User login
For MD-IQ use only
Elderly mice receive the gift of warmth
Steal from the warm, give to the cold
If there’s one constant in life other than taxes, it’s elderly people moving to Florida. The Sunshine State’s reputation as a giant retirement home needs no elaboration, but why do senior citizens gravitate there? Well, many reasons, but a big one is that, the older you get, the more susceptible and sensitive you are to the cold. And now, according to a new study, we may have identified a culprit.

Researchers from Yale University examined a group of mice and found that the older ones lacked ICL2 cells in their fatty tissue. These cells, at least in younger mice, help restore body heat when exposed to cold temperatures. Lacking these cells meant that older mice had a limited ability to burn their fat and raise their temperature in response to cold.
Well, job done, all we need to do now is stimulate production of ICL2 cells in elderly people, and they’ll be able to go outside in 80-degree weather without a sweater again. Except there’s a problem. In a cruel twist of fate, when the elderly mice were given a molecule to boost ICL2 cell production, they actually became less tolerant of the cold than at baseline. Oops.
The scientists didn’t give up though, and gave their elderly mice ICL2 cells from young mice. This finally did the trick, though we have to admit, if that treatment does eventually scale up to humans, the prospect of a bunch of senior citizens taking ICL2 cells from young people to stay warm does sound a bit like a bad vampire movie premise. “I vant to suck your immune cell group 2 innate lymphoid cells!” Not the most pithy catch phrase in the world.
Grocery store tapping your subconscious? It’s a good thing
We all know there’s marketing and functionality elements to grocery stores and how they’re set up for your shopping pleasure. But what if I told you that the good old supermarket subconscious trick works on how healthy food decisions are?

In a recent study, researchers at the University of Southampton in England found that if you placed a wider selection of fruits and vegetables near the entrances and more nonfood items near checkouts, sales decreased on the sweets and increased on the produce. “The findings of our study suggest that a healthier store layout could lead to nearly 10,000 extra portions of fruit and vegetables and approximately 1,500 fewer portions of confectionery being sold on a weekly basis in each store,” lead author Dr. Christina Vogel explained.
You’re probably thinking that food placement studies aren’t new. That’s true, but this one went above and beyond. Instead of just looking at the influence placement has on purchase, this one took it further by trying to reduce the consumers’ “calorie opportunities” and examining the effect on sales. Also, customer loyalty, patterns, and diets were taken into account across multiple household members.
The researchers think shifting the layouts in grocery stores could shift people’s food choices, producing a domino effect on the population’s overall diet. With obesity, diabetes, and cardiology concerns always looming, swaying consumers toward healthier food choices makes for better public health overall.
So if you feel like you’re being subconsciously assaulted by veggies every time you walk into Trader Joe’s, just know it’s for your own good.
TikTokers take on tics
We know TikTok is what makes a lot of teens and young adults tick, but what if TikTokers are actually catching tic disorders from other TikTokers?

TikTok blew up during the pandemic. Many people were stuck at home and had nothing better to do than make and watch TikTok videos. The pandemic brought isolation, uncertainty, and anxiety. The stress that followed may have caused many people, mostly women and young girls, to develop tic disorders.
There’s a TikTok for everything, whether it’s a new dance or a recipe. Many people even use TikTok to speak out about their illnesses. Several TikTokers have Tourette’s syndrome and show their tics on their videos. It appears that some audience members actually “catch” the tics from watching the videos and are then unable to stop certain jerking movements or saying specific words.
Neurologists at the University of Calgary (Alta.), who were hearing from colleagues and getting referrals of such patients, called it “an epidemic within the pandemic.” The behavior is not actually Tourette’s, they told Vice, but the patients “cannot stop, and we have absolutely witnessed that.”
There is, of course, controversy over the issue. One individual with the condition said, “I feel like there’s a lot of really weird, backwards stigma on TikTok about tic disorders. Like, you aren’t allowed to have one unless it’s this one.”
Who would have guessed that people would disagree over stuff on the Internet?
Look on the bright side: Obesity edition
The pandemic may have postponed “Top Gun: Maverick” and “The Marvelous Mrs. Maisel” until who-knows-when, but we here at LOTME are happy to announce the nearly-as-anticipated return of Bacteria vs. the World.

As you may recall from our last edition of BVTW, bacteria battled the ghost of Charles Darwin, who had taken the earthly form of antibiotics capable of stopping bacterial evolution. Tonight, our prokaryotic protagonists take on an equally relentless and ubiquitous challenger: obesity.
Specifically, we’re putting bacteria up against the obesity survival paradox, that phenomenon in which obesity and overweight seem to protect against – yes, you guessed it – bacterial infections.
A Swedish research team observed a group of 2,196 individual adults who received care for suspected severe bacterial infection at Skaraborg Hospital in Skövde. One year after hospitalization, 26% of normal-weight (body mass index, 18.5-24.99) patients were dead, compared with 17% of overweight (BMI, 25.0-29.99), 16% of obese (BMI, 30.0-34.99), and 9% of very obese (BMI >35) patients.
These results confirm the obesity survival paradox, but “what we don’t know is how being overweight can benefit the patient with a bacterial infection, or whether it’s connected with functions in the immune system and how they’re regulated,” lead author Dr. Åsa Alsiö said in a written statement.
A spokes-cell for the bacteria disputed the results and challenged the legitimacy of the investigators. When asked if there should be some sort of reexamination of the findings, he/she/it replied: “You bet your flagella.” We then pointed out that humans don’t have flagellum, and the representative raised his/her/its flagella in what could only be considered an obscene gesture.
Steal from the warm, give to the cold
If there’s one constant in life other than taxes, it’s elderly people moving to Florida. The Sunshine State’s reputation as a giant retirement home needs no elaboration, but why do senior citizens gravitate there? Well, many reasons, but a big one is that, the older you get, the more susceptible and sensitive you are to the cold. And now, according to a new study, we may have identified a culprit.
Researchers from Yale University examined a group of mice and found that the older ones lacked ICL2 cells in their fatty tissue. These cells, at least in younger mice, help restore body heat when exposed to cold temperatures. Lacking these cells meant that older mice had a limited ability to burn their fat and raise their temperature in response to cold.
Well, job done, all we need to do now is stimulate production of ICL2 cells in elderly people, and they’ll be able to go outside in 80-degree weather without a sweater again. Except there’s a problem. In a cruel twist of fate, when the elderly mice were given a molecule to boost ICL2 cell production, they actually became less tolerant of the cold than at baseline. Oops.
The scientists didn’t give up though, and gave their elderly mice ICL2 cells from young mice. This finally did the trick, though we have to admit, if that treatment does eventually scale up to humans, the prospect of a bunch of senior citizens taking ICL2 cells from young people to stay warm does sound a bit like a bad vampire movie premise. “I vant to suck your immune cell group 2 innate lymphoid cells!” Not the most pithy catch phrase in the world.
Grocery store tapping your subconscious? It’s a good thing
We all know there’s marketing and functionality elements to grocery stores and how they’re set up for your shopping pleasure. But what if I told you that the good old supermarket subconscious trick works on how healthy food decisions are?
In a recent study, researchers at the University of Southampton in England found that if you placed a wider selection of fruits and vegetables near the entrances and more nonfood items near checkouts, sales decreased on the sweets and increased on the produce. “The findings of our study suggest that a healthier store layout could lead to nearly 10,000 extra portions of fruit and vegetables and approximately 1,500 fewer portions of confectionery being sold on a weekly basis in each store,” lead author Dr. Christina Vogel explained.
You’re probably thinking that food placement studies aren’t new. That’s true, but this one went above and beyond. Instead of just looking at the influence placement has on purchase, this one took it further by trying to reduce the consumers’ “calorie opportunities” and examining the effect on sales. Also, customer loyalty, patterns, and diets were taken into account across multiple household members.
The researchers think shifting the layouts in grocery stores could shift people’s food choices, producing a domino effect on the population’s overall diet. With obesity, diabetes, and cardiology concerns always looming, swaying consumers toward healthier food choices makes for better public health overall.
So if you feel like you’re being subconsciously assaulted by veggies every time you walk into Trader Joe’s, just know it’s for your own good.
TikTokers take on tics
We know TikTok is what makes a lot of teens and young adults tick, but what if TikTokers are actually catching tic disorders from other TikTokers?
TikTok blew up during the pandemic. Many people were stuck at home and had nothing better to do than make and watch TikTok videos. The pandemic brought isolation, uncertainty, and anxiety. The stress that followed may have caused many people, mostly women and young girls, to develop tic disorders.
There’s a TikTok for everything, whether it’s a new dance or a recipe. Many people even use TikTok to speak out about their illnesses. Several TikTokers have Tourette’s syndrome and show their tics on their videos. It appears that some audience members actually “catch” the tics from watching the videos and are then unable to stop certain jerking movements or saying specific words.
Neurologists at the University of Calgary (Alta.), who were hearing from colleagues and getting referrals of such patients, called it “an epidemic within the pandemic.” The behavior is not actually Tourette’s, they told Vice, but the patients “cannot stop, and we have absolutely witnessed that.”
There is, of course, controversy over the issue. One individual with the condition said, “I feel like there’s a lot of really weird, backwards stigma on TikTok about tic disorders. Like, you aren’t allowed to have one unless it’s this one.”
Who would have guessed that people would disagree over stuff on the Internet?
Look on the bright side: Obesity edition
The pandemic may have postponed “Top Gun: Maverick” and “The Marvelous Mrs. Maisel” until who-knows-when, but we here at LOTME are happy to announce the nearly-as-anticipated return of Bacteria vs. the World.
As you may recall from our last edition of BVTW, bacteria battled the ghost of Charles Darwin, who had taken the earthly form of antibiotics capable of stopping bacterial evolution. Tonight, our prokaryotic protagonists take on an equally relentless and ubiquitous challenger: obesity.
Specifically, we’re putting bacteria up against the obesity survival paradox, that phenomenon in which obesity and overweight seem to protect against – yes, you guessed it – bacterial infections.
A Swedish research team observed a group of 2,196 individual adults who received care for suspected severe bacterial infection at Skaraborg Hospital in Skövde. One year after hospitalization, 26% of normal-weight (body mass index, 18.5-24.99) patients were dead, compared with 17% of overweight (BMI, 25.0-29.99), 16% of obese (BMI, 30.0-34.99), and 9% of very obese (BMI >35) patients.
These results confirm the obesity survival paradox, but “what we don’t know is how being overweight can benefit the patient with a bacterial infection, or whether it’s connected with functions in the immune system and how they’re regulated,” lead author Dr. Åsa Alsiö said in a written statement.
A spokes-cell for the bacteria disputed the results and challenged the legitimacy of the investigators. When asked if there should be some sort of reexamination of the findings, he/she/it replied: “You bet your flagella.” We then pointed out that humans don’t have flagellum, and the representative raised his/her/its flagella in what could only be considered an obscene gesture.
Steal from the warm, give to the cold
If there’s one constant in life other than taxes, it’s elderly people moving to Florida. The Sunshine State’s reputation as a giant retirement home needs no elaboration, but why do senior citizens gravitate there? Well, many reasons, but a big one is that, the older you get, the more susceptible and sensitive you are to the cold. And now, according to a new study, we may have identified a culprit.
Researchers from Yale University examined a group of mice and found that the older ones lacked ICL2 cells in their fatty tissue. These cells, at least in younger mice, help restore body heat when exposed to cold temperatures. Lacking these cells meant that older mice had a limited ability to burn their fat and raise their temperature in response to cold.
Well, job done, all we need to do now is stimulate production of ICL2 cells in elderly people, and they’ll be able to go outside in 80-degree weather without a sweater again. Except there’s a problem. In a cruel twist of fate, when the elderly mice were given a molecule to boost ICL2 cell production, they actually became less tolerant of the cold than at baseline. Oops.
The scientists didn’t give up though, and gave their elderly mice ICL2 cells from young mice. This finally did the trick, though we have to admit, if that treatment does eventually scale up to humans, the prospect of a bunch of senior citizens taking ICL2 cells from young people to stay warm does sound a bit like a bad vampire movie premise. “I vant to suck your immune cell group 2 innate lymphoid cells!” Not the most pithy catch phrase in the world.
Grocery store tapping your subconscious? It’s a good thing
We all know there’s marketing and functionality elements to grocery stores and how they’re set up for your shopping pleasure. But what if I told you that the good old supermarket subconscious trick works on how healthy food decisions are?
In a recent study, researchers at the University of Southampton in England found that if you placed a wider selection of fruits and vegetables near the entrances and more nonfood items near checkouts, sales decreased on the sweets and increased on the produce. “The findings of our study suggest that a healthier store layout could lead to nearly 10,000 extra portions of fruit and vegetables and approximately 1,500 fewer portions of confectionery being sold on a weekly basis in each store,” lead author Dr. Christina Vogel explained.
You’re probably thinking that food placement studies aren’t new. That’s true, but this one went above and beyond. Instead of just looking at the influence placement has on purchase, this one took it further by trying to reduce the consumers’ “calorie opportunities” and examining the effect on sales. Also, customer loyalty, patterns, and diets were taken into account across multiple household members.
The researchers think shifting the layouts in grocery stores could shift people’s food choices, producing a domino effect on the population’s overall diet. With obesity, diabetes, and cardiology concerns always looming, swaying consumers toward healthier food choices makes for better public health overall.
So if you feel like you’re being subconsciously assaulted by veggies every time you walk into Trader Joe’s, just know it’s for your own good.
TikTokers take on tics
We know TikTok is what makes a lot of teens and young adults tick, but what if TikTokers are actually catching tic disorders from other TikTokers?
TikTok blew up during the pandemic. Many people were stuck at home and had nothing better to do than make and watch TikTok videos. The pandemic brought isolation, uncertainty, and anxiety. The stress that followed may have caused many people, mostly women and young girls, to develop tic disorders.
There’s a TikTok for everything, whether it’s a new dance or a recipe. Many people even use TikTok to speak out about their illnesses. Several TikTokers have Tourette’s syndrome and show their tics on their videos. It appears that some audience members actually “catch” the tics from watching the videos and are then unable to stop certain jerking movements or saying specific words.
Neurologists at the University of Calgary (Alta.), who were hearing from colleagues and getting referrals of such patients, called it “an epidemic within the pandemic.” The behavior is not actually Tourette’s, they told Vice, but the patients “cannot stop, and we have absolutely witnessed that.”
There is, of course, controversy over the issue. One individual with the condition said, “I feel like there’s a lot of really weird, backwards stigma on TikTok about tic disorders. Like, you aren’t allowed to have one unless it’s this one.”
Who would have guessed that people would disagree over stuff on the Internet?
Look on the bright side: Obesity edition
The pandemic may have postponed “Top Gun: Maverick” and “The Marvelous Mrs. Maisel” until who-knows-when, but we here at LOTME are happy to announce the nearly-as-anticipated return of Bacteria vs. the World.
As you may recall from our last edition of BVTW, bacteria battled the ghost of Charles Darwin, who had taken the earthly form of antibiotics capable of stopping bacterial evolution. Tonight, our prokaryotic protagonists take on an equally relentless and ubiquitous challenger: obesity.
Specifically, we’re putting bacteria up against the obesity survival paradox, that phenomenon in which obesity and overweight seem to protect against – yes, you guessed it – bacterial infections.
A Swedish research team observed a group of 2,196 individual adults who received care for suspected severe bacterial infection at Skaraborg Hospital in Skövde. One year after hospitalization, 26% of normal-weight (body mass index, 18.5-24.99) patients were dead, compared with 17% of overweight (BMI, 25.0-29.99), 16% of obese (BMI, 30.0-34.99), and 9% of very obese (BMI >35) patients.
These results confirm the obesity survival paradox, but “what we don’t know is how being overweight can benefit the patient with a bacterial infection, or whether it’s connected with functions in the immune system and how they’re regulated,” lead author Dr. Åsa Alsiö said in a written statement.
A spokes-cell for the bacteria disputed the results and challenged the legitimacy of the investigators. When asked if there should be some sort of reexamination of the findings, he/she/it replied: “You bet your flagella.” We then pointed out that humans don’t have flagellum, and the representative raised his/her/its flagella in what could only be considered an obscene gesture.

Medical education must takes broader view of disabilities
“All physicians, regardless of specialty, will work with patients with disabilities,” Corrie Harris, MD, of the University of Louisville (Ky.), said in a plenary session presentation at the 2021 virtual Pediatric Hospital Medicine conference.
Disabilities vary in their visibility, from cognitive and sensory impairments that are not immediately obvious to an obvious physical disability, she said.
One in four adults and one in six children in the United States has a disability, said Dr. Harris. The prevalence of disability increases with age, but occurs across the lifespan, and will likely increase in the future with greater improvements in health care overall.
Dr. Harris reviewed the current conceptual model that forms the basis for the World Health Organization definition of functioning disability. This “functional model” defines disability as caused by interactions between health conditions and the environment, and the response is to “prioritize function to meet patient goals,” Dr. Harris said at the meeting, sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
This model is based on collaboration between health care providers and their patients with disabilities, and training is important to help providers make this collaboration successful, said Dr. Harris. Without training, physicians may be ineffective in communicating with patients with disabilities by not speaking directly to the patient, not speaking in a way the patient can understand clearly, and not providing accessible patient education materials. Physicians also tend to minimize the extent of the patient’s expertise in their own condition based on their lived experiences, and tend to underestimate the abilities of patients with disabilities.
However, direct experience with disabled patients and an understanding of the health disparities they endure can help physicians look at these patients “through a more intersectional lens,” that also takes into account social determinants of health, Dr. Harris said. “I have found that people with disabilities are the best teachers about disability, because they have expertise that comes from their lived experience.”
Patients are the best teachers
Several initiatives are helping physicians to bridge this gap in understanding and reduce disparities in care. One such program is FRAME: Faces Redefining the Art of Medical Education. FRAME is a web-based film library designed to present medical information to health care providers in training, clinicians, families, and communities in a dignified and humanizing way. FRAME was developed in part by fashion photographer Rick Guidotti, who was inspired after meeting a young woman with albinism to create Positive Exposure, an ongoing project featuring children and adolescents with various disabilities.
FRAME films are “short films presenting all the basic hallmark characteristics of a certain genetic condition, but presented by somebody living with that condition,” said Mr. Guidotti in his presentation during the session.
The National Curriculum Initiative in Developmental Medicine (NCIDM) is designed to incorporate care for individuals with disabilities into medical education. NCIDM is a project created by the American Academy of Developmental Medicine and Dentistry (AADMD).
“The need for this program is that there is no U.S. requirement for medical schools to teach about intellectual and developmental disabilities,” Priya Chandan, MD, also of the University of Louisville, said in her presentation during the session. “Approximately 81% of graduating medical students have no training in caring for adults with disabilities,” said Dr. Chandan, who serves as director of the NCIDM.
The current NCIDM was created as a 5-year partnership between the AADMD and Special Olympics, supported in part by the Centers for Disease Control and Prevention, Dr. Chandan said. The purpose was to provide training to medical students in the field of developmental medicine, meaning the care of individuals with intellectual/developmental disabilities (IDD) across the lifespan. The AADMD has expanded to 26 medical schools in the United States and will reach approximately 4,000 medical students by the conclusion of the current initiative.
One challenge in medical education is getting past the idea that people living with disabilities need to be fixed, said Dr. Chandan. The NCIDM approach reflects Mr. Guidotti’s approach in both the FRAME initiatives and his Positive Exposure foundation, with a focus on treating people as people, and letting individuals with disabilities represent themselves.
Dr. Chandan described the NCIDM curriculum as allowing for flexible teaching methodologies and materials, as long as they meet the NCIDM-created learning goals and objectives. The curriculum also includes standardized evaluations. Each NCIDM program in a participating medical school includes a faculty champion, and the curriculum supports meeting people with IDD not only inside medical settings, but also outside in the community.
NCIDM embraces the idea of community-engaged scholarship, which Dr. Chandan defined as “a form of scholarship that directly benefits the community and is consistent with university and unit missions.” This method combined teaching and conducting research while providing a service to the community.
The next steps for the current NCIDM initiative are to complete collection of data and course evaluations from participating schools by early 2022, followed by continued dissemination and collaboration through AADMD.
Overall, the content of the curriculum explores how and where IDD fits into clinical care, Dr. Chandan said, who also emphasized the implications of communication. “How we think affects how we communicate,” she added. Be mindful of the language used to talk to and about patients with disabilities, both to colleagues and to learners.
When talking to the patient, find something in common, beyond the diagnosis, said Dr. Chandan. Remember that some disabilities are visible and some are not. “Treat people with respect, because you won’t know what their functional level is just by looking,” she concluded.
The presenters had no financial conflicts to disclose.
“All physicians, regardless of specialty, will work with patients with disabilities,” Corrie Harris, MD, of the University of Louisville (Ky.), said in a plenary session presentation at the 2021 virtual Pediatric Hospital Medicine conference.
Disabilities vary in their visibility, from cognitive and sensory impairments that are not immediately obvious to an obvious physical disability, she said.
One in four adults and one in six children in the United States has a disability, said Dr. Harris. The prevalence of disability increases with age, but occurs across the lifespan, and will likely increase in the future with greater improvements in health care overall.
Dr. Harris reviewed the current conceptual model that forms the basis for the World Health Organization definition of functioning disability. This “functional model” defines disability as caused by interactions between health conditions and the environment, and the response is to “prioritize function to meet patient goals,” Dr. Harris said at the meeting, sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
This model is based on collaboration between health care providers and their patients with disabilities, and training is important to help providers make this collaboration successful, said Dr. Harris. Without training, physicians may be ineffective in communicating with patients with disabilities by not speaking directly to the patient, not speaking in a way the patient can understand clearly, and not providing accessible patient education materials. Physicians also tend to minimize the extent of the patient’s expertise in their own condition based on their lived experiences, and tend to underestimate the abilities of patients with disabilities.
However, direct experience with disabled patients and an understanding of the health disparities they endure can help physicians look at these patients “through a more intersectional lens,” that also takes into account social determinants of health, Dr. Harris said. “I have found that people with disabilities are the best teachers about disability, because they have expertise that comes from their lived experience.”
Patients are the best teachers
Several initiatives are helping physicians to bridge this gap in understanding and reduce disparities in care. One such program is FRAME: Faces Redefining the Art of Medical Education. FRAME is a web-based film library designed to present medical information to health care providers in training, clinicians, families, and communities in a dignified and humanizing way. FRAME was developed in part by fashion photographer Rick Guidotti, who was inspired after meeting a young woman with albinism to create Positive Exposure, an ongoing project featuring children and adolescents with various disabilities.
FRAME films are “short films presenting all the basic hallmark characteristics of a certain genetic condition, but presented by somebody living with that condition,” said Mr. Guidotti in his presentation during the session.
The National Curriculum Initiative in Developmental Medicine (NCIDM) is designed to incorporate care for individuals with disabilities into medical education. NCIDM is a project created by the American Academy of Developmental Medicine and Dentistry (AADMD).
“The need for this program is that there is no U.S. requirement for medical schools to teach about intellectual and developmental disabilities,” Priya Chandan, MD, also of the University of Louisville, said in her presentation during the session. “Approximately 81% of graduating medical students have no training in caring for adults with disabilities,” said Dr. Chandan, who serves as director of the NCIDM.
The current NCIDM was created as a 5-year partnership between the AADMD and Special Olympics, supported in part by the Centers for Disease Control and Prevention, Dr. Chandan said. The purpose was to provide training to medical students in the field of developmental medicine, meaning the care of individuals with intellectual/developmental disabilities (IDD) across the lifespan. The AADMD has expanded to 26 medical schools in the United States and will reach approximately 4,000 medical students by the conclusion of the current initiative.
One challenge in medical education is getting past the idea that people living with disabilities need to be fixed, said Dr. Chandan. The NCIDM approach reflects Mr. Guidotti’s approach in both the FRAME initiatives and his Positive Exposure foundation, with a focus on treating people as people, and letting individuals with disabilities represent themselves.
Dr. Chandan described the NCIDM curriculum as allowing for flexible teaching methodologies and materials, as long as they meet the NCIDM-created learning goals and objectives. The curriculum also includes standardized evaluations. Each NCIDM program in a participating medical school includes a faculty champion, and the curriculum supports meeting people with IDD not only inside medical settings, but also outside in the community.
NCIDM embraces the idea of community-engaged scholarship, which Dr. Chandan defined as “a form of scholarship that directly benefits the community and is consistent with university and unit missions.” This method combined teaching and conducting research while providing a service to the community.
The next steps for the current NCIDM initiative are to complete collection of data and course evaluations from participating schools by early 2022, followed by continued dissemination and collaboration through AADMD.
Overall, the content of the curriculum explores how and where IDD fits into clinical care, Dr. Chandan said, who also emphasized the implications of communication. “How we think affects how we communicate,” she added. Be mindful of the language used to talk to and about patients with disabilities, both to colleagues and to learners.
When talking to the patient, find something in common, beyond the diagnosis, said Dr. Chandan. Remember that some disabilities are visible and some are not. “Treat people with respect, because you won’t know what their functional level is just by looking,” she concluded.
The presenters had no financial conflicts to disclose.
“All physicians, regardless of specialty, will work with patients with disabilities,” Corrie Harris, MD, of the University of Louisville (Ky.), said in a plenary session presentation at the 2021 virtual Pediatric Hospital Medicine conference.
Disabilities vary in their visibility, from cognitive and sensory impairments that are not immediately obvious to an obvious physical disability, she said.
One in four adults and one in six children in the United States has a disability, said Dr. Harris. The prevalence of disability increases with age, but occurs across the lifespan, and will likely increase in the future with greater improvements in health care overall.
Dr. Harris reviewed the current conceptual model that forms the basis for the World Health Organization definition of functioning disability. This “functional model” defines disability as caused by interactions between health conditions and the environment, and the response is to “prioritize function to meet patient goals,” Dr. Harris said at the meeting, sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
This model is based on collaboration between health care providers and their patients with disabilities, and training is important to help providers make this collaboration successful, said Dr. Harris. Without training, physicians may be ineffective in communicating with patients with disabilities by not speaking directly to the patient, not speaking in a way the patient can understand clearly, and not providing accessible patient education materials. Physicians also tend to minimize the extent of the patient’s expertise in their own condition based on their lived experiences, and tend to underestimate the abilities of patients with disabilities.
However, direct experience with disabled patients and an understanding of the health disparities they endure can help physicians look at these patients “through a more intersectional lens,” that also takes into account social determinants of health, Dr. Harris said. “I have found that people with disabilities are the best teachers about disability, because they have expertise that comes from their lived experience.”
Patients are the best teachers
Several initiatives are helping physicians to bridge this gap in understanding and reduce disparities in care. One such program is FRAME: Faces Redefining the Art of Medical Education. FRAME is a web-based film library designed to present medical information to health care providers in training, clinicians, families, and communities in a dignified and humanizing way. FRAME was developed in part by fashion photographer Rick Guidotti, who was inspired after meeting a young woman with albinism to create Positive Exposure, an ongoing project featuring children and adolescents with various disabilities.
FRAME films are “short films presenting all the basic hallmark characteristics of a certain genetic condition, but presented by somebody living with that condition,” said Mr. Guidotti in his presentation during the session.
The National Curriculum Initiative in Developmental Medicine (NCIDM) is designed to incorporate care for individuals with disabilities into medical education. NCIDM is a project created by the American Academy of Developmental Medicine and Dentistry (AADMD).
“The need for this program is that there is no U.S. requirement for medical schools to teach about intellectual and developmental disabilities,” Priya Chandan, MD, also of the University of Louisville, said in her presentation during the session. “Approximately 81% of graduating medical students have no training in caring for adults with disabilities,” said Dr. Chandan, who serves as director of the NCIDM.
The current NCIDM was created as a 5-year partnership between the AADMD and Special Olympics, supported in part by the Centers for Disease Control and Prevention, Dr. Chandan said. The purpose was to provide training to medical students in the field of developmental medicine, meaning the care of individuals with intellectual/developmental disabilities (IDD) across the lifespan. The AADMD has expanded to 26 medical schools in the United States and will reach approximately 4,000 medical students by the conclusion of the current initiative.
One challenge in medical education is getting past the idea that people living with disabilities need to be fixed, said Dr. Chandan. The NCIDM approach reflects Mr. Guidotti’s approach in both the FRAME initiatives and his Positive Exposure foundation, with a focus on treating people as people, and letting individuals with disabilities represent themselves.
Dr. Chandan described the NCIDM curriculum as allowing for flexible teaching methodologies and materials, as long as they meet the NCIDM-created learning goals and objectives. The curriculum also includes standardized evaluations. Each NCIDM program in a participating medical school includes a faculty champion, and the curriculum supports meeting people with IDD not only inside medical settings, but also outside in the community.
NCIDM embraces the idea of community-engaged scholarship, which Dr. Chandan defined as “a form of scholarship that directly benefits the community and is consistent with university and unit missions.” This method combined teaching and conducting research while providing a service to the community.
The next steps for the current NCIDM initiative are to complete collection of data and course evaluations from participating schools by early 2022, followed by continued dissemination and collaboration through AADMD.
Overall, the content of the curriculum explores how and where IDD fits into clinical care, Dr. Chandan said, who also emphasized the implications of communication. “How we think affects how we communicate,” she added. Be mindful of the language used to talk to and about patients with disabilities, both to colleagues and to learners.
When talking to the patient, find something in common, beyond the diagnosis, said Dr. Chandan. Remember that some disabilities are visible and some are not. “Treat people with respect, because you won’t know what their functional level is just by looking,” she concluded.
The presenters had no financial conflicts to disclose.
FROM PHM 2021
Walking 7,000 steps per day may be enough to reduce mortality risk
based on prospective data from more than 2,000 people.
Findings were consistent regardless of race or sex, and step intensity had no impact on mortality risk, reported lead author Amanda E. Paluch, PhD, of the University of Massachusetts Amherst, and colleagues.
“In response to the need for empirical data on the associations of step volume and intensity with mortality in younger and diverse populations, we conducted a prospective study in middle-aged Black and White adults followed up for mortality for approximately 11 years,” the investigators wrote in JAMA Network Open. “The objectives of our study were to examine the associations of step volume and intensity with mortality overall and by race and sex.”
Steps per day is easy to communicate
Dr. Paluch noted that steps per day is a “very appealing metric to quantify activity,” for both researchers and laypeople.
“Steps per day is simple and easy to communicate in public health and clinical settings,” Dr. Paluch said in an interview. “Additionally, the dramatic growth of wearable devices measuring steps makes it appealing and broadens the reach of promoting physical activity to many individuals. Walking is an activity that most of the general population can pursue. It can also be accumulated throughout daily living and may seem more achievable to fit into busy lives than a structured exercise session.”
The present investigation was conducted as part of the Coronary Artery Risk Development in Young Adults (CARDIA) Study. The dataset included 2,110 participants ranging from 38-50 years of age, with a mean age of 45.2 years. A slightly higher proportion of the subjects were women (57.1%) and White (57.9%).
All participants wore an ActiGraph 7164 accelerometer for 1 week and were then followed for death of any cause, with a mean follow-up of 10.8 years. Multivariable-adjusted Cox proportional hazards models included a range of covariates, such as smoking history, body weight, alcohol intake, blood pressure, total cholesterol, and others. Step counts were grouped into low (less than 7,000 steps per day), moderate (7,000-9,999), and high (at least 10,000 steps per day) categories.
Compared with individuals who took less than 7,000 steps per day, those who took 7,000-9,000 steps per day had a 72% reduced risk of mortality (hazard ratio, 0.28; 95% confidence interval, 0.15-0.54). Going beyond 10,000 steps appeared to add no benefit, based on a 55% lower risk of all-cause mortality in the highly active group, compared with those taking less than 7,000 steps per day (HR, 0.45; 95% CI, 0.25-0.81).
Walking faster didn’t appear to help either, as stepping intensity was not associated with mortality risk; however, Dr. Paluch urged a cautious interpretation of this finding, calling it “inconclusive,” and suggesting that more research is needed.
“It is also important to note that this study only looked at premature all-cause mortality, and therefore the results may be different for other health outcomes, such as the risk of cardiovascular disease, or diabetes, cancer, or mental health outcomes,” Dr. Paluch said.
“The results from our study demonstrated that those who are least active have the most to gain,” Dr. Paluch said. “Even small incremental increases in steps per day are associated with a lower mortality risk during middle age. A walking plan that gradually works up toward 7,000-10,000 steps per day in middle-aged adults may have health benefits and lower the risk of premature mortality.”
Causality cannot be confirmed
According to Raed A. Joundi, MD, DPhil, of the University of Calgary (Alta.), the study size, diverse population, and length of follow-up should increase confidence in the findings, although a causal relationship remains elusive.
“As this study is observational, causality between step count and mortality cannot be confirmed; however, the authors accounted for many factors, and the association was consistent in different analyses and with prior literature,” Dr. Joundi said in an interview. “The authors did not assess the risk of other important events like stroke and heart attack, and these could be addressed in a future study.”
Dr. Joundi, who recently published a study linking exercise with a 50% reduction in mortality after stroke, noted that “physical activity has innumerable benefits, and it’s important that people engage in activity that can be regular and consistent, regardless of the type or intensity.”
To this end, he highlighted the use of “devices capable of monitoring step count, which can be an important motivational tool,” and suggested that these findings may bring a sigh of relief to step counters who come up a little short on a common daily goal.
“A target of 10,000 steps is often used for public health promotion, and this study now provides convincing observational evidence that it may be an optimal step count target for mortality reduction,” Dr. Joundi said. “However, if 10,000 steps per day is not feasible, 7,000 steps seems to be a very reasonable target given its association with markedly lower mortality in this study.”
Not all step counters are equal
Unfortunately, such recommendations are complicated by uncertainty in measurement, as widely used step counting devices, like smart watches, may not yield the same results as research-grade accelerometers, according to Nicole L. Spartano, PhD, of Boston University.
“Many comparison studies have been conducted in laboratory settings among young healthy adults, but these do not necessarily reflect real-life wear experiences that will be generalizable to the population as a whole,” Dr. Spartano wrote in an accompanying editorial.
She called for large-scale comparison studies to compare research-grade and consumer devices.
“The reason for conducting comparison studies is not to develop distinct guidelines for different devices or subgroups of the population, but rather to understand the variability so that we can develop one clear message that is most appropriate to the public,” Dr. Spartano wrote. “Some devices may have bias in terms of step measurement at different activity intensity and may not record steps as accurately in older adults or individuals with obesity or mobility disorders. For example, when adults who were obese wore an ActiGraph monitor in a laboratory setting, the device only recorded 80% of steps walked at a moderate pace, while other devices recorded close to 100% of steps walked. If we in the public health community are to move toward using these devices more for physical activity prescription, these details will need to be explored in more depth.”
CARDIA was conducted and supported by the National Heart, Lung, and Blood Institute in collaboration with the University of Alabama at Birmingham, Northwestern University, the University of Minnesota, and the Kaiser Foundation Research Institute. Some study authors received grants from the National Institutes of Health and the Kaiser Foundation Research Institute. Dr Spartano disclosed relationships with Novo Nordisk, the American Heart Association, the Alzheimer’s Association, and the National Institutes of Health. Dr. Joundi and Dr. Paluch disclosed no relevant financial relationships.
based on prospective data from more than 2,000 people.
Findings were consistent regardless of race or sex, and step intensity had no impact on mortality risk, reported lead author Amanda E. Paluch, PhD, of the University of Massachusetts Amherst, and colleagues.
“In response to the need for empirical data on the associations of step volume and intensity with mortality in younger and diverse populations, we conducted a prospective study in middle-aged Black and White adults followed up for mortality for approximately 11 years,” the investigators wrote in JAMA Network Open. “The objectives of our study were to examine the associations of step volume and intensity with mortality overall and by race and sex.”
Steps per day is easy to communicate
Dr. Paluch noted that steps per day is a “very appealing metric to quantify activity,” for both researchers and laypeople.
“Steps per day is simple and easy to communicate in public health and clinical settings,” Dr. Paluch said in an interview. “Additionally, the dramatic growth of wearable devices measuring steps makes it appealing and broadens the reach of promoting physical activity to many individuals. Walking is an activity that most of the general population can pursue. It can also be accumulated throughout daily living and may seem more achievable to fit into busy lives than a structured exercise session.”
The present investigation was conducted as part of the Coronary Artery Risk Development in Young Adults (CARDIA) Study. The dataset included 2,110 participants ranging from 38-50 years of age, with a mean age of 45.2 years. A slightly higher proportion of the subjects were women (57.1%) and White (57.9%).
All participants wore an ActiGraph 7164 accelerometer for 1 week and were then followed for death of any cause, with a mean follow-up of 10.8 years. Multivariable-adjusted Cox proportional hazards models included a range of covariates, such as smoking history, body weight, alcohol intake, blood pressure, total cholesterol, and others. Step counts were grouped into low (less than 7,000 steps per day), moderate (7,000-9,999), and high (at least 10,000 steps per day) categories.
Compared with individuals who took less than 7,000 steps per day, those who took 7,000-9,000 steps per day had a 72% reduced risk of mortality (hazard ratio, 0.28; 95% confidence interval, 0.15-0.54). Going beyond 10,000 steps appeared to add no benefit, based on a 55% lower risk of all-cause mortality in the highly active group, compared with those taking less than 7,000 steps per day (HR, 0.45; 95% CI, 0.25-0.81).
Walking faster didn’t appear to help either, as stepping intensity was not associated with mortality risk; however, Dr. Paluch urged a cautious interpretation of this finding, calling it “inconclusive,” and suggesting that more research is needed.
“It is also important to note that this study only looked at premature all-cause mortality, and therefore the results may be different for other health outcomes, such as the risk of cardiovascular disease, or diabetes, cancer, or mental health outcomes,” Dr. Paluch said.
“The results from our study demonstrated that those who are least active have the most to gain,” Dr. Paluch said. “Even small incremental increases in steps per day are associated with a lower mortality risk during middle age. A walking plan that gradually works up toward 7,000-10,000 steps per day in middle-aged adults may have health benefits and lower the risk of premature mortality.”
Causality cannot be confirmed
According to Raed A. Joundi, MD, DPhil, of the University of Calgary (Alta.), the study size, diverse population, and length of follow-up should increase confidence in the findings, although a causal relationship remains elusive.
“As this study is observational, causality between step count and mortality cannot be confirmed; however, the authors accounted for many factors, and the association was consistent in different analyses and with prior literature,” Dr. Joundi said in an interview. “The authors did not assess the risk of other important events like stroke and heart attack, and these could be addressed in a future study.”
Dr. Joundi, who recently published a study linking exercise with a 50% reduction in mortality after stroke, noted that “physical activity has innumerable benefits, and it’s important that people engage in activity that can be regular and consistent, regardless of the type or intensity.”
To this end, he highlighted the use of “devices capable of monitoring step count, which can be an important motivational tool,” and suggested that these findings may bring a sigh of relief to step counters who come up a little short on a common daily goal.
“A target of 10,000 steps is often used for public health promotion, and this study now provides convincing observational evidence that it may be an optimal step count target for mortality reduction,” Dr. Joundi said. “However, if 10,000 steps per day is not feasible, 7,000 steps seems to be a very reasonable target given its association with markedly lower mortality in this study.”
Not all step counters are equal
Unfortunately, such recommendations are complicated by uncertainty in measurement, as widely used step counting devices, like smart watches, may not yield the same results as research-grade accelerometers, according to Nicole L. Spartano, PhD, of Boston University.
“Many comparison studies have been conducted in laboratory settings among young healthy adults, but these do not necessarily reflect real-life wear experiences that will be generalizable to the population as a whole,” Dr. Spartano wrote in an accompanying editorial.
She called for large-scale comparison studies to compare research-grade and consumer devices.
“The reason for conducting comparison studies is not to develop distinct guidelines for different devices or subgroups of the population, but rather to understand the variability so that we can develop one clear message that is most appropriate to the public,” Dr. Spartano wrote. “Some devices may have bias in terms of step measurement at different activity intensity and may not record steps as accurately in older adults or individuals with obesity or mobility disorders. For example, when adults who were obese wore an ActiGraph monitor in a laboratory setting, the device only recorded 80% of steps walked at a moderate pace, while other devices recorded close to 100% of steps walked. If we in the public health community are to move toward using these devices more for physical activity prescription, these details will need to be explored in more depth.”
CARDIA was conducted and supported by the National Heart, Lung, and Blood Institute in collaboration with the University of Alabama at Birmingham, Northwestern University, the University of Minnesota, and the Kaiser Foundation Research Institute. Some study authors received grants from the National Institutes of Health and the Kaiser Foundation Research Institute. Dr Spartano disclosed relationships with Novo Nordisk, the American Heart Association, the Alzheimer’s Association, and the National Institutes of Health. Dr. Joundi and Dr. Paluch disclosed no relevant financial relationships.
based on prospective data from more than 2,000 people.
Findings were consistent regardless of race or sex, and step intensity had no impact on mortality risk, reported lead author Amanda E. Paluch, PhD, of the University of Massachusetts Amherst, and colleagues.
“In response to the need for empirical data on the associations of step volume and intensity with mortality in younger and diverse populations, we conducted a prospective study in middle-aged Black and White adults followed up for mortality for approximately 11 years,” the investigators wrote in JAMA Network Open. “The objectives of our study were to examine the associations of step volume and intensity with mortality overall and by race and sex.”
Steps per day is easy to communicate
Dr. Paluch noted that steps per day is a “very appealing metric to quantify activity,” for both researchers and laypeople.
“Steps per day is simple and easy to communicate in public health and clinical settings,” Dr. Paluch said in an interview. “Additionally, the dramatic growth of wearable devices measuring steps makes it appealing and broadens the reach of promoting physical activity to many individuals. Walking is an activity that most of the general population can pursue. It can also be accumulated throughout daily living and may seem more achievable to fit into busy lives than a structured exercise session.”
The present investigation was conducted as part of the Coronary Artery Risk Development in Young Adults (CARDIA) Study. The dataset included 2,110 participants ranging from 38-50 years of age, with a mean age of 45.2 years. A slightly higher proportion of the subjects were women (57.1%) and White (57.9%).
All participants wore an ActiGraph 7164 accelerometer for 1 week and were then followed for death of any cause, with a mean follow-up of 10.8 years. Multivariable-adjusted Cox proportional hazards models included a range of covariates, such as smoking history, body weight, alcohol intake, blood pressure, total cholesterol, and others. Step counts were grouped into low (less than 7,000 steps per day), moderate (7,000-9,999), and high (at least 10,000 steps per day) categories.
Compared with individuals who took less than 7,000 steps per day, those who took 7,000-9,000 steps per day had a 72% reduced risk of mortality (hazard ratio, 0.28; 95% confidence interval, 0.15-0.54). Going beyond 10,000 steps appeared to add no benefit, based on a 55% lower risk of all-cause mortality in the highly active group, compared with those taking less than 7,000 steps per day (HR, 0.45; 95% CI, 0.25-0.81).
Walking faster didn’t appear to help either, as stepping intensity was not associated with mortality risk; however, Dr. Paluch urged a cautious interpretation of this finding, calling it “inconclusive,” and suggesting that more research is needed.
“It is also important to note that this study only looked at premature all-cause mortality, and therefore the results may be different for other health outcomes, such as the risk of cardiovascular disease, or diabetes, cancer, or mental health outcomes,” Dr. Paluch said.
“The results from our study demonstrated that those who are least active have the most to gain,” Dr. Paluch said. “Even small incremental increases in steps per day are associated with a lower mortality risk during middle age. A walking plan that gradually works up toward 7,000-10,000 steps per day in middle-aged adults may have health benefits and lower the risk of premature mortality.”
Causality cannot be confirmed
According to Raed A. Joundi, MD, DPhil, of the University of Calgary (Alta.), the study size, diverse population, and length of follow-up should increase confidence in the findings, although a causal relationship remains elusive.
“As this study is observational, causality between step count and mortality cannot be confirmed; however, the authors accounted for many factors, and the association was consistent in different analyses and with prior literature,” Dr. Joundi said in an interview. “The authors did not assess the risk of other important events like stroke and heart attack, and these could be addressed in a future study.”
Dr. Joundi, who recently published a study linking exercise with a 50% reduction in mortality after stroke, noted that “physical activity has innumerable benefits, and it’s important that people engage in activity that can be regular and consistent, regardless of the type or intensity.”
To this end, he highlighted the use of “devices capable of monitoring step count, which can be an important motivational tool,” and suggested that these findings may bring a sigh of relief to step counters who come up a little short on a common daily goal.
“A target of 10,000 steps is often used for public health promotion, and this study now provides convincing observational evidence that it may be an optimal step count target for mortality reduction,” Dr. Joundi said. “However, if 10,000 steps per day is not feasible, 7,000 steps seems to be a very reasonable target given its association with markedly lower mortality in this study.”
Not all step counters are equal
Unfortunately, such recommendations are complicated by uncertainty in measurement, as widely used step counting devices, like smart watches, may not yield the same results as research-grade accelerometers, according to Nicole L. Spartano, PhD, of Boston University.
“Many comparison studies have been conducted in laboratory settings among young healthy adults, but these do not necessarily reflect real-life wear experiences that will be generalizable to the population as a whole,” Dr. Spartano wrote in an accompanying editorial.
She called for large-scale comparison studies to compare research-grade and consumer devices.
“The reason for conducting comparison studies is not to develop distinct guidelines for different devices or subgroups of the population, but rather to understand the variability so that we can develop one clear message that is most appropriate to the public,” Dr. Spartano wrote. “Some devices may have bias in terms of step measurement at different activity intensity and may not record steps as accurately in older adults or individuals with obesity or mobility disorders. For example, when adults who were obese wore an ActiGraph monitor in a laboratory setting, the device only recorded 80% of steps walked at a moderate pace, while other devices recorded close to 100% of steps walked. If we in the public health community are to move toward using these devices more for physical activity prescription, these details will need to be explored in more depth.”
CARDIA was conducted and supported by the National Heart, Lung, and Blood Institute in collaboration with the University of Alabama at Birmingham, Northwestern University, the University of Minnesota, and the Kaiser Foundation Research Institute. Some study authors received grants from the National Institutes of Health and the Kaiser Foundation Research Institute. Dr Spartano disclosed relationships with Novo Nordisk, the American Heart Association, the Alzheimer’s Association, and the National Institutes of Health. Dr. Joundi and Dr. Paluch disclosed no relevant financial relationships.
FROM JAMA NETWORK OPEN
Open notes: Legal issues
In July, I had my annual physical with my primary care physician, whose practice is based out of a large urban academic medical center. As she concluded my visit and directed me to the lab to have my blood work done, she said, “You’ll be receiving an automatic notice from MyChart by 9 am tomorrow that your medical records from today’s visit are available. I apologize if I have not yet had the opportunity to review them and enter my note, but you’ll get access to all of that, as well, as soon as it is in the system.”

This sort of interaction is increasingly common across the United States as health care institutions implement policies and procedures to comply with new regulations promulgated by the Office of the National Coordinator for Health Information Technology (ONC), which went into effect on April 5, 2021. These rules were promulgated in accordance with the 21st Century Cures Act of 2016 (Cures Act).1 The regulations, known as the Interoperability, Information Blocking, and the ONC Health IT Certification Program, implement provisions of the Cures Act intended to “support the access, exchange, and use of electronic health information.” The rule is considered a significant step in the “open notes” movement, which is intended to make health care more transparent by enabling patients to access their medical records. The drafters of the ONC regulations have carved out certain exceptions to the information blocking rule. For example, one exception allows some patient information to be withheld where making that information available might cause physical harm to the patient or another person.
Thus far, few patients have been informed about the new regulation.2 By forbidding “information blocking,” the rule enables patients to more easily access and control their health information. Records must be provided “without delay,” or at least as soon as the physician’s office receives an electronic copy. In 2022, it will be required that access to even more of a patient’s personal electronic health record be provided in real-time through a patient portal and that electronic health information be shareable across third-party apps.
The Cures Act and the regulations governing its implementation highlight the inherent tension between two core principles of bioethical inquiry: autonomy and beneficence. The first principle, autonomy, champions allowing patient access and control over their own personal information. Beneficence, which is often expressed as paternalism, ensures that the experts are able to analyze and interpret data so that patients are in the best position to then make informed decisions.
With these principles in mind, arguments against open notes have generally fallen into three related categories. First, critics worry that immediate access to one’s medical record will increase patient anxiety caused by feelings of being inundated with complex medical information that patients may be ill-equipped to analyze and understand. This is a common refrain any time policies are implemented to improve medical information sharing. For example, critics of direct-to-consumer genetic testing caution that permitting unfettered access to complex information, particularly without an intermediary to interpret the data, could lead to confusion and poor medical choices.
There may be validity to this claim. One study found that 3% of patients reported feeling very confused when granted access to their medical notes.3 Another study concluded that direct release of medical test results “sometimes leads to unnecessary anxiety.”4 While the drafters of the ONC regulations have carved out certain exceptions to the information blocking rule, those exceptions do not allow for withholding of information because of concerns about patient anxiety or psychological harms.
The second common critique of open notes is that requiring release of all clinical notes will lead to clinician self-censorship, effectively muzzling or silencing the experts whose responsibility it is to objectively interpret results in order to provide the best care for their patients. Some have expressed concern that clinicians will be forced to “code” their records to avoid addressing “sensitive” subjects that might make patients feel offended or judged. This, in turn, might lead to less complete, reliable, or useful clinician communication.3
In fact, open notes has led to changes in the documentation process for some clinicians. They have reported modifying the way they document patient visits by changing their use of critical language and sensitive information.5 One study found that open notes led physicians to adjust “their language to avoid being perceived as critical of patients; omitting certain terms, such as ‘noncompliant’ and ‘patient denies’; and modifying how they document sensitive information.”3
In response, experts recommend focusing on precise and empathetic patient notes; in other words, the clinician should not write something in the note that they would not say directly to the patient. For example, they recommend that clinicians use precise language (for example, identifying the patient’s BMI) rather than using terms that could be offensive (for example, labeling the patient as “obese”).6 The shift to more empathetic note-taking could be seen less as a burden and more as a valuable tool in the shared decision-making endeavor: It could allow physicians to document both their clinical judgments and the patient’s values and preferences, which could lead to better medical decision-making.
Third, critics of open notes point to concerns about the burden it places on clinicians’ already limited time. The ONC rule requires automatic release of test results regardless of whether the clinician has had the opportunity to review them and offer their interpretation and insight. Because physician interpretation of results has known benefits,4 this puts additional pressure on clinicians to review results and enter notes in a timely manner. But physicians have reported that often open notes necessitates that they spend more time on documentation than they would otherwise.5
Despite critiques of open notes, the benefits of allowing patients access to their medical records have been repeatedly demonstrated. And research has shown that patients benefit from accessing open notes by allowing them to access and control their own personal medical information.5 Patients report that they understand and value the information provided to them in their medical records,7 and they feel empowered to participate in their medical decision-making. In surveys, patients report that reading their doctors’ notes is useful for taking care of their health and for remembering their care plans, understanding why a medication was prescribed, and reinforcing the need to take their medications and adhere to treatment plans.8
Importantly, open notes can increase patient engagement and patients’ trust in their physicians,9 thereby improving the doctor-patient relationship.3 And allowing patients to share their medical records with care partners enables supported decision-making, particularly for older and chronically ill individuals.3 Additionally, it is predicted that open notes may, in fact, decrease legal liability.9 By improving both trust in the doctor-patient relationship and safety, some experts expect that legal claims against clinicians will, in turn, decrease.10
The modern practice of medicine necessitates a more empathetic approach to clinical note-taking, even in the absence of regulation requiring it. As the regulations implementing the Cures Act roll out, patients will have easier, and more immediate, access to their medical records. Despite earlier hesitancy, clinicians are steadily beginning to support sharing access to notes with patients.5 Change can be hard. But the change expected of clinicians because of these new regulations appears to be less onerous than originally anticipated.
Prof. Koch is codirector of Health Law & Policy Institute and assistant professor at the University of Houston Law Center, as well as director of law and ethics at the MacLean Center for Clinical Medical Ethics at the University of Chicago. She has no disclosures.
This article was updated Sept. 9, 2021.
References
1. Fed Regist. 2020 May;85(85):25642-961.
2. The Petrie-Flom Center Staff. “New Rule Puts Medical Data in Patients’ Hands.” Bill of Health. July 12, 2021. Accessed August 30, 2021. https://blog.petrieflom.law.harvard.edu/2021/07/12/new-rule-puts-medical-data-in-patients-hands/.
3. Blease C et al. Ann Intern Med. 2021 Jan;174(1):101-2.
4. Pillemer F et al. PLoS One. 2016 Jun. doi: 10.1371/journal.pone.0154743.
5. DesRoches CM et al. JAMA Netw Open. 2020 Mar. doi: 10.1001/jamanetworkopen.2020.1753.
6. Heath S. “Most Patients Understand Clinical Notes, Patient Data Access.” Patient Engagement HIT. July 29, 2020. Accessed August 30, 2021. https://patientengagementhit.com/news/most-patients-understand-clinical-notes-patient-data-access
7. Leveille SG et al. J Gen Intern Med. 2020 Dec;35(12):3510-6.
8. Walker J et al. J Med Internet Res. 2019 May. doi: 10.2196/13876.
9. Bell SK et al. BMJ Qual Saf. 2017 Apr;26(4):262-70.
10. Kachalia A, Mello MM. N Engl J Med. 2011 Apr;364(16):1564-72.
In July, I had my annual physical with my primary care physician, whose practice is based out of a large urban academic medical center. As she concluded my visit and directed me to the lab to have my blood work done, she said, “You’ll be receiving an automatic notice from MyChart by 9 am tomorrow that your medical records from today’s visit are available. I apologize if I have not yet had the opportunity to review them and enter my note, but you’ll get access to all of that, as well, as soon as it is in the system.”
This sort of interaction is increasingly common across the United States as health care institutions implement policies and procedures to comply with new regulations promulgated by the Office of the National Coordinator for Health Information Technology (ONC), which went into effect on April 5, 2021. These rules were promulgated in accordance with the 21st Century Cures Act of 2016 (Cures Act).1 The regulations, known as the Interoperability, Information Blocking, and the ONC Health IT Certification Program, implement provisions of the Cures Act intended to “support the access, exchange, and use of electronic health information.” The rule is considered a significant step in the “open notes” movement, which is intended to make health care more transparent by enabling patients to access their medical records. The drafters of the ONC regulations have carved out certain exceptions to the information blocking rule. For example, one exception allows some patient information to be withheld where making that information available might cause physical harm to the patient or another person.
Thus far, few patients have been informed about the new regulation.2 By forbidding “information blocking,” the rule enables patients to more easily access and control their health information. Records must be provided “without delay,” or at least as soon as the physician’s office receives an electronic copy. In 2022, it will be required that access to even more of a patient’s personal electronic health record be provided in real-time through a patient portal and that electronic health information be shareable across third-party apps.
The Cures Act and the regulations governing its implementation highlight the inherent tension between two core principles of bioethical inquiry: autonomy and beneficence. The first principle, autonomy, champions allowing patient access and control over their own personal information. Beneficence, which is often expressed as paternalism, ensures that the experts are able to analyze and interpret data so that patients are in the best position to then make informed decisions.
With these principles in mind, arguments against open notes have generally fallen into three related categories. First, critics worry that immediate access to one’s medical record will increase patient anxiety caused by feelings of being inundated with complex medical information that patients may be ill-equipped to analyze and understand. This is a common refrain any time policies are implemented to improve medical information sharing. For example, critics of direct-to-consumer genetic testing caution that permitting unfettered access to complex information, particularly without an intermediary to interpret the data, could lead to confusion and poor medical choices.
There may be validity to this claim. One study found that 3% of patients reported feeling very confused when granted access to their medical notes.3 Another study concluded that direct release of medical test results “sometimes leads to unnecessary anxiety.”4 While the drafters of the ONC regulations have carved out certain exceptions to the information blocking rule, those exceptions do not allow for withholding of information because of concerns about patient anxiety or psychological harms.
The second common critique of open notes is that requiring release of all clinical notes will lead to clinician self-censorship, effectively muzzling or silencing the experts whose responsibility it is to objectively interpret results in order to provide the best care for their patients. Some have expressed concern that clinicians will be forced to “code” their records to avoid addressing “sensitive” subjects that might make patients feel offended or judged. This, in turn, might lead to less complete, reliable, or useful clinician communication.3
In fact, open notes has led to changes in the documentation process for some clinicians. They have reported modifying the way they document patient visits by changing their use of critical language and sensitive information.5 One study found that open notes led physicians to adjust “their language to avoid being perceived as critical of patients; omitting certain terms, such as ‘noncompliant’ and ‘patient denies’; and modifying how they document sensitive information.”3
In response, experts recommend focusing on precise and empathetic patient notes; in other words, the clinician should not write something in the note that they would not say directly to the patient. For example, they recommend that clinicians use precise language (for example, identifying the patient’s BMI) rather than using terms that could be offensive (for example, labeling the patient as “obese”).6 The shift to more empathetic note-taking could be seen less as a burden and more as a valuable tool in the shared decision-making endeavor: It could allow physicians to document both their clinical judgments and the patient’s values and preferences, which could lead to better medical decision-making.
Third, critics of open notes point to concerns about the burden it places on clinicians’ already limited time. The ONC rule requires automatic release of test results regardless of whether the clinician has had the opportunity to review them and offer their interpretation and insight. Because physician interpretation of results has known benefits,4 this puts additional pressure on clinicians to review results and enter notes in a timely manner. But physicians have reported that often open notes necessitates that they spend more time on documentation than they would otherwise.5
Despite critiques of open notes, the benefits of allowing patients access to their medical records have been repeatedly demonstrated. And research has shown that patients benefit from accessing open notes by allowing them to access and control their own personal medical information.5 Patients report that they understand and value the information provided to them in their medical records,7 and they feel empowered to participate in their medical decision-making. In surveys, patients report that reading their doctors’ notes is useful for taking care of their health and for remembering their care plans, understanding why a medication was prescribed, and reinforcing the need to take their medications and adhere to treatment plans.8
Importantly, open notes can increase patient engagement and patients’ trust in their physicians,9 thereby improving the doctor-patient relationship.3 And allowing patients to share their medical records with care partners enables supported decision-making, particularly for older and chronically ill individuals.3 Additionally, it is predicted that open notes may, in fact, decrease legal liability.9 By improving both trust in the doctor-patient relationship and safety, some experts expect that legal claims against clinicians will, in turn, decrease.10
The modern practice of medicine necessitates a more empathetic approach to clinical note-taking, even in the absence of regulation requiring it. As the regulations implementing the Cures Act roll out, patients will have easier, and more immediate, access to their medical records. Despite earlier hesitancy, clinicians are steadily beginning to support sharing access to notes with patients.5 Change can be hard. But the change expected of clinicians because of these new regulations appears to be less onerous than originally anticipated.
Prof. Koch is codirector of Health Law & Policy Institute and assistant professor at the University of Houston Law Center, as well as director of law and ethics at the MacLean Center for Clinical Medical Ethics at the University of Chicago. She has no disclosures.
This article was updated Sept. 9, 2021.
References
1. Fed Regist. 2020 May;85(85):25642-961.
2. The Petrie-Flom Center Staff. “New Rule Puts Medical Data in Patients’ Hands.” Bill of Health. July 12, 2021. Accessed August 30, 2021. https://blog.petrieflom.law.harvard.edu/2021/07/12/new-rule-puts-medical-data-in-patients-hands/.
3. Blease C et al. Ann Intern Med. 2021 Jan;174(1):101-2.
4. Pillemer F et al. PLoS One. 2016 Jun. doi: 10.1371/journal.pone.0154743.
5. DesRoches CM et al. JAMA Netw Open. 2020 Mar. doi: 10.1001/jamanetworkopen.2020.1753.
6. Heath S. “Most Patients Understand Clinical Notes, Patient Data Access.” Patient Engagement HIT. July 29, 2020. Accessed August 30, 2021. https://patientengagementhit.com/news/most-patients-understand-clinical-notes-patient-data-access
7. Leveille SG et al. J Gen Intern Med. 2020 Dec;35(12):3510-6.
8. Walker J et al. J Med Internet Res. 2019 May. doi: 10.2196/13876.
9. Bell SK et al. BMJ Qual Saf. 2017 Apr;26(4):262-70.
10. Kachalia A, Mello MM. N Engl J Med. 2011 Apr;364(16):1564-72.
In July, I had my annual physical with my primary care physician, whose practice is based out of a large urban academic medical center. As she concluded my visit and directed me to the lab to have my blood work done, she said, “You’ll be receiving an automatic notice from MyChart by 9 am tomorrow that your medical records from today’s visit are available. I apologize if I have not yet had the opportunity to review them and enter my note, but you’ll get access to all of that, as well, as soon as it is in the system.”
This sort of interaction is increasingly common across the United States as health care institutions implement policies and procedures to comply with new regulations promulgated by the Office of the National Coordinator for Health Information Technology (ONC), which went into effect on April 5, 2021. These rules were promulgated in accordance with the 21st Century Cures Act of 2016 (Cures Act).1 The regulations, known as the Interoperability, Information Blocking, and the ONC Health IT Certification Program, implement provisions of the Cures Act intended to “support the access, exchange, and use of electronic health information.” The rule is considered a significant step in the “open notes” movement, which is intended to make health care more transparent by enabling patients to access their medical records. The drafters of the ONC regulations have carved out certain exceptions to the information blocking rule. For example, one exception allows some patient information to be withheld where making that information available might cause physical harm to the patient or another person.
Thus far, few patients have been informed about the new regulation.2 By forbidding “information blocking,” the rule enables patients to more easily access and control their health information. Records must be provided “without delay,” or at least as soon as the physician’s office receives an electronic copy. In 2022, it will be required that access to even more of a patient’s personal electronic health record be provided in real-time through a patient portal and that electronic health information be shareable across third-party apps.
The Cures Act and the regulations governing its implementation highlight the inherent tension between two core principles of bioethical inquiry: autonomy and beneficence. The first principle, autonomy, champions allowing patient access and control over their own personal information. Beneficence, which is often expressed as paternalism, ensures that the experts are able to analyze and interpret data so that patients are in the best position to then make informed decisions.
With these principles in mind, arguments against open notes have generally fallen into three related categories. First, critics worry that immediate access to one’s medical record will increase patient anxiety caused by feelings of being inundated with complex medical information that patients may be ill-equipped to analyze and understand. This is a common refrain any time policies are implemented to improve medical information sharing. For example, critics of direct-to-consumer genetic testing caution that permitting unfettered access to complex information, particularly without an intermediary to interpret the data, could lead to confusion and poor medical choices.
There may be validity to this claim. One study found that 3% of patients reported feeling very confused when granted access to their medical notes.3 Another study concluded that direct release of medical test results “sometimes leads to unnecessary anxiety.”4 While the drafters of the ONC regulations have carved out certain exceptions to the information blocking rule, those exceptions do not allow for withholding of information because of concerns about patient anxiety or psychological harms.
The second common critique of open notes is that requiring release of all clinical notes will lead to clinician self-censorship, effectively muzzling or silencing the experts whose responsibility it is to objectively interpret results in order to provide the best care for their patients. Some have expressed concern that clinicians will be forced to “code” their records to avoid addressing “sensitive” subjects that might make patients feel offended or judged. This, in turn, might lead to less complete, reliable, or useful clinician communication.3
In fact, open notes has led to changes in the documentation process for some clinicians. They have reported modifying the way they document patient visits by changing their use of critical language and sensitive information.5 One study found that open notes led physicians to adjust “their language to avoid being perceived as critical of patients; omitting certain terms, such as ‘noncompliant’ and ‘patient denies’; and modifying how they document sensitive information.”3
In response, experts recommend focusing on precise and empathetic patient notes; in other words, the clinician should not write something in the note that they would not say directly to the patient. For example, they recommend that clinicians use precise language (for example, identifying the patient’s BMI) rather than using terms that could be offensive (for example, labeling the patient as “obese”).6 The shift to more empathetic note-taking could be seen less as a burden and more as a valuable tool in the shared decision-making endeavor: It could allow physicians to document both their clinical judgments and the patient’s values and preferences, which could lead to better medical decision-making.
Third, critics of open notes point to concerns about the burden it places on clinicians’ already limited time. The ONC rule requires automatic release of test results regardless of whether the clinician has had the opportunity to review them and offer their interpretation and insight. Because physician interpretation of results has known benefits,4 this puts additional pressure on clinicians to review results and enter notes in a timely manner. But physicians have reported that often open notes necessitates that they spend more time on documentation than they would otherwise.5
Despite critiques of open notes, the benefits of allowing patients access to their medical records have been repeatedly demonstrated. And research has shown that patients benefit from accessing open notes by allowing them to access and control their own personal medical information.5 Patients report that they understand and value the information provided to them in their medical records,7 and they feel empowered to participate in their medical decision-making. In surveys, patients report that reading their doctors’ notes is useful for taking care of their health and for remembering their care plans, understanding why a medication was prescribed, and reinforcing the need to take their medications and adhere to treatment plans.8
Importantly, open notes can increase patient engagement and patients’ trust in their physicians,9 thereby improving the doctor-patient relationship.3 And allowing patients to share their medical records with care partners enables supported decision-making, particularly for older and chronically ill individuals.3 Additionally, it is predicted that open notes may, in fact, decrease legal liability.9 By improving both trust in the doctor-patient relationship and safety, some experts expect that legal claims against clinicians will, in turn, decrease.10
The modern practice of medicine necessitates a more empathetic approach to clinical note-taking, even in the absence of regulation requiring it. As the regulations implementing the Cures Act roll out, patients will have easier, and more immediate, access to their medical records. Despite earlier hesitancy, clinicians are steadily beginning to support sharing access to notes with patients.5 Change can be hard. But the change expected of clinicians because of these new regulations appears to be less onerous than originally anticipated.
Prof. Koch is codirector of Health Law & Policy Institute and assistant professor at the University of Houston Law Center, as well as director of law and ethics at the MacLean Center for Clinical Medical Ethics at the University of Chicago. She has no disclosures.
This article was updated Sept. 9, 2021.
References
1. Fed Regist. 2020 May;85(85):25642-961.
2. The Petrie-Flom Center Staff. “New Rule Puts Medical Data in Patients’ Hands.” Bill of Health. July 12, 2021. Accessed August 30, 2021. https://blog.petrieflom.law.harvard.edu/2021/07/12/new-rule-puts-medical-data-in-patients-hands/.
3. Blease C et al. Ann Intern Med. 2021 Jan;174(1):101-2.
4. Pillemer F et al. PLoS One. 2016 Jun. doi: 10.1371/journal.pone.0154743.
5. DesRoches CM et al. JAMA Netw Open. 2020 Mar. doi: 10.1001/jamanetworkopen.2020.1753.
6. Heath S. “Most Patients Understand Clinical Notes, Patient Data Access.” Patient Engagement HIT. July 29, 2020. Accessed August 30, 2021. https://patientengagementhit.com/news/most-patients-understand-clinical-notes-patient-data-access
7. Leveille SG et al. J Gen Intern Med. 2020 Dec;35(12):3510-6.
8. Walker J et al. J Med Internet Res. 2019 May. doi: 10.2196/13876.
9. Bell SK et al. BMJ Qual Saf. 2017 Apr;26(4):262-70.
10. Kachalia A, Mello MM. N Engl J Med. 2011 Apr;364(16):1564-72.
The postpandemic path forward for GI research
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) recognizes the alarming impact of COVID-19 on the biomedical research community. The Institute has taken steps to address the pandemic’s immediate challenges, such as supporting COVID-19 research within its mission and implementing policies that ease grantees’ concerns about funding and lost time. The NIDDK has also sought to balance the needs brought about by the pandemic with its responsibility to continue research on the many diseases and conditions in the NIDDK’s purview.
The NIDDK continues to support most research through unsolicited R01 awards. It also continues to support organized consortia that aim to improve our understanding and treatment of digestive diseases; research centers that provide valuable sources of collaboration among researchers investigating digestive diseases and/or nutrition and obesity; and programs that encourage transitions to different career levels.
The pandemic has shown in stark relief the devastating impact of health disparities. Because many NIDDK mission diseases place disparate burdens on minority groups and people with limited resources, the NIDDK remains committed to combating health disparities, whether pandemic related or not. The Institute recruits diverse study cohorts inclusive of those most affected. It seeks to open doors for young people from underrepresented groups through training, support, and inspiration to pursue research careers, such as through partnerships with organizations like the American Gastroenterological Association. The NIDDK is also implementing strategies to promote participant engagement, not only as study volunteers, but also in study design, recruitment, and consent. And, importantly, the Institute is supporting research to identify the causes of health disparities, including research on social determinants of health.
This year, the NIDDK embarked on the development of a 5-year Strategic Plan to develop a broad vision for accelerating research on diseases and conditions across its mission. This plan is meant to be overarching and will complement the NIDDK’s disease-specific planning efforts. The first draft of the plan is currently being developed based on the input received from a Strategic Plan Working Group (which includes several AGA members), a public Request for Information, and NIDDK’s Advisory Council. The draft will be available through the NIDDK website (niddk.nih.gov) for public comment.
By taking these actions, the NIDDK aims to continue reducing the burden of digestive diseases and improving health for all people.
Dr. Rodgers is director of the National Institute of Diabetes and Digestive and Kidney Diseases at the National Institutes of Health. He has no conflicts. Dr. Rodgers made these comments during the AGA Institute Presidential Plenary at the annual Digestive Disease Week®.
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) recognizes the alarming impact of COVID-19 on the biomedical research community. The Institute has taken steps to address the pandemic’s immediate challenges, such as supporting COVID-19 research within its mission and implementing policies that ease grantees’ concerns about funding and lost time. The NIDDK has also sought to balance the needs brought about by the pandemic with its responsibility to continue research on the many diseases and conditions in the NIDDK’s purview.
The NIDDK continues to support most research through unsolicited R01 awards. It also continues to support organized consortia that aim to improve our understanding and treatment of digestive diseases; research centers that provide valuable sources of collaboration among researchers investigating digestive diseases and/or nutrition and obesity; and programs that encourage transitions to different career levels.
The pandemic has shown in stark relief the devastating impact of health disparities. Because many NIDDK mission diseases place disparate burdens on minority groups and people with limited resources, the NIDDK remains committed to combating health disparities, whether pandemic related or not. The Institute recruits diverse study cohorts inclusive of those most affected. It seeks to open doors for young people from underrepresented groups through training, support, and inspiration to pursue research careers, such as through partnerships with organizations like the American Gastroenterological Association. The NIDDK is also implementing strategies to promote participant engagement, not only as study volunteers, but also in study design, recruitment, and consent. And, importantly, the Institute is supporting research to identify the causes of health disparities, including research on social determinants of health.
This year, the NIDDK embarked on the development of a 5-year Strategic Plan to develop a broad vision for accelerating research on diseases and conditions across its mission. This plan is meant to be overarching and will complement the NIDDK’s disease-specific planning efforts. The first draft of the plan is currently being developed based on the input received from a Strategic Plan Working Group (which includes several AGA members), a public Request for Information, and NIDDK’s Advisory Council. The draft will be available through the NIDDK website (niddk.nih.gov) for public comment.
By taking these actions, the NIDDK aims to continue reducing the burden of digestive diseases and improving health for all people.
Dr. Rodgers is director of the National Institute of Diabetes and Digestive and Kidney Diseases at the National Institutes of Health. He has no conflicts. Dr. Rodgers made these comments during the AGA Institute Presidential Plenary at the annual Digestive Disease Week®.
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) recognizes the alarming impact of COVID-19 on the biomedical research community. The Institute has taken steps to address the pandemic’s immediate challenges, such as supporting COVID-19 research within its mission and implementing policies that ease grantees’ concerns about funding and lost time. The NIDDK has also sought to balance the needs brought about by the pandemic with its responsibility to continue research on the many diseases and conditions in the NIDDK’s purview.
The NIDDK continues to support most research through unsolicited R01 awards. It also continues to support organized consortia that aim to improve our understanding and treatment of digestive diseases; research centers that provide valuable sources of collaboration among researchers investigating digestive diseases and/or nutrition and obesity; and programs that encourage transitions to different career levels.
The pandemic has shown in stark relief the devastating impact of health disparities. Because many NIDDK mission diseases place disparate burdens on minority groups and people with limited resources, the NIDDK remains committed to combating health disparities, whether pandemic related or not. The Institute recruits diverse study cohorts inclusive of those most affected. It seeks to open doors for young people from underrepresented groups through training, support, and inspiration to pursue research careers, such as through partnerships with organizations like the American Gastroenterological Association. The NIDDK is also implementing strategies to promote participant engagement, not only as study volunteers, but also in study design, recruitment, and consent. And, importantly, the Institute is supporting research to identify the causes of health disparities, including research on social determinants of health.
This year, the NIDDK embarked on the development of a 5-year Strategic Plan to develop a broad vision for accelerating research on diseases and conditions across its mission. This plan is meant to be overarching and will complement the NIDDK’s disease-specific planning efforts. The first draft of the plan is currently being developed based on the input received from a Strategic Plan Working Group (which includes several AGA members), a public Request for Information, and NIDDK’s Advisory Council. The draft will be available through the NIDDK website (niddk.nih.gov) for public comment.
By taking these actions, the NIDDK aims to continue reducing the burden of digestive diseases and improving health for all people.
Dr. Rodgers is director of the National Institute of Diabetes and Digestive and Kidney Diseases at the National Institutes of Health. He has no conflicts. Dr. Rodgers made these comments during the AGA Institute Presidential Plenary at the annual Digestive Disease Week®.
The making of the Pfizer-BioNTech COVID-19 vaccine
Days after the World Health Organization declared the COVID-19 outbreak a global pandemic, Pfizer and BioNTech announced plans to codevelop a potential mRNA-based vaccine to help prevent COVID-19. The mRNA platform was selected given its potential for high potency and capacity for rapid development. A bold decision was made to invest in R&D and manufacturing at risk.

Two candidates, BNT162b1 and BNT162b2, quickly emerged as most promising. After extensive review of preclinical and early clinical data and in consultation with regulators, we advanced BNT162b2 into a global, Phase 2/3 efficacy trial in July 2020.
Enrollment was later expanded to increase diversity, and also to include adolescents 12 and older and people with chronic, stable HIV, Hepatitis C, or Hepatitis B.
In November 2020, we announced the results of our ongoing Phase 3 study with BNT162b2 demonstrating a vaccine efficacy rate of 95% against COVID-19 beginning 28 days after dose one. This result showed our ability to leverage decades of scientific expertise to execute a rigorous Phase 3 clinical program to make a potential vaccine available as quickly and safely as possible. The emergency use authorization that followed was a big step, but our research did not stop there.
Pfizer and BioNTech continue to evaluate data from the landmark trial, which ultimately enrolled 46,331 participants. We are also conducting trials in special populations, such as pregnant women and children under 12. To date, real-world evidence has demonstrated lower COVID-19 incidence in vaccinated individuals and has not shown escape of variant viruses from BNT162b2-mediated protection. Studies are ongoing to explore the effect of a third dose on immunity and to prepare in case a variant emerges that escapes protection.
We continue to identify improvements to increase production and are on track to deliver approximately 2.5 billion doses in 2021. Next generation ready-to-use and freeze-dried formulations are in development.
This pandemic sparked an unparalleled period of innovation, investment, and partnership with lessons learned that will help us prepare for future pandemics and accelerate R&D of therapeutic candidates for other debilitating and life-threatening conditions.
The Pfizer-BioNTech COVID-19 vaccine has not been approved or licensed by the U.S. Food and Drug Administration but has been authorized for emergency use to prevent COVID-19 in individuals 12+. See conditions of use: http://cvdvaccine.com
Dr. Dolsten is the Chief Scientific Officer and President of Worldwide Research, Development and Medical at Pfizer. He has no other conflicts. Dr. Dolsten made these comments during the AGA Institute Presidential Plenary at the annual Digestive Disease Week®.
Days after the World Health Organization declared the COVID-19 outbreak a global pandemic, Pfizer and BioNTech announced plans to codevelop a potential mRNA-based vaccine to help prevent COVID-19. The mRNA platform was selected given its potential for high potency and capacity for rapid development. A bold decision was made to invest in R&D and manufacturing at risk.
Two candidates, BNT162b1 and BNT162b2, quickly emerged as most promising. After extensive review of preclinical and early clinical data and in consultation with regulators, we advanced BNT162b2 into a global, Phase 2/3 efficacy trial in July 2020.
Enrollment was later expanded to increase diversity, and also to include adolescents 12 and older and people with chronic, stable HIV, Hepatitis C, or Hepatitis B.
In November 2020, we announced the results of our ongoing Phase 3 study with BNT162b2 demonstrating a vaccine efficacy rate of 95% against COVID-19 beginning 28 days after dose one. This result showed our ability to leverage decades of scientific expertise to execute a rigorous Phase 3 clinical program to make a potential vaccine available as quickly and safely as possible. The emergency use authorization that followed was a big step, but our research did not stop there.
Pfizer and BioNTech continue to evaluate data from the landmark trial, which ultimately enrolled 46,331 participants. We are also conducting trials in special populations, such as pregnant women and children under 12. To date, real-world evidence has demonstrated lower COVID-19 incidence in vaccinated individuals and has not shown escape of variant viruses from BNT162b2-mediated protection. Studies are ongoing to explore the effect of a third dose on immunity and to prepare in case a variant emerges that escapes protection.
We continue to identify improvements to increase production and are on track to deliver approximately 2.5 billion doses in 2021. Next generation ready-to-use and freeze-dried formulations are in development.
This pandemic sparked an unparalleled period of innovation, investment, and partnership with lessons learned that will help us prepare for future pandemics and accelerate R&D of therapeutic candidates for other debilitating and life-threatening conditions.
The Pfizer-BioNTech COVID-19 vaccine has not been approved or licensed by the U.S. Food and Drug Administration but has been authorized for emergency use to prevent COVID-19 in individuals 12+. See conditions of use: http://cvdvaccine.com
Dr. Dolsten is the Chief Scientific Officer and President of Worldwide Research, Development and Medical at Pfizer. He has no other conflicts. Dr. Dolsten made these comments during the AGA Institute Presidential Plenary at the annual Digestive Disease Week®.
Days after the World Health Organization declared the COVID-19 outbreak a global pandemic, Pfizer and BioNTech announced plans to codevelop a potential mRNA-based vaccine to help prevent COVID-19. The mRNA platform was selected given its potential for high potency and capacity for rapid development. A bold decision was made to invest in R&D and manufacturing at risk.
Two candidates, BNT162b1 and BNT162b2, quickly emerged as most promising. After extensive review of preclinical and early clinical data and in consultation with regulators, we advanced BNT162b2 into a global, Phase 2/3 efficacy trial in July 2020.
Enrollment was later expanded to increase diversity, and also to include adolescents 12 and older and people with chronic, stable HIV, Hepatitis C, or Hepatitis B.
In November 2020, we announced the results of our ongoing Phase 3 study with BNT162b2 demonstrating a vaccine efficacy rate of 95% against COVID-19 beginning 28 days after dose one. This result showed our ability to leverage decades of scientific expertise to execute a rigorous Phase 3 clinical program to make a potential vaccine available as quickly and safely as possible. The emergency use authorization that followed was a big step, but our research did not stop there.
Pfizer and BioNTech continue to evaluate data from the landmark trial, which ultimately enrolled 46,331 participants. We are also conducting trials in special populations, such as pregnant women and children under 12. To date, real-world evidence has demonstrated lower COVID-19 incidence in vaccinated individuals and has not shown escape of variant viruses from BNT162b2-mediated protection. Studies are ongoing to explore the effect of a third dose on immunity and to prepare in case a variant emerges that escapes protection.
We continue to identify improvements to increase production and are on track to deliver approximately 2.5 billion doses in 2021. Next generation ready-to-use and freeze-dried formulations are in development.
This pandemic sparked an unparalleled period of innovation, investment, and partnership with lessons learned that will help us prepare for future pandemics and accelerate R&D of therapeutic candidates for other debilitating and life-threatening conditions.
The Pfizer-BioNTech COVID-19 vaccine has not been approved or licensed by the U.S. Food and Drug Administration but has been authorized for emergency use to prevent COVID-19 in individuals 12+. See conditions of use: http://cvdvaccine.com
Dr. Dolsten is the Chief Scientific Officer and President of Worldwide Research, Development and Medical at Pfizer. He has no other conflicts. Dr. Dolsten made these comments during the AGA Institute Presidential Plenary at the annual Digestive Disease Week®.
Malaria study shows remarkable 70% reduction in severe disease and death
A new study from Africa shows a remarkable 70% reduction in malaria if two treatments — a vaccine and an antimalarial medication — are combined instead of giving them individually.
Malaria is endemic in the tropics. The World Health Organization (WHO) reports that in 2019, there were 229 million cases and 409,000 deaths from this parasitic infection. Most of the burden (94%) occurs in Africa, and children younger than age 5 account for 67% of the deaths.
In the Sahel region of Africa, a broad, sub-Saharan band that stretches across the continent, high malaria transmission is seasonal. Children in some countries there are treated with monthly courses of sulfadoxine-pyrimethamine and amodiaquine chemoprophylaxis during the four higher-risk months. Such seasonal malaria chemoprophylaxis (SMC) has been shown to reduce infections by up to 88% and costs an average of $3.43 per child per year.
This double-blind, randomized controlled trial enrolled young children (5-17 months old) in Burkina Faso and Mali, where SMC is the current treatment regimen. Nearly 6,000 children received either chemoprophylaxis, the RTS,S/AS01E malaria vaccine (RTS,S), or both treatments. The study, led by investigators at the London School of Hygiene and Tropical Medicine (LSHTM), was reported in the New England Journal of Medicine.
Co-lead investigator Daniel Chandramohan, MBBS, PhD, MSc, professor of public health at LSHTM, said in an interview that SMC administration is quite labor-intensive and that “we thought we can replace these four cycles of seasonal cure prevention with one seasonal vaccination like the flu vaccine ... and that there might be some additive benefit.”
Instead, the study found the combination reduces the incidence of malaria by 62% against clinical malaria infection, 70% against severe malaria, and 73% against death from malaria compared with SMC alone. “Not in our wildest dreams would I have hypothesized that this is a possibility,” Dr. Chandramohan said. He continued that this was unlikely a “freak result” because the findings are “consistent between both countries. Two, it is consistent across the years. Three, all the malaria outcomes ... are consistently showing the protective effect at the same level.”
To maintain the blinded study design, children received injections of rabies vaccine and hepatitis A vaccine instead of a placebo for RTS,S. Both were chosen to provide additional benefits by protecting children against those infections.
With so many children followed over years, accuracy in providing the correct treatment for each study arm can be difficult. Each child was given a QR code and picture identification to facilitate drug distribution each year in this study.
Miriam K. Laufer, MD, professor and associate director for malaria research at the University of Maryland, Baltimore, who was not involved in the study, said in an interview, “This is a spectacular result, you know, decreasing disease by 60%-70% using interventions that we already have.”
RTS,S is not a new vaccine; it was developed in 2001 by GlaxoSmithKline with Path’s Malaria Vaccine Initiative, then manufactured by GSK. The Gates Foundation has supported production. Dr. Chandramohan said GSK has transferred the technology to Bharat, in India, and that it will take 2-3 years to ramp up production. Until then, enough vaccine is available to supply Kenya, Malawi, and Ghana, where the pilot studies are being done.
Dr. Laufer stressed that the “group that got RTS,S did as well as the group that received SMC.” She noted that the use of SMC is limited to specific areas of the Sahel sub-region of Africa, with a brief transmission period. In other areas of Africa where malaria has a longer transmission period, SMC isn’t as effective. “RTS,S vaccine could really have an impact” there, she added.
Asked if RTS,S might be substituted for SMC to reduce the likelihood of resistance emerging, Dr. Laufer said, “Giving RTS,S vaccine is as good as using repeated treatment of malaria drugs during the malaria season. And that’s important for two reasons. One is that the advantage of a vaccine is that you’re not producing pressure of drugs that would enable drug resistance to emerge and spread. So maybe your vaccine efficacy could last longer than drug efficacy. We don’t know the answer to that.”
Hypothesizing about the unexpectedly good trial results, Dr. Laufer explained, “We know that RTS,S decreases the number of parasites that make it into the blood when a child is bitten by an infected mosquito. When drugs like sulfadoxine-pyrimethamine and amodiaquine that have moderate efficacy only have to kill off a small number of parasites, they can work better. Maybe that explains why the combination of RTS,S and SMC created such a positive outcome.”
Dr. Laufer echoed Chandramohan, saying, “Results were much more dramatic than anybody – certainly than I anticipated.” Both physicians anticipate that WHO will give full approval for this combination this fall.
Dr. Chandramohan and Dr. Laufer have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study from Africa shows a remarkable 70% reduction in malaria if two treatments — a vaccine and an antimalarial medication — are combined instead of giving them individually.
Malaria is endemic in the tropics. The World Health Organization (WHO) reports that in 2019, there were 229 million cases and 409,000 deaths from this parasitic infection. Most of the burden (94%) occurs in Africa, and children younger than age 5 account for 67% of the deaths.
In the Sahel region of Africa, a broad, sub-Saharan band that stretches across the continent, high malaria transmission is seasonal. Children in some countries there are treated with monthly courses of sulfadoxine-pyrimethamine and amodiaquine chemoprophylaxis during the four higher-risk months. Such seasonal malaria chemoprophylaxis (SMC) has been shown to reduce infections by up to 88% and costs an average of $3.43 per child per year.
This double-blind, randomized controlled trial enrolled young children (5-17 months old) in Burkina Faso and Mali, where SMC is the current treatment regimen. Nearly 6,000 children received either chemoprophylaxis, the RTS,S/AS01E malaria vaccine (RTS,S), or both treatments. The study, led by investigators at the London School of Hygiene and Tropical Medicine (LSHTM), was reported in the New England Journal of Medicine.
Co-lead investigator Daniel Chandramohan, MBBS, PhD, MSc, professor of public health at LSHTM, said in an interview that SMC administration is quite labor-intensive and that “we thought we can replace these four cycles of seasonal cure prevention with one seasonal vaccination like the flu vaccine ... and that there might be some additive benefit.”
Instead, the study found the combination reduces the incidence of malaria by 62% against clinical malaria infection, 70% against severe malaria, and 73% against death from malaria compared with SMC alone. “Not in our wildest dreams would I have hypothesized that this is a possibility,” Dr. Chandramohan said. He continued that this was unlikely a “freak result” because the findings are “consistent between both countries. Two, it is consistent across the years. Three, all the malaria outcomes ... are consistently showing the protective effect at the same level.”
To maintain the blinded study design, children received injections of rabies vaccine and hepatitis A vaccine instead of a placebo for RTS,S. Both were chosen to provide additional benefits by protecting children against those infections.
With so many children followed over years, accuracy in providing the correct treatment for each study arm can be difficult. Each child was given a QR code and picture identification to facilitate drug distribution each year in this study.
Miriam K. Laufer, MD, professor and associate director for malaria research at the University of Maryland, Baltimore, who was not involved in the study, said in an interview, “This is a spectacular result, you know, decreasing disease by 60%-70% using interventions that we already have.”
RTS,S is not a new vaccine; it was developed in 2001 by GlaxoSmithKline with Path’s Malaria Vaccine Initiative, then manufactured by GSK. The Gates Foundation has supported production. Dr. Chandramohan said GSK has transferred the technology to Bharat, in India, and that it will take 2-3 years to ramp up production. Until then, enough vaccine is available to supply Kenya, Malawi, and Ghana, where the pilot studies are being done.
Dr. Laufer stressed that the “group that got RTS,S did as well as the group that received SMC.” She noted that the use of SMC is limited to specific areas of the Sahel sub-region of Africa, with a brief transmission period. In other areas of Africa where malaria has a longer transmission period, SMC isn’t as effective. “RTS,S vaccine could really have an impact” there, she added.
Asked if RTS,S might be substituted for SMC to reduce the likelihood of resistance emerging, Dr. Laufer said, “Giving RTS,S vaccine is as good as using repeated treatment of malaria drugs during the malaria season. And that’s important for two reasons. One is that the advantage of a vaccine is that you’re not producing pressure of drugs that would enable drug resistance to emerge and spread. So maybe your vaccine efficacy could last longer than drug efficacy. We don’t know the answer to that.”
Hypothesizing about the unexpectedly good trial results, Dr. Laufer explained, “We know that RTS,S decreases the number of parasites that make it into the blood when a child is bitten by an infected mosquito. When drugs like sulfadoxine-pyrimethamine and amodiaquine that have moderate efficacy only have to kill off a small number of parasites, they can work better. Maybe that explains why the combination of RTS,S and SMC created such a positive outcome.”
Dr. Laufer echoed Chandramohan, saying, “Results were much more dramatic than anybody – certainly than I anticipated.” Both physicians anticipate that WHO will give full approval for this combination this fall.
Dr. Chandramohan and Dr. Laufer have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study from Africa shows a remarkable 70% reduction in malaria if two treatments — a vaccine and an antimalarial medication — are combined instead of giving them individually.
Malaria is endemic in the tropics. The World Health Organization (WHO) reports that in 2019, there were 229 million cases and 409,000 deaths from this parasitic infection. Most of the burden (94%) occurs in Africa, and children younger than age 5 account for 67% of the deaths.
In the Sahel region of Africa, a broad, sub-Saharan band that stretches across the continent, high malaria transmission is seasonal. Children in some countries there are treated with monthly courses of sulfadoxine-pyrimethamine and amodiaquine chemoprophylaxis during the four higher-risk months. Such seasonal malaria chemoprophylaxis (SMC) has been shown to reduce infections by up to 88% and costs an average of $3.43 per child per year.
This double-blind, randomized controlled trial enrolled young children (5-17 months old) in Burkina Faso and Mali, where SMC is the current treatment regimen. Nearly 6,000 children received either chemoprophylaxis, the RTS,S/AS01E malaria vaccine (RTS,S), or both treatments. The study, led by investigators at the London School of Hygiene and Tropical Medicine (LSHTM), was reported in the New England Journal of Medicine.
Co-lead investigator Daniel Chandramohan, MBBS, PhD, MSc, professor of public health at LSHTM, said in an interview that SMC administration is quite labor-intensive and that “we thought we can replace these four cycles of seasonal cure prevention with one seasonal vaccination like the flu vaccine ... and that there might be some additive benefit.”
Instead, the study found the combination reduces the incidence of malaria by 62% against clinical malaria infection, 70% against severe malaria, and 73% against death from malaria compared with SMC alone. “Not in our wildest dreams would I have hypothesized that this is a possibility,” Dr. Chandramohan said. He continued that this was unlikely a “freak result” because the findings are “consistent between both countries. Two, it is consistent across the years. Three, all the malaria outcomes ... are consistently showing the protective effect at the same level.”
To maintain the blinded study design, children received injections of rabies vaccine and hepatitis A vaccine instead of a placebo for RTS,S. Both were chosen to provide additional benefits by protecting children against those infections.
With so many children followed over years, accuracy in providing the correct treatment for each study arm can be difficult. Each child was given a QR code and picture identification to facilitate drug distribution each year in this study.
Miriam K. Laufer, MD, professor and associate director for malaria research at the University of Maryland, Baltimore, who was not involved in the study, said in an interview, “This is a spectacular result, you know, decreasing disease by 60%-70% using interventions that we already have.”
RTS,S is not a new vaccine; it was developed in 2001 by GlaxoSmithKline with Path’s Malaria Vaccine Initiative, then manufactured by GSK. The Gates Foundation has supported production. Dr. Chandramohan said GSK has transferred the technology to Bharat, in India, and that it will take 2-3 years to ramp up production. Until then, enough vaccine is available to supply Kenya, Malawi, and Ghana, where the pilot studies are being done.
Dr. Laufer stressed that the “group that got RTS,S did as well as the group that received SMC.” She noted that the use of SMC is limited to specific areas of the Sahel sub-region of Africa, with a brief transmission period. In other areas of Africa where malaria has a longer transmission period, SMC isn’t as effective. “RTS,S vaccine could really have an impact” there, she added.
Asked if RTS,S might be substituted for SMC to reduce the likelihood of resistance emerging, Dr. Laufer said, “Giving RTS,S vaccine is as good as using repeated treatment of malaria drugs during the malaria season. And that’s important for two reasons. One is that the advantage of a vaccine is that you’re not producing pressure of drugs that would enable drug resistance to emerge and spread. So maybe your vaccine efficacy could last longer than drug efficacy. We don’t know the answer to that.”
Hypothesizing about the unexpectedly good trial results, Dr. Laufer explained, “We know that RTS,S decreases the number of parasites that make it into the blood when a child is bitten by an infected mosquito. When drugs like sulfadoxine-pyrimethamine and amodiaquine that have moderate efficacy only have to kill off a small number of parasites, they can work better. Maybe that explains why the combination of RTS,S and SMC created such a positive outcome.”
Dr. Laufer echoed Chandramohan, saying, “Results were much more dramatic than anybody – certainly than I anticipated.” Both physicians anticipate that WHO will give full approval for this combination this fall.
Dr. Chandramohan and Dr. Laufer have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
What’s your diagnosis?
Choledocopyloric fistula secondary to peptic ulcer disease.
This patient has a known history of prepyloric peptic ulcer disease and related gastric outlet obstruction requiring two previous dilations. Upon endoscopic examination, we observed high-grade obstruction at the pylorus similar to previous examinations. During the initial positioning of the balloon for dilation, we inadvertently cannulated the fistula located in the pyloric channel using the guidewire (arrow in Figure D) and were able to characterize its anatomy upon contrast administration (Figure C). However, after repositioning the guidewire into the duodenal lumen beyond pyloric stricture, the balloon was inflated to a maximal diameter of 15 mm under fluoroscopic guidance. Discounting other common causes, our patient presented with an infrequent occurrence of choledocopyloric fistula secondary to peptic ulcer disease.
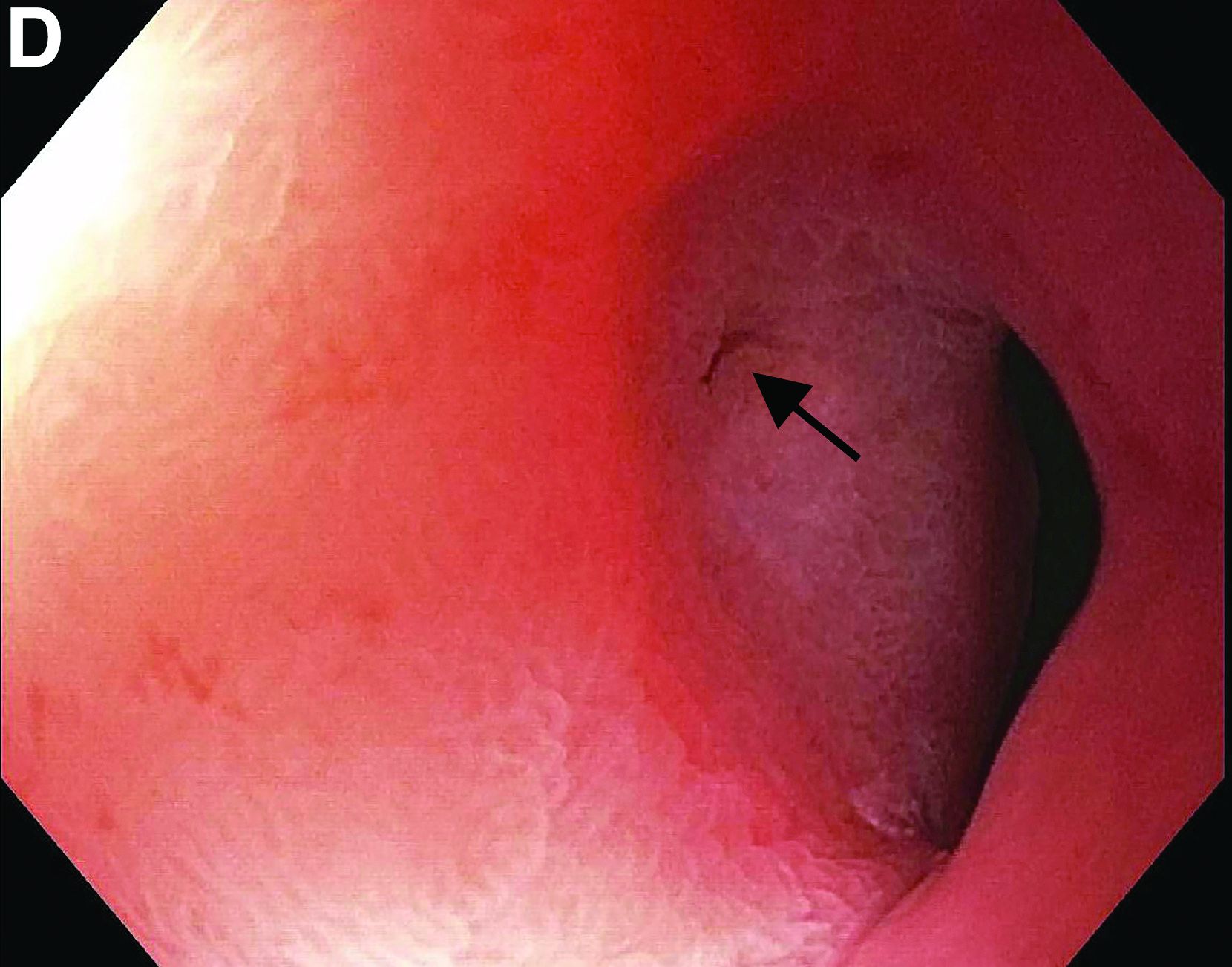
The most common cause of choledocoenteric fistula is bile duct inflammation due to gallstone formation, while other minor causes include neoplasms, ulcers, and inflammation of neighboring organs.1 Additionally, in recent years, fistula formation is a relatively rare complication of peptic ulcer disease due to the increased effectiveness of ulcer drugs.2 Similar to this patient's condition, cholangitis, jaundice, or anomaly of biological liver examinations are rarely observed. Consequently, diagnosis is mainly incidental with pneumobilia being the most helpful marker present in 50% of cases.3 Because cholangitis and biliary sequelae remain rare, choledocoenteric fistulas do not warrant prophylactic surgical treatment. As a result, treatment is generally focused on the underlying ulcer disease.
The quiz authors disclose no conflicts.
References
1. Stagnitti F et al. G Chir. 2000 Mar;21(3):110-7.
2. Wu MB et al. Ann Surg Treat Res. 2015 Nov;89(5):240-6.
3. Dewulf E et al. J Chir (Paris). 1987 Jan;124(1):19-23.
Previously published in Gastroenterology (2019 Oct;157[4]:936-7).
Choledocopyloric fistula secondary to peptic ulcer disease.
This patient has a known history of prepyloric peptic ulcer disease and related gastric outlet obstruction requiring two previous dilations. Upon endoscopic examination, we observed high-grade obstruction at the pylorus similar to previous examinations. During the initial positioning of the balloon for dilation, we inadvertently cannulated the fistula located in the pyloric channel using the guidewire (arrow in Figure D) and were able to characterize its anatomy upon contrast administration (Figure C). However, after repositioning the guidewire into the duodenal lumen beyond pyloric stricture, the balloon was inflated to a maximal diameter of 15 mm under fluoroscopic guidance. Discounting other common causes, our patient presented with an infrequent occurrence of choledocopyloric fistula secondary to peptic ulcer disease.
The most common cause of choledocoenteric fistula is bile duct inflammation due to gallstone formation, while other minor causes include neoplasms, ulcers, and inflammation of neighboring organs.1 Additionally, in recent years, fistula formation is a relatively rare complication of peptic ulcer disease due to the increased effectiveness of ulcer drugs.2 Similar to this patient's condition, cholangitis, jaundice, or anomaly of biological liver examinations are rarely observed. Consequently, diagnosis is mainly incidental with pneumobilia being the most helpful marker present in 50% of cases.3 Because cholangitis and biliary sequelae remain rare, choledocoenteric fistulas do not warrant prophylactic surgical treatment. As a result, treatment is generally focused on the underlying ulcer disease.
The quiz authors disclose no conflicts.
References
1. Stagnitti F et al. G Chir. 2000 Mar;21(3):110-7.
2. Wu MB et al. Ann Surg Treat Res. 2015 Nov;89(5):240-6.
3. Dewulf E et al. J Chir (Paris). 1987 Jan;124(1):19-23.
Previously published in Gastroenterology (2019 Oct;157[4]:936-7).
Choledocopyloric fistula secondary to peptic ulcer disease.
This patient has a known history of prepyloric peptic ulcer disease and related gastric outlet obstruction requiring two previous dilations. Upon endoscopic examination, we observed high-grade obstruction at the pylorus similar to previous examinations. During the initial positioning of the balloon for dilation, we inadvertently cannulated the fistula located in the pyloric channel using the guidewire (arrow in Figure D) and were able to characterize its anatomy upon contrast administration (Figure C). However, after repositioning the guidewire into the duodenal lumen beyond pyloric stricture, the balloon was inflated to a maximal diameter of 15 mm under fluoroscopic guidance. Discounting other common causes, our patient presented with an infrequent occurrence of choledocopyloric fistula secondary to peptic ulcer disease.
The most common cause of choledocoenteric fistula is bile duct inflammation due to gallstone formation, while other minor causes include neoplasms, ulcers, and inflammation of neighboring organs.1 Additionally, in recent years, fistula formation is a relatively rare complication of peptic ulcer disease due to the increased effectiveness of ulcer drugs.2 Similar to this patient's condition, cholangitis, jaundice, or anomaly of biological liver examinations are rarely observed. Consequently, diagnosis is mainly incidental with pneumobilia being the most helpful marker present in 50% of cases.3 Because cholangitis and biliary sequelae remain rare, choledocoenteric fistulas do not warrant prophylactic surgical treatment. As a result, treatment is generally focused on the underlying ulcer disease.
The quiz authors disclose no conflicts.
References
1. Stagnitti F et al. G Chir. 2000 Mar;21(3):110-7.
2. Wu MB et al. Ann Surg Treat Res. 2015 Nov;89(5):240-6.
3. Dewulf E et al. J Chir (Paris). 1987 Jan;124(1):19-23.
Previously published in Gastroenterology (2019 Oct;157[4]:936-7).
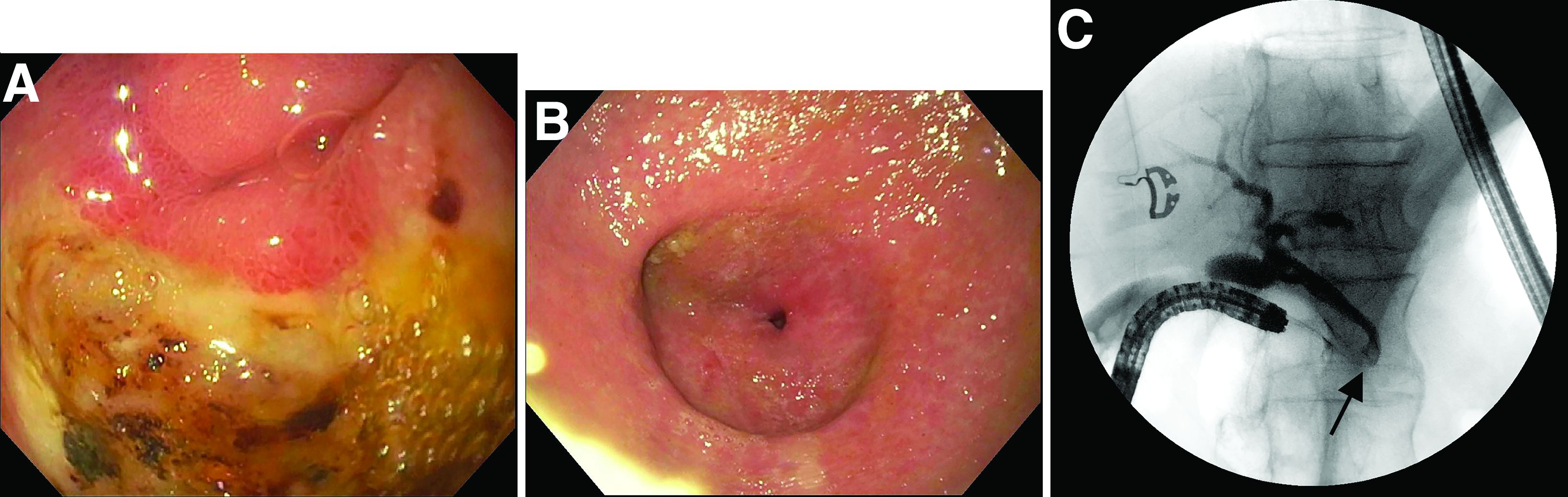
What’s the diagnosis?
Emerging data point to underlying autoimmunity in ME/CFS
Emerging evidence suggests that autoimmunity plays a role in postinfectious myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and that targeting autoantibodies could be a promising treatment approach.

The same may also apply to many cases of “long COVID,” in which many of the symptoms overlap with those of ME/CFS, Carmen Scheibenbogen, MD, professor of clinical immunology and director of the Institute for Medical Immunology, Charité University Medicine, Berlin, said during the annual meeting of the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis.
Several groups, including Dr. Scheibenbogen’s, have reported finding autoantibodies against neurotransmitter receptor antigens in people with ME/CFS. And, in a paper published in the Journal of Clinical Medicine the day that Dr. Scheibenbogen spoke at the meeting, her team reported significant correlations between autoantibodies to vasoregulative G-protein–coupled receptors and symptom severity, autonomic dysfunction, and disability among 116 patients with infection-triggered ME/CFS who were diagnosed using the symptom-based 2003 Canadian consensus criteria.
People with ME/CFS are also more likely to have genetic risk factors associated with autoimmunity and personal and/or family histories of autoimmune conditions. And, clinical trials have demonstrated early success with various immunomodulatory treatments in subsets of people with ME/CFS, including endoxan, rituximab, and immunoadsorption.
“We have evidence that ME/CFS is an autoantibody-mediated disease, and we have evidence that autoantibody targeting is effective in this disease. So far ... we have few and underfinanced clinical studies, but the good news is we have promising emerging treatment options,” Dr. Scheibenbogen said.

Asked to comment, ME/CFS expert Anthony L. Komaroff, MD, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, said: “There is already strong evidence that there are autoantibodies in ME/CFS. Dr. Scheibenbogen’s work is the latest and employs the latest technology. ... I would bet that autoantibodies to neural targets are likely to cause some of the symptoms of ME/CFS and some of the symptoms of long COVID.”
However, he cautioned, “that has not been proven, and even if it were proven you would have to demonstrate that treatments based on that theory worked.”
Dr. Komaroff said he views autoimmunity as a likely component of the ME/CFS spectrum, but not the only one. “My current view of this illness is that there’s a final common pathway in the brain that leads to the symptoms of the illness. But that final common pathway can be triggered by a variety of different things, one of which could be autoantibodies while another could be infection or inflammation in the brain.”
Emerging evidence points to autoimmunity
Dr. Scheibenbogen summarized the work published in this area over the past few years by her group and others.
In a comparison of ME/CFS patients with 201 healthy controls, significant associations were seen with two specific autoimmunity-related risk alleles only in the ME/CFS patients who reported acute onset of disease with an infection but not in those with ME/CFS without infection-triggered onset or the controls. Both genes play roles in regulating B- and T-cell activation.
Another recent study found associations with ME/CFS and major histocompatibility complex class II molecules, a typical feature of autoimmune diseases, in a comparison between 426 adult Norwegian ME/CFS patients who were diagnosed with the Canadian consensus criteria and 4,511 healthy, ethnically matched controls.
In a 2020 paper, Dr. Scheibenbogen and pharmacologist Klaus Wirth presented a “unifying hypothesis” of ME/CFS pathophysiology based on the finding of elevations in autoantibodies against beta2-adrenergic receptors and muscarinic acetylcholine receptors in some individuals with the condition. Since both of those receptors are important vasodilators, their functional disturbance would be expected to cause vasoconstriction and hypoxemia, which would explain many of the symptoms of ME/CFS. This mechanism would align with other findings of muscular and cerebral hypoperfusion that correlate with fatigue, particularly post exertion, as well as metabolic changes that are in line with the concepts of hypoxemia and ischemia.
Further evidence for vascular dysfunction in ME/CFS came from her group’s study finding evidence of peripheral endothelial dysfunction that was associated with symptom severity in 35 adult patients. “Vasoconstriction, hypovolemia, and release of vasoactive and algesic mediators is probably a key pathomechanism of the disease,” Dr. Scheibenbogen said.
Treatments: Will targeting autoantibodies work?
In the second part of her talk, Dr. Scheibenbogen summarized clinical trials of the following treatment approaches that involve targeting autoantibodies as a way to alleviate ME/CFS symptoms:
Rituximab: Work on infusions of the B-cell depleting agent has been conducted by Norwegian researchers beginning in 2011 with a small randomized trial and an open-label, phase 2 study in 2015, both showing clinical responses in ME/CFS. However, a subsequent phase 3, randomized clinical trial of 151 patients, again diagnosed using the Canadian criteria, was negative.
There are several possible explanations for this, Dr. Scheibenbogen noted. For one, the maintenance dose had to be reduced because of a lack of financial support. “This was probably critical. The lower dose was insufficient to adequately deplete B cells.” Also, there may have been a strong placebo response in the control group since they were being given better care than they normally would receive during the trial. “I think probably nobody will again do a rituximab trial. This was very disappointing for all of us. But, we still have other opportunities to follow this path,” she said.
Dr. Komaroff agreed. “I don’t think the failure of one drug that hits malignant B cells is proof against the autoimmune hypothesis per se. I think the evidence is that rituximab doesn’t work, but that doesn’t invalidate the autoimmunity hypothesis.”
Cyclophosphamide: The same Norwegian group also showed positive findings in an open-label, phase 2 trial of the immune-modifying drug cyclophosphamide in 22 of 40 patients. Interestingly, HLA risk alleles were much more common in responders than nonresponders, Dr. Scheibenbogen noted.
Immunoadsorption: This technique, similar to dialysis, involves separating out the blood plasma by centrifugation and removing IgG autoantibodies by a binding column, then returning the plasma back to the patient. It is used, primarily in Europe, to treat severe autoimmune diseases including dilative cardiomyopathy and refractory systemic lupus erythematosus (SLE).
Dr. Scheibenbogen’s group has conducted two studies of immunoadsorption in ME/CFS. In one, a 5-day procedure led to rapid symptom improvement in 7 of 10 patients, with sustained improvement in 3 patients after 2 years. Autoantibodies decreased rapidly in 9 of the 10 patients. In a follow-up study of five of the responders 2 years later, retreatment with a modified immunoadsorption protocol led to rapid and sustained improvement in four. Further study has been on hold because of the pandemic.
Next-gen IgG-targeting therapies: Another approach that could offer promise for ME/CFS involves therapies that block the Fc receptors of IgG. Several are in phase 1-3 trials for autoimmune conditions. One candidate drug, the Fc fragment efgartigimod, is currently in phase 3 trials for several conditions, including generalized myasthenia gravis, primary immune thrombocytopenia, and chronic inflammatory demyelinating polyneuropathy. Phase 3 trials are planned for the monoclonal antibody rozanolixizumab in those same conditions.
Newer-generation monoclonal antibodies targeting CD19 or CD20 that show benefit in various autoimmune conditions are another possibility for ME/CFS. These include ocrelizumab (Ocrevus), approved in the United States for treating relapsing and progressive multiple sclerosis and in trials for SLE; obinutuzumab (Gazyva), approved for treating lymphoma and also in development for SLE; and ublituximab, in phase 3 trials for multiple sclerosis.
“Most of them are more effective than rituximab,” Dr. Scheibenbogen noted, adding that “currently the data look quite promising. They are effective in different autoimmune diseases and they are quite well tolerated. There’s great hope now with COVID-19 that we can convince some companies to do such trials in ME/CFS as well.”
Dr. Scheibenbogen’s institution, the Charité Fatigue Center, has a patent for beta2-adrenergic receptor antibodies for diagnosing ME/CFS under her name together with Celltrend. Dr. Komaroff has received personal fees from Serimmune.
Emerging evidence suggests that autoimmunity plays a role in postinfectious myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and that targeting autoantibodies could be a promising treatment approach.
The same may also apply to many cases of “long COVID,” in which many of the symptoms overlap with those of ME/CFS, Carmen Scheibenbogen, MD, professor of clinical immunology and director of the Institute for Medical Immunology, Charité University Medicine, Berlin, said during the annual meeting of the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis.
Several groups, including Dr. Scheibenbogen’s, have reported finding autoantibodies against neurotransmitter receptor antigens in people with ME/CFS. And, in a paper published in the Journal of Clinical Medicine the day that Dr. Scheibenbogen spoke at the meeting, her team reported significant correlations between autoantibodies to vasoregulative G-protein–coupled receptors and symptom severity, autonomic dysfunction, and disability among 116 patients with infection-triggered ME/CFS who were diagnosed using the symptom-based 2003 Canadian consensus criteria.
People with ME/CFS are also more likely to have genetic risk factors associated with autoimmunity and personal and/or family histories of autoimmune conditions. And, clinical trials have demonstrated early success with various immunomodulatory treatments in subsets of people with ME/CFS, including endoxan, rituximab, and immunoadsorption.
“We have evidence that ME/CFS is an autoantibody-mediated disease, and we have evidence that autoantibody targeting is effective in this disease. So far ... we have few and underfinanced clinical studies, but the good news is we have promising emerging treatment options,” Dr. Scheibenbogen said.
Asked to comment, ME/CFS expert Anthony L. Komaroff, MD, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, said: “There is already strong evidence that there are autoantibodies in ME/CFS. Dr. Scheibenbogen’s work is the latest and employs the latest technology. ... I would bet that autoantibodies to neural targets are likely to cause some of the symptoms of ME/CFS and some of the symptoms of long COVID.”
However, he cautioned, “that has not been proven, and even if it were proven you would have to demonstrate that treatments based on that theory worked.”
Dr. Komaroff said he views autoimmunity as a likely component of the ME/CFS spectrum, but not the only one. “My current view of this illness is that there’s a final common pathway in the brain that leads to the symptoms of the illness. But that final common pathway can be triggered by a variety of different things, one of which could be autoantibodies while another could be infection or inflammation in the brain.”
Emerging evidence points to autoimmunity
Dr. Scheibenbogen summarized the work published in this area over the past few years by her group and others.
In a comparison of ME/CFS patients with 201 healthy controls, significant associations were seen with two specific autoimmunity-related risk alleles only in the ME/CFS patients who reported acute onset of disease with an infection but not in those with ME/CFS without infection-triggered onset or the controls. Both genes play roles in regulating B- and T-cell activation.
Another recent study found associations with ME/CFS and major histocompatibility complex class II molecules, a typical feature of autoimmune diseases, in a comparison between 426 adult Norwegian ME/CFS patients who were diagnosed with the Canadian consensus criteria and 4,511 healthy, ethnically matched controls.
In a 2020 paper, Dr. Scheibenbogen and pharmacologist Klaus Wirth presented a “unifying hypothesis” of ME/CFS pathophysiology based on the finding of elevations in autoantibodies against beta2-adrenergic receptors and muscarinic acetylcholine receptors in some individuals with the condition. Since both of those receptors are important vasodilators, their functional disturbance would be expected to cause vasoconstriction and hypoxemia, which would explain many of the symptoms of ME/CFS. This mechanism would align with other findings of muscular and cerebral hypoperfusion that correlate with fatigue, particularly post exertion, as well as metabolic changes that are in line with the concepts of hypoxemia and ischemia.
Further evidence for vascular dysfunction in ME/CFS came from her group’s study finding evidence of peripheral endothelial dysfunction that was associated with symptom severity in 35 adult patients. “Vasoconstriction, hypovolemia, and release of vasoactive and algesic mediators is probably a key pathomechanism of the disease,” Dr. Scheibenbogen said.
Treatments: Will targeting autoantibodies work?
In the second part of her talk, Dr. Scheibenbogen summarized clinical trials of the following treatment approaches that involve targeting autoantibodies as a way to alleviate ME/CFS symptoms:
Rituximab: Work on infusions of the B-cell depleting agent has been conducted by Norwegian researchers beginning in 2011 with a small randomized trial and an open-label, phase 2 study in 2015, both showing clinical responses in ME/CFS. However, a subsequent phase 3, randomized clinical trial of 151 patients, again diagnosed using the Canadian criteria, was negative.
There are several possible explanations for this, Dr. Scheibenbogen noted. For one, the maintenance dose had to be reduced because of a lack of financial support. “This was probably critical. The lower dose was insufficient to adequately deplete B cells.” Also, there may have been a strong placebo response in the control group since they were being given better care than they normally would receive during the trial. “I think probably nobody will again do a rituximab trial. This was very disappointing for all of us. But, we still have other opportunities to follow this path,” she said.
Dr. Komaroff agreed. “I don’t think the failure of one drug that hits malignant B cells is proof against the autoimmune hypothesis per se. I think the evidence is that rituximab doesn’t work, but that doesn’t invalidate the autoimmunity hypothesis.”
Cyclophosphamide: The same Norwegian group also showed positive findings in an open-label, phase 2 trial of the immune-modifying drug cyclophosphamide in 22 of 40 patients. Interestingly, HLA risk alleles were much more common in responders than nonresponders, Dr. Scheibenbogen noted.
Immunoadsorption: This technique, similar to dialysis, involves separating out the blood plasma by centrifugation and removing IgG autoantibodies by a binding column, then returning the plasma back to the patient. It is used, primarily in Europe, to treat severe autoimmune diseases including dilative cardiomyopathy and refractory systemic lupus erythematosus (SLE).
Dr. Scheibenbogen’s group has conducted two studies of immunoadsorption in ME/CFS. In one, a 5-day procedure led to rapid symptom improvement in 7 of 10 patients, with sustained improvement in 3 patients after 2 years. Autoantibodies decreased rapidly in 9 of the 10 patients. In a follow-up study of five of the responders 2 years later, retreatment with a modified immunoadsorption protocol led to rapid and sustained improvement in four. Further study has been on hold because of the pandemic.
Next-gen IgG-targeting therapies: Another approach that could offer promise for ME/CFS involves therapies that block the Fc receptors of IgG. Several are in phase 1-3 trials for autoimmune conditions. One candidate drug, the Fc fragment efgartigimod, is currently in phase 3 trials for several conditions, including generalized myasthenia gravis, primary immune thrombocytopenia, and chronic inflammatory demyelinating polyneuropathy. Phase 3 trials are planned for the monoclonal antibody rozanolixizumab in those same conditions.
Newer-generation monoclonal antibodies targeting CD19 or CD20 that show benefit in various autoimmune conditions are another possibility for ME/CFS. These include ocrelizumab (Ocrevus), approved in the United States for treating relapsing and progressive multiple sclerosis and in trials for SLE; obinutuzumab (Gazyva), approved for treating lymphoma and also in development for SLE; and ublituximab, in phase 3 trials for multiple sclerosis.
“Most of them are more effective than rituximab,” Dr. Scheibenbogen noted, adding that “currently the data look quite promising. They are effective in different autoimmune diseases and they are quite well tolerated. There’s great hope now with COVID-19 that we can convince some companies to do such trials in ME/CFS as well.”
Dr. Scheibenbogen’s institution, the Charité Fatigue Center, has a patent for beta2-adrenergic receptor antibodies for diagnosing ME/CFS under her name together with Celltrend. Dr. Komaroff has received personal fees from Serimmune.
Emerging evidence suggests that autoimmunity plays a role in postinfectious myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and that targeting autoantibodies could be a promising treatment approach.
The same may also apply to many cases of “long COVID,” in which many of the symptoms overlap with those of ME/CFS, Carmen Scheibenbogen, MD, professor of clinical immunology and director of the Institute for Medical Immunology, Charité University Medicine, Berlin, said during the annual meeting of the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis.
Several groups, including Dr. Scheibenbogen’s, have reported finding autoantibodies against neurotransmitter receptor antigens in people with ME/CFS. And, in a paper published in the Journal of Clinical Medicine the day that Dr. Scheibenbogen spoke at the meeting, her team reported significant correlations between autoantibodies to vasoregulative G-protein–coupled receptors and symptom severity, autonomic dysfunction, and disability among 116 patients with infection-triggered ME/CFS who were diagnosed using the symptom-based 2003 Canadian consensus criteria.
People with ME/CFS are also more likely to have genetic risk factors associated with autoimmunity and personal and/or family histories of autoimmune conditions. And, clinical trials have demonstrated early success with various immunomodulatory treatments in subsets of people with ME/CFS, including endoxan, rituximab, and immunoadsorption.
“We have evidence that ME/CFS is an autoantibody-mediated disease, and we have evidence that autoantibody targeting is effective in this disease. So far ... we have few and underfinanced clinical studies, but the good news is we have promising emerging treatment options,” Dr. Scheibenbogen said.
Asked to comment, ME/CFS expert Anthony L. Komaroff, MD, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, said: “There is already strong evidence that there are autoantibodies in ME/CFS. Dr. Scheibenbogen’s work is the latest and employs the latest technology. ... I would bet that autoantibodies to neural targets are likely to cause some of the symptoms of ME/CFS and some of the symptoms of long COVID.”
However, he cautioned, “that has not been proven, and even if it were proven you would have to demonstrate that treatments based on that theory worked.”
Dr. Komaroff said he views autoimmunity as a likely component of the ME/CFS spectrum, but not the only one. “My current view of this illness is that there’s a final common pathway in the brain that leads to the symptoms of the illness. But that final common pathway can be triggered by a variety of different things, one of which could be autoantibodies while another could be infection or inflammation in the brain.”
Emerging evidence points to autoimmunity
Dr. Scheibenbogen summarized the work published in this area over the past few years by her group and others.
In a comparison of ME/CFS patients with 201 healthy controls, significant associations were seen with two specific autoimmunity-related risk alleles only in the ME/CFS patients who reported acute onset of disease with an infection but not in those with ME/CFS without infection-triggered onset or the controls. Both genes play roles in regulating B- and T-cell activation.
Another recent study found associations with ME/CFS and major histocompatibility complex class II molecules, a typical feature of autoimmune diseases, in a comparison between 426 adult Norwegian ME/CFS patients who were diagnosed with the Canadian consensus criteria and 4,511 healthy, ethnically matched controls.
In a 2020 paper, Dr. Scheibenbogen and pharmacologist Klaus Wirth presented a “unifying hypothesis” of ME/CFS pathophysiology based on the finding of elevations in autoantibodies against beta2-adrenergic receptors and muscarinic acetylcholine receptors in some individuals with the condition. Since both of those receptors are important vasodilators, their functional disturbance would be expected to cause vasoconstriction and hypoxemia, which would explain many of the symptoms of ME/CFS. This mechanism would align with other findings of muscular and cerebral hypoperfusion that correlate with fatigue, particularly post exertion, as well as metabolic changes that are in line with the concepts of hypoxemia and ischemia.
Further evidence for vascular dysfunction in ME/CFS came from her group’s study finding evidence of peripheral endothelial dysfunction that was associated with symptom severity in 35 adult patients. “Vasoconstriction, hypovolemia, and release of vasoactive and algesic mediators is probably a key pathomechanism of the disease,” Dr. Scheibenbogen said.
Treatments: Will targeting autoantibodies work?
In the second part of her talk, Dr. Scheibenbogen summarized clinical trials of the following treatment approaches that involve targeting autoantibodies as a way to alleviate ME/CFS symptoms:
Rituximab: Work on infusions of the B-cell depleting agent has been conducted by Norwegian researchers beginning in 2011 with a small randomized trial and an open-label, phase 2 study in 2015, both showing clinical responses in ME/CFS. However, a subsequent phase 3, randomized clinical trial of 151 patients, again diagnosed using the Canadian criteria, was negative.
There are several possible explanations for this, Dr. Scheibenbogen noted. For one, the maintenance dose had to be reduced because of a lack of financial support. “This was probably critical. The lower dose was insufficient to adequately deplete B cells.” Also, there may have been a strong placebo response in the control group since they were being given better care than they normally would receive during the trial. “I think probably nobody will again do a rituximab trial. This was very disappointing for all of us. But, we still have other opportunities to follow this path,” she said.
Dr. Komaroff agreed. “I don’t think the failure of one drug that hits malignant B cells is proof against the autoimmune hypothesis per se. I think the evidence is that rituximab doesn’t work, but that doesn’t invalidate the autoimmunity hypothesis.”
Cyclophosphamide: The same Norwegian group also showed positive findings in an open-label, phase 2 trial of the immune-modifying drug cyclophosphamide in 22 of 40 patients. Interestingly, HLA risk alleles were much more common in responders than nonresponders, Dr. Scheibenbogen noted.
Immunoadsorption: This technique, similar to dialysis, involves separating out the blood plasma by centrifugation and removing IgG autoantibodies by a binding column, then returning the plasma back to the patient. It is used, primarily in Europe, to treat severe autoimmune diseases including dilative cardiomyopathy and refractory systemic lupus erythematosus (SLE).
Dr. Scheibenbogen’s group has conducted two studies of immunoadsorption in ME/CFS. In one, a 5-day procedure led to rapid symptom improvement in 7 of 10 patients, with sustained improvement in 3 patients after 2 years. Autoantibodies decreased rapidly in 9 of the 10 patients. In a follow-up study of five of the responders 2 years later, retreatment with a modified immunoadsorption protocol led to rapid and sustained improvement in four. Further study has been on hold because of the pandemic.
Next-gen IgG-targeting therapies: Another approach that could offer promise for ME/CFS involves therapies that block the Fc receptors of IgG. Several are in phase 1-3 trials for autoimmune conditions. One candidate drug, the Fc fragment efgartigimod, is currently in phase 3 trials for several conditions, including generalized myasthenia gravis, primary immune thrombocytopenia, and chronic inflammatory demyelinating polyneuropathy. Phase 3 trials are planned for the monoclonal antibody rozanolixizumab in those same conditions.
Newer-generation monoclonal antibodies targeting CD19 or CD20 that show benefit in various autoimmune conditions are another possibility for ME/CFS. These include ocrelizumab (Ocrevus), approved in the United States for treating relapsing and progressive multiple sclerosis and in trials for SLE; obinutuzumab (Gazyva), approved for treating lymphoma and also in development for SLE; and ublituximab, in phase 3 trials for multiple sclerosis.
“Most of them are more effective than rituximab,” Dr. Scheibenbogen noted, adding that “currently the data look quite promising. They are effective in different autoimmune diseases and they are quite well tolerated. There’s great hope now with COVID-19 that we can convince some companies to do such trials in ME/CFS as well.”
Dr. Scheibenbogen’s institution, the Charité Fatigue Center, has a patent for beta2-adrenergic receptor antibodies for diagnosing ME/CFS under her name together with Celltrend. Dr. Komaroff has received personal fees from Serimmune.
FROM IACFS/ME 2021
From past to future
This month, the current Editor-in-Chief and his Editorial Board will conclude our 5-year term. Megan Adams MD, JD, MSc, from the University of Michigan School of Medicine will assume my position. She has a stellar academic, research, and teaching record and is one of the best writers I know. She and her Board of Editors will carry on the tradition of GIHN.

The idea of an official newspaper of the AGA came from AGA staff in 2006. The goals of the newspaper were twofold: to communicate the latest news and information to practitioners to help them stay at the forefront of patient care and to develop another revenue stream for our society. The newspaper was launched in January 2007 with Charles Lightdale MD, AGAF, as the first editor and Colin W. Howden MD, AGAF, as the second (each with 5-year terms). While they wrote occasional editorials, I began writing 300-word essays for each issue. I have tried diligently to maintain a balanced viewpoint for all my editorials, although this has been difficult in the recent past and current national environment.
The paper evolved from a simple print publication to a multimedia communications vehicle that includes online-only content, videos, supplements, quizzes, and more. Last year, we published our first “Data Trends,” a supplement containing 10 or so brief articles written by content experts, covering current topics of high interest. As the paper evolved, we broadened our target audience to include research scientists, international practitioners and others interested in digestive diseases.
As I did last month, I would like to thank the AGA and Frontline Medical Communications staff for their dedication and constant work to bring you this newspaper.
Finally, I would like to pay tribute to Tadataka “Tachi” Yamada, who died this last month at the age of 76 years. He was one of the premier advocates for global health. His contributions to our field thru research, philanthropy, and leadership were enormous. We will miss him greatly.
John I Allen, MD, MBA, AGAF
Editor in Chief
This month, the current Editor-in-Chief and his Editorial Board will conclude our 5-year term. Megan Adams MD, JD, MSc, from the University of Michigan School of Medicine will assume my position. She has a stellar academic, research, and teaching record and is one of the best writers I know. She and her Board of Editors will carry on the tradition of GIHN.
The idea of an official newspaper of the AGA came from AGA staff in 2006. The goals of the newspaper were twofold: to communicate the latest news and information to practitioners to help them stay at the forefront of patient care and to develop another revenue stream for our society. The newspaper was launched in January 2007 with Charles Lightdale MD, AGAF, as the first editor and Colin W. Howden MD, AGAF, as the second (each with 5-year terms). While they wrote occasional editorials, I began writing 300-word essays for each issue. I have tried diligently to maintain a balanced viewpoint for all my editorials, although this has been difficult in the recent past and current national environment.
The paper evolved from a simple print publication to a multimedia communications vehicle that includes online-only content, videos, supplements, quizzes, and more. Last year, we published our first “Data Trends,” a supplement containing 10 or so brief articles written by content experts, covering current topics of high interest. As the paper evolved, we broadened our target audience to include research scientists, international practitioners and others interested in digestive diseases.
As I did last month, I would like to thank the AGA and Frontline Medical Communications staff for their dedication and constant work to bring you this newspaper.
Finally, I would like to pay tribute to Tadataka “Tachi” Yamada, who died this last month at the age of 76 years. He was one of the premier advocates for global health. His contributions to our field thru research, philanthropy, and leadership were enormous. We will miss him greatly.
John I Allen, MD, MBA, AGAF
Editor in Chief
This month, the current Editor-in-Chief and his Editorial Board will conclude our 5-year term. Megan Adams MD, JD, MSc, from the University of Michigan School of Medicine will assume my position. She has a stellar academic, research, and teaching record and is one of the best writers I know. She and her Board of Editors will carry on the tradition of GIHN.
The idea of an official newspaper of the AGA came from AGA staff in 2006. The goals of the newspaper were twofold: to communicate the latest news and information to practitioners to help them stay at the forefront of patient care and to develop another revenue stream for our society. The newspaper was launched in January 2007 with Charles Lightdale MD, AGAF, as the first editor and Colin W. Howden MD, AGAF, as the second (each with 5-year terms). While they wrote occasional editorials, I began writing 300-word essays for each issue. I have tried diligently to maintain a balanced viewpoint for all my editorials, although this has been difficult in the recent past and current national environment.
The paper evolved from a simple print publication to a multimedia communications vehicle that includes online-only content, videos, supplements, quizzes, and more. Last year, we published our first “Data Trends,” a supplement containing 10 or so brief articles written by content experts, covering current topics of high interest. As the paper evolved, we broadened our target audience to include research scientists, international practitioners and others interested in digestive diseases.
As I did last month, I would like to thank the AGA and Frontline Medical Communications staff for their dedication and constant work to bring you this newspaper.
Finally, I would like to pay tribute to Tadataka “Tachi” Yamada, who died this last month at the age of 76 years. He was one of the premier advocates for global health. His contributions to our field thru research, philanthropy, and leadership were enormous. We will miss him greatly.
John I Allen, MD, MBA, AGAF
Editor in Chief