User login
Even moderate exercise offers strong shield from COVID-19
in its participants.
Researchers identified 65,361 members of a South African private health plan who had a COVID-19 diagnosis from March 2020 to June 2021 and matched them with physical activity data during the 2 years prior to the country’s March 2020 lockdown captured by smart devices, and clocked gym attendance and mass event participation in a voluntary healthy lifestyle behavior program linked to the insurer.
In all, 20.4% of participants had engaged in low levels of at least moderate-intensity physical activity per week (0-59 minutes), 34.5% in moderate levels (60-149 minutes), and 45.1% in high levels (150 minutes or more).
Overall, 11.1% were hospitalized as a result of COVID-19, 2.4% were admitted to the ICU, 1.3% required a ventilator, and 1.6% died.
As reported in the British Journal of Sports Medicine, analyses adjusted for demographic and other risk factors showed that, with COVID-19 infection, people with high versus low physical activity had a 34% lower risk for hospitalization (risk ratio, 0.66; 95% confidence interval, 0.63-0.70), a 41% lower risk for ICU admission (RR, 0.59; 95% CI, 0.52-0.66), a 45% lower risk of requiring ventilation (RR, 0.55; 95% CI, 0.47-0.64), and a 42% lower risk for death (RR, 0.58; 95% CI, 0.50-0.68).
Even moderate physical exercise, below the recommended guidelines of at least 150 minutes per week, was associated with several benefits, such as a 13% lower risk for hospitalization (RR, 0.87; 95% CI, 0.82-0.91), a 20% lower risk for ICU admission (RR, 0.80; 95% CI, 0.71-0.89), a 27% lower risk of requiring ventilation (RR, 0.73; 95% CI, 0.62-0.84), and a21% lower risk for death (RR, 0.79; 95% CI, 0.69-0.91).
“Should we come across further waves of this pandemic, our advice from a medical point of view should be to promote and facilitate exercise,” senior author Jon Patricios, MD, Wits Sport and Health, University of the Witwatersrand, Johannesburg, South Africa, said in an interview. “The likelihood is that exercise and vaccination are going to be the two most significant interventions in terms of helping to offload the health care system rather than face the catastrophic events endured a year or so ago.”
The study showed that males are at greater risk than females for severe COVID-19 outcomes, as were patients with essential hypertension, diabetes, and chronic renal disease.
It also suggests that the protective benefit of exercise extends to HIV-positive patients and those with rheumatoid arthritis, two groups previously not evaluated, the authors noted.
The results are comparable with previous reports of self-reported exercise and COVID-19 from the United States and South Korea, although the effect of even moderate exercise was more significant, possibly due to the use of direct measures of exercise rather than self-report, Dr. Patricios suggested.
Previous data suggest that regular physical activity may protect against many viral infections including influenza, rhinovirus, and the reactivation of latent herpes viruses, he noted. However, emerging evidence also points to significant decreases in physical activity during the pandemic.
“Regular physical activity should be a message that is strongly, strongly advocated for, particularly in less well-developed countries where we don’t have access or the resources to afford pharmacological interventions in many of these scenarios,” Dr. Patricios said. “It’s frustrating that the message is not driven strongly enough. It should be part of every government’s agenda.”
The cohort all being members of a medical insurance plan could imply some selection bias based on affordability and limit generalizability of the results, the authors noted. Other limitations include a lack of data on sociodemographic criteria such as education, income, and race, as well as behavioral risk factors such as smoking and diet.
Dr. Patricios and one coauthor are editors of the British Journal of Sports Medicine. Several coauthors are employees of Discovery Health, Johannesburg.
A version of this article first appeared on Medscape.com.
in its participants.
Researchers identified 65,361 members of a South African private health plan who had a COVID-19 diagnosis from March 2020 to June 2021 and matched them with physical activity data during the 2 years prior to the country’s March 2020 lockdown captured by smart devices, and clocked gym attendance and mass event participation in a voluntary healthy lifestyle behavior program linked to the insurer.
In all, 20.4% of participants had engaged in low levels of at least moderate-intensity physical activity per week (0-59 minutes), 34.5% in moderate levels (60-149 minutes), and 45.1% in high levels (150 minutes or more).
Overall, 11.1% were hospitalized as a result of COVID-19, 2.4% were admitted to the ICU, 1.3% required a ventilator, and 1.6% died.
As reported in the British Journal of Sports Medicine, analyses adjusted for demographic and other risk factors showed that, with COVID-19 infection, people with high versus low physical activity had a 34% lower risk for hospitalization (risk ratio, 0.66; 95% confidence interval, 0.63-0.70), a 41% lower risk for ICU admission (RR, 0.59; 95% CI, 0.52-0.66), a 45% lower risk of requiring ventilation (RR, 0.55; 95% CI, 0.47-0.64), and a 42% lower risk for death (RR, 0.58; 95% CI, 0.50-0.68).
Even moderate physical exercise, below the recommended guidelines of at least 150 minutes per week, was associated with several benefits, such as a 13% lower risk for hospitalization (RR, 0.87; 95% CI, 0.82-0.91), a 20% lower risk for ICU admission (RR, 0.80; 95% CI, 0.71-0.89), a 27% lower risk of requiring ventilation (RR, 0.73; 95% CI, 0.62-0.84), and a21% lower risk for death (RR, 0.79; 95% CI, 0.69-0.91).
“Should we come across further waves of this pandemic, our advice from a medical point of view should be to promote and facilitate exercise,” senior author Jon Patricios, MD, Wits Sport and Health, University of the Witwatersrand, Johannesburg, South Africa, said in an interview. “The likelihood is that exercise and vaccination are going to be the two most significant interventions in terms of helping to offload the health care system rather than face the catastrophic events endured a year or so ago.”
The study showed that males are at greater risk than females for severe COVID-19 outcomes, as were patients with essential hypertension, diabetes, and chronic renal disease.
It also suggests that the protective benefit of exercise extends to HIV-positive patients and those with rheumatoid arthritis, two groups previously not evaluated, the authors noted.
The results are comparable with previous reports of self-reported exercise and COVID-19 from the United States and South Korea, although the effect of even moderate exercise was more significant, possibly due to the use of direct measures of exercise rather than self-report, Dr. Patricios suggested.
Previous data suggest that regular physical activity may protect against many viral infections including influenza, rhinovirus, and the reactivation of latent herpes viruses, he noted. However, emerging evidence also points to significant decreases in physical activity during the pandemic.
“Regular physical activity should be a message that is strongly, strongly advocated for, particularly in less well-developed countries where we don’t have access or the resources to afford pharmacological interventions in many of these scenarios,” Dr. Patricios said. “It’s frustrating that the message is not driven strongly enough. It should be part of every government’s agenda.”
The cohort all being members of a medical insurance plan could imply some selection bias based on affordability and limit generalizability of the results, the authors noted. Other limitations include a lack of data on sociodemographic criteria such as education, income, and race, as well as behavioral risk factors such as smoking and diet.
Dr. Patricios and one coauthor are editors of the British Journal of Sports Medicine. Several coauthors are employees of Discovery Health, Johannesburg.
A version of this article first appeared on Medscape.com.
in its participants.
Researchers identified 65,361 members of a South African private health plan who had a COVID-19 diagnosis from March 2020 to June 2021 and matched them with physical activity data during the 2 years prior to the country’s March 2020 lockdown captured by smart devices, and clocked gym attendance and mass event participation in a voluntary healthy lifestyle behavior program linked to the insurer.
In all, 20.4% of participants had engaged in low levels of at least moderate-intensity physical activity per week (0-59 minutes), 34.5% in moderate levels (60-149 minutes), and 45.1% in high levels (150 minutes or more).
Overall, 11.1% were hospitalized as a result of COVID-19, 2.4% were admitted to the ICU, 1.3% required a ventilator, and 1.6% died.
As reported in the British Journal of Sports Medicine, analyses adjusted for demographic and other risk factors showed that, with COVID-19 infection, people with high versus low physical activity had a 34% lower risk for hospitalization (risk ratio, 0.66; 95% confidence interval, 0.63-0.70), a 41% lower risk for ICU admission (RR, 0.59; 95% CI, 0.52-0.66), a 45% lower risk of requiring ventilation (RR, 0.55; 95% CI, 0.47-0.64), and a 42% lower risk for death (RR, 0.58; 95% CI, 0.50-0.68).
Even moderate physical exercise, below the recommended guidelines of at least 150 minutes per week, was associated with several benefits, such as a 13% lower risk for hospitalization (RR, 0.87; 95% CI, 0.82-0.91), a 20% lower risk for ICU admission (RR, 0.80; 95% CI, 0.71-0.89), a 27% lower risk of requiring ventilation (RR, 0.73; 95% CI, 0.62-0.84), and a21% lower risk for death (RR, 0.79; 95% CI, 0.69-0.91).
“Should we come across further waves of this pandemic, our advice from a medical point of view should be to promote and facilitate exercise,” senior author Jon Patricios, MD, Wits Sport and Health, University of the Witwatersrand, Johannesburg, South Africa, said in an interview. “The likelihood is that exercise and vaccination are going to be the two most significant interventions in terms of helping to offload the health care system rather than face the catastrophic events endured a year or so ago.”
The study showed that males are at greater risk than females for severe COVID-19 outcomes, as were patients with essential hypertension, diabetes, and chronic renal disease.
It also suggests that the protective benefit of exercise extends to HIV-positive patients and those with rheumatoid arthritis, two groups previously not evaluated, the authors noted.
The results are comparable with previous reports of self-reported exercise and COVID-19 from the United States and South Korea, although the effect of even moderate exercise was more significant, possibly due to the use of direct measures of exercise rather than self-report, Dr. Patricios suggested.
Previous data suggest that regular physical activity may protect against many viral infections including influenza, rhinovirus, and the reactivation of latent herpes viruses, he noted. However, emerging evidence also points to significant decreases in physical activity during the pandemic.
“Regular physical activity should be a message that is strongly, strongly advocated for, particularly in less well-developed countries where we don’t have access or the resources to afford pharmacological interventions in many of these scenarios,” Dr. Patricios said. “It’s frustrating that the message is not driven strongly enough. It should be part of every government’s agenda.”
The cohort all being members of a medical insurance plan could imply some selection bias based on affordability and limit generalizability of the results, the authors noted. Other limitations include a lack of data on sociodemographic criteria such as education, income, and race, as well as behavioral risk factors such as smoking and diet.
Dr. Patricios and one coauthor are editors of the British Journal of Sports Medicine. Several coauthors are employees of Discovery Health, Johannesburg.
A version of this article first appeared on Medscape.com.
FROM THE BRITISH JOURNAL OF SPORTS MEDICINE
Aluminum named allergen of the year
BOSTON – The . Aluminum salts, which are the major cause of allergic reactions, are “ubiquitous,” Donald Belsito, MD, professor of dermatology at Columbia University, New York, said at the annual meeting of the American Contact Dermatitis Society.
These salts can be found in sunscreen, cosmetics, dental restorations, and food, to name a few, though the most commonly identified reactions are from aluminum hydroxide, which can be found in some vaccines or preparations for allergen-specific immunotherapy. “It’s the aluminum hydroxide that seems to be more allergenic than other aluminum salts,” Dr. Belsito said in an interview.
“It’s not a dangerous allergy; It’s not a threat,” he said, “but it’s something that dermatologists need to be aware of.”
These reactions normally present as itchy nodules that can last for months and even years, like some reactions from patch testing. “We’re not talking about a vaccine allergy in such a way where people are getting anaphylaxis,” JiaDe Yu, MD, a pediatric dermatologist specializing in allergic contact dermatitis at Massachusetts General Hospital, Boston, said in an interview. “An itchy rash is what we tend to see.”
There have also been occasional reports of atopic dermatitis from aluminum in antiperspirants, astringents, as well as from the metallic aluminum.
Dr. Yu noted that aluminum allergies are not thought to be very common, but the overall prevalence is not known. Studies do suggest, however, that the allergy may be more prevalent in children. In one recent study in Sweden, 5% of children and 0.9% of adults who underwent patch testing had an aluminum contact allergy.
Recommendations for testing
Aluminum is not included in baseline patch testing in the United States, though a recent report about the allergen in the journal Dermatitis argued for its inclusion for pediatric patch testing. Both Dr. Belsito and Dr. Yu agreed that the best approach is to do targeted testing. “If there is a suspicion for it, absolutely test for it,” Dr. Yu said, but if a patient comes in with something like eyelid dermatitis or a rash after a hair care appointment, an aluminum allergy is not very likely.
Because aluminum is also present in Finn Chambers for patch testing, Dr. Belsito advised using plastic chambers in people suspected of having an aluminum allergy. He now uses only plastic chambers in children, he said, as some patients have had reactions to the Finn Chambers even if they have no history of reactions to vaccines or other aluminum-containing products.
While aluminum chloride hexahydrate (ACH) 2% in petrolatum is the commercially available preparation in patch testing, a preparation with ACH 10% is more sensitive, Dr. Belsito said. If a physician strongly suspects an aluminum allergy in a patient but the test with the ACH 2% is negative, he or she should then try a 10% solution, he noted, adding that 7-day readings are also necessary to maximize accuracy.
Vaccine safety
One of the concerns about naming aluminum as the allergen of the year is the potential to cause anxiety around vaccines. “We want to make sure that we’re not giving more fuel to people who have an excuse not to get a vaccine,” Dr. Yu said. “We certainly want to reinforce that fact that it is safe.” Dr. Belsito noted that COVID-19 vaccines do not contain aluminum.
Even on the rare chance that a patient does have a reaction to an aluminum-containing vaccine, these subcutaneous nodules resolve over time, Dr. Belsito said. In his own clinical experience, “99.99% of the time they resolve and there is no residual.” He did add that overreacting to the rash by prescribing injectable steroids can lead to steroid atrophy. In these cases, a topical steroid may be more appropriate.
All unexpected or clinically significant vaccine reactions should be reported to the Vaccine Adverse Event Reporting System, cosponsored by the Centers for Disease Control and Prevention and the Food and Drug Administration. The Clinical Immunization Project Safety Assessment Project, from the CDC, also can provide expertise and advice on aluminum-free alternatives for some vaccines.
Dr. Belsito and Dr. Yu have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BOSTON – The . Aluminum salts, which are the major cause of allergic reactions, are “ubiquitous,” Donald Belsito, MD, professor of dermatology at Columbia University, New York, said at the annual meeting of the American Contact Dermatitis Society.
These salts can be found in sunscreen, cosmetics, dental restorations, and food, to name a few, though the most commonly identified reactions are from aluminum hydroxide, which can be found in some vaccines or preparations for allergen-specific immunotherapy. “It’s the aluminum hydroxide that seems to be more allergenic than other aluminum salts,” Dr. Belsito said in an interview.
“It’s not a dangerous allergy; It’s not a threat,” he said, “but it’s something that dermatologists need to be aware of.”
These reactions normally present as itchy nodules that can last for months and even years, like some reactions from patch testing. “We’re not talking about a vaccine allergy in such a way where people are getting anaphylaxis,” JiaDe Yu, MD, a pediatric dermatologist specializing in allergic contact dermatitis at Massachusetts General Hospital, Boston, said in an interview. “An itchy rash is what we tend to see.”
There have also been occasional reports of atopic dermatitis from aluminum in antiperspirants, astringents, as well as from the metallic aluminum.
Dr. Yu noted that aluminum allergies are not thought to be very common, but the overall prevalence is not known. Studies do suggest, however, that the allergy may be more prevalent in children. In one recent study in Sweden, 5% of children and 0.9% of adults who underwent patch testing had an aluminum contact allergy.
Recommendations for testing
Aluminum is not included in baseline patch testing in the United States, though a recent report about the allergen in the journal Dermatitis argued for its inclusion for pediatric patch testing. Both Dr. Belsito and Dr. Yu agreed that the best approach is to do targeted testing. “If there is a suspicion for it, absolutely test for it,” Dr. Yu said, but if a patient comes in with something like eyelid dermatitis or a rash after a hair care appointment, an aluminum allergy is not very likely.
Because aluminum is also present in Finn Chambers for patch testing, Dr. Belsito advised using plastic chambers in people suspected of having an aluminum allergy. He now uses only plastic chambers in children, he said, as some patients have had reactions to the Finn Chambers even if they have no history of reactions to vaccines or other aluminum-containing products.
While aluminum chloride hexahydrate (ACH) 2% in petrolatum is the commercially available preparation in patch testing, a preparation with ACH 10% is more sensitive, Dr. Belsito said. If a physician strongly suspects an aluminum allergy in a patient but the test with the ACH 2% is negative, he or she should then try a 10% solution, he noted, adding that 7-day readings are also necessary to maximize accuracy.
Vaccine safety
One of the concerns about naming aluminum as the allergen of the year is the potential to cause anxiety around vaccines. “We want to make sure that we’re not giving more fuel to people who have an excuse not to get a vaccine,” Dr. Yu said. “We certainly want to reinforce that fact that it is safe.” Dr. Belsito noted that COVID-19 vaccines do not contain aluminum.
Even on the rare chance that a patient does have a reaction to an aluminum-containing vaccine, these subcutaneous nodules resolve over time, Dr. Belsito said. In his own clinical experience, “99.99% of the time they resolve and there is no residual.” He did add that overreacting to the rash by prescribing injectable steroids can lead to steroid atrophy. In these cases, a topical steroid may be more appropriate.
All unexpected or clinically significant vaccine reactions should be reported to the Vaccine Adverse Event Reporting System, cosponsored by the Centers for Disease Control and Prevention and the Food and Drug Administration. The Clinical Immunization Project Safety Assessment Project, from the CDC, also can provide expertise and advice on aluminum-free alternatives for some vaccines.
Dr. Belsito and Dr. Yu have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BOSTON – The . Aluminum salts, which are the major cause of allergic reactions, are “ubiquitous,” Donald Belsito, MD, professor of dermatology at Columbia University, New York, said at the annual meeting of the American Contact Dermatitis Society.
These salts can be found in sunscreen, cosmetics, dental restorations, and food, to name a few, though the most commonly identified reactions are from aluminum hydroxide, which can be found in some vaccines or preparations for allergen-specific immunotherapy. “It’s the aluminum hydroxide that seems to be more allergenic than other aluminum salts,” Dr. Belsito said in an interview.
“It’s not a dangerous allergy; It’s not a threat,” he said, “but it’s something that dermatologists need to be aware of.”
These reactions normally present as itchy nodules that can last for months and even years, like some reactions from patch testing. “We’re not talking about a vaccine allergy in such a way where people are getting anaphylaxis,” JiaDe Yu, MD, a pediatric dermatologist specializing in allergic contact dermatitis at Massachusetts General Hospital, Boston, said in an interview. “An itchy rash is what we tend to see.”
There have also been occasional reports of atopic dermatitis from aluminum in antiperspirants, astringents, as well as from the metallic aluminum.
Dr. Yu noted that aluminum allergies are not thought to be very common, but the overall prevalence is not known. Studies do suggest, however, that the allergy may be more prevalent in children. In one recent study in Sweden, 5% of children and 0.9% of adults who underwent patch testing had an aluminum contact allergy.
Recommendations for testing
Aluminum is not included in baseline patch testing in the United States, though a recent report about the allergen in the journal Dermatitis argued for its inclusion for pediatric patch testing. Both Dr. Belsito and Dr. Yu agreed that the best approach is to do targeted testing. “If there is a suspicion for it, absolutely test for it,” Dr. Yu said, but if a patient comes in with something like eyelid dermatitis or a rash after a hair care appointment, an aluminum allergy is not very likely.
Because aluminum is also present in Finn Chambers for patch testing, Dr. Belsito advised using plastic chambers in people suspected of having an aluminum allergy. He now uses only plastic chambers in children, he said, as some patients have had reactions to the Finn Chambers even if they have no history of reactions to vaccines or other aluminum-containing products.
While aluminum chloride hexahydrate (ACH) 2% in petrolatum is the commercially available preparation in patch testing, a preparation with ACH 10% is more sensitive, Dr. Belsito said. If a physician strongly suspects an aluminum allergy in a patient but the test with the ACH 2% is negative, he or she should then try a 10% solution, he noted, adding that 7-day readings are also necessary to maximize accuracy.
Vaccine safety
One of the concerns about naming aluminum as the allergen of the year is the potential to cause anxiety around vaccines. “We want to make sure that we’re not giving more fuel to people who have an excuse not to get a vaccine,” Dr. Yu said. “We certainly want to reinforce that fact that it is safe.” Dr. Belsito noted that COVID-19 vaccines do not contain aluminum.
Even on the rare chance that a patient does have a reaction to an aluminum-containing vaccine, these subcutaneous nodules resolve over time, Dr. Belsito said. In his own clinical experience, “99.99% of the time they resolve and there is no residual.” He did add that overreacting to the rash by prescribing injectable steroids can lead to steroid atrophy. In these cases, a topical steroid may be more appropriate.
All unexpected or clinically significant vaccine reactions should be reported to the Vaccine Adverse Event Reporting System, cosponsored by the Centers for Disease Control and Prevention and the Food and Drug Administration. The Clinical Immunization Project Safety Assessment Project, from the CDC, also can provide expertise and advice on aluminum-free alternatives for some vaccines.
Dr. Belsito and Dr. Yu have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ACDS 2022
COVID-19 infection linked to risk of cutaneous autoimmune and vascular diseases
BOSTON – . This predominately favored systemic disease states with cutaneous involvement, rather than skin-limited processes.
The findings come from a large multicenter analysis that Zachary Holcomb, MD, presented during a late-breaking abstract session at the annual meeting of the American Academy of Dermatology.

“Viral triggers have been implicated in the pathogenesis of rheumatologic disease, but information regarding development of autoimmune disease following SARS-CoV-2 infection is limited,” said Dr. Holcomb, chief resident in the Harvard Combined Internal Medicine–Dermatology Residency, Boston. “Given its proposed thromboinflammatory pathobiology, we hypothesized that SARS-CoV-2 infection increases the risk of development of autoimmune disease with cutaneous manifestations and sought to define incidence rates of newly-diagnosed autoimmune diseases following SARS-CoV-2 infection.”
The researchers drew from the TriNetX Dataworks platform, an online cloud-based system that contains aggregated and deidentified patient information from about 75 million patients across 48 health care organizations. The infected cohort was defined as having a positive lab test for severe SARS-CoV-2 within the study window using Logical Observation Identifiers Names and Codes (LOINCs). Healthy controls consisted of a documented health care contact (inpatient or outpatient visit) during the study window without a positive SARS-CoV-2 lab test. Each cohort included patients aged 18-65 at the time of the study, and patients with previously diagnosed cutaneous autoimmune or vascular diseases were excluded from the analysis.
After propensity matching, the COVID-19 infected cohort and the healthy cohort included 1,904,864 patients each, with no baseline differences in age at index event, ethnicity, race, or sex. The study window was between April 1, 2020, and Oct. 1, 2020. The index event was a COVID-19 infection for the infected group and first documented health care contact in the healthy control group. The researchers looked at a window of 60 days following this index event for new incidence of cutaneous or vascular disease.
In the realm of connective tissue and related diseases, they found the incidence was increased among the COVID-19 infected group compared with controls for dermatomyositis (risk ratio, 2.273; P = .0196), scleroderma (RR, 1.959; P = .0001), and systemic lupus erythematosus (RR, 1.401; P < .0001). They also noted a significant decrease in the new incidence of alopecia areata in the COVID-19 infected group compared with controls (RR, 0.527; P < .0001).
No significant differences in the incidence of bullous and papulosquamous diseases were observed between the two groups. However, sarcoidosis was significantly more common in the COVID-19–infected group compared with controls (RR, 2.086; P < .001). “When taking all of these autoinflammatory diseases as a whole, there was an increased incidence in the COVID-19 infected group overall with a RR of 1.168 (P < .0001),” Dr. Holcomb said.
In the realm of vascular skin diseases, there was an increased incidence in the COVID-19 infected group in acrocyanosis (RR, 2.825; P < .001), Raynaud’s phenomenon (RR, 1.462; P < .0001), cutaneous small vessel vasculitis (RR, 1.714; P < .0001), granulomatosis with polyangiitis (RR, 2.667; P = .0002), and temporal arteritis (RR, 1.900; P = .0038).
“Interestingly, despite the academic and lay press reports of COVID toes, we did not see that in our data related to the COVID-infected group,” he said.
Dr. Holcomb acknowledged certain limitations of the study, including a narrow study window with a relatively short follow-up. “We were able to propensity match based on baseline demographics but not necessarily so based on health status and prior autoimmune disease,” he said. In addition, since the study was limited to those aged 18-65, the results may not be generalizable to pediatric and elderly patients, he said.
He described the study findings as “somewhat hypothesis-generating.” For instance, “why would we have more of a systemic process [at play?]. Our theory is that the severe inflammatory nature of COVID-19 leads to a lot of internal organ damage and exposure of autoantigens in that process, with relative skin sparing.”
One of the session moderators, Robert Paul Dellavalle, MD, PhD, professor of dermatology at the University of Colorado, Aurora, characterized the findings as “intriguing” but preliminary. “It would be interesting to look at more recent cohorts and see how vaccination for COVID-19 would impact the incidence rates of some of these diseases,” he said.
When asked for comment, Jeffrey A. Sparks, MD, MMSc, a rheumatologist at Brigham and Women's Hospital and assistant professor of medicine at Harvard Medical School, both in Boston, said, "This is an interesting study that should be followed up. Viral triggers have been known to precede autoimmune diseases so it will be very important to understand whether COVID-19 also impacts systemic autoimmune rheumatic diseases. I would be interested in differences in surveillance between the infection and control groups early in the pandemic. Many patients were avoiding interaction with the health care system at that point."
Dr. Holcomb reported having no financial disclosures. Dr. Dellavalle disclosed that he is a consultant for Altus Labs and ParaPRO LLC. He has received grants and research funding from Pfizer.
* This story was updated on 3/29/22.
BOSTON – . This predominately favored systemic disease states with cutaneous involvement, rather than skin-limited processes.
The findings come from a large multicenter analysis that Zachary Holcomb, MD, presented during a late-breaking abstract session at the annual meeting of the American Academy of Dermatology.
“Viral triggers have been implicated in the pathogenesis of rheumatologic disease, but information regarding development of autoimmune disease following SARS-CoV-2 infection is limited,” said Dr. Holcomb, chief resident in the Harvard Combined Internal Medicine–Dermatology Residency, Boston. “Given its proposed thromboinflammatory pathobiology, we hypothesized that SARS-CoV-2 infection increases the risk of development of autoimmune disease with cutaneous manifestations and sought to define incidence rates of newly-diagnosed autoimmune diseases following SARS-CoV-2 infection.”
The researchers drew from the TriNetX Dataworks platform, an online cloud-based system that contains aggregated and deidentified patient information from about 75 million patients across 48 health care organizations. The infected cohort was defined as having a positive lab test for severe SARS-CoV-2 within the study window using Logical Observation Identifiers Names and Codes (LOINCs). Healthy controls consisted of a documented health care contact (inpatient or outpatient visit) during the study window without a positive SARS-CoV-2 lab test. Each cohort included patients aged 18-65 at the time of the study, and patients with previously diagnosed cutaneous autoimmune or vascular diseases were excluded from the analysis.
After propensity matching, the COVID-19 infected cohort and the healthy cohort included 1,904,864 patients each, with no baseline differences in age at index event, ethnicity, race, or sex. The study window was between April 1, 2020, and Oct. 1, 2020. The index event was a COVID-19 infection for the infected group and first documented health care contact in the healthy control group. The researchers looked at a window of 60 days following this index event for new incidence of cutaneous or vascular disease.
In the realm of connective tissue and related diseases, they found the incidence was increased among the COVID-19 infected group compared with controls for dermatomyositis (risk ratio, 2.273; P = .0196), scleroderma (RR, 1.959; P = .0001), and systemic lupus erythematosus (RR, 1.401; P < .0001). They also noted a significant decrease in the new incidence of alopecia areata in the COVID-19 infected group compared with controls (RR, 0.527; P < .0001).
No significant differences in the incidence of bullous and papulosquamous diseases were observed between the two groups. However, sarcoidosis was significantly more common in the COVID-19–infected group compared with controls (RR, 2.086; P < .001). “When taking all of these autoinflammatory diseases as a whole, there was an increased incidence in the COVID-19 infected group overall with a RR of 1.168 (P < .0001),” Dr. Holcomb said.
In the realm of vascular skin diseases, there was an increased incidence in the COVID-19 infected group in acrocyanosis (RR, 2.825; P < .001), Raynaud’s phenomenon (RR, 1.462; P < .0001), cutaneous small vessel vasculitis (RR, 1.714; P < .0001), granulomatosis with polyangiitis (RR, 2.667; P = .0002), and temporal arteritis (RR, 1.900; P = .0038).
“Interestingly, despite the academic and lay press reports of COVID toes, we did not see that in our data related to the COVID-infected group,” he said.
Dr. Holcomb acknowledged certain limitations of the study, including a narrow study window with a relatively short follow-up. “We were able to propensity match based on baseline demographics but not necessarily so based on health status and prior autoimmune disease,” he said. In addition, since the study was limited to those aged 18-65, the results may not be generalizable to pediatric and elderly patients, he said.
He described the study findings as “somewhat hypothesis-generating.” For instance, “why would we have more of a systemic process [at play?]. Our theory is that the severe inflammatory nature of COVID-19 leads to a lot of internal organ damage and exposure of autoantigens in that process, with relative skin sparing.”
One of the session moderators, Robert Paul Dellavalle, MD, PhD, professor of dermatology at the University of Colorado, Aurora, characterized the findings as “intriguing” but preliminary. “It would be interesting to look at more recent cohorts and see how vaccination for COVID-19 would impact the incidence rates of some of these diseases,” he said.
When asked for comment, Jeffrey A. Sparks, MD, MMSc, a rheumatologist at Brigham and Women's Hospital and assistant professor of medicine at Harvard Medical School, both in Boston, said, "This is an interesting study that should be followed up. Viral triggers have been known to precede autoimmune diseases so it will be very important to understand whether COVID-19 also impacts systemic autoimmune rheumatic diseases. I would be interested in differences in surveillance between the infection and control groups early in the pandemic. Many patients were avoiding interaction with the health care system at that point."
Dr. Holcomb reported having no financial disclosures. Dr. Dellavalle disclosed that he is a consultant for Altus Labs and ParaPRO LLC. He has received grants and research funding from Pfizer.
* This story was updated on 3/29/22.
BOSTON – . This predominately favored systemic disease states with cutaneous involvement, rather than skin-limited processes.
The findings come from a large multicenter analysis that Zachary Holcomb, MD, presented during a late-breaking abstract session at the annual meeting of the American Academy of Dermatology.
“Viral triggers have been implicated in the pathogenesis of rheumatologic disease, but information regarding development of autoimmune disease following SARS-CoV-2 infection is limited,” said Dr. Holcomb, chief resident in the Harvard Combined Internal Medicine–Dermatology Residency, Boston. “Given its proposed thromboinflammatory pathobiology, we hypothesized that SARS-CoV-2 infection increases the risk of development of autoimmune disease with cutaneous manifestations and sought to define incidence rates of newly-diagnosed autoimmune diseases following SARS-CoV-2 infection.”
The researchers drew from the TriNetX Dataworks platform, an online cloud-based system that contains aggregated and deidentified patient information from about 75 million patients across 48 health care organizations. The infected cohort was defined as having a positive lab test for severe SARS-CoV-2 within the study window using Logical Observation Identifiers Names and Codes (LOINCs). Healthy controls consisted of a documented health care contact (inpatient or outpatient visit) during the study window without a positive SARS-CoV-2 lab test. Each cohort included patients aged 18-65 at the time of the study, and patients with previously diagnosed cutaneous autoimmune or vascular diseases were excluded from the analysis.
After propensity matching, the COVID-19 infected cohort and the healthy cohort included 1,904,864 patients each, with no baseline differences in age at index event, ethnicity, race, or sex. The study window was between April 1, 2020, and Oct. 1, 2020. The index event was a COVID-19 infection for the infected group and first documented health care contact in the healthy control group. The researchers looked at a window of 60 days following this index event for new incidence of cutaneous or vascular disease.
In the realm of connective tissue and related diseases, they found the incidence was increased among the COVID-19 infected group compared with controls for dermatomyositis (risk ratio, 2.273; P = .0196), scleroderma (RR, 1.959; P = .0001), and systemic lupus erythematosus (RR, 1.401; P < .0001). They also noted a significant decrease in the new incidence of alopecia areata in the COVID-19 infected group compared with controls (RR, 0.527; P < .0001).
No significant differences in the incidence of bullous and papulosquamous diseases were observed between the two groups. However, sarcoidosis was significantly more common in the COVID-19–infected group compared with controls (RR, 2.086; P < .001). “When taking all of these autoinflammatory diseases as a whole, there was an increased incidence in the COVID-19 infected group overall with a RR of 1.168 (P < .0001),” Dr. Holcomb said.
In the realm of vascular skin diseases, there was an increased incidence in the COVID-19 infected group in acrocyanosis (RR, 2.825; P < .001), Raynaud’s phenomenon (RR, 1.462; P < .0001), cutaneous small vessel vasculitis (RR, 1.714; P < .0001), granulomatosis with polyangiitis (RR, 2.667; P = .0002), and temporal arteritis (RR, 1.900; P = .0038).
“Interestingly, despite the academic and lay press reports of COVID toes, we did not see that in our data related to the COVID-infected group,” he said.
Dr. Holcomb acknowledged certain limitations of the study, including a narrow study window with a relatively short follow-up. “We were able to propensity match based on baseline demographics but not necessarily so based on health status and prior autoimmune disease,” he said. In addition, since the study was limited to those aged 18-65, the results may not be generalizable to pediatric and elderly patients, he said.
He described the study findings as “somewhat hypothesis-generating.” For instance, “why would we have more of a systemic process [at play?]. Our theory is that the severe inflammatory nature of COVID-19 leads to a lot of internal organ damage and exposure of autoantigens in that process, with relative skin sparing.”
One of the session moderators, Robert Paul Dellavalle, MD, PhD, professor of dermatology at the University of Colorado, Aurora, characterized the findings as “intriguing” but preliminary. “It would be interesting to look at more recent cohorts and see how vaccination for COVID-19 would impact the incidence rates of some of these diseases,” he said.
When asked for comment, Jeffrey A. Sparks, MD, MMSc, a rheumatologist at Brigham and Women's Hospital and assistant professor of medicine at Harvard Medical School, both in Boston, said, "This is an interesting study that should be followed up. Viral triggers have been known to precede autoimmune diseases so it will be very important to understand whether COVID-19 also impacts systemic autoimmune rheumatic diseases. I would be interested in differences in surveillance between the infection and control groups early in the pandemic. Many patients were avoiding interaction with the health care system at that point."
Dr. Holcomb reported having no financial disclosures. Dr. Dellavalle disclosed that he is a consultant for Altus Labs and ParaPRO LLC. He has received grants and research funding from Pfizer.
* This story was updated on 3/29/22.
AT AAD 2022
Neuropsychiatric outcomes similar for hospitalized COVID-19 patients and non–COVID-19 patients
Hospitalized COVID-19 survivors showed greater cognitive impairment 6 months later, compared with patients hospitalized for other causes, but the overall disease burden was similar, based on data from 85 adults with COVID-19.
Previous studies have shown that cognitive and neuropsychiatric symptoms can occur from 2-6 months after COVID-19 recovery, and such symptoms are known to be associated with hospitalization for other severe medical conditions, Vardan Nersesjan, MD, of Copenhagen University Hospital, and colleagues wrote.
However, it remains unknown if COVID-19 is associated with a unique pattern of cognitive and mental impairment compared with other similarly severe medical conditions, they said.
In a study published in JAMA Psychiatry (2022 Mar 23. doi: 10.1001/jamapsychiatry.2022.0284), the researchers identified 85 adult COVID-19 survivors and 61 controls with non-COVID medical conditions who were treated and released between July 2020 and July 2021. The COVID-19 patients and controls were matched for age, sex, and ICU status. Cognitive impairment was assessed using the Mini-International Neuropsychiatric Interview, the Montreal Cognitive Assessment (MoCA), neurologic examination, and a semistructured interview to determine subjective symptoms.
The primary outcomes were the total scores on the MoCA and any new-onset psychiatric diagnoses. Secondary outcomes included specific psychiatric diagnoses such as depression, neurologic examination findings, and self-reported neuropsychiatric and cognitive symptoms. The mean age of the COVID-19 patients was 56.8 years, and 42% were women.
At 6 months’ follow-up, cognitive status was significantly lower in COVID-19 survivors, compared with controls, based on total geometric mean MoCA scores (26.7 vs. 27.5, P = .01). However, cognitive status improved significantly from 19.2 at hospital discharge to 26.1 at 6 months in 15 of the COVID-19 patients (P = .004), the researchers noted.
New-onset psychiatric diagnoses occurred in 16 COVID-19 patients and 12 of the controls (19% vs. 20%); this difference was not significant.
Secondary outcomes were not significantly different at 6 months between the groups, with the exception of anosmia, which was significantly more common in the COVID-19 patients; however, the significance disappeared in adjusted analysis, the researchers said.
The study findings were limited by several factors including the inability to prove causality because of the case-control feature and by the inability to detect small differences in neuropsychiatric outcomes, the researchers noted.
However, the results were strengthened by the use of a prospectively matched control group with similar disease severity admitted to the same hospital in the same time frame. Although the overall burden of neuropsychiatric and neurologic symptoms and diagnoses appeared similar in COVID-19 patients and those with other medical conditions, more research in larger populations is needed to determine smaller differences in neuropsychiatric profiles, the researchers noted.
Study fills research gap
The study is important at this time because, although prolonged neuropsychiatric and cognitive symptoms have been reported after COVID-19, the field lacked prospective case-control studies with well-matched controls to investigate whether these outcomes differed from those seen in other critical illnesses that had also required hospitalization, corresponding author Michael E. Benros, MD, of the Mental Health Center, Copenhagen, said in an interview.

“I was surprised that there was a significant worse cognitive functioning among COVID-19 patients 6 months after symptom onset also when compared to this well-matched control group that had been hospitalized for non–COVID-19 illness, although the absolute difference between the groups in cognition score were small,” said Dr. Benros. “Another notable finding is the large improvement in cognitive functioning from discharge to follow-up,” he added on behalf of himself and fellow corresponding author Daniel Kondziella, MD.
The study results show that cognitive function affected by COVID-19 and critical illness as observed at discharge showed a substantial improvement at 6 months after symptom onset, said Dr. Benros. “However, the cognitive function was significantly worse among severely ill COVID-19 patients 6 months after symptom onset when compared to a matched control group of individuals hospitalized for non–COVID-19 illness, although this difference in cognitive function was rather small in absolute numbers, and smaller than what had been suggested by other studies that lacked control groups. Strikingly, neuropsychiatric disorders were similar across the two groups, which was also the case when looking at neuropsychiatric symptoms.
“Larger prospective case-control studies of neuropsychiatric and cognitive functioning after COVID-19, compared with matched controls are still needed to detect smaller differences, and more detailed cognitive domains, and with longer follow-up time, which we are currently conducting,” Dr. Benros said.
Controlled studies will help planning
“Lingering neuropsychiatric complications are common after COVID-19, but only controlled studies can tell us whether these complications are specific to COVID-19, rather than a general effect of having been medically ill,” Alasdair G. Rooney, MRCPsych MD PhD, of the University of Edinburgh, said in an interview. “The answer matters ultimately because COVID-19 is a new disease; societies and health care services need to be able to plan for its specific consequences.”

The health status of the control group is important as well. “Most previous studies had compared COVID-19 survivors against healthy controls or patients from a historical database. This new study compared COVID-19 survivors against those hospitalized for other medical causes over the same period,” Dr. Rooney said. “This is a more stringent test of whether COVID-19 has specific neurocognitive and neuropsychiatric consequences.
“The study found that new-onset neuropsychiatric diagnoses and symptoms were no more likely to occur after COVID-19 than after similarly severe medical illnesses,” Dr. Rooney said. “This negative finding runs counter to some earlier studies and may surprise some.” The findings need to be replicated in larger samples, but the current study shows the importance of prospectively recruiting active controls.
“In a subgroup analysis, some patients showed good improvement in cognitive scores between discharge and follow-up. While unsurprising, this is encouraging and suggests that the early postdischarge months are an important time for neurocognitive recovery,” Dr. Rooney noted.
“The findings suggest that COVID-19 may impair attention more selectively than other medical causes of hospitalization. COVID-19 survivors may also be at higher risk of significant overall cognitive impairment than survivors of similarly severe medical illnesses, after a similar duration,” said Dr. Rooney. “If the results are replicated by other prospective studies, they would suggest that there is something about COVID-19 that causes clinically significant neurocognitive difficulties in a minority of survivors.
“Larger well-controlled studies are required, with longer follow-up and more detailed neurocognitive testing,” as the duration of impairment and scope for further recovery are not known, Dr. Rooney added. Also unknown is whether COVID-19 affects attention permanently, or whether recovery is simply slower after COVID-19 compared to other medical illnesses.
“Knowing who is at the greatest risk of severe cognitive impairment after COVID-19 is important and likely to allow tailoring of more effective shielding strategies,” said Dr. Rooney. “This study was conducted before the widespread availability of vaccines for COVID-19. Long-term neuropsychiatric outcomes in vaccinated patients remain largely unknown. Arguably, these are now more important to understand, as future COVID-19 waves will occur mainly among vaccinated individuals.”
The study was supported by the Lundbeck Foundation and the Novo Nordisk Foundation. Lead author Dr. Nersesjan had no financial conflicts to disclose. Dr. Benros reported grants from Lundbeck Foundation and Novo Nordisk Foundation during the conduct of the study. Dr. Rooney had no financial conflicts to disclose.
This article was updated 3/25/22.
Hospitalized COVID-19 survivors showed greater cognitive impairment 6 months later, compared with patients hospitalized for other causes, but the overall disease burden was similar, based on data from 85 adults with COVID-19.
Previous studies have shown that cognitive and neuropsychiatric symptoms can occur from 2-6 months after COVID-19 recovery, and such symptoms are known to be associated with hospitalization for other severe medical conditions, Vardan Nersesjan, MD, of Copenhagen University Hospital, and colleagues wrote.
However, it remains unknown if COVID-19 is associated with a unique pattern of cognitive and mental impairment compared with other similarly severe medical conditions, they said.
In a study published in JAMA Psychiatry (2022 Mar 23. doi: 10.1001/jamapsychiatry.2022.0284), the researchers identified 85 adult COVID-19 survivors and 61 controls with non-COVID medical conditions who were treated and released between July 2020 and July 2021. The COVID-19 patients and controls were matched for age, sex, and ICU status. Cognitive impairment was assessed using the Mini-International Neuropsychiatric Interview, the Montreal Cognitive Assessment (MoCA), neurologic examination, and a semistructured interview to determine subjective symptoms.
The primary outcomes were the total scores on the MoCA and any new-onset psychiatric diagnoses. Secondary outcomes included specific psychiatric diagnoses such as depression, neurologic examination findings, and self-reported neuropsychiatric and cognitive symptoms. The mean age of the COVID-19 patients was 56.8 years, and 42% were women.
At 6 months’ follow-up, cognitive status was significantly lower in COVID-19 survivors, compared with controls, based on total geometric mean MoCA scores (26.7 vs. 27.5, P = .01). However, cognitive status improved significantly from 19.2 at hospital discharge to 26.1 at 6 months in 15 of the COVID-19 patients (P = .004), the researchers noted.
New-onset psychiatric diagnoses occurred in 16 COVID-19 patients and 12 of the controls (19% vs. 20%); this difference was not significant.
Secondary outcomes were not significantly different at 6 months between the groups, with the exception of anosmia, which was significantly more common in the COVID-19 patients; however, the significance disappeared in adjusted analysis, the researchers said.
The study findings were limited by several factors including the inability to prove causality because of the case-control feature and by the inability to detect small differences in neuropsychiatric outcomes, the researchers noted.
However, the results were strengthened by the use of a prospectively matched control group with similar disease severity admitted to the same hospital in the same time frame. Although the overall burden of neuropsychiatric and neurologic symptoms and diagnoses appeared similar in COVID-19 patients and those with other medical conditions, more research in larger populations is needed to determine smaller differences in neuropsychiatric profiles, the researchers noted.
Study fills research gap
The study is important at this time because, although prolonged neuropsychiatric and cognitive symptoms have been reported after COVID-19, the field lacked prospective case-control studies with well-matched controls to investigate whether these outcomes differed from those seen in other critical illnesses that had also required hospitalization, corresponding author Michael E. Benros, MD, of the Mental Health Center, Copenhagen, said in an interview.
“I was surprised that there was a significant worse cognitive functioning among COVID-19 patients 6 months after symptom onset also when compared to this well-matched control group that had been hospitalized for non–COVID-19 illness, although the absolute difference between the groups in cognition score were small,” said Dr. Benros. “Another notable finding is the large improvement in cognitive functioning from discharge to follow-up,” he added on behalf of himself and fellow corresponding author Daniel Kondziella, MD.
The study results show that cognitive function affected by COVID-19 and critical illness as observed at discharge showed a substantial improvement at 6 months after symptom onset, said Dr. Benros. “However, the cognitive function was significantly worse among severely ill COVID-19 patients 6 months after symptom onset when compared to a matched control group of individuals hospitalized for non–COVID-19 illness, although this difference in cognitive function was rather small in absolute numbers, and smaller than what had been suggested by other studies that lacked control groups. Strikingly, neuropsychiatric disorders were similar across the two groups, which was also the case when looking at neuropsychiatric symptoms.
“Larger prospective case-control studies of neuropsychiatric and cognitive functioning after COVID-19, compared with matched controls are still needed to detect smaller differences, and more detailed cognitive domains, and with longer follow-up time, which we are currently conducting,” Dr. Benros said.
Controlled studies will help planning
“Lingering neuropsychiatric complications are common after COVID-19, but only controlled studies can tell us whether these complications are specific to COVID-19, rather than a general effect of having been medically ill,” Alasdair G. Rooney, MRCPsych MD PhD, of the University of Edinburgh, said in an interview. “The answer matters ultimately because COVID-19 is a new disease; societies and health care services need to be able to plan for its specific consequences.”
The health status of the control group is important as well. “Most previous studies had compared COVID-19 survivors against healthy controls or patients from a historical database. This new study compared COVID-19 survivors against those hospitalized for other medical causes over the same period,” Dr. Rooney said. “This is a more stringent test of whether COVID-19 has specific neurocognitive and neuropsychiatric consequences.
“The study found that new-onset neuropsychiatric diagnoses and symptoms were no more likely to occur after COVID-19 than after similarly severe medical illnesses,” Dr. Rooney said. “This negative finding runs counter to some earlier studies and may surprise some.” The findings need to be replicated in larger samples, but the current study shows the importance of prospectively recruiting active controls.
“In a subgroup analysis, some patients showed good improvement in cognitive scores between discharge and follow-up. While unsurprising, this is encouraging and suggests that the early postdischarge months are an important time for neurocognitive recovery,” Dr. Rooney noted.
“The findings suggest that COVID-19 may impair attention more selectively than other medical causes of hospitalization. COVID-19 survivors may also be at higher risk of significant overall cognitive impairment than survivors of similarly severe medical illnesses, after a similar duration,” said Dr. Rooney. “If the results are replicated by other prospective studies, they would suggest that there is something about COVID-19 that causes clinically significant neurocognitive difficulties in a minority of survivors.
“Larger well-controlled studies are required, with longer follow-up and more detailed neurocognitive testing,” as the duration of impairment and scope for further recovery are not known, Dr. Rooney added. Also unknown is whether COVID-19 affects attention permanently, or whether recovery is simply slower after COVID-19 compared to other medical illnesses.
“Knowing who is at the greatest risk of severe cognitive impairment after COVID-19 is important and likely to allow tailoring of more effective shielding strategies,” said Dr. Rooney. “This study was conducted before the widespread availability of vaccines for COVID-19. Long-term neuropsychiatric outcomes in vaccinated patients remain largely unknown. Arguably, these are now more important to understand, as future COVID-19 waves will occur mainly among vaccinated individuals.”
The study was supported by the Lundbeck Foundation and the Novo Nordisk Foundation. Lead author Dr. Nersesjan had no financial conflicts to disclose. Dr. Benros reported grants from Lundbeck Foundation and Novo Nordisk Foundation during the conduct of the study. Dr. Rooney had no financial conflicts to disclose.
This article was updated 3/25/22.
Hospitalized COVID-19 survivors showed greater cognitive impairment 6 months later, compared with patients hospitalized for other causes, but the overall disease burden was similar, based on data from 85 adults with COVID-19.
Previous studies have shown that cognitive and neuropsychiatric symptoms can occur from 2-6 months after COVID-19 recovery, and such symptoms are known to be associated with hospitalization for other severe medical conditions, Vardan Nersesjan, MD, of Copenhagen University Hospital, and colleagues wrote.
However, it remains unknown if COVID-19 is associated with a unique pattern of cognitive and mental impairment compared with other similarly severe medical conditions, they said.
In a study published in JAMA Psychiatry (2022 Mar 23. doi: 10.1001/jamapsychiatry.2022.0284), the researchers identified 85 adult COVID-19 survivors and 61 controls with non-COVID medical conditions who were treated and released between July 2020 and July 2021. The COVID-19 patients and controls were matched for age, sex, and ICU status. Cognitive impairment was assessed using the Mini-International Neuropsychiatric Interview, the Montreal Cognitive Assessment (MoCA), neurologic examination, and a semistructured interview to determine subjective symptoms.
The primary outcomes were the total scores on the MoCA and any new-onset psychiatric diagnoses. Secondary outcomes included specific psychiatric diagnoses such as depression, neurologic examination findings, and self-reported neuropsychiatric and cognitive symptoms. The mean age of the COVID-19 patients was 56.8 years, and 42% were women.
At 6 months’ follow-up, cognitive status was significantly lower in COVID-19 survivors, compared with controls, based on total geometric mean MoCA scores (26.7 vs. 27.5, P = .01). However, cognitive status improved significantly from 19.2 at hospital discharge to 26.1 at 6 months in 15 of the COVID-19 patients (P = .004), the researchers noted.
New-onset psychiatric diagnoses occurred in 16 COVID-19 patients and 12 of the controls (19% vs. 20%); this difference was not significant.
Secondary outcomes were not significantly different at 6 months between the groups, with the exception of anosmia, which was significantly more common in the COVID-19 patients; however, the significance disappeared in adjusted analysis, the researchers said.
The study findings were limited by several factors including the inability to prove causality because of the case-control feature and by the inability to detect small differences in neuropsychiatric outcomes, the researchers noted.
However, the results were strengthened by the use of a prospectively matched control group with similar disease severity admitted to the same hospital in the same time frame. Although the overall burden of neuropsychiatric and neurologic symptoms and diagnoses appeared similar in COVID-19 patients and those with other medical conditions, more research in larger populations is needed to determine smaller differences in neuropsychiatric profiles, the researchers noted.
Study fills research gap
The study is important at this time because, although prolonged neuropsychiatric and cognitive symptoms have been reported after COVID-19, the field lacked prospective case-control studies with well-matched controls to investigate whether these outcomes differed from those seen in other critical illnesses that had also required hospitalization, corresponding author Michael E. Benros, MD, of the Mental Health Center, Copenhagen, said in an interview.
“I was surprised that there was a significant worse cognitive functioning among COVID-19 patients 6 months after symptom onset also when compared to this well-matched control group that had been hospitalized for non–COVID-19 illness, although the absolute difference between the groups in cognition score were small,” said Dr. Benros. “Another notable finding is the large improvement in cognitive functioning from discharge to follow-up,” he added on behalf of himself and fellow corresponding author Daniel Kondziella, MD.
The study results show that cognitive function affected by COVID-19 and critical illness as observed at discharge showed a substantial improvement at 6 months after symptom onset, said Dr. Benros. “However, the cognitive function was significantly worse among severely ill COVID-19 patients 6 months after symptom onset when compared to a matched control group of individuals hospitalized for non–COVID-19 illness, although this difference in cognitive function was rather small in absolute numbers, and smaller than what had been suggested by other studies that lacked control groups. Strikingly, neuropsychiatric disorders were similar across the two groups, which was also the case when looking at neuropsychiatric symptoms.
“Larger prospective case-control studies of neuropsychiatric and cognitive functioning after COVID-19, compared with matched controls are still needed to detect smaller differences, and more detailed cognitive domains, and with longer follow-up time, which we are currently conducting,” Dr. Benros said.
Controlled studies will help planning
“Lingering neuropsychiatric complications are common after COVID-19, but only controlled studies can tell us whether these complications are specific to COVID-19, rather than a general effect of having been medically ill,” Alasdair G. Rooney, MRCPsych MD PhD, of the University of Edinburgh, said in an interview. “The answer matters ultimately because COVID-19 is a new disease; societies and health care services need to be able to plan for its specific consequences.”
The health status of the control group is important as well. “Most previous studies had compared COVID-19 survivors against healthy controls or patients from a historical database. This new study compared COVID-19 survivors against those hospitalized for other medical causes over the same period,” Dr. Rooney said. “This is a more stringent test of whether COVID-19 has specific neurocognitive and neuropsychiatric consequences.
“The study found that new-onset neuropsychiatric diagnoses and symptoms were no more likely to occur after COVID-19 than after similarly severe medical illnesses,” Dr. Rooney said. “This negative finding runs counter to some earlier studies and may surprise some.” The findings need to be replicated in larger samples, but the current study shows the importance of prospectively recruiting active controls.
“In a subgroup analysis, some patients showed good improvement in cognitive scores between discharge and follow-up. While unsurprising, this is encouraging and suggests that the early postdischarge months are an important time for neurocognitive recovery,” Dr. Rooney noted.
“The findings suggest that COVID-19 may impair attention more selectively than other medical causes of hospitalization. COVID-19 survivors may also be at higher risk of significant overall cognitive impairment than survivors of similarly severe medical illnesses, after a similar duration,” said Dr. Rooney. “If the results are replicated by other prospective studies, they would suggest that there is something about COVID-19 that causes clinically significant neurocognitive difficulties in a minority of survivors.
“Larger well-controlled studies are required, with longer follow-up and more detailed neurocognitive testing,” as the duration of impairment and scope for further recovery are not known, Dr. Rooney added. Also unknown is whether COVID-19 affects attention permanently, or whether recovery is simply slower after COVID-19 compared to other medical illnesses.
“Knowing who is at the greatest risk of severe cognitive impairment after COVID-19 is important and likely to allow tailoring of more effective shielding strategies,” said Dr. Rooney. “This study was conducted before the widespread availability of vaccines for COVID-19. Long-term neuropsychiatric outcomes in vaccinated patients remain largely unknown. Arguably, these are now more important to understand, as future COVID-19 waves will occur mainly among vaccinated individuals.”
The study was supported by the Lundbeck Foundation and the Novo Nordisk Foundation. Lead author Dr. Nersesjan had no financial conflicts to disclose. Dr. Benros reported grants from Lundbeck Foundation and Novo Nordisk Foundation during the conduct of the study. Dr. Rooney had no financial conflicts to disclose.
This article was updated 3/25/22.
FROM JAMA PSYCHIATRY
Natural, vaccine-induced, and hybrid immunity to COVID-19
Seroprevalence surveys suggest that, from the beginning of the pandemic to 2022, more than a third of the global population had been infected with SARS-CoV-2. As large numbers of people continue to be infected, the efficacy and duration of natural immunity, in terms of protection against SARS-CoV-2 reinfections and severe disease, are of crucial significance. The virus’s epidemiologic trajectory will be influenced by the trends in vaccine-induced and hybrid immunity.
Omicron’s immune evasion
Cases of SARS-CoV-2 reinfection are increasing around the world. According to data from the U.K. Health Security Agency, 650,000 people in England have been infected twice, and most of them were reinfected in the past 2 months. Before mid-November 2021, reinfections accounted for about 1% of reported cases, but the rate has now increased to around 10%. The reinfection risk was 16 times higher between mid-December 2021 and early January 2022. Experts believe that this spike in reinfections is related to the spread of Omicron, which overtook Delta as the dominant variant. Nonetheless, other aspects should also be considered.
Omicron’s greater propensity to spread is not unrelated to its ability to evade the body’s immune defenses. This aspect was raised in a letter recently published in the New England Journal of Medicine. The authors reported that the effectiveness of previous infection in preventing reinfection against the Alpha, Beta, and Delta variants was around 90%, but it was only 56% against Omicron.
Natural immunity
Natural immunity showed roughly similar effectiveness regarding protection against reinfection across different SARS-CoV-2 variants, with the exception of the Omicron variant. The risk of hospitalization and death was also reduced in SARS-CoV-2 reinfections versus primary infections. Observational studies indicate that natural immunity may offer equal or greater protection against SARS-CoV-2 infections, compared with immunization with two doses of an mRNA vaccine, but the data are not fully consistent.
Natural immunity seems to be relatively long-lasting. Data from Denmark and Austria show no evidence that protection against reinfections wanes after 6 months. Some investigations indicate that protection against reinfection is lowest 4-5 months after initial infection and increases thereafter, a finding that might hypothetically be explained by persistent viral shedding; that is, misclassification of prolonged SARS-CoV-2 infections as reinfections. While no comparison was made against information pertaining to unvaccinated, not previously-infected individuals, preliminary data from Israel suggest that protection from reinfection can decrease from 6 to more than 12 months after the first SARS-CoV-2 infection. Taken together, epidemiologic studies indicate that protection against reinfections by natural immunity lasts over 1 year with only moderate, if any, decline over this period. Among older individuals, immunocompromised patients, and those with certain comorbidities or exposure risk (for example, health care workers), rates of reinfection may be higher. It is plausible that reinfection risk may be a function of exposure risk.
There is accumulating evidence that reinfections may be significantly less severe than primary infections with SARS-CoV-2. Reduced clinical severity of SARS-CoV-2 reinfections naturally also makes sense from a biologic point of view, inasmuch as a previously primed immune system should be better prepared for a rechallenge with this virus.
Vaccine-induced immunity
The short-term (<4 months) efficacy of mRNA vaccines against SARS-CoV-2 is high and varies from 94.1% (Moderna) to 95% (BioNTech/Pfizer). This has been confirmed by randomized controlled trials and was subsequently confirmed in effectiveness studies in real-world settings. Waning efficacy was observed with respect to protection against SARS-CoV-2 infections (for example, only approximately 20% after about half a year in Qatar), whereas protection against severe disease was either sustained or showed only a moderate decline.
In individuals who received two doses of the BioNTech/Pfizer vaccine at least 5 months earlier, an additional vaccine dose, a so-called booster, significantly lowered mortality and severe illness. These findings suggest that the booster restored and probably exceeded the initial short-term efficacy of the initial vaccination.
Data are still emerging regarding the efficacy of boosters against the Omicron variants. Preliminary data suggest a far lower ability to restore protection from infection and vaccination. However, fatalities and hospitalizations remain low.
Natural immunity vs. vaccine-induced immunity
Comparisons of natural immunity with vaccine-induced immunity are complicated by a series of biases and by combinations of biases – for example, the biases of comparisons between infected and uninfected, plus the biases of comparisons between vaccinated and nonvaccinated, with strong potential selection biases and confounding. Of particular note, the proportion of people previously infected and/or vaccinated may influence estimates of effectiveness. Regarding this point, one study compared unvaccinated patients with a prior SARS-CoV-2 infection and vaccinated individuals followed up from a week after the second vaccine dose onward versus a group of unvaccinated, not previously infected individuals. The findings showed that, compared with unvaccinated, not previously infected individuals, the natural immunity group and the vaccinated group had similar protection of 94.8% and 92.8% against infection, of 94.1% and 94.2% against hospitalization, and of 96.4% and 94.4% against severe illness, respectively.
Hybrid immunity
The combination of a previous SARS-CoV-2 infection and a respective vaccination is called hybrid immunity. This combination seems to confer the greatest protection against SARS-CoV-2 infections, but several knowledge gaps remain regarding this issue.
Data from Israel showed that, when the time since the last immunity-conferring event (either primary infection or vaccination) was the same, the rates of SARS-CoV-2 infections were similar in the following groups: individuals who had a previous infection and no vaccination, individuals who had an infection and were then vaccinated with a single dose after at least 3 months, and individuals who were vaccinated (two doses) and then infected. Severe disease was relatively rare overall.
Data on the efficacy of hybrid immunity point in the direction of hybrid immunity being superior, as compared with either vaccine-induced (without a booster) immunity or natural immunity alone. Timing and mode of vaccination of previously infected individuals to achieve optimal hybrid immunity are central questions that remain to be addressed in future studies.
Given that vaccination rates are continuously increasing and that, by the beginning of 2022, perhaps half or more of the global population had already been infected with SARS-CoV-2, with the vast majority of this group not being officially detected, it would appear logical that future infection waves, even with highly transmissible variants of SARS-CoV-2, may be limited with respect to their maximum potential health burden. The advent of Omicron suggests that massive surges can occur even in populations with extremely high rates of previous vaccination and variable rates of prior infections. However, even then, the accompanying burden of hospitalizations and deaths is far less than what was seen in 2020 and 2021. One may argue that the pandemic has already transitioned to the endemic phase and that Omicron is an endemic wave occurring in the setting of already widespread population immunity.
A version of this article first appeared on Medscape.com.
Seroprevalence surveys suggest that, from the beginning of the pandemic to 2022, more than a third of the global population had been infected with SARS-CoV-2. As large numbers of people continue to be infected, the efficacy and duration of natural immunity, in terms of protection against SARS-CoV-2 reinfections and severe disease, are of crucial significance. The virus’s epidemiologic trajectory will be influenced by the trends in vaccine-induced and hybrid immunity.
Omicron’s immune evasion
Cases of SARS-CoV-2 reinfection are increasing around the world. According to data from the U.K. Health Security Agency, 650,000 people in England have been infected twice, and most of them were reinfected in the past 2 months. Before mid-November 2021, reinfections accounted for about 1% of reported cases, but the rate has now increased to around 10%. The reinfection risk was 16 times higher between mid-December 2021 and early January 2022. Experts believe that this spike in reinfections is related to the spread of Omicron, which overtook Delta as the dominant variant. Nonetheless, other aspects should also be considered.
Omicron’s greater propensity to spread is not unrelated to its ability to evade the body’s immune defenses. This aspect was raised in a letter recently published in the New England Journal of Medicine. The authors reported that the effectiveness of previous infection in preventing reinfection against the Alpha, Beta, and Delta variants was around 90%, but it was only 56% against Omicron.
Natural immunity
Natural immunity showed roughly similar effectiveness regarding protection against reinfection across different SARS-CoV-2 variants, with the exception of the Omicron variant. The risk of hospitalization and death was also reduced in SARS-CoV-2 reinfections versus primary infections. Observational studies indicate that natural immunity may offer equal or greater protection against SARS-CoV-2 infections, compared with immunization with two doses of an mRNA vaccine, but the data are not fully consistent.
Natural immunity seems to be relatively long-lasting. Data from Denmark and Austria show no evidence that protection against reinfections wanes after 6 months. Some investigations indicate that protection against reinfection is lowest 4-5 months after initial infection and increases thereafter, a finding that might hypothetically be explained by persistent viral shedding; that is, misclassification of prolonged SARS-CoV-2 infections as reinfections. While no comparison was made against information pertaining to unvaccinated, not previously-infected individuals, preliminary data from Israel suggest that protection from reinfection can decrease from 6 to more than 12 months after the first SARS-CoV-2 infection. Taken together, epidemiologic studies indicate that protection against reinfections by natural immunity lasts over 1 year with only moderate, if any, decline over this period. Among older individuals, immunocompromised patients, and those with certain comorbidities or exposure risk (for example, health care workers), rates of reinfection may be higher. It is plausible that reinfection risk may be a function of exposure risk.
There is accumulating evidence that reinfections may be significantly less severe than primary infections with SARS-CoV-2. Reduced clinical severity of SARS-CoV-2 reinfections naturally also makes sense from a biologic point of view, inasmuch as a previously primed immune system should be better prepared for a rechallenge with this virus.
Vaccine-induced immunity
The short-term (<4 months) efficacy of mRNA vaccines against SARS-CoV-2 is high and varies from 94.1% (Moderna) to 95% (BioNTech/Pfizer). This has been confirmed by randomized controlled trials and was subsequently confirmed in effectiveness studies in real-world settings. Waning efficacy was observed with respect to protection against SARS-CoV-2 infections (for example, only approximately 20% after about half a year in Qatar), whereas protection against severe disease was either sustained or showed only a moderate decline.
In individuals who received two doses of the BioNTech/Pfizer vaccine at least 5 months earlier, an additional vaccine dose, a so-called booster, significantly lowered mortality and severe illness. These findings suggest that the booster restored and probably exceeded the initial short-term efficacy of the initial vaccination.
Data are still emerging regarding the efficacy of boosters against the Omicron variants. Preliminary data suggest a far lower ability to restore protection from infection and vaccination. However, fatalities and hospitalizations remain low.
Natural immunity vs. vaccine-induced immunity
Comparisons of natural immunity with vaccine-induced immunity are complicated by a series of biases and by combinations of biases – for example, the biases of comparisons between infected and uninfected, plus the biases of comparisons between vaccinated and nonvaccinated, with strong potential selection biases and confounding. Of particular note, the proportion of people previously infected and/or vaccinated may influence estimates of effectiveness. Regarding this point, one study compared unvaccinated patients with a prior SARS-CoV-2 infection and vaccinated individuals followed up from a week after the second vaccine dose onward versus a group of unvaccinated, not previously infected individuals. The findings showed that, compared with unvaccinated, not previously infected individuals, the natural immunity group and the vaccinated group had similar protection of 94.8% and 92.8% against infection, of 94.1% and 94.2% against hospitalization, and of 96.4% and 94.4% against severe illness, respectively.
Hybrid immunity
The combination of a previous SARS-CoV-2 infection and a respective vaccination is called hybrid immunity. This combination seems to confer the greatest protection against SARS-CoV-2 infections, but several knowledge gaps remain regarding this issue.
Data from Israel showed that, when the time since the last immunity-conferring event (either primary infection or vaccination) was the same, the rates of SARS-CoV-2 infections were similar in the following groups: individuals who had a previous infection and no vaccination, individuals who had an infection and were then vaccinated with a single dose after at least 3 months, and individuals who were vaccinated (two doses) and then infected. Severe disease was relatively rare overall.
Data on the efficacy of hybrid immunity point in the direction of hybrid immunity being superior, as compared with either vaccine-induced (without a booster) immunity or natural immunity alone. Timing and mode of vaccination of previously infected individuals to achieve optimal hybrid immunity are central questions that remain to be addressed in future studies.
Given that vaccination rates are continuously increasing and that, by the beginning of 2022, perhaps half or more of the global population had already been infected with SARS-CoV-2, with the vast majority of this group not being officially detected, it would appear logical that future infection waves, even with highly transmissible variants of SARS-CoV-2, may be limited with respect to their maximum potential health burden. The advent of Omicron suggests that massive surges can occur even in populations with extremely high rates of previous vaccination and variable rates of prior infections. However, even then, the accompanying burden of hospitalizations and deaths is far less than what was seen in 2020 and 2021. One may argue that the pandemic has already transitioned to the endemic phase and that Omicron is an endemic wave occurring in the setting of already widespread population immunity.
A version of this article first appeared on Medscape.com.
Seroprevalence surveys suggest that, from the beginning of the pandemic to 2022, more than a third of the global population had been infected with SARS-CoV-2. As large numbers of people continue to be infected, the efficacy and duration of natural immunity, in terms of protection against SARS-CoV-2 reinfections and severe disease, are of crucial significance. The virus’s epidemiologic trajectory will be influenced by the trends in vaccine-induced and hybrid immunity.
Omicron’s immune evasion
Cases of SARS-CoV-2 reinfection are increasing around the world. According to data from the U.K. Health Security Agency, 650,000 people in England have been infected twice, and most of them were reinfected in the past 2 months. Before mid-November 2021, reinfections accounted for about 1% of reported cases, but the rate has now increased to around 10%. The reinfection risk was 16 times higher between mid-December 2021 and early January 2022. Experts believe that this spike in reinfections is related to the spread of Omicron, which overtook Delta as the dominant variant. Nonetheless, other aspects should also be considered.
Omicron’s greater propensity to spread is not unrelated to its ability to evade the body’s immune defenses. This aspect was raised in a letter recently published in the New England Journal of Medicine. The authors reported that the effectiveness of previous infection in preventing reinfection against the Alpha, Beta, and Delta variants was around 90%, but it was only 56% against Omicron.
Natural immunity
Natural immunity showed roughly similar effectiveness regarding protection against reinfection across different SARS-CoV-2 variants, with the exception of the Omicron variant. The risk of hospitalization and death was also reduced in SARS-CoV-2 reinfections versus primary infections. Observational studies indicate that natural immunity may offer equal or greater protection against SARS-CoV-2 infections, compared with immunization with two doses of an mRNA vaccine, but the data are not fully consistent.
Natural immunity seems to be relatively long-lasting. Data from Denmark and Austria show no evidence that protection against reinfections wanes after 6 months. Some investigations indicate that protection against reinfection is lowest 4-5 months after initial infection and increases thereafter, a finding that might hypothetically be explained by persistent viral shedding; that is, misclassification of prolonged SARS-CoV-2 infections as reinfections. While no comparison was made against information pertaining to unvaccinated, not previously-infected individuals, preliminary data from Israel suggest that protection from reinfection can decrease from 6 to more than 12 months after the first SARS-CoV-2 infection. Taken together, epidemiologic studies indicate that protection against reinfections by natural immunity lasts over 1 year with only moderate, if any, decline over this period. Among older individuals, immunocompromised patients, and those with certain comorbidities or exposure risk (for example, health care workers), rates of reinfection may be higher. It is plausible that reinfection risk may be a function of exposure risk.
There is accumulating evidence that reinfections may be significantly less severe than primary infections with SARS-CoV-2. Reduced clinical severity of SARS-CoV-2 reinfections naturally also makes sense from a biologic point of view, inasmuch as a previously primed immune system should be better prepared for a rechallenge with this virus.
Vaccine-induced immunity
The short-term (<4 months) efficacy of mRNA vaccines against SARS-CoV-2 is high and varies from 94.1% (Moderna) to 95% (BioNTech/Pfizer). This has been confirmed by randomized controlled trials and was subsequently confirmed in effectiveness studies in real-world settings. Waning efficacy was observed with respect to protection against SARS-CoV-2 infections (for example, only approximately 20% after about half a year in Qatar), whereas protection against severe disease was either sustained or showed only a moderate decline.
In individuals who received two doses of the BioNTech/Pfizer vaccine at least 5 months earlier, an additional vaccine dose, a so-called booster, significantly lowered mortality and severe illness. These findings suggest that the booster restored and probably exceeded the initial short-term efficacy of the initial vaccination.
Data are still emerging regarding the efficacy of boosters against the Omicron variants. Preliminary data suggest a far lower ability to restore protection from infection and vaccination. However, fatalities and hospitalizations remain low.
Natural immunity vs. vaccine-induced immunity
Comparisons of natural immunity with vaccine-induced immunity are complicated by a series of biases and by combinations of biases – for example, the biases of comparisons between infected and uninfected, plus the biases of comparisons between vaccinated and nonvaccinated, with strong potential selection biases and confounding. Of particular note, the proportion of people previously infected and/or vaccinated may influence estimates of effectiveness. Regarding this point, one study compared unvaccinated patients with a prior SARS-CoV-2 infection and vaccinated individuals followed up from a week after the second vaccine dose onward versus a group of unvaccinated, not previously infected individuals. The findings showed that, compared with unvaccinated, not previously infected individuals, the natural immunity group and the vaccinated group had similar protection of 94.8% and 92.8% against infection, of 94.1% and 94.2% against hospitalization, and of 96.4% and 94.4% against severe illness, respectively.
Hybrid immunity
The combination of a previous SARS-CoV-2 infection and a respective vaccination is called hybrid immunity. This combination seems to confer the greatest protection against SARS-CoV-2 infections, but several knowledge gaps remain regarding this issue.
Data from Israel showed that, when the time since the last immunity-conferring event (either primary infection or vaccination) was the same, the rates of SARS-CoV-2 infections were similar in the following groups: individuals who had a previous infection and no vaccination, individuals who had an infection and were then vaccinated with a single dose after at least 3 months, and individuals who were vaccinated (two doses) and then infected. Severe disease was relatively rare overall.
Data on the efficacy of hybrid immunity point in the direction of hybrid immunity being superior, as compared with either vaccine-induced (without a booster) immunity or natural immunity alone. Timing and mode of vaccination of previously infected individuals to achieve optimal hybrid immunity are central questions that remain to be addressed in future studies.
Given that vaccination rates are continuously increasing and that, by the beginning of 2022, perhaps half or more of the global population had already been infected with SARS-CoV-2, with the vast majority of this group not being officially detected, it would appear logical that future infection waves, even with highly transmissible variants of SARS-CoV-2, may be limited with respect to their maximum potential health burden. The advent of Omicron suggests that massive surges can occur even in populations with extremely high rates of previous vaccination and variable rates of prior infections. However, even then, the accompanying burden of hospitalizations and deaths is far less than what was seen in 2020 and 2021. One may argue that the pandemic has already transitioned to the endemic phase and that Omicron is an endemic wave occurring in the setting of already widespread population immunity.
A version of this article first appeared on Medscape.com.
‘Pandemic brain’ not limited to patients infected with COVID-19
The stress of living through a pandemic may cause brain inflammation even in those uninfected with SARS-CoV-2, a study suggests.
Healthy individuals who tested negative for the virus that causes COVID-19 had elevated levels of inflammatory markers known to be involved in depression, stress, and mental fatigue. The study indicates a possible link between pandemic-associated stressors and neuroimmune responses.
“The most important finding is the evidence of neuroinflammation in noninfected, otherwise healthy participants, which may explain the variety of sickness-behavior-like symptoms experienced by many during the pandemic,” lead author Ludovica Brusaferri, PhD, a postdoctoral research fellow at Massachusetts General Hospital and Harvard Medical School in Boston, told this news organization.
The study was published online Feb. 16 in Brain, Behavior, and Immunity.
Impact of pandemic stress?
Reports of psychological distress have increased considerably in the United States during the pandemic, including among those not infected with SARS-CoV-2.
To better understand the effects of the pandemic on brain and mental health, the investigators retrospectively analyzed data collected from 57 people who were enrolled as control subjects for unrelated studies before the pandemic began.
They also enrolled 15 people living in Massachusetts during that state’s 2-month lockdown/stay-at-home order from March to May 2020, all of whom had tested negative for COVID-19 antibodies.
The investigators used PET and MRI imaging and blood sample analyses to investigate whether there were any differences in the brains of healthy people before and during the pandemic following the lockdown.
Compared with the control group, the pandemic cohort had elevated levels of 18 kDa translocator protein (TSPO) and myoinositol, inflammatory markers in the brain. Increased TSPO has been associated with depression and suicidal thoughts and elevated myoinositol has been linked to schizophrenia.
Blood levels of two inflammatory markers, interleukin-16 and monocyte chemoattractant protein-1, were also elevated in the pandemic cohort, although to a lesser extent.
TSPO levels were especially high in participants in the pandemic cohort who reported moodiness and mental and physical fatigue, compared with those reporting few or no symptoms.
“These findings provide support to a role for neuroinflammation in stress, an observation that, if replicated, might help guide the development of novel treatments focused on the reduction of brain inflammation,” study author Marco Loggia, PhD, codirector of the Center for Integrative Pain NeuroImaging at Mass General and Harvard Medical School, told this news organization.
Although the data showing increased neuroinflammation were collected when participants were under a stay-at-home order, the researchers said it’s not clear that this was the cause.
“We’re not saying it is the lockdown that was causing it,” Dr. Loggia said. “It could have been social isolation, changes in diet, or changes in exercise patterns. We don’t know exactly what the cause was so, maybe.”
A significant contribution
Commenting on the study for this news organization, Ning Quan, PhD, professor of biomedical science at Florida Atlantic University, Boca Raton, said although questions remain, the findings offer valuable information.
“This study contributes significantly to our understanding of how pandemic stress might impact our brain and behavior,” Dr. Quan said. “The main advance that this paper provides is that fatigue or brain fog could be induced in individuals with COVID infection during the pandemic.”
However, Dr. Quan added, the study has a number of limitations, including a small sample size, which makes it difficult to generalize the results.
“Another issue is the subjects of the study all lived in Massachusetts,” Dr. Quan added. “Subjects from different states or different countries could yield different results.”
The study was funded by the National Institutes of Health and by the Landreth Family Foundation. The study authors and Dr. Quan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The stress of living through a pandemic may cause brain inflammation even in those uninfected with SARS-CoV-2, a study suggests.
Healthy individuals who tested negative for the virus that causes COVID-19 had elevated levels of inflammatory markers known to be involved in depression, stress, and mental fatigue. The study indicates a possible link between pandemic-associated stressors and neuroimmune responses.
“The most important finding is the evidence of neuroinflammation in noninfected, otherwise healthy participants, which may explain the variety of sickness-behavior-like symptoms experienced by many during the pandemic,” lead author Ludovica Brusaferri, PhD, a postdoctoral research fellow at Massachusetts General Hospital and Harvard Medical School in Boston, told this news organization.
The study was published online Feb. 16 in Brain, Behavior, and Immunity.
Impact of pandemic stress?
Reports of psychological distress have increased considerably in the United States during the pandemic, including among those not infected with SARS-CoV-2.
To better understand the effects of the pandemic on brain and mental health, the investigators retrospectively analyzed data collected from 57 people who were enrolled as control subjects for unrelated studies before the pandemic began.
They also enrolled 15 people living in Massachusetts during that state’s 2-month lockdown/stay-at-home order from March to May 2020, all of whom had tested negative for COVID-19 antibodies.
The investigators used PET and MRI imaging and blood sample analyses to investigate whether there were any differences in the brains of healthy people before and during the pandemic following the lockdown.
Compared with the control group, the pandemic cohort had elevated levels of 18 kDa translocator protein (TSPO) and myoinositol, inflammatory markers in the brain. Increased TSPO has been associated with depression and suicidal thoughts and elevated myoinositol has been linked to schizophrenia.
Blood levels of two inflammatory markers, interleukin-16 and monocyte chemoattractant protein-1, were also elevated in the pandemic cohort, although to a lesser extent.
TSPO levels were especially high in participants in the pandemic cohort who reported moodiness and mental and physical fatigue, compared with those reporting few or no symptoms.
“These findings provide support to a role for neuroinflammation in stress, an observation that, if replicated, might help guide the development of novel treatments focused on the reduction of brain inflammation,” study author Marco Loggia, PhD, codirector of the Center for Integrative Pain NeuroImaging at Mass General and Harvard Medical School, told this news organization.
Although the data showing increased neuroinflammation were collected when participants were under a stay-at-home order, the researchers said it’s not clear that this was the cause.
“We’re not saying it is the lockdown that was causing it,” Dr. Loggia said. “It could have been social isolation, changes in diet, or changes in exercise patterns. We don’t know exactly what the cause was so, maybe.”
A significant contribution
Commenting on the study for this news organization, Ning Quan, PhD, professor of biomedical science at Florida Atlantic University, Boca Raton, said although questions remain, the findings offer valuable information.
“This study contributes significantly to our understanding of how pandemic stress might impact our brain and behavior,” Dr. Quan said. “The main advance that this paper provides is that fatigue or brain fog could be induced in individuals with COVID infection during the pandemic.”
However, Dr. Quan added, the study has a number of limitations, including a small sample size, which makes it difficult to generalize the results.
“Another issue is the subjects of the study all lived in Massachusetts,” Dr. Quan added. “Subjects from different states or different countries could yield different results.”
The study was funded by the National Institutes of Health and by the Landreth Family Foundation. The study authors and Dr. Quan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The stress of living through a pandemic may cause brain inflammation even in those uninfected with SARS-CoV-2, a study suggests.
Healthy individuals who tested negative for the virus that causes COVID-19 had elevated levels of inflammatory markers known to be involved in depression, stress, and mental fatigue. The study indicates a possible link between pandemic-associated stressors and neuroimmune responses.
“The most important finding is the evidence of neuroinflammation in noninfected, otherwise healthy participants, which may explain the variety of sickness-behavior-like symptoms experienced by many during the pandemic,” lead author Ludovica Brusaferri, PhD, a postdoctoral research fellow at Massachusetts General Hospital and Harvard Medical School in Boston, told this news organization.
The study was published online Feb. 16 in Brain, Behavior, and Immunity.
Impact of pandemic stress?
Reports of psychological distress have increased considerably in the United States during the pandemic, including among those not infected with SARS-CoV-2.
To better understand the effects of the pandemic on brain and mental health, the investigators retrospectively analyzed data collected from 57 people who were enrolled as control subjects for unrelated studies before the pandemic began.
They also enrolled 15 people living in Massachusetts during that state’s 2-month lockdown/stay-at-home order from March to May 2020, all of whom had tested negative for COVID-19 antibodies.
The investigators used PET and MRI imaging and blood sample analyses to investigate whether there were any differences in the brains of healthy people before and during the pandemic following the lockdown.
Compared with the control group, the pandemic cohort had elevated levels of 18 kDa translocator protein (TSPO) and myoinositol, inflammatory markers in the brain. Increased TSPO has been associated with depression and suicidal thoughts and elevated myoinositol has been linked to schizophrenia.
Blood levels of two inflammatory markers, interleukin-16 and monocyte chemoattractant protein-1, were also elevated in the pandemic cohort, although to a lesser extent.
TSPO levels were especially high in participants in the pandemic cohort who reported moodiness and mental and physical fatigue, compared with those reporting few or no symptoms.
“These findings provide support to a role for neuroinflammation in stress, an observation that, if replicated, might help guide the development of novel treatments focused on the reduction of brain inflammation,” study author Marco Loggia, PhD, codirector of the Center for Integrative Pain NeuroImaging at Mass General and Harvard Medical School, told this news organization.
Although the data showing increased neuroinflammation were collected when participants were under a stay-at-home order, the researchers said it’s not clear that this was the cause.
“We’re not saying it is the lockdown that was causing it,” Dr. Loggia said. “It could have been social isolation, changes in diet, or changes in exercise patterns. We don’t know exactly what the cause was so, maybe.”
A significant contribution
Commenting on the study for this news organization, Ning Quan, PhD, professor of biomedical science at Florida Atlantic University, Boca Raton, said although questions remain, the findings offer valuable information.
“This study contributes significantly to our understanding of how pandemic stress might impact our brain and behavior,” Dr. Quan said. “The main advance that this paper provides is that fatigue or brain fog could be induced in individuals with COVID infection during the pandemic.”
However, Dr. Quan added, the study has a number of limitations, including a small sample size, which makes it difficult to generalize the results.
“Another issue is the subjects of the study all lived in Massachusetts,” Dr. Quan added. “Subjects from different states or different countries could yield different results.”
The study was funded by the National Institutes of Health and by the Landreth Family Foundation. The study authors and Dr. Quan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM BRAIN, BEHAVIOR, AND IMMUNITY
Moderna reports positive COVID-19 vaccine response in kids down to 6 months
Moderna on March 23 released interim results indicating that its mRNA-1273 COVID vaccine produced “robust” neutralizing antibody titers in children aged 6 months to 6 years – levels similar to those seen in adults.
Vaccine efficacy against infection was 43.7% in children aged 6 months to 2 years and 37.5% among children aged 2-6 years, the new data from its phase 2/3 KidCOVE study show.
The company explained the lower efficacy numbers by noting that its study involving these younger children was conducted during the Omicron wave. The same decrease in efficacy against infection was reported in adults during the Omicron surge.
A majority of COVID-19 cases were mild in the approximately 6,900 children aged 6 months to 6 years in the study. No severe COVID-19 cases, hospitalizations, or deaths were reported.
The primary series of two 25-mcg doses of the vaccine given 28 days apart was generally well tolerated. Most adverse events were mild to moderate. For example, temperature greater than 38° C (>100.4° F) was reported for 17.0% of the 6-month-old to 2-year-old group and for 14.6% of the 2- to 6-year-old group. A few children, 0.2% of each group, experienced a temperature greater than 40° C (>104° F).
Moderna plans to include these response, efficacy, and safety data in an application to the Food and Drug Administration for emergency use authorization (EUA) of the vaccine in these younger children in the coming weeks.
“We now have clinical data on the performance of our vaccine from infants 6 months of age through older adults,” Moderna CEO Stephane Bancel said in a news release. He described the interim results as “good news for parents of children under 6 years of age.”
In other news
Moderna also announced that it began the FDA EUA submission process for a 50-μg two-dose primary series for children aged 6-12 years.
The company is also updating its EUA submission for a 100-mcg two-dose primary series for children and adolescents aged 12-18 years.
Similar to its booster research in adults, Moderna plans to evaluate the potential of a booster dose for all pediatric populations, including those aged 6 months to 6 years, 6-12 years, and adolescents. The company is evaluating both a booster dose of mRNA-1273 and its bivalent booster candidate (mRNA1273.214), which includes an Omicron variant booster and mRNA-1273.
A version of this article first appeared on Medscape.com.
Moderna on March 23 released interim results indicating that its mRNA-1273 COVID vaccine produced “robust” neutralizing antibody titers in children aged 6 months to 6 years – levels similar to those seen in adults.
Vaccine efficacy against infection was 43.7% in children aged 6 months to 2 years and 37.5% among children aged 2-6 years, the new data from its phase 2/3 KidCOVE study show.
The company explained the lower efficacy numbers by noting that its study involving these younger children was conducted during the Omicron wave. The same decrease in efficacy against infection was reported in adults during the Omicron surge.
A majority of COVID-19 cases were mild in the approximately 6,900 children aged 6 months to 6 years in the study. No severe COVID-19 cases, hospitalizations, or deaths were reported.
The primary series of two 25-mcg doses of the vaccine given 28 days apart was generally well tolerated. Most adverse events were mild to moderate. For example, temperature greater than 38° C (>100.4° F) was reported for 17.0% of the 6-month-old to 2-year-old group and for 14.6% of the 2- to 6-year-old group. A few children, 0.2% of each group, experienced a temperature greater than 40° C (>104° F).
Moderna plans to include these response, efficacy, and safety data in an application to the Food and Drug Administration for emergency use authorization (EUA) of the vaccine in these younger children in the coming weeks.
“We now have clinical data on the performance of our vaccine from infants 6 months of age through older adults,” Moderna CEO Stephane Bancel said in a news release. He described the interim results as “good news for parents of children under 6 years of age.”
In other news
Moderna also announced that it began the FDA EUA submission process for a 50-μg two-dose primary series for children aged 6-12 years.
The company is also updating its EUA submission for a 100-mcg two-dose primary series for children and adolescents aged 12-18 years.
Similar to its booster research in adults, Moderna plans to evaluate the potential of a booster dose for all pediatric populations, including those aged 6 months to 6 years, 6-12 years, and adolescents. The company is evaluating both a booster dose of mRNA-1273 and its bivalent booster candidate (mRNA1273.214), which includes an Omicron variant booster and mRNA-1273.
A version of this article first appeared on Medscape.com.
Moderna on March 23 released interim results indicating that its mRNA-1273 COVID vaccine produced “robust” neutralizing antibody titers in children aged 6 months to 6 years – levels similar to those seen in adults.
Vaccine efficacy against infection was 43.7% in children aged 6 months to 2 years and 37.5% among children aged 2-6 years, the new data from its phase 2/3 KidCOVE study show.
The company explained the lower efficacy numbers by noting that its study involving these younger children was conducted during the Omicron wave. The same decrease in efficacy against infection was reported in adults during the Omicron surge.
A majority of COVID-19 cases were mild in the approximately 6,900 children aged 6 months to 6 years in the study. No severe COVID-19 cases, hospitalizations, or deaths were reported.
The primary series of two 25-mcg doses of the vaccine given 28 days apart was generally well tolerated. Most adverse events were mild to moderate. For example, temperature greater than 38° C (>100.4° F) was reported for 17.0% of the 6-month-old to 2-year-old group and for 14.6% of the 2- to 6-year-old group. A few children, 0.2% of each group, experienced a temperature greater than 40° C (>104° F).
Moderna plans to include these response, efficacy, and safety data in an application to the Food and Drug Administration for emergency use authorization (EUA) of the vaccine in these younger children in the coming weeks.
“We now have clinical data on the performance of our vaccine from infants 6 months of age through older adults,” Moderna CEO Stephane Bancel said in a news release. He described the interim results as “good news for parents of children under 6 years of age.”
In other news
Moderna also announced that it began the FDA EUA submission process for a 50-μg two-dose primary series for children aged 6-12 years.
The company is also updating its EUA submission for a 100-mcg two-dose primary series for children and adolescents aged 12-18 years.
Similar to its booster research in adults, Moderna plans to evaluate the potential of a booster dose for all pediatric populations, including those aged 6 months to 6 years, 6-12 years, and adolescents. The company is evaluating both a booster dose of mRNA-1273 and its bivalent booster candidate (mRNA1273.214), which includes an Omicron variant booster and mRNA-1273.
A version of this article first appeared on Medscape.com.
‘Profound implications’: COVID ups diabetes risk 40% a year later
COVID-19 infection appears to significantly raise the risk for diabetes by about 40% at 1 year, indicate new data from a very large Veterans Administration population.
“If patients have a prior history of COVID-19, that’s a risk factor for diabetes and they should certainly be screened for diabetes,” study coauthor Ziyad Al-Aly, MD, a nephrologist and chief of research and development at VA St. Louis Health Care, told this news organization.
“It’s still premature to make guidelines. I think we have to process the data landscape to understand what this all really means, but it’s really, really clear that all these roads are pointing in one direction, that COVID-19 increases the risk of diabetes up to a year later. The risk is small but not negligible,” he said.
The database includes over 8 million people and 180,000 with a prior COVID-19 diagnosis. Significantly increased diabetes risks compared to those not infected ranging from 31% to more than double were found in an analysis of subgroups based on diabetes risk score, body mass index, age, race, prediabetes status, and deprivation level, even after adjustment for confounding factors.
There was a gradient of diabetes risk by COVID-19 severity – i.e., whether patients had not been hospitalized, had been hospitalized, or stayed in intensive care – but a significant excess diabetes burden was seen even among those with “mild” COVID-19. The diabetes risk was also elevated compared to both contemporary and historical controls.
The study was published March 21 in The Lancet Diabetes & Endocrinology, by Yan Xie, MPH, also of VA St Louis Health Care, along with Dr. Al-Aly.
The data align with those from another study just published from a nationwide German primary care database. That study was smaller and of shorter duration than the new VA study but consistent, said Dr. Al-Aly, a clinical epidemiologist at Washington University, St. Louis.
Millions more with new diabetes as late manifestation of COVID-19
“Millions of people in the U.S. have had COVID-19, so this is going to translate to literally millions more people with new-onset diabetes. Better to identify them early so they can be adequately treated,” Dr. Al-Aly said in an interview.
“The long-term implications of SARS-CoV-2 infection increasing diabetes risk are profound,” Venkat Narayan, MD, and Lisa R. Staimez, PhD, both of the Rollins School of Public Health and Emory Global Diabetes Research Center at Emory University, Atlanta, said in an accompanying editorial.
“With large and growing numbers of people worldwide infected with SARS-CoV-2 (434,154,739 cumulative cases by Feb. 28, 2022), any COVID-19-related increases in diabetes incidence could lead to unprecedented cases of diabetes worldwide – wreaking havoc on already over-stretched and under-resourced clinical and public health systems globally, with devastating tolls in terms of deaths and suffering,” they added.
Medscape Medical News contributor Eric Topol MD, of Scripps Research Institute, La Jolla, Calif., agrees. He said these new data “are most profound. The researchers found a 40% increase in diabetes that wasn’t present at 1 month after COVID-19 but at 1 year, it was. Some kind of late manifestation is happening here.”
Dr. Al-Aly told this news organization that the mechanisms for the association are unknown and likely to be heterogeneous. Among the people who already had risk factors for type 2 diabetes, such as obesity or metabolic syndrome, SARS-CoV-2 could simply accelerate that process and “put them over the edge” to overt diabetes.
However, for those without diabetes risk factors, “COVID-19 with all the inflammation it provokes in the body could be leading to de novo disease.” (Diabetes status was ascertained by ICD-10 codes and only about 0.70% of the total were recorded as type 1 diabetes. But, since autoantibody testing wasn’t routinely conducted, it’s unknown how many of the cases may have been type 1 misclassified as type 2, Dr. Al-Aly acknowledged.)
Diabetes risk significantly increased after COVID-19 in all analyses
The analysis included 181,280 patients in the U.S. Department of Veterans Affairs health care database with a COVID-19 diagnosis who survived for at least 30 days afterward during March 2020 through Sept. 30, 2021, with 4,118,441 contemporary controls without COVID-19 seen during 2019, and a historical control group of 4,286,911 people seen at the VA in 2017. Average follow-up was about a year.
Compared with the contemporary controls, the COVID-19 group had an excess diabetes burden of 13.46 per 1,000 person-years with a hazard ratio of 1.40. They had an increased 12.35 per 1,000 person-year risk for incident use of glucose-lowering medications, with a hazard ratio of 1.85. Similar results were seen with the historical controls.
Subgroup analyses showed an increased risk for diabetes following COVID-19 infection by age (≤ 65 years and > 65 years), race (White and Black), sex (male and female), BMI categories (> 18.5 to ≤ 25 kg/m², > 25 to ≤ 30 kg/m², and > 30 kg/m²), and area deprivation index quartiles. The increased risk was also seen across diabetes risk score quartiles.
Notably, COVID-19 significantly elevated the diabetes risk by 59% even for the subgroup with BMI between 18 and 25 kg/m², and by 38% among those with the lowest diabetes risk score quartile.
The COVID-19 population included 162,096 who were not hospitalized, 15,078 hospitalized, and 4,106 admitted to intensive care. Here, the hazard ratios for diabetes compared to the contemporary controls were 1.25, 2.73, and 3.76, respectively, all significant.
Dr. Al-Aly said that his group is now further analyzing the VA data for other outcomes including cardiovascular disease and kidney disease, as well as the now well-documented long COVID symptoms including fatigue, pain, and neurocognitive dysfunction.
They’re also investigating the impact of the COVID-19 vaccine to see whether the risks are mitigated in the case of breakthrough infections: “We’re doing a broad systematic assessment. The next paper will be more comprehensive.”
Dr. Narayan and Dr. Staimez wrote: “The potential connection between COVID-19 and diabetes highlights that infectious diseases (eg, SARS-CoV-2) and chronic diseases (eg, diabetes) cannot be viewed in siloes. When we emerge out of the pandemic, the much-neglected non-communicable diseases, such as type 2 diabetes, will continue their relentless trajectory, possibly in an accelerated manner, as the leading burdens of global health.”
Dr. Al-Aly declared support from the U.S. Department of Veterans Affairs for the submitted work. He has received consultation fees from Gilead Sciences and funding (unrelated to this work) from Tonix Pharmaceuticals. He is a member of the board of directors for Veterans Research and Education Foundation of Saint Louis, associate editor for the Journal of the American Society of Nephrology, and a member of multiple editorial boards. Dr. Narayan and Dr. Staimez have received support from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
COVID-19 infection appears to significantly raise the risk for diabetes by about 40% at 1 year, indicate new data from a very large Veterans Administration population.
“If patients have a prior history of COVID-19, that’s a risk factor for diabetes and they should certainly be screened for diabetes,” study coauthor Ziyad Al-Aly, MD, a nephrologist and chief of research and development at VA St. Louis Health Care, told this news organization.
“It’s still premature to make guidelines. I think we have to process the data landscape to understand what this all really means, but it’s really, really clear that all these roads are pointing in one direction, that COVID-19 increases the risk of diabetes up to a year later. The risk is small but not negligible,” he said.
The database includes over 8 million people and 180,000 with a prior COVID-19 diagnosis. Significantly increased diabetes risks compared to those not infected ranging from 31% to more than double were found in an analysis of subgroups based on diabetes risk score, body mass index, age, race, prediabetes status, and deprivation level, even after adjustment for confounding factors.
There was a gradient of diabetes risk by COVID-19 severity – i.e., whether patients had not been hospitalized, had been hospitalized, or stayed in intensive care – but a significant excess diabetes burden was seen even among those with “mild” COVID-19. The diabetes risk was also elevated compared to both contemporary and historical controls.
The study was published March 21 in The Lancet Diabetes & Endocrinology, by Yan Xie, MPH, also of VA St Louis Health Care, along with Dr. Al-Aly.
The data align with those from another study just published from a nationwide German primary care database. That study was smaller and of shorter duration than the new VA study but consistent, said Dr. Al-Aly, a clinical epidemiologist at Washington University, St. Louis.
Millions more with new diabetes as late manifestation of COVID-19
“Millions of people in the U.S. have had COVID-19, so this is going to translate to literally millions more people with new-onset diabetes. Better to identify them early so they can be adequately treated,” Dr. Al-Aly said in an interview.
“The long-term implications of SARS-CoV-2 infection increasing diabetes risk are profound,” Venkat Narayan, MD, and Lisa R. Staimez, PhD, both of the Rollins School of Public Health and Emory Global Diabetes Research Center at Emory University, Atlanta, said in an accompanying editorial.
“With large and growing numbers of people worldwide infected with SARS-CoV-2 (434,154,739 cumulative cases by Feb. 28, 2022), any COVID-19-related increases in diabetes incidence could lead to unprecedented cases of diabetes worldwide – wreaking havoc on already over-stretched and under-resourced clinical and public health systems globally, with devastating tolls in terms of deaths and suffering,” they added.
Medscape Medical News contributor Eric Topol MD, of Scripps Research Institute, La Jolla, Calif., agrees. He said these new data “are most profound. The researchers found a 40% increase in diabetes that wasn’t present at 1 month after COVID-19 but at 1 year, it was. Some kind of late manifestation is happening here.”
Dr. Al-Aly told this news organization that the mechanisms for the association are unknown and likely to be heterogeneous. Among the people who already had risk factors for type 2 diabetes, such as obesity or metabolic syndrome, SARS-CoV-2 could simply accelerate that process and “put them over the edge” to overt diabetes.
However, for those without diabetes risk factors, “COVID-19 with all the inflammation it provokes in the body could be leading to de novo disease.” (Diabetes status was ascertained by ICD-10 codes and only about 0.70% of the total were recorded as type 1 diabetes. But, since autoantibody testing wasn’t routinely conducted, it’s unknown how many of the cases may have been type 1 misclassified as type 2, Dr. Al-Aly acknowledged.)
Diabetes risk significantly increased after COVID-19 in all analyses
The analysis included 181,280 patients in the U.S. Department of Veterans Affairs health care database with a COVID-19 diagnosis who survived for at least 30 days afterward during March 2020 through Sept. 30, 2021, with 4,118,441 contemporary controls without COVID-19 seen during 2019, and a historical control group of 4,286,911 people seen at the VA in 2017. Average follow-up was about a year.
Compared with the contemporary controls, the COVID-19 group had an excess diabetes burden of 13.46 per 1,000 person-years with a hazard ratio of 1.40. They had an increased 12.35 per 1,000 person-year risk for incident use of glucose-lowering medications, with a hazard ratio of 1.85. Similar results were seen with the historical controls.
Subgroup analyses showed an increased risk for diabetes following COVID-19 infection by age (≤ 65 years and > 65 years), race (White and Black), sex (male and female), BMI categories (> 18.5 to ≤ 25 kg/m², > 25 to ≤ 30 kg/m², and > 30 kg/m²), and area deprivation index quartiles. The increased risk was also seen across diabetes risk score quartiles.
Notably, COVID-19 significantly elevated the diabetes risk by 59% even for the subgroup with BMI between 18 and 25 kg/m², and by 38% among those with the lowest diabetes risk score quartile.
The COVID-19 population included 162,096 who were not hospitalized, 15,078 hospitalized, and 4,106 admitted to intensive care. Here, the hazard ratios for diabetes compared to the contemporary controls were 1.25, 2.73, and 3.76, respectively, all significant.
Dr. Al-Aly said that his group is now further analyzing the VA data for other outcomes including cardiovascular disease and kidney disease, as well as the now well-documented long COVID symptoms including fatigue, pain, and neurocognitive dysfunction.
They’re also investigating the impact of the COVID-19 vaccine to see whether the risks are mitigated in the case of breakthrough infections: “We’re doing a broad systematic assessment. The next paper will be more comprehensive.”
Dr. Narayan and Dr. Staimez wrote: “The potential connection between COVID-19 and diabetes highlights that infectious diseases (eg, SARS-CoV-2) and chronic diseases (eg, diabetes) cannot be viewed in siloes. When we emerge out of the pandemic, the much-neglected non-communicable diseases, such as type 2 diabetes, will continue their relentless trajectory, possibly in an accelerated manner, as the leading burdens of global health.”
Dr. Al-Aly declared support from the U.S. Department of Veterans Affairs for the submitted work. He has received consultation fees from Gilead Sciences and funding (unrelated to this work) from Tonix Pharmaceuticals. He is a member of the board of directors for Veterans Research and Education Foundation of Saint Louis, associate editor for the Journal of the American Society of Nephrology, and a member of multiple editorial boards. Dr. Narayan and Dr. Staimez have received support from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
COVID-19 infection appears to significantly raise the risk for diabetes by about 40% at 1 year, indicate new data from a very large Veterans Administration population.
“If patients have a prior history of COVID-19, that’s a risk factor for diabetes and they should certainly be screened for diabetes,” study coauthor Ziyad Al-Aly, MD, a nephrologist and chief of research and development at VA St. Louis Health Care, told this news organization.
“It’s still premature to make guidelines. I think we have to process the data landscape to understand what this all really means, but it’s really, really clear that all these roads are pointing in one direction, that COVID-19 increases the risk of diabetes up to a year later. The risk is small but not negligible,” he said.
The database includes over 8 million people and 180,000 with a prior COVID-19 diagnosis. Significantly increased diabetes risks compared to those not infected ranging from 31% to more than double were found in an analysis of subgroups based on diabetes risk score, body mass index, age, race, prediabetes status, and deprivation level, even after adjustment for confounding factors.
There was a gradient of diabetes risk by COVID-19 severity – i.e., whether patients had not been hospitalized, had been hospitalized, or stayed in intensive care – but a significant excess diabetes burden was seen even among those with “mild” COVID-19. The diabetes risk was also elevated compared to both contemporary and historical controls.
The study was published March 21 in The Lancet Diabetes & Endocrinology, by Yan Xie, MPH, also of VA St Louis Health Care, along with Dr. Al-Aly.
The data align with those from another study just published from a nationwide German primary care database. That study was smaller and of shorter duration than the new VA study but consistent, said Dr. Al-Aly, a clinical epidemiologist at Washington University, St. Louis.
Millions more with new diabetes as late manifestation of COVID-19
“Millions of people in the U.S. have had COVID-19, so this is going to translate to literally millions more people with new-onset diabetes. Better to identify them early so they can be adequately treated,” Dr. Al-Aly said in an interview.
“The long-term implications of SARS-CoV-2 infection increasing diabetes risk are profound,” Venkat Narayan, MD, and Lisa R. Staimez, PhD, both of the Rollins School of Public Health and Emory Global Diabetes Research Center at Emory University, Atlanta, said in an accompanying editorial.
“With large and growing numbers of people worldwide infected with SARS-CoV-2 (434,154,739 cumulative cases by Feb. 28, 2022), any COVID-19-related increases in diabetes incidence could lead to unprecedented cases of diabetes worldwide – wreaking havoc on already over-stretched and under-resourced clinical and public health systems globally, with devastating tolls in terms of deaths and suffering,” they added.
Medscape Medical News contributor Eric Topol MD, of Scripps Research Institute, La Jolla, Calif., agrees. He said these new data “are most profound. The researchers found a 40% increase in diabetes that wasn’t present at 1 month after COVID-19 but at 1 year, it was. Some kind of late manifestation is happening here.”
Dr. Al-Aly told this news organization that the mechanisms for the association are unknown and likely to be heterogeneous. Among the people who already had risk factors for type 2 diabetes, such as obesity or metabolic syndrome, SARS-CoV-2 could simply accelerate that process and “put them over the edge” to overt diabetes.
However, for those without diabetes risk factors, “COVID-19 with all the inflammation it provokes in the body could be leading to de novo disease.” (Diabetes status was ascertained by ICD-10 codes and only about 0.70% of the total were recorded as type 1 diabetes. But, since autoantibody testing wasn’t routinely conducted, it’s unknown how many of the cases may have been type 1 misclassified as type 2, Dr. Al-Aly acknowledged.)
Diabetes risk significantly increased after COVID-19 in all analyses
The analysis included 181,280 patients in the U.S. Department of Veterans Affairs health care database with a COVID-19 diagnosis who survived for at least 30 days afterward during March 2020 through Sept. 30, 2021, with 4,118,441 contemporary controls without COVID-19 seen during 2019, and a historical control group of 4,286,911 people seen at the VA in 2017. Average follow-up was about a year.
Compared with the contemporary controls, the COVID-19 group had an excess diabetes burden of 13.46 per 1,000 person-years with a hazard ratio of 1.40. They had an increased 12.35 per 1,000 person-year risk for incident use of glucose-lowering medications, with a hazard ratio of 1.85. Similar results were seen with the historical controls.
Subgroup analyses showed an increased risk for diabetes following COVID-19 infection by age (≤ 65 years and > 65 years), race (White and Black), sex (male and female), BMI categories (> 18.5 to ≤ 25 kg/m², > 25 to ≤ 30 kg/m², and > 30 kg/m²), and area deprivation index quartiles. The increased risk was also seen across diabetes risk score quartiles.
Notably, COVID-19 significantly elevated the diabetes risk by 59% even for the subgroup with BMI between 18 and 25 kg/m², and by 38% among those with the lowest diabetes risk score quartile.
The COVID-19 population included 162,096 who were not hospitalized, 15,078 hospitalized, and 4,106 admitted to intensive care. Here, the hazard ratios for diabetes compared to the contemporary controls were 1.25, 2.73, and 3.76, respectively, all significant.
Dr. Al-Aly said that his group is now further analyzing the VA data for other outcomes including cardiovascular disease and kidney disease, as well as the now well-documented long COVID symptoms including fatigue, pain, and neurocognitive dysfunction.
They’re also investigating the impact of the COVID-19 vaccine to see whether the risks are mitigated in the case of breakthrough infections: “We’re doing a broad systematic assessment. The next paper will be more comprehensive.”
Dr. Narayan and Dr. Staimez wrote: “The potential connection between COVID-19 and diabetes highlights that infectious diseases (eg, SARS-CoV-2) and chronic diseases (eg, diabetes) cannot be viewed in siloes. When we emerge out of the pandemic, the much-neglected non-communicable diseases, such as type 2 diabetes, will continue their relentless trajectory, possibly in an accelerated manner, as the leading burdens of global health.”
Dr. Al-Aly declared support from the U.S. Department of Veterans Affairs for the submitted work. He has received consultation fees from Gilead Sciences and funding (unrelated to this work) from Tonix Pharmaceuticals. He is a member of the board of directors for Veterans Research and Education Foundation of Saint Louis, associate editor for the Journal of the American Society of Nephrology, and a member of multiple editorial boards. Dr. Narayan and Dr. Staimez have received support from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
FROM THE LANCET DIABETES & ENDOCRINOLOGY
Children and COVID: CDC gives perspective on hospitalizations
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.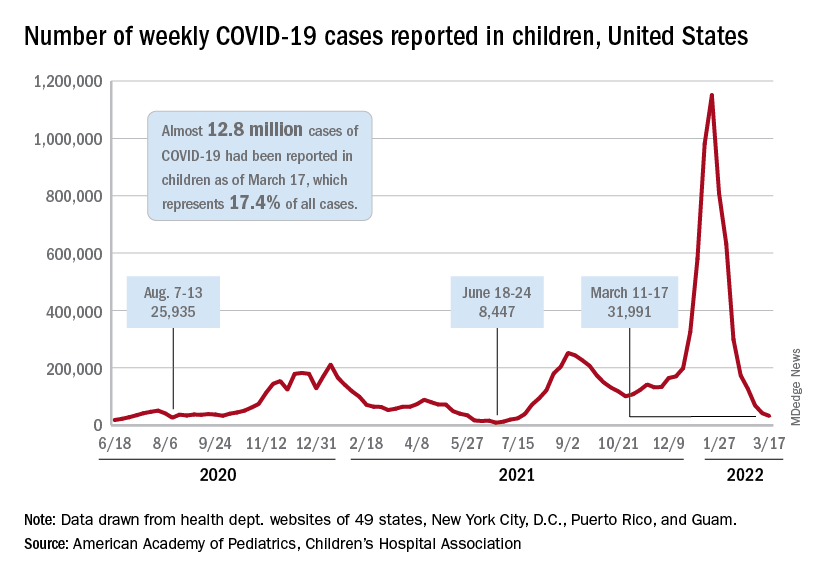
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
Mild COVID-19 infection linked to later type 2 diabetes
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
FROM DIABETOLOGIA