blue circle showing people who develop AMR infections. Where the two circles overlap would be green for those hospitalized who – because of receiving steroids, being on a ventilator, or getting a central line – develop a superinfection.
Official guidance continues
The study comes in the context of recent guidance and federal action on AMR. For example, the Infectious Diseases Society of America released new guidelines for AMR in November 2021 as part of ongoing advice on prevention and treatment of this “ongoing crisis.”
This most recent IDSA guidance addresses three pathogens in particular: AmpC beta-lactamase–producing Enterobacterales, carbapenem-resistant A. baumannii, and Stenotrophomonas maltophilia.
Also in November, the World Health Organization released an updated fact sheet on antimicrobial resistance. The WHO declared AMR one of the world’s top 10 global public health threats. The agency emphasized that misuse and overuse of antimicrobials are the main drivers in the development of drug-resistant pathogens. The WHO also pointed out that lack of clean water and sanitation in many areas of the world contribute to spread of microbes, including those resistant to current treatment options.
In September 2021, the Biden administration acknowledged the threat of AMR with allocation of more than $2 billion of the American Rescue Plan money for prevention and treatment of these infections.
Asked if there are any reasons for hope or optimism at this point, Dr. Ikuta said: “Definitely. We know what needs to be done to combat the spread of resistance. COVID-19 has demonstrated the importance of global commitment to infection control measures, such as hand washing and surveillance, and rapid investments in treatments, which can all be applied to antimicrobial resistance.”
The Bill & Melinda Gates Foundation, the Wellcome Trust, and the U.K. Department of Health and Social Care using U.K. aid funding managed by the Fleming Fund and other organizations provided funding for the study. Dr. Ikuta and Dr. Laxminarayan have disclosed no relevant financial relationships. Dr. Fowler reported receiving grants or honoraria, as well as serving as a consultant, for numerous sources. He also reported a patent pending in sepsis diagnostics and serving as chair of the V710 Scientific Advisory Committee (Merck).
A version of this article first appeared on Medscape.com.