User login
Total laparoscopic versus laparoscopic supracervical hysterectomy
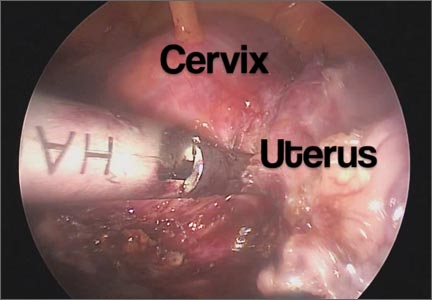
It gives me great pleasure to introduce this month’s surgical video. The following feature presentation was produced by my third-year fellow, Mireille Truong, MD, and my third-year resident, Sarah Horvath, MD. The focus of this surgical video is to compare and contrast total laparoscopic hysterectomy (TLH) with laparoscopic supracervical hysterectomy (LSH). The indication for the TLH case was refractory dysmenorrhea and for the LSH case was as part of a concomitant sacrocervicopexy. The particular methods for specimen removal demonstrated include through the colpotomy for TLH and cold knife manual morcellation within a bag using an Alexis retractor for LSH.
The objectives of this surgical video are to:
- Highlight the clinical advantages and disadvantages between cervical removal or retention at the time of a minimally invasive laparoscopic hysterectomy
- Demonstrate the surgical nuances between TLH and LSH
- Provide a potential resource for patient counseling as well as medical student and resident education.
I encourage you to share this video as an educational resource with your colleagues, residents, students, and patients alike.

I hope to see you at the AAGL Global Congress on Minimally Invasive Gynecology in Vancouver, November 17–21, 2014. Visit www.aagl.org/globalcongress for more information.
— Dr. Arnold Advincula, AAGL 2014 Scientific Program Chair
Share your thoughts on this video! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
It gives me great pleasure to introduce this month’s surgical video. The following feature presentation was produced by my third-year fellow, Mireille Truong, MD, and my third-year resident, Sarah Horvath, MD. The focus of this surgical video is to compare and contrast total laparoscopic hysterectomy (TLH) with laparoscopic supracervical hysterectomy (LSH). The indication for the TLH case was refractory dysmenorrhea and for the LSH case was as part of a concomitant sacrocervicopexy. The particular methods for specimen removal demonstrated include through the colpotomy for TLH and cold knife manual morcellation within a bag using an Alexis retractor for LSH.
The objectives of this surgical video are to:
- Highlight the clinical advantages and disadvantages between cervical removal or retention at the time of a minimally invasive laparoscopic hysterectomy
- Demonstrate the surgical nuances between TLH and LSH
- Provide a potential resource for patient counseling as well as medical student and resident education.
I encourage you to share this video as an educational resource with your colleagues, residents, students, and patients alike.
I hope to see you at the AAGL Global Congress on Minimally Invasive Gynecology in Vancouver, November 17–21, 2014. Visit www.aagl.org/globalcongress for more information.
— Dr. Arnold Advincula, AAGL 2014 Scientific Program Chair
Share your thoughts on this video! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
It gives me great pleasure to introduce this month’s surgical video. The following feature presentation was produced by my third-year fellow, Mireille Truong, MD, and my third-year resident, Sarah Horvath, MD. The focus of this surgical video is to compare and contrast total laparoscopic hysterectomy (TLH) with laparoscopic supracervical hysterectomy (LSH). The indication for the TLH case was refractory dysmenorrhea and for the LSH case was as part of a concomitant sacrocervicopexy. The particular methods for specimen removal demonstrated include through the colpotomy for TLH and cold knife manual morcellation within a bag using an Alexis retractor for LSH.
The objectives of this surgical video are to:
- Highlight the clinical advantages and disadvantages between cervical removal or retention at the time of a minimally invasive laparoscopic hysterectomy
- Demonstrate the surgical nuances between TLH and LSH
- Provide a potential resource for patient counseling as well as medical student and resident education.
I encourage you to share this video as an educational resource with your colleagues, residents, students, and patients alike.
I hope to see you at the AAGL Global Congress on Minimally Invasive Gynecology in Vancouver, November 17–21, 2014. Visit www.aagl.org/globalcongress for more information.
— Dr. Arnold Advincula, AAGL 2014 Scientific Program Chair
Share your thoughts on this video! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
VIDEO: Waiting for long-term data on pCR could be disservice to some breast cancer patients, expert says
SAN FRANCISCO – Only a fraction of patients with breast cancer who are eligible for neoadjuvant therapy are getting it, partly because of confusion around the significance of achieving a pathologic complete response, Dr. William M. Sikov said in an interview at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
Dr. Sikov of Brown University, Providence, R.I., explained why it’s been difficult for researchers to show improved outcomes even after a pathologic complete response (pCR) is obtained, but argued that waiting for long-term outcomes data for neoadjuvant therapy could be a disservice to some patients with breast cancer.
Breast cancer surgeons at his own institution have become converts in favor of neoadjuvant therapy, and Dr. Sikov explained why in this video report.
He reported having no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
SAN FRANCISCO – Only a fraction of patients with breast cancer who are eligible for neoadjuvant therapy are getting it, partly because of confusion around the significance of achieving a pathologic complete response, Dr. William M. Sikov said in an interview at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
Dr. Sikov of Brown University, Providence, R.I., explained why it’s been difficult for researchers to show improved outcomes even after a pathologic complete response (pCR) is obtained, but argued that waiting for long-term outcomes data for neoadjuvant therapy could be a disservice to some patients with breast cancer.
Breast cancer surgeons at his own institution have become converts in favor of neoadjuvant therapy, and Dr. Sikov explained why in this video report.
He reported having no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
SAN FRANCISCO – Only a fraction of patients with breast cancer who are eligible for neoadjuvant therapy are getting it, partly because of confusion around the significance of achieving a pathologic complete response, Dr. William M. Sikov said in an interview at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
Dr. Sikov of Brown University, Providence, R.I., explained why it’s been difficult for researchers to show improved outcomes even after a pathologic complete response (pCR) is obtained, but argued that waiting for long-term outcomes data for neoadjuvant therapy could be a disservice to some patients with breast cancer.
Breast cancer surgeons at his own institution have become converts in favor of neoadjuvant therapy, and Dr. Sikov explained why in this video report.
He reported having no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
AT THE ASCO BREAST CANCER SYMPOSIUM
VIDEO: Unclear if altering lifestyle affects breast cancer
SAN FRANCISCO – Physicians have multiple good reasons to suggest lifestyle changes to many patients with breast cancer, but affecting the cancer itself may not be one of them, Dr. Pamela J. Goodwin said at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
In this video interview, Dr. Goodwin summarizes the ongoing research on how changes in lifestyle such as weight loss, diet, physical activity, and drinking may or may not alter outcomes in patients with breast cancer.
The good news: A drink or two a day probably doesn’t hurt, said Dr. Goodwin, professor of medicine at the University of Toronto’s Mount Sinai Hospital.
She reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
SAN FRANCISCO – Physicians have multiple good reasons to suggest lifestyle changes to many patients with breast cancer, but affecting the cancer itself may not be one of them, Dr. Pamela J. Goodwin said at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
In this video interview, Dr. Goodwin summarizes the ongoing research on how changes in lifestyle such as weight loss, diet, physical activity, and drinking may or may not alter outcomes in patients with breast cancer.
The good news: A drink or two a day probably doesn’t hurt, said Dr. Goodwin, professor of medicine at the University of Toronto’s Mount Sinai Hospital.
She reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
SAN FRANCISCO – Physicians have multiple good reasons to suggest lifestyle changes to many patients with breast cancer, but affecting the cancer itself may not be one of them, Dr. Pamela J. Goodwin said at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
In this video interview, Dr. Goodwin summarizes the ongoing research on how changes in lifestyle such as weight loss, diet, physical activity, and drinking may or may not alter outcomes in patients with breast cancer.
The good news: A drink or two a day probably doesn’t hurt, said Dr. Goodwin, professor of medicine at the University of Toronto’s Mount Sinai Hospital.
She reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
AT THE 2014 ASCO BREAST CANCER SYMPOSIUM

New Protocol Aims to Evaluate Medication Adherence
Rusty Crawford, RPh, was one of the authors of "Protocol to Evaluate Medication Nonadherence Among Patients with Metastatic Prostate Cancer," which was presented at the AVAHO 2014 Meeting in Portland, Oregon. The presentation discusses a new AVAHO-sponsored medication adherence protocol.
According to Crawford, the protocol will look at oral therapies and will help assess prescribing patterns and adherence rates to these new, oral medications.
"That's the big buzz in medicine these days," Crawford said. "Is oral better? It keeps outpatients at home but the downside of oral therapy is that it is not observed."
Rusty Crawford, RPh, was one of the authors of "Protocol to Evaluate Medication Nonadherence Among Patients with Metastatic Prostate Cancer," which was presented at the AVAHO 2014 Meeting in Portland, Oregon. The presentation discusses a new AVAHO-sponsored medication adherence protocol.
According to Crawford, the protocol will look at oral therapies and will help assess prescribing patterns and adherence rates to these new, oral medications.
"That's the big buzz in medicine these days," Crawford said. "Is oral better? It keeps outpatients at home but the downside of oral therapy is that it is not observed."
Rusty Crawford, RPh, was one of the authors of "Protocol to Evaluate Medication Nonadherence Among Patients with Metastatic Prostate Cancer," which was presented at the AVAHO 2014 Meeting in Portland, Oregon. The presentation discusses a new AVAHO-sponsored medication adherence protocol.
According to Crawford, the protocol will look at oral therapies and will help assess prescribing patterns and adherence rates to these new, oral medications.
"That's the big buzz in medicine these days," Crawford said. "Is oral better? It keeps outpatients at home but the downside of oral therapy is that it is not observed."
Living with schizophrenia


VIDEO: Experts offer top tips for flu season 2014-2015
WASHINGTON – Options and opportunity are the keys to navigating the 2014-2015 flu season, according to a panel of experts at a press conference sponsored by the National Foundation for Infectious Diseases.
“The easier we make it for people to get vaccinated, the more likely they are to get vaccinated,” said CDC Director Thomas Frieden, who received his flu shot at the press conference.
In interviews at the conference, Dr. Frieden, Dr. Paul A. Offit of the Children’s Hospital of Philadelphia; Dr. Laura E. Riley of Massachusetts General Hospital, Boston; and Dr. William Schaffner of Vanderbilt University, Nashville, Tenn., discussed making the most of opportunities to vaccinate patients, offering reassurance about vaccine safety (especially for pregnant women), setting an example in your practice by getting vaccinated yourself, and ensuring that everyone who works in your office receives a flu vaccine as well.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – Options and opportunity are the keys to navigating the 2014-2015 flu season, according to a panel of experts at a press conference sponsored by the National Foundation for Infectious Diseases.
“The easier we make it for people to get vaccinated, the more likely they are to get vaccinated,” said CDC Director Thomas Frieden, who received his flu shot at the press conference.
In interviews at the conference, Dr. Frieden, Dr. Paul A. Offit of the Children’s Hospital of Philadelphia; Dr. Laura E. Riley of Massachusetts General Hospital, Boston; and Dr. William Schaffner of Vanderbilt University, Nashville, Tenn., discussed making the most of opportunities to vaccinate patients, offering reassurance about vaccine safety (especially for pregnant women), setting an example in your practice by getting vaccinated yourself, and ensuring that everyone who works in your office receives a flu vaccine as well.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – Options and opportunity are the keys to navigating the 2014-2015 flu season, according to a panel of experts at a press conference sponsored by the National Foundation for Infectious Diseases.
“The easier we make it for people to get vaccinated, the more likely they are to get vaccinated,” said CDC Director Thomas Frieden, who received his flu shot at the press conference.
In interviews at the conference, Dr. Frieden, Dr. Paul A. Offit of the Children’s Hospital of Philadelphia; Dr. Laura E. Riley of Massachusetts General Hospital, Boston; and Dr. William Schaffner of Vanderbilt University, Nashville, Tenn., discussed making the most of opportunities to vaccinate patients, offering reassurance about vaccine safety (especially for pregnant women), setting an example in your practice by getting vaccinated yourself, and ensuring that everyone who works in your office receives a flu vaccine as well.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

VIDEO: Insulin still mainstay of T2DM treatment
VIENNA – Although several new oral hypoglycemic drug classes have entered formularies over the past 5 years or so, none has supplanted insulin as a linchpin for managing patients with type 2 diabetes who fail to achieve adequate glycemic control with diet, exercise, and metformin treatment, Dr. David M. Nathan said in an interview during the annual meeting of the European Association for the Study of Diabetes.
Physicians should keep in mind that insulin remains a “powerful and important drug” for type 2 patients, said Dr. Nathan, chief of diabetes at Massachusetts General Hospital and professor of medicine at Harvard Medical School, both in Boston. Even though insulin’s price has risen recently, it is still a bargain, compared with the new drugs, he added.
Dr. Nathan said he had no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
VIENNA – Although several new oral hypoglycemic drug classes have entered formularies over the past 5 years or so, none has supplanted insulin as a linchpin for managing patients with type 2 diabetes who fail to achieve adequate glycemic control with diet, exercise, and metformin treatment, Dr. David M. Nathan said in an interview during the annual meeting of the European Association for the Study of Diabetes.
Physicians should keep in mind that insulin remains a “powerful and important drug” for type 2 patients, said Dr. Nathan, chief of diabetes at Massachusetts General Hospital and professor of medicine at Harvard Medical School, both in Boston. Even though insulin’s price has risen recently, it is still a bargain, compared with the new drugs, he added.
Dr. Nathan said he had no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
VIENNA – Although several new oral hypoglycemic drug classes have entered formularies over the past 5 years or so, none has supplanted insulin as a linchpin for managing patients with type 2 diabetes who fail to achieve adequate glycemic control with diet, exercise, and metformin treatment, Dr. David M. Nathan said in an interview during the annual meeting of the European Association for the Study of Diabetes.
Physicians should keep in mind that insulin remains a “powerful and important drug” for type 2 patients, said Dr. Nathan, chief of diabetes at Massachusetts General Hospital and professor of medicine at Harvard Medical School, both in Boston. Even though insulin’s price has risen recently, it is still a bargain, compared with the new drugs, he added.
Dr. Nathan said he had no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT EASD 2014
VIDEO: New diagnostic criteria catch systemic lupus earlier
LAS VEGAS – New diagnostic criteria from the Systemic Lupus International Collaborating Clinics make the difficult task of diagnosing systemic lupus easier.
SLICC’s criteria are meant to supplant years-old criteria from the American College of Rheumatology. The SLICC criteria cast a wider net, without sacrificing specificity (Arthritis Rheum. 2012;64:2677-86).
SLICC coauthor Dr. Susan Manzi, chair of the department of medicine in the Allegheny Health Network and director of the Lupus Center of Excellence, both in Pittsburgh, explained how the new criteria work, and why they are an improvement.
At the conference held by Global Academy for Medical Education, she also explained why antinuclear antibody – “the lupus test” – isn’t completely reliable when diagnosing the disease.
Global Academy for Medical Education and this news organization are owned by Frontline Medical Communications.
LAS VEGAS – New diagnostic criteria from the Systemic Lupus International Collaborating Clinics make the difficult task of diagnosing systemic lupus easier.
SLICC’s criteria are meant to supplant years-old criteria from the American College of Rheumatology. The SLICC criteria cast a wider net, without sacrificing specificity (Arthritis Rheum. 2012;64:2677-86).
SLICC coauthor Dr. Susan Manzi, chair of the department of medicine in the Allegheny Health Network and director of the Lupus Center of Excellence, both in Pittsburgh, explained how the new criteria work, and why they are an improvement.
At the conference held by Global Academy for Medical Education, she also explained why antinuclear antibody – “the lupus test” – isn’t completely reliable when diagnosing the disease.
Global Academy for Medical Education and this news organization are owned by Frontline Medical Communications.
LAS VEGAS – New diagnostic criteria from the Systemic Lupus International Collaborating Clinics make the difficult task of diagnosing systemic lupus easier.
SLICC’s criteria are meant to supplant years-old criteria from the American College of Rheumatology. The SLICC criteria cast a wider net, without sacrificing specificity (Arthritis Rheum. 2012;64:2677-86).
SLICC coauthor Dr. Susan Manzi, chair of the department of medicine in the Allegheny Health Network and director of the Lupus Center of Excellence, both in Pittsburgh, explained how the new criteria work, and why they are an improvement.
At the conference held by Global Academy for Medical Education, she also explained why antinuclear antibody – “the lupus test” – isn’t completely reliable when diagnosing the disease.
Global Academy for Medical Education and this news organization are owned by Frontline Medical Communications.
VIDEO: Resistant infection risk grows by 1% for each day of hospitalization
WASHINGTON – Length of stay seemed to have the greatest impact on contracting multidrug-resistant strains of gram-negative organisms, with risk maximizing at 10 days of hospitalization. Each day of hospitalization increased the likelihood of contracting an infection with a gram-negative, multidrug-resistant organism by 1%, with risk maximizing at 10 days of hospitalization, said John A. Bosso, Pharm.D.
Researchers led by Dr. Bosso, a professor in the College of Pharmacy at the Medical University of South Carolina, Charleston, analyzed 949 incidents of documented gram-negative infection during 1998-2014. The study is the first to quantify the potential risk of contracting a multidrug-resistant infection based on length of stay.
We caught up with Dr. Bosso, who presented his findings at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy 2014, and asked how health care providers and clinicians can mitigate the risks to patient health. Dr. Bosso said clinicians should be sure to identify which patients are most likely to contract a serious infection, advise patients on the risks associated with long hospital stays, and encourage patients to do their part in getting out of the hospital as quickly as possible.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – Length of stay seemed to have the greatest impact on contracting multidrug-resistant strains of gram-negative organisms, with risk maximizing at 10 days of hospitalization. Each day of hospitalization increased the likelihood of contracting an infection with a gram-negative, multidrug-resistant organism by 1%, with risk maximizing at 10 days of hospitalization, said John A. Bosso, Pharm.D.
Researchers led by Dr. Bosso, a professor in the College of Pharmacy at the Medical University of South Carolina, Charleston, analyzed 949 incidents of documented gram-negative infection during 1998-2014. The study is the first to quantify the potential risk of contracting a multidrug-resistant infection based on length of stay.
We caught up with Dr. Bosso, who presented his findings at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy 2014, and asked how health care providers and clinicians can mitigate the risks to patient health. Dr. Bosso said clinicians should be sure to identify which patients are most likely to contract a serious infection, advise patients on the risks associated with long hospital stays, and encourage patients to do their part in getting out of the hospital as quickly as possible.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – Length of stay seemed to have the greatest impact on contracting multidrug-resistant strains of gram-negative organisms, with risk maximizing at 10 days of hospitalization. Each day of hospitalization increased the likelihood of contracting an infection with a gram-negative, multidrug-resistant organism by 1%, with risk maximizing at 10 days of hospitalization, said John A. Bosso, Pharm.D.
Researchers led by Dr. Bosso, a professor in the College of Pharmacy at the Medical University of South Carolina, Charleston, analyzed 949 incidents of documented gram-negative infection during 1998-2014. The study is the first to quantify the potential risk of contracting a multidrug-resistant infection based on length of stay.
We caught up with Dr. Bosso, who presented his findings at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy 2014, and asked how health care providers and clinicians can mitigate the risks to patient health. Dr. Bosso said clinicians should be sure to identify which patients are most likely to contract a serious infection, advise patients on the risks associated with long hospital stays, and encourage patients to do their part in getting out of the hospital as quickly as possible.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT ICAAC 2014

VIDEO: Novel sphingosine 1-phosphate 1 receptor modulator has promising safety results
BOSTON – Treatment of relapsing-remitting multiple sclerosis patients with the investigational drug RPC1063, a selective, oral sphingosine 1-phosphate 1 receptor modulator, in the phase II RADIANCE trial generated few concerns about potential cardiac events or elevated liver enzymes.
These initial clinical trial results of RPC1063 hint at a potentially better safety profile than the approved sphingosine 1-phosphate receptor modulator fingolimod, which has a high affinity for the sphingosine 1-phosphate 1, 3, 4, and 5 receptor subtypes. Its affinity for the sphingosine 1-phosphate 3 and 4 subtypes are thought to contribute to its potential for cardiac adverse events. RPC1063 could prove to be a safer drug because of its specificity for sphingosine 1-phosphate receptor subtype 1, according to Dr. Jeffrey Cohen, director of the Mellon Center for Multiple Sclerosis at the Cleveland Clinic and primary investigator for the RADIANCE trial. Dr. Cohen spoke with us at the joint meeting of the European and Americas Committees for Treatment and Research in Multiple Sclerosis.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
BOSTON – Treatment of relapsing-remitting multiple sclerosis patients with the investigational drug RPC1063, a selective, oral sphingosine 1-phosphate 1 receptor modulator, in the phase II RADIANCE trial generated few concerns about potential cardiac events or elevated liver enzymes.
These initial clinical trial results of RPC1063 hint at a potentially better safety profile than the approved sphingosine 1-phosphate receptor modulator fingolimod, which has a high affinity for the sphingosine 1-phosphate 1, 3, 4, and 5 receptor subtypes. Its affinity for the sphingosine 1-phosphate 3 and 4 subtypes are thought to contribute to its potential for cardiac adverse events. RPC1063 could prove to be a safer drug because of its specificity for sphingosine 1-phosphate receptor subtype 1, according to Dr. Jeffrey Cohen, director of the Mellon Center for Multiple Sclerosis at the Cleveland Clinic and primary investigator for the RADIANCE trial. Dr. Cohen spoke with us at the joint meeting of the European and Americas Committees for Treatment and Research in Multiple Sclerosis.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
BOSTON – Treatment of relapsing-remitting multiple sclerosis patients with the investigational drug RPC1063, a selective, oral sphingosine 1-phosphate 1 receptor modulator, in the phase II RADIANCE trial generated few concerns about potential cardiac events or elevated liver enzymes.
These initial clinical trial results of RPC1063 hint at a potentially better safety profile than the approved sphingosine 1-phosphate receptor modulator fingolimod, which has a high affinity for the sphingosine 1-phosphate 1, 3, 4, and 5 receptor subtypes. Its affinity for the sphingosine 1-phosphate 3 and 4 subtypes are thought to contribute to its potential for cardiac adverse events. RPC1063 could prove to be a safer drug because of its specificity for sphingosine 1-phosphate receptor subtype 1, according to Dr. Jeffrey Cohen, director of the Mellon Center for Multiple Sclerosis at the Cleveland Clinic and primary investigator for the RADIANCE trial. Dr. Cohen spoke with us at the joint meeting of the European and Americas Committees for Treatment and Research in Multiple Sclerosis.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
At MSBoston 2014
