User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Neuraminidase inhibition titer a better predictor of influenza protection
Neuraminidase inhibition (NAI) titer is a better predictor of protection against influenza infection than hemagglutination inhibition (HAI) titer, according to new research, which could have implications for future flu vaccine development.
Investigators at the National Institute of Allergy and Infectious Diseases (NIAID) and the University of Pennsylvania, Philadelphia, performed a healthy volunteer challenge study with a wild-type 2009 A(H1N1)pdm influenza A challenge virus at the NIH Clinical Center in Bethesda, Md., to evaluate two groups of participants with HAI titers of greater than 1:40 and less than 1:40. The primary objective was to determine whether participants with HAI titers of greater than 1:40 were less likely to develop mild to moderate influenza disease after intranasal inoculation

In a multiple regression analysis, researchers evaluated the independent effects of both HAI and NAI titers on four diseases severity measures. In all measures – duration of shedding (HAI: P = .164; NAI: P less than .001), duration of symptoms (HAI: P = .497; NAI: P = .011), number of symptoms (HAI: P = .533; NAI: P less than .001), and symptom severity score (HAI: P = .906; NAI: P less than .001) – increasing NAI titers showed a statistically significant independent effect of decreasing severity, while HAI titers showed no significant independent effect on any of the disease severity measures examined.
When grouped by baseline NAI titers, those participants with high titers (greater than or equal to 1:40) had only minimal increases in NAI after challenge, but unlike HAI titer, every cohort with a low NAI titer had a rise in NAI titer after challenge, regardless of the outcome.
“These data further suggest that NAI titer may play a more significant role as a correlate of protection than previously thought and that the role of neuraminidase immunity should be considered when studying influenza susceptibility after vaccination and as a critical target in future influenza vaccine platforms,” Dr. Jeffery K. Taubenberger of the NIAID and his coauthors concluded.
This study was the first time the current “gold standard” for evaluating influenza vaccines – a protective HAI titer of greater than 1:40 – has been evaluated in a well-controlled healthy volunteer challenge since the cutoff was established, and the first time NAI titer has been identified in a controlled trial to be an independent predictor of a reduction in all aspects of influenza. The authors declared no conflicts of interest.
Read the full study in mBio (doi: 10.1128/mBio.00417-16).
Neuraminidase inhibition (NAI) titer is a better predictor of protection against influenza infection than hemagglutination inhibition (HAI) titer, according to new research, which could have implications for future flu vaccine development.
Investigators at the National Institute of Allergy and Infectious Diseases (NIAID) and the University of Pennsylvania, Philadelphia, performed a healthy volunteer challenge study with a wild-type 2009 A(H1N1)pdm influenza A challenge virus at the NIH Clinical Center in Bethesda, Md., to evaluate two groups of participants with HAI titers of greater than 1:40 and less than 1:40. The primary objective was to determine whether participants with HAI titers of greater than 1:40 were less likely to develop mild to moderate influenza disease after intranasal inoculation
In a multiple regression analysis, researchers evaluated the independent effects of both HAI and NAI titers on four diseases severity measures. In all measures – duration of shedding (HAI: P = .164; NAI: P less than .001), duration of symptoms (HAI: P = .497; NAI: P = .011), number of symptoms (HAI: P = .533; NAI: P less than .001), and symptom severity score (HAI: P = .906; NAI: P less than .001) – increasing NAI titers showed a statistically significant independent effect of decreasing severity, while HAI titers showed no significant independent effect on any of the disease severity measures examined.
When grouped by baseline NAI titers, those participants with high titers (greater than or equal to 1:40) had only minimal increases in NAI after challenge, but unlike HAI titer, every cohort with a low NAI titer had a rise in NAI titer after challenge, regardless of the outcome.
“These data further suggest that NAI titer may play a more significant role as a correlate of protection than previously thought and that the role of neuraminidase immunity should be considered when studying influenza susceptibility after vaccination and as a critical target in future influenza vaccine platforms,” Dr. Jeffery K. Taubenberger of the NIAID and his coauthors concluded.
This study was the first time the current “gold standard” for evaluating influenza vaccines – a protective HAI titer of greater than 1:40 – has been evaluated in a well-controlled healthy volunteer challenge since the cutoff was established, and the first time NAI titer has been identified in a controlled trial to be an independent predictor of a reduction in all aspects of influenza. The authors declared no conflicts of interest.
Read the full study in mBio (doi: 10.1128/mBio.00417-16).
Neuraminidase inhibition (NAI) titer is a better predictor of protection against influenza infection than hemagglutination inhibition (HAI) titer, according to new research, which could have implications for future flu vaccine development.
Investigators at the National Institute of Allergy and Infectious Diseases (NIAID) and the University of Pennsylvania, Philadelphia, performed a healthy volunteer challenge study with a wild-type 2009 A(H1N1)pdm influenza A challenge virus at the NIH Clinical Center in Bethesda, Md., to evaluate two groups of participants with HAI titers of greater than 1:40 and less than 1:40. The primary objective was to determine whether participants with HAI titers of greater than 1:40 were less likely to develop mild to moderate influenza disease after intranasal inoculation
In a multiple regression analysis, researchers evaluated the independent effects of both HAI and NAI titers on four diseases severity measures. In all measures – duration of shedding (HAI: P = .164; NAI: P less than .001), duration of symptoms (HAI: P = .497; NAI: P = .011), number of symptoms (HAI: P = .533; NAI: P less than .001), and symptom severity score (HAI: P = .906; NAI: P less than .001) – increasing NAI titers showed a statistically significant independent effect of decreasing severity, while HAI titers showed no significant independent effect on any of the disease severity measures examined.
When grouped by baseline NAI titers, those participants with high titers (greater than or equal to 1:40) had only minimal increases in NAI after challenge, but unlike HAI titer, every cohort with a low NAI titer had a rise in NAI titer after challenge, regardless of the outcome.
“These data further suggest that NAI titer may play a more significant role as a correlate of protection than previously thought and that the role of neuraminidase immunity should be considered when studying influenza susceptibility after vaccination and as a critical target in future influenza vaccine platforms,” Dr. Jeffery K. Taubenberger of the NIAID and his coauthors concluded.
This study was the first time the current “gold standard” for evaluating influenza vaccines – a protective HAI titer of greater than 1:40 – has been evaluated in a well-controlled healthy volunteer challenge since the cutoff was established, and the first time NAI titer has been identified in a controlled trial to be an independent predictor of a reduction in all aspects of influenza. The authors declared no conflicts of interest.
Read the full study in mBio (doi: 10.1128/mBio.00417-16).
FROM MBIO

Varenicline, bupropion not tied to significant increase in neuropsychiatric events in smokers
Neuropsychiatric adverse events do not increase significantly in smokers treated with either varenicline or bupropion, a large cohort study shows.
Both bupropion and varenicline have been tied to long-term smoking cessation in observational studies and randomized trials. However, concerns about adverse neuropsychiatric events, including aggression and suicidality, have been raised. Furthermore, data are limited on the safety of the medications in smokers with known psychiatric conditions.

At the request of the Food and Drug Administration, Dr. Robert M. Anthenelli and his colleagues conducted a randomized, double-blind, triple-dummy, placebo- and active-controlled trial to assess bupropion and varenicline in motivated smokers with and without psychiatric diagnoses for 12 weeks. The efficacy endpoint in the multinational trial, called the Evaluating Adverse Events in a Global Smoking Cessation Study (EAGLES), was abstinence for 9-12 weeks. The primary endpoint was adverse neuropsychiatric events, reported Dr. Anthenelli of the psychiatry department at the University of California, San Diego.
In total, 8,144 participants were randomized to either a nonpsychiatric (n = 4,028) or a psychiatric (n = 4,116) cohort. Men made up 44% of the study population, and the average age was 46.5 years. Most participants were white (82%) and American (52%). The psychiatric cohort included participants with diagnoses of primary mood disorders, anxiety and psychotic disorders, and borderline personality disorders, and 49% reported treatment with a psychotropic medication (Lancet. 2016 Apr 22. doi: 10.1016/S0140-6736).
Overall, the incidence of neuropsychiatric adverse events was similar in the bupropion (4.5%), varenicline (4.0%), nicotine patch (3.9%), and the placebo (3.7%) groups. However, more neuropsychiatric events were reported in the psychiatric cohort than the nonpsychiatric cohort (5.8% versus 2.1%, P less than .0001). Likewise, the psychiatric cohort reported moderate and severe neuropsychiatric adverse events more often in the bupropion group (6.7% versus 2.2%), varenicline (6.5% versus 1.3%), nicotine patch (5.2% versus 2.5%), and placebo groups (4.9% versus 2.4%) than the nonpsychiatric cohort.
In the nonpsychiatric cohort, the risk differences for moderate and severe neuropsychiatric adverse events were –1.28 (95% confidence interval, –2.40 to –0.15) for varenicline vs. placebo and –0.08 (95% CI, –1.37 to 1.21) for bupropion vs. placebo. In the psychiatric cohort, the risk differences for moderate and severe neuropsychiatric adverse events were 1.59 (95% CI, -0.42 to 3.59) for varenicline-placebo and 1.78 (95% CI, -0.24 to 3.81) for bupropion-placebo.
Rates of abstinence were higher in the participants who received varenicline, compared with placebo (OR, 3.61; 95% CI, 3.07-4.24), bupropion (OR, 1.75; 95% CI, 1.52-2.01), and the nicotine patch (OR, 1.68; 95% CI, 1.46-1.93).
The most common adverse events reported included abnormal dreams, headache, insomnia, and nausea.
Dr. Anthenelli and his associates noted several limitations. For example, participants in the psychiatric cohort were stable or in remission; they were restricted to particular psychiatric diagnoses; and participants with current substance abuse or risk for suicide were excluded.
However, they said the EAGLES trial results provide “further evidence that varenicline and bupropion can be used safely by psychiatrically stable smokers,” they wrote. “Although varenicline appears to be the most effective single pharmacotherapy available, all of the first-line medications – varenicline, bupropion, and nicotine patch – are efficacious, compared with placebo.”
The authors report relationships with several pharmaceutical companies, including Pfizer and GlaxoSmithKline. The study was funded by Pfizer and GlaxoSmithKline.
Neuropsychiatric adverse events do not increase significantly in smokers treated with either varenicline or bupropion, a large cohort study shows.
Both bupropion and varenicline have been tied to long-term smoking cessation in observational studies and randomized trials. However, concerns about adverse neuropsychiatric events, including aggression and suicidality, have been raised. Furthermore, data are limited on the safety of the medications in smokers with known psychiatric conditions.
At the request of the Food and Drug Administration, Dr. Robert M. Anthenelli and his colleagues conducted a randomized, double-blind, triple-dummy, placebo- and active-controlled trial to assess bupropion and varenicline in motivated smokers with and without psychiatric diagnoses for 12 weeks. The efficacy endpoint in the multinational trial, called the Evaluating Adverse Events in a Global Smoking Cessation Study (EAGLES), was abstinence for 9-12 weeks. The primary endpoint was adverse neuropsychiatric events, reported Dr. Anthenelli of the psychiatry department at the University of California, San Diego.
In total, 8,144 participants were randomized to either a nonpsychiatric (n = 4,028) or a psychiatric (n = 4,116) cohort. Men made up 44% of the study population, and the average age was 46.5 years. Most participants were white (82%) and American (52%). The psychiatric cohort included participants with diagnoses of primary mood disorders, anxiety and psychotic disorders, and borderline personality disorders, and 49% reported treatment with a psychotropic medication (Lancet. 2016 Apr 22. doi: 10.1016/S0140-6736).
Overall, the incidence of neuropsychiatric adverse events was similar in the bupropion (4.5%), varenicline (4.0%), nicotine patch (3.9%), and the placebo (3.7%) groups. However, more neuropsychiatric events were reported in the psychiatric cohort than the nonpsychiatric cohort (5.8% versus 2.1%, P less than .0001). Likewise, the psychiatric cohort reported moderate and severe neuropsychiatric adverse events more often in the bupropion group (6.7% versus 2.2%), varenicline (6.5% versus 1.3%), nicotine patch (5.2% versus 2.5%), and placebo groups (4.9% versus 2.4%) than the nonpsychiatric cohort.
In the nonpsychiatric cohort, the risk differences for moderate and severe neuropsychiatric adverse events were –1.28 (95% confidence interval, –2.40 to –0.15) for varenicline vs. placebo and –0.08 (95% CI, –1.37 to 1.21) for bupropion vs. placebo. In the psychiatric cohort, the risk differences for moderate and severe neuropsychiatric adverse events were 1.59 (95% CI, -0.42 to 3.59) for varenicline-placebo and 1.78 (95% CI, -0.24 to 3.81) for bupropion-placebo.
Rates of abstinence were higher in the participants who received varenicline, compared with placebo (OR, 3.61; 95% CI, 3.07-4.24), bupropion (OR, 1.75; 95% CI, 1.52-2.01), and the nicotine patch (OR, 1.68; 95% CI, 1.46-1.93).
The most common adverse events reported included abnormal dreams, headache, insomnia, and nausea.
Dr. Anthenelli and his associates noted several limitations. For example, participants in the psychiatric cohort were stable or in remission; they were restricted to particular psychiatric diagnoses; and participants with current substance abuse or risk for suicide were excluded.
However, they said the EAGLES trial results provide “further evidence that varenicline and bupropion can be used safely by psychiatrically stable smokers,” they wrote. “Although varenicline appears to be the most effective single pharmacotherapy available, all of the first-line medications – varenicline, bupropion, and nicotine patch – are efficacious, compared with placebo.”
The authors report relationships with several pharmaceutical companies, including Pfizer and GlaxoSmithKline. The study was funded by Pfizer and GlaxoSmithKline.
Neuropsychiatric adverse events do not increase significantly in smokers treated with either varenicline or bupropion, a large cohort study shows.
Both bupropion and varenicline have been tied to long-term smoking cessation in observational studies and randomized trials. However, concerns about adverse neuropsychiatric events, including aggression and suicidality, have been raised. Furthermore, data are limited on the safety of the medications in smokers with known psychiatric conditions.
At the request of the Food and Drug Administration, Dr. Robert M. Anthenelli and his colleagues conducted a randomized, double-blind, triple-dummy, placebo- and active-controlled trial to assess bupropion and varenicline in motivated smokers with and without psychiatric diagnoses for 12 weeks. The efficacy endpoint in the multinational trial, called the Evaluating Adverse Events in a Global Smoking Cessation Study (EAGLES), was abstinence for 9-12 weeks. The primary endpoint was adverse neuropsychiatric events, reported Dr. Anthenelli of the psychiatry department at the University of California, San Diego.
In total, 8,144 participants were randomized to either a nonpsychiatric (n = 4,028) or a psychiatric (n = 4,116) cohort. Men made up 44% of the study population, and the average age was 46.5 years. Most participants were white (82%) and American (52%). The psychiatric cohort included participants with diagnoses of primary mood disorders, anxiety and psychotic disorders, and borderline personality disorders, and 49% reported treatment with a psychotropic medication (Lancet. 2016 Apr 22. doi: 10.1016/S0140-6736).
Overall, the incidence of neuropsychiatric adverse events was similar in the bupropion (4.5%), varenicline (4.0%), nicotine patch (3.9%), and the placebo (3.7%) groups. However, more neuropsychiatric events were reported in the psychiatric cohort than the nonpsychiatric cohort (5.8% versus 2.1%, P less than .0001). Likewise, the psychiatric cohort reported moderate and severe neuropsychiatric adverse events more often in the bupropion group (6.7% versus 2.2%), varenicline (6.5% versus 1.3%), nicotine patch (5.2% versus 2.5%), and placebo groups (4.9% versus 2.4%) than the nonpsychiatric cohort.
In the nonpsychiatric cohort, the risk differences for moderate and severe neuropsychiatric adverse events were –1.28 (95% confidence interval, –2.40 to –0.15) for varenicline vs. placebo and –0.08 (95% CI, –1.37 to 1.21) for bupropion vs. placebo. In the psychiatric cohort, the risk differences for moderate and severe neuropsychiatric adverse events were 1.59 (95% CI, -0.42 to 3.59) for varenicline-placebo and 1.78 (95% CI, -0.24 to 3.81) for bupropion-placebo.
Rates of abstinence were higher in the participants who received varenicline, compared with placebo (OR, 3.61; 95% CI, 3.07-4.24), bupropion (OR, 1.75; 95% CI, 1.52-2.01), and the nicotine patch (OR, 1.68; 95% CI, 1.46-1.93).
The most common adverse events reported included abnormal dreams, headache, insomnia, and nausea.
Dr. Anthenelli and his associates noted several limitations. For example, participants in the psychiatric cohort were stable or in remission; they were restricted to particular psychiatric diagnoses; and participants with current substance abuse or risk for suicide were excluded.
However, they said the EAGLES trial results provide “further evidence that varenicline and bupropion can be used safely by psychiatrically stable smokers,” they wrote. “Although varenicline appears to be the most effective single pharmacotherapy available, all of the first-line medications – varenicline, bupropion, and nicotine patch – are efficacious, compared with placebo.”
The authors report relationships with several pharmaceutical companies, including Pfizer and GlaxoSmithKline. The study was funded by Pfizer and GlaxoSmithKline.
FROM THE LANCET
Key clinical point: Neuropsychiatric adverse events were not significantly increased in smokers treated with varenicline or bupropion.
Major finding: In the nonpsychiatric cohort, the risk differences for moderate and severe neuropsychiatric adverse events were –1.28 (95% CI, –2.40 to –0.15) for varenicline vs. placebo and –0.08 (95% CI, –1.37 to 1.21) for bupropion vs. placebo.
Data source: A randomized, double-blind, triple-dummy, placebo- and active-controlled trial aimed at assessing bupropion and varenicline in motivated smokers with and without psychiatric diagnoses for 12 weeks.
Disclosures: The authors report relationships to several pharmaceutical companies, including Pfizer and GlaxoSmithKline. The study was funded by Pfizer and GlaxoSmithKline.

Two Ebola vaccines effective, safe in phase I trials
Two Ebola vaccines were found safe and effective in separate international phase I trials involving healthy European and African adults, according to two reports published online April 27 in the New England Journal of Medicine.
After further testing and confirmation of these preliminary results, both vaccines should prove useful in both preventing and controlling future outbreaks, both research groups said.

Several vaccines showed promise in previous primate and preliminary human studies, including one expressing the surface glycoprotein of Zaire ebolavirus (ZEBOV). Different versions of this vaccine were assessed in the present phase I studies.
In the first trial, investigators sought to extend the durability of this vaccine by administering a single “priming” dose of the chimpanzee adenovirus 3 (ChAd3) vaccine encoding the ZEBOV surface glycoprotein, then giving a “booster” with a modified vaccinia Ankara (MVA) strain either 1 or 2 weeks later. The participants, 60 healthy adults aged 18-50 years, were randomly assigned to receive a low dose (20 subjects), an intermediate dose (20 subjects), or a high dose (20 subjects) of viral particles. Ten participants from each of these dose groups were then offered the booster. Then two additional groups of eight participants each were assessed to see whether giving the booster at 1 week vs. at 2 weeks made a difference in immunogenicity or safety.
All the study groups showed both antibody and T-cell immunogenicity after vaccination, but the groups that received the boosters showed antibody responses four times higher than those who did not. The MVA booster increased virus-specific antibodies by a factor of 12, and significantly increased neutralizing antibodies as well, said Dr. Katie Ewer of the Jenner Institute and Centre for Clinical Vaccinology and Tropical Medicine, University of Oxford (England) and the National Institute for Health Research Oxford Biomedical Research Centre and her associates.
The boosters also improved the vaccine’s cell-mediated immunity, increasing glycoprotein-specific CD8+ T cells by a factor of five.
In addition, the MVA booster markedly improved the vaccine’s durability, with 100% of recipients continuing to show seropositivity at 6 months, compared with only 50%-74% of participants who did not receive the booster.
The safety profile of the vaccine and the booster were termed “acceptable” at all dose levels and at all dosing intervals studied. There were no serious adverse events, and most adverse events were self-limited and mild. Moderate systemic adverse events included transient fever, myalgia, arthralgia, headache, fatigue, nausea, and malaise. Regarding laboratory abnormalities, four patients showed prolonged activated partial-thromboplastin time without coagulopathy, all of which resolved within 10 weeks; several patients showed mild or moderate lymphocytopenia and mild or moderate elevations in bilirubin, all of which were transient.
Overall, “We found that boosting can be immunogenic for antibodies and T cells at prime-boost intervals as short as 1 week. Such short-interval regimens may facilitate vaccine deployment in outbreak settings where both rapid onset and durable vaccine efficacy are required,” Dr. Ewer and her associates noted (N Engl J Med. 2016 Apr 27. doi: 10.1056/NEJMoa1411627).
They added that the ChAd3-plus-MVA viral vectors have other practical advantages. “Large-scale manufacturing processes concordant with Good Manufacturing Practice standards have been established, and both vectors have been assessed in large numbers of vaccines for a range of indications, without reports of any substantial safety concerns to date,” Dr. Ewer and her coauthors said.
The second report concerned four parallel studies: three open-label dose-escalation studies in Gabon, Kenya, and Germany and one randomized, double-blind trial in Geneva assessing the safety and immunogenicity of several doses of recombinant vesicular stomatitis virus (rVSV)-vectored ZEBOV. The 158 participants were followed for at least 6 months, said Dr. Selidji T. Agnandji of the Centre de Recherches Medicales de Lambarene (Gabon), the Institut für Tropenmedizin, Universitätsklinikum Tübingen (Germany), and the German Center for Infection Research, Tübingen, and his associates.
The vaccine was immunogenic in all participants across every dose and every study site, with higher glycoprotein-binding antibody titers at higher doses. These antibodies persisted through 6 months, a “promising” result suggesting that a single dose of this vaccine may be sufficient for early and possibly for long-term protection, the investigators said (N Engl J Med. 2016 Apr 27. doi: 10.1056/NEJMoa1502924).
Although there were no serious adverse events associated with this vaccine, acute vaccine reactions were common: 92% of patients reported an acute reaction, and 10%-22% (depending on the study site) reported grade 3 symptoms. The most bothersome – and unexpected – reactions involved viral seeding of joints and skin.
The joint problems manifested as arthritis, tenosynovitis, or bursitis that appeared at a median of 11 days after injection. The arthritis tended to affect one to four peripheral joints asymmetrically; pain was usually mild and dysfunction was usually moderate. Ten of the 11 affected patients in Geneva and both of the two (out of 60) affected patients at the other sites were symptom-free by 6 months. These findings “suggest a favorable long-term prognosis for these vaccine-induced arthritides,” Dr. Agnandji and his associates said.
Three participants developed maculopapular rashes mainly affecting the limbs, which appeared at 7-9 days following injection and persisted for 1-2 weeks. The rash was accompanied by a few tender vesicles on fingers or toes. Synovial fluid extracted from affected joints and material recovered from skin vesicles showed the presence of rVSV.
Given that most adverse reactions occurred soon after vaccination, were of short duration, and were amenable to treatment, this vaccine demonstrated “a favorable risk-benefit balance,” they added.
Two Ebola vaccines were found safe and effective in separate international phase I trials involving healthy European and African adults, according to two reports published online April 27 in the New England Journal of Medicine.
After further testing and confirmation of these preliminary results, both vaccines should prove useful in both preventing and controlling future outbreaks, both research groups said.
Several vaccines showed promise in previous primate and preliminary human studies, including one expressing the surface glycoprotein of Zaire ebolavirus (ZEBOV). Different versions of this vaccine were assessed in the present phase I studies.
In the first trial, investigators sought to extend the durability of this vaccine by administering a single “priming” dose of the chimpanzee adenovirus 3 (ChAd3) vaccine encoding the ZEBOV surface glycoprotein, then giving a “booster” with a modified vaccinia Ankara (MVA) strain either 1 or 2 weeks later. The participants, 60 healthy adults aged 18-50 years, were randomly assigned to receive a low dose (20 subjects), an intermediate dose (20 subjects), or a high dose (20 subjects) of viral particles. Ten participants from each of these dose groups were then offered the booster. Then two additional groups of eight participants each were assessed to see whether giving the booster at 1 week vs. at 2 weeks made a difference in immunogenicity or safety.
All the study groups showed both antibody and T-cell immunogenicity after vaccination, but the groups that received the boosters showed antibody responses four times higher than those who did not. The MVA booster increased virus-specific antibodies by a factor of 12, and significantly increased neutralizing antibodies as well, said Dr. Katie Ewer of the Jenner Institute and Centre for Clinical Vaccinology and Tropical Medicine, University of Oxford (England) and the National Institute for Health Research Oxford Biomedical Research Centre and her associates.
The boosters also improved the vaccine’s cell-mediated immunity, increasing glycoprotein-specific CD8+ T cells by a factor of five.
In addition, the MVA booster markedly improved the vaccine’s durability, with 100% of recipients continuing to show seropositivity at 6 months, compared with only 50%-74% of participants who did not receive the booster.
The safety profile of the vaccine and the booster were termed “acceptable” at all dose levels and at all dosing intervals studied. There were no serious adverse events, and most adverse events were self-limited and mild. Moderate systemic adverse events included transient fever, myalgia, arthralgia, headache, fatigue, nausea, and malaise. Regarding laboratory abnormalities, four patients showed prolonged activated partial-thromboplastin time without coagulopathy, all of which resolved within 10 weeks; several patients showed mild or moderate lymphocytopenia and mild or moderate elevations in bilirubin, all of which were transient.
Overall, “We found that boosting can be immunogenic for antibodies and T cells at prime-boost intervals as short as 1 week. Such short-interval regimens may facilitate vaccine deployment in outbreak settings where both rapid onset and durable vaccine efficacy are required,” Dr. Ewer and her associates noted (N Engl J Med. 2016 Apr 27. doi: 10.1056/NEJMoa1411627).
They added that the ChAd3-plus-MVA viral vectors have other practical advantages. “Large-scale manufacturing processes concordant with Good Manufacturing Practice standards have been established, and both vectors have been assessed in large numbers of vaccines for a range of indications, without reports of any substantial safety concerns to date,” Dr. Ewer and her coauthors said.
The second report concerned four parallel studies: three open-label dose-escalation studies in Gabon, Kenya, and Germany and one randomized, double-blind trial in Geneva assessing the safety and immunogenicity of several doses of recombinant vesicular stomatitis virus (rVSV)-vectored ZEBOV. The 158 participants were followed for at least 6 months, said Dr. Selidji T. Agnandji of the Centre de Recherches Medicales de Lambarene (Gabon), the Institut für Tropenmedizin, Universitätsklinikum Tübingen (Germany), and the German Center for Infection Research, Tübingen, and his associates.
The vaccine was immunogenic in all participants across every dose and every study site, with higher glycoprotein-binding antibody titers at higher doses. These antibodies persisted through 6 months, a “promising” result suggesting that a single dose of this vaccine may be sufficient for early and possibly for long-term protection, the investigators said (N Engl J Med. 2016 Apr 27. doi: 10.1056/NEJMoa1502924).
Although there were no serious adverse events associated with this vaccine, acute vaccine reactions were common: 92% of patients reported an acute reaction, and 10%-22% (depending on the study site) reported grade 3 symptoms. The most bothersome – and unexpected – reactions involved viral seeding of joints and skin.
The joint problems manifested as arthritis, tenosynovitis, or bursitis that appeared at a median of 11 days after injection. The arthritis tended to affect one to four peripheral joints asymmetrically; pain was usually mild and dysfunction was usually moderate. Ten of the 11 affected patients in Geneva and both of the two (out of 60) affected patients at the other sites were symptom-free by 6 months. These findings “suggest a favorable long-term prognosis for these vaccine-induced arthritides,” Dr. Agnandji and his associates said.
Three participants developed maculopapular rashes mainly affecting the limbs, which appeared at 7-9 days following injection and persisted for 1-2 weeks. The rash was accompanied by a few tender vesicles on fingers or toes. Synovial fluid extracted from affected joints and material recovered from skin vesicles showed the presence of rVSV.
Given that most adverse reactions occurred soon after vaccination, were of short duration, and were amenable to treatment, this vaccine demonstrated “a favorable risk-benefit balance,” they added.
Two Ebola vaccines were found safe and effective in separate international phase I trials involving healthy European and African adults, according to two reports published online April 27 in the New England Journal of Medicine.
After further testing and confirmation of these preliminary results, both vaccines should prove useful in both preventing and controlling future outbreaks, both research groups said.
Several vaccines showed promise in previous primate and preliminary human studies, including one expressing the surface glycoprotein of Zaire ebolavirus (ZEBOV). Different versions of this vaccine were assessed in the present phase I studies.
In the first trial, investigators sought to extend the durability of this vaccine by administering a single “priming” dose of the chimpanzee adenovirus 3 (ChAd3) vaccine encoding the ZEBOV surface glycoprotein, then giving a “booster” with a modified vaccinia Ankara (MVA) strain either 1 or 2 weeks later. The participants, 60 healthy adults aged 18-50 years, were randomly assigned to receive a low dose (20 subjects), an intermediate dose (20 subjects), or a high dose (20 subjects) of viral particles. Ten participants from each of these dose groups were then offered the booster. Then two additional groups of eight participants each were assessed to see whether giving the booster at 1 week vs. at 2 weeks made a difference in immunogenicity or safety.
All the study groups showed both antibody and T-cell immunogenicity after vaccination, but the groups that received the boosters showed antibody responses four times higher than those who did not. The MVA booster increased virus-specific antibodies by a factor of 12, and significantly increased neutralizing antibodies as well, said Dr. Katie Ewer of the Jenner Institute and Centre for Clinical Vaccinology and Tropical Medicine, University of Oxford (England) and the National Institute for Health Research Oxford Biomedical Research Centre and her associates.
The boosters also improved the vaccine’s cell-mediated immunity, increasing glycoprotein-specific CD8+ T cells by a factor of five.
In addition, the MVA booster markedly improved the vaccine’s durability, with 100% of recipients continuing to show seropositivity at 6 months, compared with only 50%-74% of participants who did not receive the booster.
The safety profile of the vaccine and the booster were termed “acceptable” at all dose levels and at all dosing intervals studied. There were no serious adverse events, and most adverse events were self-limited and mild. Moderate systemic adverse events included transient fever, myalgia, arthralgia, headache, fatigue, nausea, and malaise. Regarding laboratory abnormalities, four patients showed prolonged activated partial-thromboplastin time without coagulopathy, all of which resolved within 10 weeks; several patients showed mild or moderate lymphocytopenia and mild or moderate elevations in bilirubin, all of which were transient.
Overall, “We found that boosting can be immunogenic for antibodies and T cells at prime-boost intervals as short as 1 week. Such short-interval regimens may facilitate vaccine deployment in outbreak settings where both rapid onset and durable vaccine efficacy are required,” Dr. Ewer and her associates noted (N Engl J Med. 2016 Apr 27. doi: 10.1056/NEJMoa1411627).
They added that the ChAd3-plus-MVA viral vectors have other practical advantages. “Large-scale manufacturing processes concordant with Good Manufacturing Practice standards have been established, and both vectors have been assessed in large numbers of vaccines for a range of indications, without reports of any substantial safety concerns to date,” Dr. Ewer and her coauthors said.
The second report concerned four parallel studies: three open-label dose-escalation studies in Gabon, Kenya, and Germany and one randomized, double-blind trial in Geneva assessing the safety and immunogenicity of several doses of recombinant vesicular stomatitis virus (rVSV)-vectored ZEBOV. The 158 participants were followed for at least 6 months, said Dr. Selidji T. Agnandji of the Centre de Recherches Medicales de Lambarene (Gabon), the Institut für Tropenmedizin, Universitätsklinikum Tübingen (Germany), and the German Center for Infection Research, Tübingen, and his associates.
The vaccine was immunogenic in all participants across every dose and every study site, with higher glycoprotein-binding antibody titers at higher doses. These antibodies persisted through 6 months, a “promising” result suggesting that a single dose of this vaccine may be sufficient for early and possibly for long-term protection, the investigators said (N Engl J Med. 2016 Apr 27. doi: 10.1056/NEJMoa1502924).
Although there were no serious adverse events associated with this vaccine, acute vaccine reactions were common: 92% of patients reported an acute reaction, and 10%-22% (depending on the study site) reported grade 3 symptoms. The most bothersome – and unexpected – reactions involved viral seeding of joints and skin.
The joint problems manifested as arthritis, tenosynovitis, or bursitis that appeared at a median of 11 days after injection. The arthritis tended to affect one to four peripheral joints asymmetrically; pain was usually mild and dysfunction was usually moderate. Ten of the 11 affected patients in Geneva and both of the two (out of 60) affected patients at the other sites were symptom-free by 6 months. These findings “suggest a favorable long-term prognosis for these vaccine-induced arthritides,” Dr. Agnandji and his associates said.
Three participants developed maculopapular rashes mainly affecting the limbs, which appeared at 7-9 days following injection and persisted for 1-2 weeks. The rash was accompanied by a few tender vesicles on fingers or toes. Synovial fluid extracted from affected joints and material recovered from skin vesicles showed the presence of rVSV.
Given that most adverse reactions occurred soon after vaccination, were of short duration, and were amenable to treatment, this vaccine demonstrated “a favorable risk-benefit balance,” they added.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Two Ebola vaccines were found effective and safe in separate international phase I trials.
Major finding: The ChAd3 vaccine boosted with MVA elicited B-cell and T-cell immune responses to ZEBOV that were superior to those induced by the ChAd3 vaccine alone. The rVSV-ZEBOV vaccine was reactogenic but immunogenic after a single dose.
Data source: A single dose of the chimpanzee adenovirus 3 (ChAd3) vaccine encoding the surface glycoprotein of Zaire ebolavirus (ZEBOV) was given to 60 healthy adult volunteers in Oxford, England. Three open-label, dose-escalation phase I trials and one randomized, double-blind, controlled phase I trial to assess the safety, side-effect profile, and immunogenicity of rVSV-ZEBOV at various doses in 158 healthy adults in Europe and Africa.
Disclosures: Dr. Ewer’s study was supported by the Wellcome Trust, the U. K. Medical Research Council, the U. K. Department for International Development, the U. K. National Institute for Health Research Oxford Biomedical Research Centre, the National Health Service Blood and Transplant, and Public Health England. The ChAd3 vaccine was provided by the U.S. Vaccine Research Center of the National Institute of Allergy and Infectious Diseases and GlaxoSmithKline, and the MVA vaccine booster was provided by the NIAID and Fisher BioServices. Dr. Ewer reported having no relevant financial disclosures; some of her associates reported ties to GlaxoSmithKline and patents pending related to these and other vaccines. Dr. Agnandji’s study was supported by the Wellcome Trust, the German Center for Infection Research, the German National Department for Education and Research, the German Ministry of Health, the Bill and Melinda Gates Foundation, Universitätsklinikum Tübingen, the Austrian Federal Ministry of Science, Research, and Economy, and the U.S. Army Medical Research Institute of Infectious Diseases. The rVSV-ZEBOV vaccine used in this study was donated by the Public Health Agency of Canada and the World Health Organization. Dr. Agnandji reported having no relevant financial disclosures; his associates reported ties to Gilead, GlaxoSmithKline, Merck Sharp & Dohme, Sanaria, and Bristol-Myers Squibb.

FDA okays glycopyrrolate/formoterol combo for COPD
The Food and Drug Administration has approved glycopyrrolate and formoterol fumarate inhalation aerosol for long-term maintenance treatment of airflow obstruction in patients with chronic obstructive pulmonary disease (COPD), according to a statement from AstraZeneca.
AstraZeneca is marketing the bronchodilator as Bevespi Aerosphere. The product is a fixed-dose dual bronchodilator delivered through a pressurized, metered-dose inhaler to be used twice daily. Glycopyrrolate, a long-acting muscarinic antagonist, is available as monotherapy. The FDA also has granted the long-acting beta-2 agonist formoterol fumarate tentative approval for use as monotherapy.
The approval of glycopyrrolate/formoterol fumarate 9 mcg/4.8 mcg is based on the PINNACLE trials, which demonstrated the product achieved improvement in morning predose forced expiratory volume in 1 second at 24 weeks (P less than .001), compared with its monotherapy components and placebo, according to AstraZeneca’s statement.
The most common adverse reactions were urinary tract infection and cough. The drug is not indicated for the treatment of asthma or for the relief of acute bronchospasm.
The Food and Drug Administration has approved glycopyrrolate and formoterol fumarate inhalation aerosol for long-term maintenance treatment of airflow obstruction in patients with chronic obstructive pulmonary disease (COPD), according to a statement from AstraZeneca.
AstraZeneca is marketing the bronchodilator as Bevespi Aerosphere. The product is a fixed-dose dual bronchodilator delivered through a pressurized, metered-dose inhaler to be used twice daily. Glycopyrrolate, a long-acting muscarinic antagonist, is available as monotherapy. The FDA also has granted the long-acting beta-2 agonist formoterol fumarate tentative approval for use as monotherapy.
The approval of glycopyrrolate/formoterol fumarate 9 mcg/4.8 mcg is based on the PINNACLE trials, which demonstrated the product achieved improvement in morning predose forced expiratory volume in 1 second at 24 weeks (P less than .001), compared with its monotherapy components and placebo, according to AstraZeneca’s statement.
The most common adverse reactions were urinary tract infection and cough. The drug is not indicated for the treatment of asthma or for the relief of acute bronchospasm.
The Food and Drug Administration has approved glycopyrrolate and formoterol fumarate inhalation aerosol for long-term maintenance treatment of airflow obstruction in patients with chronic obstructive pulmonary disease (COPD), according to a statement from AstraZeneca.
AstraZeneca is marketing the bronchodilator as Bevespi Aerosphere. The product is a fixed-dose dual bronchodilator delivered through a pressurized, metered-dose inhaler to be used twice daily. Glycopyrrolate, a long-acting muscarinic antagonist, is available as monotherapy. The FDA also has granted the long-acting beta-2 agonist formoterol fumarate tentative approval for use as monotherapy.
The approval of glycopyrrolate/formoterol fumarate 9 mcg/4.8 mcg is based on the PINNACLE trials, which demonstrated the product achieved improvement in morning predose forced expiratory volume in 1 second at 24 weeks (P less than .001), compared with its monotherapy components and placebo, according to AstraZeneca’s statement.
The most common adverse reactions were urinary tract infection and cough. The drug is not indicated for the treatment of asthma or for the relief of acute bronchospasm.
Macrolide adds no benefit to pneumonia treatment in HIV patients
AMSTERDAM – Adding a macrolide to beta-lactam antibiotic treatment didn’t improve outcomes in HIV-infected patients with community-acquired bacterial pneumonia, according to the results of a Brazilian study.
Dr. Claudia Figueiredo Mello of the Instituto de Infectologia Emílio Ribas, São Paolo, said her study found no difference in in-hospital mortality between treatment with a beta-lactam alone, and treatment with the combination of a beta-lactam and a macrolide. Indeed, length of hospital stay was exactly the same. Dr. Mello reported the study results at the European Society of Clinical Microbiology and Infectious Diseases annual congress.
The study involved 228 patients with longstanding HIV infections and community-acquired bacterial pneumonia who were randomized to two treatment regimens. Protocol 1 was the standard treatment of 1 g ceftriaxone intravenously every 12 hours plus placebo for a minimum of 7 days. Protocol 2 was the same ceftriaxone treatment with the addition of azithromycin 500 mg/day or clarithromycin 500 mg every 12 hours.
Patients were a mean of 40 years old, with a median HIV duration of 12 years. Only about 20% were on regular highly active antiretroviral therapy (HAART); this was reflected in the low proportion of patients with a viral load of less than 50 copies/mL (about 16%), Dr. Mello said.
The median CD4 T-cell count varied widely in patients, but in half it was below 50 cells/mm3. Comorbidities were common in the cohort (30%); the most common were hypertension (12%) and liver disease (10%). Many patients used tobacco (41%), and illicit drug use was also common (about a third).
Most patients (60%) were risk class I-III on the Pneumonia Severity Index. Risk class III occurred in 20%, and the remainder were risk class IV and V.
In the intention-to-treat analysis, in-hospital mortality was 11% in the beta-lactam–only group and 15% in the combination therapy group – not a significant difference. The time to reach clinical stability was 5 days in each group, and the hospital length of stay, 14 days in each group.
Dr. Mello said she and her colleagues would continue to examine the data to determine if a specific subgroup might benefit from combination therapy, as extant data do suggest that adding a macrolide to beta-lactam treatment improves outcomes in a general population. She could not speculate as to why combination therapy didn’t appear to confer additional benefit on this cohort of patients living with HIV.
She had no financial disclosures.
AMSTERDAM – Adding a macrolide to beta-lactam antibiotic treatment didn’t improve outcomes in HIV-infected patients with community-acquired bacterial pneumonia, according to the results of a Brazilian study.
Dr. Claudia Figueiredo Mello of the Instituto de Infectologia Emílio Ribas, São Paolo, said her study found no difference in in-hospital mortality between treatment with a beta-lactam alone, and treatment with the combination of a beta-lactam and a macrolide. Indeed, length of hospital stay was exactly the same. Dr. Mello reported the study results at the European Society of Clinical Microbiology and Infectious Diseases annual congress.
The study involved 228 patients with longstanding HIV infections and community-acquired bacterial pneumonia who were randomized to two treatment regimens. Protocol 1 was the standard treatment of 1 g ceftriaxone intravenously every 12 hours plus placebo for a minimum of 7 days. Protocol 2 was the same ceftriaxone treatment with the addition of azithromycin 500 mg/day or clarithromycin 500 mg every 12 hours.
Patients were a mean of 40 years old, with a median HIV duration of 12 years. Only about 20% were on regular highly active antiretroviral therapy (HAART); this was reflected in the low proportion of patients with a viral load of less than 50 copies/mL (about 16%), Dr. Mello said.
The median CD4 T-cell count varied widely in patients, but in half it was below 50 cells/mm3. Comorbidities were common in the cohort (30%); the most common were hypertension (12%) and liver disease (10%). Many patients used tobacco (41%), and illicit drug use was also common (about a third).
Most patients (60%) were risk class I-III on the Pneumonia Severity Index. Risk class III occurred in 20%, and the remainder were risk class IV and V.
In the intention-to-treat analysis, in-hospital mortality was 11% in the beta-lactam–only group and 15% in the combination therapy group – not a significant difference. The time to reach clinical stability was 5 days in each group, and the hospital length of stay, 14 days in each group.
Dr. Mello said she and her colleagues would continue to examine the data to determine if a specific subgroup might benefit from combination therapy, as extant data do suggest that adding a macrolide to beta-lactam treatment improves outcomes in a general population. She could not speculate as to why combination therapy didn’t appear to confer additional benefit on this cohort of patients living with HIV.
She had no financial disclosures.
AMSTERDAM – Adding a macrolide to beta-lactam antibiotic treatment didn’t improve outcomes in HIV-infected patients with community-acquired bacterial pneumonia, according to the results of a Brazilian study.
Dr. Claudia Figueiredo Mello of the Instituto de Infectologia Emílio Ribas, São Paolo, said her study found no difference in in-hospital mortality between treatment with a beta-lactam alone, and treatment with the combination of a beta-lactam and a macrolide. Indeed, length of hospital stay was exactly the same. Dr. Mello reported the study results at the European Society of Clinical Microbiology and Infectious Diseases annual congress.
The study involved 228 patients with longstanding HIV infections and community-acquired bacterial pneumonia who were randomized to two treatment regimens. Protocol 1 was the standard treatment of 1 g ceftriaxone intravenously every 12 hours plus placebo for a minimum of 7 days. Protocol 2 was the same ceftriaxone treatment with the addition of azithromycin 500 mg/day or clarithromycin 500 mg every 12 hours.
Patients were a mean of 40 years old, with a median HIV duration of 12 years. Only about 20% were on regular highly active antiretroviral therapy (HAART); this was reflected in the low proportion of patients with a viral load of less than 50 copies/mL (about 16%), Dr. Mello said.
The median CD4 T-cell count varied widely in patients, but in half it was below 50 cells/mm3. Comorbidities were common in the cohort (30%); the most common were hypertension (12%) and liver disease (10%). Many patients used tobacco (41%), and illicit drug use was also common (about a third).
Most patients (60%) were risk class I-III on the Pneumonia Severity Index. Risk class III occurred in 20%, and the remainder were risk class IV and V.
In the intention-to-treat analysis, in-hospital mortality was 11% in the beta-lactam–only group and 15% in the combination therapy group – not a significant difference. The time to reach clinical stability was 5 days in each group, and the hospital length of stay, 14 days in each group.
Dr. Mello said she and her colleagues would continue to examine the data to determine if a specific subgroup might benefit from combination therapy, as extant data do suggest that adding a macrolide to beta-lactam treatment improves outcomes in a general population. She could not speculate as to why combination therapy didn’t appear to confer additional benefit on this cohort of patients living with HIV.
She had no financial disclosures.
AT ECCMID 2016
Key clinical point: Adding a macrolide to beta-lactam antibiotic treatment didn’t improve outcomes in HIV-positive patients with community-acquired pneumonia.
Major finding: In-hospital mortality was 11% in the combination group and 15% in the beta-lactam–only group.
Data source: A randomized, controlled trial comprising 228 patients.
Disclosures: Dr. Mello had no financial obligations.
Sublingual immunotherapy for allergy-related asthma
Immunotherapy using sublingual tablets containing house dust mite allergen extended the interval until patients developed a moderate asthma exacerbation in a manufacturer-sponsored clinical trial reported online April 26 in JAMA.
However, patients’ scores on both the Asthma Control Questionnaire and the Asthma Quality of Life Questionnaire showed no difference between active treatment and placebo. And 25%-27% of the study participants dropped out of the study, usually citing asthma exacerbations, adverse events, or “withdrawal of consent.” Further studies are needed to assess long-term efficacy and safety, said Dr. J. Christian Virchow of the department of pulmonology/intensive care medicine, University of Rostock (Germany), and his associates.

The trial, involving 834 adults with asthma related to house dust mite allergy that was not well controlled by inhaled corticosteroids and short-acting beta-agonists, was performed at 109 sites in 13 European countries during a 2-year period. These participants were randomly assigned to receive add-on daily sublingual tablets containing low-dose dust-mite extract (275 patients), high-dose extract (282 patients), or placebo (277 patients) for 7-12 months. During the final 6 months of the intervention, corticosteroids were reduced by half for 3 months and then withdrawn for 3 months.
The primary efficacy outcome (time to the first asthma exacerbation) was extended by both doses of active drug, compared with placebo, with hazard ratios of 0.69 for the lower dose and 0.66 for the higher dose, the investigators said (JAMA. 2016 Apr 26;315[16]:1715-25).
Adverse events were significantly more frequent with active treatment, affecting 39% of patients receiving the lower dose and 46% of those receiving the higher dose of active immunotherapy, compared with only 17% of patients receiving placebo. However, this study was not adequately powered to compare adverse events across groups, Dr. Virchow and his associates noted.
The most frequently reported adverse events were oral pruritus, mouth edema, and throat irritation, which developed within a median of 1-2 minutes of taking the first dose on day 1 and persisted for a median of 4-23 days. There were 32 serious adverse events, including erosive esophagitis, hepatocellular injury, arthralgia, laryngeal edema, and asthma.
This trial was limited in that treatment duration was much shorter than that for a standard course of immunotherapy, which is often 3 years. This prevents drawing conclusions regarding the sustained effect of the treatment. “Furthermore, because the ultimate aim of allergen immunotherapy is disease modification beyond the duration of treatment, a follow-up after the end of treatment would have been relevant,” the investigators said.
This study was sponsored by the Danish pharmaceutical company ALK. Dr. Virchow reported ties to 31 industry sources; his associates also reported ties to numerous industry sources.
Sublingual immunotherapy appears to be somewhat less effective than subcutaneous immunotherapy, but it offers several advantages. It doesn’t require injections, can be self-administered, doesn’t require dose escalations, and carries a much lower risk of anaphylaxis. However, in this study there were no significant differences in patients’ responses to questionnaires regarding either asthma control or quality of life.
The main disadvantage is that sublingual immunotherapy requires adherence to daily dosing, and research has consistently shown low rates of long-term adherence. In one study, 55%-82% of patients failed to complete the recommended course of sublingual immunotherapy. In another, only 44% of patients renewed their prescriptions after 1 year of treatment, only 28% did so after 2 years, and only 13% did so after 3 years.
Dr. Robert A. Wood is in the division of allergy and immunology, department of pediatrics, at Johns Hopkins University, Baltimore. He reported ties to DBV Technologies, the Immune Tolerance Network, Stallergenes, Sanofi, and UpToDate. Dr. Wood made these remarks in an editorial accompanying Dr. Virchow’s report (JAMA. 2016 Apr 26;315:1711-2).
Sublingual immunotherapy appears to be somewhat less effective than subcutaneous immunotherapy, but it offers several advantages. It doesn’t require injections, can be self-administered, doesn’t require dose escalations, and carries a much lower risk of anaphylaxis. However, in this study there were no significant differences in patients’ responses to questionnaires regarding either asthma control or quality of life.
The main disadvantage is that sublingual immunotherapy requires adherence to daily dosing, and research has consistently shown low rates of long-term adherence. In one study, 55%-82% of patients failed to complete the recommended course of sublingual immunotherapy. In another, only 44% of patients renewed their prescriptions after 1 year of treatment, only 28% did so after 2 years, and only 13% did so after 3 years.
Dr. Robert A. Wood is in the division of allergy and immunology, department of pediatrics, at Johns Hopkins University, Baltimore. He reported ties to DBV Technologies, the Immune Tolerance Network, Stallergenes, Sanofi, and UpToDate. Dr. Wood made these remarks in an editorial accompanying Dr. Virchow’s report (JAMA. 2016 Apr 26;315:1711-2).
Sublingual immunotherapy appears to be somewhat less effective than subcutaneous immunotherapy, but it offers several advantages. It doesn’t require injections, can be self-administered, doesn’t require dose escalations, and carries a much lower risk of anaphylaxis. However, in this study there were no significant differences in patients’ responses to questionnaires regarding either asthma control or quality of life.
The main disadvantage is that sublingual immunotherapy requires adherence to daily dosing, and research has consistently shown low rates of long-term adherence. In one study, 55%-82% of patients failed to complete the recommended course of sublingual immunotherapy. In another, only 44% of patients renewed their prescriptions after 1 year of treatment, only 28% did so after 2 years, and only 13% did so after 3 years.
Dr. Robert A. Wood is in the division of allergy and immunology, department of pediatrics, at Johns Hopkins University, Baltimore. He reported ties to DBV Technologies, the Immune Tolerance Network, Stallergenes, Sanofi, and UpToDate. Dr. Wood made these remarks in an editorial accompanying Dr. Virchow’s report (JAMA. 2016 Apr 26;315:1711-2).
Immunotherapy using sublingual tablets containing house dust mite allergen extended the interval until patients developed a moderate asthma exacerbation in a manufacturer-sponsored clinical trial reported online April 26 in JAMA.
However, patients’ scores on both the Asthma Control Questionnaire and the Asthma Quality of Life Questionnaire showed no difference between active treatment and placebo. And 25%-27% of the study participants dropped out of the study, usually citing asthma exacerbations, adverse events, or “withdrawal of consent.” Further studies are needed to assess long-term efficacy and safety, said Dr. J. Christian Virchow of the department of pulmonology/intensive care medicine, University of Rostock (Germany), and his associates.
The trial, involving 834 adults with asthma related to house dust mite allergy that was not well controlled by inhaled corticosteroids and short-acting beta-agonists, was performed at 109 sites in 13 European countries during a 2-year period. These participants were randomly assigned to receive add-on daily sublingual tablets containing low-dose dust-mite extract (275 patients), high-dose extract (282 patients), or placebo (277 patients) for 7-12 months. During the final 6 months of the intervention, corticosteroids were reduced by half for 3 months and then withdrawn for 3 months.
The primary efficacy outcome (time to the first asthma exacerbation) was extended by both doses of active drug, compared with placebo, with hazard ratios of 0.69 for the lower dose and 0.66 for the higher dose, the investigators said (JAMA. 2016 Apr 26;315[16]:1715-25).
Adverse events were significantly more frequent with active treatment, affecting 39% of patients receiving the lower dose and 46% of those receiving the higher dose of active immunotherapy, compared with only 17% of patients receiving placebo. However, this study was not adequately powered to compare adverse events across groups, Dr. Virchow and his associates noted.
The most frequently reported adverse events were oral pruritus, mouth edema, and throat irritation, which developed within a median of 1-2 minutes of taking the first dose on day 1 and persisted for a median of 4-23 days. There were 32 serious adverse events, including erosive esophagitis, hepatocellular injury, arthralgia, laryngeal edema, and asthma.
This trial was limited in that treatment duration was much shorter than that for a standard course of immunotherapy, which is often 3 years. This prevents drawing conclusions regarding the sustained effect of the treatment. “Furthermore, because the ultimate aim of allergen immunotherapy is disease modification beyond the duration of treatment, a follow-up after the end of treatment would have been relevant,” the investigators said.
This study was sponsored by the Danish pharmaceutical company ALK. Dr. Virchow reported ties to 31 industry sources; his associates also reported ties to numerous industry sources.
Immunotherapy using sublingual tablets containing house dust mite allergen extended the interval until patients developed a moderate asthma exacerbation in a manufacturer-sponsored clinical trial reported online April 26 in JAMA.
However, patients’ scores on both the Asthma Control Questionnaire and the Asthma Quality of Life Questionnaire showed no difference between active treatment and placebo. And 25%-27% of the study participants dropped out of the study, usually citing asthma exacerbations, adverse events, or “withdrawal of consent.” Further studies are needed to assess long-term efficacy and safety, said Dr. J. Christian Virchow of the department of pulmonology/intensive care medicine, University of Rostock (Germany), and his associates.
The trial, involving 834 adults with asthma related to house dust mite allergy that was not well controlled by inhaled corticosteroids and short-acting beta-agonists, was performed at 109 sites in 13 European countries during a 2-year period. These participants were randomly assigned to receive add-on daily sublingual tablets containing low-dose dust-mite extract (275 patients), high-dose extract (282 patients), or placebo (277 patients) for 7-12 months. During the final 6 months of the intervention, corticosteroids were reduced by half for 3 months and then withdrawn for 3 months.
The primary efficacy outcome (time to the first asthma exacerbation) was extended by both doses of active drug, compared with placebo, with hazard ratios of 0.69 for the lower dose and 0.66 for the higher dose, the investigators said (JAMA. 2016 Apr 26;315[16]:1715-25).
Adverse events were significantly more frequent with active treatment, affecting 39% of patients receiving the lower dose and 46% of those receiving the higher dose of active immunotherapy, compared with only 17% of patients receiving placebo. However, this study was not adequately powered to compare adverse events across groups, Dr. Virchow and his associates noted.
The most frequently reported adverse events were oral pruritus, mouth edema, and throat irritation, which developed within a median of 1-2 minutes of taking the first dose on day 1 and persisted for a median of 4-23 days. There were 32 serious adverse events, including erosive esophagitis, hepatocellular injury, arthralgia, laryngeal edema, and asthma.
This trial was limited in that treatment duration was much shorter than that for a standard course of immunotherapy, which is often 3 years. This prevents drawing conclusions regarding the sustained effect of the treatment. “Furthermore, because the ultimate aim of allergen immunotherapy is disease modification beyond the duration of treatment, a follow-up after the end of treatment would have been relevant,” the investigators said.
This study was sponsored by the Danish pharmaceutical company ALK. Dr. Virchow reported ties to 31 industry sources; his associates also reported ties to numerous industry sources.
FROM JAMA
Key clinical point: Sublingual tablets containing house dust mite allergen immunotherapy extended the interval until a moderate or severe asthma exacerbation.
Major finding: The primary efficacy outcome (time to the first asthma exacerbation) was extended by both doses of active drug, compared with placebo, with hazard ratios of 0.69 for the lower dose and 0.66 for the higher dose.
Data source: An industry-sponsored international randomized placebo-controlled trial involving 834 patients.
Disclosures: This study was sponsored by the Danish pharmaceutical company ALK. Dr. Virchow reported ties to 31 industry sources; his associates also reported ties to numerous industry sources.

Atopic dermatitis early in childhood tied to increased risk of autism, ADHD
Children who are diagnosed with atopic dermatitis before the age of 2 are more likely to be diagnosed with autism spectrum disorder or attention-deficit/hyperactivity disorder, according to Tzu-Chu Liao and associates.
Of the 387,262 children diagnosed with atopic dermatitis (AD) before the age of 2 included in the study, 0.5% were diagnosed with autism spectrum disorder (ASD), and 3.7% were diagnosed with attention-deficit/hyperactivity disorder (ADHD). In the control group, 0.4% were diagnosed with ASD, and 2.9% were diagnosed with ADHD. The hazard ratios for children exposed to atopic disorders before the age of 2 were 1.1 for ASD and 1.16 for ADHD.
Among children diagnosed early with AD, being male was the most significant risk factor for developing ASD (HR, 4.92) or ADHD (HR, 3.28). An urban/suburban residence was also a significant risk factor, as was persistent AD and emerging atopic respiratory disease in childhood.
“These findings suggest a possible etiologic communality between the diagnosis of allergic disorders along with comorbid ASD or ADHD. The atopic diathesis approach might influence the attention of child psychiatrists and pediatricians toward the diagnosis of ASD and ADHD. Further attention should be given to the management of allergic manifestations when treating symptoms of ASD and ADHD,” the investigators concluded.
Find the study in the Journal of Pediatrics (doi: 10.1016/j.jpeds.2015.12.063).
Children who are diagnosed with atopic dermatitis before the age of 2 are more likely to be diagnosed with autism spectrum disorder or attention-deficit/hyperactivity disorder, according to Tzu-Chu Liao and associates.
Of the 387,262 children diagnosed with atopic dermatitis (AD) before the age of 2 included in the study, 0.5% were diagnosed with autism spectrum disorder (ASD), and 3.7% were diagnosed with attention-deficit/hyperactivity disorder (ADHD). In the control group, 0.4% were diagnosed with ASD, and 2.9% were diagnosed with ADHD. The hazard ratios for children exposed to atopic disorders before the age of 2 were 1.1 for ASD and 1.16 for ADHD.
Among children diagnosed early with AD, being male was the most significant risk factor for developing ASD (HR, 4.92) or ADHD (HR, 3.28). An urban/suburban residence was also a significant risk factor, as was persistent AD and emerging atopic respiratory disease in childhood.
“These findings suggest a possible etiologic communality between the diagnosis of allergic disorders along with comorbid ASD or ADHD. The atopic diathesis approach might influence the attention of child psychiatrists and pediatricians toward the diagnosis of ASD and ADHD. Further attention should be given to the management of allergic manifestations when treating symptoms of ASD and ADHD,” the investigators concluded.
Find the study in the Journal of Pediatrics (doi: 10.1016/j.jpeds.2015.12.063).
Children who are diagnosed with atopic dermatitis before the age of 2 are more likely to be diagnosed with autism spectrum disorder or attention-deficit/hyperactivity disorder, according to Tzu-Chu Liao and associates.
Of the 387,262 children diagnosed with atopic dermatitis (AD) before the age of 2 included in the study, 0.5% were diagnosed with autism spectrum disorder (ASD), and 3.7% were diagnosed with attention-deficit/hyperactivity disorder (ADHD). In the control group, 0.4% were diagnosed with ASD, and 2.9% were diagnosed with ADHD. The hazard ratios for children exposed to atopic disorders before the age of 2 were 1.1 for ASD and 1.16 for ADHD.
Among children diagnosed early with AD, being male was the most significant risk factor for developing ASD (HR, 4.92) or ADHD (HR, 3.28). An urban/suburban residence was also a significant risk factor, as was persistent AD and emerging atopic respiratory disease in childhood.
“These findings suggest a possible etiologic communality between the diagnosis of allergic disorders along with comorbid ASD or ADHD. The atopic diathesis approach might influence the attention of child psychiatrists and pediatricians toward the diagnosis of ASD and ADHD. Further attention should be given to the management of allergic manifestations when treating symptoms of ASD and ADHD,” the investigators concluded.
Find the study in the Journal of Pediatrics (doi: 10.1016/j.jpeds.2015.12.063).
FROM THE JOURNAL OF PEDIATRICS
Improving your care of patients with spinal cord injury/disease
› Have a high index of suspicion for the leading causes of hospitalization among patients with spinal cord injury and disease (SCI/D). These include respiratory infections, urinary tract infections, and pressure ulcers. A
› Treat respiratory infections early and aggressively in patients with SCI/D; strongly consider inpatient management because of the high risk of respiratory failure. C
› Be alert to atypical signs and symptoms of urinary tract infection in patients with SCI/D, such as fever, chills, spasm, autonomic dysfunction, nausea and vomiting, abdominal discomfort, and fatigue. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
More than 5 million Americans are living with paralysis, and for nearly one in 4 of them the cause is spinal cord injury or disease (SCI/D).1 More common than multiple sclerosis (17%) as a cause for the loss of movement, SCI/D is second only to stroke (29%).1
The percentage of people living with paralysis due to SCI/D is increasing, partly because the population is aging and partly because management of infections has improved. Prior to the 1970s, life expectancy for people with SCI/D was significantly shortened, largely because of urologic and respiratory infections. But improved bladder management, in particular, has increased life expectancy—especially for the least severely injured.2 Respiratory diseases and septicemia remain the leading causes of death, but with increased longevity, other causes, such as endocrine, metabolic and nutritional diseases, accidents, nervous system diseases, and musculoskeletal disorders, are becoming increasingly common.2,3
Primary care’s pivotal role. Given the size of the population affected by SCI/D and the increase in life expectancy, family physicians (FPs) are more likely than ever before to care for these patients, most of whom have highly specific needs. However, little information about the primary care of patients with SCI/D exists. This patient population tends to consume a relatively large share of practices’ resources because of high case complexity.4
A recent Canadian report confirms our clinical experience that FPs report knowledge gaps in the area of SCI/D care, yet the same report found that 90% of people with SCI/D identify FPs as their “regular doctors.”5 Although a large number of patients with SCI/D identify their physiatrist as their primary care physician (PCP), one study reported that fewer than half of physiatrists are willing to assume that role.6 And while more than half of all patients with SCI/D have both specialists and PCPs involved in their care,5 communication breakdowns are a concern for patients receiving medical and rehabilitative direction from multiple health care professionals.
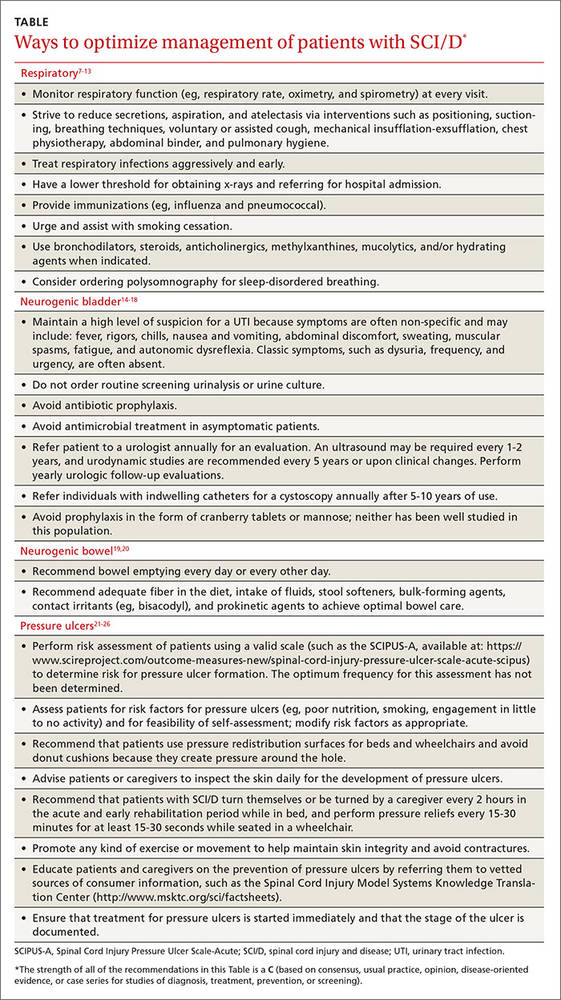
Below we take a closer look at the distinct patient populations affected by SCI/D, summarize several clinical conditions that contribute to hospitalization, and provide clinical management recommendations (TABLE7-26).
2 patient populations, one diagnosis
Paralysis due to spinal trauma occurs predominantly in non-Hispanic white and black males because of vehicular accidents, falls, violence, and sports.2 The mean age of injury has increased from 29 years during the 1970s to 42 years since 2010.2 However, this calculated average is misleading because there is an emerging bimodal distribution of people injured during early adulthood and a new increase in older adults injured primarily because of falls.27 In addition to those injured traumatically, a broader cohort of approximately 1 million patients represents a largely undefined group of people with paralysis due to diseases such as spinal stenosis, cancer, infection, multiple sclerosis, or other non-traumatic causes.
As a result, the population with SCI/D is comprised primarily of young adult males who have relatively few chronic medical conditions at the time of their injury and age with SCI/D, and older patients who are more likely to have already developed chronic medical conditions by the time of their SCI/D. Approximately 60% of SCI/Ds result in tetraplegia (ie, 4 limbs affected), although approximately two-thirds are incomplete, meaning that patients have some residual motor or sensory function below the level of injury.2 Not surprisingly, the level and severity of SCI/D impact life expectancy inversely and lifetime financial costs directly.
High health care utilization. Morbidity data largely parallel mortality data, often resulting in high health care utilization and cost among SCI/D patients.28 In a recent prospective observational study of nearly 1000 people with new traumatic SCI, 36.2% were rehospitalized at least once and 12.5% were rehospitalized at least twice during the 12-month period after discharge following injury.29
Rehospitalization, an outcome often quoted as a proxy for inadequate primary care, remains unacceptably high (36%-50%) for people with SCI/D.29,30 The leading causes of rehospitalization—pneumonia, urinary tract infection (UTI), and pressure ulcers29—have not changed over the years and persist over the lifetime of individuals with SCI/D.30
Take steps to prevent pneumonia, other respiratory complications
Many people with SCI/D are at high risk for respiratory complications because of their weakened respiratory muscles. This is particularly true for individuals who have injuries occurring above T10; those with injuries that are high on the spinal cord have the highest complication risk.7,8 In fact, pneumonia, atelectasis, and other respiratory complications are the leading causes of mortality in patients with tetraplegia, occurring in 40% to 70% of these patients.7
The diaphragm, innervated by the phrenic nerve (C3-C5), is the primary muscle of inspiration. Accessory muscles of inspiration include the scalenes (C5-C8), sternocleidomastoid and trapezius (C1-C4), and intercostals (T1-T11); whereas forced exhalation (cough) occurs with contraction of the abdominals (T5-T12).9 Diminished inspiration in individuals with higher level lesions can lead to microatelectasis, dyspnea with exertion, and even respiratory insufficiency.
In SCI/D above T8, weakened expiration can severely decrease cough effectiveness and secretion clearance, increasing susceptibility to lower respiratory tract infections. In addition, experts have described asthma-like disorders of airway function, particularly in those with higher lesions, due to unopposed parasympathetic innervation of respiratory smooth muscle.10
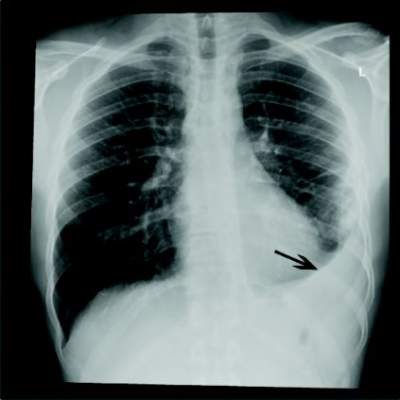
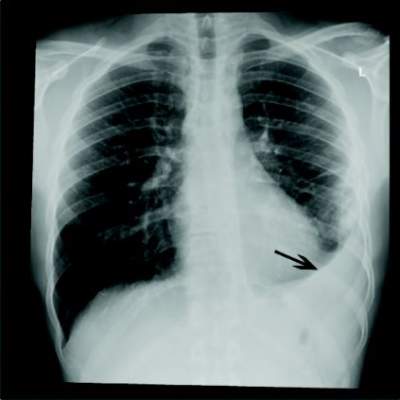
Management of this neurogenic pulmonary dysfunction after SCI/D relies on extensive preventive measures, including positioning and postural changes, breathing techniques, coughing (assisted for patients with tetraplegia), postural drainage, chest compression and percussion, and suctioning to avoid atelectasis, aspiration, and pneumonia. Ensure that patients receive influenza and pneumococcal vaccinations, and encourage smoking cessation. Obtain a chest x-ray if the patient demonstrates a decrease in respiratory function, deteriorating vital signs, reduced vital capacity, an increase in subjective dyspnea, or a change in sputum quantity. Treat respiratory infections early and aggressively,7-10 and strongly consider inpatient management because of the high risk of respiratory failure.
Pneumococcus is the most common cause of respiratory infections, although up to 21% of cases of community-acquired pneumonia in patients with SCI/D are caused by Pseudomonas.11-13 Avoid the use of antibiotics in patients who do not have signs or symptoms of a respiratory infection to minimize the development of resistant organisms. Target antibiotic therapy as per general population guidelines, as guidelines validated for use in the population with SCI/D do not currently exist.7,11
Be alert for UTIs—typical signs, symptoms don’t apply
The bladder receives innervation from S2 to S4 via the hypogastric, pudendal, and pelvic nerves. As such, the vast majority—70% to 84%—of patients with SCI/D report some degree of bladder dysfunction.14 Generally, SCI/D contributes to a combination of a failure to empty the bladder and a failure to store urine. The former is more frequent and the latter occurs more often in people with bladder outlet flaccidity, which usually occurs with low injury, such as that of the lumbar spine.14
The majority of people with SCI/D who are unable to empty their bladder require the use of some type of bladder catheter, either intermittent, indwelling (urethral or suprapubic), or condom. The choice of bladder management technique depends on gender, hand function, body habitus, caregiver assistance, and medical comorbidities. People with SCI/D are at greater risk for bladder and renal stones, UTI, vesicoureteral reflux, and bladder cancer.15,16 That said, the risk of bladder and renal stones declines somewhat after the first 6 months following an injury due to an immobility-induced loss of calcium.
Patients with SCI/D are often found to have bacteruria and even pyuria, and although they are at high risk for recurrent UTIs, these can be difficult to diagnose because signs and symptoms may differ from those seen in people with neurologically intact bladders. Symptomatic UTIs may present with fever, hematuria, abdominal discomfort, and/or increased spasticity, among other symptoms. They may cause increased bouts of autonomic dysreflexia, malaise, or a change in functional status. One cannot rely on the typical symptoms of dysuria and increased urinary frequency in this patient population. Further, the Infectious Diseases Society of America (IDSA) states that cloudy or foul-smelling urine in adults with catheters is not a symptom or sign mandating treatment.17
Because there is a lack of consensus as to what constitutes UTI symptoms in patients with SCI/D, PCPs need to be aware of changes from baseline in patients; these, combined with urine dip and culture results, should guide initiation of treatment.16
Prophylactic antibiotics have no role in the prevention of UTIs in patients with SCI/D. The minimal benefits associated with prophylaxis are outweighed by the risks of increased bacterial resistance to antibiotics. Research shows no significant benefit associated with the use of non-antibiotic prophylaxis, including the use of cranberry products and mannose, but further studies are needed in this patient population.18
Focus on bowel function; it correlates with quality of life
Bowel dysfunction is nearly universal in patients with SCI/D. The enteric nervous system is modulated via the sympathetic, parasympathetic, and somatic systems, and intrinsic control occurs via the myenteric and submucosal plexi. The loss of volitional control of defecation can result in prolonged transit time, reduced colonic motility, fecal incontinence, and difficulty with evacuation.
Because bowel care and function are highly correlated with quality of life,19 recommend bowel emptying every day or every other day, as well as adequate fiber in the diet, intake of fluids, stool softeners, bulk forming agents, contact irritants (eg, bisacodyl), and prokinetic agents to achieve optimal bowel care.
Prevent and treat pressure ulcers whenever possible
Accompanying the paralysis associated with SCI/D is often some degree of sensory loss of pain, light touch, temperature, and/or proprioception. The combination of insensate skin, immobility, and sarcopenia with resultant body composition changes places individuals with SCI/D at high risk for skin breakdown.21,22 Blood flow and oxygen tension at the skin surface are also decreased in patients with SCI/D compared to those without, further contributing to the problem.21,23 Increased latency from the time of injury correlates with increased likelihood of pressure ulcer development.21,22,24
External risk factors for pressure ulcers include prolonged pressure exposure, or intense pressure over a short period, shear forces, poor nutrition, smoking, moisture, and immobility. The incidence of pressure ulcers in patients with SCI/D is 25% to 66%, compared with 0.38% in the general population.21,22 Research indicates that US hospitals spend $11 billion annually on the treatment of the condition.22
To minimize pressure ulcers in this population, perform a risk assessment, using, for example, the Spinal Cord Injury Pressure Ulcer Scale-Acute (SCIPUS-A) available at https://www.scireproject.com/outcome-measures-new/spinal-cord-injury-pressure-ulcer-scale-acute-scipus. In addition, recommend that patients use pressure redistribution surfaces for beds and wheelchairs, turn while in bed, perform frequent (approximately every 15-30 minutes) pressure reliefs, exercise or move regularly, and that they or a caregiver inspect the skin daily. If pressure ulcers do occur, start treatment immediately and document the stage of the ulcer.
Ensure that screening efforts go beyond what’s standard
Preventive care for patients with SCI/D is similar in many ways to that recommended for the general population. Screening for colorectal cancer,31 cervical cancer, and breast cancer32 should follow the same evidence-based intervals and age ranges suggested by groups such as the US Preventive Services Task Force (USPSTF). The only difference is to give special consideration to patients’ physical limitations and the set-up of exam rooms when scheduling and conducting procedures, such as Pap smears, colonoscopies, and mammograms.33,34
Bladder cancer. Because of the high risk for bladder cancer (ie, squamous cell carcinoma, as opposed to the more common transitional cell carcinoma) in this population, experts recommend annual cystoscopy for bladder cancer surveillance in patients who have had indwelling catheters for more than 5 to 10 years.35
Osteoporosis. Screening for osteoporosis is another preventive health area in which recommendations differ from those addressing the general population. Paralysis contributes to a decrease in mechanical stress on bone and to accelerated bone loss, and, thus, to osteoporosis.36
In patients with SCI/D, osteoporosis affects primarily weight-bearing areas below the injured lesion, such as the distal femur and proximal tibia. Fractures in patients with SCI/D may occur during minor trauma (eg, during transfers from wheelchair to bed). Although screening and treatment guidelines for osteoporosis in patients with SCI/D are not established, most experts recommend early screening and early and aggressive treatment.36
Depression reportedly occurs more frequently in individuals with SCI/D than in the general population,37,38 affecting adjustment, quality of life, and social, behavioral, and physical functioning. In light of this, it’s advisable to use screening tools, such as The Patient Health Questionnaire (PHQ)-9, routinely.39
Sexuality and sexual function are often adversely affected in both men and women with SCI/D. Loss of sensation in the sexual organs, combined with difficulty with positioning and mobility and bowel and bladder dysfunction, contribute not only to sexual dysfunction, but to lower self-esteem and altered body image.40
It is important to remember that fertility is often unaffected in women, so routine discussions about contraception with women who have SCI/D and who are sexually active are imperative. At the same time, male fertility is usually profoundly affected by SCI/D; patients and their partners who are interested in having children will require specialized interventions. Address sexuality and fertility during primary care visits and refer patients to counseling or specialists as necessary.41-43
SCI/D requires a whole-person approach
The care of individuals with SCI/D requires a holistic approach that takes into consideration physical, psychological, environmental, and interpersonal factors44,45 and involves ongoing support from a variety of specialists. FPs, with their whole-person orientation, can be instrumental in ensuring the successful rehabilitation of patients affected by SCI/D, and in helping individuals attain, preserve, and enhance their health and well-being.
CORRESPONDENCE
Ranit Mishori, MD, MHS, FAAFP, Georgetown University School of Medicine, 3900 Reservoir Road, NW, Pre-clinical Building GB-01D, Washington, DC 20007; [email protected].
1. Christopher and Dana Reeve Foundation. One degree of separation. Paralysis and spinal cord injury in the United States. Available at: https://www.heart.us/uploads/userfiles/files/one-degree-of-separation.pdf. Accessed April 23, 2015.
2. National Spinal Cord Injury Statistical Center. 2014 Annual Statistical Report-Complete public version. Available at: https://www.nscisc.uab.edu/reports. Accessed November 1, 2015.
3. van den Berg ME, Castellote JM, de Pedro-Cuesta J, et al. Survival after spinal cord injury: a systematic review. J Neurotrauma. 2010;27:1517-1528.
4. Smith KM, Naumann DN, McDiarmid AL, et al. Using developmental research to design innovative knowledge translation technology for spinal cord injury in primary care: Actionable Nuggets on SkillScribe. J Spinal Cord Med. 2014;37:582-588.
5. McColl MA, Aiken A, McColl A, et al. Primary care of people with spinal cord injury: scoping review. Can Fam Physician. 2012;58:1207-1216.
6. Francisco GE, Chae JC, DeLisa JA. Physiatry as a primary care specialty. Am J Phys Med Rehabil. 1995;74:186-192.
7. Consortium for Spinal Cord Medicine. Respiratory management following spinal cord injury: A clinical practice guideline for health-care professionals. Paralyzed Veterans of America. January 2005.
8. Weaver FM, Smith B, LaVela S, et al. Interventions to increase influenza vaccination rates in veterans with spinal cord injuries and disorders. J Spinal Cord Med. 2007;30:10-19.
9. McKinley WO, Jackson AB, Cardenas DD, et al. Long-term medical complications after traumatic spinal cord injury: A regional model systems analysis. Arch Phys Med Rehabil. 1999;80:1402-1410.
10. Cardozo CP. Respiratory complications of spinal cord injury. J Spinal Cord Med. 2007;30: 307-308.
11. Burns SP, Weaver FM, Parada JP, et al. Management of community-acquired pneumonia in persons with spinal cord injury. Spinal Cord. 2004;42:450-458.
12. Schilero GJ, Spungen AM, Bauman WA, et al. Pulmonary function and spinal cord injury. Respir Physiol Neurobiol. 2009;166:129-141.
13. Waites KB, Canupp KC, Chen Y, et al. Revaccination of adults with spinal cord injury using the 23-valent pneumococcal polysaccharide vaccine. J Spinal Cord Med. 2008;31: 53-59.
14. Dorsher PT, McIntosh PM. Neurogenic bladder. Adv Urol. 2012:816274.
15. Taweel W, Seyam R. Neurogenic bladder in spinal cord injury patients. Res Rep Urol. 2015;7:85-99.
16. Klausner AP, Steers WD. The neurogenic bladder: an update with management strategies for primary care physicians. Med Clin North Am. 2011;95:111-120.
17. Hooten TM, Bradley SF, Cardenas DD, et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin Infect Dis. 2010;50:625-663.
18. Goets L, Klausner A. Strategies for prevention of urinary tract infections in neurogenic bladder dysfunction. Phys Med Rehabil Clin N Am. 2014;25:605-618.
19. Stiens SA, Bergman SB, Goetz LL. Neurogenic bowel dysfunction after spinal cord injury: clinical evaluation and rehabilitative management. Arch Phys Med Rehabil. 1997;78:S86-S102.
20. Paralyzed Veterans of America. Consortium for Spinal Cord Medicine. Neurogenic Bowel Management in Adults with Spinal Cord Injury. Available at: http://www.pva.org/site/c.ajIRK9NJbcJ2E/b.6305815/k.A19D/Publications.htm#CPG. Accessed October 30, 2015.
21. Groah SL, Schladen M, Pineda CG, et al. Prevention of Pressure Ulcers Among People With Spinal Cord Injury: A Systematic Review. PM R. 2015;7:613-636.
22. Consortium for Spinal Cord Medicine Clinical Practice Guidelines. Pressure ulcer prevention and treatment following spinal cord injury: a clinical practice guideline for health-care professionals. J Spinal Cord Med. 2001;24:S40-S101.
23. Kruger EA, Pires M, Ngann Y, et al. Comprehensive management of pressure ulcers in spinal cord injury: current concepts and future trends. J Spinal Cord Med. 2013;36:572-585.
24. Schubart JR, Hilgart M, Lyder C. Pressure ulcer prevention and management in spinal cord-injured adults: analysis of educational needs. Adv Skin Wound Care. 2008;21:322-329.
25. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and treatment of pressure ulcers: quick reference guide. 2nd ed. Cambridge Media. 2014.
26. Ghaisas S, Pyatak EA, Blanche E, et al. Lifestyle changes and pressure ulcer prevention in adults with spinal cord injury in the pressure ulcer prevention study lifestyle intervention. Am J Occup Ther. 2015;69:6901290020p1-6901290020p10.
27. Groah SL, Charlifue S, Tate D, et al. Spinal cord injury and aging: challenges and recommendations for future research. Am J Phys Med Rehabil. 2012;91:80-93.
28. Noonan VK, Fallah N, Park SE, et al. Health care utilization in persons with traumatic spinal cord injury: the importance of multimorbidity and the impact on patient outcomes. Top Spinal Cord Inj Rehabil. 2014;20:289-301.
29. DeJong G, Tian W, Hsieh CH, et al. Rehospitalization in the first year of traumatic spinal cord injury after discharge from medical rehabilitation. Arch Phys Med Rehabil. 2013;94:S87-S97.
30. Cardenas DD, Hoffman JM, Kirshblum S, et al. Etiology and incidence of rehospitalization after traumatic spinal cord injury: a multicenter analysis. Arch Phys Med Rehabil. 2004;85:1757-1763.
31. Hayman AV, Guihan M, Fisher MJ, et al. Colonoscopy is high yield in spinal cord injury. J Spinal Cord Med. 2013;36:436-442.
32. Guilcher SJ, Newman A, Jaglal SB. A comparison of cervical cancer screening rates among women with traumatic spinal cord injury and the general population. J Womens Health. 2010;19:57-63.
33. Lezzoni LI, Park ER, Kilbridge KL. Implications of mobility impairment on the diagnosis and treatment of breast cancer. J Womens Health. 2011;20:45-52.
34. Graham A, Savic G, Gardner B. Cervical and breast cancer screening in wheelchair dependent females. Spinal Cord. 1998;36:340-344.
35. Groah SL, Weitzenkamp DA, Lammertse DP, et al. Excess risk of bladder cancer in spinal cord injury: evidence for an association between indwelling catheter use and bladder cancer. Arch Phys Med Rehabil. 2002;83:346-351.
36. Charmetant C, Phaner V, Condemine A, et al. Diagnosis and treatment of osteoporosis in spinal cord injury patients: a literature review. Ann Phys Rehabil Med. 2010;53:655-668.
37. Bombardier CH, Richards JS, Krause JS, et al. Symptoms of major depression in people with spinal cord injury: implications for screening. Arch Phys Med Rehabil. 2004;85:1749-1756.
38. Elliott TR. Studying depression following spinal cord injury: evidence, policy and practice. J Spinal Cord Med. 2015;38:584-586.
39. Kalpakjian CZ, Bombardier CH, Schomer K, et al. Measuring depression in persons with spinal cord injury: a systematic review. J Spinal Cord Med. 2009;32:6-24.
40. Courtois F, Charvier K. Sexual dysfunction in patients with spinal cord lesions. Handb Clin Neurol. 2015;130:225-245.
41. Kreuter M, Taft C, Siösteen A, et al. Women’s sexual functioning and sex life after spinal cord injury. Spinal Cord. 2011;49:154-160.
42. Fritz HA, Dillaway H, Lysack CL. “Don’t think paralysis takes away your womanhood”: Sexual intimacy after spinal cord injury. Am J Occup Ther. 2015;69:6902260030p1-6902260030p10.
43. Smith AE, Molton IR, McMullen K, et al. Sexual function, satisfaction, and use of aids for sexual activity in middle-aged adults with long-term physical disability. Top Spinal Cord Inj Rehabil. 2015;21:227-232.
44. Chiodo AE, Scelza WM, Kirshblum SC, et al. Spinal cord injury medicine. 5. Long-term medical issues and health maintenance. Arch Phys Med Rehabil. 2007;88:S76-S83.
45. Middleton JW, Ramakrishnan K, Cameron ID. Health Maintenance for Adults with Spinal Cord Injuries. NSW Agency for Clinical Innovation. Chatswood, NSW, Australia. February 2014. Available at: http://www.aci.health.nsw.gov.au/__data/assets/pdf_file/0007/155167/Health-Maintenance.pdf. Accessed November 1, 2015.
› Have a high index of suspicion for the leading causes of hospitalization among patients with spinal cord injury and disease (SCI/D). These include respiratory infections, urinary tract infections, and pressure ulcers. A
› Treat respiratory infections early and aggressively in patients with SCI/D; strongly consider inpatient management because of the high risk of respiratory failure. C
› Be alert to atypical signs and symptoms of urinary tract infection in patients with SCI/D, such as fever, chills, spasm, autonomic dysfunction, nausea and vomiting, abdominal discomfort, and fatigue. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
More than 5 million Americans are living with paralysis, and for nearly one in 4 of them the cause is spinal cord injury or disease (SCI/D).1 More common than multiple sclerosis (17%) as a cause for the loss of movement, SCI/D is second only to stroke (29%).1
The percentage of people living with paralysis due to SCI/D is increasing, partly because the population is aging and partly because management of infections has improved. Prior to the 1970s, life expectancy for people with SCI/D was significantly shortened, largely because of urologic and respiratory infections. But improved bladder management, in particular, has increased life expectancy—especially for the least severely injured.2 Respiratory diseases and septicemia remain the leading causes of death, but with increased longevity, other causes, such as endocrine, metabolic and nutritional diseases, accidents, nervous system diseases, and musculoskeletal disorders, are becoming increasingly common.2,3
Primary care’s pivotal role. Given the size of the population affected by SCI/D and the increase in life expectancy, family physicians (FPs) are more likely than ever before to care for these patients, most of whom have highly specific needs. However, little information about the primary care of patients with SCI/D exists. This patient population tends to consume a relatively large share of practices’ resources because of high case complexity.4
A recent Canadian report confirms our clinical experience that FPs report knowledge gaps in the area of SCI/D care, yet the same report found that 90% of people with SCI/D identify FPs as their “regular doctors.”5 Although a large number of patients with SCI/D identify their physiatrist as their primary care physician (PCP), one study reported that fewer than half of physiatrists are willing to assume that role.6 And while more than half of all patients with SCI/D have both specialists and PCPs involved in their care,5 communication breakdowns are a concern for patients receiving medical and rehabilitative direction from multiple health care professionals.
Below we take a closer look at the distinct patient populations affected by SCI/D, summarize several clinical conditions that contribute to hospitalization, and provide clinical management recommendations (TABLE7-26).
2 patient populations, one diagnosis
Paralysis due to spinal trauma occurs predominantly in non-Hispanic white and black males because of vehicular accidents, falls, violence, and sports.2 The mean age of injury has increased from 29 years during the 1970s to 42 years since 2010.2 However, this calculated average is misleading because there is an emerging bimodal distribution of people injured during early adulthood and a new increase in older adults injured primarily because of falls.27 In addition to those injured traumatically, a broader cohort of approximately 1 million patients represents a largely undefined group of people with paralysis due to diseases such as spinal stenosis, cancer, infection, multiple sclerosis, or other non-traumatic causes.
As a result, the population with SCI/D is comprised primarily of young adult males who have relatively few chronic medical conditions at the time of their injury and age with SCI/D, and older patients who are more likely to have already developed chronic medical conditions by the time of their SCI/D. Approximately 60% of SCI/Ds result in tetraplegia (ie, 4 limbs affected), although approximately two-thirds are incomplete, meaning that patients have some residual motor or sensory function below the level of injury.2 Not surprisingly, the level and severity of SCI/D impact life expectancy inversely and lifetime financial costs directly.
High health care utilization. Morbidity data largely parallel mortality data, often resulting in high health care utilization and cost among SCI/D patients.28 In a recent prospective observational study of nearly 1000 people with new traumatic SCI, 36.2% were rehospitalized at least once and 12.5% were rehospitalized at least twice during the 12-month period after discharge following injury.29
Rehospitalization, an outcome often quoted as a proxy for inadequate primary care, remains unacceptably high (36%-50%) for people with SCI/D.29,30 The leading causes of rehospitalization—pneumonia, urinary tract infection (UTI), and pressure ulcers29—have not changed over the years and persist over the lifetime of individuals with SCI/D.30
Take steps to prevent pneumonia, other respiratory complications
Many people with SCI/D are at high risk for respiratory complications because of their weakened respiratory muscles. This is particularly true for individuals who have injuries occurring above T10; those with injuries that are high on the spinal cord have the highest complication risk.7,8 In fact, pneumonia, atelectasis, and other respiratory complications are the leading causes of mortality in patients with tetraplegia, occurring in 40% to 70% of these patients.7
The diaphragm, innervated by the phrenic nerve (C3-C5), is the primary muscle of inspiration. Accessory muscles of inspiration include the scalenes (C5-C8), sternocleidomastoid and trapezius (C1-C4), and intercostals (T1-T11); whereas forced exhalation (cough) occurs with contraction of the abdominals (T5-T12).9 Diminished inspiration in individuals with higher level lesions can lead to microatelectasis, dyspnea with exertion, and even respiratory insufficiency.
In SCI/D above T8, weakened expiration can severely decrease cough effectiveness and secretion clearance, increasing susceptibility to lower respiratory tract infections. In addition, experts have described asthma-like disorders of airway function, particularly in those with higher lesions, due to unopposed parasympathetic innervation of respiratory smooth muscle.10
Management of this neurogenic pulmonary dysfunction after SCI/D relies on extensive preventive measures, including positioning and postural changes, breathing techniques, coughing (assisted for patients with tetraplegia), postural drainage, chest compression and percussion, and suctioning to avoid atelectasis, aspiration, and pneumonia. Ensure that patients receive influenza and pneumococcal vaccinations, and encourage smoking cessation. Obtain a chest x-ray if the patient demonstrates a decrease in respiratory function, deteriorating vital signs, reduced vital capacity, an increase in subjective dyspnea, or a change in sputum quantity. Treat respiratory infections early and aggressively,7-10 and strongly consider inpatient management because of the high risk of respiratory failure.
Pneumococcus is the most common cause of respiratory infections, although up to 21% of cases of community-acquired pneumonia in patients with SCI/D are caused by Pseudomonas.11-13 Avoid the use of antibiotics in patients who do not have signs or symptoms of a respiratory infection to minimize the development of resistant organisms. Target antibiotic therapy as per general population guidelines, as guidelines validated for use in the population with SCI/D do not currently exist.7,11
Be alert for UTIs—typical signs, symptoms don’t apply
The bladder receives innervation from S2 to S4 via the hypogastric, pudendal, and pelvic nerves. As such, the vast majority—70% to 84%—of patients with SCI/D report some degree of bladder dysfunction.14 Generally, SCI/D contributes to a combination of a failure to empty the bladder and a failure to store urine. The former is more frequent and the latter occurs more often in people with bladder outlet flaccidity, which usually occurs with low injury, such as that of the lumbar spine.14
The majority of people with SCI/D who are unable to empty their bladder require the use of some type of bladder catheter, either intermittent, indwelling (urethral or suprapubic), or condom. The choice of bladder management technique depends on gender, hand function, body habitus, caregiver assistance, and medical comorbidities. People with SCI/D are at greater risk for bladder and renal stones, UTI, vesicoureteral reflux, and bladder cancer.15,16 That said, the risk of bladder and renal stones declines somewhat after the first 6 months following an injury due to an immobility-induced loss of calcium.
Patients with SCI/D are often found to have bacteruria and even pyuria, and although they are at high risk for recurrent UTIs, these can be difficult to diagnose because signs and symptoms may differ from those seen in people with neurologically intact bladders. Symptomatic UTIs may present with fever, hematuria, abdominal discomfort, and/or increased spasticity, among other symptoms. They may cause increased bouts of autonomic dysreflexia, malaise, or a change in functional status. One cannot rely on the typical symptoms of dysuria and increased urinary frequency in this patient population. Further, the Infectious Diseases Society of America (IDSA) states that cloudy or foul-smelling urine in adults with catheters is not a symptom or sign mandating treatment.17
Because there is a lack of consensus as to what constitutes UTI symptoms in patients with SCI/D, PCPs need to be aware of changes from baseline in patients; these, combined with urine dip and culture results, should guide initiation of treatment.16
Prophylactic antibiotics have no role in the prevention of UTIs in patients with SCI/D. The minimal benefits associated with prophylaxis are outweighed by the risks of increased bacterial resistance to antibiotics. Research shows no significant benefit associated with the use of non-antibiotic prophylaxis, including the use of cranberry products and mannose, but further studies are needed in this patient population.18
Focus on bowel function; it correlates with quality of life
Bowel dysfunction is nearly universal in patients with SCI/D. The enteric nervous system is modulated via the sympathetic, parasympathetic, and somatic systems, and intrinsic control occurs via the myenteric and submucosal plexi. The loss of volitional control of defecation can result in prolonged transit time, reduced colonic motility, fecal incontinence, and difficulty with evacuation.
Because bowel care and function are highly correlated with quality of life,19 recommend bowel emptying every day or every other day, as well as adequate fiber in the diet, intake of fluids, stool softeners, bulk forming agents, contact irritants (eg, bisacodyl), and prokinetic agents to achieve optimal bowel care.
Prevent and treat pressure ulcers whenever possible
Accompanying the paralysis associated with SCI/D is often some degree of sensory loss of pain, light touch, temperature, and/or proprioception. The combination of insensate skin, immobility, and sarcopenia with resultant body composition changes places individuals with SCI/D at high risk for skin breakdown.21,22 Blood flow and oxygen tension at the skin surface are also decreased in patients with SCI/D compared to those without, further contributing to the problem.21,23 Increased latency from the time of injury correlates with increased likelihood of pressure ulcer development.21,22,24
External risk factors for pressure ulcers include prolonged pressure exposure, or intense pressure over a short period, shear forces, poor nutrition, smoking, moisture, and immobility. The incidence of pressure ulcers in patients with SCI/D is 25% to 66%, compared with 0.38% in the general population.21,22 Research indicates that US hospitals spend $11 billion annually on the treatment of the condition.22
To minimize pressure ulcers in this population, perform a risk assessment, using, for example, the Spinal Cord Injury Pressure Ulcer Scale-Acute (SCIPUS-A) available at https://www.scireproject.com/outcome-measures-new/spinal-cord-injury-pressure-ulcer-scale-acute-scipus. In addition, recommend that patients use pressure redistribution surfaces for beds and wheelchairs, turn while in bed, perform frequent (approximately every 15-30 minutes) pressure reliefs, exercise or move regularly, and that they or a caregiver inspect the skin daily. If pressure ulcers do occur, start treatment immediately and document the stage of the ulcer.
Ensure that screening efforts go beyond what’s standard
Preventive care for patients with SCI/D is similar in many ways to that recommended for the general population. Screening for colorectal cancer,31 cervical cancer, and breast cancer32 should follow the same evidence-based intervals and age ranges suggested by groups such as the US Preventive Services Task Force (USPSTF). The only difference is to give special consideration to patients’ physical limitations and the set-up of exam rooms when scheduling and conducting procedures, such as Pap smears, colonoscopies, and mammograms.33,34
Bladder cancer. Because of the high risk for bladder cancer (ie, squamous cell carcinoma, as opposed to the more common transitional cell carcinoma) in this population, experts recommend annual cystoscopy for bladder cancer surveillance in patients who have had indwelling catheters for more than 5 to 10 years.35
Osteoporosis. Screening for osteoporosis is another preventive health area in which recommendations differ from those addressing the general population. Paralysis contributes to a decrease in mechanical stress on bone and to accelerated bone loss, and, thus, to osteoporosis.36
In patients with SCI/D, osteoporosis affects primarily weight-bearing areas below the injured lesion, such as the distal femur and proximal tibia. Fractures in patients with SCI/D may occur during minor trauma (eg, during transfers from wheelchair to bed). Although screening and treatment guidelines for osteoporosis in patients with SCI/D are not established, most experts recommend early screening and early and aggressive treatment.36
Depression reportedly occurs more frequently in individuals with SCI/D than in the general population,37,38 affecting adjustment, quality of life, and social, behavioral, and physical functioning. In light of this, it’s advisable to use screening tools, such as The Patient Health Questionnaire (PHQ)-9, routinely.39
Sexuality and sexual function are often adversely affected in both men and women with SCI/D. Loss of sensation in the sexual organs, combined with difficulty with positioning and mobility and bowel and bladder dysfunction, contribute not only to sexual dysfunction, but to lower self-esteem and altered body image.40
It is important to remember that fertility is often unaffected in women, so routine discussions about contraception with women who have SCI/D and who are sexually active are imperative. At the same time, male fertility is usually profoundly affected by SCI/D; patients and their partners who are interested in having children will require specialized interventions. Address sexuality and fertility during primary care visits and refer patients to counseling or specialists as necessary.41-43
SCI/D requires a whole-person approach
The care of individuals with SCI/D requires a holistic approach that takes into consideration physical, psychological, environmental, and interpersonal factors44,45 and involves ongoing support from a variety of specialists. FPs, with their whole-person orientation, can be instrumental in ensuring the successful rehabilitation of patients affected by SCI/D, and in helping individuals attain, preserve, and enhance their health and well-being.
CORRESPONDENCE
Ranit Mishori, MD, MHS, FAAFP, Georgetown University School of Medicine, 3900 Reservoir Road, NW, Pre-clinical Building GB-01D, Washington, DC 20007; [email protected].
› Have a high index of suspicion for the leading causes of hospitalization among patients with spinal cord injury and disease (SCI/D). These include respiratory infections, urinary tract infections, and pressure ulcers. A
› Treat respiratory infections early and aggressively in patients with SCI/D; strongly consider inpatient management because of the high risk of respiratory failure. C
› Be alert to atypical signs and symptoms of urinary tract infection in patients with SCI/D, such as fever, chills, spasm, autonomic dysfunction, nausea and vomiting, abdominal discomfort, and fatigue. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
More than 5 million Americans are living with paralysis, and for nearly one in 4 of them the cause is spinal cord injury or disease (SCI/D).1 More common than multiple sclerosis (17%) as a cause for the loss of movement, SCI/D is second only to stroke (29%).1
The percentage of people living with paralysis due to SCI/D is increasing, partly because the population is aging and partly because management of infections has improved. Prior to the 1970s, life expectancy for people with SCI/D was significantly shortened, largely because of urologic and respiratory infections. But improved bladder management, in particular, has increased life expectancy—especially for the least severely injured.2 Respiratory diseases and septicemia remain the leading causes of death, but with increased longevity, other causes, such as endocrine, metabolic and nutritional diseases, accidents, nervous system diseases, and musculoskeletal disorders, are becoming increasingly common.2,3
Primary care’s pivotal role. Given the size of the population affected by SCI/D and the increase in life expectancy, family physicians (FPs) are more likely than ever before to care for these patients, most of whom have highly specific needs. However, little information about the primary care of patients with SCI/D exists. This patient population tends to consume a relatively large share of practices’ resources because of high case complexity.4
A recent Canadian report confirms our clinical experience that FPs report knowledge gaps in the area of SCI/D care, yet the same report found that 90% of people with SCI/D identify FPs as their “regular doctors.”5 Although a large number of patients with SCI/D identify their physiatrist as their primary care physician (PCP), one study reported that fewer than half of physiatrists are willing to assume that role.6 And while more than half of all patients with SCI/D have both specialists and PCPs involved in their care,5 communication breakdowns are a concern for patients receiving medical and rehabilitative direction from multiple health care professionals.
Below we take a closer look at the distinct patient populations affected by SCI/D, summarize several clinical conditions that contribute to hospitalization, and provide clinical management recommendations (TABLE7-26).
2 patient populations, one diagnosis
Paralysis due to spinal trauma occurs predominantly in non-Hispanic white and black males because of vehicular accidents, falls, violence, and sports.2 The mean age of injury has increased from 29 years during the 1970s to 42 years since 2010.2 However, this calculated average is misleading because there is an emerging bimodal distribution of people injured during early adulthood and a new increase in older adults injured primarily because of falls.27 In addition to those injured traumatically, a broader cohort of approximately 1 million patients represents a largely undefined group of people with paralysis due to diseases such as spinal stenosis, cancer, infection, multiple sclerosis, or other non-traumatic causes.
As a result, the population with SCI/D is comprised primarily of young adult males who have relatively few chronic medical conditions at the time of their injury and age with SCI/D, and older patients who are more likely to have already developed chronic medical conditions by the time of their SCI/D. Approximately 60% of SCI/Ds result in tetraplegia (ie, 4 limbs affected), although approximately two-thirds are incomplete, meaning that patients have some residual motor or sensory function below the level of injury.2 Not surprisingly, the level and severity of SCI/D impact life expectancy inversely and lifetime financial costs directly.
High health care utilization. Morbidity data largely parallel mortality data, often resulting in high health care utilization and cost among SCI/D patients.28 In a recent prospective observational study of nearly 1000 people with new traumatic SCI, 36.2% were rehospitalized at least once and 12.5% were rehospitalized at least twice during the 12-month period after discharge following injury.29
Rehospitalization, an outcome often quoted as a proxy for inadequate primary care, remains unacceptably high (36%-50%) for people with SCI/D.29,30 The leading causes of rehospitalization—pneumonia, urinary tract infection (UTI), and pressure ulcers29—have not changed over the years and persist over the lifetime of individuals with SCI/D.30
Take steps to prevent pneumonia, other respiratory complications
Many people with SCI/D are at high risk for respiratory complications because of their weakened respiratory muscles. This is particularly true for individuals who have injuries occurring above T10; those with injuries that are high on the spinal cord have the highest complication risk.7,8 In fact, pneumonia, atelectasis, and other respiratory complications are the leading causes of mortality in patients with tetraplegia, occurring in 40% to 70% of these patients.7
The diaphragm, innervated by the phrenic nerve (C3-C5), is the primary muscle of inspiration. Accessory muscles of inspiration include the scalenes (C5-C8), sternocleidomastoid and trapezius (C1-C4), and intercostals (T1-T11); whereas forced exhalation (cough) occurs with contraction of the abdominals (T5-T12).9 Diminished inspiration in individuals with higher level lesions can lead to microatelectasis, dyspnea with exertion, and even respiratory insufficiency.
In SCI/D above T8, weakened expiration can severely decrease cough effectiveness and secretion clearance, increasing susceptibility to lower respiratory tract infections. In addition, experts have described asthma-like disorders of airway function, particularly in those with higher lesions, due to unopposed parasympathetic innervation of respiratory smooth muscle.10
Management of this neurogenic pulmonary dysfunction after SCI/D relies on extensive preventive measures, including positioning and postural changes, breathing techniques, coughing (assisted for patients with tetraplegia), postural drainage, chest compression and percussion, and suctioning to avoid atelectasis, aspiration, and pneumonia. Ensure that patients receive influenza and pneumococcal vaccinations, and encourage smoking cessation. Obtain a chest x-ray if the patient demonstrates a decrease in respiratory function, deteriorating vital signs, reduced vital capacity, an increase in subjective dyspnea, or a change in sputum quantity. Treat respiratory infections early and aggressively,7-10 and strongly consider inpatient management because of the high risk of respiratory failure.
Pneumococcus is the most common cause of respiratory infections, although up to 21% of cases of community-acquired pneumonia in patients with SCI/D are caused by Pseudomonas.11-13 Avoid the use of antibiotics in patients who do not have signs or symptoms of a respiratory infection to minimize the development of resistant organisms. Target antibiotic therapy as per general population guidelines, as guidelines validated for use in the population with SCI/D do not currently exist.7,11
Be alert for UTIs—typical signs, symptoms don’t apply
The bladder receives innervation from S2 to S4 via the hypogastric, pudendal, and pelvic nerves. As such, the vast majority—70% to 84%—of patients with SCI/D report some degree of bladder dysfunction.14 Generally, SCI/D contributes to a combination of a failure to empty the bladder and a failure to store urine. The former is more frequent and the latter occurs more often in people with bladder outlet flaccidity, which usually occurs with low injury, such as that of the lumbar spine.14
The majority of people with SCI/D who are unable to empty their bladder require the use of some type of bladder catheter, either intermittent, indwelling (urethral or suprapubic), or condom. The choice of bladder management technique depends on gender, hand function, body habitus, caregiver assistance, and medical comorbidities. People with SCI/D are at greater risk for bladder and renal stones, UTI, vesicoureteral reflux, and bladder cancer.15,16 That said, the risk of bladder and renal stones declines somewhat after the first 6 months following an injury due to an immobility-induced loss of calcium.
Patients with SCI/D are often found to have bacteruria and even pyuria, and although they are at high risk for recurrent UTIs, these can be difficult to diagnose because signs and symptoms may differ from those seen in people with neurologically intact bladders. Symptomatic UTIs may present with fever, hematuria, abdominal discomfort, and/or increased spasticity, among other symptoms. They may cause increased bouts of autonomic dysreflexia, malaise, or a change in functional status. One cannot rely on the typical symptoms of dysuria and increased urinary frequency in this patient population. Further, the Infectious Diseases Society of America (IDSA) states that cloudy or foul-smelling urine in adults with catheters is not a symptom or sign mandating treatment.17
Because there is a lack of consensus as to what constitutes UTI symptoms in patients with SCI/D, PCPs need to be aware of changes from baseline in patients; these, combined with urine dip and culture results, should guide initiation of treatment.16
Prophylactic antibiotics have no role in the prevention of UTIs in patients with SCI/D. The minimal benefits associated with prophylaxis are outweighed by the risks of increased bacterial resistance to antibiotics. Research shows no significant benefit associated with the use of non-antibiotic prophylaxis, including the use of cranberry products and mannose, but further studies are needed in this patient population.18
Focus on bowel function; it correlates with quality of life
Bowel dysfunction is nearly universal in patients with SCI/D. The enteric nervous system is modulated via the sympathetic, parasympathetic, and somatic systems, and intrinsic control occurs via the myenteric and submucosal plexi. The loss of volitional control of defecation can result in prolonged transit time, reduced colonic motility, fecal incontinence, and difficulty with evacuation.
Because bowel care and function are highly correlated with quality of life,19 recommend bowel emptying every day or every other day, as well as adequate fiber in the diet, intake of fluids, stool softeners, bulk forming agents, contact irritants (eg, bisacodyl), and prokinetic agents to achieve optimal bowel care.
Prevent and treat pressure ulcers whenever possible
Accompanying the paralysis associated with SCI/D is often some degree of sensory loss of pain, light touch, temperature, and/or proprioception. The combination of insensate skin, immobility, and sarcopenia with resultant body composition changes places individuals with SCI/D at high risk for skin breakdown.21,22 Blood flow and oxygen tension at the skin surface are also decreased in patients with SCI/D compared to those without, further contributing to the problem.21,23 Increased latency from the time of injury correlates with increased likelihood of pressure ulcer development.21,22,24
External risk factors for pressure ulcers include prolonged pressure exposure, or intense pressure over a short period, shear forces, poor nutrition, smoking, moisture, and immobility. The incidence of pressure ulcers in patients with SCI/D is 25% to 66%, compared with 0.38% in the general population.21,22 Research indicates that US hospitals spend $11 billion annually on the treatment of the condition.22
To minimize pressure ulcers in this population, perform a risk assessment, using, for example, the Spinal Cord Injury Pressure Ulcer Scale-Acute (SCIPUS-A) available at https://www.scireproject.com/outcome-measures-new/spinal-cord-injury-pressure-ulcer-scale-acute-scipus. In addition, recommend that patients use pressure redistribution surfaces for beds and wheelchairs, turn while in bed, perform frequent (approximately every 15-30 minutes) pressure reliefs, exercise or move regularly, and that they or a caregiver inspect the skin daily. If pressure ulcers do occur, start treatment immediately and document the stage of the ulcer.
Ensure that screening efforts go beyond what’s standard
Preventive care for patients with SCI/D is similar in many ways to that recommended for the general population. Screening for colorectal cancer,31 cervical cancer, and breast cancer32 should follow the same evidence-based intervals and age ranges suggested by groups such as the US Preventive Services Task Force (USPSTF). The only difference is to give special consideration to patients’ physical limitations and the set-up of exam rooms when scheduling and conducting procedures, such as Pap smears, colonoscopies, and mammograms.33,34
Bladder cancer. Because of the high risk for bladder cancer (ie, squamous cell carcinoma, as opposed to the more common transitional cell carcinoma) in this population, experts recommend annual cystoscopy for bladder cancer surveillance in patients who have had indwelling catheters for more than 5 to 10 years.35
Osteoporosis. Screening for osteoporosis is another preventive health area in which recommendations differ from those addressing the general population. Paralysis contributes to a decrease in mechanical stress on bone and to accelerated bone loss, and, thus, to osteoporosis.36
In patients with SCI/D, osteoporosis affects primarily weight-bearing areas below the injured lesion, such as the distal femur and proximal tibia. Fractures in patients with SCI/D may occur during minor trauma (eg, during transfers from wheelchair to bed). Although screening and treatment guidelines for osteoporosis in patients with SCI/D are not established, most experts recommend early screening and early and aggressive treatment.36
Depression reportedly occurs more frequently in individuals with SCI/D than in the general population,37,38 affecting adjustment, quality of life, and social, behavioral, and physical functioning. In light of this, it’s advisable to use screening tools, such as The Patient Health Questionnaire (PHQ)-9, routinely.39
Sexuality and sexual function are often adversely affected in both men and women with SCI/D. Loss of sensation in the sexual organs, combined with difficulty with positioning and mobility and bowel and bladder dysfunction, contribute not only to sexual dysfunction, but to lower self-esteem and altered body image.40
It is important to remember that fertility is often unaffected in women, so routine discussions about contraception with women who have SCI/D and who are sexually active are imperative. At the same time, male fertility is usually profoundly affected by SCI/D; patients and their partners who are interested in having children will require specialized interventions. Address sexuality and fertility during primary care visits and refer patients to counseling or specialists as necessary.41-43
SCI/D requires a whole-person approach
The care of individuals with SCI/D requires a holistic approach that takes into consideration physical, psychological, environmental, and interpersonal factors44,45 and involves ongoing support from a variety of specialists. FPs, with their whole-person orientation, can be instrumental in ensuring the successful rehabilitation of patients affected by SCI/D, and in helping individuals attain, preserve, and enhance their health and well-being.
CORRESPONDENCE
Ranit Mishori, MD, MHS, FAAFP, Georgetown University School of Medicine, 3900 Reservoir Road, NW, Pre-clinical Building GB-01D, Washington, DC 20007; [email protected].
1. Christopher and Dana Reeve Foundation. One degree of separation. Paralysis and spinal cord injury in the United States. Available at: https://www.heart.us/uploads/userfiles/files/one-degree-of-separation.pdf. Accessed April 23, 2015.
2. National Spinal Cord Injury Statistical Center. 2014 Annual Statistical Report-Complete public version. Available at: https://www.nscisc.uab.edu/reports. Accessed November 1, 2015.
3. van den Berg ME, Castellote JM, de Pedro-Cuesta J, et al. Survival after spinal cord injury: a systematic review. J Neurotrauma. 2010;27:1517-1528.
4. Smith KM, Naumann DN, McDiarmid AL, et al. Using developmental research to design innovative knowledge translation technology for spinal cord injury in primary care: Actionable Nuggets on SkillScribe. J Spinal Cord Med. 2014;37:582-588.
5. McColl MA, Aiken A, McColl A, et al. Primary care of people with spinal cord injury: scoping review. Can Fam Physician. 2012;58:1207-1216.
6. Francisco GE, Chae JC, DeLisa JA. Physiatry as a primary care specialty. Am J Phys Med Rehabil. 1995;74:186-192.
7. Consortium for Spinal Cord Medicine. Respiratory management following spinal cord injury: A clinical practice guideline for health-care professionals. Paralyzed Veterans of America. January 2005.
8. Weaver FM, Smith B, LaVela S, et al. Interventions to increase influenza vaccination rates in veterans with spinal cord injuries and disorders. J Spinal Cord Med. 2007;30:10-19.
9. McKinley WO, Jackson AB, Cardenas DD, et al. Long-term medical complications after traumatic spinal cord injury: A regional model systems analysis. Arch Phys Med Rehabil. 1999;80:1402-1410.
10. Cardozo CP. Respiratory complications of spinal cord injury. J Spinal Cord Med. 2007;30: 307-308.
11. Burns SP, Weaver FM, Parada JP, et al. Management of community-acquired pneumonia in persons with spinal cord injury. Spinal Cord. 2004;42:450-458.
12. Schilero GJ, Spungen AM, Bauman WA, et al. Pulmonary function and spinal cord injury. Respir Physiol Neurobiol. 2009;166:129-141.
13. Waites KB, Canupp KC, Chen Y, et al. Revaccination of adults with spinal cord injury using the 23-valent pneumococcal polysaccharide vaccine. J Spinal Cord Med. 2008;31: 53-59.
14. Dorsher PT, McIntosh PM. Neurogenic bladder. Adv Urol. 2012:816274.
15. Taweel W, Seyam R. Neurogenic bladder in spinal cord injury patients. Res Rep Urol. 2015;7:85-99.
16. Klausner AP, Steers WD. The neurogenic bladder: an update with management strategies for primary care physicians. Med Clin North Am. 2011;95:111-120.
17. Hooten TM, Bradley SF, Cardenas DD, et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin Infect Dis. 2010;50:625-663.
18. Goets L, Klausner A. Strategies for prevention of urinary tract infections in neurogenic bladder dysfunction. Phys Med Rehabil Clin N Am. 2014;25:605-618.
19. Stiens SA, Bergman SB, Goetz LL. Neurogenic bowel dysfunction after spinal cord injury: clinical evaluation and rehabilitative management. Arch Phys Med Rehabil. 1997;78:S86-S102.
20. Paralyzed Veterans of America. Consortium for Spinal Cord Medicine. Neurogenic Bowel Management in Adults with Spinal Cord Injury. Available at: http://www.pva.org/site/c.ajIRK9NJbcJ2E/b.6305815/k.A19D/Publications.htm#CPG. Accessed October 30, 2015.
21. Groah SL, Schladen M, Pineda CG, et al. Prevention of Pressure Ulcers Among People With Spinal Cord Injury: A Systematic Review. PM R. 2015;7:613-636.
22. Consortium for Spinal Cord Medicine Clinical Practice Guidelines. Pressure ulcer prevention and treatment following spinal cord injury: a clinical practice guideline for health-care professionals. J Spinal Cord Med. 2001;24:S40-S101.
23. Kruger EA, Pires M, Ngann Y, et al. Comprehensive management of pressure ulcers in spinal cord injury: current concepts and future trends. J Spinal Cord Med. 2013;36:572-585.
24. Schubart JR, Hilgart M, Lyder C. Pressure ulcer prevention and management in spinal cord-injured adults: analysis of educational needs. Adv Skin Wound Care. 2008;21:322-329.
25. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and treatment of pressure ulcers: quick reference guide. 2nd ed. Cambridge Media. 2014.
26. Ghaisas S, Pyatak EA, Blanche E, et al. Lifestyle changes and pressure ulcer prevention in adults with spinal cord injury in the pressure ulcer prevention study lifestyle intervention. Am J Occup Ther. 2015;69:6901290020p1-6901290020p10.
27. Groah SL, Charlifue S, Tate D, et al. Spinal cord injury and aging: challenges and recommendations for future research. Am J Phys Med Rehabil. 2012;91:80-93.
28. Noonan VK, Fallah N, Park SE, et al. Health care utilization in persons with traumatic spinal cord injury: the importance of multimorbidity and the impact on patient outcomes. Top Spinal Cord Inj Rehabil. 2014;20:289-301.
29. DeJong G, Tian W, Hsieh CH, et al. Rehospitalization in the first year of traumatic spinal cord injury after discharge from medical rehabilitation. Arch Phys Med Rehabil. 2013;94:S87-S97.
30. Cardenas DD, Hoffman JM, Kirshblum S, et al. Etiology and incidence of rehospitalization after traumatic spinal cord injury: a multicenter analysis. Arch Phys Med Rehabil. 2004;85:1757-1763.
31. Hayman AV, Guihan M, Fisher MJ, et al. Colonoscopy is high yield in spinal cord injury. J Spinal Cord Med. 2013;36:436-442.
32. Guilcher SJ, Newman A, Jaglal SB. A comparison of cervical cancer screening rates among women with traumatic spinal cord injury and the general population. J Womens Health. 2010;19:57-63.
33. Lezzoni LI, Park ER, Kilbridge KL. Implications of mobility impairment on the diagnosis and treatment of breast cancer. J Womens Health. 2011;20:45-52.
34. Graham A, Savic G, Gardner B. Cervical and breast cancer screening in wheelchair dependent females. Spinal Cord. 1998;36:340-344.
35. Groah SL, Weitzenkamp DA, Lammertse DP, et al. Excess risk of bladder cancer in spinal cord injury: evidence for an association between indwelling catheter use and bladder cancer. Arch Phys Med Rehabil. 2002;83:346-351.
36. Charmetant C, Phaner V, Condemine A, et al. Diagnosis and treatment of osteoporosis in spinal cord injury patients: a literature review. Ann Phys Rehabil Med. 2010;53:655-668.
37. Bombardier CH, Richards JS, Krause JS, et al. Symptoms of major depression in people with spinal cord injury: implications for screening. Arch Phys Med Rehabil. 2004;85:1749-1756.
38. Elliott TR. Studying depression following spinal cord injury: evidence, policy and practice. J Spinal Cord Med. 2015;38:584-586.
39. Kalpakjian CZ, Bombardier CH, Schomer K, et al. Measuring depression in persons with spinal cord injury: a systematic review. J Spinal Cord Med. 2009;32:6-24.
40. Courtois F, Charvier K. Sexual dysfunction in patients with spinal cord lesions. Handb Clin Neurol. 2015;130:225-245.
41. Kreuter M, Taft C, Siösteen A, et al. Women’s sexual functioning and sex life after spinal cord injury. Spinal Cord. 2011;49:154-160.
42. Fritz HA, Dillaway H, Lysack CL. “Don’t think paralysis takes away your womanhood”: Sexual intimacy after spinal cord injury. Am J Occup Ther. 2015;69:6902260030p1-6902260030p10.
43. Smith AE, Molton IR, McMullen K, et al. Sexual function, satisfaction, and use of aids for sexual activity in middle-aged adults with long-term physical disability. Top Spinal Cord Inj Rehabil. 2015;21:227-232.
44. Chiodo AE, Scelza WM, Kirshblum SC, et al. Spinal cord injury medicine. 5. Long-term medical issues and health maintenance. Arch Phys Med Rehabil. 2007;88:S76-S83.
45. Middleton JW, Ramakrishnan K, Cameron ID. Health Maintenance for Adults with Spinal Cord Injuries. NSW Agency for Clinical Innovation. Chatswood, NSW, Australia. February 2014. Available at: http://www.aci.health.nsw.gov.au/__data/assets/pdf_file/0007/155167/Health-Maintenance.pdf. Accessed November 1, 2015.
1. Christopher and Dana Reeve Foundation. One degree of separation. Paralysis and spinal cord injury in the United States. Available at: https://www.heart.us/uploads/userfiles/files/one-degree-of-separation.pdf. Accessed April 23, 2015.
2. National Spinal Cord Injury Statistical Center. 2014 Annual Statistical Report-Complete public version. Available at: https://www.nscisc.uab.edu/reports. Accessed November 1, 2015.
3. van den Berg ME, Castellote JM, de Pedro-Cuesta J, et al. Survival after spinal cord injury: a systematic review. J Neurotrauma. 2010;27:1517-1528.
4. Smith KM, Naumann DN, McDiarmid AL, et al. Using developmental research to design innovative knowledge translation technology for spinal cord injury in primary care: Actionable Nuggets on SkillScribe. J Spinal Cord Med. 2014;37:582-588.
5. McColl MA, Aiken A, McColl A, et al. Primary care of people with spinal cord injury: scoping review. Can Fam Physician. 2012;58:1207-1216.
6. Francisco GE, Chae JC, DeLisa JA. Physiatry as a primary care specialty. Am J Phys Med Rehabil. 1995;74:186-192.
7. Consortium for Spinal Cord Medicine. Respiratory management following spinal cord injury: A clinical practice guideline for health-care professionals. Paralyzed Veterans of America. January 2005.
8. Weaver FM, Smith B, LaVela S, et al. Interventions to increase influenza vaccination rates in veterans with spinal cord injuries and disorders. J Spinal Cord Med. 2007;30:10-19.
9. McKinley WO, Jackson AB, Cardenas DD, et al. Long-term medical complications after traumatic spinal cord injury: A regional model systems analysis. Arch Phys Med Rehabil. 1999;80:1402-1410.
10. Cardozo CP. Respiratory complications of spinal cord injury. J Spinal Cord Med. 2007;30: 307-308.
11. Burns SP, Weaver FM, Parada JP, et al. Management of community-acquired pneumonia in persons with spinal cord injury. Spinal Cord. 2004;42:450-458.
12. Schilero GJ, Spungen AM, Bauman WA, et al. Pulmonary function and spinal cord injury. Respir Physiol Neurobiol. 2009;166:129-141.
13. Waites KB, Canupp KC, Chen Y, et al. Revaccination of adults with spinal cord injury using the 23-valent pneumococcal polysaccharide vaccine. J Spinal Cord Med. 2008;31: 53-59.
14. Dorsher PT, McIntosh PM. Neurogenic bladder. Adv Urol. 2012:816274.
15. Taweel W, Seyam R. Neurogenic bladder in spinal cord injury patients. Res Rep Urol. 2015;7:85-99.
16. Klausner AP, Steers WD. The neurogenic bladder: an update with management strategies for primary care physicians. Med Clin North Am. 2011;95:111-120.
17. Hooten TM, Bradley SF, Cardenas DD, et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin Infect Dis. 2010;50:625-663.
18. Goets L, Klausner A. Strategies for prevention of urinary tract infections in neurogenic bladder dysfunction. Phys Med Rehabil Clin N Am. 2014;25:605-618.
19. Stiens SA, Bergman SB, Goetz LL. Neurogenic bowel dysfunction after spinal cord injury: clinical evaluation and rehabilitative management. Arch Phys Med Rehabil. 1997;78:S86-S102.
20. Paralyzed Veterans of America. Consortium for Spinal Cord Medicine. Neurogenic Bowel Management in Adults with Spinal Cord Injury. Available at: http://www.pva.org/site/c.ajIRK9NJbcJ2E/b.6305815/k.A19D/Publications.htm#CPG. Accessed October 30, 2015.
21. Groah SL, Schladen M, Pineda CG, et al. Prevention of Pressure Ulcers Among People With Spinal Cord Injury: A Systematic Review. PM R. 2015;7:613-636.
22. Consortium for Spinal Cord Medicine Clinical Practice Guidelines. Pressure ulcer prevention and treatment following spinal cord injury: a clinical practice guideline for health-care professionals. J Spinal Cord Med. 2001;24:S40-S101.
23. Kruger EA, Pires M, Ngann Y, et al. Comprehensive management of pressure ulcers in spinal cord injury: current concepts and future trends. J Spinal Cord Med. 2013;36:572-585.
24. Schubart JR, Hilgart M, Lyder C. Pressure ulcer prevention and management in spinal cord-injured adults: analysis of educational needs. Adv Skin Wound Care. 2008;21:322-329.
25. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and treatment of pressure ulcers: quick reference guide. 2nd ed. Cambridge Media. 2014.
26. Ghaisas S, Pyatak EA, Blanche E, et al. Lifestyle changes and pressure ulcer prevention in adults with spinal cord injury in the pressure ulcer prevention study lifestyle intervention. Am J Occup Ther. 2015;69:6901290020p1-6901290020p10.
27. Groah SL, Charlifue S, Tate D, et al. Spinal cord injury and aging: challenges and recommendations for future research. Am J Phys Med Rehabil. 2012;91:80-93.
28. Noonan VK, Fallah N, Park SE, et al. Health care utilization in persons with traumatic spinal cord injury: the importance of multimorbidity and the impact on patient outcomes. Top Spinal Cord Inj Rehabil. 2014;20:289-301.
29. DeJong G, Tian W, Hsieh CH, et al. Rehospitalization in the first year of traumatic spinal cord injury after discharge from medical rehabilitation. Arch Phys Med Rehabil. 2013;94:S87-S97.
30. Cardenas DD, Hoffman JM, Kirshblum S, et al. Etiology and incidence of rehospitalization after traumatic spinal cord injury: a multicenter analysis. Arch Phys Med Rehabil. 2004;85:1757-1763.
31. Hayman AV, Guihan M, Fisher MJ, et al. Colonoscopy is high yield in spinal cord injury. J Spinal Cord Med. 2013;36:436-442.
32. Guilcher SJ, Newman A, Jaglal SB. A comparison of cervical cancer screening rates among women with traumatic spinal cord injury and the general population. J Womens Health. 2010;19:57-63.
33. Lezzoni LI, Park ER, Kilbridge KL. Implications of mobility impairment on the diagnosis and treatment of breast cancer. J Womens Health. 2011;20:45-52.
34. Graham A, Savic G, Gardner B. Cervical and breast cancer screening in wheelchair dependent females. Spinal Cord. 1998;36:340-344.
35. Groah SL, Weitzenkamp DA, Lammertse DP, et al. Excess risk of bladder cancer in spinal cord injury: evidence for an association between indwelling catheter use and bladder cancer. Arch Phys Med Rehabil. 2002;83:346-351.
36. Charmetant C, Phaner V, Condemine A, et al. Diagnosis and treatment of osteoporosis in spinal cord injury patients: a literature review. Ann Phys Rehabil Med. 2010;53:655-668.
37. Bombardier CH, Richards JS, Krause JS, et al. Symptoms of major depression in people with spinal cord injury: implications for screening. Arch Phys Med Rehabil. 2004;85:1749-1756.
38. Elliott TR. Studying depression following spinal cord injury: evidence, policy and practice. J Spinal Cord Med. 2015;38:584-586.
39. Kalpakjian CZ, Bombardier CH, Schomer K, et al. Measuring depression in persons with spinal cord injury: a systematic review. J Spinal Cord Med. 2009;32:6-24.
40. Courtois F, Charvier K. Sexual dysfunction in patients with spinal cord lesions. Handb Clin Neurol. 2015;130:225-245.
41. Kreuter M, Taft C, Siösteen A, et al. Women’s sexual functioning and sex life after spinal cord injury. Spinal Cord. 2011;49:154-160.
42. Fritz HA, Dillaway H, Lysack CL. “Don’t think paralysis takes away your womanhood”: Sexual intimacy after spinal cord injury. Am J Occup Ther. 2015;69:6902260030p1-6902260030p10.
43. Smith AE, Molton IR, McMullen K, et al. Sexual function, satisfaction, and use of aids for sexual activity in middle-aged adults with long-term physical disability. Top Spinal Cord Inj Rehabil. 2015;21:227-232.
44. Chiodo AE, Scelza WM, Kirshblum SC, et al. Spinal cord injury medicine. 5. Long-term medical issues and health maintenance. Arch Phys Med Rehabil. 2007;88:S76-S83.
45. Middleton JW, Ramakrishnan K, Cameron ID. Health Maintenance for Adults with Spinal Cord Injuries. NSW Agency for Clinical Innovation. Chatswood, NSW, Australia. February 2014. Available at: http://www.aci.health.nsw.gov.au/__data/assets/pdf_file/0007/155167/Health-Maintenance.pdf. Accessed November 1, 2015.
From The Journal of Family Practice | 2016;65(5):302-306,308-309.

Surgery for PHPT improves sleep quality
BALTIMORE – Research into how primary hyperparathyroidism and parathyroidectomy affect sleep quality has been limited, but investigators at the Medical College of Wisconsin, Milwaukee, reported that primary hyperparathyroidism does indeed disrupt sleep patterns and that curative surgery can improve sleep quality in a third of patients.
“Today, most patients with primary hyperparathyroidism have what is considered asymptomatic disease,” Justin La reported at the annual meeting of the American Association of Endocrine Surgeons. “However, recent studies demonstrate that many of these asymptomatic patients commonly exhibit neuropsychological problems, including sleep disturbances.” Mr. La is a fourth-year medical student at the Medical College of Wisconsin.
This prospective study, led by Dr. Tina Yen, recruited patients between June 2013 and September 2015 and compared 110 patients who had parathyroidectomy for primary hyperparathyroidism (PHPT) with 45 controls who had thyroidectomy for benign euthyroid disease between June 2013 and September 2015.
“Multiple studies, including recent meta-analyses, have demonstrated lower quality of life in patients with primary hyperparathyroidism and have suggested that patients, regardless of symptoms or degree of hypercalcemia, report varying degrees of improvement after parathyroidectomy,” Mr. La said. “In contrast there is a relative paucity of literature on the effects of primary hyperparathyroidism on sleep quality and changes after parathyroidectomy.”
He noted studies from both the University of Texas M.D. Anderson Cancer Center, Houston, and the University of Wisconsin–Madison had demonstrated a 44%-63% incidence of sleep disturbance preoperatively and improvement postoperatively in patients with PHPT who had parathyroidectomy (Endocr Pract. 2007 Jul-Aug;13:338-44; World J Surg. 2014 Mar;38:542-8; Surgery. 2009 Dec;146:1116-22).
“However, these studies were limited by small sample sizes and lack of a control group,” La said.
The latest study had subjects complete questionnaires inquiring about quality of life and sleep patterns at three different intervals: before surgery; and 1 and 6 months after surgery. The study used the Medical Outcomes Study SF-36 to assess quality of life and the Pittsburgh Sleep Quality Index (PSQI) to evaluate sleep quality. The PSQI rates sleep quality on a scale of 0 to 21; a score of 5 or higher indicates poor sleep quality.
“Compared to the preoperative scores, sleep scores after parathyroidectomy were lower, signifying better sleep quality among the 105 patients who completed 1-month postoperative surveys and the 94 patients who completed the 6-month surveys,” La said.
Before surgery, PHPT patients had worse sleep quality than their thyroid counterparts with PSQI scores of 8.1 vs. 5.3, respectively. After surgery, sleep quality scores between the two groups were similar, with mean PSQI scores of 6.3 vs. 5.3 at 1 month after surgery for the parathyroid and thyroid groups, respectively, and 5.8 vs. 4.6 for the two groups at 6 months.
Also, the proportion of patients in both groups who had poor sleep quality after surgery showed no statistical difference. At 1 month after surgery, 50% of patients in the parathyroid group and 40% in the thyroid group continued to have poor sleep quality, La said. However, when comparing preoperative with postoperative sleep scores, 37% in the parathyroid group had a noticeable improvement in their sleep scores, while only 10% of the thyroid group demonstrated improvement.
The researchers also evaluated physical and mental function in the two groups. “Preoperative overall health status was significantly worse in the parathyroid group,” La said. At 1 and 6 months after parathyroidectomy, only two physical components, physical functioning and bodily pain, remained worse in the PHPT patients. Compared with preoperative scores, PHPT patients showed statistically significant improvement in all four mental components at both postoperative periods. “In contrast, the thyroid group demonstrated no significant changes in the preoperative to postoperative scores in all eight components,” La said.
“Our study adds to the body of literature suggesting that asymptomatic patients with primary hyperparathyroidism are unlikely to be truly asymptomatic,” La said. “All patients with primary hyperparathyroidism should be referred for surgical consultation, particularly those with neurocognitive symptoms.”
He also said that patients should be counseled that improvement in sleep quality and quality of life, if they are to occur, typically are seen within 1 month after surgery.
Mr. La, Dr. Yen, and the study coauthors had no relationships to disclose.
BALTIMORE – Research into how primary hyperparathyroidism and parathyroidectomy affect sleep quality has been limited, but investigators at the Medical College of Wisconsin, Milwaukee, reported that primary hyperparathyroidism does indeed disrupt sleep patterns and that curative surgery can improve sleep quality in a third of patients.
“Today, most patients with primary hyperparathyroidism have what is considered asymptomatic disease,” Justin La reported at the annual meeting of the American Association of Endocrine Surgeons. “However, recent studies demonstrate that many of these asymptomatic patients commonly exhibit neuropsychological problems, including sleep disturbances.” Mr. La is a fourth-year medical student at the Medical College of Wisconsin.
This prospective study, led by Dr. Tina Yen, recruited patients between June 2013 and September 2015 and compared 110 patients who had parathyroidectomy for primary hyperparathyroidism (PHPT) with 45 controls who had thyroidectomy for benign euthyroid disease between June 2013 and September 2015.
“Multiple studies, including recent meta-analyses, have demonstrated lower quality of life in patients with primary hyperparathyroidism and have suggested that patients, regardless of symptoms or degree of hypercalcemia, report varying degrees of improvement after parathyroidectomy,” Mr. La said. “In contrast there is a relative paucity of literature on the effects of primary hyperparathyroidism on sleep quality and changes after parathyroidectomy.”
He noted studies from both the University of Texas M.D. Anderson Cancer Center, Houston, and the University of Wisconsin–Madison had demonstrated a 44%-63% incidence of sleep disturbance preoperatively and improvement postoperatively in patients with PHPT who had parathyroidectomy (Endocr Pract. 2007 Jul-Aug;13:338-44; World J Surg. 2014 Mar;38:542-8; Surgery. 2009 Dec;146:1116-22).
“However, these studies were limited by small sample sizes and lack of a control group,” La said.
The latest study had subjects complete questionnaires inquiring about quality of life and sleep patterns at three different intervals: before surgery; and 1 and 6 months after surgery. The study used the Medical Outcomes Study SF-36 to assess quality of life and the Pittsburgh Sleep Quality Index (PSQI) to evaluate sleep quality. The PSQI rates sleep quality on a scale of 0 to 21; a score of 5 or higher indicates poor sleep quality.
“Compared to the preoperative scores, sleep scores after parathyroidectomy were lower, signifying better sleep quality among the 105 patients who completed 1-month postoperative surveys and the 94 patients who completed the 6-month surveys,” La said.
Before surgery, PHPT patients had worse sleep quality than their thyroid counterparts with PSQI scores of 8.1 vs. 5.3, respectively. After surgery, sleep quality scores between the two groups were similar, with mean PSQI scores of 6.3 vs. 5.3 at 1 month after surgery for the parathyroid and thyroid groups, respectively, and 5.8 vs. 4.6 for the two groups at 6 months.
Also, the proportion of patients in both groups who had poor sleep quality after surgery showed no statistical difference. At 1 month after surgery, 50% of patients in the parathyroid group and 40% in the thyroid group continued to have poor sleep quality, La said. However, when comparing preoperative with postoperative sleep scores, 37% in the parathyroid group had a noticeable improvement in their sleep scores, while only 10% of the thyroid group demonstrated improvement.
The researchers also evaluated physical and mental function in the two groups. “Preoperative overall health status was significantly worse in the parathyroid group,” La said. At 1 and 6 months after parathyroidectomy, only two physical components, physical functioning and bodily pain, remained worse in the PHPT patients. Compared with preoperative scores, PHPT patients showed statistically significant improvement in all four mental components at both postoperative periods. “In contrast, the thyroid group demonstrated no significant changes in the preoperative to postoperative scores in all eight components,” La said.
“Our study adds to the body of literature suggesting that asymptomatic patients with primary hyperparathyroidism are unlikely to be truly asymptomatic,” La said. “All patients with primary hyperparathyroidism should be referred for surgical consultation, particularly those with neurocognitive symptoms.”
He also said that patients should be counseled that improvement in sleep quality and quality of life, if they are to occur, typically are seen within 1 month after surgery.
Mr. La, Dr. Yen, and the study coauthors had no relationships to disclose.
BALTIMORE – Research into how primary hyperparathyroidism and parathyroidectomy affect sleep quality has been limited, but investigators at the Medical College of Wisconsin, Milwaukee, reported that primary hyperparathyroidism does indeed disrupt sleep patterns and that curative surgery can improve sleep quality in a third of patients.
“Today, most patients with primary hyperparathyroidism have what is considered asymptomatic disease,” Justin La reported at the annual meeting of the American Association of Endocrine Surgeons. “However, recent studies demonstrate that many of these asymptomatic patients commonly exhibit neuropsychological problems, including sleep disturbances.” Mr. La is a fourth-year medical student at the Medical College of Wisconsin.
This prospective study, led by Dr. Tina Yen, recruited patients between June 2013 and September 2015 and compared 110 patients who had parathyroidectomy for primary hyperparathyroidism (PHPT) with 45 controls who had thyroidectomy for benign euthyroid disease between June 2013 and September 2015.
“Multiple studies, including recent meta-analyses, have demonstrated lower quality of life in patients with primary hyperparathyroidism and have suggested that patients, regardless of symptoms or degree of hypercalcemia, report varying degrees of improvement after parathyroidectomy,” Mr. La said. “In contrast there is a relative paucity of literature on the effects of primary hyperparathyroidism on sleep quality and changes after parathyroidectomy.”
He noted studies from both the University of Texas M.D. Anderson Cancer Center, Houston, and the University of Wisconsin–Madison had demonstrated a 44%-63% incidence of sleep disturbance preoperatively and improvement postoperatively in patients with PHPT who had parathyroidectomy (Endocr Pract. 2007 Jul-Aug;13:338-44; World J Surg. 2014 Mar;38:542-8; Surgery. 2009 Dec;146:1116-22).
“However, these studies were limited by small sample sizes and lack of a control group,” La said.
The latest study had subjects complete questionnaires inquiring about quality of life and sleep patterns at three different intervals: before surgery; and 1 and 6 months after surgery. The study used the Medical Outcomes Study SF-36 to assess quality of life and the Pittsburgh Sleep Quality Index (PSQI) to evaluate sleep quality. The PSQI rates sleep quality on a scale of 0 to 21; a score of 5 or higher indicates poor sleep quality.
“Compared to the preoperative scores, sleep scores after parathyroidectomy were lower, signifying better sleep quality among the 105 patients who completed 1-month postoperative surveys and the 94 patients who completed the 6-month surveys,” La said.
Before surgery, PHPT patients had worse sleep quality than their thyroid counterparts with PSQI scores of 8.1 vs. 5.3, respectively. After surgery, sleep quality scores between the two groups were similar, with mean PSQI scores of 6.3 vs. 5.3 at 1 month after surgery for the parathyroid and thyroid groups, respectively, and 5.8 vs. 4.6 for the two groups at 6 months.
Also, the proportion of patients in both groups who had poor sleep quality after surgery showed no statistical difference. At 1 month after surgery, 50% of patients in the parathyroid group and 40% in the thyroid group continued to have poor sleep quality, La said. However, when comparing preoperative with postoperative sleep scores, 37% in the parathyroid group had a noticeable improvement in their sleep scores, while only 10% of the thyroid group demonstrated improvement.
The researchers also evaluated physical and mental function in the two groups. “Preoperative overall health status was significantly worse in the parathyroid group,” La said. At 1 and 6 months after parathyroidectomy, only two physical components, physical functioning and bodily pain, remained worse in the PHPT patients. Compared with preoperative scores, PHPT patients showed statistically significant improvement in all four mental components at both postoperative periods. “In contrast, the thyroid group demonstrated no significant changes in the preoperative to postoperative scores in all eight components,” La said.
“Our study adds to the body of literature suggesting that asymptomatic patients with primary hyperparathyroidism are unlikely to be truly asymptomatic,” La said. “All patients with primary hyperparathyroidism should be referred for surgical consultation, particularly those with neurocognitive symptoms.”
He also said that patients should be counseled that improvement in sleep quality and quality of life, if they are to occur, typically are seen within 1 month after surgery.
Mr. La, Dr. Yen, and the study coauthors had no relationships to disclose.
AT AAES 2016
Key clinical point: A large proportion of “asymptomatic” patients with primary hyperparathyroidism (PHPT) actually have sleep disturbances.
Major finding: Sleep scores a month after parathyroidectomy were found to improve in 50% of patients with PHPT.
Data source: Single institution, prospective study of 155 patients comparing sleep patterns in patients with PHPT and thyroid controls.
Disclosures: Mr. La and his coauthors reported having no financial disclosures.
Cochrane Review nixes specific allergen immunotherapy for atopic dermatitis
LOS ANGELES – A new Cochrane systematic review and meta-analysis has concluded there is no consistent evidence that specific allergen immunotherapy is beneficial in patients with atopic dermatitis, Dr. Herman H. Tam reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
“We know that for specific allergen immunotherapy, there have been really good results in allergic rhinitis and venom allergy. For atopic dermatitis, however, dating back almost 40 years, we found there have only been 12 randomized trials using standardized allergen extracts. The quality of evidence was low, and the study findings have been inconsistent,” Dr. Tam, first author of the Cochrane review, said in an interview.
The dozen trials included a total of 733 children and adults in nine countries. Because of insufficient follow-up in most of the studies, coupled with the use of a variety of endpoints, the analysis concluded that “specific allergen immunotherapy cannot be recommended for atopic eczema at present” (Cochrane Database Syst Rev. 2016 Feb 12;2:CD008774).
“We found no consistent evidence that specific allergen immunotherapy provides a treatment benefit for people with allergic eczema, compared with placebo or no treatment. The message of this review is that we need more large randomized trials with better controls, modern high-quality allergen extracts that have proven themselves in other allergic diseases, and patient-centered outcome measures,” according to Dr. Tam, who participated in the Cochrane review while at Imperial College London and is now a pediatric resident at the University of Manitoba, Winnipeg.
He reported having no relevant financial conflicts.
LOS ANGELES – A new Cochrane systematic review and meta-analysis has concluded there is no consistent evidence that specific allergen immunotherapy is beneficial in patients with atopic dermatitis, Dr. Herman H. Tam reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
“We know that for specific allergen immunotherapy, there have been really good results in allergic rhinitis and venom allergy. For atopic dermatitis, however, dating back almost 40 years, we found there have only been 12 randomized trials using standardized allergen extracts. The quality of evidence was low, and the study findings have been inconsistent,” Dr. Tam, first author of the Cochrane review, said in an interview.
The dozen trials included a total of 733 children and adults in nine countries. Because of insufficient follow-up in most of the studies, coupled with the use of a variety of endpoints, the analysis concluded that “specific allergen immunotherapy cannot be recommended for atopic eczema at present” (Cochrane Database Syst Rev. 2016 Feb 12;2:CD008774).
“We found no consistent evidence that specific allergen immunotherapy provides a treatment benefit for people with allergic eczema, compared with placebo or no treatment. The message of this review is that we need more large randomized trials with better controls, modern high-quality allergen extracts that have proven themselves in other allergic diseases, and patient-centered outcome measures,” according to Dr. Tam, who participated in the Cochrane review while at Imperial College London and is now a pediatric resident at the University of Manitoba, Winnipeg.
He reported having no relevant financial conflicts.
LOS ANGELES – A new Cochrane systematic review and meta-analysis has concluded there is no consistent evidence that specific allergen immunotherapy is beneficial in patients with atopic dermatitis, Dr. Herman H. Tam reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
“We know that for specific allergen immunotherapy, there have been really good results in allergic rhinitis and venom allergy. For atopic dermatitis, however, dating back almost 40 years, we found there have only been 12 randomized trials using standardized allergen extracts. The quality of evidence was low, and the study findings have been inconsistent,” Dr. Tam, first author of the Cochrane review, said in an interview.
The dozen trials included a total of 733 children and adults in nine countries. Because of insufficient follow-up in most of the studies, coupled with the use of a variety of endpoints, the analysis concluded that “specific allergen immunotherapy cannot be recommended for atopic eczema at present” (Cochrane Database Syst Rev. 2016 Feb 12;2:CD008774).
“We found no consistent evidence that specific allergen immunotherapy provides a treatment benefit for people with allergic eczema, compared with placebo or no treatment. The message of this review is that we need more large randomized trials with better controls, modern high-quality allergen extracts that have proven themselves in other allergic diseases, and patient-centered outcome measures,” according to Dr. Tam, who participated in the Cochrane review while at Imperial College London and is now a pediatric resident at the University of Manitoba, Winnipeg.
He reported having no relevant financial conflicts.
AT 2016 AAAAI ANNUAL MEETING
Key clinical point: The available evidence doesn’t support using specific allergen immunotherapy for atopic dermatitis.
Major finding: A new Cochrane systematic review and meta-analysis has found “no consistent evidence” that specific allergen immunotherapy is more effective than placebo in treating atopic dermatitis.
Data source: This was a Cochrane systematic review and meta-analysis of 12 randomized controlled trials of specific allergen immunotherapy in 733 pediatric and adult atopic dermatitis patients.
Disclosures: The presenter reported having no relevant financial conflicts of interest.