User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Scientists create ‘vagina on a chip’: What to know
For years, women’s health advocates have argued that far more research is needed on women’s bodies and health. The world’s first-ever “vagina on a chip,” recently developed at Harvard’s Wyss Institute for Biologically Inspired Engineering in Boston, could go a long way to making that happen.
“Women’s health has not received the attention it deserves,” says Don Ingber, MD, PhD, who led the team that created the vagina chip. The advance quickly drew media attention after it was reported in the journal Microbiome. But researchers hope for more than headlines. They see the chip as a way to facilitate vaginal health research and open the door to vital new treatments.
By now, you may have heard of “organs on chips”: tiny devices about the size of a flash drive that are designed to mimic the biological activity of human organs. These glass chips contain living human cells within grooves that allow the passage of fluid, to either maintain or disrupt the cells’ function. So far, Dr. Ingber and his team at the Wyss Institute have developed more than 15 organ chip models, including chips that mimic the lung, intestine, kidney, and bone marrow.
The idea to develop a vagina chip grew out of research, funded by the Gates Foundation, on a childhood disease called environmental enteric dysfunction, an intestinal disease most commonly found in low-resource nations that is the second leading cause of death in children under 5. That’s when Dr. Ingber discovered just how much the child’s microbiome influences this disease.
Stemming from that work, the Gates Foundation turned its attention to newborn health – in particular, the impact of bacterial vaginosis, an imbalance in the vagina’s bacterial makeup. Bacterial vaginosis occurs in one out of four women worldwide and has been linked to premature birth as well as HIV, HPV persistence, and cervical cancer.
The goal was to test “live biotherapeutic products,” or living microbes like probiotics, that might restore the vagina’s microbiome to health.
No other preclinical model exists to perform tests like that, says Dr. Ingber.
“The vagina chip is a way to help make some advances,” he says.
The Gates Foundation recognized that women’s reproductive health is a major issue, not only in low-income nations, but everywhere around the world. As the project evolved, Dr. Ingber began to hear from female colleagues about how neglected women’s reproductive health is in medical science.
“It is something I became sensitive to and realized this is just the starting point,” Dr. Ingber says.
Take bacterial vaginosis, for example. Since 1982, treatment has revolved around the same two antibiotics. That’s partly because there is no animal model to study. No other species has the same vaginal bacterial community as humans do.
That makes developing any new therapy “incredibly challenging,” explains Caroline Mitchell, MD, MPH, an ob.gyn. at Massachusetts General Hospital, Boston, and a member of the consortium.
It turns out, replicating the vagina in a lab dish is, to use the technical term, very hard.
“That’s where a vagina chip offers an opportunity,” Dr. Mitchell says. “It’s not super-high throughput, but it’s way more high throughput than a [human] clinical trial.”
As such, the vagina chip could help scientists find new treatments much faster.
Like Dr. Ingber, Dr. Mitchell also sees the chip as a way to bring more attention to the largely unmet needs in female reproductive medicine.
“Women’s reproductive health has been under-resourced, under-prioritized, and largely disregarded for decades,” she says. And the time may be ripe for change: Dr. Mitchell says she was encouraged by the National Institutes of Health’s Advancing NIH Research on the Health of Women conference, held in 2021 in response to a congressional request to address women’s health research efforts.
Beyond bacterial vaginosis, Dr. Mitchell imagines the chip could help scientists find new treatments for vaginal yeast infection (candidiasis), chlamydia, and endometriosis. As with bacterial vaginosis, medicines for vaginal yeast infections have not advanced in decades, Dr. Mitchell says. Efforts to develop a vaccine for chlamydia – which can cause permanent damage to a woman’s reproductive system – have dragged on for many years. And endometriosis, an often painful condition in which the tissue that makes up the uterine lining grows outside the uterus, remains under-researched despite affecting 10% of childbearing-age women.
While some mouse models are used in chlamydia research, it’s hard to say if they’ll translate to humans, given the vaginal and cervical bacterial differences.
“Our understanding of the basic physiology of the environment of the vagina and cervix is another area where we’re woefully ignorant,” Dr. Mitchell says.
To that end, Dr. Ingber’s team is developing more complex chips mimicking the vagina and the cervix. One of his team members wants to use the chips to study infertility. The researchers have already used the chips to see how bacterial vaginosis and mucous changes impact the way sperm migrates up the reproductive tract.
The lab is now linking vagina and cervix chips together to study viral infections of the cervix, like HPV, and all types of bacterial diseases of the vaginal tract. By applying cervical mucus to the vagina chip, they hope to learn more about how female reproductive tissues respond to infection and inflammation.
“I always say that organ chips are like synthetic biology at the cell tissue and organ level,” says Dr. Ingber. “You start simple and see if you [can] mimic a clinical situation.”
As they make the chips more complex – perhaps by adding blood vessel cells and female hormones – Dr. Ingber foresees being able to study the response to hormonal changes during the menstrual cycle.
“We can begin to explore the effects of cycling over time as well as other types of hormonal effects,” he says.
Dr. Ingber also envisions linking the vagina chip to other organ chips – he’s already succeeded in linking eight different organ types together. But for now, the team hopes the vagina chip will enhance our understanding of basic female reproductive biology and speed up the process of developing new treatments for women’s health.
A version of this article first appeared on WebMD.com.
For years, women’s health advocates have argued that far more research is needed on women’s bodies and health. The world’s first-ever “vagina on a chip,” recently developed at Harvard’s Wyss Institute for Biologically Inspired Engineering in Boston, could go a long way to making that happen.
“Women’s health has not received the attention it deserves,” says Don Ingber, MD, PhD, who led the team that created the vagina chip. The advance quickly drew media attention after it was reported in the journal Microbiome. But researchers hope for more than headlines. They see the chip as a way to facilitate vaginal health research and open the door to vital new treatments.
By now, you may have heard of “organs on chips”: tiny devices about the size of a flash drive that are designed to mimic the biological activity of human organs. These glass chips contain living human cells within grooves that allow the passage of fluid, to either maintain or disrupt the cells’ function. So far, Dr. Ingber and his team at the Wyss Institute have developed more than 15 organ chip models, including chips that mimic the lung, intestine, kidney, and bone marrow.
The idea to develop a vagina chip grew out of research, funded by the Gates Foundation, on a childhood disease called environmental enteric dysfunction, an intestinal disease most commonly found in low-resource nations that is the second leading cause of death in children under 5. That’s when Dr. Ingber discovered just how much the child’s microbiome influences this disease.
Stemming from that work, the Gates Foundation turned its attention to newborn health – in particular, the impact of bacterial vaginosis, an imbalance in the vagina’s bacterial makeup. Bacterial vaginosis occurs in one out of four women worldwide and has been linked to premature birth as well as HIV, HPV persistence, and cervical cancer.
The goal was to test “live biotherapeutic products,” or living microbes like probiotics, that might restore the vagina’s microbiome to health.
No other preclinical model exists to perform tests like that, says Dr. Ingber.
“The vagina chip is a way to help make some advances,” he says.
The Gates Foundation recognized that women’s reproductive health is a major issue, not only in low-income nations, but everywhere around the world. As the project evolved, Dr. Ingber began to hear from female colleagues about how neglected women’s reproductive health is in medical science.
“It is something I became sensitive to and realized this is just the starting point,” Dr. Ingber says.
Take bacterial vaginosis, for example. Since 1982, treatment has revolved around the same two antibiotics. That’s partly because there is no animal model to study. No other species has the same vaginal bacterial community as humans do.
That makes developing any new therapy “incredibly challenging,” explains Caroline Mitchell, MD, MPH, an ob.gyn. at Massachusetts General Hospital, Boston, and a member of the consortium.
It turns out, replicating the vagina in a lab dish is, to use the technical term, very hard.
“That’s where a vagina chip offers an opportunity,” Dr. Mitchell says. “It’s not super-high throughput, but it’s way more high throughput than a [human] clinical trial.”
As such, the vagina chip could help scientists find new treatments much faster.
Like Dr. Ingber, Dr. Mitchell also sees the chip as a way to bring more attention to the largely unmet needs in female reproductive medicine.
“Women’s reproductive health has been under-resourced, under-prioritized, and largely disregarded for decades,” she says. And the time may be ripe for change: Dr. Mitchell says she was encouraged by the National Institutes of Health’s Advancing NIH Research on the Health of Women conference, held in 2021 in response to a congressional request to address women’s health research efforts.
Beyond bacterial vaginosis, Dr. Mitchell imagines the chip could help scientists find new treatments for vaginal yeast infection (candidiasis), chlamydia, and endometriosis. As with bacterial vaginosis, medicines for vaginal yeast infections have not advanced in decades, Dr. Mitchell says. Efforts to develop a vaccine for chlamydia – which can cause permanent damage to a woman’s reproductive system – have dragged on for many years. And endometriosis, an often painful condition in which the tissue that makes up the uterine lining grows outside the uterus, remains under-researched despite affecting 10% of childbearing-age women.
While some mouse models are used in chlamydia research, it’s hard to say if they’ll translate to humans, given the vaginal and cervical bacterial differences.
“Our understanding of the basic physiology of the environment of the vagina and cervix is another area where we’re woefully ignorant,” Dr. Mitchell says.
To that end, Dr. Ingber’s team is developing more complex chips mimicking the vagina and the cervix. One of his team members wants to use the chips to study infertility. The researchers have already used the chips to see how bacterial vaginosis and mucous changes impact the way sperm migrates up the reproductive tract.
The lab is now linking vagina and cervix chips together to study viral infections of the cervix, like HPV, and all types of bacterial diseases of the vaginal tract. By applying cervical mucus to the vagina chip, they hope to learn more about how female reproductive tissues respond to infection and inflammation.
“I always say that organ chips are like synthetic biology at the cell tissue and organ level,” says Dr. Ingber. “You start simple and see if you [can] mimic a clinical situation.”
As they make the chips more complex – perhaps by adding blood vessel cells and female hormones – Dr. Ingber foresees being able to study the response to hormonal changes during the menstrual cycle.
“We can begin to explore the effects of cycling over time as well as other types of hormonal effects,” he says.
Dr. Ingber also envisions linking the vagina chip to other organ chips – he’s already succeeded in linking eight different organ types together. But for now, the team hopes the vagina chip will enhance our understanding of basic female reproductive biology and speed up the process of developing new treatments for women’s health.
A version of this article first appeared on WebMD.com.
For years, women’s health advocates have argued that far more research is needed on women’s bodies and health. The world’s first-ever “vagina on a chip,” recently developed at Harvard’s Wyss Institute for Biologically Inspired Engineering in Boston, could go a long way to making that happen.
“Women’s health has not received the attention it deserves,” says Don Ingber, MD, PhD, who led the team that created the vagina chip. The advance quickly drew media attention after it was reported in the journal Microbiome. But researchers hope for more than headlines. They see the chip as a way to facilitate vaginal health research and open the door to vital new treatments.
By now, you may have heard of “organs on chips”: tiny devices about the size of a flash drive that are designed to mimic the biological activity of human organs. These glass chips contain living human cells within grooves that allow the passage of fluid, to either maintain or disrupt the cells’ function. So far, Dr. Ingber and his team at the Wyss Institute have developed more than 15 organ chip models, including chips that mimic the lung, intestine, kidney, and bone marrow.
The idea to develop a vagina chip grew out of research, funded by the Gates Foundation, on a childhood disease called environmental enteric dysfunction, an intestinal disease most commonly found in low-resource nations that is the second leading cause of death in children under 5. That’s when Dr. Ingber discovered just how much the child’s microbiome influences this disease.
Stemming from that work, the Gates Foundation turned its attention to newborn health – in particular, the impact of bacterial vaginosis, an imbalance in the vagina’s bacterial makeup. Bacterial vaginosis occurs in one out of four women worldwide and has been linked to premature birth as well as HIV, HPV persistence, and cervical cancer.
The goal was to test “live biotherapeutic products,” or living microbes like probiotics, that might restore the vagina’s microbiome to health.
No other preclinical model exists to perform tests like that, says Dr. Ingber.
“The vagina chip is a way to help make some advances,” he says.
The Gates Foundation recognized that women’s reproductive health is a major issue, not only in low-income nations, but everywhere around the world. As the project evolved, Dr. Ingber began to hear from female colleagues about how neglected women’s reproductive health is in medical science.
“It is something I became sensitive to and realized this is just the starting point,” Dr. Ingber says.
Take bacterial vaginosis, for example. Since 1982, treatment has revolved around the same two antibiotics. That’s partly because there is no animal model to study. No other species has the same vaginal bacterial community as humans do.
That makes developing any new therapy “incredibly challenging,” explains Caroline Mitchell, MD, MPH, an ob.gyn. at Massachusetts General Hospital, Boston, and a member of the consortium.
It turns out, replicating the vagina in a lab dish is, to use the technical term, very hard.
“That’s where a vagina chip offers an opportunity,” Dr. Mitchell says. “It’s not super-high throughput, but it’s way more high throughput than a [human] clinical trial.”
As such, the vagina chip could help scientists find new treatments much faster.
Like Dr. Ingber, Dr. Mitchell also sees the chip as a way to bring more attention to the largely unmet needs in female reproductive medicine.
“Women’s reproductive health has been under-resourced, under-prioritized, and largely disregarded for decades,” she says. And the time may be ripe for change: Dr. Mitchell says she was encouraged by the National Institutes of Health’s Advancing NIH Research on the Health of Women conference, held in 2021 in response to a congressional request to address women’s health research efforts.
Beyond bacterial vaginosis, Dr. Mitchell imagines the chip could help scientists find new treatments for vaginal yeast infection (candidiasis), chlamydia, and endometriosis. As with bacterial vaginosis, medicines for vaginal yeast infections have not advanced in decades, Dr. Mitchell says. Efforts to develop a vaccine for chlamydia – which can cause permanent damage to a woman’s reproductive system – have dragged on for many years. And endometriosis, an often painful condition in which the tissue that makes up the uterine lining grows outside the uterus, remains under-researched despite affecting 10% of childbearing-age women.
While some mouse models are used in chlamydia research, it’s hard to say if they’ll translate to humans, given the vaginal and cervical bacterial differences.
“Our understanding of the basic physiology of the environment of the vagina and cervix is another area where we’re woefully ignorant,” Dr. Mitchell says.
To that end, Dr. Ingber’s team is developing more complex chips mimicking the vagina and the cervix. One of his team members wants to use the chips to study infertility. The researchers have already used the chips to see how bacterial vaginosis and mucous changes impact the way sperm migrates up the reproductive tract.
The lab is now linking vagina and cervix chips together to study viral infections of the cervix, like HPV, and all types of bacterial diseases of the vaginal tract. By applying cervical mucus to the vagina chip, they hope to learn more about how female reproductive tissues respond to infection and inflammation.
“I always say that organ chips are like synthetic biology at the cell tissue and organ level,” says Dr. Ingber. “You start simple and see if you [can] mimic a clinical situation.”
As they make the chips more complex – perhaps by adding blood vessel cells and female hormones – Dr. Ingber foresees being able to study the response to hormonal changes during the menstrual cycle.
“We can begin to explore the effects of cycling over time as well as other types of hormonal effects,” he says.
Dr. Ingber also envisions linking the vagina chip to other organ chips – he’s already succeeded in linking eight different organ types together. But for now, the team hopes the vagina chip will enhance our understanding of basic female reproductive biology and speed up the process of developing new treatments for women’s health.
A version of this article first appeared on WebMD.com.
FROM MICROBIOME
Vacuum device for postpartum hemorrhage works well in real world
Postpartum hemorrhage is the leading cause of maternal mortality worldwide, accounting for 25% of deaths from obstetric causes. Although balloon tamponade has been widely used to manage uncontrolled postpartum bleeding, a recent evaluation of an intrauterine vacuum-induced hemorrhage control device demonstrated impressive safety and effectiveness, researchers reported at the meeting sponsored by the Society for Maternal-Fetal Medicine.
“It’s exciting to see new technology and new potential treatment modalities. We just don’t have that many tools in our toolkit right now,” said Dena Goffman, MD, professor of women’s health and obstetrics and gynecology and vice chair of quality and patient safety at Columbia University’s Irving Medical Center, in New York, who presented the findings.
Dr. Goffman led an earlier multicenter prospective single-arm treatment study of the Jada System, a vacuum device marketed by Organon. The U.S. Food and Drug Administration approved use of the Jada System in October 2020.
Dr. Goffman said she and her colleagues felt “a next logical step would be to see what happens with real-world use.” In the new study, researchers at 16 U.S. medical centers reviewed medical charts of 800 women who underwent treatment with the Jada System between October 2020 and April 2022.
Treatment was successful in 92.5% of the vaginal births (n = 530) and 83.7% of the cesarean births (n = 270), similar to the results of the initial treatment trial that led to FDA approval, according to the researchers. For both types of delivery, bleeding was controlled in less than 5 minutes for most patients. Three serious adverse events were identified that could have been related to use of the device (two in vaginal births, one in cesarean birth), they reported.
Although the study was not designed to directly compare the Jada System with balloon tamponade, in a recent meta-analysis, it was estimated that tamponade controls postpartum hemorrhage in roughly 87% of cases, with complication rates in as many as 6.5% among women who undergo the procedure.
Dr. Goffman pointed out additional benefits. The vacuum device typically must stay in place for less time (3.1 hours for vaginal birth and 4.6 hours for cesarean birth) than balloon tamponade, allowing women to recover more quickly. In the initial trial, which Dr. Goffman helped conduct, 98% of clinicians reported that the device was easy to use, which increases its attractiveness in lower-income countries. Dr. Goffman felt that the device “has potential for huge impact” in those countries, given the high rates of maternal morbidity and mortality in these areas.
Amber Samuel, MD, medical director of OBSETRIX Maternal Fetal Medicine Specialists of Houston, said the device recently became available in the hospitals in which she works, and she has used the Jada System several times. Like Dr. Goffman, she was excited to have a new tool for treating a life-threatening condition.
Although the device has been on the market for more than 2 years, Dr. Samuel felt clinicians who were reluctant to adopt a new technology would be reassured by the findings.
“We should make sure that it’s effective, and we should know what the safety profile is,” said Dr. Samuel, adding that “the more data we have, the more we’re able to counsel patients and work this into our protocols for what is a really common obstetric problem.”
Both Dr. Goffman and Dr. Samuel agreed that more data, ideally from randomized clinical trials, are needed to convince professional groups such as the American College of Obstetricians and Gynecologists to state a clear preference for use of vacuum-induced hemorrhage control devices over balloon tamponade.
“We should be supporting further investigation,” Dr. Goffman said, “but for people who have this tool available to them now, I think they can feel confident in using it.”
The study was funded by Alydia Health, the manufacturer of the Jada System. Alydia Health was acquired by Organon in 2021. Study sites received research-related financial support, but none of the authors received direct payments from Alydia Health/Organon. Dr. Goffman serves on the scientific advisory board of Alydia Health/Organon. Dr. Samuel has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Postpartum hemorrhage is the leading cause of maternal mortality worldwide, accounting for 25% of deaths from obstetric causes. Although balloon tamponade has been widely used to manage uncontrolled postpartum bleeding, a recent evaluation of an intrauterine vacuum-induced hemorrhage control device demonstrated impressive safety and effectiveness, researchers reported at the meeting sponsored by the Society for Maternal-Fetal Medicine.
“It’s exciting to see new technology and new potential treatment modalities. We just don’t have that many tools in our toolkit right now,” said Dena Goffman, MD, professor of women’s health and obstetrics and gynecology and vice chair of quality and patient safety at Columbia University’s Irving Medical Center, in New York, who presented the findings.
Dr. Goffman led an earlier multicenter prospective single-arm treatment study of the Jada System, a vacuum device marketed by Organon. The U.S. Food and Drug Administration approved use of the Jada System in October 2020.
Dr. Goffman said she and her colleagues felt “a next logical step would be to see what happens with real-world use.” In the new study, researchers at 16 U.S. medical centers reviewed medical charts of 800 women who underwent treatment with the Jada System between October 2020 and April 2022.
Treatment was successful in 92.5% of the vaginal births (n = 530) and 83.7% of the cesarean births (n = 270), similar to the results of the initial treatment trial that led to FDA approval, according to the researchers. For both types of delivery, bleeding was controlled in less than 5 minutes for most patients. Three serious adverse events were identified that could have been related to use of the device (two in vaginal births, one in cesarean birth), they reported.
Although the study was not designed to directly compare the Jada System with balloon tamponade, in a recent meta-analysis, it was estimated that tamponade controls postpartum hemorrhage in roughly 87% of cases, with complication rates in as many as 6.5% among women who undergo the procedure.
Dr. Goffman pointed out additional benefits. The vacuum device typically must stay in place for less time (3.1 hours for vaginal birth and 4.6 hours for cesarean birth) than balloon tamponade, allowing women to recover more quickly. In the initial trial, which Dr. Goffman helped conduct, 98% of clinicians reported that the device was easy to use, which increases its attractiveness in lower-income countries. Dr. Goffman felt that the device “has potential for huge impact” in those countries, given the high rates of maternal morbidity and mortality in these areas.
Amber Samuel, MD, medical director of OBSETRIX Maternal Fetal Medicine Specialists of Houston, said the device recently became available in the hospitals in which she works, and she has used the Jada System several times. Like Dr. Goffman, she was excited to have a new tool for treating a life-threatening condition.
Although the device has been on the market for more than 2 years, Dr. Samuel felt clinicians who were reluctant to adopt a new technology would be reassured by the findings.
“We should make sure that it’s effective, and we should know what the safety profile is,” said Dr. Samuel, adding that “the more data we have, the more we’re able to counsel patients and work this into our protocols for what is a really common obstetric problem.”
Both Dr. Goffman and Dr. Samuel agreed that more data, ideally from randomized clinical trials, are needed to convince professional groups such as the American College of Obstetricians and Gynecologists to state a clear preference for use of vacuum-induced hemorrhage control devices over balloon tamponade.
“We should be supporting further investigation,” Dr. Goffman said, “but for people who have this tool available to them now, I think they can feel confident in using it.”
The study was funded by Alydia Health, the manufacturer of the Jada System. Alydia Health was acquired by Organon in 2021. Study sites received research-related financial support, but none of the authors received direct payments from Alydia Health/Organon. Dr. Goffman serves on the scientific advisory board of Alydia Health/Organon. Dr. Samuel has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Postpartum hemorrhage is the leading cause of maternal mortality worldwide, accounting for 25% of deaths from obstetric causes. Although balloon tamponade has been widely used to manage uncontrolled postpartum bleeding, a recent evaluation of an intrauterine vacuum-induced hemorrhage control device demonstrated impressive safety and effectiveness, researchers reported at the meeting sponsored by the Society for Maternal-Fetal Medicine.
“It’s exciting to see new technology and new potential treatment modalities. We just don’t have that many tools in our toolkit right now,” said Dena Goffman, MD, professor of women’s health and obstetrics and gynecology and vice chair of quality and patient safety at Columbia University’s Irving Medical Center, in New York, who presented the findings.
Dr. Goffman led an earlier multicenter prospective single-arm treatment study of the Jada System, a vacuum device marketed by Organon. The U.S. Food and Drug Administration approved use of the Jada System in October 2020.
Dr. Goffman said she and her colleagues felt “a next logical step would be to see what happens with real-world use.” In the new study, researchers at 16 U.S. medical centers reviewed medical charts of 800 women who underwent treatment with the Jada System between October 2020 and April 2022.
Treatment was successful in 92.5% of the vaginal births (n = 530) and 83.7% of the cesarean births (n = 270), similar to the results of the initial treatment trial that led to FDA approval, according to the researchers. For both types of delivery, bleeding was controlled in less than 5 minutes for most patients. Three serious adverse events were identified that could have been related to use of the device (two in vaginal births, one in cesarean birth), they reported.
Although the study was not designed to directly compare the Jada System with balloon tamponade, in a recent meta-analysis, it was estimated that tamponade controls postpartum hemorrhage in roughly 87% of cases, with complication rates in as many as 6.5% among women who undergo the procedure.
Dr. Goffman pointed out additional benefits. The vacuum device typically must stay in place for less time (3.1 hours for vaginal birth and 4.6 hours for cesarean birth) than balloon tamponade, allowing women to recover more quickly. In the initial trial, which Dr. Goffman helped conduct, 98% of clinicians reported that the device was easy to use, which increases its attractiveness in lower-income countries. Dr. Goffman felt that the device “has potential for huge impact” in those countries, given the high rates of maternal morbidity and mortality in these areas.
Amber Samuel, MD, medical director of OBSETRIX Maternal Fetal Medicine Specialists of Houston, said the device recently became available in the hospitals in which she works, and she has used the Jada System several times. Like Dr. Goffman, she was excited to have a new tool for treating a life-threatening condition.
Although the device has been on the market for more than 2 years, Dr. Samuel felt clinicians who were reluctant to adopt a new technology would be reassured by the findings.
“We should make sure that it’s effective, and we should know what the safety profile is,” said Dr. Samuel, adding that “the more data we have, the more we’re able to counsel patients and work this into our protocols for what is a really common obstetric problem.”
Both Dr. Goffman and Dr. Samuel agreed that more data, ideally from randomized clinical trials, are needed to convince professional groups such as the American College of Obstetricians and Gynecologists to state a clear preference for use of vacuum-induced hemorrhage control devices over balloon tamponade.
“We should be supporting further investigation,” Dr. Goffman said, “but for people who have this tool available to them now, I think they can feel confident in using it.”
The study was funded by Alydia Health, the manufacturer of the Jada System. Alydia Health was acquired by Organon in 2021. Study sites received research-related financial support, but none of the authors received direct payments from Alydia Health/Organon. Dr. Goffman serves on the scientific advisory board of Alydia Health/Organon. Dr. Samuel has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE PREGNANCY MEETING
More evidence suggests oxytocin can be discontinued early in labor
A new randomized, open-label French trial offers more evidence that the discontinuation of oxytocin treatment after the earliest stages of labor may be safe. Stopping oxytocin didn’t appear to affect neonatal outcomes, compared with continual use of the medication. However, the first stage of labor lasted slightly longer – not surprisingly – in those in the intervention group, and many of those who stopped oxytocin treatment resumed it later.
“Our trial did not show any impact of oxytocin discontinuation in the active [labor] stage on neonatal morbidity cesarean delivery, postpartum hemorrhage, birth experience, and postpartum depression,” said Aude Girault, MD, PhD, of Paris Cité University, in a presentation in San Francisco at the meeting sponsored by the Society for Maternal-Fetal Medicine.
The goal of the STOPOXY study is to build upon previous research that found oxytocin discontinuation didn’t boost the risk of cesarean delivery rates, uterine hyperstimulation, and abnormal fetal heart rate, Dr. Girault said. “These studies were underpowered to show any effects on neonatal morbidity,” so she and colleagues decided to dig deeper into the issue by launching the new trial.
From 2020 to 2022, researchers assigned 2,367 women who received oxytocin before 4 centimeters dilation to either continue with the drug (n = 1,192) or discontinue it before reaching 6 centimeters dilation (n = 1,175). Overall, the women were pregnant for the first time (around 55%) with a median age around 32 years and body mass index around 24.1 kg/m2. All had live, singleton, full-term babies.
More than a third – 37% – of those who discontinued oxytocin resumed treatment with the medication, while 5% of those in the control group stopped taking it.
The neonatal morbidity rate – defined via a composite variable based on umbilical arterial pH, umbilical arterial lactates, Apgar score, and/or neonatal ICU admission – was 10.0% in the intervention group and 10.1% in the control group (P = .94), the researchers reported. Cesarean delivery rates were similar (18.8% vs. 16.5%, respectively; P = .22). Apart from the duration of the active first stage, which was significantly higher in the intervention group (100 min [ interquartile range, 50-208 min] vs. 90 min [IQR, 45-150 min]; P = .001), there were no significant differences between the groups.
Dr. Girault said this increase in labor duration was “moderate and clinically debatable.”
In an interview, oncologist-gynecologist George Saade, MD, of the University of Texas Medical Branch, Galveston, noted that “oxytocin is frequently used for either induction or augmentation of labor ... with the goal of improving maternal and neonatal outcomes.”
Oxytocin itself is not expensive, Dr. Saade said. “However, when it is given, the patient requires more monitoring, which may increase cost.”
There’s debate over the proper use of oxytocin, which is available in a synthetic version as Pitocin, and researchers have been trying to understand whether it can safely be discontinued early in labor.
Potential side effects of oxytocin include heart disorders such as arrhythmia, asphyxia, neonatal seizure, and jaundice, low Apgar score, and fetal death. A boxed warning says: “Because the available data are inadequate to evaluate the benefits-to-risks considerations, oxytocin is not indicated for elective induction of labor.”
However, “overall oxytocin is commonly used and very safe as long as careful protocols are followed,” David N. Hackney, MD, MS, of University Hospitals Cleveland, said in an interview. “The medication itself does not have many negative side effects. With very high doses there can be a concern for water intoxication, though this is clinically very uncommon. Some prior studies have raised concerns about the use of oxytocin and subsequent long-term neurodevelopmental outcomes, though these associations are likely confounders and the mainstream opinion is that these are not truly biologically causative associations.”
A 2021 study in The BMJ randomly assigned 1,200 women to continue or discontinue oxytocin. There was a slight increase in cesarean sections in the discontinuation group but significantly lower risks of uterine hyperstimulation and abnormal fetal heart rate.
Dr. Hackney, who didn’t take part in the new study, said the trial is “well conducted and well executed.” However, it needs peer review before any of its findings should change practice.
He added that differences in delivery protocols between the United States and France should be considered. As he noted, Dr. Girault mentioned in a Q&A after her presentation that delayed second-stage labor is more common in France than in the United States.
The study was funded by the French National Ministry of Health. Disclosures for the authors were not provided. Dr. Saade and Dr. Hackney have no disclosures.
A new randomized, open-label French trial offers more evidence that the discontinuation of oxytocin treatment after the earliest stages of labor may be safe. Stopping oxytocin didn’t appear to affect neonatal outcomes, compared with continual use of the medication. However, the first stage of labor lasted slightly longer – not surprisingly – in those in the intervention group, and many of those who stopped oxytocin treatment resumed it later.
“Our trial did not show any impact of oxytocin discontinuation in the active [labor] stage on neonatal morbidity cesarean delivery, postpartum hemorrhage, birth experience, and postpartum depression,” said Aude Girault, MD, PhD, of Paris Cité University, in a presentation in San Francisco at the meeting sponsored by the Society for Maternal-Fetal Medicine.
The goal of the STOPOXY study is to build upon previous research that found oxytocin discontinuation didn’t boost the risk of cesarean delivery rates, uterine hyperstimulation, and abnormal fetal heart rate, Dr. Girault said. “These studies were underpowered to show any effects on neonatal morbidity,” so she and colleagues decided to dig deeper into the issue by launching the new trial.
From 2020 to 2022, researchers assigned 2,367 women who received oxytocin before 4 centimeters dilation to either continue with the drug (n = 1,192) or discontinue it before reaching 6 centimeters dilation (n = 1,175). Overall, the women were pregnant for the first time (around 55%) with a median age around 32 years and body mass index around 24.1 kg/m2. All had live, singleton, full-term babies.
More than a third – 37% – of those who discontinued oxytocin resumed treatment with the medication, while 5% of those in the control group stopped taking it.
The neonatal morbidity rate – defined via a composite variable based on umbilical arterial pH, umbilical arterial lactates, Apgar score, and/or neonatal ICU admission – was 10.0% in the intervention group and 10.1% in the control group (P = .94), the researchers reported. Cesarean delivery rates were similar (18.8% vs. 16.5%, respectively; P = .22). Apart from the duration of the active first stage, which was significantly higher in the intervention group (100 min [ interquartile range, 50-208 min] vs. 90 min [IQR, 45-150 min]; P = .001), there were no significant differences between the groups.
Dr. Girault said this increase in labor duration was “moderate and clinically debatable.”
In an interview, oncologist-gynecologist George Saade, MD, of the University of Texas Medical Branch, Galveston, noted that “oxytocin is frequently used for either induction or augmentation of labor ... with the goal of improving maternal and neonatal outcomes.”
Oxytocin itself is not expensive, Dr. Saade said. “However, when it is given, the patient requires more monitoring, which may increase cost.”
There’s debate over the proper use of oxytocin, which is available in a synthetic version as Pitocin, and researchers have been trying to understand whether it can safely be discontinued early in labor.
Potential side effects of oxytocin include heart disorders such as arrhythmia, asphyxia, neonatal seizure, and jaundice, low Apgar score, and fetal death. A boxed warning says: “Because the available data are inadequate to evaluate the benefits-to-risks considerations, oxytocin is not indicated for elective induction of labor.”
However, “overall oxytocin is commonly used and very safe as long as careful protocols are followed,” David N. Hackney, MD, MS, of University Hospitals Cleveland, said in an interview. “The medication itself does not have many negative side effects. With very high doses there can be a concern for water intoxication, though this is clinically very uncommon. Some prior studies have raised concerns about the use of oxytocin and subsequent long-term neurodevelopmental outcomes, though these associations are likely confounders and the mainstream opinion is that these are not truly biologically causative associations.”
A 2021 study in The BMJ randomly assigned 1,200 women to continue or discontinue oxytocin. There was a slight increase in cesarean sections in the discontinuation group but significantly lower risks of uterine hyperstimulation and abnormal fetal heart rate.
Dr. Hackney, who didn’t take part in the new study, said the trial is “well conducted and well executed.” However, it needs peer review before any of its findings should change practice.
He added that differences in delivery protocols between the United States and France should be considered. As he noted, Dr. Girault mentioned in a Q&A after her presentation that delayed second-stage labor is more common in France than in the United States.
The study was funded by the French National Ministry of Health. Disclosures for the authors were not provided. Dr. Saade and Dr. Hackney have no disclosures.
A new randomized, open-label French trial offers more evidence that the discontinuation of oxytocin treatment after the earliest stages of labor may be safe. Stopping oxytocin didn’t appear to affect neonatal outcomes, compared with continual use of the medication. However, the first stage of labor lasted slightly longer – not surprisingly – in those in the intervention group, and many of those who stopped oxytocin treatment resumed it later.
“Our trial did not show any impact of oxytocin discontinuation in the active [labor] stage on neonatal morbidity cesarean delivery, postpartum hemorrhage, birth experience, and postpartum depression,” said Aude Girault, MD, PhD, of Paris Cité University, in a presentation in San Francisco at the meeting sponsored by the Society for Maternal-Fetal Medicine.
The goal of the STOPOXY study is to build upon previous research that found oxytocin discontinuation didn’t boost the risk of cesarean delivery rates, uterine hyperstimulation, and abnormal fetal heart rate, Dr. Girault said. “These studies were underpowered to show any effects on neonatal morbidity,” so she and colleagues decided to dig deeper into the issue by launching the new trial.
From 2020 to 2022, researchers assigned 2,367 women who received oxytocin before 4 centimeters dilation to either continue with the drug (n = 1,192) or discontinue it before reaching 6 centimeters dilation (n = 1,175). Overall, the women were pregnant for the first time (around 55%) with a median age around 32 years and body mass index around 24.1 kg/m2. All had live, singleton, full-term babies.
More than a third – 37% – of those who discontinued oxytocin resumed treatment with the medication, while 5% of those in the control group stopped taking it.
The neonatal morbidity rate – defined via a composite variable based on umbilical arterial pH, umbilical arterial lactates, Apgar score, and/or neonatal ICU admission – was 10.0% in the intervention group and 10.1% in the control group (P = .94), the researchers reported. Cesarean delivery rates were similar (18.8% vs. 16.5%, respectively; P = .22). Apart from the duration of the active first stage, which was significantly higher in the intervention group (100 min [ interquartile range, 50-208 min] vs. 90 min [IQR, 45-150 min]; P = .001), there were no significant differences between the groups.
Dr. Girault said this increase in labor duration was “moderate and clinically debatable.”
In an interview, oncologist-gynecologist George Saade, MD, of the University of Texas Medical Branch, Galveston, noted that “oxytocin is frequently used for either induction or augmentation of labor ... with the goal of improving maternal and neonatal outcomes.”
Oxytocin itself is not expensive, Dr. Saade said. “However, when it is given, the patient requires more monitoring, which may increase cost.”
There’s debate over the proper use of oxytocin, which is available in a synthetic version as Pitocin, and researchers have been trying to understand whether it can safely be discontinued early in labor.
Potential side effects of oxytocin include heart disorders such as arrhythmia, asphyxia, neonatal seizure, and jaundice, low Apgar score, and fetal death. A boxed warning says: “Because the available data are inadequate to evaluate the benefits-to-risks considerations, oxytocin is not indicated for elective induction of labor.”
However, “overall oxytocin is commonly used and very safe as long as careful protocols are followed,” David N. Hackney, MD, MS, of University Hospitals Cleveland, said in an interview. “The medication itself does not have many negative side effects. With very high doses there can be a concern for water intoxication, though this is clinically very uncommon. Some prior studies have raised concerns about the use of oxytocin and subsequent long-term neurodevelopmental outcomes, though these associations are likely confounders and the mainstream opinion is that these are not truly biologically causative associations.”
A 2021 study in The BMJ randomly assigned 1,200 women to continue or discontinue oxytocin. There was a slight increase in cesarean sections in the discontinuation group but significantly lower risks of uterine hyperstimulation and abnormal fetal heart rate.
Dr. Hackney, who didn’t take part in the new study, said the trial is “well conducted and well executed.” However, it needs peer review before any of its findings should change practice.
He added that differences in delivery protocols between the United States and France should be considered. As he noted, Dr. Girault mentioned in a Q&A after her presentation that delayed second-stage labor is more common in France than in the United States.
The study was funded by the French National Ministry of Health. Disclosures for the authors were not provided. Dr. Saade and Dr. Hackney have no disclosures.
FROM THE PREGNANCY MEETING
USPSTF backs screening for hypertensive disorders of pregnancy
The U.S. Preventive Services Task Force (USPSTF) recommends that clinicians screen for hypertensive disorders of pregnancy, which can cause serious and fatal complications, according to a new draft statement.
All pregnant people should have their blood pressure measured at each prenatal visit to identify and prevent serious health problems. The grade B recommendation expands on the task force’s 2017 recommendation on screening for preeclampsia to include all hypertensive disorders of pregnancy.
“Hypertensive disorders of pregnancy are some of the leading causes of serious complications and death for pregnant people,” Esa Davis, MD, a USPSTF member and associate professor of medicine and clinical and translational science at the University of Pittsburgh School of Medicine, told this news organization.
In the U.S., the rate of hypertensive disorders of pregnancy has increased in recent decades, jumping from about 500 cases per 10,000 deliveries in the early 1990s to more than 1,000 cases per 10,000 deliveries in the mid-2010s.
“The U.S. Preventive Services Task Force wants to help save the lives of pregnant people and their babies by ensuring that clinicians have the most up-to-date guidance on how to find these conditions early,” she said.
The draft recommendation statement was published online .
Screening recommendation
Hypertensive disorders of pregnancy, including gestational hypertension, preeclampsia, eclampsia, and chronic hypertension with and without superimposed preeclampsia, are marked by elevated blood pressure during pregnancy.
The disorders can lead to complications for the pregnant person, such as stroke, retinal detachment, organ damage or failure, and seizures, as well as for the baby, including restricted growth, low birth weight, and stillbirth. Many complications can lead to early induction of labor, cesarean delivery, and preterm birth.
After commissioning a systematic evidence review, the USPSTF provided a grade B recommendation for clinicians to offer or provide screening for hypertensive disorders of pregnancy. The recommendation concludes with “moderate certainty” that screening with blood pressure measurements has “substantial net benefit.”
The task force notes that it is “essential” for all pregnant women and pregnant people of all genders to be screened and that those who screen positive receive evidence-based management of their condition.
Risk factors include a history of eclampsia or preeclampsia, a family history of preeclampsia, a previous adverse pregnancy outcome, having gestational diabetes or chronic hypertension, being pregnant with more than one baby, having a first pregnancy, having a high body mass index prior to pregnancy, and being 35 years of age or older.
In addition, Black, American Indian, and Alaska Native people face higher risks and are more likely both to have and to die from a hypertensive disorder of pregnancy. In particular, Black people experience higher rates of maternal and infant morbidity and perinatal mortality than other racial and ethnic groups, and hypertensive disorders of pregnancy account for a larger proportion of these outcomes.
Although measuring blood pressure throughout pregnancy is an important first step, it’s not enough to improve inequities in health outcomes, the task force notes. Identifying hypertensive disorders of pregnancy requires adequate prenatal follow-up visits, surveillance, and evidence-based care, which can be a barrier for some pregnant people.
Follow-up visits with health care providers such as nurses, nurse midwives, pediatricians, and lactation consultants could help, as well as screening and monitoring during the postpartum period. Other approaches include telehealth, connections to community resources during the perinatal period, collaborative care provided in medical homes, and multilevel interventions to address underlying health inequities that increase health risks during pregnancy.
“Since screening is not enough to address the health disparities experienced by Black, American Indian, and Alaska Native people, health care professionals should also do what they can to help address these inequities,” Dr. Davis said. “For example, the task force identified a few promising approaches, including using standardized clinical bundles of best practices for disease management to help ensure that all pregnant persons receive appropriate, equitable care.”
Additional considerations
The USPSTF looked at the evidence on additional methods of screening but continued to find that measuring blood pressure at each prenatal visit is the best approach. Other evaluations, such as testing for proteinuria when preeclampsia is suspected, have low accuracy for detecting proteinuria in pregnancy.
Although there is no currently available treatment for preeclampsia except delivery, management strategies for diagnosed hypertensive disorders of pregnancy include close fetal and maternal monitoring, antihypertension medications, and magnesium sulfate for seizure prophylaxis when indicated.
Previously, the USPSTF also recommended that pregnant Black people be considered for treatment with low-dose aspirin to prevent preeclampsia, with aspirin use recommended for those with at least one additional moderate risk factor. Clinicians should also be aware of the complications of poor health outcomes among populations who face higher risks.
The USPSTF noted several gaps for future research, including the best approaches for blood pressure monitoring during pregnancy and the postpartum period, how to address health inequities through multilevel interventions, how to increase access to care through telehealth services, and how to mitigate cardiovascular complications later in life in patients diagnosed with hypertensive disorders of pregnancy.
“Continued research is needed in these promising areas,” Dr. Davis said. “We hope all clinicians will join us in helping ensure that all parents and babies have access to the care they need to be as healthy as possible.”
The draft recommendation statement and draft evidence review were posted for public comment on the USPSTF website. Comments can be submitted until March 6.
No relevant financial relationships have been disclosed.
A version of this article originally appeared on Medscape.com.
The U.S. Preventive Services Task Force (USPSTF) recommends that clinicians screen for hypertensive disorders of pregnancy, which can cause serious and fatal complications, according to a new draft statement.
All pregnant people should have their blood pressure measured at each prenatal visit to identify and prevent serious health problems. The grade B recommendation expands on the task force’s 2017 recommendation on screening for preeclampsia to include all hypertensive disorders of pregnancy.
“Hypertensive disorders of pregnancy are some of the leading causes of serious complications and death for pregnant people,” Esa Davis, MD, a USPSTF member and associate professor of medicine and clinical and translational science at the University of Pittsburgh School of Medicine, told this news organization.
In the U.S., the rate of hypertensive disorders of pregnancy has increased in recent decades, jumping from about 500 cases per 10,000 deliveries in the early 1990s to more than 1,000 cases per 10,000 deliveries in the mid-2010s.
“The U.S. Preventive Services Task Force wants to help save the lives of pregnant people and their babies by ensuring that clinicians have the most up-to-date guidance on how to find these conditions early,” she said.
The draft recommendation statement was published online .
Screening recommendation
Hypertensive disorders of pregnancy, including gestational hypertension, preeclampsia, eclampsia, and chronic hypertension with and without superimposed preeclampsia, are marked by elevated blood pressure during pregnancy.
The disorders can lead to complications for the pregnant person, such as stroke, retinal detachment, organ damage or failure, and seizures, as well as for the baby, including restricted growth, low birth weight, and stillbirth. Many complications can lead to early induction of labor, cesarean delivery, and preterm birth.
After commissioning a systematic evidence review, the USPSTF provided a grade B recommendation for clinicians to offer or provide screening for hypertensive disorders of pregnancy. The recommendation concludes with “moderate certainty” that screening with blood pressure measurements has “substantial net benefit.”
The task force notes that it is “essential” for all pregnant women and pregnant people of all genders to be screened and that those who screen positive receive evidence-based management of their condition.
Risk factors include a history of eclampsia or preeclampsia, a family history of preeclampsia, a previous adverse pregnancy outcome, having gestational diabetes or chronic hypertension, being pregnant with more than one baby, having a first pregnancy, having a high body mass index prior to pregnancy, and being 35 years of age or older.
In addition, Black, American Indian, and Alaska Native people face higher risks and are more likely both to have and to die from a hypertensive disorder of pregnancy. In particular, Black people experience higher rates of maternal and infant morbidity and perinatal mortality than other racial and ethnic groups, and hypertensive disorders of pregnancy account for a larger proportion of these outcomes.
Although measuring blood pressure throughout pregnancy is an important first step, it’s not enough to improve inequities in health outcomes, the task force notes. Identifying hypertensive disorders of pregnancy requires adequate prenatal follow-up visits, surveillance, and evidence-based care, which can be a barrier for some pregnant people.
Follow-up visits with health care providers such as nurses, nurse midwives, pediatricians, and lactation consultants could help, as well as screening and monitoring during the postpartum period. Other approaches include telehealth, connections to community resources during the perinatal period, collaborative care provided in medical homes, and multilevel interventions to address underlying health inequities that increase health risks during pregnancy.
“Since screening is not enough to address the health disparities experienced by Black, American Indian, and Alaska Native people, health care professionals should also do what they can to help address these inequities,” Dr. Davis said. “For example, the task force identified a few promising approaches, including using standardized clinical bundles of best practices for disease management to help ensure that all pregnant persons receive appropriate, equitable care.”
Additional considerations
The USPSTF looked at the evidence on additional methods of screening but continued to find that measuring blood pressure at each prenatal visit is the best approach. Other evaluations, such as testing for proteinuria when preeclampsia is suspected, have low accuracy for detecting proteinuria in pregnancy.
Although there is no currently available treatment for preeclampsia except delivery, management strategies for diagnosed hypertensive disorders of pregnancy include close fetal and maternal monitoring, antihypertension medications, and magnesium sulfate for seizure prophylaxis when indicated.
Previously, the USPSTF also recommended that pregnant Black people be considered for treatment with low-dose aspirin to prevent preeclampsia, with aspirin use recommended for those with at least one additional moderate risk factor. Clinicians should also be aware of the complications of poor health outcomes among populations who face higher risks.
The USPSTF noted several gaps for future research, including the best approaches for blood pressure monitoring during pregnancy and the postpartum period, how to address health inequities through multilevel interventions, how to increase access to care through telehealth services, and how to mitigate cardiovascular complications later in life in patients diagnosed with hypertensive disorders of pregnancy.
“Continued research is needed in these promising areas,” Dr. Davis said. “We hope all clinicians will join us in helping ensure that all parents and babies have access to the care they need to be as healthy as possible.”
The draft recommendation statement and draft evidence review were posted for public comment on the USPSTF website. Comments can be submitted until March 6.
No relevant financial relationships have been disclosed.
A version of this article originally appeared on Medscape.com.
The U.S. Preventive Services Task Force (USPSTF) recommends that clinicians screen for hypertensive disorders of pregnancy, which can cause serious and fatal complications, according to a new draft statement.
All pregnant people should have their blood pressure measured at each prenatal visit to identify and prevent serious health problems. The grade B recommendation expands on the task force’s 2017 recommendation on screening for preeclampsia to include all hypertensive disorders of pregnancy.
“Hypertensive disorders of pregnancy are some of the leading causes of serious complications and death for pregnant people,” Esa Davis, MD, a USPSTF member and associate professor of medicine and clinical and translational science at the University of Pittsburgh School of Medicine, told this news organization.
In the U.S., the rate of hypertensive disorders of pregnancy has increased in recent decades, jumping from about 500 cases per 10,000 deliveries in the early 1990s to more than 1,000 cases per 10,000 deliveries in the mid-2010s.
“The U.S. Preventive Services Task Force wants to help save the lives of pregnant people and their babies by ensuring that clinicians have the most up-to-date guidance on how to find these conditions early,” she said.
The draft recommendation statement was published online .
Screening recommendation
Hypertensive disorders of pregnancy, including gestational hypertension, preeclampsia, eclampsia, and chronic hypertension with and without superimposed preeclampsia, are marked by elevated blood pressure during pregnancy.
The disorders can lead to complications for the pregnant person, such as stroke, retinal detachment, organ damage or failure, and seizures, as well as for the baby, including restricted growth, low birth weight, and stillbirth. Many complications can lead to early induction of labor, cesarean delivery, and preterm birth.
After commissioning a systematic evidence review, the USPSTF provided a grade B recommendation for clinicians to offer or provide screening for hypertensive disorders of pregnancy. The recommendation concludes with “moderate certainty” that screening with blood pressure measurements has “substantial net benefit.”
The task force notes that it is “essential” for all pregnant women and pregnant people of all genders to be screened and that those who screen positive receive evidence-based management of their condition.
Risk factors include a history of eclampsia or preeclampsia, a family history of preeclampsia, a previous adverse pregnancy outcome, having gestational diabetes or chronic hypertension, being pregnant with more than one baby, having a first pregnancy, having a high body mass index prior to pregnancy, and being 35 years of age or older.
In addition, Black, American Indian, and Alaska Native people face higher risks and are more likely both to have and to die from a hypertensive disorder of pregnancy. In particular, Black people experience higher rates of maternal and infant morbidity and perinatal mortality than other racial and ethnic groups, and hypertensive disorders of pregnancy account for a larger proportion of these outcomes.
Although measuring blood pressure throughout pregnancy is an important first step, it’s not enough to improve inequities in health outcomes, the task force notes. Identifying hypertensive disorders of pregnancy requires adequate prenatal follow-up visits, surveillance, and evidence-based care, which can be a barrier for some pregnant people.
Follow-up visits with health care providers such as nurses, nurse midwives, pediatricians, and lactation consultants could help, as well as screening and monitoring during the postpartum period. Other approaches include telehealth, connections to community resources during the perinatal period, collaborative care provided in medical homes, and multilevel interventions to address underlying health inequities that increase health risks during pregnancy.
“Since screening is not enough to address the health disparities experienced by Black, American Indian, and Alaska Native people, health care professionals should also do what they can to help address these inequities,” Dr. Davis said. “For example, the task force identified a few promising approaches, including using standardized clinical bundles of best practices for disease management to help ensure that all pregnant persons receive appropriate, equitable care.”
Additional considerations
The USPSTF looked at the evidence on additional methods of screening but continued to find that measuring blood pressure at each prenatal visit is the best approach. Other evaluations, such as testing for proteinuria when preeclampsia is suspected, have low accuracy for detecting proteinuria in pregnancy.
Although there is no currently available treatment for preeclampsia except delivery, management strategies for diagnosed hypertensive disorders of pregnancy include close fetal and maternal monitoring, antihypertension medications, and magnesium sulfate for seizure prophylaxis when indicated.
Previously, the USPSTF also recommended that pregnant Black people be considered for treatment with low-dose aspirin to prevent preeclampsia, with aspirin use recommended for those with at least one additional moderate risk factor. Clinicians should also be aware of the complications of poor health outcomes among populations who face higher risks.
The USPSTF noted several gaps for future research, including the best approaches for blood pressure monitoring during pregnancy and the postpartum period, how to address health inequities through multilevel interventions, how to increase access to care through telehealth services, and how to mitigate cardiovascular complications later in life in patients diagnosed with hypertensive disorders of pregnancy.
“Continued research is needed in these promising areas,” Dr. Davis said. “We hope all clinicians will join us in helping ensure that all parents and babies have access to the care they need to be as healthy as possible.”
The draft recommendation statement and draft evidence review were posted for public comment on the USPSTF website. Comments can be submitted until March 6.
No relevant financial relationships have been disclosed.
A version of this article originally appeared on Medscape.com.
Three wild technologies about to change health care
When I was a child, I watched syndicated episodes of the original “Star Trek.” I was dazzled by the space travel, sure, but also the medical technology.
A handheld “tricorder” detected diseases, while an intramuscular injector (“hypospray”) could treat them. Sickbay “biobeds” came with real-time health monitors that looked futuristic at the time but seem primitive today.
Such visions inspired a lot of us kids to pursue science. Little did we know the real-life advances many of us would see in our lifetimes.
Artificial intelligence helping to spot disease, robots performing surgery, even video calls between doctor and patient – all these once sounded fantastical but now happen in clinical care.
Now, in the 23rd year of the 21st century, you might not believe wht we’ll be capable of next. Three especially wild examples are moving closer to clinical reality.
Human hibernation
Captain America, Han Solo, and “Star Trek” villain Khan – all were preserved at low temperatures and then revived, waking up alive and well months, decades, or centuries later. These are fictional examples, to be sure, but the science they’re rooted in is real.
(In one extreme case, a climber survived after almost 9 hours of efforts to revive him.)
Useful for a space traveler? Maybe not. But it’s potentially huge for someone with life-threatening injuries from a car accident or a gunshot wound.
That’s the thinking behind a breakthrough procedure that came after decades of research on pigs and dogs, now in a clinical trial. The idea: A person with massive blood loss whose heart has stopped is injected with an ice-cold fluid, cooling them from the inside, down to about 50° F.
Doctors already induce more modest hypothermia to protect the brain and other organs after cardiac arrest and during surgery on the aortic arch (the main artery carrying blood from the heart).
But this experimental procedure – called emergency preservation and resuscitation (EPR) – goes far beyond that, dramatically “decreasing the body’s need for oxygen and blood flow,” says Samuel Tisherman, MD, a trauma surgeon at the University of Maryland Medical Center and the trial’s lead researcher. This puts the patient in a state of suspended animation that “could buy time for surgeons to stop the bleeding and save more of these patients.”
The technique has been done on at least six patients, though none were reported to survive. The trial is expected to include 20 people by the time it wraps up in December, according to the listing on the U.S. clinical trials database. Though given the strict requirements for candidates (emergency trauma victims who are not likely to survive), one can’t exactly rely on a set schedule.
Still, the technology is promising. Someday we may even use it to keep patients in suspended animation for months or years, experts predict, helping astronauts through decades-long spaceflights, or stalling death in sick patients awaiting a cure.
Artificial womb
Another sci-fi classic: growing human babies outside the womb. Think the fetus fields from “The Matrix,” or the frozen embryos in “Alien: Covenant.”
In 1923, British biologist J.B.S. Haldane coined a term for that – ectogenesis. He predicted that 70% of pregnancies would take place, from fertilization to birth, in artificial wombs by 2074. That many seems unlikely, but the timeline is on track.
Developing an embryo outside the womb is already routine in in vitro fertilization. And technology enables preterm babies to survive through much of the second half of gestation. Normal human pregnancy is 40 weeks, and the youngest preterm baby ever to survive was 21 weeks and 1 day old, just a few days younger than a smattering of others who lived.
The biggest obstacle for babies younger than that is lung viability. Mechanical ventilation can damage the lungs and lead to a chronic (sometimes fatal) lung disease known as bronchopulmonary dysplasia. Avoiding this would mean figuring out a way to maintain fetal circulation – the intricate system that delivers oxygenated blood from the placenta to the fetus via the umbilical cord. Researchers at Children’s Hospital of Philadelphia have done this using a fetal lamb.
The key to their invention is a substitute placenta: an oxygenator connected to the lamb’s umbilical cord. Tubes inserted through the umbilical vein and arteries carry oxygenated blood from the “placenta” to the fetus, and deoxygenated blood back out. The lamb resides in an artificial, fluid-filled amniotic sac until its lungs and other organs are developed.
Fertility treatment could benefit, too. “An artificial womb may substitute in situations in which a gestational carrier – surrogate – is indicated,” says Paula Amato, MD, a professor of obstetrics and gynecology at Oregon Health and Science University, Portland. (Dr. Amato is not involved in the CHOP research.) For example: when the mother is missing a uterus or can’t carry a pregnancy safely.
No date is set for clinical trials yet. But according to the research, the main difference between human and lamb may come down to size. A lamb’s umbilical vessels are larger, so feeding in a tube is easier. With today’s advances in miniaturizing surgical methods, that seems like a challenge scientists can overcome.
Messenger RNA therapeutics
Back to “Star Trek.” The hypospray injector’s contents could cure just about any disease, even one newly discovered on a strange planet. That’s not unlike messenger RNA (mRNA) technology, a breakthrough that enabled scientists to quickly develop some of the first COVID-19 vaccines.
But vaccines are just the beginning of what this technology can do.
A whole field of immunotherapy is emerging that uses mRNA to deliver instructions to produce chimeric antigen receptor–modified immune cells (CAR-modified immune cells). These cells are engineered to target diseased cells and tissues, like cancer cells and harmful fibroblasts (scar tissue) that promote fibrosis in, for example, the heart and lungs.
The field is bursting with rodent research, and clinical trials have started for treating some advanced-stage malignancies.
Actual clinical use may be years away, but if all goes well, these medicines could help treat or even cure the core medical problems facing humanity. We’re talking cancer, heart disease, neurodegenerative disease – transforming one therapy into another by simply changing the mRNA’s “nucleotide sequence,” the blueprint containing instructions telling it what to do, and what disease to attack.
As this technology matures, we may start to feel as if we’re really on “Star Trek,” where Dr. Leonard “Bones” McCoy pulls out the same device to treat just about every disease or injury.
A version of this article first appeared on WebMD.com.
When I was a child, I watched syndicated episodes of the original “Star Trek.” I was dazzled by the space travel, sure, but also the medical technology.
A handheld “tricorder” detected diseases, while an intramuscular injector (“hypospray”) could treat them. Sickbay “biobeds” came with real-time health monitors that looked futuristic at the time but seem primitive today.
Such visions inspired a lot of us kids to pursue science. Little did we know the real-life advances many of us would see in our lifetimes.
Artificial intelligence helping to spot disease, robots performing surgery, even video calls between doctor and patient – all these once sounded fantastical but now happen in clinical care.
Now, in the 23rd year of the 21st century, you might not believe wht we’ll be capable of next. Three especially wild examples are moving closer to clinical reality.
Human hibernation
Captain America, Han Solo, and “Star Trek” villain Khan – all were preserved at low temperatures and then revived, waking up alive and well months, decades, or centuries later. These are fictional examples, to be sure, but the science they’re rooted in is real.
(In one extreme case, a climber survived after almost 9 hours of efforts to revive him.)
Useful for a space traveler? Maybe not. But it’s potentially huge for someone with life-threatening injuries from a car accident or a gunshot wound.
That’s the thinking behind a breakthrough procedure that came after decades of research on pigs and dogs, now in a clinical trial. The idea: A person with massive blood loss whose heart has stopped is injected with an ice-cold fluid, cooling them from the inside, down to about 50° F.
Doctors already induce more modest hypothermia to protect the brain and other organs after cardiac arrest and during surgery on the aortic arch (the main artery carrying blood from the heart).
But this experimental procedure – called emergency preservation and resuscitation (EPR) – goes far beyond that, dramatically “decreasing the body’s need for oxygen and blood flow,” says Samuel Tisherman, MD, a trauma surgeon at the University of Maryland Medical Center and the trial’s lead researcher. This puts the patient in a state of suspended animation that “could buy time for surgeons to stop the bleeding and save more of these patients.”
The technique has been done on at least six patients, though none were reported to survive. The trial is expected to include 20 people by the time it wraps up in December, according to the listing on the U.S. clinical trials database. Though given the strict requirements for candidates (emergency trauma victims who are not likely to survive), one can’t exactly rely on a set schedule.
Still, the technology is promising. Someday we may even use it to keep patients in suspended animation for months or years, experts predict, helping astronauts through decades-long spaceflights, or stalling death in sick patients awaiting a cure.
Artificial womb
Another sci-fi classic: growing human babies outside the womb. Think the fetus fields from “The Matrix,” or the frozen embryos in “Alien: Covenant.”
In 1923, British biologist J.B.S. Haldane coined a term for that – ectogenesis. He predicted that 70% of pregnancies would take place, from fertilization to birth, in artificial wombs by 2074. That many seems unlikely, but the timeline is on track.
Developing an embryo outside the womb is already routine in in vitro fertilization. And technology enables preterm babies to survive through much of the second half of gestation. Normal human pregnancy is 40 weeks, and the youngest preterm baby ever to survive was 21 weeks and 1 day old, just a few days younger than a smattering of others who lived.
The biggest obstacle for babies younger than that is lung viability. Mechanical ventilation can damage the lungs and lead to a chronic (sometimes fatal) lung disease known as bronchopulmonary dysplasia. Avoiding this would mean figuring out a way to maintain fetal circulation – the intricate system that delivers oxygenated blood from the placenta to the fetus via the umbilical cord. Researchers at Children’s Hospital of Philadelphia have done this using a fetal lamb.
The key to their invention is a substitute placenta: an oxygenator connected to the lamb’s umbilical cord. Tubes inserted through the umbilical vein and arteries carry oxygenated blood from the “placenta” to the fetus, and deoxygenated blood back out. The lamb resides in an artificial, fluid-filled amniotic sac until its lungs and other organs are developed.
Fertility treatment could benefit, too. “An artificial womb may substitute in situations in which a gestational carrier – surrogate – is indicated,” says Paula Amato, MD, a professor of obstetrics and gynecology at Oregon Health and Science University, Portland. (Dr. Amato is not involved in the CHOP research.) For example: when the mother is missing a uterus or can’t carry a pregnancy safely.
No date is set for clinical trials yet. But according to the research, the main difference between human and lamb may come down to size. A lamb’s umbilical vessels are larger, so feeding in a tube is easier. With today’s advances in miniaturizing surgical methods, that seems like a challenge scientists can overcome.
Messenger RNA therapeutics
Back to “Star Trek.” The hypospray injector’s contents could cure just about any disease, even one newly discovered on a strange planet. That’s not unlike messenger RNA (mRNA) technology, a breakthrough that enabled scientists to quickly develop some of the first COVID-19 vaccines.
But vaccines are just the beginning of what this technology can do.
A whole field of immunotherapy is emerging that uses mRNA to deliver instructions to produce chimeric antigen receptor–modified immune cells (CAR-modified immune cells). These cells are engineered to target diseased cells and tissues, like cancer cells and harmful fibroblasts (scar tissue) that promote fibrosis in, for example, the heart and lungs.
The field is bursting with rodent research, and clinical trials have started for treating some advanced-stage malignancies.
Actual clinical use may be years away, but if all goes well, these medicines could help treat or even cure the core medical problems facing humanity. We’re talking cancer, heart disease, neurodegenerative disease – transforming one therapy into another by simply changing the mRNA’s “nucleotide sequence,” the blueprint containing instructions telling it what to do, and what disease to attack.
As this technology matures, we may start to feel as if we’re really on “Star Trek,” where Dr. Leonard “Bones” McCoy pulls out the same device to treat just about every disease or injury.
A version of this article first appeared on WebMD.com.
When I was a child, I watched syndicated episodes of the original “Star Trek.” I was dazzled by the space travel, sure, but also the medical technology.
A handheld “tricorder” detected diseases, while an intramuscular injector (“hypospray”) could treat them. Sickbay “biobeds” came with real-time health monitors that looked futuristic at the time but seem primitive today.
Such visions inspired a lot of us kids to pursue science. Little did we know the real-life advances many of us would see in our lifetimes.
Artificial intelligence helping to spot disease, robots performing surgery, even video calls between doctor and patient – all these once sounded fantastical but now happen in clinical care.
Now, in the 23rd year of the 21st century, you might not believe wht we’ll be capable of next. Three especially wild examples are moving closer to clinical reality.
Human hibernation
Captain America, Han Solo, and “Star Trek” villain Khan – all were preserved at low temperatures and then revived, waking up alive and well months, decades, or centuries later. These are fictional examples, to be sure, but the science they’re rooted in is real.
(In one extreme case, a climber survived after almost 9 hours of efforts to revive him.)
Useful for a space traveler? Maybe not. But it’s potentially huge for someone with life-threatening injuries from a car accident or a gunshot wound.
That’s the thinking behind a breakthrough procedure that came after decades of research on pigs and dogs, now in a clinical trial. The idea: A person with massive blood loss whose heart has stopped is injected with an ice-cold fluid, cooling them from the inside, down to about 50° F.
Doctors already induce more modest hypothermia to protect the brain and other organs after cardiac arrest and during surgery on the aortic arch (the main artery carrying blood from the heart).
But this experimental procedure – called emergency preservation and resuscitation (EPR) – goes far beyond that, dramatically “decreasing the body’s need for oxygen and blood flow,” says Samuel Tisherman, MD, a trauma surgeon at the University of Maryland Medical Center and the trial’s lead researcher. This puts the patient in a state of suspended animation that “could buy time for surgeons to stop the bleeding and save more of these patients.”
The technique has been done on at least six patients, though none were reported to survive. The trial is expected to include 20 people by the time it wraps up in December, according to the listing on the U.S. clinical trials database. Though given the strict requirements for candidates (emergency trauma victims who are not likely to survive), one can’t exactly rely on a set schedule.
Still, the technology is promising. Someday we may even use it to keep patients in suspended animation for months or years, experts predict, helping astronauts through decades-long spaceflights, or stalling death in sick patients awaiting a cure.
Artificial womb
Another sci-fi classic: growing human babies outside the womb. Think the fetus fields from “The Matrix,” or the frozen embryos in “Alien: Covenant.”
In 1923, British biologist J.B.S. Haldane coined a term for that – ectogenesis. He predicted that 70% of pregnancies would take place, from fertilization to birth, in artificial wombs by 2074. That many seems unlikely, but the timeline is on track.
Developing an embryo outside the womb is already routine in in vitro fertilization. And technology enables preterm babies to survive through much of the second half of gestation. Normal human pregnancy is 40 weeks, and the youngest preterm baby ever to survive was 21 weeks and 1 day old, just a few days younger than a smattering of others who lived.
The biggest obstacle for babies younger than that is lung viability. Mechanical ventilation can damage the lungs and lead to a chronic (sometimes fatal) lung disease known as bronchopulmonary dysplasia. Avoiding this would mean figuring out a way to maintain fetal circulation – the intricate system that delivers oxygenated blood from the placenta to the fetus via the umbilical cord. Researchers at Children’s Hospital of Philadelphia have done this using a fetal lamb.
The key to their invention is a substitute placenta: an oxygenator connected to the lamb’s umbilical cord. Tubes inserted through the umbilical vein and arteries carry oxygenated blood from the “placenta” to the fetus, and deoxygenated blood back out. The lamb resides in an artificial, fluid-filled amniotic sac until its lungs and other organs are developed.
Fertility treatment could benefit, too. “An artificial womb may substitute in situations in which a gestational carrier – surrogate – is indicated,” says Paula Amato, MD, a professor of obstetrics and gynecology at Oregon Health and Science University, Portland. (Dr. Amato is not involved in the CHOP research.) For example: when the mother is missing a uterus or can’t carry a pregnancy safely.
No date is set for clinical trials yet. But according to the research, the main difference between human and lamb may come down to size. A lamb’s umbilical vessels are larger, so feeding in a tube is easier. With today’s advances in miniaturizing surgical methods, that seems like a challenge scientists can overcome.
Messenger RNA therapeutics
Back to “Star Trek.” The hypospray injector’s contents could cure just about any disease, even one newly discovered on a strange planet. That’s not unlike messenger RNA (mRNA) technology, a breakthrough that enabled scientists to quickly develop some of the first COVID-19 vaccines.
But vaccines are just the beginning of what this technology can do.
A whole field of immunotherapy is emerging that uses mRNA to deliver instructions to produce chimeric antigen receptor–modified immune cells (CAR-modified immune cells). These cells are engineered to target diseased cells and tissues, like cancer cells and harmful fibroblasts (scar tissue) that promote fibrosis in, for example, the heart and lungs.
The field is bursting with rodent research, and clinical trials have started for treating some advanced-stage malignancies.
Actual clinical use may be years away, but if all goes well, these medicines could help treat or even cure the core medical problems facing humanity. We’re talking cancer, heart disease, neurodegenerative disease – transforming one therapy into another by simply changing the mRNA’s “nucleotide sequence,” the blueprint containing instructions telling it what to do, and what disease to attack.
As this technology matures, we may start to feel as if we’re really on “Star Trek,” where Dr. Leonard “Bones” McCoy pulls out the same device to treat just about every disease or injury.
A version of this article first appeared on WebMD.com.
Can a hormone shot rescue low libido?
according to results from two small randomized controlled trials.
The data suggest that injections of kisspeptin can boost sexual desire in men and women and can increase penile rigidity in men.
Together, these two studies provide proof of concept for the development of kisspeptin-based therapeutics for men and women with distressing hypoactive sexual desire disorder (HSDD), study investigator Alexander Comninos, MD, PhD, Imperial College London, said in a news release.
One study was published online Feb. 3, 2022, in JAMA Network Open. The other was published in October 2022.
Unmet need
HSDD affects up to 10% of women and 8% of men worldwide and leads to psychological and social harm, the news release noted.
“There is a real unmet need to find new, safer, and more effective therapies for this distressing condition for both women and men seeking treatment,” Dr. Comninos said.
Kisspeptin is a naturally occurring reproductive hormone that serves as a crucial activator of the reproductive system. Emerging evidence from animal models shows that kisspeptin signaling has key roles in modulating reproductive behavior, including sexual motivation and erections.
In a double-blind, placebo-controlled, crossover study, the researchers enrolled 32 healthy heterosexual men (mean age, 37.9 years) who had HSDD.
At the first study visit, the men were given an infusion of kisspeptin-54 (1 nmol/kg per hour) or placebo (saline) over 75 minutes. The participants then crossed over to the other treatment at a second study visit at least 7 days later.
The active treatment significantly increased circulating kisspeptin levels. A steady state was reached after 30-75 minutes of infusion, the researchers reported.
Similar data in men, women
While the men viewed sexual videos, kisspeptin significantly modulated brain activity on fMRI in key structures of the sexual-processing network, compared with placebo (P = .003).
In addition, the treatment led to significant increases in penile tumescence in response to sexual stimuli (by up to 56% more than placebo; P = .02) and behavioral measures of sexual desire – most notably increased happiness about sex (P = .02).
Given the significant stimulatory effect of kisspeptin administration on penile rigidity, coupled with its demonstrated proerectile effect in rodents, future studies should examine the use of kisspeptin for patients with erectile dysfunction, the researchers wrote.
The second study included 32 women with HSDD and had the same design. Its results also showed that kisspeptin restored sexual and attraction brain processing without adverse effects.
“It is highly encouraging to see the same boosting effect in both women and men, although the precise brain pathways were slightly different, as might be expected,” coinvestigator Waljit Dhillo, PhD, Imperial College London, said in the news release.
“Collectively, the results suggest that kisspeptin may offer a safe and much-needed treatment for HSDD that affects millions of people around the world; and we look forward to taking this forward in future larger studies and in other patient groups,” Dr. Dhillo added.
The study was funded by the National Institute for Health and Care Research Imperial Biomedical Research Centre and the Medical Research Council, part of UK Research and Innovation. Dr. Comninos reported no relevant financial relationships. Dr. Dhillo reported receiving consulting fees from Myovant Sciences and KaNDy Therapeutics outside the submitted work.
A version of this article first appeared on Medscape.com.
according to results from two small randomized controlled trials.
The data suggest that injections of kisspeptin can boost sexual desire in men and women and can increase penile rigidity in men.
Together, these two studies provide proof of concept for the development of kisspeptin-based therapeutics for men and women with distressing hypoactive sexual desire disorder (HSDD), study investigator Alexander Comninos, MD, PhD, Imperial College London, said in a news release.
One study was published online Feb. 3, 2022, in JAMA Network Open. The other was published in October 2022.
Unmet need
HSDD affects up to 10% of women and 8% of men worldwide and leads to psychological and social harm, the news release noted.
“There is a real unmet need to find new, safer, and more effective therapies for this distressing condition for both women and men seeking treatment,” Dr. Comninos said.
Kisspeptin is a naturally occurring reproductive hormone that serves as a crucial activator of the reproductive system. Emerging evidence from animal models shows that kisspeptin signaling has key roles in modulating reproductive behavior, including sexual motivation and erections.
In a double-blind, placebo-controlled, crossover study, the researchers enrolled 32 healthy heterosexual men (mean age, 37.9 years) who had HSDD.
At the first study visit, the men were given an infusion of kisspeptin-54 (1 nmol/kg per hour) or placebo (saline) over 75 minutes. The participants then crossed over to the other treatment at a second study visit at least 7 days later.
The active treatment significantly increased circulating kisspeptin levels. A steady state was reached after 30-75 minutes of infusion, the researchers reported.
Similar data in men, women
While the men viewed sexual videos, kisspeptin significantly modulated brain activity on fMRI in key structures of the sexual-processing network, compared with placebo (P = .003).
In addition, the treatment led to significant increases in penile tumescence in response to sexual stimuli (by up to 56% more than placebo; P = .02) and behavioral measures of sexual desire – most notably increased happiness about sex (P = .02).
Given the significant stimulatory effect of kisspeptin administration on penile rigidity, coupled with its demonstrated proerectile effect in rodents, future studies should examine the use of kisspeptin for patients with erectile dysfunction, the researchers wrote.
The second study included 32 women with HSDD and had the same design. Its results also showed that kisspeptin restored sexual and attraction brain processing without adverse effects.
“It is highly encouraging to see the same boosting effect in both women and men, although the precise brain pathways were slightly different, as might be expected,” coinvestigator Waljit Dhillo, PhD, Imperial College London, said in the news release.
“Collectively, the results suggest that kisspeptin may offer a safe and much-needed treatment for HSDD that affects millions of people around the world; and we look forward to taking this forward in future larger studies and in other patient groups,” Dr. Dhillo added.
The study was funded by the National Institute for Health and Care Research Imperial Biomedical Research Centre and the Medical Research Council, part of UK Research and Innovation. Dr. Comninos reported no relevant financial relationships. Dr. Dhillo reported receiving consulting fees from Myovant Sciences and KaNDy Therapeutics outside the submitted work.
A version of this article first appeared on Medscape.com.
according to results from two small randomized controlled trials.
The data suggest that injections of kisspeptin can boost sexual desire in men and women and can increase penile rigidity in men.
Together, these two studies provide proof of concept for the development of kisspeptin-based therapeutics for men and women with distressing hypoactive sexual desire disorder (HSDD), study investigator Alexander Comninos, MD, PhD, Imperial College London, said in a news release.
One study was published online Feb. 3, 2022, in JAMA Network Open. The other was published in October 2022.
Unmet need
HSDD affects up to 10% of women and 8% of men worldwide and leads to psychological and social harm, the news release noted.
“There is a real unmet need to find new, safer, and more effective therapies for this distressing condition for both women and men seeking treatment,” Dr. Comninos said.
Kisspeptin is a naturally occurring reproductive hormone that serves as a crucial activator of the reproductive system. Emerging evidence from animal models shows that kisspeptin signaling has key roles in modulating reproductive behavior, including sexual motivation and erections.
In a double-blind, placebo-controlled, crossover study, the researchers enrolled 32 healthy heterosexual men (mean age, 37.9 years) who had HSDD.
At the first study visit, the men were given an infusion of kisspeptin-54 (1 nmol/kg per hour) or placebo (saline) over 75 minutes. The participants then crossed over to the other treatment at a second study visit at least 7 days later.
The active treatment significantly increased circulating kisspeptin levels. A steady state was reached after 30-75 minutes of infusion, the researchers reported.
Similar data in men, women
While the men viewed sexual videos, kisspeptin significantly modulated brain activity on fMRI in key structures of the sexual-processing network, compared with placebo (P = .003).
In addition, the treatment led to significant increases in penile tumescence in response to sexual stimuli (by up to 56% more than placebo; P = .02) and behavioral measures of sexual desire – most notably increased happiness about sex (P = .02).
Given the significant stimulatory effect of kisspeptin administration on penile rigidity, coupled with its demonstrated proerectile effect in rodents, future studies should examine the use of kisspeptin for patients with erectile dysfunction, the researchers wrote.
The second study included 32 women with HSDD and had the same design. Its results also showed that kisspeptin restored sexual and attraction brain processing without adverse effects.
“It is highly encouraging to see the same boosting effect in both women and men, although the precise brain pathways were slightly different, as might be expected,” coinvestigator Waljit Dhillo, PhD, Imperial College London, said in the news release.
“Collectively, the results suggest that kisspeptin may offer a safe and much-needed treatment for HSDD that affects millions of people around the world; and we look forward to taking this forward in future larger studies and in other patient groups,” Dr. Dhillo added.
The study was funded by the National Institute for Health and Care Research Imperial Biomedical Research Centre and the Medical Research Council, part of UK Research and Innovation. Dr. Comninos reported no relevant financial relationships. Dr. Dhillo reported receiving consulting fees from Myovant Sciences and KaNDy Therapeutics outside the submitted work.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Pound of flesh buys less prison time
Pound of flesh buys less prison time
We should all have more Shakespeare in our lives. Yeah, yeah, Shakespeare is meant to be played, not read, and it can be a struggle to herd teenagers through the Bard’s interesting and bloody tragedies, but even a perfunctory reading of “The Merchant of Venice” would hopefully have prevented the dystopian nightmare Massachusetts has presented us with today.

The United States has a massive shortage of donor organs. This is an unfortunate truth. So, to combat this issue, a pair of Massachusetts congresspeople have proposed HD 3822, which would allow prisoners to donate organs and/or bone marrow (a pound of flesh, so to speak) in exchange for up to a year in reduced prison time. Yes, that’s right. Give up pieces of yourself and the state of Massachusetts will deign to reduce your long prison sentence.
Oh, and before you dismiss this as typical Republican antics, the bill was sponsored by two Democrats, and in a statement one of them hoped to address racial disparities in organ donation, as people of color are much less likely to receive organs. Never mind that Black people are imprisoned at a much higher rate than Whites.
Yeah, this whole thing is what people in the business like to call an ethical disaster.
Fortunately, the bill will likely never be passed and it’s probably illegal anyway. A federal law from 1984 (how’s that for a coincidence) prevents people from donating organs for use in human transplantation in exchange for “valuable consideration.” In other words, you can’t sell your organs for profit, and in this case, reducing prison time would probably count as valuable consideration in the eyes of the courts.
Oh, and in case you’ve never read Merchant of Venice, Shylock, the character looking for the pound of flesh as payment for a debt? He’s the villain. In fact, it’s pretty safe to say that anyone looking to extract payment from human dismemberment is probably the bad guy of the story. Apparently that wasn’t clear.
How do you stop a fungi? With a deadly guy
Thanks to the new HBO series “The Last of Us,” there’s been a lot of talk about the upcoming fungi-pocalypse, as the show depicts the real-life “zombie fungus” Cordyceps turning humans into, you know, zombies.

No need to worry, ladies and gentleman, because science has discovered a way to turn back the fungal horde. A heroic, and environmentally friendly, alternative to chemical pesticides “in the fight against resistant fungi [that] are now resistant to antimycotics – partly because they are used in large quantities in agricultural fields,” investigators at the Leibniz Institute for Natural Product Research and Infection Biology in Jena, Germany, said in a written statement.
We are, of course, talking about Keanu Reeves. Wait a second. He’s not even in “The Last of Us.” Sorry folks, we are being told that it really is Keanu Reeves. Our champion in the inevitable fungal pandemic is movie star Keanu Reeves. Sort of. It’s actually keanumycin, a substance produced by bacteria of the genus Pseudomonas.
Really? Keanumycin? “The lipopeptides kill so efficiently that we named them after Keanu Reeves because he, too, is extremely deadly in his roles,” lead author Sebastian Götze, PhD, explained.
Dr. Götze and his associates had been working with pseudomonads for quite a while before they were able to isolate the toxins responsible for their ability to kill amoebae, which resemble fungi in some characteristics. When then finally tried the keanumycin against gray mold rot on hydrangea leaves, the intensely contemplative star of “The Matrix” and “John Wick” – sorry, wrong Keanu – the bacterial derivative significantly inhibited growth of the fungus, they said.
Additional testing has shown that keanumycin is not highly toxic to human cells and is effective against fungi such as Candida albicans in very low concentrations, which makes it a good candidate for future pharmaceutical development.
To that news there can be only one response from the substance’s namesake.
High fat, bye parasites
Fat. Fat. Fat. Seems like everyone is trying to avoid it these days, but fat may be good thing when it comes to weaseling out a parasite.
The parasite in this case is the whipworm, aka Trichuris trichiura. You can find this guy in the intestines of millions of people, where it causes long-lasting infections. Yikes … Researchers have found that the plan of attack to get rid of this invasive species is to boost the immune system, but instead of vitamin C and zinc it’s fat they’re pumping in. Yes, fat.
The developing countries with poor sewage that are at the highest risk for contracting parasites such as this also are among those where people ingest cheaper diets that are generally higher in fat. The investigators were interested to see how a high-fat diet would affect immune responses to the whipworms.
And, as with almost everything else, the researchers turned to mice, which were introduced to a closely related species, Trichuris muris.
A high-fat diet, rather than obesity itself, increases a molecule on T-helper cells called ST2, and this allows an increased T-helper 2 response, effectively giving eviction notices to the parasites in the intestinal lining.
To say the least, the researchers were surprised since “high-fat diets are mostly associated with increased pathology during disease,” said senior author Richard Grencis, PhD, of the University of Manchester (England), who noted that ST2 is not normally triggered with a standard diet in mice but the high-fat diet gave it a boost and an “alternate pathway” out.
Now before you start ordering extra-large fries at the drive-through to keep the whipworms away, the researchers added that they “have previously published that weight loss can aid the expulsion of a different gut parasite worm.” Figures.
Once again, though, signs are pointing to the gut for improved health.
Pound of flesh buys less prison time
We should all have more Shakespeare in our lives. Yeah, yeah, Shakespeare is meant to be played, not read, and it can be a struggle to herd teenagers through the Bard’s interesting and bloody tragedies, but even a perfunctory reading of “The Merchant of Venice” would hopefully have prevented the dystopian nightmare Massachusetts has presented us with today.
The United States has a massive shortage of donor organs. This is an unfortunate truth. So, to combat this issue, a pair of Massachusetts congresspeople have proposed HD 3822, which would allow prisoners to donate organs and/or bone marrow (a pound of flesh, so to speak) in exchange for up to a year in reduced prison time. Yes, that’s right. Give up pieces of yourself and the state of Massachusetts will deign to reduce your long prison sentence.
Oh, and before you dismiss this as typical Republican antics, the bill was sponsored by two Democrats, and in a statement one of them hoped to address racial disparities in organ donation, as people of color are much less likely to receive organs. Never mind that Black people are imprisoned at a much higher rate than Whites.
Yeah, this whole thing is what people in the business like to call an ethical disaster.
Fortunately, the bill will likely never be passed and it’s probably illegal anyway. A federal law from 1984 (how’s that for a coincidence) prevents people from donating organs for use in human transplantation in exchange for “valuable consideration.” In other words, you can’t sell your organs for profit, and in this case, reducing prison time would probably count as valuable consideration in the eyes of the courts.
Oh, and in case you’ve never read Merchant of Venice, Shylock, the character looking for the pound of flesh as payment for a debt? He’s the villain. In fact, it’s pretty safe to say that anyone looking to extract payment from human dismemberment is probably the bad guy of the story. Apparently that wasn’t clear.
How do you stop a fungi? With a deadly guy
Thanks to the new HBO series “The Last of Us,” there’s been a lot of talk about the upcoming fungi-pocalypse, as the show depicts the real-life “zombie fungus” Cordyceps turning humans into, you know, zombies.
No need to worry, ladies and gentleman, because science has discovered a way to turn back the fungal horde. A heroic, and environmentally friendly, alternative to chemical pesticides “in the fight against resistant fungi [that] are now resistant to antimycotics – partly because they are used in large quantities in agricultural fields,” investigators at the Leibniz Institute for Natural Product Research and Infection Biology in Jena, Germany, said in a written statement.
We are, of course, talking about Keanu Reeves. Wait a second. He’s not even in “The Last of Us.” Sorry folks, we are being told that it really is Keanu Reeves. Our champion in the inevitable fungal pandemic is movie star Keanu Reeves. Sort of. It’s actually keanumycin, a substance produced by bacteria of the genus Pseudomonas.
Really? Keanumycin? “The lipopeptides kill so efficiently that we named them after Keanu Reeves because he, too, is extremely deadly in his roles,” lead author Sebastian Götze, PhD, explained.
Dr. Götze and his associates had been working with pseudomonads for quite a while before they were able to isolate the toxins responsible for their ability to kill amoebae, which resemble fungi in some characteristics. When then finally tried the keanumycin against gray mold rot on hydrangea leaves, the intensely contemplative star of “The Matrix” and “John Wick” – sorry, wrong Keanu – the bacterial derivative significantly inhibited growth of the fungus, they said.
Additional testing has shown that keanumycin is not highly toxic to human cells and is effective against fungi such as Candida albicans in very low concentrations, which makes it a good candidate for future pharmaceutical development.
To that news there can be only one response from the substance’s namesake.
High fat, bye parasites
Fat. Fat. Fat. Seems like everyone is trying to avoid it these days, but fat may be good thing when it comes to weaseling out a parasite.
The parasite in this case is the whipworm, aka Trichuris trichiura. You can find this guy in the intestines of millions of people, where it causes long-lasting infections. Yikes … Researchers have found that the plan of attack to get rid of this invasive species is to boost the immune system, but instead of vitamin C and zinc it’s fat they’re pumping in. Yes, fat.
The developing countries with poor sewage that are at the highest risk for contracting parasites such as this also are among those where people ingest cheaper diets that are generally higher in fat. The investigators were interested to see how a high-fat diet would affect immune responses to the whipworms.
And, as with almost everything else, the researchers turned to mice, which were introduced to a closely related species, Trichuris muris.
A high-fat diet, rather than obesity itself, increases a molecule on T-helper cells called ST2, and this allows an increased T-helper 2 response, effectively giving eviction notices to the parasites in the intestinal lining.
To say the least, the researchers were surprised since “high-fat diets are mostly associated with increased pathology during disease,” said senior author Richard Grencis, PhD, of the University of Manchester (England), who noted that ST2 is not normally triggered with a standard diet in mice but the high-fat diet gave it a boost and an “alternate pathway” out.
Now before you start ordering extra-large fries at the drive-through to keep the whipworms away, the researchers added that they “have previously published that weight loss can aid the expulsion of a different gut parasite worm.” Figures.
Once again, though, signs are pointing to the gut for improved health.
Pound of flesh buys less prison time
We should all have more Shakespeare in our lives. Yeah, yeah, Shakespeare is meant to be played, not read, and it can be a struggle to herd teenagers through the Bard’s interesting and bloody tragedies, but even a perfunctory reading of “The Merchant of Venice” would hopefully have prevented the dystopian nightmare Massachusetts has presented us with today.
The United States has a massive shortage of donor organs. This is an unfortunate truth. So, to combat this issue, a pair of Massachusetts congresspeople have proposed HD 3822, which would allow prisoners to donate organs and/or bone marrow (a pound of flesh, so to speak) in exchange for up to a year in reduced prison time. Yes, that’s right. Give up pieces of yourself and the state of Massachusetts will deign to reduce your long prison sentence.
Oh, and before you dismiss this as typical Republican antics, the bill was sponsored by two Democrats, and in a statement one of them hoped to address racial disparities in organ donation, as people of color are much less likely to receive organs. Never mind that Black people are imprisoned at a much higher rate than Whites.
Yeah, this whole thing is what people in the business like to call an ethical disaster.
Fortunately, the bill will likely never be passed and it’s probably illegal anyway. A federal law from 1984 (how’s that for a coincidence) prevents people from donating organs for use in human transplantation in exchange for “valuable consideration.” In other words, you can’t sell your organs for profit, and in this case, reducing prison time would probably count as valuable consideration in the eyes of the courts.
Oh, and in case you’ve never read Merchant of Venice, Shylock, the character looking for the pound of flesh as payment for a debt? He’s the villain. In fact, it’s pretty safe to say that anyone looking to extract payment from human dismemberment is probably the bad guy of the story. Apparently that wasn’t clear.
How do you stop a fungi? With a deadly guy
Thanks to the new HBO series “The Last of Us,” there’s been a lot of talk about the upcoming fungi-pocalypse, as the show depicts the real-life “zombie fungus” Cordyceps turning humans into, you know, zombies.
No need to worry, ladies and gentleman, because science has discovered a way to turn back the fungal horde. A heroic, and environmentally friendly, alternative to chemical pesticides “in the fight against resistant fungi [that] are now resistant to antimycotics – partly because they are used in large quantities in agricultural fields,” investigators at the Leibniz Institute for Natural Product Research and Infection Biology in Jena, Germany, said in a written statement.
We are, of course, talking about Keanu Reeves. Wait a second. He’s not even in “The Last of Us.” Sorry folks, we are being told that it really is Keanu Reeves. Our champion in the inevitable fungal pandemic is movie star Keanu Reeves. Sort of. It’s actually keanumycin, a substance produced by bacteria of the genus Pseudomonas.
Really? Keanumycin? “The lipopeptides kill so efficiently that we named them after Keanu Reeves because he, too, is extremely deadly in his roles,” lead author Sebastian Götze, PhD, explained.
Dr. Götze and his associates had been working with pseudomonads for quite a while before they were able to isolate the toxins responsible for their ability to kill amoebae, which resemble fungi in some characteristics. When then finally tried the keanumycin against gray mold rot on hydrangea leaves, the intensely contemplative star of “The Matrix” and “John Wick” – sorry, wrong Keanu – the bacterial derivative significantly inhibited growth of the fungus, they said.
Additional testing has shown that keanumycin is not highly toxic to human cells and is effective against fungi such as Candida albicans in very low concentrations, which makes it a good candidate for future pharmaceutical development.
To that news there can be only one response from the substance’s namesake.
High fat, bye parasites
Fat. Fat. Fat. Seems like everyone is trying to avoid it these days, but fat may be good thing when it comes to weaseling out a parasite.
The parasite in this case is the whipworm, aka Trichuris trichiura. You can find this guy in the intestines of millions of people, where it causes long-lasting infections. Yikes … Researchers have found that the plan of attack to get rid of this invasive species is to boost the immune system, but instead of vitamin C and zinc it’s fat they’re pumping in. Yes, fat.
The developing countries with poor sewage that are at the highest risk for contracting parasites such as this also are among those where people ingest cheaper diets that are generally higher in fat. The investigators were interested to see how a high-fat diet would affect immune responses to the whipworms.
And, as with almost everything else, the researchers turned to mice, which were introduced to a closely related species, Trichuris muris.
A high-fat diet, rather than obesity itself, increases a molecule on T-helper cells called ST2, and this allows an increased T-helper 2 response, effectively giving eviction notices to the parasites in the intestinal lining.
To say the least, the researchers were surprised since “high-fat diets are mostly associated with increased pathology during disease,” said senior author Richard Grencis, PhD, of the University of Manchester (England), who noted that ST2 is not normally triggered with a standard diet in mice but the high-fat diet gave it a boost and an “alternate pathway” out.
Now before you start ordering extra-large fries at the drive-through to keep the whipworms away, the researchers added that they “have previously published that weight loss can aid the expulsion of a different gut parasite worm.” Figures.
Once again, though, signs are pointing to the gut for improved health.
Maternal COVID-19 vaccine curbs infant infection
a new study shows.
Previous research has confirmed that COVID-19 neutralizing antibodies following maternal vaccination or maternal COVID-19 infection are present in umbilical cord blood, breast milk, and infant serum specimens, wrote Sarah C.J. Jorgensen, PharmD, MPH, of the University of Toronto, and colleagues in their article published in The BMJ.
In the study, the researchers identified maternal and newborn pairs using administrative databases from Canada. The study population included 8,809 infants aged younger than 6 months who were born between May 7, 2021, and March 31, 2022, and who underwent testing for COVID-19 between May 7, 2021, and September 5, 2022.
Maternal vaccination with the primary COVID-19 mRNA monovalent vaccine series was defined as two vaccine doses administered up to 14 days before delivery, with at least one of the doses after the conception date.
Maternal vaccination with the primary series plus one booster was defined as three doses administered up to 14 days before delivery, with at least one of these doses after the conception date.
The primary outcome was the presence of delta or omicron COVID-19 infection or hospital admission of the infants.
The study population included 99 COVID-19 cases with the delta variant (with 4,365 controls) and 1,501 cases with the omicron variant (with 4,847 controls).
Overall, the vaccine effectiveness of maternal doses was 95% against delta infection and 45% against omicron.
The effectiveness against hospital admission in cases of delta and omicron variants were 97% and 53%, respectively.
The effectiveness of three doses was 73% against omicron infant infection and 80% against omicron-related infant hospitalization. Data were not available for the effectiveness of three doses against the delta variant.
The effectiveness of two doses of vaccine against infant omicron infection was highest when mothers received the second dose during the third trimester of pregnancy, compared with during the first trimester or second trimester (53% vs. 47% and 53% vs. 37%, respectively).
Vaccine effectiveness with two doses against infant infection from omicron was highest in the first 8 weeks of life (57%), then decreased to 40% among infants after 16 weeks of age.
Although the study was not designed to assess the mechanism of action of the impact of maternal vaccination on infants, the current study results were consistent with other recent studies showing a reduction in infections and hospitalizations among infants whose mothers received COVID-19 vaccines during pregnancy, the researchers wrote in their discussion.
The findings were limited by several factors including the potential unmeasured confounders not available in databases, such as whether infants were breastfed, the researchers noted. Other limitations included a lack of data on home test results and the inability to assess the waning impact of the vaccine effectiveness against the delta variant because of the small number of delta cases, they said. However, the results suggest that the mRNA COVID-19 vaccine during pregnancy was moderately to highly effective for protection against omicron and delta infection and infection-related hospitalization – especially during the first 8 weeks of life.
Effectiveness is encouraging, but updates are needed
The effectiveness of maternal vaccination to prevent COVID-19 infection and related hospitalizations in infants is promising, especially since those younger than 6 months have no other source of vaccine protection against COVID-19 infection, wrote Dana Danino, MD, of Soroka University Medical Center, Israel, and Ilan Youngster, MD, of Shamir Medical Center, Israel, in an accompanying editorial also published in The BMJ.
They also noted that maternal vaccination during pregnancy is an established method of protecting infants from infections such as influenza and pertussis.
Data from previous studies show that most infants whose mothers were vaccinated against COVID-19 during pregnancy retained maternal antibodies at 6 months, “but evidence for protection against neonatal COVID-19 infection has been deficient,” they said.
The current study findings support the value of vaccination during pregnancy, and the findings were strengthened by the large study population, the editorialists wrote. However, whether the same effectiveness holds for other COVID-19 strains such as BQ.1, BQ.1.1, BF.7, XBB, and XBB.1 remains unknown, they said.
Other areas in need of exploration include the optimal timing of vaccination during pregnancy, the protective effects of a bivalent mRNA vaccine (vs. the primary monovalent vaccine in the current study), and the potential benefits of additional boosters, they added.
“Although Jorgenson and colleagues’ study reinforces the value of maternal vaccination against COVID-19 during pregnancy, more studies are needed to better inform vaccination recommendations in an evolving landscape of new SARS-CoV-2 strains and novel vaccines,” the editorialists concluded.
The study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-term Care; the study also received funding from the Canadian Immunization Research Network and the Public Health Agency of Canada. Dr. Jorgensen and the editorialists had no financial conflicts to disclose.
*This article was updated on 3/2/2023.
a new study shows.
Previous research has confirmed that COVID-19 neutralizing antibodies following maternal vaccination or maternal COVID-19 infection are present in umbilical cord blood, breast milk, and infant serum specimens, wrote Sarah C.J. Jorgensen, PharmD, MPH, of the University of Toronto, and colleagues in their article published in The BMJ.
In the study, the researchers identified maternal and newborn pairs using administrative databases from Canada. The study population included 8,809 infants aged younger than 6 months who were born between May 7, 2021, and March 31, 2022, and who underwent testing for COVID-19 between May 7, 2021, and September 5, 2022.
Maternal vaccination with the primary COVID-19 mRNA monovalent vaccine series was defined as two vaccine doses administered up to 14 days before delivery, with at least one of the doses after the conception date.
Maternal vaccination with the primary series plus one booster was defined as three doses administered up to 14 days before delivery, with at least one of these doses after the conception date.
The primary outcome was the presence of delta or omicron COVID-19 infection or hospital admission of the infants.
The study population included 99 COVID-19 cases with the delta variant (with 4,365 controls) and 1,501 cases with the omicron variant (with 4,847 controls).
Overall, the vaccine effectiveness of maternal doses was 95% against delta infection and 45% against omicron.
The effectiveness against hospital admission in cases of delta and omicron variants were 97% and 53%, respectively.
The effectiveness of three doses was 73% against omicron infant infection and 80% against omicron-related infant hospitalization. Data were not available for the effectiveness of three doses against the delta variant.
The effectiveness of two doses of vaccine against infant omicron infection was highest when mothers received the second dose during the third trimester of pregnancy, compared with during the first trimester or second trimester (53% vs. 47% and 53% vs. 37%, respectively).
Vaccine effectiveness with two doses against infant infection from omicron was highest in the first 8 weeks of life (57%), then decreased to 40% among infants after 16 weeks of age.
Although the study was not designed to assess the mechanism of action of the impact of maternal vaccination on infants, the current study results were consistent with other recent studies showing a reduction in infections and hospitalizations among infants whose mothers received COVID-19 vaccines during pregnancy, the researchers wrote in their discussion.
The findings were limited by several factors including the potential unmeasured confounders not available in databases, such as whether infants were breastfed, the researchers noted. Other limitations included a lack of data on home test results and the inability to assess the waning impact of the vaccine effectiveness against the delta variant because of the small number of delta cases, they said. However, the results suggest that the mRNA COVID-19 vaccine during pregnancy was moderately to highly effective for protection against omicron and delta infection and infection-related hospitalization – especially during the first 8 weeks of life.
Effectiveness is encouraging, but updates are needed
The effectiveness of maternal vaccination to prevent COVID-19 infection and related hospitalizations in infants is promising, especially since those younger than 6 months have no other source of vaccine protection against COVID-19 infection, wrote Dana Danino, MD, of Soroka University Medical Center, Israel, and Ilan Youngster, MD, of Shamir Medical Center, Israel, in an accompanying editorial also published in The BMJ.
They also noted that maternal vaccination during pregnancy is an established method of protecting infants from infections such as influenza and pertussis.
Data from previous studies show that most infants whose mothers were vaccinated against COVID-19 during pregnancy retained maternal antibodies at 6 months, “but evidence for protection against neonatal COVID-19 infection has been deficient,” they said.
The current study findings support the value of vaccination during pregnancy, and the findings were strengthened by the large study population, the editorialists wrote. However, whether the same effectiveness holds for other COVID-19 strains such as BQ.1, BQ.1.1, BF.7, XBB, and XBB.1 remains unknown, they said.
Other areas in need of exploration include the optimal timing of vaccination during pregnancy, the protective effects of a bivalent mRNA vaccine (vs. the primary monovalent vaccine in the current study), and the potential benefits of additional boosters, they added.
“Although Jorgenson and colleagues’ study reinforces the value of maternal vaccination against COVID-19 during pregnancy, more studies are needed to better inform vaccination recommendations in an evolving landscape of new SARS-CoV-2 strains and novel vaccines,” the editorialists concluded.
The study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-term Care; the study also received funding from the Canadian Immunization Research Network and the Public Health Agency of Canada. Dr. Jorgensen and the editorialists had no financial conflicts to disclose.
*This article was updated on 3/2/2023.
a new study shows.
Previous research has confirmed that COVID-19 neutralizing antibodies following maternal vaccination or maternal COVID-19 infection are present in umbilical cord blood, breast milk, and infant serum specimens, wrote Sarah C.J. Jorgensen, PharmD, MPH, of the University of Toronto, and colleagues in their article published in The BMJ.
In the study, the researchers identified maternal and newborn pairs using administrative databases from Canada. The study population included 8,809 infants aged younger than 6 months who were born between May 7, 2021, and March 31, 2022, and who underwent testing for COVID-19 between May 7, 2021, and September 5, 2022.
Maternal vaccination with the primary COVID-19 mRNA monovalent vaccine series was defined as two vaccine doses administered up to 14 days before delivery, with at least one of the doses after the conception date.
Maternal vaccination with the primary series plus one booster was defined as three doses administered up to 14 days before delivery, with at least one of these doses after the conception date.
The primary outcome was the presence of delta or omicron COVID-19 infection or hospital admission of the infants.
The study population included 99 COVID-19 cases with the delta variant (with 4,365 controls) and 1,501 cases with the omicron variant (with 4,847 controls).
Overall, the vaccine effectiveness of maternal doses was 95% against delta infection and 45% against omicron.
The effectiveness against hospital admission in cases of delta and omicron variants were 97% and 53%, respectively.
The effectiveness of three doses was 73% against omicron infant infection and 80% against omicron-related infant hospitalization. Data were not available for the effectiveness of three doses against the delta variant.
The effectiveness of two doses of vaccine against infant omicron infection was highest when mothers received the second dose during the third trimester of pregnancy, compared with during the first trimester or second trimester (53% vs. 47% and 53% vs. 37%, respectively).
Vaccine effectiveness with two doses against infant infection from omicron was highest in the first 8 weeks of life (57%), then decreased to 40% among infants after 16 weeks of age.
Although the study was not designed to assess the mechanism of action of the impact of maternal vaccination on infants, the current study results were consistent with other recent studies showing a reduction in infections and hospitalizations among infants whose mothers received COVID-19 vaccines during pregnancy, the researchers wrote in their discussion.
The findings were limited by several factors including the potential unmeasured confounders not available in databases, such as whether infants were breastfed, the researchers noted. Other limitations included a lack of data on home test results and the inability to assess the waning impact of the vaccine effectiveness against the delta variant because of the small number of delta cases, they said. However, the results suggest that the mRNA COVID-19 vaccine during pregnancy was moderately to highly effective for protection against omicron and delta infection and infection-related hospitalization – especially during the first 8 weeks of life.
Effectiveness is encouraging, but updates are needed
The effectiveness of maternal vaccination to prevent COVID-19 infection and related hospitalizations in infants is promising, especially since those younger than 6 months have no other source of vaccine protection against COVID-19 infection, wrote Dana Danino, MD, of Soroka University Medical Center, Israel, and Ilan Youngster, MD, of Shamir Medical Center, Israel, in an accompanying editorial also published in The BMJ.
They also noted that maternal vaccination during pregnancy is an established method of protecting infants from infections such as influenza and pertussis.
Data from previous studies show that most infants whose mothers were vaccinated against COVID-19 during pregnancy retained maternal antibodies at 6 months, “but evidence for protection against neonatal COVID-19 infection has been deficient,” they said.
The current study findings support the value of vaccination during pregnancy, and the findings were strengthened by the large study population, the editorialists wrote. However, whether the same effectiveness holds for other COVID-19 strains such as BQ.1, BQ.1.1, BF.7, XBB, and XBB.1 remains unknown, they said.
Other areas in need of exploration include the optimal timing of vaccination during pregnancy, the protective effects of a bivalent mRNA vaccine (vs. the primary monovalent vaccine in the current study), and the potential benefits of additional boosters, they added.
“Although Jorgenson and colleagues’ study reinforces the value of maternal vaccination against COVID-19 during pregnancy, more studies are needed to better inform vaccination recommendations in an evolving landscape of new SARS-CoV-2 strains and novel vaccines,” the editorialists concluded.
The study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-term Care; the study also received funding from the Canadian Immunization Research Network and the Public Health Agency of Canada. Dr. Jorgensen and the editorialists had no financial conflicts to disclose.
*This article was updated on 3/2/2023.
FROM THE BMJ
Renewed calls for fallopian tube removal to avoid ovarian cancer
All women, regardless of their risk profile, should consider prophylactic removal of the fallopian tubes at the same time as other pelvic surgery once they are finished having children, the Ovarian Cancer Research Alliance has advised.
The recommendation, announced Feb. 1, replaces the decades-old focus on symptom awareness and early detection and follows “sobering and deeply disappointing” results from a large U.K. study published 2 years ago, the organization said.
That was the UK Collaborative Trial of Ovarian Cancer Screening published in The Lancet in 2021, which followed more than 200,000 women for a median 16 years. It showed that screening average-risk women with a CA-125 blood test and ultrasound does not reduce deaths from the disease, as reported at the time by this news organization.
“We all hoped that the trial would show that early detection was effective in changing mortality rates. When the results came out, it was very hard to accept,” Audra Moran, OCRA president and CEO, said in an interview.
“We have an obligation to let people know that symptom awareness and early detection will not save lives” but considering opportunistic salpingectomy “absolutely will,” said Ms. Moran. Hence the renewed call for women to consider having their fallopian tubes removed.
What sounds new about this call is that the group is directing fallopian tube removal to all women “who are undergoing pelvic surgeries for benign conditions,” irrespective of what perceived risk they have of developing ovarian cancer (for example, based on family history).
But this advice has been in place for years for women who are known to be at higher risk for the disease.
For instance, women at high risk for ovarian cancer based on Hereditary Breast and Ovarian Cancer Syndrome (HBOC) have long been recommended to undergo surgery to remove ovaries and fallopian tubes (risk-reducing bilateral salpingo-oophorectomy or RRBSO) once there is no longer a desire for pregnancy.
Approached for comment about the new messaging, Stephanie V. Blank, MD, president of the Society of Gynecologic Oncology, says that the new recommendation – that all women who are finished childbearing consider opportunistic salpingectomy at the time of other pelvic surgery for benign conditions – is “not aggressive.”
“It’s reasonable and makes sense,” Dr. Blank said in an interview.
And she pointed out that it’s actually not “new”; it is, however, getting “new attention” based on the disappointing U.K. screening study, said Dr. Blank, director of gynecologic oncology for the Mount Sinai Health System in New York and professor of gynecologic oncology at Icahn School of Medicine at Mount Sinai.
She noted that the procedure of opportunistic salpingectomy has been endorsed by SGO since 2013 and by the American College of Obstetricians and Gynecologists since 2015.
There is increasing evidence that most high-grade serous ovarian cancers arise from cells in the fallopian tubes, William Dahut, MD, chief scientific officer for the American Cancer Society, told this news organization.
“Indirect evidence suggests a fairly strong degree of risk reduction associated with opportunistic salpingectomy for the most prevalent type of ovarian cancer (serous), and some risk reduction of epithelial ovarian cancer. At this time, these discussions seem warranted,” Dr. Dahut said.
At this point, however, the fact that leading organizations advise “consideration” means that the evidence base has “not been judged to be sufficiently strong (in terms of what we can say about benefits and harms) to advise a direct recommendation for opportunistic salpingectomy,” Dr. Dahut added.
There is no current recommendation to have fallopian tubes removed as a stand-alone procedure, he pointed out. However, he commented that “the occasion of scheduled gynecologic surgery presents an opportunity to possibly reduce the risk of ovarian cancer without known adverse effects in women who have completed childbearing. Having the discussion seems to be justified by the current evidence,” Dr. Dahut said.
Deanna Gerber, MD, a gynecologic oncologist at NYU Langone Perlmutter Cancer Center-Long Island, agrees. “In women who are scheduled to have a gynecologic or pelvic procedure, clinicians should discuss the possibility of removing the fallopian tubes at that time. A salpingectomy is a relatively low-risk procedure and adds little time to the surgery,” Dr. Gerber said in an interview.
“Women should understand that there is still ongoing research on this topic, but this low-risk procedure may reduce their risk of developing an ovarian or fallopian tube cancer,” Dr. Gerber said.
OCRA also encourages all women (or anyone born with ovaries) to know their risk for ovarian cancer. To that end, the organization has launched a pilot program offering free, at-home genetic testing kits to people with a personal or family history of breast, ovarian, uterine, or colorectal cancer.
Ms. Moran, Dr. Blank, Dr. Dahut, and Dr. Gerber report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
All women, regardless of their risk profile, should consider prophylactic removal of the fallopian tubes at the same time as other pelvic surgery once they are finished having children, the Ovarian Cancer Research Alliance has advised.
The recommendation, announced Feb. 1, replaces the decades-old focus on symptom awareness and early detection and follows “sobering and deeply disappointing” results from a large U.K. study published 2 years ago, the organization said.
That was the UK Collaborative Trial of Ovarian Cancer Screening published in The Lancet in 2021, which followed more than 200,000 women for a median 16 years. It showed that screening average-risk women with a CA-125 blood test and ultrasound does not reduce deaths from the disease, as reported at the time by this news organization.
“We all hoped that the trial would show that early detection was effective in changing mortality rates. When the results came out, it was very hard to accept,” Audra Moran, OCRA president and CEO, said in an interview.
“We have an obligation to let people know that symptom awareness and early detection will not save lives” but considering opportunistic salpingectomy “absolutely will,” said Ms. Moran. Hence the renewed call for women to consider having their fallopian tubes removed.
What sounds new about this call is that the group is directing fallopian tube removal to all women “who are undergoing pelvic surgeries for benign conditions,” irrespective of what perceived risk they have of developing ovarian cancer (for example, based on family history).
But this advice has been in place for years for women who are known to be at higher risk for the disease.
For instance, women at high risk for ovarian cancer based on Hereditary Breast and Ovarian Cancer Syndrome (HBOC) have long been recommended to undergo surgery to remove ovaries and fallopian tubes (risk-reducing bilateral salpingo-oophorectomy or RRBSO) once there is no longer a desire for pregnancy.
Approached for comment about the new messaging, Stephanie V. Blank, MD, president of the Society of Gynecologic Oncology, says that the new recommendation – that all women who are finished childbearing consider opportunistic salpingectomy at the time of other pelvic surgery for benign conditions – is “not aggressive.”
“It’s reasonable and makes sense,” Dr. Blank said in an interview.
And she pointed out that it’s actually not “new”; it is, however, getting “new attention” based on the disappointing U.K. screening study, said Dr. Blank, director of gynecologic oncology for the Mount Sinai Health System in New York and professor of gynecologic oncology at Icahn School of Medicine at Mount Sinai.
She noted that the procedure of opportunistic salpingectomy has been endorsed by SGO since 2013 and by the American College of Obstetricians and Gynecologists since 2015.
There is increasing evidence that most high-grade serous ovarian cancers arise from cells in the fallopian tubes, William Dahut, MD, chief scientific officer for the American Cancer Society, told this news organization.
“Indirect evidence suggests a fairly strong degree of risk reduction associated with opportunistic salpingectomy for the most prevalent type of ovarian cancer (serous), and some risk reduction of epithelial ovarian cancer. At this time, these discussions seem warranted,” Dr. Dahut said.
At this point, however, the fact that leading organizations advise “consideration” means that the evidence base has “not been judged to be sufficiently strong (in terms of what we can say about benefits and harms) to advise a direct recommendation for opportunistic salpingectomy,” Dr. Dahut added.
There is no current recommendation to have fallopian tubes removed as a stand-alone procedure, he pointed out. However, he commented that “the occasion of scheduled gynecologic surgery presents an opportunity to possibly reduce the risk of ovarian cancer without known adverse effects in women who have completed childbearing. Having the discussion seems to be justified by the current evidence,” Dr. Dahut said.
Deanna Gerber, MD, a gynecologic oncologist at NYU Langone Perlmutter Cancer Center-Long Island, agrees. “In women who are scheduled to have a gynecologic or pelvic procedure, clinicians should discuss the possibility of removing the fallopian tubes at that time. A salpingectomy is a relatively low-risk procedure and adds little time to the surgery,” Dr. Gerber said in an interview.
“Women should understand that there is still ongoing research on this topic, but this low-risk procedure may reduce their risk of developing an ovarian or fallopian tube cancer,” Dr. Gerber said.
OCRA also encourages all women (or anyone born with ovaries) to know their risk for ovarian cancer. To that end, the organization has launched a pilot program offering free, at-home genetic testing kits to people with a personal or family history of breast, ovarian, uterine, or colorectal cancer.
Ms. Moran, Dr. Blank, Dr. Dahut, and Dr. Gerber report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
All women, regardless of their risk profile, should consider prophylactic removal of the fallopian tubes at the same time as other pelvic surgery once they are finished having children, the Ovarian Cancer Research Alliance has advised.
The recommendation, announced Feb. 1, replaces the decades-old focus on symptom awareness and early detection and follows “sobering and deeply disappointing” results from a large U.K. study published 2 years ago, the organization said.
That was the UK Collaborative Trial of Ovarian Cancer Screening published in The Lancet in 2021, which followed more than 200,000 women for a median 16 years. It showed that screening average-risk women with a CA-125 blood test and ultrasound does not reduce deaths from the disease, as reported at the time by this news organization.
“We all hoped that the trial would show that early detection was effective in changing mortality rates. When the results came out, it was very hard to accept,” Audra Moran, OCRA president and CEO, said in an interview.
“We have an obligation to let people know that symptom awareness and early detection will not save lives” but considering opportunistic salpingectomy “absolutely will,” said Ms. Moran. Hence the renewed call for women to consider having their fallopian tubes removed.
What sounds new about this call is that the group is directing fallopian tube removal to all women “who are undergoing pelvic surgeries for benign conditions,” irrespective of what perceived risk they have of developing ovarian cancer (for example, based on family history).
But this advice has been in place for years for women who are known to be at higher risk for the disease.
For instance, women at high risk for ovarian cancer based on Hereditary Breast and Ovarian Cancer Syndrome (HBOC) have long been recommended to undergo surgery to remove ovaries and fallopian tubes (risk-reducing bilateral salpingo-oophorectomy or RRBSO) once there is no longer a desire for pregnancy.
Approached for comment about the new messaging, Stephanie V. Blank, MD, president of the Society of Gynecologic Oncology, says that the new recommendation – that all women who are finished childbearing consider opportunistic salpingectomy at the time of other pelvic surgery for benign conditions – is “not aggressive.”
“It’s reasonable and makes sense,” Dr. Blank said in an interview.
And she pointed out that it’s actually not “new”; it is, however, getting “new attention” based on the disappointing U.K. screening study, said Dr. Blank, director of gynecologic oncology for the Mount Sinai Health System in New York and professor of gynecologic oncology at Icahn School of Medicine at Mount Sinai.
She noted that the procedure of opportunistic salpingectomy has been endorsed by SGO since 2013 and by the American College of Obstetricians and Gynecologists since 2015.
There is increasing evidence that most high-grade serous ovarian cancers arise from cells in the fallopian tubes, William Dahut, MD, chief scientific officer for the American Cancer Society, told this news organization.
“Indirect evidence suggests a fairly strong degree of risk reduction associated with opportunistic salpingectomy for the most prevalent type of ovarian cancer (serous), and some risk reduction of epithelial ovarian cancer. At this time, these discussions seem warranted,” Dr. Dahut said.
At this point, however, the fact that leading organizations advise “consideration” means that the evidence base has “not been judged to be sufficiently strong (in terms of what we can say about benefits and harms) to advise a direct recommendation for opportunistic salpingectomy,” Dr. Dahut added.
There is no current recommendation to have fallopian tubes removed as a stand-alone procedure, he pointed out. However, he commented that “the occasion of scheduled gynecologic surgery presents an opportunity to possibly reduce the risk of ovarian cancer without known adverse effects in women who have completed childbearing. Having the discussion seems to be justified by the current evidence,” Dr. Dahut said.
Deanna Gerber, MD, a gynecologic oncologist at NYU Langone Perlmutter Cancer Center-Long Island, agrees. “In women who are scheduled to have a gynecologic or pelvic procedure, clinicians should discuss the possibility of removing the fallopian tubes at that time. A salpingectomy is a relatively low-risk procedure and adds little time to the surgery,” Dr. Gerber said in an interview.
“Women should understand that there is still ongoing research on this topic, but this low-risk procedure may reduce their risk of developing an ovarian or fallopian tube cancer,” Dr. Gerber said.
OCRA also encourages all women (or anyone born with ovaries) to know their risk for ovarian cancer. To that end, the organization has launched a pilot program offering free, at-home genetic testing kits to people with a personal or family history of breast, ovarian, uterine, or colorectal cancer.
Ms. Moran, Dr. Blank, Dr. Dahut, and Dr. Gerber report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Nonsurgical options for stress urinary incontinence
In the article, “Nonsurgical treatments for patients with urinary incontinence” (OBG Manag. September 2022;34:36- 42.), the authors, Ashley J. Murillo, MD, and Halina M. Zyczynski, MD, discuss the successful nonsurgical management of urge urinary incontinence, stress urinary incontinence, and mixed urinary incontinence, presenting the case of a 39-year-old woman with urine leakage during exercise. As a follow-up for readers, OBG Management posted a quiz question asking, “Which of the following is a nonsurgical treatment for stress urinary incontinence?”
A total of 129 readers cast their vote:
50.4% (65 readers) said bladder retraining
36.4% (47 readers) said periurethral bulking
13.2% (17 readers) said antimuscarinic agents
The correct answer was periurethral bulking, as bladder retraining and antimuscarinic agents, according to TABLE 1 in Murillo and Zyczynski’s article, are appropriate for managing urge urinary incontinence.
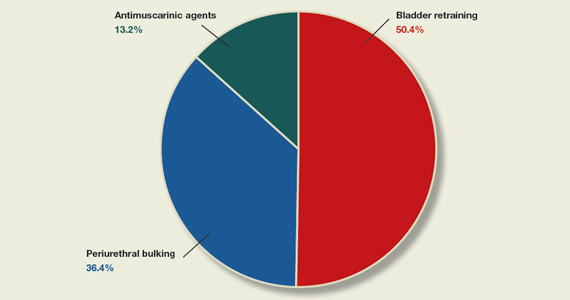
In the article, “Nonsurgical treatments for patients with urinary incontinence” (OBG Manag. September 2022;34:36- 42.), the authors, Ashley J. Murillo, MD, and Halina M. Zyczynski, MD, discuss the successful nonsurgical management of urge urinary incontinence, stress urinary incontinence, and mixed urinary incontinence, presenting the case of a 39-year-old woman with urine leakage during exercise. As a follow-up for readers, OBG Management posted a quiz question asking, “Which of the following is a nonsurgical treatment for stress urinary incontinence?”
A total of 129 readers cast their vote:
50.4% (65 readers) said bladder retraining
36.4% (47 readers) said periurethral bulking
13.2% (17 readers) said antimuscarinic agents
The correct answer was periurethral bulking, as bladder retraining and antimuscarinic agents, according to TABLE 1 in Murillo and Zyczynski’s article, are appropriate for managing urge urinary incontinence.
In the article, “Nonsurgical treatments for patients with urinary incontinence” (OBG Manag. September 2022;34:36- 42.), the authors, Ashley J. Murillo, MD, and Halina M. Zyczynski, MD, discuss the successful nonsurgical management of urge urinary incontinence, stress urinary incontinence, and mixed urinary incontinence, presenting the case of a 39-year-old woman with urine leakage during exercise. As a follow-up for readers, OBG Management posted a quiz question asking, “Which of the following is a nonsurgical treatment for stress urinary incontinence?”
A total of 129 readers cast their vote:
50.4% (65 readers) said bladder retraining
36.4% (47 readers) said periurethral bulking
13.2% (17 readers) said antimuscarinic agents
The correct answer was periurethral bulking, as bladder retraining and antimuscarinic agents, according to TABLE 1 in Murillo and Zyczynski’s article, are appropriate for managing urge urinary incontinence.